User login
AVAHO Mtg: Germline Testing Key for Vets With High-Risk PC
Not too long ago, prostate-cancer genetics didn’t mean much to patient care. But in recent years, the landscape of therapy has transformed as researchers have discovered links between multiple genes and aggressive tumors.
Now, as a hematologist-oncologist explained to attendees at an Association of VA Hematology/Oncology regional meeting in Detroit, genetic tests can guide treatment for some—but not all—men with prostate cancer.
For patients with mutations, appropriate supplemental medications “can improve overall outcomes and have a long-standing impact on patients” said Scott J. Dawsey, MD, of the John D. Dingell Veterans Affairs Medical Center in Detroit in an interview following the AVAHO meeting, which focused on the management of prostate cancer.
As Dawsey explained, about 10% of patients with prostate cancer appear to have genetic mutations, although the exact percentage is unclear. The mutations are especially common in metastatic forms of prostate cancer. They’re estimated to be present in 11.8%-16.2% of those cases.
While these proportions are relatively small, the number of overall prostate-cancer cases with mutations is large due to the high burden of the disease, Dawsey said. Prostate cancer is by far the most common cancer in men, and estimated 299,010 cases will be diagnosed in the United States this year.
According to Dawsey, genetic mutations seem to boost the risk of more aggressive disease—and the risk of other malignancies—by disrupting DNA repair. This process can lead to even more mutations that may “make the cancer behave and grow more aggressively.”
But not all prostate cancer patients need to undergo genetic testing. Dawsey urged colleagues to figure out which patients should be tested by consulting National Comprehensive Cancer Network (NCCN) guidelines and the newly updated US Department of Veterans Affairs (VA) prostate cancer clinical pathway.
The two sets of recommendations agree on germline testing in patients with cases that are metastatic, very high risk, and high risk. Lower-risk cases should only be tested if patients meet family history criteria. The sets of guidelines also recommend somatic testing in patients with metastatic cancer.
In addition to providing guidance about treatment, genetic test results can have implications regarding other potential malignancies that may affect patients, Dawsey said. The results may also have implications for cancer risk in family members.
Several drugs are now available for patients with genetic mutations, including checkpoint inhibitors and PARP inhibitors. The drugs, which have unique mechanisms of action, are given in addition to standard prostate cancer treatments, he said.
“If a patient doesn’t have one of these genetic changes,” he said, “these drugs aren’t an option.”
A long list of drugs or combinations of drugs are in clinical trials, including the poly(adenosine diphosphate–ribose) polymerase (PARP) inhibitors olaparib, abiraterone, and niraparib and the checkpoint inhibitors nivolumab and cemiplimab.
The drugs generally improve response rates and progression-free survival, Dawsey said, and patients are generally able to tolerate them. In regard to which drugs to choose, he suggested consulting the and NCCN guidelines and the VA oncology clinical pathway for prostate cancer.
Not too long ago, prostate-cancer genetics didn’t mean much to patient care. But in recent years, the landscape of therapy has transformed as researchers have discovered links between multiple genes and aggressive tumors.
Now, as a hematologist-oncologist explained to attendees at an Association of VA Hematology/Oncology regional meeting in Detroit, genetic tests can guide treatment for some—but not all—men with prostate cancer.
For patients with mutations, appropriate supplemental medications “can improve overall outcomes and have a long-standing impact on patients” said Scott J. Dawsey, MD, of the John D. Dingell Veterans Affairs Medical Center in Detroit in an interview following the AVAHO meeting, which focused on the management of prostate cancer.
As Dawsey explained, about 10% of patients with prostate cancer appear to have genetic mutations, although the exact percentage is unclear. The mutations are especially common in metastatic forms of prostate cancer. They’re estimated to be present in 11.8%-16.2% of those cases.
While these proportions are relatively small, the number of overall prostate-cancer cases with mutations is large due to the high burden of the disease, Dawsey said. Prostate cancer is by far the most common cancer in men, and estimated 299,010 cases will be diagnosed in the United States this year.
According to Dawsey, genetic mutations seem to boost the risk of more aggressive disease—and the risk of other malignancies—by disrupting DNA repair. This process can lead to even more mutations that may “make the cancer behave and grow more aggressively.”
But not all prostate cancer patients need to undergo genetic testing. Dawsey urged colleagues to figure out which patients should be tested by consulting National Comprehensive Cancer Network (NCCN) guidelines and the newly updated US Department of Veterans Affairs (VA) prostate cancer clinical pathway.
The two sets of recommendations agree on germline testing in patients with cases that are metastatic, very high risk, and high risk. Lower-risk cases should only be tested if patients meet family history criteria. The sets of guidelines also recommend somatic testing in patients with metastatic cancer.
In addition to providing guidance about treatment, genetic test results can have implications regarding other potential malignancies that may affect patients, Dawsey said. The results may also have implications for cancer risk in family members.
Several drugs are now available for patients with genetic mutations, including checkpoint inhibitors and PARP inhibitors. The drugs, which have unique mechanisms of action, are given in addition to standard prostate cancer treatments, he said.
“If a patient doesn’t have one of these genetic changes,” he said, “these drugs aren’t an option.”
A long list of drugs or combinations of drugs are in clinical trials, including the poly(adenosine diphosphate–ribose) polymerase (PARP) inhibitors olaparib, abiraterone, and niraparib and the checkpoint inhibitors nivolumab and cemiplimab.
The drugs generally improve response rates and progression-free survival, Dawsey said, and patients are generally able to tolerate them. In regard to which drugs to choose, he suggested consulting the and NCCN guidelines and the VA oncology clinical pathway for prostate cancer.
Not too long ago, prostate-cancer genetics didn’t mean much to patient care. But in recent years, the landscape of therapy has transformed as researchers have discovered links between multiple genes and aggressive tumors.
Now, as a hematologist-oncologist explained to attendees at an Association of VA Hematology/Oncology regional meeting in Detroit, genetic tests can guide treatment for some—but not all—men with prostate cancer.
For patients with mutations, appropriate supplemental medications “can improve overall outcomes and have a long-standing impact on patients” said Scott J. Dawsey, MD, of the John D. Dingell Veterans Affairs Medical Center in Detroit in an interview following the AVAHO meeting, which focused on the management of prostate cancer.
As Dawsey explained, about 10% of patients with prostate cancer appear to have genetic mutations, although the exact percentage is unclear. The mutations are especially common in metastatic forms of prostate cancer. They’re estimated to be present in 11.8%-16.2% of those cases.
While these proportions are relatively small, the number of overall prostate-cancer cases with mutations is large due to the high burden of the disease, Dawsey said. Prostate cancer is by far the most common cancer in men, and estimated 299,010 cases will be diagnosed in the United States this year.
According to Dawsey, genetic mutations seem to boost the risk of more aggressive disease—and the risk of other malignancies—by disrupting DNA repair. This process can lead to even more mutations that may “make the cancer behave and grow more aggressively.”
But not all prostate cancer patients need to undergo genetic testing. Dawsey urged colleagues to figure out which patients should be tested by consulting National Comprehensive Cancer Network (NCCN) guidelines and the newly updated US Department of Veterans Affairs (VA) prostate cancer clinical pathway.
The two sets of recommendations agree on germline testing in patients with cases that are metastatic, very high risk, and high risk. Lower-risk cases should only be tested if patients meet family history criteria. The sets of guidelines also recommend somatic testing in patients with metastatic cancer.
In addition to providing guidance about treatment, genetic test results can have implications regarding other potential malignancies that may affect patients, Dawsey said. The results may also have implications for cancer risk in family members.
Several drugs are now available for patients with genetic mutations, including checkpoint inhibitors and PARP inhibitors. The drugs, which have unique mechanisms of action, are given in addition to standard prostate cancer treatments, he said.
“If a patient doesn’t have one of these genetic changes,” he said, “these drugs aren’t an option.”
A long list of drugs or combinations of drugs are in clinical trials, including the poly(adenosine diphosphate–ribose) polymerase (PARP) inhibitors olaparib, abiraterone, and niraparib and the checkpoint inhibitors nivolumab and cemiplimab.
The drugs generally improve response rates and progression-free survival, Dawsey said, and patients are generally able to tolerate them. In regard to which drugs to choose, he suggested consulting the and NCCN guidelines and the VA oncology clinical pathway for prostate cancer.
BP Disorder in Pregnancy Tied to Young-Onset Dementia Risk
TOPLINE:
A new analysis showed that preeclampsia is associated with an increased risk for young-onset dementia.
METHODOLOGY:
- Researchers analyzed data from the French Conception study, a nationwide prospective cohort study of more than 1.9 million pregnancies.
- Mothers were followed for an average of 9 years.
TAKEAWAY:
- Nearly 3% of the mothers had preeclampsia, and 128 developed young-onset dementia.
- Preeclampsia was associated with a 2.65-fold increased risk for young-onset dementia after adjusting for obesity, diabetes, smoking, drug or alcohol addiction, and social deprivation.
- The risk was greater when preeclampsia occurred before 34 weeks of gestation (hazard ratio [HR], 4.15) or was superimposed on chronic hypertension (HR, 4.76).
- Prior research has found an association between preeclampsia and vascular dementia, but this analysis “is the first to show an increase in early-onset dementia risk,” the authors of the study wrote.
IN PRACTICE:
“Individuals who have had preeclampsia should be reassured that young-onset dementia remains a very rare condition. Their absolute risk increases only imperceptibly,” Stephen Tong, PhD, and Roxanne Hastie, PhD, both with the University of Melbourne, Melbourne, Australia, wrote in a related commentary about the findings.
“Individuals who have been affected by preeclampsia in a prior pregnancy might instead focus on reducing their risk of developing the many chronic health ailments that are far more common,” they added. “Although it is yet to be proven in clinical trials, it is plausible that after an episode of preeclampsia, adopting a healthy lifestyle may improve vascular health and reduce the risk of many serious cardiovascular conditions.”
SOURCE:
Valérie Olié, PhD, of the Santé Publique France in Saint-Maurice, France, was the corresponding author on the paper. The research letter was published online in JAMA Network Open.
LIMITATIONS:
The investigators relied on hospital records to identify cases of dementia, which may have led to underestimation of incidence of the disease.
DISCLOSURES:
The study was funded by the French Hypertension Society, the French Hypertension Research Foundation, and the French Cardiology Federation. A co-author disclosed personal fees from pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
A new analysis showed that preeclampsia is associated with an increased risk for young-onset dementia.
METHODOLOGY:
- Researchers analyzed data from the French Conception study, a nationwide prospective cohort study of more than 1.9 million pregnancies.
- Mothers were followed for an average of 9 years.
TAKEAWAY:
- Nearly 3% of the mothers had preeclampsia, and 128 developed young-onset dementia.
- Preeclampsia was associated with a 2.65-fold increased risk for young-onset dementia after adjusting for obesity, diabetes, smoking, drug or alcohol addiction, and social deprivation.
- The risk was greater when preeclampsia occurred before 34 weeks of gestation (hazard ratio [HR], 4.15) or was superimposed on chronic hypertension (HR, 4.76).
- Prior research has found an association between preeclampsia and vascular dementia, but this analysis “is the first to show an increase in early-onset dementia risk,” the authors of the study wrote.
IN PRACTICE:
“Individuals who have had preeclampsia should be reassured that young-onset dementia remains a very rare condition. Their absolute risk increases only imperceptibly,” Stephen Tong, PhD, and Roxanne Hastie, PhD, both with the University of Melbourne, Melbourne, Australia, wrote in a related commentary about the findings.
“Individuals who have been affected by preeclampsia in a prior pregnancy might instead focus on reducing their risk of developing the many chronic health ailments that are far more common,” they added. “Although it is yet to be proven in clinical trials, it is plausible that after an episode of preeclampsia, adopting a healthy lifestyle may improve vascular health and reduce the risk of many serious cardiovascular conditions.”
SOURCE:
Valérie Olié, PhD, of the Santé Publique France in Saint-Maurice, France, was the corresponding author on the paper. The research letter was published online in JAMA Network Open.
LIMITATIONS:
The investigators relied on hospital records to identify cases of dementia, which may have led to underestimation of incidence of the disease.
DISCLOSURES:
The study was funded by the French Hypertension Society, the French Hypertension Research Foundation, and the French Cardiology Federation. A co-author disclosed personal fees from pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
A new analysis showed that preeclampsia is associated with an increased risk for young-onset dementia.
METHODOLOGY:
- Researchers analyzed data from the French Conception study, a nationwide prospective cohort study of more than 1.9 million pregnancies.
- Mothers were followed for an average of 9 years.
TAKEAWAY:
- Nearly 3% of the mothers had preeclampsia, and 128 developed young-onset dementia.
- Preeclampsia was associated with a 2.65-fold increased risk for young-onset dementia after adjusting for obesity, diabetes, smoking, drug or alcohol addiction, and social deprivation.
- The risk was greater when preeclampsia occurred before 34 weeks of gestation (hazard ratio [HR], 4.15) or was superimposed on chronic hypertension (HR, 4.76).
- Prior research has found an association between preeclampsia and vascular dementia, but this analysis “is the first to show an increase in early-onset dementia risk,” the authors of the study wrote.
IN PRACTICE:
“Individuals who have had preeclampsia should be reassured that young-onset dementia remains a very rare condition. Their absolute risk increases only imperceptibly,” Stephen Tong, PhD, and Roxanne Hastie, PhD, both with the University of Melbourne, Melbourne, Australia, wrote in a related commentary about the findings.
“Individuals who have been affected by preeclampsia in a prior pregnancy might instead focus on reducing their risk of developing the many chronic health ailments that are far more common,” they added. “Although it is yet to be proven in clinical trials, it is plausible that after an episode of preeclampsia, adopting a healthy lifestyle may improve vascular health and reduce the risk of many serious cardiovascular conditions.”
SOURCE:
Valérie Olié, PhD, of the Santé Publique France in Saint-Maurice, France, was the corresponding author on the paper. The research letter was published online in JAMA Network Open.
LIMITATIONS:
The investigators relied on hospital records to identify cases of dementia, which may have led to underestimation of incidence of the disease.
DISCLOSURES:
The study was funded by the French Hypertension Society, the French Hypertension Research Foundation, and the French Cardiology Federation. A co-author disclosed personal fees from pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
ESOPEC: FLOT Bests CROSS in Resectable Esophageal Cancer
The study results, presented as a late-breaking abstract at the annual meeting of the American Society of Clinical Oncology (ASCO), help settle a long-standing debate about whether chemotherapy with FLOT — 5-florouracil, leucovorin, oxaliplatin, and docetaxel — before and after surgery, or neoadjuvant radiation plus CROSS — carboplatin and paclitaxel — followed by surgery is the best approach.
There has been “considerable disagreement as to whether giving all adjuvant therapy upfront versus ‘sandwich’ adjuvant therapy before and after surgery is the better standard of care for locally advanced resectable esophageal cancer,” Jennifer Tseng, MD, of Boston Medical Center, Boston, said in an ASCO press release. This randomized clinical trial shows the sandwich approach “provides better outcomes.”
The practice-changing ESOPEC findings will have an important effect on the management of patients with resectable esophageal adenocarcinoma and gastroesophageal junction adenocarcinoma, but local and distant failures remain a challenge in this population, explained invited discussant Karyn A. Goodman, MD.
Advances since the initiation of ESOPEC — such as immunotherapy options and personalized strategies — suggest the esophageal adenocarcinoma story is still evolving, said Dr. Goodman, professor and vice chair of research and quality in the Department of Radiation Oncology at Icahn School of Medicine at Mount Sinai, New York.
The ESOPEC trial
Both the FLOT and CROSS regimens are established standards of care in resectable esophageal adenocarcinoma, and the choice of treatment has largely varied based on geographical location.
The current randomized, prospective, open-label ESOPEC trial, however, demonstrated that FLOT can prolong overall survival, first author Jens Hoeppner, MD, from the University of Bielefeld in Detmold, Germany, reported.
Overall, 438 patients with locally advanced, resectable esophageal adenocarcinoma recruited between February 2016 and April 2020 from 25 sites in Germany and randomized to either FLOT (n = 221) or CROSS (n = 217). The median age was 63 years, and most (89.3%) were men. Patients were followed until November 2023, and median follow-up was 55 months.
Patients in the FLOT arm received four cycles — one every 2 weeks for 8 weeks — followed by surgery 4-6 weeks later. FLOT cycles were reinitiated 4-6 weeks after surgery and given every 2 weeks for 8 weeks.
Those in the CROSS arm received one cycle per week of radiation therapy for 5 weeks plus carboplatin and paclitaxel followed by surgery 4-6 weeks after the last cycle.
Overall, 86% received both neoadjuvant therapy and surgery in the FLOT arm versus 82.9% in the CROSS group. Among these patients, 16.8% in the FLOT group achieved a pathological complete remission versus 10.0% in the CROSS arm.
In the intention-to-treat population, median overall survival was almost twice as long in the FLOT group — 66 months versus 37 months. At 3 years, those who received FLOT had a 30% lower risk of dying (hazard ratio [HR], 0.70), with 57.4% of patients alive at that point, compared with 50.7% patients in the CROSS arm.
The 5-year overall survival was 50.6% in the FLOT group versus 38.7% in the CROSS group.
Patients receiving FLOT also demonstrated improved progression-free survival (PFS), with a median PFS of 38 months versus 16 months. The 3-year PFS was 51.6% with FLOT versus 35.0% with CROSS (HR, 0.66). The exploratory subgroup analyses for sex, age, ECOG status, and clinical T and N stages also favored FLOT.
The 30-day postoperative mortality was 1.0% in the FLOT group and 1.7% in the CROSS group, and the 90-day postoperative mortality rate was 3.2% and 5.6%, respectively.
Based on these findings, perioperative chemotherapy with FLOT should be preferred over neoadjuvant chemoradiation with CROSS, Dr. Hoeppner concluded.
Dr. Goodman agreed, noting that, in the wake of ESOPEC, FLOT will likely be adopted as a more standard approach in the United States for patients who are fit. And, for patients who are not candidates for FLOT, CROSS is a reasonable option, she said.
But, she asked, does it really have to be an either/or situation?
Multiple studies, including Dr. Goodman’s 2021 Alliance/CALGB 80803 study, have demonstrated promising outcomes with combined modalities and adapting therapy based on treatment response. Several trials, for instance, are evaluating combining FLOT and CROSS, with some showing the approach is feasible and comes with manageable toxicity.
It’s also important to look outside of FLOT and CROSS. During ESOPEC, new approaches entered the treatment landscape, including the use of adjuvant immunotherapy following neoadjuvant chemoradiation and surgery for noncomplete response.
Take the CheckMate 577 study, which found that adjuvant nivolumab immunotherapy after preoperative CROSS and surgery significantly reduced metastatic recurrence and doubled disease-free survival in patients who did not achieve a complete response. This approach is now a standard of care for those patients.
FLOT plus neoadjuvant nivolumab may also be a viable option, Dr. Goodman noted, but we haven’t yet seen “any benefit in survival with the combo of chemotherapy and immunotherapy for resectable esophago-gastric cancer.”
Further studies are needed to evaluate the synergy of immunotherapy and radiotherapy. The next chapter of the esophageal adenocarcinoma story may feature a “best-of-both-worlds” approach that combines induction chemotherapy, followed by personalized chemoradiation, surgery, and potentially adjuvant immunotherapy, Dr. Goodman explained.
While the ESOPEC findings are impressive, the 5-year overall survival of only 50% is still suboptimal, she noted. “Given the poor prognosis with this disease, we need to continue to develop clinical trials to identify better targets, novel treatment combinations, and select patients that will respond best to specific treatment.”
ESOPEC was funded by the Deutsche Forschungsgemeinschaft (German Research Foundation). Dr. Hoeppner reported receiving travel, accommodations, and expenses from Intuitive Surgical. Dr. Goodman reported a relationship with the National Cancer Institute and consulting or advisory roles for Novartis, Philips Healthcare, RenovoRX, and Roche/Genentech.
A version of this article first appeared on Medscape.com.
The study results, presented as a late-breaking abstract at the annual meeting of the American Society of Clinical Oncology (ASCO), help settle a long-standing debate about whether chemotherapy with FLOT — 5-florouracil, leucovorin, oxaliplatin, and docetaxel — before and after surgery, or neoadjuvant radiation plus CROSS — carboplatin and paclitaxel — followed by surgery is the best approach.
There has been “considerable disagreement as to whether giving all adjuvant therapy upfront versus ‘sandwich’ adjuvant therapy before and after surgery is the better standard of care for locally advanced resectable esophageal cancer,” Jennifer Tseng, MD, of Boston Medical Center, Boston, said in an ASCO press release. This randomized clinical trial shows the sandwich approach “provides better outcomes.”
The practice-changing ESOPEC findings will have an important effect on the management of patients with resectable esophageal adenocarcinoma and gastroesophageal junction adenocarcinoma, but local and distant failures remain a challenge in this population, explained invited discussant Karyn A. Goodman, MD.
Advances since the initiation of ESOPEC — such as immunotherapy options and personalized strategies — suggest the esophageal adenocarcinoma story is still evolving, said Dr. Goodman, professor and vice chair of research and quality in the Department of Radiation Oncology at Icahn School of Medicine at Mount Sinai, New York.
The ESOPEC trial
Both the FLOT and CROSS regimens are established standards of care in resectable esophageal adenocarcinoma, and the choice of treatment has largely varied based on geographical location.
The current randomized, prospective, open-label ESOPEC trial, however, demonstrated that FLOT can prolong overall survival, first author Jens Hoeppner, MD, from the University of Bielefeld in Detmold, Germany, reported.
Overall, 438 patients with locally advanced, resectable esophageal adenocarcinoma recruited between February 2016 and April 2020 from 25 sites in Germany and randomized to either FLOT (n = 221) or CROSS (n = 217). The median age was 63 years, and most (89.3%) were men. Patients were followed until November 2023, and median follow-up was 55 months.
Patients in the FLOT arm received four cycles — one every 2 weeks for 8 weeks — followed by surgery 4-6 weeks later. FLOT cycles were reinitiated 4-6 weeks after surgery and given every 2 weeks for 8 weeks.
Those in the CROSS arm received one cycle per week of radiation therapy for 5 weeks plus carboplatin and paclitaxel followed by surgery 4-6 weeks after the last cycle.
Overall, 86% received both neoadjuvant therapy and surgery in the FLOT arm versus 82.9% in the CROSS group. Among these patients, 16.8% in the FLOT group achieved a pathological complete remission versus 10.0% in the CROSS arm.
In the intention-to-treat population, median overall survival was almost twice as long in the FLOT group — 66 months versus 37 months. At 3 years, those who received FLOT had a 30% lower risk of dying (hazard ratio [HR], 0.70), with 57.4% of patients alive at that point, compared with 50.7% patients in the CROSS arm.
The 5-year overall survival was 50.6% in the FLOT group versus 38.7% in the CROSS group.
Patients receiving FLOT also demonstrated improved progression-free survival (PFS), with a median PFS of 38 months versus 16 months. The 3-year PFS was 51.6% with FLOT versus 35.0% with CROSS (HR, 0.66). The exploratory subgroup analyses for sex, age, ECOG status, and clinical T and N stages also favored FLOT.
The 30-day postoperative mortality was 1.0% in the FLOT group and 1.7% in the CROSS group, and the 90-day postoperative mortality rate was 3.2% and 5.6%, respectively.
Based on these findings, perioperative chemotherapy with FLOT should be preferred over neoadjuvant chemoradiation with CROSS, Dr. Hoeppner concluded.
Dr. Goodman agreed, noting that, in the wake of ESOPEC, FLOT will likely be adopted as a more standard approach in the United States for patients who are fit. And, for patients who are not candidates for FLOT, CROSS is a reasonable option, she said.
But, she asked, does it really have to be an either/or situation?
Multiple studies, including Dr. Goodman’s 2021 Alliance/CALGB 80803 study, have demonstrated promising outcomes with combined modalities and adapting therapy based on treatment response. Several trials, for instance, are evaluating combining FLOT and CROSS, with some showing the approach is feasible and comes with manageable toxicity.
It’s also important to look outside of FLOT and CROSS. During ESOPEC, new approaches entered the treatment landscape, including the use of adjuvant immunotherapy following neoadjuvant chemoradiation and surgery for noncomplete response.
Take the CheckMate 577 study, which found that adjuvant nivolumab immunotherapy after preoperative CROSS and surgery significantly reduced metastatic recurrence and doubled disease-free survival in patients who did not achieve a complete response. This approach is now a standard of care for those patients.
FLOT plus neoadjuvant nivolumab may also be a viable option, Dr. Goodman noted, but we haven’t yet seen “any benefit in survival with the combo of chemotherapy and immunotherapy for resectable esophago-gastric cancer.”
Further studies are needed to evaluate the synergy of immunotherapy and radiotherapy. The next chapter of the esophageal adenocarcinoma story may feature a “best-of-both-worlds” approach that combines induction chemotherapy, followed by personalized chemoradiation, surgery, and potentially adjuvant immunotherapy, Dr. Goodman explained.
While the ESOPEC findings are impressive, the 5-year overall survival of only 50% is still suboptimal, she noted. “Given the poor prognosis with this disease, we need to continue to develop clinical trials to identify better targets, novel treatment combinations, and select patients that will respond best to specific treatment.”
ESOPEC was funded by the Deutsche Forschungsgemeinschaft (German Research Foundation). Dr. Hoeppner reported receiving travel, accommodations, and expenses from Intuitive Surgical. Dr. Goodman reported a relationship with the National Cancer Institute and consulting or advisory roles for Novartis, Philips Healthcare, RenovoRX, and Roche/Genentech.
A version of this article first appeared on Medscape.com.
The study results, presented as a late-breaking abstract at the annual meeting of the American Society of Clinical Oncology (ASCO), help settle a long-standing debate about whether chemotherapy with FLOT — 5-florouracil, leucovorin, oxaliplatin, and docetaxel — before and after surgery, or neoadjuvant radiation plus CROSS — carboplatin and paclitaxel — followed by surgery is the best approach.
There has been “considerable disagreement as to whether giving all adjuvant therapy upfront versus ‘sandwich’ adjuvant therapy before and after surgery is the better standard of care for locally advanced resectable esophageal cancer,” Jennifer Tseng, MD, of Boston Medical Center, Boston, said in an ASCO press release. This randomized clinical trial shows the sandwich approach “provides better outcomes.”
The practice-changing ESOPEC findings will have an important effect on the management of patients with resectable esophageal adenocarcinoma and gastroesophageal junction adenocarcinoma, but local and distant failures remain a challenge in this population, explained invited discussant Karyn A. Goodman, MD.
Advances since the initiation of ESOPEC — such as immunotherapy options and personalized strategies — suggest the esophageal adenocarcinoma story is still evolving, said Dr. Goodman, professor and vice chair of research and quality in the Department of Radiation Oncology at Icahn School of Medicine at Mount Sinai, New York.
The ESOPEC trial
Both the FLOT and CROSS regimens are established standards of care in resectable esophageal adenocarcinoma, and the choice of treatment has largely varied based on geographical location.
The current randomized, prospective, open-label ESOPEC trial, however, demonstrated that FLOT can prolong overall survival, first author Jens Hoeppner, MD, from the University of Bielefeld in Detmold, Germany, reported.
Overall, 438 patients with locally advanced, resectable esophageal adenocarcinoma recruited between February 2016 and April 2020 from 25 sites in Germany and randomized to either FLOT (n = 221) or CROSS (n = 217). The median age was 63 years, and most (89.3%) were men. Patients were followed until November 2023, and median follow-up was 55 months.
Patients in the FLOT arm received four cycles — one every 2 weeks for 8 weeks — followed by surgery 4-6 weeks later. FLOT cycles were reinitiated 4-6 weeks after surgery and given every 2 weeks for 8 weeks.
Those in the CROSS arm received one cycle per week of radiation therapy for 5 weeks plus carboplatin and paclitaxel followed by surgery 4-6 weeks after the last cycle.
Overall, 86% received both neoadjuvant therapy and surgery in the FLOT arm versus 82.9% in the CROSS group. Among these patients, 16.8% in the FLOT group achieved a pathological complete remission versus 10.0% in the CROSS arm.
In the intention-to-treat population, median overall survival was almost twice as long in the FLOT group — 66 months versus 37 months. At 3 years, those who received FLOT had a 30% lower risk of dying (hazard ratio [HR], 0.70), with 57.4% of patients alive at that point, compared with 50.7% patients in the CROSS arm.
The 5-year overall survival was 50.6% in the FLOT group versus 38.7% in the CROSS group.
Patients receiving FLOT also demonstrated improved progression-free survival (PFS), with a median PFS of 38 months versus 16 months. The 3-year PFS was 51.6% with FLOT versus 35.0% with CROSS (HR, 0.66). The exploratory subgroup analyses for sex, age, ECOG status, and clinical T and N stages also favored FLOT.
The 30-day postoperative mortality was 1.0% in the FLOT group and 1.7% in the CROSS group, and the 90-day postoperative mortality rate was 3.2% and 5.6%, respectively.
Based on these findings, perioperative chemotherapy with FLOT should be preferred over neoadjuvant chemoradiation with CROSS, Dr. Hoeppner concluded.
Dr. Goodman agreed, noting that, in the wake of ESOPEC, FLOT will likely be adopted as a more standard approach in the United States for patients who are fit. And, for patients who are not candidates for FLOT, CROSS is a reasonable option, she said.
But, she asked, does it really have to be an either/or situation?
Multiple studies, including Dr. Goodman’s 2021 Alliance/CALGB 80803 study, have demonstrated promising outcomes with combined modalities and adapting therapy based on treatment response. Several trials, for instance, are evaluating combining FLOT and CROSS, with some showing the approach is feasible and comes with manageable toxicity.
It’s also important to look outside of FLOT and CROSS. During ESOPEC, new approaches entered the treatment landscape, including the use of adjuvant immunotherapy following neoadjuvant chemoradiation and surgery for noncomplete response.
Take the CheckMate 577 study, which found that adjuvant nivolumab immunotherapy after preoperative CROSS and surgery significantly reduced metastatic recurrence and doubled disease-free survival in patients who did not achieve a complete response. This approach is now a standard of care for those patients.
FLOT plus neoadjuvant nivolumab may also be a viable option, Dr. Goodman noted, but we haven’t yet seen “any benefit in survival with the combo of chemotherapy and immunotherapy for resectable esophago-gastric cancer.”
Further studies are needed to evaluate the synergy of immunotherapy and radiotherapy. The next chapter of the esophageal adenocarcinoma story may feature a “best-of-both-worlds” approach that combines induction chemotherapy, followed by personalized chemoradiation, surgery, and potentially adjuvant immunotherapy, Dr. Goodman explained.
While the ESOPEC findings are impressive, the 5-year overall survival of only 50% is still suboptimal, she noted. “Given the poor prognosis with this disease, we need to continue to develop clinical trials to identify better targets, novel treatment combinations, and select patients that will respond best to specific treatment.”
ESOPEC was funded by the Deutsche Forschungsgemeinschaft (German Research Foundation). Dr. Hoeppner reported receiving travel, accommodations, and expenses from Intuitive Surgical. Dr. Goodman reported a relationship with the National Cancer Institute and consulting or advisory roles for Novartis, Philips Healthcare, RenovoRX, and Roche/Genentech.
A version of this article first appeared on Medscape.com.
FROM ASCO 2024
Study Addresses Litigation Related to Cutaneous Energy-based Based Device Treatments
“The utilization of laser and energy-based devices (LEBD) has grown substantially,” corresponding author Scott Stratman, MD, MPH, and coauthors wrote in their study, which was published online in the Journal of the American Academy of Dermatology. “This has led to a rise in practitioners, both physicians and nonphysicians, who may lack the requisite training in LEBD procedures. Subsequently, procedures performed by these untrained practitioners have resulted in more lawsuits related to patient complications. As the demand for LEBD procedures and the number of practitioners performing these procedures increase, it remains paramount to characterize the trends of malpractice cases involving these procedures.”
Dr. Stratman, a dermatology resident at the Icahn School of Medicine at Mount Sinai, New York City, and colleagues queried the LexisNexis database from 1985 to Sept. 30, 2023, for all state, federal, and appellate cases that included the terms “negligence” or “malpractice” and “skin” and “laser.” After they removed duplicate cases and excluded cases that did not report dermatologic complications or cutaneous energy-based procedures, the final analysis included 75 cases.
Most of the appellants/plaintiffs (66; 88%) were women, a greater number of cases were in the Northeast (26; 34.7%) and the South (23; 30.7%), and the fewest cases were in the Midwest (12 [16%]). The most common anatomical sites were the face, head, and/or neck, and 43 of the cases (57.3%) were decided in favor of the appellee/defendant or the party defending against the appeal, while 29 (38.7%) were in favor of the appellant/plaintiff or the party appealing, and three cases (4%) did not report a verdict.
In other findings, plastic surgeons were the most litigated healthcare professionals (18; 24%), while 39 of the overall cases (52%) involved nonphysician operators (NPOs), 32 (42.7%) involved a physician operator, and 4 cases (5.3%) did not name a device operator. The most common procedure performed in the included cases was laser hair removal (33; 44%). Complications from energy-based devices included burns, scarring, and pigmentation changes. Statistically significant associations were neither found between verdict outcome and appellee/defendant type nor found between energy-device operator or anatomical site.
The authors acknowledged certain limitations of the study, including the fact that the LexisNexis database does not contain cases handled in out-of-court settlements and cases that underwent third-party arbitration.
“Physicians must recognize their responsibility when delegating procedures to NPOs and their role in supervision of these procedures,” they concluded. “Comprehensive training for physicians and their agents is necessary to diminish adverse outcomes and legal risks. Moreover, all practitioners should be held to the same standard of care. Familiarity with malpractice trends not only strengthens the patient-provider relationship but also equips providers with effective strategies to minimize the risk of legal repercussions.”
Mathew M. Avram, MD, JD, director of laser, cosmetics, and dermatologic surgery at Massachusetts General Hospital, Boston, who was asked to comment on the study, said that it “reaffirms previous studies which show that laser hair removal continues to be the most litigated procedure in laser surgery, and that nonphysician operators are most commonly litigated against. It further reiterates the importance of close supervision and expert training of procedures delegated by physicians.”
Neither the authors nor Dr. Avram reported having relevant financial disclosures.
A version of this article first appeared on Medscape.com.
“The utilization of laser and energy-based devices (LEBD) has grown substantially,” corresponding author Scott Stratman, MD, MPH, and coauthors wrote in their study, which was published online in the Journal of the American Academy of Dermatology. “This has led to a rise in practitioners, both physicians and nonphysicians, who may lack the requisite training in LEBD procedures. Subsequently, procedures performed by these untrained practitioners have resulted in more lawsuits related to patient complications. As the demand for LEBD procedures and the number of practitioners performing these procedures increase, it remains paramount to characterize the trends of malpractice cases involving these procedures.”
Dr. Stratman, a dermatology resident at the Icahn School of Medicine at Mount Sinai, New York City, and colleagues queried the LexisNexis database from 1985 to Sept. 30, 2023, for all state, federal, and appellate cases that included the terms “negligence” or “malpractice” and “skin” and “laser.” After they removed duplicate cases and excluded cases that did not report dermatologic complications or cutaneous energy-based procedures, the final analysis included 75 cases.
Most of the appellants/plaintiffs (66; 88%) were women, a greater number of cases were in the Northeast (26; 34.7%) and the South (23; 30.7%), and the fewest cases were in the Midwest (12 [16%]). The most common anatomical sites were the face, head, and/or neck, and 43 of the cases (57.3%) were decided in favor of the appellee/defendant or the party defending against the appeal, while 29 (38.7%) were in favor of the appellant/plaintiff or the party appealing, and three cases (4%) did not report a verdict.
In other findings, plastic surgeons were the most litigated healthcare professionals (18; 24%), while 39 of the overall cases (52%) involved nonphysician operators (NPOs), 32 (42.7%) involved a physician operator, and 4 cases (5.3%) did not name a device operator. The most common procedure performed in the included cases was laser hair removal (33; 44%). Complications from energy-based devices included burns, scarring, and pigmentation changes. Statistically significant associations were neither found between verdict outcome and appellee/defendant type nor found between energy-device operator or anatomical site.
The authors acknowledged certain limitations of the study, including the fact that the LexisNexis database does not contain cases handled in out-of-court settlements and cases that underwent third-party arbitration.
“Physicians must recognize their responsibility when delegating procedures to NPOs and their role in supervision of these procedures,” they concluded. “Comprehensive training for physicians and their agents is necessary to diminish adverse outcomes and legal risks. Moreover, all practitioners should be held to the same standard of care. Familiarity with malpractice trends not only strengthens the patient-provider relationship but also equips providers with effective strategies to minimize the risk of legal repercussions.”
Mathew M. Avram, MD, JD, director of laser, cosmetics, and dermatologic surgery at Massachusetts General Hospital, Boston, who was asked to comment on the study, said that it “reaffirms previous studies which show that laser hair removal continues to be the most litigated procedure in laser surgery, and that nonphysician operators are most commonly litigated against. It further reiterates the importance of close supervision and expert training of procedures delegated by physicians.”
Neither the authors nor Dr. Avram reported having relevant financial disclosures.
A version of this article first appeared on Medscape.com.
“The utilization of laser and energy-based devices (LEBD) has grown substantially,” corresponding author Scott Stratman, MD, MPH, and coauthors wrote in their study, which was published online in the Journal of the American Academy of Dermatology. “This has led to a rise in practitioners, both physicians and nonphysicians, who may lack the requisite training in LEBD procedures. Subsequently, procedures performed by these untrained practitioners have resulted in more lawsuits related to patient complications. As the demand for LEBD procedures and the number of practitioners performing these procedures increase, it remains paramount to characterize the trends of malpractice cases involving these procedures.”
Dr. Stratman, a dermatology resident at the Icahn School of Medicine at Mount Sinai, New York City, and colleagues queried the LexisNexis database from 1985 to Sept. 30, 2023, for all state, federal, and appellate cases that included the terms “negligence” or “malpractice” and “skin” and “laser.” After they removed duplicate cases and excluded cases that did not report dermatologic complications or cutaneous energy-based procedures, the final analysis included 75 cases.
Most of the appellants/plaintiffs (66; 88%) were women, a greater number of cases were in the Northeast (26; 34.7%) and the South (23; 30.7%), and the fewest cases were in the Midwest (12 [16%]). The most common anatomical sites were the face, head, and/or neck, and 43 of the cases (57.3%) were decided in favor of the appellee/defendant or the party defending against the appeal, while 29 (38.7%) were in favor of the appellant/plaintiff or the party appealing, and three cases (4%) did not report a verdict.
In other findings, plastic surgeons were the most litigated healthcare professionals (18; 24%), while 39 of the overall cases (52%) involved nonphysician operators (NPOs), 32 (42.7%) involved a physician operator, and 4 cases (5.3%) did not name a device operator. The most common procedure performed in the included cases was laser hair removal (33; 44%). Complications from energy-based devices included burns, scarring, and pigmentation changes. Statistically significant associations were neither found between verdict outcome and appellee/defendant type nor found between energy-device operator or anatomical site.
The authors acknowledged certain limitations of the study, including the fact that the LexisNexis database does not contain cases handled in out-of-court settlements and cases that underwent third-party arbitration.
“Physicians must recognize their responsibility when delegating procedures to NPOs and their role in supervision of these procedures,” they concluded. “Comprehensive training for physicians and their agents is necessary to diminish adverse outcomes and legal risks. Moreover, all practitioners should be held to the same standard of care. Familiarity with malpractice trends not only strengthens the patient-provider relationship but also equips providers with effective strategies to minimize the risk of legal repercussions.”
Mathew M. Avram, MD, JD, director of laser, cosmetics, and dermatologic surgery at Massachusetts General Hospital, Boston, who was asked to comment on the study, said that it “reaffirms previous studies which show that laser hair removal continues to be the most litigated procedure in laser surgery, and that nonphysician operators are most commonly litigated against. It further reiterates the importance of close supervision and expert training of procedures delegated by physicians.”
Neither the authors nor Dr. Avram reported having relevant financial disclosures.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
‘Therapeutic Continuums’ Guide Systemic Sclerosis Treatment in Updated EULAR Recommendations
VIENNA – The use of immunosuppressive and antifibrotic drugs to treat skin and lung fibrosis leads updated recommendations from the European Alliance of Associations for Rheumatology (EULAR) for the treatment of systemic sclerosis.
“The most impactful new recommendation relates to the evidence for immunosuppressive agents and antifibrotics for the treatment of skin fibrosis and lung fibrosis,” said Francesco Del Galdo, MD, PhD, professor of experimental medicine, consultant rheumatologist, and scleroderma and connective tissue diseases specialist at Leeds Teaching Hospitals NHS Trust, Leeds, England. Dr. Del Galdo presented the update at the annual European Congress of Rheumatology.
“But there are also new recommendations, including a redefined target population for hematopoietic stem cell transplantation following cyclophosphamide, the upfront combination treatment at the time of diagnosis of pulmonary arterial hypertension [PAH], and a negative recommendation for the use of anticoagulants for pulmonary arterial hypertension,” noted Dr. Del Galdo, highlighting key updates in the 2024 recommendations.
Robert B.M. Landewé, MD, PhD, professor and rheumatologist at Amsterdam University Medical Center, Amsterdam, the Netherlands, and Zuyderland Medical Center, Heerlen, the Netherlands, co-moderated the session on EULAR recommendations. “The management of systemic sclerosis is a field in which a lot is happening,” he said. “The last update goes back to 2017, and in the meantime, many new approaches have seen the light, especially pertaining to skin fibrosis and interstitial lung disease. Six new recommendations have been coined, covering drugs like mycophenolate mofetil, nintedanib, rituximab, and tocilizumab. None of these therapies were present in the 2017 recommendations. It seems the field is now ready to further expand on targeted therapies for the management of musculoskeletal and gastrointestinal manifestations, calcinosis, and the local management of digital ulcers.”
‘Therapeutic Continuums’ Aid Disease Management
Dr. Del Galdo and his colleagues grouped the various interventions across what the recommendations label as evidence-backed “therapeutic continuums.” These span six of the eight different clinical manifestations of systemic sclerosis: Raynaud’s phenomenon, digital ulcers, pulmonary hypertension, musculoskeletal manifestations, skin fibrosis, interstitial lung disease (ILD), and gastrointestinal and renal crisis.
A slide showing the different strengths of evidence for various drugs across the eight manifestations illustrated the principle behind the therapeutic continuums. “These ‘therapeutic continuums’ suggest a common pathogenetic mechanism driving the various manifestations of disease,” said Dr. Del Galdo. For example, he noted, “If rituximab had a positive response in skin and in lung, it suggests that B cells play a role in the clinical manifestations of skin and lung in this disease.”
Dr. Del Galdo highlighted the new immunosuppression continuum and associated treatments for skin and lung fibrosis. “For skin involvement, the task force recommended mycophenolate, methotrexate, and rituximab, with tocilizumab having a lower level of evidence and lower recommendation strength; similarly, in interstitial lung disease, we have rituximab, mycophenolate, cyclophosphamide, and nintedanib, and these all have the highest strength of evidence. Tocilizumab is assigned one strength of evidence below the other drugs.”
He also cited the phosphodiesterase 5 inhibitor (PDE5i) drugs that are used across Raynaud’s phenomenon, digital ulcers, and pulmonary arterial hypertension, which together form a vascular therapeutic continuum.
The complexity of systemic sclerosis and multiple manifestations was a major determinant of the recommendations, Dr. Del Galdo pointed out. “The task force realized that since this is such a complex disease, we cannot recommend one treatment unconditionally. For example, with mycophenolate mofetil, what works for most patients for the skin and lung manifestations might not for someone who experiences severe diarrhea, in which mycophenolate is contraindicated. So, the highest degree of recommendation that the task force felt comfortable with was ‘should be considered.’ ”
Dr. Del Galdo stressed that the complex nature of systemic sclerosis means that “when thinking of treating one manifestation, you also always need to consider all the other clinical manifestations as experienced by the patient, and it is this multifaceted scenario that will ultimately lead to your final choice.”
Turning to new evidence around drug use, Dr. Del Galdo said that rituximab has the highest level of evidence across skin and lung manifestations, nintedanib is new in lung, and tocilizumab is new across both skin and lung.
To treat systemic sclerosis–pulmonary arterial hypertension (SSc-PAH), as long as there are no contraindications, the task force recommends using PDE5i and endothelin receptor antagonists (ERAs) at diagnosis. Data from phase 3 trials show a better outcome when the combination is established early.
The task force suggests avoiding the use of warfarin in PAH. “This is supported by a signal from two trials showing an increase in morbidity and mortality in these patients,” noted Dr. Del Galdo.
He also pointed out that selexipag and riociguat were new and important second-line additions for the treatment of PAH, and — consistent with the ERA approach — the EULAR recommendation supports frequent follow-up to establish a treat-to-target approach to maximizing clinical outcomes in SSc-PAH and SSc-ILD. “Specifically, for the first time, we recommend monitoring the effect of any chosen intervention selected within 3-6 months of starting. The evidence suggests there is a group of patients who respond and some who respond less well and who might benefit from a second-line intervention.”
For example, results of one trial support the approach of adding an antifibrotic agent to reduce progression in people with progressive lung fibrosis. “Similarly, for pulmonary hypertension, we recommend putting patients on dual treatment, and if this fails, place them on selexipag or switch the PDE5i to riociguat,” Dr. Del Galdo said.
Systemic Sclerosis Research Agenda and Recommendations Align
Dr. Del Galdo highlighted the value of therapeutic continuums in advancing disease understanding. “It is starting to teach us what we know and what we don’t and where do we need to build more evidence. Effectively, they determine where the gaps in therapy lie, and this starts to guide the research agenda.
“In fact, what is really interesting about this recommendation update — certainly from the perspective of disease understanding — is that we are starting to have a bird’s-eye view of the clinical manifestations of scleroderma that have so often been dealt with separately. Now we are starting to build a cumulative evidence map of this disease.”
In 2017, the research agenda largely advocated identifying immune-targeting drugs for skin and lung fibrosis, Dr. Del Galdo pointed out. “Now, we’ve done that — we’ve identified appropriate immunosuppressive drugs — and this is testimony to the importance of these recommendations because what prioritized the research agenda 10 years ago ended up informing the clinical trials and made it into the recommendations.”
“We definitely are one step forward compared to this 2017 recommendation and closer to what we would like to do,” he asserted.
Remission Elusive but Getting Closer
In some respects, according to Dr. Del Galdo, research and development is making relatively slow progress, especially compared with other rheumatologic diseases such as rheumatoid arthritis. “We cannot put patients with systemic sclerosis in remission yet. But I think we are one step ahead in that we’ve now established the treat-to-target approach to maximize the efficacy with which we can stall disease progression, but we cannot yet put these patients into remission,” he said. Systemic sclerosis has multiple manifestations, and fibrotic damage cannot be reversed. “Right now, the scar will remain there forever,” he noted.
Until remission is achievable, Dr. Del Galdo advises diagnosing and treating patients earlier to prevent fibrotic manifestations.
Dr. Del Galdo explained the three leading priorities on the systemic sclerosis research agenda. “There are three because it is such a complex disease. The first is considering the patient voice — this is the most important one, and the patients say they want a more holistic approach — so trialing and treating multiple manifestations together.”
Second, Dr. Del Galdo said, he would like to see a patient-reported measure developed that can capture the entire disease.
Third, from a physician’s point of view, Dr. Del Galdo said, “We want to send the patients into remission. We need to continue to further deconvolute the clinical manifestations and find the bottleneck at the beginning of the natural history of disease.
“If we can find a drug that is effective very early on, before the patients start getting the eight different manifestations with different levels of severity, then we will be on the right road, which we hope will end in remission.”
Dr. Del Galdo has served on the speakers bureau for AstraZeneca and Janssen; consulted for AstraZeneca, Boehringer Ingelheim, Capella, Chemomab, Janssen, and Mitsubishi-Tanabe; and received grant or research support from AbbVie, AstraZeneca, Boheringer Ingelheim, Capella, Chemomab, Kymab, Janssen, and Mitsubishi-Tanabe. Dr. Landewé had no relevant disclosures.
A version of this article first appeared on Medscape.com.
VIENNA – The use of immunosuppressive and antifibrotic drugs to treat skin and lung fibrosis leads updated recommendations from the European Alliance of Associations for Rheumatology (EULAR) for the treatment of systemic sclerosis.
“The most impactful new recommendation relates to the evidence for immunosuppressive agents and antifibrotics for the treatment of skin fibrosis and lung fibrosis,” said Francesco Del Galdo, MD, PhD, professor of experimental medicine, consultant rheumatologist, and scleroderma and connective tissue diseases specialist at Leeds Teaching Hospitals NHS Trust, Leeds, England. Dr. Del Galdo presented the update at the annual European Congress of Rheumatology.
“But there are also new recommendations, including a redefined target population for hematopoietic stem cell transplantation following cyclophosphamide, the upfront combination treatment at the time of diagnosis of pulmonary arterial hypertension [PAH], and a negative recommendation for the use of anticoagulants for pulmonary arterial hypertension,” noted Dr. Del Galdo, highlighting key updates in the 2024 recommendations.
Robert B.M. Landewé, MD, PhD, professor and rheumatologist at Amsterdam University Medical Center, Amsterdam, the Netherlands, and Zuyderland Medical Center, Heerlen, the Netherlands, co-moderated the session on EULAR recommendations. “The management of systemic sclerosis is a field in which a lot is happening,” he said. “The last update goes back to 2017, and in the meantime, many new approaches have seen the light, especially pertaining to skin fibrosis and interstitial lung disease. Six new recommendations have been coined, covering drugs like mycophenolate mofetil, nintedanib, rituximab, and tocilizumab. None of these therapies were present in the 2017 recommendations. It seems the field is now ready to further expand on targeted therapies for the management of musculoskeletal and gastrointestinal manifestations, calcinosis, and the local management of digital ulcers.”
‘Therapeutic Continuums’ Aid Disease Management
Dr. Del Galdo and his colleagues grouped the various interventions across what the recommendations label as evidence-backed “therapeutic continuums.” These span six of the eight different clinical manifestations of systemic sclerosis: Raynaud’s phenomenon, digital ulcers, pulmonary hypertension, musculoskeletal manifestations, skin fibrosis, interstitial lung disease (ILD), and gastrointestinal and renal crisis.
A slide showing the different strengths of evidence for various drugs across the eight manifestations illustrated the principle behind the therapeutic continuums. “These ‘therapeutic continuums’ suggest a common pathogenetic mechanism driving the various manifestations of disease,” said Dr. Del Galdo. For example, he noted, “If rituximab had a positive response in skin and in lung, it suggests that B cells play a role in the clinical manifestations of skin and lung in this disease.”
Dr. Del Galdo highlighted the new immunosuppression continuum and associated treatments for skin and lung fibrosis. “For skin involvement, the task force recommended mycophenolate, methotrexate, and rituximab, with tocilizumab having a lower level of evidence and lower recommendation strength; similarly, in interstitial lung disease, we have rituximab, mycophenolate, cyclophosphamide, and nintedanib, and these all have the highest strength of evidence. Tocilizumab is assigned one strength of evidence below the other drugs.”
He also cited the phosphodiesterase 5 inhibitor (PDE5i) drugs that are used across Raynaud’s phenomenon, digital ulcers, and pulmonary arterial hypertension, which together form a vascular therapeutic continuum.
The complexity of systemic sclerosis and multiple manifestations was a major determinant of the recommendations, Dr. Del Galdo pointed out. “The task force realized that since this is such a complex disease, we cannot recommend one treatment unconditionally. For example, with mycophenolate mofetil, what works for most patients for the skin and lung manifestations might not for someone who experiences severe diarrhea, in which mycophenolate is contraindicated. So, the highest degree of recommendation that the task force felt comfortable with was ‘should be considered.’ ”
Dr. Del Galdo stressed that the complex nature of systemic sclerosis means that “when thinking of treating one manifestation, you also always need to consider all the other clinical manifestations as experienced by the patient, and it is this multifaceted scenario that will ultimately lead to your final choice.”
Turning to new evidence around drug use, Dr. Del Galdo said that rituximab has the highest level of evidence across skin and lung manifestations, nintedanib is new in lung, and tocilizumab is new across both skin and lung.
To treat systemic sclerosis–pulmonary arterial hypertension (SSc-PAH), as long as there are no contraindications, the task force recommends using PDE5i and endothelin receptor antagonists (ERAs) at diagnosis. Data from phase 3 trials show a better outcome when the combination is established early.
The task force suggests avoiding the use of warfarin in PAH. “This is supported by a signal from two trials showing an increase in morbidity and mortality in these patients,” noted Dr. Del Galdo.
He also pointed out that selexipag and riociguat were new and important second-line additions for the treatment of PAH, and — consistent with the ERA approach — the EULAR recommendation supports frequent follow-up to establish a treat-to-target approach to maximizing clinical outcomes in SSc-PAH and SSc-ILD. “Specifically, for the first time, we recommend monitoring the effect of any chosen intervention selected within 3-6 months of starting. The evidence suggests there is a group of patients who respond and some who respond less well and who might benefit from a second-line intervention.”
For example, results of one trial support the approach of adding an antifibrotic agent to reduce progression in people with progressive lung fibrosis. “Similarly, for pulmonary hypertension, we recommend putting patients on dual treatment, and if this fails, place them on selexipag or switch the PDE5i to riociguat,” Dr. Del Galdo said.
Systemic Sclerosis Research Agenda and Recommendations Align
Dr. Del Galdo highlighted the value of therapeutic continuums in advancing disease understanding. “It is starting to teach us what we know and what we don’t and where do we need to build more evidence. Effectively, they determine where the gaps in therapy lie, and this starts to guide the research agenda.
“In fact, what is really interesting about this recommendation update — certainly from the perspective of disease understanding — is that we are starting to have a bird’s-eye view of the clinical manifestations of scleroderma that have so often been dealt with separately. Now we are starting to build a cumulative evidence map of this disease.”
In 2017, the research agenda largely advocated identifying immune-targeting drugs for skin and lung fibrosis, Dr. Del Galdo pointed out. “Now, we’ve done that — we’ve identified appropriate immunosuppressive drugs — and this is testimony to the importance of these recommendations because what prioritized the research agenda 10 years ago ended up informing the clinical trials and made it into the recommendations.”
“We definitely are one step forward compared to this 2017 recommendation and closer to what we would like to do,” he asserted.
Remission Elusive but Getting Closer
In some respects, according to Dr. Del Galdo, research and development is making relatively slow progress, especially compared with other rheumatologic diseases such as rheumatoid arthritis. “We cannot put patients with systemic sclerosis in remission yet. But I think we are one step ahead in that we’ve now established the treat-to-target approach to maximize the efficacy with which we can stall disease progression, but we cannot yet put these patients into remission,” he said. Systemic sclerosis has multiple manifestations, and fibrotic damage cannot be reversed. “Right now, the scar will remain there forever,” he noted.
Until remission is achievable, Dr. Del Galdo advises diagnosing and treating patients earlier to prevent fibrotic manifestations.
Dr. Del Galdo explained the three leading priorities on the systemic sclerosis research agenda. “There are three because it is such a complex disease. The first is considering the patient voice — this is the most important one, and the patients say they want a more holistic approach — so trialing and treating multiple manifestations together.”
Second, Dr. Del Galdo said, he would like to see a patient-reported measure developed that can capture the entire disease.
Third, from a physician’s point of view, Dr. Del Galdo said, “We want to send the patients into remission. We need to continue to further deconvolute the clinical manifestations and find the bottleneck at the beginning of the natural history of disease.
“If we can find a drug that is effective very early on, before the patients start getting the eight different manifestations with different levels of severity, then we will be on the right road, which we hope will end in remission.”
Dr. Del Galdo has served on the speakers bureau for AstraZeneca and Janssen; consulted for AstraZeneca, Boehringer Ingelheim, Capella, Chemomab, Janssen, and Mitsubishi-Tanabe; and received grant or research support from AbbVie, AstraZeneca, Boheringer Ingelheim, Capella, Chemomab, Kymab, Janssen, and Mitsubishi-Tanabe. Dr. Landewé had no relevant disclosures.
A version of this article first appeared on Medscape.com.
VIENNA – The use of immunosuppressive and antifibrotic drugs to treat skin and lung fibrosis leads updated recommendations from the European Alliance of Associations for Rheumatology (EULAR) for the treatment of systemic sclerosis.
“The most impactful new recommendation relates to the evidence for immunosuppressive agents and antifibrotics for the treatment of skin fibrosis and lung fibrosis,” said Francesco Del Galdo, MD, PhD, professor of experimental medicine, consultant rheumatologist, and scleroderma and connective tissue diseases specialist at Leeds Teaching Hospitals NHS Trust, Leeds, England. Dr. Del Galdo presented the update at the annual European Congress of Rheumatology.
“But there are also new recommendations, including a redefined target population for hematopoietic stem cell transplantation following cyclophosphamide, the upfront combination treatment at the time of diagnosis of pulmonary arterial hypertension [PAH], and a negative recommendation for the use of anticoagulants for pulmonary arterial hypertension,” noted Dr. Del Galdo, highlighting key updates in the 2024 recommendations.
Robert B.M. Landewé, MD, PhD, professor and rheumatologist at Amsterdam University Medical Center, Amsterdam, the Netherlands, and Zuyderland Medical Center, Heerlen, the Netherlands, co-moderated the session on EULAR recommendations. “The management of systemic sclerosis is a field in which a lot is happening,” he said. “The last update goes back to 2017, and in the meantime, many new approaches have seen the light, especially pertaining to skin fibrosis and interstitial lung disease. Six new recommendations have been coined, covering drugs like mycophenolate mofetil, nintedanib, rituximab, and tocilizumab. None of these therapies were present in the 2017 recommendations. It seems the field is now ready to further expand on targeted therapies for the management of musculoskeletal and gastrointestinal manifestations, calcinosis, and the local management of digital ulcers.”
‘Therapeutic Continuums’ Aid Disease Management
Dr. Del Galdo and his colleagues grouped the various interventions across what the recommendations label as evidence-backed “therapeutic continuums.” These span six of the eight different clinical manifestations of systemic sclerosis: Raynaud’s phenomenon, digital ulcers, pulmonary hypertension, musculoskeletal manifestations, skin fibrosis, interstitial lung disease (ILD), and gastrointestinal and renal crisis.
A slide showing the different strengths of evidence for various drugs across the eight manifestations illustrated the principle behind the therapeutic continuums. “These ‘therapeutic continuums’ suggest a common pathogenetic mechanism driving the various manifestations of disease,” said Dr. Del Galdo. For example, he noted, “If rituximab had a positive response in skin and in lung, it suggests that B cells play a role in the clinical manifestations of skin and lung in this disease.”
Dr. Del Galdo highlighted the new immunosuppression continuum and associated treatments for skin and lung fibrosis. “For skin involvement, the task force recommended mycophenolate, methotrexate, and rituximab, with tocilizumab having a lower level of evidence and lower recommendation strength; similarly, in interstitial lung disease, we have rituximab, mycophenolate, cyclophosphamide, and nintedanib, and these all have the highest strength of evidence. Tocilizumab is assigned one strength of evidence below the other drugs.”
He also cited the phosphodiesterase 5 inhibitor (PDE5i) drugs that are used across Raynaud’s phenomenon, digital ulcers, and pulmonary arterial hypertension, which together form a vascular therapeutic continuum.
The complexity of systemic sclerosis and multiple manifestations was a major determinant of the recommendations, Dr. Del Galdo pointed out. “The task force realized that since this is such a complex disease, we cannot recommend one treatment unconditionally. For example, with mycophenolate mofetil, what works for most patients for the skin and lung manifestations might not for someone who experiences severe diarrhea, in which mycophenolate is contraindicated. So, the highest degree of recommendation that the task force felt comfortable with was ‘should be considered.’ ”
Dr. Del Galdo stressed that the complex nature of systemic sclerosis means that “when thinking of treating one manifestation, you also always need to consider all the other clinical manifestations as experienced by the patient, and it is this multifaceted scenario that will ultimately lead to your final choice.”
Turning to new evidence around drug use, Dr. Del Galdo said that rituximab has the highest level of evidence across skin and lung manifestations, nintedanib is new in lung, and tocilizumab is new across both skin and lung.
To treat systemic sclerosis–pulmonary arterial hypertension (SSc-PAH), as long as there are no contraindications, the task force recommends using PDE5i and endothelin receptor antagonists (ERAs) at diagnosis. Data from phase 3 trials show a better outcome when the combination is established early.
The task force suggests avoiding the use of warfarin in PAH. “This is supported by a signal from two trials showing an increase in morbidity and mortality in these patients,” noted Dr. Del Galdo.
He also pointed out that selexipag and riociguat were new and important second-line additions for the treatment of PAH, and — consistent with the ERA approach — the EULAR recommendation supports frequent follow-up to establish a treat-to-target approach to maximizing clinical outcomes in SSc-PAH and SSc-ILD. “Specifically, for the first time, we recommend monitoring the effect of any chosen intervention selected within 3-6 months of starting. The evidence suggests there is a group of patients who respond and some who respond less well and who might benefit from a second-line intervention.”
For example, results of one trial support the approach of adding an antifibrotic agent to reduce progression in people with progressive lung fibrosis. “Similarly, for pulmonary hypertension, we recommend putting patients on dual treatment, and if this fails, place them on selexipag or switch the PDE5i to riociguat,” Dr. Del Galdo said.
Systemic Sclerosis Research Agenda and Recommendations Align
Dr. Del Galdo highlighted the value of therapeutic continuums in advancing disease understanding. “It is starting to teach us what we know and what we don’t and where do we need to build more evidence. Effectively, they determine where the gaps in therapy lie, and this starts to guide the research agenda.
“In fact, what is really interesting about this recommendation update — certainly from the perspective of disease understanding — is that we are starting to have a bird’s-eye view of the clinical manifestations of scleroderma that have so often been dealt with separately. Now we are starting to build a cumulative evidence map of this disease.”
In 2017, the research agenda largely advocated identifying immune-targeting drugs for skin and lung fibrosis, Dr. Del Galdo pointed out. “Now, we’ve done that — we’ve identified appropriate immunosuppressive drugs — and this is testimony to the importance of these recommendations because what prioritized the research agenda 10 years ago ended up informing the clinical trials and made it into the recommendations.”
“We definitely are one step forward compared to this 2017 recommendation and closer to what we would like to do,” he asserted.
Remission Elusive but Getting Closer
In some respects, according to Dr. Del Galdo, research and development is making relatively slow progress, especially compared with other rheumatologic diseases such as rheumatoid arthritis. “We cannot put patients with systemic sclerosis in remission yet. But I think we are one step ahead in that we’ve now established the treat-to-target approach to maximize the efficacy with which we can stall disease progression, but we cannot yet put these patients into remission,” he said. Systemic sclerosis has multiple manifestations, and fibrotic damage cannot be reversed. “Right now, the scar will remain there forever,” he noted.
Until remission is achievable, Dr. Del Galdo advises diagnosing and treating patients earlier to prevent fibrotic manifestations.
Dr. Del Galdo explained the three leading priorities on the systemic sclerosis research agenda. “There are three because it is such a complex disease. The first is considering the patient voice — this is the most important one, and the patients say they want a more holistic approach — so trialing and treating multiple manifestations together.”
Second, Dr. Del Galdo said, he would like to see a patient-reported measure developed that can capture the entire disease.
Third, from a physician’s point of view, Dr. Del Galdo said, “We want to send the patients into remission. We need to continue to further deconvolute the clinical manifestations and find the bottleneck at the beginning of the natural history of disease.
“If we can find a drug that is effective very early on, before the patients start getting the eight different manifestations with different levels of severity, then we will be on the right road, which we hope will end in remission.”
Dr. Del Galdo has served on the speakers bureau for AstraZeneca and Janssen; consulted for AstraZeneca, Boehringer Ingelheim, Capella, Chemomab, Janssen, and Mitsubishi-Tanabe; and received grant or research support from AbbVie, AstraZeneca, Boheringer Ingelheim, Capella, Chemomab, Kymab, Janssen, and Mitsubishi-Tanabe. Dr. Landewé had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM EULAR 2024
First-line Canakinumab Without Steroids Shows Effectiveness for Systemic Juvenile Idiopathic Arthritis
VIENNA — The interleukin-1 receptor antagonist (IL-1RA) canakinumab provided control of systemic juvenile idiopathic arthritis (sJIA) without the use of glucocorticoids for up to a year in most study participants after three monthly injections.
In this study of 20 patients with newly diagnosed sJIA treated off glucocorticoids, fever was controlled after a single injection in all patients, and 16 patients reached the primary outcome of remission after three injections, said Gerd Horneff, MD, PhD, Asklepios Children’s Hospital, Sankt Augustin, Germany.
Results of this open-label study, called CANAKINUMAB FIRST, were presented as late-breaking findings at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting.
“Steroid-free, first-line treatment with canakinumab led to sustained responses in most patients, with a considerable number achieving remission,” said Dr. Horneff, adding that the observation in this group is ongoing.
Building on Earlier Data
The efficacy of canakinumab was previously reported in anecdotal experiences and one small patient series published 10 years ago. Dr. Horneff noted that he has offered this drug off label to patients with challenging cases.
The objective was to evaluate canakinumab as a first-line monotherapy administered in the absence of glucocorticoids. The study was open to children aged 2-18 years with active sJIA/juvenile Still disease confirmed with published criteria. All were naive to biologic or nonbiologic disease-modifying antirheumatic drugs as well as steroids.
The median age of the children was 8.4 years. A total of 60% were men. The median disease duration at the time of entry was 1.2 months. Most had fever (95%) and rash (80%) with high levels of inflammatory markers at baseline. The mean number of painful joints was 3.1, and the mean number of systemic manifestations was 2.8. No patient was without any systemic involvement, but four of the patients did not have any painful joints.
At enrollment, patients were scheduled to receive three injections of canakinumab at monthly intervals during an active treatment phase, after which they entered an observation phase lasting 40 weeks. In the event of nonresponse or flares in either phase, they were transitioned to usual care.
Symptoms Resolve After Single Injection
After the first injection, active joint disease and all systemic manifestations resolved in 16 (80%) of the 20 patients. Joint activity and systemic manifestations also remained controlled after the second and third injections in 16 of the 20 patients.
One patient in this series achieved inactive disease after a single injection but developed what appeared to be a treatment-related allergic reaction. He received no further treatment and was excluded from the study, although he is being followed separately.
“According to sJADAS [systemic JIA Disease Activity Score] criteria at month 3, 14 had inactive disease, three had minimal disease activity, and one patient had moderate disease activity,” Dr. Horneff said.
At week 24, or 3 months after the last injection, there was still no joint activity in 16 patients. Systemic manifestations remained controlled in 13 patients, but 1 patient by this point had a flare. Another flare occurred after this point, and other patients have not yet completed the 52-week observation period.
“Of the 10 patients who remained in the study and have completed the 52-week observation period, eight have had a drug-free remission,” Dr. Horneff said.
MAS Event Observed in One Patient
In addition to the allergic skin reaction, which was considered probably related to the study drug, there were three flares, one of which was a macrophage activation syndrome (MAS) event. The MAS occurred 8 weeks after the last injection, but it was managed successfully.
Of 30 infections that developed during the observation period, 18 involved the upper airway. All were treated successfully. There were also two injection-site reactions and one case of cytopenia.
Among the studies planned for follow-up, investigators will examine genomic and gene activation in relation to disease activity and the effect of canakinumab.
Comoderator of the abstract session and chair of the EULAR 2024 Abstract Selection Committee, Christian Dejaco, MD, PhD, a consultant rheumatologist and associate professor at the Medical University of Graz in Graz, Austria, suggested that these are highly encouraging data for a disease that does not currently have any approved therapies. Clearly, larger studies with a longer follow-up period are needed, but he pointed out that phase 3 trials in a rare disease like sJIA are challenging.
Because of the limited number of cases, “it will be difficult to conduct a placebo-controlled trial,” he pointed out. However, he hopes this study will provide the basis for larger studies and sufficient data to lead to an indication for this therapy.
In the meantime, he also believes that these data are likely to support empirical use in a difficult disease, even in advance of formal regulatory approval.
“We heard that canakinumab is already being used off label in JIA, and these data might encourage more of that,” he said.
Dr. Horneff reported financial relationships with AbbVie, Boehringer Ingelheim, Celgene, Chugai, GlaxoSmithKline, Janssen, Merck Sharpe & Dohme, Novartis, Pfizer, Roche, Sanofi, and Sobe. Dr. Dejaco reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
VIENNA — The interleukin-1 receptor antagonist (IL-1RA) canakinumab provided control of systemic juvenile idiopathic arthritis (sJIA) without the use of glucocorticoids for up to a year in most study participants after three monthly injections.
In this study of 20 patients with newly diagnosed sJIA treated off glucocorticoids, fever was controlled after a single injection in all patients, and 16 patients reached the primary outcome of remission after three injections, said Gerd Horneff, MD, PhD, Asklepios Children’s Hospital, Sankt Augustin, Germany.
Results of this open-label study, called CANAKINUMAB FIRST, were presented as late-breaking findings at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting.
“Steroid-free, first-line treatment with canakinumab led to sustained responses in most patients, with a considerable number achieving remission,” said Dr. Horneff, adding that the observation in this group is ongoing.
Building on Earlier Data
The efficacy of canakinumab was previously reported in anecdotal experiences and one small patient series published 10 years ago. Dr. Horneff noted that he has offered this drug off label to patients with challenging cases.
The objective was to evaluate canakinumab as a first-line monotherapy administered in the absence of glucocorticoids. The study was open to children aged 2-18 years with active sJIA/juvenile Still disease confirmed with published criteria. All were naive to biologic or nonbiologic disease-modifying antirheumatic drugs as well as steroids.
The median age of the children was 8.4 years. A total of 60% were men. The median disease duration at the time of entry was 1.2 months. Most had fever (95%) and rash (80%) with high levels of inflammatory markers at baseline. The mean number of painful joints was 3.1, and the mean number of systemic manifestations was 2.8. No patient was without any systemic involvement, but four of the patients did not have any painful joints.
At enrollment, patients were scheduled to receive three injections of canakinumab at monthly intervals during an active treatment phase, after which they entered an observation phase lasting 40 weeks. In the event of nonresponse or flares in either phase, they were transitioned to usual care.
Symptoms Resolve After Single Injection
After the first injection, active joint disease and all systemic manifestations resolved in 16 (80%) of the 20 patients. Joint activity and systemic manifestations also remained controlled after the second and third injections in 16 of the 20 patients.
One patient in this series achieved inactive disease after a single injection but developed what appeared to be a treatment-related allergic reaction. He received no further treatment and was excluded from the study, although he is being followed separately.
“According to sJADAS [systemic JIA Disease Activity Score] criteria at month 3, 14 had inactive disease, three had minimal disease activity, and one patient had moderate disease activity,” Dr. Horneff said.
At week 24, or 3 months after the last injection, there was still no joint activity in 16 patients. Systemic manifestations remained controlled in 13 patients, but 1 patient by this point had a flare. Another flare occurred after this point, and other patients have not yet completed the 52-week observation period.
“Of the 10 patients who remained in the study and have completed the 52-week observation period, eight have had a drug-free remission,” Dr. Horneff said.
MAS Event Observed in One Patient
In addition to the allergic skin reaction, which was considered probably related to the study drug, there were three flares, one of which was a macrophage activation syndrome (MAS) event. The MAS occurred 8 weeks after the last injection, but it was managed successfully.
Of 30 infections that developed during the observation period, 18 involved the upper airway. All were treated successfully. There were also two injection-site reactions and one case of cytopenia.
Among the studies planned for follow-up, investigators will examine genomic and gene activation in relation to disease activity and the effect of canakinumab.
Comoderator of the abstract session and chair of the EULAR 2024 Abstract Selection Committee, Christian Dejaco, MD, PhD, a consultant rheumatologist and associate professor at the Medical University of Graz in Graz, Austria, suggested that these are highly encouraging data for a disease that does not currently have any approved therapies. Clearly, larger studies with a longer follow-up period are needed, but he pointed out that phase 3 trials in a rare disease like sJIA are challenging.
Because of the limited number of cases, “it will be difficult to conduct a placebo-controlled trial,” he pointed out. However, he hopes this study will provide the basis for larger studies and sufficient data to lead to an indication for this therapy.
In the meantime, he also believes that these data are likely to support empirical use in a difficult disease, even in advance of formal regulatory approval.
“We heard that canakinumab is already being used off label in JIA, and these data might encourage more of that,” he said.
Dr. Horneff reported financial relationships with AbbVie, Boehringer Ingelheim, Celgene, Chugai, GlaxoSmithKline, Janssen, Merck Sharpe & Dohme, Novartis, Pfizer, Roche, Sanofi, and Sobe. Dr. Dejaco reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
VIENNA — The interleukin-1 receptor antagonist (IL-1RA) canakinumab provided control of systemic juvenile idiopathic arthritis (sJIA) without the use of glucocorticoids for up to a year in most study participants after three monthly injections.
In this study of 20 patients with newly diagnosed sJIA treated off glucocorticoids, fever was controlled after a single injection in all patients, and 16 patients reached the primary outcome of remission after three injections, said Gerd Horneff, MD, PhD, Asklepios Children’s Hospital, Sankt Augustin, Germany.
Results of this open-label study, called CANAKINUMAB FIRST, were presented as late-breaking findings at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting.
“Steroid-free, first-line treatment with canakinumab led to sustained responses in most patients, with a considerable number achieving remission,” said Dr. Horneff, adding that the observation in this group is ongoing.
Building on Earlier Data
The efficacy of canakinumab was previously reported in anecdotal experiences and one small patient series published 10 years ago. Dr. Horneff noted that he has offered this drug off label to patients with challenging cases.
The objective was to evaluate canakinumab as a first-line monotherapy administered in the absence of glucocorticoids. The study was open to children aged 2-18 years with active sJIA/juvenile Still disease confirmed with published criteria. All were naive to biologic or nonbiologic disease-modifying antirheumatic drugs as well as steroids.
The median age of the children was 8.4 years. A total of 60% were men. The median disease duration at the time of entry was 1.2 months. Most had fever (95%) and rash (80%) with high levels of inflammatory markers at baseline. The mean number of painful joints was 3.1, and the mean number of systemic manifestations was 2.8. No patient was without any systemic involvement, but four of the patients did not have any painful joints.
At enrollment, patients were scheduled to receive three injections of canakinumab at monthly intervals during an active treatment phase, after which they entered an observation phase lasting 40 weeks. In the event of nonresponse or flares in either phase, they were transitioned to usual care.
Symptoms Resolve After Single Injection
After the first injection, active joint disease and all systemic manifestations resolved in 16 (80%) of the 20 patients. Joint activity and systemic manifestations also remained controlled after the second and third injections in 16 of the 20 patients.
One patient in this series achieved inactive disease after a single injection but developed what appeared to be a treatment-related allergic reaction. He received no further treatment and was excluded from the study, although he is being followed separately.
“According to sJADAS [systemic JIA Disease Activity Score] criteria at month 3, 14 had inactive disease, three had minimal disease activity, and one patient had moderate disease activity,” Dr. Horneff said.
At week 24, or 3 months after the last injection, there was still no joint activity in 16 patients. Systemic manifestations remained controlled in 13 patients, but 1 patient by this point had a flare. Another flare occurred after this point, and other patients have not yet completed the 52-week observation period.
“Of the 10 patients who remained in the study and have completed the 52-week observation period, eight have had a drug-free remission,” Dr. Horneff said.
MAS Event Observed in One Patient
In addition to the allergic skin reaction, which was considered probably related to the study drug, there were three flares, one of which was a macrophage activation syndrome (MAS) event. The MAS occurred 8 weeks after the last injection, but it was managed successfully.
Of 30 infections that developed during the observation period, 18 involved the upper airway. All were treated successfully. There were also two injection-site reactions and one case of cytopenia.
Among the studies planned for follow-up, investigators will examine genomic and gene activation in relation to disease activity and the effect of canakinumab.
Comoderator of the abstract session and chair of the EULAR 2024 Abstract Selection Committee, Christian Dejaco, MD, PhD, a consultant rheumatologist and associate professor at the Medical University of Graz in Graz, Austria, suggested that these are highly encouraging data for a disease that does not currently have any approved therapies. Clearly, larger studies with a longer follow-up period are needed, but he pointed out that phase 3 trials in a rare disease like sJIA are challenging.
Because of the limited number of cases, “it will be difficult to conduct a placebo-controlled trial,” he pointed out. However, he hopes this study will provide the basis for larger studies and sufficient data to lead to an indication for this therapy.
In the meantime, he also believes that these data are likely to support empirical use in a difficult disease, even in advance of formal regulatory approval.
“We heard that canakinumab is already being used off label in JIA, and these data might encourage more of that,” he said.
Dr. Horneff reported financial relationships with AbbVie, Boehringer Ingelheim, Celgene, Chugai, GlaxoSmithKline, Janssen, Merck Sharpe & Dohme, Novartis, Pfizer, Roche, Sanofi, and Sobe. Dr. Dejaco reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM EULAR 2024
‘Critical Gaps’ Seen in Managing Moms’ Postpartum BP
TOPLINE:
Over 80% of women with new-onset hypertensive disorders during pregnancy experienced persistent hypertension in the 6 weeks after delivery.
METHODOLOGY:
- Researchers analyzed data from 2705 women in the University of Pittsburgh Medical Center system who developed new-onset hypertensive disorders during pregnancy and participated in a remote blood pressure (BP) monitoring program after discharge from the hospital.
- Nurses showed patients how to monitor their pressure at home, and patients had access to a call center that focused on BP management.
TAKEAWAY:
- Persistent hypertension postpartum — defined as an at-home BP measurement of 140/90 mmHg or greater or treatment with an antihypertensive medication — occurred in 81.8% of the participants.
- A total of 14.1% developed severe hypertension (BP of 160/110 mmHg or greater); 22.6% started an antihypertensive medication after discharge.
- Hospital readmission occurred for 13.4% of the women with severe hypertension, 4% of the women with less serious hypertension, and 2.7% of those who did not have persistent high BP.
IN PRACTICE:
Many of the patients had met criteria to initiate antihypertensive treatment during the delivery admission based on guidance from the American College of Cardiology/American Heart Association (67.9%) and the American College of Obstetricians and Gynecologists (38.7%), “yet only 23.5% were discharged with antihypertensive medications,” Sadiya S. Khan, MD, MSc, of Northwestern University Feinberg School of Medicine, in Chicago, wrote in an editor’s note accompanying the study. “These data highlight several critical gaps in evidence-based recommendations for the monitoring and management of BP following a pregnancy complicated by” hypertensive disorders of pregnancy.
SOURCE:
The study was led by Alisse Hauspurg, MD, MS, of Magee-Womens Research Institute in Pittsburgh, and appeared online in JAMA Cardiology.
LIMITATIONS:
The study was limited to data from one center, and the researchers relied on self-reported BP measurements.
DISCLOSURES:
The study was supported by the National Institutes of Health and the American Heart Association. A coauthor disclosed consulting for Organon and being a cofounder of Naima Health.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Over 80% of women with new-onset hypertensive disorders during pregnancy experienced persistent hypertension in the 6 weeks after delivery.
METHODOLOGY:
- Researchers analyzed data from 2705 women in the University of Pittsburgh Medical Center system who developed new-onset hypertensive disorders during pregnancy and participated in a remote blood pressure (BP) monitoring program after discharge from the hospital.
- Nurses showed patients how to monitor their pressure at home, and patients had access to a call center that focused on BP management.
TAKEAWAY:
- Persistent hypertension postpartum — defined as an at-home BP measurement of 140/90 mmHg or greater or treatment with an antihypertensive medication — occurred in 81.8% of the participants.
- A total of 14.1% developed severe hypertension (BP of 160/110 mmHg or greater); 22.6% started an antihypertensive medication after discharge.
- Hospital readmission occurred for 13.4% of the women with severe hypertension, 4% of the women with less serious hypertension, and 2.7% of those who did not have persistent high BP.
IN PRACTICE:
Many of the patients had met criteria to initiate antihypertensive treatment during the delivery admission based on guidance from the American College of Cardiology/American Heart Association (67.9%) and the American College of Obstetricians and Gynecologists (38.7%), “yet only 23.5% were discharged with antihypertensive medications,” Sadiya S. Khan, MD, MSc, of Northwestern University Feinberg School of Medicine, in Chicago, wrote in an editor’s note accompanying the study. “These data highlight several critical gaps in evidence-based recommendations for the monitoring and management of BP following a pregnancy complicated by” hypertensive disorders of pregnancy.
SOURCE:
The study was led by Alisse Hauspurg, MD, MS, of Magee-Womens Research Institute in Pittsburgh, and appeared online in JAMA Cardiology.
LIMITATIONS:
The study was limited to data from one center, and the researchers relied on self-reported BP measurements.
DISCLOSURES:
The study was supported by the National Institutes of Health and the American Heart Association. A coauthor disclosed consulting for Organon and being a cofounder of Naima Health.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Over 80% of women with new-onset hypertensive disorders during pregnancy experienced persistent hypertension in the 6 weeks after delivery.
METHODOLOGY:
- Researchers analyzed data from 2705 women in the University of Pittsburgh Medical Center system who developed new-onset hypertensive disorders during pregnancy and participated in a remote blood pressure (BP) monitoring program after discharge from the hospital.
- Nurses showed patients how to monitor their pressure at home, and patients had access to a call center that focused on BP management.
TAKEAWAY:
- Persistent hypertension postpartum — defined as an at-home BP measurement of 140/90 mmHg or greater or treatment with an antihypertensive medication — occurred in 81.8% of the participants.
- A total of 14.1% developed severe hypertension (BP of 160/110 mmHg or greater); 22.6% started an antihypertensive medication after discharge.
- Hospital readmission occurred for 13.4% of the women with severe hypertension, 4% of the women with less serious hypertension, and 2.7% of those who did not have persistent high BP.
IN PRACTICE:
Many of the patients had met criteria to initiate antihypertensive treatment during the delivery admission based on guidance from the American College of Cardiology/American Heart Association (67.9%) and the American College of Obstetricians and Gynecologists (38.7%), “yet only 23.5% were discharged with antihypertensive medications,” Sadiya S. Khan, MD, MSc, of Northwestern University Feinberg School of Medicine, in Chicago, wrote in an editor’s note accompanying the study. “These data highlight several critical gaps in evidence-based recommendations for the monitoring and management of BP following a pregnancy complicated by” hypertensive disorders of pregnancy.
SOURCE:
The study was led by Alisse Hauspurg, MD, MS, of Magee-Womens Research Institute in Pittsburgh, and appeared online in JAMA Cardiology.
LIMITATIONS:
The study was limited to data from one center, and the researchers relied on self-reported BP measurements.
DISCLOSURES:
The study was supported by the National Institutes of Health and the American Heart Association. A coauthor disclosed consulting for Organon and being a cofounder of Naima Health.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Which Surgery for Vaginal Vault Prolapse? No Clear Winner
TOPLINE:
Various surgical approaches to treat vaginal vault prolapse may be similarly safe and effective and can produce high rates of patient satisfaction.
METHODOLOGY:
- A randomized clinical trial at nine sites in the United States included 360 women with vaginal vault prolapse after hysterectomy (average age, 66 years).
- The women were randomly assigned to undergo native tissue repair (transvaginal repair using the sacrospinous or uterosacral ligament), sacrocolpopexy (mesh repair placed abdominally via open or minimally invasive surgery), or transvaginal mesh repair.
TAKEAWAY:
- At 36 months, a composite measure of treatment failure — based on the need for retreatment, the presence of symptoms, or prolapse beyond the hymen — had occurred in 28% of the women who received sacrocolpopexy, 29% who received transvaginal mesh, and 43% who underwent native tissue repair.
- Sacrocolpopexy was superior to native tissue repair for treatment success (adjusted hazard ratio, 0.57; P = .01), and transvaginal mesh was noninferior to sacrocolpopexy, the researchers found.
- All of the surgical approaches were associated with high rates of treatment satisfaction and improved quality of life and sexual function.
- Adverse events and mesh complications were uncommon.
IN PRACTICE:
“All approaches were associated with high treatment satisfaction; improved symptoms, quality of life, and sexual function; and low rates of regret,” the authors of the study wrote. “As such, clinicians counseling patients with prolapse can discuss the ramifications of each approach and engage in shared, individualized decision-making.”
SOURCE:
The study was led by Shawn A. Menefee, MD, Kaiser Permanente San Diego in San Diego, California. It was published online in JAMA Surgery.
LIMITATIONS:
The US Food and Drug Administration in April 2019 banned transvaginal mesh for pelvic organ prolapse because of concerns about complications such as exposure and erosion. Five trial participants who had been assigned to receive transvaginal mesh but had not yet received it at that time were rerandomized to one of the other surgical approaches.
DISCLOSURES:
The study was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health Office of Research on Women’s Health. Researchers disclosed consulting for companies that market medical devices.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Various surgical approaches to treat vaginal vault prolapse may be similarly safe and effective and can produce high rates of patient satisfaction.
METHODOLOGY:
- A randomized clinical trial at nine sites in the United States included 360 women with vaginal vault prolapse after hysterectomy (average age, 66 years).
- The women were randomly assigned to undergo native tissue repair (transvaginal repair using the sacrospinous or uterosacral ligament), sacrocolpopexy (mesh repair placed abdominally via open or minimally invasive surgery), or transvaginal mesh repair.
TAKEAWAY:
- At 36 months, a composite measure of treatment failure — based on the need for retreatment, the presence of symptoms, or prolapse beyond the hymen — had occurred in 28% of the women who received sacrocolpopexy, 29% who received transvaginal mesh, and 43% who underwent native tissue repair.
- Sacrocolpopexy was superior to native tissue repair for treatment success (adjusted hazard ratio, 0.57; P = .01), and transvaginal mesh was noninferior to sacrocolpopexy, the researchers found.
- All of the surgical approaches were associated with high rates of treatment satisfaction and improved quality of life and sexual function.
- Adverse events and mesh complications were uncommon.
IN PRACTICE:
“All approaches were associated with high treatment satisfaction; improved symptoms, quality of life, and sexual function; and low rates of regret,” the authors of the study wrote. “As such, clinicians counseling patients with prolapse can discuss the ramifications of each approach and engage in shared, individualized decision-making.”
SOURCE:
The study was led by Shawn A. Menefee, MD, Kaiser Permanente San Diego in San Diego, California. It was published online in JAMA Surgery.
LIMITATIONS:
The US Food and Drug Administration in April 2019 banned transvaginal mesh for pelvic organ prolapse because of concerns about complications such as exposure and erosion. Five trial participants who had been assigned to receive transvaginal mesh but had not yet received it at that time were rerandomized to one of the other surgical approaches.
DISCLOSURES:
The study was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health Office of Research on Women’s Health. Researchers disclosed consulting for companies that market medical devices.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Various surgical approaches to treat vaginal vault prolapse may be similarly safe and effective and can produce high rates of patient satisfaction.
METHODOLOGY:
- A randomized clinical trial at nine sites in the United States included 360 women with vaginal vault prolapse after hysterectomy (average age, 66 years).
- The women were randomly assigned to undergo native tissue repair (transvaginal repair using the sacrospinous or uterosacral ligament), sacrocolpopexy (mesh repair placed abdominally via open or minimally invasive surgery), or transvaginal mesh repair.
TAKEAWAY:
- At 36 months, a composite measure of treatment failure — based on the need for retreatment, the presence of symptoms, or prolapse beyond the hymen — had occurred in 28% of the women who received sacrocolpopexy, 29% who received transvaginal mesh, and 43% who underwent native tissue repair.
- Sacrocolpopexy was superior to native tissue repair for treatment success (adjusted hazard ratio, 0.57; P = .01), and transvaginal mesh was noninferior to sacrocolpopexy, the researchers found.
- All of the surgical approaches were associated with high rates of treatment satisfaction and improved quality of life and sexual function.
- Adverse events and mesh complications were uncommon.
IN PRACTICE:
“All approaches were associated with high treatment satisfaction; improved symptoms, quality of life, and sexual function; and low rates of regret,” the authors of the study wrote. “As such, clinicians counseling patients with prolapse can discuss the ramifications of each approach and engage in shared, individualized decision-making.”
SOURCE:
The study was led by Shawn A. Menefee, MD, Kaiser Permanente San Diego in San Diego, California. It was published online in JAMA Surgery.
LIMITATIONS:
The US Food and Drug Administration in April 2019 banned transvaginal mesh for pelvic organ prolapse because of concerns about complications such as exposure and erosion. Five trial participants who had been assigned to receive transvaginal mesh but had not yet received it at that time were rerandomized to one of the other surgical approaches.
DISCLOSURES:
The study was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health Office of Research on Women’s Health. Researchers disclosed consulting for companies that market medical devices.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Liver Resection Beats Out Alternatives in Early Multinodular HCC
TOPLINE:
METHODOLOGY:
- The presentation of HCC is often multinodular — meaning patients have two or three nodules measuring ≤ 3 cm each. Although liver resection is considered the gold standard curative treatment for early-stage disease, experts debate its efficacy in multinodular HCC, researchers explained.
- Using two large Italian registries with data from multiple centers, researchers compared the efficacy of liver resection, percutaneous radiofrequency ablation, and TACE in 720 patients with early multinodular HCC. Overall, 296 patients underwent liver resection, 240 had percutaneous radiofrequency ablation, and 184 underwent TACE.
- To avoid crossovers between groups, the researchers considered liver resection, percutaneous radiofrequency ablation, and TACE the main treatments in each population in a hierarchical order. That meant, in the liver resection group, researchers excluded patients undergoing a superior treatment during the follow-up, such as liver transplant. In the ablation group, patients undergoing surgery to treat HCC recurrences were excluded.
- The primary outcome was overall survival at 1, 3, and 5 years. The researchers used a matching-adjusted indirect comparison (MAIC) to balance data and control for confounding factors between the three treatment groups.
TAKEAWAY:
- After MAIC adjustment, the survival rate at 1 year was slightly lower in the liver resection group — 89% vs 94% in the ablation group and 91% in the TACE group. However, at 3 and 5 years, survival rates were better in the liver resection group — 71% at 3 years and 56% at 5 years vs 65% and 40%, respectively, in the ablation group and 49% and 29%, respectively, in the TACE group.
- Median overall survival was 69 months with liver resection, 54 months with ablation, and 34 months with TACE. Multivariable Cox survival analysis confirmed a significantly higher mortality risk with ablation (hazard ratio [HR], 1.41; P = .01) and TACE (HR, 1.86; P = .001) than with liver resection.
- In competing risk analyses, patients who underwent liver resection had a lower risk for HCC-related death than peers who had ablation (HR, 1.38; P = .07) or TACE (HR, 1.91; P = .006).
- In a subgroup survival analysis of patients with Child-Pugh class B cirrhosis, liver resection provided significantly better overall survival than TACE (HR, 2.79; P = .001) and higher overall survival than ablation (HR, 1.44; P = .21), but these findings were not statistically significant.
IN PRACTICE:
“The main result of the current study is the indisputable superiority” of liver resection over percutaneous radiofrequency ablation and TACE in patients with multinodular HCC, the researchers concluded. “For patients with early multinodular HCC who are ineligible for transplant, LR [liver resection] should be prioritized as the primary therapeutic option,” followed by percutaneous radiofrequency ablation and TACE, when resection is not feasible.
The authors of an invited commentary said the analysis provides “convincing” data that liver resection leads to superior 3- and 5-year survival. “All of our local therapies are getting better. Making each available under different clinical circumstances and combining these when appropriate provides patients with the best chance at cure with the least invasiveness,” the editorialists added.
SOURCE:
The study, with first author Alessandro Vitale, MD, PhD, with the Department of Surgical, Oncological and Gastroenterological Sciences, University of Padova, Padua, Italy, and the accompanying commentary were published online last month in JAMA Surgery.
LIMITATIONS:
Selection bias cannot be ruled out due to potential hidden variables that were not collected in the centers’ databases. Not all patients included in the study were potentially treatable with all three proposed approaches. The study population was derived from Italian centers, which may have limited the generalizability of the results.
DISCLOSURES:
The study reported no specific funding. The authors reported various disclosures during the conduct of the study, including ties to AstraZeneca, AbbVie, Bayer, MSD, Roche, and Eisai. An editorialist reported ties to Medtronic, Theromics, Vergent Bioscience, Imugene, Sovato Health, XDemics, and Imugene.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The presentation of HCC is often multinodular — meaning patients have two or three nodules measuring ≤ 3 cm each. Although liver resection is considered the gold standard curative treatment for early-stage disease, experts debate its efficacy in multinodular HCC, researchers explained.
- Using two large Italian registries with data from multiple centers, researchers compared the efficacy of liver resection, percutaneous radiofrequency ablation, and TACE in 720 patients with early multinodular HCC. Overall, 296 patients underwent liver resection, 240 had percutaneous radiofrequency ablation, and 184 underwent TACE.
- To avoid crossovers between groups, the researchers considered liver resection, percutaneous radiofrequency ablation, and TACE the main treatments in each population in a hierarchical order. That meant, in the liver resection group, researchers excluded patients undergoing a superior treatment during the follow-up, such as liver transplant. In the ablation group, patients undergoing surgery to treat HCC recurrences were excluded.
- The primary outcome was overall survival at 1, 3, and 5 years. The researchers used a matching-adjusted indirect comparison (MAIC) to balance data and control for confounding factors between the three treatment groups.
TAKEAWAY:
- After MAIC adjustment, the survival rate at 1 year was slightly lower in the liver resection group — 89% vs 94% in the ablation group and 91% in the TACE group. However, at 3 and 5 years, survival rates were better in the liver resection group — 71% at 3 years and 56% at 5 years vs 65% and 40%, respectively, in the ablation group and 49% and 29%, respectively, in the TACE group.
- Median overall survival was 69 months with liver resection, 54 months with ablation, and 34 months with TACE. Multivariable Cox survival analysis confirmed a significantly higher mortality risk with ablation (hazard ratio [HR], 1.41; P = .01) and TACE (HR, 1.86; P = .001) than with liver resection.
- In competing risk analyses, patients who underwent liver resection had a lower risk for HCC-related death than peers who had ablation (HR, 1.38; P = .07) or TACE (HR, 1.91; P = .006).
- In a subgroup survival analysis of patients with Child-Pugh class B cirrhosis, liver resection provided significantly better overall survival than TACE (HR, 2.79; P = .001) and higher overall survival than ablation (HR, 1.44; P = .21), but these findings were not statistically significant.
IN PRACTICE:
“The main result of the current study is the indisputable superiority” of liver resection over percutaneous radiofrequency ablation and TACE in patients with multinodular HCC, the researchers concluded. “For patients with early multinodular HCC who are ineligible for transplant, LR [liver resection] should be prioritized as the primary therapeutic option,” followed by percutaneous radiofrequency ablation and TACE, when resection is not feasible.
The authors of an invited commentary said the analysis provides “convincing” data that liver resection leads to superior 3- and 5-year survival. “All of our local therapies are getting better. Making each available under different clinical circumstances and combining these when appropriate provides patients with the best chance at cure with the least invasiveness,” the editorialists added.
SOURCE:
The study, with first author Alessandro Vitale, MD, PhD, with the Department of Surgical, Oncological and Gastroenterological Sciences, University of Padova, Padua, Italy, and the accompanying commentary were published online last month in JAMA Surgery.
LIMITATIONS:
Selection bias cannot be ruled out due to potential hidden variables that were not collected in the centers’ databases. Not all patients included in the study were potentially treatable with all three proposed approaches. The study population was derived from Italian centers, which may have limited the generalizability of the results.
DISCLOSURES:
The study reported no specific funding. The authors reported various disclosures during the conduct of the study, including ties to AstraZeneca, AbbVie, Bayer, MSD, Roche, and Eisai. An editorialist reported ties to Medtronic, Theromics, Vergent Bioscience, Imugene, Sovato Health, XDemics, and Imugene.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The presentation of HCC is often multinodular — meaning patients have two or three nodules measuring ≤ 3 cm each. Although liver resection is considered the gold standard curative treatment for early-stage disease, experts debate its efficacy in multinodular HCC, researchers explained.
- Using two large Italian registries with data from multiple centers, researchers compared the efficacy of liver resection, percutaneous radiofrequency ablation, and TACE in 720 patients with early multinodular HCC. Overall, 296 patients underwent liver resection, 240 had percutaneous radiofrequency ablation, and 184 underwent TACE.
- To avoid crossovers between groups, the researchers considered liver resection, percutaneous radiofrequency ablation, and TACE the main treatments in each population in a hierarchical order. That meant, in the liver resection group, researchers excluded patients undergoing a superior treatment during the follow-up, such as liver transplant. In the ablation group, patients undergoing surgery to treat HCC recurrences were excluded.
- The primary outcome was overall survival at 1, 3, and 5 years. The researchers used a matching-adjusted indirect comparison (MAIC) to balance data and control for confounding factors between the three treatment groups.
TAKEAWAY:
- After MAIC adjustment, the survival rate at 1 year was slightly lower in the liver resection group — 89% vs 94% in the ablation group and 91% in the TACE group. However, at 3 and 5 years, survival rates were better in the liver resection group — 71% at 3 years and 56% at 5 years vs 65% and 40%, respectively, in the ablation group and 49% and 29%, respectively, in the TACE group.
- Median overall survival was 69 months with liver resection, 54 months with ablation, and 34 months with TACE. Multivariable Cox survival analysis confirmed a significantly higher mortality risk with ablation (hazard ratio [HR], 1.41; P = .01) and TACE (HR, 1.86; P = .001) than with liver resection.
- In competing risk analyses, patients who underwent liver resection had a lower risk for HCC-related death than peers who had ablation (HR, 1.38; P = .07) or TACE (HR, 1.91; P = .006).
- In a subgroup survival analysis of patients with Child-Pugh class B cirrhosis, liver resection provided significantly better overall survival than TACE (HR, 2.79; P = .001) and higher overall survival than ablation (HR, 1.44; P = .21), but these findings were not statistically significant.
IN PRACTICE:
“The main result of the current study is the indisputable superiority” of liver resection over percutaneous radiofrequency ablation and TACE in patients with multinodular HCC, the researchers concluded. “For patients with early multinodular HCC who are ineligible for transplant, LR [liver resection] should be prioritized as the primary therapeutic option,” followed by percutaneous radiofrequency ablation and TACE, when resection is not feasible.
The authors of an invited commentary said the analysis provides “convincing” data that liver resection leads to superior 3- and 5-year survival. “All of our local therapies are getting better. Making each available under different clinical circumstances and combining these when appropriate provides patients with the best chance at cure with the least invasiveness,” the editorialists added.
SOURCE:
The study, with first author Alessandro Vitale, MD, PhD, with the Department of Surgical, Oncological and Gastroenterological Sciences, University of Padova, Padua, Italy, and the accompanying commentary were published online last month in JAMA Surgery.
LIMITATIONS:
Selection bias cannot be ruled out due to potential hidden variables that were not collected in the centers’ databases. Not all patients included in the study were potentially treatable with all three proposed approaches. The study population was derived from Italian centers, which may have limited the generalizability of the results.
DISCLOSURES:
The study reported no specific funding. The authors reported various disclosures during the conduct of the study, including ties to AstraZeneca, AbbVie, Bayer, MSD, Roche, and Eisai. An editorialist reported ties to Medtronic, Theromics, Vergent Bioscience, Imugene, Sovato Health, XDemics, and Imugene.
A version of this article first appeared on Medscape.com.
Extensive Multidrug-Resistant Dermatophytosis From Trichophyton indotineae
To the Editor:
Historically, commonly available antifungal medications have been effective for treating dermatophytosis (tinea). However, recent tinea outbreaks caused by Trichophyton indotineae—a dermatophyte often resistant to terbinafine and sometimes to other antifungals—have been reported in South Asia, Europe, the Middle East, Southeast Asia, and Australia.1-5
Three confirmed cases of T indotineae dermatophytosis in the United States were reported in 2023 in New York3,6; a fourth confirmed case was reported in 2024 in Pennsylvania.7 Post hoc laboratory testing of fungal isolates in New York in 2022 and 2023 identified an additional 11 cases.8 We present a case of extensive multidrug-resistant tinea caused by T indotineae in a man in California.
An otherwise healthy 65-year-old man who had traveled to Europe in the past 3 months presented to his primary care physician with a widespread pruritic rash (Figure 1). He was treated with 2 weeks of oral terbinafine 250 mg/d and topical medicines, including clotrimazole cream 1%, fluocinonide ointment 0.05%, and clobetasol ointment 0.05% without improvement. Subsequently, 2 weeks of oral griseofulvin microsize 500 mg/d also proved ineffective. An antibody test was negative for HIV. His hemoglobin A1c was 6.2% (reference range, ≤5.6%). The patient was referred to dermatology.
Erythematous plaques—many scaly throughout and some annular with central clearing—were present on the arms, legs, and torso as well as in the groin. Honey crust was present on some plaques on the leg. A potassium hydroxide preparation showed abundant fungal hyphae. Material for fungal and bacterial cultures was collected. The patient was treated again with oral terbinafine 250 mg/d, an oral prednisone taper starting at 60 mg/d for a presumed id reaction, and various oral antihistamines for pruritus; all were ineffective. A bacterial culture showed only mixed skin flora. Oral fluconazole 200 mg/d was prescribed. A skin biopsy specimen showed compact orthokeratosis and parakeratosis of the stratum corneum with few neutrophils and focal pustule formation (Figure 2). Superficial perivascular inflammation, including lymphocytes, histiocytes, and few neutrophils, was present. A periodic acid–Schiff stain showed fungal hyphae in the stratum corneum and a hair follicle (Figure 3). After approximately 2 weeks, mold was identified in the fungal culture. Approximately 2 weeks thereafter, the organism was reported as Trichophyton species.

The rash did not improve; resistance to terbinafine, griseofulvin, and fluconazole was suspected clinically. The fungal isolate was sent to a reference laboratory (University of Texas Health Science Center, San Antonio). Meanwhile, oral itraconazole 200 mg twice daily and ketoconazole cream 2% were prescribed; the rash began to improve. A serum itraconazole trough level obtained 4 days after treatment initiation was 0.5 μg/mL (reference range, ≥0.6 μg/mL). The evening itraconazole dose was increased to 300 mg; a subsequent trough level was 0.8 μg/mL.
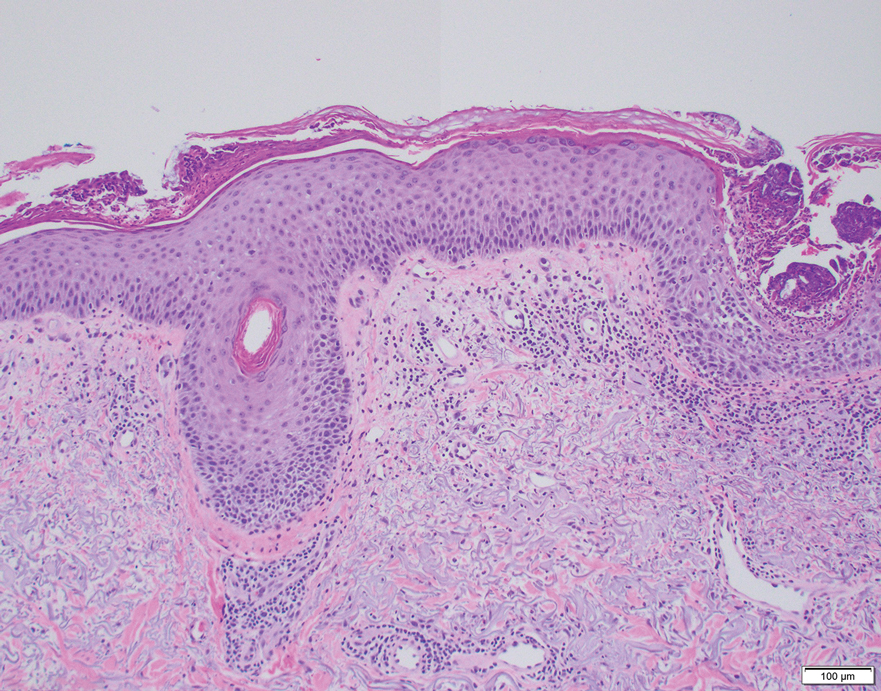
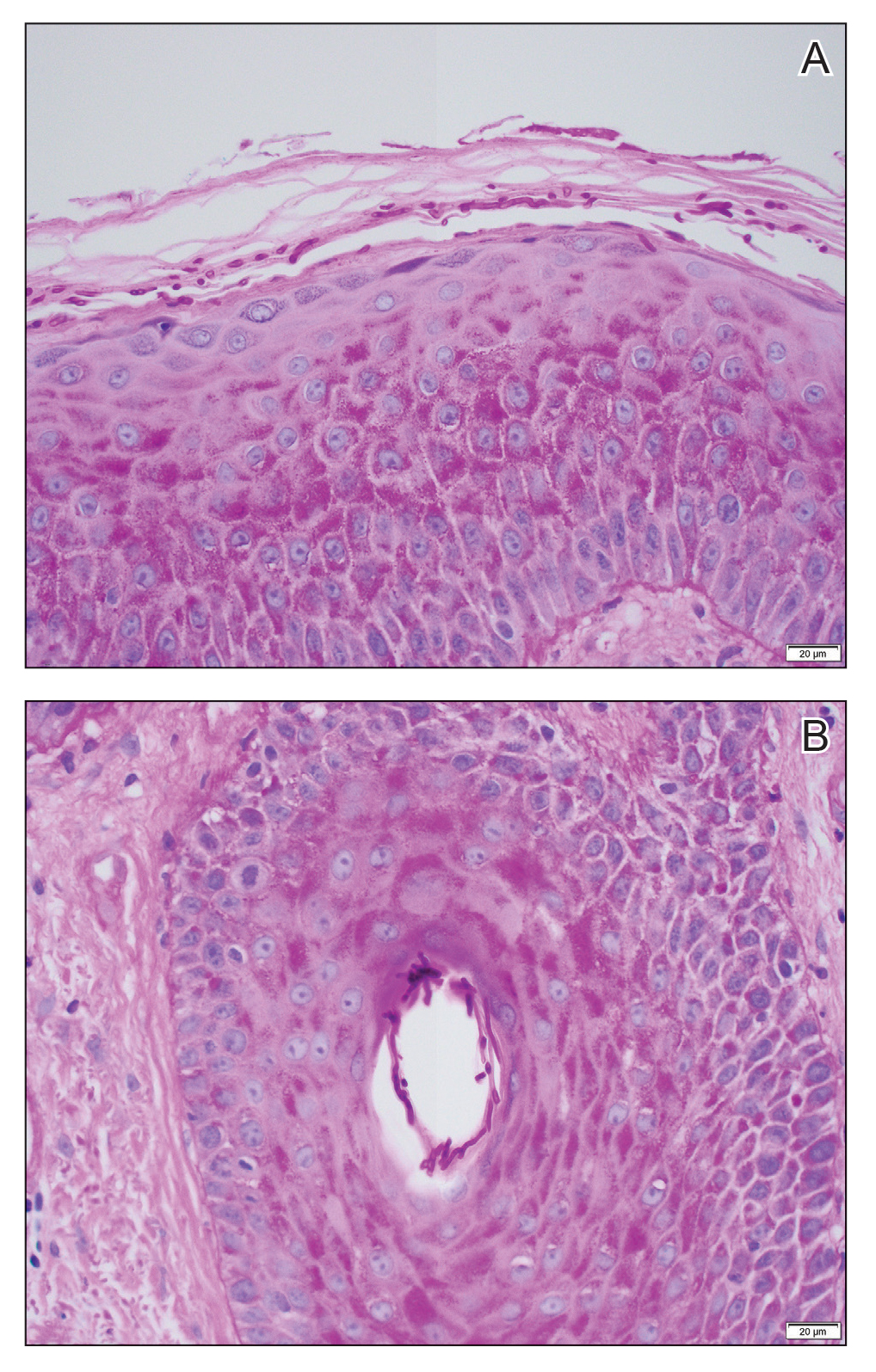
Approximately 1 month after the fungal isolate was sent to the reference laboratory, T indotineae was confirmed based on polymerase chain reaction (PCR) testing of internal transcribed spacer region sequences. Minimum inhibitory concentrations (MICs) obtained through antifungal susceptibility testing (AFST) were reported for fluconazole (8 μg/mL), griseofulvin (2 μg/mL), itraconazole (≤0.03 μg/mL), posaconazole (≤0.03 μg/mL), terbinafine (≥2 μg/mL), and voriconazole (0.125 μg/mL).
Approximately 7 weeks after itraconazole and ketoconazole were started, the rash had completely resolved. Nearly 8 months later (at the time this article was written), the rash had not recurred.
We report a unique case of T indotineae in a patient residing in California. Post hoc laboratory testing of dermatophyte isolates sent to the University of Texas reference laboratory identified terbinafine-resistant T indotineae specimens from the United States and Canada dating to 2017; clinical characteristics of patients from whom those isolates were obtained were unavailable.9
Trichophyton indotineae dermatophytosis typically is more extensive, inflamed, and pruritic, as well as likely more contagious, than tinea caused by other dermatophytes.5 Previously called Trichophyton mentagrophytes genotype VIII when first isolated in 2017, the pathogen was renamed T indotineae in 2020 after important genetic differences were discovered between it and other T mentagrophytes species.5 The emergence of T indotineae has been attributed to concomitant use of topical steroids and antifungals,5,10 inappropriate prescribing of antifungals,5 and nonadherence to antifungal treatment.5
Likely risk factors for T indotineae infection include suboptimal hygiene, overcrowded conditions, hot and humid environments, and tight-fitting synthetic clothing.4 Transmission from family members appears common,5 especially when fomites are shared.4 A case reported in Pennsylvania likely was acquired through sexual contact.7 Travel to South Asia has been associated with acquisition of T indotineae infection,3,5-7 though our patient and some others had not traveled there.3,8 It is not clear whether immunosuppression and diabetes mellitus are associated with T indotineae infection.4,5,8 Trichophyton indotineae also can affect animals,11 though zoonotic transmission has not been reported.4
Not all T indotineae isolates are resistant to one or more antifungals; furthermore, antifungal resistance in other dermatophyte species has been reported.5 Terbinafine resistance in T indotineae is conferred by mutations in the gene encoding squalene epoxidase, which helps synthesize ergosterol—a component of the cell membrane in fungi.2,4,5,12 Although clinical cut-points for MIC obtained by AFST are not well established, T indotineae MICs for terbinafine of 0.5 μg/mL or more correlate with resistance.9 Resistance to azoles has been linked to overexpression of transporter genes, which increase azole efflux from cells, as well as to mutations in the gene encoding lanosterol 14α demethylase.4,12,13
Potassium hydroxide preparations and fungal cultures cannot differentiate T indotineae from other dermatophytes that typically cause tinea.5,14 Histopathologic findings in our case were no different than those of non–T indotineae dermatophytes. Only molecular testing using PCR assays to sequence internal transcribed spacer genes can confirm T indotineae infection. However, PCR assays and AFST are not available in many US laboratories.5 Matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry has shown promise in distinguishing T indotineae from other dermatophytes, though its clinical use is limited and it cannot assess terbinafine sensitivity.15,16 Clinicians in the United States who want to test specimens from cases suspicious for T indotineae infection should contact their local or state health department or the Centers for Disease Control and Prevention for assistance.3,5
Systemic treatment typically is necessary for T indotineae infection.5 Combinations of oral and topical azoles have been used, as well as topical ciclopirox, amorolfine (not available in the United States), and luliconazole.1,5,17-21
Itraconazole has emerged as the treatment of choice for T indotineae tinea, typically at 200 mg/d and often for courses of more than 3 months.5 Testing for serum itraconazole trough levels, as done for our patient, typically is not recommended. Clinicians should counsel patients to take itraconazole with high-fat foods and an acidic beverage to increase bioavailability.5 Potential adverse effects of itraconazole include heart failure and numerous drug-drug interactions.5,22 Patients with T indotineae dermatophytosis should avoid sharing personal belongings and having skin-to-skin contact of affected areas with others.4
Dermatologists who suspect T indotineae infection should work with public health agencies that can assist with testing and undertake infection surveillance, prevention, and control.5,23 Challenges to diagnosing and managing T indotineae infection include lack of awareness among dermatology providers, the need for specialized laboratory testing to confirm infection, lack of established clinical cut-points for MICs from AFST, the need for longer duration of treatment vs what is needed for typical tinea, and potential challenges with insurance coverage for testing and treatment. Empiric treatment with itraconazole should be considered when terbinafine-resistant dermatophytosis is suspected or when terbinafine-resistant T indotineae infection is confirmed.
Acknowledgments—Jeremy Gold, MD; Dallas J. Smith, PharmD; and Shawn Lockhart, PhD, all of the Centers for Disease Control and Prevention, Mycotic Diseases Branch (Atlanta, Georgia), provided helpful comments to the authors in preparing the manuscript of this article.
- Uhrlaß S, Verma SB, Gräser Y, al. Trichophyton indotineae—an emerging pathogen causing recalcitrant dermatophytoses in India and worldwide—a multidimensional perspective. J Fungi (Basel). 2022;8:757. doi:10.3390/jof8070757
- Jabet A, Brun S, Normand A-C, et al. Extensive dermatophytosis caused by terbinafine-resistant Trichophyton indotineae, France. Emerg Infect Dis. 2022;28:229-233. doi:10.3201/eid2801.210883
- Caplan AS, Chaturvedi S, Zhu Y, et al. Notes from the field. First reported U.S. cases of tinea caused by Trichophyton indotineae—New York City, December 2021-March 2023. MMWR Morb Mortal Wkly Rep. 2023;72:536-537. doi:10.15585/mmwr.mm7219a4
- Jabet A, Normand A-C, Brun S, et al. Trichophyton indotineae, from epidemiology to therapeutic. J Mycol Med. 2023;33:101383. doi:10.1016/j.mycmed.2023.101383
- Hill RC, Caplan AS, Elewski B, et al. Expert panel review of skin and hair dermatophytoses in an era of antifungal resistance. Am J Clin Dermatol. 2024;25:359-389. doi:10.1007/s40257-024-00848-1
- Caplan AS, Zakhem GA, Pomeranz MK. Trichophyton mentagrophytes internal transcribed spacer genotype VIII. JAMA Dermatol. 2023;159:1130. doi:10.1001/jamadermatol.2023.2645
- Spivack S, Gold JAW, Lockhart SR, et al. Potential sexual transmission of antifungal-resistant Trichophyton indotineae. Emerg Infect Dis. 2024;30:807-809. doi:10.3201/eid3004.240115
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. Published online May 15, 2024. doi:10.1001/jamadermatol.2024.1126
- Cañete-Gibas CF, Mele J, Patterson HP, et al. Terbinafine-resistant dermatophytes and the presence of Trichophyton indotineae in North America. J Clin Microbiol. 2023;61:e0056223. doi:10.1128/jcm.00562-23
- Gupta AK, Venkataraman M, Hall DC, et al. The emergence of Trichophyton indotineae: implications for clinical practice. Int J Dermatol. 2023;62:857-861.
- Oladzad V, Nasrollahi Omran A, Haghani I, et al. Multi-drug resistance Trichophyton indotineae in a stray dog. Res Vet Sci. 2024;166:105105. doi:10.1016/j.rvsc.2023.105105
- Martinez-Rossi NM, Bitencourt TA, Peres NTA, et al. Dermatophyte resistance to antifungal drugs: mechanisms and prospectus. Front Microbiol. 2018;9:1108. doi:10.3389/fmicb.2018.01108
- Sacheli R, Hayette MP. Antifungal resistance in dermatophytes: genetic considerations, clinical presentations and alternative therapies. J Fungi (Basel). 2021;711:983. doi:10.3390/jof7110983
- Gupta AK, Cooper EA. Dermatophytosis (tinea) and other superficial fungal infections. In: Hospenthal DR, Rinaldi MG, eds. Diagnosis and Treatment of Human Mycoses. Humana Press; 2008:355-381.
- Normand A-C, Moreno-Sabater A, Jabet A, et al. MALDI-TOF mass spectrometry online identification of Trichophyton indotineae using the MSI-2 application. J Fungi (Basel). 2022;8:1103. doi:10.3390/jof8101103
- De Paepe R, Normand A-C, Uhrlaß S, et al. Resistance profile, terbinafine resistance screening and MALDI-TOF MS identification of the emerging pathogen Trichophyton indotineae. Mycopathologia. 2024;189:29. doi:10.1007/s11046-024-00835-4
- Rajagopalan M, Inamadar A, Mittal A, et al. Expert consensus on the management of dermatophytosis in India (ECTODERM India). BMC Dermatol. 2018;18:6. doi:10.1186/s12895-018-0073-1
- Verma SB, Panda S, Nenoff P, et al. The unprecedented epidemic-like scenario of dermatophytosis in India: III. Antifungal resistance and treatment options. Indian J Dermatol Venereol Leprol. 2021;87:468-482. doi:10.25259/IJDVL_303_20
- Shaw D, Singh S, Dogra S, et al. MIC and upper limit of wild-type distribution for 13 antifungal agents against a Trichophyton mentagrophytes–Trichophyton interdigitale complex of Indian origin. Antimicrob Agents Chemother. 2020;64:E01964-19. doi:10.1128/AAC.01964-19
- Burmester A, Hipler U-C, Uhrlaß S, et al. Indian Trichophyton mentagrophytes squalene epoxidase erg1 double mutants show high proportion of combined fluconazole and terbinafine resistance. Mycoses. 2020;63:1175-1180. doi:10.1111/myc.13150
- Khurana A, Agarwal A, Agrawal D, et al. Effect of different itraconazole dosing regimens on cure rates, treatment duration, safety, and relapse rates in adult patients with tinea corporis/cruris: a randomized clinical trial. JAMA Dermatol. 2022;158:1269-1278. doi:10.1001/jamadermatol.2022.3745
- Itraconazole capsule. DailyMed [Internet]. Updated June 3, 2024. Accessed June 19, 2024. https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=2ab38a8a-3708-4b97-9f7f-8e554a15348d
- Bui TS, Katz KA. Resistant Trichophyton indotineae dermatophytosis—an emerging pandemic, now in the US. JAMA Dermatol. Published online May 15, 2024. doi:10.1001/jamadermatol.2024.1125
To the Editor:
Historically, commonly available antifungal medications have been effective for treating dermatophytosis (tinea). However, recent tinea outbreaks caused by Trichophyton indotineae—a dermatophyte often resistant to terbinafine and sometimes to other antifungals—have been reported in South Asia, Europe, the Middle East, Southeast Asia, and Australia.1-5
Three confirmed cases of T indotineae dermatophytosis in the United States were reported in 2023 in New York3,6; a fourth confirmed case was reported in 2024 in Pennsylvania.7 Post hoc laboratory testing of fungal isolates in New York in 2022 and 2023 identified an additional 11 cases.8 We present a case of extensive multidrug-resistant tinea caused by T indotineae in a man in California.
An otherwise healthy 65-year-old man who had traveled to Europe in the past 3 months presented to his primary care physician with a widespread pruritic rash (Figure 1). He was treated with 2 weeks of oral terbinafine 250 mg/d and topical medicines, including clotrimazole cream 1%, fluocinonide ointment 0.05%, and clobetasol ointment 0.05% without improvement. Subsequently, 2 weeks of oral griseofulvin microsize 500 mg/d also proved ineffective. An antibody test was negative for HIV. His hemoglobin A1c was 6.2% (reference range, ≤5.6%). The patient was referred to dermatology.
Erythematous plaques—many scaly throughout and some annular with central clearing—were present on the arms, legs, and torso as well as in the groin. Honey crust was present on some plaques on the leg. A potassium hydroxide preparation showed abundant fungal hyphae. Material for fungal and bacterial cultures was collected. The patient was treated again with oral terbinafine 250 mg/d, an oral prednisone taper starting at 60 mg/d for a presumed id reaction, and various oral antihistamines for pruritus; all were ineffective. A bacterial culture showed only mixed skin flora. Oral fluconazole 200 mg/d was prescribed. A skin biopsy specimen showed compact orthokeratosis and parakeratosis of the stratum corneum with few neutrophils and focal pustule formation (Figure 2). Superficial perivascular inflammation, including lymphocytes, histiocytes, and few neutrophils, was present. A periodic acid–Schiff stain showed fungal hyphae in the stratum corneum and a hair follicle (Figure 3). After approximately 2 weeks, mold was identified in the fungal culture. Approximately 2 weeks thereafter, the organism was reported as Trichophyton species.
The rash did not improve; resistance to terbinafine, griseofulvin, and fluconazole was suspected clinically. The fungal isolate was sent to a reference laboratory (University of Texas Health Science Center, San Antonio). Meanwhile, oral itraconazole 200 mg twice daily and ketoconazole cream 2% were prescribed; the rash began to improve. A serum itraconazole trough level obtained 4 days after treatment initiation was 0.5 μg/mL (reference range, ≥0.6 μg/mL). The evening itraconazole dose was increased to 300 mg; a subsequent trough level was 0.8 μg/mL.
Approximately 1 month after the fungal isolate was sent to the reference laboratory, T indotineae was confirmed based on polymerase chain reaction (PCR) testing of internal transcribed spacer region sequences. Minimum inhibitory concentrations (MICs) obtained through antifungal susceptibility testing (AFST) were reported for fluconazole (8 μg/mL), griseofulvin (2 μg/mL), itraconazole (≤0.03 μg/mL), posaconazole (≤0.03 μg/mL), terbinafine (≥2 μg/mL), and voriconazole (0.125 μg/mL).
Approximately 7 weeks after itraconazole and ketoconazole were started, the rash had completely resolved. Nearly 8 months later (at the time this article was written), the rash had not recurred.
We report a unique case of T indotineae in a patient residing in California. Post hoc laboratory testing of dermatophyte isolates sent to the University of Texas reference laboratory identified terbinafine-resistant T indotineae specimens from the United States and Canada dating to 2017; clinical characteristics of patients from whom those isolates were obtained were unavailable.9
Trichophyton indotineae dermatophytosis typically is more extensive, inflamed, and pruritic, as well as likely more contagious, than tinea caused by other dermatophytes.5 Previously called Trichophyton mentagrophytes genotype VIII when first isolated in 2017, the pathogen was renamed T indotineae in 2020 after important genetic differences were discovered between it and other T mentagrophytes species.5 The emergence of T indotineae has been attributed to concomitant use of topical steroids and antifungals,5,10 inappropriate prescribing of antifungals,5 and nonadherence to antifungal treatment.5
Likely risk factors for T indotineae infection include suboptimal hygiene, overcrowded conditions, hot and humid environments, and tight-fitting synthetic clothing.4 Transmission from family members appears common,5 especially when fomites are shared.4 A case reported in Pennsylvania likely was acquired through sexual contact.7 Travel to South Asia has been associated with acquisition of T indotineae infection,3,5-7 though our patient and some others had not traveled there.3,8 It is not clear whether immunosuppression and diabetes mellitus are associated with T indotineae infection.4,5,8 Trichophyton indotineae also can affect animals,11 though zoonotic transmission has not been reported.4
Not all T indotineae isolates are resistant to one or more antifungals; furthermore, antifungal resistance in other dermatophyte species has been reported.5 Terbinafine resistance in T indotineae is conferred by mutations in the gene encoding squalene epoxidase, which helps synthesize ergosterol—a component of the cell membrane in fungi.2,4,5,12 Although clinical cut-points for MIC obtained by AFST are not well established, T indotineae MICs for terbinafine of 0.5 μg/mL or more correlate with resistance.9 Resistance to azoles has been linked to overexpression of transporter genes, which increase azole efflux from cells, as well as to mutations in the gene encoding lanosterol 14α demethylase.4,12,13
Potassium hydroxide preparations and fungal cultures cannot differentiate T indotineae from other dermatophytes that typically cause tinea.5,14 Histopathologic findings in our case were no different than those of non–T indotineae dermatophytes. Only molecular testing using PCR assays to sequence internal transcribed spacer genes can confirm T indotineae infection. However, PCR assays and AFST are not available in many US laboratories.5 Matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry has shown promise in distinguishing T indotineae from other dermatophytes, though its clinical use is limited and it cannot assess terbinafine sensitivity.15,16 Clinicians in the United States who want to test specimens from cases suspicious for T indotineae infection should contact their local or state health department or the Centers for Disease Control and Prevention for assistance.3,5
Systemic treatment typically is necessary for T indotineae infection.5 Combinations of oral and topical azoles have been used, as well as topical ciclopirox, amorolfine (not available in the United States), and luliconazole.1,5,17-21
Itraconazole has emerged as the treatment of choice for T indotineae tinea, typically at 200 mg/d and often for courses of more than 3 months.5 Testing for serum itraconazole trough levels, as done for our patient, typically is not recommended. Clinicians should counsel patients to take itraconazole with high-fat foods and an acidic beverage to increase bioavailability.5 Potential adverse effects of itraconazole include heart failure and numerous drug-drug interactions.5,22 Patients with T indotineae dermatophytosis should avoid sharing personal belongings and having skin-to-skin contact of affected areas with others.4
Dermatologists who suspect T indotineae infection should work with public health agencies that can assist with testing and undertake infection surveillance, prevention, and control.5,23 Challenges to diagnosing and managing T indotineae infection include lack of awareness among dermatology providers, the need for specialized laboratory testing to confirm infection, lack of established clinical cut-points for MICs from AFST, the need for longer duration of treatment vs what is needed for typical tinea, and potential challenges with insurance coverage for testing and treatment. Empiric treatment with itraconazole should be considered when terbinafine-resistant dermatophytosis is suspected or when terbinafine-resistant T indotineae infection is confirmed.
Acknowledgments—Jeremy Gold, MD; Dallas J. Smith, PharmD; and Shawn Lockhart, PhD, all of the Centers for Disease Control and Prevention, Mycotic Diseases Branch (Atlanta, Georgia), provided helpful comments to the authors in preparing the manuscript of this article.
To the Editor:
Historically, commonly available antifungal medications have been effective for treating dermatophytosis (tinea). However, recent tinea outbreaks caused by Trichophyton indotineae—a dermatophyte often resistant to terbinafine and sometimes to other antifungals—have been reported in South Asia, Europe, the Middle East, Southeast Asia, and Australia.1-5
Three confirmed cases of T indotineae dermatophytosis in the United States were reported in 2023 in New York3,6; a fourth confirmed case was reported in 2024 in Pennsylvania.7 Post hoc laboratory testing of fungal isolates in New York in 2022 and 2023 identified an additional 11 cases.8 We present a case of extensive multidrug-resistant tinea caused by T indotineae in a man in California.
An otherwise healthy 65-year-old man who had traveled to Europe in the past 3 months presented to his primary care physician with a widespread pruritic rash (Figure 1). He was treated with 2 weeks of oral terbinafine 250 mg/d and topical medicines, including clotrimazole cream 1%, fluocinonide ointment 0.05%, and clobetasol ointment 0.05% without improvement. Subsequently, 2 weeks of oral griseofulvin microsize 500 mg/d also proved ineffective. An antibody test was negative for HIV. His hemoglobin A1c was 6.2% (reference range, ≤5.6%). The patient was referred to dermatology.
Erythematous plaques—many scaly throughout and some annular with central clearing—were present on the arms, legs, and torso as well as in the groin. Honey crust was present on some plaques on the leg. A potassium hydroxide preparation showed abundant fungal hyphae. Material for fungal and bacterial cultures was collected. The patient was treated again with oral terbinafine 250 mg/d, an oral prednisone taper starting at 60 mg/d for a presumed id reaction, and various oral antihistamines for pruritus; all were ineffective. A bacterial culture showed only mixed skin flora. Oral fluconazole 200 mg/d was prescribed. A skin biopsy specimen showed compact orthokeratosis and parakeratosis of the stratum corneum with few neutrophils and focal pustule formation (Figure 2). Superficial perivascular inflammation, including lymphocytes, histiocytes, and few neutrophils, was present. A periodic acid–Schiff stain showed fungal hyphae in the stratum corneum and a hair follicle (Figure 3). After approximately 2 weeks, mold was identified in the fungal culture. Approximately 2 weeks thereafter, the organism was reported as Trichophyton species.
The rash did not improve; resistance to terbinafine, griseofulvin, and fluconazole was suspected clinically. The fungal isolate was sent to a reference laboratory (University of Texas Health Science Center, San Antonio). Meanwhile, oral itraconazole 200 mg twice daily and ketoconazole cream 2% were prescribed; the rash began to improve. A serum itraconazole trough level obtained 4 days after treatment initiation was 0.5 μg/mL (reference range, ≥0.6 μg/mL). The evening itraconazole dose was increased to 300 mg; a subsequent trough level was 0.8 μg/mL.
Approximately 1 month after the fungal isolate was sent to the reference laboratory, T indotineae was confirmed based on polymerase chain reaction (PCR) testing of internal transcribed spacer region sequences. Minimum inhibitory concentrations (MICs) obtained through antifungal susceptibility testing (AFST) were reported for fluconazole (8 μg/mL), griseofulvin (2 μg/mL), itraconazole (≤0.03 μg/mL), posaconazole (≤0.03 μg/mL), terbinafine (≥2 μg/mL), and voriconazole (0.125 μg/mL).
Approximately 7 weeks after itraconazole and ketoconazole were started, the rash had completely resolved. Nearly 8 months later (at the time this article was written), the rash had not recurred.
We report a unique case of T indotineae in a patient residing in California. Post hoc laboratory testing of dermatophyte isolates sent to the University of Texas reference laboratory identified terbinafine-resistant T indotineae specimens from the United States and Canada dating to 2017; clinical characteristics of patients from whom those isolates were obtained were unavailable.9
Trichophyton indotineae dermatophytosis typically is more extensive, inflamed, and pruritic, as well as likely more contagious, than tinea caused by other dermatophytes.5 Previously called Trichophyton mentagrophytes genotype VIII when first isolated in 2017, the pathogen was renamed T indotineae in 2020 after important genetic differences were discovered between it and other T mentagrophytes species.5 The emergence of T indotineae has been attributed to concomitant use of topical steroids and antifungals,5,10 inappropriate prescribing of antifungals,5 and nonadherence to antifungal treatment.5
Likely risk factors for T indotineae infection include suboptimal hygiene, overcrowded conditions, hot and humid environments, and tight-fitting synthetic clothing.4 Transmission from family members appears common,5 especially when fomites are shared.4 A case reported in Pennsylvania likely was acquired through sexual contact.7 Travel to South Asia has been associated with acquisition of T indotineae infection,3,5-7 though our patient and some others had not traveled there.3,8 It is not clear whether immunosuppression and diabetes mellitus are associated with T indotineae infection.4,5,8 Trichophyton indotineae also can affect animals,11 though zoonotic transmission has not been reported.4
Not all T indotineae isolates are resistant to one or more antifungals; furthermore, antifungal resistance in other dermatophyte species has been reported.5 Terbinafine resistance in T indotineae is conferred by mutations in the gene encoding squalene epoxidase, which helps synthesize ergosterol—a component of the cell membrane in fungi.2,4,5,12 Although clinical cut-points for MIC obtained by AFST are not well established, T indotineae MICs for terbinafine of 0.5 μg/mL or more correlate with resistance.9 Resistance to azoles has been linked to overexpression of transporter genes, which increase azole efflux from cells, as well as to mutations in the gene encoding lanosterol 14α demethylase.4,12,13
Potassium hydroxide preparations and fungal cultures cannot differentiate T indotineae from other dermatophytes that typically cause tinea.5,14 Histopathologic findings in our case were no different than those of non–T indotineae dermatophytes. Only molecular testing using PCR assays to sequence internal transcribed spacer genes can confirm T indotineae infection. However, PCR assays and AFST are not available in many US laboratories.5 Matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry has shown promise in distinguishing T indotineae from other dermatophytes, though its clinical use is limited and it cannot assess terbinafine sensitivity.15,16 Clinicians in the United States who want to test specimens from cases suspicious for T indotineae infection should contact their local or state health department or the Centers for Disease Control and Prevention for assistance.3,5
Systemic treatment typically is necessary for T indotineae infection.5 Combinations of oral and topical azoles have been used, as well as topical ciclopirox, amorolfine (not available in the United States), and luliconazole.1,5,17-21
Itraconazole has emerged as the treatment of choice for T indotineae tinea, typically at 200 mg/d and often for courses of more than 3 months.5 Testing for serum itraconazole trough levels, as done for our patient, typically is not recommended. Clinicians should counsel patients to take itraconazole with high-fat foods and an acidic beverage to increase bioavailability.5 Potential adverse effects of itraconazole include heart failure and numerous drug-drug interactions.5,22 Patients with T indotineae dermatophytosis should avoid sharing personal belongings and having skin-to-skin contact of affected areas with others.4
Dermatologists who suspect T indotineae infection should work with public health agencies that can assist with testing and undertake infection surveillance, prevention, and control.5,23 Challenges to diagnosing and managing T indotineae infection include lack of awareness among dermatology providers, the need for specialized laboratory testing to confirm infection, lack of established clinical cut-points for MICs from AFST, the need for longer duration of treatment vs what is needed for typical tinea, and potential challenges with insurance coverage for testing and treatment. Empiric treatment with itraconazole should be considered when terbinafine-resistant dermatophytosis is suspected or when terbinafine-resistant T indotineae infection is confirmed.
Acknowledgments—Jeremy Gold, MD; Dallas J. Smith, PharmD; and Shawn Lockhart, PhD, all of the Centers for Disease Control and Prevention, Mycotic Diseases Branch (Atlanta, Georgia), provided helpful comments to the authors in preparing the manuscript of this article.
- Uhrlaß S, Verma SB, Gräser Y, al. Trichophyton indotineae—an emerging pathogen causing recalcitrant dermatophytoses in India and worldwide—a multidimensional perspective. J Fungi (Basel). 2022;8:757. doi:10.3390/jof8070757
- Jabet A, Brun S, Normand A-C, et al. Extensive dermatophytosis caused by terbinafine-resistant Trichophyton indotineae, France. Emerg Infect Dis. 2022;28:229-233. doi:10.3201/eid2801.210883
- Caplan AS, Chaturvedi S, Zhu Y, et al. Notes from the field. First reported U.S. cases of tinea caused by Trichophyton indotineae—New York City, December 2021-March 2023. MMWR Morb Mortal Wkly Rep. 2023;72:536-537. doi:10.15585/mmwr.mm7219a4
- Jabet A, Normand A-C, Brun S, et al. Trichophyton indotineae, from epidemiology to therapeutic. J Mycol Med. 2023;33:101383. doi:10.1016/j.mycmed.2023.101383
- Hill RC, Caplan AS, Elewski B, et al. Expert panel review of skin and hair dermatophytoses in an era of antifungal resistance. Am J Clin Dermatol. 2024;25:359-389. doi:10.1007/s40257-024-00848-1
- Caplan AS, Zakhem GA, Pomeranz MK. Trichophyton mentagrophytes internal transcribed spacer genotype VIII. JAMA Dermatol. 2023;159:1130. doi:10.1001/jamadermatol.2023.2645
- Spivack S, Gold JAW, Lockhart SR, et al. Potential sexual transmission of antifungal-resistant Trichophyton indotineae. Emerg Infect Dis. 2024;30:807-809. doi:10.3201/eid3004.240115
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. Published online May 15, 2024. doi:10.1001/jamadermatol.2024.1126
- Cañete-Gibas CF, Mele J, Patterson HP, et al. Terbinafine-resistant dermatophytes and the presence of Trichophyton indotineae in North America. J Clin Microbiol. 2023;61:e0056223. doi:10.1128/jcm.00562-23
- Gupta AK, Venkataraman M, Hall DC, et al. The emergence of Trichophyton indotineae: implications for clinical practice. Int J Dermatol. 2023;62:857-861.
- Oladzad V, Nasrollahi Omran A, Haghani I, et al. Multi-drug resistance Trichophyton indotineae in a stray dog. Res Vet Sci. 2024;166:105105. doi:10.1016/j.rvsc.2023.105105
- Martinez-Rossi NM, Bitencourt TA, Peres NTA, et al. Dermatophyte resistance to antifungal drugs: mechanisms and prospectus. Front Microbiol. 2018;9:1108. doi:10.3389/fmicb.2018.01108
- Sacheli R, Hayette MP. Antifungal resistance in dermatophytes: genetic considerations, clinical presentations and alternative therapies. J Fungi (Basel). 2021;711:983. doi:10.3390/jof7110983
- Gupta AK, Cooper EA. Dermatophytosis (tinea) and other superficial fungal infections. In: Hospenthal DR, Rinaldi MG, eds. Diagnosis and Treatment of Human Mycoses. Humana Press; 2008:355-381.
- Normand A-C, Moreno-Sabater A, Jabet A, et al. MALDI-TOF mass spectrometry online identification of Trichophyton indotineae using the MSI-2 application. J Fungi (Basel). 2022;8:1103. doi:10.3390/jof8101103
- De Paepe R, Normand A-C, Uhrlaß S, et al. Resistance profile, terbinafine resistance screening and MALDI-TOF MS identification of the emerging pathogen Trichophyton indotineae. Mycopathologia. 2024;189:29. doi:10.1007/s11046-024-00835-4
- Rajagopalan M, Inamadar A, Mittal A, et al. Expert consensus on the management of dermatophytosis in India (ECTODERM India). BMC Dermatol. 2018;18:6. doi:10.1186/s12895-018-0073-1
- Verma SB, Panda S, Nenoff P, et al. The unprecedented epidemic-like scenario of dermatophytosis in India: III. Antifungal resistance and treatment options. Indian J Dermatol Venereol Leprol. 2021;87:468-482. doi:10.25259/IJDVL_303_20
- Shaw D, Singh S, Dogra S, et al. MIC and upper limit of wild-type distribution for 13 antifungal agents against a Trichophyton mentagrophytes–Trichophyton interdigitale complex of Indian origin. Antimicrob Agents Chemother. 2020;64:E01964-19. doi:10.1128/AAC.01964-19
- Burmester A, Hipler U-C, Uhrlaß S, et al. Indian Trichophyton mentagrophytes squalene epoxidase erg1 double mutants show high proportion of combined fluconazole and terbinafine resistance. Mycoses. 2020;63:1175-1180. doi:10.1111/myc.13150
- Khurana A, Agarwal A, Agrawal D, et al. Effect of different itraconazole dosing regimens on cure rates, treatment duration, safety, and relapse rates in adult patients with tinea corporis/cruris: a randomized clinical trial. JAMA Dermatol. 2022;158:1269-1278. doi:10.1001/jamadermatol.2022.3745
- Itraconazole capsule. DailyMed [Internet]. Updated June 3, 2024. Accessed June 19, 2024. https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=2ab38a8a-3708-4b97-9f7f-8e554a15348d
- Bui TS, Katz KA. Resistant Trichophyton indotineae dermatophytosis—an emerging pandemic, now in the US. JAMA Dermatol. Published online May 15, 2024. doi:10.1001/jamadermatol.2024.1125
- Uhrlaß S, Verma SB, Gräser Y, al. Trichophyton indotineae—an emerging pathogen causing recalcitrant dermatophytoses in India and worldwide—a multidimensional perspective. J Fungi (Basel). 2022;8:757. doi:10.3390/jof8070757
- Jabet A, Brun S, Normand A-C, et al. Extensive dermatophytosis caused by terbinafine-resistant Trichophyton indotineae, France. Emerg Infect Dis. 2022;28:229-233. doi:10.3201/eid2801.210883
- Caplan AS, Chaturvedi S, Zhu Y, et al. Notes from the field. First reported U.S. cases of tinea caused by Trichophyton indotineae—New York City, December 2021-March 2023. MMWR Morb Mortal Wkly Rep. 2023;72:536-537. doi:10.15585/mmwr.mm7219a4
- Jabet A, Normand A-C, Brun S, et al. Trichophyton indotineae, from epidemiology to therapeutic. J Mycol Med. 2023;33:101383. doi:10.1016/j.mycmed.2023.101383
- Hill RC, Caplan AS, Elewski B, et al. Expert panel review of skin and hair dermatophytoses in an era of antifungal resistance. Am J Clin Dermatol. 2024;25:359-389. doi:10.1007/s40257-024-00848-1
- Caplan AS, Zakhem GA, Pomeranz MK. Trichophyton mentagrophytes internal transcribed spacer genotype VIII. JAMA Dermatol. 2023;159:1130. doi:10.1001/jamadermatol.2023.2645
- Spivack S, Gold JAW, Lockhart SR, et al. Potential sexual transmission of antifungal-resistant Trichophyton indotineae. Emerg Infect Dis. 2024;30:807-809. doi:10.3201/eid3004.240115
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. Published online May 15, 2024. doi:10.1001/jamadermatol.2024.1126
- Cañete-Gibas CF, Mele J, Patterson HP, et al. Terbinafine-resistant dermatophytes and the presence of Trichophyton indotineae in North America. J Clin Microbiol. 2023;61:e0056223. doi:10.1128/jcm.00562-23
- Gupta AK, Venkataraman M, Hall DC, et al. The emergence of Trichophyton indotineae: implications for clinical practice. Int J Dermatol. 2023;62:857-861.
- Oladzad V, Nasrollahi Omran A, Haghani I, et al. Multi-drug resistance Trichophyton indotineae in a stray dog. Res Vet Sci. 2024;166:105105. doi:10.1016/j.rvsc.2023.105105
- Martinez-Rossi NM, Bitencourt TA, Peres NTA, et al. Dermatophyte resistance to antifungal drugs: mechanisms and prospectus. Front Microbiol. 2018;9:1108. doi:10.3389/fmicb.2018.01108
- Sacheli R, Hayette MP. Antifungal resistance in dermatophytes: genetic considerations, clinical presentations and alternative therapies. J Fungi (Basel). 2021;711:983. doi:10.3390/jof7110983
- Gupta AK, Cooper EA. Dermatophytosis (tinea) and other superficial fungal infections. In: Hospenthal DR, Rinaldi MG, eds. Diagnosis and Treatment of Human Mycoses. Humana Press; 2008:355-381.
- Normand A-C, Moreno-Sabater A, Jabet A, et al. MALDI-TOF mass spectrometry online identification of Trichophyton indotineae using the MSI-2 application. J Fungi (Basel). 2022;8:1103. doi:10.3390/jof8101103
- De Paepe R, Normand A-C, Uhrlaß S, et al. Resistance profile, terbinafine resistance screening and MALDI-TOF MS identification of the emerging pathogen Trichophyton indotineae. Mycopathologia. 2024;189:29. doi:10.1007/s11046-024-00835-4
- Rajagopalan M, Inamadar A, Mittal A, et al. Expert consensus on the management of dermatophytosis in India (ECTODERM India). BMC Dermatol. 2018;18:6. doi:10.1186/s12895-018-0073-1
- Verma SB, Panda S, Nenoff P, et al. The unprecedented epidemic-like scenario of dermatophytosis in India: III. Antifungal resistance and treatment options. Indian J Dermatol Venereol Leprol. 2021;87:468-482. doi:10.25259/IJDVL_303_20
- Shaw D, Singh S, Dogra S, et al. MIC and upper limit of wild-type distribution for 13 antifungal agents against a Trichophyton mentagrophytes–Trichophyton interdigitale complex of Indian origin. Antimicrob Agents Chemother. 2020;64:E01964-19. doi:10.1128/AAC.01964-19
- Burmester A, Hipler U-C, Uhrlaß S, et al. Indian Trichophyton mentagrophytes squalene epoxidase erg1 double mutants show high proportion of combined fluconazole and terbinafine resistance. Mycoses. 2020;63:1175-1180. doi:10.1111/myc.13150
- Khurana A, Agarwal A, Agrawal D, et al. Effect of different itraconazole dosing regimens on cure rates, treatment duration, safety, and relapse rates in adult patients with tinea corporis/cruris: a randomized clinical trial. JAMA Dermatol. 2022;158:1269-1278. doi:10.1001/jamadermatol.2022.3745
- Itraconazole capsule. DailyMed [Internet]. Updated June 3, 2024. Accessed June 19, 2024. https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=2ab38a8a-3708-4b97-9f7f-8e554a15348d
- Bui TS, Katz KA. Resistant Trichophyton indotineae dermatophytosis—an emerging pandemic, now in the US. JAMA Dermatol. Published online May 15, 2024. doi:10.1001/jamadermatol.2024.1125
Practice Points
- Trichophyton indotineae can cause extensive dermatophytosis that often is resistant to terbinafine and in some cases to other antifungals.
- Only molecular testing, which is not widely available, can distinguish T indotineae from other dermatophytes.
- Suspected or confirmed cases of T indotineae dermatophytosis should be reported to public health agencies to provide assistance with testing, as well as surveillance, prevention, and control of infection.
