User login
Neurology Reviews covers innovative and emerging news in neurology and neuroscience every month, with a focus on practical approaches to treating Parkinson's disease, epilepsy, headache, stroke, multiple sclerosis, Alzheimer's disease, and other neurologic disorders.
PML
Progressive multifocal leukoencephalopathy
Rituxan
The leading independent newspaper covering neurology news and commentary.
Low physical function tied to cardiac events in older adults
including coronary heart disease (CHD), stroke, and heart failure (HF) in older adults, according to new observational data from the Atherosclerosis Risk in Communities (ARIC) study.
“We found that physical function in older adults predicts future cardiovascular disease (CVD) beyond traditional heart disease risk factors, regardless of whether an individual has a history of cardiovascular disease,” senior author Kunihiro Matsushita, MD, PhD, division of cardiology, Johns Hopkins University, Baltimore, said in a news release.
The study was published online in the Journal of the American Heart Association.
Keeping fit with age
The researchers analyzed health data collected between 2011 and 2013 for 5,570 ARIC participants (mean age, 75 years; 58% women, 22% Black persons). They assessed physical function using the Short Physical Performance Battery (SPPB), which measures walking speed, leg strength, and balance.
On the basis of the results, participants were categorized into three physical function groups: low (score, 0-6; 13% of the cohort), intermediate (score, 7-9; 30%) and high (score, 10-12; 57%).
During a median follow up of 7 years, there were 930 composite CVD events (386 CHD, 251 stroke, and 529 HF).
Adults with lower SPPB scores had a higher cumulative incidence of composite CVD outcomes.
The 5-year cumulative incidence of the composite CVD outcome in the low- and intermediate-SPPB categories was about three times (23.4%) and two times (15.3%) higher than in the high-SPPB category (8.6%), the researchers reported.
In addition, continuous SPPB scores showed significant associations with composite and individual CVD outcomes in all models. A 1-point lower SPPB score was associated with 6%-10% higher risk for CVD events after adjusting for potential confounders.
In the fully adjusted model, the risk for composite CVD outcomes was 47% higher (hazard ratio, 1.47; 95% confidence interval, 1.20-1.79) in those with low physical function and 25% higher in those with intermediate physical function (HR, 1.25; 95% CI, 1.07-1.46) compared with peers with high physical function.
For the individual outcomes, low physical function was associated with higher risk for stroke (HR, 1.81; 95% CI, 1.24-2.64) and HF (HR, 1.33; 95% CI, 1.02-1.73), whereas the association for CHD was not significant.
The associations were largely consistent across subgroups, including those with CVD at baseline.
The addition of SPPB scores significantly improved risk prediction of CVD events beyond traditional CVD risk factors in adults regardless of prior CVD history, suggesting that this tool may be useful for classifying CVD risk in older adults, the researchers said.
Meaningful impact on care?
“Our findings highlight the value of assessing the physical function level of older adults in clinical practice,” lead author Xiao Hu, MHS, with the department of epidemiology at Johns Hopkins, said in the news release. “In addition to heart health, older adults are at higher risk for falls and disability. The assessment of physical function may also inform the risk of these concerning conditions in older adults.”
Weighing in on the study, Jonathan Halperin, MD, cardiologist at Mount Sinai Heart and professor of medicine (cardiology) at the Icahn School of Medicine at Mount Sinai, both in New York, said that “It’s known that cardiorespiratory fitness is an important predictor of cardiovascular risk, but it is one of the few physiological risk factors that are subjectively queried but not objectively assessed in routine clinical practice.”
In this study, Dr. Halperin noted, the investigators found that a battery of physical performance assessments, including a walk test, chair standing, and balance testing, improved cardiovascular risk prediction.
Dr. Halperin cautioned, however, that “since even the short sequence of tests takes time to perform and interpret, and is not currently reimbursed under most health insurance policies, it is not clear whether the report will have a meaningful impact on patient care.”
This research was funded by the National Institutes of Health. Dr. Matsushita and Dr. Halperin have no relevant disclosures.
A version of this article first appeared on Medscape.com.
including coronary heart disease (CHD), stroke, and heart failure (HF) in older adults, according to new observational data from the Atherosclerosis Risk in Communities (ARIC) study.
“We found that physical function in older adults predicts future cardiovascular disease (CVD) beyond traditional heart disease risk factors, regardless of whether an individual has a history of cardiovascular disease,” senior author Kunihiro Matsushita, MD, PhD, division of cardiology, Johns Hopkins University, Baltimore, said in a news release.
The study was published online in the Journal of the American Heart Association.
Keeping fit with age
The researchers analyzed health data collected between 2011 and 2013 for 5,570 ARIC participants (mean age, 75 years; 58% women, 22% Black persons). They assessed physical function using the Short Physical Performance Battery (SPPB), which measures walking speed, leg strength, and balance.
On the basis of the results, participants were categorized into three physical function groups: low (score, 0-6; 13% of the cohort), intermediate (score, 7-9; 30%) and high (score, 10-12; 57%).
During a median follow up of 7 years, there were 930 composite CVD events (386 CHD, 251 stroke, and 529 HF).
Adults with lower SPPB scores had a higher cumulative incidence of composite CVD outcomes.
The 5-year cumulative incidence of the composite CVD outcome in the low- and intermediate-SPPB categories was about three times (23.4%) and two times (15.3%) higher than in the high-SPPB category (8.6%), the researchers reported.
In addition, continuous SPPB scores showed significant associations with composite and individual CVD outcomes in all models. A 1-point lower SPPB score was associated with 6%-10% higher risk for CVD events after adjusting for potential confounders.
In the fully adjusted model, the risk for composite CVD outcomes was 47% higher (hazard ratio, 1.47; 95% confidence interval, 1.20-1.79) in those with low physical function and 25% higher in those with intermediate physical function (HR, 1.25; 95% CI, 1.07-1.46) compared with peers with high physical function.
For the individual outcomes, low physical function was associated with higher risk for stroke (HR, 1.81; 95% CI, 1.24-2.64) and HF (HR, 1.33; 95% CI, 1.02-1.73), whereas the association for CHD was not significant.
The associations were largely consistent across subgroups, including those with CVD at baseline.
The addition of SPPB scores significantly improved risk prediction of CVD events beyond traditional CVD risk factors in adults regardless of prior CVD history, suggesting that this tool may be useful for classifying CVD risk in older adults, the researchers said.
Meaningful impact on care?
“Our findings highlight the value of assessing the physical function level of older adults in clinical practice,” lead author Xiao Hu, MHS, with the department of epidemiology at Johns Hopkins, said in the news release. “In addition to heart health, older adults are at higher risk for falls and disability. The assessment of physical function may also inform the risk of these concerning conditions in older adults.”
Weighing in on the study, Jonathan Halperin, MD, cardiologist at Mount Sinai Heart and professor of medicine (cardiology) at the Icahn School of Medicine at Mount Sinai, both in New York, said that “It’s known that cardiorespiratory fitness is an important predictor of cardiovascular risk, but it is one of the few physiological risk factors that are subjectively queried but not objectively assessed in routine clinical practice.”
In this study, Dr. Halperin noted, the investigators found that a battery of physical performance assessments, including a walk test, chair standing, and balance testing, improved cardiovascular risk prediction.
Dr. Halperin cautioned, however, that “since even the short sequence of tests takes time to perform and interpret, and is not currently reimbursed under most health insurance policies, it is not clear whether the report will have a meaningful impact on patient care.”
This research was funded by the National Institutes of Health. Dr. Matsushita and Dr. Halperin have no relevant disclosures.
A version of this article first appeared on Medscape.com.
including coronary heart disease (CHD), stroke, and heart failure (HF) in older adults, according to new observational data from the Atherosclerosis Risk in Communities (ARIC) study.
“We found that physical function in older adults predicts future cardiovascular disease (CVD) beyond traditional heart disease risk factors, regardless of whether an individual has a history of cardiovascular disease,” senior author Kunihiro Matsushita, MD, PhD, division of cardiology, Johns Hopkins University, Baltimore, said in a news release.
The study was published online in the Journal of the American Heart Association.
Keeping fit with age
The researchers analyzed health data collected between 2011 and 2013 for 5,570 ARIC participants (mean age, 75 years; 58% women, 22% Black persons). They assessed physical function using the Short Physical Performance Battery (SPPB), which measures walking speed, leg strength, and balance.
On the basis of the results, participants were categorized into three physical function groups: low (score, 0-6; 13% of the cohort), intermediate (score, 7-9; 30%) and high (score, 10-12; 57%).
During a median follow up of 7 years, there were 930 composite CVD events (386 CHD, 251 stroke, and 529 HF).
Adults with lower SPPB scores had a higher cumulative incidence of composite CVD outcomes.
The 5-year cumulative incidence of the composite CVD outcome in the low- and intermediate-SPPB categories was about three times (23.4%) and two times (15.3%) higher than in the high-SPPB category (8.6%), the researchers reported.
In addition, continuous SPPB scores showed significant associations with composite and individual CVD outcomes in all models. A 1-point lower SPPB score was associated with 6%-10% higher risk for CVD events after adjusting for potential confounders.
In the fully adjusted model, the risk for composite CVD outcomes was 47% higher (hazard ratio, 1.47; 95% confidence interval, 1.20-1.79) in those with low physical function and 25% higher in those with intermediate physical function (HR, 1.25; 95% CI, 1.07-1.46) compared with peers with high physical function.
For the individual outcomes, low physical function was associated with higher risk for stroke (HR, 1.81; 95% CI, 1.24-2.64) and HF (HR, 1.33; 95% CI, 1.02-1.73), whereas the association for CHD was not significant.
The associations were largely consistent across subgroups, including those with CVD at baseline.
The addition of SPPB scores significantly improved risk prediction of CVD events beyond traditional CVD risk factors in adults regardless of prior CVD history, suggesting that this tool may be useful for classifying CVD risk in older adults, the researchers said.
Meaningful impact on care?
“Our findings highlight the value of assessing the physical function level of older adults in clinical practice,” lead author Xiao Hu, MHS, with the department of epidemiology at Johns Hopkins, said in the news release. “In addition to heart health, older adults are at higher risk for falls and disability. The assessment of physical function may also inform the risk of these concerning conditions in older adults.”
Weighing in on the study, Jonathan Halperin, MD, cardiologist at Mount Sinai Heart and professor of medicine (cardiology) at the Icahn School of Medicine at Mount Sinai, both in New York, said that “It’s known that cardiorespiratory fitness is an important predictor of cardiovascular risk, but it is one of the few physiological risk factors that are subjectively queried but not objectively assessed in routine clinical practice.”
In this study, Dr. Halperin noted, the investigators found that a battery of physical performance assessments, including a walk test, chair standing, and balance testing, improved cardiovascular risk prediction.
Dr. Halperin cautioned, however, that “since even the short sequence of tests takes time to perform and interpret, and is not currently reimbursed under most health insurance policies, it is not clear whether the report will have a meaningful impact on patient care.”
This research was funded by the National Institutes of Health. Dr. Matsushita and Dr. Halperin have no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN HEART ASSOCIATION
Blood type linked to higher risk for early onset stroke
Conversely, results from a meta-analysis of nearly 17,000 cases of ischemic stroke in adults younger than 60 years showed that having type O blood reduced the risk for EOS by 12%.
In addition, the associations with risk were significantly stronger in EOS than in those with late-onset stroke (LOS), pointing to a stronger role for prothrombotic factors in younger patients, the researchers noted.
“What this is telling us is that maybe what makes you susceptible to stroke as a young adult is the blood type, which is really giving you a much higher risk of clotting and stroke compared to later onset,” coinvestigator Braxton Mitchell, PhD, professor of medicine and epidemiology and public health at the University of Maryland, Baltimore, said in an interview.
The findings were published online in Neurology.
Strong association
The genome-wide association study (GWAS) was done as part of the Genetics of Early Onset Ischemic Stroke Consortium, a collaboration of 48 different studies across North America, Europe, Japan, Pakistan, and Australia. It assessed early onset ischemic stroke in patients aged 18-59 years.
Researchers included data from 16,927 patients with stroke. Of these, 5,825 had a stroke before age 60, defined as early onset. GWAS results were also examined for nearly 600,000 individuals without stroke.
Results showed two genetic variants tied to blood types A and O emerged as highly associated with risk for early stroke.
Researchers found that the protective effects of type O were significantly stronger with EOS vs. LOS (odds ratio [OR], 0.88 vs. 0.96, respectively; P = .001). Likewise, the association between type A and increased EOS risk was significantly stronger than that found in LOS (OR, 1.16 vs. 1.05; P = .005).
Using polygenic risk scores, the investigators also found that the greater genetic risk for venous thromboembolism, another prothrombotic condition, was more strongly associated with EOS compared with LOS (P = .008).
Previous studies have shown a link between stroke risk and variants of the ABO gene, which determines blood type. The new analysis suggests that type A and O gene variants represent nearly all of those genetically linked with early stroke, the researchers noted.
While the findings point to blood type as a risk factor for stroke in younger people, Dr. Mitchell cautions that “at the moment, blood group does not have implications for preventive care.”
“The risk of stroke due to blood type is smaller than other risk factors that we know about, like smoking and hypertension,” he said. “I would be much more worried about these other risk factors, especially because those may be modifiable.”
He noted the next step in the study is to assess how blood type interacts with other known risk factors to raise stroke risk.
“There may be a subset of people where, if you have blood type A and you have some of these other risk factors, it’s possible that you may be at particularly high risk,” Dr. Mitchell said.
More research needed on younger patients
In an accompanying editorial, Jennifer Juhl Majersik, MD, associate professor of neurology at the University of Utah, Salt Lake City, and Paul Lacaze, PhD, associate professor and head of the public health genomics program at Monash University, Australia, noted that the study fills a gap in stroke research, which often focuses mostly on older individuals.
“In approximately 40% of people with EOS, the stroke is cryptogenic, and there is scant data from clinical trials to guide the selection of preventative strategies in this population, as people with EOS are often excluded from trials,” Dr. Majersik and Dr. Lacaze wrote.
“This work has deepened our understanding of EOS pathophysiology,” they added.
The editorialists noted that future research can build on the results from this analysis, “with the goal of a more precise understanding of stroke pathophysiology, leading to targeted preventative treatments for EOS and a reduction in disability in patients’ most productive years.”
Dr. Mitchell echoed the call for greater inclusion of young patients with stroke in clinical trials.
“As we’re learning, stroke in older folks isn’t the same as stroke in younger people,” he said. “There are many shared risk factors but there are also some that are different ... so there really is a need to include younger people.”
A version of this article first appeared on Medscape.com.
Conversely, results from a meta-analysis of nearly 17,000 cases of ischemic stroke in adults younger than 60 years showed that having type O blood reduced the risk for EOS by 12%.
In addition, the associations with risk were significantly stronger in EOS than in those with late-onset stroke (LOS), pointing to a stronger role for prothrombotic factors in younger patients, the researchers noted.
“What this is telling us is that maybe what makes you susceptible to stroke as a young adult is the blood type, which is really giving you a much higher risk of clotting and stroke compared to later onset,” coinvestigator Braxton Mitchell, PhD, professor of medicine and epidemiology and public health at the University of Maryland, Baltimore, said in an interview.
The findings were published online in Neurology.
Strong association
The genome-wide association study (GWAS) was done as part of the Genetics of Early Onset Ischemic Stroke Consortium, a collaboration of 48 different studies across North America, Europe, Japan, Pakistan, and Australia. It assessed early onset ischemic stroke in patients aged 18-59 years.
Researchers included data from 16,927 patients with stroke. Of these, 5,825 had a stroke before age 60, defined as early onset. GWAS results were also examined for nearly 600,000 individuals without stroke.
Results showed two genetic variants tied to blood types A and O emerged as highly associated with risk for early stroke.
Researchers found that the protective effects of type O were significantly stronger with EOS vs. LOS (odds ratio [OR], 0.88 vs. 0.96, respectively; P = .001). Likewise, the association between type A and increased EOS risk was significantly stronger than that found in LOS (OR, 1.16 vs. 1.05; P = .005).
Using polygenic risk scores, the investigators also found that the greater genetic risk for venous thromboembolism, another prothrombotic condition, was more strongly associated with EOS compared with LOS (P = .008).
Previous studies have shown a link between stroke risk and variants of the ABO gene, which determines blood type. The new analysis suggests that type A and O gene variants represent nearly all of those genetically linked with early stroke, the researchers noted.
While the findings point to blood type as a risk factor for stroke in younger people, Dr. Mitchell cautions that “at the moment, blood group does not have implications for preventive care.”
“The risk of stroke due to blood type is smaller than other risk factors that we know about, like smoking and hypertension,” he said. “I would be much more worried about these other risk factors, especially because those may be modifiable.”
He noted the next step in the study is to assess how blood type interacts with other known risk factors to raise stroke risk.
“There may be a subset of people where, if you have blood type A and you have some of these other risk factors, it’s possible that you may be at particularly high risk,” Dr. Mitchell said.
More research needed on younger patients
In an accompanying editorial, Jennifer Juhl Majersik, MD, associate professor of neurology at the University of Utah, Salt Lake City, and Paul Lacaze, PhD, associate professor and head of the public health genomics program at Monash University, Australia, noted that the study fills a gap in stroke research, which often focuses mostly on older individuals.
“In approximately 40% of people with EOS, the stroke is cryptogenic, and there is scant data from clinical trials to guide the selection of preventative strategies in this population, as people with EOS are often excluded from trials,” Dr. Majersik and Dr. Lacaze wrote.
“This work has deepened our understanding of EOS pathophysiology,” they added.
The editorialists noted that future research can build on the results from this analysis, “with the goal of a more precise understanding of stroke pathophysiology, leading to targeted preventative treatments for EOS and a reduction in disability in patients’ most productive years.”
Dr. Mitchell echoed the call for greater inclusion of young patients with stroke in clinical trials.
“As we’re learning, stroke in older folks isn’t the same as stroke in younger people,” he said. “There are many shared risk factors but there are also some that are different ... so there really is a need to include younger people.”
A version of this article first appeared on Medscape.com.
Conversely, results from a meta-analysis of nearly 17,000 cases of ischemic stroke in adults younger than 60 years showed that having type O blood reduced the risk for EOS by 12%.
In addition, the associations with risk were significantly stronger in EOS than in those with late-onset stroke (LOS), pointing to a stronger role for prothrombotic factors in younger patients, the researchers noted.
“What this is telling us is that maybe what makes you susceptible to stroke as a young adult is the blood type, which is really giving you a much higher risk of clotting and stroke compared to later onset,” coinvestigator Braxton Mitchell, PhD, professor of medicine and epidemiology and public health at the University of Maryland, Baltimore, said in an interview.
The findings were published online in Neurology.
Strong association
The genome-wide association study (GWAS) was done as part of the Genetics of Early Onset Ischemic Stroke Consortium, a collaboration of 48 different studies across North America, Europe, Japan, Pakistan, and Australia. It assessed early onset ischemic stroke in patients aged 18-59 years.
Researchers included data from 16,927 patients with stroke. Of these, 5,825 had a stroke before age 60, defined as early onset. GWAS results were also examined for nearly 600,000 individuals without stroke.
Results showed two genetic variants tied to blood types A and O emerged as highly associated with risk for early stroke.
Researchers found that the protective effects of type O were significantly stronger with EOS vs. LOS (odds ratio [OR], 0.88 vs. 0.96, respectively; P = .001). Likewise, the association between type A and increased EOS risk was significantly stronger than that found in LOS (OR, 1.16 vs. 1.05; P = .005).
Using polygenic risk scores, the investigators also found that the greater genetic risk for venous thromboembolism, another prothrombotic condition, was more strongly associated with EOS compared with LOS (P = .008).
Previous studies have shown a link between stroke risk and variants of the ABO gene, which determines blood type. The new analysis suggests that type A and O gene variants represent nearly all of those genetically linked with early stroke, the researchers noted.
While the findings point to blood type as a risk factor for stroke in younger people, Dr. Mitchell cautions that “at the moment, blood group does not have implications for preventive care.”
“The risk of stroke due to blood type is smaller than other risk factors that we know about, like smoking and hypertension,” he said. “I would be much more worried about these other risk factors, especially because those may be modifiable.”
He noted the next step in the study is to assess how blood type interacts with other known risk factors to raise stroke risk.
“There may be a subset of people where, if you have blood type A and you have some of these other risk factors, it’s possible that you may be at particularly high risk,” Dr. Mitchell said.
More research needed on younger patients
In an accompanying editorial, Jennifer Juhl Majersik, MD, associate professor of neurology at the University of Utah, Salt Lake City, and Paul Lacaze, PhD, associate professor and head of the public health genomics program at Monash University, Australia, noted that the study fills a gap in stroke research, which often focuses mostly on older individuals.
“In approximately 40% of people with EOS, the stroke is cryptogenic, and there is scant data from clinical trials to guide the selection of preventative strategies in this population, as people with EOS are often excluded from trials,” Dr. Majersik and Dr. Lacaze wrote.
“This work has deepened our understanding of EOS pathophysiology,” they added.
The editorialists noted that future research can build on the results from this analysis, “with the goal of a more precise understanding of stroke pathophysiology, leading to targeted preventative treatments for EOS and a reduction in disability in patients’ most productive years.”
Dr. Mitchell echoed the call for greater inclusion of young patients with stroke in clinical trials.
“As we’re learning, stroke in older folks isn’t the same as stroke in younger people,” he said. “There are many shared risk factors but there are also some that are different ... so there really is a need to include younger people.”
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
Class I recall issued for intracranial pressure monitor
Integra is recalling the CereLink Intracranial Pressure (ICP) Monitor after reports that the device may display incorrect ICP values and out-of-range pressure readings.
The recall includes 388 monitors, with model numbers 826820 and 826820P. The devices were distributed between June 1, 2021 and May 31, 2022.
The U.S. Food and Drug Administration has identified this as a class I recall, the most serious type, because of the risk for serious injury or death.
The monitor is used in patients with head injuries and stroke as well as in surgical and postoperative neurosurgical patients and those with other conditions.
The device’s sensor is implanted in the brain and connected by a wire to an external monitor that displays ICP readings, which are used to both monitor and guide treatment.
If the CereLink ICP Monitor fails to function properly, the patient may have to undergo additional brain surgeries to replace it, which involves the risks for infection, bleeding, and damage to tissue. A malfunctioning device also creates a risk for serious injury or death, the MedWatch notes.
Global complaints
As of July 31, Integra has received 105 global complaints associated with this recall.
In addition,
According to the FDA, the patient death report in the MDR described a malfunctioning CereLink ICP Monitor during use in a critically injured patient, which was mitigated by replacing the ICP sensor.
“The cause of patient death was determined by Integra to be unrelated to the CereLink ICP Monitor malfunction,” the FDA said.
The manufacturer has sent a letter to customers advising them to stop using the recalled monitors “as soon as clinically possible.”
The letter states that continued use of a monitor already in place should be determined only by an individualized risk-benefit analysis by the attending clinician.
For any new patients, the company advises switching to an alternate patient-monitoring system.
Customers with questions or concerns about this recall should contact their Integra account manager, clinical specialist, or customer service by phone at 800-654-2873 or by email at [email protected].
Problems related to the CereLink ICP Monitor should be reported to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
Integra is recalling the CereLink Intracranial Pressure (ICP) Monitor after reports that the device may display incorrect ICP values and out-of-range pressure readings.
The recall includes 388 monitors, with model numbers 826820 and 826820P. The devices were distributed between June 1, 2021 and May 31, 2022.
The U.S. Food and Drug Administration has identified this as a class I recall, the most serious type, because of the risk for serious injury or death.
The monitor is used in patients with head injuries and stroke as well as in surgical and postoperative neurosurgical patients and those with other conditions.
The device’s sensor is implanted in the brain and connected by a wire to an external monitor that displays ICP readings, which are used to both monitor and guide treatment.
If the CereLink ICP Monitor fails to function properly, the patient may have to undergo additional brain surgeries to replace it, which involves the risks for infection, bleeding, and damage to tissue. A malfunctioning device also creates a risk for serious injury or death, the MedWatch notes.
Global complaints
As of July 31, Integra has received 105 global complaints associated with this recall.
In addition,
According to the FDA, the patient death report in the MDR described a malfunctioning CereLink ICP Monitor during use in a critically injured patient, which was mitigated by replacing the ICP sensor.
“The cause of patient death was determined by Integra to be unrelated to the CereLink ICP Monitor malfunction,” the FDA said.
The manufacturer has sent a letter to customers advising them to stop using the recalled monitors “as soon as clinically possible.”
The letter states that continued use of a monitor already in place should be determined only by an individualized risk-benefit analysis by the attending clinician.
For any new patients, the company advises switching to an alternate patient-monitoring system.
Customers with questions or concerns about this recall should contact their Integra account manager, clinical specialist, or customer service by phone at 800-654-2873 or by email at [email protected].
Problems related to the CereLink ICP Monitor should be reported to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
Integra is recalling the CereLink Intracranial Pressure (ICP) Monitor after reports that the device may display incorrect ICP values and out-of-range pressure readings.
The recall includes 388 monitors, with model numbers 826820 and 826820P. The devices were distributed between June 1, 2021 and May 31, 2022.
The U.S. Food and Drug Administration has identified this as a class I recall, the most serious type, because of the risk for serious injury or death.
The monitor is used in patients with head injuries and stroke as well as in surgical and postoperative neurosurgical patients and those with other conditions.
The device’s sensor is implanted in the brain and connected by a wire to an external monitor that displays ICP readings, which are used to both monitor and guide treatment.
If the CereLink ICP Monitor fails to function properly, the patient may have to undergo additional brain surgeries to replace it, which involves the risks for infection, bleeding, and damage to tissue. A malfunctioning device also creates a risk for serious injury or death, the MedWatch notes.
Global complaints
As of July 31, Integra has received 105 global complaints associated with this recall.
In addition,
According to the FDA, the patient death report in the MDR described a malfunctioning CereLink ICP Monitor during use in a critically injured patient, which was mitigated by replacing the ICP sensor.
“The cause of patient death was determined by Integra to be unrelated to the CereLink ICP Monitor malfunction,” the FDA said.
The manufacturer has sent a letter to customers advising them to stop using the recalled monitors “as soon as clinically possible.”
The letter states that continued use of a monitor already in place should be determined only by an individualized risk-benefit analysis by the attending clinician.
For any new patients, the company advises switching to an alternate patient-monitoring system.
Customers with questions or concerns about this recall should contact their Integra account manager, clinical specialist, or customer service by phone at 800-654-2873 or by email at [email protected].
Problems related to the CereLink ICP Monitor should be reported to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
Real medical news: Many teens trust fake medical news
The kids aren’t alright (at identifying fake news online)
If there’s one thing today’s teenagers are good at, it’s the Internet. What with their TokTiks, Fortnights, and memes whose lifespans are measured in milliseconds, it’s only natural that a contingent of people who have never known a world where the Internet wasn’t omnipresent would be highly skilled at navigating the dense, labyrinthine virtual world and the many falsehoods contained within.
Ladies and gentlemen, we’ve been duped, bamboozled, and smeckledorfed. New research from Slovakia suggests the opposite, in fact: Teenagers are just as bad as the rest of us, if not worse, at distinguishing between fake and real online health messaging.
For the study, 300 teenagers aged 16-19 years old were shown a group of messages about the health-promoting effects of fruits and vegetables; these messages were either false, true and neutral, or true with some sort of editing (a clickbait title or grammar mistakes) to mask their trustworthiness. Just under half of the subjects identified and trusted the true neutral messages over fake messages, while 41% couldn’t tell the difference and 11% trusted the fake messages more. In addition, they couldn’t tell the difference between fake and true messages when the content seemed plausible.
In a bit of good news, teenagers were just as likely to trust the edited true messages as the true neutral ones, except in instances when the edited message had a clickbait title. They were much less likely to trust those.
Based on their subjects’ rather poor performance, the study authors suggested teenagers go through health literacy and media literacy training, as well as develop their analytical and scientific reasoning. The LOTME staff rather suspects the study authors have never met a teenager. The only thing teenagers are going to get out of health literacy training is fodder for memes to put up on Myspace. Myspace is still a thing, right? We’re not old, we swear.
Can a computer help deliver babies?
Delivering babies can be a complicated business. Most doctors and midwives rely on their years of experience and training to make certain decisions for mothers in labor, but an artificial intelligence (AI) algorithm could make the entire process easier and safer.

Researchers from the Mayo Clinic recently reported that using an AI to analyze women’s labor patterns was very successful in determining whether a vaginal or cesarean delivery was appropriate.
They examined over 700 factors and over 66,000 deliveries from the National Institute of Child Health and Human Development’s multicenter Consortium on Safe Labor database to produce a risk-prediction model that may “provide an alternative to conventional labor charts and promote individualization of clinical decisions using baseline and labor characteristics of each patient,” they said in a written statement from the clinic.
It is hoped that the AI will reduce the risk of possible complications and the costs associated with maternal mortality. The AI also could be a significant tool for doctors and midwives in rural areas to determine when a patient needs to be moved to a location with a higher level of care.
“We believe the algorithm will work in real time, meaning every input of new data during an expectant woman’s labor automatically recalculates the risk of adverse outcome,” said senior author Abimbola Famuyide, MD, of the Mayo Clinic.
If it all works out, many lives and dollars could be saved, thanks to science.
Democracy, meet COVID-19
Everywhere you look, it seems, someone is trying to keep someone else from doing something: Don’t carry a gun. Don’t get an abortion. Don’t drive so fast. Don’t inhale that whipped cream. Don’t get a vaccine. Don’t put that in your mouth.
One of the biggies these days is voting rights. Some people are trying to prevent other people from voting. But why? Well, turns out that turnout can be bad for your health … at least during a worldwide pandemic event.
The evidence for that claim comes from researchers who examined the Italian national constitutional referendum conducted in September 2020 along with elections for assembly representatives in 7 of the country’s 20 regions and for mayors in about 12% of municipalities. The combination mattered: Voter turnout was higher in the municipalities that voted for both the referendum and local elections (69%), compared with municipalities voting only for the referendum (47%), the investigators reported in the Journal of Economic Behavior & Organization.
Also occurring in September of 2020 was, as we mentioned, a worldwide pandemic event. You may have heard about it.
The investigators considered the differences in election turnout between the various municipalities and compared them with new weekly COVID-19 infections at the municipality level. “Our model shows that something as fundamental as casting a vote can come at a cost,” investigator Giuseppe Moscelli, PhD, of the University of Surrey (England) said in a written statement.
What was the cost? Each 1% increase in turnout, they found, amounted to an average 1.1% increase in COVID infections after the elections.
See? More people voting means more COVID, which is bad. Which brings us to today’s lesson in people preventing other people from doing something. Don’t let COVID win. Stay in your house and never come out. And get that smeckledorf out of your mouth. You don’t know where it’s been.
The kids aren’t alright (at identifying fake news online)
If there’s one thing today’s teenagers are good at, it’s the Internet. What with their TokTiks, Fortnights, and memes whose lifespans are measured in milliseconds, it’s only natural that a contingent of people who have never known a world where the Internet wasn’t omnipresent would be highly skilled at navigating the dense, labyrinthine virtual world and the many falsehoods contained within.
Ladies and gentlemen, we’ve been duped, bamboozled, and smeckledorfed. New research from Slovakia suggests the opposite, in fact: Teenagers are just as bad as the rest of us, if not worse, at distinguishing between fake and real online health messaging.
For the study, 300 teenagers aged 16-19 years old were shown a group of messages about the health-promoting effects of fruits and vegetables; these messages were either false, true and neutral, or true with some sort of editing (a clickbait title or grammar mistakes) to mask their trustworthiness. Just under half of the subjects identified and trusted the true neutral messages over fake messages, while 41% couldn’t tell the difference and 11% trusted the fake messages more. In addition, they couldn’t tell the difference between fake and true messages when the content seemed plausible.
In a bit of good news, teenagers were just as likely to trust the edited true messages as the true neutral ones, except in instances when the edited message had a clickbait title. They were much less likely to trust those.
Based on their subjects’ rather poor performance, the study authors suggested teenagers go through health literacy and media literacy training, as well as develop their analytical and scientific reasoning. The LOTME staff rather suspects the study authors have never met a teenager. The only thing teenagers are going to get out of health literacy training is fodder for memes to put up on Myspace. Myspace is still a thing, right? We’re not old, we swear.
Can a computer help deliver babies?
Delivering babies can be a complicated business. Most doctors and midwives rely on their years of experience and training to make certain decisions for mothers in labor, but an artificial intelligence (AI) algorithm could make the entire process easier and safer.
Researchers from the Mayo Clinic recently reported that using an AI to analyze women’s labor patterns was very successful in determining whether a vaginal or cesarean delivery was appropriate.
They examined over 700 factors and over 66,000 deliveries from the National Institute of Child Health and Human Development’s multicenter Consortium on Safe Labor database to produce a risk-prediction model that may “provide an alternative to conventional labor charts and promote individualization of clinical decisions using baseline and labor characteristics of each patient,” they said in a written statement from the clinic.
It is hoped that the AI will reduce the risk of possible complications and the costs associated with maternal mortality. The AI also could be a significant tool for doctors and midwives in rural areas to determine when a patient needs to be moved to a location with a higher level of care.
“We believe the algorithm will work in real time, meaning every input of new data during an expectant woman’s labor automatically recalculates the risk of adverse outcome,” said senior author Abimbola Famuyide, MD, of the Mayo Clinic.
If it all works out, many lives and dollars could be saved, thanks to science.
Democracy, meet COVID-19
Everywhere you look, it seems, someone is trying to keep someone else from doing something: Don’t carry a gun. Don’t get an abortion. Don’t drive so fast. Don’t inhale that whipped cream. Don’t get a vaccine. Don’t put that in your mouth.
One of the biggies these days is voting rights. Some people are trying to prevent other people from voting. But why? Well, turns out that turnout can be bad for your health … at least during a worldwide pandemic event.
The evidence for that claim comes from researchers who examined the Italian national constitutional referendum conducted in September 2020 along with elections for assembly representatives in 7 of the country’s 20 regions and for mayors in about 12% of municipalities. The combination mattered: Voter turnout was higher in the municipalities that voted for both the referendum and local elections (69%), compared with municipalities voting only for the referendum (47%), the investigators reported in the Journal of Economic Behavior & Organization.
Also occurring in September of 2020 was, as we mentioned, a worldwide pandemic event. You may have heard about it.
The investigators considered the differences in election turnout between the various municipalities and compared them with new weekly COVID-19 infections at the municipality level. “Our model shows that something as fundamental as casting a vote can come at a cost,” investigator Giuseppe Moscelli, PhD, of the University of Surrey (England) said in a written statement.
What was the cost? Each 1% increase in turnout, they found, amounted to an average 1.1% increase in COVID infections after the elections.
See? More people voting means more COVID, which is bad. Which brings us to today’s lesson in people preventing other people from doing something. Don’t let COVID win. Stay in your house and never come out. And get that smeckledorf out of your mouth. You don’t know where it’s been.
The kids aren’t alright (at identifying fake news online)
If there’s one thing today’s teenagers are good at, it’s the Internet. What with their TokTiks, Fortnights, and memes whose lifespans are measured in milliseconds, it’s only natural that a contingent of people who have never known a world where the Internet wasn’t omnipresent would be highly skilled at navigating the dense, labyrinthine virtual world and the many falsehoods contained within.
Ladies and gentlemen, we’ve been duped, bamboozled, and smeckledorfed. New research from Slovakia suggests the opposite, in fact: Teenagers are just as bad as the rest of us, if not worse, at distinguishing between fake and real online health messaging.
For the study, 300 teenagers aged 16-19 years old were shown a group of messages about the health-promoting effects of fruits and vegetables; these messages were either false, true and neutral, or true with some sort of editing (a clickbait title or grammar mistakes) to mask their trustworthiness. Just under half of the subjects identified and trusted the true neutral messages over fake messages, while 41% couldn’t tell the difference and 11% trusted the fake messages more. In addition, they couldn’t tell the difference between fake and true messages when the content seemed plausible.
In a bit of good news, teenagers were just as likely to trust the edited true messages as the true neutral ones, except in instances when the edited message had a clickbait title. They were much less likely to trust those.
Based on their subjects’ rather poor performance, the study authors suggested teenagers go through health literacy and media literacy training, as well as develop their analytical and scientific reasoning. The LOTME staff rather suspects the study authors have never met a teenager. The only thing teenagers are going to get out of health literacy training is fodder for memes to put up on Myspace. Myspace is still a thing, right? We’re not old, we swear.
Can a computer help deliver babies?
Delivering babies can be a complicated business. Most doctors and midwives rely on their years of experience and training to make certain decisions for mothers in labor, but an artificial intelligence (AI) algorithm could make the entire process easier and safer.
Researchers from the Mayo Clinic recently reported that using an AI to analyze women’s labor patterns was very successful in determining whether a vaginal or cesarean delivery was appropriate.
They examined over 700 factors and over 66,000 deliveries from the National Institute of Child Health and Human Development’s multicenter Consortium on Safe Labor database to produce a risk-prediction model that may “provide an alternative to conventional labor charts and promote individualization of clinical decisions using baseline and labor characteristics of each patient,” they said in a written statement from the clinic.
It is hoped that the AI will reduce the risk of possible complications and the costs associated with maternal mortality. The AI also could be a significant tool for doctors and midwives in rural areas to determine when a patient needs to be moved to a location with a higher level of care.
“We believe the algorithm will work in real time, meaning every input of new data during an expectant woman’s labor automatically recalculates the risk of adverse outcome,” said senior author Abimbola Famuyide, MD, of the Mayo Clinic.
If it all works out, many lives and dollars could be saved, thanks to science.
Democracy, meet COVID-19
Everywhere you look, it seems, someone is trying to keep someone else from doing something: Don’t carry a gun. Don’t get an abortion. Don’t drive so fast. Don’t inhale that whipped cream. Don’t get a vaccine. Don’t put that in your mouth.
One of the biggies these days is voting rights. Some people are trying to prevent other people from voting. But why? Well, turns out that turnout can be bad for your health … at least during a worldwide pandemic event.
The evidence for that claim comes from researchers who examined the Italian national constitutional referendum conducted in September 2020 along with elections for assembly representatives in 7 of the country’s 20 regions and for mayors in about 12% of municipalities. The combination mattered: Voter turnout was higher in the municipalities that voted for both the referendum and local elections (69%), compared with municipalities voting only for the referendum (47%), the investigators reported in the Journal of Economic Behavior & Organization.
Also occurring in September of 2020 was, as we mentioned, a worldwide pandemic event. You may have heard about it.
The investigators considered the differences in election turnout between the various municipalities and compared them with new weekly COVID-19 infections at the municipality level. “Our model shows that something as fundamental as casting a vote can come at a cost,” investigator Giuseppe Moscelli, PhD, of the University of Surrey (England) said in a written statement.
What was the cost? Each 1% increase in turnout, they found, amounted to an average 1.1% increase in COVID infections after the elections.
See? More people voting means more COVID, which is bad. Which brings us to today’s lesson in people preventing other people from doing something. Don’t let COVID win. Stay in your house and never come out. And get that smeckledorf out of your mouth. You don’t know where it’s been.
Inhaled, systemic steroids linked to changes in brain structure
New research links the use of glucocorticoids with changes in white matter microstructure – which may explain the development of anxiety, depression, and other neuropsychiatric side effects related to these drugs, investigators say.
Results from a cross-sectional study showed that use of both systemic and inhaled glucocorticoids was associated with widespread reductions in fractional anisotropy (FA) and increases in mean diffusivity.
Glucocorticoids have “a whole catalogue” of adverse events, and effects on brain structure “adds to the list,” co-investigator Onno C. Meijer, PhD, professor of molecular neuroendocrinology of corticosteroids, department of medicine, Leiden University Medical Center, the Netherlands, told this news organization.

The findings should encourage clinicians to consider whether doses they are prescribing are too high, said Dr. Meijer. He added that the negative effect of glucocorticoids on the brain was also found in those using inhalers, such as patients with asthma.
The findings were published online in the BMJ Open.
Serious side effects
Glucocorticoids, a class of synthetic steroids with immunosuppressive properties, are prescribed for a wide range of conditions, including rheumatoid arthritis and asthma.
However, they are also associated with potentially serious metabolic, cardiovascular, and musculoskeletal side effects as well as neuropsychiatric side effects such as depression, mania, and cognitive impairment.
About 1 in 3 patients exposed to “quite a lot of these drugs” will experience neuropsychiatric symptoms, Dr. Meijer said.
Most previous studies that investigated effects from high levels of glucocorticoids on brain structure have been small and involved selected populations, such as those with Cushing disease.
The new study included participants from the UK Biobank, a large population-based cohort. Participants had undergone imaging and did not have a history of psychiatric disease – although they could have conditions associated with glucocorticoid use, including anxiety, depression, mania, or delirium.
The analysis included 222 patients using oral or parenteral glucocorticoids at the time of imaging (systemic group), 557 using inhaled glucocorticoids, and 24,106 not using glucocorticoids (the control group).
Inhaled steroids target the lungs, whereas a steroid in pill form “travels in the blood and reaches each and every organ and cell in the body and typically requires higher doses,” Dr. Meijer noted.
The groups were similar with respect to sex, education, and smoking status. However, the systemic glucocorticoid group was slightly older (mean age, 66.1 years vs. 63.3 years for inhaled glucocorticoid users and 63.5 years for the control group).
In addition to age, researchers adjusted for sex, education level, head position in the scanner, head size, assessment center, and year of imaging.
Imaging analyses
Imaging analyses showed systemic glucocorticoid use was associated with reduced global FA (adjusted mean difference, -3.7e-3; 95% confidence interval, -6.4e-3 to 1.0e-3), and reductions in regional FA in the body and genu of the corpus callosum versus the control group.
Inhaled glucocorticoid use was associated with reduced global FA (AMD, -2.3e-3; 95% CI, -4.0e-3 to -5.7e-4), and lower FA in the splenium of the corpus callosum and the cingulum of the hippocampus.
Global mean diffusivity was higher in systemic glucocorticoid users (AMD, 7.2e-6; 95% CI, 3.2e-6 to 1.1e-5) and inhaled glucocorticoid users (AMD, 2.7e-6; 95% CI, 1.7e-7 to 5.2e-6), compared with the control group.
The effects of glucocorticoids on white matter were “pervasive,” and the “most important finding” of the study, Dr. Meijer said. “We were impressed by the fact white matter is so sensitive to these drugs.”
He noted that it is likely that functional connectivity between brain regions is affected by use of glucocorticoids. “You could say communication between brain regions is probably somewhat impaired or challenged,” he said.
Subgroup analyses among participants using glucocorticoids chronically, defined as reported at two consecutive visits, suggested a potential dose-dependent or duration-dependent effect of glucocorticoids on white matter microstructure.
Systemic glucocorticoid use was also associated with an increase in total and grey matter volume of the caudate nucleus.
In addition, there was a significant association between inhaled glucocorticoid use and decreased grey matter volume of the amygdala, which Dr. Meijer said was surprising because studies have shown that glucocorticoids “can drive amygdala big time.”
Move away from ‘one dose for all’?
Another surprise was that the results showed no hippocampal volume differences with steroid use, Dr. Meijer noted.
The modest association between glucocorticoid use and brain volumes could indicate that white matter integrity is more sensitive to glucocorticoids than is grey matter volume, “at least at the structural level,” he said.
He added that longer use or higher doses may be necessary to also induce volumetric changes.
Participants also completed a questionnaire to assess mood over the previous 2 weeks. Systemic glucocorticoid users had more depressive symptoms, disinterest, tenseness/restlessness, and tiredness/lethargy, compared with the control group. Inhaled glucocorticoid users only reported more tiredness/lethargy.
The investigators note that mood-related effects could be linked to the condition for which glucocorticoids were prescribed: for example, rheumatoid arthritis or chronic obstructive pulmonary disease.
In terms of cognition, systemic glucocorticoid users performed significantly worse on the symbol digit substitution task, compared with participants in the control group.
In light of these findings, pharmaceutical companies that make inhaled corticosteroids “should perhaps find out if glucocorticoids can be dosed by kilogram body weight rather than simply one dose fits all,” which is currently the case, Dr. Meijer said.
Impressive, but several limitations
Commenting on the findings, E. Sherwood Brown, MD, PhD, Distinguished Chair in Psychiatric Research and professor and vice chair for clinical research, department of psychiatry, The University of Texas Southwestern Medical Center, Dallas, called the study sample size “impressive.”
In addition, the study is the first to look at systemic as well as inhaled corticosteroids, said Dr. Brown, who was not involved with the research. He noted that previously, there had been only case reports of psychiatric symptoms with inhaled corticosteroids.
That results are in the same direction but greater with systemic, compared with inhaled corticosteroids, is “particularly interesting” because this might suggest dose-dependent effects, Dr. Brown said.
He noted that cognitive differences were also only observed with systemic corticosteroids.
Some study observations, such as smaller amygdala volume with inhaled but not systemic corticosteroids, “are harder to understand,” said Dr. Brown.
However, he pointed out some study limitations. For example, data were apparently unavailable for verbal and declarative memory test data, despite corticosteroids probably affecting the hippocampus and causing memory changes.
Other drawbacks were that the dose and duration of corticosteroid use, as well as the medical histories of study participants, were not available, Dr. Brown said.
No study funding was reported. Dr. Meijer has received research grants and honorariums from Corcept Therapeutics and a speakers’ fee from Ipsen. Dr. Brown is on an advisory board for Sage Pharmaceuticals, which is developing neurosteroids (not corticosteroids) for mood disorders. He is also on a Medscape advisory board related to bipolar disorder.
A version of this article first appeared on Medscape.com.
New research links the use of glucocorticoids with changes in white matter microstructure – which may explain the development of anxiety, depression, and other neuropsychiatric side effects related to these drugs, investigators say.
Results from a cross-sectional study showed that use of both systemic and inhaled glucocorticoids was associated with widespread reductions in fractional anisotropy (FA) and increases in mean diffusivity.
Glucocorticoids have “a whole catalogue” of adverse events, and effects on brain structure “adds to the list,” co-investigator Onno C. Meijer, PhD, professor of molecular neuroendocrinology of corticosteroids, department of medicine, Leiden University Medical Center, the Netherlands, told this news organization.
The findings should encourage clinicians to consider whether doses they are prescribing are too high, said Dr. Meijer. He added that the negative effect of glucocorticoids on the brain was also found in those using inhalers, such as patients with asthma.
The findings were published online in the BMJ Open.
Serious side effects
Glucocorticoids, a class of synthetic steroids with immunosuppressive properties, are prescribed for a wide range of conditions, including rheumatoid arthritis and asthma.
However, they are also associated with potentially serious metabolic, cardiovascular, and musculoskeletal side effects as well as neuropsychiatric side effects such as depression, mania, and cognitive impairment.
About 1 in 3 patients exposed to “quite a lot of these drugs” will experience neuropsychiatric symptoms, Dr. Meijer said.
Most previous studies that investigated effects from high levels of glucocorticoids on brain structure have been small and involved selected populations, such as those with Cushing disease.
The new study included participants from the UK Biobank, a large population-based cohort. Participants had undergone imaging and did not have a history of psychiatric disease – although they could have conditions associated with glucocorticoid use, including anxiety, depression, mania, or delirium.
The analysis included 222 patients using oral or parenteral glucocorticoids at the time of imaging (systemic group), 557 using inhaled glucocorticoids, and 24,106 not using glucocorticoids (the control group).
Inhaled steroids target the lungs, whereas a steroid in pill form “travels in the blood and reaches each and every organ and cell in the body and typically requires higher doses,” Dr. Meijer noted.
The groups were similar with respect to sex, education, and smoking status. However, the systemic glucocorticoid group was slightly older (mean age, 66.1 years vs. 63.3 years for inhaled glucocorticoid users and 63.5 years for the control group).
In addition to age, researchers adjusted for sex, education level, head position in the scanner, head size, assessment center, and year of imaging.
Imaging analyses
Imaging analyses showed systemic glucocorticoid use was associated with reduced global FA (adjusted mean difference, -3.7e-3; 95% confidence interval, -6.4e-3 to 1.0e-3), and reductions in regional FA in the body and genu of the corpus callosum versus the control group.
Inhaled glucocorticoid use was associated with reduced global FA (AMD, -2.3e-3; 95% CI, -4.0e-3 to -5.7e-4), and lower FA in the splenium of the corpus callosum and the cingulum of the hippocampus.
Global mean diffusivity was higher in systemic glucocorticoid users (AMD, 7.2e-6; 95% CI, 3.2e-6 to 1.1e-5) and inhaled glucocorticoid users (AMD, 2.7e-6; 95% CI, 1.7e-7 to 5.2e-6), compared with the control group.
The effects of glucocorticoids on white matter were “pervasive,” and the “most important finding” of the study, Dr. Meijer said. “We were impressed by the fact white matter is so sensitive to these drugs.”
He noted that it is likely that functional connectivity between brain regions is affected by use of glucocorticoids. “You could say communication between brain regions is probably somewhat impaired or challenged,” he said.
Subgroup analyses among participants using glucocorticoids chronically, defined as reported at two consecutive visits, suggested a potential dose-dependent or duration-dependent effect of glucocorticoids on white matter microstructure.
Systemic glucocorticoid use was also associated with an increase in total and grey matter volume of the caudate nucleus.
In addition, there was a significant association between inhaled glucocorticoid use and decreased grey matter volume of the amygdala, which Dr. Meijer said was surprising because studies have shown that glucocorticoids “can drive amygdala big time.”
Move away from ‘one dose for all’?
Another surprise was that the results showed no hippocampal volume differences with steroid use, Dr. Meijer noted.
The modest association between glucocorticoid use and brain volumes could indicate that white matter integrity is more sensitive to glucocorticoids than is grey matter volume, “at least at the structural level,” he said.
He added that longer use or higher doses may be necessary to also induce volumetric changes.
Participants also completed a questionnaire to assess mood over the previous 2 weeks. Systemic glucocorticoid users had more depressive symptoms, disinterest, tenseness/restlessness, and tiredness/lethargy, compared with the control group. Inhaled glucocorticoid users only reported more tiredness/lethargy.
The investigators note that mood-related effects could be linked to the condition for which glucocorticoids were prescribed: for example, rheumatoid arthritis or chronic obstructive pulmonary disease.
In terms of cognition, systemic glucocorticoid users performed significantly worse on the symbol digit substitution task, compared with participants in the control group.
In light of these findings, pharmaceutical companies that make inhaled corticosteroids “should perhaps find out if glucocorticoids can be dosed by kilogram body weight rather than simply one dose fits all,” which is currently the case, Dr. Meijer said.
Impressive, but several limitations
Commenting on the findings, E. Sherwood Brown, MD, PhD, Distinguished Chair in Psychiatric Research and professor and vice chair for clinical research, department of psychiatry, The University of Texas Southwestern Medical Center, Dallas, called the study sample size “impressive.”
In addition, the study is the first to look at systemic as well as inhaled corticosteroids, said Dr. Brown, who was not involved with the research. He noted that previously, there had been only case reports of psychiatric symptoms with inhaled corticosteroids.
That results are in the same direction but greater with systemic, compared with inhaled corticosteroids, is “particularly interesting” because this might suggest dose-dependent effects, Dr. Brown said.
He noted that cognitive differences were also only observed with systemic corticosteroids.
Some study observations, such as smaller amygdala volume with inhaled but not systemic corticosteroids, “are harder to understand,” said Dr. Brown.
However, he pointed out some study limitations. For example, data were apparently unavailable for verbal and declarative memory test data, despite corticosteroids probably affecting the hippocampus and causing memory changes.
Other drawbacks were that the dose and duration of corticosteroid use, as well as the medical histories of study participants, were not available, Dr. Brown said.
No study funding was reported. Dr. Meijer has received research grants and honorariums from Corcept Therapeutics and a speakers’ fee from Ipsen. Dr. Brown is on an advisory board for Sage Pharmaceuticals, which is developing neurosteroids (not corticosteroids) for mood disorders. He is also on a Medscape advisory board related to bipolar disorder.
A version of this article first appeared on Medscape.com.
New research links the use of glucocorticoids with changes in white matter microstructure – which may explain the development of anxiety, depression, and other neuropsychiatric side effects related to these drugs, investigators say.
Results from a cross-sectional study showed that use of both systemic and inhaled glucocorticoids was associated with widespread reductions in fractional anisotropy (FA) and increases in mean diffusivity.
Glucocorticoids have “a whole catalogue” of adverse events, and effects on brain structure “adds to the list,” co-investigator Onno C. Meijer, PhD, professor of molecular neuroendocrinology of corticosteroids, department of medicine, Leiden University Medical Center, the Netherlands, told this news organization.
The findings should encourage clinicians to consider whether doses they are prescribing are too high, said Dr. Meijer. He added that the negative effect of glucocorticoids on the brain was also found in those using inhalers, such as patients with asthma.
The findings were published online in the BMJ Open.
Serious side effects
Glucocorticoids, a class of synthetic steroids with immunosuppressive properties, are prescribed for a wide range of conditions, including rheumatoid arthritis and asthma.
However, they are also associated with potentially serious metabolic, cardiovascular, and musculoskeletal side effects as well as neuropsychiatric side effects such as depression, mania, and cognitive impairment.
About 1 in 3 patients exposed to “quite a lot of these drugs” will experience neuropsychiatric symptoms, Dr. Meijer said.
Most previous studies that investigated effects from high levels of glucocorticoids on brain structure have been small and involved selected populations, such as those with Cushing disease.
The new study included participants from the UK Biobank, a large population-based cohort. Participants had undergone imaging and did not have a history of psychiatric disease – although they could have conditions associated with glucocorticoid use, including anxiety, depression, mania, or delirium.
The analysis included 222 patients using oral or parenteral glucocorticoids at the time of imaging (systemic group), 557 using inhaled glucocorticoids, and 24,106 not using glucocorticoids (the control group).
Inhaled steroids target the lungs, whereas a steroid in pill form “travels in the blood and reaches each and every organ and cell in the body and typically requires higher doses,” Dr. Meijer noted.
The groups were similar with respect to sex, education, and smoking status. However, the systemic glucocorticoid group was slightly older (mean age, 66.1 years vs. 63.3 years for inhaled glucocorticoid users and 63.5 years for the control group).
In addition to age, researchers adjusted for sex, education level, head position in the scanner, head size, assessment center, and year of imaging.
Imaging analyses
Imaging analyses showed systemic glucocorticoid use was associated with reduced global FA (adjusted mean difference, -3.7e-3; 95% confidence interval, -6.4e-3 to 1.0e-3), and reductions in regional FA in the body and genu of the corpus callosum versus the control group.
Inhaled glucocorticoid use was associated with reduced global FA (AMD, -2.3e-3; 95% CI, -4.0e-3 to -5.7e-4), and lower FA in the splenium of the corpus callosum and the cingulum of the hippocampus.
Global mean diffusivity was higher in systemic glucocorticoid users (AMD, 7.2e-6; 95% CI, 3.2e-6 to 1.1e-5) and inhaled glucocorticoid users (AMD, 2.7e-6; 95% CI, 1.7e-7 to 5.2e-6), compared with the control group.
The effects of glucocorticoids on white matter were “pervasive,” and the “most important finding” of the study, Dr. Meijer said. “We were impressed by the fact white matter is so sensitive to these drugs.”
He noted that it is likely that functional connectivity between brain regions is affected by use of glucocorticoids. “You could say communication between brain regions is probably somewhat impaired or challenged,” he said.
Subgroup analyses among participants using glucocorticoids chronically, defined as reported at two consecutive visits, suggested a potential dose-dependent or duration-dependent effect of glucocorticoids on white matter microstructure.
Systemic glucocorticoid use was also associated with an increase in total and grey matter volume of the caudate nucleus.
In addition, there was a significant association between inhaled glucocorticoid use and decreased grey matter volume of the amygdala, which Dr. Meijer said was surprising because studies have shown that glucocorticoids “can drive amygdala big time.”
Move away from ‘one dose for all’?
Another surprise was that the results showed no hippocampal volume differences with steroid use, Dr. Meijer noted.
The modest association between glucocorticoid use and brain volumes could indicate that white matter integrity is more sensitive to glucocorticoids than is grey matter volume, “at least at the structural level,” he said.
He added that longer use or higher doses may be necessary to also induce volumetric changes.
Participants also completed a questionnaire to assess mood over the previous 2 weeks. Systemic glucocorticoid users had more depressive symptoms, disinterest, tenseness/restlessness, and tiredness/lethargy, compared with the control group. Inhaled glucocorticoid users only reported more tiredness/lethargy.
The investigators note that mood-related effects could be linked to the condition for which glucocorticoids were prescribed: for example, rheumatoid arthritis or chronic obstructive pulmonary disease.
In terms of cognition, systemic glucocorticoid users performed significantly worse on the symbol digit substitution task, compared with participants in the control group.
In light of these findings, pharmaceutical companies that make inhaled corticosteroids “should perhaps find out if glucocorticoids can be dosed by kilogram body weight rather than simply one dose fits all,” which is currently the case, Dr. Meijer said.
Impressive, but several limitations
Commenting on the findings, E. Sherwood Brown, MD, PhD, Distinguished Chair in Psychiatric Research and professor and vice chair for clinical research, department of psychiatry, The University of Texas Southwestern Medical Center, Dallas, called the study sample size “impressive.”
In addition, the study is the first to look at systemic as well as inhaled corticosteroids, said Dr. Brown, who was not involved with the research. He noted that previously, there had been only case reports of psychiatric symptoms with inhaled corticosteroids.
That results are in the same direction but greater with systemic, compared with inhaled corticosteroids, is “particularly interesting” because this might suggest dose-dependent effects, Dr. Brown said.
He noted that cognitive differences were also only observed with systemic corticosteroids.
Some study observations, such as smaller amygdala volume with inhaled but not systemic corticosteroids, “are harder to understand,” said Dr. Brown.
However, he pointed out some study limitations. For example, data were apparently unavailable for verbal and declarative memory test data, despite corticosteroids probably affecting the hippocampus and causing memory changes.
Other drawbacks were that the dose and duration of corticosteroid use, as well as the medical histories of study participants, were not available, Dr. Brown said.
No study funding was reported. Dr. Meijer has received research grants and honorariums from Corcept Therapeutics and a speakers’ fee from Ipsen. Dr. Brown is on an advisory board for Sage Pharmaceuticals, which is developing neurosteroids (not corticosteroids) for mood disorders. He is also on a Medscape advisory board related to bipolar disorder.
A version of this article first appeared on Medscape.com.
FROM BMJ OPEN
Majority of muscle symptoms with statins not caused by treatment
In the vast majority of people who experience muscle pain or weakness while taking a statin, those symptoms are not related to the statin, a new individual patient data meta-analysis of randomized controlled trials shows.
The Cholesterol Trialists Collaboration meta-analysis examined 19 large randomized double-blind trials that compared statin therapy with placebo and involved almost 124,000 patients.
“Our results show that, in people who experience muscle symptoms in the first year of taking a statin, those symptoms are actually due to the statin in only 1 of 15 of those people. For the other 14 of the 15 people who experience muscle symptoms in the first year of taking a statin, that muscle pain is not due to the statin,” lead investigator Colin Baigent, MD, said.
After the first year, there was no difference in muscle symptoms between patients taking a statin or those taking placebo.
Dr. Baigent, who is director of the Population Health Research Unit at the University of Oxford (England), presented the data on Aug. 29 at the European Society of Cardiology 2022 Congress.
It was also simultaneously published online in The Lancet.
Dr. Baigent explained that statins very rarely cause serious muscle adverse effects with biochemical evidence of cellular damage, such as myopathy (which occurs in less than 1 in 10,000 patients per year) and rhabdomyolysis (which occurs in about 0.2 per 10,000 patients per year).
The effect of statins on other less serious muscle symptoms without biochemical evidence of cellular damage is less clear, but misinformation about the risks have arisen from nonrandomized studies, with social media and press reports suggesting that the risk for muscle symptoms with statins is extremely common, Dr. Baigent said.
In response to this, the Cholesterol Trialists Collaboration put together a new program of data collection, validation, and analysis to provide reliable information from large double-blind randomized trials that are free from bias and confounding.
“Overall, when we look at all these data, we find there is about a 3% relative increase in the risks of experiencing muscle pain or weakness with a statin versus with placebo,” Dr. Baigent reported.
Muscle pain or weakness was reported by 16,835 of 62,028 patients taking a statin, (27.1%), compared with 16,446 of 61,912 patients taking placebo (26.6%), for a rate ratio of 1.03 (95% confidence interval, 1.01-1.06).
In absolute terms, the results show a rate of 166 reports of muscle symptoms per 1,000 patient-years in those taking a statin, compared with 155 per 1,000-patient-years in those taking placebo in the first year. This gives a rate ratio of 1.07 and an excess of 11 cases of muscle pain or weakness per 1,000 patients in the first year of statin therapy.
“The very small excess of muscle symptoms in the statin patients were generally mild, with most patients able to continue treatment,” Dr. Baigent added.
After the first year, the rate of muscle pain or weakness was exactly the same in the statin and placebo groups, at 50 per 1,000 patient-years.
“Therefore, for the vast majority of people who experience muscle pain or weakness on a statin, those symptoms are not due to the statin itself. It is due to something else, which could be ageing, thyroid disease, or exercise,” Dr. Baigent said. “After the first year of taking a statin, there is no excess risk of muscle pain or weakness at all.”
“To summarize, the excess risk of muscle pain or weakness with statin use is tiny, and almost nonexistent after the first year,” he added.
“Muscle pain is very common in the general population, and it was very common in both patients taking a statin and those given placebo in these randomized trials. We can only detect a difference by looking at all the data combined in this enormous study. And we now know for sure that over 90% of cases of muscle symptoms experienced by people taking a statin are not due to the statin.”
The researchers also looked at statin intensity and found that the more intense statins tend to cause slightly more muscle pain. “There was also some evidence, although this was not very clear, that the muscle pain with the more intensive statins may persist for longer than 1 year,” Dr. Baigent said.
But in terms of different moderate-intensity and high-intensity statins, there was no evidence of differences in muscle pain between the individual statin brands, he added.
Better patient information needed
Dr. Baigent called for better information in statin package inserts about the real risk for muscle symptoms with these drugs.
“We need to do a better job of communicating the real risk of muscle symptom to patients who are taking statins and to their doctors. At the moment, doctors often stop statins if patients complain of muscle pain, but our data show that in 14 out of 15 times, they would be wrong for doing that. Stopping the statin is nearly always a mistake,” he commented.
“At present, the package inserts include a whole load of rubbish from observational studies, which are completely unreliable,” he added. “This is of no value to patients. They go through this information and find several symptoms they are experiencing, which they attribute to the drugs. We really need to divide up the information into the evidence that we really know for sure and then the more speculative stuff.”
Dr. Baigent also highlighted the large benefits of statins, compared with the small risk for muscle symptoms.
“While statins may cause 11 patients per 1,000 to experience some mild muscle pain in the first year of taking these drugs, and this was reduced to none in subsequent years, statins, when used for the primary prevention of cardiovascular disease, prevent 25 cardiovascular events per 1,000 patients every year they are taken. And for secondary prevention this rises to 50 events prevented per 1,000 patients each year,” he noted.
The individual participant data meta-analysis involved 23 trials with information on almost 155,000 patients. All trials included at least 1,000 patients and at least 2 years of scheduled treatment. Adverse-event data were collected for all individual participants in 19 large randomized double-blind trials comparing statin therapy with placebo (123,940 patients) and in four randomized double-blind trials comparing more-intensive with less-intensive statin therapy (30,724 patients).
In the four trials of more-intensive versus less-intensive statin therapy, high-intensity regimens (atorvastatin 40-80 mg daily or rosuvastatin 20-40 mg daily) resulted in a larger relative increase in the rate of muscle pain or weakness than moderate-intensity regimens, with rate ratios of 1.08 (95% CI, 1.04-1.13) and 1.02 (95% CI, 1.00-1.05), respectively.
‘Reassuring information’
Discussant of the study at the ESC Hotline session, Erin Bohula, MD, Brigham and Women’s Hospital, Boston, said this new analysis had many strengths and used a rigorous approach to look at the issue of muscle symptoms with statins.
She pointed out some challenges, including the fact that the definition of adverse muscle events has changed over time and differed in the various trials, with heterogeneous data capture across trials. “So, this was a Herculean task to harmonize this very complicated dataset.”
Dr. Bohula concluded: “I think this is a very significant undertaking, resulting in a rich dataset that enhances our understanding of muscle symptoms related to statin use. The take-home for me is that muscle symptoms are a common complaint in the general population but are very rarely attributable to statins. This is very reassuring to me, and I hope it is reassuring to patients and can help us encourage them with adherence, given the clear cardiovascular benefits of statins.”
Chair of the ESC Hotline session at which the study was presented, Gabriel Steg, MD, Hôpital Bichat, Paris, asked whether some statin patients who experienced muscle symptoms with the drugs in active run-in periods in the trials may have been excluded from the main trials, so that this information might not have been captured, but Dr. Baigent replied that they also examined those data, which had been accounted for in the analysis.
“That’s really good news,” Dr. Steg commented. “This study is going to be one more tool in our response to statin skeptics and I think, as such, this work is a really a service to public health.”
The meta-analysis was funded by the British Heart Foundation, the U.K. Medical Research Council, and the Australian National Health and Medical Research Council.
A version of this article first appeared on Medscape.com.
In the vast majority of people who experience muscle pain or weakness while taking a statin, those symptoms are not related to the statin, a new individual patient data meta-analysis of randomized controlled trials shows.
The Cholesterol Trialists Collaboration meta-analysis examined 19 large randomized double-blind trials that compared statin therapy with placebo and involved almost 124,000 patients.
“Our results show that, in people who experience muscle symptoms in the first year of taking a statin, those symptoms are actually due to the statin in only 1 of 15 of those people. For the other 14 of the 15 people who experience muscle symptoms in the first year of taking a statin, that muscle pain is not due to the statin,” lead investigator Colin Baigent, MD, said.
After the first year, there was no difference in muscle symptoms between patients taking a statin or those taking placebo.
Dr. Baigent, who is director of the Population Health Research Unit at the University of Oxford (England), presented the data on Aug. 29 at the European Society of Cardiology 2022 Congress.
It was also simultaneously published online in The Lancet.
Dr. Baigent explained that statins very rarely cause serious muscle adverse effects with biochemical evidence of cellular damage, such as myopathy (which occurs in less than 1 in 10,000 patients per year) and rhabdomyolysis (which occurs in about 0.2 per 10,000 patients per year).
The effect of statins on other less serious muscle symptoms without biochemical evidence of cellular damage is less clear, but misinformation about the risks have arisen from nonrandomized studies, with social media and press reports suggesting that the risk for muscle symptoms with statins is extremely common, Dr. Baigent said.
In response to this, the Cholesterol Trialists Collaboration put together a new program of data collection, validation, and analysis to provide reliable information from large double-blind randomized trials that are free from bias and confounding.
“Overall, when we look at all these data, we find there is about a 3% relative increase in the risks of experiencing muscle pain or weakness with a statin versus with placebo,” Dr. Baigent reported.
Muscle pain or weakness was reported by 16,835 of 62,028 patients taking a statin, (27.1%), compared with 16,446 of 61,912 patients taking placebo (26.6%), for a rate ratio of 1.03 (95% confidence interval, 1.01-1.06).
In absolute terms, the results show a rate of 166 reports of muscle symptoms per 1,000 patient-years in those taking a statin, compared with 155 per 1,000-patient-years in those taking placebo in the first year. This gives a rate ratio of 1.07 and an excess of 11 cases of muscle pain or weakness per 1,000 patients in the first year of statin therapy.
“The very small excess of muscle symptoms in the statin patients were generally mild, with most patients able to continue treatment,” Dr. Baigent added.
After the first year, the rate of muscle pain or weakness was exactly the same in the statin and placebo groups, at 50 per 1,000 patient-years.
“Therefore, for the vast majority of people who experience muscle pain or weakness on a statin, those symptoms are not due to the statin itself. It is due to something else, which could be ageing, thyroid disease, or exercise,” Dr. Baigent said. “After the first year of taking a statin, there is no excess risk of muscle pain or weakness at all.”
“To summarize, the excess risk of muscle pain or weakness with statin use is tiny, and almost nonexistent after the first year,” he added.
“Muscle pain is very common in the general population, and it was very common in both patients taking a statin and those given placebo in these randomized trials. We can only detect a difference by looking at all the data combined in this enormous study. And we now know for sure that over 90% of cases of muscle symptoms experienced by people taking a statin are not due to the statin.”
The researchers also looked at statin intensity and found that the more intense statins tend to cause slightly more muscle pain. “There was also some evidence, although this was not very clear, that the muscle pain with the more intensive statins may persist for longer than 1 year,” Dr. Baigent said.
But in terms of different moderate-intensity and high-intensity statins, there was no evidence of differences in muscle pain between the individual statin brands, he added.
Better patient information needed
Dr. Baigent called for better information in statin package inserts about the real risk for muscle symptoms with these drugs.
“We need to do a better job of communicating the real risk of muscle symptom to patients who are taking statins and to their doctors. At the moment, doctors often stop statins if patients complain of muscle pain, but our data show that in 14 out of 15 times, they would be wrong for doing that. Stopping the statin is nearly always a mistake,” he commented.
“At present, the package inserts include a whole load of rubbish from observational studies, which are completely unreliable,” he added. “This is of no value to patients. They go through this information and find several symptoms they are experiencing, which they attribute to the drugs. We really need to divide up the information into the evidence that we really know for sure and then the more speculative stuff.”
Dr. Baigent also highlighted the large benefits of statins, compared with the small risk for muscle symptoms.
“While statins may cause 11 patients per 1,000 to experience some mild muscle pain in the first year of taking these drugs, and this was reduced to none in subsequent years, statins, when used for the primary prevention of cardiovascular disease, prevent 25 cardiovascular events per 1,000 patients every year they are taken. And for secondary prevention this rises to 50 events prevented per 1,000 patients each year,” he noted.
The individual participant data meta-analysis involved 23 trials with information on almost 155,000 patients. All trials included at least 1,000 patients and at least 2 years of scheduled treatment. Adverse-event data were collected for all individual participants in 19 large randomized double-blind trials comparing statin therapy with placebo (123,940 patients) and in four randomized double-blind trials comparing more-intensive with less-intensive statin therapy (30,724 patients).
In the four trials of more-intensive versus less-intensive statin therapy, high-intensity regimens (atorvastatin 40-80 mg daily or rosuvastatin 20-40 mg daily) resulted in a larger relative increase in the rate of muscle pain or weakness than moderate-intensity regimens, with rate ratios of 1.08 (95% CI, 1.04-1.13) and 1.02 (95% CI, 1.00-1.05), respectively.
‘Reassuring information’
Discussant of the study at the ESC Hotline session, Erin Bohula, MD, Brigham and Women’s Hospital, Boston, said this new analysis had many strengths and used a rigorous approach to look at the issue of muscle symptoms with statins.
She pointed out some challenges, including the fact that the definition of adverse muscle events has changed over time and differed in the various trials, with heterogeneous data capture across trials. “So, this was a Herculean task to harmonize this very complicated dataset.”
Dr. Bohula concluded: “I think this is a very significant undertaking, resulting in a rich dataset that enhances our understanding of muscle symptoms related to statin use. The take-home for me is that muscle symptoms are a common complaint in the general population but are very rarely attributable to statins. This is very reassuring to me, and I hope it is reassuring to patients and can help us encourage them with adherence, given the clear cardiovascular benefits of statins.”
Chair of the ESC Hotline session at which the study was presented, Gabriel Steg, MD, Hôpital Bichat, Paris, asked whether some statin patients who experienced muscle symptoms with the drugs in active run-in periods in the trials may have been excluded from the main trials, so that this information might not have been captured, but Dr. Baigent replied that they also examined those data, which had been accounted for in the analysis.
“That’s really good news,” Dr. Steg commented. “This study is going to be one more tool in our response to statin skeptics and I think, as such, this work is a really a service to public health.”
The meta-analysis was funded by the British Heart Foundation, the U.K. Medical Research Council, and the Australian National Health and Medical Research Council.
A version of this article first appeared on Medscape.com.
In the vast majority of people who experience muscle pain or weakness while taking a statin, those symptoms are not related to the statin, a new individual patient data meta-analysis of randomized controlled trials shows.
The Cholesterol Trialists Collaboration meta-analysis examined 19 large randomized double-blind trials that compared statin therapy with placebo and involved almost 124,000 patients.
“Our results show that, in people who experience muscle symptoms in the first year of taking a statin, those symptoms are actually due to the statin in only 1 of 15 of those people. For the other 14 of the 15 people who experience muscle symptoms in the first year of taking a statin, that muscle pain is not due to the statin,” lead investigator Colin Baigent, MD, said.
After the first year, there was no difference in muscle symptoms between patients taking a statin or those taking placebo.
Dr. Baigent, who is director of the Population Health Research Unit at the University of Oxford (England), presented the data on Aug. 29 at the European Society of Cardiology 2022 Congress.
It was also simultaneously published online in The Lancet.
Dr. Baigent explained that statins very rarely cause serious muscle adverse effects with biochemical evidence of cellular damage, such as myopathy (which occurs in less than 1 in 10,000 patients per year) and rhabdomyolysis (which occurs in about 0.2 per 10,000 patients per year).
The effect of statins on other less serious muscle symptoms without biochemical evidence of cellular damage is less clear, but misinformation about the risks have arisen from nonrandomized studies, with social media and press reports suggesting that the risk for muscle symptoms with statins is extremely common, Dr. Baigent said.
In response to this, the Cholesterol Trialists Collaboration put together a new program of data collection, validation, and analysis to provide reliable information from large double-blind randomized trials that are free from bias and confounding.
“Overall, when we look at all these data, we find there is about a 3% relative increase in the risks of experiencing muscle pain or weakness with a statin versus with placebo,” Dr. Baigent reported.
Muscle pain or weakness was reported by 16,835 of 62,028 patients taking a statin, (27.1%), compared with 16,446 of 61,912 patients taking placebo (26.6%), for a rate ratio of 1.03 (95% confidence interval, 1.01-1.06).
In absolute terms, the results show a rate of 166 reports of muscle symptoms per 1,000 patient-years in those taking a statin, compared with 155 per 1,000-patient-years in those taking placebo in the first year. This gives a rate ratio of 1.07 and an excess of 11 cases of muscle pain or weakness per 1,000 patients in the first year of statin therapy.
“The very small excess of muscle symptoms in the statin patients were generally mild, with most patients able to continue treatment,” Dr. Baigent added.
After the first year, the rate of muscle pain or weakness was exactly the same in the statin and placebo groups, at 50 per 1,000 patient-years.
“Therefore, for the vast majority of people who experience muscle pain or weakness on a statin, those symptoms are not due to the statin itself. It is due to something else, which could be ageing, thyroid disease, or exercise,” Dr. Baigent said. “After the first year of taking a statin, there is no excess risk of muscle pain or weakness at all.”
“To summarize, the excess risk of muscle pain or weakness with statin use is tiny, and almost nonexistent after the first year,” he added.
“Muscle pain is very common in the general population, and it was very common in both patients taking a statin and those given placebo in these randomized trials. We can only detect a difference by looking at all the data combined in this enormous study. And we now know for sure that over 90% of cases of muscle symptoms experienced by people taking a statin are not due to the statin.”
The researchers also looked at statin intensity and found that the more intense statins tend to cause slightly more muscle pain. “There was also some evidence, although this was not very clear, that the muscle pain with the more intensive statins may persist for longer than 1 year,” Dr. Baigent said.
But in terms of different moderate-intensity and high-intensity statins, there was no evidence of differences in muscle pain between the individual statin brands, he added.
Better patient information needed
Dr. Baigent called for better information in statin package inserts about the real risk for muscle symptoms with these drugs.
“We need to do a better job of communicating the real risk of muscle symptom to patients who are taking statins and to their doctors. At the moment, doctors often stop statins if patients complain of muscle pain, but our data show that in 14 out of 15 times, they would be wrong for doing that. Stopping the statin is nearly always a mistake,” he commented.
“At present, the package inserts include a whole load of rubbish from observational studies, which are completely unreliable,” he added. “This is of no value to patients. They go through this information and find several symptoms they are experiencing, which they attribute to the drugs. We really need to divide up the information into the evidence that we really know for sure and then the more speculative stuff.”
Dr. Baigent also highlighted the large benefits of statins, compared with the small risk for muscle symptoms.
“While statins may cause 11 patients per 1,000 to experience some mild muscle pain in the first year of taking these drugs, and this was reduced to none in subsequent years, statins, when used for the primary prevention of cardiovascular disease, prevent 25 cardiovascular events per 1,000 patients every year they are taken. And for secondary prevention this rises to 50 events prevented per 1,000 patients each year,” he noted.
The individual participant data meta-analysis involved 23 trials with information on almost 155,000 patients. All trials included at least 1,000 patients and at least 2 years of scheduled treatment. Adverse-event data were collected for all individual participants in 19 large randomized double-blind trials comparing statin therapy with placebo (123,940 patients) and in four randomized double-blind trials comparing more-intensive with less-intensive statin therapy (30,724 patients).
In the four trials of more-intensive versus less-intensive statin therapy, high-intensity regimens (atorvastatin 40-80 mg daily or rosuvastatin 20-40 mg daily) resulted in a larger relative increase in the rate of muscle pain or weakness than moderate-intensity regimens, with rate ratios of 1.08 (95% CI, 1.04-1.13) and 1.02 (95% CI, 1.00-1.05), respectively.
‘Reassuring information’
Discussant of the study at the ESC Hotline session, Erin Bohula, MD, Brigham and Women’s Hospital, Boston, said this new analysis had many strengths and used a rigorous approach to look at the issue of muscle symptoms with statins.
She pointed out some challenges, including the fact that the definition of adverse muscle events has changed over time and differed in the various trials, with heterogeneous data capture across trials. “So, this was a Herculean task to harmonize this very complicated dataset.”
Dr. Bohula concluded: “I think this is a very significant undertaking, resulting in a rich dataset that enhances our understanding of muscle symptoms related to statin use. The take-home for me is that muscle symptoms are a common complaint in the general population but are very rarely attributable to statins. This is very reassuring to me, and I hope it is reassuring to patients and can help us encourage them with adherence, given the clear cardiovascular benefits of statins.”
Chair of the ESC Hotline session at which the study was presented, Gabriel Steg, MD, Hôpital Bichat, Paris, asked whether some statin patients who experienced muscle symptoms with the drugs in active run-in periods in the trials may have been excluded from the main trials, so that this information might not have been captured, but Dr. Baigent replied that they also examined those data, which had been accounted for in the analysis.
“That’s really good news,” Dr. Steg commented. “This study is going to be one more tool in our response to statin skeptics and I think, as such, this work is a really a service to public health.”
The meta-analysis was funded by the British Heart Foundation, the U.K. Medical Research Council, and the Australian National Health and Medical Research Council.
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2022

How do you live with COVID? One doctor’s personal experience
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”

“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Ublituximab bests teriflunomide in head-to-head clinical trials
Study shows ublituximab’s superiority over teriflunomide in suppressing MS relapses and MRI lesions.
Patients with relapsing multiple sclerosis (MS) treated with intravenous ublituximab had fewer relapses and brain lesions compared with those treated with oral teriflunomide, although both therapies resulted in similar rates of worsening disability, according to results of the two identical phase 3 ULTIMATE I and II trials.
“In these two 96-week trials involving participants with MS, annualized relapse rates were lower with intravenous ublituximab than with oral teriflunomide. Ublituximab was associated with infusion-related reactions. Larger and longer trials are required to determine the efficacy and safety of ublituximab in patients with relapsing MS, including comparison with other disease-modifying treatments such as existing anti-CD20 monoclonal antibodies,” noted lead author Lawrence Steinman, MD, professor of neurology and neurological sciences, pediatrics, and genetics at Stanford (Calif.) University, and colleagues.

The results, published in the New England Journal of Medicine, pave the way for ublituximab’s approval as the third high-efficacy anti-CD20 monoclonal antibody to treat relapsing forms of MS, predicted Patricia Coyle, MD, director of the MS Comprehensive Care Center, and professor of neurology, at Stony Brook (N.Y.) Neurosciences Institute, who was not involved in the research. Ublituximab will “widen the anti-CD20 monoclonal choices for MS, and should directly compete with ocrelizumab and ofatumumab,” she said.
Two trials
The double-blind, double-dummy ULTIMATE I and II trials enrolled 549 and 545 participants respectively, with a median follow-up of 95 weeks. Subjects, aged between 18 and 55 years, were randomized to receive either oral placebo and intravenous ublituximab (150 mg on day 1, followed by 450 mg on day 15 and at weeks 24, 48, and 72), or oral teriflunomide (14 mg once daily) and intravenous placebo. The primary endpoint was the annualized relapse rate, defined as the number of confirmed MS relapses per participant-year, with a range of secondary end points including number of lesions on magnetic resonance imaging (MRI) by 96 weeks, and worsening of disability confirmed at 12 weeks.
Prevention and management of infusion-related reactions was with oral antihistamine and dexamethasone, administered 30 to 60 minutes before each intravenous dose of ublituximab or placebo, as well as reductions in infusion flow rates and discretionary acetaminophen.
Results for the primary endpoint in ULTIMATE I showed the adjusted annualized relapse rate over a period of 96 weeks was 0.08 in the ublituximab group and 0.19 in the teriflunomide group (rate ratio, 0.41; P < .001). Corresponding rates for ULTIMATE II were 0.09 and 0.18 (rate ratio, 0.51; P = .002).
The mean number of lesions in both ublituximab arms of the trials was 0.02 and 0.01 compared with 0.49 and 0.25 in the teriflunomide arms (rate ratios 0.03 and 0.04 respectively; P < .001 for both).
Similar disability worsening in both groups
A pooled analysis of the two trials showed worsening disability in 5.2% of the ublituximab group, and 5.9% of the teriflunomide group (hazard ratio, 0.84; P = 0.51). “In both trials, teriflunomide was associated with a numerically lower rate of worsening of disability than that reported in previous studies with this drug, but no conclusions can be drawn from these comparisons,” noted the authors.
Infusion-related reactions occurred in 47.7% of the participants in the ublituximab group, consisting mainly of mild to moderate pyrexia, headache, chills, and influenza-like illness. “The reactions may have been related to cytokine release from immune cells (B and NK cells) on interaction of the Fc antibody domain with Fc gamma receptors on effector cells,” they suggested.
Although no opportunistic infections occurred, a higher frequency of infections, including serious infections, was observed with ublituximab (5.0%) than with teriflunomide (2.9%).
While the ULTIMATE trials showed no difference between ublituximab and teriflunomide in confirmed worsening of disability, only a small percentage of participants in either arm showed deterioration, Dr. Coyle remarked. “In a relatively short trial (96 weeks), in a relapsing population on active treatment, this result was not surprising … If the study was bigger, or longer it would increase the chances of seeing a progressive slow worsening component to affect the EDSS [Expanded Disability Status Scale],” she added.
Equivalent efficacy
Ultimately, “it appears likely” that ublituximab is “equivalent in efficacy” to the earlier anti-CD20 agents ocrelizumab and ofatumumab, Dr. Coyle said. While all three agents target B-cells, “ublituximab targets a novel CD20 binding site, and is bioengineered to have a particularly potent antibody dependent cell cytotoxicity lysis mechanism,” she added. “It has been touted to ultimately allow a short infusion of 1 hour.”
Although the serious infection rate is slightly higher with ublituximab (5.0% vs. 2.5% for ofatumumab, and 1.3% for ocrelizumab), “it is still low,” and infusion-related reactions are also higher with ublituximab, she added (47.7% vs. 20.2% and 34.3%, respectively). She suggested factors that might influence which treatment is chosen for a given patient might include cost, convenience, whether it is more or less likely to cause low IgG, interference with vaccination, or influence on cancer or COVID risk.
The trials were supported by TG Therapeutics.
Dr. Coyle has received consulting fees from Accordant, Biogen, Bristol Myers Squibb, Celgene, Genentech/Roche, GlaxoSmithKline, Horizon, Janssen, Novartis, Sanofi Genzyme, and Viela Bio and grant funding from Actelion, Alkermes, Bristol Myers Squibb, CorEvitas LLD, Genentech/Roche, Sanofi Genzyme, MedDay, NINDS, and Novartis.
Study shows ublituximab’s superiority over teriflunomide in suppressing MS relapses and MRI lesions.
Study shows ublituximab’s superiority over teriflunomide in suppressing MS relapses and MRI lesions.
Patients with relapsing multiple sclerosis (MS) treated with intravenous ublituximab had fewer relapses and brain lesions compared with those treated with oral teriflunomide, although both therapies resulted in similar rates of worsening disability, according to results of the two identical phase 3 ULTIMATE I and II trials.
“In these two 96-week trials involving participants with MS, annualized relapse rates were lower with intravenous ublituximab than with oral teriflunomide. Ublituximab was associated with infusion-related reactions. Larger and longer trials are required to determine the efficacy and safety of ublituximab in patients with relapsing MS, including comparison with other disease-modifying treatments such as existing anti-CD20 monoclonal antibodies,” noted lead author Lawrence Steinman, MD, professor of neurology and neurological sciences, pediatrics, and genetics at Stanford (Calif.) University, and colleagues.
The results, published in the New England Journal of Medicine, pave the way for ublituximab’s approval as the third high-efficacy anti-CD20 monoclonal antibody to treat relapsing forms of MS, predicted Patricia Coyle, MD, director of the MS Comprehensive Care Center, and professor of neurology, at Stony Brook (N.Y.) Neurosciences Institute, who was not involved in the research. Ublituximab will “widen the anti-CD20 monoclonal choices for MS, and should directly compete with ocrelizumab and ofatumumab,” she said.
Two trials
The double-blind, double-dummy ULTIMATE I and II trials enrolled 549 and 545 participants respectively, with a median follow-up of 95 weeks. Subjects, aged between 18 and 55 years, were randomized to receive either oral placebo and intravenous ublituximab (150 mg on day 1, followed by 450 mg on day 15 and at weeks 24, 48, and 72), or oral teriflunomide (14 mg once daily) and intravenous placebo. The primary endpoint was the annualized relapse rate, defined as the number of confirmed MS relapses per participant-year, with a range of secondary end points including number of lesions on magnetic resonance imaging (MRI) by 96 weeks, and worsening of disability confirmed at 12 weeks.
Prevention and management of infusion-related reactions was with oral antihistamine and dexamethasone, administered 30 to 60 minutes before each intravenous dose of ublituximab or placebo, as well as reductions in infusion flow rates and discretionary acetaminophen.
Results for the primary endpoint in ULTIMATE I showed the adjusted annualized relapse rate over a period of 96 weeks was 0.08 in the ublituximab group and 0.19 in the teriflunomide group (rate ratio, 0.41; P < .001). Corresponding rates for ULTIMATE II were 0.09 and 0.18 (rate ratio, 0.51; P = .002).
The mean number of lesions in both ublituximab arms of the trials was 0.02 and 0.01 compared with 0.49 and 0.25 in the teriflunomide arms (rate ratios 0.03 and 0.04 respectively; P < .001 for both).
Similar disability worsening in both groups
A pooled analysis of the two trials showed worsening disability in 5.2% of the ublituximab group, and 5.9% of the teriflunomide group (hazard ratio, 0.84; P = 0.51). “In both trials, teriflunomide was associated with a numerically lower rate of worsening of disability than that reported in previous studies with this drug, but no conclusions can be drawn from these comparisons,” noted the authors.
Infusion-related reactions occurred in 47.7% of the participants in the ublituximab group, consisting mainly of mild to moderate pyrexia, headache, chills, and influenza-like illness. “The reactions may have been related to cytokine release from immune cells (B and NK cells) on interaction of the Fc antibody domain with Fc gamma receptors on effector cells,” they suggested.
Although no opportunistic infections occurred, a higher frequency of infections, including serious infections, was observed with ublituximab (5.0%) than with teriflunomide (2.9%).
While the ULTIMATE trials showed no difference between ublituximab and teriflunomide in confirmed worsening of disability, only a small percentage of participants in either arm showed deterioration, Dr. Coyle remarked. “In a relatively short trial (96 weeks), in a relapsing population on active treatment, this result was not surprising … If the study was bigger, or longer it would increase the chances of seeing a progressive slow worsening component to affect the EDSS [Expanded Disability Status Scale],” she added.
Equivalent efficacy
Ultimately, “it appears likely” that ublituximab is “equivalent in efficacy” to the earlier anti-CD20 agents ocrelizumab and ofatumumab, Dr. Coyle said. While all three agents target B-cells, “ublituximab targets a novel CD20 binding site, and is bioengineered to have a particularly potent antibody dependent cell cytotoxicity lysis mechanism,” she added. “It has been touted to ultimately allow a short infusion of 1 hour.”
Although the serious infection rate is slightly higher with ublituximab (5.0% vs. 2.5% for ofatumumab, and 1.3% for ocrelizumab), “it is still low,” and infusion-related reactions are also higher with ublituximab, she added (47.7% vs. 20.2% and 34.3%, respectively). She suggested factors that might influence which treatment is chosen for a given patient might include cost, convenience, whether it is more or less likely to cause low IgG, interference with vaccination, or influence on cancer or COVID risk.
The trials were supported by TG Therapeutics.
Dr. Coyle has received consulting fees from Accordant, Biogen, Bristol Myers Squibb, Celgene, Genentech/Roche, GlaxoSmithKline, Horizon, Janssen, Novartis, Sanofi Genzyme, and Viela Bio and grant funding from Actelion, Alkermes, Bristol Myers Squibb, CorEvitas LLD, Genentech/Roche, Sanofi Genzyme, MedDay, NINDS, and Novartis.
Patients with relapsing multiple sclerosis (MS) treated with intravenous ublituximab had fewer relapses and brain lesions compared with those treated with oral teriflunomide, although both therapies resulted in similar rates of worsening disability, according to results of the two identical phase 3 ULTIMATE I and II trials.
“In these two 96-week trials involving participants with MS, annualized relapse rates were lower with intravenous ublituximab than with oral teriflunomide. Ublituximab was associated with infusion-related reactions. Larger and longer trials are required to determine the efficacy and safety of ublituximab in patients with relapsing MS, including comparison with other disease-modifying treatments such as existing anti-CD20 monoclonal antibodies,” noted lead author Lawrence Steinman, MD, professor of neurology and neurological sciences, pediatrics, and genetics at Stanford (Calif.) University, and colleagues.
The results, published in the New England Journal of Medicine, pave the way for ublituximab’s approval as the third high-efficacy anti-CD20 monoclonal antibody to treat relapsing forms of MS, predicted Patricia Coyle, MD, director of the MS Comprehensive Care Center, and professor of neurology, at Stony Brook (N.Y.) Neurosciences Institute, who was not involved in the research. Ublituximab will “widen the anti-CD20 monoclonal choices for MS, and should directly compete with ocrelizumab and ofatumumab,” she said.
Two trials
The double-blind, double-dummy ULTIMATE I and II trials enrolled 549 and 545 participants respectively, with a median follow-up of 95 weeks. Subjects, aged between 18 and 55 years, were randomized to receive either oral placebo and intravenous ublituximab (150 mg on day 1, followed by 450 mg on day 15 and at weeks 24, 48, and 72), or oral teriflunomide (14 mg once daily) and intravenous placebo. The primary endpoint was the annualized relapse rate, defined as the number of confirmed MS relapses per participant-year, with a range of secondary end points including number of lesions on magnetic resonance imaging (MRI) by 96 weeks, and worsening of disability confirmed at 12 weeks.
Prevention and management of infusion-related reactions was with oral antihistamine and dexamethasone, administered 30 to 60 minutes before each intravenous dose of ublituximab or placebo, as well as reductions in infusion flow rates and discretionary acetaminophen.
Results for the primary endpoint in ULTIMATE I showed the adjusted annualized relapse rate over a period of 96 weeks was 0.08 in the ublituximab group and 0.19 in the teriflunomide group (rate ratio, 0.41; P < .001). Corresponding rates for ULTIMATE II were 0.09 and 0.18 (rate ratio, 0.51; P = .002).
The mean number of lesions in both ublituximab arms of the trials was 0.02 and 0.01 compared with 0.49 and 0.25 in the teriflunomide arms (rate ratios 0.03 and 0.04 respectively; P < .001 for both).
Similar disability worsening in both groups
A pooled analysis of the two trials showed worsening disability in 5.2% of the ublituximab group, and 5.9% of the teriflunomide group (hazard ratio, 0.84; P = 0.51). “In both trials, teriflunomide was associated with a numerically lower rate of worsening of disability than that reported in previous studies with this drug, but no conclusions can be drawn from these comparisons,” noted the authors.
Infusion-related reactions occurred in 47.7% of the participants in the ublituximab group, consisting mainly of mild to moderate pyrexia, headache, chills, and influenza-like illness. “The reactions may have been related to cytokine release from immune cells (B and NK cells) on interaction of the Fc antibody domain with Fc gamma receptors on effector cells,” they suggested.
Although no opportunistic infections occurred, a higher frequency of infections, including serious infections, was observed with ublituximab (5.0%) than with teriflunomide (2.9%).
While the ULTIMATE trials showed no difference between ublituximab and teriflunomide in confirmed worsening of disability, only a small percentage of participants in either arm showed deterioration, Dr. Coyle remarked. “In a relatively short trial (96 weeks), in a relapsing population on active treatment, this result was not surprising … If the study was bigger, or longer it would increase the chances of seeing a progressive slow worsening component to affect the EDSS [Expanded Disability Status Scale],” she added.
Equivalent efficacy
Ultimately, “it appears likely” that ublituximab is “equivalent in efficacy” to the earlier anti-CD20 agents ocrelizumab and ofatumumab, Dr. Coyle said. While all three agents target B-cells, “ublituximab targets a novel CD20 binding site, and is bioengineered to have a particularly potent antibody dependent cell cytotoxicity lysis mechanism,” she added. “It has been touted to ultimately allow a short infusion of 1 hour.”
Although the serious infection rate is slightly higher with ublituximab (5.0% vs. 2.5% for ofatumumab, and 1.3% for ocrelizumab), “it is still low,” and infusion-related reactions are also higher with ublituximab, she added (47.7% vs. 20.2% and 34.3%, respectively). She suggested factors that might influence which treatment is chosen for a given patient might include cost, convenience, whether it is more or less likely to cause low IgG, interference with vaccination, or influence on cancer or COVID risk.
The trials were supported by TG Therapeutics.
Dr. Coyle has received consulting fees from Accordant, Biogen, Bristol Myers Squibb, Celgene, Genentech/Roche, GlaxoSmithKline, Horizon, Janssen, Novartis, Sanofi Genzyme, and Viela Bio and grant funding from Actelion, Alkermes, Bristol Myers Squibb, CorEvitas LLD, Genentech/Roche, Sanofi Genzyme, MedDay, NINDS, and Novartis.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Kicking the can
Medicare, like any other business (regardless of how you want to view it, it’s as much a business as any other insurance company), is dependent on cash flow. Money comes in from young people and their employers through withholding and taxes, and goes back out again in payments to doctors, hospitals, and all the others who bill Medicare for services and supplies in providing health care.
Unlike other businesses, it’s hampered by regulations and competing interests that affect its viability and capacity to adapt to changing markets and circumstances.

For a while, estimates were that Medicare would run out of cash in 2026, but with a stronger-then-expected COVID recovery, it’s been pushed back all the way to ... 2028.
Yeah.
The trouble here is that nobody wants to fix the system to keep it from happening. It’s easier to blame the other side for losing the game than it is to work together to win it. This isn’t a Republican or Democrat issue. Both of them are the problem.
Pushing it back 2 years doesn’t keep it from happening, though it does give more time to find a solution. But that’s only if you have people willing to do so.
Currently politicians favor a strategy of kicking the can down the road for the next congress to deal with. But we’re running out of road to kick it down, and the odds of the next generation of politicians being reasonable, functioning, adults seem to get lower each year.
Can you run your practice like that? In such a way that you know that in a few years your expenses will outweigh your income? And just figure that at some point you’ll get it figured out before your creditors come knocking?
Me neither.
If you were like me, or any other small business owner, you’d sit down and figure out what changes are needed so you’ll still have a viable business down the road.
Of course, that’s part of the issue. The people making these decisions for Medicare don’t have a vested interest in it. If it fails, they have other jobs and income sources to move on to, not to mention some pension-funded health insurance plan. It’s not their problem.
But for the patients, doctors, and other health care professionals who will be depending on it in 6 years, it is a problem, and a serious one.
Hopefully someone will listen before then.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Medicare, like any other business (regardless of how you want to view it, it’s as much a business as any other insurance company), is dependent on cash flow. Money comes in from young people and their employers through withholding and taxes, and goes back out again in payments to doctors, hospitals, and all the others who bill Medicare for services and supplies in providing health care.
Unlike other businesses, it’s hampered by regulations and competing interests that affect its viability and capacity to adapt to changing markets and circumstances.
For a while, estimates were that Medicare would run out of cash in 2026, but with a stronger-then-expected COVID recovery, it’s been pushed back all the way to ... 2028.
Yeah.
The trouble here is that nobody wants to fix the system to keep it from happening. It’s easier to blame the other side for losing the game than it is to work together to win it. This isn’t a Republican or Democrat issue. Both of them are the problem.
Pushing it back 2 years doesn’t keep it from happening, though it does give more time to find a solution. But that’s only if you have people willing to do so.
Currently politicians favor a strategy of kicking the can down the road for the next congress to deal with. But we’re running out of road to kick it down, and the odds of the next generation of politicians being reasonable, functioning, adults seem to get lower each year.
Can you run your practice like that? In such a way that you know that in a few years your expenses will outweigh your income? And just figure that at some point you’ll get it figured out before your creditors come knocking?
Me neither.
If you were like me, or any other small business owner, you’d sit down and figure out what changes are needed so you’ll still have a viable business down the road.
Of course, that’s part of the issue. The people making these decisions for Medicare don’t have a vested interest in it. If it fails, they have other jobs and income sources to move on to, not to mention some pension-funded health insurance plan. It’s not their problem.
But for the patients, doctors, and other health care professionals who will be depending on it in 6 years, it is a problem, and a serious one.
Hopefully someone will listen before then.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Medicare, like any other business (regardless of how you want to view it, it’s as much a business as any other insurance company), is dependent on cash flow. Money comes in from young people and their employers through withholding and taxes, and goes back out again in payments to doctors, hospitals, and all the others who bill Medicare for services and supplies in providing health care.
Unlike other businesses, it’s hampered by regulations and competing interests that affect its viability and capacity to adapt to changing markets and circumstances.
For a while, estimates were that Medicare would run out of cash in 2026, but with a stronger-then-expected COVID recovery, it’s been pushed back all the way to ... 2028.
Yeah.
The trouble here is that nobody wants to fix the system to keep it from happening. It’s easier to blame the other side for losing the game than it is to work together to win it. This isn’t a Republican or Democrat issue. Both of them are the problem.
Pushing it back 2 years doesn’t keep it from happening, though it does give more time to find a solution. But that’s only if you have people willing to do so.
Currently politicians favor a strategy of kicking the can down the road for the next congress to deal with. But we’re running out of road to kick it down, and the odds of the next generation of politicians being reasonable, functioning, adults seem to get lower each year.
Can you run your practice like that? In such a way that you know that in a few years your expenses will outweigh your income? And just figure that at some point you’ll get it figured out before your creditors come knocking?
Me neither.
If you were like me, or any other small business owner, you’d sit down and figure out what changes are needed so you’ll still have a viable business down the road.
Of course, that’s part of the issue. The people making these decisions for Medicare don’t have a vested interest in it. If it fails, they have other jobs and income sources to move on to, not to mention some pension-funded health insurance plan. It’s not their problem.
But for the patients, doctors, and other health care professionals who will be depending on it in 6 years, it is a problem, and a serious one.
Hopefully someone will listen before then.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Infographic: Is physician behavior on social media really so bad?
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
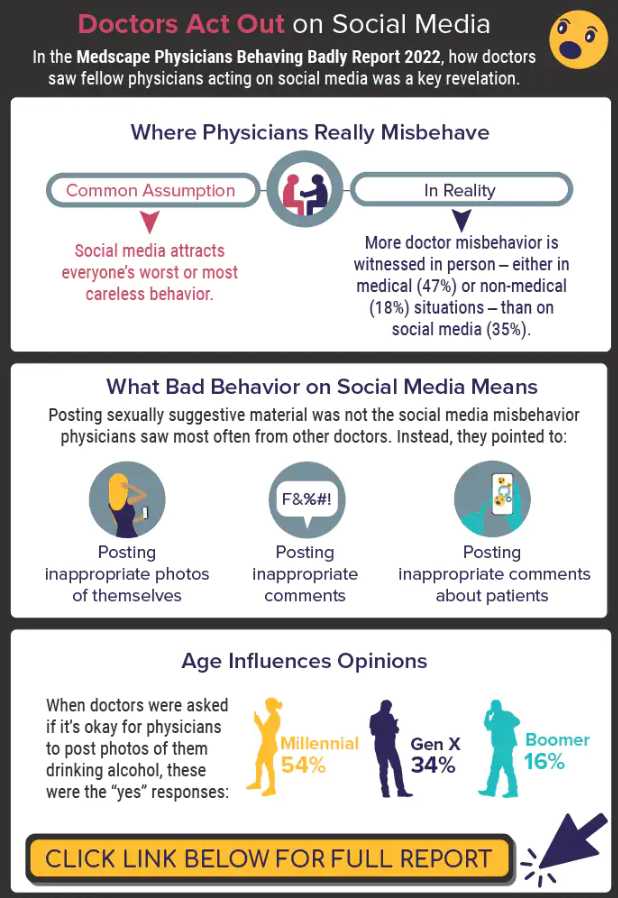
A version of this article first appeared on Medscape.com.
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.