User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Stockholm3 Prostate Test Bests PSA for Prostate Cancer Risk in North America
The Stockholm3 (A3P Biomedical) multiparametic blood test has shown accuracy in assessing the risk of prostate cancer, exceeding that of the standard prostate-specific antigen (PSA)-based test, in Swedish patients.
“The Stockholm3 outperformed the PSA test overall and in every subcohort, with an impressive reduction of unnecessary biopsies of 40% to 50%, while maintaining relative sensitivity,” first author Scott E. Eggener, MD, said in presenting the findings at the ASCO Genitourinary Cancers Symposium. The test “has attractive characteristics in a diverse cohort, including within various racial and ethnic subgroups,” added Dr. Eggener, professor of surgery and radiology at the University of Chicago.
While the PSA test, the standard-of-care in prostate cancer risk assessment, reduces mortality, the test is known to have a risk for false positive results, leading to unnecessary prostate biopsies, as well as overdiagnosis of low-risk prostate cancers, Dr. Eggener explained in his talk.
Randomized trials do show “fewer men die from prostate cancer with screening [with PSA testing], however, the likelihood of unnecessarily finding out about a cancer, undergoing treatment, and exposure to potential treatment-related side effects is significantly higher,” Dr. Eggener said in a interview.
The Stockholm3 clinical diagnostic prostate cancer test, which has been used in Sweden and Norway since 2017, was validated in a sample of nearly 60,000 men in the STHLM3 study (doi: 10.1016/S1470-2045[15]00361-7), which was published in The Lancet Oncology in December 2015. That study showed significant improvement over PSA alone detection of prostate cancers with a Gleason score of at least 7 (P < .0001), Dr. Eggener explained.
The test combines five plasma protein markers, including total and free PSA, PSP94, GDF-15 and KLK2, along with 101 genetic markers and clinical patient data, including age, previous biopsy results and family history.
Because the Stockholm3 test was validated in a Swedish population cohort, evidence on the accuracy of the test in other racial and ethnic populations is lacking, the authors noted in the abstract.
Study Methods and Results
To further investigate, Dr. Eggener and his colleagues conducted the prospective SEPTA trial, involving 2,129 men with no known prostate cancer but clinical indications for prostate biopsy, who were referred for prostate biopsy at 17 North American sites between 2019 and 2023.
Among the men, 24% were self-identified as African American/Black; 46% were White/Caucasian; 14% were Hispanic/Latina; and 16% were Asian. The men’s median age was 63; their median PSA value was 6.1 ng/mL, according to the abstract.
Of the patients, 16% received magnetic resonance imaging (MRI)-targeted biopsies and 20% had prior benign biopsies, the abstract notes.
Biopsy results showed that clinically significant prostate cancer, defined as International Society of Urological Pathology (ISUP) Gleason Grade group ≥ 2, was detected in 29% of patients, with 14% having ISUP 1 cancer and 57% of cases having been benign, according to the abstract.
Overall detection rates of grade 2 or higher were 37% for African American/Black, 28% for White/Caucasian, 29% for Hispanic/Latino, and 21% Asian.
In terms of sensitivity of the two tests, the Stockholm3 (cut-point of ≥ 15) was noninferior compared with the traditional PSA cut-point of ≥ 4 ng/mL (relative sensitivity 0.95).
Results were consistent across ethnic subgroups: noninferior sensitivity (0.91-0.98) and superior specificity (2.51-4.70), the abstract authors reported.
Compared with the use of the PSA test’s cut-point of ≥ 4 ng/mL, the use of Stockholm3’s cut-point of ≥ 15 or higher would have reduced unnecessary biopsies by 45% overall, including by 46% among Asian and Black/African American patients, by 53% in Hispanic patients and 42% in White patients, according to the abstract.
Overall, “utilization of Stockholm3 improves the net benefit:harm ratio of PSA screening by identifying nearly all men with Gleason Grade 2 or higher, while minimizing the number of men undergoing biopsy who show no cancer or an indolent cancer (Gleason Grade 1),” Dr. Eggener said in an interview.
Stockholm3 Expected to be Available in U.S. This Year
The test, which has been available in Sweden since 2018, is expected to become commercially available in the United States in early 2024. Dr. Eggener noted that “cost of the test hasn’t been finalized, but will be considerably more expensive than PSA, which is very cheap.”
Commenting on the findings, Bradley McGregor, MD, of the Dana Farber Cancer Institute and an ASCO oncology expert, noted that “ultimately, the goal [of prostate screening] is to be able to better decide when a biopsy is going to yield a clinically relevant prostate cancer, [and] this study gives us some insight of the use of the Stockholm3 tool in a more diverse population.
“How the tool will be utilized in the clinic and in guidelines is something that is a work in progress,” he added. “But I think this provides some reassurances that this will have implications beyond just the homogeneous populations in the original studies.”
Dr. McGregor noted that considerations of the issue of cost should be weighed against the potential costs involved in unnecessary biopsies and a host of other costs that can arise with an inaccurate risk assessment.
“If there is a way to avoid those costs and help us have more confidence in the prostate test results and intervene at an earlier stage, I think that’s exciting,” he said.
Dr. Eggener has consulted for A3P Biomedical but had no financial relationship with the company to disclose.
The Stockholm3 (A3P Biomedical) multiparametic blood test has shown accuracy in assessing the risk of prostate cancer, exceeding that of the standard prostate-specific antigen (PSA)-based test, in Swedish patients.
“The Stockholm3 outperformed the PSA test overall and in every subcohort, with an impressive reduction of unnecessary biopsies of 40% to 50%, while maintaining relative sensitivity,” first author Scott E. Eggener, MD, said in presenting the findings at the ASCO Genitourinary Cancers Symposium. The test “has attractive characteristics in a diverse cohort, including within various racial and ethnic subgroups,” added Dr. Eggener, professor of surgery and radiology at the University of Chicago.
While the PSA test, the standard-of-care in prostate cancer risk assessment, reduces mortality, the test is known to have a risk for false positive results, leading to unnecessary prostate biopsies, as well as overdiagnosis of low-risk prostate cancers, Dr. Eggener explained in his talk.
Randomized trials do show “fewer men die from prostate cancer with screening [with PSA testing], however, the likelihood of unnecessarily finding out about a cancer, undergoing treatment, and exposure to potential treatment-related side effects is significantly higher,” Dr. Eggener said in a interview.
The Stockholm3 clinical diagnostic prostate cancer test, which has been used in Sweden and Norway since 2017, was validated in a sample of nearly 60,000 men in the STHLM3 study (doi: 10.1016/S1470-2045[15]00361-7), which was published in The Lancet Oncology in December 2015. That study showed significant improvement over PSA alone detection of prostate cancers with a Gleason score of at least 7 (P < .0001), Dr. Eggener explained.
The test combines five plasma protein markers, including total and free PSA, PSP94, GDF-15 and KLK2, along with 101 genetic markers and clinical patient data, including age, previous biopsy results and family history.
Because the Stockholm3 test was validated in a Swedish population cohort, evidence on the accuracy of the test in other racial and ethnic populations is lacking, the authors noted in the abstract.
Study Methods and Results
To further investigate, Dr. Eggener and his colleagues conducted the prospective SEPTA trial, involving 2,129 men with no known prostate cancer but clinical indications for prostate biopsy, who were referred for prostate biopsy at 17 North American sites between 2019 and 2023.
Among the men, 24% were self-identified as African American/Black; 46% were White/Caucasian; 14% were Hispanic/Latina; and 16% were Asian. The men’s median age was 63; their median PSA value was 6.1 ng/mL, according to the abstract.
Of the patients, 16% received magnetic resonance imaging (MRI)-targeted biopsies and 20% had prior benign biopsies, the abstract notes.
Biopsy results showed that clinically significant prostate cancer, defined as International Society of Urological Pathology (ISUP) Gleason Grade group ≥ 2, was detected in 29% of patients, with 14% having ISUP 1 cancer and 57% of cases having been benign, according to the abstract.
Overall detection rates of grade 2 or higher were 37% for African American/Black, 28% for White/Caucasian, 29% for Hispanic/Latino, and 21% Asian.
In terms of sensitivity of the two tests, the Stockholm3 (cut-point of ≥ 15) was noninferior compared with the traditional PSA cut-point of ≥ 4 ng/mL (relative sensitivity 0.95).
Results were consistent across ethnic subgroups: noninferior sensitivity (0.91-0.98) and superior specificity (2.51-4.70), the abstract authors reported.
Compared with the use of the PSA test’s cut-point of ≥ 4 ng/mL, the use of Stockholm3’s cut-point of ≥ 15 or higher would have reduced unnecessary biopsies by 45% overall, including by 46% among Asian and Black/African American patients, by 53% in Hispanic patients and 42% in White patients, according to the abstract.
Overall, “utilization of Stockholm3 improves the net benefit:harm ratio of PSA screening by identifying nearly all men with Gleason Grade 2 or higher, while minimizing the number of men undergoing biopsy who show no cancer or an indolent cancer (Gleason Grade 1),” Dr. Eggener said in an interview.
Stockholm3 Expected to be Available in U.S. This Year
The test, which has been available in Sweden since 2018, is expected to become commercially available in the United States in early 2024. Dr. Eggener noted that “cost of the test hasn’t been finalized, but will be considerably more expensive than PSA, which is very cheap.”
Commenting on the findings, Bradley McGregor, MD, of the Dana Farber Cancer Institute and an ASCO oncology expert, noted that “ultimately, the goal [of prostate screening] is to be able to better decide when a biopsy is going to yield a clinically relevant prostate cancer, [and] this study gives us some insight of the use of the Stockholm3 tool in a more diverse population.
“How the tool will be utilized in the clinic and in guidelines is something that is a work in progress,” he added. “But I think this provides some reassurances that this will have implications beyond just the homogeneous populations in the original studies.”
Dr. McGregor noted that considerations of the issue of cost should be weighed against the potential costs involved in unnecessary biopsies and a host of other costs that can arise with an inaccurate risk assessment.
“If there is a way to avoid those costs and help us have more confidence in the prostate test results and intervene at an earlier stage, I think that’s exciting,” he said.
Dr. Eggener has consulted for A3P Biomedical but had no financial relationship with the company to disclose.
The Stockholm3 (A3P Biomedical) multiparametic blood test has shown accuracy in assessing the risk of prostate cancer, exceeding that of the standard prostate-specific antigen (PSA)-based test, in Swedish patients.
“The Stockholm3 outperformed the PSA test overall and in every subcohort, with an impressive reduction of unnecessary biopsies of 40% to 50%, while maintaining relative sensitivity,” first author Scott E. Eggener, MD, said in presenting the findings at the ASCO Genitourinary Cancers Symposium. The test “has attractive characteristics in a diverse cohort, including within various racial and ethnic subgroups,” added Dr. Eggener, professor of surgery and radiology at the University of Chicago.
While the PSA test, the standard-of-care in prostate cancer risk assessment, reduces mortality, the test is known to have a risk for false positive results, leading to unnecessary prostate biopsies, as well as overdiagnosis of low-risk prostate cancers, Dr. Eggener explained in his talk.
Randomized trials do show “fewer men die from prostate cancer with screening [with PSA testing], however, the likelihood of unnecessarily finding out about a cancer, undergoing treatment, and exposure to potential treatment-related side effects is significantly higher,” Dr. Eggener said in a interview.
The Stockholm3 clinical diagnostic prostate cancer test, which has been used in Sweden and Norway since 2017, was validated in a sample of nearly 60,000 men in the STHLM3 study (doi: 10.1016/S1470-2045[15]00361-7), which was published in The Lancet Oncology in December 2015. That study showed significant improvement over PSA alone detection of prostate cancers with a Gleason score of at least 7 (P < .0001), Dr. Eggener explained.
The test combines five plasma protein markers, including total and free PSA, PSP94, GDF-15 and KLK2, along with 101 genetic markers and clinical patient data, including age, previous biopsy results and family history.
Because the Stockholm3 test was validated in a Swedish population cohort, evidence on the accuracy of the test in other racial and ethnic populations is lacking, the authors noted in the abstract.
Study Methods and Results
To further investigate, Dr. Eggener and his colleagues conducted the prospective SEPTA trial, involving 2,129 men with no known prostate cancer but clinical indications for prostate biopsy, who were referred for prostate biopsy at 17 North American sites between 2019 and 2023.
Among the men, 24% were self-identified as African American/Black; 46% were White/Caucasian; 14% were Hispanic/Latina; and 16% were Asian. The men’s median age was 63; their median PSA value was 6.1 ng/mL, according to the abstract.
Of the patients, 16% received magnetic resonance imaging (MRI)-targeted biopsies and 20% had prior benign biopsies, the abstract notes.
Biopsy results showed that clinically significant prostate cancer, defined as International Society of Urological Pathology (ISUP) Gleason Grade group ≥ 2, was detected in 29% of patients, with 14% having ISUP 1 cancer and 57% of cases having been benign, according to the abstract.
Overall detection rates of grade 2 or higher were 37% for African American/Black, 28% for White/Caucasian, 29% for Hispanic/Latino, and 21% Asian.
In terms of sensitivity of the two tests, the Stockholm3 (cut-point of ≥ 15) was noninferior compared with the traditional PSA cut-point of ≥ 4 ng/mL (relative sensitivity 0.95).
Results were consistent across ethnic subgroups: noninferior sensitivity (0.91-0.98) and superior specificity (2.51-4.70), the abstract authors reported.
Compared with the use of the PSA test’s cut-point of ≥ 4 ng/mL, the use of Stockholm3’s cut-point of ≥ 15 or higher would have reduced unnecessary biopsies by 45% overall, including by 46% among Asian and Black/African American patients, by 53% in Hispanic patients and 42% in White patients, according to the abstract.
Overall, “utilization of Stockholm3 improves the net benefit:harm ratio of PSA screening by identifying nearly all men with Gleason Grade 2 or higher, while minimizing the number of men undergoing biopsy who show no cancer or an indolent cancer (Gleason Grade 1),” Dr. Eggener said in an interview.
Stockholm3 Expected to be Available in U.S. This Year
The test, which has been available in Sweden since 2018, is expected to become commercially available in the United States in early 2024. Dr. Eggener noted that “cost of the test hasn’t been finalized, but will be considerably more expensive than PSA, which is very cheap.”
Commenting on the findings, Bradley McGregor, MD, of the Dana Farber Cancer Institute and an ASCO oncology expert, noted that “ultimately, the goal [of prostate screening] is to be able to better decide when a biopsy is going to yield a clinically relevant prostate cancer, [and] this study gives us some insight of the use of the Stockholm3 tool in a more diverse population.
“How the tool will be utilized in the clinic and in guidelines is something that is a work in progress,” he added. “But I think this provides some reassurances that this will have implications beyond just the homogeneous populations in the original studies.”
Dr. McGregor noted that considerations of the issue of cost should be weighed against the potential costs involved in unnecessary biopsies and a host of other costs that can arise with an inaccurate risk assessment.
“If there is a way to avoid those costs and help us have more confidence in the prostate test results and intervene at an earlier stage, I think that’s exciting,” he said.
Dr. Eggener has consulted for A3P Biomedical but had no financial relationship with the company to disclose.
FROM ASCO GU 2024
More Young Women Being Diagnosed With Breast Cancer Than Ever Before
This transcript has been edited for clarity.
From the year 2000 until around 2016, the incidence of breast cancer among young women — those under age 50 — rose steadily, if slowly.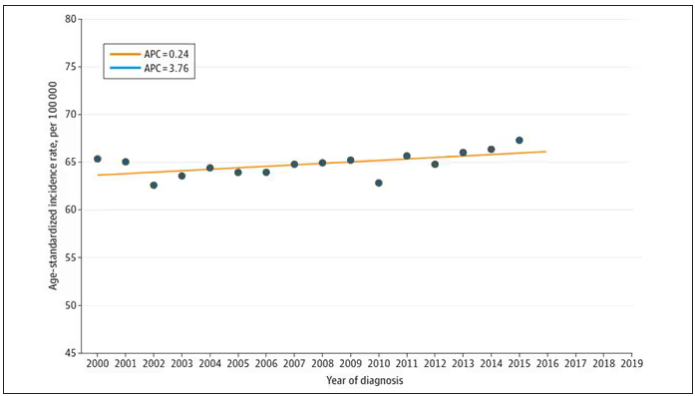
And then this happened: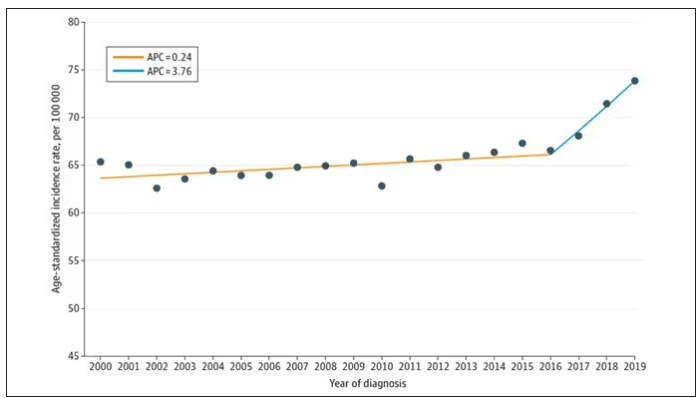
I look at a lot of graphs in my line of work, and it’s not too often that one actually makes me say “What the hell?” out loud. But this one did. Why are young women all of a sudden more likely to get breast cancer?
The graph comes from this paper, Breast cancer incidence among us women aged 20 to 49 years by race, stage, and hormone receptor status, appearing in JAMA Network Open
Researchers from Washington University in St. Louis utilized SEER registries to conduct their analyses. SEER is a public database from the National Cancer Institute with coverage of 27% of the US population and a long track record of statistical backbone to translate the data from SEER to numbers that are representative of the population at large.
From 2000 to 2019, more than 200,000 women were diagnosed with primary invasive breast cancer in the dataset, and I’ve already given you the top-line results. Of course, when you see a graph like this, the next question really needs to be why?
Fortunately, the SEER dataset contains a lot more information than simply whether someone was diagnosed with cancer. In the case of breast cancer, there is information about the patient’s demographics, the hormone status of the cancer, the stage, and so on. Using those additional data points can help the authors, and us, start to formulate some hypotheses as to what is happening here.
Let’s start with something a bit tricky about this kind of data. We see an uptick in new breast cancer diagnoses among young women in recent years. We need to tease that uptick apart a bit. It could be that it is the year that is the key factor here. In other words, it is simply that more women are getting breast cancer since 2016 and so more young women are getting breast cancer since 2016. These are known as period effects.
Or is there something unique to young women — something about their environmental exposures that put them at higher risk than they would have been had they been born at some other time? These are known as cohort effects.
The researchers teased these two effects apart, as you can see here, and concluded that, well, it’s both.
Stage of cancer at diagnosis can give us some more insight into what is happening. These results are pretty interesting. These higher cancer rates are due primarily to stage I and stage IV cancers, not stage II and stage III cancers.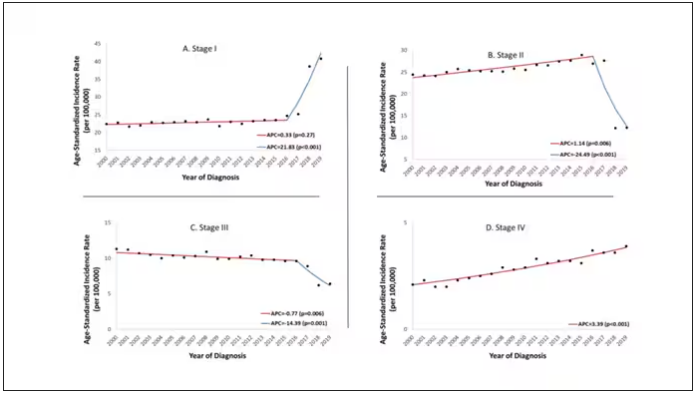
The rising incidence of stage I cancers could reflect better detection, though many of the women in this cohort would not have been old enough to quality for screening mammograms. That said, increased awareness about genetic risk and family history might be leading younger women to get screened, picking up more early cancers. Additionally, much of the increased incidence was with estrogen receptor–positive tumors, which might reflect the fact that women in this cohort are tending to have fewer children, and children later in life.
So why the rise in stage IV breast cancer? Well, precisely because younger women are not recommended to get screening mammograms; those who detect a lump on their own are likely to be at a more advanced stage. But I’m not sure why that would be changing recently. The authors argue that an increase in overweight and obesity in the country might be to blame here. Prior studies have shown that higher BMI is associated with higher stage at breast cancer diagnosis.
Of course, we can speculate as to multiple other causes as well: environmental toxins, pollution, hormone exposures, and so on. Figuring this out will be the work of multiple other studies. In the meantime, we should remember that the landscape of cancer is continuously changing. And that means we need to adapt to it. If these trends continue, national agencies may need to reconsider their guidelines for when screening mammography should begin — at least in some groups of young women.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
From the year 2000 until around 2016, the incidence of breast cancer among young women — those under age 50 — rose steadily, if slowly.
And then this happened:
I look at a lot of graphs in my line of work, and it’s not too often that one actually makes me say “What the hell?” out loud. But this one did. Why are young women all of a sudden more likely to get breast cancer?
The graph comes from this paper, Breast cancer incidence among us women aged 20 to 49 years by race, stage, and hormone receptor status, appearing in JAMA Network Open
Researchers from Washington University in St. Louis utilized SEER registries to conduct their analyses. SEER is a public database from the National Cancer Institute with coverage of 27% of the US population and a long track record of statistical backbone to translate the data from SEER to numbers that are representative of the population at large.
From 2000 to 2019, more than 200,000 women were diagnosed with primary invasive breast cancer in the dataset, and I’ve already given you the top-line results. Of course, when you see a graph like this, the next question really needs to be why?
Fortunately, the SEER dataset contains a lot more information than simply whether someone was diagnosed with cancer. In the case of breast cancer, there is information about the patient’s demographics, the hormone status of the cancer, the stage, and so on. Using those additional data points can help the authors, and us, start to formulate some hypotheses as to what is happening here.
Let’s start with something a bit tricky about this kind of data. We see an uptick in new breast cancer diagnoses among young women in recent years. We need to tease that uptick apart a bit. It could be that it is the year that is the key factor here. In other words, it is simply that more women are getting breast cancer since 2016 and so more young women are getting breast cancer since 2016. These are known as period effects.
Or is there something unique to young women — something about their environmental exposures that put them at higher risk than they would have been had they been born at some other time? These are known as cohort effects.
The researchers teased these two effects apart, as you can see here, and concluded that, well, it’s both.
Stage of cancer at diagnosis can give us some more insight into what is happening. These results are pretty interesting. These higher cancer rates are due primarily to stage I and stage IV cancers, not stage II and stage III cancers.
The rising incidence of stage I cancers could reflect better detection, though many of the women in this cohort would not have been old enough to quality for screening mammograms. That said, increased awareness about genetic risk and family history might be leading younger women to get screened, picking up more early cancers. Additionally, much of the increased incidence was with estrogen receptor–positive tumors, which might reflect the fact that women in this cohort are tending to have fewer children, and children later in life.
So why the rise in stage IV breast cancer? Well, precisely because younger women are not recommended to get screening mammograms; those who detect a lump on their own are likely to be at a more advanced stage. But I’m not sure why that would be changing recently. The authors argue that an increase in overweight and obesity in the country might be to blame here. Prior studies have shown that higher BMI is associated with higher stage at breast cancer diagnosis.
Of course, we can speculate as to multiple other causes as well: environmental toxins, pollution, hormone exposures, and so on. Figuring this out will be the work of multiple other studies. In the meantime, we should remember that the landscape of cancer is continuously changing. And that means we need to adapt to it. If these trends continue, national agencies may need to reconsider their guidelines for when screening mammography should begin — at least in some groups of young women.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
From the year 2000 until around 2016, the incidence of breast cancer among young women — those under age 50 — rose steadily, if slowly.
And then this happened:
I look at a lot of graphs in my line of work, and it’s not too often that one actually makes me say “What the hell?” out loud. But this one did. Why are young women all of a sudden more likely to get breast cancer?
The graph comes from this paper, Breast cancer incidence among us women aged 20 to 49 years by race, stage, and hormone receptor status, appearing in JAMA Network Open
Researchers from Washington University in St. Louis utilized SEER registries to conduct their analyses. SEER is a public database from the National Cancer Institute with coverage of 27% of the US population and a long track record of statistical backbone to translate the data from SEER to numbers that are representative of the population at large.
From 2000 to 2019, more than 200,000 women were diagnosed with primary invasive breast cancer in the dataset, and I’ve already given you the top-line results. Of course, when you see a graph like this, the next question really needs to be why?
Fortunately, the SEER dataset contains a lot more information than simply whether someone was diagnosed with cancer. In the case of breast cancer, there is information about the patient’s demographics, the hormone status of the cancer, the stage, and so on. Using those additional data points can help the authors, and us, start to formulate some hypotheses as to what is happening here.
Let’s start with something a bit tricky about this kind of data. We see an uptick in new breast cancer diagnoses among young women in recent years. We need to tease that uptick apart a bit. It could be that it is the year that is the key factor here. In other words, it is simply that more women are getting breast cancer since 2016 and so more young women are getting breast cancer since 2016. These are known as period effects.
Or is there something unique to young women — something about their environmental exposures that put them at higher risk than they would have been had they been born at some other time? These are known as cohort effects.
The researchers teased these two effects apart, as you can see here, and concluded that, well, it’s both.
Stage of cancer at diagnosis can give us some more insight into what is happening. These results are pretty interesting. These higher cancer rates are due primarily to stage I and stage IV cancers, not stage II and stage III cancers.
The rising incidence of stage I cancers could reflect better detection, though many of the women in this cohort would not have been old enough to quality for screening mammograms. That said, increased awareness about genetic risk and family history might be leading younger women to get screened, picking up more early cancers. Additionally, much of the increased incidence was with estrogen receptor–positive tumors, which might reflect the fact that women in this cohort are tending to have fewer children, and children later in life.
So why the rise in stage IV breast cancer? Well, precisely because younger women are not recommended to get screening mammograms; those who detect a lump on their own are likely to be at a more advanced stage. But I’m not sure why that would be changing recently. The authors argue that an increase in overweight and obesity in the country might be to blame here. Prior studies have shown that higher BMI is associated with higher stage at breast cancer diagnosis.
Of course, we can speculate as to multiple other causes as well: environmental toxins, pollution, hormone exposures, and so on. Figuring this out will be the work of multiple other studies. In the meantime, we should remember that the landscape of cancer is continuously changing. And that means we need to adapt to it. If these trends continue, national agencies may need to reconsider their guidelines for when screening mammography should begin — at least in some groups of young women.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Chemo-Free Maintenance Strategies May Boost Survival in TNBC
TOPLINE:
METHODOLOGY:
- First-line standard therapy for advanced TNBC generally includes taxane- or platinum-based chemotherapy which poses challenging toxicities. Exploring chemotherapy-free maintenance strategies may provide adequate disease control and improve patient quality of life.
- The researchers evaluated 45 patients, at five sites in the Republic of Korea, the United States, and Singapore, with TNBC who had ongoing stable disease or complete/partial response from first- or second-line platinum-based chemotherapy.
- The patients were randomized 1:1 to receive olaparib 300 mg twice daily with or without durvalumab 1500 mg on day 1 every 4 weeks.
- The authors compared PFS with a historical control of continued platinum-based therapy. An improvement to 4 months with maintenance therapy was considered clinically significant.
TAKEAWAY:
- After a follow-up of 9.8 months, patients who received olaparib alone demonstrated median PFS of 4.0 months, and those who received the combination therapy had median PFS of 6.1 months.
- Clinical benefit rates, defined as stable disease for at least 24 weeks or complete/partial response, were reported in 44% of the monotherapy group and 36% of the combination therapy group.
- Sustained clinical benefit was evident irrespective of germline BRCA mutation or programmed death-ligand 1 status, although it tended to be associated with complete or partial response to prior platinum.
- Grade 3-4 adverse events were reported in nine patients (39%) in the olaparib arm and eight patients (36%) in the combination arm. No treatment-related deaths or new safety signals were observed.
IN PRACTICE:
“Maintenance regimens are rarely used in [triple-negative breast cancer] but offer the possibility of more tolerable long-term treatment avoiding some of the chemotherapy-related side effects of more aggressive regimens, as is standard in the first-line treatment of HER2-positive advanced breast cancer,” the researchers concluded.
SOURCE:
This study, led by Tira J. Tan from Duke-NUS Medical School, Singapore, was published online on January 18, 2024, in Clinical Cancer Research.
LIMITATIONS:
The main limitations were the small sample size and lack of a standard control arm. Most patients (76%) were Asian, limiting generalizability. The trial was not designed to compare olaparib monotherapy and olaparib plus durvalumab regimens.
DISCLOSURES:
AstraZeneca Pharmaceuticals LP supported this study. Several authors reported financial support from various sources.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- First-line standard therapy for advanced TNBC generally includes taxane- or platinum-based chemotherapy which poses challenging toxicities. Exploring chemotherapy-free maintenance strategies may provide adequate disease control and improve patient quality of life.
- The researchers evaluated 45 patients, at five sites in the Republic of Korea, the United States, and Singapore, with TNBC who had ongoing stable disease or complete/partial response from first- or second-line platinum-based chemotherapy.
- The patients were randomized 1:1 to receive olaparib 300 mg twice daily with or without durvalumab 1500 mg on day 1 every 4 weeks.
- The authors compared PFS with a historical control of continued platinum-based therapy. An improvement to 4 months with maintenance therapy was considered clinically significant.
TAKEAWAY:
- After a follow-up of 9.8 months, patients who received olaparib alone demonstrated median PFS of 4.0 months, and those who received the combination therapy had median PFS of 6.1 months.
- Clinical benefit rates, defined as stable disease for at least 24 weeks or complete/partial response, were reported in 44% of the monotherapy group and 36% of the combination therapy group.
- Sustained clinical benefit was evident irrespective of germline BRCA mutation or programmed death-ligand 1 status, although it tended to be associated with complete or partial response to prior platinum.
- Grade 3-4 adverse events were reported in nine patients (39%) in the olaparib arm and eight patients (36%) in the combination arm. No treatment-related deaths or new safety signals were observed.
IN PRACTICE:
“Maintenance regimens are rarely used in [triple-negative breast cancer] but offer the possibility of more tolerable long-term treatment avoiding some of the chemotherapy-related side effects of more aggressive regimens, as is standard in the first-line treatment of HER2-positive advanced breast cancer,” the researchers concluded.
SOURCE:
This study, led by Tira J. Tan from Duke-NUS Medical School, Singapore, was published online on January 18, 2024, in Clinical Cancer Research.
LIMITATIONS:
The main limitations were the small sample size and lack of a standard control arm. Most patients (76%) were Asian, limiting generalizability. The trial was not designed to compare olaparib monotherapy and olaparib plus durvalumab regimens.
DISCLOSURES:
AstraZeneca Pharmaceuticals LP supported this study. Several authors reported financial support from various sources.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- First-line standard therapy for advanced TNBC generally includes taxane- or platinum-based chemotherapy which poses challenging toxicities. Exploring chemotherapy-free maintenance strategies may provide adequate disease control and improve patient quality of life.
- The researchers evaluated 45 patients, at five sites in the Republic of Korea, the United States, and Singapore, with TNBC who had ongoing stable disease or complete/partial response from first- or second-line platinum-based chemotherapy.
- The patients were randomized 1:1 to receive olaparib 300 mg twice daily with or without durvalumab 1500 mg on day 1 every 4 weeks.
- The authors compared PFS with a historical control of continued platinum-based therapy. An improvement to 4 months with maintenance therapy was considered clinically significant.
TAKEAWAY:
- After a follow-up of 9.8 months, patients who received olaparib alone demonstrated median PFS of 4.0 months, and those who received the combination therapy had median PFS of 6.1 months.
- Clinical benefit rates, defined as stable disease for at least 24 weeks or complete/partial response, were reported in 44% of the monotherapy group and 36% of the combination therapy group.
- Sustained clinical benefit was evident irrespective of germline BRCA mutation or programmed death-ligand 1 status, although it tended to be associated with complete or partial response to prior platinum.
- Grade 3-4 adverse events were reported in nine patients (39%) in the olaparib arm and eight patients (36%) in the combination arm. No treatment-related deaths or new safety signals were observed.
IN PRACTICE:
“Maintenance regimens are rarely used in [triple-negative breast cancer] but offer the possibility of more tolerable long-term treatment avoiding some of the chemotherapy-related side effects of more aggressive regimens, as is standard in the first-line treatment of HER2-positive advanced breast cancer,” the researchers concluded.
SOURCE:
This study, led by Tira J. Tan from Duke-NUS Medical School, Singapore, was published online on January 18, 2024, in Clinical Cancer Research.
LIMITATIONS:
The main limitations were the small sample size and lack of a standard control arm. Most patients (76%) were Asian, limiting generalizability. The trial was not designed to compare olaparib monotherapy and olaparib plus durvalumab regimens.
DISCLOSURES:
AstraZeneca Pharmaceuticals LP supported this study. Several authors reported financial support from various sources.
A version of this article appeared on Medscape.com.
Treatment Sequence May Impact Pancreatic Cancer Survival
TOPLINE:
METHODOLOGY:
- Despite therapeutic advances, survival among patients with unresectable and/or metastatic pancreatic ductal adenocarcinoma has not markedly improved in recent years.
- In the current analysis, researchers evaluated whether treatment sequence could affect survival outcomes in this patient population.
- To this end , researchers conducted a single institution, retrospective analysis of patients who received different lines of treatment between January 2015 and December 2021.
- The most common first-line therapy was nab-paclitaxel plus S-1 (58%), followed by FOLFIRINOX (10%), nab-paclitaxel plus gemcitabine (8%), gemcitabine alone (7%), gemcitabine plus oxaliplatin (6%); second-line therapies, in order of frequency, included gemcitabine combination therapy (48%), nab-paclitaxel combination therapy (19%), FOLFIRINOX (10%), and gemcitabine alone (7%); third-line treatments consisted of FOLFIRINOX (31%), irinotecan or oxaliplatin combination therapy (23%), immunotherapy (19%), and gemcitabine combination therapy (10%).
TAKEAWAY:
- Overall, progression occurred in 90% of patients, and the median overall survival was 12.0 months, with only 48% of patients able to start a third-line therapy.
- The researchers focused on three common therapy sequences: nab-paclitaxel plus gemcitabine or nab-paclitaxel combination therapy as first-line and FOLFIRINOX as second-line (line A); nab-paclitaxel combination therapy to gemcitabine combination therapy to FOLFIRINOX (line B); and nab-paclitaxel combination therapy, to gemcitabine combination therapy, to oxaliplatin or irinotecan combination therapy (line C).
- Overall, the researchers observed a median overall survival of 14 months among patients receiving line A and C sequences and 18 months with line B.
- Patients receiving line B therapy demonstrated a 52% lower risk for death compared with those receiving line A treatment (hazard ratio [HR], 0.48; P = .018) and a 75% reduced risk for death compared with those on the line C sequence (HR, 0.25; P = .040).
IN PRACTICE:
“Our study provides real-world evidence for the effectiveness of different treatment sequences and underscores the [impact of] treatment sequences on survival outcome when considering the entire management in advanced pancreatic ductal adenocarcinoma,” the authors concluded.
SOURCE:
The study, led by Guanghai Dai, MD, from the Chinese People’s Liberation Army General Hospital, Beijing, was published in BMC Cancer on January 12, 2024.
LIMITATIONS:
The study was a single-center, retrospective analysis.
DISCLOSURES:
The paper was funded by Beijing natural science foundation. The authors did not declare any relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Despite therapeutic advances, survival among patients with unresectable and/or metastatic pancreatic ductal adenocarcinoma has not markedly improved in recent years.
- In the current analysis, researchers evaluated whether treatment sequence could affect survival outcomes in this patient population.
- To this end , researchers conducted a single institution, retrospective analysis of patients who received different lines of treatment between January 2015 and December 2021.
- The most common first-line therapy was nab-paclitaxel plus S-1 (58%), followed by FOLFIRINOX (10%), nab-paclitaxel plus gemcitabine (8%), gemcitabine alone (7%), gemcitabine plus oxaliplatin (6%); second-line therapies, in order of frequency, included gemcitabine combination therapy (48%), nab-paclitaxel combination therapy (19%), FOLFIRINOX (10%), and gemcitabine alone (7%); third-line treatments consisted of FOLFIRINOX (31%), irinotecan or oxaliplatin combination therapy (23%), immunotherapy (19%), and gemcitabine combination therapy (10%).
TAKEAWAY:
- Overall, progression occurred in 90% of patients, and the median overall survival was 12.0 months, with only 48% of patients able to start a third-line therapy.
- The researchers focused on three common therapy sequences: nab-paclitaxel plus gemcitabine or nab-paclitaxel combination therapy as first-line and FOLFIRINOX as second-line (line A); nab-paclitaxel combination therapy to gemcitabine combination therapy to FOLFIRINOX (line B); and nab-paclitaxel combination therapy, to gemcitabine combination therapy, to oxaliplatin or irinotecan combination therapy (line C).
- Overall, the researchers observed a median overall survival of 14 months among patients receiving line A and C sequences and 18 months with line B.
- Patients receiving line B therapy demonstrated a 52% lower risk for death compared with those receiving line A treatment (hazard ratio [HR], 0.48; P = .018) and a 75% reduced risk for death compared with those on the line C sequence (HR, 0.25; P = .040).
IN PRACTICE:
“Our study provides real-world evidence for the effectiveness of different treatment sequences and underscores the [impact of] treatment sequences on survival outcome when considering the entire management in advanced pancreatic ductal adenocarcinoma,” the authors concluded.
SOURCE:
The study, led by Guanghai Dai, MD, from the Chinese People’s Liberation Army General Hospital, Beijing, was published in BMC Cancer on January 12, 2024.
LIMITATIONS:
The study was a single-center, retrospective analysis.
DISCLOSURES:
The paper was funded by Beijing natural science foundation. The authors did not declare any relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Despite therapeutic advances, survival among patients with unresectable and/or metastatic pancreatic ductal adenocarcinoma has not markedly improved in recent years.
- In the current analysis, researchers evaluated whether treatment sequence could affect survival outcomes in this patient population.
- To this end , researchers conducted a single institution, retrospective analysis of patients who received different lines of treatment between January 2015 and December 2021.
- The most common first-line therapy was nab-paclitaxel plus S-1 (58%), followed by FOLFIRINOX (10%), nab-paclitaxel plus gemcitabine (8%), gemcitabine alone (7%), gemcitabine plus oxaliplatin (6%); second-line therapies, in order of frequency, included gemcitabine combination therapy (48%), nab-paclitaxel combination therapy (19%), FOLFIRINOX (10%), and gemcitabine alone (7%); third-line treatments consisted of FOLFIRINOX (31%), irinotecan or oxaliplatin combination therapy (23%), immunotherapy (19%), and gemcitabine combination therapy (10%).
TAKEAWAY:
- Overall, progression occurred in 90% of patients, and the median overall survival was 12.0 months, with only 48% of patients able to start a third-line therapy.
- The researchers focused on three common therapy sequences: nab-paclitaxel plus gemcitabine or nab-paclitaxel combination therapy as first-line and FOLFIRINOX as second-line (line A); nab-paclitaxel combination therapy to gemcitabine combination therapy to FOLFIRINOX (line B); and nab-paclitaxel combination therapy, to gemcitabine combination therapy, to oxaliplatin or irinotecan combination therapy (line C).
- Overall, the researchers observed a median overall survival of 14 months among patients receiving line A and C sequences and 18 months with line B.
- Patients receiving line B therapy demonstrated a 52% lower risk for death compared with those receiving line A treatment (hazard ratio [HR], 0.48; P = .018) and a 75% reduced risk for death compared with those on the line C sequence (HR, 0.25; P = .040).
IN PRACTICE:
“Our study provides real-world evidence for the effectiveness of different treatment sequences and underscores the [impact of] treatment sequences on survival outcome when considering the entire management in advanced pancreatic ductal adenocarcinoma,” the authors concluded.
SOURCE:
The study, led by Guanghai Dai, MD, from the Chinese People’s Liberation Army General Hospital, Beijing, was published in BMC Cancer on January 12, 2024.
LIMITATIONS:
The study was a single-center, retrospective analysis.
DISCLOSURES:
The paper was funded by Beijing natural science foundation. The authors did not declare any relevant financial relationships.
A version of this article appeared on Medscape.com.
ALL: When Should MRD Trigger Stem Cell Transplants?
Allogeneic hematopoietic stem cell transplants (HSCT) are still part of the hematology armamentarium for relapsed/refractory (R/R) patients with Ph-negative ALL who are MRD positive. However, when asked about the best treatment strategy for patients who are MRD-negative, hematologist Mark R. Litzow, MD, of the Mayo Clinic in Rochester, Minnesota, said in an interview, “There is no firm consensus about that.”
Discussing how medicine has evolved over the past 20 to 30 years, Dr. Litzow recalled that HSCT used to be standard treatment for adult patients with ALL. “We felt that in most instances, chemotherapy alone was not going to be effective in curing them. A vast majority would relapse,” he said. Nowadays, however, specialists differ on the use of HSCT in patients with Ph-negative, MRD-negative ALL.
A pair of commentaries in the January issue of The Lancet Hematology tackle this topic from different perspectives. On one hand, hematologist Patrice Chevallier, MD, of the University of Nantes in France, argues that for such patients, HSCT “remains a valid option,”and MRD status shouldn’t be the sole factor used for a decision.
However, hematologist Nicolas Boissel, MD, PhD, of Paris Cité University, contends that detectable early MRD is the “only robust predictor” of HSCT benefit in patients under 60 with Ph-negative ALL, and it has “unproven” benefit in older patients.
As Dr. Chevallier notes, “allogeneic HSCT is indicated in patients defined as having a high risk of relapse. Currently, a high level of residual leukemic cells after treatment is recognized as the strongest, and sometimes sole, criterion defining high-risk patients.”
As first- and second-line therapy in pediatric patients and as first-line therapy in adults, the “rule” is to offer HSCT to MRD-positive patients but not MRD-negative ones, he writes. “In older patients and those who are relapsed or refractory, the recent demonstration of efficient immunotherapies and cell therapies has launched the debate on the role of MRD status and the question of whether or not to transplant patients who are MRD-negative in both settings.”
Dr. Chevallier notes that “there is no standard definition of an MRD-negative status,” and the best timing for evaluation is unknown. Further, he adds, a “variable proportion of MRD-negative patients still relapse after treatment — up to 25% of patients who respond early and more than 50% of patients who respond late.”
He also points out that there’s an 80% chance that patients will convert from MRD negative to MRD positive after blinatumomab therapy, and he highlights the low long-term survival rate (20%) after brexucabtagene autoleucel (Tecartus), a CAR T-cell therapy.
As for older patients, Dr. Chevallier observes that improved chemo-immunotherapy and conditioning regimens could spark a rethinking of the feasibility of HSCT. However, for now, in those patients, “MRD is not decisional, and allogeneic HSCT is not a routine practice,” he writes.
In his commentary, Dr. Boissel points out that there have been no controlled studies of HSCT in the first-remission setting, although he writes that some data suggests that HSCT may be helpful for patients in high-risk genetic subgroups, regardless of MRD status. On the other hand, “converging observations suggest no benefit of HSCT in MRD-positive patients treated with blinatumomab in the front-line setting.”
If MRD monitoring is unavailable, Dr. Boissel adds, “it seems reasonable to use early blast clearance or other baseline high-risk features to indicate HSCT.”
How can hematologists make the best decision about HSCT?
In an interview, City of Hope Medical Center (Duarte, California) hematologist-oncologist Ibrahim T. Aldoss, MD, said that chemotherapy — with or without immunotherapy — can often be enough to treat younger patients without high-risk genetic factors. “Potentially, these patients can be spared from transplants,” he said, although patients with resistant MRD “clearly need transplants.”
The risks of transplants are significant, he noted. While they can reduce the risk of relapse, the risk of dying during remission is higher vs chemotherapy. “So you have to balance the risks that you’re willing to take,” he said, keeping in mind that some patients can be cured with chemotherapy.
In addition, Dr. Aldoss said, acute graft-versus-host disease in the first few months after transplant can become chronic. “Many years later, patients can be struggling to where it actually impacts their daily activity. And unfortunately, patients can die from it.”
In the big picture, “you cannot have a generalized statement about whether you shouldn’t do transplants in every MRD-negative patient,” he said. However, “if you do achieve MRD negativity, most patients likely don’t need transplants.”
The Mayo Clinic’s Dr. Litzow urged colleagues to consider several factors when making decisions. Do patients have a high level of comorbidities that would raise the risk of death from HSCT? He noted that there’s nearly a 20% risk of death from HSCT, and comorbidities can boost the risk to 40%-50%.
Also, does the patient have a suitable donor? While advances have boosted the number of eligible donors, he said, “not everybody has an ideal donor.”
If a patient is MRD-negative but not a good candidate for a transplant, Dr. Litzow said consolidation therapy followed by maintenance therapy may be indicated. “Continue to check their bone marrow and their blood periodically as they’re going through treatment and reassess their MRD status to make sure they’re staying negative. If they turn MRD-positive during the course of their therapy, then we have to step back and rethink the role of transplant.”
As for cost, Dr. Litzow points out that HSCT is very expensive, although ALL is an accepted indication for HSCT. However, “if someone doesn’t have medical insurance, then it can be difficult to consider them having a transplant.”
What’s next? In his commentary, Dr. Boissel writes that his team aims to study whether HSCT is helpful in patients with high-risk B-cell ALL “who reach MRD negativity after a consolidation phase including blinatumomab.”
Dr. Aldoss discloses relationships with Amgen, Kite, Pfizer, Jazz, AbbVie, Sobi, Agios, Autolus, and MacroGenics. Dr. Litzow reports ties with Amgen. Dr. Boissel declares relationships with Amgen, Pfizer, Novartis, and Servier. Dr. Chevallier has no disclosures.
Allogeneic hematopoietic stem cell transplants (HSCT) are still part of the hematology armamentarium for relapsed/refractory (R/R) patients with Ph-negative ALL who are MRD positive. However, when asked about the best treatment strategy for patients who are MRD-negative, hematologist Mark R. Litzow, MD, of the Mayo Clinic in Rochester, Minnesota, said in an interview, “There is no firm consensus about that.”
Discussing how medicine has evolved over the past 20 to 30 years, Dr. Litzow recalled that HSCT used to be standard treatment for adult patients with ALL. “We felt that in most instances, chemotherapy alone was not going to be effective in curing them. A vast majority would relapse,” he said. Nowadays, however, specialists differ on the use of HSCT in patients with Ph-negative, MRD-negative ALL.
A pair of commentaries in the January issue of The Lancet Hematology tackle this topic from different perspectives. On one hand, hematologist Patrice Chevallier, MD, of the University of Nantes in France, argues that for such patients, HSCT “remains a valid option,”and MRD status shouldn’t be the sole factor used for a decision.
However, hematologist Nicolas Boissel, MD, PhD, of Paris Cité University, contends that detectable early MRD is the “only robust predictor” of HSCT benefit in patients under 60 with Ph-negative ALL, and it has “unproven” benefit in older patients.
As Dr. Chevallier notes, “allogeneic HSCT is indicated in patients defined as having a high risk of relapse. Currently, a high level of residual leukemic cells after treatment is recognized as the strongest, and sometimes sole, criterion defining high-risk patients.”
As first- and second-line therapy in pediatric patients and as first-line therapy in adults, the “rule” is to offer HSCT to MRD-positive patients but not MRD-negative ones, he writes. “In older patients and those who are relapsed or refractory, the recent demonstration of efficient immunotherapies and cell therapies has launched the debate on the role of MRD status and the question of whether or not to transplant patients who are MRD-negative in both settings.”
Dr. Chevallier notes that “there is no standard definition of an MRD-negative status,” and the best timing for evaluation is unknown. Further, he adds, a “variable proportion of MRD-negative patients still relapse after treatment — up to 25% of patients who respond early and more than 50% of patients who respond late.”
He also points out that there’s an 80% chance that patients will convert from MRD negative to MRD positive after blinatumomab therapy, and he highlights the low long-term survival rate (20%) after brexucabtagene autoleucel (Tecartus), a CAR T-cell therapy.
As for older patients, Dr. Chevallier observes that improved chemo-immunotherapy and conditioning regimens could spark a rethinking of the feasibility of HSCT. However, for now, in those patients, “MRD is not decisional, and allogeneic HSCT is not a routine practice,” he writes.
In his commentary, Dr. Boissel points out that there have been no controlled studies of HSCT in the first-remission setting, although he writes that some data suggests that HSCT may be helpful for patients in high-risk genetic subgroups, regardless of MRD status. On the other hand, “converging observations suggest no benefit of HSCT in MRD-positive patients treated with blinatumomab in the front-line setting.”
If MRD monitoring is unavailable, Dr. Boissel adds, “it seems reasonable to use early blast clearance or other baseline high-risk features to indicate HSCT.”
How can hematologists make the best decision about HSCT?
In an interview, City of Hope Medical Center (Duarte, California) hematologist-oncologist Ibrahim T. Aldoss, MD, said that chemotherapy — with or without immunotherapy — can often be enough to treat younger patients without high-risk genetic factors. “Potentially, these patients can be spared from transplants,” he said, although patients with resistant MRD “clearly need transplants.”
The risks of transplants are significant, he noted. While they can reduce the risk of relapse, the risk of dying during remission is higher vs chemotherapy. “So you have to balance the risks that you’re willing to take,” he said, keeping in mind that some patients can be cured with chemotherapy.
In addition, Dr. Aldoss said, acute graft-versus-host disease in the first few months after transplant can become chronic. “Many years later, patients can be struggling to where it actually impacts their daily activity. And unfortunately, patients can die from it.”
In the big picture, “you cannot have a generalized statement about whether you shouldn’t do transplants in every MRD-negative patient,” he said. However, “if you do achieve MRD negativity, most patients likely don’t need transplants.”
The Mayo Clinic’s Dr. Litzow urged colleagues to consider several factors when making decisions. Do patients have a high level of comorbidities that would raise the risk of death from HSCT? He noted that there’s nearly a 20% risk of death from HSCT, and comorbidities can boost the risk to 40%-50%.
Also, does the patient have a suitable donor? While advances have boosted the number of eligible donors, he said, “not everybody has an ideal donor.”
If a patient is MRD-negative but not a good candidate for a transplant, Dr. Litzow said consolidation therapy followed by maintenance therapy may be indicated. “Continue to check their bone marrow and their blood periodically as they’re going through treatment and reassess their MRD status to make sure they’re staying negative. If they turn MRD-positive during the course of their therapy, then we have to step back and rethink the role of transplant.”
As for cost, Dr. Litzow points out that HSCT is very expensive, although ALL is an accepted indication for HSCT. However, “if someone doesn’t have medical insurance, then it can be difficult to consider them having a transplant.”
What’s next? In his commentary, Dr. Boissel writes that his team aims to study whether HSCT is helpful in patients with high-risk B-cell ALL “who reach MRD negativity after a consolidation phase including blinatumomab.”
Dr. Aldoss discloses relationships with Amgen, Kite, Pfizer, Jazz, AbbVie, Sobi, Agios, Autolus, and MacroGenics. Dr. Litzow reports ties with Amgen. Dr. Boissel declares relationships with Amgen, Pfizer, Novartis, and Servier. Dr. Chevallier has no disclosures.
Allogeneic hematopoietic stem cell transplants (HSCT) are still part of the hematology armamentarium for relapsed/refractory (R/R) patients with Ph-negative ALL who are MRD positive. However, when asked about the best treatment strategy for patients who are MRD-negative, hematologist Mark R. Litzow, MD, of the Mayo Clinic in Rochester, Minnesota, said in an interview, “There is no firm consensus about that.”
Discussing how medicine has evolved over the past 20 to 30 years, Dr. Litzow recalled that HSCT used to be standard treatment for adult patients with ALL. “We felt that in most instances, chemotherapy alone was not going to be effective in curing them. A vast majority would relapse,” he said. Nowadays, however, specialists differ on the use of HSCT in patients with Ph-negative, MRD-negative ALL.
A pair of commentaries in the January issue of The Lancet Hematology tackle this topic from different perspectives. On one hand, hematologist Patrice Chevallier, MD, of the University of Nantes in France, argues that for such patients, HSCT “remains a valid option,”and MRD status shouldn’t be the sole factor used for a decision.
However, hematologist Nicolas Boissel, MD, PhD, of Paris Cité University, contends that detectable early MRD is the “only robust predictor” of HSCT benefit in patients under 60 with Ph-negative ALL, and it has “unproven” benefit in older patients.
As Dr. Chevallier notes, “allogeneic HSCT is indicated in patients defined as having a high risk of relapse. Currently, a high level of residual leukemic cells after treatment is recognized as the strongest, and sometimes sole, criterion defining high-risk patients.”
As first- and second-line therapy in pediatric patients and as first-line therapy in adults, the “rule” is to offer HSCT to MRD-positive patients but not MRD-negative ones, he writes. “In older patients and those who are relapsed or refractory, the recent demonstration of efficient immunotherapies and cell therapies has launched the debate on the role of MRD status and the question of whether or not to transplant patients who are MRD-negative in both settings.”
Dr. Chevallier notes that “there is no standard definition of an MRD-negative status,” and the best timing for evaluation is unknown. Further, he adds, a “variable proportion of MRD-negative patients still relapse after treatment — up to 25% of patients who respond early and more than 50% of patients who respond late.”
He also points out that there’s an 80% chance that patients will convert from MRD negative to MRD positive after blinatumomab therapy, and he highlights the low long-term survival rate (20%) after brexucabtagene autoleucel (Tecartus), a CAR T-cell therapy.
As for older patients, Dr. Chevallier observes that improved chemo-immunotherapy and conditioning regimens could spark a rethinking of the feasibility of HSCT. However, for now, in those patients, “MRD is not decisional, and allogeneic HSCT is not a routine practice,” he writes.
In his commentary, Dr. Boissel points out that there have been no controlled studies of HSCT in the first-remission setting, although he writes that some data suggests that HSCT may be helpful for patients in high-risk genetic subgroups, regardless of MRD status. On the other hand, “converging observations suggest no benefit of HSCT in MRD-positive patients treated with blinatumomab in the front-line setting.”
If MRD monitoring is unavailable, Dr. Boissel adds, “it seems reasonable to use early blast clearance or other baseline high-risk features to indicate HSCT.”
How can hematologists make the best decision about HSCT?
In an interview, City of Hope Medical Center (Duarte, California) hematologist-oncologist Ibrahim T. Aldoss, MD, said that chemotherapy — with or without immunotherapy — can often be enough to treat younger patients without high-risk genetic factors. “Potentially, these patients can be spared from transplants,” he said, although patients with resistant MRD “clearly need transplants.”
The risks of transplants are significant, he noted. While they can reduce the risk of relapse, the risk of dying during remission is higher vs chemotherapy. “So you have to balance the risks that you’re willing to take,” he said, keeping in mind that some patients can be cured with chemotherapy.
In addition, Dr. Aldoss said, acute graft-versus-host disease in the first few months after transplant can become chronic. “Many years later, patients can be struggling to where it actually impacts their daily activity. And unfortunately, patients can die from it.”
In the big picture, “you cannot have a generalized statement about whether you shouldn’t do transplants in every MRD-negative patient,” he said. However, “if you do achieve MRD negativity, most patients likely don’t need transplants.”
The Mayo Clinic’s Dr. Litzow urged colleagues to consider several factors when making decisions. Do patients have a high level of comorbidities that would raise the risk of death from HSCT? He noted that there’s nearly a 20% risk of death from HSCT, and comorbidities can boost the risk to 40%-50%.
Also, does the patient have a suitable donor? While advances have boosted the number of eligible donors, he said, “not everybody has an ideal donor.”
If a patient is MRD-negative but not a good candidate for a transplant, Dr. Litzow said consolidation therapy followed by maintenance therapy may be indicated. “Continue to check their bone marrow and their blood periodically as they’re going through treatment and reassess their MRD status to make sure they’re staying negative. If they turn MRD-positive during the course of their therapy, then we have to step back and rethink the role of transplant.”
As for cost, Dr. Litzow points out that HSCT is very expensive, although ALL is an accepted indication for HSCT. However, “if someone doesn’t have medical insurance, then it can be difficult to consider them having a transplant.”
What’s next? In his commentary, Dr. Boissel writes that his team aims to study whether HSCT is helpful in patients with high-risk B-cell ALL “who reach MRD negativity after a consolidation phase including blinatumomab.”
Dr. Aldoss discloses relationships with Amgen, Kite, Pfizer, Jazz, AbbVie, Sobi, Agios, Autolus, and MacroGenics. Dr. Litzow reports ties with Amgen. Dr. Boissel declares relationships with Amgen, Pfizer, Novartis, and Servier. Dr. Chevallier has no disclosures.
Two-Step Strategy Improves Early-Stage Ovarian Cancer Detection
TOPLINE:
a new analysis with a 21-year follow-up found.
METHODOLOGY:
- Detecting ovarian cancer at stage I or II could significantly reduce ovarian cancer-related deaths, but only 25%-30% of patients are diagnosed at an early stage.
- In this single-arm prospective analysis, 7,856 healthy postmenopausal women received annual screening for ovarian cancer between 2011 and 2022. Screening involved an annual blood test to detect levels of cancer antigen 125 and track these levels over time.
- Investigators used the Risk of Ovarian Cancer Algorithm (ROCA) to determine whether ovarian cancer risk was normal, intermediate, or high. Those with elevated ROCA scores were referred for transvaginal sonography; those with intermediate scores received follow-up blood tests every 3 months.
- Overall, 92.3% of women were normal risk, 5.7% were intermediate, and 2% were high risk and recommended for transvaginal sonography.
TAKEAWAY:
- Most women (95.5%) referred for transvaginal ultrasound had one. Of these ultrasounds, most (90%) were negative or revealed benign findings, 5.2% required a repeat ultrasound, and 4.8% (34 patients) showed suspicious findings.
- Of 34 patients with suspicious findings and recommended for surgery, 15 had ovarian cancer and two had borderline tumors, indicating a positive predictive value of 50% (17 of 34 patients) for ovarian cancer. Of these 17 patients, 12 (70.6%) had stage I or II disease.
- Following abnormal ROCA results, seven other women were diagnosed with endometrial tumors (six of which were stage I), indicating a positive predictive value of 74% (25 of 34) for any cancer.
- The specificity for elevated risk ROCA prompting ultrasound was 98%, and the specificity of the ROCA and ultrasound prompting surgery was 99.8%. The sensitivity for detecting ovarian and borderline cancer was 74% (17 of 23).
IN PRACTICE:
“Remarkably, 70% of ovarian cancers detected by the ROCA” were early stage,” the authors concluded. Although the trial was not powered to detect reduced mortality, the high specificity, positive predictive value, and shift to identifying earlier-stage cancers “support further development of this strategy,” the investigators said.
LIMITATIONS:
This trial was not powered to detect mortality benefit. Six ovarian cancers and borderline tumors were missed. Only 80% of ovarian cancers express cancer antigen 125, potentially limiting the sensitivity of the algorithm.
SOURCE:
This study, led by Chae Young Han from the University of Texas MD Anderson Cancer Center, Houston, was published online on January 12 in the Journal of Clinical Oncology.
DISCLOSURES:
This study was supported by funds from the NCI Early Detection Research Network, the MD Anderson Ovarian SPOREs, the National Cancer Institute, the Department of Health and Human Services, and others. The authors reported receiving research funding, grants, consulting, and personal fees from various companies, including Curio Science, Fujirebio Diagnostics, GlaxoSmithKline, AstraZeneca, and Genentech.
A version of this article appeared on Medscape.com.
TOPLINE:
a new analysis with a 21-year follow-up found.
METHODOLOGY:
- Detecting ovarian cancer at stage I or II could significantly reduce ovarian cancer-related deaths, but only 25%-30% of patients are diagnosed at an early stage.
- In this single-arm prospective analysis, 7,856 healthy postmenopausal women received annual screening for ovarian cancer between 2011 and 2022. Screening involved an annual blood test to detect levels of cancer antigen 125 and track these levels over time.
- Investigators used the Risk of Ovarian Cancer Algorithm (ROCA) to determine whether ovarian cancer risk was normal, intermediate, or high. Those with elevated ROCA scores were referred for transvaginal sonography; those with intermediate scores received follow-up blood tests every 3 months.
- Overall, 92.3% of women were normal risk, 5.7% were intermediate, and 2% were high risk and recommended for transvaginal sonography.
TAKEAWAY:
- Most women (95.5%) referred for transvaginal ultrasound had one. Of these ultrasounds, most (90%) were negative or revealed benign findings, 5.2% required a repeat ultrasound, and 4.8% (34 patients) showed suspicious findings.
- Of 34 patients with suspicious findings and recommended for surgery, 15 had ovarian cancer and two had borderline tumors, indicating a positive predictive value of 50% (17 of 34 patients) for ovarian cancer. Of these 17 patients, 12 (70.6%) had stage I or II disease.
- Following abnormal ROCA results, seven other women were diagnosed with endometrial tumors (six of which were stage I), indicating a positive predictive value of 74% (25 of 34) for any cancer.
- The specificity for elevated risk ROCA prompting ultrasound was 98%, and the specificity of the ROCA and ultrasound prompting surgery was 99.8%. The sensitivity for detecting ovarian and borderline cancer was 74% (17 of 23).
IN PRACTICE:
“Remarkably, 70% of ovarian cancers detected by the ROCA” were early stage,” the authors concluded. Although the trial was not powered to detect reduced mortality, the high specificity, positive predictive value, and shift to identifying earlier-stage cancers “support further development of this strategy,” the investigators said.
LIMITATIONS:
This trial was not powered to detect mortality benefit. Six ovarian cancers and borderline tumors were missed. Only 80% of ovarian cancers express cancer antigen 125, potentially limiting the sensitivity of the algorithm.
SOURCE:
This study, led by Chae Young Han from the University of Texas MD Anderson Cancer Center, Houston, was published online on January 12 in the Journal of Clinical Oncology.
DISCLOSURES:
This study was supported by funds from the NCI Early Detection Research Network, the MD Anderson Ovarian SPOREs, the National Cancer Institute, the Department of Health and Human Services, and others. The authors reported receiving research funding, grants, consulting, and personal fees from various companies, including Curio Science, Fujirebio Diagnostics, GlaxoSmithKline, AstraZeneca, and Genentech.
A version of this article appeared on Medscape.com.
TOPLINE:
a new analysis with a 21-year follow-up found.
METHODOLOGY:
- Detecting ovarian cancer at stage I or II could significantly reduce ovarian cancer-related deaths, but only 25%-30% of patients are diagnosed at an early stage.
- In this single-arm prospective analysis, 7,856 healthy postmenopausal women received annual screening for ovarian cancer between 2011 and 2022. Screening involved an annual blood test to detect levels of cancer antigen 125 and track these levels over time.
- Investigators used the Risk of Ovarian Cancer Algorithm (ROCA) to determine whether ovarian cancer risk was normal, intermediate, or high. Those with elevated ROCA scores were referred for transvaginal sonography; those with intermediate scores received follow-up blood tests every 3 months.
- Overall, 92.3% of women were normal risk, 5.7% were intermediate, and 2% were high risk and recommended for transvaginal sonography.
TAKEAWAY:
- Most women (95.5%) referred for transvaginal ultrasound had one. Of these ultrasounds, most (90%) were negative or revealed benign findings, 5.2% required a repeat ultrasound, and 4.8% (34 patients) showed suspicious findings.
- Of 34 patients with suspicious findings and recommended for surgery, 15 had ovarian cancer and two had borderline tumors, indicating a positive predictive value of 50% (17 of 34 patients) for ovarian cancer. Of these 17 patients, 12 (70.6%) had stage I or II disease.
- Following abnormal ROCA results, seven other women were diagnosed with endometrial tumors (six of which were stage I), indicating a positive predictive value of 74% (25 of 34) for any cancer.
- The specificity for elevated risk ROCA prompting ultrasound was 98%, and the specificity of the ROCA and ultrasound prompting surgery was 99.8%. The sensitivity for detecting ovarian and borderline cancer was 74% (17 of 23).
IN PRACTICE:
“Remarkably, 70% of ovarian cancers detected by the ROCA” were early stage,” the authors concluded. Although the trial was not powered to detect reduced mortality, the high specificity, positive predictive value, and shift to identifying earlier-stage cancers “support further development of this strategy,” the investigators said.
LIMITATIONS:
This trial was not powered to detect mortality benefit. Six ovarian cancers and borderline tumors were missed. Only 80% of ovarian cancers express cancer antigen 125, potentially limiting the sensitivity of the algorithm.
SOURCE:
This study, led by Chae Young Han from the University of Texas MD Anderson Cancer Center, Houston, was published online on January 12 in the Journal of Clinical Oncology.
DISCLOSURES:
This study was supported by funds from the NCI Early Detection Research Network, the MD Anderson Ovarian SPOREs, the National Cancer Institute, the Department of Health and Human Services, and others. The authors reported receiving research funding, grants, consulting, and personal fees from various companies, including Curio Science, Fujirebio Diagnostics, GlaxoSmithKline, AstraZeneca, and Genentech.
A version of this article appeared on Medscape.com.
Europe Is Facing a Pancreatic Cancer Emergency
“It’s a health emergency for society, with mortality rates at over 90%,” warned Professor Alfredo Carrato, MD, PhD, the chairperson of Pancreatic Cancer Europe.
There are many challenges with pancreatic cancer: Lack of awareness, difficult to diagnose, no screening programs for the general population, poor survival rate, and limited treatment options.
Life expectancy at the time of diagnosis is just 4.6 months. Only 3% of people diagnosed with pancreatic cancer will survive for 5 years.
A 2024 systematic analysis in The Lancet suggested that people living in Western Europe are more likely to develop pancreatic cancer than those living anywhere else in the world.
Dr. Carrato, emeritus professor of medical oncology at the University of Alcalá, Madrid, Spain, wasn’t surprised. He told this news organization: “I think the lifestyle in Europe plays a part. We have all of the risk factors in society like obesity, our sedentary behavior, too much red meat consumption, and excess alcohol intake.”
Other risk factors include smoking, diabetes, chronic pancreatitis, and a family history.
The incidence of pancreatic cancer increases with age, so the longer life expectancy in Western Europe could also contribute to the region’s high rates.
A Silent Killer
Pancreatic cancer is difficult to identify. It is often asymptomatic. Symptoms that do show themselves, like back pain, weight loss, and nausea, are nonspecific and make early diagnosis challenging.
Professor Mattias Löhr from the Karolinska Institutet, Stockholm, Sweden, told this news organization: “It’s a dismal disease. It’s not accessible for any easy screening or surveillance. Even early diagnosis is too late with pancreatic cancer.”
There have been few advancements in patient outcomes over the past few decades.
Only about 20% of patients are suitable candidates for surgery that could prolong their lives.
Also, cancer reoccurs in two thirds of surgical candidates, said Dr. Carrato, and oncologists don’t know how to identify them in advance. “I have patients who survive 3 months and others who survive 4 or 5 years, so there’s a need to identify these subtypes at a molecular level for personalized, clinical, and translational research and therapies.”
Dr. Löhr agreed: “All of the medical therapies are not really working well enough for pancreatic cancer in sharp contrast to other cancers.”
How Can Rates Be Reduced?
“Pancreatic Cancer Europe is working in every EU state to try to raise awareness,” said Dr. Carrato. “We should have primary prevention programs to modify lifestyle risks. We also need funds for translational and clinical research. Secondary prevention isn’t possible yet as we haven’t identified the higher-risk population who would be the target for screening.”
Screening programs are available for the 10% of people who have a family history of pancreatic cancer. But, for the vast majority, there are no tests or screenings that allow for earlier detection.
“We need blood or stool tests that have high specificity and sensitivity that are cost-effective,” said Dr. Carrato.
“It’s a type of cancer with a particular and very aggressive biology. There is a lack of pancreatic tumor tissue for research, as many patients are diagnosed by fine-needle aspiration cytology. It’s a challenge for researchers. We have no biomarkers available to direct our decisions; no precision oncology,” he added.
Still, there are some encouraging developments.
The European PANCAID project (pancreatic cancer initial detection via liquid biopsy) is trying to find biomarkers to screen at-risk groups for earlier diagnosis via a blood test.
Also, the European Union (EU)-funded PANCAIM project (pancreatic cancer artificial intelligence [AI] for genomics and personalized medicine) has developed an AI algorithm that detects small cancers in CT scans that even experienced radiologists might easily overlook.
The project’s head, Henkjan Huisman, is professor of medical imaging AI at Radboud University Medical Center, Nijmegen, the Netherlands. He told this news organization: “It’s an extremely important step, as 20% of people with pancreas cancer have the ability to undergo surgery, which means they might live substantially longer. We believe if the tumors are found earlier, thanks to the algorithm, they are smaller and more contained, and so substantially more than 20% of patients would be suitable for surgery, which would be a breakthrough.”
Dr. Löhr added that a messenger RNA vaccine is being developed in the United States to prevent pancreatic cancer from returning after surgery and is demonstrating encouraging results in its early trials.
The Road Toward Better Care
To improve cancer care in Europe, Dr. Carrato said: “Reference centers should be a requirement in health policy programs because the outcomes are much better than in centers which only perform fewer surgeries, and Pancreatic Cancer Europe is working with the EU in this direction.”
Finland is a country that appears to have succeeded in this regard. Its 2005 Health Care Act, for example, ensures that cancer patients are able to receive care in one of its five specialized hospitals.
More research funding is also needed. According to Pancreatic Cancer Europe, only 2% of EU funding on cancer is spent on pancreatic cancer.
The American Cancer Society’s Cancer Facts & Figures 2024 makes room for some optimism, with the 5-year survival rate in the United States jumping to 13% from 6% in the society’s 2014 report, as a result of earlier diagnoses and more personalized treatment. But, even with potentially longer survival rates, said Dr. Löhr, “we are still on the trajectory of pancreatic cancer being number two for cancer deaths by 2030.”
“We need more money on research, centralized surgery, and networking between European countries,” said Dr. Carrato. “This networking would need more money for prevention, better diagnosis, and treatment. The problem is pancreatic cancer incidence is increasing and mortality is also in parallel, and we are not making real progress in this scenario.”
A version of this article appeared on Medscape.com.
“It’s a health emergency for society, with mortality rates at over 90%,” warned Professor Alfredo Carrato, MD, PhD, the chairperson of Pancreatic Cancer Europe.
There are many challenges with pancreatic cancer: Lack of awareness, difficult to diagnose, no screening programs for the general population, poor survival rate, and limited treatment options.
Life expectancy at the time of diagnosis is just 4.6 months. Only 3% of people diagnosed with pancreatic cancer will survive for 5 years.
A 2024 systematic analysis in The Lancet suggested that people living in Western Europe are more likely to develop pancreatic cancer than those living anywhere else in the world.
Dr. Carrato, emeritus professor of medical oncology at the University of Alcalá, Madrid, Spain, wasn’t surprised. He told this news organization: “I think the lifestyle in Europe plays a part. We have all of the risk factors in society like obesity, our sedentary behavior, too much red meat consumption, and excess alcohol intake.”
Other risk factors include smoking, diabetes, chronic pancreatitis, and a family history.
The incidence of pancreatic cancer increases with age, so the longer life expectancy in Western Europe could also contribute to the region’s high rates.
A Silent Killer
Pancreatic cancer is difficult to identify. It is often asymptomatic. Symptoms that do show themselves, like back pain, weight loss, and nausea, are nonspecific and make early diagnosis challenging.
Professor Mattias Löhr from the Karolinska Institutet, Stockholm, Sweden, told this news organization: “It’s a dismal disease. It’s not accessible for any easy screening or surveillance. Even early diagnosis is too late with pancreatic cancer.”
There have been few advancements in patient outcomes over the past few decades.
Only about 20% of patients are suitable candidates for surgery that could prolong their lives.
Also, cancer reoccurs in two thirds of surgical candidates, said Dr. Carrato, and oncologists don’t know how to identify them in advance. “I have patients who survive 3 months and others who survive 4 or 5 years, so there’s a need to identify these subtypes at a molecular level for personalized, clinical, and translational research and therapies.”
Dr. Löhr agreed: “All of the medical therapies are not really working well enough for pancreatic cancer in sharp contrast to other cancers.”
How Can Rates Be Reduced?
“Pancreatic Cancer Europe is working in every EU state to try to raise awareness,” said Dr. Carrato. “We should have primary prevention programs to modify lifestyle risks. We also need funds for translational and clinical research. Secondary prevention isn’t possible yet as we haven’t identified the higher-risk population who would be the target for screening.”
Screening programs are available for the 10% of people who have a family history of pancreatic cancer. But, for the vast majority, there are no tests or screenings that allow for earlier detection.
“We need blood or stool tests that have high specificity and sensitivity that are cost-effective,” said Dr. Carrato.
“It’s a type of cancer with a particular and very aggressive biology. There is a lack of pancreatic tumor tissue for research, as many patients are diagnosed by fine-needle aspiration cytology. It’s a challenge for researchers. We have no biomarkers available to direct our decisions; no precision oncology,” he added.
Still, there are some encouraging developments.
The European PANCAID project (pancreatic cancer initial detection via liquid biopsy) is trying to find biomarkers to screen at-risk groups for earlier diagnosis via a blood test.
Also, the European Union (EU)-funded PANCAIM project (pancreatic cancer artificial intelligence [AI] for genomics and personalized medicine) has developed an AI algorithm that detects small cancers in CT scans that even experienced radiologists might easily overlook.
The project’s head, Henkjan Huisman, is professor of medical imaging AI at Radboud University Medical Center, Nijmegen, the Netherlands. He told this news organization: “It’s an extremely important step, as 20% of people with pancreas cancer have the ability to undergo surgery, which means they might live substantially longer. We believe if the tumors are found earlier, thanks to the algorithm, they are smaller and more contained, and so substantially more than 20% of patients would be suitable for surgery, which would be a breakthrough.”
Dr. Löhr added that a messenger RNA vaccine is being developed in the United States to prevent pancreatic cancer from returning after surgery and is demonstrating encouraging results in its early trials.
The Road Toward Better Care
To improve cancer care in Europe, Dr. Carrato said: “Reference centers should be a requirement in health policy programs because the outcomes are much better than in centers which only perform fewer surgeries, and Pancreatic Cancer Europe is working with the EU in this direction.”
Finland is a country that appears to have succeeded in this regard. Its 2005 Health Care Act, for example, ensures that cancer patients are able to receive care in one of its five specialized hospitals.
More research funding is also needed. According to Pancreatic Cancer Europe, only 2% of EU funding on cancer is spent on pancreatic cancer.
The American Cancer Society’s Cancer Facts & Figures 2024 makes room for some optimism, with the 5-year survival rate in the United States jumping to 13% from 6% in the society’s 2014 report, as a result of earlier diagnoses and more personalized treatment. But, even with potentially longer survival rates, said Dr. Löhr, “we are still on the trajectory of pancreatic cancer being number two for cancer deaths by 2030.”
“We need more money on research, centralized surgery, and networking between European countries,” said Dr. Carrato. “This networking would need more money for prevention, better diagnosis, and treatment. The problem is pancreatic cancer incidence is increasing and mortality is also in parallel, and we are not making real progress in this scenario.”
A version of this article appeared on Medscape.com.
“It’s a health emergency for society, with mortality rates at over 90%,” warned Professor Alfredo Carrato, MD, PhD, the chairperson of Pancreatic Cancer Europe.
There are many challenges with pancreatic cancer: Lack of awareness, difficult to diagnose, no screening programs for the general population, poor survival rate, and limited treatment options.
Life expectancy at the time of diagnosis is just 4.6 months. Only 3% of people diagnosed with pancreatic cancer will survive for 5 years.
A 2024 systematic analysis in The Lancet suggested that people living in Western Europe are more likely to develop pancreatic cancer than those living anywhere else in the world.
Dr. Carrato, emeritus professor of medical oncology at the University of Alcalá, Madrid, Spain, wasn’t surprised. He told this news organization: “I think the lifestyle in Europe plays a part. We have all of the risk factors in society like obesity, our sedentary behavior, too much red meat consumption, and excess alcohol intake.”
Other risk factors include smoking, diabetes, chronic pancreatitis, and a family history.
The incidence of pancreatic cancer increases with age, so the longer life expectancy in Western Europe could also contribute to the region’s high rates.
A Silent Killer
Pancreatic cancer is difficult to identify. It is often asymptomatic. Symptoms that do show themselves, like back pain, weight loss, and nausea, are nonspecific and make early diagnosis challenging.
Professor Mattias Löhr from the Karolinska Institutet, Stockholm, Sweden, told this news organization: “It’s a dismal disease. It’s not accessible for any easy screening or surveillance. Even early diagnosis is too late with pancreatic cancer.”
There have been few advancements in patient outcomes over the past few decades.
Only about 20% of patients are suitable candidates for surgery that could prolong their lives.
Also, cancer reoccurs in two thirds of surgical candidates, said Dr. Carrato, and oncologists don’t know how to identify them in advance. “I have patients who survive 3 months and others who survive 4 or 5 years, so there’s a need to identify these subtypes at a molecular level for personalized, clinical, and translational research and therapies.”
Dr. Löhr agreed: “All of the medical therapies are not really working well enough for pancreatic cancer in sharp contrast to other cancers.”
How Can Rates Be Reduced?
“Pancreatic Cancer Europe is working in every EU state to try to raise awareness,” said Dr. Carrato. “We should have primary prevention programs to modify lifestyle risks. We also need funds for translational and clinical research. Secondary prevention isn’t possible yet as we haven’t identified the higher-risk population who would be the target for screening.”
Screening programs are available for the 10% of people who have a family history of pancreatic cancer. But, for the vast majority, there are no tests or screenings that allow for earlier detection.
“We need blood or stool tests that have high specificity and sensitivity that are cost-effective,” said Dr. Carrato.
“It’s a type of cancer with a particular and very aggressive biology. There is a lack of pancreatic tumor tissue for research, as many patients are diagnosed by fine-needle aspiration cytology. It’s a challenge for researchers. We have no biomarkers available to direct our decisions; no precision oncology,” he added.
Still, there are some encouraging developments.
The European PANCAID project (pancreatic cancer initial detection via liquid biopsy) is trying to find biomarkers to screen at-risk groups for earlier diagnosis via a blood test.
Also, the European Union (EU)-funded PANCAIM project (pancreatic cancer artificial intelligence [AI] for genomics and personalized medicine) has developed an AI algorithm that detects small cancers in CT scans that even experienced radiologists might easily overlook.
The project’s head, Henkjan Huisman, is professor of medical imaging AI at Radboud University Medical Center, Nijmegen, the Netherlands. He told this news organization: “It’s an extremely important step, as 20% of people with pancreas cancer have the ability to undergo surgery, which means they might live substantially longer. We believe if the tumors are found earlier, thanks to the algorithm, they are smaller and more contained, and so substantially more than 20% of patients would be suitable for surgery, which would be a breakthrough.”
Dr. Löhr added that a messenger RNA vaccine is being developed in the United States to prevent pancreatic cancer from returning after surgery and is demonstrating encouraging results in its early trials.
The Road Toward Better Care
To improve cancer care in Europe, Dr. Carrato said: “Reference centers should be a requirement in health policy programs because the outcomes are much better than in centers which only perform fewer surgeries, and Pancreatic Cancer Europe is working with the EU in this direction.”
Finland is a country that appears to have succeeded in this regard. Its 2005 Health Care Act, for example, ensures that cancer patients are able to receive care in one of its five specialized hospitals.
More research funding is also needed. According to Pancreatic Cancer Europe, only 2% of EU funding on cancer is spent on pancreatic cancer.
The American Cancer Society’s Cancer Facts & Figures 2024 makes room for some optimism, with the 5-year survival rate in the United States jumping to 13% from 6% in the society’s 2014 report, as a result of earlier diagnoses and more personalized treatment. But, even with potentially longer survival rates, said Dr. Löhr, “we are still on the trajectory of pancreatic cancer being number two for cancer deaths by 2030.”
“We need more money on research, centralized surgery, and networking between European countries,” said Dr. Carrato. “This networking would need more money for prevention, better diagnosis, and treatment. The problem is pancreatic cancer incidence is increasing and mortality is also in parallel, and we are not making real progress in this scenario.”
A version of this article appeared on Medscape.com.
High-dose RT and long-term ADT improve survival in high-risk prostate cancer
For patients with high-risk prostate cancer, treatment with long-term androgen deprivation therapy (ADT) and high-dose radiation was associated with significantly better progression-free, cancer-specific, and overall survival compared with ADT and standard-dose radiation.
The investigators also found that the patients taking long-term ADT and high-dose radiation did not experience additional late urinary tract or gastrointestinal toxicities. Christophe Hennequin, MD, PhD, reported these and other findings of the Radiation Therapy in Treating Patients Receiving Hormone Therapy for Prostate Cancer (GETUG-AFU 18) trial, at the 2024 American Society for Clinical Oncology (ASCO) Genitourinary Cancers Symposium.
Among 505 patients randomly assigned to be treated with radiation therapy (RT) at either the standard 70 Gy dose or a high, 80 Gy dose followed by 3 years of adjuvant ADT, the 10-year progression-free survival (PFS) rate was 83.6% for patients who had received the 80 Gy dose, vs. 72.2% for patients who had received the 70 Gy dose. This translated into a hazard ratio (HR) for biochemical or clinical progression of 0.56 (P = .0005).
This PFS advantage for high-dose radiation was also reflected by an overall survival (OS) advantage, with 10-year OS rates of 77% vs. 65.9%, respectively, translating into a 39% reduction in risk of death (HR 0.61, P = .0039) for patients who had received the higher radiation dose, reported Dr. Hennequin, of the Hospital Saint Louis in Paris, France.
"We have now Level 1 evidence that high-dose RT with long-term ADT must be the standard of care in high-risk prostate cancer patients," he said at the meeting.
Dr. Hennequin noted that significantly more patients assigned to high-dose RT were treated with intensity modulated radiation therapy (IMRT) rather than conventional beam radiation, and emphasized that the superior results seen with the higher dose is likely due to the use of IMRT.
Prior evidence
Dr. Hennequin pointed to a meta-analysis published in The Lancet in 2022 which showed that among nearly 11,000 patients with a median follow-up of 11.4 years the addition of ADT to RT significantly improved metastasis-free survival, and that longer ADT reduced the risk of metastases by 16% compared with standard schedule ADT.
He also cited the DART 01/05 trial results, which were published in 2022 in The Lancet: Oncology, which found a clinically relevant benefit for 24 months vs. 4 months of adjuvant ADT following a minimum of 76 Gy radiation in patients with high-risk disease, but not among patients with intermediate-risk disease.
The GETUG-AFU 18 trial was designed to address the question of whether 80 Gy of radiation could improve outcomes compared with 70 Gy in patients treated with long-term ADT.
Study details and results
The investigators enrolled men with high-risk prostate cancer defined as either a prostate-specific antigen (PSA) level 20 ng/ml or greater, Gleason score 8 or higher, or clinical stage T3 or T4 disease, and after stratification by treatment center and lymph node resection randomly assigned them to receive either 70 Gy or 80 Gy RT followed by 3 years of ADT.
Approximately two-thirds of the patients in each study arm had one risk factor and about one-fourth had two risk factors. The remaining patients had all three high-risk defining factors.
Approximately 16.5% of patients in each arm had undergone lymph node dissection.
The median ADT duration was 33.4 months. In all, 82.9% of patients underwent pelvic lymph node radiation; lymph node radiation was not performed in those patients who had negative node dissection results.
Significantly more patients assigned to the 80 Gy dose were treated with IMRT (80.6% vs. 58.6%, P < .001).
The cancer-specific survival rate was also higher for the group receiving the 80 Gy dose, with a 10 year rate of 95.6% vs. 90% for patients treated with 70 Gy. This difference translated into a HR of 0.48 (P = .0090).
Comparable safety
The safety analysis, which included 248 patients who received 80 Gy and 251 who received 70 Gy, showed that the incidence rates of both late genitourinary and gastrointestinal toxicities were low and comparable between the groups. Grade 3 or greater late genitourinary toxicities were seen in 2.0% of patients treated with 80 Gy and 3.2% of those treated with 70 Gy. In both arms, only 1.6% of patients had grade 3 or greater later GI toxicities.
There were also no differences between the study arms in patient-reported quality of life measures related to either bowel or urinary symptoms.
Invited discussant Neha Vapiwala, MD, FACR, from Penn Medicine in Philadelphia commented that the results of the GETUG-AFU 18 trial suggest that "if you had even lower-dose systemic therapy that the radiation control at the local level - local-regional level in this case - can in fact contribute to the prevention of distant metastases and can contribute to cancer-specific survival."
She said that with the efficacy results and the comparable toxicity and quality of life measures, dose-escalated radiation therapy and long-term ADT appear to offer a synergistic benefit.
The results are "practice-affirming for many, perhaps practice-changing for some if you're not already offering this," she said.
For patients with high-risk prostate cancer, treatment with long-term androgen deprivation therapy (ADT) and high-dose radiation was associated with significantly better progression-free, cancer-specific, and overall survival compared with ADT and standard-dose radiation.
The investigators also found that the patients taking long-term ADT and high-dose radiation did not experience additional late urinary tract or gastrointestinal toxicities. Christophe Hennequin, MD, PhD, reported these and other findings of the Radiation Therapy in Treating Patients Receiving Hormone Therapy for Prostate Cancer (GETUG-AFU 18) trial, at the 2024 American Society for Clinical Oncology (ASCO) Genitourinary Cancers Symposium.
Among 505 patients randomly assigned to be treated with radiation therapy (RT) at either the standard 70 Gy dose or a high, 80 Gy dose followed by 3 years of adjuvant ADT, the 10-year progression-free survival (PFS) rate was 83.6% for patients who had received the 80 Gy dose, vs. 72.2% for patients who had received the 70 Gy dose. This translated into a hazard ratio (HR) for biochemical or clinical progression of 0.56 (P = .0005).
This PFS advantage for high-dose radiation was also reflected by an overall survival (OS) advantage, with 10-year OS rates of 77% vs. 65.9%, respectively, translating into a 39% reduction in risk of death (HR 0.61, P = .0039) for patients who had received the higher radiation dose, reported Dr. Hennequin, of the Hospital Saint Louis in Paris, France.
"We have now Level 1 evidence that high-dose RT with long-term ADT must be the standard of care in high-risk prostate cancer patients," he said at the meeting.
Dr. Hennequin noted that significantly more patients assigned to high-dose RT were treated with intensity modulated radiation therapy (IMRT) rather than conventional beam radiation, and emphasized that the superior results seen with the higher dose is likely due to the use of IMRT.
Prior evidence
Dr. Hennequin pointed to a meta-analysis published in The Lancet in 2022 which showed that among nearly 11,000 patients with a median follow-up of 11.4 years the addition of ADT to RT significantly improved metastasis-free survival, and that longer ADT reduced the risk of metastases by 16% compared with standard schedule ADT.
He also cited the DART 01/05 trial results, which were published in 2022 in The Lancet: Oncology, which found a clinically relevant benefit for 24 months vs. 4 months of adjuvant ADT following a minimum of 76 Gy radiation in patients with high-risk disease, but not among patients with intermediate-risk disease.
The GETUG-AFU 18 trial was designed to address the question of whether 80 Gy of radiation could improve outcomes compared with 70 Gy in patients treated with long-term ADT.
Study details and results
The investigators enrolled men with high-risk prostate cancer defined as either a prostate-specific antigen (PSA) level 20 ng/ml or greater, Gleason score 8 or higher, or clinical stage T3 or T4 disease, and after stratification by treatment center and lymph node resection randomly assigned them to receive either 70 Gy or 80 Gy RT followed by 3 years of ADT.
Approximately two-thirds of the patients in each study arm had one risk factor and about one-fourth had two risk factors. The remaining patients had all three high-risk defining factors.
Approximately 16.5% of patients in each arm had undergone lymph node dissection.
The median ADT duration was 33.4 months. In all, 82.9% of patients underwent pelvic lymph node radiation; lymph node radiation was not performed in those patients who had negative node dissection results.
Significantly more patients assigned to the 80 Gy dose were treated with IMRT (80.6% vs. 58.6%, P < .001).
The cancer-specific survival rate was also higher for the group receiving the 80 Gy dose, with a 10 year rate of 95.6% vs. 90% for patients treated with 70 Gy. This difference translated into a HR of 0.48 (P = .0090).
Comparable safety
The safety analysis, which included 248 patients who received 80 Gy and 251 who received 70 Gy, showed that the incidence rates of both late genitourinary and gastrointestinal toxicities were low and comparable between the groups. Grade 3 or greater late genitourinary toxicities were seen in 2.0% of patients treated with 80 Gy and 3.2% of those treated with 70 Gy. In both arms, only 1.6% of patients had grade 3 or greater later GI toxicities.
There were also no differences between the study arms in patient-reported quality of life measures related to either bowel or urinary symptoms.
Invited discussant Neha Vapiwala, MD, FACR, from Penn Medicine in Philadelphia commented that the results of the GETUG-AFU 18 trial suggest that "if you had even lower-dose systemic therapy that the radiation control at the local level - local-regional level in this case - can in fact contribute to the prevention of distant metastases and can contribute to cancer-specific survival."
She said that with the efficacy results and the comparable toxicity and quality of life measures, dose-escalated radiation therapy and long-term ADT appear to offer a synergistic benefit.
The results are "practice-affirming for many, perhaps practice-changing for some if you're not already offering this," she said.
For patients with high-risk prostate cancer, treatment with long-term androgen deprivation therapy (ADT) and high-dose radiation was associated with significantly better progression-free, cancer-specific, and overall survival compared with ADT and standard-dose radiation.
The investigators also found that the patients taking long-term ADT and high-dose radiation did not experience additional late urinary tract or gastrointestinal toxicities. Christophe Hennequin, MD, PhD, reported these and other findings of the Radiation Therapy in Treating Patients Receiving Hormone Therapy for Prostate Cancer (GETUG-AFU 18) trial, at the 2024 American Society for Clinical Oncology (ASCO) Genitourinary Cancers Symposium.
Among 505 patients randomly assigned to be treated with radiation therapy (RT) at either the standard 70 Gy dose or a high, 80 Gy dose followed by 3 years of adjuvant ADT, the 10-year progression-free survival (PFS) rate was 83.6% for patients who had received the 80 Gy dose, vs. 72.2% for patients who had received the 70 Gy dose. This translated into a hazard ratio (HR) for biochemical or clinical progression of 0.56 (P = .0005).
This PFS advantage for high-dose radiation was also reflected by an overall survival (OS) advantage, with 10-year OS rates of 77% vs. 65.9%, respectively, translating into a 39% reduction in risk of death (HR 0.61, P = .0039) for patients who had received the higher radiation dose, reported Dr. Hennequin, of the Hospital Saint Louis in Paris, France.
"We have now Level 1 evidence that high-dose RT with long-term ADT must be the standard of care in high-risk prostate cancer patients," he said at the meeting.
Dr. Hennequin noted that significantly more patients assigned to high-dose RT were treated with intensity modulated radiation therapy (IMRT) rather than conventional beam radiation, and emphasized that the superior results seen with the higher dose is likely due to the use of IMRT.
Prior evidence
Dr. Hennequin pointed to a meta-analysis published in The Lancet in 2022 which showed that among nearly 11,000 patients with a median follow-up of 11.4 years the addition of ADT to RT significantly improved metastasis-free survival, and that longer ADT reduced the risk of metastases by 16% compared with standard schedule ADT.
He also cited the DART 01/05 trial results, which were published in 2022 in The Lancet: Oncology, which found a clinically relevant benefit for 24 months vs. 4 months of adjuvant ADT following a minimum of 76 Gy radiation in patients with high-risk disease, but not among patients with intermediate-risk disease.
The GETUG-AFU 18 trial was designed to address the question of whether 80 Gy of radiation could improve outcomes compared with 70 Gy in patients treated with long-term ADT.
Study details and results
The investigators enrolled men with high-risk prostate cancer defined as either a prostate-specific antigen (PSA) level 20 ng/ml or greater, Gleason score 8 or higher, or clinical stage T3 or T4 disease, and after stratification by treatment center and lymph node resection randomly assigned them to receive either 70 Gy or 80 Gy RT followed by 3 years of ADT.
Approximately two-thirds of the patients in each study arm had one risk factor and about one-fourth had two risk factors. The remaining patients had all three high-risk defining factors.
Approximately 16.5% of patients in each arm had undergone lymph node dissection.
The median ADT duration was 33.4 months. In all, 82.9% of patients underwent pelvic lymph node radiation; lymph node radiation was not performed in those patients who had negative node dissection results.
Significantly more patients assigned to the 80 Gy dose were treated with IMRT (80.6% vs. 58.6%, P < .001).
The cancer-specific survival rate was also higher for the group receiving the 80 Gy dose, with a 10 year rate of 95.6% vs. 90% for patients treated with 70 Gy. This difference translated into a HR of 0.48 (P = .0090).
Comparable safety
The safety analysis, which included 248 patients who received 80 Gy and 251 who received 70 Gy, showed that the incidence rates of both late genitourinary and gastrointestinal toxicities were low and comparable between the groups. Grade 3 or greater late genitourinary toxicities were seen in 2.0% of patients treated with 80 Gy and 3.2% of those treated with 70 Gy. In both arms, only 1.6% of patients had grade 3 or greater later GI toxicities.
There were also no differences between the study arms in patient-reported quality of life measures related to either bowel or urinary symptoms.
Invited discussant Neha Vapiwala, MD, FACR, from Penn Medicine in Philadelphia commented that the results of the GETUG-AFU 18 trial suggest that "if you had even lower-dose systemic therapy that the radiation control at the local level - local-regional level in this case - can in fact contribute to the prevention of distant metastases and can contribute to cancer-specific survival."
She said that with the efficacy results and the comparable toxicity and quality of life measures, dose-escalated radiation therapy and long-term ADT appear to offer a synergistic benefit.
The results are "practice-affirming for many, perhaps practice-changing for some if you're not already offering this," she said.
FROM ASCO GU 2024
Dana-Farber Moves to Retract, Correct Dozens of Cancer Papers Amid Allegations
News of the investigation follows a blog post by British molecular biologist Sholto David, MD, who flagged almost 60 papers published between 1997 and 2017 that contained image manipulation and other errors. Some of the papers were published by Dana-Farber’s chief executive officer, Laurie Glimcher, MD, and chief operating officer, William Hahn, MD, on topics including multiple myeloma and immune cells.
Mr. David, who blogs about research integrity, highlighted numerous errors and irregularities, including copying and pasting images across multiple experiments to represent different days within the same experiment, sometimes rotating or stretching images.
In one case, Mr. David equated the manipulation with tactics used by “hapless Chinese papermills” and concluded that “a swathe of research coming out of [Dana-Farber] authored by the most senior researchers and managers appears to be hopelessly corrupt with errors that are obvious from just a cursory reading the papers.”
“Imagine what mistakes might be found in the raw data if anyone was allowed to look!” he wrote.
Barrett Rollins, MD, PhD, Dana-Farber Cancer Institute’s research integrity officer, declined to comment on whether the errors represent scientific misconduct, according to STAT. Rollins told ScienceInsider that the “presence of image discrepancies in a paper is not evidence of an author’s intent to deceive.”
Access to new artificial intelligence tools is making it easier for data sleuths, like Mr. David, to unearth data manipulation and errors.
The current investigation closely follows two other investigations into the published work of Harvard University’s former president, Claudine Gay, and Stanford University’s former president, Marc Tessier-Lavigne, which led both to resign their posts.
A version of this article appeared on Medscape.com.
News of the investigation follows a blog post by British molecular biologist Sholto David, MD, who flagged almost 60 papers published between 1997 and 2017 that contained image manipulation and other errors. Some of the papers were published by Dana-Farber’s chief executive officer, Laurie Glimcher, MD, and chief operating officer, William Hahn, MD, on topics including multiple myeloma and immune cells.
Mr. David, who blogs about research integrity, highlighted numerous errors and irregularities, including copying and pasting images across multiple experiments to represent different days within the same experiment, sometimes rotating or stretching images.
In one case, Mr. David equated the manipulation with tactics used by “hapless Chinese papermills” and concluded that “a swathe of research coming out of [Dana-Farber] authored by the most senior researchers and managers appears to be hopelessly corrupt with errors that are obvious from just a cursory reading the papers.”
“Imagine what mistakes might be found in the raw data if anyone was allowed to look!” he wrote.
Barrett Rollins, MD, PhD, Dana-Farber Cancer Institute’s research integrity officer, declined to comment on whether the errors represent scientific misconduct, according to STAT. Rollins told ScienceInsider that the “presence of image discrepancies in a paper is not evidence of an author’s intent to deceive.”
Access to new artificial intelligence tools is making it easier for data sleuths, like Mr. David, to unearth data manipulation and errors.
The current investigation closely follows two other investigations into the published work of Harvard University’s former president, Claudine Gay, and Stanford University’s former president, Marc Tessier-Lavigne, which led both to resign their posts.
A version of this article appeared on Medscape.com.
News of the investigation follows a blog post by British molecular biologist Sholto David, MD, who flagged almost 60 papers published between 1997 and 2017 that contained image manipulation and other errors. Some of the papers were published by Dana-Farber’s chief executive officer, Laurie Glimcher, MD, and chief operating officer, William Hahn, MD, on topics including multiple myeloma and immune cells.
Mr. David, who blogs about research integrity, highlighted numerous errors and irregularities, including copying and pasting images across multiple experiments to represent different days within the same experiment, sometimes rotating or stretching images.
In one case, Mr. David equated the manipulation with tactics used by “hapless Chinese papermills” and concluded that “a swathe of research coming out of [Dana-Farber] authored by the most senior researchers and managers appears to be hopelessly corrupt with errors that are obvious from just a cursory reading the papers.”
“Imagine what mistakes might be found in the raw data if anyone was allowed to look!” he wrote.
Barrett Rollins, MD, PhD, Dana-Farber Cancer Institute’s research integrity officer, declined to comment on whether the errors represent scientific misconduct, according to STAT. Rollins told ScienceInsider that the “presence of image discrepancies in a paper is not evidence of an author’s intent to deceive.”
Access to new artificial intelligence tools is making it easier for data sleuths, like Mr. David, to unearth data manipulation and errors.
The current investigation closely follows two other investigations into the published work of Harvard University’s former president, Claudine Gay, and Stanford University’s former president, Marc Tessier-Lavigne, which led both to resign their posts.
A version of this article appeared on Medscape.com.
Cancer Identified as a New Cardiovascular Risk Factor
A history of cancer is an independent predictor of major cardiovascular events in patients undergoing coronary angioplasty. Cancer should be considered a new cardiovascular risk factor in primary and secondary prevention, according to a study presented at the 2023 American Heart Association Congress in Philadelphia.
, for example, equating it to the situation of a patient with diabetes or chronic renal failure,” said lead author Renzo Melchiori, MD, a cardiologist at the University Hospital Austral in Pilar, Argentina.
The researchers also advocate for intensifying cardiovascular control measures in secondary prevention for these patients, reconsidering goals, and ensuring compliance with prescribed pharmacological regimens and healthy lifestyle habits.
“Previously, when a patient had oncological pathology, thinking about associated cardiovascular risk seemed somewhat superfluous. But today, oncological diseases are treated so effectively, increasing survival and life expectancy, that we begin to focus on what happens with the arteries of these patients after treatment,” said Dr. Melchiori.
Higher Incidence Density
The retrospective analysis included 937 patients of both sexes aged 18 years and older who underwent coronary angioplasty for acute coronary syndrome between 2008 and 2022 at a university hospital. Of these participants, 89 (9.5%) had a history of cancer, with a median time since oncologic diagnosis of around 2 years for solid and hematologic tumors. Most participants had treated and resolved cancer.
Over a median follow-up of 45 months (range, 14-72 months), the cumulative incidence rates of a major cardiovascular event (nonfatal stroke, nonfatal acute myocardial infarction, cardiovascular death, or new angioplasty) were 22.2% (155/698) and 28.4% (25/88) in the groups without and with a history of cancer, respectively. The incidence density was significantly higher in the group with an oncologic history than in the group without such a history: 0.78 events/100 patients/month vs 0.48 events/100 patients/month (P = .01).
Kaplan-Meier analysis showed a higher probability of a major cardiovascular event in the group of patients with cancer or a history of cancer (P = .0086). In multivariate Cox regression analysis, cancer history was an independent predictor of major cardiovascular events adjusted for other risk factors such as age, hypertension, diabetes, smoking, sedentary lifestyle, and family history (hazard ratio, 1.66; P = .025).
Dr. Melchiori clarified that the increased incidence of cardiovascular events in patients with cancer or a history of cancer cannot be attributed to differences in percutaneous intervention or the indication or compliance of post-treatment pharmacological therapy.
In addition, the specialist acknowledged that due to the sample size, discrimination by cancer type, disease stage, or therapeutic strategies couldn’t be performed. A subanalysis, which has not been presented, indicated that the effect could not be explained solely by the application of radiotherapy or chemotherapy in the 90 days before angioplasty — two factors that cause arterial inflammation.
Intensifying Prevention Measures
Two independent experts told this news organization that the new study is "interesting" and reinforces the close connection between oncologic and cardiovascular pathology.
Andrés Daniele, MD, cardiologist and president of the Argentine Cardio-Oncology Association, a local chapter of the International Cardio-Oncology Society, emphasized that the study “reiterates an observation seen in other works: A higher rate of atherosclerotic pathology and cardiovascular events in patients with a history of cancer. And that has a reason to be: Both pathologies present common risk factors, and on the other hand, there is greater endothelial dysfunction secondary to the inflammatory syndrome and oncologic therapies.”
“There needs to be a continuum in the intensification of measures in primary and secondary cardiovascular prevention in cancer survivors, whether in remission or with chronic disease. We need to be very aggressive in managing risk factors and insist that patients who have had a cardiovascular event enter cardiovascular rehabilitation therapies,” said Dr. Daniele, who also heads the Cardio-Oncology Department at the centenary Roffo Institute of Oncology at the University of Buenos Aires, Argentina.
The study provides a valuable contribution because “we need to understand the epidemiology and natural history of patients with cancer at risk of developing cardiovascular complications to implement personalized cardiovascular prevention strategies,” said Teresa López Fernández, MD, cardiologist, coordinator of the Cardio-Oncology Program at La Paz University Hospital in Madrid, member of the Cardio-Oncology Working Group of the Spanish Society of Cardiology, member of the board of the International Cardio-Oncology Society, and cochair of the first clinical practice guidelines in cardio-oncology of the European Society of Cardiology.
“We have to be aware that perhaps we should not guide ourselves in these patients with the usual risk stratification scores as cancer or cardiotoxic treatment are not included as variables. However, they require our attention and effort to improve their quality and quantity of life, avoiding potentially preventable cardiovascular events that could negatively impact the survival achieved thanks to advances in cancer treatments,” said Dr. López Fernández.
Dr. Melchiori and Dr. Daniele declared no relevant economic conflicts of interest. Dr. López Fernández reported relationships with Daiichi Sankyo, Almirall España, Janssen-Cilag, Bayer, Roche, Philips, and Incyte.
This article was translated from the Medscape Spanish edition. A version of this article appeared on Medscape.com.
A history of cancer is an independent predictor of major cardiovascular events in patients undergoing coronary angioplasty. Cancer should be considered a new cardiovascular risk factor in primary and secondary prevention, according to a study presented at the 2023 American Heart Association Congress in Philadelphia.
, for example, equating it to the situation of a patient with diabetes or chronic renal failure,” said lead author Renzo Melchiori, MD, a cardiologist at the University Hospital Austral in Pilar, Argentina.
The researchers also advocate for intensifying cardiovascular control measures in secondary prevention for these patients, reconsidering goals, and ensuring compliance with prescribed pharmacological regimens and healthy lifestyle habits.
“Previously, when a patient had oncological pathology, thinking about associated cardiovascular risk seemed somewhat superfluous. But today, oncological diseases are treated so effectively, increasing survival and life expectancy, that we begin to focus on what happens with the arteries of these patients after treatment,” said Dr. Melchiori.
Higher Incidence Density
The retrospective analysis included 937 patients of both sexes aged 18 years and older who underwent coronary angioplasty for acute coronary syndrome between 2008 and 2022 at a university hospital. Of these participants, 89 (9.5%) had a history of cancer, with a median time since oncologic diagnosis of around 2 years for solid and hematologic tumors. Most participants had treated and resolved cancer.
Over a median follow-up of 45 months (range, 14-72 months), the cumulative incidence rates of a major cardiovascular event (nonfatal stroke, nonfatal acute myocardial infarction, cardiovascular death, or new angioplasty) were 22.2% (155/698) and 28.4% (25/88) in the groups without and with a history of cancer, respectively. The incidence density was significantly higher in the group with an oncologic history than in the group without such a history: 0.78 events/100 patients/month vs 0.48 events/100 patients/month (P = .01).
Kaplan-Meier analysis showed a higher probability of a major cardiovascular event in the group of patients with cancer or a history of cancer (P = .0086). In multivariate Cox regression analysis, cancer history was an independent predictor of major cardiovascular events adjusted for other risk factors such as age, hypertension, diabetes, smoking, sedentary lifestyle, and family history (hazard ratio, 1.66; P = .025).
Dr. Melchiori clarified that the increased incidence of cardiovascular events in patients with cancer or a history of cancer cannot be attributed to differences in percutaneous intervention or the indication or compliance of post-treatment pharmacological therapy.
In addition, the specialist acknowledged that due to the sample size, discrimination by cancer type, disease stage, or therapeutic strategies couldn’t be performed. A subanalysis, which has not been presented, indicated that the effect could not be explained solely by the application of radiotherapy or chemotherapy in the 90 days before angioplasty — two factors that cause arterial inflammation.
Intensifying Prevention Measures
Two independent experts told this news organization that the new study is "interesting" and reinforces the close connection between oncologic and cardiovascular pathology.
Andrés Daniele, MD, cardiologist and president of the Argentine Cardio-Oncology Association, a local chapter of the International Cardio-Oncology Society, emphasized that the study “reiterates an observation seen in other works: A higher rate of atherosclerotic pathology and cardiovascular events in patients with a history of cancer. And that has a reason to be: Both pathologies present common risk factors, and on the other hand, there is greater endothelial dysfunction secondary to the inflammatory syndrome and oncologic therapies.”
“There needs to be a continuum in the intensification of measures in primary and secondary cardiovascular prevention in cancer survivors, whether in remission or with chronic disease. We need to be very aggressive in managing risk factors and insist that patients who have had a cardiovascular event enter cardiovascular rehabilitation therapies,” said Dr. Daniele, who also heads the Cardio-Oncology Department at the centenary Roffo Institute of Oncology at the University of Buenos Aires, Argentina.
The study provides a valuable contribution because “we need to understand the epidemiology and natural history of patients with cancer at risk of developing cardiovascular complications to implement personalized cardiovascular prevention strategies,” said Teresa López Fernández, MD, cardiologist, coordinator of the Cardio-Oncology Program at La Paz University Hospital in Madrid, member of the Cardio-Oncology Working Group of the Spanish Society of Cardiology, member of the board of the International Cardio-Oncology Society, and cochair of the first clinical practice guidelines in cardio-oncology of the European Society of Cardiology.
“We have to be aware that perhaps we should not guide ourselves in these patients with the usual risk stratification scores as cancer or cardiotoxic treatment are not included as variables. However, they require our attention and effort to improve their quality and quantity of life, avoiding potentially preventable cardiovascular events that could negatively impact the survival achieved thanks to advances in cancer treatments,” said Dr. López Fernández.
Dr. Melchiori and Dr. Daniele declared no relevant economic conflicts of interest. Dr. López Fernández reported relationships with Daiichi Sankyo, Almirall España, Janssen-Cilag, Bayer, Roche, Philips, and Incyte.
This article was translated from the Medscape Spanish edition. A version of this article appeared on Medscape.com.
A history of cancer is an independent predictor of major cardiovascular events in patients undergoing coronary angioplasty. Cancer should be considered a new cardiovascular risk factor in primary and secondary prevention, according to a study presented at the 2023 American Heart Association Congress in Philadelphia.
, for example, equating it to the situation of a patient with diabetes or chronic renal failure,” said lead author Renzo Melchiori, MD, a cardiologist at the University Hospital Austral in Pilar, Argentina.
The researchers also advocate for intensifying cardiovascular control measures in secondary prevention for these patients, reconsidering goals, and ensuring compliance with prescribed pharmacological regimens and healthy lifestyle habits.
“Previously, when a patient had oncological pathology, thinking about associated cardiovascular risk seemed somewhat superfluous. But today, oncological diseases are treated so effectively, increasing survival and life expectancy, that we begin to focus on what happens with the arteries of these patients after treatment,” said Dr. Melchiori.
Higher Incidence Density
The retrospective analysis included 937 patients of both sexes aged 18 years and older who underwent coronary angioplasty for acute coronary syndrome between 2008 and 2022 at a university hospital. Of these participants, 89 (9.5%) had a history of cancer, with a median time since oncologic diagnosis of around 2 years for solid and hematologic tumors. Most participants had treated and resolved cancer.
Over a median follow-up of 45 months (range, 14-72 months), the cumulative incidence rates of a major cardiovascular event (nonfatal stroke, nonfatal acute myocardial infarction, cardiovascular death, or new angioplasty) were 22.2% (155/698) and 28.4% (25/88) in the groups without and with a history of cancer, respectively. The incidence density was significantly higher in the group with an oncologic history than in the group without such a history: 0.78 events/100 patients/month vs 0.48 events/100 patients/month (P = .01).
Kaplan-Meier analysis showed a higher probability of a major cardiovascular event in the group of patients with cancer or a history of cancer (P = .0086). In multivariate Cox regression analysis, cancer history was an independent predictor of major cardiovascular events adjusted for other risk factors such as age, hypertension, diabetes, smoking, sedentary lifestyle, and family history (hazard ratio, 1.66; P = .025).
Dr. Melchiori clarified that the increased incidence of cardiovascular events in patients with cancer or a history of cancer cannot be attributed to differences in percutaneous intervention or the indication or compliance of post-treatment pharmacological therapy.
In addition, the specialist acknowledged that due to the sample size, discrimination by cancer type, disease stage, or therapeutic strategies couldn’t be performed. A subanalysis, which has not been presented, indicated that the effect could not be explained solely by the application of radiotherapy or chemotherapy in the 90 days before angioplasty — two factors that cause arterial inflammation.
Intensifying Prevention Measures
Two independent experts told this news organization that the new study is "interesting" and reinforces the close connection between oncologic and cardiovascular pathology.
Andrés Daniele, MD, cardiologist and president of the Argentine Cardio-Oncology Association, a local chapter of the International Cardio-Oncology Society, emphasized that the study “reiterates an observation seen in other works: A higher rate of atherosclerotic pathology and cardiovascular events in patients with a history of cancer. And that has a reason to be: Both pathologies present common risk factors, and on the other hand, there is greater endothelial dysfunction secondary to the inflammatory syndrome and oncologic therapies.”
“There needs to be a continuum in the intensification of measures in primary and secondary cardiovascular prevention in cancer survivors, whether in remission or with chronic disease. We need to be very aggressive in managing risk factors and insist that patients who have had a cardiovascular event enter cardiovascular rehabilitation therapies,” said Dr. Daniele, who also heads the Cardio-Oncology Department at the centenary Roffo Institute of Oncology at the University of Buenos Aires, Argentina.
The study provides a valuable contribution because “we need to understand the epidemiology and natural history of patients with cancer at risk of developing cardiovascular complications to implement personalized cardiovascular prevention strategies,” said Teresa López Fernández, MD, cardiologist, coordinator of the Cardio-Oncology Program at La Paz University Hospital in Madrid, member of the Cardio-Oncology Working Group of the Spanish Society of Cardiology, member of the board of the International Cardio-Oncology Society, and cochair of the first clinical practice guidelines in cardio-oncology of the European Society of Cardiology.
“We have to be aware that perhaps we should not guide ourselves in these patients with the usual risk stratification scores as cancer or cardiotoxic treatment are not included as variables. However, they require our attention and effort to improve their quality and quantity of life, avoiding potentially preventable cardiovascular events that could negatively impact the survival achieved thanks to advances in cancer treatments,” said Dr. López Fernández.
Dr. Melchiori and Dr. Daniele declared no relevant economic conflicts of interest. Dr. López Fernández reported relationships with Daiichi Sankyo, Almirall España, Janssen-Cilag, Bayer, Roche, Philips, and Incyte.
This article was translated from the Medscape Spanish edition. A version of this article appeared on Medscape.com.