User login
Renal Cell Carcinoma: What You Need to Know About Hereditary Syndromes
Renal Cell Carcinoma: What You Need to Know About Hereditary Syndromes
The role of hereditary syndromes in renal cell carcinoma (RCC) might be easily missed, a kidney cancer specialist said during a recent Association of VA Hematology and Oncology (AVAHO) seminar in Long Beach, California, though careful clinical evaluation can uncover genetic traits that may affect treatment and familial risk.
“The importance of finding or identifying hereditary forms of kidney cancer really should not be underestimated,” said urologist Brian Shuch, MD, director of the UCLA Kidney Cancer Program, on treating veterans with kidney cancer.
According to Shuch, recent data suggest that about 4.5% of patients with RCC have a hereditary syndrome: “A lot of times, these hide in plain sight. You have to really look deep and try to figure things out and understand that maybe they have a hereditary form of kidney cancer.”
It is important to consider early genetic testing, Shuch said. Red flags for hereditary syndromes include early-onset RCC (age ≤ 45 years), multifocal tumors, bilateral tumors (especially in younger individuals), or a relevant family personal history, he said.
Unusual skin conditions are also potential signs, Shuch said. These can include leiomyomas, fibrofolliculomas, and angiofibromas: “Patients have lots of lumps or bumps.”
“When I look at a patient, I go head to toe and ask if there any issues with your vision, any issues with your hearing, any issues swallowing,” he explained at the meeting. “Do you have any problems with heart issues, adrenal issues? You’ve got to go through each organ, and it can lead you to different things.”
Shuch highlighted Von Hippel-Lindau (VHL) syndrome, which affects 1 in 25,000 people. About 80% to 90% of these patients have a family history, Shuch said.
But the others do not. “Unfortunately, some get diagnosed later in life because they don’t get cascade testing starting at aged 2, which is recommended. These are the patients who might be coming into the ER with a hemangioblastoma or picking up the phone and all of a sudden being deaf in one ear due to an endolymphatic sac tumor.
“We want to limit metastatic spread and preserve the kidneys,” Shuch said. “We don’t want to be doing radical nephrectomies. We want to avoid chronic kidney disease, prevent end-stage renal disease, and maximize quality of life.”
It’s a good idea to avoid surgical removal unless a patient’s tumor grows to be > 3 cm, a line that indicates risk of metastases, he said.
In terms of treatment, Shuch highlighted a 2021 study that showed benefit in VHL from belzutifan (Welireg), an oral HIF-2 α inhibitor approved by the US Food and Drug Administration. The medication significantly reduced the need for surgical intervention.
“Patients go on this drug, and surgeons are putting their scalpels down,” said Shuch, who worked on the 2021 study.
Other hereditary syndromes include the rare hereditary papillary RCC, and Birt-Hogg-Dubé syndrome, believed to affect 1 in 200,000 people but may be more common, he said.
Birt-Hogg-Dubé syndrome is linked to lung cysts, lung collapse, and skin manifestations. The 3 cm surgery rule is appropriate in these cases, Shuch said, and metastases are rare.
Another condition, hereditary leiomyomatosis and RCC, is the most dangerous hereditary form. Originally thought to affect 1 in 200,000 people, hereditary leiomyomatosis and RCC is similar to Birt-Hogg-Dubé syndrome in that it is believed to be more common.
“You will see this,” Shuch predicted.
Shuch advised colleagues to intervene early and take a large margin during surgery.
He also highlighted familial paraganglioma syndrome, which is associated with gastrointestinal stromal tumors, and Cowden syndrome, which is linked to skin manifestations and breast, thyroid, and endometrial cancer.
Shuch reported that he had no disclosures.
The role of hereditary syndromes in renal cell carcinoma (RCC) might be easily missed, a kidney cancer specialist said during a recent Association of VA Hematology and Oncology (AVAHO) seminar in Long Beach, California, though careful clinical evaluation can uncover genetic traits that may affect treatment and familial risk.
“The importance of finding or identifying hereditary forms of kidney cancer really should not be underestimated,” said urologist Brian Shuch, MD, director of the UCLA Kidney Cancer Program, on treating veterans with kidney cancer.
According to Shuch, recent data suggest that about 4.5% of patients with RCC have a hereditary syndrome: “A lot of times, these hide in plain sight. You have to really look deep and try to figure things out and understand that maybe they have a hereditary form of kidney cancer.”
It is important to consider early genetic testing, Shuch said. Red flags for hereditary syndromes include early-onset RCC (age ≤ 45 years), multifocal tumors, bilateral tumors (especially in younger individuals), or a relevant family personal history, he said.
Unusual skin conditions are also potential signs, Shuch said. These can include leiomyomas, fibrofolliculomas, and angiofibromas: “Patients have lots of lumps or bumps.”
“When I look at a patient, I go head to toe and ask if there any issues with your vision, any issues with your hearing, any issues swallowing,” he explained at the meeting. “Do you have any problems with heart issues, adrenal issues? You’ve got to go through each organ, and it can lead you to different things.”
Shuch highlighted Von Hippel-Lindau (VHL) syndrome, which affects 1 in 25,000 people. About 80% to 90% of these patients have a family history, Shuch said.
But the others do not. “Unfortunately, some get diagnosed later in life because they don’t get cascade testing starting at aged 2, which is recommended. These are the patients who might be coming into the ER with a hemangioblastoma or picking up the phone and all of a sudden being deaf in one ear due to an endolymphatic sac tumor.
“We want to limit metastatic spread and preserve the kidneys,” Shuch said. “We don’t want to be doing radical nephrectomies. We want to avoid chronic kidney disease, prevent end-stage renal disease, and maximize quality of life.”
It’s a good idea to avoid surgical removal unless a patient’s tumor grows to be > 3 cm, a line that indicates risk of metastases, he said.
In terms of treatment, Shuch highlighted a 2021 study that showed benefit in VHL from belzutifan (Welireg), an oral HIF-2 α inhibitor approved by the US Food and Drug Administration. The medication significantly reduced the need for surgical intervention.
“Patients go on this drug, and surgeons are putting their scalpels down,” said Shuch, who worked on the 2021 study.
Other hereditary syndromes include the rare hereditary papillary RCC, and Birt-Hogg-Dubé syndrome, believed to affect 1 in 200,000 people but may be more common, he said.
Birt-Hogg-Dubé syndrome is linked to lung cysts, lung collapse, and skin manifestations. The 3 cm surgery rule is appropriate in these cases, Shuch said, and metastases are rare.
Another condition, hereditary leiomyomatosis and RCC, is the most dangerous hereditary form. Originally thought to affect 1 in 200,000 people, hereditary leiomyomatosis and RCC is similar to Birt-Hogg-Dubé syndrome in that it is believed to be more common.
“You will see this,” Shuch predicted.
Shuch advised colleagues to intervene early and take a large margin during surgery.
He also highlighted familial paraganglioma syndrome, which is associated with gastrointestinal stromal tumors, and Cowden syndrome, which is linked to skin manifestations and breast, thyroid, and endometrial cancer.
Shuch reported that he had no disclosures.
The role of hereditary syndromes in renal cell carcinoma (RCC) might be easily missed, a kidney cancer specialist said during a recent Association of VA Hematology and Oncology (AVAHO) seminar in Long Beach, California, though careful clinical evaluation can uncover genetic traits that may affect treatment and familial risk.
“The importance of finding or identifying hereditary forms of kidney cancer really should not be underestimated,” said urologist Brian Shuch, MD, director of the UCLA Kidney Cancer Program, on treating veterans with kidney cancer.
According to Shuch, recent data suggest that about 4.5% of patients with RCC have a hereditary syndrome: “A lot of times, these hide in plain sight. You have to really look deep and try to figure things out and understand that maybe they have a hereditary form of kidney cancer.”
It is important to consider early genetic testing, Shuch said. Red flags for hereditary syndromes include early-onset RCC (age ≤ 45 years), multifocal tumors, bilateral tumors (especially in younger individuals), or a relevant family personal history, he said.
Unusual skin conditions are also potential signs, Shuch said. These can include leiomyomas, fibrofolliculomas, and angiofibromas: “Patients have lots of lumps or bumps.”
“When I look at a patient, I go head to toe and ask if there any issues with your vision, any issues with your hearing, any issues swallowing,” he explained at the meeting. “Do you have any problems with heart issues, adrenal issues? You’ve got to go through each organ, and it can lead you to different things.”
Shuch highlighted Von Hippel-Lindau (VHL) syndrome, which affects 1 in 25,000 people. About 80% to 90% of these patients have a family history, Shuch said.
But the others do not. “Unfortunately, some get diagnosed later in life because they don’t get cascade testing starting at aged 2, which is recommended. These are the patients who might be coming into the ER with a hemangioblastoma or picking up the phone and all of a sudden being deaf in one ear due to an endolymphatic sac tumor.
“We want to limit metastatic spread and preserve the kidneys,” Shuch said. “We don’t want to be doing radical nephrectomies. We want to avoid chronic kidney disease, prevent end-stage renal disease, and maximize quality of life.”
It’s a good idea to avoid surgical removal unless a patient’s tumor grows to be > 3 cm, a line that indicates risk of metastases, he said.
In terms of treatment, Shuch highlighted a 2021 study that showed benefit in VHL from belzutifan (Welireg), an oral HIF-2 α inhibitor approved by the US Food and Drug Administration. The medication significantly reduced the need for surgical intervention.
“Patients go on this drug, and surgeons are putting their scalpels down,” said Shuch, who worked on the 2021 study.
Other hereditary syndromes include the rare hereditary papillary RCC, and Birt-Hogg-Dubé syndrome, believed to affect 1 in 200,000 people but may be more common, he said.
Birt-Hogg-Dubé syndrome is linked to lung cysts, lung collapse, and skin manifestations. The 3 cm surgery rule is appropriate in these cases, Shuch said, and metastases are rare.
Another condition, hereditary leiomyomatosis and RCC, is the most dangerous hereditary form. Originally thought to affect 1 in 200,000 people, hereditary leiomyomatosis and RCC is similar to Birt-Hogg-Dubé syndrome in that it is believed to be more common.
“You will see this,” Shuch predicted.
Shuch advised colleagues to intervene early and take a large margin during surgery.
He also highlighted familial paraganglioma syndrome, which is associated with gastrointestinal stromal tumors, and Cowden syndrome, which is linked to skin manifestations and breast, thyroid, and endometrial cancer.
Shuch reported that he had no disclosures.
Renal Cell Carcinoma: What You Need to Know About Hereditary Syndromes
Renal Cell Carcinoma: What You Need to Know About Hereditary Syndromes

At-Home Alzheimer’s Testing Is Here: Are Physicians Ready?
Given the opportunity, 90% of Americans say they would take a blood biomarker test for Alzheimer’s disease (AD) — even in the absence of symptoms. Notably, 80% say they wouldn’t wait for a physician to order a test, they’d request one themselves.
The findings, from a recent nationwide survey by the Alzheimer’s Association, suggest a growing desire to predict the risk for or show evidence of AD and related dementias with a simple blood test. For consumers with the inclination and the money, that desire can now become reality.
Once limited to research settings or only available via a physician’s order, blood-based diagnostics for specific biomarkers — primarily pTau-217 and beta-amyloid 42/20 — are now offered by at least four companies in the US. Several others sell blood-based “dementia” panels without those biomarkers and screens for apolipoprotein (APOE) genes, including APOE4, a variant that confers a higher risk for AD.
The companies promote testing to all comers, not just those with a family history or concerns about cognitive symptoms. Test prices range from hundreds to thousands of dollars, depending on whether they are included in a company membership, often designed to encourage repeat testing. Blood draws are conducted at home or at certified labs. Buyers don’t need a prescription or to consult with a physician after receiving results.
Knowing results of such tests could be empowering and may encourage people to prepare for their illness, Jessica Mozersky, PhD, assistant professor of medicine at the Bioethics Research Center at Washington University in St. Louis, told this news organization. A direct-to-consumer (DTC) test also eliminates potential physician-created barriers to testing, she added.
But there are also potential harms.
Based on results, individuals may interpret everyday forgetfulness — like misplacing keys — as a sign that dementia is inevitable. This can lead them to change life plans, rethink the way they spend their time, or begin viewing their future negatively. “It creates unnecessary worry and anxiety,” Mozersky said.
The growing availability of DTC tests — heralded by some experts and discouraged by others — comes as AD and dementia specialists continue to debate whether AD diagnostic and staging criteria should be based only on biomarkers or on criteria that includes both pathology and symptomology.
For many, it raises a fundamental concern: If experts haven’t reached a consensus on blood-based AD biomarker testing, how can consumers be expected to interpret at-home test results?
Growing Demand
In 2024, the number of people living with AD passed 7 million. A recent report from the Alzheimer’s Association estimates that number will nearly double by 2060.
The demand for testing also appears to be rising. Similar to the findings in the Alzheimer’s Association’s survey, a small observational study published last year showed that 90% of patients who received a cerebrospinal fluid AD biomarker test ordered by a physician said the decision to get the test was “easy.” For 82%, getting results was positive because it allowed them to plan ahead and to adopt or continue healthy behaviors such as exercise and cognitive activities.
Until now, blood biomarker tests for AD have primarily been available only through a doctor. The tests measure beta-amyloid 42/20 and pTau-217, both of which are strong biomarkers of AD. Some other blood-based biomarkers under investigation include neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP).
As reported by Medscape Medical News, the FDA approved the first blood-based AD diagnostic test in May. The Lumipulse G pTau 217/Beta-Amyloid 1-42 is for the early detection of amyloid plaques associated with AD in adults aged 55 years or older who show signs and symptoms of the disease. But it is only available by prescription.
Quest Diagnostics tested the DTC market in 2023, promoting a consumer-initiated test for beta-amyloid 42/40 that had previously been available only through physicians. It was not well-received by clinicians and ethicists. The company withdrew it later that year but continues to sell beta-amyloid 42/20 and pTau-217 tests through physicians, as does its competitor Labcorp.
Today, at least a handful of companies in the US market AD biomarkers directly to the public: Apollo Health, BetterBrain, Function Health, Neurogen Biomarking, and True Health Labs. None of the companies have disclosed ties to pharmaceutical or device companies or test developers.
What Can Consumers Get?
Some companies direct customers to a lab for blood sample collection, whereas others send a technician to customers’ homes. The extent of biomarker testing and posttest consultation also vary by company.
Apollo Health customers can order a “BrainScan” for $799, which includes screens for pTau-217, GFAP, and NfL. Buyers get a detailed report that explains each test, the result (in nanograms per liter) and optimal range (ng/L) and potential next steps. A pTau-217 result in the normal range, for instance, would come with a recommendation for repeat testing every 2 years. If someone receives an abnormal result, they are contacted by a health coach who can make a physician referral.
At Function Health, members pay $499 a year to have access to hundreds of tests and a written summary of results by a clinician. All of its “Brain Health” tests, including “Beta-Amyloid 42/40 Ratio,” pTau-217, APOE, MTHFR, DNA, and NfL, are available for an additional undisclosed charge.
BetterBrain has a $399 membership that covers an initial 75-minute consultation with cognitive tests, a “personalized brain health plan,” and a blood test that is a basic panel without AD biomarkers. A $499 membership includes all of that plus an APOE test. A pTau-217 test is available for an additional undisclosed fee.
At Neurogen Biomarking, which started in January, a consumer orders an at-home test kit, and a phlebotomist comes to their home for a blood draw. The consumer then fills out an online cognitive assessment. Test results are reviewed by a board-certified neurologist and discussed with the consumer via a virtual visit. If the person is at low-risk, they are given some educational material. Those at higher risk are referred to Neurogen’s “team of specialty-trained neurologists” for continuing care. Testing costs were not provided by the company.
Consumers can order “Beta-Amyloid 42/40” for $749 and pTau-217 for $229 directly through True Health Labs. No consultations or services are offered.
DTC Testing Raises Alarms
It’s unclear where DTC tests fall in terms of regulation. The FDA does not usually review at-home tests for low-risk medical purposes but will generally do so for diagnostics that are for higher-risk conditions “to determine the validity of test claims,” according to the agency’s website.
Consumers, however, don’t usually have easy access to information on biomarker tests’ sensitivity, specificity, or other characteristics that would be used by clinicians or regulatory authorities to assess a test’s validity.
The lack of regulation of consumer-initiated AD testing is one issue cited by critics of at-home tests, including the Alzheimer’s Association.
“None of these tests have been scientifically proven to be accurate,” the association noted in a statement, adding that “the tests can have false positive results, meaning that individuals can have results saying they have dementia when in fact they do not.”
“For these and other reasons, the Alzheimer’s Association believes that home screening tests cannot and should not be used as a substitute for a thorough examination by a skilled physician. The whole process of assessment and diagnosis should be carried out within the context of an ongoing relationship with a responsible and qualified healthcare professional,” the statement said.
The association also said that biomarker tests should not be ordered — even by physicians — for asymptomatic individuals.
The American Academy of Neurology (AAN) does not have a position on DTC tests for AD biomarkers, a spokesperson told this news organization. In a 2021 paper on ethical considerations for diagnosis and care, an AAN committee said that biomarker testing could be clinically useful for some symptomatic patients, but testing asymptomatic individuals is “recommended solely in a research setting” because of potential harms “and the absence of interventions capable of favorably altering the natural history of the disease.”
Eric Topol, MD, chair of the Department of Translational Medicine at Scripps Research in La Jolla, California, is bullish on the potential for blood-based biomarker tests. In a blog post, he called the pTau-217 biomarker “one of the most exciting advances in neurology for decades, giving us a new opportunity to accurately predict and potentially prevent (or at least substantially delay) mild cognitive impairment and Alzheimer’s.”
But, wrote Topol, who is the former editor in chief of MedscapeMedical News, “I don’t think these biomarkers are going to be useful in people at low risk.” He wrote that testing should not be used by people who are “cognitively intact” or to tell someone they have pre-AD. “More work needs to be done to determine whether lowering one’s pTau-217 will alter the brain plaque progression and be seen as a disease-modifier,” wrote Topol.
The Risks of Knowing
Some people don’t want to know their biomarker status. In a study in May in JAMA Network Open, Mozersky and colleagues reported that while 81% of a group of cognitively normal participants in a longitudinal study of dementia said they wanted to see results, only 60% ultimately opted to get results after testing. Participants said they did not want to know because they didn’t want to become a burden on their family or that they felt fine; others had concerns about whether the tests were accurate.
That low number “surprised us,” said Mozersky. “Our study certainly suggests that when you’re really faced with knowing, that your answer is more likely to possibly be no,” she added.
DTC companies tell buyers that results could motivate them to change their lifestyle to reduce their future risk for AD and dementia. But some participants in Mozersky’s study said they didn’t want to know their status because there were no preventive treatments. Test results weren’t seen as “actionable,” she said.
Some studies have shown a degree of fatalism in individuals after receiving a test result, whether it’s positive or negative.
A group of Israeli researchers studied responses of people given PET scans to detect beta-amyloid. Before testing, all participants said they were motivated to adopt lifestyle changes to fight dementia. However, after testing, both those who had elevated beta-amyloid and those who did not reported a much lower desire to change their lifestyle. Those with normal scans probably felt relieved, wrote the researchers. The group with abnormal scans was too small to fully understand their reaction, they wrote.
Concerns about insurance coverage might also deter potential test-takers. Overall, 44% of those responding to the Alzheimer’s Association survey said they were worried that insurers might not cover healthcare costs in the future if they had received a positive test earlier. Respondents also worried about test accuracy, the cost of testing, and whether a positive test might lead to a prohibition on some activities, like driving.
What About the Doctors?
The DTC companies promise buyers that results will be private and won’t be shared with insurers — or with clinicians. And that raises another issue for many who are concerned about the lack of a physician intermediary with at-home testing.
“You remove the opportunity for clinicians to both review the result and figure out how to interpret it before it’s communicated to the patient,” Jalayne J. Arias, JD, a bioethicist and associate professor of Health Policy and Behavioral Sciences at Georgia State University, Atlanta, told this news organization.
Many in the field have been “thinking really carefully about how do we provide guidance to clinicians about biomarker testing,” she said. “Those issues are just heightened when we put it into a direct-to-consumer model,” Arias said.
Arias — who with colleagues published an analysis of potential insurance issues with biomarker tests in JAMA Neurology — said that prohibitions against discrimination based on preexisting conditions means that most likely, health insurers could not use testing data to deny coverage or increase premiums.
But, she said, “there are some question marks around the discrimination risks.” This is especially true for people seeking long-term care, disability or life insurance, she added.
If a test result is not documented in a medical record, it’s not clear whether the individual has an obligation to disclose the result to an insurer, said Arias.
Given all the unanswered questions about how results should be interpreted, to whom the results should be disclosed, and when and how to have discussions with patients, “it’s hard for me to imagine that we’re quite ready for a direct-to-consumer” test, Arias said.
Mozersky noted that Washington University has a financial stake in C2N Diagnostics, which makes the PrecivityAD — biomarker tests for AD. Arias reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.
Given the opportunity, 90% of Americans say they would take a blood biomarker test for Alzheimer’s disease (AD) — even in the absence of symptoms. Notably, 80% say they wouldn’t wait for a physician to order a test, they’d request one themselves.
The findings, from a recent nationwide survey by the Alzheimer’s Association, suggest a growing desire to predict the risk for or show evidence of AD and related dementias with a simple blood test. For consumers with the inclination and the money, that desire can now become reality.
Once limited to research settings or only available via a physician’s order, blood-based diagnostics for specific biomarkers — primarily pTau-217 and beta-amyloid 42/20 — are now offered by at least four companies in the US. Several others sell blood-based “dementia” panels without those biomarkers and screens for apolipoprotein (APOE) genes, including APOE4, a variant that confers a higher risk for AD.
The companies promote testing to all comers, not just those with a family history or concerns about cognitive symptoms. Test prices range from hundreds to thousands of dollars, depending on whether they are included in a company membership, often designed to encourage repeat testing. Blood draws are conducted at home or at certified labs. Buyers don’t need a prescription or to consult with a physician after receiving results.
Knowing results of such tests could be empowering and may encourage people to prepare for their illness, Jessica Mozersky, PhD, assistant professor of medicine at the Bioethics Research Center at Washington University in St. Louis, told this news organization. A direct-to-consumer (DTC) test also eliminates potential physician-created barriers to testing, she added.
But there are also potential harms.
Based on results, individuals may interpret everyday forgetfulness — like misplacing keys — as a sign that dementia is inevitable. This can lead them to change life plans, rethink the way they spend their time, or begin viewing their future negatively. “It creates unnecessary worry and anxiety,” Mozersky said.
The growing availability of DTC tests — heralded by some experts and discouraged by others — comes as AD and dementia specialists continue to debate whether AD diagnostic and staging criteria should be based only on biomarkers or on criteria that includes both pathology and symptomology.
For many, it raises a fundamental concern: If experts haven’t reached a consensus on blood-based AD biomarker testing, how can consumers be expected to interpret at-home test results?
Growing Demand
In 2024, the number of people living with AD passed 7 million. A recent report from the Alzheimer’s Association estimates that number will nearly double by 2060.
The demand for testing also appears to be rising. Similar to the findings in the Alzheimer’s Association’s survey, a small observational study published last year showed that 90% of patients who received a cerebrospinal fluid AD biomarker test ordered by a physician said the decision to get the test was “easy.” For 82%, getting results was positive because it allowed them to plan ahead and to adopt or continue healthy behaviors such as exercise and cognitive activities.
Until now, blood biomarker tests for AD have primarily been available only through a doctor. The tests measure beta-amyloid 42/20 and pTau-217, both of which are strong biomarkers of AD. Some other blood-based biomarkers under investigation include neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP).
As reported by Medscape Medical News, the FDA approved the first blood-based AD diagnostic test in May. The Lumipulse G pTau 217/Beta-Amyloid 1-42 is for the early detection of amyloid plaques associated with AD in adults aged 55 years or older who show signs and symptoms of the disease. But it is only available by prescription.
Quest Diagnostics tested the DTC market in 2023, promoting a consumer-initiated test for beta-amyloid 42/40 that had previously been available only through physicians. It was not well-received by clinicians and ethicists. The company withdrew it later that year but continues to sell beta-amyloid 42/20 and pTau-217 tests through physicians, as does its competitor Labcorp.
Today, at least a handful of companies in the US market AD biomarkers directly to the public: Apollo Health, BetterBrain, Function Health, Neurogen Biomarking, and True Health Labs. None of the companies have disclosed ties to pharmaceutical or device companies or test developers.
What Can Consumers Get?
Some companies direct customers to a lab for blood sample collection, whereas others send a technician to customers’ homes. The extent of biomarker testing and posttest consultation also vary by company.
Apollo Health customers can order a “BrainScan” for $799, which includes screens for pTau-217, GFAP, and NfL. Buyers get a detailed report that explains each test, the result (in nanograms per liter) and optimal range (ng/L) and potential next steps. A pTau-217 result in the normal range, for instance, would come with a recommendation for repeat testing every 2 years. If someone receives an abnormal result, they are contacted by a health coach who can make a physician referral.
At Function Health, members pay $499 a year to have access to hundreds of tests and a written summary of results by a clinician. All of its “Brain Health” tests, including “Beta-Amyloid 42/40 Ratio,” pTau-217, APOE, MTHFR, DNA, and NfL, are available for an additional undisclosed charge.
BetterBrain has a $399 membership that covers an initial 75-minute consultation with cognitive tests, a “personalized brain health plan,” and a blood test that is a basic panel without AD biomarkers. A $499 membership includes all of that plus an APOE test. A pTau-217 test is available for an additional undisclosed fee.
At Neurogen Biomarking, which started in January, a consumer orders an at-home test kit, and a phlebotomist comes to their home for a blood draw. The consumer then fills out an online cognitive assessment. Test results are reviewed by a board-certified neurologist and discussed with the consumer via a virtual visit. If the person is at low-risk, they are given some educational material. Those at higher risk are referred to Neurogen’s “team of specialty-trained neurologists” for continuing care. Testing costs were not provided by the company.
Consumers can order “Beta-Amyloid 42/40” for $749 and pTau-217 for $229 directly through True Health Labs. No consultations or services are offered.
DTC Testing Raises Alarms
It’s unclear where DTC tests fall in terms of regulation. The FDA does not usually review at-home tests for low-risk medical purposes but will generally do so for diagnostics that are for higher-risk conditions “to determine the validity of test claims,” according to the agency’s website.
Consumers, however, don’t usually have easy access to information on biomarker tests’ sensitivity, specificity, or other characteristics that would be used by clinicians or regulatory authorities to assess a test’s validity.
The lack of regulation of consumer-initiated AD testing is one issue cited by critics of at-home tests, including the Alzheimer’s Association.
“None of these tests have been scientifically proven to be accurate,” the association noted in a statement, adding that “the tests can have false positive results, meaning that individuals can have results saying they have dementia when in fact they do not.”
“For these and other reasons, the Alzheimer’s Association believes that home screening tests cannot and should not be used as a substitute for a thorough examination by a skilled physician. The whole process of assessment and diagnosis should be carried out within the context of an ongoing relationship with a responsible and qualified healthcare professional,” the statement said.
The association also said that biomarker tests should not be ordered — even by physicians — for asymptomatic individuals.
The American Academy of Neurology (AAN) does not have a position on DTC tests for AD biomarkers, a spokesperson told this news organization. In a 2021 paper on ethical considerations for diagnosis and care, an AAN committee said that biomarker testing could be clinically useful for some symptomatic patients, but testing asymptomatic individuals is “recommended solely in a research setting” because of potential harms “and the absence of interventions capable of favorably altering the natural history of the disease.”
Eric Topol, MD, chair of the Department of Translational Medicine at Scripps Research in La Jolla, California, is bullish on the potential for blood-based biomarker tests. In a blog post, he called the pTau-217 biomarker “one of the most exciting advances in neurology for decades, giving us a new opportunity to accurately predict and potentially prevent (or at least substantially delay) mild cognitive impairment and Alzheimer’s.”
But, wrote Topol, who is the former editor in chief of MedscapeMedical News, “I don’t think these biomarkers are going to be useful in people at low risk.” He wrote that testing should not be used by people who are “cognitively intact” or to tell someone they have pre-AD. “More work needs to be done to determine whether lowering one’s pTau-217 will alter the brain plaque progression and be seen as a disease-modifier,” wrote Topol.
The Risks of Knowing
Some people don’t want to know their biomarker status. In a study in May in JAMA Network Open, Mozersky and colleagues reported that while 81% of a group of cognitively normal participants in a longitudinal study of dementia said they wanted to see results, only 60% ultimately opted to get results after testing. Participants said they did not want to know because they didn’t want to become a burden on their family or that they felt fine; others had concerns about whether the tests were accurate.
That low number “surprised us,” said Mozersky. “Our study certainly suggests that when you’re really faced with knowing, that your answer is more likely to possibly be no,” she added.
DTC companies tell buyers that results could motivate them to change their lifestyle to reduce their future risk for AD and dementia. But some participants in Mozersky’s study said they didn’t want to know their status because there were no preventive treatments. Test results weren’t seen as “actionable,” she said.
Some studies have shown a degree of fatalism in individuals after receiving a test result, whether it’s positive or negative.
A group of Israeli researchers studied responses of people given PET scans to detect beta-amyloid. Before testing, all participants said they were motivated to adopt lifestyle changes to fight dementia. However, after testing, both those who had elevated beta-amyloid and those who did not reported a much lower desire to change their lifestyle. Those with normal scans probably felt relieved, wrote the researchers. The group with abnormal scans was too small to fully understand their reaction, they wrote.
Concerns about insurance coverage might also deter potential test-takers. Overall, 44% of those responding to the Alzheimer’s Association survey said they were worried that insurers might not cover healthcare costs in the future if they had received a positive test earlier. Respondents also worried about test accuracy, the cost of testing, and whether a positive test might lead to a prohibition on some activities, like driving.
What About the Doctors?
The DTC companies promise buyers that results will be private and won’t be shared with insurers — or with clinicians. And that raises another issue for many who are concerned about the lack of a physician intermediary with at-home testing.
“You remove the opportunity for clinicians to both review the result and figure out how to interpret it before it’s communicated to the patient,” Jalayne J. Arias, JD, a bioethicist and associate professor of Health Policy and Behavioral Sciences at Georgia State University, Atlanta, told this news organization.
Many in the field have been “thinking really carefully about how do we provide guidance to clinicians about biomarker testing,” she said. “Those issues are just heightened when we put it into a direct-to-consumer model,” Arias said.
Arias — who with colleagues published an analysis of potential insurance issues with biomarker tests in JAMA Neurology — said that prohibitions against discrimination based on preexisting conditions means that most likely, health insurers could not use testing data to deny coverage or increase premiums.
But, she said, “there are some question marks around the discrimination risks.” This is especially true for people seeking long-term care, disability or life insurance, she added.
If a test result is not documented in a medical record, it’s not clear whether the individual has an obligation to disclose the result to an insurer, said Arias.
Given all the unanswered questions about how results should be interpreted, to whom the results should be disclosed, and when and how to have discussions with patients, “it’s hard for me to imagine that we’re quite ready for a direct-to-consumer” test, Arias said.
Mozersky noted that Washington University has a financial stake in C2N Diagnostics, which makes the PrecivityAD — biomarker tests for AD. Arias reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.
Given the opportunity, 90% of Americans say they would take a blood biomarker test for Alzheimer’s disease (AD) — even in the absence of symptoms. Notably, 80% say they wouldn’t wait for a physician to order a test, they’d request one themselves.
The findings, from a recent nationwide survey by the Alzheimer’s Association, suggest a growing desire to predict the risk for or show evidence of AD and related dementias with a simple blood test. For consumers with the inclination and the money, that desire can now become reality.
Once limited to research settings or only available via a physician’s order, blood-based diagnostics for specific biomarkers — primarily pTau-217 and beta-amyloid 42/20 — are now offered by at least four companies in the US. Several others sell blood-based “dementia” panels without those biomarkers and screens for apolipoprotein (APOE) genes, including APOE4, a variant that confers a higher risk for AD.
The companies promote testing to all comers, not just those with a family history or concerns about cognitive symptoms. Test prices range from hundreds to thousands of dollars, depending on whether they are included in a company membership, often designed to encourage repeat testing. Blood draws are conducted at home or at certified labs. Buyers don’t need a prescription or to consult with a physician after receiving results.
Knowing results of such tests could be empowering and may encourage people to prepare for their illness, Jessica Mozersky, PhD, assistant professor of medicine at the Bioethics Research Center at Washington University in St. Louis, told this news organization. A direct-to-consumer (DTC) test also eliminates potential physician-created barriers to testing, she added.
But there are also potential harms.
Based on results, individuals may interpret everyday forgetfulness — like misplacing keys — as a sign that dementia is inevitable. This can lead them to change life plans, rethink the way they spend their time, or begin viewing their future negatively. “It creates unnecessary worry and anxiety,” Mozersky said.
The growing availability of DTC tests — heralded by some experts and discouraged by others — comes as AD and dementia specialists continue to debate whether AD diagnostic and staging criteria should be based only on biomarkers or on criteria that includes both pathology and symptomology.
For many, it raises a fundamental concern: If experts haven’t reached a consensus on blood-based AD biomarker testing, how can consumers be expected to interpret at-home test results?
Growing Demand
In 2024, the number of people living with AD passed 7 million. A recent report from the Alzheimer’s Association estimates that number will nearly double by 2060.
The demand for testing also appears to be rising. Similar to the findings in the Alzheimer’s Association’s survey, a small observational study published last year showed that 90% of patients who received a cerebrospinal fluid AD biomarker test ordered by a physician said the decision to get the test was “easy.” For 82%, getting results was positive because it allowed them to plan ahead and to adopt or continue healthy behaviors such as exercise and cognitive activities.
Until now, blood biomarker tests for AD have primarily been available only through a doctor. The tests measure beta-amyloid 42/20 and pTau-217, both of which are strong biomarkers of AD. Some other blood-based biomarkers under investigation include neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP).
As reported by Medscape Medical News, the FDA approved the first blood-based AD diagnostic test in May. The Lumipulse G pTau 217/Beta-Amyloid 1-42 is for the early detection of amyloid plaques associated with AD in adults aged 55 years or older who show signs and symptoms of the disease. But it is only available by prescription.
Quest Diagnostics tested the DTC market in 2023, promoting a consumer-initiated test for beta-amyloid 42/40 that had previously been available only through physicians. It was not well-received by clinicians and ethicists. The company withdrew it later that year but continues to sell beta-amyloid 42/20 and pTau-217 tests through physicians, as does its competitor Labcorp.
Today, at least a handful of companies in the US market AD biomarkers directly to the public: Apollo Health, BetterBrain, Function Health, Neurogen Biomarking, and True Health Labs. None of the companies have disclosed ties to pharmaceutical or device companies or test developers.
What Can Consumers Get?
Some companies direct customers to a lab for blood sample collection, whereas others send a technician to customers’ homes. The extent of biomarker testing and posttest consultation also vary by company.
Apollo Health customers can order a “BrainScan” for $799, which includes screens for pTau-217, GFAP, and NfL. Buyers get a detailed report that explains each test, the result (in nanograms per liter) and optimal range (ng/L) and potential next steps. A pTau-217 result in the normal range, for instance, would come with a recommendation for repeat testing every 2 years. If someone receives an abnormal result, they are contacted by a health coach who can make a physician referral.
At Function Health, members pay $499 a year to have access to hundreds of tests and a written summary of results by a clinician. All of its “Brain Health” tests, including “Beta-Amyloid 42/40 Ratio,” pTau-217, APOE, MTHFR, DNA, and NfL, are available for an additional undisclosed charge.
BetterBrain has a $399 membership that covers an initial 75-minute consultation with cognitive tests, a “personalized brain health plan,” and a blood test that is a basic panel without AD biomarkers. A $499 membership includes all of that plus an APOE test. A pTau-217 test is available for an additional undisclosed fee.
At Neurogen Biomarking, which started in January, a consumer orders an at-home test kit, and a phlebotomist comes to their home for a blood draw. The consumer then fills out an online cognitive assessment. Test results are reviewed by a board-certified neurologist and discussed with the consumer via a virtual visit. If the person is at low-risk, they are given some educational material. Those at higher risk are referred to Neurogen’s “team of specialty-trained neurologists” for continuing care. Testing costs were not provided by the company.
Consumers can order “Beta-Amyloid 42/40” for $749 and pTau-217 for $229 directly through True Health Labs. No consultations or services are offered.
DTC Testing Raises Alarms
It’s unclear where DTC tests fall in terms of regulation. The FDA does not usually review at-home tests for low-risk medical purposes but will generally do so for diagnostics that are for higher-risk conditions “to determine the validity of test claims,” according to the agency’s website.
Consumers, however, don’t usually have easy access to information on biomarker tests’ sensitivity, specificity, or other characteristics that would be used by clinicians or regulatory authorities to assess a test’s validity.
The lack of regulation of consumer-initiated AD testing is one issue cited by critics of at-home tests, including the Alzheimer’s Association.
“None of these tests have been scientifically proven to be accurate,” the association noted in a statement, adding that “the tests can have false positive results, meaning that individuals can have results saying they have dementia when in fact they do not.”
“For these and other reasons, the Alzheimer’s Association believes that home screening tests cannot and should not be used as a substitute for a thorough examination by a skilled physician. The whole process of assessment and diagnosis should be carried out within the context of an ongoing relationship with a responsible and qualified healthcare professional,” the statement said.
The association also said that biomarker tests should not be ordered — even by physicians — for asymptomatic individuals.
The American Academy of Neurology (AAN) does not have a position on DTC tests for AD biomarkers, a spokesperson told this news organization. In a 2021 paper on ethical considerations for diagnosis and care, an AAN committee said that biomarker testing could be clinically useful for some symptomatic patients, but testing asymptomatic individuals is “recommended solely in a research setting” because of potential harms “and the absence of interventions capable of favorably altering the natural history of the disease.”
Eric Topol, MD, chair of the Department of Translational Medicine at Scripps Research in La Jolla, California, is bullish on the potential for blood-based biomarker tests. In a blog post, he called the pTau-217 biomarker “one of the most exciting advances in neurology for decades, giving us a new opportunity to accurately predict and potentially prevent (or at least substantially delay) mild cognitive impairment and Alzheimer’s.”
But, wrote Topol, who is the former editor in chief of MedscapeMedical News, “I don’t think these biomarkers are going to be useful in people at low risk.” He wrote that testing should not be used by people who are “cognitively intact” or to tell someone they have pre-AD. “More work needs to be done to determine whether lowering one’s pTau-217 will alter the brain plaque progression and be seen as a disease-modifier,” wrote Topol.
The Risks of Knowing
Some people don’t want to know their biomarker status. In a study in May in JAMA Network Open, Mozersky and colleagues reported that while 81% of a group of cognitively normal participants in a longitudinal study of dementia said they wanted to see results, only 60% ultimately opted to get results after testing. Participants said they did not want to know because they didn’t want to become a burden on their family or that they felt fine; others had concerns about whether the tests were accurate.
That low number “surprised us,” said Mozersky. “Our study certainly suggests that when you’re really faced with knowing, that your answer is more likely to possibly be no,” she added.
DTC companies tell buyers that results could motivate them to change their lifestyle to reduce their future risk for AD and dementia. But some participants in Mozersky’s study said they didn’t want to know their status because there were no preventive treatments. Test results weren’t seen as “actionable,” she said.
Some studies have shown a degree of fatalism in individuals after receiving a test result, whether it’s positive or negative.
A group of Israeli researchers studied responses of people given PET scans to detect beta-amyloid. Before testing, all participants said they were motivated to adopt lifestyle changes to fight dementia. However, after testing, both those who had elevated beta-amyloid and those who did not reported a much lower desire to change their lifestyle. Those with normal scans probably felt relieved, wrote the researchers. The group with abnormal scans was too small to fully understand their reaction, they wrote.
Concerns about insurance coverage might also deter potential test-takers. Overall, 44% of those responding to the Alzheimer’s Association survey said they were worried that insurers might not cover healthcare costs in the future if they had received a positive test earlier. Respondents also worried about test accuracy, the cost of testing, and whether a positive test might lead to a prohibition on some activities, like driving.
What About the Doctors?
The DTC companies promise buyers that results will be private and won’t be shared with insurers — or with clinicians. And that raises another issue for many who are concerned about the lack of a physician intermediary with at-home testing.
“You remove the opportunity for clinicians to both review the result and figure out how to interpret it before it’s communicated to the patient,” Jalayne J. Arias, JD, a bioethicist and associate professor of Health Policy and Behavioral Sciences at Georgia State University, Atlanta, told this news organization.
Many in the field have been “thinking really carefully about how do we provide guidance to clinicians about biomarker testing,” she said. “Those issues are just heightened when we put it into a direct-to-consumer model,” Arias said.
Arias — who with colleagues published an analysis of potential insurance issues with biomarker tests in JAMA Neurology — said that prohibitions against discrimination based on preexisting conditions means that most likely, health insurers could not use testing data to deny coverage or increase premiums.
But, she said, “there are some question marks around the discrimination risks.” This is especially true for people seeking long-term care, disability or life insurance, she added.
If a test result is not documented in a medical record, it’s not clear whether the individual has an obligation to disclose the result to an insurer, said Arias.
Given all the unanswered questions about how results should be interpreted, to whom the results should be disclosed, and when and how to have discussions with patients, “it’s hard for me to imagine that we’re quite ready for a direct-to-consumer” test, Arias said.
Mozersky noted that Washington University has a financial stake in C2N Diagnostics, which makes the PrecivityAD — biomarker tests for AD. Arias reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.

Metastases-Directed Therapy for Pancreatic Cancer: More Questions Than Answers
This transcript has been edited for clarity.
Hello. I’m Dr Maurie Markman, from City of Hope. I’d like to discuss what I consider to be an absolutely fascinating paper, and one that I will say has very interesting results but raises many more questions than it answers. I think that was the intent of the authors.
The paper is entitled, “Addition of metastasis-directed therapy to systemic therapy for oligometastatic pancreatic ductal adenocarcinoma (EXTEND): a multicenter, randomized phase 2 trial,” published in the Journal of Clinical Oncology.
You might ask what metastasis-directed therapy in pancreatic cancer means. Have we really made much of an impact on pancreatic cancer? In fact, in my earlier years of training, if somebody came up with the idea, or suggested as part of a trial or treatment of an individual patient, that they would focus on metastases in pancreas cancer, you might say they’re crazy, or you might say: “Yeah, but they probably don’t know anything about the disease and its natural history.”
Now, fast forward several decades. Even with the recognized, modest advances in systemic therapy, what we see are tremendous, really remarkable advances in innovations in radiation therapy. Of course, this includes not only the use of radiation itself but also the imaging technology that is used to direct the radiation therapy. These advances have permitted asking the questions that are addressed in the current study.
Again, this study is fascinating. They randomized a very small number. Again, it’s a randomized phase 2 study. It’s really more of a proof of principle here. They randomized 41 patients with five or fewer metastatic lesions — with oligometastatic disease, they could have numerous lesions — to undergo what they’ve described as comprehensive metastases-directed therapy.
Most of this was external beam radiation therapy and stereotactic radiation therapy, but there were some localized radiation implants as well, plus chemotherapy. This was comprehensive metastases-directed therapy to each of these sites plus chemotherapy vs chemotherapy alone.
What was shown in this trial? The progression-free survival (PFS) in the metastases-directed therapy group was 10.3 months vs 2.5 months in the group of patients who received chemotherapy only, with a hazard ratio of 0.43 and statistical significance.
Remember, this was a very small study, but we see more than a tripling in the PFS. There was no difference in overall survival, which is not at all surprising because it was a very small sample size.
Very importantly — and essential to doing this trial ethically — a crossover was permitted at the time of progression, meaning that if a patient received chemotherapy only and progressed, they could potentially get stereotactic radiation to sites of metastatic disease. They might have also benefited from that kind of strategy to the metastasis-[therapy] so that overall survival in the small population may not be different. Again, there was a tripling of the time to disease progression.
Clearly, a larger study will be required to be more definitive. We would need more centers involved and maybe some modification in the study design in this trial because of any issues that the investigators may have identified. Of course, overall survival would be a fair endpoint to look at, but again, crossover would be essential, and that might influence an ultimate outcome. PFS is a very valid endpoint.
The only other point to mention is, with these results — and as I mentioned, advances in radiation and imaging — is it reasonable to potentially consider this type of approach for individual patients as a component of aggressive standard of care? Of course, this would be with very adequate informed consent from patients, because we don’t know what the impact will be.
With the limited morbidity associated with the radiation, for an individual patient with pancreatic cancer who has an adequate performance status and limited metastases, if we give them chemotherapy and also directed radiation, is it reasonable to consider that as an appropriate treatment option outside the setting of a clinical trial?
I think this is a very valid question that needs to be addressed. In my opinion, the answer in some settings should be yes, but that needs to be discussed much more widely than simply in this randomized phase 2 trial.
Thank you for your attention.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. I’m Dr Maurie Markman, from City of Hope. I’d like to discuss what I consider to be an absolutely fascinating paper, and one that I will say has very interesting results but raises many more questions than it answers. I think that was the intent of the authors.
The paper is entitled, “Addition of metastasis-directed therapy to systemic therapy for oligometastatic pancreatic ductal adenocarcinoma (EXTEND): a multicenter, randomized phase 2 trial,” published in the Journal of Clinical Oncology.
You might ask what metastasis-directed therapy in pancreatic cancer means. Have we really made much of an impact on pancreatic cancer? In fact, in my earlier years of training, if somebody came up with the idea, or suggested as part of a trial or treatment of an individual patient, that they would focus on metastases in pancreas cancer, you might say they’re crazy, or you might say: “Yeah, but they probably don’t know anything about the disease and its natural history.”
Now, fast forward several decades. Even with the recognized, modest advances in systemic therapy, what we see are tremendous, really remarkable advances in innovations in radiation therapy. Of course, this includes not only the use of radiation itself but also the imaging technology that is used to direct the radiation therapy. These advances have permitted asking the questions that are addressed in the current study.
Again, this study is fascinating. They randomized a very small number. Again, it’s a randomized phase 2 study. It’s really more of a proof of principle here. They randomized 41 patients with five or fewer metastatic lesions — with oligometastatic disease, they could have numerous lesions — to undergo what they’ve described as comprehensive metastases-directed therapy.
Most of this was external beam radiation therapy and stereotactic radiation therapy, but there were some localized radiation implants as well, plus chemotherapy. This was comprehensive metastases-directed therapy to each of these sites plus chemotherapy vs chemotherapy alone.
What was shown in this trial? The progression-free survival (PFS) in the metastases-directed therapy group was 10.3 months vs 2.5 months in the group of patients who received chemotherapy only, with a hazard ratio of 0.43 and statistical significance.
Remember, this was a very small study, but we see more than a tripling in the PFS. There was no difference in overall survival, which is not at all surprising because it was a very small sample size.
Very importantly — and essential to doing this trial ethically — a crossover was permitted at the time of progression, meaning that if a patient received chemotherapy only and progressed, they could potentially get stereotactic radiation to sites of metastatic disease. They might have also benefited from that kind of strategy to the metastasis-[therapy] so that overall survival in the small population may not be different. Again, there was a tripling of the time to disease progression.
Clearly, a larger study will be required to be more definitive. We would need more centers involved and maybe some modification in the study design in this trial because of any issues that the investigators may have identified. Of course, overall survival would be a fair endpoint to look at, but again, crossover would be essential, and that might influence an ultimate outcome. PFS is a very valid endpoint.
The only other point to mention is, with these results — and as I mentioned, advances in radiation and imaging — is it reasonable to potentially consider this type of approach for individual patients as a component of aggressive standard of care? Of course, this would be with very adequate informed consent from patients, because we don’t know what the impact will be.
With the limited morbidity associated with the radiation, for an individual patient with pancreatic cancer who has an adequate performance status and limited metastases, if we give them chemotherapy and also directed radiation, is it reasonable to consider that as an appropriate treatment option outside the setting of a clinical trial?
I think this is a very valid question that needs to be addressed. In my opinion, the answer in some settings should be yes, but that needs to be discussed much more widely than simply in this randomized phase 2 trial.
Thank you for your attention.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. I’m Dr Maurie Markman, from City of Hope. I’d like to discuss what I consider to be an absolutely fascinating paper, and one that I will say has very interesting results but raises many more questions than it answers. I think that was the intent of the authors.
The paper is entitled, “Addition of metastasis-directed therapy to systemic therapy for oligometastatic pancreatic ductal adenocarcinoma (EXTEND): a multicenter, randomized phase 2 trial,” published in the Journal of Clinical Oncology.
You might ask what metastasis-directed therapy in pancreatic cancer means. Have we really made much of an impact on pancreatic cancer? In fact, in my earlier years of training, if somebody came up with the idea, or suggested as part of a trial or treatment of an individual patient, that they would focus on metastases in pancreas cancer, you might say they’re crazy, or you might say: “Yeah, but they probably don’t know anything about the disease and its natural history.”
Now, fast forward several decades. Even with the recognized, modest advances in systemic therapy, what we see are tremendous, really remarkable advances in innovations in radiation therapy. Of course, this includes not only the use of radiation itself but also the imaging technology that is used to direct the radiation therapy. These advances have permitted asking the questions that are addressed in the current study.
Again, this study is fascinating. They randomized a very small number. Again, it’s a randomized phase 2 study. It’s really more of a proof of principle here. They randomized 41 patients with five or fewer metastatic lesions — with oligometastatic disease, they could have numerous lesions — to undergo what they’ve described as comprehensive metastases-directed therapy.
Most of this was external beam radiation therapy and stereotactic radiation therapy, but there were some localized radiation implants as well, plus chemotherapy. This was comprehensive metastases-directed therapy to each of these sites plus chemotherapy vs chemotherapy alone.
What was shown in this trial? The progression-free survival (PFS) in the metastases-directed therapy group was 10.3 months vs 2.5 months in the group of patients who received chemotherapy only, with a hazard ratio of 0.43 and statistical significance.
Remember, this was a very small study, but we see more than a tripling in the PFS. There was no difference in overall survival, which is not at all surprising because it was a very small sample size.
Very importantly — and essential to doing this trial ethically — a crossover was permitted at the time of progression, meaning that if a patient received chemotherapy only and progressed, they could potentially get stereotactic radiation to sites of metastatic disease. They might have also benefited from that kind of strategy to the metastasis-[therapy] so that overall survival in the small population may not be different. Again, there was a tripling of the time to disease progression.
Clearly, a larger study will be required to be more definitive. We would need more centers involved and maybe some modification in the study design in this trial because of any issues that the investigators may have identified. Of course, overall survival would be a fair endpoint to look at, but again, crossover would be essential, and that might influence an ultimate outcome. PFS is a very valid endpoint.
The only other point to mention is, with these results — and as I mentioned, advances in radiation and imaging — is it reasonable to potentially consider this type of approach for individual patients as a component of aggressive standard of care? Of course, this would be with very adequate informed consent from patients, because we don’t know what the impact will be.
With the limited morbidity associated with the radiation, for an individual patient with pancreatic cancer who has an adequate performance status and limited metastases, if we give them chemotherapy and also directed radiation, is it reasonable to consider that as an appropriate treatment option outside the setting of a clinical trial?
I think this is a very valid question that needs to be addressed. In my opinion, the answer in some settings should be yes, but that needs to be discussed much more widely than simply in this randomized phase 2 trial.
Thank you for your attention.
A version of this article first appeared on Medscape.com.

Neighborhood Determinants of Health Adversely Impact MASLD

These health mediators should be considered along with individual SDOH in clinical care and healthcare quality and equity improvement, a large retrospective study of adults with MASLD at a multi-state healthcare institution concluded.
Across quartiles, patients in the most disadvantaged neighborhoods (according to home addresses) vs the least disadvantaged had worse outcomes and were also disproportionately Hispanic, Black, and Native American/Alaska Native, more often Spanish-speaking in primary language, and more often uninsured or on Medicaid, according to Karn Wijarnpreecha, MD, MPH, of the Division of Gastroenterology and Hepatology at University of Arizona College of Medicine–Phoenix, and colleagues writing in Clinical Gastroenterology and Hepatology.
Even after adjustment for measures in the Social Deprivation Index (SDI), the incidence of death, cirrhosis, diabetes mellitus (DM), and major adverse cardiovascular events (MACE) was higher in Native American/Alaska Native patients compared with their non-Hispanic White counterparts. The SDI is a composite measure of seven demographic characteristics from the American Community Survey, with scores ranging from 1 to 100 and weighted based on characteristics from national percentile rankings.
Aligning with the growing prevalence of obesity and DM, MASLD has increased substantially over the past three decades, and is now the leading cause of chronic liver disease in this country and the world.
This rise in prevalence has underscored health disparities in MASLD and prompted research into linkd between liver disease and SDOH, defined as the conditions under which people are born, grow, live, work, and age. These are fundamental drivers of health disparities, including those in MASLD.
Study Details
Primary outcomes were MASLD burden, mortality, and comorbidities by neighborhood SDOH, assessed using the SDI in cross-sectional and longitudinal analyses.
A total of 69,191 adult patients (more than 50% female) diagnosed with MASLD were included, 45,003 of whom had at least 365 days of follow-up. They were treated from July 2012 to June 2023 in Banner Health Systems, a network that includes primary-, secondary-, and tertiary-care centers in Arizona, Colorado, Wyoming, Nevada, Nebraska, and California.
The median follow-up time was 48 months. Among patients across SDI quartiles (age range 49 to 62 years), 1390 patients (3.1%) died, 902 (2.0%) developed cirrhosis, 1087 (2.4%) developed LRE, 6537 (14.5%) developed DM, 2057 (4.6%) developed cancer, and 5409 (12.0%) developed MACE.
Those living in the most disadvantaged quartile of neighborhoods compared with the least had the following higher odds:
- cirrhosis, adjusted odds ratio [aOR], 1.42 (P < .001)
- any cardiovascular (CVD) disease, aOR, 1.20 (P < .001),
- coronary artery disease, aOR, 1.17 (P < .001)
- congestive heart failure, aOR, 1.43 (P < .001)
- cerebrovascular accident, aOR, 1.19 (P = .001)
- DM, aOR, 1.57 (P < .001)
- hypertension, aOR, 1.38 (P < .001).
They also had increased incidence of death (adjusted hazard ratio [aHR], 1.47; P < .001), LRE (aHR, 1.31; P = .012), DM (aHR, 1.47; P < .001), and MACE (aHR, 1.24; P < .001).
The study expands upon previous SDOH-related research in liver disease and is the largest analysis of neighborhood-level SDOH in patients with MASLD to date. “Our findings are consistent with a recent study by Chen et al of over 15,900 patients with MASLD in Michigan that found neighborhood-level social disadvantage was associated with increased mortality and incident LREs and CVD,” Wijarnpreecha and colleagues wrote.
“Beyond screening patients for individual-level SDOH, neighborhood-level determinants of health should also be considered, as they are important mediators between the environment and the individual,” they added, calling for studies to better understand the specific neighborhood SDOH that drive the disparate outcomes. In practice, integration of these measures into medical records might inform clinicians which patients would benefit from social services or help guide quality improvement projects and community partnerships.
Wijarnpreecha had no conflicts of interest to disclose. Several coauthors reported research support, consulting/advisory work, or stock ownership for various private-sector companies.
The sprectrum of steatotic liver disease (SLD) including metabolic dysfunction associated steatotic liver disease (MASLD) is increasing in the United Statues. 38% of adults and 7-14% of children currently have MASLD and it is projected that by 2040 the prevalence rate for MASLD will be higher than 55% in US adults. Fortunately, most will not develop serious liver disease. However, even a small subset is impacted, significant liver related morbidity and mortality will be the result.

Yet, concentrating only on the liver misses the substantial impact of other metabolic outcomes associated with MASLD. Equally important, at risk MASLD is treatable with lifestyle modifications, pharmacotherapy and surgical options which improve liver related outcomes, metabolic complications, and all-cause mortality. When over half of the US has a disease that requires individuals to navigate a complex care pathway that includes screening, staging, and risk modification across multiple metabolic conditions, any factor that can help identify those in need for targeted interventions is paramount. And personalization that allows someone to effectively traverse the care pathway allows for the most successful outcome.
Social determinants of health (SDOH) are complex but not insurmountable. By recognizing the contribution of SDOH, studies can be designed to discover which factors drive disparate outcomes on a granular level. This can then support funding and policy changes to address these elements. It is already well established that food insecurity is associated with both prevalence of MASLD and liver-related mortality. Policies to address the issues related to poverty can be prioritized and their impact measured.
This study also highlights the importance of needs by neighborhood. Culture has an impact on diet which is inextricably linked to MASLD. Acculturation, or the process of adapting to a new culture, is associated with poor health, physical inactivity, and poor diet but is also recognized. Western diets are high in saturated fat and refined carbohydrates which then increase risk of obesity and MASLD. In neighborhoods where culturally tailored interventions can improve health outcomes, community-based programs are imperative. In conclusion, a holistic approach that acknowledges and integrates cultural practices and preferences into MASLD prevention and management strategies can improve treatment adherence and outcomes, particularly for high-risk populations.
Nancy S. Reau, MD, AGAF, is professor and section chief of hepatology in the Division of Digestive Diseases and Nutrition at Rush University, Chicago. She has no disclosures in relation to this commentary.
The sprectrum of steatotic liver disease (SLD) including metabolic dysfunction associated steatotic liver disease (MASLD) is increasing in the United Statues. 38% of adults and 7-14% of children currently have MASLD and it is projected that by 2040 the prevalence rate for MASLD will be higher than 55% in US adults. Fortunately, most will not develop serious liver disease. However, even a small subset is impacted, significant liver related morbidity and mortality will be the result.
Yet, concentrating only on the liver misses the substantial impact of other metabolic outcomes associated with MASLD. Equally important, at risk MASLD is treatable with lifestyle modifications, pharmacotherapy and surgical options which improve liver related outcomes, metabolic complications, and all-cause mortality. When over half of the US has a disease that requires individuals to navigate a complex care pathway that includes screening, staging, and risk modification across multiple metabolic conditions, any factor that can help identify those in need for targeted interventions is paramount. And personalization that allows someone to effectively traverse the care pathway allows for the most successful outcome.
Social determinants of health (SDOH) are complex but not insurmountable. By recognizing the contribution of SDOH, studies can be designed to discover which factors drive disparate outcomes on a granular level. This can then support funding and policy changes to address these elements. It is already well established that food insecurity is associated with both prevalence of MASLD and liver-related mortality. Policies to address the issues related to poverty can be prioritized and their impact measured.
This study also highlights the importance of needs by neighborhood. Culture has an impact on diet which is inextricably linked to MASLD. Acculturation, or the process of adapting to a new culture, is associated with poor health, physical inactivity, and poor diet but is also recognized. Western diets are high in saturated fat and refined carbohydrates which then increase risk of obesity and MASLD. In neighborhoods where culturally tailored interventions can improve health outcomes, community-based programs are imperative. In conclusion, a holistic approach that acknowledges and integrates cultural practices and preferences into MASLD prevention and management strategies can improve treatment adherence and outcomes, particularly for high-risk populations.
Nancy S. Reau, MD, AGAF, is professor and section chief of hepatology in the Division of Digestive Diseases and Nutrition at Rush University, Chicago. She has no disclosures in relation to this commentary.
The sprectrum of steatotic liver disease (SLD) including metabolic dysfunction associated steatotic liver disease (MASLD) is increasing in the United Statues. 38% of adults and 7-14% of children currently have MASLD and it is projected that by 2040 the prevalence rate for MASLD will be higher than 55% in US adults. Fortunately, most will not develop serious liver disease. However, even a small subset is impacted, significant liver related morbidity and mortality will be the result.
Yet, concentrating only on the liver misses the substantial impact of other metabolic outcomes associated with MASLD. Equally important, at risk MASLD is treatable with lifestyle modifications, pharmacotherapy and surgical options which improve liver related outcomes, metabolic complications, and all-cause mortality. When over half of the US has a disease that requires individuals to navigate a complex care pathway that includes screening, staging, and risk modification across multiple metabolic conditions, any factor that can help identify those in need for targeted interventions is paramount. And personalization that allows someone to effectively traverse the care pathway allows for the most successful outcome.
Social determinants of health (SDOH) are complex but not insurmountable. By recognizing the contribution of SDOH, studies can be designed to discover which factors drive disparate outcomes on a granular level. This can then support funding and policy changes to address these elements. It is already well established that food insecurity is associated with both prevalence of MASLD and liver-related mortality. Policies to address the issues related to poverty can be prioritized and their impact measured.
This study also highlights the importance of needs by neighborhood. Culture has an impact on diet which is inextricably linked to MASLD. Acculturation, or the process of adapting to a new culture, is associated with poor health, physical inactivity, and poor diet but is also recognized. Western diets are high in saturated fat and refined carbohydrates which then increase risk of obesity and MASLD. In neighborhoods where culturally tailored interventions can improve health outcomes, community-based programs are imperative. In conclusion, a holistic approach that acknowledges and integrates cultural practices and preferences into MASLD prevention and management strategies can improve treatment adherence and outcomes, particularly for high-risk populations.
Nancy S. Reau, MD, AGAF, is professor and section chief of hepatology in the Division of Digestive Diseases and Nutrition at Rush University, Chicago. She has no disclosures in relation to this commentary.
These health mediators should be considered along with individual SDOH in clinical care and healthcare quality and equity improvement, a large retrospective study of adults with MASLD at a multi-state healthcare institution concluded.
Across quartiles, patients in the most disadvantaged neighborhoods (according to home addresses) vs the least disadvantaged had worse outcomes and were also disproportionately Hispanic, Black, and Native American/Alaska Native, more often Spanish-speaking in primary language, and more often uninsured or on Medicaid, according to Karn Wijarnpreecha, MD, MPH, of the Division of Gastroenterology and Hepatology at University of Arizona College of Medicine–Phoenix, and colleagues writing in Clinical Gastroenterology and Hepatology.
Even after adjustment for measures in the Social Deprivation Index (SDI), the incidence of death, cirrhosis, diabetes mellitus (DM), and major adverse cardiovascular events (MACE) was higher in Native American/Alaska Native patients compared with their non-Hispanic White counterparts. The SDI is a composite measure of seven demographic characteristics from the American Community Survey, with scores ranging from 1 to 100 and weighted based on characteristics from national percentile rankings.
Aligning with the growing prevalence of obesity and DM, MASLD has increased substantially over the past three decades, and is now the leading cause of chronic liver disease in this country and the world.
This rise in prevalence has underscored health disparities in MASLD and prompted research into linkd between liver disease and SDOH, defined as the conditions under which people are born, grow, live, work, and age. These are fundamental drivers of health disparities, including those in MASLD.
Study Details
Primary outcomes were MASLD burden, mortality, and comorbidities by neighborhood SDOH, assessed using the SDI in cross-sectional and longitudinal analyses.
A total of 69,191 adult patients (more than 50% female) diagnosed with MASLD were included, 45,003 of whom had at least 365 days of follow-up. They were treated from July 2012 to June 2023 in Banner Health Systems, a network that includes primary-, secondary-, and tertiary-care centers in Arizona, Colorado, Wyoming, Nevada, Nebraska, and California.
The median follow-up time was 48 months. Among patients across SDI quartiles (age range 49 to 62 years), 1390 patients (3.1%) died, 902 (2.0%) developed cirrhosis, 1087 (2.4%) developed LRE, 6537 (14.5%) developed DM, 2057 (4.6%) developed cancer, and 5409 (12.0%) developed MACE.
Those living in the most disadvantaged quartile of neighborhoods compared with the least had the following higher odds:
- cirrhosis, adjusted odds ratio [aOR], 1.42 (P < .001)
- any cardiovascular (CVD) disease, aOR, 1.20 (P < .001),
- coronary artery disease, aOR, 1.17 (P < .001)
- congestive heart failure, aOR, 1.43 (P < .001)
- cerebrovascular accident, aOR, 1.19 (P = .001)
- DM, aOR, 1.57 (P < .001)
- hypertension, aOR, 1.38 (P < .001).
They also had increased incidence of death (adjusted hazard ratio [aHR], 1.47; P < .001), LRE (aHR, 1.31; P = .012), DM (aHR, 1.47; P < .001), and MACE (aHR, 1.24; P < .001).
The study expands upon previous SDOH-related research in liver disease and is the largest analysis of neighborhood-level SDOH in patients with MASLD to date. “Our findings are consistent with a recent study by Chen et al of over 15,900 patients with MASLD in Michigan that found neighborhood-level social disadvantage was associated with increased mortality and incident LREs and CVD,” Wijarnpreecha and colleagues wrote.
“Beyond screening patients for individual-level SDOH, neighborhood-level determinants of health should also be considered, as they are important mediators between the environment and the individual,” they added, calling for studies to better understand the specific neighborhood SDOH that drive the disparate outcomes. In practice, integration of these measures into medical records might inform clinicians which patients would benefit from social services or help guide quality improvement projects and community partnerships.
Wijarnpreecha had no conflicts of interest to disclose. Several coauthors reported research support, consulting/advisory work, or stock ownership for various private-sector companies.
These health mediators should be considered along with individual SDOH in clinical care and healthcare quality and equity improvement, a large retrospective study of adults with MASLD at a multi-state healthcare institution concluded.
Across quartiles, patients in the most disadvantaged neighborhoods (according to home addresses) vs the least disadvantaged had worse outcomes and were also disproportionately Hispanic, Black, and Native American/Alaska Native, more often Spanish-speaking in primary language, and more often uninsured or on Medicaid, according to Karn Wijarnpreecha, MD, MPH, of the Division of Gastroenterology and Hepatology at University of Arizona College of Medicine–Phoenix, and colleagues writing in Clinical Gastroenterology and Hepatology.
Even after adjustment for measures in the Social Deprivation Index (SDI), the incidence of death, cirrhosis, diabetes mellitus (DM), and major adverse cardiovascular events (MACE) was higher in Native American/Alaska Native patients compared with their non-Hispanic White counterparts. The SDI is a composite measure of seven demographic characteristics from the American Community Survey, with scores ranging from 1 to 100 and weighted based on characteristics from national percentile rankings.
Aligning with the growing prevalence of obesity and DM, MASLD has increased substantially over the past three decades, and is now the leading cause of chronic liver disease in this country and the world.
This rise in prevalence has underscored health disparities in MASLD and prompted research into linkd between liver disease and SDOH, defined as the conditions under which people are born, grow, live, work, and age. These are fundamental drivers of health disparities, including those in MASLD.
Study Details
Primary outcomes were MASLD burden, mortality, and comorbidities by neighborhood SDOH, assessed using the SDI in cross-sectional and longitudinal analyses.
A total of 69,191 adult patients (more than 50% female) diagnosed with MASLD were included, 45,003 of whom had at least 365 days of follow-up. They were treated from July 2012 to June 2023 in Banner Health Systems, a network that includes primary-, secondary-, and tertiary-care centers in Arizona, Colorado, Wyoming, Nevada, Nebraska, and California.
The median follow-up time was 48 months. Among patients across SDI quartiles (age range 49 to 62 years), 1390 patients (3.1%) died, 902 (2.0%) developed cirrhosis, 1087 (2.4%) developed LRE, 6537 (14.5%) developed DM, 2057 (4.6%) developed cancer, and 5409 (12.0%) developed MACE.
Those living in the most disadvantaged quartile of neighborhoods compared with the least had the following higher odds:
- cirrhosis, adjusted odds ratio [aOR], 1.42 (P < .001)
- any cardiovascular (CVD) disease, aOR, 1.20 (P < .001),
- coronary artery disease, aOR, 1.17 (P < .001)
- congestive heart failure, aOR, 1.43 (P < .001)
- cerebrovascular accident, aOR, 1.19 (P = .001)
- DM, aOR, 1.57 (P < .001)
- hypertension, aOR, 1.38 (P < .001).
They also had increased incidence of death (adjusted hazard ratio [aHR], 1.47; P < .001), LRE (aHR, 1.31; P = .012), DM (aHR, 1.47; P < .001), and MACE (aHR, 1.24; P < .001).
The study expands upon previous SDOH-related research in liver disease and is the largest analysis of neighborhood-level SDOH in patients with MASLD to date. “Our findings are consistent with a recent study by Chen et al of over 15,900 patients with MASLD in Michigan that found neighborhood-level social disadvantage was associated with increased mortality and incident LREs and CVD,” Wijarnpreecha and colleagues wrote.
“Beyond screening patients for individual-level SDOH, neighborhood-level determinants of health should also be considered, as they are important mediators between the environment and the individual,” they added, calling for studies to better understand the specific neighborhood SDOH that drive the disparate outcomes. In practice, integration of these measures into medical records might inform clinicians which patients would benefit from social services or help guide quality improvement projects and community partnerships.
Wijarnpreecha had no conflicts of interest to disclose. Several coauthors reported research support, consulting/advisory work, or stock ownership for various private-sector companies.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Does Tofacitinib Worsen Postoperative Complications in Acute Severe Ulcerative Colitis?
A head-to-head comparison of the JAK inhibitor drug tofacitinib and chimeric monoclonal antibody infliximab in the treatment of acute severe ulcerative colitis (ASUC) shows that, contrary to concerns, tofacitinib is not associated with worse postoperative complications and in fact may reduce the risk of the need for colectomy.
“Tofacitinib has shown efficacy in managing ASUC, but concerns about postoperative complications have limited its adoption,” reported the authors in research published in Clinical Gastroenterology and Hepatology.“, which is unfortunately common in this population,” senior author Jeffrey A. Berinstein, MD, of the Division of Gastroenterology and Hepatology, Michigan Medicine, Ann Arbor, Michigan, told GI & Hepatology News.

Recent treatment advances for UC have provided significant benefits in reducing the severity of symptoms; however, about a quarter of patients go on to experience flares, with fecal urgency, rectal bleeding, and severe abdominal pain of ASUC potentially requiring hospitalization.
The standard of care for those patients is rapid induction with intravenous (IV) corticosteroids; however, up to 30% of patients don’t respond to those interventions, and even with subsequent treatment of cyclosporine and infliximab helping to reduce the risk for an urgent colectomy, patients often don’t respond, and ultimately, up to a third of patients with ASUC end up having to receive a colectomy.
While JAK inhibitor therapies, including tofacitinib and upadacitinib, have recently emerged as potentially important treatment options in such cases, showing reductions in the risk for colectomy, concerns about the drugs’ downstream biologic effects have given many clinicians reservations about their use.
“Anecdotally, gastroenterologists and surgeons have expressed concern about JAK inhibitors leading to poor wound healing, as well as increasing both intraoperative and postoperative complications, despite limited data to support these claims,” the authors wrote.
To better understand those possible risks, first author Charlotte Larson, MD, of the Department of Internal Medicine, Michigan Medicine, and colleagues conducted a multicenter, retrospective, case-control study of 109 patients hospitalized with ASUC at two centers in the US and 14 in France.
Of the patients, 41 were treated with tofacitinib and 68 with infliximab prior to colectomy.
Among patients treated with tofacitinib, five (12.2%) received infliximab and four (9.8%) received cyclosporine rescue immediately prior to receiving tofacitinib during the index admission. In the infliximab group, one (1.5%) received rescue cyclosporine.
In a univariate analysis, the tofacitinib-treated patients showed significantly lower overall rates of postoperative complications than infliximab-treated patients (31.7% vs 64.7%; odds ratio [OR], 0.33; P = .006).
The tofacitinib-treated group also had lower rates of serious postoperative complications (12% vs 28.9; OR, 0.20; P = .016).
After adjusting for multivariate factors including age, inflammatory burden, nutrition status, 90-day cumulative corticosteroid exposure and open surgery, there was a trend favoring tofacitinib but no statistically significant difference between the two treatments in terms of serious postoperative complications (P = .061).
However, a significantly lower rate of overall postoperative complications with tofacitinib was observed after the adjustment (odds ratio, 0.38; P = .023).
Importantly, a subanalysis showed that the 63.4% of tofacitinib-treated patients receiving the standard FDA-approved induction dose of 10 mg twice daily did indeed have significantly lower rates than infliximab-treated patients in terms of serious postoperative complications (OR, .10; P = .031), as well as overall postoperative complications (OR, 0.23; P = .003), whereas neither of the outcomes were significantly improved among the 36.6% of patients who received the higher-intensity thrice-daily tofacitinib dose (P = .3 and P = .4, respectively).
Further complicating the matter, in a previous case-control study that the research team conducted, it was the off-label, 10 mg thrice-daily dose of tofacitinib that performed favorably and was associated with a significantly lower risk for colectomy than the twice-daily dose (hazard ratio 0.28; P = .018); the twice-daily dose was not protective.
Berinstein added that a hypothesis for the benefits overall, with either dose, is that tofacitinib’s anti-inflammatory properties are key.
“We believe that lowering inflammation as much as possible, with the colon less inflamed, could be providing the benefit in lowering complications rate in surgery,” he explained.
Regarding the dosing, “it’s a careful trade-off,” Berinstein added. “Obviously, we want to avoid the need for a colectomy in the first place, as it is a life-changing surgery, but we don’t want to increase the risk of infections.”
In other findings, the tofacitinib group had no increased risk for postoperative venous thrombotic embolisms (VTEs), which is important as tofacitinib exposure has previously been associated with an increased risk for VTEs independent of other prothrombotic factors common to patients with ASUC, including decreased ambulation, active inflammation, corticosteroid use, and major colorectal surgery.
“This observed absence of an increased VTE risk may alleviate some of the hypothetical postoperative safety concern attributed to JAK inhibitor therapy in this high-risk population,” the authors wrote.
Overall, the results underscore that “providers should feel comfortable using this medication if they need it and if they think it’s most likely to help their patients avoid colectomy,” Berinstein said.
“They should not give pause over concerns of postoperative complications because we didn’t show that,” he said.
Commenting on the study, Joseph D. Feuerstein, MD, AGAF, of the Department of Medicine and Division of Gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, noted that, in general, in patients with ASUC who fail on IV steroids, “the main treatments are infliximab, cyclosporine, or a JAK inhibitor like tofacitinib or upadacitinib, [and] knowing that if someone needs surgery, the complication rates are similar and that pre-operative use is okay is reassuring.”
Regarding the protective effect observed with some circumstances, “I don’t put too much weight into that,” he noted. “[One] could speculate that it is somehow related to faster half-life of the drug, and it might not sit around as long,” he said.
Feuerstein added that “the study design being retrospective is a limitation, but this is the best data we have to date.”
Berinstein and Feuerstein had no disclosures to report.
A version of this article appeared on Medscape.com .
A head-to-head comparison of the JAK inhibitor drug tofacitinib and chimeric monoclonal antibody infliximab in the treatment of acute severe ulcerative colitis (ASUC) shows that, contrary to concerns, tofacitinib is not associated with worse postoperative complications and in fact may reduce the risk of the need for colectomy.
“Tofacitinib has shown efficacy in managing ASUC, but concerns about postoperative complications have limited its adoption,” reported the authors in research published in Clinical Gastroenterology and Hepatology.“, which is unfortunately common in this population,” senior author Jeffrey A. Berinstein, MD, of the Division of Gastroenterology and Hepatology, Michigan Medicine, Ann Arbor, Michigan, told GI & Hepatology News.
Recent treatment advances for UC have provided significant benefits in reducing the severity of symptoms; however, about a quarter of patients go on to experience flares, with fecal urgency, rectal bleeding, and severe abdominal pain of ASUC potentially requiring hospitalization.
The standard of care for those patients is rapid induction with intravenous (IV) corticosteroids; however, up to 30% of patients don’t respond to those interventions, and even with subsequent treatment of cyclosporine and infliximab helping to reduce the risk for an urgent colectomy, patients often don’t respond, and ultimately, up to a third of patients with ASUC end up having to receive a colectomy.
While JAK inhibitor therapies, including tofacitinib and upadacitinib, have recently emerged as potentially important treatment options in such cases, showing reductions in the risk for colectomy, concerns about the drugs’ downstream biologic effects have given many clinicians reservations about their use.
“Anecdotally, gastroenterologists and surgeons have expressed concern about JAK inhibitors leading to poor wound healing, as well as increasing both intraoperative and postoperative complications, despite limited data to support these claims,” the authors wrote.
To better understand those possible risks, first author Charlotte Larson, MD, of the Department of Internal Medicine, Michigan Medicine, and colleagues conducted a multicenter, retrospective, case-control study of 109 patients hospitalized with ASUC at two centers in the US and 14 in France.
Of the patients, 41 were treated with tofacitinib and 68 with infliximab prior to colectomy.
Among patients treated with tofacitinib, five (12.2%) received infliximab and four (9.8%) received cyclosporine rescue immediately prior to receiving tofacitinib during the index admission. In the infliximab group, one (1.5%) received rescue cyclosporine.
In a univariate analysis, the tofacitinib-treated patients showed significantly lower overall rates of postoperative complications than infliximab-treated patients (31.7% vs 64.7%; odds ratio [OR], 0.33; P = .006).
The tofacitinib-treated group also had lower rates of serious postoperative complications (12% vs 28.9; OR, 0.20; P = .016).
After adjusting for multivariate factors including age, inflammatory burden, nutrition status, 90-day cumulative corticosteroid exposure and open surgery, there was a trend favoring tofacitinib but no statistically significant difference between the two treatments in terms of serious postoperative complications (P = .061).
However, a significantly lower rate of overall postoperative complications with tofacitinib was observed after the adjustment (odds ratio, 0.38; P = .023).
Importantly, a subanalysis showed that the 63.4% of tofacitinib-treated patients receiving the standard FDA-approved induction dose of 10 mg twice daily did indeed have significantly lower rates than infliximab-treated patients in terms of serious postoperative complications (OR, .10; P = .031), as well as overall postoperative complications (OR, 0.23; P = .003), whereas neither of the outcomes were significantly improved among the 36.6% of patients who received the higher-intensity thrice-daily tofacitinib dose (P = .3 and P = .4, respectively).
Further complicating the matter, in a previous case-control study that the research team conducted, it was the off-label, 10 mg thrice-daily dose of tofacitinib that performed favorably and was associated with a significantly lower risk for colectomy than the twice-daily dose (hazard ratio 0.28; P = .018); the twice-daily dose was not protective.
Berinstein added that a hypothesis for the benefits overall, with either dose, is that tofacitinib’s anti-inflammatory properties are key.
“We believe that lowering inflammation as much as possible, with the colon less inflamed, could be providing the benefit in lowering complications rate in surgery,” he explained.
Regarding the dosing, “it’s a careful trade-off,” Berinstein added. “Obviously, we want to avoid the need for a colectomy in the first place, as it is a life-changing surgery, but we don’t want to increase the risk of infections.”
In other findings, the tofacitinib group had no increased risk for postoperative venous thrombotic embolisms (VTEs), which is important as tofacitinib exposure has previously been associated with an increased risk for VTEs independent of other prothrombotic factors common to patients with ASUC, including decreased ambulation, active inflammation, corticosteroid use, and major colorectal surgery.
“This observed absence of an increased VTE risk may alleviate some of the hypothetical postoperative safety concern attributed to JAK inhibitor therapy in this high-risk population,” the authors wrote.
Overall, the results underscore that “providers should feel comfortable using this medication if they need it and if they think it’s most likely to help their patients avoid colectomy,” Berinstein said.
“They should not give pause over concerns of postoperative complications because we didn’t show that,” he said.
Commenting on the study, Joseph D. Feuerstein, MD, AGAF, of the Department of Medicine and Division of Gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, noted that, in general, in patients with ASUC who fail on IV steroids, “the main treatments are infliximab, cyclosporine, or a JAK inhibitor like tofacitinib or upadacitinib, [and] knowing that if someone needs surgery, the complication rates are similar and that pre-operative use is okay is reassuring.”
Regarding the protective effect observed with some circumstances, “I don’t put too much weight into that,” he noted. “[One] could speculate that it is somehow related to faster half-life of the drug, and it might not sit around as long,” he said.
Feuerstein added that “the study design being retrospective is a limitation, but this is the best data we have to date.”
Berinstein and Feuerstein had no disclosures to report.
A version of this article appeared on Medscape.com .
A head-to-head comparison of the JAK inhibitor drug tofacitinib and chimeric monoclonal antibody infliximab in the treatment of acute severe ulcerative colitis (ASUC) shows that, contrary to concerns, tofacitinib is not associated with worse postoperative complications and in fact may reduce the risk of the need for colectomy.
“Tofacitinib has shown efficacy in managing ASUC, but concerns about postoperative complications have limited its adoption,” reported the authors in research published in Clinical Gastroenterology and Hepatology.“, which is unfortunately common in this population,” senior author Jeffrey A. Berinstein, MD, of the Division of Gastroenterology and Hepatology, Michigan Medicine, Ann Arbor, Michigan, told GI & Hepatology News.
Recent treatment advances for UC have provided significant benefits in reducing the severity of symptoms; however, about a quarter of patients go on to experience flares, with fecal urgency, rectal bleeding, and severe abdominal pain of ASUC potentially requiring hospitalization.
The standard of care for those patients is rapid induction with intravenous (IV) corticosteroids; however, up to 30% of patients don’t respond to those interventions, and even with subsequent treatment of cyclosporine and infliximab helping to reduce the risk for an urgent colectomy, patients often don’t respond, and ultimately, up to a third of patients with ASUC end up having to receive a colectomy.
While JAK inhibitor therapies, including tofacitinib and upadacitinib, have recently emerged as potentially important treatment options in such cases, showing reductions in the risk for colectomy, concerns about the drugs’ downstream biologic effects have given many clinicians reservations about their use.
“Anecdotally, gastroenterologists and surgeons have expressed concern about JAK inhibitors leading to poor wound healing, as well as increasing both intraoperative and postoperative complications, despite limited data to support these claims,” the authors wrote.
To better understand those possible risks, first author Charlotte Larson, MD, of the Department of Internal Medicine, Michigan Medicine, and colleagues conducted a multicenter, retrospective, case-control study of 109 patients hospitalized with ASUC at two centers in the US and 14 in France.
Of the patients, 41 were treated with tofacitinib and 68 with infliximab prior to colectomy.
Among patients treated with tofacitinib, five (12.2%) received infliximab and four (9.8%) received cyclosporine rescue immediately prior to receiving tofacitinib during the index admission. In the infliximab group, one (1.5%) received rescue cyclosporine.
In a univariate analysis, the tofacitinib-treated patients showed significantly lower overall rates of postoperative complications than infliximab-treated patients (31.7% vs 64.7%; odds ratio [OR], 0.33; P = .006).
The tofacitinib-treated group also had lower rates of serious postoperative complications (12% vs 28.9; OR, 0.20; P = .016).
After adjusting for multivariate factors including age, inflammatory burden, nutrition status, 90-day cumulative corticosteroid exposure and open surgery, there was a trend favoring tofacitinib but no statistically significant difference between the two treatments in terms of serious postoperative complications (P = .061).
However, a significantly lower rate of overall postoperative complications with tofacitinib was observed after the adjustment (odds ratio, 0.38; P = .023).
Importantly, a subanalysis showed that the 63.4% of tofacitinib-treated patients receiving the standard FDA-approved induction dose of 10 mg twice daily did indeed have significantly lower rates than infliximab-treated patients in terms of serious postoperative complications (OR, .10; P = .031), as well as overall postoperative complications (OR, 0.23; P = .003), whereas neither of the outcomes were significantly improved among the 36.6% of patients who received the higher-intensity thrice-daily tofacitinib dose (P = .3 and P = .4, respectively).
Further complicating the matter, in a previous case-control study that the research team conducted, it was the off-label, 10 mg thrice-daily dose of tofacitinib that performed favorably and was associated with a significantly lower risk for colectomy than the twice-daily dose (hazard ratio 0.28; P = .018); the twice-daily dose was not protective.
Berinstein added that a hypothesis for the benefits overall, with either dose, is that tofacitinib’s anti-inflammatory properties are key.
“We believe that lowering inflammation as much as possible, with the colon less inflamed, could be providing the benefit in lowering complications rate in surgery,” he explained.
Regarding the dosing, “it’s a careful trade-off,” Berinstein added. “Obviously, we want to avoid the need for a colectomy in the first place, as it is a life-changing surgery, but we don’t want to increase the risk of infections.”
In other findings, the tofacitinib group had no increased risk for postoperative venous thrombotic embolisms (VTEs), which is important as tofacitinib exposure has previously been associated with an increased risk for VTEs independent of other prothrombotic factors common to patients with ASUC, including decreased ambulation, active inflammation, corticosteroid use, and major colorectal surgery.
“This observed absence of an increased VTE risk may alleviate some of the hypothetical postoperative safety concern attributed to JAK inhibitor therapy in this high-risk population,” the authors wrote.
Overall, the results underscore that “providers should feel comfortable using this medication if they need it and if they think it’s most likely to help their patients avoid colectomy,” Berinstein said.
“They should not give pause over concerns of postoperative complications because we didn’t show that,” he said.
Commenting on the study, Joseph D. Feuerstein, MD, AGAF, of the Department of Medicine and Division of Gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, noted that, in general, in patients with ASUC who fail on IV steroids, “the main treatments are infliximab, cyclosporine, or a JAK inhibitor like tofacitinib or upadacitinib, [and] knowing that if someone needs surgery, the complication rates are similar and that pre-operative use is okay is reassuring.”
Regarding the protective effect observed with some circumstances, “I don’t put too much weight into that,” he noted. “[One] could speculate that it is somehow related to faster half-life of the drug, and it might not sit around as long,” he said.
Feuerstein added that “the study design being retrospective is a limitation, but this is the best data we have to date.”
Berinstein and Feuerstein had no disclosures to report.
A version of this article appeared on Medscape.com .
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Endoscopic Lifting Agents: AGA Issues New Clinical Practice Update
Published in Clinical Gastroenterology and Hepatology, the commentary reviews available agents and provides clinically relevant commentary on their indications and use — with the caveat that it is not a formal systematic review but rather empirical advice for endoscopists. No formal rating of the quality of evidence or strength of recommendations was performed.
Led by Tobias Zuchelli, MD, a clinical associate professor at Michigan State University and a gastroenterologist at the Henry Ford Health System in Detroit, the expert panel noted that endoscopists are increasingly resecting precancerous lesions and early cancers of the gastrointestinal tract.
“Although new endoscopic procedures have been developed, there had not been much in terms of high-quality guidance on lifting agents,” panelist Amit V. Patel, MD, a professor of medicine at Duke University and director of Endoscopy at Durham Veterans Affairs Medical Center in Durham, North Carolina, told GI & Hepatology News. “With our better understanding and use of techniques, this commentary was timely. It summarizes the available data on the topic and includes our clinical experiences.”
Filling that knowledge gap, the document reviews in detail the timing and methods of agent injection according to procedure type, including the dynamic needle approach, the empirical merits of different agents such as saline (with or without blue contrast) and viscous agents, as well as lift-enhancing assistive devices — for example, the ERBEJET 2 high-pressure water jet, an adjustable hydrosurgical device to facilitate lifting. A chart provides an at-a-glance summary of agents and their pros and cons.
“The feedback from gastroenterologists so far has been quite positive on social media and on GI channels,” Patel said.
Endoscopic resection has evolved from snare polypectomy to endoscopic mucosal resection (EMR) and now, endoscopic submucosal dissection (ESD). The primary benefit of submucosal lifting is the creation of a separating submucosal cushion between the lesion and muscularis propria (MP), which reduces the risk for immediate or delayed perforation of the muscle. Adding a contrast agent also demarcates lesion margins and stains the submucosa, which is fundamental to ESD and allows for assessment of MP injury during EMR.
For decades, homemade solutions were used to lift lesions before removal, with the sentinel agent being normal saline, later mixed with a blue contrast agent, usually indigo carmine or methylene blue. The authors noted that some endoscopists performing ESD start the submucosal injection and incision using a prepackaged viscous solution. “The endoscopist may continue with the viscous fluid or transition to saline or another less expensive solution,” they wrote.
Saline tends to dissipate more quickly than viscous solutions, however. In 2015, the polymer compound SIC-8000 became the first FDA-approved submucosal injection agent. Since then, several other fluids have come on the market, although homemade agents remain available.
Among the update’s recommendations, the fluid selected for EMR should be determined by lesion size, predicted histology, and endoscopist preference. Based on the US Multi-Society Task Force (USMSTF) on Colorectal Cancer, submucosal injection is optional for nonpedunculated colorectal lesions (NPCRLs) of intermediate size (10-19 mm).
Cold snare polypectomy without submucosal injection was later found to be non-inferior to other resection methods utilizing submucosal injection for NPCRLs ≤ 15 mm.
The update noted that the USMSTF considers EMR first-line therapy for most NPCRLs ≥ 20 mm and advocates viscous solutions as preferred, while the use of lifting agents for pedunculated polyps is generally at the discretion of the endoscopist.
For Patel, the main “clinical pearls” in the update are adding a contrast agent to normal saline, using a viscous agent for cold EMR, and manipulating the injection needle first tangentially and then dynamically toward the lumen to maximize separation of the lesion.
In terms of the ideal, an optimal lifting solution would be readily available, inexpensive, and premixed, providing a sustained submucosal cushion. “However, this ideal solution currently does not exist. Injection fluids should, therefore, be selected based on planned resection method, predicted histology, local expertise and preferences, and cost,” the panelists wrote.
Added Patel, “A lot of the agents out there check most of these boxes, but we’re hoping for further development toward the ideal.”
Offering a nonparticipant’s perspective on the overview, Wasseem Skef, MD, a gastroenterologist at UTHealth Houston, found the update very useful. “It always helps to have the literature summarized,” he told GI & Hepatology News. “It’s a pretty balanced review that pulls together the various options but allows people to stick to their preferred practice.”

In his practice, the lifting agent selected depends on the type of resection. “Viscous agents are generally more popular for EMR-type resections,” Skef said. One unanswered question, he noted, is whether adding a hemostatic agent would be superior to a viscous agent alone. “But overall, this is a nice summary of available agents. Gastroenterologists should consider these different options if doing procedures like EMR.”
This review was sponsored by the AGA Institute.
Zuchelli is a consultant for Boston Scientific. Patel consults for Medpace, Renexxion, and Sanofi. Skef reported having no relevant disclosures.
A version of this article appeared on Medscape.com .
Published in Clinical Gastroenterology and Hepatology, the commentary reviews available agents and provides clinically relevant commentary on their indications and use — with the caveat that it is not a formal systematic review but rather empirical advice for endoscopists. No formal rating of the quality of evidence or strength of recommendations was performed.
Led by Tobias Zuchelli, MD, a clinical associate professor at Michigan State University and a gastroenterologist at the Henry Ford Health System in Detroit, the expert panel noted that endoscopists are increasingly resecting precancerous lesions and early cancers of the gastrointestinal tract.
“Although new endoscopic procedures have been developed, there had not been much in terms of high-quality guidance on lifting agents,” panelist Amit V. Patel, MD, a professor of medicine at Duke University and director of Endoscopy at Durham Veterans Affairs Medical Center in Durham, North Carolina, told GI & Hepatology News. “With our better understanding and use of techniques, this commentary was timely. It summarizes the available data on the topic and includes our clinical experiences.”
Filling that knowledge gap, the document reviews in detail the timing and methods of agent injection according to procedure type, including the dynamic needle approach, the empirical merits of different agents such as saline (with or without blue contrast) and viscous agents, as well as lift-enhancing assistive devices — for example, the ERBEJET 2 high-pressure water jet, an adjustable hydrosurgical device to facilitate lifting. A chart provides an at-a-glance summary of agents and their pros and cons.
“The feedback from gastroenterologists so far has been quite positive on social media and on GI channels,” Patel said.
Endoscopic resection has evolved from snare polypectomy to endoscopic mucosal resection (EMR) and now, endoscopic submucosal dissection (ESD). The primary benefit of submucosal lifting is the creation of a separating submucosal cushion between the lesion and muscularis propria (MP), which reduces the risk for immediate or delayed perforation of the muscle. Adding a contrast agent also demarcates lesion margins and stains the submucosa, which is fundamental to ESD and allows for assessment of MP injury during EMR.
For decades, homemade solutions were used to lift lesions before removal, with the sentinel agent being normal saline, later mixed with a blue contrast agent, usually indigo carmine or methylene blue. The authors noted that some endoscopists performing ESD start the submucosal injection and incision using a prepackaged viscous solution. “The endoscopist may continue with the viscous fluid or transition to saline or another less expensive solution,” they wrote.
Saline tends to dissipate more quickly than viscous solutions, however. In 2015, the polymer compound SIC-8000 became the first FDA-approved submucosal injection agent. Since then, several other fluids have come on the market, although homemade agents remain available.
Among the update’s recommendations, the fluid selected for EMR should be determined by lesion size, predicted histology, and endoscopist preference. Based on the US Multi-Society Task Force (USMSTF) on Colorectal Cancer, submucosal injection is optional for nonpedunculated colorectal lesions (NPCRLs) of intermediate size (10-19 mm).
Cold snare polypectomy without submucosal injection was later found to be non-inferior to other resection methods utilizing submucosal injection for NPCRLs ≤ 15 mm.
The update noted that the USMSTF considers EMR first-line therapy for most NPCRLs ≥ 20 mm and advocates viscous solutions as preferred, while the use of lifting agents for pedunculated polyps is generally at the discretion of the endoscopist.
For Patel, the main “clinical pearls” in the update are adding a contrast agent to normal saline, using a viscous agent for cold EMR, and manipulating the injection needle first tangentially and then dynamically toward the lumen to maximize separation of the lesion.
In terms of the ideal, an optimal lifting solution would be readily available, inexpensive, and premixed, providing a sustained submucosal cushion. “However, this ideal solution currently does not exist. Injection fluids should, therefore, be selected based on planned resection method, predicted histology, local expertise and preferences, and cost,” the panelists wrote.
Added Patel, “A lot of the agents out there check most of these boxes, but we’re hoping for further development toward the ideal.”
Offering a nonparticipant’s perspective on the overview, Wasseem Skef, MD, a gastroenterologist at UTHealth Houston, found the update very useful. “It always helps to have the literature summarized,” he told GI & Hepatology News. “It’s a pretty balanced review that pulls together the various options but allows people to stick to their preferred practice.”
In his practice, the lifting agent selected depends on the type of resection. “Viscous agents are generally more popular for EMR-type resections,” Skef said. One unanswered question, he noted, is whether adding a hemostatic agent would be superior to a viscous agent alone. “But overall, this is a nice summary of available agents. Gastroenterologists should consider these different options if doing procedures like EMR.”
This review was sponsored by the AGA Institute.
Zuchelli is a consultant for Boston Scientific. Patel consults for Medpace, Renexxion, and Sanofi. Skef reported having no relevant disclosures.
A version of this article appeared on Medscape.com .
Published in Clinical Gastroenterology and Hepatology, the commentary reviews available agents and provides clinically relevant commentary on their indications and use — with the caveat that it is not a formal systematic review but rather empirical advice for endoscopists. No formal rating of the quality of evidence or strength of recommendations was performed.
Led by Tobias Zuchelli, MD, a clinical associate professor at Michigan State University and a gastroenterologist at the Henry Ford Health System in Detroit, the expert panel noted that endoscopists are increasingly resecting precancerous lesions and early cancers of the gastrointestinal tract.
“Although new endoscopic procedures have been developed, there had not been much in terms of high-quality guidance on lifting agents,” panelist Amit V. Patel, MD, a professor of medicine at Duke University and director of Endoscopy at Durham Veterans Affairs Medical Center in Durham, North Carolina, told GI & Hepatology News. “With our better understanding and use of techniques, this commentary was timely. It summarizes the available data on the topic and includes our clinical experiences.”
Filling that knowledge gap, the document reviews in detail the timing and methods of agent injection according to procedure type, including the dynamic needle approach, the empirical merits of different agents such as saline (with or without blue contrast) and viscous agents, as well as lift-enhancing assistive devices — for example, the ERBEJET 2 high-pressure water jet, an adjustable hydrosurgical device to facilitate lifting. A chart provides an at-a-glance summary of agents and their pros and cons.
“The feedback from gastroenterologists so far has been quite positive on social media and on GI channels,” Patel said.
Endoscopic resection has evolved from snare polypectomy to endoscopic mucosal resection (EMR) and now, endoscopic submucosal dissection (ESD). The primary benefit of submucosal lifting is the creation of a separating submucosal cushion between the lesion and muscularis propria (MP), which reduces the risk for immediate or delayed perforation of the muscle. Adding a contrast agent also demarcates lesion margins and stains the submucosa, which is fundamental to ESD and allows for assessment of MP injury during EMR.
For decades, homemade solutions were used to lift lesions before removal, with the sentinel agent being normal saline, later mixed with a blue contrast agent, usually indigo carmine or methylene blue. The authors noted that some endoscopists performing ESD start the submucosal injection and incision using a prepackaged viscous solution. “The endoscopist may continue with the viscous fluid or transition to saline or another less expensive solution,” they wrote.
Saline tends to dissipate more quickly than viscous solutions, however. In 2015, the polymer compound SIC-8000 became the first FDA-approved submucosal injection agent. Since then, several other fluids have come on the market, although homemade agents remain available.
Among the update’s recommendations, the fluid selected for EMR should be determined by lesion size, predicted histology, and endoscopist preference. Based on the US Multi-Society Task Force (USMSTF) on Colorectal Cancer, submucosal injection is optional for nonpedunculated colorectal lesions (NPCRLs) of intermediate size (10-19 mm).
Cold snare polypectomy without submucosal injection was later found to be non-inferior to other resection methods utilizing submucosal injection for NPCRLs ≤ 15 mm.
The update noted that the USMSTF considers EMR first-line therapy for most NPCRLs ≥ 20 mm and advocates viscous solutions as preferred, while the use of lifting agents for pedunculated polyps is generally at the discretion of the endoscopist.
For Patel, the main “clinical pearls” in the update are adding a contrast agent to normal saline, using a viscous agent for cold EMR, and manipulating the injection needle first tangentially and then dynamically toward the lumen to maximize separation of the lesion.
In terms of the ideal, an optimal lifting solution would be readily available, inexpensive, and premixed, providing a sustained submucosal cushion. “However, this ideal solution currently does not exist. Injection fluids should, therefore, be selected based on planned resection method, predicted histology, local expertise and preferences, and cost,” the panelists wrote.
Added Patel, “A lot of the agents out there check most of these boxes, but we’re hoping for further development toward the ideal.”
Offering a nonparticipant’s perspective on the overview, Wasseem Skef, MD, a gastroenterologist at UTHealth Houston, found the update very useful. “It always helps to have the literature summarized,” he told GI & Hepatology News. “It’s a pretty balanced review that pulls together the various options but allows people to stick to their preferred practice.”
In his practice, the lifting agent selected depends on the type of resection. “Viscous agents are generally more popular for EMR-type resections,” Skef said. One unanswered question, he noted, is whether adding a hemostatic agent would be superior to a viscous agent alone. “But overall, this is a nice summary of available agents. Gastroenterologists should consider these different options if doing procedures like EMR.”
This review was sponsored by the AGA Institute.
Zuchelli is a consultant for Boston Scientific. Patel consults for Medpace, Renexxion, and Sanofi. Skef reported having no relevant disclosures.
A version of this article appeared on Medscape.com .
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
IBS, Chronic Idiopathic Constipation Surged During Pandemic
, with a near doubling of the national rate of IBS over 2 years, a study has found.
The uptick is probably due to not only the direct impact of SARS-CoV-2 infection on the gastrointestinal tract but also to the psychological stress associated with pandemic life, the study team said.
“COVID infection itself can definitely cause gastrointestinal symptoms like diarrhea, nausea, and abdominal pain — and for some people, those symptoms can linger and lead to chronic conditions like IBS,” Christopher V. Almario, MD, MSHPM, lead author and gastroenterologist at Cedars-Sinai Medical Center, Los Angeles, California, told GI & Hepatology News.

“But the stress of living through the pandemic — lockdowns, fear, isolation — also likely played a major role as well in the increased prevalence of digestive disorders. Both the infection itself and the psychological toll of the pandemic can disrupt the gut-brain axis and trigger chronic digestive disorders like IBS,” Almario said.
The study was published in Neurogastroenterology & Motility.
Growing Burden of Gut Disorders
Disorders of gut-brain interaction (DGBIs) are a heterogeneous group of conditions in which gastrointestinal symptoms occur without any detectable structural or biochemical abnormalities in the digestive tract. They include IBS, functional dyspepsia, and chronic idiopathic constipation, among others.
DGBIs are highly prevalent. Research has shown that nearly 40% of people in the US meet Rome IV criteria for at least one DGBI.
Almario and colleagues assessed trends in prevalence of these conditions during the COVID-19 pandemic. Starting in May 2020 through May 2022, they conducted a series of online surveys with more than 160,000 adults aged 18 or older using validated Rome IV diagnostic questionnaires.
Results showed that during the pandemic, IBS prevalence rose from 6.1% in May 2020 to 11.0% by May 2022, an increase of 0.188% per month (adjusted P < .001).
Chronic idiopathic constipation showed a smaller but statistically significant increase, from 6.0% to 6.4% (0.056% per month; adjusted P < .001).
Within the IBS subtypes, mixed-type IBS showed the largest relative increase (0.085% per month), followed by IBS with constipation (0.041% per month) and IBS with diarrhea (0.037% per month).
There were no significant changes in the prevalence of other DGBIs, such as functional bloating, functional diarrhea, or functional dyspepsia, during the study period.
Almario told GI & Hepatology News only about 9% of those surveyed reported a positive COVID test at the time of the surveys, but that figure probably underrepresents actual infections, especially in the early months of the pandemic. “Most of the survey responses came in during the earlier phases of the pandemic, and the percentage reporting a positive test increased over time,” he explained.
Almario also noted that this study did not directly compare digestive disorder rates between infected and uninfected individuals. However, a separate study by the Cedars-Sinai team currently undergoing peer review addresses that question more directly. “That study, along with several other studies, show that having COVID increases the risk of developing conditions like IBS and functional dyspepsia,” Almario said.
Taken together, the findings “underscore the increasing healthcare and economic burden of DGBI in the post-pandemic era, emphasizing the need for targeted efforts to effectively diagnose and manage these complex conditions,” they wrote.
“This will be especially challenging for healthcare systems to address, given the existing shortage of primary care physicians and gastroenterologists — clinicians who primarily manage individuals with DGBI,” they noted.
Support for this study was received from Ironwood Pharmaceuticals and Salix Pharmaceuticals in the form of institutional research grants to Cedars-Sinai. Almario has consulted for Exact Sciences, Greenspace Labs, Owlstone Medical, Salix Pharmaceuticals, and Universal DX.
A version of this article appeared on Medscape.com.
, with a near doubling of the national rate of IBS over 2 years, a study has found.
The uptick is probably due to not only the direct impact of SARS-CoV-2 infection on the gastrointestinal tract but also to the psychological stress associated with pandemic life, the study team said.
“COVID infection itself can definitely cause gastrointestinal symptoms like diarrhea, nausea, and abdominal pain — and for some people, those symptoms can linger and lead to chronic conditions like IBS,” Christopher V. Almario, MD, MSHPM, lead author and gastroenterologist at Cedars-Sinai Medical Center, Los Angeles, California, told GI & Hepatology News.
“But the stress of living through the pandemic — lockdowns, fear, isolation — also likely played a major role as well in the increased prevalence of digestive disorders. Both the infection itself and the psychological toll of the pandemic can disrupt the gut-brain axis and trigger chronic digestive disorders like IBS,” Almario said.
The study was published in Neurogastroenterology & Motility.
Growing Burden of Gut Disorders
Disorders of gut-brain interaction (DGBIs) are a heterogeneous group of conditions in which gastrointestinal symptoms occur without any detectable structural or biochemical abnormalities in the digestive tract. They include IBS, functional dyspepsia, and chronic idiopathic constipation, among others.
DGBIs are highly prevalent. Research has shown that nearly 40% of people in the US meet Rome IV criteria for at least one DGBI.
Almario and colleagues assessed trends in prevalence of these conditions during the COVID-19 pandemic. Starting in May 2020 through May 2022, they conducted a series of online surveys with more than 160,000 adults aged 18 or older using validated Rome IV diagnostic questionnaires.
Results showed that during the pandemic, IBS prevalence rose from 6.1% in May 2020 to 11.0% by May 2022, an increase of 0.188% per month (adjusted P < .001).
Chronic idiopathic constipation showed a smaller but statistically significant increase, from 6.0% to 6.4% (0.056% per month; adjusted P < .001).
Within the IBS subtypes, mixed-type IBS showed the largest relative increase (0.085% per month), followed by IBS with constipation (0.041% per month) and IBS with diarrhea (0.037% per month).
There were no significant changes in the prevalence of other DGBIs, such as functional bloating, functional diarrhea, or functional dyspepsia, during the study period.
Almario told GI & Hepatology News only about 9% of those surveyed reported a positive COVID test at the time of the surveys, but that figure probably underrepresents actual infections, especially in the early months of the pandemic. “Most of the survey responses came in during the earlier phases of the pandemic, and the percentage reporting a positive test increased over time,” he explained.
Almario also noted that this study did not directly compare digestive disorder rates between infected and uninfected individuals. However, a separate study by the Cedars-Sinai team currently undergoing peer review addresses that question more directly. “That study, along with several other studies, show that having COVID increases the risk of developing conditions like IBS and functional dyspepsia,” Almario said.
Taken together, the findings “underscore the increasing healthcare and economic burden of DGBI in the post-pandemic era, emphasizing the need for targeted efforts to effectively diagnose and manage these complex conditions,” they wrote.
“This will be especially challenging for healthcare systems to address, given the existing shortage of primary care physicians and gastroenterologists — clinicians who primarily manage individuals with DGBI,” they noted.
Support for this study was received from Ironwood Pharmaceuticals and Salix Pharmaceuticals in the form of institutional research grants to Cedars-Sinai. Almario has consulted for Exact Sciences, Greenspace Labs, Owlstone Medical, Salix Pharmaceuticals, and Universal DX.
A version of this article appeared on Medscape.com.
, with a near doubling of the national rate of IBS over 2 years, a study has found.
The uptick is probably due to not only the direct impact of SARS-CoV-2 infection on the gastrointestinal tract but also to the psychological stress associated with pandemic life, the study team said.
“COVID infection itself can definitely cause gastrointestinal symptoms like diarrhea, nausea, and abdominal pain — and for some people, those symptoms can linger and lead to chronic conditions like IBS,” Christopher V. Almario, MD, MSHPM, lead author and gastroenterologist at Cedars-Sinai Medical Center, Los Angeles, California, told GI & Hepatology News.
“But the stress of living through the pandemic — lockdowns, fear, isolation — also likely played a major role as well in the increased prevalence of digestive disorders. Both the infection itself and the psychological toll of the pandemic can disrupt the gut-brain axis and trigger chronic digestive disorders like IBS,” Almario said.
The study was published in Neurogastroenterology & Motility.
Growing Burden of Gut Disorders
Disorders of gut-brain interaction (DGBIs) are a heterogeneous group of conditions in which gastrointestinal symptoms occur without any detectable structural or biochemical abnormalities in the digestive tract. They include IBS, functional dyspepsia, and chronic idiopathic constipation, among others.
DGBIs are highly prevalent. Research has shown that nearly 40% of people in the US meet Rome IV criteria for at least one DGBI.
Almario and colleagues assessed trends in prevalence of these conditions during the COVID-19 pandemic. Starting in May 2020 through May 2022, they conducted a series of online surveys with more than 160,000 adults aged 18 or older using validated Rome IV diagnostic questionnaires.
Results showed that during the pandemic, IBS prevalence rose from 6.1% in May 2020 to 11.0% by May 2022, an increase of 0.188% per month (adjusted P < .001).
Chronic idiopathic constipation showed a smaller but statistically significant increase, from 6.0% to 6.4% (0.056% per month; adjusted P < .001).
Within the IBS subtypes, mixed-type IBS showed the largest relative increase (0.085% per month), followed by IBS with constipation (0.041% per month) and IBS with diarrhea (0.037% per month).
There were no significant changes in the prevalence of other DGBIs, such as functional bloating, functional diarrhea, or functional dyspepsia, during the study period.
Almario told GI & Hepatology News only about 9% of those surveyed reported a positive COVID test at the time of the surveys, but that figure probably underrepresents actual infections, especially in the early months of the pandemic. “Most of the survey responses came in during the earlier phases of the pandemic, and the percentage reporting a positive test increased over time,” he explained.
Almario also noted that this study did not directly compare digestive disorder rates between infected and uninfected individuals. However, a separate study by the Cedars-Sinai team currently undergoing peer review addresses that question more directly. “That study, along with several other studies, show that having COVID increases the risk of developing conditions like IBS and functional dyspepsia,” Almario said.
Taken together, the findings “underscore the increasing healthcare and economic burden of DGBI in the post-pandemic era, emphasizing the need for targeted efforts to effectively diagnose and manage these complex conditions,” they wrote.
“This will be especially challenging for healthcare systems to address, given the existing shortage of primary care physicians and gastroenterologists — clinicians who primarily manage individuals with DGBI,” they noted.
Support for this study was received from Ironwood Pharmaceuticals and Salix Pharmaceuticals in the form of institutional research grants to Cedars-Sinai. Almario has consulted for Exact Sciences, Greenspace Labs, Owlstone Medical, Salix Pharmaceuticals, and Universal DX.
A version of this article appeared on Medscape.com.
FDA Issues Early Alert for Medtronic pH-Monitoring Capsules
The notice follows two letters sent in June to customers by the devices’ manufacturer Medtronic and its subsidiary Given Imaging Inc., recommending that customers using certain Bravo CF Capsule Delivery Devices (lot numbers below) for esophageal pH monitoring be removed from all sites of use and sale.
All three of the capsule models listed below are thought to pose a potential risk because the capsules fail to attach to the esophagus’s mucosal wall or to detach from the delivery device as intended owing to a misapplication of adhesive during manufacture. The devices transmit pH data to a recorder attached to the waist of the patient, who interacts with the recorder to indicate symptoms, thereby allowing the physician to compare the symptoms with the occurrence of reflux episodes.
Risks associated with the devices include aspiration/inhalation, perforation of the esophagus, obstruction of the airway, hemorrhage/blood loss/bleeding, laceration of the esophagus, a delay in diagnosis, and foreign bodies remaining in the patient.
Medtronic has reported 33 serious injuries but no deaths associated with the devices.
The lot numbers of the three affected units, which should be identified and quarantined immediately are:
- Bravo CF Capsule Delivery Device, 5-pk, Product Number FGS-0635, Unique Device Identifier-Device Identifier (UDI-DI) 07290101369707
- Bravo CF Capsule Delivery Device 5-pk, FGS-0635, UDI-DI 10613994000009
- Bravo CF Capsule Delivery Device 1-pk, FGS-0636, UDI-DI 07290101369714
These lot identifiers can be found on both the 5-pks’ FGS-0635 outer labels and on the 1-pk FGS-036 individual unit. Customers are advised to return all unused affected products to Medtronic for replacement or credit. In addition, they should pass on this notice to all those who need to be aware within their organizations or to any organizations to which the affected products have been distributed.
They are also advised to check the FDA recall website above for updates as it continues to review information about this potentially high-risk device issue.
Healthcare professionals with concerns or reports of adverse events can contact Medtronic at 800-448-3644 or MedWatch: The FDA Safety Information and Adverse Event Reporting Program.
A version of this article appeared on Medscape.com.
The notice follows two letters sent in June to customers by the devices’ manufacturer Medtronic and its subsidiary Given Imaging Inc., recommending that customers using certain Bravo CF Capsule Delivery Devices (lot numbers below) for esophageal pH monitoring be removed from all sites of use and sale.
All three of the capsule models listed below are thought to pose a potential risk because the capsules fail to attach to the esophagus’s mucosal wall or to detach from the delivery device as intended owing to a misapplication of adhesive during manufacture. The devices transmit pH data to a recorder attached to the waist of the patient, who interacts with the recorder to indicate symptoms, thereby allowing the physician to compare the symptoms with the occurrence of reflux episodes.
Risks associated with the devices include aspiration/inhalation, perforation of the esophagus, obstruction of the airway, hemorrhage/blood loss/bleeding, laceration of the esophagus, a delay in diagnosis, and foreign bodies remaining in the patient.
Medtronic has reported 33 serious injuries but no deaths associated with the devices.
The lot numbers of the three affected units, which should be identified and quarantined immediately are:
- Bravo CF Capsule Delivery Device, 5-pk, Product Number FGS-0635, Unique Device Identifier-Device Identifier (UDI-DI) 07290101369707
- Bravo CF Capsule Delivery Device 5-pk, FGS-0635, UDI-DI 10613994000009
- Bravo CF Capsule Delivery Device 1-pk, FGS-0636, UDI-DI 07290101369714
These lot identifiers can be found on both the 5-pks’ FGS-0635 outer labels and on the 1-pk FGS-036 individual unit. Customers are advised to return all unused affected products to Medtronic for replacement or credit. In addition, they should pass on this notice to all those who need to be aware within their organizations or to any organizations to which the affected products have been distributed.
They are also advised to check the FDA recall website above for updates as it continues to review information about this potentially high-risk device issue.
Healthcare professionals with concerns or reports of adverse events can contact Medtronic at 800-448-3644 or MedWatch: The FDA Safety Information and Adverse Event Reporting Program.
A version of this article appeared on Medscape.com.
The notice follows two letters sent in June to customers by the devices’ manufacturer Medtronic and its subsidiary Given Imaging Inc., recommending that customers using certain Bravo CF Capsule Delivery Devices (lot numbers below) for esophageal pH monitoring be removed from all sites of use and sale.
All three of the capsule models listed below are thought to pose a potential risk because the capsules fail to attach to the esophagus’s mucosal wall or to detach from the delivery device as intended owing to a misapplication of adhesive during manufacture. The devices transmit pH data to a recorder attached to the waist of the patient, who interacts with the recorder to indicate symptoms, thereby allowing the physician to compare the symptoms with the occurrence of reflux episodes.
Risks associated with the devices include aspiration/inhalation, perforation of the esophagus, obstruction of the airway, hemorrhage/blood loss/bleeding, laceration of the esophagus, a delay in diagnosis, and foreign bodies remaining in the patient.
Medtronic has reported 33 serious injuries but no deaths associated with the devices.
The lot numbers of the three affected units, which should be identified and quarantined immediately are:
- Bravo CF Capsule Delivery Device, 5-pk, Product Number FGS-0635, Unique Device Identifier-Device Identifier (UDI-DI) 07290101369707
- Bravo CF Capsule Delivery Device 5-pk, FGS-0635, UDI-DI 10613994000009
- Bravo CF Capsule Delivery Device 1-pk, FGS-0636, UDI-DI 07290101369714
These lot identifiers can be found on both the 5-pks’ FGS-0635 outer labels and on the 1-pk FGS-036 individual unit. Customers are advised to return all unused affected products to Medtronic for replacement or credit. In addition, they should pass on this notice to all those who need to be aware within their organizations or to any organizations to which the affected products have been distributed.
They are also advised to check the FDA recall website above for updates as it continues to review information about this potentially high-risk device issue.
Healthcare professionals with concerns or reports of adverse events can contact Medtronic at 800-448-3644 or MedWatch: The FDA Safety Information and Adverse Event Reporting Program.
A version of this article appeared on Medscape.com.
Help Sustain GI Research
Scientists are working hard to develop new treatments and therapies, and to discover cures to advance the field and better patient care. But they can’t do this without research funding.
A lack of funding can prevent talented individuals from pursuing a research career, thereby denying them the opportunity to conduct work that will ultimately benefit patients with critical needs.
Treatment options for digestive diseases begin with rigorous research, but the limited funding available for physician-scientists to conduct research puts the field at risk of losing talented investigators.
As an AGA member, you have the power to make a difference. By increasing the number of talented women and men doing state-of-the-art research, you can help improve care for all patients suffering from digestive diseases.
Your gift to the AGA Research Foundation will catalyze discovery and career growth for a promising researcher in gastroenterology and hepatology. Please help us fund the next generation of GI researchers by donating today at https://foundation.gastro.org.
Scientists are working hard to develop new treatments and therapies, and to discover cures to advance the field and better patient care. But they can’t do this without research funding.
A lack of funding can prevent talented individuals from pursuing a research career, thereby denying them the opportunity to conduct work that will ultimately benefit patients with critical needs.
Treatment options for digestive diseases begin with rigorous research, but the limited funding available for physician-scientists to conduct research puts the field at risk of losing talented investigators.
As an AGA member, you have the power to make a difference. By increasing the number of talented women and men doing state-of-the-art research, you can help improve care for all patients suffering from digestive diseases.
Your gift to the AGA Research Foundation will catalyze discovery and career growth for a promising researcher in gastroenterology and hepatology. Please help us fund the next generation of GI researchers by donating today at https://foundation.gastro.org.
Scientists are working hard to develop new treatments and therapies, and to discover cures to advance the field and better patient care. But they can’t do this without research funding.
A lack of funding can prevent talented individuals from pursuing a research career, thereby denying them the opportunity to conduct work that will ultimately benefit patients with critical needs.
Treatment options for digestive diseases begin with rigorous research, but the limited funding available for physician-scientists to conduct research puts the field at risk of losing talented investigators.
As an AGA member, you have the power to make a difference. By increasing the number of talented women and men doing state-of-the-art research, you can help improve care for all patients suffering from digestive diseases.
Your gift to the AGA Research Foundation will catalyze discovery and career growth for a promising researcher in gastroenterology and hepatology. Please help us fund the next generation of GI researchers by donating today at https://foundation.gastro.org.
Impact of Rapid Blood Culture Identification on Antibiotic De-escalation at a Veterans Affairs Medical Center
Impact of Rapid Blood Culture Identification on Antibiotic De-escalation at a Veterans Affairs Medical Center
About 530,000 to 628,000 episodes of bloodstream infections (BSI) occur annually in the US.1 Early identification and treatment of bacteremia are essential to improve patient outcomes because it allows for more timely targeted antibiotic therapy.2 Organism identification and susceptibility testing can take 2 to 5 days, prolonging the use of broad-spectrum empiric antibiotics and increasing the risk of adverse events.3,4 The Infectious Disease Society of America recommends the use of rapid diagnostic testing and antimicrobial stewardship programs (ASPs) to improve rates of antibiotic susceptibilities to targeted antibiotics and optimize resource utilization.3 Rapid blood culture identification (BCID) technologies reduce the duration of empiric antibiotics in patients with contaminated blood cultures, resulting in shorter hospital stays and saving money per each patient tested.4
In March 2023, Veteran Health Indiana (VHI) implemented the BioFire FilmArray Blood Culture Identification (BCID2), a BSI panel test that identifies select gram-negative bacteria, gram-positive bacteria, yeast, and antimicrobial resistance genes with an aggregate sensitivity of 99% and a specificity of 99.8%. The BCID2 presents clinically relevant information faster than traditional culture methods, allowing clinicians to make more efficient and educated antibiotic regimen decisions than with previous methods.5
It takes 24 to 48 hours from blood collection for culture incubation, positivity, and gram staining to occur at VHI. If the gram stain is positive, the blood culture is placed on the BioFire BCID2 in addition to traditional culture medium. BioFire BCID2 results are ready in 45 to 60 minutes. Results are uploaded into the electronic health record (EHR) ≤ 2 hours after they are obtained and the primary team is notified if the test is positive for certain critical results. Susceptibility testing of an identified organism typically requires an additional 24 to 48 hours for finalization. VHI Infectious Disease created an evidence-based antibiotic recommendation chart for certain medication(s) and alternate therapies based on the reported organism and its interpreted presence of resistance markers (eg, ceftriaxone for Escherichia coli when extended-spectrum beta lactamases are not detected vs meropenem if extended-spectrum beta lactamases marker are present). These charts optimize the antibiotic regimen while awaiting susceptibility finalizations.
Two previous studies describe the impact of rapid diagnostic testing technology at US Department of Veterans Affairs (VA) medical centers.6,7 In Texas, the ASP reviewed BCID panel results via clinical decision support software for about 1 hour per day.6 A Los Angeles study analyzed the impact of Biofire BCID with an interpretation guide centered on unnecessary vancomycin use and determined that shorter duration of the medication may have been the result of more frequent infectious disease consultation.7
This study assessed the time to optimal antibiotic de-escalation before and after the implementation of BioFire BCID2 with results reviewed by the ASP without active notification or assistance of any clinical decision support technology. The primary objective was to evaluate difference in time to optimal antibiotics from blood culture draw pre- vs postintervention. Secondary objectives included differences in time to organism identification, difference in time on broad-spectrum antibiotics, and difference in time to appropriate antibiotics.
Methods
This quasi-experimental retrospective chart review assessed the impact of BioFire BCID2 use on timely antibiotic de-escalation for patients who experienced a BSI at VHI between March 1, 2022, and October 1, 2023. Microbiology laboratory records identified eligible patients with positive blood cultures within the study time frame. Data were collected from the VHI EHR.
Patients were included if they had a positive bacterial blood culture and received ≥ 1 antibiotic indicated for bacteremia while receiving inpatient care. Patients were excluded if they died prior to blood culture results, transferred out of VHI, left against medical advice, or had untreated contaminants in blood culture results (ie, never received antibiotics aimed at the contaminated culture).
Patient lists were generated for before and after implementation of BioFire BCID2 (pre- and postintervention) using the VHI EHR and microbiology laboratory record system. The pre- and postinterventions groups were different sizes. As a result, a random sampling of the preintervention group was selected and included patients from March 1, 2022, through March 26, 2023. The postintervention group was smaller due to time constraints between initiation of BioFire BCID2 for data collection and included all patients from March 27, 2023, through October 1, 2023.
Optimal antibiotics were defined as escalation from inappropriate therapy to broader agent(s), de-escalation from broad-spectrum therapy to targeted agent(s), discontinuation of therapy due to an organism being identified as a contaminant, or optimization of a regimen to the preferred antimicrobial agent based on evidence-based consensus guidelines. Broad-spectrum antibiotics included: piperacillin/tazobactam, cefepime, ceftazidime, ceftazidime-avibactam, cefiderocol, carbapenems, fluroquinolones, vancomycin, daptomycin, ceftaroline, linezolid, or aztreonam. Appropriate antibiotics were defined as those with activity toward the final identified organism(s).
Deidentified participant data were entered into Microsoft Excel and kept on a secure VA server to complete statistical analyses. Parametric continuous data, such as age, were analyzed using the t-test, while nonparametric continuous data, such as time to optimal antibiotics, were analyzed using the Mann-Whitney U test. Categorical data, like sex and race, were analyzed using either Fisher exact test for small sample sizes or X2 test for a larger sample size. Statistical significance levels was defined as P < .05.
Results
Using patient lists drawn from the EHR and the microbiology laboratory records, 110 electronic charts were randomly selected for review. Fifteen patients were excluded: 8 had untreated contaminants, 4 died, and 3 were transferred out of VHI. Of the 95 patients included, 48 were in the preintervention group and 47 were in the postintervention group (Figure 1).
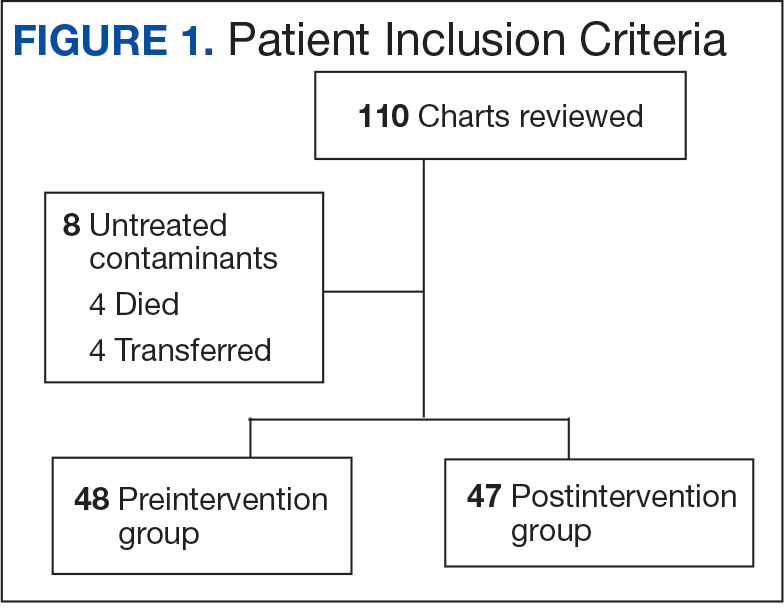
Baseline characteristics were similar between the 2 groups (Table 1). Most patients were White males aged > 70 years in the EHR. The urinary tract was the most common source of infection, impacting 12 patients in each group (Figure 2). Escherichia coli, Klebsiella, Staphylococcus, and Streptococcus were the most common bloodstream isolates identified.
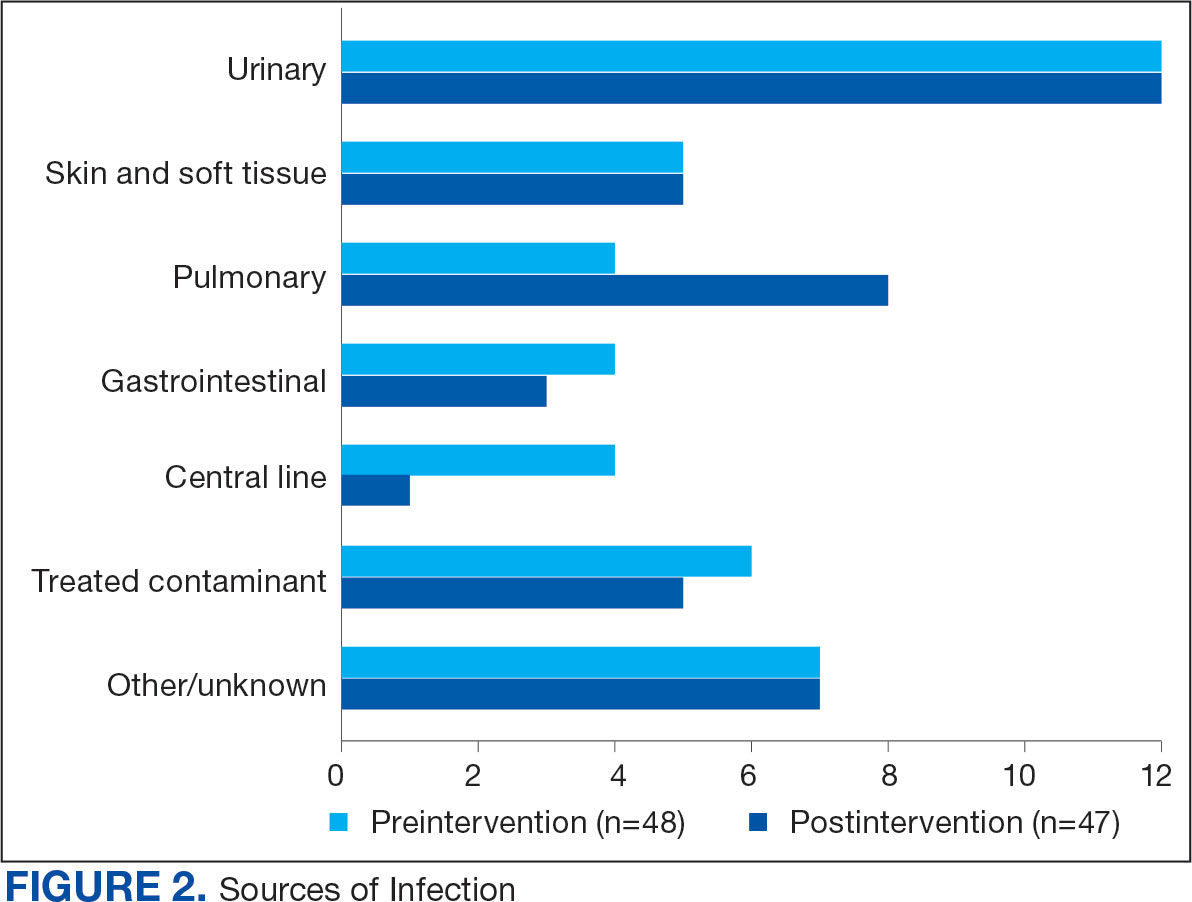
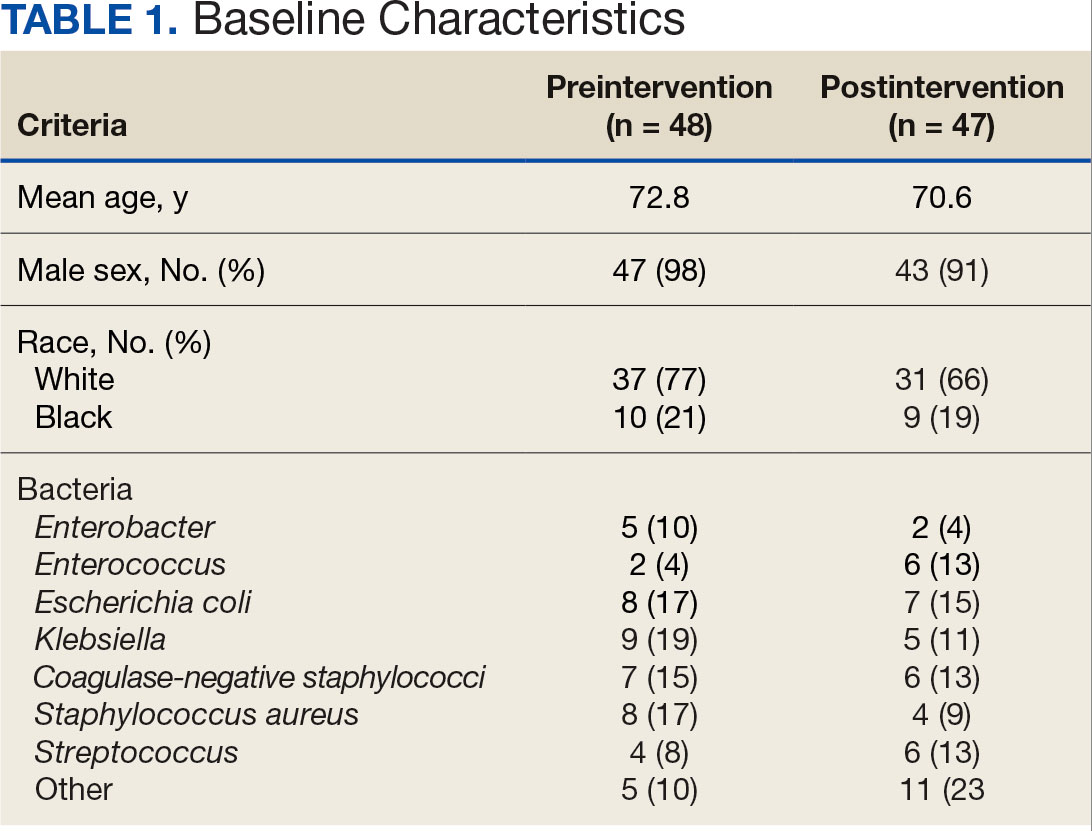
The median time to optimal antibiotics in the preintervention group was 58.5 hours vs 43.4 hours in the postintervention group (P = .11). The median time to organism identification was 37.8 hours in the preintervention group vs 16.9 hours in the postintervention group (P < .001). The median time on broad-spectrum antibiotics was 45.2 hours in the preintervention group vs 46.6 hours in the postintervention group (P = .99). The median time on appropriate antibiotics in the preintervention group was 2.3 hours vs 1.9 hours in the postintervention group (P = .79). Differences in other measured outcomes between the groups were not statistically significant (Table 2).
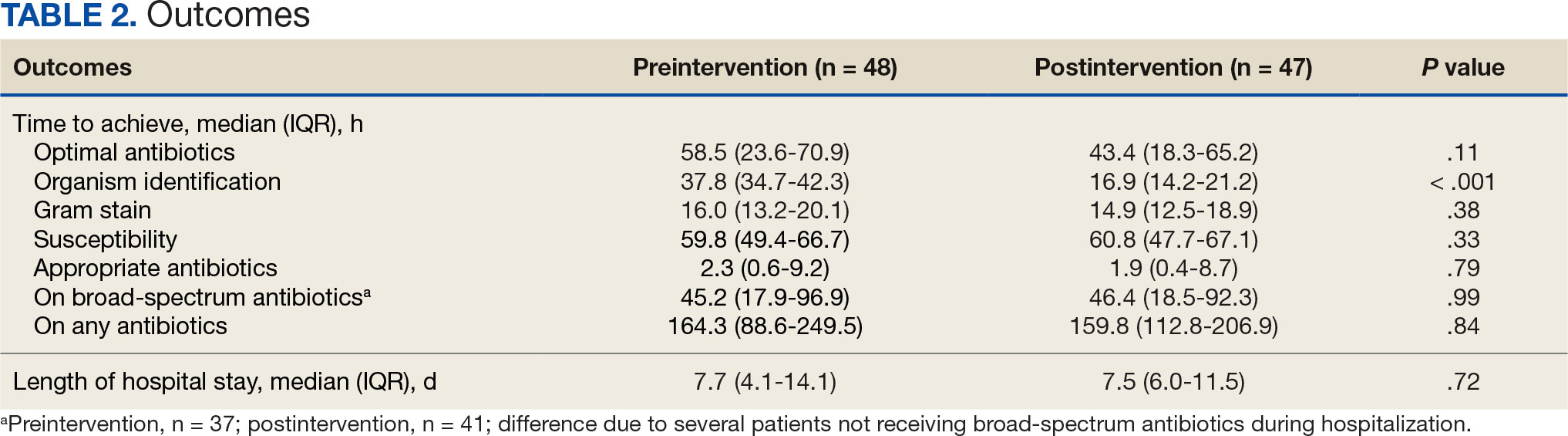
Although implementation of rapid diagnostic technology reduced the median time to optimal antibiotics, the results were not statistically significant. Shorter time to organism identification in the postintervention group compared to the preintervention group was the lone statistically significant metric (P < .001).
Discussion
A lack of statistical significance in the primary outcome may have been due to nonadherence to facility de-escalation protocols or a suboptimal BioFire BCID2 result notification system. Additionally, use of rapid BCID at VHI may improve over time as clinicians become more familiar with the technology. Gaps in clinical pharmacy coverage during the night shift may have also contributed to delays in antibiotic optimization, particularly if other clinicians are not equipped with the knowledge or training to appropriately deescalate antibiotics based on microorganisms identified. A 2017 study by Donner et al concluded that physician interpretation of BCID results is suboptimal and should be augmented with clinical decision support tools as new technology becomes available.8 Despite the statistically insignificant results of this study, it did highlight potential areas of improvement which can lead to improved patient care.
Previous research has evaluated the impact of rapid BCID technology on antibiotic treatment and clinical outcomes. Chiasson et al found that median time to optimal therapy was 73.8 hours in the pre-BCID arm compared to 34.7 hours in the post- BCID arm (P ≤ .001), emphasizing the importance of combining rapid BCID with clinical decision support tools and pharmacy input.6 Senok et al found that BCID2 implementation led to a significant decrease in median time to culture result, which informed optimal antibiotic therapy and decreased 30-day mortality in the intensive care setting.9 In contrast, the current study did not stratify patients according to medical ward or illness severity even though clinicians may be less likely to de-escalate antibiotic therapy in critically ill patients.
Bae et al reported findings consistent with the current study and concluded that BCID did not affect the clinical outcomes of overall BSIs; however, it contributed to early administration of effective antibiotics in cases of BSIs caused by multidrug-resistant organisms.10 Results of this study were not stratified according to multidrug-resistant organisms because the sample size was too small. The current study also included patients with polymicrobial infections, which may have impacted the results due to a less streamlined approach to antibiotic optimization.
Limitations
This single-center, retrospective study had a small sample size, short time frame, and lacked patient diversity, and therefore may not be generalizable to other health care systems. The sample size was limited by shorter date range and smaller patient list between BioFire BCID2 implementation and data collection, which was used to determine the number of charts selected in each group. Some patients received antibiotics prior to blood cultures being drawn, which may falsely decrease time to optimal/ appropriate antibiotics and falsely increase time on broad spectrum/any antibiotics due to early antibiotic administration. The total number of patients on broad-spectrum antibiotics differed from the total number of patients for other outcomes because several patients never received the defined broad spectrum antibiotics.
Conclusions
When combined with a pre-existing ASP without active notification, the implementation of BioFire BCID2 did not return statistically significant data showing a decrease in time to optimal antibiotics, time to appropriate antibiotics, or time on broad-spectrum antibiotics at VHI. To make this program more successful, pharmacist intervention and clinical decision support tools may be needed.
Additional research is required to determine the optimal integration of antimicrobial stewardship, rapid diagnostic technology, and pharmacy services for maximum benefit. Even though the primary outcome was not statistically significant, the results may be clinically significant from a stewardship perspective. Realigning microbiology workflows to mimic other research, which emphasizes the importance of funneling rapid BCID results through the ASP, may improve outcomes. Future studies may be warranted following the implementation of clinical decision support tools to assess their impact on stewardship practices and patient outcomes.
- Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect. 2013;19(6):501- 509. doi:10.1111/1469-0691.12195
- Pardo J, Klinker KP, Borgert SJ, Butler BM, Giglio PG, Rand KH. Clinical and economic impact of antimicrobial stewardship interventions with the FilmArray blood culture identification panel. Diagn Microbiol Infect Dis. 2016;84(2):159-164. doi:10.1016/j.diagmicrobio.2015.10.023.
- Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program: guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77. doi:10.1093/cid/ciw118
- BIOFIRE® Blood Culture Identification 2 (BCID2) Panel. Biomerierux. Updated 2025. Accessed May 10, 2025. https://www.biofiredx.com/products/the-filmarray-panels/filmarraybcid/
- Huang AM, Newton D, Kunapuli A, et al. Impact of rapid organism identification via matrix-assisted laser desorption/ionization time-of-flight combined with antimicrobial stewardship team intervention in adult patients with bacteremia and candidemia. Clin Infect Dis. 2013;57(9):1237-1245. doi:10.1093/cid/cit498
- Chiasson JM, Smith WJ, Jodlowski TZ, Kouma MA, Cutrell JB. Impact of a rapid blood culture diagnostic panel on time to optimal antimicrobial therapy at a veterans affairs medical center. J Pharm Pract. 2022;35(5):722-729. doi:10.1177/08971900211000686
- Wu S, Watson RL, Graber CJ. 2007. Impact of combining rapid diagnostics with an interpretation guide on vancomycin usage for contaminant blood cultures growing coagulase- negative staphylococci (CoNS). Open Forum Infect Dis. 2019;6(Suppl 2):S674. doi:10.1093/ofid/ofz360.1687
- Donner LM, Campbell WS, Lyden E, Van Schooneveld TC. Assessment of rapid-blood-culture-identification result interpretation and antibiotic prescribing practices. J Clin Microbiol. 2017;55(5):1496-1507. doi:10.1128/JCM.02395-16
- Senok A, Dabal LA, Alfaresi M, et al. Clinical impact of the BIOFIRE blood culture identification 2 panel in adult patients with bloodstream infection: a multicentre observational study in the United Arab Emirates. Diagnostics (Basel). 2023;13(14):2433. doi:10.3390/diagnostics13142433
- Bae JY, Bae J, So MK, Choi HJ, Lee M. The impact of the rapid blood culture identification panel on antibiotic treatment and clinical outcomes in bloodstream infections, particularly those associated with multidrug-resistant micro-organisms. Diagnostics (Basel). 2023;13(23):3504. doi:10.3390/diagnostics13233504
About 530,000 to 628,000 episodes of bloodstream infections (BSI) occur annually in the US.1 Early identification and treatment of bacteremia are essential to improve patient outcomes because it allows for more timely targeted antibiotic therapy.2 Organism identification and susceptibility testing can take 2 to 5 days, prolonging the use of broad-spectrum empiric antibiotics and increasing the risk of adverse events.3,4 The Infectious Disease Society of America recommends the use of rapid diagnostic testing and antimicrobial stewardship programs (ASPs) to improve rates of antibiotic susceptibilities to targeted antibiotics and optimize resource utilization.3 Rapid blood culture identification (BCID) technologies reduce the duration of empiric antibiotics in patients with contaminated blood cultures, resulting in shorter hospital stays and saving money per each patient tested.4
In March 2023, Veteran Health Indiana (VHI) implemented the BioFire FilmArray Blood Culture Identification (BCID2), a BSI panel test that identifies select gram-negative bacteria, gram-positive bacteria, yeast, and antimicrobial resistance genes with an aggregate sensitivity of 99% and a specificity of 99.8%. The BCID2 presents clinically relevant information faster than traditional culture methods, allowing clinicians to make more efficient and educated antibiotic regimen decisions than with previous methods.5
It takes 24 to 48 hours from blood collection for culture incubation, positivity, and gram staining to occur at VHI. If the gram stain is positive, the blood culture is placed on the BioFire BCID2 in addition to traditional culture medium. BioFire BCID2 results are ready in 45 to 60 minutes. Results are uploaded into the electronic health record (EHR) ≤ 2 hours after they are obtained and the primary team is notified if the test is positive for certain critical results. Susceptibility testing of an identified organism typically requires an additional 24 to 48 hours for finalization. VHI Infectious Disease created an evidence-based antibiotic recommendation chart for certain medication(s) and alternate therapies based on the reported organism and its interpreted presence of resistance markers (eg, ceftriaxone for Escherichia coli when extended-spectrum beta lactamases are not detected vs meropenem if extended-spectrum beta lactamases marker are present). These charts optimize the antibiotic regimen while awaiting susceptibility finalizations.
Two previous studies describe the impact of rapid diagnostic testing technology at US Department of Veterans Affairs (VA) medical centers.6,7 In Texas, the ASP reviewed BCID panel results via clinical decision support software for about 1 hour per day.6 A Los Angeles study analyzed the impact of Biofire BCID with an interpretation guide centered on unnecessary vancomycin use and determined that shorter duration of the medication may have been the result of more frequent infectious disease consultation.7
This study assessed the time to optimal antibiotic de-escalation before and after the implementation of BioFire BCID2 with results reviewed by the ASP without active notification or assistance of any clinical decision support technology. The primary objective was to evaluate difference in time to optimal antibiotics from blood culture draw pre- vs postintervention. Secondary objectives included differences in time to organism identification, difference in time on broad-spectrum antibiotics, and difference in time to appropriate antibiotics.
Methods
This quasi-experimental retrospective chart review assessed the impact of BioFire BCID2 use on timely antibiotic de-escalation for patients who experienced a BSI at VHI between March 1, 2022, and October 1, 2023. Microbiology laboratory records identified eligible patients with positive blood cultures within the study time frame. Data were collected from the VHI EHR.
Patients were included if they had a positive bacterial blood culture and received ≥ 1 antibiotic indicated for bacteremia while receiving inpatient care. Patients were excluded if they died prior to blood culture results, transferred out of VHI, left against medical advice, or had untreated contaminants in blood culture results (ie, never received antibiotics aimed at the contaminated culture).
Patient lists were generated for before and after implementation of BioFire BCID2 (pre- and postintervention) using the VHI EHR and microbiology laboratory record system. The pre- and postinterventions groups were different sizes. As a result, a random sampling of the preintervention group was selected and included patients from March 1, 2022, through March 26, 2023. The postintervention group was smaller due to time constraints between initiation of BioFire BCID2 for data collection and included all patients from March 27, 2023, through October 1, 2023.
Optimal antibiotics were defined as escalation from inappropriate therapy to broader agent(s), de-escalation from broad-spectrum therapy to targeted agent(s), discontinuation of therapy due to an organism being identified as a contaminant, or optimization of a regimen to the preferred antimicrobial agent based on evidence-based consensus guidelines. Broad-spectrum antibiotics included: piperacillin/tazobactam, cefepime, ceftazidime, ceftazidime-avibactam, cefiderocol, carbapenems, fluroquinolones, vancomycin, daptomycin, ceftaroline, linezolid, or aztreonam. Appropriate antibiotics were defined as those with activity toward the final identified organism(s).
Deidentified participant data were entered into Microsoft Excel and kept on a secure VA server to complete statistical analyses. Parametric continuous data, such as age, were analyzed using the t-test, while nonparametric continuous data, such as time to optimal antibiotics, were analyzed using the Mann-Whitney U test. Categorical data, like sex and race, were analyzed using either Fisher exact test for small sample sizes or X2 test for a larger sample size. Statistical significance levels was defined as P < .05.
Results
Using patient lists drawn from the EHR and the microbiology laboratory records, 110 electronic charts were randomly selected for review. Fifteen patients were excluded: 8 had untreated contaminants, 4 died, and 3 were transferred out of VHI. Of the 95 patients included, 48 were in the preintervention group and 47 were in the postintervention group (Figure 1).
Baseline characteristics were similar between the 2 groups (Table 1). Most patients were White males aged > 70 years in the EHR. The urinary tract was the most common source of infection, impacting 12 patients in each group (Figure 2). Escherichia coli, Klebsiella, Staphylococcus, and Streptococcus were the most common bloodstream isolates identified.
The median time to optimal antibiotics in the preintervention group was 58.5 hours vs 43.4 hours in the postintervention group (P = .11). The median time to organism identification was 37.8 hours in the preintervention group vs 16.9 hours in the postintervention group (P < .001). The median time on broad-spectrum antibiotics was 45.2 hours in the preintervention group vs 46.6 hours in the postintervention group (P = .99). The median time on appropriate antibiotics in the preintervention group was 2.3 hours vs 1.9 hours in the postintervention group (P = .79). Differences in other measured outcomes between the groups were not statistically significant (Table 2).
Although implementation of rapid diagnostic technology reduced the median time to optimal antibiotics, the results were not statistically significant. Shorter time to organism identification in the postintervention group compared to the preintervention group was the lone statistically significant metric (P < .001).
Discussion
A lack of statistical significance in the primary outcome may have been due to nonadherence to facility de-escalation protocols or a suboptimal BioFire BCID2 result notification system. Additionally, use of rapid BCID at VHI may improve over time as clinicians become more familiar with the technology. Gaps in clinical pharmacy coverage during the night shift may have also contributed to delays in antibiotic optimization, particularly if other clinicians are not equipped with the knowledge or training to appropriately deescalate antibiotics based on microorganisms identified. A 2017 study by Donner et al concluded that physician interpretation of BCID results is suboptimal and should be augmented with clinical decision support tools as new technology becomes available.8 Despite the statistically insignificant results of this study, it did highlight potential areas of improvement which can lead to improved patient care.
Previous research has evaluated the impact of rapid BCID technology on antibiotic treatment and clinical outcomes. Chiasson et al found that median time to optimal therapy was 73.8 hours in the pre-BCID arm compared to 34.7 hours in the post- BCID arm (P ≤ .001), emphasizing the importance of combining rapid BCID with clinical decision support tools and pharmacy input.6 Senok et al found that BCID2 implementation led to a significant decrease in median time to culture result, which informed optimal antibiotic therapy and decreased 30-day mortality in the intensive care setting.9 In contrast, the current study did not stratify patients according to medical ward or illness severity even though clinicians may be less likely to de-escalate antibiotic therapy in critically ill patients.
Bae et al reported findings consistent with the current study and concluded that BCID did not affect the clinical outcomes of overall BSIs; however, it contributed to early administration of effective antibiotics in cases of BSIs caused by multidrug-resistant organisms.10 Results of this study were not stratified according to multidrug-resistant organisms because the sample size was too small. The current study also included patients with polymicrobial infections, which may have impacted the results due to a less streamlined approach to antibiotic optimization.
Limitations
This single-center, retrospective study had a small sample size, short time frame, and lacked patient diversity, and therefore may not be generalizable to other health care systems. The sample size was limited by shorter date range and smaller patient list between BioFire BCID2 implementation and data collection, which was used to determine the number of charts selected in each group. Some patients received antibiotics prior to blood cultures being drawn, which may falsely decrease time to optimal/ appropriate antibiotics and falsely increase time on broad spectrum/any antibiotics due to early antibiotic administration. The total number of patients on broad-spectrum antibiotics differed from the total number of patients for other outcomes because several patients never received the defined broad spectrum antibiotics.
Conclusions
When combined with a pre-existing ASP without active notification, the implementation of BioFire BCID2 did not return statistically significant data showing a decrease in time to optimal antibiotics, time to appropriate antibiotics, or time on broad-spectrum antibiotics at VHI. To make this program more successful, pharmacist intervention and clinical decision support tools may be needed.
Additional research is required to determine the optimal integration of antimicrobial stewardship, rapid diagnostic technology, and pharmacy services for maximum benefit. Even though the primary outcome was not statistically significant, the results may be clinically significant from a stewardship perspective. Realigning microbiology workflows to mimic other research, which emphasizes the importance of funneling rapid BCID results through the ASP, may improve outcomes. Future studies may be warranted following the implementation of clinical decision support tools to assess their impact on stewardship practices and patient outcomes.
About 530,000 to 628,000 episodes of bloodstream infections (BSI) occur annually in the US.1 Early identification and treatment of bacteremia are essential to improve patient outcomes because it allows for more timely targeted antibiotic therapy.2 Organism identification and susceptibility testing can take 2 to 5 days, prolonging the use of broad-spectrum empiric antibiotics and increasing the risk of adverse events.3,4 The Infectious Disease Society of America recommends the use of rapid diagnostic testing and antimicrobial stewardship programs (ASPs) to improve rates of antibiotic susceptibilities to targeted antibiotics and optimize resource utilization.3 Rapid blood culture identification (BCID) technologies reduce the duration of empiric antibiotics in patients with contaminated blood cultures, resulting in shorter hospital stays and saving money per each patient tested.4
In March 2023, Veteran Health Indiana (VHI) implemented the BioFire FilmArray Blood Culture Identification (BCID2), a BSI panel test that identifies select gram-negative bacteria, gram-positive bacteria, yeast, and antimicrobial resistance genes with an aggregate sensitivity of 99% and a specificity of 99.8%. The BCID2 presents clinically relevant information faster than traditional culture methods, allowing clinicians to make more efficient and educated antibiotic regimen decisions than with previous methods.5
It takes 24 to 48 hours from blood collection for culture incubation, positivity, and gram staining to occur at VHI. If the gram stain is positive, the blood culture is placed on the BioFire BCID2 in addition to traditional culture medium. BioFire BCID2 results are ready in 45 to 60 minutes. Results are uploaded into the electronic health record (EHR) ≤ 2 hours after they are obtained and the primary team is notified if the test is positive for certain critical results. Susceptibility testing of an identified organism typically requires an additional 24 to 48 hours for finalization. VHI Infectious Disease created an evidence-based antibiotic recommendation chart for certain medication(s) and alternate therapies based on the reported organism and its interpreted presence of resistance markers (eg, ceftriaxone for Escherichia coli when extended-spectrum beta lactamases are not detected vs meropenem if extended-spectrum beta lactamases marker are present). These charts optimize the antibiotic regimen while awaiting susceptibility finalizations.
Two previous studies describe the impact of rapid diagnostic testing technology at US Department of Veterans Affairs (VA) medical centers.6,7 In Texas, the ASP reviewed BCID panel results via clinical decision support software for about 1 hour per day.6 A Los Angeles study analyzed the impact of Biofire BCID with an interpretation guide centered on unnecessary vancomycin use and determined that shorter duration of the medication may have been the result of more frequent infectious disease consultation.7
This study assessed the time to optimal antibiotic de-escalation before and after the implementation of BioFire BCID2 with results reviewed by the ASP without active notification or assistance of any clinical decision support technology. The primary objective was to evaluate difference in time to optimal antibiotics from blood culture draw pre- vs postintervention. Secondary objectives included differences in time to organism identification, difference in time on broad-spectrum antibiotics, and difference in time to appropriate antibiotics.
Methods
This quasi-experimental retrospective chart review assessed the impact of BioFire BCID2 use on timely antibiotic de-escalation for patients who experienced a BSI at VHI between March 1, 2022, and October 1, 2023. Microbiology laboratory records identified eligible patients with positive blood cultures within the study time frame. Data were collected from the VHI EHR.
Patients were included if they had a positive bacterial blood culture and received ≥ 1 antibiotic indicated for bacteremia while receiving inpatient care. Patients were excluded if they died prior to blood culture results, transferred out of VHI, left against medical advice, or had untreated contaminants in blood culture results (ie, never received antibiotics aimed at the contaminated culture).
Patient lists were generated for before and after implementation of BioFire BCID2 (pre- and postintervention) using the VHI EHR and microbiology laboratory record system. The pre- and postinterventions groups were different sizes. As a result, a random sampling of the preintervention group was selected and included patients from March 1, 2022, through March 26, 2023. The postintervention group was smaller due to time constraints between initiation of BioFire BCID2 for data collection and included all patients from March 27, 2023, through October 1, 2023.
Optimal antibiotics were defined as escalation from inappropriate therapy to broader agent(s), de-escalation from broad-spectrum therapy to targeted agent(s), discontinuation of therapy due to an organism being identified as a contaminant, or optimization of a regimen to the preferred antimicrobial agent based on evidence-based consensus guidelines. Broad-spectrum antibiotics included: piperacillin/tazobactam, cefepime, ceftazidime, ceftazidime-avibactam, cefiderocol, carbapenems, fluroquinolones, vancomycin, daptomycin, ceftaroline, linezolid, or aztreonam. Appropriate antibiotics were defined as those with activity toward the final identified organism(s).
Deidentified participant data were entered into Microsoft Excel and kept on a secure VA server to complete statistical analyses. Parametric continuous data, such as age, were analyzed using the t-test, while nonparametric continuous data, such as time to optimal antibiotics, were analyzed using the Mann-Whitney U test. Categorical data, like sex and race, were analyzed using either Fisher exact test for small sample sizes or X2 test for a larger sample size. Statistical significance levels was defined as P < .05.
Results
Using patient lists drawn from the EHR and the microbiology laboratory records, 110 electronic charts were randomly selected for review. Fifteen patients were excluded: 8 had untreated contaminants, 4 died, and 3 were transferred out of VHI. Of the 95 patients included, 48 were in the preintervention group and 47 were in the postintervention group (Figure 1).
Baseline characteristics were similar between the 2 groups (Table 1). Most patients were White males aged > 70 years in the EHR. The urinary tract was the most common source of infection, impacting 12 patients in each group (Figure 2). Escherichia coli, Klebsiella, Staphylococcus, and Streptococcus were the most common bloodstream isolates identified.
The median time to optimal antibiotics in the preintervention group was 58.5 hours vs 43.4 hours in the postintervention group (P = .11). The median time to organism identification was 37.8 hours in the preintervention group vs 16.9 hours in the postintervention group (P < .001). The median time on broad-spectrum antibiotics was 45.2 hours in the preintervention group vs 46.6 hours in the postintervention group (P = .99). The median time on appropriate antibiotics in the preintervention group was 2.3 hours vs 1.9 hours in the postintervention group (P = .79). Differences in other measured outcomes between the groups were not statistically significant (Table 2).
Although implementation of rapid diagnostic technology reduced the median time to optimal antibiotics, the results were not statistically significant. Shorter time to organism identification in the postintervention group compared to the preintervention group was the lone statistically significant metric (P < .001).
Discussion
A lack of statistical significance in the primary outcome may have been due to nonadherence to facility de-escalation protocols or a suboptimal BioFire BCID2 result notification system. Additionally, use of rapid BCID at VHI may improve over time as clinicians become more familiar with the technology. Gaps in clinical pharmacy coverage during the night shift may have also contributed to delays in antibiotic optimization, particularly if other clinicians are not equipped with the knowledge or training to appropriately deescalate antibiotics based on microorganisms identified. A 2017 study by Donner et al concluded that physician interpretation of BCID results is suboptimal and should be augmented with clinical decision support tools as new technology becomes available.8 Despite the statistically insignificant results of this study, it did highlight potential areas of improvement which can lead to improved patient care.
Previous research has evaluated the impact of rapid BCID technology on antibiotic treatment and clinical outcomes. Chiasson et al found that median time to optimal therapy was 73.8 hours in the pre-BCID arm compared to 34.7 hours in the post- BCID arm (P ≤ .001), emphasizing the importance of combining rapid BCID with clinical decision support tools and pharmacy input.6 Senok et al found that BCID2 implementation led to a significant decrease in median time to culture result, which informed optimal antibiotic therapy and decreased 30-day mortality in the intensive care setting.9 In contrast, the current study did not stratify patients according to medical ward or illness severity even though clinicians may be less likely to de-escalate antibiotic therapy in critically ill patients.
Bae et al reported findings consistent with the current study and concluded that BCID did not affect the clinical outcomes of overall BSIs; however, it contributed to early administration of effective antibiotics in cases of BSIs caused by multidrug-resistant organisms.10 Results of this study were not stratified according to multidrug-resistant organisms because the sample size was too small. The current study also included patients with polymicrobial infections, which may have impacted the results due to a less streamlined approach to antibiotic optimization.
Limitations
This single-center, retrospective study had a small sample size, short time frame, and lacked patient diversity, and therefore may not be generalizable to other health care systems. The sample size was limited by shorter date range and smaller patient list between BioFire BCID2 implementation and data collection, which was used to determine the number of charts selected in each group. Some patients received antibiotics prior to blood cultures being drawn, which may falsely decrease time to optimal/ appropriate antibiotics and falsely increase time on broad spectrum/any antibiotics due to early antibiotic administration. The total number of patients on broad-spectrum antibiotics differed from the total number of patients for other outcomes because several patients never received the defined broad spectrum antibiotics.
Conclusions
When combined with a pre-existing ASP without active notification, the implementation of BioFire BCID2 did not return statistically significant data showing a decrease in time to optimal antibiotics, time to appropriate antibiotics, or time on broad-spectrum antibiotics at VHI. To make this program more successful, pharmacist intervention and clinical decision support tools may be needed.
Additional research is required to determine the optimal integration of antimicrobial stewardship, rapid diagnostic technology, and pharmacy services for maximum benefit. Even though the primary outcome was not statistically significant, the results may be clinically significant from a stewardship perspective. Realigning microbiology workflows to mimic other research, which emphasizes the importance of funneling rapid BCID results through the ASP, may improve outcomes. Future studies may be warranted following the implementation of clinical decision support tools to assess their impact on stewardship practices and patient outcomes.
- Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect. 2013;19(6):501- 509. doi:10.1111/1469-0691.12195
- Pardo J, Klinker KP, Borgert SJ, Butler BM, Giglio PG, Rand KH. Clinical and economic impact of antimicrobial stewardship interventions with the FilmArray blood culture identification panel. Diagn Microbiol Infect Dis. 2016;84(2):159-164. doi:10.1016/j.diagmicrobio.2015.10.023.
- Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program: guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77. doi:10.1093/cid/ciw118
- BIOFIRE® Blood Culture Identification 2 (BCID2) Panel. Biomerierux. Updated 2025. Accessed May 10, 2025. https://www.biofiredx.com/products/the-filmarray-panels/filmarraybcid/
- Huang AM, Newton D, Kunapuli A, et al. Impact of rapid organism identification via matrix-assisted laser desorption/ionization time-of-flight combined with antimicrobial stewardship team intervention in adult patients with bacteremia and candidemia. Clin Infect Dis. 2013;57(9):1237-1245. doi:10.1093/cid/cit498
- Chiasson JM, Smith WJ, Jodlowski TZ, Kouma MA, Cutrell JB. Impact of a rapid blood culture diagnostic panel on time to optimal antimicrobial therapy at a veterans affairs medical center. J Pharm Pract. 2022;35(5):722-729. doi:10.1177/08971900211000686
- Wu S, Watson RL, Graber CJ. 2007. Impact of combining rapid diagnostics with an interpretation guide on vancomycin usage for contaminant blood cultures growing coagulase- negative staphylococci (CoNS). Open Forum Infect Dis. 2019;6(Suppl 2):S674. doi:10.1093/ofid/ofz360.1687
- Donner LM, Campbell WS, Lyden E, Van Schooneveld TC. Assessment of rapid-blood-culture-identification result interpretation and antibiotic prescribing practices. J Clin Microbiol. 2017;55(5):1496-1507. doi:10.1128/JCM.02395-16
- Senok A, Dabal LA, Alfaresi M, et al. Clinical impact of the BIOFIRE blood culture identification 2 panel in adult patients with bloodstream infection: a multicentre observational study in the United Arab Emirates. Diagnostics (Basel). 2023;13(14):2433. doi:10.3390/diagnostics13142433
- Bae JY, Bae J, So MK, Choi HJ, Lee M. The impact of the rapid blood culture identification panel on antibiotic treatment and clinical outcomes in bloodstream infections, particularly those associated with multidrug-resistant micro-organisms. Diagnostics (Basel). 2023;13(23):3504. doi:10.3390/diagnostics13233504
- Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect. 2013;19(6):501- 509. doi:10.1111/1469-0691.12195
- Pardo J, Klinker KP, Borgert SJ, Butler BM, Giglio PG, Rand KH. Clinical and economic impact of antimicrobial stewardship interventions with the FilmArray blood culture identification panel. Diagn Microbiol Infect Dis. 2016;84(2):159-164. doi:10.1016/j.diagmicrobio.2015.10.023.
- Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program: guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77. doi:10.1093/cid/ciw118
- BIOFIRE® Blood Culture Identification 2 (BCID2) Panel. Biomerierux. Updated 2025. Accessed May 10, 2025. https://www.biofiredx.com/products/the-filmarray-panels/filmarraybcid/
- Huang AM, Newton D, Kunapuli A, et al. Impact of rapid organism identification via matrix-assisted laser desorption/ionization time-of-flight combined with antimicrobial stewardship team intervention in adult patients with bacteremia and candidemia. Clin Infect Dis. 2013;57(9):1237-1245. doi:10.1093/cid/cit498
- Chiasson JM, Smith WJ, Jodlowski TZ, Kouma MA, Cutrell JB. Impact of a rapid blood culture diagnostic panel on time to optimal antimicrobial therapy at a veterans affairs medical center. J Pharm Pract. 2022;35(5):722-729. doi:10.1177/08971900211000686
- Wu S, Watson RL, Graber CJ. 2007. Impact of combining rapid diagnostics with an interpretation guide on vancomycin usage for contaminant blood cultures growing coagulase- negative staphylococci (CoNS). Open Forum Infect Dis. 2019;6(Suppl 2):S674. doi:10.1093/ofid/ofz360.1687
- Donner LM, Campbell WS, Lyden E, Van Schooneveld TC. Assessment of rapid-blood-culture-identification result interpretation and antibiotic prescribing practices. J Clin Microbiol. 2017;55(5):1496-1507. doi:10.1128/JCM.02395-16
- Senok A, Dabal LA, Alfaresi M, et al. Clinical impact of the BIOFIRE blood culture identification 2 panel in adult patients with bloodstream infection: a multicentre observational study in the United Arab Emirates. Diagnostics (Basel). 2023;13(14):2433. doi:10.3390/diagnostics13142433
- Bae JY, Bae J, So MK, Choi HJ, Lee M. The impact of the rapid blood culture identification panel on antibiotic treatment and clinical outcomes in bloodstream infections, particularly those associated with multidrug-resistant micro-organisms. Diagnostics (Basel). 2023;13(23):3504. doi:10.3390/diagnostics13233504
Impact of Rapid Blood Culture Identification on Antibiotic De-escalation at a Veterans Affairs Medical Center
Impact of Rapid Blood Culture Identification on Antibiotic De-escalation at a Veterans Affairs Medical Center
