User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
‘My boss is my son’s age’: Age differences in medical practices
Morton J, MD, a 68-year-old cardiologist based in the Midwest, saw things become dramatically worse when his nine-physician practice was taken over by a large health system.
“Everything changed. My partners and I lost a lot of autonomy. We had a say – but not the final say-so in who we hired as medical assistants or receptionists. We had to change how long we spent with patients and justify procedures or tests – not just to the insurance companies, which is an old story, but to our new employer,” said Dr. J, who asked to remain anonymous.
Worst of all, “I had to report to a kid – a doctor in his 30s, someone young enough to be my son, someone with a fraction of the clinical training and experience I had but who now got to tell me what to do and how to run my practice.”
The “final straw” for Dr. J came when the practice had to change to a new electronic health record (EHR) system. “Learning this new system was like pulling teeth,” he said. His youthful supervisor was “obviously impatient and irritated – his whole attitude and demeanor reflected a sense that he was saddled with a dinosaur.”
After much anguishing and soul-searching, Dr. J decided to retire. “I was already close to retirement age, and I thought it would be nice to spend more time with my grandchildren. Feeling so disrespected was simply the catalyst that brought the decision to a head a couple of years sooner than I had planned.”
Getting through a delicate discussion
This unfortunate situation could have been avoided had the younger supervisor shown more sensitivity, says otolaryngologist Mark Wallace, DO.
Dr. Wallace is speaking from personal experience. Early in his career, he was a younger physician who was forced to discuss a practice management issue with an older physician.
Dr. Wallace was a member of a committee that was responsible for “maximizing the efficiency of good care, while still being aware of cost issues.” When the committee “wanted one of the physicians in the group to change their behavior to improve cost savings, it was my job to discuss that with them.”
Dr. Wallace, who today is a locum tenens physician and a medical practice consultant to Physicians Thrive – an advisory group that helps physicians with financial and practice management problems – recalls feeling uncomfortable about broaching the subject to his supervisee. In this case, the older physician was prescribing name brand medications, and the committee that appointed Dr. Wallace wanted him to encourage the physician to prescribe a generic medication first and reserve brand prescriptions only for cases in which the generic was ineffective.
He acknowledges that he thought the generic was equivalent to the branded product in safety and efficacy.
“I always felt this to be a delicate discussion, whatever the age of the physician, because I didn’t like the idea of telling a doctor that they have to change how they practice so as to save money. I would never want anyone to feel they’re providing a lower level of care.”
The fact that this was an older physician – in his 60s – compounded his hesitancy. “Older physicians have a lot more experience than what I had in my 30s,” Dr. Wallace said. “I could talk to them about studies and outcomes and things like that, but a large part of medicine is the experience you gain over time.
“I presented it simply as a cost issue raised by the committee and asked him to consider experimenting with changing his prescribing behavior, while emphasizing that ultimately, it was his decision,” says Dr. Wallace.
The supervisee understood the concern and agreed to the experiment. He ended up prescribing the generic more frequently, although perhaps not as frequently as the committee would have liked.
, says Ted Epperly, MD, a family physician in Boise, Idaho, and president and CEO of Family Medicine Residency of Idaho.
Dr. Wallace said that older physicians, on coming out of training, felt more respected, were better paid, and didn’t have to continually adjust to new regulations and new complicated insurance requirements. Today’s young physicians coming out of training may not find the practice of medicine as enjoyable as their older counterparts did, but they are accustomed to increasingly complex rules and regulations, so it’s less of an adjustment. But many may not feel they want to work 80 hours per week, as their older counterparts did.
Challenges of technology
Technology is one of the most central areas where intergenerational differences play out, says Tracy Clarke, chief human resources officer at Kitsap Mental Health Services, a large nonprofit organization in Bremerton, Wash., that employs roughly 500 individuals. “The younger physicians in our practice are really prepared, already engaged in technology, and used to using technology for documentation, and it is already integrated into the way they do business in general and practice,” she said.
Dr. Epperly noted that Gen X-ers are typically comfortable with digital technology, although not quite as much as the following generation, the millennials, who have grown up with smartphones and computers quite literally at their fingertips from earliest childhood.
Dr. Epperly, now 67, described the experience of having his organization convert to a new EHR system. “Although the younger physicians were not my supervisors, the dynamic that occurred when we were switching to the new system is typical of what might happen in a more formal reporting structure of older ‘supervisee’ and younger supervisor,” he said. In fact, his experience was similar to that of Dr. J.
“Some of the millennials were so quick to learn the new system that they forgot to check in with the older ones about how they were doing, or they were frustrated with our slow pace of learning the new technology,” said Dr. Epperly. “In fact, I was struggling to master it, and so were many others of my generation, and I felt very dumb, slow, and vulnerable, even though I usually regard myself as a pretty bright guy.”
Dr. Epperly encourages younger physicians not to think, “He’s asked me five times how to do this – what’s his problem?” This impatience can be intuited by the older physician, who may take it personally and feel devalued and disrespected.
Joy Engblade, an internal medicine physician and CMO of Northern Inyo Hospital, Bishop, Calif., said that when her institution was transitioning to a new EHR system this past May, she was worried that the older physicians would have the most difficulty.
Ironically, that turned out not to be the case. In fact, the younger physicians struggled more because the older physicians recognized their limitations and “were willing to do whatever we asked them to do. They watched the tutorials about how to use the new EHR. They went to every class that was offered and did all the practice sessions.” By contrast, many of the younger ones thought, “I know how to work an EHR, I’ve been doing it for years, so how hard could it be?” By the time they needed to actually use it, the instructional resources and tutorials were no longer available.
Dr. Epperly’s experience is different. He noted that some older physicians may be embarrassed to acknowledge that they are technologically challenged and may say, “I got it, I understand,” when they are still struggling to master the new technology.
Ms. Clarke notes that the leadership in her organization is younger than many of the physicians who report to them. “For the leadership, the biggest challenge is that many older physicians are set in their ways, and they haven’t really seen a reason to change their practice or ways of doing things.” For example, some still prefer paper charting or making voice recordings of patient visits for other people to transcribe.
Ms. Clarke has some advice for younger leaders: “Really explore what the pain points are of these older physicians. Beyond their saying, ‘because I’ve always done it this way,’ what really is the advantage of, for example, paper charting when using the EHR is more efficient?”
Daniel DeBehnke, MD, is an emergency medicine physician and vice president and chief physician executive for Premier Inc., where he helps hospitals improve quality, safety, and financial performance. Before joining Premier, he was both a practicing physician and CEO of a health system consisting of more than 1,500 physicians.
“Having been on both sides of the spectrum as manager/leader within a physician group, some of whom are senior to me and some of whom are junior, I can tell you that I have never had any issues related to the age gap.” In fact, it is less about age per se and more about “the expertise that you, as a manager, bring to the table in understanding the nuances of the medical practice and for the individual being ‘managed.’ It is about trusting the expertise of the manager.”
Before and after hourly caps
Dr. Engblade regards “generational” issues to be less about age and birth year and more about the cap on hours worked during residency.
Dr. Engblade, who is 45 years old, said she did her internship year with no hourly restrictions. Such restrictions only went into effect during her second year of residency. “This created a paradigm shift in how much people wanted to work and created a consciousness of work-life balance that hadn’t been part of the conversation before,” she said.
When she interviews an older physician, a typical response is, “Of course I’ll be available any time,” whereas younger physicians, who went through residency after hourly restrictions had been established, are more likely to ask how many hours they will be on and how many they’ll be off.
Matt Lambert, MD, an independent emergency medicine physician and CMO of Curation Health, Washington, agreed, noting that differences in the cap on hours during training “can create a bit of an undertow, a tension between younger managers who are better adjusted in terms of work-life balance and older physicians being managed, who have a different work ethic and also might regard their managers as being less trained because they put in fewer hours during training.”
It is also important to be cognizant of differences in style and priorities that each generation brings to the table. Jaciel Keltgen, PhD, assistant professor of business administration, Augustana University, Sioux Falls, S.D., has heard older physicians say, “We did this the hard way, we sacrificed for our organization, and we expect the same values of younger physicians.” The younger ones tend to say, “We need to use all the tools at our disposal, and medicine doesn’t have to be practiced the way it’s always been.”
Dr. Keltgen, whose PhD is in political science and who has studied public administration, said that younger physicians may also question the mores and protocols that older physicians take for granted. For example, when her physician son was beginning his career, he was told by his senior supervisors that although he was “performing beautifully as a physician, he needed to shave more frequently, wear his white coat more often, and introduce himself as ‘Doctor’ rather than by his first name. Although he did wear his white coat more often, he didn’t change how he introduced himself to patients.”
Flexibility and mutual understanding of each generation’s needs, the type, structure, and amount of training they underwent, and the prevailing values will smooth supervisory interactions and optimize outcomes, experts agree.
Every generation’s No. 1 concern
For her dissertation, Dr. Keltgen used a large dataset of physicians and sought to draw a predictive model by generation and gender as to what physicians were seeking in order to be satisfied in their careers. One “overwhelming finding” of her research into generational differences in physicians is that “every single generation and gender is there to promote the health of their patients, and providing excellent care is their No. 1 concern. That is the common focus and the foundation that everyone can build on.”
Dr. J agreed. “Had I felt like a valued collaborator, I might have made a different decision.” He has begun to consider reentering clinical practice, perhaps as locum tenens or on a part-time basis. “I don’t want to feel that I’ve been driven out of a field that I love. I will see if I can find some type of context where my experience will be valued and learn to bring myself up to speed with technology if necessary. I believe I still have much to offer patients, and I would like to find a context to do so.”
A version of this article first appeared on Medscape.com.
Morton J, MD, a 68-year-old cardiologist based in the Midwest, saw things become dramatically worse when his nine-physician practice was taken over by a large health system.
“Everything changed. My partners and I lost a lot of autonomy. We had a say – but not the final say-so in who we hired as medical assistants or receptionists. We had to change how long we spent with patients and justify procedures or tests – not just to the insurance companies, which is an old story, but to our new employer,” said Dr. J, who asked to remain anonymous.
Worst of all, “I had to report to a kid – a doctor in his 30s, someone young enough to be my son, someone with a fraction of the clinical training and experience I had but who now got to tell me what to do and how to run my practice.”
The “final straw” for Dr. J came when the practice had to change to a new electronic health record (EHR) system. “Learning this new system was like pulling teeth,” he said. His youthful supervisor was “obviously impatient and irritated – his whole attitude and demeanor reflected a sense that he was saddled with a dinosaur.”
After much anguishing and soul-searching, Dr. J decided to retire. “I was already close to retirement age, and I thought it would be nice to spend more time with my grandchildren. Feeling so disrespected was simply the catalyst that brought the decision to a head a couple of years sooner than I had planned.”
Getting through a delicate discussion
This unfortunate situation could have been avoided had the younger supervisor shown more sensitivity, says otolaryngologist Mark Wallace, DO.
Dr. Wallace is speaking from personal experience. Early in his career, he was a younger physician who was forced to discuss a practice management issue with an older physician.
Dr. Wallace was a member of a committee that was responsible for “maximizing the efficiency of good care, while still being aware of cost issues.” When the committee “wanted one of the physicians in the group to change their behavior to improve cost savings, it was my job to discuss that with them.”
Dr. Wallace, who today is a locum tenens physician and a medical practice consultant to Physicians Thrive – an advisory group that helps physicians with financial and practice management problems – recalls feeling uncomfortable about broaching the subject to his supervisee. In this case, the older physician was prescribing name brand medications, and the committee that appointed Dr. Wallace wanted him to encourage the physician to prescribe a generic medication first and reserve brand prescriptions only for cases in which the generic was ineffective.
He acknowledges that he thought the generic was equivalent to the branded product in safety and efficacy.
“I always felt this to be a delicate discussion, whatever the age of the physician, because I didn’t like the idea of telling a doctor that they have to change how they practice so as to save money. I would never want anyone to feel they’re providing a lower level of care.”
The fact that this was an older physician – in his 60s – compounded his hesitancy. “Older physicians have a lot more experience than what I had in my 30s,” Dr. Wallace said. “I could talk to them about studies and outcomes and things like that, but a large part of medicine is the experience you gain over time.
“I presented it simply as a cost issue raised by the committee and asked him to consider experimenting with changing his prescribing behavior, while emphasizing that ultimately, it was his decision,” says Dr. Wallace.
The supervisee understood the concern and agreed to the experiment. He ended up prescribing the generic more frequently, although perhaps not as frequently as the committee would have liked.
, says Ted Epperly, MD, a family physician in Boise, Idaho, and president and CEO of Family Medicine Residency of Idaho.
Dr. Wallace said that older physicians, on coming out of training, felt more respected, were better paid, and didn’t have to continually adjust to new regulations and new complicated insurance requirements. Today’s young physicians coming out of training may not find the practice of medicine as enjoyable as their older counterparts did, but they are accustomed to increasingly complex rules and regulations, so it’s less of an adjustment. But many may not feel they want to work 80 hours per week, as their older counterparts did.
Challenges of technology
Technology is one of the most central areas where intergenerational differences play out, says Tracy Clarke, chief human resources officer at Kitsap Mental Health Services, a large nonprofit organization in Bremerton, Wash., that employs roughly 500 individuals. “The younger physicians in our practice are really prepared, already engaged in technology, and used to using technology for documentation, and it is already integrated into the way they do business in general and practice,” she said.
Dr. Epperly noted that Gen X-ers are typically comfortable with digital technology, although not quite as much as the following generation, the millennials, who have grown up with smartphones and computers quite literally at their fingertips from earliest childhood.
Dr. Epperly, now 67, described the experience of having his organization convert to a new EHR system. “Although the younger physicians were not my supervisors, the dynamic that occurred when we were switching to the new system is typical of what might happen in a more formal reporting structure of older ‘supervisee’ and younger supervisor,” he said. In fact, his experience was similar to that of Dr. J.
“Some of the millennials were so quick to learn the new system that they forgot to check in with the older ones about how they were doing, or they were frustrated with our slow pace of learning the new technology,” said Dr. Epperly. “In fact, I was struggling to master it, and so were many others of my generation, and I felt very dumb, slow, and vulnerable, even though I usually regard myself as a pretty bright guy.”
Dr. Epperly encourages younger physicians not to think, “He’s asked me five times how to do this – what’s his problem?” This impatience can be intuited by the older physician, who may take it personally and feel devalued and disrespected.
Joy Engblade, an internal medicine physician and CMO of Northern Inyo Hospital, Bishop, Calif., said that when her institution was transitioning to a new EHR system this past May, she was worried that the older physicians would have the most difficulty.
Ironically, that turned out not to be the case. In fact, the younger physicians struggled more because the older physicians recognized their limitations and “were willing to do whatever we asked them to do. They watched the tutorials about how to use the new EHR. They went to every class that was offered and did all the practice sessions.” By contrast, many of the younger ones thought, “I know how to work an EHR, I’ve been doing it for years, so how hard could it be?” By the time they needed to actually use it, the instructional resources and tutorials were no longer available.
Dr. Epperly’s experience is different. He noted that some older physicians may be embarrassed to acknowledge that they are technologically challenged and may say, “I got it, I understand,” when they are still struggling to master the new technology.
Ms. Clarke notes that the leadership in her organization is younger than many of the physicians who report to them. “For the leadership, the biggest challenge is that many older physicians are set in their ways, and they haven’t really seen a reason to change their practice or ways of doing things.” For example, some still prefer paper charting or making voice recordings of patient visits for other people to transcribe.
Ms. Clarke has some advice for younger leaders: “Really explore what the pain points are of these older physicians. Beyond their saying, ‘because I’ve always done it this way,’ what really is the advantage of, for example, paper charting when using the EHR is more efficient?”
Daniel DeBehnke, MD, is an emergency medicine physician and vice president and chief physician executive for Premier Inc., where he helps hospitals improve quality, safety, and financial performance. Before joining Premier, he was both a practicing physician and CEO of a health system consisting of more than 1,500 physicians.
“Having been on both sides of the spectrum as manager/leader within a physician group, some of whom are senior to me and some of whom are junior, I can tell you that I have never had any issues related to the age gap.” In fact, it is less about age per se and more about “the expertise that you, as a manager, bring to the table in understanding the nuances of the medical practice and for the individual being ‘managed.’ It is about trusting the expertise of the manager.”
Before and after hourly caps
Dr. Engblade regards “generational” issues to be less about age and birth year and more about the cap on hours worked during residency.
Dr. Engblade, who is 45 years old, said she did her internship year with no hourly restrictions. Such restrictions only went into effect during her second year of residency. “This created a paradigm shift in how much people wanted to work and created a consciousness of work-life balance that hadn’t been part of the conversation before,” she said.
When she interviews an older physician, a typical response is, “Of course I’ll be available any time,” whereas younger physicians, who went through residency after hourly restrictions had been established, are more likely to ask how many hours they will be on and how many they’ll be off.
Matt Lambert, MD, an independent emergency medicine physician and CMO of Curation Health, Washington, agreed, noting that differences in the cap on hours during training “can create a bit of an undertow, a tension between younger managers who are better adjusted in terms of work-life balance and older physicians being managed, who have a different work ethic and also might regard their managers as being less trained because they put in fewer hours during training.”
It is also important to be cognizant of differences in style and priorities that each generation brings to the table. Jaciel Keltgen, PhD, assistant professor of business administration, Augustana University, Sioux Falls, S.D., has heard older physicians say, “We did this the hard way, we sacrificed for our organization, and we expect the same values of younger physicians.” The younger ones tend to say, “We need to use all the tools at our disposal, and medicine doesn’t have to be practiced the way it’s always been.”
Dr. Keltgen, whose PhD is in political science and who has studied public administration, said that younger physicians may also question the mores and protocols that older physicians take for granted. For example, when her physician son was beginning his career, he was told by his senior supervisors that although he was “performing beautifully as a physician, he needed to shave more frequently, wear his white coat more often, and introduce himself as ‘Doctor’ rather than by his first name. Although he did wear his white coat more often, he didn’t change how he introduced himself to patients.”
Flexibility and mutual understanding of each generation’s needs, the type, structure, and amount of training they underwent, and the prevailing values will smooth supervisory interactions and optimize outcomes, experts agree.
Every generation’s No. 1 concern
For her dissertation, Dr. Keltgen used a large dataset of physicians and sought to draw a predictive model by generation and gender as to what physicians were seeking in order to be satisfied in their careers. One “overwhelming finding” of her research into generational differences in physicians is that “every single generation and gender is there to promote the health of their patients, and providing excellent care is their No. 1 concern. That is the common focus and the foundation that everyone can build on.”
Dr. J agreed. “Had I felt like a valued collaborator, I might have made a different decision.” He has begun to consider reentering clinical practice, perhaps as locum tenens or on a part-time basis. “I don’t want to feel that I’ve been driven out of a field that I love. I will see if I can find some type of context where my experience will be valued and learn to bring myself up to speed with technology if necessary. I believe I still have much to offer patients, and I would like to find a context to do so.”
A version of this article first appeared on Medscape.com.
Morton J, MD, a 68-year-old cardiologist based in the Midwest, saw things become dramatically worse when his nine-physician practice was taken over by a large health system.
“Everything changed. My partners and I lost a lot of autonomy. We had a say – but not the final say-so in who we hired as medical assistants or receptionists. We had to change how long we spent with patients and justify procedures or tests – not just to the insurance companies, which is an old story, but to our new employer,” said Dr. J, who asked to remain anonymous.
Worst of all, “I had to report to a kid – a doctor in his 30s, someone young enough to be my son, someone with a fraction of the clinical training and experience I had but who now got to tell me what to do and how to run my practice.”
The “final straw” for Dr. J came when the practice had to change to a new electronic health record (EHR) system. “Learning this new system was like pulling teeth,” he said. His youthful supervisor was “obviously impatient and irritated – his whole attitude and demeanor reflected a sense that he was saddled with a dinosaur.”
After much anguishing and soul-searching, Dr. J decided to retire. “I was already close to retirement age, and I thought it would be nice to spend more time with my grandchildren. Feeling so disrespected was simply the catalyst that brought the decision to a head a couple of years sooner than I had planned.”
Getting through a delicate discussion
This unfortunate situation could have been avoided had the younger supervisor shown more sensitivity, says otolaryngologist Mark Wallace, DO.
Dr. Wallace is speaking from personal experience. Early in his career, he was a younger physician who was forced to discuss a practice management issue with an older physician.
Dr. Wallace was a member of a committee that was responsible for “maximizing the efficiency of good care, while still being aware of cost issues.” When the committee “wanted one of the physicians in the group to change their behavior to improve cost savings, it was my job to discuss that with them.”
Dr. Wallace, who today is a locum tenens physician and a medical practice consultant to Physicians Thrive – an advisory group that helps physicians with financial and practice management problems – recalls feeling uncomfortable about broaching the subject to his supervisee. In this case, the older physician was prescribing name brand medications, and the committee that appointed Dr. Wallace wanted him to encourage the physician to prescribe a generic medication first and reserve brand prescriptions only for cases in which the generic was ineffective.
He acknowledges that he thought the generic was equivalent to the branded product in safety and efficacy.
“I always felt this to be a delicate discussion, whatever the age of the physician, because I didn’t like the idea of telling a doctor that they have to change how they practice so as to save money. I would never want anyone to feel they’re providing a lower level of care.”
The fact that this was an older physician – in his 60s – compounded his hesitancy. “Older physicians have a lot more experience than what I had in my 30s,” Dr. Wallace said. “I could talk to them about studies and outcomes and things like that, but a large part of medicine is the experience you gain over time.
“I presented it simply as a cost issue raised by the committee and asked him to consider experimenting with changing his prescribing behavior, while emphasizing that ultimately, it was his decision,” says Dr. Wallace.
The supervisee understood the concern and agreed to the experiment. He ended up prescribing the generic more frequently, although perhaps not as frequently as the committee would have liked.
, says Ted Epperly, MD, a family physician in Boise, Idaho, and president and CEO of Family Medicine Residency of Idaho.
Dr. Wallace said that older physicians, on coming out of training, felt more respected, were better paid, and didn’t have to continually adjust to new regulations and new complicated insurance requirements. Today’s young physicians coming out of training may not find the practice of medicine as enjoyable as their older counterparts did, but they are accustomed to increasingly complex rules and regulations, so it’s less of an adjustment. But many may not feel they want to work 80 hours per week, as their older counterparts did.
Challenges of technology
Technology is one of the most central areas where intergenerational differences play out, says Tracy Clarke, chief human resources officer at Kitsap Mental Health Services, a large nonprofit organization in Bremerton, Wash., that employs roughly 500 individuals. “The younger physicians in our practice are really prepared, already engaged in technology, and used to using technology for documentation, and it is already integrated into the way they do business in general and practice,” she said.
Dr. Epperly noted that Gen X-ers are typically comfortable with digital technology, although not quite as much as the following generation, the millennials, who have grown up with smartphones and computers quite literally at their fingertips from earliest childhood.
Dr. Epperly, now 67, described the experience of having his organization convert to a new EHR system. “Although the younger physicians were not my supervisors, the dynamic that occurred when we were switching to the new system is typical of what might happen in a more formal reporting structure of older ‘supervisee’ and younger supervisor,” he said. In fact, his experience was similar to that of Dr. J.
“Some of the millennials were so quick to learn the new system that they forgot to check in with the older ones about how they were doing, or they were frustrated with our slow pace of learning the new technology,” said Dr. Epperly. “In fact, I was struggling to master it, and so were many others of my generation, and I felt very dumb, slow, and vulnerable, even though I usually regard myself as a pretty bright guy.”
Dr. Epperly encourages younger physicians not to think, “He’s asked me five times how to do this – what’s his problem?” This impatience can be intuited by the older physician, who may take it personally and feel devalued and disrespected.
Joy Engblade, an internal medicine physician and CMO of Northern Inyo Hospital, Bishop, Calif., said that when her institution was transitioning to a new EHR system this past May, she was worried that the older physicians would have the most difficulty.
Ironically, that turned out not to be the case. In fact, the younger physicians struggled more because the older physicians recognized their limitations and “were willing to do whatever we asked them to do. They watched the tutorials about how to use the new EHR. They went to every class that was offered and did all the practice sessions.” By contrast, many of the younger ones thought, “I know how to work an EHR, I’ve been doing it for years, so how hard could it be?” By the time they needed to actually use it, the instructional resources and tutorials were no longer available.
Dr. Epperly’s experience is different. He noted that some older physicians may be embarrassed to acknowledge that they are technologically challenged and may say, “I got it, I understand,” when they are still struggling to master the new technology.
Ms. Clarke notes that the leadership in her organization is younger than many of the physicians who report to them. “For the leadership, the biggest challenge is that many older physicians are set in their ways, and they haven’t really seen a reason to change their practice or ways of doing things.” For example, some still prefer paper charting or making voice recordings of patient visits for other people to transcribe.
Ms. Clarke has some advice for younger leaders: “Really explore what the pain points are of these older physicians. Beyond their saying, ‘because I’ve always done it this way,’ what really is the advantage of, for example, paper charting when using the EHR is more efficient?”
Daniel DeBehnke, MD, is an emergency medicine physician and vice president and chief physician executive for Premier Inc., where he helps hospitals improve quality, safety, and financial performance. Before joining Premier, he was both a practicing physician and CEO of a health system consisting of more than 1,500 physicians.
“Having been on both sides of the spectrum as manager/leader within a physician group, some of whom are senior to me and some of whom are junior, I can tell you that I have never had any issues related to the age gap.” In fact, it is less about age per se and more about “the expertise that you, as a manager, bring to the table in understanding the nuances of the medical practice and for the individual being ‘managed.’ It is about trusting the expertise of the manager.”
Before and after hourly caps
Dr. Engblade regards “generational” issues to be less about age and birth year and more about the cap on hours worked during residency.
Dr. Engblade, who is 45 years old, said she did her internship year with no hourly restrictions. Such restrictions only went into effect during her second year of residency. “This created a paradigm shift in how much people wanted to work and created a consciousness of work-life balance that hadn’t been part of the conversation before,” she said.
When she interviews an older physician, a typical response is, “Of course I’ll be available any time,” whereas younger physicians, who went through residency after hourly restrictions had been established, are more likely to ask how many hours they will be on and how many they’ll be off.
Matt Lambert, MD, an independent emergency medicine physician and CMO of Curation Health, Washington, agreed, noting that differences in the cap on hours during training “can create a bit of an undertow, a tension between younger managers who are better adjusted in terms of work-life balance and older physicians being managed, who have a different work ethic and also might regard their managers as being less trained because they put in fewer hours during training.”
It is also important to be cognizant of differences in style and priorities that each generation brings to the table. Jaciel Keltgen, PhD, assistant professor of business administration, Augustana University, Sioux Falls, S.D., has heard older physicians say, “We did this the hard way, we sacrificed for our organization, and we expect the same values of younger physicians.” The younger ones tend to say, “We need to use all the tools at our disposal, and medicine doesn’t have to be practiced the way it’s always been.”
Dr. Keltgen, whose PhD is in political science and who has studied public administration, said that younger physicians may also question the mores and protocols that older physicians take for granted. For example, when her physician son was beginning his career, he was told by his senior supervisors that although he was “performing beautifully as a physician, he needed to shave more frequently, wear his white coat more often, and introduce himself as ‘Doctor’ rather than by his first name. Although he did wear his white coat more often, he didn’t change how he introduced himself to patients.”
Flexibility and mutual understanding of each generation’s needs, the type, structure, and amount of training they underwent, and the prevailing values will smooth supervisory interactions and optimize outcomes, experts agree.
Every generation’s No. 1 concern
For her dissertation, Dr. Keltgen used a large dataset of physicians and sought to draw a predictive model by generation and gender as to what physicians were seeking in order to be satisfied in their careers. One “overwhelming finding” of her research into generational differences in physicians is that “every single generation and gender is there to promote the health of their patients, and providing excellent care is their No. 1 concern. That is the common focus and the foundation that everyone can build on.”
Dr. J agreed. “Had I felt like a valued collaborator, I might have made a different decision.” He has begun to consider reentering clinical practice, perhaps as locum tenens or on a part-time basis. “I don’t want to feel that I’ve been driven out of a field that I love. I will see if I can find some type of context where my experience will be valued and learn to bring myself up to speed with technology if necessary. I believe I still have much to offer patients, and I would like to find a context to do so.”
A version of this article first appeared on Medscape.com.
Boring is good. Boring is right. Boring is … interesting
Can you keep it down? I’m trying to be boring
He chides his friends for not looking both ways before crossing the road. He is never questioned by the police because they fall asleep listening to him talk. He has won the office’s coveted perfect attendance award 10 years running. Look out, Dos Equis guy, you’ve got some new competition. That’s right, it’s the most boring man in the world.
For this boring study (sorry, study on boredom) conducted by English researchers and published in Personality and Social Psychology Bulletin, people were surveyed on various jobs and hobbies, ranking them by how exciting or boring they are, as well as how competent someone with those jobs/hobbies would be, their willingness to avoid someone with those jobs/hobbies, and how much they’d need to be paid to spend time with someone who had an undesirable job/hobby.
According to the British public, the most boring person in the world is a religious data analyst who likes to sleep and lives in a small town. In fact, spending time with this person is almost a full-time job on its own: To make it worth their while, survey subjects wanted 35 pounds a day. The boring person also was viewed as less competent, as is anyone with a boring job.
Now, there probably aren’t a lot of religious data analysts out there, but don’t worry, there are plenty of other boring jobs – accounting, tax/insurance, cleaning, and banking rounded out the top five (apparently people don’t like finances) – and hobbies – watching TV, observing animals, and mathematics filled out the top five. In case you’re curious, performing artists, scientists, journalists, health professionals, and teachers were viewed as having exciting jobs; exciting hobbies included gaming, reading, domestic tasks (really?), gardening, and writing.
Lead researcher Wijnand Van Tilburg, PhD, made an excellent point about people with boring jobs: They “have power in society – perhaps we should try not to upset them and stereotype them as boring!”
We think they should lean into it and make The Most Boring Man in the World ads: “When I drive a car off the lot, its value increases because I used the correct lending association. Batman trusts me with his Batmobile insurance. I can make those Cuban cigars tax exempt. Stay financially solvent, my friends.”
Fungi, but make it fashion
Fashion is an expensive and costly industry to sustain. Cotton production takes a toll on the environment, leather production comes with environmental and ethical/moral conundrums, and thanks to fast fashion, about 85% of textiles are being thrown away in the United States.
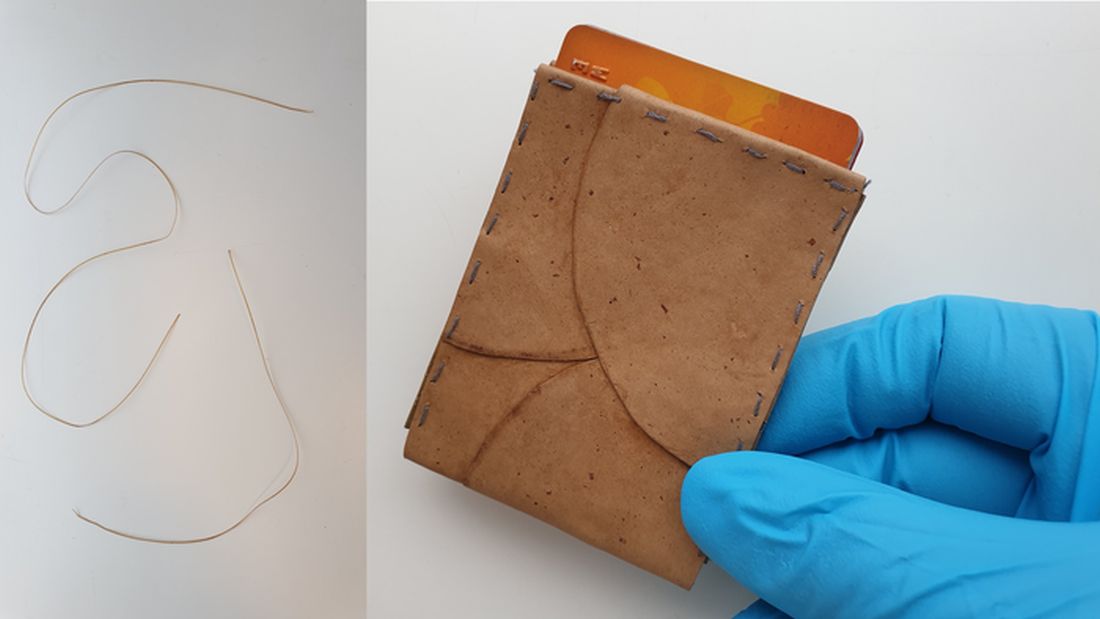
Researchers at the University of Borås in Sweden, however, have found a newish solution to create leather, cotton, and other textiles. And as with so many of the finer things, it starts with unsold bread from the grocery store.
Akram Zamani, PhD, and her team take that bread and turn it into breadcrumbs, then combine it with water and Rhizopus delemar, a fungus typically found in decaying food. After a couple of days of feasting on the bread, the fungus produces natural fibers made of chitin and chitosan that accumulate in the cell walls. After proteins, lipids, and other byproducts are removed, the team is left with a jelly-like substance made of those fibrous cell walls that can be spun into a fabric.
The researchers started small with very thin nonpliable sheets, but with a little layering by using tree tannins for softness and alkali for strength, their fungal leather is more like real leather than competing fungal leathers. Not to mention its being able to be produced in a fraction of the time.
This new fungal leather is fast to produce, it’s biodegradable, and it uses only natural ingredients to treat the materials. It’s the ultimate environmental fashion statement.
Who’s afraid of cancer? Not C. elegans
And now, we bring you part 2 of our ongoing series: Creatures that can diagnose cancer. Last week, we discovered that ants are well on their way to replacing dogs in our medical labs and in our hearts. This week, we present the even-more-lovable nematode.
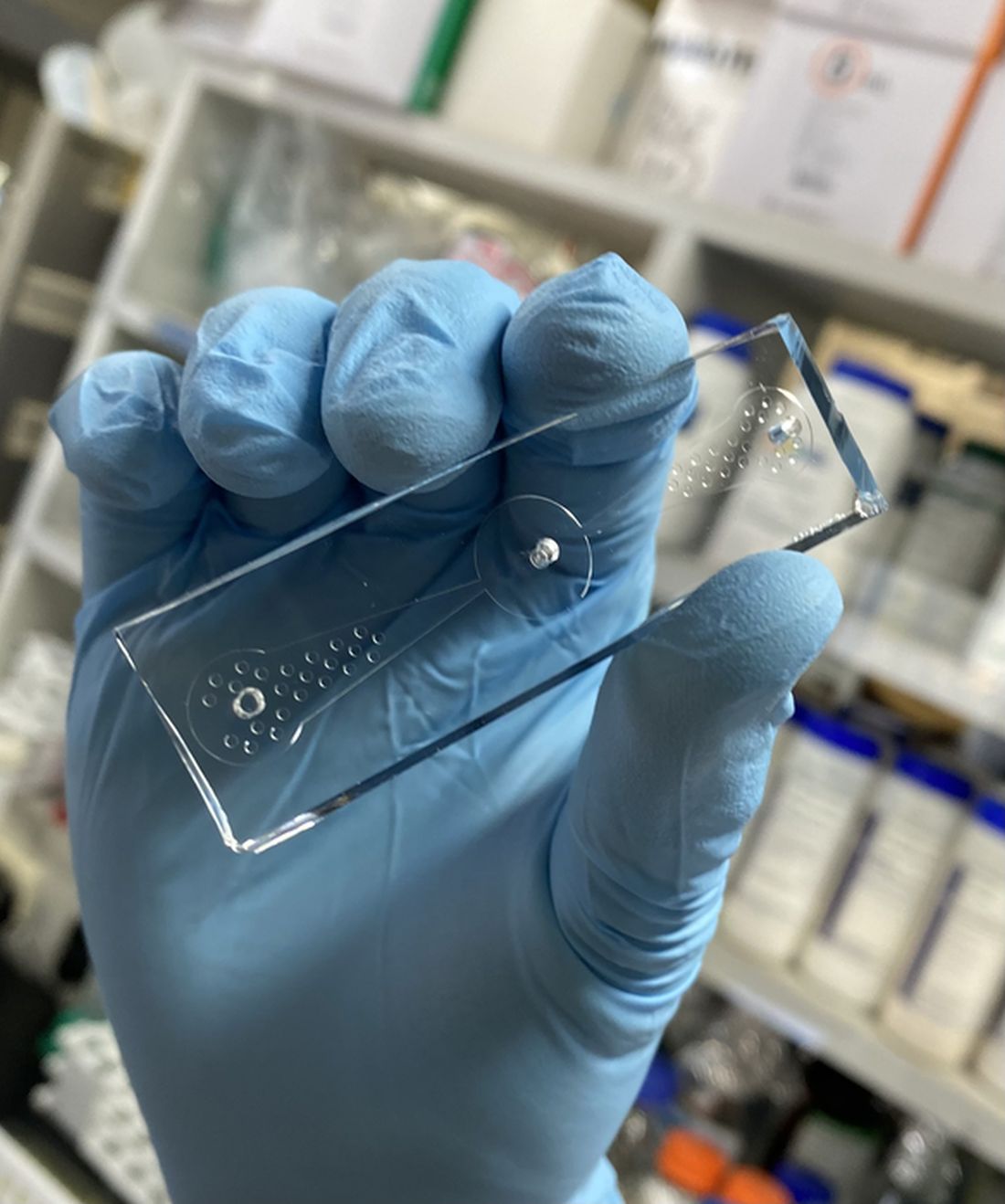
The soil-dwelling nematode Caenorhabditis elegans, which is less than 1 mm long, is known to be “attracted or repelled by certain odors, so we came up with an idea that the roundworm could be used to detect lung cancer,” Shin Sik Choi, PhD, of Myongji University in South Korea, who is the project’s principal investigator, said in a statement on Eurekalert.
Dr. Choi’s team created a “worm-on-a-chip” that allowed the nematodes to choose between a drop of culture media from lung cancer cells and media from normal lung fibroblasts. An hour after being placed in the chip’s central chamber, more nematodes had crawled toward the lung cancer media than the normal-cell sample.
The investigators estimate that the device is about 70% effective at detecting cancer cells, but “they hope to increase both the accuracy and sensitivity of the method by using worms that were previously exposed to cancer cell media and therefore have a ‘memory’ of cancer-specific odor molecules,” according to the statement from the American Chemical Society.
Since C. elegans is easy to grow in a lab and, apparently, easy to train, the researchers hope that the worm-on-a-chip can become a quick, easy, economical, and noninvasive cancer screen.
So watch out cancer, because we never bet against the creepy crawlies.
Mosquitoes have us figured out
We are nearing mosquito season; quite possibly the most annoying and itchy time of the year. We stock up on bottles of bug spray, but somehow we still get bite after bite. It appears that mosquitoes are basically able to ignore our bug sprays, which explains why we’re still covered in bites after the Fourth of July fireworks. It turns out mosquitoes are more complex than we thought for such tiny creatures.

There’s plenty of research on the best ways to keep mosquitoes away, because not only are they incredibly annoying, but they also carry potentially harmful diseases. In a recent experiment, researchers used mosquitoes that were genetically modified to have an excessive amount of an odor receptor called AgOR2, which responds to the smell of humans.
“AgOR2 overexpression threw a wrench in the whole system by inactivating olfactory receptors in these mosquitoes,” Christopher Potter, PhD, associate professor of neuroscience at Johns Hopkins University, said in a written statement.
After testing how these genetically modified mosquitoes reacted to some of the common smells of bug spray such as lemongrass, they discovered that it’s easy for the mosquitoes to ignore the smell. We wish it were that easy for us to ignore that chemically fruity smell.
Researchers continue to work hard to figure out how to repel mosquitoes and we’re rooting for them as summer approaches, despite the mosquito’s status as a creepy crawly.
Can you keep it down? I’m trying to be boring
He chides his friends for not looking both ways before crossing the road. He is never questioned by the police because they fall asleep listening to him talk. He has won the office’s coveted perfect attendance award 10 years running. Look out, Dos Equis guy, you’ve got some new competition. That’s right, it’s the most boring man in the world.
For this boring study (sorry, study on boredom) conducted by English researchers and published in Personality and Social Psychology Bulletin, people were surveyed on various jobs and hobbies, ranking them by how exciting or boring they are, as well as how competent someone with those jobs/hobbies would be, their willingness to avoid someone with those jobs/hobbies, and how much they’d need to be paid to spend time with someone who had an undesirable job/hobby.
According to the British public, the most boring person in the world is a religious data analyst who likes to sleep and lives in a small town. In fact, spending time with this person is almost a full-time job on its own: To make it worth their while, survey subjects wanted 35 pounds a day. The boring person also was viewed as less competent, as is anyone with a boring job.
Now, there probably aren’t a lot of religious data analysts out there, but don’t worry, there are plenty of other boring jobs – accounting, tax/insurance, cleaning, and banking rounded out the top five (apparently people don’t like finances) – and hobbies – watching TV, observing animals, and mathematics filled out the top five. In case you’re curious, performing artists, scientists, journalists, health professionals, and teachers were viewed as having exciting jobs; exciting hobbies included gaming, reading, domestic tasks (really?), gardening, and writing.
Lead researcher Wijnand Van Tilburg, PhD, made an excellent point about people with boring jobs: They “have power in society – perhaps we should try not to upset them and stereotype them as boring!”
We think they should lean into it and make The Most Boring Man in the World ads: “When I drive a car off the lot, its value increases because I used the correct lending association. Batman trusts me with his Batmobile insurance. I can make those Cuban cigars tax exempt. Stay financially solvent, my friends.”
Fungi, but make it fashion
Fashion is an expensive and costly industry to sustain. Cotton production takes a toll on the environment, leather production comes with environmental and ethical/moral conundrums, and thanks to fast fashion, about 85% of textiles are being thrown away in the United States.
Researchers at the University of Borås in Sweden, however, have found a newish solution to create leather, cotton, and other textiles. And as with so many of the finer things, it starts with unsold bread from the grocery store.
Akram Zamani, PhD, and her team take that bread and turn it into breadcrumbs, then combine it with water and Rhizopus delemar, a fungus typically found in decaying food. After a couple of days of feasting on the bread, the fungus produces natural fibers made of chitin and chitosan that accumulate in the cell walls. After proteins, lipids, and other byproducts are removed, the team is left with a jelly-like substance made of those fibrous cell walls that can be spun into a fabric.
The researchers started small with very thin nonpliable sheets, but with a little layering by using tree tannins for softness and alkali for strength, their fungal leather is more like real leather than competing fungal leathers. Not to mention its being able to be produced in a fraction of the time.
This new fungal leather is fast to produce, it’s biodegradable, and it uses only natural ingredients to treat the materials. It’s the ultimate environmental fashion statement.
Who’s afraid of cancer? Not C. elegans
And now, we bring you part 2 of our ongoing series: Creatures that can diagnose cancer. Last week, we discovered that ants are well on their way to replacing dogs in our medical labs and in our hearts. This week, we present the even-more-lovable nematode.
The soil-dwelling nematode Caenorhabditis elegans, which is less than 1 mm long, is known to be “attracted or repelled by certain odors, so we came up with an idea that the roundworm could be used to detect lung cancer,” Shin Sik Choi, PhD, of Myongji University in South Korea, who is the project’s principal investigator, said in a statement on Eurekalert.
Dr. Choi’s team created a “worm-on-a-chip” that allowed the nematodes to choose between a drop of culture media from lung cancer cells and media from normal lung fibroblasts. An hour after being placed in the chip’s central chamber, more nematodes had crawled toward the lung cancer media than the normal-cell sample.
The investigators estimate that the device is about 70% effective at detecting cancer cells, but “they hope to increase both the accuracy and sensitivity of the method by using worms that were previously exposed to cancer cell media and therefore have a ‘memory’ of cancer-specific odor molecules,” according to the statement from the American Chemical Society.
Since C. elegans is easy to grow in a lab and, apparently, easy to train, the researchers hope that the worm-on-a-chip can become a quick, easy, economical, and noninvasive cancer screen.
So watch out cancer, because we never bet against the creepy crawlies.
Mosquitoes have us figured out
We are nearing mosquito season; quite possibly the most annoying and itchy time of the year. We stock up on bottles of bug spray, but somehow we still get bite after bite. It appears that mosquitoes are basically able to ignore our bug sprays, which explains why we’re still covered in bites after the Fourth of July fireworks. It turns out mosquitoes are more complex than we thought for such tiny creatures.
There’s plenty of research on the best ways to keep mosquitoes away, because not only are they incredibly annoying, but they also carry potentially harmful diseases. In a recent experiment, researchers used mosquitoes that were genetically modified to have an excessive amount of an odor receptor called AgOR2, which responds to the smell of humans.
“AgOR2 overexpression threw a wrench in the whole system by inactivating olfactory receptors in these mosquitoes,” Christopher Potter, PhD, associate professor of neuroscience at Johns Hopkins University, said in a written statement.
After testing how these genetically modified mosquitoes reacted to some of the common smells of bug spray such as lemongrass, they discovered that it’s easy for the mosquitoes to ignore the smell. We wish it were that easy for us to ignore that chemically fruity smell.
Researchers continue to work hard to figure out how to repel mosquitoes and we’re rooting for them as summer approaches, despite the mosquito’s status as a creepy crawly.
Can you keep it down? I’m trying to be boring
He chides his friends for not looking both ways before crossing the road. He is never questioned by the police because they fall asleep listening to him talk. He has won the office’s coveted perfect attendance award 10 years running. Look out, Dos Equis guy, you’ve got some new competition. That’s right, it’s the most boring man in the world.
For this boring study (sorry, study on boredom) conducted by English researchers and published in Personality and Social Psychology Bulletin, people were surveyed on various jobs and hobbies, ranking them by how exciting or boring they are, as well as how competent someone with those jobs/hobbies would be, their willingness to avoid someone with those jobs/hobbies, and how much they’d need to be paid to spend time with someone who had an undesirable job/hobby.
According to the British public, the most boring person in the world is a religious data analyst who likes to sleep and lives in a small town. In fact, spending time with this person is almost a full-time job on its own: To make it worth their while, survey subjects wanted 35 pounds a day. The boring person also was viewed as less competent, as is anyone with a boring job.
Now, there probably aren’t a lot of religious data analysts out there, but don’t worry, there are plenty of other boring jobs – accounting, tax/insurance, cleaning, and banking rounded out the top five (apparently people don’t like finances) – and hobbies – watching TV, observing animals, and mathematics filled out the top five. In case you’re curious, performing artists, scientists, journalists, health professionals, and teachers were viewed as having exciting jobs; exciting hobbies included gaming, reading, domestic tasks (really?), gardening, and writing.
Lead researcher Wijnand Van Tilburg, PhD, made an excellent point about people with boring jobs: They “have power in society – perhaps we should try not to upset them and stereotype them as boring!”
We think they should lean into it and make The Most Boring Man in the World ads: “When I drive a car off the lot, its value increases because I used the correct lending association. Batman trusts me with his Batmobile insurance. I can make those Cuban cigars tax exempt. Stay financially solvent, my friends.”
Fungi, but make it fashion
Fashion is an expensive and costly industry to sustain. Cotton production takes a toll on the environment, leather production comes with environmental and ethical/moral conundrums, and thanks to fast fashion, about 85% of textiles are being thrown away in the United States.
Researchers at the University of Borås in Sweden, however, have found a newish solution to create leather, cotton, and other textiles. And as with so many of the finer things, it starts with unsold bread from the grocery store.
Akram Zamani, PhD, and her team take that bread and turn it into breadcrumbs, then combine it with water and Rhizopus delemar, a fungus typically found in decaying food. After a couple of days of feasting on the bread, the fungus produces natural fibers made of chitin and chitosan that accumulate in the cell walls. After proteins, lipids, and other byproducts are removed, the team is left with a jelly-like substance made of those fibrous cell walls that can be spun into a fabric.
The researchers started small with very thin nonpliable sheets, but with a little layering by using tree tannins for softness and alkali for strength, their fungal leather is more like real leather than competing fungal leathers. Not to mention its being able to be produced in a fraction of the time.
This new fungal leather is fast to produce, it’s biodegradable, and it uses only natural ingredients to treat the materials. It’s the ultimate environmental fashion statement.
Who’s afraid of cancer? Not C. elegans
And now, we bring you part 2 of our ongoing series: Creatures that can diagnose cancer. Last week, we discovered that ants are well on their way to replacing dogs in our medical labs and in our hearts. This week, we present the even-more-lovable nematode.
The soil-dwelling nematode Caenorhabditis elegans, which is less than 1 mm long, is known to be “attracted or repelled by certain odors, so we came up with an idea that the roundworm could be used to detect lung cancer,” Shin Sik Choi, PhD, of Myongji University in South Korea, who is the project’s principal investigator, said in a statement on Eurekalert.
Dr. Choi’s team created a “worm-on-a-chip” that allowed the nematodes to choose between a drop of culture media from lung cancer cells and media from normal lung fibroblasts. An hour after being placed in the chip’s central chamber, more nematodes had crawled toward the lung cancer media than the normal-cell sample.
The investigators estimate that the device is about 70% effective at detecting cancer cells, but “they hope to increase both the accuracy and sensitivity of the method by using worms that were previously exposed to cancer cell media and therefore have a ‘memory’ of cancer-specific odor molecules,” according to the statement from the American Chemical Society.
Since C. elegans is easy to grow in a lab and, apparently, easy to train, the researchers hope that the worm-on-a-chip can become a quick, easy, economical, and noninvasive cancer screen.
So watch out cancer, because we never bet against the creepy crawlies.
Mosquitoes have us figured out
We are nearing mosquito season; quite possibly the most annoying and itchy time of the year. We stock up on bottles of bug spray, but somehow we still get bite after bite. It appears that mosquitoes are basically able to ignore our bug sprays, which explains why we’re still covered in bites after the Fourth of July fireworks. It turns out mosquitoes are more complex than we thought for such tiny creatures.
There’s plenty of research on the best ways to keep mosquitoes away, because not only are they incredibly annoying, but they also carry potentially harmful diseases. In a recent experiment, researchers used mosquitoes that were genetically modified to have an excessive amount of an odor receptor called AgOR2, which responds to the smell of humans.
“AgOR2 overexpression threw a wrench in the whole system by inactivating olfactory receptors in these mosquitoes,” Christopher Potter, PhD, associate professor of neuroscience at Johns Hopkins University, said in a written statement.
After testing how these genetically modified mosquitoes reacted to some of the common smells of bug spray such as lemongrass, they discovered that it’s easy for the mosquitoes to ignore the smell. We wish it were that easy for us to ignore that chemically fruity smell.
Researchers continue to work hard to figure out how to repel mosquitoes and we’re rooting for them as summer approaches, despite the mosquito’s status as a creepy crawly.
Natural, vaccine-induced, and hybrid immunity to COVID-19
Seroprevalence surveys suggest that, from the beginning of the pandemic to 2022, more than a third of the global population had been infected with SARS-CoV-2. As large numbers of people continue to be infected, the efficacy and duration of natural immunity, in terms of protection against SARS-CoV-2 reinfections and severe disease, are of crucial significance. The virus’s epidemiologic trajectory will be influenced by the trends in vaccine-induced and hybrid immunity.
Omicron’s immune evasion
Cases of SARS-CoV-2 reinfection are increasing around the world. According to data from the U.K. Health Security Agency, 650,000 people in England have been infected twice, and most of them were reinfected in the past 2 months. Before mid-November 2021, reinfections accounted for about 1% of reported cases, but the rate has now increased to around 10%. The reinfection risk was 16 times higher between mid-December 2021 and early January 2022. Experts believe that this spike in reinfections is related to the spread of Omicron, which overtook Delta as the dominant variant. Nonetheless, other aspects should also be considered.
Omicron’s greater propensity to spread is not unrelated to its ability to evade the body’s immune defenses. This aspect was raised in a letter recently published in the New England Journal of Medicine. The authors reported that the effectiveness of previous infection in preventing reinfection against the Alpha, Beta, and Delta variants was around 90%, but it was only 56% against Omicron.
Natural immunity
Natural immunity showed roughly similar effectiveness regarding protection against reinfection across different SARS-CoV-2 variants, with the exception of the Omicron variant. The risk of hospitalization and death was also reduced in SARS-CoV-2 reinfections versus primary infections. Observational studies indicate that natural immunity may offer equal or greater protection against SARS-CoV-2 infections, compared with immunization with two doses of an mRNA vaccine, but the data are not fully consistent.
Natural immunity seems to be relatively long-lasting. Data from Denmark and Austria show no evidence that protection against reinfections wanes after 6 months. Some investigations indicate that protection against reinfection is lowest 4-5 months after initial infection and increases thereafter, a finding that might hypothetically be explained by persistent viral shedding; that is, misclassification of prolonged SARS-CoV-2 infections as reinfections. While no comparison was made against information pertaining to unvaccinated, not previously-infected individuals, preliminary data from Israel suggest that protection from reinfection can decrease from 6 to more than 12 months after the first SARS-CoV-2 infection. Taken together, epidemiologic studies indicate that protection against reinfections by natural immunity lasts over 1 year with only moderate, if any, decline over this period. Among older individuals, immunocompromised patients, and those with certain comorbidities or exposure risk (for example, health care workers), rates of reinfection may be higher. It is plausible that reinfection risk may be a function of exposure risk.
There is accumulating evidence that reinfections may be significantly less severe than primary infections with SARS-CoV-2. Reduced clinical severity of SARS-CoV-2 reinfections naturally also makes sense from a biologic point of view, inasmuch as a previously primed immune system should be better prepared for a rechallenge with this virus.
Vaccine-induced immunity
The short-term (<4 months) efficacy of mRNA vaccines against SARS-CoV-2 is high and varies from 94.1% (Moderna) to 95% (BioNTech/Pfizer). This has been confirmed by randomized controlled trials and was subsequently confirmed in effectiveness studies in real-world settings. Waning efficacy was observed with respect to protection against SARS-CoV-2 infections (for example, only approximately 20% after about half a year in Qatar), whereas protection against severe disease was either sustained or showed only a moderate decline.
In individuals who received two doses of the BioNTech/Pfizer vaccine at least 5 months earlier, an additional vaccine dose, a so-called booster, significantly lowered mortality and severe illness. These findings suggest that the booster restored and probably exceeded the initial short-term efficacy of the initial vaccination.
Data are still emerging regarding the efficacy of boosters against the Omicron variants. Preliminary data suggest a far lower ability to restore protection from infection and vaccination. However, fatalities and hospitalizations remain low.
Natural immunity vs. vaccine-induced immunity
Comparisons of natural immunity with vaccine-induced immunity are complicated by a series of biases and by combinations of biases – for example, the biases of comparisons between infected and uninfected, plus the biases of comparisons between vaccinated and nonvaccinated, with strong potential selection biases and confounding. Of particular note, the proportion of people previously infected and/or vaccinated may influence estimates of effectiveness. Regarding this point, one study compared unvaccinated patients with a prior SARS-CoV-2 infection and vaccinated individuals followed up from a week after the second vaccine dose onward versus a group of unvaccinated, not previously infected individuals. The findings showed that, compared with unvaccinated, not previously infected individuals, the natural immunity group and the vaccinated group had similar protection of 94.8% and 92.8% against infection, of 94.1% and 94.2% against hospitalization, and of 96.4% and 94.4% against severe illness, respectively.
Hybrid immunity
The combination of a previous SARS-CoV-2 infection and a respective vaccination is called hybrid immunity. This combination seems to confer the greatest protection against SARS-CoV-2 infections, but several knowledge gaps remain regarding this issue.
Data from Israel showed that, when the time since the last immunity-conferring event (either primary infection or vaccination) was the same, the rates of SARS-CoV-2 infections were similar in the following groups: individuals who had a previous infection and no vaccination, individuals who had an infection and were then vaccinated with a single dose after at least 3 months, and individuals who were vaccinated (two doses) and then infected. Severe disease was relatively rare overall.
Data on the efficacy of hybrid immunity point in the direction of hybrid immunity being superior, as compared with either vaccine-induced (without a booster) immunity or natural immunity alone. Timing and mode of vaccination of previously infected individuals to achieve optimal hybrid immunity are central questions that remain to be addressed in future studies.
Given that vaccination rates are continuously increasing and that, by the beginning of 2022, perhaps half or more of the global population had already been infected with SARS-CoV-2, with the vast majority of this group not being officially detected, it would appear logical that future infection waves, even with highly transmissible variants of SARS-CoV-2, may be limited with respect to their maximum potential health burden. The advent of Omicron suggests that massive surges can occur even in populations with extremely high rates of previous vaccination and variable rates of prior infections. However, even then, the accompanying burden of hospitalizations and deaths is far less than what was seen in 2020 and 2021. One may argue that the pandemic has already transitioned to the endemic phase and that Omicron is an endemic wave occurring in the setting of already widespread population immunity.
A version of this article first appeared on Medscape.com.
Seroprevalence surveys suggest that, from the beginning of the pandemic to 2022, more than a third of the global population had been infected with SARS-CoV-2. As large numbers of people continue to be infected, the efficacy and duration of natural immunity, in terms of protection against SARS-CoV-2 reinfections and severe disease, are of crucial significance. The virus’s epidemiologic trajectory will be influenced by the trends in vaccine-induced and hybrid immunity.
Omicron’s immune evasion
Cases of SARS-CoV-2 reinfection are increasing around the world. According to data from the U.K. Health Security Agency, 650,000 people in England have been infected twice, and most of them were reinfected in the past 2 months. Before mid-November 2021, reinfections accounted for about 1% of reported cases, but the rate has now increased to around 10%. The reinfection risk was 16 times higher between mid-December 2021 and early January 2022. Experts believe that this spike in reinfections is related to the spread of Omicron, which overtook Delta as the dominant variant. Nonetheless, other aspects should also be considered.
Omicron’s greater propensity to spread is not unrelated to its ability to evade the body’s immune defenses. This aspect was raised in a letter recently published in the New England Journal of Medicine. The authors reported that the effectiveness of previous infection in preventing reinfection against the Alpha, Beta, and Delta variants was around 90%, but it was only 56% against Omicron.
Natural immunity
Natural immunity showed roughly similar effectiveness regarding protection against reinfection across different SARS-CoV-2 variants, with the exception of the Omicron variant. The risk of hospitalization and death was also reduced in SARS-CoV-2 reinfections versus primary infections. Observational studies indicate that natural immunity may offer equal or greater protection against SARS-CoV-2 infections, compared with immunization with two doses of an mRNA vaccine, but the data are not fully consistent.
Natural immunity seems to be relatively long-lasting. Data from Denmark and Austria show no evidence that protection against reinfections wanes after 6 months. Some investigations indicate that protection against reinfection is lowest 4-5 months after initial infection and increases thereafter, a finding that might hypothetically be explained by persistent viral shedding; that is, misclassification of prolonged SARS-CoV-2 infections as reinfections. While no comparison was made against information pertaining to unvaccinated, not previously-infected individuals, preliminary data from Israel suggest that protection from reinfection can decrease from 6 to more than 12 months after the first SARS-CoV-2 infection. Taken together, epidemiologic studies indicate that protection against reinfections by natural immunity lasts over 1 year with only moderate, if any, decline over this period. Among older individuals, immunocompromised patients, and those with certain comorbidities or exposure risk (for example, health care workers), rates of reinfection may be higher. It is plausible that reinfection risk may be a function of exposure risk.
There is accumulating evidence that reinfections may be significantly less severe than primary infections with SARS-CoV-2. Reduced clinical severity of SARS-CoV-2 reinfections naturally also makes sense from a biologic point of view, inasmuch as a previously primed immune system should be better prepared for a rechallenge with this virus.
Vaccine-induced immunity
The short-term (<4 months) efficacy of mRNA vaccines against SARS-CoV-2 is high and varies from 94.1% (Moderna) to 95% (BioNTech/Pfizer). This has been confirmed by randomized controlled trials and was subsequently confirmed in effectiveness studies in real-world settings. Waning efficacy was observed with respect to protection against SARS-CoV-2 infections (for example, only approximately 20% after about half a year in Qatar), whereas protection against severe disease was either sustained or showed only a moderate decline.
In individuals who received two doses of the BioNTech/Pfizer vaccine at least 5 months earlier, an additional vaccine dose, a so-called booster, significantly lowered mortality and severe illness. These findings suggest that the booster restored and probably exceeded the initial short-term efficacy of the initial vaccination.
Data are still emerging regarding the efficacy of boosters against the Omicron variants. Preliminary data suggest a far lower ability to restore protection from infection and vaccination. However, fatalities and hospitalizations remain low.
Natural immunity vs. vaccine-induced immunity
Comparisons of natural immunity with vaccine-induced immunity are complicated by a series of biases and by combinations of biases – for example, the biases of comparisons between infected and uninfected, plus the biases of comparisons between vaccinated and nonvaccinated, with strong potential selection biases and confounding. Of particular note, the proportion of people previously infected and/or vaccinated may influence estimates of effectiveness. Regarding this point, one study compared unvaccinated patients with a prior SARS-CoV-2 infection and vaccinated individuals followed up from a week after the second vaccine dose onward versus a group of unvaccinated, not previously infected individuals. The findings showed that, compared with unvaccinated, not previously infected individuals, the natural immunity group and the vaccinated group had similar protection of 94.8% and 92.8% against infection, of 94.1% and 94.2% against hospitalization, and of 96.4% and 94.4% against severe illness, respectively.
Hybrid immunity
The combination of a previous SARS-CoV-2 infection and a respective vaccination is called hybrid immunity. This combination seems to confer the greatest protection against SARS-CoV-2 infections, but several knowledge gaps remain regarding this issue.
Data from Israel showed that, when the time since the last immunity-conferring event (either primary infection or vaccination) was the same, the rates of SARS-CoV-2 infections were similar in the following groups: individuals who had a previous infection and no vaccination, individuals who had an infection and were then vaccinated with a single dose after at least 3 months, and individuals who were vaccinated (two doses) and then infected. Severe disease was relatively rare overall.
Data on the efficacy of hybrid immunity point in the direction of hybrid immunity being superior, as compared with either vaccine-induced (without a booster) immunity or natural immunity alone. Timing and mode of vaccination of previously infected individuals to achieve optimal hybrid immunity are central questions that remain to be addressed in future studies.
Given that vaccination rates are continuously increasing and that, by the beginning of 2022, perhaps half or more of the global population had already been infected with SARS-CoV-2, with the vast majority of this group not being officially detected, it would appear logical that future infection waves, even with highly transmissible variants of SARS-CoV-2, may be limited with respect to their maximum potential health burden. The advent of Omicron suggests that massive surges can occur even in populations with extremely high rates of previous vaccination and variable rates of prior infections. However, even then, the accompanying burden of hospitalizations and deaths is far less than what was seen in 2020 and 2021. One may argue that the pandemic has already transitioned to the endemic phase and that Omicron is an endemic wave occurring in the setting of already widespread population immunity.
A version of this article first appeared on Medscape.com.
Seroprevalence surveys suggest that, from the beginning of the pandemic to 2022, more than a third of the global population had been infected with SARS-CoV-2. As large numbers of people continue to be infected, the efficacy and duration of natural immunity, in terms of protection against SARS-CoV-2 reinfections and severe disease, are of crucial significance. The virus’s epidemiologic trajectory will be influenced by the trends in vaccine-induced and hybrid immunity.
Omicron’s immune evasion
Cases of SARS-CoV-2 reinfection are increasing around the world. According to data from the U.K. Health Security Agency, 650,000 people in England have been infected twice, and most of them were reinfected in the past 2 months. Before mid-November 2021, reinfections accounted for about 1% of reported cases, but the rate has now increased to around 10%. The reinfection risk was 16 times higher between mid-December 2021 and early January 2022. Experts believe that this spike in reinfections is related to the spread of Omicron, which overtook Delta as the dominant variant. Nonetheless, other aspects should also be considered.
Omicron’s greater propensity to spread is not unrelated to its ability to evade the body’s immune defenses. This aspect was raised in a letter recently published in the New England Journal of Medicine. The authors reported that the effectiveness of previous infection in preventing reinfection against the Alpha, Beta, and Delta variants was around 90%, but it was only 56% against Omicron.
Natural immunity
Natural immunity showed roughly similar effectiveness regarding protection against reinfection across different SARS-CoV-2 variants, with the exception of the Omicron variant. The risk of hospitalization and death was also reduced in SARS-CoV-2 reinfections versus primary infections. Observational studies indicate that natural immunity may offer equal or greater protection against SARS-CoV-2 infections, compared with immunization with two doses of an mRNA vaccine, but the data are not fully consistent.
Natural immunity seems to be relatively long-lasting. Data from Denmark and Austria show no evidence that protection against reinfections wanes after 6 months. Some investigations indicate that protection against reinfection is lowest 4-5 months after initial infection and increases thereafter, a finding that might hypothetically be explained by persistent viral shedding; that is, misclassification of prolonged SARS-CoV-2 infections as reinfections. While no comparison was made against information pertaining to unvaccinated, not previously-infected individuals, preliminary data from Israel suggest that protection from reinfection can decrease from 6 to more than 12 months after the first SARS-CoV-2 infection. Taken together, epidemiologic studies indicate that protection against reinfections by natural immunity lasts over 1 year with only moderate, if any, decline over this period. Among older individuals, immunocompromised patients, and those with certain comorbidities or exposure risk (for example, health care workers), rates of reinfection may be higher. It is plausible that reinfection risk may be a function of exposure risk.
There is accumulating evidence that reinfections may be significantly less severe than primary infections with SARS-CoV-2. Reduced clinical severity of SARS-CoV-2 reinfections naturally also makes sense from a biologic point of view, inasmuch as a previously primed immune system should be better prepared for a rechallenge with this virus.
Vaccine-induced immunity
The short-term (<4 months) efficacy of mRNA vaccines against SARS-CoV-2 is high and varies from 94.1% (Moderna) to 95% (BioNTech/Pfizer). This has been confirmed by randomized controlled trials and was subsequently confirmed in effectiveness studies in real-world settings. Waning efficacy was observed with respect to protection against SARS-CoV-2 infections (for example, only approximately 20% after about half a year in Qatar), whereas protection against severe disease was either sustained or showed only a moderate decline.
In individuals who received two doses of the BioNTech/Pfizer vaccine at least 5 months earlier, an additional vaccine dose, a so-called booster, significantly lowered mortality and severe illness. These findings suggest that the booster restored and probably exceeded the initial short-term efficacy of the initial vaccination.
Data are still emerging regarding the efficacy of boosters against the Omicron variants. Preliminary data suggest a far lower ability to restore protection from infection and vaccination. However, fatalities and hospitalizations remain low.
Natural immunity vs. vaccine-induced immunity
Comparisons of natural immunity with vaccine-induced immunity are complicated by a series of biases and by combinations of biases – for example, the biases of comparisons between infected and uninfected, plus the biases of comparisons between vaccinated and nonvaccinated, with strong potential selection biases and confounding. Of particular note, the proportion of people previously infected and/or vaccinated may influence estimates of effectiveness. Regarding this point, one study compared unvaccinated patients with a prior SARS-CoV-2 infection and vaccinated individuals followed up from a week after the second vaccine dose onward versus a group of unvaccinated, not previously infected individuals. The findings showed that, compared with unvaccinated, not previously infected individuals, the natural immunity group and the vaccinated group had similar protection of 94.8% and 92.8% against infection, of 94.1% and 94.2% against hospitalization, and of 96.4% and 94.4% against severe illness, respectively.
Hybrid immunity
The combination of a previous SARS-CoV-2 infection and a respective vaccination is called hybrid immunity. This combination seems to confer the greatest protection against SARS-CoV-2 infections, but several knowledge gaps remain regarding this issue.
Data from Israel showed that, when the time since the last immunity-conferring event (either primary infection or vaccination) was the same, the rates of SARS-CoV-2 infections were similar in the following groups: individuals who had a previous infection and no vaccination, individuals who had an infection and were then vaccinated with a single dose after at least 3 months, and individuals who were vaccinated (two doses) and then infected. Severe disease was relatively rare overall.
Data on the efficacy of hybrid immunity point in the direction of hybrid immunity being superior, as compared with either vaccine-induced (without a booster) immunity or natural immunity alone. Timing and mode of vaccination of previously infected individuals to achieve optimal hybrid immunity are central questions that remain to be addressed in future studies.
Given that vaccination rates are continuously increasing and that, by the beginning of 2022, perhaps half or more of the global population had already been infected with SARS-CoV-2, with the vast majority of this group not being officially detected, it would appear logical that future infection waves, even with highly transmissible variants of SARS-CoV-2, may be limited with respect to their maximum potential health burden. The advent of Omicron suggests that massive surges can occur even in populations with extremely high rates of previous vaccination and variable rates of prior infections. However, even then, the accompanying burden of hospitalizations and deaths is far less than what was seen in 2020 and 2021. One may argue that the pandemic has already transitioned to the endemic phase and that Omicron is an endemic wave occurring in the setting of already widespread population immunity.
A version of this article first appeared on Medscape.com.
Maternal obesity promotes risk of perinatal death
The infants of obese pregnant women had a 55% higher adjusted perinatal death rate, compared with those of normal-weight pregnant women, but lower gestational age had a mediating effect, based on data from nearly 400,000 women-infant pairs.
“While some obesity-related causes of fetal death are known, the exact pathophysiology behind the effects of obesity on perinatal death are not completely understood,” Jeffrey N. Bone, MD, of the University of British Columbia, Vancouver, and colleagues wrote. Higher body mass index prior to pregnancy also is associated with preterm delivery, but the effect of gestational age on the association between BMI and infant mortality has not been well explored.
In a study published in PLOS ONE, the researchers reviewed data from nearly 400,000 women obtained through the British Columbia Perinatal Database Registry, which collects obstetric and neonatal data from hospital charts and from delivery records of home births. Births at less than 20 weeks’ gestation and late pregnancy terminations were excluded.
BMI was based on self-reported prepregnancy height and weight; of the 392,820 included women, 12.8% were classified as obese, 20.6% were overweight, 60.6% were normal weight, and 6.0% were underweight. Infants of women with higher BMI had a lower gestational age at delivery. Perinatal mortality occurred in 1,834 pregnancies (0.5%). In adjusted analysis, infant perinatal death was significantly more likely for obese women (adjusted odds ratio, 1.55) and overweight women (aOR, 1.22).
However, 63.1% of this association in obese women was mediated by gestational age of the infant at delivery, with aORs of 1.32 and 1.18 for natural indirect and natural direct effects, respectively, compared with that of normal-weight women. Similar, but lesser effects were noted for overweight women, with aORs of 1.11 and 1.10, respectively. “Direct effects were higher, and mediation was lower for stillbirth than for neonatal death, where the total effect was entirely indirect,” but the confidence intervals remained consistent with the primary analyses, the researchers noted.
The increased perinatal death rates of infants of obese and overweight women reflect data from previous studies, but the current study’s use of mediation analysis offers new insight on the mechanism by which perinatal death rates increase with higher maternal BMI, the researchers wrote.
The study findings were limited by several factors including the need to consider potential common risk factors for both perinatal death and early delivery that would be affected by maternal obesity, the researchers noted. Other limitations included the use of gestational age at stillbirth, which represents an approximation of fetal death in some cases, and the use of self-reports for prepregnancy maternal BMI.
However, the results were strengthened by the large, population-based design and information on potential confounding variables, and suggest that early gestational age at delivery may play a role in maternal obesity-related perinatal death risk.
“To better inform the pregnancy management in obese women, further studies should continue to disentangle the causal pathways under which obesity increases the risk of perinatal death, including, for example, gestational diabetes and other obesity-related pregnancy complications,” they concluded.
More testing and counseling are needed
The current study is important because obesity rates continue to increase in the reproductive-age population, Marissa Platner, MD, of Emory University, Atlanta, said in an interview. “Obesity has become a known risk factor for adverse pregnancy outcomes, specifically the risk of stillbirth and perinatal death. However, the authors correctly point out that the underlying cause of these perinatal deaths in women with obesity is unclear. Additionally, ACOG recently updated their clinical guidelines to recommend routine antenatal testing for women with obesity due to these increased rates of stillbirth.
“I was not surprised by these findings; similar to previous literature, the risks of perinatal death seem to have a dose-response relationship with increasing BMI. We know that women with prepregnancy obesity are also at higher risk of perinatal complications in the preterm period, which would increase the risk of perinatal death,” Dr. Platner said
“I think the take-home message for clinicians is twofold,” Dr. Platner said. First, “we need to take the updated antenatal testing guidelines from ACOG very seriously and implement these in our practices.” Second, “in the preconception or early antepartum period, these patients should be thoroughly counseled on the associated risks of pregnancy and discuss appropriate gestational weight gain guidelines and lifestyle modifications.”
However, “additional research is needed in a U.S. population with higher rates of obesity to determine the true effects of obesity on perinatal deaths and to further elucidate the underlying pathophysiology and disease processes that may lead to increased risk of both stillbirth and perinatal deaths,” Dr. Platner emphasized.
*This story was updated on March 23, 2022.
The study was supported by the Sick Kids Foundation and the Canadian Institute of Health Research. The researchers had no financial conflicts to disclose. Dr. Platner had no financial conflicts to disclose.
The infants of obese pregnant women had a 55% higher adjusted perinatal death rate, compared with those of normal-weight pregnant women, but lower gestational age had a mediating effect, based on data from nearly 400,000 women-infant pairs.
“While some obesity-related causes of fetal death are known, the exact pathophysiology behind the effects of obesity on perinatal death are not completely understood,” Jeffrey N. Bone, MD, of the University of British Columbia, Vancouver, and colleagues wrote. Higher body mass index prior to pregnancy also is associated with preterm delivery, but the effect of gestational age on the association between BMI and infant mortality has not been well explored.
In a study published in PLOS ONE, the researchers reviewed data from nearly 400,000 women obtained through the British Columbia Perinatal Database Registry, which collects obstetric and neonatal data from hospital charts and from delivery records of home births. Births at less than 20 weeks’ gestation and late pregnancy terminations were excluded.
BMI was based on self-reported prepregnancy height and weight; of the 392,820 included women, 12.8% were classified as obese, 20.6% were overweight, 60.6% were normal weight, and 6.0% were underweight. Infants of women with higher BMI had a lower gestational age at delivery. Perinatal mortality occurred in 1,834 pregnancies (0.5%). In adjusted analysis, infant perinatal death was significantly more likely for obese women (adjusted odds ratio, 1.55) and overweight women (aOR, 1.22).
However, 63.1% of this association in obese women was mediated by gestational age of the infant at delivery, with aORs of 1.32 and 1.18 for natural indirect and natural direct effects, respectively, compared with that of normal-weight women. Similar, but lesser effects were noted for overweight women, with aORs of 1.11 and 1.10, respectively. “Direct effects were higher, and mediation was lower for stillbirth than for neonatal death, where the total effect was entirely indirect,” but the confidence intervals remained consistent with the primary analyses, the researchers noted.
The increased perinatal death rates of infants of obese and overweight women reflect data from previous studies, but the current study’s use of mediation analysis offers new insight on the mechanism by which perinatal death rates increase with higher maternal BMI, the researchers wrote.
The study findings were limited by several factors including the need to consider potential common risk factors for both perinatal death and early delivery that would be affected by maternal obesity, the researchers noted. Other limitations included the use of gestational age at stillbirth, which represents an approximation of fetal death in some cases, and the use of self-reports for prepregnancy maternal BMI.
However, the results were strengthened by the large, population-based design and information on potential confounding variables, and suggest that early gestational age at delivery may play a role in maternal obesity-related perinatal death risk.
“To better inform the pregnancy management in obese women, further studies should continue to disentangle the causal pathways under which obesity increases the risk of perinatal death, including, for example, gestational diabetes and other obesity-related pregnancy complications,” they concluded.
More testing and counseling are needed
The current study is important because obesity rates continue to increase in the reproductive-age population, Marissa Platner, MD, of Emory University, Atlanta, said in an interview. “Obesity has become a known risk factor for adverse pregnancy outcomes, specifically the risk of stillbirth and perinatal death. However, the authors correctly point out that the underlying cause of these perinatal deaths in women with obesity is unclear. Additionally, ACOG recently updated their clinical guidelines to recommend routine antenatal testing for women with obesity due to these increased rates of stillbirth.
“I was not surprised by these findings; similar to previous literature, the risks of perinatal death seem to have a dose-response relationship with increasing BMI. We know that women with prepregnancy obesity are also at higher risk of perinatal complications in the preterm period, which would increase the risk of perinatal death,” Dr. Platner said
“I think the take-home message for clinicians is twofold,” Dr. Platner said. First, “we need to take the updated antenatal testing guidelines from ACOG very seriously and implement these in our practices.” Second, “in the preconception or early antepartum period, these patients should be thoroughly counseled on the associated risks of pregnancy and discuss appropriate gestational weight gain guidelines and lifestyle modifications.”
However, “additional research is needed in a U.S. population with higher rates of obesity to determine the true effects of obesity on perinatal deaths and to further elucidate the underlying pathophysiology and disease processes that may lead to increased risk of both stillbirth and perinatal deaths,” Dr. Platner emphasized.
*This story was updated on March 23, 2022.
The study was supported by the Sick Kids Foundation and the Canadian Institute of Health Research. The researchers had no financial conflicts to disclose. Dr. Platner had no financial conflicts to disclose.
The infants of obese pregnant women had a 55% higher adjusted perinatal death rate, compared with those of normal-weight pregnant women, but lower gestational age had a mediating effect, based on data from nearly 400,000 women-infant pairs.
“While some obesity-related causes of fetal death are known, the exact pathophysiology behind the effects of obesity on perinatal death are not completely understood,” Jeffrey N. Bone, MD, of the University of British Columbia, Vancouver, and colleagues wrote. Higher body mass index prior to pregnancy also is associated with preterm delivery, but the effect of gestational age on the association between BMI and infant mortality has not been well explored.
In a study published in PLOS ONE, the researchers reviewed data from nearly 400,000 women obtained through the British Columbia Perinatal Database Registry, which collects obstetric and neonatal data from hospital charts and from delivery records of home births. Births at less than 20 weeks’ gestation and late pregnancy terminations were excluded.
BMI was based on self-reported prepregnancy height and weight; of the 392,820 included women, 12.8% were classified as obese, 20.6% were overweight, 60.6% were normal weight, and 6.0% were underweight. Infants of women with higher BMI had a lower gestational age at delivery. Perinatal mortality occurred in 1,834 pregnancies (0.5%). In adjusted analysis, infant perinatal death was significantly more likely for obese women (adjusted odds ratio, 1.55) and overweight women (aOR, 1.22).
However, 63.1% of this association in obese women was mediated by gestational age of the infant at delivery, with aORs of 1.32 and 1.18 for natural indirect and natural direct effects, respectively, compared with that of normal-weight women. Similar, but lesser effects were noted for overweight women, with aORs of 1.11 and 1.10, respectively. “Direct effects were higher, and mediation was lower for stillbirth than for neonatal death, where the total effect was entirely indirect,” but the confidence intervals remained consistent with the primary analyses, the researchers noted.
The increased perinatal death rates of infants of obese and overweight women reflect data from previous studies, but the current study’s use of mediation analysis offers new insight on the mechanism by which perinatal death rates increase with higher maternal BMI, the researchers wrote.
The study findings were limited by several factors including the need to consider potential common risk factors for both perinatal death and early delivery that would be affected by maternal obesity, the researchers noted. Other limitations included the use of gestational age at stillbirth, which represents an approximation of fetal death in some cases, and the use of self-reports for prepregnancy maternal BMI.
However, the results were strengthened by the large, population-based design and information on potential confounding variables, and suggest that early gestational age at delivery may play a role in maternal obesity-related perinatal death risk.
“To better inform the pregnancy management in obese women, further studies should continue to disentangle the causal pathways under which obesity increases the risk of perinatal death, including, for example, gestational diabetes and other obesity-related pregnancy complications,” they concluded.
More testing and counseling are needed
The current study is important because obesity rates continue to increase in the reproductive-age population, Marissa Platner, MD, of Emory University, Atlanta, said in an interview. “Obesity has become a known risk factor for adverse pregnancy outcomes, specifically the risk of stillbirth and perinatal death. However, the authors correctly point out that the underlying cause of these perinatal deaths in women with obesity is unclear. Additionally, ACOG recently updated their clinical guidelines to recommend routine antenatal testing for women with obesity due to these increased rates of stillbirth.
“I was not surprised by these findings; similar to previous literature, the risks of perinatal death seem to have a dose-response relationship with increasing BMI. We know that women with prepregnancy obesity are also at higher risk of perinatal complications in the preterm period, which would increase the risk of perinatal death,” Dr. Platner said
“I think the take-home message for clinicians is twofold,” Dr. Platner said. First, “we need to take the updated antenatal testing guidelines from ACOG very seriously and implement these in our practices.” Second, “in the preconception or early antepartum period, these patients should be thoroughly counseled on the associated risks of pregnancy and discuss appropriate gestational weight gain guidelines and lifestyle modifications.”
However, “additional research is needed in a U.S. population with higher rates of obesity to determine the true effects of obesity on perinatal deaths and to further elucidate the underlying pathophysiology and disease processes that may lead to increased risk of both stillbirth and perinatal deaths,” Dr. Platner emphasized.
*This story was updated on March 23, 2022.
The study was supported by the Sick Kids Foundation and the Canadian Institute of Health Research. The researchers had no financial conflicts to disclose. Dr. Platner had no financial conflicts to disclose.
FROM PLOS ONE
‘Profound implications’: COVID ups diabetes risk 40% a year later
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
Sit-to-stand BP spike tied to CV events in young adults
A sudden drop in blood pressure when standing is a common and concerning problem in elderly hypertensive people. Now, research suggests a large BP swing in the opposite direction on standing may be equally concerning in younger hypertensive people.
Young and middle-aged adults with a systolic BP response to standing greater than 6.5 mm Hg had almost double the risk of major adverse cardiovascular events (MACE) during follow-up, compared with other participants.
An exaggerated BP response remained an independent predictor of MACE, even after adjusting for traditional risk factors, including 24-hour BP (hazard ratio, 1.94; 95% confidence interval, 1.10 to 3.44), the study showed.
“The clinical implication is important, because now doctors measure blood pressure in young people in the upright posture, but what we say is it must be measured also while standing,” said Paolo Palatini, MD, a professor of internal medicine at the University of Padova, Italy, who led the study.
Previous studies have found that an exaggerated BP response to standing is a predictor of future hypertension, CV events, and mortality, particularly in older patients, but few prognostic data exist in those who are young to middle age, he noted.
The study, published in Hypertension, included 1,207 participants ages 18-45 years with untreated stage 1 hypertension (systolic BP 140-159 mm Hg or diastolic BP 90-100 mm Hg) in the prospective multicenter HARVEST study that began in Italy in 1990. The average age at enrollment was 33 years.
BP was measured at two visits 2 weeks apart, with each visit including three supine measurements taken after the patient had lain down for a minimum of 5 minutes, followed by three standing measurements taken 1 minute apart.
Based on the average of standing-lying BP differences during the two visits, participants were then classified as having a normal or exaggerated (top decile, lower limit > 6.5 mm Hg) systolic BP response to standing.
The 120 participants classified as “hyper-reactors” averaged an 11.4 mm Hg systolic BP increase upon standing, whereas the rest of the participants averaged a 3.8 mm Hg fall in systolic BP upon standing.
At their initial visit, hyper-reactors were more likely to be smokers (32.1% vs. 19.9%) and coffee drinkers (81.7% vs. 73%) and to have ambulatory hypertension (90.8% vs. 76.4%).
They were, however, no more likely to have a family history of cardiovascular events and had a lower supine systolic BP (140.5 mm Hg vs. 146.0 mm Hg), lower total cholesterol (4.93 mmol/L vs. 5.13 mmol/L), and higher HDL cholesterol (1.42 mmol/L vs. 1.35 mmol/L).
Age, sex, and body mass index were similar between the two groups, as was BP variability, nocturnal BP dip, and the frequency of extreme dippers. Participants with a normal systolic BP response were more likely to be treated for hypertension during follow-up (81.7% vs. 69.7%; P = .003).
In 630 participants who had catecholamines measured from 24-hour urine samples, the epinephrine/creatinine ratio was higher in hyper-reactors than normal responders (118.4 nmol/mol vs. 77.0 nmol/mol; P = .005).
During a median follow-up of 17.3 years, there were 105 major cardiovascular events, broadly defined to include acute coronary syndromes (48), any stroke (13), heart failure requiring hospitalization (3), aortic aneurysms (3), peripheral vascular disease (6), chronic kidney disease (12), and permanent atrial fibrillation (20).
The near doubling of MACE risk among hyper-reactors remained when atrial fibrillation was excluded and when 24-hour ambulatory systolic BP was included in the model, the author reported.
The results are in line with previous studies, indicating that hyper-reactors to standing have normal sympathetic activity at rest but an increased sympathetic response to stressors, observed Dr. Palatini and colleagues. This neurohumoral overshoot seems to be peculiar to young adults, whereas vascular stiffness seems to be the driving mechanism of orthostatic hypertension in older adults.
If a young person’s BP spikes upon standing, “then you have to treat them according to the average of the lying and the standing pressure,” Dr. Palatini said. “In these people, blood pressure should be treated earlier than in the past.”
“The study is important because it identified a new marker for hypertension that is easily evaluated in clinical practice,” Nieca Goldberg, MD, medical director of the Atria Institute, New York, and an associate professor of medicine at New York University Grossman School of Medicine, commented via email.
She noted that standing blood pressures are usually not taken as part of a medical visit and, in fact, seated blood pressures are often taken incorrectly while the patient is seated on the exam table rather than with their feet on the floor and using the proper cuff size.
“By incorporating standing BP, we will improve our diagnosis for hypertension, and with interventions such as diet and exercise, salt reduction, and medication when indicated, lower risk for heart attack, stroke, heart failure, [and] kidney and eye disease,” said Dr. Goldberg, who is also a spokesperson for the American Heart Association.
“The biggest barrier is that office visits are limited to 15 minutes, and not enough time is spent on the vital signs,” she noted. “We need changes to the health care system that value our ability to diagnose BP and take the time to counsel patients and explain treatment options.”
Limitations of the present study are that 72.7% of participants were men and all were White, Dr. Palatini said. Future work is also needed to create a uniform definition of BP hyper-reactivity to standing, possibly based on risk estimates, for inclusion in future hypertension guidelines.
The study was funded by the Association 18 Maggio 1370 in Italy. The authors have disclosed no relevant financial relationships. Dr. Goldberg reported being a spokesperson for the American Heart Association.
A version of this article first appeared on Medscape.com.
A sudden drop in blood pressure when standing is a common and concerning problem in elderly hypertensive people. Now, research suggests a large BP swing in the opposite direction on standing may be equally concerning in younger hypertensive people.
Young and middle-aged adults with a systolic BP response to standing greater than 6.5 mm Hg had almost double the risk of major adverse cardiovascular events (MACE) during follow-up, compared with other participants.
An exaggerated BP response remained an independent predictor of MACE, even after adjusting for traditional risk factors, including 24-hour BP (hazard ratio, 1.94; 95% confidence interval, 1.10 to 3.44), the study showed.
“The clinical implication is important, because now doctors measure blood pressure in young people in the upright posture, but what we say is it must be measured also while standing,” said Paolo Palatini, MD, a professor of internal medicine at the University of Padova, Italy, who led the study.
Previous studies have found that an exaggerated BP response to standing is a predictor of future hypertension, CV events, and mortality, particularly in older patients, but few prognostic data exist in those who are young to middle age, he noted.
The study, published in Hypertension, included 1,207 participants ages 18-45 years with untreated stage 1 hypertension (systolic BP 140-159 mm Hg or diastolic BP 90-100 mm Hg) in the prospective multicenter HARVEST study that began in Italy in 1990. The average age at enrollment was 33 years.
BP was measured at two visits 2 weeks apart, with each visit including three supine measurements taken after the patient had lain down for a minimum of 5 minutes, followed by three standing measurements taken 1 minute apart.
Based on the average of standing-lying BP differences during the two visits, participants were then classified as having a normal or exaggerated (top decile, lower limit > 6.5 mm Hg) systolic BP response to standing.
The 120 participants classified as “hyper-reactors” averaged an 11.4 mm Hg systolic BP increase upon standing, whereas the rest of the participants averaged a 3.8 mm Hg fall in systolic BP upon standing.
At their initial visit, hyper-reactors were more likely to be smokers (32.1% vs. 19.9%) and coffee drinkers (81.7% vs. 73%) and to have ambulatory hypertension (90.8% vs. 76.4%).
They were, however, no more likely to have a family history of cardiovascular events and had a lower supine systolic BP (140.5 mm Hg vs. 146.0 mm Hg), lower total cholesterol (4.93 mmol/L vs. 5.13 mmol/L), and higher HDL cholesterol (1.42 mmol/L vs. 1.35 mmol/L).
Age, sex, and body mass index were similar between the two groups, as was BP variability, nocturnal BP dip, and the frequency of extreme dippers. Participants with a normal systolic BP response were more likely to be treated for hypertension during follow-up (81.7% vs. 69.7%; P = .003).
In 630 participants who had catecholamines measured from 24-hour urine samples, the epinephrine/creatinine ratio was higher in hyper-reactors than normal responders (118.4 nmol/mol vs. 77.0 nmol/mol; P = .005).
During a median follow-up of 17.3 years, there were 105 major cardiovascular events, broadly defined to include acute coronary syndromes (48), any stroke (13), heart failure requiring hospitalization (3), aortic aneurysms (3), peripheral vascular disease (6), chronic kidney disease (12), and permanent atrial fibrillation (20).
The near doubling of MACE risk among hyper-reactors remained when atrial fibrillation was excluded and when 24-hour ambulatory systolic BP was included in the model, the author reported.
The results are in line with previous studies, indicating that hyper-reactors to standing have normal sympathetic activity at rest but an increased sympathetic response to stressors, observed Dr. Palatini and colleagues. This neurohumoral overshoot seems to be peculiar to young adults, whereas vascular stiffness seems to be the driving mechanism of orthostatic hypertension in older adults.
If a young person’s BP spikes upon standing, “then you have to treat them according to the average of the lying and the standing pressure,” Dr. Palatini said. “In these people, blood pressure should be treated earlier than in the past.”
“The study is important because it identified a new marker for hypertension that is easily evaluated in clinical practice,” Nieca Goldberg, MD, medical director of the Atria Institute, New York, and an associate professor of medicine at New York University Grossman School of Medicine, commented via email.
She noted that standing blood pressures are usually not taken as part of a medical visit and, in fact, seated blood pressures are often taken incorrectly while the patient is seated on the exam table rather than with their feet on the floor and using the proper cuff size.
“By incorporating standing BP, we will improve our diagnosis for hypertension, and with interventions such as diet and exercise, salt reduction, and medication when indicated, lower risk for heart attack, stroke, heart failure, [and] kidney and eye disease,” said Dr. Goldberg, who is also a spokesperson for the American Heart Association.
“The biggest barrier is that office visits are limited to 15 minutes, and not enough time is spent on the vital signs,” she noted. “We need changes to the health care system that value our ability to diagnose BP and take the time to counsel patients and explain treatment options.”
Limitations of the present study are that 72.7% of participants were men and all were White, Dr. Palatini said. Future work is also needed to create a uniform definition of BP hyper-reactivity to standing, possibly based on risk estimates, for inclusion in future hypertension guidelines.
The study was funded by the Association 18 Maggio 1370 in Italy. The authors have disclosed no relevant financial relationships. Dr. Goldberg reported being a spokesperson for the American Heart Association.
A version of this article first appeared on Medscape.com.
A sudden drop in blood pressure when standing is a common and concerning problem in elderly hypertensive people. Now, research suggests a large BP swing in the opposite direction on standing may be equally concerning in younger hypertensive people.
Young and middle-aged adults with a systolic BP response to standing greater than 6.5 mm Hg had almost double the risk of major adverse cardiovascular events (MACE) during follow-up, compared with other participants.
An exaggerated BP response remained an independent predictor of MACE, even after adjusting for traditional risk factors, including 24-hour BP (hazard ratio, 1.94; 95% confidence interval, 1.10 to 3.44), the study showed.
“The clinical implication is important, because now doctors measure blood pressure in young people in the upright posture, but what we say is it must be measured also while standing,” said Paolo Palatini, MD, a professor of internal medicine at the University of Padova, Italy, who led the study.
Previous studies have found that an exaggerated BP response to standing is a predictor of future hypertension, CV events, and mortality, particularly in older patients, but few prognostic data exist in those who are young to middle age, he noted.
The study, published in Hypertension, included 1,207 participants ages 18-45 years with untreated stage 1 hypertension (systolic BP 140-159 mm Hg or diastolic BP 90-100 mm Hg) in the prospective multicenter HARVEST study that began in Italy in 1990. The average age at enrollment was 33 years.
BP was measured at two visits 2 weeks apart, with each visit including three supine measurements taken after the patient had lain down for a minimum of 5 minutes, followed by three standing measurements taken 1 minute apart.
Based on the average of standing-lying BP differences during the two visits, participants were then classified as having a normal or exaggerated (top decile, lower limit > 6.5 mm Hg) systolic BP response to standing.
The 120 participants classified as “hyper-reactors” averaged an 11.4 mm Hg systolic BP increase upon standing, whereas the rest of the participants averaged a 3.8 mm Hg fall in systolic BP upon standing.
At their initial visit, hyper-reactors were more likely to be smokers (32.1% vs. 19.9%) and coffee drinkers (81.7% vs. 73%) and to have ambulatory hypertension (90.8% vs. 76.4%).
They were, however, no more likely to have a family history of cardiovascular events and had a lower supine systolic BP (140.5 mm Hg vs. 146.0 mm Hg), lower total cholesterol (4.93 mmol/L vs. 5.13 mmol/L), and higher HDL cholesterol (1.42 mmol/L vs. 1.35 mmol/L).
Age, sex, and body mass index were similar between the two groups, as was BP variability, nocturnal BP dip, and the frequency of extreme dippers. Participants with a normal systolic BP response were more likely to be treated for hypertension during follow-up (81.7% vs. 69.7%; P = .003).
In 630 participants who had catecholamines measured from 24-hour urine samples, the epinephrine/creatinine ratio was higher in hyper-reactors than normal responders (118.4 nmol/mol vs. 77.0 nmol/mol; P = .005).
During a median follow-up of 17.3 years, there were 105 major cardiovascular events, broadly defined to include acute coronary syndromes (48), any stroke (13), heart failure requiring hospitalization (3), aortic aneurysms (3), peripheral vascular disease (6), chronic kidney disease (12), and permanent atrial fibrillation (20).
The near doubling of MACE risk among hyper-reactors remained when atrial fibrillation was excluded and when 24-hour ambulatory systolic BP was included in the model, the author reported.
The results are in line with previous studies, indicating that hyper-reactors to standing have normal sympathetic activity at rest but an increased sympathetic response to stressors, observed Dr. Palatini and colleagues. This neurohumoral overshoot seems to be peculiar to young adults, whereas vascular stiffness seems to be the driving mechanism of orthostatic hypertension in older adults.
If a young person’s BP spikes upon standing, “then you have to treat them according to the average of the lying and the standing pressure,” Dr. Palatini said. “In these people, blood pressure should be treated earlier than in the past.”
“The study is important because it identified a new marker for hypertension that is easily evaluated in clinical practice,” Nieca Goldberg, MD, medical director of the Atria Institute, New York, and an associate professor of medicine at New York University Grossman School of Medicine, commented via email.
She noted that standing blood pressures are usually not taken as part of a medical visit and, in fact, seated blood pressures are often taken incorrectly while the patient is seated on the exam table rather than with their feet on the floor and using the proper cuff size.
“By incorporating standing BP, we will improve our diagnosis for hypertension, and with interventions such as diet and exercise, salt reduction, and medication when indicated, lower risk for heart attack, stroke, heart failure, [and] kidney and eye disease,” said Dr. Goldberg, who is also a spokesperson for the American Heart Association.
“The biggest barrier is that office visits are limited to 15 minutes, and not enough time is spent on the vital signs,” she noted. “We need changes to the health care system that value our ability to diagnose BP and take the time to counsel patients and explain treatment options.”
Limitations of the present study are that 72.7% of participants were men and all were White, Dr. Palatini said. Future work is also needed to create a uniform definition of BP hyper-reactivity to standing, possibly based on risk estimates, for inclusion in future hypertension guidelines.
The study was funded by the Association 18 Maggio 1370 in Italy. The authors have disclosed no relevant financial relationships. Dr. Goldberg reported being a spokesperson for the American Heart Association.
A version of this article first appeared on Medscape.com.
Pfizer recalls BP drugs because of potential carcinogen
Pfizer is voluntarily recalling some antihypertensive medications because of unacceptable levels of a potential carcinogen, the company announced.
The affected products are quinapril HCI/hydrochlorothiazide (Accuretic) tablets that Pfizer distributes, and two authorized generics, quinapril plus hydrochlorothiazide and quinapril HCI/hydrochlorothiazide, distributed by Greenstone. The drugs have been withdrawn because of the presence of nitrosamine, N-nitroso-quinapril.
“Although long-term ingestion of N-nitroso-quinapril may be associated with a potential increased cancer risk in humans, there is no immediate risk to patients taking this medication,” Pfizer said in a news release.
The tablets are indicated for the treatment of hypertension. Patients currently taking the products are asked to consult with their doctor about alternative treatment options.
To date, there have been no reports of adverse events related to the recall, the company said.
In all, Pfizer is recalling six lots of Accuretic tablets (two at 10 mg/12.5 mg, three at 20 mg/12.5 mg, and one at 20 mg/25 mg), one lot of quinapril plus hydrochlorothiazide 20-mg/25-mg tablets, and four lots of quinapril HCl/ hydrochlorothiazide tablets (three at 20 mg/12.5 mg and one at 20 mg/25 mg)
The recalled tablets were sold in 90-count bottles distributed in the United States and Puerto Rico between November 2019 and March 2022. Product codes and lot numbers of the recalled medications are listed on the Pfizer website.
Patients who are taking this product should consult with their health care provider or pharmacy to determine if they have the affected product. Those with the affected tablets should contact claims management firm Sedgwick by phone at 888-843-0247 Monday through Friday from 8 a.m. to 5 p.m. ET for instructions on how to return their product and obtain reimbursement.
Health care providers with medical questions regarding the recall can contact Pfizer by telephone at 800-438-1985, option 3, Monday through Friday 8 a.m. to 9 p.m. ET.
Providers should report adverse reactions or quality problems they experience using these tablets to Pfizer either by telephone at 800-438-1985, option 1, by regular mail or by fax, or to the Food and Drug Administration’s MedWatch program.
A version of this article first appeared on Medscape.com.
Pfizer is voluntarily recalling some antihypertensive medications because of unacceptable levels of a potential carcinogen, the company announced.
The affected products are quinapril HCI/hydrochlorothiazide (Accuretic) tablets that Pfizer distributes, and two authorized generics, quinapril plus hydrochlorothiazide and quinapril HCI/hydrochlorothiazide, distributed by Greenstone. The drugs have been withdrawn because of the presence of nitrosamine, N-nitroso-quinapril.
“Although long-term ingestion of N-nitroso-quinapril may be associated with a potential increased cancer risk in humans, there is no immediate risk to patients taking this medication,” Pfizer said in a news release.
The tablets are indicated for the treatment of hypertension. Patients currently taking the products are asked to consult with their doctor about alternative treatment options.
To date, there have been no reports of adverse events related to the recall, the company said.
In all, Pfizer is recalling six lots of Accuretic tablets (two at 10 mg/12.5 mg, three at 20 mg/12.5 mg, and one at 20 mg/25 mg), one lot of quinapril plus hydrochlorothiazide 20-mg/25-mg tablets, and four lots of quinapril HCl/ hydrochlorothiazide tablets (three at 20 mg/12.5 mg and one at 20 mg/25 mg)
The recalled tablets were sold in 90-count bottles distributed in the United States and Puerto Rico between November 2019 and March 2022. Product codes and lot numbers of the recalled medications are listed on the Pfizer website.
Patients who are taking this product should consult with their health care provider or pharmacy to determine if they have the affected product. Those with the affected tablets should contact claims management firm Sedgwick by phone at 888-843-0247 Monday through Friday from 8 a.m. to 5 p.m. ET for instructions on how to return their product and obtain reimbursement.
Health care providers with medical questions regarding the recall can contact Pfizer by telephone at 800-438-1985, option 3, Monday through Friday 8 a.m. to 9 p.m. ET.
Providers should report adverse reactions or quality problems they experience using these tablets to Pfizer either by telephone at 800-438-1985, option 1, by regular mail or by fax, or to the Food and Drug Administration’s MedWatch program.
A version of this article first appeared on Medscape.com.
Pfizer is voluntarily recalling some antihypertensive medications because of unacceptable levels of a potential carcinogen, the company announced.
The affected products are quinapril HCI/hydrochlorothiazide (Accuretic) tablets that Pfizer distributes, and two authorized generics, quinapril plus hydrochlorothiazide and quinapril HCI/hydrochlorothiazide, distributed by Greenstone. The drugs have been withdrawn because of the presence of nitrosamine, N-nitroso-quinapril.
“Although long-term ingestion of N-nitroso-quinapril may be associated with a potential increased cancer risk in humans, there is no immediate risk to patients taking this medication,” Pfizer said in a news release.
The tablets are indicated for the treatment of hypertension. Patients currently taking the products are asked to consult with their doctor about alternative treatment options.
To date, there have been no reports of adverse events related to the recall, the company said.
In all, Pfizer is recalling six lots of Accuretic tablets (two at 10 mg/12.5 mg, three at 20 mg/12.5 mg, and one at 20 mg/25 mg), one lot of quinapril plus hydrochlorothiazide 20-mg/25-mg tablets, and four lots of quinapril HCl/ hydrochlorothiazide tablets (three at 20 mg/12.5 mg and one at 20 mg/25 mg)
The recalled tablets were sold in 90-count bottles distributed in the United States and Puerto Rico between November 2019 and March 2022. Product codes and lot numbers of the recalled medications are listed on the Pfizer website.
Patients who are taking this product should consult with their health care provider or pharmacy to determine if they have the affected product. Those with the affected tablets should contact claims management firm Sedgwick by phone at 888-843-0247 Monday through Friday from 8 a.m. to 5 p.m. ET for instructions on how to return their product and obtain reimbursement.
Health care providers with medical questions regarding the recall can contact Pfizer by telephone at 800-438-1985, option 3, Monday through Friday 8 a.m. to 9 p.m. ET.
Providers should report adverse reactions or quality problems they experience using these tablets to Pfizer either by telephone at 800-438-1985, option 1, by regular mail or by fax, or to the Food and Drug Administration’s MedWatch program.
A version of this article first appeared on Medscape.com.
Intermittent fasting good for weight loss, at least short term
The health benefits of intermittent fasting are slowly being clarified as more evidence continues to emerge, say the authors of a new review of 21 studies. Initial findings suggest that fasting might be effective for mild to moderate weight loss for certain groups of people, at least in the short term.
And data so far at least dispel the myth that “people are going to feel weak and not be able to concentrate during fasting,” lead researcher Krista A. Varady, PhD, professor of nutrition in the University of Illinois at Chicago, noted in a press release from her university.
“We’ve shown it is the opposite,” she said. “They actually have a better ability to concentrate.”
Yet much longer-term data are needed on issues such as safety, Dr. Varady and colleagues note in their review in Nature Reviews: Endocrinology .
The trials so far have only been conducted in adults – generally with overweight or obesity and sometimes hypertension, dyslipidemia, and/or diabetes – but some have been performed in those of normal weight.
Dr. Varady and colleague recommend that those with type 1 diabetes, type 2 diabetes, or other comorbidities, or patients who need to take medications with meals at certain times of the day, should seek clinical supervision when considering intermittent fasting.
And currently, based on existing evidence, intermittent fasting is contraindicated for children under age 12 and those who have a history of an eating disorder or a body mass index <18.5 kg/m2. Opinions vary about the safety of supervised fasting in adolescents with obesity. Also, safety has not been evaluated in those older than age 70, and in women who are pregnant or lactating.
‘A few studies’ show 3%-8% weight loss over 2-3 months
Despite the recent surge in the popularity of intermittent fasting, “only a few studies have examined the health benefits of these diets in humans,” Dr. Varady and coauthors emphasize.
They identified 21 clinical trials of three types of intermittent fasting strategies:
Alternate day fasting (alternating between consuming 0-500 kcal on “fasting” days, followed by unlimited food on “feasting” days), six trials.
5:2 diet (“feasting” on 5 days and “fasting” on 2 days), seven trials.
Time-restricted eating (eating during a 4- to 8- hour window), nine trials.
The trials were short (mostly 5-12 weeks long) and small (10-150 participants), and mostly conducted in the United States.
They found these strategies can all produce a mild to moderate 3%-8% weight loss during 8-12 weeks, similar to that attained with a calorie-restricted diet.
Some studies found that patients had improvements in blood pressure, LDL cholesterol, triglycerides, insulin resistance, and hemoglobin A1c.
These weight-loss strategies produced few gastrointestinal, neurological, hormonal, or metabolic adverse effects; “however, as adverse outcomes are not regularly assessed in human trials of fasting, definitive conclusions regarding the safety of these diets are difficult to draw at present,” the researchers caution.
Practical advice, great anecdotes
Typically, 1-2 weeks of adjustment is needed when individuals start intermittent fasting, the researchers say.
While following this eating pattern, patients should be encouraged to consume plenty of fruits, vegetables, and whole grains to boost their fiber and micronutrient intake.
On fasting days, they should consume at least 50 g of lean protein to help control hunger and prevent excessive loss of lean mass. On those days, alcohol is permitted but not recommended. Energy drinks and coffee or tea without sugar, milk, or cream are allowed, and diet soda should be limited to two servings a day because it can increase sugar cravings.
Ideally, clinicians should regularly assess patients for adverse effects during the first 3 months of intermittent fasting. They should also monitor patients for deficiencies in vitamin D, vitamin B12, and electrolytes, as well as for changes in medications for blood pressure, lipids, and glucose that may be needed if patients lose weight.
Patients who reach their weight-loss goals and wish to stop intermittent fasting need to transition to a weight-maintenance program, possibly by increasing energy intake on fasting days to 1,000-1,200 kcal/day or widening the eating window to 12 hours in time-restricted eating.
“I get lots of emails from people saying that they have been on the diet for 10-15 years, and it reversed their type 2 diabetes, and they lost 60 pounds, and it was the only diet they could stick to,” Dr. Varady noted.
“That is always nice to hear, but we really do need long-term data to see if people can do intermittent fasting for the long term,” she reiterated.
The review was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Varady received author fees from the Hachette Book Group for the book, “The Every Other Day Diet.” The other authors have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The health benefits of intermittent fasting are slowly being clarified as more evidence continues to emerge, say the authors of a new review of 21 studies. Initial findings suggest that fasting might be effective for mild to moderate weight loss for certain groups of people, at least in the short term.
And data so far at least dispel the myth that “people are going to feel weak and not be able to concentrate during fasting,” lead researcher Krista A. Varady, PhD, professor of nutrition in the University of Illinois at Chicago, noted in a press release from her university.
“We’ve shown it is the opposite,” she said. “They actually have a better ability to concentrate.”
Yet much longer-term data are needed on issues such as safety, Dr. Varady and colleagues note in their review in Nature Reviews: Endocrinology .
The trials so far have only been conducted in adults – generally with overweight or obesity and sometimes hypertension, dyslipidemia, and/or diabetes – but some have been performed in those of normal weight.
Dr. Varady and colleague recommend that those with type 1 diabetes, type 2 diabetes, or other comorbidities, or patients who need to take medications with meals at certain times of the day, should seek clinical supervision when considering intermittent fasting.
And currently, based on existing evidence, intermittent fasting is contraindicated for children under age 12 and those who have a history of an eating disorder or a body mass index <18.5 kg/m2. Opinions vary about the safety of supervised fasting in adolescents with obesity. Also, safety has not been evaluated in those older than age 70, and in women who are pregnant or lactating.
‘A few studies’ show 3%-8% weight loss over 2-3 months
Despite the recent surge in the popularity of intermittent fasting, “only a few studies have examined the health benefits of these diets in humans,” Dr. Varady and coauthors emphasize.
They identified 21 clinical trials of three types of intermittent fasting strategies:
Alternate day fasting (alternating between consuming 0-500 kcal on “fasting” days, followed by unlimited food on “feasting” days), six trials.
5:2 diet (“feasting” on 5 days and “fasting” on 2 days), seven trials.
Time-restricted eating (eating during a 4- to 8- hour window), nine trials.
The trials were short (mostly 5-12 weeks long) and small (10-150 participants), and mostly conducted in the United States.
They found these strategies can all produce a mild to moderate 3%-8% weight loss during 8-12 weeks, similar to that attained with a calorie-restricted diet.
Some studies found that patients had improvements in blood pressure, LDL cholesterol, triglycerides, insulin resistance, and hemoglobin A1c.
These weight-loss strategies produced few gastrointestinal, neurological, hormonal, or metabolic adverse effects; “however, as adverse outcomes are not regularly assessed in human trials of fasting, definitive conclusions regarding the safety of these diets are difficult to draw at present,” the researchers caution.
Practical advice, great anecdotes
Typically, 1-2 weeks of adjustment is needed when individuals start intermittent fasting, the researchers say.
While following this eating pattern, patients should be encouraged to consume plenty of fruits, vegetables, and whole grains to boost their fiber and micronutrient intake.
On fasting days, they should consume at least 50 g of lean protein to help control hunger and prevent excessive loss of lean mass. On those days, alcohol is permitted but not recommended. Energy drinks and coffee or tea without sugar, milk, or cream are allowed, and diet soda should be limited to two servings a day because it can increase sugar cravings.
Ideally, clinicians should regularly assess patients for adverse effects during the first 3 months of intermittent fasting. They should also monitor patients for deficiencies in vitamin D, vitamin B12, and electrolytes, as well as for changes in medications for blood pressure, lipids, and glucose that may be needed if patients lose weight.
Patients who reach their weight-loss goals and wish to stop intermittent fasting need to transition to a weight-maintenance program, possibly by increasing energy intake on fasting days to 1,000-1,200 kcal/day or widening the eating window to 12 hours in time-restricted eating.
“I get lots of emails from people saying that they have been on the diet for 10-15 years, and it reversed their type 2 diabetes, and they lost 60 pounds, and it was the only diet they could stick to,” Dr. Varady noted.
“That is always nice to hear, but we really do need long-term data to see if people can do intermittent fasting for the long term,” she reiterated.
The review was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Varady received author fees from the Hachette Book Group for the book, “The Every Other Day Diet.” The other authors have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The health benefits of intermittent fasting are slowly being clarified as more evidence continues to emerge, say the authors of a new review of 21 studies. Initial findings suggest that fasting might be effective for mild to moderate weight loss for certain groups of people, at least in the short term.
And data so far at least dispel the myth that “people are going to feel weak and not be able to concentrate during fasting,” lead researcher Krista A. Varady, PhD, professor of nutrition in the University of Illinois at Chicago, noted in a press release from her university.
“We’ve shown it is the opposite,” she said. “They actually have a better ability to concentrate.”
Yet much longer-term data are needed on issues such as safety, Dr. Varady and colleagues note in their review in Nature Reviews: Endocrinology .
The trials so far have only been conducted in adults – generally with overweight or obesity and sometimes hypertension, dyslipidemia, and/or diabetes – but some have been performed in those of normal weight.
Dr. Varady and colleague recommend that those with type 1 diabetes, type 2 diabetes, or other comorbidities, or patients who need to take medications with meals at certain times of the day, should seek clinical supervision when considering intermittent fasting.
And currently, based on existing evidence, intermittent fasting is contraindicated for children under age 12 and those who have a history of an eating disorder or a body mass index <18.5 kg/m2. Opinions vary about the safety of supervised fasting in adolescents with obesity. Also, safety has not been evaluated in those older than age 70, and in women who are pregnant or lactating.
‘A few studies’ show 3%-8% weight loss over 2-3 months
Despite the recent surge in the popularity of intermittent fasting, “only a few studies have examined the health benefits of these diets in humans,” Dr. Varady and coauthors emphasize.
They identified 21 clinical trials of three types of intermittent fasting strategies:
Alternate day fasting (alternating between consuming 0-500 kcal on “fasting” days, followed by unlimited food on “feasting” days), six trials.
5:2 diet (“feasting” on 5 days and “fasting” on 2 days), seven trials.
Time-restricted eating (eating during a 4- to 8- hour window), nine trials.
The trials were short (mostly 5-12 weeks long) and small (10-150 participants), and mostly conducted in the United States.
They found these strategies can all produce a mild to moderate 3%-8% weight loss during 8-12 weeks, similar to that attained with a calorie-restricted diet.
Some studies found that patients had improvements in blood pressure, LDL cholesterol, triglycerides, insulin resistance, and hemoglobin A1c.
These weight-loss strategies produced few gastrointestinal, neurological, hormonal, or metabolic adverse effects; “however, as adverse outcomes are not regularly assessed in human trials of fasting, definitive conclusions regarding the safety of these diets are difficult to draw at present,” the researchers caution.
Practical advice, great anecdotes
Typically, 1-2 weeks of adjustment is needed when individuals start intermittent fasting, the researchers say.
While following this eating pattern, patients should be encouraged to consume plenty of fruits, vegetables, and whole grains to boost their fiber and micronutrient intake.
On fasting days, they should consume at least 50 g of lean protein to help control hunger and prevent excessive loss of lean mass. On those days, alcohol is permitted but not recommended. Energy drinks and coffee or tea without sugar, milk, or cream are allowed, and diet soda should be limited to two servings a day because it can increase sugar cravings.
Ideally, clinicians should regularly assess patients for adverse effects during the first 3 months of intermittent fasting. They should also monitor patients for deficiencies in vitamin D, vitamin B12, and electrolytes, as well as for changes in medications for blood pressure, lipids, and glucose that may be needed if patients lose weight.
Patients who reach their weight-loss goals and wish to stop intermittent fasting need to transition to a weight-maintenance program, possibly by increasing energy intake on fasting days to 1,000-1,200 kcal/day or widening the eating window to 12 hours in time-restricted eating.
“I get lots of emails from people saying that they have been on the diet for 10-15 years, and it reversed their type 2 diabetes, and they lost 60 pounds, and it was the only diet they could stick to,” Dr. Varady noted.
“That is always nice to hear, but we really do need long-term data to see if people can do intermittent fasting for the long term,” she reiterated.
The review was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Varady received author fees from the Hachette Book Group for the book, “The Every Other Day Diet.” The other authors have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE REVIEWS: ENDOCRINOLOGY
Mild COVID-19 infection linked to later type 2 diabetes
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
FROM DIABETOLOGIA
COVID-19 doesn’t spike A1c levels
Key takeaways
Results from a retrospective, observational, case-control study of more than 20,000 people from a single U.S. medical center showed a statistically significant but clinically insignificant increase in A1c in people following COVID-19 infection, in both those with and without diabetes.
After people received a diagnosis of COVID-19 infection, they were 40% more likely to also receive a diagnosis of type 2 diabetes, compared with people who tested negative for COVID-19, a difference that was significant and could be explained by the increased medical care received by people who test positive for COVID-19.
The risk of incident diabetic ketoacidosis (DKA) among people who tested positive for COVID-19 was significantly higher among those with pre-existing type 2 diabetes, those using insulin, and among Black individuals.
Why this matters
The authors said that their study is the first report of evidence that infection with COVID-19 affects A1c levels in a large, real-world clinical cohort.
Until now, the impact of COVID-19 infection on A1c remained unclear. Results from previous studies indicated that COVID-19 infection may increase A1c levels, but the studied cohorts were small and lacked uninfected controls.
The current study included 8,755 people infected with COVID-19, had data from both before and after the infection on diabetes status and A1c levels, and also included many matched, uninfected people who served as controls.
Study design
Data came from a Cleveland Clinic registry that included 81,093 people who tested positive for COVID-19 between March 2020 and May 2021 and 153,034 matched individuals who tested negative for COVID-19 during the same period.
The researchers retrospectively selected patients with an A1c recorded within 12 months before their COVID-19 test, as well as a second A1c value recorded within 12 months after COVID-19 testing. This produced a study cohort of 8,755 COVID-positive people and 11,998 matched people who tested negative for COVID-19.
To evaluate the risk of DKA onset after COVID-19 infection, the authors identified two sub-cohorts that excluded those with a history of DKA. The sub-cohorts were 701 people with type 1 diabetes and 21,830 with type 2 diabetes.
Key results
The investigators found a statistically significant but clinically insignificant A1c increase following a positive COVID-19 test, an average A1c increase of 0.06 percentage points. Those who tested negative for COVID-19 had a clinically insignificant change in their average A1c level that was of borderline statistical significance, an average increase of 0.02 percentage points (P = .05).
The statistically significant but clinically insignificant increase in A1c following infection with COVID-19 was similar in people with and without type 2 diabetes prior to infection.
In patients with type 2 diabetes who became infected with COVID-19, the researchers saw significant positive associations between higher A1c levels before infection and time to hospitalization (hazard ratio, 1.07), need for assisted breathing (HR, 1.06), and ICU admission (HR, 1.07).
Following a COVID-19 infection, people were 40% more likely to receive a diagnosis of incident type 2 diabetes, compared with matched uninfected people. The authors said a possible explanation is that after diagnosis of COVID-19, infected people in general received more intensified care that led to better identification of those with underlying type 2 diabetes.
The 701 people included with pre-existing type 1 diabetes showed no significant difference in their rate of developing DKA between those infected and not infected with COVID-19.
Among the 21,830 people with pre-existing type 2 diabetes, the DKA risk was a significant 35% greater for those who were infected with COVID-19, compared with those who were uninfected. The magnitude of this increased relative risk was even higher among the patients with type 2 diabetes who used insulin as part of their treatment.
The difference in DKA risk didn’t differ between Black and White patients who were not infected with COVID-19, but among those infected by COVID-19, Black patients were more than twice as likely to be diagnosed with DKA, compared with White patients, a significant difference.
Black patients with type 2 diabetes who became infected with COVID-19 had a significant (63%) increased rate of DKA compared with Black patients with type 2 diabetes who remained uninfected.
Limitations
The study included patients with A1c measurements made up to 12 months prior to their COVID-19 test, and hence comorbid conditions, medication changes during this period, or other factors may have affected subsequent A1c levels. To address this, the authors also assessed outcomes at 3- and 6-month intervals, which produced results consistent with the 12-month findings.
The researchers did not have A1c values for many of the more than 234,000 people in the entire registry who underwent COVID-19 testing from March 2020-May 2021 at the Cleveland Clinic, omissions that may have biased the study cohort.
This was a single-center study. Some patients may have received care outside of the center, hence records of those episodes could not be included.
Disclosures
The study received no commercial funding. Four authors received consulting and speaker honoraria and research funding from AstraZeneca, Bayer, Boehringer Ingelheim, Corcept Therapeutics, Diasome, Eli Lilly, Merck, Novo Nordisk, and Sanofi. Three authors have intellectual property related to treatment decisionmaking in the context of type 2 diabetes.
This is a summary of a preprint research study “Impacts of COVID-19 on glycemia and risk of diabetic ketoacidosis,” written by researchers at the Cleveland Clinic on medRxiv. The study has not yet been peer reviewed. The full text of the study can be found on medRxiv.org.
A version of this article first appeared on Medscape.com.
Key takeaways
Results from a retrospective, observational, case-control study of more than 20,000 people from a single U.S. medical center showed a statistically significant but clinically insignificant increase in A1c in people following COVID-19 infection, in both those with and without diabetes.
After people received a diagnosis of COVID-19 infection, they were 40% more likely to also receive a diagnosis of type 2 diabetes, compared with people who tested negative for COVID-19, a difference that was significant and could be explained by the increased medical care received by people who test positive for COVID-19.
The risk of incident diabetic ketoacidosis (DKA) among people who tested positive for COVID-19 was significantly higher among those with pre-existing type 2 diabetes, those using insulin, and among Black individuals.
Why this matters
The authors said that their study is the first report of evidence that infection with COVID-19 affects A1c levels in a large, real-world clinical cohort.
Until now, the impact of COVID-19 infection on A1c remained unclear. Results from previous studies indicated that COVID-19 infection may increase A1c levels, but the studied cohorts were small and lacked uninfected controls.
The current study included 8,755 people infected with COVID-19, had data from both before and after the infection on diabetes status and A1c levels, and also included many matched, uninfected people who served as controls.
Study design
Data came from a Cleveland Clinic registry that included 81,093 people who tested positive for COVID-19 between March 2020 and May 2021 and 153,034 matched individuals who tested negative for COVID-19 during the same period.
The researchers retrospectively selected patients with an A1c recorded within 12 months before their COVID-19 test, as well as a second A1c value recorded within 12 months after COVID-19 testing. This produced a study cohort of 8,755 COVID-positive people and 11,998 matched people who tested negative for COVID-19.
To evaluate the risk of DKA onset after COVID-19 infection, the authors identified two sub-cohorts that excluded those with a history of DKA. The sub-cohorts were 701 people with type 1 diabetes and 21,830 with type 2 diabetes.
Key results
The investigators found a statistically significant but clinically insignificant A1c increase following a positive COVID-19 test, an average A1c increase of 0.06 percentage points. Those who tested negative for COVID-19 had a clinically insignificant change in their average A1c level that was of borderline statistical significance, an average increase of 0.02 percentage points (P = .05).
The statistically significant but clinically insignificant increase in A1c following infection with COVID-19 was similar in people with and without type 2 diabetes prior to infection.
In patients with type 2 diabetes who became infected with COVID-19, the researchers saw significant positive associations between higher A1c levels before infection and time to hospitalization (hazard ratio, 1.07), need for assisted breathing (HR, 1.06), and ICU admission (HR, 1.07).
Following a COVID-19 infection, people were 40% more likely to receive a diagnosis of incident type 2 diabetes, compared with matched uninfected people. The authors said a possible explanation is that after diagnosis of COVID-19, infected people in general received more intensified care that led to better identification of those with underlying type 2 diabetes.
The 701 people included with pre-existing type 1 diabetes showed no significant difference in their rate of developing DKA between those infected and not infected with COVID-19.
Among the 21,830 people with pre-existing type 2 diabetes, the DKA risk was a significant 35% greater for those who were infected with COVID-19, compared with those who were uninfected. The magnitude of this increased relative risk was even higher among the patients with type 2 diabetes who used insulin as part of their treatment.
The difference in DKA risk didn’t differ between Black and White patients who were not infected with COVID-19, but among those infected by COVID-19, Black patients were more than twice as likely to be diagnosed with DKA, compared with White patients, a significant difference.
Black patients with type 2 diabetes who became infected with COVID-19 had a significant (63%) increased rate of DKA compared with Black patients with type 2 diabetes who remained uninfected.
Limitations
The study included patients with A1c measurements made up to 12 months prior to their COVID-19 test, and hence comorbid conditions, medication changes during this period, or other factors may have affected subsequent A1c levels. To address this, the authors also assessed outcomes at 3- and 6-month intervals, which produced results consistent with the 12-month findings.
The researchers did not have A1c values for many of the more than 234,000 people in the entire registry who underwent COVID-19 testing from March 2020-May 2021 at the Cleveland Clinic, omissions that may have biased the study cohort.
This was a single-center study. Some patients may have received care outside of the center, hence records of those episodes could not be included.
Disclosures
The study received no commercial funding. Four authors received consulting and speaker honoraria and research funding from AstraZeneca, Bayer, Boehringer Ingelheim, Corcept Therapeutics, Diasome, Eli Lilly, Merck, Novo Nordisk, and Sanofi. Three authors have intellectual property related to treatment decisionmaking in the context of type 2 diabetes.
This is a summary of a preprint research study “Impacts of COVID-19 on glycemia and risk of diabetic ketoacidosis,” written by researchers at the Cleveland Clinic on medRxiv. The study has not yet been peer reviewed. The full text of the study can be found on medRxiv.org.
A version of this article first appeared on Medscape.com.
Key takeaways
Results from a retrospective, observational, case-control study of more than 20,000 people from a single U.S. medical center showed a statistically significant but clinically insignificant increase in A1c in people following COVID-19 infection, in both those with and without diabetes.
After people received a diagnosis of COVID-19 infection, they were 40% more likely to also receive a diagnosis of type 2 diabetes, compared with people who tested negative for COVID-19, a difference that was significant and could be explained by the increased medical care received by people who test positive for COVID-19.
The risk of incident diabetic ketoacidosis (DKA) among people who tested positive for COVID-19 was significantly higher among those with pre-existing type 2 diabetes, those using insulin, and among Black individuals.
Why this matters
The authors said that their study is the first report of evidence that infection with COVID-19 affects A1c levels in a large, real-world clinical cohort.
Until now, the impact of COVID-19 infection on A1c remained unclear. Results from previous studies indicated that COVID-19 infection may increase A1c levels, but the studied cohorts were small and lacked uninfected controls.
The current study included 8,755 people infected with COVID-19, had data from both before and after the infection on diabetes status and A1c levels, and also included many matched, uninfected people who served as controls.
Study design
Data came from a Cleveland Clinic registry that included 81,093 people who tested positive for COVID-19 between March 2020 and May 2021 and 153,034 matched individuals who tested negative for COVID-19 during the same period.
The researchers retrospectively selected patients with an A1c recorded within 12 months before their COVID-19 test, as well as a second A1c value recorded within 12 months after COVID-19 testing. This produced a study cohort of 8,755 COVID-positive people and 11,998 matched people who tested negative for COVID-19.
To evaluate the risk of DKA onset after COVID-19 infection, the authors identified two sub-cohorts that excluded those with a history of DKA. The sub-cohorts were 701 people with type 1 diabetes and 21,830 with type 2 diabetes.
Key results
The investigators found a statistically significant but clinically insignificant A1c increase following a positive COVID-19 test, an average A1c increase of 0.06 percentage points. Those who tested negative for COVID-19 had a clinically insignificant change in their average A1c level that was of borderline statistical significance, an average increase of 0.02 percentage points (P = .05).
The statistically significant but clinically insignificant increase in A1c following infection with COVID-19 was similar in people with and without type 2 diabetes prior to infection.
In patients with type 2 diabetes who became infected with COVID-19, the researchers saw significant positive associations between higher A1c levels before infection and time to hospitalization (hazard ratio, 1.07), need for assisted breathing (HR, 1.06), and ICU admission (HR, 1.07).
Following a COVID-19 infection, people were 40% more likely to receive a diagnosis of incident type 2 diabetes, compared with matched uninfected people. The authors said a possible explanation is that after diagnosis of COVID-19, infected people in general received more intensified care that led to better identification of those with underlying type 2 diabetes.
The 701 people included with pre-existing type 1 diabetes showed no significant difference in their rate of developing DKA between those infected and not infected with COVID-19.
Among the 21,830 people with pre-existing type 2 diabetes, the DKA risk was a significant 35% greater for those who were infected with COVID-19, compared with those who were uninfected. The magnitude of this increased relative risk was even higher among the patients with type 2 diabetes who used insulin as part of their treatment.
The difference in DKA risk didn’t differ between Black and White patients who were not infected with COVID-19, but among those infected by COVID-19, Black patients were more than twice as likely to be diagnosed with DKA, compared with White patients, a significant difference.
Black patients with type 2 diabetes who became infected with COVID-19 had a significant (63%) increased rate of DKA compared with Black patients with type 2 diabetes who remained uninfected.
Limitations
The study included patients with A1c measurements made up to 12 months prior to their COVID-19 test, and hence comorbid conditions, medication changes during this period, or other factors may have affected subsequent A1c levels. To address this, the authors also assessed outcomes at 3- and 6-month intervals, which produced results consistent with the 12-month findings.
The researchers did not have A1c values for many of the more than 234,000 people in the entire registry who underwent COVID-19 testing from March 2020-May 2021 at the Cleveland Clinic, omissions that may have biased the study cohort.
This was a single-center study. Some patients may have received care outside of the center, hence records of those episodes could not be included.
Disclosures
The study received no commercial funding. Four authors received consulting and speaker honoraria and research funding from AstraZeneca, Bayer, Boehringer Ingelheim, Corcept Therapeutics, Diasome, Eli Lilly, Merck, Novo Nordisk, and Sanofi. Three authors have intellectual property related to treatment decisionmaking in the context of type 2 diabetes.
This is a summary of a preprint research study “Impacts of COVID-19 on glycemia and risk of diabetic ketoacidosis,” written by researchers at the Cleveland Clinic on medRxiv. The study has not yet been peer reviewed. The full text of the study can be found on medRxiv.org.
A version of this article first appeared on Medscape.com.