User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
SPRINT-type BP control provides up to 3 years of additional life
PHILADELPHIA – in age-dependent fashion, compared with the older target standard BP, according to a novel analysis of data from the landmark SPRINT trial.

SPRINT randomized 9,361 hypertensive patients aged 50 years or older with at least one additional cardiovascular risk factor to intensive control with a target systolic BP of less than 120 mm Hg or to the then-standard target of less than 140 mm Hg. The trial was stopped early for ethical reasons when an interim analysis showed intensive control was associated with a 27% reduction in mortality. But that 27% reduction in mortality risk is a tough concept for many patients to interpret in practical terms, Muthiah Vaduganathan, MD, observed at the American Heart Association scientific sessions.
So he and his coinvestigators sliced and diced the mountainous SPRINT data in a novel way, using an actuarial statistical analysis.
“These actuarial data from SPRINT support the survival benefits of intensive blood pressure control, especially when initiated in middle-aged, high-risk adults. Our analysis really reaffirms the original SPRINT trial results [N Engl J Med. 2015 Nov 26;373(22):2103-16] and helps present them in an alternative format that can potentially be more easily communicated to clinicians, patients, and the public at large,” explained Dr. Vaduganathan, a cardiologist at Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
The impact of intensive BP control on residual survival was magnified in patients who were younger, since they intrinsically have a longer expected survival and will apply the antihypertensive regimen over a longer period. For example, the actuarial analysis concluded that the mean survival benefit of starting intensive BP lowering, rather than settling for a target systolic BP of less than 140 mm Hg starting at age 50 years, was 3 additional years of life, as compared with 1.1 additional years in 65-year-olds and 0.5 years in patients aged 85 years or older. The same approach can be applied to patients at any individual age from 50 to 95 years at the time of enrollment.
“This is very helpful in conveying messages to individual patients. Often if you tell a patient: ‘Your risk is going to go down by 27%,’ it’s tough for them to recognize what the baseline is and if that actually applied to them. So this may personalize that decision-making conversation,” according to the cardiologist.
One audience member commented that this SPRINT analysis might actually underestimate the true survival advantage of intensive BP lowering. He noted that SPRINT, which was halted after an average of 3.3 years, didn’t show a significant benefit for intensive BP lowering in terms of stroke reduction, whereas the ACCORD trial did, but that benefit didn’t occur until after 3 years into the study (Hypertension. 2018 Aug;72[2]:323-30).
Dr. Vaduganathan conceded that’s a limitation of his analysis.
“The assumption we’ve used is that long-term cardiovascular benefits are going to be as seen in the trial, but since SPRINT was stopped early, some benefits may be exaggerated and some may not have been observed yet,” he agreed.
Another audience member observed, “I think a lot of patients will think: ‘Okay, you’re tacking on a year at the end, when I’m going to be 89 and demented.’ The National Institute on Aging is focusing a lot more now on nondisabled life expectancy or healthy life expectancy.’”
Dr. Vaduganathan offered a degree of reassurance on this score. Because of time limitations, he said, he only presented the life expectancy results. But he and his coworkers have performed the same actuarial analysis of the SPRINT data for other endpoints related to freedom from various forms of disease or disability and found a consistent effect: Intensive BP control was associated with a longer time to onset of morbidity.
SPRINT was sponsored primarily by the National Heart, Lung, and Blood Institute. Dr. Vaduganathan reported that he receives research support from/and or serves on advisory boards for Amgen, AstraZeneca, Baxter Healthcare, Bayer, Boehringer Ingelheim, and Relypsa.
SOURCE: Vaduganathan M et al. AHA 2019, Abstract MDP233.
PHILADELPHIA – in age-dependent fashion, compared with the older target standard BP, according to a novel analysis of data from the landmark SPRINT trial.
SPRINT randomized 9,361 hypertensive patients aged 50 years or older with at least one additional cardiovascular risk factor to intensive control with a target systolic BP of less than 120 mm Hg or to the then-standard target of less than 140 mm Hg. The trial was stopped early for ethical reasons when an interim analysis showed intensive control was associated with a 27% reduction in mortality. But that 27% reduction in mortality risk is a tough concept for many patients to interpret in practical terms, Muthiah Vaduganathan, MD, observed at the American Heart Association scientific sessions.
So he and his coinvestigators sliced and diced the mountainous SPRINT data in a novel way, using an actuarial statistical analysis.
“These actuarial data from SPRINT support the survival benefits of intensive blood pressure control, especially when initiated in middle-aged, high-risk adults. Our analysis really reaffirms the original SPRINT trial results [N Engl J Med. 2015 Nov 26;373(22):2103-16] and helps present them in an alternative format that can potentially be more easily communicated to clinicians, patients, and the public at large,” explained Dr. Vaduganathan, a cardiologist at Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
The impact of intensive BP control on residual survival was magnified in patients who were younger, since they intrinsically have a longer expected survival and will apply the antihypertensive regimen over a longer period. For example, the actuarial analysis concluded that the mean survival benefit of starting intensive BP lowering, rather than settling for a target systolic BP of less than 140 mm Hg starting at age 50 years, was 3 additional years of life, as compared with 1.1 additional years in 65-year-olds and 0.5 years in patients aged 85 years or older. The same approach can be applied to patients at any individual age from 50 to 95 years at the time of enrollment.
“This is very helpful in conveying messages to individual patients. Often if you tell a patient: ‘Your risk is going to go down by 27%,’ it’s tough for them to recognize what the baseline is and if that actually applied to them. So this may personalize that decision-making conversation,” according to the cardiologist.
One audience member commented that this SPRINT analysis might actually underestimate the true survival advantage of intensive BP lowering. He noted that SPRINT, which was halted after an average of 3.3 years, didn’t show a significant benefit for intensive BP lowering in terms of stroke reduction, whereas the ACCORD trial did, but that benefit didn’t occur until after 3 years into the study (Hypertension. 2018 Aug;72[2]:323-30).
Dr. Vaduganathan conceded that’s a limitation of his analysis.
“The assumption we’ve used is that long-term cardiovascular benefits are going to be as seen in the trial, but since SPRINT was stopped early, some benefits may be exaggerated and some may not have been observed yet,” he agreed.
Another audience member observed, “I think a lot of patients will think: ‘Okay, you’re tacking on a year at the end, when I’m going to be 89 and demented.’ The National Institute on Aging is focusing a lot more now on nondisabled life expectancy or healthy life expectancy.’”
Dr. Vaduganathan offered a degree of reassurance on this score. Because of time limitations, he said, he only presented the life expectancy results. But he and his coworkers have performed the same actuarial analysis of the SPRINT data for other endpoints related to freedom from various forms of disease or disability and found a consistent effect: Intensive BP control was associated with a longer time to onset of morbidity.
SPRINT was sponsored primarily by the National Heart, Lung, and Blood Institute. Dr. Vaduganathan reported that he receives research support from/and or serves on advisory boards for Amgen, AstraZeneca, Baxter Healthcare, Bayer, Boehringer Ingelheim, and Relypsa.
SOURCE: Vaduganathan M et al. AHA 2019, Abstract MDP233.
PHILADELPHIA – in age-dependent fashion, compared with the older target standard BP, according to a novel analysis of data from the landmark SPRINT trial.
SPRINT randomized 9,361 hypertensive patients aged 50 years or older with at least one additional cardiovascular risk factor to intensive control with a target systolic BP of less than 120 mm Hg or to the then-standard target of less than 140 mm Hg. The trial was stopped early for ethical reasons when an interim analysis showed intensive control was associated with a 27% reduction in mortality. But that 27% reduction in mortality risk is a tough concept for many patients to interpret in practical terms, Muthiah Vaduganathan, MD, observed at the American Heart Association scientific sessions.
So he and his coinvestigators sliced and diced the mountainous SPRINT data in a novel way, using an actuarial statistical analysis.
“These actuarial data from SPRINT support the survival benefits of intensive blood pressure control, especially when initiated in middle-aged, high-risk adults. Our analysis really reaffirms the original SPRINT trial results [N Engl J Med. 2015 Nov 26;373(22):2103-16] and helps present them in an alternative format that can potentially be more easily communicated to clinicians, patients, and the public at large,” explained Dr. Vaduganathan, a cardiologist at Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
The impact of intensive BP control on residual survival was magnified in patients who were younger, since they intrinsically have a longer expected survival and will apply the antihypertensive regimen over a longer period. For example, the actuarial analysis concluded that the mean survival benefit of starting intensive BP lowering, rather than settling for a target systolic BP of less than 140 mm Hg starting at age 50 years, was 3 additional years of life, as compared with 1.1 additional years in 65-year-olds and 0.5 years in patients aged 85 years or older. The same approach can be applied to patients at any individual age from 50 to 95 years at the time of enrollment.
“This is very helpful in conveying messages to individual patients. Often if you tell a patient: ‘Your risk is going to go down by 27%,’ it’s tough for them to recognize what the baseline is and if that actually applied to them. So this may personalize that decision-making conversation,” according to the cardiologist.
One audience member commented that this SPRINT analysis might actually underestimate the true survival advantage of intensive BP lowering. He noted that SPRINT, which was halted after an average of 3.3 years, didn’t show a significant benefit for intensive BP lowering in terms of stroke reduction, whereas the ACCORD trial did, but that benefit didn’t occur until after 3 years into the study (Hypertension. 2018 Aug;72[2]:323-30).
Dr. Vaduganathan conceded that’s a limitation of his analysis.
“The assumption we’ve used is that long-term cardiovascular benefits are going to be as seen in the trial, but since SPRINT was stopped early, some benefits may be exaggerated and some may not have been observed yet,” he agreed.
Another audience member observed, “I think a lot of patients will think: ‘Okay, you’re tacking on a year at the end, when I’m going to be 89 and demented.’ The National Institute on Aging is focusing a lot more now on nondisabled life expectancy or healthy life expectancy.’”
Dr. Vaduganathan offered a degree of reassurance on this score. Because of time limitations, he said, he only presented the life expectancy results. But he and his coworkers have performed the same actuarial analysis of the SPRINT data for other endpoints related to freedom from various forms of disease or disability and found a consistent effect: Intensive BP control was associated with a longer time to onset of morbidity.
SPRINT was sponsored primarily by the National Heart, Lung, and Blood Institute. Dr. Vaduganathan reported that he receives research support from/and or serves on advisory boards for Amgen, AstraZeneca, Baxter Healthcare, Bayer, Boehringer Ingelheim, and Relypsa.
SOURCE: Vaduganathan M et al. AHA 2019, Abstract MDP233.
REPORTING FROM AHA 2019
Expedited review programs not shortening drug development
Drug development times are not showing any signs of decreasing even though application review times at the Food and Drug Administration are improving, new research has shown.

“Despite the accumulation of expedited programs that have reduced FDA review times, overall clinical development times have not become shorter, although it is not possible to know what role these programs may have played in preventing an increase in development times,” Jonathan Darrow of Harvard Medical School, Boston, and colleagues wrote in a study published Jan. 14 in JAMA.
Researchers noted that FDA approval times declined from more than 3 years in 1983 to less than 1 year in 2017, although total time from the authorization of clinical testing to approval has remained steady across that period at about 8 years.
“The resistance of total development times to efforts to shorten them could be the result of more submissions of applications for rare disease drugs, which can sometimes pose trial recruitment challenges; a shifting emphasis to more challenging therapeutic categories, such as central nervous system disorder treatments; longer time horizons needed to establish efficacy when early intervention is important (e.g., cancer); or other factors,” wrote Mr. Darrow and colleagues.
The authors also note that the value of the expanded review toolbox the FDA now employs is “unclear” as “the number of new drug approvals has not increased substantially over the past three decades.” This observation does not count biologics or generic approvals.
Research revealed that the mean annual number of new drug approvals (including biologics) was 34 from 1990 to 1999, 25 from 2000 to 2009, and 41 from 2010 to 2018. In addition, while the number of new drug approvals has remained at or below 60 per year, the portion of drugs using at least one expedited review program increased over time, with more than 80% of the 59 new drugs approved in 2018 being subject to at least one expedited review program.
“Although the FDA has on average applied its expedited programs to drugs offering larger health gains, it is difficult to assess whether these programs have incentivized greater therapeutic innovation or merely allowed more appropriate agency prioritization,” noted Mr. Darrow and colleagues.
And while it may be hard to truly understand the impact of the many expedited review programs that have been introduced at the FDA, there is still room for improvement in the process.
In an editorial published in JAMA, Joshua Sharfstein, MD, of Johns Hopkins University, Baltimore, suggested four reforms the FDA could examine.
“First, Congress and the FDA should rationalize the various programs for expedited review,” he wrote, noting that companies are using the Orphan Drug Act to prevent competition. “Fixing the system requires, at a minimum, promoting meaningful competition for non-orphan uses.”
Second, he wrote, the FDA needs to strengthen oversight of postmarket safety though more diligence in the operation of its Risk Evaluation and Management Strategies (REMS) program.
“Third, Congress should recalibrate the programs that provide companies with special marketing protections,” added Dr. Sharfstein, former FDA principal deputy commissioner. “One place to look is pediatric exclusivity, which has been estimated to cost the health care system more than $6 for every $1 spent by a company on a pediatric trial.”
And finally, “Congress should use patent and pricing incentives to accelerate the generation of definitive evidence under accelerated approval,” citing proposals to limit pricing or market exclusivity until companies complete studies that assess clinically relevant endpoints.
“These changes would reflect an evolution, not a revolution, of the FDA’s approach to new drug approval,” Dr. Sharfstein said. “These reforms could also bring greater order and thoughtfulness to the regulation of important new therapies, while enhancing safety and creating greater capability to afford truly transformative medical products.”
SOURCE: Jonathan Darrow et al. JAMA 2020 Jan 14. doi: 10.1001/jama.2019.20288.
Drug development times are not showing any signs of decreasing even though application review times at the Food and Drug Administration are improving, new research has shown.
“Despite the accumulation of expedited programs that have reduced FDA review times, overall clinical development times have not become shorter, although it is not possible to know what role these programs may have played in preventing an increase in development times,” Jonathan Darrow of Harvard Medical School, Boston, and colleagues wrote in a study published Jan. 14 in JAMA.
Researchers noted that FDA approval times declined from more than 3 years in 1983 to less than 1 year in 2017, although total time from the authorization of clinical testing to approval has remained steady across that period at about 8 years.
“The resistance of total development times to efforts to shorten them could be the result of more submissions of applications for rare disease drugs, which can sometimes pose trial recruitment challenges; a shifting emphasis to more challenging therapeutic categories, such as central nervous system disorder treatments; longer time horizons needed to establish efficacy when early intervention is important (e.g., cancer); or other factors,” wrote Mr. Darrow and colleagues.
The authors also note that the value of the expanded review toolbox the FDA now employs is “unclear” as “the number of new drug approvals has not increased substantially over the past three decades.” This observation does not count biologics or generic approvals.
Research revealed that the mean annual number of new drug approvals (including biologics) was 34 from 1990 to 1999, 25 from 2000 to 2009, and 41 from 2010 to 2018. In addition, while the number of new drug approvals has remained at or below 60 per year, the portion of drugs using at least one expedited review program increased over time, with more than 80% of the 59 new drugs approved in 2018 being subject to at least one expedited review program.
“Although the FDA has on average applied its expedited programs to drugs offering larger health gains, it is difficult to assess whether these programs have incentivized greater therapeutic innovation or merely allowed more appropriate agency prioritization,” noted Mr. Darrow and colleagues.
And while it may be hard to truly understand the impact of the many expedited review programs that have been introduced at the FDA, there is still room for improvement in the process.
In an editorial published in JAMA, Joshua Sharfstein, MD, of Johns Hopkins University, Baltimore, suggested four reforms the FDA could examine.
“First, Congress and the FDA should rationalize the various programs for expedited review,” he wrote, noting that companies are using the Orphan Drug Act to prevent competition. “Fixing the system requires, at a minimum, promoting meaningful competition for non-orphan uses.”
Second, he wrote, the FDA needs to strengthen oversight of postmarket safety though more diligence in the operation of its Risk Evaluation and Management Strategies (REMS) program.
“Third, Congress should recalibrate the programs that provide companies with special marketing protections,” added Dr. Sharfstein, former FDA principal deputy commissioner. “One place to look is pediatric exclusivity, which has been estimated to cost the health care system more than $6 for every $1 spent by a company on a pediatric trial.”
And finally, “Congress should use patent and pricing incentives to accelerate the generation of definitive evidence under accelerated approval,” citing proposals to limit pricing or market exclusivity until companies complete studies that assess clinically relevant endpoints.
“These changes would reflect an evolution, not a revolution, of the FDA’s approach to new drug approval,” Dr. Sharfstein said. “These reforms could also bring greater order and thoughtfulness to the regulation of important new therapies, while enhancing safety and creating greater capability to afford truly transformative medical products.”
SOURCE: Jonathan Darrow et al. JAMA 2020 Jan 14. doi: 10.1001/jama.2019.20288.
Drug development times are not showing any signs of decreasing even though application review times at the Food and Drug Administration are improving, new research has shown.
“Despite the accumulation of expedited programs that have reduced FDA review times, overall clinical development times have not become shorter, although it is not possible to know what role these programs may have played in preventing an increase in development times,” Jonathan Darrow of Harvard Medical School, Boston, and colleagues wrote in a study published Jan. 14 in JAMA.
Researchers noted that FDA approval times declined from more than 3 years in 1983 to less than 1 year in 2017, although total time from the authorization of clinical testing to approval has remained steady across that period at about 8 years.
“The resistance of total development times to efforts to shorten them could be the result of more submissions of applications for rare disease drugs, which can sometimes pose trial recruitment challenges; a shifting emphasis to more challenging therapeutic categories, such as central nervous system disorder treatments; longer time horizons needed to establish efficacy when early intervention is important (e.g., cancer); or other factors,” wrote Mr. Darrow and colleagues.
The authors also note that the value of the expanded review toolbox the FDA now employs is “unclear” as “the number of new drug approvals has not increased substantially over the past three decades.” This observation does not count biologics or generic approvals.
Research revealed that the mean annual number of new drug approvals (including biologics) was 34 from 1990 to 1999, 25 from 2000 to 2009, and 41 from 2010 to 2018. In addition, while the number of new drug approvals has remained at or below 60 per year, the portion of drugs using at least one expedited review program increased over time, with more than 80% of the 59 new drugs approved in 2018 being subject to at least one expedited review program.
“Although the FDA has on average applied its expedited programs to drugs offering larger health gains, it is difficult to assess whether these programs have incentivized greater therapeutic innovation or merely allowed more appropriate agency prioritization,” noted Mr. Darrow and colleagues.
And while it may be hard to truly understand the impact of the many expedited review programs that have been introduced at the FDA, there is still room for improvement in the process.
In an editorial published in JAMA, Joshua Sharfstein, MD, of Johns Hopkins University, Baltimore, suggested four reforms the FDA could examine.
“First, Congress and the FDA should rationalize the various programs for expedited review,” he wrote, noting that companies are using the Orphan Drug Act to prevent competition. “Fixing the system requires, at a minimum, promoting meaningful competition for non-orphan uses.”
Second, he wrote, the FDA needs to strengthen oversight of postmarket safety though more diligence in the operation of its Risk Evaluation and Management Strategies (REMS) program.
“Third, Congress should recalibrate the programs that provide companies with special marketing protections,” added Dr. Sharfstein, former FDA principal deputy commissioner. “One place to look is pediatric exclusivity, which has been estimated to cost the health care system more than $6 for every $1 spent by a company on a pediatric trial.”
And finally, “Congress should use patent and pricing incentives to accelerate the generation of definitive evidence under accelerated approval,” citing proposals to limit pricing or market exclusivity until companies complete studies that assess clinically relevant endpoints.
“These changes would reflect an evolution, not a revolution, of the FDA’s approach to new drug approval,” Dr. Sharfstein said. “These reforms could also bring greater order and thoughtfulness to the regulation of important new therapies, while enhancing safety and creating greater capability to afford truly transformative medical products.”
SOURCE: Jonathan Darrow et al. JAMA 2020 Jan 14. doi: 10.1001/jama.2019.20288.
FROM JAMA
APPRENTICE registry: Wide variation exists in acute pancreatitis treatment, outcomes
Etiologies, demographics, management, and outcomes vary widely among patients with acute pancreatitis around the world, according to an analysis of data from the prospective, international APPRENTICE patient registry.
In some cases – particularly in regard to therapeutic interventions – the differences are “strikingly divergent” and demonstrate a “lag behind current evidence,” Bassem Matta, MD, of the University of Pittsburgh Medical Center, and colleagues reported in Clinical Gastroenterology and Hepatology.
Findings of a disproportionately higher rate of opioid prescribing during hospitalization and at discharge at North American sites are especially alarming, the investigators said.
Demographics and etiologies
The most common etiologies among 1,612 patients in the registry, which collects data from individuals with acute pancreatitis at six centers in Europe, three centers in India, five centers in Latin America, and eight centers in North America, were biliary (45%) and alcoholic (21%), and severity was mild in 65% of patients, moderate in 23%, and severe in 12%, they noted.
The predominant etiology in Latin America was biliary (78%), whereas the predominant etiology in India was alcoholic (45%).
The mean age of patients in Europe was 58 years, which is older than the mean age of 46 years for all regions represented in the registry, and comorbid conditions were also more common among patients in Europe (73% vs. 50% overall), the investigators found.
In addition to age differences, significant geographic differences were seen with respect to sex, ethnicity, and race distributions. Patients from Indian sites, for example, were mostly men (75%), were younger in age (median, 39 years), and were more likely to have alcoholic etiology (45% vs. 14% in the other areas). Most of the Latin American patients were women (67%), were young (median, 43 years), and most often had biliary etiology (78% vs. 37% elsewhere).
In contrast, European and North American subjects had a relatively equal sex distribution and an overall older age (median, 58 years).
“Observed differences in etiology and demographics likely reflect a tight interconnection between age, sex, and etiology,” the investigators wrote.
Management
Analgesic utilization was “markedly variable” across the world, they said, explaining that nonsteroidal anti-inflammatory drugs (NSAIDs) were the mainstay of pain management in Europe (68%), whereas Indian sites used tramadol in 91% of patients.
Latin American centers frequently used opioids (59%), NSAIDs (48%), and tramadol (34%).
However, opioid analgesics were used in 93% of patients in North America, compared with 27% of patients in the other regions, and 64% vs. 2.7% of patients in North American vs. the other regions were discharged on opioid analgesics.
This is of particular concern in light of a meta-analysis showing no difference in efficacy between opioids and nonsteroidal anti-inflammatory drugs for pain control in acute pancreatitis, the investigators said, noting that “[i]t is not entirely clear why such divergences exist between North American centers compared to the rest of the world.
“Notably, no clear statements are included in the current societal guidelines addressing optimal strategies for analgesia in [acute pancreatitis],” they added.
Also of note, the rate of endoscopic retrograde cholangiopancreatography (ERCP) – which guidelines based on strong evidence say should be limited to urgent cases among biliary acute pancreatitis patients with suspected cholangitis or biliary obstruction – was much higher at North American sites (44.7% vs. 21.9% overall) and post-ERCP pancreatitis was significantly more common at North American sites (19% vs. 2.8% in the other geographic areas), they said.
However, these differences were mostly driven by two North American sites, which classified 50 out of 90 and 22 out of 62 enrolled patients, respectively, as having post-ERCP pancreatitis.
Further, cholecystectomies were performed at the time of hospital admission in 60% of patients in Latin America, compared with 15% overall.
Another notable difference in management related to intravenous fluid use; similar amounts were administered during the first 24 hours in India and Latin America (3-3.2 liters), but in Europe the average was 2.5 liters, and while lactated Ringers and normal saline were the main types of fluid used, lactated Ringers was the dominant type used in India (92%), but was rarely used in Latin America (7%).
Outcomes
The overall median length of stay was 8 days, and overall mortality during hospitalization was 2.8%. In patients with mild disease, the shortest lengths of stay were in North America (4 vs. 7 days in other regions), and severe disease was more common in India (23% vs. 9% elsewhere).
Intensive care unit admissions were highest at Indian centers, and in-hospital mortality was highest in Europe (5.7%), compared with 3.3% in India, 2.3% in Latin America, and 0.6% in North America, they said.
Mortality during the initial hospital stay among patients with severe acute pancreatitis was 44% in Europe, compared with 15% in the other three regions.
Multivariable regression analyses adjusting for potential confounders such as age, sex, body mass index, Charlson score, etiology, and transfer status showed that the odds of severe acute pancreatitis were 11.2 times higher in Europe, 7 times higher in India, and 5.6 times higher in Latin America, compared with North America.
The odds ratios for mortality during hospitalization among patients with severe disease were 10.4 in Europe, 4.2 in India, and 8.3 in Latin America, compared with North America.
Implications of the findings
Around the world, acute pancreatitis is a leading cause of gastrointestinal-related hospital admissions, and incidence is reportedly increasing in the United States and Europe, the investigators said, noting that about 20% of patients develop severe disease with relatively high morbidity and mortality.
Multiple advances in management have emerged over the last decade, but it is unclear whether those recent advances have gained traction worldwide, they added.
The APPRENTICE registry was created as a response to the lack of prospective, multinational data and the current study aimed to assess the geographic differences in patient characteristics, management, and outcomes across four geographic areas.
The findings, which represent “a bird’s eye view” of regional variation, underscore a need for “adequately powered, multicenter, randomized controlled trials comparing the efficacy of different fluid resuscitation protocols” in acute pancreatitis patients, the investigators said.
Further, “the interventions specific to each region are in certain aspects strikingly divergent, and in many occasions lag behind current evidence,” they wrote, noting the largely variable length-of-stay outcomes and mortality rates.
“In addition to depicting key features of [acute pancreatitis], the results from this study may serve as a reference guide for designing future clinical trials,” they concluded.
The authors reported having no disclosures.
SOURCE: Matt B et al. Clin Gastroenterol Hepatol. 2019. doi: 10.1016/j.cgh.2019.11.017.
Etiologies, demographics, management, and outcomes vary widely among patients with acute pancreatitis around the world, according to an analysis of data from the prospective, international APPRENTICE patient registry.
In some cases – particularly in regard to therapeutic interventions – the differences are “strikingly divergent” and demonstrate a “lag behind current evidence,” Bassem Matta, MD, of the University of Pittsburgh Medical Center, and colleagues reported in Clinical Gastroenterology and Hepatology.
Findings of a disproportionately higher rate of opioid prescribing during hospitalization and at discharge at North American sites are especially alarming, the investigators said.
Demographics and etiologies
The most common etiologies among 1,612 patients in the registry, which collects data from individuals with acute pancreatitis at six centers in Europe, three centers in India, five centers in Latin America, and eight centers in North America, were biliary (45%) and alcoholic (21%), and severity was mild in 65% of patients, moderate in 23%, and severe in 12%, they noted.
The predominant etiology in Latin America was biliary (78%), whereas the predominant etiology in India was alcoholic (45%).
The mean age of patients in Europe was 58 years, which is older than the mean age of 46 years for all regions represented in the registry, and comorbid conditions were also more common among patients in Europe (73% vs. 50% overall), the investigators found.
In addition to age differences, significant geographic differences were seen with respect to sex, ethnicity, and race distributions. Patients from Indian sites, for example, were mostly men (75%), were younger in age (median, 39 years), and were more likely to have alcoholic etiology (45% vs. 14% in the other areas). Most of the Latin American patients were women (67%), were young (median, 43 years), and most often had biliary etiology (78% vs. 37% elsewhere).
In contrast, European and North American subjects had a relatively equal sex distribution and an overall older age (median, 58 years).
“Observed differences in etiology and demographics likely reflect a tight interconnection between age, sex, and etiology,” the investigators wrote.
Management
Analgesic utilization was “markedly variable” across the world, they said, explaining that nonsteroidal anti-inflammatory drugs (NSAIDs) were the mainstay of pain management in Europe (68%), whereas Indian sites used tramadol in 91% of patients.
Latin American centers frequently used opioids (59%), NSAIDs (48%), and tramadol (34%).
However, opioid analgesics were used in 93% of patients in North America, compared with 27% of patients in the other regions, and 64% vs. 2.7% of patients in North American vs. the other regions were discharged on opioid analgesics.
This is of particular concern in light of a meta-analysis showing no difference in efficacy between opioids and nonsteroidal anti-inflammatory drugs for pain control in acute pancreatitis, the investigators said, noting that “[i]t is not entirely clear why such divergences exist between North American centers compared to the rest of the world.
“Notably, no clear statements are included in the current societal guidelines addressing optimal strategies for analgesia in [acute pancreatitis],” they added.
Also of note, the rate of endoscopic retrograde cholangiopancreatography (ERCP) – which guidelines based on strong evidence say should be limited to urgent cases among biliary acute pancreatitis patients with suspected cholangitis or biliary obstruction – was much higher at North American sites (44.7% vs. 21.9% overall) and post-ERCP pancreatitis was significantly more common at North American sites (19% vs. 2.8% in the other geographic areas), they said.
However, these differences were mostly driven by two North American sites, which classified 50 out of 90 and 22 out of 62 enrolled patients, respectively, as having post-ERCP pancreatitis.
Further, cholecystectomies were performed at the time of hospital admission in 60% of patients in Latin America, compared with 15% overall.
Another notable difference in management related to intravenous fluid use; similar amounts were administered during the first 24 hours in India and Latin America (3-3.2 liters), but in Europe the average was 2.5 liters, and while lactated Ringers and normal saline were the main types of fluid used, lactated Ringers was the dominant type used in India (92%), but was rarely used in Latin America (7%).
Outcomes
The overall median length of stay was 8 days, and overall mortality during hospitalization was 2.8%. In patients with mild disease, the shortest lengths of stay were in North America (4 vs. 7 days in other regions), and severe disease was more common in India (23% vs. 9% elsewhere).
Intensive care unit admissions were highest at Indian centers, and in-hospital mortality was highest in Europe (5.7%), compared with 3.3% in India, 2.3% in Latin America, and 0.6% in North America, they said.
Mortality during the initial hospital stay among patients with severe acute pancreatitis was 44% in Europe, compared with 15% in the other three regions.
Multivariable regression analyses adjusting for potential confounders such as age, sex, body mass index, Charlson score, etiology, and transfer status showed that the odds of severe acute pancreatitis were 11.2 times higher in Europe, 7 times higher in India, and 5.6 times higher in Latin America, compared with North America.
The odds ratios for mortality during hospitalization among patients with severe disease were 10.4 in Europe, 4.2 in India, and 8.3 in Latin America, compared with North America.
Implications of the findings
Around the world, acute pancreatitis is a leading cause of gastrointestinal-related hospital admissions, and incidence is reportedly increasing in the United States and Europe, the investigators said, noting that about 20% of patients develop severe disease with relatively high morbidity and mortality.
Multiple advances in management have emerged over the last decade, but it is unclear whether those recent advances have gained traction worldwide, they added.
The APPRENTICE registry was created as a response to the lack of prospective, multinational data and the current study aimed to assess the geographic differences in patient characteristics, management, and outcomes across four geographic areas.
The findings, which represent “a bird’s eye view” of regional variation, underscore a need for “adequately powered, multicenter, randomized controlled trials comparing the efficacy of different fluid resuscitation protocols” in acute pancreatitis patients, the investigators said.
Further, “the interventions specific to each region are in certain aspects strikingly divergent, and in many occasions lag behind current evidence,” they wrote, noting the largely variable length-of-stay outcomes and mortality rates.
“In addition to depicting key features of [acute pancreatitis], the results from this study may serve as a reference guide for designing future clinical trials,” they concluded.
The authors reported having no disclosures.
SOURCE: Matt B et al. Clin Gastroenterol Hepatol. 2019. doi: 10.1016/j.cgh.2019.11.017.
Etiologies, demographics, management, and outcomes vary widely among patients with acute pancreatitis around the world, according to an analysis of data from the prospective, international APPRENTICE patient registry.
In some cases – particularly in regard to therapeutic interventions – the differences are “strikingly divergent” and demonstrate a “lag behind current evidence,” Bassem Matta, MD, of the University of Pittsburgh Medical Center, and colleagues reported in Clinical Gastroenterology and Hepatology.
Findings of a disproportionately higher rate of opioid prescribing during hospitalization and at discharge at North American sites are especially alarming, the investigators said.
Demographics and etiologies
The most common etiologies among 1,612 patients in the registry, which collects data from individuals with acute pancreatitis at six centers in Europe, three centers in India, five centers in Latin America, and eight centers in North America, were biliary (45%) and alcoholic (21%), and severity was mild in 65% of patients, moderate in 23%, and severe in 12%, they noted.
The predominant etiology in Latin America was biliary (78%), whereas the predominant etiology in India was alcoholic (45%).
The mean age of patients in Europe was 58 years, which is older than the mean age of 46 years for all regions represented in the registry, and comorbid conditions were also more common among patients in Europe (73% vs. 50% overall), the investigators found.
In addition to age differences, significant geographic differences were seen with respect to sex, ethnicity, and race distributions. Patients from Indian sites, for example, were mostly men (75%), were younger in age (median, 39 years), and were more likely to have alcoholic etiology (45% vs. 14% in the other areas). Most of the Latin American patients were women (67%), were young (median, 43 years), and most often had biliary etiology (78% vs. 37% elsewhere).
In contrast, European and North American subjects had a relatively equal sex distribution and an overall older age (median, 58 years).
“Observed differences in etiology and demographics likely reflect a tight interconnection between age, sex, and etiology,” the investigators wrote.
Management
Analgesic utilization was “markedly variable” across the world, they said, explaining that nonsteroidal anti-inflammatory drugs (NSAIDs) were the mainstay of pain management in Europe (68%), whereas Indian sites used tramadol in 91% of patients.
Latin American centers frequently used opioids (59%), NSAIDs (48%), and tramadol (34%).
However, opioid analgesics were used in 93% of patients in North America, compared with 27% of patients in the other regions, and 64% vs. 2.7% of patients in North American vs. the other regions were discharged on opioid analgesics.
This is of particular concern in light of a meta-analysis showing no difference in efficacy between opioids and nonsteroidal anti-inflammatory drugs for pain control in acute pancreatitis, the investigators said, noting that “[i]t is not entirely clear why such divergences exist between North American centers compared to the rest of the world.
“Notably, no clear statements are included in the current societal guidelines addressing optimal strategies for analgesia in [acute pancreatitis],” they added.
Also of note, the rate of endoscopic retrograde cholangiopancreatography (ERCP) – which guidelines based on strong evidence say should be limited to urgent cases among biliary acute pancreatitis patients with suspected cholangitis or biliary obstruction – was much higher at North American sites (44.7% vs. 21.9% overall) and post-ERCP pancreatitis was significantly more common at North American sites (19% vs. 2.8% in the other geographic areas), they said.
However, these differences were mostly driven by two North American sites, which classified 50 out of 90 and 22 out of 62 enrolled patients, respectively, as having post-ERCP pancreatitis.
Further, cholecystectomies were performed at the time of hospital admission in 60% of patients in Latin America, compared with 15% overall.
Another notable difference in management related to intravenous fluid use; similar amounts were administered during the first 24 hours in India and Latin America (3-3.2 liters), but in Europe the average was 2.5 liters, and while lactated Ringers and normal saline were the main types of fluid used, lactated Ringers was the dominant type used in India (92%), but was rarely used in Latin America (7%).
Outcomes
The overall median length of stay was 8 days, and overall mortality during hospitalization was 2.8%. In patients with mild disease, the shortest lengths of stay were in North America (4 vs. 7 days in other regions), and severe disease was more common in India (23% vs. 9% elsewhere).
Intensive care unit admissions were highest at Indian centers, and in-hospital mortality was highest in Europe (5.7%), compared with 3.3% in India, 2.3% in Latin America, and 0.6% in North America, they said.
Mortality during the initial hospital stay among patients with severe acute pancreatitis was 44% in Europe, compared with 15% in the other three regions.
Multivariable regression analyses adjusting for potential confounders such as age, sex, body mass index, Charlson score, etiology, and transfer status showed that the odds of severe acute pancreatitis were 11.2 times higher in Europe, 7 times higher in India, and 5.6 times higher in Latin America, compared with North America.
The odds ratios for mortality during hospitalization among patients with severe disease were 10.4 in Europe, 4.2 in India, and 8.3 in Latin America, compared with North America.
Implications of the findings
Around the world, acute pancreatitis is a leading cause of gastrointestinal-related hospital admissions, and incidence is reportedly increasing in the United States and Europe, the investigators said, noting that about 20% of patients develop severe disease with relatively high morbidity and mortality.
Multiple advances in management have emerged over the last decade, but it is unclear whether those recent advances have gained traction worldwide, they added.
The APPRENTICE registry was created as a response to the lack of prospective, multinational data and the current study aimed to assess the geographic differences in patient characteristics, management, and outcomes across four geographic areas.
The findings, which represent “a bird’s eye view” of regional variation, underscore a need for “adequately powered, multicenter, randomized controlled trials comparing the efficacy of different fluid resuscitation protocols” in acute pancreatitis patients, the investigators said.
Further, “the interventions specific to each region are in certain aspects strikingly divergent, and in many occasions lag behind current evidence,” they wrote, noting the largely variable length-of-stay outcomes and mortality rates.
“In addition to depicting key features of [acute pancreatitis], the results from this study may serve as a reference guide for designing future clinical trials,” they concluded.
The authors reported having no disclosures.
SOURCE: Matt B et al. Clin Gastroenterol Hepatol. 2019. doi: 10.1016/j.cgh.2019.11.017.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Comorbidity rates remain stable over 10 years in childhood-onset epilepsy
BALTIMORE – , according to research presented at the annual meeting of the American Epilepsy Society. Compared with controls, however, young adults with childhood-onset epilepsy have higher rates of psychiatric comorbidity.
The findings suggest that “diagnoses that are identified at baseline continue to be a problem over time,” said Jana E. Jones, PhD, associate professor of neuropsychology at the University of Wisconsin in Madison. Although neurologists understand that comorbidities are common among patients with childhood-onset epilepsy, “it would be good for us to continue to learn what factors are influencing this,” she added.
Investigators sought predictors of outcomes at 10 years
Since 2004, Dr. Jones and her colleagues at the University of Wisconsin have been conducting a study of patients with childhood-onset epilepsy. After the population had completed 10 years of follow-up, the researchers analyzed the data to identify potential patterns of medical and psychiatric comorbidities. One question that they sought to answer was whether any baseline factors could predict outcomes at 10 years.
The researchers analyzed data for 53 patients with childhood-onset epilepsy and 55 controls without epilepsy. At baseline, participants were between ages 8 years and 18 years and had no intellectual disability or neurologic impairment. Within 1 year of epilepsy diagnosis, each participant underwent a psychiatric interview based on the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS). Ten years later, participants underwent the Composite International Diagnostic Interview (CIDI), a psychiatric interview for adults. Information about medical comorbidities was collected through interviews and record review at baseline and through an online survey at the 10-year follow-up.
Participants’ mean age at baseline was 12 years. Mean IQ was 105 for the epilepsy group and 109 for the control group. At 10 years, participants’ mean age was about 23 years. Among patients with epilepsy, 55% had focal epilepsy, and 42% had generalized epilepsy. About 40% of participants with epilepsy were in remission at 10 years, which Dr. Jones and colleagues defined as having achieved 5 years without taking medications and without having seizures. At 10 years after diagnosis, 51% of patients with epilepsy were not taking any seizure medication, including approximately 11% of patients with epilepsy who were not categorized as in remission. Most patients taking medication were on monotherapy.
Trends in psychiatric and medical comorbidities
At baseline, approximately 75% of children with epilepsy had a psychiatric or medical diagnosis, compared with 40% of controls. At the 10-year follow-up, 62% of children with epilepsy had a psychiatric diagnosis, compared with 35% of controls. Among controls, 4% had a medical comorbidity (i.e., asthma) alone at baseline. Asthma was the most common medical comorbidity at baseline among patients with epilepsy, and other comorbidities included sleep disorder, head injury, and scoliosis. Six percent of patients had a medical comorbidity alone at baseline. The proportion of patients with both psychiatric and medical comorbidity was 8% at baseline. Patients with epilepsy at baseline had an increased risk of psychiatric comorbidity.
At 10 years, the most common medical comorbidity among patients with epilepsy was head injury (18.9%), followed by allergies and asthma. The rate of migraine was about 13% among controls and slightly less in the epilepsy group. Dr. Jones and colleagues found no significant differences in medical comorbidities between groups at 10 years. At that point, the rate of medical comorbidity was 4% among patients and 11% among controls.
The rate of psychiatric comorbidity remained relatively stable over 10 years, said Dr. Jones. Approximately 47% of patients with epilepsy had a psychiatric diagnosis at 10 years, compared with 29% of controls. In addition, 38% of patients with epilepsy had both psychiatric and medical diagnoses, compared with 29% of controls. Epilepsy increased the risk of psychiatric comorbidity at the 10-year follow-up. Neither medications, remission status, nor seizure type predicted any comorbidity at 10 years.
Dr. Jones and colleagues compared comorbidity rates between the study sample and the National Comorbidity Survey Replication (NCS-R), which reported population-based data that included an epilepsy sample. About 47% of the epilepsy group had an anxiety disorder, compared with 40.7% in the NCS-R. The rate of anxiety disorders was higher in the control group (45.5%) than in the control group (30.8%) in the NCS-R. Approximately 26.4% of the population in Dr. Jones’s study had a mood disorder, compared with 25.9% in the National Comorbidity Survey.
Dr. Jones and colleagues are conducting 15-year follow-up of their original population. One question they will examine is whether medical comorbidities will increase in patients with childhood-onset epilepsy as they approach age 30 years.
Two of the investigators received funding in the form of a grant from the National Institutes of Health.
SOURCE: Kesselmayer RF et al. AES 2019. Abstract 1.288.
BALTIMORE – , according to research presented at the annual meeting of the American Epilepsy Society. Compared with controls, however, young adults with childhood-onset epilepsy have higher rates of psychiatric comorbidity.
The findings suggest that “diagnoses that are identified at baseline continue to be a problem over time,” said Jana E. Jones, PhD, associate professor of neuropsychology at the University of Wisconsin in Madison. Although neurologists understand that comorbidities are common among patients with childhood-onset epilepsy, “it would be good for us to continue to learn what factors are influencing this,” she added.
Investigators sought predictors of outcomes at 10 years
Since 2004, Dr. Jones and her colleagues at the University of Wisconsin have been conducting a study of patients with childhood-onset epilepsy. After the population had completed 10 years of follow-up, the researchers analyzed the data to identify potential patterns of medical and psychiatric comorbidities. One question that they sought to answer was whether any baseline factors could predict outcomes at 10 years.
The researchers analyzed data for 53 patients with childhood-onset epilepsy and 55 controls without epilepsy. At baseline, participants were between ages 8 years and 18 years and had no intellectual disability or neurologic impairment. Within 1 year of epilepsy diagnosis, each participant underwent a psychiatric interview based on the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS). Ten years later, participants underwent the Composite International Diagnostic Interview (CIDI), a psychiatric interview for adults. Information about medical comorbidities was collected through interviews and record review at baseline and through an online survey at the 10-year follow-up.
Participants’ mean age at baseline was 12 years. Mean IQ was 105 for the epilepsy group and 109 for the control group. At 10 years, participants’ mean age was about 23 years. Among patients with epilepsy, 55% had focal epilepsy, and 42% had generalized epilepsy. About 40% of participants with epilepsy were in remission at 10 years, which Dr. Jones and colleagues defined as having achieved 5 years without taking medications and without having seizures. At 10 years after diagnosis, 51% of patients with epilepsy were not taking any seizure medication, including approximately 11% of patients with epilepsy who were not categorized as in remission. Most patients taking medication were on monotherapy.
Trends in psychiatric and medical comorbidities
At baseline, approximately 75% of children with epilepsy had a psychiatric or medical diagnosis, compared with 40% of controls. At the 10-year follow-up, 62% of children with epilepsy had a psychiatric diagnosis, compared with 35% of controls. Among controls, 4% had a medical comorbidity (i.e., asthma) alone at baseline. Asthma was the most common medical comorbidity at baseline among patients with epilepsy, and other comorbidities included sleep disorder, head injury, and scoliosis. Six percent of patients had a medical comorbidity alone at baseline. The proportion of patients with both psychiatric and medical comorbidity was 8% at baseline. Patients with epilepsy at baseline had an increased risk of psychiatric comorbidity.
At 10 years, the most common medical comorbidity among patients with epilepsy was head injury (18.9%), followed by allergies and asthma. The rate of migraine was about 13% among controls and slightly less in the epilepsy group. Dr. Jones and colleagues found no significant differences in medical comorbidities between groups at 10 years. At that point, the rate of medical comorbidity was 4% among patients and 11% among controls.
The rate of psychiatric comorbidity remained relatively stable over 10 years, said Dr. Jones. Approximately 47% of patients with epilepsy had a psychiatric diagnosis at 10 years, compared with 29% of controls. In addition, 38% of patients with epilepsy had both psychiatric and medical diagnoses, compared with 29% of controls. Epilepsy increased the risk of psychiatric comorbidity at the 10-year follow-up. Neither medications, remission status, nor seizure type predicted any comorbidity at 10 years.
Dr. Jones and colleagues compared comorbidity rates between the study sample and the National Comorbidity Survey Replication (NCS-R), which reported population-based data that included an epilepsy sample. About 47% of the epilepsy group had an anxiety disorder, compared with 40.7% in the NCS-R. The rate of anxiety disorders was higher in the control group (45.5%) than in the control group (30.8%) in the NCS-R. Approximately 26.4% of the population in Dr. Jones’s study had a mood disorder, compared with 25.9% in the National Comorbidity Survey.
Dr. Jones and colleagues are conducting 15-year follow-up of their original population. One question they will examine is whether medical comorbidities will increase in patients with childhood-onset epilepsy as they approach age 30 years.
Two of the investigators received funding in the form of a grant from the National Institutes of Health.
SOURCE: Kesselmayer RF et al. AES 2019. Abstract 1.288.
BALTIMORE – , according to research presented at the annual meeting of the American Epilepsy Society. Compared with controls, however, young adults with childhood-onset epilepsy have higher rates of psychiatric comorbidity.
The findings suggest that “diagnoses that are identified at baseline continue to be a problem over time,” said Jana E. Jones, PhD, associate professor of neuropsychology at the University of Wisconsin in Madison. Although neurologists understand that comorbidities are common among patients with childhood-onset epilepsy, “it would be good for us to continue to learn what factors are influencing this,” she added.
Investigators sought predictors of outcomes at 10 years
Since 2004, Dr. Jones and her colleagues at the University of Wisconsin have been conducting a study of patients with childhood-onset epilepsy. After the population had completed 10 years of follow-up, the researchers analyzed the data to identify potential patterns of medical and psychiatric comorbidities. One question that they sought to answer was whether any baseline factors could predict outcomes at 10 years.
The researchers analyzed data for 53 patients with childhood-onset epilepsy and 55 controls without epilepsy. At baseline, participants were between ages 8 years and 18 years and had no intellectual disability or neurologic impairment. Within 1 year of epilepsy diagnosis, each participant underwent a psychiatric interview based on the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS). Ten years later, participants underwent the Composite International Diagnostic Interview (CIDI), a psychiatric interview for adults. Information about medical comorbidities was collected through interviews and record review at baseline and through an online survey at the 10-year follow-up.
Participants’ mean age at baseline was 12 years. Mean IQ was 105 for the epilepsy group and 109 for the control group. At 10 years, participants’ mean age was about 23 years. Among patients with epilepsy, 55% had focal epilepsy, and 42% had generalized epilepsy. About 40% of participants with epilepsy were in remission at 10 years, which Dr. Jones and colleagues defined as having achieved 5 years without taking medications and without having seizures. At 10 years after diagnosis, 51% of patients with epilepsy were not taking any seizure medication, including approximately 11% of patients with epilepsy who were not categorized as in remission. Most patients taking medication were on monotherapy.
Trends in psychiatric and medical comorbidities
At baseline, approximately 75% of children with epilepsy had a psychiatric or medical diagnosis, compared with 40% of controls. At the 10-year follow-up, 62% of children with epilepsy had a psychiatric diagnosis, compared with 35% of controls. Among controls, 4% had a medical comorbidity (i.e., asthma) alone at baseline. Asthma was the most common medical comorbidity at baseline among patients with epilepsy, and other comorbidities included sleep disorder, head injury, and scoliosis. Six percent of patients had a medical comorbidity alone at baseline. The proportion of patients with both psychiatric and medical comorbidity was 8% at baseline. Patients with epilepsy at baseline had an increased risk of psychiatric comorbidity.
At 10 years, the most common medical comorbidity among patients with epilepsy was head injury (18.9%), followed by allergies and asthma. The rate of migraine was about 13% among controls and slightly less in the epilepsy group. Dr. Jones and colleagues found no significant differences in medical comorbidities between groups at 10 years. At that point, the rate of medical comorbidity was 4% among patients and 11% among controls.
The rate of psychiatric comorbidity remained relatively stable over 10 years, said Dr. Jones. Approximately 47% of patients with epilepsy had a psychiatric diagnosis at 10 years, compared with 29% of controls. In addition, 38% of patients with epilepsy had both psychiatric and medical diagnoses, compared with 29% of controls. Epilepsy increased the risk of psychiatric comorbidity at the 10-year follow-up. Neither medications, remission status, nor seizure type predicted any comorbidity at 10 years.
Dr. Jones and colleagues compared comorbidity rates between the study sample and the National Comorbidity Survey Replication (NCS-R), which reported population-based data that included an epilepsy sample. About 47% of the epilepsy group had an anxiety disorder, compared with 40.7% in the NCS-R. The rate of anxiety disorders was higher in the control group (45.5%) than in the control group (30.8%) in the NCS-R. Approximately 26.4% of the population in Dr. Jones’s study had a mood disorder, compared with 25.9% in the National Comorbidity Survey.
Dr. Jones and colleagues are conducting 15-year follow-up of their original population. One question they will examine is whether medical comorbidities will increase in patients with childhood-onset epilepsy as they approach age 30 years.
Two of the investigators received funding in the form of a grant from the National Institutes of Health.
SOURCE: Kesselmayer RF et al. AES 2019. Abstract 1.288.
REPORTING FROM AES 2019
Patient-reported outcomes highlight long-term impacts of prostatectomy
For men with prostate cancer, prostatectomy is more likely to cause long-term, clinically meaningful incontinence than are other treatment modalities, based on patient-reported outcomes from more than 2,000 men.
Patients with high-risk disease who underwent prostatectomy also reported worse sexual function at every time point over 5 years, reported Karen E. Hoffman, MD, of the University of Texas MD Anderson Cancer Center in Houston, and colleagues. Other functional differences between treatments faded over time, they said.
“These estimates of the long-term bowel, bladder, and sexual function after localized prostate cancer treatment may clarify expectations and enable men to make informed choices about care,” the investigators wrote. Their report is in JAMA.
The prospective, population-based cohort study involved 1,386 men with favorable-risk prostate cancer and 619 men with unfavorable-risk disease. For men with favorable-risk disease, treatments included low-dose brachytherapy, external beam radiation therapy (EBRT), nerve-sparing prostatectomy, and active surveillance. Men with unfavorable-risk disease were treated with either prostatectomy or EBRT plus androgen deprivation therapy (ADT).
At multiple time points for 5 years, patients completed the 26-item Expanded Prostate Index Composite questionnaire (EPIC; range, 0-100). Clinically significant functional differences between treatment modalities were defined for bowel and hormonal function (4-6), urinary irritative symptoms (5-7), urinary incontinence (6-9), and sexual function (10-12). All 2,005 men completed at least one questionnaire, with about 3 out of 4 men (77%) still responding after 5 years.
Across all patients, prostatectomy was associated with a relatively higher risk of long-term, clinically meaningful urinary incontinence.
For men with favorable-risk disease, the adjusted mean difference for incontinence between nerve-sparing prostatectomy and active surveillance was –10.9 (P less than .001). Patients in this group who elected prostatectomy over active surveillance had a higher rate of urinary leakage (10% vs. 7%; P = .04); however, there was no significant difference in rates of moderate or big problems with urinary function, which suggests that incontinence issues were typically mild.
For men with unfavorable risk disease, prostatectomy carried a higher risk of more severe incontinence. The adjusted mean difference between prostatectomy and EBRT plus ADT was –23.2 (P less than .001), and patients treated with prostatectomy were more likely to report moderate or big problems with urinary function (17% vs. 13%; P = .005). In addition to these urinary issues, men with unfavorable-risk disease who underwent prostatectomy were more likely to report worse sexual function at 5 years, compared with those who were treated with EBRT plus ADT (adjusted mean difference, –12.5).
While other clinically meaningful differences were found between treatments for other functional categories, these differences lost statistical significance by the 5-year time point.
The Agency for Healthcare Research and Quality, the Patient-Centered Outcomes Research Institute, and the National Cancer Institute funded the study. The investigators reported additional relationships with Dendreon, Bayer, AstraZeneca, and others.
SOURCE: Hoffman et al. JAMA. 2020 Jan 14. doi: 10.1001/jama.2019.20675.
For men with prostate cancer, prostatectomy is more likely to cause long-term, clinically meaningful incontinence than are other treatment modalities, based on patient-reported outcomes from more than 2,000 men.
Patients with high-risk disease who underwent prostatectomy also reported worse sexual function at every time point over 5 years, reported Karen E. Hoffman, MD, of the University of Texas MD Anderson Cancer Center in Houston, and colleagues. Other functional differences between treatments faded over time, they said.
“These estimates of the long-term bowel, bladder, and sexual function after localized prostate cancer treatment may clarify expectations and enable men to make informed choices about care,” the investigators wrote. Their report is in JAMA.
The prospective, population-based cohort study involved 1,386 men with favorable-risk prostate cancer and 619 men with unfavorable-risk disease. For men with favorable-risk disease, treatments included low-dose brachytherapy, external beam radiation therapy (EBRT), nerve-sparing prostatectomy, and active surveillance. Men with unfavorable-risk disease were treated with either prostatectomy or EBRT plus androgen deprivation therapy (ADT).
At multiple time points for 5 years, patients completed the 26-item Expanded Prostate Index Composite questionnaire (EPIC; range, 0-100). Clinically significant functional differences between treatment modalities were defined for bowel and hormonal function (4-6), urinary irritative symptoms (5-7), urinary incontinence (6-9), and sexual function (10-12). All 2,005 men completed at least one questionnaire, with about 3 out of 4 men (77%) still responding after 5 years.
Across all patients, prostatectomy was associated with a relatively higher risk of long-term, clinically meaningful urinary incontinence.
For men with favorable-risk disease, the adjusted mean difference for incontinence between nerve-sparing prostatectomy and active surveillance was –10.9 (P less than .001). Patients in this group who elected prostatectomy over active surveillance had a higher rate of urinary leakage (10% vs. 7%; P = .04); however, there was no significant difference in rates of moderate or big problems with urinary function, which suggests that incontinence issues were typically mild.
For men with unfavorable risk disease, prostatectomy carried a higher risk of more severe incontinence. The adjusted mean difference between prostatectomy and EBRT plus ADT was –23.2 (P less than .001), and patients treated with prostatectomy were more likely to report moderate or big problems with urinary function (17% vs. 13%; P = .005). In addition to these urinary issues, men with unfavorable-risk disease who underwent prostatectomy were more likely to report worse sexual function at 5 years, compared with those who were treated with EBRT plus ADT (adjusted mean difference, –12.5).
While other clinically meaningful differences were found between treatments for other functional categories, these differences lost statistical significance by the 5-year time point.
The Agency for Healthcare Research and Quality, the Patient-Centered Outcomes Research Institute, and the National Cancer Institute funded the study. The investigators reported additional relationships with Dendreon, Bayer, AstraZeneca, and others.
SOURCE: Hoffman et al. JAMA. 2020 Jan 14. doi: 10.1001/jama.2019.20675.
For men with prostate cancer, prostatectomy is more likely to cause long-term, clinically meaningful incontinence than are other treatment modalities, based on patient-reported outcomes from more than 2,000 men.
Patients with high-risk disease who underwent prostatectomy also reported worse sexual function at every time point over 5 years, reported Karen E. Hoffman, MD, of the University of Texas MD Anderson Cancer Center in Houston, and colleagues. Other functional differences between treatments faded over time, they said.
“These estimates of the long-term bowel, bladder, and sexual function after localized prostate cancer treatment may clarify expectations and enable men to make informed choices about care,” the investigators wrote. Their report is in JAMA.
The prospective, population-based cohort study involved 1,386 men with favorable-risk prostate cancer and 619 men with unfavorable-risk disease. For men with favorable-risk disease, treatments included low-dose brachytherapy, external beam radiation therapy (EBRT), nerve-sparing prostatectomy, and active surveillance. Men with unfavorable-risk disease were treated with either prostatectomy or EBRT plus androgen deprivation therapy (ADT).
At multiple time points for 5 years, patients completed the 26-item Expanded Prostate Index Composite questionnaire (EPIC; range, 0-100). Clinically significant functional differences between treatment modalities were defined for bowel and hormonal function (4-6), urinary irritative symptoms (5-7), urinary incontinence (6-9), and sexual function (10-12). All 2,005 men completed at least one questionnaire, with about 3 out of 4 men (77%) still responding after 5 years.
Across all patients, prostatectomy was associated with a relatively higher risk of long-term, clinically meaningful urinary incontinence.
For men with favorable-risk disease, the adjusted mean difference for incontinence between nerve-sparing prostatectomy and active surveillance was –10.9 (P less than .001). Patients in this group who elected prostatectomy over active surveillance had a higher rate of urinary leakage (10% vs. 7%; P = .04); however, there was no significant difference in rates of moderate or big problems with urinary function, which suggests that incontinence issues were typically mild.
For men with unfavorable risk disease, prostatectomy carried a higher risk of more severe incontinence. The adjusted mean difference between prostatectomy and EBRT plus ADT was –23.2 (P less than .001), and patients treated with prostatectomy were more likely to report moderate or big problems with urinary function (17% vs. 13%; P = .005). In addition to these urinary issues, men with unfavorable-risk disease who underwent prostatectomy were more likely to report worse sexual function at 5 years, compared with those who were treated with EBRT plus ADT (adjusted mean difference, –12.5).
While other clinically meaningful differences were found between treatments for other functional categories, these differences lost statistical significance by the 5-year time point.
The Agency for Healthcare Research and Quality, the Patient-Centered Outcomes Research Institute, and the National Cancer Institute funded the study. The investigators reported additional relationships with Dendreon, Bayer, AstraZeneca, and others.
SOURCE: Hoffman et al. JAMA. 2020 Jan 14. doi: 10.1001/jama.2019.20675.
FROM JAMA
Key clinical point: For men with prostate cancer, prostatectomy is significantly more likely to cause long-term incontinence than are other treatment modalities.
Major finding: For each time point through 5 years, men with unfavorable-risk prostate cancer who underwent prostatectomy had significantly worse incontinence scores than did those who underwent external beam radiation therapy (EBRT) and androgen deprivation therapy (ADT) (adjusted mean difference, –23.2).
Study details: A prospective, population-based cohort study involving 2,005 men prostate cancer.
Disclosures: The Agency for Healthcare Research and Quality, the Patient-Centered Outcomes Research Institute, and the National Cancer Institute funded the study. The investigators reported additional relationships with Dendreon, Bayer, AstraZeneca, and others.
Source: Hoffman et al. JAMA. 2020 Jan 14. doi: 10.1001/jama.2019.20675.
NCCN guidelines highlight ‘complicated’ treatment for pediatric lymphomas
The National Comprehensive Cancer Network (NCCN) has released its first set of guidelines for managing pediatric aggressive mature B-cell lymphomas.
The guidelines highlight the complexities of treating pediatric Burkitt lymphoma (BL) and diffuse large B-cell lymphoma (DLBCL), as recommendations include a range of multiagent regimens for different patient groups at various time points.
“The treatment of this disease is relatively complicated,” said Kimberly J. Davies, MD, a pediatric hematologist/oncologist at Dana-Farber Cancer Institute in Boston and chair of the guidelines panel. “The chemotherapy regimens have a lot of drugs, a lot of nuances to how they’re supposed to be given. These guidelines delineate that treatment and help the provider … make sure they are delivering the treatment a patient needs.”
The guidelines recommend different regimens according to a patient’s risk group, but the same treatment approach should be used for patients with BL and those with DLBCL.

“The biggest difference between pediatric and adult patients is that pediatric patients are more uniformly treated, regardless of what type of aggressive B-cell lymphoma they have,” said Matthew Barth, MD, a pediatric hematologist/oncologist at Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., and vice chair of the NCCN guidelines panel.
“Adults with diffuse large B-cell lymphoma and Burkitt lymphoma are generally treated with different chemotherapy regimens, but, in pediatrics, we use the same treatment regimens for both diffuse large B-cell lymphoma and Burkitt lymphoma,” he added.
As an example, the new guidelines recommend that pediatric patients with low-risk BL/DLBCL receive the POG9219 regimen (N Engl J Med. 1997 Oct 30;337[18]:1259-66) or FAB/LMB96 regimen A (Br J Haematol. 2008 Jun;141[6]:840-7) as induction, or they should be enrolled in a clinical trial.
On the other hand, induction for high-risk pediatric BL/DLBCL patients should consist of rituximab and a chemotherapy regimen used in the COG ANHL1131 trial. The recommendation to incorporate rituximab in high-risk pediatric patients is based on results from that trial (J Clin Oncol. 2016 May 20. doi: 10.1200/JCO.2016.34.15_suppl.10507).
“Until recent clinical trial data was available, we weren’t really sure how to incorporate rituximab into the treatment of pediatric patients with mature B-cell lymphomas,” Dr. Barth said. “We now have evidence that rituximab is clearly beneficial for patients who are in higher-risk groups.”
Dr. Barth and Dr. Davies both noted that pediatric BL and DLBCL have high cure rates. Long-term survival rates range from about 80% to more than 90%, according to the American Cancer Society. However, the patients who do relapse or progress can be difficult to treat.
“We have quite good cure rates at this point in time, which is a great success, but that means that a very small population of patients don’t respond to initial therapy, and … it’s hard to know what the best treatment for those patients is,” Dr. Davies said.
She noted that studies are underway to determine if immunotherapies, including chimeric antigen receptor T-cell therapy, might improve outcomes in patients with relapsed or refractory disease.
For now, the NCCN guidelines recommend clinical trial enrollment for relapsed/refractory patients. Alternatively, these patients can receive additional chemotherapy, and responders can proceed to transplant. Patients who don’t achieve at least a partial response may go on to a clinical trial or receive best supportive care.
Dr. Davies and Dr. Barth reported having no conflicts of interest.
The National Comprehensive Cancer Network (NCCN) has released its first set of guidelines for managing pediatric aggressive mature B-cell lymphomas.
The guidelines highlight the complexities of treating pediatric Burkitt lymphoma (BL) and diffuse large B-cell lymphoma (DLBCL), as recommendations include a range of multiagent regimens for different patient groups at various time points.
“The treatment of this disease is relatively complicated,” said Kimberly J. Davies, MD, a pediatric hematologist/oncologist at Dana-Farber Cancer Institute in Boston and chair of the guidelines panel. “The chemotherapy regimens have a lot of drugs, a lot of nuances to how they’re supposed to be given. These guidelines delineate that treatment and help the provider … make sure they are delivering the treatment a patient needs.”
The guidelines recommend different regimens according to a patient’s risk group, but the same treatment approach should be used for patients with BL and those with DLBCL.
“The biggest difference between pediatric and adult patients is that pediatric patients are more uniformly treated, regardless of what type of aggressive B-cell lymphoma they have,” said Matthew Barth, MD, a pediatric hematologist/oncologist at Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., and vice chair of the NCCN guidelines panel.
“Adults with diffuse large B-cell lymphoma and Burkitt lymphoma are generally treated with different chemotherapy regimens, but, in pediatrics, we use the same treatment regimens for both diffuse large B-cell lymphoma and Burkitt lymphoma,” he added.
As an example, the new guidelines recommend that pediatric patients with low-risk BL/DLBCL receive the POG9219 regimen (N Engl J Med. 1997 Oct 30;337[18]:1259-66) or FAB/LMB96 regimen A (Br J Haematol. 2008 Jun;141[6]:840-7) as induction, or they should be enrolled in a clinical trial.
On the other hand, induction for high-risk pediatric BL/DLBCL patients should consist of rituximab and a chemotherapy regimen used in the COG ANHL1131 trial. The recommendation to incorporate rituximab in high-risk pediatric patients is based on results from that trial (J Clin Oncol. 2016 May 20. doi: 10.1200/JCO.2016.34.15_suppl.10507).
“Until recent clinical trial data was available, we weren’t really sure how to incorporate rituximab into the treatment of pediatric patients with mature B-cell lymphomas,” Dr. Barth said. “We now have evidence that rituximab is clearly beneficial for patients who are in higher-risk groups.”
Dr. Barth and Dr. Davies both noted that pediatric BL and DLBCL have high cure rates. Long-term survival rates range from about 80% to more than 90%, according to the American Cancer Society. However, the patients who do relapse or progress can be difficult to treat.
“We have quite good cure rates at this point in time, which is a great success, but that means that a very small population of patients don’t respond to initial therapy, and … it’s hard to know what the best treatment for those patients is,” Dr. Davies said.
She noted that studies are underway to determine if immunotherapies, including chimeric antigen receptor T-cell therapy, might improve outcomes in patients with relapsed or refractory disease.
For now, the NCCN guidelines recommend clinical trial enrollment for relapsed/refractory patients. Alternatively, these patients can receive additional chemotherapy, and responders can proceed to transplant. Patients who don’t achieve at least a partial response may go on to a clinical trial or receive best supportive care.
Dr. Davies and Dr. Barth reported having no conflicts of interest.
The National Comprehensive Cancer Network (NCCN) has released its first set of guidelines for managing pediatric aggressive mature B-cell lymphomas.
The guidelines highlight the complexities of treating pediatric Burkitt lymphoma (BL) and diffuse large B-cell lymphoma (DLBCL), as recommendations include a range of multiagent regimens for different patient groups at various time points.
“The treatment of this disease is relatively complicated,” said Kimberly J. Davies, MD, a pediatric hematologist/oncologist at Dana-Farber Cancer Institute in Boston and chair of the guidelines panel. “The chemotherapy regimens have a lot of drugs, a lot of nuances to how they’re supposed to be given. These guidelines delineate that treatment and help the provider … make sure they are delivering the treatment a patient needs.”
The guidelines recommend different regimens according to a patient’s risk group, but the same treatment approach should be used for patients with BL and those with DLBCL.
“The biggest difference between pediatric and adult patients is that pediatric patients are more uniformly treated, regardless of what type of aggressive B-cell lymphoma they have,” said Matthew Barth, MD, a pediatric hematologist/oncologist at Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., and vice chair of the NCCN guidelines panel.
“Adults with diffuse large B-cell lymphoma and Burkitt lymphoma are generally treated with different chemotherapy regimens, but, in pediatrics, we use the same treatment regimens for both diffuse large B-cell lymphoma and Burkitt lymphoma,” he added.
As an example, the new guidelines recommend that pediatric patients with low-risk BL/DLBCL receive the POG9219 regimen (N Engl J Med. 1997 Oct 30;337[18]:1259-66) or FAB/LMB96 regimen A (Br J Haematol. 2008 Jun;141[6]:840-7) as induction, or they should be enrolled in a clinical trial.
On the other hand, induction for high-risk pediatric BL/DLBCL patients should consist of rituximab and a chemotherapy regimen used in the COG ANHL1131 trial. The recommendation to incorporate rituximab in high-risk pediatric patients is based on results from that trial (J Clin Oncol. 2016 May 20. doi: 10.1200/JCO.2016.34.15_suppl.10507).
“Until recent clinical trial data was available, we weren’t really sure how to incorporate rituximab into the treatment of pediatric patients with mature B-cell lymphomas,” Dr. Barth said. “We now have evidence that rituximab is clearly beneficial for patients who are in higher-risk groups.”
Dr. Barth and Dr. Davies both noted that pediatric BL and DLBCL have high cure rates. Long-term survival rates range from about 80% to more than 90%, according to the American Cancer Society. However, the patients who do relapse or progress can be difficult to treat.
“We have quite good cure rates at this point in time, which is a great success, but that means that a very small population of patients don’t respond to initial therapy, and … it’s hard to know what the best treatment for those patients is,” Dr. Davies said.
She noted that studies are underway to determine if immunotherapies, including chimeric antigen receptor T-cell therapy, might improve outcomes in patients with relapsed or refractory disease.
For now, the NCCN guidelines recommend clinical trial enrollment for relapsed/refractory patients. Alternatively, these patients can receive additional chemotherapy, and responders can proceed to transplant. Patients who don’t achieve at least a partial response may go on to a clinical trial or receive best supportive care.
Dr. Davies and Dr. Barth reported having no conflicts of interest.
Half of SLE patients have incident neuropsychiatric events
Neuropsychiatric events occurred in just over half of all patients recently diagnosed with systemic lupus erythematosus and followed for an average of nearly 8 years in an international study of more than 1,800 patients.
Up to 30% of these neuropsychiatric (NP) events in up to 20% of the followed cohort were directly attributable to systemic lupus erythematosus (SLE) in a representative patient population, wrote John G. Hanly, MD, and associates in Annals of the Rheumatic Diseases. Their findings were consistent with prior reports, they added.
Another notable finding from follow-up of these 1,827 SLE patients was that among those without a history of SLE-related NP events at baseline, 74% remained free of NP events during the subsequent 10 years, wrote Dr. Hanly, professor of medicine and director of the lupus clinic at Dalhousie University, Halifax, N.S., and coauthors. Among patients free from SLE-associated NP events after 2 years, 84% remained event free during their remaining follow-up. SLE patients with a history of an NP event that subsequently resolved had a 72% rate of freedom from another NP event during 10 years of follow-up.
These findings came from patients recently diagnosed with SLE (within the preceding 15 months) and enrolled at any of 31 participating academic medical centers in North America, Europe, and Asia. The investigators considered preenrollment NP events to include those starting from 6 months prior to diagnosis of SLE until the time patients entered the study. They used case definitions for 19 SLE-associated NP events published by the American College of Rheumatology (Arthritis Rheum. 1999 Apr;42[4]:599-608). All enrolled patients underwent annual assessment for NP events, with follow-up continuing as long as 18 years.
The researchers identified NP events in 955 of the 1,827 enrolled patients, a 52% incidence, including 1,910 unique NP events that included episodes from each of the 19 NP event types, with 92% involving the central nervous system and 8% involving the peripheral nervous system. The percentage of NP events attributable to SLE ranged from 17% to 31%, and they occurred in 14%-21% of the studied patients, with the range reflecting various attribution models used in the analyses. Some patients remained in the same NP state, while others progressed through more than one state.
The study did not receive commercial funding. Dr. Hanly had no disclosures.
SOURCE: Hanly JG et al. Ann Rheum Dis. 2020 Jan 8. doi: 10.1136/annrheumdis-2019-216150.
Neuropsychiatric events occurred in just over half of all patients recently diagnosed with systemic lupus erythematosus and followed for an average of nearly 8 years in an international study of more than 1,800 patients.
Up to 30% of these neuropsychiatric (NP) events in up to 20% of the followed cohort were directly attributable to systemic lupus erythematosus (SLE) in a representative patient population, wrote John G. Hanly, MD, and associates in Annals of the Rheumatic Diseases. Their findings were consistent with prior reports, they added.
Another notable finding from follow-up of these 1,827 SLE patients was that among those without a history of SLE-related NP events at baseline, 74% remained free of NP events during the subsequent 10 years, wrote Dr. Hanly, professor of medicine and director of the lupus clinic at Dalhousie University, Halifax, N.S., and coauthors. Among patients free from SLE-associated NP events after 2 years, 84% remained event free during their remaining follow-up. SLE patients with a history of an NP event that subsequently resolved had a 72% rate of freedom from another NP event during 10 years of follow-up.
These findings came from patients recently diagnosed with SLE (within the preceding 15 months) and enrolled at any of 31 participating academic medical centers in North America, Europe, and Asia. The investigators considered preenrollment NP events to include those starting from 6 months prior to diagnosis of SLE until the time patients entered the study. They used case definitions for 19 SLE-associated NP events published by the American College of Rheumatology (Arthritis Rheum. 1999 Apr;42[4]:599-608). All enrolled patients underwent annual assessment for NP events, with follow-up continuing as long as 18 years.
The researchers identified NP events in 955 of the 1,827 enrolled patients, a 52% incidence, including 1,910 unique NP events that included episodes from each of the 19 NP event types, with 92% involving the central nervous system and 8% involving the peripheral nervous system. The percentage of NP events attributable to SLE ranged from 17% to 31%, and they occurred in 14%-21% of the studied patients, with the range reflecting various attribution models used in the analyses. Some patients remained in the same NP state, while others progressed through more than one state.
The study did not receive commercial funding. Dr. Hanly had no disclosures.
SOURCE: Hanly JG et al. Ann Rheum Dis. 2020 Jan 8. doi: 10.1136/annrheumdis-2019-216150.
Neuropsychiatric events occurred in just over half of all patients recently diagnosed with systemic lupus erythematosus and followed for an average of nearly 8 years in an international study of more than 1,800 patients.
Up to 30% of these neuropsychiatric (NP) events in up to 20% of the followed cohort were directly attributable to systemic lupus erythematosus (SLE) in a representative patient population, wrote John G. Hanly, MD, and associates in Annals of the Rheumatic Diseases. Their findings were consistent with prior reports, they added.
Another notable finding from follow-up of these 1,827 SLE patients was that among those without a history of SLE-related NP events at baseline, 74% remained free of NP events during the subsequent 10 years, wrote Dr. Hanly, professor of medicine and director of the lupus clinic at Dalhousie University, Halifax, N.S., and coauthors. Among patients free from SLE-associated NP events after 2 years, 84% remained event free during their remaining follow-up. SLE patients with a history of an NP event that subsequently resolved had a 72% rate of freedom from another NP event during 10 years of follow-up.
These findings came from patients recently diagnosed with SLE (within the preceding 15 months) and enrolled at any of 31 participating academic medical centers in North America, Europe, and Asia. The investigators considered preenrollment NP events to include those starting from 6 months prior to diagnosis of SLE until the time patients entered the study. They used case definitions for 19 SLE-associated NP events published by the American College of Rheumatology (Arthritis Rheum. 1999 Apr;42[4]:599-608). All enrolled patients underwent annual assessment for NP events, with follow-up continuing as long as 18 years.
The researchers identified NP events in 955 of the 1,827 enrolled patients, a 52% incidence, including 1,910 unique NP events that included episodes from each of the 19 NP event types, with 92% involving the central nervous system and 8% involving the peripheral nervous system. The percentage of NP events attributable to SLE ranged from 17% to 31%, and they occurred in 14%-21% of the studied patients, with the range reflecting various attribution models used in the analyses. Some patients remained in the same NP state, while others progressed through more than one state.
The study did not receive commercial funding. Dr. Hanly had no disclosures.
SOURCE: Hanly JG et al. Ann Rheum Dis. 2020 Jan 8. doi: 10.1136/annrheumdis-2019-216150.
FROM ANNALS OF THE RHEUMATIC DISEASES
Gout rates reduced with SGLT2 inhibitors
The incidence of gout was approximately 40% lower in diabetes patients who were prescribed sodium-glucose cotransporter 2 inhibitors (SGLT2) than it was in those who were prescribed glucagonlike peptide–1 receptor (GLP-1) agonists in a population-based new-user cohort study.
Hyperuricemia is a known cause of gout and common in type 2 diabetes patients. SGLT2 inhibitors may reduce the risk of gout by preventing the reabsorption of glucose and lowering serum uric acid levels; however, the impact on gout risk remains uncertain, wrote Michael Fralick, MD, of Brigham and Women’s Hospital, Boston, and colleagues.
In a study published in the Annals of Internal Medicine, the researchers compared SGLT2 inhibitors and GLP-1 agonists in patients with type 2 diabetes to assess protection against gout.
The study population included adults with type 2 diabetes mellitus who had a new prescription for an SGTL2 inhibitor or GLP-1 agonist. The average age of the patients was 54 years; approximately half were women. Baseline characteristics were similar between the groups.
Overall, the researchers found a relative risk reduction of approximately 40% and an absolute risk reduction of approximately three fewer cases per 1,000 person-years in patients who received SGLT2 inhibitors, compared with those who received GLP-1 agonists. The incidence rate for gout in the SGLT2 and GLP-1 groups were 4.9 per 1,000 person-years and 7.8 per 1,000 person-years, respectively.
The study findings were limited by the investigators’ inability to measure potential confounding variables such as body mass index, alcohol use, and high purine diet; incomplete lab data on creatinine and hemoglobin A; and a low baseline risk for gout in the study population, the researchers noted. However, the results persisted across sensitivity analysis and, if replicated, suggest that “SGLT2 inhibitors might be an effective class of medication for the prevention of gout for patients with diabetes or metabolic disorders,” they wrote.
The study was supported in part by Brigham and Women’s Hospital; lead author Dr. Fralick disclosed funding from the Eliot Phillipson Clinician-Scientist Training Program at the University of Toronto and the Canadian Institutes of Health Research.
SOURCE: Fralick M et al. Ann Intern Med. 2020 Jan 14. doi: 10.7326/M19-2610.
The incidence of gout was approximately 40% lower in diabetes patients who were prescribed sodium-glucose cotransporter 2 inhibitors (SGLT2) than it was in those who were prescribed glucagonlike peptide–1 receptor (GLP-1) agonists in a population-based new-user cohort study.
Hyperuricemia is a known cause of gout and common in type 2 diabetes patients. SGLT2 inhibitors may reduce the risk of gout by preventing the reabsorption of glucose and lowering serum uric acid levels; however, the impact on gout risk remains uncertain, wrote Michael Fralick, MD, of Brigham and Women’s Hospital, Boston, and colleagues.
In a study published in the Annals of Internal Medicine, the researchers compared SGLT2 inhibitors and GLP-1 agonists in patients with type 2 diabetes to assess protection against gout.
The study population included adults with type 2 diabetes mellitus who had a new prescription for an SGTL2 inhibitor or GLP-1 agonist. The average age of the patients was 54 years; approximately half were women. Baseline characteristics were similar between the groups.
Overall, the researchers found a relative risk reduction of approximately 40% and an absolute risk reduction of approximately three fewer cases per 1,000 person-years in patients who received SGLT2 inhibitors, compared with those who received GLP-1 agonists. The incidence rate for gout in the SGLT2 and GLP-1 groups were 4.9 per 1,000 person-years and 7.8 per 1,000 person-years, respectively.
The study findings were limited by the investigators’ inability to measure potential confounding variables such as body mass index, alcohol use, and high purine diet; incomplete lab data on creatinine and hemoglobin A; and a low baseline risk for gout in the study population, the researchers noted. However, the results persisted across sensitivity analysis and, if replicated, suggest that “SGLT2 inhibitors might be an effective class of medication for the prevention of gout for patients with diabetes or metabolic disorders,” they wrote.
The study was supported in part by Brigham and Women’s Hospital; lead author Dr. Fralick disclosed funding from the Eliot Phillipson Clinician-Scientist Training Program at the University of Toronto and the Canadian Institutes of Health Research.
SOURCE: Fralick M et al. Ann Intern Med. 2020 Jan 14. doi: 10.7326/M19-2610.
The incidence of gout was approximately 40% lower in diabetes patients who were prescribed sodium-glucose cotransporter 2 inhibitors (SGLT2) than it was in those who were prescribed glucagonlike peptide–1 receptor (GLP-1) agonists in a population-based new-user cohort study.
Hyperuricemia is a known cause of gout and common in type 2 diabetes patients. SGLT2 inhibitors may reduce the risk of gout by preventing the reabsorption of glucose and lowering serum uric acid levels; however, the impact on gout risk remains uncertain, wrote Michael Fralick, MD, of Brigham and Women’s Hospital, Boston, and colleagues.
In a study published in the Annals of Internal Medicine, the researchers compared SGLT2 inhibitors and GLP-1 agonists in patients with type 2 diabetes to assess protection against gout.
The study population included adults with type 2 diabetes mellitus who had a new prescription for an SGTL2 inhibitor or GLP-1 agonist. The average age of the patients was 54 years; approximately half were women. Baseline characteristics were similar between the groups.
Overall, the researchers found a relative risk reduction of approximately 40% and an absolute risk reduction of approximately three fewer cases per 1,000 person-years in patients who received SGLT2 inhibitors, compared with those who received GLP-1 agonists. The incidence rate for gout in the SGLT2 and GLP-1 groups were 4.9 per 1,000 person-years and 7.8 per 1,000 person-years, respectively.
The study findings were limited by the investigators’ inability to measure potential confounding variables such as body mass index, alcohol use, and high purine diet; incomplete lab data on creatinine and hemoglobin A; and a low baseline risk for gout in the study population, the researchers noted. However, the results persisted across sensitivity analysis and, if replicated, suggest that “SGLT2 inhibitors might be an effective class of medication for the prevention of gout for patients with diabetes or metabolic disorders,” they wrote.
The study was supported in part by Brigham and Women’s Hospital; lead author Dr. Fralick disclosed funding from the Eliot Phillipson Clinician-Scientist Training Program at the University of Toronto and the Canadian Institutes of Health Research.
SOURCE: Fralick M et al. Ann Intern Med. 2020 Jan 14. doi: 10.7326/M19-2610.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: Sodium-glucose cotransporter 2 (SGLT2) inhibitor use was associated with lower rates of gout in type 2 diabetes patients compared with glucagonlike peptide–1 (GLP-1) agonist use.
Major finding: The incidence of gout was 4.9 per 1,000 person-years in patients on SGLT2 inhibitors and 7.8 per 1,000 person-years in patients on GLP1 agonists.
Study details: The data come from a population-based cohort study of 295,907 adults with type 2 diabetes.
Disclosures: The study was supported in part by Brigham and Women’s Hospital; lead author Dr. Fralick disclosed funding from the Eliot Phillipson Clinician-Scientist Training Program at the University of Toronto and the Canadian Institutes of Health Research.
Source: Fralick M et al. Ann Intern Med. 2020 Jan 14. doi: 10.7326/M19-2610.
Draft ACR Takayasu’s guidelines: Surgery is the last resort
ATLANTA – One of the goals in soon-to-be-published Takayasu’s arteritis guidelines from the American College of Rheumatology is to wean patients off high-dose steroids once they are in remission.

This recommendation is in opposition to another option – namely, switching these patients to low-dose glucocorticoids. The idea is to prevent long-term side effects, particularly in children. The guidelines also recommend against escalating immunotherapy for asymptomatic increases in inflammatory markers and generally recommend against surgery – stenting in most cases – unless there is threat to life, limb, or organ and also if limb pain is so severe it cramps quality of life and dose escalation doesn’t get the job done. If surgery is planned, patients should be on perioperative steroids if there’s active disease.
It’s draft guidance for now, but it’s probably what the final document will say when it’s published in 2020, according to a presentation at the annual meeting of the American College of Rheumatology by one of the authors, Anisha Dua, MD, an associate professor of rheumatology at Northwestern University, Chicago. She gave a sneak preview at the meeting.
In general, severe, active Takayasu’s calls for high-dose oral steroids in conjunction with a nonsteroid immunosuppressive, such as methotrexate, azathioprine, leflunomide, or mycophenolate mofetil. There’s evidence that dual therapy gives a more durable remission and also reduces the need for steroids.
When that approach doesn’t do the trick, the next step is a tumor necrosis factor (TNF) inhibitor. There’s evidence for infliximab, adalimumab, certolizumab, and etanercept. Dr. Dua noted, “We still can consider” tocilizumab, but it failed to meet its primary endpoint in a randomized trial, and evidence for other biologics is sparse or nonexistent. “TNF inhibitors are the first line” for refractory disease, Dr. Dua said.
The steroid taper comes after 6-12 months of remission. Given their toxicity, “our goal for steroids is zero,” especially in pediatric populations. Even in remission, patients should have a clinical assessment, including inflammatory markers, every 3-12 months.
A rise in C-reactive protein or erythrocyte sedimentation rate, with no new symptoms, might be a reason for more frequent monitoring, but it’s not a reason to escalate immunosuppression. That should be kept in reserve for new vascular lesions, rapid progression on an old one, or worsening of organ or limb ischemia.
“We recommend [escalation] over surgical intervention” because patients often develop collateral circulation that solves the problem; it also gives the disease time to quiet down should the patient eventually go into surgery. Immediate surgery is reserved for organ or life-threatening disease, Dr. Dua said.
“Takayasu’s is different from other vasculitides in the sense that patients often present with certain nonspecific constitutional symptoms,” and there’s not a lot of pathology or histology to work with, “so we do tend to rely on imaging a lot,” Dr. Dua said.
Angiography has fallen out of favor because it’s invasive and exposes patients to radiation, among other problems. The field has moved to noninvasive imaging such as color Doppler ultrasound, CT angiography, magnetic resonance angiography, and PET CT.
“We do recommend regularly scheduled, noninvasive imaging every 6-12 months, in addition to the routine clinical assessment,” except in children with inactive disease; the risk of sedation outweighs the imaging benefit, Dr. Dua said.
In patients with single-vessel cranial or cervical stenosis, without symptoms, “we recommend medical over surgical management because of the risk of surgery. Surgery can be considered for multivessel involvement,” she said.
She and her colleagues also recommend medical management for renal artery stenosis, including antihypertensives and immunotherapy escalation for active disease. Surgery is considered for refractory hypertension or worsening kidney function
Dr. Dua is a primary investigator and adviser for Chemocentryx and an adviser for Novartis and AbbVie.
ATLANTA – One of the goals in soon-to-be-published Takayasu’s arteritis guidelines from the American College of Rheumatology is to wean patients off high-dose steroids once they are in remission.
This recommendation is in opposition to another option – namely, switching these patients to low-dose glucocorticoids. The idea is to prevent long-term side effects, particularly in children. The guidelines also recommend against escalating immunotherapy for asymptomatic increases in inflammatory markers and generally recommend against surgery – stenting in most cases – unless there is threat to life, limb, or organ and also if limb pain is so severe it cramps quality of life and dose escalation doesn’t get the job done. If surgery is planned, patients should be on perioperative steroids if there’s active disease.
It’s draft guidance for now, but it’s probably what the final document will say when it’s published in 2020, according to a presentation at the annual meeting of the American College of Rheumatology by one of the authors, Anisha Dua, MD, an associate professor of rheumatology at Northwestern University, Chicago. She gave a sneak preview at the meeting.
In general, severe, active Takayasu’s calls for high-dose oral steroids in conjunction with a nonsteroid immunosuppressive, such as methotrexate, azathioprine, leflunomide, or mycophenolate mofetil. There’s evidence that dual therapy gives a more durable remission and also reduces the need for steroids.
When that approach doesn’t do the trick, the next step is a tumor necrosis factor (TNF) inhibitor. There’s evidence for infliximab, adalimumab, certolizumab, and etanercept. Dr. Dua noted, “We still can consider” tocilizumab, but it failed to meet its primary endpoint in a randomized trial, and evidence for other biologics is sparse or nonexistent. “TNF inhibitors are the first line” for refractory disease, Dr. Dua said.
The steroid taper comes after 6-12 months of remission. Given their toxicity, “our goal for steroids is zero,” especially in pediatric populations. Even in remission, patients should have a clinical assessment, including inflammatory markers, every 3-12 months.
A rise in C-reactive protein or erythrocyte sedimentation rate, with no new symptoms, might be a reason for more frequent monitoring, but it’s not a reason to escalate immunosuppression. That should be kept in reserve for new vascular lesions, rapid progression on an old one, or worsening of organ or limb ischemia.
“We recommend [escalation] over surgical intervention” because patients often develop collateral circulation that solves the problem; it also gives the disease time to quiet down should the patient eventually go into surgery. Immediate surgery is reserved for organ or life-threatening disease, Dr. Dua said.
“Takayasu’s is different from other vasculitides in the sense that patients often present with certain nonspecific constitutional symptoms,” and there’s not a lot of pathology or histology to work with, “so we do tend to rely on imaging a lot,” Dr. Dua said.
Angiography has fallen out of favor because it’s invasive and exposes patients to radiation, among other problems. The field has moved to noninvasive imaging such as color Doppler ultrasound, CT angiography, magnetic resonance angiography, and PET CT.
“We do recommend regularly scheduled, noninvasive imaging every 6-12 months, in addition to the routine clinical assessment,” except in children with inactive disease; the risk of sedation outweighs the imaging benefit, Dr. Dua said.
In patients with single-vessel cranial or cervical stenosis, without symptoms, “we recommend medical over surgical management because of the risk of surgery. Surgery can be considered for multivessel involvement,” she said.
She and her colleagues also recommend medical management for renal artery stenosis, including antihypertensives and immunotherapy escalation for active disease. Surgery is considered for refractory hypertension or worsening kidney function
Dr. Dua is a primary investigator and adviser for Chemocentryx and an adviser for Novartis and AbbVie.
ATLANTA – One of the goals in soon-to-be-published Takayasu’s arteritis guidelines from the American College of Rheumatology is to wean patients off high-dose steroids once they are in remission.
This recommendation is in opposition to another option – namely, switching these patients to low-dose glucocorticoids. The idea is to prevent long-term side effects, particularly in children. The guidelines also recommend against escalating immunotherapy for asymptomatic increases in inflammatory markers and generally recommend against surgery – stenting in most cases – unless there is threat to life, limb, or organ and also if limb pain is so severe it cramps quality of life and dose escalation doesn’t get the job done. If surgery is planned, patients should be on perioperative steroids if there’s active disease.
It’s draft guidance for now, but it’s probably what the final document will say when it’s published in 2020, according to a presentation at the annual meeting of the American College of Rheumatology by one of the authors, Anisha Dua, MD, an associate professor of rheumatology at Northwestern University, Chicago. She gave a sneak preview at the meeting.
In general, severe, active Takayasu’s calls for high-dose oral steroids in conjunction with a nonsteroid immunosuppressive, such as methotrexate, azathioprine, leflunomide, or mycophenolate mofetil. There’s evidence that dual therapy gives a more durable remission and also reduces the need for steroids.
When that approach doesn’t do the trick, the next step is a tumor necrosis factor (TNF) inhibitor. There’s evidence for infliximab, adalimumab, certolizumab, and etanercept. Dr. Dua noted, “We still can consider” tocilizumab, but it failed to meet its primary endpoint in a randomized trial, and evidence for other biologics is sparse or nonexistent. “TNF inhibitors are the first line” for refractory disease, Dr. Dua said.
The steroid taper comes after 6-12 months of remission. Given their toxicity, “our goal for steroids is zero,” especially in pediatric populations. Even in remission, patients should have a clinical assessment, including inflammatory markers, every 3-12 months.
A rise in C-reactive protein or erythrocyte sedimentation rate, with no new symptoms, might be a reason for more frequent monitoring, but it’s not a reason to escalate immunosuppression. That should be kept in reserve for new vascular lesions, rapid progression on an old one, or worsening of organ or limb ischemia.
“We recommend [escalation] over surgical intervention” because patients often develop collateral circulation that solves the problem; it also gives the disease time to quiet down should the patient eventually go into surgery. Immediate surgery is reserved for organ or life-threatening disease, Dr. Dua said.
“Takayasu’s is different from other vasculitides in the sense that patients often present with certain nonspecific constitutional symptoms,” and there’s not a lot of pathology or histology to work with, “so we do tend to rely on imaging a lot,” Dr. Dua said.
Angiography has fallen out of favor because it’s invasive and exposes patients to radiation, among other problems. The field has moved to noninvasive imaging such as color Doppler ultrasound, CT angiography, magnetic resonance angiography, and PET CT.
“We do recommend regularly scheduled, noninvasive imaging every 6-12 months, in addition to the routine clinical assessment,” except in children with inactive disease; the risk of sedation outweighs the imaging benefit, Dr. Dua said.
In patients with single-vessel cranial or cervical stenosis, without symptoms, “we recommend medical over surgical management because of the risk of surgery. Surgery can be considered for multivessel involvement,” she said.
She and her colleagues also recommend medical management for renal artery stenosis, including antihypertensives and immunotherapy escalation for active disease. Surgery is considered for refractory hypertension or worsening kidney function
Dr. Dua is a primary investigator and adviser for Chemocentryx and an adviser for Novartis and AbbVie.
REPORTING FROM ACR 2019
Drop in flu activity may not signal seasonal peak
A key indicator of flu activity dropped but remains high, but measures of severity have not yet shown any unusual increases, according to the Centers for Disease Control and Prevention.
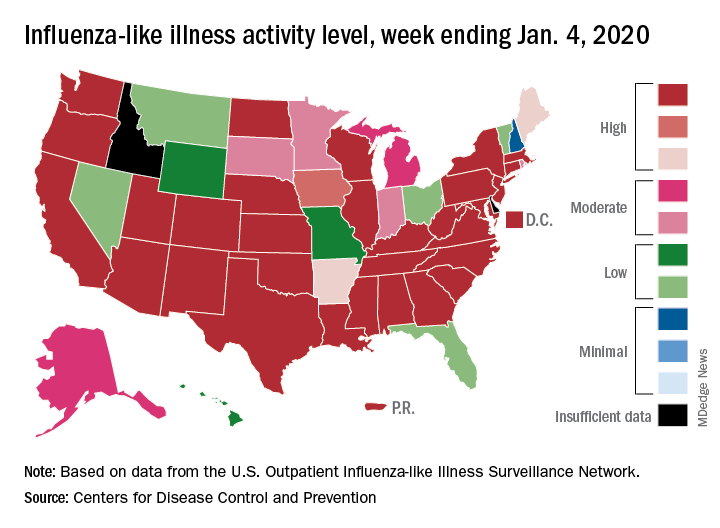
Patients with influenza-like illness (ILI) made up an estimated 5.8% of the visits to outpatient providers during the week ending Jan. 4, and that’s a decline from 7.0% for the last full week of 2019, the CDC’s influenza division reported.
That 7.0% outpatient ILI visit rate was the highest seen in December since 2003, but “hospitalization rates and percent of deaths due to pneumonia and influenza remain low,” the influenza division said in its weekly report.
Influenza B/Victoria and influenza A(H1N1)pdm09 viruses have been the predominant strains so far this season, and they “are more likely to affect children and younger adults than the elderly. Because the majority of hospitalizations and deaths occur among people age 65 and older, with fewer illnesses among that group, we expect, on a population level, to see less impact in flu-related hospitalizations and deaths,” the CDC said.
Last year, there was a similar drop in the outpatient ILI rate in early January after visits rose through December. The rate then increased for another 5 weeks before peaking at 5.0% in February. A similar pattern also occurred during the 2016-2017 and 2015-2016 seasons, CDC data show.
The nationwide ILI hospitalization rate, which is cumulative through the season, was up to 14.6 per 100,000 population for the week ending Jan. 4, the CDC said. Here are the corresponding rates for each of the last five seasons:
- 11.6 (2018-2019).
- 30.5 (2017-2018).
- 12.2 (2016-2017).
- 1.8 (2015-2016).
- 38.3 (2014-2015).
There were five new ILI-related pediatric deaths reported for the week ending Jan. 4, two of which occurred the week before. The total is now up to 32 for the 2019-2020 season, the CDC said in the weekly report. Last season, there were 21 pediatric deaths through the first January report, compared with 42 during the 2017-2018 season and 13 in 2016-2017.
A key indicator of flu activity dropped but remains high, but measures of severity have not yet shown any unusual increases, according to the Centers for Disease Control and Prevention.
Patients with influenza-like illness (ILI) made up an estimated 5.8% of the visits to outpatient providers during the week ending Jan. 4, and that’s a decline from 7.0% for the last full week of 2019, the CDC’s influenza division reported.
That 7.0% outpatient ILI visit rate was the highest seen in December since 2003, but “hospitalization rates and percent of deaths due to pneumonia and influenza remain low,” the influenza division said in its weekly report.
Influenza B/Victoria and influenza A(H1N1)pdm09 viruses have been the predominant strains so far this season, and they “are more likely to affect children and younger adults than the elderly. Because the majority of hospitalizations and deaths occur among people age 65 and older, with fewer illnesses among that group, we expect, on a population level, to see less impact in flu-related hospitalizations and deaths,” the CDC said.
Last year, there was a similar drop in the outpatient ILI rate in early January after visits rose through December. The rate then increased for another 5 weeks before peaking at 5.0% in February. A similar pattern also occurred during the 2016-2017 and 2015-2016 seasons, CDC data show.
The nationwide ILI hospitalization rate, which is cumulative through the season, was up to 14.6 per 100,000 population for the week ending Jan. 4, the CDC said. Here are the corresponding rates for each of the last five seasons:
- 11.6 (2018-2019).
- 30.5 (2017-2018).
- 12.2 (2016-2017).
- 1.8 (2015-2016).
- 38.3 (2014-2015).
There were five new ILI-related pediatric deaths reported for the week ending Jan. 4, two of which occurred the week before. The total is now up to 32 for the 2019-2020 season, the CDC said in the weekly report. Last season, there were 21 pediatric deaths through the first January report, compared with 42 during the 2017-2018 season and 13 in 2016-2017.
A key indicator of flu activity dropped but remains high, but measures of severity have not yet shown any unusual increases, according to the Centers for Disease Control and Prevention.
Patients with influenza-like illness (ILI) made up an estimated 5.8% of the visits to outpatient providers during the week ending Jan. 4, and that’s a decline from 7.0% for the last full week of 2019, the CDC’s influenza division reported.
That 7.0% outpatient ILI visit rate was the highest seen in December since 2003, but “hospitalization rates and percent of deaths due to pneumonia and influenza remain low,” the influenza division said in its weekly report.
Influenza B/Victoria and influenza A(H1N1)pdm09 viruses have been the predominant strains so far this season, and they “are more likely to affect children and younger adults than the elderly. Because the majority of hospitalizations and deaths occur among people age 65 and older, with fewer illnesses among that group, we expect, on a population level, to see less impact in flu-related hospitalizations and deaths,” the CDC said.
Last year, there was a similar drop in the outpatient ILI rate in early January after visits rose through December. The rate then increased for another 5 weeks before peaking at 5.0% in February. A similar pattern also occurred during the 2016-2017 and 2015-2016 seasons, CDC data show.
The nationwide ILI hospitalization rate, which is cumulative through the season, was up to 14.6 per 100,000 population for the week ending Jan. 4, the CDC said. Here are the corresponding rates for each of the last five seasons:
- 11.6 (2018-2019).
- 30.5 (2017-2018).
- 12.2 (2016-2017).
- 1.8 (2015-2016).
- 38.3 (2014-2015).
There were five new ILI-related pediatric deaths reported for the week ending Jan. 4, two of which occurred the week before. The total is now up to 32 for the 2019-2020 season, the CDC said in the weekly report. Last season, there were 21 pediatric deaths through the first January report, compared with 42 during the 2017-2018 season and 13 in 2016-2017.