User login
The Official Newspaper of the American Association for Thoracic Surgery
Docs to CMS: Delay Meaningful Use Stage 3
The American Medical Association is asking the Centers for Medicare & Medicaid Services to revise the meaningful use program to better align with requirements of last year’s Medicare Access and CHIP Reauthorization Act (MACRA) and to allow for smoother transition to value-based payment models.
In a Dec. 15 letter to CMS, the AMA issued a list of recommendations for meaningful use Stage 3 that aim to address challenges with using electronic health records (EHRs) and to help move toward MACRA’s alternative payment models (APM) and Merit-Based Incentive Payment System (MIPS).

“Doctors want to spend their time with patients, not measuring the number of clicks,” Dr. Steven J. Stack, AMA president, said in a statement. “We want a successful transition to digital health records, and we also want the new Medicare law to succeed. It will take thoughtful changes in the regulations to support physicians as they treat patients through new models of care.”
The AMA’s recommendations come in response to CMS’ final rule for meaningful use Stage 3, effective Dec. 15. The final rule simplified Stage 3 and gave doctors 1 more year – until Jan. 1, 2018 – to comply.
The AMA requested that CMS immediately adopt the association’s revisions for meaningful use Stage 3, including that the agency provide more flexibility and allow for multiple methods/paths to achieve desired end goals; remove threshold requirements for measures outside physicians’ control; and eliminate its pass-fail program design. Scrapping a pass-fail approach is the only way the ... program can align and operate within MIPS and APMs, Dr. James L. Madara, AMA executive vice president and CEO wrote in the letter.

The AMA also criticized Stage 3 for taking a poor approach to interoperability. The current measures are too focused on the quantity of information moved and “not the relevance of exchanges or the underlying business case for transmitting data,” Dr. Madara wrote. The AMA wants the measures to be refocused to address specific instances of data exchange, such as closing the referral loop, team-based care, and notification of tests/admissions.
According to the AMA, CMS should:
• Re-orient measures away from process-based tasks to highlight goals that are useful to patients and physicians.
• Encourage new technology functions to be the focus of certification rather than placing requirements on physicians and patients that may not yet be feasible.
• Support the reuse of data to reduce the burden on documentation.
The AMA’s recommendations are in line with concerns by the American Academy of Family Physicians over Stage 3, according to Dr. Robert L. Wergin, AAFP board chair. In a Dec. 2 letter to CMS, the AAFP said the final rule fell short of expectations and, in fact, places further obstacles in the way of improved health, better health care, and lower cost.
Interoperability challenges remain a top concern with the program, Dr. Wergin said in an interview. He cited a 27% decrease in physician satisfaction with EHRs since the launch of the meaningful use program, according to a 2014 survey.
“The whole concept of electronic health records, as family physicians, we saw the potential to help us care for our patients and help us track their progress,” Dr. Wergin said. “I would call it a potential unrealized. It really hasn’t developed into what we thought it could do. There’s a lot of frustrations.”
The AAFP calls for CMS to hit the pause button on meaningful use until 2019 – long enough to allow:
• The health care industry time to focus on interoperability issues.
• Vendors, physicians, and other health care professionals time to focus on designing and implementing the functionality and work flows necessary to achieve value-based payment.
• Regulators time to modify meaningful use regulations and align them with pending MACRA rules.

Similar concerns were expressed in a Nov. 20 letter from the GOP Doctors Caucus to Speaker of the House Paul Ryan (R-Wisc.). The 18-member caucus requested Speaker Ryan’s help in pressing for a delay of Stage 3 and a blanket hardship waiver exception for Stage 2. Implementation of more-stringent criteria is likely to create “a chilling effect on further EMR adoption as physicians conclude that the cost of implementation is simply not worth the bureaucratic hassle,” according to the letter. “Members of our caucus, as well as numerous congressional health care leaders, have engaged CMS on these issues to warn them of the potential negative consequences of placing these new requirements on providers in order to meet an arbitrary deadline. CMS has ignored Congress. Congressional action is the only solution left for preserving patient access, choice and quality.”
But Dr. Rocky D. Bilhartz, an interventional cardiologist in private practice in College Station, Tex., does not believe that the AMA’s recommendations nor other changes to the meaningful use program will make it better.
“I think they’re going about this entirely the wrong way,” said Dr. Bilhartz who blogs at bilhartzmd.com. “Meaningful use should not be delayed, but frankly abandoned. I don’t necessarily believe that the Department of Health & Human Service set out to try to design a system that would impair a physician’s ability to care for patients. I do believe without a doubt, that is exactly what has happened.”
On Twitter @legal_med
The American Medical Association is asking the Centers for Medicare & Medicaid Services to revise the meaningful use program to better align with requirements of last year’s Medicare Access and CHIP Reauthorization Act (MACRA) and to allow for smoother transition to value-based payment models.
In a Dec. 15 letter to CMS, the AMA issued a list of recommendations for meaningful use Stage 3 that aim to address challenges with using electronic health records (EHRs) and to help move toward MACRA’s alternative payment models (APM) and Merit-Based Incentive Payment System (MIPS).
“Doctors want to spend their time with patients, not measuring the number of clicks,” Dr. Steven J. Stack, AMA president, said in a statement. “We want a successful transition to digital health records, and we also want the new Medicare law to succeed. It will take thoughtful changes in the regulations to support physicians as they treat patients through new models of care.”
The AMA’s recommendations come in response to CMS’ final rule for meaningful use Stage 3, effective Dec. 15. The final rule simplified Stage 3 and gave doctors 1 more year – until Jan. 1, 2018 – to comply.
The AMA requested that CMS immediately adopt the association’s revisions for meaningful use Stage 3, including that the agency provide more flexibility and allow for multiple methods/paths to achieve desired end goals; remove threshold requirements for measures outside physicians’ control; and eliminate its pass-fail program design. Scrapping a pass-fail approach is the only way the ... program can align and operate within MIPS and APMs, Dr. James L. Madara, AMA executive vice president and CEO wrote in the letter.
The AMA also criticized Stage 3 for taking a poor approach to interoperability. The current measures are too focused on the quantity of information moved and “not the relevance of exchanges or the underlying business case for transmitting data,” Dr. Madara wrote. The AMA wants the measures to be refocused to address specific instances of data exchange, such as closing the referral loop, team-based care, and notification of tests/admissions.
According to the AMA, CMS should:
• Re-orient measures away from process-based tasks to highlight goals that are useful to patients and physicians.
• Encourage new technology functions to be the focus of certification rather than placing requirements on physicians and patients that may not yet be feasible.
• Support the reuse of data to reduce the burden on documentation.
The AMA’s recommendations are in line with concerns by the American Academy of Family Physicians over Stage 3, according to Dr. Robert L. Wergin, AAFP board chair. In a Dec. 2 letter to CMS, the AAFP said the final rule fell short of expectations and, in fact, places further obstacles in the way of improved health, better health care, and lower cost.
Interoperability challenges remain a top concern with the program, Dr. Wergin said in an interview. He cited a 27% decrease in physician satisfaction with EHRs since the launch of the meaningful use program, according to a 2014 survey.
“The whole concept of electronic health records, as family physicians, we saw the potential to help us care for our patients and help us track their progress,” Dr. Wergin said. “I would call it a potential unrealized. It really hasn’t developed into what we thought it could do. There’s a lot of frustrations.”
The AAFP calls for CMS to hit the pause button on meaningful use until 2019 – long enough to allow:
• The health care industry time to focus on interoperability issues.
• Vendors, physicians, and other health care professionals time to focus on designing and implementing the functionality and work flows necessary to achieve value-based payment.
• Regulators time to modify meaningful use regulations and align them with pending MACRA rules.
Similar concerns were expressed in a Nov. 20 letter from the GOP Doctors Caucus to Speaker of the House Paul Ryan (R-Wisc.). The 18-member caucus requested Speaker Ryan’s help in pressing for a delay of Stage 3 and a blanket hardship waiver exception for Stage 2. Implementation of more-stringent criteria is likely to create “a chilling effect on further EMR adoption as physicians conclude that the cost of implementation is simply not worth the bureaucratic hassle,” according to the letter. “Members of our caucus, as well as numerous congressional health care leaders, have engaged CMS on these issues to warn them of the potential negative consequences of placing these new requirements on providers in order to meet an arbitrary deadline. CMS has ignored Congress. Congressional action is the only solution left for preserving patient access, choice and quality.”
But Dr. Rocky D. Bilhartz, an interventional cardiologist in private practice in College Station, Tex., does not believe that the AMA’s recommendations nor other changes to the meaningful use program will make it better.
“I think they’re going about this entirely the wrong way,” said Dr. Bilhartz who blogs at bilhartzmd.com. “Meaningful use should not be delayed, but frankly abandoned. I don’t necessarily believe that the Department of Health & Human Service set out to try to design a system that would impair a physician’s ability to care for patients. I do believe without a doubt, that is exactly what has happened.”
On Twitter @legal_med
The American Medical Association is asking the Centers for Medicare & Medicaid Services to revise the meaningful use program to better align with requirements of last year’s Medicare Access and CHIP Reauthorization Act (MACRA) and to allow for smoother transition to value-based payment models.
In a Dec. 15 letter to CMS, the AMA issued a list of recommendations for meaningful use Stage 3 that aim to address challenges with using electronic health records (EHRs) and to help move toward MACRA’s alternative payment models (APM) and Merit-Based Incentive Payment System (MIPS).
“Doctors want to spend their time with patients, not measuring the number of clicks,” Dr. Steven J. Stack, AMA president, said in a statement. “We want a successful transition to digital health records, and we also want the new Medicare law to succeed. It will take thoughtful changes in the regulations to support physicians as they treat patients through new models of care.”
The AMA’s recommendations come in response to CMS’ final rule for meaningful use Stage 3, effective Dec. 15. The final rule simplified Stage 3 and gave doctors 1 more year – until Jan. 1, 2018 – to comply.
The AMA requested that CMS immediately adopt the association’s revisions for meaningful use Stage 3, including that the agency provide more flexibility and allow for multiple methods/paths to achieve desired end goals; remove threshold requirements for measures outside physicians’ control; and eliminate its pass-fail program design. Scrapping a pass-fail approach is the only way the ... program can align and operate within MIPS and APMs, Dr. James L. Madara, AMA executive vice president and CEO wrote in the letter.
The AMA also criticized Stage 3 for taking a poor approach to interoperability. The current measures are too focused on the quantity of information moved and “not the relevance of exchanges or the underlying business case for transmitting data,” Dr. Madara wrote. The AMA wants the measures to be refocused to address specific instances of data exchange, such as closing the referral loop, team-based care, and notification of tests/admissions.
According to the AMA, CMS should:
• Re-orient measures away from process-based tasks to highlight goals that are useful to patients and physicians.
• Encourage new technology functions to be the focus of certification rather than placing requirements on physicians and patients that may not yet be feasible.
• Support the reuse of data to reduce the burden on documentation.
The AMA’s recommendations are in line with concerns by the American Academy of Family Physicians over Stage 3, according to Dr. Robert L. Wergin, AAFP board chair. In a Dec. 2 letter to CMS, the AAFP said the final rule fell short of expectations and, in fact, places further obstacles in the way of improved health, better health care, and lower cost.
Interoperability challenges remain a top concern with the program, Dr. Wergin said in an interview. He cited a 27% decrease in physician satisfaction with EHRs since the launch of the meaningful use program, according to a 2014 survey.
“The whole concept of electronic health records, as family physicians, we saw the potential to help us care for our patients and help us track their progress,” Dr. Wergin said. “I would call it a potential unrealized. It really hasn’t developed into what we thought it could do. There’s a lot of frustrations.”
The AAFP calls for CMS to hit the pause button on meaningful use until 2019 – long enough to allow:
• The health care industry time to focus on interoperability issues.
• Vendors, physicians, and other health care professionals time to focus on designing and implementing the functionality and work flows necessary to achieve value-based payment.
• Regulators time to modify meaningful use regulations and align them with pending MACRA rules.
Similar concerns were expressed in a Nov. 20 letter from the GOP Doctors Caucus to Speaker of the House Paul Ryan (R-Wisc.). The 18-member caucus requested Speaker Ryan’s help in pressing for a delay of Stage 3 and a blanket hardship waiver exception for Stage 2. Implementation of more-stringent criteria is likely to create “a chilling effect on further EMR adoption as physicians conclude that the cost of implementation is simply not worth the bureaucratic hassle,” according to the letter. “Members of our caucus, as well as numerous congressional health care leaders, have engaged CMS on these issues to warn them of the potential negative consequences of placing these new requirements on providers in order to meet an arbitrary deadline. CMS has ignored Congress. Congressional action is the only solution left for preserving patient access, choice and quality.”
But Dr. Rocky D. Bilhartz, an interventional cardiologist in private practice in College Station, Tex., does not believe that the AMA’s recommendations nor other changes to the meaningful use program will make it better.
“I think they’re going about this entirely the wrong way,” said Dr. Bilhartz who blogs at bilhartzmd.com. “Meaningful use should not be delayed, but frankly abandoned. I don’t necessarily believe that the Department of Health & Human Service set out to try to design a system that would impair a physician’s ability to care for patients. I do believe without a doubt, that is exactly what has happened.”
On Twitter @legal_med

Bystander CPR rising in children with cardiac arrest
ORLANDO – Bystander CPR was provided in 49% of U.S. cases of pediatric out-of-hospital cardiac arrest during 2013-2014, a major improvement over the 35% rate in a prior study 15 years ago, Dr. Maryam Y. Naim reported at the American Heart Association scientific sessions.
She presented an analysis of 2,176 out-of-hospital cardiac arrests (OHCA) in patients up to age 18 years who were included in the Cardiac Arrest Registry to Enhance Survival (CARES), the nation’s largest OHCA registry. Patients with traumatic OHCA and those whose bystander CPR (BCPR) was provided by a health care professional weren’t included.

Overall, the rate of neurologically favorable survival in pediatric recipients of BCPR was 11%, compared with 7% when BCPR wasn’t provided. But the results were far more impressive in the 14% of cardiac arrests that occurred outside the home, where the rate of neurologically favorable survival in BCPR recipients was 34%, more than twice the 15% figure for nonrecipients, according to Dr. Naim, a pediatrician and cardiac intensivist at Children’s Hospital of Philadelphia and the University of Pennsylvania.
Infants accounted for 47% of all pediatric OHCA, and in these youngest patients BCPR was of no benefit.
“The most common etiology of cardiac arrest in infants is sudden infant death syndrome. These are children who are found unresponsive in their cribs, and sometimes they’ve been dead a long time. We need to find something different for this population: perhaps developing a monitor to signal when an infant stops breathing or the heart rate goes down,” she said.
The fact that the BCPR rate in pediatric OHCA has climbed to 49% speaks well for public health efforts to improve education and awareness. Of those who received BCPR during 2013 and 2014, half got compression-only CPR, suggesting increasing adherence to the 2010 AHA guidelines for CPR and emergency cardiovascular care, which emphasized compression-only CPR as a viable alternative to conventional CPR, Dr. Naim added.
Her study highlighted a racial disparity in the application of BCPR in children and adolescents: Sixty percent of white youths with OHCA received BCPR, compared with 42% of blacks and 48% of Hispanics.
“About 70% of all bystander CPR was provided by a family member at home. So there’s really an opportunity there, especially in minority communities, to further increase education and awareness about bystander CPR, teaching family members to do it and also how to call 911 to start the chain of response,” she said.
Dr. Naim reported having no financial conflicts regarding her study.
ORLANDO – Bystander CPR was provided in 49% of U.S. cases of pediatric out-of-hospital cardiac arrest during 2013-2014, a major improvement over the 35% rate in a prior study 15 years ago, Dr. Maryam Y. Naim reported at the American Heart Association scientific sessions.
She presented an analysis of 2,176 out-of-hospital cardiac arrests (OHCA) in patients up to age 18 years who were included in the Cardiac Arrest Registry to Enhance Survival (CARES), the nation’s largest OHCA registry. Patients with traumatic OHCA and those whose bystander CPR (BCPR) was provided by a health care professional weren’t included.
Overall, the rate of neurologically favorable survival in pediatric recipients of BCPR was 11%, compared with 7% when BCPR wasn’t provided. But the results were far more impressive in the 14% of cardiac arrests that occurred outside the home, where the rate of neurologically favorable survival in BCPR recipients was 34%, more than twice the 15% figure for nonrecipients, according to Dr. Naim, a pediatrician and cardiac intensivist at Children’s Hospital of Philadelphia and the University of Pennsylvania.
Infants accounted for 47% of all pediatric OHCA, and in these youngest patients BCPR was of no benefit.
“The most common etiology of cardiac arrest in infants is sudden infant death syndrome. These are children who are found unresponsive in their cribs, and sometimes they’ve been dead a long time. We need to find something different for this population: perhaps developing a monitor to signal when an infant stops breathing or the heart rate goes down,” she said.
The fact that the BCPR rate in pediatric OHCA has climbed to 49% speaks well for public health efforts to improve education and awareness. Of those who received BCPR during 2013 and 2014, half got compression-only CPR, suggesting increasing adherence to the 2010 AHA guidelines for CPR and emergency cardiovascular care, which emphasized compression-only CPR as a viable alternative to conventional CPR, Dr. Naim added.
Her study highlighted a racial disparity in the application of BCPR in children and adolescents: Sixty percent of white youths with OHCA received BCPR, compared with 42% of blacks and 48% of Hispanics.
“About 70% of all bystander CPR was provided by a family member at home. So there’s really an opportunity there, especially in minority communities, to further increase education and awareness about bystander CPR, teaching family members to do it and also how to call 911 to start the chain of response,” she said.
Dr. Naim reported having no financial conflicts regarding her study.
ORLANDO – Bystander CPR was provided in 49% of U.S. cases of pediatric out-of-hospital cardiac arrest during 2013-2014, a major improvement over the 35% rate in a prior study 15 years ago, Dr. Maryam Y. Naim reported at the American Heart Association scientific sessions.
She presented an analysis of 2,176 out-of-hospital cardiac arrests (OHCA) in patients up to age 18 years who were included in the Cardiac Arrest Registry to Enhance Survival (CARES), the nation’s largest OHCA registry. Patients with traumatic OHCA and those whose bystander CPR (BCPR) was provided by a health care professional weren’t included.
Overall, the rate of neurologically favorable survival in pediatric recipients of BCPR was 11%, compared with 7% when BCPR wasn’t provided. But the results were far more impressive in the 14% of cardiac arrests that occurred outside the home, where the rate of neurologically favorable survival in BCPR recipients was 34%, more than twice the 15% figure for nonrecipients, according to Dr. Naim, a pediatrician and cardiac intensivist at Children’s Hospital of Philadelphia and the University of Pennsylvania.
Infants accounted for 47% of all pediatric OHCA, and in these youngest patients BCPR was of no benefit.
“The most common etiology of cardiac arrest in infants is sudden infant death syndrome. These are children who are found unresponsive in their cribs, and sometimes they’ve been dead a long time. We need to find something different for this population: perhaps developing a monitor to signal when an infant stops breathing or the heart rate goes down,” she said.
The fact that the BCPR rate in pediatric OHCA has climbed to 49% speaks well for public health efforts to improve education and awareness. Of those who received BCPR during 2013 and 2014, half got compression-only CPR, suggesting increasing adherence to the 2010 AHA guidelines for CPR and emergency cardiovascular care, which emphasized compression-only CPR as a viable alternative to conventional CPR, Dr. Naim added.
Her study highlighted a racial disparity in the application of BCPR in children and adolescents: Sixty percent of white youths with OHCA received BCPR, compared with 42% of blacks and 48% of Hispanics.
“About 70% of all bystander CPR was provided by a family member at home. So there’s really an opportunity there, especially in minority communities, to further increase education and awareness about bystander CPR, teaching family members to do it and also how to call 911 to start the chain of response,” she said.
Dr. Naim reported having no financial conflicts regarding her study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Nearly half of all children and adolescents with out-of-hospital cardiac arrest in 2013-2014 got bystander CPR.
Major finding: The rate of neurologically favorable survival in pediatric patients with out-of-hospital cardiac arrest who receive bystander CPR is 34%, compared with 15% in those who don’t get the intervention.
Data source: An analysis of 2,176 out-of-hospital cardiac arrests in the Cardiac Arrest Registry to Enhance Survival during 2013 and 2014.
Disclosures: The presenter reported having no financial conflicts regarding her study.

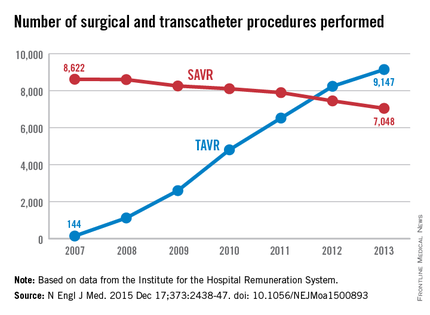
Aortic valve replacement: Transcatheter soars past surgical
In Germany, almost all of the marked increase in the use of transcatheter aortic valve replacement (TAVR) since the procedure’s introduction in 2007 occurred in patients unsuited to a surgical approach because of their advanced age or elevated risk, according to an analysis published online Dec. 17 in the New England Journal of Medicine.
The surgical aortic valve replacement (SAVR) is still the standard of care, but many have questioned how the relatively new transcatheter approach has affected clinical practice overall, said Dr. Jochen Reinöhl of the Heart Center, University of Freiburg (Germany) and his associates.
To assess the evolution of treatment since TAVR was introduced, the investigators analyzed data from the Institute for the Hospital Remuneration System, which tracks all patient data regarding diagnoses, comorbidities, and procedures throughout the country. They focused on all 88,573 admissions for isolated surgical aortic valve replacements (55,992 procedures) and for isolated TAVR (32,581 procedures) performed in Germany during 2007-2013.
The number of TAVR procedures increased markedly over time, from 144 to 9,147 per year, while the number of SAVRs declined only slightly, from 8,622 to 7,048 per year. Patients aged 80 years and older accounted for almost all of the dramatic increase in transcatheter procedures, the investigators said (N Engl J Med. 2015 Dec 17;373:2438-47 [doi:10.1056/NEJMoa1500893]).
Overall in-hospital mortality was significantly higher with TAVR (6.5%) than with SAVR (2.8%), for an odds ratio of 2.41. This likely reflects the significantly greater risk of patients selected for TAVR, compared with those undergoing surgery, they said.
Mortality decreased over time in both patient groups, from 3.8% to 2.2% with surgery and from 13.2% to 5.4% with TAVR. In the case of TAVR, this decline is likely from a “learning curve” effect among clinicians, improvements in patient care, and advances in treatment devices. In the case of surgery, the mortality decline is probably due in part to the shift of high-risk patients from SAVR to the transcatheter approach, Dr. Reinöhl and his associates said.
Similarly, complications were significantly more common with TAVR. The need for permanent pacemaker implantation was the most frequently reported complication of TAVR, occurring in 17.7% of the transcatheter group but only 4.0% of the surgical group. Stroke rates (2.5% vs. 1.8%) and rates of acute kidney injury (5.5% vs. 3.0%) followed a similar pattern. In contrast, bleeding complications were more frequent with surgery (14.0% vs. 8.2%).
In Germany, almost all of the marked increase in the use of transcatheter aortic valve replacement (TAVR) since the procedure’s introduction in 2007 occurred in patients unsuited to a surgical approach because of their advanced age or elevated risk, according to an analysis published online Dec. 17 in the New England Journal of Medicine.
The surgical aortic valve replacement (SAVR) is still the standard of care, but many have questioned how the relatively new transcatheter approach has affected clinical practice overall, said Dr. Jochen Reinöhl of the Heart Center, University of Freiburg (Germany) and his associates.
To assess the evolution of treatment since TAVR was introduced, the investigators analyzed data from the Institute for the Hospital Remuneration System, which tracks all patient data regarding diagnoses, comorbidities, and procedures throughout the country. They focused on all 88,573 admissions for isolated surgical aortic valve replacements (55,992 procedures) and for isolated TAVR (32,581 procedures) performed in Germany during 2007-2013.
The number of TAVR procedures increased markedly over time, from 144 to 9,147 per year, while the number of SAVRs declined only slightly, from 8,622 to 7,048 per year. Patients aged 80 years and older accounted for almost all of the dramatic increase in transcatheter procedures, the investigators said (N Engl J Med. 2015 Dec 17;373:2438-47 [doi:10.1056/NEJMoa1500893]).
Overall in-hospital mortality was significantly higher with TAVR (6.5%) than with SAVR (2.8%), for an odds ratio of 2.41. This likely reflects the significantly greater risk of patients selected for TAVR, compared with those undergoing surgery, they said.
Mortality decreased over time in both patient groups, from 3.8% to 2.2% with surgery and from 13.2% to 5.4% with TAVR. In the case of TAVR, this decline is likely from a “learning curve” effect among clinicians, improvements in patient care, and advances in treatment devices. In the case of surgery, the mortality decline is probably due in part to the shift of high-risk patients from SAVR to the transcatheter approach, Dr. Reinöhl and his associates said.
Similarly, complications were significantly more common with TAVR. The need for permanent pacemaker implantation was the most frequently reported complication of TAVR, occurring in 17.7% of the transcatheter group but only 4.0% of the surgical group. Stroke rates (2.5% vs. 1.8%) and rates of acute kidney injury (5.5% vs. 3.0%) followed a similar pattern. In contrast, bleeding complications were more frequent with surgery (14.0% vs. 8.2%).
In Germany, almost all of the marked increase in the use of transcatheter aortic valve replacement (TAVR) since the procedure’s introduction in 2007 occurred in patients unsuited to a surgical approach because of their advanced age or elevated risk, according to an analysis published online Dec. 17 in the New England Journal of Medicine.
The surgical aortic valve replacement (SAVR) is still the standard of care, but many have questioned how the relatively new transcatheter approach has affected clinical practice overall, said Dr. Jochen Reinöhl of the Heart Center, University of Freiburg (Germany) and his associates.
To assess the evolution of treatment since TAVR was introduced, the investigators analyzed data from the Institute for the Hospital Remuneration System, which tracks all patient data regarding diagnoses, comorbidities, and procedures throughout the country. They focused on all 88,573 admissions for isolated surgical aortic valve replacements (55,992 procedures) and for isolated TAVR (32,581 procedures) performed in Germany during 2007-2013.
The number of TAVR procedures increased markedly over time, from 144 to 9,147 per year, while the number of SAVRs declined only slightly, from 8,622 to 7,048 per year. Patients aged 80 years and older accounted for almost all of the dramatic increase in transcatheter procedures, the investigators said (N Engl J Med. 2015 Dec 17;373:2438-47 [doi:10.1056/NEJMoa1500893]).
Overall in-hospital mortality was significantly higher with TAVR (6.5%) than with SAVR (2.8%), for an odds ratio of 2.41. This likely reflects the significantly greater risk of patients selected for TAVR, compared with those undergoing surgery, they said.
Mortality decreased over time in both patient groups, from 3.8% to 2.2% with surgery and from 13.2% to 5.4% with TAVR. In the case of TAVR, this decline is likely from a “learning curve” effect among clinicians, improvements in patient care, and advances in treatment devices. In the case of surgery, the mortality decline is probably due in part to the shift of high-risk patients from SAVR to the transcatheter approach, Dr. Reinöhl and his associates said.
Similarly, complications were significantly more common with TAVR. The need for permanent pacemaker implantation was the most frequently reported complication of TAVR, occurring in 17.7% of the transcatheter group but only 4.0% of the surgical group. Stroke rates (2.5% vs. 1.8%) and rates of acute kidney injury (5.5% vs. 3.0%) followed a similar pattern. In contrast, bleeding complications were more frequent with surgery (14.0% vs. 8.2%).
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: In Germany, almost all of the marked increase in the use of transcatheter aortic valve replacement occurred among patients unsuited for a surgical approach.
Major finding: The number of TAVR procedures increased markedly over time, from 144 to 9,147 per year, while the number of surgical procedures declined only slightly, from 8,622 to 7,048 per year.
Data source: A retrospective analysis of all 88,573 surgical and TAVR performed in Germany in 2007-2013.
Disclosures: This study was supported by the Heart Center at Freiburg University. Dr. Reinöhl and one of his associates reported receiving personal fees from Edwards Lifesciences and Direct Flow Medical.

Sugammadex OK’d to reverse neuromuscular blockade during surgery
The Food and Drug Administration approved on Dec. 15 Merck’s sugammadex (Bridion) injection to reverse the effects of neuromuscular blockade induced by rocuronium bromide and vecuronium bromide during surgery.
The safety and efficacy of sugammadex were evaluated in three phase III trials involving 456 participants; most recovered within 5 minutes. An FDA review of the drug found that there was less residual neuromuscular blockade with sugammadex compared to neostigmine, and a 4-minute time savings to extubation and operating room discharge.
“Bridion provides a new treatment option that may help patients recover sooner from medications used for intubation or ventilation during surgery. This drug enables medical personnel to reverse the effects of neuromuscular blocking drugs and restore spontaneous breathing after surgery,” Dr. Sharon Hertz, director of the FDA’s Division of Anesthesia, Analgesia, and Addiction Products, said in a statement.
Although approved in other countries, sugammadex has been in the FDA’s review process since 2007, previously rejected and held up by concerns over anaphylaxis and other issues.
Because of that, sugammadex was further evaluated in a randomized, double-blind, parallel-group, repeat-dose trial. Of the 299 participants treated with Bridion, one person had an anaphylactic reaction. “Clinicians should be aware of the possibility of a hypersensitivity reaction or anaphylaxis and should intervene as appropriate,” the agency said in its statement.
Cases of marked bradycardia, some of which have resulted in cardiac arrest, have also been observed within minutes after the administration of Bridion. Tachycardia and bradycardia have been associated with cases of anaphylaxis. “Patients should be closely monitored for hemodynamic changes during and after reversal of neuromuscular blockade, and treatment with anticholinergic agents, such as atropine, should be administered if clinically significant bradycardia is observed,” the agency said.
The most common side effects reported in trials were vomiting, hypotension, pain, headache, and nausea. “Doctors should also advise women using hormonal contraceptives that Bridion may temporarily reduce the contraceptive effect so they must use an alternate method of birth control for a period of time,” the agency said.
Rocuronium bromide and vecuronium bromide are used to paralyze the vocal cords for tracheal intubation, as well as to paralyze patients under general anesthesia and prevent spontaneous breathing during ventilation. Sugammadex is a new molecular entity of the gamma-cyclodextrin class, designed to bind rocuronium and vecuronium.
The Food and Drug Administration approved on Dec. 15 Merck’s sugammadex (Bridion) injection to reverse the effects of neuromuscular blockade induced by rocuronium bromide and vecuronium bromide during surgery.
The safety and efficacy of sugammadex were evaluated in three phase III trials involving 456 participants; most recovered within 5 minutes. An FDA review of the drug found that there was less residual neuromuscular blockade with sugammadex compared to neostigmine, and a 4-minute time savings to extubation and operating room discharge.
“Bridion provides a new treatment option that may help patients recover sooner from medications used for intubation or ventilation during surgery. This drug enables medical personnel to reverse the effects of neuromuscular blocking drugs and restore spontaneous breathing after surgery,” Dr. Sharon Hertz, director of the FDA’s Division of Anesthesia, Analgesia, and Addiction Products, said in a statement.
Although approved in other countries, sugammadex has been in the FDA’s review process since 2007, previously rejected and held up by concerns over anaphylaxis and other issues.
Because of that, sugammadex was further evaluated in a randomized, double-blind, parallel-group, repeat-dose trial. Of the 299 participants treated with Bridion, one person had an anaphylactic reaction. “Clinicians should be aware of the possibility of a hypersensitivity reaction or anaphylaxis and should intervene as appropriate,” the agency said in its statement.
Cases of marked bradycardia, some of which have resulted in cardiac arrest, have also been observed within minutes after the administration of Bridion. Tachycardia and bradycardia have been associated with cases of anaphylaxis. “Patients should be closely monitored for hemodynamic changes during and after reversal of neuromuscular blockade, and treatment with anticholinergic agents, such as atropine, should be administered if clinically significant bradycardia is observed,” the agency said.
The most common side effects reported in trials were vomiting, hypotension, pain, headache, and nausea. “Doctors should also advise women using hormonal contraceptives that Bridion may temporarily reduce the contraceptive effect so they must use an alternate method of birth control for a period of time,” the agency said.
Rocuronium bromide and vecuronium bromide are used to paralyze the vocal cords for tracheal intubation, as well as to paralyze patients under general anesthesia and prevent spontaneous breathing during ventilation. Sugammadex is a new molecular entity of the gamma-cyclodextrin class, designed to bind rocuronium and vecuronium.
The Food and Drug Administration approved on Dec. 15 Merck’s sugammadex (Bridion) injection to reverse the effects of neuromuscular blockade induced by rocuronium bromide and vecuronium bromide during surgery.
The safety and efficacy of sugammadex were evaluated in three phase III trials involving 456 participants; most recovered within 5 minutes. An FDA review of the drug found that there was less residual neuromuscular blockade with sugammadex compared to neostigmine, and a 4-minute time savings to extubation and operating room discharge.
“Bridion provides a new treatment option that may help patients recover sooner from medications used for intubation or ventilation during surgery. This drug enables medical personnel to reverse the effects of neuromuscular blocking drugs and restore spontaneous breathing after surgery,” Dr. Sharon Hertz, director of the FDA’s Division of Anesthesia, Analgesia, and Addiction Products, said in a statement.
Although approved in other countries, sugammadex has been in the FDA’s review process since 2007, previously rejected and held up by concerns over anaphylaxis and other issues.
Because of that, sugammadex was further evaluated in a randomized, double-blind, parallel-group, repeat-dose trial. Of the 299 participants treated with Bridion, one person had an anaphylactic reaction. “Clinicians should be aware of the possibility of a hypersensitivity reaction or anaphylaxis and should intervene as appropriate,” the agency said in its statement.
Cases of marked bradycardia, some of which have resulted in cardiac arrest, have also been observed within minutes after the administration of Bridion. Tachycardia and bradycardia have been associated with cases of anaphylaxis. “Patients should be closely monitored for hemodynamic changes during and after reversal of neuromuscular blockade, and treatment with anticholinergic agents, such as atropine, should be administered if clinically significant bradycardia is observed,” the agency said.
The most common side effects reported in trials were vomiting, hypotension, pain, headache, and nausea. “Doctors should also advise women using hormonal contraceptives that Bridion may temporarily reduce the contraceptive effect so they must use an alternate method of birth control for a period of time,” the agency said.
Rocuronium bromide and vecuronium bromide are used to paralyze the vocal cords for tracheal intubation, as well as to paralyze patients under general anesthesia and prevent spontaneous breathing during ventilation. Sugammadex is a new molecular entity of the gamma-cyclodextrin class, designed to bind rocuronium and vecuronium.
Six-year Norwood-RVPA results in matched patients outperformed BT-shunt
Concerns with delayed right ventricle dysfunction have offset the early survival advantages after Norwood procedure with right ventricle to pulmonary artery conduit (NW-RVPA) over the Norwood with Blalock-Taussig shunt (NW-BT) in newborns with left ventricular outflow tract obstruction, but a recent report provides evidence that RV function between the two procedures is comparable for up to six years.
Reporting in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 Dec;150:1440–52), investigators for the Congenital Heart Surgeons’ Society (CHSS) trial found that NW-RVPA has better overall six-year survival and superior right ventricle function in the short term after surgery than NW-BT. The study involved 454 newborns with critical left ventricular outflow tract obstruction (LVOTO) in the CHSS database who had Norwood stage-1 from 2005 to 2014. Propensity matching paired 169 NW-RVPA patients with the same number of NW-BT patients for comparison. CHSS along with the Hospital for Sick Children in Toronto provided funding for the study.

“For neonates with critical LVOTO and similar baseline characteristics undergoing a Norwood stage-1 operation, the six-year overall survival and transplant-free survival were significantly better after NW-RVPA vs. NW-BT,” said Dr. Travis J. Wilder and his colleagues from the Hospital for Sick Children in Toronto.
Key questions the study sought to answer involved the clinical implications of the small variations in RV function between the two procedures, as well as the association between Norwood procedures and tricuspid valve regurgitation (TR) and overall survival.
Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group. Right ventricle dysfunction rates three months after the procedure were lower for the NW-RVPA group, 6% vs. 16%, but rates of late RV dysfunction were less than 5% for both groups. Likewise, rates of moderate or greater TR at two years were lower in the NW-RVPA group: 11% vs. 16%.
Rates of Fontan operation after six years were higher among the NW-RVPA group (54% vs. 49%), as were transplantation rates (6% vs. 2%). Overall, 2% converted to a biventricular repair, but only after NW-RVPA; and seven patients who had NW-RVPA underwent a tricuspid valve repair, compared with four in the NW-BT group.
“For all survivors not undergoing transplantation or biventricular repair, the prevalence of late moderate or greater RV dysfunction and TR were similar between NW-BT and NW-RVPA at six years, without evidence of increased RV dysfunction for patients who underwent NW-RVPA,” Dr. Wilder and his colleagues said.
Consistent with previous studies, the CHSS study showed an early risk of death after a Norwood stage-1 operation, which may be due to a greater prevalence of significant RV dysfunction as the operation transitions from stage 1 to stage 2, Dr. Wilder and his coauthors said. “Although causation between these two time-related events cannot directly be made, it suggests that poor RV function contributes to early hazard for death,” they said.
The authors acknowledge a number of limitations with their study: the variation in the quality of echocardiogram reports from the multiple institutions involved, the inability of propensity matching to account for unmeasured factors and the influence of center and surgeon volume among participating sites. They also said that the ventriculotomy the NW-RVPA involves can lead to late aneurysm, arrhythmias, and ventricular failure. The adverse effects of ventriculotomy on long-term RV function “may not become apparent for years,” Dr. Wilder and his coauthors said.
Dr. Wilder presented a report of the original results at the 2015 American Association for Thoracic Surgery Annual meeting.
The authors had no relationships to disclose.
“It is time to have the courage to confess that we need a more overarching quality improvement strategy,” Dr. James S. Tweddell of the Children’s Hospital of Wisconsin said of the results of the Congenital Heart Surgeons’ Society (CHSS) study in his invited commentary (J Thorac Cardiovasc Surg. 2015 Dec;150:1453–4).
Dr. Tweddell said the findings of the CHSS study and the earlier Single Ventricle Reconstruction (SVR) trial (N Engl J Med. 2010;362:1980-1992) are similar in terms of transplant-free survival in newborns. And while the dates of the studies’ enrollments overlap – 2005-2008 for SVR and 2005-2014 for CHSS – the more recent findings of the CHSS study would imply an advantage in terms of survival and right ventricle function. Nonetheless, the survival rates are similar, he said. “Only about 60% of patients remain alive.”

|
Dr. James S. Tweddell |
Dr. Tweddell pointed out the CHSS study is not a randomized, controlled trial, “and the shortcomings of the prospective observational study are well known.”
In calling for a “more overarching” quality improvement measure, Dr. Tweddell said that many programs use Norwood performance as a benchmark for outcomes. He proposed collaboration among high and low performing centers, imitating the adult cardiology model. He also suggested consolidation of programs performing the Norwood procedure to eliminate low-volume centers and develop centers of excellence. “The outcome of the Norwood procedure is dependent on both program and surgeon volume,” Dr. Tweddell said.
The CHSS study “is important and identifies a potentially durable benefit to the NW-RVPA,” Dr. Tweddell said, “but perhaps now is the time to focus on strategies between programs rather than solely within programs.”
“It is time to have the courage to confess that we need a more overarching quality improvement strategy,” Dr. James S. Tweddell of the Children’s Hospital of Wisconsin said of the results of the Congenital Heart Surgeons’ Society (CHSS) study in his invited commentary (J Thorac Cardiovasc Surg. 2015 Dec;150:1453–4).
Dr. Tweddell said the findings of the CHSS study and the earlier Single Ventricle Reconstruction (SVR) trial (N Engl J Med. 2010;362:1980-1992) are similar in terms of transplant-free survival in newborns. And while the dates of the studies’ enrollments overlap – 2005-2008 for SVR and 2005-2014 for CHSS – the more recent findings of the CHSS study would imply an advantage in terms of survival and right ventricle function. Nonetheless, the survival rates are similar, he said. “Only about 60% of patients remain alive.”
|
|
Dr. James S. Tweddell |
Dr. Tweddell pointed out the CHSS study is not a randomized, controlled trial, “and the shortcomings of the prospective observational study are well known.”
In calling for a “more overarching” quality improvement measure, Dr. Tweddell said that many programs use Norwood performance as a benchmark for outcomes. He proposed collaboration among high and low performing centers, imitating the adult cardiology model. He also suggested consolidation of programs performing the Norwood procedure to eliminate low-volume centers and develop centers of excellence. “The outcome of the Norwood procedure is dependent on both program and surgeon volume,” Dr. Tweddell said.
The CHSS study “is important and identifies a potentially durable benefit to the NW-RVPA,” Dr. Tweddell said, “but perhaps now is the time to focus on strategies between programs rather than solely within programs.”
“It is time to have the courage to confess that we need a more overarching quality improvement strategy,” Dr. James S. Tweddell of the Children’s Hospital of Wisconsin said of the results of the Congenital Heart Surgeons’ Society (CHSS) study in his invited commentary (J Thorac Cardiovasc Surg. 2015 Dec;150:1453–4).
Dr. Tweddell said the findings of the CHSS study and the earlier Single Ventricle Reconstruction (SVR) trial (N Engl J Med. 2010;362:1980-1992) are similar in terms of transplant-free survival in newborns. And while the dates of the studies’ enrollments overlap – 2005-2008 for SVR and 2005-2014 for CHSS – the more recent findings of the CHSS study would imply an advantage in terms of survival and right ventricle function. Nonetheless, the survival rates are similar, he said. “Only about 60% of patients remain alive.”
|
|
Dr. James S. Tweddell |
Dr. Tweddell pointed out the CHSS study is not a randomized, controlled trial, “and the shortcomings of the prospective observational study are well known.”
In calling for a “more overarching” quality improvement measure, Dr. Tweddell said that many programs use Norwood performance as a benchmark for outcomes. He proposed collaboration among high and low performing centers, imitating the adult cardiology model. He also suggested consolidation of programs performing the Norwood procedure to eliminate low-volume centers and develop centers of excellence. “The outcome of the Norwood procedure is dependent on both program and surgeon volume,” Dr. Tweddell said.
The CHSS study “is important and identifies a potentially durable benefit to the NW-RVPA,” Dr. Tweddell said, “but perhaps now is the time to focus on strategies between programs rather than solely within programs.”
Concerns with delayed right ventricle dysfunction have offset the early survival advantages after Norwood procedure with right ventricle to pulmonary artery conduit (NW-RVPA) over the Norwood with Blalock-Taussig shunt (NW-BT) in newborns with left ventricular outflow tract obstruction, but a recent report provides evidence that RV function between the two procedures is comparable for up to six years.
Reporting in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 Dec;150:1440–52), investigators for the Congenital Heart Surgeons’ Society (CHSS) trial found that NW-RVPA has better overall six-year survival and superior right ventricle function in the short term after surgery than NW-BT. The study involved 454 newborns with critical left ventricular outflow tract obstruction (LVOTO) in the CHSS database who had Norwood stage-1 from 2005 to 2014. Propensity matching paired 169 NW-RVPA patients with the same number of NW-BT patients for comparison. CHSS along with the Hospital for Sick Children in Toronto provided funding for the study.
“For neonates with critical LVOTO and similar baseline characteristics undergoing a Norwood stage-1 operation, the six-year overall survival and transplant-free survival were significantly better after NW-RVPA vs. NW-BT,” said Dr. Travis J. Wilder and his colleagues from the Hospital for Sick Children in Toronto.
Key questions the study sought to answer involved the clinical implications of the small variations in RV function between the two procedures, as well as the association between Norwood procedures and tricuspid valve regurgitation (TR) and overall survival.
Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group. Right ventricle dysfunction rates three months after the procedure were lower for the NW-RVPA group, 6% vs. 16%, but rates of late RV dysfunction were less than 5% for both groups. Likewise, rates of moderate or greater TR at two years were lower in the NW-RVPA group: 11% vs. 16%.
Rates of Fontan operation after six years were higher among the NW-RVPA group (54% vs. 49%), as were transplantation rates (6% vs. 2%). Overall, 2% converted to a biventricular repair, but only after NW-RVPA; and seven patients who had NW-RVPA underwent a tricuspid valve repair, compared with four in the NW-BT group.
“For all survivors not undergoing transplantation or biventricular repair, the prevalence of late moderate or greater RV dysfunction and TR were similar between NW-BT and NW-RVPA at six years, without evidence of increased RV dysfunction for patients who underwent NW-RVPA,” Dr. Wilder and his colleagues said.
Consistent with previous studies, the CHSS study showed an early risk of death after a Norwood stage-1 operation, which may be due to a greater prevalence of significant RV dysfunction as the operation transitions from stage 1 to stage 2, Dr. Wilder and his coauthors said. “Although causation between these two time-related events cannot directly be made, it suggests that poor RV function contributes to early hazard for death,” they said.
The authors acknowledge a number of limitations with their study: the variation in the quality of echocardiogram reports from the multiple institutions involved, the inability of propensity matching to account for unmeasured factors and the influence of center and surgeon volume among participating sites. They also said that the ventriculotomy the NW-RVPA involves can lead to late aneurysm, arrhythmias, and ventricular failure. The adverse effects of ventriculotomy on long-term RV function “may not become apparent for years,” Dr. Wilder and his coauthors said.
Dr. Wilder presented a report of the original results at the 2015 American Association for Thoracic Surgery Annual meeting.
The authors had no relationships to disclose.
Concerns with delayed right ventricle dysfunction have offset the early survival advantages after Norwood procedure with right ventricle to pulmonary artery conduit (NW-RVPA) over the Norwood with Blalock-Taussig shunt (NW-BT) in newborns with left ventricular outflow tract obstruction, but a recent report provides evidence that RV function between the two procedures is comparable for up to six years.
Reporting in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 Dec;150:1440–52), investigators for the Congenital Heart Surgeons’ Society (CHSS) trial found that NW-RVPA has better overall six-year survival and superior right ventricle function in the short term after surgery than NW-BT. The study involved 454 newborns with critical left ventricular outflow tract obstruction (LVOTO) in the CHSS database who had Norwood stage-1 from 2005 to 2014. Propensity matching paired 169 NW-RVPA patients with the same number of NW-BT patients for comparison. CHSS along with the Hospital for Sick Children in Toronto provided funding for the study.
“For neonates with critical LVOTO and similar baseline characteristics undergoing a Norwood stage-1 operation, the six-year overall survival and transplant-free survival were significantly better after NW-RVPA vs. NW-BT,” said Dr. Travis J. Wilder and his colleagues from the Hospital for Sick Children in Toronto.
Key questions the study sought to answer involved the clinical implications of the small variations in RV function between the two procedures, as well as the association between Norwood procedures and tricuspid valve regurgitation (TR) and overall survival.
Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group. Right ventricle dysfunction rates three months after the procedure were lower for the NW-RVPA group, 6% vs. 16%, but rates of late RV dysfunction were less than 5% for both groups. Likewise, rates of moderate or greater TR at two years were lower in the NW-RVPA group: 11% vs. 16%.
Rates of Fontan operation after six years were higher among the NW-RVPA group (54% vs. 49%), as were transplantation rates (6% vs. 2%). Overall, 2% converted to a biventricular repair, but only after NW-RVPA; and seven patients who had NW-RVPA underwent a tricuspid valve repair, compared with four in the NW-BT group.
“For all survivors not undergoing transplantation or biventricular repair, the prevalence of late moderate or greater RV dysfunction and TR were similar between NW-BT and NW-RVPA at six years, without evidence of increased RV dysfunction for patients who underwent NW-RVPA,” Dr. Wilder and his colleagues said.
Consistent with previous studies, the CHSS study showed an early risk of death after a Norwood stage-1 operation, which may be due to a greater prevalence of significant RV dysfunction as the operation transitions from stage 1 to stage 2, Dr. Wilder and his coauthors said. “Although causation between these two time-related events cannot directly be made, it suggests that poor RV function contributes to early hazard for death,” they said.
The authors acknowledge a number of limitations with their study: the variation in the quality of echocardiogram reports from the multiple institutions involved, the inability of propensity matching to account for unmeasured factors and the influence of center and surgeon volume among participating sites. They also said that the ventriculotomy the NW-RVPA involves can lead to late aneurysm, arrhythmias, and ventricular failure. The adverse effects of ventriculotomy on long-term RV function “may not become apparent for years,” Dr. Wilder and his coauthors said.
Dr. Wilder presented a report of the original results at the 2015 American Association for Thoracic Surgery Annual meeting.
The authors had no relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOTHORACIC SURGERY
Key clinical point: For newborns with critical left ventricular outflow tract obstruction (LVOTO) undergoing Norwood stage-1 procedures, Norwood with right ventricle to pulmonary artery conduit (NW-RVPA) resulted in better survival and less short-term right-ventricle dysfunction than matched patients who had the Norwood procedure with Blalock-Taussig shunt (NW-BT).
Major finding: Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group, and RV dysfunction rates three months after the procedure were 6% for NW-RVPA vs. 16% for NW-BT.
Data source: Prospective group of 454 newborns with LVOTO in the Congenital Heart Surgeons’ Society database.
Disclosures: The Congenital Heart Surgeons’ Society and Hospital for Sick Children, Toronto, provided funding for the study. The authors had no relationships to disclose.

AHA/ACC: Consensus recommendations for young athletes with congenital heart disease
Most children and young adult patients with congenital heart disease can and should engage in some form of physical activity and should avoid a sedentary lifestyle, according to a task force scientific statement from the American Heart Association and the American College of Cardiology (AHA/ACC).
This recommendation comes despite the fears of sudden cardiac death (SCD) in young athletes, which formed the initial impetus of the entire series of task force reports.
The recommended level of sports participation for patients with treated or untreated congenital heart defect, however, should consider the training and the competitive aspects of the sport itself and must be individualized to the patient. This means taking into account the patient’s current functional status, history of surgery, and the presence of implanted cardiac devices, according to the report by Dr. George F. Van Hare of Washington University, St. Louis, and his colleagues, which was published online in the Journal of the American College of Cardiology.

The report breaks down its specific recommendations based upon the various types of congenital heart defect (CHD). Full details and nuances of the recommendations and their specific levels of evidence for each individual condition and the many variants can be found in the online publication. Below is a brief and selected summary for some of the most common defects and some of those most pertinent to sudden cardiac death in young athletes.
Simple shunting lesions (atrial septal defect, ventricular septal defect, patent ductus arteriosus): Treated and untreated
In addressing the three most common subtypes of CHD – ventricular septal defect (VSD, 34%), atrial septal defect (ASD, 13%), and patent ductus arteriosus (PDA, 10%) – the committee found no data that children with these lesions are related to acknowledged episodes of sudden cardiac death (SCD). This applied whether the defects were closed or remained open. “With rare exceptions, patients with hemodynamically insignificant CHD such as VSD, ASD, and PDA may participate competitively in all sports,” it concluded. These recommendations fall under class I; level of evidence C for almost all of these patients, according to the writing committee.
Congenital coronary anomalies: Treated and untreated
Anomalies of coronary arteries are the second-most commonly identified structural causes of SCD in competitive athletes, accounting for about 17% of such deaths in the United States, according to the report. The vast majority of sudden deaths associated with coronary anomalies occur during or shortly after exercise. Despite being less commonly represented in patients, among athletes who have died suddenly, anomalous origin of the left main or left anterior descending coronary artery from the right sinus of Valsalva is far more prevalent. In addition, SCDs are most strongly associated with the pattern in which the anomalous left coronary artery passes between the aorta and main pulmonary artery. Recommended return to intense athletic activities is only to be permitted at least 3 months after surgery, and with a demonstration of the absence of ischemia on postoperative stress testing, with evidence levels depending on the type of anomaly. Of note, in contrast, the committee indicated that athletes with an anomalous origin of a right coronary artery from the left sinus of Valsalva should simply be evaluated by an exercise stress test, and for those without symptoms or a positive exercise stress test, permission to compete can be considered after adequate counseling (class IIa; level of evidence C).
Pulmonary valve stenosis: Treated and untreated
The committee determined that athletes with mild pulmonary stenosis (PS) and normal right ventricular (RV) function can participate in all competitive sports, although annual reevaluation also is recommended (class I; level of evidence B). In addition, athletes treated by operation or balloon valvuloplasty who have achieved adequate relief of PS (gradient less than 40 mm Hg by Doppler) can participate in all competitive sports (class I; level of evidence B). Other patients should be restricted to low-intensity sports, according to the committee.
Aortic valve stenosis: Treated and untreated
Children and adolescents with aortic stenosis (AS) are differentiated between those with mild, moderate, and severe AS by physical examination, ECG, and Doppler echocardiography. In all cases, regardless of the degree of stenosis, patients with a history of fatigue, light-headedness, dizziness, syncope, chest pain, or pallor on exercise deserve a full evaluation. Annual re-evaluation is required for all patients with AS because the disease can progress. Patients with severe AS are at risk of sudden death, particularly with exercise. The committee determined that athletes with mild AS can participate in all competitive sports (class I; level of evidence B), but that athletes with severe AS should be restricted from all competitive sports, with the possible exception of low-intensity sports (class III; level of evidence B).
Coarctation of the aorta: Treated and untreated
Before a decision is made regarding exercise participation, a detailed evaluation should be conducted, including a physical examination, ECG, chest radiograph, exercise testing, transthoracic echocardiographic evaluation of the aortic valve and aorta, and either magnetic resonance imaging or computed tomography angiography, according to the committee. The determination as to the level of sports participation permitted requires a complex assessment of these various test results and can range from full participation in the case of the least affected to restrictions to low-intensity sports in those more severely affected.
Cyanotic CHD, including tetralogy of Fallot
Full clinical assessment, including laboratory and exercise testing, should be considered before any physical activity because this population is at very high risk of sudden death, according to the committee. Recommendations are complex and depend on the level of repair and its success, but, in general, significant restrictions are recommended for all but the most effectively treated patients.
Transposition of the great arteries after atrial switch (Mustard or Senning operation)
This is a population highly at risk, according to the committee. They appear to have a unique response to exercise with reports that a high proportion of sudden death events occur during exertion. In addition, evidence of exercise-induced arrhythmias on routine clinical testing has not been shown to reliably predict exercise-induced SCD events. Although recommendations vary, including strong restrictions for many, at best the most successful of these patients should only be considered for low- to moderate-intensity competitive sports, according to the committee.
Other conditions assessed and evaluated by the committee included congenitally corrected TGA, TGA after the arterial switch, Fontan procedure, elevated pulmonary vascular resistence in CHD, ventricular dysfunction after CHD surgery, and Ebstein anomaly of the tricuspid valve.
In all cases, complete physical assessment of these patients is recommended, especially due to the often highly individualized nature of the patient’s presentation of these conditions and the variety and variability of interventions that may have been performed. Such differentials make recommendations regarding sports participation a complex calculus, which the committee attempts to provide, listing whatever evidence is available.
The majority of these patients, however, will not be considered for the highest levels of competitive sports participation. Although, in almost all cases, the need for physical activity as a contributor to patient health and well-being is stressed at whatever level of performance is possible.
The report ”Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: Task Force 4: congenital heart disease: a scientific statement from the American Heart Association and American College of Cardiology,” was prepared by Dr. Van Hare and his colleagues on behalf of the American Heart Association Electrocardiography and Arrhythmias Committee of the Council on Clinical Cardiology, Council on Cardiovascular Disease in the Young, Council on Cardiovascular and Stroke Nursing, Council on Functional Genomics and Translational Biology, and the American College of Cardiology (doi: 10.1016/j.jacc.2015.09.032).
This report is one of the assessments and recommendations of 15 task forces on eligibility and disqualification recommendations for young athletes, nine of which are disease or multidisease related. The other six task forces focus on a variety of relevant topics and issues regarding the risks of young athletes on the field, including screening, the use of automated external defibrillators on the field, the use of dietary supplements and performance-enhancing drugs, sudden death, and the medical-legal perspectives involved.
All 15 task force reports were simultaneously published online in the Journal of the American College of Cardiology and the journal Circulation.
Dr. Van Hare and all but one member of the writing group had no disclosures. One member disclosed consultant/advisory committee associations with a variety of medical device companies.
For many busy clinicians, societal guidelines, task force recommendations, expert consensus statements, and similar authoritative tomes are resources that are scarcely ever read carefully. This is likely not a reflection of the inherent value of such documents, but rather related to the observation that updated guidelines generally reflect, at most, a small change from predecessor versions. (It also should be mentioned that many such contributions are fairly heavy going for even the most determined reader.)
Occasionally, however, a new guideline may signal a dramatic shift in practice, and the recently published AHA/ACC Scientific Statement on Eligibility and Disqualification Recommendations for Competitive Athletes with Cardiovascular Abnormalities (Congenital Heart Disease) contains such a change.

|
Dr. Robert Jaquiss |
In particular, the new recommendation suggests that athletes with anomalous aortic origin of the right coronary from the left coronary sinus, who have neither symptoms nor a positive stress test, may be allowed to participate in competitive athletics without undergoing surgical repair. As before, those with anomalous left coronary should not be allowed to participate until after surgical treatment.
Prior guidelines suggested that all patients, both anomalous left from right sinus and right from left sinus, be restricted prior to surgery. Because anomalous right coronary is five to six times more common than anomalous left coronary and because it is certainly much less ominous, the previous “one size fits all” approach almost certainly resulted in overtreatment, unnecessary restriction of participation, or both. Furthermore, because anomalous aortic of a coronary artery is so common, occurring in 0.1%-0.2% of the population (300,000 to 600,000 people in the United States), many thousands of competitive athletes will be impacted by the changed guidelines.
Most cardiologists, surgeons, and, most especially, patients will welcome the updated recommendations. Nonetheless, it must be emphasized that anomalous coronary arteries, even anomalous right coronary arteries, may indicate an increased risk of sudden death and that a complete assessment, including stress testing when feasible, and thorough discussion with expert clinicians is still absolutely necessary for such patients and their families.
Dr. Robert Jaquiss of Duke University, Durham, N.C., is the congenital heart section associate medical editor for Thoracic Surgery News.
For many busy clinicians, societal guidelines, task force recommendations, expert consensus statements, and similar authoritative tomes are resources that are scarcely ever read carefully. This is likely not a reflection of the inherent value of such documents, but rather related to the observation that updated guidelines generally reflect, at most, a small change from predecessor versions. (It also should be mentioned that many such contributions are fairly heavy going for even the most determined reader.)
Occasionally, however, a new guideline may signal a dramatic shift in practice, and the recently published AHA/ACC Scientific Statement on Eligibility and Disqualification Recommendations for Competitive Athletes with Cardiovascular Abnormalities (Congenital Heart Disease) contains such a change.
|
|
Dr. Robert Jaquiss |
In particular, the new recommendation suggests that athletes with anomalous aortic origin of the right coronary from the left coronary sinus, who have neither symptoms nor a positive stress test, may be allowed to participate in competitive athletics without undergoing surgical repair. As before, those with anomalous left coronary should not be allowed to participate until after surgical treatment.
Prior guidelines suggested that all patients, both anomalous left from right sinus and right from left sinus, be restricted prior to surgery. Because anomalous right coronary is five to six times more common than anomalous left coronary and because it is certainly much less ominous, the previous “one size fits all” approach almost certainly resulted in overtreatment, unnecessary restriction of participation, or both. Furthermore, because anomalous aortic of a coronary artery is so common, occurring in 0.1%-0.2% of the population (300,000 to 600,000 people in the United States), many thousands of competitive athletes will be impacted by the changed guidelines.
Most cardiologists, surgeons, and, most especially, patients will welcome the updated recommendations. Nonetheless, it must be emphasized that anomalous coronary arteries, even anomalous right coronary arteries, may indicate an increased risk of sudden death and that a complete assessment, including stress testing when feasible, and thorough discussion with expert clinicians is still absolutely necessary for such patients and their families.
Dr. Robert Jaquiss of Duke University, Durham, N.C., is the congenital heart section associate medical editor for Thoracic Surgery News.
For many busy clinicians, societal guidelines, task force recommendations, expert consensus statements, and similar authoritative tomes are resources that are scarcely ever read carefully. This is likely not a reflection of the inherent value of such documents, but rather related to the observation that updated guidelines generally reflect, at most, a small change from predecessor versions. (It also should be mentioned that many such contributions are fairly heavy going for even the most determined reader.)
Occasionally, however, a new guideline may signal a dramatic shift in practice, and the recently published AHA/ACC Scientific Statement on Eligibility and Disqualification Recommendations for Competitive Athletes with Cardiovascular Abnormalities (Congenital Heart Disease) contains such a change.
|
|
Dr. Robert Jaquiss |
In particular, the new recommendation suggests that athletes with anomalous aortic origin of the right coronary from the left coronary sinus, who have neither symptoms nor a positive stress test, may be allowed to participate in competitive athletics without undergoing surgical repair. As before, those with anomalous left coronary should not be allowed to participate until after surgical treatment.
Prior guidelines suggested that all patients, both anomalous left from right sinus and right from left sinus, be restricted prior to surgery. Because anomalous right coronary is five to six times more common than anomalous left coronary and because it is certainly much less ominous, the previous “one size fits all” approach almost certainly resulted in overtreatment, unnecessary restriction of participation, or both. Furthermore, because anomalous aortic of a coronary artery is so common, occurring in 0.1%-0.2% of the population (300,000 to 600,000 people in the United States), many thousands of competitive athletes will be impacted by the changed guidelines.
Most cardiologists, surgeons, and, most especially, patients will welcome the updated recommendations. Nonetheless, it must be emphasized that anomalous coronary arteries, even anomalous right coronary arteries, may indicate an increased risk of sudden death and that a complete assessment, including stress testing when feasible, and thorough discussion with expert clinicians is still absolutely necessary for such patients and their families.
Dr. Robert Jaquiss of Duke University, Durham, N.C., is the congenital heart section associate medical editor for Thoracic Surgery News.
Most children and young adult patients with congenital heart disease can and should engage in some form of physical activity and should avoid a sedentary lifestyle, according to a task force scientific statement from the American Heart Association and the American College of Cardiology (AHA/ACC).
This recommendation comes despite the fears of sudden cardiac death (SCD) in young athletes, which formed the initial impetus of the entire series of task force reports.
The recommended level of sports participation for patients with treated or untreated congenital heart defect, however, should consider the training and the competitive aspects of the sport itself and must be individualized to the patient. This means taking into account the patient’s current functional status, history of surgery, and the presence of implanted cardiac devices, according to the report by Dr. George F. Van Hare of Washington University, St. Louis, and his colleagues, which was published online in the Journal of the American College of Cardiology.
The report breaks down its specific recommendations based upon the various types of congenital heart defect (CHD). Full details and nuances of the recommendations and their specific levels of evidence for each individual condition and the many variants can be found in the online publication. Below is a brief and selected summary for some of the most common defects and some of those most pertinent to sudden cardiac death in young athletes.
Simple shunting lesions (atrial septal defect, ventricular septal defect, patent ductus arteriosus): Treated and untreated
In addressing the three most common subtypes of CHD – ventricular septal defect (VSD, 34%), atrial septal defect (ASD, 13%), and patent ductus arteriosus (PDA, 10%) – the committee found no data that children with these lesions are related to acknowledged episodes of sudden cardiac death (SCD). This applied whether the defects were closed or remained open. “With rare exceptions, patients with hemodynamically insignificant CHD such as VSD, ASD, and PDA may participate competitively in all sports,” it concluded. These recommendations fall under class I; level of evidence C for almost all of these patients, according to the writing committee.
Congenital coronary anomalies: Treated and untreated
Anomalies of coronary arteries are the second-most commonly identified structural causes of SCD in competitive athletes, accounting for about 17% of such deaths in the United States, according to the report. The vast majority of sudden deaths associated with coronary anomalies occur during or shortly after exercise. Despite being less commonly represented in patients, among athletes who have died suddenly, anomalous origin of the left main or left anterior descending coronary artery from the right sinus of Valsalva is far more prevalent. In addition, SCDs are most strongly associated with the pattern in which the anomalous left coronary artery passes between the aorta and main pulmonary artery. Recommended return to intense athletic activities is only to be permitted at least 3 months after surgery, and with a demonstration of the absence of ischemia on postoperative stress testing, with evidence levels depending on the type of anomaly. Of note, in contrast, the committee indicated that athletes with an anomalous origin of a right coronary artery from the left sinus of Valsalva should simply be evaluated by an exercise stress test, and for those without symptoms or a positive exercise stress test, permission to compete can be considered after adequate counseling (class IIa; level of evidence C).
Pulmonary valve stenosis: Treated and untreated
The committee determined that athletes with mild pulmonary stenosis (PS) and normal right ventricular (RV) function can participate in all competitive sports, although annual reevaluation also is recommended (class I; level of evidence B). In addition, athletes treated by operation or balloon valvuloplasty who have achieved adequate relief of PS (gradient less than 40 mm Hg by Doppler) can participate in all competitive sports (class I; level of evidence B). Other patients should be restricted to low-intensity sports, according to the committee.
Aortic valve stenosis: Treated and untreated
Children and adolescents with aortic stenosis (AS) are differentiated between those with mild, moderate, and severe AS by physical examination, ECG, and Doppler echocardiography. In all cases, regardless of the degree of stenosis, patients with a history of fatigue, light-headedness, dizziness, syncope, chest pain, or pallor on exercise deserve a full evaluation. Annual re-evaluation is required for all patients with AS because the disease can progress. Patients with severe AS are at risk of sudden death, particularly with exercise. The committee determined that athletes with mild AS can participate in all competitive sports (class I; level of evidence B), but that athletes with severe AS should be restricted from all competitive sports, with the possible exception of low-intensity sports (class III; level of evidence B).
Coarctation of the aorta: Treated and untreated
Before a decision is made regarding exercise participation, a detailed evaluation should be conducted, including a physical examination, ECG, chest radiograph, exercise testing, transthoracic echocardiographic evaluation of the aortic valve and aorta, and either magnetic resonance imaging or computed tomography angiography, according to the committee. The determination as to the level of sports participation permitted requires a complex assessment of these various test results and can range from full participation in the case of the least affected to restrictions to low-intensity sports in those more severely affected.
Cyanotic CHD, including tetralogy of Fallot
Full clinical assessment, including laboratory and exercise testing, should be considered before any physical activity because this population is at very high risk of sudden death, according to the committee. Recommendations are complex and depend on the level of repair and its success, but, in general, significant restrictions are recommended for all but the most effectively treated patients.
Transposition of the great arteries after atrial switch (Mustard or Senning operation)
This is a population highly at risk, according to the committee. They appear to have a unique response to exercise with reports that a high proportion of sudden death events occur during exertion. In addition, evidence of exercise-induced arrhythmias on routine clinical testing has not been shown to reliably predict exercise-induced SCD events. Although recommendations vary, including strong restrictions for many, at best the most successful of these patients should only be considered for low- to moderate-intensity competitive sports, according to the committee.
Other conditions assessed and evaluated by the committee included congenitally corrected TGA, TGA after the arterial switch, Fontan procedure, elevated pulmonary vascular resistence in CHD, ventricular dysfunction after CHD surgery, and Ebstein anomaly of the tricuspid valve.
In all cases, complete physical assessment of these patients is recommended, especially due to the often highly individualized nature of the patient’s presentation of these conditions and the variety and variability of interventions that may have been performed. Such differentials make recommendations regarding sports participation a complex calculus, which the committee attempts to provide, listing whatever evidence is available.
The majority of these patients, however, will not be considered for the highest levels of competitive sports participation. Although, in almost all cases, the need for physical activity as a contributor to patient health and well-being is stressed at whatever level of performance is possible.
The report ”Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: Task Force 4: congenital heart disease: a scientific statement from the American Heart Association and American College of Cardiology,” was prepared by Dr. Van Hare and his colleagues on behalf of the American Heart Association Electrocardiography and Arrhythmias Committee of the Council on Clinical Cardiology, Council on Cardiovascular Disease in the Young, Council on Cardiovascular and Stroke Nursing, Council on Functional Genomics and Translational Biology, and the American College of Cardiology (doi: 10.1016/j.jacc.2015.09.032).
This report is one of the assessments and recommendations of 15 task forces on eligibility and disqualification recommendations for young athletes, nine of which are disease or multidisease related. The other six task forces focus on a variety of relevant topics and issues regarding the risks of young athletes on the field, including screening, the use of automated external defibrillators on the field, the use of dietary supplements and performance-enhancing drugs, sudden death, and the medical-legal perspectives involved.
All 15 task force reports were simultaneously published online in the Journal of the American College of Cardiology and the journal Circulation.
Dr. Van Hare and all but one member of the writing group had no disclosures. One member disclosed consultant/advisory committee associations with a variety of medical device companies.
Most children and young adult patients with congenital heart disease can and should engage in some form of physical activity and should avoid a sedentary lifestyle, according to a task force scientific statement from the American Heart Association and the American College of Cardiology (AHA/ACC).
This recommendation comes despite the fears of sudden cardiac death (SCD) in young athletes, which formed the initial impetus of the entire series of task force reports.
The recommended level of sports participation for patients with treated or untreated congenital heart defect, however, should consider the training and the competitive aspects of the sport itself and must be individualized to the patient. This means taking into account the patient’s current functional status, history of surgery, and the presence of implanted cardiac devices, according to the report by Dr. George F. Van Hare of Washington University, St. Louis, and his colleagues, which was published online in the Journal of the American College of Cardiology.
The report breaks down its specific recommendations based upon the various types of congenital heart defect (CHD). Full details and nuances of the recommendations and their specific levels of evidence for each individual condition and the many variants can be found in the online publication. Below is a brief and selected summary for some of the most common defects and some of those most pertinent to sudden cardiac death in young athletes.
Simple shunting lesions (atrial septal defect, ventricular septal defect, patent ductus arteriosus): Treated and untreated
In addressing the three most common subtypes of CHD – ventricular septal defect (VSD, 34%), atrial septal defect (ASD, 13%), and patent ductus arteriosus (PDA, 10%) – the committee found no data that children with these lesions are related to acknowledged episodes of sudden cardiac death (SCD). This applied whether the defects were closed or remained open. “With rare exceptions, patients with hemodynamically insignificant CHD such as VSD, ASD, and PDA may participate competitively in all sports,” it concluded. These recommendations fall under class I; level of evidence C for almost all of these patients, according to the writing committee.
Congenital coronary anomalies: Treated and untreated
Anomalies of coronary arteries are the second-most commonly identified structural causes of SCD in competitive athletes, accounting for about 17% of such deaths in the United States, according to the report. The vast majority of sudden deaths associated with coronary anomalies occur during or shortly after exercise. Despite being less commonly represented in patients, among athletes who have died suddenly, anomalous origin of the left main or left anterior descending coronary artery from the right sinus of Valsalva is far more prevalent. In addition, SCDs are most strongly associated with the pattern in which the anomalous left coronary artery passes between the aorta and main pulmonary artery. Recommended return to intense athletic activities is only to be permitted at least 3 months after surgery, and with a demonstration of the absence of ischemia on postoperative stress testing, with evidence levels depending on the type of anomaly. Of note, in contrast, the committee indicated that athletes with an anomalous origin of a right coronary artery from the left sinus of Valsalva should simply be evaluated by an exercise stress test, and for those without symptoms or a positive exercise stress test, permission to compete can be considered after adequate counseling (class IIa; level of evidence C).
Pulmonary valve stenosis: Treated and untreated
The committee determined that athletes with mild pulmonary stenosis (PS) and normal right ventricular (RV) function can participate in all competitive sports, although annual reevaluation also is recommended (class I; level of evidence B). In addition, athletes treated by operation or balloon valvuloplasty who have achieved adequate relief of PS (gradient less than 40 mm Hg by Doppler) can participate in all competitive sports (class I; level of evidence B). Other patients should be restricted to low-intensity sports, according to the committee.
Aortic valve stenosis: Treated and untreated
Children and adolescents with aortic stenosis (AS) are differentiated between those with mild, moderate, and severe AS by physical examination, ECG, and Doppler echocardiography. In all cases, regardless of the degree of stenosis, patients with a history of fatigue, light-headedness, dizziness, syncope, chest pain, or pallor on exercise deserve a full evaluation. Annual re-evaluation is required for all patients with AS because the disease can progress. Patients with severe AS are at risk of sudden death, particularly with exercise. The committee determined that athletes with mild AS can participate in all competitive sports (class I; level of evidence B), but that athletes with severe AS should be restricted from all competitive sports, with the possible exception of low-intensity sports (class III; level of evidence B).
Coarctation of the aorta: Treated and untreated
Before a decision is made regarding exercise participation, a detailed evaluation should be conducted, including a physical examination, ECG, chest radiograph, exercise testing, transthoracic echocardiographic evaluation of the aortic valve and aorta, and either magnetic resonance imaging or computed tomography angiography, according to the committee. The determination as to the level of sports participation permitted requires a complex assessment of these various test results and can range from full participation in the case of the least affected to restrictions to low-intensity sports in those more severely affected.
Cyanotic CHD, including tetralogy of Fallot
Full clinical assessment, including laboratory and exercise testing, should be considered before any physical activity because this population is at very high risk of sudden death, according to the committee. Recommendations are complex and depend on the level of repair and its success, but, in general, significant restrictions are recommended for all but the most effectively treated patients.
Transposition of the great arteries after atrial switch (Mustard or Senning operation)
This is a population highly at risk, according to the committee. They appear to have a unique response to exercise with reports that a high proportion of sudden death events occur during exertion. In addition, evidence of exercise-induced arrhythmias on routine clinical testing has not been shown to reliably predict exercise-induced SCD events. Although recommendations vary, including strong restrictions for many, at best the most successful of these patients should only be considered for low- to moderate-intensity competitive sports, according to the committee.
Other conditions assessed and evaluated by the committee included congenitally corrected TGA, TGA after the arterial switch, Fontan procedure, elevated pulmonary vascular resistence in CHD, ventricular dysfunction after CHD surgery, and Ebstein anomaly of the tricuspid valve.
In all cases, complete physical assessment of these patients is recommended, especially due to the often highly individualized nature of the patient’s presentation of these conditions and the variety and variability of interventions that may have been performed. Such differentials make recommendations regarding sports participation a complex calculus, which the committee attempts to provide, listing whatever evidence is available.
The majority of these patients, however, will not be considered for the highest levels of competitive sports participation. Although, in almost all cases, the need for physical activity as a contributor to patient health and well-being is stressed at whatever level of performance is possible.
The report ”Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: Task Force 4: congenital heart disease: a scientific statement from the American Heart Association and American College of Cardiology,” was prepared by Dr. Van Hare and his colleagues on behalf of the American Heart Association Electrocardiography and Arrhythmias Committee of the Council on Clinical Cardiology, Council on Cardiovascular Disease in the Young, Council on Cardiovascular and Stroke Nursing, Council on Functional Genomics and Translational Biology, and the American College of Cardiology (doi: 10.1016/j.jacc.2015.09.032).
This report is one of the assessments and recommendations of 15 task forces on eligibility and disqualification recommendations for young athletes, nine of which are disease or multidisease related. The other six task forces focus on a variety of relevant topics and issues regarding the risks of young athletes on the field, including screening, the use of automated external defibrillators on the field, the use of dietary supplements and performance-enhancing drugs, sudden death, and the medical-legal perspectives involved.
All 15 task force reports were simultaneously published online in the Journal of the American College of Cardiology and the journal Circulation.
Dr. Van Hare and all but one member of the writing group had no disclosures. One member disclosed consultant/advisory committee associations with a variety of medical device companies.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Key clinical point: Recommendations for sports participation should consider the activity itself and take into account the patient’s functional status, history of surgery, and implanted devices.
Major finding: Congenital heart disease is the most common form of serious birth defect (8 per 1,000 live births) and, with dramatic improvements in survival, the issue of youth and young-adult participation in competitive sports must be addressed.
Data source: The AHA/ACC expert consensus recommendations were developed using the experience of the writing-group members and the available scientific evidence in the literature.
Disclosures: The review was sponsored by the AHA and the ACC. Dr. Van Hare and all but one member of the writing group had no disclosures. One member disclosed consultant/advisory committee associations with a variety of medical device companies.

Residents’ Forum: Searching for a Thoracic Job in 2016
In the thick of a job search for this coming July, I fondly remember my first experience at the 47th Annual STS meeting in San Diego in 2011. The presidential address was delivered by Dr. Mathisen and focused nearly an entire hour on encouraging and mentoring young trainees to pursue a career in cardiothoracic surgery. Citing concerns about job availability and security, declining compensation, and increasing scrutiny on outcome measures, the president attempted to individually address these.
Most vividly I remember the emphasis on baby boomers getting older, median CT surgeon age approaching the retirement point, and the overall increased need for young, motivated, and highly skilled junior attendings. Until this year, the number of STS and CTSnet job posts was abysmally low. This led many new graduates to consider advanced fellowships or alternative avenues. Half a decade after Dr. Mathisen’s prediction at STS, the proverbial flood gates have opened.

This past year, I’ve seen at least a dozen quality academic positions looking for new graduates in thoracic surgery. Additionally, at least another dozen hybrid practice or private/community practice groups are looking to hire junior attendings. What is also interesting is the direction that many practices are headed: thoracic service lines, where volume is accrued from surrounding community practices and brought to centralized, multidisciplinary tertiary care institutions.
In many models, mentorship has been built in with involved senior partners, especially now that expertise in advanced techniques in bronchoscopy (EBUS, navigational bronchoscopy), endoscopy (RFA, EMR, and other ablative strategies) and minimally invasive surgery (VATS, MIS esophagectomy, robotic) are commonly expected by patients. These skills are initially learned in training and, with the right support structure, are perfected early in practice.
With more precise earlier stage screening and detection of esophageal and lung malignancies and the general stability or increase in the year-to-year incidence of these cancers, I expect the job market will continue to accommodate a growing need for thoracic surgeons in the United States. This should greatly help recruitment of the best young medical talent into what is truly an exciting and blossoming field of surgery.
Reference
Mathisen DJ. “It’s Not the Destination, It’s the Journey: Lessons Learned”. 47th Annual STS Presidential Address. San Diego, CA. January 2011. www.sts.org/news/mathisen-delivers-presidential-address.
Dr. Shersher is at Rush University Medical Center, Chicago.
In the thick of a job search for this coming July, I fondly remember my first experience at the 47th Annual STS meeting in San Diego in 2011. The presidential address was delivered by Dr. Mathisen and focused nearly an entire hour on encouraging and mentoring young trainees to pursue a career in cardiothoracic surgery. Citing concerns about job availability and security, declining compensation, and increasing scrutiny on outcome measures, the president attempted to individually address these.
Most vividly I remember the emphasis on baby boomers getting older, median CT surgeon age approaching the retirement point, and the overall increased need for young, motivated, and highly skilled junior attendings. Until this year, the number of STS and CTSnet job posts was abysmally low. This led many new graduates to consider advanced fellowships or alternative avenues. Half a decade after Dr. Mathisen’s prediction at STS, the proverbial flood gates have opened.
This past year, I’ve seen at least a dozen quality academic positions looking for new graduates in thoracic surgery. Additionally, at least another dozen hybrid practice or private/community practice groups are looking to hire junior attendings. What is also interesting is the direction that many practices are headed: thoracic service lines, where volume is accrued from surrounding community practices and brought to centralized, multidisciplinary tertiary care institutions.
In many models, mentorship has been built in with involved senior partners, especially now that expertise in advanced techniques in bronchoscopy (EBUS, navigational bronchoscopy), endoscopy (RFA, EMR, and other ablative strategies) and minimally invasive surgery (VATS, MIS esophagectomy, robotic) are commonly expected by patients. These skills are initially learned in training and, with the right support structure, are perfected early in practice.
With more precise earlier stage screening and detection of esophageal and lung malignancies and the general stability or increase in the year-to-year incidence of these cancers, I expect the job market will continue to accommodate a growing need for thoracic surgeons in the United States. This should greatly help recruitment of the best young medical talent into what is truly an exciting and blossoming field of surgery.
Reference
Mathisen DJ. “It’s Not the Destination, It’s the Journey: Lessons Learned”. 47th Annual STS Presidential Address. San Diego, CA. January 2011. www.sts.org/news/mathisen-delivers-presidential-address.
Dr. Shersher is at Rush University Medical Center, Chicago.
In the thick of a job search for this coming July, I fondly remember my first experience at the 47th Annual STS meeting in San Diego in 2011. The presidential address was delivered by Dr. Mathisen and focused nearly an entire hour on encouraging and mentoring young trainees to pursue a career in cardiothoracic surgery. Citing concerns about job availability and security, declining compensation, and increasing scrutiny on outcome measures, the president attempted to individually address these.
Most vividly I remember the emphasis on baby boomers getting older, median CT surgeon age approaching the retirement point, and the overall increased need for young, motivated, and highly skilled junior attendings. Until this year, the number of STS and CTSnet job posts was abysmally low. This led many new graduates to consider advanced fellowships or alternative avenues. Half a decade after Dr. Mathisen’s prediction at STS, the proverbial flood gates have opened.
This past year, I’ve seen at least a dozen quality academic positions looking for new graduates in thoracic surgery. Additionally, at least another dozen hybrid practice or private/community practice groups are looking to hire junior attendings. What is also interesting is the direction that many practices are headed: thoracic service lines, where volume is accrued from surrounding community practices and brought to centralized, multidisciplinary tertiary care institutions.
In many models, mentorship has been built in with involved senior partners, especially now that expertise in advanced techniques in bronchoscopy (EBUS, navigational bronchoscopy), endoscopy (RFA, EMR, and other ablative strategies) and minimally invasive surgery (VATS, MIS esophagectomy, robotic) are commonly expected by patients. These skills are initially learned in training and, with the right support structure, are perfected early in practice.
With more precise earlier stage screening and detection of esophageal and lung malignancies and the general stability or increase in the year-to-year incidence of these cancers, I expect the job market will continue to accommodate a growing need for thoracic surgeons in the United States. This should greatly help recruitment of the best young medical talent into what is truly an exciting and blossoming field of surgery.
Reference
Mathisen DJ. “It’s Not the Destination, It’s the Journey: Lessons Learned”. 47th Annual STS Presidential Address. San Diego, CA. January 2011. www.sts.org/news/mathisen-delivers-presidential-address.
Dr. Shersher is at Rush University Medical Center, Chicago.

Setting a new standard for aortic root repair?
Over the past 3 decades surgery for aortic root replacement has seen a dramatic decline in rates of death and complications, but there have been few studies comparing which technique would be best for specific patients, and those that have been done have been limited by selection bias or small patient numbers.
But a team of investigators from Weill Cornell Medical College in New York have analyzed results of three different aortic root replacement (ARR) procedures over a 17-year period and found that the rates of death during surgery and complications were less than 1% regardless of the technique. They published their results in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1120-9).

“In the current era, aortic root replacement can be performed with very low perioperative risk in high-volume aortic centers,” said Dr. Mario Gaudino and coauthors. “The type of operation performed does not affect early or late survival.”
They compared results of three different approaches to ARR performed in 890 consecutive patients in their institution from May 1997 to January 2014: mechanical composite valved graft (mCVG) in 289 patients; biologic composite valved graft (bCVG) in 421; and valve-sparing reconstruction (VSR) in 180. Then the researchers applied propensity matching to neutralize the differences in the baseline characteristics between the different procedures.
The overall rate of death from the operation was 0.2%, but the two patients who died did so in the first 5 years of the study. There were no deaths in the VSR group, and the incidence of complications after surgery was less than 0.5%. Three-year survival was 94.8% and 5-year survival was 89.4%, and reintervention rates at 5 years were 0% for the mCVG group, 2.4% for the bCVG group, and 7.3% for those who had VSR. “Although mCVG remains the gold standard for durability, bCVG and VSR are excellent options for those who either cannot take or wish to avoid long-term anticoagulation,” Dr. Gaudino and colleagues said.
At the time of surgery, 332 patients (37.3%) had at least one associated cardiac procedure, led by arch replacement (149 patients) and coronary artery bypass (81 patients). Eighty-four patients (9.4%) had two or more associated procedures. The bCVG and mCVG groups had the highest rates of associated cardiac procedures.
Before propensity matching, bCVG patients were older and had more comorbidities and worse functional class, while the mCVG group had higher rates of redo procedures and urgent or emergent operations. Connective tissue disorders were most common in the VSR group.
The results paralleled data from the Society of Thoracic Surgery’s Adult Cardiac Surgery Database, Dr. Gaudino and colleagues said, including a fivefold increase in the number of root replacements performed annually during the study period and a shift away from the traditional mCVG operation to widespread adoption of the bCVG and VSR procedures in the later years of the study.
“Surgeons with extensive experience in aortic surgery can tailor their choice of ARR to the procedure that best suits the individual patient based on their baseline characteristics,” Dr. Gaudino and coauthors said.
Dr. Gaudino and his coauthors had no disclosures.
The results of elective aortic root surgery that Dr. Mario Gaudino and his colleagues reported are “the most impressive … ever published and probably difficult, if not impossible, to reproduce,” Dr. Tirone David of the University of Toronto said in his invited commentary in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1130-1).
Dr. David cited the study’s low rates of deaths and complications. “They had only two deaths early on in their experience and no deaths among the most recent 804 patients operated on since 2002,” he said. “And there is more,” he said: only four strokes, one heart attack, one sternal infection, and only 11.2% of patients receiving blood transfusion. “And to make us ordinary surgeons even more envious, more than one-third of their patients had combined procedures,” Dr. David said.
|
Dr. Tirone David |
He said Dr. Gaudino and his colleagues have set a new standard for early outcomes of elective aortic root surgery. “These outcomes are difficult to emulate but we have to try,” Dr. David said. “To be an obsessive-compulsive surgeon who pays enormous attention to technical details is not enough because even patients who have perfectly executed operations may suffer serious and occasionally fatal postoperative complications.”
The results of elective aortic root surgery that Dr. Mario Gaudino and his colleagues reported are “the most impressive … ever published and probably difficult, if not impossible, to reproduce,” Dr. Tirone David of the University of Toronto said in his invited commentary in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1130-1).
Dr. David cited the study’s low rates of deaths and complications. “They had only two deaths early on in their experience and no deaths among the most recent 804 patients operated on since 2002,” he said. “And there is more,” he said: only four strokes, one heart attack, one sternal infection, and only 11.2% of patients receiving blood transfusion. “And to make us ordinary surgeons even more envious, more than one-third of their patients had combined procedures,” Dr. David said.
|
|
Dr. Tirone David |
He said Dr. Gaudino and his colleagues have set a new standard for early outcomes of elective aortic root surgery. “These outcomes are difficult to emulate but we have to try,” Dr. David said. “To be an obsessive-compulsive surgeon who pays enormous attention to technical details is not enough because even patients who have perfectly executed operations may suffer serious and occasionally fatal postoperative complications.”
The results of elective aortic root surgery that Dr. Mario Gaudino and his colleagues reported are “the most impressive … ever published and probably difficult, if not impossible, to reproduce,” Dr. Tirone David of the University of Toronto said in his invited commentary in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1130-1).
Dr. David cited the study’s low rates of deaths and complications. “They had only two deaths early on in their experience and no deaths among the most recent 804 patients operated on since 2002,” he said. “And there is more,” he said: only four strokes, one heart attack, one sternal infection, and only 11.2% of patients receiving blood transfusion. “And to make us ordinary surgeons even more envious, more than one-third of their patients had combined procedures,” Dr. David said.
|
|
Dr. Tirone David |
He said Dr. Gaudino and his colleagues have set a new standard for early outcomes of elective aortic root surgery. “These outcomes are difficult to emulate but we have to try,” Dr. David said. “To be an obsessive-compulsive surgeon who pays enormous attention to technical details is not enough because even patients who have perfectly executed operations may suffer serious and occasionally fatal postoperative complications.”
Over the past 3 decades surgery for aortic root replacement has seen a dramatic decline in rates of death and complications, but there have been few studies comparing which technique would be best for specific patients, and those that have been done have been limited by selection bias or small patient numbers.
But a team of investigators from Weill Cornell Medical College in New York have analyzed results of three different aortic root replacement (ARR) procedures over a 17-year period and found that the rates of death during surgery and complications were less than 1% regardless of the technique. They published their results in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1120-9).
“In the current era, aortic root replacement can be performed with very low perioperative risk in high-volume aortic centers,” said Dr. Mario Gaudino and coauthors. “The type of operation performed does not affect early or late survival.”
They compared results of three different approaches to ARR performed in 890 consecutive patients in their institution from May 1997 to January 2014: mechanical composite valved graft (mCVG) in 289 patients; biologic composite valved graft (bCVG) in 421; and valve-sparing reconstruction (VSR) in 180. Then the researchers applied propensity matching to neutralize the differences in the baseline characteristics between the different procedures.
The overall rate of death from the operation was 0.2%, but the two patients who died did so in the first 5 years of the study. There were no deaths in the VSR group, and the incidence of complications after surgery was less than 0.5%. Three-year survival was 94.8% and 5-year survival was 89.4%, and reintervention rates at 5 years were 0% for the mCVG group, 2.4% for the bCVG group, and 7.3% for those who had VSR. “Although mCVG remains the gold standard for durability, bCVG and VSR are excellent options for those who either cannot take or wish to avoid long-term anticoagulation,” Dr. Gaudino and colleagues said.
At the time of surgery, 332 patients (37.3%) had at least one associated cardiac procedure, led by arch replacement (149 patients) and coronary artery bypass (81 patients). Eighty-four patients (9.4%) had two or more associated procedures. The bCVG and mCVG groups had the highest rates of associated cardiac procedures.
Before propensity matching, bCVG patients were older and had more comorbidities and worse functional class, while the mCVG group had higher rates of redo procedures and urgent or emergent operations. Connective tissue disorders were most common in the VSR group.
The results paralleled data from the Society of Thoracic Surgery’s Adult Cardiac Surgery Database, Dr. Gaudino and colleagues said, including a fivefold increase in the number of root replacements performed annually during the study period and a shift away from the traditional mCVG operation to widespread adoption of the bCVG and VSR procedures in the later years of the study.
“Surgeons with extensive experience in aortic surgery can tailor their choice of ARR to the procedure that best suits the individual patient based on their baseline characteristics,” Dr. Gaudino and coauthors said.
Dr. Gaudino and his coauthors had no disclosures.
Over the past 3 decades surgery for aortic root replacement has seen a dramatic decline in rates of death and complications, but there have been few studies comparing which technique would be best for specific patients, and those that have been done have been limited by selection bias or small patient numbers.
But a team of investigators from Weill Cornell Medical College in New York have analyzed results of three different aortic root replacement (ARR) procedures over a 17-year period and found that the rates of death during surgery and complications were less than 1% regardless of the technique. They published their results in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1120-9).
“In the current era, aortic root replacement can be performed with very low perioperative risk in high-volume aortic centers,” said Dr. Mario Gaudino and coauthors. “The type of operation performed does not affect early or late survival.”
They compared results of three different approaches to ARR performed in 890 consecutive patients in their institution from May 1997 to January 2014: mechanical composite valved graft (mCVG) in 289 patients; biologic composite valved graft (bCVG) in 421; and valve-sparing reconstruction (VSR) in 180. Then the researchers applied propensity matching to neutralize the differences in the baseline characteristics between the different procedures.
The overall rate of death from the operation was 0.2%, but the two patients who died did so in the first 5 years of the study. There were no deaths in the VSR group, and the incidence of complications after surgery was less than 0.5%. Three-year survival was 94.8% and 5-year survival was 89.4%, and reintervention rates at 5 years were 0% for the mCVG group, 2.4% for the bCVG group, and 7.3% for those who had VSR. “Although mCVG remains the gold standard for durability, bCVG and VSR are excellent options for those who either cannot take or wish to avoid long-term anticoagulation,” Dr. Gaudino and colleagues said.
At the time of surgery, 332 patients (37.3%) had at least one associated cardiac procedure, led by arch replacement (149 patients) and coronary artery bypass (81 patients). Eighty-four patients (9.4%) had two or more associated procedures. The bCVG and mCVG groups had the highest rates of associated cardiac procedures.
Before propensity matching, bCVG patients were older and had more comorbidities and worse functional class, while the mCVG group had higher rates of redo procedures and urgent or emergent operations. Connective tissue disorders were most common in the VSR group.
The results paralleled data from the Society of Thoracic Surgery’s Adult Cardiac Surgery Database, Dr. Gaudino and colleagues said, including a fivefold increase in the number of root replacements performed annually during the study period and a shift away from the traditional mCVG operation to widespread adoption of the bCVG and VSR procedures in the later years of the study.
“Surgeons with extensive experience in aortic surgery can tailor their choice of ARR to the procedure that best suits the individual patient based on their baseline characteristics,” Dr. Gaudino and coauthors said.
Dr. Gaudino and his coauthors had no disclosures.
Key clinical point: Aortic root replacement surgery can be performed with minimal risk of death and complications regardless of the approach taken.
Major finding: Overall rate of death was 0.2%, with none since 2002, and the overall rate of complications was below 0.5% in the study cohort.
Data source: Review of prospective data on 890 aortic root replacement operations performed over a 17-year period at a single center.
Disclosures: The study authors had no relationships to disclose.

Self-reported poor functional status predicts perioperative morbidity
SAN DIEGO – Among patients with pulmonary hypertension presenting for elective surgery, self-reported poor functional status is associated with multiple comorbidities and is independently predictive of longer hospital length of stay, results from an ongoing single-center study suggest.
“Patients with pulmonary hypertension (PHTN) presenting for elective surgery are at significantly higher risk for adverse perioperative outcomes, including increased hospital length of stay, right ventricular failure, cardiac arrhythmia, persistent postoperative hypoxemia, coronary ischemia and death,” researchers led by Dr. Aalap C. Shah wrote in an abstract presented at the at the annual meeting of the American Society of Anesthesiologists. “The diagnosis of PHTN is based on costly echocardiographic examination and right heart catheterization and should be reserved for high-risk patients. No studies have assessed the role of self-reported functional classification on PHTN severity stratification, and few studies have achieved a sufficiently large patient sample size.”

In an effort to evaluate the predictive value of self-reported exercise tolerance on echocardiogram findings, outcomes, and length of stay (LOS) after noncardiac, nonobstetric surgery, the researchers queried the University of Washington database for all PHTN seen in preoperative anesthesia clinic for noncardiac, nonobstetric procedures from April 2007 through September 2013. Inclusion criteria required an echocardiogram less than 1 year prior to the procedure and available patient-reported functional status, which was defined as less than four metabolic equivalents (METS) in exercise testing or four METS or greater. Dr. Shah, formerly a resident in the University of Washington’s department of anesthesiology and pain medicine, and his associates used univariate analyses to compare functional status with echocardiographic findings, complication rates, and length of stay (LOS). At the meeting he presented results from 294 patients evaluated to date: 143 with normal functional status and 151 with poor functional status. Their mean age was 62 years, and 51% of patients were female.
Compared with their counterparts with normal functional status, patients with poor functional status trended toward a higher complication rate at hospital discharge (14.6% vs. 7%, respectively; P = .041) and had a higher cumulative rate of complications (33 vs. 15; P = .035). However, no association between functional status and complications was observed 30 days postoperatively.
Patients with poor functional status had a significantly longer average LOS, compared with patients with normal functional status (7.21 vs. 4.73 days; P = .047). Open surgical approach was also an independent predictor of increased LOS (odds ratio 2.39; P = .005). No significant independent predictors of complications were observed at discharge or 30 days postoperatively.
“Going forward, the goal is to use these data to create a risk stratification algorithm to figure out: Does a patient with good functional status and pulmonary hypertension undergoing toe surgery, for example, really need an echocardiogram before getting surgery?” said Dr. Shah said, who is now an anesthesiology fellow at Boston Children’s Hospital. “Hopefully we can show that using these risk stratification algorithms can decrease the costs and decrease the time to actually getting surgery.”
The researchers reported having no financial disclosures.
SAN DIEGO – Among patients with pulmonary hypertension presenting for elective surgery, self-reported poor functional status is associated with multiple comorbidities and is independently predictive of longer hospital length of stay, results from an ongoing single-center study suggest.
“Patients with pulmonary hypertension (PHTN) presenting for elective surgery are at significantly higher risk for adverse perioperative outcomes, including increased hospital length of stay, right ventricular failure, cardiac arrhythmia, persistent postoperative hypoxemia, coronary ischemia and death,” researchers led by Dr. Aalap C. Shah wrote in an abstract presented at the at the annual meeting of the American Society of Anesthesiologists. “The diagnosis of PHTN is based on costly echocardiographic examination and right heart catheterization and should be reserved for high-risk patients. No studies have assessed the role of self-reported functional classification on PHTN severity stratification, and few studies have achieved a sufficiently large patient sample size.”
In an effort to evaluate the predictive value of self-reported exercise tolerance on echocardiogram findings, outcomes, and length of stay (LOS) after noncardiac, nonobstetric surgery, the researchers queried the University of Washington database for all PHTN seen in preoperative anesthesia clinic for noncardiac, nonobstetric procedures from April 2007 through September 2013. Inclusion criteria required an echocardiogram less than 1 year prior to the procedure and available patient-reported functional status, which was defined as less than four metabolic equivalents (METS) in exercise testing or four METS or greater. Dr. Shah, formerly a resident in the University of Washington’s department of anesthesiology and pain medicine, and his associates used univariate analyses to compare functional status with echocardiographic findings, complication rates, and length of stay (LOS). At the meeting he presented results from 294 patients evaluated to date: 143 with normal functional status and 151 with poor functional status. Their mean age was 62 years, and 51% of patients were female.
Compared with their counterparts with normal functional status, patients with poor functional status trended toward a higher complication rate at hospital discharge (14.6% vs. 7%, respectively; P = .041) and had a higher cumulative rate of complications (33 vs. 15; P = .035). However, no association between functional status and complications was observed 30 days postoperatively.
Patients with poor functional status had a significantly longer average LOS, compared with patients with normal functional status (7.21 vs. 4.73 days; P = .047). Open surgical approach was also an independent predictor of increased LOS (odds ratio 2.39; P = .005). No significant independent predictors of complications were observed at discharge or 30 days postoperatively.
“Going forward, the goal is to use these data to create a risk stratification algorithm to figure out: Does a patient with good functional status and pulmonary hypertension undergoing toe surgery, for example, really need an echocardiogram before getting surgery?” said Dr. Shah said, who is now an anesthesiology fellow at Boston Children’s Hospital. “Hopefully we can show that using these risk stratification algorithms can decrease the costs and decrease the time to actually getting surgery.”
The researchers reported having no financial disclosures.
SAN DIEGO – Among patients with pulmonary hypertension presenting for elective surgery, self-reported poor functional status is associated with multiple comorbidities and is independently predictive of longer hospital length of stay, results from an ongoing single-center study suggest.
“Patients with pulmonary hypertension (PHTN) presenting for elective surgery are at significantly higher risk for adverse perioperative outcomes, including increased hospital length of stay, right ventricular failure, cardiac arrhythmia, persistent postoperative hypoxemia, coronary ischemia and death,” researchers led by Dr. Aalap C. Shah wrote in an abstract presented at the at the annual meeting of the American Society of Anesthesiologists. “The diagnosis of PHTN is based on costly echocardiographic examination and right heart catheterization and should be reserved for high-risk patients. No studies have assessed the role of self-reported functional classification on PHTN severity stratification, and few studies have achieved a sufficiently large patient sample size.”
In an effort to evaluate the predictive value of self-reported exercise tolerance on echocardiogram findings, outcomes, and length of stay (LOS) after noncardiac, nonobstetric surgery, the researchers queried the University of Washington database for all PHTN seen in preoperative anesthesia clinic for noncardiac, nonobstetric procedures from April 2007 through September 2013. Inclusion criteria required an echocardiogram less than 1 year prior to the procedure and available patient-reported functional status, which was defined as less than four metabolic equivalents (METS) in exercise testing or four METS or greater. Dr. Shah, formerly a resident in the University of Washington’s department of anesthesiology and pain medicine, and his associates used univariate analyses to compare functional status with echocardiographic findings, complication rates, and length of stay (LOS). At the meeting he presented results from 294 patients evaluated to date: 143 with normal functional status and 151 with poor functional status. Their mean age was 62 years, and 51% of patients were female.
Compared with their counterparts with normal functional status, patients with poor functional status trended toward a higher complication rate at hospital discharge (14.6% vs. 7%, respectively; P = .041) and had a higher cumulative rate of complications (33 vs. 15; P = .035). However, no association between functional status and complications was observed 30 days postoperatively.
Patients with poor functional status had a significantly longer average LOS, compared with patients with normal functional status (7.21 vs. 4.73 days; P = .047). Open surgical approach was also an independent predictor of increased LOS (odds ratio 2.39; P = .005). No significant independent predictors of complications were observed at discharge or 30 days postoperatively.
“Going forward, the goal is to use these data to create a risk stratification algorithm to figure out: Does a patient with good functional status and pulmonary hypertension undergoing toe surgery, for example, really need an echocardiogram before getting surgery?” said Dr. Shah said, who is now an anesthesiology fellow at Boston Children’s Hospital. “Hopefully we can show that using these risk stratification algorithms can decrease the costs and decrease the time to actually getting surgery.”
The researchers reported having no financial disclosures.
AT THE ASA ANNUAL MEETING
Key clinical point:Poor self-reported exercise tolerance by patients with pulmonary hypertension is associated with multiple comorbidities and increased hospital length of stay.
Major finding: Compared with their counterparts with normal functional status, patients with poor functional status trended toward a higher complication rate at hospital discharge (14.6% vs. 7%, respectively; P = .041) and had a higher cumulative rate of complications (33 vs. 15; P = .035).
Data source: A study 294 PHTN patients seen in preoperative anesthesia clinic at the University of Washington for non-cardiac, nonobstetric procedures from April 2007 through September 2013.
Disclosures: The researchers reported having no financial disclosures.

ACC/AHA risk estimator underpredicts in HIV+ individuals
ORLANDO – The 2013 ACC/AHA atherosclerotic cardiovascular disease risk calculator isn’t reliably applicable to HIV-positive adults in its present form because it consistently underpredicts their MI risk, Dr. Michael J. Feinstein reported at the American Heart Association scientific sessions.
That’s the bad news. The good news is that “a simple, data-derived refit of the pooled cohort equations may improve the model’s performance in HIV-positive individuals,” said Dr. Feinstein of Northwestern University, Chicago.

Tweaking the risk calculator to enhance its accuracy in the HIV-positive population is particularly important because this population is growing in size and aging. And as Dr. Feinstein and coinvestigators showed in another study presented at the AHA meeting, the proportion of deaths due to cardiovascular disease in HIV-positive adults is shooting upward as they live longer because of treatment advances.
The investigators’ analysis of data from the Centers for Disease Control and Prevention national Wonder database showed that the proportion of deaths due to cardiovascular disease more than doubled between 1999 and 2013. Meanwhile, proportionate cardiovascular disease mortality declined by 22% in the general population and by 28% among individuals with inflammatory polyarthropathies.
That the ACC/AHA risk calculator in its present form doesn’t perform adequately in HIV-positive individuals hadn’t previously been shown, but it doesn’t really come as a surprise, according to Dr. Feinstein. After all, it’s known that this population is at 1.5- to 2-fold increased risk for MI and roughly 5-fold increased risk for sudden cardiac death, compared to the general population, where the risk calculator works best.
“Most data suggest that even in the setting of optimally treated HIV and undetectable viral load there’s still an underlying viral reservoir that appears to be driving inflammation and atherothrombotic and even nonatherothrombotic events in this population,” he said.
Dr. Feinstein and coworkers evaluated the 2013 ACC/AHA risk calculator in 11,901 HIV-positive black or white adults enrolled in the Centers for AIDS Research Network of Integrated Clinical Systems (CNICS) database for whom 5-year follow-up was available; 52% of the subjects were aged 40 or older at baseline.
Running each of these nearly 12,000 subjects through the risk calculator, the predicted result was that 103 of them would have an acute MI during the 5-year follow-up period. In reality, 132 MIs were observed. The discrepancy between the risk calculator predictions and observed MI rates was greatest in the 63% of HIV-positive subjects deemed at low risk, with an estimated 10-year risk of atherosclerotic cardiovascular disease of less than 5%.
Among white men, the risk calculator was remarkably consistent in underpredicting MIs. Regardless of whether the risk calculator put their estimated 10-year risk at less than 5%, 5% to less than 7.5%, 7.5% to less than 10%, or at least 10%, the actual observed MI rates were 67%-68% greater across the board than predicted.
Dr. Feinstein and coworkers refit the ACC/AHA risk calculator on a trial basis by incorporating variables related to HIV-positivity into the risk equations. Then they reanalyzed the tool’s performance in the same nearly 12,000 HIV-infected subjects. They found the discrimination and calibration of the revised risk equations improved substantially and met the standard of “acceptable” by statisticians’ standards.
The next step in this ongoing CNICS project will be to validate the provisionally refit risk calculator’s performance in a separate database of HIV-infected adults with adjudicated MIs. If the results are again positive, it will be a relatively straightforward matter to introduce the revisions into the ACC/AHA risk calculator, particularly since the senior coinvestigator in this project is Dr. Donald M. Lloyd-Jones, also of Northwestern University, who played a central role in developing the 2013 risk calculator.
Dr. Feinstein reported having no financial conflicts regarding this study.
ORLANDO – The 2013 ACC/AHA atherosclerotic cardiovascular disease risk calculator isn’t reliably applicable to HIV-positive adults in its present form because it consistently underpredicts their MI risk, Dr. Michael J. Feinstein reported at the American Heart Association scientific sessions.
That’s the bad news. The good news is that “a simple, data-derived refit of the pooled cohort equations may improve the model’s performance in HIV-positive individuals,” said Dr. Feinstein of Northwestern University, Chicago.
Tweaking the risk calculator to enhance its accuracy in the HIV-positive population is particularly important because this population is growing in size and aging. And as Dr. Feinstein and coinvestigators showed in another study presented at the AHA meeting, the proportion of deaths due to cardiovascular disease in HIV-positive adults is shooting upward as they live longer because of treatment advances.
The investigators’ analysis of data from the Centers for Disease Control and Prevention national Wonder database showed that the proportion of deaths due to cardiovascular disease more than doubled between 1999 and 2013. Meanwhile, proportionate cardiovascular disease mortality declined by 22% in the general population and by 28% among individuals with inflammatory polyarthropathies.
That the ACC/AHA risk calculator in its present form doesn’t perform adequately in HIV-positive individuals hadn’t previously been shown, but it doesn’t really come as a surprise, according to Dr. Feinstein. After all, it’s known that this population is at 1.5- to 2-fold increased risk for MI and roughly 5-fold increased risk for sudden cardiac death, compared to the general population, where the risk calculator works best.
“Most data suggest that even in the setting of optimally treated HIV and undetectable viral load there’s still an underlying viral reservoir that appears to be driving inflammation and atherothrombotic and even nonatherothrombotic events in this population,” he said.
Dr. Feinstein and coworkers evaluated the 2013 ACC/AHA risk calculator in 11,901 HIV-positive black or white adults enrolled in the Centers for AIDS Research Network of Integrated Clinical Systems (CNICS) database for whom 5-year follow-up was available; 52% of the subjects were aged 40 or older at baseline.
Running each of these nearly 12,000 subjects through the risk calculator, the predicted result was that 103 of them would have an acute MI during the 5-year follow-up period. In reality, 132 MIs were observed. The discrepancy between the risk calculator predictions and observed MI rates was greatest in the 63% of HIV-positive subjects deemed at low risk, with an estimated 10-year risk of atherosclerotic cardiovascular disease of less than 5%.
Among white men, the risk calculator was remarkably consistent in underpredicting MIs. Regardless of whether the risk calculator put their estimated 10-year risk at less than 5%, 5% to less than 7.5%, 7.5% to less than 10%, or at least 10%, the actual observed MI rates were 67%-68% greater across the board than predicted.
Dr. Feinstein and coworkers refit the ACC/AHA risk calculator on a trial basis by incorporating variables related to HIV-positivity into the risk equations. Then they reanalyzed the tool’s performance in the same nearly 12,000 HIV-infected subjects. They found the discrimination and calibration of the revised risk equations improved substantially and met the standard of “acceptable” by statisticians’ standards.
The next step in this ongoing CNICS project will be to validate the provisionally refit risk calculator’s performance in a separate database of HIV-infected adults with adjudicated MIs. If the results are again positive, it will be a relatively straightforward matter to introduce the revisions into the ACC/AHA risk calculator, particularly since the senior coinvestigator in this project is Dr. Donald M. Lloyd-Jones, also of Northwestern University, who played a central role in developing the 2013 risk calculator.
Dr. Feinstein reported having no financial conflicts regarding this study.
ORLANDO – The 2013 ACC/AHA atherosclerotic cardiovascular disease risk calculator isn’t reliably applicable to HIV-positive adults in its present form because it consistently underpredicts their MI risk, Dr. Michael J. Feinstein reported at the American Heart Association scientific sessions.
That’s the bad news. The good news is that “a simple, data-derived refit of the pooled cohort equations may improve the model’s performance in HIV-positive individuals,” said Dr. Feinstein of Northwestern University, Chicago.
Tweaking the risk calculator to enhance its accuracy in the HIV-positive population is particularly important because this population is growing in size and aging. And as Dr. Feinstein and coinvestigators showed in another study presented at the AHA meeting, the proportion of deaths due to cardiovascular disease in HIV-positive adults is shooting upward as they live longer because of treatment advances.
The investigators’ analysis of data from the Centers for Disease Control and Prevention national Wonder database showed that the proportion of deaths due to cardiovascular disease more than doubled between 1999 and 2013. Meanwhile, proportionate cardiovascular disease mortality declined by 22% in the general population and by 28% among individuals with inflammatory polyarthropathies.
That the ACC/AHA risk calculator in its present form doesn’t perform adequately in HIV-positive individuals hadn’t previously been shown, but it doesn’t really come as a surprise, according to Dr. Feinstein. After all, it’s known that this population is at 1.5- to 2-fold increased risk for MI and roughly 5-fold increased risk for sudden cardiac death, compared to the general population, where the risk calculator works best.
“Most data suggest that even in the setting of optimally treated HIV and undetectable viral load there’s still an underlying viral reservoir that appears to be driving inflammation and atherothrombotic and even nonatherothrombotic events in this population,” he said.
Dr. Feinstein and coworkers evaluated the 2013 ACC/AHA risk calculator in 11,901 HIV-positive black or white adults enrolled in the Centers for AIDS Research Network of Integrated Clinical Systems (CNICS) database for whom 5-year follow-up was available; 52% of the subjects were aged 40 or older at baseline.
Running each of these nearly 12,000 subjects through the risk calculator, the predicted result was that 103 of them would have an acute MI during the 5-year follow-up period. In reality, 132 MIs were observed. The discrepancy between the risk calculator predictions and observed MI rates was greatest in the 63% of HIV-positive subjects deemed at low risk, with an estimated 10-year risk of atherosclerotic cardiovascular disease of less than 5%.
Among white men, the risk calculator was remarkably consistent in underpredicting MIs. Regardless of whether the risk calculator put their estimated 10-year risk at less than 5%, 5% to less than 7.5%, 7.5% to less than 10%, or at least 10%, the actual observed MI rates were 67%-68% greater across the board than predicted.
Dr. Feinstein and coworkers refit the ACC/AHA risk calculator on a trial basis by incorporating variables related to HIV-positivity into the risk equations. Then they reanalyzed the tool’s performance in the same nearly 12,000 HIV-infected subjects. They found the discrimination and calibration of the revised risk equations improved substantially and met the standard of “acceptable” by statisticians’ standards.
The next step in this ongoing CNICS project will be to validate the provisionally refit risk calculator’s performance in a separate database of HIV-infected adults with adjudicated MIs. If the results are again positive, it will be a relatively straightforward matter to introduce the revisions into the ACC/AHA risk calculator, particularly since the senior coinvestigator in this project is Dr. Donald M. Lloyd-Jones, also of Northwestern University, who played a central role in developing the 2013 risk calculator.
Dr. Feinstein reported having no financial conflicts regarding this study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: The 2013 ACC/AHA risk estimator needs a tune-up before it can be reliably applied to HIV-infected adults.
Major finding: Observed rates of acute MI over time in HIV-positive white men were 67%-68% higher than predicted by the 2013 ACC/AHA atherosclerotic cardiovascular disease risk calculator regardless of whether the men were deemed at low, intermediate, or high baseline risk.
Data source: A study comparing the predicted number of acute MIs in a population of nearly 12,000 HIV-positive adults over a 5-year period as determined via the 2013 ACC/AHA atherosclerotic cardiovascular disease risk calculator with the actual observed number of adjudicated MIs.
Disclosures: The study was conducted free of commercial support. The presenter reported having no financial conflicts of interest.
