User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
RYGB tops sleeve gastrectomy in long-term outcomes for diabetes
Patients with type 2 diabetes who underwent Roux-en-Y gastric bypass (RYGB) surgery experienced higher rates of diabetes remission, improved glycemic control, greater weight loss, and fewer diabetes relapse events, compared with those who had sleeve gastrectomy, according to findings from nearly 10,000 patients.
“Remission of type 2 diabetes is common after bariatric surgery and may reduce risk for subsequent microvascular and macrovascular disease,” but it is not clear which of the two most common procedures, RYGB or sleeve gastrectomy, has better long-term diabetes and weight outcomes, wrote Kathleen M. McTigue, MD, of the University of Pittsburgh, and colleagues in JAMA Surgery.
To examine the effectiveness of the two procedures, the researchers identified 9,710 adults with type 2 diabetes who were part of the National Patient-Centered Clinical Research Network Bariatric Study. They compared diabetes outcomes for up to 5 years after surgery for 6,233 patients who underwent RYGB and 3,477 who underwent sleeve gastrectomy. The average age of the patients was 50 years, and 73% were women. The average preoperative body mass index was 49 kg/m2.
Overall, 6,141 patients experienced diabetes remission. The estimated adjusted cumulative remission rates for the RYGB and sleeve gastrectomy groups after 1 year were 59% and 56%, respectively, and after 5 years were 86% and 84%.
Weight loss was significantly greater in RYGB patients, compared with those who had the sleeve gastrectomy, with average differences in percentage points of 6.3 at 1 year and 8.1 at year 5. RYGB patients also showed significantly better long-term glycemic control, compared with sleeve gastrectomy patients. At 5 years, hemoglobin A1c levels were 0.80 percentage points below baseline in the RYGB group, and 0.35 percentage points below baseline in the sleeve gastrectomy group.
In addition, after 1 year, diabetes relapse rates in the RYGB and sleeve gastrectomy groups were 8% and 11%, respectively, and 33% and 42% after 5 years.
The findings were limited by several factors, including the observational design of the study and the potential for confounding and coding inaccuracies, the researchers noted, adding that future studies should address the impact of weight loss on diabetes remission and relapse in bariatric surgery patients.
They also noted that their results were in contrast to findings in previous studies that established no significant differences in outcomes between the procedures, but emphasized that most previous studies were smaller and controlled and that outcome differences may be greater in clinical practice.
“For patients, clinicians, and policy makers to make informed decisions about which procedure is best suited to patients’ personal situations, additional data are needed to understand the adverse event profile of the procedures, as well as patient values regarding procedure choice and the role of surgery relative to other aspects of lifelong weight management,” they concluded.
In an accompanying commentary, Natalie Liu, MD, and Luke M. Funk, MD, of the department of surgery, University of Wisconsin–Madison, said the analysis made an important contribution to the existing literature, despite its limitations.
“It included long-term electronic health record data from a large cohort of U.S. patients who had bariatric surgery in a real-world setting,” they wrote, adding that, although the remission rates were high, the relapse rate in both treatment groups deserved further study.
Dr. Liu and Dr. Funk emphasized that the overall high remission rates for either surgery, compared with lifestyle interventions, suggest the need for continued advocacy for better insurance coverage of, and access to, bariatric surgery procedures for patients with type 2 diabetes, notably those with class 1 obesity.
The study was conducted using the National Patient-Centered Clinical Research Network, which was funded by the Patient-Centered Outcomes Research Institute. Dr. McTigue and Dr. Liu had reported no conflicts of interest. Dr. Funk disclosed a Veterans Affairs Health Services Research & Development Career Development Award, and grants from the VA, National Institutes of Health, and American College of Surgeons.
SOURCES: McTigue KM et al. JAMA Surg. 2020 Mar 4. doi: 10.1001/jamasurg.2020.0087; Lui N, Funk LM. JAMA Surg. 2020 Mar 4. doi: 10.1001/jamasurg.2020.0088.
Patients with type 2 diabetes who underwent Roux-en-Y gastric bypass (RYGB) surgery experienced higher rates of diabetes remission, improved glycemic control, greater weight loss, and fewer diabetes relapse events, compared with those who had sleeve gastrectomy, according to findings from nearly 10,000 patients.
“Remission of type 2 diabetes is common after bariatric surgery and may reduce risk for subsequent microvascular and macrovascular disease,” but it is not clear which of the two most common procedures, RYGB or sleeve gastrectomy, has better long-term diabetes and weight outcomes, wrote Kathleen M. McTigue, MD, of the University of Pittsburgh, and colleagues in JAMA Surgery.
To examine the effectiveness of the two procedures, the researchers identified 9,710 adults with type 2 diabetes who were part of the National Patient-Centered Clinical Research Network Bariatric Study. They compared diabetes outcomes for up to 5 years after surgery for 6,233 patients who underwent RYGB and 3,477 who underwent sleeve gastrectomy. The average age of the patients was 50 years, and 73% were women. The average preoperative body mass index was 49 kg/m2.
Overall, 6,141 patients experienced diabetes remission. The estimated adjusted cumulative remission rates for the RYGB and sleeve gastrectomy groups after 1 year were 59% and 56%, respectively, and after 5 years were 86% and 84%.
Weight loss was significantly greater in RYGB patients, compared with those who had the sleeve gastrectomy, with average differences in percentage points of 6.3 at 1 year and 8.1 at year 5. RYGB patients also showed significantly better long-term glycemic control, compared with sleeve gastrectomy patients. At 5 years, hemoglobin A1c levels were 0.80 percentage points below baseline in the RYGB group, and 0.35 percentage points below baseline in the sleeve gastrectomy group.
In addition, after 1 year, diabetes relapse rates in the RYGB and sleeve gastrectomy groups were 8% and 11%, respectively, and 33% and 42% after 5 years.
The findings were limited by several factors, including the observational design of the study and the potential for confounding and coding inaccuracies, the researchers noted, adding that future studies should address the impact of weight loss on diabetes remission and relapse in bariatric surgery patients.
They also noted that their results were in contrast to findings in previous studies that established no significant differences in outcomes between the procedures, but emphasized that most previous studies were smaller and controlled and that outcome differences may be greater in clinical practice.
“For patients, clinicians, and policy makers to make informed decisions about which procedure is best suited to patients’ personal situations, additional data are needed to understand the adverse event profile of the procedures, as well as patient values regarding procedure choice and the role of surgery relative to other aspects of lifelong weight management,” they concluded.
In an accompanying commentary, Natalie Liu, MD, and Luke M. Funk, MD, of the department of surgery, University of Wisconsin–Madison, said the analysis made an important contribution to the existing literature, despite its limitations.
“It included long-term electronic health record data from a large cohort of U.S. patients who had bariatric surgery in a real-world setting,” they wrote, adding that, although the remission rates were high, the relapse rate in both treatment groups deserved further study.
Dr. Liu and Dr. Funk emphasized that the overall high remission rates for either surgery, compared with lifestyle interventions, suggest the need for continued advocacy for better insurance coverage of, and access to, bariatric surgery procedures for patients with type 2 diabetes, notably those with class 1 obesity.
The study was conducted using the National Patient-Centered Clinical Research Network, which was funded by the Patient-Centered Outcomes Research Institute. Dr. McTigue and Dr. Liu had reported no conflicts of interest. Dr. Funk disclosed a Veterans Affairs Health Services Research & Development Career Development Award, and grants from the VA, National Institutes of Health, and American College of Surgeons.
SOURCES: McTigue KM et al. JAMA Surg. 2020 Mar 4. doi: 10.1001/jamasurg.2020.0087; Lui N, Funk LM. JAMA Surg. 2020 Mar 4. doi: 10.1001/jamasurg.2020.0088.
Patients with type 2 diabetes who underwent Roux-en-Y gastric bypass (RYGB) surgery experienced higher rates of diabetes remission, improved glycemic control, greater weight loss, and fewer diabetes relapse events, compared with those who had sleeve gastrectomy, according to findings from nearly 10,000 patients.
“Remission of type 2 diabetes is common after bariatric surgery and may reduce risk for subsequent microvascular and macrovascular disease,” but it is not clear which of the two most common procedures, RYGB or sleeve gastrectomy, has better long-term diabetes and weight outcomes, wrote Kathleen M. McTigue, MD, of the University of Pittsburgh, and colleagues in JAMA Surgery.
To examine the effectiveness of the two procedures, the researchers identified 9,710 adults with type 2 diabetes who were part of the National Patient-Centered Clinical Research Network Bariatric Study. They compared diabetes outcomes for up to 5 years after surgery for 6,233 patients who underwent RYGB and 3,477 who underwent sleeve gastrectomy. The average age of the patients was 50 years, and 73% were women. The average preoperative body mass index was 49 kg/m2.
Overall, 6,141 patients experienced diabetes remission. The estimated adjusted cumulative remission rates for the RYGB and sleeve gastrectomy groups after 1 year were 59% and 56%, respectively, and after 5 years were 86% and 84%.
Weight loss was significantly greater in RYGB patients, compared with those who had the sleeve gastrectomy, with average differences in percentage points of 6.3 at 1 year and 8.1 at year 5. RYGB patients also showed significantly better long-term glycemic control, compared with sleeve gastrectomy patients. At 5 years, hemoglobin A1c levels were 0.80 percentage points below baseline in the RYGB group, and 0.35 percentage points below baseline in the sleeve gastrectomy group.
In addition, after 1 year, diabetes relapse rates in the RYGB and sleeve gastrectomy groups were 8% and 11%, respectively, and 33% and 42% after 5 years.
The findings were limited by several factors, including the observational design of the study and the potential for confounding and coding inaccuracies, the researchers noted, adding that future studies should address the impact of weight loss on diabetes remission and relapse in bariatric surgery patients.
They also noted that their results were in contrast to findings in previous studies that established no significant differences in outcomes between the procedures, but emphasized that most previous studies were smaller and controlled and that outcome differences may be greater in clinical practice.
“For patients, clinicians, and policy makers to make informed decisions about which procedure is best suited to patients’ personal situations, additional data are needed to understand the adverse event profile of the procedures, as well as patient values regarding procedure choice and the role of surgery relative to other aspects of lifelong weight management,” they concluded.
In an accompanying commentary, Natalie Liu, MD, and Luke M. Funk, MD, of the department of surgery, University of Wisconsin–Madison, said the analysis made an important contribution to the existing literature, despite its limitations.
“It included long-term electronic health record data from a large cohort of U.S. patients who had bariatric surgery in a real-world setting,” they wrote, adding that, although the remission rates were high, the relapse rate in both treatment groups deserved further study.
Dr. Liu and Dr. Funk emphasized that the overall high remission rates for either surgery, compared with lifestyle interventions, suggest the need for continued advocacy for better insurance coverage of, and access to, bariatric surgery procedures for patients with type 2 diabetes, notably those with class 1 obesity.
The study was conducted using the National Patient-Centered Clinical Research Network, which was funded by the Patient-Centered Outcomes Research Institute. Dr. McTigue and Dr. Liu had reported no conflicts of interest. Dr. Funk disclosed a Veterans Affairs Health Services Research & Development Career Development Award, and grants from the VA, National Institutes of Health, and American College of Surgeons.
SOURCES: McTigue KM et al. JAMA Surg. 2020 Mar 4. doi: 10.1001/jamasurg.2020.0087; Lui N, Funk LM. JAMA Surg. 2020 Mar 4. doi: 10.1001/jamasurg.2020.0088.
FROM JAMA SURGERY
2020 Update on gynecologic cancer
Over the past year, major strides have been made in the treatment of gynecologic malignancies. In this Update, we highlight 3 notable studies. The first is a phase 3, multicenter, international, randomized clinical trial that demonstrated a significant improvement in both overall and failure-free survival with the use of adjuvant chemoradiation versus radiotherapy alone in patients with stage III or high-risk uterine cancer. Additionally, we describe the results of 2 phase 3, multicenter, international, randomized clinical trials in ovarian cancer treatment: use of poly(adenosine diphosphate-ribose) polymerase (PARP) inhibitors in combination with platinum and taxane-based chemotherapy followed by the PARP inhibitor as maintenance therapy, and secondary cytoreductive surgery in platinum-sensitive, recurrent ovarian cancer.
We provide a brief overview of current treatment strategies, summarize the key findings of these trials, and establish how these findings have changed our management of these gynecologic malignancies.
Adjuvant chemotherapy and radiotherapy improves survival in women with high-risk endometrial cancer
de Boer SM, Powell ME, Mileshkin L, et al; on behalf of the PORTEC Study Group. Adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3): patterns of recurrence and post-hoc survival analysis of a randomised phase 3 trial. Lancet Oncol. 2019;1273-1285.
In the United States, it is estimated that more than 61,000 women were diagnosed with endometrial cancer in 2019.1 Women with endometrial cancer usually have a favorable prognosis; more than 65% are diagnosed with early-stage disease, which is associated with a 95% 5-year survival rate.1 However, 15% to 20% of patients have disease with high-risk features, including advanced stage (stage II-IV), high tumor grade, lymphovascular space invasion, deep myometrial invasion, or nonendometrioid histologic subtypes (serous or clear cell).2 The presence of these high-risk disease features is associated with an increased incidence of distant metastases and cancer-related death.
Adjuvant therapy in high-risk endometrial cancer
To date, the optimal adjuvant therapy for patients with high-risk endometrial cancer remains controversial. Prior data from Gynecologic Oncology Group (GOG) protocol 122 demonstrated that chemotherapy significantly improved progression-free survival and overall survival when compared with radiotherapy in patients with advanced-stage endometrial cancer.3 As such, chemotherapy now is frequently used in this population, often in combination with radiation, although data describing the benefit of chemoradiation are limited.4 For women with earlier-stage disease with high-risk features, the value of chemotherapy plus radiation is uncertain.5,6
Continue to: Benefit observed with adjuvant chemoradiotherapy...
Benefit observed with adjuvant chemoradiotherapy
In a multicenter, international, randomized phase 3 trial, known as the PORTEC-3 trial, de Boer and colleagues sought to determine if combined adjuvant chemoradiation improved overall survival (OS) and failure-free survival when compared with external-beam radiation therapy (EBRT) alone in the treatment of women with high-risk endometrial cancer.7 Women were eligible for the study if they had histologically confirmed stage I, grade 3 endometrioid endometrial cancer with deep invasion and/or lymphovascular space invasion, stage II or III disease, or stage I-III disease with serous or clear cell histology.
Participants were randomly assigned in a 1:1 ratio; 330 women received adjuvant EBRT alone (total dose of 48.6 Gy administered in 27 fractions), and 330 received adjuvant chemotherapy during and after radiation therapy (CTRT) (2 cycles of cisplatin 50 mg/m2 IV given on days 1 and 22 of EBRT followed by 4 cycles of carboplatin AUC 5 and paclitaxel 175 mg/m2 IV every 3 weeks).
At a median follow-up of 73 months, treatment with adjuvant CTRT, compared with adjuvant EBRT alone, was associated with a significant improvement in both overall survival (5-year OS: 81.4% vs 76.1%, P = .034 [FIGURE]) and failure-free survival (5-year failure-free survival: 76.5% vs 69.1%, P = .016).
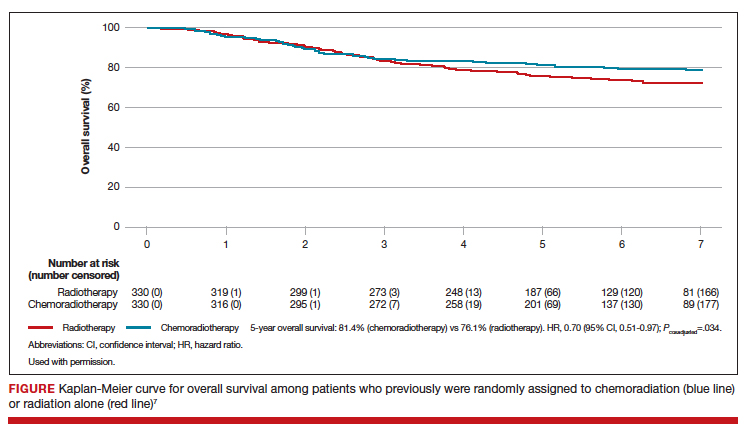
The greatest absolute benefit of adjuvant CTRT, compared with EBRT alone, in survival was among women with stage III endometrial cancer (5-year OS: 78.5% vs 68.5%, P = .043) or serous cancers (19% absolute improvement in 5-year OS), or both. Significant differences in 5-year OS and failure-free survival in women with stage I-II cancer were not observed with adjuvant CTRT when compared with adjuvant EBRT alone. At 5 years, significantly more adverse events of grade 2 or worse were reported in the adjuvant CTRT arm.
Results from similar trials
Since the publication of results from the updated analysis of PORTEC-3, results from 2 pertinent trials have been published.8,9 In the GOG 249 trial, women with stage I-II endometrial cancer with high-risk features were randomly assigned to receive 3 cycles of carboplatin-paclitaxel chemotherapy with vaginal brachytherapy or EBRT.8 There was no difference in survival, but a significant increase in both pelvic and para-aortic recurrences were seen after the combination of chemotherapy and vaginal brachytherapy.8
In GOG 258, women with stage III-IVA endometrial cancer were randomly assigned to receive chemotherapy alone (carboplatin-paclitaxel) or adjuvant chemotherapy after EBRT.9 No differences in recurrence-free or overall survival were noted, but there was a significant increase in the number of vaginal and pelvic or para-aortic recurrences in patients in the chemotherapy-only arm.9
The conflicting data regarding the ideal adjuvant therapy for endometrial cancer suggests that treatment decisions should be individualized. Pelvic EBRT with concurrent adjuvant chemotherapy should be considered in women with stage III endometrial cancer or serous cancers as combination therapy improves survival, although dual modality treatment is associated with increased toxicity. Chemoradiation appears to have less benefit for women with stage I–II cancers with other pathologic risk factors.
Role for PARP inhibitor plus first-line chemotherapy, and as maintenance therapy, in ovarian cancer treatment
Coleman RL, Fleming GF, Brady MF, et al. Veliparib with first-line chemotherapy and as maintenance therapy in ovarian cancer. N Engl J Med. 2019;381:2403-2415.
Ovarian cancer is the leading cause of gynecologic cancer-related deaths among women in the United States.10 Treatment consists of cytoreductive surgery combined with platinum and taxane-based chemotherapy.11 Despite favorable initial responses, more than 80% of patients experience a recurrence, with an 18-month median time to progression.12 As a result, recent efforts have focused on finding novel therapeutic approaches to improve treatment outcomes and mitigate the risk of disease recurrence.
Continue to: PARP inhibitors are changing the face of treatment...
PARP inhibitors are changing the face of treatment
Poly(adenosine diphosphate-ribose) polymerases (PARPs) are a family of enzymes that play a critical role in DNA damage repair. These enzymes promote DNA repair by recruiting proteins involved in repairing single-strand and double-strand DNA breaks and in protecting and restarting stalled DNA replication forks.13 The predominant mechanisms of action of PARP inhibitors in cells with homologous-recombination deficiency (HRD) include inhibiting repair of single-strand DNA breaks and trapping PARP-DNA complexes at stalled DNA replication forks.14
Germline or somatic BRCA1/2 mutations and genetic alterations resulting in HRD are present in about 20% and 30% of ovarian carcinomas, respectively, and increase the susceptibility of tumors to platinum-based agents and PARP inhibitors.15,16 Based on multiple clinical trials that demonstrated the efficacy of single-agent PARP in the treatment of recurrent ovarian carcinoma and as maintenance therapy after an initial response to platinum-based therapy, the US Food and Drug Administration approved olaparib, niraparib, and rucaparib for the treatment of high-grade epithelial ovarian cancer.17-19 Only olaparib is approved for maintenance therapy after initial adjuvant therapy in patients with BRCA mutations.20
Given the robust response to PARP inhibitors, there has been great interest in using these agents earlier in the disease course in combination with chemotherapy.
Efficacy of veliparib with chemotherapy and as maintenance monotherapy
In a randomized, double-blind, placebo-controlled phase 3 trial, Coleman and colleagues sought to determine the efficacy of the PARP inhibitor veliparib when administered with first-line carboplatin and paclitaxel induction chemotherapy and subsequently continued as maintenance monotherapy.21
Women with stage III or IV high-grade epithelial ovarian, fallopian tube, or primary peritoneal carcinoma were eligible for the study. Cytoreductive surgery could be performed prior to the initiation of trial treatment or after 3 cycles of chemotherapy.
Participants were randomized in a 1:1:1 ratio: 371 women received carboplatin and paclitaxel plus placebo followed by placebo maintenance (control arm); 376 received chemotherapy plus veliparib followed by placebo maintenance (veliparib combination-only arm); and 377 received chemotherapy plus veliparib followed by veliparib maintenance therapy (veliparib-throughout arm). Combination chemotherapy consisted of 6 cycles, and maintenance therapy was an additional 30 cycles.
Progression-free survival extended
At a median follow-up of 28 months, investigators observed a significant improvement in progression-free survival in the veliparib-throughout (initial and maintenance therapy) arm compared with the control arm in 3 cohorts: the BRCA-mutation cohort, the HRD cohort, and the intention-to-treat population (all participants undergoing randomization).
In the BRCA-mutation cohort, the median progression-free survival was 12.7 months longer in the veliparib-throughout arm than in the control arm. Similarly, in the HRD cohort, the median progression-free survival was 11.4 months longer in the veliparib-throughout arm than in the control group. In the intention-to-treat population, the median progression-free survival increased from 17.3 to 23.5 months in the veliparib-throughout arm compared with the control arm.
Women who received veliparib experienced increased rates of nausea, anemia, and fatigue and were more likely to require dose reductions and treatment interruptions. Myelodysplastic syndrome was reported in 1 patient (BRCA1 positive) in the veliparib combination-only arm.
For women with newly diagnosed, previously untreated stage III or IV high-grade serous ovarian carcinoma, carboplatin, paclitaxel, and veliparib induction therapy followed by single-agent veliparib maintenance therapy resulted in a significant improvement in median progression-free survival compared with induction chemotherapy alone. However, veliparib use was also associated with a higher incidence of adverse effects that required dose reduction and/or interruption during both the combination and maintenance phases of treatment.
Secondary cytoreductive surgery or chemotherapy alone for platinum-sensitive recurrent ovarian carcinoma?
Coleman RL, Spirtos NM, Enserro D, et al. Secondary surgical cytoreduction for recurrent ovarian cancer. N Engl J Med. 2019;381:1929-1939.
Primary surgical cytoreduction combined with platinum and taxane-based chemotherapy remains the mainstay of ovarian cancer treatment.11 The role of surgery for women with recurrent ovarian cancer, so-called secondary cytoreduction, remains controversial.22
Data have shown that among women who undergo secondary surgery, those with little or no postoperative residual disease benefit the most from a secondary debulking.23-26 Prior work largely is based on small retrospective reports and is limited by substantial bias in the selection of patients undergoing surgery. Additionally, with the availability of targeted therapies such as bevacizumab and PARP inhibitors as maintenance—medical interventions with a demonstrated benefit in progression-free survival17-19,27—the role of secondary cytoreduction in the treatment of ovarian carcinoma needs to be clarified.
Continue to: Overall survival after secondary cytoreduction followed by chemotherapy...
Overall survival after secondary cytoreduction followed by chemotherapy
Coleman and colleagues conducted a prospective, multicenter, international, randomized phase 3 trial to assess whether secondary cytoreductive surgery followed by chemotherapy would improve overall survival versus chemotherapy alone among women with resectable platinum-sensitive, recurrent ovarian cancer.22 Platinum sensitivity was defined as a disease-free interval of at least 6 months after the last cycle of platinum-based chemotherapy.
All women had recurrent epithelial ovarian carcinoma considered to be amenable to complete gross surgical resection by the investigator and a history of complete response to at least 3 cycles of platinum-based chemotherapy as determined by a normal CA-125 value or negative imaging studies (if obtained).
Participants were randomly assigned 1:1, with 240 women assigned to secondary surgical cytoreduction followed by platinum-based chemotherapy, and 245 assigned to chemotherapy alone. The type of adjuvant chemotherapy used (carboplatin-paclitaxel or carboplatin-gemcitabine) and whether or not bevacizumab was administered were at the investigators' discretion.
Shorter survival, decline in quality of life
Among the participants assigned to and who underwent surgery, complete gross resection was achieved in 67%. Eighty-four percent of the entire study population received platinum-based chemotherapy with bevacizumab followed by bevacizumab maintenance therapy, which was equally distributed between the 2 study arms.
At a median follow-up of 48.1 months, median overall survival was 50.6 months in the surgery arm compared with 64.7 months in the chemotherapy arm, corresponding to a hazard ratio (HR) for death of 1.29 (95% confidence interval [CI], 0.97-1.72; P = .08). This effect was unchanged after adjusting for platinum-free interval, chemotherapy choice, and restricting the analysis to women who had a complete gross resection.
Similarly, the adjusted HR for disease progression or death was 0.82 (95% CI, 0.66-1.01) and corresponded to a median progression-free survival of 18.9 months for the surgery group and 16.2 months for the chemotherapy group. Surgical morbidity was reported in 9% of patients who underwent surgery, and 1 patient (0.4%) died from postoperative complications.
While a significant decline in both quality of life and patient-reported outcomes was reported immediately after surgery, significant differences were not noted between the 2 groups after the initial postoperative recovery period.
For women with platinum-sensitive, recurrent ovarian cancer, a secondary cytoreductive surgery followed by chemotherapy was not associated with an improvement in overall survival when compared with chemotherapy alone. Secondary cytoreductive surgery should not be used routinely in women with recurrent ovarian cancer.
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;20:7-34.
- Colombo N, Creutzberg C, Amant F, et al; ESMO-ESGOESTRO Endometrial Consensus Conference Working Group. ESMO-ESGO-ESTRO consensus conference on endometrial cancer: diagnosis, treatment and follow-up. Ann Oncol. 2016;27:16-41.
- Randall ME, Filiaci VL, Muss H, et al; Gynecologic Oncology Group Study. Randomized phase III trial of whole-abdominal irradiation versus doxorubicin and cisplatin chemotherapy in advanced endometrial carcinoma: a Gynecologic Oncology Group study. J Clin Oncol. 2006;24:36-44.
- Syeda S, Chen L, Hou JY, et al. Chemotherapy, radiation, or combination therapy for stage III uterine cancer. Obstet Gynecol. 2019;134:17-29.
- Maggi R, Lissoni A, Spina F, et al. Adjuvant chemotherapy vs radiotherapy in high-risk endometrial carcinoma: results of a randomised trial. Br J Cancer. 2006;95:266-271.
- Susumu N, Sagae S, Udagawa Y, et al; Japanese Gynecologic Oncology Group. Randomized phase III trial of pelvic radiotherapy versus cisplatin-based combined chemotherapy in patients with intermediate- and high-risk endometrial cancer: a Japanese Gynecologic Oncology Group study. Gynecol Oncol. 2008;108:226-233.
- de Boer SM, Powell ME, Mileshkin L, et al; PORTEC Study Group. Adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3): patterns of recurrence and post-hoc survival analysis of a randomised phase 3 trial. Lancet Oncol. 2019;20:1273-1285.
- Randall ME, Filiaci V, McMeekin DS, et al. Phase III trial: adjuvant pelvic radiation therapy versus vaginal brachytherapy plus paclitaxel/carboplatin in high-intermediate and high-risk early stage endometrial cancer. J Clin Oncol. 2019;37:1810-1818.
- Matei D, Filiaci V, Randall ME, et al. Adjuvant chemotherapy plus radiation for locally advanced endometrial cancer. N Engl J Med. 2019;380:2317-2326.
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-424.
- Armstrong DK, Alvarez RD, Bakkum-Gamez JN, et al. NCCN guidelines insights: ovarian cancer, version 1.2019. J Natl Compr Canc Netw. 2019;17:896-909.
- Ledermann JA, Raja FA, Fotopoulou C, et al. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(suppl 6):vi24-vi32.
- Moore KN, Mirza MR, Matulonis UA. The poly (ADP ribose) polymerase inhibitor niraparib: management of toxicities. Gynecol Oncol. 2018;149:214-220.
- Konstantinopoulos PA, Matulonis UA. PARP inhibitors in ovarian cancer: a trailblazing and transformative journey. Clin Cancer Res. 2018;24:4062-4065.
- Pennington KP, Walsh T, Harrell MI, et al. Germline and somatic mutations in homologous recombination genes predict platinum response and survival in ovarian, fallopian tube, and peritoneal carcinomas. Clin Cancer Res. 2014;20:764-775.
- Mukhopadhyay A, Plummer ER, Elattar A, et al. Clinicopathological features of homologous recombination-deficient epithelial ovarian cancers: sensitivity to PARP inhibitors, platinum, and survival. Cancer Res. 2012;72:5675-5682.
- Mirza MR, Monk BJ, Herrstedt J, et al; ENGOT-OV16/ NOVA Investigators. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N Engl J Med. 2016;375:2154-2164.
- Pujade-Lauraine E, Ledermann JA, Selle F, et al; SOLO2/ ENGOT-Ov21 Investigators. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017;18:1274-1284.
- Coleman RL, Oza AM, Lorusso D, et al; ARIEL3 Investigators. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;390:1949-1961.
- Moore K, Colombo N, Scambia G, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med. 2018;379:2495-2505.
- Coleman RL, Fleming GF, Brady MF, et al. Veliparib with firstline chemotherapy and as maintenance therapy in ovarian cancer. N Engl J Med. 2019;381:2403-2415.
- Coleman RL, Spirtos NM, Enserro D, et al. Secondary surgical cytoreduction for recurrent ovarian cancer. N Engl J Med. 2019;381:1929-1939.
- Bommert M, Harter P, Heitz F, et al. When should surgery be used for recurrent ovarian carcinoma? Clin Oncol (R Coll Radiol). 2018;30:493-497.
- Santillan A, Karam AK, Li AJ, et al. Secondary cytoreductive surgery for isolated nodal recurrence in patients with epithelial ovarian cancer. Gynecol Oncol. 2007;104:686-690.
- Zang RY, Harter P, Chi DS, et al. Predictors of survival in patients with recurrent ovarian cancer undergoing secondary cytoreductive surgery based on the pooled analysis of an international collaborative cohort. Br J Cancer. 2011;105:890-896.
- Chi DS, McCaughty K, Diaz JP, et al. Guidelines and selection criteria for secondary cytoreductive surgery in patients with recurrent, platinum-sensitive epithelial ovarian carcinoma. Cancer. 2006;106:1933-1939.
- Aghajanian C, Blank SV, Goff BA, et al. OCEANS: a randomized, double-blind, placebo-controlled phase III trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube cancer. J Clin Oncol. 2012;30: 2039-2045.
Zhen Ni Zhou, MD, PhD
Dr. Zhou is a Fellow in the
Division of Gynecologic
Oncology, New York–
Presbyterian/Columbia
University Medical Center and
Weill Cornell Medical Center,
New York, New York.

Jason D. Wright, MD
Dr. Wright is the Sol Goldman
Associate Professor, Chief of
the Division of Gynecologic
Oncology, Vice Chair of
Academic Affairs, Department
of Obstetrics and Gynecology,
Columbia University College of
Physicians and Surgeons,
New York, New York.
Dr. Wright reports that he is a consultant to Clovis Oncology and Tesaro, Inc, and has received research funding from Merck. Dr. Zhou reports no financial relationships relevant to this article.
Zhen Ni Zhou, MD, PhD
Dr. Zhou is a Fellow in the
Division of Gynecologic
Oncology, New York–
Presbyterian/Columbia
University Medical Center and
Weill Cornell Medical Center,
New York, New York.
Jason D. Wright, MD
Dr. Wright is the Sol Goldman
Associate Professor, Chief of
the Division of Gynecologic
Oncology, Vice Chair of
Academic Affairs, Department
of Obstetrics and Gynecology,
Columbia University College of
Physicians and Surgeons,
New York, New York.
Dr. Wright reports that he is a consultant to Clovis Oncology and Tesaro, Inc, and has received research funding from Merck. Dr. Zhou reports no financial relationships relevant to this article.
Zhen Ni Zhou, MD, PhD
Dr. Zhou is a Fellow in the
Division of Gynecologic
Oncology, New York–
Presbyterian/Columbia
University Medical Center and
Weill Cornell Medical Center,
New York, New York.
Jason D. Wright, MD
Dr. Wright is the Sol Goldman
Associate Professor, Chief of
the Division of Gynecologic
Oncology, Vice Chair of
Academic Affairs, Department
of Obstetrics and Gynecology,
Columbia University College of
Physicians and Surgeons,
New York, New York.
Dr. Wright reports that he is a consultant to Clovis Oncology and Tesaro, Inc, and has received research funding from Merck. Dr. Zhou reports no financial relationships relevant to this article.
Over the past year, major strides have been made in the treatment of gynecologic malignancies. In this Update, we highlight 3 notable studies. The first is a phase 3, multicenter, international, randomized clinical trial that demonstrated a significant improvement in both overall and failure-free survival with the use of adjuvant chemoradiation versus radiotherapy alone in patients with stage III or high-risk uterine cancer. Additionally, we describe the results of 2 phase 3, multicenter, international, randomized clinical trials in ovarian cancer treatment: use of poly(adenosine diphosphate-ribose) polymerase (PARP) inhibitors in combination with platinum and taxane-based chemotherapy followed by the PARP inhibitor as maintenance therapy, and secondary cytoreductive surgery in platinum-sensitive, recurrent ovarian cancer.
We provide a brief overview of current treatment strategies, summarize the key findings of these trials, and establish how these findings have changed our management of these gynecologic malignancies.
Adjuvant chemotherapy and radiotherapy improves survival in women with high-risk endometrial cancer
de Boer SM, Powell ME, Mileshkin L, et al; on behalf of the PORTEC Study Group. Adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3): patterns of recurrence and post-hoc survival analysis of a randomised phase 3 trial. Lancet Oncol. 2019;1273-1285.
In the United States, it is estimated that more than 61,000 women were diagnosed with endometrial cancer in 2019.1 Women with endometrial cancer usually have a favorable prognosis; more than 65% are diagnosed with early-stage disease, which is associated with a 95% 5-year survival rate.1 However, 15% to 20% of patients have disease with high-risk features, including advanced stage (stage II-IV), high tumor grade, lymphovascular space invasion, deep myometrial invasion, or nonendometrioid histologic subtypes (serous or clear cell).2 The presence of these high-risk disease features is associated with an increased incidence of distant metastases and cancer-related death.
Adjuvant therapy in high-risk endometrial cancer
To date, the optimal adjuvant therapy for patients with high-risk endometrial cancer remains controversial. Prior data from Gynecologic Oncology Group (GOG) protocol 122 demonstrated that chemotherapy significantly improved progression-free survival and overall survival when compared with radiotherapy in patients with advanced-stage endometrial cancer.3 As such, chemotherapy now is frequently used in this population, often in combination with radiation, although data describing the benefit of chemoradiation are limited.4 For women with earlier-stage disease with high-risk features, the value of chemotherapy plus radiation is uncertain.5,6
Continue to: Benefit observed with adjuvant chemoradiotherapy...
Benefit observed with adjuvant chemoradiotherapy
In a multicenter, international, randomized phase 3 trial, known as the PORTEC-3 trial, de Boer and colleagues sought to determine if combined adjuvant chemoradiation improved overall survival (OS) and failure-free survival when compared with external-beam radiation therapy (EBRT) alone in the treatment of women with high-risk endometrial cancer.7 Women were eligible for the study if they had histologically confirmed stage I, grade 3 endometrioid endometrial cancer with deep invasion and/or lymphovascular space invasion, stage II or III disease, or stage I-III disease with serous or clear cell histology.
Participants were randomly assigned in a 1:1 ratio; 330 women received adjuvant EBRT alone (total dose of 48.6 Gy administered in 27 fractions), and 330 received adjuvant chemotherapy during and after radiation therapy (CTRT) (2 cycles of cisplatin 50 mg/m2 IV given on days 1 and 22 of EBRT followed by 4 cycles of carboplatin AUC 5 and paclitaxel 175 mg/m2 IV every 3 weeks).
At a median follow-up of 73 months, treatment with adjuvant CTRT, compared with adjuvant EBRT alone, was associated with a significant improvement in both overall survival (5-year OS: 81.4% vs 76.1%, P = .034 [FIGURE]) and failure-free survival (5-year failure-free survival: 76.5% vs 69.1%, P = .016).
The greatest absolute benefit of adjuvant CTRT, compared with EBRT alone, in survival was among women with stage III endometrial cancer (5-year OS: 78.5% vs 68.5%, P = .043) or serous cancers (19% absolute improvement in 5-year OS), or both. Significant differences in 5-year OS and failure-free survival in women with stage I-II cancer were not observed with adjuvant CTRT when compared with adjuvant EBRT alone. At 5 years, significantly more adverse events of grade 2 or worse were reported in the adjuvant CTRT arm.
Results from similar trials
Since the publication of results from the updated analysis of PORTEC-3, results from 2 pertinent trials have been published.8,9 In the GOG 249 trial, women with stage I-II endometrial cancer with high-risk features were randomly assigned to receive 3 cycles of carboplatin-paclitaxel chemotherapy with vaginal brachytherapy or EBRT.8 There was no difference in survival, but a significant increase in both pelvic and para-aortic recurrences were seen after the combination of chemotherapy and vaginal brachytherapy.8
In GOG 258, women with stage III-IVA endometrial cancer were randomly assigned to receive chemotherapy alone (carboplatin-paclitaxel) or adjuvant chemotherapy after EBRT.9 No differences in recurrence-free or overall survival were noted, but there was a significant increase in the number of vaginal and pelvic or para-aortic recurrences in patients in the chemotherapy-only arm.9
The conflicting data regarding the ideal adjuvant therapy for endometrial cancer suggests that treatment decisions should be individualized. Pelvic EBRT with concurrent adjuvant chemotherapy should be considered in women with stage III endometrial cancer or serous cancers as combination therapy improves survival, although dual modality treatment is associated with increased toxicity. Chemoradiation appears to have less benefit for women with stage I–II cancers with other pathologic risk factors.
Role for PARP inhibitor plus first-line chemotherapy, and as maintenance therapy, in ovarian cancer treatment
Coleman RL, Fleming GF, Brady MF, et al. Veliparib with first-line chemotherapy and as maintenance therapy in ovarian cancer. N Engl J Med. 2019;381:2403-2415.
Ovarian cancer is the leading cause of gynecologic cancer-related deaths among women in the United States.10 Treatment consists of cytoreductive surgery combined with platinum and taxane-based chemotherapy.11 Despite favorable initial responses, more than 80% of patients experience a recurrence, with an 18-month median time to progression.12 As a result, recent efforts have focused on finding novel therapeutic approaches to improve treatment outcomes and mitigate the risk of disease recurrence.
Continue to: PARP inhibitors are changing the face of treatment...
PARP inhibitors are changing the face of treatment
Poly(adenosine diphosphate-ribose) polymerases (PARPs) are a family of enzymes that play a critical role in DNA damage repair. These enzymes promote DNA repair by recruiting proteins involved in repairing single-strand and double-strand DNA breaks and in protecting and restarting stalled DNA replication forks.13 The predominant mechanisms of action of PARP inhibitors in cells with homologous-recombination deficiency (HRD) include inhibiting repair of single-strand DNA breaks and trapping PARP-DNA complexes at stalled DNA replication forks.14
Germline or somatic BRCA1/2 mutations and genetic alterations resulting in HRD are present in about 20% and 30% of ovarian carcinomas, respectively, and increase the susceptibility of tumors to platinum-based agents and PARP inhibitors.15,16 Based on multiple clinical trials that demonstrated the efficacy of single-agent PARP in the treatment of recurrent ovarian carcinoma and as maintenance therapy after an initial response to platinum-based therapy, the US Food and Drug Administration approved olaparib, niraparib, and rucaparib for the treatment of high-grade epithelial ovarian cancer.17-19 Only olaparib is approved for maintenance therapy after initial adjuvant therapy in patients with BRCA mutations.20
Given the robust response to PARP inhibitors, there has been great interest in using these agents earlier in the disease course in combination with chemotherapy.
Efficacy of veliparib with chemotherapy and as maintenance monotherapy
In a randomized, double-blind, placebo-controlled phase 3 trial, Coleman and colleagues sought to determine the efficacy of the PARP inhibitor veliparib when administered with first-line carboplatin and paclitaxel induction chemotherapy and subsequently continued as maintenance monotherapy.21
Women with stage III or IV high-grade epithelial ovarian, fallopian tube, or primary peritoneal carcinoma were eligible for the study. Cytoreductive surgery could be performed prior to the initiation of trial treatment or after 3 cycles of chemotherapy.
Participants were randomized in a 1:1:1 ratio: 371 women received carboplatin and paclitaxel plus placebo followed by placebo maintenance (control arm); 376 received chemotherapy plus veliparib followed by placebo maintenance (veliparib combination-only arm); and 377 received chemotherapy plus veliparib followed by veliparib maintenance therapy (veliparib-throughout arm). Combination chemotherapy consisted of 6 cycles, and maintenance therapy was an additional 30 cycles.
Progression-free survival extended
At a median follow-up of 28 months, investigators observed a significant improvement in progression-free survival in the veliparib-throughout (initial and maintenance therapy) arm compared with the control arm in 3 cohorts: the BRCA-mutation cohort, the HRD cohort, and the intention-to-treat population (all participants undergoing randomization).
In the BRCA-mutation cohort, the median progression-free survival was 12.7 months longer in the veliparib-throughout arm than in the control arm. Similarly, in the HRD cohort, the median progression-free survival was 11.4 months longer in the veliparib-throughout arm than in the control group. In the intention-to-treat population, the median progression-free survival increased from 17.3 to 23.5 months in the veliparib-throughout arm compared with the control arm.
Women who received veliparib experienced increased rates of nausea, anemia, and fatigue and were more likely to require dose reductions and treatment interruptions. Myelodysplastic syndrome was reported in 1 patient (BRCA1 positive) in the veliparib combination-only arm.
For women with newly diagnosed, previously untreated stage III or IV high-grade serous ovarian carcinoma, carboplatin, paclitaxel, and veliparib induction therapy followed by single-agent veliparib maintenance therapy resulted in a significant improvement in median progression-free survival compared with induction chemotherapy alone. However, veliparib use was also associated with a higher incidence of adverse effects that required dose reduction and/or interruption during both the combination and maintenance phases of treatment.
Secondary cytoreductive surgery or chemotherapy alone for platinum-sensitive recurrent ovarian carcinoma?
Coleman RL, Spirtos NM, Enserro D, et al. Secondary surgical cytoreduction for recurrent ovarian cancer. N Engl J Med. 2019;381:1929-1939.
Primary surgical cytoreduction combined with platinum and taxane-based chemotherapy remains the mainstay of ovarian cancer treatment.11 The role of surgery for women with recurrent ovarian cancer, so-called secondary cytoreduction, remains controversial.22
Data have shown that among women who undergo secondary surgery, those with little or no postoperative residual disease benefit the most from a secondary debulking.23-26 Prior work largely is based on small retrospective reports and is limited by substantial bias in the selection of patients undergoing surgery. Additionally, with the availability of targeted therapies such as bevacizumab and PARP inhibitors as maintenance—medical interventions with a demonstrated benefit in progression-free survival17-19,27—the role of secondary cytoreduction in the treatment of ovarian carcinoma needs to be clarified.
Continue to: Overall survival after secondary cytoreduction followed by chemotherapy...
Overall survival after secondary cytoreduction followed by chemotherapy
Coleman and colleagues conducted a prospective, multicenter, international, randomized phase 3 trial to assess whether secondary cytoreductive surgery followed by chemotherapy would improve overall survival versus chemotherapy alone among women with resectable platinum-sensitive, recurrent ovarian cancer.22 Platinum sensitivity was defined as a disease-free interval of at least 6 months after the last cycle of platinum-based chemotherapy.
All women had recurrent epithelial ovarian carcinoma considered to be amenable to complete gross surgical resection by the investigator and a history of complete response to at least 3 cycles of platinum-based chemotherapy as determined by a normal CA-125 value or negative imaging studies (if obtained).
Participants were randomly assigned 1:1, with 240 women assigned to secondary surgical cytoreduction followed by platinum-based chemotherapy, and 245 assigned to chemotherapy alone. The type of adjuvant chemotherapy used (carboplatin-paclitaxel or carboplatin-gemcitabine) and whether or not bevacizumab was administered were at the investigators' discretion.
Shorter survival, decline in quality of life
Among the participants assigned to and who underwent surgery, complete gross resection was achieved in 67%. Eighty-four percent of the entire study population received platinum-based chemotherapy with bevacizumab followed by bevacizumab maintenance therapy, which was equally distributed between the 2 study arms.
At a median follow-up of 48.1 months, median overall survival was 50.6 months in the surgery arm compared with 64.7 months in the chemotherapy arm, corresponding to a hazard ratio (HR) for death of 1.29 (95% confidence interval [CI], 0.97-1.72; P = .08). This effect was unchanged after adjusting for platinum-free interval, chemotherapy choice, and restricting the analysis to women who had a complete gross resection.
Similarly, the adjusted HR for disease progression or death was 0.82 (95% CI, 0.66-1.01) and corresponded to a median progression-free survival of 18.9 months for the surgery group and 16.2 months for the chemotherapy group. Surgical morbidity was reported in 9% of patients who underwent surgery, and 1 patient (0.4%) died from postoperative complications.
While a significant decline in both quality of life and patient-reported outcomes was reported immediately after surgery, significant differences were not noted between the 2 groups after the initial postoperative recovery period.
For women with platinum-sensitive, recurrent ovarian cancer, a secondary cytoreductive surgery followed by chemotherapy was not associated with an improvement in overall survival when compared with chemotherapy alone. Secondary cytoreductive surgery should not be used routinely in women with recurrent ovarian cancer.
Over the past year, major strides have been made in the treatment of gynecologic malignancies. In this Update, we highlight 3 notable studies. The first is a phase 3, multicenter, international, randomized clinical trial that demonstrated a significant improvement in both overall and failure-free survival with the use of adjuvant chemoradiation versus radiotherapy alone in patients with stage III or high-risk uterine cancer. Additionally, we describe the results of 2 phase 3, multicenter, international, randomized clinical trials in ovarian cancer treatment: use of poly(adenosine diphosphate-ribose) polymerase (PARP) inhibitors in combination with platinum and taxane-based chemotherapy followed by the PARP inhibitor as maintenance therapy, and secondary cytoreductive surgery in platinum-sensitive, recurrent ovarian cancer.
We provide a brief overview of current treatment strategies, summarize the key findings of these trials, and establish how these findings have changed our management of these gynecologic malignancies.
Adjuvant chemotherapy and radiotherapy improves survival in women with high-risk endometrial cancer
de Boer SM, Powell ME, Mileshkin L, et al; on behalf of the PORTEC Study Group. Adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3): patterns of recurrence and post-hoc survival analysis of a randomised phase 3 trial. Lancet Oncol. 2019;1273-1285.
In the United States, it is estimated that more than 61,000 women were diagnosed with endometrial cancer in 2019.1 Women with endometrial cancer usually have a favorable prognosis; more than 65% are diagnosed with early-stage disease, which is associated with a 95% 5-year survival rate.1 However, 15% to 20% of patients have disease with high-risk features, including advanced stage (stage II-IV), high tumor grade, lymphovascular space invasion, deep myometrial invasion, or nonendometrioid histologic subtypes (serous or clear cell).2 The presence of these high-risk disease features is associated with an increased incidence of distant metastases and cancer-related death.
Adjuvant therapy in high-risk endometrial cancer
To date, the optimal adjuvant therapy for patients with high-risk endometrial cancer remains controversial. Prior data from Gynecologic Oncology Group (GOG) protocol 122 demonstrated that chemotherapy significantly improved progression-free survival and overall survival when compared with radiotherapy in patients with advanced-stage endometrial cancer.3 As such, chemotherapy now is frequently used in this population, often in combination with radiation, although data describing the benefit of chemoradiation are limited.4 For women with earlier-stage disease with high-risk features, the value of chemotherapy plus radiation is uncertain.5,6
Continue to: Benefit observed with adjuvant chemoradiotherapy...
Benefit observed with adjuvant chemoradiotherapy
In a multicenter, international, randomized phase 3 trial, known as the PORTEC-3 trial, de Boer and colleagues sought to determine if combined adjuvant chemoradiation improved overall survival (OS) and failure-free survival when compared with external-beam radiation therapy (EBRT) alone in the treatment of women with high-risk endometrial cancer.7 Women were eligible for the study if they had histologically confirmed stage I, grade 3 endometrioid endometrial cancer with deep invasion and/or lymphovascular space invasion, stage II or III disease, or stage I-III disease with serous or clear cell histology.
Participants were randomly assigned in a 1:1 ratio; 330 women received adjuvant EBRT alone (total dose of 48.6 Gy administered in 27 fractions), and 330 received adjuvant chemotherapy during and after radiation therapy (CTRT) (2 cycles of cisplatin 50 mg/m2 IV given on days 1 and 22 of EBRT followed by 4 cycles of carboplatin AUC 5 and paclitaxel 175 mg/m2 IV every 3 weeks).
At a median follow-up of 73 months, treatment with adjuvant CTRT, compared with adjuvant EBRT alone, was associated with a significant improvement in both overall survival (5-year OS: 81.4% vs 76.1%, P = .034 [FIGURE]) and failure-free survival (5-year failure-free survival: 76.5% vs 69.1%, P = .016).
The greatest absolute benefit of adjuvant CTRT, compared with EBRT alone, in survival was among women with stage III endometrial cancer (5-year OS: 78.5% vs 68.5%, P = .043) or serous cancers (19% absolute improvement in 5-year OS), or both. Significant differences in 5-year OS and failure-free survival in women with stage I-II cancer were not observed with adjuvant CTRT when compared with adjuvant EBRT alone. At 5 years, significantly more adverse events of grade 2 or worse were reported in the adjuvant CTRT arm.
Results from similar trials
Since the publication of results from the updated analysis of PORTEC-3, results from 2 pertinent trials have been published.8,9 In the GOG 249 trial, women with stage I-II endometrial cancer with high-risk features were randomly assigned to receive 3 cycles of carboplatin-paclitaxel chemotherapy with vaginal brachytherapy or EBRT.8 There was no difference in survival, but a significant increase in both pelvic and para-aortic recurrences were seen after the combination of chemotherapy and vaginal brachytherapy.8
In GOG 258, women with stage III-IVA endometrial cancer were randomly assigned to receive chemotherapy alone (carboplatin-paclitaxel) or adjuvant chemotherapy after EBRT.9 No differences in recurrence-free or overall survival were noted, but there was a significant increase in the number of vaginal and pelvic or para-aortic recurrences in patients in the chemotherapy-only arm.9
The conflicting data regarding the ideal adjuvant therapy for endometrial cancer suggests that treatment decisions should be individualized. Pelvic EBRT with concurrent adjuvant chemotherapy should be considered in women with stage III endometrial cancer or serous cancers as combination therapy improves survival, although dual modality treatment is associated with increased toxicity. Chemoradiation appears to have less benefit for women with stage I–II cancers with other pathologic risk factors.
Role for PARP inhibitor plus first-line chemotherapy, and as maintenance therapy, in ovarian cancer treatment
Coleman RL, Fleming GF, Brady MF, et al. Veliparib with first-line chemotherapy and as maintenance therapy in ovarian cancer. N Engl J Med. 2019;381:2403-2415.
Ovarian cancer is the leading cause of gynecologic cancer-related deaths among women in the United States.10 Treatment consists of cytoreductive surgery combined with platinum and taxane-based chemotherapy.11 Despite favorable initial responses, more than 80% of patients experience a recurrence, with an 18-month median time to progression.12 As a result, recent efforts have focused on finding novel therapeutic approaches to improve treatment outcomes and mitigate the risk of disease recurrence.
Continue to: PARP inhibitors are changing the face of treatment...
PARP inhibitors are changing the face of treatment
Poly(adenosine diphosphate-ribose) polymerases (PARPs) are a family of enzymes that play a critical role in DNA damage repair. These enzymes promote DNA repair by recruiting proteins involved in repairing single-strand and double-strand DNA breaks and in protecting and restarting stalled DNA replication forks.13 The predominant mechanisms of action of PARP inhibitors in cells with homologous-recombination deficiency (HRD) include inhibiting repair of single-strand DNA breaks and trapping PARP-DNA complexes at stalled DNA replication forks.14
Germline or somatic BRCA1/2 mutations and genetic alterations resulting in HRD are present in about 20% and 30% of ovarian carcinomas, respectively, and increase the susceptibility of tumors to platinum-based agents and PARP inhibitors.15,16 Based on multiple clinical trials that demonstrated the efficacy of single-agent PARP in the treatment of recurrent ovarian carcinoma and as maintenance therapy after an initial response to platinum-based therapy, the US Food and Drug Administration approved olaparib, niraparib, and rucaparib for the treatment of high-grade epithelial ovarian cancer.17-19 Only olaparib is approved for maintenance therapy after initial adjuvant therapy in patients with BRCA mutations.20
Given the robust response to PARP inhibitors, there has been great interest in using these agents earlier in the disease course in combination with chemotherapy.
Efficacy of veliparib with chemotherapy and as maintenance monotherapy
In a randomized, double-blind, placebo-controlled phase 3 trial, Coleman and colleagues sought to determine the efficacy of the PARP inhibitor veliparib when administered with first-line carboplatin and paclitaxel induction chemotherapy and subsequently continued as maintenance monotherapy.21
Women with stage III or IV high-grade epithelial ovarian, fallopian tube, or primary peritoneal carcinoma were eligible for the study. Cytoreductive surgery could be performed prior to the initiation of trial treatment or after 3 cycles of chemotherapy.
Participants were randomized in a 1:1:1 ratio: 371 women received carboplatin and paclitaxel plus placebo followed by placebo maintenance (control arm); 376 received chemotherapy plus veliparib followed by placebo maintenance (veliparib combination-only arm); and 377 received chemotherapy plus veliparib followed by veliparib maintenance therapy (veliparib-throughout arm). Combination chemotherapy consisted of 6 cycles, and maintenance therapy was an additional 30 cycles.
Progression-free survival extended
At a median follow-up of 28 months, investigators observed a significant improvement in progression-free survival in the veliparib-throughout (initial and maintenance therapy) arm compared with the control arm in 3 cohorts: the BRCA-mutation cohort, the HRD cohort, and the intention-to-treat population (all participants undergoing randomization).
In the BRCA-mutation cohort, the median progression-free survival was 12.7 months longer in the veliparib-throughout arm than in the control arm. Similarly, in the HRD cohort, the median progression-free survival was 11.4 months longer in the veliparib-throughout arm than in the control group. In the intention-to-treat population, the median progression-free survival increased from 17.3 to 23.5 months in the veliparib-throughout arm compared with the control arm.
Women who received veliparib experienced increased rates of nausea, anemia, and fatigue and were more likely to require dose reductions and treatment interruptions. Myelodysplastic syndrome was reported in 1 patient (BRCA1 positive) in the veliparib combination-only arm.
For women with newly diagnosed, previously untreated stage III or IV high-grade serous ovarian carcinoma, carboplatin, paclitaxel, and veliparib induction therapy followed by single-agent veliparib maintenance therapy resulted in a significant improvement in median progression-free survival compared with induction chemotherapy alone. However, veliparib use was also associated with a higher incidence of adverse effects that required dose reduction and/or interruption during both the combination and maintenance phases of treatment.
Secondary cytoreductive surgery or chemotherapy alone for platinum-sensitive recurrent ovarian carcinoma?
Coleman RL, Spirtos NM, Enserro D, et al. Secondary surgical cytoreduction for recurrent ovarian cancer. N Engl J Med. 2019;381:1929-1939.
Primary surgical cytoreduction combined with platinum and taxane-based chemotherapy remains the mainstay of ovarian cancer treatment.11 The role of surgery for women with recurrent ovarian cancer, so-called secondary cytoreduction, remains controversial.22
Data have shown that among women who undergo secondary surgery, those with little or no postoperative residual disease benefit the most from a secondary debulking.23-26 Prior work largely is based on small retrospective reports and is limited by substantial bias in the selection of patients undergoing surgery. Additionally, with the availability of targeted therapies such as bevacizumab and PARP inhibitors as maintenance—medical interventions with a demonstrated benefit in progression-free survival17-19,27—the role of secondary cytoreduction in the treatment of ovarian carcinoma needs to be clarified.
Continue to: Overall survival after secondary cytoreduction followed by chemotherapy...
Overall survival after secondary cytoreduction followed by chemotherapy
Coleman and colleagues conducted a prospective, multicenter, international, randomized phase 3 trial to assess whether secondary cytoreductive surgery followed by chemotherapy would improve overall survival versus chemotherapy alone among women with resectable platinum-sensitive, recurrent ovarian cancer.22 Platinum sensitivity was defined as a disease-free interval of at least 6 months after the last cycle of platinum-based chemotherapy.
All women had recurrent epithelial ovarian carcinoma considered to be amenable to complete gross surgical resection by the investigator and a history of complete response to at least 3 cycles of platinum-based chemotherapy as determined by a normal CA-125 value or negative imaging studies (if obtained).
Participants were randomly assigned 1:1, with 240 women assigned to secondary surgical cytoreduction followed by platinum-based chemotherapy, and 245 assigned to chemotherapy alone. The type of adjuvant chemotherapy used (carboplatin-paclitaxel or carboplatin-gemcitabine) and whether or not bevacizumab was administered were at the investigators' discretion.
Shorter survival, decline in quality of life
Among the participants assigned to and who underwent surgery, complete gross resection was achieved in 67%. Eighty-four percent of the entire study population received platinum-based chemotherapy with bevacizumab followed by bevacizumab maintenance therapy, which was equally distributed between the 2 study arms.
At a median follow-up of 48.1 months, median overall survival was 50.6 months in the surgery arm compared with 64.7 months in the chemotherapy arm, corresponding to a hazard ratio (HR) for death of 1.29 (95% confidence interval [CI], 0.97-1.72; P = .08). This effect was unchanged after adjusting for platinum-free interval, chemotherapy choice, and restricting the analysis to women who had a complete gross resection.
Similarly, the adjusted HR for disease progression or death was 0.82 (95% CI, 0.66-1.01) and corresponded to a median progression-free survival of 18.9 months for the surgery group and 16.2 months for the chemotherapy group. Surgical morbidity was reported in 9% of patients who underwent surgery, and 1 patient (0.4%) died from postoperative complications.
While a significant decline in both quality of life and patient-reported outcomes was reported immediately after surgery, significant differences were not noted between the 2 groups after the initial postoperative recovery period.
For women with platinum-sensitive, recurrent ovarian cancer, a secondary cytoreductive surgery followed by chemotherapy was not associated with an improvement in overall survival when compared with chemotherapy alone. Secondary cytoreductive surgery should not be used routinely in women with recurrent ovarian cancer.
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;20:7-34.
- Colombo N, Creutzberg C, Amant F, et al; ESMO-ESGOESTRO Endometrial Consensus Conference Working Group. ESMO-ESGO-ESTRO consensus conference on endometrial cancer: diagnosis, treatment and follow-up. Ann Oncol. 2016;27:16-41.
- Randall ME, Filiaci VL, Muss H, et al; Gynecologic Oncology Group Study. Randomized phase III trial of whole-abdominal irradiation versus doxorubicin and cisplatin chemotherapy in advanced endometrial carcinoma: a Gynecologic Oncology Group study. J Clin Oncol. 2006;24:36-44.
- Syeda S, Chen L, Hou JY, et al. Chemotherapy, radiation, or combination therapy for stage III uterine cancer. Obstet Gynecol. 2019;134:17-29.
- Maggi R, Lissoni A, Spina F, et al. Adjuvant chemotherapy vs radiotherapy in high-risk endometrial carcinoma: results of a randomised trial. Br J Cancer. 2006;95:266-271.
- Susumu N, Sagae S, Udagawa Y, et al; Japanese Gynecologic Oncology Group. Randomized phase III trial of pelvic radiotherapy versus cisplatin-based combined chemotherapy in patients with intermediate- and high-risk endometrial cancer: a Japanese Gynecologic Oncology Group study. Gynecol Oncol. 2008;108:226-233.
- de Boer SM, Powell ME, Mileshkin L, et al; PORTEC Study Group. Adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3): patterns of recurrence and post-hoc survival analysis of a randomised phase 3 trial. Lancet Oncol. 2019;20:1273-1285.
- Randall ME, Filiaci V, McMeekin DS, et al. Phase III trial: adjuvant pelvic radiation therapy versus vaginal brachytherapy plus paclitaxel/carboplatin in high-intermediate and high-risk early stage endometrial cancer. J Clin Oncol. 2019;37:1810-1818.
- Matei D, Filiaci V, Randall ME, et al. Adjuvant chemotherapy plus radiation for locally advanced endometrial cancer. N Engl J Med. 2019;380:2317-2326.
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-424.
- Armstrong DK, Alvarez RD, Bakkum-Gamez JN, et al. NCCN guidelines insights: ovarian cancer, version 1.2019. J Natl Compr Canc Netw. 2019;17:896-909.
- Ledermann JA, Raja FA, Fotopoulou C, et al. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(suppl 6):vi24-vi32.
- Moore KN, Mirza MR, Matulonis UA. The poly (ADP ribose) polymerase inhibitor niraparib: management of toxicities. Gynecol Oncol. 2018;149:214-220.
- Konstantinopoulos PA, Matulonis UA. PARP inhibitors in ovarian cancer: a trailblazing and transformative journey. Clin Cancer Res. 2018;24:4062-4065.
- Pennington KP, Walsh T, Harrell MI, et al. Germline and somatic mutations in homologous recombination genes predict platinum response and survival in ovarian, fallopian tube, and peritoneal carcinomas. Clin Cancer Res. 2014;20:764-775.
- Mukhopadhyay A, Plummer ER, Elattar A, et al. Clinicopathological features of homologous recombination-deficient epithelial ovarian cancers: sensitivity to PARP inhibitors, platinum, and survival. Cancer Res. 2012;72:5675-5682.
- Mirza MR, Monk BJ, Herrstedt J, et al; ENGOT-OV16/ NOVA Investigators. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N Engl J Med. 2016;375:2154-2164.
- Pujade-Lauraine E, Ledermann JA, Selle F, et al; SOLO2/ ENGOT-Ov21 Investigators. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017;18:1274-1284.
- Coleman RL, Oza AM, Lorusso D, et al; ARIEL3 Investigators. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;390:1949-1961.
- Moore K, Colombo N, Scambia G, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med. 2018;379:2495-2505.
- Coleman RL, Fleming GF, Brady MF, et al. Veliparib with firstline chemotherapy and as maintenance therapy in ovarian cancer. N Engl J Med. 2019;381:2403-2415.
- Coleman RL, Spirtos NM, Enserro D, et al. Secondary surgical cytoreduction for recurrent ovarian cancer. N Engl J Med. 2019;381:1929-1939.
- Bommert M, Harter P, Heitz F, et al. When should surgery be used for recurrent ovarian carcinoma? Clin Oncol (R Coll Radiol). 2018;30:493-497.
- Santillan A, Karam AK, Li AJ, et al. Secondary cytoreductive surgery for isolated nodal recurrence in patients with epithelial ovarian cancer. Gynecol Oncol. 2007;104:686-690.
- Zang RY, Harter P, Chi DS, et al. Predictors of survival in patients with recurrent ovarian cancer undergoing secondary cytoreductive surgery based on the pooled analysis of an international collaborative cohort. Br J Cancer. 2011;105:890-896.
- Chi DS, McCaughty K, Diaz JP, et al. Guidelines and selection criteria for secondary cytoreductive surgery in patients with recurrent, platinum-sensitive epithelial ovarian carcinoma. Cancer. 2006;106:1933-1939.
- Aghajanian C, Blank SV, Goff BA, et al. OCEANS: a randomized, double-blind, placebo-controlled phase III trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube cancer. J Clin Oncol. 2012;30: 2039-2045.
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;20:7-34.
- Colombo N, Creutzberg C, Amant F, et al; ESMO-ESGOESTRO Endometrial Consensus Conference Working Group. ESMO-ESGO-ESTRO consensus conference on endometrial cancer: diagnosis, treatment and follow-up. Ann Oncol. 2016;27:16-41.
- Randall ME, Filiaci VL, Muss H, et al; Gynecologic Oncology Group Study. Randomized phase III trial of whole-abdominal irradiation versus doxorubicin and cisplatin chemotherapy in advanced endometrial carcinoma: a Gynecologic Oncology Group study. J Clin Oncol. 2006;24:36-44.
- Syeda S, Chen L, Hou JY, et al. Chemotherapy, radiation, or combination therapy for stage III uterine cancer. Obstet Gynecol. 2019;134:17-29.
- Maggi R, Lissoni A, Spina F, et al. Adjuvant chemotherapy vs radiotherapy in high-risk endometrial carcinoma: results of a randomised trial. Br J Cancer. 2006;95:266-271.
- Susumu N, Sagae S, Udagawa Y, et al; Japanese Gynecologic Oncology Group. Randomized phase III trial of pelvic radiotherapy versus cisplatin-based combined chemotherapy in patients with intermediate- and high-risk endometrial cancer: a Japanese Gynecologic Oncology Group study. Gynecol Oncol. 2008;108:226-233.
- de Boer SM, Powell ME, Mileshkin L, et al; PORTEC Study Group. Adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3): patterns of recurrence and post-hoc survival analysis of a randomised phase 3 trial. Lancet Oncol. 2019;20:1273-1285.
- Randall ME, Filiaci V, McMeekin DS, et al. Phase III trial: adjuvant pelvic radiation therapy versus vaginal brachytherapy plus paclitaxel/carboplatin in high-intermediate and high-risk early stage endometrial cancer. J Clin Oncol. 2019;37:1810-1818.
- Matei D, Filiaci V, Randall ME, et al. Adjuvant chemotherapy plus radiation for locally advanced endometrial cancer. N Engl J Med. 2019;380:2317-2326.
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-424.
- Armstrong DK, Alvarez RD, Bakkum-Gamez JN, et al. NCCN guidelines insights: ovarian cancer, version 1.2019. J Natl Compr Canc Netw. 2019;17:896-909.
- Ledermann JA, Raja FA, Fotopoulou C, et al. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(suppl 6):vi24-vi32.
- Moore KN, Mirza MR, Matulonis UA. The poly (ADP ribose) polymerase inhibitor niraparib: management of toxicities. Gynecol Oncol. 2018;149:214-220.
- Konstantinopoulos PA, Matulonis UA. PARP inhibitors in ovarian cancer: a trailblazing and transformative journey. Clin Cancer Res. 2018;24:4062-4065.
- Pennington KP, Walsh T, Harrell MI, et al. Germline and somatic mutations in homologous recombination genes predict platinum response and survival in ovarian, fallopian tube, and peritoneal carcinomas. Clin Cancer Res. 2014;20:764-775.
- Mukhopadhyay A, Plummer ER, Elattar A, et al. Clinicopathological features of homologous recombination-deficient epithelial ovarian cancers: sensitivity to PARP inhibitors, platinum, and survival. Cancer Res. 2012;72:5675-5682.
- Mirza MR, Monk BJ, Herrstedt J, et al; ENGOT-OV16/ NOVA Investigators. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N Engl J Med. 2016;375:2154-2164.
- Pujade-Lauraine E, Ledermann JA, Selle F, et al; SOLO2/ ENGOT-Ov21 Investigators. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017;18:1274-1284.
- Coleman RL, Oza AM, Lorusso D, et al; ARIEL3 Investigators. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;390:1949-1961.
- Moore K, Colombo N, Scambia G, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med. 2018;379:2495-2505.
- Coleman RL, Fleming GF, Brady MF, et al. Veliparib with firstline chemotherapy and as maintenance therapy in ovarian cancer. N Engl J Med. 2019;381:2403-2415.
- Coleman RL, Spirtos NM, Enserro D, et al. Secondary surgical cytoreduction for recurrent ovarian cancer. N Engl J Med. 2019;381:1929-1939.
- Bommert M, Harter P, Heitz F, et al. When should surgery be used for recurrent ovarian carcinoma? Clin Oncol (R Coll Radiol). 2018;30:493-497.
- Santillan A, Karam AK, Li AJ, et al. Secondary cytoreductive surgery for isolated nodal recurrence in patients with epithelial ovarian cancer. Gynecol Oncol. 2007;104:686-690.
- Zang RY, Harter P, Chi DS, et al. Predictors of survival in patients with recurrent ovarian cancer undergoing secondary cytoreductive surgery based on the pooled analysis of an international collaborative cohort. Br J Cancer. 2011;105:890-896.
- Chi DS, McCaughty K, Diaz JP, et al. Guidelines and selection criteria for secondary cytoreductive surgery in patients with recurrent, platinum-sensitive epithelial ovarian carcinoma. Cancer. 2006;106:1933-1939.
- Aghajanian C, Blank SV, Goff BA, et al. OCEANS: a randomized, double-blind, placebo-controlled phase III trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube cancer. J Clin Oncol. 2012;30: 2039-2045.
Novel coronavirus may cause environmental contamination through fecal shedding
The toilet bowl, sink, and bathroom door handle of an isolation room housing a patient with the novel coronavirus tested positive for the virus, raising the possibility that viral shedding in the stool could represent another route of transmission, investigators reported.
Air outlet fans and other room sites also tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), though an anteroom, a corridor, and most personal protective equipment (PPE) worn by health care providers tested negative, according to the researchers, led by Sean Wei Xiang Ong, MBBS, of the National Centre for Infectious Diseases, Singapore.
Taken together, these findings suggest a “need for strict adherence to environmental and hand hygiene” to combat significant environmental contamination through respiratory droplets and fecal shedding, Dr. Ong and colleagues wrote in JAMA.
Aaron Eli Glatt, MD, chair of medicine at Mount Sinai South Nassau in New York, said these results demonstrate that SARS-CoV-2 is “clearly capable” of contaminating bathroom sinks and toilets.
“That wouldn’t have been the first place I would have thought of, before this study,” he said in an interview. “You need to pay attention to cleaning the bathrooms, which we obviously do, but that’s an important reminder.”
The report by Dr. Ong and coauthors included a total of three patients housed in airborne infection isolation rooms in a dedicated SARS-CoV-2 outbreak center in Singapore. For each patient, surface samples were taken from 26 sites in the isolation room, an anteroom, and a bathroom. Samples were also taken from PPE on physicians as they left the patient rooms.
Samples for the first patient, taken right after routine cleaning, were all negative, according to researchers. That room was sampled twice, on days 4 and 10 of the illness, while the patient was still symptomatic. Likewise, for the second patient, postcleaning samples were negative; those samples were taken 2 days after cleaning.
However, for the third patient, samples were taken before routine cleaning. In this case, Dr. Ong and colleagues said 13 of 15 room sites (87%) were positive, including air outlet fans, while 3 of 5 toilet sites (60%) were positive as well, though no contamination was found in the anteroom, corridor, or in air samples.
That patient had two stool samples that were positive for SARS-CoV-2, but no diarrhea, authors said, and had upper respiratory tract involvement without pneumonia.
The fact that swabs of the air exhaust outlets tested positive suggests that virus-laden droplets could be “displaced by airflows” and end up on vents or other equipment, Dr. Ong and coauthors reported.
All PPE samples tested negative, except for the front of one shoe.
“The risk of transmission from contaminated footwear is likely low, as evidenced by negative results in the anteroom and corridor,” they wrote.
While this study included only a small number of patients, Dr. Glatt said the findings represent an important and useful contribution to the literature on coronavirus disease 2019 (COVID-19).
“Every day we’re getting more information, and each little piece of the puzzle helps us in the overall management of individuals with COVID-19,” he said in the interview. “They’re adding to our ability to manage, control, and mitigate further spread of the disease.”
Funding for the study came from the National Medical Research Council in Singapore and DSO National Laboratories. Dr. Ong and colleagues reported no conflicts of interest.
SOURCE: Ong SWX et al. JAMA. 2020 Mar 4. doi: 10.1001/jama.2020.3227.
The toilet bowl, sink, and bathroom door handle of an isolation room housing a patient with the novel coronavirus tested positive for the virus, raising the possibility that viral shedding in the stool could represent another route of transmission, investigators reported.
Air outlet fans and other room sites also tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), though an anteroom, a corridor, and most personal protective equipment (PPE) worn by health care providers tested negative, according to the researchers, led by Sean Wei Xiang Ong, MBBS, of the National Centre for Infectious Diseases, Singapore.
Taken together, these findings suggest a “need for strict adherence to environmental and hand hygiene” to combat significant environmental contamination through respiratory droplets and fecal shedding, Dr. Ong and colleagues wrote in JAMA.
Aaron Eli Glatt, MD, chair of medicine at Mount Sinai South Nassau in New York, said these results demonstrate that SARS-CoV-2 is “clearly capable” of contaminating bathroom sinks and toilets.
“That wouldn’t have been the first place I would have thought of, before this study,” he said in an interview. “You need to pay attention to cleaning the bathrooms, which we obviously do, but that’s an important reminder.”
The report by Dr. Ong and coauthors included a total of three patients housed in airborne infection isolation rooms in a dedicated SARS-CoV-2 outbreak center in Singapore. For each patient, surface samples were taken from 26 sites in the isolation room, an anteroom, and a bathroom. Samples were also taken from PPE on physicians as they left the patient rooms.
Samples for the first patient, taken right after routine cleaning, were all negative, according to researchers. That room was sampled twice, on days 4 and 10 of the illness, while the patient was still symptomatic. Likewise, for the second patient, postcleaning samples were negative; those samples were taken 2 days after cleaning.
However, for the third patient, samples were taken before routine cleaning. In this case, Dr. Ong and colleagues said 13 of 15 room sites (87%) were positive, including air outlet fans, while 3 of 5 toilet sites (60%) were positive as well, though no contamination was found in the anteroom, corridor, or in air samples.
That patient had two stool samples that were positive for SARS-CoV-2, but no diarrhea, authors said, and had upper respiratory tract involvement without pneumonia.
The fact that swabs of the air exhaust outlets tested positive suggests that virus-laden droplets could be “displaced by airflows” and end up on vents or other equipment, Dr. Ong and coauthors reported.
All PPE samples tested negative, except for the front of one shoe.
“The risk of transmission from contaminated footwear is likely low, as evidenced by negative results in the anteroom and corridor,” they wrote.
While this study included only a small number of patients, Dr. Glatt said the findings represent an important and useful contribution to the literature on coronavirus disease 2019 (COVID-19).
“Every day we’re getting more information, and each little piece of the puzzle helps us in the overall management of individuals with COVID-19,” he said in the interview. “They’re adding to our ability to manage, control, and mitigate further spread of the disease.”
Funding for the study came from the National Medical Research Council in Singapore and DSO National Laboratories. Dr. Ong and colleagues reported no conflicts of interest.
SOURCE: Ong SWX et al. JAMA. 2020 Mar 4. doi: 10.1001/jama.2020.3227.
The toilet bowl, sink, and bathroom door handle of an isolation room housing a patient with the novel coronavirus tested positive for the virus, raising the possibility that viral shedding in the stool could represent another route of transmission, investigators reported.
Air outlet fans and other room sites also tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), though an anteroom, a corridor, and most personal protective equipment (PPE) worn by health care providers tested negative, according to the researchers, led by Sean Wei Xiang Ong, MBBS, of the National Centre for Infectious Diseases, Singapore.
Taken together, these findings suggest a “need for strict adherence to environmental and hand hygiene” to combat significant environmental contamination through respiratory droplets and fecal shedding, Dr. Ong and colleagues wrote in JAMA.
Aaron Eli Glatt, MD, chair of medicine at Mount Sinai South Nassau in New York, said these results demonstrate that SARS-CoV-2 is “clearly capable” of contaminating bathroom sinks and toilets.
“That wouldn’t have been the first place I would have thought of, before this study,” he said in an interview. “You need to pay attention to cleaning the bathrooms, which we obviously do, but that’s an important reminder.”
The report by Dr. Ong and coauthors included a total of three patients housed in airborne infection isolation rooms in a dedicated SARS-CoV-2 outbreak center in Singapore. For each patient, surface samples were taken from 26 sites in the isolation room, an anteroom, and a bathroom. Samples were also taken from PPE on physicians as they left the patient rooms.
Samples for the first patient, taken right after routine cleaning, were all negative, according to researchers. That room was sampled twice, on days 4 and 10 of the illness, while the patient was still symptomatic. Likewise, for the second patient, postcleaning samples were negative; those samples were taken 2 days after cleaning.
However, for the third patient, samples were taken before routine cleaning. In this case, Dr. Ong and colleagues said 13 of 15 room sites (87%) were positive, including air outlet fans, while 3 of 5 toilet sites (60%) were positive as well, though no contamination was found in the anteroom, corridor, or in air samples.
That patient had two stool samples that were positive for SARS-CoV-2, but no diarrhea, authors said, and had upper respiratory tract involvement without pneumonia.
The fact that swabs of the air exhaust outlets tested positive suggests that virus-laden droplets could be “displaced by airflows” and end up on vents or other equipment, Dr. Ong and coauthors reported.
All PPE samples tested negative, except for the front of one shoe.
“The risk of transmission from contaminated footwear is likely low, as evidenced by negative results in the anteroom and corridor,” they wrote.
While this study included only a small number of patients, Dr. Glatt said the findings represent an important and useful contribution to the literature on coronavirus disease 2019 (COVID-19).
“Every day we’re getting more information, and each little piece of the puzzle helps us in the overall management of individuals with COVID-19,” he said in the interview. “They’re adding to our ability to manage, control, and mitigate further spread of the disease.”
Funding for the study came from the National Medical Research Council in Singapore and DSO National Laboratories. Dr. Ong and colleagues reported no conflicts of interest.
SOURCE: Ong SWX et al. JAMA. 2020 Mar 4. doi: 10.1001/jama.2020.3227.
FROM JAMA

Telehealth seen as a key tool to help fight COVID-19
Telehealth is increasingly being viewed as a key way to help fight the COVID-19 outbreak in the United States. Recognizing the potential of this technology to slow the spread of the disease, the House of Representatives included a provision in an $8.3 billion emergency response bill it approved today that would temporarily lift restrictions on Medicare telehealth coverage to assist in the efforts to contain the virus.
Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention (CDC), said that hospitals should be prepared to use telehealth as one of their tools in fighting the outbreak, according to a recent news release from the American Hospital Association (AHA).
Congress is responding to that need by including the service in the new coronavirus legislation now headed to the Senate, after the funding bill was approved in a 415-2 vote by the House.
The bill empowers the Secretary of Health and Human Services (HHS) to “waive or modify application of certain Medicare requirements with respect to telehealth services furnished during certain emergency periods.”
While the measure adds telehealth to the waiver authority that the HHS secretary currently has during national emergencies, it’s only for the coronavirus crisis in this case, Krista Drobac, executive director of the Alliance for Connected Care, told Medscape Medical News.
The waiver would apply to originating sites of telehealth visits, she noted. Thus Medicare coverage of telemedicine would be expanded beyond rural areas.
In addition, the waiver would allow coverage of virtual visits conducted on smartphones with audio and video capabilities. A “qualified provider,” as defined by the legislation, would be a practitioner who has an established relationship with the patient or who is in the same practice as the provider who has that relationship.
An advantage of telehealth, proponents say, is that it can enable people who believe they have COVID-19 to be seen at home rather than visit offices or emergency departments (EDs) where they might spread the disease or be in proximity to others who have it.
In an editorial published March 2 in Modern Healthcare, medical directors from Stanford Medicine, MedStar Health, and Intermountain Healthcare also noted that telehealth can give patients 24/7 access to care, allow surveillance of patients at risk while keeping them at home, ensure that treatment in hospitals is reserved for high-need patients, and enable providers to triage and screen more patients than can be handled in brick-and-mortar care settings.
However, telehealth screening would allow physicians only to judge whether a patient’s symptoms might be indicative of COVID-19, the Alliance for Connected Care, a telehealth advocacy group, noted in a letter to Congressional leaders. Patients would still have to be seen in person to be tested for the disease.
The group, which represents technology companies, health insurers, pharmacies, and other healthcare players, has been lobbying Congress to include telehealth in federal funds to combat the outbreak.
The American Telemedicine Association (ATA) also supports this goal, ATA President Joseph Kvedar, MD, told Medscape Medical News. And the authors of the Modern Healthcare editorial also advocated for this legislative solution. Because the fatality rate for COVID-19 is significantly higher for older people than for other age groups, they noted, telehealth should be an economically viable option for all seniors.
The Centers for Medicare and Medicaid Services (CMS) long covered telemedicine only in rural areas and only when initiated in healthcare settings. Recently, however, CMS loosened its approach to some extent. Virtual “check-in visits” can now be initiated from any location, including home, to determine whether a Medicare patient needs to be seen in the office. In addition, CMS allows Medicare Advantage plans to offer telemedicine as a core benefit.
Are healthcare systems prepared?
Some large healthcare systems such as Stanford, MedStar, and Intermountain are already using telehealth to diagnose and treat patients who have traditional influenza. Telehealth providers at Stanford estimate that almost 50% of these patients are being prescribed the antiviral drug Tamiflu.
It’s unclear whether other healthcare systems are this well prepared to offer telehealth on a large scale. But, according to an AHA survey, Kvedar noted, three quarters of AHA members are engaged in some form of telehealth.
Drobac said “it wouldn’t require too much effort” to ramp up a wide-scale telehealth program that could help reduce the impact of the outbreak. “The technology is there,” she noted. “You need a HIPAA-compliant telehealth platform, but there are so many out there.”
Kvedar agreed. To begin with, he said, hospitals might sequester patients who visit the ED with COVID-19 symptoms in a video-equipped “isolation room.” Staff members could then do the patient intake from a different location in the hospital.
He admitted that this approach would be infeasible if a lot of patients arrived in EDs with coronavirus symptoms. However, Kvedar noted, “All the tools are in place to go well beyond that. American Well, Teladoc, and others are all offering ways to get out in front of this. There are plenty of vendors out there, and most people have a connected cell phone that you can do a video call on.”
Hospital leaders would have to decide whether to embrace telehealth, which would mean less use of services in their institutions, he said. “But it would be for the greater good of the public.”
Kvedar recalled that there was some use of telehealth in the New York area after 9/11. Telehealth was also used in the aftermath of Hurricane Katrina in 2005. But the ATA president, who is also vice president of connected health at Partners HealthCare in Boston, noted that the COVID-19 outbreak is the first public health emergency to occur in the era of Skype and smartphones.
If Congress does ultimately authorize CMS to cover telehealth across the board during this emergency, might that lead to a permanent change in Medicare coverage policy? Kvedar wouldn’t venture an opinion. “However, the current CMS leadership has been incredibly telehealth friendly,” he said. “So it’s possible they would [embrace a lifting of restrictions]. As patients get a sense of this modality of care and how convenient it is for them, they’ll start asking for more.”
Meanwhile, he said, the telehealth opportunity goes beyond video visits with doctors to mitigate the outbreak. Telehealth data could also be used to track disease spread, similar to how researchers have studied Google searches to predict the spread of the flu, he noted.
Teladoc, a major telehealth vendor, recently told stock analysts it’s already working with the CDC on disease surveillance, according to a report in FierceHealthcare.
This article first appeared on Medscape.com.
Telehealth is increasingly being viewed as a key way to help fight the COVID-19 outbreak in the United States. Recognizing the potential of this technology to slow the spread of the disease, the House of Representatives included a provision in an $8.3 billion emergency response bill it approved today that would temporarily lift restrictions on Medicare telehealth coverage to assist in the efforts to contain the virus.
Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention (CDC), said that hospitals should be prepared to use telehealth as one of their tools in fighting the outbreak, according to a recent news release from the American Hospital Association (AHA).
Congress is responding to that need by including the service in the new coronavirus legislation now headed to the Senate, after the funding bill was approved in a 415-2 vote by the House.
The bill empowers the Secretary of Health and Human Services (HHS) to “waive or modify application of certain Medicare requirements with respect to telehealth services furnished during certain emergency periods.”
While the measure adds telehealth to the waiver authority that the HHS secretary currently has during national emergencies, it’s only for the coronavirus crisis in this case, Krista Drobac, executive director of the Alliance for Connected Care, told Medscape Medical News.
The waiver would apply to originating sites of telehealth visits, she noted. Thus Medicare coverage of telemedicine would be expanded beyond rural areas.
In addition, the waiver would allow coverage of virtual visits conducted on smartphones with audio and video capabilities. A “qualified provider,” as defined by the legislation, would be a practitioner who has an established relationship with the patient or who is in the same practice as the provider who has that relationship.
An advantage of telehealth, proponents say, is that it can enable people who believe they have COVID-19 to be seen at home rather than visit offices or emergency departments (EDs) where they might spread the disease or be in proximity to others who have it.
In an editorial published March 2 in Modern Healthcare, medical directors from Stanford Medicine, MedStar Health, and Intermountain Healthcare also noted that telehealth can give patients 24/7 access to care, allow surveillance of patients at risk while keeping them at home, ensure that treatment in hospitals is reserved for high-need patients, and enable providers to triage and screen more patients than can be handled in brick-and-mortar care settings.
However, telehealth screening would allow physicians only to judge whether a patient’s symptoms might be indicative of COVID-19, the Alliance for Connected Care, a telehealth advocacy group, noted in a letter to Congressional leaders. Patients would still have to be seen in person to be tested for the disease.
The group, which represents technology companies, health insurers, pharmacies, and other healthcare players, has been lobbying Congress to include telehealth in federal funds to combat the outbreak.
The American Telemedicine Association (ATA) also supports this goal, ATA President Joseph Kvedar, MD, told Medscape Medical News. And the authors of the Modern Healthcare editorial also advocated for this legislative solution. Because the fatality rate for COVID-19 is significantly higher for older people than for other age groups, they noted, telehealth should be an economically viable option for all seniors.
The Centers for Medicare and Medicaid Services (CMS) long covered telemedicine only in rural areas and only when initiated in healthcare settings. Recently, however, CMS loosened its approach to some extent. Virtual “check-in visits” can now be initiated from any location, including home, to determine whether a Medicare patient needs to be seen in the office. In addition, CMS allows Medicare Advantage plans to offer telemedicine as a core benefit.
Are healthcare systems prepared?
Some large healthcare systems such as Stanford, MedStar, and Intermountain are already using telehealth to diagnose and treat patients who have traditional influenza. Telehealth providers at Stanford estimate that almost 50% of these patients are being prescribed the antiviral drug Tamiflu.
It’s unclear whether other healthcare systems are this well prepared to offer telehealth on a large scale. But, according to an AHA survey, Kvedar noted, three quarters of AHA members are engaged in some form of telehealth.
Drobac said “it wouldn’t require too much effort” to ramp up a wide-scale telehealth program that could help reduce the impact of the outbreak. “The technology is there,” she noted. “You need a HIPAA-compliant telehealth platform, but there are so many out there.”
Kvedar agreed. To begin with, he said, hospitals might sequester patients who visit the ED with COVID-19 symptoms in a video-equipped “isolation room.” Staff members could then do the patient intake from a different location in the hospital.
He admitted that this approach would be infeasible if a lot of patients arrived in EDs with coronavirus symptoms. However, Kvedar noted, “All the tools are in place to go well beyond that. American Well, Teladoc, and others are all offering ways to get out in front of this. There are plenty of vendors out there, and most people have a connected cell phone that you can do a video call on.”
Hospital leaders would have to decide whether to embrace telehealth, which would mean less use of services in their institutions, he said. “But it would be for the greater good of the public.”
Kvedar recalled that there was some use of telehealth in the New York area after 9/11. Telehealth was also used in the aftermath of Hurricane Katrina in 2005. But the ATA president, who is also vice president of connected health at Partners HealthCare in Boston, noted that the COVID-19 outbreak is the first public health emergency to occur in the era of Skype and smartphones.
If Congress does ultimately authorize CMS to cover telehealth across the board during this emergency, might that lead to a permanent change in Medicare coverage policy? Kvedar wouldn’t venture an opinion. “However, the current CMS leadership has been incredibly telehealth friendly,” he said. “So it’s possible they would [embrace a lifting of restrictions]. As patients get a sense of this modality of care and how convenient it is for them, they’ll start asking for more.”
Meanwhile, he said, the telehealth opportunity goes beyond video visits with doctors to mitigate the outbreak. Telehealth data could also be used to track disease spread, similar to how researchers have studied Google searches to predict the spread of the flu, he noted.
Teladoc, a major telehealth vendor, recently told stock analysts it’s already working with the CDC on disease surveillance, according to a report in FierceHealthcare.
This article first appeared on Medscape.com.
Telehealth is increasingly being viewed as a key way to help fight the COVID-19 outbreak in the United States. Recognizing the potential of this technology to slow the spread of the disease, the House of Representatives included a provision in an $8.3 billion emergency response bill it approved today that would temporarily lift restrictions on Medicare telehealth coverage to assist in the efforts to contain the virus.
Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention (CDC), said that hospitals should be prepared to use telehealth as one of their tools in fighting the outbreak, according to a recent news release from the American Hospital Association (AHA).
Congress is responding to that need by including the service in the new coronavirus legislation now headed to the Senate, after the funding bill was approved in a 415-2 vote by the House.
The bill empowers the Secretary of Health and Human Services (HHS) to “waive or modify application of certain Medicare requirements with respect to telehealth services furnished during certain emergency periods.”
While the measure adds telehealth to the waiver authority that the HHS secretary currently has during national emergencies, it’s only for the coronavirus crisis in this case, Krista Drobac, executive director of the Alliance for Connected Care, told Medscape Medical News.
The waiver would apply to originating sites of telehealth visits, she noted. Thus Medicare coverage of telemedicine would be expanded beyond rural areas.
In addition, the waiver would allow coverage of virtual visits conducted on smartphones with audio and video capabilities. A “qualified provider,” as defined by the legislation, would be a practitioner who has an established relationship with the patient or who is in the same practice as the provider who has that relationship.
An advantage of telehealth, proponents say, is that it can enable people who believe they have COVID-19 to be seen at home rather than visit offices or emergency departments (EDs) where they might spread the disease or be in proximity to others who have it.
In an editorial published March 2 in Modern Healthcare, medical directors from Stanford Medicine, MedStar Health, and Intermountain Healthcare also noted that telehealth can give patients 24/7 access to care, allow surveillance of patients at risk while keeping them at home, ensure that treatment in hospitals is reserved for high-need patients, and enable providers to triage and screen more patients than can be handled in brick-and-mortar care settings.
However, telehealth screening would allow physicians only to judge whether a patient’s symptoms might be indicative of COVID-19, the Alliance for Connected Care, a telehealth advocacy group, noted in a letter to Congressional leaders. Patients would still have to be seen in person to be tested for the disease.
The group, which represents technology companies, health insurers, pharmacies, and other healthcare players, has been lobbying Congress to include telehealth in federal funds to combat the outbreak.
The American Telemedicine Association (ATA) also supports this goal, ATA President Joseph Kvedar, MD, told Medscape Medical News. And the authors of the Modern Healthcare editorial also advocated for this legislative solution. Because the fatality rate for COVID-19 is significantly higher for older people than for other age groups, they noted, telehealth should be an economically viable option for all seniors.
The Centers for Medicare and Medicaid Services (CMS) long covered telemedicine only in rural areas and only when initiated in healthcare settings. Recently, however, CMS loosened its approach to some extent. Virtual “check-in visits” can now be initiated from any location, including home, to determine whether a Medicare patient needs to be seen in the office. In addition, CMS allows Medicare Advantage plans to offer telemedicine as a core benefit.
Are healthcare systems prepared?
Some large healthcare systems such as Stanford, MedStar, and Intermountain are already using telehealth to diagnose and treat patients who have traditional influenza. Telehealth providers at Stanford estimate that almost 50% of these patients are being prescribed the antiviral drug Tamiflu.
It’s unclear whether other healthcare systems are this well prepared to offer telehealth on a large scale. But, according to an AHA survey, Kvedar noted, three quarters of AHA members are engaged in some form of telehealth.
Drobac said “it wouldn’t require too much effort” to ramp up a wide-scale telehealth program that could help reduce the impact of the outbreak. “The technology is there,” she noted. “You need a HIPAA-compliant telehealth platform, but there are so many out there.”
Kvedar agreed. To begin with, he said, hospitals might sequester patients who visit the ED with COVID-19 symptoms in a video-equipped “isolation room.” Staff members could then do the patient intake from a different location in the hospital.
He admitted that this approach would be infeasible if a lot of patients arrived in EDs with coronavirus symptoms. However, Kvedar noted, “All the tools are in place to go well beyond that. American Well, Teladoc, and others are all offering ways to get out in front of this. There are plenty of vendors out there, and most people have a connected cell phone that you can do a video call on.”
Hospital leaders would have to decide whether to embrace telehealth, which would mean less use of services in their institutions, he said. “But it would be for the greater good of the public.”
Kvedar recalled that there was some use of telehealth in the New York area after 9/11. Telehealth was also used in the aftermath of Hurricane Katrina in 2005. But the ATA president, who is also vice president of connected health at Partners HealthCare in Boston, noted that the COVID-19 outbreak is the first public health emergency to occur in the era of Skype and smartphones.
If Congress does ultimately authorize CMS to cover telehealth across the board during this emergency, might that lead to a permanent change in Medicare coverage policy? Kvedar wouldn’t venture an opinion. “However, the current CMS leadership has been incredibly telehealth friendly,” he said. “So it’s possible they would [embrace a lifting of restrictions]. As patients get a sense of this modality of care and how convenient it is for them, they’ll start asking for more.”
Meanwhile, he said, the telehealth opportunity goes beyond video visits with doctors to mitigate the outbreak. Telehealth data could also be used to track disease spread, similar to how researchers have studied Google searches to predict the spread of the flu, he noted.
Teladoc, a major telehealth vendor, recently told stock analysts it’s already working with the CDC on disease surveillance, according to a report in FierceHealthcare.
This article first appeared on Medscape.com.
Effective osteoarthritis therapy remains elusive
MAUI, HAWAII – Osteoarthritis therapy remains a barren landscape where conventional medicine has so little to offer that many affected patients eagerly embrace unproven Internet claims for costly out-of-pocket intra-articular injections of platelet-rich plasma, oxygen ozone, and mesenchymal stem cells, Eric M. Ruderman, MD, said at the 2020 Rheumatology Winter Clinical Symposium.

He presented a whirlwind review of the evidence – or lack thereof – for a wide range of contemporary OA therapies, ranging from acupuncture to cupping, lateral wedge insoles, various substances for intra-articular injection, radiofrequency therapy, medical leeches, and several widely ballyhooed medications that are well along in the developmental pipeline but whose placebo-subtracted efficacy is actually quite modest.
“I’ve shown you the evidence, such as it is – it’s not very much. The question is, have we really moved the needle in this disease in the last 30 years? The answer is I’m not so sure we have,” concluded Dr. Ruderman, professor of medicine and associate chief for clinical affairs in the division of rheumatology at Northwestern University, Chicago.
Several audience members were less restrained in their assessments.
“You have not moved the needle in osteoarthritis,” stated orthopedic surgeon William Bugbee, MD, chief of joint reconstruction at the Scripps Clinic in La Jolla, Calif., adding that he’s not much impressed by the long-term impact of intra-articular injections, be they of glucocorticoid, hyaluronic acid, or anything else being put into osteoarthritic joints.

“To me, and to most orthopedic surgeons, an injection is a handshake. It’s like: ‘How do you do? Let’s get to know each other.’ But you know where this interaction is going – it’s going to end up in surgery. But that’s okay. Surgery is great. Let’s face it: It’s the only disease-modifying treatment for OA,” Dr. Bugbee declared.
Roy Fleischmann, MD, rose from the audience to assert that “the biggest need in rheumatology right now is a medication for OA that actually works and is actually disease modifying.”
That’s not going to happen until clinical trialists and the pharmaceutical industry learn how to subgroup OA and separate inflammatory OA from noninflammatory OA. Lumping the two together tends to wash out any strong efficacy signal an investigational agent might have, added Dr. Fleischmann, a rheumatologist at the University of Texas and medical director of the Metroplex Clinical Research Center, both in Dallas.
Dr. Ruderman noted that his own analysis of the contemporary evidence base for OA pharmacotherapies reached conclusions generally similar to those contained in the new American College of Rheumatology/Arthritis Foundation “Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee”. The list of pharmacotherapies that were strongly recommended in the guidelines was slim and rather tired: oral NSAIDs, intra-articular glucocorticoid injections, and – for knee OA only – topical NSAIDs. The strength of those favorable recommendations was based more upon solid evidence of safety rather than impressive efficacy, in his view. And the guidelines’ list of therapies whose use was strongly discouraged was much longer.
A factor in the flimsy evidence base for OA treatment is the strikingly large across-the-board placebo effect. This was nicely captured in a meta-analysis of 215 randomized, controlled trials of various therapies totaling more than 41,000 participants. Drilling down into the data, the British and Chinese investigators concluded that on average 75% of the overall treatment effect seen in the trials was caused by the placebo effect and only 25% represented a treatment-specific effect. The “winner” was intra-articular glucocorticoid, where the placebo effect was a mere 47%.
In the OA pipeline
“There’s a lot of interest in DMOADs – disease-modifying osteoarthritis drugs – but not a lot of success so far,” Dr. Ruderman observed.
Case in point: intra-articular sprifermin, a recombinant human fibroblast growth factor 18. In a 549-patient, multicenter, dose-ranging study, the two highest doses achieved a modest yet statistically significant advantage over placebo in total femorotibial joint cartilage thickness on MRI at 2 years. However, the investigators added that the result was of “uncertain clinical importance,” given the lack of a difference from baseline in total Western Ontario and McMaster Universities OA Index score.
“I’m not sure this is going anywhere,” Dr. Ruderman commented.
Tanezumab, a novel subcutaneously injected monoclonal antibody directed against nerve growth factor, has drawn a lot of attention. In an initial multicenter, phase 3, randomized trial it showed what Dr. Ruderman termed “some modest benefit” on pain and function.
“Very much like everything else in OA, you see a huge placebo effect buried in there,” according to the rheumatologist.
This modest clinical benefit was accompanied by a safety signal at the higher 5-mg dose of tanezumab. Moreover, a second phase 3 trial, this one conducted in nearly 3,000 OA patients and presented at the 2019 annual meeting of the American College of Rheumatology, also raised significant safety concerns at the higher dose. And while the 2.5-mg dose was safer, it was disappointingly no more effective in terms of improvement in pain and function scores than diclofenac at 75 mg twice daily, Dr. Ruderman noted.
Dr. Fleischmann predicted that, given the enormous unmet need for new OA treatments, tanezumab at 2.5 mg will win regulatory approval, but it will be a costly niche drug reserved for the challenging subset of patients who can’t take an NSAID and are poor surgical candidates. (On March 2, 2020, Eli Lilly announced that the Food and Drug Administration had accepted its Biologics License Application for tanezumab for the treatment of chronic pain caused by moderate to severe OA.)
Intra-articular FX006, a microsphere-based, extended-release formulation of triamcinolone, outperformed conventional triamcinolone in a phase 3 clinical trial. However, the placebo-subtracted improvement in pain was modest.
“There’s some marginal benefit here, but over time I’m not sure this adds much to just straight-up triamcinolone,” Dr. Ruderman opined.
Welcome to the wild, wild West
Patients with knee OA ask Dr. Ruderman all the time about the intra-articular injections of platelet-rich plasma (PRP) or mesenchymal stem cells they’ve seen touted on the Internet. As an evidence-based physician, he’s not a fan. A meta-analysis of 14 controlled trials of PRP, none double blind, showed some benefit in terms of pain and function at 3, 6, and 12 months, with little risk of adverse events. However, PRP is being marketed with a hype and claimed efficacy out of all proportion to the actual evidence.
“It’s the wild, wild West out there,” the rheumatologist warned.
He cited a study involving a scripted survey of 179 U.S. clinics offering PRP. The mean price quoted for a unilateral knee injection in a hypothetical 52-year-old man with knee OA was $714, and it’s a cash business, since insurance companies won’t cover PRP. Out of 84 centers that were willing to share their claimed efficacy, 10 quoted 90%-100% rates of good results or symptomatic improvement, 27 claimed 80%-90% efficacy, and 29 quoted figures of 70%-80%, all of which are well above the success rates achieved in the flawed clinical trials.
As for mesenchymal stem cells, “if PRP is the wild, wild West, this is the surface of Mars,” Dr. Ruderman quipped.
These stem cell injections are neither FDA regulated nor approved. There are no barriers to setting up a mesenchymal stem cell injection center, and the number of such centers is skyrocketing. Anybody can set up a center, and there’s essentially no oversight.
“The evidence in this area is really terrible,” the rheumatologist said. He pointed to a meta-analysis of five trials, only two of which were rated by the researchers as having a low risk of bias. The conclusion: There was limited evidence of short-term benefit in pain and function, but no evidence of cartilage repair, which is the chief claimed benefit.
The same group of investigators who queried the PRP clinics also successfully contacted 273 of the proliferating U.S. centers offering direct-to-consumer mesenchymal stem cell therapy. The mean price quoted for a unilateral knee injection was a whopping $5,156, which – like PRP – isn’t covered by insurance. At the 36 clinics responding to a request for their efficacy rates, the mean claim was good results or symptomatic improvement in 82% of treated patients.
Dr. Bugbee didn’t endorse this intervention, which is increasingly popular among his fellow orthopedic surgeons.
“The regulatory pathway drives this. Mesenchymal stem cells are categorized as a minimally manipulated tissue, so the regulatory pathway is easy,” explained Dr. Bugbee. “I talk 9 out of 10 patients out of it because there’s no evidence of disease modification.”
On a brighter note
Radiofrequency ablation and neuromodulation procedures for treatment of symptomatic knee OA make no pretense of being disease modifying, but a new systematic review of 33 published studies deemed of moderate or high methodological quality totaling 1,512 patients documented improved pain, function, and disease-specific quality of life for 3-12 months with minimal complications.
Most of these procedures target the genicular nerve, the sensory nerve that innervates the knee.
“There’s some value here to this,” Dr. Ruderman said. “Our pain folks are actually pretty interested in this. At our center, they’re using this for patients with persistent knee pain after knee replacement, with some success. It’s not an unreasonable approach.”
As part of his examination of the evidence base for OA treatment, Dr. Ruderman looked into an intervention he wasn’t familiar with: acupuncture. He was pleasantly surprised.
“There’s quite a bit of data. There is decent evidence that acupuncture has significant benefit, at least for pain, and is certainly without significant side effects,” according to the rheumatologist.
He cited a review of a dozen systematic reviews of randomized, controlled trials of acupuncture for OA. The Chinese investigators rated the overall quality of the evidence as moderate to low, but with some studies being rated high quality. “That’s not as bad as some of the other stuff I looked at,” Dr. Ruderman said.
Acupuncture was found to be 2.4 times more effective than Western medicine for short-term pain relief, and 4.1 times better in terms of total efficacy, with a lower risk of adverse events than with Western medicine.
Dr. Ruderman reported serving as a consultant for and/or receiving research grants from more than a half-dozen pharmaceutical companies.
MAUI, HAWAII – Osteoarthritis therapy remains a barren landscape where conventional medicine has so little to offer that many affected patients eagerly embrace unproven Internet claims for costly out-of-pocket intra-articular injections of platelet-rich plasma, oxygen ozone, and mesenchymal stem cells, Eric M. Ruderman, MD, said at the 2020 Rheumatology Winter Clinical Symposium.
He presented a whirlwind review of the evidence – or lack thereof – for a wide range of contemporary OA therapies, ranging from acupuncture to cupping, lateral wedge insoles, various substances for intra-articular injection, radiofrequency therapy, medical leeches, and several widely ballyhooed medications that are well along in the developmental pipeline but whose placebo-subtracted efficacy is actually quite modest.
“I’ve shown you the evidence, such as it is – it’s not very much. The question is, have we really moved the needle in this disease in the last 30 years? The answer is I’m not so sure we have,” concluded Dr. Ruderman, professor of medicine and associate chief for clinical affairs in the division of rheumatology at Northwestern University, Chicago.
Several audience members were less restrained in their assessments.
“You have not moved the needle in osteoarthritis,” stated orthopedic surgeon William Bugbee, MD, chief of joint reconstruction at the Scripps Clinic in La Jolla, Calif., adding that he’s not much impressed by the long-term impact of intra-articular injections, be they of glucocorticoid, hyaluronic acid, or anything else being put into osteoarthritic joints.
“To me, and to most orthopedic surgeons, an injection is a handshake. It’s like: ‘How do you do? Let’s get to know each other.’ But you know where this interaction is going – it’s going to end up in surgery. But that’s okay. Surgery is great. Let’s face it: It’s the only disease-modifying treatment for OA,” Dr. Bugbee declared.
Roy Fleischmann, MD, rose from the audience to assert that “the biggest need in rheumatology right now is a medication for OA that actually works and is actually disease modifying.”
That’s not going to happen until clinical trialists and the pharmaceutical industry learn how to subgroup OA and separate inflammatory OA from noninflammatory OA. Lumping the two together tends to wash out any strong efficacy signal an investigational agent might have, added Dr. Fleischmann, a rheumatologist at the University of Texas and medical director of the Metroplex Clinical Research Center, both in Dallas.
Dr. Ruderman noted that his own analysis of the contemporary evidence base for OA pharmacotherapies reached conclusions generally similar to those contained in the new American College of Rheumatology/Arthritis Foundation “Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee”. The list of pharmacotherapies that were strongly recommended in the guidelines was slim and rather tired: oral NSAIDs, intra-articular glucocorticoid injections, and – for knee OA only – topical NSAIDs. The strength of those favorable recommendations was based more upon solid evidence of safety rather than impressive efficacy, in his view. And the guidelines’ list of therapies whose use was strongly discouraged was much longer.
A factor in the flimsy evidence base for OA treatment is the strikingly large across-the-board placebo effect. This was nicely captured in a meta-analysis of 215 randomized, controlled trials of various therapies totaling more than 41,000 participants. Drilling down into the data, the British and Chinese investigators concluded that on average 75% of the overall treatment effect seen in the trials was caused by the placebo effect and only 25% represented a treatment-specific effect. The “winner” was intra-articular glucocorticoid, where the placebo effect was a mere 47%.
In the OA pipeline
“There’s a lot of interest in DMOADs – disease-modifying osteoarthritis drugs – but not a lot of success so far,” Dr. Ruderman observed.
Case in point: intra-articular sprifermin, a recombinant human fibroblast growth factor 18. In a 549-patient, multicenter, dose-ranging study, the two highest doses achieved a modest yet statistically significant advantage over placebo in total femorotibial joint cartilage thickness on MRI at 2 years. However, the investigators added that the result was of “uncertain clinical importance,” given the lack of a difference from baseline in total Western Ontario and McMaster Universities OA Index score.
“I’m not sure this is going anywhere,” Dr. Ruderman commented.
Tanezumab, a novel subcutaneously injected monoclonal antibody directed against nerve growth factor, has drawn a lot of attention. In an initial multicenter, phase 3, randomized trial it showed what Dr. Ruderman termed “some modest benefit” on pain and function.
“Very much like everything else in OA, you see a huge placebo effect buried in there,” according to the rheumatologist.
This modest clinical benefit was accompanied by a safety signal at the higher 5-mg dose of tanezumab. Moreover, a second phase 3 trial, this one conducted in nearly 3,000 OA patients and presented at the 2019 annual meeting of the American College of Rheumatology, also raised significant safety concerns at the higher dose. And while the 2.5-mg dose was safer, it was disappointingly no more effective in terms of improvement in pain and function scores than diclofenac at 75 mg twice daily, Dr. Ruderman noted.
Dr. Fleischmann predicted that, given the enormous unmet need for new OA treatments, tanezumab at 2.5 mg will win regulatory approval, but it will be a costly niche drug reserved for the challenging subset of patients who can’t take an NSAID and are poor surgical candidates. (On March 2, 2020, Eli Lilly announced that the Food and Drug Administration had accepted its Biologics License Application for tanezumab for the treatment of chronic pain caused by moderate to severe OA.)
Intra-articular FX006, a microsphere-based, extended-release formulation of triamcinolone, outperformed conventional triamcinolone in a phase 3 clinical trial. However, the placebo-subtracted improvement in pain was modest.
“There’s some marginal benefit here, but over time I’m not sure this adds much to just straight-up triamcinolone,” Dr. Ruderman opined.
Welcome to the wild, wild West
Patients with knee OA ask Dr. Ruderman all the time about the intra-articular injections of platelet-rich plasma (PRP) or mesenchymal stem cells they’ve seen touted on the Internet. As an evidence-based physician, he’s not a fan. A meta-analysis of 14 controlled trials of PRP, none double blind, showed some benefit in terms of pain and function at 3, 6, and 12 months, with little risk of adverse events. However, PRP is being marketed with a hype and claimed efficacy out of all proportion to the actual evidence.
“It’s the wild, wild West out there,” the rheumatologist warned.
He cited a study involving a scripted survey of 179 U.S. clinics offering PRP. The mean price quoted for a unilateral knee injection in a hypothetical 52-year-old man with knee OA was $714, and it’s a cash business, since insurance companies won’t cover PRP. Out of 84 centers that were willing to share their claimed efficacy, 10 quoted 90%-100% rates of good results or symptomatic improvement, 27 claimed 80%-90% efficacy, and 29 quoted figures of 70%-80%, all of which are well above the success rates achieved in the flawed clinical trials.
As for mesenchymal stem cells, “if PRP is the wild, wild West, this is the surface of Mars,” Dr. Ruderman quipped.
These stem cell injections are neither FDA regulated nor approved. There are no barriers to setting up a mesenchymal stem cell injection center, and the number of such centers is skyrocketing. Anybody can set up a center, and there’s essentially no oversight.
“The evidence in this area is really terrible,” the rheumatologist said. He pointed to a meta-analysis of five trials, only two of which were rated by the researchers as having a low risk of bias. The conclusion: There was limited evidence of short-term benefit in pain and function, but no evidence of cartilage repair, which is the chief claimed benefit.
The same group of investigators who queried the PRP clinics also successfully contacted 273 of the proliferating U.S. centers offering direct-to-consumer mesenchymal stem cell therapy. The mean price quoted for a unilateral knee injection was a whopping $5,156, which – like PRP – isn’t covered by insurance. At the 36 clinics responding to a request for their efficacy rates, the mean claim was good results or symptomatic improvement in 82% of treated patients.
Dr. Bugbee didn’t endorse this intervention, which is increasingly popular among his fellow orthopedic surgeons.
“The regulatory pathway drives this. Mesenchymal stem cells are categorized as a minimally manipulated tissue, so the regulatory pathway is easy,” explained Dr. Bugbee. “I talk 9 out of 10 patients out of it because there’s no evidence of disease modification.”
On a brighter note
Radiofrequency ablation and neuromodulation procedures for treatment of symptomatic knee OA make no pretense of being disease modifying, but a new systematic review of 33 published studies deemed of moderate or high methodological quality totaling 1,512 patients documented improved pain, function, and disease-specific quality of life for 3-12 months with minimal complications.
Most of these procedures target the genicular nerve, the sensory nerve that innervates the knee.
“There’s some value here to this,” Dr. Ruderman said. “Our pain folks are actually pretty interested in this. At our center, they’re using this for patients with persistent knee pain after knee replacement, with some success. It’s not an unreasonable approach.”
As part of his examination of the evidence base for OA treatment, Dr. Ruderman looked into an intervention he wasn’t familiar with: acupuncture. He was pleasantly surprised.
“There’s quite a bit of data. There is decent evidence that acupuncture has significant benefit, at least for pain, and is certainly without significant side effects,” according to the rheumatologist.
He cited a review of a dozen systematic reviews of randomized, controlled trials of acupuncture for OA. The Chinese investigators rated the overall quality of the evidence as moderate to low, but with some studies being rated high quality. “That’s not as bad as some of the other stuff I looked at,” Dr. Ruderman said.
Acupuncture was found to be 2.4 times more effective than Western medicine for short-term pain relief, and 4.1 times better in terms of total efficacy, with a lower risk of adverse events than with Western medicine.
Dr. Ruderman reported serving as a consultant for and/or receiving research grants from more than a half-dozen pharmaceutical companies.
MAUI, HAWAII – Osteoarthritis therapy remains a barren landscape where conventional medicine has so little to offer that many affected patients eagerly embrace unproven Internet claims for costly out-of-pocket intra-articular injections of platelet-rich plasma, oxygen ozone, and mesenchymal stem cells, Eric M. Ruderman, MD, said at the 2020 Rheumatology Winter Clinical Symposium.
He presented a whirlwind review of the evidence – or lack thereof – for a wide range of contemporary OA therapies, ranging from acupuncture to cupping, lateral wedge insoles, various substances for intra-articular injection, radiofrequency therapy, medical leeches, and several widely ballyhooed medications that are well along in the developmental pipeline but whose placebo-subtracted efficacy is actually quite modest.
“I’ve shown you the evidence, such as it is – it’s not very much. The question is, have we really moved the needle in this disease in the last 30 years? The answer is I’m not so sure we have,” concluded Dr. Ruderman, professor of medicine and associate chief for clinical affairs in the division of rheumatology at Northwestern University, Chicago.
Several audience members were less restrained in their assessments.
“You have not moved the needle in osteoarthritis,” stated orthopedic surgeon William Bugbee, MD, chief of joint reconstruction at the Scripps Clinic in La Jolla, Calif., adding that he’s not much impressed by the long-term impact of intra-articular injections, be they of glucocorticoid, hyaluronic acid, or anything else being put into osteoarthritic joints.
“To me, and to most orthopedic surgeons, an injection is a handshake. It’s like: ‘How do you do? Let’s get to know each other.’ But you know where this interaction is going – it’s going to end up in surgery. But that’s okay. Surgery is great. Let’s face it: It’s the only disease-modifying treatment for OA,” Dr. Bugbee declared.
Roy Fleischmann, MD, rose from the audience to assert that “the biggest need in rheumatology right now is a medication for OA that actually works and is actually disease modifying.”
That’s not going to happen until clinical trialists and the pharmaceutical industry learn how to subgroup OA and separate inflammatory OA from noninflammatory OA. Lumping the two together tends to wash out any strong efficacy signal an investigational agent might have, added Dr. Fleischmann, a rheumatologist at the University of Texas and medical director of the Metroplex Clinical Research Center, both in Dallas.
Dr. Ruderman noted that his own analysis of the contemporary evidence base for OA pharmacotherapies reached conclusions generally similar to those contained in the new American College of Rheumatology/Arthritis Foundation “Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee”. The list of pharmacotherapies that were strongly recommended in the guidelines was slim and rather tired: oral NSAIDs, intra-articular glucocorticoid injections, and – for knee OA only – topical NSAIDs. The strength of those favorable recommendations was based more upon solid evidence of safety rather than impressive efficacy, in his view. And the guidelines’ list of therapies whose use was strongly discouraged was much longer.
A factor in the flimsy evidence base for OA treatment is the strikingly large across-the-board placebo effect. This was nicely captured in a meta-analysis of 215 randomized, controlled trials of various therapies totaling more than 41,000 participants. Drilling down into the data, the British and Chinese investigators concluded that on average 75% of the overall treatment effect seen in the trials was caused by the placebo effect and only 25% represented a treatment-specific effect. The “winner” was intra-articular glucocorticoid, where the placebo effect was a mere 47%.
In the OA pipeline
“There’s a lot of interest in DMOADs – disease-modifying osteoarthritis drugs – but not a lot of success so far,” Dr. Ruderman observed.
Case in point: intra-articular sprifermin, a recombinant human fibroblast growth factor 18. In a 549-patient, multicenter, dose-ranging study, the two highest doses achieved a modest yet statistically significant advantage over placebo in total femorotibial joint cartilage thickness on MRI at 2 years. However, the investigators added that the result was of “uncertain clinical importance,” given the lack of a difference from baseline in total Western Ontario and McMaster Universities OA Index score.
“I’m not sure this is going anywhere,” Dr. Ruderman commented.
Tanezumab, a novel subcutaneously injected monoclonal antibody directed against nerve growth factor, has drawn a lot of attention. In an initial multicenter, phase 3, randomized trial it showed what Dr. Ruderman termed “some modest benefit” on pain and function.
“Very much like everything else in OA, you see a huge placebo effect buried in there,” according to the rheumatologist.
This modest clinical benefit was accompanied by a safety signal at the higher 5-mg dose of tanezumab. Moreover, a second phase 3 trial, this one conducted in nearly 3,000 OA patients and presented at the 2019 annual meeting of the American College of Rheumatology, also raised significant safety concerns at the higher dose. And while the 2.5-mg dose was safer, it was disappointingly no more effective in terms of improvement in pain and function scores than diclofenac at 75 mg twice daily, Dr. Ruderman noted.
Dr. Fleischmann predicted that, given the enormous unmet need for new OA treatments, tanezumab at 2.5 mg will win regulatory approval, but it will be a costly niche drug reserved for the challenging subset of patients who can’t take an NSAID and are poor surgical candidates. (On March 2, 2020, Eli Lilly announced that the Food and Drug Administration had accepted its Biologics License Application for tanezumab for the treatment of chronic pain caused by moderate to severe OA.)
Intra-articular FX006, a microsphere-based, extended-release formulation of triamcinolone, outperformed conventional triamcinolone in a phase 3 clinical trial. However, the placebo-subtracted improvement in pain was modest.
“There’s some marginal benefit here, but over time I’m not sure this adds much to just straight-up triamcinolone,” Dr. Ruderman opined.
Welcome to the wild, wild West
Patients with knee OA ask Dr. Ruderman all the time about the intra-articular injections of platelet-rich plasma (PRP) or mesenchymal stem cells they’ve seen touted on the Internet. As an evidence-based physician, he’s not a fan. A meta-analysis of 14 controlled trials of PRP, none double blind, showed some benefit in terms of pain and function at 3, 6, and 12 months, with little risk of adverse events. However, PRP is being marketed with a hype and claimed efficacy out of all proportion to the actual evidence.
“It’s the wild, wild West out there,” the rheumatologist warned.
He cited a study involving a scripted survey of 179 U.S. clinics offering PRP. The mean price quoted for a unilateral knee injection in a hypothetical 52-year-old man with knee OA was $714, and it’s a cash business, since insurance companies won’t cover PRP. Out of 84 centers that were willing to share their claimed efficacy, 10 quoted 90%-100% rates of good results or symptomatic improvement, 27 claimed 80%-90% efficacy, and 29 quoted figures of 70%-80%, all of which are well above the success rates achieved in the flawed clinical trials.
As for mesenchymal stem cells, “if PRP is the wild, wild West, this is the surface of Mars,” Dr. Ruderman quipped.
These stem cell injections are neither FDA regulated nor approved. There are no barriers to setting up a mesenchymal stem cell injection center, and the number of such centers is skyrocketing. Anybody can set up a center, and there’s essentially no oversight.
“The evidence in this area is really terrible,” the rheumatologist said. He pointed to a meta-analysis of five trials, only two of which were rated by the researchers as having a low risk of bias. The conclusion: There was limited evidence of short-term benefit in pain and function, but no evidence of cartilage repair, which is the chief claimed benefit.
The same group of investigators who queried the PRP clinics also successfully contacted 273 of the proliferating U.S. centers offering direct-to-consumer mesenchymal stem cell therapy. The mean price quoted for a unilateral knee injection was a whopping $5,156, which – like PRP – isn’t covered by insurance. At the 36 clinics responding to a request for their efficacy rates, the mean claim was good results or symptomatic improvement in 82% of treated patients.
Dr. Bugbee didn’t endorse this intervention, which is increasingly popular among his fellow orthopedic surgeons.
“The regulatory pathway drives this. Mesenchymal stem cells are categorized as a minimally manipulated tissue, so the regulatory pathway is easy,” explained Dr. Bugbee. “I talk 9 out of 10 patients out of it because there’s no evidence of disease modification.”
On a brighter note
Radiofrequency ablation and neuromodulation procedures for treatment of symptomatic knee OA make no pretense of being disease modifying, but a new systematic review of 33 published studies deemed of moderate or high methodological quality totaling 1,512 patients documented improved pain, function, and disease-specific quality of life for 3-12 months with minimal complications.
Most of these procedures target the genicular nerve, the sensory nerve that innervates the knee.
“There’s some value here to this,” Dr. Ruderman said. “Our pain folks are actually pretty interested in this. At our center, they’re using this for patients with persistent knee pain after knee replacement, with some success. It’s not an unreasonable approach.”
As part of his examination of the evidence base for OA treatment, Dr. Ruderman looked into an intervention he wasn’t familiar with: acupuncture. He was pleasantly surprised.
“There’s quite a bit of data. There is decent evidence that acupuncture has significant benefit, at least for pain, and is certainly without significant side effects,” according to the rheumatologist.
He cited a review of a dozen systematic reviews of randomized, controlled trials of acupuncture for OA. The Chinese investigators rated the overall quality of the evidence as moderate to low, but with some studies being rated high quality. “That’s not as bad as some of the other stuff I looked at,” Dr. Ruderman said.
Acupuncture was found to be 2.4 times more effective than Western medicine for short-term pain relief, and 4.1 times better in terms of total efficacy, with a lower risk of adverse events than with Western medicine.
Dr. Ruderman reported serving as a consultant for and/or receiving research grants from more than a half-dozen pharmaceutical companies.
EXPERT ANALYSIS FROM RWCS 2020
Exercise needn’t be strenuous to reduce heart risk
PHOENIX – results from two studies presented at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting showed.
In one study, women who walked 2,100-4,500 steps each day reduced their risk of dying from cardiovascular disease by up to 38%, compared with those who walked fewer than 2,100 steps each day. In addition, women who walked more than 4,500 steps each day reduced their risk of cardiovascular disease (CVD) mortality risk by 48%.
The findings come from an ancillary analysis of the Women’s Health Study known as the Objective Physical Activity and Cardiovascular Health (OPACH) Study.
“Our work shows that both light-intensity and moderate-/vigorous-intensity steps are associated with reduced risk of cardiovascular disease death,” lead author Andrea Z. LaCroix, PhD, said in an interview. “And our previous studies show that all movement while standing, stepping, or just moving about at whatever intensity you choose, appears to have cardiovascular benefits, whereas long hours spent sedentary, especially prolonged sitting bouts are associated with increased risk of cardiovascular disease. These new findings on steps are best interpreted as showing that moving instead of sitting is good for your heart and blood vessels as we get older. Find the things you love to do and get moving.”
For OPACH, 6,379 women with an average age of 79 years wore ActiGraph GT3X+ triaxial accelerometers on their wrist for 7 days during 2012-2014, as a way to ascertain the number of steps they took. The researchers followed the study participants to March 1, 2019, and used Cox proportional hazard models to estimate CVD mortality across four quartiles of steps per day, adjusted for age, race/ethnicity, education, smoking, alcohol consumption, self-reported health, comorbidities, and physical function. The lowest quartile reference category was less than 2,108 steps per day. The second, third and fourth quartiles were: 2,108 to fewer than 3,136 steps, 3,136 to fewer than 4,499, and 4,500 and above.
Dr. LaCroix, distinguished professor and chief of epidemiology at the University of California, San Diego, reported that women who walked 2,100-4,500 steps daily reduced their risk of dying from CVD by up to up to 38%, compared with women who walked fewer than 2,100 daily steps. The women who walked more than 4,500 steps per day reduced their risk by 48%.
She noted that, for many years, common wisdom was that 10,000 steps per day should be used as a general fitness target, [but] that goal “was never evidence based, and so far, emerging evidence using accelerometers to measure steps shows benefit way below the level of 10,000 steps.” Dr. LaCroix added that, in this study, “we were able separate steps taken at a light intensity of energy expenditure versus a moderate or vigorous level of energy expenditure. This is like comparing slower versus faster steps. Both influenced the risk of CVD death and we found no evidence that faster steps were more beneficial for reducing risk of CVD death than slower steps. So, the main message I want my demographic [women aged over 60] to understand is that all movement appears to be good for your heart.”
Barry A. Franklin, PhD, director of preventive cardiology and cardiac rehabilitation at Beaumont Health in Royal Oak, Mich., characterized the study findings as “good news” but not entirely surprising. “It goes along with other research showing that the biggest bang from the buck is going from the least fit, least active cohort, which we call the bottom 20%, to the next lowest level,” he said in an interview. “So, by simply doing some steps, certainly less than 10,000, there were significant benefits for this older age group.”
Dr. LaCroix acknowledged certain limitations of the OPACH study, including the fact that it did not include men or women aged younger than 60 years. In addition, the accelerometer used in this and other studies may measure fewer steps than women are actually taking. “Devices vary in their accuracy,” she said. “If you are tracking steps, try to aim for 4,500 or a little more, but know that every step counts.”
In a separate study, researchers found that an increase of 30 minutes per day of low-intensity physical activity (LIPA) may lower the risk of death among older adults, regardless of the amount of moderate to vigorous physical activity (MVPA) participants are involved in or whether they have impaired physical function. In addition, an increase of 30 minutes of sedentary time per day may increase the risk of death regardless of the amount of MVPA or whether participants have impaired physical function.
Those are key findings from an analysis of 1,262 participants in the Framingham Offspring Study.

“Given that MVPA tends to decline with age, particularly during the mid- to late-life transition, promoting LIPA and reducing sedentary time may be a more practical alternative among older adults for reducing the risk of mortality,” lead author Joowon Lee, PhD, said in an interview at the meeting sponsored by the American Heart Association.
According to Dr. Lee, a postdoctoral fellow at Boston University, prior studies found that the inverse association between MVPA and cardiovascular and all-cause mortality among older adults. “However, we focused on sedentary and light-intensity physical activity, which is prevalent in older adult population,” he said. “Additionally, we looked at the association between physical activity and mortality after excluding participants with frailty as a sensitivity analysis.”
The researchers drew from accelerometry-derived physical activity data from 1,262 Framingham Offspring Study participants at their ninth examination (2011-2014). The mean age of the subjects was 69 years, 54% were women, and they had worn the accelerometers at least 10 hours per day for at least 4 days prior to the exam visit. The researchers used multivariable Cox proportional hazards regression models to relate physician activity and sedentary time with all-cause mortality adjusting for potential confounders.
During a median follow-up of 4.8 years, 67 study participants died. Dr. Lee and colleagues observed that higher total physical activity, LIPA, adherence to physical activity guidelines (at least 150 minutes of activity each week), and lower sedentary time were associated with a lower risk of all-cause mortality. Specifically, they were 67% less likely to die of any cause if they spent at least 150 minutes per week in moderate to vigorous physical activity, compared with those who did not. In addition, the researchers found that each 30-minute interval of LIPA, such as doing household chores or casual walking, was associated with a 20% lower risk of dying from any cause. On the other hand, every additional 30 minutes of being sedentary was related to a 32% higher risk of dying from any cause. The results remained statistically significant even after excluding those with frailty.
“In the present analysis, an increase of 10 minutes in MVPA was not associated with the risk of all-cause mortality although meeting physical activity guidelines [MVPA of at least 150 minutes per week] was the strongest factor associated with the risk of all-cause mortality,” Dr. Lee said.
He acknowledged certain limitations of the analysis, including the fact that the study participants were white individuals with European ancestry. “Additionally, a small number of mortality events were observed in the current investigation,” he said. “So, an additional study of larger multiethnic samples of older adults is warranted to confirm our findings.”
“We tell people: ‘You need 30 minutes of moderate intensity exercise most days of the week,’ ” Dr. Franklin said. “That’s true, but a classic study in Lancet showed that if you do 12 or 15 minutes of moderate exercise, not 30 minutes, you also get a 14% reduction in mortality. Some exercise is better than none, and for older adults, they don’t even have to do moderate intensity exercise to get benefits.”
Dr. LaCroix’s study was funded by the National Heart, Lung, and Blood Institute; Dr. LaCroix reported having no financial disclosures. Dr. Lee’s study was supported by the National Heart, Lung, and Blood Institute; Dr. Lee reported having no disclosures.
SOURCES: LaCroix A et al. Epi/Lifestyle 2020, Abstract 30; Lee J et al. Epi/Lifestyle 2020, Abstract 31.
PHOENIX – results from two studies presented at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting showed.
In one study, women who walked 2,100-4,500 steps each day reduced their risk of dying from cardiovascular disease by up to 38%, compared with those who walked fewer than 2,100 steps each day. In addition, women who walked more than 4,500 steps each day reduced their risk of cardiovascular disease (CVD) mortality risk by 48%.
The findings come from an ancillary analysis of the Women’s Health Study known as the Objective Physical Activity and Cardiovascular Health (OPACH) Study.
“Our work shows that both light-intensity and moderate-/vigorous-intensity steps are associated with reduced risk of cardiovascular disease death,” lead author Andrea Z. LaCroix, PhD, said in an interview. “And our previous studies show that all movement while standing, stepping, or just moving about at whatever intensity you choose, appears to have cardiovascular benefits, whereas long hours spent sedentary, especially prolonged sitting bouts are associated with increased risk of cardiovascular disease. These new findings on steps are best interpreted as showing that moving instead of sitting is good for your heart and blood vessels as we get older. Find the things you love to do and get moving.”
For OPACH, 6,379 women with an average age of 79 years wore ActiGraph GT3X+ triaxial accelerometers on their wrist for 7 days during 2012-2014, as a way to ascertain the number of steps they took. The researchers followed the study participants to March 1, 2019, and used Cox proportional hazard models to estimate CVD mortality across four quartiles of steps per day, adjusted for age, race/ethnicity, education, smoking, alcohol consumption, self-reported health, comorbidities, and physical function. The lowest quartile reference category was less than 2,108 steps per day. The second, third and fourth quartiles were: 2,108 to fewer than 3,136 steps, 3,136 to fewer than 4,499, and 4,500 and above.
Dr. LaCroix, distinguished professor and chief of epidemiology at the University of California, San Diego, reported that women who walked 2,100-4,500 steps daily reduced their risk of dying from CVD by up to up to 38%, compared with women who walked fewer than 2,100 daily steps. The women who walked more than 4,500 steps per day reduced their risk by 48%.
She noted that, for many years, common wisdom was that 10,000 steps per day should be used as a general fitness target, [but] that goal “was never evidence based, and so far, emerging evidence using accelerometers to measure steps shows benefit way below the level of 10,000 steps.” Dr. LaCroix added that, in this study, “we were able separate steps taken at a light intensity of energy expenditure versus a moderate or vigorous level of energy expenditure. This is like comparing slower versus faster steps. Both influenced the risk of CVD death and we found no evidence that faster steps were more beneficial for reducing risk of CVD death than slower steps. So, the main message I want my demographic [women aged over 60] to understand is that all movement appears to be good for your heart.”
Barry A. Franklin, PhD, director of preventive cardiology and cardiac rehabilitation at Beaumont Health in Royal Oak, Mich., characterized the study findings as “good news” but not entirely surprising. “It goes along with other research showing that the biggest bang from the buck is going from the least fit, least active cohort, which we call the bottom 20%, to the next lowest level,” he said in an interview. “So, by simply doing some steps, certainly less than 10,000, there were significant benefits for this older age group.”
Dr. LaCroix acknowledged certain limitations of the OPACH study, including the fact that it did not include men or women aged younger than 60 years. In addition, the accelerometer used in this and other studies may measure fewer steps than women are actually taking. “Devices vary in their accuracy,” she said. “If you are tracking steps, try to aim for 4,500 or a little more, but know that every step counts.”
In a separate study, researchers found that an increase of 30 minutes per day of low-intensity physical activity (LIPA) may lower the risk of death among older adults, regardless of the amount of moderate to vigorous physical activity (MVPA) participants are involved in or whether they have impaired physical function. In addition, an increase of 30 minutes of sedentary time per day may increase the risk of death regardless of the amount of MVPA or whether participants have impaired physical function.
Those are key findings from an analysis of 1,262 participants in the Framingham Offspring Study.
“Given that MVPA tends to decline with age, particularly during the mid- to late-life transition, promoting LIPA and reducing sedentary time may be a more practical alternative among older adults for reducing the risk of mortality,” lead author Joowon Lee, PhD, said in an interview at the meeting sponsored by the American Heart Association.
According to Dr. Lee, a postdoctoral fellow at Boston University, prior studies found that the inverse association between MVPA and cardiovascular and all-cause mortality among older adults. “However, we focused on sedentary and light-intensity physical activity, which is prevalent in older adult population,” he said. “Additionally, we looked at the association between physical activity and mortality after excluding participants with frailty as a sensitivity analysis.”
The researchers drew from accelerometry-derived physical activity data from 1,262 Framingham Offspring Study participants at their ninth examination (2011-2014). The mean age of the subjects was 69 years, 54% were women, and they had worn the accelerometers at least 10 hours per day for at least 4 days prior to the exam visit. The researchers used multivariable Cox proportional hazards regression models to relate physician activity and sedentary time with all-cause mortality adjusting for potential confounders.
During a median follow-up of 4.8 years, 67 study participants died. Dr. Lee and colleagues observed that higher total physical activity, LIPA, adherence to physical activity guidelines (at least 150 minutes of activity each week), and lower sedentary time were associated with a lower risk of all-cause mortality. Specifically, they were 67% less likely to die of any cause if they spent at least 150 minutes per week in moderate to vigorous physical activity, compared with those who did not. In addition, the researchers found that each 30-minute interval of LIPA, such as doing household chores or casual walking, was associated with a 20% lower risk of dying from any cause. On the other hand, every additional 30 minutes of being sedentary was related to a 32% higher risk of dying from any cause. The results remained statistically significant even after excluding those with frailty.
“In the present analysis, an increase of 10 minutes in MVPA was not associated with the risk of all-cause mortality although meeting physical activity guidelines [MVPA of at least 150 minutes per week] was the strongest factor associated with the risk of all-cause mortality,” Dr. Lee said.
He acknowledged certain limitations of the analysis, including the fact that the study participants were white individuals with European ancestry. “Additionally, a small number of mortality events were observed in the current investigation,” he said. “So, an additional study of larger multiethnic samples of older adults is warranted to confirm our findings.”
“We tell people: ‘You need 30 minutes of moderate intensity exercise most days of the week,’ ” Dr. Franklin said. “That’s true, but a classic study in Lancet showed that if you do 12 or 15 minutes of moderate exercise, not 30 minutes, you also get a 14% reduction in mortality. Some exercise is better than none, and for older adults, they don’t even have to do moderate intensity exercise to get benefits.”
Dr. LaCroix’s study was funded by the National Heart, Lung, and Blood Institute; Dr. LaCroix reported having no financial disclosures. Dr. Lee’s study was supported by the National Heart, Lung, and Blood Institute; Dr. Lee reported having no disclosures.
SOURCES: LaCroix A et al. Epi/Lifestyle 2020, Abstract 30; Lee J et al. Epi/Lifestyle 2020, Abstract 31.
PHOENIX – results from two studies presented at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting showed.
In one study, women who walked 2,100-4,500 steps each day reduced their risk of dying from cardiovascular disease by up to 38%, compared with those who walked fewer than 2,100 steps each day. In addition, women who walked more than 4,500 steps each day reduced their risk of cardiovascular disease (CVD) mortality risk by 48%.
The findings come from an ancillary analysis of the Women’s Health Study known as the Objective Physical Activity and Cardiovascular Health (OPACH) Study.
“Our work shows that both light-intensity and moderate-/vigorous-intensity steps are associated with reduced risk of cardiovascular disease death,” lead author Andrea Z. LaCroix, PhD, said in an interview. “And our previous studies show that all movement while standing, stepping, or just moving about at whatever intensity you choose, appears to have cardiovascular benefits, whereas long hours spent sedentary, especially prolonged sitting bouts are associated with increased risk of cardiovascular disease. These new findings on steps are best interpreted as showing that moving instead of sitting is good for your heart and blood vessels as we get older. Find the things you love to do and get moving.”
For OPACH, 6,379 women with an average age of 79 years wore ActiGraph GT3X+ triaxial accelerometers on their wrist for 7 days during 2012-2014, as a way to ascertain the number of steps they took. The researchers followed the study participants to March 1, 2019, and used Cox proportional hazard models to estimate CVD mortality across four quartiles of steps per day, adjusted for age, race/ethnicity, education, smoking, alcohol consumption, self-reported health, comorbidities, and physical function. The lowest quartile reference category was less than 2,108 steps per day. The second, third and fourth quartiles were: 2,108 to fewer than 3,136 steps, 3,136 to fewer than 4,499, and 4,500 and above.
Dr. LaCroix, distinguished professor and chief of epidemiology at the University of California, San Diego, reported that women who walked 2,100-4,500 steps daily reduced their risk of dying from CVD by up to up to 38%, compared with women who walked fewer than 2,100 daily steps. The women who walked more than 4,500 steps per day reduced their risk by 48%.
She noted that, for many years, common wisdom was that 10,000 steps per day should be used as a general fitness target, [but] that goal “was never evidence based, and so far, emerging evidence using accelerometers to measure steps shows benefit way below the level of 10,000 steps.” Dr. LaCroix added that, in this study, “we were able separate steps taken at a light intensity of energy expenditure versus a moderate or vigorous level of energy expenditure. This is like comparing slower versus faster steps. Both influenced the risk of CVD death and we found no evidence that faster steps were more beneficial for reducing risk of CVD death than slower steps. So, the main message I want my demographic [women aged over 60] to understand is that all movement appears to be good for your heart.”
Barry A. Franklin, PhD, director of preventive cardiology and cardiac rehabilitation at Beaumont Health in Royal Oak, Mich., characterized the study findings as “good news” but not entirely surprising. “It goes along with other research showing that the biggest bang from the buck is going from the least fit, least active cohort, which we call the bottom 20%, to the next lowest level,” he said in an interview. “So, by simply doing some steps, certainly less than 10,000, there were significant benefits for this older age group.”
Dr. LaCroix acknowledged certain limitations of the OPACH study, including the fact that it did not include men or women aged younger than 60 years. In addition, the accelerometer used in this and other studies may measure fewer steps than women are actually taking. “Devices vary in their accuracy,” she said. “If you are tracking steps, try to aim for 4,500 or a little more, but know that every step counts.”
In a separate study, researchers found that an increase of 30 minutes per day of low-intensity physical activity (LIPA) may lower the risk of death among older adults, regardless of the amount of moderate to vigorous physical activity (MVPA) participants are involved in or whether they have impaired physical function. In addition, an increase of 30 minutes of sedentary time per day may increase the risk of death regardless of the amount of MVPA or whether participants have impaired physical function.
Those are key findings from an analysis of 1,262 participants in the Framingham Offspring Study.
“Given that MVPA tends to decline with age, particularly during the mid- to late-life transition, promoting LIPA and reducing sedentary time may be a more practical alternative among older adults for reducing the risk of mortality,” lead author Joowon Lee, PhD, said in an interview at the meeting sponsored by the American Heart Association.
According to Dr. Lee, a postdoctoral fellow at Boston University, prior studies found that the inverse association between MVPA and cardiovascular and all-cause mortality among older adults. “However, we focused on sedentary and light-intensity physical activity, which is prevalent in older adult population,” he said. “Additionally, we looked at the association between physical activity and mortality after excluding participants with frailty as a sensitivity analysis.”
The researchers drew from accelerometry-derived physical activity data from 1,262 Framingham Offspring Study participants at their ninth examination (2011-2014). The mean age of the subjects was 69 years, 54% were women, and they had worn the accelerometers at least 10 hours per day for at least 4 days prior to the exam visit. The researchers used multivariable Cox proportional hazards regression models to relate physician activity and sedentary time with all-cause mortality adjusting for potential confounders.
During a median follow-up of 4.8 years, 67 study participants died. Dr. Lee and colleagues observed that higher total physical activity, LIPA, adherence to physical activity guidelines (at least 150 minutes of activity each week), and lower sedentary time were associated with a lower risk of all-cause mortality. Specifically, they were 67% less likely to die of any cause if they spent at least 150 minutes per week in moderate to vigorous physical activity, compared with those who did not. In addition, the researchers found that each 30-minute interval of LIPA, such as doing household chores or casual walking, was associated with a 20% lower risk of dying from any cause. On the other hand, every additional 30 minutes of being sedentary was related to a 32% higher risk of dying from any cause. The results remained statistically significant even after excluding those with frailty.
“In the present analysis, an increase of 10 minutes in MVPA was not associated with the risk of all-cause mortality although meeting physical activity guidelines [MVPA of at least 150 minutes per week] was the strongest factor associated with the risk of all-cause mortality,” Dr. Lee said.
He acknowledged certain limitations of the analysis, including the fact that the study participants were white individuals with European ancestry. “Additionally, a small number of mortality events were observed in the current investigation,” he said. “So, an additional study of larger multiethnic samples of older adults is warranted to confirm our findings.”
“We tell people: ‘You need 30 minutes of moderate intensity exercise most days of the week,’ ” Dr. Franklin said. “That’s true, but a classic study in Lancet showed that if you do 12 or 15 minutes of moderate exercise, not 30 minutes, you also get a 14% reduction in mortality. Some exercise is better than none, and for older adults, they don’t even have to do moderate intensity exercise to get benefits.”
Dr. LaCroix’s study was funded by the National Heart, Lung, and Blood Institute; Dr. LaCroix reported having no financial disclosures. Dr. Lee’s study was supported by the National Heart, Lung, and Blood Institute; Dr. Lee reported having no disclosures.
SOURCES: LaCroix A et al. Epi/Lifestyle 2020, Abstract 30; Lee J et al. Epi/Lifestyle 2020, Abstract 31.
REPORTING FROM EPI/LIFESTYLE 2020
SARS epidemiology provides clues to potential treatment for COVID-19
A team of researchers has discovered important commonalities between SARS-CoV-2 and SARS-CoV infection that could lead to a potential targets for antiviral intervention.

Markus Hoffmann, of the Leibniz Institute for Primate Research, Göttingen, Germany, and a team of investigators also found that antibody responses raised against SARS-S during infection or vaccination might offer some level of protection against SARS-CoV-2 infection. Their findings were published in Cell.
In order for coronaviruses to enter a cell, they must first bind their viral spike (S) proteins to cellular receptors and depend on S protein priming by host cell proteases. The study found that the SARS-CoV-2, causal agent for COVID-19, uses the same SARS-CoV receptor, ACE2, for entry and uses the serine protease TMPRSS2 for S protein priming as the original SARS-CoV-1 (SARS). Importantly, the researchers also found that the cellular serine protease TMPRSS2 primes SARS-CoV-2-S for entry and that a serine protease inhibitor blocks SARS-CoV-2 infection of lung cells, providing opportunities for potential therapeutic intervention.
The researchers performed a sequence analysis that showed SARS-CoV-2 clusters with SARS-CoV–related viruses from bats, of which some – but not all – can use ACE2 for host cell entry. Further analysis of the receptor binding motif known to make contact with ACE2 showed that most amino acid residues essential for ACE2 binding by SARS-S were conserved in SARS-2-S but were absent from S proteins of those SARS-related coronaviruses previously found not to use ACE2.
In addition, the researchers found that SARS-CoV-2–infected BHK-21 cells transfected to express ACE2 with high efficiency, but not the parental BHK-21 cells indicating that SARS-CoV-2-S, like the original SARS virus S protein, uses ACE2 for cellular entry.
Using cultured cells, the researchers found that the protease inhibitor, camostat mesylate, inhibited SARS-S and SARS-2-S entry into primary human lung cells, demonstrating that SARS-CoV-2 can use TMPRSS2 for S protein priming and that camostat mesylate can block SARS-CoV-2 infection of lung cells. Camostat mesylate has been used as a therapy for some forms of cancer and other viral infections.
In addition to their research on the protease inhibitor, the researchers also found that sera from convalescent SARS patients cross-neutralized SARS-2-S–driven entry. They found that four sera obtained from three convalescent SARS patients inhibited SARS-S entry into cell lines in a concentration dependent fashion.
“We demonstrate that SARS-CoV-2 uses the SARS55 CoV receptor, ACE2, for entry and the serine protease TMPRSS2 for S protein priming. A TMPRSS2 inhibitor approved for clinical use blocked entry and might constitute a treatment option. Finally, we show that the sera from convalescent SARS patients cross-neutralized SARS-2-S–driven entry,” the authors concluded.
The study was supported by BMBF (RAPID Consortium) and German Research Foundation (DFG). The authors reported that they had no conflicts.
SOURCE: Hoffmann M et al. Cell 2020. doi: 10.1016/j.cell.2020.02.052.
A team of researchers has discovered important commonalities between SARS-CoV-2 and SARS-CoV infection that could lead to a potential targets for antiviral intervention.
Markus Hoffmann, of the Leibniz Institute for Primate Research, Göttingen, Germany, and a team of investigators also found that antibody responses raised against SARS-S during infection or vaccination might offer some level of protection against SARS-CoV-2 infection. Their findings were published in Cell.
In order for coronaviruses to enter a cell, they must first bind their viral spike (S) proteins to cellular receptors and depend on S protein priming by host cell proteases. The study found that the SARS-CoV-2, causal agent for COVID-19, uses the same SARS-CoV receptor, ACE2, for entry and uses the serine protease TMPRSS2 for S protein priming as the original SARS-CoV-1 (SARS). Importantly, the researchers also found that the cellular serine protease TMPRSS2 primes SARS-CoV-2-S for entry and that a serine protease inhibitor blocks SARS-CoV-2 infection of lung cells, providing opportunities for potential therapeutic intervention.
The researchers performed a sequence analysis that showed SARS-CoV-2 clusters with SARS-CoV–related viruses from bats, of which some – but not all – can use ACE2 for host cell entry. Further analysis of the receptor binding motif known to make contact with ACE2 showed that most amino acid residues essential for ACE2 binding by SARS-S were conserved in SARS-2-S but were absent from S proteins of those SARS-related coronaviruses previously found not to use ACE2.
In addition, the researchers found that SARS-CoV-2–infected BHK-21 cells transfected to express ACE2 with high efficiency, but not the parental BHK-21 cells indicating that SARS-CoV-2-S, like the original SARS virus S protein, uses ACE2 for cellular entry.
Using cultured cells, the researchers found that the protease inhibitor, camostat mesylate, inhibited SARS-S and SARS-2-S entry into primary human lung cells, demonstrating that SARS-CoV-2 can use TMPRSS2 for S protein priming and that camostat mesylate can block SARS-CoV-2 infection of lung cells. Camostat mesylate has been used as a therapy for some forms of cancer and other viral infections.
In addition to their research on the protease inhibitor, the researchers also found that sera from convalescent SARS patients cross-neutralized SARS-2-S–driven entry. They found that four sera obtained from three convalescent SARS patients inhibited SARS-S entry into cell lines in a concentration dependent fashion.
“We demonstrate that SARS-CoV-2 uses the SARS55 CoV receptor, ACE2, for entry and the serine protease TMPRSS2 for S protein priming. A TMPRSS2 inhibitor approved for clinical use blocked entry and might constitute a treatment option. Finally, we show that the sera from convalescent SARS patients cross-neutralized SARS-2-S–driven entry,” the authors concluded.
The study was supported by BMBF (RAPID Consortium) and German Research Foundation (DFG). The authors reported that they had no conflicts.
SOURCE: Hoffmann M et al. Cell 2020. doi: 10.1016/j.cell.2020.02.052.
A team of researchers has discovered important commonalities between SARS-CoV-2 and SARS-CoV infection that could lead to a potential targets for antiviral intervention.
Markus Hoffmann, of the Leibniz Institute for Primate Research, Göttingen, Germany, and a team of investigators also found that antibody responses raised against SARS-S during infection or vaccination might offer some level of protection against SARS-CoV-2 infection. Their findings were published in Cell.
In order for coronaviruses to enter a cell, they must first bind their viral spike (S) proteins to cellular receptors and depend on S protein priming by host cell proteases. The study found that the SARS-CoV-2, causal agent for COVID-19, uses the same SARS-CoV receptor, ACE2, for entry and uses the serine protease TMPRSS2 for S protein priming as the original SARS-CoV-1 (SARS). Importantly, the researchers also found that the cellular serine protease TMPRSS2 primes SARS-CoV-2-S for entry and that a serine protease inhibitor blocks SARS-CoV-2 infection of lung cells, providing opportunities for potential therapeutic intervention.
The researchers performed a sequence analysis that showed SARS-CoV-2 clusters with SARS-CoV–related viruses from bats, of which some – but not all – can use ACE2 for host cell entry. Further analysis of the receptor binding motif known to make contact with ACE2 showed that most amino acid residues essential for ACE2 binding by SARS-S were conserved in SARS-2-S but were absent from S proteins of those SARS-related coronaviruses previously found not to use ACE2.
In addition, the researchers found that SARS-CoV-2–infected BHK-21 cells transfected to express ACE2 with high efficiency, but not the parental BHK-21 cells indicating that SARS-CoV-2-S, like the original SARS virus S protein, uses ACE2 for cellular entry.
Using cultured cells, the researchers found that the protease inhibitor, camostat mesylate, inhibited SARS-S and SARS-2-S entry into primary human lung cells, demonstrating that SARS-CoV-2 can use TMPRSS2 for S protein priming and that camostat mesylate can block SARS-CoV-2 infection of lung cells. Camostat mesylate has been used as a therapy for some forms of cancer and other viral infections.
In addition to their research on the protease inhibitor, the researchers also found that sera from convalescent SARS patients cross-neutralized SARS-2-S–driven entry. They found that four sera obtained from three convalescent SARS patients inhibited SARS-S entry into cell lines in a concentration dependent fashion.
“We demonstrate that SARS-CoV-2 uses the SARS55 CoV receptor, ACE2, for entry and the serine protease TMPRSS2 for S protein priming. A TMPRSS2 inhibitor approved for clinical use blocked entry and might constitute a treatment option. Finally, we show that the sera from convalescent SARS patients cross-neutralized SARS-2-S–driven entry,” the authors concluded.
The study was supported by BMBF (RAPID Consortium) and German Research Foundation (DFG). The authors reported that they had no conflicts.
SOURCE: Hoffmann M et al. Cell 2020. doi: 10.1016/j.cell.2020.02.052.
FROM CELL
Infection control protects hospital staff from COVID-19, study shows
Hospital-related infections have been widely reported during the ongoing coronavirus outbreak, with healthcare professionals bearing a disproportionate risk. However, a proactive response in Hong Kong’s public hospital system appears to have bucked this trend and successfully protected both patients and staff from SARS-CoV-2, according to a study published online today in Infection Control & Hospital Epidemiology.
During the first 42 days of the outbreak, the 43 hospitals in the network tested 1275 suspected cases and treated 42 patients with confirmed COVID-19, the disease caused by SARS-CoV-2 infection. Yet, there were no nosocomial infections or infections among healthcare personnel, report Vincent C.C. Cheng, MD, FRCPath, the hospital’s infection control officer, and colleagues.
Cheng and colleagues note that 11 out of 413 healthcare workers who treat patients with confirmed infections had unprotected exposure and were in quarantine for 14 days, but none became ill.
In comparison, they note, the 2003 SARS outbreak saw almost 60% of nosocomial cases occurring in healthcare workers.
Proactive bundle
The Hong Kong success story may be due to a stepped-up proactive bundle of measures that included enhanced laboratory surveillance, early airborne infection isolation, and rapid-turnaround molecular diagnostics. Other strategies included staff forums and one-on-one discussions about infection control, employee training in protective equipment use, hand-hygiene compliance enforcement, and contact tracing for workers with unprotected exposure.
In addition, surgical masks were provided for all healthcare workers, patients, and visitors to clinical areas, a practice previously associated with reduced in-hospital transmission during influenza outbreaks, the authors note.
Hospitals also mandated use of personal protective equipment (PPE) for aerosol-generating procedures (AGPs), such as endotracheal intubation, open suctioning, and high-flow oxygen use, as AGPs had been linked to nosocomial transmission to healthcare workers during the 2003 SARS outbreak.
The infection control measures, which were part of a preparedness plan developed after the SARS outbreak, were initiated on December 31, when the first reports of a cluster of infections came from Wuhan, China.
As the outbreak evolved, the Hong Kong hospitals quickly widened the epidemiologic criteria for screening, from initially including only those who had been to a wet market in Wuhan within 14 days of symptom onset, to eventually including anyone who had been to Hubei province, been in a medical facility in mainland China, or in contact with a known case.
All suspected cases were sent to an airborne-infection isolation room (AIIR) or a ward with at least a meter of space between patients.
“Appropriate hospital infection control measures could prevent nosocomial transmission of SARS-CoV-2,” the authors write. “Vigilance in hand hygiene practice, wearing of surgical mask in the hospital, and appropriate use of PPE in patient care, especially [when] performing AGPs, are the key infection control measures to prevent nosocomial transmission of SARS-CoV-2 even before the availability of effective antiviral agents and vaccine.”
Asked for his perspective on the report, Aaron E. Glatt, MD, chairman of the department of medicine and chief of infectious diseases at Mount Sinai South Nassau in Oceanside, New York, said that apart from the widespread issuing of surgical masks to workers, patients, and visitors, the measures taken in Hong Kong are not different from standard infection-control practices in American hospitals. Glatt, who is also a hospital epidemiologist, said it was unclear how much impact the masks would have.
“Although the infection control was impressive, I don’t see any evidence of a difference in care,” he told Medscape Medical News.
Could zero infection transmission be achieved in the more far-flung and variable settings of hospitals across the United States? “The ability to get zero transmission is only possible if people adhere to the strictest infection-control guidelines,” Glatt said. “That is clearly the goal, and it will take time to see if our existing strict guidelines are sufficient to maintain zero or close to zero contamination and transmission rates in our hospitals.”
Rather than looking to change US practices, he stressed adherence to widely established tenets of care. “It’s critically important to keep paying close attention to the basics, to the simple blocking and tackling, and to identify which patients are at risk, and therefore, when workers need protective equipment,” he said.
“Follow the recommended standards,” continued Glatt, who is also a spokesperson for the Infectious Diseases Society of America and did not participate in this study.
In a finding from an ancillary pilot experiment, the Hong Kong researchers found exhaled air from a patient with a moderate coronavirus load showed no evidence of the virus, whether the patient was breathing normally or heavily, speaking, or coughing. And spot tests around the room detected the virus in just one location.
“We may not be able to make a definite conclusion based on the analysis of a single patient,” the authors write. “However, it may help to reassure our staff that the exhaled air may be rapidly diluted inside the AIIR with 12 air changes per hour, or probably the SARS-CoV-2 may not be predominantly transmitted by [the] airborne route.”
However, a recent Singapore study showed widespread environmental contamination by SARS-CoV-2 through respiratory droplets and fecal shedding, underlining the need for strict adherence to environmental and hand hygiene. Post-cleaning samples tested negative, suggesting that standard decontamination practices are effective.
This work was partly supported by the Consultancy Service for Enhancing Laboratory Surveillance of Emerging Infectious Diseases of the Department of Health, Hong Kong Special Administrative Region; and the Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, Ministry of Education of China. The authors and Glatt have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Hospital-related infections have been widely reported during the ongoing coronavirus outbreak, with healthcare professionals bearing a disproportionate risk. However, a proactive response in Hong Kong’s public hospital system appears to have bucked this trend and successfully protected both patients and staff from SARS-CoV-2, according to a study published online today in Infection Control & Hospital Epidemiology.
During the first 42 days of the outbreak, the 43 hospitals in the network tested 1275 suspected cases and treated 42 patients with confirmed COVID-19, the disease caused by SARS-CoV-2 infection. Yet, there were no nosocomial infections or infections among healthcare personnel, report Vincent C.C. Cheng, MD, FRCPath, the hospital’s infection control officer, and colleagues.
Cheng and colleagues note that 11 out of 413 healthcare workers who treat patients with confirmed infections had unprotected exposure and were in quarantine for 14 days, but none became ill.
In comparison, they note, the 2003 SARS outbreak saw almost 60% of nosocomial cases occurring in healthcare workers.
Proactive bundle
The Hong Kong success story may be due to a stepped-up proactive bundle of measures that included enhanced laboratory surveillance, early airborne infection isolation, and rapid-turnaround molecular diagnostics. Other strategies included staff forums and one-on-one discussions about infection control, employee training in protective equipment use, hand-hygiene compliance enforcement, and contact tracing for workers with unprotected exposure.
In addition, surgical masks were provided for all healthcare workers, patients, and visitors to clinical areas, a practice previously associated with reduced in-hospital transmission during influenza outbreaks, the authors note.
Hospitals also mandated use of personal protective equipment (PPE) for aerosol-generating procedures (AGPs), such as endotracheal intubation, open suctioning, and high-flow oxygen use, as AGPs had been linked to nosocomial transmission to healthcare workers during the 2003 SARS outbreak.
The infection control measures, which were part of a preparedness plan developed after the SARS outbreak, were initiated on December 31, when the first reports of a cluster of infections came from Wuhan, China.
As the outbreak evolved, the Hong Kong hospitals quickly widened the epidemiologic criteria for screening, from initially including only those who had been to a wet market in Wuhan within 14 days of symptom onset, to eventually including anyone who had been to Hubei province, been in a medical facility in mainland China, or in contact with a known case.
All suspected cases were sent to an airborne-infection isolation room (AIIR) or a ward with at least a meter of space between patients.
“Appropriate hospital infection control measures could prevent nosocomial transmission of SARS-CoV-2,” the authors write. “Vigilance in hand hygiene practice, wearing of surgical mask in the hospital, and appropriate use of PPE in patient care, especially [when] performing AGPs, are the key infection control measures to prevent nosocomial transmission of SARS-CoV-2 even before the availability of effective antiviral agents and vaccine.”
Asked for his perspective on the report, Aaron E. Glatt, MD, chairman of the department of medicine and chief of infectious diseases at Mount Sinai South Nassau in Oceanside, New York, said that apart from the widespread issuing of surgical masks to workers, patients, and visitors, the measures taken in Hong Kong are not different from standard infection-control practices in American hospitals. Glatt, who is also a hospital epidemiologist, said it was unclear how much impact the masks would have.
“Although the infection control was impressive, I don’t see any evidence of a difference in care,” he told Medscape Medical News.
Could zero infection transmission be achieved in the more far-flung and variable settings of hospitals across the United States? “The ability to get zero transmission is only possible if people adhere to the strictest infection-control guidelines,” Glatt said. “That is clearly the goal, and it will take time to see if our existing strict guidelines are sufficient to maintain zero or close to zero contamination and transmission rates in our hospitals.”
Rather than looking to change US practices, he stressed adherence to widely established tenets of care. “It’s critically important to keep paying close attention to the basics, to the simple blocking and tackling, and to identify which patients are at risk, and therefore, when workers need protective equipment,” he said.
“Follow the recommended standards,” continued Glatt, who is also a spokesperson for the Infectious Diseases Society of America and did not participate in this study.
In a finding from an ancillary pilot experiment, the Hong Kong researchers found exhaled air from a patient with a moderate coronavirus load showed no evidence of the virus, whether the patient was breathing normally or heavily, speaking, or coughing. And spot tests around the room detected the virus in just one location.
“We may not be able to make a definite conclusion based on the analysis of a single patient,” the authors write. “However, it may help to reassure our staff that the exhaled air may be rapidly diluted inside the AIIR with 12 air changes per hour, or probably the SARS-CoV-2 may not be predominantly transmitted by [the] airborne route.”
However, a recent Singapore study showed widespread environmental contamination by SARS-CoV-2 through respiratory droplets and fecal shedding, underlining the need for strict adherence to environmental and hand hygiene. Post-cleaning samples tested negative, suggesting that standard decontamination practices are effective.
This work was partly supported by the Consultancy Service for Enhancing Laboratory Surveillance of Emerging Infectious Diseases of the Department of Health, Hong Kong Special Administrative Region; and the Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, Ministry of Education of China. The authors and Glatt have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Hospital-related infections have been widely reported during the ongoing coronavirus outbreak, with healthcare professionals bearing a disproportionate risk. However, a proactive response in Hong Kong’s public hospital system appears to have bucked this trend and successfully protected both patients and staff from SARS-CoV-2, according to a study published online today in Infection Control & Hospital Epidemiology.
During the first 42 days of the outbreak, the 43 hospitals in the network tested 1275 suspected cases and treated 42 patients with confirmed COVID-19, the disease caused by SARS-CoV-2 infection. Yet, there were no nosocomial infections or infections among healthcare personnel, report Vincent C.C. Cheng, MD, FRCPath, the hospital’s infection control officer, and colleagues.
Cheng and colleagues note that 11 out of 413 healthcare workers who treat patients with confirmed infections had unprotected exposure and were in quarantine for 14 days, but none became ill.
In comparison, they note, the 2003 SARS outbreak saw almost 60% of nosocomial cases occurring in healthcare workers.
Proactive bundle
The Hong Kong success story may be due to a stepped-up proactive bundle of measures that included enhanced laboratory surveillance, early airborne infection isolation, and rapid-turnaround molecular diagnostics. Other strategies included staff forums and one-on-one discussions about infection control, employee training in protective equipment use, hand-hygiene compliance enforcement, and contact tracing for workers with unprotected exposure.
In addition, surgical masks were provided for all healthcare workers, patients, and visitors to clinical areas, a practice previously associated with reduced in-hospital transmission during influenza outbreaks, the authors note.
Hospitals also mandated use of personal protective equipment (PPE) for aerosol-generating procedures (AGPs), such as endotracheal intubation, open suctioning, and high-flow oxygen use, as AGPs had been linked to nosocomial transmission to healthcare workers during the 2003 SARS outbreak.
The infection control measures, which were part of a preparedness plan developed after the SARS outbreak, were initiated on December 31, when the first reports of a cluster of infections came from Wuhan, China.
As the outbreak evolved, the Hong Kong hospitals quickly widened the epidemiologic criteria for screening, from initially including only those who had been to a wet market in Wuhan within 14 days of symptom onset, to eventually including anyone who had been to Hubei province, been in a medical facility in mainland China, or in contact with a known case.
All suspected cases were sent to an airborne-infection isolation room (AIIR) or a ward with at least a meter of space between patients.
“Appropriate hospital infection control measures could prevent nosocomial transmission of SARS-CoV-2,” the authors write. “Vigilance in hand hygiene practice, wearing of surgical mask in the hospital, and appropriate use of PPE in patient care, especially [when] performing AGPs, are the key infection control measures to prevent nosocomial transmission of SARS-CoV-2 even before the availability of effective antiviral agents and vaccine.”
Asked for his perspective on the report, Aaron E. Glatt, MD, chairman of the department of medicine and chief of infectious diseases at Mount Sinai South Nassau in Oceanside, New York, said that apart from the widespread issuing of surgical masks to workers, patients, and visitors, the measures taken in Hong Kong are not different from standard infection-control practices in American hospitals. Glatt, who is also a hospital epidemiologist, said it was unclear how much impact the masks would have.
“Although the infection control was impressive, I don’t see any evidence of a difference in care,” he told Medscape Medical News.
Could zero infection transmission be achieved in the more far-flung and variable settings of hospitals across the United States? “The ability to get zero transmission is only possible if people adhere to the strictest infection-control guidelines,” Glatt said. “That is clearly the goal, and it will take time to see if our existing strict guidelines are sufficient to maintain zero or close to zero contamination and transmission rates in our hospitals.”
Rather than looking to change US practices, he stressed adherence to widely established tenets of care. “It’s critically important to keep paying close attention to the basics, to the simple blocking and tackling, and to identify which patients are at risk, and therefore, when workers need protective equipment,” he said.
“Follow the recommended standards,” continued Glatt, who is also a spokesperson for the Infectious Diseases Society of America and did not participate in this study.
In a finding from an ancillary pilot experiment, the Hong Kong researchers found exhaled air from a patient with a moderate coronavirus load showed no evidence of the virus, whether the patient was breathing normally or heavily, speaking, or coughing. And spot tests around the room detected the virus in just one location.
“We may not be able to make a definite conclusion based on the analysis of a single patient,” the authors write. “However, it may help to reassure our staff that the exhaled air may be rapidly diluted inside the AIIR with 12 air changes per hour, or probably the SARS-CoV-2 may not be predominantly transmitted by [the] airborne route.”
However, a recent Singapore study showed widespread environmental contamination by SARS-CoV-2 through respiratory droplets and fecal shedding, underlining the need for strict adherence to environmental and hand hygiene. Post-cleaning samples tested negative, suggesting that standard decontamination practices are effective.
This work was partly supported by the Consultancy Service for Enhancing Laboratory Surveillance of Emerging Infectious Diseases of the Department of Health, Hong Kong Special Administrative Region; and the Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, Ministry of Education of China. The authors and Glatt have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
What are the most prescribed medications for type 2 diabetes?
new research shows.
The findings, from U.S.-based administrative claims data, were published online in Diabetes Care by Chintan V. Dave, PharmD, PhD, and colleagues.
Among patients initiating oral sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors) over the 5-year period, empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) became the most commonly prescribed glucose-lowering drug, primarily driven by an increasing proportion of patients with diabetes who had a diagnosis of myocardial infarction, stroke, or heart failure (collectively called cardiovascular disease-heart failure [CVD-HF]).
And within the subcutaneous injectable glucagonlike peptide–1 receptor (GLP-1) agonist class, initiations of dulaglutide (Trulicity, Lilly) surpassed liraglutide in 2013-2018, although patients starting liraglutide (Victoza, Novo Nordisk) were more likely to have a CVD-HF diagnosis.
“This study shows that by preferring empagliflozin, prescribers have largely reacted in accordance with the available evidence and drug labels, while other factors such as lower price, frequency of administration [dulaglutide is given weekly and liraglutide is given daily], or prior authorizations may have led prescribers to select dulaglutide over liraglutide,” Dr. Dave, of the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, and colleagues wrote.
Internists and endocrinologists were the most frequent prescribers of both drug classes, but cardiologists rarely prescribed them, even for patients with established CVD-HF. “As patients with co-occurring diabetes and CVD are likely to see their cardiologist, these encounters may provide an additional opportunity to optimize their treatment,” the authors emphasized.
SGLT2 inhibitors and label changes
Over the study period, the proportion of patients who had CVD-HF and who received SGLT2 inhibitors rose by 3.4 percentage points, from 8.8% to 12.2% (P trend < .001).
The proportion of overall prescriptions for SGLT2 inhibitors written by endocrinologists dropped by 12.0%, although the absolute number of SGLT2-inhibitor prescriptions written by endocrinologists increased (P < .001).
The proportion written by internists did not change (P = .58), whereas it increased slightly among cardiologists but still barely exceeded 1% (P < .001). The findings were similar for the subgroup of patients with CVD-HF who initiated SGLT2 inhibitors.
By individual agents, canagliflozin (Invokana, Janssen) prescriptions dropped by 75.1 percentage points over the study period, from 100% in 2013 to just 24.9% by 2018 (P < .001), whereas empagliflozin initiation rose by 51.7 percentage points, from 13.9% to 65.6% of all SGLT2 inhibitor initiations (P < .001).
Among those initiating empagliflozin, the proportion with CVD-HF rose by 5.3 percentage points, from 8.8% to 14.1% (P < .001), mostly after the additional indication for reducing CV events and death was added to the U.S. label in December 2016.
In contrast, there were no significant changes in the proportions of those with CVD-HF who initiated canagliflozin (P = 065), dapagliflozin (P = .87), or other medications (P = .060).
“Changes in the drug label for canagliflozin (boxed warning for amputation) and empagliflozin (for reduction in CV events and death) in 2016 likely contributed to a rapid change in prescribing preference for empagliflozin,” Dr. Dave and colleagues wrote.
GLP-1 agonists and frequency
Among the patients starting GLP-1 agonists, the proportion with CVD-HF increased by 3.9 percentage points, from 10.5% to 14.4% (P < .001) during the study period.
Prescriptions by endocrinologists declined as a proportion, but rose in absolute numbers (P < .001), and remained consistent for internists (> 55%; P = .12).
Prescribing of GLP-1 agonists by cardiologists remained low (< 0.5%) and was not higher for individuals with CVD-HF.
By individual GLP-1 agonist, liraglutide initiation declined by 32.1 percentage points, from 72.4% to 40.3% of GLP-1 agonist initiations (P < .001), whereas dulaglutide initiation rose by 43.8 percentage points, from 5.0% to 48.8% (P < .001). Again, these trends were similar in the subgroup of patients with CVD-HF.
The proportion of patients with CVD-HF in liraglutide initiators increased by 5.1 percentage points, from 10.5% to 15.6% (P = .018), and in exenatide initiators by 2.1 percentage points, from 10.3% to 13.8% (P = .77).
“Due to the reduced frequency of administration and possible formulary preferences, dulaglutide initiations surpassed liraglutide, the only GLP-1 agonist with evidence of CV benefit at the time,” Dr. Dave and colleagues noted.
Dulaglutide has just been granted an additional approval by the Food and Drug Administration for reducing the risk of major adverse cardiovascular events in adults with type 2 diabetes with and without established CVD or multiple CV risk factors. That makes it the first and only type 2 diabetes medicine approved to reduce the risk of CV events for both primary and secondary prevention populations.
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston. Dr. Dave has reported receiving support from the New Jersey Alliance for Clinical and Translational Science.
This article first appeared on Medscape.com.
new research shows.
The findings, from U.S.-based administrative claims data, were published online in Diabetes Care by Chintan V. Dave, PharmD, PhD, and colleagues.
Among patients initiating oral sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors) over the 5-year period, empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) became the most commonly prescribed glucose-lowering drug, primarily driven by an increasing proportion of patients with diabetes who had a diagnosis of myocardial infarction, stroke, or heart failure (collectively called cardiovascular disease-heart failure [CVD-HF]).
And within the subcutaneous injectable glucagonlike peptide–1 receptor (GLP-1) agonist class, initiations of dulaglutide (Trulicity, Lilly) surpassed liraglutide in 2013-2018, although patients starting liraglutide (Victoza, Novo Nordisk) were more likely to have a CVD-HF diagnosis.
“This study shows that by preferring empagliflozin, prescribers have largely reacted in accordance with the available evidence and drug labels, while other factors such as lower price, frequency of administration [dulaglutide is given weekly and liraglutide is given daily], or prior authorizations may have led prescribers to select dulaglutide over liraglutide,” Dr. Dave, of the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, and colleagues wrote.
Internists and endocrinologists were the most frequent prescribers of both drug classes, but cardiologists rarely prescribed them, even for patients with established CVD-HF. “As patients with co-occurring diabetes and CVD are likely to see their cardiologist, these encounters may provide an additional opportunity to optimize their treatment,” the authors emphasized.
SGLT2 inhibitors and label changes
Over the study period, the proportion of patients who had CVD-HF and who received SGLT2 inhibitors rose by 3.4 percentage points, from 8.8% to 12.2% (P trend < .001).
The proportion of overall prescriptions for SGLT2 inhibitors written by endocrinologists dropped by 12.0%, although the absolute number of SGLT2-inhibitor prescriptions written by endocrinologists increased (P < .001).
The proportion written by internists did not change (P = .58), whereas it increased slightly among cardiologists but still barely exceeded 1% (P < .001). The findings were similar for the subgroup of patients with CVD-HF who initiated SGLT2 inhibitors.
By individual agents, canagliflozin (Invokana, Janssen) prescriptions dropped by 75.1 percentage points over the study period, from 100% in 2013 to just 24.9% by 2018 (P < .001), whereas empagliflozin initiation rose by 51.7 percentage points, from 13.9% to 65.6% of all SGLT2 inhibitor initiations (P < .001).
Among those initiating empagliflozin, the proportion with CVD-HF rose by 5.3 percentage points, from 8.8% to 14.1% (P < .001), mostly after the additional indication for reducing CV events and death was added to the U.S. label in December 2016.
In contrast, there were no significant changes in the proportions of those with CVD-HF who initiated canagliflozin (P = 065), dapagliflozin (P = .87), or other medications (P = .060).
“Changes in the drug label for canagliflozin (boxed warning for amputation) and empagliflozin (for reduction in CV events and death) in 2016 likely contributed to a rapid change in prescribing preference for empagliflozin,” Dr. Dave and colleagues wrote.
GLP-1 agonists and frequency
Among the patients starting GLP-1 agonists, the proportion with CVD-HF increased by 3.9 percentage points, from 10.5% to 14.4% (P < .001) during the study period.
Prescriptions by endocrinologists declined as a proportion, but rose in absolute numbers (P < .001), and remained consistent for internists (> 55%; P = .12).
Prescribing of GLP-1 agonists by cardiologists remained low (< 0.5%) and was not higher for individuals with CVD-HF.
By individual GLP-1 agonist, liraglutide initiation declined by 32.1 percentage points, from 72.4% to 40.3% of GLP-1 agonist initiations (P < .001), whereas dulaglutide initiation rose by 43.8 percentage points, from 5.0% to 48.8% (P < .001). Again, these trends were similar in the subgroup of patients with CVD-HF.
The proportion of patients with CVD-HF in liraglutide initiators increased by 5.1 percentage points, from 10.5% to 15.6% (P = .018), and in exenatide initiators by 2.1 percentage points, from 10.3% to 13.8% (P = .77).
“Due to the reduced frequency of administration and possible formulary preferences, dulaglutide initiations surpassed liraglutide, the only GLP-1 agonist with evidence of CV benefit at the time,” Dr. Dave and colleagues noted.
Dulaglutide has just been granted an additional approval by the Food and Drug Administration for reducing the risk of major adverse cardiovascular events in adults with type 2 diabetes with and without established CVD or multiple CV risk factors. That makes it the first and only type 2 diabetes medicine approved to reduce the risk of CV events for both primary and secondary prevention populations.
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston. Dr. Dave has reported receiving support from the New Jersey Alliance for Clinical and Translational Science.
This article first appeared on Medscape.com.
new research shows.
The findings, from U.S.-based administrative claims data, were published online in Diabetes Care by Chintan V. Dave, PharmD, PhD, and colleagues.
Among patients initiating oral sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors) over the 5-year period, empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) became the most commonly prescribed glucose-lowering drug, primarily driven by an increasing proportion of patients with diabetes who had a diagnosis of myocardial infarction, stroke, or heart failure (collectively called cardiovascular disease-heart failure [CVD-HF]).
And within the subcutaneous injectable glucagonlike peptide–1 receptor (GLP-1) agonist class, initiations of dulaglutide (Trulicity, Lilly) surpassed liraglutide in 2013-2018, although patients starting liraglutide (Victoza, Novo Nordisk) were more likely to have a CVD-HF diagnosis.
“This study shows that by preferring empagliflozin, prescribers have largely reacted in accordance with the available evidence and drug labels, while other factors such as lower price, frequency of administration [dulaglutide is given weekly and liraglutide is given daily], or prior authorizations may have led prescribers to select dulaglutide over liraglutide,” Dr. Dave, of the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, and colleagues wrote.
Internists and endocrinologists were the most frequent prescribers of both drug classes, but cardiologists rarely prescribed them, even for patients with established CVD-HF. “As patients with co-occurring diabetes and CVD are likely to see their cardiologist, these encounters may provide an additional opportunity to optimize their treatment,” the authors emphasized.
SGLT2 inhibitors and label changes
Over the study period, the proportion of patients who had CVD-HF and who received SGLT2 inhibitors rose by 3.4 percentage points, from 8.8% to 12.2% (P trend < .001).
The proportion of overall prescriptions for SGLT2 inhibitors written by endocrinologists dropped by 12.0%, although the absolute number of SGLT2-inhibitor prescriptions written by endocrinologists increased (P < .001).
The proportion written by internists did not change (P = .58), whereas it increased slightly among cardiologists but still barely exceeded 1% (P < .001). The findings were similar for the subgroup of patients with CVD-HF who initiated SGLT2 inhibitors.
By individual agents, canagliflozin (Invokana, Janssen) prescriptions dropped by 75.1 percentage points over the study period, from 100% in 2013 to just 24.9% by 2018 (P < .001), whereas empagliflozin initiation rose by 51.7 percentage points, from 13.9% to 65.6% of all SGLT2 inhibitor initiations (P < .001).
Among those initiating empagliflozin, the proportion with CVD-HF rose by 5.3 percentage points, from 8.8% to 14.1% (P < .001), mostly after the additional indication for reducing CV events and death was added to the U.S. label in December 2016.
In contrast, there were no significant changes in the proportions of those with CVD-HF who initiated canagliflozin (P = 065), dapagliflozin (P = .87), or other medications (P = .060).
“Changes in the drug label for canagliflozin (boxed warning for amputation) and empagliflozin (for reduction in CV events and death) in 2016 likely contributed to a rapid change in prescribing preference for empagliflozin,” Dr. Dave and colleagues wrote.
GLP-1 agonists and frequency
Among the patients starting GLP-1 agonists, the proportion with CVD-HF increased by 3.9 percentage points, from 10.5% to 14.4% (P < .001) during the study period.
Prescriptions by endocrinologists declined as a proportion, but rose in absolute numbers (P < .001), and remained consistent for internists (> 55%; P = .12).
Prescribing of GLP-1 agonists by cardiologists remained low (< 0.5%) and was not higher for individuals with CVD-HF.
By individual GLP-1 agonist, liraglutide initiation declined by 32.1 percentage points, from 72.4% to 40.3% of GLP-1 agonist initiations (P < .001), whereas dulaglutide initiation rose by 43.8 percentage points, from 5.0% to 48.8% (P < .001). Again, these trends were similar in the subgroup of patients with CVD-HF.
The proportion of patients with CVD-HF in liraglutide initiators increased by 5.1 percentage points, from 10.5% to 15.6% (P = .018), and in exenatide initiators by 2.1 percentage points, from 10.3% to 13.8% (P = .77).
“Due to the reduced frequency of administration and possible formulary preferences, dulaglutide initiations surpassed liraglutide, the only GLP-1 agonist with evidence of CV benefit at the time,” Dr. Dave and colleagues noted.
Dulaglutide has just been granted an additional approval by the Food and Drug Administration for reducing the risk of major adverse cardiovascular events in adults with type 2 diabetes with and without established CVD or multiple CV risk factors. That makes it the first and only type 2 diabetes medicine approved to reduce the risk of CV events for both primary and secondary prevention populations.
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston. Dr. Dave has reported receiving support from the New Jersey Alliance for Clinical and Translational Science.
This article first appeared on Medscape.com.
CMS issues guidance on containing spread of coronavirus
The first guidance document, “Guidance for Infection Control and Prevention Concerning Coronavirus Disease (COVID-19): FAQs and Considerations for Patient Triage, Placement and Hospital Discharge,” issued March 4, provides some basic guidance, including identifying which patients are at risk, how facilities should screen for COVID-19, how facilities should monitor or restrict health care facility staff, and other recommendations for infection prevention and control.
“Hospitals should identify visitors and patients at risk for having COVID-19 infection before or immediately upon arrival to the healthcare facility,” the guidance document notes. “For patients, implement respiratory hygiene and cough etiquette (i.e., placing a face mask over the patient’s nose and mouth if that has not already been done) and isolate the patient in an examination room with the door closed. If the patient cannot be immediately moved to an examination room, ensure they are not allowed to wait among other patients seeking care.”
The document offers further information regarding the care of patients and provides numerous links to existing guidance from the Centers for Disease Control and Prevention.
The second document, “Guidance for Infection Control and Prevention of Coronavirus Disease 2019 (COVID-19) in Nursing Homes,” issued the same day, provides information on how to limit and monitor visitors as well as monitor and restrict health staff. It details when to transfer residents with suspected or confirmed coronavirus infection, and when a nursing home should accept a resident diagnosed with COVID-19.
Facilities “should contact their local health department if they have questions or suspect a resident of a nursing home has COVID-19,” the document states. “Per CDC, prompt detection, triage and isolation of potentially infectious patients are essential to prevent unnecessary exposure among patients, healthcare personnel, and visitors at the facility.”
The CMS also announced that it is suspending all nonemergency survey activity.
“CMS is suspending nonemergency inspections across the country, allowing inspectors to turn their focus on the most serious health and safety threats like infectious diseases and abuse,” the agency stated in a March 4 memo. “This shift in approach will also allow inspectors to focus on addressing the spread of ... COVID-19. CMS is issuing this memorandum to State Survey Agencies to provide important guidelines for the inspection process in situations in which a COVID-19 is suspected.”

In a statement, CMS Administrator Seema Verma said these actions “represent a call to action across the health care system. All health care providers must immediately review their procedures to ensure compliance with CMS’ infection control requirements, as well as the guidelines from the Centers for Disease Control and Prevention.”
The first guidance document, “Guidance for Infection Control and Prevention Concerning Coronavirus Disease (COVID-19): FAQs and Considerations for Patient Triage, Placement and Hospital Discharge,” issued March 4, provides some basic guidance, including identifying which patients are at risk, how facilities should screen for COVID-19, how facilities should monitor or restrict health care facility staff, and other recommendations for infection prevention and control.
“Hospitals should identify visitors and patients at risk for having COVID-19 infection before or immediately upon arrival to the healthcare facility,” the guidance document notes. “For patients, implement respiratory hygiene and cough etiquette (i.e., placing a face mask over the patient’s nose and mouth if that has not already been done) and isolate the patient in an examination room with the door closed. If the patient cannot be immediately moved to an examination room, ensure they are not allowed to wait among other patients seeking care.”
The document offers further information regarding the care of patients and provides numerous links to existing guidance from the Centers for Disease Control and Prevention.
The second document, “Guidance for Infection Control and Prevention of Coronavirus Disease 2019 (COVID-19) in Nursing Homes,” issued the same day, provides information on how to limit and monitor visitors as well as monitor and restrict health staff. It details when to transfer residents with suspected or confirmed coronavirus infection, and when a nursing home should accept a resident diagnosed with COVID-19.
Facilities “should contact their local health department if they have questions or suspect a resident of a nursing home has COVID-19,” the document states. “Per CDC, prompt detection, triage and isolation of potentially infectious patients are essential to prevent unnecessary exposure among patients, healthcare personnel, and visitors at the facility.”
The CMS also announced that it is suspending all nonemergency survey activity.
“CMS is suspending nonemergency inspections across the country, allowing inspectors to turn their focus on the most serious health and safety threats like infectious diseases and abuse,” the agency stated in a March 4 memo. “This shift in approach will also allow inspectors to focus on addressing the spread of ... COVID-19. CMS is issuing this memorandum to State Survey Agencies to provide important guidelines for the inspection process in situations in which a COVID-19 is suspected.”
In a statement, CMS Administrator Seema Verma said these actions “represent a call to action across the health care system. All health care providers must immediately review their procedures to ensure compliance with CMS’ infection control requirements, as well as the guidelines from the Centers for Disease Control and Prevention.”
The first guidance document, “Guidance for Infection Control and Prevention Concerning Coronavirus Disease (COVID-19): FAQs and Considerations for Patient Triage, Placement and Hospital Discharge,” issued March 4, provides some basic guidance, including identifying which patients are at risk, how facilities should screen for COVID-19, how facilities should monitor or restrict health care facility staff, and other recommendations for infection prevention and control.
“Hospitals should identify visitors and patients at risk for having COVID-19 infection before or immediately upon arrival to the healthcare facility,” the guidance document notes. “For patients, implement respiratory hygiene and cough etiquette (i.e., placing a face mask over the patient’s nose and mouth if that has not already been done) and isolate the patient in an examination room with the door closed. If the patient cannot be immediately moved to an examination room, ensure they are not allowed to wait among other patients seeking care.”
The document offers further information regarding the care of patients and provides numerous links to existing guidance from the Centers for Disease Control and Prevention.
The second document, “Guidance for Infection Control and Prevention of Coronavirus Disease 2019 (COVID-19) in Nursing Homes,” issued the same day, provides information on how to limit and monitor visitors as well as monitor and restrict health staff. It details when to transfer residents with suspected or confirmed coronavirus infection, and when a nursing home should accept a resident diagnosed with COVID-19.
Facilities “should contact their local health department if they have questions or suspect a resident of a nursing home has COVID-19,” the document states. “Per CDC, prompt detection, triage and isolation of potentially infectious patients are essential to prevent unnecessary exposure among patients, healthcare personnel, and visitors at the facility.”
The CMS also announced that it is suspending all nonemergency survey activity.
“CMS is suspending nonemergency inspections across the country, allowing inspectors to turn their focus on the most serious health and safety threats like infectious diseases and abuse,” the agency stated in a March 4 memo. “This shift in approach will also allow inspectors to focus on addressing the spread of ... COVID-19. CMS is issuing this memorandum to State Survey Agencies to provide important guidelines for the inspection process in situations in which a COVID-19 is suspected.”
In a statement, CMS Administrator Seema Verma said these actions “represent a call to action across the health care system. All health care providers must immediately review their procedures to ensure compliance with CMS’ infection control requirements, as well as the guidelines from the Centers for Disease Control and Prevention.”