User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Healthy lifestyle may offset genetic risk in prostate cancer
In men at the highest risk of dying from prostate cancer, having the highest healthy lifestyle scores cut the risk of fatal disease in half, said study author Anna Plym, PhD, of Brigham and Women’s Hospital and Harvard School of Public Health, both in Boston. She presented these findings at the American Association for Cancer Research Annual Meeting 2021: Week 1 (Abstract 822).
Dr. Plym noted that about 58% of the variability in prostate cancer risk is accounted for by genetic factors, with common single-nucleotide polymorphisms (SNPs) accounting for a substantial proportion of prostate cancer susceptibility.
A recent study showed that a polygenic risk score (PRS) derived by combining information from 269 SNPs was “highly predictive” of prostate cancer, Dr. Plym said. There was a 10-fold gradient in disease risk between the lowest and highest genetic risk deciles, and the pattern was consistent across ethnic groups.
In addition, Dr. Plym noted, previous studies have suggested that a healthy lifestyle reduces lethal prostate cancer risk.
What has remained unclear is whether the risk for both developing prostate cancer and experiencing progression to lethal disease can be offset by adherence to a healthy lifestyle.
To investigate, Dr. Plym and colleagues used the 269-SNP PRS to quantify the genetic risk of prostate cancer in 10,443 men enrolled in the Health Professionals Follow-up Study. The men were divided into quartiles according to genetic risk.
The investigators also classified the men using a validated lifestyle score. For this score, one point was given for each of the following: not currently smoking or having quit 10 or more years ago, body mass index under 30 kg/m2, high vigorous physical activity, high intake of tomatoes and fatty fish, and low intake of processed meat. Patients with 1-2 points were considered the least healthy, those with 3 points were moderately healthy, and those with 4-6 points were the most healthy.
The outcomes assessed were overall prostate cancer and lethal prostate cancer (i.e., metastatic disease or prostate cancer–specific death).
No overall benefit of healthy lifestyle
At a median follow-up of 18 years, 2,111 cases of prostate cancer were observed. And at a median follow-up of 22 years, 238 lethal prostate cancer events occurred.
Men in the highest genetic risk quartile were five times more likely to develop prostate cancer (hazard ratio, 5.39; 95% confidence interval, 4.59-6.34) and three times more likely to develop lethal prostate cancer (HR, 3.43; 95% CI, 2.29-5.14), when compared with men in the lowest genetic risk quartile.
Adherence to a healthy lifestyle did not decrease the risk of prostate cancer overall (HR, 1.01; 95% CI, 0.84-1.22), nor did it affect men in the lower genetic risk quartiles.
However, healthy lifestyle did appear to affect men in the highest genetic risk quartile. Men with the highest healthy lifestyle scores had roughly half the risk of lethal prostate cancer, compared to men with the lowest lifestyle scores (3% vs. 6%).
A counterbalance to genetic risk
Dr. Plym observed that the rate of lethal disease in men with the best lifestyle scores matched the rate for the study population as a whole (3%), suggesting that healthy lifestyle may counterbalance high genetic risk.
She added that previous research has confirmed physical activity as a protective factor, but more study is needed to shed light on the relative benefit of the healthy lifestyle components.
In addition, further research is necessary to explain why the benefit was limited to lethal prostate cancer risk in men with the highest genetic risk.
Dr. Plym speculated that the genetic variants contributing to a high PRS may also be the variants that have the strongest interaction with lifestyle factors. For men with a genetic predisposition to prostate cancer, she added, these findings underscore the potential value of surveillance.
“Our findings add to current evidence suggesting that men with a high genetic risk may benefit from a targeted prostate cancer screening program, aiming at detecting a potentially lethal prostate cancer while it is still curable,” she said.
Charles Swanton, MBPhD, of the Francis Crick Institute and UCL Cancer Institute in London, raised the possibility that competing risk issues could be at play.
If a healthy lifestyle leads to longer life, he asked, does that make it more likely that patients will live long enough to die from their prostate cancer because they are not dying from cardiovascular disease, complications of diabetes, etc.? In that case, is the healthy lifestyle really affecting prostate cancer at all?
Dr. Plym responded that, among those in the highest genetic risk group with an unhealthy lifestyle, the increased risk for prostate cancer exceeded the risk for other illnesses.
This study was funded by the DiNovi Family Foundation, the National Cancer Institute, the William Casey Foundation, the Swedish Society for Medical Research, and the Prostate Cancer Foundation. Dr. Plym declared no conflicts of interest. Dr. Swanton disclosed relationships with numerous companies, including Pfizer, Novartis, and GlaxoSmithKline.
In men at the highest risk of dying from prostate cancer, having the highest healthy lifestyle scores cut the risk of fatal disease in half, said study author Anna Plym, PhD, of Brigham and Women’s Hospital and Harvard School of Public Health, both in Boston. She presented these findings at the American Association for Cancer Research Annual Meeting 2021: Week 1 (Abstract 822).
Dr. Plym noted that about 58% of the variability in prostate cancer risk is accounted for by genetic factors, with common single-nucleotide polymorphisms (SNPs) accounting for a substantial proportion of prostate cancer susceptibility.
A recent study showed that a polygenic risk score (PRS) derived by combining information from 269 SNPs was “highly predictive” of prostate cancer, Dr. Plym said. There was a 10-fold gradient in disease risk between the lowest and highest genetic risk deciles, and the pattern was consistent across ethnic groups.
In addition, Dr. Plym noted, previous studies have suggested that a healthy lifestyle reduces lethal prostate cancer risk.
What has remained unclear is whether the risk for both developing prostate cancer and experiencing progression to lethal disease can be offset by adherence to a healthy lifestyle.
To investigate, Dr. Plym and colleagues used the 269-SNP PRS to quantify the genetic risk of prostate cancer in 10,443 men enrolled in the Health Professionals Follow-up Study. The men were divided into quartiles according to genetic risk.
The investigators also classified the men using a validated lifestyle score. For this score, one point was given for each of the following: not currently smoking or having quit 10 or more years ago, body mass index under 30 kg/m2, high vigorous physical activity, high intake of tomatoes and fatty fish, and low intake of processed meat. Patients with 1-2 points were considered the least healthy, those with 3 points were moderately healthy, and those with 4-6 points were the most healthy.
The outcomes assessed were overall prostate cancer and lethal prostate cancer (i.e., metastatic disease or prostate cancer–specific death).
No overall benefit of healthy lifestyle
At a median follow-up of 18 years, 2,111 cases of prostate cancer were observed. And at a median follow-up of 22 years, 238 lethal prostate cancer events occurred.
Men in the highest genetic risk quartile were five times more likely to develop prostate cancer (hazard ratio, 5.39; 95% confidence interval, 4.59-6.34) and three times more likely to develop lethal prostate cancer (HR, 3.43; 95% CI, 2.29-5.14), when compared with men in the lowest genetic risk quartile.
Adherence to a healthy lifestyle did not decrease the risk of prostate cancer overall (HR, 1.01; 95% CI, 0.84-1.22), nor did it affect men in the lower genetic risk quartiles.
However, healthy lifestyle did appear to affect men in the highest genetic risk quartile. Men with the highest healthy lifestyle scores had roughly half the risk of lethal prostate cancer, compared to men with the lowest lifestyle scores (3% vs. 6%).
A counterbalance to genetic risk
Dr. Plym observed that the rate of lethal disease in men with the best lifestyle scores matched the rate for the study population as a whole (3%), suggesting that healthy lifestyle may counterbalance high genetic risk.
She added that previous research has confirmed physical activity as a protective factor, but more study is needed to shed light on the relative benefit of the healthy lifestyle components.
In addition, further research is necessary to explain why the benefit was limited to lethal prostate cancer risk in men with the highest genetic risk.
Dr. Plym speculated that the genetic variants contributing to a high PRS may also be the variants that have the strongest interaction with lifestyle factors. For men with a genetic predisposition to prostate cancer, she added, these findings underscore the potential value of surveillance.
“Our findings add to current evidence suggesting that men with a high genetic risk may benefit from a targeted prostate cancer screening program, aiming at detecting a potentially lethal prostate cancer while it is still curable,” she said.
Charles Swanton, MBPhD, of the Francis Crick Institute and UCL Cancer Institute in London, raised the possibility that competing risk issues could be at play.
If a healthy lifestyle leads to longer life, he asked, does that make it more likely that patients will live long enough to die from their prostate cancer because they are not dying from cardiovascular disease, complications of diabetes, etc.? In that case, is the healthy lifestyle really affecting prostate cancer at all?
Dr. Plym responded that, among those in the highest genetic risk group with an unhealthy lifestyle, the increased risk for prostate cancer exceeded the risk for other illnesses.
This study was funded by the DiNovi Family Foundation, the National Cancer Institute, the William Casey Foundation, the Swedish Society for Medical Research, and the Prostate Cancer Foundation. Dr. Plym declared no conflicts of interest. Dr. Swanton disclosed relationships with numerous companies, including Pfizer, Novartis, and GlaxoSmithKline.
In men at the highest risk of dying from prostate cancer, having the highest healthy lifestyle scores cut the risk of fatal disease in half, said study author Anna Plym, PhD, of Brigham and Women’s Hospital and Harvard School of Public Health, both in Boston. She presented these findings at the American Association for Cancer Research Annual Meeting 2021: Week 1 (Abstract 822).
Dr. Plym noted that about 58% of the variability in prostate cancer risk is accounted for by genetic factors, with common single-nucleotide polymorphisms (SNPs) accounting for a substantial proportion of prostate cancer susceptibility.
A recent study showed that a polygenic risk score (PRS) derived by combining information from 269 SNPs was “highly predictive” of prostate cancer, Dr. Plym said. There was a 10-fold gradient in disease risk between the lowest and highest genetic risk deciles, and the pattern was consistent across ethnic groups.
In addition, Dr. Plym noted, previous studies have suggested that a healthy lifestyle reduces lethal prostate cancer risk.
What has remained unclear is whether the risk for both developing prostate cancer and experiencing progression to lethal disease can be offset by adherence to a healthy lifestyle.
To investigate, Dr. Plym and colleagues used the 269-SNP PRS to quantify the genetic risk of prostate cancer in 10,443 men enrolled in the Health Professionals Follow-up Study. The men were divided into quartiles according to genetic risk.
The investigators also classified the men using a validated lifestyle score. For this score, one point was given for each of the following: not currently smoking or having quit 10 or more years ago, body mass index under 30 kg/m2, high vigorous physical activity, high intake of tomatoes and fatty fish, and low intake of processed meat. Patients with 1-2 points were considered the least healthy, those with 3 points were moderately healthy, and those with 4-6 points were the most healthy.
The outcomes assessed were overall prostate cancer and lethal prostate cancer (i.e., metastatic disease or prostate cancer–specific death).
No overall benefit of healthy lifestyle
At a median follow-up of 18 years, 2,111 cases of prostate cancer were observed. And at a median follow-up of 22 years, 238 lethal prostate cancer events occurred.
Men in the highest genetic risk quartile were five times more likely to develop prostate cancer (hazard ratio, 5.39; 95% confidence interval, 4.59-6.34) and three times more likely to develop lethal prostate cancer (HR, 3.43; 95% CI, 2.29-5.14), when compared with men in the lowest genetic risk quartile.
Adherence to a healthy lifestyle did not decrease the risk of prostate cancer overall (HR, 1.01; 95% CI, 0.84-1.22), nor did it affect men in the lower genetic risk quartiles.
However, healthy lifestyle did appear to affect men in the highest genetic risk quartile. Men with the highest healthy lifestyle scores had roughly half the risk of lethal prostate cancer, compared to men with the lowest lifestyle scores (3% vs. 6%).
A counterbalance to genetic risk
Dr. Plym observed that the rate of lethal disease in men with the best lifestyle scores matched the rate for the study population as a whole (3%), suggesting that healthy lifestyle may counterbalance high genetic risk.
She added that previous research has confirmed physical activity as a protective factor, but more study is needed to shed light on the relative benefit of the healthy lifestyle components.
In addition, further research is necessary to explain why the benefit was limited to lethal prostate cancer risk in men with the highest genetic risk.
Dr. Plym speculated that the genetic variants contributing to a high PRS may also be the variants that have the strongest interaction with lifestyle factors. For men with a genetic predisposition to prostate cancer, she added, these findings underscore the potential value of surveillance.
“Our findings add to current evidence suggesting that men with a high genetic risk may benefit from a targeted prostate cancer screening program, aiming at detecting a potentially lethal prostate cancer while it is still curable,” she said.
Charles Swanton, MBPhD, of the Francis Crick Institute and UCL Cancer Institute in London, raised the possibility that competing risk issues could be at play.
If a healthy lifestyle leads to longer life, he asked, does that make it more likely that patients will live long enough to die from their prostate cancer because they are not dying from cardiovascular disease, complications of diabetes, etc.? In that case, is the healthy lifestyle really affecting prostate cancer at all?
Dr. Plym responded that, among those in the highest genetic risk group with an unhealthy lifestyle, the increased risk for prostate cancer exceeded the risk for other illnesses.
This study was funded by the DiNovi Family Foundation, the National Cancer Institute, the William Casey Foundation, the Swedish Society for Medical Research, and the Prostate Cancer Foundation. Dr. Plym declared no conflicts of interest. Dr. Swanton disclosed relationships with numerous companies, including Pfizer, Novartis, and GlaxoSmithKline.
FROM AACR 2021
Deadly brain tumor: Survival extended by oncolytic virus product
This is a rapidly fatal form of brain cancer. Among historical control patients, the median overall survival was only 5.3 months.
The new results show a median overall survival of 12.2 months.
They come from a phase 1 trial conducted in 12 patients aged 7-18 years who had high-grade gliomas. All of the patients received the experimental therapy, dubbed G207, which was infused directly into the brain tumors.
“In our secondary objectives, we saw promising overall survival data ... [and] we saw that G207 turned immunologically ‘cold’ tumors to ‘hot,’ ” said lead investigator Gregory K. Friedman, MD, from the University of Alabama at Birmingham.
Dr. Friedman presented the new data at the American Association for Cancer Research Annual Meeting 2021: Week 1 (Abstract CT018). The study was also published simultaneously online in the New England Journal of Medicine.
Although the number of patients in the study was small, the data from this early trial look promising, commented Howard Kaufman, MD, director of the Oncolytic Virus Research Laboratory at Massachusetts General Hospital, Boston, who was not involved in the study.
“This is just a horrendous disease that hasn’t really responded to anything, so seeing some signs of benefit as well as a pretty tolerable safety profile is a very important observation that I think merits further investigation,” he said in an interview.
Engineered virus
G207 is an oncolytic form of HSV-1 created through genetic engineering in which a neurovirulence gene was deleted and viral nucleotide reductase was disabled. The engineered mutations prevent HSV-1 from infecting normal cells while allowing the virus to replicate in tumor cells.
The oncolytic virus product can be inoculated directly into tumors to circumvent the blood-brain barrier, and it preferentially infects neural tissue, making it ideal for treating brain tumors, the investigators explain.
One example of this type of product is already on the market. Talimogene laherparepvec is an oncolytic HSV-1 therapy that was approved in 2015 by the Food and Drug Administration for local treatment (i.e., injection directly into the skin lesion) of unresectable cutaneous, subcutaneous, and nodal lesions in patients with melanoma that recurs after initial surgery.
In their article, Dr. Friedman and colleagues summarized some of the data with G207 that “provided a strong rationale for conducting a trial involving children and adolescents.
“In addition to infecting and lysing tumor cells directly, G207 can reverse tumor immune evasion, increase cross-presentation of tumor antigens, and promote an antitumor immune response even in the absence of virus permissivity,” they wrote. “A single radiation dose enhances G207 efficacy in animal models by increasing viral replication and spread.”
In preclinical studies using tumor xenografts, pediatric brain tumors were 11-fold more sensitive to G207, compared with glioblastomas in adults.
The researchers hypothesized that intratumoral G207 would increase the amount of tumor-infiltrating lymphocytes and thereby convert immunologically “cold” pediatric brain tumors to “hot” and “inflamed” tumors.
Phase 1 trial
The phase 1 trial included four dose cohorts of children and adolescents with a pathologically proven malignant supratentorial brain tumor of at least 1 cm in diameter that had progressed after surgery, radiotherapy, or chemotherapy.
There were three patients in each dose cohort. One cohort received 107 plaque-forming units, the second received 108 PFU, the third received 107 PFU with 5 Gy of radiation, and the fourth received 108 PFU with 5 Gy radiation.
The patients first underwent stereotactic placement of up to four intratumoral catheters. The next day, they underwent infusion of the assigned PFU doses by controlled-rate infusion over 6 hours.
For the patients who received radiation, 5 Gy were administered to the gross tumor volume within 24 hours following G207 administration.
Among the 12 patients, tumors included 10 glioblastomas, one anaplastic astrocytoma, and one high-grade glioma not otherwise specified.
Responses (radiographic, neuropathologic, or clinical) occurred in 11 of the 12 patients.
Four patients were still alive 18 months after treatment, “which exceeds the life expectancy for newly diagnosed patients,” Dr. Friedman noted. Most patients die within 1 year of being diagnosed with pediatric glioma.
The investigators also found evidence to suggest that survival may be improved for patients who experience seroconversion after exposure to HSV-1 in comparison to patients with HSV-1 antibodies from prior HSV-1 infection. The median overall survival was 18.3 months for patients who experienced seroconversion, compared with 5.1 months for three patients who, at baseline, had IgG antibodies to HSV-1.
No dose-limiting toxicities or serious adverse events attributable to G207 occurred. There were 20 grade 1 adverse events that were potentially related to G207.
There was no evidence of peripheral G207 shedding or viremia, the investigators reported.
Radiation effect?
Commenting on the results in an interview, Dr. Kaufman noted that the sample size (12 patients) in this study was too small to determine whether the radiation received by patients in two of the four cohorts had any additive effect.
“Whether to move forward with virus alone or to add the radiation remains an open question that I don’t think was adequately answered,” he said.
Regarding the evidence suggesting that survival was better among patients who did not have antibodies to HSV-1 at baseline, Dr. Kaufman said, “We’ve looked at that in the melanoma population but haven’t seen any correlation there, so that’s interesting.”
The finding could be related to the fact that this was a pediatric population, or it could be related to the location of the tumors in the brain.
“It’s an interesting finding, and it suggests that, in future studies, they might want to select patients who are HSV seronegative up front,” he said.
Dr. Friedman and colleagues are currently planning a phase 2 trial of G207 with 5 Gy of radiation for children and adolescents with recurrent or progressive high-grade gliomas.
The study was supported by grants from the FDA, the National Institutes of Health, Cannonball Kids’ Cancer Foundation, the Rally Foundation for Childhood Cancer Research, Hyundai Hope on Wheels, St. Baldrick’s Foundation, the Department of Defense, the Andrew McDonough B+ Foundation, and the Kaul Pediatric Research Institute; by NIH/National Cancer Institute Cancer Center support grants to the University of Alabama at Birmingham and to the Memorial Sloan Kettering Cancer Center; and by Kelsie’s Crew, Eli’s Block Party Childhood Cancer Foundation, the Eli Jackson Foundation, Jaxon’s FROG Foundation, Battle for a Cure Foundation, and Sandcastle Kids. Dr. Friedman has received grants/support from the organizations listed above, as well as from Eli Lilly and Pfizer. Dr. Kaufman disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This is a rapidly fatal form of brain cancer. Among historical control patients, the median overall survival was only 5.3 months.
The new results show a median overall survival of 12.2 months.
They come from a phase 1 trial conducted in 12 patients aged 7-18 years who had high-grade gliomas. All of the patients received the experimental therapy, dubbed G207, which was infused directly into the brain tumors.
“In our secondary objectives, we saw promising overall survival data ... [and] we saw that G207 turned immunologically ‘cold’ tumors to ‘hot,’ ” said lead investigator Gregory K. Friedman, MD, from the University of Alabama at Birmingham.
Dr. Friedman presented the new data at the American Association for Cancer Research Annual Meeting 2021: Week 1 (Abstract CT018). The study was also published simultaneously online in the New England Journal of Medicine.
Although the number of patients in the study was small, the data from this early trial look promising, commented Howard Kaufman, MD, director of the Oncolytic Virus Research Laboratory at Massachusetts General Hospital, Boston, who was not involved in the study.
“This is just a horrendous disease that hasn’t really responded to anything, so seeing some signs of benefit as well as a pretty tolerable safety profile is a very important observation that I think merits further investigation,” he said in an interview.
Engineered virus
G207 is an oncolytic form of HSV-1 created through genetic engineering in which a neurovirulence gene was deleted and viral nucleotide reductase was disabled. The engineered mutations prevent HSV-1 from infecting normal cells while allowing the virus to replicate in tumor cells.
The oncolytic virus product can be inoculated directly into tumors to circumvent the blood-brain barrier, and it preferentially infects neural tissue, making it ideal for treating brain tumors, the investigators explain.
One example of this type of product is already on the market. Talimogene laherparepvec is an oncolytic HSV-1 therapy that was approved in 2015 by the Food and Drug Administration for local treatment (i.e., injection directly into the skin lesion) of unresectable cutaneous, subcutaneous, and nodal lesions in patients with melanoma that recurs after initial surgery.
In their article, Dr. Friedman and colleagues summarized some of the data with G207 that “provided a strong rationale for conducting a trial involving children and adolescents.
“In addition to infecting and lysing tumor cells directly, G207 can reverse tumor immune evasion, increase cross-presentation of tumor antigens, and promote an antitumor immune response even in the absence of virus permissivity,” they wrote. “A single radiation dose enhances G207 efficacy in animal models by increasing viral replication and spread.”
In preclinical studies using tumor xenografts, pediatric brain tumors were 11-fold more sensitive to G207, compared with glioblastomas in adults.
The researchers hypothesized that intratumoral G207 would increase the amount of tumor-infiltrating lymphocytes and thereby convert immunologically “cold” pediatric brain tumors to “hot” and “inflamed” tumors.
Phase 1 trial
The phase 1 trial included four dose cohorts of children and adolescents with a pathologically proven malignant supratentorial brain tumor of at least 1 cm in diameter that had progressed after surgery, radiotherapy, or chemotherapy.
There were three patients in each dose cohort. One cohort received 107 plaque-forming units, the second received 108 PFU, the third received 107 PFU with 5 Gy of radiation, and the fourth received 108 PFU with 5 Gy radiation.
The patients first underwent stereotactic placement of up to four intratumoral catheters. The next day, they underwent infusion of the assigned PFU doses by controlled-rate infusion over 6 hours.
For the patients who received radiation, 5 Gy were administered to the gross tumor volume within 24 hours following G207 administration.
Among the 12 patients, tumors included 10 glioblastomas, one anaplastic astrocytoma, and one high-grade glioma not otherwise specified.
Responses (radiographic, neuropathologic, or clinical) occurred in 11 of the 12 patients.
Four patients were still alive 18 months after treatment, “which exceeds the life expectancy for newly diagnosed patients,” Dr. Friedman noted. Most patients die within 1 year of being diagnosed with pediatric glioma.
The investigators also found evidence to suggest that survival may be improved for patients who experience seroconversion after exposure to HSV-1 in comparison to patients with HSV-1 antibodies from prior HSV-1 infection. The median overall survival was 18.3 months for patients who experienced seroconversion, compared with 5.1 months for three patients who, at baseline, had IgG antibodies to HSV-1.
No dose-limiting toxicities or serious adverse events attributable to G207 occurred. There were 20 grade 1 adverse events that were potentially related to G207.
There was no evidence of peripheral G207 shedding or viremia, the investigators reported.
Radiation effect?
Commenting on the results in an interview, Dr. Kaufman noted that the sample size (12 patients) in this study was too small to determine whether the radiation received by patients in two of the four cohorts had any additive effect.
“Whether to move forward with virus alone or to add the radiation remains an open question that I don’t think was adequately answered,” he said.
Regarding the evidence suggesting that survival was better among patients who did not have antibodies to HSV-1 at baseline, Dr. Kaufman said, “We’ve looked at that in the melanoma population but haven’t seen any correlation there, so that’s interesting.”
The finding could be related to the fact that this was a pediatric population, or it could be related to the location of the tumors in the brain.
“It’s an interesting finding, and it suggests that, in future studies, they might want to select patients who are HSV seronegative up front,” he said.
Dr. Friedman and colleagues are currently planning a phase 2 trial of G207 with 5 Gy of radiation for children and adolescents with recurrent or progressive high-grade gliomas.
The study was supported by grants from the FDA, the National Institutes of Health, Cannonball Kids’ Cancer Foundation, the Rally Foundation for Childhood Cancer Research, Hyundai Hope on Wheels, St. Baldrick’s Foundation, the Department of Defense, the Andrew McDonough B+ Foundation, and the Kaul Pediatric Research Institute; by NIH/National Cancer Institute Cancer Center support grants to the University of Alabama at Birmingham and to the Memorial Sloan Kettering Cancer Center; and by Kelsie’s Crew, Eli’s Block Party Childhood Cancer Foundation, the Eli Jackson Foundation, Jaxon’s FROG Foundation, Battle for a Cure Foundation, and Sandcastle Kids. Dr. Friedman has received grants/support from the organizations listed above, as well as from Eli Lilly and Pfizer. Dr. Kaufman disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This is a rapidly fatal form of brain cancer. Among historical control patients, the median overall survival was only 5.3 months.
The new results show a median overall survival of 12.2 months.
They come from a phase 1 trial conducted in 12 patients aged 7-18 years who had high-grade gliomas. All of the patients received the experimental therapy, dubbed G207, which was infused directly into the brain tumors.
“In our secondary objectives, we saw promising overall survival data ... [and] we saw that G207 turned immunologically ‘cold’ tumors to ‘hot,’ ” said lead investigator Gregory K. Friedman, MD, from the University of Alabama at Birmingham.
Dr. Friedman presented the new data at the American Association for Cancer Research Annual Meeting 2021: Week 1 (Abstract CT018). The study was also published simultaneously online in the New England Journal of Medicine.
Although the number of patients in the study was small, the data from this early trial look promising, commented Howard Kaufman, MD, director of the Oncolytic Virus Research Laboratory at Massachusetts General Hospital, Boston, who was not involved in the study.
“This is just a horrendous disease that hasn’t really responded to anything, so seeing some signs of benefit as well as a pretty tolerable safety profile is a very important observation that I think merits further investigation,” he said in an interview.
Engineered virus
G207 is an oncolytic form of HSV-1 created through genetic engineering in which a neurovirulence gene was deleted and viral nucleotide reductase was disabled. The engineered mutations prevent HSV-1 from infecting normal cells while allowing the virus to replicate in tumor cells.
The oncolytic virus product can be inoculated directly into tumors to circumvent the blood-brain barrier, and it preferentially infects neural tissue, making it ideal for treating brain tumors, the investigators explain.
One example of this type of product is already on the market. Talimogene laherparepvec is an oncolytic HSV-1 therapy that was approved in 2015 by the Food and Drug Administration for local treatment (i.e., injection directly into the skin lesion) of unresectable cutaneous, subcutaneous, and nodal lesions in patients with melanoma that recurs after initial surgery.
In their article, Dr. Friedman and colleagues summarized some of the data with G207 that “provided a strong rationale for conducting a trial involving children and adolescents.
“In addition to infecting and lysing tumor cells directly, G207 can reverse tumor immune evasion, increase cross-presentation of tumor antigens, and promote an antitumor immune response even in the absence of virus permissivity,” they wrote. “A single radiation dose enhances G207 efficacy in animal models by increasing viral replication and spread.”
In preclinical studies using tumor xenografts, pediatric brain tumors were 11-fold more sensitive to G207, compared with glioblastomas in adults.
The researchers hypothesized that intratumoral G207 would increase the amount of tumor-infiltrating lymphocytes and thereby convert immunologically “cold” pediatric brain tumors to “hot” and “inflamed” tumors.
Phase 1 trial
The phase 1 trial included four dose cohorts of children and adolescents with a pathologically proven malignant supratentorial brain tumor of at least 1 cm in diameter that had progressed after surgery, radiotherapy, or chemotherapy.
There were three patients in each dose cohort. One cohort received 107 plaque-forming units, the second received 108 PFU, the third received 107 PFU with 5 Gy of radiation, and the fourth received 108 PFU with 5 Gy radiation.
The patients first underwent stereotactic placement of up to four intratumoral catheters. The next day, they underwent infusion of the assigned PFU doses by controlled-rate infusion over 6 hours.
For the patients who received radiation, 5 Gy were administered to the gross tumor volume within 24 hours following G207 administration.
Among the 12 patients, tumors included 10 glioblastomas, one anaplastic astrocytoma, and one high-grade glioma not otherwise specified.
Responses (radiographic, neuropathologic, or clinical) occurred in 11 of the 12 patients.
Four patients were still alive 18 months after treatment, “which exceeds the life expectancy for newly diagnosed patients,” Dr. Friedman noted. Most patients die within 1 year of being diagnosed with pediatric glioma.
The investigators also found evidence to suggest that survival may be improved for patients who experience seroconversion after exposure to HSV-1 in comparison to patients with HSV-1 antibodies from prior HSV-1 infection. The median overall survival was 18.3 months for patients who experienced seroconversion, compared with 5.1 months for three patients who, at baseline, had IgG antibodies to HSV-1.
No dose-limiting toxicities or serious adverse events attributable to G207 occurred. There were 20 grade 1 adverse events that were potentially related to G207.
There was no evidence of peripheral G207 shedding or viremia, the investigators reported.
Radiation effect?
Commenting on the results in an interview, Dr. Kaufman noted that the sample size (12 patients) in this study was too small to determine whether the radiation received by patients in two of the four cohorts had any additive effect.
“Whether to move forward with virus alone or to add the radiation remains an open question that I don’t think was adequately answered,” he said.
Regarding the evidence suggesting that survival was better among patients who did not have antibodies to HSV-1 at baseline, Dr. Kaufman said, “We’ve looked at that in the melanoma population but haven’t seen any correlation there, so that’s interesting.”
The finding could be related to the fact that this was a pediatric population, or it could be related to the location of the tumors in the brain.
“It’s an interesting finding, and it suggests that, in future studies, they might want to select patients who are HSV seronegative up front,” he said.
Dr. Friedman and colleagues are currently planning a phase 2 trial of G207 with 5 Gy of radiation for children and adolescents with recurrent or progressive high-grade gliomas.
The study was supported by grants from the FDA, the National Institutes of Health, Cannonball Kids’ Cancer Foundation, the Rally Foundation for Childhood Cancer Research, Hyundai Hope on Wheels, St. Baldrick’s Foundation, the Department of Defense, the Andrew McDonough B+ Foundation, and the Kaul Pediatric Research Institute; by NIH/National Cancer Institute Cancer Center support grants to the University of Alabama at Birmingham and to the Memorial Sloan Kettering Cancer Center; and by Kelsie’s Crew, Eli’s Block Party Childhood Cancer Foundation, the Eli Jackson Foundation, Jaxon’s FROG Foundation, Battle for a Cure Foundation, and Sandcastle Kids. Dr. Friedman has received grants/support from the organizations listed above, as well as from Eli Lilly and Pfizer. Dr. Kaufman disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AACR 2021
FDA approves first AI device to detect colon lesions
The GI Genius (Cosmo Artificial Intelligence) identifies areas of the colon where a colorectal polyp or tumor might be located. Clinicians then follow up with a closer examination and possible treatment.
“With the FDA’s authorization of this device today, clinicians now have a tool that could help improve their ability to detect gastrointestinal lesions they may have missed otherwise,” said Courtney H. Lias, PhD, acting director of the FDA’s gastrorenal, ob.gyn., general hospital, and urology devices office, in a media release.
The GI Genius consists of both hardware and software designed to work with an endoscope. It uses machine learning to recognize possible polyps during a colonoscopy. It marks these areas with green squares on the video generated by the endoscope’s camera and emits a short, low-volume sound. Clinicians decide if a lesion is truly present and whether to sample or remove such a lesion.
The device does not diagnose the lesions or recommend treatments and is not intended to take the place of laboratory sampling
The FDA based its approval on a trial in which 700 people aged 40-80 years underwent colonoscopies for colorectal cancer screening, surveillance, follow-up from positive results of a fecal occult blood test, or gastrointestinal symptoms of possible colon cancer.
Of these participants, 263 were being screened or surveilled every 3 years or more. The researchers randomly divided patients into a group of 136 who underwent white-light standard colonoscopy with the GI Genius, and 127 who underwent white-light standard colonoscopy without the GI Genius.
Using the GI Genius, clinicians identified adenomas or carcinomas that were later confirmed through lab results in 55.1% of patients. Without the GI Genius, the clinicians identified such lesions in 42.0% of patients.
The patients examined with the GI Genius received more biopsies, including slightly more that were not adenomas. But the biopsies did not lead to any adverse events such as perforations, infections, bleeding, or further biopsies.
More information on the GI Genius is available on the FDA website.
A version of this article first appeared on Medscape.com .
The GI Genius (Cosmo Artificial Intelligence) identifies areas of the colon where a colorectal polyp or tumor might be located. Clinicians then follow up with a closer examination and possible treatment.
“With the FDA’s authorization of this device today, clinicians now have a tool that could help improve their ability to detect gastrointestinal lesions they may have missed otherwise,” said Courtney H. Lias, PhD, acting director of the FDA’s gastrorenal, ob.gyn., general hospital, and urology devices office, in a media release.
The GI Genius consists of both hardware and software designed to work with an endoscope. It uses machine learning to recognize possible polyps during a colonoscopy. It marks these areas with green squares on the video generated by the endoscope’s camera and emits a short, low-volume sound. Clinicians decide if a lesion is truly present and whether to sample or remove such a lesion.
The device does not diagnose the lesions or recommend treatments and is not intended to take the place of laboratory sampling
The FDA based its approval on a trial in which 700 people aged 40-80 years underwent colonoscopies for colorectal cancer screening, surveillance, follow-up from positive results of a fecal occult blood test, or gastrointestinal symptoms of possible colon cancer.
Of these participants, 263 were being screened or surveilled every 3 years or more. The researchers randomly divided patients into a group of 136 who underwent white-light standard colonoscopy with the GI Genius, and 127 who underwent white-light standard colonoscopy without the GI Genius.
Using the GI Genius, clinicians identified adenomas or carcinomas that were later confirmed through lab results in 55.1% of patients. Without the GI Genius, the clinicians identified such lesions in 42.0% of patients.
The patients examined with the GI Genius received more biopsies, including slightly more that were not adenomas. But the biopsies did not lead to any adverse events such as perforations, infections, bleeding, or further biopsies.
More information on the GI Genius is available on the FDA website.
A version of this article first appeared on Medscape.com .
The GI Genius (Cosmo Artificial Intelligence) identifies areas of the colon where a colorectal polyp or tumor might be located. Clinicians then follow up with a closer examination and possible treatment.
“With the FDA’s authorization of this device today, clinicians now have a tool that could help improve their ability to detect gastrointestinal lesions they may have missed otherwise,” said Courtney H. Lias, PhD, acting director of the FDA’s gastrorenal, ob.gyn., general hospital, and urology devices office, in a media release.
The GI Genius consists of both hardware and software designed to work with an endoscope. It uses machine learning to recognize possible polyps during a colonoscopy. It marks these areas with green squares on the video generated by the endoscope’s camera and emits a short, low-volume sound. Clinicians decide if a lesion is truly present and whether to sample or remove such a lesion.
The device does not diagnose the lesions or recommend treatments and is not intended to take the place of laboratory sampling
The FDA based its approval on a trial in which 700 people aged 40-80 years underwent colonoscopies for colorectal cancer screening, surveillance, follow-up from positive results of a fecal occult blood test, or gastrointestinal symptoms of possible colon cancer.
Of these participants, 263 were being screened or surveilled every 3 years or more. The researchers randomly divided patients into a group of 136 who underwent white-light standard colonoscopy with the GI Genius, and 127 who underwent white-light standard colonoscopy without the GI Genius.
Using the GI Genius, clinicians identified adenomas or carcinomas that were later confirmed through lab results in 55.1% of patients. Without the GI Genius, the clinicians identified such lesions in 42.0% of patients.
The patients examined with the GI Genius received more biopsies, including slightly more that were not adenomas. But the biopsies did not lead to any adverse events such as perforations, infections, bleeding, or further biopsies.
More information on the GI Genius is available on the FDA website.
A version of this article first appeared on Medscape.com .
Endometrial thickness could predict cancer, guide lymph node assessment
In a retrospective study of 378 patients who had hysterectomies for EIN, those with a preoperative endometrial stripe of 20 mm or greater were two times more likely to have endometrial cancer on final pathology, and those with an endometrial thickness of 15 mm or greater were 1.8 times more likely to have cancer.
“This data suggests that increasing endometrial thickness may be a useful preoperative marker to identify who’s at higher risk of concurrent endometrial cancer. It could also be considered a criterion for selectively using a sentinel lymph node algorithm in patients with a preoperative diagnosis of EIN. However, prospective studies are warranted to further establish this association,” said Devon Abt, MD, of Beth Israel Deaconess Medical Center in Boston.
She presented the data at the Society of Gynecologic Oncology’s Virtual Annual Meeting on Women’s Cancer (Abstract 11103).
Risk of overtreatment
There are no clear consensus guidelines on lymph node assessment for patients with EIN, Dr. Abt noted. She pointed out that roughly 40% of patients with EIN are diagnosed with endometrial cancer. However, it’s usually low-stage, low-grade disease, and only about 10% of patients will have high-risk features that warrant lymph node evaluation.
“Typically, we identify patients with concurrent endometrial cancer based on intraoperative pathology, or frozen section,” Dr. Abt explained. “We then apply the Mayo criteria, which stratifies patients as high or low risk for lymph node metastasis based on pathologic criteria. ... This information helps guide our intraoperative decisions to perform, or not perform, pelvic and para-aortic lymphadenectomy.”
Dr. Abt noted, however, that “lymphadenectomy is not benign” and increases surgical time as well as the risk of complications.
Taking these factors into account, some centers have implemented routine sentinel lymph node algorithms for staging endometrial cancers, Dr. Abt said.
What she and her colleagues wanted to determine is if there is value in this practice. Should sentinel lymph node mapping and biopsy be offered routinely to all patients with a preoperative diagnosis of EIN?
Study details
Dr. Abt and colleagues conducted a retrospective, single-center study of 378 patients with EIN. Ultimately, 27% (n = 103) of the patients were diagnosed with endometrial cancer – 95% with stage 1a disease and 5% with stage 1b.
Increasing age, White race, and hypertension were significantly associated with the presence of endometrial cancer. Body mass index, parity, hormone therapy exposure, and baseline CA 125 were not.
The median preoperative endometrial thickness was 14 mm among patients with endometrial cancer and 11 mm in patients without cancer (P = .002).
Overall, 31% of the cancer cases were considered high risk for nodal metastases by Mayo criteria, but an endometrial stripe of 15 mm or higher increased the chance of being considered high risk.
The risk of cancer was 47% among patients with an endometrial stripe of at least 20 mm versus 21% among patients with a measurement below 15 mm.
Only 10 patients underwent lymph node evaluation, 5 with sentinel lymph node dissection and 5 with lymphadenectomy. Six of the 10 patients had endometrial cancer on final pathology, but none had positive lymph nodes.
“Given the low-grade and early-stage disease in this cohort, adherence to a routine sentinel lymph node algorithm in all patients with EIN would result in overtreatment,” Dr. Abt said.
Discussant Nicole Fleming, MD, of the University of Texas MD Anderson Cancer Center, Houston, said she would advocate for more selective use of sentinel lymph node biopsies in EIN as well.
Dr. Fleming said, in general, lymph node biopsy may be reasonable in settings where frozen sections are unreliable and the patient seems to be at high risk of invasive cancer. However, at academic centers with dedicated gynecologic pathologists, given the low risk of invasive cancer and the fact that lymph nodes “are probably not going to provide you a lot of useful therapeutic decision-making tools,” potentially eliminating sentinel lymph node biopsy might make sense, Dr. Fleming said.
Dr. Fleming disclosed relationships with Tesaro, Bristol-Myers Squibb, Pfizer, and GlaxoSmithKline. Dr. Abt reported having no relevant disclosures and did not report any study funding.
In a retrospective study of 378 patients who had hysterectomies for EIN, those with a preoperative endometrial stripe of 20 mm or greater were two times more likely to have endometrial cancer on final pathology, and those with an endometrial thickness of 15 mm or greater were 1.8 times more likely to have cancer.
“This data suggests that increasing endometrial thickness may be a useful preoperative marker to identify who’s at higher risk of concurrent endometrial cancer. It could also be considered a criterion for selectively using a sentinel lymph node algorithm in patients with a preoperative diagnosis of EIN. However, prospective studies are warranted to further establish this association,” said Devon Abt, MD, of Beth Israel Deaconess Medical Center in Boston.
She presented the data at the Society of Gynecologic Oncology’s Virtual Annual Meeting on Women’s Cancer (Abstract 11103).
Risk of overtreatment
There are no clear consensus guidelines on lymph node assessment for patients with EIN, Dr. Abt noted. She pointed out that roughly 40% of patients with EIN are diagnosed with endometrial cancer. However, it’s usually low-stage, low-grade disease, and only about 10% of patients will have high-risk features that warrant lymph node evaluation.
“Typically, we identify patients with concurrent endometrial cancer based on intraoperative pathology, or frozen section,” Dr. Abt explained. “We then apply the Mayo criteria, which stratifies patients as high or low risk for lymph node metastasis based on pathologic criteria. ... This information helps guide our intraoperative decisions to perform, or not perform, pelvic and para-aortic lymphadenectomy.”
Dr. Abt noted, however, that “lymphadenectomy is not benign” and increases surgical time as well as the risk of complications.
Taking these factors into account, some centers have implemented routine sentinel lymph node algorithms for staging endometrial cancers, Dr. Abt said.
What she and her colleagues wanted to determine is if there is value in this practice. Should sentinel lymph node mapping and biopsy be offered routinely to all patients with a preoperative diagnosis of EIN?
Study details
Dr. Abt and colleagues conducted a retrospective, single-center study of 378 patients with EIN. Ultimately, 27% (n = 103) of the patients were diagnosed with endometrial cancer – 95% with stage 1a disease and 5% with stage 1b.
Increasing age, White race, and hypertension were significantly associated with the presence of endometrial cancer. Body mass index, parity, hormone therapy exposure, and baseline CA 125 were not.
The median preoperative endometrial thickness was 14 mm among patients with endometrial cancer and 11 mm in patients without cancer (P = .002).
Overall, 31% of the cancer cases were considered high risk for nodal metastases by Mayo criteria, but an endometrial stripe of 15 mm or higher increased the chance of being considered high risk.
The risk of cancer was 47% among patients with an endometrial stripe of at least 20 mm versus 21% among patients with a measurement below 15 mm.
Only 10 patients underwent lymph node evaluation, 5 with sentinel lymph node dissection and 5 with lymphadenectomy. Six of the 10 patients had endometrial cancer on final pathology, but none had positive lymph nodes.
“Given the low-grade and early-stage disease in this cohort, adherence to a routine sentinel lymph node algorithm in all patients with EIN would result in overtreatment,” Dr. Abt said.
Discussant Nicole Fleming, MD, of the University of Texas MD Anderson Cancer Center, Houston, said she would advocate for more selective use of sentinel lymph node biopsies in EIN as well.
Dr. Fleming said, in general, lymph node biopsy may be reasonable in settings where frozen sections are unreliable and the patient seems to be at high risk of invasive cancer. However, at academic centers with dedicated gynecologic pathologists, given the low risk of invasive cancer and the fact that lymph nodes “are probably not going to provide you a lot of useful therapeutic decision-making tools,” potentially eliminating sentinel lymph node biopsy might make sense, Dr. Fleming said.
Dr. Fleming disclosed relationships with Tesaro, Bristol-Myers Squibb, Pfizer, and GlaxoSmithKline. Dr. Abt reported having no relevant disclosures and did not report any study funding.
In a retrospective study of 378 patients who had hysterectomies for EIN, those with a preoperative endometrial stripe of 20 mm or greater were two times more likely to have endometrial cancer on final pathology, and those with an endometrial thickness of 15 mm or greater were 1.8 times more likely to have cancer.
“This data suggests that increasing endometrial thickness may be a useful preoperative marker to identify who’s at higher risk of concurrent endometrial cancer. It could also be considered a criterion for selectively using a sentinel lymph node algorithm in patients with a preoperative diagnosis of EIN. However, prospective studies are warranted to further establish this association,” said Devon Abt, MD, of Beth Israel Deaconess Medical Center in Boston.
She presented the data at the Society of Gynecologic Oncology’s Virtual Annual Meeting on Women’s Cancer (Abstract 11103).
Risk of overtreatment
There are no clear consensus guidelines on lymph node assessment for patients with EIN, Dr. Abt noted. She pointed out that roughly 40% of patients with EIN are diagnosed with endometrial cancer. However, it’s usually low-stage, low-grade disease, and only about 10% of patients will have high-risk features that warrant lymph node evaluation.
“Typically, we identify patients with concurrent endometrial cancer based on intraoperative pathology, or frozen section,” Dr. Abt explained. “We then apply the Mayo criteria, which stratifies patients as high or low risk for lymph node metastasis based on pathologic criteria. ... This information helps guide our intraoperative decisions to perform, or not perform, pelvic and para-aortic lymphadenectomy.”
Dr. Abt noted, however, that “lymphadenectomy is not benign” and increases surgical time as well as the risk of complications.
Taking these factors into account, some centers have implemented routine sentinel lymph node algorithms for staging endometrial cancers, Dr. Abt said.
What she and her colleagues wanted to determine is if there is value in this practice. Should sentinel lymph node mapping and biopsy be offered routinely to all patients with a preoperative diagnosis of EIN?
Study details
Dr. Abt and colleagues conducted a retrospective, single-center study of 378 patients with EIN. Ultimately, 27% (n = 103) of the patients were diagnosed with endometrial cancer – 95% with stage 1a disease and 5% with stage 1b.
Increasing age, White race, and hypertension were significantly associated with the presence of endometrial cancer. Body mass index, parity, hormone therapy exposure, and baseline CA 125 were not.
The median preoperative endometrial thickness was 14 mm among patients with endometrial cancer and 11 mm in patients without cancer (P = .002).
Overall, 31% of the cancer cases were considered high risk for nodal metastases by Mayo criteria, but an endometrial stripe of 15 mm or higher increased the chance of being considered high risk.
The risk of cancer was 47% among patients with an endometrial stripe of at least 20 mm versus 21% among patients with a measurement below 15 mm.
Only 10 patients underwent lymph node evaluation, 5 with sentinel lymph node dissection and 5 with lymphadenectomy. Six of the 10 patients had endometrial cancer on final pathology, but none had positive lymph nodes.
“Given the low-grade and early-stage disease in this cohort, adherence to a routine sentinel lymph node algorithm in all patients with EIN would result in overtreatment,” Dr. Abt said.
Discussant Nicole Fleming, MD, of the University of Texas MD Anderson Cancer Center, Houston, said she would advocate for more selective use of sentinel lymph node biopsies in EIN as well.
Dr. Fleming said, in general, lymph node biopsy may be reasonable in settings where frozen sections are unreliable and the patient seems to be at high risk of invasive cancer. However, at academic centers with dedicated gynecologic pathologists, given the low risk of invasive cancer and the fact that lymph nodes “are probably not going to provide you a lot of useful therapeutic decision-making tools,” potentially eliminating sentinel lymph node biopsy might make sense, Dr. Fleming said.
Dr. Fleming disclosed relationships with Tesaro, Bristol-Myers Squibb, Pfizer, and GlaxoSmithKline. Dr. Abt reported having no relevant disclosures and did not report any study funding.
FROM SGO 2021
Low-risk adenomas may not elevate risk of CRC-related death
Unlike high-risk adenomas (HRAs), low-risk adenomas (LRAs) have a minimal association with risk of metachronous colorectal cancer (CRC), and no relationship with odds of metachronous CRC-related mortality, according to a meta-analysis of more than 500,000 individuals.

These findings should impact surveillance guidelines and make follow-up the same for individuals with LRAs or no adenomas, reported lead author Abhiram Duvvuri, MD, of the division of gastroenterology and hepatology at the University of Kansas, Kansas City, and colleagues. Currently, the United States Multi-Society Task Force on Colorectal Cancer advises colonoscopy intervals of 3 years for individuals with HRAs, 7-10 years for those with LRAs, and 10 years for those without adenomas.
“The evidence supporting these surveillance recommendations for clinically relevant endpoints such as cancer and cancer-related deaths among patients who undergo adenoma removal, particularly LRA, is minimal, because most of the evidence was based on the surrogate risk of metachronous advanced neoplasia,” the investigators wrote in Gastroenterology.
To provide more solid evidence, the investigators performed a systematic review and meta-analysis, ultimately analyzing 12 studies with data from 510,019 individuals at a mean age of 59.2 years. All studies reported rates of LRA, HRA, or no adenoma at baseline colonoscopy, plus incidence of metachronous CRC and/or CRC-related mortality. With these data, the investigators determined incidence of metachronous CRC and CRC-related mortality for each of the adenoma groups and also compared these incidences per 10,000 person-years of follow-up across groups.
After a mean follow-up of 8.5 years, patients with HRAs had a significantly higher rate of CRC compared with patients who had LRAs (13.81 vs. 4.5; odds ratio, 2.35; 95% confidence interval, 1.72-3.20) or no adenomas (13.81 vs. 3.4; OR, 2.92; 95% CI, 2.31-3.69). Similarly, but to a lesser degree, LRAs were associated with significantly greater risk of CRC than that of no adenomas (4.5 vs. 3.4; OR, 1.26; 95% CI, 1.06-1.51).
Data on CRC- related mortality further supported these minimal risk profiles because LRAs did not significantly increase the risk of CRC-related mortality compared with no adenomas (OR, 1.15; 95% CI, 0.76-1.74). In contrast, HRAs were associated with significantly greater risk of CRC-related death than that of both LRAs (OR, 2.48; 95% CI, 1.30-4.75) and no adenomas (OR, 2.69; 95% CI, 1.87-3.87).
The investigators acknowledged certain limitations of their study. For one, there were no randomized controlled trials in the meta-analysis, which can introduce bias. Loss of patients to follow-up is also possible; however, the investigators noted that there was a robust sample of patients available for study outcomes all the same. There is also risk of comparability bias in that HRA and LRA groups underwent more colonoscopies; however, the duration of follow-up and timing of last colonoscopy were similar among groups. Lastly, it’s possible the patient sample wasn’t representative because of healthy screenee bias, but the investigators compared groups against general population to minimize that bias.
The investigators also highlighted several strengths of their study that make their findings more reliable than those of past meta-analyses. For one, their study is the largest of its kind to date, and involved a significantly higher number of patients with LRA and no adenomas. Also, in contrast with previous studies, CRC and CRC-related mortality were evaluated rather than advanced adenomas, they noted.
“Furthermore, we also analyzed CRC incidence and mortality in the LRA group compared with the general population, with the [standardized incidence ratio] being lower and [standardized mortality ratio] being comparable, confirming that it is indeed a low-risk group,” they wrote.
Considering these strengths and the nature of their findings, Dr. Duvvuri and colleagues called for a more conservative approach to CRC surveillance among individuals with LRAs, and more research to investigate extending colonoscopy intervals even further.
“We recommend that the interval for follow-up colonoscopy should be the same in patients with LRAs or no adenomas but that the HRA group should have a more frequent surveillance interval for CRC surveillance compared with these groups,” they concluded. “Future studies should evaluate whether surveillance intervals could be lengthened beyond 10 years in the no-adenoma and LRA groups after an initial high-quality index colonoscopy.”
One author disclosed affiliations with Erbe, Cdx Labs, Aries, and others. Dr. Duvvuri and the remaining authors disclosed no conflicts.
Unlike high-risk adenomas (HRAs), low-risk adenomas (LRAs) have a minimal association with risk of metachronous colorectal cancer (CRC), and no relationship with odds of metachronous CRC-related mortality, according to a meta-analysis of more than 500,000 individuals.
These findings should impact surveillance guidelines and make follow-up the same for individuals with LRAs or no adenomas, reported lead author Abhiram Duvvuri, MD, of the division of gastroenterology and hepatology at the University of Kansas, Kansas City, and colleagues. Currently, the United States Multi-Society Task Force on Colorectal Cancer advises colonoscopy intervals of 3 years for individuals with HRAs, 7-10 years for those with LRAs, and 10 years for those without adenomas.
“The evidence supporting these surveillance recommendations for clinically relevant endpoints such as cancer and cancer-related deaths among patients who undergo adenoma removal, particularly LRA, is minimal, because most of the evidence was based on the surrogate risk of metachronous advanced neoplasia,” the investigators wrote in Gastroenterology.
To provide more solid evidence, the investigators performed a systematic review and meta-analysis, ultimately analyzing 12 studies with data from 510,019 individuals at a mean age of 59.2 years. All studies reported rates of LRA, HRA, or no adenoma at baseline colonoscopy, plus incidence of metachronous CRC and/or CRC-related mortality. With these data, the investigators determined incidence of metachronous CRC and CRC-related mortality for each of the adenoma groups and also compared these incidences per 10,000 person-years of follow-up across groups.
After a mean follow-up of 8.5 years, patients with HRAs had a significantly higher rate of CRC compared with patients who had LRAs (13.81 vs. 4.5; odds ratio, 2.35; 95% confidence interval, 1.72-3.20) or no adenomas (13.81 vs. 3.4; OR, 2.92; 95% CI, 2.31-3.69). Similarly, but to a lesser degree, LRAs were associated with significantly greater risk of CRC than that of no adenomas (4.5 vs. 3.4; OR, 1.26; 95% CI, 1.06-1.51).
Data on CRC- related mortality further supported these minimal risk profiles because LRAs did not significantly increase the risk of CRC-related mortality compared with no adenomas (OR, 1.15; 95% CI, 0.76-1.74). In contrast, HRAs were associated with significantly greater risk of CRC-related death than that of both LRAs (OR, 2.48; 95% CI, 1.30-4.75) and no adenomas (OR, 2.69; 95% CI, 1.87-3.87).
The investigators acknowledged certain limitations of their study. For one, there were no randomized controlled trials in the meta-analysis, which can introduce bias. Loss of patients to follow-up is also possible; however, the investigators noted that there was a robust sample of patients available for study outcomes all the same. There is also risk of comparability bias in that HRA and LRA groups underwent more colonoscopies; however, the duration of follow-up and timing of last colonoscopy were similar among groups. Lastly, it’s possible the patient sample wasn’t representative because of healthy screenee bias, but the investigators compared groups against general population to minimize that bias.
The investigators also highlighted several strengths of their study that make their findings more reliable than those of past meta-analyses. For one, their study is the largest of its kind to date, and involved a significantly higher number of patients with LRA and no adenomas. Also, in contrast with previous studies, CRC and CRC-related mortality were evaluated rather than advanced adenomas, they noted.
“Furthermore, we also analyzed CRC incidence and mortality in the LRA group compared with the general population, with the [standardized incidence ratio] being lower and [standardized mortality ratio] being comparable, confirming that it is indeed a low-risk group,” they wrote.
Considering these strengths and the nature of their findings, Dr. Duvvuri and colleagues called for a more conservative approach to CRC surveillance among individuals with LRAs, and more research to investigate extending colonoscopy intervals even further.
“We recommend that the interval for follow-up colonoscopy should be the same in patients with LRAs or no adenomas but that the HRA group should have a more frequent surveillance interval for CRC surveillance compared with these groups,” they concluded. “Future studies should evaluate whether surveillance intervals could be lengthened beyond 10 years in the no-adenoma and LRA groups after an initial high-quality index colonoscopy.”
One author disclosed affiliations with Erbe, Cdx Labs, Aries, and others. Dr. Duvvuri and the remaining authors disclosed no conflicts.
Unlike high-risk adenomas (HRAs), low-risk adenomas (LRAs) have a minimal association with risk of metachronous colorectal cancer (CRC), and no relationship with odds of metachronous CRC-related mortality, according to a meta-analysis of more than 500,000 individuals.
These findings should impact surveillance guidelines and make follow-up the same for individuals with LRAs or no adenomas, reported lead author Abhiram Duvvuri, MD, of the division of gastroenterology and hepatology at the University of Kansas, Kansas City, and colleagues. Currently, the United States Multi-Society Task Force on Colorectal Cancer advises colonoscopy intervals of 3 years for individuals with HRAs, 7-10 years for those with LRAs, and 10 years for those without adenomas.
“The evidence supporting these surveillance recommendations for clinically relevant endpoints such as cancer and cancer-related deaths among patients who undergo adenoma removal, particularly LRA, is minimal, because most of the evidence was based on the surrogate risk of metachronous advanced neoplasia,” the investigators wrote in Gastroenterology.
To provide more solid evidence, the investigators performed a systematic review and meta-analysis, ultimately analyzing 12 studies with data from 510,019 individuals at a mean age of 59.2 years. All studies reported rates of LRA, HRA, or no adenoma at baseline colonoscopy, plus incidence of metachronous CRC and/or CRC-related mortality. With these data, the investigators determined incidence of metachronous CRC and CRC-related mortality for each of the adenoma groups and also compared these incidences per 10,000 person-years of follow-up across groups.
After a mean follow-up of 8.5 years, patients with HRAs had a significantly higher rate of CRC compared with patients who had LRAs (13.81 vs. 4.5; odds ratio, 2.35; 95% confidence interval, 1.72-3.20) or no adenomas (13.81 vs. 3.4; OR, 2.92; 95% CI, 2.31-3.69). Similarly, but to a lesser degree, LRAs were associated with significantly greater risk of CRC than that of no adenomas (4.5 vs. 3.4; OR, 1.26; 95% CI, 1.06-1.51).
Data on CRC- related mortality further supported these minimal risk profiles because LRAs did not significantly increase the risk of CRC-related mortality compared with no adenomas (OR, 1.15; 95% CI, 0.76-1.74). In contrast, HRAs were associated with significantly greater risk of CRC-related death than that of both LRAs (OR, 2.48; 95% CI, 1.30-4.75) and no adenomas (OR, 2.69; 95% CI, 1.87-3.87).
The investigators acknowledged certain limitations of their study. For one, there were no randomized controlled trials in the meta-analysis, which can introduce bias. Loss of patients to follow-up is also possible; however, the investigators noted that there was a robust sample of patients available for study outcomes all the same. There is also risk of comparability bias in that HRA and LRA groups underwent more colonoscopies; however, the duration of follow-up and timing of last colonoscopy were similar among groups. Lastly, it’s possible the patient sample wasn’t representative because of healthy screenee bias, but the investigators compared groups against general population to minimize that bias.
The investigators also highlighted several strengths of their study that make their findings more reliable than those of past meta-analyses. For one, their study is the largest of its kind to date, and involved a significantly higher number of patients with LRA and no adenomas. Also, in contrast with previous studies, CRC and CRC-related mortality were evaluated rather than advanced adenomas, they noted.
“Furthermore, we also analyzed CRC incidence and mortality in the LRA group compared with the general population, with the [standardized incidence ratio] being lower and [standardized mortality ratio] being comparable, confirming that it is indeed a low-risk group,” they wrote.
Considering these strengths and the nature of their findings, Dr. Duvvuri and colleagues called for a more conservative approach to CRC surveillance among individuals with LRAs, and more research to investigate extending colonoscopy intervals even further.
“We recommend that the interval for follow-up colonoscopy should be the same in patients with LRAs or no adenomas but that the HRA group should have a more frequent surveillance interval for CRC surveillance compared with these groups,” they concluded. “Future studies should evaluate whether surveillance intervals could be lengthened beyond 10 years in the no-adenoma and LRA groups after an initial high-quality index colonoscopy.”
One author disclosed affiliations with Erbe, Cdx Labs, Aries, and others. Dr. Duvvuri and the remaining authors disclosed no conflicts.
FROM GASTROENTEROLOGY
Bariatric surgery may cut cancer in obesity with liver disease
In a large cohort of insured working adults with severe obesity and nonalcoholic fatty liver disease (NAFLD), the rate of incident cancer was lower during a 10-month median follow-up period among those who underwent bariatric surgery. The rate was especially lower with regard to obesity-related cancers. The risk reduction was greater among patients with cirrhosis.
Among almost 100,000 patients with severe obesity (body mass index >40 kg/m2) and NAFLD, those who underwent bariatric surgery had an 18% and 35% lower risk of developing any cancer or obesity-related cancer, respectively.
Bariatric surgery was associated with a significantly lower risk of being diagnosed with colorectal, pancreatic, endometrial, and thyroid cancer, as well as hepatocellular carcinoma and multiple myeloma (all obesity-related cancers). The findings are from an observational study by Vinod K. Rustgi, MD, MBA, and colleagues, which was published online March 17, 2021, in Gastroenterology.
It was not surprising that bariatric surgery is effective in reducing the malignancy rate among patients with cirrhosis, the researchers wrote, because the surgery results in long-term weight loss, resolution of nonalcoholic steatohepatitis (NASH), and regression of fibrosis.
“Cirrhosis can happen from fatty liver disease or NASH,” Dr. Rustgi, a hepatologist at Robert Wood Johnson Medical School, New Brunswick, N.J., explained to this news organization. “It’s becoming the fastest growing indication for liver transplant, but also the reason for increased rates of hepatocellular carcinoma.”
Current treatment for patients with obesity and fatty liver disease begins with lifestyle changes to lose weight, he continued. “As people lose 10% of their weight, they actually start to see regression of fibrosis in the liver that is correlated with [lower rates of] malignancy outcomes and other deleterious outcomes.” But long-lasting weight loss is extremely difficult to achieve.
Future studies “may identify new targets and treatments, such as antidiabetic-, satiety-, or GLP-1-based medications, for chemoprevention in NAFLD/NASH,” the investigators suggested. However, pharmaceutical agents will likely be very expensive when they eventually get marketed, Dr. Rustgi observed.
Although “bariatric surgery is a more aggressive approach than lifestyle modifications, surgery may provide additional benefits, such as improved quality of life and decreased long-term health care costs,” he and his coauthors concluded.
Rising rates of fatty liver disease, obesity
An estimated 30% of the population of the United States has NAFLD, the most common chronic liver disease, the researchers noted in their article. The prevalence of NAFLD increased 2.8-fold in the United States between 2003 and 2011, in parallel with increasing obesity.
NAFLD is more common among male patients with obesity and diabetes and Hispanic patients; “70% of [patients with diabetes] may have fatty liver disease, according to certain surveys,” Dr. Rustgi noted.
Cancer is the second greatest cause of mortality among patients with obesity and NAFLD, he continued, after cardiovascular disease. Cancer mortality is higher than mortality from liver disease.
Obesity-related cancers include adenocarcinoma of the esophagus, cancers of the breast (in postmenopausal women), colon, rectum, endometrium (corpus uterus), gallbladder, gastric cardia, kidney (renal cell), liver, ovary, pancreas, and thyroid, as well as meningioma and multiple myeloma, according to a 2016 report from the International Agency for Research on Cancer working group.
Obesity-related cancer accounted for 40% of all cancer in the United States in 2014 – 55% of cancers in women, and 24% of cancers in men, according to a study published in Morbidity and Mortality Weekly Report in 2017, as previously reported by this news organization.
Several studies, including one presented at Obesity Week in 2019 and later published, have shown that bariatric surgery is linked with a lower risk for cancer in general populations.
One meta-analysis reported that NAFLD is an independent risk factor for cholangiocarcinoma and colorectal, breast, gastric, pancreatic, prostate, and esophageal cancers. In another study, NAFLD was associated with a twofold increased risk for hepatocellular carcinoma and uterine, stomach, pancreatic, and colon cancers, Dr. Rustgi and colleagues noted.
Until now, the impact of bariatric surgery on the risk for cancer among patients with obesity and NAFLD was unknown.
Does bariatric surgery curb cancer risk in liver disease?
The researchers examined insurance claims data from the national MarketScan database from Jan. 1, 2007, to Dec. 31, 2017, for patients aged 18-64 years who had health insurance from 350 employers and 100 insurers. They identified 98,090 patients with severe obesity who were newly diagnosed with NAFLD during 2008-2017.
Roughly a third of the cohort (33,435 patients) underwent bariatric surgery. From 2008 to 2017, laparoscopic sleeve gastrectomies increased from 4% of bariatric procedures to 68% of all surgeries. Laparoscopic adjustable gastric band and laparoscopic Roux-en-Y gastric bypass procedures fell from 35% to less than 1% and from 49% to 28%, respectively.
Patients who underwent bariatric surgery were younger (mean age, 44 vs. 46 years), were more likely to be women (74% vs. 62%), and were less likely to have a history of smoking (6% vs. 10%).
During a mean follow-up of 22 months (and a median follow-up of 10 months), there were 911 incident cases of obesity-related cancers. These included cancer of the colon (116 cases), rectum (15), breast (in postmenopausal women; 131), kidney (120), esophagus (16), gastric cardia (8), gallbladder (4), pancreas (44), ovaries (74), endometrium (135), and thyroid (143), as well as hepatocellular carcinoma (49), multiple myeloma (50), and meningioma (6). There were 1,912 incident cases of other cancers, such as brain and lung cancers and leukemia.
A total of 258 patients who underwent bariatric surgery developed an obesity-related cancer (an incidence of 3.83 per 1,000 person-years), compared with 653 patients who did not have bariatric surgery (an incidence of 5.63 per 1,000 person-years).
The researchers noted that study limitations include the fact that it was restricted to privately insured individuals aged 18-64 years with severe obesity. In addition, “the short median follow-up may underestimate the full effect of bariatric surgery on cancer risk,” they wrote.
The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a large cohort of insured working adults with severe obesity and nonalcoholic fatty liver disease (NAFLD), the rate of incident cancer was lower during a 10-month median follow-up period among those who underwent bariatric surgery. The rate was especially lower with regard to obesity-related cancers. The risk reduction was greater among patients with cirrhosis.
Among almost 100,000 patients with severe obesity (body mass index >40 kg/m2) and NAFLD, those who underwent bariatric surgery had an 18% and 35% lower risk of developing any cancer or obesity-related cancer, respectively.
Bariatric surgery was associated with a significantly lower risk of being diagnosed with colorectal, pancreatic, endometrial, and thyroid cancer, as well as hepatocellular carcinoma and multiple myeloma (all obesity-related cancers). The findings are from an observational study by Vinod K. Rustgi, MD, MBA, and colleagues, which was published online March 17, 2021, in Gastroenterology.
It was not surprising that bariatric surgery is effective in reducing the malignancy rate among patients with cirrhosis, the researchers wrote, because the surgery results in long-term weight loss, resolution of nonalcoholic steatohepatitis (NASH), and regression of fibrosis.
“Cirrhosis can happen from fatty liver disease or NASH,” Dr. Rustgi, a hepatologist at Robert Wood Johnson Medical School, New Brunswick, N.J., explained to this news organization. “It’s becoming the fastest growing indication for liver transplant, but also the reason for increased rates of hepatocellular carcinoma.”
Current treatment for patients with obesity and fatty liver disease begins with lifestyle changes to lose weight, he continued. “As people lose 10% of their weight, they actually start to see regression of fibrosis in the liver that is correlated with [lower rates of] malignancy outcomes and other deleterious outcomes.” But long-lasting weight loss is extremely difficult to achieve.
Future studies “may identify new targets and treatments, such as antidiabetic-, satiety-, or GLP-1-based medications, for chemoprevention in NAFLD/NASH,” the investigators suggested. However, pharmaceutical agents will likely be very expensive when they eventually get marketed, Dr. Rustgi observed.
Although “bariatric surgery is a more aggressive approach than lifestyle modifications, surgery may provide additional benefits, such as improved quality of life and decreased long-term health care costs,” he and his coauthors concluded.
Rising rates of fatty liver disease, obesity
An estimated 30% of the population of the United States has NAFLD, the most common chronic liver disease, the researchers noted in their article. The prevalence of NAFLD increased 2.8-fold in the United States between 2003 and 2011, in parallel with increasing obesity.
NAFLD is more common among male patients with obesity and diabetes and Hispanic patients; “70% of [patients with diabetes] may have fatty liver disease, according to certain surveys,” Dr. Rustgi noted.
Cancer is the second greatest cause of mortality among patients with obesity and NAFLD, he continued, after cardiovascular disease. Cancer mortality is higher than mortality from liver disease.
Obesity-related cancers include adenocarcinoma of the esophagus, cancers of the breast (in postmenopausal women), colon, rectum, endometrium (corpus uterus), gallbladder, gastric cardia, kidney (renal cell), liver, ovary, pancreas, and thyroid, as well as meningioma and multiple myeloma, according to a 2016 report from the International Agency for Research on Cancer working group.
Obesity-related cancer accounted for 40% of all cancer in the United States in 2014 – 55% of cancers in women, and 24% of cancers in men, according to a study published in Morbidity and Mortality Weekly Report in 2017, as previously reported by this news organization.
Several studies, including one presented at Obesity Week in 2019 and later published, have shown that bariatric surgery is linked with a lower risk for cancer in general populations.
One meta-analysis reported that NAFLD is an independent risk factor for cholangiocarcinoma and colorectal, breast, gastric, pancreatic, prostate, and esophageal cancers. In another study, NAFLD was associated with a twofold increased risk for hepatocellular carcinoma and uterine, stomach, pancreatic, and colon cancers, Dr. Rustgi and colleagues noted.
Until now, the impact of bariatric surgery on the risk for cancer among patients with obesity and NAFLD was unknown.
Does bariatric surgery curb cancer risk in liver disease?
The researchers examined insurance claims data from the national MarketScan database from Jan. 1, 2007, to Dec. 31, 2017, for patients aged 18-64 years who had health insurance from 350 employers and 100 insurers. They identified 98,090 patients with severe obesity who were newly diagnosed with NAFLD during 2008-2017.
Roughly a third of the cohort (33,435 patients) underwent bariatric surgery. From 2008 to 2017, laparoscopic sleeve gastrectomies increased from 4% of bariatric procedures to 68% of all surgeries. Laparoscopic adjustable gastric band and laparoscopic Roux-en-Y gastric bypass procedures fell from 35% to less than 1% and from 49% to 28%, respectively.
Patients who underwent bariatric surgery were younger (mean age, 44 vs. 46 years), were more likely to be women (74% vs. 62%), and were less likely to have a history of smoking (6% vs. 10%).
During a mean follow-up of 22 months (and a median follow-up of 10 months), there were 911 incident cases of obesity-related cancers. These included cancer of the colon (116 cases), rectum (15), breast (in postmenopausal women; 131), kidney (120), esophagus (16), gastric cardia (8), gallbladder (4), pancreas (44), ovaries (74), endometrium (135), and thyroid (143), as well as hepatocellular carcinoma (49), multiple myeloma (50), and meningioma (6). There were 1,912 incident cases of other cancers, such as brain and lung cancers and leukemia.
A total of 258 patients who underwent bariatric surgery developed an obesity-related cancer (an incidence of 3.83 per 1,000 person-years), compared with 653 patients who did not have bariatric surgery (an incidence of 5.63 per 1,000 person-years).
The researchers noted that study limitations include the fact that it was restricted to privately insured individuals aged 18-64 years with severe obesity. In addition, “the short median follow-up may underestimate the full effect of bariatric surgery on cancer risk,” they wrote.
The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a large cohort of insured working adults with severe obesity and nonalcoholic fatty liver disease (NAFLD), the rate of incident cancer was lower during a 10-month median follow-up period among those who underwent bariatric surgery. The rate was especially lower with regard to obesity-related cancers. The risk reduction was greater among patients with cirrhosis.
Among almost 100,000 patients with severe obesity (body mass index >40 kg/m2) and NAFLD, those who underwent bariatric surgery had an 18% and 35% lower risk of developing any cancer or obesity-related cancer, respectively.
Bariatric surgery was associated with a significantly lower risk of being diagnosed with colorectal, pancreatic, endometrial, and thyroid cancer, as well as hepatocellular carcinoma and multiple myeloma (all obesity-related cancers). The findings are from an observational study by Vinod K. Rustgi, MD, MBA, and colleagues, which was published online March 17, 2021, in Gastroenterology.
It was not surprising that bariatric surgery is effective in reducing the malignancy rate among patients with cirrhosis, the researchers wrote, because the surgery results in long-term weight loss, resolution of nonalcoholic steatohepatitis (NASH), and regression of fibrosis.
“Cirrhosis can happen from fatty liver disease or NASH,” Dr. Rustgi, a hepatologist at Robert Wood Johnson Medical School, New Brunswick, N.J., explained to this news organization. “It’s becoming the fastest growing indication for liver transplant, but also the reason for increased rates of hepatocellular carcinoma.”
Current treatment for patients with obesity and fatty liver disease begins with lifestyle changes to lose weight, he continued. “As people lose 10% of their weight, they actually start to see regression of fibrosis in the liver that is correlated with [lower rates of] malignancy outcomes and other deleterious outcomes.” But long-lasting weight loss is extremely difficult to achieve.
Future studies “may identify new targets and treatments, such as antidiabetic-, satiety-, or GLP-1-based medications, for chemoprevention in NAFLD/NASH,” the investigators suggested. However, pharmaceutical agents will likely be very expensive when they eventually get marketed, Dr. Rustgi observed.
Although “bariatric surgery is a more aggressive approach than lifestyle modifications, surgery may provide additional benefits, such as improved quality of life and decreased long-term health care costs,” he and his coauthors concluded.
Rising rates of fatty liver disease, obesity
An estimated 30% of the population of the United States has NAFLD, the most common chronic liver disease, the researchers noted in their article. The prevalence of NAFLD increased 2.8-fold in the United States between 2003 and 2011, in parallel with increasing obesity.
NAFLD is more common among male patients with obesity and diabetes and Hispanic patients; “70% of [patients with diabetes] may have fatty liver disease, according to certain surveys,” Dr. Rustgi noted.
Cancer is the second greatest cause of mortality among patients with obesity and NAFLD, he continued, after cardiovascular disease. Cancer mortality is higher than mortality from liver disease.
Obesity-related cancers include adenocarcinoma of the esophagus, cancers of the breast (in postmenopausal women), colon, rectum, endometrium (corpus uterus), gallbladder, gastric cardia, kidney (renal cell), liver, ovary, pancreas, and thyroid, as well as meningioma and multiple myeloma, according to a 2016 report from the International Agency for Research on Cancer working group.
Obesity-related cancer accounted for 40% of all cancer in the United States in 2014 – 55% of cancers in women, and 24% of cancers in men, according to a study published in Morbidity and Mortality Weekly Report in 2017, as previously reported by this news organization.
Several studies, including one presented at Obesity Week in 2019 and later published, have shown that bariatric surgery is linked with a lower risk for cancer in general populations.
One meta-analysis reported that NAFLD is an independent risk factor for cholangiocarcinoma and colorectal, breast, gastric, pancreatic, prostate, and esophageal cancers. In another study, NAFLD was associated with a twofold increased risk for hepatocellular carcinoma and uterine, stomach, pancreatic, and colon cancers, Dr. Rustgi and colleagues noted.
Until now, the impact of bariatric surgery on the risk for cancer among patients with obesity and NAFLD was unknown.
Does bariatric surgery curb cancer risk in liver disease?
The researchers examined insurance claims data from the national MarketScan database from Jan. 1, 2007, to Dec. 31, 2017, for patients aged 18-64 years who had health insurance from 350 employers and 100 insurers. They identified 98,090 patients with severe obesity who were newly diagnosed with NAFLD during 2008-2017.
Roughly a third of the cohort (33,435 patients) underwent bariatric surgery. From 2008 to 2017, laparoscopic sleeve gastrectomies increased from 4% of bariatric procedures to 68% of all surgeries. Laparoscopic adjustable gastric band and laparoscopic Roux-en-Y gastric bypass procedures fell from 35% to less than 1% and from 49% to 28%, respectively.
Patients who underwent bariatric surgery were younger (mean age, 44 vs. 46 years), were more likely to be women (74% vs. 62%), and were less likely to have a history of smoking (6% vs. 10%).
During a mean follow-up of 22 months (and a median follow-up of 10 months), there were 911 incident cases of obesity-related cancers. These included cancer of the colon (116 cases), rectum (15), breast (in postmenopausal women; 131), kidney (120), esophagus (16), gastric cardia (8), gallbladder (4), pancreas (44), ovaries (74), endometrium (135), and thyroid (143), as well as hepatocellular carcinoma (49), multiple myeloma (50), and meningioma (6). There were 1,912 incident cases of other cancers, such as brain and lung cancers and leukemia.
A total of 258 patients who underwent bariatric surgery developed an obesity-related cancer (an incidence of 3.83 per 1,000 person-years), compared with 653 patients who did not have bariatric surgery (an incidence of 5.63 per 1,000 person-years).
The researchers noted that study limitations include the fact that it was restricted to privately insured individuals aged 18-64 years with severe obesity. In addition, “the short median follow-up may underestimate the full effect of bariatric surgery on cancer risk,” they wrote.
The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Increased cancer risk from night shift due to gene dysregulation?
Working night shifts has been associated with an increased risk for certain cancers, as well as other health disorders. Indeed, the World Health Organization’s International Agency for Research on Cancer (IARC) has classified night shift work as “probably carcinogenic to humans.”
But why night shift should elevate the risk for cancer has been unclear.
A new study shows that a simulated night shift schedule significantly altered the normal circadian rhythmicity of genes that are involved in cancer hallmark pathways. It also found that this circadian misalignment caused circadian dysregulation of genes involved in key DNA repair pathways.
“Taken together, these findings suggest that night shift schedules throw off the timing of expression of cancer-related genes in a way that reduces the effectiveness of the body’s DNA repair processes when they are most needed,” said co-corresponding author Jason McDermott, a computational scientist with the Pacific Northwest National Laboratory’s biological sciences division in Richland, Wash.
The study was published online in the Journal of Pineal Research.
Study conducted among volunteers
The study was carried out among healthy volunteers who were subjected to simulated night shift or day shift schedules.
The cohort comprised 14 adults between the ages of 22 and 34 years who had normal nighttime sleep schedules. They were randomly assigned (seven in each group) to a simulated day shift schedule that involved 3 days of daytime wakefulness (6 a.m.-10 p.m.), or a simulated night shift schedule involving 3 days of nighttime wakefulness (6 p.m.-10 a.m.).
After the 3 days of simulated shift work, all participants were then kept in a constant routine protocol (used to study humans’ internally generated biological rhythms independent of any external influences). As part of the protocol, they were kept awake for 24 hours in a semi-reclined posture under laboratory conditions with constant light exposure and room temperature and evenly distributed food intake (hourly isocaloric snacks).
Blood samples were collected at 3-hour intervals and used for leukocyte transcriptome analysis and DNA damage assessment.
The authors found that the circadian expression of canonical clock genes was substantially altered by the simulated night shift schedule vs. the day shift schedule. Four genes (CRY1, CRY2, PER2, and NR1D2) lost their normal day-shift rhythmicity following the night shift schedule, and NPAS2 gene expression was not rhythmic during the day shift but exhibited circadian rhythmicity in the simulated night shift condition. Three other genes (NR1D1, PER3, and DBP) were significantly rhythmic during both shifts.
The team also looked at the effect of night shift on circadian rhythmicity in cancer hallmark genes, using a panel of 726 genes. The analysis showed that:
- 257 (35.4%) were rhythmic after at least one of the two simulated shift work conditions.
- 113 (15.6%) were rhythmic in day shift only.
- 96 (13.2%) were rhythmic during night shift only.
- 48 (6.6%) were rhythmic during both shifts.
A subset of 10 (1.4%) genes exhibited a significant phase advance (3.7 to 8.3 hours) or phase delay (2.8 to 7.0 hours) during the night shift vs. the day shift.
Thus, the authors concluded, shift work caused significant disturbances in the rhythmicity of gene expression in cancer hallmark pathways.
Findings also showed that night shift work increases endogenous and exogenous DNA damage. Endogenous DNA damage was generally higher after the night shift compared to the day shift, and across the 24-hour constant routine the percentage of cells with BRCA1 and g H2AX foci was significantly higher for night shift.
Next steps
The team said that the next step is to conduct the same experiment with real-world shift workers who have been consistently on day or night shifts for many years to determine whether in night workers the unrepaired DNA damage builds up over time, which could ultimately increase the risk for cancer.
If what happens in real-world shift workers is consistent with the current findings, this work could eventually be used to develop prevention strategies and drugs that could address the mistiming of DNA repair processes, they suggested.
“Night shift workers face considerable health disparities, ranging from increased risks of metabolic and cardiovascular disease to mental health disorders and cancer,” co-senior author Hans Van Dongen, PhD, a professor at Washington State University in Pullman and director of the WSU Sleep and Performance Research Center, Spokane, said in a statement. “It is high time that we find diagnosis and treatment solutions for this underserved group of essential workers so that the medical community can address their unique health challenges.”
The study was supported by start-up funds from Washington State University and a Center for Human Health and the Environment grant from North Carolina State University, and in part by the United States Army Medical Research and Development Command, the National Institutes of Health, CDMRP (Congressionally Directed Medical Research Programs) Peer Reviewed Cancer Research Program award, and the BRAVE investment.
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Working night shifts has been associated with an increased risk for certain cancers, as well as other health disorders. Indeed, the World Health Organization’s International Agency for Research on Cancer (IARC) has classified night shift work as “probably carcinogenic to humans.”
But why night shift should elevate the risk for cancer has been unclear.
A new study shows that a simulated night shift schedule significantly altered the normal circadian rhythmicity of genes that are involved in cancer hallmark pathways. It also found that this circadian misalignment caused circadian dysregulation of genes involved in key DNA repair pathways.
“Taken together, these findings suggest that night shift schedules throw off the timing of expression of cancer-related genes in a way that reduces the effectiveness of the body’s DNA repair processes when they are most needed,” said co-corresponding author Jason McDermott, a computational scientist with the Pacific Northwest National Laboratory’s biological sciences division in Richland, Wash.
The study was published online in the Journal of Pineal Research.
Study conducted among volunteers
The study was carried out among healthy volunteers who were subjected to simulated night shift or day shift schedules.
The cohort comprised 14 adults between the ages of 22 and 34 years who had normal nighttime sleep schedules. They were randomly assigned (seven in each group) to a simulated day shift schedule that involved 3 days of daytime wakefulness (6 a.m.-10 p.m.), or a simulated night shift schedule involving 3 days of nighttime wakefulness (6 p.m.-10 a.m.).
After the 3 days of simulated shift work, all participants were then kept in a constant routine protocol (used to study humans’ internally generated biological rhythms independent of any external influences). As part of the protocol, they were kept awake for 24 hours in a semi-reclined posture under laboratory conditions with constant light exposure and room temperature and evenly distributed food intake (hourly isocaloric snacks).
Blood samples were collected at 3-hour intervals and used for leukocyte transcriptome analysis and DNA damage assessment.
The authors found that the circadian expression of canonical clock genes was substantially altered by the simulated night shift schedule vs. the day shift schedule. Four genes (CRY1, CRY2, PER2, and NR1D2) lost their normal day-shift rhythmicity following the night shift schedule, and NPAS2 gene expression was not rhythmic during the day shift but exhibited circadian rhythmicity in the simulated night shift condition. Three other genes (NR1D1, PER3, and DBP) were significantly rhythmic during both shifts.
The team also looked at the effect of night shift on circadian rhythmicity in cancer hallmark genes, using a panel of 726 genes. The analysis showed that:
- 257 (35.4%) were rhythmic after at least one of the two simulated shift work conditions.
- 113 (15.6%) were rhythmic in day shift only.
- 96 (13.2%) were rhythmic during night shift only.
- 48 (6.6%) were rhythmic during both shifts.
A subset of 10 (1.4%) genes exhibited a significant phase advance (3.7 to 8.3 hours) or phase delay (2.8 to 7.0 hours) during the night shift vs. the day shift.
Thus, the authors concluded, shift work caused significant disturbances in the rhythmicity of gene expression in cancer hallmark pathways.
Findings also showed that night shift work increases endogenous and exogenous DNA damage. Endogenous DNA damage was generally higher after the night shift compared to the day shift, and across the 24-hour constant routine the percentage of cells with BRCA1 and g H2AX foci was significantly higher for night shift.
Next steps
The team said that the next step is to conduct the same experiment with real-world shift workers who have been consistently on day or night shifts for many years to determine whether in night workers the unrepaired DNA damage builds up over time, which could ultimately increase the risk for cancer.
If what happens in real-world shift workers is consistent with the current findings, this work could eventually be used to develop prevention strategies and drugs that could address the mistiming of DNA repair processes, they suggested.
“Night shift workers face considerable health disparities, ranging from increased risks of metabolic and cardiovascular disease to mental health disorders and cancer,” co-senior author Hans Van Dongen, PhD, a professor at Washington State University in Pullman and director of the WSU Sleep and Performance Research Center, Spokane, said in a statement. “It is high time that we find diagnosis and treatment solutions for this underserved group of essential workers so that the medical community can address their unique health challenges.”
The study was supported by start-up funds from Washington State University and a Center for Human Health and the Environment grant from North Carolina State University, and in part by the United States Army Medical Research and Development Command, the National Institutes of Health, CDMRP (Congressionally Directed Medical Research Programs) Peer Reviewed Cancer Research Program award, and the BRAVE investment.
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Working night shifts has been associated with an increased risk for certain cancers, as well as other health disorders. Indeed, the World Health Organization’s International Agency for Research on Cancer (IARC) has classified night shift work as “probably carcinogenic to humans.”
But why night shift should elevate the risk for cancer has been unclear.
A new study shows that a simulated night shift schedule significantly altered the normal circadian rhythmicity of genes that are involved in cancer hallmark pathways. It also found that this circadian misalignment caused circadian dysregulation of genes involved in key DNA repair pathways.
“Taken together, these findings suggest that night shift schedules throw off the timing of expression of cancer-related genes in a way that reduces the effectiveness of the body’s DNA repair processes when they are most needed,” said co-corresponding author Jason McDermott, a computational scientist with the Pacific Northwest National Laboratory’s biological sciences division in Richland, Wash.
The study was published online in the Journal of Pineal Research.
Study conducted among volunteers
The study was carried out among healthy volunteers who were subjected to simulated night shift or day shift schedules.
The cohort comprised 14 adults between the ages of 22 and 34 years who had normal nighttime sleep schedules. They were randomly assigned (seven in each group) to a simulated day shift schedule that involved 3 days of daytime wakefulness (6 a.m.-10 p.m.), or a simulated night shift schedule involving 3 days of nighttime wakefulness (6 p.m.-10 a.m.).
After the 3 days of simulated shift work, all participants were then kept in a constant routine protocol (used to study humans’ internally generated biological rhythms independent of any external influences). As part of the protocol, they were kept awake for 24 hours in a semi-reclined posture under laboratory conditions with constant light exposure and room temperature and evenly distributed food intake (hourly isocaloric snacks).
Blood samples were collected at 3-hour intervals and used for leukocyte transcriptome analysis and DNA damage assessment.
The authors found that the circadian expression of canonical clock genes was substantially altered by the simulated night shift schedule vs. the day shift schedule. Four genes (CRY1, CRY2, PER2, and NR1D2) lost their normal day-shift rhythmicity following the night shift schedule, and NPAS2 gene expression was not rhythmic during the day shift but exhibited circadian rhythmicity in the simulated night shift condition. Three other genes (NR1D1, PER3, and DBP) were significantly rhythmic during both shifts.
The team also looked at the effect of night shift on circadian rhythmicity in cancer hallmark genes, using a panel of 726 genes. The analysis showed that:
- 257 (35.4%) were rhythmic after at least one of the two simulated shift work conditions.
- 113 (15.6%) were rhythmic in day shift only.
- 96 (13.2%) were rhythmic during night shift only.
- 48 (6.6%) were rhythmic during both shifts.
A subset of 10 (1.4%) genes exhibited a significant phase advance (3.7 to 8.3 hours) or phase delay (2.8 to 7.0 hours) during the night shift vs. the day shift.
Thus, the authors concluded, shift work caused significant disturbances in the rhythmicity of gene expression in cancer hallmark pathways.
Findings also showed that night shift work increases endogenous and exogenous DNA damage. Endogenous DNA damage was generally higher after the night shift compared to the day shift, and across the 24-hour constant routine the percentage of cells with BRCA1 and g H2AX foci was significantly higher for night shift.
Next steps
The team said that the next step is to conduct the same experiment with real-world shift workers who have been consistently on day or night shifts for many years to determine whether in night workers the unrepaired DNA damage builds up over time, which could ultimately increase the risk for cancer.
If what happens in real-world shift workers is consistent with the current findings, this work could eventually be used to develop prevention strategies and drugs that could address the mistiming of DNA repair processes, they suggested.
“Night shift workers face considerable health disparities, ranging from increased risks of metabolic and cardiovascular disease to mental health disorders and cancer,” co-senior author Hans Van Dongen, PhD, a professor at Washington State University in Pullman and director of the WSU Sleep and Performance Research Center, Spokane, said in a statement. “It is high time that we find diagnosis and treatment solutions for this underserved group of essential workers so that the medical community can address their unique health challenges.”
The study was supported by start-up funds from Washington State University and a Center for Human Health and the Environment grant from North Carolina State University, and in part by the United States Army Medical Research and Development Command, the National Institutes of Health, CDMRP (Congressionally Directed Medical Research Programs) Peer Reviewed Cancer Research Program award, and the BRAVE investment.
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Palliative care helpful but underutilized for blood cancer patients
Specialty palliative care interventions improve outcomes in patients with hematologic malignancies but are underutilized, according to findings from a systematic literature review.
Outcomes that were improved, as demonstrated by 16 studies that met inclusion criteria for the review, included symptom management, inpatient mortality, health care utilization, health care costs, and caregiver-reported outcomes, Elizabeth Elliott, DO, a hematology and oncology fellow at the Cardinal Bernardin Cancer Center, Loyola University, Maywood, Ill., and colleagues reported.
The findings were published online in the Journal of Pain and Symptom Management.
Palliative care needs
Patients with hematologic malignancies, including leukemia, myeloma, and lymphoma, have a high need for supportive care, the authors noted, adding that, although its use has increased over time, palliative care (PC) is often provided late in the disease course – sometimes only in the final days of life.
“Compared with their solid tumor counterparts, patients with hematologic malignancies experience higher symptom burdens, have higher rates of cancer-directed care near death, and are more likely to die while hospitalized than at home or in hospice,” they wrote. “Despite this need, specialist palliative care is less commonly utilized in patients with hematologic malignancies than other cancer types.”
Given the high health care utilization among patients with hematologic malignancies, earlier and more widespread utilization of PC in this population may significantly reduce health care costs, they added.
Palliative care benefits
Of 5,345 studies published between 2005 and 2020 and screened for the current review, 16 met inclusion criteria, including 10 retrospective cohort studies; 4 prospective cohort studies; and 2 randomized, controlled studies.
Nine studies included only patients with hematologic malignancies and seven included both patients with solid tumors and patients with hematologic malignancies. Each study assessed as being of moderate quality.
Benefits of PC as demonstrated in the studies included:
Symptom management: One study, for example, showed that an integrated psychological and PC intervention improved traumatic stress levels, degree and number of physical symptoms, pain intensity, depressive symptoms, and quality of life, compared with no intervention. Another showed that the percentage of patients reporting moderate to severe pain improved from 57% to 18% with a PC intervention, and the number reporting depressive episodes improved from 13% to 5%.
Reduced in-patient death: Findings from eight studies showed that 21.9%-83% of those receiving PC died at home, compared with 6.0%-8.9% of controls. Two studies showed that PC provided at least 20 days prior to death decreased the likelihood of inpatient death and death in an ICU, compared with controls, and one showed that the rate of in-hospital deaths was 30% for those with home PC or hospice, compared with 80% of controls.
Health care utilization: The studies showed that hospitalization occurred in 45%-76.3% of hematologic malignancy patients who received PC, compared with 98% of controls. The odds ratio for hospitalization among acute leukemia patients receiving PC was 0.64, compared with 2.53 among those in a historical control group.
Caregiver-reported outcomes: One randomized, controlled study showed that PC was associated with smaller increases in depression scores, improved coping, and improved scores in multiple quality of life domains in caregivers versus controls.
Survival: One study showed that a larger percentage of hematologic malignancy patients who died 1-6 months after diagnosis had not received PC (28% vs. 23%), whereas more of those who died 6-12 months or 12 or more months after diagnosis had received PC (23.9 vs. 14.9% and 42.5% vs. 22.0%).
Health care costs: Two studies showed a decrease in inpatient costs after a palliative care consultation. Decreases in hospitalization costs were $2,321 and $1,506 for less medically complex patients and $3,515 and $5,617 for more medically complex patient.
Improving PC utilization
One potential strategy to promote earlier referrals to PC is improved education for hematologists, the authors said, citing a study showing that 98% of oncology fellows at one center reported improvement in their ability to assess and manage patient symptoms after completion of a 4-week mandatory PC rotation.
“Another strategy to improve referrals to PC of hematologic malignancies patients could be the creation of programs which facilitate collaboration between PC providers and hematologists, such as the palliative and supportive care special interest group within the American Society for Transplantation and Cellular Therapy,” they wrote.
A third strategy “could be to provide a concurrent care model, in which cancer directed therapy (such as transfusions) is provided at the same time as hospice care,” they added, explaining that such an approach was shown in a study of patients with advanced non–small cell lung cancer to be associated with less aggressive medical treatment and lower costs.
The authors also stressed that patient with solid tumors and those with hematologic malignancies have differing supportive care needs and health care utilization, but several studies included in the current review included both types of cancer.
“Further studies investigating PC use exclusively in patients with hematologic malignancies are needed. Our results demonstrate a strong argument for hematologists to refer their patients early and often for specialized PC,” they concluded.
Indeed, when PC is integrated within hematologic malignancies, impacts occur that are similar to those seen in a variety of other diseases and include improved symptom control, enhanced caregiver experience, and reduced burdens on the health care system, Toby C Campbell, MD, said in an interview.
“The benefits of providing palliative care concurrent with standard cancer care is felt by all the major stakeholders in this care: the patients, their caregivers, and the health care system around them,” said Dr. Campbell, a thoracic medical oncologist and professor in the division of hematology, medical oncology, and palliative care at the University of Wisconsin–Madison.
Overcoming challenges
However, this is “new territory” for most programs, added Dr. Campbell, who also is the University of Wisconsin health chief of palliative care and holds the Ellen and Peter O. Johnson Chair in Palliative Care .
“The palliative care clinicians have a lot of learning to do if they’re going to enter this space and provide expert care,” he said, adding that expert care is what is needed and what was studied in this review. “Providing palliative care to patients with hematologic malignancies has a unique pace and a number of subspecialized therapeutic options with which the palliative care clinician must become familiar.”
Examples include bone marrow transplantation with prolonged hospitalizations and transfusion support, he said.
“Palliative care programs, in order to provide high quality care, will need to familiarize themselves with these therapies and develop close partnership with hematologists to integrate seamlessly into the patient’s care,” he added. “At some centers, culture changes will be necessary concurrent with the clinical practice change of integrating palliative care and it is the responsibility of the palliative care clinicians to bring their very best to these new relationships and patient populations.”
The authors reported having no disclosures. Dr. Campbell also reported having no disclosures.
Specialty palliative care interventions improve outcomes in patients with hematologic malignancies but are underutilized, according to findings from a systematic literature review.
Outcomes that were improved, as demonstrated by 16 studies that met inclusion criteria for the review, included symptom management, inpatient mortality, health care utilization, health care costs, and caregiver-reported outcomes, Elizabeth Elliott, DO, a hematology and oncology fellow at the Cardinal Bernardin Cancer Center, Loyola University, Maywood, Ill., and colleagues reported.
The findings were published online in the Journal of Pain and Symptom Management.
Palliative care needs
Patients with hematologic malignancies, including leukemia, myeloma, and lymphoma, have a high need for supportive care, the authors noted, adding that, although its use has increased over time, palliative care (PC) is often provided late in the disease course – sometimes only in the final days of life.
“Compared with their solid tumor counterparts, patients with hematologic malignancies experience higher symptom burdens, have higher rates of cancer-directed care near death, and are more likely to die while hospitalized than at home or in hospice,” they wrote. “Despite this need, specialist palliative care is less commonly utilized in patients with hematologic malignancies than other cancer types.”
Given the high health care utilization among patients with hematologic malignancies, earlier and more widespread utilization of PC in this population may significantly reduce health care costs, they added.
Palliative care benefits
Of 5,345 studies published between 2005 and 2020 and screened for the current review, 16 met inclusion criteria, including 10 retrospective cohort studies; 4 prospective cohort studies; and 2 randomized, controlled studies.
Nine studies included only patients with hematologic malignancies and seven included both patients with solid tumors and patients with hematologic malignancies. Each study assessed as being of moderate quality.
Benefits of PC as demonstrated in the studies included:
Symptom management: One study, for example, showed that an integrated psychological and PC intervention improved traumatic stress levels, degree and number of physical symptoms, pain intensity, depressive symptoms, and quality of life, compared with no intervention. Another showed that the percentage of patients reporting moderate to severe pain improved from 57% to 18% with a PC intervention, and the number reporting depressive episodes improved from 13% to 5%.
Reduced in-patient death: Findings from eight studies showed that 21.9%-83% of those receiving PC died at home, compared with 6.0%-8.9% of controls. Two studies showed that PC provided at least 20 days prior to death decreased the likelihood of inpatient death and death in an ICU, compared with controls, and one showed that the rate of in-hospital deaths was 30% for those with home PC or hospice, compared with 80% of controls.
Health care utilization: The studies showed that hospitalization occurred in 45%-76.3% of hematologic malignancy patients who received PC, compared with 98% of controls. The odds ratio for hospitalization among acute leukemia patients receiving PC was 0.64, compared with 2.53 among those in a historical control group.
Caregiver-reported outcomes: One randomized, controlled study showed that PC was associated with smaller increases in depression scores, improved coping, and improved scores in multiple quality of life domains in caregivers versus controls.
Survival: One study showed that a larger percentage of hematologic malignancy patients who died 1-6 months after diagnosis had not received PC (28% vs. 23%), whereas more of those who died 6-12 months or 12 or more months after diagnosis had received PC (23.9 vs. 14.9% and 42.5% vs. 22.0%).
Health care costs: Two studies showed a decrease in inpatient costs after a palliative care consultation. Decreases in hospitalization costs were $2,321 and $1,506 for less medically complex patients and $3,515 and $5,617 for more medically complex patient.
Improving PC utilization
One potential strategy to promote earlier referrals to PC is improved education for hematologists, the authors said, citing a study showing that 98% of oncology fellows at one center reported improvement in their ability to assess and manage patient symptoms after completion of a 4-week mandatory PC rotation.
“Another strategy to improve referrals to PC of hematologic malignancies patients could be the creation of programs which facilitate collaboration between PC providers and hematologists, such as the palliative and supportive care special interest group within the American Society for Transplantation and Cellular Therapy,” they wrote.
A third strategy “could be to provide a concurrent care model, in which cancer directed therapy (such as transfusions) is provided at the same time as hospice care,” they added, explaining that such an approach was shown in a study of patients with advanced non–small cell lung cancer to be associated with less aggressive medical treatment and lower costs.
The authors also stressed that patient with solid tumors and those with hematologic malignancies have differing supportive care needs and health care utilization, but several studies included in the current review included both types of cancer.
“Further studies investigating PC use exclusively in patients with hematologic malignancies are needed. Our results demonstrate a strong argument for hematologists to refer their patients early and often for specialized PC,” they concluded.
Indeed, when PC is integrated within hematologic malignancies, impacts occur that are similar to those seen in a variety of other diseases and include improved symptom control, enhanced caregiver experience, and reduced burdens on the health care system, Toby C Campbell, MD, said in an interview.
“The benefits of providing palliative care concurrent with standard cancer care is felt by all the major stakeholders in this care: the patients, their caregivers, and the health care system around them,” said Dr. Campbell, a thoracic medical oncologist and professor in the division of hematology, medical oncology, and palliative care at the University of Wisconsin–Madison.
Overcoming challenges
However, this is “new territory” for most programs, added Dr. Campbell, who also is the University of Wisconsin health chief of palliative care and holds the Ellen and Peter O. Johnson Chair in Palliative Care .
“The palliative care clinicians have a lot of learning to do if they’re going to enter this space and provide expert care,” he said, adding that expert care is what is needed and what was studied in this review. “Providing palliative care to patients with hematologic malignancies has a unique pace and a number of subspecialized therapeutic options with which the palliative care clinician must become familiar.”
Examples include bone marrow transplantation with prolonged hospitalizations and transfusion support, he said.
“Palliative care programs, in order to provide high quality care, will need to familiarize themselves with these therapies and develop close partnership with hematologists to integrate seamlessly into the patient’s care,” he added. “At some centers, culture changes will be necessary concurrent with the clinical practice change of integrating palliative care and it is the responsibility of the palliative care clinicians to bring their very best to these new relationships and patient populations.”
The authors reported having no disclosures. Dr. Campbell also reported having no disclosures.
Specialty palliative care interventions improve outcomes in patients with hematologic malignancies but are underutilized, according to findings from a systematic literature review.
Outcomes that were improved, as demonstrated by 16 studies that met inclusion criteria for the review, included symptom management, inpatient mortality, health care utilization, health care costs, and caregiver-reported outcomes, Elizabeth Elliott, DO, a hematology and oncology fellow at the Cardinal Bernardin Cancer Center, Loyola University, Maywood, Ill., and colleagues reported.
The findings were published online in the Journal of Pain and Symptom Management.
Palliative care needs
Patients with hematologic malignancies, including leukemia, myeloma, and lymphoma, have a high need for supportive care, the authors noted, adding that, although its use has increased over time, palliative care (PC) is often provided late in the disease course – sometimes only in the final days of life.
“Compared with their solid tumor counterparts, patients with hematologic malignancies experience higher symptom burdens, have higher rates of cancer-directed care near death, and are more likely to die while hospitalized than at home or in hospice,” they wrote. “Despite this need, specialist palliative care is less commonly utilized in patients with hematologic malignancies than other cancer types.”
Given the high health care utilization among patients with hematologic malignancies, earlier and more widespread utilization of PC in this population may significantly reduce health care costs, they added.
Palliative care benefits
Of 5,345 studies published between 2005 and 2020 and screened for the current review, 16 met inclusion criteria, including 10 retrospective cohort studies; 4 prospective cohort studies; and 2 randomized, controlled studies.
Nine studies included only patients with hematologic malignancies and seven included both patients with solid tumors and patients with hematologic malignancies. Each study assessed as being of moderate quality.
Benefits of PC as demonstrated in the studies included:
Symptom management: One study, for example, showed that an integrated psychological and PC intervention improved traumatic stress levels, degree and number of physical symptoms, pain intensity, depressive symptoms, and quality of life, compared with no intervention. Another showed that the percentage of patients reporting moderate to severe pain improved from 57% to 18% with a PC intervention, and the number reporting depressive episodes improved from 13% to 5%.
Reduced in-patient death: Findings from eight studies showed that 21.9%-83% of those receiving PC died at home, compared with 6.0%-8.9% of controls. Two studies showed that PC provided at least 20 days prior to death decreased the likelihood of inpatient death and death in an ICU, compared with controls, and one showed that the rate of in-hospital deaths was 30% for those with home PC or hospice, compared with 80% of controls.
Health care utilization: The studies showed that hospitalization occurred in 45%-76.3% of hematologic malignancy patients who received PC, compared with 98% of controls. The odds ratio for hospitalization among acute leukemia patients receiving PC was 0.64, compared with 2.53 among those in a historical control group.
Caregiver-reported outcomes: One randomized, controlled study showed that PC was associated with smaller increases in depression scores, improved coping, and improved scores in multiple quality of life domains in caregivers versus controls.
Survival: One study showed that a larger percentage of hematologic malignancy patients who died 1-6 months after diagnosis had not received PC (28% vs. 23%), whereas more of those who died 6-12 months or 12 or more months after diagnosis had received PC (23.9 vs. 14.9% and 42.5% vs. 22.0%).
Health care costs: Two studies showed a decrease in inpatient costs after a palliative care consultation. Decreases in hospitalization costs were $2,321 and $1,506 for less medically complex patients and $3,515 and $5,617 for more medically complex patient.
Improving PC utilization
One potential strategy to promote earlier referrals to PC is improved education for hematologists, the authors said, citing a study showing that 98% of oncology fellows at one center reported improvement in their ability to assess and manage patient symptoms after completion of a 4-week mandatory PC rotation.
“Another strategy to improve referrals to PC of hematologic malignancies patients could be the creation of programs which facilitate collaboration between PC providers and hematologists, such as the palliative and supportive care special interest group within the American Society for Transplantation and Cellular Therapy,” they wrote.
A third strategy “could be to provide a concurrent care model, in which cancer directed therapy (such as transfusions) is provided at the same time as hospice care,” they added, explaining that such an approach was shown in a study of patients with advanced non–small cell lung cancer to be associated with less aggressive medical treatment and lower costs.
The authors also stressed that patient with solid tumors and those with hematologic malignancies have differing supportive care needs and health care utilization, but several studies included in the current review included both types of cancer.
“Further studies investigating PC use exclusively in patients with hematologic malignancies are needed. Our results demonstrate a strong argument for hematologists to refer their patients early and often for specialized PC,” they concluded.
Indeed, when PC is integrated within hematologic malignancies, impacts occur that are similar to those seen in a variety of other diseases and include improved symptom control, enhanced caregiver experience, and reduced burdens on the health care system, Toby C Campbell, MD, said in an interview.
“The benefits of providing palliative care concurrent with standard cancer care is felt by all the major stakeholders in this care: the patients, their caregivers, and the health care system around them,” said Dr. Campbell, a thoracic medical oncologist and professor in the division of hematology, medical oncology, and palliative care at the University of Wisconsin–Madison.
Overcoming challenges
However, this is “new territory” for most programs, added Dr. Campbell, who also is the University of Wisconsin health chief of palliative care and holds the Ellen and Peter O. Johnson Chair in Palliative Care .
“The palliative care clinicians have a lot of learning to do if they’re going to enter this space and provide expert care,” he said, adding that expert care is what is needed and what was studied in this review. “Providing palliative care to patients with hematologic malignancies has a unique pace and a number of subspecialized therapeutic options with which the palliative care clinician must become familiar.”
Examples include bone marrow transplantation with prolonged hospitalizations and transfusion support, he said.
“Palliative care programs, in order to provide high quality care, will need to familiarize themselves with these therapies and develop close partnership with hematologists to integrate seamlessly into the patient’s care,” he added. “At some centers, culture changes will be necessary concurrent with the clinical practice change of integrating palliative care and it is the responsibility of the palliative care clinicians to bring their very best to these new relationships and patient populations.”
The authors reported having no disclosures. Dr. Campbell also reported having no disclosures.
FROM THE JOURNAL OF PAIN AND SYMPTOM MANAGEMENT
Cancer screening stopped by pandemic: Repercussions to come?
Last year, cancer screening programs around the world ground to a halt as SARS-CoV-2 infection rates surged globally. The effect of this slowdown is now becoming clear.
Thousands of cancer diagnoses are “missing,” and oncologists worry that this will lead to more advanced cancers and higher mortality for years to come.
“I feel like this is an earthquake that’s rocked our health care system. My guess is that you’ll probably still see repercussions of this over the next couple of years at least,” said Sharon Chang, MD, an attending surgical oncologist in the Permanente Medical Group, Fremont, Calif.
She was senior author of a study that analyzed the effects of the slowdown in mammography screening as a result of California’s “shelter-in-place” order on March 17, 2020. In the 2 months that followed, there were 64% fewer breast cancer diagnoses at 21 Kaiser Permanente medical centers, compared with the same period in 2019 (250 vs. 703).
In effect, approximately 450 breast cancer patients had “disappeared,” said coauthor Annie Tang, MD, a research fellow at the University of California, San Francisco, East Bay surgery program.
“What surprised me most from our data was the sheer number of breast cancer patients that were missing,” Dr. Tang said in an interview.
A similar picture has emerged elsewhere.
In Boston, an estimated 1,438 cancerous and precancerous lesions “went missing” during the first 3 months of pandemic shutdown, according to a study from the Massachusetts General Brigham health care system.
In this study, the investigators assessed screening rates for five cancers – breast cancer (mammography), prostate cancer (prostate-specific antigen testing), colorectal cancer (colonoscopy), cervical cancer (Papanicolaou tests), and lung cancer (low-dose CT).
Screening rates during the first peak of the pandemic (March 2 to June 2, 2020) were compared with those during the preceding and following 3 months and during the same 3 months in 2019.
The results showed a pronounced drop in screening rates during the peak pandemic period, compared with the three control periods. Decreases occurred for all screening tests and ranged from –60% to –82%.
There were also significant decreases in cancer diagnoses resulting from the decreases in screening tests, ranging from –19% to –78%.
“Quantifying the actual problem made us realize how much work needs to be done to get us back to prepandemic numbers,” said senior author Quoc-Dien Trinh, MD, FACS, codirector of the Dana Farber/Brigham and Women’s prostate cancer program.
In the Canadian province of Alberta, a similar decrease in cancer diagnoses occurred during the early days of the pandemic.
By the end of 2020, Alberta was “missing” approximately 2,000 cases of invasive cancers and 1,000 cases of noninvasive cancers, Doug Stewart, MD, senior medical director at the Cancer Strategic Clinical Network (SCN) of Alberta Health Services, told this news organization.
Dr. Stewart is able to track cancer diagnoses in Alberta almost in real time through a mandatory cancer registry. Within a month of shutdown, there was a 30% decrease in diagnoses of invasive cancers and a 50% decrease “in the kind of preinvasive cancers that, for the most part, are picked up by screening programs,” said Dr. Stewart.
After the health care system opened up again in the summer, Stewart said, noninvasive cancer diagnoses continued to be 20% lower than expected. There was a 10% shortfall in invasive cancer diagnoses.
The number of diagnoses had returned to normal by December 2020. However, Dr. Stewart is worried that this fact conceals a terrible truth.
The worry is over the backlog. Although the number of diagnoses is now similar to what it was before the pandemic, “people are presenting later, and maybe the cancer is more advanced,” he speculated.
His team at Alberta Health Services is assessing whether the cancers that are being diagnosed now are more advanced. Initial results are anticipated by late April 2021.
In the United Kingdom, there was a similar halt in cancer screening as a result of the country’s lockdown. Researchers now predict an uptick in cancer diagnoses.
Ajay Aggarwal, MD, PhD, consultant clinical oncologist and associate professor at the London School of Hygiene and Tropical Medicine, and colleagues have estimated that at least 3,500 deaths from breast, colorectal, esophageal, and lung cancer will occur during the next 5 years in England that could have been avoided had it not been for the lockdown measures necessitated by the pandemic.
Speaking to this news organization, Dr. Aggarwal warned that these numbers, which are from a modeling study published in August 2020, are “extremely conservative,” because the investigators considered diagnostic delays over only a 3-month period, the analysis involved only four cancers, and it did not reflect deferral of cancer treatment.
“It felt like it was the tip of the iceberg,” Dr. Aggarwal said. He warns that more recent data suggest that “diagnostic delays are probably worse than we predicted.”
He suspects that there is more at play than screening cancellations.
In another study conducted in the United Kingdom, data show “a falling edge of referrals” from primary care to cancer centers early in the pandemic. In that study, investigators analyzed real-time weekly hospital data from eight large British hospitals and found that urgent cancer referrals fell 70% at their lowest point.
“It really surprised me that the urgent referrals dropped so drastically,” said lead author Alvina Lai, PhD, a lecturer in health data analytics at University College London.
She attributed this in part to patients’ adherence to lockdown rules. “Patients are trying to follow government guidelines to stay home and not go to [general practitioners] unless necessary,” Dr. Lai explained in an interview.
Canada, like the United Kingdom, has a publicly funded health care system. Dr. Stewart came to a similar conclusion. “Some patients who have been diagnosed with cancer ... have told me it took them an extra couple of months to even contact the family doc, because they ... didn’t want to bother the family doctor with something that wasn’t COVID, this kind of guilt. They want to do something good for society. You know, most people are just really nice people, and they don’t want to bother the health care system if they don’t have COVID,” Dr. Stewart said.
Shelley Fuld Nasso, CEO of the National Coalition for Cancer Survivorship, a nonprofit organization based in Silver Spring, Md., agreed that screening shutdowns are not the only danger. “While we agree that screening is really important, we also want to make sure patients are following up with their physicians about symptoms that they have,” she said.
“Some of the speculation or concern about increased mortality for cancer is related to screening, but some of it is related to delayed diagnosis because of not following up on symptoms. ... What concerns me is not everyone has that ability or willingness to advocate for themselves,” she said.
Speaking at a press briefing held by the American Society for Radiation Oncology on March 30, Dr. Nasso related a case involving a patient who experienced severe arm pain. In a teleconsultation with her primary care physician, her condition was diagnosed as arthritis. She was subsequently diagnosed in the ED as having multiple myeloma.
Patients who “feel fine” may postpone their checkups to avoid going to the hospital and risking exposure to COVID-19.
“Some patients are still hesitant about returning for their mammograms or coming in if they feel a breast lump,” Dr. Tang said. “That fear of COVID-19 is still out there, and we don’t know how long patients are going to delay.”
In London, Dr. Aggarwal saw a similar response to the pandemic. “People were overestimating quite significantly what their risk of death was from acquiring COVID-19, and I think that balance was never [redressed] explicitly,” he said.
Public health initiatives to rebalance the messaging are now underway.
Public Health England and National Health Service England launched their Help Us Help You campaign in October 2020. The public information campaign urges people to speak to their doctors if they were “worried about a symptom that could be cancer.”
In Canada, the provincial government in Alberta has launched a public awareness campaign that conveys the message, “cancer has not gone away.”
“Cancer is still the No. 1 cause of potential life-years lost, despite COVID,” Dr. Stewart said. “We need to do what we can to make sure there’s no slippage in survival rates.”
Dr. Tang, Dr. Chang, Dr. Lai, Dr. Stewart, and Dr. Aggarwal have disclosed no relevant financial relationship. Dr. Trinh has received personal fees from Astellas, Bayer, and Janssen and grants from Intuitive Surgical.
A version of this article first appeared on Medscape.com.
Last year, cancer screening programs around the world ground to a halt as SARS-CoV-2 infection rates surged globally. The effect of this slowdown is now becoming clear.
Thousands of cancer diagnoses are “missing,” and oncologists worry that this will lead to more advanced cancers and higher mortality for years to come.
“I feel like this is an earthquake that’s rocked our health care system. My guess is that you’ll probably still see repercussions of this over the next couple of years at least,” said Sharon Chang, MD, an attending surgical oncologist in the Permanente Medical Group, Fremont, Calif.
She was senior author of a study that analyzed the effects of the slowdown in mammography screening as a result of California’s “shelter-in-place” order on March 17, 2020. In the 2 months that followed, there were 64% fewer breast cancer diagnoses at 21 Kaiser Permanente medical centers, compared with the same period in 2019 (250 vs. 703).
In effect, approximately 450 breast cancer patients had “disappeared,” said coauthor Annie Tang, MD, a research fellow at the University of California, San Francisco, East Bay surgery program.
“What surprised me most from our data was the sheer number of breast cancer patients that were missing,” Dr. Tang said in an interview.
A similar picture has emerged elsewhere.
In Boston, an estimated 1,438 cancerous and precancerous lesions “went missing” during the first 3 months of pandemic shutdown, according to a study from the Massachusetts General Brigham health care system.
In this study, the investigators assessed screening rates for five cancers – breast cancer (mammography), prostate cancer (prostate-specific antigen testing), colorectal cancer (colonoscopy), cervical cancer (Papanicolaou tests), and lung cancer (low-dose CT).
Screening rates during the first peak of the pandemic (March 2 to June 2, 2020) were compared with those during the preceding and following 3 months and during the same 3 months in 2019.
The results showed a pronounced drop in screening rates during the peak pandemic period, compared with the three control periods. Decreases occurred for all screening tests and ranged from –60% to –82%.
There were also significant decreases in cancer diagnoses resulting from the decreases in screening tests, ranging from –19% to –78%.
“Quantifying the actual problem made us realize how much work needs to be done to get us back to prepandemic numbers,” said senior author Quoc-Dien Trinh, MD, FACS, codirector of the Dana Farber/Brigham and Women’s prostate cancer program.
In the Canadian province of Alberta, a similar decrease in cancer diagnoses occurred during the early days of the pandemic.
By the end of 2020, Alberta was “missing” approximately 2,000 cases of invasive cancers and 1,000 cases of noninvasive cancers, Doug Stewart, MD, senior medical director at the Cancer Strategic Clinical Network (SCN) of Alberta Health Services, told this news organization.
Dr. Stewart is able to track cancer diagnoses in Alberta almost in real time through a mandatory cancer registry. Within a month of shutdown, there was a 30% decrease in diagnoses of invasive cancers and a 50% decrease “in the kind of preinvasive cancers that, for the most part, are picked up by screening programs,” said Dr. Stewart.
After the health care system opened up again in the summer, Stewart said, noninvasive cancer diagnoses continued to be 20% lower than expected. There was a 10% shortfall in invasive cancer diagnoses.
The number of diagnoses had returned to normal by December 2020. However, Dr. Stewart is worried that this fact conceals a terrible truth.
The worry is over the backlog. Although the number of diagnoses is now similar to what it was before the pandemic, “people are presenting later, and maybe the cancer is more advanced,” he speculated.
His team at Alberta Health Services is assessing whether the cancers that are being diagnosed now are more advanced. Initial results are anticipated by late April 2021.
In the United Kingdom, there was a similar halt in cancer screening as a result of the country’s lockdown. Researchers now predict an uptick in cancer diagnoses.
Ajay Aggarwal, MD, PhD, consultant clinical oncologist and associate professor at the London School of Hygiene and Tropical Medicine, and colleagues have estimated that at least 3,500 deaths from breast, colorectal, esophageal, and lung cancer will occur during the next 5 years in England that could have been avoided had it not been for the lockdown measures necessitated by the pandemic.
Speaking to this news organization, Dr. Aggarwal warned that these numbers, which are from a modeling study published in August 2020, are “extremely conservative,” because the investigators considered diagnostic delays over only a 3-month period, the analysis involved only four cancers, and it did not reflect deferral of cancer treatment.
“It felt like it was the tip of the iceberg,” Dr. Aggarwal said. He warns that more recent data suggest that “diagnostic delays are probably worse than we predicted.”
He suspects that there is more at play than screening cancellations.
In another study conducted in the United Kingdom, data show “a falling edge of referrals” from primary care to cancer centers early in the pandemic. In that study, investigators analyzed real-time weekly hospital data from eight large British hospitals and found that urgent cancer referrals fell 70% at their lowest point.
“It really surprised me that the urgent referrals dropped so drastically,” said lead author Alvina Lai, PhD, a lecturer in health data analytics at University College London.
She attributed this in part to patients’ adherence to lockdown rules. “Patients are trying to follow government guidelines to stay home and not go to [general practitioners] unless necessary,” Dr. Lai explained in an interview.
Canada, like the United Kingdom, has a publicly funded health care system. Dr. Stewart came to a similar conclusion. “Some patients who have been diagnosed with cancer ... have told me it took them an extra couple of months to even contact the family doc, because they ... didn’t want to bother the family doctor with something that wasn’t COVID, this kind of guilt. They want to do something good for society. You know, most people are just really nice people, and they don’t want to bother the health care system if they don’t have COVID,” Dr. Stewart said.
Shelley Fuld Nasso, CEO of the National Coalition for Cancer Survivorship, a nonprofit organization based in Silver Spring, Md., agreed that screening shutdowns are not the only danger. “While we agree that screening is really important, we also want to make sure patients are following up with their physicians about symptoms that they have,” she said.
“Some of the speculation or concern about increased mortality for cancer is related to screening, but some of it is related to delayed diagnosis because of not following up on symptoms. ... What concerns me is not everyone has that ability or willingness to advocate for themselves,” she said.
Speaking at a press briefing held by the American Society for Radiation Oncology on March 30, Dr. Nasso related a case involving a patient who experienced severe arm pain. In a teleconsultation with her primary care physician, her condition was diagnosed as arthritis. She was subsequently diagnosed in the ED as having multiple myeloma.
Patients who “feel fine” may postpone their checkups to avoid going to the hospital and risking exposure to COVID-19.
“Some patients are still hesitant about returning for their mammograms or coming in if they feel a breast lump,” Dr. Tang said. “That fear of COVID-19 is still out there, and we don’t know how long patients are going to delay.”
In London, Dr. Aggarwal saw a similar response to the pandemic. “People were overestimating quite significantly what their risk of death was from acquiring COVID-19, and I think that balance was never [redressed] explicitly,” he said.
Public health initiatives to rebalance the messaging are now underway.
Public Health England and National Health Service England launched their Help Us Help You campaign in October 2020. The public information campaign urges people to speak to their doctors if they were “worried about a symptom that could be cancer.”
In Canada, the provincial government in Alberta has launched a public awareness campaign that conveys the message, “cancer has not gone away.”
“Cancer is still the No. 1 cause of potential life-years lost, despite COVID,” Dr. Stewart said. “We need to do what we can to make sure there’s no slippage in survival rates.”
Dr. Tang, Dr. Chang, Dr. Lai, Dr. Stewart, and Dr. Aggarwal have disclosed no relevant financial relationship. Dr. Trinh has received personal fees from Astellas, Bayer, and Janssen and grants from Intuitive Surgical.
A version of this article first appeared on Medscape.com.
Last year, cancer screening programs around the world ground to a halt as SARS-CoV-2 infection rates surged globally. The effect of this slowdown is now becoming clear.
Thousands of cancer diagnoses are “missing,” and oncologists worry that this will lead to more advanced cancers and higher mortality for years to come.
“I feel like this is an earthquake that’s rocked our health care system. My guess is that you’ll probably still see repercussions of this over the next couple of years at least,” said Sharon Chang, MD, an attending surgical oncologist in the Permanente Medical Group, Fremont, Calif.
She was senior author of a study that analyzed the effects of the slowdown in mammography screening as a result of California’s “shelter-in-place” order on March 17, 2020. In the 2 months that followed, there were 64% fewer breast cancer diagnoses at 21 Kaiser Permanente medical centers, compared with the same period in 2019 (250 vs. 703).
In effect, approximately 450 breast cancer patients had “disappeared,” said coauthor Annie Tang, MD, a research fellow at the University of California, San Francisco, East Bay surgery program.
“What surprised me most from our data was the sheer number of breast cancer patients that were missing,” Dr. Tang said in an interview.
A similar picture has emerged elsewhere.
In Boston, an estimated 1,438 cancerous and precancerous lesions “went missing” during the first 3 months of pandemic shutdown, according to a study from the Massachusetts General Brigham health care system.
In this study, the investigators assessed screening rates for five cancers – breast cancer (mammography), prostate cancer (prostate-specific antigen testing), colorectal cancer (colonoscopy), cervical cancer (Papanicolaou tests), and lung cancer (low-dose CT).
Screening rates during the first peak of the pandemic (March 2 to June 2, 2020) were compared with those during the preceding and following 3 months and during the same 3 months in 2019.
The results showed a pronounced drop in screening rates during the peak pandemic period, compared with the three control periods. Decreases occurred for all screening tests and ranged from –60% to –82%.
There were also significant decreases in cancer diagnoses resulting from the decreases in screening tests, ranging from –19% to –78%.
“Quantifying the actual problem made us realize how much work needs to be done to get us back to prepandemic numbers,” said senior author Quoc-Dien Trinh, MD, FACS, codirector of the Dana Farber/Brigham and Women’s prostate cancer program.
In the Canadian province of Alberta, a similar decrease in cancer diagnoses occurred during the early days of the pandemic.
By the end of 2020, Alberta was “missing” approximately 2,000 cases of invasive cancers and 1,000 cases of noninvasive cancers, Doug Stewart, MD, senior medical director at the Cancer Strategic Clinical Network (SCN) of Alberta Health Services, told this news organization.
Dr. Stewart is able to track cancer diagnoses in Alberta almost in real time through a mandatory cancer registry. Within a month of shutdown, there was a 30% decrease in diagnoses of invasive cancers and a 50% decrease “in the kind of preinvasive cancers that, for the most part, are picked up by screening programs,” said Dr. Stewart.
After the health care system opened up again in the summer, Stewart said, noninvasive cancer diagnoses continued to be 20% lower than expected. There was a 10% shortfall in invasive cancer diagnoses.
The number of diagnoses had returned to normal by December 2020. However, Dr. Stewart is worried that this fact conceals a terrible truth.
The worry is over the backlog. Although the number of diagnoses is now similar to what it was before the pandemic, “people are presenting later, and maybe the cancer is more advanced,” he speculated.
His team at Alberta Health Services is assessing whether the cancers that are being diagnosed now are more advanced. Initial results are anticipated by late April 2021.
In the United Kingdom, there was a similar halt in cancer screening as a result of the country’s lockdown. Researchers now predict an uptick in cancer diagnoses.
Ajay Aggarwal, MD, PhD, consultant clinical oncologist and associate professor at the London School of Hygiene and Tropical Medicine, and colleagues have estimated that at least 3,500 deaths from breast, colorectal, esophageal, and lung cancer will occur during the next 5 years in England that could have been avoided had it not been for the lockdown measures necessitated by the pandemic.
Speaking to this news organization, Dr. Aggarwal warned that these numbers, which are from a modeling study published in August 2020, are “extremely conservative,” because the investigators considered diagnostic delays over only a 3-month period, the analysis involved only four cancers, and it did not reflect deferral of cancer treatment.
“It felt like it was the tip of the iceberg,” Dr. Aggarwal said. He warns that more recent data suggest that “diagnostic delays are probably worse than we predicted.”
He suspects that there is more at play than screening cancellations.
In another study conducted in the United Kingdom, data show “a falling edge of referrals” from primary care to cancer centers early in the pandemic. In that study, investigators analyzed real-time weekly hospital data from eight large British hospitals and found that urgent cancer referrals fell 70% at their lowest point.
“It really surprised me that the urgent referrals dropped so drastically,” said lead author Alvina Lai, PhD, a lecturer in health data analytics at University College London.
She attributed this in part to patients’ adherence to lockdown rules. “Patients are trying to follow government guidelines to stay home and not go to [general practitioners] unless necessary,” Dr. Lai explained in an interview.
Canada, like the United Kingdom, has a publicly funded health care system. Dr. Stewart came to a similar conclusion. “Some patients who have been diagnosed with cancer ... have told me it took them an extra couple of months to even contact the family doc, because they ... didn’t want to bother the family doctor with something that wasn’t COVID, this kind of guilt. They want to do something good for society. You know, most people are just really nice people, and they don’t want to bother the health care system if they don’t have COVID,” Dr. Stewart said.
Shelley Fuld Nasso, CEO of the National Coalition for Cancer Survivorship, a nonprofit organization based in Silver Spring, Md., agreed that screening shutdowns are not the only danger. “While we agree that screening is really important, we also want to make sure patients are following up with their physicians about symptoms that they have,” she said.
“Some of the speculation or concern about increased mortality for cancer is related to screening, but some of it is related to delayed diagnosis because of not following up on symptoms. ... What concerns me is not everyone has that ability or willingness to advocate for themselves,” she said.
Speaking at a press briefing held by the American Society for Radiation Oncology on March 30, Dr. Nasso related a case involving a patient who experienced severe arm pain. In a teleconsultation with her primary care physician, her condition was diagnosed as arthritis. She was subsequently diagnosed in the ED as having multiple myeloma.
Patients who “feel fine” may postpone their checkups to avoid going to the hospital and risking exposure to COVID-19.
“Some patients are still hesitant about returning for their mammograms or coming in if they feel a breast lump,” Dr. Tang said. “That fear of COVID-19 is still out there, and we don’t know how long patients are going to delay.”
In London, Dr. Aggarwal saw a similar response to the pandemic. “People were overestimating quite significantly what their risk of death was from acquiring COVID-19, and I think that balance was never [redressed] explicitly,” he said.
Public health initiatives to rebalance the messaging are now underway.
Public Health England and National Health Service England launched their Help Us Help You campaign in October 2020. The public information campaign urges people to speak to their doctors if they were “worried about a symptom that could be cancer.”
In Canada, the provincial government in Alberta has launched a public awareness campaign that conveys the message, “cancer has not gone away.”
“Cancer is still the No. 1 cause of potential life-years lost, despite COVID,” Dr. Stewart said. “We need to do what we can to make sure there’s no slippage in survival rates.”
Dr. Tang, Dr. Chang, Dr. Lai, Dr. Stewart, and Dr. Aggarwal have disclosed no relevant financial relationship. Dr. Trinh has received personal fees from Astellas, Bayer, and Janssen and grants from Intuitive Surgical.
A version of this article first appeared on Medscape.com.
VEXAS: A novel rheumatologic, hematologic syndrome that’s making waves
Older men with a novel adult-onset, severe autoinflammatory syndrome known by the acronym VEXAS are likely hiding in plain sight in many adult rheumatology, hematology, and dermatology practices. New clinical features are being described to fill out the clinical profile of such patients who may be currently misdiagnosed with other conditions, according to researchers who first described the syndrome in the last quarter of 2020.

VEXAS is often misdiagnosed as treatment-refractory relapsing polychondritis, polyarteritis nodosa, Sweet syndrome, or giant cell arteritis. These seemingly unrelated disorders are actually tied together by a single thread recently unraveled by David B. Beck, MD, PhD, a clinical fellow at the National Human Genome Research Institute, and colleagues, including rheumatologist Marcela Ferrada, MD, and others at institutes of the National Institutes of Health, Bethesda, Md. The connection between these disparate clinical presentations lies in somatic mutations in UBA1, a gene that initiates cytoplasmic ubiquitylation, a process by which misfolded proteins are tagged for degradation. VEXAS appears primarily limited to men because the UBA1 gene lies on the X chromosome, although it may be possible for women to have it because of an acquired loss of X chromosome.
VEXAS is an acronym for:
- Vacuoles in bone marrow cells
- E-1 activating enzyme, which is what UBA1 encodes for
- X-linked
- Autoinflammatory
- Somatic mutation featuring hematologic mosaicism
Dr. Beck said that VEXAS is “probably affecting thousands of Americans,” but it is tough to say this early in the understanding of the disease. He estimated that the prevalence of VEXAS could be 1 per 20,000-30,000 individuals.
A new way of looking for disease
VEXAS has caused a major stir among geneticists because of the novel manner in which Dr. Beck and his coinvestigators made their discovery. Instead of starting out in the traditional path to discovery of a new genetic disease – that is, by looking for clinical similarities among patients with undiagnosed diseases and then conducting a search for a gene or genes that might explain the shared patient symptoms – the investigators took a genotype-first approach. They scanned the mapped genomic sequences of patients in the National Institutes of Health Undiagnosed Diseases Network, which led them to zero in on mutations in UBA1 as their top candidate.
“We targeted the ubiquitin-proteasome pathway, because it has been implicated in many autoinflammatory diseases – for example, HA20 [A20 haploinsufficiency] and CANDLE syndrome [Chronic Atypical Neutrophilic Dermatosis with Lipodystrophy and Elevated temperature]. Many of these recurrent inflammatory diseases are caused by mutations within this pathway,” Dr. Beck said in an interview.
Next, they analyzed the genomes of patients in other NIH databases and patients from other study populations at the University College London and Leeds Teaching Hospitals NHS Trust in the United Kingdom in a search for UBA1 somatic mutations, eventually identifying 25 men with the shared features they called VEXAS. These 25 formed the basis for their initial report on the syndrome in the New England Journal of Medicine.
Most autoinflammatory diseases appear in childhood because they stem from germline mutations. VEXAS syndrome, because of somatic mutations with mosaicism, appears to manifest later in life: The median age of the initial 25-man cohort was 64 years, ranging from 45 to 80 years. It’s a severe disorder. By the time the investigators were preparing their paper for publication, 10 of the 25 patients, or 40%, had died.
“I think that somatic mutations may account for a significant percentage of severe. adult-onset rheumatologic diseases, and it may change the way we think about treating them based on having a genetic diagnosis,” Dr. Beck said.
“This approach could be expanded to look at other pathways we know are important in inflammation, or alternatively, it could be completely unbiased and look for any shared variation that occurs across undiagnosed patients with inflammatory diseases. I think that one thing that’s important about our study is that previously we had been looking for mutations that really in most cases were the same sort of germline mutations present in [pediatric] patients who have disease at early onset, but now we’re thinking about things differently. There may be a different type of genetics that drives adult-onset rheumatologic disease, and this would be somatic mutations which are not present in every cell of the body, just in the blood, and that’s why there’s just this blood-based disease.”
When to suspect VEXAS syndrome
Consider the possibility of VEXAS in middle-aged or older men in a rheumatology clinic with characteristics suggestive of treatment-refractory relapsing polychondritis, giant cell arteritis, polyarteritis nodosa, or Sweet syndrome. In the original series of 25 men, 15 were diagnosed with relapsing polychondritis, 8 with Sweet syndrome, 3 with polyarteritis nodosa, and 1 with giant cell arteritis.
Men with VEXAS often have periodic fevers, pulmonary infiltrates, a history of unprovoked venous thromboembolic events, neutrophilic dermatoses, and/or hematologic abnormalities such as myelodysplastic syndrome, multiple myeloma, or monoclonal gammopathy of unknown origin.
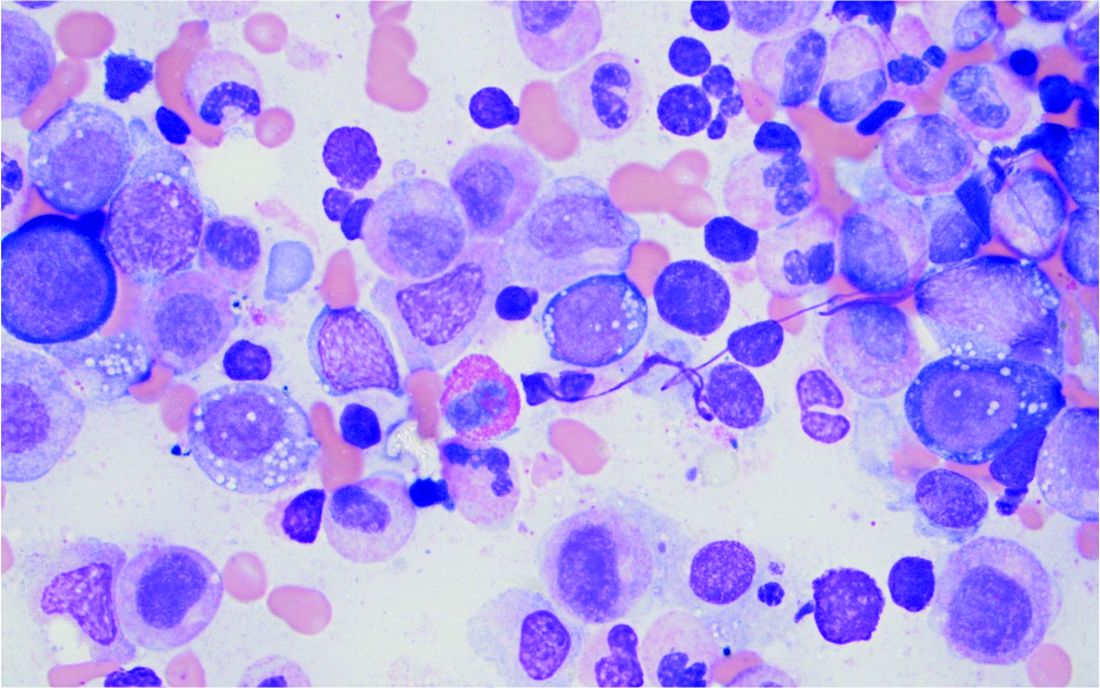
Bone marrow biopsy will show vacuoles in myeloid and erythroid precursor cells. Inflammatory marker levels are very high: In the NIH series, the median C-reactive protein was 73 mg/L and median erythrocyte sedimentation rate was 97 mm/hr. The diagnosis of VEXAS can be confirmed by genetic testing performed by Dr. Beck and his NIH coworkers ([email protected]).
In interviews, Dr. Beck and Dr. Ferrada emphasized that management of VEXAS requires a multidisciplinary team of clinicians including rheumatologists, hematologists, and dermatologists.
Dr. Ferrada said that rheumatologists could suspect VEXAS in patients who have very high inflammatory markers and do not have a clear diagnosis or do not meet all criteria for other rheumatologic diseases, particularly in older men, but it’s possible in younger men as well. Hematologists could also consider VEXAS in patients with macrocytic anemia or macrocytosis without an explanation and inflammatory features, she said.
Dr. Ferrada, Dr. Beck, and colleagues also published a study in Arthritis & Rheumatology that presents a useful clinical algorithm for deciding whether to order genetic screening for VEXAS in patients with relapsing polychondritis.
First off, Dr. Ferrada and colleagues performed whole-exome sequencing and testing for UBA1 variants in an observational cohort of 92 relapsing polychondritis patients to determine the prevalence of VEXAS, which turned out to be 8%. They added an additional 6 patients with relapsing polychondritis and VEXAS from other cohorts, for a total of 13. The investigators determined that patients with VEXAS were older at disease onset, and more likely to have fever, ear chondritis, DVT, pulmonary infiltrates, skin involvement, and periorbital edema. In contrast, the RP cohort had a significantly higher prevalence of airway chondritis, joint involvement, and vestibular symptoms.

Dr. Ferrada’s algorithm for picking out VEXAS in patients who meet diagnostic criteria for relapsing polychondritis is based upon a few simple factors readily apparent in screening patient charts: male sex; age at onset older than 50 years; macrocytic anemia; and thrombocytopenia. Those four variables, when present, identify VEXAS within an RP cohort with 100% sensitivity and 96% specificity. “As we learn more about [VEXAS] and how it presents earlier, I think we are going to be able to find different manifestations or laboratory data that are going to allow us to diagnose these patients earlier,” she said. “The whole role of that algorithm was to guide clinicians who see patients with relapsing polychondritis to test these patients for the mutation, but I think over time that is going to evolve.”
Researchers are taking similar approaches for other clinical diagnoses to see which should be referred for UBA1 testing, Dr. Beck said.
Myelodysplastic syndrome and hematologic abnormalities
While patients with both myelodysplastic syndrome and relapsing polychondritis have been known in the literature for many years, it’s not until now that researchers are seeing a connection between the two, Dr. Ferrada said.
A majority of the VEXAS patients in the NEJM study had a workup for myelodysplastic syndrome, but only 24% met criteria. However, many were within the spectrum of myelodysplastic disease and some did not meet criteria because their anemia was attributed to a rheumatologic diagnosis and they did not have a known genetic driver of myelodysplastic syndrome, Dr. Beck said. It also fits with this new evidence that UBA1 is probably a driver of myelodysplastic syndrome in and of itself, and that anemia and hematologic involvement are not secondary to the rheumatologic disease; they are linked to the same disease process.
Dr. Beck said that there may be a subset of patients who present with primarily hematologic manifestations, noting the NEJM study could have ascertainment bias because the researchers analyzed mainly patients presenting to their clinic with relapsing polychondritis and severe inflammation. NIH researchers also are still looking in their cohort for any association with hematologic malignancies that preceded clinical manifestations, he said.
More cases reported
As of early April, another 27 cases had been reported in the literature as more researchers have begun to look for patients with UBA1 mutations, some with additional presenting clinical features associated with VEXAS, including chronic progressive inflammatory arthritis, Kikuchi-Fujimoto disease, spondyloarthritis, and bacterial pneumonia.
“Many times with rare diseases, we can’t get enough patients to understand the full spectrum of the disease, but this disease seems to be far more common than we would have expected. We’re actually getting many referrals,” Dr. Beck said.
It appears so far that the range of somatic UBA1 mutations that have been discovered in VEXAS patients does make a difference in the severity of clinical presentation and could potentially be useful in prognosis, Dr. Beck said.
Right now, NIH researchers are asking patients about their natural clinical course, assessing disease activity, and determining which treatments get a response, with the ultimate goal of a treatment trial at the NIH.
Treatment
Developing better treatments for VEXAS syndrome is a priority. In the initial report on VEXAS, the researchers found that the only reliably effective therapy is high-dose corticosteroids. Dr. Ferrada said that NIH investigators have begun thinking about agents that target both the hematologic and inflammatory features of VEXAS. “Most patients get exposed to treatments that are targeted to decrease the inflammatory process, and some of these treatments help partially but not completely to decrease the amount of steroids that patients are taking. For example, one of the medications is tocilizumab. [It was used in] patients who had previous diagnosis of relapsing polychondritis, but they still had to take steroids and their hematologic manifestations keep progressing. We’re in the process of figuring out medications that may help in treating both.” Dr. Ferrada added that because the source of the mutation is in the bone marrow, transplantation may be an effective option.
Laboratory work to identify potential treatments for VEXAS in studies of model organisms could identify treatments outside of the classic anti-inflammatory agents, such as targeting certain cell types in the bone marrow or the ubiquitin-proteasome pathway, Dr. Beck said. “We think that however UBA1 works to initiate inflammation may be important not just in VEXAS but in other diseases. Rare diseases may be informing the mechanisms in common diseases.”
The VEXAS NEJM study was sponsored by the NIH Intramural Research Programs and by an EU Horizon 2020 Research and Innovation Program grant. Dr. Beck reported a patent pending on “Diagnosis and Treatment of VEXAS with Mosaic Missense Mutations in UBA1.”
Older men with a novel adult-onset, severe autoinflammatory syndrome known by the acronym VEXAS are likely hiding in plain sight in many adult rheumatology, hematology, and dermatology practices. New clinical features are being described to fill out the clinical profile of such patients who may be currently misdiagnosed with other conditions, according to researchers who first described the syndrome in the last quarter of 2020.
VEXAS is often misdiagnosed as treatment-refractory relapsing polychondritis, polyarteritis nodosa, Sweet syndrome, or giant cell arteritis. These seemingly unrelated disorders are actually tied together by a single thread recently unraveled by David B. Beck, MD, PhD, a clinical fellow at the National Human Genome Research Institute, and colleagues, including rheumatologist Marcela Ferrada, MD, and others at institutes of the National Institutes of Health, Bethesda, Md. The connection between these disparate clinical presentations lies in somatic mutations in UBA1, a gene that initiates cytoplasmic ubiquitylation, a process by which misfolded proteins are tagged for degradation. VEXAS appears primarily limited to men because the UBA1 gene lies on the X chromosome, although it may be possible for women to have it because of an acquired loss of X chromosome.
VEXAS is an acronym for:
- Vacuoles in bone marrow cells
- E-1 activating enzyme, which is what UBA1 encodes for
- X-linked
- Autoinflammatory
- Somatic mutation featuring hematologic mosaicism
Dr. Beck said that VEXAS is “probably affecting thousands of Americans,” but it is tough to say this early in the understanding of the disease. He estimated that the prevalence of VEXAS could be 1 per 20,000-30,000 individuals.
A new way of looking for disease
VEXAS has caused a major stir among geneticists because of the novel manner in which Dr. Beck and his coinvestigators made their discovery. Instead of starting out in the traditional path to discovery of a new genetic disease – that is, by looking for clinical similarities among patients with undiagnosed diseases and then conducting a search for a gene or genes that might explain the shared patient symptoms – the investigators took a genotype-first approach. They scanned the mapped genomic sequences of patients in the National Institutes of Health Undiagnosed Diseases Network, which led them to zero in on mutations in UBA1 as their top candidate.
“We targeted the ubiquitin-proteasome pathway, because it has been implicated in many autoinflammatory diseases – for example, HA20 [A20 haploinsufficiency] and CANDLE syndrome [Chronic Atypical Neutrophilic Dermatosis with Lipodystrophy and Elevated temperature]. Many of these recurrent inflammatory diseases are caused by mutations within this pathway,” Dr. Beck said in an interview.
Next, they analyzed the genomes of patients in other NIH databases and patients from other study populations at the University College London and Leeds Teaching Hospitals NHS Trust in the United Kingdom in a search for UBA1 somatic mutations, eventually identifying 25 men with the shared features they called VEXAS. These 25 formed the basis for their initial report on the syndrome in the New England Journal of Medicine.
Most autoinflammatory diseases appear in childhood because they stem from germline mutations. VEXAS syndrome, because of somatic mutations with mosaicism, appears to manifest later in life: The median age of the initial 25-man cohort was 64 years, ranging from 45 to 80 years. It’s a severe disorder. By the time the investigators were preparing their paper for publication, 10 of the 25 patients, or 40%, had died.
“I think that somatic mutations may account for a significant percentage of severe. adult-onset rheumatologic diseases, and it may change the way we think about treating them based on having a genetic diagnosis,” Dr. Beck said.
“This approach could be expanded to look at other pathways we know are important in inflammation, or alternatively, it could be completely unbiased and look for any shared variation that occurs across undiagnosed patients with inflammatory diseases. I think that one thing that’s important about our study is that previously we had been looking for mutations that really in most cases were the same sort of germline mutations present in [pediatric] patients who have disease at early onset, but now we’re thinking about things differently. There may be a different type of genetics that drives adult-onset rheumatologic disease, and this would be somatic mutations which are not present in every cell of the body, just in the blood, and that’s why there’s just this blood-based disease.”
When to suspect VEXAS syndrome
Consider the possibility of VEXAS in middle-aged or older men in a rheumatology clinic with characteristics suggestive of treatment-refractory relapsing polychondritis, giant cell arteritis, polyarteritis nodosa, or Sweet syndrome. In the original series of 25 men, 15 were diagnosed with relapsing polychondritis, 8 with Sweet syndrome, 3 with polyarteritis nodosa, and 1 with giant cell arteritis.
Men with VEXAS often have periodic fevers, pulmonary infiltrates, a history of unprovoked venous thromboembolic events, neutrophilic dermatoses, and/or hematologic abnormalities such as myelodysplastic syndrome, multiple myeloma, or monoclonal gammopathy of unknown origin.
Bone marrow biopsy will show vacuoles in myeloid and erythroid precursor cells. Inflammatory marker levels are very high: In the NIH series, the median C-reactive protein was 73 mg/L and median erythrocyte sedimentation rate was 97 mm/hr. The diagnosis of VEXAS can be confirmed by genetic testing performed by Dr. Beck and his NIH coworkers ([email protected]).
In interviews, Dr. Beck and Dr. Ferrada emphasized that management of VEXAS requires a multidisciplinary team of clinicians including rheumatologists, hematologists, and dermatologists.
Dr. Ferrada said that rheumatologists could suspect VEXAS in patients who have very high inflammatory markers and do not have a clear diagnosis or do not meet all criteria for other rheumatologic diseases, particularly in older men, but it’s possible in younger men as well. Hematologists could also consider VEXAS in patients with macrocytic anemia or macrocytosis without an explanation and inflammatory features, she said.
Dr. Ferrada, Dr. Beck, and colleagues also published a study in Arthritis & Rheumatology that presents a useful clinical algorithm for deciding whether to order genetic screening for VEXAS in patients with relapsing polychondritis.
First off, Dr. Ferrada and colleagues performed whole-exome sequencing and testing for UBA1 variants in an observational cohort of 92 relapsing polychondritis patients to determine the prevalence of VEXAS, which turned out to be 8%. They added an additional 6 patients with relapsing polychondritis and VEXAS from other cohorts, for a total of 13. The investigators determined that patients with VEXAS were older at disease onset, and more likely to have fever, ear chondritis, DVT, pulmonary infiltrates, skin involvement, and periorbital edema. In contrast, the RP cohort had a significantly higher prevalence of airway chondritis, joint involvement, and vestibular symptoms.
Dr. Ferrada’s algorithm for picking out VEXAS in patients who meet diagnostic criteria for relapsing polychondritis is based upon a few simple factors readily apparent in screening patient charts: male sex; age at onset older than 50 years; macrocytic anemia; and thrombocytopenia. Those four variables, when present, identify VEXAS within an RP cohort with 100% sensitivity and 96% specificity. “As we learn more about [VEXAS] and how it presents earlier, I think we are going to be able to find different manifestations or laboratory data that are going to allow us to diagnose these patients earlier,” she said. “The whole role of that algorithm was to guide clinicians who see patients with relapsing polychondritis to test these patients for the mutation, but I think over time that is going to evolve.”
Researchers are taking similar approaches for other clinical diagnoses to see which should be referred for UBA1 testing, Dr. Beck said.
Myelodysplastic syndrome and hematologic abnormalities
While patients with both myelodysplastic syndrome and relapsing polychondritis have been known in the literature for many years, it’s not until now that researchers are seeing a connection between the two, Dr. Ferrada said.
A majority of the VEXAS patients in the NEJM study had a workup for myelodysplastic syndrome, but only 24% met criteria. However, many were within the spectrum of myelodysplastic disease and some did not meet criteria because their anemia was attributed to a rheumatologic diagnosis and they did not have a known genetic driver of myelodysplastic syndrome, Dr. Beck said. It also fits with this new evidence that UBA1 is probably a driver of myelodysplastic syndrome in and of itself, and that anemia and hematologic involvement are not secondary to the rheumatologic disease; they are linked to the same disease process.
Dr. Beck said that there may be a subset of patients who present with primarily hematologic manifestations, noting the NEJM study could have ascertainment bias because the researchers analyzed mainly patients presenting to their clinic with relapsing polychondritis and severe inflammation. NIH researchers also are still looking in their cohort for any association with hematologic malignancies that preceded clinical manifestations, he said.
More cases reported
As of early April, another 27 cases had been reported in the literature as more researchers have begun to look for patients with UBA1 mutations, some with additional presenting clinical features associated with VEXAS, including chronic progressive inflammatory arthritis, Kikuchi-Fujimoto disease, spondyloarthritis, and bacterial pneumonia.
“Many times with rare diseases, we can’t get enough patients to understand the full spectrum of the disease, but this disease seems to be far more common than we would have expected. We’re actually getting many referrals,” Dr. Beck said.
It appears so far that the range of somatic UBA1 mutations that have been discovered in VEXAS patients does make a difference in the severity of clinical presentation and could potentially be useful in prognosis, Dr. Beck said.
Right now, NIH researchers are asking patients about their natural clinical course, assessing disease activity, and determining which treatments get a response, with the ultimate goal of a treatment trial at the NIH.
Treatment
Developing better treatments for VEXAS syndrome is a priority. In the initial report on VEXAS, the researchers found that the only reliably effective therapy is high-dose corticosteroids. Dr. Ferrada said that NIH investigators have begun thinking about agents that target both the hematologic and inflammatory features of VEXAS. “Most patients get exposed to treatments that are targeted to decrease the inflammatory process, and some of these treatments help partially but not completely to decrease the amount of steroids that patients are taking. For example, one of the medications is tocilizumab. [It was used in] patients who had previous diagnosis of relapsing polychondritis, but they still had to take steroids and their hematologic manifestations keep progressing. We’re in the process of figuring out medications that may help in treating both.” Dr. Ferrada added that because the source of the mutation is in the bone marrow, transplantation may be an effective option.
Laboratory work to identify potential treatments for VEXAS in studies of model organisms could identify treatments outside of the classic anti-inflammatory agents, such as targeting certain cell types in the bone marrow or the ubiquitin-proteasome pathway, Dr. Beck said. “We think that however UBA1 works to initiate inflammation may be important not just in VEXAS but in other diseases. Rare diseases may be informing the mechanisms in common diseases.”
The VEXAS NEJM study was sponsored by the NIH Intramural Research Programs and by an EU Horizon 2020 Research and Innovation Program grant. Dr. Beck reported a patent pending on “Diagnosis and Treatment of VEXAS with Mosaic Missense Mutations in UBA1.”
Older men with a novel adult-onset, severe autoinflammatory syndrome known by the acronym VEXAS are likely hiding in plain sight in many adult rheumatology, hematology, and dermatology practices. New clinical features are being described to fill out the clinical profile of such patients who may be currently misdiagnosed with other conditions, according to researchers who first described the syndrome in the last quarter of 2020.
VEXAS is often misdiagnosed as treatment-refractory relapsing polychondritis, polyarteritis nodosa, Sweet syndrome, or giant cell arteritis. These seemingly unrelated disorders are actually tied together by a single thread recently unraveled by David B. Beck, MD, PhD, a clinical fellow at the National Human Genome Research Institute, and colleagues, including rheumatologist Marcela Ferrada, MD, and others at institutes of the National Institutes of Health, Bethesda, Md. The connection between these disparate clinical presentations lies in somatic mutations in UBA1, a gene that initiates cytoplasmic ubiquitylation, a process by which misfolded proteins are tagged for degradation. VEXAS appears primarily limited to men because the UBA1 gene lies on the X chromosome, although it may be possible for women to have it because of an acquired loss of X chromosome.
VEXAS is an acronym for:
- Vacuoles in bone marrow cells
- E-1 activating enzyme, which is what UBA1 encodes for
- X-linked
- Autoinflammatory
- Somatic mutation featuring hematologic mosaicism
Dr. Beck said that VEXAS is “probably affecting thousands of Americans,” but it is tough to say this early in the understanding of the disease. He estimated that the prevalence of VEXAS could be 1 per 20,000-30,000 individuals.
A new way of looking for disease
VEXAS has caused a major stir among geneticists because of the novel manner in which Dr. Beck and his coinvestigators made their discovery. Instead of starting out in the traditional path to discovery of a new genetic disease – that is, by looking for clinical similarities among patients with undiagnosed diseases and then conducting a search for a gene or genes that might explain the shared patient symptoms – the investigators took a genotype-first approach. They scanned the mapped genomic sequences of patients in the National Institutes of Health Undiagnosed Diseases Network, which led them to zero in on mutations in UBA1 as their top candidate.
“We targeted the ubiquitin-proteasome pathway, because it has been implicated in many autoinflammatory diseases – for example, HA20 [A20 haploinsufficiency] and CANDLE syndrome [Chronic Atypical Neutrophilic Dermatosis with Lipodystrophy and Elevated temperature]. Many of these recurrent inflammatory diseases are caused by mutations within this pathway,” Dr. Beck said in an interview.
Next, they analyzed the genomes of patients in other NIH databases and patients from other study populations at the University College London and Leeds Teaching Hospitals NHS Trust in the United Kingdom in a search for UBA1 somatic mutations, eventually identifying 25 men with the shared features they called VEXAS. These 25 formed the basis for their initial report on the syndrome in the New England Journal of Medicine.
Most autoinflammatory diseases appear in childhood because they stem from germline mutations. VEXAS syndrome, because of somatic mutations with mosaicism, appears to manifest later in life: The median age of the initial 25-man cohort was 64 years, ranging from 45 to 80 years. It’s a severe disorder. By the time the investigators were preparing their paper for publication, 10 of the 25 patients, or 40%, had died.
“I think that somatic mutations may account for a significant percentage of severe. adult-onset rheumatologic diseases, and it may change the way we think about treating them based on having a genetic diagnosis,” Dr. Beck said.
“This approach could be expanded to look at other pathways we know are important in inflammation, or alternatively, it could be completely unbiased and look for any shared variation that occurs across undiagnosed patients with inflammatory diseases. I think that one thing that’s important about our study is that previously we had been looking for mutations that really in most cases were the same sort of germline mutations present in [pediatric] patients who have disease at early onset, but now we’re thinking about things differently. There may be a different type of genetics that drives adult-onset rheumatologic disease, and this would be somatic mutations which are not present in every cell of the body, just in the blood, and that’s why there’s just this blood-based disease.”
When to suspect VEXAS syndrome
Consider the possibility of VEXAS in middle-aged or older men in a rheumatology clinic with characteristics suggestive of treatment-refractory relapsing polychondritis, giant cell arteritis, polyarteritis nodosa, or Sweet syndrome. In the original series of 25 men, 15 were diagnosed with relapsing polychondritis, 8 with Sweet syndrome, 3 with polyarteritis nodosa, and 1 with giant cell arteritis.
Men with VEXAS often have periodic fevers, pulmonary infiltrates, a history of unprovoked venous thromboembolic events, neutrophilic dermatoses, and/or hematologic abnormalities such as myelodysplastic syndrome, multiple myeloma, or monoclonal gammopathy of unknown origin.
Bone marrow biopsy will show vacuoles in myeloid and erythroid precursor cells. Inflammatory marker levels are very high: In the NIH series, the median C-reactive protein was 73 mg/L and median erythrocyte sedimentation rate was 97 mm/hr. The diagnosis of VEXAS can be confirmed by genetic testing performed by Dr. Beck and his NIH coworkers ([email protected]).
In interviews, Dr. Beck and Dr. Ferrada emphasized that management of VEXAS requires a multidisciplinary team of clinicians including rheumatologists, hematologists, and dermatologists.
Dr. Ferrada said that rheumatologists could suspect VEXAS in patients who have very high inflammatory markers and do not have a clear diagnosis or do not meet all criteria for other rheumatologic diseases, particularly in older men, but it’s possible in younger men as well. Hematologists could also consider VEXAS in patients with macrocytic anemia or macrocytosis without an explanation and inflammatory features, she said.
Dr. Ferrada, Dr. Beck, and colleagues also published a study in Arthritis & Rheumatology that presents a useful clinical algorithm for deciding whether to order genetic screening for VEXAS in patients with relapsing polychondritis.
First off, Dr. Ferrada and colleagues performed whole-exome sequencing and testing for UBA1 variants in an observational cohort of 92 relapsing polychondritis patients to determine the prevalence of VEXAS, which turned out to be 8%. They added an additional 6 patients with relapsing polychondritis and VEXAS from other cohorts, for a total of 13. The investigators determined that patients with VEXAS were older at disease onset, and more likely to have fever, ear chondritis, DVT, pulmonary infiltrates, skin involvement, and periorbital edema. In contrast, the RP cohort had a significantly higher prevalence of airway chondritis, joint involvement, and vestibular symptoms.
Dr. Ferrada’s algorithm for picking out VEXAS in patients who meet diagnostic criteria for relapsing polychondritis is based upon a few simple factors readily apparent in screening patient charts: male sex; age at onset older than 50 years; macrocytic anemia; and thrombocytopenia. Those four variables, when present, identify VEXAS within an RP cohort with 100% sensitivity and 96% specificity. “As we learn more about [VEXAS] and how it presents earlier, I think we are going to be able to find different manifestations or laboratory data that are going to allow us to diagnose these patients earlier,” she said. “The whole role of that algorithm was to guide clinicians who see patients with relapsing polychondritis to test these patients for the mutation, but I think over time that is going to evolve.”
Researchers are taking similar approaches for other clinical diagnoses to see which should be referred for UBA1 testing, Dr. Beck said.
Myelodysplastic syndrome and hematologic abnormalities
While patients with both myelodysplastic syndrome and relapsing polychondritis have been known in the literature for many years, it’s not until now that researchers are seeing a connection between the two, Dr. Ferrada said.
A majority of the VEXAS patients in the NEJM study had a workup for myelodysplastic syndrome, but only 24% met criteria. However, many were within the spectrum of myelodysplastic disease and some did not meet criteria because their anemia was attributed to a rheumatologic diagnosis and they did not have a known genetic driver of myelodysplastic syndrome, Dr. Beck said. It also fits with this new evidence that UBA1 is probably a driver of myelodysplastic syndrome in and of itself, and that anemia and hematologic involvement are not secondary to the rheumatologic disease; they are linked to the same disease process.
Dr. Beck said that there may be a subset of patients who present with primarily hematologic manifestations, noting the NEJM study could have ascertainment bias because the researchers analyzed mainly patients presenting to their clinic with relapsing polychondritis and severe inflammation. NIH researchers also are still looking in their cohort for any association with hematologic malignancies that preceded clinical manifestations, he said.
More cases reported
As of early April, another 27 cases had been reported in the literature as more researchers have begun to look for patients with UBA1 mutations, some with additional presenting clinical features associated with VEXAS, including chronic progressive inflammatory arthritis, Kikuchi-Fujimoto disease, spondyloarthritis, and bacterial pneumonia.
“Many times with rare diseases, we can’t get enough patients to understand the full spectrum of the disease, but this disease seems to be far more common than we would have expected. We’re actually getting many referrals,” Dr. Beck said.
It appears so far that the range of somatic UBA1 mutations that have been discovered in VEXAS patients does make a difference in the severity of clinical presentation and could potentially be useful in prognosis, Dr. Beck said.
Right now, NIH researchers are asking patients about their natural clinical course, assessing disease activity, and determining which treatments get a response, with the ultimate goal of a treatment trial at the NIH.
Treatment
Developing better treatments for VEXAS syndrome is a priority. In the initial report on VEXAS, the researchers found that the only reliably effective therapy is high-dose corticosteroids. Dr. Ferrada said that NIH investigators have begun thinking about agents that target both the hematologic and inflammatory features of VEXAS. “Most patients get exposed to treatments that are targeted to decrease the inflammatory process, and some of these treatments help partially but not completely to decrease the amount of steroids that patients are taking. For example, one of the medications is tocilizumab. [It was used in] patients who had previous diagnosis of relapsing polychondritis, but they still had to take steroids and their hematologic manifestations keep progressing. We’re in the process of figuring out medications that may help in treating both.” Dr. Ferrada added that because the source of the mutation is in the bone marrow, transplantation may be an effective option.
Laboratory work to identify potential treatments for VEXAS in studies of model organisms could identify treatments outside of the classic anti-inflammatory agents, such as targeting certain cell types in the bone marrow or the ubiquitin-proteasome pathway, Dr. Beck said. “We think that however UBA1 works to initiate inflammation may be important not just in VEXAS but in other diseases. Rare diseases may be informing the mechanisms in common diseases.”
The VEXAS NEJM study was sponsored by the NIH Intramural Research Programs and by an EU Horizon 2020 Research and Innovation Program grant. Dr. Beck reported a patent pending on “Diagnosis and Treatment of VEXAS with Mosaic Missense Mutations in UBA1.”