User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
COVID-19 mitigation measures led to shifts in typical annual respiratory virus patterns
Nonpharmaceutical interventions, such as masking, staying home, limiting travel, and social distancing, have been doing more than reducing the risk for COVID-19. They’re also having an impact on infection rates and the timing of seasonal surges of other common respiratory diseases, according to an article published July 23 in Morbidity and Mortality Weekly Report.
Typically, respiratory pathogens such as respiratory syncytial virus (RSV), common cold coronaviruses, parainfluenza viruses, and respiratory adenoviruses increase in the fall and remain high throughout winter, following the same basic patterns as influenza. Although the historically low rates of influenza remained low into spring 2021, that’s not the case for several other common respiratory viruses.
“Clinicians should be aware of increases in some respiratory virus activity and remain vigilant for off-season increases,” wrote Sonja J. Olsen, PhD, and her colleagues at the Centers for Disease Control and Prevention. She told this news organization that clinicians should use multipathogen testing to help guide treatment.
The authors also underscore the importance of fall influenza vaccination campaigns for anyone aged 6 months or older.
Timothy Brewer, MD, MPH, a professor of medicine in the Division of Infectious Diseases at the University of California, Los Angeles (UCLA), and of epidemiology at the UCLA Fielding School of Public Health, agreed that it’s important for health care professionals to consider off-season illnesses in their patients.
“Practitioners should be aware that if they see a sick child in the summer, outside of what normally might be influenza season, but they look like they have influenza, consider potentially influenza and test for it, because it might be possible that we may have disrupted that natural pattern,” Dr. Brewer told this news organization. Dr. Brewer, who was not involved in the CDC research, said it’s also “critically important” to encourage influenza vaccination as the season approaches.
The CDC researchers used the U.S. World Health Organization Collaborating Laboratories System and the CDC’s National Respiratory and Enteric Virus Surveillance System to analyze virologic data from Oct. 3, 2020, to May 22, 2021, for influenza and Jan. 4, 2020, to May 22, 2021, for other respiratory viruses. The authors compared virus circulation during these periods to circulation during the same dates from four previous years.
Data to calculate influenza and RSV hospitalization rates came from the Influenza Hospitalization Surveillance Network and RSV Hospitalization Surveillance Network.
The authors report that flu activity dropped dramatically in March 2020 to its lowest levels since 1997, the earliest season for which data are available. Only 0.2% of more than 1 million specimens tested positive for influenza; the rate of hospitalizations for lab-confirmed flu was 0.8 per 100,000 people. Flu levels remained low through the summer, fall, and on to May 2021.
A potential drawback to this low activity, however, is a more prevalent and severe upcoming flu season, the authors write. The repeated exposure to flu viruses every year often “does not lead to illness, but it does serve to boost our immune response to influenza viruses,” Dr. Olsen said in an interview. “The absence of influenza viruses in the community over the last year means that we are not getting these regular boosts to our immune system. When we finally get exposed, our body may mount a weak response, and this could mean we develop a more clinically severe illness.”
Children are most susceptible to that phenomenon because they haven’t had a lifetime of exposure to flu viruses, Dr. Olsen said.
“An immunologically naive child may be more likely to develop a severe illness than someone who has lived through several influenza seasons,” she said. “This is why it is especially important for everyone 6 months and older to get vaccinated against influenza this season.”
Rhinovirus and enterovirus infections rebounded fairly quickly after their decline in March 2020 and started increasing in May 2020 until they reached “near prepandemic seasonal levels,” the authors write.
RSV infections dropped from 15.3% of weekly positive results in January 2020 to 1.4% by April and then stayed below 1% through the end of 2020. In past years, weekly positive results climbed to 3% in October and peaked at 12.5% to 16.7% in late December. Instead, RSV weekly positive results began increasing in April 2021, rising from 1.1% to 2.8% in May.
The “unusually timed” late spring increase in RSV “is probably associated with various nonpharmaceutical measures that have been in place but are now relaxing,” Dr. Olsen stated.
The RSV hospitalization rate was 0.3 per 100,000 people from October 2020 to April 2021, compared to 27.1 and 33.4 per 100,000 people in the previous 2 years. Of all RSV hospitalizations in the past year, 76.5% occurred in April-May 2021.
Rates of illness caused by the four common human coronaviruses (OC43, NL63, 229E, and HKU1) dropped from 7.5% of weekly positive results in January 2020 to 1.3% in April 2020 and stayed below 1% through February 2021. Then they climbed to 6.6% by May 2021. Infection rates of parainfluenza viruses types 1-4 similarly dropped from 2.6% in January 2020 to 1% in March 2020 and stayed below 1% until April 2021. Since then, rates of the common coronaviruses increased to 6.6% and parainfluenza viruses to 10.9% in May 2021.
Normally, parainfluenza viruses peak in October-November and May-June, so “the current increase could represent a return to prepandemic seasonality,” the authors write.
Human pneumoviruses’ weekly positive results initially increased from 4.2% in January 2020 to 7% in March and then fell to 1.9% the second week of April and remained below 1% through May 2021. In typical years, these viruses peak from 6.2% to 7.7% in March-April. Respiratory adenovirus activity similarly dropped to historically low levels in April 2021 and then began increasing to reach 3% by May 2021, the usual level for that month.
“The different circulation patterns observed across respiratory viruses probably also reflect differences in the virus transmission routes and how effective various nonpharmaceutical measures are at stopping transmission,” Dr. Olsen said in an interview. “As pandemic mitigation measures continue to be adjusted, we expect to see more changes in the circulation of these viruses, including a return to prepandemic circulation, as seen for rhinoviruses and enteroviruses.”
Rhinovirus and enterovirus rates dropped from 14.9% in March 2020 to 3.2% in May – lower than typical – and then climbed to a peak in October 2020. The peak (21.7% weekly positive results) was, however, still lower than the usual median of 32.8%. After dropping to 9.9% in January 2021, it then rose 19.1% in May, potentially reflecting “the usual spring peak that has occurred in previous years,” the authors write.
The authors note that it’s not yet clear how the COVID-19 pandemic and related mitigation measures will continue to affect respiratory virus circulation.
The authors hypothesize that the reasons for a seeming return to seasonal activity of respiratory adenoviruses, rhinoviruses, and enteroviruses could involve “different transmission mechanisms, the role of asymptomatic transmission, and prolonged survival of these nonenveloped viruses on surfaces, all of which might make these viruses less susceptible to nonpharmaceutical interventions.”
Dr. Brewer, of UCLA, agreed.
All the viruses basically “flatline except for adenoviruses and enteroviruses, and they behave a little differently in terms of how they spread,” he said. “Enteroviruses are much more likely to be fecal-oral spread than the other viruses [in the study].”
The delayed circulation of parainfluenza and human coronaviruses may have resulted from suspension of in-person classes through late winter 2020, they write, but that doesn’t explain the relative absence of pneumovirus activity, which usually affects the same young pediatric populations as RSV.
Dr. Brewer said California is seeing a surge of RSV right now, as are many states, especially throughout in the South. He’s not surprised by RSV’s deferred season, because those most affected – children younger than 2 years – are less likely to wear masks now and were “not going to daycare, not being out in public” in 2020. “As people are doing more activities, that’s probably why RSV has been starting to go up since April,” he said.
Despite the fact that, unlike many East Asian cultures, the United States has not traditionally been a mask-wearing culture, Dr. Brewer wouldn’t be surprised if more Americans begin wearing masks during flu season. “Hopefully another thing that will come out of this is better hand hygiene, with people just getting used to washing their hands more, particularly after they come home from being out,” he added.
Dr. Brewer similarly emphasized the importance of flu vaccination for the upcoming season, especially for younger children who may have poorer natural immunity to influenza, owing to its low circulation rates in 2020-2021.
The study was funded by the CDC. Dr. Brewer and Dr. Olsen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nonpharmaceutical interventions, such as masking, staying home, limiting travel, and social distancing, have been doing more than reducing the risk for COVID-19. They’re also having an impact on infection rates and the timing of seasonal surges of other common respiratory diseases, according to an article published July 23 in Morbidity and Mortality Weekly Report.
Typically, respiratory pathogens such as respiratory syncytial virus (RSV), common cold coronaviruses, parainfluenza viruses, and respiratory adenoviruses increase in the fall and remain high throughout winter, following the same basic patterns as influenza. Although the historically low rates of influenza remained low into spring 2021, that’s not the case for several other common respiratory viruses.
“Clinicians should be aware of increases in some respiratory virus activity and remain vigilant for off-season increases,” wrote Sonja J. Olsen, PhD, and her colleagues at the Centers for Disease Control and Prevention. She told this news organization that clinicians should use multipathogen testing to help guide treatment.
The authors also underscore the importance of fall influenza vaccination campaigns for anyone aged 6 months or older.
Timothy Brewer, MD, MPH, a professor of medicine in the Division of Infectious Diseases at the University of California, Los Angeles (UCLA), and of epidemiology at the UCLA Fielding School of Public Health, agreed that it’s important for health care professionals to consider off-season illnesses in their patients.
“Practitioners should be aware that if they see a sick child in the summer, outside of what normally might be influenza season, but they look like they have influenza, consider potentially influenza and test for it, because it might be possible that we may have disrupted that natural pattern,” Dr. Brewer told this news organization. Dr. Brewer, who was not involved in the CDC research, said it’s also “critically important” to encourage influenza vaccination as the season approaches.
The CDC researchers used the U.S. World Health Organization Collaborating Laboratories System and the CDC’s National Respiratory and Enteric Virus Surveillance System to analyze virologic data from Oct. 3, 2020, to May 22, 2021, for influenza and Jan. 4, 2020, to May 22, 2021, for other respiratory viruses. The authors compared virus circulation during these periods to circulation during the same dates from four previous years.
Data to calculate influenza and RSV hospitalization rates came from the Influenza Hospitalization Surveillance Network and RSV Hospitalization Surveillance Network.
The authors report that flu activity dropped dramatically in March 2020 to its lowest levels since 1997, the earliest season for which data are available. Only 0.2% of more than 1 million specimens tested positive for influenza; the rate of hospitalizations for lab-confirmed flu was 0.8 per 100,000 people. Flu levels remained low through the summer, fall, and on to May 2021.
A potential drawback to this low activity, however, is a more prevalent and severe upcoming flu season, the authors write. The repeated exposure to flu viruses every year often “does not lead to illness, but it does serve to boost our immune response to influenza viruses,” Dr. Olsen said in an interview. “The absence of influenza viruses in the community over the last year means that we are not getting these regular boosts to our immune system. When we finally get exposed, our body may mount a weak response, and this could mean we develop a more clinically severe illness.”
Children are most susceptible to that phenomenon because they haven’t had a lifetime of exposure to flu viruses, Dr. Olsen said.
“An immunologically naive child may be more likely to develop a severe illness than someone who has lived through several influenza seasons,” she said. “This is why it is especially important for everyone 6 months and older to get vaccinated against influenza this season.”
Rhinovirus and enterovirus infections rebounded fairly quickly after their decline in March 2020 and started increasing in May 2020 until they reached “near prepandemic seasonal levels,” the authors write.
RSV infections dropped from 15.3% of weekly positive results in January 2020 to 1.4% by April and then stayed below 1% through the end of 2020. In past years, weekly positive results climbed to 3% in October and peaked at 12.5% to 16.7% in late December. Instead, RSV weekly positive results began increasing in April 2021, rising from 1.1% to 2.8% in May.
The “unusually timed” late spring increase in RSV “is probably associated with various nonpharmaceutical measures that have been in place but are now relaxing,” Dr. Olsen stated.
The RSV hospitalization rate was 0.3 per 100,000 people from October 2020 to April 2021, compared to 27.1 and 33.4 per 100,000 people in the previous 2 years. Of all RSV hospitalizations in the past year, 76.5% occurred in April-May 2021.
Rates of illness caused by the four common human coronaviruses (OC43, NL63, 229E, and HKU1) dropped from 7.5% of weekly positive results in January 2020 to 1.3% in April 2020 and stayed below 1% through February 2021. Then they climbed to 6.6% by May 2021. Infection rates of parainfluenza viruses types 1-4 similarly dropped from 2.6% in January 2020 to 1% in March 2020 and stayed below 1% until April 2021. Since then, rates of the common coronaviruses increased to 6.6% and parainfluenza viruses to 10.9% in May 2021.
Normally, parainfluenza viruses peak in October-November and May-June, so “the current increase could represent a return to prepandemic seasonality,” the authors write.
Human pneumoviruses’ weekly positive results initially increased from 4.2% in January 2020 to 7% in March and then fell to 1.9% the second week of April and remained below 1% through May 2021. In typical years, these viruses peak from 6.2% to 7.7% in March-April. Respiratory adenovirus activity similarly dropped to historically low levels in April 2021 and then began increasing to reach 3% by May 2021, the usual level for that month.
“The different circulation patterns observed across respiratory viruses probably also reflect differences in the virus transmission routes and how effective various nonpharmaceutical measures are at stopping transmission,” Dr. Olsen said in an interview. “As pandemic mitigation measures continue to be adjusted, we expect to see more changes in the circulation of these viruses, including a return to prepandemic circulation, as seen for rhinoviruses and enteroviruses.”
Rhinovirus and enterovirus rates dropped from 14.9% in March 2020 to 3.2% in May – lower than typical – and then climbed to a peak in October 2020. The peak (21.7% weekly positive results) was, however, still lower than the usual median of 32.8%. After dropping to 9.9% in January 2021, it then rose 19.1% in May, potentially reflecting “the usual spring peak that has occurred in previous years,” the authors write.
The authors note that it’s not yet clear how the COVID-19 pandemic and related mitigation measures will continue to affect respiratory virus circulation.
The authors hypothesize that the reasons for a seeming return to seasonal activity of respiratory adenoviruses, rhinoviruses, and enteroviruses could involve “different transmission mechanisms, the role of asymptomatic transmission, and prolonged survival of these nonenveloped viruses on surfaces, all of which might make these viruses less susceptible to nonpharmaceutical interventions.”
Dr. Brewer, of UCLA, agreed.
All the viruses basically “flatline except for adenoviruses and enteroviruses, and they behave a little differently in terms of how they spread,” he said. “Enteroviruses are much more likely to be fecal-oral spread than the other viruses [in the study].”
The delayed circulation of parainfluenza and human coronaviruses may have resulted from suspension of in-person classes through late winter 2020, they write, but that doesn’t explain the relative absence of pneumovirus activity, which usually affects the same young pediatric populations as RSV.
Dr. Brewer said California is seeing a surge of RSV right now, as are many states, especially throughout in the South. He’s not surprised by RSV’s deferred season, because those most affected – children younger than 2 years – are less likely to wear masks now and were “not going to daycare, not being out in public” in 2020. “As people are doing more activities, that’s probably why RSV has been starting to go up since April,” he said.
Despite the fact that, unlike many East Asian cultures, the United States has not traditionally been a mask-wearing culture, Dr. Brewer wouldn’t be surprised if more Americans begin wearing masks during flu season. “Hopefully another thing that will come out of this is better hand hygiene, with people just getting used to washing their hands more, particularly after they come home from being out,” he added.
Dr. Brewer similarly emphasized the importance of flu vaccination for the upcoming season, especially for younger children who may have poorer natural immunity to influenza, owing to its low circulation rates in 2020-2021.
The study was funded by the CDC. Dr. Brewer and Dr. Olsen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nonpharmaceutical interventions, such as masking, staying home, limiting travel, and social distancing, have been doing more than reducing the risk for COVID-19. They’re also having an impact on infection rates and the timing of seasonal surges of other common respiratory diseases, according to an article published July 23 in Morbidity and Mortality Weekly Report.
Typically, respiratory pathogens such as respiratory syncytial virus (RSV), common cold coronaviruses, parainfluenza viruses, and respiratory adenoviruses increase in the fall and remain high throughout winter, following the same basic patterns as influenza. Although the historically low rates of influenza remained low into spring 2021, that’s not the case for several other common respiratory viruses.
“Clinicians should be aware of increases in some respiratory virus activity and remain vigilant for off-season increases,” wrote Sonja J. Olsen, PhD, and her colleagues at the Centers for Disease Control and Prevention. She told this news organization that clinicians should use multipathogen testing to help guide treatment.
The authors also underscore the importance of fall influenza vaccination campaigns for anyone aged 6 months or older.
Timothy Brewer, MD, MPH, a professor of medicine in the Division of Infectious Diseases at the University of California, Los Angeles (UCLA), and of epidemiology at the UCLA Fielding School of Public Health, agreed that it’s important for health care professionals to consider off-season illnesses in their patients.
“Practitioners should be aware that if they see a sick child in the summer, outside of what normally might be influenza season, but they look like they have influenza, consider potentially influenza and test for it, because it might be possible that we may have disrupted that natural pattern,” Dr. Brewer told this news organization. Dr. Brewer, who was not involved in the CDC research, said it’s also “critically important” to encourage influenza vaccination as the season approaches.
The CDC researchers used the U.S. World Health Organization Collaborating Laboratories System and the CDC’s National Respiratory and Enteric Virus Surveillance System to analyze virologic data from Oct. 3, 2020, to May 22, 2021, for influenza and Jan. 4, 2020, to May 22, 2021, for other respiratory viruses. The authors compared virus circulation during these periods to circulation during the same dates from four previous years.
Data to calculate influenza and RSV hospitalization rates came from the Influenza Hospitalization Surveillance Network and RSV Hospitalization Surveillance Network.
The authors report that flu activity dropped dramatically in March 2020 to its lowest levels since 1997, the earliest season for which data are available. Only 0.2% of more than 1 million specimens tested positive for influenza; the rate of hospitalizations for lab-confirmed flu was 0.8 per 100,000 people. Flu levels remained low through the summer, fall, and on to May 2021.
A potential drawback to this low activity, however, is a more prevalent and severe upcoming flu season, the authors write. The repeated exposure to flu viruses every year often “does not lead to illness, but it does serve to boost our immune response to influenza viruses,” Dr. Olsen said in an interview. “The absence of influenza viruses in the community over the last year means that we are not getting these regular boosts to our immune system. When we finally get exposed, our body may mount a weak response, and this could mean we develop a more clinically severe illness.”
Children are most susceptible to that phenomenon because they haven’t had a lifetime of exposure to flu viruses, Dr. Olsen said.
“An immunologically naive child may be more likely to develop a severe illness than someone who has lived through several influenza seasons,” she said. “This is why it is especially important for everyone 6 months and older to get vaccinated against influenza this season.”
Rhinovirus and enterovirus infections rebounded fairly quickly after their decline in March 2020 and started increasing in May 2020 until they reached “near prepandemic seasonal levels,” the authors write.
RSV infections dropped from 15.3% of weekly positive results in January 2020 to 1.4% by April and then stayed below 1% through the end of 2020. In past years, weekly positive results climbed to 3% in October and peaked at 12.5% to 16.7% in late December. Instead, RSV weekly positive results began increasing in April 2021, rising from 1.1% to 2.8% in May.
The “unusually timed” late spring increase in RSV “is probably associated with various nonpharmaceutical measures that have been in place but are now relaxing,” Dr. Olsen stated.
The RSV hospitalization rate was 0.3 per 100,000 people from October 2020 to April 2021, compared to 27.1 and 33.4 per 100,000 people in the previous 2 years. Of all RSV hospitalizations in the past year, 76.5% occurred in April-May 2021.
Rates of illness caused by the four common human coronaviruses (OC43, NL63, 229E, and HKU1) dropped from 7.5% of weekly positive results in January 2020 to 1.3% in April 2020 and stayed below 1% through February 2021. Then they climbed to 6.6% by May 2021. Infection rates of parainfluenza viruses types 1-4 similarly dropped from 2.6% in January 2020 to 1% in March 2020 and stayed below 1% until April 2021. Since then, rates of the common coronaviruses increased to 6.6% and parainfluenza viruses to 10.9% in May 2021.
Normally, parainfluenza viruses peak in October-November and May-June, so “the current increase could represent a return to prepandemic seasonality,” the authors write.
Human pneumoviruses’ weekly positive results initially increased from 4.2% in January 2020 to 7% in March and then fell to 1.9% the second week of April and remained below 1% through May 2021. In typical years, these viruses peak from 6.2% to 7.7% in March-April. Respiratory adenovirus activity similarly dropped to historically low levels in April 2021 and then began increasing to reach 3% by May 2021, the usual level for that month.
“The different circulation patterns observed across respiratory viruses probably also reflect differences in the virus transmission routes and how effective various nonpharmaceutical measures are at stopping transmission,” Dr. Olsen said in an interview. “As pandemic mitigation measures continue to be adjusted, we expect to see more changes in the circulation of these viruses, including a return to prepandemic circulation, as seen for rhinoviruses and enteroviruses.”
Rhinovirus and enterovirus rates dropped from 14.9% in March 2020 to 3.2% in May – lower than typical – and then climbed to a peak in October 2020. The peak (21.7% weekly positive results) was, however, still lower than the usual median of 32.8%. After dropping to 9.9% in January 2021, it then rose 19.1% in May, potentially reflecting “the usual spring peak that has occurred in previous years,” the authors write.
The authors note that it’s not yet clear how the COVID-19 pandemic and related mitigation measures will continue to affect respiratory virus circulation.
The authors hypothesize that the reasons for a seeming return to seasonal activity of respiratory adenoviruses, rhinoviruses, and enteroviruses could involve “different transmission mechanisms, the role of asymptomatic transmission, and prolonged survival of these nonenveloped viruses on surfaces, all of which might make these viruses less susceptible to nonpharmaceutical interventions.”
Dr. Brewer, of UCLA, agreed.
All the viruses basically “flatline except for adenoviruses and enteroviruses, and they behave a little differently in terms of how they spread,” he said. “Enteroviruses are much more likely to be fecal-oral spread than the other viruses [in the study].”
The delayed circulation of parainfluenza and human coronaviruses may have resulted from suspension of in-person classes through late winter 2020, they write, but that doesn’t explain the relative absence of pneumovirus activity, which usually affects the same young pediatric populations as RSV.
Dr. Brewer said California is seeing a surge of RSV right now, as are many states, especially throughout in the South. He’s not surprised by RSV’s deferred season, because those most affected – children younger than 2 years – are less likely to wear masks now and were “not going to daycare, not being out in public” in 2020. “As people are doing more activities, that’s probably why RSV has been starting to go up since April,” he said.
Despite the fact that, unlike many East Asian cultures, the United States has not traditionally been a mask-wearing culture, Dr. Brewer wouldn’t be surprised if more Americans begin wearing masks during flu season. “Hopefully another thing that will come out of this is better hand hygiene, with people just getting used to washing their hands more, particularly after they come home from being out,” he added.
Dr. Brewer similarly emphasized the importance of flu vaccination for the upcoming season, especially for younger children who may have poorer natural immunity to influenza, owing to its low circulation rates in 2020-2021.
The study was funded by the CDC. Dr. Brewer and Dr. Olsen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
NetWorks Compete to Combat Health Disparities
One way members get involved in CHEST’s philanthropic efforts takes place each year with the start of the NetWorks Challenge. CHEST members compete through their NetWorks – special interest groups that focus on particular areas of chest medicine – to raise funds that support Foundation microgrants.
NetWorks Challenge 2021 kicked off in June with a special twist to celebrate the Foundation’s 25th anniversary. Each NetWork is asked to complete a 25k virtual physical challenge. This can be done by walking, running, biking, swimming—or any other physical activity.
Through the challenge, members engage in friendly competition while supporting the goals of the Foundation. This year, money raised will directly help the Foundation in addressing health disparities through our microgrants program. In addition, the funds will support travel grants for doctors in training looking to attend CHEST 2021.
By participating in the NetWorks Challenge, members help fund grants that aim to lend a hand to those who need it the most. Expanding research capabilities, improving patient care, and giving access to medical equipment are just a few ways microgrants from the CHEST Foundation have been used in the past.
Inspired by the Listening Tour and the struggles experienced by underserved communities, money raised through the Network Challenge will go to a new pilot microgrant program called Rita’s Fund. The grants aim to supplement community-based projects that provide resources to individuals to help drastically change their quality of life. Funding will assist with coverage for medical equipment, transportation, and access to technology for those living with lung disease and other medical complications.
NetWork members are asked to encourage one another to join in this summer’s race to 25k.
To learn more about this initiative and this year’s NetWorks Challenge, visit chestfoundation.org/nwc21. And, don’t miss the summer issue of Donor Spotlight.
One way members get involved in CHEST’s philanthropic efforts takes place each year with the start of the NetWorks Challenge. CHEST members compete through their NetWorks – special interest groups that focus on particular areas of chest medicine – to raise funds that support Foundation microgrants.
NetWorks Challenge 2021 kicked off in June with a special twist to celebrate the Foundation’s 25th anniversary. Each NetWork is asked to complete a 25k virtual physical challenge. This can be done by walking, running, biking, swimming—or any other physical activity.
Through the challenge, members engage in friendly competition while supporting the goals of the Foundation. This year, money raised will directly help the Foundation in addressing health disparities through our microgrants program. In addition, the funds will support travel grants for doctors in training looking to attend CHEST 2021.
By participating in the NetWorks Challenge, members help fund grants that aim to lend a hand to those who need it the most. Expanding research capabilities, improving patient care, and giving access to medical equipment are just a few ways microgrants from the CHEST Foundation have been used in the past.
Inspired by the Listening Tour and the struggles experienced by underserved communities, money raised through the Network Challenge will go to a new pilot microgrant program called Rita’s Fund. The grants aim to supplement community-based projects that provide resources to individuals to help drastically change their quality of life. Funding will assist with coverage for medical equipment, transportation, and access to technology for those living with lung disease and other medical complications.
NetWork members are asked to encourage one another to join in this summer’s race to 25k.
To learn more about this initiative and this year’s NetWorks Challenge, visit chestfoundation.org/nwc21. And, don’t miss the summer issue of Donor Spotlight.
One way members get involved in CHEST’s philanthropic efforts takes place each year with the start of the NetWorks Challenge. CHEST members compete through their NetWorks – special interest groups that focus on particular areas of chest medicine – to raise funds that support Foundation microgrants.
NetWorks Challenge 2021 kicked off in June with a special twist to celebrate the Foundation’s 25th anniversary. Each NetWork is asked to complete a 25k virtual physical challenge. This can be done by walking, running, biking, swimming—or any other physical activity.
Through the challenge, members engage in friendly competition while supporting the goals of the Foundation. This year, money raised will directly help the Foundation in addressing health disparities through our microgrants program. In addition, the funds will support travel grants for doctors in training looking to attend CHEST 2021.
By participating in the NetWorks Challenge, members help fund grants that aim to lend a hand to those who need it the most. Expanding research capabilities, improving patient care, and giving access to medical equipment are just a few ways microgrants from the CHEST Foundation have been used in the past.
Inspired by the Listening Tour and the struggles experienced by underserved communities, money raised through the Network Challenge will go to a new pilot microgrant program called Rita’s Fund. The grants aim to supplement community-based projects that provide resources to individuals to help drastically change their quality of life. Funding will assist with coverage for medical equipment, transportation, and access to technology for those living with lung disease and other medical complications.
NetWork members are asked to encourage one another to join in this summer’s race to 25k.
To learn more about this initiative and this year’s NetWorks Challenge, visit chestfoundation.org/nwc21. And, don’t miss the summer issue of Donor Spotlight.
This month in the journal CHEST®Editor’s Picks
Peak inspiratory flow as a predictive therapeutic biomarker in COPD. By Drs. D. Mahler and D. Halpin.Family presence for critically ill patients during a pandemic. By Drs. J. Hart and S. Taylor.
Executive summary: diagnosis and evaluation of hypersensitivity pneumonitis: CHEST guideline and expert panel report. By Dr. L. Fernandez Perez et al.
The usefulness of chest CT imaging in patients with suspected or diagnosed COVID-19: A review of literature. By Dr. S. Machnicki et al.
Oxygen therapy in sleep-disordered breathing. By Dr. S. Zeineddine et al.
Peak inspiratory flow as a predictive therapeutic biomarker in COPD. By Drs. D. Mahler and D. Halpin.Family presence for critically ill patients during a pandemic. By Drs. J. Hart and S. Taylor.
Executive summary: diagnosis and evaluation of hypersensitivity pneumonitis: CHEST guideline and expert panel report. By Dr. L. Fernandez Perez et al.
The usefulness of chest CT imaging in patients with suspected or diagnosed COVID-19: A review of literature. By Dr. S. Machnicki et al.
Oxygen therapy in sleep-disordered breathing. By Dr. S. Zeineddine et al.
Peak inspiratory flow as a predictive therapeutic biomarker in COPD. By Drs. D. Mahler and D. Halpin.Family presence for critically ill patients during a pandemic. By Drs. J. Hart and S. Taylor.
Executive summary: diagnosis and evaluation of hypersensitivity pneumonitis: CHEST guideline and expert panel report. By Dr. L. Fernandez Perez et al.
The usefulness of chest CT imaging in patients with suspected or diagnosed COVID-19: A review of literature. By Dr. S. Machnicki et al.
Oxygen therapy in sleep-disordered breathing. By Dr. S. Zeineddine et al.
Delirium in the ICU: Best sedation practices lead to the best outcomes
Delirium is a frequent form of organ failure among the critically ill, impacting up to 80% of mechanically ventilated patients (Ely EW et al. JAMA. 2004;291[14]:1753-62). Its cardinal manifestations include disturbances in attention and cognition that occur acutely (e.g., hours to days) that are not better explained by another disease process (such as a toxidrome or dementia) (American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders. 5th ed., 2013). Duration of delirium in the intensive care unit (ICU) is independently associated with poor outcomes, such as mortality and hospital length of stay, even when accounting for comorbidities, coma duration, sedative use, and severity of illness. Delirium during critical illness is an important bellwether for a patient’s clinical status, often serving as a harbinger for severe or worsening disease.
Over the last two decades, the critical care community has come to understand the importance of recognizing delirium, which is often underdiagnosed, as well as delirium prevention. In the ICU, several factors coalesce to form the perfect environment for the development of delirium. Patients often have preexisting comorbidities that predispose to delirium, such as preexisting cognitive impairment, and the severity of critical illness increases the risk of delirium further. There are also bedside factors, however, that are important for the intensivist to address, many of which are modifiable. These include routinely screening for delirium and assessing level of consciousness, implementing early mobility and rehabilitation, targeting light sedation, and avoiding deliriogenic medications such as benzodiazepines. These evidence-based care practices form the foundation of the 2018 Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU (i.e., PADIS guidelines), which aim to reduce delirium and iatrogenesis from critical care (Devlin JW et al. Crit Care Med. 2018;46[9]:e825-e873). The severe acute respiratory syndrome–coronavirus 2 (SARS-CoV-2) pathogen that has caused the coronavirus disease 2019 (COVID-19) pandemic, however, has brought unprecedented challenges to critical care. One unfortunate side effect has been increased use of deep sedation and, thus, a greater incidence of delirium (Pun BT et al. Lancet Respir Med. 2021;9[3]:239-50). While the impact of the pandemic is unprecedented, thoughtful and careful sedation use remains vital to providing optimal care for the critically ill patient.
The link between sedation and delirium
The advent of modern mechanical ventilation brought critical care medicine into a period of rapid growth. Practices derived from the operating room, such as deep sedation and paralysis, became commonplace. Yet, starting in the late 1990s and early 2000s, evidence started growing regarding the impact of delirium and the unique aspects of the ICU that made it so prevalent. Delirium is strongly linked to inpatient mortality in mechanically ventilated adults, and it is best understood as an additional form of organ failure, much like other organ failures commonly recognized and treated by intensivists, such as respiratory or renal failure. Certain medications and sedation practices are associated with the development and duration of delirium. Benzodiazepines, a common sedative medication, are strongly linked to the development of delirium. In a study comparing commonly used sedative and analgesic agents, the use of lorazepam was associated with a greater risk of delirium the following day among critically ill, mechanically ventilated patients (Pandhariphande PP et al. Anesthesiology. 2006;104[1]:21-6). Given how commonly benzodiazepines are used and delirium develops in the ICU, this association has striking implications for clinical care and outcomes such as mortality. It is also significant, given that benzodiazepine use has increased during the pandemic, potentially creating significant downstream consequences. Benzodiazepines should be actively avoided when at all possible, given their propensity to lead to delirium, in accordance with the most recent guidelines.
Which sedation agent to choose?
While the negative effects of benzodiazepine-based sedation are well established, the optimal sedation agent remains unclear. Several other drugs are commonly used in the ICU, including propofol, dexmedetomidine, and opioid agents such as fentanyl and morphine. Propofol and dexmedetomidine are used specifically for their sedative properties, though they have dramatically different effects on the depth of sedation and different mechanisms of action. Opioid agents are most commonly used for their analgesic effect; however, in higher doses or combined with other medications, they have the secondary effect of inducing sedation. No particular sedation agent, however, beyond the avoidance of benzodiazepines has been recommended for use in the most recent guidelines. In the PRODEX and MIDEX studies, dexmedetomidine was noninferior to both midazolam and propofol in achieving targeted light to moderate sedation, and dexmedetomidine was associated with a shorter duration of mechanical ventilation compared to midazolam (Jakob SM et al. JAMA. 2012;307[11]:1151-60). More recently, the SPICE-III trial studied dexmedetomidine vs. usual care and found no difference in 90-day mortality (Shehabi Y et al. N Engl J Med. 2019;380[26]:2506-17).
In choosing the best sedation agent to avoid delirium, the largest and most applicable trial to date is the “Maximizing the Efficacy of Sedation and Reducing Neurological Dysfunction and Mortality in Septic Patients with Acute Respiratory Failure,” or MENDS2 trial (Hughes CG et al. N Engl J Med. 2021;384:1424-36). This study was a double-blind, multicenter randomized controlled trial of dexmedetomidine vs propofol in critically ill patients with sepsis receiving mechanical ventilation. The primary outcome was days alive without delirium or coma over the 14-day intervention period. The study enrolled 438 patients between 13 sites, with 422 patients receiving either dexmedetomidine or propofol. Hughes and colleagues found no difference in the primary outcome of days alive without delirium or coma between the dexmedetomidine and the propofol arms. The study also found no difference in secondary outcomes, including ventilator-free days, 90-day mortality, and 6-month global cognition, as well as no difference in safety endpoints. Importantly, there was excellent compliance with guideline-recommended practices of spontaneous awakening and breathing trials and early mobility, both of which are associated with reduced sedation exposure. The study did have some notable nuances, however. The overall doses of trial drugs were relatively low, and there was a moderate use of rescue sedation. There was also a small amount of crossover use of propofol and dexmedetomidine between treatment arms (10%), although the authors note that this was lower than in prior related studies. Overall, the MENDS2 study suggests there is likely clinical equipoise between propofol and dexmedetomidine in terms of delirium outcomes when combined with best practices, such targeted light sedation, paired awakening and breathing trials, and early mobility.
How should we manage sedation to prevent delirium?
Building off of the recent MENDS2 study and earlier work in the field, along with the 2018 PADIS guidelines, the general paradigm of sedation management should be focused on using light sedation with sedation interruptions to minimize overall sedation exposure. Based on the best available evidence to date, targeting less overall sedation leads to improved outcomes in critically ill patients, including mortality and duration of mechanical ventilation. Benzodiazepines should be avoided due to their association with delirium, but currently there is no evidence to suggest one nonbenzodiazepine sedative is better than another. Intensivists can feel comfortable choosing between agents based on a patient’s individual clinical needs, especially when patients are receiving paired spontaneous awakening and breathing trials and early rehabilitation. These same principles should be applied to sedation management and delirium patients in COVID-19 patients as well. While certain circumstances will necessitate deeper sedation at times (e.g., refractory hypoxemia due to ARDS from COVID-19), clinicians should continually reassess the actual sedation needs of the patient with the goal of reducing overall sedation. Focusing effort on these evidence-based practices will help reduce the incidence of delirium and ultimately improve patient outcomes.
Dr. Mart is with the Division of Allergy, Pulmonary, and Critical Care Medicine, Vanderbilt University Medical Center; Critical Illness, Brain Dysfunction, and Survivorship (CIBS) Center; and VA Tennessee Valley Healthcare System Geriatric Research Education and Clinical Center (GRECC), Nashville, Tennessee.
Delirium is a frequent form of organ failure among the critically ill, impacting up to 80% of mechanically ventilated patients (Ely EW et al. JAMA. 2004;291[14]:1753-62). Its cardinal manifestations include disturbances in attention and cognition that occur acutely (e.g., hours to days) that are not better explained by another disease process (such as a toxidrome or dementia) (American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders. 5th ed., 2013). Duration of delirium in the intensive care unit (ICU) is independently associated with poor outcomes, such as mortality and hospital length of stay, even when accounting for comorbidities, coma duration, sedative use, and severity of illness. Delirium during critical illness is an important bellwether for a patient’s clinical status, often serving as a harbinger for severe or worsening disease.
Over the last two decades, the critical care community has come to understand the importance of recognizing delirium, which is often underdiagnosed, as well as delirium prevention. In the ICU, several factors coalesce to form the perfect environment for the development of delirium. Patients often have preexisting comorbidities that predispose to delirium, such as preexisting cognitive impairment, and the severity of critical illness increases the risk of delirium further. There are also bedside factors, however, that are important for the intensivist to address, many of which are modifiable. These include routinely screening for delirium and assessing level of consciousness, implementing early mobility and rehabilitation, targeting light sedation, and avoiding deliriogenic medications such as benzodiazepines. These evidence-based care practices form the foundation of the 2018 Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU (i.e., PADIS guidelines), which aim to reduce delirium and iatrogenesis from critical care (Devlin JW et al. Crit Care Med. 2018;46[9]:e825-e873). The severe acute respiratory syndrome–coronavirus 2 (SARS-CoV-2) pathogen that has caused the coronavirus disease 2019 (COVID-19) pandemic, however, has brought unprecedented challenges to critical care. One unfortunate side effect has been increased use of deep sedation and, thus, a greater incidence of delirium (Pun BT et al. Lancet Respir Med. 2021;9[3]:239-50). While the impact of the pandemic is unprecedented, thoughtful and careful sedation use remains vital to providing optimal care for the critically ill patient.
The link between sedation and delirium
The advent of modern mechanical ventilation brought critical care medicine into a period of rapid growth. Practices derived from the operating room, such as deep sedation and paralysis, became commonplace. Yet, starting in the late 1990s and early 2000s, evidence started growing regarding the impact of delirium and the unique aspects of the ICU that made it so prevalent. Delirium is strongly linked to inpatient mortality in mechanically ventilated adults, and it is best understood as an additional form of organ failure, much like other organ failures commonly recognized and treated by intensivists, such as respiratory or renal failure. Certain medications and sedation practices are associated with the development and duration of delirium. Benzodiazepines, a common sedative medication, are strongly linked to the development of delirium. In a study comparing commonly used sedative and analgesic agents, the use of lorazepam was associated with a greater risk of delirium the following day among critically ill, mechanically ventilated patients (Pandhariphande PP et al. Anesthesiology. 2006;104[1]:21-6). Given how commonly benzodiazepines are used and delirium develops in the ICU, this association has striking implications for clinical care and outcomes such as mortality. It is also significant, given that benzodiazepine use has increased during the pandemic, potentially creating significant downstream consequences. Benzodiazepines should be actively avoided when at all possible, given their propensity to lead to delirium, in accordance with the most recent guidelines.
Which sedation agent to choose?
While the negative effects of benzodiazepine-based sedation are well established, the optimal sedation agent remains unclear. Several other drugs are commonly used in the ICU, including propofol, dexmedetomidine, and opioid agents such as fentanyl and morphine. Propofol and dexmedetomidine are used specifically for their sedative properties, though they have dramatically different effects on the depth of sedation and different mechanisms of action. Opioid agents are most commonly used for their analgesic effect; however, in higher doses or combined with other medications, they have the secondary effect of inducing sedation. No particular sedation agent, however, beyond the avoidance of benzodiazepines has been recommended for use in the most recent guidelines. In the PRODEX and MIDEX studies, dexmedetomidine was noninferior to both midazolam and propofol in achieving targeted light to moderate sedation, and dexmedetomidine was associated with a shorter duration of mechanical ventilation compared to midazolam (Jakob SM et al. JAMA. 2012;307[11]:1151-60). More recently, the SPICE-III trial studied dexmedetomidine vs. usual care and found no difference in 90-day mortality (Shehabi Y et al. N Engl J Med. 2019;380[26]:2506-17).
In choosing the best sedation agent to avoid delirium, the largest and most applicable trial to date is the “Maximizing the Efficacy of Sedation and Reducing Neurological Dysfunction and Mortality in Septic Patients with Acute Respiratory Failure,” or MENDS2 trial (Hughes CG et al. N Engl J Med. 2021;384:1424-36). This study was a double-blind, multicenter randomized controlled trial of dexmedetomidine vs propofol in critically ill patients with sepsis receiving mechanical ventilation. The primary outcome was days alive without delirium or coma over the 14-day intervention period. The study enrolled 438 patients between 13 sites, with 422 patients receiving either dexmedetomidine or propofol. Hughes and colleagues found no difference in the primary outcome of days alive without delirium or coma between the dexmedetomidine and the propofol arms. The study also found no difference in secondary outcomes, including ventilator-free days, 90-day mortality, and 6-month global cognition, as well as no difference in safety endpoints. Importantly, there was excellent compliance with guideline-recommended practices of spontaneous awakening and breathing trials and early mobility, both of which are associated with reduced sedation exposure. The study did have some notable nuances, however. The overall doses of trial drugs were relatively low, and there was a moderate use of rescue sedation. There was also a small amount of crossover use of propofol and dexmedetomidine between treatment arms (10%), although the authors note that this was lower than in prior related studies. Overall, the MENDS2 study suggests there is likely clinical equipoise between propofol and dexmedetomidine in terms of delirium outcomes when combined with best practices, such targeted light sedation, paired awakening and breathing trials, and early mobility.
How should we manage sedation to prevent delirium?
Building off of the recent MENDS2 study and earlier work in the field, along with the 2018 PADIS guidelines, the general paradigm of sedation management should be focused on using light sedation with sedation interruptions to minimize overall sedation exposure. Based on the best available evidence to date, targeting less overall sedation leads to improved outcomes in critically ill patients, including mortality and duration of mechanical ventilation. Benzodiazepines should be avoided due to their association with delirium, but currently there is no evidence to suggest one nonbenzodiazepine sedative is better than another. Intensivists can feel comfortable choosing between agents based on a patient’s individual clinical needs, especially when patients are receiving paired spontaneous awakening and breathing trials and early rehabilitation. These same principles should be applied to sedation management and delirium patients in COVID-19 patients as well. While certain circumstances will necessitate deeper sedation at times (e.g., refractory hypoxemia due to ARDS from COVID-19), clinicians should continually reassess the actual sedation needs of the patient with the goal of reducing overall sedation. Focusing effort on these evidence-based practices will help reduce the incidence of delirium and ultimately improve patient outcomes.
Dr. Mart is with the Division of Allergy, Pulmonary, and Critical Care Medicine, Vanderbilt University Medical Center; Critical Illness, Brain Dysfunction, and Survivorship (CIBS) Center; and VA Tennessee Valley Healthcare System Geriatric Research Education and Clinical Center (GRECC), Nashville, Tennessee.
Delirium is a frequent form of organ failure among the critically ill, impacting up to 80% of mechanically ventilated patients (Ely EW et al. JAMA. 2004;291[14]:1753-62). Its cardinal manifestations include disturbances in attention and cognition that occur acutely (e.g., hours to days) that are not better explained by another disease process (such as a toxidrome or dementia) (American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders. 5th ed., 2013). Duration of delirium in the intensive care unit (ICU) is independently associated with poor outcomes, such as mortality and hospital length of stay, even when accounting for comorbidities, coma duration, sedative use, and severity of illness. Delirium during critical illness is an important bellwether for a patient’s clinical status, often serving as a harbinger for severe or worsening disease.
Over the last two decades, the critical care community has come to understand the importance of recognizing delirium, which is often underdiagnosed, as well as delirium prevention. In the ICU, several factors coalesce to form the perfect environment for the development of delirium. Patients often have preexisting comorbidities that predispose to delirium, such as preexisting cognitive impairment, and the severity of critical illness increases the risk of delirium further. There are also bedside factors, however, that are important for the intensivist to address, many of which are modifiable. These include routinely screening for delirium and assessing level of consciousness, implementing early mobility and rehabilitation, targeting light sedation, and avoiding deliriogenic medications such as benzodiazepines. These evidence-based care practices form the foundation of the 2018 Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU (i.e., PADIS guidelines), which aim to reduce delirium and iatrogenesis from critical care (Devlin JW et al. Crit Care Med. 2018;46[9]:e825-e873). The severe acute respiratory syndrome–coronavirus 2 (SARS-CoV-2) pathogen that has caused the coronavirus disease 2019 (COVID-19) pandemic, however, has brought unprecedented challenges to critical care. One unfortunate side effect has been increased use of deep sedation and, thus, a greater incidence of delirium (Pun BT et al. Lancet Respir Med. 2021;9[3]:239-50). While the impact of the pandemic is unprecedented, thoughtful and careful sedation use remains vital to providing optimal care for the critically ill patient.
The link between sedation and delirium
The advent of modern mechanical ventilation brought critical care medicine into a period of rapid growth. Practices derived from the operating room, such as deep sedation and paralysis, became commonplace. Yet, starting in the late 1990s and early 2000s, evidence started growing regarding the impact of delirium and the unique aspects of the ICU that made it so prevalent. Delirium is strongly linked to inpatient mortality in mechanically ventilated adults, and it is best understood as an additional form of organ failure, much like other organ failures commonly recognized and treated by intensivists, such as respiratory or renal failure. Certain medications and sedation practices are associated with the development and duration of delirium. Benzodiazepines, a common sedative medication, are strongly linked to the development of delirium. In a study comparing commonly used sedative and analgesic agents, the use of lorazepam was associated with a greater risk of delirium the following day among critically ill, mechanically ventilated patients (Pandhariphande PP et al. Anesthesiology. 2006;104[1]:21-6). Given how commonly benzodiazepines are used and delirium develops in the ICU, this association has striking implications for clinical care and outcomes such as mortality. It is also significant, given that benzodiazepine use has increased during the pandemic, potentially creating significant downstream consequences. Benzodiazepines should be actively avoided when at all possible, given their propensity to lead to delirium, in accordance with the most recent guidelines.
Which sedation agent to choose?
While the negative effects of benzodiazepine-based sedation are well established, the optimal sedation agent remains unclear. Several other drugs are commonly used in the ICU, including propofol, dexmedetomidine, and opioid agents such as fentanyl and morphine. Propofol and dexmedetomidine are used specifically for their sedative properties, though they have dramatically different effects on the depth of sedation and different mechanisms of action. Opioid agents are most commonly used for their analgesic effect; however, in higher doses or combined with other medications, they have the secondary effect of inducing sedation. No particular sedation agent, however, beyond the avoidance of benzodiazepines has been recommended for use in the most recent guidelines. In the PRODEX and MIDEX studies, dexmedetomidine was noninferior to both midazolam and propofol in achieving targeted light to moderate sedation, and dexmedetomidine was associated with a shorter duration of mechanical ventilation compared to midazolam (Jakob SM et al. JAMA. 2012;307[11]:1151-60). More recently, the SPICE-III trial studied dexmedetomidine vs. usual care and found no difference in 90-day mortality (Shehabi Y et al. N Engl J Med. 2019;380[26]:2506-17).
In choosing the best sedation agent to avoid delirium, the largest and most applicable trial to date is the “Maximizing the Efficacy of Sedation and Reducing Neurological Dysfunction and Mortality in Septic Patients with Acute Respiratory Failure,” or MENDS2 trial (Hughes CG et al. N Engl J Med. 2021;384:1424-36). This study was a double-blind, multicenter randomized controlled trial of dexmedetomidine vs propofol in critically ill patients with sepsis receiving mechanical ventilation. The primary outcome was days alive without delirium or coma over the 14-day intervention period. The study enrolled 438 patients between 13 sites, with 422 patients receiving either dexmedetomidine or propofol. Hughes and colleagues found no difference in the primary outcome of days alive without delirium or coma between the dexmedetomidine and the propofol arms. The study also found no difference in secondary outcomes, including ventilator-free days, 90-day mortality, and 6-month global cognition, as well as no difference in safety endpoints. Importantly, there was excellent compliance with guideline-recommended practices of spontaneous awakening and breathing trials and early mobility, both of which are associated with reduced sedation exposure. The study did have some notable nuances, however. The overall doses of trial drugs were relatively low, and there was a moderate use of rescue sedation. There was also a small amount of crossover use of propofol and dexmedetomidine between treatment arms (10%), although the authors note that this was lower than in prior related studies. Overall, the MENDS2 study suggests there is likely clinical equipoise between propofol and dexmedetomidine in terms of delirium outcomes when combined with best practices, such targeted light sedation, paired awakening and breathing trials, and early mobility.
How should we manage sedation to prevent delirium?
Building off of the recent MENDS2 study and earlier work in the field, along with the 2018 PADIS guidelines, the general paradigm of sedation management should be focused on using light sedation with sedation interruptions to minimize overall sedation exposure. Based on the best available evidence to date, targeting less overall sedation leads to improved outcomes in critically ill patients, including mortality and duration of mechanical ventilation. Benzodiazepines should be avoided due to their association with delirium, but currently there is no evidence to suggest one nonbenzodiazepine sedative is better than another. Intensivists can feel comfortable choosing between agents based on a patient’s individual clinical needs, especially when patients are receiving paired spontaneous awakening and breathing trials and early rehabilitation. These same principles should be applied to sedation management and delirium patients in COVID-19 patients as well. While certain circumstances will necessitate deeper sedation at times (e.g., refractory hypoxemia due to ARDS from COVID-19), clinicians should continually reassess the actual sedation needs of the patient with the goal of reducing overall sedation. Focusing effort on these evidence-based practices will help reduce the incidence of delirium and ultimately improve patient outcomes.
Dr. Mart is with the Division of Allergy, Pulmonary, and Critical Care Medicine, Vanderbilt University Medical Center; Critical Illness, Brain Dysfunction, and Survivorship (CIBS) Center; and VA Tennessee Valley Healthcare System Geriatric Research Education and Clinical Center (GRECC), Nashville, Tennessee.
CHEST website redesign puts the user first
You’ve probably noticed that we recently rolled out a new website – one that is updated, streamlined, and user-friendly (and if you haven’t, go check it out!). Our goal for this project was to ensure that chestnet.org remains your go-to resource when it comes to pulmonary, critical care, and sleep medicine, and to accomplish that, we recognized that some major changes were needed. In short, while we were on the cutting-edge of chest medicine, our website definitely was not.
That’s why we’ve redesigned everything from the ground up. Our very best tools, resources, and offerings are now front and center, which means that you’ll be able to find everything you’re looking for, plus some extras you aren’t, with a few simple clicks.
While there are a lot of new features on the site that we can’t wait for you to discover, here are the upgrades that we’re most excited about.
Mobile responsiveness
One of the biggest changes to the site is that it is now mobile responsive. That means you’ll have a seamless experience regardless of what device you’re on. Whether that’s a phone or a tablet, you’ll be able to log in to your account, view any of our resources, and purchase products – functions that used to be only accessible from a desktop.
Intuitive navigation
We have so much content to offer that finding a place for everything can be difficult, and, in the past, resources often got buried within the navigation. That’s why we spent months taking an inventory of our entire site so that we could reorganize all of our resources in a way that would make more sense to you – our users.
Community-centered
We know that you joined CHEST for more than our top-tier resources; you joined to be part of a community. That’s why the new site includes more community-based hubs and opportunities for peer-to-peer interaction. We’ll continue to add more features like blog commenting and Twitter feeds so that you can continue to engage with your colleagues, let your voice be heard, and expand your circle of peers.
User-focused design
What are you hoping to find when coming to our site? What do you want to accomplish? What features would make that easier? By asking these questions, employing a succinct set of design principles, and completing several rounds of member prototype testing, we believe that we redesigned the site not only for you, but with you.
While we’ve made some major upgrades, we’re not done yet. We’ll continue to enhance the site in the upcoming month with one goal in mind – to ensure you’re getting more out of your membership than ever before.
You’ve probably noticed that we recently rolled out a new website – one that is updated, streamlined, and user-friendly (and if you haven’t, go check it out!). Our goal for this project was to ensure that chestnet.org remains your go-to resource when it comes to pulmonary, critical care, and sleep medicine, and to accomplish that, we recognized that some major changes were needed. In short, while we were on the cutting-edge of chest medicine, our website definitely was not.
That’s why we’ve redesigned everything from the ground up. Our very best tools, resources, and offerings are now front and center, which means that you’ll be able to find everything you’re looking for, plus some extras you aren’t, with a few simple clicks.
While there are a lot of new features on the site that we can’t wait for you to discover, here are the upgrades that we’re most excited about.
Mobile responsiveness
One of the biggest changes to the site is that it is now mobile responsive. That means you’ll have a seamless experience regardless of what device you’re on. Whether that’s a phone or a tablet, you’ll be able to log in to your account, view any of our resources, and purchase products – functions that used to be only accessible from a desktop.
Intuitive navigation
We have so much content to offer that finding a place for everything can be difficult, and, in the past, resources often got buried within the navigation. That’s why we spent months taking an inventory of our entire site so that we could reorganize all of our resources in a way that would make more sense to you – our users.
Community-centered
We know that you joined CHEST for more than our top-tier resources; you joined to be part of a community. That’s why the new site includes more community-based hubs and opportunities for peer-to-peer interaction. We’ll continue to add more features like blog commenting and Twitter feeds so that you can continue to engage with your colleagues, let your voice be heard, and expand your circle of peers.
User-focused design
What are you hoping to find when coming to our site? What do you want to accomplish? What features would make that easier? By asking these questions, employing a succinct set of design principles, and completing several rounds of member prototype testing, we believe that we redesigned the site not only for you, but with you.
While we’ve made some major upgrades, we’re not done yet. We’ll continue to enhance the site in the upcoming month with one goal in mind – to ensure you’re getting more out of your membership than ever before.
You’ve probably noticed that we recently rolled out a new website – one that is updated, streamlined, and user-friendly (and if you haven’t, go check it out!). Our goal for this project was to ensure that chestnet.org remains your go-to resource when it comes to pulmonary, critical care, and sleep medicine, and to accomplish that, we recognized that some major changes were needed. In short, while we were on the cutting-edge of chest medicine, our website definitely was not.
That’s why we’ve redesigned everything from the ground up. Our very best tools, resources, and offerings are now front and center, which means that you’ll be able to find everything you’re looking for, plus some extras you aren’t, with a few simple clicks.
While there are a lot of new features on the site that we can’t wait for you to discover, here are the upgrades that we’re most excited about.
Mobile responsiveness
One of the biggest changes to the site is that it is now mobile responsive. That means you’ll have a seamless experience regardless of what device you’re on. Whether that’s a phone or a tablet, you’ll be able to log in to your account, view any of our resources, and purchase products – functions that used to be only accessible from a desktop.
Intuitive navigation
We have so much content to offer that finding a place for everything can be difficult, and, in the past, resources often got buried within the navigation. That’s why we spent months taking an inventory of our entire site so that we could reorganize all of our resources in a way that would make more sense to you – our users.
Community-centered
We know that you joined CHEST for more than our top-tier resources; you joined to be part of a community. That’s why the new site includes more community-based hubs and opportunities for peer-to-peer interaction. We’ll continue to add more features like blog commenting and Twitter feeds so that you can continue to engage with your colleagues, let your voice be heard, and expand your circle of peers.
User-focused design
What are you hoping to find when coming to our site? What do you want to accomplish? What features would make that easier? By asking these questions, employing a succinct set of design principles, and completing several rounds of member prototype testing, we believe that we redesigned the site not only for you, but with you.
While we’ve made some major upgrades, we’re not done yet. We’ll continue to enhance the site in the upcoming month with one goal in mind – to ensure you’re getting more out of your membership than ever before.
Advancing bronchoscopy: Reaching the unreachable
As of 2019, lung cancer remained the leading cause of cancer death in the United States. In March 2021, the USPSTF updated the guidelines for lung cancer screening, increasing the number of eligible patients in order to identify malignancies in the early stages when more treatment options exist. With the growth of lung cancer screening, increasingly smaller pulmonary nodules are being identified in more peripheral locations previously thought to be unreachable with bronchoscopy. While bronchoscopy has been utilized for over a century for therapeutic interventions, the development of the fiberoptic bronchoscope in 1967 ushered in an era of evolving diagnostic functions. From the initial endobronchial and transbronchial biopsy techniques, to the introduction of endobronchial ultrasound, and now the latest navigational and robotic modalities, these advances have opened a new realm of interventions available in our diagnostic approach to lung cancer.

Bronchoscopy has become essential in the diagnosis of thoracic malignancies, providing both diagnostic and staging information in one procedural setting. By first assessing the mediastinal and hilar lymph nodes with endobronchial ultrasound and transbronchial needle aspiration, involved lymph nodes can give both diagnosis and staging information required to guide treatment. This is particularly important in the case of non-small cell lung cancer, which utilizes the TNM staging system. Through the use of convex probe endobronchial ultrasound (CP-EBUS), combined with rapid on-site evaluation (ROSE) by pathologic condition, we can more accurately target the individual lymph nodes for biopsy without the need for any additional procedures that are often more complex and invasive, such as mediastinoscopy. It is important to note the role of CP-EBUS extends beyond the lymph node assessment and can also be utilized for the evaluation of other mediastinal lesions, such as central parenchymal masses. These would otherwise be difficult to access due to the lack of a clear airway to the lesion (Argento and Puchalski. Respir Med. 2016;116:55-8).
While EBUS has improved the sampling of lymph nodes, advanced imaging technologies and subsequent increases in lung cancer screening have increased the number of lung malignancies identified in earlier stages before extension to the lymph nodes occurs. This scenario requires a direct biopsy of the primary nodule or lung mass. While CP-EBUS can be utilized for some central parenchymal lesions, peripheral nodules pose a greater challenge to the bronchoscopist as they cannot be directly visualized with the conventional bronchoscope. These lesions are amenable to traditional sampling techniques such as bronchial brushings and washings in addition to transbronchial needle aspiration and transbronchial biopsy. However, the yield for peripheral lesions is less than that for central tumors and depends on lesion size, distance from hilum, spatial positioning from bronchus, and operator experience. To help localize peripheral lesions, a separate form of endobronchial ultrasound is available that can be used in combination with fluoroscopy to target a lesion. Radial probe endobronchial ultrasound (RP-EBUS) utilizes a rotating ultrasound transducer that can be advanced either through the working channel of the bronchoscope or through a guide sheath to extend to airways beyond what the conventional bronchoscope can reach. This assists the bronchoscopist with locating the correct airway and, therefore, increases the yield of sampling techniques. The use of RP-EBUS has reported diagnostic yields of almost 85% if the ultrasound is located within the lesion, but less than 50% if adjacent to the lesion (Chen et al. Ann Am Thorac Soc. 2014;11[4]:578-82). While this improves the yield beyond that achieved with conventional bronchoscopy alone, it continues to challenge the bronchoscopist to locate an accessible airway from a series of branching bronchi that are beyond the level of direct visualization.
Due to the historical difficulty in accurately reaching peripheral lesions, alternative technologies for sampling these lesions, such as image-guided biopsies or surgical resection, were employed. While CT scan-guided biopsies traditionally have high diagnostic yields, they also carry a higher rate of complications, including pneumothorax and bleeding. This has led to a significant increase over the past 2 decades in new bronchoscopic technologies targeting safer and more accurate sampling of increasingly smaller, peripheral lesions.
Traditionally, any new technologies created were intended to be used alongside flexible fiberoptic bronchoscopy. The more recently introduced technologies, however, aim to provide a safer, more accurate procedure through virtual bronchoscopy. By obtaining CT scan images prior to the procedure, a 3D visualization is constructed of the tracheobronchial tree, allowing for directed guidance of endobronchial accessories to more distal airways. Where the bronchoscopist was previously limited in navigating the bronchial tree to the subsegmental bronchi, virtual bronchoscopy can depict the airways up to the 7th order subdivision. This is a significant improvement in airway visualization – however, only when partnered with guidance technologies can the model be accurately navigated.
One modality that is often coupled with virtual bronchoscopy to accurately reach peripheral lesions is electromagnetic navigation bronchoscopy (ENB). Multiple ENB software systems have been created and continue to be highly utilized by bronchoscopists to target peripheral lesions, as it has often been likened to a GPS for the lungs. With the addition of specific hardware components, a magnetic field is created around the patient where the sensor position can be elicited to within 1-mm accuracy. When overlaid with the CT scan images, the bronchoscopist can have real-time positioning of the probe in all three planes and guide the necessary sampling tools to the lesion of interest. The reported yields for ENB vary but have been shown to increase in the presence of specific image findings such as a positive bronchus sign – an air-filled bronchus leading into the lesion. The presence of this finding can increase the yield up to almost 75% from just under 50% in the absence of a positive bronchus sign. (Ali et al. Ann Am Thorac Soc. 2018;15[8]:978-87). However, regardless of this finding, the overall diagnostic yields for ENB continue to fall below that seen with other image-guided biopsy techniques. The procedural complications, however, are significantly less and, therefore, many physicians continue to advocate for ENB as the initial procedure in attempt to decrease risk for the patient.
The newest technology to be introduced to target peripheral lung lesions and to improve upon the shortcomings of other techniques is robotic-assisted bronchoscopy. While surgical specialties have seen success with robotic techniques over many years, the first robotic bronchoscopy system was not introduced until 2018. At present, there are two systems available: the Monarch® system by Auris Health and the Ion Endoluminal® System by Intuitive Surgical. These systems allow for increased bronchoscope stability, improved visualization, adjustable angulation of biopsy tools, and an improved ability to make even subtle turns in the airways. Early studies on both systems were cadaver based, but an increasing number of patient trials are now being reported or actively enrolling. Both systems have shown high rates of lesion localization, greater than 85%, with varying diagnostic yields from 69-79%. Some cadaver studies that utilized artificial tumors reported higher diagnostic yields – over 90% – but this was not seen in initial patient-based studies. (Agrawal et al. J Thorac Dis. 2020;12[6]:3279-86) More data related to the robotic-assisted bronchoscopy systems can be expected in the future as more experience is gained, but initial results are promising in the system’s ability to diagnose early lung cancers safely and accurately.
With increasing technologies and equipment available, bronchoscopy has quickly become an essential step in the diagnosis of lung cancer. While other techniques exist beyond those described here, these are some of the more widely used options currently available. It is not possible at this time to define one technology as the best tool for the diagnosis of lung cancer, as patient factors will always have to be taken into consideration to ensure safety and accuracy. However, with constantly changing technologies, the bronchoscopist now has a variety of tools available to help target previously “unreachable” lesions as we aim to decrease the historically high mortality rates of lung cancer.
Dr. Jewani and Dr. Johnson are from Loyola University Medical Center, Department of Pulmonary and Critical Care Medicine, Maywood, Illinois.
1. Agrawal, Abhinav et al. “Robotic bronchoscopy for pulmonary lesions: a review of existing technologies and clinical data.” Journal of thoracic disease vol. 12,6 (2020): 3279-3286. doi:10.21037/jtd.2020.03.35
2. Ali MS, Sethi J, Taneja A, Musani A, Maldonado F. Computed Tomography Bronchus Sign and the Diagnostic Yield of Guided Bronchoscopy for Peripheral Pulmonary Lesions. A Systematic Review and Meta-Analysis. Ann Am Thorac Soc. 2018 Aug;15(8):978-987. doi: 10.1513/AnnalsATS.201711-856OC. PMID: 29877715.
3. Argento AC, Puchalski J. Convex probe EBUS for centrally located parenchymal lesions without a bronchus sign. Respir Med. 2016 Jul;116:55-8. doi: 10.1016/j.rmed.2016.04.012. Epub 2016 Apr 29. PMID: 27296821.
4. Chen A, Chenna P, Loiselle A, Massoni J, Mayse M, Misselhorn D. Radial probe endobronchial ultrasound for peripheral pulmonary lesions. A 5-year institutional experience. Ann Am Thorac Soc. 2014 May;11(4):578-82. doi: 10.1513/AnnalsATS.201311-384OC. PMID: 24635641.
As of 2019, lung cancer remained the leading cause of cancer death in the United States. In March 2021, the USPSTF updated the guidelines for lung cancer screening, increasing the number of eligible patients in order to identify malignancies in the early stages when more treatment options exist. With the growth of lung cancer screening, increasingly smaller pulmonary nodules are being identified in more peripheral locations previously thought to be unreachable with bronchoscopy. While bronchoscopy has been utilized for over a century for therapeutic interventions, the development of the fiberoptic bronchoscope in 1967 ushered in an era of evolving diagnostic functions. From the initial endobronchial and transbronchial biopsy techniques, to the introduction of endobronchial ultrasound, and now the latest navigational and robotic modalities, these advances have opened a new realm of interventions available in our diagnostic approach to lung cancer.
Bronchoscopy has become essential in the diagnosis of thoracic malignancies, providing both diagnostic and staging information in one procedural setting. By first assessing the mediastinal and hilar lymph nodes with endobronchial ultrasound and transbronchial needle aspiration, involved lymph nodes can give both diagnosis and staging information required to guide treatment. This is particularly important in the case of non-small cell lung cancer, which utilizes the TNM staging system. Through the use of convex probe endobronchial ultrasound (CP-EBUS), combined with rapid on-site evaluation (ROSE) by pathologic condition, we can more accurately target the individual lymph nodes for biopsy without the need for any additional procedures that are often more complex and invasive, such as mediastinoscopy. It is important to note the role of CP-EBUS extends beyond the lymph node assessment and can also be utilized for the evaluation of other mediastinal lesions, such as central parenchymal masses. These would otherwise be difficult to access due to the lack of a clear airway to the lesion (Argento and Puchalski. Respir Med. 2016;116:55-8).
While EBUS has improved the sampling of lymph nodes, advanced imaging technologies and subsequent increases in lung cancer screening have increased the number of lung malignancies identified in earlier stages before extension to the lymph nodes occurs. This scenario requires a direct biopsy of the primary nodule or lung mass. While CP-EBUS can be utilized for some central parenchymal lesions, peripheral nodules pose a greater challenge to the bronchoscopist as they cannot be directly visualized with the conventional bronchoscope. These lesions are amenable to traditional sampling techniques such as bronchial brushings and washings in addition to transbronchial needle aspiration and transbronchial biopsy. However, the yield for peripheral lesions is less than that for central tumors and depends on lesion size, distance from hilum, spatial positioning from bronchus, and operator experience. To help localize peripheral lesions, a separate form of endobronchial ultrasound is available that can be used in combination with fluoroscopy to target a lesion. Radial probe endobronchial ultrasound (RP-EBUS) utilizes a rotating ultrasound transducer that can be advanced either through the working channel of the bronchoscope or through a guide sheath to extend to airways beyond what the conventional bronchoscope can reach. This assists the bronchoscopist with locating the correct airway and, therefore, increases the yield of sampling techniques. The use of RP-EBUS has reported diagnostic yields of almost 85% if the ultrasound is located within the lesion, but less than 50% if adjacent to the lesion (Chen et al. Ann Am Thorac Soc. 2014;11[4]:578-82). While this improves the yield beyond that achieved with conventional bronchoscopy alone, it continues to challenge the bronchoscopist to locate an accessible airway from a series of branching bronchi that are beyond the level of direct visualization.
Due to the historical difficulty in accurately reaching peripheral lesions, alternative technologies for sampling these lesions, such as image-guided biopsies or surgical resection, were employed. While CT scan-guided biopsies traditionally have high diagnostic yields, they also carry a higher rate of complications, including pneumothorax and bleeding. This has led to a significant increase over the past 2 decades in new bronchoscopic technologies targeting safer and more accurate sampling of increasingly smaller, peripheral lesions.
Traditionally, any new technologies created were intended to be used alongside flexible fiberoptic bronchoscopy. The more recently introduced technologies, however, aim to provide a safer, more accurate procedure through virtual bronchoscopy. By obtaining CT scan images prior to the procedure, a 3D visualization is constructed of the tracheobronchial tree, allowing for directed guidance of endobronchial accessories to more distal airways. Where the bronchoscopist was previously limited in navigating the bronchial tree to the subsegmental bronchi, virtual bronchoscopy can depict the airways up to the 7th order subdivision. This is a significant improvement in airway visualization – however, only when partnered with guidance technologies can the model be accurately navigated.
One modality that is often coupled with virtual bronchoscopy to accurately reach peripheral lesions is electromagnetic navigation bronchoscopy (ENB). Multiple ENB software systems have been created and continue to be highly utilized by bronchoscopists to target peripheral lesions, as it has often been likened to a GPS for the lungs. With the addition of specific hardware components, a magnetic field is created around the patient where the sensor position can be elicited to within 1-mm accuracy. When overlaid with the CT scan images, the bronchoscopist can have real-time positioning of the probe in all three planes and guide the necessary sampling tools to the lesion of interest. The reported yields for ENB vary but have been shown to increase in the presence of specific image findings such as a positive bronchus sign – an air-filled bronchus leading into the lesion. The presence of this finding can increase the yield up to almost 75% from just under 50% in the absence of a positive bronchus sign. (Ali et al. Ann Am Thorac Soc. 2018;15[8]:978-87). However, regardless of this finding, the overall diagnostic yields for ENB continue to fall below that seen with other image-guided biopsy techniques. The procedural complications, however, are significantly less and, therefore, many physicians continue to advocate for ENB as the initial procedure in attempt to decrease risk for the patient.
The newest technology to be introduced to target peripheral lung lesions and to improve upon the shortcomings of other techniques is robotic-assisted bronchoscopy. While surgical specialties have seen success with robotic techniques over many years, the first robotic bronchoscopy system was not introduced until 2018. At present, there are two systems available: the Monarch® system by Auris Health and the Ion Endoluminal® System by Intuitive Surgical. These systems allow for increased bronchoscope stability, improved visualization, adjustable angulation of biopsy tools, and an improved ability to make even subtle turns in the airways. Early studies on both systems were cadaver based, but an increasing number of patient trials are now being reported or actively enrolling. Both systems have shown high rates of lesion localization, greater than 85%, with varying diagnostic yields from 69-79%. Some cadaver studies that utilized artificial tumors reported higher diagnostic yields – over 90% – but this was not seen in initial patient-based studies. (Agrawal et al. J Thorac Dis. 2020;12[6]:3279-86) More data related to the robotic-assisted bronchoscopy systems can be expected in the future as more experience is gained, but initial results are promising in the system’s ability to diagnose early lung cancers safely and accurately.
With increasing technologies and equipment available, bronchoscopy has quickly become an essential step in the diagnosis of lung cancer. While other techniques exist beyond those described here, these are some of the more widely used options currently available. It is not possible at this time to define one technology as the best tool for the diagnosis of lung cancer, as patient factors will always have to be taken into consideration to ensure safety and accuracy. However, with constantly changing technologies, the bronchoscopist now has a variety of tools available to help target previously “unreachable” lesions as we aim to decrease the historically high mortality rates of lung cancer.
Dr. Jewani and Dr. Johnson are from Loyola University Medical Center, Department of Pulmonary and Critical Care Medicine, Maywood, Illinois.
1. Agrawal, Abhinav et al. “Robotic bronchoscopy for pulmonary lesions: a review of existing technologies and clinical data.” Journal of thoracic disease vol. 12,6 (2020): 3279-3286. doi:10.21037/jtd.2020.03.35
2. Ali MS, Sethi J, Taneja A, Musani A, Maldonado F. Computed Tomography Bronchus Sign and the Diagnostic Yield of Guided Bronchoscopy for Peripheral Pulmonary Lesions. A Systematic Review and Meta-Analysis. Ann Am Thorac Soc. 2018 Aug;15(8):978-987. doi: 10.1513/AnnalsATS.201711-856OC. PMID: 29877715.
3. Argento AC, Puchalski J. Convex probe EBUS for centrally located parenchymal lesions without a bronchus sign. Respir Med. 2016 Jul;116:55-8. doi: 10.1016/j.rmed.2016.04.012. Epub 2016 Apr 29. PMID: 27296821.
4. Chen A, Chenna P, Loiselle A, Massoni J, Mayse M, Misselhorn D. Radial probe endobronchial ultrasound for peripheral pulmonary lesions. A 5-year institutional experience. Ann Am Thorac Soc. 2014 May;11(4):578-82. doi: 10.1513/AnnalsATS.201311-384OC. PMID: 24635641.
As of 2019, lung cancer remained the leading cause of cancer death in the United States. In March 2021, the USPSTF updated the guidelines for lung cancer screening, increasing the number of eligible patients in order to identify malignancies in the early stages when more treatment options exist. With the growth of lung cancer screening, increasingly smaller pulmonary nodules are being identified in more peripheral locations previously thought to be unreachable with bronchoscopy. While bronchoscopy has been utilized for over a century for therapeutic interventions, the development of the fiberoptic bronchoscope in 1967 ushered in an era of evolving diagnostic functions. From the initial endobronchial and transbronchial biopsy techniques, to the introduction of endobronchial ultrasound, and now the latest navigational and robotic modalities, these advances have opened a new realm of interventions available in our diagnostic approach to lung cancer.
Bronchoscopy has become essential in the diagnosis of thoracic malignancies, providing both diagnostic and staging information in one procedural setting. By first assessing the mediastinal and hilar lymph nodes with endobronchial ultrasound and transbronchial needle aspiration, involved lymph nodes can give both diagnosis and staging information required to guide treatment. This is particularly important in the case of non-small cell lung cancer, which utilizes the TNM staging system. Through the use of convex probe endobronchial ultrasound (CP-EBUS), combined with rapid on-site evaluation (ROSE) by pathologic condition, we can more accurately target the individual lymph nodes for biopsy without the need for any additional procedures that are often more complex and invasive, such as mediastinoscopy. It is important to note the role of CP-EBUS extends beyond the lymph node assessment and can also be utilized for the evaluation of other mediastinal lesions, such as central parenchymal masses. These would otherwise be difficult to access due to the lack of a clear airway to the lesion (Argento and Puchalski. Respir Med. 2016;116:55-8).
While EBUS has improved the sampling of lymph nodes, advanced imaging technologies and subsequent increases in lung cancer screening have increased the number of lung malignancies identified in earlier stages before extension to the lymph nodes occurs. This scenario requires a direct biopsy of the primary nodule or lung mass. While CP-EBUS can be utilized for some central parenchymal lesions, peripheral nodules pose a greater challenge to the bronchoscopist as they cannot be directly visualized with the conventional bronchoscope. These lesions are amenable to traditional sampling techniques such as bronchial brushings and washings in addition to transbronchial needle aspiration and transbronchial biopsy. However, the yield for peripheral lesions is less than that for central tumors and depends on lesion size, distance from hilum, spatial positioning from bronchus, and operator experience. To help localize peripheral lesions, a separate form of endobronchial ultrasound is available that can be used in combination with fluoroscopy to target a lesion. Radial probe endobronchial ultrasound (RP-EBUS) utilizes a rotating ultrasound transducer that can be advanced either through the working channel of the bronchoscope or through a guide sheath to extend to airways beyond what the conventional bronchoscope can reach. This assists the bronchoscopist with locating the correct airway and, therefore, increases the yield of sampling techniques. The use of RP-EBUS has reported diagnostic yields of almost 85% if the ultrasound is located within the lesion, but less than 50% if adjacent to the lesion (Chen et al. Ann Am Thorac Soc. 2014;11[4]:578-82). While this improves the yield beyond that achieved with conventional bronchoscopy alone, it continues to challenge the bronchoscopist to locate an accessible airway from a series of branching bronchi that are beyond the level of direct visualization.
Due to the historical difficulty in accurately reaching peripheral lesions, alternative technologies for sampling these lesions, such as image-guided biopsies or surgical resection, were employed. While CT scan-guided biopsies traditionally have high diagnostic yields, they also carry a higher rate of complications, including pneumothorax and bleeding. This has led to a significant increase over the past 2 decades in new bronchoscopic technologies targeting safer and more accurate sampling of increasingly smaller, peripheral lesions.
Traditionally, any new technologies created were intended to be used alongside flexible fiberoptic bronchoscopy. The more recently introduced technologies, however, aim to provide a safer, more accurate procedure through virtual bronchoscopy. By obtaining CT scan images prior to the procedure, a 3D visualization is constructed of the tracheobronchial tree, allowing for directed guidance of endobronchial accessories to more distal airways. Where the bronchoscopist was previously limited in navigating the bronchial tree to the subsegmental bronchi, virtual bronchoscopy can depict the airways up to the 7th order subdivision. This is a significant improvement in airway visualization – however, only when partnered with guidance technologies can the model be accurately navigated.
One modality that is often coupled with virtual bronchoscopy to accurately reach peripheral lesions is electromagnetic navigation bronchoscopy (ENB). Multiple ENB software systems have been created and continue to be highly utilized by bronchoscopists to target peripheral lesions, as it has often been likened to a GPS for the lungs. With the addition of specific hardware components, a magnetic field is created around the patient where the sensor position can be elicited to within 1-mm accuracy. When overlaid with the CT scan images, the bronchoscopist can have real-time positioning of the probe in all three planes and guide the necessary sampling tools to the lesion of interest. The reported yields for ENB vary but have been shown to increase in the presence of specific image findings such as a positive bronchus sign – an air-filled bronchus leading into the lesion. The presence of this finding can increase the yield up to almost 75% from just under 50% in the absence of a positive bronchus sign. (Ali et al. Ann Am Thorac Soc. 2018;15[8]:978-87). However, regardless of this finding, the overall diagnostic yields for ENB continue to fall below that seen with other image-guided biopsy techniques. The procedural complications, however, are significantly less and, therefore, many physicians continue to advocate for ENB as the initial procedure in attempt to decrease risk for the patient.
The newest technology to be introduced to target peripheral lung lesions and to improve upon the shortcomings of other techniques is robotic-assisted bronchoscopy. While surgical specialties have seen success with robotic techniques over many years, the first robotic bronchoscopy system was not introduced until 2018. At present, there are two systems available: the Monarch® system by Auris Health and the Ion Endoluminal® System by Intuitive Surgical. These systems allow for increased bronchoscope stability, improved visualization, adjustable angulation of biopsy tools, and an improved ability to make even subtle turns in the airways. Early studies on both systems were cadaver based, but an increasing number of patient trials are now being reported or actively enrolling. Both systems have shown high rates of lesion localization, greater than 85%, with varying diagnostic yields from 69-79%. Some cadaver studies that utilized artificial tumors reported higher diagnostic yields – over 90% – but this was not seen in initial patient-based studies. (Agrawal et al. J Thorac Dis. 2020;12[6]:3279-86) More data related to the robotic-assisted bronchoscopy systems can be expected in the future as more experience is gained, but initial results are promising in the system’s ability to diagnose early lung cancers safely and accurately.
With increasing technologies and equipment available, bronchoscopy has quickly become an essential step in the diagnosis of lung cancer. While other techniques exist beyond those described here, these are some of the more widely used options currently available. It is not possible at this time to define one technology as the best tool for the diagnosis of lung cancer, as patient factors will always have to be taken into consideration to ensure safety and accuracy. However, with constantly changing technologies, the bronchoscopist now has a variety of tools available to help target previously “unreachable” lesions as we aim to decrease the historically high mortality rates of lung cancer.
Dr. Jewani and Dr. Johnson are from Loyola University Medical Center, Department of Pulmonary and Critical Care Medicine, Maywood, Illinois.
1. Agrawal, Abhinav et al. “Robotic bronchoscopy for pulmonary lesions: a review of existing technologies and clinical data.” Journal of thoracic disease vol. 12,6 (2020): 3279-3286. doi:10.21037/jtd.2020.03.35
2. Ali MS, Sethi J, Taneja A, Musani A, Maldonado F. Computed Tomography Bronchus Sign and the Diagnostic Yield of Guided Bronchoscopy for Peripheral Pulmonary Lesions. A Systematic Review and Meta-Analysis. Ann Am Thorac Soc. 2018 Aug;15(8):978-987. doi: 10.1513/AnnalsATS.201711-856OC. PMID: 29877715.
3. Argento AC, Puchalski J. Convex probe EBUS for centrally located parenchymal lesions without a bronchus sign. Respir Med. 2016 Jul;116:55-8. doi: 10.1016/j.rmed.2016.04.012. Epub 2016 Apr 29. PMID: 27296821.
4. Chen A, Chenna P, Loiselle A, Massoni J, Mayse M, Misselhorn D. Radial probe endobronchial ultrasound for peripheral pulmonary lesions. A 5-year institutional experience. Ann Am Thorac Soc. 2014 May;11(4):578-82. doi: 10.1513/AnnalsATS.201311-384OC. PMID: 24635641.
Disaster medicine in the pandemic; telehealth; rise in lung transplants for older patients; women’s lung health; and more
Disaster response
Advancing disaster medicine and global health in times of pandemic
Worldwide hardships due to COVID-19 have revealed opportunities for improvement. Disaster education, telemedicine, knowledge sharing, and resource allocation have been highlighted as such areas. In an August 2020 publication, Hart et al. argue, “Every hospital needs a Disaster Medicine physician now” (Hart et al. “Why Every US Hospital Needs a Disaster Medicine Physician Now”).

Every physician must be prepared to be the expert in times of disaster. A survey of U.S. medical students showed that despite few respondents (<27%) feeling adequately educated, >90% are willing to respond to a natural disaster or a pandemic (Kaiser et al. Disaster Med Pub Health Prep. 2009;3[4]:210-16). While natural disasters have increased by almost 35% since the 1990s, a robust approach to disaster education is not routinely implemented across the fields of medicine, nursing, allied health, and health administration (Freebairn. World Disasters Report 2020: Executive Summary. 2020 ed. IFRC. ). Notably, disaster education provides opportunities for multidisciplinary team-building where learners build a foundation of knowledge together. While no ideal educational model has been fully adopted, high-quality educational opportunities include National Disaster Life Support Foundation courses, SALT triage, and ATLS (Homer et al. Prehospital and Disaster Medicine).

Telemedicine has emerged as a very effective means of disaster support through both direct patient encounters and provider education. Tele-triage used to delineate patients requiring urgent hospitalization from those who can be managed at home has proven effective in areas with limited health care facilities (World Health Organization. Coronavirus disease.). Knowledge sharing opportunities from organizations like Project ECHO have allowed for >368,000 learners from 146 countries to exchange information during >8,000 learning sessions (Project ECHO COVID-19 response.).
Physicians of all specialties should continue to develop skills in triage, surge capacity management, ethical/legal issues surrounding disasters, organizational interoperability, and telemedicine, and emphasize skills to ensure their own personal protection.
Christopher Miller, DO, MPH
Steering Committee Fellow-in-Training Member
Sarang Patil, MD
Steering Committee Member
Practice operations
Telehealth and postpandemic care
Telehealth is the use of electronic information and telecommunication technologies to provide care when the physician and the patient are not in the same place. Telehealth has been available for 40 years. The COVID-19 pandemic forced health care providers, systems, and patients to quickly adapt to virtual audio and visual visits, new documentation parameters, billing, and reimbursement structures. Emergency rules have removed the barriers to adoption of home-based diagnostics and virtual visits. It is expected that 20% to 30% post-pandemic care will be provided via telehealth.

Telehealth is particularly beneficial in providing counseling services or managing chronic illnesses, such as COPD and heart failure. There has been an explosion of monitoring devices both wearable and implantable. Some devices, which monitor PA pressure, have been shown to reduce heart failure hospitalizations and all-cause hospitalizations (Shavelle DM, et al. Circ Heart Fail. 2020;13: e006863). Studies have been conducted on home spirometry and oximetry devices in post-lung transplant, ILD (Russell AM et al. Am J Respir Crit Care Med. 2016 Oct 15; 194[8]:989-997), and CF patients (Compton M et al. Telemed J E Health . 2020 Aug;26[8]:978-84). As we move forward, we will have to ascertain what data acquisition is relevant and develop processes to address it in real time.
In this changing landscape of health care delivery, we can anticipate an increase in virtual visits and a trend toward e-consults, which will necessitate further advancements in remote monitoring and assessment and will require us to adopt new practice models.
Caitlin Baxter, MBBS
Steering Committee Fellow-in-Training
Namita Sood, MBBCh, FCCP
Steering Committee Member
Transplant network
The rise in lung transplant for older patients
Over the past 20 years, there has been a dramatic increase in lung transplantation in elderly patients, with wide variability in age limit amongst transplant centers. The number of recipients over the age of 65 has risen from 6.9% in 2004 to 29.6% in 2016 in the United States, and 2.6% to 17% internationally. There is a number of factors driving this increase; the prevalence of advanced lung disease with increasing age, advances in targeted therapies to treat cystic fibrosis, an increased willingness of centers to perform transplants in older patients, and the 2005 revision of the Lung Allocation Scoring System (Courtwright A, Cantu E. J Thoracic Dis. 2017:9[9]:3346-51).

In the past, outcomes posttransplant for elderly patients have been conflicting in single-center studies. More recently, Hayanga et al. found no difference in survival up to 1 year between individuals 60-69 and those over 70 (J Heart Lung Transplant. 2015;34[2]:182-88). Mosher et al., however, found the median survival dropped from 4.64 years for patients aged 65-69 to 3.07 years for patients ≥74 (J Heart Lung Transplant. 2021;40[1]:42-55). Notably, older recipients were more likely to be readmitted at 30 and 90 days, and more likely to be discharged to an inpatient rehabilitation facility following transplant (McCarthy et al. J Heart Lung Transplant. 2017;36:S115; Tang et al. Clin Transplant. 2015;29:581-587).

The use of transplant in elderly patients comes with many concerns regarding neurocognitive status, frailty, and other comorbidities, all of which must be rigorously tested prior to consideration(Biswas R et al. Ann Thorac Surg. 2015;100:443-51). Recipient age, creatinine level, bilirubin level, steroid use at the time of transplant, and hospitalization at the time of transplant were associated with increased mortality (Mosher et al. J Heart Lung Transplant. 2021;40[1]:42-55). Further research is warranted in this evolving area.
Melissa B. Lesko, DO
Grant Turner, MD, MHA
Steering Committee Members
Women’s lung health
Will the new pulmonary hypertension hemodynamic classification temper the PH ‘sex-paradox’?
Older and contemporary PH registries have consistently shown that PH predominantly affects women ~2 to 3.5 times than men, with female patients having better survival compared with men (Kozu K et al. Heart Vessels. 2018;33[8]:93), a fact attributed to better RV function in female than male subjects. This PH sex-paradox denotes that while estrogen leads to increased susceptibility to PH, it appears to confer better outcomes after PH develops due to improved RV function, since RV dysfunction is a strong predictor of poor outcomes in PH. Multiple preclinical studies have described how estrogen provides protective effects on the RV (Cheng TC et al. Am J Physiol Heart Circ Physiol. 2020;319:H1459; Frump AL et al. Am J Physiol Lung Cell Mol Physiol. 2015;308:L873).
The recent recommended updates to the hemodynamic definition reflect acknowledgment of irrefutable evidence that even mildly elevated mPAP (between 19 and 24 mm Hg) is associated with increased morbidity and mortality based on consistent data from pulmonary arterial hypertension (PAH) as well as from other forms of PH [Simonneau G et al. Eur Respir J. 2019;(Jan 24);53(1):1801913). With incorporation of the updated definition that more accurately captures the disease state and its progression, an unaddressed question still remains as to how the new classification will change PH treatment algorithm and outcomes in women compared with men. Setting the definition of PH at a mPAP of 20 mm Hg not only better represents the typical patients with PH in practice, such as those with PH due to left-sided heart disease (Group 2) or PH associated with chronic lung disease (Group 3), but incorporates the preclinical pathologic disease state of PH, in which symptoms may not be evident (Maron BA, et al. Circulation. 2016;133:1240). In adhering to the new PH definition, will earlier diagnosis across the spectrum of all individuals with PH before RV dysfunction has developed improve outcomes for all those afflicted with PH and equalize outcomes between men and women? As future studies continue to investigate the direct effects of sex hormones on the RV and dissect the mechanisms leading to the sex differences in RV function in PH, a pre-clinical diagnosis in all PH patients, particularly male patients with Group 2/3 disease, may mitigate some of the previously observed advantages of estrogen on outcomes in PH.
Lavannya Pandit, MD, FCCP
Disaster response
Advancing disaster medicine and global health in times of pandemic
Worldwide hardships due to COVID-19 have revealed opportunities for improvement. Disaster education, telemedicine, knowledge sharing, and resource allocation have been highlighted as such areas. In an August 2020 publication, Hart et al. argue, “Every hospital needs a Disaster Medicine physician now” (Hart et al. “Why Every US Hospital Needs a Disaster Medicine Physician Now”).
Every physician must be prepared to be the expert in times of disaster. A survey of U.S. medical students showed that despite few respondents (<27%) feeling adequately educated, >90% are willing to respond to a natural disaster or a pandemic (Kaiser et al. Disaster Med Pub Health Prep. 2009;3[4]:210-16). While natural disasters have increased by almost 35% since the 1990s, a robust approach to disaster education is not routinely implemented across the fields of medicine, nursing, allied health, and health administration (Freebairn. World Disasters Report 2020: Executive Summary. 2020 ed. IFRC. ). Notably, disaster education provides opportunities for multidisciplinary team-building where learners build a foundation of knowledge together. While no ideal educational model has been fully adopted, high-quality educational opportunities include National Disaster Life Support Foundation courses, SALT triage, and ATLS (Homer et al. Prehospital and Disaster Medicine).
Telemedicine has emerged as a very effective means of disaster support through both direct patient encounters and provider education. Tele-triage used to delineate patients requiring urgent hospitalization from those who can be managed at home has proven effective in areas with limited health care facilities (World Health Organization. Coronavirus disease.). Knowledge sharing opportunities from organizations like Project ECHO have allowed for >368,000 learners from 146 countries to exchange information during >8,000 learning sessions (Project ECHO COVID-19 response.).
Physicians of all specialties should continue to develop skills in triage, surge capacity management, ethical/legal issues surrounding disasters, organizational interoperability, and telemedicine, and emphasize skills to ensure their own personal protection.
Christopher Miller, DO, MPH
Steering Committee Fellow-in-Training Member
Sarang Patil, MD
Steering Committee Member
Practice operations
Telehealth and postpandemic care
Telehealth is the use of electronic information and telecommunication technologies to provide care when the physician and the patient are not in the same place. Telehealth has been available for 40 years. The COVID-19 pandemic forced health care providers, systems, and patients to quickly adapt to virtual audio and visual visits, new documentation parameters, billing, and reimbursement structures. Emergency rules have removed the barriers to adoption of home-based diagnostics and virtual visits. It is expected that 20% to 30% post-pandemic care will be provided via telehealth.
Telehealth is particularly beneficial in providing counseling services or managing chronic illnesses, such as COPD and heart failure. There has been an explosion of monitoring devices both wearable and implantable. Some devices, which monitor PA pressure, have been shown to reduce heart failure hospitalizations and all-cause hospitalizations (Shavelle DM, et al. Circ Heart Fail. 2020;13: e006863). Studies have been conducted on home spirometry and oximetry devices in post-lung transplant, ILD (Russell AM et al. Am J Respir Crit Care Med. 2016 Oct 15; 194[8]:989-997), and CF patients (Compton M et al. Telemed J E Health . 2020 Aug;26[8]:978-84). As we move forward, we will have to ascertain what data acquisition is relevant and develop processes to address it in real time.
In this changing landscape of health care delivery, we can anticipate an increase in virtual visits and a trend toward e-consults, which will necessitate further advancements in remote monitoring and assessment and will require us to adopt new practice models.
Caitlin Baxter, MBBS
Steering Committee Fellow-in-Training
Namita Sood, MBBCh, FCCP
Steering Committee Member
Transplant network
The rise in lung transplant for older patients
Over the past 20 years, there has been a dramatic increase in lung transplantation in elderly patients, with wide variability in age limit amongst transplant centers. The number of recipients over the age of 65 has risen from 6.9% in 2004 to 29.6% in 2016 in the United States, and 2.6% to 17% internationally. There is a number of factors driving this increase; the prevalence of advanced lung disease with increasing age, advances in targeted therapies to treat cystic fibrosis, an increased willingness of centers to perform transplants in older patients, and the 2005 revision of the Lung Allocation Scoring System (Courtwright A, Cantu E. J Thoracic Dis. 2017:9[9]:3346-51).
In the past, outcomes posttransplant for elderly patients have been conflicting in single-center studies. More recently, Hayanga et al. found no difference in survival up to 1 year between individuals 60-69 and those over 70 (J Heart Lung Transplant. 2015;34[2]:182-88). Mosher et al., however, found the median survival dropped from 4.64 years for patients aged 65-69 to 3.07 years for patients ≥74 (J Heart Lung Transplant. 2021;40[1]:42-55). Notably, older recipients were more likely to be readmitted at 30 and 90 days, and more likely to be discharged to an inpatient rehabilitation facility following transplant (McCarthy et al. J Heart Lung Transplant. 2017;36:S115; Tang et al. Clin Transplant. 2015;29:581-587).
The use of transplant in elderly patients comes with many concerns regarding neurocognitive status, frailty, and other comorbidities, all of which must be rigorously tested prior to consideration(Biswas R et al. Ann Thorac Surg. 2015;100:443-51). Recipient age, creatinine level, bilirubin level, steroid use at the time of transplant, and hospitalization at the time of transplant were associated with increased mortality (Mosher et al. J Heart Lung Transplant. 2021;40[1]:42-55). Further research is warranted in this evolving area.
Melissa B. Lesko, DO
Grant Turner, MD, MHA
Steering Committee Members
Women’s lung health
Will the new pulmonary hypertension hemodynamic classification temper the PH ‘sex-paradox’?
Older and contemporary PH registries have consistently shown that PH predominantly affects women ~2 to 3.5 times than men, with female patients having better survival compared with men (Kozu K et al. Heart Vessels. 2018;33[8]:93), a fact attributed to better RV function in female than male subjects. This PH sex-paradox denotes that while estrogen leads to increased susceptibility to PH, it appears to confer better outcomes after PH develops due to improved RV function, since RV dysfunction is a strong predictor of poor outcomes in PH. Multiple preclinical studies have described how estrogen provides protective effects on the RV (Cheng TC et al. Am J Physiol Heart Circ Physiol. 2020;319:H1459; Frump AL et al. Am J Physiol Lung Cell Mol Physiol. 2015;308:L873).
The recent recommended updates to the hemodynamic definition reflect acknowledgment of irrefutable evidence that even mildly elevated mPAP (between 19 and 24 mm Hg) is associated with increased morbidity and mortality based on consistent data from pulmonary arterial hypertension (PAH) as well as from other forms of PH [Simonneau G et al. Eur Respir J. 2019;(Jan 24);53(1):1801913). With incorporation of the updated definition that more accurately captures the disease state and its progression, an unaddressed question still remains as to how the new classification will change PH treatment algorithm and outcomes in women compared with men. Setting the definition of PH at a mPAP of 20 mm Hg not only better represents the typical patients with PH in practice, such as those with PH due to left-sided heart disease (Group 2) or PH associated with chronic lung disease (Group 3), but incorporates the preclinical pathologic disease state of PH, in which symptoms may not be evident (Maron BA, et al. Circulation. 2016;133:1240). In adhering to the new PH definition, will earlier diagnosis across the spectrum of all individuals with PH before RV dysfunction has developed improve outcomes for all those afflicted with PH and equalize outcomes between men and women? As future studies continue to investigate the direct effects of sex hormones on the RV and dissect the mechanisms leading to the sex differences in RV function in PH, a pre-clinical diagnosis in all PH patients, particularly male patients with Group 2/3 disease, may mitigate some of the previously observed advantages of estrogen on outcomes in PH.
Lavannya Pandit, MD, FCCP
Disaster response
Advancing disaster medicine and global health in times of pandemic
Worldwide hardships due to COVID-19 have revealed opportunities for improvement. Disaster education, telemedicine, knowledge sharing, and resource allocation have been highlighted as such areas. In an August 2020 publication, Hart et al. argue, “Every hospital needs a Disaster Medicine physician now” (Hart et al. “Why Every US Hospital Needs a Disaster Medicine Physician Now”).
Every physician must be prepared to be the expert in times of disaster. A survey of U.S. medical students showed that despite few respondents (<27%) feeling adequately educated, >90% are willing to respond to a natural disaster or a pandemic (Kaiser et al. Disaster Med Pub Health Prep. 2009;3[4]:210-16). While natural disasters have increased by almost 35% since the 1990s, a robust approach to disaster education is not routinely implemented across the fields of medicine, nursing, allied health, and health administration (Freebairn. World Disasters Report 2020: Executive Summary. 2020 ed. IFRC. ). Notably, disaster education provides opportunities for multidisciplinary team-building where learners build a foundation of knowledge together. While no ideal educational model has been fully adopted, high-quality educational opportunities include National Disaster Life Support Foundation courses, SALT triage, and ATLS (Homer et al. Prehospital and Disaster Medicine).
Telemedicine has emerged as a very effective means of disaster support through both direct patient encounters and provider education. Tele-triage used to delineate patients requiring urgent hospitalization from those who can be managed at home has proven effective in areas with limited health care facilities (World Health Organization. Coronavirus disease.). Knowledge sharing opportunities from organizations like Project ECHO have allowed for >368,000 learners from 146 countries to exchange information during >8,000 learning sessions (Project ECHO COVID-19 response.).
Physicians of all specialties should continue to develop skills in triage, surge capacity management, ethical/legal issues surrounding disasters, organizational interoperability, and telemedicine, and emphasize skills to ensure their own personal protection.
Christopher Miller, DO, MPH
Steering Committee Fellow-in-Training Member
Sarang Patil, MD
Steering Committee Member
Practice operations
Telehealth and postpandemic care
Telehealth is the use of electronic information and telecommunication technologies to provide care when the physician and the patient are not in the same place. Telehealth has been available for 40 years. The COVID-19 pandemic forced health care providers, systems, and patients to quickly adapt to virtual audio and visual visits, new documentation parameters, billing, and reimbursement structures. Emergency rules have removed the barriers to adoption of home-based diagnostics and virtual visits. It is expected that 20% to 30% post-pandemic care will be provided via telehealth.
Telehealth is particularly beneficial in providing counseling services or managing chronic illnesses, such as COPD and heart failure. There has been an explosion of monitoring devices both wearable and implantable. Some devices, which monitor PA pressure, have been shown to reduce heart failure hospitalizations and all-cause hospitalizations (Shavelle DM, et al. Circ Heart Fail. 2020;13: e006863). Studies have been conducted on home spirometry and oximetry devices in post-lung transplant, ILD (Russell AM et al. Am J Respir Crit Care Med. 2016 Oct 15; 194[8]:989-997), and CF patients (Compton M et al. Telemed J E Health . 2020 Aug;26[8]:978-84). As we move forward, we will have to ascertain what data acquisition is relevant and develop processes to address it in real time.
In this changing landscape of health care delivery, we can anticipate an increase in virtual visits and a trend toward e-consults, which will necessitate further advancements in remote monitoring and assessment and will require us to adopt new practice models.
Caitlin Baxter, MBBS
Steering Committee Fellow-in-Training
Namita Sood, MBBCh, FCCP
Steering Committee Member
Transplant network
The rise in lung transplant for older patients
Over the past 20 years, there has been a dramatic increase in lung transplantation in elderly patients, with wide variability in age limit amongst transplant centers. The number of recipients over the age of 65 has risen from 6.9% in 2004 to 29.6% in 2016 in the United States, and 2.6% to 17% internationally. There is a number of factors driving this increase; the prevalence of advanced lung disease with increasing age, advances in targeted therapies to treat cystic fibrosis, an increased willingness of centers to perform transplants in older patients, and the 2005 revision of the Lung Allocation Scoring System (Courtwright A, Cantu E. J Thoracic Dis. 2017:9[9]:3346-51).
In the past, outcomes posttransplant for elderly patients have been conflicting in single-center studies. More recently, Hayanga et al. found no difference in survival up to 1 year between individuals 60-69 and those over 70 (J Heart Lung Transplant. 2015;34[2]:182-88). Mosher et al., however, found the median survival dropped from 4.64 years for patients aged 65-69 to 3.07 years for patients ≥74 (J Heart Lung Transplant. 2021;40[1]:42-55). Notably, older recipients were more likely to be readmitted at 30 and 90 days, and more likely to be discharged to an inpatient rehabilitation facility following transplant (McCarthy et al. J Heart Lung Transplant. 2017;36:S115; Tang et al. Clin Transplant. 2015;29:581-587).
The use of transplant in elderly patients comes with many concerns regarding neurocognitive status, frailty, and other comorbidities, all of which must be rigorously tested prior to consideration(Biswas R et al. Ann Thorac Surg. 2015;100:443-51). Recipient age, creatinine level, bilirubin level, steroid use at the time of transplant, and hospitalization at the time of transplant were associated with increased mortality (Mosher et al. J Heart Lung Transplant. 2021;40[1]:42-55). Further research is warranted in this evolving area.
Melissa B. Lesko, DO
Grant Turner, MD, MHA
Steering Committee Members
Women’s lung health
Will the new pulmonary hypertension hemodynamic classification temper the PH ‘sex-paradox’?
Older and contemporary PH registries have consistently shown that PH predominantly affects women ~2 to 3.5 times than men, with female patients having better survival compared with men (Kozu K et al. Heart Vessels. 2018;33[8]:93), a fact attributed to better RV function in female than male subjects. This PH sex-paradox denotes that while estrogen leads to increased susceptibility to PH, it appears to confer better outcomes after PH develops due to improved RV function, since RV dysfunction is a strong predictor of poor outcomes in PH. Multiple preclinical studies have described how estrogen provides protective effects on the RV (Cheng TC et al. Am J Physiol Heart Circ Physiol. 2020;319:H1459; Frump AL et al. Am J Physiol Lung Cell Mol Physiol. 2015;308:L873).
The recent recommended updates to the hemodynamic definition reflect acknowledgment of irrefutable evidence that even mildly elevated mPAP (between 19 and 24 mm Hg) is associated with increased morbidity and mortality based on consistent data from pulmonary arterial hypertension (PAH) as well as from other forms of PH [Simonneau G et al. Eur Respir J. 2019;(Jan 24);53(1):1801913). With incorporation of the updated definition that more accurately captures the disease state and its progression, an unaddressed question still remains as to how the new classification will change PH treatment algorithm and outcomes in women compared with men. Setting the definition of PH at a mPAP of 20 mm Hg not only better represents the typical patients with PH in practice, such as those with PH due to left-sided heart disease (Group 2) or PH associated with chronic lung disease (Group 3), but incorporates the preclinical pathologic disease state of PH, in which symptoms may not be evident (Maron BA, et al. Circulation. 2016;133:1240). In adhering to the new PH definition, will earlier diagnosis across the spectrum of all individuals with PH before RV dysfunction has developed improve outcomes for all those afflicted with PH and equalize outcomes between men and women? As future studies continue to investigate the direct effects of sex hormones on the RV and dissect the mechanisms leading to the sex differences in RV function in PH, a pre-clinical diagnosis in all PH patients, particularly male patients with Group 2/3 disease, may mitigate some of the previously observed advantages of estrogen on outcomes in PH.
Lavannya Pandit, MD, FCCP
Surge of new child COVID cases continues for 6th consecutive week
The current COVID-19 surge has brought new cases in children to their highest level since February, according to a new report.
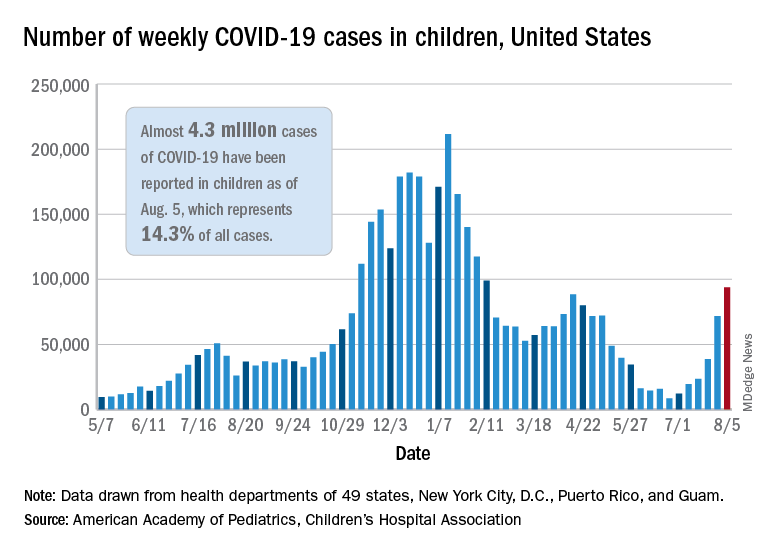
New pediatric cases rose for the 6th straight week, with almost 94,000 reported for the week ending Aug. 5.
That weekly total was up by 31% over the previous week and by over 1,000% since late June, when the new-case figure was at its lowest point (8,447) since early in the pandemic, the American Academy of Pediatrics and the Children’s Hospital Association said. COVID-related deaths – 13 for the week – were also higher than at any time since March 2021.
Almost 4.3 million children have been infected with SARS-CoV-2, which is 14.3% of all cases reported in 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. Children represented 15.0% of the new cases reported in those jurisdictions during the week ending Aug. 5, the AAP and CHA said in their weekly report.
Another measure that has been trending upward recently is vaccine initiation among 12- to 15-year-olds, although the latest weekly total is still well below the high of 1.4 million seen in May. First-time vaccinations reached almost 411,000 for the week of Aug. 3-9, marking the fourth consecutive increase in that age group, the Centers for Disease Control and Prevention said on its COVID Data Tracker. Vaccinations also increased, although more modestly, for 16- and 17-year-olds in the most recent week.
Cumulative figures for children aged 12-17 show that almost 10.4 million have received at least one dose and that 7.7 million are fully vaccinated as of Aug. 9. By age group, 42.2% of those aged 12-15 have received at least one dose, and 30.4% have completed the vaccine regimen. Among those aged 16-17 years, 52.2% have gotten their first dose, and 41.4% are fully vaccinated, according to the COVID Data Tracker.
Looking at vaccination rates on the state level shows that only 20% of children aged 12-17 in Wyoming and 21% in Mississippi have gotten at least one dose as of Aug. 4, while Massachusetts is up to 68% and Vermont reports 70%. Rates for full vaccination range from 11% in Mississippi and Alabama to 61% in Vermont, based on an AAP analysis of CDC data, which is not available for Idaho.
The current COVID-19 surge has brought new cases in children to their highest level since February, according to a new report.
New pediatric cases rose for the 6th straight week, with almost 94,000 reported for the week ending Aug. 5.
That weekly total was up by 31% over the previous week and by over 1,000% since late June, when the new-case figure was at its lowest point (8,447) since early in the pandemic, the American Academy of Pediatrics and the Children’s Hospital Association said. COVID-related deaths – 13 for the week – were also higher than at any time since March 2021.
Almost 4.3 million children have been infected with SARS-CoV-2, which is 14.3% of all cases reported in 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. Children represented 15.0% of the new cases reported in those jurisdictions during the week ending Aug. 5, the AAP and CHA said in their weekly report.
Another measure that has been trending upward recently is vaccine initiation among 12- to 15-year-olds, although the latest weekly total is still well below the high of 1.4 million seen in May. First-time vaccinations reached almost 411,000 for the week of Aug. 3-9, marking the fourth consecutive increase in that age group, the Centers for Disease Control and Prevention said on its COVID Data Tracker. Vaccinations also increased, although more modestly, for 16- and 17-year-olds in the most recent week.
Cumulative figures for children aged 12-17 show that almost 10.4 million have received at least one dose and that 7.7 million are fully vaccinated as of Aug. 9. By age group, 42.2% of those aged 12-15 have received at least one dose, and 30.4% have completed the vaccine regimen. Among those aged 16-17 years, 52.2% have gotten their first dose, and 41.4% are fully vaccinated, according to the COVID Data Tracker.
Looking at vaccination rates on the state level shows that only 20% of children aged 12-17 in Wyoming and 21% in Mississippi have gotten at least one dose as of Aug. 4, while Massachusetts is up to 68% and Vermont reports 70%. Rates for full vaccination range from 11% in Mississippi and Alabama to 61% in Vermont, based on an AAP analysis of CDC data, which is not available for Idaho.
The current COVID-19 surge has brought new cases in children to their highest level since February, according to a new report.
New pediatric cases rose for the 6th straight week, with almost 94,000 reported for the week ending Aug. 5.
That weekly total was up by 31% over the previous week and by over 1,000% since late June, when the new-case figure was at its lowest point (8,447) since early in the pandemic, the American Academy of Pediatrics and the Children’s Hospital Association said. COVID-related deaths – 13 for the week – were also higher than at any time since March 2021.
Almost 4.3 million children have been infected with SARS-CoV-2, which is 14.3% of all cases reported in 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. Children represented 15.0% of the new cases reported in those jurisdictions during the week ending Aug. 5, the AAP and CHA said in their weekly report.
Another measure that has been trending upward recently is vaccine initiation among 12- to 15-year-olds, although the latest weekly total is still well below the high of 1.4 million seen in May. First-time vaccinations reached almost 411,000 for the week of Aug. 3-9, marking the fourth consecutive increase in that age group, the Centers for Disease Control and Prevention said on its COVID Data Tracker. Vaccinations also increased, although more modestly, for 16- and 17-year-olds in the most recent week.
Cumulative figures for children aged 12-17 show that almost 10.4 million have received at least one dose and that 7.7 million are fully vaccinated as of Aug. 9. By age group, 42.2% of those aged 12-15 have received at least one dose, and 30.4% have completed the vaccine regimen. Among those aged 16-17 years, 52.2% have gotten their first dose, and 41.4% are fully vaccinated, according to the COVID Data Tracker.
Looking at vaccination rates on the state level shows that only 20% of children aged 12-17 in Wyoming and 21% in Mississippi have gotten at least one dose as of Aug. 4, while Massachusetts is up to 68% and Vermont reports 70%. Rates for full vaccination range from 11% in Mississippi and Alabama to 61% in Vermont, based on an AAP analysis of CDC data, which is not available for Idaho.
Exposure to marijuana smoke linked to increased risk of respiratory infections in children
Exposure to secondhand marijuana smoke is more strongly associated with viral respiratory infections in children, compared with children who were exposed to tobacco smoke and those with no smoke exposure, new research shows.
“The findings of this study are interesting and pleasantly raise further questions,” said Kristen Miller, MD, attending physician in the division of pulmonary and sleep medicine at Children’s Hospital of Philadelphia, who was not involved in the study. “Given the robust literature regarding secondhand smoke exposure and the current landscape surrounding marijuana, this is a timely study to evaluate the prevalence of marijuana use and the associated effects of marijuana exposure among children.”
Prior research has linked primary marijuana use with respiratory effects. A 2020 study associated cannabis use with an increased risk of severe bronchitis, lung hyperinflation, and increased central airway resistance. However, according to the Centers for Disease Control and Prevention, there are still a lot of unanswered questions surrounding secondhand marijuana smoke exposure and its effects.
“If kids are exposed to enough secondhand smoke, regardless of what the substance is, they’re going to have some negative health outcomes with it,” study author Adam Johnson, MD, of Wake Forest University, Winston-Salem, N.C., said in an interview.
The study, published in Pediatric Research, looked at rates of reported ED and urgent care visits and specific illnesses – such as otitis media, viral respiratory infections, and asthma exacerbations – among children with marijuana exposure and tobacco exposure.
For the study, Dr. Johnson and colleagues surveyed 1,500 parents and caregivers who went to an academic children’s hospital between Dec. 1, 2015, and July 30, 2017. Researchers found that children exposed to marijuana smoke had higher rates of ED visits at 2.21 within the past 12 months, compared with those exposed to tobacco smoke (2.14 within the past 12 months) and those with no smoke exposure (1.94 within the past 12 months). However, the difference in these visits were not statistically significant.
Researchers saw that children exposed to secondhand marijuana smoke saw a 30% increase in viral respiratory infections, compared with those who were not exposed to tobacco or marijuana smoke, Dr. Johnson said. Caregivers who smoked marijuana reported a rate of 1.31 viral infections in their children within the last year. Meanwhile those who smoked tobacco reported a rate of 1.00 infections within the last 12 months and caregivers who did not smoke reported 1.04 infections within the year.
“It suggests that components in marijuana smoke may depress the body’s immune responses to viral infections in children,” Dr. Miller said in an interview.
When it came to otitis media episodes, children exposed to marijuana had a rate of 0.96 episodes within the past 12 months. Children experiencing secondhand tobacco smoke had a rate of 0.83 episodes and those with no smoke exposure had 0.75 episodes within the past 12 months. Researchers did not note this difference as statistically significant.
When it came to asthma exacerbations, children exposed to marijuana smoke also had statistically insignificantly higher rates of exacerbations, compared with those exposed to tobacco smoke and those not exposed to smoke.
“I think it was surprising that the survey results found that marijuana seemed to be more strongly associated with the viral respiratory infections than tobacco,” Dr. Johnson said. “We know that secondhand tobacco smoke exposure in kids does lead to things like otitis media or ear infections, asthma attacks, and other processes, including colds. It was interesting that we didn’t find that association [in the new study], but we found that with marijuana.”
Dr. Johnson said the findings are especially concerning with increases in the acceptance and accessibility of marijuana as it becomes legalized in many states.
A 2015 study examined the effect of secondhand marijuana smoke exposure. Researchers found that exposure to secondhand marijuana smoke can increase heart rate, have mild to moderate sedative effects and can produce detectable cannabinoid levels in blood and urine. However, another study published in 2012 found that low to moderate primary marijuana use is less harmful to users’ lungs than tobacco exposure.
Dr. Miller added that little is known about how exposure to marijuana smoke can affect the innate responses to pathogens and there is a need to “study this in more detail” to figure out if secondhand marijuana smoke is a risk factor for either an increase in respiratory virus infections or their severity.
“These questions could have considerable implications for the health of our children and public health measures regarding marijuana use,” she explained. “As documented marijuana use increases, health care providers need to be aware of the effects of marijuana use and exposure.”
Neither Dr. Johnson nor Dr. Miller has any relevant financial disclosures.
Exposure to secondhand marijuana smoke is more strongly associated with viral respiratory infections in children, compared with children who were exposed to tobacco smoke and those with no smoke exposure, new research shows.
“The findings of this study are interesting and pleasantly raise further questions,” said Kristen Miller, MD, attending physician in the division of pulmonary and sleep medicine at Children’s Hospital of Philadelphia, who was not involved in the study. “Given the robust literature regarding secondhand smoke exposure and the current landscape surrounding marijuana, this is a timely study to evaluate the prevalence of marijuana use and the associated effects of marijuana exposure among children.”
Prior research has linked primary marijuana use with respiratory effects. A 2020 study associated cannabis use with an increased risk of severe bronchitis, lung hyperinflation, and increased central airway resistance. However, according to the Centers for Disease Control and Prevention, there are still a lot of unanswered questions surrounding secondhand marijuana smoke exposure and its effects.
“If kids are exposed to enough secondhand smoke, regardless of what the substance is, they’re going to have some negative health outcomes with it,” study author Adam Johnson, MD, of Wake Forest University, Winston-Salem, N.C., said in an interview.
The study, published in Pediatric Research, looked at rates of reported ED and urgent care visits and specific illnesses – such as otitis media, viral respiratory infections, and asthma exacerbations – among children with marijuana exposure and tobacco exposure.
For the study, Dr. Johnson and colleagues surveyed 1,500 parents and caregivers who went to an academic children’s hospital between Dec. 1, 2015, and July 30, 2017. Researchers found that children exposed to marijuana smoke had higher rates of ED visits at 2.21 within the past 12 months, compared with those exposed to tobacco smoke (2.14 within the past 12 months) and those with no smoke exposure (1.94 within the past 12 months). However, the difference in these visits were not statistically significant.
Researchers saw that children exposed to secondhand marijuana smoke saw a 30% increase in viral respiratory infections, compared with those who were not exposed to tobacco or marijuana smoke, Dr. Johnson said. Caregivers who smoked marijuana reported a rate of 1.31 viral infections in their children within the last year. Meanwhile those who smoked tobacco reported a rate of 1.00 infections within the last 12 months and caregivers who did not smoke reported 1.04 infections within the year.
“It suggests that components in marijuana smoke may depress the body’s immune responses to viral infections in children,” Dr. Miller said in an interview.
When it came to otitis media episodes, children exposed to marijuana had a rate of 0.96 episodes within the past 12 months. Children experiencing secondhand tobacco smoke had a rate of 0.83 episodes and those with no smoke exposure had 0.75 episodes within the past 12 months. Researchers did not note this difference as statistically significant.
When it came to asthma exacerbations, children exposed to marijuana smoke also had statistically insignificantly higher rates of exacerbations, compared with those exposed to tobacco smoke and those not exposed to smoke.
“I think it was surprising that the survey results found that marijuana seemed to be more strongly associated with the viral respiratory infections than tobacco,” Dr. Johnson said. “We know that secondhand tobacco smoke exposure in kids does lead to things like otitis media or ear infections, asthma attacks, and other processes, including colds. It was interesting that we didn’t find that association [in the new study], but we found that with marijuana.”
Dr. Johnson said the findings are especially concerning with increases in the acceptance and accessibility of marijuana as it becomes legalized in many states.
A 2015 study examined the effect of secondhand marijuana smoke exposure. Researchers found that exposure to secondhand marijuana smoke can increase heart rate, have mild to moderate sedative effects and can produce detectable cannabinoid levels in blood and urine. However, another study published in 2012 found that low to moderate primary marijuana use is less harmful to users’ lungs than tobacco exposure.
Dr. Miller added that little is known about how exposure to marijuana smoke can affect the innate responses to pathogens and there is a need to “study this in more detail” to figure out if secondhand marijuana smoke is a risk factor for either an increase in respiratory virus infections or their severity.
“These questions could have considerable implications for the health of our children and public health measures regarding marijuana use,” she explained. “As documented marijuana use increases, health care providers need to be aware of the effects of marijuana use and exposure.”
Neither Dr. Johnson nor Dr. Miller has any relevant financial disclosures.
Exposure to secondhand marijuana smoke is more strongly associated with viral respiratory infections in children, compared with children who were exposed to tobacco smoke and those with no smoke exposure, new research shows.
“The findings of this study are interesting and pleasantly raise further questions,” said Kristen Miller, MD, attending physician in the division of pulmonary and sleep medicine at Children’s Hospital of Philadelphia, who was not involved in the study. “Given the robust literature regarding secondhand smoke exposure and the current landscape surrounding marijuana, this is a timely study to evaluate the prevalence of marijuana use and the associated effects of marijuana exposure among children.”
Prior research has linked primary marijuana use with respiratory effects. A 2020 study associated cannabis use with an increased risk of severe bronchitis, lung hyperinflation, and increased central airway resistance. However, according to the Centers for Disease Control and Prevention, there are still a lot of unanswered questions surrounding secondhand marijuana smoke exposure and its effects.
“If kids are exposed to enough secondhand smoke, regardless of what the substance is, they’re going to have some negative health outcomes with it,” study author Adam Johnson, MD, of Wake Forest University, Winston-Salem, N.C., said in an interview.
The study, published in Pediatric Research, looked at rates of reported ED and urgent care visits and specific illnesses – such as otitis media, viral respiratory infections, and asthma exacerbations – among children with marijuana exposure and tobacco exposure.
For the study, Dr. Johnson and colleagues surveyed 1,500 parents and caregivers who went to an academic children’s hospital between Dec. 1, 2015, and July 30, 2017. Researchers found that children exposed to marijuana smoke had higher rates of ED visits at 2.21 within the past 12 months, compared with those exposed to tobacco smoke (2.14 within the past 12 months) and those with no smoke exposure (1.94 within the past 12 months). However, the difference in these visits were not statistically significant.
Researchers saw that children exposed to secondhand marijuana smoke saw a 30% increase in viral respiratory infections, compared with those who were not exposed to tobacco or marijuana smoke, Dr. Johnson said. Caregivers who smoked marijuana reported a rate of 1.31 viral infections in their children within the last year. Meanwhile those who smoked tobacco reported a rate of 1.00 infections within the last 12 months and caregivers who did not smoke reported 1.04 infections within the year.
“It suggests that components in marijuana smoke may depress the body’s immune responses to viral infections in children,” Dr. Miller said in an interview.
When it came to otitis media episodes, children exposed to marijuana had a rate of 0.96 episodes within the past 12 months. Children experiencing secondhand tobacco smoke had a rate of 0.83 episodes and those with no smoke exposure had 0.75 episodes within the past 12 months. Researchers did not note this difference as statistically significant.
When it came to asthma exacerbations, children exposed to marijuana smoke also had statistically insignificantly higher rates of exacerbations, compared with those exposed to tobacco smoke and those not exposed to smoke.
“I think it was surprising that the survey results found that marijuana seemed to be more strongly associated with the viral respiratory infections than tobacco,” Dr. Johnson said. “We know that secondhand tobacco smoke exposure in kids does lead to things like otitis media or ear infections, asthma attacks, and other processes, including colds. It was interesting that we didn’t find that association [in the new study], but we found that with marijuana.”
Dr. Johnson said the findings are especially concerning with increases in the acceptance and accessibility of marijuana as it becomes legalized in many states.
A 2015 study examined the effect of secondhand marijuana smoke exposure. Researchers found that exposure to secondhand marijuana smoke can increase heart rate, have mild to moderate sedative effects and can produce detectable cannabinoid levels in blood and urine. However, another study published in 2012 found that low to moderate primary marijuana use is less harmful to users’ lungs than tobacco exposure.
Dr. Miller added that little is known about how exposure to marijuana smoke can affect the innate responses to pathogens and there is a need to “study this in more detail” to figure out if secondhand marijuana smoke is a risk factor for either an increase in respiratory virus infections or their severity.
“These questions could have considerable implications for the health of our children and public health measures regarding marijuana use,” she explained. “As documented marijuana use increases, health care providers need to be aware of the effects of marijuana use and exposure.”
Neither Dr. Johnson nor Dr. Miller has any relevant financial disclosures.
FROM PEDIATRIC RESEARCH
CDC: Vaccination may cut risk of COVID reinfection in half
The Centers for Disease Control and Prevention has recommended that everyone get a COVID-19 vaccine, even if they’ve had the virus before. Yet many skeptics have held off getting the shots, believing that immunity generated by their previous infection will protect them if they should encounter the virus again.
A new study published in the CDC’s Morbidity and Mortality Weekly Report pokes holes in this notion. It shows people who have recovered from COVID-19 but haven’t been vaccinated have more than double the risk of testing positive for the virus again, compared with someone who was vaccinated after an initial infection.
The study looked at 738 Kentucky residents who had an initial bout of COVID-19 in 2020. About 250 of them tested positive for COVID-19 a second time between May and July of 2021, when the Delta variant became dominant in the United States.
The study matched each person who’d been reinfected with two people of the same sex and roughly the same age who had caught their initial COVID infection within the same week. The researchers then cross-matched those cases with data from Kentucky’s Immunization Registry.
They found that those who were unvaccinated had more than double the risk of being reinfected during the Delta wave. Partial vaccination appeared to have no significant impact on the risk of reinfection.
Among those who were reinfected, 20% were fully vaccinated, while 34% of those who did not get reinfected were fully vaccinated.
The study is observational, meaning it can’t show cause and effect; and the researchers had no information on the severity of the infections. Alyson Cavanaugh, PhD, a member of the CDC’s Epidemic Intelligence Service who led the study, said it is possible that some of the people who tested positive a second time had asymptomatic infections that were picked up through routine screening.
Still, the study backs up previous research and suggests that vaccination offers important additional protection.
“Our laboratory studies have shown that there’s an added benefit of vaccine for people who’ve had previous COVID-19. This is a real-world, epidemiologic study that found that among people who’d previously already had COVID-19, those who were vaccinated had lower odds of being reinfected,” Dr. Cavanaugh said.
“If you have had COVID-19 before, please still get vaccinated,” said CDC Director Rochelle Walensky, MD, in a written media statement. “This study shows you are twice as likely to get infected again if you are unvaccinated. Getting the vaccine is the best way to protect yourself and others around you, especially as the more contagious Delta variant spreads around the country.”
In a White House COVID-19 Response Team briefing in May, Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Disease, explained why vaccines create stronger immunity than infection. He highlighted new research showing that two doses of an mRNA vaccine produce levels of neutralizing antibodies that are up to 10 times higher than the levels found in the blood of people who’ve recovered from COVID-19. Vaccines also enhance B cells and T cells in people who’ve recovered from COVID-19, which broadens the spectrum of protection and helps to fend off variants.
The study has some important limitations, which the authors acknowledged. The first is that second infections weren’t confirmed with genetic sequencing, so the researchers couldn’t definitively tell if a person tested positive a second time because they caught a new virus, or if they were somehow still shedding virus from their first infection. Given that the tests were at least 5 months apart, though, the researchers think reinfection is the most likely explanation.
Another bias in the study could have something to do with vaccination. Vaccinated people may have been less likely to be tested for COVID-19 after their vaccines, so the association or reinfection with a lack of vaccination may be overestimated.
Also, people who were vaccinated at federal sites or in another state were not logged in the state’s immunization registry, which may have skewed the data.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has recommended that everyone get a COVID-19 vaccine, even if they’ve had the virus before. Yet many skeptics have held off getting the shots, believing that immunity generated by their previous infection will protect them if they should encounter the virus again.
A new study published in the CDC’s Morbidity and Mortality Weekly Report pokes holes in this notion. It shows people who have recovered from COVID-19 but haven’t been vaccinated have more than double the risk of testing positive for the virus again, compared with someone who was vaccinated after an initial infection.
The study looked at 738 Kentucky residents who had an initial bout of COVID-19 in 2020. About 250 of them tested positive for COVID-19 a second time between May and July of 2021, when the Delta variant became dominant in the United States.
The study matched each person who’d been reinfected with two people of the same sex and roughly the same age who had caught their initial COVID infection within the same week. The researchers then cross-matched those cases with data from Kentucky’s Immunization Registry.
They found that those who were unvaccinated had more than double the risk of being reinfected during the Delta wave. Partial vaccination appeared to have no significant impact on the risk of reinfection.
Among those who were reinfected, 20% were fully vaccinated, while 34% of those who did not get reinfected were fully vaccinated.
The study is observational, meaning it can’t show cause and effect; and the researchers had no information on the severity of the infections. Alyson Cavanaugh, PhD, a member of the CDC’s Epidemic Intelligence Service who led the study, said it is possible that some of the people who tested positive a second time had asymptomatic infections that were picked up through routine screening.
Still, the study backs up previous research and suggests that vaccination offers important additional protection.
“Our laboratory studies have shown that there’s an added benefit of vaccine for people who’ve had previous COVID-19. This is a real-world, epidemiologic study that found that among people who’d previously already had COVID-19, those who were vaccinated had lower odds of being reinfected,” Dr. Cavanaugh said.
“If you have had COVID-19 before, please still get vaccinated,” said CDC Director Rochelle Walensky, MD, in a written media statement. “This study shows you are twice as likely to get infected again if you are unvaccinated. Getting the vaccine is the best way to protect yourself and others around you, especially as the more contagious Delta variant spreads around the country.”
In a White House COVID-19 Response Team briefing in May, Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Disease, explained why vaccines create stronger immunity than infection. He highlighted new research showing that two doses of an mRNA vaccine produce levels of neutralizing antibodies that are up to 10 times higher than the levels found in the blood of people who’ve recovered from COVID-19. Vaccines also enhance B cells and T cells in people who’ve recovered from COVID-19, which broadens the spectrum of protection and helps to fend off variants.
The study has some important limitations, which the authors acknowledged. The first is that second infections weren’t confirmed with genetic sequencing, so the researchers couldn’t definitively tell if a person tested positive a second time because they caught a new virus, or if they were somehow still shedding virus from their first infection. Given that the tests were at least 5 months apart, though, the researchers think reinfection is the most likely explanation.
Another bias in the study could have something to do with vaccination. Vaccinated people may have been less likely to be tested for COVID-19 after their vaccines, so the association or reinfection with a lack of vaccination may be overestimated.
Also, people who were vaccinated at federal sites or in another state were not logged in the state’s immunization registry, which may have skewed the data.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has recommended that everyone get a COVID-19 vaccine, even if they’ve had the virus before. Yet many skeptics have held off getting the shots, believing that immunity generated by their previous infection will protect them if they should encounter the virus again.
A new study published in the CDC’s Morbidity and Mortality Weekly Report pokes holes in this notion. It shows people who have recovered from COVID-19 but haven’t been vaccinated have more than double the risk of testing positive for the virus again, compared with someone who was vaccinated after an initial infection.
The study looked at 738 Kentucky residents who had an initial bout of COVID-19 in 2020. About 250 of them tested positive for COVID-19 a second time between May and July of 2021, when the Delta variant became dominant in the United States.
The study matched each person who’d been reinfected with two people of the same sex and roughly the same age who had caught their initial COVID infection within the same week. The researchers then cross-matched those cases with data from Kentucky’s Immunization Registry.
They found that those who were unvaccinated had more than double the risk of being reinfected during the Delta wave. Partial vaccination appeared to have no significant impact on the risk of reinfection.
Among those who were reinfected, 20% were fully vaccinated, while 34% of those who did not get reinfected were fully vaccinated.
The study is observational, meaning it can’t show cause and effect; and the researchers had no information on the severity of the infections. Alyson Cavanaugh, PhD, a member of the CDC’s Epidemic Intelligence Service who led the study, said it is possible that some of the people who tested positive a second time had asymptomatic infections that were picked up through routine screening.
Still, the study backs up previous research and suggests that vaccination offers important additional protection.
“Our laboratory studies have shown that there’s an added benefit of vaccine for people who’ve had previous COVID-19. This is a real-world, epidemiologic study that found that among people who’d previously already had COVID-19, those who were vaccinated had lower odds of being reinfected,” Dr. Cavanaugh said.
“If you have had COVID-19 before, please still get vaccinated,” said CDC Director Rochelle Walensky, MD, in a written media statement. “This study shows you are twice as likely to get infected again if you are unvaccinated. Getting the vaccine is the best way to protect yourself and others around you, especially as the more contagious Delta variant spreads around the country.”
In a White House COVID-19 Response Team briefing in May, Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Disease, explained why vaccines create stronger immunity than infection. He highlighted new research showing that two doses of an mRNA vaccine produce levels of neutralizing antibodies that are up to 10 times higher than the levels found in the blood of people who’ve recovered from COVID-19. Vaccines also enhance B cells and T cells in people who’ve recovered from COVID-19, which broadens the spectrum of protection and helps to fend off variants.
The study has some important limitations, which the authors acknowledged. The first is that second infections weren’t confirmed with genetic sequencing, so the researchers couldn’t definitively tell if a person tested positive a second time because they caught a new virus, or if they were somehow still shedding virus from their first infection. Given that the tests were at least 5 months apart, though, the researchers think reinfection is the most likely explanation.
Another bias in the study could have something to do with vaccination. Vaccinated people may have been less likely to be tested for COVID-19 after their vaccines, so the association or reinfection with a lack of vaccination may be overestimated.
Also, people who were vaccinated at federal sites or in another state were not logged in the state’s immunization registry, which may have skewed the data.
A version of this article first appeared on Medscape.com.