User login
Intensive BP lowering harmful in acute ischemic stroke: ENCHANTED2/MT
“Intensive control of systolic blood pressure to lower than 120 mm Hg should be avoided to prevent compromising the functional recovery of patients who have received endovascular thrombectomy for acute ischemic stroke due to intracranial large-vessel occlusion,” the investigators conclude.
Results from the ENCHANTED2/MT trial were presented by Craig Anderson, MD, professor of neurology and epidemiology, University of New South Wales, Sydney, during the 14th World Stroke Congress (WSC) in Singapore.
The study was simultaneously published online in The Lancet.
“What our results have pretty convincingly shown is that in acute stroke patients who have undergone mechanical thrombectomy, lowering blood pressure down to a systolic of 120 mm Hg for 3 days is too low for too long. We shouldn’t go that far down,” Dr. Anderson said in an interview.
Dr. Anderson said the trial has provided an important message for clinical practice.
“This result is not what we expected, but it is a definitive result and gives us a lower safety margin for blood pressure in acute ischemic stroke patients. This, in itself, is a big step forward.”
He noted that the optimum blood pressure for these patients is not known.
“We need to do further trials to determine optimum blood pressure in these acute patients, but perhaps we should be aiming more towards 140 mm Hg,” he suggested.
“But this trial shows us that in patients who have had successful clot retrieval with endovascular treatment for acute ischemic stroke, careful blood pressure management is important to avoid levels becoming too low. We have to make sure we don’t overshoot down to 120 mm Hg or below.”
The chair of the WSC session at which the trial was presented, Jeyaraj Pandian, MD, head of neurology at Christian Medical College, Ludhiana, India, who is the current vice-president of the World Stroke Organization, said: “This is a very important result. It has major practical implications.”
As background, Dr. Anderson explained that elevated blood pressure is very common in patients who have an acute ischemic stroke, and the higher the blood pressure, the higher the chances of having a worse outcome.
“Theoretically, if we can control the blood pressure, we may be able to improve outcomes,” he said.
In 2019, the first ENCHANTED trial reported that controlling blood pressure by a moderate amount – to around 140 mm Hg, which is lower than currently recommended in the guidelines – was linked to a reduction in bleeding complications of thrombolysis and appeared safe, but it did not improve recovery, Dr. Anderson noted.
“This trial was done before mechanical thrombectomy became routinely adopted, and this procedure has now become the standard of care for large-vessel occlusion strokes, but we don’t know what we should do about blood pressure in these patients,” he added.
A smaller French trial has suggested lowering blood pressure to 130 mm Hg, rather than a more liberal 130-180 mm Hg, was safe after successful mechanical thrombectomy, but there was no effect on functional outcome.
“In stroke patients with a large-vessel occlusion, blood pressure is often elevated to very high levels. There are wide ranges of opinions on what to do about this – whether it should be lowered, and by how much,” Dr. Anderson said. “We conducted the current ENCHANTED2/MT trial to look at this issue.”
The trial randomly assigned patients who had undergone successful mechanical clot retrieval and reperfusion but whose blood pressure was still elevated to two groups. In one group, blood pressure was aggressively lowered to less than 120 mm Hg within 1 hour of reperfusion, and blood pressure was kept at this level for 3 days. In the other group, a more liberal approach was used: Blood pressure was kept at 140-180 mm Hg.
The primary endpoint was disability, as measured by the Modified Rankin Scale (mRS) score at 90 days.
The study was started in China with the intention of expanding recruitment internationally. The planned enrollment was more than 2,000 patients.
However, in March of 2022, after 821 patients had been enrolled, the data safety monitoring board (DSMB) recommended that recruitment into the trial be suspended because of a safety signal. All of the patients who had been recruited were from China.
These patients were followed to obtain the 3-month outcome results, after which the DSMB recommended that the trial be stopped because safety was still a problem.
Mean systolic blood pressure was 125 mm Hg at 1 hour and 121 mm Hg at 24 hours in the more intensive-treatment group; it was 143 mm Hg at 1 hour and 139 mm Hg at 24 hours in the less intensive-treatment group, giving an adjusted mean difference over 24 hours of 18 mm Hg.
Worse disability scores
Results showed that the patients who underwent the more intensive blood pressure lowering had more disability at 3-month follow-up, with worse scores on a shift analysis of the mRS than those in the less intensive group (common odds ratio, 1.37; 95% confidence interval, 1.07-1.76).
The unfavorable shift in mRS scores in the more intensive group was consistent in adjusted sensitivity analysis, and there was no significant heterogeneity in the treatment effect on the primary outcome across all prespecified subgroups.
The incidence of death or neurologic deterioration at 7 days was higher in the more intensive-treatment group than the less intensive-treatment group (common OR, 1.53), and a between-group difference emerged at 24 hours.
The incidence of death or disability (mRS scores, 3-6) at 90 days was higher among patients in the more intensive-treatment group than the less intensive-treatment group (53% vs. 39%; OR, 1.85; P = .0001).
Among those who survived, more patients in the more intensive-treatment group had major disability (mRS scores, 3-5) at 90 days than did patients in the less intensive-treatment group (43% vs. 28%; OR, 2.07; P = .0001).
No difference in ICH or severe hypotension episodes
The incidence of symptomatic intracranial hemorrhage, mortality, and serious adverse events did not significantly differ between the two groups. There were no significant differences in recurrent ischemic stroke events at 90 days, and no episodes of severe hypotension were reported as a serious adverse event.
“Our results show that intensive lowering of blood pressure appears to be associated with worsening physical disability. While there was no difference in mortality rates between the two groups, the lower blood pressure appeared to compromise the ability to recover from the stroke,” Dr. Anderson said.
On the possible mechanism of harm, he suggested that the intensive blood pressure reduction might be interfering with blood flow through the injured part of the brain and impeding the ability to recover from the clot removal procedure.
What levels should be aimed for?
Dr. Anderson stressed that it was important to have conducted this trial.
“Current guidelines recommend very conservative level of blood pressure in acute ischemic stroke patients – to below 180 mm Hg. But no lower limit is recommended.
“Most clinicians aim for about the 140 mm Hg mark, but there is a large variation in opinion on what to do,” he said. “Some doctors treat aggressively, believing that lower pressures could be beneficial in preventing bleeding and swelling, and others prefer to keep levels higher. Our results have helped to give some guidance on this.”
Asked what he thought an optimum target would be, Dr. Anderson replied: “For now, I think a target of around 140 mm Hg systolic would be reasonable, and there is no evidence to move below that.”
Yvo Roos, MD, professor of acute neurology at University Medical Center, Amsterdam, a co-author of the ENCHANTED2/MT trial, also commented: “The real importance of these study results is that they show that lowering blood pressure too much is detrimental on outcome. My personal interpretation, looking at the results of this study but also on the previous studies, is that we should aim for a target of 140-150 mm Hg. This is true for patients with recanalization therapy. For patients without any therapy, I would even be more careful in lowering blood pressure and recommend just staying below 180 mm Hg.”
As to whether these results are generalizable to other populations, given that the patients were Chinese, Dr. Anderson noted that Asian people have higher rates of intracranial atherosclerosis and more blood pressure complications in the heart and kidney than White patients. Stroke management patterns also differ.
“These points raise questions about generalizability, and while I think this is an issue for consideration, I do not think it should detract from the clarity of these results,” he commented.
The study is supported by grants from the Shanghai Hospital Development Center, the National Health and Medical Research Council of Australia, the China Stroke Prevention Project, Shanghai Changhai Hospital, the Science and Technology Commission of Shanghai Municipality, Takeda China, Genesis Medtech, and Penumbra. Dr. Anderson has received grants from the National Health and Medical Research Council and Medical Research Futures Fund of Australia, the UK Medical Research Council, Penumbra, and Takeda China.
A version of this article first appeared on Medscape.com.
“Intensive control of systolic blood pressure to lower than 120 mm Hg should be avoided to prevent compromising the functional recovery of patients who have received endovascular thrombectomy for acute ischemic stroke due to intracranial large-vessel occlusion,” the investigators conclude.
Results from the ENCHANTED2/MT trial were presented by Craig Anderson, MD, professor of neurology and epidemiology, University of New South Wales, Sydney, during the 14th World Stroke Congress (WSC) in Singapore.
The study was simultaneously published online in The Lancet.
“What our results have pretty convincingly shown is that in acute stroke patients who have undergone mechanical thrombectomy, lowering blood pressure down to a systolic of 120 mm Hg for 3 days is too low for too long. We shouldn’t go that far down,” Dr. Anderson said in an interview.
Dr. Anderson said the trial has provided an important message for clinical practice.
“This result is not what we expected, but it is a definitive result and gives us a lower safety margin for blood pressure in acute ischemic stroke patients. This, in itself, is a big step forward.”
He noted that the optimum blood pressure for these patients is not known.
“We need to do further trials to determine optimum blood pressure in these acute patients, but perhaps we should be aiming more towards 140 mm Hg,” he suggested.
“But this trial shows us that in patients who have had successful clot retrieval with endovascular treatment for acute ischemic stroke, careful blood pressure management is important to avoid levels becoming too low. We have to make sure we don’t overshoot down to 120 mm Hg or below.”
The chair of the WSC session at which the trial was presented, Jeyaraj Pandian, MD, head of neurology at Christian Medical College, Ludhiana, India, who is the current vice-president of the World Stroke Organization, said: “This is a very important result. It has major practical implications.”
As background, Dr. Anderson explained that elevated blood pressure is very common in patients who have an acute ischemic stroke, and the higher the blood pressure, the higher the chances of having a worse outcome.
“Theoretically, if we can control the blood pressure, we may be able to improve outcomes,” he said.
In 2019, the first ENCHANTED trial reported that controlling blood pressure by a moderate amount – to around 140 mm Hg, which is lower than currently recommended in the guidelines – was linked to a reduction in bleeding complications of thrombolysis and appeared safe, but it did not improve recovery, Dr. Anderson noted.
“This trial was done before mechanical thrombectomy became routinely adopted, and this procedure has now become the standard of care for large-vessel occlusion strokes, but we don’t know what we should do about blood pressure in these patients,” he added.
A smaller French trial has suggested lowering blood pressure to 130 mm Hg, rather than a more liberal 130-180 mm Hg, was safe after successful mechanical thrombectomy, but there was no effect on functional outcome.
“In stroke patients with a large-vessel occlusion, blood pressure is often elevated to very high levels. There are wide ranges of opinions on what to do about this – whether it should be lowered, and by how much,” Dr. Anderson said. “We conducted the current ENCHANTED2/MT trial to look at this issue.”
The trial randomly assigned patients who had undergone successful mechanical clot retrieval and reperfusion but whose blood pressure was still elevated to two groups. In one group, blood pressure was aggressively lowered to less than 120 mm Hg within 1 hour of reperfusion, and blood pressure was kept at this level for 3 days. In the other group, a more liberal approach was used: Blood pressure was kept at 140-180 mm Hg.
The primary endpoint was disability, as measured by the Modified Rankin Scale (mRS) score at 90 days.
The study was started in China with the intention of expanding recruitment internationally. The planned enrollment was more than 2,000 patients.
However, in March of 2022, after 821 patients had been enrolled, the data safety monitoring board (DSMB) recommended that recruitment into the trial be suspended because of a safety signal. All of the patients who had been recruited were from China.
These patients were followed to obtain the 3-month outcome results, after which the DSMB recommended that the trial be stopped because safety was still a problem.
Mean systolic blood pressure was 125 mm Hg at 1 hour and 121 mm Hg at 24 hours in the more intensive-treatment group; it was 143 mm Hg at 1 hour and 139 mm Hg at 24 hours in the less intensive-treatment group, giving an adjusted mean difference over 24 hours of 18 mm Hg.
Worse disability scores
Results showed that the patients who underwent the more intensive blood pressure lowering had more disability at 3-month follow-up, with worse scores on a shift analysis of the mRS than those in the less intensive group (common odds ratio, 1.37; 95% confidence interval, 1.07-1.76).
The unfavorable shift in mRS scores in the more intensive group was consistent in adjusted sensitivity analysis, and there was no significant heterogeneity in the treatment effect on the primary outcome across all prespecified subgroups.
The incidence of death or neurologic deterioration at 7 days was higher in the more intensive-treatment group than the less intensive-treatment group (common OR, 1.53), and a between-group difference emerged at 24 hours.
The incidence of death or disability (mRS scores, 3-6) at 90 days was higher among patients in the more intensive-treatment group than the less intensive-treatment group (53% vs. 39%; OR, 1.85; P = .0001).
Among those who survived, more patients in the more intensive-treatment group had major disability (mRS scores, 3-5) at 90 days than did patients in the less intensive-treatment group (43% vs. 28%; OR, 2.07; P = .0001).
No difference in ICH or severe hypotension episodes
The incidence of symptomatic intracranial hemorrhage, mortality, and serious adverse events did not significantly differ between the two groups. There were no significant differences in recurrent ischemic stroke events at 90 days, and no episodes of severe hypotension were reported as a serious adverse event.
“Our results show that intensive lowering of blood pressure appears to be associated with worsening physical disability. While there was no difference in mortality rates between the two groups, the lower blood pressure appeared to compromise the ability to recover from the stroke,” Dr. Anderson said.
On the possible mechanism of harm, he suggested that the intensive blood pressure reduction might be interfering with blood flow through the injured part of the brain and impeding the ability to recover from the clot removal procedure.
What levels should be aimed for?
Dr. Anderson stressed that it was important to have conducted this trial.
“Current guidelines recommend very conservative level of blood pressure in acute ischemic stroke patients – to below 180 mm Hg. But no lower limit is recommended.
“Most clinicians aim for about the 140 mm Hg mark, but there is a large variation in opinion on what to do,” he said. “Some doctors treat aggressively, believing that lower pressures could be beneficial in preventing bleeding and swelling, and others prefer to keep levels higher. Our results have helped to give some guidance on this.”
Asked what he thought an optimum target would be, Dr. Anderson replied: “For now, I think a target of around 140 mm Hg systolic would be reasonable, and there is no evidence to move below that.”
Yvo Roos, MD, professor of acute neurology at University Medical Center, Amsterdam, a co-author of the ENCHANTED2/MT trial, also commented: “The real importance of these study results is that they show that lowering blood pressure too much is detrimental on outcome. My personal interpretation, looking at the results of this study but also on the previous studies, is that we should aim for a target of 140-150 mm Hg. This is true for patients with recanalization therapy. For patients without any therapy, I would even be more careful in lowering blood pressure and recommend just staying below 180 mm Hg.”
As to whether these results are generalizable to other populations, given that the patients were Chinese, Dr. Anderson noted that Asian people have higher rates of intracranial atherosclerosis and more blood pressure complications in the heart and kidney than White patients. Stroke management patterns also differ.
“These points raise questions about generalizability, and while I think this is an issue for consideration, I do not think it should detract from the clarity of these results,” he commented.
The study is supported by grants from the Shanghai Hospital Development Center, the National Health and Medical Research Council of Australia, the China Stroke Prevention Project, Shanghai Changhai Hospital, the Science and Technology Commission of Shanghai Municipality, Takeda China, Genesis Medtech, and Penumbra. Dr. Anderson has received grants from the National Health and Medical Research Council and Medical Research Futures Fund of Australia, the UK Medical Research Council, Penumbra, and Takeda China.
A version of this article first appeared on Medscape.com.
“Intensive control of systolic blood pressure to lower than 120 mm Hg should be avoided to prevent compromising the functional recovery of patients who have received endovascular thrombectomy for acute ischemic stroke due to intracranial large-vessel occlusion,” the investigators conclude.
Results from the ENCHANTED2/MT trial were presented by Craig Anderson, MD, professor of neurology and epidemiology, University of New South Wales, Sydney, during the 14th World Stroke Congress (WSC) in Singapore.
The study was simultaneously published online in The Lancet.
“What our results have pretty convincingly shown is that in acute stroke patients who have undergone mechanical thrombectomy, lowering blood pressure down to a systolic of 120 mm Hg for 3 days is too low for too long. We shouldn’t go that far down,” Dr. Anderson said in an interview.
Dr. Anderson said the trial has provided an important message for clinical practice.
“This result is not what we expected, but it is a definitive result and gives us a lower safety margin for blood pressure in acute ischemic stroke patients. This, in itself, is a big step forward.”
He noted that the optimum blood pressure for these patients is not known.
“We need to do further trials to determine optimum blood pressure in these acute patients, but perhaps we should be aiming more towards 140 mm Hg,” he suggested.
“But this trial shows us that in patients who have had successful clot retrieval with endovascular treatment for acute ischemic stroke, careful blood pressure management is important to avoid levels becoming too low. We have to make sure we don’t overshoot down to 120 mm Hg or below.”
The chair of the WSC session at which the trial was presented, Jeyaraj Pandian, MD, head of neurology at Christian Medical College, Ludhiana, India, who is the current vice-president of the World Stroke Organization, said: “This is a very important result. It has major practical implications.”
As background, Dr. Anderson explained that elevated blood pressure is very common in patients who have an acute ischemic stroke, and the higher the blood pressure, the higher the chances of having a worse outcome.
“Theoretically, if we can control the blood pressure, we may be able to improve outcomes,” he said.
In 2019, the first ENCHANTED trial reported that controlling blood pressure by a moderate amount – to around 140 mm Hg, which is lower than currently recommended in the guidelines – was linked to a reduction in bleeding complications of thrombolysis and appeared safe, but it did not improve recovery, Dr. Anderson noted.
“This trial was done before mechanical thrombectomy became routinely adopted, and this procedure has now become the standard of care for large-vessel occlusion strokes, but we don’t know what we should do about blood pressure in these patients,” he added.
A smaller French trial has suggested lowering blood pressure to 130 mm Hg, rather than a more liberal 130-180 mm Hg, was safe after successful mechanical thrombectomy, but there was no effect on functional outcome.
“In stroke patients with a large-vessel occlusion, blood pressure is often elevated to very high levels. There are wide ranges of opinions on what to do about this – whether it should be lowered, and by how much,” Dr. Anderson said. “We conducted the current ENCHANTED2/MT trial to look at this issue.”
The trial randomly assigned patients who had undergone successful mechanical clot retrieval and reperfusion but whose blood pressure was still elevated to two groups. In one group, blood pressure was aggressively lowered to less than 120 mm Hg within 1 hour of reperfusion, and blood pressure was kept at this level for 3 days. In the other group, a more liberal approach was used: Blood pressure was kept at 140-180 mm Hg.
The primary endpoint was disability, as measured by the Modified Rankin Scale (mRS) score at 90 days.
The study was started in China with the intention of expanding recruitment internationally. The planned enrollment was more than 2,000 patients.
However, in March of 2022, after 821 patients had been enrolled, the data safety monitoring board (DSMB) recommended that recruitment into the trial be suspended because of a safety signal. All of the patients who had been recruited were from China.
These patients were followed to obtain the 3-month outcome results, after which the DSMB recommended that the trial be stopped because safety was still a problem.
Mean systolic blood pressure was 125 mm Hg at 1 hour and 121 mm Hg at 24 hours in the more intensive-treatment group; it was 143 mm Hg at 1 hour and 139 mm Hg at 24 hours in the less intensive-treatment group, giving an adjusted mean difference over 24 hours of 18 mm Hg.
Worse disability scores
Results showed that the patients who underwent the more intensive blood pressure lowering had more disability at 3-month follow-up, with worse scores on a shift analysis of the mRS than those in the less intensive group (common odds ratio, 1.37; 95% confidence interval, 1.07-1.76).
The unfavorable shift in mRS scores in the more intensive group was consistent in adjusted sensitivity analysis, and there was no significant heterogeneity in the treatment effect on the primary outcome across all prespecified subgroups.
The incidence of death or neurologic deterioration at 7 days was higher in the more intensive-treatment group than the less intensive-treatment group (common OR, 1.53), and a between-group difference emerged at 24 hours.
The incidence of death or disability (mRS scores, 3-6) at 90 days was higher among patients in the more intensive-treatment group than the less intensive-treatment group (53% vs. 39%; OR, 1.85; P = .0001).
Among those who survived, more patients in the more intensive-treatment group had major disability (mRS scores, 3-5) at 90 days than did patients in the less intensive-treatment group (43% vs. 28%; OR, 2.07; P = .0001).
No difference in ICH or severe hypotension episodes
The incidence of symptomatic intracranial hemorrhage, mortality, and serious adverse events did not significantly differ between the two groups. There were no significant differences in recurrent ischemic stroke events at 90 days, and no episodes of severe hypotension were reported as a serious adverse event.
“Our results show that intensive lowering of blood pressure appears to be associated with worsening physical disability. While there was no difference in mortality rates between the two groups, the lower blood pressure appeared to compromise the ability to recover from the stroke,” Dr. Anderson said.
On the possible mechanism of harm, he suggested that the intensive blood pressure reduction might be interfering with blood flow through the injured part of the brain and impeding the ability to recover from the clot removal procedure.
What levels should be aimed for?
Dr. Anderson stressed that it was important to have conducted this trial.
“Current guidelines recommend very conservative level of blood pressure in acute ischemic stroke patients – to below 180 mm Hg. But no lower limit is recommended.
“Most clinicians aim for about the 140 mm Hg mark, but there is a large variation in opinion on what to do,” he said. “Some doctors treat aggressively, believing that lower pressures could be beneficial in preventing bleeding and swelling, and others prefer to keep levels higher. Our results have helped to give some guidance on this.”
Asked what he thought an optimum target would be, Dr. Anderson replied: “For now, I think a target of around 140 mm Hg systolic would be reasonable, and there is no evidence to move below that.”
Yvo Roos, MD, professor of acute neurology at University Medical Center, Amsterdam, a co-author of the ENCHANTED2/MT trial, also commented: “The real importance of these study results is that they show that lowering blood pressure too much is detrimental on outcome. My personal interpretation, looking at the results of this study but also on the previous studies, is that we should aim for a target of 140-150 mm Hg. This is true for patients with recanalization therapy. For patients without any therapy, I would even be more careful in lowering blood pressure and recommend just staying below 180 mm Hg.”
As to whether these results are generalizable to other populations, given that the patients were Chinese, Dr. Anderson noted that Asian people have higher rates of intracranial atherosclerosis and more blood pressure complications in the heart and kidney than White patients. Stroke management patterns also differ.
“These points raise questions about generalizability, and while I think this is an issue for consideration, I do not think it should detract from the clarity of these results,” he commented.
The study is supported by grants from the Shanghai Hospital Development Center, the National Health and Medical Research Council of Australia, the China Stroke Prevention Project, Shanghai Changhai Hospital, the Science and Technology Commission of Shanghai Municipality, Takeda China, Genesis Medtech, and Penumbra. Dr. Anderson has received grants from the National Health and Medical Research Council and Medical Research Futures Fund of Australia, the UK Medical Research Council, Penumbra, and Takeda China.
A version of this article first appeared on Medscape.com.
FROM THE WORLD STROKE CONGRESS
Poor control of serum urate linked to cardiovascular risk in patients with gout
A new study based on U.S. veterans’ medical records adds to the evidence for a link between gout – especially poorly controlled cases – and cardiovascular disease (CVD) risk, Tate Johnson, MD, reported at the annual research symposium of the Gout, Hyperuricemia, and Crystal Associated Disease Network.
Gout was associated with a 68% increased risk of heart failure (HF) hospitalization, 25% increased risk of HF-related death, and a 22% increased risk of major adverse cardiovascular events (MACE), said Dr. Johnson, of the division of rheumatology at the University of Nebraska, Omaha.
Poorly controlled serum urate was associated with a higher risk of cardiovascular events, regardless of the use of urate-lowering therapy (ULT). He said more research is needed to see if there is a causal link between gout, hyperuricemia – or its treatment – and CVD risk.

Dr. Johnson and colleagues used records from the Veterans Health Administration for this study. They created a retrospective, matched cohort study that looked at records dating from January 1999 to September 2015. Patients with gout (≥ 2 ICD-9 codes) were matched 1:10 on age, sex, and year of VHA enrollment to patients without a gout ICD-9 code or a record of receiving ULT. They matched 559,243 people with gout to 5,407,379 people who did not have a diagnosis or a recorded treatment for this condition.
Over 43,331,604 person-years, Dr. Johnson and colleagues observed 137,162 CVD events in gout (incidence rate 33.96 per 1,000 person-years) vs. 879,903 in non-gout patients (IR 22.37 per 1,000 person-years). Gout was most strongly associated with HF hospitalization, with a nearly threefold higher risk (hazard ratio, 2.78; 95% confidence interval, 2.73-2.83), which attenuated but persisted after adjustment for additional CVD risk factors (adjusted hazard ratio, 1.68; 95% CI, 1.65-1.70) and excluding patients with prevalent HF (aHR, 1.60; 95% CI, 1.57-1.64).
People with gout were also at higher risk of HF-related death (aHR, 1.25; 95% CI, 1.21-1.29), MACE (aHR, 1.22; 95% CI, 1.21-1.23), and coronary artery disease–related death (aHR, 1.21; 95% CI, 1.20-1.22).
Among people with gout in the study, poor serum urate control was associated with a higher risk of all CVD events, with the highest CVD risk occurring in patients with inadequately controlled serum urate despite receipt of ULT, particularly related to HF hospitalization (aHR, 1.43; 95% CI, 1.34-1.52) and HF-related death (aHR, 1.47; 95% CI, 1.34-1.61).
Limits of the study include the generalizability of the study population. Reflecting the VHA’s patient population, 99% of the cohort were men, with 62% of the gout group and 59.4% of the control group identifying as White and non-Hispanic.
The study provides evidence that may be found only by studying medical records, Richard J. Johnson, MD, of the University of Colorado at Denver, Aurora, said in an interview.
Dr. Richard Johnson, who is not related to the author, said that only about one-third of people with gout are adequately treated, and about another one-third take urate-lowering therapy (ULT) but fail to get their serum urate level under control. But it would be unethical to design a clinical trial to study CVD risk and poorly controlled serum urate without ULT treatment.
“The only way you can figure out if uric acid lowering is going to help these guys is to actually do a study like this where you see the ones who don’t get adequate treatment versus adequate treatment and you show that there’s going to be a difference in outcome,” he said.
Dr. Richard Johnson contrasted this approach with the one used in the recently reported study that appeared to cast doubt on the link between serum uric acid levels and cardiovascular disease. The ALL-HEART trial found that allopurinol, a drug commonly used to treat gout, provided no benefit in terms of reducing cardiovascular events in patients with ischemic heart disease. But these patients did not have gout, and that was a critical difference, he said.
He noted that it was not surprising that the results of ALL-HEART were negative, given the study design.
“The ALL-HEART study treated people regardless of their uric acid level, and they also excluded subjects who had a history of gout,” he said. “Yet the risk associated with uric acid occurs primarily among those with elevated serum uric acid levels and those with gout.”
The study received funding from the Rheumatology Research Foundation and the VHA. Neither Dr. Tate Johnson nor Dr. Richard Johnson had any relevant disclosures.
A new study based on U.S. veterans’ medical records adds to the evidence for a link between gout – especially poorly controlled cases – and cardiovascular disease (CVD) risk, Tate Johnson, MD, reported at the annual research symposium of the Gout, Hyperuricemia, and Crystal Associated Disease Network.
Gout was associated with a 68% increased risk of heart failure (HF) hospitalization, 25% increased risk of HF-related death, and a 22% increased risk of major adverse cardiovascular events (MACE), said Dr. Johnson, of the division of rheumatology at the University of Nebraska, Omaha.
Poorly controlled serum urate was associated with a higher risk of cardiovascular events, regardless of the use of urate-lowering therapy (ULT). He said more research is needed to see if there is a causal link between gout, hyperuricemia – or its treatment – and CVD risk.
Dr. Johnson and colleagues used records from the Veterans Health Administration for this study. They created a retrospective, matched cohort study that looked at records dating from January 1999 to September 2015. Patients with gout (≥ 2 ICD-9 codes) were matched 1:10 on age, sex, and year of VHA enrollment to patients without a gout ICD-9 code or a record of receiving ULT. They matched 559,243 people with gout to 5,407,379 people who did not have a diagnosis or a recorded treatment for this condition.
Over 43,331,604 person-years, Dr. Johnson and colleagues observed 137,162 CVD events in gout (incidence rate 33.96 per 1,000 person-years) vs. 879,903 in non-gout patients (IR 22.37 per 1,000 person-years). Gout was most strongly associated with HF hospitalization, with a nearly threefold higher risk (hazard ratio, 2.78; 95% confidence interval, 2.73-2.83), which attenuated but persisted after adjustment for additional CVD risk factors (adjusted hazard ratio, 1.68; 95% CI, 1.65-1.70) and excluding patients with prevalent HF (aHR, 1.60; 95% CI, 1.57-1.64).
People with gout were also at higher risk of HF-related death (aHR, 1.25; 95% CI, 1.21-1.29), MACE (aHR, 1.22; 95% CI, 1.21-1.23), and coronary artery disease–related death (aHR, 1.21; 95% CI, 1.20-1.22).
Among people with gout in the study, poor serum urate control was associated with a higher risk of all CVD events, with the highest CVD risk occurring in patients with inadequately controlled serum urate despite receipt of ULT, particularly related to HF hospitalization (aHR, 1.43; 95% CI, 1.34-1.52) and HF-related death (aHR, 1.47; 95% CI, 1.34-1.61).
Limits of the study include the generalizability of the study population. Reflecting the VHA’s patient population, 99% of the cohort were men, with 62% of the gout group and 59.4% of the control group identifying as White and non-Hispanic.
The study provides evidence that may be found only by studying medical records, Richard J. Johnson, MD, of the University of Colorado at Denver, Aurora, said in an interview.
Dr. Richard Johnson, who is not related to the author, said that only about one-third of people with gout are adequately treated, and about another one-third take urate-lowering therapy (ULT) but fail to get their serum urate level under control. But it would be unethical to design a clinical trial to study CVD risk and poorly controlled serum urate without ULT treatment.
“The only way you can figure out if uric acid lowering is going to help these guys is to actually do a study like this where you see the ones who don’t get adequate treatment versus adequate treatment and you show that there’s going to be a difference in outcome,” he said.
Dr. Richard Johnson contrasted this approach with the one used in the recently reported study that appeared to cast doubt on the link between serum uric acid levels and cardiovascular disease. The ALL-HEART trial found that allopurinol, a drug commonly used to treat gout, provided no benefit in terms of reducing cardiovascular events in patients with ischemic heart disease. But these patients did not have gout, and that was a critical difference, he said.
He noted that it was not surprising that the results of ALL-HEART were negative, given the study design.
“The ALL-HEART study treated people regardless of their uric acid level, and they also excluded subjects who had a history of gout,” he said. “Yet the risk associated with uric acid occurs primarily among those with elevated serum uric acid levels and those with gout.”
The study received funding from the Rheumatology Research Foundation and the VHA. Neither Dr. Tate Johnson nor Dr. Richard Johnson had any relevant disclosures.
A new study based on U.S. veterans’ medical records adds to the evidence for a link between gout – especially poorly controlled cases – and cardiovascular disease (CVD) risk, Tate Johnson, MD, reported at the annual research symposium of the Gout, Hyperuricemia, and Crystal Associated Disease Network.
Gout was associated with a 68% increased risk of heart failure (HF) hospitalization, 25% increased risk of HF-related death, and a 22% increased risk of major adverse cardiovascular events (MACE), said Dr. Johnson, of the division of rheumatology at the University of Nebraska, Omaha.
Poorly controlled serum urate was associated with a higher risk of cardiovascular events, regardless of the use of urate-lowering therapy (ULT). He said more research is needed to see if there is a causal link between gout, hyperuricemia – or its treatment – and CVD risk.
Dr. Johnson and colleagues used records from the Veterans Health Administration for this study. They created a retrospective, matched cohort study that looked at records dating from January 1999 to September 2015. Patients with gout (≥ 2 ICD-9 codes) were matched 1:10 on age, sex, and year of VHA enrollment to patients without a gout ICD-9 code or a record of receiving ULT. They matched 559,243 people with gout to 5,407,379 people who did not have a diagnosis or a recorded treatment for this condition.
Over 43,331,604 person-years, Dr. Johnson and colleagues observed 137,162 CVD events in gout (incidence rate 33.96 per 1,000 person-years) vs. 879,903 in non-gout patients (IR 22.37 per 1,000 person-years). Gout was most strongly associated with HF hospitalization, with a nearly threefold higher risk (hazard ratio, 2.78; 95% confidence interval, 2.73-2.83), which attenuated but persisted after adjustment for additional CVD risk factors (adjusted hazard ratio, 1.68; 95% CI, 1.65-1.70) and excluding patients with prevalent HF (aHR, 1.60; 95% CI, 1.57-1.64).
People with gout were also at higher risk of HF-related death (aHR, 1.25; 95% CI, 1.21-1.29), MACE (aHR, 1.22; 95% CI, 1.21-1.23), and coronary artery disease–related death (aHR, 1.21; 95% CI, 1.20-1.22).
Among people with gout in the study, poor serum urate control was associated with a higher risk of all CVD events, with the highest CVD risk occurring in patients with inadequately controlled serum urate despite receipt of ULT, particularly related to HF hospitalization (aHR, 1.43; 95% CI, 1.34-1.52) and HF-related death (aHR, 1.47; 95% CI, 1.34-1.61).
Limits of the study include the generalizability of the study population. Reflecting the VHA’s patient population, 99% of the cohort were men, with 62% of the gout group and 59.4% of the control group identifying as White and non-Hispanic.
The study provides evidence that may be found only by studying medical records, Richard J. Johnson, MD, of the University of Colorado at Denver, Aurora, said in an interview.
Dr. Richard Johnson, who is not related to the author, said that only about one-third of people with gout are adequately treated, and about another one-third take urate-lowering therapy (ULT) but fail to get their serum urate level under control. But it would be unethical to design a clinical trial to study CVD risk and poorly controlled serum urate without ULT treatment.
“The only way you can figure out if uric acid lowering is going to help these guys is to actually do a study like this where you see the ones who don’t get adequate treatment versus adequate treatment and you show that there’s going to be a difference in outcome,” he said.
Dr. Richard Johnson contrasted this approach with the one used in the recently reported study that appeared to cast doubt on the link between serum uric acid levels and cardiovascular disease. The ALL-HEART trial found that allopurinol, a drug commonly used to treat gout, provided no benefit in terms of reducing cardiovascular events in patients with ischemic heart disease. But these patients did not have gout, and that was a critical difference, he said.
He noted that it was not surprising that the results of ALL-HEART were negative, given the study design.
“The ALL-HEART study treated people regardless of their uric acid level, and they also excluded subjects who had a history of gout,” he said. “Yet the risk associated with uric acid occurs primarily among those with elevated serum uric acid levels and those with gout.”
The study received funding from the Rheumatology Research Foundation and the VHA. Neither Dr. Tate Johnson nor Dr. Richard Johnson had any relevant disclosures.
FROM G-CAN 2022
Endoscopic severity score helps guide treatment in immune-mediated colitis
, according to new research presented at the annual meeting of the American College of Gastroenterology.
An endoscopy score cutoff of 4 or higher had a specificity of 82.8% across all colitis grades, and a cutoff of 5 or higher had a specificity of 87.6%, said Yinghong Wang, MD, PhD, a gastroenterologist at the University of Texas MD Anderson Cancer Center, Houston.
Immune-mediated colitis (IMC) is a common immune-related adverse event associated with immune checkpoint inhibitors. Dr. Wang and colleagues previously reported on endoscopic presentations of IMC, including severe inflammation with deep ulcerated mucosa; moderate to severe inflammation with diffuse erythema, superficial ulcers, exudate, and loss of vasculature; and mild inflammation with patchy erythema, aphtha, edema, or normal mucosa associated with histological inflammation.

Endoscopic scoring systems haven’t been established for IMC, but previous studies have shown benefits from early endoscopic evaluation. The current Common Terminology Criteria for Adverse Events (CTCAE) grading system for clinical symptoms alone has been poorly correlated with endoscopic findings and unable to provide accurate assessments, Dr. Wang said.
“There is a critical and urgent need to develop a new scoring system that could provide accurate and comprehensive assessment for IMC severity to better predict the requirement of more aggressive selective immunosuppressive therapy (SIT), which includes infliximab and vedolizumab,” she said.
Dr. Wang and colleagues conducted a retrospective international study across 14 centers to develop a new comprehensive endoscopic scoring system to assess the severity of IMC and explore its utility in predicting the need for aggressive treatment with SIT. They included 674 adult cancer patients in the United States, United Kingdom, Germany, and Australia with IMC who underwent endoscopic evaluation between 2010 and 2020.
All patients had received immune checkpoint inhibitors, an IMC diagnosis, and endoscopy and histology evaluations for IMC. In addition, all patients had diarrhea, including 92% who had grade 2 diarrhea and higher and 80% who had grade 2 colitis and higher. About 85% were treated with corticosteroids, 31% were treated with infliximab, 10% were treated with vedolizumab, and 5% were treated with both treatment types, corticosteroids and SIT.
Based on endoscopic reports, the research team looked at 10 endoscopic features and assigned one point each for erythema, edema, loss of vasculature, friability, erosions, exudate, any ulcers, large ulcers, deep ulcers, and more than two ulcers. The median IMC endoscopic score was 2.
The scoring system was devised by measuring the specificity of a selected score cutoff in predicting the need for SIT based on clinical consensus from the study group.
The researchers divided the cohort into a training set and a validation set. In the training set, an IMC endoscopy score cutoff of 4 or more had a specificity of 82.8% across all colitis grades and 96.4% among grade 1 colitis to predict SIT use. A cutoff of 5 or more had a specificity of 87.6% across all colitis grades and 98.2% among grade 1. These specificities were comparable to those of the validation sets.
At the same time, the CTCAE score was poorly associated with prediction of future SIT use, with a specificity of 27.4% for clinical colitis grading and 12.3% for diarrhea grading.
In addition, an IMC endoscopic score of 4 or 5 plus ulcer factors had a numerically higher specificity than a Mayo Endoscopic Score of 3. The IMC endoscopic score had a specificity of 85% at a cutoff of 4 and 88.2% at a cutoff of 5, as compared with 74.6% for the Mayo score.
Early endoscopic evaluation in disease course was associated with early SIT use, with a P value of less than .001.
“Implementation of this novel endoscopic scoring system could guide future IMC treatment more precisely,” Dr. Wang said.
The study funding was not disclosed. The authors reported consultant roles, advisory roles, and research support from several pharmaceutical companies.
, according to new research presented at the annual meeting of the American College of Gastroenterology.
An endoscopy score cutoff of 4 or higher had a specificity of 82.8% across all colitis grades, and a cutoff of 5 or higher had a specificity of 87.6%, said Yinghong Wang, MD, PhD, a gastroenterologist at the University of Texas MD Anderson Cancer Center, Houston.
Immune-mediated colitis (IMC) is a common immune-related adverse event associated with immune checkpoint inhibitors. Dr. Wang and colleagues previously reported on endoscopic presentations of IMC, including severe inflammation with deep ulcerated mucosa; moderate to severe inflammation with diffuse erythema, superficial ulcers, exudate, and loss of vasculature; and mild inflammation with patchy erythema, aphtha, edema, or normal mucosa associated with histological inflammation.
Endoscopic scoring systems haven’t been established for IMC, but previous studies have shown benefits from early endoscopic evaluation. The current Common Terminology Criteria for Adverse Events (CTCAE) grading system for clinical symptoms alone has been poorly correlated with endoscopic findings and unable to provide accurate assessments, Dr. Wang said.
“There is a critical and urgent need to develop a new scoring system that could provide accurate and comprehensive assessment for IMC severity to better predict the requirement of more aggressive selective immunosuppressive therapy (SIT), which includes infliximab and vedolizumab,” she said.
Dr. Wang and colleagues conducted a retrospective international study across 14 centers to develop a new comprehensive endoscopic scoring system to assess the severity of IMC and explore its utility in predicting the need for aggressive treatment with SIT. They included 674 adult cancer patients in the United States, United Kingdom, Germany, and Australia with IMC who underwent endoscopic evaluation between 2010 and 2020.
All patients had received immune checkpoint inhibitors, an IMC diagnosis, and endoscopy and histology evaluations for IMC. In addition, all patients had diarrhea, including 92% who had grade 2 diarrhea and higher and 80% who had grade 2 colitis and higher. About 85% were treated with corticosteroids, 31% were treated with infliximab, 10% were treated with vedolizumab, and 5% were treated with both treatment types, corticosteroids and SIT.
Based on endoscopic reports, the research team looked at 10 endoscopic features and assigned one point each for erythema, edema, loss of vasculature, friability, erosions, exudate, any ulcers, large ulcers, deep ulcers, and more than two ulcers. The median IMC endoscopic score was 2.
The scoring system was devised by measuring the specificity of a selected score cutoff in predicting the need for SIT based on clinical consensus from the study group.
The researchers divided the cohort into a training set and a validation set. In the training set, an IMC endoscopy score cutoff of 4 or more had a specificity of 82.8% across all colitis grades and 96.4% among grade 1 colitis to predict SIT use. A cutoff of 5 or more had a specificity of 87.6% across all colitis grades and 98.2% among grade 1. These specificities were comparable to those of the validation sets.
At the same time, the CTCAE score was poorly associated with prediction of future SIT use, with a specificity of 27.4% for clinical colitis grading and 12.3% for diarrhea grading.
In addition, an IMC endoscopic score of 4 or 5 plus ulcer factors had a numerically higher specificity than a Mayo Endoscopic Score of 3. The IMC endoscopic score had a specificity of 85% at a cutoff of 4 and 88.2% at a cutoff of 5, as compared with 74.6% for the Mayo score.
Early endoscopic evaluation in disease course was associated with early SIT use, with a P value of less than .001.
“Implementation of this novel endoscopic scoring system could guide future IMC treatment more precisely,” Dr. Wang said.
The study funding was not disclosed. The authors reported consultant roles, advisory roles, and research support from several pharmaceutical companies.
, according to new research presented at the annual meeting of the American College of Gastroenterology.
An endoscopy score cutoff of 4 or higher had a specificity of 82.8% across all colitis grades, and a cutoff of 5 or higher had a specificity of 87.6%, said Yinghong Wang, MD, PhD, a gastroenterologist at the University of Texas MD Anderson Cancer Center, Houston.
Immune-mediated colitis (IMC) is a common immune-related adverse event associated with immune checkpoint inhibitors. Dr. Wang and colleagues previously reported on endoscopic presentations of IMC, including severe inflammation with deep ulcerated mucosa; moderate to severe inflammation with diffuse erythema, superficial ulcers, exudate, and loss of vasculature; and mild inflammation with patchy erythema, aphtha, edema, or normal mucosa associated with histological inflammation.
Endoscopic scoring systems haven’t been established for IMC, but previous studies have shown benefits from early endoscopic evaluation. The current Common Terminology Criteria for Adverse Events (CTCAE) grading system for clinical symptoms alone has been poorly correlated with endoscopic findings and unable to provide accurate assessments, Dr. Wang said.
“There is a critical and urgent need to develop a new scoring system that could provide accurate and comprehensive assessment for IMC severity to better predict the requirement of more aggressive selective immunosuppressive therapy (SIT), which includes infliximab and vedolizumab,” she said.
Dr. Wang and colleagues conducted a retrospective international study across 14 centers to develop a new comprehensive endoscopic scoring system to assess the severity of IMC and explore its utility in predicting the need for aggressive treatment with SIT. They included 674 adult cancer patients in the United States, United Kingdom, Germany, and Australia with IMC who underwent endoscopic evaluation between 2010 and 2020.
All patients had received immune checkpoint inhibitors, an IMC diagnosis, and endoscopy and histology evaluations for IMC. In addition, all patients had diarrhea, including 92% who had grade 2 diarrhea and higher and 80% who had grade 2 colitis and higher. About 85% were treated with corticosteroids, 31% were treated with infliximab, 10% were treated with vedolizumab, and 5% were treated with both treatment types, corticosteroids and SIT.
Based on endoscopic reports, the research team looked at 10 endoscopic features and assigned one point each for erythema, edema, loss of vasculature, friability, erosions, exudate, any ulcers, large ulcers, deep ulcers, and more than two ulcers. The median IMC endoscopic score was 2.
The scoring system was devised by measuring the specificity of a selected score cutoff in predicting the need for SIT based on clinical consensus from the study group.
The researchers divided the cohort into a training set and a validation set. In the training set, an IMC endoscopy score cutoff of 4 or more had a specificity of 82.8% across all colitis grades and 96.4% among grade 1 colitis to predict SIT use. A cutoff of 5 or more had a specificity of 87.6% across all colitis grades and 98.2% among grade 1. These specificities were comparable to those of the validation sets.
At the same time, the CTCAE score was poorly associated with prediction of future SIT use, with a specificity of 27.4% for clinical colitis grading and 12.3% for diarrhea grading.
In addition, an IMC endoscopic score of 4 or 5 plus ulcer factors had a numerically higher specificity than a Mayo Endoscopic Score of 3. The IMC endoscopic score had a specificity of 85% at a cutoff of 4 and 88.2% at a cutoff of 5, as compared with 74.6% for the Mayo score.
Early endoscopic evaluation in disease course was associated with early SIT use, with a P value of less than .001.
“Implementation of this novel endoscopic scoring system could guide future IMC treatment more precisely,” Dr. Wang said.
The study funding was not disclosed. The authors reported consultant roles, advisory roles, and research support from several pharmaceutical companies.
FROM ACG 2022
Guselkumab induction improves moderate to severe active UC at week 12
according to findings presented at the annual meeting of the American College of Gastroenterology.
The efficacy of the 200-mg dose and the 400-mg dose was comparable, said David Rubin, MD, a gastroenterologist at the University of Chicago Medicine Inflammatory Bowel Disease Center. Outcomes improved in all patients, with or without a history of inadequate response or intolerance to advanced therapy.
Guselkumab, an interleukin-12 p19 subunit antagonist, is currently being investigated in inflammatory bowel disease.
The QUASAR Induction Study 1 (NCT04033445) is a phase 2b, randomized, double-blind, placebo-controlled study that evaluates guselkumab as induction therapy in patients with moderately to severely active UC. Inclusion criteria specify a demonstrated inadequate response or intolerance to conventional therapy, such as thiopurines or corticosteroids, or to advanced therapy, such as tumor necrosis factor–alpha antagonists, vedolizumab, or tofacitinib. The study didn’t include patients exposed to ustekinumab.
Study participants were age 18 and older with moderately to severely active UC, defined as a modified Mayo score of 5-9 with a Mayo rectal bleeding subscore of 1 or greater and a Mayo endoscopy subscore of 2 or greater at baseline. The groups were randomized 1:1:1 to receive 400 mg of IV guselkumab, 200 mg of guselkumab, or placebo at weeks 0, 4, and 8.
At week 12, the research team looked for several key endpoints. Clinical response was defined as a modified Mayo score decrease of 30% or more and a drop in 2 or more points, with either a 1-point decrease or more in the rectal bleeding subscore or a rectal bleeding subscore of 0 or 1.
Clinical remission was defined as a stool frequency subscore of 0 or 1 that hadn’t increased from baseline, a rectal bleeding subscore of 0, and an endoscopy subscore of 0 or 1 with no friability present on the endoscopy.
In addition, symptomatic remission was defined as a stool subscore of 0 or 1 that hadn’t increased from baseline and rectal bleeding subscore of 0.
Endoscopic improvement was defined as an endoscopy subscore of 0 or 1 with no friability present on the endoscopy. Endoscopic normalization was an endoscopy subscore of 0.
Notably, the research team looked at histoendoscopic mucosal improvement, which includes a combination of endoscopic improvement and histologic improvement (neutrophil infiltration in less than 5% of crypts, no crypt destruction, and no erosions, ulcerations, or granulation tissue, according to the Geboes grading system).
Among the 313 total patients, 47% had a history of inadequate response or intolerance to advanced therapy, and about half of these patients had prior inadequate response or intolerance to two or more advanced therapy classes.
At baseline, about 90% of patients had an endoscopic subscore of 3 (severe). More than half had extensive UC, and the average UC duration was 9 years. About 20% overall had extraintestinal manifestations present, which were noted in 33% of the 400 mg guselkumab treatment arm.
At week 12, clinical response was achieved by a higher proportion of patients treated with guselkumab versus placebo, at 50.5% versus 25.5% for patients with prior inadequate response or intolerance to advanced therapy and 70.3% versus 29.6% for those without prior inadequate response or intolerance to advanced therapy, the authors reported in the abstract.
Compared with placebo, higher proportions of patients treated with guselkumab achieved clinical, endoscopic, and histologic outcomes in both groups with or without inadequate response or intolerance to advanced therapy. Generally, those without a history of inadequate response had higher response rates across all endpoints.
Overall, both the 200-mg and 400-mg doses of guselkumab were statistically superior to the placebo across all endpoints for both groups (with or without inadequate response or intolerance). Although the efficacy was comparable for the two doses, the 400-mg dose was associated with greater histoendoscopic mucosal improvement in both groups.
“It’s of interest to think about how we position and sequence our therapies with this additional data,” Dr. Rubin said.
The study was sponsored by Janssen Research & Development. Several authors are employees for and have stock options with Johnson & Johnson and Janssen. The other authors reported consultant roles, advisory roles, and research support from numerous pharmaceutical companies, including Janssen.
according to findings presented at the annual meeting of the American College of Gastroenterology.
The efficacy of the 200-mg dose and the 400-mg dose was comparable, said David Rubin, MD, a gastroenterologist at the University of Chicago Medicine Inflammatory Bowel Disease Center. Outcomes improved in all patients, with or without a history of inadequate response or intolerance to advanced therapy.
Guselkumab, an interleukin-12 p19 subunit antagonist, is currently being investigated in inflammatory bowel disease.
The QUASAR Induction Study 1 (NCT04033445) is a phase 2b, randomized, double-blind, placebo-controlled study that evaluates guselkumab as induction therapy in patients with moderately to severely active UC. Inclusion criteria specify a demonstrated inadequate response or intolerance to conventional therapy, such as thiopurines or corticosteroids, or to advanced therapy, such as tumor necrosis factor–alpha antagonists, vedolizumab, or tofacitinib. The study didn’t include patients exposed to ustekinumab.
Study participants were age 18 and older with moderately to severely active UC, defined as a modified Mayo score of 5-9 with a Mayo rectal bleeding subscore of 1 or greater and a Mayo endoscopy subscore of 2 or greater at baseline. The groups were randomized 1:1:1 to receive 400 mg of IV guselkumab, 200 mg of guselkumab, or placebo at weeks 0, 4, and 8.
At week 12, the research team looked for several key endpoints. Clinical response was defined as a modified Mayo score decrease of 30% or more and a drop in 2 or more points, with either a 1-point decrease or more in the rectal bleeding subscore or a rectal bleeding subscore of 0 or 1.
Clinical remission was defined as a stool frequency subscore of 0 or 1 that hadn’t increased from baseline, a rectal bleeding subscore of 0, and an endoscopy subscore of 0 or 1 with no friability present on the endoscopy.
In addition, symptomatic remission was defined as a stool subscore of 0 or 1 that hadn’t increased from baseline and rectal bleeding subscore of 0.
Endoscopic improvement was defined as an endoscopy subscore of 0 or 1 with no friability present on the endoscopy. Endoscopic normalization was an endoscopy subscore of 0.
Notably, the research team looked at histoendoscopic mucosal improvement, which includes a combination of endoscopic improvement and histologic improvement (neutrophil infiltration in less than 5% of crypts, no crypt destruction, and no erosions, ulcerations, or granulation tissue, according to the Geboes grading system).
Among the 313 total patients, 47% had a history of inadequate response or intolerance to advanced therapy, and about half of these patients had prior inadequate response or intolerance to two or more advanced therapy classes.
At baseline, about 90% of patients had an endoscopic subscore of 3 (severe). More than half had extensive UC, and the average UC duration was 9 years. About 20% overall had extraintestinal manifestations present, which were noted in 33% of the 400 mg guselkumab treatment arm.
At week 12, clinical response was achieved by a higher proportion of patients treated with guselkumab versus placebo, at 50.5% versus 25.5% for patients with prior inadequate response or intolerance to advanced therapy and 70.3% versus 29.6% for those without prior inadequate response or intolerance to advanced therapy, the authors reported in the abstract.
Compared with placebo, higher proportions of patients treated with guselkumab achieved clinical, endoscopic, and histologic outcomes in both groups with or without inadequate response or intolerance to advanced therapy. Generally, those without a history of inadequate response had higher response rates across all endpoints.
Overall, both the 200-mg and 400-mg doses of guselkumab were statistically superior to the placebo across all endpoints for both groups (with or without inadequate response or intolerance). Although the efficacy was comparable for the two doses, the 400-mg dose was associated with greater histoendoscopic mucosal improvement in both groups.
“It’s of interest to think about how we position and sequence our therapies with this additional data,” Dr. Rubin said.
The study was sponsored by Janssen Research & Development. Several authors are employees for and have stock options with Johnson & Johnson and Janssen. The other authors reported consultant roles, advisory roles, and research support from numerous pharmaceutical companies, including Janssen.
according to findings presented at the annual meeting of the American College of Gastroenterology.
The efficacy of the 200-mg dose and the 400-mg dose was comparable, said David Rubin, MD, a gastroenterologist at the University of Chicago Medicine Inflammatory Bowel Disease Center. Outcomes improved in all patients, with or without a history of inadequate response or intolerance to advanced therapy.
Guselkumab, an interleukin-12 p19 subunit antagonist, is currently being investigated in inflammatory bowel disease.
The QUASAR Induction Study 1 (NCT04033445) is a phase 2b, randomized, double-blind, placebo-controlled study that evaluates guselkumab as induction therapy in patients with moderately to severely active UC. Inclusion criteria specify a demonstrated inadequate response or intolerance to conventional therapy, such as thiopurines or corticosteroids, or to advanced therapy, such as tumor necrosis factor–alpha antagonists, vedolizumab, or tofacitinib. The study didn’t include patients exposed to ustekinumab.
Study participants were age 18 and older with moderately to severely active UC, defined as a modified Mayo score of 5-9 with a Mayo rectal bleeding subscore of 1 or greater and a Mayo endoscopy subscore of 2 or greater at baseline. The groups were randomized 1:1:1 to receive 400 mg of IV guselkumab, 200 mg of guselkumab, or placebo at weeks 0, 4, and 8.
At week 12, the research team looked for several key endpoints. Clinical response was defined as a modified Mayo score decrease of 30% or more and a drop in 2 or more points, with either a 1-point decrease or more in the rectal bleeding subscore or a rectal bleeding subscore of 0 or 1.
Clinical remission was defined as a stool frequency subscore of 0 or 1 that hadn’t increased from baseline, a rectal bleeding subscore of 0, and an endoscopy subscore of 0 or 1 with no friability present on the endoscopy.
In addition, symptomatic remission was defined as a stool subscore of 0 or 1 that hadn’t increased from baseline and rectal bleeding subscore of 0.
Endoscopic improvement was defined as an endoscopy subscore of 0 or 1 with no friability present on the endoscopy. Endoscopic normalization was an endoscopy subscore of 0.
Notably, the research team looked at histoendoscopic mucosal improvement, which includes a combination of endoscopic improvement and histologic improvement (neutrophil infiltration in less than 5% of crypts, no crypt destruction, and no erosions, ulcerations, or granulation tissue, according to the Geboes grading system).
Among the 313 total patients, 47% had a history of inadequate response or intolerance to advanced therapy, and about half of these patients had prior inadequate response or intolerance to two or more advanced therapy classes.
At baseline, about 90% of patients had an endoscopic subscore of 3 (severe). More than half had extensive UC, and the average UC duration was 9 years. About 20% overall had extraintestinal manifestations present, which were noted in 33% of the 400 mg guselkumab treatment arm.
At week 12, clinical response was achieved by a higher proportion of patients treated with guselkumab versus placebo, at 50.5% versus 25.5% for patients with prior inadequate response or intolerance to advanced therapy and 70.3% versus 29.6% for those without prior inadequate response or intolerance to advanced therapy, the authors reported in the abstract.
Compared with placebo, higher proportions of patients treated with guselkumab achieved clinical, endoscopic, and histologic outcomes in both groups with or without inadequate response or intolerance to advanced therapy. Generally, those without a history of inadequate response had higher response rates across all endpoints.
Overall, both the 200-mg and 400-mg doses of guselkumab were statistically superior to the placebo across all endpoints for both groups (with or without inadequate response or intolerance). Although the efficacy was comparable for the two doses, the 400-mg dose was associated with greater histoendoscopic mucosal improvement in both groups.
“It’s of interest to think about how we position and sequence our therapies with this additional data,” Dr. Rubin said.
The study was sponsored by Janssen Research & Development. Several authors are employees for and have stock options with Johnson & Johnson and Janssen. The other authors reported consultant roles, advisory roles, and research support from numerous pharmaceutical companies, including Janssen.
FROM ACG 2022
Dupilumab improves eosinophilic esophagitis up to 24 weeks
Dupilumab appears to improve clinical, symptomatic, histologic, and endoscopic aspects of eosinophilic esophagitis (EoE) up to 24 weeks, according to findings presented at the annual meeting of the American College of Gastroenterology.
The drug was also well tolerated, demonstrating consistency with the known dupilumab safety profile, said Evan S. Dellon, MD, a gastroenterologist at the University of North Carolina at Chapel Hill.

In May, the Food and Drug Administration approved dupilumab (Dupixent) for the treatment of EoE in adults and adolescents who are 12 years and older and weigh at least 40 kg (about 88 pounds), based on safety and efficacy data previously presented by Dr. Dellon and colleagues as part of the phase 3 LIBERTY-EoE-TREET study (NCT03633617).
“Dupilumab is now the only medication FDA approved to treat EoE in the U.S.,” Dr. Dellon said. “The findings here are that the pooled efficacy and safety data for parts A and B of the phase 3 trial are consistent with the results of the individual parts of the study that were previously reported, and which led to the drug being approved for EoE.”
EoE is a chronic, progressive, type 2 inflammatory disease of the esophagus, which can lead to symptoms of esophageal dysfunction that affect quality of life. Current treatment options often lack specificity, present adherence challenges, and provide suboptimal long-term disease control, Dr. Dellon said.
Dupilumab, a fully human monoclonal antibody manufactured by Regeneron Pharmaceuticals, blocks the shared receptor component for interleukin-4 and IL-13, which are central drivers of type 2 inflammation in EoE.
Study population difficult to treat
In the three-part, double-blind, placebo-controlled, phase 3 study, dupilumab was administered to 122 patients as 300-mg weekly doses through subcutaneous injection. In parts A and B, dupilumab demonstrated statistically significant and clinically meaningful improvement in adults and adolescents up to 24 weeks. In patients from part A who continued to an extended active treatment period called part C, efficacy was sustained to week 52.
Participants were included if they had EoE that hadn’t responded to high-dose proton pump inhibitors, had baseline esophageal biopsies with a peak intraepithelial eosinophilic count of 15 eosinophils per high-power field (eos/HPF) or higher in two or more esophageal regions, had a history of an average of two or more episodes of dysphagia per week in the 4 weeks prior to screening, had four or more episodes of dysphagia in the 2 weeks prior to randomization with two or more episodes that required liquids or medical attention, and had a baseline Dysphagia Symptom Questionnaire (DSQ) score of 10 or higher.
On the other hand, participants were excluded if they initiated or changed a food-elimination diet regimen or reintroduced a previously eliminated food group in the 6 weeks before screening, had other causes of esophageal eosinophilia, had a history of other inflammatory diseases such as Crohn’s disease or ulcerative colitis, or were treated with swallowed topical corticosteroids within 8 weeks prior to baseline.
Dr. Dellon and colleagues focused on co–primary endpoints: The proportion of patients who achieved peak esophageal intraepithelial eosinophil count of 6 eos/HPF or less, and the absolute change in DSQ score from baseline to week 24.
Key secondary endpoints included percentage change in eos/HPF, absolute change in EoE-Endoscopic Reference Score (EREFS), absolute change in EoE-Histologic Scoring System (EoE-HSS) grade score, and EoE-HSS stage score. Other secondary endpoints included percentage change in DSQ score and proportion of patients achieving less than 15 eos/HPF.
The baseline demographics and clinical characteristics were similar between the treatment and placebo groups. Importantly, about 70% had been treated with topical corticosteroids, and about 40% had a history of esophageal dilation, Dr. Dellon said. The DSQ scores, peak eosinophil counts, and EREFS scores were high, indicating an inflamed, symptomatic, and difficult-to-treat population.
Pooled parts A and B findings
Overall, dupilumab reduced peak esophageal intraepithelial eosinophil counts at week 24. In the dupilumab group, 59% of patients were down to 6 eos/HPF or less, compared with 5.9% in the placebo group. In a secondary endpoint, 77% of dupilumab patients were down to 15 eos/HPF, compared with 7.6% in the placebo group. The dupilumab group saw an 80% drop in baseline change, compared with 1.5% in the placebo group.
Dupilumab also reduced dysphagia symptoms and improved endoscopic features of EoE at week 24. The absolute change in DSQ score was –23.21 in the dupilumab group, compared with –12.69 in the placebo group. The percent change in DSQ score was –65.5% in the dupilumab group, compared with –38.2% in the placebo group. The absolute change in EREFS score was –3.95 in the dupilumab group, compared with –0.41 in the placebo group.
In addition, dupilumab reduced histologic scores at week 24. The absolute change in EoE-HSS grade score was –0.82 in the dupilumab group, compared with –0.1 in the placebo group. The absolute change in EoE-HSS stage score was –0.79 in the dupilumab group, compared with –0.09 in the placebo group.
Dupilumab demonstrated an acceptable safety profile, and no new safety signals were noted, Dr. Dellon said. The most common adverse events was injection-site reaction at 37.5% in the dupilumab group and 33.3% in the placebo group. The severe adverse events were not related to the medication.
“If patients have EoE, dupilumab might be an option for treatment. However, it’s important to realize that, in the phase 3 study, all patients were PPI nonresponders, most had been treated with topical steroids [and many were not responsive], and many had prior esophageal dilation,” Dr. Dellon said. “We don’t have a lot of data in more mild EoE patients, and insurances are currently requiring a series of authorization before patients might be able to get this medication. It’s best to talk to their doctor about whether the medication is a good fit for not.”
The study was sponsored by Sanofi and Regeneron Pharmaceuticals. Three of the authors are employees for and have stock options with Regeneron or Sanofi. The other authors reported consultant roles, advisory roles, and research support from numerous pharmaceutical companies, including Regeneron and Sanofi.
Dupilumab appears to improve clinical, symptomatic, histologic, and endoscopic aspects of eosinophilic esophagitis (EoE) up to 24 weeks, according to findings presented at the annual meeting of the American College of Gastroenterology.
The drug was also well tolerated, demonstrating consistency with the known dupilumab safety profile, said Evan S. Dellon, MD, a gastroenterologist at the University of North Carolina at Chapel Hill.
In May, the Food and Drug Administration approved dupilumab (Dupixent) for the treatment of EoE in adults and adolescents who are 12 years and older and weigh at least 40 kg (about 88 pounds), based on safety and efficacy data previously presented by Dr. Dellon and colleagues as part of the phase 3 LIBERTY-EoE-TREET study (NCT03633617).
“Dupilumab is now the only medication FDA approved to treat EoE in the U.S.,” Dr. Dellon said. “The findings here are that the pooled efficacy and safety data for parts A and B of the phase 3 trial are consistent with the results of the individual parts of the study that were previously reported, and which led to the drug being approved for EoE.”
EoE is a chronic, progressive, type 2 inflammatory disease of the esophagus, which can lead to symptoms of esophageal dysfunction that affect quality of life. Current treatment options often lack specificity, present adherence challenges, and provide suboptimal long-term disease control, Dr. Dellon said.
Dupilumab, a fully human monoclonal antibody manufactured by Regeneron Pharmaceuticals, blocks the shared receptor component for interleukin-4 and IL-13, which are central drivers of type 2 inflammation in EoE.
Study population difficult to treat
In the three-part, double-blind, placebo-controlled, phase 3 study, dupilumab was administered to 122 patients as 300-mg weekly doses through subcutaneous injection. In parts A and B, dupilumab demonstrated statistically significant and clinically meaningful improvement in adults and adolescents up to 24 weeks. In patients from part A who continued to an extended active treatment period called part C, efficacy was sustained to week 52.
Participants were included if they had EoE that hadn’t responded to high-dose proton pump inhibitors, had baseline esophageal biopsies with a peak intraepithelial eosinophilic count of 15 eosinophils per high-power field (eos/HPF) or higher in two or more esophageal regions, had a history of an average of two or more episodes of dysphagia per week in the 4 weeks prior to screening, had four or more episodes of dysphagia in the 2 weeks prior to randomization with two or more episodes that required liquids or medical attention, and had a baseline Dysphagia Symptom Questionnaire (DSQ) score of 10 or higher.
On the other hand, participants were excluded if they initiated or changed a food-elimination diet regimen or reintroduced a previously eliminated food group in the 6 weeks before screening, had other causes of esophageal eosinophilia, had a history of other inflammatory diseases such as Crohn’s disease or ulcerative colitis, or were treated with swallowed topical corticosteroids within 8 weeks prior to baseline.
Dr. Dellon and colleagues focused on co–primary endpoints: The proportion of patients who achieved peak esophageal intraepithelial eosinophil count of 6 eos/HPF or less, and the absolute change in DSQ score from baseline to week 24.
Key secondary endpoints included percentage change in eos/HPF, absolute change in EoE-Endoscopic Reference Score (EREFS), absolute change in EoE-Histologic Scoring System (EoE-HSS) grade score, and EoE-HSS stage score. Other secondary endpoints included percentage change in DSQ score and proportion of patients achieving less than 15 eos/HPF.
The baseline demographics and clinical characteristics were similar between the treatment and placebo groups. Importantly, about 70% had been treated with topical corticosteroids, and about 40% had a history of esophageal dilation, Dr. Dellon said. The DSQ scores, peak eosinophil counts, and EREFS scores were high, indicating an inflamed, symptomatic, and difficult-to-treat population.
Pooled parts A and B findings
Overall, dupilumab reduced peak esophageal intraepithelial eosinophil counts at week 24. In the dupilumab group, 59% of patients were down to 6 eos/HPF or less, compared with 5.9% in the placebo group. In a secondary endpoint, 77% of dupilumab patients were down to 15 eos/HPF, compared with 7.6% in the placebo group. The dupilumab group saw an 80% drop in baseline change, compared with 1.5% in the placebo group.
Dupilumab also reduced dysphagia symptoms and improved endoscopic features of EoE at week 24. The absolute change in DSQ score was –23.21 in the dupilumab group, compared with –12.69 in the placebo group. The percent change in DSQ score was –65.5% in the dupilumab group, compared with –38.2% in the placebo group. The absolute change in EREFS score was –3.95 in the dupilumab group, compared with –0.41 in the placebo group.
In addition, dupilumab reduced histologic scores at week 24. The absolute change in EoE-HSS grade score was –0.82 in the dupilumab group, compared with –0.1 in the placebo group. The absolute change in EoE-HSS stage score was –0.79 in the dupilumab group, compared with –0.09 in the placebo group.
Dupilumab demonstrated an acceptable safety profile, and no new safety signals were noted, Dr. Dellon said. The most common adverse events was injection-site reaction at 37.5% in the dupilumab group and 33.3% in the placebo group. The severe adverse events were not related to the medication.
“If patients have EoE, dupilumab might be an option for treatment. However, it’s important to realize that, in the phase 3 study, all patients were PPI nonresponders, most had been treated with topical steroids [and many were not responsive], and many had prior esophageal dilation,” Dr. Dellon said. “We don’t have a lot of data in more mild EoE patients, and insurances are currently requiring a series of authorization before patients might be able to get this medication. It’s best to talk to their doctor about whether the medication is a good fit for not.”
The study was sponsored by Sanofi and Regeneron Pharmaceuticals. Three of the authors are employees for and have stock options with Regeneron or Sanofi. The other authors reported consultant roles, advisory roles, and research support from numerous pharmaceutical companies, including Regeneron and Sanofi.
Dupilumab appears to improve clinical, symptomatic, histologic, and endoscopic aspects of eosinophilic esophagitis (EoE) up to 24 weeks, according to findings presented at the annual meeting of the American College of Gastroenterology.
The drug was also well tolerated, demonstrating consistency with the known dupilumab safety profile, said Evan S. Dellon, MD, a gastroenterologist at the University of North Carolina at Chapel Hill.
In May, the Food and Drug Administration approved dupilumab (Dupixent) for the treatment of EoE in adults and adolescents who are 12 years and older and weigh at least 40 kg (about 88 pounds), based on safety and efficacy data previously presented by Dr. Dellon and colleagues as part of the phase 3 LIBERTY-EoE-TREET study (NCT03633617).
“Dupilumab is now the only medication FDA approved to treat EoE in the U.S.,” Dr. Dellon said. “The findings here are that the pooled efficacy and safety data for parts A and B of the phase 3 trial are consistent with the results of the individual parts of the study that were previously reported, and which led to the drug being approved for EoE.”
EoE is a chronic, progressive, type 2 inflammatory disease of the esophagus, which can lead to symptoms of esophageal dysfunction that affect quality of life. Current treatment options often lack specificity, present adherence challenges, and provide suboptimal long-term disease control, Dr. Dellon said.
Dupilumab, a fully human monoclonal antibody manufactured by Regeneron Pharmaceuticals, blocks the shared receptor component for interleukin-4 and IL-13, which are central drivers of type 2 inflammation in EoE.
Study population difficult to treat
In the three-part, double-blind, placebo-controlled, phase 3 study, dupilumab was administered to 122 patients as 300-mg weekly doses through subcutaneous injection. In parts A and B, dupilumab demonstrated statistically significant and clinically meaningful improvement in adults and adolescents up to 24 weeks. In patients from part A who continued to an extended active treatment period called part C, efficacy was sustained to week 52.
Participants were included if they had EoE that hadn’t responded to high-dose proton pump inhibitors, had baseline esophageal biopsies with a peak intraepithelial eosinophilic count of 15 eosinophils per high-power field (eos/HPF) or higher in two or more esophageal regions, had a history of an average of two or more episodes of dysphagia per week in the 4 weeks prior to screening, had four or more episodes of dysphagia in the 2 weeks prior to randomization with two or more episodes that required liquids or medical attention, and had a baseline Dysphagia Symptom Questionnaire (DSQ) score of 10 or higher.
On the other hand, participants were excluded if they initiated or changed a food-elimination diet regimen or reintroduced a previously eliminated food group in the 6 weeks before screening, had other causes of esophageal eosinophilia, had a history of other inflammatory diseases such as Crohn’s disease or ulcerative colitis, or were treated with swallowed topical corticosteroids within 8 weeks prior to baseline.
Dr. Dellon and colleagues focused on co–primary endpoints: The proportion of patients who achieved peak esophageal intraepithelial eosinophil count of 6 eos/HPF or less, and the absolute change in DSQ score from baseline to week 24.
Key secondary endpoints included percentage change in eos/HPF, absolute change in EoE-Endoscopic Reference Score (EREFS), absolute change in EoE-Histologic Scoring System (EoE-HSS) grade score, and EoE-HSS stage score. Other secondary endpoints included percentage change in DSQ score and proportion of patients achieving less than 15 eos/HPF.
The baseline demographics and clinical characteristics were similar between the treatment and placebo groups. Importantly, about 70% had been treated with topical corticosteroids, and about 40% had a history of esophageal dilation, Dr. Dellon said. The DSQ scores, peak eosinophil counts, and EREFS scores were high, indicating an inflamed, symptomatic, and difficult-to-treat population.
Pooled parts A and B findings
Overall, dupilumab reduced peak esophageal intraepithelial eosinophil counts at week 24. In the dupilumab group, 59% of patients were down to 6 eos/HPF or less, compared with 5.9% in the placebo group. In a secondary endpoint, 77% of dupilumab patients were down to 15 eos/HPF, compared with 7.6% in the placebo group. The dupilumab group saw an 80% drop in baseline change, compared with 1.5% in the placebo group.
Dupilumab also reduced dysphagia symptoms and improved endoscopic features of EoE at week 24. The absolute change in DSQ score was –23.21 in the dupilumab group, compared with –12.69 in the placebo group. The percent change in DSQ score was –65.5% in the dupilumab group, compared with –38.2% in the placebo group. The absolute change in EREFS score was –3.95 in the dupilumab group, compared with –0.41 in the placebo group.
In addition, dupilumab reduced histologic scores at week 24. The absolute change in EoE-HSS grade score was –0.82 in the dupilumab group, compared with –0.1 in the placebo group. The absolute change in EoE-HSS stage score was –0.79 in the dupilumab group, compared with –0.09 in the placebo group.
Dupilumab demonstrated an acceptable safety profile, and no new safety signals were noted, Dr. Dellon said. The most common adverse events was injection-site reaction at 37.5% in the dupilumab group and 33.3% in the placebo group. The severe adverse events were not related to the medication.
“If patients have EoE, dupilumab might be an option for treatment. However, it’s important to realize that, in the phase 3 study, all patients were PPI nonresponders, most had been treated with topical steroids [and many were not responsive], and many had prior esophageal dilation,” Dr. Dellon said. “We don’t have a lot of data in more mild EoE patients, and insurances are currently requiring a series of authorization before patients might be able to get this medication. It’s best to talk to their doctor about whether the medication is a good fit for not.”
The study was sponsored by Sanofi and Regeneron Pharmaceuticals. Three of the authors are employees for and have stock options with Regeneron or Sanofi. The other authors reported consultant roles, advisory roles, and research support from numerous pharmaceutical companies, including Regeneron and Sanofi.
FROM ACG 2022

Despite Katie Couric’s advice, doctors say ultrasound breast exams may not be needed
When Katie Couric shared the news of her breast cancer diagnosis, the former co-host of NBC’s “Today” show said she considered this new health challenge to be a teachable moment to encourage people to get needed cancer screenings.
“Please get your annual mammogram,” she wrote on her website in September. “But just as importantly, please find out if you need additional screening.”
In the essay, Couric, 65, explained that because she tends to have dense breast tissue, she gets an ultrasound test in addition to a mammogram when screening for breast cancer. A breast ultrasound, sometimes called a sonogram, uses sound waves to take images of the breast tissue. It can sometimes identify malignancies that are hard to spot on a mammogram in women whose breasts are dense – that is, having a high proportion of fibrous tissue and glands vs. fatty tissue.
Ms. Couric, who famously underwent a colonoscopy on live television after her first husband died of colon cancer and who lost her sister to pancreatic cancer, has long pushed for cancer screening and better detection options.
“We don’t have evidence that auxiliary screening reduces breast cancer mortality or improves quality of life,” said Dr. Carol Mangione, a professor of medicine and public health at the University of California, Los Angeles, who chairs the U.S. Preventive Services Task Force, a group of medical experts who make recommendations for preventive services after weighing their benefits and harms.
Ms. Couric’s office did not respond to requests for comment.
In addition to an annual mammogram, some women with dense breasts get a breast ultrasound or MRI to help identify cancerous cells missed by the mammogram. Dense fibrous tissue appears white on a mammogram and makes it harder to see cancers, which also appear white. Fatty breast tissue, which appears dark on the mammogram, doesn’t obscure breast malignancies.
As digital breast tomosynthesis, or 3-D mammography, has become more widely available, a growing number of women are getting that screening test rather than the standard 2-D mammography. The 3-D mammography has been found to reduce the number of false-positive results and identify more cancers in some women with dense breasts, though the impact on mortality is unknown.
The task force gives an “I” rating to supplemental screening for women with dense breasts whose mammogram results don’t indicate a problem. That means the current evidence is “insufficient” to assess whether the benefits outweigh the harms of the extra screening. (The task force is updating its recommendation for breast cancer screening, including supplemental screening for women with dense breasts.)
One key harm that researchers are concerned about, besides the possible extra cost, is the chance of a false-positive result. Supplemental imaging in women who aren’t at high risk for breast cancer may identify potential trouble spots, which can lead to follow-up testing such as breast biopsies that are invasive and raise cancer fears for many patients. But research has found that very often these results turn out to be false alarms.
If 1,000 women with dense breasts get an ultrasound after a negative mammogram, the ultrasound will identify two to three cancers, studies show. But the extra imaging will also identify up to 117 potential problems that lead to recall visits and tests but are ultimately determined to be false positives.
“On the one hand, we want to do everything we can to improve detection,” said Dr. Sharon Mass, an ob.gyn. in Morristown, N.J., and the former chair of the American College of Obstetricians and Gynecologists’ New Jersey section. “But on the other hand, there are lots of costs and emotional distress” associated with false-positive results.
The professional group doesn’t recommend supplemental screening for women with dense breasts who don’t have any additional risk factors for cancer.
Many other professional groups take a similar position.
“We recommend having a conversation with a health care provider, and for patients to understand whether their breasts are dense,” Dr. Mass said. “But we do not recommend everyone get tested.”
In particular, for the roughly 8% of women who have extremely dense breasts, it’s worth having a conversation with a doctor about additional screening, said Dr. Mass.
Similarly, for women with dense breasts who have additional risk factors for breast cancer, such as a family history of the disease or a personal history of breast biopsies to check suspected cancers, supplemental screening may make sense, she said.
Dense breasts are relatively common. In the United States, an estimated 43% of women 40 and older have breasts that are considered dense or extremely dense. In addition to making it harder to interpret mammograms, women with dense breasts are up to twice as likely to develop breast cancer as women with average-density breasts, research shows.
Studies have shown that mammograms reduce breast cancer mortality. But even though it seems intuitive that more testing would improve someone’s odds of beating cancer, research hasn’t found that women are any less likely to die from breast cancer if they get a supplemental ultrasound or MRI after a negative mammogram result.
A few studies have found that women with dense or very dense breasts who got an ultrasound or an MRI in addition to a mammogram had fewer so-called interval cancers between regular screening mammograms. But it’s unclear whether those results have any effect on their risk of dying from breast cancer.
“Not every small abnormality is going to lead to something that needs treatment,” said Dr. Mangione.
Thirty-eight states and the District of Columbia have laws requiring that patients be notified about breast density after a mammogram, though some require only a general notice rather than mandate that individual women be informed about their own status. Some states require insurers to cover supplemental testing, but others do not.
In 2019, the FDA proposed that information about breast density be incorporated into the letters patients receive after a mammogram. That rule hasn’t yet been finalized, but the agency told lawmakers that it expects to issue the rule no later than early next year.
In a statement to KHN, FDA spokesperson Carly Kempler said, “The FDA is committed to improving mammography services for patients and working diligently to finalize the rule to amend the existing mammography regulations.”
The cost of additional testing is another factor to consider. Because the Preventive Services Task Force recommends women get regular screening mammograms, health plans are generally required to cover them without charging people anything out-of-pocket. That’s not the case with supplemental screening for women with dense breasts, which the task force does not recommend. Some states require insurance coverage of those tests, but those laws don’t apply to the many plans in which employers “self-fund” workers’ benefits rather than buy state-regulated insurance coverage.
Supplemental imaging can be pricey if your health plan doesn’t cover it. A screening ultrasound might cost $250 out-of-pocket while a breast MRI could cost $1,084, according to the Brem Foundation to Defeat Breast Cancer.
Rep. Rosa DeLauro (D-Conn.) recently tweeted that she is working on a bill with Ms. Couric that would cover MRIs and ultrasounds for women with dense breasts without any out-of-pocket costs.
Some doctors recommend other steps that may be more effective than extra screening for women with dense breasts who want to reduce their breast cancer risk.
“If you really want to help yourself, lose weight,” said Dr. Karla Kerlikowske, a professor of medicine and epidemiology/biostatistics at the University of California, San Francisco, who has worked with other researchers to develop calculators that help providers assess patients’ breast cancer risk. “Moderate your alcohol intake and avoid long-term hormone replacement. Those are things you can control.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
When Katie Couric shared the news of her breast cancer diagnosis, the former co-host of NBC’s “Today” show said she considered this new health challenge to be a teachable moment to encourage people to get needed cancer screenings.
“Please get your annual mammogram,” she wrote on her website in September. “But just as importantly, please find out if you need additional screening.”
In the essay, Couric, 65, explained that because she tends to have dense breast tissue, she gets an ultrasound test in addition to a mammogram when screening for breast cancer. A breast ultrasound, sometimes called a sonogram, uses sound waves to take images of the breast tissue. It can sometimes identify malignancies that are hard to spot on a mammogram in women whose breasts are dense – that is, having a high proportion of fibrous tissue and glands vs. fatty tissue.
Ms. Couric, who famously underwent a colonoscopy on live television after her first husband died of colon cancer and who lost her sister to pancreatic cancer, has long pushed for cancer screening and better detection options.
“We don’t have evidence that auxiliary screening reduces breast cancer mortality or improves quality of life,” said Dr. Carol Mangione, a professor of medicine and public health at the University of California, Los Angeles, who chairs the U.S. Preventive Services Task Force, a group of medical experts who make recommendations for preventive services after weighing their benefits and harms.
Ms. Couric’s office did not respond to requests for comment.
In addition to an annual mammogram, some women with dense breasts get a breast ultrasound or MRI to help identify cancerous cells missed by the mammogram. Dense fibrous tissue appears white on a mammogram and makes it harder to see cancers, which also appear white. Fatty breast tissue, which appears dark on the mammogram, doesn’t obscure breast malignancies.
As digital breast tomosynthesis, or 3-D mammography, has become more widely available, a growing number of women are getting that screening test rather than the standard 2-D mammography. The 3-D mammography has been found to reduce the number of false-positive results and identify more cancers in some women with dense breasts, though the impact on mortality is unknown.
The task force gives an “I” rating to supplemental screening for women with dense breasts whose mammogram results don’t indicate a problem. That means the current evidence is “insufficient” to assess whether the benefits outweigh the harms of the extra screening. (The task force is updating its recommendation for breast cancer screening, including supplemental screening for women with dense breasts.)
One key harm that researchers are concerned about, besides the possible extra cost, is the chance of a false-positive result. Supplemental imaging in women who aren’t at high risk for breast cancer may identify potential trouble spots, which can lead to follow-up testing such as breast biopsies that are invasive and raise cancer fears for many patients. But research has found that very often these results turn out to be false alarms.
If 1,000 women with dense breasts get an ultrasound after a negative mammogram, the ultrasound will identify two to three cancers, studies show. But the extra imaging will also identify up to 117 potential problems that lead to recall visits and tests but are ultimately determined to be false positives.
“On the one hand, we want to do everything we can to improve detection,” said Dr. Sharon Mass, an ob.gyn. in Morristown, N.J., and the former chair of the American College of Obstetricians and Gynecologists’ New Jersey section. “But on the other hand, there are lots of costs and emotional distress” associated with false-positive results.
The professional group doesn’t recommend supplemental screening for women with dense breasts who don’t have any additional risk factors for cancer.
Many other professional groups take a similar position.
“We recommend having a conversation with a health care provider, and for patients to understand whether their breasts are dense,” Dr. Mass said. “But we do not recommend everyone get tested.”
In particular, for the roughly 8% of women who have extremely dense breasts, it’s worth having a conversation with a doctor about additional screening, said Dr. Mass.
Similarly, for women with dense breasts who have additional risk factors for breast cancer, such as a family history of the disease or a personal history of breast biopsies to check suspected cancers, supplemental screening may make sense, she said.
Dense breasts are relatively common. In the United States, an estimated 43% of women 40 and older have breasts that are considered dense or extremely dense. In addition to making it harder to interpret mammograms, women with dense breasts are up to twice as likely to develop breast cancer as women with average-density breasts, research shows.
Studies have shown that mammograms reduce breast cancer mortality. But even though it seems intuitive that more testing would improve someone’s odds of beating cancer, research hasn’t found that women are any less likely to die from breast cancer if they get a supplemental ultrasound or MRI after a negative mammogram result.
A few studies have found that women with dense or very dense breasts who got an ultrasound or an MRI in addition to a mammogram had fewer so-called interval cancers between regular screening mammograms. But it’s unclear whether those results have any effect on their risk of dying from breast cancer.
“Not every small abnormality is going to lead to something that needs treatment,” said Dr. Mangione.
Thirty-eight states and the District of Columbia have laws requiring that patients be notified about breast density after a mammogram, though some require only a general notice rather than mandate that individual women be informed about their own status. Some states require insurers to cover supplemental testing, but others do not.
In 2019, the FDA proposed that information about breast density be incorporated into the letters patients receive after a mammogram. That rule hasn’t yet been finalized, but the agency told lawmakers that it expects to issue the rule no later than early next year.
In a statement to KHN, FDA spokesperson Carly Kempler said, “The FDA is committed to improving mammography services for patients and working diligently to finalize the rule to amend the existing mammography regulations.”
The cost of additional testing is another factor to consider. Because the Preventive Services Task Force recommends women get regular screening mammograms, health plans are generally required to cover them without charging people anything out-of-pocket. That’s not the case with supplemental screening for women with dense breasts, which the task force does not recommend. Some states require insurance coverage of those tests, but those laws don’t apply to the many plans in which employers “self-fund” workers’ benefits rather than buy state-regulated insurance coverage.
Supplemental imaging can be pricey if your health plan doesn’t cover it. A screening ultrasound might cost $250 out-of-pocket while a breast MRI could cost $1,084, according to the Brem Foundation to Defeat Breast Cancer.
Rep. Rosa DeLauro (D-Conn.) recently tweeted that she is working on a bill with Ms. Couric that would cover MRIs and ultrasounds for women with dense breasts without any out-of-pocket costs.
Some doctors recommend other steps that may be more effective than extra screening for women with dense breasts who want to reduce their breast cancer risk.
“If you really want to help yourself, lose weight,” said Dr. Karla Kerlikowske, a professor of medicine and epidemiology/biostatistics at the University of California, San Francisco, who has worked with other researchers to develop calculators that help providers assess patients’ breast cancer risk. “Moderate your alcohol intake and avoid long-term hormone replacement. Those are things you can control.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
When Katie Couric shared the news of her breast cancer diagnosis, the former co-host of NBC’s “Today” show said she considered this new health challenge to be a teachable moment to encourage people to get needed cancer screenings.
“Please get your annual mammogram,” she wrote on her website in September. “But just as importantly, please find out if you need additional screening.”
In the essay, Couric, 65, explained that because she tends to have dense breast tissue, she gets an ultrasound test in addition to a mammogram when screening for breast cancer. A breast ultrasound, sometimes called a sonogram, uses sound waves to take images of the breast tissue. It can sometimes identify malignancies that are hard to spot on a mammogram in women whose breasts are dense – that is, having a high proportion of fibrous tissue and glands vs. fatty tissue.
Ms. Couric, who famously underwent a colonoscopy on live television after her first husband died of colon cancer and who lost her sister to pancreatic cancer, has long pushed for cancer screening and better detection options.
“We don’t have evidence that auxiliary screening reduces breast cancer mortality or improves quality of life,” said Dr. Carol Mangione, a professor of medicine and public health at the University of California, Los Angeles, who chairs the U.S. Preventive Services Task Force, a group of medical experts who make recommendations for preventive services after weighing their benefits and harms.
Ms. Couric’s office did not respond to requests for comment.
In addition to an annual mammogram, some women with dense breasts get a breast ultrasound or MRI to help identify cancerous cells missed by the mammogram. Dense fibrous tissue appears white on a mammogram and makes it harder to see cancers, which also appear white. Fatty breast tissue, which appears dark on the mammogram, doesn’t obscure breast malignancies.
As digital breast tomosynthesis, or 3-D mammography, has become more widely available, a growing number of women are getting that screening test rather than the standard 2-D mammography. The 3-D mammography has been found to reduce the number of false-positive results and identify more cancers in some women with dense breasts, though the impact on mortality is unknown.
The task force gives an “I” rating to supplemental screening for women with dense breasts whose mammogram results don’t indicate a problem. That means the current evidence is “insufficient” to assess whether the benefits outweigh the harms of the extra screening. (The task force is updating its recommendation for breast cancer screening, including supplemental screening for women with dense breasts.)
One key harm that researchers are concerned about, besides the possible extra cost, is the chance of a false-positive result. Supplemental imaging in women who aren’t at high risk for breast cancer may identify potential trouble spots, which can lead to follow-up testing such as breast biopsies that are invasive and raise cancer fears for many patients. But research has found that very often these results turn out to be false alarms.
If 1,000 women with dense breasts get an ultrasound after a negative mammogram, the ultrasound will identify two to three cancers, studies show. But the extra imaging will also identify up to 117 potential problems that lead to recall visits and tests but are ultimately determined to be false positives.
“On the one hand, we want to do everything we can to improve detection,” said Dr. Sharon Mass, an ob.gyn. in Morristown, N.J., and the former chair of the American College of Obstetricians and Gynecologists’ New Jersey section. “But on the other hand, there are lots of costs and emotional distress” associated with false-positive results.
The professional group doesn’t recommend supplemental screening for women with dense breasts who don’t have any additional risk factors for cancer.
Many other professional groups take a similar position.
“We recommend having a conversation with a health care provider, and for patients to understand whether their breasts are dense,” Dr. Mass said. “But we do not recommend everyone get tested.”
In particular, for the roughly 8% of women who have extremely dense breasts, it’s worth having a conversation with a doctor about additional screening, said Dr. Mass.
Similarly, for women with dense breasts who have additional risk factors for breast cancer, such as a family history of the disease or a personal history of breast biopsies to check suspected cancers, supplemental screening may make sense, she said.
Dense breasts are relatively common. In the United States, an estimated 43% of women 40 and older have breasts that are considered dense or extremely dense. In addition to making it harder to interpret mammograms, women with dense breasts are up to twice as likely to develop breast cancer as women with average-density breasts, research shows.
Studies have shown that mammograms reduce breast cancer mortality. But even though it seems intuitive that more testing would improve someone’s odds of beating cancer, research hasn’t found that women are any less likely to die from breast cancer if they get a supplemental ultrasound or MRI after a negative mammogram result.
A few studies have found that women with dense or very dense breasts who got an ultrasound or an MRI in addition to a mammogram had fewer so-called interval cancers between regular screening mammograms. But it’s unclear whether those results have any effect on their risk of dying from breast cancer.
“Not every small abnormality is going to lead to something that needs treatment,” said Dr. Mangione.
Thirty-eight states and the District of Columbia have laws requiring that patients be notified about breast density after a mammogram, though some require only a general notice rather than mandate that individual women be informed about their own status. Some states require insurers to cover supplemental testing, but others do not.
In 2019, the FDA proposed that information about breast density be incorporated into the letters patients receive after a mammogram. That rule hasn’t yet been finalized, but the agency told lawmakers that it expects to issue the rule no later than early next year.
In a statement to KHN, FDA spokesperson Carly Kempler said, “The FDA is committed to improving mammography services for patients and working diligently to finalize the rule to amend the existing mammography regulations.”
The cost of additional testing is another factor to consider. Because the Preventive Services Task Force recommends women get regular screening mammograms, health plans are generally required to cover them without charging people anything out-of-pocket. That’s not the case with supplemental screening for women with dense breasts, which the task force does not recommend. Some states require insurance coverage of those tests, but those laws don’t apply to the many plans in which employers “self-fund” workers’ benefits rather than buy state-regulated insurance coverage.
Supplemental imaging can be pricey if your health plan doesn’t cover it. A screening ultrasound might cost $250 out-of-pocket while a breast MRI could cost $1,084, according to the Brem Foundation to Defeat Breast Cancer.
Rep. Rosa DeLauro (D-Conn.) recently tweeted that she is working on a bill with Ms. Couric that would cover MRIs and ultrasounds for women with dense breasts without any out-of-pocket costs.
Some doctors recommend other steps that may be more effective than extra screening for women with dense breasts who want to reduce their breast cancer risk.
“If you really want to help yourself, lose weight,” said Dr. Karla Kerlikowske, a professor of medicine and epidemiology/biostatistics at the University of California, San Francisco, who has worked with other researchers to develop calculators that help providers assess patients’ breast cancer risk. “Moderate your alcohol intake and avoid long-term hormone replacement. Those are things you can control.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Commentary: Multifocal Hepatocellular Carcinoma, November 2022

Orimo and colleagues addressed the use of liver resection in patients with more than one HCC in the liver. Patients with no or Child-Pugh A/B cirrhosis were included in this single-center retrospective study of 1088 patients who underwent hepatectomy for Barcelona Clinic Liver Cancer (BCLC) stage 0 (n = 88), A (n = 750), or B (n = 250) HCC, with stages A and B subcategorized into A1 (single nodule 2-5 cm or ≤ 3 nodules ≤ 3 cm), A2 (single nodule 5-10 cm), A3 (single nodule ≥ 10 cm), B1 (2-3 nodules > 3 cm), and B2 (≥ 4 nodules). The 5-year overall survival (OS) rates for stage 0, A1, A2, A3, B1, and B2 patients were 70.4%, 74.2%, 63.8%, 47.7%, 47.5%, and 31.9%, respectively (P < .0001). Significant differences in overall survival (OS) were found between stages A1 and A2 (P = .0118), A2 and A3 (P = .0013), and B1 and B2 (P = .0050), but not between stages A3 and B1 (P = .4742). In stage B1 patients, Child-Pugh B cirrhosis was the only independent prognostic factor for OS. The authors concluded that hepatectomy is beneficial in patients with three or fewer hepatocellular carcinomas and either no or Child-Pugh class A cirrhosis, with the long-term results being comparable to those in patients who underwent a resection of a single HCC. Therefore, resection of up to three HCC is safe and should be considered in clinically appropriate patients.
Many patients with multifocal HCC are not eligible for liver-directed therapies. The standard of care for first-line systemic therapy is the combination of atezolizumab and bevacizumab, as reported in the IMbrave150 clinical trial. Fulgenzi and colleagues published the results of a multicenter prospective observational study, AB-Real, that included 433 patients who received atezolizumab and bevacizumab in routine clinical practice. The investigators confirmed the efficacy of the combination and found that portal vein tumor thrombosis and worse albumin-bilirubin grade were independent prognostic factors for poor OS and were associated with an increased risk for hemorrhagic events. In addition, the authors reported that the overall response rate (ORR) predicted better outcomes, including longer OS. Therefore, atezolizumab and bevacizumab remains a safe and effective first-line treatment for many patients with unresectable HCC.
Finally, Finn and colleagues reported the results of an open-label, noncomparative cohort of the REACH-2 study of ramucirumab in 47 patients with advanced HCC and an alpha-fetoprotein (AFP) level ≥ 400 ng/mL. These patients had previously received one to two lines of systemic therapy, excluding sorafenib or chemotherapy. Lenvatinib was the most common prior systemic therapy (n = 20; 43%). Others included immune checkpoint inhibitor (CPI) monotherapies (n = 11), CPI/antiangiogenic therapy (n = 14), or dual CPI therapy (n = 5). The ORR was 10.6% (95% CI 1.8-19.5) and disease control rate was 46.8% (95% CI 32.5-61.1), with a median duration of response of 8.3 months [95% CI 2.4 to not reached). The grade 3 or more adverse event rate was 57%, with hypertension (11%) being the most common, allowing the authors to conclude that ramucirumab offers clinically significant efficacy with no new safety signals in this setting. Therefore, ramucirumab remains as a safe and effective later-line treatment option for patients with unresectable HCC and an AFP ≥ 400 ng/mL.
Orimo and colleagues addressed the use of liver resection in patients with more than one HCC in the liver. Patients with no or Child-Pugh A/B cirrhosis were included in this single-center retrospective study of 1088 patients who underwent hepatectomy for Barcelona Clinic Liver Cancer (BCLC) stage 0 (n = 88), A (n = 750), or B (n = 250) HCC, with stages A and B subcategorized into A1 (single nodule 2-5 cm or ≤ 3 nodules ≤ 3 cm), A2 (single nodule 5-10 cm), A3 (single nodule ≥ 10 cm), B1 (2-3 nodules > 3 cm), and B2 (≥ 4 nodules). The 5-year overall survival (OS) rates for stage 0, A1, A2, A3, B1, and B2 patients were 70.4%, 74.2%, 63.8%, 47.7%, 47.5%, and 31.9%, respectively (P < .0001). Significant differences in overall survival (OS) were found between stages A1 and A2 (P = .0118), A2 and A3 (P = .0013), and B1 and B2 (P = .0050), but not between stages A3 and B1 (P = .4742). In stage B1 patients, Child-Pugh B cirrhosis was the only independent prognostic factor for OS. The authors concluded that hepatectomy is beneficial in patients with three or fewer hepatocellular carcinomas and either no or Child-Pugh class A cirrhosis, with the long-term results being comparable to those in patients who underwent a resection of a single HCC. Therefore, resection of up to three HCC is safe and should be considered in clinically appropriate patients.
Many patients with multifocal HCC are not eligible for liver-directed therapies. The standard of care for first-line systemic therapy is the combination of atezolizumab and bevacizumab, as reported in the IMbrave150 clinical trial. Fulgenzi and colleagues published the results of a multicenter prospective observational study, AB-Real, that included 433 patients who received atezolizumab and bevacizumab in routine clinical practice. The investigators confirmed the efficacy of the combination and found that portal vein tumor thrombosis and worse albumin-bilirubin grade were independent prognostic factors for poor OS and were associated with an increased risk for hemorrhagic events. In addition, the authors reported that the overall response rate (ORR) predicted better outcomes, including longer OS. Therefore, atezolizumab and bevacizumab remains a safe and effective first-line treatment for many patients with unresectable HCC.
Finally, Finn and colleagues reported the results of an open-label, noncomparative cohort of the REACH-2 study of ramucirumab in 47 patients with advanced HCC and an alpha-fetoprotein (AFP) level ≥ 400 ng/mL. These patients had previously received one to two lines of systemic therapy, excluding sorafenib or chemotherapy. Lenvatinib was the most common prior systemic therapy (n = 20; 43%). Others included immune checkpoint inhibitor (CPI) monotherapies (n = 11), CPI/antiangiogenic therapy (n = 14), or dual CPI therapy (n = 5). The ORR was 10.6% (95% CI 1.8-19.5) and disease control rate was 46.8% (95% CI 32.5-61.1), with a median duration of response of 8.3 months [95% CI 2.4 to not reached). The grade 3 or more adverse event rate was 57%, with hypertension (11%) being the most common, allowing the authors to conclude that ramucirumab offers clinically significant efficacy with no new safety signals in this setting. Therefore, ramucirumab remains as a safe and effective later-line treatment option for patients with unresectable HCC and an AFP ≥ 400 ng/mL.
Orimo and colleagues addressed the use of liver resection in patients with more than one HCC in the liver. Patients with no or Child-Pugh A/B cirrhosis were included in this single-center retrospective study of 1088 patients who underwent hepatectomy for Barcelona Clinic Liver Cancer (BCLC) stage 0 (n = 88), A (n = 750), or B (n = 250) HCC, with stages A and B subcategorized into A1 (single nodule 2-5 cm or ≤ 3 nodules ≤ 3 cm), A2 (single nodule 5-10 cm), A3 (single nodule ≥ 10 cm), B1 (2-3 nodules > 3 cm), and B2 (≥ 4 nodules). The 5-year overall survival (OS) rates for stage 0, A1, A2, A3, B1, and B2 patients were 70.4%, 74.2%, 63.8%, 47.7%, 47.5%, and 31.9%, respectively (P < .0001). Significant differences in overall survival (OS) were found between stages A1 and A2 (P = .0118), A2 and A3 (P = .0013), and B1 and B2 (P = .0050), but not between stages A3 and B1 (P = .4742). In stage B1 patients, Child-Pugh B cirrhosis was the only independent prognostic factor for OS. The authors concluded that hepatectomy is beneficial in patients with three or fewer hepatocellular carcinomas and either no or Child-Pugh class A cirrhosis, with the long-term results being comparable to those in patients who underwent a resection of a single HCC. Therefore, resection of up to three HCC is safe and should be considered in clinically appropriate patients.
Many patients with multifocal HCC are not eligible for liver-directed therapies. The standard of care for first-line systemic therapy is the combination of atezolizumab and bevacizumab, as reported in the IMbrave150 clinical trial. Fulgenzi and colleagues published the results of a multicenter prospective observational study, AB-Real, that included 433 patients who received atezolizumab and bevacizumab in routine clinical practice. The investigators confirmed the efficacy of the combination and found that portal vein tumor thrombosis and worse albumin-bilirubin grade were independent prognostic factors for poor OS and were associated with an increased risk for hemorrhagic events. In addition, the authors reported that the overall response rate (ORR) predicted better outcomes, including longer OS. Therefore, atezolizumab and bevacizumab remains a safe and effective first-line treatment for many patients with unresectable HCC.
Finally, Finn and colleagues reported the results of an open-label, noncomparative cohort of the REACH-2 study of ramucirumab in 47 patients with advanced HCC and an alpha-fetoprotein (AFP) level ≥ 400 ng/mL. These patients had previously received one to two lines of systemic therapy, excluding sorafenib or chemotherapy. Lenvatinib was the most common prior systemic therapy (n = 20; 43%). Others included immune checkpoint inhibitor (CPI) monotherapies (n = 11), CPI/antiangiogenic therapy (n = 14), or dual CPI therapy (n = 5). The ORR was 10.6% (95% CI 1.8-19.5) and disease control rate was 46.8% (95% CI 32.5-61.1), with a median duration of response of 8.3 months [95% CI 2.4 to not reached). The grade 3 or more adverse event rate was 57%, with hypertension (11%) being the most common, allowing the authors to conclude that ramucirumab offers clinically significant efficacy with no new safety signals in this setting. Therefore, ramucirumab remains as a safe and effective later-line treatment option for patients with unresectable HCC and an AFP ≥ 400 ng/mL.
Commentary: Multifocal Hepatocellular Carcinoma, November 2022

Orimo and colleagues addressed the use of liver resection in patients with more than one HCC in the liver. Patients with no or Child-Pugh A/B cirrhosis were included in this single-center retrospective study of 1088 patients who underwent hepatectomy for Barcelona Clinic Liver Cancer (BCLC) stage 0 (n = 88), A (n = 750), or B (n = 250) HCC, with stages A and B subcategorized into A1 (single nodule 2-5 cm or ≤ 3 nodules ≤ 3 cm), A2 (single nodule 5-10 cm), A3 (single nodule ≥ 10 cm), B1 (2-3 nodules > 3 cm), and B2 (≥ 4 nodules). The 5-year overall survival (OS) rates for stage 0, A1, A2, A3, B1, and B2 patients were 70.4%, 74.2%, 63.8%, 47.7%, 47.5%, and 31.9%, respectively (P < .0001). Significant differences in overall survival (OS) were found between stages A1 and A2 (P = .0118), A2 and A3 (P = .0013), and B1 and B2 (P = .0050), but not between stages A3 and B1 (P = .4742). In stage B1 patients, Child-Pugh B cirrhosis was the only independent prognostic factor for OS. The authors concluded that hepatectomy is beneficial in patients with three or fewer hepatocellular carcinomas and either no or Child-Pugh class A cirrhosis, with the long-term results being comparable to those in patients who underwent a resection of a single HCC. Therefore, resection of up to three HCC is safe and should be considered in clinically appropriate patients.
Many patients with multifocal HCC are not eligible for liver-directed therapies. The standard of care for first-line systemic therapy is the combination of atezolizumab and bevacizumab, as reported in the IMbrave150 clinical trial. Fulgenzi and colleagues published the results of a multicenter prospective observational study, AB-Real, that included 433 patients who received atezolizumab and bevacizumab in routine clinical practice. The investigators confirmed the efficacy of the combination and found that portal vein tumor thrombosis and worse albumin-bilirubin grade were independent prognostic factors for poor OS and were associated with an increased risk for hemorrhagic events. In addition, the authors reported that the overall response rate (ORR) predicted better outcomes, including longer OS. Therefore, atezolizumab and bevacizumab remains a safe and effective first-line treatment for many patients with unresectable HCC.
Finally, Finn and colleagues reported the results of an open-label, noncomparative cohort of the REACH-2 study of ramucirumab in 47 patients with advanced HCC and an alpha-fetoprotein (AFP) level ≥ 400 ng/mL. These patients had previously received one to two lines of systemic therapy, excluding sorafenib or chemotherapy. Lenvatinib was the most common prior systemic therapy (n = 20; 43%). Others included immune checkpoint inhibitor (CPI) monotherapies (n = 11), CPI/antiangiogenic therapy (n = 14), or dual CPI therapy (n = 5). The ORR was 10.6% (95% CI 1.8-19.5) and disease control rate was 46.8% (95% CI 32.5-61.1), with a median duration of response of 8.3 months (95% CI 2.4 to not reached). The grade 3 or more adverse event rate was 57%, with hypertension (11%) being the most common, allowing the authors to conclude that ramucirumab offers clinically significant efficacy with no new safety signals in this setting. Therefore, ramucirumab remains as a safe and effective later-line treatment option for patients with unresectable HCC and an AFP ≥ 400 ng/mL.
Orimo and colleagues addressed the use of liver resection in patients with more than one HCC in the liver. Patients with no or Child-Pugh A/B cirrhosis were included in this single-center retrospective study of 1088 patients who underwent hepatectomy for Barcelona Clinic Liver Cancer (BCLC) stage 0 (n = 88), A (n = 750), or B (n = 250) HCC, with stages A and B subcategorized into A1 (single nodule 2-5 cm or ≤ 3 nodules ≤ 3 cm), A2 (single nodule 5-10 cm), A3 (single nodule ≥ 10 cm), B1 (2-3 nodules > 3 cm), and B2 (≥ 4 nodules). The 5-year overall survival (OS) rates for stage 0, A1, A2, A3, B1, and B2 patients were 70.4%, 74.2%, 63.8%, 47.7%, 47.5%, and 31.9%, respectively (P < .0001). Significant differences in overall survival (OS) were found between stages A1 and A2 (P = .0118), A2 and A3 (P = .0013), and B1 and B2 (P = .0050), but not between stages A3 and B1 (P = .4742). In stage B1 patients, Child-Pugh B cirrhosis was the only independent prognostic factor for OS. The authors concluded that hepatectomy is beneficial in patients with three or fewer hepatocellular carcinomas and either no or Child-Pugh class A cirrhosis, with the long-term results being comparable to those in patients who underwent a resection of a single HCC. Therefore, resection of up to three HCC is safe and should be considered in clinically appropriate patients.
Many patients with multifocal HCC are not eligible for liver-directed therapies. The standard of care for first-line systemic therapy is the combination of atezolizumab and bevacizumab, as reported in the IMbrave150 clinical trial. Fulgenzi and colleagues published the results of a multicenter prospective observational study, AB-Real, that included 433 patients who received atezolizumab and bevacizumab in routine clinical practice. The investigators confirmed the efficacy of the combination and found that portal vein tumor thrombosis and worse albumin-bilirubin grade were independent prognostic factors for poor OS and were associated with an increased risk for hemorrhagic events. In addition, the authors reported that the overall response rate (ORR) predicted better outcomes, including longer OS. Therefore, atezolizumab and bevacizumab remains a safe and effective first-line treatment for many patients with unresectable HCC.
Finally, Finn and colleagues reported the results of an open-label, noncomparative cohort of the REACH-2 study of ramucirumab in 47 patients with advanced HCC and an alpha-fetoprotein (AFP) level ≥ 400 ng/mL. These patients had previously received one to two lines of systemic therapy, excluding sorafenib or chemotherapy. Lenvatinib was the most common prior systemic therapy (n = 20; 43%). Others included immune checkpoint inhibitor (CPI) monotherapies (n = 11), CPI/antiangiogenic therapy (n = 14), or dual CPI therapy (n = 5). The ORR was 10.6% (95% CI 1.8-19.5) and disease control rate was 46.8% (95% CI 32.5-61.1), with a median duration of response of 8.3 months (95% CI 2.4 to not reached). The grade 3 or more adverse event rate was 57%, with hypertension (11%) being the most common, allowing the authors to conclude that ramucirumab offers clinically significant efficacy with no new safety signals in this setting. Therefore, ramucirumab remains as a safe and effective later-line treatment option for patients with unresectable HCC and an AFP ≥ 400 ng/mL.
Orimo and colleagues addressed the use of liver resection in patients with more than one HCC in the liver. Patients with no or Child-Pugh A/B cirrhosis were included in this single-center retrospective study of 1088 patients who underwent hepatectomy for Barcelona Clinic Liver Cancer (BCLC) stage 0 (n = 88), A (n = 750), or B (n = 250) HCC, with stages A and B subcategorized into A1 (single nodule 2-5 cm or ≤ 3 nodules ≤ 3 cm), A2 (single nodule 5-10 cm), A3 (single nodule ≥ 10 cm), B1 (2-3 nodules > 3 cm), and B2 (≥ 4 nodules). The 5-year overall survival (OS) rates for stage 0, A1, A2, A3, B1, and B2 patients were 70.4%, 74.2%, 63.8%, 47.7%, 47.5%, and 31.9%, respectively (P < .0001). Significant differences in overall survival (OS) were found between stages A1 and A2 (P = .0118), A2 and A3 (P = .0013), and B1 and B2 (P = .0050), but not between stages A3 and B1 (P = .4742). In stage B1 patients, Child-Pugh B cirrhosis was the only independent prognostic factor for OS. The authors concluded that hepatectomy is beneficial in patients with three or fewer hepatocellular carcinomas and either no or Child-Pugh class A cirrhosis, with the long-term results being comparable to those in patients who underwent a resection of a single HCC. Therefore, resection of up to three HCC is safe and should be considered in clinically appropriate patients.
Many patients with multifocal HCC are not eligible for liver-directed therapies. The standard of care for first-line systemic therapy is the combination of atezolizumab and bevacizumab, as reported in the IMbrave150 clinical trial. Fulgenzi and colleagues published the results of a multicenter prospective observational study, AB-Real, that included 433 patients who received atezolizumab and bevacizumab in routine clinical practice. The investigators confirmed the efficacy of the combination and found that portal vein tumor thrombosis and worse albumin-bilirubin grade were independent prognostic factors for poor OS and were associated with an increased risk for hemorrhagic events. In addition, the authors reported that the overall response rate (ORR) predicted better outcomes, including longer OS. Therefore, atezolizumab and bevacizumab remains a safe and effective first-line treatment for many patients with unresectable HCC.
Finally, Finn and colleagues reported the results of an open-label, noncomparative cohort of the REACH-2 study of ramucirumab in 47 patients with advanced HCC and an alpha-fetoprotein (AFP) level ≥ 400 ng/mL. These patients had previously received one to two lines of systemic therapy, excluding sorafenib or chemotherapy. Lenvatinib was the most common prior systemic therapy (n = 20; 43%). Others included immune checkpoint inhibitor (CPI) monotherapies (n = 11), CPI/antiangiogenic therapy (n = 14), or dual CPI therapy (n = 5). The ORR was 10.6% (95% CI 1.8-19.5) and disease control rate was 46.8% (95% CI 32.5-61.1), with a median duration of response of 8.3 months (95% CI 2.4 to not reached). The grade 3 or more adverse event rate was 57%, with hypertension (11%) being the most common, allowing the authors to conclude that ramucirumab offers clinically significant efficacy with no new safety signals in this setting. Therefore, ramucirumab remains as a safe and effective later-line treatment option for patients with unresectable HCC and an AFP ≥ 400 ng/mL.
Strategies to treat food allergy with oral immunotherapy
according to a new review.
In OIT, a patient who is allergic to a specific food consumes increasing amounts of the allergen over time to reduce their risk for allergic reaction.
“OIT is an elective, usually noncurative procedure with inherent risks that require families to function as amateur medical professionals. Preparing them for this role is essential to protect patients and ensure the long-term success of this life-changing procedure,” lead author Douglas P. Mack, MD, MSc, a pediatric allergy, asthma, and immunology specialist at McMaster University in Hamilton, Ont., and colleagues write in Clinical & Experimental Allergy.
From strict avoidance to desensitization
Food allergy treatment has traditionally involved avoiding accidental exposure that may lead to anaphylaxis and providing rescue medication. In recent years, OIT “has been recommended by several guidelines as a primary option,” Dr. Mack and coauthors write. And with the “approval by European and USA regulators of [peanut allergen powder] Palforzia [Aimmune Therapeutics], there are now commercial and noncommercial forms of OIT available for use in several countries.”
They advise physicians to take a proactive, educational, supportive approach to patients and their families throughout the therapy.
“Ultimately, the decision to pursue OIT or continue avoidance strategies remains the responsibility of the family and the patients,” they write. “Some families may not be prepared for the role that they have to play in actively managing their child’s food allergy treatment.”
Strategies to overcome OIT challenges
Reviewing the literature about OIT for food allergy, the authors suggest various strategies physicians can use to help OIT patients and their families prepare for and overcome common treatment-related challenges.
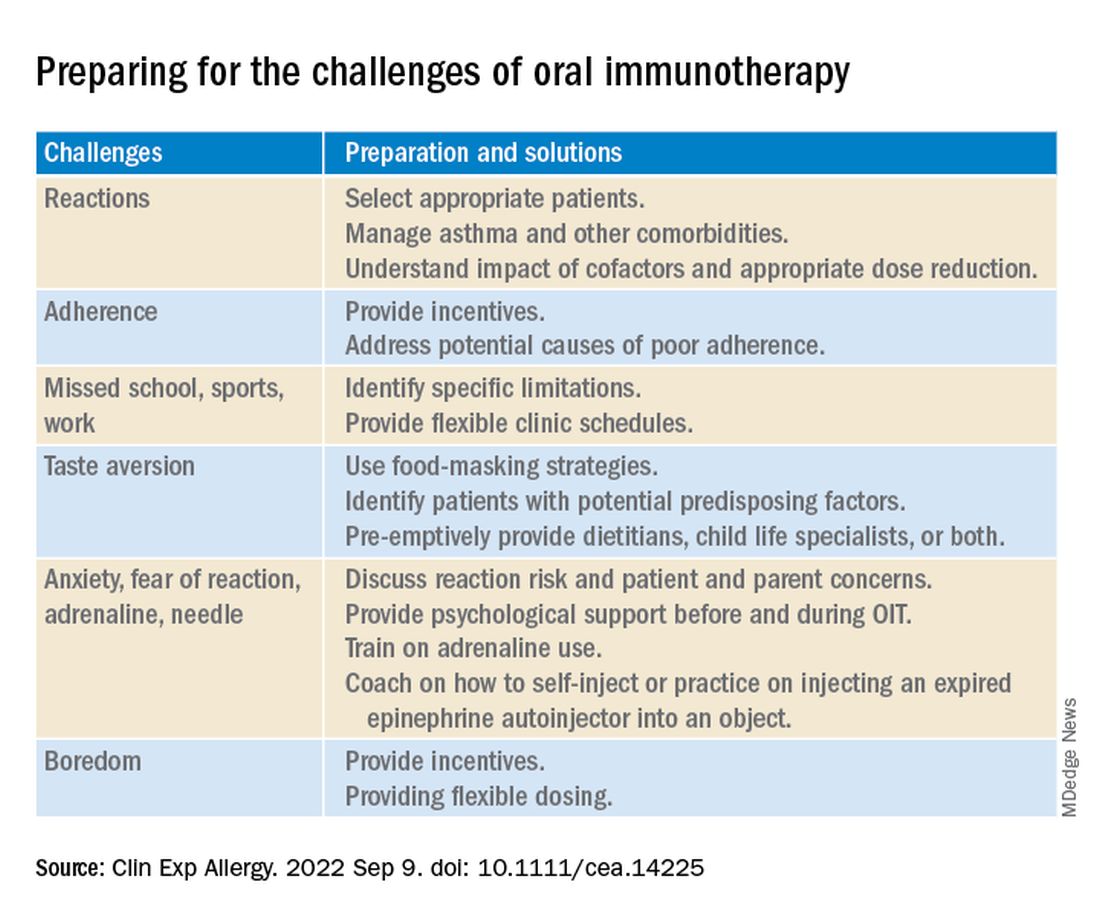
Two experts welcome the report
Rita Kachru, MD, a specialist in allergy and immunology and a codirector of the food allergy program at UCLA Health in Los Angeles, called this “an excellent report about a wonderful, individualized option in food allergy management.
“The authors did an excellent job delineating OIT terminology, outlining the goals, risks, and benefits of OIT, noting that it’s not a cure, and emphasizing the crucial importance of discussions with each family throughout the process,” Dr. Kachru, who was not involved in developing the report, told this news organization.
“I thoroughly agree with their assessment,” she added. “The more you do OIT research and clinical care, the more you realize the pitfalls, the benefits, and the importance of patient goals and family dynamics. Discussing the goals, risks, benefits, and alternatives to OIT in detail with the family is crucial so they fully understand the process.”
Basil M. Kahwash, MD, an allergy, pulmonary, and critical care medicine specialist at Vanderbilt University Medical Center in Nashville, Tenn., said that providers in the immunology community have been discussing OIT for years and that he welcomes the well-written report that summarizes the evidence.
“It’s important to periodically summarize the evidence, as well as the consensus expert opinion about the evidence, so we may better inform our colleagues and patients,” said Dr. Kahwash, who was not involved in developing the report. “The authors are well-known experts in our field who have experience with OIT and with reviewing the evidence of food allergy.
“OIT can be a fantastic option for some patients, especially those who are very highly motivated and understand the process from start to finish. But OIT is not the best option for every child, and it’s not much of an option for adults,” he explained. “Patients need to be chosen carefully and understand the level of motivation required to safely follow through with the treatment.
“The report will hopefully affect patient care positively and allow patients to understand the limitations around OIT when they consider their candidacy for it,” he added. “In most cases, OIT patients will still need to avoid the allergen, but if a small amount accidentally gets into their food, they probably won’t have a very severe reaction to it.”
Dr. Kahwash would like to see data on patients who have seen long-term remission with OIT.
“Clearly, some patients benefit from OIT. What differentiates patients who benefit from OIT from those who do not?” he asked. “In the future, we need to consider possible biomarkers of patients who are and who aren’t good candidates for OIT.
“Regardless of OIT’s limitations, the potential for desensitization rather than strict avoidance represents a big step in the evolution of food allergy treatment,” Dr. Kahwash noted.
No funding details were provided. Dr. Mack and three coauthors report financial relationships with Aimmune. Aimmune Therapeutics is the manufacturer of Palforzia OIT (AR101 powder provided in capsules and sachets). Most coauthors also report financial relationships with other pharmaceutical companies. The full list can be found with the original article. Dr. Kachru was an investigator in the PALISADES clinical trial of AR101. Dr. Kahwash reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new review.
In OIT, a patient who is allergic to a specific food consumes increasing amounts of the allergen over time to reduce their risk for allergic reaction.
“OIT is an elective, usually noncurative procedure with inherent risks that require families to function as amateur medical professionals. Preparing them for this role is essential to protect patients and ensure the long-term success of this life-changing procedure,” lead author Douglas P. Mack, MD, MSc, a pediatric allergy, asthma, and immunology specialist at McMaster University in Hamilton, Ont., and colleagues write in Clinical & Experimental Allergy.
From strict avoidance to desensitization
Food allergy treatment has traditionally involved avoiding accidental exposure that may lead to anaphylaxis and providing rescue medication. In recent years, OIT “has been recommended by several guidelines as a primary option,” Dr. Mack and coauthors write. And with the “approval by European and USA regulators of [peanut allergen powder] Palforzia [Aimmune Therapeutics], there are now commercial and noncommercial forms of OIT available for use in several countries.”
They advise physicians to take a proactive, educational, supportive approach to patients and their families throughout the therapy.
“Ultimately, the decision to pursue OIT or continue avoidance strategies remains the responsibility of the family and the patients,” they write. “Some families may not be prepared for the role that they have to play in actively managing their child’s food allergy treatment.”
Strategies to overcome OIT challenges
Reviewing the literature about OIT for food allergy, the authors suggest various strategies physicians can use to help OIT patients and their families prepare for and overcome common treatment-related challenges.
Two experts welcome the report
Rita Kachru, MD, a specialist in allergy and immunology and a codirector of the food allergy program at UCLA Health in Los Angeles, called this “an excellent report about a wonderful, individualized option in food allergy management.
“The authors did an excellent job delineating OIT terminology, outlining the goals, risks, and benefits of OIT, noting that it’s not a cure, and emphasizing the crucial importance of discussions with each family throughout the process,” Dr. Kachru, who was not involved in developing the report, told this news organization.
“I thoroughly agree with their assessment,” she added. “The more you do OIT research and clinical care, the more you realize the pitfalls, the benefits, and the importance of patient goals and family dynamics. Discussing the goals, risks, benefits, and alternatives to OIT in detail with the family is crucial so they fully understand the process.”
Basil M. Kahwash, MD, an allergy, pulmonary, and critical care medicine specialist at Vanderbilt University Medical Center in Nashville, Tenn., said that providers in the immunology community have been discussing OIT for years and that he welcomes the well-written report that summarizes the evidence.
“It’s important to periodically summarize the evidence, as well as the consensus expert opinion about the evidence, so we may better inform our colleagues and patients,” said Dr. Kahwash, who was not involved in developing the report. “The authors are well-known experts in our field who have experience with OIT and with reviewing the evidence of food allergy.
“OIT can be a fantastic option for some patients, especially those who are very highly motivated and understand the process from start to finish. But OIT is not the best option for every child, and it’s not much of an option for adults,” he explained. “Patients need to be chosen carefully and understand the level of motivation required to safely follow through with the treatment.
“The report will hopefully affect patient care positively and allow patients to understand the limitations around OIT when they consider their candidacy for it,” he added. “In most cases, OIT patients will still need to avoid the allergen, but if a small amount accidentally gets into their food, they probably won’t have a very severe reaction to it.”
Dr. Kahwash would like to see data on patients who have seen long-term remission with OIT.
“Clearly, some patients benefit from OIT. What differentiates patients who benefit from OIT from those who do not?” he asked. “In the future, we need to consider possible biomarkers of patients who are and who aren’t good candidates for OIT.
“Regardless of OIT’s limitations, the potential for desensitization rather than strict avoidance represents a big step in the evolution of food allergy treatment,” Dr. Kahwash noted.
No funding details were provided. Dr. Mack and three coauthors report financial relationships with Aimmune. Aimmune Therapeutics is the manufacturer of Palforzia OIT (AR101 powder provided in capsules and sachets). Most coauthors also report financial relationships with other pharmaceutical companies. The full list can be found with the original article. Dr. Kachru was an investigator in the PALISADES clinical trial of AR101. Dr. Kahwash reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new review.
In OIT, a patient who is allergic to a specific food consumes increasing amounts of the allergen over time to reduce their risk for allergic reaction.
“OIT is an elective, usually noncurative procedure with inherent risks that require families to function as amateur medical professionals. Preparing them for this role is essential to protect patients and ensure the long-term success of this life-changing procedure,” lead author Douglas P. Mack, MD, MSc, a pediatric allergy, asthma, and immunology specialist at McMaster University in Hamilton, Ont., and colleagues write in Clinical & Experimental Allergy.
From strict avoidance to desensitization
Food allergy treatment has traditionally involved avoiding accidental exposure that may lead to anaphylaxis and providing rescue medication. In recent years, OIT “has been recommended by several guidelines as a primary option,” Dr. Mack and coauthors write. And with the “approval by European and USA regulators of [peanut allergen powder] Palforzia [Aimmune Therapeutics], there are now commercial and noncommercial forms of OIT available for use in several countries.”
They advise physicians to take a proactive, educational, supportive approach to patients and their families throughout the therapy.
“Ultimately, the decision to pursue OIT or continue avoidance strategies remains the responsibility of the family and the patients,” they write. “Some families may not be prepared for the role that they have to play in actively managing their child’s food allergy treatment.”
Strategies to overcome OIT challenges
Reviewing the literature about OIT for food allergy, the authors suggest various strategies physicians can use to help OIT patients and their families prepare for and overcome common treatment-related challenges.
Two experts welcome the report
Rita Kachru, MD, a specialist in allergy and immunology and a codirector of the food allergy program at UCLA Health in Los Angeles, called this “an excellent report about a wonderful, individualized option in food allergy management.
“The authors did an excellent job delineating OIT terminology, outlining the goals, risks, and benefits of OIT, noting that it’s not a cure, and emphasizing the crucial importance of discussions with each family throughout the process,” Dr. Kachru, who was not involved in developing the report, told this news organization.
“I thoroughly agree with their assessment,” she added. “The more you do OIT research and clinical care, the more you realize the pitfalls, the benefits, and the importance of patient goals and family dynamics. Discussing the goals, risks, benefits, and alternatives to OIT in detail with the family is crucial so they fully understand the process.”
Basil M. Kahwash, MD, an allergy, pulmonary, and critical care medicine specialist at Vanderbilt University Medical Center in Nashville, Tenn., said that providers in the immunology community have been discussing OIT for years and that he welcomes the well-written report that summarizes the evidence.
“It’s important to periodically summarize the evidence, as well as the consensus expert opinion about the evidence, so we may better inform our colleagues and patients,” said Dr. Kahwash, who was not involved in developing the report. “The authors are well-known experts in our field who have experience with OIT and with reviewing the evidence of food allergy.
“OIT can be a fantastic option for some patients, especially those who are very highly motivated and understand the process from start to finish. But OIT is not the best option for every child, and it’s not much of an option for adults,” he explained. “Patients need to be chosen carefully and understand the level of motivation required to safely follow through with the treatment.
“The report will hopefully affect patient care positively and allow patients to understand the limitations around OIT when they consider their candidacy for it,” he added. “In most cases, OIT patients will still need to avoid the allergen, but if a small amount accidentally gets into their food, they probably won’t have a very severe reaction to it.”
Dr. Kahwash would like to see data on patients who have seen long-term remission with OIT.
“Clearly, some patients benefit from OIT. What differentiates patients who benefit from OIT from those who do not?” he asked. “In the future, we need to consider possible biomarkers of patients who are and who aren’t good candidates for OIT.
“Regardless of OIT’s limitations, the potential for desensitization rather than strict avoidance represents a big step in the evolution of food allergy treatment,” Dr. Kahwash noted.
No funding details were provided. Dr. Mack and three coauthors report financial relationships with Aimmune. Aimmune Therapeutics is the manufacturer of Palforzia OIT (AR101 powder provided in capsules and sachets). Most coauthors also report financial relationships with other pharmaceutical companies. The full list can be found with the original article. Dr. Kachru was an investigator in the PALISADES clinical trial of AR101. Dr. Kahwash reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CLINICAL & EXPERIMENTAL ALLERGY
Legal and malpractice risks when taking call
Taking call is one of the more challenging - and annoying - aspects of the job for many physicians. Calls may wake them up in the middle of the night and can interfere with their at-home activities. In Medscape’s Employed Physicians Report, 37% of respondents said they have from 1 to 5 hours of call per month; 19% said they have 6 to 10 hours; and 12% have 11 hours or more.
“Even if you don’t have to come in to the ED, you can get calls in the middle of the night, and you may get paid very little, if anything,” said Robert Bitterman MD, JD, an emergency physician and attorney in Harbor Springs, Mich.
And responding to the calls is not optional. Dr. Bitterman said
On-call activities are regulated by the federal Emergency Medical Treatment and Active Labor Act (EMTALA). Dr. Bitterman said it’s rare for the federal government to prosecute on-call physicians for violating EMTALA. Instead, it’s more likely that the hospital will be fined for EMTALA violations committed by on-call physicians.
However, the hospital passes the on-call obligation on to individual physicians through medical staff bylaws. Physicians who violate the bylaws may have their privileges restricted or removed, Dr. Bitterman said. Physicians could also be sued for malpractice, even if they never treated the patient, he added.
After-hours call duty in physicians’ practices
A very different type of call duty is having to respond to calls from one’s own patients after regular hours. Unlike doctors on ED call, who usually deal with patients they have never met, these physicians deal with their established patients or those of a colleague in their practice.
Courts have established that physicians have to provide an answering service or other means for their patients to contact them after hours, and the doctor must respond to these calls in a timely manner.
In a 2015 Louisiana ruling, a cardiologist was found liable for malpractice because he didn’t respond to an after-hours call from his patient. The patient tried several times to contact the cardiologist but got no reply.
Physicians may also be responsible if their answering service does not send critical messages to them immediately, if it fails to make appropriate documentation, or if it sends inaccurate data to the doctor.
Cases when on-call doctors didn’t respond
The Office of the Inspector General (OIG) of the U.S. Health and Human Services Administration oversees federal EMTALA violations and regularly reports them.
In 2018, the OIG fined a hospital in Waterloo, Iowa, $90,000 when an on-call cardiologist failed to implant a pacemaker for an ED patient. According to the OIG’s report, the patient arrived at the hospital with heart problems. Reached by phone, the cardiologist directed the ED physician to begin transcutaneous pacing but asked that the patient be transferred to another hospital for placement of the pacemaker. The patient died after transfer.
The OIG found that the original cardiologist could have placed the pacemaker, but, as often happens, it only fined the hospital, not the on-call physician for the EMTALA violation.
EMTALA requires that hospitals provide on-call specialists to assist emergency physicians with care of patients who arrive in the ED. In specialties for which there are few doctors to choose from, the on-call specialist may be on duty every third night and every third weekend. This can be daunting, especially for specialists who’ve had a grueling day of work.
Occasionally, on-call physicians, fearful they could make a medical error, request that the patient be transferred to another hospital for treatment. This is what a neurosurgeon who was on call at a Topeka, Kan., hospital did in 2001. Transferred to another hospital, the patient underwent an operation but lost sensation in his lower extremities. The patient sued the on-call neurosurgeon for negligence.
During the trial, the on-call neurosurgeon testified that he was “feeling run-down because he had been an on-call physician every third night for more than 10 years.” He also said this was the first time he had refused to see a patient because of fatigue, and he had decided that the patient “would be better off at a trauma center that had a trauma team and a fresher surgeon.”
The neurosurgeon successfully defended the malpractice suit, but Dr. Bitterman said he might have lost had there not been some unusual circumstances in the case. The court ruled that the hospital had not clearly defined the duties of on-call physicians, and the lawsuit didn’t cite the neurosurgeon’s EMTALA duty.
On-call duties defined by EMTALA
EMTALA sets the overall rules for on-call duties, which each hospital is expected to fine-tune on the basis of its own particular circumstances. Here are some of those rules, issued by the Centers for Medicare & Medicaid Services and the OIG.
Only an individual physician can be on call. The hospital’s on-call schedule cannot name a physician practice.
Call applies to all ED patients. Physicians cannot limit their on-call responsibilities to their own patients, to patients in their insurance network, or to paying patients.
There may be some gaps in the call schedule. The OIG is not specific as to how many gaps are allowed, said Nick Healey, an attorney in Cheyenne, Wyo., who has written about on-call duties. Among other things, adequate coverage depends on the number of available physicians and the demand for their services. Mr. Healey added that states may require more extensive availability of on-call physicians at high-level trauma centers.
Hospitals must have made arrangements for transfer. Whenever there is a gap in the schedule, hospitals need to have a designated hospital to send the patient to. Hospitals that unnecessarily transfer patients will be penalized.
The ED physician calls the shots. The emergency physician handling the case decides if the on-call doctor has to come in and treat the patient firsthand.
The on-call physician may delegate the work to others. On-call physicians may designate a nurse practitioner or physician assistant, but the on-call physician is ultimately responsible. The ED doctor may require the physician to come in anyway, according to Todd B. Taylor, MD, an emergency physician in Phoenix, who has written about on-call duties. Dr. Bitterman noted that the physician may designate a colleague to take their call, but the substitute has to have privileges at the hospital.
Physicians may do their own work while on call. Physicians can perform elective surgery while on call, provided they have made arrangements if they then become unavailable for duty, Dr. Taylor said. He added that physicians can also have simultaneous call at other hospitals, provided they make arrangements.
The hospital fine-tunes call obligations
The hospital is expected to further define the federal rules. For instance, the CMS says physicians should respond to calls within a “reasonable period of time” and requires hospitals to specify response times, which may be 15-30 minutes for responding to phone calls and traveling to the ED, Dr. Bitterman said.
The CMS says older physicians can be exempted from call. The hospital determines the age at which physicians can be exempted. “Hospitals typically exempt physicians over age 65 or 70, or when they have certain medical conditions,” said Lowell Brown, a Los Angeles attorney who deals with on-call duties.
The hospital also sets the call schedule, which may result in uncovered periods in specialties in which there are few physicians to draw from, according to Mr. Healey. He said many hospitals still use a simple rule of thumb, even though it has been dismissed by the CMS. Under this so-called “rule of three,” hospitals that have three doctors or fewer in a specialty do not have to provide constant call coverage.
On-call rules are part of the medical staff bylaws, and they have to be approved by the medical staff. This may require delicate negotiations between the staff’s leadership and administrators, Dr. Bitterman said.
It is often up to the emergency physician on duty to enforce the hospital’s on-call rules, Dr. Taylor said. “If the ED physician is having trouble, he or she may contact the on-call physician’s department chairman or, if necessary, the chief of the medical staff and ask that person to deal with the physician,” Dr. Taylor said.
The ED physician has to determine whether the patient needs to be transferred to another hospital. Dr. Taylor said the ED physician must fill out a transfer form and obtain consent from the receiving hospital.
If a patient has to be transferred because an on-call physician failed to appear, the originating hospital has to report this to the CMS, and the physician and the hospital can be cited for an inappropriate transfer and fined, Mr. Brown said. “The possibility of being identified in this way should be a powerful incentive to accept call duty,” he added.
Malpractice exposure of on-call physicians
When on-call doctors provide medical advice regarding an ED patient, that advice may be subject to malpractice litigation, Dr. Taylor said. “Even if you only give the ED doctor advice over the phone, that may establish a patient-physician relationship and a duty that patient can cite in a malpractice case,” he noted.
Refusing to take call may also be grounds for a malpractice lawsuit, Dr. Bitterman said. Refusing to see a patient would not be considered medical negligence, he continued, because no medical decision is made. Rather, it involves general negligence, which occurs when physicians fail to carry out duties expected of them.
Dr. Bitterman cited a 2006 malpractice judgment in which an on-call neurosurgeon in Missouri was found to be generally negligent. The neurosurgeon had arranged for a colleague in his practice to take his call, but the colleague did not have privileges at the hospital.
A patient with a brain bleed came in and the substitute was on duty. The patient had to be transferred to another hospital, where the patient died. The court ordered that the on-call doctor and the originating hospital had to split a fine of $400,800.
On-call physicians can be charged with abandonment
Dr. Bitterman said that if on-call physicians do not provide expected follow-up treatment for an ED patient, they could be charged with abandonment, which is a matter of state law and involves filing a malpractice lawsuit.
Abandonment involves unilaterally terminating the patient relationship without providing notice. There must be an established relationship, which, in the case of call, is formed when the doctor comes to the ED to examine or admit the patient, Dr. Bitterman said. He added that the on-call doctor’s obligation applies only to the medical condition the patient came in for.
Even when an on-call doctor does not see a patient, a relationship can be established if the hospital requires its on-call doctors to make follow-up visits for ED patients, Dr. Taylor said. At some hospitals, he said, on-call doctors have blanket agreements to provide follow-up care in return for not having to arrive in the middle of the night during the ED visit.
Dr. Taylor gave an example of the on-call doctor’s obligation: “The ED doctor puts a splint on the patient’s ankle fracture, and the orthopedic surgeon on call agrees to follow up with the patient within the next few days. If the orthopedic surgeon refuses to follow up without making a reasonable accommodation, it may become an issue of patient abandonment.”
Now everyone has a good grasp of the rules
Fifteen years ago, many doctors were in open revolt against on-call duties, but they are more accepting now and understand the rules better, Mr. Healey said.
“Many hospitals have begun paying some specialists for call and designating hospitalists and surgicalists to do at least some of the work that used to be expected of on-call doctors,” he said.
According to Dr. Taylor, today’s on-call doctors often have less to do than in the past. “For example,” he said, “the hospitalist may admit an orthopedic patient at night, and then the orthopedic surgeon does the operation the next day. We’ve had EMTALA for 36 years now, and hospitals and doctors know how call works.”
A version of this article first appeared on Medscape.com.
Taking call is one of the more challenging - and annoying - aspects of the job for many physicians. Calls may wake them up in the middle of the night and can interfere with their at-home activities. In Medscape’s Employed Physicians Report, 37% of respondents said they have from 1 to 5 hours of call per month; 19% said they have 6 to 10 hours; and 12% have 11 hours or more.
“Even if you don’t have to come in to the ED, you can get calls in the middle of the night, and you may get paid very little, if anything,” said Robert Bitterman MD, JD, an emergency physician and attorney in Harbor Springs, Mich.
And responding to the calls is not optional. Dr. Bitterman said
On-call activities are regulated by the federal Emergency Medical Treatment and Active Labor Act (EMTALA). Dr. Bitterman said it’s rare for the federal government to prosecute on-call physicians for violating EMTALA. Instead, it’s more likely that the hospital will be fined for EMTALA violations committed by on-call physicians.
However, the hospital passes the on-call obligation on to individual physicians through medical staff bylaws. Physicians who violate the bylaws may have their privileges restricted or removed, Dr. Bitterman said. Physicians could also be sued for malpractice, even if they never treated the patient, he added.
After-hours call duty in physicians’ practices
A very different type of call duty is having to respond to calls from one’s own patients after regular hours. Unlike doctors on ED call, who usually deal with patients they have never met, these physicians deal with their established patients or those of a colleague in their practice.
Courts have established that physicians have to provide an answering service or other means for their patients to contact them after hours, and the doctor must respond to these calls in a timely manner.
In a 2015 Louisiana ruling, a cardiologist was found liable for malpractice because he didn’t respond to an after-hours call from his patient. The patient tried several times to contact the cardiologist but got no reply.
Physicians may also be responsible if their answering service does not send critical messages to them immediately, if it fails to make appropriate documentation, or if it sends inaccurate data to the doctor.
Cases when on-call doctors didn’t respond
The Office of the Inspector General (OIG) of the U.S. Health and Human Services Administration oversees federal EMTALA violations and regularly reports them.
In 2018, the OIG fined a hospital in Waterloo, Iowa, $90,000 when an on-call cardiologist failed to implant a pacemaker for an ED patient. According to the OIG’s report, the patient arrived at the hospital with heart problems. Reached by phone, the cardiologist directed the ED physician to begin transcutaneous pacing but asked that the patient be transferred to another hospital for placement of the pacemaker. The patient died after transfer.
The OIG found that the original cardiologist could have placed the pacemaker, but, as often happens, it only fined the hospital, not the on-call physician for the EMTALA violation.
EMTALA requires that hospitals provide on-call specialists to assist emergency physicians with care of patients who arrive in the ED. In specialties for which there are few doctors to choose from, the on-call specialist may be on duty every third night and every third weekend. This can be daunting, especially for specialists who’ve had a grueling day of work.
Occasionally, on-call physicians, fearful they could make a medical error, request that the patient be transferred to another hospital for treatment. This is what a neurosurgeon who was on call at a Topeka, Kan., hospital did in 2001. Transferred to another hospital, the patient underwent an operation but lost sensation in his lower extremities. The patient sued the on-call neurosurgeon for negligence.
During the trial, the on-call neurosurgeon testified that he was “feeling run-down because he had been an on-call physician every third night for more than 10 years.” He also said this was the first time he had refused to see a patient because of fatigue, and he had decided that the patient “would be better off at a trauma center that had a trauma team and a fresher surgeon.”
The neurosurgeon successfully defended the malpractice suit, but Dr. Bitterman said he might have lost had there not been some unusual circumstances in the case. The court ruled that the hospital had not clearly defined the duties of on-call physicians, and the lawsuit didn’t cite the neurosurgeon’s EMTALA duty.
On-call duties defined by EMTALA
EMTALA sets the overall rules for on-call duties, which each hospital is expected to fine-tune on the basis of its own particular circumstances. Here are some of those rules, issued by the Centers for Medicare & Medicaid Services and the OIG.
Only an individual physician can be on call. The hospital’s on-call schedule cannot name a physician practice.
Call applies to all ED patients. Physicians cannot limit their on-call responsibilities to their own patients, to patients in their insurance network, or to paying patients.
There may be some gaps in the call schedule. The OIG is not specific as to how many gaps are allowed, said Nick Healey, an attorney in Cheyenne, Wyo., who has written about on-call duties. Among other things, adequate coverage depends on the number of available physicians and the demand for their services. Mr. Healey added that states may require more extensive availability of on-call physicians at high-level trauma centers.
Hospitals must have made arrangements for transfer. Whenever there is a gap in the schedule, hospitals need to have a designated hospital to send the patient to. Hospitals that unnecessarily transfer patients will be penalized.
The ED physician calls the shots. The emergency physician handling the case decides if the on-call doctor has to come in and treat the patient firsthand.
The on-call physician may delegate the work to others. On-call physicians may designate a nurse practitioner or physician assistant, but the on-call physician is ultimately responsible. The ED doctor may require the physician to come in anyway, according to Todd B. Taylor, MD, an emergency physician in Phoenix, who has written about on-call duties. Dr. Bitterman noted that the physician may designate a colleague to take their call, but the substitute has to have privileges at the hospital.
Physicians may do their own work while on call. Physicians can perform elective surgery while on call, provided they have made arrangements if they then become unavailable for duty, Dr. Taylor said. He added that physicians can also have simultaneous call at other hospitals, provided they make arrangements.
The hospital fine-tunes call obligations
The hospital is expected to further define the federal rules. For instance, the CMS says physicians should respond to calls within a “reasonable period of time” and requires hospitals to specify response times, which may be 15-30 minutes for responding to phone calls and traveling to the ED, Dr. Bitterman said.
The CMS says older physicians can be exempted from call. The hospital determines the age at which physicians can be exempted. “Hospitals typically exempt physicians over age 65 or 70, or when they have certain medical conditions,” said Lowell Brown, a Los Angeles attorney who deals with on-call duties.
The hospital also sets the call schedule, which may result in uncovered periods in specialties in which there are few physicians to draw from, according to Mr. Healey. He said many hospitals still use a simple rule of thumb, even though it has been dismissed by the CMS. Under this so-called “rule of three,” hospitals that have three doctors or fewer in a specialty do not have to provide constant call coverage.
On-call rules are part of the medical staff bylaws, and they have to be approved by the medical staff. This may require delicate negotiations between the staff’s leadership and administrators, Dr. Bitterman said.
It is often up to the emergency physician on duty to enforce the hospital’s on-call rules, Dr. Taylor said. “If the ED physician is having trouble, he or she may contact the on-call physician’s department chairman or, if necessary, the chief of the medical staff and ask that person to deal with the physician,” Dr. Taylor said.
The ED physician has to determine whether the patient needs to be transferred to another hospital. Dr. Taylor said the ED physician must fill out a transfer form and obtain consent from the receiving hospital.
If a patient has to be transferred because an on-call physician failed to appear, the originating hospital has to report this to the CMS, and the physician and the hospital can be cited for an inappropriate transfer and fined, Mr. Brown said. “The possibility of being identified in this way should be a powerful incentive to accept call duty,” he added.
Malpractice exposure of on-call physicians
When on-call doctors provide medical advice regarding an ED patient, that advice may be subject to malpractice litigation, Dr. Taylor said. “Even if you only give the ED doctor advice over the phone, that may establish a patient-physician relationship and a duty that patient can cite in a malpractice case,” he noted.
Refusing to take call may also be grounds for a malpractice lawsuit, Dr. Bitterman said. Refusing to see a patient would not be considered medical negligence, he continued, because no medical decision is made. Rather, it involves general negligence, which occurs when physicians fail to carry out duties expected of them.
Dr. Bitterman cited a 2006 malpractice judgment in which an on-call neurosurgeon in Missouri was found to be generally negligent. The neurosurgeon had arranged for a colleague in his practice to take his call, but the colleague did not have privileges at the hospital.
A patient with a brain bleed came in and the substitute was on duty. The patient had to be transferred to another hospital, where the patient died. The court ordered that the on-call doctor and the originating hospital had to split a fine of $400,800.
On-call physicians can be charged with abandonment
Dr. Bitterman said that if on-call physicians do not provide expected follow-up treatment for an ED patient, they could be charged with abandonment, which is a matter of state law and involves filing a malpractice lawsuit.
Abandonment involves unilaterally terminating the patient relationship without providing notice. There must be an established relationship, which, in the case of call, is formed when the doctor comes to the ED to examine or admit the patient, Dr. Bitterman said. He added that the on-call doctor’s obligation applies only to the medical condition the patient came in for.
Even when an on-call doctor does not see a patient, a relationship can be established if the hospital requires its on-call doctors to make follow-up visits for ED patients, Dr. Taylor said. At some hospitals, he said, on-call doctors have blanket agreements to provide follow-up care in return for not having to arrive in the middle of the night during the ED visit.
Dr. Taylor gave an example of the on-call doctor’s obligation: “The ED doctor puts a splint on the patient’s ankle fracture, and the orthopedic surgeon on call agrees to follow up with the patient within the next few days. If the orthopedic surgeon refuses to follow up without making a reasonable accommodation, it may become an issue of patient abandonment.”
Now everyone has a good grasp of the rules
Fifteen years ago, many doctors were in open revolt against on-call duties, but they are more accepting now and understand the rules better, Mr. Healey said.
“Many hospitals have begun paying some specialists for call and designating hospitalists and surgicalists to do at least some of the work that used to be expected of on-call doctors,” he said.
According to Dr. Taylor, today’s on-call doctors often have less to do than in the past. “For example,” he said, “the hospitalist may admit an orthopedic patient at night, and then the orthopedic surgeon does the operation the next day. We’ve had EMTALA for 36 years now, and hospitals and doctors know how call works.”
A version of this article first appeared on Medscape.com.
Taking call is one of the more challenging - and annoying - aspects of the job for many physicians. Calls may wake them up in the middle of the night and can interfere with their at-home activities. In Medscape’s Employed Physicians Report, 37% of respondents said they have from 1 to 5 hours of call per month; 19% said they have 6 to 10 hours; and 12% have 11 hours or more.
“Even if you don’t have to come in to the ED, you can get calls in the middle of the night, and you may get paid very little, if anything,” said Robert Bitterman MD, JD, an emergency physician and attorney in Harbor Springs, Mich.
And responding to the calls is not optional. Dr. Bitterman said
On-call activities are regulated by the federal Emergency Medical Treatment and Active Labor Act (EMTALA). Dr. Bitterman said it’s rare for the federal government to prosecute on-call physicians for violating EMTALA. Instead, it’s more likely that the hospital will be fined for EMTALA violations committed by on-call physicians.
However, the hospital passes the on-call obligation on to individual physicians through medical staff bylaws. Physicians who violate the bylaws may have their privileges restricted or removed, Dr. Bitterman said. Physicians could also be sued for malpractice, even if they never treated the patient, he added.
After-hours call duty in physicians’ practices
A very different type of call duty is having to respond to calls from one’s own patients after regular hours. Unlike doctors on ED call, who usually deal with patients they have never met, these physicians deal with their established patients or those of a colleague in their practice.
Courts have established that physicians have to provide an answering service or other means for their patients to contact them after hours, and the doctor must respond to these calls in a timely manner.
In a 2015 Louisiana ruling, a cardiologist was found liable for malpractice because he didn’t respond to an after-hours call from his patient. The patient tried several times to contact the cardiologist but got no reply.
Physicians may also be responsible if their answering service does not send critical messages to them immediately, if it fails to make appropriate documentation, or if it sends inaccurate data to the doctor.
Cases when on-call doctors didn’t respond
The Office of the Inspector General (OIG) of the U.S. Health and Human Services Administration oversees federal EMTALA violations and regularly reports them.
In 2018, the OIG fined a hospital in Waterloo, Iowa, $90,000 when an on-call cardiologist failed to implant a pacemaker for an ED patient. According to the OIG’s report, the patient arrived at the hospital with heart problems. Reached by phone, the cardiologist directed the ED physician to begin transcutaneous pacing but asked that the patient be transferred to another hospital for placement of the pacemaker. The patient died after transfer.
The OIG found that the original cardiologist could have placed the pacemaker, but, as often happens, it only fined the hospital, not the on-call physician for the EMTALA violation.
EMTALA requires that hospitals provide on-call specialists to assist emergency physicians with care of patients who arrive in the ED. In specialties for which there are few doctors to choose from, the on-call specialist may be on duty every third night and every third weekend. This can be daunting, especially for specialists who’ve had a grueling day of work.
Occasionally, on-call physicians, fearful they could make a medical error, request that the patient be transferred to another hospital for treatment. This is what a neurosurgeon who was on call at a Topeka, Kan., hospital did in 2001. Transferred to another hospital, the patient underwent an operation but lost sensation in his lower extremities. The patient sued the on-call neurosurgeon for negligence.
During the trial, the on-call neurosurgeon testified that he was “feeling run-down because he had been an on-call physician every third night for more than 10 years.” He also said this was the first time he had refused to see a patient because of fatigue, and he had decided that the patient “would be better off at a trauma center that had a trauma team and a fresher surgeon.”
The neurosurgeon successfully defended the malpractice suit, but Dr. Bitterman said he might have lost had there not been some unusual circumstances in the case. The court ruled that the hospital had not clearly defined the duties of on-call physicians, and the lawsuit didn’t cite the neurosurgeon’s EMTALA duty.
On-call duties defined by EMTALA
EMTALA sets the overall rules for on-call duties, which each hospital is expected to fine-tune on the basis of its own particular circumstances. Here are some of those rules, issued by the Centers for Medicare & Medicaid Services and the OIG.
Only an individual physician can be on call. The hospital’s on-call schedule cannot name a physician practice.
Call applies to all ED patients. Physicians cannot limit their on-call responsibilities to their own patients, to patients in their insurance network, or to paying patients.
There may be some gaps in the call schedule. The OIG is not specific as to how many gaps are allowed, said Nick Healey, an attorney in Cheyenne, Wyo., who has written about on-call duties. Among other things, adequate coverage depends on the number of available physicians and the demand for their services. Mr. Healey added that states may require more extensive availability of on-call physicians at high-level trauma centers.
Hospitals must have made arrangements for transfer. Whenever there is a gap in the schedule, hospitals need to have a designated hospital to send the patient to. Hospitals that unnecessarily transfer patients will be penalized.
The ED physician calls the shots. The emergency physician handling the case decides if the on-call doctor has to come in and treat the patient firsthand.
The on-call physician may delegate the work to others. On-call physicians may designate a nurse practitioner or physician assistant, but the on-call physician is ultimately responsible. The ED doctor may require the physician to come in anyway, according to Todd B. Taylor, MD, an emergency physician in Phoenix, who has written about on-call duties. Dr. Bitterman noted that the physician may designate a colleague to take their call, but the substitute has to have privileges at the hospital.
Physicians may do their own work while on call. Physicians can perform elective surgery while on call, provided they have made arrangements if they then become unavailable for duty, Dr. Taylor said. He added that physicians can also have simultaneous call at other hospitals, provided they make arrangements.
The hospital fine-tunes call obligations
The hospital is expected to further define the federal rules. For instance, the CMS says physicians should respond to calls within a “reasonable period of time” and requires hospitals to specify response times, which may be 15-30 minutes for responding to phone calls and traveling to the ED, Dr. Bitterman said.
The CMS says older physicians can be exempted from call. The hospital determines the age at which physicians can be exempted. “Hospitals typically exempt physicians over age 65 or 70, or when they have certain medical conditions,” said Lowell Brown, a Los Angeles attorney who deals with on-call duties.
The hospital also sets the call schedule, which may result in uncovered periods in specialties in which there are few physicians to draw from, according to Mr. Healey. He said many hospitals still use a simple rule of thumb, even though it has been dismissed by the CMS. Under this so-called “rule of three,” hospitals that have three doctors or fewer in a specialty do not have to provide constant call coverage.
On-call rules are part of the medical staff bylaws, and they have to be approved by the medical staff. This may require delicate negotiations between the staff’s leadership and administrators, Dr. Bitterman said.
It is often up to the emergency physician on duty to enforce the hospital’s on-call rules, Dr. Taylor said. “If the ED physician is having trouble, he or she may contact the on-call physician’s department chairman or, if necessary, the chief of the medical staff and ask that person to deal with the physician,” Dr. Taylor said.
The ED physician has to determine whether the patient needs to be transferred to another hospital. Dr. Taylor said the ED physician must fill out a transfer form and obtain consent from the receiving hospital.
If a patient has to be transferred because an on-call physician failed to appear, the originating hospital has to report this to the CMS, and the physician and the hospital can be cited for an inappropriate transfer and fined, Mr. Brown said. “The possibility of being identified in this way should be a powerful incentive to accept call duty,” he added.
Malpractice exposure of on-call physicians
When on-call doctors provide medical advice regarding an ED patient, that advice may be subject to malpractice litigation, Dr. Taylor said. “Even if you only give the ED doctor advice over the phone, that may establish a patient-physician relationship and a duty that patient can cite in a malpractice case,” he noted.
Refusing to take call may also be grounds for a malpractice lawsuit, Dr. Bitterman said. Refusing to see a patient would not be considered medical negligence, he continued, because no medical decision is made. Rather, it involves general negligence, which occurs when physicians fail to carry out duties expected of them.
Dr. Bitterman cited a 2006 malpractice judgment in which an on-call neurosurgeon in Missouri was found to be generally negligent. The neurosurgeon had arranged for a colleague in his practice to take his call, but the colleague did not have privileges at the hospital.
A patient with a brain bleed came in and the substitute was on duty. The patient had to be transferred to another hospital, where the patient died. The court ordered that the on-call doctor and the originating hospital had to split a fine of $400,800.
On-call physicians can be charged with abandonment
Dr. Bitterman said that if on-call physicians do not provide expected follow-up treatment for an ED patient, they could be charged with abandonment, which is a matter of state law and involves filing a malpractice lawsuit.
Abandonment involves unilaterally terminating the patient relationship without providing notice. There must be an established relationship, which, in the case of call, is formed when the doctor comes to the ED to examine or admit the patient, Dr. Bitterman said. He added that the on-call doctor’s obligation applies only to the medical condition the patient came in for.
Even when an on-call doctor does not see a patient, a relationship can be established if the hospital requires its on-call doctors to make follow-up visits for ED patients, Dr. Taylor said. At some hospitals, he said, on-call doctors have blanket agreements to provide follow-up care in return for not having to arrive in the middle of the night during the ED visit.
Dr. Taylor gave an example of the on-call doctor’s obligation: “The ED doctor puts a splint on the patient’s ankle fracture, and the orthopedic surgeon on call agrees to follow up with the patient within the next few days. If the orthopedic surgeon refuses to follow up without making a reasonable accommodation, it may become an issue of patient abandonment.”
Now everyone has a good grasp of the rules
Fifteen years ago, many doctors were in open revolt against on-call duties, but they are more accepting now and understand the rules better, Mr. Healey said.
“Many hospitals have begun paying some specialists for call and designating hospitalists and surgicalists to do at least some of the work that used to be expected of on-call doctors,” he said.
According to Dr. Taylor, today’s on-call doctors often have less to do than in the past. “For example,” he said, “the hospitalist may admit an orthopedic patient at night, and then the orthopedic surgeon does the operation the next day. We’ve had EMTALA for 36 years now, and hospitals and doctors know how call works.”
A version of this article first appeared on Medscape.com.