User login
In Case You Missed It: COVID
New reports guide return to play in athletes with COVID-19
Increasingly, clinicians are being called upon to advise athletes who have recovered from COVID-19 on when it is safe for them to return to play.
Now, they have two reports that offer more insights into the cardiotoxic effects of COVID-19 on the athletic heart.
In the first report, researchers report a high prevalence of pericardial involvement in college-student athletes who have recovered from COVID-19 and give their practical advice on how to let these athletes return to play safely.
In the second report, an expert panel of sports cardiologists provides a comprehensive guide to the appropriate imaging of athletes who may have cardiovascular complications from COVID-19.
Both are published in JACC: Cardiovascular Imaging.
“We were asked by the editors of JACC to submit this paper, and the impetus for it was the fact that there are so many athletes returning after being infected with COVID-19, we need to try and give guidance to cardiologists as to how best to evaluate these athletes,” Dermot Phelan, MD, PhD, Sanger Heart and Vascular Institute, Atrium Health, Charlotte, N.C., and lead author of the consensus statement, said in an interview.
The consensus statement acknowledges that information about the cardiovascular complications of COVID-19 continues to evolve. Meanwhile, pathologies such as myocarditis, pericarditis, and right ventricular dysfunction, in the absence of significant clinical symptoms, in athletes who have been affected by COVID-19 remain of considerable concern.
It also emphasizes the unique challenges the average cardiologist faces in distinguishing between what is normal for an athlete’s heart and what is true pathology after COVID-19 infection; details how different imaging modalities can help in screening, evaluating, and monitoring athletes with suspected cardiovascular complications of COVID-19 infection; and discusses the strengths and limitations of these modalities.
Finally, the consensus statement provides some well-needed guidance on return-to-play decision-making, for both the athlete and the clinician.
Athletic remodeling or covid-19 damage?
Athletes can develop certain cardiovascular characteristics because of their athletic activity, and sometimes, this can cloud the diagnostic picture.
“Is this change due to the effects of COVID-19, or is it just because this is an athlete’s heart? This was an international expert consensus, made up of sports cardiologists from all over the world who have a lot of experience in dealing with athletes,” Dr. Phelan said. “We were trying to relay the important information to the cardiologist who is not used to dealing with athletes on a day-to-day basis, as to what they might expect to find in that athlete, and what is not an expected finding and should be tested further.”
Phelan, a sports cardiologist, is familiar with what is normal for an athlete’s heart and what is pathology.
“We know that athletes, particularly long-term endurance athletes, develop changes in the heart that can affect not only the electrics but the structure of the heart, and sometimes, that overlaps with abnormalities with pathology. This can be a challenge for the nonsports cardiologist to differentiate,” he said.
Phelan and his group have written two other consensus documents on the management of cardiovascular problems that develop in some athletes who have been infected with COVID-19.
The first was published in May in JAMA Cardiology, and the second, which revised some of the original recommendations made in the first document, was published online Oct. 26 in JAMA Cardiology.
The first set of recommendations called for imaging studies to be done in all athletes, but the second set states that athletes who recover and are asymptomatic do not need extensive (and expensive) imaging tests.
“These two papers work hand in hand,” Dr. Phelan said. “In May, we had very little experience with COVID, and there was a lot of concern about hospitalized patients having a very high incidence of heart disease. We published those recommendations, but we recognized at the time that we had very little data and that we would reconsider once we had more experience with data.
“This current set of recommendations that we have put forth here are for those athletes who do need to get further testing, so it’s a step beyond,” Dr. Phelan added. “So the second iteration states that young athletes who had mild or no symptoms didn’t need to go through all of that cardiac testing, but others do need it.”
To do widespread cardiovascular imaging for many individuals would be very costly. Realistically, there are not that many centers in the United States that have all the sophisticated equipment required to do such testing, Dr. Phelan noted.
“One of our major points is difficulty obtaining the test, but also the cost; these are very expensive tests. There are limitations. They are useful when used in the correct context,” he said.
To play or not to play, that is the question
Partho P. Sengupta, MD, DM, had to answer that question for more than 50 young athletes who were returning to college at West Virginia University, anxious to be back with their teams and on the playing field. They had been infected with COVID-19 and needed to know when they could return to play.
Dr. Sengupta, who is also an author for the Phelan et al consensus statement on imaging, said there was a lot of pressure – from all the various stakeholders, and from anxious parents, worried college athletes, their teammates, and the university – to determine if the youngsters could return to play.
The fear was that COVID-19 infection left the young athlete’s heart vulnerable to myocarditis and, thus, sudden death on the playing field after strenuous activity.
“At the time we were doing this imaging, there was a lot of concern in the media, and papers were coming out reporting a lot of cardiac involvement or myocarditis associated with COVID-19. Nobody really knew what to do,” he explained.
“There were all kinds of questions, concerns. The parents were putting pressure on us, the athletes wanted to know, the teams, the university. So we put together a team and completed all of the examinations, including testing of blood markers, within a 2-week period. These young athletes, they’re scared, they’re worried and anxious, they don’t know what’s going to happen with their scholarship, so there was some urgency to this work,” Dr. Sengupta said.
“We had to screen all comers within a very short period. We had 54 consecutive patients, gave them full screening, full battery of tests, blood tests, all in a 2-week period,” he said.
Speed was of the essence, and Dr. Sengupta and his team rolled up their sleeves and got to work “We had to know who was safe to clear to return to play and who might need extra follow-up.”
Screening echocardiograms
They performed screening echocardiograms on 54 consecutive college athletes who had tested positive for COVID-19 on reverse transcription polymerase chain reaction nasal swab testing or who showed that they had IgG antibodies against COVID-19. The screening echocardiograms were done after the athletes had quarantined for at least 14 days and were no longer infectious.
Most (85%) were male, and the mean age was 19 years. A total of 16 (30%) athletes were asymptomatic, 36 (66%) reported mild COVID-19 related symptoms, and two (4%) reported moderate symptoms.
Of the 54 athletes who were initially screened with echocardiography, 48 (11 asymptomatic, 37 symptomatic), went on to have cardiac magnetic resonance imaging.
Results showed that more than half the athletes (27; 56.3%), showed some cardiac abnormality. The most common was pericardial late enhancement with associated pericardial effusion, affecting 19 (39.5%) athletes.
Of these, six (12.5%) had reduced global longitudinal strain (GLS) or an increased native T1.
One patient showed myocardial enhancement.
Additionally, seven athletes (14.6%) had reduced left ventricular ejection fraction or reduced GLS with or without increased native T1. Native T2 levels were normal in all subjects and no specific imaging features of myocardial inflammation were identified.
Participants were brought back to receive the results of their tests and to get an individualized plan about their safe return to play 3 to 5 weeks after they had ceased to be infectious with COVID-19.
“We saw pericardial inflammation that was resolving. We did not see any blood biomarkers to suggest that there was active inflammation going on,” he said. “We also did not see any muscle inflammation, but we did see pockets of fluid in over a third of our athletes.”
Fortunately, most were deemed able to get back to playing safely, despite having evidence of pericardial inflammation.
This was on strict condition that they be monitored very closely for any adverse events that might occur as they began to exercise again.
“Once they go back to the field to start exercising and practicing, it is under great supervision. We instructed all of our sports physicians and other team managers that these people need to be observed very carefully. So as long as they were asymptomatic, even though the signs of pericardial inflammation were there, if there were no signs of inflammation in the blood, we let them go back to play, closely monitored,” Dr. Sengupta said.
A small number remained very symptomatic at the end of the 5 weeks and were referred to cardiac rehabilitation, Dr. Sengupta said. “They were tired, fatigued, short of breath, even 5 weeks after they got over COVID, so we sent them for cardiac rehab to help them get conditioned again.”
The researchers plan to reevaluate and reimage all of the athletes in another 3 months to monitor their cardiac health.
Dr. Sengupta acknowledged the limitations of this single-center, nonrandomized, controlled report, but insists reports such as this add a bit more to what we are learning about COVID-19 every day.
“These kids were coming to us and asking questions. You have to use the best science you have available to you at that point in time. Some people ask why we did not have a control group, but how do you design a control population in the midst of a pandemic? The science may or may not be perfect, I agree, but the information we obtained is important,” he said.
“Right now, I don’t think we have enough science, and we are still learning. It is very difficult to predict who will develop the heart muscle disease or the pericardial disease,” Dr. Sengupta said. “We had to do our work quickly to give answers to the young athletes, their parents, their teammates, their university, as soon as possible, and we were doing this under pandemic conditions.”
The work was supported by the National Science Foundation National Institute of General Medical Sciences of the National Institutes of Health. Dr. Phelan reported no relevant financial relationships. Dr. Sengupta reported that he is a consultant for HeartSciences, Kencor Health, and Ultromics.
This article first appeared on Medscape.com.
Increasingly, clinicians are being called upon to advise athletes who have recovered from COVID-19 on when it is safe for them to return to play.
Now, they have two reports that offer more insights into the cardiotoxic effects of COVID-19 on the athletic heart.
In the first report, researchers report a high prevalence of pericardial involvement in college-student athletes who have recovered from COVID-19 and give their practical advice on how to let these athletes return to play safely.
In the second report, an expert panel of sports cardiologists provides a comprehensive guide to the appropriate imaging of athletes who may have cardiovascular complications from COVID-19.
Both are published in JACC: Cardiovascular Imaging.
“We were asked by the editors of JACC to submit this paper, and the impetus for it was the fact that there are so many athletes returning after being infected with COVID-19, we need to try and give guidance to cardiologists as to how best to evaluate these athletes,” Dermot Phelan, MD, PhD, Sanger Heart and Vascular Institute, Atrium Health, Charlotte, N.C., and lead author of the consensus statement, said in an interview.
The consensus statement acknowledges that information about the cardiovascular complications of COVID-19 continues to evolve. Meanwhile, pathologies such as myocarditis, pericarditis, and right ventricular dysfunction, in the absence of significant clinical symptoms, in athletes who have been affected by COVID-19 remain of considerable concern.
It also emphasizes the unique challenges the average cardiologist faces in distinguishing between what is normal for an athlete’s heart and what is true pathology after COVID-19 infection; details how different imaging modalities can help in screening, evaluating, and monitoring athletes with suspected cardiovascular complications of COVID-19 infection; and discusses the strengths and limitations of these modalities.
Finally, the consensus statement provides some well-needed guidance on return-to-play decision-making, for both the athlete and the clinician.
Athletic remodeling or covid-19 damage?
Athletes can develop certain cardiovascular characteristics because of their athletic activity, and sometimes, this can cloud the diagnostic picture.
“Is this change due to the effects of COVID-19, or is it just because this is an athlete’s heart? This was an international expert consensus, made up of sports cardiologists from all over the world who have a lot of experience in dealing with athletes,” Dr. Phelan said. “We were trying to relay the important information to the cardiologist who is not used to dealing with athletes on a day-to-day basis, as to what they might expect to find in that athlete, and what is not an expected finding and should be tested further.”
Phelan, a sports cardiologist, is familiar with what is normal for an athlete’s heart and what is pathology.
“We know that athletes, particularly long-term endurance athletes, develop changes in the heart that can affect not only the electrics but the structure of the heart, and sometimes, that overlaps with abnormalities with pathology. This can be a challenge for the nonsports cardiologist to differentiate,” he said.
Phelan and his group have written two other consensus documents on the management of cardiovascular problems that develop in some athletes who have been infected with COVID-19.
The first was published in May in JAMA Cardiology, and the second, which revised some of the original recommendations made in the first document, was published online Oct. 26 in JAMA Cardiology.
The first set of recommendations called for imaging studies to be done in all athletes, but the second set states that athletes who recover and are asymptomatic do not need extensive (and expensive) imaging tests.
“These two papers work hand in hand,” Dr. Phelan said. “In May, we had very little experience with COVID, and there was a lot of concern about hospitalized patients having a very high incidence of heart disease. We published those recommendations, but we recognized at the time that we had very little data and that we would reconsider once we had more experience with data.
“This current set of recommendations that we have put forth here are for those athletes who do need to get further testing, so it’s a step beyond,” Dr. Phelan added. “So the second iteration states that young athletes who had mild or no symptoms didn’t need to go through all of that cardiac testing, but others do need it.”
To do widespread cardiovascular imaging for many individuals would be very costly. Realistically, there are not that many centers in the United States that have all the sophisticated equipment required to do such testing, Dr. Phelan noted.
“One of our major points is difficulty obtaining the test, but also the cost; these are very expensive tests. There are limitations. They are useful when used in the correct context,” he said.
To play or not to play, that is the question
Partho P. Sengupta, MD, DM, had to answer that question for more than 50 young athletes who were returning to college at West Virginia University, anxious to be back with their teams and on the playing field. They had been infected with COVID-19 and needed to know when they could return to play.
Dr. Sengupta, who is also an author for the Phelan et al consensus statement on imaging, said there was a lot of pressure – from all the various stakeholders, and from anxious parents, worried college athletes, their teammates, and the university – to determine if the youngsters could return to play.
The fear was that COVID-19 infection left the young athlete’s heart vulnerable to myocarditis and, thus, sudden death on the playing field after strenuous activity.
“At the time we were doing this imaging, there was a lot of concern in the media, and papers were coming out reporting a lot of cardiac involvement or myocarditis associated with COVID-19. Nobody really knew what to do,” he explained.
“There were all kinds of questions, concerns. The parents were putting pressure on us, the athletes wanted to know, the teams, the university. So we put together a team and completed all of the examinations, including testing of blood markers, within a 2-week period. These young athletes, they’re scared, they’re worried and anxious, they don’t know what’s going to happen with their scholarship, so there was some urgency to this work,” Dr. Sengupta said.
“We had to screen all comers within a very short period. We had 54 consecutive patients, gave them full screening, full battery of tests, blood tests, all in a 2-week period,” he said.
Speed was of the essence, and Dr. Sengupta and his team rolled up their sleeves and got to work “We had to know who was safe to clear to return to play and who might need extra follow-up.”
Screening echocardiograms
They performed screening echocardiograms on 54 consecutive college athletes who had tested positive for COVID-19 on reverse transcription polymerase chain reaction nasal swab testing or who showed that they had IgG antibodies against COVID-19. The screening echocardiograms were done after the athletes had quarantined for at least 14 days and were no longer infectious.
Most (85%) were male, and the mean age was 19 years. A total of 16 (30%) athletes were asymptomatic, 36 (66%) reported mild COVID-19 related symptoms, and two (4%) reported moderate symptoms.
Of the 54 athletes who were initially screened with echocardiography, 48 (11 asymptomatic, 37 symptomatic), went on to have cardiac magnetic resonance imaging.
Results showed that more than half the athletes (27; 56.3%), showed some cardiac abnormality. The most common was pericardial late enhancement with associated pericardial effusion, affecting 19 (39.5%) athletes.
Of these, six (12.5%) had reduced global longitudinal strain (GLS) or an increased native T1.
One patient showed myocardial enhancement.
Additionally, seven athletes (14.6%) had reduced left ventricular ejection fraction or reduced GLS with or without increased native T1. Native T2 levels were normal in all subjects and no specific imaging features of myocardial inflammation were identified.
Participants were brought back to receive the results of their tests and to get an individualized plan about their safe return to play 3 to 5 weeks after they had ceased to be infectious with COVID-19.
“We saw pericardial inflammation that was resolving. We did not see any blood biomarkers to suggest that there was active inflammation going on,” he said. “We also did not see any muscle inflammation, but we did see pockets of fluid in over a third of our athletes.”
Fortunately, most were deemed able to get back to playing safely, despite having evidence of pericardial inflammation.
This was on strict condition that they be monitored very closely for any adverse events that might occur as they began to exercise again.
“Once they go back to the field to start exercising and practicing, it is under great supervision. We instructed all of our sports physicians and other team managers that these people need to be observed very carefully. So as long as they were asymptomatic, even though the signs of pericardial inflammation were there, if there were no signs of inflammation in the blood, we let them go back to play, closely monitored,” Dr. Sengupta said.
A small number remained very symptomatic at the end of the 5 weeks and were referred to cardiac rehabilitation, Dr. Sengupta said. “They were tired, fatigued, short of breath, even 5 weeks after they got over COVID, so we sent them for cardiac rehab to help them get conditioned again.”
The researchers plan to reevaluate and reimage all of the athletes in another 3 months to monitor their cardiac health.
Dr. Sengupta acknowledged the limitations of this single-center, nonrandomized, controlled report, but insists reports such as this add a bit more to what we are learning about COVID-19 every day.
“These kids were coming to us and asking questions. You have to use the best science you have available to you at that point in time. Some people ask why we did not have a control group, but how do you design a control population in the midst of a pandemic? The science may or may not be perfect, I agree, but the information we obtained is important,” he said.
“Right now, I don’t think we have enough science, and we are still learning. It is very difficult to predict who will develop the heart muscle disease or the pericardial disease,” Dr. Sengupta said. “We had to do our work quickly to give answers to the young athletes, their parents, their teammates, their university, as soon as possible, and we were doing this under pandemic conditions.”
The work was supported by the National Science Foundation National Institute of General Medical Sciences of the National Institutes of Health. Dr. Phelan reported no relevant financial relationships. Dr. Sengupta reported that he is a consultant for HeartSciences, Kencor Health, and Ultromics.
This article first appeared on Medscape.com.
Increasingly, clinicians are being called upon to advise athletes who have recovered from COVID-19 on when it is safe for them to return to play.
Now, they have two reports that offer more insights into the cardiotoxic effects of COVID-19 on the athletic heart.
In the first report, researchers report a high prevalence of pericardial involvement in college-student athletes who have recovered from COVID-19 and give their practical advice on how to let these athletes return to play safely.
In the second report, an expert panel of sports cardiologists provides a comprehensive guide to the appropriate imaging of athletes who may have cardiovascular complications from COVID-19.
Both are published in JACC: Cardiovascular Imaging.
“We were asked by the editors of JACC to submit this paper, and the impetus for it was the fact that there are so many athletes returning after being infected with COVID-19, we need to try and give guidance to cardiologists as to how best to evaluate these athletes,” Dermot Phelan, MD, PhD, Sanger Heart and Vascular Institute, Atrium Health, Charlotte, N.C., and lead author of the consensus statement, said in an interview.
The consensus statement acknowledges that information about the cardiovascular complications of COVID-19 continues to evolve. Meanwhile, pathologies such as myocarditis, pericarditis, and right ventricular dysfunction, in the absence of significant clinical symptoms, in athletes who have been affected by COVID-19 remain of considerable concern.
It also emphasizes the unique challenges the average cardiologist faces in distinguishing between what is normal for an athlete’s heart and what is true pathology after COVID-19 infection; details how different imaging modalities can help in screening, evaluating, and monitoring athletes with suspected cardiovascular complications of COVID-19 infection; and discusses the strengths and limitations of these modalities.
Finally, the consensus statement provides some well-needed guidance on return-to-play decision-making, for both the athlete and the clinician.
Athletic remodeling or covid-19 damage?
Athletes can develop certain cardiovascular characteristics because of their athletic activity, and sometimes, this can cloud the diagnostic picture.
“Is this change due to the effects of COVID-19, or is it just because this is an athlete’s heart? This was an international expert consensus, made up of sports cardiologists from all over the world who have a lot of experience in dealing with athletes,” Dr. Phelan said. “We were trying to relay the important information to the cardiologist who is not used to dealing with athletes on a day-to-day basis, as to what they might expect to find in that athlete, and what is not an expected finding and should be tested further.”
Phelan, a sports cardiologist, is familiar with what is normal for an athlete’s heart and what is pathology.
“We know that athletes, particularly long-term endurance athletes, develop changes in the heart that can affect not only the electrics but the structure of the heart, and sometimes, that overlaps with abnormalities with pathology. This can be a challenge for the nonsports cardiologist to differentiate,” he said.
Phelan and his group have written two other consensus documents on the management of cardiovascular problems that develop in some athletes who have been infected with COVID-19.
The first was published in May in JAMA Cardiology, and the second, which revised some of the original recommendations made in the first document, was published online Oct. 26 in JAMA Cardiology.
The first set of recommendations called for imaging studies to be done in all athletes, but the second set states that athletes who recover and are asymptomatic do not need extensive (and expensive) imaging tests.
“These two papers work hand in hand,” Dr. Phelan said. “In May, we had very little experience with COVID, and there was a lot of concern about hospitalized patients having a very high incidence of heart disease. We published those recommendations, but we recognized at the time that we had very little data and that we would reconsider once we had more experience with data.
“This current set of recommendations that we have put forth here are for those athletes who do need to get further testing, so it’s a step beyond,” Dr. Phelan added. “So the second iteration states that young athletes who had mild or no symptoms didn’t need to go through all of that cardiac testing, but others do need it.”
To do widespread cardiovascular imaging for many individuals would be very costly. Realistically, there are not that many centers in the United States that have all the sophisticated equipment required to do such testing, Dr. Phelan noted.
“One of our major points is difficulty obtaining the test, but also the cost; these are very expensive tests. There are limitations. They are useful when used in the correct context,” he said.
To play or not to play, that is the question
Partho P. Sengupta, MD, DM, had to answer that question for more than 50 young athletes who were returning to college at West Virginia University, anxious to be back with their teams and on the playing field. They had been infected with COVID-19 and needed to know when they could return to play.
Dr. Sengupta, who is also an author for the Phelan et al consensus statement on imaging, said there was a lot of pressure – from all the various stakeholders, and from anxious parents, worried college athletes, their teammates, and the university – to determine if the youngsters could return to play.
The fear was that COVID-19 infection left the young athlete’s heart vulnerable to myocarditis and, thus, sudden death on the playing field after strenuous activity.
“At the time we were doing this imaging, there was a lot of concern in the media, and papers were coming out reporting a lot of cardiac involvement or myocarditis associated with COVID-19. Nobody really knew what to do,” he explained.
“There were all kinds of questions, concerns. The parents were putting pressure on us, the athletes wanted to know, the teams, the university. So we put together a team and completed all of the examinations, including testing of blood markers, within a 2-week period. These young athletes, they’re scared, they’re worried and anxious, they don’t know what’s going to happen with their scholarship, so there was some urgency to this work,” Dr. Sengupta said.
“We had to screen all comers within a very short period. We had 54 consecutive patients, gave them full screening, full battery of tests, blood tests, all in a 2-week period,” he said.
Speed was of the essence, and Dr. Sengupta and his team rolled up their sleeves and got to work “We had to know who was safe to clear to return to play and who might need extra follow-up.”
Screening echocardiograms
They performed screening echocardiograms on 54 consecutive college athletes who had tested positive for COVID-19 on reverse transcription polymerase chain reaction nasal swab testing or who showed that they had IgG antibodies against COVID-19. The screening echocardiograms were done after the athletes had quarantined for at least 14 days and were no longer infectious.
Most (85%) were male, and the mean age was 19 years. A total of 16 (30%) athletes were asymptomatic, 36 (66%) reported mild COVID-19 related symptoms, and two (4%) reported moderate symptoms.
Of the 54 athletes who were initially screened with echocardiography, 48 (11 asymptomatic, 37 symptomatic), went on to have cardiac magnetic resonance imaging.
Results showed that more than half the athletes (27; 56.3%), showed some cardiac abnormality. The most common was pericardial late enhancement with associated pericardial effusion, affecting 19 (39.5%) athletes.
Of these, six (12.5%) had reduced global longitudinal strain (GLS) or an increased native T1.
One patient showed myocardial enhancement.
Additionally, seven athletes (14.6%) had reduced left ventricular ejection fraction or reduced GLS with or without increased native T1. Native T2 levels were normal in all subjects and no specific imaging features of myocardial inflammation were identified.
Participants were brought back to receive the results of their tests and to get an individualized plan about their safe return to play 3 to 5 weeks after they had ceased to be infectious with COVID-19.
“We saw pericardial inflammation that was resolving. We did not see any blood biomarkers to suggest that there was active inflammation going on,” he said. “We also did not see any muscle inflammation, but we did see pockets of fluid in over a third of our athletes.”
Fortunately, most were deemed able to get back to playing safely, despite having evidence of pericardial inflammation.
This was on strict condition that they be monitored very closely for any adverse events that might occur as they began to exercise again.
“Once they go back to the field to start exercising and practicing, it is under great supervision. We instructed all of our sports physicians and other team managers that these people need to be observed very carefully. So as long as they were asymptomatic, even though the signs of pericardial inflammation were there, if there were no signs of inflammation in the blood, we let them go back to play, closely monitored,” Dr. Sengupta said.
A small number remained very symptomatic at the end of the 5 weeks and were referred to cardiac rehabilitation, Dr. Sengupta said. “They were tired, fatigued, short of breath, even 5 weeks after they got over COVID, so we sent them for cardiac rehab to help them get conditioned again.”
The researchers plan to reevaluate and reimage all of the athletes in another 3 months to monitor their cardiac health.
Dr. Sengupta acknowledged the limitations of this single-center, nonrandomized, controlled report, but insists reports such as this add a bit more to what we are learning about COVID-19 every day.
“These kids were coming to us and asking questions. You have to use the best science you have available to you at that point in time. Some people ask why we did not have a control group, but how do you design a control population in the midst of a pandemic? The science may or may not be perfect, I agree, but the information we obtained is important,” he said.
“Right now, I don’t think we have enough science, and we are still learning. It is very difficult to predict who will develop the heart muscle disease or the pericardial disease,” Dr. Sengupta said. “We had to do our work quickly to give answers to the young athletes, their parents, their teammates, their university, as soon as possible, and we were doing this under pandemic conditions.”
The work was supported by the National Science Foundation National Institute of General Medical Sciences of the National Institutes of Health. Dr. Phelan reported no relevant financial relationships. Dr. Sengupta reported that he is a consultant for HeartSciences, Kencor Health, and Ultromics.
This article first appeared on Medscape.com.
AMA creates COVID-19 CPT codes for Pfizer, Moderna vaccines
The largest U.S. physician organization on Tuesday took a step to prepare for future payments for administration of two leading COVID-19 vaccine candidates, publishing new billing codes tailored to track each use of these medications.
The The new codes apply to the experimental vaccine being developed by Pfizer, in collaboration with a smaller German firm BioNTech, and to the similar product expected from Moderna, according to an AMA press release.
Positive news has emerged this week about both of these vaccines, which were developed using a newer – and as yet unproven – approach. They seek to use messenger RNA to instruct cells to produce a target protein for SARS-CoV-2.
New York–based Pfizer on Monday announced interim phase 3 data that was widely viewed as promising. Pfizer said the vaccine appeared to be 90% effective in preventing COVID-19 in trial volunteers who were without evidence of prior infection of the virus.
In a press release, Pfizer said it plans to ask the Food and Drug Administration to consider a special clearance, known as an emergency-use authorization, “soon after” a safety milestone is achieved in its vaccine trial. That milestone could be reached this month.
Moderna said it was on track to report early data from a late-stage trial of its experimental coronavirus vaccine later this month, and could file with the FDA for an emergency-use authorization in early December, according to a Reuters report.
The severity of the global pandemic has put the FDA under pressure to move quickly on approval of COVID-19 vaccines, based on limited data, while also working to make sure these products are safe. The creation of CPT codes for each of two coronavirus vaccines, as well as accompanying administration codes, will set up a way to keep tabs on each dose of each of these shots, the AMA said.

“Correlating each coronavirus vaccine with its own unique CPT code provides analytical advantages to help track, allocate and optimize resources as an immunization program ramps up in the United States,” AMA President Susan R. Bailey, MD, said in the release.
AMA plans to introduce more vaccine-specific CPT codes as more vaccine candidates approach FDA review. These vaccine-specific CPT codes can go into effect only after the FDA grants a clearance.
The newly created Category I CPT codes and long descriptors for the vaccine products are:
- 91300; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3mL dosage, diluent reconstituted, for intramuscular use (Pfizer/BioNTech)
- 91301; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5mL dosage, for intramuscular use (Moderna)
These two administrative codes would apply to the Pfizer-BioNTech shot:
- 0001A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3 mL dosage, diluent reconstituted; first dose.
- 0002A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3 mL dosage, diluent reconstituted; second dose.
And these two administrative codes would apply to the Moderna shot:
- 0011A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5 mL dosage; first dose.
- 0012A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5 mL dosage; second dose.
A version of this article originally appeared on Medscape.com.
The largest U.S. physician organization on Tuesday took a step to prepare for future payments for administration of two leading COVID-19 vaccine candidates, publishing new billing codes tailored to track each use of these medications.
The The new codes apply to the experimental vaccine being developed by Pfizer, in collaboration with a smaller German firm BioNTech, and to the similar product expected from Moderna, according to an AMA press release.
Positive news has emerged this week about both of these vaccines, which were developed using a newer – and as yet unproven – approach. They seek to use messenger RNA to instruct cells to produce a target protein for SARS-CoV-2.
New York–based Pfizer on Monday announced interim phase 3 data that was widely viewed as promising. Pfizer said the vaccine appeared to be 90% effective in preventing COVID-19 in trial volunteers who were without evidence of prior infection of the virus.
In a press release, Pfizer said it plans to ask the Food and Drug Administration to consider a special clearance, known as an emergency-use authorization, “soon after” a safety milestone is achieved in its vaccine trial. That milestone could be reached this month.
Moderna said it was on track to report early data from a late-stage trial of its experimental coronavirus vaccine later this month, and could file with the FDA for an emergency-use authorization in early December, according to a Reuters report.
The severity of the global pandemic has put the FDA under pressure to move quickly on approval of COVID-19 vaccines, based on limited data, while also working to make sure these products are safe. The creation of CPT codes for each of two coronavirus vaccines, as well as accompanying administration codes, will set up a way to keep tabs on each dose of each of these shots, the AMA said.
“Correlating each coronavirus vaccine with its own unique CPT code provides analytical advantages to help track, allocate and optimize resources as an immunization program ramps up in the United States,” AMA President Susan R. Bailey, MD, said in the release.
AMA plans to introduce more vaccine-specific CPT codes as more vaccine candidates approach FDA review. These vaccine-specific CPT codes can go into effect only after the FDA grants a clearance.
The newly created Category I CPT codes and long descriptors for the vaccine products are:
- 91300; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3mL dosage, diluent reconstituted, for intramuscular use (Pfizer/BioNTech)
- 91301; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5mL dosage, for intramuscular use (Moderna)
These two administrative codes would apply to the Pfizer-BioNTech shot:
- 0001A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3 mL dosage, diluent reconstituted; first dose.
- 0002A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3 mL dosage, diluent reconstituted; second dose.
And these two administrative codes would apply to the Moderna shot:
- 0011A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5 mL dosage; first dose.
- 0012A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5 mL dosage; second dose.
A version of this article originally appeared on Medscape.com.
The largest U.S. physician organization on Tuesday took a step to prepare for future payments for administration of two leading COVID-19 vaccine candidates, publishing new billing codes tailored to track each use of these medications.
The The new codes apply to the experimental vaccine being developed by Pfizer, in collaboration with a smaller German firm BioNTech, and to the similar product expected from Moderna, according to an AMA press release.
Positive news has emerged this week about both of these vaccines, which were developed using a newer – and as yet unproven – approach. They seek to use messenger RNA to instruct cells to produce a target protein for SARS-CoV-2.
New York–based Pfizer on Monday announced interim phase 3 data that was widely viewed as promising. Pfizer said the vaccine appeared to be 90% effective in preventing COVID-19 in trial volunteers who were without evidence of prior infection of the virus.
In a press release, Pfizer said it plans to ask the Food and Drug Administration to consider a special clearance, known as an emergency-use authorization, “soon after” a safety milestone is achieved in its vaccine trial. That milestone could be reached this month.
Moderna said it was on track to report early data from a late-stage trial of its experimental coronavirus vaccine later this month, and could file with the FDA for an emergency-use authorization in early December, according to a Reuters report.
The severity of the global pandemic has put the FDA under pressure to move quickly on approval of COVID-19 vaccines, based on limited data, while also working to make sure these products are safe. The creation of CPT codes for each of two coronavirus vaccines, as well as accompanying administration codes, will set up a way to keep tabs on each dose of each of these shots, the AMA said.
“Correlating each coronavirus vaccine with its own unique CPT code provides analytical advantages to help track, allocate and optimize resources as an immunization program ramps up in the United States,” AMA President Susan R. Bailey, MD, said in the release.
AMA plans to introduce more vaccine-specific CPT codes as more vaccine candidates approach FDA review. These vaccine-specific CPT codes can go into effect only after the FDA grants a clearance.
The newly created Category I CPT codes and long descriptors for the vaccine products are:
- 91300; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3mL dosage, diluent reconstituted, for intramuscular use (Pfizer/BioNTech)
- 91301; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5mL dosage, for intramuscular use (Moderna)
These two administrative codes would apply to the Pfizer-BioNTech shot:
- 0001A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3 mL dosage, diluent reconstituted; first dose.
- 0002A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3 mL dosage, diluent reconstituted; second dose.
And these two administrative codes would apply to the Moderna shot:
- 0011A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5 mL dosage; first dose.
- 0012A; Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5 mL dosage; second dose.
A version of this article originally appeared on Medscape.com.
Nearly 10% of hospitalized patients with COVID-19 later readmitted
About 1 in 11 patients discharged after COVID-19 treatment is readmitted to the same hospital, according to researchers from the Centers for Disease Control and Prevention (CDC).
Older age and chronic diseases are associated with increased risk, said senior author Adi V. Gundlapalli, MD, PhD, chief public health informatics officer of the CDC’s Center for Surveillance, Epidemiology, and Laboratory Services.
Gundlapalli and colleagues published the finding November 9 in Morbidity and Mortality Weekly Report.
To get a picture of readmission after COVID-19 hospitalization, the researchers analyzed records of 126,137 patients hospitalized with COVID-19 between March and July and included in the Premier Healthcare Database, which covers discharge records from 865 nongovernmental, community, and teaching hospitals.
Overall, 15% of the patients died during hospitalization. Of those who survived to discharge, 9% were readmitted to the same hospital within 2 months of discharge; 1.6% of patients were readmitted more than once. The median interval from discharge to first readmission was 8 days (interquartile range, 3-20 days). This short interval suggests that patients are probably not suffering a relapse, Gundlapalli said in an interview. More likely they experienced some adverse event, such as difficulty breathing, that led their caretakers to send them back to the hospital.
Forty-five percent of the primary discharge diagnoses after readmission were infectious and parasitic diseases, primarily COVID-19. The next most common were circulatory system symptoms (11%) and digestive symptoms (7%).
After controlling for covariates, the researchers found that patients were more likely to be readmitted if they had chronic obstructive pulmonary disease (odds ratio [OR], 1.4), heart failure (OR, 1.6), diabetes (OR, 1.2), or chronic kidney disease (OR, 1.6).
They also found increased odds among patients discharged from the index hospitalization to a skilled nursing facility (OR, 1.4) or with home health organization support (OR, 1.3), compared with being discharged to home or self-care. Looked at another way, the rate of readmission was 15% among those discharged to a skilled nursing facility, 12% among those needing home health care and 7% of those discharged to home or self-care.
The researchers also found that people who had been hospitalized within 3 months prior to the index hospitalization were 2.6 times more likely to be readmitted than were those without prior inpatient care.
Further, the odds of readmission increased significantly among people over 65 years of age, compared with people aged 18 to 39 years.
“The results are not surprising,” Gundlapalli said. “We have known from before that elderly patients, especially with chronic conditions, certain clinical conditions, and those who have been hospitalized before, are at risk for readmission.”
But admitting COVID-19 patients requires special planning because they must be isolated and because more personal protective equipment (PPE) is required, he pointed out.
One unexpected finding from the report is that non-Hispanic White people were more likely to be readmitted than were people of other racial or ethnic groups. This contrasts with other research showing Hispanic and Black individuals are more severely affected by COVID-19 than White people. More research is needed to explain this result, Gundlapalli said.
The authors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
About 1 in 11 patients discharged after COVID-19 treatment is readmitted to the same hospital, according to researchers from the Centers for Disease Control and Prevention (CDC).
Older age and chronic diseases are associated with increased risk, said senior author Adi V. Gundlapalli, MD, PhD, chief public health informatics officer of the CDC’s Center for Surveillance, Epidemiology, and Laboratory Services.
Gundlapalli and colleagues published the finding November 9 in Morbidity and Mortality Weekly Report.
To get a picture of readmission after COVID-19 hospitalization, the researchers analyzed records of 126,137 patients hospitalized with COVID-19 between March and July and included in the Premier Healthcare Database, which covers discharge records from 865 nongovernmental, community, and teaching hospitals.
Overall, 15% of the patients died during hospitalization. Of those who survived to discharge, 9% were readmitted to the same hospital within 2 months of discharge; 1.6% of patients were readmitted more than once. The median interval from discharge to first readmission was 8 days (interquartile range, 3-20 days). This short interval suggests that patients are probably not suffering a relapse, Gundlapalli said in an interview. More likely they experienced some adverse event, such as difficulty breathing, that led their caretakers to send them back to the hospital.
Forty-five percent of the primary discharge diagnoses after readmission were infectious and parasitic diseases, primarily COVID-19. The next most common were circulatory system symptoms (11%) and digestive symptoms (7%).
After controlling for covariates, the researchers found that patients were more likely to be readmitted if they had chronic obstructive pulmonary disease (odds ratio [OR], 1.4), heart failure (OR, 1.6), diabetes (OR, 1.2), or chronic kidney disease (OR, 1.6).
They also found increased odds among patients discharged from the index hospitalization to a skilled nursing facility (OR, 1.4) or with home health organization support (OR, 1.3), compared with being discharged to home or self-care. Looked at another way, the rate of readmission was 15% among those discharged to a skilled nursing facility, 12% among those needing home health care and 7% of those discharged to home or self-care.
The researchers also found that people who had been hospitalized within 3 months prior to the index hospitalization were 2.6 times more likely to be readmitted than were those without prior inpatient care.
Further, the odds of readmission increased significantly among people over 65 years of age, compared with people aged 18 to 39 years.
“The results are not surprising,” Gundlapalli said. “We have known from before that elderly patients, especially with chronic conditions, certain clinical conditions, and those who have been hospitalized before, are at risk for readmission.”
But admitting COVID-19 patients requires special planning because they must be isolated and because more personal protective equipment (PPE) is required, he pointed out.
One unexpected finding from the report is that non-Hispanic White people were more likely to be readmitted than were people of other racial or ethnic groups. This contrasts with other research showing Hispanic and Black individuals are more severely affected by COVID-19 than White people. More research is needed to explain this result, Gundlapalli said.
The authors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
About 1 in 11 patients discharged after COVID-19 treatment is readmitted to the same hospital, according to researchers from the Centers for Disease Control and Prevention (CDC).
Older age and chronic diseases are associated with increased risk, said senior author Adi V. Gundlapalli, MD, PhD, chief public health informatics officer of the CDC’s Center for Surveillance, Epidemiology, and Laboratory Services.
Gundlapalli and colleagues published the finding November 9 in Morbidity and Mortality Weekly Report.
To get a picture of readmission after COVID-19 hospitalization, the researchers analyzed records of 126,137 patients hospitalized with COVID-19 between March and July and included in the Premier Healthcare Database, which covers discharge records from 865 nongovernmental, community, and teaching hospitals.
Overall, 15% of the patients died during hospitalization. Of those who survived to discharge, 9% were readmitted to the same hospital within 2 months of discharge; 1.6% of patients were readmitted more than once. The median interval from discharge to first readmission was 8 days (interquartile range, 3-20 days). This short interval suggests that patients are probably not suffering a relapse, Gundlapalli said in an interview. More likely they experienced some adverse event, such as difficulty breathing, that led their caretakers to send them back to the hospital.
Forty-five percent of the primary discharge diagnoses after readmission were infectious and parasitic diseases, primarily COVID-19. The next most common were circulatory system symptoms (11%) and digestive symptoms (7%).
After controlling for covariates, the researchers found that patients were more likely to be readmitted if they had chronic obstructive pulmonary disease (odds ratio [OR], 1.4), heart failure (OR, 1.6), diabetes (OR, 1.2), or chronic kidney disease (OR, 1.6).
They also found increased odds among patients discharged from the index hospitalization to a skilled nursing facility (OR, 1.4) or with home health organization support (OR, 1.3), compared with being discharged to home or self-care. Looked at another way, the rate of readmission was 15% among those discharged to a skilled nursing facility, 12% among those needing home health care and 7% of those discharged to home or self-care.
The researchers also found that people who had been hospitalized within 3 months prior to the index hospitalization were 2.6 times more likely to be readmitted than were those without prior inpatient care.
Further, the odds of readmission increased significantly among people over 65 years of age, compared with people aged 18 to 39 years.
“The results are not surprising,” Gundlapalli said. “We have known from before that elderly patients, especially with chronic conditions, certain clinical conditions, and those who have been hospitalized before, are at risk for readmission.”
But admitting COVID-19 patients requires special planning because they must be isolated and because more personal protective equipment (PPE) is required, he pointed out.
One unexpected finding from the report is that non-Hispanic White people were more likely to be readmitted than were people of other racial or ethnic groups. This contrasts with other research showing Hispanic and Black individuals are more severely affected by COVID-19 than White people. More research is needed to explain this result, Gundlapalli said.
The authors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Should our patients really go home for the holidays?
As an East Coast transplant residing in Texas, I look forward to the annual sojourn home to celebrate the holidays with family and friends – as do many of our patients and their families. But this is 2020. SARS-CoV-2, the causative agent of COVID-19, is still circulating. To make matters worse, cases are rising in 45 states and internationally. The day of this writing 102,831 new cases were reported in the United States. 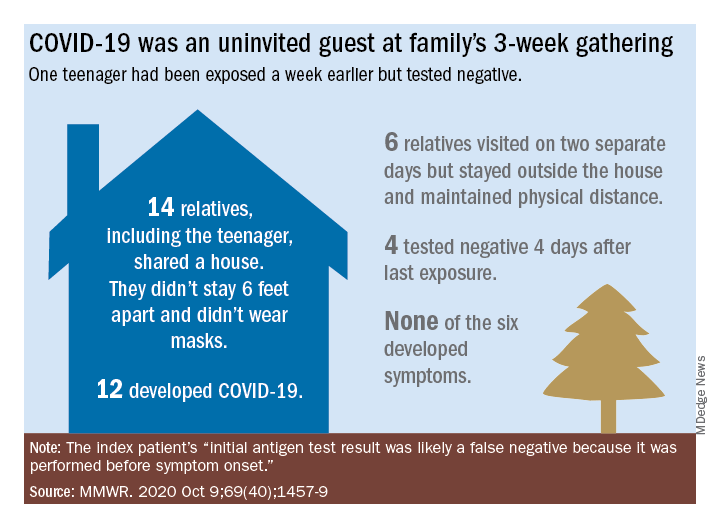
Social distancing, wearing masks, and hand washing have been strategies recommended to help mitigate the spread of the virus. We know adherence is not always 100%. The reality is that several families will consider traveling and gathering with others over the holidays. Their actions may lead to increased infections, hospitalizations, and even deaths. It behooves us to at least remind them of the potential consequences of the activity, and if travel and/or holiday gatherings are inevitable, to provide some guidance to help them look at both the risks and benefits and offer strategies to minimize infection and spread.
What should be considered prior to travel?
Here is a list of points to ponder:
- Is your patient is in a high-risk group for developing severe disease or visiting someone who is in a high-risk group?
- What is their mode of transportation?
- What is their destination?
- How prevalent is the disease at their destination, compared with their community?
- What will be their accommodations?
- How will attendees prepare for the gathering, if at all?
- Will multiple families congregate after quarantining for 2 weeks or simply arrive?
- At the destination, will people wear masks and socially distance?
- Is an outdoor venue an option?
All of these questions should be considered by patients.
Review high-risk groups
In terms of high-risk groups, we usually focus on underlying medical conditions or extremes of age, but Black and LatinX children and their families have been diagnosed with COVID-19 and hospitalized more frequently than other racial/ ethnic groups in the United States. Of 277,285 school-aged children infected between March 1 and Sept. 19, 2020, 42% were LatinX, 32% White, and 17% Black, yet they comprise 18%, 60%, and 11% of the U.S. population, respectively. Of those hospitalized, 45% were LatinX, 22% White, and 24% Black. LatinX and Black children also have disproportionately higher mortality rates.
Think about transmission and how to mitigate it
Many patients erroneously think combining multiple households for small group gatherings is inconsequential. These types of gatherings serve as a continued source of SARS-CoV-2 spread. For example, a person in Illinois with mild upper respiratory infection symptoms attended a funeral; he reported embracing the family members after the funeral. He dined with two people the evening prior to the funeral, sharing the meal using common serving dishes. Four days later, he attended a birthday party with nine family members. Some of the family members with symptoms subsequently attended church, infecting another church attendee. A cluster of 16 cases of COVID-19 was subsequently identified, including three deaths likely resulting from this one introduction of COVID-19 at these two family gatherings.

In Tennessee and Wisconsin, household transmission of SARS-CoV-2 was studied prospectively. A total of 101 index cases and 191 asymptomatic household contacts were enrolled between April and Sept. 2020; 102 of 191 (53%) had SARS-CoV-2 detected during the 14-day follow-up. Most infections (75%) were identified within 5 days and occurred whether the index case was an adult or child.
Lastly, one adolescent was identified as the source for an outbreak at a family gathering where 15 persons from five households and four states shared a house between 8 and 25 days in July 2020. Six additional members visited the house. The index case had an exposure to COVID-19 and had a negative antigen test 4 days after exposure. She was asymptomatic when tested. She developed nasal congestion 2 days later, the same day she and her family departed for the gathering. A total of 11 household contacts developed confirmed, suspected, or probable COVID-19, and the teen developed symptoms. This report illustrates how easily SARS-CoV-2 is transmitted, and how when implemented, mitigation strategies work because none of the six who only visited the house was infected. It also serves as a reminder that antigen testing is indicated only for use within the first 5-12 days of onset of symptoms. In this case, the adolescent was asymptomatic when tested and had a false-negative test result.
Ponder modes of transportation
How will your patient arrive to their holiday destination? Nonstop travel by car with household members is probably the safest way. However, for many families, buses and trains are the only options, and social distancing may be challenging. Air travel is a must for others. Acquisition of COVID-19 during air travel appears to be low, but not absent based on how air enters and leaves the cabin. The challenge is socially distancing throughout the check in and boarding processes, as well as minimizing contact with common surfaces. There also is loss of social distancing once on board. Ideally, masks should be worn during the flight. Additionally, for those with international destinations, most countries now require a negative polymerase chain reaction COVID-19 test within a specified time frame for entry.
Essentially the safest place for your patients during the holidays is celebrating at home with their household contacts. The risk for disease acquisition increases with travel. You will not have the opportunity to discuss holiday plans with most parents. However, you can encourage them to consider the pros and cons of travel with reminders via telephone, e-mail, and /or social messaging directly from your practices similar to those sent for other medically necessary interventions. As for me, I will be celebrating virtually this year. There is a first time for everything.
For additional information that also is patient friendly, the Centers for Disease Control and Prevention offers information about travel within the United States and international travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at [email protected].
As an East Coast transplant residing in Texas, I look forward to the annual sojourn home to celebrate the holidays with family and friends – as do many of our patients and their families. But this is 2020. SARS-CoV-2, the causative agent of COVID-19, is still circulating. To make matters worse, cases are rising in 45 states and internationally. The day of this writing 102,831 new cases were reported in the United States.
Social distancing, wearing masks, and hand washing have been strategies recommended to help mitigate the spread of the virus. We know adherence is not always 100%. The reality is that several families will consider traveling and gathering with others over the holidays. Their actions may lead to increased infections, hospitalizations, and even deaths. It behooves us to at least remind them of the potential consequences of the activity, and if travel and/or holiday gatherings are inevitable, to provide some guidance to help them look at both the risks and benefits and offer strategies to minimize infection and spread.
What should be considered prior to travel?
Here is a list of points to ponder:
- Is your patient is in a high-risk group for developing severe disease or visiting someone who is in a high-risk group?
- What is their mode of transportation?
- What is their destination?
- How prevalent is the disease at their destination, compared with their community?
- What will be their accommodations?
- How will attendees prepare for the gathering, if at all?
- Will multiple families congregate after quarantining for 2 weeks or simply arrive?
- At the destination, will people wear masks and socially distance?
- Is an outdoor venue an option?
All of these questions should be considered by patients.
Review high-risk groups
In terms of high-risk groups, we usually focus on underlying medical conditions or extremes of age, but Black and LatinX children and their families have been diagnosed with COVID-19 and hospitalized more frequently than other racial/ ethnic groups in the United States. Of 277,285 school-aged children infected between March 1 and Sept. 19, 2020, 42% were LatinX, 32% White, and 17% Black, yet they comprise 18%, 60%, and 11% of the U.S. population, respectively. Of those hospitalized, 45% were LatinX, 22% White, and 24% Black. LatinX and Black children also have disproportionately higher mortality rates.
Think about transmission and how to mitigate it
Many patients erroneously think combining multiple households for small group gatherings is inconsequential. These types of gatherings serve as a continued source of SARS-CoV-2 spread. For example, a person in Illinois with mild upper respiratory infection symptoms attended a funeral; he reported embracing the family members after the funeral. He dined with two people the evening prior to the funeral, sharing the meal using common serving dishes. Four days later, he attended a birthday party with nine family members. Some of the family members with symptoms subsequently attended church, infecting another church attendee. A cluster of 16 cases of COVID-19 was subsequently identified, including three deaths likely resulting from this one introduction of COVID-19 at these two family gatherings.
In Tennessee and Wisconsin, household transmission of SARS-CoV-2 was studied prospectively. A total of 101 index cases and 191 asymptomatic household contacts were enrolled between April and Sept. 2020; 102 of 191 (53%) had SARS-CoV-2 detected during the 14-day follow-up. Most infections (75%) were identified within 5 days and occurred whether the index case was an adult or child.
Lastly, one adolescent was identified as the source for an outbreak at a family gathering where 15 persons from five households and four states shared a house between 8 and 25 days in July 2020. Six additional members visited the house. The index case had an exposure to COVID-19 and had a negative antigen test 4 days after exposure. She was asymptomatic when tested. She developed nasal congestion 2 days later, the same day she and her family departed for the gathering. A total of 11 household contacts developed confirmed, suspected, or probable COVID-19, and the teen developed symptoms. This report illustrates how easily SARS-CoV-2 is transmitted, and how when implemented, mitigation strategies work because none of the six who only visited the house was infected. It also serves as a reminder that antigen testing is indicated only for use within the first 5-12 days of onset of symptoms. In this case, the adolescent was asymptomatic when tested and had a false-negative test result.
Ponder modes of transportation
How will your patient arrive to their holiday destination? Nonstop travel by car with household members is probably the safest way. However, for many families, buses and trains are the only options, and social distancing may be challenging. Air travel is a must for others. Acquisition of COVID-19 during air travel appears to be low, but not absent based on how air enters and leaves the cabin. The challenge is socially distancing throughout the check in and boarding processes, as well as minimizing contact with common surfaces. There also is loss of social distancing once on board. Ideally, masks should be worn during the flight. Additionally, for those with international destinations, most countries now require a negative polymerase chain reaction COVID-19 test within a specified time frame for entry.
Essentially the safest place for your patients during the holidays is celebrating at home with their household contacts. The risk for disease acquisition increases with travel. You will not have the opportunity to discuss holiday plans with most parents. However, you can encourage them to consider the pros and cons of travel with reminders via telephone, e-mail, and /or social messaging directly from your practices similar to those sent for other medically necessary interventions. As for me, I will be celebrating virtually this year. There is a first time for everything.
For additional information that also is patient friendly, the Centers for Disease Control and Prevention offers information about travel within the United States and international travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at [email protected].
As an East Coast transplant residing in Texas, I look forward to the annual sojourn home to celebrate the holidays with family and friends – as do many of our patients and their families. But this is 2020. SARS-CoV-2, the causative agent of COVID-19, is still circulating. To make matters worse, cases are rising in 45 states and internationally. The day of this writing 102,831 new cases were reported in the United States.
Social distancing, wearing masks, and hand washing have been strategies recommended to help mitigate the spread of the virus. We know adherence is not always 100%. The reality is that several families will consider traveling and gathering with others over the holidays. Their actions may lead to increased infections, hospitalizations, and even deaths. It behooves us to at least remind them of the potential consequences of the activity, and if travel and/or holiday gatherings are inevitable, to provide some guidance to help them look at both the risks and benefits and offer strategies to minimize infection and spread.
What should be considered prior to travel?
Here is a list of points to ponder:
- Is your patient is in a high-risk group for developing severe disease or visiting someone who is in a high-risk group?
- What is their mode of transportation?
- What is their destination?
- How prevalent is the disease at their destination, compared with their community?
- What will be their accommodations?
- How will attendees prepare for the gathering, if at all?
- Will multiple families congregate after quarantining for 2 weeks or simply arrive?
- At the destination, will people wear masks and socially distance?
- Is an outdoor venue an option?
All of these questions should be considered by patients.
Review high-risk groups
In terms of high-risk groups, we usually focus on underlying medical conditions or extremes of age, but Black and LatinX children and their families have been diagnosed with COVID-19 and hospitalized more frequently than other racial/ ethnic groups in the United States. Of 277,285 school-aged children infected between March 1 and Sept. 19, 2020, 42% were LatinX, 32% White, and 17% Black, yet they comprise 18%, 60%, and 11% of the U.S. population, respectively. Of those hospitalized, 45% were LatinX, 22% White, and 24% Black. LatinX and Black children also have disproportionately higher mortality rates.
Think about transmission and how to mitigate it
Many patients erroneously think combining multiple households for small group gatherings is inconsequential. These types of gatherings serve as a continued source of SARS-CoV-2 spread. For example, a person in Illinois with mild upper respiratory infection symptoms attended a funeral; he reported embracing the family members after the funeral. He dined with two people the evening prior to the funeral, sharing the meal using common serving dishes. Four days later, he attended a birthday party with nine family members. Some of the family members with symptoms subsequently attended church, infecting another church attendee. A cluster of 16 cases of COVID-19 was subsequently identified, including three deaths likely resulting from this one introduction of COVID-19 at these two family gatherings.
In Tennessee and Wisconsin, household transmission of SARS-CoV-2 was studied prospectively. A total of 101 index cases and 191 asymptomatic household contacts were enrolled between April and Sept. 2020; 102 of 191 (53%) had SARS-CoV-2 detected during the 14-day follow-up. Most infections (75%) were identified within 5 days and occurred whether the index case was an adult or child.
Lastly, one adolescent was identified as the source for an outbreak at a family gathering where 15 persons from five households and four states shared a house between 8 and 25 days in July 2020. Six additional members visited the house. The index case had an exposure to COVID-19 and had a negative antigen test 4 days after exposure. She was asymptomatic when tested. She developed nasal congestion 2 days later, the same day she and her family departed for the gathering. A total of 11 household contacts developed confirmed, suspected, or probable COVID-19, and the teen developed symptoms. This report illustrates how easily SARS-CoV-2 is transmitted, and how when implemented, mitigation strategies work because none of the six who only visited the house was infected. It also serves as a reminder that antigen testing is indicated only for use within the first 5-12 days of onset of symptoms. In this case, the adolescent was asymptomatic when tested and had a false-negative test result.
Ponder modes of transportation
How will your patient arrive to their holiday destination? Nonstop travel by car with household members is probably the safest way. However, for many families, buses and trains are the only options, and social distancing may be challenging. Air travel is a must for others. Acquisition of COVID-19 during air travel appears to be low, but not absent based on how air enters and leaves the cabin. The challenge is socially distancing throughout the check in and boarding processes, as well as minimizing contact with common surfaces. There also is loss of social distancing once on board. Ideally, masks should be worn during the flight. Additionally, for those with international destinations, most countries now require a negative polymerase chain reaction COVID-19 test within a specified time frame for entry.
Essentially the safest place for your patients during the holidays is celebrating at home with their household contacts. The risk for disease acquisition increases with travel. You will not have the opportunity to discuss holiday plans with most parents. However, you can encourage them to consider the pros and cons of travel with reminders via telephone, e-mail, and /or social messaging directly from your practices similar to those sent for other medically necessary interventions. As for me, I will be celebrating virtually this year. There is a first time for everything.
For additional information that also is patient friendly, the Centers for Disease Control and Prevention offers information about travel within the United States and international travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at [email protected].
Patients with mental illness a priority for COVID vaccine, experts say
With this week’s announcement that Pfizer’s vaccine candidate against SARS-CoV-2 was 90% effective in preventing COVID-19, the world is one step closer to an effective vaccine.
Nevertheless, with a limited supply of initial doses, the question becomes, who should get it first? Individuals with severe mental illness should be a priority group to receive a COVID-19 vaccine, assert the authors of a perspective article published Nov. 1 in World Psychiatry.
Patients with underlying physical conditions, such as cardiovascular disease, chronic obstructive pulmonary disease, diabetes, chronic kidney disease, obesity, immunodeficiency, and cancer, are particularly vulnerable to developing more severe illness and dying from COVID-19.
In these populations, the risk of a more severe course of infection or early death is significant enough for the U.S. National Academies of Sciences, Engineering, and Medicine to make these patients priority recipients of a vaccine against COVID-19.
Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors argued that those with severe mental illness also fit into this group.
Even without factoring COVID-19 into the calculation, those with severe mental illness have a two- to threefold higher mortality rate than the general population, resulting in reduction in life expectancy of 10-20 years, they noted. This is largely because of physical diseases including cardiovascular disease, type 2 diabetes, and respiratory ailments.
Individuals with severe mental illness also have higher rates of obesity than the general population and obesity is a risk factor for dying from COVID-19.
High-risk population
Like their peers with physical illnesses, recent studies suggest that those with severe mental illness are also at increased risk of morbidity and mortality from COVID-19.
For example, a recent U.S. case-control study with over 61 million adults showed that those recently diagnosed with a mental health disorder had a significantly increased risk for COVID-19 infection, an effect strongest for depression and schizophrenia.
Other recent studies have confirmed these data, including one linking a psychiatric diagnosis in patients hospitalized with COVID-19 to a significantly increased risk for death, as reported by Medscape Medical News.
Dr. De Hert and colleagues put these findings into perspective with this example: In 2017, there were an estimated 11.2 million adults in the United States with severe mental illness. Taking into account the 8.5% death rate in COVID-19 patients recently diagnosed with a severe mental illness, this means that about 1 million patients with severe mental illness in the United States would die if all were infected with the virus.
In light of this knowledge, and taking into account published ethical principles that should guide vaccine allocation, Dr. De Hert and colleagues said it is “paramount” that persons with severe mental illness be prioritized to guarantee that they receive a COVID-19 vaccine during the first phase of its distribution.
“It is our responsibility as psychiatrists in this global health crisis to advocate for the needs of our patients with governments and public health policy bodies,” they wrote.
The authors also encourage public health agencies to develop and implement targeted programs to ensure that patients with severe mental illness and their health care providers “are made aware of these increased risks as well as the benefits of vaccination.”
An argument for fairness
Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, also believes those with severe mental illness should be a priority group for a COVID vaccine.
“When we’re prioritizing groups for a COVID-19 vaccine, let’s not forget that people with serious mental illness have much lower life expectancies, more obesity, and more undiagnosed chronic conditions. They should be a priority group,” Dr. Appelbaum said in an interview.
“The argument for including people with severe mental illnesses among the vulnerable populations who should be prioritized for receipt of a COVID-19 vaccine is an argument for fairness in constructing that group,” he added.
“Like people with other chronic conditions associated with poor outcomes after SARS-CoV-2 infection, people with severe mental illnesses are more likely to be hospitalized and more likely to die. Although they are often systematically ignored when decisions are made about allocation of resources, there is some hope that, with enough public attention to this issue, they can be included this time,” Dr. Appelbaum said.
Dr. De Hert and Dr. Applebaum disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
With this week’s announcement that Pfizer’s vaccine candidate against SARS-CoV-2 was 90% effective in preventing COVID-19, the world is one step closer to an effective vaccine.
Nevertheless, with a limited supply of initial doses, the question becomes, who should get it first? Individuals with severe mental illness should be a priority group to receive a COVID-19 vaccine, assert the authors of a perspective article published Nov. 1 in World Psychiatry.
Patients with underlying physical conditions, such as cardiovascular disease, chronic obstructive pulmonary disease, diabetes, chronic kidney disease, obesity, immunodeficiency, and cancer, are particularly vulnerable to developing more severe illness and dying from COVID-19.
In these populations, the risk of a more severe course of infection or early death is significant enough for the U.S. National Academies of Sciences, Engineering, and Medicine to make these patients priority recipients of a vaccine against COVID-19.
Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors argued that those with severe mental illness also fit into this group.
Even without factoring COVID-19 into the calculation, those with severe mental illness have a two- to threefold higher mortality rate than the general population, resulting in reduction in life expectancy of 10-20 years, they noted. This is largely because of physical diseases including cardiovascular disease, type 2 diabetes, and respiratory ailments.
Individuals with severe mental illness also have higher rates of obesity than the general population and obesity is a risk factor for dying from COVID-19.
High-risk population
Like their peers with physical illnesses, recent studies suggest that those with severe mental illness are also at increased risk of morbidity and mortality from COVID-19.
For example, a recent U.S. case-control study with over 61 million adults showed that those recently diagnosed with a mental health disorder had a significantly increased risk for COVID-19 infection, an effect strongest for depression and schizophrenia.
Other recent studies have confirmed these data, including one linking a psychiatric diagnosis in patients hospitalized with COVID-19 to a significantly increased risk for death, as reported by Medscape Medical News.
Dr. De Hert and colleagues put these findings into perspective with this example: In 2017, there were an estimated 11.2 million adults in the United States with severe mental illness. Taking into account the 8.5% death rate in COVID-19 patients recently diagnosed with a severe mental illness, this means that about 1 million patients with severe mental illness in the United States would die if all were infected with the virus.
In light of this knowledge, and taking into account published ethical principles that should guide vaccine allocation, Dr. De Hert and colleagues said it is “paramount” that persons with severe mental illness be prioritized to guarantee that they receive a COVID-19 vaccine during the first phase of its distribution.
“It is our responsibility as psychiatrists in this global health crisis to advocate for the needs of our patients with governments and public health policy bodies,” they wrote.
The authors also encourage public health agencies to develop and implement targeted programs to ensure that patients with severe mental illness and their health care providers “are made aware of these increased risks as well as the benefits of vaccination.”
An argument for fairness
Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, also believes those with severe mental illness should be a priority group for a COVID vaccine.
“When we’re prioritizing groups for a COVID-19 vaccine, let’s not forget that people with serious mental illness have much lower life expectancies, more obesity, and more undiagnosed chronic conditions. They should be a priority group,” Dr. Appelbaum said in an interview.
“The argument for including people with severe mental illnesses among the vulnerable populations who should be prioritized for receipt of a COVID-19 vaccine is an argument for fairness in constructing that group,” he added.
“Like people with other chronic conditions associated with poor outcomes after SARS-CoV-2 infection, people with severe mental illnesses are more likely to be hospitalized and more likely to die. Although they are often systematically ignored when decisions are made about allocation of resources, there is some hope that, with enough public attention to this issue, they can be included this time,” Dr. Appelbaum said.
Dr. De Hert and Dr. Applebaum disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
With this week’s announcement that Pfizer’s vaccine candidate against SARS-CoV-2 was 90% effective in preventing COVID-19, the world is one step closer to an effective vaccine.
Nevertheless, with a limited supply of initial doses, the question becomes, who should get it first? Individuals with severe mental illness should be a priority group to receive a COVID-19 vaccine, assert the authors of a perspective article published Nov. 1 in World Psychiatry.
Patients with underlying physical conditions, such as cardiovascular disease, chronic obstructive pulmonary disease, diabetes, chronic kidney disease, obesity, immunodeficiency, and cancer, are particularly vulnerable to developing more severe illness and dying from COVID-19.
In these populations, the risk of a more severe course of infection or early death is significant enough for the U.S. National Academies of Sciences, Engineering, and Medicine to make these patients priority recipients of a vaccine against COVID-19.
Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors argued that those with severe mental illness also fit into this group.
Even without factoring COVID-19 into the calculation, those with severe mental illness have a two- to threefold higher mortality rate than the general population, resulting in reduction in life expectancy of 10-20 years, they noted. This is largely because of physical diseases including cardiovascular disease, type 2 diabetes, and respiratory ailments.
Individuals with severe mental illness also have higher rates of obesity than the general population and obesity is a risk factor for dying from COVID-19.
High-risk population
Like their peers with physical illnesses, recent studies suggest that those with severe mental illness are also at increased risk of morbidity and mortality from COVID-19.
For example, a recent U.S. case-control study with over 61 million adults showed that those recently diagnosed with a mental health disorder had a significantly increased risk for COVID-19 infection, an effect strongest for depression and schizophrenia.
Other recent studies have confirmed these data, including one linking a psychiatric diagnosis in patients hospitalized with COVID-19 to a significantly increased risk for death, as reported by Medscape Medical News.
Dr. De Hert and colleagues put these findings into perspective with this example: In 2017, there were an estimated 11.2 million adults in the United States with severe mental illness. Taking into account the 8.5% death rate in COVID-19 patients recently diagnosed with a severe mental illness, this means that about 1 million patients with severe mental illness in the United States would die if all were infected with the virus.
In light of this knowledge, and taking into account published ethical principles that should guide vaccine allocation, Dr. De Hert and colleagues said it is “paramount” that persons with severe mental illness be prioritized to guarantee that they receive a COVID-19 vaccine during the first phase of its distribution.
“It is our responsibility as psychiatrists in this global health crisis to advocate for the needs of our patients with governments and public health policy bodies,” they wrote.
The authors also encourage public health agencies to develop and implement targeted programs to ensure that patients with severe mental illness and their health care providers “are made aware of these increased risks as well as the benefits of vaccination.”
An argument for fairness
Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, also believes those with severe mental illness should be a priority group for a COVID vaccine.
“When we’re prioritizing groups for a COVID-19 vaccine, let’s not forget that people with serious mental illness have much lower life expectancies, more obesity, and more undiagnosed chronic conditions. They should be a priority group,” Dr. Appelbaum said in an interview.
“The argument for including people with severe mental illnesses among the vulnerable populations who should be prioritized for receipt of a COVID-19 vaccine is an argument for fairness in constructing that group,” he added.
“Like people with other chronic conditions associated with poor outcomes after SARS-CoV-2 infection, people with severe mental illnesses are more likely to be hospitalized and more likely to die. Although they are often systematically ignored when decisions are made about allocation of resources, there is some hope that, with enough public attention to this issue, they can be included this time,” Dr. Appelbaum said.
Dr. De Hert and Dr. Applebaum disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The Cell’s Waste Disposal System May be Key to Killing Coronavirus
Normally, the lysosome, known as the cells’ “trash compactor,” destroys viruses before they can leave the cell. However, researchers at the National Institutes of Health (NIH) have discovered that SARS-CoV-2 is not like other viruses. The virus can deactivate that waste disposal system, exit without hindrance, and spread freely throughout the body.
“To our shock, these coronaviruses got out of the cells just fine,” said Nihal Altan-Bonnet, PhD, chief of the Laboratory of Host-Pathogen Dynamics at the National Heart, Lung, and Blood Institute, who coauthored the study report.
Most viruses exit via the biosynthetic secretory pathway, used to transport hormones, growth factors and other materials. The researchers wanted to learn whether coronaviruses took an alternate route. To find out, they conducted further studies, using microscopy and virus-specific markers. They discovered that coronaviruses somehow target the lysosome and congregate there. Although lysosomes are highly acidic, the coronaviruses were not destroyed.
That question led to more experiments. The researchers next found that lysosomes get “de-acidified” in coronavirus-infected cells, which weakens their destructive enzymes. The result: The coronavirus remains intact, ready to infect other cells upon exiting.
The coronaviruses are “very sneaky,” Altan-Bonnet says. “They’re using these lysosomes to get out, but they’re also disrupting the lysosome so it can’t do its job or function.” It’s possible that the way the coronavirus interferes with the lysosome’s “immunological machinery” underlies some of the immune system abnormalities seen in COVID-19 patients, such as cytokine storms.
Studying this coronavirus's heterodox ways may mean that researchers can figure out how to keep it from getting out unscathed, or restore the lysosome’s killing ability by re-acidifying it. Altan-Bonnet and coauthor Sourish Ghosh, PhD, say they have already identified one experimental enzyme inhibitor that potently blocks coronaviruses from exiting the cell.
The lysosome pathway, Altan-Bonnet says, “offers a whole different way of thinking about targeted therapeutics.”
Normally, the lysosome, known as the cells’ “trash compactor,” destroys viruses before they can leave the cell. However, researchers at the National Institutes of Health (NIH) have discovered that SARS-CoV-2 is not like other viruses. The virus can deactivate that waste disposal system, exit without hindrance, and spread freely throughout the body.
“To our shock, these coronaviruses got out of the cells just fine,” said Nihal Altan-Bonnet, PhD, chief of the Laboratory of Host-Pathogen Dynamics at the National Heart, Lung, and Blood Institute, who coauthored the study report.
Most viruses exit via the biosynthetic secretory pathway, used to transport hormones, growth factors and other materials. The researchers wanted to learn whether coronaviruses took an alternate route. To find out, they conducted further studies, using microscopy and virus-specific markers. They discovered that coronaviruses somehow target the lysosome and congregate there. Although lysosomes are highly acidic, the coronaviruses were not destroyed.
That question led to more experiments. The researchers next found that lysosomes get “de-acidified” in coronavirus-infected cells, which weakens their destructive enzymes. The result: The coronavirus remains intact, ready to infect other cells upon exiting.
The coronaviruses are “very sneaky,” Altan-Bonnet says. “They’re using these lysosomes to get out, but they’re also disrupting the lysosome so it can’t do its job or function.” It’s possible that the way the coronavirus interferes with the lysosome’s “immunological machinery” underlies some of the immune system abnormalities seen in COVID-19 patients, such as cytokine storms.
Studying this coronavirus's heterodox ways may mean that researchers can figure out how to keep it from getting out unscathed, or restore the lysosome’s killing ability by re-acidifying it. Altan-Bonnet and coauthor Sourish Ghosh, PhD, say they have already identified one experimental enzyme inhibitor that potently blocks coronaviruses from exiting the cell.
The lysosome pathway, Altan-Bonnet says, “offers a whole different way of thinking about targeted therapeutics.”
Normally, the lysosome, known as the cells’ “trash compactor,” destroys viruses before they can leave the cell. However, researchers at the National Institutes of Health (NIH) have discovered that SARS-CoV-2 is not like other viruses. The virus can deactivate that waste disposal system, exit without hindrance, and spread freely throughout the body.
“To our shock, these coronaviruses got out of the cells just fine,” said Nihal Altan-Bonnet, PhD, chief of the Laboratory of Host-Pathogen Dynamics at the National Heart, Lung, and Blood Institute, who coauthored the study report.
Most viruses exit via the biosynthetic secretory pathway, used to transport hormones, growth factors and other materials. The researchers wanted to learn whether coronaviruses took an alternate route. To find out, they conducted further studies, using microscopy and virus-specific markers. They discovered that coronaviruses somehow target the lysosome and congregate there. Although lysosomes are highly acidic, the coronaviruses were not destroyed.
That question led to more experiments. The researchers next found that lysosomes get “de-acidified” in coronavirus-infected cells, which weakens their destructive enzymes. The result: The coronavirus remains intact, ready to infect other cells upon exiting.
The coronaviruses are “very sneaky,” Altan-Bonnet says. “They’re using these lysosomes to get out, but they’re also disrupting the lysosome so it can’t do its job or function.” It’s possible that the way the coronavirus interferes with the lysosome’s “immunological machinery” underlies some of the immune system abnormalities seen in COVID-19 patients, such as cytokine storms.
Studying this coronavirus's heterodox ways may mean that researchers can figure out how to keep it from getting out unscathed, or restore the lysosome’s killing ability by re-acidifying it. Altan-Bonnet and coauthor Sourish Ghosh, PhD, say they have already identified one experimental enzyme inhibitor that potently blocks coronaviruses from exiting the cell.
The lysosome pathway, Altan-Bonnet says, “offers a whole different way of thinking about targeted therapeutics.”
Treatments for COVID-19: Update for hospitalists
Most patients with COVID-19 will have a mild presentation and not require hospitalization or any treatment. Inpatient management revolves around the supportive management of the most common complications of severe COVID-19, which includes pneumonia, hypoxemic respiratory failure, acute respiratory distress syndrome (ARDS), and septic shock.

Currently, there is no clinically proven specific antiviral treatment for COVID-19. A few antivirals and treatment modalities have been studied and used, with the hope of decreasing mortality and improving recovery time for those with moderate to severe cases of COVID-19.
Remdesivir
The antiviral remdesivir was the second drug to receive emergency use authorization by the Food and Drug Administration for the treatment of suspected or laboratory-confirmed COVID-19 in adults and children hospitalized with severe disease. Severe disease is defined as patients with an oxygen saturation less than 94% on room air or requiring supplemental oxygen or requiring mechanical ventilation or requiring extracorporeal membrane oxygenation (ECMO).
Remdesivir is a nucleotide analogue that has shown in vitro antiviral activity against a range of RNA viruses. It acts by causing premature termination of viral RNA transcription. Remdesivir is administered intravenously and the recommended dose is 200 mg on day 1, followed by 100 mg daily for various time courses.
A few clinical studies have reported benefits of remdesivir rather than no remdesivir for treatment of severe COVID-19 in hospitalized patients. The Infectious Diseases Society of America (IDSA) recommends 5 days of remdesivir in patients with severe COVID-19 on noninvasive supplemental oxygen and 10 days treatment for those on mechanical ventilation and ECMO. In a randomized, uncontrolled, phase 3 trial, investigators compared 5-day (n = 200) versus 10-day (n = 197) courses of remdesivir in patients with severe COVID-19. Clinical data revealed no differences in outcomes in the two groups.

Common reported adverse effects of the drug include elevated alanine aminotransferase (ALT) and/or aspartate aminotransferase (AST) and gastrointestinal symptoms including nausea, vomiting, and hematochezia. There is insufficient data on using remdesivir in patients requiring dialysis.
Corticosteroids
Is dexamethasone effective for treating COVID-19? In the early days of the COVID-19 pandemic, corticosteroids were not recommended with the fear that, if started too soon, you could blunt the body’s natural defense system and that could allow the virus to thrive. Recent clinical data has shown clinical benefits and decreased mortality with the use of dexamethasone in patients with severe COVID-19 infection because glucocorticoids may modulate inflammation-mediated lung injury and reduce progression to respiratory failure and death.
The Recovery Trial was an open label study which used 6-mg once-daily doses of dexamethasone for up to 10 days or until hospital discharge if sooner. The study concluded that the use of dexamethasone for up to 10 days in hospitalized patients with severe COVID-19 resulted in lower 28-day mortality than usual care.
Dexamethasone is recommended in COVID-19 patients who require supplemental oxygen. If dexamethasone is not available, alternative forms of steroids – prednisone, methylprednisolone, or hydrocortisone – can be used. However, there is no clear evidence that the use of other steroids provides the same benefit as dexamethasone.
Both the IDSA and National Institutes of Health guidelines have recommended the use of steroids. However, clinicians should closely monitor the adverse effects like hyperglycemia, secondary infections, psychiatric effects, and avascular necrosis.
Convalescent plasma
Convalescent plasma is a blood product believed to provide passive antibody therapy through the transmission of neutralizing viral antibodies. Convalescent plasma has been used for decades for different viral infections including the treatment of H1N1 influenza virus, polio, chicken pox, measles, SARS-CoV-1, and MERS-CoV.

On Aug. 23, 2020, the FDA issued an emergency use authorization for investigational convalescent plasma for the treatment of COVID-19 in hospitalized patients. The FDA recommends neutralizing antibodies of at least 1:160. However, such assays have not been widely available and titers in plasma have often not been assessed prior to infusion.
There is no current standard recommended dosing. Most study protocols infuse 1-2 units of convalescent plasma for persons with COVID-19.
There is insufficient data to recommend either for or against the use of convalescent plasma for the treatment of COVID-19. Existing data suggest that, if a benefit exists, convalescent plasma is most useful when given early and with a high titer of neutralizing antibodies.
The adverse effects of convalescent plasma is very similar to the receipt of other blood products, including allergic reactions to the plasma, transfusion-associated circulatory overload (TACO), transfusion-related acute lung injury (TRALI), and acquisition of infections, though the latter is rare because of the rigorous screening process.
Tocilizumab
Tocilizumab is a recombinant humanized monoclonal antibody that binds to interleukin (IL)-6 receptors. Tocilizumab is currently FDA approved for the treatment of severe or life-threatening cytokine release syndrome that is associated with chimeric antigen–receptor (CAR) T-cell therapy and for the treatment of rheumatologic disorders.
The interest in using tocilizumab to treat persons with COVID-19 is based on the observations that a subset of patients with COVID-19 develop a severe inflammatory response that can result in cytokine storm resulting in ARDS, multiorgan failure, and potentially death. Very high levels of IL-6 have been observed in these individuals, thereby suggesting IL-6 may play a central role in the acute clinical decompensation seen with severe COVID-19.
The optimal dosing of tocilizumab in patients with COVID-19 is not known. The FDA recommends dosing of tocilizumab for cytokine release syndrome should not exceed 800 mg. There is limited data about the potential benefit of tocilizumab in patients with COVID-19. The COVACTA trial showed no difference between tocilizumab and placebo in regard to mortality. The time to hospital discharge was shorter in patients treated with tocilizumab; however, the difference was not statistically significant.
Reported adverse effects of tocilizumab include increase in ALT and AST, increased risk of serious infections (especially tuberculosis and invasive fungal infections), reactivation of hepatitis B virus, and rare reports of gastrointestinal perforation.
Hydroxychloroquine

Hydroxycholoroquine (HCQ) and its sister drug chloroquine, have been used for many decades as treatment for malaria and autoimmune diseases. HCQ gained widespread popularity in the early days of the COVID-19 pandemic when clinical studies showed that it had significant in vitro activity against SARS-CoV-2, which provided the rationale for its use in the treatment and prevention of COVID-19 infection.
It was the first drug that was authorized for emergency use by the FDA during the COVID-19 pandemic. However, On June 15, 2020, because of accumulating harmful data, the FDA revoked the emergency authorization use of HCQ as a COVID-19 treatment.
Randomized controlled trials showed that patients treated with HCQ experienced a longer hospital stay with increase in mortality rates and increased likelihood of being placed on mechanical ventilation. In addition, studies revealed an increase in QT prolongation in patients treated with HCQ, especially when coadministered with azithromycin, which can lead to torsades de pointes, ventricular tachycardia, and sudden cardiac death.
The IDSA and National Institutes of Health, both recommend against the use of hydroxychloroquine with or without azithromycin to treat COVID-19 because the harms outweigh the benefits, even if high quality RCTs were to become available in the future.
Other drugs
There have been experimental studies on other medications for the treatment of COVID-19, including losartan, amlodipine, ivermectin, famotidine, Anakinra, Bruton’s tyrosine kinase inhibitors such as ibrutinib, and Janus kinase inhibitors, such as tofacitinib. Additionally, a few supplements such as vitamin C, vitamin D, and zinc have been used in both inpatient and outpatient settings for COVID-19 treatment. Polyclonal antibodies are being investigated in phase 3 trials. However, the data is insufficient, and the effectiveness of these drugs is unknown. The COVID-19 treatment guidelines panel recommends against the use of these treatment modalities.
Dr Tiyouh is an infectious diseases physician at Keystone Health in Chambersburg, Pa. Dr. Tenneti completed medical school at Vydehi Institute of Medical Sciences and Research Centre in Karnataka, India, and is interested in pursuing internal medicine residency. Dr. Tirupathi is the medical director of Keystone Infectious Diseases/HIV in Chambersburg, Pa., and currently chair of infection prevention at Wellspan Chambersburg Hospital and Waynesboro (Pa.) Hospitals. Dr. Palabindala is hospital medicine division chief at the University of Mississippi Medical Center, Jackson, and a member of the editorial advisory board for The Hospitalist.
Sources
Goldman JD et al. Remdesivir for 5 or 10 Days in Patients with Severe Covid-19. N Engl J Med. 2020 May 27. doi: 10.1056/NEJMoa2015301.
Beigel JH et al. Remdesivir for the Treatment of Covid-19 - Final Report. N Engl J Med. 2020 Oct 8. doi: 10.1056/NEJMoa2007764
Wang Y et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2020 May 16;395(10236):1569-78.
National Institutes of Health. COVID-19 Treatment Guidelines.
Infectious Diseases Society of America. Infectious Diseases Society of America guidelines on the treatment and management of patients with COVID-19.
Joyner et al. Early safety indicators of COVID-19 convalescent plasma in 5000 patients. J Clin Invest. 2020;130(9):4791-7.
Luo P et al. Tocilizumab treatment in COVID-19: A single center experience. J Med Virol. 2020 Jul;92(7):814-8.
Centers for Disease Control and Prevention. Healthcare Workers: Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19).
University of Washington. COVID-19 Treatments: Prescribing Information, Clinical Studies, and Slide Decks.
Most patients with COVID-19 will have a mild presentation and not require hospitalization or any treatment. Inpatient management revolves around the supportive management of the most common complications of severe COVID-19, which includes pneumonia, hypoxemic respiratory failure, acute respiratory distress syndrome (ARDS), and septic shock.
Currently, there is no clinically proven specific antiviral treatment for COVID-19. A few antivirals and treatment modalities have been studied and used, with the hope of decreasing mortality and improving recovery time for those with moderate to severe cases of COVID-19.
Remdesivir
The antiviral remdesivir was the second drug to receive emergency use authorization by the Food and Drug Administration for the treatment of suspected or laboratory-confirmed COVID-19 in adults and children hospitalized with severe disease. Severe disease is defined as patients with an oxygen saturation less than 94% on room air or requiring supplemental oxygen or requiring mechanical ventilation or requiring extracorporeal membrane oxygenation (ECMO).
Remdesivir is a nucleotide analogue that has shown in vitro antiviral activity against a range of RNA viruses. It acts by causing premature termination of viral RNA transcription. Remdesivir is administered intravenously and the recommended dose is 200 mg on day 1, followed by 100 mg daily for various time courses.
A few clinical studies have reported benefits of remdesivir rather than no remdesivir for treatment of severe COVID-19 in hospitalized patients. The Infectious Diseases Society of America (IDSA) recommends 5 days of remdesivir in patients with severe COVID-19 on noninvasive supplemental oxygen and 10 days treatment for those on mechanical ventilation and ECMO. In a randomized, uncontrolled, phase 3 trial, investigators compared 5-day (n = 200) versus 10-day (n = 197) courses of remdesivir in patients with severe COVID-19. Clinical data revealed no differences in outcomes in the two groups.
Common reported adverse effects of the drug include elevated alanine aminotransferase (ALT) and/or aspartate aminotransferase (AST) and gastrointestinal symptoms including nausea, vomiting, and hematochezia. There is insufficient data on using remdesivir in patients requiring dialysis.
Corticosteroids
Is dexamethasone effective for treating COVID-19? In the early days of the COVID-19 pandemic, corticosteroids were not recommended with the fear that, if started too soon, you could blunt the body’s natural defense system and that could allow the virus to thrive. Recent clinical data has shown clinical benefits and decreased mortality with the use of dexamethasone in patients with severe COVID-19 infection because glucocorticoids may modulate inflammation-mediated lung injury and reduce progression to respiratory failure and death.
The Recovery Trial was an open label study which used 6-mg once-daily doses of dexamethasone for up to 10 days or until hospital discharge if sooner. The study concluded that the use of dexamethasone for up to 10 days in hospitalized patients with severe COVID-19 resulted in lower 28-day mortality than usual care.
Dexamethasone is recommended in COVID-19 patients who require supplemental oxygen. If dexamethasone is not available, alternative forms of steroids – prednisone, methylprednisolone, or hydrocortisone – can be used. However, there is no clear evidence that the use of other steroids provides the same benefit as dexamethasone.
Both the IDSA and National Institutes of Health guidelines have recommended the use of steroids. However, clinicians should closely monitor the adverse effects like hyperglycemia, secondary infections, psychiatric effects, and avascular necrosis.
Convalescent plasma
Convalescent plasma is a blood product believed to provide passive antibody therapy through the transmission of neutralizing viral antibodies. Convalescent plasma has been used for decades for different viral infections including the treatment of H1N1 influenza virus, polio, chicken pox, measles, SARS-CoV-1, and MERS-CoV.
On Aug. 23, 2020, the FDA issued an emergency use authorization for investigational convalescent plasma for the treatment of COVID-19 in hospitalized patients. The FDA recommends neutralizing antibodies of at least 1:160. However, such assays have not been widely available and titers in plasma have often not been assessed prior to infusion.
There is no current standard recommended dosing. Most study protocols infuse 1-2 units of convalescent plasma for persons with COVID-19.
There is insufficient data to recommend either for or against the use of convalescent plasma for the treatment of COVID-19. Existing data suggest that, if a benefit exists, convalescent plasma is most useful when given early and with a high titer of neutralizing antibodies.
The adverse effects of convalescent plasma is very similar to the receipt of other blood products, including allergic reactions to the plasma, transfusion-associated circulatory overload (TACO), transfusion-related acute lung injury (TRALI), and acquisition of infections, though the latter is rare because of the rigorous screening process.
Tocilizumab
Tocilizumab is a recombinant humanized monoclonal antibody that binds to interleukin (IL)-6 receptors. Tocilizumab is currently FDA approved for the treatment of severe or life-threatening cytokine release syndrome that is associated with chimeric antigen–receptor (CAR) T-cell therapy and for the treatment of rheumatologic disorders.
The interest in using tocilizumab to treat persons with COVID-19 is based on the observations that a subset of patients with COVID-19 develop a severe inflammatory response that can result in cytokine storm resulting in ARDS, multiorgan failure, and potentially death. Very high levels of IL-6 have been observed in these individuals, thereby suggesting IL-6 may play a central role in the acute clinical decompensation seen with severe COVID-19.
The optimal dosing of tocilizumab in patients with COVID-19 is not known. The FDA recommends dosing of tocilizumab for cytokine release syndrome should not exceed 800 mg. There is limited data about the potential benefit of tocilizumab in patients with COVID-19. The COVACTA trial showed no difference between tocilizumab and placebo in regard to mortality. The time to hospital discharge was shorter in patients treated with tocilizumab; however, the difference was not statistically significant.
Reported adverse effects of tocilizumab include increase in ALT and AST, increased risk of serious infections (especially tuberculosis and invasive fungal infections), reactivation of hepatitis B virus, and rare reports of gastrointestinal perforation.
Hydroxychloroquine
Hydroxycholoroquine (HCQ) and its sister drug chloroquine, have been used for many decades as treatment for malaria and autoimmune diseases. HCQ gained widespread popularity in the early days of the COVID-19 pandemic when clinical studies showed that it had significant in vitro activity against SARS-CoV-2, which provided the rationale for its use in the treatment and prevention of COVID-19 infection.
It was the first drug that was authorized for emergency use by the FDA during the COVID-19 pandemic. However, On June 15, 2020, because of accumulating harmful data, the FDA revoked the emergency authorization use of HCQ as a COVID-19 treatment.
Randomized controlled trials showed that patients treated with HCQ experienced a longer hospital stay with increase in mortality rates and increased likelihood of being placed on mechanical ventilation. In addition, studies revealed an increase in QT prolongation in patients treated with HCQ, especially when coadministered with azithromycin, which can lead to torsades de pointes, ventricular tachycardia, and sudden cardiac death.
The IDSA and National Institutes of Health, both recommend against the use of hydroxychloroquine with or without azithromycin to treat COVID-19 because the harms outweigh the benefits, even if high quality RCTs were to become available in the future.
Other drugs
There have been experimental studies on other medications for the treatment of COVID-19, including losartan, amlodipine, ivermectin, famotidine, Anakinra, Bruton’s tyrosine kinase inhibitors such as ibrutinib, and Janus kinase inhibitors, such as tofacitinib. Additionally, a few supplements such as vitamin C, vitamin D, and zinc have been used in both inpatient and outpatient settings for COVID-19 treatment. Polyclonal antibodies are being investigated in phase 3 trials. However, the data is insufficient, and the effectiveness of these drugs is unknown. The COVID-19 treatment guidelines panel recommends against the use of these treatment modalities.
Dr Tiyouh is an infectious diseases physician at Keystone Health in Chambersburg, Pa. Dr. Tenneti completed medical school at Vydehi Institute of Medical Sciences and Research Centre in Karnataka, India, and is interested in pursuing internal medicine residency. Dr. Tirupathi is the medical director of Keystone Infectious Diseases/HIV in Chambersburg, Pa., and currently chair of infection prevention at Wellspan Chambersburg Hospital and Waynesboro (Pa.) Hospitals. Dr. Palabindala is hospital medicine division chief at the University of Mississippi Medical Center, Jackson, and a member of the editorial advisory board for The Hospitalist.
Sources
Goldman JD et al. Remdesivir for 5 or 10 Days in Patients with Severe Covid-19. N Engl J Med. 2020 May 27. doi: 10.1056/NEJMoa2015301.
Beigel JH et al. Remdesivir for the Treatment of Covid-19 - Final Report. N Engl J Med. 2020 Oct 8. doi: 10.1056/NEJMoa2007764
Wang Y et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2020 May 16;395(10236):1569-78.
National Institutes of Health. COVID-19 Treatment Guidelines.
Infectious Diseases Society of America. Infectious Diseases Society of America guidelines on the treatment and management of patients with COVID-19.
Joyner et al. Early safety indicators of COVID-19 convalescent plasma in 5000 patients. J Clin Invest. 2020;130(9):4791-7.
Luo P et al. Tocilizumab treatment in COVID-19: A single center experience. J Med Virol. 2020 Jul;92(7):814-8.
Centers for Disease Control and Prevention. Healthcare Workers: Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19).
University of Washington. COVID-19 Treatments: Prescribing Information, Clinical Studies, and Slide Decks.
Most patients with COVID-19 will have a mild presentation and not require hospitalization or any treatment. Inpatient management revolves around the supportive management of the most common complications of severe COVID-19, which includes pneumonia, hypoxemic respiratory failure, acute respiratory distress syndrome (ARDS), and septic shock.
Currently, there is no clinically proven specific antiviral treatment for COVID-19. A few antivirals and treatment modalities have been studied and used, with the hope of decreasing mortality and improving recovery time for those with moderate to severe cases of COVID-19.
Remdesivir
The antiviral remdesivir was the second drug to receive emergency use authorization by the Food and Drug Administration for the treatment of suspected or laboratory-confirmed COVID-19 in adults and children hospitalized with severe disease. Severe disease is defined as patients with an oxygen saturation less than 94% on room air or requiring supplemental oxygen or requiring mechanical ventilation or requiring extracorporeal membrane oxygenation (ECMO).
Remdesivir is a nucleotide analogue that has shown in vitro antiviral activity against a range of RNA viruses. It acts by causing premature termination of viral RNA transcription. Remdesivir is administered intravenously and the recommended dose is 200 mg on day 1, followed by 100 mg daily for various time courses.
A few clinical studies have reported benefits of remdesivir rather than no remdesivir for treatment of severe COVID-19 in hospitalized patients. The Infectious Diseases Society of America (IDSA) recommends 5 days of remdesivir in patients with severe COVID-19 on noninvasive supplemental oxygen and 10 days treatment for those on mechanical ventilation and ECMO. In a randomized, uncontrolled, phase 3 trial, investigators compared 5-day (n = 200) versus 10-day (n = 197) courses of remdesivir in patients with severe COVID-19. Clinical data revealed no differences in outcomes in the two groups.
Common reported adverse effects of the drug include elevated alanine aminotransferase (ALT) and/or aspartate aminotransferase (AST) and gastrointestinal symptoms including nausea, vomiting, and hematochezia. There is insufficient data on using remdesivir in patients requiring dialysis.
Corticosteroids
Is dexamethasone effective for treating COVID-19? In the early days of the COVID-19 pandemic, corticosteroids were not recommended with the fear that, if started too soon, you could blunt the body’s natural defense system and that could allow the virus to thrive. Recent clinical data has shown clinical benefits and decreased mortality with the use of dexamethasone in patients with severe COVID-19 infection because glucocorticoids may modulate inflammation-mediated lung injury and reduce progression to respiratory failure and death.
The Recovery Trial was an open label study which used 6-mg once-daily doses of dexamethasone for up to 10 days or until hospital discharge if sooner. The study concluded that the use of dexamethasone for up to 10 days in hospitalized patients with severe COVID-19 resulted in lower 28-day mortality than usual care.
Dexamethasone is recommended in COVID-19 patients who require supplemental oxygen. If dexamethasone is not available, alternative forms of steroids – prednisone, methylprednisolone, or hydrocortisone – can be used. However, there is no clear evidence that the use of other steroids provides the same benefit as dexamethasone.
Both the IDSA and National Institutes of Health guidelines have recommended the use of steroids. However, clinicians should closely monitor the adverse effects like hyperglycemia, secondary infections, psychiatric effects, and avascular necrosis.
Convalescent plasma
Convalescent plasma is a blood product believed to provide passive antibody therapy through the transmission of neutralizing viral antibodies. Convalescent plasma has been used for decades for different viral infections including the treatment of H1N1 influenza virus, polio, chicken pox, measles, SARS-CoV-1, and MERS-CoV.
On Aug. 23, 2020, the FDA issued an emergency use authorization for investigational convalescent plasma for the treatment of COVID-19 in hospitalized patients. The FDA recommends neutralizing antibodies of at least 1:160. However, such assays have not been widely available and titers in plasma have often not been assessed prior to infusion.
There is no current standard recommended dosing. Most study protocols infuse 1-2 units of convalescent plasma for persons with COVID-19.
There is insufficient data to recommend either for or against the use of convalescent plasma for the treatment of COVID-19. Existing data suggest that, if a benefit exists, convalescent plasma is most useful when given early and with a high titer of neutralizing antibodies.
The adverse effects of convalescent plasma is very similar to the receipt of other blood products, including allergic reactions to the plasma, transfusion-associated circulatory overload (TACO), transfusion-related acute lung injury (TRALI), and acquisition of infections, though the latter is rare because of the rigorous screening process.
Tocilizumab
Tocilizumab is a recombinant humanized monoclonal antibody that binds to interleukin (IL)-6 receptors. Tocilizumab is currently FDA approved for the treatment of severe or life-threatening cytokine release syndrome that is associated with chimeric antigen–receptor (CAR) T-cell therapy and for the treatment of rheumatologic disorders.
The interest in using tocilizumab to treat persons with COVID-19 is based on the observations that a subset of patients with COVID-19 develop a severe inflammatory response that can result in cytokine storm resulting in ARDS, multiorgan failure, and potentially death. Very high levels of IL-6 have been observed in these individuals, thereby suggesting IL-6 may play a central role in the acute clinical decompensation seen with severe COVID-19.
The optimal dosing of tocilizumab in patients with COVID-19 is not known. The FDA recommends dosing of tocilizumab for cytokine release syndrome should not exceed 800 mg. There is limited data about the potential benefit of tocilizumab in patients with COVID-19. The COVACTA trial showed no difference between tocilizumab and placebo in regard to mortality. The time to hospital discharge was shorter in patients treated with tocilizumab; however, the difference was not statistically significant.
Reported adverse effects of tocilizumab include increase in ALT and AST, increased risk of serious infections (especially tuberculosis and invasive fungal infections), reactivation of hepatitis B virus, and rare reports of gastrointestinal perforation.
Hydroxychloroquine
Hydroxycholoroquine (HCQ) and its sister drug chloroquine, have been used for many decades as treatment for malaria and autoimmune diseases. HCQ gained widespread popularity in the early days of the COVID-19 pandemic when clinical studies showed that it had significant in vitro activity against SARS-CoV-2, which provided the rationale for its use in the treatment and prevention of COVID-19 infection.
It was the first drug that was authorized for emergency use by the FDA during the COVID-19 pandemic. However, On June 15, 2020, because of accumulating harmful data, the FDA revoked the emergency authorization use of HCQ as a COVID-19 treatment.
Randomized controlled trials showed that patients treated with HCQ experienced a longer hospital stay with increase in mortality rates and increased likelihood of being placed on mechanical ventilation. In addition, studies revealed an increase in QT prolongation in patients treated with HCQ, especially when coadministered with azithromycin, which can lead to torsades de pointes, ventricular tachycardia, and sudden cardiac death.
The IDSA and National Institutes of Health, both recommend against the use of hydroxychloroquine with or without azithromycin to treat COVID-19 because the harms outweigh the benefits, even if high quality RCTs were to become available in the future.
Other drugs
There have been experimental studies on other medications for the treatment of COVID-19, including losartan, amlodipine, ivermectin, famotidine, Anakinra, Bruton’s tyrosine kinase inhibitors such as ibrutinib, and Janus kinase inhibitors, such as tofacitinib. Additionally, a few supplements such as vitamin C, vitamin D, and zinc have been used in both inpatient and outpatient settings for COVID-19 treatment. Polyclonal antibodies are being investigated in phase 3 trials. However, the data is insufficient, and the effectiveness of these drugs is unknown. The COVID-19 treatment guidelines panel recommends against the use of these treatment modalities.
Dr Tiyouh is an infectious diseases physician at Keystone Health in Chambersburg, Pa. Dr. Tenneti completed medical school at Vydehi Institute of Medical Sciences and Research Centre in Karnataka, India, and is interested in pursuing internal medicine residency. Dr. Tirupathi is the medical director of Keystone Infectious Diseases/HIV in Chambersburg, Pa., and currently chair of infection prevention at Wellspan Chambersburg Hospital and Waynesboro (Pa.) Hospitals. Dr. Palabindala is hospital medicine division chief at the University of Mississippi Medical Center, Jackson, and a member of the editorial advisory board for The Hospitalist.
Sources
Goldman JD et al. Remdesivir for 5 or 10 Days in Patients with Severe Covid-19. N Engl J Med. 2020 May 27. doi: 10.1056/NEJMoa2015301.
Beigel JH et al. Remdesivir for the Treatment of Covid-19 - Final Report. N Engl J Med. 2020 Oct 8. doi: 10.1056/NEJMoa2007764
Wang Y et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2020 May 16;395(10236):1569-78.
National Institutes of Health. COVID-19 Treatment Guidelines.
Infectious Diseases Society of America. Infectious Diseases Society of America guidelines on the treatment and management of patients with COVID-19.
Joyner et al. Early safety indicators of COVID-19 convalescent plasma in 5000 patients. J Clin Invest. 2020;130(9):4791-7.
Luo P et al. Tocilizumab treatment in COVID-19: A single center experience. J Med Virol. 2020 Jul;92(7):814-8.
Centers for Disease Control and Prevention. Healthcare Workers: Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19).
University of Washington. COVID-19 Treatments: Prescribing Information, Clinical Studies, and Slide Decks.
Search for a snakebite drug might lead to a COVID treatment, too
Matthew Lewin, MD, PhD, founder of the Center for Exploration and Travel Health at the California Academy of Sciences, was researching snakebite treatments in rural locations in preparation for an expedition to the Philippines in 2011.
The story of a renowned herpetologist from the academy, Joseph Slowinski, who was bitten by a highly venomous krait in Myanmar and couldn’t get to a hospital in time to save his life a decade earlier, weighed on the emergency room doctor.
“I concluded that I needed something small and compact and that doesn’t care what kind of snake,” Dr. Lewin said.
It didn’t exist. That set Dr. Lewin in pursuit of a modern snakebite drug, a journey that finds his Corte Madera, Calif., company, Ophirex, nearing a promising oral treatment that fits in a pocket; is stable, easy to use, and affordable; and treats the venom from many species. “That’s the holy grail of snakebite treatment,” he said.
His work has gotten a boost with multimillion-dollar grants from a British charity and the U.S. Army. If it works – and it has been shown to work extremely well in mice and pigs – it could save tens of thousands of lives a year.
Dr. Lewin and Ophirex are not alone in their quest. Snakebites kill nearly 140,000 people a year, overwhelmingly in impoverished rural areas of Asia and Africa without adequate medical infrastructure and knowledge to administer antivenom. Though just a few people die each year in the United States from snakebites, the problem has risen to the top of the list of global health concerns in recent years. Funding has soared, and other research groups have also done promising work on new treatments. Herpetologists say deforestation and climate change are increasing human-snake encounters by forcing snakes to move to new habitats.
Dr. Lewin’s research is centered on a drug called varespladib. The enzyme inhibitor has proven itself in in-vitro lab studies and has effectively saved mice and pigs dosed with venom.
Along the way, Dr. Lewin and his team have come across another potential use for the drug. Varespladib has a positive effect on acute respiratory distress syndrome, associated with COVID-19. Next year, Ophirex will conduct human trials for the possible treatment of the condition funded with $9.9 million from the Army.
The link to a snakebite? The inflammation of the lungs caused by the coronavirus produces the sPLA2 enzyme. A more deadly version of the same enzyme is produced by snake venom.
The other companies that have come up with promising approaches to snakebite aren’t as far along as Ophirex. At the University of California-Irvine, chemist Ken Shea and his team created a nanogel – a kind of polymer used in medical applications – that blocks key proteins in the venom that cause cell destruction. At the Technical University of Denmark, Copenhagen, Andreas Laustsen is looking at engineering bacteria to manufacture anti-venom in fermentation tanks.
The days of incising a snakebite and sucking out the poison are long over, but the current treatment for venomous snakebites remains archaic.
Since the early 1900s, antivenom has been made by injecting horses or other animals with venom milked from snakes and diluted. The animals’ immune systems generate antibodies over several months, and blood plasma is taken from the animals and antibodies extracted from it.
It’s extremely expensive. Hospitals in the United States can charge as much as $15,000 a vial – and a single snakebite might require anywhere from 4 to 50 vials. Moreover, antivenom exists for little more than half the world’s species of venomous snakes.
A major problem is the roughly 2 hours it takes on average for a snakebite victim to reach a hospital and begin treatment. The chemical weapon that is venom starts immediately to destroy cells as it digests its next meal, making fast treatment essential to saving lives and preventing tissue loss.
“The two-hour window between fang and needle is where the most damage occurs,” said Leslie Boyer, director of the University of Arizona’s Venom Immunochemistry, Pharmacology and Emergency Response (VIPER) Institute. “We have a saying, ‘Time is tissue.’ ”
That’s why the search for a new snakebite drug has focused on an inexpensive treatment that can be taken into the field. Dr. Lewin’s drug wouldn’t replace antivenom. Instead, he thinks of it as the first line of defense until the victim can reach a hospital for antivenom treatment.
Dr. Lewin said he expects the drug to be inexpensive, so people in regions where snakebites are common can afford it.
Venom is extremely complicated chemically, and Dr. Lewin began his search by sussing out which of its myriad components to block. He zeroed in on the sPLA2 enzyme.
Surveying the literature about drugs that had been clinically tested for other conditions, he came across varespladib. It had been developed jointly by Eli Lilly and Shionogi, a Japanese pharmaceutical company, as a possible treatment for sepsis. They had never taken it to market.
If it worked, Dr. Lewin could license the right to produce the drug, which had already been thoroughly studied and was shown to be safe.
He placed venom in an array of test tubes. Varespladib and other drugs were added to the venom. He then added a reagent. If the venom was still active, the solution would turn yellow; if it was neutralized, it would remain clear.
The vials with varespladib “came up completely blank,” he said. “It was so stunning I said, ‘I must have made a mistake.’ ”
With a small grant, he sent the drug to the Yale Center for Molecular Discovery and found that varespladib effectively neutralized the venom of snakes found on six continents. The results were published in the journal Toxins and sent ripples through the small community of snakebite researchers.
Dr. Lewin then conducted tests on mice and pigs. Both were successful.
Human clinical trials are next, but they have been delayed by the pandemic. They are scheduled to get underway next spring.
Along the way, Dr. Lewin was fortunate enough to make some good connections that led to funding. In 2012, he attended a party at the Mill Valley, Calif., home of Jerry Harrison, the former guitarist and keyboardist for Talking Heads. Mr. Harrison had long been interested in business and start-ups – he said he was the most careful reader of the ’80s band’s contracts – and at the party he asked “if anyone had any ideas lying fallow,” Mr. Harrison said.
“And Matt pipes up and says, ‘I have this idea how to prevent people from dying from snakebites,’ ” Mr. Harrison said.
The musician said he was a bit taken aback by such an unusual and dire problem, but “I thought if it can save lives we have to do it,” he said. He became an investor and cofounder of Ophirex with Dr. Lewin.
Dr. Lewin met Lt. Col. Rebecca Carter, a biochemist who was assigned to lead the Medical Modernization Division of Air Force Special Operations Command, in 2016 when she attended a Venom Week conference in Greenville, N.C. He was presenting the results of his mouse studies. She told him about her first mission: to find a universal antivenom for medics on special operations teams in Africa. She persuaded the Special Operations Command Biomedical Research Advisory Group, which specializes in getting critical projects to production, to grant Ophirex $148,000 in 2017. She later retired from the Air Force and now works for Ophirex as vice president.
More multimillion-dollar grants followed, including the Army’s COVID grant. Clinical trials are scheduled to begin this winter.
Despite the progress and the sudden cash flow, Dr. Lewin tamps down talk of a universal snakebite cure. “There’s enough evidence to say the drug deserves to have its day in clinical trials,” he said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Matthew Lewin, MD, PhD, founder of the Center for Exploration and Travel Health at the California Academy of Sciences, was researching snakebite treatments in rural locations in preparation for an expedition to the Philippines in 2011.
The story of a renowned herpetologist from the academy, Joseph Slowinski, who was bitten by a highly venomous krait in Myanmar and couldn’t get to a hospital in time to save his life a decade earlier, weighed on the emergency room doctor.
“I concluded that I needed something small and compact and that doesn’t care what kind of snake,” Dr. Lewin said.
It didn’t exist. That set Dr. Lewin in pursuit of a modern snakebite drug, a journey that finds his Corte Madera, Calif., company, Ophirex, nearing a promising oral treatment that fits in a pocket; is stable, easy to use, and affordable; and treats the venom from many species. “That’s the holy grail of snakebite treatment,” he said.
His work has gotten a boost with multimillion-dollar grants from a British charity and the U.S. Army. If it works – and it has been shown to work extremely well in mice and pigs – it could save tens of thousands of lives a year.
Dr. Lewin and Ophirex are not alone in their quest. Snakebites kill nearly 140,000 people a year, overwhelmingly in impoverished rural areas of Asia and Africa without adequate medical infrastructure and knowledge to administer antivenom. Though just a few people die each year in the United States from snakebites, the problem has risen to the top of the list of global health concerns in recent years. Funding has soared, and other research groups have also done promising work on new treatments. Herpetologists say deforestation and climate change are increasing human-snake encounters by forcing snakes to move to new habitats.
Dr. Lewin’s research is centered on a drug called varespladib. The enzyme inhibitor has proven itself in in-vitro lab studies and has effectively saved mice and pigs dosed with venom.
Along the way, Dr. Lewin and his team have come across another potential use for the drug. Varespladib has a positive effect on acute respiratory distress syndrome, associated with COVID-19. Next year, Ophirex will conduct human trials for the possible treatment of the condition funded with $9.9 million from the Army.
The link to a snakebite? The inflammation of the lungs caused by the coronavirus produces the sPLA2 enzyme. A more deadly version of the same enzyme is produced by snake venom.
The other companies that have come up with promising approaches to snakebite aren’t as far along as Ophirex. At the University of California-Irvine, chemist Ken Shea and his team created a nanogel – a kind of polymer used in medical applications – that blocks key proteins in the venom that cause cell destruction. At the Technical University of Denmark, Copenhagen, Andreas Laustsen is looking at engineering bacteria to manufacture anti-venom in fermentation tanks.
The days of incising a snakebite and sucking out the poison are long over, but the current treatment for venomous snakebites remains archaic.
Since the early 1900s, antivenom has been made by injecting horses or other animals with venom milked from snakes and diluted. The animals’ immune systems generate antibodies over several months, and blood plasma is taken from the animals and antibodies extracted from it.
It’s extremely expensive. Hospitals in the United States can charge as much as $15,000 a vial – and a single snakebite might require anywhere from 4 to 50 vials. Moreover, antivenom exists for little more than half the world’s species of venomous snakes.
A major problem is the roughly 2 hours it takes on average for a snakebite victim to reach a hospital and begin treatment. The chemical weapon that is venom starts immediately to destroy cells as it digests its next meal, making fast treatment essential to saving lives and preventing tissue loss.
“The two-hour window between fang and needle is where the most damage occurs,” said Leslie Boyer, director of the University of Arizona’s Venom Immunochemistry, Pharmacology and Emergency Response (VIPER) Institute. “We have a saying, ‘Time is tissue.’ ”
That’s why the search for a new snakebite drug has focused on an inexpensive treatment that can be taken into the field. Dr. Lewin’s drug wouldn’t replace antivenom. Instead, he thinks of it as the first line of defense until the victim can reach a hospital for antivenom treatment.
Dr. Lewin said he expects the drug to be inexpensive, so people in regions where snakebites are common can afford it.
Venom is extremely complicated chemically, and Dr. Lewin began his search by sussing out which of its myriad components to block. He zeroed in on the sPLA2 enzyme.
Surveying the literature about drugs that had been clinically tested for other conditions, he came across varespladib. It had been developed jointly by Eli Lilly and Shionogi, a Japanese pharmaceutical company, as a possible treatment for sepsis. They had never taken it to market.
If it worked, Dr. Lewin could license the right to produce the drug, which had already been thoroughly studied and was shown to be safe.
He placed venom in an array of test tubes. Varespladib and other drugs were added to the venom. He then added a reagent. If the venom was still active, the solution would turn yellow; if it was neutralized, it would remain clear.
The vials with varespladib “came up completely blank,” he said. “It was so stunning I said, ‘I must have made a mistake.’ ”
With a small grant, he sent the drug to the Yale Center for Molecular Discovery and found that varespladib effectively neutralized the venom of snakes found on six continents. The results were published in the journal Toxins and sent ripples through the small community of snakebite researchers.
Dr. Lewin then conducted tests on mice and pigs. Both were successful.
Human clinical trials are next, but they have been delayed by the pandemic. They are scheduled to get underway next spring.
Along the way, Dr. Lewin was fortunate enough to make some good connections that led to funding. In 2012, he attended a party at the Mill Valley, Calif., home of Jerry Harrison, the former guitarist and keyboardist for Talking Heads. Mr. Harrison had long been interested in business and start-ups – he said he was the most careful reader of the ’80s band’s contracts – and at the party he asked “if anyone had any ideas lying fallow,” Mr. Harrison said.
“And Matt pipes up and says, ‘I have this idea how to prevent people from dying from snakebites,’ ” Mr. Harrison said.
The musician said he was a bit taken aback by such an unusual and dire problem, but “I thought if it can save lives we have to do it,” he said. He became an investor and cofounder of Ophirex with Dr. Lewin.
Dr. Lewin met Lt. Col. Rebecca Carter, a biochemist who was assigned to lead the Medical Modernization Division of Air Force Special Operations Command, in 2016 when she attended a Venom Week conference in Greenville, N.C. He was presenting the results of his mouse studies. She told him about her first mission: to find a universal antivenom for medics on special operations teams in Africa. She persuaded the Special Operations Command Biomedical Research Advisory Group, which specializes in getting critical projects to production, to grant Ophirex $148,000 in 2017. She later retired from the Air Force and now works for Ophirex as vice president.
More multimillion-dollar grants followed, including the Army’s COVID grant. Clinical trials are scheduled to begin this winter.
Despite the progress and the sudden cash flow, Dr. Lewin tamps down talk of a universal snakebite cure. “There’s enough evidence to say the drug deserves to have its day in clinical trials,” he said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Matthew Lewin, MD, PhD, founder of the Center for Exploration and Travel Health at the California Academy of Sciences, was researching snakebite treatments in rural locations in preparation for an expedition to the Philippines in 2011.
The story of a renowned herpetologist from the academy, Joseph Slowinski, who was bitten by a highly venomous krait in Myanmar and couldn’t get to a hospital in time to save his life a decade earlier, weighed on the emergency room doctor.
“I concluded that I needed something small and compact and that doesn’t care what kind of snake,” Dr. Lewin said.
It didn’t exist. That set Dr. Lewin in pursuit of a modern snakebite drug, a journey that finds his Corte Madera, Calif., company, Ophirex, nearing a promising oral treatment that fits in a pocket; is stable, easy to use, and affordable; and treats the venom from many species. “That’s the holy grail of snakebite treatment,” he said.
His work has gotten a boost with multimillion-dollar grants from a British charity and the U.S. Army. If it works – and it has been shown to work extremely well in mice and pigs – it could save tens of thousands of lives a year.
Dr. Lewin and Ophirex are not alone in their quest. Snakebites kill nearly 140,000 people a year, overwhelmingly in impoverished rural areas of Asia and Africa without adequate medical infrastructure and knowledge to administer antivenom. Though just a few people die each year in the United States from snakebites, the problem has risen to the top of the list of global health concerns in recent years. Funding has soared, and other research groups have also done promising work on new treatments. Herpetologists say deforestation and climate change are increasing human-snake encounters by forcing snakes to move to new habitats.
Dr. Lewin’s research is centered on a drug called varespladib. The enzyme inhibitor has proven itself in in-vitro lab studies and has effectively saved mice and pigs dosed with venom.
Along the way, Dr. Lewin and his team have come across another potential use for the drug. Varespladib has a positive effect on acute respiratory distress syndrome, associated with COVID-19. Next year, Ophirex will conduct human trials for the possible treatment of the condition funded with $9.9 million from the Army.
The link to a snakebite? The inflammation of the lungs caused by the coronavirus produces the sPLA2 enzyme. A more deadly version of the same enzyme is produced by snake venom.
The other companies that have come up with promising approaches to snakebite aren’t as far along as Ophirex. At the University of California-Irvine, chemist Ken Shea and his team created a nanogel – a kind of polymer used in medical applications – that blocks key proteins in the venom that cause cell destruction. At the Technical University of Denmark, Copenhagen, Andreas Laustsen is looking at engineering bacteria to manufacture anti-venom in fermentation tanks.
The days of incising a snakebite and sucking out the poison are long over, but the current treatment for venomous snakebites remains archaic.
Since the early 1900s, antivenom has been made by injecting horses or other animals with venom milked from snakes and diluted. The animals’ immune systems generate antibodies over several months, and blood plasma is taken from the animals and antibodies extracted from it.
It’s extremely expensive. Hospitals in the United States can charge as much as $15,000 a vial – and a single snakebite might require anywhere from 4 to 50 vials. Moreover, antivenom exists for little more than half the world’s species of venomous snakes.
A major problem is the roughly 2 hours it takes on average for a snakebite victim to reach a hospital and begin treatment. The chemical weapon that is venom starts immediately to destroy cells as it digests its next meal, making fast treatment essential to saving lives and preventing tissue loss.
“The two-hour window between fang and needle is where the most damage occurs,” said Leslie Boyer, director of the University of Arizona’s Venom Immunochemistry, Pharmacology and Emergency Response (VIPER) Institute. “We have a saying, ‘Time is tissue.’ ”
That’s why the search for a new snakebite drug has focused on an inexpensive treatment that can be taken into the field. Dr. Lewin’s drug wouldn’t replace antivenom. Instead, he thinks of it as the first line of defense until the victim can reach a hospital for antivenom treatment.
Dr. Lewin said he expects the drug to be inexpensive, so people in regions where snakebites are common can afford it.
Venom is extremely complicated chemically, and Dr. Lewin began his search by sussing out which of its myriad components to block. He zeroed in on the sPLA2 enzyme.
Surveying the literature about drugs that had been clinically tested for other conditions, he came across varespladib. It had been developed jointly by Eli Lilly and Shionogi, a Japanese pharmaceutical company, as a possible treatment for sepsis. They had never taken it to market.
If it worked, Dr. Lewin could license the right to produce the drug, which had already been thoroughly studied and was shown to be safe.
He placed venom in an array of test tubes. Varespladib and other drugs were added to the venom. He then added a reagent. If the venom was still active, the solution would turn yellow; if it was neutralized, it would remain clear.
The vials with varespladib “came up completely blank,” he said. “It was so stunning I said, ‘I must have made a mistake.’ ”
With a small grant, he sent the drug to the Yale Center for Molecular Discovery and found that varespladib effectively neutralized the venom of snakes found on six continents. The results were published in the journal Toxins and sent ripples through the small community of snakebite researchers.
Dr. Lewin then conducted tests on mice and pigs. Both were successful.
Human clinical trials are next, but they have been delayed by the pandemic. They are scheduled to get underway next spring.
Along the way, Dr. Lewin was fortunate enough to make some good connections that led to funding. In 2012, he attended a party at the Mill Valley, Calif., home of Jerry Harrison, the former guitarist and keyboardist for Talking Heads. Mr. Harrison had long been interested in business and start-ups – he said he was the most careful reader of the ’80s band’s contracts – and at the party he asked “if anyone had any ideas lying fallow,” Mr. Harrison said.
“And Matt pipes up and says, ‘I have this idea how to prevent people from dying from snakebites,’ ” Mr. Harrison said.
The musician said he was a bit taken aback by such an unusual and dire problem, but “I thought if it can save lives we have to do it,” he said. He became an investor and cofounder of Ophirex with Dr. Lewin.
Dr. Lewin met Lt. Col. Rebecca Carter, a biochemist who was assigned to lead the Medical Modernization Division of Air Force Special Operations Command, in 2016 when she attended a Venom Week conference in Greenville, N.C. He was presenting the results of his mouse studies. She told him about her first mission: to find a universal antivenom for medics on special operations teams in Africa. She persuaded the Special Operations Command Biomedical Research Advisory Group, which specializes in getting critical projects to production, to grant Ophirex $148,000 in 2017. She later retired from the Air Force and now works for Ophirex as vice president.
More multimillion-dollar grants followed, including the Army’s COVID grant. Clinical trials are scheduled to begin this winter.
Despite the progress and the sudden cash flow, Dr. Lewin tamps down talk of a universal snakebite cure. “There’s enough evidence to say the drug deserves to have its day in clinical trials,” he said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Moral distress: COVID-19 shortages prompt tough decisions at bedside
Choosing which hospitalized COVID-19 patients receive potentially lifesaving care, making urgent calls for ventilators and other equipment, and triaging care based on patient age and comorbidities were among the challenges revealed in new feedback from health care leaders and frontline workers.
Even though many hospitals have contingency plans for how to allocate resources and triage patient care during crisis capacity, for many providers during the real-world COVID-19 trial of these protocols, they fell short.
Many hospital crisis capacity plans, for example, were too general to address all the specific challenges arising during the pandemic, investigators report in a study published online Nov. 6 in JAMA Network Open.
“Our research shows that the types of challenges and approach to resource limitation in real-world clinical settings during the pandemic differed in practice from how we had prepared in theory,” lead author Catherine Butler, MD, told Medscape Medical News. Insufficient dialysis treatment time, staff shortages, and routine supply scarcity are examples “for which there was not an established plan or approach for appropriate allocation.”
“This left frontline clinicians to determine what constituted an acceptable standard of care and to make difficult allocation decisions at the bedside,” added Butler, acting instructor in the Division of Nephrology at the University of Washington in Seattle and a research fellow at the VA Health Services Research and Development Seattle-Denver Center of Innovation.
The investigators conducted semistructured interviews in April and May with 61 clinicians and health leaders. Mean age was 46 years, 63% were women, and participants practiced in 15 states. Most participants hailed from locations hard-hit by the pandemic at the time, including Seattle, New York City, and New Orleans.
Triage tribulations
The qualitative study included comments from respondents on three major themes that emerged: planning for crisis capacity, adapting to resource limitation, and the multiple unprecedented barriers to care delivery.
Overall, planning and support from institutional leaders varied. One provider said, “Talking to administration, and they just seemed really disengaged with the problem. We asked multiple times if there was a triage command center or a plan for what would occur if we got to the point where we had to triage resources. They said there was, but they wouldn’t provide it to us.”
Another had a more positive experience. “The biggest deal in the ethics world in the last 2 months has been preparing in case we need to triage. So, we have a very detailed, elaborate, well thought-out triage policy … that was done at the highest levels of the system.”
Clinicians said they participate on triage teams – despite the moral weight and likely emotional burden – out of a sense of duty.
Interestingly, some providers on these teams also reported a reluctance to reveal their participation to colleagues. “I didn’t feel like I should tell anybody … even some of my close friends who are physicians and nurses here … that I’ve been asked to be on this [triage team],” one respondent said. “I didn’t feel like I should make it known.”
Adapting to scarce resources
Multiple providers said they faced difficult care decisions because of limited dialysis or supply shortages. “They felt that this patient had the greatest likelihood of benefiting from most aggressive therapy. … I think there was probably like 5 or 6 patients in the ICU … and then you had this 35-year-old with no comorbidities,” one respondent said. “That’s who the ICU dialyzed, and I couldn’t really disagree.”
“I emailed all of [my colleagues], and I said ‘Help! We need X, we need CRRT [continuous renal replacement therapy] machines, we need dialysates,’ “ another responded.
“One of the attendings had a tweet when we were running out of CRRT. He had a tweet about, ‘Can anybody give us supplies for CRRT?’ So, it got to that. You do anything. You get really desperate,” the clinician said.
Other providers reported getting innovative under the circumstances. “My partner’s son, he actually borrowed a couple of 3D printers. He printed some of these face shields, and then they got the formula, or the specifics as to how to make this particular connection to connect to a dialysis machine to generate dialysate. So, he also printed some of those from the 3D printer.”
Dire situations with dialysis
Another respondent understood the focus on ventilators and ICU beds throughout the crisis, but said “no one has acknowledged that dialysis has been one of the most, if not the most, limited resources.”
Another clinician expressed surprise at a decision made in the face of limited availability of traditional dialysis. “A month ago, people said we were going to do acute peritoneal dialysis [PD]. And I said, ‘No, we’re not going to do acute PD. PD, it’s not that great for acute patients, sick people in the ICUs. I don’t think we’re going to do PD.’
“Three days later we were doing acute PD. I mean, that was unbelievable!”
Some institutions rationed dialysis therapy. “We went through the entire list at the beginning of the week and [said], this person has to dialyze these days, this person would probably benefit from a dialysis session, a third group person we could probably just string along and medically manage if we needed to,” one provider said.
Another respondent reported a different strategy. “No one was not getting dialysis, but there were a lot of people getting minimal dialysis. Even though people were getting treated, resources were very stretched.”
Changing family dynamics
COVID-19 has naturally changed how clinicians speak with families. One respondent recalled looking at the ICU physician and being like, ‘Have you talked to the son this week?’ And she’s like, ‘Oh my God, no. … Did you talk to the son?’ I’m like, ‘Oh my God, no.’ “
They realized, the respondent added, “that none of us had called the family because it’s just not in your workflow. You’re so used to the family being there.”
Multiple providers also feared a conversation with family regarding necessary changes to care given the limitation of resources during the pandemic.
“Most families have been actually very understanding. This is a crisis, and we’re in a pandemic, and we’re all doing things we wouldn’t normally do.”
Another respondent said, “We were pretty honest about how resources were limited and how we were doing with this COVID-19 surge. And I think we talked about how the usual ability to provide aggressive dialysis was not the case with COVID-19. There was a lot of understanding, sometimes to my surprise. I would think people would be more upset when hearing something like that.”
Many clinicians facing these challenges experience moral distress, the researchers noted.
“Early in the pandemic, it became quickly apparent that possible resource limitation, such as scarce ventilators, was a major ethical concern. There was robust debate and discussion published in medical journals and the popular press about how to appropriately allocate health care resources,” the University of Washington’s Butler said.
“Transparency, accountability, and standardized processes for rationing these resources in ‘crisis capacity’ settings were seen as key to avoiding the impact of implicit bias and moral distress for clinicians,” she added.
Lessons learned
In terms of potential solutions that could mitigate these challenges in the future, health care leaders “could develop standardized protocols or guidelines for allocating a broader range of potentially scarce health care resources even before ‘crisis capacity’ is declared,” Butler said.
Furthermore, no frontline worker should have to go it alone. “Medical ethicists and/or other clinicians familiar with ethical considerations in settings of scarce health care resources might provide bedside consultation and collaborate with frontline providers who must grapple with the impact of more subtle forms of resource limitation on clinical decision-making.”
The study was partially funded by grants from the National Institute of Diabetes and Digestive and Kidney Diseases and a COVID-19 Research Award from the University of Washington Institute of Translational Health Sciences given to Butler.
This article first appeared on Medscape.com.
Choosing which hospitalized COVID-19 patients receive potentially lifesaving care, making urgent calls for ventilators and other equipment, and triaging care based on patient age and comorbidities were among the challenges revealed in new feedback from health care leaders and frontline workers.
Even though many hospitals have contingency plans for how to allocate resources and triage patient care during crisis capacity, for many providers during the real-world COVID-19 trial of these protocols, they fell short.
Many hospital crisis capacity plans, for example, were too general to address all the specific challenges arising during the pandemic, investigators report in a study published online Nov. 6 in JAMA Network Open.
“Our research shows that the types of challenges and approach to resource limitation in real-world clinical settings during the pandemic differed in practice from how we had prepared in theory,” lead author Catherine Butler, MD, told Medscape Medical News. Insufficient dialysis treatment time, staff shortages, and routine supply scarcity are examples “for which there was not an established plan or approach for appropriate allocation.”
“This left frontline clinicians to determine what constituted an acceptable standard of care and to make difficult allocation decisions at the bedside,” added Butler, acting instructor in the Division of Nephrology at the University of Washington in Seattle and a research fellow at the VA Health Services Research and Development Seattle-Denver Center of Innovation.
The investigators conducted semistructured interviews in April and May with 61 clinicians and health leaders. Mean age was 46 years, 63% were women, and participants practiced in 15 states. Most participants hailed from locations hard-hit by the pandemic at the time, including Seattle, New York City, and New Orleans.
Triage tribulations
The qualitative study included comments from respondents on three major themes that emerged: planning for crisis capacity, adapting to resource limitation, and the multiple unprecedented barriers to care delivery.
Overall, planning and support from institutional leaders varied. One provider said, “Talking to administration, and they just seemed really disengaged with the problem. We asked multiple times if there was a triage command center or a plan for what would occur if we got to the point where we had to triage resources. They said there was, but they wouldn’t provide it to us.”
Another had a more positive experience. “The biggest deal in the ethics world in the last 2 months has been preparing in case we need to triage. So, we have a very detailed, elaborate, well thought-out triage policy … that was done at the highest levels of the system.”
Clinicians said they participate on triage teams – despite the moral weight and likely emotional burden – out of a sense of duty.
Interestingly, some providers on these teams also reported a reluctance to reveal their participation to colleagues. “I didn’t feel like I should tell anybody … even some of my close friends who are physicians and nurses here … that I’ve been asked to be on this [triage team],” one respondent said. “I didn’t feel like I should make it known.”
Adapting to scarce resources
Multiple providers said they faced difficult care decisions because of limited dialysis or supply shortages. “They felt that this patient had the greatest likelihood of benefiting from most aggressive therapy. … I think there was probably like 5 or 6 patients in the ICU … and then you had this 35-year-old with no comorbidities,” one respondent said. “That’s who the ICU dialyzed, and I couldn’t really disagree.”
“I emailed all of [my colleagues], and I said ‘Help! We need X, we need CRRT [continuous renal replacement therapy] machines, we need dialysates,’ “ another responded.
“One of the attendings had a tweet when we were running out of CRRT. He had a tweet about, ‘Can anybody give us supplies for CRRT?’ So, it got to that. You do anything. You get really desperate,” the clinician said.
Other providers reported getting innovative under the circumstances. “My partner’s son, he actually borrowed a couple of 3D printers. He printed some of these face shields, and then they got the formula, or the specifics as to how to make this particular connection to connect to a dialysis machine to generate dialysate. So, he also printed some of those from the 3D printer.”
Dire situations with dialysis
Another respondent understood the focus on ventilators and ICU beds throughout the crisis, but said “no one has acknowledged that dialysis has been one of the most, if not the most, limited resources.”
Another clinician expressed surprise at a decision made in the face of limited availability of traditional dialysis. “A month ago, people said we were going to do acute peritoneal dialysis [PD]. And I said, ‘No, we’re not going to do acute PD. PD, it’s not that great for acute patients, sick people in the ICUs. I don’t think we’re going to do PD.’
“Three days later we were doing acute PD. I mean, that was unbelievable!”
Some institutions rationed dialysis therapy. “We went through the entire list at the beginning of the week and [said], this person has to dialyze these days, this person would probably benefit from a dialysis session, a third group person we could probably just string along and medically manage if we needed to,” one provider said.
Another respondent reported a different strategy. “No one was not getting dialysis, but there were a lot of people getting minimal dialysis. Even though people were getting treated, resources were very stretched.”
Changing family dynamics
COVID-19 has naturally changed how clinicians speak with families. One respondent recalled looking at the ICU physician and being like, ‘Have you talked to the son this week?’ And she’s like, ‘Oh my God, no. … Did you talk to the son?’ I’m like, ‘Oh my God, no.’ “
They realized, the respondent added, “that none of us had called the family because it’s just not in your workflow. You’re so used to the family being there.”
Multiple providers also feared a conversation with family regarding necessary changes to care given the limitation of resources during the pandemic.
“Most families have been actually very understanding. This is a crisis, and we’re in a pandemic, and we’re all doing things we wouldn’t normally do.”
Another respondent said, “We were pretty honest about how resources were limited and how we were doing with this COVID-19 surge. And I think we talked about how the usual ability to provide aggressive dialysis was not the case with COVID-19. There was a lot of understanding, sometimes to my surprise. I would think people would be more upset when hearing something like that.”
Many clinicians facing these challenges experience moral distress, the researchers noted.
“Early in the pandemic, it became quickly apparent that possible resource limitation, such as scarce ventilators, was a major ethical concern. There was robust debate and discussion published in medical journals and the popular press about how to appropriately allocate health care resources,” the University of Washington’s Butler said.
“Transparency, accountability, and standardized processes for rationing these resources in ‘crisis capacity’ settings were seen as key to avoiding the impact of implicit bias and moral distress for clinicians,” she added.
Lessons learned
In terms of potential solutions that could mitigate these challenges in the future, health care leaders “could develop standardized protocols or guidelines for allocating a broader range of potentially scarce health care resources even before ‘crisis capacity’ is declared,” Butler said.
Furthermore, no frontline worker should have to go it alone. “Medical ethicists and/or other clinicians familiar with ethical considerations in settings of scarce health care resources might provide bedside consultation and collaborate with frontline providers who must grapple with the impact of more subtle forms of resource limitation on clinical decision-making.”
The study was partially funded by grants from the National Institute of Diabetes and Digestive and Kidney Diseases and a COVID-19 Research Award from the University of Washington Institute of Translational Health Sciences given to Butler.
This article first appeared on Medscape.com.
Choosing which hospitalized COVID-19 patients receive potentially lifesaving care, making urgent calls for ventilators and other equipment, and triaging care based on patient age and comorbidities were among the challenges revealed in new feedback from health care leaders and frontline workers.
Even though many hospitals have contingency plans for how to allocate resources and triage patient care during crisis capacity, for many providers during the real-world COVID-19 trial of these protocols, they fell short.
Many hospital crisis capacity plans, for example, were too general to address all the specific challenges arising during the pandemic, investigators report in a study published online Nov. 6 in JAMA Network Open.
“Our research shows that the types of challenges and approach to resource limitation in real-world clinical settings during the pandemic differed in practice from how we had prepared in theory,” lead author Catherine Butler, MD, told Medscape Medical News. Insufficient dialysis treatment time, staff shortages, and routine supply scarcity are examples “for which there was not an established plan or approach for appropriate allocation.”
“This left frontline clinicians to determine what constituted an acceptable standard of care and to make difficult allocation decisions at the bedside,” added Butler, acting instructor in the Division of Nephrology at the University of Washington in Seattle and a research fellow at the VA Health Services Research and Development Seattle-Denver Center of Innovation.
The investigators conducted semistructured interviews in April and May with 61 clinicians and health leaders. Mean age was 46 years, 63% were women, and participants practiced in 15 states. Most participants hailed from locations hard-hit by the pandemic at the time, including Seattle, New York City, and New Orleans.
Triage tribulations
The qualitative study included comments from respondents on three major themes that emerged: planning for crisis capacity, adapting to resource limitation, and the multiple unprecedented barriers to care delivery.
Overall, planning and support from institutional leaders varied. One provider said, “Talking to administration, and they just seemed really disengaged with the problem. We asked multiple times if there was a triage command center or a plan for what would occur if we got to the point where we had to triage resources. They said there was, but they wouldn’t provide it to us.”
Another had a more positive experience. “The biggest deal in the ethics world in the last 2 months has been preparing in case we need to triage. So, we have a very detailed, elaborate, well thought-out triage policy … that was done at the highest levels of the system.”
Clinicians said they participate on triage teams – despite the moral weight and likely emotional burden – out of a sense of duty.
Interestingly, some providers on these teams also reported a reluctance to reveal their participation to colleagues. “I didn’t feel like I should tell anybody … even some of my close friends who are physicians and nurses here … that I’ve been asked to be on this [triage team],” one respondent said. “I didn’t feel like I should make it known.”
Adapting to scarce resources
Multiple providers said they faced difficult care decisions because of limited dialysis or supply shortages. “They felt that this patient had the greatest likelihood of benefiting from most aggressive therapy. … I think there was probably like 5 or 6 patients in the ICU … and then you had this 35-year-old with no comorbidities,” one respondent said. “That’s who the ICU dialyzed, and I couldn’t really disagree.”
“I emailed all of [my colleagues], and I said ‘Help! We need X, we need CRRT [continuous renal replacement therapy] machines, we need dialysates,’ “ another responded.
“One of the attendings had a tweet when we were running out of CRRT. He had a tweet about, ‘Can anybody give us supplies for CRRT?’ So, it got to that. You do anything. You get really desperate,” the clinician said.
Other providers reported getting innovative under the circumstances. “My partner’s son, he actually borrowed a couple of 3D printers. He printed some of these face shields, and then they got the formula, or the specifics as to how to make this particular connection to connect to a dialysis machine to generate dialysate. So, he also printed some of those from the 3D printer.”
Dire situations with dialysis
Another respondent understood the focus on ventilators and ICU beds throughout the crisis, but said “no one has acknowledged that dialysis has been one of the most, if not the most, limited resources.”
Another clinician expressed surprise at a decision made in the face of limited availability of traditional dialysis. “A month ago, people said we were going to do acute peritoneal dialysis [PD]. And I said, ‘No, we’re not going to do acute PD. PD, it’s not that great for acute patients, sick people in the ICUs. I don’t think we’re going to do PD.’
“Three days later we were doing acute PD. I mean, that was unbelievable!”
Some institutions rationed dialysis therapy. “We went through the entire list at the beginning of the week and [said], this person has to dialyze these days, this person would probably benefit from a dialysis session, a third group person we could probably just string along and medically manage if we needed to,” one provider said.
Another respondent reported a different strategy. “No one was not getting dialysis, but there were a lot of people getting minimal dialysis. Even though people were getting treated, resources were very stretched.”
Changing family dynamics
COVID-19 has naturally changed how clinicians speak with families. One respondent recalled looking at the ICU physician and being like, ‘Have you talked to the son this week?’ And she’s like, ‘Oh my God, no. … Did you talk to the son?’ I’m like, ‘Oh my God, no.’ “
They realized, the respondent added, “that none of us had called the family because it’s just not in your workflow. You’re so used to the family being there.”
Multiple providers also feared a conversation with family regarding necessary changes to care given the limitation of resources during the pandemic.
“Most families have been actually very understanding. This is a crisis, and we’re in a pandemic, and we’re all doing things we wouldn’t normally do.”
Another respondent said, “We were pretty honest about how resources were limited and how we were doing with this COVID-19 surge. And I think we talked about how the usual ability to provide aggressive dialysis was not the case with COVID-19. There was a lot of understanding, sometimes to my surprise. I would think people would be more upset when hearing something like that.”
Many clinicians facing these challenges experience moral distress, the researchers noted.
“Early in the pandemic, it became quickly apparent that possible resource limitation, such as scarce ventilators, was a major ethical concern. There was robust debate and discussion published in medical journals and the popular press about how to appropriately allocate health care resources,” the University of Washington’s Butler said.
“Transparency, accountability, and standardized processes for rationing these resources in ‘crisis capacity’ settings were seen as key to avoiding the impact of implicit bias and moral distress for clinicians,” she added.
Lessons learned
In terms of potential solutions that could mitigate these challenges in the future, health care leaders “could develop standardized protocols or guidelines for allocating a broader range of potentially scarce health care resources even before ‘crisis capacity’ is declared,” Butler said.
Furthermore, no frontline worker should have to go it alone. “Medical ethicists and/or other clinicians familiar with ethical considerations in settings of scarce health care resources might provide bedside consultation and collaborate with frontline providers who must grapple with the impact of more subtle forms of resource limitation on clinical decision-making.”
The study was partially funded by grants from the National Institute of Diabetes and Digestive and Kidney Diseases and a COVID-19 Research Award from the University of Washington Institute of Translational Health Sciences given to Butler.
This article first appeared on Medscape.com.
What happened to melanoma care during COVID-19 sequestration
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.

This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.

Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”

“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.
This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.
Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”
“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.
This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.
Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”
“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
REPORTING FROM THE CUTANEOUS MALIGNANCIES FORUM