User login
Hookah, snus users more likely to start smoking
Smoking water pipe tobacco, or hookahs, more than doubles the odds that a non–cigarette smoker will begin smoking within 2 years, according to a recent study. Using snus increases the risk of starting smoking by more than sixfold.
“Our study demonstrates that [water pipe tobacco] and snus use among non–cigarette smoking adolescents and young adults were longitudinally associated with subsequent cigarette smoking,” Samir S. Soneji, Ph.D., of Dartmouth University, Lebanon, N.H., and his associates reported online [JAMA Pediatr. 2014 Dec. 8 [doi:10.1001/jamapediatrics.2014.2697]).
“Yet, water pipe tobacco remains largely unregulated by the [Food and Drug Administration], and snus is less regulated than other smokeless tobacco,” Dr. Soneji and colleagues wrote. “The success of FDA tobacco regulatory control policies will depend, in part, on their ability to reduce the use of alternative tobacco products that may lead to subsequent cigarette smoking.”

The researchers interviewed 2,541 respondents between October 2010 and June 2011 and then gathered follow-up data 2 years later from 1,596 respondents. Of the original sample, 39% had never tried smoking cigarettes, and 15% were current smokers. Two thirds of follow-up respondents (1,048 of 1,596) were non–cigarette smokers at baseline: 20 of these individuals had used snus, and 71 had smoked water pipe tobacco.
At follow-up, among those who did not smoke cigarettes at baseline, 39% of hookah users had begun smoking, compared with 20% of those who had not used water pipes. Similarly, among baseline nonsmokers, 55% of snus users had begun smoking at follow-up, compared with 21% of those who did not use snus.
After accounting for sociodemographic and behavioral risk factors, those who used hookahs at baseline, compared with non–hookah users, were 2.6 times more likely to start smoking 2 years later; snus users were 3.7 times more likely than non–snus users. Similarly, hookah users were 2.5 times more likely to be current smokers and 2.6 times more likely to be higher-intensity cigarette smokers at follow-up. Snus users were 6.2 times more likely to be current smokers and 4.5 times more likely to be higher-intensity cigarette smokers.
The sociodemographic factors controlled for included age, sex, race/ethnicity, region, urbanicity, and socioeconomic status as based on maternal educational level and annual household income. Behavioral risk factors considered included smoking status of friends and parents, and respondents’ answers to questions about risk taking, sensation seeking, and binge drinking.
The research was funded by the National Cancer Institute and the National Center for Advancing Translational Sciences. The authors reported no disclosures.
Smoking water pipe tobacco, or hookahs, more than doubles the odds that a non–cigarette smoker will begin smoking within 2 years, according to a recent study. Using snus increases the risk of starting smoking by more than sixfold.
“Our study demonstrates that [water pipe tobacco] and snus use among non–cigarette smoking adolescents and young adults were longitudinally associated with subsequent cigarette smoking,” Samir S. Soneji, Ph.D., of Dartmouth University, Lebanon, N.H., and his associates reported online [JAMA Pediatr. 2014 Dec. 8 [doi:10.1001/jamapediatrics.2014.2697]).
“Yet, water pipe tobacco remains largely unregulated by the [Food and Drug Administration], and snus is less regulated than other smokeless tobacco,” Dr. Soneji and colleagues wrote. “The success of FDA tobacco regulatory control policies will depend, in part, on their ability to reduce the use of alternative tobacco products that may lead to subsequent cigarette smoking.”
The researchers interviewed 2,541 respondents between October 2010 and June 2011 and then gathered follow-up data 2 years later from 1,596 respondents. Of the original sample, 39% had never tried smoking cigarettes, and 15% were current smokers. Two thirds of follow-up respondents (1,048 of 1,596) were non–cigarette smokers at baseline: 20 of these individuals had used snus, and 71 had smoked water pipe tobacco.
At follow-up, among those who did not smoke cigarettes at baseline, 39% of hookah users had begun smoking, compared with 20% of those who had not used water pipes. Similarly, among baseline nonsmokers, 55% of snus users had begun smoking at follow-up, compared with 21% of those who did not use snus.
After accounting for sociodemographic and behavioral risk factors, those who used hookahs at baseline, compared with non–hookah users, were 2.6 times more likely to start smoking 2 years later; snus users were 3.7 times more likely than non–snus users. Similarly, hookah users were 2.5 times more likely to be current smokers and 2.6 times more likely to be higher-intensity cigarette smokers at follow-up. Snus users were 6.2 times more likely to be current smokers and 4.5 times more likely to be higher-intensity cigarette smokers.
The sociodemographic factors controlled for included age, sex, race/ethnicity, region, urbanicity, and socioeconomic status as based on maternal educational level and annual household income. Behavioral risk factors considered included smoking status of friends and parents, and respondents’ answers to questions about risk taking, sensation seeking, and binge drinking.
The research was funded by the National Cancer Institute and the National Center for Advancing Translational Sciences. The authors reported no disclosures.
Smoking water pipe tobacco, or hookahs, more than doubles the odds that a non–cigarette smoker will begin smoking within 2 years, according to a recent study. Using snus increases the risk of starting smoking by more than sixfold.
“Our study demonstrates that [water pipe tobacco] and snus use among non–cigarette smoking adolescents and young adults were longitudinally associated with subsequent cigarette smoking,” Samir S. Soneji, Ph.D., of Dartmouth University, Lebanon, N.H., and his associates reported online [JAMA Pediatr. 2014 Dec. 8 [doi:10.1001/jamapediatrics.2014.2697]).
“Yet, water pipe tobacco remains largely unregulated by the [Food and Drug Administration], and snus is less regulated than other smokeless tobacco,” Dr. Soneji and colleagues wrote. “The success of FDA tobacco regulatory control policies will depend, in part, on their ability to reduce the use of alternative tobacco products that may lead to subsequent cigarette smoking.”
The researchers interviewed 2,541 respondents between October 2010 and June 2011 and then gathered follow-up data 2 years later from 1,596 respondents. Of the original sample, 39% had never tried smoking cigarettes, and 15% were current smokers. Two thirds of follow-up respondents (1,048 of 1,596) were non–cigarette smokers at baseline: 20 of these individuals had used snus, and 71 had smoked water pipe tobacco.
At follow-up, among those who did not smoke cigarettes at baseline, 39% of hookah users had begun smoking, compared with 20% of those who had not used water pipes. Similarly, among baseline nonsmokers, 55% of snus users had begun smoking at follow-up, compared with 21% of those who did not use snus.
After accounting for sociodemographic and behavioral risk factors, those who used hookahs at baseline, compared with non–hookah users, were 2.6 times more likely to start smoking 2 years later; snus users were 3.7 times more likely than non–snus users. Similarly, hookah users were 2.5 times more likely to be current smokers and 2.6 times more likely to be higher-intensity cigarette smokers at follow-up. Snus users were 6.2 times more likely to be current smokers and 4.5 times more likely to be higher-intensity cigarette smokers.
The sociodemographic factors controlled for included age, sex, race/ethnicity, region, urbanicity, and socioeconomic status as based on maternal educational level and annual household income. Behavioral risk factors considered included smoking status of friends and parents, and respondents’ answers to questions about risk taking, sensation seeking, and binge drinking.
The research was funded by the National Cancer Institute and the National Center for Advancing Translational Sciences. The authors reported no disclosures.
FROM JAMA PEDIATRICS
Key clinical point: “The increasing use of novel alternative tobacco products introduces new harms to adolescents and young adults.”
Major finding: Hookah users were 2.6 times more likely to start smoking cigarettes and be high-intensity cigarette smokers; snus users were 6.2 times more likely to start smoking and 4.5 times more likely to be high-intensity smokers.
Data source: The findings are based on a prospective longitudinal study of 1,596 individuals aged 15 to 23 between October 2010 and March 2013.
Disclosures: The research was funded by the National Cancer Institute and the National Center for Advancing Translational Sciences. The authors reported no disclosures.

Antibiotic delivery time improved through hospital initiative
The average time it takes to deliver antibiotics to febrile children with a central line can be improved with an appropriately planned hospital intervention, a recent study found.
The University of North Carolina Hospitals, Chapel Hill, emergency department, which cares for approximately 14,000 patients under 19 years each year, set out to identify barriers to timely administration of antibiotics to pediatric patients with a central line who presented with fever. An 8-month baseline analysis showed only 63% of patients received antibiotics within 60 minutes, and the average time to receive antibiotics was 65 minutes.
The hospital formed an improvement team that included nursing staff, attending physicians, and volunteer research assistants to improve timing of antibiotic delivery to these patients. Their goals included delivering antibiotics within 60 minutes to 90% of patients, reducing the average delivery time to less than 60 minutes and reducing variation of times among different demographic groups. From January 2010, when the baseline analysis began, through June 2013, the team tracked 479 patient encounters.
“Key areas for improvement included patient identification at triage, appropriate level of triage assigned, antibiotic availability, and a standard management process,” reported Meghan Jobson, Ph.D., and her associates at the University of North Carolina, Chapel Hill, reported online Dec. 8 (Pediatrics 2014 [doi: 10.1542/peds.2014-1192]). The three-phase initiative involved communicating the baseline analysis and goals to the staff, removing the step of contacting patients’ subspecialists before treatment, addressing patient identification and triage issues, and continually refining procedures with ongoing staff coaching.
Eight months after the initiative began, 99% of patients received antibiotics within 60 minutes and average time to delivery dropped to 30 minutes. Since meeting that goal, the hospital has maintained antibiotic delivery within 60 minutes for more than 90% of patients for 24 subsequent months. Further, the significantly longer delays in antibiotic delivery to black patients that had shown up in the baseline analysis no longer existed once the initiative had been fully implemented.
The study did not receive external funding, and the authors reported no disclosures.
The average time it takes to deliver antibiotics to febrile children with a central line can be improved with an appropriately planned hospital intervention, a recent study found.
The University of North Carolina Hospitals, Chapel Hill, emergency department, which cares for approximately 14,000 patients under 19 years each year, set out to identify barriers to timely administration of antibiotics to pediatric patients with a central line who presented with fever. An 8-month baseline analysis showed only 63% of patients received antibiotics within 60 minutes, and the average time to receive antibiotics was 65 minutes.
The hospital formed an improvement team that included nursing staff, attending physicians, and volunteer research assistants to improve timing of antibiotic delivery to these patients. Their goals included delivering antibiotics within 60 minutes to 90% of patients, reducing the average delivery time to less than 60 minutes and reducing variation of times among different demographic groups. From January 2010, when the baseline analysis began, through June 2013, the team tracked 479 patient encounters.
“Key areas for improvement included patient identification at triage, appropriate level of triage assigned, antibiotic availability, and a standard management process,” reported Meghan Jobson, Ph.D., and her associates at the University of North Carolina, Chapel Hill, reported online Dec. 8 (Pediatrics 2014 [doi: 10.1542/peds.2014-1192]). The three-phase initiative involved communicating the baseline analysis and goals to the staff, removing the step of contacting patients’ subspecialists before treatment, addressing patient identification and triage issues, and continually refining procedures with ongoing staff coaching.
Eight months after the initiative began, 99% of patients received antibiotics within 60 minutes and average time to delivery dropped to 30 minutes. Since meeting that goal, the hospital has maintained antibiotic delivery within 60 minutes for more than 90% of patients for 24 subsequent months. Further, the significantly longer delays in antibiotic delivery to black patients that had shown up in the baseline analysis no longer existed once the initiative had been fully implemented.
The study did not receive external funding, and the authors reported no disclosures.
The average time it takes to deliver antibiotics to febrile children with a central line can be improved with an appropriately planned hospital intervention, a recent study found.
The University of North Carolina Hospitals, Chapel Hill, emergency department, which cares for approximately 14,000 patients under 19 years each year, set out to identify barriers to timely administration of antibiotics to pediatric patients with a central line who presented with fever. An 8-month baseline analysis showed only 63% of patients received antibiotics within 60 minutes, and the average time to receive antibiotics was 65 minutes.
The hospital formed an improvement team that included nursing staff, attending physicians, and volunteer research assistants to improve timing of antibiotic delivery to these patients. Their goals included delivering antibiotics within 60 minutes to 90% of patients, reducing the average delivery time to less than 60 minutes and reducing variation of times among different demographic groups. From January 2010, when the baseline analysis began, through June 2013, the team tracked 479 patient encounters.
“Key areas for improvement included patient identification at triage, appropriate level of triage assigned, antibiotic availability, and a standard management process,” reported Meghan Jobson, Ph.D., and her associates at the University of North Carolina, Chapel Hill, reported online Dec. 8 (Pediatrics 2014 [doi: 10.1542/peds.2014-1192]). The three-phase initiative involved communicating the baseline analysis and goals to the staff, removing the step of contacting patients’ subspecialists before treatment, addressing patient identification and triage issues, and continually refining procedures with ongoing staff coaching.
Eight months after the initiative began, 99% of patients received antibiotics within 60 minutes and average time to delivery dropped to 30 minutes. Since meeting that goal, the hospital has maintained antibiotic delivery within 60 minutes for more than 90% of patients for 24 subsequent months. Further, the significantly longer delays in antibiotic delivery to black patients that had shown up in the baseline analysis no longer existed once the initiative had been fully implemented.
The study did not receive external funding, and the authors reported no disclosures.
FROM PEDIATRICS
Key clinical point: An hospital initiative successfully improved time for antibiotic delivery to febrile pediatric patients with central lines.
Major finding: The proportion of febrile patients receiving antibiotics within 60 minutes increased from 63% to 99%.
Data source: The findings are based on a prospective evaluation of a three-phase hospital initiative to improve antibiotic delivery time in an academic ED between January 2010 and June 2013.
Disclosures: The study did not receive external funding, and the authors reported no disclosures.
Exclusively breastfed neonate weight loss graphed
Losing more than 10% of birthweight early in the postnatal course is common among neonates delivered vaginally and by cesarean section who have been exclusively breastfed, nomograms developed by a team of researchers show. Those graphical depictions of hourly weight loss “may inform clinical care,” Dr. Valerie J. Flaherman and her colleagues reported in Pediatrics.
“The availability of detailed data on weight and feeding for a large cohort allows this study to present the first graphical depiction of hourly weight loss for exclusively breastfed newborns from a large, diverse population,” wrote Dr. Flaherman of the University of California, San Francisco, and her colleagues. “Our curves demonstrate that expected weight loss differs substantially by method of delivery and that this difference persists over time” (Pediatrics 2014 Dec. 1 [doi:10.1542/peds.2014-1532]).

Using available weight data from the births of 108,907 singleton neonates born at 36 weeks’ gestation or later at Northern California Kaiser Permanente hospitals between 2009 and 2013, the researchers created nomograms that estimate percentiles of weight loss among exclusively breastfed infants who were vaginally delivery or delivered by cesarean section.
Dr. Flaherman’s team estimated 50th, 75th, 90th, and 95th percentiles based on analysis of 83,433 vaginally born neonates and 25,474 infants delivered by C-section, all exclusively breastfed. The study excluded infants who received any formula, those weighing less than 2,000 g or more than 5,000 g, and those whose weight, delivery mode, or feeding status was unknown.
Median weight loss for vaginally delivered newborns was 4.2%, 7.1%, and 6.4% at 24, 48, and 72 hours after birth, respectively. Among cesarean section–born newborns, median percent weight loss was 4.9%, 8%, 8.6%, and 5.8% at 24, 48, 72, and 96 hours after birth.
Nearly 5% of vaginally delivered newborns and nearly 10% of newborns delivered by cesarean section had lost at least 10% of their birthweight at 48 hours after birth. Percentile curves began to rise shortly after 48 hours for vaginally delivered newborns and by 72 hours after birth for cesarean section–delivered newborns, although more than 25% of the latter remained at least 10% below their birthweight by the third day.
The research was funded by the U.S. Department of Health & Human Services and the National Institute of Child Health and Human Development. The authors reported no disclosures.
“A major focus of contemporary care during the birth hospitalization is the management of breastfed infants. Although much effort is centered on the provision of optimal instruction and support to mothers initiating breastfeeding, an equally important goal is to appropriately diagnose and manage newborns with breastfeeding difficulties,” Dr. James A. Taylor and Dr. Elizabeth A. Simpson wrote in an accompanying editorial (Pediatrics 2014 Dec. 1 [doi:10.1542/peds.2014-3354]).“The results of the study by Flaherman et al in this issue of Pediatrics provide much needed data for both of these efforts.”
Dr. Flaherman and her colleagues have “normalized weight loss in breastfed infants. The data can be used to allay the anxiety of a new mother. ... More important, using the nomograms, neonates with significant breastfeeding problems may be identified because their weight loss is ≥ 95th percentile for age or because the trajectory of weight loss is atypical.”
Dr. Taylor is at the department of pediatrics at University of Washington in Seattle and Dr. Simpson is at the department of pediatrics at Children’s Mercy Hospital in Kansas City, Mo. Both authors reported no disclosures.
“A major focus of contemporary care during the birth hospitalization is the management of breastfed infants. Although much effort is centered on the provision of optimal instruction and support to mothers initiating breastfeeding, an equally important goal is to appropriately diagnose and manage newborns with breastfeeding difficulties,” Dr. James A. Taylor and Dr. Elizabeth A. Simpson wrote in an accompanying editorial (Pediatrics 2014 Dec. 1 [doi:10.1542/peds.2014-3354]).“The results of the study by Flaherman et al in this issue of Pediatrics provide much needed data for both of these efforts.”
Dr. Flaherman and her colleagues have “normalized weight loss in breastfed infants. The data can be used to allay the anxiety of a new mother. ... More important, using the nomograms, neonates with significant breastfeeding problems may be identified because their weight loss is ≥ 95th percentile for age or because the trajectory of weight loss is atypical.”
Dr. Taylor is at the department of pediatrics at University of Washington in Seattle and Dr. Simpson is at the department of pediatrics at Children’s Mercy Hospital in Kansas City, Mo. Both authors reported no disclosures.
“A major focus of contemporary care during the birth hospitalization is the management of breastfed infants. Although much effort is centered on the provision of optimal instruction and support to mothers initiating breastfeeding, an equally important goal is to appropriately diagnose and manage newborns with breastfeeding difficulties,” Dr. James A. Taylor and Dr. Elizabeth A. Simpson wrote in an accompanying editorial (Pediatrics 2014 Dec. 1 [doi:10.1542/peds.2014-3354]).“The results of the study by Flaherman et al in this issue of Pediatrics provide much needed data for both of these efforts.”
Dr. Flaherman and her colleagues have “normalized weight loss in breastfed infants. The data can be used to allay the anxiety of a new mother. ... More important, using the nomograms, neonates with significant breastfeeding problems may be identified because their weight loss is ≥ 95th percentile for age or because the trajectory of weight loss is atypical.”
Dr. Taylor is at the department of pediatrics at University of Washington in Seattle and Dr. Simpson is at the department of pediatrics at Children’s Mercy Hospital in Kansas City, Mo. Both authors reported no disclosures.
Losing more than 10% of birthweight early in the postnatal course is common among neonates delivered vaginally and by cesarean section who have been exclusively breastfed, nomograms developed by a team of researchers show. Those graphical depictions of hourly weight loss “may inform clinical care,” Dr. Valerie J. Flaherman and her colleagues reported in Pediatrics.
“The availability of detailed data on weight and feeding for a large cohort allows this study to present the first graphical depiction of hourly weight loss for exclusively breastfed newborns from a large, diverse population,” wrote Dr. Flaherman of the University of California, San Francisco, and her colleagues. “Our curves demonstrate that expected weight loss differs substantially by method of delivery and that this difference persists over time” (Pediatrics 2014 Dec. 1 [doi:10.1542/peds.2014-1532]).
Using available weight data from the births of 108,907 singleton neonates born at 36 weeks’ gestation or later at Northern California Kaiser Permanente hospitals between 2009 and 2013, the researchers created nomograms that estimate percentiles of weight loss among exclusively breastfed infants who were vaginally delivery or delivered by cesarean section.
Dr. Flaherman’s team estimated 50th, 75th, 90th, and 95th percentiles based on analysis of 83,433 vaginally born neonates and 25,474 infants delivered by C-section, all exclusively breastfed. The study excluded infants who received any formula, those weighing less than 2,000 g or more than 5,000 g, and those whose weight, delivery mode, or feeding status was unknown.
Median weight loss for vaginally delivered newborns was 4.2%, 7.1%, and 6.4% at 24, 48, and 72 hours after birth, respectively. Among cesarean section–born newborns, median percent weight loss was 4.9%, 8%, 8.6%, and 5.8% at 24, 48, 72, and 96 hours after birth.
Nearly 5% of vaginally delivered newborns and nearly 10% of newborns delivered by cesarean section had lost at least 10% of their birthweight at 48 hours after birth. Percentile curves began to rise shortly after 48 hours for vaginally delivered newborns and by 72 hours after birth for cesarean section–delivered newborns, although more than 25% of the latter remained at least 10% below their birthweight by the third day.
The research was funded by the U.S. Department of Health & Human Services and the National Institute of Child Health and Human Development. The authors reported no disclosures.
Losing more than 10% of birthweight early in the postnatal course is common among neonates delivered vaginally and by cesarean section who have been exclusively breastfed, nomograms developed by a team of researchers show. Those graphical depictions of hourly weight loss “may inform clinical care,” Dr. Valerie J. Flaherman and her colleagues reported in Pediatrics.
“The availability of detailed data on weight and feeding for a large cohort allows this study to present the first graphical depiction of hourly weight loss for exclusively breastfed newborns from a large, diverse population,” wrote Dr. Flaherman of the University of California, San Francisco, and her colleagues. “Our curves demonstrate that expected weight loss differs substantially by method of delivery and that this difference persists over time” (Pediatrics 2014 Dec. 1 [doi:10.1542/peds.2014-1532]).
Using available weight data from the births of 108,907 singleton neonates born at 36 weeks’ gestation or later at Northern California Kaiser Permanente hospitals between 2009 and 2013, the researchers created nomograms that estimate percentiles of weight loss among exclusively breastfed infants who were vaginally delivery or delivered by cesarean section.
Dr. Flaherman’s team estimated 50th, 75th, 90th, and 95th percentiles based on analysis of 83,433 vaginally born neonates and 25,474 infants delivered by C-section, all exclusively breastfed. The study excluded infants who received any formula, those weighing less than 2,000 g or more than 5,000 g, and those whose weight, delivery mode, or feeding status was unknown.
Median weight loss for vaginally delivered newborns was 4.2%, 7.1%, and 6.4% at 24, 48, and 72 hours after birth, respectively. Among cesarean section–born newborns, median percent weight loss was 4.9%, 8%, 8.6%, and 5.8% at 24, 48, 72, and 96 hours after birth.
Nearly 5% of vaginally delivered newborns and nearly 10% of newborns delivered by cesarean section had lost at least 10% of their birthweight at 48 hours after birth. Percentile curves began to rise shortly after 48 hours for vaginally delivered newborns and by 72 hours after birth for cesarean section–delivered newborns, although more than 25% of the latter remained at least 10% below their birthweight by the third day.
The research was funded by the U.S. Department of Health & Human Services and the National Institute of Child Health and Human Development. The authors reported no disclosures.
FROM PEDIATRICS
Key clinical point: Newborn weight loss of at least 10% of birth weight is common in exclusively breastfed infants.
Major finding: Nearly 5% of vaginally delivered newborns and more than 10% of cesarean section–born newborns lost at least 10% of their birth weight 48 hours after birth.
Data source: Prospective cohort study of 161,471 term, singleton neonates born ≥ 36 weeks gestation at Northern California Kaiser Permanente hospitals in 2009-2013.
Disclosures: The research was funded by the U.S. Department of Health & Human Services and the National Institute of Child Health and Human Development. The authors reported no disclosures.

Parents continue practice that increases SIDS risk
Despite a decline in use of soft bedding in infant sleep environments since 1993, more than half of parents continue the practice, putting their children at risk, according to a recent study.
“The use of certain types of bedding in the infant sleep environment is a modifiable risk factor for SIDS [sudden infant death syndrome] and unintentional sleep-related suffocation,” reported Carrie Shapiro-Mendoza, Ph.D., of the Centers for Disease Control and Prevention, Atlanta, and her colleagues.
The American Academy of Pediatrics recommends that soft objects – such as blankets, pillows, soft toys, quilts, comforters, and sheepskin – not be placed in infants’ sleeping areas.

“However, despite such recommendations, the use of bedding over and under the infant for sleep seems to have remained a common practice,” the authors wrote (Pediatrics 2014 [doi:10.1542/peds.2014-1793]).
The authors analyzed data from the annual, cross-sectional National Infant Sleep Position telephone survey data from 1993 to 2010. Among the 18,952 respondents – all of whom were parents of children under 8 months old – 83% were white, 45% had a college education, and 52% had a previous child.
Use of soft bedding dropped from an average 86% in 1993-1995 to 55% in 2008-2010. Thick blankets and quilts/comforters were the most common covers used, and blankets and cushions were the most common items used under infants.
Although use of thick blanket coverings declined from 56% to 27% during that time and quilt/comforter cover use declined from 39% to 8%, the use of blankets and cushions under sleeping infants actually increased, from 26% to 32% and 3% to 5%, respectively.
Risk factors for soft bedding use included lack of college education, nonwhite race, and younger maternal age, with 84% of teenage mothers reporting soft bedding use. In 1993-2010, an average 64% of white parents, 76% of Hispanic parents, and 75% of black parents used bedding.
The study was funded by the National Institutes of Health and the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The authors reported no disclosures.
“Studies that measure trends in infant care practices are helpful in providing a window into our patients’ behaviors and guiding us as we provide education on a public as well as individual level. The article by Shapiro-Mendoza and colleagues is the first to report trends in the use of potentially hazardous bedding in the infant sleep environment.
“There were several disturbing findings described in the study. Of course, the next question for us to ask is, Why do parents feel the need to use soft bedding? Qualitative studies are helpful in this regard. The major reasons for using soft bedding are comfort/warmth and safety. Many parents worry that their infant will become cold or otherwise be uncomfortable if they do not use bedding.
“In addition, parents may be incorrectly interpreting the recommendation against using thick blankets or comforters as meaning only over the infant, rather than under as well. Ironically, parents believe that soft bedding makes the sleep area safer for their infant. Unfortunately, if infants roll into these objects, they may not be able to roll back out and may accidentally suffocate.
“The groups at highest risk of SIDS are also those that were found in this study to be more likely to be using potentially hazardous bedding in their infants’ sleep environment: teenage, black, or less-educated mothers. Counseling is likely more effective if we understand parental concerns and misgivings about infant health and safety recommendations and can address these. Discussion of potentially hazardous bedding should be included whenever we talk to parents about the infant’s sleep environment and safe sleep practices. Only then will we be able to achieve improvements in these worrisome trends and further reductions in the incidence of SIDS and suffocation deaths.”
Dr. Rachel Y. Moon is at the Goldberg Center for Community Pediatric Health at Children’s National Medical Center in Washington and George Washington University. Dr. Fern R. Hauck is a professor of family medicine at University of Virginia in Charlottesville. These comments are from an editorial accompanying the study. Both authors reported no disclosures.
“Studies that measure trends in infant care practices are helpful in providing a window into our patients’ behaviors and guiding us as we provide education on a public as well as individual level. The article by Shapiro-Mendoza and colleagues is the first to report trends in the use of potentially hazardous bedding in the infant sleep environment.
“There were several disturbing findings described in the study. Of course, the next question for us to ask is, Why do parents feel the need to use soft bedding? Qualitative studies are helpful in this regard. The major reasons for using soft bedding are comfort/warmth and safety. Many parents worry that their infant will become cold or otherwise be uncomfortable if they do not use bedding.
“In addition, parents may be incorrectly interpreting the recommendation against using thick blankets or comforters as meaning only over the infant, rather than under as well. Ironically, parents believe that soft bedding makes the sleep area safer for their infant. Unfortunately, if infants roll into these objects, they may not be able to roll back out and may accidentally suffocate.
“The groups at highest risk of SIDS are also those that were found in this study to be more likely to be using potentially hazardous bedding in their infants’ sleep environment: teenage, black, or less-educated mothers. Counseling is likely more effective if we understand parental concerns and misgivings about infant health and safety recommendations and can address these. Discussion of potentially hazardous bedding should be included whenever we talk to parents about the infant’s sleep environment and safe sleep practices. Only then will we be able to achieve improvements in these worrisome trends and further reductions in the incidence of SIDS and suffocation deaths.”
Dr. Rachel Y. Moon is at the Goldberg Center for Community Pediatric Health at Children’s National Medical Center in Washington and George Washington University. Dr. Fern R. Hauck is a professor of family medicine at University of Virginia in Charlottesville. These comments are from an editorial accompanying the study. Both authors reported no disclosures.
“Studies that measure trends in infant care practices are helpful in providing a window into our patients’ behaviors and guiding us as we provide education on a public as well as individual level. The article by Shapiro-Mendoza and colleagues is the first to report trends in the use of potentially hazardous bedding in the infant sleep environment.
“There were several disturbing findings described in the study. Of course, the next question for us to ask is, Why do parents feel the need to use soft bedding? Qualitative studies are helpful in this regard. The major reasons for using soft bedding are comfort/warmth and safety. Many parents worry that their infant will become cold or otherwise be uncomfortable if they do not use bedding.
“In addition, parents may be incorrectly interpreting the recommendation against using thick blankets or comforters as meaning only over the infant, rather than under as well. Ironically, parents believe that soft bedding makes the sleep area safer for their infant. Unfortunately, if infants roll into these objects, they may not be able to roll back out and may accidentally suffocate.
“The groups at highest risk of SIDS are also those that were found in this study to be more likely to be using potentially hazardous bedding in their infants’ sleep environment: teenage, black, or less-educated mothers. Counseling is likely more effective if we understand parental concerns and misgivings about infant health and safety recommendations and can address these. Discussion of potentially hazardous bedding should be included whenever we talk to parents about the infant’s sleep environment and safe sleep practices. Only then will we be able to achieve improvements in these worrisome trends and further reductions in the incidence of SIDS and suffocation deaths.”
Dr. Rachel Y. Moon is at the Goldberg Center for Community Pediatric Health at Children’s National Medical Center in Washington and George Washington University. Dr. Fern R. Hauck is a professor of family medicine at University of Virginia in Charlottesville. These comments are from an editorial accompanying the study. Both authors reported no disclosures.
Despite a decline in use of soft bedding in infant sleep environments since 1993, more than half of parents continue the practice, putting their children at risk, according to a recent study.
“The use of certain types of bedding in the infant sleep environment is a modifiable risk factor for SIDS [sudden infant death syndrome] and unintentional sleep-related suffocation,” reported Carrie Shapiro-Mendoza, Ph.D., of the Centers for Disease Control and Prevention, Atlanta, and her colleagues.
The American Academy of Pediatrics recommends that soft objects – such as blankets, pillows, soft toys, quilts, comforters, and sheepskin – not be placed in infants’ sleeping areas.
“However, despite such recommendations, the use of bedding over and under the infant for sleep seems to have remained a common practice,” the authors wrote (Pediatrics 2014 [doi:10.1542/peds.2014-1793]).
The authors analyzed data from the annual, cross-sectional National Infant Sleep Position telephone survey data from 1993 to 2010. Among the 18,952 respondents – all of whom were parents of children under 8 months old – 83% were white, 45% had a college education, and 52% had a previous child.
Use of soft bedding dropped from an average 86% in 1993-1995 to 55% in 2008-2010. Thick blankets and quilts/comforters were the most common covers used, and blankets and cushions were the most common items used under infants.
Although use of thick blanket coverings declined from 56% to 27% during that time and quilt/comforter cover use declined from 39% to 8%, the use of blankets and cushions under sleeping infants actually increased, from 26% to 32% and 3% to 5%, respectively.
Risk factors for soft bedding use included lack of college education, nonwhite race, and younger maternal age, with 84% of teenage mothers reporting soft bedding use. In 1993-2010, an average 64% of white parents, 76% of Hispanic parents, and 75% of black parents used bedding.
The study was funded by the National Institutes of Health and the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The authors reported no disclosures.
Despite a decline in use of soft bedding in infant sleep environments since 1993, more than half of parents continue the practice, putting their children at risk, according to a recent study.
“The use of certain types of bedding in the infant sleep environment is a modifiable risk factor for SIDS [sudden infant death syndrome] and unintentional sleep-related suffocation,” reported Carrie Shapiro-Mendoza, Ph.D., of the Centers for Disease Control and Prevention, Atlanta, and her colleagues.
The American Academy of Pediatrics recommends that soft objects – such as blankets, pillows, soft toys, quilts, comforters, and sheepskin – not be placed in infants’ sleeping areas.
“However, despite such recommendations, the use of bedding over and under the infant for sleep seems to have remained a common practice,” the authors wrote (Pediatrics 2014 [doi:10.1542/peds.2014-1793]).
The authors analyzed data from the annual, cross-sectional National Infant Sleep Position telephone survey data from 1993 to 2010. Among the 18,952 respondents – all of whom were parents of children under 8 months old – 83% were white, 45% had a college education, and 52% had a previous child.
Use of soft bedding dropped from an average 86% in 1993-1995 to 55% in 2008-2010. Thick blankets and quilts/comforters were the most common covers used, and blankets and cushions were the most common items used under infants.
Although use of thick blanket coverings declined from 56% to 27% during that time and quilt/comforter cover use declined from 39% to 8%, the use of blankets and cushions under sleeping infants actually increased, from 26% to 32% and 3% to 5%, respectively.
Risk factors for soft bedding use included lack of college education, nonwhite race, and younger maternal age, with 84% of teenage mothers reporting soft bedding use. In 1993-2010, an average 64% of white parents, 76% of Hispanic parents, and 75% of black parents used bedding.
The study was funded by the National Institutes of Health and the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The authors reported no disclosures.
FROM PEDIATRICS
Key clinical point: Many infants still sleeping with soft bedding, a SIDS risk factor.
Major finding: 54.7% of parents used soft bedding with their sleeping infants.
Data source: Annual, cross-sectional National Infant Sleep Position telephone survey data from 1993 to 2010, including 18,952 parents of children under 8 months old.
Disclosures: The study was funded by the National Institutes of Health and the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The authors reported no disclosures.

Heart attack survival better with basic vs. advanced life support
Patients who experience a heart attack outside of the hospital are more likely to survive and have better neurologic function when they receive basic rather than advanced life support, according to a recent study.
Emergency medical services respond to an estimated 380,000 cardiac arrests outside of the hospital each year, but 90% of these patients do not survive to hospital discharge, noted Prachi Sanghavi and her associates at Harvard University, Cambridge, Mass.

“Our study calls into question the widespread assumption that advanced prehospital care improves the outcomes of out-of-hospital cardiac arrest relative to the care following the principles of basic life support, including rapid transport and basic interventions such as effective chest compressions, bag valve mask ventilation, and automated external defibrillation,” the authors wrote (JAMA Intern. Med. 2014 Nov. 24 [doi:10.1001/jamainternmed.2014.5420]). Advanced life support involves use of interventions such as endotracheal intubation, intravenous fluid and drug delivery, and semiautomatic defibrillation.
From among more than 4 million emergency rides to the hospital billed under Medicare, the authors analyzed 31,292 involving cardiac arrest where advanced life support was provided and 1,643 cardiac arrests where basic life support was provided. All cases occurred in nonrural counties.
They found 13.1% of those receiving basic life support and 9.2% of those receiving advanced life support survived to hospital discharge. Similarly, 8% who received basic life support and 5.4% who received advanced life support survived to 90 days.
Neurological functioning was also superior in those receiving basic rather than advanced interventions: 21.8% who received basic life support had poor functioning, compared with 44.8% of those who received advanced life support.
“Mean medical spending was higher among beneficiaries receiving basic life support ($11,875 for BLS vs. $9,097 for ALS), in part because individuals who received basic life support survived longer and had more opportunity to receive medical care,” the authors reported.
The study was funded by the National Science Foundation, the Agency for Healthcare Research and Quality, and the National Institutes of Health. A coauthor, Joseph P. Newhouse, holds equity in and is a director at Aetna.
Is it possible that basic life support – with automatic defibrillators, cardiopulmonary resuscitation, and airway management without intubation – could be as good or better [than advanced life support]? Sanghavi et al. have provided us with provocative data in answer to this question. The authors found that patients receiving advanced life support had 43% lower survival to hospital discharge, 51% had poorer neurologic function, and 30% had higher costs. The likelihood that their findings are true is strengthened by the study’s consistency with a growing body of research demonstrating the ineffectiveness of many advanced life support therapies.
How can outcomes of basic life support be equal or superior to “advanced” life support? For one, the handful of therapies with solid proof are all components of basic life support; most advanced life support interventions rely on tenuous evidence. Basic life support teams may take crucial basic skills more seriously and perform them better. Most importantly, advanced life support procedures are distracting, take extra time, and interrupt critical and effective basic life support measures. Unless advanced life support interventions were decisively proven to have major benefit (compared with “hail Mary” hopes), it would be inherently harmful to interrupt basic life support to perform them. In most EMS systems, many advanced life support providers have insufficient clinical experience to be truly adept at advanced procedures, many of which are done infrequently. Also, paramedics are not as well supervised or monitored as would be mandatory in a hospital environment.
How should we proceed now? The last 15 years have produced high-quality studies, all with similar conclusions. The most beneficial treatment changes in out-of-hospital cardiac arrest treatment have not involved new modalities, but instead the progressive removal of multiple unproven medications (e.g., antiarrhythmics) and interventions (pulse checks, precordial thumps) once mandated in protocols but now found to be ineffective or even harmful. We should complete the process of removing unproven and ineffective interventions from guidelines and practice until better interventions are backed up by evidence that meets contemporary standards. Using them where we know they will almost always fail is neither efficient nor ethical.
Dr. Michael Callaham is chair of emergency medicine at the University of California, San Francisco. These comments are excerpted from an editorial accompanying the study in the Nov. 24 online issue of JAMA Internal Medicine (doi:10.1001/jamainternmed.2014.6590). He reported no disclosures.
Is it possible that basic life support – with automatic defibrillators, cardiopulmonary resuscitation, and airway management without intubation – could be as good or better [than advanced life support]? Sanghavi et al. have provided us with provocative data in answer to this question. The authors found that patients receiving advanced life support had 43% lower survival to hospital discharge, 51% had poorer neurologic function, and 30% had higher costs. The likelihood that their findings are true is strengthened by the study’s consistency with a growing body of research demonstrating the ineffectiveness of many advanced life support therapies.
How can outcomes of basic life support be equal or superior to “advanced” life support? For one, the handful of therapies with solid proof are all components of basic life support; most advanced life support interventions rely on tenuous evidence. Basic life support teams may take crucial basic skills more seriously and perform them better. Most importantly, advanced life support procedures are distracting, take extra time, and interrupt critical and effective basic life support measures. Unless advanced life support interventions were decisively proven to have major benefit (compared with “hail Mary” hopes), it would be inherently harmful to interrupt basic life support to perform them. In most EMS systems, many advanced life support providers have insufficient clinical experience to be truly adept at advanced procedures, many of which are done infrequently. Also, paramedics are not as well supervised or monitored as would be mandatory in a hospital environment.
How should we proceed now? The last 15 years have produced high-quality studies, all with similar conclusions. The most beneficial treatment changes in out-of-hospital cardiac arrest treatment have not involved new modalities, but instead the progressive removal of multiple unproven medications (e.g., antiarrhythmics) and interventions (pulse checks, precordial thumps) once mandated in protocols but now found to be ineffective or even harmful. We should complete the process of removing unproven and ineffective interventions from guidelines and practice until better interventions are backed up by evidence that meets contemporary standards. Using them where we know they will almost always fail is neither efficient nor ethical.
Dr. Michael Callaham is chair of emergency medicine at the University of California, San Francisco. These comments are excerpted from an editorial accompanying the study in the Nov. 24 online issue of JAMA Internal Medicine (doi:10.1001/jamainternmed.2014.6590). He reported no disclosures.
Is it possible that basic life support – with automatic defibrillators, cardiopulmonary resuscitation, and airway management without intubation – could be as good or better [than advanced life support]? Sanghavi et al. have provided us with provocative data in answer to this question. The authors found that patients receiving advanced life support had 43% lower survival to hospital discharge, 51% had poorer neurologic function, and 30% had higher costs. The likelihood that their findings are true is strengthened by the study’s consistency with a growing body of research demonstrating the ineffectiveness of many advanced life support therapies.
How can outcomes of basic life support be equal or superior to “advanced” life support? For one, the handful of therapies with solid proof are all components of basic life support; most advanced life support interventions rely on tenuous evidence. Basic life support teams may take crucial basic skills more seriously and perform them better. Most importantly, advanced life support procedures are distracting, take extra time, and interrupt critical and effective basic life support measures. Unless advanced life support interventions were decisively proven to have major benefit (compared with “hail Mary” hopes), it would be inherently harmful to interrupt basic life support to perform them. In most EMS systems, many advanced life support providers have insufficient clinical experience to be truly adept at advanced procedures, many of which are done infrequently. Also, paramedics are not as well supervised or monitored as would be mandatory in a hospital environment.
How should we proceed now? The last 15 years have produced high-quality studies, all with similar conclusions. The most beneficial treatment changes in out-of-hospital cardiac arrest treatment have not involved new modalities, but instead the progressive removal of multiple unproven medications (e.g., antiarrhythmics) and interventions (pulse checks, precordial thumps) once mandated in protocols but now found to be ineffective or even harmful. We should complete the process of removing unproven and ineffective interventions from guidelines and practice until better interventions are backed up by evidence that meets contemporary standards. Using them where we know they will almost always fail is neither efficient nor ethical.
Dr. Michael Callaham is chair of emergency medicine at the University of California, San Francisco. These comments are excerpted from an editorial accompanying the study in the Nov. 24 online issue of JAMA Internal Medicine (doi:10.1001/jamainternmed.2014.6590). He reported no disclosures.
Patients who experience a heart attack outside of the hospital are more likely to survive and have better neurologic function when they receive basic rather than advanced life support, according to a recent study.
Emergency medical services respond to an estimated 380,000 cardiac arrests outside of the hospital each year, but 90% of these patients do not survive to hospital discharge, noted Prachi Sanghavi and her associates at Harvard University, Cambridge, Mass.
“Our study calls into question the widespread assumption that advanced prehospital care improves the outcomes of out-of-hospital cardiac arrest relative to the care following the principles of basic life support, including rapid transport and basic interventions such as effective chest compressions, bag valve mask ventilation, and automated external defibrillation,” the authors wrote (JAMA Intern. Med. 2014 Nov. 24 [doi:10.1001/jamainternmed.2014.5420]). Advanced life support involves use of interventions such as endotracheal intubation, intravenous fluid and drug delivery, and semiautomatic defibrillation.
From among more than 4 million emergency rides to the hospital billed under Medicare, the authors analyzed 31,292 involving cardiac arrest where advanced life support was provided and 1,643 cardiac arrests where basic life support was provided. All cases occurred in nonrural counties.
They found 13.1% of those receiving basic life support and 9.2% of those receiving advanced life support survived to hospital discharge. Similarly, 8% who received basic life support and 5.4% who received advanced life support survived to 90 days.
Neurological functioning was also superior in those receiving basic rather than advanced interventions: 21.8% who received basic life support had poor functioning, compared with 44.8% of those who received advanced life support.
“Mean medical spending was higher among beneficiaries receiving basic life support ($11,875 for BLS vs. $9,097 for ALS), in part because individuals who received basic life support survived longer and had more opportunity to receive medical care,” the authors reported.
The study was funded by the National Science Foundation, the Agency for Healthcare Research and Quality, and the National Institutes of Health. A coauthor, Joseph P. Newhouse, holds equity in and is a director at Aetna.
Patients who experience a heart attack outside of the hospital are more likely to survive and have better neurologic function when they receive basic rather than advanced life support, according to a recent study.
Emergency medical services respond to an estimated 380,000 cardiac arrests outside of the hospital each year, but 90% of these patients do not survive to hospital discharge, noted Prachi Sanghavi and her associates at Harvard University, Cambridge, Mass.
“Our study calls into question the widespread assumption that advanced prehospital care improves the outcomes of out-of-hospital cardiac arrest relative to the care following the principles of basic life support, including rapid transport and basic interventions such as effective chest compressions, bag valve mask ventilation, and automated external defibrillation,” the authors wrote (JAMA Intern. Med. 2014 Nov. 24 [doi:10.1001/jamainternmed.2014.5420]). Advanced life support involves use of interventions such as endotracheal intubation, intravenous fluid and drug delivery, and semiautomatic defibrillation.
From among more than 4 million emergency rides to the hospital billed under Medicare, the authors analyzed 31,292 involving cardiac arrest where advanced life support was provided and 1,643 cardiac arrests where basic life support was provided. All cases occurred in nonrural counties.
They found 13.1% of those receiving basic life support and 9.2% of those receiving advanced life support survived to hospital discharge. Similarly, 8% who received basic life support and 5.4% who received advanced life support survived to 90 days.
Neurological functioning was also superior in those receiving basic rather than advanced interventions: 21.8% who received basic life support had poor functioning, compared with 44.8% of those who received advanced life support.
“Mean medical spending was higher among beneficiaries receiving basic life support ($11,875 for BLS vs. $9,097 for ALS), in part because individuals who received basic life support survived longer and had more opportunity to receive medical care,” the authors reported.
The study was funded by the National Science Foundation, the Agency for Healthcare Research and Quality, and the National Institutes of Health. A coauthor, Joseph P. Newhouse, holds equity in and is a director at Aetna.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Out-of-hospital cardiac arrests result in better survival with basic life support.
Major finding: Survival to discharge was 13.1% with basic life support and 9.2% with advanced life support; 90-day survival was 8% with basic life support and 5.4% with advanced life support.
Data source: Observational cohort study of 32,935 nationally representative nonrural Medicare beneficiaries who had an out-of-hospital cardiac arrest between Jan. 1, 2009, and Oct. 2, 2011.
Disclosures: The study was funded by the National Science Foundation, the Agency for Healthcare Research and Quality, and the National Institutes of Health. Dr. Newhouse holds equity in and is a director at Aetna.

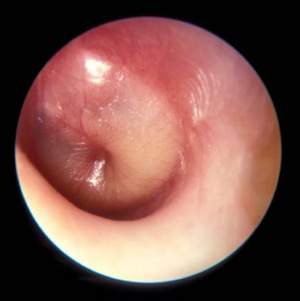
Otitis media prescribing patterns differ by race
Black children were less likely to be diagnosed with otitis media and more likely to be prescribed narrow-spectrum, rather than broad-spectrum, antibiotics compared with nonblack children, according to a recent study.
“These findings raise concerns that differences in care for otitis media based on race may reflect inappropriate treatment of otitis media with the use of broad-spectrum antibiotics in a majority of U.S. children,” wrote Dr. Katherine E. Fleming-Dutra of Emory University, Atlanta (Pediatrics 2014 [doi:10.1542/peds.2014-1781]).
After a study in the Philadelphia area showed lower otitis media diagnosis rates and less use of

broad-spectrum antibiotics for blacks compared with nonblacks, these researchers investigated race, diagnosis, and prescribing patterns nationwide.
They analyzed visits for children 14 years old and younger between 2008 and 2010 using data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, both data sets from the National Center for Health Statistics at the Centers for Disease Control and Prevention.
Based on 4,178 visits in the database, the researchers estimated that 19.2 million visits for otitis media occurred from 2008 to 2010 in the United States. However, only 7% of black children’s visits included an otitis media diagnosis, compared with 10% of nonblack children’s visits (P = .004).
While black and nonblack children with otitis media were prescribed antibiotics at similar rates (81% vs. 76%, respectively, P = .30), black children were prescribed broad-spectrum antibiotics 42% of the time, compared with 52% for nonblack children (P = .01). Broad-spectrum cephalosporins were prescribed for otitis media for 12% of black children and 21% of nonblack children; broad-spectrum penicillins were prescribed for 10% of black children and 16% of nonblack children with otitis media.
After adjustment for age, gender, region, insurance, care setting, metropolitan area, and year, black children had 41% lower odds than did nonblack children of receiving a broad-spectrum antibiotic prescription for otitis media.
The study was funded by the CDC. Dr. Gerber and Dr. Hersh received a Pfizer research grant to implement antibiotic stewardship in children’s hospitals. The remaining authors had no relevant financial disclosures.
“At face value, these data could indicate a ‘reversal’ in direction of the health care disparity usually identified in the United States. Fleming-Dutra et al. found no differences in care-seeking by black children versus nonblack children for upper respiratory tract conditions, suggesting that the difference in prescribing for acute otitis media was not due to differences in care-seeking behaviors among the families of black and nonblack children.
“We as physicians may enter the patient-provider relationship with our own set of biases, stereotypes, and expectations. We may subconsciously use the strategy of socialization to put people into categories (i.e., race) to use cognitive shortcuts that have been previously created in decision-making.
“We develop our own perceptions of what our patients and their families may want or need and form images related to their understanding of medical information and whether a particular family can participate in a shared-decision model. These shortcuts in imagery may act as facilitators or could have the opposite effect for minority populations, resulting in disparities of care.
“What is the true basis for the observed ‘reverse’ guideline-adherent disparity reported by Fleming-Dutra et al.? We hope it is due at least in part to conscious application of guideline recommendations among the practitioners caring for black children. We suspect it is partially due to perceptions of parent expectations or other influences on overprescribing of broad-spectrum antimicrobial agents for nonblack children.
“Regardless, these data provide an opportunity for all of us to reflect upon the beliefs and practices regarding race/ethnicity that may consciously or unconsciously influence clinical decision-making within ourselves and the institutional cultures in which we practice.”
Charles R. Woods, M.D., and V. Faye Jones, M.D., are in the department of pediatrics at the University of Louisville (Ky.). These comments are taken from an accompanying editorial (Pediatrics 2014 [doi:10.1542/peds.2014-3056]). The authors reported no disclosures or external funding.
“At face value, these data could indicate a ‘reversal’ in direction of the health care disparity usually identified in the United States. Fleming-Dutra et al. found no differences in care-seeking by black children versus nonblack children for upper respiratory tract conditions, suggesting that the difference in prescribing for acute otitis media was not due to differences in care-seeking behaviors among the families of black and nonblack children.
“We as physicians may enter the patient-provider relationship with our own set of biases, stereotypes, and expectations. We may subconsciously use the strategy of socialization to put people into categories (i.e., race) to use cognitive shortcuts that have been previously created in decision-making.
“We develop our own perceptions of what our patients and their families may want or need and form images related to their understanding of medical information and whether a particular family can participate in a shared-decision model. These shortcuts in imagery may act as facilitators or could have the opposite effect for minority populations, resulting in disparities of care.
“What is the true basis for the observed ‘reverse’ guideline-adherent disparity reported by Fleming-Dutra et al.? We hope it is due at least in part to conscious application of guideline recommendations among the practitioners caring for black children. We suspect it is partially due to perceptions of parent expectations or other influences on overprescribing of broad-spectrum antimicrobial agents for nonblack children.
“Regardless, these data provide an opportunity for all of us to reflect upon the beliefs and practices regarding race/ethnicity that may consciously or unconsciously influence clinical decision-making within ourselves and the institutional cultures in which we practice.”
Charles R. Woods, M.D., and V. Faye Jones, M.D., are in the department of pediatrics at the University of Louisville (Ky.). These comments are taken from an accompanying editorial (Pediatrics 2014 [doi:10.1542/peds.2014-3056]). The authors reported no disclosures or external funding.
“At face value, these data could indicate a ‘reversal’ in direction of the health care disparity usually identified in the United States. Fleming-Dutra et al. found no differences in care-seeking by black children versus nonblack children for upper respiratory tract conditions, suggesting that the difference in prescribing for acute otitis media was not due to differences in care-seeking behaviors among the families of black and nonblack children.
“We as physicians may enter the patient-provider relationship with our own set of biases, stereotypes, and expectations. We may subconsciously use the strategy of socialization to put people into categories (i.e., race) to use cognitive shortcuts that have been previously created in decision-making.
“We develop our own perceptions of what our patients and their families may want or need and form images related to their understanding of medical information and whether a particular family can participate in a shared-decision model. These shortcuts in imagery may act as facilitators or could have the opposite effect for minority populations, resulting in disparities of care.
“What is the true basis for the observed ‘reverse’ guideline-adherent disparity reported by Fleming-Dutra et al.? We hope it is due at least in part to conscious application of guideline recommendations among the practitioners caring for black children. We suspect it is partially due to perceptions of parent expectations or other influences on overprescribing of broad-spectrum antimicrobial agents for nonblack children.
“Regardless, these data provide an opportunity for all of us to reflect upon the beliefs and practices regarding race/ethnicity that may consciously or unconsciously influence clinical decision-making within ourselves and the institutional cultures in which we practice.”
Charles R. Woods, M.D., and V. Faye Jones, M.D., are in the department of pediatrics at the University of Louisville (Ky.). These comments are taken from an accompanying editorial (Pediatrics 2014 [doi:10.1542/peds.2014-3056]). The authors reported no disclosures or external funding.
Black children were less likely to be diagnosed with otitis media and more likely to be prescribed narrow-spectrum, rather than broad-spectrum, antibiotics compared with nonblack children, according to a recent study.
“These findings raise concerns that differences in care for otitis media based on race may reflect inappropriate treatment of otitis media with the use of broad-spectrum antibiotics in a majority of U.S. children,” wrote Dr. Katherine E. Fleming-Dutra of Emory University, Atlanta (Pediatrics 2014 [doi:10.1542/peds.2014-1781]).
After a study in the Philadelphia area showed lower otitis media diagnosis rates and less use of
broad-spectrum antibiotics for blacks compared with nonblacks, these researchers investigated race, diagnosis, and prescribing patterns nationwide.
They analyzed visits for children 14 years old and younger between 2008 and 2010 using data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, both data sets from the National Center for Health Statistics at the Centers for Disease Control and Prevention.
Based on 4,178 visits in the database, the researchers estimated that 19.2 million visits for otitis media occurred from 2008 to 2010 in the United States. However, only 7% of black children’s visits included an otitis media diagnosis, compared with 10% of nonblack children’s visits (P = .004).
While black and nonblack children with otitis media were prescribed antibiotics at similar rates (81% vs. 76%, respectively, P = .30), black children were prescribed broad-spectrum antibiotics 42% of the time, compared with 52% for nonblack children (P = .01). Broad-spectrum cephalosporins were prescribed for otitis media for 12% of black children and 21% of nonblack children; broad-spectrum penicillins were prescribed for 10% of black children and 16% of nonblack children with otitis media.
After adjustment for age, gender, region, insurance, care setting, metropolitan area, and year, black children had 41% lower odds than did nonblack children of receiving a broad-spectrum antibiotic prescription for otitis media.
The study was funded by the CDC. Dr. Gerber and Dr. Hersh received a Pfizer research grant to implement antibiotic stewardship in children’s hospitals. The remaining authors had no relevant financial disclosures.
Black children were less likely to be diagnosed with otitis media and more likely to be prescribed narrow-spectrum, rather than broad-spectrum, antibiotics compared with nonblack children, according to a recent study.
“These findings raise concerns that differences in care for otitis media based on race may reflect inappropriate treatment of otitis media with the use of broad-spectrum antibiotics in a majority of U.S. children,” wrote Dr. Katherine E. Fleming-Dutra of Emory University, Atlanta (Pediatrics 2014 [doi:10.1542/peds.2014-1781]).
After a study in the Philadelphia area showed lower otitis media diagnosis rates and less use of
broad-spectrum antibiotics for blacks compared with nonblacks, these researchers investigated race, diagnosis, and prescribing patterns nationwide.
They analyzed visits for children 14 years old and younger between 2008 and 2010 using data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, both data sets from the National Center for Health Statistics at the Centers for Disease Control and Prevention.
Based on 4,178 visits in the database, the researchers estimated that 19.2 million visits for otitis media occurred from 2008 to 2010 in the United States. However, only 7% of black children’s visits included an otitis media diagnosis, compared with 10% of nonblack children’s visits (P = .004).
While black and nonblack children with otitis media were prescribed antibiotics at similar rates (81% vs. 76%, respectively, P = .30), black children were prescribed broad-spectrum antibiotics 42% of the time, compared with 52% for nonblack children (P = .01). Broad-spectrum cephalosporins were prescribed for otitis media for 12% of black children and 21% of nonblack children; broad-spectrum penicillins were prescribed for 10% of black children and 16% of nonblack children with otitis media.
After adjustment for age, gender, region, insurance, care setting, metropolitan area, and year, black children had 41% lower odds than did nonblack children of receiving a broad-spectrum antibiotic prescription for otitis media.
The study was funded by the CDC. Dr. Gerber and Dr. Hersh received a Pfizer research grant to implement antibiotic stewardship in children’s hospitals. The remaining authors had no relevant financial disclosures.
FROM PEDIATRICS
Key clinical point: Black children are less likely than nonblack children to receive otitis media diagnosis and broad-spectrum antibiotics.
Major finding: Black children are 30% less likely to be diagnosed with otitis media (P = .004) and 41% less likely to be prescribed broad-spectrum antibiotics.
Data source: Analysis of 4,178 visits for children aged 14 years and younger between 2008 and 2010 in two Centers for Disease Control and Prevention database sets.
Disclosures: The study was funded by the CDC. Dr. Gerber and Dr. Hersh received a Pfizer research grant to implement antibiotic stewardship in children’s hospitals. The remaining authors had no relevant financial disclosures.
Energy drink poison control calls involved cardiac, neurologic effects
Children under 6 years old are among those at the highest risk for poison control calls related to energy drinks, yet those most likely to experience moderate or major clinical effects from energy drinks are adults and often involve mixing with alcohol, according to a recent study.
Approximately 40% of all calls involving single-product energy drinks (not mixed with alcohol) were unintentional exposures by children under 6 years old, according to researchers led by Dr. Steven E. Lipshultz, chair of the department of pediatrics at Wayne State University in Detroit.

“We recommend improved labeling of caffeine content and continued efforts to decrease pediatric exposures to these products,” the researchers concluded in a presentation at the American Heart Association scientific sessions Nov. 16.
Emergency department visits involving caffeinated energy drinks in children under 12 years of age increased “exponentially” between 2005 and 2011, from 840 cases of adverse reactions in 2005 to 14,042 cases in 2011, according to Drug Abuse Warning Network background information in the presentation.
For their study, the researchers analyzed all cases of energy drink exposure reported to the U.S. National Poison Data System during October 2010 and September 2013. These include calls to 55 poison control centers in the United States.
Among the total 10,610 cases reported, 5,156 (49%) were single-product exposures with ingredients that could be identified, thereby excluding exposures related to alcoholic mixes or other combinations.
Mixtures of energy drinks and alcohol produced the most serious problems, with moderate to major effects occurring in 42% of cases involving alcohol and 19% of cases without alcohol (P < .001). Exposures involving alcohol have fallen sharply, though, since a 2010 Food and Drug Administration ban on prepackaged energy drinks containing alcohol, the researchers reported.
Both pharmaceutical-grade caffeine and caffeine from other sources may be in energy drinks, according to a statement from the American Heart Association. In this study, 23% of cases related to drinks with both pharmaceutical and additional caffeine resulted in moderate or major outcomes, compared with 15% of cases involving drinks with only pharmaceutical-grade caffeine (P < .001).
Children were least likely to experience major problems, with only 4% of cases with major or moderate effects involving children under age 12 years. Meanwhile, 64% of cases resulting in moderate or major clinical effects involved adults aged 20 years and older.
The most commonly affected organ system for non–alcohol-related energy drink exposures was neurologic, composing 20% of all clinical effects reported. These symptoms included agitation/irritability, dizziness, lethargy, headache, seizures, and tremors.
In addition, 15% of the cases involved gastrointestinal effects, such as abdominal pain, diarrhea, nausea, and vomiting, and 12% involved cardiovascular effects, which included chest pain, hypertension, arrhythmia, and tachycardia, among others.
Among the cases involving major clinical effects, 57% were cardiovascular, 54% were neurologic, and 14% were gastrointestinal. Some patients had multiple effects in more than one organ system.
Children younger than age 6 years represented the highest proportion of unintentional exposures, 75% of the total, while 10% of unintentional exposures occurred to children aged 6-12 years. Among intentional exposures, on the other hand, 45% included teenagers aged 13-19 years, and 41% included people aged 20 years and older.
These findings, based on poison control center reports, underestimate the problem, the researchers noted, because “many people who become ill from energy drinks don’t call the hotlines and emergency room visits are not included.” Those that are reported may, however, be biased in favor of greater toxicity, they said.
Information on funding and disclosures was unavailable.
Children under 6 years old are among those at the highest risk for poison control calls related to energy drinks, yet those most likely to experience moderate or major clinical effects from energy drinks are adults and often involve mixing with alcohol, according to a recent study.
Approximately 40% of all calls involving single-product energy drinks (not mixed with alcohol) were unintentional exposures by children under 6 years old, according to researchers led by Dr. Steven E. Lipshultz, chair of the department of pediatrics at Wayne State University in Detroit.
“We recommend improved labeling of caffeine content and continued efforts to decrease pediatric exposures to these products,” the researchers concluded in a presentation at the American Heart Association scientific sessions Nov. 16.
Emergency department visits involving caffeinated energy drinks in children under 12 years of age increased “exponentially” between 2005 and 2011, from 840 cases of adverse reactions in 2005 to 14,042 cases in 2011, according to Drug Abuse Warning Network background information in the presentation.
For their study, the researchers analyzed all cases of energy drink exposure reported to the U.S. National Poison Data System during October 2010 and September 2013. These include calls to 55 poison control centers in the United States.
Among the total 10,610 cases reported, 5,156 (49%) were single-product exposures with ingredients that could be identified, thereby excluding exposures related to alcoholic mixes or other combinations.
Mixtures of energy drinks and alcohol produced the most serious problems, with moderate to major effects occurring in 42% of cases involving alcohol and 19% of cases without alcohol (P < .001). Exposures involving alcohol have fallen sharply, though, since a 2010 Food and Drug Administration ban on prepackaged energy drinks containing alcohol, the researchers reported.
Both pharmaceutical-grade caffeine and caffeine from other sources may be in energy drinks, according to a statement from the American Heart Association. In this study, 23% of cases related to drinks with both pharmaceutical and additional caffeine resulted in moderate or major outcomes, compared with 15% of cases involving drinks with only pharmaceutical-grade caffeine (P < .001).
Children were least likely to experience major problems, with only 4% of cases with major or moderate effects involving children under age 12 years. Meanwhile, 64% of cases resulting in moderate or major clinical effects involved adults aged 20 years and older.
The most commonly affected organ system for non–alcohol-related energy drink exposures was neurologic, composing 20% of all clinical effects reported. These symptoms included agitation/irritability, dizziness, lethargy, headache, seizures, and tremors.
In addition, 15% of the cases involved gastrointestinal effects, such as abdominal pain, diarrhea, nausea, and vomiting, and 12% involved cardiovascular effects, which included chest pain, hypertension, arrhythmia, and tachycardia, among others.
Among the cases involving major clinical effects, 57% were cardiovascular, 54% were neurologic, and 14% were gastrointestinal. Some patients had multiple effects in more than one organ system.
Children younger than age 6 years represented the highest proportion of unintentional exposures, 75% of the total, while 10% of unintentional exposures occurred to children aged 6-12 years. Among intentional exposures, on the other hand, 45% included teenagers aged 13-19 years, and 41% included people aged 20 years and older.
These findings, based on poison control center reports, underestimate the problem, the researchers noted, because “many people who become ill from energy drinks don’t call the hotlines and emergency room visits are not included.” Those that are reported may, however, be biased in favor of greater toxicity, they said.
Information on funding and disclosures was unavailable.
Children under 6 years old are among those at the highest risk for poison control calls related to energy drinks, yet those most likely to experience moderate or major clinical effects from energy drinks are adults and often involve mixing with alcohol, according to a recent study.
Approximately 40% of all calls involving single-product energy drinks (not mixed with alcohol) were unintentional exposures by children under 6 years old, according to researchers led by Dr. Steven E. Lipshultz, chair of the department of pediatrics at Wayne State University in Detroit.
“We recommend improved labeling of caffeine content and continued efforts to decrease pediatric exposures to these products,” the researchers concluded in a presentation at the American Heart Association scientific sessions Nov. 16.
Emergency department visits involving caffeinated energy drinks in children under 12 years of age increased “exponentially” between 2005 and 2011, from 840 cases of adverse reactions in 2005 to 14,042 cases in 2011, according to Drug Abuse Warning Network background information in the presentation.
For their study, the researchers analyzed all cases of energy drink exposure reported to the U.S. National Poison Data System during October 2010 and September 2013. These include calls to 55 poison control centers in the United States.
Among the total 10,610 cases reported, 5,156 (49%) were single-product exposures with ingredients that could be identified, thereby excluding exposures related to alcoholic mixes or other combinations.
Mixtures of energy drinks and alcohol produced the most serious problems, with moderate to major effects occurring in 42% of cases involving alcohol and 19% of cases without alcohol (P < .001). Exposures involving alcohol have fallen sharply, though, since a 2010 Food and Drug Administration ban on prepackaged energy drinks containing alcohol, the researchers reported.
Both pharmaceutical-grade caffeine and caffeine from other sources may be in energy drinks, according to a statement from the American Heart Association. In this study, 23% of cases related to drinks with both pharmaceutical and additional caffeine resulted in moderate or major outcomes, compared with 15% of cases involving drinks with only pharmaceutical-grade caffeine (P < .001).
Children were least likely to experience major problems, with only 4% of cases with major or moderate effects involving children under age 12 years. Meanwhile, 64% of cases resulting in moderate or major clinical effects involved adults aged 20 years and older.
The most commonly affected organ system for non–alcohol-related energy drink exposures was neurologic, composing 20% of all clinical effects reported. These symptoms included agitation/irritability, dizziness, lethargy, headache, seizures, and tremors.
In addition, 15% of the cases involved gastrointestinal effects, such as abdominal pain, diarrhea, nausea, and vomiting, and 12% involved cardiovascular effects, which included chest pain, hypertension, arrhythmia, and tachycardia, among others.
Among the cases involving major clinical effects, 57% were cardiovascular, 54% were neurologic, and 14% were gastrointestinal. Some patients had multiple effects in more than one organ system.
Children younger than age 6 years represented the highest proportion of unintentional exposures, 75% of the total, while 10% of unintentional exposures occurred to children aged 6-12 years. Among intentional exposures, on the other hand, 45% included teenagers aged 13-19 years, and 41% included people aged 20 years and older.
These findings, based on poison control center reports, underestimate the problem, the researchers noted, because “many people who become ill from energy drinks don’t call the hotlines and emergency room visits are not included.” Those that are reported may, however, be biased in favor of greater toxicity, they said.
Information on funding and disclosures was unavailable.
FROM THE AHA SCIENTIFIC SESSIONS
Key clinical point: Energy drink exposures commonly involve children and may lead to serious cardiac and neurologic effects in adults.
Major finding: A total of 40% of unintentional energy drink exposures involved children under 6 years; 42% of energy drink exposures involving alcohol and 19% without alcohol resulted in moderate to major clinical effects.
Data source: Retrospective analysis of 10,610 exposures reported to the U.S. National Poison Data System between October 2010 and September 2013.
Disclosures: Information on funding and disclosures was unavailable.

Multitarget induction therapy superior over short term for lupus nephritis
A multitarget therapy of mycophenolate mofetil and tacrolimus for lupus nephritis induction therapy led to almost twice as many complete remissions as did intravenous cyclophosphamide in an open-label, randomized, controlled trial.
“Because immune dysregulation is fundamental to pathogenesis of lupus nephritis, with both B and T cells involved in the development of the disease, it may be necessary to target multiple aspects of the immune response using combined immunosuppressants,” wrote Dr. Zhi-Hong Liu of Nanjing (China) University and her colleagues (Ann. Intern. Med. 2014 Nov. 11 [doi:10.7326/M14-1030]).

Between April 2009 and June 2011, 368 adults aged 18-65 years from 26 renal centers in China were randomized to receive mycophenolate mofetil (MMF) and tacrolimus with a steroid or IV cyclophosphamide with a steroid for 24 weeks. A total of 362 received medication (6 did not receive their assigned cyclophosphamide treatment for unknown reasons), and 310 completed the whole 24-week course of treatment. All participants in the study had biopsy-proven lupus nephritis diagnosed within the previous 6 months and had not been previously treated with MMF, cyclophosphamide, tacrolimus, or high-dose methylprednisolone, nor had they had renal replacement therapy, plasmapheresis, or IV gamma globulin therapy in the previous 12 weeks.
All patients began by receiving IV methylprednisolone pulse therapy (0.5 g/day) for 3 days and then oral prednisone (0.6 mg/kg) daily for 4 weeks, with prednisone tapering to 10 mg/day for the remainder of the study period. Following methylprednisolone pulse therapy, the multitarget group received MMF (0.5 g twice daily) and tacrolimus (2 mg twice daily) while the comparison group received IV cyclophosphamide (initially 0.75 g/m2 body surface area, then adjusted to 0.5-1.0 g/m2).
Nearly half – 45.9% – of patients in the multitarget group achieved full remission, whereas 25.6% of patients receiving IV cyclophosphamide showed complete remission (P < .001). The investigators defined complete remission as a 24-hour urinary protein excretion of 0.4 g or less, the absence of active urine sediments, a serum albumin level of 35 g/L or greater, and normal serum creatinine.
Results on secondary endpoints also favored multitarget therapy. The percentage of patients who had an overall response to treatment (complete and partial remissions) was 83.5% for multitarget therapy and 63% for cyclophosphamide (P < .001). Multitarget therapy patients responded to treatment at a median of 8.9 weeks, compared with cyclophosphamide-treated patients at 13 weeks. The investigators defined partial response as a 50% or greater reduction in proteinuria and urine protein less than 3.5 g/24 hours, a serum albumin level of 30 g/L or higher, and a normal or 25% or lower increase in serum creatinine level from baseline.
After treatment, patients in the multitarget therapy group also had significantly better results on other secondary endpoints, including changes in urine protein, serum albumin, systemic lupus erythematosus disease activity score, and C3 levels.
Adverse events occurred among 50.3% of multitarget recipients and 52.5% of cyclophosphamide recipients. More patients who received multitarget therapy had a serious adverse event (7.2% vs. 2.8%, respectively), and more patients withdrew from the multitarget therapy group (5.5% vs. 1.7%), but there were no statistically significant differences between the groups for either comparison.
The study was supported by the National Basic Research Program of China and the National Key Technology R&D Programs. Information on disclosures was unavailable at the time of publication.
During the last decades, trials in lupus nephritis have been blessed by the publication of large studies involving hundreds of patients. While this is certainly a major achievement, yet it has not been paralleled by long-enough follow-ups. Experience has shown that in lupus nephritis, a large number of patients is “silver” but long-term follow-up is “gold.”
The very good 6-month results of Dr. Liu and colleagues’ study is an example of this aphorism. The importance of this finding is emphasized by data showing that early (within 3-6 months) response to immunosuppressive treatment has good positive predictive value for long-term (10 years) preservation of renal function (Arthritis Rheum. 2004;50:3934-40).
So, should multitarget therapy with combination of tacrolimus with mycophenolate become the new “standard of care” in lupus nephritis?
The authors of this commentary are painfully aware of the unmet needs in the treatment of lupus nephritis and certainly welcome these data. However, our enthusiasm is tempered by the following concerns.
First, there are some methodology issues to be considered such as the fact that six patients randomized to cyclophosphamide for unknown reasons did not receive the treatment and were excluded from the study, or that there were 80 missing visits in the cyclophosphamide group and 38 in the multitarget group. Nonetheless, the researchers handled these issues by data imputation and sensitivity analyses, which confirmed their findings.
Second, the results of this trial may not be generalized to all patients with lupus nephritis. As the authors discuss in the paper, this study was performed in Chinese patients who tend to respond favorably to calcineurin inhibitors. Previous lupus nephritis trials have suggested differences in the efficacy of immunosuppressive agents across patients from different ethnic backgrounds (Rheumatology [Oxford] 2010;49:128-40). Furthermore, included patients had median disease duration of 2 months, only 20.7% had glomerular filtration rate < 60 mL/min per 1.73m2, and most of them did not have high-risk histological features in kidney biopsy (median activity index of 7, chronicity index of 1). Further studies will be required to determine the efficacy of multitarget therapy in patients with adverse prognostic factors such as moderate or severe impairment of renal function, or presence of crescents.
The current study was an induction-only trial. The podocyte-preserving and anti-proteinuric effects of calcineurin inhibitors may account for the higher and faster rates of resolution of proteinuria and complete renal remission in the multitarget group. The clinical significance of this finding, especially in view of the slow-mode of action of cyclophosphamide, remains to be seen. In fact, several studies have shown that in spite of the lower rates of renal remission with cyclophosphamide, the majority of patients maintain their renal function if proteinuria is less than 2 g/day (Ann. Intern. Med. 2001;135:248-57). Whether there is a benefit of the multitarget therapy in terms of renal flares and long-term stabilization of the renal function remains to be seen. To this end, the authors do not indicate how the renal remission in these patients will be maintained and the optimal dosage and duration of immunosuppressive treatment. This is of particular importance considering also the potential nephrotoxic effects of calcineurin inhibitors when used for long time periods.
Thus, at this point, while the use of multitarget therapy from the beginning may increase the rates of complete renal remission, it increases the cost and the complexity of lupus nephritis treatment. One may consider adding calcineurin inhibitors if the patient does not reach partial renal response after 3-6 months. Meanwhile, we are eagerly awaiting longer follow-up of this most valuable cohort of patients and information of how this remission can be maintained, how durable it is, and more importantly, whether after 5 years of therapy there is a difference in the preservation of renal function.
Dr. George Bertsias is with the department of rheumatology, clinical immunology, and allergy at the University of Crete Medical School, Heraklion, Greece. Dr. John Boletis is with the nephrology department and renal transplant unit at Laiko General Hospital, University of Athens. Dr. Dimitrios T. Boumpas is with the fourth department of internal medicine, Attikon Hospital, University of Athens. They had nothing to disclose.
During the last decades, trials in lupus nephritis have been blessed by the publication of large studies involving hundreds of patients. While this is certainly a major achievement, yet it has not been paralleled by long-enough follow-ups. Experience has shown that in lupus nephritis, a large number of patients is “silver” but long-term follow-up is “gold.”
The very good 6-month results of Dr. Liu and colleagues’ study is an example of this aphorism. The importance of this finding is emphasized by data showing that early (within 3-6 months) response to immunosuppressive treatment has good positive predictive value for long-term (10 years) preservation of renal function (Arthritis Rheum. 2004;50:3934-40).
So, should multitarget therapy with combination of tacrolimus with mycophenolate become the new “standard of care” in lupus nephritis?
The authors of this commentary are painfully aware of the unmet needs in the treatment of lupus nephritis and certainly welcome these data. However, our enthusiasm is tempered by the following concerns.
First, there are some methodology issues to be considered such as the fact that six patients randomized to cyclophosphamide for unknown reasons did not receive the treatment and were excluded from the study, or that there were 80 missing visits in the cyclophosphamide group and 38 in the multitarget group. Nonetheless, the researchers handled these issues by data imputation and sensitivity analyses, which confirmed their findings.
Second, the results of this trial may not be generalized to all patients with lupus nephritis. As the authors discuss in the paper, this study was performed in Chinese patients who tend to respond favorably to calcineurin inhibitors. Previous lupus nephritis trials have suggested differences in the efficacy of immunosuppressive agents across patients from different ethnic backgrounds (Rheumatology [Oxford] 2010;49:128-40). Furthermore, included patients had median disease duration of 2 months, only 20.7% had glomerular filtration rate < 60 mL/min per 1.73m2, and most of them did not have high-risk histological features in kidney biopsy (median activity index of 7, chronicity index of 1). Further studies will be required to determine the efficacy of multitarget therapy in patients with adverse prognostic factors such as moderate or severe impairment of renal function, or presence of crescents.
The current study was an induction-only trial. The podocyte-preserving and anti-proteinuric effects of calcineurin inhibitors may account for the higher and faster rates of resolution of proteinuria and complete renal remission in the multitarget group. The clinical significance of this finding, especially in view of the slow-mode of action of cyclophosphamide, remains to be seen. In fact, several studies have shown that in spite of the lower rates of renal remission with cyclophosphamide, the majority of patients maintain their renal function if proteinuria is less than 2 g/day (Ann. Intern. Med. 2001;135:248-57). Whether there is a benefit of the multitarget therapy in terms of renal flares and long-term stabilization of the renal function remains to be seen. To this end, the authors do not indicate how the renal remission in these patients will be maintained and the optimal dosage and duration of immunosuppressive treatment. This is of particular importance considering also the potential nephrotoxic effects of calcineurin inhibitors when used for long time periods.
Thus, at this point, while the use of multitarget therapy from the beginning may increase the rates of complete renal remission, it increases the cost and the complexity of lupus nephritis treatment. One may consider adding calcineurin inhibitors if the patient does not reach partial renal response after 3-6 months. Meanwhile, we are eagerly awaiting longer follow-up of this most valuable cohort of patients and information of how this remission can be maintained, how durable it is, and more importantly, whether after 5 years of therapy there is a difference in the preservation of renal function.
Dr. George Bertsias is with the department of rheumatology, clinical immunology, and allergy at the University of Crete Medical School, Heraklion, Greece. Dr. John Boletis is with the nephrology department and renal transplant unit at Laiko General Hospital, University of Athens. Dr. Dimitrios T. Boumpas is with the fourth department of internal medicine, Attikon Hospital, University of Athens. They had nothing to disclose.
During the last decades, trials in lupus nephritis have been blessed by the publication of large studies involving hundreds of patients. While this is certainly a major achievement, yet it has not been paralleled by long-enough follow-ups. Experience has shown that in lupus nephritis, a large number of patients is “silver” but long-term follow-up is “gold.”
The very good 6-month results of Dr. Liu and colleagues’ study is an example of this aphorism. The importance of this finding is emphasized by data showing that early (within 3-6 months) response to immunosuppressive treatment has good positive predictive value for long-term (10 years) preservation of renal function (Arthritis Rheum. 2004;50:3934-40).
So, should multitarget therapy with combination of tacrolimus with mycophenolate become the new “standard of care” in lupus nephritis?
The authors of this commentary are painfully aware of the unmet needs in the treatment of lupus nephritis and certainly welcome these data. However, our enthusiasm is tempered by the following concerns.
First, there are some methodology issues to be considered such as the fact that six patients randomized to cyclophosphamide for unknown reasons did not receive the treatment and were excluded from the study, or that there were 80 missing visits in the cyclophosphamide group and 38 in the multitarget group. Nonetheless, the researchers handled these issues by data imputation and sensitivity analyses, which confirmed their findings.
Second, the results of this trial may not be generalized to all patients with lupus nephritis. As the authors discuss in the paper, this study was performed in Chinese patients who tend to respond favorably to calcineurin inhibitors. Previous lupus nephritis trials have suggested differences in the efficacy of immunosuppressive agents across patients from different ethnic backgrounds (Rheumatology [Oxford] 2010;49:128-40). Furthermore, included patients had median disease duration of 2 months, only 20.7% had glomerular filtration rate < 60 mL/min per 1.73m2, and most of them did not have high-risk histological features in kidney biopsy (median activity index of 7, chronicity index of 1). Further studies will be required to determine the efficacy of multitarget therapy in patients with adverse prognostic factors such as moderate or severe impairment of renal function, or presence of crescents.
The current study was an induction-only trial. The podocyte-preserving and anti-proteinuric effects of calcineurin inhibitors may account for the higher and faster rates of resolution of proteinuria and complete renal remission in the multitarget group. The clinical significance of this finding, especially in view of the slow-mode of action of cyclophosphamide, remains to be seen. In fact, several studies have shown that in spite of the lower rates of renal remission with cyclophosphamide, the majority of patients maintain their renal function if proteinuria is less than 2 g/day (Ann. Intern. Med. 2001;135:248-57). Whether there is a benefit of the multitarget therapy in terms of renal flares and long-term stabilization of the renal function remains to be seen. To this end, the authors do not indicate how the renal remission in these patients will be maintained and the optimal dosage and duration of immunosuppressive treatment. This is of particular importance considering also the potential nephrotoxic effects of calcineurin inhibitors when used for long time periods.
Thus, at this point, while the use of multitarget therapy from the beginning may increase the rates of complete renal remission, it increases the cost and the complexity of lupus nephritis treatment. One may consider adding calcineurin inhibitors if the patient does not reach partial renal response after 3-6 months. Meanwhile, we are eagerly awaiting longer follow-up of this most valuable cohort of patients and information of how this remission can be maintained, how durable it is, and more importantly, whether after 5 years of therapy there is a difference in the preservation of renal function.
Dr. George Bertsias is with the department of rheumatology, clinical immunology, and allergy at the University of Crete Medical School, Heraklion, Greece. Dr. John Boletis is with the nephrology department and renal transplant unit at Laiko General Hospital, University of Athens. Dr. Dimitrios T. Boumpas is with the fourth department of internal medicine, Attikon Hospital, University of Athens. They had nothing to disclose.
A multitarget therapy of mycophenolate mofetil and tacrolimus for lupus nephritis induction therapy led to almost twice as many complete remissions as did intravenous cyclophosphamide in an open-label, randomized, controlled trial.
“Because immune dysregulation is fundamental to pathogenesis of lupus nephritis, with both B and T cells involved in the development of the disease, it may be necessary to target multiple aspects of the immune response using combined immunosuppressants,” wrote Dr. Zhi-Hong Liu of Nanjing (China) University and her colleagues (Ann. Intern. Med. 2014 Nov. 11 [doi:10.7326/M14-1030]).
Between April 2009 and June 2011, 368 adults aged 18-65 years from 26 renal centers in China were randomized to receive mycophenolate mofetil (MMF) and tacrolimus with a steroid or IV cyclophosphamide with a steroid for 24 weeks. A total of 362 received medication (6 did not receive their assigned cyclophosphamide treatment for unknown reasons), and 310 completed the whole 24-week course of treatment. All participants in the study had biopsy-proven lupus nephritis diagnosed within the previous 6 months and had not been previously treated with MMF, cyclophosphamide, tacrolimus, or high-dose methylprednisolone, nor had they had renal replacement therapy, plasmapheresis, or IV gamma globulin therapy in the previous 12 weeks.
All patients began by receiving IV methylprednisolone pulse therapy (0.5 g/day) for 3 days and then oral prednisone (0.6 mg/kg) daily for 4 weeks, with prednisone tapering to 10 mg/day for the remainder of the study period. Following methylprednisolone pulse therapy, the multitarget group received MMF (0.5 g twice daily) and tacrolimus (2 mg twice daily) while the comparison group received IV cyclophosphamide (initially 0.75 g/m2 body surface area, then adjusted to 0.5-1.0 g/m2).
Nearly half – 45.9% – of patients in the multitarget group achieved full remission, whereas 25.6% of patients receiving IV cyclophosphamide showed complete remission (P < .001). The investigators defined complete remission as a 24-hour urinary protein excretion of 0.4 g or less, the absence of active urine sediments, a serum albumin level of 35 g/L or greater, and normal serum creatinine.
Results on secondary endpoints also favored multitarget therapy. The percentage of patients who had an overall response to treatment (complete and partial remissions) was 83.5% for multitarget therapy and 63% for cyclophosphamide (P < .001). Multitarget therapy patients responded to treatment at a median of 8.9 weeks, compared with cyclophosphamide-treated patients at 13 weeks. The investigators defined partial response as a 50% or greater reduction in proteinuria and urine protein less than 3.5 g/24 hours, a serum albumin level of 30 g/L or higher, and a normal or 25% or lower increase in serum creatinine level from baseline.
After treatment, patients in the multitarget therapy group also had significantly better results on other secondary endpoints, including changes in urine protein, serum albumin, systemic lupus erythematosus disease activity score, and C3 levels.
Adverse events occurred among 50.3% of multitarget recipients and 52.5% of cyclophosphamide recipients. More patients who received multitarget therapy had a serious adverse event (7.2% vs. 2.8%, respectively), and more patients withdrew from the multitarget therapy group (5.5% vs. 1.7%), but there were no statistically significant differences between the groups for either comparison.
The study was supported by the National Basic Research Program of China and the National Key Technology R&D Programs. Information on disclosures was unavailable at the time of publication.
A multitarget therapy of mycophenolate mofetil and tacrolimus for lupus nephritis induction therapy led to almost twice as many complete remissions as did intravenous cyclophosphamide in an open-label, randomized, controlled trial.
“Because immune dysregulation is fundamental to pathogenesis of lupus nephritis, with both B and T cells involved in the development of the disease, it may be necessary to target multiple aspects of the immune response using combined immunosuppressants,” wrote Dr. Zhi-Hong Liu of Nanjing (China) University and her colleagues (Ann. Intern. Med. 2014 Nov. 11 [doi:10.7326/M14-1030]).
Between April 2009 and June 2011, 368 adults aged 18-65 years from 26 renal centers in China were randomized to receive mycophenolate mofetil (MMF) and tacrolimus with a steroid or IV cyclophosphamide with a steroid for 24 weeks. A total of 362 received medication (6 did not receive their assigned cyclophosphamide treatment for unknown reasons), and 310 completed the whole 24-week course of treatment. All participants in the study had biopsy-proven lupus nephritis diagnosed within the previous 6 months and had not been previously treated with MMF, cyclophosphamide, tacrolimus, or high-dose methylprednisolone, nor had they had renal replacement therapy, plasmapheresis, or IV gamma globulin therapy in the previous 12 weeks.
All patients began by receiving IV methylprednisolone pulse therapy (0.5 g/day) for 3 days and then oral prednisone (0.6 mg/kg) daily for 4 weeks, with prednisone tapering to 10 mg/day for the remainder of the study period. Following methylprednisolone pulse therapy, the multitarget group received MMF (0.5 g twice daily) and tacrolimus (2 mg twice daily) while the comparison group received IV cyclophosphamide (initially 0.75 g/m2 body surface area, then adjusted to 0.5-1.0 g/m2).
Nearly half – 45.9% – of patients in the multitarget group achieved full remission, whereas 25.6% of patients receiving IV cyclophosphamide showed complete remission (P < .001). The investigators defined complete remission as a 24-hour urinary protein excretion of 0.4 g or less, the absence of active urine sediments, a serum albumin level of 35 g/L or greater, and normal serum creatinine.
Results on secondary endpoints also favored multitarget therapy. The percentage of patients who had an overall response to treatment (complete and partial remissions) was 83.5% for multitarget therapy and 63% for cyclophosphamide (P < .001). Multitarget therapy patients responded to treatment at a median of 8.9 weeks, compared with cyclophosphamide-treated patients at 13 weeks. The investigators defined partial response as a 50% or greater reduction in proteinuria and urine protein less than 3.5 g/24 hours, a serum albumin level of 30 g/L or higher, and a normal or 25% or lower increase in serum creatinine level from baseline.
After treatment, patients in the multitarget therapy group also had significantly better results on other secondary endpoints, including changes in urine protein, serum albumin, systemic lupus erythematosus disease activity score, and C3 levels.
Adverse events occurred among 50.3% of multitarget recipients and 52.5% of cyclophosphamide recipients. More patients who received multitarget therapy had a serious adverse event (7.2% vs. 2.8%, respectively), and more patients withdrew from the multitarget therapy group (5.5% vs. 1.7%), but there were no statistically significant differences between the groups for either comparison.
The study was supported by the National Basic Research Program of China and the National Key Technology R&D Programs. Information on disclosures was unavailable at the time of publication.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: Multitarget treatment is superior to intravenous cyclophosphamide as induction therapy for lupus nephritis.
Major finding: Among of patients receiving mycophenolate mofetil and tacrolimus, 45.9% achieved complete remission, compared with 25.6% receiving IV cyclophosphamide (P < .001).
Data source: A 24-week, open-label, randomized, controlled trial of 368 adults from 26 centers in China between April 2009 and June 2011.
Disclosures: The National Basic Research Program of China and the National Key Technology R&D Programs funded the study. Information on disclosures was unavailable at the time of publication.

Adenotonsillectomy offers moderate cardiac benefits in children
Children with obstructive sleep apnea appear to gain moderate cardiac benefits based on echocardiographic findings following an adenotonsillectomy, according to a recent meta-analysis.
“This review showed cardiovascular repercussions mostly on pulmonary circulation, right heart dimensions and diastolic function, with improvement after treatment,” Dr. Silke Anna Theresa Weber of Universidade Estadual Paulisita–UNESP in Botucatu, Brazil, and her colleagues reported (Int. J. Pediatr. Otorhinolaryngol. 2014;78:1571-8).
From a search of PUBMED, Embase, and LILACS in studies of cohorts ranging from 55 to 110 subjects, the researchers identified seven cohort studies meeting their criteria. Each study included children 12 years old or younger with obstructive sleep apnea (OSA) who received an adenotonsillectomy, and a comparison group of children without OSA.
Before the surgery, children with OSA had 8.67 greater mean pulmonary arterial pressure levels, compared with those without OSA, according to data in two studies. After surgery, the groups’ levels did not differ with statistical significance. Preoperatively, children with OSA had a mean 0.60-mm thicker increased interventricular septum and a mean 0.19-cm/m right ventricular dimension, compared with children with OSA in those two studies.
After the operation through 6 months’ follow-up, two studies “showed improvement of the mean arterial pulmonary blood pressure” in OSA children, and three other studies “showed improvement of cardiac structure and heart functions, mostly on the right heart, as right ventricle dimensions, tricuspid E/A ratio, and estimated pulmonary pressure,” the authors wrote.
Yet, the evidence for postoperative positive cardiovascular outcomes were limited, the authors wrote. None of the studies mentioned confounding factors for cardiovascular disease, such as obesity, and many did not use polysomnography for sleep apnea diagnoses.
The study was supported by FAPESP – Fundação de Amparo á Pesquisa do Estado de São Paulo. The authors reported no disclosures.
Children with obstructive sleep apnea appear to gain moderate cardiac benefits based on echocardiographic findings following an adenotonsillectomy, according to a recent meta-analysis.
“This review showed cardiovascular repercussions mostly on pulmonary circulation, right heart dimensions and diastolic function, with improvement after treatment,” Dr. Silke Anna Theresa Weber of Universidade Estadual Paulisita–UNESP in Botucatu, Brazil, and her colleagues reported (Int. J. Pediatr. Otorhinolaryngol. 2014;78:1571-8).
From a search of PUBMED, Embase, and LILACS in studies of cohorts ranging from 55 to 110 subjects, the researchers identified seven cohort studies meeting their criteria. Each study included children 12 years old or younger with obstructive sleep apnea (OSA) who received an adenotonsillectomy, and a comparison group of children without OSA.
Before the surgery, children with OSA had 8.67 greater mean pulmonary arterial pressure levels, compared with those without OSA, according to data in two studies. After surgery, the groups’ levels did not differ with statistical significance. Preoperatively, children with OSA had a mean 0.60-mm thicker increased interventricular septum and a mean 0.19-cm/m right ventricular dimension, compared with children with OSA in those two studies.
After the operation through 6 months’ follow-up, two studies “showed improvement of the mean arterial pulmonary blood pressure” in OSA children, and three other studies “showed improvement of cardiac structure and heart functions, mostly on the right heart, as right ventricle dimensions, tricuspid E/A ratio, and estimated pulmonary pressure,” the authors wrote.
Yet, the evidence for postoperative positive cardiovascular outcomes were limited, the authors wrote. None of the studies mentioned confounding factors for cardiovascular disease, such as obesity, and many did not use polysomnography for sleep apnea diagnoses.
The study was supported by FAPESP – Fundação de Amparo á Pesquisa do Estado de São Paulo. The authors reported no disclosures.
Children with obstructive sleep apnea appear to gain moderate cardiac benefits based on echocardiographic findings following an adenotonsillectomy, according to a recent meta-analysis.
“This review showed cardiovascular repercussions mostly on pulmonary circulation, right heart dimensions and diastolic function, with improvement after treatment,” Dr. Silke Anna Theresa Weber of Universidade Estadual Paulisita–UNESP in Botucatu, Brazil, and her colleagues reported (Int. J. Pediatr. Otorhinolaryngol. 2014;78:1571-8).
From a search of PUBMED, Embase, and LILACS in studies of cohorts ranging from 55 to 110 subjects, the researchers identified seven cohort studies meeting their criteria. Each study included children 12 years old or younger with obstructive sleep apnea (OSA) who received an adenotonsillectomy, and a comparison group of children without OSA.
Before the surgery, children with OSA had 8.67 greater mean pulmonary arterial pressure levels, compared with those without OSA, according to data in two studies. After surgery, the groups’ levels did not differ with statistical significance. Preoperatively, children with OSA had a mean 0.60-mm thicker increased interventricular septum and a mean 0.19-cm/m right ventricular dimension, compared with children with OSA in those two studies.
After the operation through 6 months’ follow-up, two studies “showed improvement of the mean arterial pulmonary blood pressure” in OSA children, and three other studies “showed improvement of cardiac structure and heart functions, mostly on the right heart, as right ventricle dimensions, tricuspid E/A ratio, and estimated pulmonary pressure,” the authors wrote.
Yet, the evidence for postoperative positive cardiovascular outcomes were limited, the authors wrote. None of the studies mentioned confounding factors for cardiovascular disease, such as obesity, and many did not use polysomnography for sleep apnea diagnoses.
The study was supported by FAPESP – Fundação de Amparo á Pesquisa do Estado de São Paulo. The authors reported no disclosures.
FROM THE INTERNATIONAL JOURNAL OF PEDIATRIC OTORHINOLARYNGOLOGY
Key clinical point: Adenotonsillectomy in children with obstructive sleep apnea has moderate cardiac benefit.
Major finding: No statistically significant difference in elevated mean pulmonary arterial pressure between OSA and non-OSA children after surgery.
Data source: Based on a meta-analysis of seven cohort studies, each involving 55 to 110 participants.
Disclosures: The study was supported by FAPESP – Fundação de Amparo á Pesquisa do Estado de São Paulo. The authors reported no disclosures.
Guidelines for children’s bronchiolitis treatment issued by AAP
The main treatment for bronchiolitis in young children should be support and observation, according to new clinical practice guidelines for diagnosing, managing, and preventing bronchiolitis.
The guidelines apply to children aged 1-23 months and emphasize clinical diagnosis and no medications except nebulized hypertonic saline for infants hospitalized with bronchiolitis, wrote Dr. Shawn L. Ralston, Dr. Allan S. Lieberthal, and their associates (Pediatrics 2014 October 27 [doi:10.1542/peds.2014-2742]). These guidelines update and replace the ones issued by the American Academy of Pediatrics in 2006 (Pediatrics 2006 118:1774-93). The findings are based on a review of the evidence in the Cochrane Library, Medline, and the Cumulative Index of Nursing and Allied Health Literature (CINAHL) from 2004 through May 2014.

The most notable change to these updated guidelines, according to Dr. Lieberthal, is the preventive recommendation for palivizumab, which is now not indicated for children born at 29 weeks’ gestation or older unless they have hemodynamically significant heart disease or chronic lung disease of prematurity (those born at less than 32 weeks’ gestation who needed at least 21% oxygen for their first month). Infants who qualify for prophylactic palivizumab should receive five monthly doses during respiratory syncytial virus season.
Dr. Lieberthal noted in an interview that several other recommendations state that certain treatments should not be used at all rather than simply not being routinely used. These include albuterol, epinephrine, corticosteroids, chest physiotherapy, and antibiotics.
“Bronchiolitis is a self-limited viral illness,” he said. Because it is diagnosed by signs and symptoms, no lab tests, oximetry, imaging, or other tests are needed, and treatment involves only support and observation. “None of the treatments that have been tested have been shown to affect the outcome of the illness,” said Dr. Lieberthal, who practices general pediatrics and clinical pediatric pulmonology at Kaiser-Permanente in Panorama City, Calif.
Dr. Ralston noted in an interview that a new recommendation exists for using hypertonic saline to children who are hospitalized for bronchiolitis (although not in the emergency department), but the evidence for it is weak and its therapeutic value limited.
“This medication appears to have a slow onset and to provide a favorable response only in settings where patients are hospitalized for longer than is typical in most U.S. hospitals, as most of the studies were performed outside the U.S.,” said Dr. Ralston, a pediatrician at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The guidelines also note that clinicians “may choose not to administer supplemental oxygen if the oxyhemoglobin saturation exceeds 90%” in children, although the evidence for this recommendation is also weak. Children should receive nasogastric or intravenous fluids if they cannot maintain oral hydration.
Parents should be advised that children who avoid secondhand tobacco smoke and are exclusively breastfed for at least 6 months have a reduced risk of bronchiolitis. Further, anyone caring for a child with bronchiolitis should disinfect their hands using an alcohol-based rub or soap and water after direct contact with the child and the child’s immediate environment.
Dr. Ralston said that important points stressed in both this recommendation and in the previous one include clinical diagnosis and avoiding exposure to tobacco smoke to reduce children’s risk of bronchiolitis.
“This guideline is mostly about what you shouldn’t do for the disease since because of the high volume of disease bronchiolitis represents a major area of unnecessary medical intervention in children,” she said. “We know that the vast majority of children will suffer only side effects from the medications or testing typically used in bronchiolitis care.”
Funding was provided by the American Academy of Pediatrics with travel support from the American Academy of Family Physicians, the American College of Chest Physicians, the American Thoracic Society, and the American College of Emergency Physicians for their representatives.
These guidelines, written with clarity, give incredibly direct and helpful direction on the diagnosis and treatment of bronchiolitis. It is great that they are coming out now, prior to RSV season. Bronchiolitis is a clinical diagnosis and these guidelines reaffirm that there is not usually any need for x-ray or laboratory confirmation of the diagnosis. The guidelines are primarily important for clarifying, based on the evidence, that many commonly used treatments, including albuterol, epinephrine, and steroids are not recommended for treatment of bronchiolitis as they are simply not helpful.
The guidance on administration of palivizumab is also important. It should not be administered in infants with a gestational age of > 29 weeks, and it should be reserved for infants in the first year of life who had a gestational age < 32 weeks and who had hemodynamically significant heart disease or chronic lung disease of prematurity.
Neil Skolnik, M.D., is the associate director of the family medicine program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
These guidelines, written with clarity, give incredibly direct and helpful direction on the diagnosis and treatment of bronchiolitis. It is great that they are coming out now, prior to RSV season. Bronchiolitis is a clinical diagnosis and these guidelines reaffirm that there is not usually any need for x-ray or laboratory confirmation of the diagnosis. The guidelines are primarily important for clarifying, based on the evidence, that many commonly used treatments, including albuterol, epinephrine, and steroids are not recommended for treatment of bronchiolitis as they are simply not helpful.
The guidance on administration of palivizumab is also important. It should not be administered in infants with a gestational age of > 29 weeks, and it should be reserved for infants in the first year of life who had a gestational age < 32 weeks and who had hemodynamically significant heart disease or chronic lung disease of prematurity.
Neil Skolnik, M.D., is the associate director of the family medicine program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
These guidelines, written with clarity, give incredibly direct and helpful direction on the diagnosis and treatment of bronchiolitis. It is great that they are coming out now, prior to RSV season. Bronchiolitis is a clinical diagnosis and these guidelines reaffirm that there is not usually any need for x-ray or laboratory confirmation of the diagnosis. The guidelines are primarily important for clarifying, based on the evidence, that many commonly used treatments, including albuterol, epinephrine, and steroids are not recommended for treatment of bronchiolitis as they are simply not helpful.
The guidance on administration of palivizumab is also important. It should not be administered in infants with a gestational age of > 29 weeks, and it should be reserved for infants in the first year of life who had a gestational age < 32 weeks and who had hemodynamically significant heart disease or chronic lung disease of prematurity.
Neil Skolnik, M.D., is the associate director of the family medicine program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
The main treatment for bronchiolitis in young children should be support and observation, according to new clinical practice guidelines for diagnosing, managing, and preventing bronchiolitis.
The guidelines apply to children aged 1-23 months and emphasize clinical diagnosis and no medications except nebulized hypertonic saline for infants hospitalized with bronchiolitis, wrote Dr. Shawn L. Ralston, Dr. Allan S. Lieberthal, and their associates (Pediatrics 2014 October 27 [doi:10.1542/peds.2014-2742]). These guidelines update and replace the ones issued by the American Academy of Pediatrics in 2006 (Pediatrics 2006 118:1774-93). The findings are based on a review of the evidence in the Cochrane Library, Medline, and the Cumulative Index of Nursing and Allied Health Literature (CINAHL) from 2004 through May 2014.
The most notable change to these updated guidelines, according to Dr. Lieberthal, is the preventive recommendation for palivizumab, which is now not indicated for children born at 29 weeks’ gestation or older unless they have hemodynamically significant heart disease or chronic lung disease of prematurity (those born at less than 32 weeks’ gestation who needed at least 21% oxygen for their first month). Infants who qualify for prophylactic palivizumab should receive five monthly doses during respiratory syncytial virus season.
Dr. Lieberthal noted in an interview that several other recommendations state that certain treatments should not be used at all rather than simply not being routinely used. These include albuterol, epinephrine, corticosteroids, chest physiotherapy, and antibiotics.
“Bronchiolitis is a self-limited viral illness,” he said. Because it is diagnosed by signs and symptoms, no lab tests, oximetry, imaging, or other tests are needed, and treatment involves only support and observation. “None of the treatments that have been tested have been shown to affect the outcome of the illness,” said Dr. Lieberthal, who practices general pediatrics and clinical pediatric pulmonology at Kaiser-Permanente in Panorama City, Calif.
Dr. Ralston noted in an interview that a new recommendation exists for using hypertonic saline to children who are hospitalized for bronchiolitis (although not in the emergency department), but the evidence for it is weak and its therapeutic value limited.
“This medication appears to have a slow onset and to provide a favorable response only in settings where patients are hospitalized for longer than is typical in most U.S. hospitals, as most of the studies were performed outside the U.S.,” said Dr. Ralston, a pediatrician at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The guidelines also note that clinicians “may choose not to administer supplemental oxygen if the oxyhemoglobin saturation exceeds 90%” in children, although the evidence for this recommendation is also weak. Children should receive nasogastric or intravenous fluids if they cannot maintain oral hydration.
Parents should be advised that children who avoid secondhand tobacco smoke and are exclusively breastfed for at least 6 months have a reduced risk of bronchiolitis. Further, anyone caring for a child with bronchiolitis should disinfect their hands using an alcohol-based rub or soap and water after direct contact with the child and the child’s immediate environment.
Dr. Ralston said that important points stressed in both this recommendation and in the previous one include clinical diagnosis and avoiding exposure to tobacco smoke to reduce children’s risk of bronchiolitis.
“This guideline is mostly about what you shouldn’t do for the disease since because of the high volume of disease bronchiolitis represents a major area of unnecessary medical intervention in children,” she said. “We know that the vast majority of children will suffer only side effects from the medications or testing typically used in bronchiolitis care.”
Funding was provided by the American Academy of Pediatrics with travel support from the American Academy of Family Physicians, the American College of Chest Physicians, the American Thoracic Society, and the American College of Emergency Physicians for their representatives.
The main treatment for bronchiolitis in young children should be support and observation, according to new clinical practice guidelines for diagnosing, managing, and preventing bronchiolitis.
The guidelines apply to children aged 1-23 months and emphasize clinical diagnosis and no medications except nebulized hypertonic saline for infants hospitalized with bronchiolitis, wrote Dr. Shawn L. Ralston, Dr. Allan S. Lieberthal, and their associates (Pediatrics 2014 October 27 [doi:10.1542/peds.2014-2742]). These guidelines update and replace the ones issued by the American Academy of Pediatrics in 2006 (Pediatrics 2006 118:1774-93). The findings are based on a review of the evidence in the Cochrane Library, Medline, and the Cumulative Index of Nursing and Allied Health Literature (CINAHL) from 2004 through May 2014.
The most notable change to these updated guidelines, according to Dr. Lieberthal, is the preventive recommendation for palivizumab, which is now not indicated for children born at 29 weeks’ gestation or older unless they have hemodynamically significant heart disease or chronic lung disease of prematurity (those born at less than 32 weeks’ gestation who needed at least 21% oxygen for their first month). Infants who qualify for prophylactic palivizumab should receive five monthly doses during respiratory syncytial virus season.
Dr. Lieberthal noted in an interview that several other recommendations state that certain treatments should not be used at all rather than simply not being routinely used. These include albuterol, epinephrine, corticosteroids, chest physiotherapy, and antibiotics.
“Bronchiolitis is a self-limited viral illness,” he said. Because it is diagnosed by signs and symptoms, no lab tests, oximetry, imaging, or other tests are needed, and treatment involves only support and observation. “None of the treatments that have been tested have been shown to affect the outcome of the illness,” said Dr. Lieberthal, who practices general pediatrics and clinical pediatric pulmonology at Kaiser-Permanente in Panorama City, Calif.
Dr. Ralston noted in an interview that a new recommendation exists for using hypertonic saline to children who are hospitalized for bronchiolitis (although not in the emergency department), but the evidence for it is weak and its therapeutic value limited.
“This medication appears to have a slow onset and to provide a favorable response only in settings where patients are hospitalized for longer than is typical in most U.S. hospitals, as most of the studies were performed outside the U.S.,” said Dr. Ralston, a pediatrician at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The guidelines also note that clinicians “may choose not to administer supplemental oxygen if the oxyhemoglobin saturation exceeds 90%” in children, although the evidence for this recommendation is also weak. Children should receive nasogastric or intravenous fluids if they cannot maintain oral hydration.
Parents should be advised that children who avoid secondhand tobacco smoke and are exclusively breastfed for at least 6 months have a reduced risk of bronchiolitis. Further, anyone caring for a child with bronchiolitis should disinfect their hands using an alcohol-based rub or soap and water after direct contact with the child and the child’s immediate environment.
Dr. Ralston said that important points stressed in both this recommendation and in the previous one include clinical diagnosis and avoiding exposure to tobacco smoke to reduce children’s risk of bronchiolitis.
“This guideline is mostly about what you shouldn’t do for the disease since because of the high volume of disease bronchiolitis represents a major area of unnecessary medical intervention in children,” she said. “We know that the vast majority of children will suffer only side effects from the medications or testing typically used in bronchiolitis care.”
Funding was provided by the American Academy of Pediatrics with travel support from the American Academy of Family Physicians, the American College of Chest Physicians, the American Thoracic Society, and the American College of Emergency Physicians for their representatives.
FROM PEDIATRICS
Key clinical point: Bronchiolitis should be diagnosed clinically and treated with support.
Major finding: Most treatments should not be administered because outcomes are not improved.
Data source: The findings are based on a review of the evidence in the Cochrane Library, Medline, and CINAHL from 2004 through May 2014.
Disclosures: Funding was provided by the American Academy of Pediatrics with travel support from the American Academy of Family Physicians, the American College of Chest Physicians, the American Thoracic Society, and the American College of Emergency Physicians for their representatives.
