User login
In Case You Missed It: COVID
Heart Attack, Stroke Survivors at High Risk for Long COVID
Primary care doctors and specialists should advise patients who have already experienced a heart attack or stroke that they are at a higher risk for long COVID and need to take steps to avoid contracting the virus, according to new research.
The study, led by researchers at Columbia University, New York City, suggests that anyone with cardiovascular disease (CVD) — defined as having experienced a heart attack or stroke — should consider getting the updated COVID vaccine boosters. They also suggest patients with CVD take other steps to avoid an acute infection, such as avoiding crowded indoor spaces.
There is no specific test or treatment for long COVID, which can become disabling and chronic. Long COVID is defined by the failure to recover from acute COVID-19 in 90 days.
The scientists used data from nearly 5000 people enrolled in 14 established, ongoing research programs, including the 76-year-old Framingham Heart Study. The results of the analysis of the “mega-cohort” were published in JAMA Network Open.
Most of the 14 studies already had 10-20 years of data on the cardiac health of thousands of enrollees, said Norrina B. Allen, one of the authors and a cardiac epidemiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“This is a particularly strong study that looked at risk factors — or individual health — prior to developing COVID and their impact on the likely of recovering from COVID,” she said.
In addition to those with CVD, women and adults with preexisting chronic illnesses took longer to recover.
More than 20% of those in the large, racially and ethnically diverse US population–based study did not recover from COVID in 90 days. The researchers found that the median self-reported time to recovery from acute infection was 20 days.
While women and those with chronic illness had a higher risk for long COVID, vaccination and infection with the Omicron variant wave were associated with shorter recovery times.
These findings make sense, said Ziyad Al-Aly, MD, chief of research at Veterans Affairs St. Louis Health Care System and clinical epidemiologist at Washington University in St. Louis, Missouri.
“We also see that COVID-19 can lead to new-onset cardiovascular disease,” said Al-Aly, who was not involved in the study. “There is clearly a (link) between COVID and cardiovascular disease. These two seem to be intimately intertwined. In my view, this emphasizes the importance of targeting these individuals for vaccination and potentially antivirals (when they get infected) to help reduce their risk of adverse events and ameliorate their chance of full and fast recovery.”
The study used data from the Collaborative Cohort of Cohorts for COVID-19 Research. The long list of researchers contributing to this study includes epidemiologists, biostatisticians, neurologists, pulmonologists, and cardiologists. The data come from a list of cohorts like the Framingham Heart Study, which identified key risk factors for CVD, including cholesterol levels. Other studies include the Atherosclerosis Risk in Communities study, which began in the mid-1980s. Researchers there recruited a cohort of 15,792 men and women in rural North Carolina and Mississippi and suburban Minneapolis. They enrolled a high number of African American participants, who have been underrepresented in past studies. Other cohorts focused on young adults with CVD and Hispanics, while another focused on people with chronic obstructive pulmonary disease.
Lead author Elizabeth C. Oelsner, MD, of Columbia University Irving Medical Center in New York City, said she was not surprised by the CVD-long COVID link.
“We were aware that individuals with CVD were at higher risk of a more severe acute infection,” she said. “We were also seeing evidence that long and severe infection led to persistent symptoms.”
Oelsner noted that many patients still take more than 3 months to recover, even during the Omicron wave.
“While that has improved over the course of the pandemic, many individuals are taking a very long time to recover, and that can have a huge burden on the patient,” she said.
She encourages healthcare providers to tell patients at higher risk to take steps to avoid the virus, including vaccination and boosters.
A version of this article first appeared on Medscape.com.
Primary care doctors and specialists should advise patients who have already experienced a heart attack or stroke that they are at a higher risk for long COVID and need to take steps to avoid contracting the virus, according to new research.
The study, led by researchers at Columbia University, New York City, suggests that anyone with cardiovascular disease (CVD) — defined as having experienced a heart attack or stroke — should consider getting the updated COVID vaccine boosters. They also suggest patients with CVD take other steps to avoid an acute infection, such as avoiding crowded indoor spaces.
There is no specific test or treatment for long COVID, which can become disabling and chronic. Long COVID is defined by the failure to recover from acute COVID-19 in 90 days.
The scientists used data from nearly 5000 people enrolled in 14 established, ongoing research programs, including the 76-year-old Framingham Heart Study. The results of the analysis of the “mega-cohort” were published in JAMA Network Open.
Most of the 14 studies already had 10-20 years of data on the cardiac health of thousands of enrollees, said Norrina B. Allen, one of the authors and a cardiac epidemiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“This is a particularly strong study that looked at risk factors — or individual health — prior to developing COVID and their impact on the likely of recovering from COVID,” she said.
In addition to those with CVD, women and adults with preexisting chronic illnesses took longer to recover.
More than 20% of those in the large, racially and ethnically diverse US population–based study did not recover from COVID in 90 days. The researchers found that the median self-reported time to recovery from acute infection was 20 days.
While women and those with chronic illness had a higher risk for long COVID, vaccination and infection with the Omicron variant wave were associated with shorter recovery times.
These findings make sense, said Ziyad Al-Aly, MD, chief of research at Veterans Affairs St. Louis Health Care System and clinical epidemiologist at Washington University in St. Louis, Missouri.
“We also see that COVID-19 can lead to new-onset cardiovascular disease,” said Al-Aly, who was not involved in the study. “There is clearly a (link) between COVID and cardiovascular disease. These two seem to be intimately intertwined. In my view, this emphasizes the importance of targeting these individuals for vaccination and potentially antivirals (when they get infected) to help reduce their risk of adverse events and ameliorate their chance of full and fast recovery.”
The study used data from the Collaborative Cohort of Cohorts for COVID-19 Research. The long list of researchers contributing to this study includes epidemiologists, biostatisticians, neurologists, pulmonologists, and cardiologists. The data come from a list of cohorts like the Framingham Heart Study, which identified key risk factors for CVD, including cholesterol levels. Other studies include the Atherosclerosis Risk in Communities study, which began in the mid-1980s. Researchers there recruited a cohort of 15,792 men and women in rural North Carolina and Mississippi and suburban Minneapolis. They enrolled a high number of African American participants, who have been underrepresented in past studies. Other cohorts focused on young adults with CVD and Hispanics, while another focused on people with chronic obstructive pulmonary disease.
Lead author Elizabeth C. Oelsner, MD, of Columbia University Irving Medical Center in New York City, said she was not surprised by the CVD-long COVID link.
“We were aware that individuals with CVD were at higher risk of a more severe acute infection,” she said. “We were also seeing evidence that long and severe infection led to persistent symptoms.”
Oelsner noted that many patients still take more than 3 months to recover, even during the Omicron wave.
“While that has improved over the course of the pandemic, many individuals are taking a very long time to recover, and that can have a huge burden on the patient,” she said.
She encourages healthcare providers to tell patients at higher risk to take steps to avoid the virus, including vaccination and boosters.
A version of this article first appeared on Medscape.com.
Primary care doctors and specialists should advise patients who have already experienced a heart attack or stroke that they are at a higher risk for long COVID and need to take steps to avoid contracting the virus, according to new research.
The study, led by researchers at Columbia University, New York City, suggests that anyone with cardiovascular disease (CVD) — defined as having experienced a heart attack or stroke — should consider getting the updated COVID vaccine boosters. They also suggest patients with CVD take other steps to avoid an acute infection, such as avoiding crowded indoor spaces.
There is no specific test or treatment for long COVID, which can become disabling and chronic. Long COVID is defined by the failure to recover from acute COVID-19 in 90 days.
The scientists used data from nearly 5000 people enrolled in 14 established, ongoing research programs, including the 76-year-old Framingham Heart Study. The results of the analysis of the “mega-cohort” were published in JAMA Network Open.
Most of the 14 studies already had 10-20 years of data on the cardiac health of thousands of enrollees, said Norrina B. Allen, one of the authors and a cardiac epidemiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“This is a particularly strong study that looked at risk factors — or individual health — prior to developing COVID and their impact on the likely of recovering from COVID,” she said.
In addition to those with CVD, women and adults with preexisting chronic illnesses took longer to recover.
More than 20% of those in the large, racially and ethnically diverse US population–based study did not recover from COVID in 90 days. The researchers found that the median self-reported time to recovery from acute infection was 20 days.
While women and those with chronic illness had a higher risk for long COVID, vaccination and infection with the Omicron variant wave were associated with shorter recovery times.
These findings make sense, said Ziyad Al-Aly, MD, chief of research at Veterans Affairs St. Louis Health Care System and clinical epidemiologist at Washington University in St. Louis, Missouri.
“We also see that COVID-19 can lead to new-onset cardiovascular disease,” said Al-Aly, who was not involved in the study. “There is clearly a (link) between COVID and cardiovascular disease. These two seem to be intimately intertwined. In my view, this emphasizes the importance of targeting these individuals for vaccination and potentially antivirals (when they get infected) to help reduce their risk of adverse events and ameliorate their chance of full and fast recovery.”
The study used data from the Collaborative Cohort of Cohorts for COVID-19 Research. The long list of researchers contributing to this study includes epidemiologists, biostatisticians, neurologists, pulmonologists, and cardiologists. The data come from a list of cohorts like the Framingham Heart Study, which identified key risk factors for CVD, including cholesterol levels. Other studies include the Atherosclerosis Risk in Communities study, which began in the mid-1980s. Researchers there recruited a cohort of 15,792 men and women in rural North Carolina and Mississippi and suburban Minneapolis. They enrolled a high number of African American participants, who have been underrepresented in past studies. Other cohorts focused on young adults with CVD and Hispanics, while another focused on people with chronic obstructive pulmonary disease.
Lead author Elizabeth C. Oelsner, MD, of Columbia University Irving Medical Center in New York City, said she was not surprised by the CVD-long COVID link.
“We were aware that individuals with CVD were at higher risk of a more severe acute infection,” she said. “We were also seeing evidence that long and severe infection led to persistent symptoms.”
Oelsner noted that many patients still take more than 3 months to recover, even during the Omicron wave.
“While that has improved over the course of the pandemic, many individuals are taking a very long time to recover, and that can have a huge burden on the patient,” she said.
She encourages healthcare providers to tell patients at higher risk to take steps to avoid the virus, including vaccination and boosters.
A version of this article first appeared on Medscape.com.
Sperm Appear to Have a Nonreproductive Function
Brazilian researchers have identified a previously unrecognized function of sperm that is unrelated to reproduction. A study of 13 patients admitted to the Hospital das Clínicas da Universidade de São Paulo with moderate to severe COVID-19 showed that male gametes released extracellular traps (in a process called ETosis) in response to the infection. This immune response, which is common to macrophages and neutrophils, had never been observed in mammalian reproductive cells.
“It opens up a new line of research,” said Jorge Hallak, a professor at the University of São Paulo School of Medicine, São Paulo, Brazil, and first author of the article published in Andrology. “This may be an innovative mechanism, or it may have always existed, and no one knew.”
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified in cells more than 3 months after infection in 11 participants, although polymerase chain reaction tests were negative. These findings suggest the potential for drafting a protocol or guidance on when to attempt a pregnancy. “My concern is with assisted reproduction, in which, in general, only one basic spermogram is done, without diagnostic investigation or serology for coronavirus,” said Hallak.
Symptomatic infections hinder the reproductive process because symptoms such as high fever impair cell function by triggering increased DNA fragmentation, reduced mitochondrial activity, decreased acrosome reaction, and cell death, thus affecting sperm count and gamete mobility.
The new findings indicate that the impact of SARS-CoV-2 infection can continue for as long as 90 days after symptoms and signs disappear and affect sperm count and gamete quality for even longer. “With the sperm selection technique, you are at risk of taking a cell with viruses and injecting it into the egg. It is not known what changes this may cause to the embryo,” said Hallak.
The expert emphasized that the finding contributes to the understanding of reproductive difficulties that previously had no plausible explanation. It serves as a warning against negligence in the evaluation of men in assisted reproductive treatments.
Daniel Zylberstein, urologist and member of the Brazilian Association of Assisted Reproduction, who did not participate in the research, noted that the result comes from a small study that should be expanded to try to develop guidance for doctors.
“There is still no protocol for these cases. The ideal approach would be to wait for complete spermatogenesis, which takes about 3 months, before putting patients on treatment. This often does not happen, and treatment begins shortly after clinical recovery. In the case of moderate to severe COVID-19, this period should be longer than 90 days,” he said.
The study suggests establishing a quarantine period for reproduction until the sperm are free of the virus, said Zylberstein. “With infected sperm, it makes no sense to start reproductive treatment. This sperm is spending energy to fight the pathogen. Assisted reproduction is expensive and exhaustive and may not have the expected outcome because of SARS-CoV-2 infectivity.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Brazilian researchers have identified a previously unrecognized function of sperm that is unrelated to reproduction. A study of 13 patients admitted to the Hospital das Clínicas da Universidade de São Paulo with moderate to severe COVID-19 showed that male gametes released extracellular traps (in a process called ETosis) in response to the infection. This immune response, which is common to macrophages and neutrophils, had never been observed in mammalian reproductive cells.
“It opens up a new line of research,” said Jorge Hallak, a professor at the University of São Paulo School of Medicine, São Paulo, Brazil, and first author of the article published in Andrology. “This may be an innovative mechanism, or it may have always existed, and no one knew.”
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified in cells more than 3 months after infection in 11 participants, although polymerase chain reaction tests were negative. These findings suggest the potential for drafting a protocol or guidance on when to attempt a pregnancy. “My concern is with assisted reproduction, in which, in general, only one basic spermogram is done, without diagnostic investigation or serology for coronavirus,” said Hallak.
Symptomatic infections hinder the reproductive process because symptoms such as high fever impair cell function by triggering increased DNA fragmentation, reduced mitochondrial activity, decreased acrosome reaction, and cell death, thus affecting sperm count and gamete mobility.
The new findings indicate that the impact of SARS-CoV-2 infection can continue for as long as 90 days after symptoms and signs disappear and affect sperm count and gamete quality for even longer. “With the sperm selection technique, you are at risk of taking a cell with viruses and injecting it into the egg. It is not known what changes this may cause to the embryo,” said Hallak.
The expert emphasized that the finding contributes to the understanding of reproductive difficulties that previously had no plausible explanation. It serves as a warning against negligence in the evaluation of men in assisted reproductive treatments.
Daniel Zylberstein, urologist and member of the Brazilian Association of Assisted Reproduction, who did not participate in the research, noted that the result comes from a small study that should be expanded to try to develop guidance for doctors.
“There is still no protocol for these cases. The ideal approach would be to wait for complete spermatogenesis, which takes about 3 months, before putting patients on treatment. This often does not happen, and treatment begins shortly after clinical recovery. In the case of moderate to severe COVID-19, this period should be longer than 90 days,” he said.
The study suggests establishing a quarantine period for reproduction until the sperm are free of the virus, said Zylberstein. “With infected sperm, it makes no sense to start reproductive treatment. This sperm is spending energy to fight the pathogen. Assisted reproduction is expensive and exhaustive and may not have the expected outcome because of SARS-CoV-2 infectivity.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Brazilian researchers have identified a previously unrecognized function of sperm that is unrelated to reproduction. A study of 13 patients admitted to the Hospital das Clínicas da Universidade de São Paulo with moderate to severe COVID-19 showed that male gametes released extracellular traps (in a process called ETosis) in response to the infection. This immune response, which is common to macrophages and neutrophils, had never been observed in mammalian reproductive cells.
“It opens up a new line of research,” said Jorge Hallak, a professor at the University of São Paulo School of Medicine, São Paulo, Brazil, and first author of the article published in Andrology. “This may be an innovative mechanism, or it may have always existed, and no one knew.”
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified in cells more than 3 months after infection in 11 participants, although polymerase chain reaction tests were negative. These findings suggest the potential for drafting a protocol or guidance on when to attempt a pregnancy. “My concern is with assisted reproduction, in which, in general, only one basic spermogram is done, without diagnostic investigation or serology for coronavirus,” said Hallak.
Symptomatic infections hinder the reproductive process because symptoms such as high fever impair cell function by triggering increased DNA fragmentation, reduced mitochondrial activity, decreased acrosome reaction, and cell death, thus affecting sperm count and gamete mobility.
The new findings indicate that the impact of SARS-CoV-2 infection can continue for as long as 90 days after symptoms and signs disappear and affect sperm count and gamete quality for even longer. “With the sperm selection technique, you are at risk of taking a cell with viruses and injecting it into the egg. It is not known what changes this may cause to the embryo,” said Hallak.
The expert emphasized that the finding contributes to the understanding of reproductive difficulties that previously had no plausible explanation. It serves as a warning against negligence in the evaluation of men in assisted reproductive treatments.
Daniel Zylberstein, urologist and member of the Brazilian Association of Assisted Reproduction, who did not participate in the research, noted that the result comes from a small study that should be expanded to try to develop guidance for doctors.
“There is still no protocol for these cases. The ideal approach would be to wait for complete spermatogenesis, which takes about 3 months, before putting patients on treatment. This often does not happen, and treatment begins shortly after clinical recovery. In the case of moderate to severe COVID-19, this period should be longer than 90 days,” he said.
The study suggests establishing a quarantine period for reproduction until the sperm are free of the virus, said Zylberstein. “With infected sperm, it makes no sense to start reproductive treatment. This sperm is spending energy to fight the pathogen. Assisted reproduction is expensive and exhaustive and may not have the expected outcome because of SARS-CoV-2 infectivity.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
FROM ANDROLOGY
Maternal Immunization to Prevent Serious Respiratory Illness
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.

Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.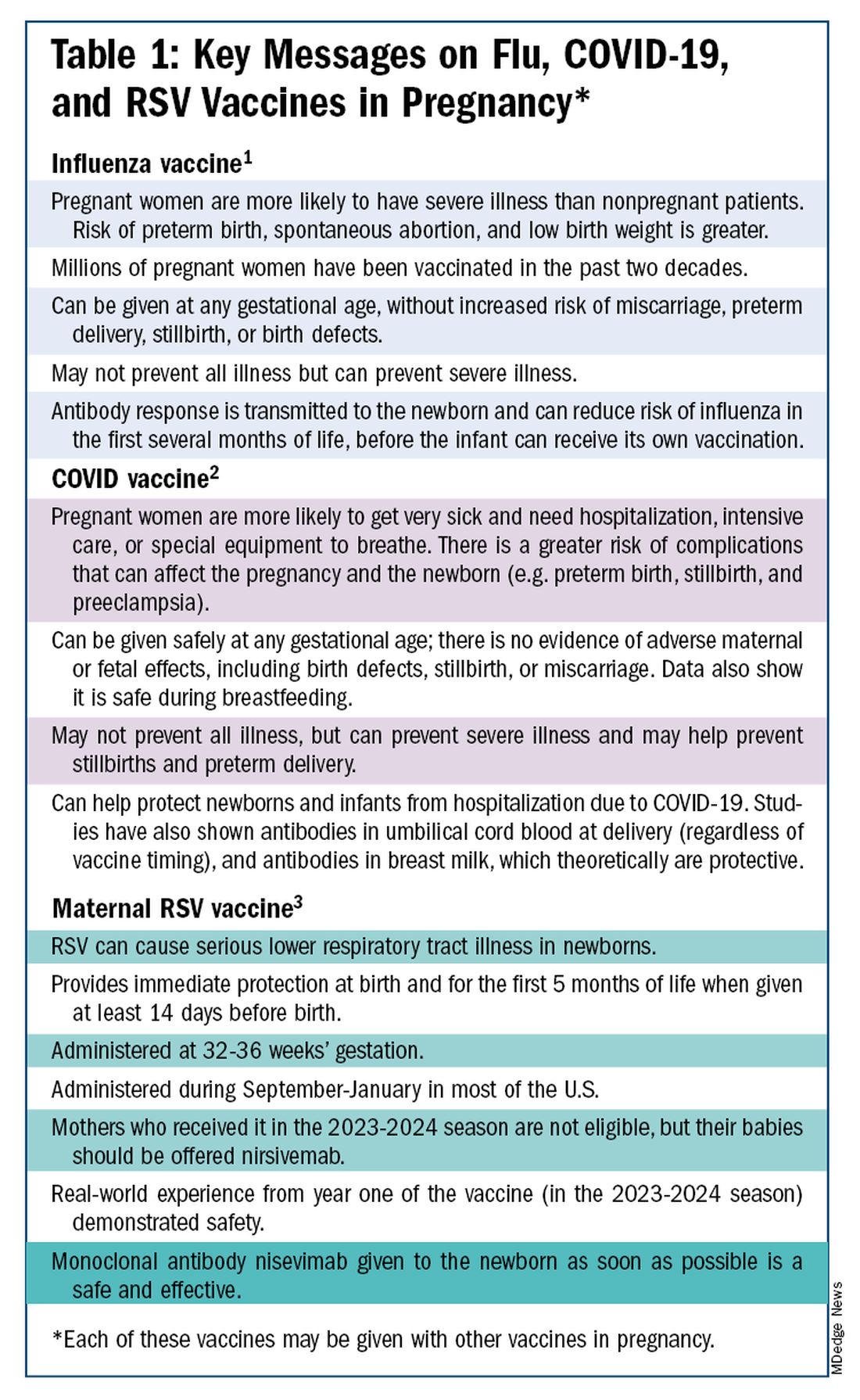
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.

With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)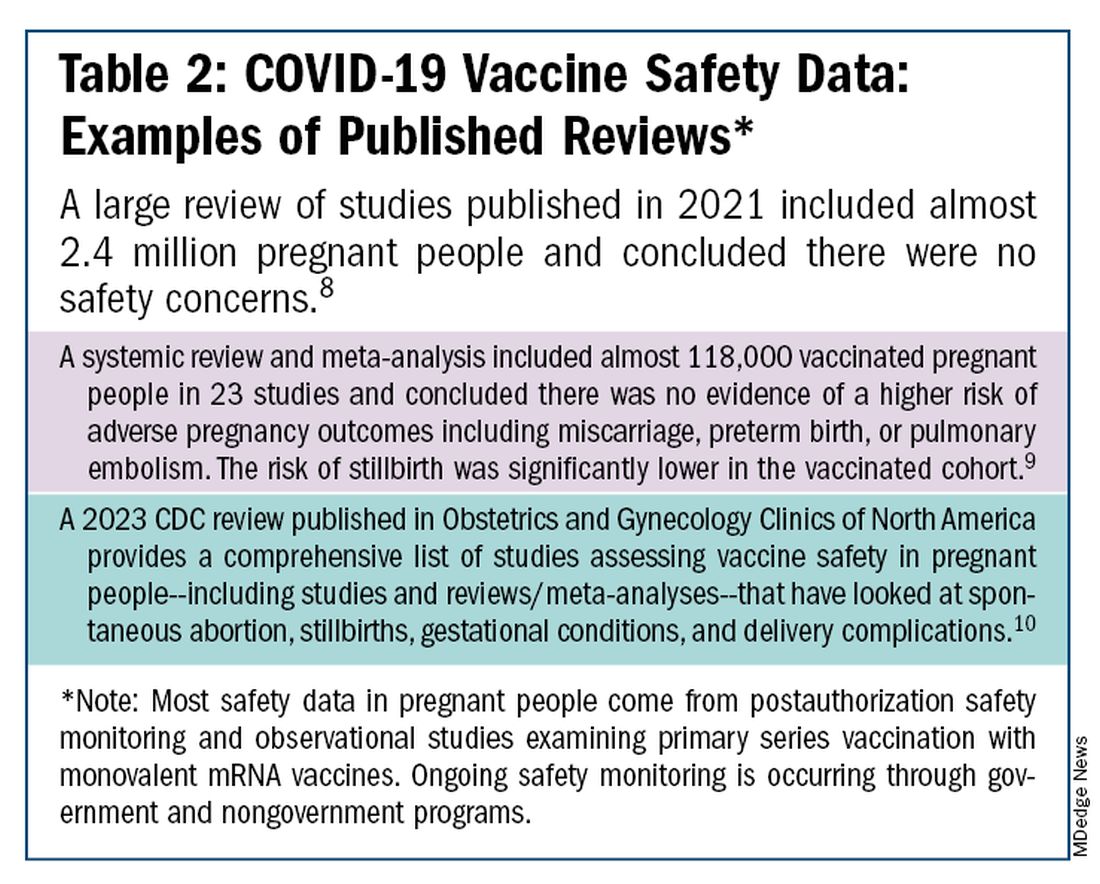
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.
Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.
With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.
Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.
With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
COVID-19 Booster Vaccine Shortens Menstrual Cycles in Teens
TOPLINE:
The vaccine did not appear to be associated with shifts in menstrual flow, pain, or other symptoms.
METHODOLOGY:
- Reports of menstrual cycle changes following the COVID-19 vaccination began to emerge in early 2021, raising concerns about the impact of the vaccine on menstrual health.
- Researchers conducted a prospective study including 65 adolescent girls (mean age, 17.3 years), of whom 47 had received an initial series of COVID-19 vaccination at least 6 months prior to receiving a booster dose (booster group), and 18 had not received the booster vaccine (control group), two of whom had never received any COVID-19 vaccine, four who had received an initial vaccine but not a booster, and 12 who had received an initial vaccine and booster but more than 6 months prior to the study.
- Menstrual cycle length was measured for three cycles prior to and four cycles after vaccination in the booster group and for seven cycles in the control group.
- Menstrual flow, pain, and stress were measured at baseline and monthly for 3 months post vaccination.
TAKEAWAY:
- Participants in the booster group experienced shorter cycles by an average of 5.35 days after receiving the COVID-19 booster vaccine (P = .03), particularly during the second cycle. In contrast, those in the control group did not experience any changes in the menstrual cycle length.
- Receiving the booster dose in the follicular phase was associated with significantly shorter menstrual cycles, compared with pre-booster cycles (P = .0157).
- Menstrual flow, pain, and other symptoms remained unaffected after the COVID-19 booster vaccination.
- Higher stress levels at baseline were also associated with a shorter length of the menstrual cycle (P = .03) in both groups, regardless of the booster vaccination status.
IN PRACTICE:
“These data are potentially important for counseling parents regarding potential vaccine refusal in the future for their teen daughters,” the authors wrote.
SOURCE:
This study was led by Laura A. Payne, PhD, from McLean Hospital in Boston, and was published online in the Journal of Adolescent Health.
LIMITATIONS:
The sample size for the booster and control groups was relatively small and homogeneous. The study did not include the height, weight, birth control use, or other chronic conditions of the participants, which may have influenced the functioning of the menstrual cycle. The control group included a majority of teens who had previously received a vaccine and even a booster, which could have affected results.
DISCLOSURES:
This study was supported by grants from the Eunice Kennedy Shriver National Institute for Child Health and Human Development. Some authors received consulting fees, travel reimbursements, honoraria, research funding, and royalties from Bayer Healthcare, Mahana Therapeutics, Gates, and Merck, among others.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
The vaccine did not appear to be associated with shifts in menstrual flow, pain, or other symptoms.
METHODOLOGY:
- Reports of menstrual cycle changes following the COVID-19 vaccination began to emerge in early 2021, raising concerns about the impact of the vaccine on menstrual health.
- Researchers conducted a prospective study including 65 adolescent girls (mean age, 17.3 years), of whom 47 had received an initial series of COVID-19 vaccination at least 6 months prior to receiving a booster dose (booster group), and 18 had not received the booster vaccine (control group), two of whom had never received any COVID-19 vaccine, four who had received an initial vaccine but not a booster, and 12 who had received an initial vaccine and booster but more than 6 months prior to the study.
- Menstrual cycle length was measured for three cycles prior to and four cycles after vaccination in the booster group and for seven cycles in the control group.
- Menstrual flow, pain, and stress were measured at baseline and monthly for 3 months post vaccination.
TAKEAWAY:
- Participants in the booster group experienced shorter cycles by an average of 5.35 days after receiving the COVID-19 booster vaccine (P = .03), particularly during the second cycle. In contrast, those in the control group did not experience any changes in the menstrual cycle length.
- Receiving the booster dose in the follicular phase was associated with significantly shorter menstrual cycles, compared with pre-booster cycles (P = .0157).
- Menstrual flow, pain, and other symptoms remained unaffected after the COVID-19 booster vaccination.
- Higher stress levels at baseline were also associated with a shorter length of the menstrual cycle (P = .03) in both groups, regardless of the booster vaccination status.
IN PRACTICE:
“These data are potentially important for counseling parents regarding potential vaccine refusal in the future for their teen daughters,” the authors wrote.
SOURCE:
This study was led by Laura A. Payne, PhD, from McLean Hospital in Boston, and was published online in the Journal of Adolescent Health.
LIMITATIONS:
The sample size for the booster and control groups was relatively small and homogeneous. The study did not include the height, weight, birth control use, or other chronic conditions of the participants, which may have influenced the functioning of the menstrual cycle. The control group included a majority of teens who had previously received a vaccine and even a booster, which could have affected results.
DISCLOSURES:
This study was supported by grants from the Eunice Kennedy Shriver National Institute for Child Health and Human Development. Some authors received consulting fees, travel reimbursements, honoraria, research funding, and royalties from Bayer Healthcare, Mahana Therapeutics, Gates, and Merck, among others.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
The vaccine did not appear to be associated with shifts in menstrual flow, pain, or other symptoms.
METHODOLOGY:
- Reports of menstrual cycle changes following the COVID-19 vaccination began to emerge in early 2021, raising concerns about the impact of the vaccine on menstrual health.
- Researchers conducted a prospective study including 65 adolescent girls (mean age, 17.3 years), of whom 47 had received an initial series of COVID-19 vaccination at least 6 months prior to receiving a booster dose (booster group), and 18 had not received the booster vaccine (control group), two of whom had never received any COVID-19 vaccine, four who had received an initial vaccine but not a booster, and 12 who had received an initial vaccine and booster but more than 6 months prior to the study.
- Menstrual cycle length was measured for three cycles prior to and four cycles after vaccination in the booster group and for seven cycles in the control group.
- Menstrual flow, pain, and stress were measured at baseline and monthly for 3 months post vaccination.
TAKEAWAY:
- Participants in the booster group experienced shorter cycles by an average of 5.35 days after receiving the COVID-19 booster vaccine (P = .03), particularly during the second cycle. In contrast, those in the control group did not experience any changes in the menstrual cycle length.
- Receiving the booster dose in the follicular phase was associated with significantly shorter menstrual cycles, compared with pre-booster cycles (P = .0157).
- Menstrual flow, pain, and other symptoms remained unaffected after the COVID-19 booster vaccination.
- Higher stress levels at baseline were also associated with a shorter length of the menstrual cycle (P = .03) in both groups, regardless of the booster vaccination status.
IN PRACTICE:
“These data are potentially important for counseling parents regarding potential vaccine refusal in the future for their teen daughters,” the authors wrote.
SOURCE:
This study was led by Laura A. Payne, PhD, from McLean Hospital in Boston, and was published online in the Journal of Adolescent Health.
LIMITATIONS:
The sample size for the booster and control groups was relatively small and homogeneous. The study did not include the height, weight, birth control use, or other chronic conditions of the participants, which may have influenced the functioning of the menstrual cycle. The control group included a majority of teens who had previously received a vaccine and even a booster, which could have affected results.
DISCLOSURES:
This study was supported by grants from the Eunice Kennedy Shriver National Institute for Child Health and Human Development. Some authors received consulting fees, travel reimbursements, honoraria, research funding, and royalties from Bayer Healthcare, Mahana Therapeutics, Gates, and Merck, among others.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Viral Season 2024-2025: Try for An Ounce of Prevention
We are quickly approaching the typical cold and flu season. But can we call anything typical since 2020? Since 2020, there have been different recommendations for prevention, testing, return to work, and treatment since our world was rocked by the pandemic. Now that we are in the “post-pandemic” era, family physicians and other primary care professionals are the front line for discussions on prevention, evaluation, and treatment of the typical upper-respiratory infections, influenza, and COVID-19.
Let’s start with prevention. We have all heard the old adage, an ounce of prevention is worth a pound of cure. In primary care, we need to focus on prevention. Vaccination is often one of our best tools against the myriad of infections we are hoping to help patients prevent during cold and flu season. Most recently, we have fall vaccinations aimed to prevent COVID-19, influenza, and respiratory syncytial virus (RSV).
The number and timing of each of these vaccinations has different recommendations based on a variety of factors including age, pregnancy status, and whether or not the patient is immunocompromised. For the 2024-2025 season, the Centers for Disease Control and Prevention has recommended updated vaccines for both influenza and COVID-19.1
They have also updated the RSV vaccine recommendations to “People 75 or older, or between 60-74 with certain chronic health conditions or living in a nursing home should get one dose of the RSV vaccine to provide an extra layer of protection.”2
In addition to vaccines as prevention, there is also hygiene, staying home when sick and away from others who are sick, following guidelines for where and when to wear a face mask, and the general tools of eating well, and getting sufficient sleep and exercise to help maintain the healthiest immune system.
Despite the best of intentions, there will still be many who experience viral infections in this upcoming season. The CDC is currently recommending persons to stay away from others for at least 24 hours after their symptoms improve and they are fever-free without antipyretics. In addition to isolation while sick, general symptom management is something that we can recommend for all of these illnesses.
There is more to consider, though, as our patients face these illnesses. The first question is how to determine the diagnosis — and if that diagnosis is even necessary. Unfortunately, many of these viral illnesses can look the same. They can all cause fevers, chills, and other upper respiratory symptoms. They are all fairly contagious. All of these viruses can cause serious illness associated with additional complications. It is not truly possible to determine which virus someone has by symptoms alone, our patients can have multiple viruses at the same time and diagnosis of one does not preclude having another.3
Instead, we truly do need a test for diagnosis. In-office testing is available for RSV, influenza, and COVID-19. Additionally, despite not being as freely available as they were during the pandemic, patients are able to do home COVID tests and then call in with their results. At the time of writing this, at-home rapid influenza tests have also been approved by the FDA but are not yet readily available to the public. These tests are important for determining if the patient is eligible for treatment. Both influenza and COVID-19 have antiviral treatments available to help decrease the severity of the illness and potentially the length of illness and time contagious. According to the CDC, both treatments are underutilized.
This could be because of a lack of testing and diagnosis. It may also be because of a lack of familiarity with the available treatments.4,5
Influenza treatment is recommended as soon as possible for those with suspected or confirmed diagnosis, immediately for anyone hospitalized, anyone with severe, complicated, or progressing illness, and for those at high risk of severe illness including but not limited to those under 2 years old, those over 65, those who are pregnant, and those with many chronic conditions.
Treatment can also be used for those who are not high risk when diagnosed within 48 hours. In the United States, four antivirals are recommended to treat influenza: oseltamivir phosphate, zanamivir, peramivir, and baloxavir marboxil. For COVID-19, treatments are also available for mild or moderate disease in those at risk for severe disease. Both remdesivir and nimatrelvir with ritonavir are treatment options that can be used for COVID-19 infection. Unfortunately, no specific antiviral is available for the other viral illnesses we see often during this season.
In primary care, we have some important roles to play. We need to continue to discuss all methods of prevention. Not only do vaccine recommendations change at least annually, our patients’ situations change and we have to reassess them. Additionally, people often need to hear things more than once before committing — so it never hurts to continue having those conversations. Combining the conversation about vaccines with other prevention measures is also important so that it does not seem like we are only recommending one thing. We should also start talking about treatment options before our patients are sick. We can communicate what is available as long as they let us know they are sick early. We can also be there to help our patients determine when they are at risk for severe illness and when they should consider a higher level of care.
The availability of home testing gives us the opportunity to provide these treatments via telehealth and even potentially in times when these illnesses are everywhere — with standing orders with our clinical teams. Although it is a busy time for us in the clinic, “cold and flu” season is definitely one of those times when our primary care relationship can truly help our patients.
References
1. CDC Recommends Updated 2024-2025 COVID-19 and Flu Vaccines for Fall/Winter Virus Season. https://www.cdc.gov/media/releases/2024/s-t0627-vaccine-recommendations.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
2. CDC Updates RSV Vaccination Recommendation for Adults. https://www.cdc.gov/media/releases/2024/s-0626-vaccination-adults.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
3. Similarities and Differences between Flu and COVID-19. https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases.
4. Respiratory Virus Guidance. https://www.cdc.gov/respiratory-viruses/guidance/index.html. Accessed August 9, 2024. Source: National Center for Immunization and Respiratory Diseases.
5. Provider Toolkit: Preparing Patients for the Fall and Winter Virus Season. https://www.cdc.gov/respiratory-viruses/hcp/tools-resources/index.html. Accessed August 9, 2024. Source: Centers for Disease Control and Prevention.
We are quickly approaching the typical cold and flu season. But can we call anything typical since 2020? Since 2020, there have been different recommendations for prevention, testing, return to work, and treatment since our world was rocked by the pandemic. Now that we are in the “post-pandemic” era, family physicians and other primary care professionals are the front line for discussions on prevention, evaluation, and treatment of the typical upper-respiratory infections, influenza, and COVID-19.
Let’s start with prevention. We have all heard the old adage, an ounce of prevention is worth a pound of cure. In primary care, we need to focus on prevention. Vaccination is often one of our best tools against the myriad of infections we are hoping to help patients prevent during cold and flu season. Most recently, we have fall vaccinations aimed to prevent COVID-19, influenza, and respiratory syncytial virus (RSV).
The number and timing of each of these vaccinations has different recommendations based on a variety of factors including age, pregnancy status, and whether or not the patient is immunocompromised. For the 2024-2025 season, the Centers for Disease Control and Prevention has recommended updated vaccines for both influenza and COVID-19.1
They have also updated the RSV vaccine recommendations to “People 75 or older, or between 60-74 with certain chronic health conditions or living in a nursing home should get one dose of the RSV vaccine to provide an extra layer of protection.”2
In addition to vaccines as prevention, there is also hygiene, staying home when sick and away from others who are sick, following guidelines for where and when to wear a face mask, and the general tools of eating well, and getting sufficient sleep and exercise to help maintain the healthiest immune system.
Despite the best of intentions, there will still be many who experience viral infections in this upcoming season. The CDC is currently recommending persons to stay away from others for at least 24 hours after their symptoms improve and they are fever-free without antipyretics. In addition to isolation while sick, general symptom management is something that we can recommend for all of these illnesses.
There is more to consider, though, as our patients face these illnesses. The first question is how to determine the diagnosis — and if that diagnosis is even necessary. Unfortunately, many of these viral illnesses can look the same. They can all cause fevers, chills, and other upper respiratory symptoms. They are all fairly contagious. All of these viruses can cause serious illness associated with additional complications. It is not truly possible to determine which virus someone has by symptoms alone, our patients can have multiple viruses at the same time and diagnosis of one does not preclude having another.3
Instead, we truly do need a test for diagnosis. In-office testing is available for RSV, influenza, and COVID-19. Additionally, despite not being as freely available as they were during the pandemic, patients are able to do home COVID tests and then call in with their results. At the time of writing this, at-home rapid influenza tests have also been approved by the FDA but are not yet readily available to the public. These tests are important for determining if the patient is eligible for treatment. Both influenza and COVID-19 have antiviral treatments available to help decrease the severity of the illness and potentially the length of illness and time contagious. According to the CDC, both treatments are underutilized.
This could be because of a lack of testing and diagnosis. It may also be because of a lack of familiarity with the available treatments.4,5
Influenza treatment is recommended as soon as possible for those with suspected or confirmed diagnosis, immediately for anyone hospitalized, anyone with severe, complicated, or progressing illness, and for those at high risk of severe illness including but not limited to those under 2 years old, those over 65, those who are pregnant, and those with many chronic conditions.
Treatment can also be used for those who are not high risk when diagnosed within 48 hours. In the United States, four antivirals are recommended to treat influenza: oseltamivir phosphate, zanamivir, peramivir, and baloxavir marboxil. For COVID-19, treatments are also available for mild or moderate disease in those at risk for severe disease. Both remdesivir and nimatrelvir with ritonavir are treatment options that can be used for COVID-19 infection. Unfortunately, no specific antiviral is available for the other viral illnesses we see often during this season.
In primary care, we have some important roles to play. We need to continue to discuss all methods of prevention. Not only do vaccine recommendations change at least annually, our patients’ situations change and we have to reassess them. Additionally, people often need to hear things more than once before committing — so it never hurts to continue having those conversations. Combining the conversation about vaccines with other prevention measures is also important so that it does not seem like we are only recommending one thing. We should also start talking about treatment options before our patients are sick. We can communicate what is available as long as they let us know they are sick early. We can also be there to help our patients determine when they are at risk for severe illness and when they should consider a higher level of care.
The availability of home testing gives us the opportunity to provide these treatments via telehealth and even potentially in times when these illnesses are everywhere — with standing orders with our clinical teams. Although it is a busy time for us in the clinic, “cold and flu” season is definitely one of those times when our primary care relationship can truly help our patients.
References
1. CDC Recommends Updated 2024-2025 COVID-19 and Flu Vaccines for Fall/Winter Virus Season. https://www.cdc.gov/media/releases/2024/s-t0627-vaccine-recommendations.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
2. CDC Updates RSV Vaccination Recommendation for Adults. https://www.cdc.gov/media/releases/2024/s-0626-vaccination-adults.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
3. Similarities and Differences between Flu and COVID-19. https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases.
4. Respiratory Virus Guidance. https://www.cdc.gov/respiratory-viruses/guidance/index.html. Accessed August 9, 2024. Source: National Center for Immunization and Respiratory Diseases.
5. Provider Toolkit: Preparing Patients for the Fall and Winter Virus Season. https://www.cdc.gov/respiratory-viruses/hcp/tools-resources/index.html. Accessed August 9, 2024. Source: Centers for Disease Control and Prevention.
We are quickly approaching the typical cold and flu season. But can we call anything typical since 2020? Since 2020, there have been different recommendations for prevention, testing, return to work, and treatment since our world was rocked by the pandemic. Now that we are in the “post-pandemic” era, family physicians and other primary care professionals are the front line for discussions on prevention, evaluation, and treatment of the typical upper-respiratory infections, influenza, and COVID-19.
Let’s start with prevention. We have all heard the old adage, an ounce of prevention is worth a pound of cure. In primary care, we need to focus on prevention. Vaccination is often one of our best tools against the myriad of infections we are hoping to help patients prevent during cold and flu season. Most recently, we have fall vaccinations aimed to prevent COVID-19, influenza, and respiratory syncytial virus (RSV).
The number and timing of each of these vaccinations has different recommendations based on a variety of factors including age, pregnancy status, and whether or not the patient is immunocompromised. For the 2024-2025 season, the Centers for Disease Control and Prevention has recommended updated vaccines for both influenza and COVID-19.1
They have also updated the RSV vaccine recommendations to “People 75 or older, or between 60-74 with certain chronic health conditions or living in a nursing home should get one dose of the RSV vaccine to provide an extra layer of protection.”2
In addition to vaccines as prevention, there is also hygiene, staying home when sick and away from others who are sick, following guidelines for where and when to wear a face mask, and the general tools of eating well, and getting sufficient sleep and exercise to help maintain the healthiest immune system.
Despite the best of intentions, there will still be many who experience viral infections in this upcoming season. The CDC is currently recommending persons to stay away from others for at least 24 hours after their symptoms improve and they are fever-free without antipyretics. In addition to isolation while sick, general symptom management is something that we can recommend for all of these illnesses.
There is more to consider, though, as our patients face these illnesses. The first question is how to determine the diagnosis — and if that diagnosis is even necessary. Unfortunately, many of these viral illnesses can look the same. They can all cause fevers, chills, and other upper respiratory symptoms. They are all fairly contagious. All of these viruses can cause serious illness associated with additional complications. It is not truly possible to determine which virus someone has by symptoms alone, our patients can have multiple viruses at the same time and diagnosis of one does not preclude having another.3
Instead, we truly do need a test for diagnosis. In-office testing is available for RSV, influenza, and COVID-19. Additionally, despite not being as freely available as they were during the pandemic, patients are able to do home COVID tests and then call in with their results. At the time of writing this, at-home rapid influenza tests have also been approved by the FDA but are not yet readily available to the public. These tests are important for determining if the patient is eligible for treatment. Both influenza and COVID-19 have antiviral treatments available to help decrease the severity of the illness and potentially the length of illness and time contagious. According to the CDC, both treatments are underutilized.
This could be because of a lack of testing and diagnosis. It may also be because of a lack of familiarity with the available treatments.4,5
Influenza treatment is recommended as soon as possible for those with suspected or confirmed diagnosis, immediately for anyone hospitalized, anyone with severe, complicated, or progressing illness, and for those at high risk of severe illness including but not limited to those under 2 years old, those over 65, those who are pregnant, and those with many chronic conditions.
Treatment can also be used for those who are not high risk when diagnosed within 48 hours. In the United States, four antivirals are recommended to treat influenza: oseltamivir phosphate, zanamivir, peramivir, and baloxavir marboxil. For COVID-19, treatments are also available for mild or moderate disease in those at risk for severe disease. Both remdesivir and nimatrelvir with ritonavir are treatment options that can be used for COVID-19 infection. Unfortunately, no specific antiviral is available for the other viral illnesses we see often during this season.
In primary care, we have some important roles to play. We need to continue to discuss all methods of prevention. Not only do vaccine recommendations change at least annually, our patients’ situations change and we have to reassess them. Additionally, people often need to hear things more than once before committing — so it never hurts to continue having those conversations. Combining the conversation about vaccines with other prevention measures is also important so that it does not seem like we are only recommending one thing. We should also start talking about treatment options before our patients are sick. We can communicate what is available as long as they let us know they are sick early. We can also be there to help our patients determine when they are at risk for severe illness and when they should consider a higher level of care.
The availability of home testing gives us the opportunity to provide these treatments via telehealth and even potentially in times when these illnesses are everywhere — with standing orders with our clinical teams. Although it is a busy time for us in the clinic, “cold and flu” season is definitely one of those times when our primary care relationship can truly help our patients.
References
1. CDC Recommends Updated 2024-2025 COVID-19 and Flu Vaccines for Fall/Winter Virus Season. https://www.cdc.gov/media/releases/2024/s-t0627-vaccine-recommendations.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
2. CDC Updates RSV Vaccination Recommendation for Adults. https://www.cdc.gov/media/releases/2024/s-0626-vaccination-adults.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
3. Similarities and Differences between Flu and COVID-19. https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases.
4. Respiratory Virus Guidance. https://www.cdc.gov/respiratory-viruses/guidance/index.html. Accessed August 9, 2024. Source: National Center for Immunization and Respiratory Diseases.
5. Provider Toolkit: Preparing Patients for the Fall and Winter Virus Season. https://www.cdc.gov/respiratory-viruses/hcp/tools-resources/index.html. Accessed August 9, 2024. Source: Centers for Disease Control and Prevention.
How Safe is Anti–IL-6 Therapy During Pregnancy?
TOPLINE:
The maternal and neonatal outcomes in pregnant women treated with anti–interleukin (IL)-6 therapy for COVID-19 are largely favorable, with transient neonatal cytopenia observed in around one third of the babies being the only possible adverse outcome that could be related to anti–IL-6 therapy.
METHODOLOGY:
- Despite guidance, very few pregnant women with COVID-19 are offered evidence-based therapies such as anti–IL-6 due to concerns regarding fetal safety in later pregnancy.
- In this retrospective study, researchers evaluated maternal and neonatal outcomes in 25 pregnant women with COVID-19 (mean age at admission, 33 years) treated with anti–IL-6 (tocilizumab or sarilumab) at two tertiary hospitals in London.
- Most women (n = 16) received anti–IL-6 in the third trimester of pregnancy, whereas nine received it during the second trimester.
- Maternal and neonatal outcomes were assessed through medical record reviews and maternal medicine networks, with follow-up for 12 months.
- The women included in the study constituted a high-risk population with severe COVID-19; 24 required level two or three critical care. All women were receiving at least three concomitant medications due to their critical illness.
TAKEAWAY:
- Overall, 24 of 25 women treated with IL-6 receptor antibodies survived until hospital discharge.
- The sole death occurred in a woman with severe COVID-19 pneumonitis who later developed myocarditis and cardiac arrest. The physicians believed that these complications were more likely due to severe COVID-19 rather than anti–IL-6 therapy.
- All pregnancies resulted in live births; however, 16 babies had to be delivered preterm due to COVID-19 complications.
- Transient cytopenia was observed in 6 of 19 babies in whom a full blood count was performed. All the six babies were premature, with cytopenia resolving within 7 days in four babies; one baby died from complications associated with extreme prematurity.
IN PRACTICE:
“Although the authors found mild, transitory cytopenia in some (6 of 19) exposed infants, most had been delivered prematurely due to progressive COVID-19–related morbidity, and distinguishing drug effects from similar prematurity-related effects is difficult,” wrote Steven L. Clark, MD, from the Department of Obstetrics and Gynecology, Baylor College of Medicine, Houston, in an accompanying editorial.
SOURCE:
The study was led by Melanie Nana, MRCP, from the Department of Obstetric Medicine, St Thomas’ Hospital, London, England. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study was retrospective in design, which may have introduced bias. The small sample size of 25 women may have limited the generalizability of the findings. Additionally, the study did not include a control group, which made it difficult to attribute outcomes solely to anti–IL-6 therapy. The lack of long-term follow-up data on the neonates also limited the understanding of potential long-term effects.
DISCLOSURES:
This study did not receive any funding. Some authors, including the lead author, received speaker fees, grants, or consultancy fees from academic institutions or pharmaceutical companies or had other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The maternal and neonatal outcomes in pregnant women treated with anti–interleukin (IL)-6 therapy for COVID-19 are largely favorable, with transient neonatal cytopenia observed in around one third of the babies being the only possible adverse outcome that could be related to anti–IL-6 therapy.
METHODOLOGY:
- Despite guidance, very few pregnant women with COVID-19 are offered evidence-based therapies such as anti–IL-6 due to concerns regarding fetal safety in later pregnancy.
- In this retrospective study, researchers evaluated maternal and neonatal outcomes in 25 pregnant women with COVID-19 (mean age at admission, 33 years) treated with anti–IL-6 (tocilizumab or sarilumab) at two tertiary hospitals in London.
- Most women (n = 16) received anti–IL-6 in the third trimester of pregnancy, whereas nine received it during the second trimester.
- Maternal and neonatal outcomes were assessed through medical record reviews and maternal medicine networks, with follow-up for 12 months.
- The women included in the study constituted a high-risk population with severe COVID-19; 24 required level two or three critical care. All women were receiving at least three concomitant medications due to their critical illness.
TAKEAWAY:
- Overall, 24 of 25 women treated with IL-6 receptor antibodies survived until hospital discharge.
- The sole death occurred in a woman with severe COVID-19 pneumonitis who later developed myocarditis and cardiac arrest. The physicians believed that these complications were more likely due to severe COVID-19 rather than anti–IL-6 therapy.
- All pregnancies resulted in live births; however, 16 babies had to be delivered preterm due to COVID-19 complications.
- Transient cytopenia was observed in 6 of 19 babies in whom a full blood count was performed. All the six babies were premature, with cytopenia resolving within 7 days in four babies; one baby died from complications associated with extreme prematurity.
IN PRACTICE:
“Although the authors found mild, transitory cytopenia in some (6 of 19) exposed infants, most had been delivered prematurely due to progressive COVID-19–related morbidity, and distinguishing drug effects from similar prematurity-related effects is difficult,” wrote Steven L. Clark, MD, from the Department of Obstetrics and Gynecology, Baylor College of Medicine, Houston, in an accompanying editorial.
SOURCE:
The study was led by Melanie Nana, MRCP, from the Department of Obstetric Medicine, St Thomas’ Hospital, London, England. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study was retrospective in design, which may have introduced bias. The small sample size of 25 women may have limited the generalizability of the findings. Additionally, the study did not include a control group, which made it difficult to attribute outcomes solely to anti–IL-6 therapy. The lack of long-term follow-up data on the neonates also limited the understanding of potential long-term effects.
DISCLOSURES:
This study did not receive any funding. Some authors, including the lead author, received speaker fees, grants, or consultancy fees from academic institutions or pharmaceutical companies or had other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The maternal and neonatal outcomes in pregnant women treated with anti–interleukin (IL)-6 therapy for COVID-19 are largely favorable, with transient neonatal cytopenia observed in around one third of the babies being the only possible adverse outcome that could be related to anti–IL-6 therapy.
METHODOLOGY:
- Despite guidance, very few pregnant women with COVID-19 are offered evidence-based therapies such as anti–IL-6 due to concerns regarding fetal safety in later pregnancy.
- In this retrospective study, researchers evaluated maternal and neonatal outcomes in 25 pregnant women with COVID-19 (mean age at admission, 33 years) treated with anti–IL-6 (tocilizumab or sarilumab) at two tertiary hospitals in London.
- Most women (n = 16) received anti–IL-6 in the third trimester of pregnancy, whereas nine received it during the second trimester.
- Maternal and neonatal outcomes were assessed through medical record reviews and maternal medicine networks, with follow-up for 12 months.
- The women included in the study constituted a high-risk population with severe COVID-19; 24 required level two or three critical care. All women were receiving at least three concomitant medications due to their critical illness.
TAKEAWAY:
- Overall, 24 of 25 women treated with IL-6 receptor antibodies survived until hospital discharge.
- The sole death occurred in a woman with severe COVID-19 pneumonitis who later developed myocarditis and cardiac arrest. The physicians believed that these complications were more likely due to severe COVID-19 rather than anti–IL-6 therapy.
- All pregnancies resulted in live births; however, 16 babies had to be delivered preterm due to COVID-19 complications.
- Transient cytopenia was observed in 6 of 19 babies in whom a full blood count was performed. All the six babies were premature, with cytopenia resolving within 7 days in four babies; one baby died from complications associated with extreme prematurity.
IN PRACTICE:
“Although the authors found mild, transitory cytopenia in some (6 of 19) exposed infants, most had been delivered prematurely due to progressive COVID-19–related morbidity, and distinguishing drug effects from similar prematurity-related effects is difficult,” wrote Steven L. Clark, MD, from the Department of Obstetrics and Gynecology, Baylor College of Medicine, Houston, in an accompanying editorial.
SOURCE:
The study was led by Melanie Nana, MRCP, from the Department of Obstetric Medicine, St Thomas’ Hospital, London, England. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study was retrospective in design, which may have introduced bias. The small sample size of 25 women may have limited the generalizability of the findings. Additionally, the study did not include a control group, which made it difficult to attribute outcomes solely to anti–IL-6 therapy. The lack of long-term follow-up data on the neonates also limited the understanding of potential long-term effects.
DISCLOSURES:
This study did not receive any funding. Some authors, including the lead author, received speaker fees, grants, or consultancy fees from academic institutions or pharmaceutical companies or had other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Long COVID & Chronic Fatigue: The Similarities are Uncanny
An estimated two million people in England and Scotland were experiencing symptoms of long COVID as of March 2024, according to the Office for National Statistics. Of these, 1.5 million said the condition was adversely affecting their day-to-day activities.
As more research emerges about long COVID, some experts are noticing that its trigger factors, symptoms, and causative mechanisms overlap with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).
ME/CFS is characterized by severe fatigue that does not improve with rest, in addition to pain and cognitive problems. One in four patients are bed- or house-bound with severe forms of the condition, sometimes experiencing atypical seizures, and speech and swallowing difficulties.
Despite affecting around 250,000 people in the UK and around 2 million people in the European Union (EU), it is a relatively poorly funded disease research area. Increased research into long COVID is thus providing a much-needed boost to ME/CFS research.
“What we already know about the possible causation of ME/CFS is helping research into the causes of long COVID. At the same time, research into long COVID is opening up new avenues of research that may also be relevant to ME/CFS. It is becoming a two-way process,” Dr. Charles Shepherd, honorary medical adviser to the UK-based ME Association, told this news organization.
While funding remains an issue, promising research is currently underway in the UK to improve diagnosis, treatment, and understanding of the pathology of ME/CFS.
Viral Reactivation
Dr. David Newton is research director at ME Research UK. “Viral infection is commonly reported as a trigger for [ME/CFS, meaning that the disease] may be caused by reactivation of latent viruses, including human herpes viruses and enteroviruses,” he said.
Herpes viruses can lie dormant in their host’s immune system for long periods of time. They can be reactivated by factors including infections, stress, and a weakened immune system, and may cause temporary symptoms or persistent disease.
A 2021 pilot study found that people with ME/CFS have a higher concentration of human herpesvirus 6B (HHV-6B) DNA in their saliva, and that concentration correlates with symptom severity. HHV-6B is a common virus typically contracted during infancy and childhood.
A continuation of this research is now underway at Brunel University to improve understanding of HHV-6B’s role in the onset and progression of ME/CFS, and to support the development of diagnostic and prognostic markers, as well as therapeutics such as antiviral therapies.
Mitochondrial Dysfunction
Dr. Shepherd explained that there is now sound evidence demonstrating that biochemical abnormalities in ME/CFS affect how mitochondria produce energy after physical exertion. Research is thus underway to see if treating mitochondrial dysfunction improves ME/CFS symptoms.
A phase 2a placebo-controlled clinical trial from 2023 found that AXA1125, a drug that works by modulating energy metabolism, significantly improved symptoms of fatigue in patients with fatigue-dominant long COVID, although it did not improve mitochondrial respiration.
“[The findings suggest] that improving mitochondrial health may be one way to restore normal functioning among people with long COVID, and by extension CFS,” study author Betty Raman, associate professor of cardiovascular medicine at the University of Oxford, told this news organization. She noted, however, that plans for a phase III trial have stalled due to insufficient funding.
Meanwhile, researchers from the Quadram Institute in Norwich and the University of East Anglia are conducting a pilot study to see if red light therapy can relieve symptoms of ME/CFS. Red light can be absorbed by mitochondria and is used to boost energy production. The trial will monitor patients remotely from their homes and will assess cognitive function and physical activity levels.
Gut Dysbiosis
Many studies have found that people with ME/CFS have altered gut microbiota, which suggests that changes in gut bacteria may contribute to the condition. Researchers at the Quadram Institute will thus conduct a clinical trial called RESTORE-ME to see whether fecal microbiota transplants (FMT) can treat the condition.
Rik Haagmans is a research scientist and PhD candidate at the Quadram Institute. He told this news organization: “Our FMT studies, if effective, could provide a longer lasting or even permanent relief of ME/CFS, as restoring the gut microbial composition wouldn’t require continuous medication,” he said.
Biobank and Biomarkers
Europe’s first ME/CFS-specific biobank is in the UK and is called UKMEB. It now has more than 30,000 blood samples from patients with ME/CFS, multiple sclerosis, and healthy controls. Uniquely, it includes samples from people with ME/CFS who are house- and bed-bound. Caroline Kingdon, RN, MSc, a research fellow and biobank lead at the London School of Hygiene and Tropical Medicine, told this news organization that samples and data from the UKMEB have been provided to research groups all over the world and have contributed to widely cited literature.
One group making use of these samples is led by Fatima Labeed, PhD, senior lecturer in human biology at the University of Surrey. Dr. Labeed and her team are developing a diagnostic test for ME/CFS based on electrical properties in white blood cells.
“To date, studies of ME/CFS have focused on the biochemical behavior of cells: the amount and type of proteins that cells use. We have taken a different approach, studying the electrical properties,” she explained to this news organization.
Her research builds on initial observations from 2019 that found differences in the electrical impedance of white blood cells between people with ME/CFS and controls. While the biological implications remain unknown, the findings may represent a biomarker for the condition.
Using blood samples from the UKMEB, the researchers are now investigating this potential biomarker with improved techniques and a larger patient cohort, including those with mild/moderate and severe forms of ME/CFS. So far, they have received more than 100 blood samples and have analyzed the electrical properties of 42.
“Based on the results we have so far, we are very close to having a biomarker for diagnosis. Our results so far show a high degree of accuracy and are able to distinguish between ME/CFS and other diseases,” said Dr. Labeed.
Genetic Test
Another promising avenue for diagnostics comes from a research team at the University of Edinburgh led by Professor Chris Ponting at the university’s Institute of Genetics and Cancer. They are currently working on DecodeMe, a large genetic study of ME using data from more than 26,000 people.
“We are studying blood-based biomarkers that distinguish people with ME from population controls. We’ve found a large number — including some found previously in other studies — and are writing these results up for publication,” said Ponting. The results should be published in early 2025.
The Future
While research into ME/CFS has picked up pace in recent years, funding remains a key bottleneck.
“Over the last 10 years, only £8.05m has been spent on ME research,” Sonya Chowdhury, chief executive of UK charity Action for ME told this news organization. She believes this amount is not equitably comparable to research funding allocated to other diseases.
In 2022, the UK government announced its intention to develop a cross-government interim delivery plan on ME/CFS for England, however publication of the final plan has been delayed numerous times.
Dr. Shepherd agreed that increased funding is crucial for progress to be made. He said the biggest help to ME/CFS research would be to end the disparity in government research funding for the disease, and match what is given for many other disabling long-term conditions.
“It’s not fair to continue to rely on the charity sector to fund almost all of the biomedical research into ME/CFS here in the UK,” he said.
A version of this article appeared on Medscape.com.
An estimated two million people in England and Scotland were experiencing symptoms of long COVID as of March 2024, according to the Office for National Statistics. Of these, 1.5 million said the condition was adversely affecting their day-to-day activities.
As more research emerges about long COVID, some experts are noticing that its trigger factors, symptoms, and causative mechanisms overlap with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).
ME/CFS is characterized by severe fatigue that does not improve with rest, in addition to pain and cognitive problems. One in four patients are bed- or house-bound with severe forms of the condition, sometimes experiencing atypical seizures, and speech and swallowing difficulties.
Despite affecting around 250,000 people in the UK and around 2 million people in the European Union (EU), it is a relatively poorly funded disease research area. Increased research into long COVID is thus providing a much-needed boost to ME/CFS research.
“What we already know about the possible causation of ME/CFS is helping research into the causes of long COVID. At the same time, research into long COVID is opening up new avenues of research that may also be relevant to ME/CFS. It is becoming a two-way process,” Dr. Charles Shepherd, honorary medical adviser to the UK-based ME Association, told this news organization.
While funding remains an issue, promising research is currently underway in the UK to improve diagnosis, treatment, and understanding of the pathology of ME/CFS.
Viral Reactivation
Dr. David Newton is research director at ME Research UK. “Viral infection is commonly reported as a trigger for [ME/CFS, meaning that the disease] may be caused by reactivation of latent viruses, including human herpes viruses and enteroviruses,” he said.
Herpes viruses can lie dormant in their host’s immune system for long periods of time. They can be reactivated by factors including infections, stress, and a weakened immune system, and may cause temporary symptoms or persistent disease.
A 2021 pilot study found that people with ME/CFS have a higher concentration of human herpesvirus 6B (HHV-6B) DNA in their saliva, and that concentration correlates with symptom severity. HHV-6B is a common virus typically contracted during infancy and childhood.
A continuation of this research is now underway at Brunel University to improve understanding of HHV-6B’s role in the onset and progression of ME/CFS, and to support the development of diagnostic and prognostic markers, as well as therapeutics such as antiviral therapies.
Mitochondrial Dysfunction
Dr. Shepherd explained that there is now sound evidence demonstrating that biochemical abnormalities in ME/CFS affect how mitochondria produce energy after physical exertion. Research is thus underway to see if treating mitochondrial dysfunction improves ME/CFS symptoms.
A phase 2a placebo-controlled clinical trial from 2023 found that AXA1125, a drug that works by modulating energy metabolism, significantly improved symptoms of fatigue in patients with fatigue-dominant long COVID, although it did not improve mitochondrial respiration.
“[The findings suggest] that improving mitochondrial health may be one way to restore normal functioning among people with long COVID, and by extension CFS,” study author Betty Raman, associate professor of cardiovascular medicine at the University of Oxford, told this news organization. She noted, however, that plans for a phase III trial have stalled due to insufficient funding.
Meanwhile, researchers from the Quadram Institute in Norwich and the University of East Anglia are conducting a pilot study to see if red light therapy can relieve symptoms of ME/CFS. Red light can be absorbed by mitochondria and is used to boost energy production. The trial will monitor patients remotely from their homes and will assess cognitive function and physical activity levels.
Gut Dysbiosis
Many studies have found that people with ME/CFS have altered gut microbiota, which suggests that changes in gut bacteria may contribute to the condition. Researchers at the Quadram Institute will thus conduct a clinical trial called RESTORE-ME to see whether fecal microbiota transplants (FMT) can treat the condition.
Rik Haagmans is a research scientist and PhD candidate at the Quadram Institute. He told this news organization: “Our FMT studies, if effective, could provide a longer lasting or even permanent relief of ME/CFS, as restoring the gut microbial composition wouldn’t require continuous medication,” he said.
Biobank and Biomarkers
Europe’s first ME/CFS-specific biobank is in the UK and is called UKMEB. It now has more than 30,000 blood samples from patients with ME/CFS, multiple sclerosis, and healthy controls. Uniquely, it includes samples from people with ME/CFS who are house- and bed-bound. Caroline Kingdon, RN, MSc, a research fellow and biobank lead at the London School of Hygiene and Tropical Medicine, told this news organization that samples and data from the UKMEB have been provided to research groups all over the world and have contributed to widely cited literature.
One group making use of these samples is led by Fatima Labeed, PhD, senior lecturer in human biology at the University of Surrey. Dr. Labeed and her team are developing a diagnostic test for ME/CFS based on electrical properties in white blood cells.
“To date, studies of ME/CFS have focused on the biochemical behavior of cells: the amount and type of proteins that cells use. We have taken a different approach, studying the electrical properties,” she explained to this news organization.
Her research builds on initial observations from 2019 that found differences in the electrical impedance of white blood cells between people with ME/CFS and controls. While the biological implications remain unknown, the findings may represent a biomarker for the condition.
Using blood samples from the UKMEB, the researchers are now investigating this potential biomarker with improved techniques and a larger patient cohort, including those with mild/moderate and severe forms of ME/CFS. So far, they have received more than 100 blood samples and have analyzed the electrical properties of 42.
“Based on the results we have so far, we are very close to having a biomarker for diagnosis. Our results so far show a high degree of accuracy and are able to distinguish between ME/CFS and other diseases,” said Dr. Labeed.
Genetic Test
Another promising avenue for diagnostics comes from a research team at the University of Edinburgh led by Professor Chris Ponting at the university’s Institute of Genetics and Cancer. They are currently working on DecodeMe, a large genetic study of ME using data from more than 26,000 people.
“We are studying blood-based biomarkers that distinguish people with ME from population controls. We’ve found a large number — including some found previously in other studies — and are writing these results up for publication,” said Ponting. The results should be published in early 2025.
The Future
While research into ME/CFS has picked up pace in recent years, funding remains a key bottleneck.
“Over the last 10 years, only £8.05m has been spent on ME research,” Sonya Chowdhury, chief executive of UK charity Action for ME told this news organization. She believes this amount is not equitably comparable to research funding allocated to other diseases.
In 2022, the UK government announced its intention to develop a cross-government interim delivery plan on ME/CFS for England, however publication of the final plan has been delayed numerous times.
Dr. Shepherd agreed that increased funding is crucial for progress to be made. He said the biggest help to ME/CFS research would be to end the disparity in government research funding for the disease, and match what is given for many other disabling long-term conditions.
“It’s not fair to continue to rely on the charity sector to fund almost all of the biomedical research into ME/CFS here in the UK,” he said.
A version of this article appeared on Medscape.com.
An estimated two million people in England and Scotland were experiencing symptoms of long COVID as of March 2024, according to the Office for National Statistics. Of these, 1.5 million said the condition was adversely affecting their day-to-day activities.
As more research emerges about long COVID, some experts are noticing that its trigger factors, symptoms, and causative mechanisms overlap with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).
ME/CFS is characterized by severe fatigue that does not improve with rest, in addition to pain and cognitive problems. One in four patients are bed- or house-bound with severe forms of the condition, sometimes experiencing atypical seizures, and speech and swallowing difficulties.
Despite affecting around 250,000 people in the UK and around 2 million people in the European Union (EU), it is a relatively poorly funded disease research area. Increased research into long COVID is thus providing a much-needed boost to ME/CFS research.
“What we already know about the possible causation of ME/CFS is helping research into the causes of long COVID. At the same time, research into long COVID is opening up new avenues of research that may also be relevant to ME/CFS. It is becoming a two-way process,” Dr. Charles Shepherd, honorary medical adviser to the UK-based ME Association, told this news organization.
While funding remains an issue, promising research is currently underway in the UK to improve diagnosis, treatment, and understanding of the pathology of ME/CFS.
Viral Reactivation
Dr. David Newton is research director at ME Research UK. “Viral infection is commonly reported as a trigger for [ME/CFS, meaning that the disease] may be caused by reactivation of latent viruses, including human herpes viruses and enteroviruses,” he said.
Herpes viruses can lie dormant in their host’s immune system for long periods of time. They can be reactivated by factors including infections, stress, and a weakened immune system, and may cause temporary symptoms or persistent disease.
A 2021 pilot study found that people with ME/CFS have a higher concentration of human herpesvirus 6B (HHV-6B) DNA in their saliva, and that concentration correlates with symptom severity. HHV-6B is a common virus typically contracted during infancy and childhood.
A continuation of this research is now underway at Brunel University to improve understanding of HHV-6B’s role in the onset and progression of ME/CFS, and to support the development of diagnostic and prognostic markers, as well as therapeutics such as antiviral therapies.
Mitochondrial Dysfunction
Dr. Shepherd explained that there is now sound evidence demonstrating that biochemical abnormalities in ME/CFS affect how mitochondria produce energy after physical exertion. Research is thus underway to see if treating mitochondrial dysfunction improves ME/CFS symptoms.
A phase 2a placebo-controlled clinical trial from 2023 found that AXA1125, a drug that works by modulating energy metabolism, significantly improved symptoms of fatigue in patients with fatigue-dominant long COVID, although it did not improve mitochondrial respiration.
“[The findings suggest] that improving mitochondrial health may be one way to restore normal functioning among people with long COVID, and by extension CFS,” study author Betty Raman, associate professor of cardiovascular medicine at the University of Oxford, told this news organization. She noted, however, that plans for a phase III trial have stalled due to insufficient funding.
Meanwhile, researchers from the Quadram Institute in Norwich and the University of East Anglia are conducting a pilot study to see if red light therapy can relieve symptoms of ME/CFS. Red light can be absorbed by mitochondria and is used to boost energy production. The trial will monitor patients remotely from their homes and will assess cognitive function and physical activity levels.
Gut Dysbiosis
Many studies have found that people with ME/CFS have altered gut microbiota, which suggests that changes in gut bacteria may contribute to the condition. Researchers at the Quadram Institute will thus conduct a clinical trial called RESTORE-ME to see whether fecal microbiota transplants (FMT) can treat the condition.
Rik Haagmans is a research scientist and PhD candidate at the Quadram Institute. He told this news organization: “Our FMT studies, if effective, could provide a longer lasting or even permanent relief of ME/CFS, as restoring the gut microbial composition wouldn’t require continuous medication,” he said.
Biobank and Biomarkers
Europe’s first ME/CFS-specific biobank is in the UK and is called UKMEB. It now has more than 30,000 blood samples from patients with ME/CFS, multiple sclerosis, and healthy controls. Uniquely, it includes samples from people with ME/CFS who are house- and bed-bound. Caroline Kingdon, RN, MSc, a research fellow and biobank lead at the London School of Hygiene and Tropical Medicine, told this news organization that samples and data from the UKMEB have been provided to research groups all over the world and have contributed to widely cited literature.
One group making use of these samples is led by Fatima Labeed, PhD, senior lecturer in human biology at the University of Surrey. Dr. Labeed and her team are developing a diagnostic test for ME/CFS based on electrical properties in white blood cells.
“To date, studies of ME/CFS have focused on the biochemical behavior of cells: the amount and type of proteins that cells use. We have taken a different approach, studying the electrical properties,” she explained to this news organization.
Her research builds on initial observations from 2019 that found differences in the electrical impedance of white blood cells between people with ME/CFS and controls. While the biological implications remain unknown, the findings may represent a biomarker for the condition.
Using blood samples from the UKMEB, the researchers are now investigating this potential biomarker with improved techniques and a larger patient cohort, including those with mild/moderate and severe forms of ME/CFS. So far, they have received more than 100 blood samples and have analyzed the electrical properties of 42.
“Based on the results we have so far, we are very close to having a biomarker for diagnosis. Our results so far show a high degree of accuracy and are able to distinguish between ME/CFS and other diseases,” said Dr. Labeed.
Genetic Test
Another promising avenue for diagnostics comes from a research team at the University of Edinburgh led by Professor Chris Ponting at the university’s Institute of Genetics and Cancer. They are currently working on DecodeMe, a large genetic study of ME using data from more than 26,000 people.
“We are studying blood-based biomarkers that distinguish people with ME from population controls. We’ve found a large number — including some found previously in other studies — and are writing these results up for publication,” said Ponting. The results should be published in early 2025.
The Future
While research into ME/CFS has picked up pace in recent years, funding remains a key bottleneck.
“Over the last 10 years, only £8.05m has been spent on ME research,” Sonya Chowdhury, chief executive of UK charity Action for ME told this news organization. She believes this amount is not equitably comparable to research funding allocated to other diseases.
In 2022, the UK government announced its intention to develop a cross-government interim delivery plan on ME/CFS for England, however publication of the final plan has been delayed numerous times.
Dr. Shepherd agreed that increased funding is crucial for progress to be made. He said the biggest help to ME/CFS research would be to end the disparity in government research funding for the disease, and match what is given for many other disabling long-term conditions.
“It’s not fair to continue to rely on the charity sector to fund almost all of the biomedical research into ME/CFS here in the UK,” he said.
A version of this article appeared on Medscape.com.
Almost 10% of Infected Pregnant People Develop Long COVID
Almost 1 in 10 pregnant people infected with COVID-19 end up developing long COVID, according to a study published in Obstetrics & Gynecology.
Researchers at University of Utah Health looked at the medical records of more than 1500 people who got COVID-19 while pregnant and checked their self-reported symptoms at least 6 months after infection, according to a news release from the school.
The scientists discovered that 9.3% of those people reported long COVID symptoms, such as fatigue and issues in their gut.
To make sure those long COVID symptoms were not actually symptoms of pregnancy, the research team did a second analysis of people who reported symptoms more than 12 weeks after giving birth. The risk of long COVID was about the same as in the first analysis.
“It was surprising to me that the prevalence was that high,” Torri D. Metz, MD, vice chair for research of obstetrics and gynecology at the school and co-leader of the study, said in the release. “This is something that does continue to affect otherwise reasonably healthy and young populations.”
The school said this is the first study to look at long COVID risks in pregnant people. Previous research found other dangers for pregnant people who get COVID, such as a higher chance of hospitalization or death, or complications such as preterm birth.
In the general population, research shows that 10%-20% of people who get COVID develop long COVID.
Dr. Metz said healthcare providers need to remain alert about long COVID, including in pregnant people.
“We need to have this on our radar as we’re seeing patients. It’s something we really don’t want to miss. And we want to get people referred to appropriate specialists who treat long COVID,” she said.
A version of this article first appeared on WebMD.com.
Almost 1 in 10 pregnant people infected with COVID-19 end up developing long COVID, according to a study published in Obstetrics & Gynecology.
Researchers at University of Utah Health looked at the medical records of more than 1500 people who got COVID-19 while pregnant and checked their self-reported symptoms at least 6 months after infection, according to a news release from the school.
The scientists discovered that 9.3% of those people reported long COVID symptoms, such as fatigue and issues in their gut.
To make sure those long COVID symptoms were not actually symptoms of pregnancy, the research team did a second analysis of people who reported symptoms more than 12 weeks after giving birth. The risk of long COVID was about the same as in the first analysis.
“It was surprising to me that the prevalence was that high,” Torri D. Metz, MD, vice chair for research of obstetrics and gynecology at the school and co-leader of the study, said in the release. “This is something that does continue to affect otherwise reasonably healthy and young populations.”
The school said this is the first study to look at long COVID risks in pregnant people. Previous research found other dangers for pregnant people who get COVID, such as a higher chance of hospitalization or death, or complications such as preterm birth.
In the general population, research shows that 10%-20% of people who get COVID develop long COVID.
Dr. Metz said healthcare providers need to remain alert about long COVID, including in pregnant people.
“We need to have this on our radar as we’re seeing patients. It’s something we really don’t want to miss. And we want to get people referred to appropriate specialists who treat long COVID,” she said.
A version of this article first appeared on WebMD.com.
Almost 1 in 10 pregnant people infected with COVID-19 end up developing long COVID, according to a study published in Obstetrics & Gynecology.
Researchers at University of Utah Health looked at the medical records of more than 1500 people who got COVID-19 while pregnant and checked their self-reported symptoms at least 6 months after infection, according to a news release from the school.
The scientists discovered that 9.3% of those people reported long COVID symptoms, such as fatigue and issues in their gut.
To make sure those long COVID symptoms were not actually symptoms of pregnancy, the research team did a second analysis of people who reported symptoms more than 12 weeks after giving birth. The risk of long COVID was about the same as in the first analysis.
“It was surprising to me that the prevalence was that high,” Torri D. Metz, MD, vice chair for research of obstetrics and gynecology at the school and co-leader of the study, said in the release. “This is something that does continue to affect otherwise reasonably healthy and young populations.”
The school said this is the first study to look at long COVID risks in pregnant people. Previous research found other dangers for pregnant people who get COVID, such as a higher chance of hospitalization or death, or complications such as preterm birth.
In the general population, research shows that 10%-20% of people who get COVID develop long COVID.
Dr. Metz said healthcare providers need to remain alert about long COVID, including in pregnant people.
“We need to have this on our radar as we’re seeing patients. It’s something we really don’t want to miss. And we want to get people referred to appropriate specialists who treat long COVID,” she said.
A version of this article first appeared on WebMD.com.
FROM OBSTETRICS & GYNECOLOGY
National Academies Issue New Broad Definition of Long COVID
A new broadly inclusive definition of long COVID from the National Academies of Sciences, Engineering, and Medicine (NASEM) has been developed with the aim of improving consistency, documentation, and treatment for both adults and children.
According to the 2024 NASEM definition of long COVID issued on June 11, 2024, “Long COVID is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
People with long COVID may present with one or more of a long list of symptoms, such as shortness of breath, rapid heartbeat, extreme fatigue, post-exertional malaise, or sleep disturbance and with single or multiple diagnosable conditions, including interstitial lung disease, arrhythmias, postural orthostatic tachycardia syndrome (POTS), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), diabetes, or autoimmune disorders. The condition can exacerbate preexisting health conditions or present as new ones.
The definition does not require laboratory confirmation or other proof of initial infection. Long COVID can follow SARS-CoV-2 infection of any severity, including asymptomatic infections, whether or not they were initially recognized.
Several working definitions and terms for long COVID had previously been proposed, including those from the World Health Organization (WHO) and the US Centers for Disease Control and Prevention, but no common definition or terminology had been established.
The new definition was developed at the request of the Administration for Strategic Preparedness and Response and the Office of the Assistant Secretary for Health (OASH). It was written by a multi-stakeholder panel convened by NASEM, which recommended that the new definition be universally adopted by the federal government, clinical societies and associations, public health practitioners, clinicians, payers, the drug industry, and others using the term long COVID.
Recent surveys suggest that approximately 7% of Americans have experienced or are experiencing long COVID. “It’s millions of people,” panel chair Harvey V. Fineberg, MD, president of the Gordon and Betty Moore Foundation, told this news organization.
The new definition “does not erase the problem of clinical judgment ... But we think this definition has the real advantage of elevating to the clinician’s mind the real likelihood in the current environment of prevalence of this virus that a presenting patient’s strange symptoms are both real and maybe related as an expression of long COVID,” Dr. Fineberg noted.
One way this new definition differs from previous ones such as WHO’s, he said, is “they talk about a diagnosis of exclusion. One of the important points in our definition is that other diagnosable conditions like ME/CFS or POTS can be part of the picture of long COVID. They are not alternative. They are, in fact, an expression of long COVID.”
Indeed, the NASEM report also introduces the term infection-associated chronic condition (IACC). This was important, Dr. Fineberg said, “because it’s the larger family of conditions of which long COVID is a part. It emphasizes a relatedness of long COVID to other conditions that can follow from a variety of infections. We also adopted the term ‘disease state’ to convey the seriousness and reality of this condition in the lives of patients.”
Comments on New Definition
In a statement provided to this news organization, Lucinda Bateman, MD, and Brayden Yellman, MD, co-medical directors of the Bateman-Horne Center in Salt Lake City, said that “describing long COVID as an IACC ... not only meets the NASEM goal of allowing clinicians, researchers, and public health officials to meaningfully identify and serve all persons who suffer illness or disability in the wake of a SARS-CoV-2 infection, but also draws direct comparison to other known IACC’s (such as ME/CFS, post-treatment Lyme, POTS) that have been plaguing many for decades.”
Dr. Fineberg noted another important aspect of the NASEM report: “Our definition includes an explicit statement on equity, explaining that long COVID can affect anyone, young and old, different races, different ages, different sexes, different genders, different orientations, different socioeconomic conditions ... This does not mean that every single person is at equal risk. There are risk factors, but the important point is the universal nature of this as a condition.”
Two clinical directors of long COVID programs who were contacted by this news organization praised the new definition. Zijian Chen, MD, director of Mount Sinai’s Center for Post-COVID Care, New York, said that it’s “very similar to the definition that we have used for our clinical practice since 2020. It is very important that the broad definition helps to be inclusive of all patients that may be affected. The inclusion of children as a consideration is important as well, since there is routinely less focus on children because they tend to have less disease frequency ... The creation of a unified definition helps both with clinical practice and research.”
Nisha Viswanathan, MD, director of the long COVID program at the University of California, Los Angeles, said: “I think they left it intentionally broad for the medical practitioner to not necessarily use the definition to rule out individuals, but to perhaps use more of a clinical gestalt to help rule in this diagnosis ... I think this definition is providing clarity to health care providers on what exactly would be falling under the long-COVID diagnosis header.”
Dr. Viswanathan also said that she anticipates this definition to help patients make their case in filing disability claims. “Because long COVID has not previously had a good fleshed-out definition, it was very easy for disability providers to reject claims for patients who continue to have symptoms ... I actually think this might help our patients ultimately in their attempt to be able to have the ability to care for themselves when they’re disabled enough to not be able to work.”
Written into the report is the expectation that the definition “will evolve as new evidence emerges and the understanding of long COVID matures.” The writing committee calls for reexamination in “no more than 3 years.” Factors that would prompt a reevaluation could include improved testing methods, discovery of medical factors and/or biomarkers that distinguish long COVID from other conditions, and new treatments.
Meanwhile, Dr. Fineberg told this news organization, “If this definition adds to the readiness, awareness, openness, and response to the patient with long COVID, it will have done its job.”
Dr. Fineberg, Dr. Bateman, Dr. Yellman, Dr. Viswanathan, and Dr. Chen have no relevant disclosures.
A version of this article appeared on Medscape.com.
A new broadly inclusive definition of long COVID from the National Academies of Sciences, Engineering, and Medicine (NASEM) has been developed with the aim of improving consistency, documentation, and treatment for both adults and children.
According to the 2024 NASEM definition of long COVID issued on June 11, 2024, “Long COVID is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
People with long COVID may present with one or more of a long list of symptoms, such as shortness of breath, rapid heartbeat, extreme fatigue, post-exertional malaise, or sleep disturbance and with single or multiple diagnosable conditions, including interstitial lung disease, arrhythmias, postural orthostatic tachycardia syndrome (POTS), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), diabetes, or autoimmune disorders. The condition can exacerbate preexisting health conditions or present as new ones.
The definition does not require laboratory confirmation or other proof of initial infection. Long COVID can follow SARS-CoV-2 infection of any severity, including asymptomatic infections, whether or not they were initially recognized.
Several working definitions and terms for long COVID had previously been proposed, including those from the World Health Organization (WHO) and the US Centers for Disease Control and Prevention, but no common definition or terminology had been established.
The new definition was developed at the request of the Administration for Strategic Preparedness and Response and the Office of the Assistant Secretary for Health (OASH). It was written by a multi-stakeholder panel convened by NASEM, which recommended that the new definition be universally adopted by the federal government, clinical societies and associations, public health practitioners, clinicians, payers, the drug industry, and others using the term long COVID.
Recent surveys suggest that approximately 7% of Americans have experienced or are experiencing long COVID. “It’s millions of people,” panel chair Harvey V. Fineberg, MD, president of the Gordon and Betty Moore Foundation, told this news organization.
The new definition “does not erase the problem of clinical judgment ... But we think this definition has the real advantage of elevating to the clinician’s mind the real likelihood in the current environment of prevalence of this virus that a presenting patient’s strange symptoms are both real and maybe related as an expression of long COVID,” Dr. Fineberg noted.
One way this new definition differs from previous ones such as WHO’s, he said, is “they talk about a diagnosis of exclusion. One of the important points in our definition is that other diagnosable conditions like ME/CFS or POTS can be part of the picture of long COVID. They are not alternative. They are, in fact, an expression of long COVID.”
Indeed, the NASEM report also introduces the term infection-associated chronic condition (IACC). This was important, Dr. Fineberg said, “because it’s the larger family of conditions of which long COVID is a part. It emphasizes a relatedness of long COVID to other conditions that can follow from a variety of infections. We also adopted the term ‘disease state’ to convey the seriousness and reality of this condition in the lives of patients.”
Comments on New Definition
In a statement provided to this news organization, Lucinda Bateman, MD, and Brayden Yellman, MD, co-medical directors of the Bateman-Horne Center in Salt Lake City, said that “describing long COVID as an IACC ... not only meets the NASEM goal of allowing clinicians, researchers, and public health officials to meaningfully identify and serve all persons who suffer illness or disability in the wake of a SARS-CoV-2 infection, but also draws direct comparison to other known IACC’s (such as ME/CFS, post-treatment Lyme, POTS) that have been plaguing many for decades.”
Dr. Fineberg noted another important aspect of the NASEM report: “Our definition includes an explicit statement on equity, explaining that long COVID can affect anyone, young and old, different races, different ages, different sexes, different genders, different orientations, different socioeconomic conditions ... This does not mean that every single person is at equal risk. There are risk factors, but the important point is the universal nature of this as a condition.”
Two clinical directors of long COVID programs who were contacted by this news organization praised the new definition. Zijian Chen, MD, director of Mount Sinai’s Center for Post-COVID Care, New York, said that it’s “very similar to the definition that we have used for our clinical practice since 2020. It is very important that the broad definition helps to be inclusive of all patients that may be affected. The inclusion of children as a consideration is important as well, since there is routinely less focus on children because they tend to have less disease frequency ... The creation of a unified definition helps both with clinical practice and research.”
Nisha Viswanathan, MD, director of the long COVID program at the University of California, Los Angeles, said: “I think they left it intentionally broad for the medical practitioner to not necessarily use the definition to rule out individuals, but to perhaps use more of a clinical gestalt to help rule in this diagnosis ... I think this definition is providing clarity to health care providers on what exactly would be falling under the long-COVID diagnosis header.”
Dr. Viswanathan also said that she anticipates this definition to help patients make their case in filing disability claims. “Because long COVID has not previously had a good fleshed-out definition, it was very easy for disability providers to reject claims for patients who continue to have symptoms ... I actually think this might help our patients ultimately in their attempt to be able to have the ability to care for themselves when they’re disabled enough to not be able to work.”
Written into the report is the expectation that the definition “will evolve as new evidence emerges and the understanding of long COVID matures.” The writing committee calls for reexamination in “no more than 3 years.” Factors that would prompt a reevaluation could include improved testing methods, discovery of medical factors and/or biomarkers that distinguish long COVID from other conditions, and new treatments.
Meanwhile, Dr. Fineberg told this news organization, “If this definition adds to the readiness, awareness, openness, and response to the patient with long COVID, it will have done its job.”
Dr. Fineberg, Dr. Bateman, Dr. Yellman, Dr. Viswanathan, and Dr. Chen have no relevant disclosures.
A version of this article appeared on Medscape.com.
A new broadly inclusive definition of long COVID from the National Academies of Sciences, Engineering, and Medicine (NASEM) has been developed with the aim of improving consistency, documentation, and treatment for both adults and children.
According to the 2024 NASEM definition of long COVID issued on June 11, 2024, “Long COVID is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
People with long COVID may present with one or more of a long list of symptoms, such as shortness of breath, rapid heartbeat, extreme fatigue, post-exertional malaise, or sleep disturbance and with single or multiple diagnosable conditions, including interstitial lung disease, arrhythmias, postural orthostatic tachycardia syndrome (POTS), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), diabetes, or autoimmune disorders. The condition can exacerbate preexisting health conditions or present as new ones.
The definition does not require laboratory confirmation or other proof of initial infection. Long COVID can follow SARS-CoV-2 infection of any severity, including asymptomatic infections, whether or not they were initially recognized.
Several working definitions and terms for long COVID had previously been proposed, including those from the World Health Organization (WHO) and the US Centers for Disease Control and Prevention, but no common definition or terminology had been established.
The new definition was developed at the request of the Administration for Strategic Preparedness and Response and the Office of the Assistant Secretary for Health (OASH). It was written by a multi-stakeholder panel convened by NASEM, which recommended that the new definition be universally adopted by the federal government, clinical societies and associations, public health practitioners, clinicians, payers, the drug industry, and others using the term long COVID.
Recent surveys suggest that approximately 7% of Americans have experienced or are experiencing long COVID. “It’s millions of people,” panel chair Harvey V. Fineberg, MD, president of the Gordon and Betty Moore Foundation, told this news organization.
The new definition “does not erase the problem of clinical judgment ... But we think this definition has the real advantage of elevating to the clinician’s mind the real likelihood in the current environment of prevalence of this virus that a presenting patient’s strange symptoms are both real and maybe related as an expression of long COVID,” Dr. Fineberg noted.
One way this new definition differs from previous ones such as WHO’s, he said, is “they talk about a diagnosis of exclusion. One of the important points in our definition is that other diagnosable conditions like ME/CFS or POTS can be part of the picture of long COVID. They are not alternative. They are, in fact, an expression of long COVID.”
Indeed, the NASEM report also introduces the term infection-associated chronic condition (IACC). This was important, Dr. Fineberg said, “because it’s the larger family of conditions of which long COVID is a part. It emphasizes a relatedness of long COVID to other conditions that can follow from a variety of infections. We also adopted the term ‘disease state’ to convey the seriousness and reality of this condition in the lives of patients.”
Comments on New Definition
In a statement provided to this news organization, Lucinda Bateman, MD, and Brayden Yellman, MD, co-medical directors of the Bateman-Horne Center in Salt Lake City, said that “describing long COVID as an IACC ... not only meets the NASEM goal of allowing clinicians, researchers, and public health officials to meaningfully identify and serve all persons who suffer illness or disability in the wake of a SARS-CoV-2 infection, but also draws direct comparison to other known IACC’s (such as ME/CFS, post-treatment Lyme, POTS) that have been plaguing many for decades.”
Dr. Fineberg noted another important aspect of the NASEM report: “Our definition includes an explicit statement on equity, explaining that long COVID can affect anyone, young and old, different races, different ages, different sexes, different genders, different orientations, different socioeconomic conditions ... This does not mean that every single person is at equal risk. There are risk factors, but the important point is the universal nature of this as a condition.”
Two clinical directors of long COVID programs who were contacted by this news organization praised the new definition. Zijian Chen, MD, director of Mount Sinai’s Center for Post-COVID Care, New York, said that it’s “very similar to the definition that we have used for our clinical practice since 2020. It is very important that the broad definition helps to be inclusive of all patients that may be affected. The inclusion of children as a consideration is important as well, since there is routinely less focus on children because they tend to have less disease frequency ... The creation of a unified definition helps both with clinical practice and research.”
Nisha Viswanathan, MD, director of the long COVID program at the University of California, Los Angeles, said: “I think they left it intentionally broad for the medical practitioner to not necessarily use the definition to rule out individuals, but to perhaps use more of a clinical gestalt to help rule in this diagnosis ... I think this definition is providing clarity to health care providers on what exactly would be falling under the long-COVID diagnosis header.”
Dr. Viswanathan also said that she anticipates this definition to help patients make their case in filing disability claims. “Because long COVID has not previously had a good fleshed-out definition, it was very easy for disability providers to reject claims for patients who continue to have symptoms ... I actually think this might help our patients ultimately in their attempt to be able to have the ability to care for themselves when they’re disabled enough to not be able to work.”
Written into the report is the expectation that the definition “will evolve as new evidence emerges and the understanding of long COVID matures.” The writing committee calls for reexamination in “no more than 3 years.” Factors that would prompt a reevaluation could include improved testing methods, discovery of medical factors and/or biomarkers that distinguish long COVID from other conditions, and new treatments.
Meanwhile, Dr. Fineberg told this news organization, “If this definition adds to the readiness, awareness, openness, and response to the patient with long COVID, it will have done its job.”
Dr. Fineberg, Dr. Bateman, Dr. Yellman, Dr. Viswanathan, and Dr. Chen have no relevant disclosures.
A version of this article appeared on Medscape.com.
MDs’ One-Word Summary of Long COVID Progress: ‘Frustration’
Stuart Malcolm, MD, a primary care physician who practices in Oregon and northern California, started seeing patients with long COVID early in the pandemic. Back then, he was frustrated by the obstacles and lack of standard diagnostic tests and treatments. Four years later, well, he still is.
“Something I learned the last few years is the logistics to get people care is really, really hard,” he said. “There’s a lot of frustration. It’s mostly frustration.”
For long COVID doctors and patients, there has been little to no progress addressing the challenges, leaving many discouraged. Researchers and clinicians now have a greater understanding of what health agencies formally call post-COVID condition, but the wide spectrum of symptoms, slow progress in launching pharmacologic clinical trials, and the research toward understanding the underlying causes mean standardized diagnostic tests and definitive treatments remain elusive.
“The frustration is that we aren’t able to help everyone with our current knowledge base. And I think the frustration lies not just with us physicians but also with patients because they’re at the point where if they tried everything, literally everything and haven’t gotten better,” said Zijian Chen, MD, director of the Mount Sinai Center for Post-COVID Care in New York City.
Wanted: More Funding, More Doctors, More Clinics
Between 10% and 20% of the estimated hundreds of millions of people infected worldwide with SARS-CoV-2 in the first 2 years went on to develop long-term symptoms. While many recover over time, doctors who have treated long COVID since 2020 said they see some patients still wrestling with the condition after 4 years.
The latest Centers for Disease Control and Prevention Household Pulse Survey, taken between March 5 and April 1, 2024, estimated that nearly 7% of the adult population — more than 18 million people — currently have long COVID. Data from other countries also suggest that millions have been living with long COVID for years now, and hundreds of thousands have seen their day-to-day activities significantly affected.
There is an urgent need for more funding, long COVID clinicians, multidisciplinary clinics, and education for non–long COVID physicians and specialists, doctors said. Instead, funding remains limited, clinics are closing, wait times are “horrendously long,” patients are left in limbo, and physicians are burning out.
“What’s changed in some ways is that there’s even less access to COVID rehab, which sounds crazy because there was very little to begin with,” said Alexandra Rendely, MD, a physical medicine and rehabilitation physician with the interdisciplinary Toronto Rehab, a part of the University Health Network of teaching hospitals in Toronto, Ontario, Canada.
“Patients are still being diagnosed every day, yet the resources available are becoming less and less.”
COVID-19 money earmarked during the pandemic was mostly limited to temporary emergency measures. As those funds dwindled, governments and institutions have decreased financial support. The Long COVID Moonshot campaign, organized by patients with long COVID, is pushing Congress to support $1 billion in annual research funding to close the financial chasm.
The Clinical Trial Conundrum
While long COVID clinics have come a long way in helping patients, gaps remain. Doctors may be unwilling to prescribe off-label treatments without proper clinical trials due to the potential risks and liabilities involved or due to the controversial or unconventional nature of the therapies, said Dr. Malcolm, who left his primary care practice more than 2 years ago to focus on long COVID.
In the absence of standard treatments, Dr. Malcolm and other doctors said they must take a trial-and-error approach in treating patients with long COVID that centers on addressing symptoms and not the underlying condition.
“There are actually a lot of treatments and a lot of them are not curative, but they can help people,” he said.
Dr. Malcolm, who is a medical director at Real Time Health Monitoring, a private clinic in the San Francisco Bay Area that specializes in long COVID and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), said it was important for him to be with a clinical team that understood and was supportive of his treatment decisions and was able to offer clinical support for those treatments if needed.
For physicians looking for clinical data before prescribing certain medications, the wait may be long. More than $1.5 billion in US federal funding has been earmarked to study long COVID, but the National Institutes of Health (NIH) has faced criticism from patients and scientists alike for its slow progress and emphasis on observational studies instead of research that could unravel the biological roots of long COVID. Among the clinical trials announced by the NIH’s RECOVER initiative, only a handful involve studying pharmaceutical treatments.
A 2023 editorial published in The Lancet called out the “dismal state of clinical research relative to the substantial burden of [long COVID]” and said, “we are clearly lacking tested pharmacological interventions that treat the underlying pathophysiology.” At the time of publication, it noted that of the 386 long COVID trials listed on ClinicalTrials.gov, only 12 were actually testing pharmacologic interventions.
There are also diagnostic and insurance barriers. The specialized tests that can detect long COVID anomalies are neither commonly known by primary care practitioners nor easily requested at the local lab, can be expensive, and are typically not covered by insurance, Dr. Malcolm explained.
Patients with long COVID also have the added barrier of being unable to advocate as easily because of their energy limitations, doctors said. Patients may appear outwardly fine, but fatigue and brain fog are among the many problems that cannot be measured in appearances. The condition has upended lives, some losing jobs, even homes, and the mental toll is why there is a “not insignificant” suicide rate.
One Patient’s 4-Year Journey
Charlie McCone, 34, used to be a tennis player and an active musician. But he’s spent the past 4 years mostly housebound, grappling with the aftermath of a SARS-CoV-2 infection he contracted in March 2020. He went from biking daily to work 10 miles and back to having at most 2 hours of energy per day.
In the first year alone, Mr. McCone saw more than two dozen doctors and specialists. The conditions now associated with long COVID, like ME/CFS, mast cell activation syndrome (a condition in which a patient experiences episodes of allergic symptoms such as hives, swelling, low blood pressure, and difficulty breathing), or dysautonomia (conditions that affect the autonomic nervous system, which controls automatic processes in the body) were not on physicians’ radars.
Then in 2021, he became bedbound for more than half a year after a Delta variant reinfection. He developed neurologic symptoms, including incapacitating fatigue, post-exertional malaise (where symptoms worsened after minimal physical or mental activity), left-sided weakness, and cognitive impairment. He stopped working altogether. But the worst was the shortness of breath he felt 24/7, even at rest. A battery of lab tests revealed nothing abnormal. He tried numerous drugs and the classic respiratory treatments.
Mr. McCone eventually connected with Dr. Malcolm over X and developed what he describes as an effective patient-doctor collaboration. When studies came out suggesting microclots were a common issue with patients with long COVID and positive outcomes were reported from anticoagulant therapy, they knew it could be one of the answers.
“After 3 weeks on [the antiplatelet drug], I was like, oh my god, my lungs are finally opening up,” said Mr. McCone. He has taken the medication for more than a year and a half, and some days he doesn’t even think about his respiratory symptoms.
“That trial-and-error process is just really long and hard and costly,” said Dr. Malcolm.
Today, fatigue and cognitive stamina are Mr. McCone’s main challenges, and he is far from recovered.
“[I had a] very fulfilling, happy life and now, it’s hard to think about. I’ve come a long way with my mental health and all this, but I’ve lost 4 years,” Mr. McCone said. “The prospect of me being here when I’m 40 seems very real ... so it’s pretty devastating.”
Lessons Learned, Hope Amid Ongoing Research
Despite the daunting obstacle, doctors said the science has come a long way for a new disease. We now know long COVID is likely caused by a combination of triggers, including viral reservoir in the tissue, inflammation, autoimmunity, and microclots; severity of infection is not necessarily an accurate risk factor predictor — long COVID can strike even those who had a mild infection; upward of 200 symptoms have been identified; and we know more about potential biomarkers that could lead to better diagnostic tools.
Unlike many other diseases and conditions with standard treatment protocols, long COVID treatments are typically aimed at addressing individual symptoms.
“It is very detailed and individualized to the patient’s specific symptoms and to the patient’s specific needs,” Dr. Rendely said. Symptoms can also fluctuate, relapse, or wax and wane, for example, so what ails a patient at their first doctor’s appointment could be completely different at the next appointment 2 months later.
Doctors are still hopeful the RECOVER research, which includes trials that look at autonomic and cognitive dysfunctions, will pave the way for more effective long COVID therapies. In Canada, Dr. Rendely is also eying the RECLAIM trial that is currently testing the effectiveness of pentoxifylline, which helps blood flow, and ibudilast, an anti-inflammatory drug.
Doctors are also hopeful when they see patients who have made “tremendous gains” or even full recoveries through their clinics. “It’s a new diagnosis, so I always tell my patients to think of this as a journey because I’m learning along with you,” said Jai Marathe, MD, an infectious disease physician at Boston Medical Center and an assistant professor of infectious diseases at Boston University Chobanian & Avedisian School of Medicine.
“Now we have 4 years of experience, but at the same time, no two long COVID patients are alike.”
Long COVID has also changed the way physicians view healthcare and how they practice medicine.
“I am a completely different person than I used to be because of this illness, and I don’t even have it. That is how profoundly it has affected how I view the universe,” said Dr. Malcolm. “I’ve been doing this for 4 years, and I’m very hopeful. But I don’t think about this in terms of months anymore. I think about this in terms of years.”
A version of this article first appeared on Medscape.com.
Stuart Malcolm, MD, a primary care physician who practices in Oregon and northern California, started seeing patients with long COVID early in the pandemic. Back then, he was frustrated by the obstacles and lack of standard diagnostic tests and treatments. Four years later, well, he still is.
“Something I learned the last few years is the logistics to get people care is really, really hard,” he said. “There’s a lot of frustration. It’s mostly frustration.”
For long COVID doctors and patients, there has been little to no progress addressing the challenges, leaving many discouraged. Researchers and clinicians now have a greater understanding of what health agencies formally call post-COVID condition, but the wide spectrum of symptoms, slow progress in launching pharmacologic clinical trials, and the research toward understanding the underlying causes mean standardized diagnostic tests and definitive treatments remain elusive.
“The frustration is that we aren’t able to help everyone with our current knowledge base. And I think the frustration lies not just with us physicians but also with patients because they’re at the point where if they tried everything, literally everything and haven’t gotten better,” said Zijian Chen, MD, director of the Mount Sinai Center for Post-COVID Care in New York City.
Wanted: More Funding, More Doctors, More Clinics
Between 10% and 20% of the estimated hundreds of millions of people infected worldwide with SARS-CoV-2 in the first 2 years went on to develop long-term symptoms. While many recover over time, doctors who have treated long COVID since 2020 said they see some patients still wrestling with the condition after 4 years.
The latest Centers for Disease Control and Prevention Household Pulse Survey, taken between March 5 and April 1, 2024, estimated that nearly 7% of the adult population — more than 18 million people — currently have long COVID. Data from other countries also suggest that millions have been living with long COVID for years now, and hundreds of thousands have seen their day-to-day activities significantly affected.
There is an urgent need for more funding, long COVID clinicians, multidisciplinary clinics, and education for non–long COVID physicians and specialists, doctors said. Instead, funding remains limited, clinics are closing, wait times are “horrendously long,” patients are left in limbo, and physicians are burning out.
“What’s changed in some ways is that there’s even less access to COVID rehab, which sounds crazy because there was very little to begin with,” said Alexandra Rendely, MD, a physical medicine and rehabilitation physician with the interdisciplinary Toronto Rehab, a part of the University Health Network of teaching hospitals in Toronto, Ontario, Canada.
“Patients are still being diagnosed every day, yet the resources available are becoming less and less.”
COVID-19 money earmarked during the pandemic was mostly limited to temporary emergency measures. As those funds dwindled, governments and institutions have decreased financial support. The Long COVID Moonshot campaign, organized by patients with long COVID, is pushing Congress to support $1 billion in annual research funding to close the financial chasm.
The Clinical Trial Conundrum
While long COVID clinics have come a long way in helping patients, gaps remain. Doctors may be unwilling to prescribe off-label treatments without proper clinical trials due to the potential risks and liabilities involved or due to the controversial or unconventional nature of the therapies, said Dr. Malcolm, who left his primary care practice more than 2 years ago to focus on long COVID.
In the absence of standard treatments, Dr. Malcolm and other doctors said they must take a trial-and-error approach in treating patients with long COVID that centers on addressing symptoms and not the underlying condition.
“There are actually a lot of treatments and a lot of them are not curative, but they can help people,” he said.
Dr. Malcolm, who is a medical director at Real Time Health Monitoring, a private clinic in the San Francisco Bay Area that specializes in long COVID and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), said it was important for him to be with a clinical team that understood and was supportive of his treatment decisions and was able to offer clinical support for those treatments if needed.
For physicians looking for clinical data before prescribing certain medications, the wait may be long. More than $1.5 billion in US federal funding has been earmarked to study long COVID, but the National Institutes of Health (NIH) has faced criticism from patients and scientists alike for its slow progress and emphasis on observational studies instead of research that could unravel the biological roots of long COVID. Among the clinical trials announced by the NIH’s RECOVER initiative, only a handful involve studying pharmaceutical treatments.
A 2023 editorial published in The Lancet called out the “dismal state of clinical research relative to the substantial burden of [long COVID]” and said, “we are clearly lacking tested pharmacological interventions that treat the underlying pathophysiology.” At the time of publication, it noted that of the 386 long COVID trials listed on ClinicalTrials.gov, only 12 were actually testing pharmacologic interventions.
There are also diagnostic and insurance barriers. The specialized tests that can detect long COVID anomalies are neither commonly known by primary care practitioners nor easily requested at the local lab, can be expensive, and are typically not covered by insurance, Dr. Malcolm explained.
Patients with long COVID also have the added barrier of being unable to advocate as easily because of their energy limitations, doctors said. Patients may appear outwardly fine, but fatigue and brain fog are among the many problems that cannot be measured in appearances. The condition has upended lives, some losing jobs, even homes, and the mental toll is why there is a “not insignificant” suicide rate.
One Patient’s 4-Year Journey
Charlie McCone, 34, used to be a tennis player and an active musician. But he’s spent the past 4 years mostly housebound, grappling with the aftermath of a SARS-CoV-2 infection he contracted in March 2020. He went from biking daily to work 10 miles and back to having at most 2 hours of energy per day.
In the first year alone, Mr. McCone saw more than two dozen doctors and specialists. The conditions now associated with long COVID, like ME/CFS, mast cell activation syndrome (a condition in which a patient experiences episodes of allergic symptoms such as hives, swelling, low blood pressure, and difficulty breathing), or dysautonomia (conditions that affect the autonomic nervous system, which controls automatic processes in the body) were not on physicians’ radars.
Then in 2021, he became bedbound for more than half a year after a Delta variant reinfection. He developed neurologic symptoms, including incapacitating fatigue, post-exertional malaise (where symptoms worsened after minimal physical or mental activity), left-sided weakness, and cognitive impairment. He stopped working altogether. But the worst was the shortness of breath he felt 24/7, even at rest. A battery of lab tests revealed nothing abnormal. He tried numerous drugs and the classic respiratory treatments.
Mr. McCone eventually connected with Dr. Malcolm over X and developed what he describes as an effective patient-doctor collaboration. When studies came out suggesting microclots were a common issue with patients with long COVID and positive outcomes were reported from anticoagulant therapy, they knew it could be one of the answers.
“After 3 weeks on [the antiplatelet drug], I was like, oh my god, my lungs are finally opening up,” said Mr. McCone. He has taken the medication for more than a year and a half, and some days he doesn’t even think about his respiratory symptoms.
“That trial-and-error process is just really long and hard and costly,” said Dr. Malcolm.
Today, fatigue and cognitive stamina are Mr. McCone’s main challenges, and he is far from recovered.
“[I had a] very fulfilling, happy life and now, it’s hard to think about. I’ve come a long way with my mental health and all this, but I’ve lost 4 years,” Mr. McCone said. “The prospect of me being here when I’m 40 seems very real ... so it’s pretty devastating.”
Lessons Learned, Hope Amid Ongoing Research
Despite the daunting obstacle, doctors said the science has come a long way for a new disease. We now know long COVID is likely caused by a combination of triggers, including viral reservoir in the tissue, inflammation, autoimmunity, and microclots; severity of infection is not necessarily an accurate risk factor predictor — long COVID can strike even those who had a mild infection; upward of 200 symptoms have been identified; and we know more about potential biomarkers that could lead to better diagnostic tools.
Unlike many other diseases and conditions with standard treatment protocols, long COVID treatments are typically aimed at addressing individual symptoms.
“It is very detailed and individualized to the patient’s specific symptoms and to the patient’s specific needs,” Dr. Rendely said. Symptoms can also fluctuate, relapse, or wax and wane, for example, so what ails a patient at their first doctor’s appointment could be completely different at the next appointment 2 months later.
Doctors are still hopeful the RECOVER research, which includes trials that look at autonomic and cognitive dysfunctions, will pave the way for more effective long COVID therapies. In Canada, Dr. Rendely is also eying the RECLAIM trial that is currently testing the effectiveness of pentoxifylline, which helps blood flow, and ibudilast, an anti-inflammatory drug.
Doctors are also hopeful when they see patients who have made “tremendous gains” or even full recoveries through their clinics. “It’s a new diagnosis, so I always tell my patients to think of this as a journey because I’m learning along with you,” said Jai Marathe, MD, an infectious disease physician at Boston Medical Center and an assistant professor of infectious diseases at Boston University Chobanian & Avedisian School of Medicine.
“Now we have 4 years of experience, but at the same time, no two long COVID patients are alike.”
Long COVID has also changed the way physicians view healthcare and how they practice medicine.
“I am a completely different person than I used to be because of this illness, and I don’t even have it. That is how profoundly it has affected how I view the universe,” said Dr. Malcolm. “I’ve been doing this for 4 years, and I’m very hopeful. But I don’t think about this in terms of months anymore. I think about this in terms of years.”
A version of this article first appeared on Medscape.com.
Stuart Malcolm, MD, a primary care physician who practices in Oregon and northern California, started seeing patients with long COVID early in the pandemic. Back then, he was frustrated by the obstacles and lack of standard diagnostic tests and treatments. Four years later, well, he still is.
“Something I learned the last few years is the logistics to get people care is really, really hard,” he said. “There’s a lot of frustration. It’s mostly frustration.”
For long COVID doctors and patients, there has been little to no progress addressing the challenges, leaving many discouraged. Researchers and clinicians now have a greater understanding of what health agencies formally call post-COVID condition, but the wide spectrum of symptoms, slow progress in launching pharmacologic clinical trials, and the research toward understanding the underlying causes mean standardized diagnostic tests and definitive treatments remain elusive.
“The frustration is that we aren’t able to help everyone with our current knowledge base. And I think the frustration lies not just with us physicians but also with patients because they’re at the point where if they tried everything, literally everything and haven’t gotten better,” said Zijian Chen, MD, director of the Mount Sinai Center for Post-COVID Care in New York City.
Wanted: More Funding, More Doctors, More Clinics
Between 10% and 20% of the estimated hundreds of millions of people infected worldwide with SARS-CoV-2 in the first 2 years went on to develop long-term symptoms. While many recover over time, doctors who have treated long COVID since 2020 said they see some patients still wrestling with the condition after 4 years.
The latest Centers for Disease Control and Prevention Household Pulse Survey, taken between March 5 and April 1, 2024, estimated that nearly 7% of the adult population — more than 18 million people — currently have long COVID. Data from other countries also suggest that millions have been living with long COVID for years now, and hundreds of thousands have seen their day-to-day activities significantly affected.
There is an urgent need for more funding, long COVID clinicians, multidisciplinary clinics, and education for non–long COVID physicians and specialists, doctors said. Instead, funding remains limited, clinics are closing, wait times are “horrendously long,” patients are left in limbo, and physicians are burning out.
“What’s changed in some ways is that there’s even less access to COVID rehab, which sounds crazy because there was very little to begin with,” said Alexandra Rendely, MD, a physical medicine and rehabilitation physician with the interdisciplinary Toronto Rehab, a part of the University Health Network of teaching hospitals in Toronto, Ontario, Canada.
“Patients are still being diagnosed every day, yet the resources available are becoming less and less.”
COVID-19 money earmarked during the pandemic was mostly limited to temporary emergency measures. As those funds dwindled, governments and institutions have decreased financial support. The Long COVID Moonshot campaign, organized by patients with long COVID, is pushing Congress to support $1 billion in annual research funding to close the financial chasm.
The Clinical Trial Conundrum
While long COVID clinics have come a long way in helping patients, gaps remain. Doctors may be unwilling to prescribe off-label treatments without proper clinical trials due to the potential risks and liabilities involved or due to the controversial or unconventional nature of the therapies, said Dr. Malcolm, who left his primary care practice more than 2 years ago to focus on long COVID.
In the absence of standard treatments, Dr. Malcolm and other doctors said they must take a trial-and-error approach in treating patients with long COVID that centers on addressing symptoms and not the underlying condition.
“There are actually a lot of treatments and a lot of them are not curative, but they can help people,” he said.
Dr. Malcolm, who is a medical director at Real Time Health Monitoring, a private clinic in the San Francisco Bay Area that specializes in long COVID and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), said it was important for him to be with a clinical team that understood and was supportive of his treatment decisions and was able to offer clinical support for those treatments if needed.
For physicians looking for clinical data before prescribing certain medications, the wait may be long. More than $1.5 billion in US federal funding has been earmarked to study long COVID, but the National Institutes of Health (NIH) has faced criticism from patients and scientists alike for its slow progress and emphasis on observational studies instead of research that could unravel the biological roots of long COVID. Among the clinical trials announced by the NIH’s RECOVER initiative, only a handful involve studying pharmaceutical treatments.
A 2023 editorial published in The Lancet called out the “dismal state of clinical research relative to the substantial burden of [long COVID]” and said, “we are clearly lacking tested pharmacological interventions that treat the underlying pathophysiology.” At the time of publication, it noted that of the 386 long COVID trials listed on ClinicalTrials.gov, only 12 were actually testing pharmacologic interventions.
There are also diagnostic and insurance barriers. The specialized tests that can detect long COVID anomalies are neither commonly known by primary care practitioners nor easily requested at the local lab, can be expensive, and are typically not covered by insurance, Dr. Malcolm explained.
Patients with long COVID also have the added barrier of being unable to advocate as easily because of their energy limitations, doctors said. Patients may appear outwardly fine, but fatigue and brain fog are among the many problems that cannot be measured in appearances. The condition has upended lives, some losing jobs, even homes, and the mental toll is why there is a “not insignificant” suicide rate.
One Patient’s 4-Year Journey
Charlie McCone, 34, used to be a tennis player and an active musician. But he’s spent the past 4 years mostly housebound, grappling with the aftermath of a SARS-CoV-2 infection he contracted in March 2020. He went from biking daily to work 10 miles and back to having at most 2 hours of energy per day.
In the first year alone, Mr. McCone saw more than two dozen doctors and specialists. The conditions now associated with long COVID, like ME/CFS, mast cell activation syndrome (a condition in which a patient experiences episodes of allergic symptoms such as hives, swelling, low blood pressure, and difficulty breathing), or dysautonomia (conditions that affect the autonomic nervous system, which controls automatic processes in the body) were not on physicians’ radars.
Then in 2021, he became bedbound for more than half a year after a Delta variant reinfection. He developed neurologic symptoms, including incapacitating fatigue, post-exertional malaise (where symptoms worsened after minimal physical or mental activity), left-sided weakness, and cognitive impairment. He stopped working altogether. But the worst was the shortness of breath he felt 24/7, even at rest. A battery of lab tests revealed nothing abnormal. He tried numerous drugs and the classic respiratory treatments.
Mr. McCone eventually connected with Dr. Malcolm over X and developed what he describes as an effective patient-doctor collaboration. When studies came out suggesting microclots were a common issue with patients with long COVID and positive outcomes were reported from anticoagulant therapy, they knew it could be one of the answers.
“After 3 weeks on [the antiplatelet drug], I was like, oh my god, my lungs are finally opening up,” said Mr. McCone. He has taken the medication for more than a year and a half, and some days he doesn’t even think about his respiratory symptoms.
“That trial-and-error process is just really long and hard and costly,” said Dr. Malcolm.
Today, fatigue and cognitive stamina are Mr. McCone’s main challenges, and he is far from recovered.
“[I had a] very fulfilling, happy life and now, it’s hard to think about. I’ve come a long way with my mental health and all this, but I’ve lost 4 years,” Mr. McCone said. “The prospect of me being here when I’m 40 seems very real ... so it’s pretty devastating.”
Lessons Learned, Hope Amid Ongoing Research
Despite the daunting obstacle, doctors said the science has come a long way for a new disease. We now know long COVID is likely caused by a combination of triggers, including viral reservoir in the tissue, inflammation, autoimmunity, and microclots; severity of infection is not necessarily an accurate risk factor predictor — long COVID can strike even those who had a mild infection; upward of 200 symptoms have been identified; and we know more about potential biomarkers that could lead to better diagnostic tools.
Unlike many other diseases and conditions with standard treatment protocols, long COVID treatments are typically aimed at addressing individual symptoms.
“It is very detailed and individualized to the patient’s specific symptoms and to the patient’s specific needs,” Dr. Rendely said. Symptoms can also fluctuate, relapse, or wax and wane, for example, so what ails a patient at their first doctor’s appointment could be completely different at the next appointment 2 months later.
Doctors are still hopeful the RECOVER research, which includes trials that look at autonomic and cognitive dysfunctions, will pave the way for more effective long COVID therapies. In Canada, Dr. Rendely is also eying the RECLAIM trial that is currently testing the effectiveness of pentoxifylline, which helps blood flow, and ibudilast, an anti-inflammatory drug.
Doctors are also hopeful when they see patients who have made “tremendous gains” or even full recoveries through their clinics. “It’s a new diagnosis, so I always tell my patients to think of this as a journey because I’m learning along with you,” said Jai Marathe, MD, an infectious disease physician at Boston Medical Center and an assistant professor of infectious diseases at Boston University Chobanian & Avedisian School of Medicine.
“Now we have 4 years of experience, but at the same time, no two long COVID patients are alike.”
Long COVID has also changed the way physicians view healthcare and how they practice medicine.
“I am a completely different person than I used to be because of this illness, and I don’t even have it. That is how profoundly it has affected how I view the universe,” said Dr. Malcolm. “I’ve been doing this for 4 years, and I’m very hopeful. But I don’t think about this in terms of months anymore. I think about this in terms of years.”
A version of this article first appeared on Medscape.com.