User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
New age of CHEST philanthropy to focus on education, impact, community
In a time echoing with the constant call for transformation, CHEST delved deep into its essence, questioning its potential for impact. This pivotal introspection led to a crucial inquiry…
Are we harnessing every opportunity to make a difference?
It’s a familiar question, yet its resonance urged a deeper evaluation.
Philanthropy has long been entwined in CHEST’s identity. Commemorating 25 years of the CHEST Foundation at CHEST 2022 spotlighted our history of generosity. Stories of transformative community initiatives and pivotal clinical research grants narrated a tale of empowered change and fostering healthier communities worldwide.

However, amid these achievements, more pressing inquiries surfaced:
- What unique role can CHEST play?
- Where do unmet needs persist?
- Which causes deeply resonate within our community?
CHEST’s leadership and dedicated staff embarked on a comprehensive review, scrutinizing past triumphs, donor commitments, and the evolving aspirations of our members. Themes of social responsibility, professional diversity, community impact, and expanded partnerships emerged as pivotal points. This extensive process, spanning nearly a year, resembled a reflective pause amid the rapid cadence of change.
Achieving these aspirations meant reimagining our approach, thereby streamlining efforts for maximal impact by…
- Integrating philanthropy as an integral facet of our mission, and amplifying the culture of giving within CHEST
- Consolidating philanthropic initiatives under CHEST to maximize resources for direct, substantial impact
- Defining clear avenues for giving that deeply resonate with our members
With endorsement from the Board of Regents, the CHEST Foundation seamlessly merged into CHEST, inaugurating a new chapter in our philanthropic endeavors.
Central to this transformative shift is the crystallization of our giving strategy, fortified by four pillars: Clinical Research, Community Impact, Support to the Profession, and Dedication to Education. These pillars encapsulate our commitment to nurturing clinicians, supporting trainees, and enhancing patient care.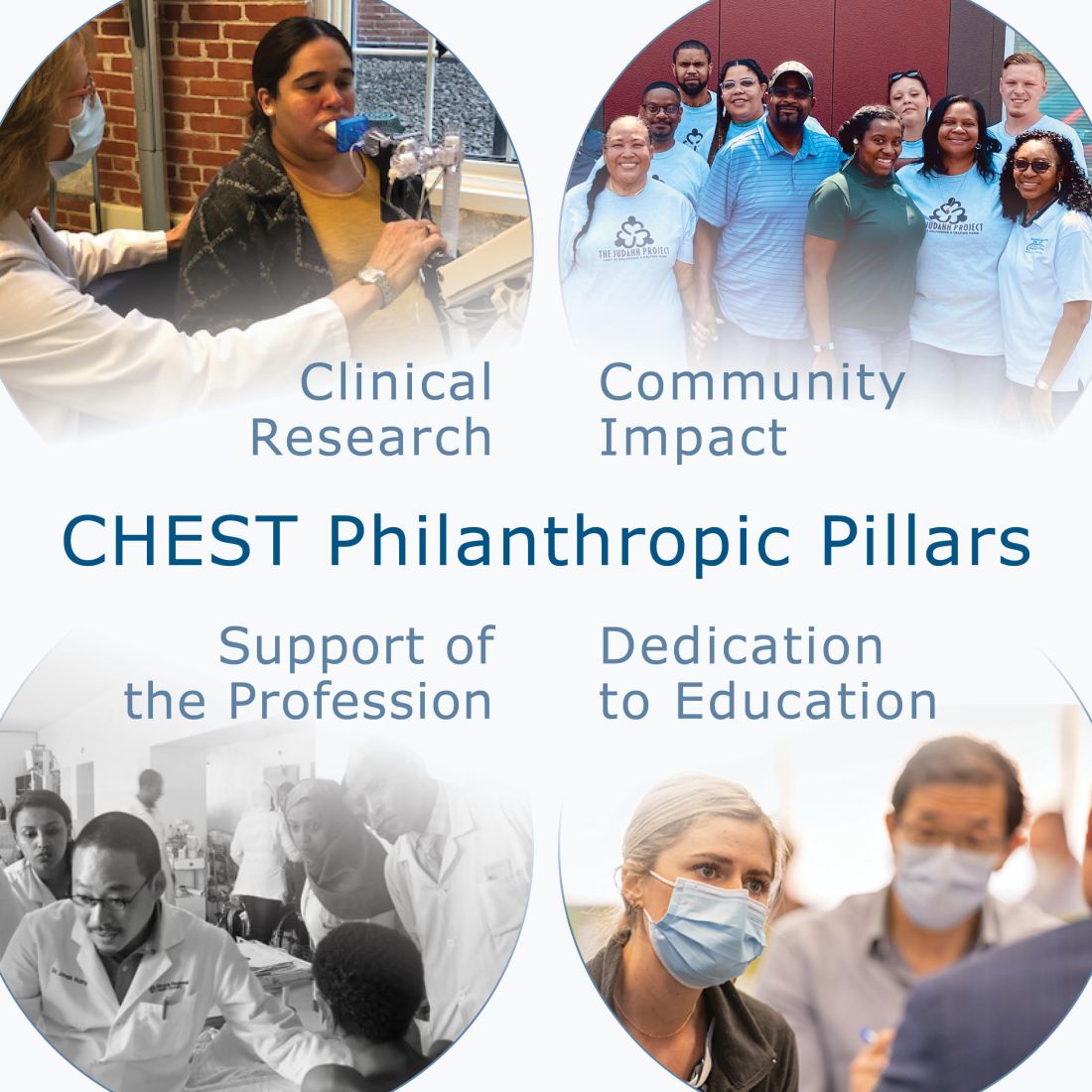
Clinical Research emerges as the cornerstone, transcending boundaries to empower researchers in their pursuit of groundbreaking insights. Through strategic grants, we embolden early career investigators to delve into uncharted territories, unraveling mysteries that underpin advancements in chest medicine. The ripple effect extends beyond labs; it traverses communities, amplifying equitable health care solutions and bridging disparities in patient care. Our commitment to nurturing this pillar springs from the belief that every breakthrough, regardless of scale, is a catalyst for transformative change.
Community Impact extends CHEST’s reach far beyond clinical settings, fostering alliances with local organizations. Together, we forge a tapestry of collaboration, weaving essential services and imparting knowledge on crucial lung health issues into the fabric of diverse communities. This engagement not only elevates awareness but also empowers individuals and communities to take charge of their respiratory well-being. It’s the grassroots unity that amplifies our impact, creating enduring shifts in local landscapes.
Support of the Profession epitomizes our dedication to fortifying the backbone of pulmonary, critical care, and sleep medicine. By offering unparalleled clinical education and mentorship, we empower emerging clinicians from diverse backgrounds with the latest knowledge and resources. Fueling their professional growth is pivotal to nurturing a robust and inclusive cadre of health care professionals, ensuring comprehensive and culturally sensitive care for patients worldwide.
Dedication to Education isn’t just a commitment—it’s a bridge spanning the gap between knowledge and application, patient and clinician. Strengthening this connection involves equipping clinicians with tools for effective communication and partnering with patient-centered organizations. Our focus transcends textbooks; it embodies a relentless pursuit to refine patient-clinician interactions, enhancing patient understanding and, ultimately, elevating their quality of life.
CHEST’s philanthropic evolution signifies not just growth but a resolute commitment to effecting tangible change in chest medicine and patient care. These pillars stand as guiding beacons, steering us toward a future that mirrors our mission, vision, and values. Each pillar represents a pathway to meaningful, enduring change within chest medicine, ensuring a lasting impact on patient well-being.
In a time echoing with the constant call for transformation, CHEST delved deep into its essence, questioning its potential for impact. This pivotal introspection led to a crucial inquiry…
Are we harnessing every opportunity to make a difference?
It’s a familiar question, yet its resonance urged a deeper evaluation.
Philanthropy has long been entwined in CHEST’s identity. Commemorating 25 years of the CHEST Foundation at CHEST 2022 spotlighted our history of generosity. Stories of transformative community initiatives and pivotal clinical research grants narrated a tale of empowered change and fostering healthier communities worldwide.
However, amid these achievements, more pressing inquiries surfaced:
- What unique role can CHEST play?
- Where do unmet needs persist?
- Which causes deeply resonate within our community?
CHEST’s leadership and dedicated staff embarked on a comprehensive review, scrutinizing past triumphs, donor commitments, and the evolving aspirations of our members. Themes of social responsibility, professional diversity, community impact, and expanded partnerships emerged as pivotal points. This extensive process, spanning nearly a year, resembled a reflective pause amid the rapid cadence of change.
Achieving these aspirations meant reimagining our approach, thereby streamlining efforts for maximal impact by…
- Integrating philanthropy as an integral facet of our mission, and amplifying the culture of giving within CHEST
- Consolidating philanthropic initiatives under CHEST to maximize resources for direct, substantial impact
- Defining clear avenues for giving that deeply resonate with our members
With endorsement from the Board of Regents, the CHEST Foundation seamlessly merged into CHEST, inaugurating a new chapter in our philanthropic endeavors.
Central to this transformative shift is the crystallization of our giving strategy, fortified by four pillars: Clinical Research, Community Impact, Support to the Profession, and Dedication to Education. These pillars encapsulate our commitment to nurturing clinicians, supporting trainees, and enhancing patient care.
Clinical Research emerges as the cornerstone, transcending boundaries to empower researchers in their pursuit of groundbreaking insights. Through strategic grants, we embolden early career investigators to delve into uncharted territories, unraveling mysteries that underpin advancements in chest medicine. The ripple effect extends beyond labs; it traverses communities, amplifying equitable health care solutions and bridging disparities in patient care. Our commitment to nurturing this pillar springs from the belief that every breakthrough, regardless of scale, is a catalyst for transformative change.
Community Impact extends CHEST’s reach far beyond clinical settings, fostering alliances with local organizations. Together, we forge a tapestry of collaboration, weaving essential services and imparting knowledge on crucial lung health issues into the fabric of diverse communities. This engagement not only elevates awareness but also empowers individuals and communities to take charge of their respiratory well-being. It’s the grassroots unity that amplifies our impact, creating enduring shifts in local landscapes.
Support of the Profession epitomizes our dedication to fortifying the backbone of pulmonary, critical care, and sleep medicine. By offering unparalleled clinical education and mentorship, we empower emerging clinicians from diverse backgrounds with the latest knowledge and resources. Fueling their professional growth is pivotal to nurturing a robust and inclusive cadre of health care professionals, ensuring comprehensive and culturally sensitive care for patients worldwide.
Dedication to Education isn’t just a commitment—it’s a bridge spanning the gap between knowledge and application, patient and clinician. Strengthening this connection involves equipping clinicians with tools for effective communication and partnering with patient-centered organizations. Our focus transcends textbooks; it embodies a relentless pursuit to refine patient-clinician interactions, enhancing patient understanding and, ultimately, elevating their quality of life.
CHEST’s philanthropic evolution signifies not just growth but a resolute commitment to effecting tangible change in chest medicine and patient care. These pillars stand as guiding beacons, steering us toward a future that mirrors our mission, vision, and values. Each pillar represents a pathway to meaningful, enduring change within chest medicine, ensuring a lasting impact on patient well-being.
In a time echoing with the constant call for transformation, CHEST delved deep into its essence, questioning its potential for impact. This pivotal introspection led to a crucial inquiry…
Are we harnessing every opportunity to make a difference?
It’s a familiar question, yet its resonance urged a deeper evaluation.
Philanthropy has long been entwined in CHEST’s identity. Commemorating 25 years of the CHEST Foundation at CHEST 2022 spotlighted our history of generosity. Stories of transformative community initiatives and pivotal clinical research grants narrated a tale of empowered change and fostering healthier communities worldwide.
However, amid these achievements, more pressing inquiries surfaced:
- What unique role can CHEST play?
- Where do unmet needs persist?
- Which causes deeply resonate within our community?
CHEST’s leadership and dedicated staff embarked on a comprehensive review, scrutinizing past triumphs, donor commitments, and the evolving aspirations of our members. Themes of social responsibility, professional diversity, community impact, and expanded partnerships emerged as pivotal points. This extensive process, spanning nearly a year, resembled a reflective pause amid the rapid cadence of change.
Achieving these aspirations meant reimagining our approach, thereby streamlining efforts for maximal impact by…
- Integrating philanthropy as an integral facet of our mission, and amplifying the culture of giving within CHEST
- Consolidating philanthropic initiatives under CHEST to maximize resources for direct, substantial impact
- Defining clear avenues for giving that deeply resonate with our members
With endorsement from the Board of Regents, the CHEST Foundation seamlessly merged into CHEST, inaugurating a new chapter in our philanthropic endeavors.
Central to this transformative shift is the crystallization of our giving strategy, fortified by four pillars: Clinical Research, Community Impact, Support to the Profession, and Dedication to Education. These pillars encapsulate our commitment to nurturing clinicians, supporting trainees, and enhancing patient care.
Clinical Research emerges as the cornerstone, transcending boundaries to empower researchers in their pursuit of groundbreaking insights. Through strategic grants, we embolden early career investigators to delve into uncharted territories, unraveling mysteries that underpin advancements in chest medicine. The ripple effect extends beyond labs; it traverses communities, amplifying equitable health care solutions and bridging disparities in patient care. Our commitment to nurturing this pillar springs from the belief that every breakthrough, regardless of scale, is a catalyst for transformative change.
Community Impact extends CHEST’s reach far beyond clinical settings, fostering alliances with local organizations. Together, we forge a tapestry of collaboration, weaving essential services and imparting knowledge on crucial lung health issues into the fabric of diverse communities. This engagement not only elevates awareness but also empowers individuals and communities to take charge of their respiratory well-being. It’s the grassroots unity that amplifies our impact, creating enduring shifts in local landscapes.
Support of the Profession epitomizes our dedication to fortifying the backbone of pulmonary, critical care, and sleep medicine. By offering unparalleled clinical education and mentorship, we empower emerging clinicians from diverse backgrounds with the latest knowledge and resources. Fueling their professional growth is pivotal to nurturing a robust and inclusive cadre of health care professionals, ensuring comprehensive and culturally sensitive care for patients worldwide.
Dedication to Education isn’t just a commitment—it’s a bridge spanning the gap between knowledge and application, patient and clinician. Strengthening this connection involves equipping clinicians with tools for effective communication and partnering with patient-centered organizations. Our focus transcends textbooks; it embodies a relentless pursuit to refine patient-clinician interactions, enhancing patient understanding and, ultimately, elevating their quality of life.
CHEST’s philanthropic evolution signifies not just growth but a resolute commitment to effecting tangible change in chest medicine and patient care. These pillars stand as guiding beacons, steering us toward a future that mirrors our mission, vision, and values. Each pillar represents a pathway to meaningful, enduring change within chest medicine, ensuring a lasting impact on patient well-being.
Biomarker checklist seeks to expedite NSCLC diagnoses
Drs. Tamer Said Ahmed and Adam Fox receive funding for quality improvement projects in biomarker testing
Establishing a systematic biomarker testing program for patients with suspected non-small cell lung cancer (NSCLC) takes both time and collaboration across specialties. To standardize this process, the American College of Chest Physicians (CHEST) created two clinician checklists for use in practice.
The case-by-case checklist helps guide physicians to ensure timely and comprehensive biomarker testing for individual patients, and the programmatic/institutional checklist is for multidisciplinary teams to enable clear expectations and processes across hand-offs to aid in the testing process.
To substantiate best practices for ordering biomarker tests using the checklists, CHEST issued quality improvement demonstration grants for implementation at two institutions. This year, Tamer Said Ahmed, MD, FCCP, pulmonary and sleep physician at Toledo Hospital (ProMedica Health System) and Assistant Professor at the University of Toledo, and Adam Fox, MD, MS, Assistant Professor of Medicine at the Medical University of South Carolina, will begin projects to improve biomarker testing.
“Biomarker testing allows for tailored treatment plans that drastically impact the progression of lung cancer, but every hospital system and practice is following a different procedure for testing,” Dr. Said Ahmed said. “To best serve the patient, our project aims to streamline the approach to biomarker testing to bridge health care inconsistencies. Given the intense progression of some forms of lung cancer where every week matters, the more streamlined we can make the biomarker testing process, the earlier we will get to an accurate diagnosis, begin treatment, and likely extend the life of a patient.”
Discrepancies in the testing process stem from existing silos between specialties, including pathology, oncology, interventional radiology, and more. Care is fragmented, leading to delays like repeat biopsies because a large enough sample was not taken the first time.
This is the exact problem that checklist implementation will seek to solve.
“By intent, these checklists help to provide a systematic approach to timely and comprehensive biomarker testing,” said Dr. Fox, who was also part of the team that developed the checklists. “What we need now is to implement them into clinical practice to gain metrics that can be studied, identified, and will lead to the process being widely accepted. To truly impact practice, we need to be able to provide strong evidence for interventions that work for clinicians to implement.”
To learn more and download the checklists, visit CHEST’s Thoracic Oncology Topic Collection onlineThis project is supported in part by AstraZeneca, Sanofi, and Pfizer.
Drs. Tamer Said Ahmed and Adam Fox receive funding for quality improvement projects in biomarker testing
Drs. Tamer Said Ahmed and Adam Fox receive funding for quality improvement projects in biomarker testing
Establishing a systematic biomarker testing program for patients with suspected non-small cell lung cancer (NSCLC) takes both time and collaboration across specialties. To standardize this process, the American College of Chest Physicians (CHEST) created two clinician checklists for use in practice.
The case-by-case checklist helps guide physicians to ensure timely and comprehensive biomarker testing for individual patients, and the programmatic/institutional checklist is for multidisciplinary teams to enable clear expectations and processes across hand-offs to aid in the testing process.
To substantiate best practices for ordering biomarker tests using the checklists, CHEST issued quality improvement demonstration grants for implementation at two institutions. This year, Tamer Said Ahmed, MD, FCCP, pulmonary and sleep physician at Toledo Hospital (ProMedica Health System) and Assistant Professor at the University of Toledo, and Adam Fox, MD, MS, Assistant Professor of Medicine at the Medical University of South Carolina, will begin projects to improve biomarker testing.
“Biomarker testing allows for tailored treatment plans that drastically impact the progression of lung cancer, but every hospital system and practice is following a different procedure for testing,” Dr. Said Ahmed said. “To best serve the patient, our project aims to streamline the approach to biomarker testing to bridge health care inconsistencies. Given the intense progression of some forms of lung cancer where every week matters, the more streamlined we can make the biomarker testing process, the earlier we will get to an accurate diagnosis, begin treatment, and likely extend the life of a patient.”
Discrepancies in the testing process stem from existing silos between specialties, including pathology, oncology, interventional radiology, and more. Care is fragmented, leading to delays like repeat biopsies because a large enough sample was not taken the first time.
This is the exact problem that checklist implementation will seek to solve.
“By intent, these checklists help to provide a systematic approach to timely and comprehensive biomarker testing,” said Dr. Fox, who was also part of the team that developed the checklists. “What we need now is to implement them into clinical practice to gain metrics that can be studied, identified, and will lead to the process being widely accepted. To truly impact practice, we need to be able to provide strong evidence for interventions that work for clinicians to implement.”
To learn more and download the checklists, visit CHEST’s Thoracic Oncology Topic Collection onlineThis project is supported in part by AstraZeneca, Sanofi, and Pfizer.
Establishing a systematic biomarker testing program for patients with suspected non-small cell lung cancer (NSCLC) takes both time and collaboration across specialties. To standardize this process, the American College of Chest Physicians (CHEST) created two clinician checklists for use in practice.
The case-by-case checklist helps guide physicians to ensure timely and comprehensive biomarker testing for individual patients, and the programmatic/institutional checklist is for multidisciplinary teams to enable clear expectations and processes across hand-offs to aid in the testing process.
To substantiate best practices for ordering biomarker tests using the checklists, CHEST issued quality improvement demonstration grants for implementation at two institutions. This year, Tamer Said Ahmed, MD, FCCP, pulmonary and sleep physician at Toledo Hospital (ProMedica Health System) and Assistant Professor at the University of Toledo, and Adam Fox, MD, MS, Assistant Professor of Medicine at the Medical University of South Carolina, will begin projects to improve biomarker testing.
“Biomarker testing allows for tailored treatment plans that drastically impact the progression of lung cancer, but every hospital system and practice is following a different procedure for testing,” Dr. Said Ahmed said. “To best serve the patient, our project aims to streamline the approach to biomarker testing to bridge health care inconsistencies. Given the intense progression of some forms of lung cancer where every week matters, the more streamlined we can make the biomarker testing process, the earlier we will get to an accurate diagnosis, begin treatment, and likely extend the life of a patient.”
Discrepancies in the testing process stem from existing silos between specialties, including pathology, oncology, interventional radiology, and more. Care is fragmented, leading to delays like repeat biopsies because a large enough sample was not taken the first time.
This is the exact problem that checklist implementation will seek to solve.
“By intent, these checklists help to provide a systematic approach to timely and comprehensive biomarker testing,” said Dr. Fox, who was also part of the team that developed the checklists. “What we need now is to implement them into clinical practice to gain metrics that can be studied, identified, and will lead to the process being widely accepted. To truly impact practice, we need to be able to provide strong evidence for interventions that work for clinicians to implement.”
To learn more and download the checklists, visit CHEST’s Thoracic Oncology Topic Collection onlineThis project is supported in part by AstraZeneca, Sanofi, and Pfizer.
Examining the past and looking toward the future: The need for quality data in interventional pulmonology
THORACIC ONCOLOGY AND CHEST PROCEDURES NETWORK
Interventional Procedures Section
During the last decade, the explosion of technological advancements in the field of interventional pulmonary (IP) has afforded patients the opportunity to undergo novel, minimally invasive diagnostic and therapeutic procedures. However, these unprecedented technological advances have often been introduced without the support of high-quality research on safety and efficacy, and without evaluating their impact on meaningful patient outcomes. Encouraging and participating in high-quality IP research should remain a top priority for those practicing in the field.

Structured research networks, such as the UK Pleural Society and more recently the Interventional Pulmonary Outcome Group, have facilitated the transition of IP research from observational case series and single-center experiences to multicenter, randomized controlled trials to generate level I evidence and inform patient care (Laskawiec-Szkonter M, et al. Br J Hosp Med (Lond). 2019 Apr 2;80[4]:186-7) (Maldonado F, et al. J Bronchology Interv Pulmonol. 2019 Jul;26(3):150-2). In the bronchoscopy space, important investigator-initiated clinical trial results anticipated in 2024 include VERITAS (NCT04250194), FROSTBITE2 (NCT05751278), and RELIANT (NCT05705544), among others. These research efforts complement industry-sponsored clinical trials (such as RheSolve, NCT04677465) and aim to emulate the extraordinary track record achieved in the field of pleural disease that has led to recently updated evidence-based guidelines for the management of challenging diseases like malignant pleural effusions, pleural space infections, and pneumothorax (Davies HE, et a l. JAMA. 2012 Jun 13;307[22]:2383-9, Mishra EK, et al. Am J Respir Crit Care Med. 2018 Feb 15;197[4]:502-8) (Rahman NM, et al. N Engl J Med. 2011 Aug 11;365[6]:518-26) (Hallifax RJ, et al. Lancet. 2020 Jul 4;396[10243]:39-49).
Ultimately, the rapidly evolving technological advancements in interventional pulmonology must be supported by research based on high-quality clinical trials, which will be contingent on appropriate trial funding requiring partnership with industry and federal funding agencies. Only through such collaboration can researchers design robust clinical trials based on complex methodology, which will advance patient care and lead to improved patient outcomes.
– Jennifer D. Duke, MD
Section Fellow-in-Training
– Fabien Maldonado, MD, MSc, FCCP
Section Member
THORACIC ONCOLOGY AND CHEST PROCEDURES NETWORK
Interventional Procedures Section
During the last decade, the explosion of technological advancements in the field of interventional pulmonary (IP) has afforded patients the opportunity to undergo novel, minimally invasive diagnostic and therapeutic procedures. However, these unprecedented technological advances have often been introduced without the support of high-quality research on safety and efficacy, and without evaluating their impact on meaningful patient outcomes. Encouraging and participating in high-quality IP research should remain a top priority for those practicing in the field.
Structured research networks, such as the UK Pleural Society and more recently the Interventional Pulmonary Outcome Group, have facilitated the transition of IP research from observational case series and single-center experiences to multicenter, randomized controlled trials to generate level I evidence and inform patient care (Laskawiec-Szkonter M, et al. Br J Hosp Med (Lond). 2019 Apr 2;80[4]:186-7) (Maldonado F, et al. J Bronchology Interv Pulmonol. 2019 Jul;26(3):150-2). In the bronchoscopy space, important investigator-initiated clinical trial results anticipated in 2024 include VERITAS (NCT04250194), FROSTBITE2 (NCT05751278), and RELIANT (NCT05705544), among others. These research efforts complement industry-sponsored clinical trials (such as RheSolve, NCT04677465) and aim to emulate the extraordinary track record achieved in the field of pleural disease that has led to recently updated evidence-based guidelines for the management of challenging diseases like malignant pleural effusions, pleural space infections, and pneumothorax (Davies HE, et a l. JAMA. 2012 Jun 13;307[22]:2383-9, Mishra EK, et al. Am J Respir Crit Care Med. 2018 Feb 15;197[4]:502-8) (Rahman NM, et al. N Engl J Med. 2011 Aug 11;365[6]:518-26) (Hallifax RJ, et al. Lancet. 2020 Jul 4;396[10243]:39-49).
Ultimately, the rapidly evolving technological advancements in interventional pulmonology must be supported by research based on high-quality clinical trials, which will be contingent on appropriate trial funding requiring partnership with industry and federal funding agencies. Only through such collaboration can researchers design robust clinical trials based on complex methodology, which will advance patient care and lead to improved patient outcomes.
– Jennifer D. Duke, MD
Section Fellow-in-Training
– Fabien Maldonado, MD, MSc, FCCP
Section Member
THORACIC ONCOLOGY AND CHEST PROCEDURES NETWORK
Interventional Procedures Section
During the last decade, the explosion of technological advancements in the field of interventional pulmonary (IP) has afforded patients the opportunity to undergo novel, minimally invasive diagnostic and therapeutic procedures. However, these unprecedented technological advances have often been introduced without the support of high-quality research on safety and efficacy, and without evaluating their impact on meaningful patient outcomes. Encouraging and participating in high-quality IP research should remain a top priority for those practicing in the field.
Structured research networks, such as the UK Pleural Society and more recently the Interventional Pulmonary Outcome Group, have facilitated the transition of IP research from observational case series and single-center experiences to multicenter, randomized controlled trials to generate level I evidence and inform patient care (Laskawiec-Szkonter M, et al. Br J Hosp Med (Lond). 2019 Apr 2;80[4]:186-7) (Maldonado F, et al. J Bronchology Interv Pulmonol. 2019 Jul;26(3):150-2). In the bronchoscopy space, important investigator-initiated clinical trial results anticipated in 2024 include VERITAS (NCT04250194), FROSTBITE2 (NCT05751278), and RELIANT (NCT05705544), among others. These research efforts complement industry-sponsored clinical trials (such as RheSolve, NCT04677465) and aim to emulate the extraordinary track record achieved in the field of pleural disease that has led to recently updated evidence-based guidelines for the management of challenging diseases like malignant pleural effusions, pleural space infections, and pneumothorax (Davies HE, et a l. JAMA. 2012 Jun 13;307[22]:2383-9, Mishra EK, et al. Am J Respir Crit Care Med. 2018 Feb 15;197[4]:502-8) (Rahman NM, et al. N Engl J Med. 2011 Aug 11;365[6]:518-26) (Hallifax RJ, et al. Lancet. 2020 Jul 4;396[10243]:39-49).
Ultimately, the rapidly evolving technological advancements in interventional pulmonology must be supported by research based on high-quality clinical trials, which will be contingent on appropriate trial funding requiring partnership with industry and federal funding agencies. Only through such collaboration can researchers design robust clinical trials based on complex methodology, which will advance patient care and lead to improved patient outcomes.
– Jennifer D. Duke, MD
Section Fellow-in-Training
– Fabien Maldonado, MD, MSc, FCCP
Section Member
Updates in evidence for rituximab in interstitial lung disease
DIFFUSE LUNG DISEASE AND LUNG TRANSPLANT NETWORK
Interstitial Lung Disease Section
Interstitial lung diseases (ILD) are a heterogeneous group of fibro-inflammatory disorders that can be progressive despite available therapies. The cornerstones of pharmacologic therapy include immunosuppression and antifibrotics.

Data on the use of rituximab, a B-lymphocyte-depleting monoclonal antibody, often utilized as rescue therapy in progressive and severe ILD, was limited until recently. The RECITAL trial reported the first randomized controlled trial investigating rituximab in severe or progressive autoimmune ILD. Though rituximab was not superior to cyclophosphamide, both agents improved forced vital capacity (FVC) at 24 weeks and respiratory-related quality of life. Rituximab was associated with less adverse events and lower corticosteroid exposure (Maher et al. Lancet Respir Med. 2023;11:45-54). In the DESIRES trial, patients with systemic sclerosis-associated ILD treated with rituximab had preservation of FVC at 24 and 48 weeks compared to placebo (Ebata et al. Lancet Rheumatol. 2021;3:e489-97; Lancet Rheumatol. 2022;4:e546-55). The EVER-ILD investigators compared mycophenolate mofetil (MMF) alone vs addition of rituximab in patients with autoimmune and idiopathic nonspecific interstitial pneumonia (NSIP). Combination therapy was superior to MMF alone in improving FVC and progression-free survival. Combination regimen was well tolerated though nonserious viral and bacterial infections were more frequent (Mankikian et al. Eur Respir J. 2023;61[6]:2202071).
These findings, primarily in autoimmune ILD, are promising and provide clinicians with evidence for utilizing rituximab in patients with severe and progressive ILD. Nonetheless, they highlight the need for additional research and standardized guidance regarding the target population who stands to most benefit from rituximab.
–Tessy K. Paul, MD
Section Member-at-Large
–Tejaswini Kulkarni, MD, MBBS, FCCP
Section Chair
DIFFUSE LUNG DISEASE AND LUNG TRANSPLANT NETWORK
Interstitial Lung Disease Section
Interstitial lung diseases (ILD) are a heterogeneous group of fibro-inflammatory disorders that can be progressive despite available therapies. The cornerstones of pharmacologic therapy include immunosuppression and antifibrotics.
Data on the use of rituximab, a B-lymphocyte-depleting monoclonal antibody, often utilized as rescue therapy in progressive and severe ILD, was limited until recently. The RECITAL trial reported the first randomized controlled trial investigating rituximab in severe or progressive autoimmune ILD. Though rituximab was not superior to cyclophosphamide, both agents improved forced vital capacity (FVC) at 24 weeks and respiratory-related quality of life. Rituximab was associated with less adverse events and lower corticosteroid exposure (Maher et al. Lancet Respir Med. 2023;11:45-54). In the DESIRES trial, patients with systemic sclerosis-associated ILD treated with rituximab had preservation of FVC at 24 and 48 weeks compared to placebo (Ebata et al. Lancet Rheumatol. 2021;3:e489-97; Lancet Rheumatol. 2022;4:e546-55). The EVER-ILD investigators compared mycophenolate mofetil (MMF) alone vs addition of rituximab in patients with autoimmune and idiopathic nonspecific interstitial pneumonia (NSIP). Combination therapy was superior to MMF alone in improving FVC and progression-free survival. Combination regimen was well tolerated though nonserious viral and bacterial infections were more frequent (Mankikian et al. Eur Respir J. 2023;61[6]:2202071).
These findings, primarily in autoimmune ILD, are promising and provide clinicians with evidence for utilizing rituximab in patients with severe and progressive ILD. Nonetheless, they highlight the need for additional research and standardized guidance regarding the target population who stands to most benefit from rituximab.
–Tessy K. Paul, MD
Section Member-at-Large
–Tejaswini Kulkarni, MD, MBBS, FCCP
Section Chair
DIFFUSE LUNG DISEASE AND LUNG TRANSPLANT NETWORK
Interstitial Lung Disease Section
Interstitial lung diseases (ILD) are a heterogeneous group of fibro-inflammatory disorders that can be progressive despite available therapies. The cornerstones of pharmacologic therapy include immunosuppression and antifibrotics.
Data on the use of rituximab, a B-lymphocyte-depleting monoclonal antibody, often utilized as rescue therapy in progressive and severe ILD, was limited until recently. The RECITAL trial reported the first randomized controlled trial investigating rituximab in severe or progressive autoimmune ILD. Though rituximab was not superior to cyclophosphamide, both agents improved forced vital capacity (FVC) at 24 weeks and respiratory-related quality of life. Rituximab was associated with less adverse events and lower corticosteroid exposure (Maher et al. Lancet Respir Med. 2023;11:45-54). In the DESIRES trial, patients with systemic sclerosis-associated ILD treated with rituximab had preservation of FVC at 24 and 48 weeks compared to placebo (Ebata et al. Lancet Rheumatol. 2021;3:e489-97; Lancet Rheumatol. 2022;4:e546-55). The EVER-ILD investigators compared mycophenolate mofetil (MMF) alone vs addition of rituximab in patients with autoimmune and idiopathic nonspecific interstitial pneumonia (NSIP). Combination therapy was superior to MMF alone in improving FVC and progression-free survival. Combination regimen was well tolerated though nonserious viral and bacterial infections were more frequent (Mankikian et al. Eur Respir J. 2023;61[6]:2202071).
These findings, primarily in autoimmune ILD, are promising and provide clinicians with evidence for utilizing rituximab in patients with severe and progressive ILD. Nonetheless, they highlight the need for additional research and standardized guidance regarding the target population who stands to most benefit from rituximab.
–Tessy K. Paul, MD
Section Member-at-Large
–Tejaswini Kulkarni, MD, MBBS, FCCP
Section Chair
The emergence of postgraduate training programs for APPs in pulmonary and critical care
APP Intersection
Postgraduate training for advanced practice providers (APPs) has existed in one form or another since the genesis of the allied professions. They are typically referred to as residencies, fellowships, postgraduate programs, and transition-to-practice.
The desire and necessity for these programs has increased in the past decade with workforce changes; namely the increasing number of nurse practitioners (NPs) graduating with fewer years of experience at the bedside compared with previous eras, a similar decrease in patient contact hours for graduating PAs, the transition of physician colleagues from employers to employees and the subsequent change in priorities in training new graduate APPs, and resident work hour restrictions necessitating more APPs to staff inpatient units and work in various specialties.
The goal of these programs is to provide postgraduate training to physician assistants/associates (PAs) and NPs across myriad medical specialties to both newly graduated APPs and those looking to transition specialties. Current programs exist in family medicine, emergency medicine, urgent care, critical care medicine, pulmonary medicine, oncology, surgery, and various surgical subspecialties, to name a few. Program length is highly variable, though most programs advertise as lasting around 12 months, with varying ratios of clinical and didactic education. Postgraduate APP programs are largely advertise as salaried, benefitted positions, though usually at a rate below that of a so-called “direct hire” due to the protected learning time associated with the postgraduate training year.

Accreditation for these programs is still disjointed, although unifying efforts have been made as of late, and is currently available through the Advanced Practice Provider Fellowship Accreditation, Association of Postgraduate Physician Assistant Programs, ARC-PA, the Accreditation Commission for Education in Nursing, and the Consortium for Advanced Practice Providers. Other organizations, such as the Association of Post Graduate APRN Programs, host regular conferences to discuss the formulation of postgraduate APP education curricula and program development.
While accreditation offers guidance for fledgling programs, many utilize the standards published by the American College of Graduate Medical Education to ensure that appropriate clinical milestones are being met and that a common language among APPs and physicians who are involved in the evaluation of the postgraduate APP trainee is being used. Programs also seek to utilize other well-established curricula and certification programs published by various national and international organizations. A key distinction from physician postgraduate training is that there is currently no fiscal or legislative support for postgraduate APP programs; these issues have been cited as reasons for the limited scope and number of programs.
When starting APP Fellowship programs, it is important to consider why this would be beneficial to a specific division and health care organization. Usually, fellowship programs develop out of a need to train and retain APPs. It is no secret that turnover and retention of skilled APPs is a nationwide problem associated with significant costs to organizations. The ability to retain fellowship-trained APPs will result in cost savings due to the reduction in onboarding time and orientation costs, as these APP fellows finish their programs ready to be fully productive team members.
Additional considerations for the development of an APP fellowship include improving access to care and increasing the quality of the care provided. Fellowship programs encourage a smoother transition to practice by offering more support through education, closer evaluation, and frequent feedback, which improves competence and confidence of these providers. A supported APP is more likely to practice to the fullest extent of their license and have improved personal and professional satisfaction, leading to employee retention and better patient care.
When developing a budget for these types of programs, it is important to include the full-time equivalent (FTE) for the fellow, benefits, onboarding/licensure, simulations, and fellowship faculty costs.
Faculty compensation varies by institution but can include salary support, FTE reduction, and nonclinical appointments. Tracking metrics such as fellow billing, length of stay, and access to care during the fellowship year are helpful to highlight the benefit of these programs to the organization.
Initiating a program like those described may seem like a Herculean feat, but motivated individuals have been able to accomplish similar goals in both adequately and poorly resourced areas. For those aspiring to start a postgraduate APP program at their instruction, these authors suggest the following approach.
First, identify your institution’s need for such a program. Next, define your curriculum, evaluation process, and expectations. Then, create buy-in from stakeholders, including administrative and clinical personnel. Finally, focus on recruitment. Seeking accreditation may be challenging for new programs, but identifying the accreditation standard you plan to pursue early will pay dividends when the time comes for the program to apply. Those starting down this path should realistically expect an 18- to 24-month period between their first efforts and the start of the first class.
“APP Intersection” is a new quarterly column focusing on areas of interest for the entire chest medicine health care team.
APP Intersection
Postgraduate training for advanced practice providers (APPs) has existed in one form or another since the genesis of the allied professions. They are typically referred to as residencies, fellowships, postgraduate programs, and transition-to-practice.
The desire and necessity for these programs has increased in the past decade with workforce changes; namely the increasing number of nurse practitioners (NPs) graduating with fewer years of experience at the bedside compared with previous eras, a similar decrease in patient contact hours for graduating PAs, the transition of physician colleagues from employers to employees and the subsequent change in priorities in training new graduate APPs, and resident work hour restrictions necessitating more APPs to staff inpatient units and work in various specialties.
The goal of these programs is to provide postgraduate training to physician assistants/associates (PAs) and NPs across myriad medical specialties to both newly graduated APPs and those looking to transition specialties. Current programs exist in family medicine, emergency medicine, urgent care, critical care medicine, pulmonary medicine, oncology, surgery, and various surgical subspecialties, to name a few. Program length is highly variable, though most programs advertise as lasting around 12 months, with varying ratios of clinical and didactic education. Postgraduate APP programs are largely advertise as salaried, benefitted positions, though usually at a rate below that of a so-called “direct hire” due to the protected learning time associated with the postgraduate training year.
Accreditation for these programs is still disjointed, although unifying efforts have been made as of late, and is currently available through the Advanced Practice Provider Fellowship Accreditation, Association of Postgraduate Physician Assistant Programs, ARC-PA, the Accreditation Commission for Education in Nursing, and the Consortium for Advanced Practice Providers. Other organizations, such as the Association of Post Graduate APRN Programs, host regular conferences to discuss the formulation of postgraduate APP education curricula and program development.
While accreditation offers guidance for fledgling programs, many utilize the standards published by the American College of Graduate Medical Education to ensure that appropriate clinical milestones are being met and that a common language among APPs and physicians who are involved in the evaluation of the postgraduate APP trainee is being used. Programs also seek to utilize other well-established curricula and certification programs published by various national and international organizations. A key distinction from physician postgraduate training is that there is currently no fiscal or legislative support for postgraduate APP programs; these issues have been cited as reasons for the limited scope and number of programs.
When starting APP Fellowship programs, it is important to consider why this would be beneficial to a specific division and health care organization. Usually, fellowship programs develop out of a need to train and retain APPs. It is no secret that turnover and retention of skilled APPs is a nationwide problem associated with significant costs to organizations. The ability to retain fellowship-trained APPs will result in cost savings due to the reduction in onboarding time and orientation costs, as these APP fellows finish their programs ready to be fully productive team members.
Additional considerations for the development of an APP fellowship include improving access to care and increasing the quality of the care provided. Fellowship programs encourage a smoother transition to practice by offering more support through education, closer evaluation, and frequent feedback, which improves competence and confidence of these providers. A supported APP is more likely to practice to the fullest extent of their license and have improved personal and professional satisfaction, leading to employee retention and better patient care.
When developing a budget for these types of programs, it is important to include the full-time equivalent (FTE) for the fellow, benefits, onboarding/licensure, simulations, and fellowship faculty costs.
Faculty compensation varies by institution but can include salary support, FTE reduction, and nonclinical appointments. Tracking metrics such as fellow billing, length of stay, and access to care during the fellowship year are helpful to highlight the benefit of these programs to the organization.
Initiating a program like those described may seem like a Herculean feat, but motivated individuals have been able to accomplish similar goals in both adequately and poorly resourced areas. For those aspiring to start a postgraduate APP program at their instruction, these authors suggest the following approach.
First, identify your institution’s need for such a program. Next, define your curriculum, evaluation process, and expectations. Then, create buy-in from stakeholders, including administrative and clinical personnel. Finally, focus on recruitment. Seeking accreditation may be challenging for new programs, but identifying the accreditation standard you plan to pursue early will pay dividends when the time comes for the program to apply. Those starting down this path should realistically expect an 18- to 24-month period between their first efforts and the start of the first class.
“APP Intersection” is a new quarterly column focusing on areas of interest for the entire chest medicine health care team.
APP Intersection
Postgraduate training for advanced practice providers (APPs) has existed in one form or another since the genesis of the allied professions. They are typically referred to as residencies, fellowships, postgraduate programs, and transition-to-practice.
The desire and necessity for these programs has increased in the past decade with workforce changes; namely the increasing number of nurse practitioners (NPs) graduating with fewer years of experience at the bedside compared with previous eras, a similar decrease in patient contact hours for graduating PAs, the transition of physician colleagues from employers to employees and the subsequent change in priorities in training new graduate APPs, and resident work hour restrictions necessitating more APPs to staff inpatient units and work in various specialties.
The goal of these programs is to provide postgraduate training to physician assistants/associates (PAs) and NPs across myriad medical specialties to both newly graduated APPs and those looking to transition specialties. Current programs exist in family medicine, emergency medicine, urgent care, critical care medicine, pulmonary medicine, oncology, surgery, and various surgical subspecialties, to name a few. Program length is highly variable, though most programs advertise as lasting around 12 months, with varying ratios of clinical and didactic education. Postgraduate APP programs are largely advertise as salaried, benefitted positions, though usually at a rate below that of a so-called “direct hire” due to the protected learning time associated with the postgraduate training year.
Accreditation for these programs is still disjointed, although unifying efforts have been made as of late, and is currently available through the Advanced Practice Provider Fellowship Accreditation, Association of Postgraduate Physician Assistant Programs, ARC-PA, the Accreditation Commission for Education in Nursing, and the Consortium for Advanced Practice Providers. Other organizations, such as the Association of Post Graduate APRN Programs, host regular conferences to discuss the formulation of postgraduate APP education curricula and program development.
While accreditation offers guidance for fledgling programs, many utilize the standards published by the American College of Graduate Medical Education to ensure that appropriate clinical milestones are being met and that a common language among APPs and physicians who are involved in the evaluation of the postgraduate APP trainee is being used. Programs also seek to utilize other well-established curricula and certification programs published by various national and international organizations. A key distinction from physician postgraduate training is that there is currently no fiscal or legislative support for postgraduate APP programs; these issues have been cited as reasons for the limited scope and number of programs.
When starting APP Fellowship programs, it is important to consider why this would be beneficial to a specific division and health care organization. Usually, fellowship programs develop out of a need to train and retain APPs. It is no secret that turnover and retention of skilled APPs is a nationwide problem associated with significant costs to organizations. The ability to retain fellowship-trained APPs will result in cost savings due to the reduction in onboarding time and orientation costs, as these APP fellows finish their programs ready to be fully productive team members.
Additional considerations for the development of an APP fellowship include improving access to care and increasing the quality of the care provided. Fellowship programs encourage a smoother transition to practice by offering more support through education, closer evaluation, and frequent feedback, which improves competence and confidence of these providers. A supported APP is more likely to practice to the fullest extent of their license and have improved personal and professional satisfaction, leading to employee retention and better patient care.
When developing a budget for these types of programs, it is important to include the full-time equivalent (FTE) for the fellow, benefits, onboarding/licensure, simulations, and fellowship faculty costs.
Faculty compensation varies by institution but can include salary support, FTE reduction, and nonclinical appointments. Tracking metrics such as fellow billing, length of stay, and access to care during the fellowship year are helpful to highlight the benefit of these programs to the organization.
Initiating a program like those described may seem like a Herculean feat, but motivated individuals have been able to accomplish similar goals in both adequately and poorly resourced areas. For those aspiring to start a postgraduate APP program at their instruction, these authors suggest the following approach.
First, identify your institution’s need for such a program. Next, define your curriculum, evaluation process, and expectations. Then, create buy-in from stakeholders, including administrative and clinical personnel. Finally, focus on recruitment. Seeking accreditation may be challenging for new programs, but identifying the accreditation standard you plan to pursue early will pay dividends when the time comes for the program to apply. Those starting down this path should realistically expect an 18- to 24-month period between their first efforts and the start of the first class.
“APP Intersection” is a new quarterly column focusing on areas of interest for the entire chest medicine health care team.
Bivalent COVID Vaccine Protected Children, Adolescents
Children and adolescents ages 5-17 who received a bivalent COVID-19 mRNA vaccine were less likely to become infected with SARS-CoV-2 compared with those who were unvaccinated or received only the monovalent COVID-19 vaccine, according to new data published February 6 in JAMA.
“All eligible children and adolescents should remain up to date with recommended COVID-19 vaccinations,” wrote the authors, led by Leora R. Feldstein, PhD, with the US Centers for Disease Control and Prevention (CDC) in Atlanta.
By the end of 2023, at least 911 youths ages 5-17 had died from COVID-related causes.
Researchers found that compared with participants who did not receive the COVID-19 vaccine or got monovalent-only doses 180 days or more before, the adjusted vaccine effectiveness of a bivalent COVID-19 vaccine dose against SARS-CoV-2 infection was 51.3% (95% confidence interval [CI], 23.6%-71.9%) 7-60 days after vaccination. Relative effectiveness was 62.4% (95% CI, 38.5%-81.1%) 61-150 days after vaccination. The researchers said the confidence intervals were wide because of the small sample size.
The information can help inform public health strategies, the authors noted, especially as new variants emerge.
Bivalent Dose Recommended in Fall of 2022
Bivalent mRNA COVID vaccines were recommended in the United States for children and adolescents ages 12 years or older on Sept. 1, 2022, and for children ages 5-11 on Oct. 12, 2022, when Omicron BA.4/5 types were the predominant circulating variant.
The study included 2,959 participants who completed periodic surveys (answering questions on demographics, household details, chronic medical conditions, and COVID-19 symptoms) and submitted weekly self-collected nasal swabs (whether or not they had symptoms). Those in the study submitted additional nasal swabs if they developed any symptoms.
Median adherence to weekly upper respiratory specimen swabbing was high throughout the study period at 93.8%.
Data from Sept. 4, 2022, to Jan. 31, 2023, were combined from three prospective US cohort studies at six sites. In addition to the surveys, researchers used information from state immunization information systems and electronic medical records.
Most of the Infected Were Unvaccinated or Had Monovalent Vax
Of the 426 participants (14.4% of the combined cohorts) infected with SARS-CoV-2, 383 (89.9%) were either unvaccinated or received monovalent vaccine doses only.
Calculations were adjusted for age, sex, race, ethnicity, health conditions, prior SARS-CoV-2 infections, geographic location, proportion of circulating variants by site, and local virus prevalence.
Participants living in Oregon, for example, had the highest uptake of bivalent COVID-19 vaccine (56.2%), whereas those in Texas had the lowest (2.4%). Participants reporting Hispanic ethnicity had lower bivalent uptake (17.1%) compared with non-Hispanic participants of all races (27.1%).
Of the 2,207 participants who did not receive a bivalent dose, 24.2% were unvaccinated and 1,672 (75.8%) received at least 1 monovalent dose.
The researchers said they saw no sign of waning effectiveness 61-150 days (the limit for this analysis) after receipt of the bivalent COVID-19 vaccine.
They wrote that continuation of the cohorts will allow study of waning patterns, which could help inform vaccine recommendations.
Among the limitations of the study are that testing methods and the COVID-19 symptoms surveyed varied among the three cohorts, so there may be some differences in defining infection or symptomatic COVID. In addition, the researchers were not able to account for the social vulnerability index and immunocompromised status, which could have affected vaccine uptake and risk of SARS-CoV-2 infection.
This study was supported by the National Center for Immunization and Respiratory Diseases, US Centers for Disease Control and Prevention, and by the National Institute of Allergy and Infectious Diseases. Coauthor Dr. Caban-Martinez reported grants from the Florida Firefighter Cancer Initiative and the Florida Department of Health. Coauthors Dr. Chu, Dr. Englund, Dr. Martin, and Dr. Monto reported receiving personal fees or grants from multiple pharmaceutical companies. Dr. Hegmann reported being the editor of the American College of Occupational and Environmental Medicine practice guidelines. Coauthor Dr. Gaglani reported serving as cochair of the infectious diseases and immunization committee and the respiratory syncytial virus task force lead for the Texas Pediatric Society and the Texas Chapter of the American Academy of Pediatrics. No other disclosures were reported.
Children and adolescents ages 5-17 who received a bivalent COVID-19 mRNA vaccine were less likely to become infected with SARS-CoV-2 compared with those who were unvaccinated or received only the monovalent COVID-19 vaccine, according to new data published February 6 in JAMA.
“All eligible children and adolescents should remain up to date with recommended COVID-19 vaccinations,” wrote the authors, led by Leora R. Feldstein, PhD, with the US Centers for Disease Control and Prevention (CDC) in Atlanta.
By the end of 2023, at least 911 youths ages 5-17 had died from COVID-related causes.
Researchers found that compared with participants who did not receive the COVID-19 vaccine or got monovalent-only doses 180 days or more before, the adjusted vaccine effectiveness of a bivalent COVID-19 vaccine dose against SARS-CoV-2 infection was 51.3% (95% confidence interval [CI], 23.6%-71.9%) 7-60 days after vaccination. Relative effectiveness was 62.4% (95% CI, 38.5%-81.1%) 61-150 days after vaccination. The researchers said the confidence intervals were wide because of the small sample size.
The information can help inform public health strategies, the authors noted, especially as new variants emerge.
Bivalent Dose Recommended in Fall of 2022
Bivalent mRNA COVID vaccines were recommended in the United States for children and adolescents ages 12 years or older on Sept. 1, 2022, and for children ages 5-11 on Oct. 12, 2022, when Omicron BA.4/5 types were the predominant circulating variant.
The study included 2,959 participants who completed periodic surveys (answering questions on demographics, household details, chronic medical conditions, and COVID-19 symptoms) and submitted weekly self-collected nasal swabs (whether or not they had symptoms). Those in the study submitted additional nasal swabs if they developed any symptoms.
Median adherence to weekly upper respiratory specimen swabbing was high throughout the study period at 93.8%.
Data from Sept. 4, 2022, to Jan. 31, 2023, were combined from three prospective US cohort studies at six sites. In addition to the surveys, researchers used information from state immunization information systems and electronic medical records.
Most of the Infected Were Unvaccinated or Had Monovalent Vax
Of the 426 participants (14.4% of the combined cohorts) infected with SARS-CoV-2, 383 (89.9%) were either unvaccinated or received monovalent vaccine doses only.
Calculations were adjusted for age, sex, race, ethnicity, health conditions, prior SARS-CoV-2 infections, geographic location, proportion of circulating variants by site, and local virus prevalence.
Participants living in Oregon, for example, had the highest uptake of bivalent COVID-19 vaccine (56.2%), whereas those in Texas had the lowest (2.4%). Participants reporting Hispanic ethnicity had lower bivalent uptake (17.1%) compared with non-Hispanic participants of all races (27.1%).
Of the 2,207 participants who did not receive a bivalent dose, 24.2% were unvaccinated and 1,672 (75.8%) received at least 1 monovalent dose.
The researchers said they saw no sign of waning effectiveness 61-150 days (the limit for this analysis) after receipt of the bivalent COVID-19 vaccine.
They wrote that continuation of the cohorts will allow study of waning patterns, which could help inform vaccine recommendations.
Among the limitations of the study are that testing methods and the COVID-19 symptoms surveyed varied among the three cohorts, so there may be some differences in defining infection or symptomatic COVID. In addition, the researchers were not able to account for the social vulnerability index and immunocompromised status, which could have affected vaccine uptake and risk of SARS-CoV-2 infection.
This study was supported by the National Center for Immunization and Respiratory Diseases, US Centers for Disease Control and Prevention, and by the National Institute of Allergy and Infectious Diseases. Coauthor Dr. Caban-Martinez reported grants from the Florida Firefighter Cancer Initiative and the Florida Department of Health. Coauthors Dr. Chu, Dr. Englund, Dr. Martin, and Dr. Monto reported receiving personal fees or grants from multiple pharmaceutical companies. Dr. Hegmann reported being the editor of the American College of Occupational and Environmental Medicine practice guidelines. Coauthor Dr. Gaglani reported serving as cochair of the infectious diseases and immunization committee and the respiratory syncytial virus task force lead for the Texas Pediatric Society and the Texas Chapter of the American Academy of Pediatrics. No other disclosures were reported.
Children and adolescents ages 5-17 who received a bivalent COVID-19 mRNA vaccine were less likely to become infected with SARS-CoV-2 compared with those who were unvaccinated or received only the monovalent COVID-19 vaccine, according to new data published February 6 in JAMA.
“All eligible children and adolescents should remain up to date with recommended COVID-19 vaccinations,” wrote the authors, led by Leora R. Feldstein, PhD, with the US Centers for Disease Control and Prevention (CDC) in Atlanta.
By the end of 2023, at least 911 youths ages 5-17 had died from COVID-related causes.
Researchers found that compared with participants who did not receive the COVID-19 vaccine or got monovalent-only doses 180 days or more before, the adjusted vaccine effectiveness of a bivalent COVID-19 vaccine dose against SARS-CoV-2 infection was 51.3% (95% confidence interval [CI], 23.6%-71.9%) 7-60 days after vaccination. Relative effectiveness was 62.4% (95% CI, 38.5%-81.1%) 61-150 days after vaccination. The researchers said the confidence intervals were wide because of the small sample size.
The information can help inform public health strategies, the authors noted, especially as new variants emerge.
Bivalent Dose Recommended in Fall of 2022
Bivalent mRNA COVID vaccines were recommended in the United States for children and adolescents ages 12 years or older on Sept. 1, 2022, and for children ages 5-11 on Oct. 12, 2022, when Omicron BA.4/5 types were the predominant circulating variant.
The study included 2,959 participants who completed periodic surveys (answering questions on demographics, household details, chronic medical conditions, and COVID-19 symptoms) and submitted weekly self-collected nasal swabs (whether or not they had symptoms). Those in the study submitted additional nasal swabs if they developed any symptoms.
Median adherence to weekly upper respiratory specimen swabbing was high throughout the study period at 93.8%.
Data from Sept. 4, 2022, to Jan. 31, 2023, were combined from three prospective US cohort studies at six sites. In addition to the surveys, researchers used information from state immunization information systems and electronic medical records.
Most of the Infected Were Unvaccinated or Had Monovalent Vax
Of the 426 participants (14.4% of the combined cohorts) infected with SARS-CoV-2, 383 (89.9%) were either unvaccinated or received monovalent vaccine doses only.
Calculations were adjusted for age, sex, race, ethnicity, health conditions, prior SARS-CoV-2 infections, geographic location, proportion of circulating variants by site, and local virus prevalence.
Participants living in Oregon, for example, had the highest uptake of bivalent COVID-19 vaccine (56.2%), whereas those in Texas had the lowest (2.4%). Participants reporting Hispanic ethnicity had lower bivalent uptake (17.1%) compared with non-Hispanic participants of all races (27.1%).
Of the 2,207 participants who did not receive a bivalent dose, 24.2% were unvaccinated and 1,672 (75.8%) received at least 1 monovalent dose.
The researchers said they saw no sign of waning effectiveness 61-150 days (the limit for this analysis) after receipt of the bivalent COVID-19 vaccine.
They wrote that continuation of the cohorts will allow study of waning patterns, which could help inform vaccine recommendations.
Among the limitations of the study are that testing methods and the COVID-19 symptoms surveyed varied among the three cohorts, so there may be some differences in defining infection or symptomatic COVID. In addition, the researchers were not able to account for the social vulnerability index and immunocompromised status, which could have affected vaccine uptake and risk of SARS-CoV-2 infection.
This study was supported by the National Center for Immunization and Respiratory Diseases, US Centers for Disease Control and Prevention, and by the National Institute of Allergy and Infectious Diseases. Coauthor Dr. Caban-Martinez reported grants from the Florida Firefighter Cancer Initiative and the Florida Department of Health. Coauthors Dr. Chu, Dr. Englund, Dr. Martin, and Dr. Monto reported receiving personal fees or grants from multiple pharmaceutical companies. Dr. Hegmann reported being the editor of the American College of Occupational and Environmental Medicine practice guidelines. Coauthor Dr. Gaglani reported serving as cochair of the infectious diseases and immunization committee and the respiratory syncytial virus task force lead for the Texas Pediatric Society and the Texas Chapter of the American Academy of Pediatrics. No other disclosures were reported.
FROM JAMA
Gabapentinoids Increase Exacerbation in COPD
TOPLINE:
Gabapentinoid use significantly increased the risk for exacerbations in adults with chronic obstructive pulmonary disease (COPD).
METHODOLOGY:
- Previous research has prompted warnings from North American and European health agencies of severe exacerbations associated with gabapentinoid use by patients with COPD.
- The researchers compared data from patients with COPD in Canadian databases between 1994 and 2015 who were new to gabapentinoids and matched them to patients who did not use gabapentinoids.
- The primary outcome was exacerbation of COPD that required hospitalization in a propensity score-matched study.
TAKEAWAY:
- The study population included 356 epilepsy patients, 9411 neuropathic pain patients, and 3737 patients with other chronic pain.
- Use of gabapentinoids was significantly associated with an overall increased risk for severe COPD exacerbation (hazard ratio, 1.49) compared with nonuse.
- Gabapentinoid use was associated with a significantly increased COPD exacerbation risk for each group of users compared with nonusers, with hazard ratios of 1.58, 1.35, and 1.49 for epilepsy, neuropathic pain, and other chronic pain, respectively.
IN PRACTICE:
“This study supports the warnings from regulatory agencies and highlights the importance of considering this potential risk when prescribing gabapentin and pregabalin to patients with COPD,” the researchers wrote.
SOURCE:
The lead author on the study was Alvi A. Rahman, MSc, of Jewish General Hospital, Montreal. The study was published online on January 16, 2024, in Annals of Internal Medicine.
LIMITATIONS:
A lack of data on smoking status and other residual confounding factors limited the study findings.
DISCLOSURES:
The study was supported by the Canadian Institutes of Health Research and the Canadian Lung Association. Mr. Rahman had no financial conflicts to disclose, but some coauthors disclosed consulting and advisory relationships with various companies, including Merck, Pfizer, Seqirus, Boehringer-Ingelheim, and Novartis outside of the current work.
A version of this article appeared on Medscape.com.
TOPLINE:
Gabapentinoid use significantly increased the risk for exacerbations in adults with chronic obstructive pulmonary disease (COPD).
METHODOLOGY:
- Previous research has prompted warnings from North American and European health agencies of severe exacerbations associated with gabapentinoid use by patients with COPD.
- The researchers compared data from patients with COPD in Canadian databases between 1994 and 2015 who were new to gabapentinoids and matched them to patients who did not use gabapentinoids.
- The primary outcome was exacerbation of COPD that required hospitalization in a propensity score-matched study.
TAKEAWAY:
- The study population included 356 epilepsy patients, 9411 neuropathic pain patients, and 3737 patients with other chronic pain.
- Use of gabapentinoids was significantly associated with an overall increased risk for severe COPD exacerbation (hazard ratio, 1.49) compared with nonuse.
- Gabapentinoid use was associated with a significantly increased COPD exacerbation risk for each group of users compared with nonusers, with hazard ratios of 1.58, 1.35, and 1.49 for epilepsy, neuropathic pain, and other chronic pain, respectively.
IN PRACTICE:
“This study supports the warnings from regulatory agencies and highlights the importance of considering this potential risk when prescribing gabapentin and pregabalin to patients with COPD,” the researchers wrote.
SOURCE:
The lead author on the study was Alvi A. Rahman, MSc, of Jewish General Hospital, Montreal. The study was published online on January 16, 2024, in Annals of Internal Medicine.
LIMITATIONS:
A lack of data on smoking status and other residual confounding factors limited the study findings.
DISCLOSURES:
The study was supported by the Canadian Institutes of Health Research and the Canadian Lung Association. Mr. Rahman had no financial conflicts to disclose, but some coauthors disclosed consulting and advisory relationships with various companies, including Merck, Pfizer, Seqirus, Boehringer-Ingelheim, and Novartis outside of the current work.
A version of this article appeared on Medscape.com.
TOPLINE:
Gabapentinoid use significantly increased the risk for exacerbations in adults with chronic obstructive pulmonary disease (COPD).
METHODOLOGY:
- Previous research has prompted warnings from North American and European health agencies of severe exacerbations associated with gabapentinoid use by patients with COPD.
- The researchers compared data from patients with COPD in Canadian databases between 1994 and 2015 who were new to gabapentinoids and matched them to patients who did not use gabapentinoids.
- The primary outcome was exacerbation of COPD that required hospitalization in a propensity score-matched study.
TAKEAWAY:
- The study population included 356 epilepsy patients, 9411 neuropathic pain patients, and 3737 patients with other chronic pain.
- Use of gabapentinoids was significantly associated with an overall increased risk for severe COPD exacerbation (hazard ratio, 1.49) compared with nonuse.
- Gabapentinoid use was associated with a significantly increased COPD exacerbation risk for each group of users compared with nonusers, with hazard ratios of 1.58, 1.35, and 1.49 for epilepsy, neuropathic pain, and other chronic pain, respectively.
IN PRACTICE:
“This study supports the warnings from regulatory agencies and highlights the importance of considering this potential risk when prescribing gabapentin and pregabalin to patients with COPD,” the researchers wrote.
SOURCE:
The lead author on the study was Alvi A. Rahman, MSc, of Jewish General Hospital, Montreal. The study was published online on January 16, 2024, in Annals of Internal Medicine.
LIMITATIONS:
A lack of data on smoking status and other residual confounding factors limited the study findings.
DISCLOSURES:
The study was supported by the Canadian Institutes of Health Research and the Canadian Lung Association. Mr. Rahman had no financial conflicts to disclose, but some coauthors disclosed consulting and advisory relationships with various companies, including Merck, Pfizer, Seqirus, Boehringer-Ingelheim, and Novartis outside of the current work.
A version of this article appeared on Medscape.com.
Doc Sues State Over ‘Antiquated’ Telehealth Rules
Telemedicine visits skyrocketed during the pandemic, but
In the complaint filed on December 13 in New Jersey District Court, plaintiff Shannon MacDonald, MD, radiation oncologist at Massachusetts General Hospital, Boston, said that New Jersey’s telehealth rules make it illegal for her and other out-of-state specialists to consult with and treat residents who could benefit from their unique expertise, unless they first obtain licensure through the medical board.
While she currently maintains licenses in six states, New Jersey’s application process can take several months and requires an initial fee of $550, plus additional expenses for a background check and fingerprinting, court documents said.
Physicians providing telehealth services to New Jersey residents without a state-authorized medical license are subject to up to 5 years in prison and criminal and civil fines exceeding $10,000.
“Every day, my ethical obligations to my patients are in direct conflict with the legal framework,” said Dr. MacDonald.
She and coplaintiff Paul Gardner, MD, neurosurgical codirector of the Center for Cranial Base Surgery at the University of Pittsburgh Medical Center, are represented by the public interest law firm Pacific Legal Foundation, which recently sued Louisiana’s governor over its medical board diversity rules.
The lawsuit names Otto Sabando, DO, president of the New Jersey State Board of Medical Examiners. Representatives for Dr. Sabando and the medical board did not respond to a request for comment.
The complaint describes the care Dr. MacDonald provided several years before the pandemic for an out-of-state patient, J.A., also named as a plaintiff, who was diagnosed with pineoblastoma at 18 months old.
After initially undergoing treatment in New York, court documents indicate that J.A.’s medical team referred him to Dr. MacDonald “because of her nationally recognized expertise in proton therapy” targeting rare childhood cancers. Dr. MacDonald remotely reviewed J.A.’s scans and discussed options before his family pursued treatment with her in Boston.
Dr. MacDonald said that allowing more patients like J.A. to use telehealth to access services when specialists are unavailable in their state would go a long way toward achieving health equity. She says it could reduce the financial burden of travel and lodging expenses and provide timely consultations and follow-up care.
Many states, including New Jersey, waived or eased licensing regulations during the pandemic so physicians could temporarily practice in other states. Since those emergency orders have ended, physicians must again seek licensure in the states where their patients are located or potentially be subjected to fines or other penalties by state medical boards.
New Jersey Governor Phil Murphy signed a law in 2022 joining the Interstate Medical Licensure Compact, an agreement that offers a streamlined process for physicians already licensed in their home states to obtain licensure in 37 other member states as well as the District of Columbia and Territory of Guam. However, the lawsuit alleges that applications still take weeks and pose significant administrative and financial barriers for physicians.
Telehealth in a Post-COVID World
“Until COVID, we didn’t realize that a telephone call really was practicing medicine,” said Dr. MacDonald. “After being allowed to do telemedicine consultations across state lines for a year and 2 years for follow-ups, I thought it would last forever, but it’s placed a spotlight on what we cannot do.”
Dr. MacDonald, who recently penned a related editorial in the Wall Street Journal, said laws regarding interstate practice are outdated.
“They made sense in the preindustrial era when you had to be in the same location as your patient, but they make little sense in the modern era when distance disappears over the Internet or telephone,” she said.
The issue isn’t unique to New Jersey. Caleb Trotter, JD, attorney for the Pacific Legal Foundation, said that 30 states prohibit doctors from conducting telemedicine services in states where they are not licensed.
“Some hospitals instruct doctors and administrators to ask the patient where they are physically located at the beginning of a telehealth appointment, and if it isn’t a state where the physician is licensed, they are instructed to end the appointment immediately,” Mr. Trotter said. “A win in New Jersey would solve a very real problem for these [patients] of not having convenient legal access to specialists.”
Neither Dr. MacDonald nor Dr. Gardner have had any enforcement actions taken against them, said Mr. Trotter. Still, he said the New Jersey attorney general’s office reminded physicians last year that state licensure rules apply to out-of-state doctors using telemedicine to conduct follow-up appointments.
In November, the Center for Health Law and Policy Innovation at Harvard Law School, Cambridge, Massachusetts, proposed telemedicine reforms, including exceptions for the care of established patients and screening for specialty referrals.
Dr. MacDonald hopes the lawsuit will increase awareness of telehealth laws and spur changes.
A version of this article appeared on Medscape.com.
Telemedicine visits skyrocketed during the pandemic, but
In the complaint filed on December 13 in New Jersey District Court, plaintiff Shannon MacDonald, MD, radiation oncologist at Massachusetts General Hospital, Boston, said that New Jersey’s telehealth rules make it illegal for her and other out-of-state specialists to consult with and treat residents who could benefit from their unique expertise, unless they first obtain licensure through the medical board.
While she currently maintains licenses in six states, New Jersey’s application process can take several months and requires an initial fee of $550, plus additional expenses for a background check and fingerprinting, court documents said.
Physicians providing telehealth services to New Jersey residents without a state-authorized medical license are subject to up to 5 years in prison and criminal and civil fines exceeding $10,000.
“Every day, my ethical obligations to my patients are in direct conflict with the legal framework,” said Dr. MacDonald.
She and coplaintiff Paul Gardner, MD, neurosurgical codirector of the Center for Cranial Base Surgery at the University of Pittsburgh Medical Center, are represented by the public interest law firm Pacific Legal Foundation, which recently sued Louisiana’s governor over its medical board diversity rules.
The lawsuit names Otto Sabando, DO, president of the New Jersey State Board of Medical Examiners. Representatives for Dr. Sabando and the medical board did not respond to a request for comment.
The complaint describes the care Dr. MacDonald provided several years before the pandemic for an out-of-state patient, J.A., also named as a plaintiff, who was diagnosed with pineoblastoma at 18 months old.
After initially undergoing treatment in New York, court documents indicate that J.A.’s medical team referred him to Dr. MacDonald “because of her nationally recognized expertise in proton therapy” targeting rare childhood cancers. Dr. MacDonald remotely reviewed J.A.’s scans and discussed options before his family pursued treatment with her in Boston.
Dr. MacDonald said that allowing more patients like J.A. to use telehealth to access services when specialists are unavailable in their state would go a long way toward achieving health equity. She says it could reduce the financial burden of travel and lodging expenses and provide timely consultations and follow-up care.
Many states, including New Jersey, waived or eased licensing regulations during the pandemic so physicians could temporarily practice in other states. Since those emergency orders have ended, physicians must again seek licensure in the states where their patients are located or potentially be subjected to fines or other penalties by state medical boards.
New Jersey Governor Phil Murphy signed a law in 2022 joining the Interstate Medical Licensure Compact, an agreement that offers a streamlined process for physicians already licensed in their home states to obtain licensure in 37 other member states as well as the District of Columbia and Territory of Guam. However, the lawsuit alleges that applications still take weeks and pose significant administrative and financial barriers for physicians.
Telehealth in a Post-COVID World
“Until COVID, we didn’t realize that a telephone call really was practicing medicine,” said Dr. MacDonald. “After being allowed to do telemedicine consultations across state lines for a year and 2 years for follow-ups, I thought it would last forever, but it’s placed a spotlight on what we cannot do.”
Dr. MacDonald, who recently penned a related editorial in the Wall Street Journal, said laws regarding interstate practice are outdated.
“They made sense in the preindustrial era when you had to be in the same location as your patient, but they make little sense in the modern era when distance disappears over the Internet or telephone,” she said.
The issue isn’t unique to New Jersey. Caleb Trotter, JD, attorney for the Pacific Legal Foundation, said that 30 states prohibit doctors from conducting telemedicine services in states where they are not licensed.
“Some hospitals instruct doctors and administrators to ask the patient where they are physically located at the beginning of a telehealth appointment, and if it isn’t a state where the physician is licensed, they are instructed to end the appointment immediately,” Mr. Trotter said. “A win in New Jersey would solve a very real problem for these [patients] of not having convenient legal access to specialists.”
Neither Dr. MacDonald nor Dr. Gardner have had any enforcement actions taken against them, said Mr. Trotter. Still, he said the New Jersey attorney general’s office reminded physicians last year that state licensure rules apply to out-of-state doctors using telemedicine to conduct follow-up appointments.
In November, the Center for Health Law and Policy Innovation at Harvard Law School, Cambridge, Massachusetts, proposed telemedicine reforms, including exceptions for the care of established patients and screening for specialty referrals.
Dr. MacDonald hopes the lawsuit will increase awareness of telehealth laws and spur changes.
A version of this article appeared on Medscape.com.
Telemedicine visits skyrocketed during the pandemic, but
In the complaint filed on December 13 in New Jersey District Court, plaintiff Shannon MacDonald, MD, radiation oncologist at Massachusetts General Hospital, Boston, said that New Jersey’s telehealth rules make it illegal for her and other out-of-state specialists to consult with and treat residents who could benefit from their unique expertise, unless they first obtain licensure through the medical board.
While she currently maintains licenses in six states, New Jersey’s application process can take several months and requires an initial fee of $550, plus additional expenses for a background check and fingerprinting, court documents said.
Physicians providing telehealth services to New Jersey residents without a state-authorized medical license are subject to up to 5 years in prison and criminal and civil fines exceeding $10,000.
“Every day, my ethical obligations to my patients are in direct conflict with the legal framework,” said Dr. MacDonald.
She and coplaintiff Paul Gardner, MD, neurosurgical codirector of the Center for Cranial Base Surgery at the University of Pittsburgh Medical Center, are represented by the public interest law firm Pacific Legal Foundation, which recently sued Louisiana’s governor over its medical board diversity rules.
The lawsuit names Otto Sabando, DO, president of the New Jersey State Board of Medical Examiners. Representatives for Dr. Sabando and the medical board did not respond to a request for comment.
The complaint describes the care Dr. MacDonald provided several years before the pandemic for an out-of-state patient, J.A., also named as a plaintiff, who was diagnosed with pineoblastoma at 18 months old.
After initially undergoing treatment in New York, court documents indicate that J.A.’s medical team referred him to Dr. MacDonald “because of her nationally recognized expertise in proton therapy” targeting rare childhood cancers. Dr. MacDonald remotely reviewed J.A.’s scans and discussed options before his family pursued treatment with her in Boston.
Dr. MacDonald said that allowing more patients like J.A. to use telehealth to access services when specialists are unavailable in their state would go a long way toward achieving health equity. She says it could reduce the financial burden of travel and lodging expenses and provide timely consultations and follow-up care.
Many states, including New Jersey, waived or eased licensing regulations during the pandemic so physicians could temporarily practice in other states. Since those emergency orders have ended, physicians must again seek licensure in the states where their patients are located or potentially be subjected to fines or other penalties by state medical boards.
New Jersey Governor Phil Murphy signed a law in 2022 joining the Interstate Medical Licensure Compact, an agreement that offers a streamlined process for physicians already licensed in their home states to obtain licensure in 37 other member states as well as the District of Columbia and Territory of Guam. However, the lawsuit alleges that applications still take weeks and pose significant administrative and financial barriers for physicians.
Telehealth in a Post-COVID World
“Until COVID, we didn’t realize that a telephone call really was practicing medicine,” said Dr. MacDonald. “After being allowed to do telemedicine consultations across state lines for a year and 2 years for follow-ups, I thought it would last forever, but it’s placed a spotlight on what we cannot do.”
Dr. MacDonald, who recently penned a related editorial in the Wall Street Journal, said laws regarding interstate practice are outdated.
“They made sense in the preindustrial era when you had to be in the same location as your patient, but they make little sense in the modern era when distance disappears over the Internet or telephone,” she said.
The issue isn’t unique to New Jersey. Caleb Trotter, JD, attorney for the Pacific Legal Foundation, said that 30 states prohibit doctors from conducting telemedicine services in states where they are not licensed.
“Some hospitals instruct doctors and administrators to ask the patient where they are physically located at the beginning of a telehealth appointment, and if it isn’t a state where the physician is licensed, they are instructed to end the appointment immediately,” Mr. Trotter said. “A win in New Jersey would solve a very real problem for these [patients] of not having convenient legal access to specialists.”
Neither Dr. MacDonald nor Dr. Gardner have had any enforcement actions taken against them, said Mr. Trotter. Still, he said the New Jersey attorney general’s office reminded physicians last year that state licensure rules apply to out-of-state doctors using telemedicine to conduct follow-up appointments.
In November, the Center for Health Law and Policy Innovation at Harvard Law School, Cambridge, Massachusetts, proposed telemedicine reforms, including exceptions for the care of established patients and screening for specialty referrals.
Dr. MacDonald hopes the lawsuit will increase awareness of telehealth laws and spur changes.
A version of this article appeared on Medscape.com.
Success with Sirolimus in Treating Skin Sarcoidosis Could Spur Studies in Other Organs
Sirolimus may be an effective treatment for patients with persistent cutaneous sarcoidosis.
In a small clinical trial, 7 of 10 patients treated with sirolimus via oral solution had improvements in skin lesions after 4 months, which was sustained for up to 2 years after the study concluded.
The results suggested that mechanistic target of rapamycin (mTOR) inhibition is a potential therapeutic avenue for sarcoidosis, which the authors said should be explored in larger clinical trials.
In the past decade, there has been a growing amount of evidence suggesting mTOR’s role in sarcoidosis. In 2017, researchers showed that activation of mTOR in macrophages could cause progressive sarcoidosis in mice. In additional studies, high levels of mTOR activity were detected in human sarcoidosis granulomas in various organs, including the skin, lung, and heart.
Three case reports also documented using the mTOR inhibitor sirolimus to effectively treat systemic sarcoidosis.
“Although all reports observed improvement of the disease following the treatment, no clinical trial investigating the efficacy and safety of sirolimus in patients with sarcoidosis had been published” prior to this study, wrote senior author Georg Stary, MD, of the Medical University of Vienna and the Research Center for Molecular Medicine of the Austrian Academy of Sciences, Vienna, Austria, and colleagues.
The findings were published in the The Lancet Rheumatology.
For the study, researchers recruited 16 individuals with persistent and glucocorticoid-refractory cutaneous sarcoidosis between September 2019 and June 2021. A total of 14 participants were randomly assigned to the topical phase of the study, whereas two immediately received systemic treatment. All treatment was conducted at Vienna General Hospital.
In the placebo-controlled, double-blinded topical treatment arm, patients received either 0.1% topical sirolimus in Vaseline or Vaseline alone (placebo) twice daily for 2 months. After a 1-month washout period, participants were switched to the alternate treatment arm for an additional 2 months.
Following this topical phase and an additional 1-month washout period, all remaining participants received systemic sirolimus via a 1-mg/mL solution, starting with a 6-mg loading dose and continuing with 2 mg once daily for 4 months. The primary outcome was change in Cutaneous Sarcoidosis Activity and Morphology Index (CSAMI) from baseline, with decrease of more than five points representing a response to treatment.
A total of 10 patients completed the trial.
There was no change in CSAMI in either topical treatment groups. In the systemic group, 70% of patients had clinical improvement in skin lesions, with three responders in this group having complete resolution of skin lesions. The median change in CSAMI was −7.0 points (P = .018).
This improvement persisted for 2 months following study conclusion, with more pronounced improvement from baseline after 2 years of drug-free follow-up (−11.5 points).
There were no serious adverse events reported during the study, but 42% of patients treated with systemic sirolimus reported mild skin reactions, such as acne and eczema. Other related adverse events were hypertriglyceridemia (17%), hyperglycemia (17%), and proteinuria (8%).
Compared with clinical outcomes with tofacitinib and tumor necrosis factor (TNF) inhibitors, “the strength of our study lies in the sustained treatment effect after drug withdrawal among all responders. This prolonged effect has not yet been explored with tofacitinib, whereas with TNF inhibitors disease relapse was seen in more than 50% of patients at 3-8 months,” the authors wrote.
The researchers also analyzed participants’ skin biopsies to gain a better understanding of how mTOR inhibition affected granuloma structures. They found that, at baseline, mTOR activity was significantly lower in the fibroblasts of treatment nonresponders than in responders. They speculated that lower expression of mTOR could make these granuloma-associated cells resistant to systemic sirolimus.
These promising findings combine “clinical response with a molecular analysis,” Avrom Caplan, MD, co-director of the Sarcoidosis Program at NYU Langone in New York City, told this news organization. He was not involved with the research. Adding molecular information to clinical outcome data “helps solidify that [the mTOR] pathway has relevance in the sarcoid granuloma formation.”
The study had a limited sample size — a challenge for many clinical trials of rare diseases, Dr. Caplan said. Larger clinical trials are necessary to explore mTOR inhibition in sarcoidosis, both he and the authors agreed. A larger trial could also include greater heterogeneity of patients, including varied sarcoid presentation and demographics, Dr. Caplan noted. In this study, all but one participants were White individuals, and 63% of participants were female.
Larger studies could also address important questions on ideal length of therapy, dosing, and where this therapy “would fall within the therapeutic step ladder,” Dr. Caplan continued.
Whether mTOR inhibition could be effective at treating individuals with sarcoidosis in other organs beyond the skin is also unknown.
“If the pathogenesis of sarcoid granuloma formation does include mTOR upregulation, which they are showing here…then you could hypothesize that, yes, using this therapy could benefit other organs,” he said. “But that has to be investigated in larger trials.”
The study was funded in part by a Vienna Science and Technology Fund project. Several authors report receiving grants from the Austrian Science Fund and one from the Ann Theodore Foundation Breakthrough Sarcoidosis Initiative. Dr. Caplan reported no relevant financial relationships.
A version of this article appeared on Medscape.com .
Sirolimus may be an effective treatment for patients with persistent cutaneous sarcoidosis.
In a small clinical trial, 7 of 10 patients treated with sirolimus via oral solution had improvements in skin lesions after 4 months, which was sustained for up to 2 years after the study concluded.
The results suggested that mechanistic target of rapamycin (mTOR) inhibition is a potential therapeutic avenue for sarcoidosis, which the authors said should be explored in larger clinical trials.
In the past decade, there has been a growing amount of evidence suggesting mTOR’s role in sarcoidosis. In 2017, researchers showed that activation of mTOR in macrophages could cause progressive sarcoidosis in mice. In additional studies, high levels of mTOR activity were detected in human sarcoidosis granulomas in various organs, including the skin, lung, and heart.
Three case reports also documented using the mTOR inhibitor sirolimus to effectively treat systemic sarcoidosis.
“Although all reports observed improvement of the disease following the treatment, no clinical trial investigating the efficacy and safety of sirolimus in patients with sarcoidosis had been published” prior to this study, wrote senior author Georg Stary, MD, of the Medical University of Vienna and the Research Center for Molecular Medicine of the Austrian Academy of Sciences, Vienna, Austria, and colleagues.
The findings were published in the The Lancet Rheumatology.
For the study, researchers recruited 16 individuals with persistent and glucocorticoid-refractory cutaneous sarcoidosis between September 2019 and June 2021. A total of 14 participants were randomly assigned to the topical phase of the study, whereas two immediately received systemic treatment. All treatment was conducted at Vienna General Hospital.
In the placebo-controlled, double-blinded topical treatment arm, patients received either 0.1% topical sirolimus in Vaseline or Vaseline alone (placebo) twice daily for 2 months. After a 1-month washout period, participants were switched to the alternate treatment arm for an additional 2 months.
Following this topical phase and an additional 1-month washout period, all remaining participants received systemic sirolimus via a 1-mg/mL solution, starting with a 6-mg loading dose and continuing with 2 mg once daily for 4 months. The primary outcome was change in Cutaneous Sarcoidosis Activity and Morphology Index (CSAMI) from baseline, with decrease of more than five points representing a response to treatment.
A total of 10 patients completed the trial.
There was no change in CSAMI in either topical treatment groups. In the systemic group, 70% of patients had clinical improvement in skin lesions, with three responders in this group having complete resolution of skin lesions. The median change in CSAMI was −7.0 points (P = .018).
This improvement persisted for 2 months following study conclusion, with more pronounced improvement from baseline after 2 years of drug-free follow-up (−11.5 points).
There were no serious adverse events reported during the study, but 42% of patients treated with systemic sirolimus reported mild skin reactions, such as acne and eczema. Other related adverse events were hypertriglyceridemia (17%), hyperglycemia (17%), and proteinuria (8%).
Compared with clinical outcomes with tofacitinib and tumor necrosis factor (TNF) inhibitors, “the strength of our study lies in the sustained treatment effect after drug withdrawal among all responders. This prolonged effect has not yet been explored with tofacitinib, whereas with TNF inhibitors disease relapse was seen in more than 50% of patients at 3-8 months,” the authors wrote.
The researchers also analyzed participants’ skin biopsies to gain a better understanding of how mTOR inhibition affected granuloma structures. They found that, at baseline, mTOR activity was significantly lower in the fibroblasts of treatment nonresponders than in responders. They speculated that lower expression of mTOR could make these granuloma-associated cells resistant to systemic sirolimus.
These promising findings combine “clinical response with a molecular analysis,” Avrom Caplan, MD, co-director of the Sarcoidosis Program at NYU Langone in New York City, told this news organization. He was not involved with the research. Adding molecular information to clinical outcome data “helps solidify that [the mTOR] pathway has relevance in the sarcoid granuloma formation.”
The study had a limited sample size — a challenge for many clinical trials of rare diseases, Dr. Caplan said. Larger clinical trials are necessary to explore mTOR inhibition in sarcoidosis, both he and the authors agreed. A larger trial could also include greater heterogeneity of patients, including varied sarcoid presentation and demographics, Dr. Caplan noted. In this study, all but one participants were White individuals, and 63% of participants were female.
Larger studies could also address important questions on ideal length of therapy, dosing, and where this therapy “would fall within the therapeutic step ladder,” Dr. Caplan continued.
Whether mTOR inhibition could be effective at treating individuals with sarcoidosis in other organs beyond the skin is also unknown.
“If the pathogenesis of sarcoid granuloma formation does include mTOR upregulation, which they are showing here…then you could hypothesize that, yes, using this therapy could benefit other organs,” he said. “But that has to be investigated in larger trials.”
The study was funded in part by a Vienna Science and Technology Fund project. Several authors report receiving grants from the Austrian Science Fund and one from the Ann Theodore Foundation Breakthrough Sarcoidosis Initiative. Dr. Caplan reported no relevant financial relationships.
A version of this article appeared on Medscape.com .
Sirolimus may be an effective treatment for patients with persistent cutaneous sarcoidosis.
In a small clinical trial, 7 of 10 patients treated with sirolimus via oral solution had improvements in skin lesions after 4 months, which was sustained for up to 2 years after the study concluded.
The results suggested that mechanistic target of rapamycin (mTOR) inhibition is a potential therapeutic avenue for sarcoidosis, which the authors said should be explored in larger clinical trials.
In the past decade, there has been a growing amount of evidence suggesting mTOR’s role in sarcoidosis. In 2017, researchers showed that activation of mTOR in macrophages could cause progressive sarcoidosis in mice. In additional studies, high levels of mTOR activity were detected in human sarcoidosis granulomas in various organs, including the skin, lung, and heart.
Three case reports also documented using the mTOR inhibitor sirolimus to effectively treat systemic sarcoidosis.
“Although all reports observed improvement of the disease following the treatment, no clinical trial investigating the efficacy and safety of sirolimus in patients with sarcoidosis had been published” prior to this study, wrote senior author Georg Stary, MD, of the Medical University of Vienna and the Research Center for Molecular Medicine of the Austrian Academy of Sciences, Vienna, Austria, and colleagues.
The findings were published in the The Lancet Rheumatology.
For the study, researchers recruited 16 individuals with persistent and glucocorticoid-refractory cutaneous sarcoidosis between September 2019 and June 2021. A total of 14 participants were randomly assigned to the topical phase of the study, whereas two immediately received systemic treatment. All treatment was conducted at Vienna General Hospital.
In the placebo-controlled, double-blinded topical treatment arm, patients received either 0.1% topical sirolimus in Vaseline or Vaseline alone (placebo) twice daily for 2 months. After a 1-month washout period, participants were switched to the alternate treatment arm for an additional 2 months.
Following this topical phase and an additional 1-month washout period, all remaining participants received systemic sirolimus via a 1-mg/mL solution, starting with a 6-mg loading dose and continuing with 2 mg once daily for 4 months. The primary outcome was change in Cutaneous Sarcoidosis Activity and Morphology Index (CSAMI) from baseline, with decrease of more than five points representing a response to treatment.
A total of 10 patients completed the trial.
There was no change in CSAMI in either topical treatment groups. In the systemic group, 70% of patients had clinical improvement in skin lesions, with three responders in this group having complete resolution of skin lesions. The median change in CSAMI was −7.0 points (P = .018).
This improvement persisted for 2 months following study conclusion, with more pronounced improvement from baseline after 2 years of drug-free follow-up (−11.5 points).
There were no serious adverse events reported during the study, but 42% of patients treated with systemic sirolimus reported mild skin reactions, such as acne and eczema. Other related adverse events were hypertriglyceridemia (17%), hyperglycemia (17%), and proteinuria (8%).
Compared with clinical outcomes with tofacitinib and tumor necrosis factor (TNF) inhibitors, “the strength of our study lies in the sustained treatment effect after drug withdrawal among all responders. This prolonged effect has not yet been explored with tofacitinib, whereas with TNF inhibitors disease relapse was seen in more than 50% of patients at 3-8 months,” the authors wrote.
The researchers also analyzed participants’ skin biopsies to gain a better understanding of how mTOR inhibition affected granuloma structures. They found that, at baseline, mTOR activity was significantly lower in the fibroblasts of treatment nonresponders than in responders. They speculated that lower expression of mTOR could make these granuloma-associated cells resistant to systemic sirolimus.
These promising findings combine “clinical response with a molecular analysis,” Avrom Caplan, MD, co-director of the Sarcoidosis Program at NYU Langone in New York City, told this news organization. He was not involved with the research. Adding molecular information to clinical outcome data “helps solidify that [the mTOR] pathway has relevance in the sarcoid granuloma formation.”
The study had a limited sample size — a challenge for many clinical trials of rare diseases, Dr. Caplan said. Larger clinical trials are necessary to explore mTOR inhibition in sarcoidosis, both he and the authors agreed. A larger trial could also include greater heterogeneity of patients, including varied sarcoid presentation and demographics, Dr. Caplan noted. In this study, all but one participants were White individuals, and 63% of participants were female.
Larger studies could also address important questions on ideal length of therapy, dosing, and where this therapy “would fall within the therapeutic step ladder,” Dr. Caplan continued.
Whether mTOR inhibition could be effective at treating individuals with sarcoidosis in other organs beyond the skin is also unknown.
“If the pathogenesis of sarcoid granuloma formation does include mTOR upregulation, which they are showing here…then you could hypothesize that, yes, using this therapy could benefit other organs,” he said. “But that has to be investigated in larger trials.”
The study was funded in part by a Vienna Science and Technology Fund project. Several authors report receiving grants from the Austrian Science Fund and one from the Ann Theodore Foundation Breakthrough Sarcoidosis Initiative. Dr. Caplan reported no relevant financial relationships.
A version of this article appeared on Medscape.com .
FROM THE LANCET RHEUMATOLOGY
Mega Malpractice Verdicts Against Physicians on the Rise
In December, in what’s known as the “Take Care of Maya” case, a Florida jury returned a record $261 million verdict against Johns Hopkins All Children’s Hospital, St. Petersburg, Florida, for its treatment of a young patient and her family after an emergency room visit.
A month earlier, in New York, a jury ordered Westchester Medical Center Health Network to pay $120 million to a patient and his family following delayed stroke care that resulted in brain damage.
Mega malpractice awards like these are rising against physicians and hospitals around the country, according to new data from TransRe, an international reinsurance company that tracks large verdicts.
“2023 blew away every record previously set among high medical malpractice verdicts,” said Richard Henderson, senior vice president for TransRe.
In 2023, there were 57 medical malpractice verdicts of $10 million or more in the United States, the data showed. Slightly more than half of those reached $25 million or more.
From 2012 to 2022, verdicts of $10 million or more ranged from 34 in 2013 to 52 in 2022, TransRe research found.
While New York, Illinois, and Florida typically saw the highest dollar verdicts in previous years, so-called “nuclear” verdicts now occur in states like Utah and Georgia where they once were uncommon, said Robert E. White Jr., president of TDC Group and The Doctors Company, a national medical liability insurer for physicians.
A rollback of tort reforms across the country is one contributor, he said. For example, Georgia’s cap on noneconomic damages is among those that have been ruled unconstitutional by courts. Utah’s cap on noneconomic damages still stands, but the limit was deemed unconstitutional in wrongful death cases. In 2019, a portion of Utah›s pre-litigation panel process was also struck down by the state’s Supreme Court.
“We used to be able to predict where these high verdicts would occur,” Mr. White said. “We can’t predict it anymore.”
Research shows a majority of malpractice cases are dropped or settled before trial, and claims that go before juries usually end in doctors’ favor. Plaintiffs’ attorneys cite large jury verdicts in similar cases to induce settlements and higher payouts, Mr. White said.
And while mega verdicts rarely stick, they can have lasting effects on future claims. The awards lead to larger settlement demands from plaintiffs and drive up the cost to resolve claims, according to Mr. Henderson and Mr. White.
“Verdicts are the yardstick by which all settlements are measured,” Mr. White said. “That’s where the damage is done.” The prospect of a mega verdict can make insurers leery of fighting some malpractice cases and motivate them to offer bigger settlements to stay out of the courtroom, he added.
Why Are Juries Awarding Higher Verdicts?
There’s no single reason for the rise in nuclear verdicts, Mr. Henderson said.
One theory is that plaintiffs’ attorneys held back on resolving high-dollar cases during the COVID pandemic and let loose with high-demand claims when courts returned to normal, he said.
Another theory is that people emerged from the pandemic angrier.
“Whether it was political dynamics, masking [mandates], or differences in opinions, people came out of it angry, and generally speaking, you don’t want an angry jury,” Mr. Henderson said. “For a while, there was the halo effect, where health professionals were seen as heroes. That went away, and all of a sudden [they] became ‘the bad guys.’ ”
“People are angry at the healthcare system, and this anger manifests itself in [liability] suits,” added Bill Burns, vice president of research for the Medical Professional Liability Association, an industry group for medical liability insurers.
Hospital and medical group consolidation also reduces the personal connection juries may have with healthcare providers, Mr. Burns said.
“Healthcare has become a big business, and the corporatization of medicine now puts companies on the stand and not your local community hospital or your family doctor that you have known since birth,” he said.
Plaintiffs’ attorneys also deploy tactics that can prompt higher verdicts, Mr. White said. They may tell a jury that the provider or hospital is a threat to the community and that awarding a large verdict will deter others in the healthcare community from repeating the same actions.
Juries may then want to punish the defendant in addition to assessing damages for economic harm or pain and suffering, Mr. White said.
“I am concerned that jurors are trying to right social wrongs rather than judging cases on the facts presented to them,” added Mike Stinson, vice president for policy and legal affairs for the Medical Professional Liability Association.
Third-party litigation financing also can lead to mega verdicts. That’s an emerging practice in which companies unrelated to a lawsuit provide capital to plaintiffs in return for a portion of any financial award. The firms essentially “invest” in the litigation.
“What this does is provide an additional financial backdrop for plaintiffs,” Mr. Henderson said. “It allows them to dig in harder on cases. They can hold out for higher numbers, and if nothing else, it can prolong litigation.”
Do High Awards Actually Stick?
Multimillion-dollar verdicts may grab headlines, but do plaintiffs actually receive them?
Rarely, said TransRe, which tracks the final outcomes of verdicts. In many cases, large verdicts are reduced on appeal.
In the Maya case, which involved child protection authorities, a judge later lowered the damages against Johns Hopkins All Children’s Hospital by $47.5 million.
A federal judge in October, for example, rejected a record $110 million medical malpractice award in Minnesota, reducing it to $10 million. The district judge ruled the award was “shockingly excessive” and that the plaintiff should either accept the $10 million award or retry the case.
After a verdict is awarded, the defendant typically challenges the award, and the case goes through the appellate pipeline, Mr. Henderson explained. A judge may reduce some elements of the verdict, he said, but more often, the plaintiff and defendant agree on a compromised figure.
Seattle medical liability defense attorney Jennifer Crisera has experienced this firsthand. She recalled a recent case where a plaintiff’s attorney demanded what she describes as an unreasonable amount to settle a claim. Ms. Crisera did not want to give exact numbers but said the plaintiff made an 8-figure demand and the defense offered a low 7-figure range.
“My impression was that plaintiff’s counsel believed that they could get a nuclear verdict from the jury, so they kept their settlement demand artificially high,” she said. “The division between the numbers was way too high. Ultimately, we had to let a jury decide the value.”
The plaintiff won the case, and the verdict was much less than the settlement demand, she said. Even so, the defense incurred trial costs, and the health provider was forced to endure the emotional stress of a trial that could have been avoided, Ms. Crisera said.
Higher medical malpractice premiums are another consequence of massive awards.
Premium rates are associated with how much insurers pay on average for cases and how frequently they are making payouts, Mr. White said.
Medical liability insurance premiums for physicians have steadily increased since 2019, according to data from the Medical Liability Monitor, a national publication that analyzes liability insurance premiums. The Monitor studies insurance premium data from insurers that cover internists, general surgeons, and obstetrician-gynecologists.
From 2019 to 2023, average premium rates for physicians increased between 1.1% and 3% each year in states without patient compensation funds, according to Monitor data.
“Nuclear verdicts are a real driver of the industry’s underwriting losses and remain top of mind for every malpractice insurance company,” said Michael Matray, editor for the Medical Liability Monitor. “Responses to this year’s rate survey questionnaire indicate that most responding companies have experienced an increase in claims greater than $1 million and claims greater than $5 million during the past 2 years.”
However, increases vary widely by region and among counties. In Montgomery County, Alabama, for instance, premiums for internists rose by 24% from 2022 to 2023, from $8,231 to $10,240. Premiums for Montgomery County general surgeons rose by 11.9% from 2022 to 2023, from $30,761 to $34,426, according to survey data.
In several counties in Illinois (Adams, Knox, Peoria, and Rock Island), premiums for some internists rose by 15% from $24,041 to $27,783, and premiums for some surgeons increased by 27% from $60,202 to $76,461, according to survey data. Some internists in Catoosa County, Georgia, meanwhile, paid $17,831 in 2023, up from $16,313 in 2022. Some surgeons in Catoosa County paid $65,616 in 2023, up from $60,032 in 2022. Inflation could be one factor behind higher liability premium rates. Claim severity is a key driver of higher premium rates, Mr. White added.
“We have not seen stability in claims severity,” he said. “It is continuing to go up and, in all likelihood, it will drive [premium] rates up further from this point.”
A version of this article appeared on Medscape.com.
In December, in what’s known as the “Take Care of Maya” case, a Florida jury returned a record $261 million verdict against Johns Hopkins All Children’s Hospital, St. Petersburg, Florida, for its treatment of a young patient and her family after an emergency room visit.
A month earlier, in New York, a jury ordered Westchester Medical Center Health Network to pay $120 million to a patient and his family following delayed stroke care that resulted in brain damage.
Mega malpractice awards like these are rising against physicians and hospitals around the country, according to new data from TransRe, an international reinsurance company that tracks large verdicts.
“2023 blew away every record previously set among high medical malpractice verdicts,” said Richard Henderson, senior vice president for TransRe.
In 2023, there were 57 medical malpractice verdicts of $10 million or more in the United States, the data showed. Slightly more than half of those reached $25 million or more.
From 2012 to 2022, verdicts of $10 million or more ranged from 34 in 2013 to 52 in 2022, TransRe research found.
While New York, Illinois, and Florida typically saw the highest dollar verdicts in previous years, so-called “nuclear” verdicts now occur in states like Utah and Georgia where they once were uncommon, said Robert E. White Jr., president of TDC Group and The Doctors Company, a national medical liability insurer for physicians.
A rollback of tort reforms across the country is one contributor, he said. For example, Georgia’s cap on noneconomic damages is among those that have been ruled unconstitutional by courts. Utah’s cap on noneconomic damages still stands, but the limit was deemed unconstitutional in wrongful death cases. In 2019, a portion of Utah›s pre-litigation panel process was also struck down by the state’s Supreme Court.
“We used to be able to predict where these high verdicts would occur,” Mr. White said. “We can’t predict it anymore.”
Research shows a majority of malpractice cases are dropped or settled before trial, and claims that go before juries usually end in doctors’ favor. Plaintiffs’ attorneys cite large jury verdicts in similar cases to induce settlements and higher payouts, Mr. White said.
And while mega verdicts rarely stick, they can have lasting effects on future claims. The awards lead to larger settlement demands from plaintiffs and drive up the cost to resolve claims, according to Mr. Henderson and Mr. White.
“Verdicts are the yardstick by which all settlements are measured,” Mr. White said. “That’s where the damage is done.” The prospect of a mega verdict can make insurers leery of fighting some malpractice cases and motivate them to offer bigger settlements to stay out of the courtroom, he added.
Why Are Juries Awarding Higher Verdicts?
There’s no single reason for the rise in nuclear verdicts, Mr. Henderson said.
One theory is that plaintiffs’ attorneys held back on resolving high-dollar cases during the COVID pandemic and let loose with high-demand claims when courts returned to normal, he said.
Another theory is that people emerged from the pandemic angrier.
“Whether it was political dynamics, masking [mandates], or differences in opinions, people came out of it angry, and generally speaking, you don’t want an angry jury,” Mr. Henderson said. “For a while, there was the halo effect, where health professionals were seen as heroes. That went away, and all of a sudden [they] became ‘the bad guys.’ ”
“People are angry at the healthcare system, and this anger manifests itself in [liability] suits,” added Bill Burns, vice president of research for the Medical Professional Liability Association, an industry group for medical liability insurers.
Hospital and medical group consolidation also reduces the personal connection juries may have with healthcare providers, Mr. Burns said.
“Healthcare has become a big business, and the corporatization of medicine now puts companies on the stand and not your local community hospital or your family doctor that you have known since birth,” he said.
Plaintiffs’ attorneys also deploy tactics that can prompt higher verdicts, Mr. White said. They may tell a jury that the provider or hospital is a threat to the community and that awarding a large verdict will deter others in the healthcare community from repeating the same actions.
Juries may then want to punish the defendant in addition to assessing damages for economic harm or pain and suffering, Mr. White said.
“I am concerned that jurors are trying to right social wrongs rather than judging cases on the facts presented to them,” added Mike Stinson, vice president for policy and legal affairs for the Medical Professional Liability Association.
Third-party litigation financing also can lead to mega verdicts. That’s an emerging practice in which companies unrelated to a lawsuit provide capital to plaintiffs in return for a portion of any financial award. The firms essentially “invest” in the litigation.
“What this does is provide an additional financial backdrop for plaintiffs,” Mr. Henderson said. “It allows them to dig in harder on cases. They can hold out for higher numbers, and if nothing else, it can prolong litigation.”
Do High Awards Actually Stick?
Multimillion-dollar verdicts may grab headlines, but do plaintiffs actually receive them?
Rarely, said TransRe, which tracks the final outcomes of verdicts. In many cases, large verdicts are reduced on appeal.
In the Maya case, which involved child protection authorities, a judge later lowered the damages against Johns Hopkins All Children’s Hospital by $47.5 million.
A federal judge in October, for example, rejected a record $110 million medical malpractice award in Minnesota, reducing it to $10 million. The district judge ruled the award was “shockingly excessive” and that the plaintiff should either accept the $10 million award or retry the case.
After a verdict is awarded, the defendant typically challenges the award, and the case goes through the appellate pipeline, Mr. Henderson explained. A judge may reduce some elements of the verdict, he said, but more often, the plaintiff and defendant agree on a compromised figure.
Seattle medical liability defense attorney Jennifer Crisera has experienced this firsthand. She recalled a recent case where a plaintiff’s attorney demanded what she describes as an unreasonable amount to settle a claim. Ms. Crisera did not want to give exact numbers but said the plaintiff made an 8-figure demand and the defense offered a low 7-figure range.
“My impression was that plaintiff’s counsel believed that they could get a nuclear verdict from the jury, so they kept their settlement demand artificially high,” she said. “The division between the numbers was way too high. Ultimately, we had to let a jury decide the value.”
The plaintiff won the case, and the verdict was much less than the settlement demand, she said. Even so, the defense incurred trial costs, and the health provider was forced to endure the emotional stress of a trial that could have been avoided, Ms. Crisera said.
Higher medical malpractice premiums are another consequence of massive awards.
Premium rates are associated with how much insurers pay on average for cases and how frequently they are making payouts, Mr. White said.
Medical liability insurance premiums for physicians have steadily increased since 2019, according to data from the Medical Liability Monitor, a national publication that analyzes liability insurance premiums. The Monitor studies insurance premium data from insurers that cover internists, general surgeons, and obstetrician-gynecologists.
From 2019 to 2023, average premium rates for physicians increased between 1.1% and 3% each year in states without patient compensation funds, according to Monitor data.
“Nuclear verdicts are a real driver of the industry’s underwriting losses and remain top of mind for every malpractice insurance company,” said Michael Matray, editor for the Medical Liability Monitor. “Responses to this year’s rate survey questionnaire indicate that most responding companies have experienced an increase in claims greater than $1 million and claims greater than $5 million during the past 2 years.”
However, increases vary widely by region and among counties. In Montgomery County, Alabama, for instance, premiums for internists rose by 24% from 2022 to 2023, from $8,231 to $10,240. Premiums for Montgomery County general surgeons rose by 11.9% from 2022 to 2023, from $30,761 to $34,426, according to survey data.
In several counties in Illinois (Adams, Knox, Peoria, and Rock Island), premiums for some internists rose by 15% from $24,041 to $27,783, and premiums for some surgeons increased by 27% from $60,202 to $76,461, according to survey data. Some internists in Catoosa County, Georgia, meanwhile, paid $17,831 in 2023, up from $16,313 in 2022. Some surgeons in Catoosa County paid $65,616 in 2023, up from $60,032 in 2022. Inflation could be one factor behind higher liability premium rates. Claim severity is a key driver of higher premium rates, Mr. White added.
“We have not seen stability in claims severity,” he said. “It is continuing to go up and, in all likelihood, it will drive [premium] rates up further from this point.”
A version of this article appeared on Medscape.com.
In December, in what’s known as the “Take Care of Maya” case, a Florida jury returned a record $261 million verdict against Johns Hopkins All Children’s Hospital, St. Petersburg, Florida, for its treatment of a young patient and her family after an emergency room visit.
A month earlier, in New York, a jury ordered Westchester Medical Center Health Network to pay $120 million to a patient and his family following delayed stroke care that resulted in brain damage.
Mega malpractice awards like these are rising against physicians and hospitals around the country, according to new data from TransRe, an international reinsurance company that tracks large verdicts.
“2023 blew away every record previously set among high medical malpractice verdicts,” said Richard Henderson, senior vice president for TransRe.
In 2023, there were 57 medical malpractice verdicts of $10 million or more in the United States, the data showed. Slightly more than half of those reached $25 million or more.
From 2012 to 2022, verdicts of $10 million or more ranged from 34 in 2013 to 52 in 2022, TransRe research found.
While New York, Illinois, and Florida typically saw the highest dollar verdicts in previous years, so-called “nuclear” verdicts now occur in states like Utah and Georgia where they once were uncommon, said Robert E. White Jr., president of TDC Group and The Doctors Company, a national medical liability insurer for physicians.
A rollback of tort reforms across the country is one contributor, he said. For example, Georgia’s cap on noneconomic damages is among those that have been ruled unconstitutional by courts. Utah’s cap on noneconomic damages still stands, but the limit was deemed unconstitutional in wrongful death cases. In 2019, a portion of Utah›s pre-litigation panel process was also struck down by the state’s Supreme Court.
“We used to be able to predict where these high verdicts would occur,” Mr. White said. “We can’t predict it anymore.”
Research shows a majority of malpractice cases are dropped or settled before trial, and claims that go before juries usually end in doctors’ favor. Plaintiffs’ attorneys cite large jury verdicts in similar cases to induce settlements and higher payouts, Mr. White said.
And while mega verdicts rarely stick, they can have lasting effects on future claims. The awards lead to larger settlement demands from plaintiffs and drive up the cost to resolve claims, according to Mr. Henderson and Mr. White.
“Verdicts are the yardstick by which all settlements are measured,” Mr. White said. “That’s where the damage is done.” The prospect of a mega verdict can make insurers leery of fighting some malpractice cases and motivate them to offer bigger settlements to stay out of the courtroom, he added.
Why Are Juries Awarding Higher Verdicts?
There’s no single reason for the rise in nuclear verdicts, Mr. Henderson said.
One theory is that plaintiffs’ attorneys held back on resolving high-dollar cases during the COVID pandemic and let loose with high-demand claims when courts returned to normal, he said.
Another theory is that people emerged from the pandemic angrier.
“Whether it was political dynamics, masking [mandates], or differences in opinions, people came out of it angry, and generally speaking, you don’t want an angry jury,” Mr. Henderson said. “For a while, there was the halo effect, where health professionals were seen as heroes. That went away, and all of a sudden [they] became ‘the bad guys.’ ”
“People are angry at the healthcare system, and this anger manifests itself in [liability] suits,” added Bill Burns, vice president of research for the Medical Professional Liability Association, an industry group for medical liability insurers.
Hospital and medical group consolidation also reduces the personal connection juries may have with healthcare providers, Mr. Burns said.
“Healthcare has become a big business, and the corporatization of medicine now puts companies on the stand and not your local community hospital or your family doctor that you have known since birth,” he said.
Plaintiffs’ attorneys also deploy tactics that can prompt higher verdicts, Mr. White said. They may tell a jury that the provider or hospital is a threat to the community and that awarding a large verdict will deter others in the healthcare community from repeating the same actions.
Juries may then want to punish the defendant in addition to assessing damages for economic harm or pain and suffering, Mr. White said.
“I am concerned that jurors are trying to right social wrongs rather than judging cases on the facts presented to them,” added Mike Stinson, vice president for policy and legal affairs for the Medical Professional Liability Association.
Third-party litigation financing also can lead to mega verdicts. That’s an emerging practice in which companies unrelated to a lawsuit provide capital to plaintiffs in return for a portion of any financial award. The firms essentially “invest” in the litigation.
“What this does is provide an additional financial backdrop for plaintiffs,” Mr. Henderson said. “It allows them to dig in harder on cases. They can hold out for higher numbers, and if nothing else, it can prolong litigation.”
Do High Awards Actually Stick?
Multimillion-dollar verdicts may grab headlines, but do plaintiffs actually receive them?
Rarely, said TransRe, which tracks the final outcomes of verdicts. In many cases, large verdicts are reduced on appeal.
In the Maya case, which involved child protection authorities, a judge later lowered the damages against Johns Hopkins All Children’s Hospital by $47.5 million.
A federal judge in October, for example, rejected a record $110 million medical malpractice award in Minnesota, reducing it to $10 million. The district judge ruled the award was “shockingly excessive” and that the plaintiff should either accept the $10 million award or retry the case.
After a verdict is awarded, the defendant typically challenges the award, and the case goes through the appellate pipeline, Mr. Henderson explained. A judge may reduce some elements of the verdict, he said, but more often, the plaintiff and defendant agree on a compromised figure.
Seattle medical liability defense attorney Jennifer Crisera has experienced this firsthand. She recalled a recent case where a plaintiff’s attorney demanded what she describes as an unreasonable amount to settle a claim. Ms. Crisera did not want to give exact numbers but said the plaintiff made an 8-figure demand and the defense offered a low 7-figure range.
“My impression was that plaintiff’s counsel believed that they could get a nuclear verdict from the jury, so they kept their settlement demand artificially high,” she said. “The division between the numbers was way too high. Ultimately, we had to let a jury decide the value.”
The plaintiff won the case, and the verdict was much less than the settlement demand, she said. Even so, the defense incurred trial costs, and the health provider was forced to endure the emotional stress of a trial that could have been avoided, Ms. Crisera said.
Higher medical malpractice premiums are another consequence of massive awards.
Premium rates are associated with how much insurers pay on average for cases and how frequently they are making payouts, Mr. White said.
Medical liability insurance premiums for physicians have steadily increased since 2019, according to data from the Medical Liability Monitor, a national publication that analyzes liability insurance premiums. The Monitor studies insurance premium data from insurers that cover internists, general surgeons, and obstetrician-gynecologists.
From 2019 to 2023, average premium rates for physicians increased between 1.1% and 3% each year in states without patient compensation funds, according to Monitor data.
“Nuclear verdicts are a real driver of the industry’s underwriting losses and remain top of mind for every malpractice insurance company,” said Michael Matray, editor for the Medical Liability Monitor. “Responses to this year’s rate survey questionnaire indicate that most responding companies have experienced an increase in claims greater than $1 million and claims greater than $5 million during the past 2 years.”
However, increases vary widely by region and among counties. In Montgomery County, Alabama, for instance, premiums for internists rose by 24% from 2022 to 2023, from $8,231 to $10,240. Premiums for Montgomery County general surgeons rose by 11.9% from 2022 to 2023, from $30,761 to $34,426, according to survey data.
In several counties in Illinois (Adams, Knox, Peoria, and Rock Island), premiums for some internists rose by 15% from $24,041 to $27,783, and premiums for some surgeons increased by 27% from $60,202 to $76,461, according to survey data. Some internists in Catoosa County, Georgia, meanwhile, paid $17,831 in 2023, up from $16,313 in 2022. Some surgeons in Catoosa County paid $65,616 in 2023, up from $60,032 in 2022. Inflation could be one factor behind higher liability premium rates. Claim severity is a key driver of higher premium rates, Mr. White added.
“We have not seen stability in claims severity,” he said. “It is continuing to go up and, in all likelihood, it will drive [premium] rates up further from this point.”
A version of this article appeared on Medscape.com.