User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Uncomplicated pediatric chest infection: Antibiotics don’t help
Unless pneumonia is suspected, clinicians should not prescribe antibiotics for most children with chest infections, according to findings of the ARTIC-PC randomized controlled trial, published in The Lancet.
“Prescribing for children with uncomplicated chest infections is still common in most countries,” said lead author Paul Little, MD, professor of primary care research at the University of Southampton, England, in an interview.
But there are barriers to stopping this practice, he said. “If you prescribe an antibiotic and the child gets better, even if the antibiotic was not doing that much, the parents then think that it was the antibiotic that was responsible for the recovery and so expect antibiotics the next time. So, physician prescribing of antibiotics in effect medicalizes illness and keeps the cycle of expectations, reconsultations, and prescriptions going.”
The study included 432 children aged 6 months to 12 years (median age, 3.2 years) who presented at 56 general practices in England with acute, uncomplicated lower respiratory tract infection (LRTI) of less than 21 days’ duration and in whom pneumonia was not suspected clinically. The children were randomly assigned to undergo 7 days of treatment with either amoxicillin 50 mg/kg or placebo. The primary outcome was duration of symptoms rated moderately bad or worse.
For up to 4 weeks, parents scored symptoms – including cough, phlegm, shortness of breath, wheeze, blocked or runny nose, disturbed sleep, feeling generally unwell, fever, and interference with normal activities – in a daily diary. The secondary outcome was symptom severity. Prespecified analyses were made for key clinical subgroups of patients for whom clinicians commonly prescribe (those with chest signs, fever, physician rating of unwell, sputum or chest rattle, and shortness of breath).
There was no significant difference in outcome between children treated with antibiotics and those treated with placebo. The median duration of moderately bad or worse symptoms was similar between the antibiotics group and the placebo group (5 vs. 6 days; hazard ratio, 1.13), as was the median time until symptoms were rated absent or as causing very little problem (7 vs. 8 days; HR, 1.09). There was a small significant difference between the groups in symptom severity score on days 2-4 after seeing the doctor (1.8 in the antibiotics group vs. 2.1 in the placebo group), “which was equivalent to less than one child in three rating symptoms a slight problem rather than very little problem,” the study authors report. “The treatment effects for all outcomes were similar for most subgroups ... but the effect of antibiotics was slightly, but not significantly, greater among those with fever or those who were unwell,” they add.
The investigators conclude that “similar to adults, antibiotics are unlikely to make a clinically important difference to the symptom burden for uncomplicated lower respiratory tract infections in children – both overall, and for the key clinical subgroups where antibiotic prescribing is most common.” They recommend that clinicians provide “safety-netting advice” to parents, such as explaining what illness course to expect and when a return visit would be necessary.
The findings provide “more evidence to do less,” wrote Rianne Oostenbrink, MD, PhD, from Erasmus MC-Sophia, in Rotterdam, the Netherlands, and Lina Jankauskaite, MD, PhD, from Lithuanian University of Health Sciences, Kaunas, in an accompanying comment.
“Overtesting and overtreatment of children are especially prominent in infectious diseases, when fever or other symptoms such as cough can be unspecific and can be of viral or bacterial origin,” they write.
The commenters note that despite antibiotics, most children did have moderately bad or worse symptoms on day 3, and symptoms had improved in about 75% of children in both groups at day 14. “A notable finding of this study is that only a few children had moderately bad or worse symptoms by day 14, and antibiotics did not alleviate the symptoms compared with placebo. Additionally, this trial aligns with other studies that have shown that reducing antibiotic treatment for LRTI is not associated with prolonged morbidity or higher incidence of complications.”
The study was funded by the UK National Institute for Health Research. Dr. Little, Dr. Jankauskaite, and Dr. Oostenbrink have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Unless pneumonia is suspected, clinicians should not prescribe antibiotics for most children with chest infections, according to findings of the ARTIC-PC randomized controlled trial, published in The Lancet.
“Prescribing for children with uncomplicated chest infections is still common in most countries,” said lead author Paul Little, MD, professor of primary care research at the University of Southampton, England, in an interview.
But there are barriers to stopping this practice, he said. “If you prescribe an antibiotic and the child gets better, even if the antibiotic was not doing that much, the parents then think that it was the antibiotic that was responsible for the recovery and so expect antibiotics the next time. So, physician prescribing of antibiotics in effect medicalizes illness and keeps the cycle of expectations, reconsultations, and prescriptions going.”
The study included 432 children aged 6 months to 12 years (median age, 3.2 years) who presented at 56 general practices in England with acute, uncomplicated lower respiratory tract infection (LRTI) of less than 21 days’ duration and in whom pneumonia was not suspected clinically. The children were randomly assigned to undergo 7 days of treatment with either amoxicillin 50 mg/kg or placebo. The primary outcome was duration of symptoms rated moderately bad or worse.
For up to 4 weeks, parents scored symptoms – including cough, phlegm, shortness of breath, wheeze, blocked or runny nose, disturbed sleep, feeling generally unwell, fever, and interference with normal activities – in a daily diary. The secondary outcome was symptom severity. Prespecified analyses were made for key clinical subgroups of patients for whom clinicians commonly prescribe (those with chest signs, fever, physician rating of unwell, sputum or chest rattle, and shortness of breath).
There was no significant difference in outcome between children treated with antibiotics and those treated with placebo. The median duration of moderately bad or worse symptoms was similar between the antibiotics group and the placebo group (5 vs. 6 days; hazard ratio, 1.13), as was the median time until symptoms were rated absent or as causing very little problem (7 vs. 8 days; HR, 1.09). There was a small significant difference between the groups in symptom severity score on days 2-4 after seeing the doctor (1.8 in the antibiotics group vs. 2.1 in the placebo group), “which was equivalent to less than one child in three rating symptoms a slight problem rather than very little problem,” the study authors report. “The treatment effects for all outcomes were similar for most subgroups ... but the effect of antibiotics was slightly, but not significantly, greater among those with fever or those who were unwell,” they add.
The investigators conclude that “similar to adults, antibiotics are unlikely to make a clinically important difference to the symptom burden for uncomplicated lower respiratory tract infections in children – both overall, and for the key clinical subgroups where antibiotic prescribing is most common.” They recommend that clinicians provide “safety-netting advice” to parents, such as explaining what illness course to expect and when a return visit would be necessary.
The findings provide “more evidence to do less,” wrote Rianne Oostenbrink, MD, PhD, from Erasmus MC-Sophia, in Rotterdam, the Netherlands, and Lina Jankauskaite, MD, PhD, from Lithuanian University of Health Sciences, Kaunas, in an accompanying comment.
“Overtesting and overtreatment of children are especially prominent in infectious diseases, when fever or other symptoms such as cough can be unspecific and can be of viral or bacterial origin,” they write.
The commenters note that despite antibiotics, most children did have moderately bad or worse symptoms on day 3, and symptoms had improved in about 75% of children in both groups at day 14. “A notable finding of this study is that only a few children had moderately bad or worse symptoms by day 14, and antibiotics did not alleviate the symptoms compared with placebo. Additionally, this trial aligns with other studies that have shown that reducing antibiotic treatment for LRTI is not associated with prolonged morbidity or higher incidence of complications.”
The study was funded by the UK National Institute for Health Research. Dr. Little, Dr. Jankauskaite, and Dr. Oostenbrink have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Unless pneumonia is suspected, clinicians should not prescribe antibiotics for most children with chest infections, according to findings of the ARTIC-PC randomized controlled trial, published in The Lancet.
“Prescribing for children with uncomplicated chest infections is still common in most countries,” said lead author Paul Little, MD, professor of primary care research at the University of Southampton, England, in an interview.
But there are barriers to stopping this practice, he said. “If you prescribe an antibiotic and the child gets better, even if the antibiotic was not doing that much, the parents then think that it was the antibiotic that was responsible for the recovery and so expect antibiotics the next time. So, physician prescribing of antibiotics in effect medicalizes illness and keeps the cycle of expectations, reconsultations, and prescriptions going.”
The study included 432 children aged 6 months to 12 years (median age, 3.2 years) who presented at 56 general practices in England with acute, uncomplicated lower respiratory tract infection (LRTI) of less than 21 days’ duration and in whom pneumonia was not suspected clinically. The children were randomly assigned to undergo 7 days of treatment with either amoxicillin 50 mg/kg or placebo. The primary outcome was duration of symptoms rated moderately bad or worse.
For up to 4 weeks, parents scored symptoms – including cough, phlegm, shortness of breath, wheeze, blocked or runny nose, disturbed sleep, feeling generally unwell, fever, and interference with normal activities – in a daily diary. The secondary outcome was symptom severity. Prespecified analyses were made for key clinical subgroups of patients for whom clinicians commonly prescribe (those with chest signs, fever, physician rating of unwell, sputum or chest rattle, and shortness of breath).
There was no significant difference in outcome between children treated with antibiotics and those treated with placebo. The median duration of moderately bad or worse symptoms was similar between the antibiotics group and the placebo group (5 vs. 6 days; hazard ratio, 1.13), as was the median time until symptoms were rated absent or as causing very little problem (7 vs. 8 days; HR, 1.09). There was a small significant difference between the groups in symptom severity score on days 2-4 after seeing the doctor (1.8 in the antibiotics group vs. 2.1 in the placebo group), “which was equivalent to less than one child in three rating symptoms a slight problem rather than very little problem,” the study authors report. “The treatment effects for all outcomes were similar for most subgroups ... but the effect of antibiotics was slightly, but not significantly, greater among those with fever or those who were unwell,” they add.
The investigators conclude that “similar to adults, antibiotics are unlikely to make a clinically important difference to the symptom burden for uncomplicated lower respiratory tract infections in children – both overall, and for the key clinical subgroups where antibiotic prescribing is most common.” They recommend that clinicians provide “safety-netting advice” to parents, such as explaining what illness course to expect and when a return visit would be necessary.
The findings provide “more evidence to do less,” wrote Rianne Oostenbrink, MD, PhD, from Erasmus MC-Sophia, in Rotterdam, the Netherlands, and Lina Jankauskaite, MD, PhD, from Lithuanian University of Health Sciences, Kaunas, in an accompanying comment.
“Overtesting and overtreatment of children are especially prominent in infectious diseases, when fever or other symptoms such as cough can be unspecific and can be of viral or bacterial origin,” they write.
The commenters note that despite antibiotics, most children did have moderately bad or worse symptoms on day 3, and symptoms had improved in about 75% of children in both groups at day 14. “A notable finding of this study is that only a few children had moderately bad or worse symptoms by day 14, and antibiotics did not alleviate the symptoms compared with placebo. Additionally, this trial aligns with other studies that have shown that reducing antibiotic treatment for LRTI is not associated with prolonged morbidity or higher incidence of complications.”
The study was funded by the UK National Institute for Health Research. Dr. Little, Dr. Jankauskaite, and Dr. Oostenbrink have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Omega-3s tame inflammation in elderly COVID-19 patients
results of a small randomized controlled trial suggest.
Results of the study, which included 22 patients with multiple comorbidities, were presented at the European Geriatric Medicine Society annual congress, a hybrid live and online meeting.
The patients, who had a median age of 81 years, were randomized to receive an intravenous infusion of an omega-3 polyunsaturated fatty acid (PUFA) emulsion containing 10 g of fish oil per 100 mL or a saline placebo.
Those who received the intravenous infusion had significant decreases from baseline to end of treatment in the neutrophil-to-lymphocyte ratio (NLR), indicating marked reductions in systemic inflammation.
In contrast, patients randomized to a saline placebo had no significant improvements in NLR, Magnus Bäck, MD, PhD, from the Karolinska Institute in Stockholm reported at the meeting.
“Our lipidomic analysis also showed that omega-3 treatment skewed the lipid response, with reduced levels of proinflammatory lipid mediators, and increased levels of proresolving mediators,” according to a late-breaking abstract, which Dr. Bäck presented during the session.
Omega-3 treatment was not significantly associated with reduction in either C-reactive protein (CRP) or the proinflammatory cytokine interleukin-6, however.
‘Eicosanoid storm’
In a review article published in January 2021 in the open-access journal Frontiers in Physiology, Dr. Bäck and colleagues outlined the rationale for their randomized trial.
“Excessive inflammation has been reported in severe cases with respiratory failure and cardiovascular complications,” they wrote. “In addition to the release of cytokines, referred to as cytokine release syndrome or ‘cytokine storm,’ increased proinflammatory lipid mediators derived from the omega-6 polyunsaturated fatty acid (PUFA) arachidonic acid may cause an ‘eicosanoid storm,’ which contributes to the uncontrolled systemic inflammation.”
Omega-3 PUFA contains proresolving mediators that can limit inflammatory reactions, suggesting the possibility of an inflammation-resolving benefit in patients with COVID-19 without concerns about immunosuppression, the authors hypothesized.
Trial details
In the trial, COVID-Omega-F, they enrolled patients with a COVID-19 diagnosis requiring hospitalization. Patients with an allergy to fish oil or who had contraindications to intravenous PUFA administration (for example, risk for bleeding, shock, or emboli) were excluded.
Ten patients were randomly assigned to receive infusions of the omega-3 PUFA and 12 were assigned to receive infusions of the placebo, once daily for 5 days. The primary outcome measure was change in inflammatory biomarkers, including white blood cell counts, CRP, cytokines, and lipid mediators.
Baseline demographic and clinical characteristics were similar between the two study arms, with a median of about 7 days since the onset of symptoms, and 3.5 days since a diagnosis of COVID-19.
All patients had low lymphocyte responses reflected by a high NLR, a prognostic measure for worse outcomes in patients with COVID-19 infections, Dr. Bäck said.
Inflammation was moderate, with a CRP of 65 mg/L in the placebo group and 62 mg/L in the omega-3 group.
Seven patients in each study arm received concomitant corticoid treatment. Two patients in each arm died in hospital, but there were no serious treatment-related adverse events.
Inflammatory markers improve
As noted before, there was a significant decline in NLR from baseline among patients randomized to omega-3 (P = .02) but no corresponding decrease in patients assigned to placebo infusions.
“The significant decrease was largely driven by an increase in the lymphocyte count in the omega-3 treated group (P = .004), whereas lymphocytes did not significantly change,” Dr. Bäck said.
As expected, patients in the omega-3 group had pronounced increases in omega-3 fatty acids, including eicosapentaenoic acid and docosahexaenoic acid.
The metabolism of fatty acids also differed markedly between the groups, with a significant decrease in the omega-3 group but not the placebo group in proinflammatory mediators, and an increase in precursors to proresolving mediators, Dr. Bäck noted.
AFib concerns
In a question-and-answer part of the session, a physician who identified herself as “Senya from Russia” questioned the safety of omega-3 treatment in this population, “because recently there was a meta-analysis which showed that omega-3 fatty acids will increase the risk of atrial fibrillation in older adults especially.”
The systematic review and meta-analysis she referred to, published in Circulation and reported on by this news organization, showed that, among 81,210 patients with a mean age of 65 enrolled in seven randomized controlled trials, omega-3 fatty acid supplementation was associated with a 25% increase in risk for atrial fibrillation. This risk appeared to be higher in trials testing doses greater than 1 g/day, according to the paper.
“This was not monitored in this study,” Dr. Bäck replied. “It is true that the meta-analysis showed an increased incidence of atrial fibrillation, so it would be something to monitor in case this trial would be expanded to a larger population.”
The study was supported by the Karolinska Institute. Dr. Bäck disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
results of a small randomized controlled trial suggest.
Results of the study, which included 22 patients with multiple comorbidities, were presented at the European Geriatric Medicine Society annual congress, a hybrid live and online meeting.
The patients, who had a median age of 81 years, were randomized to receive an intravenous infusion of an omega-3 polyunsaturated fatty acid (PUFA) emulsion containing 10 g of fish oil per 100 mL or a saline placebo.
Those who received the intravenous infusion had significant decreases from baseline to end of treatment in the neutrophil-to-lymphocyte ratio (NLR), indicating marked reductions in systemic inflammation.
In contrast, patients randomized to a saline placebo had no significant improvements in NLR, Magnus Bäck, MD, PhD, from the Karolinska Institute in Stockholm reported at the meeting.
“Our lipidomic analysis also showed that omega-3 treatment skewed the lipid response, with reduced levels of proinflammatory lipid mediators, and increased levels of proresolving mediators,” according to a late-breaking abstract, which Dr. Bäck presented during the session.
Omega-3 treatment was not significantly associated with reduction in either C-reactive protein (CRP) or the proinflammatory cytokine interleukin-6, however.
‘Eicosanoid storm’
In a review article published in January 2021 in the open-access journal Frontiers in Physiology, Dr. Bäck and colleagues outlined the rationale for their randomized trial.
“Excessive inflammation has been reported in severe cases with respiratory failure and cardiovascular complications,” they wrote. “In addition to the release of cytokines, referred to as cytokine release syndrome or ‘cytokine storm,’ increased proinflammatory lipid mediators derived from the omega-6 polyunsaturated fatty acid (PUFA) arachidonic acid may cause an ‘eicosanoid storm,’ which contributes to the uncontrolled systemic inflammation.”
Omega-3 PUFA contains proresolving mediators that can limit inflammatory reactions, suggesting the possibility of an inflammation-resolving benefit in patients with COVID-19 without concerns about immunosuppression, the authors hypothesized.
Trial details
In the trial, COVID-Omega-F, they enrolled patients with a COVID-19 diagnosis requiring hospitalization. Patients with an allergy to fish oil or who had contraindications to intravenous PUFA administration (for example, risk for bleeding, shock, or emboli) were excluded.
Ten patients were randomly assigned to receive infusions of the omega-3 PUFA and 12 were assigned to receive infusions of the placebo, once daily for 5 days. The primary outcome measure was change in inflammatory biomarkers, including white blood cell counts, CRP, cytokines, and lipid mediators.
Baseline demographic and clinical characteristics were similar between the two study arms, with a median of about 7 days since the onset of symptoms, and 3.5 days since a diagnosis of COVID-19.
All patients had low lymphocyte responses reflected by a high NLR, a prognostic measure for worse outcomes in patients with COVID-19 infections, Dr. Bäck said.
Inflammation was moderate, with a CRP of 65 mg/L in the placebo group and 62 mg/L in the omega-3 group.
Seven patients in each study arm received concomitant corticoid treatment. Two patients in each arm died in hospital, but there were no serious treatment-related adverse events.
Inflammatory markers improve
As noted before, there was a significant decline in NLR from baseline among patients randomized to omega-3 (P = .02) but no corresponding decrease in patients assigned to placebo infusions.
“The significant decrease was largely driven by an increase in the lymphocyte count in the omega-3 treated group (P = .004), whereas lymphocytes did not significantly change,” Dr. Bäck said.
As expected, patients in the omega-3 group had pronounced increases in omega-3 fatty acids, including eicosapentaenoic acid and docosahexaenoic acid.
The metabolism of fatty acids also differed markedly between the groups, with a significant decrease in the omega-3 group but not the placebo group in proinflammatory mediators, and an increase in precursors to proresolving mediators, Dr. Bäck noted.
AFib concerns
In a question-and-answer part of the session, a physician who identified herself as “Senya from Russia” questioned the safety of omega-3 treatment in this population, “because recently there was a meta-analysis which showed that omega-3 fatty acids will increase the risk of atrial fibrillation in older adults especially.”
The systematic review and meta-analysis she referred to, published in Circulation and reported on by this news organization, showed that, among 81,210 patients with a mean age of 65 enrolled in seven randomized controlled trials, omega-3 fatty acid supplementation was associated with a 25% increase in risk for atrial fibrillation. This risk appeared to be higher in trials testing doses greater than 1 g/day, according to the paper.
“This was not monitored in this study,” Dr. Bäck replied. “It is true that the meta-analysis showed an increased incidence of atrial fibrillation, so it would be something to monitor in case this trial would be expanded to a larger population.”
The study was supported by the Karolinska Institute. Dr. Bäck disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
results of a small randomized controlled trial suggest.
Results of the study, which included 22 patients with multiple comorbidities, were presented at the European Geriatric Medicine Society annual congress, a hybrid live and online meeting.
The patients, who had a median age of 81 years, were randomized to receive an intravenous infusion of an omega-3 polyunsaturated fatty acid (PUFA) emulsion containing 10 g of fish oil per 100 mL or a saline placebo.
Those who received the intravenous infusion had significant decreases from baseline to end of treatment in the neutrophil-to-lymphocyte ratio (NLR), indicating marked reductions in systemic inflammation.
In contrast, patients randomized to a saline placebo had no significant improvements in NLR, Magnus Bäck, MD, PhD, from the Karolinska Institute in Stockholm reported at the meeting.
“Our lipidomic analysis also showed that omega-3 treatment skewed the lipid response, with reduced levels of proinflammatory lipid mediators, and increased levels of proresolving mediators,” according to a late-breaking abstract, which Dr. Bäck presented during the session.
Omega-3 treatment was not significantly associated with reduction in either C-reactive protein (CRP) or the proinflammatory cytokine interleukin-6, however.
‘Eicosanoid storm’
In a review article published in January 2021 in the open-access journal Frontiers in Physiology, Dr. Bäck and colleagues outlined the rationale for their randomized trial.
“Excessive inflammation has been reported in severe cases with respiratory failure and cardiovascular complications,” they wrote. “In addition to the release of cytokines, referred to as cytokine release syndrome or ‘cytokine storm,’ increased proinflammatory lipid mediators derived from the omega-6 polyunsaturated fatty acid (PUFA) arachidonic acid may cause an ‘eicosanoid storm,’ which contributes to the uncontrolled systemic inflammation.”
Omega-3 PUFA contains proresolving mediators that can limit inflammatory reactions, suggesting the possibility of an inflammation-resolving benefit in patients with COVID-19 without concerns about immunosuppression, the authors hypothesized.
Trial details
In the trial, COVID-Omega-F, they enrolled patients with a COVID-19 diagnosis requiring hospitalization. Patients with an allergy to fish oil or who had contraindications to intravenous PUFA administration (for example, risk for bleeding, shock, or emboli) were excluded.
Ten patients were randomly assigned to receive infusions of the omega-3 PUFA and 12 were assigned to receive infusions of the placebo, once daily for 5 days. The primary outcome measure was change in inflammatory biomarkers, including white blood cell counts, CRP, cytokines, and lipid mediators.
Baseline demographic and clinical characteristics were similar between the two study arms, with a median of about 7 days since the onset of symptoms, and 3.5 days since a diagnosis of COVID-19.
All patients had low lymphocyte responses reflected by a high NLR, a prognostic measure for worse outcomes in patients with COVID-19 infections, Dr. Bäck said.
Inflammation was moderate, with a CRP of 65 mg/L in the placebo group and 62 mg/L in the omega-3 group.
Seven patients in each study arm received concomitant corticoid treatment. Two patients in each arm died in hospital, but there were no serious treatment-related adverse events.
Inflammatory markers improve
As noted before, there was a significant decline in NLR from baseline among patients randomized to omega-3 (P = .02) but no corresponding decrease in patients assigned to placebo infusions.
“The significant decrease was largely driven by an increase in the lymphocyte count in the omega-3 treated group (P = .004), whereas lymphocytes did not significantly change,” Dr. Bäck said.
As expected, patients in the omega-3 group had pronounced increases in omega-3 fatty acids, including eicosapentaenoic acid and docosahexaenoic acid.
The metabolism of fatty acids also differed markedly between the groups, with a significant decrease in the omega-3 group but not the placebo group in proinflammatory mediators, and an increase in precursors to proresolving mediators, Dr. Bäck noted.
AFib concerns
In a question-and-answer part of the session, a physician who identified herself as “Senya from Russia” questioned the safety of omega-3 treatment in this population, “because recently there was a meta-analysis which showed that omega-3 fatty acids will increase the risk of atrial fibrillation in older adults especially.”
The systematic review and meta-analysis she referred to, published in Circulation and reported on by this news organization, showed that, among 81,210 patients with a mean age of 65 enrolled in seven randomized controlled trials, omega-3 fatty acid supplementation was associated with a 25% increase in risk for atrial fibrillation. This risk appeared to be higher in trials testing doses greater than 1 g/day, according to the paper.
“This was not monitored in this study,” Dr. Bäck replied. “It is true that the meta-analysis showed an increased incidence of atrial fibrillation, so it would be something to monitor in case this trial would be expanded to a larger population.”
The study was supported by the Karolinska Institute. Dr. Bäck disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EUGMS
USPSTF rules out aspirin for over 60s in primary CVD prevention
New draft recommendations from the U.S. Preventive Services Task Force (USPSTF) on the use of aspirin for the primary prevention of cardiovascular disease (CVD) have been released and appear to limit the population in which it should be considered.

“The USPSTF concludes with moderate certainty that aspirin use for the primary prevention of CVD events in adults ages 40 to 59 years who have a 10% or greater 10-year CVD risk has a small net benefit,” the recommendation notes. They conclude that for these patients, the decision to use aspirin “should be an individual one.”
“Persons who are not at increased risk for bleeding and are willing to take low-dose aspirin daily are more likely to benefit,” they note.
For older individuals, however, the task force concludes.
The new recommendations were posted online Oct. 12 and will be available for public comment until November 8. Once it is finalized, the recommendation will replace the 2016 USPSTF recommendation on aspirin use to prevent CVD and colorectal cancer (CRC), they note.
In that document, the task force recommended initiating low-dose aspirin for the primary prevention of both CVD and CRC in adults 50-59 years of age who had a 10% or greater 10-year CVD risk, were not at increased risk for bleeding, had a life expectancy of at least 10 years, and were willing to take daily low-dose aspirin for at least 10 years, with the decision to start being an individual one.
For older and younger patients, they found at that time that the evidence was “insufficient to assess the balance of benefits and harms of initiating aspirin use for the primary prevention of CVD and CRC in adults younger than age 50 years or adults aged 70 years or older.”
In the new draft document, “the USPSTF has changed the age ranges and grades of its recommendation on aspirin use.” Besides the recommendations for CVD prevention, they have also changed the previous recommendation of aspirin for the prevention of CRC given evidence generated from large primary CVD prevention trials.
“Based on new analyses of the evidence from primary CVD prevention populations, longer-term follow-up data from the Women’s Health Study (WHS) (JE Buring, personal communication, November 23, 2020), and new trial evidence, the USPSTF concluded that the evidence is inadequate that low-dose aspirin use reduces CRC incidence or mortality,” it states.
Optimum dose
On the optimum dose for primary CVD prevention, the task force says the benefit appears similar for a low dose (≤100 mg/d) and all doses that have been studied in CVD prevention trials (50 to 500 mg/d). “A pragmatic approach would be to use 81 mg/d, which is the most commonly prescribed dose in the United States,” it states.
The USPSTF recommends using the ACC/AHA Pooled Cohort Equations to estimate cardiovascular risk but it points out that these equations are imperfect for risk prediction at the individual level, and suggests using these risk estimates as a starting point to discuss with appropriate candidates their desire for daily aspirin use. The benefits of initiating aspirin use are greater for individuals at higher risk for CVD events (eg, those with >15% or >20% 10-year CVD risk), they note.
“Decisions about initiating aspirin use should be based on shared decision-making between clinicians and patients about the potential benefits and harms. Persons who place a higher value on the potential benefits than the potential harms may choose to initiate low-dose aspirin use. Persons who place a higher value on the potential harms or on the burden of taking a daily preventive medication than the potential benefits may choose not to initiate low-dose aspirin use,” the task force says.
It also points out that the risk for bleeding increases modestly with advancing age. “For persons who have initiated aspirin use, the net benefits continue to accrue over time in the absence of a bleeding event. The net benefits, however, become smaller with advancing age because of an increased risk for bleeding, so modeling data suggest that it may be reasonable to consider stopping aspirin use around age 75 years,” it states.
Systematic review
The updated draft recommendations are based on a new systematic review commissioned by the USPSTF on the effectiveness of aspirin to reduce the risk of CVD events (myocardial infarction and stroke), cardiovascular mortality, and all-cause mortality in persons without a history of CVD.
The systematic review also investigated the effect of aspirin use on CRC incidence and mortality in primary CVD prevention populations, as well as the harms, particularly bleeding harms, associated with aspirin use.
In addition to the systematic evidence review, the USPSTF commissioned a microsimulation modeling study to assess the net balance of benefits and harms from aspirin use for primary prevention of CVD and CRC, stratified by age, sex, and CVD risk level. Modeling study parameter inputs were informed by the results of the systematic review, and the primary outcomes were net benefits expressed as quality-adjusted life-years and life-years.
The USPSTF found 13 randomized clinical trials (RCTs) that reported on the benefits of aspirin use for the primary prevention of cardiovascular morbidity and mortality. The total number of participants was 161,680, and most trials used low-dose aspirin of 100 mg/d or less or aspirin every other day. The 13 primary prevention trials included a balanced number of male and female participants and included a broad distribution of ages, with mean age ranging from 53 years in the Physicians’ Health Study to 74 years in the ASPREE trial.
This body of evidence shows that aspirin use for primary prevention of CVD is associated with a decreased risk of myocardial infarction and stroke but not cardiovascular mortality or all-cause mortality. Results are quite similar when including studies using all doses of aspirin compared with studies using low-dose aspirin.
The USPSTF reviewed 14 RCTs in CVD primary prevention populations that reported on the bleeding harms of aspirin.
When looking at studies reporting on the harms of low-dose aspirin use (≤100 mg/d), which is most relevant to current practice, a pooled analysis of 10 trials showed that aspirin use was associated with a 58% increase in major gastrointestinal bleeding, and a pooled analysis of 11 trials showed a 31% increase in intracranial bleeds in the aspirin group compared with the control group. Low-dose aspirin use was not associated with a statistically significant increase in risk of fatal hemorrhagic stroke.
Data suggested that the increased risk of bleeding associated with aspirin use occurs relatively quickly after initiating aspirin, and data do not suggest that aspirin has a differential relative bleeding risk based on age, sex, presence of diabetes, level of CVD risk, or race or ethnicity. Although the increase in relative risk does not appear to differ based on age, the absolute risk of bleeding, and thus the magnitude of bleeding harm, does increase with age, and more so in adults age 60 years or older, they note.
The microsimulation model to estimate the magnitude of net benefit of low-dose aspirin use incorporated findings from the systematic review.
Modeling data demonstrated that aspirin use in both men and women ages 40-59 years with 10% or greater 10-year CVD risk generally provides a modest net benefit in both quality-adjusted life-years and life-years gained. Initiation of aspirin use in persons aged 60-69 years results in quality-adjusted life-years gained that range from slightly negative to slightly positive depending on CVD risk level, and life-years gained are generally negative.
In persons aged 70-79 years, initiation of aspirin use results in a loss of both quality-adjusted life-years and life-years at essentially all CVD risk levels modeled (ie, up to 20% 10-year CVD risk).
The USPSTF thus determined that aspirin use has a small net benefit in persons aged 40-59 years with 10% or greater 10-year CVD risk, and initiation of aspirin use has no net benefit in persons age 60 years or older.
When looking at net lifetime benefit of continuous aspirin use until stopping at age 65, 70, 75, 80, or 85 years, modeling data suggest that there is generally little incremental lifetime net benefit in continuing aspirin use beyond the age of 75-80 years.
The task force points out that the net benefit of continuing aspirin use by a person in their 60s or 70s is not the same as the net benefit of initiating aspirin use by a person in their 60s or 70s. This is because, in part, of the fact that CVD risk is heavily influenced by age. Persons who meet the eligibility criteria for aspirin use at a younger age (ie, ≥10% 10-year CVD risk in their 40s or 50s) typically have even higher CVD risk by their 60s or 70s compared with persons who first reach a 10% or greater 10-year CVD risk in their 60s or 70s, and may gain more benefit by continuing aspirin use than a person at lower risk might gain by initiating aspirin use, the USPSTF explains.
A version of this article first appeared on Medscape.com.
New draft recommendations from the U.S. Preventive Services Task Force (USPSTF) on the use of aspirin for the primary prevention of cardiovascular disease (CVD) have been released and appear to limit the population in which it should be considered.
“The USPSTF concludes with moderate certainty that aspirin use for the primary prevention of CVD events in adults ages 40 to 59 years who have a 10% or greater 10-year CVD risk has a small net benefit,” the recommendation notes. They conclude that for these patients, the decision to use aspirin “should be an individual one.”
“Persons who are not at increased risk for bleeding and are willing to take low-dose aspirin daily are more likely to benefit,” they note.
For older individuals, however, the task force concludes.
The new recommendations were posted online Oct. 12 and will be available for public comment until November 8. Once it is finalized, the recommendation will replace the 2016 USPSTF recommendation on aspirin use to prevent CVD and colorectal cancer (CRC), they note.
In that document, the task force recommended initiating low-dose aspirin for the primary prevention of both CVD and CRC in adults 50-59 years of age who had a 10% or greater 10-year CVD risk, were not at increased risk for bleeding, had a life expectancy of at least 10 years, and were willing to take daily low-dose aspirin for at least 10 years, with the decision to start being an individual one.
For older and younger patients, they found at that time that the evidence was “insufficient to assess the balance of benefits and harms of initiating aspirin use for the primary prevention of CVD and CRC in adults younger than age 50 years or adults aged 70 years or older.”
In the new draft document, “the USPSTF has changed the age ranges and grades of its recommendation on aspirin use.” Besides the recommendations for CVD prevention, they have also changed the previous recommendation of aspirin for the prevention of CRC given evidence generated from large primary CVD prevention trials.
“Based on new analyses of the evidence from primary CVD prevention populations, longer-term follow-up data from the Women’s Health Study (WHS) (JE Buring, personal communication, November 23, 2020), and new trial evidence, the USPSTF concluded that the evidence is inadequate that low-dose aspirin use reduces CRC incidence or mortality,” it states.
Optimum dose
On the optimum dose for primary CVD prevention, the task force says the benefit appears similar for a low dose (≤100 mg/d) and all doses that have been studied in CVD prevention trials (50 to 500 mg/d). “A pragmatic approach would be to use 81 mg/d, which is the most commonly prescribed dose in the United States,” it states.
The USPSTF recommends using the ACC/AHA Pooled Cohort Equations to estimate cardiovascular risk but it points out that these equations are imperfect for risk prediction at the individual level, and suggests using these risk estimates as a starting point to discuss with appropriate candidates their desire for daily aspirin use. The benefits of initiating aspirin use are greater for individuals at higher risk for CVD events (eg, those with >15% or >20% 10-year CVD risk), they note.
“Decisions about initiating aspirin use should be based on shared decision-making between clinicians and patients about the potential benefits and harms. Persons who place a higher value on the potential benefits than the potential harms may choose to initiate low-dose aspirin use. Persons who place a higher value on the potential harms or on the burden of taking a daily preventive medication than the potential benefits may choose not to initiate low-dose aspirin use,” the task force says.
It also points out that the risk for bleeding increases modestly with advancing age. “For persons who have initiated aspirin use, the net benefits continue to accrue over time in the absence of a bleeding event. The net benefits, however, become smaller with advancing age because of an increased risk for bleeding, so modeling data suggest that it may be reasonable to consider stopping aspirin use around age 75 years,” it states.
Systematic review
The updated draft recommendations are based on a new systematic review commissioned by the USPSTF on the effectiveness of aspirin to reduce the risk of CVD events (myocardial infarction and stroke), cardiovascular mortality, and all-cause mortality in persons without a history of CVD.
The systematic review also investigated the effect of aspirin use on CRC incidence and mortality in primary CVD prevention populations, as well as the harms, particularly bleeding harms, associated with aspirin use.
In addition to the systematic evidence review, the USPSTF commissioned a microsimulation modeling study to assess the net balance of benefits and harms from aspirin use for primary prevention of CVD and CRC, stratified by age, sex, and CVD risk level. Modeling study parameter inputs were informed by the results of the systematic review, and the primary outcomes were net benefits expressed as quality-adjusted life-years and life-years.
The USPSTF found 13 randomized clinical trials (RCTs) that reported on the benefits of aspirin use for the primary prevention of cardiovascular morbidity and mortality. The total number of participants was 161,680, and most trials used low-dose aspirin of 100 mg/d or less or aspirin every other day. The 13 primary prevention trials included a balanced number of male and female participants and included a broad distribution of ages, with mean age ranging from 53 years in the Physicians’ Health Study to 74 years in the ASPREE trial.
This body of evidence shows that aspirin use for primary prevention of CVD is associated with a decreased risk of myocardial infarction and stroke but not cardiovascular mortality or all-cause mortality. Results are quite similar when including studies using all doses of aspirin compared with studies using low-dose aspirin.
The USPSTF reviewed 14 RCTs in CVD primary prevention populations that reported on the bleeding harms of aspirin.
When looking at studies reporting on the harms of low-dose aspirin use (≤100 mg/d), which is most relevant to current practice, a pooled analysis of 10 trials showed that aspirin use was associated with a 58% increase in major gastrointestinal bleeding, and a pooled analysis of 11 trials showed a 31% increase in intracranial bleeds in the aspirin group compared with the control group. Low-dose aspirin use was not associated with a statistically significant increase in risk of fatal hemorrhagic stroke.
Data suggested that the increased risk of bleeding associated with aspirin use occurs relatively quickly after initiating aspirin, and data do not suggest that aspirin has a differential relative bleeding risk based on age, sex, presence of diabetes, level of CVD risk, or race or ethnicity. Although the increase in relative risk does not appear to differ based on age, the absolute risk of bleeding, and thus the magnitude of bleeding harm, does increase with age, and more so in adults age 60 years or older, they note.
The microsimulation model to estimate the magnitude of net benefit of low-dose aspirin use incorporated findings from the systematic review.
Modeling data demonstrated that aspirin use in both men and women ages 40-59 years with 10% or greater 10-year CVD risk generally provides a modest net benefit in both quality-adjusted life-years and life-years gained. Initiation of aspirin use in persons aged 60-69 years results in quality-adjusted life-years gained that range from slightly negative to slightly positive depending on CVD risk level, and life-years gained are generally negative.
In persons aged 70-79 years, initiation of aspirin use results in a loss of both quality-adjusted life-years and life-years at essentially all CVD risk levels modeled (ie, up to 20% 10-year CVD risk).
The USPSTF thus determined that aspirin use has a small net benefit in persons aged 40-59 years with 10% or greater 10-year CVD risk, and initiation of aspirin use has no net benefit in persons age 60 years or older.
When looking at net lifetime benefit of continuous aspirin use until stopping at age 65, 70, 75, 80, or 85 years, modeling data suggest that there is generally little incremental lifetime net benefit in continuing aspirin use beyond the age of 75-80 years.
The task force points out that the net benefit of continuing aspirin use by a person in their 60s or 70s is not the same as the net benefit of initiating aspirin use by a person in their 60s or 70s. This is because, in part, of the fact that CVD risk is heavily influenced by age. Persons who meet the eligibility criteria for aspirin use at a younger age (ie, ≥10% 10-year CVD risk in their 40s or 50s) typically have even higher CVD risk by their 60s or 70s compared with persons who first reach a 10% or greater 10-year CVD risk in their 60s or 70s, and may gain more benefit by continuing aspirin use than a person at lower risk might gain by initiating aspirin use, the USPSTF explains.
A version of this article first appeared on Medscape.com.
New draft recommendations from the U.S. Preventive Services Task Force (USPSTF) on the use of aspirin for the primary prevention of cardiovascular disease (CVD) have been released and appear to limit the population in which it should be considered.
“The USPSTF concludes with moderate certainty that aspirin use for the primary prevention of CVD events in adults ages 40 to 59 years who have a 10% or greater 10-year CVD risk has a small net benefit,” the recommendation notes. They conclude that for these patients, the decision to use aspirin “should be an individual one.”
“Persons who are not at increased risk for bleeding and are willing to take low-dose aspirin daily are more likely to benefit,” they note.
For older individuals, however, the task force concludes.
The new recommendations were posted online Oct. 12 and will be available for public comment until November 8. Once it is finalized, the recommendation will replace the 2016 USPSTF recommendation on aspirin use to prevent CVD and colorectal cancer (CRC), they note.
In that document, the task force recommended initiating low-dose aspirin for the primary prevention of both CVD and CRC in adults 50-59 years of age who had a 10% or greater 10-year CVD risk, were not at increased risk for bleeding, had a life expectancy of at least 10 years, and were willing to take daily low-dose aspirin for at least 10 years, with the decision to start being an individual one.
For older and younger patients, they found at that time that the evidence was “insufficient to assess the balance of benefits and harms of initiating aspirin use for the primary prevention of CVD and CRC in adults younger than age 50 years or adults aged 70 years or older.”
In the new draft document, “the USPSTF has changed the age ranges and grades of its recommendation on aspirin use.” Besides the recommendations for CVD prevention, they have also changed the previous recommendation of aspirin for the prevention of CRC given evidence generated from large primary CVD prevention trials.
“Based on new analyses of the evidence from primary CVD prevention populations, longer-term follow-up data from the Women’s Health Study (WHS) (JE Buring, personal communication, November 23, 2020), and new trial evidence, the USPSTF concluded that the evidence is inadequate that low-dose aspirin use reduces CRC incidence or mortality,” it states.
Optimum dose
On the optimum dose for primary CVD prevention, the task force says the benefit appears similar for a low dose (≤100 mg/d) and all doses that have been studied in CVD prevention trials (50 to 500 mg/d). “A pragmatic approach would be to use 81 mg/d, which is the most commonly prescribed dose in the United States,” it states.
The USPSTF recommends using the ACC/AHA Pooled Cohort Equations to estimate cardiovascular risk but it points out that these equations are imperfect for risk prediction at the individual level, and suggests using these risk estimates as a starting point to discuss with appropriate candidates their desire for daily aspirin use. The benefits of initiating aspirin use are greater for individuals at higher risk for CVD events (eg, those with >15% or >20% 10-year CVD risk), they note.
“Decisions about initiating aspirin use should be based on shared decision-making between clinicians and patients about the potential benefits and harms. Persons who place a higher value on the potential benefits than the potential harms may choose to initiate low-dose aspirin use. Persons who place a higher value on the potential harms or on the burden of taking a daily preventive medication than the potential benefits may choose not to initiate low-dose aspirin use,” the task force says.
It also points out that the risk for bleeding increases modestly with advancing age. “For persons who have initiated aspirin use, the net benefits continue to accrue over time in the absence of a bleeding event. The net benefits, however, become smaller with advancing age because of an increased risk for bleeding, so modeling data suggest that it may be reasonable to consider stopping aspirin use around age 75 years,” it states.
Systematic review
The updated draft recommendations are based on a new systematic review commissioned by the USPSTF on the effectiveness of aspirin to reduce the risk of CVD events (myocardial infarction and stroke), cardiovascular mortality, and all-cause mortality in persons without a history of CVD.
The systematic review also investigated the effect of aspirin use on CRC incidence and mortality in primary CVD prevention populations, as well as the harms, particularly bleeding harms, associated with aspirin use.
In addition to the systematic evidence review, the USPSTF commissioned a microsimulation modeling study to assess the net balance of benefits and harms from aspirin use for primary prevention of CVD and CRC, stratified by age, sex, and CVD risk level. Modeling study parameter inputs were informed by the results of the systematic review, and the primary outcomes were net benefits expressed as quality-adjusted life-years and life-years.
The USPSTF found 13 randomized clinical trials (RCTs) that reported on the benefits of aspirin use for the primary prevention of cardiovascular morbidity and mortality. The total number of participants was 161,680, and most trials used low-dose aspirin of 100 mg/d or less or aspirin every other day. The 13 primary prevention trials included a balanced number of male and female participants and included a broad distribution of ages, with mean age ranging from 53 years in the Physicians’ Health Study to 74 years in the ASPREE trial.
This body of evidence shows that aspirin use for primary prevention of CVD is associated with a decreased risk of myocardial infarction and stroke but not cardiovascular mortality or all-cause mortality. Results are quite similar when including studies using all doses of aspirin compared with studies using low-dose aspirin.
The USPSTF reviewed 14 RCTs in CVD primary prevention populations that reported on the bleeding harms of aspirin.
When looking at studies reporting on the harms of low-dose aspirin use (≤100 mg/d), which is most relevant to current practice, a pooled analysis of 10 trials showed that aspirin use was associated with a 58% increase in major gastrointestinal bleeding, and a pooled analysis of 11 trials showed a 31% increase in intracranial bleeds in the aspirin group compared with the control group. Low-dose aspirin use was not associated with a statistically significant increase in risk of fatal hemorrhagic stroke.
Data suggested that the increased risk of bleeding associated with aspirin use occurs relatively quickly after initiating aspirin, and data do not suggest that aspirin has a differential relative bleeding risk based on age, sex, presence of diabetes, level of CVD risk, or race or ethnicity. Although the increase in relative risk does not appear to differ based on age, the absolute risk of bleeding, and thus the magnitude of bleeding harm, does increase with age, and more so in adults age 60 years or older, they note.
The microsimulation model to estimate the magnitude of net benefit of low-dose aspirin use incorporated findings from the systematic review.
Modeling data demonstrated that aspirin use in both men and women ages 40-59 years with 10% or greater 10-year CVD risk generally provides a modest net benefit in both quality-adjusted life-years and life-years gained. Initiation of aspirin use in persons aged 60-69 years results in quality-adjusted life-years gained that range from slightly negative to slightly positive depending on CVD risk level, and life-years gained are generally negative.
In persons aged 70-79 years, initiation of aspirin use results in a loss of both quality-adjusted life-years and life-years at essentially all CVD risk levels modeled (ie, up to 20% 10-year CVD risk).
The USPSTF thus determined that aspirin use has a small net benefit in persons aged 40-59 years with 10% or greater 10-year CVD risk, and initiation of aspirin use has no net benefit in persons age 60 years or older.
When looking at net lifetime benefit of continuous aspirin use until stopping at age 65, 70, 75, 80, or 85 years, modeling data suggest that there is generally little incremental lifetime net benefit in continuing aspirin use beyond the age of 75-80 years.
The task force points out that the net benefit of continuing aspirin use by a person in their 60s or 70s is not the same as the net benefit of initiating aspirin use by a person in their 60s or 70s. This is because, in part, of the fact that CVD risk is heavily influenced by age. Persons who meet the eligibility criteria for aspirin use at a younger age (ie, ≥10% 10-year CVD risk in their 40s or 50s) typically have even higher CVD risk by their 60s or 70s compared with persons who first reach a 10% or greater 10-year CVD risk in their 60s or 70s, and may gain more benefit by continuing aspirin use than a person at lower risk might gain by initiating aspirin use, the USPSTF explains.
A version of this article first appeared on Medscape.com.
Synthetic chemical in consumer products linked to early death, study says
Daily exposure to phthalates, which are synthetic chemicals founds in many consumer products, may lead to hundreds of thousands of early deaths each year among older adults in the United States, according to a new study published Oct. 12, 2021, in the peer-reviewed journal Environmental Pollution.
The chemicals are found in hundreds of types of products, including children’s toys, food storage containers, makeup, perfume, and shampoo. In the study, those with the highest levels of phthalates had a greater risk of death from any cause, especially heart disease.
“This study adds to the growing database on the impact of plastics on the human body and bolsters public health and business cases for reducing or eliminating the use of plastics,” Leonardo Trasande, MD, the lead author and a professor of environmental medicine and population health at New York University Langone Health, told CNN.
Dr. Trasande and colleagues measured the urine concentration of phthalates in more than 5,000 adults aged 55-64 and compared the levels with the risk of early death over an average of 10 years. The research team controlled for preexisting heart diseases, diabetes, cancer, poor eating habits, physical activity, body mass, and other known hormone disruptors such as bisphenol A, or BPA, an industrial chemical that’s been used since the 1950s to make certain plastics and resins, according to the Mayo Clinic
The research team found that phthalates could contribute to 91,000-107,000 premature deaths per year in the United States. These early deaths could cost the nation $40 billion to $47 billion each year in lost economic productivity.
Phthalates interrupt the body’s endocrine system and hormone production. Previous studies have found that the chemicals are linked with developmental, reproductive, and immune system problems, according to NYU Langone Health. They’ve also been linked with asthma, childhood obesity, heart issues, and cancer.
“These chemicals have a rap sheet,” Dr. Trasande told CNN. “And the fact of the matter is that when you look at the entire body of evidence, it provides a haunting pattern of concern.”
Phthalates are often called “everywhere chemicals” because they are so common, CNN reported. Also called “plasticizers,” they are added to products to make them more durable, including PVC plumbing, vinyl flooring, medical tubing, garden hoses, food packaging, detergents, clothing, furniture, and automotive materials.
People are often exposed when they breathe contaminated air or consume food that comes into contact with the chemical, according to the Centers for Disease Control and Prevention. Children may be exposed by touching plastic items and putting their hands in their mouth.
Dr. Trasande told CNN that it’s possible to lessen exposure to phthalates and other endocrine disruptors such as BPA by using unscented lotions, laundry detergents, and cleaning supplies, as well as substituting glass, stainless steel, ceramic, and wood for plastic food storage.
“First, avoid plastics as much as you can. Never put plastic containers in the microwave or dishwasher, where the heat can break down the linings so they might be absorbed more readily,” he said. “In addition, cooking at home and reducing your use of processed foods can reduce the levels of the chemical exposures you come in contact with.”
A version of this article first appeared on WebMD.com.
Daily exposure to phthalates, which are synthetic chemicals founds in many consumer products, may lead to hundreds of thousands of early deaths each year among older adults in the United States, according to a new study published Oct. 12, 2021, in the peer-reviewed journal Environmental Pollution.
The chemicals are found in hundreds of types of products, including children’s toys, food storage containers, makeup, perfume, and shampoo. In the study, those with the highest levels of phthalates had a greater risk of death from any cause, especially heart disease.
“This study adds to the growing database on the impact of plastics on the human body and bolsters public health and business cases for reducing or eliminating the use of plastics,” Leonardo Trasande, MD, the lead author and a professor of environmental medicine and population health at New York University Langone Health, told CNN.
Dr. Trasande and colleagues measured the urine concentration of phthalates in more than 5,000 adults aged 55-64 and compared the levels with the risk of early death over an average of 10 years. The research team controlled for preexisting heart diseases, diabetes, cancer, poor eating habits, physical activity, body mass, and other known hormone disruptors such as bisphenol A, or BPA, an industrial chemical that’s been used since the 1950s to make certain plastics and resins, according to the Mayo Clinic
The research team found that phthalates could contribute to 91,000-107,000 premature deaths per year in the United States. These early deaths could cost the nation $40 billion to $47 billion each year in lost economic productivity.
Phthalates interrupt the body’s endocrine system and hormone production. Previous studies have found that the chemicals are linked with developmental, reproductive, and immune system problems, according to NYU Langone Health. They’ve also been linked with asthma, childhood obesity, heart issues, and cancer.
“These chemicals have a rap sheet,” Dr. Trasande told CNN. “And the fact of the matter is that when you look at the entire body of evidence, it provides a haunting pattern of concern.”
Phthalates are often called “everywhere chemicals” because they are so common, CNN reported. Also called “plasticizers,” they are added to products to make them more durable, including PVC plumbing, vinyl flooring, medical tubing, garden hoses, food packaging, detergents, clothing, furniture, and automotive materials.
People are often exposed when they breathe contaminated air or consume food that comes into contact with the chemical, according to the Centers for Disease Control and Prevention. Children may be exposed by touching plastic items and putting their hands in their mouth.
Dr. Trasande told CNN that it’s possible to lessen exposure to phthalates and other endocrine disruptors such as BPA by using unscented lotions, laundry detergents, and cleaning supplies, as well as substituting glass, stainless steel, ceramic, and wood for plastic food storage.
“First, avoid plastics as much as you can. Never put plastic containers in the microwave or dishwasher, where the heat can break down the linings so they might be absorbed more readily,” he said. “In addition, cooking at home and reducing your use of processed foods can reduce the levels of the chemical exposures you come in contact with.”
A version of this article first appeared on WebMD.com.
Daily exposure to phthalates, which are synthetic chemicals founds in many consumer products, may lead to hundreds of thousands of early deaths each year among older adults in the United States, according to a new study published Oct. 12, 2021, in the peer-reviewed journal Environmental Pollution.
The chemicals are found in hundreds of types of products, including children’s toys, food storage containers, makeup, perfume, and shampoo. In the study, those with the highest levels of phthalates had a greater risk of death from any cause, especially heart disease.
“This study adds to the growing database on the impact of plastics on the human body and bolsters public health and business cases for reducing or eliminating the use of plastics,” Leonardo Trasande, MD, the lead author and a professor of environmental medicine and population health at New York University Langone Health, told CNN.
Dr. Trasande and colleagues measured the urine concentration of phthalates in more than 5,000 adults aged 55-64 and compared the levels with the risk of early death over an average of 10 years. The research team controlled for preexisting heart diseases, diabetes, cancer, poor eating habits, physical activity, body mass, and other known hormone disruptors such as bisphenol A, or BPA, an industrial chemical that’s been used since the 1950s to make certain plastics and resins, according to the Mayo Clinic
The research team found that phthalates could contribute to 91,000-107,000 premature deaths per year in the United States. These early deaths could cost the nation $40 billion to $47 billion each year in lost economic productivity.
Phthalates interrupt the body’s endocrine system and hormone production. Previous studies have found that the chemicals are linked with developmental, reproductive, and immune system problems, according to NYU Langone Health. They’ve also been linked with asthma, childhood obesity, heart issues, and cancer.
“These chemicals have a rap sheet,” Dr. Trasande told CNN. “And the fact of the matter is that when you look at the entire body of evidence, it provides a haunting pattern of concern.”
Phthalates are often called “everywhere chemicals” because they are so common, CNN reported. Also called “plasticizers,” they are added to products to make them more durable, including PVC plumbing, vinyl flooring, medical tubing, garden hoses, food packaging, detergents, clothing, furniture, and automotive materials.
People are often exposed when they breathe contaminated air or consume food that comes into contact with the chemical, according to the Centers for Disease Control and Prevention. Children may be exposed by touching plastic items and putting their hands in their mouth.
Dr. Trasande told CNN that it’s possible to lessen exposure to phthalates and other endocrine disruptors such as BPA by using unscented lotions, laundry detergents, and cleaning supplies, as well as substituting glass, stainless steel, ceramic, and wood for plastic food storage.
“First, avoid plastics as much as you can. Never put plastic containers in the microwave or dishwasher, where the heat can break down the linings so they might be absorbed more readily,” he said. “In addition, cooking at home and reducing your use of processed foods can reduce the levels of the chemical exposures you come in contact with.”
A version of this article first appeared on WebMD.com.
Children and COVID-19: U.S. adds latest million cases in record time
The United States just passed the 6-million mark in COVID-19 cases among children, with the last million cases taking less time to record than any of the first five, according to new data from the American Academy of Pediatrics and the Children’s Hospital Association.
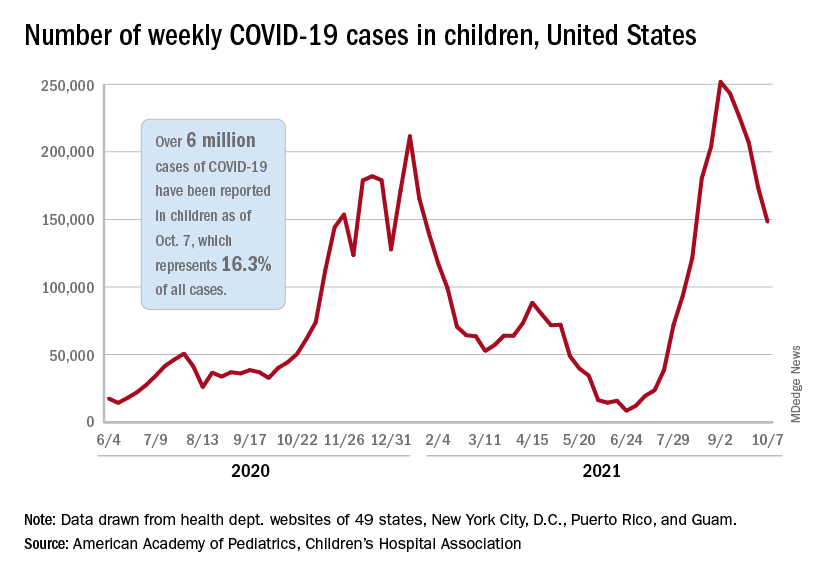
The five-millionth case was reported during the week of Aug. 27 to Sept. 2, and case number 6 million came during the week of Oct. 1-7, just 5 weeks later, compared with the 6 weeks it took to go from 1 million to 2 million last November and December, the AAP and CHA said in their weekly COVID-19 report.
New cases continued to drop, however, and that weekly count was down by 14.6% from the previous week and by 41.1% from the peak of almost 252,000 reached in early September, the two groups said while also noting limitations to the data, such as three states (Alabama, Nebraska, and Texas) that are no longer updating their COVID-19 dashboards.
Other metrics show similar drops in recent weeks. Among children aged 0-11 years, emergency department visits involving a COVID-19 diagnosis dropped from 4.1% of all ED visits in late August to 1.4% of ED visits on Oct. 6. ED visits with a COVID-19 diagnosis fell from a peak of 8.5% on Aug. 22 to 1.5% on Oct. 6 for 12- to 15-year-olds and from 8.5% to 1.5% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
The rate of new hospital admissions for children aged 0-17 years was down to 0.26 per 100,000 population on Oct. 9 after reaching 0.51 per 100,000 on Sept. 4. Hospitalizations in children totaled just over 64,000 from Aug. 1, 2020, to Oct. 9, 2021, which is just over 2% of all COVID-19–related admissions over that time period, the CDC said on its COVID Data Tracker.
That pattern, unfortunately, also applies to vaccinations. “The number of children receiving their first COVID-19 vaccine this week [Sept. 30 to Oct. 6], about 156,000, was the lowest number since vaccines were available,” the AAP said in a separate report on vaccination trends, adding that “the number of children receiving their first dose has steadily declined from 8 weeks ago when 586,000 children received their initial dose the week ending Aug. 11.”
The United States just passed the 6-million mark in COVID-19 cases among children, with the last million cases taking less time to record than any of the first five, according to new data from the American Academy of Pediatrics and the Children’s Hospital Association.
The five-millionth case was reported during the week of Aug. 27 to Sept. 2, and case number 6 million came during the week of Oct. 1-7, just 5 weeks later, compared with the 6 weeks it took to go from 1 million to 2 million last November and December, the AAP and CHA said in their weekly COVID-19 report.
New cases continued to drop, however, and that weekly count was down by 14.6% from the previous week and by 41.1% from the peak of almost 252,000 reached in early September, the two groups said while also noting limitations to the data, such as three states (Alabama, Nebraska, and Texas) that are no longer updating their COVID-19 dashboards.
Other metrics show similar drops in recent weeks. Among children aged 0-11 years, emergency department visits involving a COVID-19 diagnosis dropped from 4.1% of all ED visits in late August to 1.4% of ED visits on Oct. 6. ED visits with a COVID-19 diagnosis fell from a peak of 8.5% on Aug. 22 to 1.5% on Oct. 6 for 12- to 15-year-olds and from 8.5% to 1.5% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
The rate of new hospital admissions for children aged 0-17 years was down to 0.26 per 100,000 population on Oct. 9 after reaching 0.51 per 100,000 on Sept. 4. Hospitalizations in children totaled just over 64,000 from Aug. 1, 2020, to Oct. 9, 2021, which is just over 2% of all COVID-19–related admissions over that time period, the CDC said on its COVID Data Tracker.
That pattern, unfortunately, also applies to vaccinations. “The number of children receiving their first COVID-19 vaccine this week [Sept. 30 to Oct. 6], about 156,000, was the lowest number since vaccines were available,” the AAP said in a separate report on vaccination trends, adding that “the number of children receiving their first dose has steadily declined from 8 weeks ago when 586,000 children received their initial dose the week ending Aug. 11.”
The United States just passed the 6-million mark in COVID-19 cases among children, with the last million cases taking less time to record than any of the first five, according to new data from the American Academy of Pediatrics and the Children’s Hospital Association.
The five-millionth case was reported during the week of Aug. 27 to Sept. 2, and case number 6 million came during the week of Oct. 1-7, just 5 weeks later, compared with the 6 weeks it took to go from 1 million to 2 million last November and December, the AAP and CHA said in their weekly COVID-19 report.
New cases continued to drop, however, and that weekly count was down by 14.6% from the previous week and by 41.1% from the peak of almost 252,000 reached in early September, the two groups said while also noting limitations to the data, such as three states (Alabama, Nebraska, and Texas) that are no longer updating their COVID-19 dashboards.
Other metrics show similar drops in recent weeks. Among children aged 0-11 years, emergency department visits involving a COVID-19 diagnosis dropped from 4.1% of all ED visits in late August to 1.4% of ED visits on Oct. 6. ED visits with a COVID-19 diagnosis fell from a peak of 8.5% on Aug. 22 to 1.5% on Oct. 6 for 12- to 15-year-olds and from 8.5% to 1.5% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
The rate of new hospital admissions for children aged 0-17 years was down to 0.26 per 100,000 population on Oct. 9 after reaching 0.51 per 100,000 on Sept. 4. Hospitalizations in children totaled just over 64,000 from Aug. 1, 2020, to Oct. 9, 2021, which is just over 2% of all COVID-19–related admissions over that time period, the CDC said on its COVID Data Tracker.
That pattern, unfortunately, also applies to vaccinations. “The number of children receiving their first COVID-19 vaccine this week [Sept. 30 to Oct. 6], about 156,000, was the lowest number since vaccines were available,” the AAP said in a separate report on vaccination trends, adding that “the number of children receiving their first dose has steadily declined from 8 weeks ago when 586,000 children received their initial dose the week ending Aug. 11.”
Is the end near for surgical and transbronchial biopsies? Challenges in the pediatric workforce; Cascade testing in PAH; and more ...
Interventional chest/diagnostic procedures
Endobronchial optical coherence tomography and interstitial lung diseases: Is the end near for surgical and transbronchial lung biopsies?
The early diagnosis of interstitial lung diseases (ILD) is paramount to initiating appropriate treatment and preventing irreversible pulmonary damage. Specific ILD subtypes may be diagnosed based on clinical evaluation, high resolution chest CT (HRCT) patterns, and serologic testing, but many patients require invasive procedures for histopathologic evaluation of lung tissue. Current modalities for obtaining tissue include transbronchial lung cryobiopsy (TBLC) and surgical lung biopsy (SLB), both of which carry a risk of potential complications (Troy LK, et al. Lancet Respir Med. 2020;8:171-81; Hutchinson JP, et al. Am J Respir Crit Care Med. 2016;193[10]:1161-7).

Recently, genomic classifiers applied to transbronchial biopsies have been proposed to facilitate the diagnosis of usual interstitial pneumonia (UIP), but the limited information provided still does not obviate the need for tissue diagnosis when needed (Raghu G, et al. Lancet Respir Med. 2019;7[6]:487-96). It is in this context that endobronchial optical coherence tomography (EB-OCT) was proposed as a real-time, in vivo, optical biopsy method for ILD.

EB-OCT uses near infrared light to generate large volumes of in-vivo three-dimensional tissue imaging with microscopic resolution (Goorsenberg A, et al. Respiration. 2020;99:190-205; Nandy S, et al. Am J Respir Crit Care Med. 2021;article in press). The OCT catheter is advanced through the bronchoscope working channel and can be used during outpatient procedures under conscious sedation. Available data suggests that minimal training is necessary, both for proceduralists and interpreting pathologists, but this will need to be confirmed in larger studies and various practice settings. Early studies suggest that OCT can identify microscopic honeycombing and other abnormalities even before they are evident on HRCT scans (Goorsenberg A, et al. Respiration. 2020;99:190-205). Newer research comparing ILD diagnosis from EB-OCT cross-sectional images with that obtained from SLB specimens revealed EB-OCT can distinguish UIP from non-UIP ILD with high sensitivity and specificity (Nandy S, et al. Am J Respir Crit Care Med. 2021;article in press). Could this mean the end of SLB and TBLC for the diagnosis of ILD? While the ability to diagnose ILD subtypes with high reliability and low risk of complications is certainly promising, studies remain admittedly small and the technique itself is only available to highly select individuals and specialized ILD centers. Let’s not pack up the cryoprobe just yet.
Audra J. Schwalk, MD, MBA: Steering Committee Member
Fabien Maldonado, MD, FCCP: Steering Committee Member
Pediatric chest medicine
Challenges in the pediatric pulmonary workforce
The future of the pediatric workforce has been the source of extensive discussion within the pediatric community and resulted in a considerable body of medical literature (Vinci RJ. Pediatrics. 2021;147[6]:e2020013292). In pediatric pulmonology, there is growing concern that current trends will lead to a workforce shortage resulting in patients having difficulty accessing subspecialty care (Harris C, et al. Pediatric Pulmonol. 2019;54[4]:444-50). The etiology of this shortage is multifactorial. Duration of fellowship training and subsequent financial implications are reported potential barriers to pursuing a fellowship (Nelson BA, et al. Pediatric Pulmonol. 2020;1-7). Discrepancies between pediatric and adult compensation may be another barrier. Insightful recruitment strategies based on the results of a recent study included maximizing resident interaction with pulmonary faculty, early identification and support of interested trainees, and consideration of flexible training models (Nelson BA, et al. ATS Sch. 2020;1:372-83). Lifestyle has also been a factor that contributes to a trainee’s decision to go into pediatric pulmonology (Freed GL, et al. Pediatrics. 2009;123(suppl 1):S31‐S37).

As our field addresses the critical need to recruit more trainees in light of the unfilled fellowship positions and the increasing average age of members of the field, we should not underestimate the prevalence of systemic racism and bias in medicine (Chiel L, et al. ATS Sch. 2020;1[4]:337-39) nor gender discrimination. Instead, we should seize the opportunity to understand and knock down barriers that trainees who are underrepresented in medicine face in pursuing pediatric subspecialty careers and build upon the excellent recent body of literature in this field to help recruit, support , and grow a robust, diverse workforce to provide the best pediatric care to all.
Anne C. Coates, MD – Steering Committee Member
Pulmonary vascular disease
Cascade testing in PAH: Is there a role?
Pediatric guidelines for pulmonary arterial hypertension (PAH) recommends genetic screening as a part of the evaluation for the newly diagnosed, with expansion to first-degree relatives as indicated. Currently, this is not mandated, and implementation is variable. In adults, genetic screening is not routinely offered, and family screening is rare. This reflects a lack of definitive guidelines (Abman SH, et al. Circulation. 2015:24;132[21]:2037-99). However, it is intuitive that if carriers are not identified by screening, they will come to attention after pulmonary vascular disease burden causes symptoms and affects outcomes.

Cascade testing is a screening methodology that is used in heritable cancers (George RM, et al. Genet Couns. 2015;24[3]:388-99). In cascade testing, identification of an index case prompts screening of at-risk family members. If these relatives are positive for mutations, the cycle is repeated (cascaded) to their immediate relatives, allowing for targeted screening. This approach is especially effective in genetic mutations that are inherited in an autosomal dominant fashion, such as in BMPR2 gene mutation. Cascade testing is an effective way to capture relatives who would otherwise be overlooked.

Unfortunately, in the United States, the cost of genetic testing is a significant obstacle to universal implementation. A new diagnosis of heritable pulmonary arterial hypertension (HPAH) is often followed by a multigene panel with costs exceeding $1000 and may prompt subsequent targeted testing resulting in additional expense (Chung WK, et al. Can J Cardiol. 2015;31[4]:544-47). Furthermore, a positive mutation detected on screening is not definitively associated with disease due to variable penetrance (Morrell NW, et al. Eur Respir J. 2019;53[1]:1801899]. As such, mass screening strategies are not recommended. The recent DELPHI-2 study [Montani D, et al. Eur Respir J. 2021;58[1]:2004229) have demonstrated that genetic screening is impactful in families with HPAH. A genetic screening algorithm should be considered, and cascade testing could be a cost-effective targeted approach.
Sandeep Sahay, MD, MSc, FCCP: Steering Committee Member
Jean M. Elwing, MD, FCCP: Chair
Pulmonary physiology, function, and rehabilitation network
Physiological benefits of awake proning: Its role and relevance in the COVID-19 pandemic
The advent of the COVID-19 pandemic has put a significant strain on the health care systems and critical care services across several countries, including the United States. Amidst this, several concerted efforts to reduce the need for mechanical ventilation has resulted in the emergence of awake proning as a strategy to improve oxygenation, which has been instituted in critical care units, in-patient settings, as well as in EDs. Although the evidence on this strategy has been vastly limited to case series and observational studies, several societies have incorporated awake proning as an initial management strategy in hypoxemic respiratory failure within their clinical guidelines (Chalmers JD, et al. Eur Respir J. 2021;57:2100048; Koeckerling D, et al. Thorax. 2020;75:833-4) and consensus statements (Nasa P, et al. Crit Care. 2021;25:106).

Physiological benefits of awake proning include improvement in ventilation-perfusion matching secondary to relative increase in ventilation in dorsal nondependent areas in the setting of higher density of perfusion within these units, thus reducing shunt and, hence, improving oxygenation. Other physiological mechanisms include homogenization of transpulmonary pressures, reduction of ventilator-induced lung injury (VILI) or patient self-inflicted lung injury (P-SILI), and possibly lung injury from pendelluft (Telias I, et al. JAMA. 2020;323[22]:2265-67).
A recent meta-trial involving randomized controlled trials done across six countries compared prone positioning with standard care in patients with hypoxemic respiratory failure (defined as SpO2/ FiO2 < 315 and on high flow oxygen therapy) showed a reduced incidence of treatment failure and need for intubation without any signal of harm; although no mortality benefit was reported (Ehrmann S, et al. Lancet Respir Med. 2021 Aug 20;S2213-2600(21)00356-8). The number needed to treat to prevent one intubation was 14. While promising and reinforcing the safety of this relatively easy maneuver, several questions remain—which patients would benefit the most? Can it be applied within general wards safely? Does institution of awake proning delay intubation rates with consequent worse outcomes? Several ongoing (NCT 04402879) and completed studies (NCT 04383613 and NCT 04350723) may shed light on these important questions (Weatherald J, et al. Lancet Respir Med. 2021 Aug 20;S2213-2600[21]00368-4).
Sujith Cherian, MD, FCCP: Steering Committee Member
Interventional chest/diagnostic procedures
Endobronchial optical coherence tomography and interstitial lung diseases: Is the end near for surgical and transbronchial lung biopsies?
The early diagnosis of interstitial lung diseases (ILD) is paramount to initiating appropriate treatment and preventing irreversible pulmonary damage. Specific ILD subtypes may be diagnosed based on clinical evaluation, high resolution chest CT (HRCT) patterns, and serologic testing, but many patients require invasive procedures for histopathologic evaluation of lung tissue. Current modalities for obtaining tissue include transbronchial lung cryobiopsy (TBLC) and surgical lung biopsy (SLB), both of which carry a risk of potential complications (Troy LK, et al. Lancet Respir Med. 2020;8:171-81; Hutchinson JP, et al. Am J Respir Crit Care Med. 2016;193[10]:1161-7).
Recently, genomic classifiers applied to transbronchial biopsies have been proposed to facilitate the diagnosis of usual interstitial pneumonia (UIP), but the limited information provided still does not obviate the need for tissue diagnosis when needed (Raghu G, et al. Lancet Respir Med. 2019;7[6]:487-96). It is in this context that endobronchial optical coherence tomography (EB-OCT) was proposed as a real-time, in vivo, optical biopsy method for ILD.
EB-OCT uses near infrared light to generate large volumes of in-vivo three-dimensional tissue imaging with microscopic resolution (Goorsenberg A, et al. Respiration. 2020;99:190-205; Nandy S, et al. Am J Respir Crit Care Med. 2021;article in press). The OCT catheter is advanced through the bronchoscope working channel and can be used during outpatient procedures under conscious sedation. Available data suggests that minimal training is necessary, both for proceduralists and interpreting pathologists, but this will need to be confirmed in larger studies and various practice settings. Early studies suggest that OCT can identify microscopic honeycombing and other abnormalities even before they are evident on HRCT scans (Goorsenberg A, et al. Respiration. 2020;99:190-205). Newer research comparing ILD diagnosis from EB-OCT cross-sectional images with that obtained from SLB specimens revealed EB-OCT can distinguish UIP from non-UIP ILD with high sensitivity and specificity (Nandy S, et al. Am J Respir Crit Care Med. 2021;article in press). Could this mean the end of SLB and TBLC for the diagnosis of ILD? While the ability to diagnose ILD subtypes with high reliability and low risk of complications is certainly promising, studies remain admittedly small and the technique itself is only available to highly select individuals and specialized ILD centers. Let’s not pack up the cryoprobe just yet.
Audra J. Schwalk, MD, MBA: Steering Committee Member
Fabien Maldonado, MD, FCCP: Steering Committee Member
Pediatric chest medicine
Challenges in the pediatric pulmonary workforce
The future of the pediatric workforce has been the source of extensive discussion within the pediatric community and resulted in a considerable body of medical literature (Vinci RJ. Pediatrics. 2021;147[6]:e2020013292). In pediatric pulmonology, there is growing concern that current trends will lead to a workforce shortage resulting in patients having difficulty accessing subspecialty care (Harris C, et al. Pediatric Pulmonol. 2019;54[4]:444-50). The etiology of this shortage is multifactorial. Duration of fellowship training and subsequent financial implications are reported potential barriers to pursuing a fellowship (Nelson BA, et al. Pediatric Pulmonol. 2020;1-7). Discrepancies between pediatric and adult compensation may be another barrier. Insightful recruitment strategies based on the results of a recent study included maximizing resident interaction with pulmonary faculty, early identification and support of interested trainees, and consideration of flexible training models (Nelson BA, et al. ATS Sch. 2020;1:372-83). Lifestyle has also been a factor that contributes to a trainee’s decision to go into pediatric pulmonology (Freed GL, et al. Pediatrics. 2009;123(suppl 1):S31‐S37).
As our field addresses the critical need to recruit more trainees in light of the unfilled fellowship positions and the increasing average age of members of the field, we should not underestimate the prevalence of systemic racism and bias in medicine (Chiel L, et al. ATS Sch. 2020;1[4]:337-39) nor gender discrimination. Instead, we should seize the opportunity to understand and knock down barriers that trainees who are underrepresented in medicine face in pursuing pediatric subspecialty careers and build upon the excellent recent body of literature in this field to help recruit, support , and grow a robust, diverse workforce to provide the best pediatric care to all.
Anne C. Coates, MD – Steering Committee Member
Pulmonary vascular disease
Cascade testing in PAH: Is there a role?
Pediatric guidelines for pulmonary arterial hypertension (PAH) recommends genetic screening as a part of the evaluation for the newly diagnosed, with expansion to first-degree relatives as indicated. Currently, this is not mandated, and implementation is variable. In adults, genetic screening is not routinely offered, and family screening is rare. This reflects a lack of definitive guidelines (Abman SH, et al. Circulation. 2015:24;132[21]:2037-99). However, it is intuitive that if carriers are not identified by screening, they will come to attention after pulmonary vascular disease burden causes symptoms and affects outcomes.
Cascade testing is a screening methodology that is used in heritable cancers (George RM, et al. Genet Couns. 2015;24[3]:388-99). In cascade testing, identification of an index case prompts screening of at-risk family members. If these relatives are positive for mutations, the cycle is repeated (cascaded) to their immediate relatives, allowing for targeted screening. This approach is especially effective in genetic mutations that are inherited in an autosomal dominant fashion, such as in BMPR2 gene mutation. Cascade testing is an effective way to capture relatives who would otherwise be overlooked.
Unfortunately, in the United States, the cost of genetic testing is a significant obstacle to universal implementation. A new diagnosis of heritable pulmonary arterial hypertension (HPAH) is often followed by a multigene panel with costs exceeding $1000 and may prompt subsequent targeted testing resulting in additional expense (Chung WK, et al. Can J Cardiol. 2015;31[4]:544-47). Furthermore, a positive mutation detected on screening is not definitively associated with disease due to variable penetrance (Morrell NW, et al. Eur Respir J. 2019;53[1]:1801899]. As such, mass screening strategies are not recommended. The recent DELPHI-2 study [Montani D, et al. Eur Respir J. 2021;58[1]:2004229) have demonstrated that genetic screening is impactful in families with HPAH. A genetic screening algorithm should be considered, and cascade testing could be a cost-effective targeted approach.
Sandeep Sahay, MD, MSc, FCCP: Steering Committee Member
Jean M. Elwing, MD, FCCP: Chair
Pulmonary physiology, function, and rehabilitation network
Physiological benefits of awake proning: Its role and relevance in the COVID-19 pandemic
The advent of the COVID-19 pandemic has put a significant strain on the health care systems and critical care services across several countries, including the United States. Amidst this, several concerted efforts to reduce the need for mechanical ventilation has resulted in the emergence of awake proning as a strategy to improve oxygenation, which has been instituted in critical care units, in-patient settings, as well as in EDs. Although the evidence on this strategy has been vastly limited to case series and observational studies, several societies have incorporated awake proning as an initial management strategy in hypoxemic respiratory failure within their clinical guidelines (Chalmers JD, et al. Eur Respir J. 2021;57:2100048; Koeckerling D, et al. Thorax. 2020;75:833-4) and consensus statements (Nasa P, et al. Crit Care. 2021;25:106).
Physiological benefits of awake proning include improvement in ventilation-perfusion matching secondary to relative increase in ventilation in dorsal nondependent areas in the setting of higher density of perfusion within these units, thus reducing shunt and, hence, improving oxygenation. Other physiological mechanisms include homogenization of transpulmonary pressures, reduction of ventilator-induced lung injury (VILI) or patient self-inflicted lung injury (P-SILI), and possibly lung injury from pendelluft (Telias I, et al. JAMA. 2020;323[22]:2265-67).
A recent meta-trial involving randomized controlled trials done across six countries compared prone positioning with standard care in patients with hypoxemic respiratory failure (defined as SpO2/ FiO2 < 315 and on high flow oxygen therapy) showed a reduced incidence of treatment failure and need for intubation without any signal of harm; although no mortality benefit was reported (Ehrmann S, et al. Lancet Respir Med. 2021 Aug 20;S2213-2600(21)00356-8). The number needed to treat to prevent one intubation was 14. While promising and reinforcing the safety of this relatively easy maneuver, several questions remain—which patients would benefit the most? Can it be applied within general wards safely? Does institution of awake proning delay intubation rates with consequent worse outcomes? Several ongoing (NCT 04402879) and completed studies (NCT 04383613 and NCT 04350723) may shed light on these important questions (Weatherald J, et al. Lancet Respir Med. 2021 Aug 20;S2213-2600[21]00368-4).
Sujith Cherian, MD, FCCP: Steering Committee Member
Interventional chest/diagnostic procedures
Endobronchial optical coherence tomography and interstitial lung diseases: Is the end near for surgical and transbronchial lung biopsies?
The early diagnosis of interstitial lung diseases (ILD) is paramount to initiating appropriate treatment and preventing irreversible pulmonary damage. Specific ILD subtypes may be diagnosed based on clinical evaluation, high resolution chest CT (HRCT) patterns, and serologic testing, but many patients require invasive procedures for histopathologic evaluation of lung tissue. Current modalities for obtaining tissue include transbronchial lung cryobiopsy (TBLC) and surgical lung biopsy (SLB), both of which carry a risk of potential complications (Troy LK, et al. Lancet Respir Med. 2020;8:171-81; Hutchinson JP, et al. Am J Respir Crit Care Med. 2016;193[10]:1161-7).
Recently, genomic classifiers applied to transbronchial biopsies have been proposed to facilitate the diagnosis of usual interstitial pneumonia (UIP), but the limited information provided still does not obviate the need for tissue diagnosis when needed (Raghu G, et al. Lancet Respir Med. 2019;7[6]:487-96). It is in this context that endobronchial optical coherence tomography (EB-OCT) was proposed as a real-time, in vivo, optical biopsy method for ILD.
EB-OCT uses near infrared light to generate large volumes of in-vivo three-dimensional tissue imaging with microscopic resolution (Goorsenberg A, et al. Respiration. 2020;99:190-205; Nandy S, et al. Am J Respir Crit Care Med. 2021;article in press). The OCT catheter is advanced through the bronchoscope working channel and can be used during outpatient procedures under conscious sedation. Available data suggests that minimal training is necessary, both for proceduralists and interpreting pathologists, but this will need to be confirmed in larger studies and various practice settings. Early studies suggest that OCT can identify microscopic honeycombing and other abnormalities even before they are evident on HRCT scans (Goorsenberg A, et al. Respiration. 2020;99:190-205). Newer research comparing ILD diagnosis from EB-OCT cross-sectional images with that obtained from SLB specimens revealed EB-OCT can distinguish UIP from non-UIP ILD with high sensitivity and specificity (Nandy S, et al. Am J Respir Crit Care Med. 2021;article in press). Could this mean the end of SLB and TBLC for the diagnosis of ILD? While the ability to diagnose ILD subtypes with high reliability and low risk of complications is certainly promising, studies remain admittedly small and the technique itself is only available to highly select individuals and specialized ILD centers. Let’s not pack up the cryoprobe just yet.
Audra J. Schwalk, MD, MBA: Steering Committee Member
Fabien Maldonado, MD, FCCP: Steering Committee Member
Pediatric chest medicine
Challenges in the pediatric pulmonary workforce
The future of the pediatric workforce has been the source of extensive discussion within the pediatric community and resulted in a considerable body of medical literature (Vinci RJ. Pediatrics. 2021;147[6]:e2020013292). In pediatric pulmonology, there is growing concern that current trends will lead to a workforce shortage resulting in patients having difficulty accessing subspecialty care (Harris C, et al. Pediatric Pulmonol. 2019;54[4]:444-50). The etiology of this shortage is multifactorial. Duration of fellowship training and subsequent financial implications are reported potential barriers to pursuing a fellowship (Nelson BA, et al. Pediatric Pulmonol. 2020;1-7). Discrepancies between pediatric and adult compensation may be another barrier. Insightful recruitment strategies based on the results of a recent study included maximizing resident interaction with pulmonary faculty, early identification and support of interested trainees, and consideration of flexible training models (Nelson BA, et al. ATS Sch. 2020;1:372-83). Lifestyle has also been a factor that contributes to a trainee’s decision to go into pediatric pulmonology (Freed GL, et al. Pediatrics. 2009;123(suppl 1):S31‐S37).
As our field addresses the critical need to recruit more trainees in light of the unfilled fellowship positions and the increasing average age of members of the field, we should not underestimate the prevalence of systemic racism and bias in medicine (Chiel L, et al. ATS Sch. 2020;1[4]:337-39) nor gender discrimination. Instead, we should seize the opportunity to understand and knock down barriers that trainees who are underrepresented in medicine face in pursuing pediatric subspecialty careers and build upon the excellent recent body of literature in this field to help recruit, support , and grow a robust, diverse workforce to provide the best pediatric care to all.
Anne C. Coates, MD – Steering Committee Member
Pulmonary vascular disease
Cascade testing in PAH: Is there a role?
Pediatric guidelines for pulmonary arterial hypertension (PAH) recommends genetic screening as a part of the evaluation for the newly diagnosed, with expansion to first-degree relatives as indicated. Currently, this is not mandated, and implementation is variable. In adults, genetic screening is not routinely offered, and family screening is rare. This reflects a lack of definitive guidelines (Abman SH, et al. Circulation. 2015:24;132[21]:2037-99). However, it is intuitive that if carriers are not identified by screening, they will come to attention after pulmonary vascular disease burden causes symptoms and affects outcomes.
Cascade testing is a screening methodology that is used in heritable cancers (George RM, et al. Genet Couns. 2015;24[3]:388-99). In cascade testing, identification of an index case prompts screening of at-risk family members. If these relatives are positive for mutations, the cycle is repeated (cascaded) to their immediate relatives, allowing for targeted screening. This approach is especially effective in genetic mutations that are inherited in an autosomal dominant fashion, such as in BMPR2 gene mutation. Cascade testing is an effective way to capture relatives who would otherwise be overlooked.
Unfortunately, in the United States, the cost of genetic testing is a significant obstacle to universal implementation. A new diagnosis of heritable pulmonary arterial hypertension (HPAH) is often followed by a multigene panel with costs exceeding $1000 and may prompt subsequent targeted testing resulting in additional expense (Chung WK, et al. Can J Cardiol. 2015;31[4]:544-47). Furthermore, a positive mutation detected on screening is not definitively associated with disease due to variable penetrance (Morrell NW, et al. Eur Respir J. 2019;53[1]:1801899]. As such, mass screening strategies are not recommended. The recent DELPHI-2 study [Montani D, et al. Eur Respir J. 2021;58[1]:2004229) have demonstrated that genetic screening is impactful in families with HPAH. A genetic screening algorithm should be considered, and cascade testing could be a cost-effective targeted approach.
Sandeep Sahay, MD, MSc, FCCP: Steering Committee Member
Jean M. Elwing, MD, FCCP: Chair
Pulmonary physiology, function, and rehabilitation network
Physiological benefits of awake proning: Its role and relevance in the COVID-19 pandemic
The advent of the COVID-19 pandemic has put a significant strain on the health care systems and critical care services across several countries, including the United States. Amidst this, several concerted efforts to reduce the need for mechanical ventilation has resulted in the emergence of awake proning as a strategy to improve oxygenation, which has been instituted in critical care units, in-patient settings, as well as in EDs. Although the evidence on this strategy has been vastly limited to case series and observational studies, several societies have incorporated awake proning as an initial management strategy in hypoxemic respiratory failure within their clinical guidelines (Chalmers JD, et al. Eur Respir J. 2021;57:2100048; Koeckerling D, et al. Thorax. 2020;75:833-4) and consensus statements (Nasa P, et al. Crit Care. 2021;25:106).
Physiological benefits of awake proning include improvement in ventilation-perfusion matching secondary to relative increase in ventilation in dorsal nondependent areas in the setting of higher density of perfusion within these units, thus reducing shunt and, hence, improving oxygenation. Other physiological mechanisms include homogenization of transpulmonary pressures, reduction of ventilator-induced lung injury (VILI) or patient self-inflicted lung injury (P-SILI), and possibly lung injury from pendelluft (Telias I, et al. JAMA. 2020;323[22]:2265-67).
A recent meta-trial involving randomized controlled trials done across six countries compared prone positioning with standard care in patients with hypoxemic respiratory failure (defined as SpO2/ FiO2 < 315 and on high flow oxygen therapy) showed a reduced incidence of treatment failure and need for intubation without any signal of harm; although no mortality benefit was reported (Ehrmann S, et al. Lancet Respir Med. 2021 Aug 20;S2213-2600(21)00356-8). The number needed to treat to prevent one intubation was 14. While promising and reinforcing the safety of this relatively easy maneuver, several questions remain—which patients would benefit the most? Can it be applied within general wards safely? Does institution of awake proning delay intubation rates with consequent worse outcomes? Several ongoing (NCT 04402879) and completed studies (NCT 04383613 and NCT 04350723) may shed light on these important questions (Weatherald J, et al. Lancet Respir Med. 2021 Aug 20;S2213-2600[21]00368-4).
Sujith Cherian, MD, FCCP: Steering Committee Member
Thoughts on becoming CHEST President
I am honored to have the privilege of serving as the 84th President of the American College of Chest Physicians. When I attended my first CHEST meeting, I sat in the opening plenary session with thousands of other members, never imagining that I would have the opportunity to lead the organization just two decades later. And while I don’t recall many sessions from that meeting, I vividly remember the way it made an emotional impact. I never felt like one of a drove of nameless learners; both faculty and staff made it a collegial experience, much like attending pulmonary grand rounds at my own institution. Speakers would stay after their presentations to answer questions from even the most junior members. Leadership made themselves available over coffee or in the hallways between sessions. And that experience was the first of a great many memorable interactions I have had with CHEST.

CHEST has meant a great deal to me personally; it served as my first professional home away from home. I had the opportunity to grow in a number of different areas through my service to CHEST, in ways that I would not have been able to do easily at my own institution. I’ve worked with incredible staff and volunteers in my service on a number of our committees, including the Council of NetWorks, the Training and Transitions Committee, the Education Committee, and the Program Committee, to name a few. While I’ve had a chance to learn what role each of these component parts of the College serves during my tenure on those committees, it wasn’t until far more recently that I better understood the role of the President. Before I get into what I’d like to achieve during my year as President, I’d like to briefly review what that role entails.
Contrary to popular belief, the President does not set the organizational goals for CHEST; those are set by the Board of Regents. While I will have the privilege of running the Board meetings, it is the seventeen incredibly talented folks who serve as voting members of the Board that set the College’s direction. Once the organizational goals are set, it is our committees that take charge of designing and implementing plans to work toward those goals. Concomitantly, Dr. Robert Musacchio (CHEST chief executive officer and executive vice president) meets with his own executive leadership team to design a structure that lets the CHEST staff work, both on their own and in tandem with our members, to achieve these goals. One of the President’s main roles, as I see it, is to serve as a liaison. When the Board makes decisions that affect the membership, it will be my job to communicate changes and why they are being made. When our members have challenges that the College might be able to help solve, it is my role to work with the Board and the CEO to see what we can do about them. And when there is need to interface with other organizations, the President (or their designee) can speak on behalf of the College in those interactions.
In the context of those duties, what are the things that I would like to accomplish during my tenure as CHEST president? First, I want to spend more time with our committees and you, our members. CHEST is a member-focused organization; I believe that this is the main thing that sets our professional society apart from its sister societies. I have always found CHEST to be very collegial and welcoming. But I am aware that some of our members haven’t always found it accessible. And I get that; our structure is complex. That’s the reason I provided a description of my role, and the reason that I intend to spend time making CHEST more accessible to all of you. We’ve already developed dedicated social media channels for a number of our NetWorks in order to make you all more aware of their activities. In the coming year, I’ll provide regular updates to membership about ongoing CHEST activities. I’ll work to provide more member awareness of what role each of our committees plays in forwarding the College’s goals. And I’ll provide you with more information about the type of qualifications that each committee seeks in its nominees, in an effort to encourage you to run for a leadership position that best suits your interests and skill set.
While improving our members’ understanding of the inner workings at CHEST will help each of you better see how the College can meet your needs, my hope is that this increase in organizational accessibility will motivate each of you to engage more actively with us. This is my second goal as President. For some of you, that engagement may take the form of joining our Twitter chats; for others, it could mean attending one of our live learning courses in Chicago for the first time. But I hope that some of you will consider submitting session proposals to our annual meeting for the first time, or running for an available leadership position within the College when nominations open in the Spring.
As our organization grows (now almost twenty thousand members strong!), I want to provide a second home for all our members, spanning the range from medical students to full professors, from lifelong academic physicians to those just starting out in community practices, from busy clinicians to physician scientists, and including all members of the healthcare team. Although the makeup of our volunteer leadership is becoming more representative of the full breadth of our membership, we are not fully there yet. Until we get to that intended target, I would like to ask each of you to reach out to me with any thoughts about how CHEST can better meet your professional needs. Creating greater access to leadership to let each of your opinions be heard is my third goal as President of CHEST. I’ll provide more details about how I’m hoping to achieve this in the coming months.
The world has been a crazy place over the last eighteen months, filled with challenges that we could never have foreseen even a year prior. Our members have been on the front lines of the pandemic; in addition to the professional stresses related to caring for innumerable critically ill patients, many of us have suffered personal losses. Although none of us knows what 2022 holds, I look forward to a brighter future, knowing that regardless of what the coming year brings, we will face it together.
I am honored to have the privilege of serving as the 84th President of the American College of Chest Physicians. When I attended my first CHEST meeting, I sat in the opening plenary session with thousands of other members, never imagining that I would have the opportunity to lead the organization just two decades later. And while I don’t recall many sessions from that meeting, I vividly remember the way it made an emotional impact. I never felt like one of a drove of nameless learners; both faculty and staff made it a collegial experience, much like attending pulmonary grand rounds at my own institution. Speakers would stay after their presentations to answer questions from even the most junior members. Leadership made themselves available over coffee or in the hallways between sessions. And that experience was the first of a great many memorable interactions I have had with CHEST.
CHEST has meant a great deal to me personally; it served as my first professional home away from home. I had the opportunity to grow in a number of different areas through my service to CHEST, in ways that I would not have been able to do easily at my own institution. I’ve worked with incredible staff and volunteers in my service on a number of our committees, including the Council of NetWorks, the Training and Transitions Committee, the Education Committee, and the Program Committee, to name a few. While I’ve had a chance to learn what role each of these component parts of the College serves during my tenure on those committees, it wasn’t until far more recently that I better understood the role of the President. Before I get into what I’d like to achieve during my year as President, I’d like to briefly review what that role entails.
Contrary to popular belief, the President does not set the organizational goals for CHEST; those are set by the Board of Regents. While I will have the privilege of running the Board meetings, it is the seventeen incredibly talented folks who serve as voting members of the Board that set the College’s direction. Once the organizational goals are set, it is our committees that take charge of designing and implementing plans to work toward those goals. Concomitantly, Dr. Robert Musacchio (CHEST chief executive officer and executive vice president) meets with his own executive leadership team to design a structure that lets the CHEST staff work, both on their own and in tandem with our members, to achieve these goals. One of the President’s main roles, as I see it, is to serve as a liaison. When the Board makes decisions that affect the membership, it will be my job to communicate changes and why they are being made. When our members have challenges that the College might be able to help solve, it is my role to work with the Board and the CEO to see what we can do about them. And when there is need to interface with other organizations, the President (or their designee) can speak on behalf of the College in those interactions.
In the context of those duties, what are the things that I would like to accomplish during my tenure as CHEST president? First, I want to spend more time with our committees and you, our members. CHEST is a member-focused organization; I believe that this is the main thing that sets our professional society apart from its sister societies. I have always found CHEST to be very collegial and welcoming. But I am aware that some of our members haven’t always found it accessible. And I get that; our structure is complex. That’s the reason I provided a description of my role, and the reason that I intend to spend time making CHEST more accessible to all of you. We’ve already developed dedicated social media channels for a number of our NetWorks in order to make you all more aware of their activities. In the coming year, I’ll provide regular updates to membership about ongoing CHEST activities. I’ll work to provide more member awareness of what role each of our committees plays in forwarding the College’s goals. And I’ll provide you with more information about the type of qualifications that each committee seeks in its nominees, in an effort to encourage you to run for a leadership position that best suits your interests and skill set.
While improving our members’ understanding of the inner workings at CHEST will help each of you better see how the College can meet your needs, my hope is that this increase in organizational accessibility will motivate each of you to engage more actively with us. This is my second goal as President. For some of you, that engagement may take the form of joining our Twitter chats; for others, it could mean attending one of our live learning courses in Chicago for the first time. But I hope that some of you will consider submitting session proposals to our annual meeting for the first time, or running for an available leadership position within the College when nominations open in the Spring.
As our organization grows (now almost twenty thousand members strong!), I want to provide a second home for all our members, spanning the range from medical students to full professors, from lifelong academic physicians to those just starting out in community practices, from busy clinicians to physician scientists, and including all members of the healthcare team. Although the makeup of our volunteer leadership is becoming more representative of the full breadth of our membership, we are not fully there yet. Until we get to that intended target, I would like to ask each of you to reach out to me with any thoughts about how CHEST can better meet your professional needs. Creating greater access to leadership to let each of your opinions be heard is my third goal as President of CHEST. I’ll provide more details about how I’m hoping to achieve this in the coming months.
The world has been a crazy place over the last eighteen months, filled with challenges that we could never have foreseen even a year prior. Our members have been on the front lines of the pandemic; in addition to the professional stresses related to caring for innumerable critically ill patients, many of us have suffered personal losses. Although none of us knows what 2022 holds, I look forward to a brighter future, knowing that regardless of what the coming year brings, we will face it together.
I am honored to have the privilege of serving as the 84th President of the American College of Chest Physicians. When I attended my first CHEST meeting, I sat in the opening plenary session with thousands of other members, never imagining that I would have the opportunity to lead the organization just two decades later. And while I don’t recall many sessions from that meeting, I vividly remember the way it made an emotional impact. I never felt like one of a drove of nameless learners; both faculty and staff made it a collegial experience, much like attending pulmonary grand rounds at my own institution. Speakers would stay after their presentations to answer questions from even the most junior members. Leadership made themselves available over coffee or in the hallways between sessions. And that experience was the first of a great many memorable interactions I have had with CHEST.
CHEST has meant a great deal to me personally; it served as my first professional home away from home. I had the opportunity to grow in a number of different areas through my service to CHEST, in ways that I would not have been able to do easily at my own institution. I’ve worked with incredible staff and volunteers in my service on a number of our committees, including the Council of NetWorks, the Training and Transitions Committee, the Education Committee, and the Program Committee, to name a few. While I’ve had a chance to learn what role each of these component parts of the College serves during my tenure on those committees, it wasn’t until far more recently that I better understood the role of the President. Before I get into what I’d like to achieve during my year as President, I’d like to briefly review what that role entails.
Contrary to popular belief, the President does not set the organizational goals for CHEST; those are set by the Board of Regents. While I will have the privilege of running the Board meetings, it is the seventeen incredibly talented folks who serve as voting members of the Board that set the College’s direction. Once the organizational goals are set, it is our committees that take charge of designing and implementing plans to work toward those goals. Concomitantly, Dr. Robert Musacchio (CHEST chief executive officer and executive vice president) meets with his own executive leadership team to design a structure that lets the CHEST staff work, both on their own and in tandem with our members, to achieve these goals. One of the President’s main roles, as I see it, is to serve as a liaison. When the Board makes decisions that affect the membership, it will be my job to communicate changes and why they are being made. When our members have challenges that the College might be able to help solve, it is my role to work with the Board and the CEO to see what we can do about them. And when there is need to interface with other organizations, the President (or their designee) can speak on behalf of the College in those interactions.
In the context of those duties, what are the things that I would like to accomplish during my tenure as CHEST president? First, I want to spend more time with our committees and you, our members. CHEST is a member-focused organization; I believe that this is the main thing that sets our professional society apart from its sister societies. I have always found CHEST to be very collegial and welcoming. But I am aware that some of our members haven’t always found it accessible. And I get that; our structure is complex. That’s the reason I provided a description of my role, and the reason that I intend to spend time making CHEST more accessible to all of you. We’ve already developed dedicated social media channels for a number of our NetWorks in order to make you all more aware of their activities. In the coming year, I’ll provide regular updates to membership about ongoing CHEST activities. I’ll work to provide more member awareness of what role each of our committees plays in forwarding the College’s goals. And I’ll provide you with more information about the type of qualifications that each committee seeks in its nominees, in an effort to encourage you to run for a leadership position that best suits your interests and skill set.
While improving our members’ understanding of the inner workings at CHEST will help each of you better see how the College can meet your needs, my hope is that this increase in organizational accessibility will motivate each of you to engage more actively with us. This is my second goal as President. For some of you, that engagement may take the form of joining our Twitter chats; for others, it could mean attending one of our live learning courses in Chicago for the first time. But I hope that some of you will consider submitting session proposals to our annual meeting for the first time, or running for an available leadership position within the College when nominations open in the Spring.
As our organization grows (now almost twenty thousand members strong!), I want to provide a second home for all our members, spanning the range from medical students to full professors, from lifelong academic physicians to those just starting out in community practices, from busy clinicians to physician scientists, and including all members of the healthcare team. Although the makeup of our volunteer leadership is becoming more representative of the full breadth of our membership, we are not fully there yet. Until we get to that intended target, I would like to ask each of you to reach out to me with any thoughts about how CHEST can better meet your professional needs. Creating greater access to leadership to let each of your opinions be heard is my third goal as President of CHEST. I’ll provide more details about how I’m hoping to achieve this in the coming months.
The world has been a crazy place over the last eighteen months, filled with challenges that we could never have foreseen even a year prior. Our members have been on the front lines of the pandemic; in addition to the professional stresses related to caring for innumerable critically ill patients, many of us have suffered personal losses. Although none of us knows what 2022 holds, I look forward to a brighter future, knowing that regardless of what the coming year brings, we will face it together.
TTM2: Is there anything therapeutic about therapeutic hypothermia?
Animal and human models of the effects of therapeutic hypothermia, now called targeted temperature management (TTM), began to surface in the late 1980s. The first randomized clinical trial employing TTM as a neuroprotective strategy following cardiac arrest did not appear until the early 2000s. When compared with normothermia, the HACA trial (Holzer M, et al. N Engl J Med. 2002;346[8]:549-56) demonstrated a 14% reduction in mortality and improved neurologic outcomes following out of hospital cardiac arrest (OHCA) due to ventricular fibrillation (VF) or ventricular tachycardia (VT) when maintaining body temperature between 32˚C and 34˚C post-arrest. Following the results of this trial, TTM in comatose patients following cardiac arrest was recommended by international guidelines and became the standard of care. It was not until the publication of the TTM1 trial (Nielsen N, et al. N Engl J Med. 2013;369[23]:2197-206) about a decade later, that serious questions regarding the efficacy of TTM were raised. The TTM1 trial showed no difference in mortality or neurologic outcomes when comparing TTM at 33˚C vs 36˚C for OHCA. The results of this trial heralded widespread practice change, with many abandoning deep cooling, and often active cooling measures, in favor of fever avoidance. The HYPERION trial (Lascarrou J, et al. N Engl J Med. 2019;381:2327-37) came next, comparing TTM at 33˚C to normothermia (<37.5˚C) for cardiac arrest with non-hockable rhythm. This study did not identify any improvement in mortality with utilization of TTM but suggested it may be associated with more favorable neurologic outcomes, albeit in a small number of patients.

The TTM2 trial (Dankiewicz J, et al. N Engl J Med. 2021;384:2283-94) is the most recent trial to address the question of TTM post-cardiac arrest. The TTM2 trial was an international, randomized controlled superiority trial of TTM at 33˚C vs normothermia (≤37.8˚C) for patients with coma following OHCA with any initial rhythm. It was conducted by the same group as the TTM1 trial and, to date, represents the largest (N= 1,850) and most robust trial conducted in this area. The trial spanned 61 institutions across 14 countries and had nearly complete follow-up at 6 months. Once again, there was no significant difference in all-cause mortality at 6 months in the TTM group when compared with the normothermia group. Equally important, there were no differences observed in secondary outcomes, including functional neurologic status and health-related quality of life at 6 months. With the results of the TTM1 and TTM2 trials failing to show any neurologic or mortality benefit to TTM, we are left wondering, is there anything therapeutic about “therapeutic hypothermia”?
Both the 2020 American Heart Association (AHA) and 2021 European Resuscitation Council (ERC) guidelines predate this trial; they recommend cooling any OHCA or in-hospital cardiac arrest (IHCA) patient who remains unresponsive after return of spontaneous circulation (ROSC) regardless of initial rhythm. They further suggest maintaining a target temperature between 32˚C and 36˚C for at least 24 hours, followed by avoidance of fever (>37.7˚C) for at least 72 hours after ROSC in patients who remain comatose. While it will be interesting to see what future iterations of the guidelines recommend, the results from the TTM1 and TTM2 trials support a shift in clinical practice away from TTM and toward more active fever avoidance. Additionally, careful review of adverse events in the TTM2 trial suggests that induced hypothermia is not without risk of harm. When compared with the normothermia group in the TTM2 trial, the hypothermia group experienced higher rates of arrhythmias with hemodynamic instability (16% vs 24%), increased exposure to sedation, increased use of neuromuscular blockade, and increased duration of mechanical ventilation.
While the results of the TTM2 trial move the needle away from therapeutic hypothermia for OHCA patients, there is some nuance that warrants further discussion. First, the initial HACA trial, upon which the standard of TTM was based, included only patients with an initial shockable rhythm (VT/VF). Inherently, the etiology of these arrests is likely to be cardiac and more reversible in nature. Most subsequent landmark trials on TTM, including the TTM2 trial, have included OHCA patients with both shockable and nonshockable initial rhythms. Still, the majority of patients in the TTM2 trial had an initial shockable rhythm on presentation (72% hypothermia vs 75% normothermia). This may limit broad generalizability of study findings as an increasing number of OHCA patients are presenting with nonshockable initial rhythms. Next, it is well known that bystander CPR improves outcomes following OHCA. Impressively, over 75% of patients in both groups in the TTM2 trial received bystander CPR compared with an average of 46% of arrest patients in the US according to AHA data. Finally, like most of its predecessors, the TTM2 trial only included OHCA patients meaning no real conclusions can be drawn regarding application of TTM to IHCA patients. Of the major trials to date, only the HYPERION trial included IHCA patients – representing about 25% of the study population. Thus, the utility of TTM in the setting of IHCA remains largely unknown.
Taken in summation, recent trials, including TTM2, suggest that fever-avoidance post-cardiac arrest is likely the best option for improving mortality and neurologic outcomes while mitigating risk to the patient. We must remain vigilant in our enforcement of normothermia though as worse neurologic outcomes have been observed with hyperthermia in the early post-arrest period (Zeiner A, et al. Arch Intern Med. 2001;161[16]:2007-12). A key takeaway from recent trials is that maintaining normothermia without active temperature control measures is likely to be difficult to achieve. A criticism of the HYPERION trial was that a “substantial proportion” of patients in the normothermia group had temperatures above 38˚C. Similarly, 10% to15% of patients in the TTM2 trial had body temperatures above 37.7˚C, 40 to 72 hours after randomization and, ultimately, 46% of patients in the normothermia group required cooling with a temperature management device. Thus, we can conclude that maintenance of strict normothermia will likely continue to require active control with a temperature management device.
Despite an increasing number of well conducted studies in this area, there are several questions that remain unanswered. The first is whether cooling patients even earlier post-arrest is felt to increase the likelihood of survival with improved neurologic outcomes. Like HACA and HYPERION, the rate of cooling in the TTM2 trial was relatively quick with a time to randomization after onset of cardiac arrest of about 2 hours in both groups and a median time from intervention until reaching target temperature of 3 hours. While some retrospective data suggest ultra-early cooling may be beneficial, neither induction of therapeutic hypothermia during OHCA using a rapid infusion of cold saline (Bernard SA, et al. Circulation. 2016;134[11]:797-805) nor transnasal evaporative cooling in the pre-hospital setting (Nordeberg P, et al. JAMA. 2019;321(17):1677-85) has shown improvement in survival with good neurologic outcomes. Next, if we are going to continue TTM, the TTM2 trial does not provide guidance on optimal duration of cooling. Although the current guidelines are to cool for at least 24 hours after ROSC, it is unclear for how long strict temperature control should be continued. The currently enrolling ICECAP study aims to further elucidate the optimal duration of TTM for OHCA patients with both shockable and non-shockable initial rhythms.
Post-cardiac arrest management continues to be a significant area of interest in clinical research and for good reason. Although steady improvement has occurred with regards to survival and neurologic function for IHCA, of the approximately 350,000 nontraumatic OHCA that occur in a year in the United States, only about 10.2% of those patients will survive their initial hospitalization, and only about 8.2% of those who survive will have good functional status (American Heart Association. Circulation. 2020;142(suppl 2):S366-S468). There remains much room for continued study and improvement.
Dr. Capp is a Pulmonary and Critical Care Fellow; and Dr. Pendleton is Assistant Professor of Medicine; Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine; University of Minnesota, Minneapolis, Minnesota.
Animal and human models of the effects of therapeutic hypothermia, now called targeted temperature management (TTM), began to surface in the late 1980s. The first randomized clinical trial employing TTM as a neuroprotective strategy following cardiac arrest did not appear until the early 2000s. When compared with normothermia, the HACA trial (Holzer M, et al. N Engl J Med. 2002;346[8]:549-56) demonstrated a 14% reduction in mortality and improved neurologic outcomes following out of hospital cardiac arrest (OHCA) due to ventricular fibrillation (VF) or ventricular tachycardia (VT) when maintaining body temperature between 32˚C and 34˚C post-arrest. Following the results of this trial, TTM in comatose patients following cardiac arrest was recommended by international guidelines and became the standard of care. It was not until the publication of the TTM1 trial (Nielsen N, et al. N Engl J Med. 2013;369[23]:2197-206) about a decade later, that serious questions regarding the efficacy of TTM were raised. The TTM1 trial showed no difference in mortality or neurologic outcomes when comparing TTM at 33˚C vs 36˚C for OHCA. The results of this trial heralded widespread practice change, with many abandoning deep cooling, and often active cooling measures, in favor of fever avoidance. The HYPERION trial (Lascarrou J, et al. N Engl J Med. 2019;381:2327-37) came next, comparing TTM at 33˚C to normothermia (<37.5˚C) for cardiac arrest with non-hockable rhythm. This study did not identify any improvement in mortality with utilization of TTM but suggested it may be associated with more favorable neurologic outcomes, albeit in a small number of patients.
The TTM2 trial (Dankiewicz J, et al. N Engl J Med. 2021;384:2283-94) is the most recent trial to address the question of TTM post-cardiac arrest. The TTM2 trial was an international, randomized controlled superiority trial of TTM at 33˚C vs normothermia (≤37.8˚C) for patients with coma following OHCA with any initial rhythm. It was conducted by the same group as the TTM1 trial and, to date, represents the largest (N= 1,850) and most robust trial conducted in this area. The trial spanned 61 institutions across 14 countries and had nearly complete follow-up at 6 months. Once again, there was no significant difference in all-cause mortality at 6 months in the TTM group when compared with the normothermia group. Equally important, there were no differences observed in secondary outcomes, including functional neurologic status and health-related quality of life at 6 months. With the results of the TTM1 and TTM2 trials failing to show any neurologic or mortality benefit to TTM, we are left wondering, is there anything therapeutic about “therapeutic hypothermia”?
Both the 2020 American Heart Association (AHA) and 2021 European Resuscitation Council (ERC) guidelines predate this trial; they recommend cooling any OHCA or in-hospital cardiac arrest (IHCA) patient who remains unresponsive after return of spontaneous circulation (ROSC) regardless of initial rhythm. They further suggest maintaining a target temperature between 32˚C and 36˚C for at least 24 hours, followed by avoidance of fever (>37.7˚C) for at least 72 hours after ROSC in patients who remain comatose. While it will be interesting to see what future iterations of the guidelines recommend, the results from the TTM1 and TTM2 trials support a shift in clinical practice away from TTM and toward more active fever avoidance. Additionally, careful review of adverse events in the TTM2 trial suggests that induced hypothermia is not without risk of harm. When compared with the normothermia group in the TTM2 trial, the hypothermia group experienced higher rates of arrhythmias with hemodynamic instability (16% vs 24%), increased exposure to sedation, increased use of neuromuscular blockade, and increased duration of mechanical ventilation.
While the results of the TTM2 trial move the needle away from therapeutic hypothermia for OHCA patients, there is some nuance that warrants further discussion. First, the initial HACA trial, upon which the standard of TTM was based, included only patients with an initial shockable rhythm (VT/VF). Inherently, the etiology of these arrests is likely to be cardiac and more reversible in nature. Most subsequent landmark trials on TTM, including the TTM2 trial, have included OHCA patients with both shockable and nonshockable initial rhythms. Still, the majority of patients in the TTM2 trial had an initial shockable rhythm on presentation (72% hypothermia vs 75% normothermia). This may limit broad generalizability of study findings as an increasing number of OHCA patients are presenting with nonshockable initial rhythms. Next, it is well known that bystander CPR improves outcomes following OHCA. Impressively, over 75% of patients in both groups in the TTM2 trial received bystander CPR compared with an average of 46% of arrest patients in the US according to AHA data. Finally, like most of its predecessors, the TTM2 trial only included OHCA patients meaning no real conclusions can be drawn regarding application of TTM to IHCA patients. Of the major trials to date, only the HYPERION trial included IHCA patients – representing about 25% of the study population. Thus, the utility of TTM in the setting of IHCA remains largely unknown.
Taken in summation, recent trials, including TTM2, suggest that fever-avoidance post-cardiac arrest is likely the best option for improving mortality and neurologic outcomes while mitigating risk to the patient. We must remain vigilant in our enforcement of normothermia though as worse neurologic outcomes have been observed with hyperthermia in the early post-arrest period (Zeiner A, et al. Arch Intern Med. 2001;161[16]:2007-12). A key takeaway from recent trials is that maintaining normothermia without active temperature control measures is likely to be difficult to achieve. A criticism of the HYPERION trial was that a “substantial proportion” of patients in the normothermia group had temperatures above 38˚C. Similarly, 10% to15% of patients in the TTM2 trial had body temperatures above 37.7˚C, 40 to 72 hours after randomization and, ultimately, 46% of patients in the normothermia group required cooling with a temperature management device. Thus, we can conclude that maintenance of strict normothermia will likely continue to require active control with a temperature management device.
Despite an increasing number of well conducted studies in this area, there are several questions that remain unanswered. The first is whether cooling patients even earlier post-arrest is felt to increase the likelihood of survival with improved neurologic outcomes. Like HACA and HYPERION, the rate of cooling in the TTM2 trial was relatively quick with a time to randomization after onset of cardiac arrest of about 2 hours in both groups and a median time from intervention until reaching target temperature of 3 hours. While some retrospective data suggest ultra-early cooling may be beneficial, neither induction of therapeutic hypothermia during OHCA using a rapid infusion of cold saline (Bernard SA, et al. Circulation. 2016;134[11]:797-805) nor transnasal evaporative cooling in the pre-hospital setting (Nordeberg P, et al. JAMA. 2019;321(17):1677-85) has shown improvement in survival with good neurologic outcomes. Next, if we are going to continue TTM, the TTM2 trial does not provide guidance on optimal duration of cooling. Although the current guidelines are to cool for at least 24 hours after ROSC, it is unclear for how long strict temperature control should be continued. The currently enrolling ICECAP study aims to further elucidate the optimal duration of TTM for OHCA patients with both shockable and non-shockable initial rhythms.
Post-cardiac arrest management continues to be a significant area of interest in clinical research and for good reason. Although steady improvement has occurred with regards to survival and neurologic function for IHCA, of the approximately 350,000 nontraumatic OHCA that occur in a year in the United States, only about 10.2% of those patients will survive their initial hospitalization, and only about 8.2% of those who survive will have good functional status (American Heart Association. Circulation. 2020;142(suppl 2):S366-S468). There remains much room for continued study and improvement.
Dr. Capp is a Pulmonary and Critical Care Fellow; and Dr. Pendleton is Assistant Professor of Medicine; Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine; University of Minnesota, Minneapolis, Minnesota.
Animal and human models of the effects of therapeutic hypothermia, now called targeted temperature management (TTM), began to surface in the late 1980s. The first randomized clinical trial employing TTM as a neuroprotective strategy following cardiac arrest did not appear until the early 2000s. When compared with normothermia, the HACA trial (Holzer M, et al. N Engl J Med. 2002;346[8]:549-56) demonstrated a 14% reduction in mortality and improved neurologic outcomes following out of hospital cardiac arrest (OHCA) due to ventricular fibrillation (VF) or ventricular tachycardia (VT) when maintaining body temperature between 32˚C and 34˚C post-arrest. Following the results of this trial, TTM in comatose patients following cardiac arrest was recommended by international guidelines and became the standard of care. It was not until the publication of the TTM1 trial (Nielsen N, et al. N Engl J Med. 2013;369[23]:2197-206) about a decade later, that serious questions regarding the efficacy of TTM were raised. The TTM1 trial showed no difference in mortality or neurologic outcomes when comparing TTM at 33˚C vs 36˚C for OHCA. The results of this trial heralded widespread practice change, with many abandoning deep cooling, and often active cooling measures, in favor of fever avoidance. The HYPERION trial (Lascarrou J, et al. N Engl J Med. 2019;381:2327-37) came next, comparing TTM at 33˚C to normothermia (<37.5˚C) for cardiac arrest with non-hockable rhythm. This study did not identify any improvement in mortality with utilization of TTM but suggested it may be associated with more favorable neurologic outcomes, albeit in a small number of patients.
The TTM2 trial (Dankiewicz J, et al. N Engl J Med. 2021;384:2283-94) is the most recent trial to address the question of TTM post-cardiac arrest. The TTM2 trial was an international, randomized controlled superiority trial of TTM at 33˚C vs normothermia (≤37.8˚C) for patients with coma following OHCA with any initial rhythm. It was conducted by the same group as the TTM1 trial and, to date, represents the largest (N= 1,850) and most robust trial conducted in this area. The trial spanned 61 institutions across 14 countries and had nearly complete follow-up at 6 months. Once again, there was no significant difference in all-cause mortality at 6 months in the TTM group when compared with the normothermia group. Equally important, there were no differences observed in secondary outcomes, including functional neurologic status and health-related quality of life at 6 months. With the results of the TTM1 and TTM2 trials failing to show any neurologic or mortality benefit to TTM, we are left wondering, is there anything therapeutic about “therapeutic hypothermia”?
Both the 2020 American Heart Association (AHA) and 2021 European Resuscitation Council (ERC) guidelines predate this trial; they recommend cooling any OHCA or in-hospital cardiac arrest (IHCA) patient who remains unresponsive after return of spontaneous circulation (ROSC) regardless of initial rhythm. They further suggest maintaining a target temperature between 32˚C and 36˚C for at least 24 hours, followed by avoidance of fever (>37.7˚C) for at least 72 hours after ROSC in patients who remain comatose. While it will be interesting to see what future iterations of the guidelines recommend, the results from the TTM1 and TTM2 trials support a shift in clinical practice away from TTM and toward more active fever avoidance. Additionally, careful review of adverse events in the TTM2 trial suggests that induced hypothermia is not without risk of harm. When compared with the normothermia group in the TTM2 trial, the hypothermia group experienced higher rates of arrhythmias with hemodynamic instability (16% vs 24%), increased exposure to sedation, increased use of neuromuscular blockade, and increased duration of mechanical ventilation.
While the results of the TTM2 trial move the needle away from therapeutic hypothermia for OHCA patients, there is some nuance that warrants further discussion. First, the initial HACA trial, upon which the standard of TTM was based, included only patients with an initial shockable rhythm (VT/VF). Inherently, the etiology of these arrests is likely to be cardiac and more reversible in nature. Most subsequent landmark trials on TTM, including the TTM2 trial, have included OHCA patients with both shockable and nonshockable initial rhythms. Still, the majority of patients in the TTM2 trial had an initial shockable rhythm on presentation (72% hypothermia vs 75% normothermia). This may limit broad generalizability of study findings as an increasing number of OHCA patients are presenting with nonshockable initial rhythms. Next, it is well known that bystander CPR improves outcomes following OHCA. Impressively, over 75% of patients in both groups in the TTM2 trial received bystander CPR compared with an average of 46% of arrest patients in the US according to AHA data. Finally, like most of its predecessors, the TTM2 trial only included OHCA patients meaning no real conclusions can be drawn regarding application of TTM to IHCA patients. Of the major trials to date, only the HYPERION trial included IHCA patients – representing about 25% of the study population. Thus, the utility of TTM in the setting of IHCA remains largely unknown.
Taken in summation, recent trials, including TTM2, suggest that fever-avoidance post-cardiac arrest is likely the best option for improving mortality and neurologic outcomes while mitigating risk to the patient. We must remain vigilant in our enforcement of normothermia though as worse neurologic outcomes have been observed with hyperthermia in the early post-arrest period (Zeiner A, et al. Arch Intern Med. 2001;161[16]:2007-12). A key takeaway from recent trials is that maintaining normothermia without active temperature control measures is likely to be difficult to achieve. A criticism of the HYPERION trial was that a “substantial proportion” of patients in the normothermia group had temperatures above 38˚C. Similarly, 10% to15% of patients in the TTM2 trial had body temperatures above 37.7˚C, 40 to 72 hours after randomization and, ultimately, 46% of patients in the normothermia group required cooling with a temperature management device. Thus, we can conclude that maintenance of strict normothermia will likely continue to require active control with a temperature management device.
Despite an increasing number of well conducted studies in this area, there are several questions that remain unanswered. The first is whether cooling patients even earlier post-arrest is felt to increase the likelihood of survival with improved neurologic outcomes. Like HACA and HYPERION, the rate of cooling in the TTM2 trial was relatively quick with a time to randomization after onset of cardiac arrest of about 2 hours in both groups and a median time from intervention until reaching target temperature of 3 hours. While some retrospective data suggest ultra-early cooling may be beneficial, neither induction of therapeutic hypothermia during OHCA using a rapid infusion of cold saline (Bernard SA, et al. Circulation. 2016;134[11]:797-805) nor transnasal evaporative cooling in the pre-hospital setting (Nordeberg P, et al. JAMA. 2019;321(17):1677-85) has shown improvement in survival with good neurologic outcomes. Next, if we are going to continue TTM, the TTM2 trial does not provide guidance on optimal duration of cooling. Although the current guidelines are to cool for at least 24 hours after ROSC, it is unclear for how long strict temperature control should be continued. The currently enrolling ICECAP study aims to further elucidate the optimal duration of TTM for OHCA patients with both shockable and non-shockable initial rhythms.
Post-cardiac arrest management continues to be a significant area of interest in clinical research and for good reason. Although steady improvement has occurred with regards to survival and neurologic function for IHCA, of the approximately 350,000 nontraumatic OHCA that occur in a year in the United States, only about 10.2% of those patients will survive their initial hospitalization, and only about 8.2% of those who survive will have good functional status (American Heart Association. Circulation. 2020;142(suppl 2):S366-S468). There remains much room for continued study and improvement.
Dr. Capp is a Pulmonary and Critical Care Fellow; and Dr. Pendleton is Assistant Professor of Medicine; Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine; University of Minnesota, Minneapolis, Minnesota.
Lung transplantation for patients with severe COVID-19
As of September 2021, over 222 million people worldwide (WHO, 2021) and 40 million Americans (CDC, 2021) have been infected with the novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). The total number of infections in the United States began climbing again this summer with the persistence of vaccine reluctance among a significant proportion of the population and the emergence of the much more infectious B.1.617.2 (Delta) variant. While the clinical illness caused by the SARS-CoV-2 virus, referred to as the Coronavirus disease 2019 (COVID-19), is mostly mild, approximately 10% of cases develop acute respiratory distress syndrome (ARDS) (Remuzzi A, et al. Lancet. 2020;395[10231]:1225-8). A small but substantial proportion of patients with COVID-19 ARDS fails to respond to the various supportive measures and requires extracorporeal membrane oxygenation (ECMO) support. The overarching goal of the different support strategies, including ECMO, is to provide time for the lungs to recover from ARDS. ECMO has the theoretical advantage over other strategies in facilitating recovery by allowing the injured lungs to ‘rest’ as the oxygenation and ventilation needs are met in an extracorporeal fashion. Regardless, a small number of patients with COVID-19 ARDS will not recover enough pulmonary function to allow them to be weaned from the various respiratory support strategies.
For patients with irreversible lung injury, lung transplantation (LT) is a potential consideration. Earlier in the pandemic, older patients with significant comorbid illnesses were more vulnerable to severe COVID-19, often precluding consideration for transplantation. However, the emergence of the Delta variant may have altered this dynamic via a substantial increase in the incidence of COVID-19 ARDS among younger and healthier patients. A handful of patients with COVID-19 ARDS have already had successful transplantation. However, the overall number is still small (Bharat A, et al. Sci Translat Med. 2020 Dec 16;12[574]:eabe4282. doi: 10.1126/scitranslmed.abe4282. Epub 2020 Nov 30; and Hawkins R, et al. Transplantation. 2021;6:1381-7), and there is a lack of long-term outcomes data among these patients.
There is currently little guidance regarding criteria for patient selection and consideration for LT among patients with COVID-19 ARDS. Given that the SARS-CoV-2 virus is a novel pathogen that leads to an illness that is unique from other forms of viral pneumonia, specific considerations regarding LT should be made among these patients. In the current article, we discuss some of the pertinent issues related to the consideration of LT among patients with COVID-19 ARDS.
The timing for considering LT is one of the most important aspects. First, patients with COVID-19 ARDS must not be actively infected at the time of transplantation consideration. It has been suggested that LT should only be considered in patients with two separate negative polymerase chain reaction (PCR) test results for SARS-CoV-2 from bronchoalveolar lavage fluid 24 hours apart and at least 4 weeks after the onset of COVID-19 symptoms (Bharat A, et al. Sci Translat Med. 2020 Dec 16;12[574]:eabe4282. doi: 10.1126/scitranslmed.abe4282. Epub 2020 Nov 30). Among patients with persistently positive SARS-CoV-2 PCR 4 to 6 weeks after symptom onset, a negative viral culture from a bronchoalveolar lavage (BAL) can be used to confirm viral inactivity (Lang C, et al. Lancet Respir Med. 2020;8[10]:1057-60).
Despite the sparse data in this domain, there seems to be a consensus in the literature that LT could be considered once 4 to 6 weeks have elapsed since the onset of the respiratory failure (Cypel M, et al. Lancet Respir Med. 2020;8[10]:944-6). This timeline is felt to be long enough to alleviate the concerns regarding ongoing inflammatory processes that may be reversible while not so long to risk the development of non-pulmonary complications or severe debility that may become significant barriers to transplant candidacy. An exception may be made in patients with medically unmanageable complications such as recalcitrant bronchopleural fistulae in the background of fibrotic changes or right ventricular failure from severe pulmonary hypertension. Regardless, this timeline is borrowed from the approach to irreversible ARDS from other forms of viral pneumonia. It is not clear if it is appropriate to extrapolate past experience to COVID-19, which is a disease unlike any other seen during the LT era: a profound inflammatory phase mediated by a cytokine storm as the etiologic basis for the organ dysfunction, activation of coagulation pathways in pulmonary circulation leading to immunothrombosis contributing to the refractory hypoxemia, favorable effects of anticoagulants, diverse pulmonary physiologic phenotypes of ARDS, an increased risk of pleural complications, and utilization of novel anti-inflammatory therapies with consequent risks ofsecondary infections are all unique to COVID-19. A recent study found that patients requiring ECMO for COVID-19 ARDS took longer to recover lung function but had similar survival rates to patients on ECMO with other virus-induced ARDS (Raff LA, et al. Am J Surg. 2021;S0002-9610[21]00233-6. doi: 10.1016/j.amjsurg.2021.04.004. Online ahead of print).These data support pursuing a more conservative timeline for consideration of LT.
Determining the reversibility of pulmonary impairment in COVID-19 ARDS is another challenge. The nature of the pulmonary opacities should be assessed on CT scan imaging as close as possible to the time of LT consideration. Differentiating the extent of irreversible parenchymal scarring vs salvageability during acute illness can be challenging. The presence of extensive architectural distortion with or without bullous changes, while being the best indicator of irreversibility, may not be sensitive enough. The standard of care in such situations remains serial assessments, often weekly, by a dedicated multidisciplinary group. We have found it useful to augment the imaging data with pulmonary physiologic assessments, including the extent of ventilator and ECMO support as well as dynamic and static compliance trends. Improvement in physiologic data often precedes radiologic improvement. Nonetheless, an important area of future research is to identify objective markers for determining reversibility, which could include novel biomarkers in serum or bronchoalveolar lavage fluid.
When a determination is made regarding the irreversibility of pulmonary impairment, the LT evaluation should begin promptly. Pre-transplant deconditioning and debility is associated with worse post-transplant outcomes. In this regard, patients managed using an ambulatory ECMO strategy may have superior rehabilitation potential. Furthermore, an attempt should be made during the evaluation to wean sedation in order to facilitate discussions regarding the rigors of LT with the patient alongside present family members. An additional consideration, given the use of immunomodulatory medications for COVID-19 and prolonged intubation, is the dramatically increased risk of multi-drug resistant infections in this population; these must be aggressively managed for patients to remain eligible for LT.
The degree of pulmonary impairment and frequent colonization of the airways will likely dictate bilateral LT as the preferred strategy, although surgical feasibility may, at times, be the overriding determinant. Regardless of the type of transplant, certain unique aspects should be anticipated. The inflammatory responses during COVID-19 that often spill outside the confines of the pulmonary parenchyma, along with potentially frequent thoracic interventions prior to transplant, create significant technical challenges during the operation. Native pneumonectomy can take longer than usual leading to prolonged ischemic time, increased need for intra-operative blood products, and raised risk for primary graft dysfunction. All of these factors have a significant impact on early and late outcomes. Finally, the long-term immunologic consequences of severe infection from a novel virus remain unknown, and it is unclear if COVID-19 ARDS patients bridged to transplant will enjoy comparable survival. It is pertinent to acknowledge that the high-risk nature of such transplants is substantially accentuated due to several unique characteristics of the illness related to COVID-19.
The emergence of the COVID-19 pandemic has led to an increase in the number of urgent inpatient lung transplant consultations for refractory ARDS. While the basic principles of LT candidate selection should continue to guide us, the unique characteristics of this illness merit using a customized approach. There are few validated predictors to guide decision-making, and longitudinal assessments by a dedicated multidisciplinary group remain the best strategy. Finally, in the absence of systemic studies and lack of longitudinal outcomes data, there is an emergent need to establish consensus guidelines regarding the approach to LT consideration in these patients.
Dr. Quinn and Dr. Banga are with the Lung Transplant Program, Divisions of Pulmonary and Critical Care Medicine, University of Texas Southwestern Medical Center, Dallas.
As of September 2021, over 222 million people worldwide (WHO, 2021) and 40 million Americans (CDC, 2021) have been infected with the novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). The total number of infections in the United States began climbing again this summer with the persistence of vaccine reluctance among a significant proportion of the population and the emergence of the much more infectious B.1.617.2 (Delta) variant. While the clinical illness caused by the SARS-CoV-2 virus, referred to as the Coronavirus disease 2019 (COVID-19), is mostly mild, approximately 10% of cases develop acute respiratory distress syndrome (ARDS) (Remuzzi A, et al. Lancet. 2020;395[10231]:1225-8). A small but substantial proportion of patients with COVID-19 ARDS fails to respond to the various supportive measures and requires extracorporeal membrane oxygenation (ECMO) support. The overarching goal of the different support strategies, including ECMO, is to provide time for the lungs to recover from ARDS. ECMO has the theoretical advantage over other strategies in facilitating recovery by allowing the injured lungs to ‘rest’ as the oxygenation and ventilation needs are met in an extracorporeal fashion. Regardless, a small number of patients with COVID-19 ARDS will not recover enough pulmonary function to allow them to be weaned from the various respiratory support strategies.
For patients with irreversible lung injury, lung transplantation (LT) is a potential consideration. Earlier in the pandemic, older patients with significant comorbid illnesses were more vulnerable to severe COVID-19, often precluding consideration for transplantation. However, the emergence of the Delta variant may have altered this dynamic via a substantial increase in the incidence of COVID-19 ARDS among younger and healthier patients. A handful of patients with COVID-19 ARDS have already had successful transplantation. However, the overall number is still small (Bharat A, et al. Sci Translat Med. 2020 Dec 16;12[574]:eabe4282. doi: 10.1126/scitranslmed.abe4282. Epub 2020 Nov 30; and Hawkins R, et al. Transplantation. 2021;6:1381-7), and there is a lack of long-term outcomes data among these patients.
There is currently little guidance regarding criteria for patient selection and consideration for LT among patients with COVID-19 ARDS. Given that the SARS-CoV-2 virus is a novel pathogen that leads to an illness that is unique from other forms of viral pneumonia, specific considerations regarding LT should be made among these patients. In the current article, we discuss some of the pertinent issues related to the consideration of LT among patients with COVID-19 ARDS.
The timing for considering LT is one of the most important aspects. First, patients with COVID-19 ARDS must not be actively infected at the time of transplantation consideration. It has been suggested that LT should only be considered in patients with two separate negative polymerase chain reaction (PCR) test results for SARS-CoV-2 from bronchoalveolar lavage fluid 24 hours apart and at least 4 weeks after the onset of COVID-19 symptoms (Bharat A, et al. Sci Translat Med. 2020 Dec 16;12[574]:eabe4282. doi: 10.1126/scitranslmed.abe4282. Epub 2020 Nov 30). Among patients with persistently positive SARS-CoV-2 PCR 4 to 6 weeks after symptom onset, a negative viral culture from a bronchoalveolar lavage (BAL) can be used to confirm viral inactivity (Lang C, et al. Lancet Respir Med. 2020;8[10]:1057-60).
Despite the sparse data in this domain, there seems to be a consensus in the literature that LT could be considered once 4 to 6 weeks have elapsed since the onset of the respiratory failure (Cypel M, et al. Lancet Respir Med. 2020;8[10]:944-6). This timeline is felt to be long enough to alleviate the concerns regarding ongoing inflammatory processes that may be reversible while not so long to risk the development of non-pulmonary complications or severe debility that may become significant barriers to transplant candidacy. An exception may be made in patients with medically unmanageable complications such as recalcitrant bronchopleural fistulae in the background of fibrotic changes or right ventricular failure from severe pulmonary hypertension. Regardless, this timeline is borrowed from the approach to irreversible ARDS from other forms of viral pneumonia. It is not clear if it is appropriate to extrapolate past experience to COVID-19, which is a disease unlike any other seen during the LT era: a profound inflammatory phase mediated by a cytokine storm as the etiologic basis for the organ dysfunction, activation of coagulation pathways in pulmonary circulation leading to immunothrombosis contributing to the refractory hypoxemia, favorable effects of anticoagulants, diverse pulmonary physiologic phenotypes of ARDS, an increased risk of pleural complications, and utilization of novel anti-inflammatory therapies with consequent risks ofsecondary infections are all unique to COVID-19. A recent study found that patients requiring ECMO for COVID-19 ARDS took longer to recover lung function but had similar survival rates to patients on ECMO with other virus-induced ARDS (Raff LA, et al. Am J Surg. 2021;S0002-9610[21]00233-6. doi: 10.1016/j.amjsurg.2021.04.004. Online ahead of print).These data support pursuing a more conservative timeline for consideration of LT.
Determining the reversibility of pulmonary impairment in COVID-19 ARDS is another challenge. The nature of the pulmonary opacities should be assessed on CT scan imaging as close as possible to the time of LT consideration. Differentiating the extent of irreversible parenchymal scarring vs salvageability during acute illness can be challenging. The presence of extensive architectural distortion with or without bullous changes, while being the best indicator of irreversibility, may not be sensitive enough. The standard of care in such situations remains serial assessments, often weekly, by a dedicated multidisciplinary group. We have found it useful to augment the imaging data with pulmonary physiologic assessments, including the extent of ventilator and ECMO support as well as dynamic and static compliance trends. Improvement in physiologic data often precedes radiologic improvement. Nonetheless, an important area of future research is to identify objective markers for determining reversibility, which could include novel biomarkers in serum or bronchoalveolar lavage fluid.
When a determination is made regarding the irreversibility of pulmonary impairment, the LT evaluation should begin promptly. Pre-transplant deconditioning and debility is associated with worse post-transplant outcomes. In this regard, patients managed using an ambulatory ECMO strategy may have superior rehabilitation potential. Furthermore, an attempt should be made during the evaluation to wean sedation in order to facilitate discussions regarding the rigors of LT with the patient alongside present family members. An additional consideration, given the use of immunomodulatory medications for COVID-19 and prolonged intubation, is the dramatically increased risk of multi-drug resistant infections in this population; these must be aggressively managed for patients to remain eligible for LT.
The degree of pulmonary impairment and frequent colonization of the airways will likely dictate bilateral LT as the preferred strategy, although surgical feasibility may, at times, be the overriding determinant. Regardless of the type of transplant, certain unique aspects should be anticipated. The inflammatory responses during COVID-19 that often spill outside the confines of the pulmonary parenchyma, along with potentially frequent thoracic interventions prior to transplant, create significant technical challenges during the operation. Native pneumonectomy can take longer than usual leading to prolonged ischemic time, increased need for intra-operative blood products, and raised risk for primary graft dysfunction. All of these factors have a significant impact on early and late outcomes. Finally, the long-term immunologic consequences of severe infection from a novel virus remain unknown, and it is unclear if COVID-19 ARDS patients bridged to transplant will enjoy comparable survival. It is pertinent to acknowledge that the high-risk nature of such transplants is substantially accentuated due to several unique characteristics of the illness related to COVID-19.
The emergence of the COVID-19 pandemic has led to an increase in the number of urgent inpatient lung transplant consultations for refractory ARDS. While the basic principles of LT candidate selection should continue to guide us, the unique characteristics of this illness merit using a customized approach. There are few validated predictors to guide decision-making, and longitudinal assessments by a dedicated multidisciplinary group remain the best strategy. Finally, in the absence of systemic studies and lack of longitudinal outcomes data, there is an emergent need to establish consensus guidelines regarding the approach to LT consideration in these patients.
Dr. Quinn and Dr. Banga are with the Lung Transplant Program, Divisions of Pulmonary and Critical Care Medicine, University of Texas Southwestern Medical Center, Dallas.
As of September 2021, over 222 million people worldwide (WHO, 2021) and 40 million Americans (CDC, 2021) have been infected with the novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). The total number of infections in the United States began climbing again this summer with the persistence of vaccine reluctance among a significant proportion of the population and the emergence of the much more infectious B.1.617.2 (Delta) variant. While the clinical illness caused by the SARS-CoV-2 virus, referred to as the Coronavirus disease 2019 (COVID-19), is mostly mild, approximately 10% of cases develop acute respiratory distress syndrome (ARDS) (Remuzzi A, et al. Lancet. 2020;395[10231]:1225-8). A small but substantial proportion of patients with COVID-19 ARDS fails to respond to the various supportive measures and requires extracorporeal membrane oxygenation (ECMO) support. The overarching goal of the different support strategies, including ECMO, is to provide time for the lungs to recover from ARDS. ECMO has the theoretical advantage over other strategies in facilitating recovery by allowing the injured lungs to ‘rest’ as the oxygenation and ventilation needs are met in an extracorporeal fashion. Regardless, a small number of patients with COVID-19 ARDS will not recover enough pulmonary function to allow them to be weaned from the various respiratory support strategies.
For patients with irreversible lung injury, lung transplantation (LT) is a potential consideration. Earlier in the pandemic, older patients with significant comorbid illnesses were more vulnerable to severe COVID-19, often precluding consideration for transplantation. However, the emergence of the Delta variant may have altered this dynamic via a substantial increase in the incidence of COVID-19 ARDS among younger and healthier patients. A handful of patients with COVID-19 ARDS have already had successful transplantation. However, the overall number is still small (Bharat A, et al. Sci Translat Med. 2020 Dec 16;12[574]:eabe4282. doi: 10.1126/scitranslmed.abe4282. Epub 2020 Nov 30; and Hawkins R, et al. Transplantation. 2021;6:1381-7), and there is a lack of long-term outcomes data among these patients.
There is currently little guidance regarding criteria for patient selection and consideration for LT among patients with COVID-19 ARDS. Given that the SARS-CoV-2 virus is a novel pathogen that leads to an illness that is unique from other forms of viral pneumonia, specific considerations regarding LT should be made among these patients. In the current article, we discuss some of the pertinent issues related to the consideration of LT among patients with COVID-19 ARDS.
The timing for considering LT is one of the most important aspects. First, patients with COVID-19 ARDS must not be actively infected at the time of transplantation consideration. It has been suggested that LT should only be considered in patients with two separate negative polymerase chain reaction (PCR) test results for SARS-CoV-2 from bronchoalveolar lavage fluid 24 hours apart and at least 4 weeks after the onset of COVID-19 symptoms (Bharat A, et al. Sci Translat Med. 2020 Dec 16;12[574]:eabe4282. doi: 10.1126/scitranslmed.abe4282. Epub 2020 Nov 30). Among patients with persistently positive SARS-CoV-2 PCR 4 to 6 weeks after symptom onset, a negative viral culture from a bronchoalveolar lavage (BAL) can be used to confirm viral inactivity (Lang C, et al. Lancet Respir Med. 2020;8[10]:1057-60).
Despite the sparse data in this domain, there seems to be a consensus in the literature that LT could be considered once 4 to 6 weeks have elapsed since the onset of the respiratory failure (Cypel M, et al. Lancet Respir Med. 2020;8[10]:944-6). This timeline is felt to be long enough to alleviate the concerns regarding ongoing inflammatory processes that may be reversible while not so long to risk the development of non-pulmonary complications or severe debility that may become significant barriers to transplant candidacy. An exception may be made in patients with medically unmanageable complications such as recalcitrant bronchopleural fistulae in the background of fibrotic changes or right ventricular failure from severe pulmonary hypertension. Regardless, this timeline is borrowed from the approach to irreversible ARDS from other forms of viral pneumonia. It is not clear if it is appropriate to extrapolate past experience to COVID-19, which is a disease unlike any other seen during the LT era: a profound inflammatory phase mediated by a cytokine storm as the etiologic basis for the organ dysfunction, activation of coagulation pathways in pulmonary circulation leading to immunothrombosis contributing to the refractory hypoxemia, favorable effects of anticoagulants, diverse pulmonary physiologic phenotypes of ARDS, an increased risk of pleural complications, and utilization of novel anti-inflammatory therapies with consequent risks ofsecondary infections are all unique to COVID-19. A recent study found that patients requiring ECMO for COVID-19 ARDS took longer to recover lung function but had similar survival rates to patients on ECMO with other virus-induced ARDS (Raff LA, et al. Am J Surg. 2021;S0002-9610[21]00233-6. doi: 10.1016/j.amjsurg.2021.04.004. Online ahead of print).These data support pursuing a more conservative timeline for consideration of LT.
Determining the reversibility of pulmonary impairment in COVID-19 ARDS is another challenge. The nature of the pulmonary opacities should be assessed on CT scan imaging as close as possible to the time of LT consideration. Differentiating the extent of irreversible parenchymal scarring vs salvageability during acute illness can be challenging. The presence of extensive architectural distortion with or without bullous changes, while being the best indicator of irreversibility, may not be sensitive enough. The standard of care in such situations remains serial assessments, often weekly, by a dedicated multidisciplinary group. We have found it useful to augment the imaging data with pulmonary physiologic assessments, including the extent of ventilator and ECMO support as well as dynamic and static compliance trends. Improvement in physiologic data often precedes radiologic improvement. Nonetheless, an important area of future research is to identify objective markers for determining reversibility, which could include novel biomarkers in serum or bronchoalveolar lavage fluid.
When a determination is made regarding the irreversibility of pulmonary impairment, the LT evaluation should begin promptly. Pre-transplant deconditioning and debility is associated with worse post-transplant outcomes. In this regard, patients managed using an ambulatory ECMO strategy may have superior rehabilitation potential. Furthermore, an attempt should be made during the evaluation to wean sedation in order to facilitate discussions regarding the rigors of LT with the patient alongside present family members. An additional consideration, given the use of immunomodulatory medications for COVID-19 and prolonged intubation, is the dramatically increased risk of multi-drug resistant infections in this population; these must be aggressively managed for patients to remain eligible for LT.
The degree of pulmonary impairment and frequent colonization of the airways will likely dictate bilateral LT as the preferred strategy, although surgical feasibility may, at times, be the overriding determinant. Regardless of the type of transplant, certain unique aspects should be anticipated. The inflammatory responses during COVID-19 that often spill outside the confines of the pulmonary parenchyma, along with potentially frequent thoracic interventions prior to transplant, create significant technical challenges during the operation. Native pneumonectomy can take longer than usual leading to prolonged ischemic time, increased need for intra-operative blood products, and raised risk for primary graft dysfunction. All of these factors have a significant impact on early and late outcomes. Finally, the long-term immunologic consequences of severe infection from a novel virus remain unknown, and it is unclear if COVID-19 ARDS patients bridged to transplant will enjoy comparable survival. It is pertinent to acknowledge that the high-risk nature of such transplants is substantially accentuated due to several unique characteristics of the illness related to COVID-19.
The emergence of the COVID-19 pandemic has led to an increase in the number of urgent inpatient lung transplant consultations for refractory ARDS. While the basic principles of LT candidate selection should continue to guide us, the unique characteristics of this illness merit using a customized approach. There are few validated predictors to guide decision-making, and longitudinal assessments by a dedicated multidisciplinary group remain the best strategy. Finally, in the absence of systemic studies and lack of longitudinal outcomes data, there is an emergent need to establish consensus guidelines regarding the approach to LT consideration in these patients.
Dr. Quinn and Dr. Banga are with the Lung Transplant Program, Divisions of Pulmonary and Critical Care Medicine, University of Texas Southwestern Medical Center, Dallas.
This month in the journal CHEST®
Editor’s picks
How I do it: Transitioning asthma care from adolescents to adults: Severe Asthma Series. By Dr. A. Nanzer.
Outpatient management of patients with COVID-19: Multicenter prospective validation of the HOME-CoV Rule to safely discharge patients. By Dr. D. Douillet, et al.
Emphysema progression and lung function decline among angiotensin converting enzyme inhibitors (ACEi) and angiotensin-receptor blockade (ARB) users in the COPDGene Cohort. By Dr. V. Tejwani, et al.
Sarcoidosis: An occupational disease? By Dr. C.L. Oliver, et al.
Pulmonary thrombosis and thromboembolism in COVID-19. By Dr. H. Poor.
How I do it: Mediastinal staging for lung cancer. By Dr. F. Farjah, et al.
Editor’s picks
Editor’s picks
How I do it: Transitioning asthma care from adolescents to adults: Severe Asthma Series. By Dr. A. Nanzer.
Outpatient management of patients with COVID-19: Multicenter prospective validation of the HOME-CoV Rule to safely discharge patients. By Dr. D. Douillet, et al.
Emphysema progression and lung function decline among angiotensin converting enzyme inhibitors (ACEi) and angiotensin-receptor blockade (ARB) users in the COPDGene Cohort. By Dr. V. Tejwani, et al.
Sarcoidosis: An occupational disease? By Dr. C.L. Oliver, et al.
Pulmonary thrombosis and thromboembolism in COVID-19. By Dr. H. Poor.
How I do it: Mediastinal staging for lung cancer. By Dr. F. Farjah, et al.
How I do it: Transitioning asthma care from adolescents to adults: Severe Asthma Series. By Dr. A. Nanzer.
Outpatient management of patients with COVID-19: Multicenter prospective validation of the HOME-CoV Rule to safely discharge patients. By Dr. D. Douillet, et al.
Emphysema progression and lung function decline among angiotensin converting enzyme inhibitors (ACEi) and angiotensin-receptor blockade (ARB) users in the COPDGene Cohort. By Dr. V. Tejwani, et al.
Sarcoidosis: An occupational disease? By Dr. C.L. Oliver, et al.
Pulmonary thrombosis and thromboembolism in COVID-19. By Dr. H. Poor.
How I do it: Mediastinal staging for lung cancer. By Dr. F. Farjah, et al.