User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Paxlovid tied to benefits in high-risk patients with COVID
In a cohort study from British Columbia that included nearly 7,000 patients with COVID-19, nirmatrelvir-ritonavir was associated with a 2.5% reduction in risk for death or emergency hospitalization in clinically extremely vulnerable (CEV) patients who were severely immunocompromised. No significant benefit was observed in patients who were not immunocompromised.
“This finding could help substantially limit unnecessary use of nirmatrelvir and ritonavir in older, otherwise healthy individuals,” lead author Colin R. Dormuth, ScD, associate professor of anesthesiology, pharmacology, and therapeutics at the University of British Columbia, Vancouver, told this news organization. “Another finding that was surprising and might help place the role of nirmatrelvir and ritonavir in context is that even in severely immunocompromised individuals who did not take [the drug], the risk of death or hospitalization with COVID-19 was less than 4% in our study population.”
The study was published online in JAMA Network Open.
Who benefits?
The investigators analyzed medical records for 6,866 patients in British Columbia (median age, 70 years; 57% women) who presented between Feb. 1, 2022, and Feb. 3, 2023. Eligible patients belonged to one of four higher-risk groups who received priority for COVID-19 vaccination.
Two groups included CEV patients who were severely (CEV1) or moderately (CEV2) immunocompromised. The CEV3 group was not immunocompromised but had medical conditions associated with a high risk for complications from COVID-19. A fourth expanded eligibility (EXEL) group included higher-risk patients who were not in one of the other groups, such as unvaccinated patients older than age 70 years.
The investigators matched treated patients to untreated patients in the same vulnerability group according to age, sex, and month of infection. The primary outcome was death from any cause or emergency hospitalization with COVID-19 within 28 days.
Treatment with nirmatrelvir-ritonavir was associated with statistically significant relative reductions in the primary outcome, compared with no treatment, for patients in the CEV1 (risk difference, −2.5%) and CEV2 (RD, −1.7%) groups. In the CEV3 group, the RD of −1.3% was not statistically significant. In the EXEL group, treatment was associated with a higher risk for the primary outcome (RD, 1.0%), but the result was not statistically significant.
The results were “robust across sex and older vs. younger age,” the authors note. “No reduction in the primary outcome was observed in lower-risk individuals, including those aged 70 years or older without serious comorbidities.”
The combination of nirmatrelvir-ritonavir was approved for use in Canada based on interim efficacy and safety data from the Evaluation of Inhibition for COVID-19 in High-Risk Patients (EPIC-HR) trial, said Dr. Dormuth.
British Columbia’s eligibility criteria for nirmatrelvir-ritonavir coverage differ substantially from the criteria for participants in the EPIC-HR trial, he noted. Those patients were unvaccinated, had no natural immunity from a previous COVID-19 infection, and were infected with COVID-19 variants that were different from those now circulating. The current study was prompted by the need to look at a broader population of individuals in British Columbia with varying risks of complications from COVID-19 infection.
Before the study, a common view was that patients aged 70 and older would benefit from the drug, said Dr. Dormuth. “Our study, which accounted for medical conditions related to an individual’s vulnerability to complications, showed that older age on its own was not a reason to use nirmatrelvir and ritonavir once relevant medical conditions were taken into consideration.”
The researchers are working on a study to identify with greater specificity which comorbid conditions are most associated with nirmatrelvir-ritonavir effectiveness, he added. “It could be that a relatively small number of conditions can be used to identify most individuals who would benefit from the drug.”
‘Signal toward benefit’
Commenting on the findings for this news organization, Abhijit Duggal, MD, vice chair of critical care at the Cleveland Clinic, who was not involved in this study, said, “I’m always very wary when we look at observational data and we start saying the effectiveness is not really as high as was seen in other studies. We are seeing an effect with all these studies that seems to be in the right direction.
“Having said that,” he added, “is the effect going to be potentially more in patients at higher risk? Absolutely. I think these postmarket studies are really showing that after vaccination, if someone does get infected, this is a secondary option available to us that can prevent progression of the disease, which would likely be more severe in immunocompromised patients.”
Dr. Duggal was a coinvestigator on a recent study of more than 68,000 patients that showed that nirmatrelvir-ritonavir or molnupiravir was associated with reductions in mortality and hospitalization in nonhospitalized patients infected with the Omicron variant, regardless of age, race and ethnicity, virus strain, vaccination status, previous infection status, or coexisting conditions.
“In all groups, there was a signal toward benefit,” said Dr. Duggal. “These studies tell us that these drugs do remain valid options. But their use needs to be discussed on a case-by-case basis with patients we feel are deteriorating or at a higher risk because of underlying disease processes.”
The study was supported by funding from the British Columbia Ministry of Health. Dr. Dormuth and Dr. Duggal report no relevant financial relationships.
A version of this article appeared on Medscape.com.
In a cohort study from British Columbia that included nearly 7,000 patients with COVID-19, nirmatrelvir-ritonavir was associated with a 2.5% reduction in risk for death or emergency hospitalization in clinically extremely vulnerable (CEV) patients who were severely immunocompromised. No significant benefit was observed in patients who were not immunocompromised.
“This finding could help substantially limit unnecessary use of nirmatrelvir and ritonavir in older, otherwise healthy individuals,” lead author Colin R. Dormuth, ScD, associate professor of anesthesiology, pharmacology, and therapeutics at the University of British Columbia, Vancouver, told this news organization. “Another finding that was surprising and might help place the role of nirmatrelvir and ritonavir in context is that even in severely immunocompromised individuals who did not take [the drug], the risk of death or hospitalization with COVID-19 was less than 4% in our study population.”
The study was published online in JAMA Network Open.
Who benefits?
The investigators analyzed medical records for 6,866 patients in British Columbia (median age, 70 years; 57% women) who presented between Feb. 1, 2022, and Feb. 3, 2023. Eligible patients belonged to one of four higher-risk groups who received priority for COVID-19 vaccination.
Two groups included CEV patients who were severely (CEV1) or moderately (CEV2) immunocompromised. The CEV3 group was not immunocompromised but had medical conditions associated with a high risk for complications from COVID-19. A fourth expanded eligibility (EXEL) group included higher-risk patients who were not in one of the other groups, such as unvaccinated patients older than age 70 years.
The investigators matched treated patients to untreated patients in the same vulnerability group according to age, sex, and month of infection. The primary outcome was death from any cause or emergency hospitalization with COVID-19 within 28 days.
Treatment with nirmatrelvir-ritonavir was associated with statistically significant relative reductions in the primary outcome, compared with no treatment, for patients in the CEV1 (risk difference, −2.5%) and CEV2 (RD, −1.7%) groups. In the CEV3 group, the RD of −1.3% was not statistically significant. In the EXEL group, treatment was associated with a higher risk for the primary outcome (RD, 1.0%), but the result was not statistically significant.
The results were “robust across sex and older vs. younger age,” the authors note. “No reduction in the primary outcome was observed in lower-risk individuals, including those aged 70 years or older without serious comorbidities.”
The combination of nirmatrelvir-ritonavir was approved for use in Canada based on interim efficacy and safety data from the Evaluation of Inhibition for COVID-19 in High-Risk Patients (EPIC-HR) trial, said Dr. Dormuth.
British Columbia’s eligibility criteria for nirmatrelvir-ritonavir coverage differ substantially from the criteria for participants in the EPIC-HR trial, he noted. Those patients were unvaccinated, had no natural immunity from a previous COVID-19 infection, and were infected with COVID-19 variants that were different from those now circulating. The current study was prompted by the need to look at a broader population of individuals in British Columbia with varying risks of complications from COVID-19 infection.
Before the study, a common view was that patients aged 70 and older would benefit from the drug, said Dr. Dormuth. “Our study, which accounted for medical conditions related to an individual’s vulnerability to complications, showed that older age on its own was not a reason to use nirmatrelvir and ritonavir once relevant medical conditions were taken into consideration.”
The researchers are working on a study to identify with greater specificity which comorbid conditions are most associated with nirmatrelvir-ritonavir effectiveness, he added. “It could be that a relatively small number of conditions can be used to identify most individuals who would benefit from the drug.”
‘Signal toward benefit’
Commenting on the findings for this news organization, Abhijit Duggal, MD, vice chair of critical care at the Cleveland Clinic, who was not involved in this study, said, “I’m always very wary when we look at observational data and we start saying the effectiveness is not really as high as was seen in other studies. We are seeing an effect with all these studies that seems to be in the right direction.
“Having said that,” he added, “is the effect going to be potentially more in patients at higher risk? Absolutely. I think these postmarket studies are really showing that after vaccination, if someone does get infected, this is a secondary option available to us that can prevent progression of the disease, which would likely be more severe in immunocompromised patients.”
Dr. Duggal was a coinvestigator on a recent study of more than 68,000 patients that showed that nirmatrelvir-ritonavir or molnupiravir was associated with reductions in mortality and hospitalization in nonhospitalized patients infected with the Omicron variant, regardless of age, race and ethnicity, virus strain, vaccination status, previous infection status, or coexisting conditions.
“In all groups, there was a signal toward benefit,” said Dr. Duggal. “These studies tell us that these drugs do remain valid options. But their use needs to be discussed on a case-by-case basis with patients we feel are deteriorating or at a higher risk because of underlying disease processes.”
The study was supported by funding from the British Columbia Ministry of Health. Dr. Dormuth and Dr. Duggal report no relevant financial relationships.
A version of this article appeared on Medscape.com.
In a cohort study from British Columbia that included nearly 7,000 patients with COVID-19, nirmatrelvir-ritonavir was associated with a 2.5% reduction in risk for death or emergency hospitalization in clinically extremely vulnerable (CEV) patients who were severely immunocompromised. No significant benefit was observed in patients who were not immunocompromised.
“This finding could help substantially limit unnecessary use of nirmatrelvir and ritonavir in older, otherwise healthy individuals,” lead author Colin R. Dormuth, ScD, associate professor of anesthesiology, pharmacology, and therapeutics at the University of British Columbia, Vancouver, told this news organization. “Another finding that was surprising and might help place the role of nirmatrelvir and ritonavir in context is that even in severely immunocompromised individuals who did not take [the drug], the risk of death or hospitalization with COVID-19 was less than 4% in our study population.”
The study was published online in JAMA Network Open.
Who benefits?
The investigators analyzed medical records for 6,866 patients in British Columbia (median age, 70 years; 57% women) who presented between Feb. 1, 2022, and Feb. 3, 2023. Eligible patients belonged to one of four higher-risk groups who received priority for COVID-19 vaccination.
Two groups included CEV patients who were severely (CEV1) or moderately (CEV2) immunocompromised. The CEV3 group was not immunocompromised but had medical conditions associated with a high risk for complications from COVID-19. A fourth expanded eligibility (EXEL) group included higher-risk patients who were not in one of the other groups, such as unvaccinated patients older than age 70 years.
The investigators matched treated patients to untreated patients in the same vulnerability group according to age, sex, and month of infection. The primary outcome was death from any cause or emergency hospitalization with COVID-19 within 28 days.
Treatment with nirmatrelvir-ritonavir was associated with statistically significant relative reductions in the primary outcome, compared with no treatment, for patients in the CEV1 (risk difference, −2.5%) and CEV2 (RD, −1.7%) groups. In the CEV3 group, the RD of −1.3% was not statistically significant. In the EXEL group, treatment was associated with a higher risk for the primary outcome (RD, 1.0%), but the result was not statistically significant.
The results were “robust across sex and older vs. younger age,” the authors note. “No reduction in the primary outcome was observed in lower-risk individuals, including those aged 70 years or older without serious comorbidities.”
The combination of nirmatrelvir-ritonavir was approved for use in Canada based on interim efficacy and safety data from the Evaluation of Inhibition for COVID-19 in High-Risk Patients (EPIC-HR) trial, said Dr. Dormuth.
British Columbia’s eligibility criteria for nirmatrelvir-ritonavir coverage differ substantially from the criteria for participants in the EPIC-HR trial, he noted. Those patients were unvaccinated, had no natural immunity from a previous COVID-19 infection, and were infected with COVID-19 variants that were different from those now circulating. The current study was prompted by the need to look at a broader population of individuals in British Columbia with varying risks of complications from COVID-19 infection.
Before the study, a common view was that patients aged 70 and older would benefit from the drug, said Dr. Dormuth. “Our study, which accounted for medical conditions related to an individual’s vulnerability to complications, showed that older age on its own was not a reason to use nirmatrelvir and ritonavir once relevant medical conditions were taken into consideration.”
The researchers are working on a study to identify with greater specificity which comorbid conditions are most associated with nirmatrelvir-ritonavir effectiveness, he added. “It could be that a relatively small number of conditions can be used to identify most individuals who would benefit from the drug.”
‘Signal toward benefit’
Commenting on the findings for this news organization, Abhijit Duggal, MD, vice chair of critical care at the Cleveland Clinic, who was not involved in this study, said, “I’m always very wary when we look at observational data and we start saying the effectiveness is not really as high as was seen in other studies. We are seeing an effect with all these studies that seems to be in the right direction.
“Having said that,” he added, “is the effect going to be potentially more in patients at higher risk? Absolutely. I think these postmarket studies are really showing that after vaccination, if someone does get infected, this is a secondary option available to us that can prevent progression of the disease, which would likely be more severe in immunocompromised patients.”
Dr. Duggal was a coinvestigator on a recent study of more than 68,000 patients that showed that nirmatrelvir-ritonavir or molnupiravir was associated with reductions in mortality and hospitalization in nonhospitalized patients infected with the Omicron variant, regardless of age, race and ethnicity, virus strain, vaccination status, previous infection status, or coexisting conditions.
“In all groups, there was a signal toward benefit,” said Dr. Duggal. “These studies tell us that these drugs do remain valid options. But their use needs to be discussed on a case-by-case basis with patients we feel are deteriorating or at a higher risk because of underlying disease processes.”
The study was supported by funding from the British Columbia Ministry of Health. Dr. Dormuth and Dr. Duggal report no relevant financial relationships.
A version of this article appeared on Medscape.com.
Don’t fear POTS: Tips for diagnosis and treatment
This transcript has been edited for clarity.
Michelle L. O’Donoghue, MD, MPH: I’m here in Amsterdam at the European Society of Cardiology (ESC) Congress 2023. Joining me for a great discussion is my friend Dr. Pam Taub, who is a cardiologist and a professor of medicine at UC San Diego. She has a particular interest in postural orthostatic tachycardia syndrome (POTS), so that’s what we’ll be talking about today.
Thanks for joining me, Pam. When we think about POTS, for those who are not familiar with the term, what does it actually mean and how do you diagnose it?
No tilt table required
Pam R. Taub, MD: That’s typically associated with symptoms such as lightheadedness, dizziness, and cognitive difficulties such as brain fog. The diagnosis can be made by tilt-table testing, but it can also be made in the office with simple orthostats.
In my clinic, I have people lie down for 3-5 minutes. At the end of that period, you get a heart rate and blood pressure. Then you have them stand up for 3-5 minutes and then get heart rate and blood pressure, and you look at the differences. If the heart rate goes up by 30 points – so maybe they’re 80 beats/min when they’re lying down and when they stand up, it goes to 110 beats/min – that’s POTS, so very objective criteria. Typically, these people don’t have what we call orthostatic hypotension, where there is a significant decrease in the blood pressure. It’s more a heart rate issue.
Dr. O’Donoghue: How symptomatically do they usually present?
Dr. Taub: It’s a spectrum. Some people have mild symptoms. After they’re in the upright position for maybe 10 minutes, they get symptoms. There are some people who, when they go from a lying to standing position, they’re extremely symptomatic and can’t really do any activities. There are some people that are even wheelchair-bound because the symptoms are so debilitating. There’s a wide spectrum.
Dr. O’Donoghue: There has been more discussion, I feel like, about the rising prevalence of POTS as a diagnosis, and in particular since the COVID pandemic. What’s our understanding of the relationship between COVID and POTS and what the mechanism might be?
Dr. Taub: We’ve known that POTS can be triggered by a viral infection. Before COVID, we knew that in certain individuals that we think have an underlying genetic predisposition, usually some autoimmune substrate, when they get certain types of infections, whether it’s influenza or mononucleosis, they get POTS.
Typically, when they get an infection, they start getting deconditioned. They don’t feel well, so they’re on bed rest. When they get long periods of bed rest, when they start to become active, they start to have overactivation of their sympathetic nervous system, and they have a large amount of cardiovascular deconditioning. It’s a cycle that is often triggered after an infection.
A huge increase of POTS has been seen after COVID-19 because we had so many people exposed to this virus. With COVID-19, there is a period where people don’t feel great and they are getting bed rest, so they’re getting deconditioned. We’ve seen so many patients referred for post-COVID POTS and also long COVID or the post-acute sequelae of COVID-19, where POTS is a part of that presentation.
Female sex and autoimmune conditions
Dr. O’Donoghue: We know that POTS seems to disproportionately affect women. Is that understood? Is it thought that that’s related to the perhaps the autoimmune component of that illness?
Dr. Taub: Yes. The theory is because women tend to have more autoimmune conditions, that’s why they’re more predisposed. There’s a large amount of genetic susceptibility. For instance, we know that there’s an association between POTS and conditions like Ehlers-Danlos syndrome and between POTS and mast cell activation. Some of those conditions are more prevalent in women as well.
Dr. O’Donoghue: I feel like many physicians don’t know how to manage POTS, and they’re actually a little fearful perhaps to take it on. Fortunately, there have been a growing number of POTS clinics with specialists that focus on that area. For the average practitioner who maybe can’t refer to a POTS clinic, how should they approach that?
Dr. Taub: The first thing is its diagnosis. When someone tells you that they have symptoms of orthostatic intolerance – so, activities that involve standing – you need to first have that on your differential diagnosis. You can make the diagnosis in the office with orthostats. You don’t need a tilt table. It’s sometimes helpful if you’re unsure about the diagnosis, but you can make the diagnosis.
Many times, you’re finding people that have very mild symptoms. You can treat that with some good lifestyle recommendations, such as increased hydration, increasing salt in their diet, and compression. And the exercise component is really important.
Many people with POTS are told to go exercise, go for a run, or go for a walk. That’s incorrect, because these people have symptoms when they’re in the upright position. The type of exercise they need to do initially is exercise in the lying or seated position – so exercises like rowing or a seated bike, and strength training. As they start to feel better, then they can do upright exercise.
You should never tell a person that has POTS to just initially start with upright exercise, because they’re going to feel so much worse and then they’re never going to want to exercise. It’s really important to give them the right exercise recommendations. I find that for many of these mild cases, if they do the right exercise and engage in the right lifestyle strategies, they get better.
Compression wear and drug therapy
Dr. O’Donoghue: When it comes to compression stockings, do you usually start with a particular length?
Dr. Taub: It’s interesting. There are many different compression stockings, medical grade. Through patients with POTS, I’ve gotten feedback on certain types of athletic wear that have built-in compression, and that’s a little bit easier for people to wear every day because they can do their errands and it doesn’t look like they’re wearing medical-grade compression stockings.
Basically, I’ve collected all the different recommendations that patients say help, and I give them a list. The medical-grade compression stockings sometimes are very challenging to put on, and sometimes people just need light compression or even just socks. Any kind of compression is going to help.
Dr. O’Donoghue: That’s a great tip, because I know there are many patients who refuse to wear the compression stockings. If there’s a fashionable alternative, that’s always good to reach for.
Dr. Taub: Another thing that patients have told me is that abdominal compression is also very helpful. There are many commercially available abdominal compression options, like shapewear. Many patients with POTS use that and that helps, too.
Dr. O’Donoghue: Good. For those patients with POTS that is refractory to the measures you’ve already discussed, what are the next steps after that?
Dr. Taub: Pharmacotherapy is very synergistic with lifestyle, and there are many different pharmacotherapy options. One of the first things that you want to think about is lowering that heart rate. The reason people feel horrible is because their heart rate is usually very high when they’re upright. If they’re upright for long periods of time and they’re having very high heart rates, they’re going to get really tired because it’s like they’re exercising for hours when they’re upright.
Heart rate lowering is the cornerstone of therapy. Traditionally, we’ve used beta-blockers for heart rate lowering. The problem is they also lower blood pressure. They can also cause fatigue, so not the ideal agent for patients with POTS.
One of the clinical trials that I led was with a drug called ivabradine, which selectively works on the SA node and decreases heart rate without affecting blood pressure. What’s really elegant about ivabradine is it has a more potent effect when the heart rate is higher. When the patient is standing, it’s going to have a more potent effect on heart rate lowering. It’s really well tolerated in patients with POTS. In our study, we showed an improvement in quality of life metrics. That’s one of the first-line drugs that I use for patients with POTS.
The other thing is some of them will also have a concomitant lowering of blood pressure. You can think about medications that increase blood pressure, like midodrine, fludrocortisone, and droxidopa. Sometimes that combination of a heart rate-lowering medication and a medication that increases blood pressure really works well.
Dr. O’Donoghue: That’s very helpful. I think that those kinds of practical tips are the ones that practitioners really want to reach for, because they need to have that algorithm in their mind to take on this condition. Thanks again for walking us through that.
I think it’s a very interesting space, and there’s more that we’re going to be learning over the next few years as we further flesh out these post-COVID cases and what we learn from that as well.
Dr. Taub: There are many clinical trials now starting in POTS, so it’s exciting.
Dr. O’Donoghue: Absolutely. Thank you again for joining me today. Signing off, this is Dr Michelle O’Donoghue.
Dr. O’Donoghue is a cardiologist at Brigham and Women’s Hospital and senior investigator with the TIMI Study Group. A strong believer in evidence-based medicine, she relishes discussions about the published literature. A native Canadian, Dr. O’Donoghue loves spending time outdoors with her family but admits with shame that she’s never strapped on hockey skates. She disclosed ties with Amgen, AstraZeneca Pharmaceuticals LP, CVS Minute Clinic, Eisai, GlaxoSmithKline, Janssen Pharmaceuticals, Merck, Novartis, and The Medicines Company. Dr. Taub is professor of Medicine, University of California San Diego Health, La Jolla. She disclosed ties with Amgen, Bayer, Boehringer Ingelheim, Medtronic, Merck, Novartis, Novo Nordisk, and Sanofi.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Michelle L. O’Donoghue, MD, MPH: I’m here in Amsterdam at the European Society of Cardiology (ESC) Congress 2023. Joining me for a great discussion is my friend Dr. Pam Taub, who is a cardiologist and a professor of medicine at UC San Diego. She has a particular interest in postural orthostatic tachycardia syndrome (POTS), so that’s what we’ll be talking about today.
Thanks for joining me, Pam. When we think about POTS, for those who are not familiar with the term, what does it actually mean and how do you diagnose it?
No tilt table required
Pam R. Taub, MD: That’s typically associated with symptoms such as lightheadedness, dizziness, and cognitive difficulties such as brain fog. The diagnosis can be made by tilt-table testing, but it can also be made in the office with simple orthostats.
In my clinic, I have people lie down for 3-5 minutes. At the end of that period, you get a heart rate and blood pressure. Then you have them stand up for 3-5 minutes and then get heart rate and blood pressure, and you look at the differences. If the heart rate goes up by 30 points – so maybe they’re 80 beats/min when they’re lying down and when they stand up, it goes to 110 beats/min – that’s POTS, so very objective criteria. Typically, these people don’t have what we call orthostatic hypotension, where there is a significant decrease in the blood pressure. It’s more a heart rate issue.
Dr. O’Donoghue: How symptomatically do they usually present?
Dr. Taub: It’s a spectrum. Some people have mild symptoms. After they’re in the upright position for maybe 10 minutes, they get symptoms. There are some people who, when they go from a lying to standing position, they’re extremely symptomatic and can’t really do any activities. There are some people that are even wheelchair-bound because the symptoms are so debilitating. There’s a wide spectrum.
Dr. O’Donoghue: There has been more discussion, I feel like, about the rising prevalence of POTS as a diagnosis, and in particular since the COVID pandemic. What’s our understanding of the relationship between COVID and POTS and what the mechanism might be?
Dr. Taub: We’ve known that POTS can be triggered by a viral infection. Before COVID, we knew that in certain individuals that we think have an underlying genetic predisposition, usually some autoimmune substrate, when they get certain types of infections, whether it’s influenza or mononucleosis, they get POTS.
Typically, when they get an infection, they start getting deconditioned. They don’t feel well, so they’re on bed rest. When they get long periods of bed rest, when they start to become active, they start to have overactivation of their sympathetic nervous system, and they have a large amount of cardiovascular deconditioning. It’s a cycle that is often triggered after an infection.
A huge increase of POTS has been seen after COVID-19 because we had so many people exposed to this virus. With COVID-19, there is a period where people don’t feel great and they are getting bed rest, so they’re getting deconditioned. We’ve seen so many patients referred for post-COVID POTS and also long COVID or the post-acute sequelae of COVID-19, where POTS is a part of that presentation.
Female sex and autoimmune conditions
Dr. O’Donoghue: We know that POTS seems to disproportionately affect women. Is that understood? Is it thought that that’s related to the perhaps the autoimmune component of that illness?
Dr. Taub: Yes. The theory is because women tend to have more autoimmune conditions, that’s why they’re more predisposed. There’s a large amount of genetic susceptibility. For instance, we know that there’s an association between POTS and conditions like Ehlers-Danlos syndrome and between POTS and mast cell activation. Some of those conditions are more prevalent in women as well.
Dr. O’Donoghue: I feel like many physicians don’t know how to manage POTS, and they’re actually a little fearful perhaps to take it on. Fortunately, there have been a growing number of POTS clinics with specialists that focus on that area. For the average practitioner who maybe can’t refer to a POTS clinic, how should they approach that?
Dr. Taub: The first thing is its diagnosis. When someone tells you that they have symptoms of orthostatic intolerance – so, activities that involve standing – you need to first have that on your differential diagnosis. You can make the diagnosis in the office with orthostats. You don’t need a tilt table. It’s sometimes helpful if you’re unsure about the diagnosis, but you can make the diagnosis.
Many times, you’re finding people that have very mild symptoms. You can treat that with some good lifestyle recommendations, such as increased hydration, increasing salt in their diet, and compression. And the exercise component is really important.
Many people with POTS are told to go exercise, go for a run, or go for a walk. That’s incorrect, because these people have symptoms when they’re in the upright position. The type of exercise they need to do initially is exercise in the lying or seated position – so exercises like rowing or a seated bike, and strength training. As they start to feel better, then they can do upright exercise.
You should never tell a person that has POTS to just initially start with upright exercise, because they’re going to feel so much worse and then they’re never going to want to exercise. It’s really important to give them the right exercise recommendations. I find that for many of these mild cases, if they do the right exercise and engage in the right lifestyle strategies, they get better.
Compression wear and drug therapy
Dr. O’Donoghue: When it comes to compression stockings, do you usually start with a particular length?
Dr. Taub: It’s interesting. There are many different compression stockings, medical grade. Through patients with POTS, I’ve gotten feedback on certain types of athletic wear that have built-in compression, and that’s a little bit easier for people to wear every day because they can do their errands and it doesn’t look like they’re wearing medical-grade compression stockings.
Basically, I’ve collected all the different recommendations that patients say help, and I give them a list. The medical-grade compression stockings sometimes are very challenging to put on, and sometimes people just need light compression or even just socks. Any kind of compression is going to help.
Dr. O’Donoghue: That’s a great tip, because I know there are many patients who refuse to wear the compression stockings. If there’s a fashionable alternative, that’s always good to reach for.
Dr. Taub: Another thing that patients have told me is that abdominal compression is also very helpful. There are many commercially available abdominal compression options, like shapewear. Many patients with POTS use that and that helps, too.
Dr. O’Donoghue: Good. For those patients with POTS that is refractory to the measures you’ve already discussed, what are the next steps after that?
Dr. Taub: Pharmacotherapy is very synergistic with lifestyle, and there are many different pharmacotherapy options. One of the first things that you want to think about is lowering that heart rate. The reason people feel horrible is because their heart rate is usually very high when they’re upright. If they’re upright for long periods of time and they’re having very high heart rates, they’re going to get really tired because it’s like they’re exercising for hours when they’re upright.
Heart rate lowering is the cornerstone of therapy. Traditionally, we’ve used beta-blockers for heart rate lowering. The problem is they also lower blood pressure. They can also cause fatigue, so not the ideal agent for patients with POTS.
One of the clinical trials that I led was with a drug called ivabradine, which selectively works on the SA node and decreases heart rate without affecting blood pressure. What’s really elegant about ivabradine is it has a more potent effect when the heart rate is higher. When the patient is standing, it’s going to have a more potent effect on heart rate lowering. It’s really well tolerated in patients with POTS. In our study, we showed an improvement in quality of life metrics. That’s one of the first-line drugs that I use for patients with POTS.
The other thing is some of them will also have a concomitant lowering of blood pressure. You can think about medications that increase blood pressure, like midodrine, fludrocortisone, and droxidopa. Sometimes that combination of a heart rate-lowering medication and a medication that increases blood pressure really works well.
Dr. O’Donoghue: That’s very helpful. I think that those kinds of practical tips are the ones that practitioners really want to reach for, because they need to have that algorithm in their mind to take on this condition. Thanks again for walking us through that.
I think it’s a very interesting space, and there’s more that we’re going to be learning over the next few years as we further flesh out these post-COVID cases and what we learn from that as well.
Dr. Taub: There are many clinical trials now starting in POTS, so it’s exciting.
Dr. O’Donoghue: Absolutely. Thank you again for joining me today. Signing off, this is Dr Michelle O’Donoghue.
Dr. O’Donoghue is a cardiologist at Brigham and Women’s Hospital and senior investigator with the TIMI Study Group. A strong believer in evidence-based medicine, she relishes discussions about the published literature. A native Canadian, Dr. O’Donoghue loves spending time outdoors with her family but admits with shame that she’s never strapped on hockey skates. She disclosed ties with Amgen, AstraZeneca Pharmaceuticals LP, CVS Minute Clinic, Eisai, GlaxoSmithKline, Janssen Pharmaceuticals, Merck, Novartis, and The Medicines Company. Dr. Taub is professor of Medicine, University of California San Diego Health, La Jolla. She disclosed ties with Amgen, Bayer, Boehringer Ingelheim, Medtronic, Merck, Novartis, Novo Nordisk, and Sanofi.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Michelle L. O’Donoghue, MD, MPH: I’m here in Amsterdam at the European Society of Cardiology (ESC) Congress 2023. Joining me for a great discussion is my friend Dr. Pam Taub, who is a cardiologist and a professor of medicine at UC San Diego. She has a particular interest in postural orthostatic tachycardia syndrome (POTS), so that’s what we’ll be talking about today.
Thanks for joining me, Pam. When we think about POTS, for those who are not familiar with the term, what does it actually mean and how do you diagnose it?
No tilt table required
Pam R. Taub, MD: That’s typically associated with symptoms such as lightheadedness, dizziness, and cognitive difficulties such as brain fog. The diagnosis can be made by tilt-table testing, but it can also be made in the office with simple orthostats.
In my clinic, I have people lie down for 3-5 minutes. At the end of that period, you get a heart rate and blood pressure. Then you have them stand up for 3-5 minutes and then get heart rate and blood pressure, and you look at the differences. If the heart rate goes up by 30 points – so maybe they’re 80 beats/min when they’re lying down and when they stand up, it goes to 110 beats/min – that’s POTS, so very objective criteria. Typically, these people don’t have what we call orthostatic hypotension, where there is a significant decrease in the blood pressure. It’s more a heart rate issue.
Dr. O’Donoghue: How symptomatically do they usually present?
Dr. Taub: It’s a spectrum. Some people have mild symptoms. After they’re in the upright position for maybe 10 minutes, they get symptoms. There are some people who, when they go from a lying to standing position, they’re extremely symptomatic and can’t really do any activities. There are some people that are even wheelchair-bound because the symptoms are so debilitating. There’s a wide spectrum.
Dr. O’Donoghue: There has been more discussion, I feel like, about the rising prevalence of POTS as a diagnosis, and in particular since the COVID pandemic. What’s our understanding of the relationship between COVID and POTS and what the mechanism might be?
Dr. Taub: We’ve known that POTS can be triggered by a viral infection. Before COVID, we knew that in certain individuals that we think have an underlying genetic predisposition, usually some autoimmune substrate, when they get certain types of infections, whether it’s influenza or mononucleosis, they get POTS.
Typically, when they get an infection, they start getting deconditioned. They don’t feel well, so they’re on bed rest. When they get long periods of bed rest, when they start to become active, they start to have overactivation of their sympathetic nervous system, and they have a large amount of cardiovascular deconditioning. It’s a cycle that is often triggered after an infection.
A huge increase of POTS has been seen after COVID-19 because we had so many people exposed to this virus. With COVID-19, there is a period where people don’t feel great and they are getting bed rest, so they’re getting deconditioned. We’ve seen so many patients referred for post-COVID POTS and also long COVID or the post-acute sequelae of COVID-19, where POTS is a part of that presentation.
Female sex and autoimmune conditions
Dr. O’Donoghue: We know that POTS seems to disproportionately affect women. Is that understood? Is it thought that that’s related to the perhaps the autoimmune component of that illness?
Dr. Taub: Yes. The theory is because women tend to have more autoimmune conditions, that’s why they’re more predisposed. There’s a large amount of genetic susceptibility. For instance, we know that there’s an association between POTS and conditions like Ehlers-Danlos syndrome and between POTS and mast cell activation. Some of those conditions are more prevalent in women as well.
Dr. O’Donoghue: I feel like many physicians don’t know how to manage POTS, and they’re actually a little fearful perhaps to take it on. Fortunately, there have been a growing number of POTS clinics with specialists that focus on that area. For the average practitioner who maybe can’t refer to a POTS clinic, how should they approach that?
Dr. Taub: The first thing is its diagnosis. When someone tells you that they have symptoms of orthostatic intolerance – so, activities that involve standing – you need to first have that on your differential diagnosis. You can make the diagnosis in the office with orthostats. You don’t need a tilt table. It’s sometimes helpful if you’re unsure about the diagnosis, but you can make the diagnosis.
Many times, you’re finding people that have very mild symptoms. You can treat that with some good lifestyle recommendations, such as increased hydration, increasing salt in their diet, and compression. And the exercise component is really important.
Many people with POTS are told to go exercise, go for a run, or go for a walk. That’s incorrect, because these people have symptoms when they’re in the upright position. The type of exercise they need to do initially is exercise in the lying or seated position – so exercises like rowing or a seated bike, and strength training. As they start to feel better, then they can do upright exercise.
You should never tell a person that has POTS to just initially start with upright exercise, because they’re going to feel so much worse and then they’re never going to want to exercise. It’s really important to give them the right exercise recommendations. I find that for many of these mild cases, if they do the right exercise and engage in the right lifestyle strategies, they get better.
Compression wear and drug therapy
Dr. O’Donoghue: When it comes to compression stockings, do you usually start with a particular length?
Dr. Taub: It’s interesting. There are many different compression stockings, medical grade. Through patients with POTS, I’ve gotten feedback on certain types of athletic wear that have built-in compression, and that’s a little bit easier for people to wear every day because they can do their errands and it doesn’t look like they’re wearing medical-grade compression stockings.
Basically, I’ve collected all the different recommendations that patients say help, and I give them a list. The medical-grade compression stockings sometimes are very challenging to put on, and sometimes people just need light compression or even just socks. Any kind of compression is going to help.
Dr. O’Donoghue: That’s a great tip, because I know there are many patients who refuse to wear the compression stockings. If there’s a fashionable alternative, that’s always good to reach for.
Dr. Taub: Another thing that patients have told me is that abdominal compression is also very helpful. There are many commercially available abdominal compression options, like shapewear. Many patients with POTS use that and that helps, too.
Dr. O’Donoghue: Good. For those patients with POTS that is refractory to the measures you’ve already discussed, what are the next steps after that?
Dr. Taub: Pharmacotherapy is very synergistic with lifestyle, and there are many different pharmacotherapy options. One of the first things that you want to think about is lowering that heart rate. The reason people feel horrible is because their heart rate is usually very high when they’re upright. If they’re upright for long periods of time and they’re having very high heart rates, they’re going to get really tired because it’s like they’re exercising for hours when they’re upright.
Heart rate lowering is the cornerstone of therapy. Traditionally, we’ve used beta-blockers for heart rate lowering. The problem is they also lower blood pressure. They can also cause fatigue, so not the ideal agent for patients with POTS.
One of the clinical trials that I led was with a drug called ivabradine, which selectively works on the SA node and decreases heart rate without affecting blood pressure. What’s really elegant about ivabradine is it has a more potent effect when the heart rate is higher. When the patient is standing, it’s going to have a more potent effect on heart rate lowering. It’s really well tolerated in patients with POTS. In our study, we showed an improvement in quality of life metrics. That’s one of the first-line drugs that I use for patients with POTS.
The other thing is some of them will also have a concomitant lowering of blood pressure. You can think about medications that increase blood pressure, like midodrine, fludrocortisone, and droxidopa. Sometimes that combination of a heart rate-lowering medication and a medication that increases blood pressure really works well.
Dr. O’Donoghue: That’s very helpful. I think that those kinds of practical tips are the ones that practitioners really want to reach for, because they need to have that algorithm in their mind to take on this condition. Thanks again for walking us through that.
I think it’s a very interesting space, and there’s more that we’re going to be learning over the next few years as we further flesh out these post-COVID cases and what we learn from that as well.
Dr. Taub: There are many clinical trials now starting in POTS, so it’s exciting.
Dr. O’Donoghue: Absolutely. Thank you again for joining me today. Signing off, this is Dr Michelle O’Donoghue.
Dr. O’Donoghue is a cardiologist at Brigham and Women’s Hospital and senior investigator with the TIMI Study Group. A strong believer in evidence-based medicine, she relishes discussions about the published literature. A native Canadian, Dr. O’Donoghue loves spending time outdoors with her family but admits with shame that she’s never strapped on hockey skates. She disclosed ties with Amgen, AstraZeneca Pharmaceuticals LP, CVS Minute Clinic, Eisai, GlaxoSmithKline, Janssen Pharmaceuticals, Merck, Novartis, and The Medicines Company. Dr. Taub is professor of Medicine, University of California San Diego Health, La Jolla. She disclosed ties with Amgen, Bayer, Boehringer Ingelheim, Medtronic, Merck, Novartis, Novo Nordisk, and Sanofi.
A version of this article appeared on Medscape.com.
Supplemental oxygen fails to improve echocardiographic measures in PE patients
compared with ambient oxygen in a pilot study of 70 individuals.
Anticoagulation monotherapy is the standard of care for patients with intermediate-risk pulmonary embolism (PE), but persistent short-term complication rates may approach 10%, wrote Deisy Barrios, MD, of Hospital Ramón y Cajal (IRYCIS), Madrid, and colleagues. Additional strategies are needed, and the use of supplemental oxygen in non-hypoxemic patients with intermediate-risk PE has not been explored, they said.
In a study published in the journal Chest, the researchers recruited 36 women and 34 men who were non-hypoxemic with stable PE and intermediate risk, defined as echocardiographic RV enlargement. The study recruitment ended prematurely because of the COVID-19 pandemic. The mean age of the participants was 67.3 years. Patients were randomized within 24 hours of hospital admission to anticoagulation plus supplemental oxygen or anticoagulation alone. The groups were similar in echocardiographic mean RV end-diameter and RV/LV ratios at baseline.
The intervention patients received supplemental oxygen at a 35% concentration (7 L/min) continuously for 48 hours via a face mask, and through a nasal cannula during meal times.
The primary outcome was normalization of right ventricle size (defined as an RV/LV diameter ratio less than 1.0 from the subcostal or apical view) at 48 hours after randomization. Secondary outcomes included change in the right ventricle/left ventricle diameter as measured at 48 hours and 7 days after randomization compared to baseline.
The proportion of patients with an RV/LV ratio of 1.0 or less at 48 hours was not significantly different between the intervention and control groups (42.4% vs. 21.6%, P = .08). Similarly, the proportion of patients with an RV/LV ratio of 1.0 or less at 7 days was not significantly different between the groups (76% vs. 70%).
The between-group reduction in RV/LV ratio was significantly greater in the supplemental oxygen group vs. the control group from baseline to 48 hours (0.28 vs. 0.12 P = .02).
However, the within-group mean RV/LV ratio was significantly reduced in both the supplemental oxygen group and the control group compared to baseline at 48 hours and at 7 days after randomization.
None of the patients experienced hemodynamic collapse or recurrent venous thromboembolism during the follow-up period.
The findings were limited by several factors including the small sample size and open-label design, and lack of power to detect clinical outcomes, the researchers noted.
However, the results suggest that although supplemental oxygen had no significant impact of RV/LV normalization, “supplemental oxygen might increase the likelihood of reducing echocardiographic RV dilatation,” and the findings warrant a definitive clinical outcomes trial of supplemental oxygen vs. ambient air to improve outcomes in non-hypoxemic patients with intermediate-risk PE, they concluded.
The study was supported by the Instituto de Salud Carlos III. Dr. Barrios had no financial conflicts to disclose.
compared with ambient oxygen in a pilot study of 70 individuals.
Anticoagulation monotherapy is the standard of care for patients with intermediate-risk pulmonary embolism (PE), but persistent short-term complication rates may approach 10%, wrote Deisy Barrios, MD, of Hospital Ramón y Cajal (IRYCIS), Madrid, and colleagues. Additional strategies are needed, and the use of supplemental oxygen in non-hypoxemic patients with intermediate-risk PE has not been explored, they said.
In a study published in the journal Chest, the researchers recruited 36 women and 34 men who were non-hypoxemic with stable PE and intermediate risk, defined as echocardiographic RV enlargement. The study recruitment ended prematurely because of the COVID-19 pandemic. The mean age of the participants was 67.3 years. Patients were randomized within 24 hours of hospital admission to anticoagulation plus supplemental oxygen or anticoagulation alone. The groups were similar in echocardiographic mean RV end-diameter and RV/LV ratios at baseline.
The intervention patients received supplemental oxygen at a 35% concentration (7 L/min) continuously for 48 hours via a face mask, and through a nasal cannula during meal times.
The primary outcome was normalization of right ventricle size (defined as an RV/LV diameter ratio less than 1.0 from the subcostal or apical view) at 48 hours after randomization. Secondary outcomes included change in the right ventricle/left ventricle diameter as measured at 48 hours and 7 days after randomization compared to baseline.
The proportion of patients with an RV/LV ratio of 1.0 or less at 48 hours was not significantly different between the intervention and control groups (42.4% vs. 21.6%, P = .08). Similarly, the proportion of patients with an RV/LV ratio of 1.0 or less at 7 days was not significantly different between the groups (76% vs. 70%).
The between-group reduction in RV/LV ratio was significantly greater in the supplemental oxygen group vs. the control group from baseline to 48 hours (0.28 vs. 0.12 P = .02).
However, the within-group mean RV/LV ratio was significantly reduced in both the supplemental oxygen group and the control group compared to baseline at 48 hours and at 7 days after randomization.
None of the patients experienced hemodynamic collapse or recurrent venous thromboembolism during the follow-up period.
The findings were limited by several factors including the small sample size and open-label design, and lack of power to detect clinical outcomes, the researchers noted.
However, the results suggest that although supplemental oxygen had no significant impact of RV/LV normalization, “supplemental oxygen might increase the likelihood of reducing echocardiographic RV dilatation,” and the findings warrant a definitive clinical outcomes trial of supplemental oxygen vs. ambient air to improve outcomes in non-hypoxemic patients with intermediate-risk PE, they concluded.
The study was supported by the Instituto de Salud Carlos III. Dr. Barrios had no financial conflicts to disclose.
compared with ambient oxygen in a pilot study of 70 individuals.
Anticoagulation monotherapy is the standard of care for patients with intermediate-risk pulmonary embolism (PE), but persistent short-term complication rates may approach 10%, wrote Deisy Barrios, MD, of Hospital Ramón y Cajal (IRYCIS), Madrid, and colleagues. Additional strategies are needed, and the use of supplemental oxygen in non-hypoxemic patients with intermediate-risk PE has not been explored, they said.
In a study published in the journal Chest, the researchers recruited 36 women and 34 men who were non-hypoxemic with stable PE and intermediate risk, defined as echocardiographic RV enlargement. The study recruitment ended prematurely because of the COVID-19 pandemic. The mean age of the participants was 67.3 years. Patients were randomized within 24 hours of hospital admission to anticoagulation plus supplemental oxygen or anticoagulation alone. The groups were similar in echocardiographic mean RV end-diameter and RV/LV ratios at baseline.
The intervention patients received supplemental oxygen at a 35% concentration (7 L/min) continuously for 48 hours via a face mask, and through a nasal cannula during meal times.
The primary outcome was normalization of right ventricle size (defined as an RV/LV diameter ratio less than 1.0 from the subcostal or apical view) at 48 hours after randomization. Secondary outcomes included change in the right ventricle/left ventricle diameter as measured at 48 hours and 7 days after randomization compared to baseline.
The proportion of patients with an RV/LV ratio of 1.0 or less at 48 hours was not significantly different between the intervention and control groups (42.4% vs. 21.6%, P = .08). Similarly, the proportion of patients with an RV/LV ratio of 1.0 or less at 7 days was not significantly different between the groups (76% vs. 70%).
The between-group reduction in RV/LV ratio was significantly greater in the supplemental oxygen group vs. the control group from baseline to 48 hours (0.28 vs. 0.12 P = .02).
However, the within-group mean RV/LV ratio was significantly reduced in both the supplemental oxygen group and the control group compared to baseline at 48 hours and at 7 days after randomization.
None of the patients experienced hemodynamic collapse or recurrent venous thromboembolism during the follow-up period.
The findings were limited by several factors including the small sample size and open-label design, and lack of power to detect clinical outcomes, the researchers noted.
However, the results suggest that although supplemental oxygen had no significant impact of RV/LV normalization, “supplemental oxygen might increase the likelihood of reducing echocardiographic RV dilatation,” and the findings warrant a definitive clinical outcomes trial of supplemental oxygen vs. ambient air to improve outcomes in non-hypoxemic patients with intermediate-risk PE, they concluded.
The study was supported by the Instituto de Salud Carlos III. Dr. Barrios had no financial conflicts to disclose.
FROM THE JOURNAL CHEST
This is how you get patients back for follow-up cancer testing
according to authors of a new study published in the Journal of the American Medical Association.
Results from the clustered, randomized clinical trial indicate that systems-based interventions, such as automating reminders in electronic health records (EHRs), outreach in the form of phone calls or letters, and assistance with barriers to health care, such as housing insecurity, can increase the number of patients who complete appropriate diagnostic follow-up after an abnormal result.
Patients who received an EHR reminder, outreach call or letter, and additional calls to screen for and assist with nine barriers to health care – housing insecurity, food insecurity, paying for basic utilities, family caregiving, legal issues, transportation, financial compensation for treatment, education, and employment – completed follow-up within 120 days of study enrollment at a rate of 31.4%. The follow-up rate was 31% for those who received only an EHR reminder and outreach, 22.7% for those who received only an EHR reminder, and 22.9% for those who received usual care.
“The benefits of cancer screening won’t be fully realized without systems to ensure timely follow-up of abnormal results,” said Anna Tosteson, ScD, director of the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H., a coauthor of the study.
Current payment incentives and quality-of-care indicators focus on getting people in for screening but should also address completion of screening – meaning timely and appropriate follow-up of results that could be indicative of cancer, Dr. Tosteson said.
“There’s a disconnect if you have screening rates that are high but once people have an abnormal result, which is potentially one step closer to a cancer diagnosis, there are no systems in place to help clinicians track them,” said study coauthor Jennifer Haas, MD, director of the Center for Primary Care Research at Massachusetts General Hospital in Boston.
In a 2016 study, researchers found that follow-up rates after abnormal cancer screenings varied widely. While 95.6% of patients with abnormal breast cancer screenings underwent timely follow-up testing, only 68.1% of patients with colorectal abnormalities and 44.8% of patients with cervical abnormalities did so.
Researchers for the new study used guideline recommendations and specialist input to create automated EHR algorithms that determined a follow-up period and diagnostic test.
They put the algorithm into practice with 11,980 patients who were part of 44 primary care practices within three health networks between August 2020 and December 2021. All patients had received abnormal test results for colorectal, breast, cervical, or lung cancer in varying risk categories.
All patients received usual care from their providers, which consisted of a “hodgepodge of whatever their clinic usually does,” Dr. Haas said. Without standards and systems in place for follow-up, the burden of testing and tracking patients with abnormal results typically falls on the primary care provider.
The researchers intervened only when patients were overdue for completion of follow-up. They then staggered the interventions sequentially.
All study participants received an automated, algorithm-triggered EHR reminder for follow-up in their patient portal along with routine health maintenance reminders. To view the reminder, patients had to log into their portal. Participants in the outreach and outreach and navigation groups also received a phone call, an EHR message, or a physical letter 2 weeks after receiving an EHR notification if they hadn’t completed follow-up. Research assistants performed the outreach after having been prompted by the algorithm.
After another 4 weeks, those in the EHR, outreach, and navigation group received a call from a patient navigator who helped them address nine barriers to health care, chiefly by providing them with referrals to free resources.
Among patients who received navigation, outcomes were not significantly better than among those who received EHR and outreach, indicating social determinants of health did not significantly affect the population studied or that the modest approach to navigation and the resources provided were insufficient, Dr. Haas said.
The complexity of an automated platform that encompasses many types of cancers, test results, and other data elements could prove difficult to apply in settings with less infrastructure, said Steven Atlas, MD, MPH, director of the Practice-Based Research and Quality Improvement Network in the division of general internal medicine at Mass General.
“I think there’s a role for the federal government to take on these initiatives,” Dr. Atlas said. Government intervention could help create “national IT systems to create standards for creating code for what an abnormal result is and how it should be followed,” he said.
While interventions improved patient follow-up, the overall rates were still low.
“What concerns me is that despite the various interventions implemented to encourage and support patients to return for follow-up testing, over 60% of patients still did not return for the recommended testing,” said Joann G. Elmore, MD, MPH, professor of medicine at the University of California, Los Angeles. Dr. Elmore was not involved with the study.
The research took place during the COVID-19 pandemic, which may have reduced follow-up, the study authors wrote. Still, given that previous research has shown that follow-up tends to be low, the rates highlight “the need to understand factors associated with not completing follow-up that go beyond reminder effort,” they wrote. These include a need for patient education about the meaning of test results and what follow-up procedures involve.
The study was supported by the National Cancer Institute and the American Cancer Society. The authors have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
according to authors of a new study published in the Journal of the American Medical Association.
Results from the clustered, randomized clinical trial indicate that systems-based interventions, such as automating reminders in electronic health records (EHRs), outreach in the form of phone calls or letters, and assistance with barriers to health care, such as housing insecurity, can increase the number of patients who complete appropriate diagnostic follow-up after an abnormal result.
Patients who received an EHR reminder, outreach call or letter, and additional calls to screen for and assist with nine barriers to health care – housing insecurity, food insecurity, paying for basic utilities, family caregiving, legal issues, transportation, financial compensation for treatment, education, and employment – completed follow-up within 120 days of study enrollment at a rate of 31.4%. The follow-up rate was 31% for those who received only an EHR reminder and outreach, 22.7% for those who received only an EHR reminder, and 22.9% for those who received usual care.
“The benefits of cancer screening won’t be fully realized without systems to ensure timely follow-up of abnormal results,” said Anna Tosteson, ScD, director of the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H., a coauthor of the study.
Current payment incentives and quality-of-care indicators focus on getting people in for screening but should also address completion of screening – meaning timely and appropriate follow-up of results that could be indicative of cancer, Dr. Tosteson said.
“There’s a disconnect if you have screening rates that are high but once people have an abnormal result, which is potentially one step closer to a cancer diagnosis, there are no systems in place to help clinicians track them,” said study coauthor Jennifer Haas, MD, director of the Center for Primary Care Research at Massachusetts General Hospital in Boston.
In a 2016 study, researchers found that follow-up rates after abnormal cancer screenings varied widely. While 95.6% of patients with abnormal breast cancer screenings underwent timely follow-up testing, only 68.1% of patients with colorectal abnormalities and 44.8% of patients with cervical abnormalities did so.
Researchers for the new study used guideline recommendations and specialist input to create automated EHR algorithms that determined a follow-up period and diagnostic test.
They put the algorithm into practice with 11,980 patients who were part of 44 primary care practices within three health networks between August 2020 and December 2021. All patients had received abnormal test results for colorectal, breast, cervical, or lung cancer in varying risk categories.
All patients received usual care from their providers, which consisted of a “hodgepodge of whatever their clinic usually does,” Dr. Haas said. Without standards and systems in place for follow-up, the burden of testing and tracking patients with abnormal results typically falls on the primary care provider.
The researchers intervened only when patients were overdue for completion of follow-up. They then staggered the interventions sequentially.
All study participants received an automated, algorithm-triggered EHR reminder for follow-up in their patient portal along with routine health maintenance reminders. To view the reminder, patients had to log into their portal. Participants in the outreach and outreach and navigation groups also received a phone call, an EHR message, or a physical letter 2 weeks after receiving an EHR notification if they hadn’t completed follow-up. Research assistants performed the outreach after having been prompted by the algorithm.
After another 4 weeks, those in the EHR, outreach, and navigation group received a call from a patient navigator who helped them address nine barriers to health care, chiefly by providing them with referrals to free resources.
Among patients who received navigation, outcomes were not significantly better than among those who received EHR and outreach, indicating social determinants of health did not significantly affect the population studied or that the modest approach to navigation and the resources provided were insufficient, Dr. Haas said.
The complexity of an automated platform that encompasses many types of cancers, test results, and other data elements could prove difficult to apply in settings with less infrastructure, said Steven Atlas, MD, MPH, director of the Practice-Based Research and Quality Improvement Network in the division of general internal medicine at Mass General.
“I think there’s a role for the federal government to take on these initiatives,” Dr. Atlas said. Government intervention could help create “national IT systems to create standards for creating code for what an abnormal result is and how it should be followed,” he said.
While interventions improved patient follow-up, the overall rates were still low.
“What concerns me is that despite the various interventions implemented to encourage and support patients to return for follow-up testing, over 60% of patients still did not return for the recommended testing,” said Joann G. Elmore, MD, MPH, professor of medicine at the University of California, Los Angeles. Dr. Elmore was not involved with the study.
The research took place during the COVID-19 pandemic, which may have reduced follow-up, the study authors wrote. Still, given that previous research has shown that follow-up tends to be low, the rates highlight “the need to understand factors associated with not completing follow-up that go beyond reminder effort,” they wrote. These include a need for patient education about the meaning of test results and what follow-up procedures involve.
The study was supported by the National Cancer Institute and the American Cancer Society. The authors have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
according to authors of a new study published in the Journal of the American Medical Association.
Results from the clustered, randomized clinical trial indicate that systems-based interventions, such as automating reminders in electronic health records (EHRs), outreach in the form of phone calls or letters, and assistance with barriers to health care, such as housing insecurity, can increase the number of patients who complete appropriate diagnostic follow-up after an abnormal result.
Patients who received an EHR reminder, outreach call or letter, and additional calls to screen for and assist with nine barriers to health care – housing insecurity, food insecurity, paying for basic utilities, family caregiving, legal issues, transportation, financial compensation for treatment, education, and employment – completed follow-up within 120 days of study enrollment at a rate of 31.4%. The follow-up rate was 31% for those who received only an EHR reminder and outreach, 22.7% for those who received only an EHR reminder, and 22.9% for those who received usual care.
“The benefits of cancer screening won’t be fully realized without systems to ensure timely follow-up of abnormal results,” said Anna Tosteson, ScD, director of the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H., a coauthor of the study.
Current payment incentives and quality-of-care indicators focus on getting people in for screening but should also address completion of screening – meaning timely and appropriate follow-up of results that could be indicative of cancer, Dr. Tosteson said.
“There’s a disconnect if you have screening rates that are high but once people have an abnormal result, which is potentially one step closer to a cancer diagnosis, there are no systems in place to help clinicians track them,” said study coauthor Jennifer Haas, MD, director of the Center for Primary Care Research at Massachusetts General Hospital in Boston.
In a 2016 study, researchers found that follow-up rates after abnormal cancer screenings varied widely. While 95.6% of patients with abnormal breast cancer screenings underwent timely follow-up testing, only 68.1% of patients with colorectal abnormalities and 44.8% of patients with cervical abnormalities did so.
Researchers for the new study used guideline recommendations and specialist input to create automated EHR algorithms that determined a follow-up period and diagnostic test.
They put the algorithm into practice with 11,980 patients who were part of 44 primary care practices within three health networks between August 2020 and December 2021. All patients had received abnormal test results for colorectal, breast, cervical, or lung cancer in varying risk categories.
All patients received usual care from their providers, which consisted of a “hodgepodge of whatever their clinic usually does,” Dr. Haas said. Without standards and systems in place for follow-up, the burden of testing and tracking patients with abnormal results typically falls on the primary care provider.
The researchers intervened only when patients were overdue for completion of follow-up. They then staggered the interventions sequentially.
All study participants received an automated, algorithm-triggered EHR reminder for follow-up in their patient portal along with routine health maintenance reminders. To view the reminder, patients had to log into their portal. Participants in the outreach and outreach and navigation groups also received a phone call, an EHR message, or a physical letter 2 weeks after receiving an EHR notification if they hadn’t completed follow-up. Research assistants performed the outreach after having been prompted by the algorithm.
After another 4 weeks, those in the EHR, outreach, and navigation group received a call from a patient navigator who helped them address nine barriers to health care, chiefly by providing them with referrals to free resources.
Among patients who received navigation, outcomes were not significantly better than among those who received EHR and outreach, indicating social determinants of health did not significantly affect the population studied or that the modest approach to navigation and the resources provided were insufficient, Dr. Haas said.
The complexity of an automated platform that encompasses many types of cancers, test results, and other data elements could prove difficult to apply in settings with less infrastructure, said Steven Atlas, MD, MPH, director of the Practice-Based Research and Quality Improvement Network in the division of general internal medicine at Mass General.
“I think there’s a role for the federal government to take on these initiatives,” Dr. Atlas said. Government intervention could help create “national IT systems to create standards for creating code for what an abnormal result is and how it should be followed,” he said.
While interventions improved patient follow-up, the overall rates were still low.
“What concerns me is that despite the various interventions implemented to encourage and support patients to return for follow-up testing, over 60% of patients still did not return for the recommended testing,” said Joann G. Elmore, MD, MPH, professor of medicine at the University of California, Los Angeles. Dr. Elmore was not involved with the study.
The research took place during the COVID-19 pandemic, which may have reduced follow-up, the study authors wrote. Still, given that previous research has shown that follow-up tends to be low, the rates highlight “the need to understand factors associated with not completing follow-up that go beyond reminder effort,” they wrote. These include a need for patient education about the meaning of test results and what follow-up procedures involve.
The study was supported by the National Cancer Institute and the American Cancer Society. The authors have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM JAMA
Dietary changes to microbiome may improve lung function
HONOLULU – , and the days immediately following the 9/11 attacks.
Among NYC firefighters enrolled in the randomized FIREHOUSE (Food Intake Restriction for Health Outcome Support and Education) study who took part in a microbiome substudy, those who followed a low-calorie, Mediterranean-style diet had higher levels in stools samples at 6 months of Bacteroides ovatus, a bacterial species associated with protection against bowel inflammation.
In contrast, participants who followed a usual-care diet had elevated 6-month levels of a species associated with high-fat diets and inflammation, reported Rachel Lam, a predoctoral fellow in the Nolan Lab at NYU Langone Medical Center, at the annual meeting of the American College of Chest Physicians (CHEST).
“Overall, we found that in our validation cohort, Bacteroides ovatus was increased in the LoCalMed arm after 6 months, and this bacterial species is associated with fewer negative health effects,” she said.
Ms. Lam noted that in a murine model of high-fat diets, mice gavaged with Bacteroides ovatus had reductions in body mass index and decreased serum LDL cholesterol and triglyceride levels.
FIREHOUSE cohort
Senior author Anna Nolan, MD, whose lab members study predictors of lung function loss in a cohort of firefighters who were exposed to the particulate matter clouding the air of lower Manhattan on 9/11 and the ensuing days, told this news organization that the findings, while preliminary, support previous research findings on potential links between intestinal microbiota and lung function.
“It’s interesting that we saw this done in other models, like mouse models and such, where certain bacteria were viewed as healthy for the system, and if they were able to bring that bacteria out in larger amounts they saw anti-inflammatory effects, so we’re hoping to mirror that and also do a mouse model,” she said.
Dr. Nolan’s group has previously shown that markers for the metabolic syndrome, inflammation, and vascular injury detected in serum samples taken within 6 months of 9/11 were predictive for later abnormal lung function. In addition, their group has found that elevated serum levels of an LDL metabolite after intense World Trade Center dust exposure is a risk factor for future impaired lung function as measured by forced expiratory volume in 1 second (FEV1).
In the FIREHOUSE trial, 89 patients were randomly assigned either to a technology-supported educational and behavioral intervention targeting calorie restriction for weight loss while following a low-calorie Mediterranean diet, or to usual care. The usual-care arm included participants who were informed about their weight, BMI, and other standard measures at annual visits and were given general advice about healthy eating, but were not assigned to a specific diet.
Participants in the LoCalMed group had significant decreases in BMI and increases in FEV1, compared with those in the usual-care group. In addition, the LoCalMed group had improved vascular health, better dietary habits, decreases in fats and calories from sweets, and decreases in inflammation as measured by a lower white blood cell count.
Microbiome substudy
At CHEST 2023, Ms. Lam reported on microbiome pilot and validation substudies of FIREHOUSE.
The pilot study included five patients in each arm. The validation sample included 15 participants in the Mediterranean diet group and 16 in the usual-care diet group.
Each participant’s microbiome was assessed with genomic sequencing with sequences aligned to a bacterial database. The number and diversity of bacterial species in each sample were determined with the Chao1 Index and Shannon Index, respectively.
There were no significant differences among the study groups in mean age, exposure at the World Trade Center site, or years of service.
Although bacterial diversity did not differ between the study arms either at baseline or at 6 months, in both groups it significantly decreased over time (P = .02 in the pilot, P < .0001 in the validation arm).
In the pilot study, there was an increase over 6 months in the usual care arm only of Bilophila wadsworthia, a species associated with high-fat diets and inflammation.
In the validation study, patients in the LoCalMed arm had significant reductions in Ruminococcaceae (P = .015) and increases in both Bacteroides ovatus (P = .03) and Alistipes shahii (P = .038), a recently identified species with uncertain protective or pathogenic potential.
In contrast, there were no significant increases in species in the usual-care group, but there were significant declines in several other bacterial species; Ms.Lam, however, did not say whether these changes had clinical significance. “Future studies will assess microbial association with clinical outcomes,” Ms. Lam said.
Confounding factors
Samuel Evans, MD, a pulmonologist at Straub Medical Center in Honolulu who moderated the oral abstract session where the data were presented, commented that the data are interesting but added that associations are difficult to determine given the heterogeneity of exposures that firefighters encounter.
“I think it’s interesting that clearly diet is influencing the type of bacteria in the biome in the gut, and perhaps some are favorable, and some are not favorable,” he told this news organization “We already know that the Mediterranean diet is associated with better health outcomes, so it makes sense, but can we tease out in the microbiome which bacteria are harmful and which are helpful.”
He noted that there are a lot of confounding factors and that “it’s hard to find the right signal when you have so many variables.”
The FIREHOUSE study is supported by the Centers for Disease Control and Prevention’s National Institute of Occupational Safety & Health and the National Heart, Lung, and Blood Institute. Ms. Lam, Dr. Nolan, and Dr. Evans report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
HONOLULU – , and the days immediately following the 9/11 attacks.
Among NYC firefighters enrolled in the randomized FIREHOUSE (Food Intake Restriction for Health Outcome Support and Education) study who took part in a microbiome substudy, those who followed a low-calorie, Mediterranean-style diet had higher levels in stools samples at 6 months of Bacteroides ovatus, a bacterial species associated with protection against bowel inflammation.
In contrast, participants who followed a usual-care diet had elevated 6-month levels of a species associated with high-fat diets and inflammation, reported Rachel Lam, a predoctoral fellow in the Nolan Lab at NYU Langone Medical Center, at the annual meeting of the American College of Chest Physicians (CHEST).
“Overall, we found that in our validation cohort, Bacteroides ovatus was increased in the LoCalMed arm after 6 months, and this bacterial species is associated with fewer negative health effects,” she said.
Ms. Lam noted that in a murine model of high-fat diets, mice gavaged with Bacteroides ovatus had reductions in body mass index and decreased serum LDL cholesterol and triglyceride levels.
FIREHOUSE cohort
Senior author Anna Nolan, MD, whose lab members study predictors of lung function loss in a cohort of firefighters who were exposed to the particulate matter clouding the air of lower Manhattan on 9/11 and the ensuing days, told this news organization that the findings, while preliminary, support previous research findings on potential links between intestinal microbiota and lung function.
“It’s interesting that we saw this done in other models, like mouse models and such, where certain bacteria were viewed as healthy for the system, and if they were able to bring that bacteria out in larger amounts they saw anti-inflammatory effects, so we’re hoping to mirror that and also do a mouse model,” she said.
Dr. Nolan’s group has previously shown that markers for the metabolic syndrome, inflammation, and vascular injury detected in serum samples taken within 6 months of 9/11 were predictive for later abnormal lung function. In addition, their group has found that elevated serum levels of an LDL metabolite after intense World Trade Center dust exposure is a risk factor for future impaired lung function as measured by forced expiratory volume in 1 second (FEV1).
In the FIREHOUSE trial, 89 patients were randomly assigned either to a technology-supported educational and behavioral intervention targeting calorie restriction for weight loss while following a low-calorie Mediterranean diet, or to usual care. The usual-care arm included participants who were informed about their weight, BMI, and other standard measures at annual visits and were given general advice about healthy eating, but were not assigned to a specific diet.
Participants in the LoCalMed group had significant decreases in BMI and increases in FEV1, compared with those in the usual-care group. In addition, the LoCalMed group had improved vascular health, better dietary habits, decreases in fats and calories from sweets, and decreases in inflammation as measured by a lower white blood cell count.
Microbiome substudy
At CHEST 2023, Ms. Lam reported on microbiome pilot and validation substudies of FIREHOUSE.
The pilot study included five patients in each arm. The validation sample included 15 participants in the Mediterranean diet group and 16 in the usual-care diet group.
Each participant’s microbiome was assessed with genomic sequencing with sequences aligned to a bacterial database. The number and diversity of bacterial species in each sample were determined with the Chao1 Index and Shannon Index, respectively.
There were no significant differences among the study groups in mean age, exposure at the World Trade Center site, or years of service.
Although bacterial diversity did not differ between the study arms either at baseline or at 6 months, in both groups it significantly decreased over time (P = .02 in the pilot, P < .0001 in the validation arm).
In the pilot study, there was an increase over 6 months in the usual care arm only of Bilophila wadsworthia, a species associated with high-fat diets and inflammation.
In the validation study, patients in the LoCalMed arm had significant reductions in Ruminococcaceae (P = .015) and increases in both Bacteroides ovatus (P = .03) and Alistipes shahii (P = .038), a recently identified species with uncertain protective or pathogenic potential.
In contrast, there were no significant increases in species in the usual-care group, but there were significant declines in several other bacterial species; Ms.Lam, however, did not say whether these changes had clinical significance. “Future studies will assess microbial association with clinical outcomes,” Ms. Lam said.
Confounding factors
Samuel Evans, MD, a pulmonologist at Straub Medical Center in Honolulu who moderated the oral abstract session where the data were presented, commented that the data are interesting but added that associations are difficult to determine given the heterogeneity of exposures that firefighters encounter.
“I think it’s interesting that clearly diet is influencing the type of bacteria in the biome in the gut, and perhaps some are favorable, and some are not favorable,” he told this news organization “We already know that the Mediterranean diet is associated with better health outcomes, so it makes sense, but can we tease out in the microbiome which bacteria are harmful and which are helpful.”
He noted that there are a lot of confounding factors and that “it’s hard to find the right signal when you have so many variables.”
The FIREHOUSE study is supported by the Centers for Disease Control and Prevention’s National Institute of Occupational Safety & Health and the National Heart, Lung, and Blood Institute. Ms. Lam, Dr. Nolan, and Dr. Evans report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
HONOLULU – , and the days immediately following the 9/11 attacks.
Among NYC firefighters enrolled in the randomized FIREHOUSE (Food Intake Restriction for Health Outcome Support and Education) study who took part in a microbiome substudy, those who followed a low-calorie, Mediterranean-style diet had higher levels in stools samples at 6 months of Bacteroides ovatus, a bacterial species associated with protection against bowel inflammation.
In contrast, participants who followed a usual-care diet had elevated 6-month levels of a species associated with high-fat diets and inflammation, reported Rachel Lam, a predoctoral fellow in the Nolan Lab at NYU Langone Medical Center, at the annual meeting of the American College of Chest Physicians (CHEST).
“Overall, we found that in our validation cohort, Bacteroides ovatus was increased in the LoCalMed arm after 6 months, and this bacterial species is associated with fewer negative health effects,” she said.
Ms. Lam noted that in a murine model of high-fat diets, mice gavaged with Bacteroides ovatus had reductions in body mass index and decreased serum LDL cholesterol and triglyceride levels.
FIREHOUSE cohort
Senior author Anna Nolan, MD, whose lab members study predictors of lung function loss in a cohort of firefighters who were exposed to the particulate matter clouding the air of lower Manhattan on 9/11 and the ensuing days, told this news organization that the findings, while preliminary, support previous research findings on potential links between intestinal microbiota and lung function.
“It’s interesting that we saw this done in other models, like mouse models and such, where certain bacteria were viewed as healthy for the system, and if they were able to bring that bacteria out in larger amounts they saw anti-inflammatory effects, so we’re hoping to mirror that and also do a mouse model,” she said.
Dr. Nolan’s group has previously shown that markers for the metabolic syndrome, inflammation, and vascular injury detected in serum samples taken within 6 months of 9/11 were predictive for later abnormal lung function. In addition, their group has found that elevated serum levels of an LDL metabolite after intense World Trade Center dust exposure is a risk factor for future impaired lung function as measured by forced expiratory volume in 1 second (FEV1).
In the FIREHOUSE trial, 89 patients were randomly assigned either to a technology-supported educational and behavioral intervention targeting calorie restriction for weight loss while following a low-calorie Mediterranean diet, or to usual care. The usual-care arm included participants who were informed about their weight, BMI, and other standard measures at annual visits and were given general advice about healthy eating, but were not assigned to a specific diet.
Participants in the LoCalMed group had significant decreases in BMI and increases in FEV1, compared with those in the usual-care group. In addition, the LoCalMed group had improved vascular health, better dietary habits, decreases in fats and calories from sweets, and decreases in inflammation as measured by a lower white blood cell count.
Microbiome substudy
At CHEST 2023, Ms. Lam reported on microbiome pilot and validation substudies of FIREHOUSE.
The pilot study included five patients in each arm. The validation sample included 15 participants in the Mediterranean diet group and 16 in the usual-care diet group.
Each participant’s microbiome was assessed with genomic sequencing with sequences aligned to a bacterial database. The number and diversity of bacterial species in each sample were determined with the Chao1 Index and Shannon Index, respectively.
There were no significant differences among the study groups in mean age, exposure at the World Trade Center site, or years of service.
Although bacterial diversity did not differ between the study arms either at baseline or at 6 months, in both groups it significantly decreased over time (P = .02 in the pilot, P < .0001 in the validation arm).
In the pilot study, there was an increase over 6 months in the usual care arm only of Bilophila wadsworthia, a species associated with high-fat diets and inflammation.
In the validation study, patients in the LoCalMed arm had significant reductions in Ruminococcaceae (P = .015) and increases in both Bacteroides ovatus (P = .03) and Alistipes shahii (P = .038), a recently identified species with uncertain protective or pathogenic potential.
In contrast, there were no significant increases in species in the usual-care group, but there were significant declines in several other bacterial species; Ms.Lam, however, did not say whether these changes had clinical significance. “Future studies will assess microbial association with clinical outcomes,” Ms. Lam said.
Confounding factors
Samuel Evans, MD, a pulmonologist at Straub Medical Center in Honolulu who moderated the oral abstract session where the data were presented, commented that the data are interesting but added that associations are difficult to determine given the heterogeneity of exposures that firefighters encounter.
“I think it’s interesting that clearly diet is influencing the type of bacteria in the biome in the gut, and perhaps some are favorable, and some are not favorable,” he told this news organization “We already know that the Mediterranean diet is associated with better health outcomes, so it makes sense, but can we tease out in the microbiome which bacteria are harmful and which are helpful.”
He noted that there are a lot of confounding factors and that “it’s hard to find the right signal when you have so many variables.”
The FIREHOUSE study is supported by the Centers for Disease Control and Prevention’s National Institute of Occupational Safety & Health and the National Heart, Lung, and Blood Institute. Ms. Lam, Dr. Nolan, and Dr. Evans report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT CHEST 2023
IPF pipeline crowded with new drug candidates
With the emergence of pirfenidone and nintedanib over the past decade or so, pulmonologists now have at their disposal two breakthrough antifibrotic agents for the treatment of idiopathic pulmonary fibrosis.

But these two drugs have a number of shortcomings that a host of investigative agents are aiming to address. For one, while pirfenidone and nintedanib have been shown to slow disease progression and improve symptoms, they don’t stop or reverse the disease. Also, a large number of patients with IPF don’t tolerate these drugs well. And, their high cost is a barrier for many patients.
in terms of therapies or interventions that have better efficacy, better long-term tolerability, and that improve symptoms and quality of life for our patients with IPF disease,” said Joyce Lee, MD, associate professor of medicine–pulmonary at the University of Colorado at Denver, Aurora, and senior medical adviser for research and health care quality for the Pulmonary Fibrosis Foundation.
The National Institutes of Health estimates that more than 30,000 new cases of IPF are diagnosed in the United States annually, and as many as 3 million people have the disease worldwide. The 5-year survival rate is less than 40% after diagnosis. Bloomberg News reported that more than 80 pharmaceutical companies are working on IPF treatments. iHealthcareAnalyst estimates the global market for IPF will reach $10.1 billion by 2029 thanks to rapidly increasing prevalence and incidence with age, premium-priced drugs, and rapid approval of new treatments.
The perils of phase 3 studies
A search on ClinicalTrials.gov turned up 89 investigative IPF treatments in human trials. However, the search for alternatives can be perilous. “In the field, we have gotten used to promising phase 2 studies that failed in the phase 3 stage of development,” Dr. Lee said. “I don’t hold my breath these days just in terms of trying to predict whether or not the efficacy will be present in the phase 3 clinical trial.”
Three notable phase 3 flops include the ISABELA 1 and 2 trials of the autotaxin inhibitor ziritaxestat, which failed to meet their primary endpoint and were halted early (JAMA. 2023;329:1567-78). The phase 3 ZEPHYRUS-1 trial failed to show any benefit of pamrevlumab to improve percent predicted force vital capacity (ppFVC) at week 48, causing discontinuation of a second phase 3 trial. The phase 3 STARSCAPE-OLE study of intravenous recombinant human pentraxin-2 was terminated earlier this year when the sponsor, Hoffmann-LaRoche, decided it was unable to meet its primary objective (NCT04594707).
In the meantime, these six other phase 3 programs in IPF are still in the field:
Anlotinib. A phase 2 and 3 trial in China is evaluating 1-year outcomes of once-daily oral anlotinib for treatment of IPF/progressive fibrosis-interstitial lung disease (PF-ILDS) (NCT05828953). Anlotinib is a tyrosine kinase inhibitor (TKI) that targets four factors: vascular endothelial growth factor receptor (VEGR), fibroblast growth factor receptor (FGFR), platelet-derived growth factor receptors (PDGFR), and c-kit. It’s approved in China as a third-line therapy for non–small cell lung cancer (NSCLC).
BI 101550. Enrollment in the FIBRONEER-IPF trial commenced last fall (NCT05321069), with completion scheduled for late next year. BI 1015550 is an oral phosphodiesterase 4B (PDE4B) inhibitor. FIBRONEER-ILD is a separate phase 3 trial in fibrosing idiopathic lung disease (NCT05321082). In both trials, the primary endpoint is the absolute change from baseline in FVC at week 52.
BMS-986278. Results of a phase 2 trial showed that twice-daily treatment with oral BMS-986278 60 mg over 26 weeks reduced the rate of decline in ppFVC by 69% vs. placebo. The phase 3 ALOFT trial has been approved but hasn’t yet started recruiting patients (NCT06003426). BMS-986278 is a lysophosphatidic acid receptor 1 (LPA1) antagonist.
Lanxoprazole. Commonly used to treat and prevent gastrointestinal problems like stomach ulcers and esophagitis, this oral proton pump inhibitor (PPI) is the focus of a trial in the United Kingdom evaluating if PPIs can slow the progression of IPF (NCT04965298).
N-acetylcysteine (NAC). The PRECISIONS trial is evaluating the effect of NAC plus standard-of-care treatment in IPF patients who have the TOLLIP rs3750910 TT genotype (NCT04300920). Participants receive 600 mg NAC orally or matched placebo three times daily for 24 months. Trial completion is scheduled for 2025.
Treprostinil. Already approved to treat pulmonary arterial hypertension and pulmonary hypertension associated with interstitial lung disease, inhaled Treprostinil is the subject of the TETON 1 and 2 trials evaluating its impact on ppFVC after 52 weeks of treatment (NCT04708782, NCT05255991).
Phase 2 candidates
The primary endpoint in most of the phase 2 trials is change in ppFVC capacity from baseline to week 24. The following investigative therapies are in phase 2 trials:
Bexotegrast (PLN-74809), an oral, small molecule, dual-selective inhibitor of alphav/beta6 and alphav/beta1 (NCT04396756).
BBT-877, described as a potent autotaxin (ATX) inhibitor, demonstrated its ability to inhibit lysophosphatidic acid (LPA) production by as much as 90 percent (NCT05483907).
CC-90001, an oral, once-daily c-Jun N-terminal kinases (JNK) inhibitor. JNKs have been implicated in the underlying mechanisms of fibrosis, including epithelial cell death, inflammation and polarization of profibrotic macrophages, fibroblast activation, and collagen production (NCT03142191).
C21 targets the underlying fibrosis in IPF by stimulating the protective arm of the renin-angiotensin system. It also has an upstream effect by promoting alveolar repair by which it can reduce fibrosis formation, stabilize disease, and increase lung capacity (NCT04533022).
CSL312 (garadacimab) is a humanized anti-FXIIa monoclonal antibody administrated intravenously (NCT05130970).
Cudetaxestat, a noncompetitive autotaxin inhibitor (NCT05373914).
Bersiposocin/DWN12088, an inhibitor of prolyl-tRNA synthetase 1 (PARS1), which is suspected to control the pathologic accumulation of collagen containing high amounts of proline in fibrotic diseases (NCT05389215).
ENV-101, a small-molecule inhibitor of the Hedgehog (Hh) signaling pathway, which plays a key role in IPF. This agent was originally developed to target Hh-driven cancers (NCT04968574).
GKT137831 (setanaxib) inhibits nicotinamide adenine dinucleotide phosphate (NADPH) oxidase (NOX) isoforms. (NCT03865927).
HZN-825, a lysophosphatidic acid receptor 1 (LPAR1) antagonist. (NCT05032066)
Ifetroban, a potent and selective thromboxane-prostanoid receptor (TPr) antagonist, which exhibits a high affinity for TPr on platelets, vascular and airway smooth muscle, and fibroblasts, and lacks agonistic activity (NCT05571059).
INS018_055, a small-molecule, oral antifibrotic candidate notable for being the first entirely AI-generated drug to enter phase 2 trials. Trial enrollment started in October (NCT05975983, NCT05983920)
Jaktinib dihydrochloride monohydrate, an oral JAK1, JAK2, and JAK3 inhibitor (NCT04312594).
Leramistat, an anti–tumor necrosis factor (TNF) agent (NCT05951296).
LTP001, an oral, selectively deuterated form of pirfenidone designed to retain the antifibrotic and anti-inflammatory activity of pirfenidone with a differentiated pharmacokinetic profile (NCT05497284, NCT05321420).
ME-015 (suplatast tosilate) aims to stabilize ion channels in the neuronal endings in the lungs that mediate IPF-related cough (NCT05983471).
Nalbuphine, a small-molecule, dual-mechanism treatment for chronic cough in IPF. It acts as both a mu opioid receptor antagonist and a kappa opioid receptor agonist (NCT05964335). The CANAL trial, complete last year, is evaluating an extended-release formulation (NCT04030026).
NP-120 (ifenprodil), a small-molecule N-methyl-D-aspartate (NMDA) receptor antagonist, specifically targets the NMDA-type subunit 2B (GluN2B) (NCT04318704).
Orvepitant, a selective antagonist for the NK₁ receptor, is being evaluated to treat IPF-related cough (NCT05815089).
RXC007 (zelasudil), a Rho-associated coiled-coil–containing protein kinase 2 (ROCK2) selective inhibitor, was granted FDA orphan drug designation in August 2023 (NCT05570058).
Saracatinib, a selective Src kinase inhibitor originally developed for oncological indications (NCT04598919).
SHR-1906, an intravenous treatment, inhibits binding of a target protein to a variety of cytokines and growth factors, affects downstream signaling pathways, and reduces cell proliferation and migration (NCT05722964).
TTI-101, an oral, small-molecule inhibitor of signal transducer and activator of transcription (STAT3), which has been found to accumulate in the lungs of IPF patients (NCT05671835).
VAY736 (lanalumab), a BAFF-R inhibitor (NCT03287414).
Vixarelimab, a human monoclonal oncastatin M receptor beta antibody (NCT05785624).
Some investigative programs, however, didn’t make it out of phase 2. The trial evaluating inhaled GB0139, a selective functional antagonist of G-protein–coupled receptor 84, which plays a key role in fibrosis, failed to meet its primary endpoint (NCT03832946). Likewise, oral GLPG1205 failed to show a significant difference in FVC decline vs. placebo (NCT03725852). The program to develop SAR156597, also known as romilkimab, was halted (NCT02345070). ND-L02-s0201n, an siRNA oligonucleotide drug designed to inhibit heat shock protein 47 (HSP47), which regulates collagen synthesis and secretion that causes fibrosis, didn’t show the expected efficacy (NCT03538301).
Phase 1 trials
No fewer than 27 phase 1 trials are evaluating investigative treatments for IPF, many in the early phase or not yet recruiting. According to GlobalData, phase 1 drugs for IPF have a 66% chance of moving onto phase 2. Among the advanced phase 1 trials that have gained corporate backing are:
9MW3811, an anti–interleukin-11 monoclonal antibody IV injection (NCT05912049).
ANG-3070, an oral tyrosine kinase inhibitor targeting platelet-derived growth factor (PDGFR) alpha and beta (NCT05387785).
C106, an angiotensin II type 2 receptor agonist (NCT05427253).
HuL001, which targets alpha-enolase (NCT04540770).
LTI-03, a Caveolin-1 (Cav1)-related peptide designed to restore Cav1 expression in lung tissue (NCT05954988).
ORIN1001, a first-in-class small molecule that selectively blocks the inositol requiring enzyme 1alphase (IRE1) RNAse and blocks X-box binding protein 1 (XBP1) activation (NCT04643769).
PRS-220 is an orally inhaled anticalin protein targeting connective tissue growth factor (CTGF) (NTC05473533).
TRK-250, a single-strand, long-chain nucleic acid that selectively suppresses expression of transforming growth factor-beta 1 (TGF-beta1) protein (NCT03727802).
“While we have therapies that we’re able to give patients, we need to do more and we need to do better,” Dr. Lee said. “We’re all hopeful the next phase 3 clinical trial will be something that will help change the treatment paradigm for our patients. We’re very patient, and hopefully those that are interested in improving this treatment landscape will continue to persist.”
Dr. Lee disclosed financial relationships with Boehringer Ingelheim, Pliant Therapeutics, Blade Therapeutics, United Therapeutics, Eleven P15. and Avalyn Pharma.
With the emergence of pirfenidone and nintedanib over the past decade or so, pulmonologists now have at their disposal two breakthrough antifibrotic agents for the treatment of idiopathic pulmonary fibrosis.
But these two drugs have a number of shortcomings that a host of investigative agents are aiming to address. For one, while pirfenidone and nintedanib have been shown to slow disease progression and improve symptoms, they don’t stop or reverse the disease. Also, a large number of patients with IPF don’t tolerate these drugs well. And, their high cost is a barrier for many patients.
in terms of therapies or interventions that have better efficacy, better long-term tolerability, and that improve symptoms and quality of life for our patients with IPF disease,” said Joyce Lee, MD, associate professor of medicine–pulmonary at the University of Colorado at Denver, Aurora, and senior medical adviser for research and health care quality for the Pulmonary Fibrosis Foundation.
The National Institutes of Health estimates that more than 30,000 new cases of IPF are diagnosed in the United States annually, and as many as 3 million people have the disease worldwide. The 5-year survival rate is less than 40% after diagnosis. Bloomberg News reported that more than 80 pharmaceutical companies are working on IPF treatments. iHealthcareAnalyst estimates the global market for IPF will reach $10.1 billion by 2029 thanks to rapidly increasing prevalence and incidence with age, premium-priced drugs, and rapid approval of new treatments.
The perils of phase 3 studies
A search on ClinicalTrials.gov turned up 89 investigative IPF treatments in human trials. However, the search for alternatives can be perilous. “In the field, we have gotten used to promising phase 2 studies that failed in the phase 3 stage of development,” Dr. Lee said. “I don’t hold my breath these days just in terms of trying to predict whether or not the efficacy will be present in the phase 3 clinical trial.”
Three notable phase 3 flops include the ISABELA 1 and 2 trials of the autotaxin inhibitor ziritaxestat, which failed to meet their primary endpoint and were halted early (JAMA. 2023;329:1567-78). The phase 3 ZEPHYRUS-1 trial failed to show any benefit of pamrevlumab to improve percent predicted force vital capacity (ppFVC) at week 48, causing discontinuation of a second phase 3 trial. The phase 3 STARSCAPE-OLE study of intravenous recombinant human pentraxin-2 was terminated earlier this year when the sponsor, Hoffmann-LaRoche, decided it was unable to meet its primary objective (NCT04594707).
In the meantime, these six other phase 3 programs in IPF are still in the field:
Anlotinib. A phase 2 and 3 trial in China is evaluating 1-year outcomes of once-daily oral anlotinib for treatment of IPF/progressive fibrosis-interstitial lung disease (PF-ILDS) (NCT05828953). Anlotinib is a tyrosine kinase inhibitor (TKI) that targets four factors: vascular endothelial growth factor receptor (VEGR), fibroblast growth factor receptor (FGFR), platelet-derived growth factor receptors (PDGFR), and c-kit. It’s approved in China as a third-line therapy for non–small cell lung cancer (NSCLC).
BI 101550. Enrollment in the FIBRONEER-IPF trial commenced last fall (NCT05321069), with completion scheduled for late next year. BI 1015550 is an oral phosphodiesterase 4B (PDE4B) inhibitor. FIBRONEER-ILD is a separate phase 3 trial in fibrosing idiopathic lung disease (NCT05321082). In both trials, the primary endpoint is the absolute change from baseline in FVC at week 52.
BMS-986278. Results of a phase 2 trial showed that twice-daily treatment with oral BMS-986278 60 mg over 26 weeks reduced the rate of decline in ppFVC by 69% vs. placebo. The phase 3 ALOFT trial has been approved but hasn’t yet started recruiting patients (NCT06003426). BMS-986278 is a lysophosphatidic acid receptor 1 (LPA1) antagonist.
Lanxoprazole. Commonly used to treat and prevent gastrointestinal problems like stomach ulcers and esophagitis, this oral proton pump inhibitor (PPI) is the focus of a trial in the United Kingdom evaluating if PPIs can slow the progression of IPF (NCT04965298).
N-acetylcysteine (NAC). The PRECISIONS trial is evaluating the effect of NAC plus standard-of-care treatment in IPF patients who have the TOLLIP rs3750910 TT genotype (NCT04300920). Participants receive 600 mg NAC orally or matched placebo three times daily for 24 months. Trial completion is scheduled for 2025.
Treprostinil. Already approved to treat pulmonary arterial hypertension and pulmonary hypertension associated with interstitial lung disease, inhaled Treprostinil is the subject of the TETON 1 and 2 trials evaluating its impact on ppFVC after 52 weeks of treatment (NCT04708782, NCT05255991).
Phase 2 candidates
The primary endpoint in most of the phase 2 trials is change in ppFVC capacity from baseline to week 24. The following investigative therapies are in phase 2 trials:
Bexotegrast (PLN-74809), an oral, small molecule, dual-selective inhibitor of alphav/beta6 and alphav/beta1 (NCT04396756).
BBT-877, described as a potent autotaxin (ATX) inhibitor, demonstrated its ability to inhibit lysophosphatidic acid (LPA) production by as much as 90 percent (NCT05483907).
CC-90001, an oral, once-daily c-Jun N-terminal kinases (JNK) inhibitor. JNKs have been implicated in the underlying mechanisms of fibrosis, including epithelial cell death, inflammation and polarization of profibrotic macrophages, fibroblast activation, and collagen production (NCT03142191).
C21 targets the underlying fibrosis in IPF by stimulating the protective arm of the renin-angiotensin system. It also has an upstream effect by promoting alveolar repair by which it can reduce fibrosis formation, stabilize disease, and increase lung capacity (NCT04533022).
CSL312 (garadacimab) is a humanized anti-FXIIa monoclonal antibody administrated intravenously (NCT05130970).
Cudetaxestat, a noncompetitive autotaxin inhibitor (NCT05373914).
Bersiposocin/DWN12088, an inhibitor of prolyl-tRNA synthetase 1 (PARS1), which is suspected to control the pathologic accumulation of collagen containing high amounts of proline in fibrotic diseases (NCT05389215).
ENV-101, a small-molecule inhibitor of the Hedgehog (Hh) signaling pathway, which plays a key role in IPF. This agent was originally developed to target Hh-driven cancers (NCT04968574).
GKT137831 (setanaxib) inhibits nicotinamide adenine dinucleotide phosphate (NADPH) oxidase (NOX) isoforms. (NCT03865927).
HZN-825, a lysophosphatidic acid receptor 1 (LPAR1) antagonist. (NCT05032066)
Ifetroban, a potent and selective thromboxane-prostanoid receptor (TPr) antagonist, which exhibits a high affinity for TPr on platelets, vascular and airway smooth muscle, and fibroblasts, and lacks agonistic activity (NCT05571059).
INS018_055, a small-molecule, oral antifibrotic candidate notable for being the first entirely AI-generated drug to enter phase 2 trials. Trial enrollment started in October (NCT05975983, NCT05983920)
Jaktinib dihydrochloride monohydrate, an oral JAK1, JAK2, and JAK3 inhibitor (NCT04312594).
Leramistat, an anti–tumor necrosis factor (TNF) agent (NCT05951296).
LTP001, an oral, selectively deuterated form of pirfenidone designed to retain the antifibrotic and anti-inflammatory activity of pirfenidone with a differentiated pharmacokinetic profile (NCT05497284, NCT05321420).
ME-015 (suplatast tosilate) aims to stabilize ion channels in the neuronal endings in the lungs that mediate IPF-related cough (NCT05983471).
Nalbuphine, a small-molecule, dual-mechanism treatment for chronic cough in IPF. It acts as both a mu opioid receptor antagonist and a kappa opioid receptor agonist (NCT05964335). The CANAL trial, complete last year, is evaluating an extended-release formulation (NCT04030026).
NP-120 (ifenprodil), a small-molecule N-methyl-D-aspartate (NMDA) receptor antagonist, specifically targets the NMDA-type subunit 2B (GluN2B) (NCT04318704).
Orvepitant, a selective antagonist for the NK₁ receptor, is being evaluated to treat IPF-related cough (NCT05815089).
RXC007 (zelasudil), a Rho-associated coiled-coil–containing protein kinase 2 (ROCK2) selective inhibitor, was granted FDA orphan drug designation in August 2023 (NCT05570058).
Saracatinib, a selective Src kinase inhibitor originally developed for oncological indications (NCT04598919).
SHR-1906, an intravenous treatment, inhibits binding of a target protein to a variety of cytokines and growth factors, affects downstream signaling pathways, and reduces cell proliferation and migration (NCT05722964).
TTI-101, an oral, small-molecule inhibitor of signal transducer and activator of transcription (STAT3), which has been found to accumulate in the lungs of IPF patients (NCT05671835).
VAY736 (lanalumab), a BAFF-R inhibitor (NCT03287414).
Vixarelimab, a human monoclonal oncastatin M receptor beta antibody (NCT05785624).
Some investigative programs, however, didn’t make it out of phase 2. The trial evaluating inhaled GB0139, a selective functional antagonist of G-protein–coupled receptor 84, which plays a key role in fibrosis, failed to meet its primary endpoint (NCT03832946). Likewise, oral GLPG1205 failed to show a significant difference in FVC decline vs. placebo (NCT03725852). The program to develop SAR156597, also known as romilkimab, was halted (NCT02345070). ND-L02-s0201n, an siRNA oligonucleotide drug designed to inhibit heat shock protein 47 (HSP47), which regulates collagen synthesis and secretion that causes fibrosis, didn’t show the expected efficacy (NCT03538301).
Phase 1 trials
No fewer than 27 phase 1 trials are evaluating investigative treatments for IPF, many in the early phase or not yet recruiting. According to GlobalData, phase 1 drugs for IPF have a 66% chance of moving onto phase 2. Among the advanced phase 1 trials that have gained corporate backing are:
9MW3811, an anti–interleukin-11 monoclonal antibody IV injection (NCT05912049).
ANG-3070, an oral tyrosine kinase inhibitor targeting platelet-derived growth factor (PDGFR) alpha and beta (NCT05387785).
C106, an angiotensin II type 2 receptor agonist (NCT05427253).
HuL001, which targets alpha-enolase (NCT04540770).
LTI-03, a Caveolin-1 (Cav1)-related peptide designed to restore Cav1 expression in lung tissue (NCT05954988).
ORIN1001, a first-in-class small molecule that selectively blocks the inositol requiring enzyme 1alphase (IRE1) RNAse and blocks X-box binding protein 1 (XBP1) activation (NCT04643769).
PRS-220 is an orally inhaled anticalin protein targeting connective tissue growth factor (CTGF) (NTC05473533).
TRK-250, a single-strand, long-chain nucleic acid that selectively suppresses expression of transforming growth factor-beta 1 (TGF-beta1) protein (NCT03727802).
“While we have therapies that we’re able to give patients, we need to do more and we need to do better,” Dr. Lee said. “We’re all hopeful the next phase 3 clinical trial will be something that will help change the treatment paradigm for our patients. We’re very patient, and hopefully those that are interested in improving this treatment landscape will continue to persist.”
Dr. Lee disclosed financial relationships with Boehringer Ingelheim, Pliant Therapeutics, Blade Therapeutics, United Therapeutics, Eleven P15. and Avalyn Pharma.
With the emergence of pirfenidone and nintedanib over the past decade or so, pulmonologists now have at their disposal two breakthrough antifibrotic agents for the treatment of idiopathic pulmonary fibrosis.
But these two drugs have a number of shortcomings that a host of investigative agents are aiming to address. For one, while pirfenidone and nintedanib have been shown to slow disease progression and improve symptoms, they don’t stop or reverse the disease. Also, a large number of patients with IPF don’t tolerate these drugs well. And, their high cost is a barrier for many patients.
in terms of therapies or interventions that have better efficacy, better long-term tolerability, and that improve symptoms and quality of life for our patients with IPF disease,” said Joyce Lee, MD, associate professor of medicine–pulmonary at the University of Colorado at Denver, Aurora, and senior medical adviser for research and health care quality for the Pulmonary Fibrosis Foundation.
The National Institutes of Health estimates that more than 30,000 new cases of IPF are diagnosed in the United States annually, and as many as 3 million people have the disease worldwide. The 5-year survival rate is less than 40% after diagnosis. Bloomberg News reported that more than 80 pharmaceutical companies are working on IPF treatments. iHealthcareAnalyst estimates the global market for IPF will reach $10.1 billion by 2029 thanks to rapidly increasing prevalence and incidence with age, premium-priced drugs, and rapid approval of new treatments.
The perils of phase 3 studies
A search on ClinicalTrials.gov turned up 89 investigative IPF treatments in human trials. However, the search for alternatives can be perilous. “In the field, we have gotten used to promising phase 2 studies that failed in the phase 3 stage of development,” Dr. Lee said. “I don’t hold my breath these days just in terms of trying to predict whether or not the efficacy will be present in the phase 3 clinical trial.”
Three notable phase 3 flops include the ISABELA 1 and 2 trials of the autotaxin inhibitor ziritaxestat, which failed to meet their primary endpoint and were halted early (JAMA. 2023;329:1567-78). The phase 3 ZEPHYRUS-1 trial failed to show any benefit of pamrevlumab to improve percent predicted force vital capacity (ppFVC) at week 48, causing discontinuation of a second phase 3 trial. The phase 3 STARSCAPE-OLE study of intravenous recombinant human pentraxin-2 was terminated earlier this year when the sponsor, Hoffmann-LaRoche, decided it was unable to meet its primary objective (NCT04594707).
In the meantime, these six other phase 3 programs in IPF are still in the field:
Anlotinib. A phase 2 and 3 trial in China is evaluating 1-year outcomes of once-daily oral anlotinib for treatment of IPF/progressive fibrosis-interstitial lung disease (PF-ILDS) (NCT05828953). Anlotinib is a tyrosine kinase inhibitor (TKI) that targets four factors: vascular endothelial growth factor receptor (VEGR), fibroblast growth factor receptor (FGFR), platelet-derived growth factor receptors (PDGFR), and c-kit. It’s approved in China as a third-line therapy for non–small cell lung cancer (NSCLC).
BI 101550. Enrollment in the FIBRONEER-IPF trial commenced last fall (NCT05321069), with completion scheduled for late next year. BI 1015550 is an oral phosphodiesterase 4B (PDE4B) inhibitor. FIBRONEER-ILD is a separate phase 3 trial in fibrosing idiopathic lung disease (NCT05321082). In both trials, the primary endpoint is the absolute change from baseline in FVC at week 52.
BMS-986278. Results of a phase 2 trial showed that twice-daily treatment with oral BMS-986278 60 mg over 26 weeks reduced the rate of decline in ppFVC by 69% vs. placebo. The phase 3 ALOFT trial has been approved but hasn’t yet started recruiting patients (NCT06003426). BMS-986278 is a lysophosphatidic acid receptor 1 (LPA1) antagonist.
Lanxoprazole. Commonly used to treat and prevent gastrointestinal problems like stomach ulcers and esophagitis, this oral proton pump inhibitor (PPI) is the focus of a trial in the United Kingdom evaluating if PPIs can slow the progression of IPF (NCT04965298).
N-acetylcysteine (NAC). The PRECISIONS trial is evaluating the effect of NAC plus standard-of-care treatment in IPF patients who have the TOLLIP rs3750910 TT genotype (NCT04300920). Participants receive 600 mg NAC orally or matched placebo three times daily for 24 months. Trial completion is scheduled for 2025.
Treprostinil. Already approved to treat pulmonary arterial hypertension and pulmonary hypertension associated with interstitial lung disease, inhaled Treprostinil is the subject of the TETON 1 and 2 trials evaluating its impact on ppFVC after 52 weeks of treatment (NCT04708782, NCT05255991).
Phase 2 candidates
The primary endpoint in most of the phase 2 trials is change in ppFVC capacity from baseline to week 24. The following investigative therapies are in phase 2 trials:
Bexotegrast (PLN-74809), an oral, small molecule, dual-selective inhibitor of alphav/beta6 and alphav/beta1 (NCT04396756).
BBT-877, described as a potent autotaxin (ATX) inhibitor, demonstrated its ability to inhibit lysophosphatidic acid (LPA) production by as much as 90 percent (NCT05483907).
CC-90001, an oral, once-daily c-Jun N-terminal kinases (JNK) inhibitor. JNKs have been implicated in the underlying mechanisms of fibrosis, including epithelial cell death, inflammation and polarization of profibrotic macrophages, fibroblast activation, and collagen production (NCT03142191).
C21 targets the underlying fibrosis in IPF by stimulating the protective arm of the renin-angiotensin system. It also has an upstream effect by promoting alveolar repair by which it can reduce fibrosis formation, stabilize disease, and increase lung capacity (NCT04533022).
CSL312 (garadacimab) is a humanized anti-FXIIa monoclonal antibody administrated intravenously (NCT05130970).
Cudetaxestat, a noncompetitive autotaxin inhibitor (NCT05373914).
Bersiposocin/DWN12088, an inhibitor of prolyl-tRNA synthetase 1 (PARS1), which is suspected to control the pathologic accumulation of collagen containing high amounts of proline in fibrotic diseases (NCT05389215).
ENV-101, a small-molecule inhibitor of the Hedgehog (Hh) signaling pathway, which plays a key role in IPF. This agent was originally developed to target Hh-driven cancers (NCT04968574).
GKT137831 (setanaxib) inhibits nicotinamide adenine dinucleotide phosphate (NADPH) oxidase (NOX) isoforms. (NCT03865927).
HZN-825, a lysophosphatidic acid receptor 1 (LPAR1) antagonist. (NCT05032066)
Ifetroban, a potent and selective thromboxane-prostanoid receptor (TPr) antagonist, which exhibits a high affinity for TPr on platelets, vascular and airway smooth muscle, and fibroblasts, and lacks agonistic activity (NCT05571059).
INS018_055, a small-molecule, oral antifibrotic candidate notable for being the first entirely AI-generated drug to enter phase 2 trials. Trial enrollment started in October (NCT05975983, NCT05983920)
Jaktinib dihydrochloride monohydrate, an oral JAK1, JAK2, and JAK3 inhibitor (NCT04312594).
Leramistat, an anti–tumor necrosis factor (TNF) agent (NCT05951296).
LTP001, an oral, selectively deuterated form of pirfenidone designed to retain the antifibrotic and anti-inflammatory activity of pirfenidone with a differentiated pharmacokinetic profile (NCT05497284, NCT05321420).
ME-015 (suplatast tosilate) aims to stabilize ion channels in the neuronal endings in the lungs that mediate IPF-related cough (NCT05983471).
Nalbuphine, a small-molecule, dual-mechanism treatment for chronic cough in IPF. It acts as both a mu opioid receptor antagonist and a kappa opioid receptor agonist (NCT05964335). The CANAL trial, complete last year, is evaluating an extended-release formulation (NCT04030026).
NP-120 (ifenprodil), a small-molecule N-methyl-D-aspartate (NMDA) receptor antagonist, specifically targets the NMDA-type subunit 2B (GluN2B) (NCT04318704).
Orvepitant, a selective antagonist for the NK₁ receptor, is being evaluated to treat IPF-related cough (NCT05815089).
RXC007 (zelasudil), a Rho-associated coiled-coil–containing protein kinase 2 (ROCK2) selective inhibitor, was granted FDA orphan drug designation in August 2023 (NCT05570058).
Saracatinib, a selective Src kinase inhibitor originally developed for oncological indications (NCT04598919).
SHR-1906, an intravenous treatment, inhibits binding of a target protein to a variety of cytokines and growth factors, affects downstream signaling pathways, and reduces cell proliferation and migration (NCT05722964).
TTI-101, an oral, small-molecule inhibitor of signal transducer and activator of transcription (STAT3), which has been found to accumulate in the lungs of IPF patients (NCT05671835).
VAY736 (lanalumab), a BAFF-R inhibitor (NCT03287414).
Vixarelimab, a human monoclonal oncastatin M receptor beta antibody (NCT05785624).
Some investigative programs, however, didn’t make it out of phase 2. The trial evaluating inhaled GB0139, a selective functional antagonist of G-protein–coupled receptor 84, which plays a key role in fibrosis, failed to meet its primary endpoint (NCT03832946). Likewise, oral GLPG1205 failed to show a significant difference in FVC decline vs. placebo (NCT03725852). The program to develop SAR156597, also known as romilkimab, was halted (NCT02345070). ND-L02-s0201n, an siRNA oligonucleotide drug designed to inhibit heat shock protein 47 (HSP47), which regulates collagen synthesis and secretion that causes fibrosis, didn’t show the expected efficacy (NCT03538301).
Phase 1 trials
No fewer than 27 phase 1 trials are evaluating investigative treatments for IPF, many in the early phase or not yet recruiting. According to GlobalData, phase 1 drugs for IPF have a 66% chance of moving onto phase 2. Among the advanced phase 1 trials that have gained corporate backing are:
9MW3811, an anti–interleukin-11 monoclonal antibody IV injection (NCT05912049).
ANG-3070, an oral tyrosine kinase inhibitor targeting platelet-derived growth factor (PDGFR) alpha and beta (NCT05387785).
C106, an angiotensin II type 2 receptor agonist (NCT05427253).
HuL001, which targets alpha-enolase (NCT04540770).
LTI-03, a Caveolin-1 (Cav1)-related peptide designed to restore Cav1 expression in lung tissue (NCT05954988).
ORIN1001, a first-in-class small molecule that selectively blocks the inositol requiring enzyme 1alphase (IRE1) RNAse and blocks X-box binding protein 1 (XBP1) activation (NCT04643769).
PRS-220 is an orally inhaled anticalin protein targeting connective tissue growth factor (CTGF) (NTC05473533).
TRK-250, a single-strand, long-chain nucleic acid that selectively suppresses expression of transforming growth factor-beta 1 (TGF-beta1) protein (NCT03727802).
“While we have therapies that we’re able to give patients, we need to do more and we need to do better,” Dr. Lee said. “We’re all hopeful the next phase 3 clinical trial will be something that will help change the treatment paradigm for our patients. We’re very patient, and hopefully those that are interested in improving this treatment landscape will continue to persist.”
Dr. Lee disclosed financial relationships with Boehringer Ingelheim, Pliant Therapeutics, Blade Therapeutics, United Therapeutics, Eleven P15. and Avalyn Pharma.
Short, long-lasting bronchodilators similar for exacerbated COPD
HONOLULU – in safety and efficacy to a short-acting combination of albuterol and ipratropium.
The 2023 Gold Report on prevention, management, and diagnosis of COPD recommended switching to long-acting bronchodilators despite a lack of clinical evidence showing safety in patients hospitalized for COPD exacerbation, according to Rajiv Dhand, MD, who presented the new study at the annual meeting of the American College of Chest Physicians (CHEST).
“We wanted to establish the safety, because long-acting agents are approved only for use in nonhospitalized patients. We established that it was safe and that it was comparably effective, but you could give 30% lower doses. Patients don’t have to be woken up to get the medication, and there’s a better chance that all the doses will be administered to these patients. So I think that it provides convenience with similar efficacy and safety,” said Dr. Dhand, a pulmonologist and professor of medicine at the University of Tennessee, Knoxville.
The researchers randomized 60 patients to receive nebulized albuterol (2.5 mg) and ipratropium (0.5 mg) every 6 hours (short-acting group) or nebulized formoterol (20 mcg) every 12 hours and revefenacin (175 mcg) every 24 hours (long-acting group). The mean age was 63.2 years, 58.3% were male, and 65% were current smokers.
The median decrease between day 1 and day 3 in the Modified Borg Dyspnea score was 4.0 in the long-acting group (P < .001), and 2.0 in the short-acting group, though the latter was not statistically significant (P = .134). Both groups had a decrease in supplemental oxygen requirement, with no difference between the two groups. There was also no difference in the number of respiratory visits for rescue therapy.
Respiratory therapists in the audience welcomed the new evidence. “As a respiratory therapist, I feel that we should move away from giving good short acting [therapies] ... the new guidelines state that we should move away from them, but I think that physicians in general have not gone that way. The way that we’re working, giving short acting every four hours – I don’t see that it’s a benefit to our patients,” said Sharon Armstead, who attended the session and was asked to comment on the study. She is a respiratory therapist at Ascension Health and an instructor at Concordia University, Austin, Texas. Ms. Armstead has asthma, and has first-hand experience as a patient when respiratory therapists are unable to attend to the patient every 4 hours.
She suggested that continued use of short-acting therapies may be due to inertia. “It’s easier [for a physician] to click a button on [a computer screen] than to actually slow down and write the order. If we need a rescue, then we’ll call for a rescue,” Ms. Armstead said.
She anticipates that long-acting therapies will ultimately lead to better outcomes because they will increase the time that respiratory therapists can spend with patients. “That’s what we really want to do. We want to spend time with our patients and stay there and watch our patients. But if you’re just telling us to [administer a therapy] every 4 hours, it’s not really giving the patient what they need.”
Specifically, there were concerns about cardiovascular safety, but the researchers found no between-group differences.
Asked for comment, session co-moderator Brittany Duchene, MD remarked: “It’s super interesting, but I worry about the cost. From a practical perspective, it’s challenging to get those drugs placed on an outpatient basis. They are very expensive, and they’re newer [drugs], but I think overall it’s good to give less,” said Dr. Duchene, a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
A potential concern raised by one audience member is that some patients are used to frequent treatment and may grow anxious with less frequent therapy. “I think we just need some reeducation that this is like a long-acting medicine. It also decreases the burden on our respiratory therapists, which is very good,” said Dr. Duchene.
The study was funded by Mylan/Theravance Biopharma. Dr. Dhand has received research support from Theravance, Mylan, and Viatris. He has received honoraria from Teva and UpToDate. Ms. Armstead and Dr. Duchene have no relevant financial disclosures.
HONOLULU – in safety and efficacy to a short-acting combination of albuterol and ipratropium.
The 2023 Gold Report on prevention, management, and diagnosis of COPD recommended switching to long-acting bronchodilators despite a lack of clinical evidence showing safety in patients hospitalized for COPD exacerbation, according to Rajiv Dhand, MD, who presented the new study at the annual meeting of the American College of Chest Physicians (CHEST).
“We wanted to establish the safety, because long-acting agents are approved only for use in nonhospitalized patients. We established that it was safe and that it was comparably effective, but you could give 30% lower doses. Patients don’t have to be woken up to get the medication, and there’s a better chance that all the doses will be administered to these patients. So I think that it provides convenience with similar efficacy and safety,” said Dr. Dhand, a pulmonologist and professor of medicine at the University of Tennessee, Knoxville.
The researchers randomized 60 patients to receive nebulized albuterol (2.5 mg) and ipratropium (0.5 mg) every 6 hours (short-acting group) or nebulized formoterol (20 mcg) every 12 hours and revefenacin (175 mcg) every 24 hours (long-acting group). The mean age was 63.2 years, 58.3% were male, and 65% were current smokers.
The median decrease between day 1 and day 3 in the Modified Borg Dyspnea score was 4.0 in the long-acting group (P < .001), and 2.0 in the short-acting group, though the latter was not statistically significant (P = .134). Both groups had a decrease in supplemental oxygen requirement, with no difference between the two groups. There was also no difference in the number of respiratory visits for rescue therapy.
Respiratory therapists in the audience welcomed the new evidence. “As a respiratory therapist, I feel that we should move away from giving good short acting [therapies] ... the new guidelines state that we should move away from them, but I think that physicians in general have not gone that way. The way that we’re working, giving short acting every four hours – I don’t see that it’s a benefit to our patients,” said Sharon Armstead, who attended the session and was asked to comment on the study. She is a respiratory therapist at Ascension Health and an instructor at Concordia University, Austin, Texas. Ms. Armstead has asthma, and has first-hand experience as a patient when respiratory therapists are unable to attend to the patient every 4 hours.
She suggested that continued use of short-acting therapies may be due to inertia. “It’s easier [for a physician] to click a button on [a computer screen] than to actually slow down and write the order. If we need a rescue, then we’ll call for a rescue,” Ms. Armstead said.
She anticipates that long-acting therapies will ultimately lead to better outcomes because they will increase the time that respiratory therapists can spend with patients. “That’s what we really want to do. We want to spend time with our patients and stay there and watch our patients. But if you’re just telling us to [administer a therapy] every 4 hours, it’s not really giving the patient what they need.”
Specifically, there were concerns about cardiovascular safety, but the researchers found no between-group differences.
Asked for comment, session co-moderator Brittany Duchene, MD remarked: “It’s super interesting, but I worry about the cost. From a practical perspective, it’s challenging to get those drugs placed on an outpatient basis. They are very expensive, and they’re newer [drugs], but I think overall it’s good to give less,” said Dr. Duchene, a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
A potential concern raised by one audience member is that some patients are used to frequent treatment and may grow anxious with less frequent therapy. “I think we just need some reeducation that this is like a long-acting medicine. It also decreases the burden on our respiratory therapists, which is very good,” said Dr. Duchene.
The study was funded by Mylan/Theravance Biopharma. Dr. Dhand has received research support from Theravance, Mylan, and Viatris. He has received honoraria from Teva and UpToDate. Ms. Armstead and Dr. Duchene have no relevant financial disclosures.
HONOLULU – in safety and efficacy to a short-acting combination of albuterol and ipratropium.
The 2023 Gold Report on prevention, management, and diagnosis of COPD recommended switching to long-acting bronchodilators despite a lack of clinical evidence showing safety in patients hospitalized for COPD exacerbation, according to Rajiv Dhand, MD, who presented the new study at the annual meeting of the American College of Chest Physicians (CHEST).
“We wanted to establish the safety, because long-acting agents are approved only for use in nonhospitalized patients. We established that it was safe and that it was comparably effective, but you could give 30% lower doses. Patients don’t have to be woken up to get the medication, and there’s a better chance that all the doses will be administered to these patients. So I think that it provides convenience with similar efficacy and safety,” said Dr. Dhand, a pulmonologist and professor of medicine at the University of Tennessee, Knoxville.
The researchers randomized 60 patients to receive nebulized albuterol (2.5 mg) and ipratropium (0.5 mg) every 6 hours (short-acting group) or nebulized formoterol (20 mcg) every 12 hours and revefenacin (175 mcg) every 24 hours (long-acting group). The mean age was 63.2 years, 58.3% were male, and 65% were current smokers.
The median decrease between day 1 and day 3 in the Modified Borg Dyspnea score was 4.0 in the long-acting group (P < .001), and 2.0 in the short-acting group, though the latter was not statistically significant (P = .134). Both groups had a decrease in supplemental oxygen requirement, with no difference between the two groups. There was also no difference in the number of respiratory visits for rescue therapy.
Respiratory therapists in the audience welcomed the new evidence. “As a respiratory therapist, I feel that we should move away from giving good short acting [therapies] ... the new guidelines state that we should move away from them, but I think that physicians in general have not gone that way. The way that we’re working, giving short acting every four hours – I don’t see that it’s a benefit to our patients,” said Sharon Armstead, who attended the session and was asked to comment on the study. She is a respiratory therapist at Ascension Health and an instructor at Concordia University, Austin, Texas. Ms. Armstead has asthma, and has first-hand experience as a patient when respiratory therapists are unable to attend to the patient every 4 hours.
She suggested that continued use of short-acting therapies may be due to inertia. “It’s easier [for a physician] to click a button on [a computer screen] than to actually slow down and write the order. If we need a rescue, then we’ll call for a rescue,” Ms. Armstead said.
She anticipates that long-acting therapies will ultimately lead to better outcomes because they will increase the time that respiratory therapists can spend with patients. “That’s what we really want to do. We want to spend time with our patients and stay there and watch our patients. But if you’re just telling us to [administer a therapy] every 4 hours, it’s not really giving the patient what they need.”
Specifically, there were concerns about cardiovascular safety, but the researchers found no between-group differences.
Asked for comment, session co-moderator Brittany Duchene, MD remarked: “It’s super interesting, but I worry about the cost. From a practical perspective, it’s challenging to get those drugs placed on an outpatient basis. They are very expensive, and they’re newer [drugs], but I think overall it’s good to give less,” said Dr. Duchene, a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
A potential concern raised by one audience member is that some patients are used to frequent treatment and may grow anxious with less frequent therapy. “I think we just need some reeducation that this is like a long-acting medicine. It also decreases the burden on our respiratory therapists, which is very good,” said Dr. Duchene.
The study was funded by Mylan/Theravance Biopharma. Dr. Dhand has received research support from Theravance, Mylan, and Viatris. He has received honoraria from Teva and UpToDate. Ms. Armstead and Dr. Duchene have no relevant financial disclosures.
AT CHEST 2023
Respiratory infections, asthma rise before type 2 diabetes
HAMBURG, GERMANY – , shows a longitudinal study looking at comorbidities both 25 years before and 25 years after a type 2 diabetes diagnosis.
About 40% of people had respiratory tract infections at the time of diagnosis with type 2 diabetes, compared with 4% who were not diagnosed. Likewise, ear, nose, and throat infections were present in 20% of people at type 2 diabetes diagnosis, compared with around 2% who were not diagnosed. A similar pattern was seen with asthma.
Taken together, the data suggest that subacute inflammation manifesting in asthma as well as the onset of asthma or an acute infection may be a precursor to a type 2 diabetes diagnosis.
“We have also found that in the years prior to diagnosis, there are associations with infections and inflammatory disorders to a much greater degree than in those people who do not get a diabetes diagnosis but who have very similar demographics,” Adrian Heald, MD, study lead and diabetes consultant from Salford (England) Royal Hospital, said in an interview.
Five years prior to diagnosis, respiratory tract infections were documented in around 23% of patients who were later diagnosed with type 2 diabetes versus 2.5% in those not diagnosed, and a similar pattern was seen for ear, nose, and throat infections and asthma. The findings suggest that patients reporting infections, in addition to other known risk factors for type 2 diabetes, might benefit from diabetes tests and early interventions, if needed.
“These novel insights offer a fascinating and fresh perspective on the onset and natural progression to type 2 diabetes and beyond, suggesting an early phase of inflammation-related disease activity long before any clinical diagnosis of type 2 diabetes is made.”
Dr. Heald points out that clinicians may intervene to stave off progression to a type 2 diabetes diagnosis in at risk patients. “At this point, an intervention could relate to lifestyle changes and involve highlighting to the patient that the morbidity they have already accumulated is suggestive of diabetes risk,” he said, adding that, “they may have dyslipidemia, hypertension, and most often excess weight so annual checks of their HbA1c, weight management, and blood pressure would need checking,” he explained.
Moderator Coen Stehouwer, MD, professor of internal medicine at Maastricht University, the Netherlands, commented, “Before clinical diagnosis of type 2 diabetes there is often a lengthy period of undiagnosed disease and before that, prediabetes, because glucose can be abnormal up to 10 years prior to clinical diagnosis.”
But he added that, “It’s not entirely clear whether the rise seen before clinical diagnosis in this study correlates with undiagnosed diabetes or prediabetes or even if it precedes type 2 diabetes – it might be because inflammation is a common origin for type 2 diabetes and various comorbidities. This might explain how they go together.”
Longitudinal study 25 years before and 25 years after type 2 diagnosis
Dr. Heald presented the findings at a session on inflammation in diabetes at the annual meeting of the European Association for the Study of Diabetes. The work was also published in Diabetes Therapy.
The researchers wanted to investigate the pattern of comorbidities in the years and decades prior to a diagnosis of type 2 diabetes as well as after: “With the database we used, called DARE [Diabetes Alliance for Research in England], we are able to explore phenomena longitudinally going right back to the beginning of their digital health records, looking at phenotypes over time.”
By mapping significant health issues in people who went on to develop type 2 diabetes alongside those that did not, Dr. Heald managed to develop a continuum spanning 25 years prior and 25 years after diagnosis of type 2 diabetes. The researchers also examined relationships between sociodemographic factors and longitudinal health outcomes of relevance to cardiac conditions and lower respiratory tract infections. His talk in Hamburg primarily addressed clinical phenotypes before the point of diagnosis.
Data were drawn from 1,932 people with (1,196) and without (736) type 2 diabetes. Participants in both groups were aged 66-67 years, 43%-46% were women, age at diagnosis was 50-52 years, and participants lived in Greater Manchester, United Kingdom.
In the years leading up to type 2 diagnosis, individuals consistently exhibited a considerable increase in several clinical phenotypes, reported Dr. Heald. Of note, he added, “immediately prior to type 2 diagnosis, there was a significantly greater proportion of hypertension at 35%, respiratory tract infection at 34%, heart disease at 17%, ear, nose, and throat infection at 19%, and asthma at 12%. And by comparison, the corresponding disease trajectory in matched controls was much less dramatic.”
“There is a huge difference in people who went on to receive a diagnosis of type 2 diabetes and those who did not, and not just what we’d expect – so hypertension for example or manifestations of renal disease, but importantly inflammatory disorders are more common,” he emphasized.
In addition, a larger signal for ischemic heart disease was seen just before type 2 diabetes diagnosis.
These data suggest that longitudinal clinical histories prior to a diagnosis of type 2 diabetes might offer new information, both genetic and nongenetic, about development of type 2 diabetes in relation to comorbidities.
After type 2 diabetes diagnosis, the proportion of people exhibiting coronary artery disease, hypertension, chronic kidney disease, retinopathy, and infections climbed rapidly before plateauing, reported Dr. Heald. “We also know that individuals with coronary artery disease are more highly represented in socially disadvantaged groups, and this is borne out in the data at 25 years prior and after type 2 diagnosis.”
Dr. Heald has received speaker fees or contributed to advisory boards from Lilly, AstraZeneca, Janssen, Bristol-Myers Squibb, Besins, Bayer, Sanofi, and Recordati. Research grants from Novo Nordisk, Pfizer, and Besins. Professor Stehouwer has declared no relevant conflicts.
A version of this article first appeared on Medscape.com.
HAMBURG, GERMANY – , shows a longitudinal study looking at comorbidities both 25 years before and 25 years after a type 2 diabetes diagnosis.
About 40% of people had respiratory tract infections at the time of diagnosis with type 2 diabetes, compared with 4% who were not diagnosed. Likewise, ear, nose, and throat infections were present in 20% of people at type 2 diabetes diagnosis, compared with around 2% who were not diagnosed. A similar pattern was seen with asthma.
Taken together, the data suggest that subacute inflammation manifesting in asthma as well as the onset of asthma or an acute infection may be a precursor to a type 2 diabetes diagnosis.
“We have also found that in the years prior to diagnosis, there are associations with infections and inflammatory disorders to a much greater degree than in those people who do not get a diabetes diagnosis but who have very similar demographics,” Adrian Heald, MD, study lead and diabetes consultant from Salford (England) Royal Hospital, said in an interview.
Five years prior to diagnosis, respiratory tract infections were documented in around 23% of patients who were later diagnosed with type 2 diabetes versus 2.5% in those not diagnosed, and a similar pattern was seen for ear, nose, and throat infections and asthma. The findings suggest that patients reporting infections, in addition to other known risk factors for type 2 diabetes, might benefit from diabetes tests and early interventions, if needed.
“These novel insights offer a fascinating and fresh perspective on the onset and natural progression to type 2 diabetes and beyond, suggesting an early phase of inflammation-related disease activity long before any clinical diagnosis of type 2 diabetes is made.”
Dr. Heald points out that clinicians may intervene to stave off progression to a type 2 diabetes diagnosis in at risk patients. “At this point, an intervention could relate to lifestyle changes and involve highlighting to the patient that the morbidity they have already accumulated is suggestive of diabetes risk,” he said, adding that, “they may have dyslipidemia, hypertension, and most often excess weight so annual checks of their HbA1c, weight management, and blood pressure would need checking,” he explained.
Moderator Coen Stehouwer, MD, professor of internal medicine at Maastricht University, the Netherlands, commented, “Before clinical diagnosis of type 2 diabetes there is often a lengthy period of undiagnosed disease and before that, prediabetes, because glucose can be abnormal up to 10 years prior to clinical diagnosis.”
But he added that, “It’s not entirely clear whether the rise seen before clinical diagnosis in this study correlates with undiagnosed diabetes or prediabetes or even if it precedes type 2 diabetes – it might be because inflammation is a common origin for type 2 diabetes and various comorbidities. This might explain how they go together.”
Longitudinal study 25 years before and 25 years after type 2 diagnosis
Dr. Heald presented the findings at a session on inflammation in diabetes at the annual meeting of the European Association for the Study of Diabetes. The work was also published in Diabetes Therapy.
The researchers wanted to investigate the pattern of comorbidities in the years and decades prior to a diagnosis of type 2 diabetes as well as after: “With the database we used, called DARE [Diabetes Alliance for Research in England], we are able to explore phenomena longitudinally going right back to the beginning of their digital health records, looking at phenotypes over time.”
By mapping significant health issues in people who went on to develop type 2 diabetes alongside those that did not, Dr. Heald managed to develop a continuum spanning 25 years prior and 25 years after diagnosis of type 2 diabetes. The researchers also examined relationships between sociodemographic factors and longitudinal health outcomes of relevance to cardiac conditions and lower respiratory tract infections. His talk in Hamburg primarily addressed clinical phenotypes before the point of diagnosis.
Data were drawn from 1,932 people with (1,196) and without (736) type 2 diabetes. Participants in both groups were aged 66-67 years, 43%-46% were women, age at diagnosis was 50-52 years, and participants lived in Greater Manchester, United Kingdom.
In the years leading up to type 2 diagnosis, individuals consistently exhibited a considerable increase in several clinical phenotypes, reported Dr. Heald. Of note, he added, “immediately prior to type 2 diagnosis, there was a significantly greater proportion of hypertension at 35%, respiratory tract infection at 34%, heart disease at 17%, ear, nose, and throat infection at 19%, and asthma at 12%. And by comparison, the corresponding disease trajectory in matched controls was much less dramatic.”
“There is a huge difference in people who went on to receive a diagnosis of type 2 diabetes and those who did not, and not just what we’d expect – so hypertension for example or manifestations of renal disease, but importantly inflammatory disorders are more common,” he emphasized.
In addition, a larger signal for ischemic heart disease was seen just before type 2 diabetes diagnosis.
These data suggest that longitudinal clinical histories prior to a diagnosis of type 2 diabetes might offer new information, both genetic and nongenetic, about development of type 2 diabetes in relation to comorbidities.
After type 2 diabetes diagnosis, the proportion of people exhibiting coronary artery disease, hypertension, chronic kidney disease, retinopathy, and infections climbed rapidly before plateauing, reported Dr. Heald. “We also know that individuals with coronary artery disease are more highly represented in socially disadvantaged groups, and this is borne out in the data at 25 years prior and after type 2 diagnosis.”
Dr. Heald has received speaker fees or contributed to advisory boards from Lilly, AstraZeneca, Janssen, Bristol-Myers Squibb, Besins, Bayer, Sanofi, and Recordati. Research grants from Novo Nordisk, Pfizer, and Besins. Professor Stehouwer has declared no relevant conflicts.
A version of this article first appeared on Medscape.com.
HAMBURG, GERMANY – , shows a longitudinal study looking at comorbidities both 25 years before and 25 years after a type 2 diabetes diagnosis.
About 40% of people had respiratory tract infections at the time of diagnosis with type 2 diabetes, compared with 4% who were not diagnosed. Likewise, ear, nose, and throat infections were present in 20% of people at type 2 diabetes diagnosis, compared with around 2% who were not diagnosed. A similar pattern was seen with asthma.
Taken together, the data suggest that subacute inflammation manifesting in asthma as well as the onset of asthma or an acute infection may be a precursor to a type 2 diabetes diagnosis.
“We have also found that in the years prior to diagnosis, there are associations with infections and inflammatory disorders to a much greater degree than in those people who do not get a diabetes diagnosis but who have very similar demographics,” Adrian Heald, MD, study lead and diabetes consultant from Salford (England) Royal Hospital, said in an interview.
Five years prior to diagnosis, respiratory tract infections were documented in around 23% of patients who were later diagnosed with type 2 diabetes versus 2.5% in those not diagnosed, and a similar pattern was seen for ear, nose, and throat infections and asthma. The findings suggest that patients reporting infections, in addition to other known risk factors for type 2 diabetes, might benefit from diabetes tests and early interventions, if needed.
“These novel insights offer a fascinating and fresh perspective on the onset and natural progression to type 2 diabetes and beyond, suggesting an early phase of inflammation-related disease activity long before any clinical diagnosis of type 2 diabetes is made.”
Dr. Heald points out that clinicians may intervene to stave off progression to a type 2 diabetes diagnosis in at risk patients. “At this point, an intervention could relate to lifestyle changes and involve highlighting to the patient that the morbidity they have already accumulated is suggestive of diabetes risk,” he said, adding that, “they may have dyslipidemia, hypertension, and most often excess weight so annual checks of their HbA1c, weight management, and blood pressure would need checking,” he explained.
Moderator Coen Stehouwer, MD, professor of internal medicine at Maastricht University, the Netherlands, commented, “Before clinical diagnosis of type 2 diabetes there is often a lengthy period of undiagnosed disease and before that, prediabetes, because glucose can be abnormal up to 10 years prior to clinical diagnosis.”
But he added that, “It’s not entirely clear whether the rise seen before clinical diagnosis in this study correlates with undiagnosed diabetes or prediabetes or even if it precedes type 2 diabetes – it might be because inflammation is a common origin for type 2 diabetes and various comorbidities. This might explain how they go together.”
Longitudinal study 25 years before and 25 years after type 2 diagnosis
Dr. Heald presented the findings at a session on inflammation in diabetes at the annual meeting of the European Association for the Study of Diabetes. The work was also published in Diabetes Therapy.
The researchers wanted to investigate the pattern of comorbidities in the years and decades prior to a diagnosis of type 2 diabetes as well as after: “With the database we used, called DARE [Diabetes Alliance for Research in England], we are able to explore phenomena longitudinally going right back to the beginning of their digital health records, looking at phenotypes over time.”
By mapping significant health issues in people who went on to develop type 2 diabetes alongside those that did not, Dr. Heald managed to develop a continuum spanning 25 years prior and 25 years after diagnosis of type 2 diabetes. The researchers also examined relationships between sociodemographic factors and longitudinal health outcomes of relevance to cardiac conditions and lower respiratory tract infections. His talk in Hamburg primarily addressed clinical phenotypes before the point of diagnosis.
Data were drawn from 1,932 people with (1,196) and without (736) type 2 diabetes. Participants in both groups were aged 66-67 years, 43%-46% were women, age at diagnosis was 50-52 years, and participants lived in Greater Manchester, United Kingdom.
In the years leading up to type 2 diagnosis, individuals consistently exhibited a considerable increase in several clinical phenotypes, reported Dr. Heald. Of note, he added, “immediately prior to type 2 diagnosis, there was a significantly greater proportion of hypertension at 35%, respiratory tract infection at 34%, heart disease at 17%, ear, nose, and throat infection at 19%, and asthma at 12%. And by comparison, the corresponding disease trajectory in matched controls was much less dramatic.”
“There is a huge difference in people who went on to receive a diagnosis of type 2 diabetes and those who did not, and not just what we’d expect – so hypertension for example or manifestations of renal disease, but importantly inflammatory disorders are more common,” he emphasized.
In addition, a larger signal for ischemic heart disease was seen just before type 2 diabetes diagnosis.
These data suggest that longitudinal clinical histories prior to a diagnosis of type 2 diabetes might offer new information, both genetic and nongenetic, about development of type 2 diabetes in relation to comorbidities.
After type 2 diabetes diagnosis, the proportion of people exhibiting coronary artery disease, hypertension, chronic kidney disease, retinopathy, and infections climbed rapidly before plateauing, reported Dr. Heald. “We also know that individuals with coronary artery disease are more highly represented in socially disadvantaged groups, and this is borne out in the data at 25 years prior and after type 2 diagnosis.”
Dr. Heald has received speaker fees or contributed to advisory boards from Lilly, AstraZeneca, Janssen, Bristol-Myers Squibb, Besins, Bayer, Sanofi, and Recordati. Research grants from Novo Nordisk, Pfizer, and Besins. Professor Stehouwer has declared no relevant conflicts.
A version of this article first appeared on Medscape.com.
AT EASD 2023
Progressive Pulmonary Fibrosis: Understanding Its Many Forms
- Raghu G et al. Am J Respir Crit Care Med. 2022;205(9):e18-e47. doi:10.1164/rccm.202202-0399ST
- Cottin V et al. Front Med (Lausanne). 2022;9:799912. doi:10.3389/fmed.2022.799912
- Molina-Molina M et al. Expert Rev Respir Med. 2022;16(7):765-774. doi:10.1080/17476348.2022.2107508
- Cottin V. Am J Respir Crit Care Med. 2023;207(1):11-13. doi:10.1164/rccm.202208-1639ED
- Wijsenbeek M, Cottin V. N Engl J Med. 2020;383(10):958-968. doi:10.1056/NEJMra2005230
- Chiu YH et al. Front Med (Lausanne). 2023;10:1106560. doi:10.3389/fmed.2023.1106560
- Wong AW et al. BMC Pulm Med. 2022;22(1):148. doi:10.1186/s12890-022-01922-2
- Raghu G et al. Am J Respir Crit Care Med. 2022;205(9):e18-e47. doi:10.1164/rccm.202202-0399ST
- Cottin V et al. Front Med (Lausanne). 2022;9:799912. doi:10.3389/fmed.2022.799912
- Molina-Molina M et al. Expert Rev Respir Med. 2022;16(7):765-774. doi:10.1080/17476348.2022.2107508
- Cottin V. Am J Respir Crit Care Med. 2023;207(1):11-13. doi:10.1164/rccm.202208-1639ED
- Wijsenbeek M, Cottin V. N Engl J Med. 2020;383(10):958-968. doi:10.1056/NEJMra2005230
- Chiu YH et al. Front Med (Lausanne). 2023;10:1106560. doi:10.3389/fmed.2023.1106560
- Wong AW et al. BMC Pulm Med. 2022;22(1):148. doi:10.1186/s12890-022-01922-2
- Raghu G et al. Am J Respir Crit Care Med. 2022;205(9):e18-e47. doi:10.1164/rccm.202202-0399ST
- Cottin V et al. Front Med (Lausanne). 2022;9:799912. doi:10.3389/fmed.2022.799912
- Molina-Molina M et al. Expert Rev Respir Med. 2022;16(7):765-774. doi:10.1080/17476348.2022.2107508
- Cottin V. Am J Respir Crit Care Med. 2023;207(1):11-13. doi:10.1164/rccm.202208-1639ED
- Wijsenbeek M, Cottin V. N Engl J Med. 2020;383(10):958-968. doi:10.1056/NEJMra2005230
- Chiu YH et al. Front Med (Lausanne). 2023;10:1106560. doi:10.3389/fmed.2023.1106560
- Wong AW et al. BMC Pulm Med. 2022;22(1):148. doi:10.1186/s12890-022-01922-2
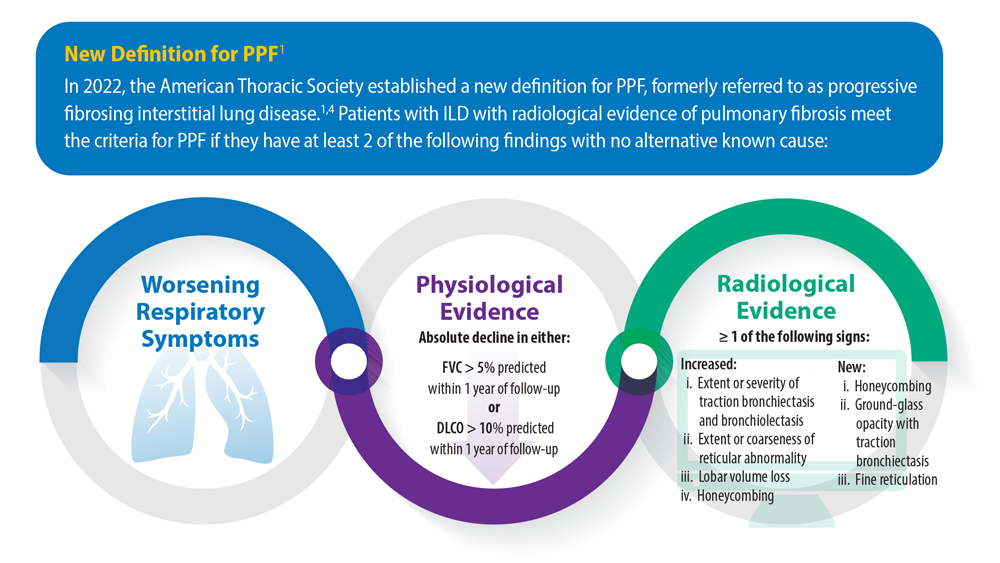
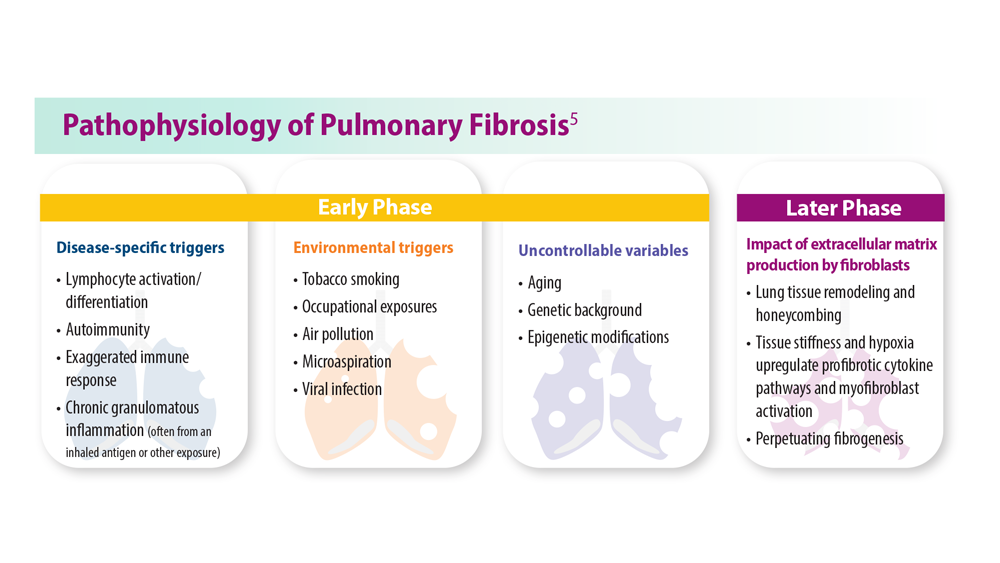
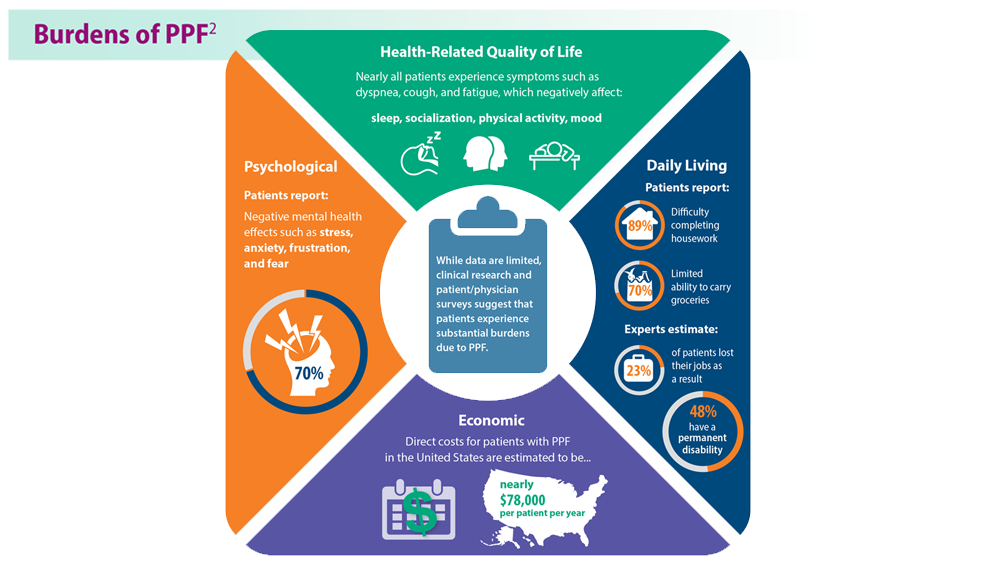
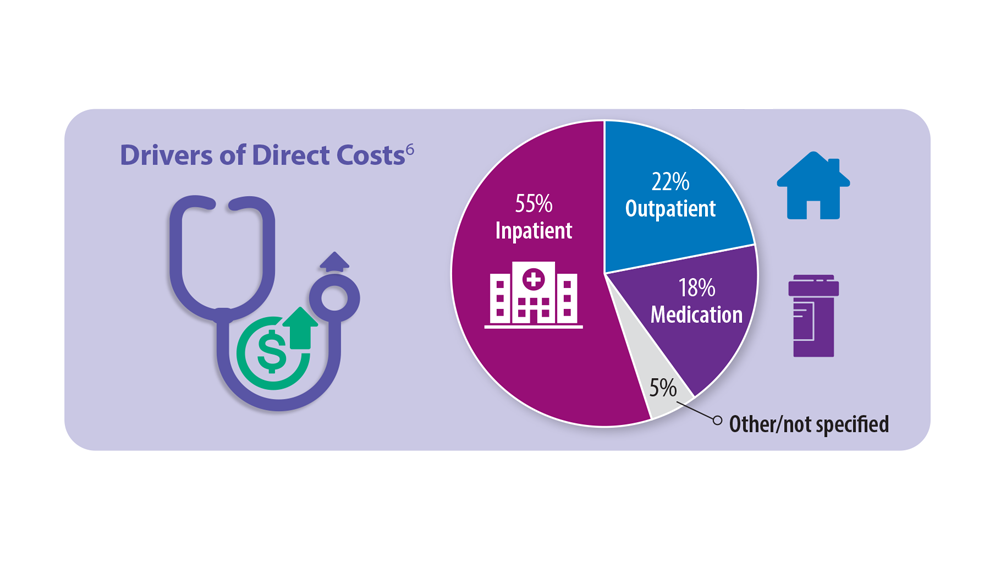
Long COVID: Advocating for Patients and Implementing Effective Techniques
1. Lutchmansingh DD et al. Semin Respir Crit Care Med. 2023;44(1):130-142. doi:10.1055/s-0042-1759568
2. Davis HE et al. Nat Rev Microbiol. 2023;21(3):133-146. doi:10.1038/s41579-022-00846-2
3. Ahmed H et al. J Rehabil Med. 2020;52(5):jrm00063. doi:10.2340/16501977-2694
4. Resources. Long COVID Physio. Accessed May 31, 2023. https://longcovid.physio/resources
5. Long COVID: What do the latest data show? KFF. Published January 26, 2023. Accessed May 31, 2023. https://www.kff.org/policy-watch/long-covid-what-do-latest-data-show/
6. Castanares-Zapatero D et al. Ann Med. 2022;54(1):1473-1487. doi:10.1080/07853890.2022.2076901
7. Mehandru S, Merad M. Nat Immunol. 2022;23(2):194-202. doi:10.1038/s41590-021-01104-y
8. Dhooria S et al. Eur Respir J. 2022;59(2):2102930. doi:10.1183/13993003.02930-2021
9. Researching COVID to enhance recovery. RECOVER. Accessed May 31, 2023. https://recovercovid.org/
1. Lutchmansingh DD et al. Semin Respir Crit Care Med. 2023;44(1):130-142. doi:10.1055/s-0042-1759568
2. Davis HE et al. Nat Rev Microbiol. 2023;21(3):133-146. doi:10.1038/s41579-022-00846-2
3. Ahmed H et al. J Rehabil Med. 2020;52(5):jrm00063. doi:10.2340/16501977-2694
4. Resources. Long COVID Physio. Accessed May 31, 2023. https://longcovid.physio/resources
5. Long COVID: What do the latest data show? KFF. Published January 26, 2023. Accessed May 31, 2023. https://www.kff.org/policy-watch/long-covid-what-do-latest-data-show/
6. Castanares-Zapatero D et al. Ann Med. 2022;54(1):1473-1487. doi:10.1080/07853890.2022.2076901
7. Mehandru S, Merad M. Nat Immunol. 2022;23(2):194-202. doi:10.1038/s41590-021-01104-y
8. Dhooria S et al. Eur Respir J. 2022;59(2):2102930. doi:10.1183/13993003.02930-2021
9. Researching COVID to enhance recovery. RECOVER. Accessed May 31, 2023. https://recovercovid.org/
1. Lutchmansingh DD et al. Semin Respir Crit Care Med. 2023;44(1):130-142. doi:10.1055/s-0042-1759568
2. Davis HE et al. Nat Rev Microbiol. 2023;21(3):133-146. doi:10.1038/s41579-022-00846-2
3. Ahmed H et al. J Rehabil Med. 2020;52(5):jrm00063. doi:10.2340/16501977-2694
4. Resources. Long COVID Physio. Accessed May 31, 2023. https://longcovid.physio/resources
5. Long COVID: What do the latest data show? KFF. Published January 26, 2023. Accessed May 31, 2023. https://www.kff.org/policy-watch/long-covid-what-do-latest-data-show/
6. Castanares-Zapatero D et al. Ann Med. 2022;54(1):1473-1487. doi:10.1080/07853890.2022.2076901
7. Mehandru S, Merad M. Nat Immunol. 2022;23(2):194-202. doi:10.1038/s41590-021-01104-y
8. Dhooria S et al. Eur Respir J. 2022;59(2):2102930. doi:10.1183/13993003.02930-2021
9. Researching COVID to enhance recovery. RECOVER. Accessed May 31, 2023. https://recovercovid.org/