User login
ER+ HER2− early BC: Patients with PEPI 0-1/pCR can safely skip adjuvant chemotherapy
Key clinical point: Postmenopausal patients with estrogen receptor-positive (ER+), human epidermal growth factor receptor 2-negative (HER2−) breast cancer (BC) who achieve a preoperative endocrine prognostic index (PEPI) score of 0-1/pathological complete response (pCR) with only neoadjuvant endocrine therapy (NET) can be safely treated without adjuvant chemotherapy.
Major finding: After a median follow-up of 60 months, the 5-year recurrence-free survival (RFS) improved significantly in patients who had PEPI 0-1/pCR without chemotherapy vs PEPI ≥2 (hazard ratio 0.18; P = .028). In patients who had PEPI ≥2, the 5-year RFS was similar regardless of the receipt of adjuvant chemotherapy (P = .432).
Study details: Findings are from a phase 2 trial including 352 postmenopausal women with early-stage, strongly ER+ and HER2− BC who received NET for 4 months before surgery; after surgery, patients with PEPI 0-1/pCR and PEPI ≥2 were recommended only adjuvant ET and adjuvant ET±chemotherapy, respectively.
Disclosures: This study was supported by Novartis. The authors declared no conflicts of interest.
Source: Wang X et al. Neoadjuvant endocrine therapy for strongly hormone receptor-positive and HER2-negative early breast cancer: results of a prospective multi-center study. Breast Cancer Res Treat. 2022 (Aug 2(. Doi: 10.1007/s10549-022-06686-1
Key clinical point: Postmenopausal patients with estrogen receptor-positive (ER+), human epidermal growth factor receptor 2-negative (HER2−) breast cancer (BC) who achieve a preoperative endocrine prognostic index (PEPI) score of 0-1/pathological complete response (pCR) with only neoadjuvant endocrine therapy (NET) can be safely treated without adjuvant chemotherapy.
Major finding: After a median follow-up of 60 months, the 5-year recurrence-free survival (RFS) improved significantly in patients who had PEPI 0-1/pCR without chemotherapy vs PEPI ≥2 (hazard ratio 0.18; P = .028). In patients who had PEPI ≥2, the 5-year RFS was similar regardless of the receipt of adjuvant chemotherapy (P = .432).
Study details: Findings are from a phase 2 trial including 352 postmenopausal women with early-stage, strongly ER+ and HER2− BC who received NET for 4 months before surgery; after surgery, patients with PEPI 0-1/pCR and PEPI ≥2 were recommended only adjuvant ET and adjuvant ET±chemotherapy, respectively.
Disclosures: This study was supported by Novartis. The authors declared no conflicts of interest.
Source: Wang X et al. Neoadjuvant endocrine therapy for strongly hormone receptor-positive and HER2-negative early breast cancer: results of a prospective multi-center study. Breast Cancer Res Treat. 2022 (Aug 2(. Doi: 10.1007/s10549-022-06686-1
Key clinical point: Postmenopausal patients with estrogen receptor-positive (ER+), human epidermal growth factor receptor 2-negative (HER2−) breast cancer (BC) who achieve a preoperative endocrine prognostic index (PEPI) score of 0-1/pathological complete response (pCR) with only neoadjuvant endocrine therapy (NET) can be safely treated without adjuvant chemotherapy.
Major finding: After a median follow-up of 60 months, the 5-year recurrence-free survival (RFS) improved significantly in patients who had PEPI 0-1/pCR without chemotherapy vs PEPI ≥2 (hazard ratio 0.18; P = .028). In patients who had PEPI ≥2, the 5-year RFS was similar regardless of the receipt of adjuvant chemotherapy (P = .432).
Study details: Findings are from a phase 2 trial including 352 postmenopausal women with early-stage, strongly ER+ and HER2− BC who received NET for 4 months before surgery; after surgery, patients with PEPI 0-1/pCR and PEPI ≥2 were recommended only adjuvant ET and adjuvant ET±chemotherapy, respectively.
Disclosures: This study was supported by Novartis. The authors declared no conflicts of interest.
Source: Wang X et al. Neoadjuvant endocrine therapy for strongly hormone receptor-positive and HER2-negative early breast cancer: results of a prospective multi-center study. Breast Cancer Res Treat. 2022 (Aug 2(. Doi: 10.1007/s10549-022-06686-1
Oral paclitaxel+encequidar offers a possible alternative to IV paclitaxel in metastatic BC
Key clinical point: Patients with metastatic breast cancer (BC) who received oral paclitaxel plus encequidar to facilitate the absorption of oral paclitaxel showed higher confirmed tumor response compared with 3 weekly intravenous (IV) paclitaxel doses.
Major finding: Confirmed tumor response rate improved significantly with oral paclitaxel+encequidar vs IV paclitaxel (36% vs 23%; P = .011). The incidence of grade ≥2 neuropathy (31% vs 8%) and grade 2 alopecia (48% vs 29%) were higher with IV paclitaxel vs oral paclitaxel+encequidar; however, the incidence of grade ≥3 gastrointestinal disorders (11.7% vs 3.7%) was higher with oral paclitaxel+encequidar vs IV paclitaxel.
Study details: Findings are from the open-label, phase 3 study including 402 postmenopausal women with metastatic BC who were randomly assigned to receive oral paclitaxel+encequidar or IV paclitaxel.
Disclosures: This study was supported by Athenex, Inc. Four authors declared being employees and owning stocks in Athenex, and the other authors reported ties with several sources, including Athenex.
Source: Rugo HS et al. Open-label, randomized, multicenter, phase III study comparing oral paclitaxel plus encequidar versus intravenous paclitaxel in patients with metastatic breast cancer. J Clin Oncol. 2022 (Jul 20). Doi: 10.1200/JCO.21.02953
Key clinical point: Patients with metastatic breast cancer (BC) who received oral paclitaxel plus encequidar to facilitate the absorption of oral paclitaxel showed higher confirmed tumor response compared with 3 weekly intravenous (IV) paclitaxel doses.
Major finding: Confirmed tumor response rate improved significantly with oral paclitaxel+encequidar vs IV paclitaxel (36% vs 23%; P = .011). The incidence of grade ≥2 neuropathy (31% vs 8%) and grade 2 alopecia (48% vs 29%) were higher with IV paclitaxel vs oral paclitaxel+encequidar; however, the incidence of grade ≥3 gastrointestinal disorders (11.7% vs 3.7%) was higher with oral paclitaxel+encequidar vs IV paclitaxel.
Study details: Findings are from the open-label, phase 3 study including 402 postmenopausal women with metastatic BC who were randomly assigned to receive oral paclitaxel+encequidar or IV paclitaxel.
Disclosures: This study was supported by Athenex, Inc. Four authors declared being employees and owning stocks in Athenex, and the other authors reported ties with several sources, including Athenex.
Source: Rugo HS et al. Open-label, randomized, multicenter, phase III study comparing oral paclitaxel plus encequidar versus intravenous paclitaxel in patients with metastatic breast cancer. J Clin Oncol. 2022 (Jul 20). Doi: 10.1200/JCO.21.02953
Key clinical point: Patients with metastatic breast cancer (BC) who received oral paclitaxel plus encequidar to facilitate the absorption of oral paclitaxel showed higher confirmed tumor response compared with 3 weekly intravenous (IV) paclitaxel doses.
Major finding: Confirmed tumor response rate improved significantly with oral paclitaxel+encequidar vs IV paclitaxel (36% vs 23%; P = .011). The incidence of grade ≥2 neuropathy (31% vs 8%) and grade 2 alopecia (48% vs 29%) were higher with IV paclitaxel vs oral paclitaxel+encequidar; however, the incidence of grade ≥3 gastrointestinal disorders (11.7% vs 3.7%) was higher with oral paclitaxel+encequidar vs IV paclitaxel.
Study details: Findings are from the open-label, phase 3 study including 402 postmenopausal women with metastatic BC who were randomly assigned to receive oral paclitaxel+encequidar or IV paclitaxel.
Disclosures: This study was supported by Athenex, Inc. Four authors declared being employees and owning stocks in Athenex, and the other authors reported ties with several sources, including Athenex.
Source: Rugo HS et al. Open-label, randomized, multicenter, phase III study comparing oral paclitaxel plus encequidar versus intravenous paclitaxel in patients with metastatic breast cancer. J Clin Oncol. 2022 (Jul 20). Doi: 10.1200/JCO.21.02953
ERBB2-positive BC: Adding atezolizumab to PATH shows acceptable pCR rate in phase 2
Key clinical point: Neoadjuvant atezolizumab plus docetaxel, trastuzumab, and pertuzumab (PATH) demonstrated an acceptable pathological complete response (pCR) rate and a modest safety profile in patients with human epidermal growth factor receptor 2 (ERBB2)-positive early breast cancer (BC).
Major finding: Rate of pCR was 61% in the overall cohort and was higher in patients with hormone receptor-negative vs -positive subtype (77% vs 44%), stages IIA and IIB vs stage III BC (69% and 70% vs 39% respectively), and positive vs negative programmed cell death 1 expression (100% vs 53%). Few patients reported grade ≥3 neutropenia (12%) and febrile neutropenia (8%).
Study details: Findings are from a single-arm phase 2 trial including 67 patients with ERBB2-positive stage II/III BC who initiated 6 cycles of PATH+atezolizumab every 3 weeks.
Disclosures: This study was supported by the Ministry of Health and Welfare, Republic of Korea, and other sources. The authors declared serving on advisory boards or receiving personal fees, grants, honoraria, consulting fees, or nonfinancial support from several sources.
Source: Ahn HK et al. Response rate and safety of a neoadjuvant pertuzumab, atezolizumab, docetaxel, and trastuzumab regimen for patients with ERBB2-positive stage II/III breast cancer: The neo-PATH phase 2 nonrandomized clinical trial. JAMA Oncol. 2022 (Jul 7). Doi: 10.1001/jamaoncol.2022.2310
Key clinical point: Neoadjuvant atezolizumab plus docetaxel, trastuzumab, and pertuzumab (PATH) demonstrated an acceptable pathological complete response (pCR) rate and a modest safety profile in patients with human epidermal growth factor receptor 2 (ERBB2)-positive early breast cancer (BC).
Major finding: Rate of pCR was 61% in the overall cohort and was higher in patients with hormone receptor-negative vs -positive subtype (77% vs 44%), stages IIA and IIB vs stage III BC (69% and 70% vs 39% respectively), and positive vs negative programmed cell death 1 expression (100% vs 53%). Few patients reported grade ≥3 neutropenia (12%) and febrile neutropenia (8%).
Study details: Findings are from a single-arm phase 2 trial including 67 patients with ERBB2-positive stage II/III BC who initiated 6 cycles of PATH+atezolizumab every 3 weeks.
Disclosures: This study was supported by the Ministry of Health and Welfare, Republic of Korea, and other sources. The authors declared serving on advisory boards or receiving personal fees, grants, honoraria, consulting fees, or nonfinancial support from several sources.
Source: Ahn HK et al. Response rate and safety of a neoadjuvant pertuzumab, atezolizumab, docetaxel, and trastuzumab regimen for patients with ERBB2-positive stage II/III breast cancer: The neo-PATH phase 2 nonrandomized clinical trial. JAMA Oncol. 2022 (Jul 7). Doi: 10.1001/jamaoncol.2022.2310
Key clinical point: Neoadjuvant atezolizumab plus docetaxel, trastuzumab, and pertuzumab (PATH) demonstrated an acceptable pathological complete response (pCR) rate and a modest safety profile in patients with human epidermal growth factor receptor 2 (ERBB2)-positive early breast cancer (BC).
Major finding: Rate of pCR was 61% in the overall cohort and was higher in patients with hormone receptor-negative vs -positive subtype (77% vs 44%), stages IIA and IIB vs stage III BC (69% and 70% vs 39% respectively), and positive vs negative programmed cell death 1 expression (100% vs 53%). Few patients reported grade ≥3 neutropenia (12%) and febrile neutropenia (8%).
Study details: Findings are from a single-arm phase 2 trial including 67 patients with ERBB2-positive stage II/III BC who initiated 6 cycles of PATH+atezolizumab every 3 weeks.
Disclosures: This study was supported by the Ministry of Health and Welfare, Republic of Korea, and other sources. The authors declared serving on advisory boards or receiving personal fees, grants, honoraria, consulting fees, or nonfinancial support from several sources.
Source: Ahn HK et al. Response rate and safety of a neoadjuvant pertuzumab, atezolizumab, docetaxel, and trastuzumab regimen for patients with ERBB2-positive stage II/III breast cancer: The neo-PATH phase 2 nonrandomized clinical trial. JAMA Oncol. 2022 (Jul 7). Doi: 10.1001/jamaoncol.2022.2310
TNBC: First-line nab-paclitaxel+cisplatin effective and safe in phase 3
Key clinical point: In patients with metastatic triple-negative breast cancer (TNBC), first-line treatment with nanoparticle albumin-bound (nab)-paclitaxel+cisplatin significantly reduced the risk for disease progression/death compared with gemcitabine+cisplatin, with both the combinations showing a consistent safety profile.
Major finding: Progression-free survival (stratified hazard ratio 0.67; P = .004) and objective response rate (81.1% vs 56.3%; P < .001) improved significantly in patients receiving nab-paclitaxel+cisplatin vs gemcitabine+cisplatin. Grade ≥3 only neuropathy (19% vs 0%) and nausea and vomiting (6% vs 1%) were higher in the nab-paclitaxel+cisplatin vs gemcitabine+cisplatin arm, whereas grade ≥3 thrombocytopenia (29.4% vs 3.9%) was more common in the gemcitabine+cisplatin vs nab-paclitaxel+cisplatin arm.
Study details: Findings are from an open-label phase 3 study including 254 patients with untreated metastatic TNBC who were randomly assigned to receive nab-paclitaxel+cisplatin or gemcitabine+cisplatin.
Disclosures: This study was funded by the National Natural Science Foundation of China. The authors declared no conflicts of interest.
Source: Wang B et al. A randomized phase 3 trial of gemcitabine or nab-paclitaxel combined with cisplatin as first-line treatment in patients with metastatic triple-negative breast cancer. Nat Commun. 2022;13:4025 (Jul 12). Doi: 10.1038/s41467-022-31704-7
Key clinical point: In patients with metastatic triple-negative breast cancer (TNBC), first-line treatment with nanoparticle albumin-bound (nab)-paclitaxel+cisplatin significantly reduced the risk for disease progression/death compared with gemcitabine+cisplatin, with both the combinations showing a consistent safety profile.
Major finding: Progression-free survival (stratified hazard ratio 0.67; P = .004) and objective response rate (81.1% vs 56.3%; P < .001) improved significantly in patients receiving nab-paclitaxel+cisplatin vs gemcitabine+cisplatin. Grade ≥3 only neuropathy (19% vs 0%) and nausea and vomiting (6% vs 1%) were higher in the nab-paclitaxel+cisplatin vs gemcitabine+cisplatin arm, whereas grade ≥3 thrombocytopenia (29.4% vs 3.9%) was more common in the gemcitabine+cisplatin vs nab-paclitaxel+cisplatin arm.
Study details: Findings are from an open-label phase 3 study including 254 patients with untreated metastatic TNBC who were randomly assigned to receive nab-paclitaxel+cisplatin or gemcitabine+cisplatin.
Disclosures: This study was funded by the National Natural Science Foundation of China. The authors declared no conflicts of interest.
Source: Wang B et al. A randomized phase 3 trial of gemcitabine or nab-paclitaxel combined with cisplatin as first-line treatment in patients with metastatic triple-negative breast cancer. Nat Commun. 2022;13:4025 (Jul 12). Doi: 10.1038/s41467-022-31704-7
Key clinical point: In patients with metastatic triple-negative breast cancer (TNBC), first-line treatment with nanoparticle albumin-bound (nab)-paclitaxel+cisplatin significantly reduced the risk for disease progression/death compared with gemcitabine+cisplatin, with both the combinations showing a consistent safety profile.
Major finding: Progression-free survival (stratified hazard ratio 0.67; P = .004) and objective response rate (81.1% vs 56.3%; P < .001) improved significantly in patients receiving nab-paclitaxel+cisplatin vs gemcitabine+cisplatin. Grade ≥3 only neuropathy (19% vs 0%) and nausea and vomiting (6% vs 1%) were higher in the nab-paclitaxel+cisplatin vs gemcitabine+cisplatin arm, whereas grade ≥3 thrombocytopenia (29.4% vs 3.9%) was more common in the gemcitabine+cisplatin vs nab-paclitaxel+cisplatin arm.
Study details: Findings are from an open-label phase 3 study including 254 patients with untreated metastatic TNBC who were randomly assigned to receive nab-paclitaxel+cisplatin or gemcitabine+cisplatin.
Disclosures: This study was funded by the National Natural Science Foundation of China. The authors declared no conflicts of interest.
Source: Wang B et al. A randomized phase 3 trial of gemcitabine or nab-paclitaxel combined with cisplatin as first-line treatment in patients with metastatic triple-negative breast cancer. Nat Commun. 2022;13:4025 (Jul 12). Doi: 10.1038/s41467-022-31704-7
New panic disorder model flags risk for recurrence, persistence
Investigators based in France and the United States analyzed data for almost 800 patients with DSM-IV–diagnosed PD.
Results showed that having a “general psychopathology factor,” defined as the shared effects of all comorbid conditions, or PD liability, significantly and independently predicted 3-year recurrence or persistence of PD symptoms.

Having a lower physical health-related quality of life (QOL), a greater number of stressful life events, and not seeking treatment at baseline were also significant and independent predictors.
“This integrative model could help clinicians to identify individuals at high risk of recurrence or persistence of panic disorder and provide content for future research,” Valentin Scheer, MD, MPH, a resident in psychiatry at AP-HP, Assistance Publique, Hôpitaux de Paris, and colleagues wrote.
The findings were published online in the Journal of Clinical Psychiatry.
Integration needed
PD is a disabling disorder with a “chronic course” – and a recurrence rate ranging from 25% to 50%, the investigators noted.
“Because of the heterogeneous course of PD, there is a need to develop a comprehensive predictive model of recurrence or persistence,” they wrote. This could “help practitioners adapt therapeutic strategies and develop prevention strategies in high-risk individuals.”
Most previous studies that have investigated risk factors for PD recurrence and persistence have relied on clinical samples, often with limited sample sizes.
Moreover, each risk factor, when considered individually, accounts for only a “small proportion” of the variance in risk, the researchers noted. The co-occurrence of these risk factors “suggests the need to combine them into a broad multivariable model.”
However, currently proposed integrative models do not identify independent predictors or mitigate the influence of confounding variables. To fill this gap, the investigators conducted a study using structural equation modeling “to take into account multiple correlations across predictors.”
They drew on data from 775 participants (mean age, 40 years) in the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). For the current analysis, they examined two waves of NESARC (2001-2002 and 2004-2005) to “build a comprehensive model” of the 3-year recurrence or persistence of PD.
The researchers used a “latent variable approach” that simultaneously examined the effect of the following five groups of potential predictors of recurrence or persistence: PD severity, severity of comorbidity, family history of psychiatric disorders, sociodemographic characteristics, and treatment-seeking behavior.
They also distinguished between risk factors responsible for recurrence and those responsible for persistence.
Psychiatric diagnoses were determined on the basis of the Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV. Participants also completed Version 2 of the Short Form 12-Item Health Survey, which assesses both mental and physical QOL over the previous 4 weeks.
Early treatment needed
Among participants with a 12-month diagnosis of PD at wave 1, 13% had persistent PD and 27.6% had recurrent PD during the 3-year period. The mean duration of illness was 9.5 years.
A greater number of lifetime panic attacks, the presence of any Axis I or II comorbid disorder, and any Axis I disorder, especially social anxiety disorder, were significantly associated with 3-year risk for recurrence and for persistence.
Sweating, choking, paresthesias, the comorbid disorders of mania/hypomania and general anxiety disorder, nicotine dependence, lower mental and physical QOL scores, and exposure to a greater number of stressful life events in the previous year were all significantly associated with 3-year risk for recurrence.
Only variables shown with a P value were statistically significant, “with the a priori fixed at .05,” the researchers noted.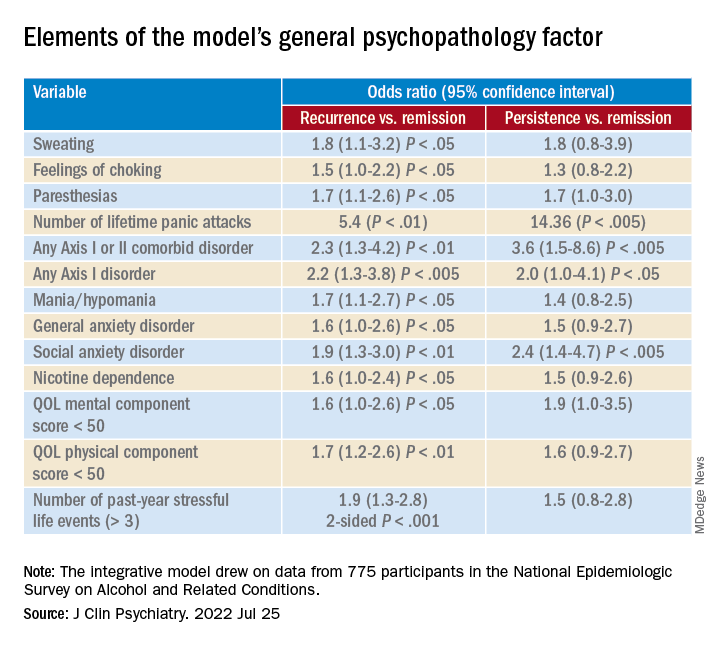
A combination of psychopathology factors, such as the shared effect of all comorbid psychiatric conditions, PD liability, lower physical health-related QOL, more life stressors during the past year, and not seeking treatment at baseline “significantly and independently” predicted recurrence or persistence of symptoms between the two waves (all Ps < .05), the investigators reported.
One study limitation cited was that several psychiatric disorders known to be associated with PD recurrence or persistence, such as borderline personality disorder, were not examined. Additionally, the study used a 3-year follow-up period – and the results might have differed for other follow-up time frames, the researchers noted.
Nevertheless, the findings constitute a “comprehensive model” to predict recurrence and persistence of PD, they wrote. Moreover, early treatment-seeking behavior “should be promoted, as it may reduce the risk of recurrence.”
Not much new?
Commenting on the study, Peter Roy-Byrne, MD, professor of psychiatry, University of Washington, Seattle, noted, “there is not much that is new here.”
Dr. Roy-Byrne, who was not involved with the study, said that a “general theme for years has been that more severe illness, whether you measure it by greater number of other Axis I disorders or symptom severity or a general psychopathology factor, usually predicts worse outcome – here codified as persistence and recurrence.”
Greater stress and reluctance to seek treatment may also predict worse outcomes, he noted.
In addition, the study “did not examine another very important factor: the degree of social connection/social support that someone has,” Dr. Roy-Byrne said. However, “perhaps some of this was contained in specific life events.”
A version of this article first appeared on Medscape.com.
Investigators based in France and the United States analyzed data for almost 800 patients with DSM-IV–diagnosed PD.
Results showed that having a “general psychopathology factor,” defined as the shared effects of all comorbid conditions, or PD liability, significantly and independently predicted 3-year recurrence or persistence of PD symptoms.
Having a lower physical health-related quality of life (QOL), a greater number of stressful life events, and not seeking treatment at baseline were also significant and independent predictors.
“This integrative model could help clinicians to identify individuals at high risk of recurrence or persistence of panic disorder and provide content for future research,” Valentin Scheer, MD, MPH, a resident in psychiatry at AP-HP, Assistance Publique, Hôpitaux de Paris, and colleagues wrote.
The findings were published online in the Journal of Clinical Psychiatry.
Integration needed
PD is a disabling disorder with a “chronic course” – and a recurrence rate ranging from 25% to 50%, the investigators noted.
“Because of the heterogeneous course of PD, there is a need to develop a comprehensive predictive model of recurrence or persistence,” they wrote. This could “help practitioners adapt therapeutic strategies and develop prevention strategies in high-risk individuals.”
Most previous studies that have investigated risk factors for PD recurrence and persistence have relied on clinical samples, often with limited sample sizes.
Moreover, each risk factor, when considered individually, accounts for only a “small proportion” of the variance in risk, the researchers noted. The co-occurrence of these risk factors “suggests the need to combine them into a broad multivariable model.”
However, currently proposed integrative models do not identify independent predictors or mitigate the influence of confounding variables. To fill this gap, the investigators conducted a study using structural equation modeling “to take into account multiple correlations across predictors.”
They drew on data from 775 participants (mean age, 40 years) in the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). For the current analysis, they examined two waves of NESARC (2001-2002 and 2004-2005) to “build a comprehensive model” of the 3-year recurrence or persistence of PD.
The researchers used a “latent variable approach” that simultaneously examined the effect of the following five groups of potential predictors of recurrence or persistence: PD severity, severity of comorbidity, family history of psychiatric disorders, sociodemographic characteristics, and treatment-seeking behavior.
They also distinguished between risk factors responsible for recurrence and those responsible for persistence.
Psychiatric diagnoses were determined on the basis of the Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV. Participants also completed Version 2 of the Short Form 12-Item Health Survey, which assesses both mental and physical QOL over the previous 4 weeks.
Early treatment needed
Among participants with a 12-month diagnosis of PD at wave 1, 13% had persistent PD and 27.6% had recurrent PD during the 3-year period. The mean duration of illness was 9.5 years.
A greater number of lifetime panic attacks, the presence of any Axis I or II comorbid disorder, and any Axis I disorder, especially social anxiety disorder, were significantly associated with 3-year risk for recurrence and for persistence.
Sweating, choking, paresthesias, the comorbid disorders of mania/hypomania and general anxiety disorder, nicotine dependence, lower mental and physical QOL scores, and exposure to a greater number of stressful life events in the previous year were all significantly associated with 3-year risk for recurrence.
Only variables shown with a P value were statistically significant, “with the a priori fixed at .05,” the researchers noted.
A combination of psychopathology factors, such as the shared effect of all comorbid psychiatric conditions, PD liability, lower physical health-related QOL, more life stressors during the past year, and not seeking treatment at baseline “significantly and independently” predicted recurrence or persistence of symptoms between the two waves (all Ps < .05), the investigators reported.
One study limitation cited was that several psychiatric disorders known to be associated with PD recurrence or persistence, such as borderline personality disorder, were not examined. Additionally, the study used a 3-year follow-up period – and the results might have differed for other follow-up time frames, the researchers noted.
Nevertheless, the findings constitute a “comprehensive model” to predict recurrence and persistence of PD, they wrote. Moreover, early treatment-seeking behavior “should be promoted, as it may reduce the risk of recurrence.”
Not much new?
Commenting on the study, Peter Roy-Byrne, MD, professor of psychiatry, University of Washington, Seattle, noted, “there is not much that is new here.”
Dr. Roy-Byrne, who was not involved with the study, said that a “general theme for years has been that more severe illness, whether you measure it by greater number of other Axis I disorders or symptom severity or a general psychopathology factor, usually predicts worse outcome – here codified as persistence and recurrence.”
Greater stress and reluctance to seek treatment may also predict worse outcomes, he noted.
In addition, the study “did not examine another very important factor: the degree of social connection/social support that someone has,” Dr. Roy-Byrne said. However, “perhaps some of this was contained in specific life events.”
A version of this article first appeared on Medscape.com.
Investigators based in France and the United States analyzed data for almost 800 patients with DSM-IV–diagnosed PD.
Results showed that having a “general psychopathology factor,” defined as the shared effects of all comorbid conditions, or PD liability, significantly and independently predicted 3-year recurrence or persistence of PD symptoms.
Having a lower physical health-related quality of life (QOL), a greater number of stressful life events, and not seeking treatment at baseline were also significant and independent predictors.
“This integrative model could help clinicians to identify individuals at high risk of recurrence or persistence of panic disorder and provide content for future research,” Valentin Scheer, MD, MPH, a resident in psychiatry at AP-HP, Assistance Publique, Hôpitaux de Paris, and colleagues wrote.
The findings were published online in the Journal of Clinical Psychiatry.
Integration needed
PD is a disabling disorder with a “chronic course” – and a recurrence rate ranging from 25% to 50%, the investigators noted.
“Because of the heterogeneous course of PD, there is a need to develop a comprehensive predictive model of recurrence or persistence,” they wrote. This could “help practitioners adapt therapeutic strategies and develop prevention strategies in high-risk individuals.”
Most previous studies that have investigated risk factors for PD recurrence and persistence have relied on clinical samples, often with limited sample sizes.
Moreover, each risk factor, when considered individually, accounts for only a “small proportion” of the variance in risk, the researchers noted. The co-occurrence of these risk factors “suggests the need to combine them into a broad multivariable model.”
However, currently proposed integrative models do not identify independent predictors or mitigate the influence of confounding variables. To fill this gap, the investigators conducted a study using structural equation modeling “to take into account multiple correlations across predictors.”
They drew on data from 775 participants (mean age, 40 years) in the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). For the current analysis, they examined two waves of NESARC (2001-2002 and 2004-2005) to “build a comprehensive model” of the 3-year recurrence or persistence of PD.
The researchers used a “latent variable approach” that simultaneously examined the effect of the following five groups of potential predictors of recurrence or persistence: PD severity, severity of comorbidity, family history of psychiatric disorders, sociodemographic characteristics, and treatment-seeking behavior.
They also distinguished between risk factors responsible for recurrence and those responsible for persistence.
Psychiatric diagnoses were determined on the basis of the Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV. Participants also completed Version 2 of the Short Form 12-Item Health Survey, which assesses both mental and physical QOL over the previous 4 weeks.
Early treatment needed
Among participants with a 12-month diagnosis of PD at wave 1, 13% had persistent PD and 27.6% had recurrent PD during the 3-year period. The mean duration of illness was 9.5 years.
A greater number of lifetime panic attacks, the presence of any Axis I or II comorbid disorder, and any Axis I disorder, especially social anxiety disorder, were significantly associated with 3-year risk for recurrence and for persistence.
Sweating, choking, paresthesias, the comorbid disorders of mania/hypomania and general anxiety disorder, nicotine dependence, lower mental and physical QOL scores, and exposure to a greater number of stressful life events in the previous year were all significantly associated with 3-year risk for recurrence.
Only variables shown with a P value were statistically significant, “with the a priori fixed at .05,” the researchers noted.
A combination of psychopathology factors, such as the shared effect of all comorbid psychiatric conditions, PD liability, lower physical health-related QOL, more life stressors during the past year, and not seeking treatment at baseline “significantly and independently” predicted recurrence or persistence of symptoms between the two waves (all Ps < .05), the investigators reported.
One study limitation cited was that several psychiatric disorders known to be associated with PD recurrence or persistence, such as borderline personality disorder, were not examined. Additionally, the study used a 3-year follow-up period – and the results might have differed for other follow-up time frames, the researchers noted.
Nevertheless, the findings constitute a “comprehensive model” to predict recurrence and persistence of PD, they wrote. Moreover, early treatment-seeking behavior “should be promoted, as it may reduce the risk of recurrence.”
Not much new?
Commenting on the study, Peter Roy-Byrne, MD, professor of psychiatry, University of Washington, Seattle, noted, “there is not much that is new here.”
Dr. Roy-Byrne, who was not involved with the study, said that a “general theme for years has been that more severe illness, whether you measure it by greater number of other Axis I disorders or symptom severity or a general psychopathology factor, usually predicts worse outcome – here codified as persistence and recurrence.”
Greater stress and reluctance to seek treatment may also predict worse outcomes, he noted.
In addition, the study “did not examine another very important factor: the degree of social connection/social support that someone has,” Dr. Roy-Byrne said. However, “perhaps some of this was contained in specific life events.”
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Bed boost after WBI reduces local recurrence of ductal carcinoma in situ in the breast
Key clinical point: In patients with ductal carcinoma in situ (DCIS), tumor bed boost after postoperative whole breast irradiation (WBI) reduced local recurrence but with higher toxicity. Hypofractionated WBI was as effective as conventional WBI.
Major finding: The 5-year free-from-local-recurrence rates improved significantly with vs without tumor bed boost after postoperative WBI (hazard ratio 0.47; P < .001) and did not worsen with hypofractionated vs conventional WBI (P = .85). The rates of grade ≥2 breast pain (P = .003) and induration (P < .001) were higher with vs without tumor bed boost.
Study details: Findings are from a multicenter, phase 3 study including 1608 adult women with unilateral, non-low-risk DCIS who underwent breast-conserving surgery and were randomly assigned to receive WBI (conventional or hypofractionated) with or without tumor bed boost.
Disclosures: This study was funded by the National Health and Medical Research Council of Australia and other sources. Some authors declared receiving research grants, funding, or non-direct financial support from several sources.
Source: Chua BH et al. Radiation doses and fractionation schedules in non-low-risk ductal carcinoma in situ in the breast (BIG 3–07/TROG 07.01): A randomised, factorial, multicentre, open-label, phase 3 study Lancet. 2022;400(10350):431-440 (Aug 6). Doi: 10.1016/S0140-6736(22)01246-6
Key clinical point: In patients with ductal carcinoma in situ (DCIS), tumor bed boost after postoperative whole breast irradiation (WBI) reduced local recurrence but with higher toxicity. Hypofractionated WBI was as effective as conventional WBI.
Major finding: The 5-year free-from-local-recurrence rates improved significantly with vs without tumor bed boost after postoperative WBI (hazard ratio 0.47; P < .001) and did not worsen with hypofractionated vs conventional WBI (P = .85). The rates of grade ≥2 breast pain (P = .003) and induration (P < .001) were higher with vs without tumor bed boost.
Study details: Findings are from a multicenter, phase 3 study including 1608 adult women with unilateral, non-low-risk DCIS who underwent breast-conserving surgery and were randomly assigned to receive WBI (conventional or hypofractionated) with or without tumor bed boost.
Disclosures: This study was funded by the National Health and Medical Research Council of Australia and other sources. Some authors declared receiving research grants, funding, or non-direct financial support from several sources.
Source: Chua BH et al. Radiation doses and fractionation schedules in non-low-risk ductal carcinoma in situ in the breast (BIG 3–07/TROG 07.01): A randomised, factorial, multicentre, open-label, phase 3 study Lancet. 2022;400(10350):431-440 (Aug 6). Doi: 10.1016/S0140-6736(22)01246-6
Key clinical point: In patients with ductal carcinoma in situ (DCIS), tumor bed boost after postoperative whole breast irradiation (WBI) reduced local recurrence but with higher toxicity. Hypofractionated WBI was as effective as conventional WBI.
Major finding: The 5-year free-from-local-recurrence rates improved significantly with vs without tumor bed boost after postoperative WBI (hazard ratio 0.47; P < .001) and did not worsen with hypofractionated vs conventional WBI (P = .85). The rates of grade ≥2 breast pain (P = .003) and induration (P < .001) were higher with vs without tumor bed boost.
Study details: Findings are from a multicenter, phase 3 study including 1608 adult women with unilateral, non-low-risk DCIS who underwent breast-conserving surgery and were randomly assigned to receive WBI (conventional or hypofractionated) with or without tumor bed boost.
Disclosures: This study was funded by the National Health and Medical Research Council of Australia and other sources. Some authors declared receiving research grants, funding, or non-direct financial support from several sources.
Source: Chua BH et al. Radiation doses and fractionation schedules in non-low-risk ductal carcinoma in situ in the breast (BIG 3–07/TROG 07.01): A randomised, factorial, multicentre, open-label, phase 3 study Lancet. 2022;400(10350):431-440 (Aug 6). Doi: 10.1016/S0140-6736(22)01246-6
Pembrolizumab+chemotherapy improves OS in a subgroup of patients with advanced TNBC
Key clinical point: First-line treatment with pembrolizumab and chemotherapy improved overall survival (OS) compared with chemotherapy alone in patients with advanced triple-negative breast cancer (TNBC) whose tumors expressed programmed death ligand 1 (PD-L1) with a combined positive score (CPS) of ≥10.
Major finding: Pembrolizumab+chemotherapy vs placebo+chemotherapy improved OS in patients whose tumors expressed PD-L1 with a CPS of ≥10 (hazard ratio for death 0.73; P = .0185); however, no survival benefits were observed in patients with PD-L1 CPS of ≥1 (P = .1125). Grade ≥3 adverse events were reported by 68.1% and 66.9% of patients in the pembrolizumab+chemotherapy and placebo+chemotherapy groups, respectively.
Study details: Findings are from an interim analysis of the phase 3 KEYNOTE-355 trial including 847 patients with locally recurrent inoperable or metastatic TNBC who were randomly assigned to receive pembrolizumab+chemotherapy or placebo+chemotherapy.
Disclosures: This study was funded by Merck Sharp and Dohme. Four authors declared being employees of or owning stocks in Merck, and the other authors reported ties with several sources, including Merck.
Source: Cortes J et al. Pembrolizumab plus chemotherapy in advanced triple-negative breast cancer. N Engl J Med. 2022;387:217-226 (Jul 21). Doi: 10.1056/NEJMoa2202809
Key clinical point: First-line treatment with pembrolizumab and chemotherapy improved overall survival (OS) compared with chemotherapy alone in patients with advanced triple-negative breast cancer (TNBC) whose tumors expressed programmed death ligand 1 (PD-L1) with a combined positive score (CPS) of ≥10.
Major finding: Pembrolizumab+chemotherapy vs placebo+chemotherapy improved OS in patients whose tumors expressed PD-L1 with a CPS of ≥10 (hazard ratio for death 0.73; P = .0185); however, no survival benefits were observed in patients with PD-L1 CPS of ≥1 (P = .1125). Grade ≥3 adverse events were reported by 68.1% and 66.9% of patients in the pembrolizumab+chemotherapy and placebo+chemotherapy groups, respectively.
Study details: Findings are from an interim analysis of the phase 3 KEYNOTE-355 trial including 847 patients with locally recurrent inoperable or metastatic TNBC who were randomly assigned to receive pembrolizumab+chemotherapy or placebo+chemotherapy.
Disclosures: This study was funded by Merck Sharp and Dohme. Four authors declared being employees of or owning stocks in Merck, and the other authors reported ties with several sources, including Merck.
Source: Cortes J et al. Pembrolizumab plus chemotherapy in advanced triple-negative breast cancer. N Engl J Med. 2022;387:217-226 (Jul 21). Doi: 10.1056/NEJMoa2202809
Key clinical point: First-line treatment with pembrolizumab and chemotherapy improved overall survival (OS) compared with chemotherapy alone in patients with advanced triple-negative breast cancer (TNBC) whose tumors expressed programmed death ligand 1 (PD-L1) with a combined positive score (CPS) of ≥10.
Major finding: Pembrolizumab+chemotherapy vs placebo+chemotherapy improved OS in patients whose tumors expressed PD-L1 with a CPS of ≥10 (hazard ratio for death 0.73; P = .0185); however, no survival benefits were observed in patients with PD-L1 CPS of ≥1 (P = .1125). Grade ≥3 adverse events were reported by 68.1% and 66.9% of patients in the pembrolizumab+chemotherapy and placebo+chemotherapy groups, respectively.
Study details: Findings are from an interim analysis of the phase 3 KEYNOTE-355 trial including 847 patients with locally recurrent inoperable or metastatic TNBC who were randomly assigned to receive pembrolizumab+chemotherapy or placebo+chemotherapy.
Disclosures: This study was funded by Merck Sharp and Dohme. Four authors declared being employees of or owning stocks in Merck, and the other authors reported ties with several sources, including Merck.
Source: Cortes J et al. Pembrolizumab plus chemotherapy in advanced triple-negative breast cancer. N Engl J Med. 2022;387:217-226 (Jul 21). Doi: 10.1056/NEJMoa2202809
Which state had the lowest primary cesarean delivery rate (15.5%) in 2021?
[polldaddy:11183184]
[polldaddy:11183184]
[polldaddy:11183184]
Is childhood maltreatment a risk factor for adult atopic dermatitis?
Key clinical point: Childhood maltreatment (CM) is associated with poor physical and mental health outcomes in adults; however, it was not found to be a risk factor for the development of adult atopic dermatitis (AD).
Major finding: Similar proportion of adults with and without AD (20.6% and 21.6%, respectively; P = .80) reported experiencing ≥1 type of moderate-to-severe CM, such as emotional, physical, and sexual abuse and emotional and physical neglect. Neither type of CM was associated with the development of AD in adults.
Study details: Findings are from an analysis of a cross-sectional population-based study including 2973 adults, of which 131 were diagnosed with AD.
Disclosures: This study was funded by the Federal Ministry of Education and Research and other sources. Some authors declared receiving honoraria, research funding, consulting fees, or support for attending meetings or travel from several sources.
Source: Piontek K et al. J Childhood maltreatment is not associated with atopic dermatitis in adults: Results from a cross-sectional population-based cohort study. Eur Acad Dermatol Venereol. 2022 (Aug 3). Doi: 10.1111/jdv.18480
Key clinical point: Childhood maltreatment (CM) is associated with poor physical and mental health outcomes in adults; however, it was not found to be a risk factor for the development of adult atopic dermatitis (AD).
Major finding: Similar proportion of adults with and without AD (20.6% and 21.6%, respectively; P = .80) reported experiencing ≥1 type of moderate-to-severe CM, such as emotional, physical, and sexual abuse and emotional and physical neglect. Neither type of CM was associated with the development of AD in adults.
Study details: Findings are from an analysis of a cross-sectional population-based study including 2973 adults, of which 131 were diagnosed with AD.
Disclosures: This study was funded by the Federal Ministry of Education and Research and other sources. Some authors declared receiving honoraria, research funding, consulting fees, or support for attending meetings or travel from several sources.
Source: Piontek K et al. J Childhood maltreatment is not associated with atopic dermatitis in adults: Results from a cross-sectional population-based cohort study. Eur Acad Dermatol Venereol. 2022 (Aug 3). Doi: 10.1111/jdv.18480
Key clinical point: Childhood maltreatment (CM) is associated with poor physical and mental health outcomes in adults; however, it was not found to be a risk factor for the development of adult atopic dermatitis (AD).
Major finding: Similar proportion of adults with and without AD (20.6% and 21.6%, respectively; P = .80) reported experiencing ≥1 type of moderate-to-severe CM, such as emotional, physical, and sexual abuse and emotional and physical neglect. Neither type of CM was associated with the development of AD in adults.
Study details: Findings are from an analysis of a cross-sectional population-based study including 2973 adults, of which 131 were diagnosed with AD.
Disclosures: This study was funded by the Federal Ministry of Education and Research and other sources. Some authors declared receiving honoraria, research funding, consulting fees, or support for attending meetings or travel from several sources.
Source: Piontek K et al. J Childhood maltreatment is not associated with atopic dermatitis in adults: Results from a cross-sectional population-based cohort study. Eur Acad Dermatol Venereol. 2022 (Aug 3). Doi: 10.1111/jdv.18480
Atopic dermatitis and immune abnormalities in children born to mothers with nickel exposure
Key clinical point: Maternal exposure to nickel was associated with increased serum interleukin (IL)-2 levels but decreased serum eotaxin-1 levels and was negatively associated with the development of atopic dermatitis (AD) in children aged 3 years.
Major finding: Maternal nickel exposure was associated with increased serum levels of IL-2 (β 16.820; P < .001) but decreased serum levels of eotaxin-1 (β −5.065; P < .01) and was negatively associated with the development of AD (P = .024) in children aged 3 years.
Study details: Findings are from the analysis of an ongoing birth cohort study including 140 mother-child pairs.
Disclosures: This work was supported by grants from the Ministry of Science and Technology, Taiwan, and National Health Research Institutes. The authors declared no conflicts of interest.
Source: Ho JC et al. Prenatal exposure to nickel and atopic dermatitis at age 3 years: A birth cohort study with cytokine profiles. J Eur Acad Dermatol Venereol. 2022 (Jul 16). Doi: 10.1111/jdv.18425
Key clinical point: Maternal exposure to nickel was associated with increased serum interleukin (IL)-2 levels but decreased serum eotaxin-1 levels and was negatively associated with the development of atopic dermatitis (AD) in children aged 3 years.
Major finding: Maternal nickel exposure was associated with increased serum levels of IL-2 (β 16.820; P < .001) but decreased serum levels of eotaxin-1 (β −5.065; P < .01) and was negatively associated with the development of AD (P = .024) in children aged 3 years.
Study details: Findings are from the analysis of an ongoing birth cohort study including 140 mother-child pairs.
Disclosures: This work was supported by grants from the Ministry of Science and Technology, Taiwan, and National Health Research Institutes. The authors declared no conflicts of interest.
Source: Ho JC et al. Prenatal exposure to nickel and atopic dermatitis at age 3 years: A birth cohort study with cytokine profiles. J Eur Acad Dermatol Venereol. 2022 (Jul 16). Doi: 10.1111/jdv.18425
Key clinical point: Maternal exposure to nickel was associated with increased serum interleukin (IL)-2 levels but decreased serum eotaxin-1 levels and was negatively associated with the development of atopic dermatitis (AD) in children aged 3 years.
Major finding: Maternal nickel exposure was associated with increased serum levels of IL-2 (β 16.820; P < .001) but decreased serum levels of eotaxin-1 (β −5.065; P < .01) and was negatively associated with the development of AD (P = .024) in children aged 3 years.
Study details: Findings are from the analysis of an ongoing birth cohort study including 140 mother-child pairs.
Disclosures: This work was supported by grants from the Ministry of Science and Technology, Taiwan, and National Health Research Institutes. The authors declared no conflicts of interest.
Source: Ho JC et al. Prenatal exposure to nickel and atopic dermatitis at age 3 years: A birth cohort study with cytokine profiles. J Eur Acad Dermatol Venereol. 2022 (Jul 16). Doi: 10.1111/jdv.18425