User login
Clinical Psychiatry News is the online destination and multimedia properties of Clinica Psychiatry News, the independent news publication for psychiatrists. Since 1971, Clinical Psychiatry News has been the leading source of news and commentary about clinical developments in psychiatry as well as health care policy and regulations that affect the physician's practice.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
ketamine
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
suicide
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-cpn')]
div[contains(@class, 'pane-pub-home-cpn')]
div[contains(@class, 'pane-pub-topic-cpn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Tough to tell COVID from smoke inhalation symptoms — And flu season’s coming
The patients walk into Dr. Melissa Marshall’s community clinics in Northern California with the telltale symptoms. They’re having trouble breathing. It may even hurt to inhale. They’ve got a cough, and the sore throat is definitely there.
A straight case of COVID-19? Not so fast. This is wildfire country.
Up and down the West Coast, hospitals and health facilities are reporting an influx of patients with problems most likely related to smoke inhalation. As fires rage largely uncontrolled amid dry heat and high winds, smoke and ash are billowing and settling on coastal areas like San Francisco and cities and towns hundreds of miles inland as well, turning the sky orange or gray and making even ordinary breathing difficult.
But that, Marshall said, is only part of the challenge.
“Obviously, there’s overlap in the symptoms,” said Marshall, the CEO of CommuniCare, a collection of six clinics in Yolo County, near Sacramento, that treats mostly underinsured and uninsured patients. “Any time someone comes in with even some of those symptoms, we ask ourselves, ‘Is it COVID?’ At the end of the day, clinically speaking, I still want to rule out the virus.”
The protocol is to treat the symptoms, whatever their cause, while recommending that the patient quarantine until test results for the virus come back, she said.
It is a scene playing out in numerous hospitals. Administrators and physicians, finely attuned to COVID-19’s ability to spread quickly and wreak havoc, simply won’t take a chance when they recognize symptoms that could emanate from the virus.
“We’ve seen an increase in patients presenting to the emergency department with respiratory distress,” said Dr. Nanette Mickiewicz, president and CEO of Dominican Hospital in Santa Cruz. “As this can also be a symptom of COVID-19, we’re treating these patients as we would any person under investigation for coronavirus until we can rule them out through our screening process.” During the workup, symptoms that are more specific to COVID-19, like fever, would become apparent.
For the workers at Dominican, the issue moved to the top of the list quickly. Santa Cruz and San Mateo counties have borne the brunt of the CZU Lightning Complex fires, which as of Sept. 10 had burned more than 86,000 acres, destroying 1,100 structures and threatening more than 7,600 others. Nearly a month after they began, the fires were approximately 84% contained, but thousands of people remained evacuated.
Dominican, a Dignity Health hospital, is “open, safe and providing care,” Mickiewicz said. Multiple tents erected outside the building serve as an extension of its ER waiting room. They also are used to perform what has come to be understood as an essential role: separating those with symptoms of COVID-19 from those without.
At the two Solano County hospitals operated by NorthBay Healthcare, the path of some of the wildfires prompted officials to review their evacuation procedures, said spokesperson Steve Huddleston. They ultimately avoided the need to evacuate patients, and new ones arrived with COVID-like symptoms that may actually have been from smoke inhalation.
Huddleston said NorthBay’s intake process “calls for anyone with COVID characteristics to be handled as [a] patient under investigation for COVID, which means they’re separated, screened and managed by staff in special PPE.” At the two hospitals, which have handled nearly 200 COVID cases so far, the protocol is well established.
Hospitals in California, though not under siege in most cases, are dealing with multiple issues they might typically face only sporadically. In Napa County, Adventist Health St. Helena Hospital evacuated 51 patients on a single August night as a fire approached, moving them to 10 other facilities according to their needs and bed space. After a 10-day closure, the hospital was allowed to reopen as evacuation orders were lifted, the fire having been contained some distance away.
The wildfires are also taking a personal toll on health care workers. CommuniCare’s Marshall lost her family’s home in rural Winters, along with 20 acres of olive trees and other plantings that surrounded it, in the Aug. 19 fires that swept through Solano County.
“They called it a ‘firenado,’ ” Marshall said. An apparent confluence of three fires raged out of control, demolishing thousands of acres. With her family safely accounted for and temporary housing arranged by a friend, she returned to work. “Our clinics interact with a very vulnerable population,” she said, “and this is a critical time for them.”
While she pondered how her family would rebuild, the CEO was faced with another immediate crisis: the clinic’s shortage of supplies. Last month, CommuniCare got down to 19 COVID test kits on hand, and ran so low on swabs “that we were literally turning to our veterinary friends for reinforcements,” the doctor said. The clinic’s COVID test results, meanwhile, were taking nearly two weeks to be returned from an overwhelmed outside lab, rendering contact tracing almost useless.
Those situations have been addressed, at least temporarily, Marshall said. But although the West Coast is in the most dangerous time of year for wildfires, generally September to December, another complication for health providers lies on the horizon: flu season.
The Southern Hemisphere, whose influenza trends during our summer months typically predict what’s to come for the U.S., has had very little of the disease this year, presumably because of restricted travel, social distancing and face masks. But it’s too early to be sure what the U.S. flu season will entail.
“You can start to see some cases of the flu in late October,” said Marshall, “and the reality is that it’s going to carry a number of characteristics that could also be symptomatic of COVID. And nothing changes: You have to rule it out, just to eliminate the risk.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente. This KHN story first published on California Healthline, a service of the California Health Care Foundation.
The patients walk into Dr. Melissa Marshall’s community clinics in Northern California with the telltale symptoms. They’re having trouble breathing. It may even hurt to inhale. They’ve got a cough, and the sore throat is definitely there.
A straight case of COVID-19? Not so fast. This is wildfire country.
Up and down the West Coast, hospitals and health facilities are reporting an influx of patients with problems most likely related to smoke inhalation. As fires rage largely uncontrolled amid dry heat and high winds, smoke and ash are billowing and settling on coastal areas like San Francisco and cities and towns hundreds of miles inland as well, turning the sky orange or gray and making even ordinary breathing difficult.
But that, Marshall said, is only part of the challenge.
“Obviously, there’s overlap in the symptoms,” said Marshall, the CEO of CommuniCare, a collection of six clinics in Yolo County, near Sacramento, that treats mostly underinsured and uninsured patients. “Any time someone comes in with even some of those symptoms, we ask ourselves, ‘Is it COVID?’ At the end of the day, clinically speaking, I still want to rule out the virus.”
The protocol is to treat the symptoms, whatever their cause, while recommending that the patient quarantine until test results for the virus come back, she said.
It is a scene playing out in numerous hospitals. Administrators and physicians, finely attuned to COVID-19’s ability to spread quickly and wreak havoc, simply won’t take a chance when they recognize symptoms that could emanate from the virus.
“We’ve seen an increase in patients presenting to the emergency department with respiratory distress,” said Dr. Nanette Mickiewicz, president and CEO of Dominican Hospital in Santa Cruz. “As this can also be a symptom of COVID-19, we’re treating these patients as we would any person under investigation for coronavirus until we can rule them out through our screening process.” During the workup, symptoms that are more specific to COVID-19, like fever, would become apparent.
For the workers at Dominican, the issue moved to the top of the list quickly. Santa Cruz and San Mateo counties have borne the brunt of the CZU Lightning Complex fires, which as of Sept. 10 had burned more than 86,000 acres, destroying 1,100 structures and threatening more than 7,600 others. Nearly a month after they began, the fires were approximately 84% contained, but thousands of people remained evacuated.
Dominican, a Dignity Health hospital, is “open, safe and providing care,” Mickiewicz said. Multiple tents erected outside the building serve as an extension of its ER waiting room. They also are used to perform what has come to be understood as an essential role: separating those with symptoms of COVID-19 from those without.
At the two Solano County hospitals operated by NorthBay Healthcare, the path of some of the wildfires prompted officials to review their evacuation procedures, said spokesperson Steve Huddleston. They ultimately avoided the need to evacuate patients, and new ones arrived with COVID-like symptoms that may actually have been from smoke inhalation.
Huddleston said NorthBay’s intake process “calls for anyone with COVID characteristics to be handled as [a] patient under investigation for COVID, which means they’re separated, screened and managed by staff in special PPE.” At the two hospitals, which have handled nearly 200 COVID cases so far, the protocol is well established.
Hospitals in California, though not under siege in most cases, are dealing with multiple issues they might typically face only sporadically. In Napa County, Adventist Health St. Helena Hospital evacuated 51 patients on a single August night as a fire approached, moving them to 10 other facilities according to their needs and bed space. After a 10-day closure, the hospital was allowed to reopen as evacuation orders were lifted, the fire having been contained some distance away.
The wildfires are also taking a personal toll on health care workers. CommuniCare’s Marshall lost her family’s home in rural Winters, along with 20 acres of olive trees and other plantings that surrounded it, in the Aug. 19 fires that swept through Solano County.
“They called it a ‘firenado,’ ” Marshall said. An apparent confluence of three fires raged out of control, demolishing thousands of acres. With her family safely accounted for and temporary housing arranged by a friend, she returned to work. “Our clinics interact with a very vulnerable population,” she said, “and this is a critical time for them.”
While she pondered how her family would rebuild, the CEO was faced with another immediate crisis: the clinic’s shortage of supplies. Last month, CommuniCare got down to 19 COVID test kits on hand, and ran so low on swabs “that we were literally turning to our veterinary friends for reinforcements,” the doctor said. The clinic’s COVID test results, meanwhile, were taking nearly two weeks to be returned from an overwhelmed outside lab, rendering contact tracing almost useless.
Those situations have been addressed, at least temporarily, Marshall said. But although the West Coast is in the most dangerous time of year for wildfires, generally September to December, another complication for health providers lies on the horizon: flu season.
The Southern Hemisphere, whose influenza trends during our summer months typically predict what’s to come for the U.S., has had very little of the disease this year, presumably because of restricted travel, social distancing and face masks. But it’s too early to be sure what the U.S. flu season will entail.
“You can start to see some cases of the flu in late October,” said Marshall, “and the reality is that it’s going to carry a number of characteristics that could also be symptomatic of COVID. And nothing changes: You have to rule it out, just to eliminate the risk.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente. This KHN story first published on California Healthline, a service of the California Health Care Foundation.
The patients walk into Dr. Melissa Marshall’s community clinics in Northern California with the telltale symptoms. They’re having trouble breathing. It may even hurt to inhale. They’ve got a cough, and the sore throat is definitely there.
A straight case of COVID-19? Not so fast. This is wildfire country.
Up and down the West Coast, hospitals and health facilities are reporting an influx of patients with problems most likely related to smoke inhalation. As fires rage largely uncontrolled amid dry heat and high winds, smoke and ash are billowing and settling on coastal areas like San Francisco and cities and towns hundreds of miles inland as well, turning the sky orange or gray and making even ordinary breathing difficult.
But that, Marshall said, is only part of the challenge.
“Obviously, there’s overlap in the symptoms,” said Marshall, the CEO of CommuniCare, a collection of six clinics in Yolo County, near Sacramento, that treats mostly underinsured and uninsured patients. “Any time someone comes in with even some of those symptoms, we ask ourselves, ‘Is it COVID?’ At the end of the day, clinically speaking, I still want to rule out the virus.”
The protocol is to treat the symptoms, whatever their cause, while recommending that the patient quarantine until test results for the virus come back, she said.
It is a scene playing out in numerous hospitals. Administrators and physicians, finely attuned to COVID-19’s ability to spread quickly and wreak havoc, simply won’t take a chance when they recognize symptoms that could emanate from the virus.
“We’ve seen an increase in patients presenting to the emergency department with respiratory distress,” said Dr. Nanette Mickiewicz, president and CEO of Dominican Hospital in Santa Cruz. “As this can also be a symptom of COVID-19, we’re treating these patients as we would any person under investigation for coronavirus until we can rule them out through our screening process.” During the workup, symptoms that are more specific to COVID-19, like fever, would become apparent.
For the workers at Dominican, the issue moved to the top of the list quickly. Santa Cruz and San Mateo counties have borne the brunt of the CZU Lightning Complex fires, which as of Sept. 10 had burned more than 86,000 acres, destroying 1,100 structures and threatening more than 7,600 others. Nearly a month after they began, the fires were approximately 84% contained, but thousands of people remained evacuated.
Dominican, a Dignity Health hospital, is “open, safe and providing care,” Mickiewicz said. Multiple tents erected outside the building serve as an extension of its ER waiting room. They also are used to perform what has come to be understood as an essential role: separating those with symptoms of COVID-19 from those without.
At the two Solano County hospitals operated by NorthBay Healthcare, the path of some of the wildfires prompted officials to review their evacuation procedures, said spokesperson Steve Huddleston. They ultimately avoided the need to evacuate patients, and new ones arrived with COVID-like symptoms that may actually have been from smoke inhalation.
Huddleston said NorthBay’s intake process “calls for anyone with COVID characteristics to be handled as [a] patient under investigation for COVID, which means they’re separated, screened and managed by staff in special PPE.” At the two hospitals, which have handled nearly 200 COVID cases so far, the protocol is well established.
Hospitals in California, though not under siege in most cases, are dealing with multiple issues they might typically face only sporadically. In Napa County, Adventist Health St. Helena Hospital evacuated 51 patients on a single August night as a fire approached, moving them to 10 other facilities according to their needs and bed space. After a 10-day closure, the hospital was allowed to reopen as evacuation orders were lifted, the fire having been contained some distance away.
The wildfires are also taking a personal toll on health care workers. CommuniCare’s Marshall lost her family’s home in rural Winters, along with 20 acres of olive trees and other plantings that surrounded it, in the Aug. 19 fires that swept through Solano County.
“They called it a ‘firenado,’ ” Marshall said. An apparent confluence of three fires raged out of control, demolishing thousands of acres. With her family safely accounted for and temporary housing arranged by a friend, she returned to work. “Our clinics interact with a very vulnerable population,” she said, “and this is a critical time for them.”
While she pondered how her family would rebuild, the CEO was faced with another immediate crisis: the clinic’s shortage of supplies. Last month, CommuniCare got down to 19 COVID test kits on hand, and ran so low on swabs “that we were literally turning to our veterinary friends for reinforcements,” the doctor said. The clinic’s COVID test results, meanwhile, were taking nearly two weeks to be returned from an overwhelmed outside lab, rendering contact tracing almost useless.
Those situations have been addressed, at least temporarily, Marshall said. But although the West Coast is in the most dangerous time of year for wildfires, generally September to December, another complication for health providers lies on the horizon: flu season.
The Southern Hemisphere, whose influenza trends during our summer months typically predict what’s to come for the U.S., has had very little of the disease this year, presumably because of restricted travel, social distancing and face masks. But it’s too early to be sure what the U.S. flu season will entail.
“You can start to see some cases of the flu in late October,” said Marshall, “and the reality is that it’s going to carry a number of characteristics that could also be symptomatic of COVID. And nothing changes: You have to rule it out, just to eliminate the risk.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente. This KHN story first published on California Healthline, a service of the California Health Care Foundation.
COVID-19 outcomes no worse in patients on TNF inhibitors or methotrexate
Continued use of tumor necrosis factor inhibitors or methotrexate is acceptable in most patients who acquire COVID-19, results of a recent cohort study suggest.
Among patients on tumor necrosis factor inhibitors (TNFi) or methotrexate who developed COVID-19, death and hospitalization rates were similar to matched COVID-19 patients not on those medications, according to authors of the multicenter research network study.
Reassuringly, likelihood of hospitalization and mortality were not significantly different between 214 patients with COVID-19 taking TNFi or methotrexate and 31,862 matched COVID-19 patients not on those medications, according to the investigators, whose findings were published recently in the Journal of the American Academy of Dermatology.
Zachary Zinn, MD, corresponding author on the study, said in an interview that the findings suggest these medicines can be safely continued in the majority of patients taking them during the COVID-19 pandemic.
“If you’re a prescribing physician who’s giving patients TNF inhibitors or methotrexate or both, I think you can comfortably tell your patients there is good data that these do not lead to worse outcomes if you get COVID-19,” said Dr. Zinn, associate professor in the department of dermatology at West Virginia University, Morgantown.
The findings from these researchers corroborate a growing body of evidence suggesting that immunosuppressive treatments can be continued in patients with dermatologic and rheumatic conditions.
In recent guidance from the National Psoriasis Foundation, released Sept. 4, an expert consensus panel cited 15 studies that they said suggested that treatments for psoriasis or psoriatic arthritis “do not meaningfully alter the risk of acquiring SARS-CoV-2 infection or having worse COVID-19 outcomes.”
That said, the data to date are mainly from small case series and registry studies based on spontaneously reported COVID-19 cases, which suggests a continued need for shared decision making. In addition, chronic systemic corticosteroids should be avoided for management of psoriatic arthritis, the guidance states, based on rheumatology and gastroenterology literature suggesting this treatment is linked to worse COVID-19 outcomes.
In the interview, Dr. Zinn noted that some previous studies of immunosuppressive treatments in patients who acquire COVID-19 have aggregated data on numerous classes of biologic medications, lessening the strength of data for each specific medication.
“By focusing specifically on TNF inhibitors and methotrexate, this study gives better guidance to prescribers of these medications,” he said.
To see whether TNFi or methotrexate increased risk of worsened COVID-19 outcomes, Dr. Zinn and coinvestigators evaluated data from TriNetX, a research network that includes approximately 53 million unique patient records, predominantly in the United States.
They identified 32,076 adult patients with COVID-19, of whom 214 had recent exposure to TNFi or methotrexate. The patients in the TNFi/methotrexate group were similar in age to those without exposure to those drugs, at 55.1 versus 53.2 years, respectively. However, patients in the drug exposure group were more frequently White, female, and had substantially more comorbidities, including diabetes and obesity, according to the investigators.
Nevertheless, the likelihood of hospitalization was not statistically different in the TNFi/methotrexate group versus the non-TNFi/methotrexate group, with a risk ratio of 0.91 (95% confidence interval, 0.68-1.22; P = .5260).
Likewise, the likelihood of death was not different between groups, with a RR of 0.87 (95% CI, 0.42-1.78; P = .6958). Looking at subgroups of patients exposed to TNFi or methotrexate only didn’t change the results, the investigators added.
Taken together, the findings argue against interruption of these treatments because of the fear of the possibly worse COVID-19 outcomes, the investigators concluded, although they emphasized the need for more research.
“Because the COVID-19 pandemic is ongoing, there is a desperate need for evidence-based data on biologic and immunomodulator exposure in the setting of COVID-19 infection,” they wrote.
Dr. Zinn and coauthors reported no conflicts of interest and no funding sources related to the study.
SOURCE: Zinn Z et al. J Am Acad Dermatol. 2020 Sep 11. doi: 10.1016/j.jaad.2020.09.009.
Continued use of tumor necrosis factor inhibitors or methotrexate is acceptable in most patients who acquire COVID-19, results of a recent cohort study suggest.
Among patients on tumor necrosis factor inhibitors (TNFi) or methotrexate who developed COVID-19, death and hospitalization rates were similar to matched COVID-19 patients not on those medications, according to authors of the multicenter research network study.
Reassuringly, likelihood of hospitalization and mortality were not significantly different between 214 patients with COVID-19 taking TNFi or methotrexate and 31,862 matched COVID-19 patients not on those medications, according to the investigators, whose findings were published recently in the Journal of the American Academy of Dermatology.
Zachary Zinn, MD, corresponding author on the study, said in an interview that the findings suggest these medicines can be safely continued in the majority of patients taking them during the COVID-19 pandemic.
“If you’re a prescribing physician who’s giving patients TNF inhibitors or methotrexate or both, I think you can comfortably tell your patients there is good data that these do not lead to worse outcomes if you get COVID-19,” said Dr. Zinn, associate professor in the department of dermatology at West Virginia University, Morgantown.
The findings from these researchers corroborate a growing body of evidence suggesting that immunosuppressive treatments can be continued in patients with dermatologic and rheumatic conditions.
In recent guidance from the National Psoriasis Foundation, released Sept. 4, an expert consensus panel cited 15 studies that they said suggested that treatments for psoriasis or psoriatic arthritis “do not meaningfully alter the risk of acquiring SARS-CoV-2 infection or having worse COVID-19 outcomes.”
That said, the data to date are mainly from small case series and registry studies based on spontaneously reported COVID-19 cases, which suggests a continued need for shared decision making. In addition, chronic systemic corticosteroids should be avoided for management of psoriatic arthritis, the guidance states, based on rheumatology and gastroenterology literature suggesting this treatment is linked to worse COVID-19 outcomes.
In the interview, Dr. Zinn noted that some previous studies of immunosuppressive treatments in patients who acquire COVID-19 have aggregated data on numerous classes of biologic medications, lessening the strength of data for each specific medication.
“By focusing specifically on TNF inhibitors and methotrexate, this study gives better guidance to prescribers of these medications,” he said.
To see whether TNFi or methotrexate increased risk of worsened COVID-19 outcomes, Dr. Zinn and coinvestigators evaluated data from TriNetX, a research network that includes approximately 53 million unique patient records, predominantly in the United States.
They identified 32,076 adult patients with COVID-19, of whom 214 had recent exposure to TNFi or methotrexate. The patients in the TNFi/methotrexate group were similar in age to those without exposure to those drugs, at 55.1 versus 53.2 years, respectively. However, patients in the drug exposure group were more frequently White, female, and had substantially more comorbidities, including diabetes and obesity, according to the investigators.
Nevertheless, the likelihood of hospitalization was not statistically different in the TNFi/methotrexate group versus the non-TNFi/methotrexate group, with a risk ratio of 0.91 (95% confidence interval, 0.68-1.22; P = .5260).
Likewise, the likelihood of death was not different between groups, with a RR of 0.87 (95% CI, 0.42-1.78; P = .6958). Looking at subgroups of patients exposed to TNFi or methotrexate only didn’t change the results, the investigators added.
Taken together, the findings argue against interruption of these treatments because of the fear of the possibly worse COVID-19 outcomes, the investigators concluded, although they emphasized the need for more research.
“Because the COVID-19 pandemic is ongoing, there is a desperate need for evidence-based data on biologic and immunomodulator exposure in the setting of COVID-19 infection,” they wrote.
Dr. Zinn and coauthors reported no conflicts of interest and no funding sources related to the study.
SOURCE: Zinn Z et al. J Am Acad Dermatol. 2020 Sep 11. doi: 10.1016/j.jaad.2020.09.009.
Continued use of tumor necrosis factor inhibitors or methotrexate is acceptable in most patients who acquire COVID-19, results of a recent cohort study suggest.
Among patients on tumor necrosis factor inhibitors (TNFi) or methotrexate who developed COVID-19, death and hospitalization rates were similar to matched COVID-19 patients not on those medications, according to authors of the multicenter research network study.
Reassuringly, likelihood of hospitalization and mortality were not significantly different between 214 patients with COVID-19 taking TNFi or methotrexate and 31,862 matched COVID-19 patients not on those medications, according to the investigators, whose findings were published recently in the Journal of the American Academy of Dermatology.
Zachary Zinn, MD, corresponding author on the study, said in an interview that the findings suggest these medicines can be safely continued in the majority of patients taking them during the COVID-19 pandemic.
“If you’re a prescribing physician who’s giving patients TNF inhibitors or methotrexate or both, I think you can comfortably tell your patients there is good data that these do not lead to worse outcomes if you get COVID-19,” said Dr. Zinn, associate professor in the department of dermatology at West Virginia University, Morgantown.
The findings from these researchers corroborate a growing body of evidence suggesting that immunosuppressive treatments can be continued in patients with dermatologic and rheumatic conditions.
In recent guidance from the National Psoriasis Foundation, released Sept. 4, an expert consensus panel cited 15 studies that they said suggested that treatments for psoriasis or psoriatic arthritis “do not meaningfully alter the risk of acquiring SARS-CoV-2 infection or having worse COVID-19 outcomes.”
That said, the data to date are mainly from small case series and registry studies based on spontaneously reported COVID-19 cases, which suggests a continued need for shared decision making. In addition, chronic systemic corticosteroids should be avoided for management of psoriatic arthritis, the guidance states, based on rheumatology and gastroenterology literature suggesting this treatment is linked to worse COVID-19 outcomes.
In the interview, Dr. Zinn noted that some previous studies of immunosuppressive treatments in patients who acquire COVID-19 have aggregated data on numerous classes of biologic medications, lessening the strength of data for each specific medication.
“By focusing specifically on TNF inhibitors and methotrexate, this study gives better guidance to prescribers of these medications,” he said.
To see whether TNFi or methotrexate increased risk of worsened COVID-19 outcomes, Dr. Zinn and coinvestigators evaluated data from TriNetX, a research network that includes approximately 53 million unique patient records, predominantly in the United States.
They identified 32,076 adult patients with COVID-19, of whom 214 had recent exposure to TNFi or methotrexate. The patients in the TNFi/methotrexate group were similar in age to those without exposure to those drugs, at 55.1 versus 53.2 years, respectively. However, patients in the drug exposure group were more frequently White, female, and had substantially more comorbidities, including diabetes and obesity, according to the investigators.
Nevertheless, the likelihood of hospitalization was not statistically different in the TNFi/methotrexate group versus the non-TNFi/methotrexate group, with a risk ratio of 0.91 (95% confidence interval, 0.68-1.22; P = .5260).
Likewise, the likelihood of death was not different between groups, with a RR of 0.87 (95% CI, 0.42-1.78; P = .6958). Looking at subgroups of patients exposed to TNFi or methotrexate only didn’t change the results, the investigators added.
Taken together, the findings argue against interruption of these treatments because of the fear of the possibly worse COVID-19 outcomes, the investigators concluded, although they emphasized the need for more research.
“Because the COVID-19 pandemic is ongoing, there is a desperate need for evidence-based data on biologic and immunomodulator exposure in the setting of COVID-19 infection,” they wrote.
Dr. Zinn and coauthors reported no conflicts of interest and no funding sources related to the study.
SOURCE: Zinn Z et al. J Am Acad Dermatol. 2020 Sep 11. doi: 10.1016/j.jaad.2020.09.009.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Study confirms link between PAP apnea treatment and dementia onset
Obstructive sleep apnea (OSA) treatment with positive airway pressure (PAP) therapy was associated with a lower odds of incident Alzheimer’s disease and other dementia in a large retrospective cohort study of Medicare patients with the sleep disorder.

The study builds on research linking OSA to poor cognitive outcomes and dementia syndromes. With use of a 5% random sample of Medicare beneficiaries (more than 2.7 million) and their claims data, investigators identified approximately 53,000 who had an OSA diagnosis prior to 2011.
Of these Medicare beneficiaries, 78% with OSA were identified as “PAP-treated” based on having at least one durable medical equipment claim for PAP equipment. And of those treated, 74% were identified as “PAP adherent” based on having more than two PAP equipment claims separated by at least a month, said Galit Levi Dunietz, PhD, MPH, at the virtual annual meeting of the Associated Professional Sleep Societies.
Dr. Dunietz and her coinvestigators used logistic regression to examine the associations between PAP treatment and PAP treatment adherence, and incident ICD-9 diagnoses of Alzheimer’s disease (AD), mild cognitive impairment (MCI), and dementia not otherwise specified (DNOS) over the period 2011-2013.
After adjustments for potential confounders (age, sex, race, stroke, hypertension, cardiovascular disease, and depression), OSA treatment was associated with a significantly lower odds of a diagnosis of AD (odds ratio, 0.78; 95% confidence interval 0.69-0.89) or DNOS (OR, 0.69; 95% CI, 0.55-0.85), as well as nonsignificantly lower odds of MCI diagnosis (OR, 0.82; 95% CI, 0.66-1.02).
“People who are treated for OSA have a 22% reduced odds of being diagnosed with AD and a 31% reduced odds of getting DNOS,” said Dr. Dunietz, from the University of Michigan in Ann Arbor, in an interview after the meeting. “The 18% reduced odds of mild cognitive disorder is not really significant because the upper bound is 1.02, but we consider it approaching significance.”
Adherence to treatment was significantly associated with lower odds of AD, but not with significantly lower odds of DNOS or MCI, she said. OSA was confirmed by ICD-9 diagnosis codes plus the presence of relevant polysomnography current procedural terminology code.
All told, the findings “suggest that PAP therapy for OSA may lower short-term risk for dementia in older persons,” Dr. Dunietz and her co-nvestigators said in their poster presentation. “If a causal pathway exists between OSA and dementia, treatment of OSA may offer new opportunities to improve cognitive outcomes in older adults with OSA.”
Andrew W. Varga, MD, of the division of pulmonary, critical care, and sleep medicine at the Icahn School of Medicine at Mount Sinai and the Mount Sinai Integrative Sleep Center, both in New York, said that cognitive impairment is now a recognized clinical consequence of OSA and that OSA treatment could be a target for the prevention of cognitive impairment and Alzheimer’s disease in particular.
“I absolutely bring it up with patients in their 60s and 70s. I’m honest – I say, there seems to be more and more evidence for links between apnea and Alzheimer’s in particular. I tell them we don’t know 100% whether PAP reverses any of this, but it stands to reason that it does,” said Dr. Varga, who was asked to comment on the study and related research.
An analysis published several years ago in Neurology from the Alzheimer’s Disease Neuroimaging Initiative cohort found that patients with self-reported sleep apnea had a younger age of MCI or AD onset (about 10 years) and that patients who used continuous positive airway pressure had a delayed age of onset. “Those who had a subjective diagnosis of sleep apnea and who also reported using CPAP as treatment seemed to go in the opposite direction,” said Dr. Varga, a coauthor of that study. “They had an onset of AD that looked just like people who had no sleep apnea.”
While this study was limited by sleep apnea being self-reported – and by the lack of severity data – the newly reported study may be limited by the use of ICD codes and the fact that OSA is often entered into patient’s chart before diagnosis is confirmed through a sleep study, Dr. Varga said.
“The field is mature enough that we should be thinking of doing honest and rigorous clinical trials for sleep apnea with cognitive outcomes being a main measure of interest,” he said. “The issue we’re struggling with in the field is that such a trial would not be short.”
There are several theories for the link between OSA and cognitive impairment, he said, including disruptions in sleep architecture leading to increased production of amyloid and tau and/or decreased “clearance” of extracellular amyloid, neuronal sensitivity to hypoxia, and cardiovascular comorbidities.
Dr. Dunietz’s study was supported by The American Academy of Sleep Medicine Foundation. She reported having no disclosures. Dr. Varga said he has no relevant disclosures.
Obstructive sleep apnea (OSA) treatment with positive airway pressure (PAP) therapy was associated with a lower odds of incident Alzheimer’s disease and other dementia in a large retrospective cohort study of Medicare patients with the sleep disorder.
The study builds on research linking OSA to poor cognitive outcomes and dementia syndromes. With use of a 5% random sample of Medicare beneficiaries (more than 2.7 million) and their claims data, investigators identified approximately 53,000 who had an OSA diagnosis prior to 2011.
Of these Medicare beneficiaries, 78% with OSA were identified as “PAP-treated” based on having at least one durable medical equipment claim for PAP equipment. And of those treated, 74% were identified as “PAP adherent” based on having more than two PAP equipment claims separated by at least a month, said Galit Levi Dunietz, PhD, MPH, at the virtual annual meeting of the Associated Professional Sleep Societies.
Dr. Dunietz and her coinvestigators used logistic regression to examine the associations between PAP treatment and PAP treatment adherence, and incident ICD-9 diagnoses of Alzheimer’s disease (AD), mild cognitive impairment (MCI), and dementia not otherwise specified (DNOS) over the period 2011-2013.
After adjustments for potential confounders (age, sex, race, stroke, hypertension, cardiovascular disease, and depression), OSA treatment was associated with a significantly lower odds of a diagnosis of AD (odds ratio, 0.78; 95% confidence interval 0.69-0.89) or DNOS (OR, 0.69; 95% CI, 0.55-0.85), as well as nonsignificantly lower odds of MCI diagnosis (OR, 0.82; 95% CI, 0.66-1.02).
“People who are treated for OSA have a 22% reduced odds of being diagnosed with AD and a 31% reduced odds of getting DNOS,” said Dr. Dunietz, from the University of Michigan in Ann Arbor, in an interview after the meeting. “The 18% reduced odds of mild cognitive disorder is not really significant because the upper bound is 1.02, but we consider it approaching significance.”
Adherence to treatment was significantly associated with lower odds of AD, but not with significantly lower odds of DNOS or MCI, she said. OSA was confirmed by ICD-9 diagnosis codes plus the presence of relevant polysomnography current procedural terminology code.
All told, the findings “suggest that PAP therapy for OSA may lower short-term risk for dementia in older persons,” Dr. Dunietz and her co-nvestigators said in their poster presentation. “If a causal pathway exists between OSA and dementia, treatment of OSA may offer new opportunities to improve cognitive outcomes in older adults with OSA.”
Andrew W. Varga, MD, of the division of pulmonary, critical care, and sleep medicine at the Icahn School of Medicine at Mount Sinai and the Mount Sinai Integrative Sleep Center, both in New York, said that cognitive impairment is now a recognized clinical consequence of OSA and that OSA treatment could be a target for the prevention of cognitive impairment and Alzheimer’s disease in particular.
“I absolutely bring it up with patients in their 60s and 70s. I’m honest – I say, there seems to be more and more evidence for links between apnea and Alzheimer’s in particular. I tell them we don’t know 100% whether PAP reverses any of this, but it stands to reason that it does,” said Dr. Varga, who was asked to comment on the study and related research.
An analysis published several years ago in Neurology from the Alzheimer’s Disease Neuroimaging Initiative cohort found that patients with self-reported sleep apnea had a younger age of MCI or AD onset (about 10 years) and that patients who used continuous positive airway pressure had a delayed age of onset. “Those who had a subjective diagnosis of sleep apnea and who also reported using CPAP as treatment seemed to go in the opposite direction,” said Dr. Varga, a coauthor of that study. “They had an onset of AD that looked just like people who had no sleep apnea.”
While this study was limited by sleep apnea being self-reported – and by the lack of severity data – the newly reported study may be limited by the use of ICD codes and the fact that OSA is often entered into patient’s chart before diagnosis is confirmed through a sleep study, Dr. Varga said.
“The field is mature enough that we should be thinking of doing honest and rigorous clinical trials for sleep apnea with cognitive outcomes being a main measure of interest,” he said. “The issue we’re struggling with in the field is that such a trial would not be short.”
There are several theories for the link between OSA and cognitive impairment, he said, including disruptions in sleep architecture leading to increased production of amyloid and tau and/or decreased “clearance” of extracellular amyloid, neuronal sensitivity to hypoxia, and cardiovascular comorbidities.
Dr. Dunietz’s study was supported by The American Academy of Sleep Medicine Foundation. She reported having no disclosures. Dr. Varga said he has no relevant disclosures.
Obstructive sleep apnea (OSA) treatment with positive airway pressure (PAP) therapy was associated with a lower odds of incident Alzheimer’s disease and other dementia in a large retrospective cohort study of Medicare patients with the sleep disorder.
The study builds on research linking OSA to poor cognitive outcomes and dementia syndromes. With use of a 5% random sample of Medicare beneficiaries (more than 2.7 million) and their claims data, investigators identified approximately 53,000 who had an OSA diagnosis prior to 2011.
Of these Medicare beneficiaries, 78% with OSA were identified as “PAP-treated” based on having at least one durable medical equipment claim for PAP equipment. And of those treated, 74% were identified as “PAP adherent” based on having more than two PAP equipment claims separated by at least a month, said Galit Levi Dunietz, PhD, MPH, at the virtual annual meeting of the Associated Professional Sleep Societies.
Dr. Dunietz and her coinvestigators used logistic regression to examine the associations between PAP treatment and PAP treatment adherence, and incident ICD-9 diagnoses of Alzheimer’s disease (AD), mild cognitive impairment (MCI), and dementia not otherwise specified (DNOS) over the period 2011-2013.
After adjustments for potential confounders (age, sex, race, stroke, hypertension, cardiovascular disease, and depression), OSA treatment was associated with a significantly lower odds of a diagnosis of AD (odds ratio, 0.78; 95% confidence interval 0.69-0.89) or DNOS (OR, 0.69; 95% CI, 0.55-0.85), as well as nonsignificantly lower odds of MCI diagnosis (OR, 0.82; 95% CI, 0.66-1.02).
“People who are treated for OSA have a 22% reduced odds of being diagnosed with AD and a 31% reduced odds of getting DNOS,” said Dr. Dunietz, from the University of Michigan in Ann Arbor, in an interview after the meeting. “The 18% reduced odds of mild cognitive disorder is not really significant because the upper bound is 1.02, but we consider it approaching significance.”
Adherence to treatment was significantly associated with lower odds of AD, but not with significantly lower odds of DNOS or MCI, she said. OSA was confirmed by ICD-9 diagnosis codes plus the presence of relevant polysomnography current procedural terminology code.
All told, the findings “suggest that PAP therapy for OSA may lower short-term risk for dementia in older persons,” Dr. Dunietz and her co-nvestigators said in their poster presentation. “If a causal pathway exists between OSA and dementia, treatment of OSA may offer new opportunities to improve cognitive outcomes in older adults with OSA.”
Andrew W. Varga, MD, of the division of pulmonary, critical care, and sleep medicine at the Icahn School of Medicine at Mount Sinai and the Mount Sinai Integrative Sleep Center, both in New York, said that cognitive impairment is now a recognized clinical consequence of OSA and that OSA treatment could be a target for the prevention of cognitive impairment and Alzheimer’s disease in particular.
“I absolutely bring it up with patients in their 60s and 70s. I’m honest – I say, there seems to be more and more evidence for links between apnea and Alzheimer’s in particular. I tell them we don’t know 100% whether PAP reverses any of this, but it stands to reason that it does,” said Dr. Varga, who was asked to comment on the study and related research.
An analysis published several years ago in Neurology from the Alzheimer’s Disease Neuroimaging Initiative cohort found that patients with self-reported sleep apnea had a younger age of MCI or AD onset (about 10 years) and that patients who used continuous positive airway pressure had a delayed age of onset. “Those who had a subjective diagnosis of sleep apnea and who also reported using CPAP as treatment seemed to go in the opposite direction,” said Dr. Varga, a coauthor of that study. “They had an onset of AD that looked just like people who had no sleep apnea.”
While this study was limited by sleep apnea being self-reported – and by the lack of severity data – the newly reported study may be limited by the use of ICD codes and the fact that OSA is often entered into patient’s chart before diagnosis is confirmed through a sleep study, Dr. Varga said.
“The field is mature enough that we should be thinking of doing honest and rigorous clinical trials for sleep apnea with cognitive outcomes being a main measure of interest,” he said. “The issue we’re struggling with in the field is that such a trial would not be short.”
There are several theories for the link between OSA and cognitive impairment, he said, including disruptions in sleep architecture leading to increased production of amyloid and tau and/or decreased “clearance” of extracellular amyloid, neuronal sensitivity to hypoxia, and cardiovascular comorbidities.
Dr. Dunietz’s study was supported by The American Academy of Sleep Medicine Foundation. She reported having no disclosures. Dr. Varga said he has no relevant disclosures.
FROM SLEEP 2020

Watch for nonsuicidal self-injury in girls with ADHD, comorbidities
Recent studies constitute a clarion call for clinicians to routinely screen adolescents with ADHD for nonsuicidal self-injury (NSSI) and its risk factors, Judit Balazs, MD, PhD, said at the virtual congress of the European College of Neuropsychopharmacology.
She was lead author of one of these studies, which drew a remarkable and disturbing conclusion: “We found – and it’s a very alarming result – that more than 70% of those people who had ADHD and [nonsuicidal self-injury] were girls. The girls with ADHD seem to be a high-risk population,” observed Dr. Balazs, professor and chair of the department of developmental psychology at Eotvos Lorand University, Budapest.
NSSI first became a specific diagnosis in the DSM-5. It is defined as deliberate, nonculturally sanctioned, nonsuicidal self-injury on at least five occasions within the past year and carried out with the aim of improving one’s emotional state as a result. The prevalence of NSSI among the general population of adolescents is high, with various investigators reporting rates of 15%-45%. Among adolescents with mental disorders, the reported prevalence climbs to 40%-80%. even though it’s now clear that many cases of pediatric-onset ADHD continue on well into adulthood, albeit often undiagnosed.
Whether NSSI and suicidal behavior are actually the same entity is currently a topic of intense research, according to Dr. Balazs, who is both a child and adolescent psychiatrist, as well as an adult psychiatrist.
She presented highlights of her cross-sectional study of 202 adolescent inpatients, 51% of them female, at the Vadaskert Child and Adolescent Psychiatry Hospital, a tertiary care center in Budapest. Using the structured diagnostic Mini International Neuropsychiatric Interview for Children and Adolescents (MINI Kid) and the self-rated Deliberate Self-Harm Inventory, Dr. Balazs and her coinvestigators determined that 52 of the adolescents, including 23 boys and 29 girls, met full diagnostic criteria for ADHD and another 77 demonstrated more than five subthreshold ADHD symptoms.
Strikingly, 35 of the 52 teens diagnosed with ADHD, or 67%, had current NSSI. Only 10 of these patients were boys. The other 25, or 71% of the total, were girls.
Psychiatric comorbidities proved to be the rule rather than the exception in the adolescent inpatients with ADHD plus NSSI. Among these inpatients, 94% had a history of suicidal behavior. In addition, 66% carried the diagnosis of oppositional defiant disorder, 63% generalized anxiety disorder, 60% had a psychotic disorder, and 51% had experienced a manic episode. Among them, 49% were diagnosed with social anxiety disorder, 46% with obsessive-compulsive disorder, 31% with panic disorder, 23% with conduct disorder, and an equal percentage with agoraphobia. Furthermore, 43% had a major depressive disorder and 34%, dysthymia. Alcohol abuse or dependence was present in 20%, and an equal percentage had psychoactive substance use disorder.
Dr. Balazs said she and her coinvestigators were surprised by the high prevalence of symptoms of comorbid psychotic disorder in conjunction with NSSI and ADHD. One possible explanation, she opined, is that as inpatients the study participants were at the more severe end of the disease spectrum, and some patients may have been admitted not solely because of the severity of their comorbidities. Another possibility is that, in some cases, what was labeled psychotic disorder may actually have been prodromal unipolar depression.
A key finding in Dr. Balazs’s study was that, according to a regression analysis, the relationship between ADHD and NSSI was mediated entirely by the symptoms of the ADHD comorbidities. Specifically, the significant risk factors for NSSI in patients with ADHD were affective disorders, suicidality, and psychotic disorders in both sexes, with the addition of comorbid alcohol abuse or dependence in girls only. There was no evidence of a direct causal relationship between ADHD, per se, and NSSI.
‘Findings warrant further investigation’
The study, which looks at the association between NSSI and adolescents is interesting, yet preliminary, said David Fassler, MD, in an interview.
“The authors conclude that girls with ADHD are at particularly high risk of NSSI,” said Dr. Fassler, clinical professor of psychiatry at the University of Vermont, Burlington. Dr. Fassler was not involved with the study.
“It is limited by sample size, acuity, and the incidence of comorbidities,” said Dr. Fassler, who had no conflicts of interest. “Nonetheless, the findings are intriguing and warrant further investigation with larger samples in diverse clinical settings.”
The study was supported by the Hungarian Scientific Research Fund. In addition, Dr. Balazs received funding from the Hungarian Academy of Sciences. The full details of the study have been published (BMC Psychiatry. 2018 Feb 6;18[1]:34).
SOURCE: Balazs J et al. ECNP 2020, Abstract EDU.02.
Recent studies constitute a clarion call for clinicians to routinely screen adolescents with ADHD for nonsuicidal self-injury (NSSI) and its risk factors, Judit Balazs, MD, PhD, said at the virtual congress of the European College of Neuropsychopharmacology.
She was lead author of one of these studies, which drew a remarkable and disturbing conclusion: “We found – and it’s a very alarming result – that more than 70% of those people who had ADHD and [nonsuicidal self-injury] were girls. The girls with ADHD seem to be a high-risk population,” observed Dr. Balazs, professor and chair of the department of developmental psychology at Eotvos Lorand University, Budapest.
NSSI first became a specific diagnosis in the DSM-5. It is defined as deliberate, nonculturally sanctioned, nonsuicidal self-injury on at least five occasions within the past year and carried out with the aim of improving one’s emotional state as a result. The prevalence of NSSI among the general population of adolescents is high, with various investigators reporting rates of 15%-45%. Among adolescents with mental disorders, the reported prevalence climbs to 40%-80%. even though it’s now clear that many cases of pediatric-onset ADHD continue on well into adulthood, albeit often undiagnosed.
Whether NSSI and suicidal behavior are actually the same entity is currently a topic of intense research, according to Dr. Balazs, who is both a child and adolescent psychiatrist, as well as an adult psychiatrist.
She presented highlights of her cross-sectional study of 202 adolescent inpatients, 51% of them female, at the Vadaskert Child and Adolescent Psychiatry Hospital, a tertiary care center in Budapest. Using the structured diagnostic Mini International Neuropsychiatric Interview for Children and Adolescents (MINI Kid) and the self-rated Deliberate Self-Harm Inventory, Dr. Balazs and her coinvestigators determined that 52 of the adolescents, including 23 boys and 29 girls, met full diagnostic criteria for ADHD and another 77 demonstrated more than five subthreshold ADHD symptoms.
Strikingly, 35 of the 52 teens diagnosed with ADHD, or 67%, had current NSSI. Only 10 of these patients were boys. The other 25, or 71% of the total, were girls.
Psychiatric comorbidities proved to be the rule rather than the exception in the adolescent inpatients with ADHD plus NSSI. Among these inpatients, 94% had a history of suicidal behavior. In addition, 66% carried the diagnosis of oppositional defiant disorder, 63% generalized anxiety disorder, 60% had a psychotic disorder, and 51% had experienced a manic episode. Among them, 49% were diagnosed with social anxiety disorder, 46% with obsessive-compulsive disorder, 31% with panic disorder, 23% with conduct disorder, and an equal percentage with agoraphobia. Furthermore, 43% had a major depressive disorder and 34%, dysthymia. Alcohol abuse or dependence was present in 20%, and an equal percentage had psychoactive substance use disorder.
Dr. Balazs said she and her coinvestigators were surprised by the high prevalence of symptoms of comorbid psychotic disorder in conjunction with NSSI and ADHD. One possible explanation, she opined, is that as inpatients the study participants were at the more severe end of the disease spectrum, and some patients may have been admitted not solely because of the severity of their comorbidities. Another possibility is that, in some cases, what was labeled psychotic disorder may actually have been prodromal unipolar depression.
A key finding in Dr. Balazs’s study was that, according to a regression analysis, the relationship between ADHD and NSSI was mediated entirely by the symptoms of the ADHD comorbidities. Specifically, the significant risk factors for NSSI in patients with ADHD were affective disorders, suicidality, and psychotic disorders in both sexes, with the addition of comorbid alcohol abuse or dependence in girls only. There was no evidence of a direct causal relationship between ADHD, per se, and NSSI.
‘Findings warrant further investigation’
The study, which looks at the association between NSSI and adolescents is interesting, yet preliminary, said David Fassler, MD, in an interview.
“The authors conclude that girls with ADHD are at particularly high risk of NSSI,” said Dr. Fassler, clinical professor of psychiatry at the University of Vermont, Burlington. Dr. Fassler was not involved with the study.
“It is limited by sample size, acuity, and the incidence of comorbidities,” said Dr. Fassler, who had no conflicts of interest. “Nonetheless, the findings are intriguing and warrant further investigation with larger samples in diverse clinical settings.”
The study was supported by the Hungarian Scientific Research Fund. In addition, Dr. Balazs received funding from the Hungarian Academy of Sciences. The full details of the study have been published (BMC Psychiatry. 2018 Feb 6;18[1]:34).
SOURCE: Balazs J et al. ECNP 2020, Abstract EDU.02.
Recent studies constitute a clarion call for clinicians to routinely screen adolescents with ADHD for nonsuicidal self-injury (NSSI) and its risk factors, Judit Balazs, MD, PhD, said at the virtual congress of the European College of Neuropsychopharmacology.
She was lead author of one of these studies, which drew a remarkable and disturbing conclusion: “We found – and it’s a very alarming result – that more than 70% of those people who had ADHD and [nonsuicidal self-injury] were girls. The girls with ADHD seem to be a high-risk population,” observed Dr. Balazs, professor and chair of the department of developmental psychology at Eotvos Lorand University, Budapest.
NSSI first became a specific diagnosis in the DSM-5. It is defined as deliberate, nonculturally sanctioned, nonsuicidal self-injury on at least five occasions within the past year and carried out with the aim of improving one’s emotional state as a result. The prevalence of NSSI among the general population of adolescents is high, with various investigators reporting rates of 15%-45%. Among adolescents with mental disorders, the reported prevalence climbs to 40%-80%. even though it’s now clear that many cases of pediatric-onset ADHD continue on well into adulthood, albeit often undiagnosed.
Whether NSSI and suicidal behavior are actually the same entity is currently a topic of intense research, according to Dr. Balazs, who is both a child and adolescent psychiatrist, as well as an adult psychiatrist.
She presented highlights of her cross-sectional study of 202 adolescent inpatients, 51% of them female, at the Vadaskert Child and Adolescent Psychiatry Hospital, a tertiary care center in Budapest. Using the structured diagnostic Mini International Neuropsychiatric Interview for Children and Adolescents (MINI Kid) and the self-rated Deliberate Self-Harm Inventory, Dr. Balazs and her coinvestigators determined that 52 of the adolescents, including 23 boys and 29 girls, met full diagnostic criteria for ADHD and another 77 demonstrated more than five subthreshold ADHD symptoms.
Strikingly, 35 of the 52 teens diagnosed with ADHD, or 67%, had current NSSI. Only 10 of these patients were boys. The other 25, or 71% of the total, were girls.
Psychiatric comorbidities proved to be the rule rather than the exception in the adolescent inpatients with ADHD plus NSSI. Among these inpatients, 94% had a history of suicidal behavior. In addition, 66% carried the diagnosis of oppositional defiant disorder, 63% generalized anxiety disorder, 60% had a psychotic disorder, and 51% had experienced a manic episode. Among them, 49% were diagnosed with social anxiety disorder, 46% with obsessive-compulsive disorder, 31% with panic disorder, 23% with conduct disorder, and an equal percentage with agoraphobia. Furthermore, 43% had a major depressive disorder and 34%, dysthymia. Alcohol abuse or dependence was present in 20%, and an equal percentage had psychoactive substance use disorder.
Dr. Balazs said she and her coinvestigators were surprised by the high prevalence of symptoms of comorbid psychotic disorder in conjunction with NSSI and ADHD. One possible explanation, she opined, is that as inpatients the study participants were at the more severe end of the disease spectrum, and some patients may have been admitted not solely because of the severity of their comorbidities. Another possibility is that, in some cases, what was labeled psychotic disorder may actually have been prodromal unipolar depression.
A key finding in Dr. Balazs’s study was that, according to a regression analysis, the relationship between ADHD and NSSI was mediated entirely by the symptoms of the ADHD comorbidities. Specifically, the significant risk factors for NSSI in patients with ADHD were affective disorders, suicidality, and psychotic disorders in both sexes, with the addition of comorbid alcohol abuse or dependence in girls only. There was no evidence of a direct causal relationship between ADHD, per se, and NSSI.
‘Findings warrant further investigation’
The study, which looks at the association between NSSI and adolescents is interesting, yet preliminary, said David Fassler, MD, in an interview.
“The authors conclude that girls with ADHD are at particularly high risk of NSSI,” said Dr. Fassler, clinical professor of psychiatry at the University of Vermont, Burlington. Dr. Fassler was not involved with the study.
“It is limited by sample size, acuity, and the incidence of comorbidities,” said Dr. Fassler, who had no conflicts of interest. “Nonetheless, the findings are intriguing and warrant further investigation with larger samples in diverse clinical settings.”
The study was supported by the Hungarian Scientific Research Fund. In addition, Dr. Balazs received funding from the Hungarian Academy of Sciences. The full details of the study have been published (BMC Psychiatry. 2018 Feb 6;18[1]:34).
SOURCE: Balazs J et al. ECNP 2020, Abstract EDU.02.
FROM ECNP 2020
Physician income drops, burnout spikes globally in pandemic
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
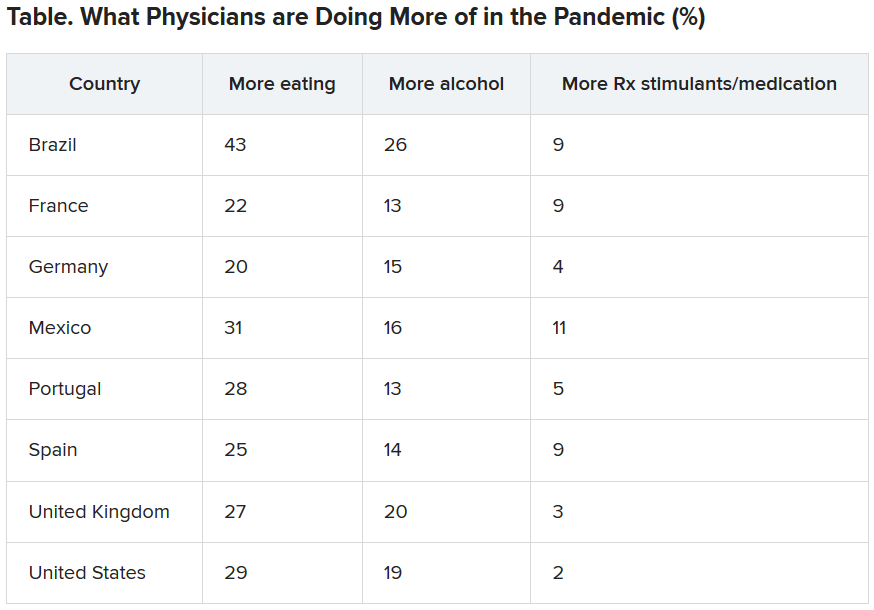
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
Reworked OxyContin fails to cut overall opioid abuse, FDA panel says
The long-awaited postmarketing studies of the abuse-deterrent formulation (ADF) of OxyContin (Perdue Pharma) received mixed reviews from a Food and Drug Administration joint advisory committee.

After a 2-day discussion of new research submitted by Perdue, as well as other relevant published data, most members of the Drug Safety and Risk Management and Anesthetic and Analgesic Drug Products advisory committees came to the conclusion that the reformulated drug “meaningfully” reduced abuse via intranasal administration and intravenous injection, but not overall opioid abuse or overdose.
The reformulated OxyContin “was the first out of the gate,” and “has the greatest market penetration of any ADF” so “it gives us the greatest opportunity to measure change before and after reformulation,” said committee member Traci C. Green, PhD, MSc, professor and director of the Opioid Policy Research Collaborative at Brandeis University, Waltham, Mass.
The FDA approved the original formulation of OxyContin (oxycodone hydrochloride), a mu-receptor opioid agonist, in December 1995 for the management of pain requiring daily round-the-clock opioid treatment in cases where other treatments were inadequate. It approved an ADF version of the product in April 2010.
The updated formulation incorporates polyethylene oxide, an inactive polymer that makes the tablet harder and more crush resistant. The tablet turns into a gel or glue-like substance when wet.
At the request of the FDA, the company carried out four postmarketing studies, which the FDA also reviewed.
- A National Addictions Vigilance Intervention and Prevention Program study that included 66,897 assessments in patients undergoing evaluation for substance use or entering an opioid addiction program. Results showed a drop in up to 52% of self-reported past 30-day OxyContin injection and snorting versus comparators, including extended-release morphine and immediate-release hydrocodone.
- An analysis of 308,465 calls to U.S. poison centers showing a reduction of up to 28% for calls regarding intentional OxyContin-related exposures immediately following the drug’s reformulation. However, the FDA analysis concluded it is unclear whether the decline was attributable to the drug’s reformulation or co-occurring trends.
- A study of 63,528 individuals entering methadone clinics or treatment programs that showed a reduction of up to 27% in OxyContin abuse versus comparators. There was no information on route of abuse. Here, the FDA analysis determined the results were mixed and didn’t provide compelling evidence.
- A claims-based analysis of patients who were dispensed an opioid (297,836 OxyContin; 659,673 a comparator) that showed no evidence that the updated product affected the rate of fatal and nonfatal opioid overdoses.

During the meeting, committee members heard that opioid use in the United States peaked in 2012, with 260 million prescriptions dispensed, then declined by 41% by 2019. ADFs accounted for only 2% of prescriptions in 2019. They also heard that results of a wide variety of studies and surveys support the conclusion that misuse, abuse, and diversion of OxyContin decreased after it was reformulated.
Ultimately, the joint committee voted 20 to 7 (with 1 abstention) that the reformulated drug reduced nonoral abuse. Most members who voted in favor cited the NAVIPPRO study as a reason for their decision, but few found the strength of the evidence better than moderate.
Meeting chair Sonia Hernandez-Diaz, MD, professor of epidemiology, Harvard School of Public Health, Boston, noted the reduction in abuse may, in part, be a result of the overall reduction in opioid use.
Jon E. Zibbell, PhD, senior public health scientist, behavioral health research division, RTI International, Atlanta, who voted “no,” was disappointed there was not more data.
“We had a bunch of years for this and so many of us could have done some amazing studies” related to how abuse changed post reformulation, he said.
As for overall abuse deterrence, the committee believed the evidence was less compelling. Only two members voted that the reformulated version of the drug reduced overall abuse and only one member voted that the reformulated tablets reduced opioid overdose.
Members generally agreed that all of the studies had limitations, including retrospective designs, confounding, and potential misclassifications. Many noted the challenge of assessing abuse pre- and post reformulation given the evolving situation.
For instance, at the time the reformulated drug was launched, public health initiatives targeting opioid abuse were introduced, more treatment centers were opening, and there was a crackdown on “pill-mill” doctors.
In addition, prescribing and consumption habits were changing. Some doctors may have switched only “at-risk” patients to the reformulated opioid and there may have been “self-selection” among patients – with some potentially opting for another drug such as immediate-release oxycodone.
During the meeting, there was discussion about how to interpret a “meaningful” abuse reduction. However, there was no consensus of a percentage the reduction had to reach in order to be deemed meaningful.
Another issue discussed was the term “abuse deterrent,” which some members believed was stigmatizing and should be changed to crush resistant.

There was also concern that prescribers might consider the ADF a “safe” or less addictive opioid. Michael Sprintz, DO, clinical assistant professor, division of geriatric and palliative medicine, University of Texas Health Science Center, Houston, said ADFs might provide physicians with “a false sense of security.”
Dr. Sprintz, also founder of the Sprintz Center for Pain and Recovery, noted the importance of pain medicine physicians understanding addiction and addiction specialists understanding pain management.
Other committee members voiced concern that the reformulation results in patients switching from intravenous and intranasal abuse to oral abuse. Committed abusers can still swallow multiple pills.
Some members noted that reformulated OxyContin coincided with increased transition to heroin, which is relatively cheap and readily available. However, they recognized that proving causality is difficult.
The committee was reminded that the reformulated drug provides a significant barrier against, but doesn’t altogether eliminate, opioid abuse. With hot water and the right tools, the tablets can still be manipulated.
In addition, the reformulated drug will not solve the U.S. opioid epidemic, which requires a multifaceted approach. The opioid crisis, said Wilson Compton, MD, deputy director at the National Institute on Drug Abuse, has resulted in a “skyrocketing” of deaths linked to “tremendously potent” forms of fentanyl, emerging stimulant use issues, and the possible increase in drug overdoses linked to COVID-19.
A version of this article originally appeared on Medscape.com.
The long-awaited postmarketing studies of the abuse-deterrent formulation (ADF) of OxyContin (Perdue Pharma) received mixed reviews from a Food and Drug Administration joint advisory committee.
After a 2-day discussion of new research submitted by Perdue, as well as other relevant published data, most members of the Drug Safety and Risk Management and Anesthetic and Analgesic Drug Products advisory committees came to the conclusion that the reformulated drug “meaningfully” reduced abuse via intranasal administration and intravenous injection, but not overall opioid abuse or overdose.
The reformulated OxyContin “was the first out of the gate,” and “has the greatest market penetration of any ADF” so “it gives us the greatest opportunity to measure change before and after reformulation,” said committee member Traci C. Green, PhD, MSc, professor and director of the Opioid Policy Research Collaborative at Brandeis University, Waltham, Mass.
The FDA approved the original formulation of OxyContin (oxycodone hydrochloride), a mu-receptor opioid agonist, in December 1995 for the management of pain requiring daily round-the-clock opioid treatment in cases where other treatments were inadequate. It approved an ADF version of the product in April 2010.
The updated formulation incorporates polyethylene oxide, an inactive polymer that makes the tablet harder and more crush resistant. The tablet turns into a gel or glue-like substance when wet.
At the request of the FDA, the company carried out four postmarketing studies, which the FDA also reviewed.
- A National Addictions Vigilance Intervention and Prevention Program study that included 66,897 assessments in patients undergoing evaluation for substance use or entering an opioid addiction program. Results showed a drop in up to 52% of self-reported past 30-day OxyContin injection and snorting versus comparators, including extended-release morphine and immediate-release hydrocodone.
- An analysis of 308,465 calls to U.S. poison centers showing a reduction of up to 28% for calls regarding intentional OxyContin-related exposures immediately following the drug’s reformulation. However, the FDA analysis concluded it is unclear whether the decline was attributable to the drug’s reformulation or co-occurring trends.
- A study of 63,528 individuals entering methadone clinics or treatment programs that showed a reduction of up to 27% in OxyContin abuse versus comparators. There was no information on route of abuse. Here, the FDA analysis determined the results were mixed and didn’t provide compelling evidence.
- A claims-based analysis of patients who were dispensed an opioid (297,836 OxyContin; 659,673 a comparator) that showed no evidence that the updated product affected the rate of fatal and nonfatal opioid overdoses.
During the meeting, committee members heard that opioid use in the United States peaked in 2012, with 260 million prescriptions dispensed, then declined by 41% by 2019. ADFs accounted for only 2% of prescriptions in 2019. They also heard that results of a wide variety of studies and surveys support the conclusion that misuse, abuse, and diversion of OxyContin decreased after it was reformulated.
Ultimately, the joint committee voted 20 to 7 (with 1 abstention) that the reformulated drug reduced nonoral abuse. Most members who voted in favor cited the NAVIPPRO study as a reason for their decision, but few found the strength of the evidence better than moderate.
Meeting chair Sonia Hernandez-Diaz, MD, professor of epidemiology, Harvard School of Public Health, Boston, noted the reduction in abuse may, in part, be a result of the overall reduction in opioid use.
Jon E. Zibbell, PhD, senior public health scientist, behavioral health research division, RTI International, Atlanta, who voted “no,” was disappointed there was not more data.
“We had a bunch of years for this and so many of us could have done some amazing studies” related to how abuse changed post reformulation, he said.
As for overall abuse deterrence, the committee believed the evidence was less compelling. Only two members voted that the reformulated version of the drug reduced overall abuse and only one member voted that the reformulated tablets reduced opioid overdose.
Members generally agreed that all of the studies had limitations, including retrospective designs, confounding, and potential misclassifications. Many noted the challenge of assessing abuse pre- and post reformulation given the evolving situation.
For instance, at the time the reformulated drug was launched, public health initiatives targeting opioid abuse were introduced, more treatment centers were opening, and there was a crackdown on “pill-mill” doctors.
In addition, prescribing and consumption habits were changing. Some doctors may have switched only “at-risk” patients to the reformulated opioid and there may have been “self-selection” among patients – with some potentially opting for another drug such as immediate-release oxycodone.
During the meeting, there was discussion about how to interpret a “meaningful” abuse reduction. However, there was no consensus of a percentage the reduction had to reach in order to be deemed meaningful.
Another issue discussed was the term “abuse deterrent,” which some members believed was stigmatizing and should be changed to crush resistant.
There was also concern that prescribers might consider the ADF a “safe” or less addictive opioid. Michael Sprintz, DO, clinical assistant professor, division of geriatric and palliative medicine, University of Texas Health Science Center, Houston, said ADFs might provide physicians with “a false sense of security.”
Dr. Sprintz, also founder of the Sprintz Center for Pain and Recovery, noted the importance of pain medicine physicians understanding addiction and addiction specialists understanding pain management.
Other committee members voiced concern that the reformulation results in patients switching from intravenous and intranasal abuse to oral abuse. Committed abusers can still swallow multiple pills.
Some members noted that reformulated OxyContin coincided with increased transition to heroin, which is relatively cheap and readily available. However, they recognized that proving causality is difficult.
The committee was reminded that the reformulated drug provides a significant barrier against, but doesn’t altogether eliminate, opioid abuse. With hot water and the right tools, the tablets can still be manipulated.
In addition, the reformulated drug will not solve the U.S. opioid epidemic, which requires a multifaceted approach. The opioid crisis, said Wilson Compton, MD, deputy director at the National Institute on Drug Abuse, has resulted in a “skyrocketing” of deaths linked to “tremendously potent” forms of fentanyl, emerging stimulant use issues, and the possible increase in drug overdoses linked to COVID-19.
A version of this article originally appeared on Medscape.com.
The long-awaited postmarketing studies of the abuse-deterrent formulation (ADF) of OxyContin (Perdue Pharma) received mixed reviews from a Food and Drug Administration joint advisory committee.
After a 2-day discussion of new research submitted by Perdue, as well as other relevant published data, most members of the Drug Safety and Risk Management and Anesthetic and Analgesic Drug Products advisory committees came to the conclusion that the reformulated drug “meaningfully” reduced abuse via intranasal administration and intravenous injection, but not overall opioid abuse or overdose.
The reformulated OxyContin “was the first out of the gate,” and “has the greatest market penetration of any ADF” so “it gives us the greatest opportunity to measure change before and after reformulation,” said committee member Traci C. Green, PhD, MSc, professor and director of the Opioid Policy Research Collaborative at Brandeis University, Waltham, Mass.
The FDA approved the original formulation of OxyContin (oxycodone hydrochloride), a mu-receptor opioid agonist, in December 1995 for the management of pain requiring daily round-the-clock opioid treatment in cases where other treatments were inadequate. It approved an ADF version of the product in April 2010.
The updated formulation incorporates polyethylene oxide, an inactive polymer that makes the tablet harder and more crush resistant. The tablet turns into a gel or glue-like substance when wet.
At the request of the FDA, the company carried out four postmarketing studies, which the FDA also reviewed.
- A National Addictions Vigilance Intervention and Prevention Program study that included 66,897 assessments in patients undergoing evaluation for substance use or entering an opioid addiction program. Results showed a drop in up to 52% of self-reported past 30-day OxyContin injection and snorting versus comparators, including extended-release morphine and immediate-release hydrocodone.
- An analysis of 308,465 calls to U.S. poison centers showing a reduction of up to 28% for calls regarding intentional OxyContin-related exposures immediately following the drug’s reformulation. However, the FDA analysis concluded it is unclear whether the decline was attributable to the drug’s reformulation or co-occurring trends.
- A study of 63,528 individuals entering methadone clinics or treatment programs that showed a reduction of up to 27% in OxyContin abuse versus comparators. There was no information on route of abuse. Here, the FDA analysis determined the results were mixed and didn’t provide compelling evidence.
- A claims-based analysis of patients who were dispensed an opioid (297,836 OxyContin; 659,673 a comparator) that showed no evidence that the updated product affected the rate of fatal and nonfatal opioid overdoses.
During the meeting, committee members heard that opioid use in the United States peaked in 2012, with 260 million prescriptions dispensed, then declined by 41% by 2019. ADFs accounted for only 2% of prescriptions in 2019. They also heard that results of a wide variety of studies and surveys support the conclusion that misuse, abuse, and diversion of OxyContin decreased after it was reformulated.
Ultimately, the joint committee voted 20 to 7 (with 1 abstention) that the reformulated drug reduced nonoral abuse. Most members who voted in favor cited the NAVIPPRO study as a reason for their decision, but few found the strength of the evidence better than moderate.
Meeting chair Sonia Hernandez-Diaz, MD, professor of epidemiology, Harvard School of Public Health, Boston, noted the reduction in abuse may, in part, be a result of the overall reduction in opioid use.
Jon E. Zibbell, PhD, senior public health scientist, behavioral health research division, RTI International, Atlanta, who voted “no,” was disappointed there was not more data.
“We had a bunch of years for this and so many of us could have done some amazing studies” related to how abuse changed post reformulation, he said.
As for overall abuse deterrence, the committee believed the evidence was less compelling. Only two members voted that the reformulated version of the drug reduced overall abuse and only one member voted that the reformulated tablets reduced opioid overdose.
Members generally agreed that all of the studies had limitations, including retrospective designs, confounding, and potential misclassifications. Many noted the challenge of assessing abuse pre- and post reformulation given the evolving situation.
For instance, at the time the reformulated drug was launched, public health initiatives targeting opioid abuse were introduced, more treatment centers were opening, and there was a crackdown on “pill-mill” doctors.
In addition, prescribing and consumption habits were changing. Some doctors may have switched only “at-risk” patients to the reformulated opioid and there may have been “self-selection” among patients – with some potentially opting for another drug such as immediate-release oxycodone.
During the meeting, there was discussion about how to interpret a “meaningful” abuse reduction. However, there was no consensus of a percentage the reduction had to reach in order to be deemed meaningful.
Another issue discussed was the term “abuse deterrent,” which some members believed was stigmatizing and should be changed to crush resistant.
There was also concern that prescribers might consider the ADF a “safe” or less addictive opioid. Michael Sprintz, DO, clinical assistant professor, division of geriatric and palliative medicine, University of Texas Health Science Center, Houston, said ADFs might provide physicians with “a false sense of security.”
Dr. Sprintz, also founder of the Sprintz Center for Pain and Recovery, noted the importance of pain medicine physicians understanding addiction and addiction specialists understanding pain management.
Other committee members voiced concern that the reformulation results in patients switching from intravenous and intranasal abuse to oral abuse. Committed abusers can still swallow multiple pills.
Some members noted that reformulated OxyContin coincided with increased transition to heroin, which is relatively cheap and readily available. However, they recognized that proving causality is difficult.
The committee was reminded that the reformulated drug provides a significant barrier against, but doesn’t altogether eliminate, opioid abuse. With hot water and the right tools, the tablets can still be manipulated.
In addition, the reformulated drug will not solve the U.S. opioid epidemic, which requires a multifaceted approach. The opioid crisis, said Wilson Compton, MD, deputy director at the National Institute on Drug Abuse, has resulted in a “skyrocketing” of deaths linked to “tremendously potent” forms of fentanyl, emerging stimulant use issues, and the possible increase in drug overdoses linked to COVID-19.
A version of this article originally appeared on Medscape.com.
Infectious COVID-19 can persist in gut for weeks
Stool tests were positive among people with no GI symptoms, and in some cases up to 6 days after nasopharyngeal swabs yielded negative results.
The small pilot study suggests a quiescent but active infection in the gut. Stool testing revealed genomic evidence of active infection in 7 of the 15 participants tested in one of two hospitals in Hong Kong.
“We found active and prolonged SARS-CoV-2 infection in the stool of patients with COVID-19, even after recovery, suggesting that coronavirus could remain in the gut of asymptomatic carriers,” senior author Siew C. Ng, MBBS, PhD, told Medscape Medical News.
“Due to the potential threat of fecal-oral transmission, it is important to maintain long-term coronavirus and health surveillance,” said Ng, Associate Director of the Centre for Gut Microbiota Research at the Chinese University of Hong Kong (CUHK).
“Discharged patients and their caretakers should remain vigilant and observe strict personal and toileting hygiene,” she added.
The prospective, observational study was published online July 20 in Gut.
Ramping up COVID-19 testing
As a follow-up to these and other findings – including the testing of more than 2,000 stool samples in children and the needy arriving at Hong Kong airports starting March 29 – the same investigators are establishing a CUHK Coronavirus Testing Center.
As of Aug. 31, the detection rate in tested children was 0.28%. The Center plans to offer as many as 2,000 COVID-19 tests daily going forward to help identify asymptomatic carriers, the investigators announced in a Sept. 7 news release.
In contrast to nasopharyngeal sampling, stool specimens are “more convenient, safe and non-invasive to collect in the pediatric population,” professor Paul Chan, chairman of the Department of Microbiology, CU Medicine, said in the release. “This makes the stool test a better option for COVID-19 screening in babies, young children and those whose respiratory samples are difficult to collect.”
Even though previous researchers identified SARS-CoV-2 in the stool, the activity and infectivity of the virus in the gastrointestinal tract during and after COVID-19 respiratory positivity remained largely unknown.
Active infection detected in stool
This prospective study involved 15 people hospitalized with COVID-19 in March and April. Participants were a median 55 years old (range, 22-71 years) and all presented with respiratory symptoms. Only one patient had concurrent GI symptoms at admission. Median length of stay was 21 days.
Investigators collected fecal samples serially until discharge. They extracted viral DNA to test for transcriptional genetic evidence of active infection, which they detected in 7 of 15 patients. The patient with GI symptoms was not in this positive group.
The findings suggest a “quiescent but active GI infection,” the researchers note.
Three of the seven patients continued to test positive for active infection in their stool up to 6 days after respiratory clearance of SARS-CoV-2.
Microbiome matters
The investigators also extracted, amplified, and sequenced DNA from the stool samples. Their “metagenomic” profile revealed the type and amounts of bacterial strains in each patient’s gut microbiome.
Interestingly, bacterial strains differed between people with high SARS-CoV-2 infectivity versus participants with low to no evidence of active infection.
“Stool with high viral activity had higher abundance of pathogenic bacteria,” Ng said. In contrast, people with low or no infectivity had more beneficial bacterial strains, including bacteria that play critical roles in boosting host immunity.
Each patient’s microbiome composition changed during the course of the study. Whether the microbiome alters the course of COVID-19 or COVID-19 alters the composition of the microbiome requires further study, the authors note.
The U.S. Food and Drug Administration and officials in other countries have contacted the Hong Kong investigators for more details on their stool testing strategy, professor Francis K.L. Chan, dean of the faculty of medicine and director of the Centre for Gut Microbiota Research at CUHK, stated in the news release.
Further research into revealing the infectivity and pathogenesis of SARS-CoV-2 in the GI tract is warranted. The value of modulating the human gut microbiome in this patient population could be worthwhile to investigate as well, the researchers said.
Novel finding
“Some of it is not-so-new news and some is new,” David A. Johnson, MD, told Medscape Medical News when asked to comment on the study.
For example, previous researchers have detected SARS-CoV-2 virus in the stool. However, this study takes it a step further and shows that the virus present in stool can remain infectious on the basis of metagenomic signatures.
Furthermore, the virus can remain infectious in the gut even after a patient tests negative for COVID-19 through nasopharyngeal sampling – in this report up to 6 days later, said Johnson, professor of medicine, chief of gastroenterology, Eastern Virginia Medical School in Norfolk, Va.
The study carries important implications for people who currently test negative following active COVID-19 infection, he added. Centers for Disease Control and Prevention criteria clear a person as negative after two nasopharyngeal swabs at least 24 hours apart.
People in this category could believe they are no longer infectious and might return to a setting where they could infect others, Johnson said.
One potential means for spreading SARS-CoV-2 from the gut is from a toilet plume, as Johnson previously highlighted in a video report for Medscape Medical News.
The study authors disclosed no relevant financial relationships. Johnson serves as an adviser to WebMD/Medscape.
This article first appeared on Medscape.com.
Stool tests were positive among people with no GI symptoms, and in some cases up to 6 days after nasopharyngeal swabs yielded negative results.
The small pilot study suggests a quiescent but active infection in the gut. Stool testing revealed genomic evidence of active infection in 7 of the 15 participants tested in one of two hospitals in Hong Kong.
“We found active and prolonged SARS-CoV-2 infection in the stool of patients with COVID-19, even after recovery, suggesting that coronavirus could remain in the gut of asymptomatic carriers,” senior author Siew C. Ng, MBBS, PhD, told Medscape Medical News.
“Due to the potential threat of fecal-oral transmission, it is important to maintain long-term coronavirus and health surveillance,” said Ng, Associate Director of the Centre for Gut Microbiota Research at the Chinese University of Hong Kong (CUHK).
“Discharged patients and their caretakers should remain vigilant and observe strict personal and toileting hygiene,” she added.
The prospective, observational study was published online July 20 in Gut.
Ramping up COVID-19 testing
As a follow-up to these and other findings – including the testing of more than 2,000 stool samples in children and the needy arriving at Hong Kong airports starting March 29 – the same investigators are establishing a CUHK Coronavirus Testing Center.
As of Aug. 31, the detection rate in tested children was 0.28%. The Center plans to offer as many as 2,000 COVID-19 tests daily going forward to help identify asymptomatic carriers, the investigators announced in a Sept. 7 news release.
In contrast to nasopharyngeal sampling, stool specimens are “more convenient, safe and non-invasive to collect in the pediatric population,” professor Paul Chan, chairman of the Department of Microbiology, CU Medicine, said in the release. “This makes the stool test a better option for COVID-19 screening in babies, young children and those whose respiratory samples are difficult to collect.”
Even though previous researchers identified SARS-CoV-2 in the stool, the activity and infectivity of the virus in the gastrointestinal tract during and after COVID-19 respiratory positivity remained largely unknown.
Active infection detected in stool
This prospective study involved 15 people hospitalized with COVID-19 in March and April. Participants were a median 55 years old (range, 22-71 years) and all presented with respiratory symptoms. Only one patient had concurrent GI symptoms at admission. Median length of stay was 21 days.
Investigators collected fecal samples serially until discharge. They extracted viral DNA to test for transcriptional genetic evidence of active infection, which they detected in 7 of 15 patients. The patient with GI symptoms was not in this positive group.
The findings suggest a “quiescent but active GI infection,” the researchers note.
Three of the seven patients continued to test positive for active infection in their stool up to 6 days after respiratory clearance of SARS-CoV-2.
Microbiome matters
The investigators also extracted, amplified, and sequenced DNA from the stool samples. Their “metagenomic” profile revealed the type and amounts of bacterial strains in each patient’s gut microbiome.
Interestingly, bacterial strains differed between people with high SARS-CoV-2 infectivity versus participants with low to no evidence of active infection.
“Stool with high viral activity had higher abundance of pathogenic bacteria,” Ng said. In contrast, people with low or no infectivity had more beneficial bacterial strains, including bacteria that play critical roles in boosting host immunity.
Each patient’s microbiome composition changed during the course of the study. Whether the microbiome alters the course of COVID-19 or COVID-19 alters the composition of the microbiome requires further study, the authors note.
The U.S. Food and Drug Administration and officials in other countries have contacted the Hong Kong investigators for more details on their stool testing strategy, professor Francis K.L. Chan, dean of the faculty of medicine and director of the Centre for Gut Microbiota Research at CUHK, stated in the news release.
Further research into revealing the infectivity and pathogenesis of SARS-CoV-2 in the GI tract is warranted. The value of modulating the human gut microbiome in this patient population could be worthwhile to investigate as well, the researchers said.
Novel finding
“Some of it is not-so-new news and some is new,” David A. Johnson, MD, told Medscape Medical News when asked to comment on the study.
For example, previous researchers have detected SARS-CoV-2 virus in the stool. However, this study takes it a step further and shows that the virus present in stool can remain infectious on the basis of metagenomic signatures.
Furthermore, the virus can remain infectious in the gut even after a patient tests negative for COVID-19 through nasopharyngeal sampling – in this report up to 6 days later, said Johnson, professor of medicine, chief of gastroenterology, Eastern Virginia Medical School in Norfolk, Va.
The study carries important implications for people who currently test negative following active COVID-19 infection, he added. Centers for Disease Control and Prevention criteria clear a person as negative after two nasopharyngeal swabs at least 24 hours apart.
People in this category could believe they are no longer infectious and might return to a setting where they could infect others, Johnson said.
One potential means for spreading SARS-CoV-2 from the gut is from a toilet plume, as Johnson previously highlighted in a video report for Medscape Medical News.
The study authors disclosed no relevant financial relationships. Johnson serves as an adviser to WebMD/Medscape.
This article first appeared on Medscape.com.
Stool tests were positive among people with no GI symptoms, and in some cases up to 6 days after nasopharyngeal swabs yielded negative results.
The small pilot study suggests a quiescent but active infection in the gut. Stool testing revealed genomic evidence of active infection in 7 of the 15 participants tested in one of two hospitals in Hong Kong.
“We found active and prolonged SARS-CoV-2 infection in the stool of patients with COVID-19, even after recovery, suggesting that coronavirus could remain in the gut of asymptomatic carriers,” senior author Siew C. Ng, MBBS, PhD, told Medscape Medical News.
“Due to the potential threat of fecal-oral transmission, it is important to maintain long-term coronavirus and health surveillance,” said Ng, Associate Director of the Centre for Gut Microbiota Research at the Chinese University of Hong Kong (CUHK).
“Discharged patients and their caretakers should remain vigilant and observe strict personal and toileting hygiene,” she added.
The prospective, observational study was published online July 20 in Gut.
Ramping up COVID-19 testing
As a follow-up to these and other findings – including the testing of more than 2,000 stool samples in children and the needy arriving at Hong Kong airports starting March 29 – the same investigators are establishing a CUHK Coronavirus Testing Center.
As of Aug. 31, the detection rate in tested children was 0.28%. The Center plans to offer as many as 2,000 COVID-19 tests daily going forward to help identify asymptomatic carriers, the investigators announced in a Sept. 7 news release.
In contrast to nasopharyngeal sampling, stool specimens are “more convenient, safe and non-invasive to collect in the pediatric population,” professor Paul Chan, chairman of the Department of Microbiology, CU Medicine, said in the release. “This makes the stool test a better option for COVID-19 screening in babies, young children and those whose respiratory samples are difficult to collect.”
Even though previous researchers identified SARS-CoV-2 in the stool, the activity and infectivity of the virus in the gastrointestinal tract during and after COVID-19 respiratory positivity remained largely unknown.
Active infection detected in stool
This prospective study involved 15 people hospitalized with COVID-19 in March and April. Participants were a median 55 years old (range, 22-71 years) and all presented with respiratory symptoms. Only one patient had concurrent GI symptoms at admission. Median length of stay was 21 days.
Investigators collected fecal samples serially until discharge. They extracted viral DNA to test for transcriptional genetic evidence of active infection, which they detected in 7 of 15 patients. The patient with GI symptoms was not in this positive group.
The findings suggest a “quiescent but active GI infection,” the researchers note.
Three of the seven patients continued to test positive for active infection in their stool up to 6 days after respiratory clearance of SARS-CoV-2.
Microbiome matters
The investigators also extracted, amplified, and sequenced DNA from the stool samples. Their “metagenomic” profile revealed the type and amounts of bacterial strains in each patient’s gut microbiome.
Interestingly, bacterial strains differed between people with high SARS-CoV-2 infectivity versus participants with low to no evidence of active infection.
“Stool with high viral activity had higher abundance of pathogenic bacteria,” Ng said. In contrast, people with low or no infectivity had more beneficial bacterial strains, including bacteria that play critical roles in boosting host immunity.
Each patient’s microbiome composition changed during the course of the study. Whether the microbiome alters the course of COVID-19 or COVID-19 alters the composition of the microbiome requires further study, the authors note.
The U.S. Food and Drug Administration and officials in other countries have contacted the Hong Kong investigators for more details on their stool testing strategy, professor Francis K.L. Chan, dean of the faculty of medicine and director of the Centre for Gut Microbiota Research at CUHK, stated in the news release.
Further research into revealing the infectivity and pathogenesis of SARS-CoV-2 in the GI tract is warranted. The value of modulating the human gut microbiome in this patient population could be worthwhile to investigate as well, the researchers said.
Novel finding
“Some of it is not-so-new news and some is new,” David A. Johnson, MD, told Medscape Medical News when asked to comment on the study.
For example, previous researchers have detected SARS-CoV-2 virus in the stool. However, this study takes it a step further and shows that the virus present in stool can remain infectious on the basis of metagenomic signatures.
Furthermore, the virus can remain infectious in the gut even after a patient tests negative for COVID-19 through nasopharyngeal sampling – in this report up to 6 days later, said Johnson, professor of medicine, chief of gastroenterology, Eastern Virginia Medical School in Norfolk, Va.
The study carries important implications for people who currently test negative following active COVID-19 infection, he added. Centers for Disease Control and Prevention criteria clear a person as negative after two nasopharyngeal swabs at least 24 hours apart.
People in this category could believe they are no longer infectious and might return to a setting where they could infect others, Johnson said.
One potential means for spreading SARS-CoV-2 from the gut is from a toilet plume, as Johnson previously highlighted in a video report for Medscape Medical News.
The study authors disclosed no relevant financial relationships. Johnson serves as an adviser to WebMD/Medscape.
This article first appeared on Medscape.com.
Can experiencing bigotry and racism lead to PTSD?
I have been studying, writing about, and treating posttraumatic stress disorder for many years. Over this time, I have seen PTSD expand to more and more areas of life, including my own view of a “subthreshold” version, which occurs in vulnerable people who experience a job loss, divorce, financial setbacks, or any number of painful life events.

As I noted in my recent book, “Find Freedom Fast,” for some people, PTSD can be triggered in the wake of events that are not life-threatening yet catastrophic for them and not tied to manmade or natural disasters, torture, assault, or war zone experiences.
The expansion of PTSD has led to the disorder being recognized in ICU patients during and after recovery (Crit Care Med. 2015 May;43[5]:1121-9), as well as in people diagnosed with cancer (Lancet Psychiatry. 2017 Apr;4[4]:330-8) and other illnesses that may cause emotional trauma – where one feels that one’s life is threatened. In some instances, the person’s life might indeed be in danger, not unlike what can happen in disasters, wars, torture, and even in some encounters with law enforcement.
This leads me to yet another circumstance that in some, may be tied to PTSD – and that is racial, religious, ethnic, and gender-related bigotry. In these cases, individuals feel threatened just for who they are in a society. Being on the receiving end of a circumstance that threatens a person’s very existence would seem to me to place a person as a potential survivor of PTSD, as well as any number of disorders, including anxiety, depression, or even paranoia.
Yes, discrimination and prejudice have been with us for a long time, and what concerns me is the psychological effect it has on children as well as adults. Friends of Irish descent remind me of hearing stories from parents and grandparents about employment signs reading, “Irish need not apply.” Certainly, those of Italian ancestry will easily recall the prejudice focused against them. And members of the Jewish community also can easily remember the bigotry and exclusion they have been subject to in certain neighborhoods and organizations, in addition to the horrors of the Holocaust during World War II, and the anti-Semitic chants in Charlottesville, Va., from just 3 years ago – with gun-carrying militants doing the chanting.
Obviously, in certain circles, we still have private clubs, plus neighborhoods and residential buildings that exclude people for a variety of reasons.
Coming from a medical family, years ago I heard stories that, if you were Roman Catholic, it would be hard to get into certain medical schools – which might explain the establishment of Catholic medical schools that often were open to people of other faiths. Then we had medical school discrimination toward Jewish students, which was followed by the establishment of medical schools focused on admitting more Jewish students. The African American community also responded to discrimination by establishing medical schools, such as the school at Howard University in Washington.
Furthermore, we cannot forget the discrimination that women faced in institutions of higher learning. My father had two women in his medical school class, I was told. In my era, I would say at least 30% were women, and today, in the United States, medical school classes are more equally balanced with men and women. Some schools have more women than men.
The question I ask, is: How did all those women feel for so many years knowing that, for reasons beyond their control, they were prevented from achieving their chosen goals? Some might have felt badly, and others might have internalized the rejection. Others might have developed PTSD based on feelings of rejection.
However, the question here mainly is: Can PTSD result when exclusion and prejudice induce fear and terror in those on the receiving end – especially innocent children? Children separated from their parents at the U.S.-Mexico border and those who witness their parents being shot immediately come to mind. This trauma can last well beyond childhood.
and make us realize the extent to which the African American community has been traumatized. Perhaps we should not be surprised by a study that found that the prevalence of PTSD among African Americans is 9.1%, compared with 6.8% for Whites (J Anxiety Dis. 2009 Jun;23[5]:573-90). Speaking with Black colleagues, friends, and patients, reading books such “The Warmth of Other Suns,” and watching films such as “Green Book,” give us a sense of how dangerous it was for Black families to travel in certain parts of the country in the recent past. I recall as a child hearing that, in Miami Beach, people of color could not stay overnight. (Even as a child I was surprised – having never heard anything like that. After all, I went to school with people of many religions and backgrounds. My parents thought those practices were terrible, and were appalled when they learned that some hotels were closed to Jews and others closed to Catholics.)
DSM-5, ICD-10 fall short
The DSM-5 describes trauma using a more or less one-dimensional set of guidelines as the focus. Those guidelines include exposure to direct violence, manmade or natural disasters, war, or torture, as well as exposure to a disaster or a life-threatening situation affecting a loved one. The ICD-10 is less restrictive about trauma but still has some limitations.
While considering potential PTSD, I try to use a less rigid diagnostic multidimensional approach, where I assess individual differences and experiences that play a role in those experiences as well as the patient’s vulnerability to the causation of PTSD – which also has to include any exposure to trauma (Curr Opin Psychol. 2017 Apr;14:29-34) before age 11 or 12. The data suggest that such early exposure leaves people more vulnerable to PTSD as adults (Soc Sci Med. 2018 Feb;199:230-40).
In my view, if individuals are frightened because of who they are – be it tied to their religion, race, sexual identity, or ethnicity – and what harm may come to them, and if they live in fear and avoidance of these potential traumatic situations that affect their mental stability and the way they live their lives, they might fit the PTSD model.
If we clinicians focus on what’s currently being brought vividly into the public eye today regarding the African American community, we would see that some of the ongoing fears of racism – whether tied to residential or workplace discrimination, unfair treatment by figures of authority, harassment, health inequities, or microaggressions – may give rise to PTSD. I know we can do better. We should broaden our definition and awareness of this very serious disorder – and be prepared to treat it.
Dr. London has been a practicing psychiatrist for 4 decades and a newspaper columnist for almost as long. He has a private practice in New York and is author of “Find Freedom Fast: Short-Term Therapy That Works” (New York: Kettlehole Publishing, 2019). Dr. London has no conflicts of interest.
I have been studying, writing about, and treating posttraumatic stress disorder for many years. Over this time, I have seen PTSD expand to more and more areas of life, including my own view of a “subthreshold” version, which occurs in vulnerable people who experience a job loss, divorce, financial setbacks, or any number of painful life events.
As I noted in my recent book, “Find Freedom Fast,” for some people, PTSD can be triggered in the wake of events that are not life-threatening yet catastrophic for them and not tied to manmade or natural disasters, torture, assault, or war zone experiences.
The expansion of PTSD has led to the disorder being recognized in ICU patients during and after recovery (Crit Care Med. 2015 May;43[5]:1121-9), as well as in people diagnosed with cancer (Lancet Psychiatry. 2017 Apr;4[4]:330-8) and other illnesses that may cause emotional trauma – where one feels that one’s life is threatened. In some instances, the person’s life might indeed be in danger, not unlike what can happen in disasters, wars, torture, and even in some encounters with law enforcement.
This leads me to yet another circumstance that in some, may be tied to PTSD – and that is racial, religious, ethnic, and gender-related bigotry. In these cases, individuals feel threatened just for who they are in a society. Being on the receiving end of a circumstance that threatens a person’s very existence would seem to me to place a person as a potential survivor of PTSD, as well as any number of disorders, including anxiety, depression, or even paranoia.
Yes, discrimination and prejudice have been with us for a long time, and what concerns me is the psychological effect it has on children as well as adults. Friends of Irish descent remind me of hearing stories from parents and grandparents about employment signs reading, “Irish need not apply.” Certainly, those of Italian ancestry will easily recall the prejudice focused against them. And members of the Jewish community also can easily remember the bigotry and exclusion they have been subject to in certain neighborhoods and organizations, in addition to the horrors of the Holocaust during World War II, and the anti-Semitic chants in Charlottesville, Va., from just 3 years ago – with gun-carrying militants doing the chanting.
Obviously, in certain circles, we still have private clubs, plus neighborhoods and residential buildings that exclude people for a variety of reasons.
Coming from a medical family, years ago I heard stories that, if you were Roman Catholic, it would be hard to get into certain medical schools – which might explain the establishment of Catholic medical schools that often were open to people of other faiths. Then we had medical school discrimination toward Jewish students, which was followed by the establishment of medical schools focused on admitting more Jewish students. The African American community also responded to discrimination by establishing medical schools, such as the school at Howard University in Washington.
Furthermore, we cannot forget the discrimination that women faced in institutions of higher learning. My father had two women in his medical school class, I was told. In my era, I would say at least 30% were women, and today, in the United States, medical school classes are more equally balanced with men and women. Some schools have more women than men.
The question I ask, is: How did all those women feel for so many years knowing that, for reasons beyond their control, they were prevented from achieving their chosen goals? Some might have felt badly, and others might have internalized the rejection. Others might have developed PTSD based on feelings of rejection.
However, the question here mainly is: Can PTSD result when exclusion and prejudice induce fear and terror in those on the receiving end – especially innocent children? Children separated from their parents at the U.S.-Mexico border and those who witness their parents being shot immediately come to mind. This trauma can last well beyond childhood.
and make us realize the extent to which the African American community has been traumatized. Perhaps we should not be surprised by a study that found that the prevalence of PTSD among African Americans is 9.1%, compared with 6.8% for Whites (J Anxiety Dis. 2009 Jun;23[5]:573-90). Speaking with Black colleagues, friends, and patients, reading books such “The Warmth of Other Suns,” and watching films such as “Green Book,” give us a sense of how dangerous it was for Black families to travel in certain parts of the country in the recent past. I recall as a child hearing that, in Miami Beach, people of color could not stay overnight. (Even as a child I was surprised – having never heard anything like that. After all, I went to school with people of many religions and backgrounds. My parents thought those practices were terrible, and were appalled when they learned that some hotels were closed to Jews and others closed to Catholics.)
DSM-5, ICD-10 fall short
The DSM-5 describes trauma using a more or less one-dimensional set of guidelines as the focus. Those guidelines include exposure to direct violence, manmade or natural disasters, war, or torture, as well as exposure to a disaster or a life-threatening situation affecting a loved one. The ICD-10 is less restrictive about trauma but still has some limitations.
While considering potential PTSD, I try to use a less rigid diagnostic multidimensional approach, where I assess individual differences and experiences that play a role in those experiences as well as the patient’s vulnerability to the causation of PTSD – which also has to include any exposure to trauma (Curr Opin Psychol. 2017 Apr;14:29-34) before age 11 or 12. The data suggest that such early exposure leaves people more vulnerable to PTSD as adults (Soc Sci Med. 2018 Feb;199:230-40).
In my view, if individuals are frightened because of who they are – be it tied to their religion, race, sexual identity, or ethnicity – and what harm may come to them, and if they live in fear and avoidance of these potential traumatic situations that affect their mental stability and the way they live their lives, they might fit the PTSD model.
If we clinicians focus on what’s currently being brought vividly into the public eye today regarding the African American community, we would see that some of the ongoing fears of racism – whether tied to residential or workplace discrimination, unfair treatment by figures of authority, harassment, health inequities, or microaggressions – may give rise to PTSD. I know we can do better. We should broaden our definition and awareness of this very serious disorder – and be prepared to treat it.
Dr. London has been a practicing psychiatrist for 4 decades and a newspaper columnist for almost as long. He has a private practice in New York and is author of “Find Freedom Fast: Short-Term Therapy That Works” (New York: Kettlehole Publishing, 2019). Dr. London has no conflicts of interest.
I have been studying, writing about, and treating posttraumatic stress disorder for many years. Over this time, I have seen PTSD expand to more and more areas of life, including my own view of a “subthreshold” version, which occurs in vulnerable people who experience a job loss, divorce, financial setbacks, or any number of painful life events.
As I noted in my recent book, “Find Freedom Fast,” for some people, PTSD can be triggered in the wake of events that are not life-threatening yet catastrophic for them and not tied to manmade or natural disasters, torture, assault, or war zone experiences.
The expansion of PTSD has led to the disorder being recognized in ICU patients during and after recovery (Crit Care Med. 2015 May;43[5]:1121-9), as well as in people diagnosed with cancer (Lancet Psychiatry. 2017 Apr;4[4]:330-8) and other illnesses that may cause emotional trauma – where one feels that one’s life is threatened. In some instances, the person’s life might indeed be in danger, not unlike what can happen in disasters, wars, torture, and even in some encounters with law enforcement.
This leads me to yet another circumstance that in some, may be tied to PTSD – and that is racial, religious, ethnic, and gender-related bigotry. In these cases, individuals feel threatened just for who they are in a society. Being on the receiving end of a circumstance that threatens a person’s very existence would seem to me to place a person as a potential survivor of PTSD, as well as any number of disorders, including anxiety, depression, or even paranoia.
Yes, discrimination and prejudice have been with us for a long time, and what concerns me is the psychological effect it has on children as well as adults. Friends of Irish descent remind me of hearing stories from parents and grandparents about employment signs reading, “Irish need not apply.” Certainly, those of Italian ancestry will easily recall the prejudice focused against them. And members of the Jewish community also can easily remember the bigotry and exclusion they have been subject to in certain neighborhoods and organizations, in addition to the horrors of the Holocaust during World War II, and the anti-Semitic chants in Charlottesville, Va., from just 3 years ago – with gun-carrying militants doing the chanting.
Obviously, in certain circles, we still have private clubs, plus neighborhoods and residential buildings that exclude people for a variety of reasons.
Coming from a medical family, years ago I heard stories that, if you were Roman Catholic, it would be hard to get into certain medical schools – which might explain the establishment of Catholic medical schools that often were open to people of other faiths. Then we had medical school discrimination toward Jewish students, which was followed by the establishment of medical schools focused on admitting more Jewish students. The African American community also responded to discrimination by establishing medical schools, such as the school at Howard University in Washington.
Furthermore, we cannot forget the discrimination that women faced in institutions of higher learning. My father had two women in his medical school class, I was told. In my era, I would say at least 30% were women, and today, in the United States, medical school classes are more equally balanced with men and women. Some schools have more women than men.
The question I ask, is: How did all those women feel for so many years knowing that, for reasons beyond their control, they were prevented from achieving their chosen goals? Some might have felt badly, and others might have internalized the rejection. Others might have developed PTSD based on feelings of rejection.
However, the question here mainly is: Can PTSD result when exclusion and prejudice induce fear and terror in those on the receiving end – especially innocent children? Children separated from their parents at the U.S.-Mexico border and those who witness their parents being shot immediately come to mind. This trauma can last well beyond childhood.
and make us realize the extent to which the African American community has been traumatized. Perhaps we should not be surprised by a study that found that the prevalence of PTSD among African Americans is 9.1%, compared with 6.8% for Whites (J Anxiety Dis. 2009 Jun;23[5]:573-90). Speaking with Black colleagues, friends, and patients, reading books such “The Warmth of Other Suns,” and watching films such as “Green Book,” give us a sense of how dangerous it was for Black families to travel in certain parts of the country in the recent past. I recall as a child hearing that, in Miami Beach, people of color could not stay overnight. (Even as a child I was surprised – having never heard anything like that. After all, I went to school with people of many religions and backgrounds. My parents thought those practices were terrible, and were appalled when they learned that some hotels were closed to Jews and others closed to Catholics.)
DSM-5, ICD-10 fall short
The DSM-5 describes trauma using a more or less one-dimensional set of guidelines as the focus. Those guidelines include exposure to direct violence, manmade or natural disasters, war, or torture, as well as exposure to a disaster or a life-threatening situation affecting a loved one. The ICD-10 is less restrictive about trauma but still has some limitations.
While considering potential PTSD, I try to use a less rigid diagnostic multidimensional approach, where I assess individual differences and experiences that play a role in those experiences as well as the patient’s vulnerability to the causation of PTSD – which also has to include any exposure to trauma (Curr Opin Psychol. 2017 Apr;14:29-34) before age 11 or 12. The data suggest that such early exposure leaves people more vulnerable to PTSD as adults (Soc Sci Med. 2018 Feb;199:230-40).
In my view, if individuals are frightened because of who they are – be it tied to their religion, race, sexual identity, or ethnicity – and what harm may come to them, and if they live in fear and avoidance of these potential traumatic situations that affect their mental stability and the way they live their lives, they might fit the PTSD model.
If we clinicians focus on what’s currently being brought vividly into the public eye today regarding the African American community, we would see that some of the ongoing fears of racism – whether tied to residential or workplace discrimination, unfair treatment by figures of authority, harassment, health inequities, or microaggressions – may give rise to PTSD. I know we can do better. We should broaden our definition and awareness of this very serious disorder – and be prepared to treat it.
Dr. London has been a practicing psychiatrist for 4 decades and a newspaper columnist for almost as long. He has a private practice in New York and is author of “Find Freedom Fast: Short-Term Therapy That Works” (New York: Kettlehole Publishing, 2019). Dr. London has no conflicts of interest.
Worry over family, friends the main driver of COVID-19 stress
Individuals are more worried about family members becoming ill with COVID-19 or about unknowingly transmitting the disease to family members than they are about contracting it themselves, results of a new survey show.
Investigators surveyed over 3,000 adults, using an online questionnaire. Of the respondents, about 20% were health care workers, and most were living in locations with active stay-at-home orders at the time of the survey.

Close to half of participants were worried about family members contracting the virus, one third were worried about unknowingly infecting others, and 20% were worried about contracting the virus themselves.
“We were a little surprised to see that people were more concerned about others than about themselves, specifically worrying about whether a family member would contract COVID-19 and whether they might unintentionally infect others,” lead author Ran Barzilay, MD, PhD, child and adolescent psychiatrist at the Children’s Hospital of Philadelphia (CHOP), told Medscape Medical News.
The study was published online August 20 in Translational Psychiatry.
Interactive platform
“The pandemic has provided a unique opportunity to study resilience in healthcare professionals and others,” said Barzilay, assistant professor at the Lifespan Brain Institute, a collaboration between CHOP and the University of Pennsylvania, under the directorship of Raquel Gur, MD, PhD.
“After the pandemic broke out in March, we launched a website in early April where we surveyed people for levels of resilience, mental health, and well-being during the outbreak,” he added.

Survey participants then shared it with their contacts.
“To date, over 7000 people have completed it – mostly from the US but also from Israel,” Barzilay said.
The survey was anonymous, but participants could choose to have follow-up contact. The survey included an interactive 21-item resilience questionnaire and an assessment of COVID-19-related items related to worries concerning the following: contracting, dying from, or currently having the illness; having a family member contract the illness; unknowingly infecting others; and experiencing significant financial burden.
A total of 1350 participants took a second survey on anxiety and depression that utilized the Generalized Anxiety Disorder–7 and the Patient Health Questionnaire–2.
“What makes the survey unique is that it’s not just a means of collecting data but also an interactive platform that gives participants immediate personalized feedback, based on their responses to the resilience and well-being surveys, with practical tips and recommendations for stress management and ways of boosting resilience,” Barzilay said.
Tend and befriend
Ten days into the survey, data were available on 3,042 participants (64% women, 54% with advanced education, 20.5% health care providers), who ranged in age from 18 to 70 years (mean [SD], 38.9 [11.9] years).
After accounting for covariates, the researchers found that participants reported more distress about family members contracting COVID-19 and about unknowingly infecting others than about getting COVID-19 themselves (48.5% and 36% vs. 19.9%, respectively; P < .0005).
Increased COVID-19-related worries were associated with 22% higher anxiety and 16.1% higher depression scores; women had higher scores than men on both.
Each 1-SD increase in the composite score of COVID-19 worries was associated with over twice the increased probability of generalized anxiety and depression (odds ratio, 2.23; 95% confidence interval, 1.88-2.65; and OR, 1.67; 95% CI, 1.41-1.98, respectively; for both, P < .001).
On the other hand, for every 1-SD increase in the resilience score, there was a 64.9% decrease in the possibility of screening positive for generalized anxiety disorder and a 69.3% decrease in the possibility of screening positive for depression (for both, P < .0001).
Compared to participants from Israel, US participants were “more stressed” about contracting, dying from, and currently having COVID-19 themselves. Overall, Israeli participants scored higher than US participants on the resilience scale.
Rates of anxiety and depression did not differ significantly between healthcare providers and others. Health care providers worried more about contracting COVID-19 themselves and worried less about finances after COVID-19.
The authors propose that survey participants were more worried about others than about themselves because of “prosocial behavior under stress” and “tend-and-befriend,” whereby, “in response to threat, humans tend to protect their close ones (tending) and seek out their social group for mutual defense (befriending).”
This type of altruistic behavior has been “described in acute situations throughout history” and has been “linked to mechanisms of resilience for overcoming adversity,” the authors indicate.
Demographic biases
Commenting on the findings for Medscape Medical News, Golnaz Tabibnia, PhD, a neuroscientist at the University of California, Irvine, who was not involved in the research, suggested that although higher resilience scores were associated with lower COVID-related worries, it is possible, “as the authors suggest, that having more resilience resources makes you less worried, but the causality could go the other direction as well, and less worry/rumination may lead to more resilience.”

Also commenting on the study for Medscape Medical News, Christiaan Vinkers, MD, PhD, a psychiatrist at the Amsterdam University Medical Center, Amsterdam, the Netherlands, said it was noteworthy that healthcare providers reported similar levels of mood and anxiety symptoms, compared to others.
“This is encouraging, as it suggests adequate resilience levels in professionals who work in the front lines of the COVID-19 pandemic,” he said.
Resilience occurs not only at the individual level but also at the community level, which may help explain the striking differences in COVID-19-related worries and anxiety between participants from the United States and Israel, Vinkers added.
E. Alison Holman, PhD, professor, Sue and Bill Gross School of Nursing, University of California, Irvine, noted that respondents were predominantly white, female, and had relatively high incomes, “suggesting strong demographic biases in those who chose to participate.”

Holman, who was not involved with the study, told Medscape Medical News that the “findings do not address the real impact of COVID-19 on the hardest-hit communities in America – poor, Black, and Latinx communities, where a large proportion of essential workers live.”
Barzilay acknowledged that, “unfortunately, because of the way the study was circulated, it did not reach minorities, which is one of the things we want to improve.”
The study is ongoing and has been translated into Spanish, French, and Hebrew. The team plans to collect data on diverse populations.
The study was supported by grants from the National Institute of Mental Health, the Lifespan Brain Institute of Children’s Hospital of Philadelphia, Penn Medicine, the University of Pennsylvania, and in part by the Zuckerman STEM Leadership Program. Barzilay serves on the scientific board and reports stock ownership in Taliaz Health. The other authors, Golnaz, Vinkers, and Holman have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Individuals are more worried about family members becoming ill with COVID-19 or about unknowingly transmitting the disease to family members than they are about contracting it themselves, results of a new survey show.
Investigators surveyed over 3,000 adults, using an online questionnaire. Of the respondents, about 20% were health care workers, and most were living in locations with active stay-at-home orders at the time of the survey.
Close to half of participants were worried about family members contracting the virus, one third were worried about unknowingly infecting others, and 20% were worried about contracting the virus themselves.
“We were a little surprised to see that people were more concerned about others than about themselves, specifically worrying about whether a family member would contract COVID-19 and whether they might unintentionally infect others,” lead author Ran Barzilay, MD, PhD, child and adolescent psychiatrist at the Children’s Hospital of Philadelphia (CHOP), told Medscape Medical News.
The study was published online August 20 in Translational Psychiatry.
Interactive platform
“The pandemic has provided a unique opportunity to study resilience in healthcare professionals and others,” said Barzilay, assistant professor at the Lifespan Brain Institute, a collaboration between CHOP and the University of Pennsylvania, under the directorship of Raquel Gur, MD, PhD.
“After the pandemic broke out in March, we launched a website in early April where we surveyed people for levels of resilience, mental health, and well-being during the outbreak,” he added.
Survey participants then shared it with their contacts.
“To date, over 7000 people have completed it – mostly from the US but also from Israel,” Barzilay said.
The survey was anonymous, but participants could choose to have follow-up contact. The survey included an interactive 21-item resilience questionnaire and an assessment of COVID-19-related items related to worries concerning the following: contracting, dying from, or currently having the illness; having a family member contract the illness; unknowingly infecting others; and experiencing significant financial burden.
A total of 1350 participants took a second survey on anxiety and depression that utilized the Generalized Anxiety Disorder–7 and the Patient Health Questionnaire–2.
“What makes the survey unique is that it’s not just a means of collecting data but also an interactive platform that gives participants immediate personalized feedback, based on their responses to the resilience and well-being surveys, with practical tips and recommendations for stress management and ways of boosting resilience,” Barzilay said.
Tend and befriend
Ten days into the survey, data were available on 3,042 participants (64% women, 54% with advanced education, 20.5% health care providers), who ranged in age from 18 to 70 years (mean [SD], 38.9 [11.9] years).
After accounting for covariates, the researchers found that participants reported more distress about family members contracting COVID-19 and about unknowingly infecting others than about getting COVID-19 themselves (48.5% and 36% vs. 19.9%, respectively; P < .0005).
Increased COVID-19-related worries were associated with 22% higher anxiety and 16.1% higher depression scores; women had higher scores than men on both.
Each 1-SD increase in the composite score of COVID-19 worries was associated with over twice the increased probability of generalized anxiety and depression (odds ratio, 2.23; 95% confidence interval, 1.88-2.65; and OR, 1.67; 95% CI, 1.41-1.98, respectively; for both, P < .001).
On the other hand, for every 1-SD increase in the resilience score, there was a 64.9% decrease in the possibility of screening positive for generalized anxiety disorder and a 69.3% decrease in the possibility of screening positive for depression (for both, P < .0001).
Compared to participants from Israel, US participants were “more stressed” about contracting, dying from, and currently having COVID-19 themselves. Overall, Israeli participants scored higher than US participants on the resilience scale.
Rates of anxiety and depression did not differ significantly between healthcare providers and others. Health care providers worried more about contracting COVID-19 themselves and worried less about finances after COVID-19.
The authors propose that survey participants were more worried about others than about themselves because of “prosocial behavior under stress” and “tend-and-befriend,” whereby, “in response to threat, humans tend to protect their close ones (tending) and seek out their social group for mutual defense (befriending).”
This type of altruistic behavior has been “described in acute situations throughout history” and has been “linked to mechanisms of resilience for overcoming adversity,” the authors indicate.
Demographic biases
Commenting on the findings for Medscape Medical News, Golnaz Tabibnia, PhD, a neuroscientist at the University of California, Irvine, who was not involved in the research, suggested that although higher resilience scores were associated with lower COVID-related worries, it is possible, “as the authors suggest, that having more resilience resources makes you less worried, but the causality could go the other direction as well, and less worry/rumination may lead to more resilience.”
Also commenting on the study for Medscape Medical News, Christiaan Vinkers, MD, PhD, a psychiatrist at the Amsterdam University Medical Center, Amsterdam, the Netherlands, said it was noteworthy that healthcare providers reported similar levels of mood and anxiety symptoms, compared to others.
“This is encouraging, as it suggests adequate resilience levels in professionals who work in the front lines of the COVID-19 pandemic,” he said.
Resilience occurs not only at the individual level but also at the community level, which may help explain the striking differences in COVID-19-related worries and anxiety between participants from the United States and Israel, Vinkers added.
E. Alison Holman, PhD, professor, Sue and Bill Gross School of Nursing, University of California, Irvine, noted that respondents were predominantly white, female, and had relatively high incomes, “suggesting strong demographic biases in those who chose to participate.”
Holman, who was not involved with the study, told Medscape Medical News that the “findings do not address the real impact of COVID-19 on the hardest-hit communities in America – poor, Black, and Latinx communities, where a large proportion of essential workers live.”
Barzilay acknowledged that, “unfortunately, because of the way the study was circulated, it did not reach minorities, which is one of the things we want to improve.”
The study is ongoing and has been translated into Spanish, French, and Hebrew. The team plans to collect data on diverse populations.
The study was supported by grants from the National Institute of Mental Health, the Lifespan Brain Institute of Children’s Hospital of Philadelphia, Penn Medicine, the University of Pennsylvania, and in part by the Zuckerman STEM Leadership Program. Barzilay serves on the scientific board and reports stock ownership in Taliaz Health. The other authors, Golnaz, Vinkers, and Holman have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Individuals are more worried about family members becoming ill with COVID-19 or about unknowingly transmitting the disease to family members than they are about contracting it themselves, results of a new survey show.
Investigators surveyed over 3,000 adults, using an online questionnaire. Of the respondents, about 20% were health care workers, and most were living in locations with active stay-at-home orders at the time of the survey.
Close to half of participants were worried about family members contracting the virus, one third were worried about unknowingly infecting others, and 20% were worried about contracting the virus themselves.
“We were a little surprised to see that people were more concerned about others than about themselves, specifically worrying about whether a family member would contract COVID-19 and whether they might unintentionally infect others,” lead author Ran Barzilay, MD, PhD, child and adolescent psychiatrist at the Children’s Hospital of Philadelphia (CHOP), told Medscape Medical News.
The study was published online August 20 in Translational Psychiatry.
Interactive platform
“The pandemic has provided a unique opportunity to study resilience in healthcare professionals and others,” said Barzilay, assistant professor at the Lifespan Brain Institute, a collaboration between CHOP and the University of Pennsylvania, under the directorship of Raquel Gur, MD, PhD.
“After the pandemic broke out in March, we launched a website in early April where we surveyed people for levels of resilience, mental health, and well-being during the outbreak,” he added.
Survey participants then shared it with their contacts.
“To date, over 7000 people have completed it – mostly from the US but also from Israel,” Barzilay said.
The survey was anonymous, but participants could choose to have follow-up contact. The survey included an interactive 21-item resilience questionnaire and an assessment of COVID-19-related items related to worries concerning the following: contracting, dying from, or currently having the illness; having a family member contract the illness; unknowingly infecting others; and experiencing significant financial burden.
A total of 1350 participants took a second survey on anxiety and depression that utilized the Generalized Anxiety Disorder–7 and the Patient Health Questionnaire–2.
“What makes the survey unique is that it’s not just a means of collecting data but also an interactive platform that gives participants immediate personalized feedback, based on their responses to the resilience and well-being surveys, with practical tips and recommendations for stress management and ways of boosting resilience,” Barzilay said.
Tend and befriend
Ten days into the survey, data were available on 3,042 participants (64% women, 54% with advanced education, 20.5% health care providers), who ranged in age from 18 to 70 years (mean [SD], 38.9 [11.9] years).
After accounting for covariates, the researchers found that participants reported more distress about family members contracting COVID-19 and about unknowingly infecting others than about getting COVID-19 themselves (48.5% and 36% vs. 19.9%, respectively; P < .0005).
Increased COVID-19-related worries were associated with 22% higher anxiety and 16.1% higher depression scores; women had higher scores than men on both.
Each 1-SD increase in the composite score of COVID-19 worries was associated with over twice the increased probability of generalized anxiety and depression (odds ratio, 2.23; 95% confidence interval, 1.88-2.65; and OR, 1.67; 95% CI, 1.41-1.98, respectively; for both, P < .001).
On the other hand, for every 1-SD increase in the resilience score, there was a 64.9% decrease in the possibility of screening positive for generalized anxiety disorder and a 69.3% decrease in the possibility of screening positive for depression (for both, P < .0001).
Compared to participants from Israel, US participants were “more stressed” about contracting, dying from, and currently having COVID-19 themselves. Overall, Israeli participants scored higher than US participants on the resilience scale.
Rates of anxiety and depression did not differ significantly between healthcare providers and others. Health care providers worried more about contracting COVID-19 themselves and worried less about finances after COVID-19.
The authors propose that survey participants were more worried about others than about themselves because of “prosocial behavior under stress” and “tend-and-befriend,” whereby, “in response to threat, humans tend to protect their close ones (tending) and seek out their social group for mutual defense (befriending).”
This type of altruistic behavior has been “described in acute situations throughout history” and has been “linked to mechanisms of resilience for overcoming adversity,” the authors indicate.
Demographic biases
Commenting on the findings for Medscape Medical News, Golnaz Tabibnia, PhD, a neuroscientist at the University of California, Irvine, who was not involved in the research, suggested that although higher resilience scores were associated with lower COVID-related worries, it is possible, “as the authors suggest, that having more resilience resources makes you less worried, but the causality could go the other direction as well, and less worry/rumination may lead to more resilience.”
Also commenting on the study for Medscape Medical News, Christiaan Vinkers, MD, PhD, a psychiatrist at the Amsterdam University Medical Center, Amsterdam, the Netherlands, said it was noteworthy that healthcare providers reported similar levels of mood and anxiety symptoms, compared to others.
“This is encouraging, as it suggests adequate resilience levels in professionals who work in the front lines of the COVID-19 pandemic,” he said.
Resilience occurs not only at the individual level but also at the community level, which may help explain the striking differences in COVID-19-related worries and anxiety between participants from the United States and Israel, Vinkers added.
E. Alison Holman, PhD, professor, Sue and Bill Gross School of Nursing, University of California, Irvine, noted that respondents were predominantly white, female, and had relatively high incomes, “suggesting strong demographic biases in those who chose to participate.”
Holman, who was not involved with the study, told Medscape Medical News that the “findings do not address the real impact of COVID-19 on the hardest-hit communities in America – poor, Black, and Latinx communities, where a large proportion of essential workers live.”
Barzilay acknowledged that, “unfortunately, because of the way the study was circulated, it did not reach minorities, which is one of the things we want to improve.”
The study is ongoing and has been translated into Spanish, French, and Hebrew. The team plans to collect data on diverse populations.
The study was supported by grants from the National Institute of Mental Health, the Lifespan Brain Institute of Children’s Hospital of Philadelphia, Penn Medicine, the University of Pennsylvania, and in part by the Zuckerman STEM Leadership Program. Barzilay serves on the scientific board and reports stock ownership in Taliaz Health. The other authors, Golnaz, Vinkers, and Holman have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Sleep EEG may predict later antidepressant response
A change in rapid eye movement sleeping pattern as measured by quantitative EEG in patients with major depressive disorder after just a single week on a first-line antidepressant predicts eventual clinical response or nonresponse to the medication weeks later, Thorsten Mikoteit, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.

This finding from a small, randomized, controlled trial opens the door to a novel biomarker-based treatment strategy: namely, an immediate switch to a different antidepressant in predicted nonresponders to the first agent. The goal is to improve the final treatment response rate while collapsing the time required to get there, explained Dr. Mikoteit, a psychiatrist affiliated with the University of Basel (Switzerland).
“In real terms, it means that patients, often in the depths of despair, might not need to wait weeks to see if their therapy is working before modifying their treatment,” he observed.
There is a huge unmet need for a biomarker predictive of response to antidepressant medication in patients with major depression, the psychiatrist added. At present, the treatment response rate is unsatisfactory. Moreover, clinical improvement takes a long time to achieve, often requiring several rounds of therapeutic trials during which patients are exposed to weeks of unpleasant side effects of drugs that are ultimately switched out for lack of efficacy or poor tolerance.
The quantitative EEG biomarker under investigation is prefrontal theta cordance (PTC) during REM sleep. It is computed from the absolute and relative theta power in tonic REM sleep. PTC has been shown to correlate with frontocingulate brain activity and cerebral blood perfusion. In an earlier pilot study, Dr. Mikoteit and coinvestigators demonstrated in 33 patients who were experiencing a depressive episode that an increase in PTC after their first week on an antidepressant was associated a significantly increased treatment response rate at the end of the fourth week on the drug, while nonresponders failed to show such increase (J Psychiatr Res. 2017 Sep;92:64-73).
At ECNP 2020, Dr. Mikoteit presented preliminary results from an ongoing randomized, controlled trial including 37 patients hospitalized for major depressive disorder. All underwent baseline evaluation using the Hamilton Depression Rating Scale (HAMD) and were placed on the first-line antidepressant of their psychiatrist’s choice. After 1 week of therapy, participants underwent polysomnography with PTC measurement during tonic REM sleep.
Twenty-two patients were randomized to the intervention arm, in which investigators informed treating psychiatrists of the PTC results. The clinicians were instructed to change to another antidepressant if the biomarker predicted nonresponse or stay the course if the PTC results were favorable. Polysomnography was repeated 1 week later in the intervention arm, and the second-line antidepressant was either continued or switched out depending on the PTC findings. In the control arm, psychiatrists weren’t informed of the PTC results and patients continued on their initial antidepressant. The intervention and control groups were comparable in terms of age, sex, and severity of depression, with an average baseline HAMD score of 22.
A treatment response was defined as at least a 50% reduction in HAMD score from baseline to week 5. About 86% of patients who switched antidepressants based upon their 1-week quantitative EEG findings were categorized as treatment responders at week 5, compared with 20% of controls.
The overall 5-week response rate in the intervention group was 73%, compared with 60% in the control arm. This favorable trend didn’t achieve statistical significance, presumably because of the study’s sample size; however, the study is continuing to enroll participants in order to achieve a definitive result.
Dr. Mikoteit noted that the cost and inconvenience of spending a night in a sleep laboratory would be worthwhile if it resulted in the ability to give effective treatment much sooner. This would be particularly advantageous in patients at increased risk for suicide.
he said.
Study could have “enormous implications”
Of note, in the landmark National Institute of Mental Health–sponsored Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, slightly less than half of patients with major depressive disorder achieved a treatment response to their first-line antidepressant, and it took an average of 6 weeks of therapy to do. About one in four nonresponders who chose to switch to a different antidepressant got better.

“The STAR*D trial is still the gold standard for understanding antidepressant response, and so being able to see if an antidepressant works within 1 week would be a real breakthrough,” Catherine Harmer, DPhil, said in an interview.
“Most of the time, patients need to wait for around 4 weeks before they can tell if they are responding to a particular antidepressant or not. This is a hugely disabling and lengthy process, and often a different treatment then needs to be started,” added Dr. Harmer, professor of cognitive neuroscience and director of the Psychopharmacology and Emotional Research Lab at the University of Oxford (England).
“If the study results presented by Dr. Mikoteit are replicated in a larger blinded study, then it would have enormous implications for the future treatment of individuals with depression,” according to Dr. Harmer, who was not involved in the study and has no conflicts of interest related to it.
Dr. Mikoteit reported having no financial conflicts regarding the study, funded by the Psychiatric University Hospital of Basel.
SOURCE: Mikoteit T et al. ECNP 2020, Abstract P.733.
A change in rapid eye movement sleeping pattern as measured by quantitative EEG in patients with major depressive disorder after just a single week on a first-line antidepressant predicts eventual clinical response or nonresponse to the medication weeks later, Thorsten Mikoteit, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.
This finding from a small, randomized, controlled trial opens the door to a novel biomarker-based treatment strategy: namely, an immediate switch to a different antidepressant in predicted nonresponders to the first agent. The goal is to improve the final treatment response rate while collapsing the time required to get there, explained Dr. Mikoteit, a psychiatrist affiliated with the University of Basel (Switzerland).
“In real terms, it means that patients, often in the depths of despair, might not need to wait weeks to see if their therapy is working before modifying their treatment,” he observed.
There is a huge unmet need for a biomarker predictive of response to antidepressant medication in patients with major depression, the psychiatrist added. At present, the treatment response rate is unsatisfactory. Moreover, clinical improvement takes a long time to achieve, often requiring several rounds of therapeutic trials during which patients are exposed to weeks of unpleasant side effects of drugs that are ultimately switched out for lack of efficacy or poor tolerance.
The quantitative EEG biomarker under investigation is prefrontal theta cordance (PTC) during REM sleep. It is computed from the absolute and relative theta power in tonic REM sleep. PTC has been shown to correlate with frontocingulate brain activity and cerebral blood perfusion. In an earlier pilot study, Dr. Mikoteit and coinvestigators demonstrated in 33 patients who were experiencing a depressive episode that an increase in PTC after their first week on an antidepressant was associated a significantly increased treatment response rate at the end of the fourth week on the drug, while nonresponders failed to show such increase (J Psychiatr Res. 2017 Sep;92:64-73).
At ECNP 2020, Dr. Mikoteit presented preliminary results from an ongoing randomized, controlled trial including 37 patients hospitalized for major depressive disorder. All underwent baseline evaluation using the Hamilton Depression Rating Scale (HAMD) and were placed on the first-line antidepressant of their psychiatrist’s choice. After 1 week of therapy, participants underwent polysomnography with PTC measurement during tonic REM sleep.
Twenty-two patients were randomized to the intervention arm, in which investigators informed treating psychiatrists of the PTC results. The clinicians were instructed to change to another antidepressant if the biomarker predicted nonresponse or stay the course if the PTC results were favorable. Polysomnography was repeated 1 week later in the intervention arm, and the second-line antidepressant was either continued or switched out depending on the PTC findings. In the control arm, psychiatrists weren’t informed of the PTC results and patients continued on their initial antidepressant. The intervention and control groups were comparable in terms of age, sex, and severity of depression, with an average baseline HAMD score of 22.
A treatment response was defined as at least a 50% reduction in HAMD score from baseline to week 5. About 86% of patients who switched antidepressants based upon their 1-week quantitative EEG findings were categorized as treatment responders at week 5, compared with 20% of controls.
The overall 5-week response rate in the intervention group was 73%, compared with 60% in the control arm. This favorable trend didn’t achieve statistical significance, presumably because of the study’s sample size; however, the study is continuing to enroll participants in order to achieve a definitive result.
Dr. Mikoteit noted that the cost and inconvenience of spending a night in a sleep laboratory would be worthwhile if it resulted in the ability to give effective treatment much sooner. This would be particularly advantageous in patients at increased risk for suicide.
he said.
Study could have “enormous implications”
Of note, in the landmark National Institute of Mental Health–sponsored Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, slightly less than half of patients with major depressive disorder achieved a treatment response to their first-line antidepressant, and it took an average of 6 weeks of therapy to do. About one in four nonresponders who chose to switch to a different antidepressant got better.
“The STAR*D trial is still the gold standard for understanding antidepressant response, and so being able to see if an antidepressant works within 1 week would be a real breakthrough,” Catherine Harmer, DPhil, said in an interview.
“Most of the time, patients need to wait for around 4 weeks before they can tell if they are responding to a particular antidepressant or not. This is a hugely disabling and lengthy process, and often a different treatment then needs to be started,” added Dr. Harmer, professor of cognitive neuroscience and director of the Psychopharmacology and Emotional Research Lab at the University of Oxford (England).
“If the study results presented by Dr. Mikoteit are replicated in a larger blinded study, then it would have enormous implications for the future treatment of individuals with depression,” according to Dr. Harmer, who was not involved in the study and has no conflicts of interest related to it.
Dr. Mikoteit reported having no financial conflicts regarding the study, funded by the Psychiatric University Hospital of Basel.
SOURCE: Mikoteit T et al. ECNP 2020, Abstract P.733.
A change in rapid eye movement sleeping pattern as measured by quantitative EEG in patients with major depressive disorder after just a single week on a first-line antidepressant predicts eventual clinical response or nonresponse to the medication weeks later, Thorsten Mikoteit, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.
This finding from a small, randomized, controlled trial opens the door to a novel biomarker-based treatment strategy: namely, an immediate switch to a different antidepressant in predicted nonresponders to the first agent. The goal is to improve the final treatment response rate while collapsing the time required to get there, explained Dr. Mikoteit, a psychiatrist affiliated with the University of Basel (Switzerland).
“In real terms, it means that patients, often in the depths of despair, might not need to wait weeks to see if their therapy is working before modifying their treatment,” he observed.
There is a huge unmet need for a biomarker predictive of response to antidepressant medication in patients with major depression, the psychiatrist added. At present, the treatment response rate is unsatisfactory. Moreover, clinical improvement takes a long time to achieve, often requiring several rounds of therapeutic trials during which patients are exposed to weeks of unpleasant side effects of drugs that are ultimately switched out for lack of efficacy or poor tolerance.
The quantitative EEG biomarker under investigation is prefrontal theta cordance (PTC) during REM sleep. It is computed from the absolute and relative theta power in tonic REM sleep. PTC has been shown to correlate with frontocingulate brain activity and cerebral blood perfusion. In an earlier pilot study, Dr. Mikoteit and coinvestigators demonstrated in 33 patients who were experiencing a depressive episode that an increase in PTC after their first week on an antidepressant was associated a significantly increased treatment response rate at the end of the fourth week on the drug, while nonresponders failed to show such increase (J Psychiatr Res. 2017 Sep;92:64-73).
At ECNP 2020, Dr. Mikoteit presented preliminary results from an ongoing randomized, controlled trial including 37 patients hospitalized for major depressive disorder. All underwent baseline evaluation using the Hamilton Depression Rating Scale (HAMD) and were placed on the first-line antidepressant of their psychiatrist’s choice. After 1 week of therapy, participants underwent polysomnography with PTC measurement during tonic REM sleep.
Twenty-two patients were randomized to the intervention arm, in which investigators informed treating psychiatrists of the PTC results. The clinicians were instructed to change to another antidepressant if the biomarker predicted nonresponse or stay the course if the PTC results were favorable. Polysomnography was repeated 1 week later in the intervention arm, and the second-line antidepressant was either continued or switched out depending on the PTC findings. In the control arm, psychiatrists weren’t informed of the PTC results and patients continued on their initial antidepressant. The intervention and control groups were comparable in terms of age, sex, and severity of depression, with an average baseline HAMD score of 22.
A treatment response was defined as at least a 50% reduction in HAMD score from baseline to week 5. About 86% of patients who switched antidepressants based upon their 1-week quantitative EEG findings were categorized as treatment responders at week 5, compared with 20% of controls.
The overall 5-week response rate in the intervention group was 73%, compared with 60% in the control arm. This favorable trend didn’t achieve statistical significance, presumably because of the study’s sample size; however, the study is continuing to enroll participants in order to achieve a definitive result.
Dr. Mikoteit noted that the cost and inconvenience of spending a night in a sleep laboratory would be worthwhile if it resulted in the ability to give effective treatment much sooner. This would be particularly advantageous in patients at increased risk for suicide.
he said.
Study could have “enormous implications”
Of note, in the landmark National Institute of Mental Health–sponsored Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study, slightly less than half of patients with major depressive disorder achieved a treatment response to their first-line antidepressant, and it took an average of 6 weeks of therapy to do. About one in four nonresponders who chose to switch to a different antidepressant got better.
“The STAR*D trial is still the gold standard for understanding antidepressant response, and so being able to see if an antidepressant works within 1 week would be a real breakthrough,” Catherine Harmer, DPhil, said in an interview.
“Most of the time, patients need to wait for around 4 weeks before they can tell if they are responding to a particular antidepressant or not. This is a hugely disabling and lengthy process, and often a different treatment then needs to be started,” added Dr. Harmer, professor of cognitive neuroscience and director of the Psychopharmacology and Emotional Research Lab at the University of Oxford (England).
“If the study results presented by Dr. Mikoteit are replicated in a larger blinded study, then it would have enormous implications for the future treatment of individuals with depression,” according to Dr. Harmer, who was not involved in the study and has no conflicts of interest related to it.
Dr. Mikoteit reported having no financial conflicts regarding the study, funded by the Psychiatric University Hospital of Basel.
SOURCE: Mikoteit T et al. ECNP 2020, Abstract P.733.
FROM ECNP 2020