User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
New developments and barriers to palliative care
As we enter into this new year, it is a good time to review the past few years of living through a pandemic and the impact this has had on the field of palliative care.

According to the World Health Organization, “Palliative care is an approach that improves the quality of life of patients and their families who are facing the problems associated with life-threatening illness, by the prevention and relief of suffering through early identification, assessment and treatment of pain and other problems whether physical, psychosocial and spiritual.”1 They identify a global need and recognize palliative care as a “human right to health and as a standard of care particularly for individuals living with a serious illness.1 However, the WHO goes further to recognize palliative care as an essential part of the response team during crises and health emergencies like a pandemic, noting that a response team without palliative care is “medically deficient and ethically indefensible.”2
The need for palliative care in the United States is projected to grow significantly in the next decades.3 However, there has been insufficient staffing to meet these needs, even prior to the pandemic.4 The demand for palliative care reached further unprecedented levels during the pandemic as palliative care teams played an integral role and were well situated to support not only patients and families with COVID-19,5 but to also support the well-being of health care teams caring for COVID-19 patients.6,7
A recent survey that was conducted by the Center to Advance Palliative Care among palliative care leadership captured the experiences of leading their teams through a pandemic. Below are the results of this survey, which highlighted important issues and developments to palliative care during the pandemic.6
Increasing need for palliative care
One of the main findings from the national survey of palliative care leaders corroborated that the demands for palliative care have increased significantly from 2020 through the pandemic.
As with many areas in the health care system, the pandemic has emphasized the strain and short staffing of the palliative care teams. In the survey, 61% of leaders reported that palliative care consults significantly increased from prepandemic levels. But only 26% of these leaders said they had the staffing support to meet these needs.
Value of palliative care
The value of palliative care along with understanding of the role of palliative care has been better recognized during the pandemic and has been evidenced by the increase in palliative care referrals from clinical providers, compared with prepandemic levels. In addition, data collected showed that earlier palliative care consultations reduced length of hospital stay, decreased ICU admissions, and improved patient, family, and provider satisfaction.
Well-being of the workforce
The pandemic has been a tremendously stressful time for the health care workforce that has undoubtedly led to burnout. A nationwide study of physicians,8 found that 61% of physicians experienced burnout. This is a significant increase from prepandemic levels with impacts on mental health (that is, anxiety, depression). This study did not include palliative care specialists, but the CAPC survey indicates a similar feeling of burnout. Because of this, some palliative care specialists have left the field altogether, or are leaving leadership positions because of burnout and exhaustion from the pandemic. This was featured as a concern among palliative care leaders, where 93% reported concern for the emotional well-being of the palliative care team.
Telehealth
A permanent operational change that has been well-utilized and implemented across multiple health care settings has been providing palliative care through telehealth. Prior to the pandemic, the baseline use of telehealth was less than 5% with the use now greater than 75% – a modality that is favored by both patients and clinicians. This has offered a broader scope of practice, reaching individuals who may have no other means, have limitations to accessing palliative care, or were in circumstances where patients required isolation during the pandemic. However, there are limitations to this platform, including in equity of access to devices and ease of use for those with limited exposure to technology.9
Barriers to implementation
Although the important role and value of palliative care has been well recognized, there have been barriers identified in a qualitative study of the integration of palliative care into COVID-19 action plans that are mentioned below.5
- Patients and families were identified as barriers to integration of palliative care if they were not open to palliative care referral, mainly because of misperceptions of palliative care as end-of-life care.
- Palliative care knowledge among providers was identified as another barrier to integration of palliative care. There are still misperceptions among providers that palliative care is end-of-life care and palliative care involvement is stigmatized as hastening death. In addition, some felt that COVID-19 was not a traditional “palliative diagnosis” thus were less likely to integrate palliative care into care plans.
- Lack of availability of a primary provider to conduct primary palliative care and lack of motivation “not to give up” were identified as other barriers. On the other hand, palliative care provider availability and accessibility to care teams affected the integration into COVID-19 care plans.
- COVID-19 itself was identified to be a barrier because of the uncertainty of illness trajectory and outcomes, which made it difficult for doctors to ascertain when to involve palliative care.
- Leadership and institution were important factors to consider in integration of palliative care into long-term care plans, which depended on leadership engagement and institutional culture.
Takeaways
The past few years have taught us a lot, but there is still much to learn. The COVID-19 pandemic has called attention to the challenges and barriers of health care delivery and has magnified the needs of the health care system including its infrastructure, preparedness, and staffing, including the field of palliative care. More work needs to be done, but leaders have taken steps to initiate national and international preparedness plans including the integration of palliative care, which has been identified as a vital role in any humanitarian crises.10,11
Dr. Kang is a geriatrician and palliative care provider at the University of Washington, Seattle, in the division of geriatrics and gerontology. She has no conflicts related to the content of this article.
References
1. Palliative care. World Health Organization. Aug 5, 2020. https://www.who.int/news-room/fact-sheets/detail/palliative-care
2. World Health Organization. Integrating palliative care and symptom relief into the response to humanitarian emergencies and crises: A WHO guide. Geneva: World Health Organization, 2018. https://apps.who.int/iris/handle/10665/274565.
3. Hughes MT, Smith TJ. The growth of palliative care in the United States. Annual Review Public Health. 2014;35:459-75.
4. Pastrana T et al. The impact of COVID-19 on palliative care workers across the world: A qualitative analysis of responses to open-ended questions. Palliative and Supportive Care. 2021:1-6.
5. Wentlandt K et al. Identifying barriers and facilitators to palliative care integration in the management of hospitalized patients with COVID-19: A qualitative study. Palliat Med. 2022;36(6):945-54.
6. Rogers M et al. Palliative care leadership during the pandemic: Results from a recent survey. Center to Advance Palliative Care. 2022 Sept 8. https://www.capc.org/blog/palliative-care-leadership-during-the-pandemic-results-from-a-recent-survey
7. Fogelman P. Reflections form a palliative care program leader two years into the pandemic. Center to Advance Palliative Care. 2023 Jan 15. https://www.capc.org/blog/reflections-from-a-palliative-care-program-leader-two-years-into-the-pandemic
8. 2021 survey of America’s physicians Covid-19 impact edition: A year later. The Physicians Foundation. 2021.
9. Caraceni A et al. Telemedicine for outpatient palliative care during Covid-19 pandemics: A longitudinal study. BMJ Supportive & Palliative Care. 2022;0:1-7.
10. Bausewein C et al. National strategy for palliative care of severely ill and dying people and their relatives in pandemics (PallPan) in Germany – study protocol of a mixed-methods project. BMC Palliative Care. 2022;21(10).
11. Powell RA et al. Palliative care in humanitarian crises: Always something to offer. The Lancet. 2017;389(10078):1498-9.
As we enter into this new year, it is a good time to review the past few years of living through a pandemic and the impact this has had on the field of palliative care.
According to the World Health Organization, “Palliative care is an approach that improves the quality of life of patients and their families who are facing the problems associated with life-threatening illness, by the prevention and relief of suffering through early identification, assessment and treatment of pain and other problems whether physical, psychosocial and spiritual.”1 They identify a global need and recognize palliative care as a “human right to health and as a standard of care particularly for individuals living with a serious illness.1 However, the WHO goes further to recognize palliative care as an essential part of the response team during crises and health emergencies like a pandemic, noting that a response team without palliative care is “medically deficient and ethically indefensible.”2
The need for palliative care in the United States is projected to grow significantly in the next decades.3 However, there has been insufficient staffing to meet these needs, even prior to the pandemic.4 The demand for palliative care reached further unprecedented levels during the pandemic as palliative care teams played an integral role and were well situated to support not only patients and families with COVID-19,5 but to also support the well-being of health care teams caring for COVID-19 patients.6,7
A recent survey that was conducted by the Center to Advance Palliative Care among palliative care leadership captured the experiences of leading their teams through a pandemic. Below are the results of this survey, which highlighted important issues and developments to palliative care during the pandemic.6
Increasing need for palliative care
One of the main findings from the national survey of palliative care leaders corroborated that the demands for palliative care have increased significantly from 2020 through the pandemic.
As with many areas in the health care system, the pandemic has emphasized the strain and short staffing of the palliative care teams. In the survey, 61% of leaders reported that palliative care consults significantly increased from prepandemic levels. But only 26% of these leaders said they had the staffing support to meet these needs.
Value of palliative care
The value of palliative care along with understanding of the role of palliative care has been better recognized during the pandemic and has been evidenced by the increase in palliative care referrals from clinical providers, compared with prepandemic levels. In addition, data collected showed that earlier palliative care consultations reduced length of hospital stay, decreased ICU admissions, and improved patient, family, and provider satisfaction.
Well-being of the workforce
The pandemic has been a tremendously stressful time for the health care workforce that has undoubtedly led to burnout. A nationwide study of physicians,8 found that 61% of physicians experienced burnout. This is a significant increase from prepandemic levels with impacts on mental health (that is, anxiety, depression). This study did not include palliative care specialists, but the CAPC survey indicates a similar feeling of burnout. Because of this, some palliative care specialists have left the field altogether, or are leaving leadership positions because of burnout and exhaustion from the pandemic. This was featured as a concern among palliative care leaders, where 93% reported concern for the emotional well-being of the palliative care team.
Telehealth
A permanent operational change that has been well-utilized and implemented across multiple health care settings has been providing palliative care through telehealth. Prior to the pandemic, the baseline use of telehealth was less than 5% with the use now greater than 75% – a modality that is favored by both patients and clinicians. This has offered a broader scope of practice, reaching individuals who may have no other means, have limitations to accessing palliative care, or were in circumstances where patients required isolation during the pandemic. However, there are limitations to this platform, including in equity of access to devices and ease of use for those with limited exposure to technology.9
Barriers to implementation
Although the important role and value of palliative care has been well recognized, there have been barriers identified in a qualitative study of the integration of palliative care into COVID-19 action plans that are mentioned below.5
- Patients and families were identified as barriers to integration of palliative care if they were not open to palliative care referral, mainly because of misperceptions of palliative care as end-of-life care.
- Palliative care knowledge among providers was identified as another barrier to integration of palliative care. There are still misperceptions among providers that palliative care is end-of-life care and palliative care involvement is stigmatized as hastening death. In addition, some felt that COVID-19 was not a traditional “palliative diagnosis” thus were less likely to integrate palliative care into care plans.
- Lack of availability of a primary provider to conduct primary palliative care and lack of motivation “not to give up” were identified as other barriers. On the other hand, palliative care provider availability and accessibility to care teams affected the integration into COVID-19 care plans.
- COVID-19 itself was identified to be a barrier because of the uncertainty of illness trajectory and outcomes, which made it difficult for doctors to ascertain when to involve palliative care.
- Leadership and institution were important factors to consider in integration of palliative care into long-term care plans, which depended on leadership engagement and institutional culture.
Takeaways
The past few years have taught us a lot, but there is still much to learn. The COVID-19 pandemic has called attention to the challenges and barriers of health care delivery and has magnified the needs of the health care system including its infrastructure, preparedness, and staffing, including the field of palliative care. More work needs to be done, but leaders have taken steps to initiate national and international preparedness plans including the integration of palliative care, which has been identified as a vital role in any humanitarian crises.10,11
Dr. Kang is a geriatrician and palliative care provider at the University of Washington, Seattle, in the division of geriatrics and gerontology. She has no conflicts related to the content of this article.
References
1. Palliative care. World Health Organization. Aug 5, 2020. https://www.who.int/news-room/fact-sheets/detail/palliative-care
2. World Health Organization. Integrating palliative care and symptom relief into the response to humanitarian emergencies and crises: A WHO guide. Geneva: World Health Organization, 2018. https://apps.who.int/iris/handle/10665/274565.
3. Hughes MT, Smith TJ. The growth of palliative care in the United States. Annual Review Public Health. 2014;35:459-75.
4. Pastrana T et al. The impact of COVID-19 on palliative care workers across the world: A qualitative analysis of responses to open-ended questions. Palliative and Supportive Care. 2021:1-6.
5. Wentlandt K et al. Identifying barriers and facilitators to palliative care integration in the management of hospitalized patients with COVID-19: A qualitative study. Palliat Med. 2022;36(6):945-54.
6. Rogers M et al. Palliative care leadership during the pandemic: Results from a recent survey. Center to Advance Palliative Care. 2022 Sept 8. https://www.capc.org/blog/palliative-care-leadership-during-the-pandemic-results-from-a-recent-survey
7. Fogelman P. Reflections form a palliative care program leader two years into the pandemic. Center to Advance Palliative Care. 2023 Jan 15. https://www.capc.org/blog/reflections-from-a-palliative-care-program-leader-two-years-into-the-pandemic
8. 2021 survey of America’s physicians Covid-19 impact edition: A year later. The Physicians Foundation. 2021.
9. Caraceni A et al. Telemedicine for outpatient palliative care during Covid-19 pandemics: A longitudinal study. BMJ Supportive & Palliative Care. 2022;0:1-7.
10. Bausewein C et al. National strategy for palliative care of severely ill and dying people and their relatives in pandemics (PallPan) in Germany – study protocol of a mixed-methods project. BMC Palliative Care. 2022;21(10).
11. Powell RA et al. Palliative care in humanitarian crises: Always something to offer. The Lancet. 2017;389(10078):1498-9.
As we enter into this new year, it is a good time to review the past few years of living through a pandemic and the impact this has had on the field of palliative care.
According to the World Health Organization, “Palliative care is an approach that improves the quality of life of patients and their families who are facing the problems associated with life-threatening illness, by the prevention and relief of suffering through early identification, assessment and treatment of pain and other problems whether physical, psychosocial and spiritual.”1 They identify a global need and recognize palliative care as a “human right to health and as a standard of care particularly for individuals living with a serious illness.1 However, the WHO goes further to recognize palliative care as an essential part of the response team during crises and health emergencies like a pandemic, noting that a response team without palliative care is “medically deficient and ethically indefensible.”2
The need for palliative care in the United States is projected to grow significantly in the next decades.3 However, there has been insufficient staffing to meet these needs, even prior to the pandemic.4 The demand for palliative care reached further unprecedented levels during the pandemic as palliative care teams played an integral role and were well situated to support not only patients and families with COVID-19,5 but to also support the well-being of health care teams caring for COVID-19 patients.6,7
A recent survey that was conducted by the Center to Advance Palliative Care among palliative care leadership captured the experiences of leading their teams through a pandemic. Below are the results of this survey, which highlighted important issues and developments to palliative care during the pandemic.6
Increasing need for palliative care
One of the main findings from the national survey of palliative care leaders corroborated that the demands for palliative care have increased significantly from 2020 through the pandemic.
As with many areas in the health care system, the pandemic has emphasized the strain and short staffing of the palliative care teams. In the survey, 61% of leaders reported that palliative care consults significantly increased from prepandemic levels. But only 26% of these leaders said they had the staffing support to meet these needs.
Value of palliative care
The value of palliative care along with understanding of the role of palliative care has been better recognized during the pandemic and has been evidenced by the increase in palliative care referrals from clinical providers, compared with prepandemic levels. In addition, data collected showed that earlier palliative care consultations reduced length of hospital stay, decreased ICU admissions, and improved patient, family, and provider satisfaction.
Well-being of the workforce
The pandemic has been a tremendously stressful time for the health care workforce that has undoubtedly led to burnout. A nationwide study of physicians,8 found that 61% of physicians experienced burnout. This is a significant increase from prepandemic levels with impacts on mental health (that is, anxiety, depression). This study did not include palliative care specialists, but the CAPC survey indicates a similar feeling of burnout. Because of this, some palliative care specialists have left the field altogether, or are leaving leadership positions because of burnout and exhaustion from the pandemic. This was featured as a concern among palliative care leaders, where 93% reported concern for the emotional well-being of the palliative care team.
Telehealth
A permanent operational change that has been well-utilized and implemented across multiple health care settings has been providing palliative care through telehealth. Prior to the pandemic, the baseline use of telehealth was less than 5% with the use now greater than 75% – a modality that is favored by both patients and clinicians. This has offered a broader scope of practice, reaching individuals who may have no other means, have limitations to accessing palliative care, or were in circumstances where patients required isolation during the pandemic. However, there are limitations to this platform, including in equity of access to devices and ease of use for those with limited exposure to technology.9
Barriers to implementation
Although the important role and value of palliative care has been well recognized, there have been barriers identified in a qualitative study of the integration of palliative care into COVID-19 action plans that are mentioned below.5
- Patients and families were identified as barriers to integration of palliative care if they were not open to palliative care referral, mainly because of misperceptions of palliative care as end-of-life care.
- Palliative care knowledge among providers was identified as another barrier to integration of palliative care. There are still misperceptions among providers that palliative care is end-of-life care and palliative care involvement is stigmatized as hastening death. In addition, some felt that COVID-19 was not a traditional “palliative diagnosis” thus were less likely to integrate palliative care into care plans.
- Lack of availability of a primary provider to conduct primary palliative care and lack of motivation “not to give up” were identified as other barriers. On the other hand, palliative care provider availability and accessibility to care teams affected the integration into COVID-19 care plans.
- COVID-19 itself was identified to be a barrier because of the uncertainty of illness trajectory and outcomes, which made it difficult for doctors to ascertain when to involve palliative care.
- Leadership and institution were important factors to consider in integration of palliative care into long-term care plans, which depended on leadership engagement and institutional culture.
Takeaways
The past few years have taught us a lot, but there is still much to learn. The COVID-19 pandemic has called attention to the challenges and barriers of health care delivery and has magnified the needs of the health care system including its infrastructure, preparedness, and staffing, including the field of palliative care. More work needs to be done, but leaders have taken steps to initiate national and international preparedness plans including the integration of palliative care, which has been identified as a vital role in any humanitarian crises.10,11
Dr. Kang is a geriatrician and palliative care provider at the University of Washington, Seattle, in the division of geriatrics and gerontology. She has no conflicts related to the content of this article.
References
1. Palliative care. World Health Organization. Aug 5, 2020. https://www.who.int/news-room/fact-sheets/detail/palliative-care
2. World Health Organization. Integrating palliative care and symptom relief into the response to humanitarian emergencies and crises: A WHO guide. Geneva: World Health Organization, 2018. https://apps.who.int/iris/handle/10665/274565.
3. Hughes MT, Smith TJ. The growth of palliative care in the United States. Annual Review Public Health. 2014;35:459-75.
4. Pastrana T et al. The impact of COVID-19 on palliative care workers across the world: A qualitative analysis of responses to open-ended questions. Palliative and Supportive Care. 2021:1-6.
5. Wentlandt K et al. Identifying barriers and facilitators to palliative care integration in the management of hospitalized patients with COVID-19: A qualitative study. Palliat Med. 2022;36(6):945-54.
6. Rogers M et al. Palliative care leadership during the pandemic: Results from a recent survey. Center to Advance Palliative Care. 2022 Sept 8. https://www.capc.org/blog/palliative-care-leadership-during-the-pandemic-results-from-a-recent-survey
7. Fogelman P. Reflections form a palliative care program leader two years into the pandemic. Center to Advance Palliative Care. 2023 Jan 15. https://www.capc.org/blog/reflections-from-a-palliative-care-program-leader-two-years-into-the-pandemic
8. 2021 survey of America’s physicians Covid-19 impact edition: A year later. The Physicians Foundation. 2021.
9. Caraceni A et al. Telemedicine for outpatient palliative care during Covid-19 pandemics: A longitudinal study. BMJ Supportive & Palliative Care. 2022;0:1-7.
10. Bausewein C et al. National strategy for palliative care of severely ill and dying people and their relatives in pandemics (PallPan) in Germany – study protocol of a mixed-methods project. BMC Palliative Care. 2022;21(10).
11. Powell RA et al. Palliative care in humanitarian crises: Always something to offer. The Lancet. 2017;389(10078):1498-9.
Frequent visits to green spaces linked to lower use of some meds
Frequent visits to green spaces such as parks and community gardens are associated with a reduced use of certain prescription medications among city dwellers, a new analysis suggests.
In a cross-sectional cohort study, frequent green space visits were associated with less frequent use of psychotropic, antihypertensive, and asthma medications in urban environments.
Viewing green or so called “blue” spaces (views of lakes, rivers, or other water views) from the home was not associated with reduced medication use.

The growing scientific evidence supporting the health benefits of nature exposure is likely to increase the availability of high-quality green spaces in urban environments and promote the use of these spaces, lead author Anu W. Turunen, PhD, from the Finnish Institute for Health and Welfare, Kuopio, Finland, told this news organization.
This might be one way to improve health and well-being among city dwellers, Dr. Turunen added.
The findings were published online in Occupational and Environmental Medicine.
Nature exposure a timely topic
Exposure to natural environments is thought to be beneficial for human health, but the evidence is inconsistent, Dr. Turunen said.
“The potential health benefits of nature exposure is a very timely topic in environmental epidemiology. Scientific evidence indicates that residential exposure to greenery and water bodies might be beneficial, especially for mental, cardiovascular, and respiratory health, but the findings are partly inconsistent and thus, more detailed information is needed,” she said.
In the current cross-sectional study, the investigators surveyed 16,000 residents of three urban areas in Finland – Helsinki, Espoo, and Vantaa – over the period of 12 months from 2015 to 2016, about their exposure to green and blue spaces.
Of this number, 43% responded, resulting in 7,321 participants.
In the questionnaire, green areas were defined as forests, parks, fields, meadows, boglands, and rocks, as well as any playgrounds or playing fields within those areas, and blue areas were defined as sea, lakes, and rivers.
Residents were asked about their use of anxiolytics, hypnotics, antidepressants, antihypertensives, and asthma medication within the past 7 to 52 weeks.
They were also asked if they had any green and blue views from any of the windows of their home, and if so, how often did they look out of those windows, selecting “seldom” to “often.”
They were also asked about how much time they spent outdoors in green spaces during the months of May and September. If so, did they spend any of that time exercising? Options ranged from never to five or more times a week.
In addition, amounts of residential green and blue spaces located within a 1 km radius of the respondents’ homes were assessed from land use and land cover data.
Covariates included health behaviors, outdoor air pollution and noise, and socioeconomic status, including household income and educational attainment.
Results showed that the presence of green and blue spaces at home, and the amount of time spent viewing them, had no association with the use of the prescribed medicines.
However, greater frequency of green space visits was associated with lower odds of using the medications surveyed.
For psychotropic medications, the odds ratios were 0.67 (95% confidence interval, 0.55-0.82) for 3-4 times per week and 0.78 (95% CI, 0.63-0.96) for 5 or more times per week.
For antihypertensive meds, the ORs were 0.64 (95% CI, 0.52-0.78) for 3-4 times per week and 0.59 (95% CI, 0.48-0.74) for 5 or more times per week.
For asthma medications, the ORs were 0.74 (95% CI, 0.58-0.94) for 3-4 times per week and 0.76 (95% CI, 0.59-0.99) for 5 or more times per week.
The observed associations were attenuated by body mass index.
“We observed that those who reported visiting green spaces often had a slightly lower BMI than those who visited green spaces less often,” Dr. Turunen said. However, no consistent interactions with socioeconomic status indicators were observed.
“We are hoping to see new results from different countries and different settings,” she noted. “Longitudinal studies, especially, are needed. In epidemiology, a large body of consistent evidence is needed to draw strong conclusions and to make recommendations.”
Evidence mounts on the benefits of nature
There is growing evidence that exposure to nature could benefit human health, especially mental and cardiovascular health, says Jochem Klompmaker, PhD, a postdoctoral researcher in the department of environmental health at the Harvard T.H. Chan School of Public Health, Boston.
Dr. Klompmaker has researched the association between exposure to green spaces and health outcomes related to neurological diseases.
In a study recently published in JAMA Network Open, and reported by this news organization, Dr. Klompmaker and his team found that among a large cohort of about 6.7 million fee-for-service Medicare beneficiaries in the United States aged 65 or older, living in areas rich with greenery, parks, and waterways was associated with fewer hospitalizations for certain neurological disorders, including Parkinson’s disease, Alzheimer’s disease, and related dementias.
Commenting on the current study, Dr. Klompmaker noted its strengths.
“A particular strength of this study is that they used data about the amount of green and blue spaces around the residential addresses of the participants, data about green space visit frequency, and data about green and blue views from home. Most other studies only have data about the amount of green and blue spaces in general,” he said.
“The strong protective associations of frequency of green space visits make sense to me and indicate the importance of one’s actual nature exposure,” he added. “Like the results of our study, these results provide clinicians with more evidence of the importance of being close to nature and of encouraging patients to take more walks. If they live near a park, that could be a good place to be more physically active and reduce stress levels.”
The study was supported by the Academy of Finland and the Ministry of the Environment. Dr. Turunen and Dr. Klompmaker report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Frequent visits to green spaces such as parks and community gardens are associated with a reduced use of certain prescription medications among city dwellers, a new analysis suggests.
In a cross-sectional cohort study, frequent green space visits were associated with less frequent use of psychotropic, antihypertensive, and asthma medications in urban environments.
Viewing green or so called “blue” spaces (views of lakes, rivers, or other water views) from the home was not associated with reduced medication use.
The growing scientific evidence supporting the health benefits of nature exposure is likely to increase the availability of high-quality green spaces in urban environments and promote the use of these spaces, lead author Anu W. Turunen, PhD, from the Finnish Institute for Health and Welfare, Kuopio, Finland, told this news organization.
This might be one way to improve health and well-being among city dwellers, Dr. Turunen added.
The findings were published online in Occupational and Environmental Medicine.
Nature exposure a timely topic
Exposure to natural environments is thought to be beneficial for human health, but the evidence is inconsistent, Dr. Turunen said.
“The potential health benefits of nature exposure is a very timely topic in environmental epidemiology. Scientific evidence indicates that residential exposure to greenery and water bodies might be beneficial, especially for mental, cardiovascular, and respiratory health, but the findings are partly inconsistent and thus, more detailed information is needed,” she said.
In the current cross-sectional study, the investigators surveyed 16,000 residents of three urban areas in Finland – Helsinki, Espoo, and Vantaa – over the period of 12 months from 2015 to 2016, about their exposure to green and blue spaces.
Of this number, 43% responded, resulting in 7,321 participants.
In the questionnaire, green areas were defined as forests, parks, fields, meadows, boglands, and rocks, as well as any playgrounds or playing fields within those areas, and blue areas were defined as sea, lakes, and rivers.
Residents were asked about their use of anxiolytics, hypnotics, antidepressants, antihypertensives, and asthma medication within the past 7 to 52 weeks.
They were also asked if they had any green and blue views from any of the windows of their home, and if so, how often did they look out of those windows, selecting “seldom” to “often.”
They were also asked about how much time they spent outdoors in green spaces during the months of May and September. If so, did they spend any of that time exercising? Options ranged from never to five or more times a week.
In addition, amounts of residential green and blue spaces located within a 1 km radius of the respondents’ homes were assessed from land use and land cover data.
Covariates included health behaviors, outdoor air pollution and noise, and socioeconomic status, including household income and educational attainment.
Results showed that the presence of green and blue spaces at home, and the amount of time spent viewing them, had no association with the use of the prescribed medicines.
However, greater frequency of green space visits was associated with lower odds of using the medications surveyed.
For psychotropic medications, the odds ratios were 0.67 (95% confidence interval, 0.55-0.82) for 3-4 times per week and 0.78 (95% CI, 0.63-0.96) for 5 or more times per week.
For antihypertensive meds, the ORs were 0.64 (95% CI, 0.52-0.78) for 3-4 times per week and 0.59 (95% CI, 0.48-0.74) for 5 or more times per week.
For asthma medications, the ORs were 0.74 (95% CI, 0.58-0.94) for 3-4 times per week and 0.76 (95% CI, 0.59-0.99) for 5 or more times per week.
The observed associations were attenuated by body mass index.
“We observed that those who reported visiting green spaces often had a slightly lower BMI than those who visited green spaces less often,” Dr. Turunen said. However, no consistent interactions with socioeconomic status indicators were observed.
“We are hoping to see new results from different countries and different settings,” she noted. “Longitudinal studies, especially, are needed. In epidemiology, a large body of consistent evidence is needed to draw strong conclusions and to make recommendations.”
Evidence mounts on the benefits of nature
There is growing evidence that exposure to nature could benefit human health, especially mental and cardiovascular health, says Jochem Klompmaker, PhD, a postdoctoral researcher in the department of environmental health at the Harvard T.H. Chan School of Public Health, Boston.
Dr. Klompmaker has researched the association between exposure to green spaces and health outcomes related to neurological diseases.
In a study recently published in JAMA Network Open, and reported by this news organization, Dr. Klompmaker and his team found that among a large cohort of about 6.7 million fee-for-service Medicare beneficiaries in the United States aged 65 or older, living in areas rich with greenery, parks, and waterways was associated with fewer hospitalizations for certain neurological disorders, including Parkinson’s disease, Alzheimer’s disease, and related dementias.
Commenting on the current study, Dr. Klompmaker noted its strengths.
“A particular strength of this study is that they used data about the amount of green and blue spaces around the residential addresses of the participants, data about green space visit frequency, and data about green and blue views from home. Most other studies only have data about the amount of green and blue spaces in general,” he said.
“The strong protective associations of frequency of green space visits make sense to me and indicate the importance of one’s actual nature exposure,” he added. “Like the results of our study, these results provide clinicians with more evidence of the importance of being close to nature and of encouraging patients to take more walks. If they live near a park, that could be a good place to be more physically active and reduce stress levels.”
The study was supported by the Academy of Finland and the Ministry of the Environment. Dr. Turunen and Dr. Klompmaker report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Frequent visits to green spaces such as parks and community gardens are associated with a reduced use of certain prescription medications among city dwellers, a new analysis suggests.
In a cross-sectional cohort study, frequent green space visits were associated with less frequent use of psychotropic, antihypertensive, and asthma medications in urban environments.
Viewing green or so called “blue” spaces (views of lakes, rivers, or other water views) from the home was not associated with reduced medication use.
The growing scientific evidence supporting the health benefits of nature exposure is likely to increase the availability of high-quality green spaces in urban environments and promote the use of these spaces, lead author Anu W. Turunen, PhD, from the Finnish Institute for Health and Welfare, Kuopio, Finland, told this news organization.
This might be one way to improve health and well-being among city dwellers, Dr. Turunen added.
The findings were published online in Occupational and Environmental Medicine.
Nature exposure a timely topic
Exposure to natural environments is thought to be beneficial for human health, but the evidence is inconsistent, Dr. Turunen said.
“The potential health benefits of nature exposure is a very timely topic in environmental epidemiology. Scientific evidence indicates that residential exposure to greenery and water bodies might be beneficial, especially for mental, cardiovascular, and respiratory health, but the findings are partly inconsistent and thus, more detailed information is needed,” she said.
In the current cross-sectional study, the investigators surveyed 16,000 residents of three urban areas in Finland – Helsinki, Espoo, and Vantaa – over the period of 12 months from 2015 to 2016, about their exposure to green and blue spaces.
Of this number, 43% responded, resulting in 7,321 participants.
In the questionnaire, green areas were defined as forests, parks, fields, meadows, boglands, and rocks, as well as any playgrounds or playing fields within those areas, and blue areas were defined as sea, lakes, and rivers.
Residents were asked about their use of anxiolytics, hypnotics, antidepressants, antihypertensives, and asthma medication within the past 7 to 52 weeks.
They were also asked if they had any green and blue views from any of the windows of their home, and if so, how often did they look out of those windows, selecting “seldom” to “often.”
They were also asked about how much time they spent outdoors in green spaces during the months of May and September. If so, did they spend any of that time exercising? Options ranged from never to five or more times a week.
In addition, amounts of residential green and blue spaces located within a 1 km radius of the respondents’ homes were assessed from land use and land cover data.
Covariates included health behaviors, outdoor air pollution and noise, and socioeconomic status, including household income and educational attainment.
Results showed that the presence of green and blue spaces at home, and the amount of time spent viewing them, had no association with the use of the prescribed medicines.
However, greater frequency of green space visits was associated with lower odds of using the medications surveyed.
For psychotropic medications, the odds ratios were 0.67 (95% confidence interval, 0.55-0.82) for 3-4 times per week and 0.78 (95% CI, 0.63-0.96) for 5 or more times per week.
For antihypertensive meds, the ORs were 0.64 (95% CI, 0.52-0.78) for 3-4 times per week and 0.59 (95% CI, 0.48-0.74) for 5 or more times per week.
For asthma medications, the ORs were 0.74 (95% CI, 0.58-0.94) for 3-4 times per week and 0.76 (95% CI, 0.59-0.99) for 5 or more times per week.
The observed associations were attenuated by body mass index.
“We observed that those who reported visiting green spaces often had a slightly lower BMI than those who visited green spaces less often,” Dr. Turunen said. However, no consistent interactions with socioeconomic status indicators were observed.
“We are hoping to see new results from different countries and different settings,” she noted. “Longitudinal studies, especially, are needed. In epidemiology, a large body of consistent evidence is needed to draw strong conclusions and to make recommendations.”
Evidence mounts on the benefits of nature
There is growing evidence that exposure to nature could benefit human health, especially mental and cardiovascular health, says Jochem Klompmaker, PhD, a postdoctoral researcher in the department of environmental health at the Harvard T.H. Chan School of Public Health, Boston.
Dr. Klompmaker has researched the association between exposure to green spaces and health outcomes related to neurological diseases.
In a study recently published in JAMA Network Open, and reported by this news organization, Dr. Klompmaker and his team found that among a large cohort of about 6.7 million fee-for-service Medicare beneficiaries in the United States aged 65 or older, living in areas rich with greenery, parks, and waterways was associated with fewer hospitalizations for certain neurological disorders, including Parkinson’s disease, Alzheimer’s disease, and related dementias.
Commenting on the current study, Dr. Klompmaker noted its strengths.
“A particular strength of this study is that they used data about the amount of green and blue spaces around the residential addresses of the participants, data about green space visit frequency, and data about green and blue views from home. Most other studies only have data about the amount of green and blue spaces in general,” he said.
“The strong protective associations of frequency of green space visits make sense to me and indicate the importance of one’s actual nature exposure,” he added. “Like the results of our study, these results provide clinicians with more evidence of the importance of being close to nature and of encouraging patients to take more walks. If they live near a park, that could be a good place to be more physically active and reduce stress levels.”
The study was supported by the Academy of Finland and the Ministry of the Environment. Dr. Turunen and Dr. Klompmaker report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Genetic testing in the PICU prompts meaningful changes in care
according to a new study presented at the Society of Critical Care Medicine’s 2023 Critical Care Congress.
“We have had a lot of success using genome sequencing to help not only with diagnosis, but also changes in management,” lead author Katherine Rodriguez, MD, a pediatric critical care fellow physician at Rady Children’s Hospital, San Diego, told this news organization.
However, data on the use of rapid whole genome sequencing (rWGS) in the pediatric intensive care unit (PICU) are limited, and data from multiple institutions are lacking, Dr. Rodriguez said. In the current study, data from multiple hospitals allowed the researchers to examine differences in management across institutions, she said.
Dr. Rodriguez, with principal investigator Nicole Coufal, MD, also of Rady Children’s, and colleagues conducted the study at three children’s hospitals from March 2019 to July 2022. The study population included 80 children whose origin of illness was uncertain. The patients underwent rWGS testing in the PICU or cardiac ICU setting. The patients ranged in age from 0 to 17 years; 64% were younger than 1 year, (mean age, 2.8 years); 56% were male, and 59% were White.
After rWGS testing, 65% of the children were positive for a genetic variant. The data prompted changes to care for 42% of these patients; 38% of the changes occurred during the patient’s PICU stay, including medication changes and procedures that were either avoided or completed.
The remaining 62% of the changes were subacute and affected management for the remainder of the child’s hospitalization and after discharge, Dr. Rodriguez explained in her presentation.
The average turnaround time for the testing was 10 days, which is important to an intensivist, who may have been hesitant to order tests because of the time involved, Dr. Rodriguez said. The current study shows that “we can get test results in a reasonable time to make meaningful changes in care,” she told this news organization.
Choosing which patients to test can be a challenge for clinicians, Dr. Rodriguez acknowledged. “We have gotten a sense of which patients are likely to have diagnostic or not diagnostic genomes, but it is also a gut feeling,” she said.
“If this child is your patient and you are concerned, if they seem sicker than expected, or have a concerning family history, then send the test,” she said. “It is becoming more affordable, and can come back quickly enough to guide treatment while the patient is still in the ICU.”
In the current study, the greatest diagnostic utility appeared in patients with cardiac symptoms, such as congenital heart disease, sudden cardiac arrest, or suspected channelopathy, Dr. Rodriguez said in her presentation.
Patients with suspected neurological disease had a 50% rate of molecular diagnosis. “Interestingly, 74% of patients with respiratory disease where an underlying genetic etiology was suspected received a molecular diagnosis,” although rWGS was not applied to general populations with RSV or other respiratory illnesses, she said.
In her presentation, Dr. Rodriguez shared examples of how genetic testing had a dramatic impact on patient survival. In one case, a 14-year-old girl presented in cardiac arrest and was found to have new-onset dilated cardiomyopathy. Whether the etiology was acquired or infectious and possibly reversible or genetic was unclear, she said.
“A diagnostic genome result within 48 hours indicated a genetic etiology,” she said. The patient was listed for heart transplant despite the incomplete infectious workup, and received a successful heart transplant 1 week after admission, Dr. Rodriguez said.
Guidelines for which PICU patients should undergo genetic testing do not yet exist, Dr. Rodriguez told this news organization. “We are trying to find some more meaningful parameters where we can say that a patient has a high pretest possibility of a genetic condition,” she said.
“Increasing availability of rWGS can significantly impact patient care and assist families in making difficult decisions during times of critical illness,” she said.
Insurance coverage and testing access are improving, said Dr. Rodriguez. Medicaid policies exist for neonates/infants in the ICU in several states, including Oregon, California, Michigan, Maryland, and Louisiana, she said. In some areas, hospitals may pay for testing for these children if insurance will not, she added.
Dr. Rodriguez and colleagues are continuing to enroll patients in a prospective study of the impact of rWGS, with the addition of a fourth study site and inclusion of family surveys. “We also will be looking at a secondary analysis of cost savings and benefits,” she said.
Ultimately, the current study should be empowering to physicians, “especially if they don’t have good access to geneticists,” Dr. Rodriguez said in an interview.
The study received no outside funding. Dr. Rodriguez reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new study presented at the Society of Critical Care Medicine’s 2023 Critical Care Congress.
“We have had a lot of success using genome sequencing to help not only with diagnosis, but also changes in management,” lead author Katherine Rodriguez, MD, a pediatric critical care fellow physician at Rady Children’s Hospital, San Diego, told this news organization.
However, data on the use of rapid whole genome sequencing (rWGS) in the pediatric intensive care unit (PICU) are limited, and data from multiple institutions are lacking, Dr. Rodriguez said. In the current study, data from multiple hospitals allowed the researchers to examine differences in management across institutions, she said.
Dr. Rodriguez, with principal investigator Nicole Coufal, MD, also of Rady Children’s, and colleagues conducted the study at three children’s hospitals from March 2019 to July 2022. The study population included 80 children whose origin of illness was uncertain. The patients underwent rWGS testing in the PICU or cardiac ICU setting. The patients ranged in age from 0 to 17 years; 64% were younger than 1 year, (mean age, 2.8 years); 56% were male, and 59% were White.
After rWGS testing, 65% of the children were positive for a genetic variant. The data prompted changes to care for 42% of these patients; 38% of the changes occurred during the patient’s PICU stay, including medication changes and procedures that were either avoided or completed.
The remaining 62% of the changes were subacute and affected management for the remainder of the child’s hospitalization and after discharge, Dr. Rodriguez explained in her presentation.
The average turnaround time for the testing was 10 days, which is important to an intensivist, who may have been hesitant to order tests because of the time involved, Dr. Rodriguez said. The current study shows that “we can get test results in a reasonable time to make meaningful changes in care,” she told this news organization.
Choosing which patients to test can be a challenge for clinicians, Dr. Rodriguez acknowledged. “We have gotten a sense of which patients are likely to have diagnostic or not diagnostic genomes, but it is also a gut feeling,” she said.
“If this child is your patient and you are concerned, if they seem sicker than expected, or have a concerning family history, then send the test,” she said. “It is becoming more affordable, and can come back quickly enough to guide treatment while the patient is still in the ICU.”
In the current study, the greatest diagnostic utility appeared in patients with cardiac symptoms, such as congenital heart disease, sudden cardiac arrest, or suspected channelopathy, Dr. Rodriguez said in her presentation.
Patients with suspected neurological disease had a 50% rate of molecular diagnosis. “Interestingly, 74% of patients with respiratory disease where an underlying genetic etiology was suspected received a molecular diagnosis,” although rWGS was not applied to general populations with RSV or other respiratory illnesses, she said.
In her presentation, Dr. Rodriguez shared examples of how genetic testing had a dramatic impact on patient survival. In one case, a 14-year-old girl presented in cardiac arrest and was found to have new-onset dilated cardiomyopathy. Whether the etiology was acquired or infectious and possibly reversible or genetic was unclear, she said.
“A diagnostic genome result within 48 hours indicated a genetic etiology,” she said. The patient was listed for heart transplant despite the incomplete infectious workup, and received a successful heart transplant 1 week after admission, Dr. Rodriguez said.
Guidelines for which PICU patients should undergo genetic testing do not yet exist, Dr. Rodriguez told this news organization. “We are trying to find some more meaningful parameters where we can say that a patient has a high pretest possibility of a genetic condition,” she said.
“Increasing availability of rWGS can significantly impact patient care and assist families in making difficult decisions during times of critical illness,” she said.
Insurance coverage and testing access are improving, said Dr. Rodriguez. Medicaid policies exist for neonates/infants in the ICU in several states, including Oregon, California, Michigan, Maryland, and Louisiana, she said. In some areas, hospitals may pay for testing for these children if insurance will not, she added.
Dr. Rodriguez and colleagues are continuing to enroll patients in a prospective study of the impact of rWGS, with the addition of a fourth study site and inclusion of family surveys. “We also will be looking at a secondary analysis of cost savings and benefits,” she said.
Ultimately, the current study should be empowering to physicians, “especially if they don’t have good access to geneticists,” Dr. Rodriguez said in an interview.
The study received no outside funding. Dr. Rodriguez reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new study presented at the Society of Critical Care Medicine’s 2023 Critical Care Congress.
“We have had a lot of success using genome sequencing to help not only with diagnosis, but also changes in management,” lead author Katherine Rodriguez, MD, a pediatric critical care fellow physician at Rady Children’s Hospital, San Diego, told this news organization.
However, data on the use of rapid whole genome sequencing (rWGS) in the pediatric intensive care unit (PICU) are limited, and data from multiple institutions are lacking, Dr. Rodriguez said. In the current study, data from multiple hospitals allowed the researchers to examine differences in management across institutions, she said.
Dr. Rodriguez, with principal investigator Nicole Coufal, MD, also of Rady Children’s, and colleagues conducted the study at three children’s hospitals from March 2019 to July 2022. The study population included 80 children whose origin of illness was uncertain. The patients underwent rWGS testing in the PICU or cardiac ICU setting. The patients ranged in age from 0 to 17 years; 64% were younger than 1 year, (mean age, 2.8 years); 56% were male, and 59% were White.
After rWGS testing, 65% of the children were positive for a genetic variant. The data prompted changes to care for 42% of these patients; 38% of the changes occurred during the patient’s PICU stay, including medication changes and procedures that were either avoided or completed.
The remaining 62% of the changes were subacute and affected management for the remainder of the child’s hospitalization and after discharge, Dr. Rodriguez explained in her presentation.
The average turnaround time for the testing was 10 days, which is important to an intensivist, who may have been hesitant to order tests because of the time involved, Dr. Rodriguez said. The current study shows that “we can get test results in a reasonable time to make meaningful changes in care,” she told this news organization.
Choosing which patients to test can be a challenge for clinicians, Dr. Rodriguez acknowledged. “We have gotten a sense of which patients are likely to have diagnostic or not diagnostic genomes, but it is also a gut feeling,” she said.
“If this child is your patient and you are concerned, if they seem sicker than expected, or have a concerning family history, then send the test,” she said. “It is becoming more affordable, and can come back quickly enough to guide treatment while the patient is still in the ICU.”
In the current study, the greatest diagnostic utility appeared in patients with cardiac symptoms, such as congenital heart disease, sudden cardiac arrest, or suspected channelopathy, Dr. Rodriguez said in her presentation.
Patients with suspected neurological disease had a 50% rate of molecular diagnosis. “Interestingly, 74% of patients with respiratory disease where an underlying genetic etiology was suspected received a molecular diagnosis,” although rWGS was not applied to general populations with RSV or other respiratory illnesses, she said.
In her presentation, Dr. Rodriguez shared examples of how genetic testing had a dramatic impact on patient survival. In one case, a 14-year-old girl presented in cardiac arrest and was found to have new-onset dilated cardiomyopathy. Whether the etiology was acquired or infectious and possibly reversible or genetic was unclear, she said.
“A diagnostic genome result within 48 hours indicated a genetic etiology,” she said. The patient was listed for heart transplant despite the incomplete infectious workup, and received a successful heart transplant 1 week after admission, Dr. Rodriguez said.
Guidelines for which PICU patients should undergo genetic testing do not yet exist, Dr. Rodriguez told this news organization. “We are trying to find some more meaningful parameters where we can say that a patient has a high pretest possibility of a genetic condition,” she said.
“Increasing availability of rWGS can significantly impact patient care and assist families in making difficult decisions during times of critical illness,” she said.
Insurance coverage and testing access are improving, said Dr. Rodriguez. Medicaid policies exist for neonates/infants in the ICU in several states, including Oregon, California, Michigan, Maryland, and Louisiana, she said. In some areas, hospitals may pay for testing for these children if insurance will not, she added.
Dr. Rodriguez and colleagues are continuing to enroll patients in a prospective study of the impact of rWGS, with the addition of a fourth study site and inclusion of family surveys. “We also will be looking at a secondary analysis of cost savings and benefits,” she said.
Ultimately, the current study should be empowering to physicians, “especially if they don’t have good access to geneticists,” Dr. Rodriguez said in an interview.
The study received no outside funding. Dr. Rodriguez reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SCCM 2023
Restricted fluid failed to reduce mortality in sepsis-induced hypotension
A restrictive fluid strategy had no significant impact on mortality in patients with sepsis-induced hypotension compared to the typical liberal fluid strategy, based on data from 1,563 individuals.
Intravenous fluids are standard in the early resuscitation of sepsis patients, as are vasopressor agents, but data comparing restrictive or liberal use in these patients are limited, wrote Nathan I. Shapiro, MD, of Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, and colleagues.
In a study published in the New England Journal of Medicine the researchers randomized 782 patients to the restrictive fluid group and 781 to the liberal fluid group. Patients aged 18 years and older were enrolled between March 7, 2018, and Jan. 31, 2022, at 60 centers in the United States. Participants were randomized within 4 hours of meeting the criteria for sepsis-induced hypotension that was refractory to initial treatment with 1-3 L of intravenous fluid. Baseline characteristics were similar between the groups. At randomization, 21% of patients in the restrictive fluid group and 18% in the liberal fluid group received vasopressors.
The primary outcome was 90-day all-cause mortality, which occurred in 109 and 116 patients in the liberal and restricted groups, respectively (approximately 14% of each group). No significant differences were noted among subgroups based on factors including systolic blood pressure and the use of vasopressors at randomization, chronic heart failure, end-stage renal disease, and pneumonia.
The restrictive fluid protocol called for vasopressors as the primary treatment for sepsis-induced hypotension, with “rescue fluids” to be used for prespecified situations of severe intravascular volume depletion. The liberal fluid protocol was a recommended initial intravenous infusion of 2,000 mL of isotonic crystalloid, followed by fluid boluses given based on clinical triggers such as tachycardia, along with “rescue vasopressors,” the researchers wrote.
The median volume of fluid administered in the first 24-hour period after randomization was 1,267 mL in the restrictive group and 3,400 mL in the liberal group. Adherence to the treatment protocols was greater than 90% for both groups.
The current study is distinct in its enrollment of patients with primary presentations of sepsis to a hospital emergency department, the researchers wrote in their discussion. we expect our findings to be generalizable to these types of patients,” they said.
Reported serious adverse events were similar between the groups, though fewer episodes of fluid overload and pulmonary edema occurred in the restricted group.
The findings were limited by several factors including some cases in which patients in the restrictive group received more fluid than called for by the protocol, the researchers noted. Other limitations included the lack of subgroups with different coexisting conditions, the lack of blinding, and the lack of a control with no instructions for treatment protocol, they said. However, the results suggest that a restrictive fluid strategy had no significant advantage over a liberal strategy in terms of mortality for patients with sepsis-induced hypotension, they concluded.
The study was supported by the National Heart, Lung, and Blood Institute. Dr. Shapiro disclosed serving as a consultant for and having stock options in Diagnostic Robotics, as well as grant support from Inflammatrix and Rapid Pathogen Screening, and serving as a consultant for Prenosis.
A restrictive fluid strategy had no significant impact on mortality in patients with sepsis-induced hypotension compared to the typical liberal fluid strategy, based on data from 1,563 individuals.
Intravenous fluids are standard in the early resuscitation of sepsis patients, as are vasopressor agents, but data comparing restrictive or liberal use in these patients are limited, wrote Nathan I. Shapiro, MD, of Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, and colleagues.
In a study published in the New England Journal of Medicine the researchers randomized 782 patients to the restrictive fluid group and 781 to the liberal fluid group. Patients aged 18 years and older were enrolled between March 7, 2018, and Jan. 31, 2022, at 60 centers in the United States. Participants were randomized within 4 hours of meeting the criteria for sepsis-induced hypotension that was refractory to initial treatment with 1-3 L of intravenous fluid. Baseline characteristics were similar between the groups. At randomization, 21% of patients in the restrictive fluid group and 18% in the liberal fluid group received vasopressors.
The primary outcome was 90-day all-cause mortality, which occurred in 109 and 116 patients in the liberal and restricted groups, respectively (approximately 14% of each group). No significant differences were noted among subgroups based on factors including systolic blood pressure and the use of vasopressors at randomization, chronic heart failure, end-stage renal disease, and pneumonia.
The restrictive fluid protocol called for vasopressors as the primary treatment for sepsis-induced hypotension, with “rescue fluids” to be used for prespecified situations of severe intravascular volume depletion. The liberal fluid protocol was a recommended initial intravenous infusion of 2,000 mL of isotonic crystalloid, followed by fluid boluses given based on clinical triggers such as tachycardia, along with “rescue vasopressors,” the researchers wrote.
The median volume of fluid administered in the first 24-hour period after randomization was 1,267 mL in the restrictive group and 3,400 mL in the liberal group. Adherence to the treatment protocols was greater than 90% for both groups.
The current study is distinct in its enrollment of patients with primary presentations of sepsis to a hospital emergency department, the researchers wrote in their discussion. we expect our findings to be generalizable to these types of patients,” they said.
Reported serious adverse events were similar between the groups, though fewer episodes of fluid overload and pulmonary edema occurred in the restricted group.
The findings were limited by several factors including some cases in which patients in the restrictive group received more fluid than called for by the protocol, the researchers noted. Other limitations included the lack of subgroups with different coexisting conditions, the lack of blinding, and the lack of a control with no instructions for treatment protocol, they said. However, the results suggest that a restrictive fluid strategy had no significant advantage over a liberal strategy in terms of mortality for patients with sepsis-induced hypotension, they concluded.
The study was supported by the National Heart, Lung, and Blood Institute. Dr. Shapiro disclosed serving as a consultant for and having stock options in Diagnostic Robotics, as well as grant support from Inflammatrix and Rapid Pathogen Screening, and serving as a consultant for Prenosis.
A restrictive fluid strategy had no significant impact on mortality in patients with sepsis-induced hypotension compared to the typical liberal fluid strategy, based on data from 1,563 individuals.
Intravenous fluids are standard in the early resuscitation of sepsis patients, as are vasopressor agents, but data comparing restrictive or liberal use in these patients are limited, wrote Nathan I. Shapiro, MD, of Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, and colleagues.
In a study published in the New England Journal of Medicine the researchers randomized 782 patients to the restrictive fluid group and 781 to the liberal fluid group. Patients aged 18 years and older were enrolled between March 7, 2018, and Jan. 31, 2022, at 60 centers in the United States. Participants were randomized within 4 hours of meeting the criteria for sepsis-induced hypotension that was refractory to initial treatment with 1-3 L of intravenous fluid. Baseline characteristics were similar between the groups. At randomization, 21% of patients in the restrictive fluid group and 18% in the liberal fluid group received vasopressors.
The primary outcome was 90-day all-cause mortality, which occurred in 109 and 116 patients in the liberal and restricted groups, respectively (approximately 14% of each group). No significant differences were noted among subgroups based on factors including systolic blood pressure and the use of vasopressors at randomization, chronic heart failure, end-stage renal disease, and pneumonia.
The restrictive fluid protocol called for vasopressors as the primary treatment for sepsis-induced hypotension, with “rescue fluids” to be used for prespecified situations of severe intravascular volume depletion. The liberal fluid protocol was a recommended initial intravenous infusion of 2,000 mL of isotonic crystalloid, followed by fluid boluses given based on clinical triggers such as tachycardia, along with “rescue vasopressors,” the researchers wrote.
The median volume of fluid administered in the first 24-hour period after randomization was 1,267 mL in the restrictive group and 3,400 mL in the liberal group. Adherence to the treatment protocols was greater than 90% for both groups.
The current study is distinct in its enrollment of patients with primary presentations of sepsis to a hospital emergency department, the researchers wrote in their discussion. we expect our findings to be generalizable to these types of patients,” they said.
Reported serious adverse events were similar between the groups, though fewer episodes of fluid overload and pulmonary edema occurred in the restricted group.
The findings were limited by several factors including some cases in which patients in the restrictive group received more fluid than called for by the protocol, the researchers noted. Other limitations included the lack of subgroups with different coexisting conditions, the lack of blinding, and the lack of a control with no instructions for treatment protocol, they said. However, the results suggest that a restrictive fluid strategy had no significant advantage over a liberal strategy in terms of mortality for patients with sepsis-induced hypotension, they concluded.
The study was supported by the National Heart, Lung, and Blood Institute. Dr. Shapiro disclosed serving as a consultant for and having stock options in Diagnostic Robotics, as well as grant support from Inflammatrix and Rapid Pathogen Screening, and serving as a consultant for Prenosis.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Three wishes: The changes health professionals want
As physicians well know, magic wands don’t exist. If they did, every patient would recover in the exam room, prior authorization wouldn’t exist, and continuing medical education credits would be printed on bearer bonds.
But Because, hey – we all need to dream.
Suzanne C. Boulter, MD, adjunct professor of pediatrics and community and family medicine, Geisel School of Medicine at Dartmouth, Hanover, N.H.
Patients: An end to gun violence.
Practice/hospital: Adequate staffing and pediatric bed availability.
Health system: Universal access to health insurance.
Sarah G. Candler, MD, MPH, care team medical director and director of academic relations, Iora Primary Care, Northside Clinic, Houston
Patients: Systems of health that start with communities of safety, including access to affordable housing, food, transportation, and health care.
Practice/hospital: I.N.T.E.R.O.P.E.R.A.B.I.L.I.T.Y.
Health system: Clinician leadership that has the power (often aka funding) to do what’s right, not just what’s right in front of us.
Arthur L. Caplan, PhD, bioethicist, New York University Langone Health
Patients: I wish for patients in the United States greater access to affordable primary care. There are still too many people without insurance or a reasonably accessible quality provider. And I especially wish for the rapid expansion of affordable training programs to meet staffing needs, including more scholarships, 3-year programs, and more new primary care–oriented schools.
Hospital: Increased staffing, especially nursing. There are too many retirements, too much burnout, and too much privatization into boutique practices to ensure the ability to provide high-quality, safe, patient-oriented care.
Health system: I wish for health systems to seriously move into electronic medicine. While billing has become electronic, there is still much to be done to supplement diagnosis, training, and standardized data collection on key metrics. Systems are not yet behaving in a manner consistent with the hype in this regard.
Stephen Devries, MD, executive director, Gaples Institute (nonprofit) and adjunct associate professor of nutrition, Harvard School of Public Health, Boston
Patients: Patients continue to demand more from their health care professionals and insist that they are offered evidence-based counseling on nutrition and lifestyle strategies.
Practice: Quality-based reimbursement for medical services will take hold that will incentivize much-needed preventive care.
Hospital: Hospitals will more fully embrace the role of serving as true centers of health and focus as much on preventive medicine as on the more lucrative areas of high-tech treatment.
Peter D. Friedmann, MD, MPH, chief research officer, Baystate Health, Springfield, Mass.
Seconded by: Elisabeth Poorman, MD, general internist, University of Washington Clinic, Kent
Patients: Don’t forget the ongoing epidemic of substance use disorder, a major cause of premature mortality. Descheduling of cannabis and expungement of cannabis-related convictions.
Practice/hospital: Commitment of hospitals and practices to address stigma and ensure delivery of medications for opioid use disorder in primary care, the emergency department, and inpatient settings.
Health system: Reform of antiquated methadone regulations to permit office-based prescription and pharmacy dispensing to treat opioid use disorder, as is the case in most of the world.
Robert Glatter, MD, emergency physician, New York
Patients: I want all patients to understand the enormous strain the health care system has been under – not just with the pandemic, the tripledemic, and mpox [previously called monkeypox], but well before the onset of these public health crises.
Hospital: The medical profession has endured not only burnout but a growing mental health crisis, staffing shortages, a physician addiction crisis, and increased attrition in the decade leading up to the pandemic. The pandemic was like a punch in the gut, occurring at the most inopportune time one could imagine.
Health system: The intersection of health and the state of our public health deserves important mention. Unless we take action to bolster our public health infrastructure, our health care system will be in jeopardy, unable to handle the next pandemic, which could be just around the corner.
William E. Golden, MD, medical director of Arkansas Medicaid, professor of medicine and public health, University of Arkansas for Medical Sciences, Little Rock
Patients: Affordable options for diabetes and obesity management.
Health system: Greater investment by health systems and third-party payers in primary care infrastructure.
Gregory A. Hood, MD, Baptist Health, Lexington, Ky.
Patients: To embrace the gift of getting out in the world, being active, and connecting with others – having put down the screens.
Health system: To be freed from the financial gamesmanship of the insurers as they continue to serve their goals of promoting their hedge fund investing over meaningful and productive partnering with primary care physicians, and that they gain insight that they are one of the main reasons they can’t find PCPs to connect with to render care in disadvantaged environments – because they made it economically impossible to do so.
Robert H. Hopkins Jr., MD, associate professor of internal medicine and pediatrics and director of the division of general internal medicine, University of Arkansas for Medical Sciences, Little Rock
Patients/Health system: I would wish for staged implementation of universal basic health coverage for all, perhaps closest to the French or Canadian model. This would need to be coupled with expanded funding for nursing education, graduate medical education, and tracing of other health-related professionals.
Harvey Hsu, MD, Banner Health, Phoenix
Patients: More clear guidelines that are simple to understand. This can apply to colonoscopy (now age 45), immunizations, blood pressure goals. I wish medications were not as expensive so patients can take the best medicine for them and not stop taking them when they hit their donut hole in coverage.
Practice: We have been functioning on a leaner basis to cut down costs. When the pandemic hit, turnover was high and we lost PAs, nurses, front-office staff, and physicians. Having adequate staffing is probably number one on many lists. One way we dealt with lack of staffing was converting in-person visits to telehealth. Video visits are paid the same as in-person visits, but if the patient could not get their video to work, then it would be a telephone visit. Now many insurances do not even pay for telephone visits. So I would wish that we could still be reimbursed for telehealth visits.
Health system: I would wish for our health system to recognize the extra work required to take care of patients while improving quality and meeting quality measures. Allowing more time for patient visits could be one way to meet those goals or having more support staff to make sure patients get their colonoscopy/mammograms done, improve their sugars, and take their medications.
Jan L. Shifren, MD, Vincent Trustees Professor, obstetrics, gynecology, and reproductive biology, Harvard Medical School, and director of the Midlife Women’s Health Center at Massachusetts General Hospital, Boston
Patients: I wish for patients to be actively involved in all aspects of their care, well informed with shared decision-making.
Practice: I wish for the enormous time demands of electronic medical records and documentation to not distract from the pleasure of caring for patients.
Health system: Patient care remains at the center of decisions and programs.
Timothy J. Joos, MD, MPH, internal medicine/pediatrics, Seattle
Health system: I wish someone could figure out how we could be reimbursed for the quality of care we provide instead of the volume of patients we see. I wish EMRs could become less complicated and more user-friendly rather than needing advanced training to use.
Peter Kovacs, MD, medical director, Kaali Institute IVF Center, Budapest
Patients: I work as an infertility specialist, so when we talk about infectious diseases and associated risks, we talk about a minimum of two (female and male partner) and ideally three (plus the pregnancy) individuals. We have learned that SARS-CoV-2 affects reproductive health. It may compromise sperm production, could delay fertility treatment, could be associated with lower success rates; and if the treatment is successful, it may harm the pregnant woman/fetus/newborn. The best preventive measure that we can offer is vaccination. One cannot overemphasize the importance of preventive measures, paying attention to personal hygiene and social distancing. Therefore, I wish those planning to become pregnant to listen to their health care provider and accept the recommended vaccines to minimize the risk of getting infected and to minimize the risk for severe disease, especially if one undergoes successful fertility treatment and achieves a long-desired pregnancy.
Practice: During the 2022 calendar year we had many days when one or more employees were out of work on sick leave. This puts extra stress on the others to allow uncompromised work in the clinic. In addition, we all have to work in a less-comfortable environment if we consider mask use every day, all day. For health care workers, vaccination is mandated but many still are affected by milder forms of coronavirus infection and other respiratory diseases. Therefore, I wish my colleagues patience toward the preventive measures to lower the individual risk for infections. As a result, hopefully we will have a less stressful 2023.
Health system: Many resources had to be delegated to dealing with acute and chronic COVID, and this was at the expense of routine daily elective and preventive medical services. I wish the health care system to return to normal daily operations, to have the personnel and financial resources to carry on with the required preventive and elective medical services to avoid long-term consequences of not being able to provide such services. It would be sad if we had to treat otherwise preventable illnesses in the upcoming years that went undiagnosed and/or were not properly managed due to limited resources as the result of the pandemic.
Alan R. Nelson, MD, internist-endocrinologist, retired
Patients: Expansion of the FDA’s authority into over-the-counter drugs, including the veracity of their advertising claims.
Practice: Make diabetes drugs available at a reasonable cost.
Health system: With the expansion of Medicaid eligibility during COVID-19 coming to a close, federal government actions are necessary for those who once again have been dropped from coverage to have their legitimate needs met.
Kevin Powell, MD, PhD, St. Louis
Patients: To be cared for and about, and not just medically, even when illness strikes and health fails.
Hospitals: To hear the thankfulness of a grateful public for the care you provide, and to hear that above the angry noise of outraged individuals who spout vitriol and focus on how they believe others have harmed them.
Health system: A truer understanding of mercy and justice.
Margaret Thew, DNP, FNP-BC, director, department of adolescent medicine, Children’s Hospital of Wisconsin, Milwaukee
Seconded by: M. Susan Jay, MD, professor of pediatrics, chief of adolescent medicine, Medical College of Wisconsin and Children’s Hospital of Wisconsin, Milwaukee
My wish for patients, hospital, and system: health, calm, and grace.
Mark P. Trolice, MD, director of Fertility CARE, the IVF Center, Winter Park, Fla.
Patients: To be proactive in their health care and be their own advocates. Question when unclear and only consult credible resources.
Practice/hospital: Improve support of physicians and all health care providers to allow more input in their practice operations and growth.
Health system: Reduce interference of the “business of medicine” and ensure that the patient experience is the priority.
Charles P. Vega, MD, University of California, Irvine
Three minutes on a routine basis for everyone in health care to reflect on our blessings and the honor and gravity – as well as joy – that are integral to health care. Three minutes that will also help us to recognize our challenges and put them in the proper context. I know 3 minutes is not meeting any standard for reflective practice. But it’s 3 minutes more than I have right now.
Karen Breach Washington, MD, medical director of WellCare of North Carolina/Centene, Charlotte
Seconded by: Lillian M. Beard, MD, physician director, Children’s Pediatricians and Associates, Silver Spring, Md.
Patients: Access to affordable health care.
Hospital: Resources to care for patients (sufficient number of beds and a healthy staff).
Health system: Equity for all.
Andrew Wilner, MD, host of the podcast “The Art of Medicine with Dr. Andrew Wilner,” www.andrewwilner.com
Let’s put patients first! Too many extraneous considerations other than the patient’s best interest obstruct optimal patient care.
Here are just a few examples of patients coming last instead of first.
- If a patient needs to start a new medication in hospital, we shouldn’t have to wait until the patient is an outpatient because “that’s when insurance will pay.”
- If there’s a new medication that’s better than the old medication, we shouldn’t be forced to choose the old medication and provide inferior care because “that’s when insurance will pay.”
- If patients need to stay in hospital, we shouldn’t be pressured to discharge them because the hospital has decided that decreasing “length of stay” is its highest priority.
Dr. Francis Peabody said it best in 1927: “The secret of the care of the patient is in caring for the patient.” How hard is that?
In 2023, why don’t we follow Dr. Peabody’s sage advice from nearly 100 years ago and see what happens?
James M. Wooten, PharmD, University of Missouri–Kansas City, University Health, Kansas City, Mo.
Patients: I want patients to understand and properly realize the advantage of vaccinations – not only for COVID-19 but also for influenza. There is so much misinformation that I spend a lot of time trying to convince patients to get vaccinated. Most patients don’t realize that through their lives, most of them have already been vaccinated for something just to be able to attend school. How the COVID-19 vaccine created so much stigma makes little sense to me. I also want patients to understand that COVID-19 vaccination and boosters do not always prevent infection but will many times prevent severe infection. I believe that better patient communication and education is the key and will always be the key to improving vaccination numbers. Not only communicating and educating patients on vaccination itself but also making patients realize that personal vaccination decisions may affect what happens to your neighbor. Allowing infection means that you may be more likely to infect someone else. As a society, we must take care of each other.
Health system: It will be interesting to see what happens when vaccines are no longer reimbursed by the federal government. Understanding which vaccines work best and are better tolerated will be key to choosing appropriate vaccine brands. Health care providers will need to be very selective regarding which vaccines are selected for formulary inclusion. Thorough meta-analysis studies must be done to provide more evaluable information to allow for appropriate selection. “Knowledge is power!” Appropriate knowledge will help distinguish which vaccines work best for various patient populations.
A version of this article first appeared on Medscape.com.
As physicians well know, magic wands don’t exist. If they did, every patient would recover in the exam room, prior authorization wouldn’t exist, and continuing medical education credits would be printed on bearer bonds.
But Because, hey – we all need to dream.
Suzanne C. Boulter, MD, adjunct professor of pediatrics and community and family medicine, Geisel School of Medicine at Dartmouth, Hanover, N.H.
Patients: An end to gun violence.
Practice/hospital: Adequate staffing and pediatric bed availability.
Health system: Universal access to health insurance.
Sarah G. Candler, MD, MPH, care team medical director and director of academic relations, Iora Primary Care, Northside Clinic, Houston
Patients: Systems of health that start with communities of safety, including access to affordable housing, food, transportation, and health care.
Practice/hospital: I.N.T.E.R.O.P.E.R.A.B.I.L.I.T.Y.
Health system: Clinician leadership that has the power (often aka funding) to do what’s right, not just what’s right in front of us.
Arthur L. Caplan, PhD, bioethicist, New York University Langone Health
Patients: I wish for patients in the United States greater access to affordable primary care. There are still too many people without insurance or a reasonably accessible quality provider. And I especially wish for the rapid expansion of affordable training programs to meet staffing needs, including more scholarships, 3-year programs, and more new primary care–oriented schools.
Hospital: Increased staffing, especially nursing. There are too many retirements, too much burnout, and too much privatization into boutique practices to ensure the ability to provide high-quality, safe, patient-oriented care.
Health system: I wish for health systems to seriously move into electronic medicine. While billing has become electronic, there is still much to be done to supplement diagnosis, training, and standardized data collection on key metrics. Systems are not yet behaving in a manner consistent with the hype in this regard.
Stephen Devries, MD, executive director, Gaples Institute (nonprofit) and adjunct associate professor of nutrition, Harvard School of Public Health, Boston
Patients: Patients continue to demand more from their health care professionals and insist that they are offered evidence-based counseling on nutrition and lifestyle strategies.
Practice: Quality-based reimbursement for medical services will take hold that will incentivize much-needed preventive care.
Hospital: Hospitals will more fully embrace the role of serving as true centers of health and focus as much on preventive medicine as on the more lucrative areas of high-tech treatment.
Peter D. Friedmann, MD, MPH, chief research officer, Baystate Health, Springfield, Mass.
Seconded by: Elisabeth Poorman, MD, general internist, University of Washington Clinic, Kent
Patients: Don’t forget the ongoing epidemic of substance use disorder, a major cause of premature mortality. Descheduling of cannabis and expungement of cannabis-related convictions.
Practice/hospital: Commitment of hospitals and practices to address stigma and ensure delivery of medications for opioid use disorder in primary care, the emergency department, and inpatient settings.
Health system: Reform of antiquated methadone regulations to permit office-based prescription and pharmacy dispensing to treat opioid use disorder, as is the case in most of the world.
Robert Glatter, MD, emergency physician, New York
Patients: I want all patients to understand the enormous strain the health care system has been under – not just with the pandemic, the tripledemic, and mpox [previously called monkeypox], but well before the onset of these public health crises.
Hospital: The medical profession has endured not only burnout but a growing mental health crisis, staffing shortages, a physician addiction crisis, and increased attrition in the decade leading up to the pandemic. The pandemic was like a punch in the gut, occurring at the most inopportune time one could imagine.
Health system: The intersection of health and the state of our public health deserves important mention. Unless we take action to bolster our public health infrastructure, our health care system will be in jeopardy, unable to handle the next pandemic, which could be just around the corner.
William E. Golden, MD, medical director of Arkansas Medicaid, professor of medicine and public health, University of Arkansas for Medical Sciences, Little Rock
Patients: Affordable options for diabetes and obesity management.
Health system: Greater investment by health systems and third-party payers in primary care infrastructure.
Gregory A. Hood, MD, Baptist Health, Lexington, Ky.
Patients: To embrace the gift of getting out in the world, being active, and connecting with others – having put down the screens.
Health system: To be freed from the financial gamesmanship of the insurers as they continue to serve their goals of promoting their hedge fund investing over meaningful and productive partnering with primary care physicians, and that they gain insight that they are one of the main reasons they can’t find PCPs to connect with to render care in disadvantaged environments – because they made it economically impossible to do so.
Robert H. Hopkins Jr., MD, associate professor of internal medicine and pediatrics and director of the division of general internal medicine, University of Arkansas for Medical Sciences, Little Rock
Patients/Health system: I would wish for staged implementation of universal basic health coverage for all, perhaps closest to the French or Canadian model. This would need to be coupled with expanded funding for nursing education, graduate medical education, and tracing of other health-related professionals.
Harvey Hsu, MD, Banner Health, Phoenix
Patients: More clear guidelines that are simple to understand. This can apply to colonoscopy (now age 45), immunizations, blood pressure goals. I wish medications were not as expensive so patients can take the best medicine for them and not stop taking them when they hit their donut hole in coverage.
Practice: We have been functioning on a leaner basis to cut down costs. When the pandemic hit, turnover was high and we lost PAs, nurses, front-office staff, and physicians. Having adequate staffing is probably number one on many lists. One way we dealt with lack of staffing was converting in-person visits to telehealth. Video visits are paid the same as in-person visits, but if the patient could not get their video to work, then it would be a telephone visit. Now many insurances do not even pay for telephone visits. So I would wish that we could still be reimbursed for telehealth visits.
Health system: I would wish for our health system to recognize the extra work required to take care of patients while improving quality and meeting quality measures. Allowing more time for patient visits could be one way to meet those goals or having more support staff to make sure patients get their colonoscopy/mammograms done, improve their sugars, and take their medications.
Jan L. Shifren, MD, Vincent Trustees Professor, obstetrics, gynecology, and reproductive biology, Harvard Medical School, and director of the Midlife Women’s Health Center at Massachusetts General Hospital, Boston
Patients: I wish for patients to be actively involved in all aspects of their care, well informed with shared decision-making.
Practice: I wish for the enormous time demands of electronic medical records and documentation to not distract from the pleasure of caring for patients.
Health system: Patient care remains at the center of decisions and programs.
Timothy J. Joos, MD, MPH, internal medicine/pediatrics, Seattle
Health system: I wish someone could figure out how we could be reimbursed for the quality of care we provide instead of the volume of patients we see. I wish EMRs could become less complicated and more user-friendly rather than needing advanced training to use.
Peter Kovacs, MD, medical director, Kaali Institute IVF Center, Budapest
Patients: I work as an infertility specialist, so when we talk about infectious diseases and associated risks, we talk about a minimum of two (female and male partner) and ideally three (plus the pregnancy) individuals. We have learned that SARS-CoV-2 affects reproductive health. It may compromise sperm production, could delay fertility treatment, could be associated with lower success rates; and if the treatment is successful, it may harm the pregnant woman/fetus/newborn. The best preventive measure that we can offer is vaccination. One cannot overemphasize the importance of preventive measures, paying attention to personal hygiene and social distancing. Therefore, I wish those planning to become pregnant to listen to their health care provider and accept the recommended vaccines to minimize the risk of getting infected and to minimize the risk for severe disease, especially if one undergoes successful fertility treatment and achieves a long-desired pregnancy.
Practice: During the 2022 calendar year we had many days when one or more employees were out of work on sick leave. This puts extra stress on the others to allow uncompromised work in the clinic. In addition, we all have to work in a less-comfortable environment if we consider mask use every day, all day. For health care workers, vaccination is mandated but many still are affected by milder forms of coronavirus infection and other respiratory diseases. Therefore, I wish my colleagues patience toward the preventive measures to lower the individual risk for infections. As a result, hopefully we will have a less stressful 2023.
Health system: Many resources had to be delegated to dealing with acute and chronic COVID, and this was at the expense of routine daily elective and preventive medical services. I wish the health care system to return to normal daily operations, to have the personnel and financial resources to carry on with the required preventive and elective medical services to avoid long-term consequences of not being able to provide such services. It would be sad if we had to treat otherwise preventable illnesses in the upcoming years that went undiagnosed and/or were not properly managed due to limited resources as the result of the pandemic.
Alan R. Nelson, MD, internist-endocrinologist, retired
Patients: Expansion of the FDA’s authority into over-the-counter drugs, including the veracity of their advertising claims.
Practice: Make diabetes drugs available at a reasonable cost.
Health system: With the expansion of Medicaid eligibility during COVID-19 coming to a close, federal government actions are necessary for those who once again have been dropped from coverage to have their legitimate needs met.
Kevin Powell, MD, PhD, St. Louis
Patients: To be cared for and about, and not just medically, even when illness strikes and health fails.
Hospitals: To hear the thankfulness of a grateful public for the care you provide, and to hear that above the angry noise of outraged individuals who spout vitriol and focus on how they believe others have harmed them.
Health system: A truer understanding of mercy and justice.
Margaret Thew, DNP, FNP-BC, director, department of adolescent medicine, Children’s Hospital of Wisconsin, Milwaukee
Seconded by: M. Susan Jay, MD, professor of pediatrics, chief of adolescent medicine, Medical College of Wisconsin and Children’s Hospital of Wisconsin, Milwaukee
My wish for patients, hospital, and system: health, calm, and grace.
Mark P. Trolice, MD, director of Fertility CARE, the IVF Center, Winter Park, Fla.
Patients: To be proactive in their health care and be their own advocates. Question when unclear and only consult credible resources.
Practice/hospital: Improve support of physicians and all health care providers to allow more input in their practice operations and growth.
Health system: Reduce interference of the “business of medicine” and ensure that the patient experience is the priority.
Charles P. Vega, MD, University of California, Irvine
Three minutes on a routine basis for everyone in health care to reflect on our blessings and the honor and gravity – as well as joy – that are integral to health care. Three minutes that will also help us to recognize our challenges and put them in the proper context. I know 3 minutes is not meeting any standard for reflective practice. But it’s 3 minutes more than I have right now.
Karen Breach Washington, MD, medical director of WellCare of North Carolina/Centene, Charlotte
Seconded by: Lillian M. Beard, MD, physician director, Children’s Pediatricians and Associates, Silver Spring, Md.
Patients: Access to affordable health care.
Hospital: Resources to care for patients (sufficient number of beds and a healthy staff).
Health system: Equity for all.
Andrew Wilner, MD, host of the podcast “The Art of Medicine with Dr. Andrew Wilner,” www.andrewwilner.com
Let’s put patients first! Too many extraneous considerations other than the patient’s best interest obstruct optimal patient care.
Here are just a few examples of patients coming last instead of first.
- If a patient needs to start a new medication in hospital, we shouldn’t have to wait until the patient is an outpatient because “that’s when insurance will pay.”
- If there’s a new medication that’s better than the old medication, we shouldn’t be forced to choose the old medication and provide inferior care because “that’s when insurance will pay.”
- If patients need to stay in hospital, we shouldn’t be pressured to discharge them because the hospital has decided that decreasing “length of stay” is its highest priority.
Dr. Francis Peabody said it best in 1927: “The secret of the care of the patient is in caring for the patient.” How hard is that?
In 2023, why don’t we follow Dr. Peabody’s sage advice from nearly 100 years ago and see what happens?
James M. Wooten, PharmD, University of Missouri–Kansas City, University Health, Kansas City, Mo.
Patients: I want patients to understand and properly realize the advantage of vaccinations – not only for COVID-19 but also for influenza. There is so much misinformation that I spend a lot of time trying to convince patients to get vaccinated. Most patients don’t realize that through their lives, most of them have already been vaccinated for something just to be able to attend school. How the COVID-19 vaccine created so much stigma makes little sense to me. I also want patients to understand that COVID-19 vaccination and boosters do not always prevent infection but will many times prevent severe infection. I believe that better patient communication and education is the key and will always be the key to improving vaccination numbers. Not only communicating and educating patients on vaccination itself but also making patients realize that personal vaccination decisions may affect what happens to your neighbor. Allowing infection means that you may be more likely to infect someone else. As a society, we must take care of each other.
Health system: It will be interesting to see what happens when vaccines are no longer reimbursed by the federal government. Understanding which vaccines work best and are better tolerated will be key to choosing appropriate vaccine brands. Health care providers will need to be very selective regarding which vaccines are selected for formulary inclusion. Thorough meta-analysis studies must be done to provide more evaluable information to allow for appropriate selection. “Knowledge is power!” Appropriate knowledge will help distinguish which vaccines work best for various patient populations.
A version of this article first appeared on Medscape.com.
As physicians well know, magic wands don’t exist. If they did, every patient would recover in the exam room, prior authorization wouldn’t exist, and continuing medical education credits would be printed on bearer bonds.
But Because, hey – we all need to dream.
Suzanne C. Boulter, MD, adjunct professor of pediatrics and community and family medicine, Geisel School of Medicine at Dartmouth, Hanover, N.H.
Patients: An end to gun violence.
Practice/hospital: Adequate staffing and pediatric bed availability.
Health system: Universal access to health insurance.
Sarah G. Candler, MD, MPH, care team medical director and director of academic relations, Iora Primary Care, Northside Clinic, Houston
Patients: Systems of health that start with communities of safety, including access to affordable housing, food, transportation, and health care.
Practice/hospital: I.N.T.E.R.O.P.E.R.A.B.I.L.I.T.Y.
Health system: Clinician leadership that has the power (often aka funding) to do what’s right, not just what’s right in front of us.
Arthur L. Caplan, PhD, bioethicist, New York University Langone Health
Patients: I wish for patients in the United States greater access to affordable primary care. There are still too many people without insurance or a reasonably accessible quality provider. And I especially wish for the rapid expansion of affordable training programs to meet staffing needs, including more scholarships, 3-year programs, and more new primary care–oriented schools.
Hospital: Increased staffing, especially nursing. There are too many retirements, too much burnout, and too much privatization into boutique practices to ensure the ability to provide high-quality, safe, patient-oriented care.
Health system: I wish for health systems to seriously move into electronic medicine. While billing has become electronic, there is still much to be done to supplement diagnosis, training, and standardized data collection on key metrics. Systems are not yet behaving in a manner consistent with the hype in this regard.
Stephen Devries, MD, executive director, Gaples Institute (nonprofit) and adjunct associate professor of nutrition, Harvard School of Public Health, Boston
Patients: Patients continue to demand more from their health care professionals and insist that they are offered evidence-based counseling on nutrition and lifestyle strategies.
Practice: Quality-based reimbursement for medical services will take hold that will incentivize much-needed preventive care.
Hospital: Hospitals will more fully embrace the role of serving as true centers of health and focus as much on preventive medicine as on the more lucrative areas of high-tech treatment.
Peter D. Friedmann, MD, MPH, chief research officer, Baystate Health, Springfield, Mass.
Seconded by: Elisabeth Poorman, MD, general internist, University of Washington Clinic, Kent
Patients: Don’t forget the ongoing epidemic of substance use disorder, a major cause of premature mortality. Descheduling of cannabis and expungement of cannabis-related convictions.
Practice/hospital: Commitment of hospitals and practices to address stigma and ensure delivery of medications for opioid use disorder in primary care, the emergency department, and inpatient settings.
Health system: Reform of antiquated methadone regulations to permit office-based prescription and pharmacy dispensing to treat opioid use disorder, as is the case in most of the world.
Robert Glatter, MD, emergency physician, New York
Patients: I want all patients to understand the enormous strain the health care system has been under – not just with the pandemic, the tripledemic, and mpox [previously called monkeypox], but well before the onset of these public health crises.
Hospital: The medical profession has endured not only burnout but a growing mental health crisis, staffing shortages, a physician addiction crisis, and increased attrition in the decade leading up to the pandemic. The pandemic was like a punch in the gut, occurring at the most inopportune time one could imagine.
Health system: The intersection of health and the state of our public health deserves important mention. Unless we take action to bolster our public health infrastructure, our health care system will be in jeopardy, unable to handle the next pandemic, which could be just around the corner.
William E. Golden, MD, medical director of Arkansas Medicaid, professor of medicine and public health, University of Arkansas for Medical Sciences, Little Rock
Patients: Affordable options for diabetes and obesity management.
Health system: Greater investment by health systems and third-party payers in primary care infrastructure.
Gregory A. Hood, MD, Baptist Health, Lexington, Ky.
Patients: To embrace the gift of getting out in the world, being active, and connecting with others – having put down the screens.
Health system: To be freed from the financial gamesmanship of the insurers as they continue to serve their goals of promoting their hedge fund investing over meaningful and productive partnering with primary care physicians, and that they gain insight that they are one of the main reasons they can’t find PCPs to connect with to render care in disadvantaged environments – because they made it economically impossible to do so.
Robert H. Hopkins Jr., MD, associate professor of internal medicine and pediatrics and director of the division of general internal medicine, University of Arkansas for Medical Sciences, Little Rock
Patients/Health system: I would wish for staged implementation of universal basic health coverage for all, perhaps closest to the French or Canadian model. This would need to be coupled with expanded funding for nursing education, graduate medical education, and tracing of other health-related professionals.
Harvey Hsu, MD, Banner Health, Phoenix
Patients: More clear guidelines that are simple to understand. This can apply to colonoscopy (now age 45), immunizations, blood pressure goals. I wish medications were not as expensive so patients can take the best medicine for them and not stop taking them when they hit their donut hole in coverage.
Practice: We have been functioning on a leaner basis to cut down costs. When the pandemic hit, turnover was high and we lost PAs, nurses, front-office staff, and physicians. Having adequate staffing is probably number one on many lists. One way we dealt with lack of staffing was converting in-person visits to telehealth. Video visits are paid the same as in-person visits, but if the patient could not get their video to work, then it would be a telephone visit. Now many insurances do not even pay for telephone visits. So I would wish that we could still be reimbursed for telehealth visits.
Health system: I would wish for our health system to recognize the extra work required to take care of patients while improving quality and meeting quality measures. Allowing more time for patient visits could be one way to meet those goals or having more support staff to make sure patients get their colonoscopy/mammograms done, improve their sugars, and take their medications.
Jan L. Shifren, MD, Vincent Trustees Professor, obstetrics, gynecology, and reproductive biology, Harvard Medical School, and director of the Midlife Women’s Health Center at Massachusetts General Hospital, Boston
Patients: I wish for patients to be actively involved in all aspects of their care, well informed with shared decision-making.
Practice: I wish for the enormous time demands of electronic medical records and documentation to not distract from the pleasure of caring for patients.
Health system: Patient care remains at the center of decisions and programs.
Timothy J. Joos, MD, MPH, internal medicine/pediatrics, Seattle
Health system: I wish someone could figure out how we could be reimbursed for the quality of care we provide instead of the volume of patients we see. I wish EMRs could become less complicated and more user-friendly rather than needing advanced training to use.
Peter Kovacs, MD, medical director, Kaali Institute IVF Center, Budapest
Patients: I work as an infertility specialist, so when we talk about infectious diseases and associated risks, we talk about a minimum of two (female and male partner) and ideally three (plus the pregnancy) individuals. We have learned that SARS-CoV-2 affects reproductive health. It may compromise sperm production, could delay fertility treatment, could be associated with lower success rates; and if the treatment is successful, it may harm the pregnant woman/fetus/newborn. The best preventive measure that we can offer is vaccination. One cannot overemphasize the importance of preventive measures, paying attention to personal hygiene and social distancing. Therefore, I wish those planning to become pregnant to listen to their health care provider and accept the recommended vaccines to minimize the risk of getting infected and to minimize the risk for severe disease, especially if one undergoes successful fertility treatment and achieves a long-desired pregnancy.
Practice: During the 2022 calendar year we had many days when one or more employees were out of work on sick leave. This puts extra stress on the others to allow uncompromised work in the clinic. In addition, we all have to work in a less-comfortable environment if we consider mask use every day, all day. For health care workers, vaccination is mandated but many still are affected by milder forms of coronavirus infection and other respiratory diseases. Therefore, I wish my colleagues patience toward the preventive measures to lower the individual risk for infections. As a result, hopefully we will have a less stressful 2023.
Health system: Many resources had to be delegated to dealing with acute and chronic COVID, and this was at the expense of routine daily elective and preventive medical services. I wish the health care system to return to normal daily operations, to have the personnel and financial resources to carry on with the required preventive and elective medical services to avoid long-term consequences of not being able to provide such services. It would be sad if we had to treat otherwise preventable illnesses in the upcoming years that went undiagnosed and/or were not properly managed due to limited resources as the result of the pandemic.
Alan R. Nelson, MD, internist-endocrinologist, retired
Patients: Expansion of the FDA’s authority into over-the-counter drugs, including the veracity of their advertising claims.
Practice: Make diabetes drugs available at a reasonable cost.
Health system: With the expansion of Medicaid eligibility during COVID-19 coming to a close, federal government actions are necessary for those who once again have been dropped from coverage to have their legitimate needs met.
Kevin Powell, MD, PhD, St. Louis
Patients: To be cared for and about, and not just medically, even when illness strikes and health fails.
Hospitals: To hear the thankfulness of a grateful public for the care you provide, and to hear that above the angry noise of outraged individuals who spout vitriol and focus on how they believe others have harmed them.
Health system: A truer understanding of mercy and justice.
Margaret Thew, DNP, FNP-BC, director, department of adolescent medicine, Children’s Hospital of Wisconsin, Milwaukee
Seconded by: M. Susan Jay, MD, professor of pediatrics, chief of adolescent medicine, Medical College of Wisconsin and Children’s Hospital of Wisconsin, Milwaukee
My wish for patients, hospital, and system: health, calm, and grace.
Mark P. Trolice, MD, director of Fertility CARE, the IVF Center, Winter Park, Fla.
Patients: To be proactive in their health care and be their own advocates. Question when unclear and only consult credible resources.
Practice/hospital: Improve support of physicians and all health care providers to allow more input in their practice operations and growth.
Health system: Reduce interference of the “business of medicine” and ensure that the patient experience is the priority.
Charles P. Vega, MD, University of California, Irvine
Three minutes on a routine basis for everyone in health care to reflect on our blessings and the honor and gravity – as well as joy – that are integral to health care. Three minutes that will also help us to recognize our challenges and put them in the proper context. I know 3 minutes is not meeting any standard for reflective practice. But it’s 3 minutes more than I have right now.
Karen Breach Washington, MD, medical director of WellCare of North Carolina/Centene, Charlotte
Seconded by: Lillian M. Beard, MD, physician director, Children’s Pediatricians and Associates, Silver Spring, Md.
Patients: Access to affordable health care.
Hospital: Resources to care for patients (sufficient number of beds and a healthy staff).
Health system: Equity for all.
Andrew Wilner, MD, host of the podcast “The Art of Medicine with Dr. Andrew Wilner,” www.andrewwilner.com
Let’s put patients first! Too many extraneous considerations other than the patient’s best interest obstruct optimal patient care.
Here are just a few examples of patients coming last instead of first.
- If a patient needs to start a new medication in hospital, we shouldn’t have to wait until the patient is an outpatient because “that’s when insurance will pay.”
- If there’s a new medication that’s better than the old medication, we shouldn’t be forced to choose the old medication and provide inferior care because “that’s when insurance will pay.”
- If patients need to stay in hospital, we shouldn’t be pressured to discharge them because the hospital has decided that decreasing “length of stay” is its highest priority.
Dr. Francis Peabody said it best in 1927: “The secret of the care of the patient is in caring for the patient.” How hard is that?
In 2023, why don’t we follow Dr. Peabody’s sage advice from nearly 100 years ago and see what happens?
James M. Wooten, PharmD, University of Missouri–Kansas City, University Health, Kansas City, Mo.
Patients: I want patients to understand and properly realize the advantage of vaccinations – not only for COVID-19 but also for influenza. There is so much misinformation that I spend a lot of time trying to convince patients to get vaccinated. Most patients don’t realize that through their lives, most of them have already been vaccinated for something just to be able to attend school. How the COVID-19 vaccine created so much stigma makes little sense to me. I also want patients to understand that COVID-19 vaccination and boosters do not always prevent infection but will many times prevent severe infection. I believe that better patient communication and education is the key and will always be the key to improving vaccination numbers. Not only communicating and educating patients on vaccination itself but also making patients realize that personal vaccination decisions may affect what happens to your neighbor. Allowing infection means that you may be more likely to infect someone else. As a society, we must take care of each other.
Health system: It will be interesting to see what happens when vaccines are no longer reimbursed by the federal government. Understanding which vaccines work best and are better tolerated will be key to choosing appropriate vaccine brands. Health care providers will need to be very selective regarding which vaccines are selected for formulary inclusion. Thorough meta-analysis studies must be done to provide more evaluable information to allow for appropriate selection. “Knowledge is power!” Appropriate knowledge will help distinguish which vaccines work best for various patient populations.
A version of this article first appeared on Medscape.com.
Universal testing for Lp(a): What are we waiting for?
It soon became clear that Lp(a) was associated with atherosclerotic cardiovascular disease (ASCVD), but whether an elevated blood level was a biomarker or a causal factor proved difficult to determine. Studies of inheritance patterns confirmed that blood levels were primarily genetically determined and largely resistant to lifestyle and pharmacologic intervention. It seemed senseless to test for something that was deemed “unmodifiable,” so untreatable. That label stuck for decades.
Fortunately, a resurgent interest in molecular pathophysiology this past decade has clarified Lp(a)’s unique contribution to atherothrombotic disease and calcific aortic stenosis. While there remains much to be learned about this complex, highly atherogenic molecule and its role in cardiac disease, it seems shortsighted not to take the simple step of identifying who carries this risk. Why are we not testing everyone for an extremely common and potent risk factor for the most lethal disease on the planet?
Epidemiologic studies project a stunning number of people in the United States to be at increased risk for Lp(a)-mediated coronary and cerebrovascular events. Because the LPA gene which codes for the apo(a) component of the Lp(a) molecule is fully expressed at age 2, this is a truly lifelong risk factor for a projected 64 million individuals with blood levels (> 60 mg/dL) high enough to double their risk for ASCVD. Because risk increases linearly, this includes 16 million, like me, with levels > 116 mg/dL, who are at four times the risk for ASCVD as those with normal levels (< 30 mg/dL).
Because Lp(a) level remains relatively constant throughout life, a single blood test would help stratify the risk it confers on millions of people who, under current U.S. guidelines, would never be tested. Until Lp(a) is integrated into its algorithms, the commonly used ASCVD Risk Calculator will substantially underestimate risk in 20% of the population.
A potential barrier to universal testing is that the ideal method to measure Lp(a) has yet to be determined. Lp(a) comprises an apoB particle bonded to an apo(a) particle. Apo(a) is complex and has a number of isoforms that can result in large heterogeneity in apo(a) size between, as well as within, individuals. This contributes to controversy about the ideal assay and whether Lp(a) levels should be expressed as mass (mg/dL) or number of particles (nmols/L). This should not, however, deter universal testing.
One-time cost, lifetime benefit?
Absent universal testing, it’s impossible to estimate the economic toll that Lp(a) exacts, but it’s surely an extraordinary number, particularly because the highest-risk individuals are prone to recurrent, nonfatal vascular events. The substantial price tag for my personal decade of Lp(a)-induced vascular havoc included four percutaneous coronary interventions with rapid stent restenosis, an eventual bypass surgery, and an aborted left hemispheric stroke, requiring an urgent carotid endarterectomy.
As a frame of reference, U.S. expenditures related to ASCVD are estimated to be $351 billion annually. If everyone in the United States over the age of 18 were tested for Lp(a) at a cost of $100 per person, this would be a $21 billion expenditure. This nonrecurring expense would identify the 20% – or almost 42 million individuals – at high risk for ASCVD, a number of whom would have already had vascular events. This one-time cost would be a foundational step in securing year-after-year savings from enhanced ASCVD prevention and reduction in recurrent vascular events.
Such savings would be significantly enhanced if and when targeted, effective Lp(a) treatments become available, but it seems shortsighted to make this the linchpin for universal testing. It’s noteworthy that Canadian and European guidelines already endorse one-time testing for all.
The confirmation of Lp(a)’s causal role in ASCVD remains underappreciated by medical providers across all specialties. Much of the elegant Lp(a)-related science of the past decade has yet to translate to the clinical world. What better way to rectify this than by identifying those with high Lp(a)? Since the advent of the statin era, “good” and “bad” cholesterol values are common conversational fare, in part because virtually every adult has had not one, but many lipid panels. Universal Lp(a) testing would spotlight this pervasive and important risk factor that was referred to as the “horrible” cholesterol in a recent review.
U.S. guidelines need updating
To foster this, U.S. guidelines, which influence every aspect of care, including testing, prevention, treatment, reimbursement, and medical legal issues, need to be simplified. The discussion of Lp(a) testing in the 2018 U.S. guidelines on cholesterol management is already obsolete. The contingencies on when testing is “reasonable” or “may be reasonable” are dated and cumbersome. In contrast, a recommendation to test everyone once, perhaps in adolescence, would be a useful, forward-looking strategy.
To date, trials of an antisense oligonucleotide and a small interfering RNA molecule targeting hepatic LPA messenger RNA have confirmed that plasma Lp(a) levels can be significantly and safely lowered. If the ongoing Lp(a) HORIZON and OCEAN(a) phase 3 trials have positive outcomes in patients with known ASCVD, this would spawn a host of clinical trials to explore the possibilities of these therapies in primary prevention as well. These will require tens of thousands of enrollees, and universal testing would expand the pool of potential participants.
The majority of at-risk individuals identified through universal testing would be candidates for primary prevention. This large, currently unidentified cohort should have all coexisting risk factors assessed and managed; lowering elevated LDL cholesterol early and aggressively is paramount. Recent data from the United Kingdom suggest that attainment of specific LDL cholesterol levels may offset the risk for vascular events in those with high Lp(a) levels.
Of note, this was the advice given to the small fraction of high-risk individuals like me, who had their Lp(a) level tested long before its ominous implications were understood. This recommendation was informed mostly by common sense. For any number of reasons, the same might be said for universal testing.
Dr. Leahy, a retired cardiologist in San Diego, has an abiding professional and personal interest in Lp(a), which has been responsible for a number of cardiovascular events in his own life over the past 2 decades. He was a participant in the phase 2 clinical trial of the Lp(a)-lowering antisense oligonucleotide being studied in the Lp(a) HORIZON trial, funded by Novartis, and is currently undergoing apheresis treatment. A version of this article originally appeared on Medscape.com.
It soon became clear that Lp(a) was associated with atherosclerotic cardiovascular disease (ASCVD), but whether an elevated blood level was a biomarker or a causal factor proved difficult to determine. Studies of inheritance patterns confirmed that blood levels were primarily genetically determined and largely resistant to lifestyle and pharmacologic intervention. It seemed senseless to test for something that was deemed “unmodifiable,” so untreatable. That label stuck for decades.
Fortunately, a resurgent interest in molecular pathophysiology this past decade has clarified Lp(a)’s unique contribution to atherothrombotic disease and calcific aortic stenosis. While there remains much to be learned about this complex, highly atherogenic molecule and its role in cardiac disease, it seems shortsighted not to take the simple step of identifying who carries this risk. Why are we not testing everyone for an extremely common and potent risk factor for the most lethal disease on the planet?
Epidemiologic studies project a stunning number of people in the United States to be at increased risk for Lp(a)-mediated coronary and cerebrovascular events. Because the LPA gene which codes for the apo(a) component of the Lp(a) molecule is fully expressed at age 2, this is a truly lifelong risk factor for a projected 64 million individuals with blood levels (> 60 mg/dL) high enough to double their risk for ASCVD. Because risk increases linearly, this includes 16 million, like me, with levels > 116 mg/dL, who are at four times the risk for ASCVD as those with normal levels (< 30 mg/dL).
Because Lp(a) level remains relatively constant throughout life, a single blood test would help stratify the risk it confers on millions of people who, under current U.S. guidelines, would never be tested. Until Lp(a) is integrated into its algorithms, the commonly used ASCVD Risk Calculator will substantially underestimate risk in 20% of the population.
A potential barrier to universal testing is that the ideal method to measure Lp(a) has yet to be determined. Lp(a) comprises an apoB particle bonded to an apo(a) particle. Apo(a) is complex and has a number of isoforms that can result in large heterogeneity in apo(a) size between, as well as within, individuals. This contributes to controversy about the ideal assay and whether Lp(a) levels should be expressed as mass (mg/dL) or number of particles (nmols/L). This should not, however, deter universal testing.
One-time cost, lifetime benefit?
Absent universal testing, it’s impossible to estimate the economic toll that Lp(a) exacts, but it’s surely an extraordinary number, particularly because the highest-risk individuals are prone to recurrent, nonfatal vascular events. The substantial price tag for my personal decade of Lp(a)-induced vascular havoc included four percutaneous coronary interventions with rapid stent restenosis, an eventual bypass surgery, and an aborted left hemispheric stroke, requiring an urgent carotid endarterectomy.
As a frame of reference, U.S. expenditures related to ASCVD are estimated to be $351 billion annually. If everyone in the United States over the age of 18 were tested for Lp(a) at a cost of $100 per person, this would be a $21 billion expenditure. This nonrecurring expense would identify the 20% – or almost 42 million individuals – at high risk for ASCVD, a number of whom would have already had vascular events. This one-time cost would be a foundational step in securing year-after-year savings from enhanced ASCVD prevention and reduction in recurrent vascular events.
Such savings would be significantly enhanced if and when targeted, effective Lp(a) treatments become available, but it seems shortsighted to make this the linchpin for universal testing. It’s noteworthy that Canadian and European guidelines already endorse one-time testing for all.
The confirmation of Lp(a)’s causal role in ASCVD remains underappreciated by medical providers across all specialties. Much of the elegant Lp(a)-related science of the past decade has yet to translate to the clinical world. What better way to rectify this than by identifying those with high Lp(a)? Since the advent of the statin era, “good” and “bad” cholesterol values are common conversational fare, in part because virtually every adult has had not one, but many lipid panels. Universal Lp(a) testing would spotlight this pervasive and important risk factor that was referred to as the “horrible” cholesterol in a recent review.
U.S. guidelines need updating
To foster this, U.S. guidelines, which influence every aspect of care, including testing, prevention, treatment, reimbursement, and medical legal issues, need to be simplified. The discussion of Lp(a) testing in the 2018 U.S. guidelines on cholesterol management is already obsolete. The contingencies on when testing is “reasonable” or “may be reasonable” are dated and cumbersome. In contrast, a recommendation to test everyone once, perhaps in adolescence, would be a useful, forward-looking strategy.
To date, trials of an antisense oligonucleotide and a small interfering RNA molecule targeting hepatic LPA messenger RNA have confirmed that plasma Lp(a) levels can be significantly and safely lowered. If the ongoing Lp(a) HORIZON and OCEAN(a) phase 3 trials have positive outcomes in patients with known ASCVD, this would spawn a host of clinical trials to explore the possibilities of these therapies in primary prevention as well. These will require tens of thousands of enrollees, and universal testing would expand the pool of potential participants.
The majority of at-risk individuals identified through universal testing would be candidates for primary prevention. This large, currently unidentified cohort should have all coexisting risk factors assessed and managed; lowering elevated LDL cholesterol early and aggressively is paramount. Recent data from the United Kingdom suggest that attainment of specific LDL cholesterol levels may offset the risk for vascular events in those with high Lp(a) levels.
Of note, this was the advice given to the small fraction of high-risk individuals like me, who had their Lp(a) level tested long before its ominous implications were understood. This recommendation was informed mostly by common sense. For any number of reasons, the same might be said for universal testing.
Dr. Leahy, a retired cardiologist in San Diego, has an abiding professional and personal interest in Lp(a), which has been responsible for a number of cardiovascular events in his own life over the past 2 decades. He was a participant in the phase 2 clinical trial of the Lp(a)-lowering antisense oligonucleotide being studied in the Lp(a) HORIZON trial, funded by Novartis, and is currently undergoing apheresis treatment. A version of this article originally appeared on Medscape.com.
It soon became clear that Lp(a) was associated with atherosclerotic cardiovascular disease (ASCVD), but whether an elevated blood level was a biomarker or a causal factor proved difficult to determine. Studies of inheritance patterns confirmed that blood levels were primarily genetically determined and largely resistant to lifestyle and pharmacologic intervention. It seemed senseless to test for something that was deemed “unmodifiable,” so untreatable. That label stuck for decades.
Fortunately, a resurgent interest in molecular pathophysiology this past decade has clarified Lp(a)’s unique contribution to atherothrombotic disease and calcific aortic stenosis. While there remains much to be learned about this complex, highly atherogenic molecule and its role in cardiac disease, it seems shortsighted not to take the simple step of identifying who carries this risk. Why are we not testing everyone for an extremely common and potent risk factor for the most lethal disease on the planet?
Epidemiologic studies project a stunning number of people in the United States to be at increased risk for Lp(a)-mediated coronary and cerebrovascular events. Because the LPA gene which codes for the apo(a) component of the Lp(a) molecule is fully expressed at age 2, this is a truly lifelong risk factor for a projected 64 million individuals with blood levels (> 60 mg/dL) high enough to double their risk for ASCVD. Because risk increases linearly, this includes 16 million, like me, with levels > 116 mg/dL, who are at four times the risk for ASCVD as those with normal levels (< 30 mg/dL).
Because Lp(a) level remains relatively constant throughout life, a single blood test would help stratify the risk it confers on millions of people who, under current U.S. guidelines, would never be tested. Until Lp(a) is integrated into its algorithms, the commonly used ASCVD Risk Calculator will substantially underestimate risk in 20% of the population.
A potential barrier to universal testing is that the ideal method to measure Lp(a) has yet to be determined. Lp(a) comprises an apoB particle bonded to an apo(a) particle. Apo(a) is complex and has a number of isoforms that can result in large heterogeneity in apo(a) size between, as well as within, individuals. This contributes to controversy about the ideal assay and whether Lp(a) levels should be expressed as mass (mg/dL) or number of particles (nmols/L). This should not, however, deter universal testing.
One-time cost, lifetime benefit?
Absent universal testing, it’s impossible to estimate the economic toll that Lp(a) exacts, but it’s surely an extraordinary number, particularly because the highest-risk individuals are prone to recurrent, nonfatal vascular events. The substantial price tag for my personal decade of Lp(a)-induced vascular havoc included four percutaneous coronary interventions with rapid stent restenosis, an eventual bypass surgery, and an aborted left hemispheric stroke, requiring an urgent carotid endarterectomy.
As a frame of reference, U.S. expenditures related to ASCVD are estimated to be $351 billion annually. If everyone in the United States over the age of 18 were tested for Lp(a) at a cost of $100 per person, this would be a $21 billion expenditure. This nonrecurring expense would identify the 20% – or almost 42 million individuals – at high risk for ASCVD, a number of whom would have already had vascular events. This one-time cost would be a foundational step in securing year-after-year savings from enhanced ASCVD prevention and reduction in recurrent vascular events.
Such savings would be significantly enhanced if and when targeted, effective Lp(a) treatments become available, but it seems shortsighted to make this the linchpin for universal testing. It’s noteworthy that Canadian and European guidelines already endorse one-time testing for all.
The confirmation of Lp(a)’s causal role in ASCVD remains underappreciated by medical providers across all specialties. Much of the elegant Lp(a)-related science of the past decade has yet to translate to the clinical world. What better way to rectify this than by identifying those with high Lp(a)? Since the advent of the statin era, “good” and “bad” cholesterol values are common conversational fare, in part because virtually every adult has had not one, but many lipid panels. Universal Lp(a) testing would spotlight this pervasive and important risk factor that was referred to as the “horrible” cholesterol in a recent review.
U.S. guidelines need updating
To foster this, U.S. guidelines, which influence every aspect of care, including testing, prevention, treatment, reimbursement, and medical legal issues, need to be simplified. The discussion of Lp(a) testing in the 2018 U.S. guidelines on cholesterol management is already obsolete. The contingencies on when testing is “reasonable” or “may be reasonable” are dated and cumbersome. In contrast, a recommendation to test everyone once, perhaps in adolescence, would be a useful, forward-looking strategy.
To date, trials of an antisense oligonucleotide and a small interfering RNA molecule targeting hepatic LPA messenger RNA have confirmed that plasma Lp(a) levels can be significantly and safely lowered. If the ongoing Lp(a) HORIZON and OCEAN(a) phase 3 trials have positive outcomes in patients with known ASCVD, this would spawn a host of clinical trials to explore the possibilities of these therapies in primary prevention as well. These will require tens of thousands of enrollees, and universal testing would expand the pool of potential participants.
The majority of at-risk individuals identified through universal testing would be candidates for primary prevention. This large, currently unidentified cohort should have all coexisting risk factors assessed and managed; lowering elevated LDL cholesterol early and aggressively is paramount. Recent data from the United Kingdom suggest that attainment of specific LDL cholesterol levels may offset the risk for vascular events in those with high Lp(a) levels.
Of note, this was the advice given to the small fraction of high-risk individuals like me, who had their Lp(a) level tested long before its ominous implications were understood. This recommendation was informed mostly by common sense. For any number of reasons, the same might be said for universal testing.
Dr. Leahy, a retired cardiologist in San Diego, has an abiding professional and personal interest in Lp(a), which has been responsible for a number of cardiovascular events in his own life over the past 2 decades. He was a participant in the phase 2 clinical trial of the Lp(a)-lowering antisense oligonucleotide being studied in the Lp(a) HORIZON trial, funded by Novartis, and is currently undergoing apheresis treatment. A version of this article originally appeared on Medscape.com.
Inflammation and immunity troubles top long-COVID suspect list
“I think that it’s a much more complex picture than just inflammation, or just autoimmunity, or just immune dysregulation. And it’s probably a combination of all three causing a cascade of effects that then manifests itself as brain fog, or shortness of breath, or chronic fatigue,” says Alexander Truong, MD, a pulmonologist and assistant professor at Emory University, Atlanta, who also runs a long-COVID clinic.
Long COVID, post–COVID-19 condition, and postacute sequelae of SARS-CoV-2 (PASC) are among the terms used by the National Institutes of Health to describe the long-term health issues faced by an estimated 10%-30% of people infected with COVID-19. Symptoms – as many as 200 – can range from inconvenient to crippling, damage multiple organ systems, come and go, and relapse. Long COVID increases the risk of worsening existing health problems and triggering new ones, including cardiovascular disease and type 2 diabetes.
So far, research suggests there is no single cause, condition, or disease that explains why some people have an extensive range of symptoms long after the early COVID-19 infection has cleared up. Many experts believe some combination of biological processes – including the virus hanging around in our bodies, inflammation, autoimmunity, tiny blood clots, immune system problems, and even the reactivation of dormant viruses such as the Epstein-Barr virus – could be the culprit, a theory also supported by a comprehensive and in-depth review of long-COVID studies published in the journal Nature Reviews Microbiology.
“It’s become clear over the last couple of years that there are different [symptoms] of long COVID … that cannot all be lumped together,” says Michael Peluso, MD, an assistant professor of medicine and an infectious diseases doctor at the University of California, San Francisco.
Inflammation and a virus that hangs around
Multiple studies have shown that the virus or pieces of it can remain in many parts of the body, including the kidneys, brain, heart, and gastrointestinal system, long after the early infection.
“One major question that I think is the area of most intense investigation now is whether there is viral persistence that is driving immune dysregulation and therefore symptoms,” says Dr. Peluso.
A small Harvard University study, for example, found evidence that reservoirs of the coronavirus could linger in patients up to a year after they’re first diagnosed.
An earlier German study found that patients with post-COVID-19 symptoms had higher levels of three cytokines – small proteins that tell the body’s immune system what to do and are involved in the growth and activity of immune system cells and blood cells. Researchers said the results supported the theory that there is persistent reprogramming of certain immune cells, and that the uncontrolled “self-fueled hyperinflammation” during the early COVID-19 infection can become continued immune cell disruption that drives long-COVID symptoms.
“Long COVID is more likely due to either an inflammatory response by the body or reservoirs of virus that the body is still trying to clear … and the symptoms we’re seeing are a side effect of that,” says Rainu Kaushal, MD, senior associate dean for clinical research at Weill Cornell Medicine in New York.
Australian researchers found that immune system recovery appeared different, compared with those who were infected with other common coronaviruses.
These findings also support concerns that some experts express over the long-term risks of COVID-19 infections in general, but especially repeat infections.
“Anything that kind of revs up inflammation in the body can boil that pot over and make the symptoms worse. That’s very easily an infection or some other insult to the body. So that’s the generalized hypothesis as to why insults to the body may worsen the symptoms,” says Dr. Truong.
An autoimmune condition?
But inflammation alone does not fully explain post–COVID-19 problems.
Dr. Truong and his team, for example, have been documenting inflammatory markers in patients at the post-COVID clinic he cofounded more than 2 years ago at Emory Executive Park in Atlanta. When the clinic was first launched, high-dose nonsteroidal anti-inflammatory drugs – including ibuprofen – and prednisone were prescribed to long-COVID patients.
“It didn’t make a difference at all for any of these folks,” he says, adding that there are signs that autoimmunity is at play. But he cautions that it is still too early to suggest treating long-COVID patients with medications used for other autoimmune conditions.
In autoimmune conditions such as rheumatoid arthritis, lupus, and type 1 diabetes, a person’s immune system can’t tell normal cells from foreign pathogens and attacks healthy cells. There is typically no single diagnostic test, and many share similar symptoms, making detection and diagnosis potentially difficult, according to Johns Hopkins Medicine.
A small study published in the journal Science Translational Medicine found that, among patients who failed to regain their sense of smell long after their initial infection, there was inflammation in the nose tissue where smell nerve cells are found, even though no detectable virus remained. Fewer olfactory sensory neurons were seen, as well – findings that researchers said resembled some kind of “autoimmune-like process.”
Meanwhile, scientists in Canada found signs of autoimmunity in blood samples taken from patients who still had fatigue and shortness of breath after their initial COVID-19 infection. Two specific proteins were present a year after infection in up to 30% of patients, many of whom still had shortness of breath and fatigue, the researchers reported in the Jan. 1 issue of the European Respiratory Journal. These patients had been healthy and had no autoimmune condition or other diseases before they were infected.
Immune system problems
A number of studies have suggested that a problematic immune response could also explain why symptoms persist for some people.
Researchers in France, for example, found that the immune response problems in those with severe COVID-19 infections caused exaggerated or uncontrolled formation of a type of bug-fighting defense mechanism called a neutrophil extracellular trap (NET), which in turn triggers harmful inflammation that can result in multiorgan damage. These traps are netlike structures made from fibers composed mostly of DNA strings that bind, or trap, pathogens.
Long COVID is not like an acute infectious disease, says Alexander Charney, MD, PhD, the lead principal investigator of the RECOVER adult cohort at Mount Sinai in New York, and an associate professor at Icahn School of Medicine at Mount Sinai. It is more similar to other complex chronic diseases that have taken decades to understand, such as heart disease, mental illness, and rheumatologic diseases, he says.
Biomarkers and blood clots
Scientists are homing in on biomarkers, or detectable and measurable traits – in this case, molecular indicators – that can make diagnosing long COVID easier and give better direction for treatment. These biomarkers are also key to helping sort out the complex biology of long COVID.
In one study, data from blood samples taken from hundreds of hospitalized COVID-19 patients suggests changes are happening at the molecular level during initial severe infections. These changes may be tied to the development of longer-term symptoms, according to the study by Dr. Charney and his team at Mount Sinai published in Nature Medicine
Blood clotting issues have also been detected in long COVID patients. At least one study found signs that long-COVID patients had higher levels of a type of auto-antibody linked to the abnormal formation of clots. Researchers suspect that tiny, persistent microclots – undetectable via regular pathology tests – may be cutting off oxygen flow to tissue by blocking capillaries – and could explain many of the post-COVID symptoms described by patients.
While enormous progress has been made toward understanding long COVID, the research is still considered early and faces many challenges, including varying criteria used to define the condition, the types and quality of data used, differences in how patients are defined and recruited, and the small size of many studies. Some research also appears to conflict with other studies. And while there are specialized tools for diagnosing some aspects of the condition, standard tests often don’t detect many of the signs seen in long-COVID patients. But given the urgency and global scale of the problem, experts say more funding and support should be prioritized.
“People are suffering now, and they want answers now. ... It’s not like with COVID, where the path towards a great and meaningful solution to this unbelievable problem was clear – we need a vaccine,” says Dr. Charney.
“It’s going to be a long haul to figure out what is going on.”
A version of this article originally appeared on WebMD.com.
“I think that it’s a much more complex picture than just inflammation, or just autoimmunity, or just immune dysregulation. And it’s probably a combination of all three causing a cascade of effects that then manifests itself as brain fog, or shortness of breath, or chronic fatigue,” says Alexander Truong, MD, a pulmonologist and assistant professor at Emory University, Atlanta, who also runs a long-COVID clinic.
Long COVID, post–COVID-19 condition, and postacute sequelae of SARS-CoV-2 (PASC) are among the terms used by the National Institutes of Health to describe the long-term health issues faced by an estimated 10%-30% of people infected with COVID-19. Symptoms – as many as 200 – can range from inconvenient to crippling, damage multiple organ systems, come and go, and relapse. Long COVID increases the risk of worsening existing health problems and triggering new ones, including cardiovascular disease and type 2 diabetes.
So far, research suggests there is no single cause, condition, or disease that explains why some people have an extensive range of symptoms long after the early COVID-19 infection has cleared up. Many experts believe some combination of biological processes – including the virus hanging around in our bodies, inflammation, autoimmunity, tiny blood clots, immune system problems, and even the reactivation of dormant viruses such as the Epstein-Barr virus – could be the culprit, a theory also supported by a comprehensive and in-depth review of long-COVID studies published in the journal Nature Reviews Microbiology.
“It’s become clear over the last couple of years that there are different [symptoms] of long COVID … that cannot all be lumped together,” says Michael Peluso, MD, an assistant professor of medicine and an infectious diseases doctor at the University of California, San Francisco.
Inflammation and a virus that hangs around
Multiple studies have shown that the virus or pieces of it can remain in many parts of the body, including the kidneys, brain, heart, and gastrointestinal system, long after the early infection.
“One major question that I think is the area of most intense investigation now is whether there is viral persistence that is driving immune dysregulation and therefore symptoms,” says Dr. Peluso.
A small Harvard University study, for example, found evidence that reservoirs of the coronavirus could linger in patients up to a year after they’re first diagnosed.
An earlier German study found that patients with post-COVID-19 symptoms had higher levels of three cytokines – small proteins that tell the body’s immune system what to do and are involved in the growth and activity of immune system cells and blood cells. Researchers said the results supported the theory that there is persistent reprogramming of certain immune cells, and that the uncontrolled “self-fueled hyperinflammation” during the early COVID-19 infection can become continued immune cell disruption that drives long-COVID symptoms.
“Long COVID is more likely due to either an inflammatory response by the body or reservoirs of virus that the body is still trying to clear … and the symptoms we’re seeing are a side effect of that,” says Rainu Kaushal, MD, senior associate dean for clinical research at Weill Cornell Medicine in New York.
Australian researchers found that immune system recovery appeared different, compared with those who were infected with other common coronaviruses.
These findings also support concerns that some experts express over the long-term risks of COVID-19 infections in general, but especially repeat infections.
“Anything that kind of revs up inflammation in the body can boil that pot over and make the symptoms worse. That’s very easily an infection or some other insult to the body. So that’s the generalized hypothesis as to why insults to the body may worsen the symptoms,” says Dr. Truong.
An autoimmune condition?
But inflammation alone does not fully explain post–COVID-19 problems.
Dr. Truong and his team, for example, have been documenting inflammatory markers in patients at the post-COVID clinic he cofounded more than 2 years ago at Emory Executive Park in Atlanta. When the clinic was first launched, high-dose nonsteroidal anti-inflammatory drugs – including ibuprofen – and prednisone were prescribed to long-COVID patients.
“It didn’t make a difference at all for any of these folks,” he says, adding that there are signs that autoimmunity is at play. But he cautions that it is still too early to suggest treating long-COVID patients with medications used for other autoimmune conditions.
In autoimmune conditions such as rheumatoid arthritis, lupus, and type 1 diabetes, a person’s immune system can’t tell normal cells from foreign pathogens and attacks healthy cells. There is typically no single diagnostic test, and many share similar symptoms, making detection and diagnosis potentially difficult, according to Johns Hopkins Medicine.
A small study published in the journal Science Translational Medicine found that, among patients who failed to regain their sense of smell long after their initial infection, there was inflammation in the nose tissue where smell nerve cells are found, even though no detectable virus remained. Fewer olfactory sensory neurons were seen, as well – findings that researchers said resembled some kind of “autoimmune-like process.”
Meanwhile, scientists in Canada found signs of autoimmunity in blood samples taken from patients who still had fatigue and shortness of breath after their initial COVID-19 infection. Two specific proteins were present a year after infection in up to 30% of patients, many of whom still had shortness of breath and fatigue, the researchers reported in the Jan. 1 issue of the European Respiratory Journal. These patients had been healthy and had no autoimmune condition or other diseases before they were infected.
Immune system problems
A number of studies have suggested that a problematic immune response could also explain why symptoms persist for some people.
Researchers in France, for example, found that the immune response problems in those with severe COVID-19 infections caused exaggerated or uncontrolled formation of a type of bug-fighting defense mechanism called a neutrophil extracellular trap (NET), which in turn triggers harmful inflammation that can result in multiorgan damage. These traps are netlike structures made from fibers composed mostly of DNA strings that bind, or trap, pathogens.
Long COVID is not like an acute infectious disease, says Alexander Charney, MD, PhD, the lead principal investigator of the RECOVER adult cohort at Mount Sinai in New York, and an associate professor at Icahn School of Medicine at Mount Sinai. It is more similar to other complex chronic diseases that have taken decades to understand, such as heart disease, mental illness, and rheumatologic diseases, he says.
Biomarkers and blood clots
Scientists are homing in on biomarkers, or detectable and measurable traits – in this case, molecular indicators – that can make diagnosing long COVID easier and give better direction for treatment. These biomarkers are also key to helping sort out the complex biology of long COVID.
In one study, data from blood samples taken from hundreds of hospitalized COVID-19 patients suggests changes are happening at the molecular level during initial severe infections. These changes may be tied to the development of longer-term symptoms, according to the study by Dr. Charney and his team at Mount Sinai published in Nature Medicine
Blood clotting issues have also been detected in long COVID patients. At least one study found signs that long-COVID patients had higher levels of a type of auto-antibody linked to the abnormal formation of clots. Researchers suspect that tiny, persistent microclots – undetectable via regular pathology tests – may be cutting off oxygen flow to tissue by blocking capillaries – and could explain many of the post-COVID symptoms described by patients.
While enormous progress has been made toward understanding long COVID, the research is still considered early and faces many challenges, including varying criteria used to define the condition, the types and quality of data used, differences in how patients are defined and recruited, and the small size of many studies. Some research also appears to conflict with other studies. And while there are specialized tools for diagnosing some aspects of the condition, standard tests often don’t detect many of the signs seen in long-COVID patients. But given the urgency and global scale of the problem, experts say more funding and support should be prioritized.
“People are suffering now, and they want answers now. ... It’s not like with COVID, where the path towards a great and meaningful solution to this unbelievable problem was clear – we need a vaccine,” says Dr. Charney.
“It’s going to be a long haul to figure out what is going on.”
A version of this article originally appeared on WebMD.com.
“I think that it’s a much more complex picture than just inflammation, or just autoimmunity, or just immune dysregulation. And it’s probably a combination of all three causing a cascade of effects that then manifests itself as brain fog, or shortness of breath, or chronic fatigue,” says Alexander Truong, MD, a pulmonologist and assistant professor at Emory University, Atlanta, who also runs a long-COVID clinic.
Long COVID, post–COVID-19 condition, and postacute sequelae of SARS-CoV-2 (PASC) are among the terms used by the National Institutes of Health to describe the long-term health issues faced by an estimated 10%-30% of people infected with COVID-19. Symptoms – as many as 200 – can range from inconvenient to crippling, damage multiple organ systems, come and go, and relapse. Long COVID increases the risk of worsening existing health problems and triggering new ones, including cardiovascular disease and type 2 diabetes.
So far, research suggests there is no single cause, condition, or disease that explains why some people have an extensive range of symptoms long after the early COVID-19 infection has cleared up. Many experts believe some combination of biological processes – including the virus hanging around in our bodies, inflammation, autoimmunity, tiny blood clots, immune system problems, and even the reactivation of dormant viruses such as the Epstein-Barr virus – could be the culprit, a theory also supported by a comprehensive and in-depth review of long-COVID studies published in the journal Nature Reviews Microbiology.
“It’s become clear over the last couple of years that there are different [symptoms] of long COVID … that cannot all be lumped together,” says Michael Peluso, MD, an assistant professor of medicine and an infectious diseases doctor at the University of California, San Francisco.
Inflammation and a virus that hangs around
Multiple studies have shown that the virus or pieces of it can remain in many parts of the body, including the kidneys, brain, heart, and gastrointestinal system, long after the early infection.
“One major question that I think is the area of most intense investigation now is whether there is viral persistence that is driving immune dysregulation and therefore symptoms,” says Dr. Peluso.
A small Harvard University study, for example, found evidence that reservoirs of the coronavirus could linger in patients up to a year after they’re first diagnosed.
An earlier German study found that patients with post-COVID-19 symptoms had higher levels of three cytokines – small proteins that tell the body’s immune system what to do and are involved in the growth and activity of immune system cells and blood cells. Researchers said the results supported the theory that there is persistent reprogramming of certain immune cells, and that the uncontrolled “self-fueled hyperinflammation” during the early COVID-19 infection can become continued immune cell disruption that drives long-COVID symptoms.
“Long COVID is more likely due to either an inflammatory response by the body or reservoirs of virus that the body is still trying to clear … and the symptoms we’re seeing are a side effect of that,” says Rainu Kaushal, MD, senior associate dean for clinical research at Weill Cornell Medicine in New York.
Australian researchers found that immune system recovery appeared different, compared with those who were infected with other common coronaviruses.
These findings also support concerns that some experts express over the long-term risks of COVID-19 infections in general, but especially repeat infections.
“Anything that kind of revs up inflammation in the body can boil that pot over and make the symptoms worse. That’s very easily an infection or some other insult to the body. So that’s the generalized hypothesis as to why insults to the body may worsen the symptoms,” says Dr. Truong.
An autoimmune condition?
But inflammation alone does not fully explain post–COVID-19 problems.
Dr. Truong and his team, for example, have been documenting inflammatory markers in patients at the post-COVID clinic he cofounded more than 2 years ago at Emory Executive Park in Atlanta. When the clinic was first launched, high-dose nonsteroidal anti-inflammatory drugs – including ibuprofen – and prednisone were prescribed to long-COVID patients.
“It didn’t make a difference at all for any of these folks,” he says, adding that there are signs that autoimmunity is at play. But he cautions that it is still too early to suggest treating long-COVID patients with medications used for other autoimmune conditions.
In autoimmune conditions such as rheumatoid arthritis, lupus, and type 1 diabetes, a person’s immune system can’t tell normal cells from foreign pathogens and attacks healthy cells. There is typically no single diagnostic test, and many share similar symptoms, making detection and diagnosis potentially difficult, according to Johns Hopkins Medicine.
A small study published in the journal Science Translational Medicine found that, among patients who failed to regain their sense of smell long after their initial infection, there was inflammation in the nose tissue where smell nerve cells are found, even though no detectable virus remained. Fewer olfactory sensory neurons were seen, as well – findings that researchers said resembled some kind of “autoimmune-like process.”
Meanwhile, scientists in Canada found signs of autoimmunity in blood samples taken from patients who still had fatigue and shortness of breath after their initial COVID-19 infection. Two specific proteins were present a year after infection in up to 30% of patients, many of whom still had shortness of breath and fatigue, the researchers reported in the Jan. 1 issue of the European Respiratory Journal. These patients had been healthy and had no autoimmune condition or other diseases before they were infected.
Immune system problems
A number of studies have suggested that a problematic immune response could also explain why symptoms persist for some people.
Researchers in France, for example, found that the immune response problems in those with severe COVID-19 infections caused exaggerated or uncontrolled formation of a type of bug-fighting defense mechanism called a neutrophil extracellular trap (NET), which in turn triggers harmful inflammation that can result in multiorgan damage. These traps are netlike structures made from fibers composed mostly of DNA strings that bind, or trap, pathogens.
Long COVID is not like an acute infectious disease, says Alexander Charney, MD, PhD, the lead principal investigator of the RECOVER adult cohort at Mount Sinai in New York, and an associate professor at Icahn School of Medicine at Mount Sinai. It is more similar to other complex chronic diseases that have taken decades to understand, such as heart disease, mental illness, and rheumatologic diseases, he says.
Biomarkers and blood clots
Scientists are homing in on biomarkers, or detectable and measurable traits – in this case, molecular indicators – that can make diagnosing long COVID easier and give better direction for treatment. These biomarkers are also key to helping sort out the complex biology of long COVID.
In one study, data from blood samples taken from hundreds of hospitalized COVID-19 patients suggests changes are happening at the molecular level during initial severe infections. These changes may be tied to the development of longer-term symptoms, according to the study by Dr. Charney and his team at Mount Sinai published in Nature Medicine
Blood clotting issues have also been detected in long COVID patients. At least one study found signs that long-COVID patients had higher levels of a type of auto-antibody linked to the abnormal formation of clots. Researchers suspect that tiny, persistent microclots – undetectable via regular pathology tests – may be cutting off oxygen flow to tissue by blocking capillaries – and could explain many of the post-COVID symptoms described by patients.
While enormous progress has been made toward understanding long COVID, the research is still considered early and faces many challenges, including varying criteria used to define the condition, the types and quality of data used, differences in how patients are defined and recruited, and the small size of many studies. Some research also appears to conflict with other studies. And while there are specialized tools for diagnosing some aspects of the condition, standard tests often don’t detect many of the signs seen in long-COVID patients. But given the urgency and global scale of the problem, experts say more funding and support should be prioritized.
“People are suffering now, and they want answers now. ... It’s not like with COVID, where the path towards a great and meaningful solution to this unbelievable problem was clear – we need a vaccine,” says Dr. Charney.
“It’s going to be a long haul to figure out what is going on.”
A version of this article originally appeared on WebMD.com.
Using live pigs in residency training sparks heated debate
Pigs have been long used in medical schools to teach surgical techniques and, more recently, in research trials and experimental xenotransplantation procedures. But
Just last month, the Physicians Committee for Responsible Medicine, a nonprofit group with a decades-long stance against the use of animals in medical education and research, placed billboards around the Portland, Ore., area demanding that Oregon Health and Science University stop using pigs to teach surgical residents.
Undergraduate medical programs no longer use live animals. But a small number of graduate medical education programs still use animals, predominantly pigs, to train physicians in subspecialties like internal medicine, emergency medicine, surgery, and anesthesiology, John Pippin, MD, FACC, director of academic affairs at PCRM, told this news organization.
Dr. Pippin says residents practice establishing emergency airways, inserting chest tubes, and accessing blood vessels on anesthetized pigs before euthanizing them.
Swine lab advocates say pigs make ideal training subjects because of their similarities to humans, including comparably sized organs like the heart, lungs, and kidneys. Pigs share about 85% of their DNA with people. Where pig skin alternatives may suffice for less invasive procedures, supporters say residents’ experiences with live tissue are irreplaceable.
In a statement, Sara Hottman, associate director of media relations at Oregon Health and Science University, told this news organization the school “only uses animal models in its surgical training program when nonanimal methods are inadequate or too dangerous for human participants.”
“We believe that the education and experience surgical trainees gain through the use of relevant animal models are essential to ensuring future surgeons have the knowledge and skills necessary to provide safe, high-quality care.”
Ms. Hottman also noted that the university continues to evaluate alternatives and looks forward to when nonanimal “surgical training methods are capable of faithfully modeling the complexity of a living system,” such as in the management of critical internal complications.
But Dr. Pippin argues that residents can gain sufficient expertise through simulators and hands-on training in the operating room, and that the differences between humans and pigs are too vast to provide meaningful clinical data or skills.
“Pigs have different genetic influences and very thick, tough skin,” he said. If you use the same pressure on a human that you learned on a pig, he added, “you’d slice right through the trachea. Whatever you think you find out in animals, you have to learn all over again with humans.”
Undergraduate medical education programs in the United States and Canada abandoned the practice of using live animals, including pigs, by 2016, with Johns Hopkins University, Baltimore, and the University of Tennessee, Chattanooga, last to announce their shift away from the controversial teaching model following campaigns by PCRM.
Today, most residency training programs have followed suit. Pippin said that pediatric residencies no longer use animals, and all trauma and anesthesiology programs have ceased such practices except two. Just 3% of emergency medicine programs continue to use animals, as do about 21% of surgical residencies, he said, based on PCRM’s latest surveys.
A public debate
Occasionally, PCRM goes public with a campaign against a residency program “if that’s the only way to win,” Dr. Pippin said.
In addition to billboards, the group has held protests, circulated petitions, and filed complaints with the U.S. Department of Agriculture’s Animal and Plant Health Inspection Service, the entity responsible for overseeing the health and welfare of animals used in medical training and research.
In 2021, spurred by a complaint from PCRM, APHIS launched an investigation into the University of Cincinnati’s surgical residency program. At the time, a university spokesperson acknowledged the school’s limited use of pigs to train “highly-skilled, well-prepared surgeons in the most advanced, complex, real-world needs, procedures, and techniques,” adding that the training methods were endorsed by the American College of Surgeons and in compliance with federal guidelines.
Residency programs have caught the attention of state lawmakers, too. In 2020, bills introduced in both the Rhode Island House and Senate sought to ban the use of live animals in medical training when “there is an alternate teaching method that teaches the medical procedure or lesson without the use of an animal.” Violators would incur misdemeanor charges and monetary fines of up to $1,000 per animal.
The bills – backed by PCRM – targeted Brown University’s emergency medicine residency program, Providence, R.I., which sponsoring legislators said was the last program in New England still using the “outdated” and “unnecessary” method.
In testimony before lawmakers, the school said fewer than 15 pigs participate in the annual training, and faculty spoke about the benefits of the experience.
“If it was your brother or sister, or your mother or father who had to come in and get this procedure done, would you want the physician who’s doing it to be the one who does it for the very first time on a human being, on live tissue? Or do you want that provider to have only practiced on plastic and rubber?” said Nicholas Musisca, MD, an assistant program director with Brown University’s emergency medicine residency, NBC affiliate WJAR reported.
The bills have since stalled, and PCRM held a protest at Brown University in October 2022. In response, a university spokesperson told the Brown Daily Herald, “effective synthetic model alternatives simply do not exist for every complex medical procedure that an emergency physician must be prepared to perform,” including establishing an airway in adults and pediatric patients with severe facial trauma.
By the numbers
Annual reports from APHIS do not show the number of pigs dedicated solely to residency training. Instead, reporting indicates the number of animals “upon which experiments, teaching, research, surgery, or tests were conducted involving accompanying pain or distress to the animals and for which appropriate anesthetic, analgesic, or tranquilizing drugs were used.”
For fiscal year 2021 – the most recent data available – Oregon Health and Science University had 154 pigs under its control, while the University of Cincinnati and Brown University had 118 and 71 pigs, respectively, according to APHIS. Primates were more commonly used at Oregon Health and Science University and guinea pigs at the University of Cincinnati.
Similarly, the Association of American Medical Colleges supports the “use of animals to meet essential educational objectives [across] the medical education continuum. ... Further restrictions on the use of animals in biomedical and behavioral research and education threatens progress in health care and disease prevention.”
The debate will likely rage on. “The one thing we don’t do is give up,” Dr. Pippin said.
A version of this article originally appeared on Medscape.com.
Pigs have been long used in medical schools to teach surgical techniques and, more recently, in research trials and experimental xenotransplantation procedures. But
Just last month, the Physicians Committee for Responsible Medicine, a nonprofit group with a decades-long stance against the use of animals in medical education and research, placed billboards around the Portland, Ore., area demanding that Oregon Health and Science University stop using pigs to teach surgical residents.
Undergraduate medical programs no longer use live animals. But a small number of graduate medical education programs still use animals, predominantly pigs, to train physicians in subspecialties like internal medicine, emergency medicine, surgery, and anesthesiology, John Pippin, MD, FACC, director of academic affairs at PCRM, told this news organization.
Dr. Pippin says residents practice establishing emergency airways, inserting chest tubes, and accessing blood vessels on anesthetized pigs before euthanizing them.
Swine lab advocates say pigs make ideal training subjects because of their similarities to humans, including comparably sized organs like the heart, lungs, and kidneys. Pigs share about 85% of their DNA with people. Where pig skin alternatives may suffice for less invasive procedures, supporters say residents’ experiences with live tissue are irreplaceable.
In a statement, Sara Hottman, associate director of media relations at Oregon Health and Science University, told this news organization the school “only uses animal models in its surgical training program when nonanimal methods are inadequate or too dangerous for human participants.”
“We believe that the education and experience surgical trainees gain through the use of relevant animal models are essential to ensuring future surgeons have the knowledge and skills necessary to provide safe, high-quality care.”
Ms. Hottman also noted that the university continues to evaluate alternatives and looks forward to when nonanimal “surgical training methods are capable of faithfully modeling the complexity of a living system,” such as in the management of critical internal complications.
But Dr. Pippin argues that residents can gain sufficient expertise through simulators and hands-on training in the operating room, and that the differences between humans and pigs are too vast to provide meaningful clinical data or skills.
“Pigs have different genetic influences and very thick, tough skin,” he said. If you use the same pressure on a human that you learned on a pig, he added, “you’d slice right through the trachea. Whatever you think you find out in animals, you have to learn all over again with humans.”
Undergraduate medical education programs in the United States and Canada abandoned the practice of using live animals, including pigs, by 2016, with Johns Hopkins University, Baltimore, and the University of Tennessee, Chattanooga, last to announce their shift away from the controversial teaching model following campaigns by PCRM.
Today, most residency training programs have followed suit. Pippin said that pediatric residencies no longer use animals, and all trauma and anesthesiology programs have ceased such practices except two. Just 3% of emergency medicine programs continue to use animals, as do about 21% of surgical residencies, he said, based on PCRM’s latest surveys.
A public debate
Occasionally, PCRM goes public with a campaign against a residency program “if that’s the only way to win,” Dr. Pippin said.
In addition to billboards, the group has held protests, circulated petitions, and filed complaints with the U.S. Department of Agriculture’s Animal and Plant Health Inspection Service, the entity responsible for overseeing the health and welfare of animals used in medical training and research.
In 2021, spurred by a complaint from PCRM, APHIS launched an investigation into the University of Cincinnati’s surgical residency program. At the time, a university spokesperson acknowledged the school’s limited use of pigs to train “highly-skilled, well-prepared surgeons in the most advanced, complex, real-world needs, procedures, and techniques,” adding that the training methods were endorsed by the American College of Surgeons and in compliance with federal guidelines.
Residency programs have caught the attention of state lawmakers, too. In 2020, bills introduced in both the Rhode Island House and Senate sought to ban the use of live animals in medical training when “there is an alternate teaching method that teaches the medical procedure or lesson without the use of an animal.” Violators would incur misdemeanor charges and monetary fines of up to $1,000 per animal.
The bills – backed by PCRM – targeted Brown University’s emergency medicine residency program, Providence, R.I., which sponsoring legislators said was the last program in New England still using the “outdated” and “unnecessary” method.
In testimony before lawmakers, the school said fewer than 15 pigs participate in the annual training, and faculty spoke about the benefits of the experience.
“If it was your brother or sister, or your mother or father who had to come in and get this procedure done, would you want the physician who’s doing it to be the one who does it for the very first time on a human being, on live tissue? Or do you want that provider to have only practiced on plastic and rubber?” said Nicholas Musisca, MD, an assistant program director with Brown University’s emergency medicine residency, NBC affiliate WJAR reported.
The bills have since stalled, and PCRM held a protest at Brown University in October 2022. In response, a university spokesperson told the Brown Daily Herald, “effective synthetic model alternatives simply do not exist for every complex medical procedure that an emergency physician must be prepared to perform,” including establishing an airway in adults and pediatric patients with severe facial trauma.
By the numbers
Annual reports from APHIS do not show the number of pigs dedicated solely to residency training. Instead, reporting indicates the number of animals “upon which experiments, teaching, research, surgery, or tests were conducted involving accompanying pain or distress to the animals and for which appropriate anesthetic, analgesic, or tranquilizing drugs were used.”
For fiscal year 2021 – the most recent data available – Oregon Health and Science University had 154 pigs under its control, while the University of Cincinnati and Brown University had 118 and 71 pigs, respectively, according to APHIS. Primates were more commonly used at Oregon Health and Science University and guinea pigs at the University of Cincinnati.
Similarly, the Association of American Medical Colleges supports the “use of animals to meet essential educational objectives [across] the medical education continuum. ... Further restrictions on the use of animals in biomedical and behavioral research and education threatens progress in health care and disease prevention.”
The debate will likely rage on. “The one thing we don’t do is give up,” Dr. Pippin said.
A version of this article originally appeared on Medscape.com.
Pigs have been long used in medical schools to teach surgical techniques and, more recently, in research trials and experimental xenotransplantation procedures. But
Just last month, the Physicians Committee for Responsible Medicine, a nonprofit group with a decades-long stance against the use of animals in medical education and research, placed billboards around the Portland, Ore., area demanding that Oregon Health and Science University stop using pigs to teach surgical residents.
Undergraduate medical programs no longer use live animals. But a small number of graduate medical education programs still use animals, predominantly pigs, to train physicians in subspecialties like internal medicine, emergency medicine, surgery, and anesthesiology, John Pippin, MD, FACC, director of academic affairs at PCRM, told this news organization.
Dr. Pippin says residents practice establishing emergency airways, inserting chest tubes, and accessing blood vessels on anesthetized pigs before euthanizing them.
Swine lab advocates say pigs make ideal training subjects because of their similarities to humans, including comparably sized organs like the heart, lungs, and kidneys. Pigs share about 85% of their DNA with people. Where pig skin alternatives may suffice for less invasive procedures, supporters say residents’ experiences with live tissue are irreplaceable.
In a statement, Sara Hottman, associate director of media relations at Oregon Health and Science University, told this news organization the school “only uses animal models in its surgical training program when nonanimal methods are inadequate or too dangerous for human participants.”
“We believe that the education and experience surgical trainees gain through the use of relevant animal models are essential to ensuring future surgeons have the knowledge and skills necessary to provide safe, high-quality care.”
Ms. Hottman also noted that the university continues to evaluate alternatives and looks forward to when nonanimal “surgical training methods are capable of faithfully modeling the complexity of a living system,” such as in the management of critical internal complications.
But Dr. Pippin argues that residents can gain sufficient expertise through simulators and hands-on training in the operating room, and that the differences between humans and pigs are too vast to provide meaningful clinical data or skills.
“Pigs have different genetic influences and very thick, tough skin,” he said. If you use the same pressure on a human that you learned on a pig, he added, “you’d slice right through the trachea. Whatever you think you find out in animals, you have to learn all over again with humans.”
Undergraduate medical education programs in the United States and Canada abandoned the practice of using live animals, including pigs, by 2016, with Johns Hopkins University, Baltimore, and the University of Tennessee, Chattanooga, last to announce their shift away from the controversial teaching model following campaigns by PCRM.
Today, most residency training programs have followed suit. Pippin said that pediatric residencies no longer use animals, and all trauma and anesthesiology programs have ceased such practices except two. Just 3% of emergency medicine programs continue to use animals, as do about 21% of surgical residencies, he said, based on PCRM’s latest surveys.
A public debate
Occasionally, PCRM goes public with a campaign against a residency program “if that’s the only way to win,” Dr. Pippin said.
In addition to billboards, the group has held protests, circulated petitions, and filed complaints with the U.S. Department of Agriculture’s Animal and Plant Health Inspection Service, the entity responsible for overseeing the health and welfare of animals used in medical training and research.
In 2021, spurred by a complaint from PCRM, APHIS launched an investigation into the University of Cincinnati’s surgical residency program. At the time, a university spokesperson acknowledged the school’s limited use of pigs to train “highly-skilled, well-prepared surgeons in the most advanced, complex, real-world needs, procedures, and techniques,” adding that the training methods were endorsed by the American College of Surgeons and in compliance with federal guidelines.
Residency programs have caught the attention of state lawmakers, too. In 2020, bills introduced in both the Rhode Island House and Senate sought to ban the use of live animals in medical training when “there is an alternate teaching method that teaches the medical procedure or lesson without the use of an animal.” Violators would incur misdemeanor charges and monetary fines of up to $1,000 per animal.
The bills – backed by PCRM – targeted Brown University’s emergency medicine residency program, Providence, R.I., which sponsoring legislators said was the last program in New England still using the “outdated” and “unnecessary” method.
In testimony before lawmakers, the school said fewer than 15 pigs participate in the annual training, and faculty spoke about the benefits of the experience.
“If it was your brother or sister, or your mother or father who had to come in and get this procedure done, would you want the physician who’s doing it to be the one who does it for the very first time on a human being, on live tissue? Or do you want that provider to have only practiced on plastic and rubber?” said Nicholas Musisca, MD, an assistant program director with Brown University’s emergency medicine residency, NBC affiliate WJAR reported.
The bills have since stalled, and PCRM held a protest at Brown University in October 2022. In response, a university spokesperson told the Brown Daily Herald, “effective synthetic model alternatives simply do not exist for every complex medical procedure that an emergency physician must be prepared to perform,” including establishing an airway in adults and pediatric patients with severe facial trauma.
By the numbers
Annual reports from APHIS do not show the number of pigs dedicated solely to residency training. Instead, reporting indicates the number of animals “upon which experiments, teaching, research, surgery, or tests were conducted involving accompanying pain or distress to the animals and for which appropriate anesthetic, analgesic, or tranquilizing drugs were used.”
For fiscal year 2021 – the most recent data available – Oregon Health and Science University had 154 pigs under its control, while the University of Cincinnati and Brown University had 118 and 71 pigs, respectively, according to APHIS. Primates were more commonly used at Oregon Health and Science University and guinea pigs at the University of Cincinnati.
Similarly, the Association of American Medical Colleges supports the “use of animals to meet essential educational objectives [across] the medical education continuum. ... Further restrictions on the use of animals in biomedical and behavioral research and education threatens progress in health care and disease prevention.”
The debate will likely rage on. “The one thing we don’t do is give up,” Dr. Pippin said.
A version of this article originally appeared on Medscape.com.
COVID emergency orders ending: What’s next?
It’s the end of an era.
The orders spanned two presidencies. The Trump administration’s Health and Human Services Secretary Alex Azar issued a public health emergency in January 2020. Then-President Donald Trump declared the COVID-19 pandemic a national emergency 2 months later. Both emergency declarations – which remained in effect under President Joe Biden – are set to expire May 11.
Read on for an overview of how the end of the public health emergency will trigger multiple federal policy changes.
Changes that affect everyone
- There will be cost-sharing changes for COVID-19 vaccines, testing, and certain treatments. One hundred–percent coverage for COVID testing, including free at-home tests, will expire May 11.
- Telemedicine cannot be used to prescribe controlled substances after May 11, 2023.
- Enhanced federal funding will be phased down through Dec. 31, 2023. This extends the time states must receive federally matched funds for COVID-related services and products, through the Consolidated Appropriations Act of 2023. Otherwise, this would have expired June 30, 2023.
- Emergency use authorizations for COVID-19 treatments and vaccinations will not be affected and/or end on May 11.
Changes that affect people with private health insurance
- Many will likely see higher costs for COVID-19 tests, as free testing expires and cost-sharing begins in the coming months.
- COVID-19 vaccinations and boosters will continue to be covered until the federal government’s vaccination supply is depleted. If that happens, you will need an in-network provider.
- You will still have access to COVID-19 treatments – but that could change when the federal supply dwindles.
Changes that affect Medicare recipients
- Medicare telehealth flexibilities will be extended through Dec. 31, 2024, regardless of public health emergency status. This means people can access telehealth services from anywhere, not just rural areas; can use a smartphone for telehealth; and can access telehealth in their homes.
- Medicare cost-sharing for testing and treatments will expire May 11, except for oral antivirals.
Changes that affect Medicaid/CHIP recipients
- Medicaid and Children’s Health Insurance Program (CHIP) recipients will continue to receive approved vaccinations free of charge, but testing and treatment without cost-sharing will expire during the third quarter of 2024.
- The Medicaid continuous enrollment provision will be separated from the public health emergency, and continuous enrollment will end March 31, 2023.
Changes that affect uninsured people
- The uninsured will no longer have access to 100% coverage for these products and services (free COVID-19 treatments, vaccines, and testing).
Changes that affect health care providers
- There will be changes to how much providers get paid for diagnosing people with COVID-19, ending the enhanced Inpatient Prospective Payment System reimbursement rate, as of May 11, 2023.
- Health Insurance Portability and Accountability Act (HIPAA) potential penalty waivers will end. This allows providers to communicate with patients through telehealth on a smartphone, for example, without violating privacy laws and incurring penalties.
What the experts are saying
This news organization asked several health experts for their thoughts on ending the emergency health declarations for COVID, and what effects this could have. Many expressed concerns about the timing of the ending, saying that the move could limit access to COVID-related treatments. Others said the move was inevitable but raised concerns about federal guidance related to the decision.
Question: Do you agree with the timing of the end to the emergency order?
Answer: Robert Atmar, MD, professor of infectious diseases at Baylor College of Medicine in Houston: “A lead time to prepare and anticipate these consequences may ease the transition, compared to an abrupt declaration that ends the declaration.”
Answer: Georges C. Benjamin, MD, executive director of the American Public Health Association: “I think it’s time to do so. It has to be done in a great, thoughtful, and organized way because we’ve attached so many different things to this public health emergency. It’s going to take time for the system to adapt. [Centers for Disease Control and Prevention] data collection most likely will continue. People are used to reporting now. The CDC needs to give guidance to the states so that we’re clear about what we’re reporting, what we’re not. If we did that abruptly, it would just be a mess.”
Answer: Bruce Farber, MD, chief public health and epidemiology officer at Northwell Health in Manhasset, N.Y.: “I would have hoped to see it delayed.”
Answer: Steven Newmark, JD, chief legal officer and director of policy at the Global Healthy Living Foundation: “While we understand that an emergency cannot last forever, we hope that expanded services such as free vaccination, promotion of widespread vaccination, increased use of pharmacists to administer vaccines, telehealth availability and reimbursement, flexibility in work-from-home opportunities, and more continues. Access to equitable health care should never backtrack or be reduced.”
Q: What will the end of free COVID vaccinations and free testing mean?
A: Dr. Farber: “There will likely be a decrease in vaccinations and testing. The vaccination rates are very low to begin with, and this will likely lower it further.”
A: Dr. Atmar: “I think it will mean that fewer people will get tested and vaccinated,” which “could lead to increased transmission, although wastewater testing suggests that there is a lot of unrecognized infection already occurring.”
A: Dr. Benjamin: “That is a big concern. It means that for people, particularly for people who are uninsured and underinsured, we’ve got to make sure they have access to those. There’s a lot of discussion and debate about what the cost of those tests and vaccines will be, and it looks like the companies are going to impose very steep, increasing costs.”
Q: How will this affect higher-risk populations, like people with weakened immune systems?
A: Dr. Farber: “Without monoclonals [drugs to treat COVID] and free Paxlovid,” people with weakened immune systems “may be undertreated.”
A: Dr. Atmar: “The implications of ongoing widespread virus transmission are that immunocompromised individuals may be more likely to be exposed and infected and to suffer the consequences of such infection, including severe illness. However, to a certain degree, this may already be happening. We are still seeing about 500 deaths/day, primarily in persons at highest risk of severe disease.”
A: Dr. Benjamin: “People who have good insurance, can afford to get immunized, and have good relations with practitioners probably will continue to be covered. But lower-income individuals and people who really can’t afford to get tested or get immunized would likely become underimmunized and more infected.
“So even though the federal emergency declaration will go away, I’m hoping that the federal government will continue to encourage all of us to emphasize those populations at the highest risk – those with chronic disease and those who are immunocompromised.”
A: Mr. Newmark: “People who are immunocompromised by their chronic illness or the medicines they take to treat acute or chronic conditions remain at higher risk for COVID-19 and its serious complications. The administration needs to support continued development of effective treatments and updated vaccines to protect the individual and public health. We’re also concerned that increased health care services - such as vaccination or telehealth – may fall back to prepandemic levels while the burden of protection, such as masking, may fall to chronic disease patients alone, which adds to the burden of living with disease.”
Q: What effect will ending Medicaid expansion money have?
A: Dr. Benjamin: Anywhere from 16 to 20 million people are going to lose in coverage. I’m hoping that states will look at their experience over these last 2 years or so and come to the decision that there were improvements in healthier populations.
Q: Will this have any effect on how the public perceives the pandemic?
A: Dr. Farber: “It is likely to give the impression that COVID is gone, which clearly is not the case.”
A: Dr. Benjamin: “It’ll be another argument by some that the pandemic is over. People should think about this as kind of like a hurricane. A hurricane comes through and tragically tears up communities, and we have an emergency during that time. But then we have to go through a period of recovery. I’m hoping people will realize that even though the public health emergencies have gone away, that we still need to go through a period of transition ... and that means that they still need to protect themselves, get vaccinated, and wear a mask when appropriate.”
A: Dr. Atmar: “There needs to be messaging that while we are transitioning away from emergency management of COVID-19, it is still a significant public health concern.”
A version of this article originally appeared on WebMD.com.
It’s the end of an era.
The orders spanned two presidencies. The Trump administration’s Health and Human Services Secretary Alex Azar issued a public health emergency in January 2020. Then-President Donald Trump declared the COVID-19 pandemic a national emergency 2 months later. Both emergency declarations – which remained in effect under President Joe Biden – are set to expire May 11.
Read on for an overview of how the end of the public health emergency will trigger multiple federal policy changes.
Changes that affect everyone
- There will be cost-sharing changes for COVID-19 vaccines, testing, and certain treatments. One hundred–percent coverage for COVID testing, including free at-home tests, will expire May 11.
- Telemedicine cannot be used to prescribe controlled substances after May 11, 2023.
- Enhanced federal funding will be phased down through Dec. 31, 2023. This extends the time states must receive federally matched funds for COVID-related services and products, through the Consolidated Appropriations Act of 2023. Otherwise, this would have expired June 30, 2023.
- Emergency use authorizations for COVID-19 treatments and vaccinations will not be affected and/or end on May 11.
Changes that affect people with private health insurance
- Many will likely see higher costs for COVID-19 tests, as free testing expires and cost-sharing begins in the coming months.
- COVID-19 vaccinations and boosters will continue to be covered until the federal government’s vaccination supply is depleted. If that happens, you will need an in-network provider.
- You will still have access to COVID-19 treatments – but that could change when the federal supply dwindles.
Changes that affect Medicare recipients
- Medicare telehealth flexibilities will be extended through Dec. 31, 2024, regardless of public health emergency status. This means people can access telehealth services from anywhere, not just rural areas; can use a smartphone for telehealth; and can access telehealth in their homes.
- Medicare cost-sharing for testing and treatments will expire May 11, except for oral antivirals.
Changes that affect Medicaid/CHIP recipients
- Medicaid and Children’s Health Insurance Program (CHIP) recipients will continue to receive approved vaccinations free of charge, but testing and treatment without cost-sharing will expire during the third quarter of 2024.
- The Medicaid continuous enrollment provision will be separated from the public health emergency, and continuous enrollment will end March 31, 2023.
Changes that affect uninsured people
- The uninsured will no longer have access to 100% coverage for these products and services (free COVID-19 treatments, vaccines, and testing).
Changes that affect health care providers
- There will be changes to how much providers get paid for diagnosing people with COVID-19, ending the enhanced Inpatient Prospective Payment System reimbursement rate, as of May 11, 2023.
- Health Insurance Portability and Accountability Act (HIPAA) potential penalty waivers will end. This allows providers to communicate with patients through telehealth on a smartphone, for example, without violating privacy laws and incurring penalties.
What the experts are saying
This news organization asked several health experts for their thoughts on ending the emergency health declarations for COVID, and what effects this could have. Many expressed concerns about the timing of the ending, saying that the move could limit access to COVID-related treatments. Others said the move was inevitable but raised concerns about federal guidance related to the decision.
Question: Do you agree with the timing of the end to the emergency order?
Answer: Robert Atmar, MD, professor of infectious diseases at Baylor College of Medicine in Houston: “A lead time to prepare and anticipate these consequences may ease the transition, compared to an abrupt declaration that ends the declaration.”
Answer: Georges C. Benjamin, MD, executive director of the American Public Health Association: “I think it’s time to do so. It has to be done in a great, thoughtful, and organized way because we’ve attached so many different things to this public health emergency. It’s going to take time for the system to adapt. [Centers for Disease Control and Prevention] data collection most likely will continue. People are used to reporting now. The CDC needs to give guidance to the states so that we’re clear about what we’re reporting, what we’re not. If we did that abruptly, it would just be a mess.”
Answer: Bruce Farber, MD, chief public health and epidemiology officer at Northwell Health in Manhasset, N.Y.: “I would have hoped to see it delayed.”
Answer: Steven Newmark, JD, chief legal officer and director of policy at the Global Healthy Living Foundation: “While we understand that an emergency cannot last forever, we hope that expanded services such as free vaccination, promotion of widespread vaccination, increased use of pharmacists to administer vaccines, telehealth availability and reimbursement, flexibility in work-from-home opportunities, and more continues. Access to equitable health care should never backtrack or be reduced.”
Q: What will the end of free COVID vaccinations and free testing mean?
A: Dr. Farber: “There will likely be a decrease in vaccinations and testing. The vaccination rates are very low to begin with, and this will likely lower it further.”
A: Dr. Atmar: “I think it will mean that fewer people will get tested and vaccinated,” which “could lead to increased transmission, although wastewater testing suggests that there is a lot of unrecognized infection already occurring.”
A: Dr. Benjamin: “That is a big concern. It means that for people, particularly for people who are uninsured and underinsured, we’ve got to make sure they have access to those. There’s a lot of discussion and debate about what the cost of those tests and vaccines will be, and it looks like the companies are going to impose very steep, increasing costs.”
Q: How will this affect higher-risk populations, like people with weakened immune systems?
A: Dr. Farber: “Without monoclonals [drugs to treat COVID] and free Paxlovid,” people with weakened immune systems “may be undertreated.”
A: Dr. Atmar: “The implications of ongoing widespread virus transmission are that immunocompromised individuals may be more likely to be exposed and infected and to suffer the consequences of such infection, including severe illness. However, to a certain degree, this may already be happening. We are still seeing about 500 deaths/day, primarily in persons at highest risk of severe disease.”
A: Dr. Benjamin: “People who have good insurance, can afford to get immunized, and have good relations with practitioners probably will continue to be covered. But lower-income individuals and people who really can’t afford to get tested or get immunized would likely become underimmunized and more infected.
“So even though the federal emergency declaration will go away, I’m hoping that the federal government will continue to encourage all of us to emphasize those populations at the highest risk – those with chronic disease and those who are immunocompromised.”
A: Mr. Newmark: “People who are immunocompromised by their chronic illness or the medicines they take to treat acute or chronic conditions remain at higher risk for COVID-19 and its serious complications. The administration needs to support continued development of effective treatments and updated vaccines to protect the individual and public health. We’re also concerned that increased health care services - such as vaccination or telehealth – may fall back to prepandemic levels while the burden of protection, such as masking, may fall to chronic disease patients alone, which adds to the burden of living with disease.”
Q: What effect will ending Medicaid expansion money have?
A: Dr. Benjamin: Anywhere from 16 to 20 million people are going to lose in coverage. I’m hoping that states will look at their experience over these last 2 years or so and come to the decision that there were improvements in healthier populations.
Q: Will this have any effect on how the public perceives the pandemic?
A: Dr. Farber: “It is likely to give the impression that COVID is gone, which clearly is not the case.”
A: Dr. Benjamin: “It’ll be another argument by some that the pandemic is over. People should think about this as kind of like a hurricane. A hurricane comes through and tragically tears up communities, and we have an emergency during that time. But then we have to go through a period of recovery. I’m hoping people will realize that even though the public health emergencies have gone away, that we still need to go through a period of transition ... and that means that they still need to protect themselves, get vaccinated, and wear a mask when appropriate.”
A: Dr. Atmar: “There needs to be messaging that while we are transitioning away from emergency management of COVID-19, it is still a significant public health concern.”
A version of this article originally appeared on WebMD.com.
It’s the end of an era.
The orders spanned two presidencies. The Trump administration’s Health and Human Services Secretary Alex Azar issued a public health emergency in January 2020. Then-President Donald Trump declared the COVID-19 pandemic a national emergency 2 months later. Both emergency declarations – which remained in effect under President Joe Biden – are set to expire May 11.
Read on for an overview of how the end of the public health emergency will trigger multiple federal policy changes.
Changes that affect everyone
- There will be cost-sharing changes for COVID-19 vaccines, testing, and certain treatments. One hundred–percent coverage for COVID testing, including free at-home tests, will expire May 11.
- Telemedicine cannot be used to prescribe controlled substances after May 11, 2023.
- Enhanced federal funding will be phased down through Dec. 31, 2023. This extends the time states must receive federally matched funds for COVID-related services and products, through the Consolidated Appropriations Act of 2023. Otherwise, this would have expired June 30, 2023.
- Emergency use authorizations for COVID-19 treatments and vaccinations will not be affected and/or end on May 11.
Changes that affect people with private health insurance
- Many will likely see higher costs for COVID-19 tests, as free testing expires and cost-sharing begins in the coming months.
- COVID-19 vaccinations and boosters will continue to be covered until the federal government’s vaccination supply is depleted. If that happens, you will need an in-network provider.
- You will still have access to COVID-19 treatments – but that could change when the federal supply dwindles.
Changes that affect Medicare recipients
- Medicare telehealth flexibilities will be extended through Dec. 31, 2024, regardless of public health emergency status. This means people can access telehealth services from anywhere, not just rural areas; can use a smartphone for telehealth; and can access telehealth in their homes.
- Medicare cost-sharing for testing and treatments will expire May 11, except for oral antivirals.
Changes that affect Medicaid/CHIP recipients
- Medicaid and Children’s Health Insurance Program (CHIP) recipients will continue to receive approved vaccinations free of charge, but testing and treatment without cost-sharing will expire during the third quarter of 2024.
- The Medicaid continuous enrollment provision will be separated from the public health emergency, and continuous enrollment will end March 31, 2023.
Changes that affect uninsured people
- The uninsured will no longer have access to 100% coverage for these products and services (free COVID-19 treatments, vaccines, and testing).
Changes that affect health care providers
- There will be changes to how much providers get paid for diagnosing people with COVID-19, ending the enhanced Inpatient Prospective Payment System reimbursement rate, as of May 11, 2023.
- Health Insurance Portability and Accountability Act (HIPAA) potential penalty waivers will end. This allows providers to communicate with patients through telehealth on a smartphone, for example, without violating privacy laws and incurring penalties.
What the experts are saying
This news organization asked several health experts for their thoughts on ending the emergency health declarations for COVID, and what effects this could have. Many expressed concerns about the timing of the ending, saying that the move could limit access to COVID-related treatments. Others said the move was inevitable but raised concerns about federal guidance related to the decision.
Question: Do you agree with the timing of the end to the emergency order?
Answer: Robert Atmar, MD, professor of infectious diseases at Baylor College of Medicine in Houston: “A lead time to prepare and anticipate these consequences may ease the transition, compared to an abrupt declaration that ends the declaration.”
Answer: Georges C. Benjamin, MD, executive director of the American Public Health Association: “I think it’s time to do so. It has to be done in a great, thoughtful, and organized way because we’ve attached so many different things to this public health emergency. It’s going to take time for the system to adapt. [Centers for Disease Control and Prevention] data collection most likely will continue. People are used to reporting now. The CDC needs to give guidance to the states so that we’re clear about what we’re reporting, what we’re not. If we did that abruptly, it would just be a mess.”
Answer: Bruce Farber, MD, chief public health and epidemiology officer at Northwell Health in Manhasset, N.Y.: “I would have hoped to see it delayed.”
Answer: Steven Newmark, JD, chief legal officer and director of policy at the Global Healthy Living Foundation: “While we understand that an emergency cannot last forever, we hope that expanded services such as free vaccination, promotion of widespread vaccination, increased use of pharmacists to administer vaccines, telehealth availability and reimbursement, flexibility in work-from-home opportunities, and more continues. Access to equitable health care should never backtrack or be reduced.”
Q: What will the end of free COVID vaccinations and free testing mean?
A: Dr. Farber: “There will likely be a decrease in vaccinations and testing. The vaccination rates are very low to begin with, and this will likely lower it further.”
A: Dr. Atmar: “I think it will mean that fewer people will get tested and vaccinated,” which “could lead to increased transmission, although wastewater testing suggests that there is a lot of unrecognized infection already occurring.”
A: Dr. Benjamin: “That is a big concern. It means that for people, particularly for people who are uninsured and underinsured, we’ve got to make sure they have access to those. There’s a lot of discussion and debate about what the cost of those tests and vaccines will be, and it looks like the companies are going to impose very steep, increasing costs.”
Q: How will this affect higher-risk populations, like people with weakened immune systems?
A: Dr. Farber: “Without monoclonals [drugs to treat COVID] and free Paxlovid,” people with weakened immune systems “may be undertreated.”
A: Dr. Atmar: “The implications of ongoing widespread virus transmission are that immunocompromised individuals may be more likely to be exposed and infected and to suffer the consequences of such infection, including severe illness. However, to a certain degree, this may already be happening. We are still seeing about 500 deaths/day, primarily in persons at highest risk of severe disease.”
A: Dr. Benjamin: “People who have good insurance, can afford to get immunized, and have good relations with practitioners probably will continue to be covered. But lower-income individuals and people who really can’t afford to get tested or get immunized would likely become underimmunized and more infected.
“So even though the federal emergency declaration will go away, I’m hoping that the federal government will continue to encourage all of us to emphasize those populations at the highest risk – those with chronic disease and those who are immunocompromised.”
A: Mr. Newmark: “People who are immunocompromised by their chronic illness or the medicines they take to treat acute or chronic conditions remain at higher risk for COVID-19 and its serious complications. The administration needs to support continued development of effective treatments and updated vaccines to protect the individual and public health. We’re also concerned that increased health care services - such as vaccination or telehealth – may fall back to prepandemic levels while the burden of protection, such as masking, may fall to chronic disease patients alone, which adds to the burden of living with disease.”
Q: What effect will ending Medicaid expansion money have?
A: Dr. Benjamin: Anywhere from 16 to 20 million people are going to lose in coverage. I’m hoping that states will look at their experience over these last 2 years or so and come to the decision that there were improvements in healthier populations.
Q: Will this have any effect on how the public perceives the pandemic?
A: Dr. Farber: “It is likely to give the impression that COVID is gone, which clearly is not the case.”
A: Dr. Benjamin: “It’ll be another argument by some that the pandemic is over. People should think about this as kind of like a hurricane. A hurricane comes through and tragically tears up communities, and we have an emergency during that time. But then we have to go through a period of recovery. I’m hoping people will realize that even though the public health emergencies have gone away, that we still need to go through a period of transition ... and that means that they still need to protect themselves, get vaccinated, and wear a mask when appropriate.”
A: Dr. Atmar: “There needs to be messaging that while we are transitioning away from emergency management of COVID-19, it is still a significant public health concern.”
A version of this article originally appeared on WebMD.com.
The long-range thrombolysis forecast calls for tiny ultrasonic tornadoes
Sticks and stones may break my bones, but clots will never hurt me
You’ve probably seen “Ghostbusters” or at least heard the theme song. Maybe you even know about the Discovery Channel’s “Mythbusters.” But now there’s a new buster in town, and it eats platitudes for breakfast: Meet Cliche-busters, LOTME’s new recurring feature.
This week, Cliche-busters takes on “Two wrongs don’t make a right.” Yum.
We start with blood clots, which are bad. Doctors go to a lot of trouble to get rid of the things because they are dangerous. A blood clot, then, is a bodily function gone wrong.
Tornadoes are also bad. Out there in the world, these violently rotating columns of air can destroy buildings, toss large objects long distances, and inspire mediocre action movies. They are examples of nature gone wrong.
Seemingly, these two wrongs – blood clots and tornadoes – are not about to make a right. Has Cliche-busters bitten off more than it can chew?
Not according to Xiaoning Jiang of North Carolina State University, Raleigh, and his team of researchers. They’ve figured out a way to use a tiny ultrasonic tornado to break down clots in the brain. “Our new work uses vortex ultrasound, where the ultrasound waves have a helical wavefront. In other words, the ultrasound is swirling as it moves forward,” he said in a statement from the university.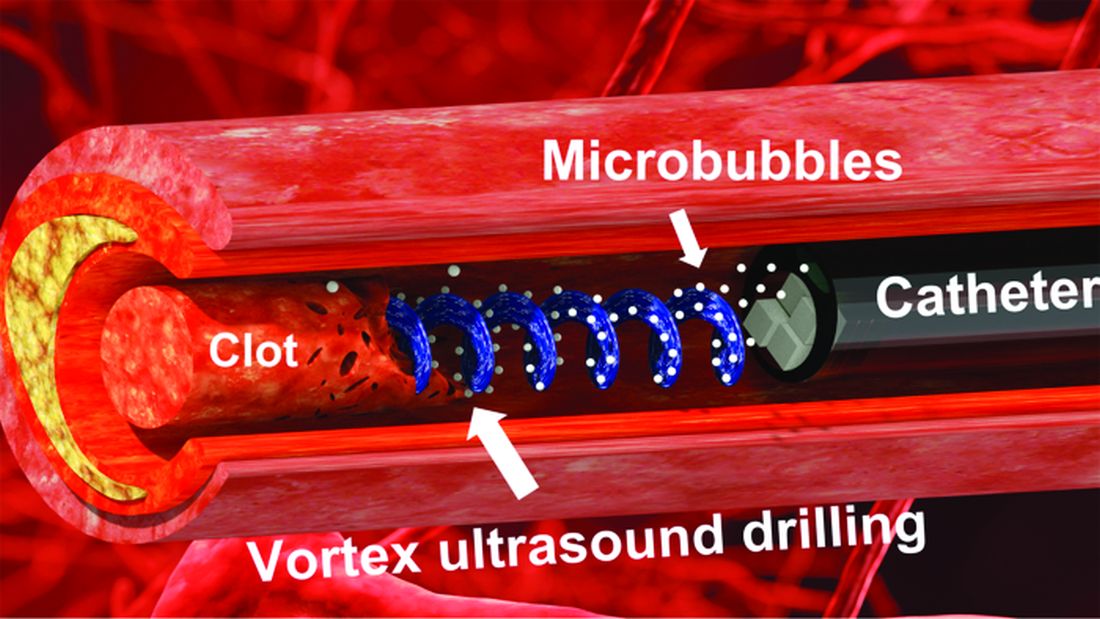
Their new tool’s single transducer is small enough to fit in a catheter, and its “vortex ultrasound-induced shear force has the potential to break down clots safely and improve the efficacy of thrombolysis,” they explained in the open-access journal Research.
The investigators used cow blood in a 3D-printed model of the cerebral venous sinus for the proof-of-concept study and were able to dissolve an acute blood clot in less than 30 minutes, compared with the 15-30 hours needed with a pharmaceutical intervention, according to the written statement.
Can you hear the sound of two wrongs making a right? We can, and that closes the curtain on this cliche.
With age does not come wisdom
We’ve all met this person before. The sort of person who takes a 10-minute IQ test on a shifty-looking website and then proceeds to brag about a 180 IQ until the heat death of the universe. The one who worships at the altar of Mensa. Yeah, that guy. They’re never as smart as they think they are, but they’ll never, ever admit it.
It’s not exactly a secret that IQ as a measurement of intelligence is highly overrated. A lot of scientists doubt we should bother measuring it at all. That said, a higher IQ is associated with greater success in academic and financial endeavors, so it’s not absolutely worthless. And if we’re stuck with it, we may as well study it.
That brings us neatly to new research published in Brain and Behavior. Most studies into IQ and self-estimated intelligence have focused on younger adults, and the author of this study was curious if the stereotype of young men inflating their IQ, a stereotype backed up by research, persisted into older adulthood. So she conducted a survey of 159 younger adults and 152 older adults to find out.
The results in younger adults were not surprising: Younger men overestimated their actual IQ by 5-15 points, which tracks with previous research. We’re in for a bit of a surprise with the older adults, though, because the older men were more humble about their intelligence, with their estimation falling in line with their actual IQ. Older women, however, not so much. In fact, they overestimated their intelligence just as much as the younger men.
In addition, older women who perceived themselves as more attractive reported the highest self-estimated intelligence of all. That isn’t how intelligence works, but honestly, if Grandma’s out and about thinking she looks good and has the brains to go and win “Jeopardy!” do you really have the heart to tell her otherwise?
Fight temptation with empathy … and shoes
Relationships are tough. They all go through their respective ups and downs, but what happens when one person is feeling so down in the partnership that cheating comes to mind? Is there any way to stop it from happening?
Well, a recent study suggests that there is, and it’s as simple as putting yourself in the other person’s shoes. By observing 408 heterosexual, monogamous participants in a series of experiments, psychologists in Israel and New York found that practicing empathy and “perspective taking” doesn’t necessarily stop people from cheating but it does reduces the desire.
People cheat on their significant others for many different reasons – men for a lack of sexual needs being met and women for shortfalls regarding emotional needs – but prioritizing the other person’s perspective gives the idea of being unfaithful a different view and could make one act differently, the investigators said.
Perspective taking also promotes other positive attributes to the relationship, such as the promotion of compassion and the feeling of being understood, lead author Gurit Birnbaum of Reichman University in Herzliya, Israel, said in a written statement. These things ultimately help couples navigate the rough patches and strengthen bonds, making them even less likely to cheat.
The researchers noted that even people in satisfying relationships do cheat, but this approach does encourage people to stop and think before they act. It could ultimately prevent what might be a huge mistake.
Think before they act. Hmm, that’s kind of like look before they leap, right? Sounds like a job for the Cliche-busters.
Sticks and stones may break my bones, but clots will never hurt me
You’ve probably seen “Ghostbusters” or at least heard the theme song. Maybe you even know about the Discovery Channel’s “Mythbusters.” But now there’s a new buster in town, and it eats platitudes for breakfast: Meet Cliche-busters, LOTME’s new recurring feature.
This week, Cliche-busters takes on “Two wrongs don’t make a right.” Yum.
We start with blood clots, which are bad. Doctors go to a lot of trouble to get rid of the things because they are dangerous. A blood clot, then, is a bodily function gone wrong.
Tornadoes are also bad. Out there in the world, these violently rotating columns of air can destroy buildings, toss large objects long distances, and inspire mediocre action movies. They are examples of nature gone wrong.
Seemingly, these two wrongs – blood clots and tornadoes – are not about to make a right. Has Cliche-busters bitten off more than it can chew?
Not according to Xiaoning Jiang of North Carolina State University, Raleigh, and his team of researchers. They’ve figured out a way to use a tiny ultrasonic tornado to break down clots in the brain. “Our new work uses vortex ultrasound, where the ultrasound waves have a helical wavefront. In other words, the ultrasound is swirling as it moves forward,” he said in a statement from the university.
Their new tool’s single transducer is small enough to fit in a catheter, and its “vortex ultrasound-induced shear force has the potential to break down clots safely and improve the efficacy of thrombolysis,” they explained in the open-access journal Research.
The investigators used cow blood in a 3D-printed model of the cerebral venous sinus for the proof-of-concept study and were able to dissolve an acute blood clot in less than 30 minutes, compared with the 15-30 hours needed with a pharmaceutical intervention, according to the written statement.
Can you hear the sound of two wrongs making a right? We can, and that closes the curtain on this cliche.
With age does not come wisdom
We’ve all met this person before. The sort of person who takes a 10-minute IQ test on a shifty-looking website and then proceeds to brag about a 180 IQ until the heat death of the universe. The one who worships at the altar of Mensa. Yeah, that guy. They’re never as smart as they think they are, but they’ll never, ever admit it.
It’s not exactly a secret that IQ as a measurement of intelligence is highly overrated. A lot of scientists doubt we should bother measuring it at all. That said, a higher IQ is associated with greater success in academic and financial endeavors, so it’s not absolutely worthless. And if we’re stuck with it, we may as well study it.
That brings us neatly to new research published in Brain and Behavior. Most studies into IQ and self-estimated intelligence have focused on younger adults, and the author of this study was curious if the stereotype of young men inflating their IQ, a stereotype backed up by research, persisted into older adulthood. So she conducted a survey of 159 younger adults and 152 older adults to find out.
The results in younger adults were not surprising: Younger men overestimated their actual IQ by 5-15 points, which tracks with previous research. We’re in for a bit of a surprise with the older adults, though, because the older men were more humble about their intelligence, with their estimation falling in line with their actual IQ. Older women, however, not so much. In fact, they overestimated their intelligence just as much as the younger men.
In addition, older women who perceived themselves as more attractive reported the highest self-estimated intelligence of all. That isn’t how intelligence works, but honestly, if Grandma’s out and about thinking she looks good and has the brains to go and win “Jeopardy!” do you really have the heart to tell her otherwise?
Fight temptation with empathy … and shoes
Relationships are tough. They all go through their respective ups and downs, but what happens when one person is feeling so down in the partnership that cheating comes to mind? Is there any way to stop it from happening?
Well, a recent study suggests that there is, and it’s as simple as putting yourself in the other person’s shoes. By observing 408 heterosexual, monogamous participants in a series of experiments, psychologists in Israel and New York found that practicing empathy and “perspective taking” doesn’t necessarily stop people from cheating but it does reduces the desire.
People cheat on their significant others for many different reasons – men for a lack of sexual needs being met and women for shortfalls regarding emotional needs – but prioritizing the other person’s perspective gives the idea of being unfaithful a different view and could make one act differently, the investigators said.
Perspective taking also promotes other positive attributes to the relationship, such as the promotion of compassion and the feeling of being understood, lead author Gurit Birnbaum of Reichman University in Herzliya, Israel, said in a written statement. These things ultimately help couples navigate the rough patches and strengthen bonds, making them even less likely to cheat.
The researchers noted that even people in satisfying relationships do cheat, but this approach does encourage people to stop and think before they act. It could ultimately prevent what might be a huge mistake.
Think before they act. Hmm, that’s kind of like look before they leap, right? Sounds like a job for the Cliche-busters.
Sticks and stones may break my bones, but clots will never hurt me
You’ve probably seen “Ghostbusters” or at least heard the theme song. Maybe you even know about the Discovery Channel’s “Mythbusters.” But now there’s a new buster in town, and it eats platitudes for breakfast: Meet Cliche-busters, LOTME’s new recurring feature.
This week, Cliche-busters takes on “Two wrongs don’t make a right.” Yum.
We start with blood clots, which are bad. Doctors go to a lot of trouble to get rid of the things because they are dangerous. A blood clot, then, is a bodily function gone wrong.
Tornadoes are also bad. Out there in the world, these violently rotating columns of air can destroy buildings, toss large objects long distances, and inspire mediocre action movies. They are examples of nature gone wrong.
Seemingly, these two wrongs – blood clots and tornadoes – are not about to make a right. Has Cliche-busters bitten off more than it can chew?
Not according to Xiaoning Jiang of North Carolina State University, Raleigh, and his team of researchers. They’ve figured out a way to use a tiny ultrasonic tornado to break down clots in the brain. “Our new work uses vortex ultrasound, where the ultrasound waves have a helical wavefront. In other words, the ultrasound is swirling as it moves forward,” he said in a statement from the university.
Their new tool’s single transducer is small enough to fit in a catheter, and its “vortex ultrasound-induced shear force has the potential to break down clots safely and improve the efficacy of thrombolysis,” they explained in the open-access journal Research.
The investigators used cow blood in a 3D-printed model of the cerebral venous sinus for the proof-of-concept study and were able to dissolve an acute blood clot in less than 30 minutes, compared with the 15-30 hours needed with a pharmaceutical intervention, according to the written statement.
Can you hear the sound of two wrongs making a right? We can, and that closes the curtain on this cliche.
With age does not come wisdom
We’ve all met this person before. The sort of person who takes a 10-minute IQ test on a shifty-looking website and then proceeds to brag about a 180 IQ until the heat death of the universe. The one who worships at the altar of Mensa. Yeah, that guy. They’re never as smart as they think they are, but they’ll never, ever admit it.
It’s not exactly a secret that IQ as a measurement of intelligence is highly overrated. A lot of scientists doubt we should bother measuring it at all. That said, a higher IQ is associated with greater success in academic and financial endeavors, so it’s not absolutely worthless. And if we’re stuck with it, we may as well study it.
That brings us neatly to new research published in Brain and Behavior. Most studies into IQ and self-estimated intelligence have focused on younger adults, and the author of this study was curious if the stereotype of young men inflating their IQ, a stereotype backed up by research, persisted into older adulthood. So she conducted a survey of 159 younger adults and 152 older adults to find out.
The results in younger adults were not surprising: Younger men overestimated their actual IQ by 5-15 points, which tracks with previous research. We’re in for a bit of a surprise with the older adults, though, because the older men were more humble about their intelligence, with their estimation falling in line with their actual IQ. Older women, however, not so much. In fact, they overestimated their intelligence just as much as the younger men.
In addition, older women who perceived themselves as more attractive reported the highest self-estimated intelligence of all. That isn’t how intelligence works, but honestly, if Grandma’s out and about thinking she looks good and has the brains to go and win “Jeopardy!” do you really have the heart to tell her otherwise?
Fight temptation with empathy … and shoes
Relationships are tough. They all go through their respective ups and downs, but what happens when one person is feeling so down in the partnership that cheating comes to mind? Is there any way to stop it from happening?
Well, a recent study suggests that there is, and it’s as simple as putting yourself in the other person’s shoes. By observing 408 heterosexual, monogamous participants in a series of experiments, psychologists in Israel and New York found that practicing empathy and “perspective taking” doesn’t necessarily stop people from cheating but it does reduces the desire.
People cheat on their significant others for many different reasons – men for a lack of sexual needs being met and women for shortfalls regarding emotional needs – but prioritizing the other person’s perspective gives the idea of being unfaithful a different view and could make one act differently, the investigators said.
Perspective taking also promotes other positive attributes to the relationship, such as the promotion of compassion and the feeling of being understood, lead author Gurit Birnbaum of Reichman University in Herzliya, Israel, said in a written statement. These things ultimately help couples navigate the rough patches and strengthen bonds, making them even less likely to cheat.
The researchers noted that even people in satisfying relationships do cheat, but this approach does encourage people to stop and think before they act. It could ultimately prevent what might be a huge mistake.
Think before they act. Hmm, that’s kind of like look before they leap, right? Sounds like a job for the Cliche-busters.