User login
Surgery has edge over surveillance for micropapillary thyroid cancer
BALTIMORE – Hemithyroidectomy for low-risk micropapillary thyroid cancer can have advantages over active surveillance, according to findings from a study that examined outcomes by cost and quality of life data.
Endocrinologists and surgeons need to have in-depth conversations with their patients to determine their level of anxiety about cancer, surgery, and about their quality of life, to determine the best course of treatment, researchers at the University of California, San Francisco (UCSF) reported at the annual meeting of the American Association of Endocrine Surgeons.

“Our study found that hemithyroidectomy is cost effective in the majority of scenarios,” presenter Shriya Venkatesh said. “However, patient perception of micropapillary thyroid cancer as well as [the patient’s] life expectancy can play a major role in deciding which therapeutic option to choose.”
The study involved a cost-effectiveness analysis of the surgery vs. active surveillance, “which is especially relevant in our current times,” Ms. Venkatesh said in an interview. “What we wanted to do is give physicians information for when they approach their patients, not only in assessing the tumor from the medical aspect but also when looking at it from quality-of-life and cost-benefit perspectives.”
Both courses of management were modeled over a 20-year period with Medicare data and literature review to calculate costs and health utilities. The UCSF researchers used Markov statistical models for both approaches in which the reference case was a 40-year-old, otherwise healthy patient with a recent diagnosis of micropapillary thyroid cancer without high-risk factors. Either hemithyroidectomy or surveillance would be reasonable treatment options.
“We found that hemithyroidectomy was about $8,000 more costly than active surveillance, but it also afforded an increase in about 1.09 quality-adjusted life years,” Ms. Venkatesh said. Hemithyroidectomy is most cost effective for patients with a life expectancy of 3 years or more and who perceive that living with low-grade thyroid cancer would have even a modest detriment on their quality of life, she said.
“Unfortunately there is no current published quality-of-life assessment of active surveillance for thyroid cancer,” Ms. Venkatesh said. “We believe that estimating active surveillance to the equivalent of surgery underestimates the anxiety some patients may feel upon receiving their diagnosis.”
The paucity of literature on active surveillance for thyroid cancer prompted the UCSF researchers to turn to the prostate cancer literature, which has more data on active surveillance, to try to determine the disutility of active surveillance for micropapillary thyroid cancer. “Our extrapolation from the literature yields a mean disutility of 0.11,” she said.
However, the utility estimates the researchers came up with were variable, Ms. Venkatesh said. “This really pushes physicians to have that conversation with their patients, not only about the physical aspects of how they’re doing but also the mental aspects,” she said.

But quality of life is difficult to quantify, senior author Dr. Insoo Suh said in an interview. “What we found is that no matter how one measures quality of life, the qualitative degree of quality of life decrease that people associate with ‘living with cancer’ need not be that significant in order for surgery to be a potentially cost-effective treatment for them,” said Dr. Suh, an endocrine surgeon at UCSF and an ACS Fellow.
During the discussion, Dr. Peter Angelos of the University of Chicago and an ACS Fellow, said, “I’m curious how this information should impact the individual decision-making and informed consent for a specific patient, because I’m not sure that an individual patient would care if active surveillance is more cost effective or not.”
“When speaking to your patients, obviously discussing the rates of progression of the disease is important and then [so is] talking to them about different therapeutic options,” Ms. Venkatesh said. “The physician should also make an assessment about the patient’s quality of life to see if there are likely to be any changes due to the diagnosis.”
The limitations of the study include the extrapolation of data from the prostate cancer literature to define a utility scale and also the reference case used in the Markov model. Other utility measures showed variability as well.
Ms. Venkatesh, Dr. Suh and their coauthors had no financial relationships to disclose.
BALTIMORE – Hemithyroidectomy for low-risk micropapillary thyroid cancer can have advantages over active surveillance, according to findings from a study that examined outcomes by cost and quality of life data.
Endocrinologists and surgeons need to have in-depth conversations with their patients to determine their level of anxiety about cancer, surgery, and about their quality of life, to determine the best course of treatment, researchers at the University of California, San Francisco (UCSF) reported at the annual meeting of the American Association of Endocrine Surgeons.
“Our study found that hemithyroidectomy is cost effective in the majority of scenarios,” presenter Shriya Venkatesh said. “However, patient perception of micropapillary thyroid cancer as well as [the patient’s] life expectancy can play a major role in deciding which therapeutic option to choose.”
The study involved a cost-effectiveness analysis of the surgery vs. active surveillance, “which is especially relevant in our current times,” Ms. Venkatesh said in an interview. “What we wanted to do is give physicians information for when they approach their patients, not only in assessing the tumor from the medical aspect but also when looking at it from quality-of-life and cost-benefit perspectives.”
Both courses of management were modeled over a 20-year period with Medicare data and literature review to calculate costs and health utilities. The UCSF researchers used Markov statistical models for both approaches in which the reference case was a 40-year-old, otherwise healthy patient with a recent diagnosis of micropapillary thyroid cancer without high-risk factors. Either hemithyroidectomy or surveillance would be reasonable treatment options.
“We found that hemithyroidectomy was about $8,000 more costly than active surveillance, but it also afforded an increase in about 1.09 quality-adjusted life years,” Ms. Venkatesh said. Hemithyroidectomy is most cost effective for patients with a life expectancy of 3 years or more and who perceive that living with low-grade thyroid cancer would have even a modest detriment on their quality of life, she said.
“Unfortunately there is no current published quality-of-life assessment of active surveillance for thyroid cancer,” Ms. Venkatesh said. “We believe that estimating active surveillance to the equivalent of surgery underestimates the anxiety some patients may feel upon receiving their diagnosis.”
The paucity of literature on active surveillance for thyroid cancer prompted the UCSF researchers to turn to the prostate cancer literature, which has more data on active surveillance, to try to determine the disutility of active surveillance for micropapillary thyroid cancer. “Our extrapolation from the literature yields a mean disutility of 0.11,” she said.
However, the utility estimates the researchers came up with were variable, Ms. Venkatesh said. “This really pushes physicians to have that conversation with their patients, not only about the physical aspects of how they’re doing but also the mental aspects,” she said.
But quality of life is difficult to quantify, senior author Dr. Insoo Suh said in an interview. “What we found is that no matter how one measures quality of life, the qualitative degree of quality of life decrease that people associate with ‘living with cancer’ need not be that significant in order for surgery to be a potentially cost-effective treatment for them,” said Dr. Suh, an endocrine surgeon at UCSF and an ACS Fellow.
During the discussion, Dr. Peter Angelos of the University of Chicago and an ACS Fellow, said, “I’m curious how this information should impact the individual decision-making and informed consent for a specific patient, because I’m not sure that an individual patient would care if active surveillance is more cost effective or not.”
“When speaking to your patients, obviously discussing the rates of progression of the disease is important and then [so is] talking to them about different therapeutic options,” Ms. Venkatesh said. “The physician should also make an assessment about the patient’s quality of life to see if there are likely to be any changes due to the diagnosis.”
The limitations of the study include the extrapolation of data from the prostate cancer literature to define a utility scale and also the reference case used in the Markov model. Other utility measures showed variability as well.
Ms. Venkatesh, Dr. Suh and their coauthors had no financial relationships to disclose.
BALTIMORE – Hemithyroidectomy for low-risk micropapillary thyroid cancer can have advantages over active surveillance, according to findings from a study that examined outcomes by cost and quality of life data.
Endocrinologists and surgeons need to have in-depth conversations with their patients to determine their level of anxiety about cancer, surgery, and about their quality of life, to determine the best course of treatment, researchers at the University of California, San Francisco (UCSF) reported at the annual meeting of the American Association of Endocrine Surgeons.
“Our study found that hemithyroidectomy is cost effective in the majority of scenarios,” presenter Shriya Venkatesh said. “However, patient perception of micropapillary thyroid cancer as well as [the patient’s] life expectancy can play a major role in deciding which therapeutic option to choose.”
The study involved a cost-effectiveness analysis of the surgery vs. active surveillance, “which is especially relevant in our current times,” Ms. Venkatesh said in an interview. “What we wanted to do is give physicians information for when they approach their patients, not only in assessing the tumor from the medical aspect but also when looking at it from quality-of-life and cost-benefit perspectives.”
Both courses of management were modeled over a 20-year period with Medicare data and literature review to calculate costs and health utilities. The UCSF researchers used Markov statistical models for both approaches in which the reference case was a 40-year-old, otherwise healthy patient with a recent diagnosis of micropapillary thyroid cancer without high-risk factors. Either hemithyroidectomy or surveillance would be reasonable treatment options.
“We found that hemithyroidectomy was about $8,000 more costly than active surveillance, but it also afforded an increase in about 1.09 quality-adjusted life years,” Ms. Venkatesh said. Hemithyroidectomy is most cost effective for patients with a life expectancy of 3 years or more and who perceive that living with low-grade thyroid cancer would have even a modest detriment on their quality of life, she said.
“Unfortunately there is no current published quality-of-life assessment of active surveillance for thyroid cancer,” Ms. Venkatesh said. “We believe that estimating active surveillance to the equivalent of surgery underestimates the anxiety some patients may feel upon receiving their diagnosis.”
The paucity of literature on active surveillance for thyroid cancer prompted the UCSF researchers to turn to the prostate cancer literature, which has more data on active surveillance, to try to determine the disutility of active surveillance for micropapillary thyroid cancer. “Our extrapolation from the literature yields a mean disutility of 0.11,” she said.
However, the utility estimates the researchers came up with were variable, Ms. Venkatesh said. “This really pushes physicians to have that conversation with their patients, not only about the physical aspects of how they’re doing but also the mental aspects,” she said.
But quality of life is difficult to quantify, senior author Dr. Insoo Suh said in an interview. “What we found is that no matter how one measures quality of life, the qualitative degree of quality of life decrease that people associate with ‘living with cancer’ need not be that significant in order for surgery to be a potentially cost-effective treatment for them,” said Dr. Suh, an endocrine surgeon at UCSF and an ACS Fellow.
During the discussion, Dr. Peter Angelos of the University of Chicago and an ACS Fellow, said, “I’m curious how this information should impact the individual decision-making and informed consent for a specific patient, because I’m not sure that an individual patient would care if active surveillance is more cost effective or not.”
“When speaking to your patients, obviously discussing the rates of progression of the disease is important and then [so is] talking to them about different therapeutic options,” Ms. Venkatesh said. “The physician should also make an assessment about the patient’s quality of life to see if there are likely to be any changes due to the diagnosis.”
The limitations of the study include the extrapolation of data from the prostate cancer literature to define a utility scale and also the reference case used in the Markov model. Other utility measures showed variability as well.
Ms. Venkatesh, Dr. Suh and their coauthors had no financial relationships to disclose.
AT AAES 2016
Key clinical point: Patient psychological factors are key determinants in choosing a course of management for low-risk micropapillary thyroid cancer.
Major finding: Hemithyroidectomy typically costs about $8,000 more than active surveillance but also accounts for improved quality of life in these patients.
Data source: Markov models for both courses of management over a 20-year period with Medicare data and literature review to calculate costs and health utilities.
Disclosures: Ms. Venkatesh and her coauthors reported having no financial disclosures.

Post-parathyroidectomy follow-up may need to be open-ended
BALTIMORE – Patients who have had parathyroidectomy for primary hyperparathyroidism can have disease recurrence 10 years or longer after surgery, raising the possibility that postop follow-up should never end, according to a study presented at the annual meeting of the American Association of Endocrine Surgeons.
Dr. Irene Lou of the University of Wisconsin–Madison reported on results of a retrospective study of 196 patients who had a presumably “curative” parathyroidectomy at the institution between November 2000 and June 2005. The mean age of the study population was 61 years.

“The long-term recurrences of primary hyperparathyroidism after curative parathyroidectomy is likely higher than previously reported, with over a third of recurrences occurring 10 years after their operation,” Dr. Lou said.
The study also identified independent predictors of recurrence, among them younger age, a drop in intraoperative parathyroid hormone less than 70%, and double adenoma, Dr. Lou said. All patients after parathyroidectomy should have at minimum an annual serum calcium test, especially younger patients with longer life expectancies, she said. This recommendation, however, may be altered for older patients or those with additional comorbidities.
The study defined recurrence as serum calcium of 10.2 mg/dL or greater 6 months or longer after the initial operation. The overall 10-year recurrence rate was 14.8% and the median time to recurrence was 6.3 years. “We found that 41.4% of patients who recurred did so by 5 years and 65.5% by 10 years,” Dr. Lou said.
The University of Wisconsin and University of Alabama at Birmingham investigators undertook the study because the recent data on recurrence was limited, with the longest study topping out at 7 years, Dr. Lou said. “We previously looked at this problem in other perspectives and we found that a lot of curves separated at around 8 years,” she said.
With regard to the type of operation the patients had, whether unilateral minimally invasive parathyroidectomy or bilateral open surgery, the study found no significant differences in recurrence rates, Dr. Lou said. “This is an excellent study,” Dr. Samuel K. Snyder of Temple, Tex., said during the discussion. “You’re telling us we need to follow patients much longer than perhaps we did previously, but we all see patients who have normal calcium and still have a residual elevated parathyroid hormone level.” He asked if the study considered parathyroid hormone levels at 6 months or more after surgery or vitamin D levels, but Dr. Lou said this information was not available, therefore could not be evaluated.
Dr. Lou and her coauthors had no financial relationships to disclose.
BALTIMORE – Patients who have had parathyroidectomy for primary hyperparathyroidism can have disease recurrence 10 years or longer after surgery, raising the possibility that postop follow-up should never end, according to a study presented at the annual meeting of the American Association of Endocrine Surgeons.
Dr. Irene Lou of the University of Wisconsin–Madison reported on results of a retrospective study of 196 patients who had a presumably “curative” parathyroidectomy at the institution between November 2000 and June 2005. The mean age of the study population was 61 years.
“The long-term recurrences of primary hyperparathyroidism after curative parathyroidectomy is likely higher than previously reported, with over a third of recurrences occurring 10 years after their operation,” Dr. Lou said.
The study also identified independent predictors of recurrence, among them younger age, a drop in intraoperative parathyroid hormone less than 70%, and double adenoma, Dr. Lou said. All patients after parathyroidectomy should have at minimum an annual serum calcium test, especially younger patients with longer life expectancies, she said. This recommendation, however, may be altered for older patients or those with additional comorbidities.
The study defined recurrence as serum calcium of 10.2 mg/dL or greater 6 months or longer after the initial operation. The overall 10-year recurrence rate was 14.8% and the median time to recurrence was 6.3 years. “We found that 41.4% of patients who recurred did so by 5 years and 65.5% by 10 years,” Dr. Lou said.
The University of Wisconsin and University of Alabama at Birmingham investigators undertook the study because the recent data on recurrence was limited, with the longest study topping out at 7 years, Dr. Lou said. “We previously looked at this problem in other perspectives and we found that a lot of curves separated at around 8 years,” she said.
With regard to the type of operation the patients had, whether unilateral minimally invasive parathyroidectomy or bilateral open surgery, the study found no significant differences in recurrence rates, Dr. Lou said. “This is an excellent study,” Dr. Samuel K. Snyder of Temple, Tex., said during the discussion. “You’re telling us we need to follow patients much longer than perhaps we did previously, but we all see patients who have normal calcium and still have a residual elevated parathyroid hormone level.” He asked if the study considered parathyroid hormone levels at 6 months or more after surgery or vitamin D levels, but Dr. Lou said this information was not available, therefore could not be evaluated.
Dr. Lou and her coauthors had no financial relationships to disclose.
BALTIMORE – Patients who have had parathyroidectomy for primary hyperparathyroidism can have disease recurrence 10 years or longer after surgery, raising the possibility that postop follow-up should never end, according to a study presented at the annual meeting of the American Association of Endocrine Surgeons.
Dr. Irene Lou of the University of Wisconsin–Madison reported on results of a retrospective study of 196 patients who had a presumably “curative” parathyroidectomy at the institution between November 2000 and June 2005. The mean age of the study population was 61 years.
“The long-term recurrences of primary hyperparathyroidism after curative parathyroidectomy is likely higher than previously reported, with over a third of recurrences occurring 10 years after their operation,” Dr. Lou said.
The study also identified independent predictors of recurrence, among them younger age, a drop in intraoperative parathyroid hormone less than 70%, and double adenoma, Dr. Lou said. All patients after parathyroidectomy should have at minimum an annual serum calcium test, especially younger patients with longer life expectancies, she said. This recommendation, however, may be altered for older patients or those with additional comorbidities.
The study defined recurrence as serum calcium of 10.2 mg/dL or greater 6 months or longer after the initial operation. The overall 10-year recurrence rate was 14.8% and the median time to recurrence was 6.3 years. “We found that 41.4% of patients who recurred did so by 5 years and 65.5% by 10 years,” Dr. Lou said.
The University of Wisconsin and University of Alabama at Birmingham investigators undertook the study because the recent data on recurrence was limited, with the longest study topping out at 7 years, Dr. Lou said. “We previously looked at this problem in other perspectives and we found that a lot of curves separated at around 8 years,” she said.
With regard to the type of operation the patients had, whether unilateral minimally invasive parathyroidectomy or bilateral open surgery, the study found no significant differences in recurrence rates, Dr. Lou said. “This is an excellent study,” Dr. Samuel K. Snyder of Temple, Tex., said during the discussion. “You’re telling us we need to follow patients much longer than perhaps we did previously, but we all see patients who have normal calcium and still have a residual elevated parathyroid hormone level.” He asked if the study considered parathyroid hormone levels at 6 months or more after surgery or vitamin D levels, but Dr. Lou said this information was not available, therefore could not be evaluated.
Dr. Lou and her coauthors had no financial relationships to disclose.
FROM AAES 2016
Key clinical point: Long-term recurrence rates for hyperparathyroidism (HPT) after “curative” parathyroidectomy are likely higher than previously reported.
Major finding: Approximately one-third of patients were found to have recurrences 10 or more years after the initial operation.
Data source: Single-institution cohort of 196 patients who had initial parathyroidectomy for HPT between November 2000 and June 2005.
Disclosures: Dr. Lou and her study coauthors reported having no financial disclosures.

Negative sestamibi scan for primary hyperparathyroidism can mean no referral or surgery
BALTIMORE – In the treatment of primary hyperparathyroidism, clinical guidelines recommend using sestamibi scan for localizing adenoma, but increasingly endocrinologists are using sestamibi results to determine whether or not to refer a patient for parathyroidectomy surgery, while surgeons are using the scans as a factor in deciding whether to perform the operation.
That was the conclusion of a paper Dr. Susana Wu presented at the American Association of Endocrine Surgeons annual meeting. Dr. Wu reported on behalf of her colleagues at Kaiser Permanente Los Angeles Medical Center and at Scripps Clinic in San Diego.

“This study suggests that negative sestamibi scan (SS) results influence management of patients with primary hyperparathyroidism,” Dr. Wu said. “Endocrinologists were less likely to refer to surgeons and surgeons were less likely to offer parathyroidectomy to a patient with a negative sestamibi scan.”
The study involved a retrospective chart review of all 539 patients with primary hyperparathyroidism in the Kaiser Permanente Southern California database from December 2011 to December 2013, 452 of whom were seen by 63 endocrinologists at 14 centers. Among these patients, 260 had SS – 120 negative and 140 positive. The study identified statistically significant variations in how both endocrinologists and surgeons managed patients depending on SS results. The researchers used Kaiser Permanente’s electronic referral system to track referrals.
“The most significant negative predictor for endocrinologists referring to surgeons was a negative sestamibi scan, with an odds ratio of 0.36,” Dr. Wu said.
Endocrinologists referred 86% of patients with positive SS to surgeons, but only 68% of those with negative SS. Surgeons exhibited a similar practice pattern. “Surgeons were less likely to recommend parathyroidectomy for patients with a negative sestamibi scan, with an odds ratio of 0.20,” Dr. Wu said. Surgeons operated on 87% of patients with a negative SS scan but 96% with a positive SS.

In an interview, study coauthor Dr. Philip Haigh explained that parathyroidectomy when the SS is negative is a more difficult operation for the surgeon, and that might make some physicians hesitate before going forward with surgery. “It has been previously shown by other studies that it is a more difficult operation when the sestamibi scan is negative because you have to look at four glands instead of removing just one, but if the surgeon is experienced, it should achieve a high success rate,” Dr. Haigh said. He said that parathyroidectomy in sestamibi-negative hyperparathyroidism had a cure rate as high as 98% in the study presented.
He offered two thoughts on how clinicians should use the study results. “To the endocrinologist, if you’re going to order a sestamibi scan, don’t change your referral practice depending on the result,” Dr. Haigh said. “To the surgeon, if you’re not comfortable operating on a patient with a negative sestamibi scan, then find someone who is.”
The study had a few limitations, Dr. Wu said. Along with its retrospective nature, the study also did not account for potential disparity in radiological vs. surgeon interpretation of the scans.
During the discussion, Dr. Samuel Snyder, of Baylor Scott & White Health, Temple, Tex., said he concurred with the results Dr. Wu reported. “It really worries me about what is happening to patients who have negative scans,” he said. “What I’ve seen in patients referred for surgery is a lot of variation in how the sestamibi scan is done.” He asked if the study accounted for the different types of sestamibi scans and how they were performed, but Dr. Wu said it did not.
Dr. Christopher McHenry of MetroHealth Medical Center, Cleveland, also concurred. “I think this is a phenomenon that occurs more often than we think or we’re aware of,” he said. “I continue to be amazed with how clinicians equate a negative sestamibi scan with not having primary hyperparathyroidism. I think it needs to reemphasized that the sestamibi scan is not diagnostic; it’s for localization.”
He asked Dr. Wu, “How do we change behavior to deal with this problem?”
Dr. Wu said her institution is developing a safety-net program that would aim to increase the identification and chart coding of patients with primary hyperparathyroidism, automate essential labs to be ordered in patients with high calcium, and automate referral to endocrinologists. The study and its findings will be disseminated to endocrinologists in the region.
The study authors had no disclosures.
BALTIMORE – In the treatment of primary hyperparathyroidism, clinical guidelines recommend using sestamibi scan for localizing adenoma, but increasingly endocrinologists are using sestamibi results to determine whether or not to refer a patient for parathyroidectomy surgery, while surgeons are using the scans as a factor in deciding whether to perform the operation.
That was the conclusion of a paper Dr. Susana Wu presented at the American Association of Endocrine Surgeons annual meeting. Dr. Wu reported on behalf of her colleagues at Kaiser Permanente Los Angeles Medical Center and at Scripps Clinic in San Diego.
“This study suggests that negative sestamibi scan (SS) results influence management of patients with primary hyperparathyroidism,” Dr. Wu said. “Endocrinologists were less likely to refer to surgeons and surgeons were less likely to offer parathyroidectomy to a patient with a negative sestamibi scan.”
The study involved a retrospective chart review of all 539 patients with primary hyperparathyroidism in the Kaiser Permanente Southern California database from December 2011 to December 2013, 452 of whom were seen by 63 endocrinologists at 14 centers. Among these patients, 260 had SS – 120 negative and 140 positive. The study identified statistically significant variations in how both endocrinologists and surgeons managed patients depending on SS results. The researchers used Kaiser Permanente’s electronic referral system to track referrals.
“The most significant negative predictor for endocrinologists referring to surgeons was a negative sestamibi scan, with an odds ratio of 0.36,” Dr. Wu said.
Endocrinologists referred 86% of patients with positive SS to surgeons, but only 68% of those with negative SS. Surgeons exhibited a similar practice pattern. “Surgeons were less likely to recommend parathyroidectomy for patients with a negative sestamibi scan, with an odds ratio of 0.20,” Dr. Wu said. Surgeons operated on 87% of patients with a negative SS scan but 96% with a positive SS.
In an interview, study coauthor Dr. Philip Haigh explained that parathyroidectomy when the SS is negative is a more difficult operation for the surgeon, and that might make some physicians hesitate before going forward with surgery. “It has been previously shown by other studies that it is a more difficult operation when the sestamibi scan is negative because you have to look at four glands instead of removing just one, but if the surgeon is experienced, it should achieve a high success rate,” Dr. Haigh said. He said that parathyroidectomy in sestamibi-negative hyperparathyroidism had a cure rate as high as 98% in the study presented.
He offered two thoughts on how clinicians should use the study results. “To the endocrinologist, if you’re going to order a sestamibi scan, don’t change your referral practice depending on the result,” Dr. Haigh said. “To the surgeon, if you’re not comfortable operating on a patient with a negative sestamibi scan, then find someone who is.”
The study had a few limitations, Dr. Wu said. Along with its retrospective nature, the study also did not account for potential disparity in radiological vs. surgeon interpretation of the scans.
During the discussion, Dr. Samuel Snyder, of Baylor Scott & White Health, Temple, Tex., said he concurred with the results Dr. Wu reported. “It really worries me about what is happening to patients who have negative scans,” he said. “What I’ve seen in patients referred for surgery is a lot of variation in how the sestamibi scan is done.” He asked if the study accounted for the different types of sestamibi scans and how they were performed, but Dr. Wu said it did not.
Dr. Christopher McHenry of MetroHealth Medical Center, Cleveland, also concurred. “I think this is a phenomenon that occurs more often than we think or we’re aware of,” he said. “I continue to be amazed with how clinicians equate a negative sestamibi scan with not having primary hyperparathyroidism. I think it needs to reemphasized that the sestamibi scan is not diagnostic; it’s for localization.”
He asked Dr. Wu, “How do we change behavior to deal with this problem?”
Dr. Wu said her institution is developing a safety-net program that would aim to increase the identification and chart coding of patients with primary hyperparathyroidism, automate essential labs to be ordered in patients with high calcium, and automate referral to endocrinologists. The study and its findings will be disseminated to endocrinologists in the region.
The study authors had no disclosures.
BALTIMORE – In the treatment of primary hyperparathyroidism, clinical guidelines recommend using sestamibi scan for localizing adenoma, but increasingly endocrinologists are using sestamibi results to determine whether or not to refer a patient for parathyroidectomy surgery, while surgeons are using the scans as a factor in deciding whether to perform the operation.
That was the conclusion of a paper Dr. Susana Wu presented at the American Association of Endocrine Surgeons annual meeting. Dr. Wu reported on behalf of her colleagues at Kaiser Permanente Los Angeles Medical Center and at Scripps Clinic in San Diego.
“This study suggests that negative sestamibi scan (SS) results influence management of patients with primary hyperparathyroidism,” Dr. Wu said. “Endocrinologists were less likely to refer to surgeons and surgeons were less likely to offer parathyroidectomy to a patient with a negative sestamibi scan.”
The study involved a retrospective chart review of all 539 patients with primary hyperparathyroidism in the Kaiser Permanente Southern California database from December 2011 to December 2013, 452 of whom were seen by 63 endocrinologists at 14 centers. Among these patients, 260 had SS – 120 negative and 140 positive. The study identified statistically significant variations in how both endocrinologists and surgeons managed patients depending on SS results. The researchers used Kaiser Permanente’s electronic referral system to track referrals.
“The most significant negative predictor for endocrinologists referring to surgeons was a negative sestamibi scan, with an odds ratio of 0.36,” Dr. Wu said.
Endocrinologists referred 86% of patients with positive SS to surgeons, but only 68% of those with negative SS. Surgeons exhibited a similar practice pattern. “Surgeons were less likely to recommend parathyroidectomy for patients with a negative sestamibi scan, with an odds ratio of 0.20,” Dr. Wu said. Surgeons operated on 87% of patients with a negative SS scan but 96% with a positive SS.
In an interview, study coauthor Dr. Philip Haigh explained that parathyroidectomy when the SS is negative is a more difficult operation for the surgeon, and that might make some physicians hesitate before going forward with surgery. “It has been previously shown by other studies that it is a more difficult operation when the sestamibi scan is negative because you have to look at four glands instead of removing just one, but if the surgeon is experienced, it should achieve a high success rate,” Dr. Haigh said. He said that parathyroidectomy in sestamibi-negative hyperparathyroidism had a cure rate as high as 98% in the study presented.
He offered two thoughts on how clinicians should use the study results. “To the endocrinologist, if you’re going to order a sestamibi scan, don’t change your referral practice depending on the result,” Dr. Haigh said. “To the surgeon, if you’re not comfortable operating on a patient with a negative sestamibi scan, then find someone who is.”
The study had a few limitations, Dr. Wu said. Along with its retrospective nature, the study also did not account for potential disparity in radiological vs. surgeon interpretation of the scans.
During the discussion, Dr. Samuel Snyder, of Baylor Scott & White Health, Temple, Tex., said he concurred with the results Dr. Wu reported. “It really worries me about what is happening to patients who have negative scans,” he said. “What I’ve seen in patients referred for surgery is a lot of variation in how the sestamibi scan is done.” He asked if the study accounted for the different types of sestamibi scans and how they were performed, but Dr. Wu said it did not.
Dr. Christopher McHenry of MetroHealth Medical Center, Cleveland, also concurred. “I think this is a phenomenon that occurs more often than we think or we’re aware of,” he said. “I continue to be amazed with how clinicians equate a negative sestamibi scan with not having primary hyperparathyroidism. I think it needs to reemphasized that the sestamibi scan is not diagnostic; it’s for localization.”
He asked Dr. Wu, “How do we change behavior to deal with this problem?”
Dr. Wu said her institution is developing a safety-net program that would aim to increase the identification and chart coding of patients with primary hyperparathyroidism, automate essential labs to be ordered in patients with high calcium, and automate referral to endocrinologists. The study and its findings will be disseminated to endocrinologists in the region.
The study authors had no disclosures.
AT AAES 2016
Key clinical point: Endocrinologists and surgeons are less likely to order surgery when patients with primary hyperparathyroidism have negative sestamibi scan (SS) results.
Major finding: Endocrinologists referred 86% of patients with positive SS to surgeons, but only 68% of those with negative SS.
Data source: A retrospective chart review of all 539 patients with primary hyperparathyroidism in the Kaiser Permanente Southern California database over a 2-year period.
Disclosures: Dr. Wu and her coauthors reported having no financial disclosures.

Choice of cardiac ‘operative mortality’ definition affects outcomes reporting
Reporting of outcomes has grown in importance as clinical registries collect data and establish benchmarks for quality care, but exactly what those data report can vary depending on the definition of a specific outcome, even for an outcome as seemingly straightforward as death after an intervention.
Dr. Steven Maximus of the University of California Irvine Medical Center, and colleagues reported on this phenomenon in the April issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:1101-10). Specifically, they showed how rates of postoperative mortality after five different cardiac interventions can vary within the same data set depending on the definition of postoperative mortality.
“A significant percentage of procedural deaths occur after transfer or discharge from the index hospital,” Dr. Maximus and colleagues said. “These findings illustrate the importance of the definition of ‘operative’ mortality and the need to ensure accuracy in the reporting of data to volunteer clinical registries.”
They calculated outcomes based on five different definitions of postoperative mortality for five different cardiac interventions, depending on when and where the patient died, each of which showed slightly different results. The five different definitions of postoperative mortality are: during the index hospitalization only; during the index hospitalization or in a hospital the patient was transferred to on the same day or within 24 hours of discharge; during the index hospitalization or within 30 days after the procedure; during the index hospitalization or transfer hospitalization or during readmission within 30 days; and during the index hospitalization, transfer, and within 30 days after the procedure regardless of readmission.
As an example, mortality rates for percutaneous coronary intervention (PCI) with acute coronary syndrome (ACS) ranged from 3.25% for the first definition listed to 4.51% for the fifth definition. For isolated coronary artery bypass grafting, the rates ranged from 1.71% for the first definition to 2.15% for the fifth.
The fifth definition “is the most encompassing and is the current definition used by the STS [Society of Thoracic Surgeons] and should be applied to other clinical registries, such as the American College of Cardiology National Cardiovascular Data Registry,” Dr. Maximus and colleagues said.
The study noted that the Society of Thoracic Surgeons National Database (STS-NDB) has revised its definition of operative mortality to more accurately measure outcomes. Originally, the STS-NDB definition included all deaths during the index hospitalization, even those after 30 days, and postdischarge deaths within 30 days unless the cause of death was not related to the operation. In 2011, the definition was updated to include patients transferred to other acute care facilities. STS-NDB updated the definition again in 2014 to include all deaths, regardless of cause, during the index hospitalization, even if after 30 days, and including patients transferred to other acute care facilities, and all deaths, again regardless of cause, after discharge and within 30 days of the operation.
The analyses by Dr. Maximus and colleagues used data from the California Office of Statewide Health Planning and Development hospitalized patient discharge database for the year 2009. The first analysis the researchers performed did not exclude any patients and found a significant number of cardiac procedural deaths occurred after transfer at discharge from the index hospitalization, 17% in the surgical group vs. 31% in the PCI group. In the second analysis, which excluded untrackable patients, hospital deaths included 12% for PCI and 4% for surgery.
“PCI mortality was more dependent on the method used to define mortality, compared with the surgical patients, and a larger percentage of deaths occurred after hospital discharge and within 30 days of the procedure,” Dr. Maximus and colleagues said.
Another key factor in calculating mortality rates was the ability of hospitals to follow patients. “We found that up to 20% of hospitals were not able to track their patients long-term,” Dr. Maximus and coauthors said.
Study coauthor Dr. Junaid Kahn disclosed consulting fees from Edwards Lifesciences. The other authors have no financial relationships to disclose.
“The public, our patients, and their families might be surprised to discover that doctors have difficulty tallying how many people die after cardiac interventions, and that the question merited a piece of published statistical analysis,” Dr. Tom Treasure of University College London and Dr. Samer Nashef of Papworth Hospital, Cambridge, said in their invited commentary (J Thorac Cardiovasc Surg. 2016;151:1110-1).
Dr. Maximus and colleagues showed that the wider they cast their net to account for postoperative death, the more deaths they found, Dr. Treasure and Dr. Nashef said. That may penalize institutions that are more fastidious in collecting outcomes data. “When we require institutions with scarce resources to chase long-term outcome data for the purposes of treatment quality comparison, we immediately penalize those institutions that comply; more extensive data retrieval will find more deaths,” the commentators said.
The “perfect system” would capture death following a procedure no matter where it occurs, they added. “For the sake of compliance and simplicity, and until data systems are adequately robust and comprehensive, quality monitoring of cardiac surgery may have to be based pragmatically on data that are universally available and difficult to falsify, such as death at the base hospital during the same hospital admission as the intervention.”
Dr. Treasure and Dr. Nashef also accounted for another “quirk” in measuring outcomes. “Humans make errors in data entry, transcription and transfer and computers have ‘glitches’ and ‘gremlins,’ ” they said. “An apparent improvement in clinical outcome in fact may be merely the result of better record keeping.”
The commentators reported that they had no relationships to disclose.
“The public, our patients, and their families might be surprised to discover that doctors have difficulty tallying how many people die after cardiac interventions, and that the question merited a piece of published statistical analysis,” Dr. Tom Treasure of University College London and Dr. Samer Nashef of Papworth Hospital, Cambridge, said in their invited commentary (J Thorac Cardiovasc Surg. 2016;151:1110-1).
Dr. Maximus and colleagues showed that the wider they cast their net to account for postoperative death, the more deaths they found, Dr. Treasure and Dr. Nashef said. That may penalize institutions that are more fastidious in collecting outcomes data. “When we require institutions with scarce resources to chase long-term outcome data for the purposes of treatment quality comparison, we immediately penalize those institutions that comply; more extensive data retrieval will find more deaths,” the commentators said.
The “perfect system” would capture death following a procedure no matter where it occurs, they added. “For the sake of compliance and simplicity, and until data systems are adequately robust and comprehensive, quality monitoring of cardiac surgery may have to be based pragmatically on data that are universally available and difficult to falsify, such as death at the base hospital during the same hospital admission as the intervention.”
Dr. Treasure and Dr. Nashef also accounted for another “quirk” in measuring outcomes. “Humans make errors in data entry, transcription and transfer and computers have ‘glitches’ and ‘gremlins,’ ” they said. “An apparent improvement in clinical outcome in fact may be merely the result of better record keeping.”
The commentators reported that they had no relationships to disclose.
“The public, our patients, and their families might be surprised to discover that doctors have difficulty tallying how many people die after cardiac interventions, and that the question merited a piece of published statistical analysis,” Dr. Tom Treasure of University College London and Dr. Samer Nashef of Papworth Hospital, Cambridge, said in their invited commentary (J Thorac Cardiovasc Surg. 2016;151:1110-1).
Dr. Maximus and colleagues showed that the wider they cast their net to account for postoperative death, the more deaths they found, Dr. Treasure and Dr. Nashef said. That may penalize institutions that are more fastidious in collecting outcomes data. “When we require institutions with scarce resources to chase long-term outcome data for the purposes of treatment quality comparison, we immediately penalize those institutions that comply; more extensive data retrieval will find more deaths,” the commentators said.
The “perfect system” would capture death following a procedure no matter where it occurs, they added. “For the sake of compliance and simplicity, and until data systems are adequately robust and comprehensive, quality monitoring of cardiac surgery may have to be based pragmatically on data that are universally available and difficult to falsify, such as death at the base hospital during the same hospital admission as the intervention.”
Dr. Treasure and Dr. Nashef also accounted for another “quirk” in measuring outcomes. “Humans make errors in data entry, transcription and transfer and computers have ‘glitches’ and ‘gremlins,’ ” they said. “An apparent improvement in clinical outcome in fact may be merely the result of better record keeping.”
The commentators reported that they had no relationships to disclose.
Reporting of outcomes has grown in importance as clinical registries collect data and establish benchmarks for quality care, but exactly what those data report can vary depending on the definition of a specific outcome, even for an outcome as seemingly straightforward as death after an intervention.
Dr. Steven Maximus of the University of California Irvine Medical Center, and colleagues reported on this phenomenon in the April issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:1101-10). Specifically, they showed how rates of postoperative mortality after five different cardiac interventions can vary within the same data set depending on the definition of postoperative mortality.
“A significant percentage of procedural deaths occur after transfer or discharge from the index hospital,” Dr. Maximus and colleagues said. “These findings illustrate the importance of the definition of ‘operative’ mortality and the need to ensure accuracy in the reporting of data to volunteer clinical registries.”
They calculated outcomes based on five different definitions of postoperative mortality for five different cardiac interventions, depending on when and where the patient died, each of which showed slightly different results. The five different definitions of postoperative mortality are: during the index hospitalization only; during the index hospitalization or in a hospital the patient was transferred to on the same day or within 24 hours of discharge; during the index hospitalization or within 30 days after the procedure; during the index hospitalization or transfer hospitalization or during readmission within 30 days; and during the index hospitalization, transfer, and within 30 days after the procedure regardless of readmission.
As an example, mortality rates for percutaneous coronary intervention (PCI) with acute coronary syndrome (ACS) ranged from 3.25% for the first definition listed to 4.51% for the fifth definition. For isolated coronary artery bypass grafting, the rates ranged from 1.71% for the first definition to 2.15% for the fifth.
The fifth definition “is the most encompassing and is the current definition used by the STS [Society of Thoracic Surgeons] and should be applied to other clinical registries, such as the American College of Cardiology National Cardiovascular Data Registry,” Dr. Maximus and colleagues said.
The study noted that the Society of Thoracic Surgeons National Database (STS-NDB) has revised its definition of operative mortality to more accurately measure outcomes. Originally, the STS-NDB definition included all deaths during the index hospitalization, even those after 30 days, and postdischarge deaths within 30 days unless the cause of death was not related to the operation. In 2011, the definition was updated to include patients transferred to other acute care facilities. STS-NDB updated the definition again in 2014 to include all deaths, regardless of cause, during the index hospitalization, even if after 30 days, and including patients transferred to other acute care facilities, and all deaths, again regardless of cause, after discharge and within 30 days of the operation.
The analyses by Dr. Maximus and colleagues used data from the California Office of Statewide Health Planning and Development hospitalized patient discharge database for the year 2009. The first analysis the researchers performed did not exclude any patients and found a significant number of cardiac procedural deaths occurred after transfer at discharge from the index hospitalization, 17% in the surgical group vs. 31% in the PCI group. In the second analysis, which excluded untrackable patients, hospital deaths included 12% for PCI and 4% for surgery.
“PCI mortality was more dependent on the method used to define mortality, compared with the surgical patients, and a larger percentage of deaths occurred after hospital discharge and within 30 days of the procedure,” Dr. Maximus and colleagues said.
Another key factor in calculating mortality rates was the ability of hospitals to follow patients. “We found that up to 20% of hospitals were not able to track their patients long-term,” Dr. Maximus and coauthors said.
Study coauthor Dr. Junaid Kahn disclosed consulting fees from Edwards Lifesciences. The other authors have no financial relationships to disclose.
Reporting of outcomes has grown in importance as clinical registries collect data and establish benchmarks for quality care, but exactly what those data report can vary depending on the definition of a specific outcome, even for an outcome as seemingly straightforward as death after an intervention.
Dr. Steven Maximus of the University of California Irvine Medical Center, and colleagues reported on this phenomenon in the April issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:1101-10). Specifically, they showed how rates of postoperative mortality after five different cardiac interventions can vary within the same data set depending on the definition of postoperative mortality.
“A significant percentage of procedural deaths occur after transfer or discharge from the index hospital,” Dr. Maximus and colleagues said. “These findings illustrate the importance of the definition of ‘operative’ mortality and the need to ensure accuracy in the reporting of data to volunteer clinical registries.”
They calculated outcomes based on five different definitions of postoperative mortality for five different cardiac interventions, depending on when and where the patient died, each of which showed slightly different results. The five different definitions of postoperative mortality are: during the index hospitalization only; during the index hospitalization or in a hospital the patient was transferred to on the same day or within 24 hours of discharge; during the index hospitalization or within 30 days after the procedure; during the index hospitalization or transfer hospitalization or during readmission within 30 days; and during the index hospitalization, transfer, and within 30 days after the procedure regardless of readmission.
As an example, mortality rates for percutaneous coronary intervention (PCI) with acute coronary syndrome (ACS) ranged from 3.25% for the first definition listed to 4.51% for the fifth definition. For isolated coronary artery bypass grafting, the rates ranged from 1.71% for the first definition to 2.15% for the fifth.
The fifth definition “is the most encompassing and is the current definition used by the STS [Society of Thoracic Surgeons] and should be applied to other clinical registries, such as the American College of Cardiology National Cardiovascular Data Registry,” Dr. Maximus and colleagues said.
The study noted that the Society of Thoracic Surgeons National Database (STS-NDB) has revised its definition of operative mortality to more accurately measure outcomes. Originally, the STS-NDB definition included all deaths during the index hospitalization, even those after 30 days, and postdischarge deaths within 30 days unless the cause of death was not related to the operation. In 2011, the definition was updated to include patients transferred to other acute care facilities. STS-NDB updated the definition again in 2014 to include all deaths, regardless of cause, during the index hospitalization, even if after 30 days, and including patients transferred to other acute care facilities, and all deaths, again regardless of cause, after discharge and within 30 days of the operation.
The analyses by Dr. Maximus and colleagues used data from the California Office of Statewide Health Planning and Development hospitalized patient discharge database for the year 2009. The first analysis the researchers performed did not exclude any patients and found a significant number of cardiac procedural deaths occurred after transfer at discharge from the index hospitalization, 17% in the surgical group vs. 31% in the PCI group. In the second analysis, which excluded untrackable patients, hospital deaths included 12% for PCI and 4% for surgery.
“PCI mortality was more dependent on the method used to define mortality, compared with the surgical patients, and a larger percentage of deaths occurred after hospital discharge and within 30 days of the procedure,” Dr. Maximus and colleagues said.
Another key factor in calculating mortality rates was the ability of hospitals to follow patients. “We found that up to 20% of hospitals were not able to track their patients long-term,” Dr. Maximus and coauthors said.
Study coauthor Dr. Junaid Kahn disclosed consulting fees from Edwards Lifesciences. The other authors have no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Mortality rates for various coronary procedures can vary depending on the definition chosen.
Major finding: The mortality rate for percutaneous coronary intervention with acute coronary syndrome ranged from 3.25% to 4.51% depending on which of five definitions was used.
Data source: California Office of Statewide Health Planning and Development Hospitalized Patient Discharge Data Base for 2009.
Disclosures: Study coauthor Dr. Junaid Kahn reports receiving consulting fees for Edwards Lifesciences. The other authors have no financial relationships to disclose.
Ripple effect of complications in lung transplant
As the frequency of lung transplants rises, so too has the strain on resources to manage in-hospital complications after those operations. Researchers from the University of Pittsburgh have identified independent predictors of short-term complications that can compromise long-term survival in these patients in what they said is the first study to systematically evaluate and profile such complications.
“These results may identify important targets for best practice guidelines and quality-of-care measures after lung transplantation,” reported Dr. Ernest G. Chan and colleagues (J Thorac Cardiovasc Surg 2016 April;151:1171-80).
The study involved 748 patients in the University of Pittsburgh Medical Center Transplant Patient Management System database who had in-hospital complications after single- or double-lung transplant from January 2007 to October 2013. The researchers analyzed 3,381 such complications in 92.78% of these patients, grading the complications via the extended Accordion Severity Grading System (ASGS). The median follow-up of the cohort was 5.4 years.
The researchers also classified complications that carried significant decrease in 5-year survival into three categories: renal complications, with a hazard ratio (HR) of 2.58; hepatic, with an HR of 4.08; and cardiac, with an HR of 1.95.
“Multivariate analysis identified a weighted ASGS sum of greater than 10 and renal, cardiac, and vascular complications as predictors of decreased long-term survival,” Dr. Chan and colleagues noted.
In-hospital complications are important predictors of long-term survival, Dr. Chan and coauthors wrote, citing studies from Memorial Sloan-Kettering Cancer Center in New York and the University of Minnesota. (N Engl J Med. 2001;345:181-8;Ann Surg. 2011;254:368-74). They also noted variable findings of several studies with regard to the impact center volume can have on long-term survival, particularly because high-volume centers may be better prepared to manage those complications.
“These important finding highlight the need for further in-depth analysis into an intriguing aspect of surgical management of complications after high-risk procedures,” the researchers wrote. Their goal was to create a postoperative complication profile for lung transplant patients.
Of the 748 patients in the study, 7.22% (54) had an uneventful postoperative course. The noncomplication group had a cumulative 5-year survival of around 73.8% vs. 53.3% for the complications group. On average, each patient in the complication group had almost five different complications. The most common were pulmonary in nature (71.66%), followed by infections (69.52%), pleural space–related problems (46.12%), renal complications (36.23%), and cardiac (35.83%). Renal complications accounted for the greatest decrease in 5-year survival at 35.4% vs. 64.4% in patients who did not have renal complications.
Survival rates for other categories of complications vs. the absence of those complications were: hepatic, 18.1% vs. 57.3%; cardiac, 39.5% vs. 62.3%; vascular, 29.4% vs. 58.5%; neurologic, 32.6% vs. 57.1%; musculoskeletal, 27.4% vs. 56.8%; and pleural-space complications, 48.7% vs. 60.3%.
The multivariate analysis assigned hazard ratios to these predictors: age older than 65 years, 1.01; renal events, 1.70; cardiac events, 1.29; vascular events, 1.33; and weighted ASGS sum, 1.08. Besides ASGS severity, the researchers considered Charlson Comorbidity Index analysis, but found that it had no significant effect on hazard ratio, the researchers said.
“With appropriate patients selection and contemporary surgical techniques, vigilant postoperative management and avoidance of adverse events may potentially offer patients better long-term outcomes,” Dr. Chan and colleagues noted. “The overall 90-day postoperative course has an influence on long-term survival.”
Among those factors that influence survival are the severity of the intervention to treat the complication and the occurrence of less-severe complications, they added. “The next step is to identify interventions that effectively reduce the incidence, as well as severity, of in-hospital, postoperative complications.”
The researchers had no financial relationships to disclose.
The study findings show not only that complications after lung transplantation “are nearly ubiquitous” but also that clinicians need better management strategies to address them, Katie Kinaschuk and Dr. Jayan Nagendran said in their invited commentary (J Thorac Cardiovasc Surg. 2016;151:1181-2).
The multivariate analysis by Dr. Chan and colleagues shows a strong correlation between nonpulmonary complications and decreased long-term survival in patients who have had lung transplants, but this does not downplay the significance of pulmonary and infectious complications, Ms. Kinaschuk and Dr. Nagendran noted. “Thus, despite the need to improve treatment algorithms of highly predictive non–allograft-related complications, the greatest opportunity to decrease the overall rates of complications still exists within pulmonary and infectious etiologies.”
Noteworthy among the study findings was that the Charlson Comorbidity Index values were not a predictor for long-term survival, they wrote. That may suggest that factors of the operation itself, along with donor tissue, may have important roles in the link between postoperative complications and decreased long-term survival. “This may represent the need for careful reporting and consideration of non–allograft-related postoperative complications in assessing new technologies for donor lung management,” they said.
The “ripple effect” of early postoperative complications “may warrant more vigilant long-term surveillance once a complication has occurred,” the commentators noted. “Ultimately, determination of preventive measures by identifying predictors of complications will have the greatest positive effect on survival,” an area that needs further investigation, they wrote.
Ms. Kinaschuk and Dr. Nagendran had no relationships to disclose.
The study findings show not only that complications after lung transplantation “are nearly ubiquitous” but also that clinicians need better management strategies to address them, Katie Kinaschuk and Dr. Jayan Nagendran said in their invited commentary (J Thorac Cardiovasc Surg. 2016;151:1181-2).
The multivariate analysis by Dr. Chan and colleagues shows a strong correlation between nonpulmonary complications and decreased long-term survival in patients who have had lung transplants, but this does not downplay the significance of pulmonary and infectious complications, Ms. Kinaschuk and Dr. Nagendran noted. “Thus, despite the need to improve treatment algorithms of highly predictive non–allograft-related complications, the greatest opportunity to decrease the overall rates of complications still exists within pulmonary and infectious etiologies.”
Noteworthy among the study findings was that the Charlson Comorbidity Index values were not a predictor for long-term survival, they wrote. That may suggest that factors of the operation itself, along with donor tissue, may have important roles in the link between postoperative complications and decreased long-term survival. “This may represent the need for careful reporting and consideration of non–allograft-related postoperative complications in assessing new technologies for donor lung management,” they said.
The “ripple effect” of early postoperative complications “may warrant more vigilant long-term surveillance once a complication has occurred,” the commentators noted. “Ultimately, determination of preventive measures by identifying predictors of complications will have the greatest positive effect on survival,” an area that needs further investigation, they wrote.
Ms. Kinaschuk and Dr. Nagendran had no relationships to disclose.
The study findings show not only that complications after lung transplantation “are nearly ubiquitous” but also that clinicians need better management strategies to address them, Katie Kinaschuk and Dr. Jayan Nagendran said in their invited commentary (J Thorac Cardiovasc Surg. 2016;151:1181-2).
The multivariate analysis by Dr. Chan and colleagues shows a strong correlation between nonpulmonary complications and decreased long-term survival in patients who have had lung transplants, but this does not downplay the significance of pulmonary and infectious complications, Ms. Kinaschuk and Dr. Nagendran noted. “Thus, despite the need to improve treatment algorithms of highly predictive non–allograft-related complications, the greatest opportunity to decrease the overall rates of complications still exists within pulmonary and infectious etiologies.”
Noteworthy among the study findings was that the Charlson Comorbidity Index values were not a predictor for long-term survival, they wrote. That may suggest that factors of the operation itself, along with donor tissue, may have important roles in the link between postoperative complications and decreased long-term survival. “This may represent the need for careful reporting and consideration of non–allograft-related postoperative complications in assessing new technologies for donor lung management,” they said.
The “ripple effect” of early postoperative complications “may warrant more vigilant long-term surveillance once a complication has occurred,” the commentators noted. “Ultimately, determination of preventive measures by identifying predictors of complications will have the greatest positive effect on survival,” an area that needs further investigation, they wrote.
Ms. Kinaschuk and Dr. Nagendran had no relationships to disclose.
As the frequency of lung transplants rises, so too has the strain on resources to manage in-hospital complications after those operations. Researchers from the University of Pittsburgh have identified independent predictors of short-term complications that can compromise long-term survival in these patients in what they said is the first study to systematically evaluate and profile such complications.
“These results may identify important targets for best practice guidelines and quality-of-care measures after lung transplantation,” reported Dr. Ernest G. Chan and colleagues (J Thorac Cardiovasc Surg 2016 April;151:1171-80).
The study involved 748 patients in the University of Pittsburgh Medical Center Transplant Patient Management System database who had in-hospital complications after single- or double-lung transplant from January 2007 to October 2013. The researchers analyzed 3,381 such complications in 92.78% of these patients, grading the complications via the extended Accordion Severity Grading System (ASGS). The median follow-up of the cohort was 5.4 years.
The researchers also classified complications that carried significant decrease in 5-year survival into three categories: renal complications, with a hazard ratio (HR) of 2.58; hepatic, with an HR of 4.08; and cardiac, with an HR of 1.95.
“Multivariate analysis identified a weighted ASGS sum of greater than 10 and renal, cardiac, and vascular complications as predictors of decreased long-term survival,” Dr. Chan and colleagues noted.
In-hospital complications are important predictors of long-term survival, Dr. Chan and coauthors wrote, citing studies from Memorial Sloan-Kettering Cancer Center in New York and the University of Minnesota. (N Engl J Med. 2001;345:181-8;Ann Surg. 2011;254:368-74). They also noted variable findings of several studies with regard to the impact center volume can have on long-term survival, particularly because high-volume centers may be better prepared to manage those complications.
“These important finding highlight the need for further in-depth analysis into an intriguing aspect of surgical management of complications after high-risk procedures,” the researchers wrote. Their goal was to create a postoperative complication profile for lung transplant patients.
Of the 748 patients in the study, 7.22% (54) had an uneventful postoperative course. The noncomplication group had a cumulative 5-year survival of around 73.8% vs. 53.3% for the complications group. On average, each patient in the complication group had almost five different complications. The most common were pulmonary in nature (71.66%), followed by infections (69.52%), pleural space–related problems (46.12%), renal complications (36.23%), and cardiac (35.83%). Renal complications accounted for the greatest decrease in 5-year survival at 35.4% vs. 64.4% in patients who did not have renal complications.
Survival rates for other categories of complications vs. the absence of those complications were: hepatic, 18.1% vs. 57.3%; cardiac, 39.5% vs. 62.3%; vascular, 29.4% vs. 58.5%; neurologic, 32.6% vs. 57.1%; musculoskeletal, 27.4% vs. 56.8%; and pleural-space complications, 48.7% vs. 60.3%.
The multivariate analysis assigned hazard ratios to these predictors: age older than 65 years, 1.01; renal events, 1.70; cardiac events, 1.29; vascular events, 1.33; and weighted ASGS sum, 1.08. Besides ASGS severity, the researchers considered Charlson Comorbidity Index analysis, but found that it had no significant effect on hazard ratio, the researchers said.
“With appropriate patients selection and contemporary surgical techniques, vigilant postoperative management and avoidance of adverse events may potentially offer patients better long-term outcomes,” Dr. Chan and colleagues noted. “The overall 90-day postoperative course has an influence on long-term survival.”
Among those factors that influence survival are the severity of the intervention to treat the complication and the occurrence of less-severe complications, they added. “The next step is to identify interventions that effectively reduce the incidence, as well as severity, of in-hospital, postoperative complications.”
The researchers had no financial relationships to disclose.
As the frequency of lung transplants rises, so too has the strain on resources to manage in-hospital complications after those operations. Researchers from the University of Pittsburgh have identified independent predictors of short-term complications that can compromise long-term survival in these patients in what they said is the first study to systematically evaluate and profile such complications.
“These results may identify important targets for best practice guidelines and quality-of-care measures after lung transplantation,” reported Dr. Ernest G. Chan and colleagues (J Thorac Cardiovasc Surg 2016 April;151:1171-80).
The study involved 748 patients in the University of Pittsburgh Medical Center Transplant Patient Management System database who had in-hospital complications after single- or double-lung transplant from January 2007 to October 2013. The researchers analyzed 3,381 such complications in 92.78% of these patients, grading the complications via the extended Accordion Severity Grading System (ASGS). The median follow-up of the cohort was 5.4 years.
The researchers also classified complications that carried significant decrease in 5-year survival into three categories: renal complications, with a hazard ratio (HR) of 2.58; hepatic, with an HR of 4.08; and cardiac, with an HR of 1.95.
“Multivariate analysis identified a weighted ASGS sum of greater than 10 and renal, cardiac, and vascular complications as predictors of decreased long-term survival,” Dr. Chan and colleagues noted.
In-hospital complications are important predictors of long-term survival, Dr. Chan and coauthors wrote, citing studies from Memorial Sloan-Kettering Cancer Center in New York and the University of Minnesota. (N Engl J Med. 2001;345:181-8;Ann Surg. 2011;254:368-74). They also noted variable findings of several studies with regard to the impact center volume can have on long-term survival, particularly because high-volume centers may be better prepared to manage those complications.
“These important finding highlight the need for further in-depth analysis into an intriguing aspect of surgical management of complications after high-risk procedures,” the researchers wrote. Their goal was to create a postoperative complication profile for lung transplant patients.
Of the 748 patients in the study, 7.22% (54) had an uneventful postoperative course. The noncomplication group had a cumulative 5-year survival of around 73.8% vs. 53.3% for the complications group. On average, each patient in the complication group had almost five different complications. The most common were pulmonary in nature (71.66%), followed by infections (69.52%), pleural space–related problems (46.12%), renal complications (36.23%), and cardiac (35.83%). Renal complications accounted for the greatest decrease in 5-year survival at 35.4% vs. 64.4% in patients who did not have renal complications.
Survival rates for other categories of complications vs. the absence of those complications were: hepatic, 18.1% vs. 57.3%; cardiac, 39.5% vs. 62.3%; vascular, 29.4% vs. 58.5%; neurologic, 32.6% vs. 57.1%; musculoskeletal, 27.4% vs. 56.8%; and pleural-space complications, 48.7% vs. 60.3%.
The multivariate analysis assigned hazard ratios to these predictors: age older than 65 years, 1.01; renal events, 1.70; cardiac events, 1.29; vascular events, 1.33; and weighted ASGS sum, 1.08. Besides ASGS severity, the researchers considered Charlson Comorbidity Index analysis, but found that it had no significant effect on hazard ratio, the researchers said.
“With appropriate patients selection and contemporary surgical techniques, vigilant postoperative management and avoidance of adverse events may potentially offer patients better long-term outcomes,” Dr. Chan and colleagues noted. “The overall 90-day postoperative course has an influence on long-term survival.”
Among those factors that influence survival are the severity of the intervention to treat the complication and the occurrence of less-severe complications, they added. “The next step is to identify interventions that effectively reduce the incidence, as well as severity, of in-hospital, postoperative complications.”
The researchers had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Early complications after lung transplant surgery can negatively impact survival and long-term outcomes.
Major finding: Postoperative complications occurred in 92.78% of patients. Median follow-up was 5.4 years.
Data source: Retrospective analysis of 748 patients in the University of Pittsburgh Medical Center Transplant Patient Management System who had lung transplants from January 2007 to October 2013.
Disclosures: The study investigators had no relationships to disclose.
Hybrid option ‘reasonable’ for HLHS?
Although the classic Norwood palliation for infants with hypoplastic left heart syndrome (HLHS) has been well established, the procedure has had its drawbacks, namely the need for cardiopulmonary bypass with hypothermia and a because it rules out biventricular correction months later. A hybrid procedure avoids the need for bypass and accommodates short-term biventricular correction, but it has lacked strong evidence.
Researchers from Justus-Liebig University Giessen, Germany, reported on 182 patients with HLHS who had the three-stage Giessen hybrid procedure, noting 10-year survival of almost 80% with almost a third of patients requiring no artery intervention in that time (J Thorac Cardiovasc Surg. 2016 April;151:1112-23).
“In view of the early results and long-term outcome after Giessen hybrid palliation, the hybrid approach has become a reasonable alternative to the conventional strategy to treat neonates with HLHS and variants,” wrote Dr. Can Yerebakan and colleagues. “Further refinements are warranted to decrease patient morbidity.”
The Giessen hybrid procedure uses a technique to control pulmonary blood flow that is different from the Norwood procedure. The hybrid approach involves stenting of the arterial duct or prostaglandin therapy to maintain systemic perfusion combined with off-pump bilateral banding of the pulmonary arteries (bPAB) in the neonatal period. The Giessen hybrid operation defers the Norwood-type palliation using cardiopulmonary bypass that involves an aortic arch reconstruction, including a superior cavopulmonary connection or a biventricular correction, if indicated, until the infant is 4-8 months of age.
“In recent years, hybrid treatment has moved from a myth to an alternative modality in a growing number of institutions globally,” Dr. Yerebakan and colleagues said. The hybrid procedure has been used in high-risk patients. One report claimed higher morbidity in the hybrid procedure due to bPAB (Ann Thorac Surg. 2013;96:1382-8). Another study raised concerns about an adequate pulmonary artery rehabilitation at the time of the Fontan operation, the third stage in the hybrid strategy (J Thorac Cardiovasc Surg. 2014;147:706-12).
But with the hybrid approach, patients retain the potential to receive a biventricular correction up to 8 months later without compromising survival, “postponing an immediate definitive decision in the newborn period in comparison with the classic Norwood palliation,” Dr. Yerebakan and coauthors noted.
The doctors at the Pediatric Heart Center Giessen treat all types and variants of HLHS with the modified Giessen hybrid strategy. Between 1998 and 2015, 182 patients with HLHS had the Giessen hybrid stage I operation, including 126 patients who received univentricular palliation or a heart transplant. The median age of stage I recipients was 6 days, and median weight 3.2 kg. The stage II operation was performed at 4.5 months, with a range of 2.9 to 39.5 months, and Fontan completion was established at 33.7 months, with a range of 21 to 108 months.
Median follow-up after the stage I procedure was 4.6 years, and the death rate was 2.5%. After stage II, mortality was 4.9%; no deaths were reported after Fontan completion. Body weight less than 2.5 kg and aortic atresia had no significant effect on survival. Mortality rates were 8.9% between stages I and II and 5.3% between stage II and Fontan completion. “Cumulative interstage mortality was 14.2%,” Dr. Yerebakan and colleagues noted. “At 10 years, the probability of survival is 77.8%.”
Also at 10 years, 32.2% of patients were free from further pulmonary artery intervention, and 16.7% needed aortic arch reconstruction. Two patients required reoperations for aortic arch reconstruction.
Dr. Yerebakan and colleagues suggested several steps to improve outcomes with the hybrid approach: “intense collaboration” with anesthesiology and pediatric cardiology during and after the procedure to risk stratify individual patients; implementation of standards for management of all stages, including out-of-hospital care, in all departments that participate in a case; and liberalized indications for use of MRI before the stage II and Fontan completion.
Among the limitations of the study the authors noted were its retrospective nature and a median follow-up of only 5 years when the center has some cases with up to 15 years of follow-up. But Dr. Yerebakan and coauthors said they could not determine if the patients benefit from the hybrid treatment in the long-term.
The researchers had no disclosures.
The study by Dr. Yerebakan and colleagues is one of the largest single-center series of patients with HLHS who routinely undergo a hybrid palliation to date, and while the study is open to criticisms, “the authors should be applauded,” Dr. Ralph S. Mosca of New York University said in his invited commentary (J Thorac Cardiovasc Surg. 2016;151:1123-25).
Among the criticisms Dr. Mosca mentioned are that the hybrid approach requires a more extensive stage II reconstruction, “often further complicated by the presence of significant branch PA stenosis and a difficult aortic arch reconstruction”; that there is “appreciable” interstage mortality at 12.2%; and that there is an absence of data on renal or respiratory insufficiency, infection rates, and neurologic outcomes.
Dr. Mosca cited the cause for applause, however: “Through their persistence and collective experience, [the authors] have achieved commendable results in this difficult patient population.”
Yet, Dr. Mosca also noted a number of “potential problems” with the hybrid approach: bilateral banding of the pulmonary artery is a “crude procedure”; arterial duct stenting can lead to retrograde aortic arch reduction; and the interstage mortality “remains significant.”
Results of the hybrid and Norwood procedures are “strikingly similar,” Dr. Mosca said. While the hybrid approach may lower neonatal mortality, it may also carry longer-term consequences “predicated upon the need to closely observe and intervene,” he said. Clinicians need more information on hybrid outcomes, but in time it will likely take its place as an option for HLHS alongside the Norwood procedure, Dr. Mosca said.
The study by Dr. Yerebakan and colleagues is one of the largest single-center series of patients with HLHS who routinely undergo a hybrid palliation to date, and while the study is open to criticisms, “the authors should be applauded,” Dr. Ralph S. Mosca of New York University said in his invited commentary (J Thorac Cardiovasc Surg. 2016;151:1123-25).
Among the criticisms Dr. Mosca mentioned are that the hybrid approach requires a more extensive stage II reconstruction, “often further complicated by the presence of significant branch PA stenosis and a difficult aortic arch reconstruction”; that there is “appreciable” interstage mortality at 12.2%; and that there is an absence of data on renal or respiratory insufficiency, infection rates, and neurologic outcomes.
Dr. Mosca cited the cause for applause, however: “Through their persistence and collective experience, [the authors] have achieved commendable results in this difficult patient population.”
Yet, Dr. Mosca also noted a number of “potential problems” with the hybrid approach: bilateral banding of the pulmonary artery is a “crude procedure”; arterial duct stenting can lead to retrograde aortic arch reduction; and the interstage mortality “remains significant.”
Results of the hybrid and Norwood procedures are “strikingly similar,” Dr. Mosca said. While the hybrid approach may lower neonatal mortality, it may also carry longer-term consequences “predicated upon the need to closely observe and intervene,” he said. Clinicians need more information on hybrid outcomes, but in time it will likely take its place as an option for HLHS alongside the Norwood procedure, Dr. Mosca said.
The study by Dr. Yerebakan and colleagues is one of the largest single-center series of patients with HLHS who routinely undergo a hybrid palliation to date, and while the study is open to criticisms, “the authors should be applauded,” Dr. Ralph S. Mosca of New York University said in his invited commentary (J Thorac Cardiovasc Surg. 2016;151:1123-25).
Among the criticisms Dr. Mosca mentioned are that the hybrid approach requires a more extensive stage II reconstruction, “often further complicated by the presence of significant branch PA stenosis and a difficult aortic arch reconstruction”; that there is “appreciable” interstage mortality at 12.2%; and that there is an absence of data on renal or respiratory insufficiency, infection rates, and neurologic outcomes.
Dr. Mosca cited the cause for applause, however: “Through their persistence and collective experience, [the authors] have achieved commendable results in this difficult patient population.”
Yet, Dr. Mosca also noted a number of “potential problems” with the hybrid approach: bilateral banding of the pulmonary artery is a “crude procedure”; arterial duct stenting can lead to retrograde aortic arch reduction; and the interstage mortality “remains significant.”
Results of the hybrid and Norwood procedures are “strikingly similar,” Dr. Mosca said. While the hybrid approach may lower neonatal mortality, it may also carry longer-term consequences “predicated upon the need to closely observe and intervene,” he said. Clinicians need more information on hybrid outcomes, but in time it will likely take its place as an option for HLHS alongside the Norwood procedure, Dr. Mosca said.
Although the classic Norwood palliation for infants with hypoplastic left heart syndrome (HLHS) has been well established, the procedure has had its drawbacks, namely the need for cardiopulmonary bypass with hypothermia and a because it rules out biventricular correction months later. A hybrid procedure avoids the need for bypass and accommodates short-term biventricular correction, but it has lacked strong evidence.
Researchers from Justus-Liebig University Giessen, Germany, reported on 182 patients with HLHS who had the three-stage Giessen hybrid procedure, noting 10-year survival of almost 80% with almost a third of patients requiring no artery intervention in that time (J Thorac Cardiovasc Surg. 2016 April;151:1112-23).
“In view of the early results and long-term outcome after Giessen hybrid palliation, the hybrid approach has become a reasonable alternative to the conventional strategy to treat neonates with HLHS and variants,” wrote Dr. Can Yerebakan and colleagues. “Further refinements are warranted to decrease patient morbidity.”
The Giessen hybrid procedure uses a technique to control pulmonary blood flow that is different from the Norwood procedure. The hybrid approach involves stenting of the arterial duct or prostaglandin therapy to maintain systemic perfusion combined with off-pump bilateral banding of the pulmonary arteries (bPAB) in the neonatal period. The Giessen hybrid operation defers the Norwood-type palliation using cardiopulmonary bypass that involves an aortic arch reconstruction, including a superior cavopulmonary connection or a biventricular correction, if indicated, until the infant is 4-8 months of age.
“In recent years, hybrid treatment has moved from a myth to an alternative modality in a growing number of institutions globally,” Dr. Yerebakan and colleagues said. The hybrid procedure has been used in high-risk patients. One report claimed higher morbidity in the hybrid procedure due to bPAB (Ann Thorac Surg. 2013;96:1382-8). Another study raised concerns about an adequate pulmonary artery rehabilitation at the time of the Fontan operation, the third stage in the hybrid strategy (J Thorac Cardiovasc Surg. 2014;147:706-12).
But with the hybrid approach, patients retain the potential to receive a biventricular correction up to 8 months later without compromising survival, “postponing an immediate definitive decision in the newborn period in comparison with the classic Norwood palliation,” Dr. Yerebakan and coauthors noted.
The doctors at the Pediatric Heart Center Giessen treat all types and variants of HLHS with the modified Giessen hybrid strategy. Between 1998 and 2015, 182 patients with HLHS had the Giessen hybrid stage I operation, including 126 patients who received univentricular palliation or a heart transplant. The median age of stage I recipients was 6 days, and median weight 3.2 kg. The stage II operation was performed at 4.5 months, with a range of 2.9 to 39.5 months, and Fontan completion was established at 33.7 months, with a range of 21 to 108 months.
Median follow-up after the stage I procedure was 4.6 years, and the death rate was 2.5%. After stage II, mortality was 4.9%; no deaths were reported after Fontan completion. Body weight less than 2.5 kg and aortic atresia had no significant effect on survival. Mortality rates were 8.9% between stages I and II and 5.3% between stage II and Fontan completion. “Cumulative interstage mortality was 14.2%,” Dr. Yerebakan and colleagues noted. “At 10 years, the probability of survival is 77.8%.”
Also at 10 years, 32.2% of patients were free from further pulmonary artery intervention, and 16.7% needed aortic arch reconstruction. Two patients required reoperations for aortic arch reconstruction.
Dr. Yerebakan and colleagues suggested several steps to improve outcomes with the hybrid approach: “intense collaboration” with anesthesiology and pediatric cardiology during and after the procedure to risk stratify individual patients; implementation of standards for management of all stages, including out-of-hospital care, in all departments that participate in a case; and liberalized indications for use of MRI before the stage II and Fontan completion.
Among the limitations of the study the authors noted were its retrospective nature and a median follow-up of only 5 years when the center has some cases with up to 15 years of follow-up. But Dr. Yerebakan and coauthors said they could not determine if the patients benefit from the hybrid treatment in the long-term.
The researchers had no disclosures.
Although the classic Norwood palliation for infants with hypoplastic left heart syndrome (HLHS) has been well established, the procedure has had its drawbacks, namely the need for cardiopulmonary bypass with hypothermia and a because it rules out biventricular correction months later. A hybrid procedure avoids the need for bypass and accommodates short-term biventricular correction, but it has lacked strong evidence.
Researchers from Justus-Liebig University Giessen, Germany, reported on 182 patients with HLHS who had the three-stage Giessen hybrid procedure, noting 10-year survival of almost 80% with almost a third of patients requiring no artery intervention in that time (J Thorac Cardiovasc Surg. 2016 April;151:1112-23).
“In view of the early results and long-term outcome after Giessen hybrid palliation, the hybrid approach has become a reasonable alternative to the conventional strategy to treat neonates with HLHS and variants,” wrote Dr. Can Yerebakan and colleagues. “Further refinements are warranted to decrease patient morbidity.”
The Giessen hybrid procedure uses a technique to control pulmonary blood flow that is different from the Norwood procedure. The hybrid approach involves stenting of the arterial duct or prostaglandin therapy to maintain systemic perfusion combined with off-pump bilateral banding of the pulmonary arteries (bPAB) in the neonatal period. The Giessen hybrid operation defers the Norwood-type palliation using cardiopulmonary bypass that involves an aortic arch reconstruction, including a superior cavopulmonary connection or a biventricular correction, if indicated, until the infant is 4-8 months of age.
“In recent years, hybrid treatment has moved from a myth to an alternative modality in a growing number of institutions globally,” Dr. Yerebakan and colleagues said. The hybrid procedure has been used in high-risk patients. One report claimed higher morbidity in the hybrid procedure due to bPAB (Ann Thorac Surg. 2013;96:1382-8). Another study raised concerns about an adequate pulmonary artery rehabilitation at the time of the Fontan operation, the third stage in the hybrid strategy (J Thorac Cardiovasc Surg. 2014;147:706-12).
But with the hybrid approach, patients retain the potential to receive a biventricular correction up to 8 months later without compromising survival, “postponing an immediate definitive decision in the newborn period in comparison with the classic Norwood palliation,” Dr. Yerebakan and coauthors noted.
The doctors at the Pediatric Heart Center Giessen treat all types and variants of HLHS with the modified Giessen hybrid strategy. Between 1998 and 2015, 182 patients with HLHS had the Giessen hybrid stage I operation, including 126 patients who received univentricular palliation or a heart transplant. The median age of stage I recipients was 6 days, and median weight 3.2 kg. The stage II operation was performed at 4.5 months, with a range of 2.9 to 39.5 months, and Fontan completion was established at 33.7 months, with a range of 21 to 108 months.
Median follow-up after the stage I procedure was 4.6 years, and the death rate was 2.5%. After stage II, mortality was 4.9%; no deaths were reported after Fontan completion. Body weight less than 2.5 kg and aortic atresia had no significant effect on survival. Mortality rates were 8.9% between stages I and II and 5.3% between stage II and Fontan completion. “Cumulative interstage mortality was 14.2%,” Dr. Yerebakan and colleagues noted. “At 10 years, the probability of survival is 77.8%.”
Also at 10 years, 32.2% of patients were free from further pulmonary artery intervention, and 16.7% needed aortic arch reconstruction. Two patients required reoperations for aortic arch reconstruction.
Dr. Yerebakan and colleagues suggested several steps to improve outcomes with the hybrid approach: “intense collaboration” with anesthesiology and pediatric cardiology during and after the procedure to risk stratify individual patients; implementation of standards for management of all stages, including out-of-hospital care, in all departments that participate in a case; and liberalized indications for use of MRI before the stage II and Fontan completion.
Among the limitations of the study the authors noted were its retrospective nature and a median follow-up of only 5 years when the center has some cases with up to 15 years of follow-up. But Dr. Yerebakan and coauthors said they could not determine if the patients benefit from the hybrid treatment in the long-term.
The researchers had no disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: A hybrid operation for hypoplastic left heart syndrome (HLHS) and variants in neonates is emerging as an alternative to the Norwood palliation.
Major finding: At 10 years, the probability of survival with the hybrid procedure was 77.8%. Low body weight (less than 2.5 kg) and aortic atresia had no significant impact on survival.
Data source: Retrospective study of 182 patients who had the hybrid procedure at a single center between June 1998 and February 2015.
Disclosures: The study investigators had no relationships to disclose.
Carpal tunnel syndrome: Guidelines rate evidence for diagnosis, treatment
The American Academy of Orthopaedic Surgeons has adopted clinical practice guidelines that assign evidence-based ratings for common strategies used to diagnose and treat carpal tunnel syndrome (CTS).
The 982-page comprehensive guidelines have been endorsed by the American Society for the Surgery of the Hand and the American College of Radiology. The guidelines address the burden of CTS, the second most common cause of sick days from work, according to AAOS, and its etiology, risk factors, emotional and physical impact, potential benefits, harms, contraindications, and future research. The document is available on the OrthoGuidelines Web-based app at orthoguidelines.org.

The assessments of evidence are based upon a systematic review of the current scientific and clinical information and accepted approaches to treatment and/or diagnosis of carpal tunnel syndrome. In addition to a concise summary, the report includes an exhaustive list of studies used to establish levels of evidence and a summary of the evidence in each. Also included is a list of studies not included, many because of poor study design or very small samples.
The guidelines make recommendations on practices to diagnose and manage CTS based on four levels of evidence:
• Strong: Supported by two or more “high-quality” studies with consistent findings.
• Moderate: Supported by two or more “moderate-quality” studies or one “high-quality” study.
• Limited: Supported by two or more “low-quality” studies or one “moderate-quality” study, or the evidence is considered insufficient or conflicting.
• Consensus: No supporting evidence but the guidelines development group made a recommendation based on clinical opinion.
Diagnosis and risk evidence
For diagnosis of CTS, the guidelines rate the evidence for the value of both observation and physical signs as strong, but assign ratings of moderate to MRI and limited to ultrasound. Evidence is strong for thenar atrophy, or diminished thumb muscle mass, being associated with CTS, but a lack of thenar atrophy is not enough to rule out a diagnosis. Common evaluation tools such the Phalen test, Tinel sign, Flick sign, or Upper-Limb Neurodynamic/Nerve Tension test (ULNT) are weakly supported as independent physical examination maneuvers to rule in or rule out carpal tunnel and the guidelines suggest that they not be used as sole diagnostic tools.
Moderate evidence supports exercise and physical activity to reduce the risk of developing CTS. The guidelines consider obesity a strong risk factor for CTS, but assign moderate ratings to evidence for a host of other factors, perimenopausal status, wrist ratio/index, rheumatoid arthritis, psychosocial factors, and activities such as gardening and computer use among them.
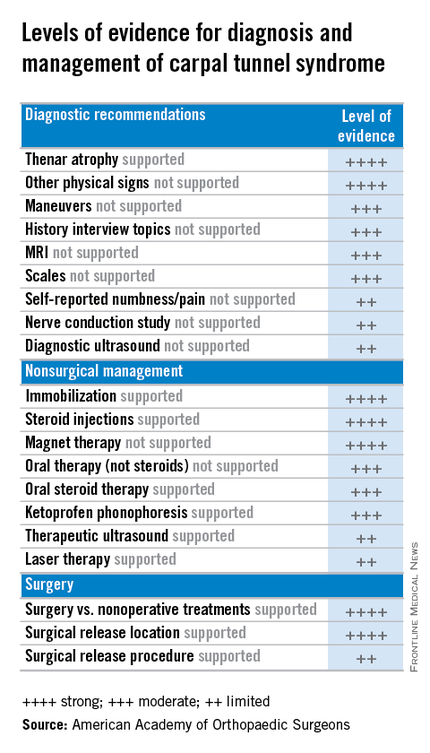
Treatment evidence
For treatment, the guidelines evaluate evidence for both surgical and nonsurgical strategies. In general, evidence for the efficacy of splinting, steroids (oral or injection), the use of ketoprofen phonophoresis gel, and magnetic therapy is strong. But therapeutic ultrasound and laser therapy are backed up with only limited evidence from the literature.
As might be expected, the evidence is strong for the efficacy of surgery to release the transverse carpal ligament. “Strong evidence supports that surgical treatment of carpal tunnel syndrome should have a greater treatment benefit at 6 and 12 months as compared to splinting, NSAIDs/therapy, and a single steroid injection.” But the value of adjunctive techniques such as epineurotomy, neurolysis, flexor tenosynovectomy, and lengthening/reconstruction of the flexor retinaculum (transverse carpal ligament) is not supported with strong evidence at this point. And the superiority of the endoscopic surgical approach is supported with only limited evidence.
“The impetus for this came from trying to help physicians cull through literally thousands and thousands of published research papers concerning various diagnoses,” said Dr. Allan E. Peljovich, vice-chair of the Guideline Work Group and AAOS representative to the group. It’s a tool to help orthopedic surgeons and other practitioners “understand what our best evidence tells us about diagnosing and treating a variety of conditions,” he said.
The effort to develop the CTS guidelines started February 2013 and involved the Guideline Work Group formulating a set of questions that, as Dr. Peljovich explained, were “the most pertinent questions that anybody interested in a particular diagnosis would want to have answered.” Then a team of statisticians and epidemiologists culled through the “incredible expanse of English language literature” to correlate data to answer those questions.
In May 2015 the work group then met to review the evidence and draft final recommendations. After a period of editing, the draft was submitted for peer review in September. The AAOS board of directors adopted the guidelines in February.
“The guidelines are not intended to be a cookbook on how to treat a condition,” Dr. Peljovich said. “They are really designed to tell you what the best evidence says about a particular set of questions. It helps you to be as updated as you want to be; it’s not designed to tell you this is the only way to do anything. ... It’s an educational tool.”
Members of the Guideline Work Group, AAOS staff, and contributing members submitted their disclosures to the AAOS.
The American Academy of Orthopaedic Surgeons has adopted clinical practice guidelines that assign evidence-based ratings for common strategies used to diagnose and treat carpal tunnel syndrome (CTS).
The 982-page comprehensive guidelines have been endorsed by the American Society for the Surgery of the Hand and the American College of Radiology. The guidelines address the burden of CTS, the second most common cause of sick days from work, according to AAOS, and its etiology, risk factors, emotional and physical impact, potential benefits, harms, contraindications, and future research. The document is available on the OrthoGuidelines Web-based app at orthoguidelines.org.
The assessments of evidence are based upon a systematic review of the current scientific and clinical information and accepted approaches to treatment and/or diagnosis of carpal tunnel syndrome. In addition to a concise summary, the report includes an exhaustive list of studies used to establish levels of evidence and a summary of the evidence in each. Also included is a list of studies not included, many because of poor study design or very small samples.
The guidelines make recommendations on practices to diagnose and manage CTS based on four levels of evidence:
• Strong: Supported by two or more “high-quality” studies with consistent findings.
• Moderate: Supported by two or more “moderate-quality” studies or one “high-quality” study.
• Limited: Supported by two or more “low-quality” studies or one “moderate-quality” study, or the evidence is considered insufficient or conflicting.
• Consensus: No supporting evidence but the guidelines development group made a recommendation based on clinical opinion.
Diagnosis and risk evidence
For diagnosis of CTS, the guidelines rate the evidence for the value of both observation and physical signs as strong, but assign ratings of moderate to MRI and limited to ultrasound. Evidence is strong for thenar atrophy, or diminished thumb muscle mass, being associated with CTS, but a lack of thenar atrophy is not enough to rule out a diagnosis. Common evaluation tools such the Phalen test, Tinel sign, Flick sign, or Upper-Limb Neurodynamic/Nerve Tension test (ULNT) are weakly supported as independent physical examination maneuvers to rule in or rule out carpal tunnel and the guidelines suggest that they not be used as sole diagnostic tools.
Moderate evidence supports exercise and physical activity to reduce the risk of developing CTS. The guidelines consider obesity a strong risk factor for CTS, but assign moderate ratings to evidence for a host of other factors, perimenopausal status, wrist ratio/index, rheumatoid arthritis, psychosocial factors, and activities such as gardening and computer use among them.
Treatment evidence
For treatment, the guidelines evaluate evidence for both surgical and nonsurgical strategies. In general, evidence for the efficacy of splinting, steroids (oral or injection), the use of ketoprofen phonophoresis gel, and magnetic therapy is strong. But therapeutic ultrasound and laser therapy are backed up with only limited evidence from the literature.
As might be expected, the evidence is strong for the efficacy of surgery to release the transverse carpal ligament. “Strong evidence supports that surgical treatment of carpal tunnel syndrome should have a greater treatment benefit at 6 and 12 months as compared to splinting, NSAIDs/therapy, and a single steroid injection.” But the value of adjunctive techniques such as epineurotomy, neurolysis, flexor tenosynovectomy, and lengthening/reconstruction of the flexor retinaculum (transverse carpal ligament) is not supported with strong evidence at this point. And the superiority of the endoscopic surgical approach is supported with only limited evidence.
“The impetus for this came from trying to help physicians cull through literally thousands and thousands of published research papers concerning various diagnoses,” said Dr. Allan E. Peljovich, vice-chair of the Guideline Work Group and AAOS representative to the group. It’s a tool to help orthopedic surgeons and other practitioners “understand what our best evidence tells us about diagnosing and treating a variety of conditions,” he said.
The effort to develop the CTS guidelines started February 2013 and involved the Guideline Work Group formulating a set of questions that, as Dr. Peljovich explained, were “the most pertinent questions that anybody interested in a particular diagnosis would want to have answered.” Then a team of statisticians and epidemiologists culled through the “incredible expanse of English language literature” to correlate data to answer those questions.
In May 2015 the work group then met to review the evidence and draft final recommendations. After a period of editing, the draft was submitted for peer review in September. The AAOS board of directors adopted the guidelines in February.
“The guidelines are not intended to be a cookbook on how to treat a condition,” Dr. Peljovich said. “They are really designed to tell you what the best evidence says about a particular set of questions. It helps you to be as updated as you want to be; it’s not designed to tell you this is the only way to do anything. ... It’s an educational tool.”
Members of the Guideline Work Group, AAOS staff, and contributing members submitted their disclosures to the AAOS.
The American Academy of Orthopaedic Surgeons has adopted clinical practice guidelines that assign evidence-based ratings for common strategies used to diagnose and treat carpal tunnel syndrome (CTS).
The 982-page comprehensive guidelines have been endorsed by the American Society for the Surgery of the Hand and the American College of Radiology. The guidelines address the burden of CTS, the second most common cause of sick days from work, according to AAOS, and its etiology, risk factors, emotional and physical impact, potential benefits, harms, contraindications, and future research. The document is available on the OrthoGuidelines Web-based app at orthoguidelines.org.
The assessments of evidence are based upon a systematic review of the current scientific and clinical information and accepted approaches to treatment and/or diagnosis of carpal tunnel syndrome. In addition to a concise summary, the report includes an exhaustive list of studies used to establish levels of evidence and a summary of the evidence in each. Also included is a list of studies not included, many because of poor study design or very small samples.
The guidelines make recommendations on practices to diagnose and manage CTS based on four levels of evidence:
• Strong: Supported by two or more “high-quality” studies with consistent findings.
• Moderate: Supported by two or more “moderate-quality” studies or one “high-quality” study.
• Limited: Supported by two or more “low-quality” studies or one “moderate-quality” study, or the evidence is considered insufficient or conflicting.
• Consensus: No supporting evidence but the guidelines development group made a recommendation based on clinical opinion.
Diagnosis and risk evidence
For diagnosis of CTS, the guidelines rate the evidence for the value of both observation and physical signs as strong, but assign ratings of moderate to MRI and limited to ultrasound. Evidence is strong for thenar atrophy, or diminished thumb muscle mass, being associated with CTS, but a lack of thenar atrophy is not enough to rule out a diagnosis. Common evaluation tools such the Phalen test, Tinel sign, Flick sign, or Upper-Limb Neurodynamic/Nerve Tension test (ULNT) are weakly supported as independent physical examination maneuvers to rule in or rule out carpal tunnel and the guidelines suggest that they not be used as sole diagnostic tools.
Moderate evidence supports exercise and physical activity to reduce the risk of developing CTS. The guidelines consider obesity a strong risk factor for CTS, but assign moderate ratings to evidence for a host of other factors, perimenopausal status, wrist ratio/index, rheumatoid arthritis, psychosocial factors, and activities such as gardening and computer use among them.
Treatment evidence
For treatment, the guidelines evaluate evidence for both surgical and nonsurgical strategies. In general, evidence for the efficacy of splinting, steroids (oral or injection), the use of ketoprofen phonophoresis gel, and magnetic therapy is strong. But therapeutic ultrasound and laser therapy are backed up with only limited evidence from the literature.
As might be expected, the evidence is strong for the efficacy of surgery to release the transverse carpal ligament. “Strong evidence supports that surgical treatment of carpal tunnel syndrome should have a greater treatment benefit at 6 and 12 months as compared to splinting, NSAIDs/therapy, and a single steroid injection.” But the value of adjunctive techniques such as epineurotomy, neurolysis, flexor tenosynovectomy, and lengthening/reconstruction of the flexor retinaculum (transverse carpal ligament) is not supported with strong evidence at this point. And the superiority of the endoscopic surgical approach is supported with only limited evidence.
“The impetus for this came from trying to help physicians cull through literally thousands and thousands of published research papers concerning various diagnoses,” said Dr. Allan E. Peljovich, vice-chair of the Guideline Work Group and AAOS representative to the group. It’s a tool to help orthopedic surgeons and other practitioners “understand what our best evidence tells us about diagnosing and treating a variety of conditions,” he said.
The effort to develop the CTS guidelines started February 2013 and involved the Guideline Work Group formulating a set of questions that, as Dr. Peljovich explained, were “the most pertinent questions that anybody interested in a particular diagnosis would want to have answered.” Then a team of statisticians and epidemiologists culled through the “incredible expanse of English language literature” to correlate data to answer those questions.
In May 2015 the work group then met to review the evidence and draft final recommendations. After a period of editing, the draft was submitted for peer review in September. The AAOS board of directors adopted the guidelines in February.
“The guidelines are not intended to be a cookbook on how to treat a condition,” Dr. Peljovich said. “They are really designed to tell you what the best evidence says about a particular set of questions. It helps you to be as updated as you want to be; it’s not designed to tell you this is the only way to do anything. ... It’s an educational tool.”
Members of the Guideline Work Group, AAOS staff, and contributing members submitted their disclosures to the AAOS.

Should esophageal cancer follow-up ever end?
About one third of patients who have esophagectomy for locally advanced esophageal cancer can survive disease-free for 5 years or longer, and once they reach that milestone, they have a good chance of living another 5 years, but previous studies have not explored if these patients continue disease-free or determined any independent predictors for long-term survival.
To get answers, investigators at Cornell University, New York conducted a retrospective review of a prospective database of 355 patients who underwent esophagectomy for cT2N0M0 or higher disease between 1988 and 2009, 126 of whom were alive and disease-free after 5 years.
The actuarial overall survival of this group was 94% at 7 years and 80% at 10 years, according to results published in the March issue of the Journal of Thoracic and Cardiovascular Surgery (2016 Mar;151:726-32). The findings were first presented at the 95th annual meeting of the American Association for Thoracic Surgery in April 2015 in Seattle. A video of the presentation is available at the AATS website (www.aats.org).
The 33% disease-free survival rate of these patients is “promising,” Dr. Galal Ghaly and colleagues said. “These excellent results are likely the result of accurate preoperative staging, standardization of surgical and perioperative management, and the use of multimodality treatment strategies,” they said.
But even after 5 years without disease, these patients were at risk of recurrence or other problems. Twenty-three patients (18%) experienced a second primary cancer elsewhere and eight (6.3%) had recurrence of esophageal cancer. Pulmonary-related deaths accounted for 10 (7.9%) of 22 (17.5%) non-cancer deaths after 5 years. “Careful follow-up is necessary for these patients, even after the 5-year mark,” Dr. Ghaly and colleagues said.
The study identified en bloc resection as the sole independent predictor of disease-free survival in these patients, a finding the investigators called “surprising,” but one with an explanation: “It is possible that patients undergoing en bloc resection were selected for that surgical procedure because of better performance status, fewer comorbidities or less frail appearance,” Dr. Ghaly and colleagues said. “Such a group might be expected to have a longer [overall survival] on the basis of those differences alone.”
Dr. Ghaly and coauthors acknowledged that over the 20-year term of the study changes in treatment approaches could have influenced patient outcomes, but a multivariable analysis accounted for that. They did find variability in preoperative staging, however. “Another limitation is the lack of a consistent method of preoperative staging, with 55% to 63% of patients staged by endoscopic ultrasonography and PET scanning,” Dr. Ghaly and coauthors said. However, that only resulted in 13 patients (10%) eventually found to have pT1N0 disease, and the results remained the same after those patients were excluded from the analysis.
Coauthor Dr. Paul J. Christos disclosed he had received a grant from the Clinical and Translational Science Center at Cornell University, New York. The other coauthors had no financial relationships to disclose.
The study by Dr. Ghaly and colleagues “provides some much-needed good news in esophageal cancer,” Dr. Gail Darling of the University of Toronto said in her invited commentary (J Thorac Cardiovasc Surg. 2016 Mar;151:733-4). She noted that 5-year survival after esophagectomy was once considered a cure, but increased survival after 5 years thanks to the use of neoadjuvant therapy raises the question: Has it simply delayed recurrence?

|
Dr. Gail Darling |
The study has shown that not all patients are cured even if they’re disease-free after 5 years, Dr. Darling said, making the case for follow-up beyond 5 years. Besides the risk of recurrence of esophageal cancer, a second reason for longer-term follow-up is the risk of second cancers. “This paper reminds us that we should not give up on our patients,” Dr. Darling said. “What a terrible thing it would be to be cured of one of the deadliest cancers, only to die from one that is more often curable.”
The role of pulmonary disease as a leading cause of death in these patients after 5 years cannot be ignored either, she said. People who have had esophagectomy often have chronic cough and reflux, and 25% of 5-year survivors had preexisting pulmonary disease. “Did patients die of their preexisting pulmonary disease, or did chronic reflux and aspiration contribute to their deaths?” she asked. “Perhaps chronic reflux is more than a quality-of-life issue.”
Dr. Darling acknowledged the study delivers “some much needed good news in esophageal cancer.” At the same time, “much work needs to be done.” That work includes addressing surgical quality. “We count lymph nodes and measure margins,” she said. “Is this enough? Is en bloc esophagectomy the answer?” The infrequency of esophageal cancer probably obviates a randomized trial, but the capabilities for collaborating on data collection and analysis provide an opportunity to determine the best surgical approach, she said. “At that point, the task of delivering high-quality surgery will rest with us.”
Dr. Darling had no financial relationships to disclose.
The study by Dr. Ghaly and colleagues “provides some much-needed good news in esophageal cancer,” Dr. Gail Darling of the University of Toronto said in her invited commentary (J Thorac Cardiovasc Surg. 2016 Mar;151:733-4). She noted that 5-year survival after esophagectomy was once considered a cure, but increased survival after 5 years thanks to the use of neoadjuvant therapy raises the question: Has it simply delayed recurrence?
|
|
Dr. Gail Darling |
The study has shown that not all patients are cured even if they’re disease-free after 5 years, Dr. Darling said, making the case for follow-up beyond 5 years. Besides the risk of recurrence of esophageal cancer, a second reason for longer-term follow-up is the risk of second cancers. “This paper reminds us that we should not give up on our patients,” Dr. Darling said. “What a terrible thing it would be to be cured of one of the deadliest cancers, only to die from one that is more often curable.”
The role of pulmonary disease as a leading cause of death in these patients after 5 years cannot be ignored either, she said. People who have had esophagectomy often have chronic cough and reflux, and 25% of 5-year survivors had preexisting pulmonary disease. “Did patients die of their preexisting pulmonary disease, or did chronic reflux and aspiration contribute to their deaths?” she asked. “Perhaps chronic reflux is more than a quality-of-life issue.”
Dr. Darling acknowledged the study delivers “some much needed good news in esophageal cancer.” At the same time, “much work needs to be done.” That work includes addressing surgical quality. “We count lymph nodes and measure margins,” she said. “Is this enough? Is en bloc esophagectomy the answer?” The infrequency of esophageal cancer probably obviates a randomized trial, but the capabilities for collaborating on data collection and analysis provide an opportunity to determine the best surgical approach, she said. “At that point, the task of delivering high-quality surgery will rest with us.”
Dr. Darling had no financial relationships to disclose.
The study by Dr. Ghaly and colleagues “provides some much-needed good news in esophageal cancer,” Dr. Gail Darling of the University of Toronto said in her invited commentary (J Thorac Cardiovasc Surg. 2016 Mar;151:733-4). She noted that 5-year survival after esophagectomy was once considered a cure, but increased survival after 5 years thanks to the use of neoadjuvant therapy raises the question: Has it simply delayed recurrence?
|
|
Dr. Gail Darling |
The study has shown that not all patients are cured even if they’re disease-free after 5 years, Dr. Darling said, making the case for follow-up beyond 5 years. Besides the risk of recurrence of esophageal cancer, a second reason for longer-term follow-up is the risk of second cancers. “This paper reminds us that we should not give up on our patients,” Dr. Darling said. “What a terrible thing it would be to be cured of one of the deadliest cancers, only to die from one that is more often curable.”
The role of pulmonary disease as a leading cause of death in these patients after 5 years cannot be ignored either, she said. People who have had esophagectomy often have chronic cough and reflux, and 25% of 5-year survivors had preexisting pulmonary disease. “Did patients die of their preexisting pulmonary disease, or did chronic reflux and aspiration contribute to their deaths?” she asked. “Perhaps chronic reflux is more than a quality-of-life issue.”
Dr. Darling acknowledged the study delivers “some much needed good news in esophageal cancer.” At the same time, “much work needs to be done.” That work includes addressing surgical quality. “We count lymph nodes and measure margins,” she said. “Is this enough? Is en bloc esophagectomy the answer?” The infrequency of esophageal cancer probably obviates a randomized trial, but the capabilities for collaborating on data collection and analysis provide an opportunity to determine the best surgical approach, she said. “At that point, the task of delivering high-quality surgery will rest with us.”
Dr. Darling had no financial relationships to disclose.
About one third of patients who have esophagectomy for locally advanced esophageal cancer can survive disease-free for 5 years or longer, and once they reach that milestone, they have a good chance of living another 5 years, but previous studies have not explored if these patients continue disease-free or determined any independent predictors for long-term survival.
To get answers, investigators at Cornell University, New York conducted a retrospective review of a prospective database of 355 patients who underwent esophagectomy for cT2N0M0 or higher disease between 1988 and 2009, 126 of whom were alive and disease-free after 5 years.
The actuarial overall survival of this group was 94% at 7 years and 80% at 10 years, according to results published in the March issue of the Journal of Thoracic and Cardiovascular Surgery (2016 Mar;151:726-32). The findings were first presented at the 95th annual meeting of the American Association for Thoracic Surgery in April 2015 in Seattle. A video of the presentation is available at the AATS website (www.aats.org).
The 33% disease-free survival rate of these patients is “promising,” Dr. Galal Ghaly and colleagues said. “These excellent results are likely the result of accurate preoperative staging, standardization of surgical and perioperative management, and the use of multimodality treatment strategies,” they said.
But even after 5 years without disease, these patients were at risk of recurrence or other problems. Twenty-three patients (18%) experienced a second primary cancer elsewhere and eight (6.3%) had recurrence of esophageal cancer. Pulmonary-related deaths accounted for 10 (7.9%) of 22 (17.5%) non-cancer deaths after 5 years. “Careful follow-up is necessary for these patients, even after the 5-year mark,” Dr. Ghaly and colleagues said.
The study identified en bloc resection as the sole independent predictor of disease-free survival in these patients, a finding the investigators called “surprising,” but one with an explanation: “It is possible that patients undergoing en bloc resection were selected for that surgical procedure because of better performance status, fewer comorbidities or less frail appearance,” Dr. Ghaly and colleagues said. “Such a group might be expected to have a longer [overall survival] on the basis of those differences alone.”
Dr. Ghaly and coauthors acknowledged that over the 20-year term of the study changes in treatment approaches could have influenced patient outcomes, but a multivariable analysis accounted for that. They did find variability in preoperative staging, however. “Another limitation is the lack of a consistent method of preoperative staging, with 55% to 63% of patients staged by endoscopic ultrasonography and PET scanning,” Dr. Ghaly and coauthors said. However, that only resulted in 13 patients (10%) eventually found to have pT1N0 disease, and the results remained the same after those patients were excluded from the analysis.
Coauthor Dr. Paul J. Christos disclosed he had received a grant from the Clinical and Translational Science Center at Cornell University, New York. The other coauthors had no financial relationships to disclose.
About one third of patients who have esophagectomy for locally advanced esophageal cancer can survive disease-free for 5 years or longer, and once they reach that milestone, they have a good chance of living another 5 years, but previous studies have not explored if these patients continue disease-free or determined any independent predictors for long-term survival.
To get answers, investigators at Cornell University, New York conducted a retrospective review of a prospective database of 355 patients who underwent esophagectomy for cT2N0M0 or higher disease between 1988 and 2009, 126 of whom were alive and disease-free after 5 years.
The actuarial overall survival of this group was 94% at 7 years and 80% at 10 years, according to results published in the March issue of the Journal of Thoracic and Cardiovascular Surgery (2016 Mar;151:726-32). The findings were first presented at the 95th annual meeting of the American Association for Thoracic Surgery in April 2015 in Seattle. A video of the presentation is available at the AATS website (www.aats.org).
The 33% disease-free survival rate of these patients is “promising,” Dr. Galal Ghaly and colleagues said. “These excellent results are likely the result of accurate preoperative staging, standardization of surgical and perioperative management, and the use of multimodality treatment strategies,” they said.
But even after 5 years without disease, these patients were at risk of recurrence or other problems. Twenty-three patients (18%) experienced a second primary cancer elsewhere and eight (6.3%) had recurrence of esophageal cancer. Pulmonary-related deaths accounted for 10 (7.9%) of 22 (17.5%) non-cancer deaths after 5 years. “Careful follow-up is necessary for these patients, even after the 5-year mark,” Dr. Ghaly and colleagues said.
The study identified en bloc resection as the sole independent predictor of disease-free survival in these patients, a finding the investigators called “surprising,” but one with an explanation: “It is possible that patients undergoing en bloc resection were selected for that surgical procedure because of better performance status, fewer comorbidities or less frail appearance,” Dr. Ghaly and colleagues said. “Such a group might be expected to have a longer [overall survival] on the basis of those differences alone.”
Dr. Ghaly and coauthors acknowledged that over the 20-year term of the study changes in treatment approaches could have influenced patient outcomes, but a multivariable analysis accounted for that. They did find variability in preoperative staging, however. “Another limitation is the lack of a consistent method of preoperative staging, with 55% to 63% of patients staged by endoscopic ultrasonography and PET scanning,” Dr. Ghaly and coauthors said. However, that only resulted in 13 patients (10%) eventually found to have pT1N0 disease, and the results remained the same after those patients were excluded from the analysis.
Coauthor Dr. Paul J. Christos disclosed he had received a grant from the Clinical and Translational Science Center at Cornell University, New York. The other coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Patients who achieve 5-year disease-free survival after esophagectomy for cancer should continue on follow-up beyond 5 years.
Major finding: After 5 years of disease-free survival, 6.3% of patients had recurrence of esophageal cancer, 18% had a second cancer elsewhere, and 7.9% died of pulmonary-related problems.
Data source: Retrospective review of a prospectively assembled thoracic surgery database of 355 patients who had esophagectomy for cT2N0M0 esophageal cancer from 1988 to 2009.
Disclosures: Coauthor Dr. Paul J. Christos disclosed partial support of a grant from Cornell University, New York. The other authors had no relationships to disclose.

Study: Tricuspid annuloplasty with mitral replacement appeared safe and effective
Controversy has surrounded the idea of concomitant tricuspid annuloplasty (TAP) with mitral valve surgery (MVR) as a way to prevent further progression of tricuspid regurgitation, and while several reports have suggested the procedures can be done safely and effectively, few reports have explored the idea of concomitant procedures in people with moderate or mild tricuspid regurgitation (TR) as a measure to prevent progression to more severe TR.
But investigators at Sungkyunkwan University in Seoul have found that TAP at the same time as MVR can be done without increasing surgical risks for patients, according to a report in the March issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:788-95).
“Although prophylactic TAP showed marginal clinical benefits for patients with less than moderate TR, we believe it is plausible to anticipate a long-term trend of a benefit of TAP in longer-term follow-up studies,“ Dr. Heemoon Lee and coauthors wrote. “Many other longer-term prospective randomized studies are needed to confirm our study findings and to ascertain clinical benefits of prophylactic TAP during mitral valve surgery.”
Despite existing clinical guidelines that recommend tricuspid valve repair for severe TR associated with mitral valve disease that requires MVR, prophylactic TAP for patients with less than moderate TR at the time of left-side valve surgery remains controversial because TR has been linked to multiple complex factors. They include etiology, whether degenerative or rheumatic; concomitant atrial fibrillation (AF); unreliable TR grading; or measurement of tricuspid annular diameter.
The investigators performed primary mechanical MVR on two groups of patients between November 1994 and December 2010: 151 with TAP; and 142 without TAP. All operations were performed through a standard median sternotomy and median follow-up was 107 months.
They looked at both early and late outcomes. There was no early mortality in either group; two bleeding episodes that required further surgery and one pacemaker insertion in the no-TAP group; and no bleeding complications and heart blocks requiring pacemaker insertion in the TAP group. While ICU stays were similar for both groups, the TAP group had significantly shorter hospital stays: 9 days vs. 11 days (P less than .001).
In terms of overall and cardiac-related deaths at 10 years, the investigators reported no significant differences between the two groups. “TAP did not appear to improve cardiac-related mortality,” Dr. Lee and coauthors said. Nor did freedom from tricuspid valve–related events differ appreciably between the two groups: 84.8% in TAP and 77.5% in no-TAP at year 10 (P = .087).
But the TAP group showed far lower rates of progression to late TR at 10 years – one in the TAP group; one (less than 1%) vs. nine (6.3%) in the no-TAP group; 96.8% in the TAP group were free from TR recurrence of grade 2 or greater vs. 85.6% in no-TAP.
“TAP can be performed safely without increases in early mortality and morbidities, including heart block,” Dr. Lee and coauthors said. “We also found that prophylactic TAP can prevent progression of late moderate or greater TR. TAP showed a tendency to prevent tricuspid valve–related events and was marginally significant.”
The researchers also evaluated the role of AF as a risk factor for progression of late TR; the effects of TAP on recurrence of moderate or greater TR were “prominent” in patients with sinus rhythm vs. AF at discharge. “These findings may reflect that the maze procedure is more important than prophylactic TAP in improving late outcomes in mitral valve disease with AF,” Dr. Lee and colleagues wrote.
The investigators acknowledged a number of limits of their study: its retrospective nature; how indications and techniques of MVR, TAP, and the maze procedure evolved over the study duration; and that the maze procedure and prophylactic TAP were not widely embraced in the early years of the study.
Dr. Lee and colleagues had no financial relationships to disclose.
The proposition of performing a concomitant TAP during MVR to prevent late progression of tricuspid regurgitation (TR) “raises safety concerns, Dr. J. Hunter Mehaffey and Dr. Irving L. Kron of the University of Virginia, Charlottesville, said in their invited commentary (J. Thorac. Cardiovasc. Surg. 2016;151:796-7). They cited their own study of 400 patients that reported higher death and complication rates in concomitant TAP-MVR procedures than in MVR alone (Ann. Thorac. Surg. 2012;52-8).

|
| M. Alex Otto/Frontline Medical News Dr. Hunter Mehaffey |
While Dr. Mehaffey and Dr. Kron commended Dr. Lee and colleagues for including atrial fibrillation in their risk analysis, they also questioned why the investigators did not address how to identify patients who would benefit from TAP to reduce the potential for long-term tricuspid, valve-related problems like reoperation for TR, right heart failure and pacemaker insertion. Nor do the investigators explain why they performed TAP in some patients and not others.
They called the study by Dr. Lee and colleagues an “interesting retrospective analysis” of concomitant TAP with MVR. “Unfortunately, this study raises numerous questions that cannot be adequately answered by propensity matching,” the coauthors wrote. A randomized, prospective trial would resolve many of these issues, they said.
Dr. Mehaffey and Dr. Kron had no financial relationships to disclose.
The proposition of performing a concomitant TAP during MVR to prevent late progression of tricuspid regurgitation (TR) “raises safety concerns, Dr. J. Hunter Mehaffey and Dr. Irving L. Kron of the University of Virginia, Charlottesville, said in their invited commentary (J. Thorac. Cardiovasc. Surg. 2016;151:796-7). They cited their own study of 400 patients that reported higher death and complication rates in concomitant TAP-MVR procedures than in MVR alone (Ann. Thorac. Surg. 2012;52-8).
|
|
| M. Alex Otto/Frontline Medical News Dr. Hunter Mehaffey |
While Dr. Mehaffey and Dr. Kron commended Dr. Lee and colleagues for including atrial fibrillation in their risk analysis, they also questioned why the investigators did not address how to identify patients who would benefit from TAP to reduce the potential for long-term tricuspid, valve-related problems like reoperation for TR, right heart failure and pacemaker insertion. Nor do the investigators explain why they performed TAP in some patients and not others.
They called the study by Dr. Lee and colleagues an “interesting retrospective analysis” of concomitant TAP with MVR. “Unfortunately, this study raises numerous questions that cannot be adequately answered by propensity matching,” the coauthors wrote. A randomized, prospective trial would resolve many of these issues, they said.
Dr. Mehaffey and Dr. Kron had no financial relationships to disclose.
The proposition of performing a concomitant TAP during MVR to prevent late progression of tricuspid regurgitation (TR) “raises safety concerns, Dr. J. Hunter Mehaffey and Dr. Irving L. Kron of the University of Virginia, Charlottesville, said in their invited commentary (J. Thorac. Cardiovasc. Surg. 2016;151:796-7). They cited their own study of 400 patients that reported higher death and complication rates in concomitant TAP-MVR procedures than in MVR alone (Ann. Thorac. Surg. 2012;52-8).
|
|
| M. Alex Otto/Frontline Medical News Dr. Hunter Mehaffey |
While Dr. Mehaffey and Dr. Kron commended Dr. Lee and colleagues for including atrial fibrillation in their risk analysis, they also questioned why the investigators did not address how to identify patients who would benefit from TAP to reduce the potential for long-term tricuspid, valve-related problems like reoperation for TR, right heart failure and pacemaker insertion. Nor do the investigators explain why they performed TAP in some patients and not others.
They called the study by Dr. Lee and colleagues an “interesting retrospective analysis” of concomitant TAP with MVR. “Unfortunately, this study raises numerous questions that cannot be adequately answered by propensity matching,” the coauthors wrote. A randomized, prospective trial would resolve many of these issues, they said.
Dr. Mehaffey and Dr. Kron had no financial relationships to disclose.
Controversy has surrounded the idea of concomitant tricuspid annuloplasty (TAP) with mitral valve surgery (MVR) as a way to prevent further progression of tricuspid regurgitation, and while several reports have suggested the procedures can be done safely and effectively, few reports have explored the idea of concomitant procedures in people with moderate or mild tricuspid regurgitation (TR) as a measure to prevent progression to more severe TR.
But investigators at Sungkyunkwan University in Seoul have found that TAP at the same time as MVR can be done without increasing surgical risks for patients, according to a report in the March issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:788-95).
“Although prophylactic TAP showed marginal clinical benefits for patients with less than moderate TR, we believe it is plausible to anticipate a long-term trend of a benefit of TAP in longer-term follow-up studies,“ Dr. Heemoon Lee and coauthors wrote. “Many other longer-term prospective randomized studies are needed to confirm our study findings and to ascertain clinical benefits of prophylactic TAP during mitral valve surgery.”
Despite existing clinical guidelines that recommend tricuspid valve repair for severe TR associated with mitral valve disease that requires MVR, prophylactic TAP for patients with less than moderate TR at the time of left-side valve surgery remains controversial because TR has been linked to multiple complex factors. They include etiology, whether degenerative or rheumatic; concomitant atrial fibrillation (AF); unreliable TR grading; or measurement of tricuspid annular diameter.
The investigators performed primary mechanical MVR on two groups of patients between November 1994 and December 2010: 151 with TAP; and 142 without TAP. All operations were performed through a standard median sternotomy and median follow-up was 107 months.
They looked at both early and late outcomes. There was no early mortality in either group; two bleeding episodes that required further surgery and one pacemaker insertion in the no-TAP group; and no bleeding complications and heart blocks requiring pacemaker insertion in the TAP group. While ICU stays were similar for both groups, the TAP group had significantly shorter hospital stays: 9 days vs. 11 days (P less than .001).
In terms of overall and cardiac-related deaths at 10 years, the investigators reported no significant differences between the two groups. “TAP did not appear to improve cardiac-related mortality,” Dr. Lee and coauthors said. Nor did freedom from tricuspid valve–related events differ appreciably between the two groups: 84.8% in TAP and 77.5% in no-TAP at year 10 (P = .087).
But the TAP group showed far lower rates of progression to late TR at 10 years – one in the TAP group; one (less than 1%) vs. nine (6.3%) in the no-TAP group; 96.8% in the TAP group were free from TR recurrence of grade 2 or greater vs. 85.6% in no-TAP.
“TAP can be performed safely without increases in early mortality and morbidities, including heart block,” Dr. Lee and coauthors said. “We also found that prophylactic TAP can prevent progression of late moderate or greater TR. TAP showed a tendency to prevent tricuspid valve–related events and was marginally significant.”
The researchers also evaluated the role of AF as a risk factor for progression of late TR; the effects of TAP on recurrence of moderate or greater TR were “prominent” in patients with sinus rhythm vs. AF at discharge. “These findings may reflect that the maze procedure is more important than prophylactic TAP in improving late outcomes in mitral valve disease with AF,” Dr. Lee and colleagues wrote.
The investigators acknowledged a number of limits of their study: its retrospective nature; how indications and techniques of MVR, TAP, and the maze procedure evolved over the study duration; and that the maze procedure and prophylactic TAP were not widely embraced in the early years of the study.
Dr. Lee and colleagues had no financial relationships to disclose.
Controversy has surrounded the idea of concomitant tricuspid annuloplasty (TAP) with mitral valve surgery (MVR) as a way to prevent further progression of tricuspid regurgitation, and while several reports have suggested the procedures can be done safely and effectively, few reports have explored the idea of concomitant procedures in people with moderate or mild tricuspid regurgitation (TR) as a measure to prevent progression to more severe TR.
But investigators at Sungkyunkwan University in Seoul have found that TAP at the same time as MVR can be done without increasing surgical risks for patients, according to a report in the March issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:788-95).
“Although prophylactic TAP showed marginal clinical benefits for patients with less than moderate TR, we believe it is plausible to anticipate a long-term trend of a benefit of TAP in longer-term follow-up studies,“ Dr. Heemoon Lee and coauthors wrote. “Many other longer-term prospective randomized studies are needed to confirm our study findings and to ascertain clinical benefits of prophylactic TAP during mitral valve surgery.”
Despite existing clinical guidelines that recommend tricuspid valve repair for severe TR associated with mitral valve disease that requires MVR, prophylactic TAP for patients with less than moderate TR at the time of left-side valve surgery remains controversial because TR has been linked to multiple complex factors. They include etiology, whether degenerative or rheumatic; concomitant atrial fibrillation (AF); unreliable TR grading; or measurement of tricuspid annular diameter.
The investigators performed primary mechanical MVR on two groups of patients between November 1994 and December 2010: 151 with TAP; and 142 without TAP. All operations were performed through a standard median sternotomy and median follow-up was 107 months.
They looked at both early and late outcomes. There was no early mortality in either group; two bleeding episodes that required further surgery and one pacemaker insertion in the no-TAP group; and no bleeding complications and heart blocks requiring pacemaker insertion in the TAP group. While ICU stays were similar for both groups, the TAP group had significantly shorter hospital stays: 9 days vs. 11 days (P less than .001).
In terms of overall and cardiac-related deaths at 10 years, the investigators reported no significant differences between the two groups. “TAP did not appear to improve cardiac-related mortality,” Dr. Lee and coauthors said. Nor did freedom from tricuspid valve–related events differ appreciably between the two groups: 84.8% in TAP and 77.5% in no-TAP at year 10 (P = .087).
But the TAP group showed far lower rates of progression to late TR at 10 years – one in the TAP group; one (less than 1%) vs. nine (6.3%) in the no-TAP group; 96.8% in the TAP group were free from TR recurrence of grade 2 or greater vs. 85.6% in no-TAP.
“TAP can be performed safely without increases in early mortality and morbidities, including heart block,” Dr. Lee and coauthors said. “We also found that prophylactic TAP can prevent progression of late moderate or greater TR. TAP showed a tendency to prevent tricuspid valve–related events and was marginally significant.”
The researchers also evaluated the role of AF as a risk factor for progression of late TR; the effects of TAP on recurrence of moderate or greater TR were “prominent” in patients with sinus rhythm vs. AF at discharge. “These findings may reflect that the maze procedure is more important than prophylactic TAP in improving late outcomes in mitral valve disease with AF,” Dr. Lee and colleagues wrote.
The investigators acknowledged a number of limits of their study: its retrospective nature; how indications and techniques of MVR, TAP, and the maze procedure evolved over the study duration; and that the maze procedure and prophylactic TAP were not widely embraced in the early years of the study.
Dr. Lee and colleagues had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Tricuspid annuloplasty performed at the same time as mitral valve surgery in people with moderate or less tricuspid regurgitation can be performed safely and achieve its clinical objective.
Major finding: Patients who had the concomitant procedure had similar rates of surgery-related death and complications as did those who had mitral valve surgery only and lower rates of late progression of tricuspid regurgitation.
Data source: Retrospective review of data for 293 patients who underwent primary mitral valve repair with mechanical prosthesis at a single center from November 1994 to December 2010.
Disclosures: The study authors had no financial relationships to disclose.

Wanted: Better evidence on fast-track lung resection
A host of medical specialties have adopted strategies to speed recovery of surgical patients, reduce length of hospital stays, and cut costs, known as fast-track or enhanced-recovery pathways, but when it comes to elective lung resection, the medical evidence has yet to establish if patients in expedited recovery protocols fare any better than do those in a conventional recovery course, a systematic review in the March issue of the Journal of Thoracic and Cardiovascular Surgery reported (2016 Mar;151:708-15).
A team of investigators from McGill University in Montreal performed a systematic review of six studies that evaluated patient outcomes of both traditional and enhanced-recovery pathways (ERPs) in elective lung resection. They concluded that ERPs may reduce the length of hospital stays and hospital costs but that well-designed trials are needed to overcome limitations of existing studies.
“The influence of ERPs on postoperative outcomes after lung resection has not been extensively studied in comparative studies involving a control group receiving traditional care,” lead author Julio F. Fiore Jr., Ph.D., and his colleagues said. One of the six studies they reviewed was a randomized clinical trial. The six studies involved a total of 1,612 participants (821 ERP, 791 control).
The researchers also reported that the studies they analyzed shared a significant limitation. “Risk of bias favoring enhanced-recovery pathways was high,” Dr. Fiore and his colleagues wrote. The studies were unclear if patient selection may have factored into the results.
Five studies reported shorter hospital length of stay (LOS) for the ERP group. “The majority of the studies reported that LOS was significantly shorter when patients undergoing lung resection were treated within an ERP, which corroborates the results observed in other surgical populations,” Dr. Fiore and his colleagues said.
Three nonrandomized studies also evaluated costs per patient. Two reported significantly lower costs for ERP patients: $13,093 vs. $14,439 for controls; and $13,432 vs. $17,103 for controls (Jpn. J. Thorac. Cardiovasc. Surg. 2006 Sep;54:387-90; Ann. Thorac. Surg. 1998 Sep;66:914-9). The third showed what the authors said was no statistically significant cost differential between the two groups: $14,792 for ERP vs. $16,063 for controls (Ann. Thorac. Surg. 1997 Aug;64:299-302).
Three studies evaluated readmission rates, but only one showed measurably lower rates for the ERP group: 3% vs. 10% for controls (Lung Cancer. 2012 Dec;78:270-5). Three studies measured complication rates in both groups. Two reported cardiopulmonary complication rates of 18% and 17% in the ERP group vs. 16% and 14% in the control group, respectively (Eur. J. Cardiothorac. Surg. 2012 May;41:1083-7; Lung Cancer. 2012 Dec;78:270-5). One reported rates of pulmonary complications of 7% for ERP vs. 36% for controls (Eur. J. Cardiothorac. Surg. 2008 Jul;34:174-80).
Dr. Fiore and his colleagues pointed out that some of the studies they reviewed were completed before video-assisted thoracic surgery became routine for lung resection. But they acknowledged that research in other surgical specialties have validated the role of ERP, along with minimally invasive surgery, to improve outcomes. “Future research should investigate whether this holds true for patients undergoing lung resection,” they said.
The study authors had no financial relationships to disclose.
The task that Dr. Fiore and colleagues undertook to evaluate and compare disparate studies of fast-track surgery in lung resection is “akin to comparing not just apples and oranges but apples to zucchini,” Dr. Lisa M. Brown of University of California, Davis, Medical Center said in her invited analysis (J. Thorac. Cardiovasc. Surg. 2016 Mar;151:715-16). Without the authors’ “descriptive approach,” Dr. Brown said, “the results of a true meta-analysis would be uninterpretable.”

|
Dr. Lisa M. Brown |
Nonetheless, the systematic review underscores the need for a blinded, randomized trial, Dr. Brown said. “Furthermore, rather than measuring [hospital] stay, subjects should be evaluated for readiness for discharge, because this would reduce the effect of systems-based obstacles to discharge,” she said. Enhanced recovery pathways (ERPs) in colorectal surgery have been used as models for other specialties, but the novelty of these pathways versus traditional care may be difficult to replicate in thoracic surgery, she said. Strategies such as antibiotic prophylaxis and epidural analgesia in thoracic surgery “are not dissimilar enough from standard care to elicit a difference in outcome,” she said.
In thoracic surgery, ERPs must consider the challenges of pain control and chest tube management unique in these patients, Dr. Brown said. For pain control, paravertebral blockade rather than epidural analgesia could lead to earlier hospital discharges. Use of chest tubes is commonly a matter of surgeon preference, she said, but chest tubes without an air leak and with acceptable fluid output can be safely removed, and even patients with an air leak but no pneumothorax on water seal can go home with a chest tube, Dr. Brown said.
Dr. Brown had no financial relationships to disclose.
The task that Dr. Fiore and colleagues undertook to evaluate and compare disparate studies of fast-track surgery in lung resection is “akin to comparing not just apples and oranges but apples to zucchini,” Dr. Lisa M. Brown of University of California, Davis, Medical Center said in her invited analysis (J. Thorac. Cardiovasc. Surg. 2016 Mar;151:715-16). Without the authors’ “descriptive approach,” Dr. Brown said, “the results of a true meta-analysis would be uninterpretable.”
|
|
Dr. Lisa M. Brown |
Nonetheless, the systematic review underscores the need for a blinded, randomized trial, Dr. Brown said. “Furthermore, rather than measuring [hospital] stay, subjects should be evaluated for readiness for discharge, because this would reduce the effect of systems-based obstacles to discharge,” she said. Enhanced recovery pathways (ERPs) in colorectal surgery have been used as models for other specialties, but the novelty of these pathways versus traditional care may be difficult to replicate in thoracic surgery, she said. Strategies such as antibiotic prophylaxis and epidural analgesia in thoracic surgery “are not dissimilar enough from standard care to elicit a difference in outcome,” she said.
In thoracic surgery, ERPs must consider the challenges of pain control and chest tube management unique in these patients, Dr. Brown said. For pain control, paravertebral blockade rather than epidural analgesia could lead to earlier hospital discharges. Use of chest tubes is commonly a matter of surgeon preference, she said, but chest tubes without an air leak and with acceptable fluid output can be safely removed, and even patients with an air leak but no pneumothorax on water seal can go home with a chest tube, Dr. Brown said.
Dr. Brown had no financial relationships to disclose.
The task that Dr. Fiore and colleagues undertook to evaluate and compare disparate studies of fast-track surgery in lung resection is “akin to comparing not just apples and oranges but apples to zucchini,” Dr. Lisa M. Brown of University of California, Davis, Medical Center said in her invited analysis (J. Thorac. Cardiovasc. Surg. 2016 Mar;151:715-16). Without the authors’ “descriptive approach,” Dr. Brown said, “the results of a true meta-analysis would be uninterpretable.”
|
|
Dr. Lisa M. Brown |
Nonetheless, the systematic review underscores the need for a blinded, randomized trial, Dr. Brown said. “Furthermore, rather than measuring [hospital] stay, subjects should be evaluated for readiness for discharge, because this would reduce the effect of systems-based obstacles to discharge,” she said. Enhanced recovery pathways (ERPs) in colorectal surgery have been used as models for other specialties, but the novelty of these pathways versus traditional care may be difficult to replicate in thoracic surgery, she said. Strategies such as antibiotic prophylaxis and epidural analgesia in thoracic surgery “are not dissimilar enough from standard care to elicit a difference in outcome,” she said.
In thoracic surgery, ERPs must consider the challenges of pain control and chest tube management unique in these patients, Dr. Brown said. For pain control, paravertebral blockade rather than epidural analgesia could lead to earlier hospital discharges. Use of chest tubes is commonly a matter of surgeon preference, she said, but chest tubes without an air leak and with acceptable fluid output can be safely removed, and even patients with an air leak but no pneumothorax on water seal can go home with a chest tube, Dr. Brown said.
Dr. Brown had no financial relationships to disclose.
A host of medical specialties have adopted strategies to speed recovery of surgical patients, reduce length of hospital stays, and cut costs, known as fast-track or enhanced-recovery pathways, but when it comes to elective lung resection, the medical evidence has yet to establish if patients in expedited recovery protocols fare any better than do those in a conventional recovery course, a systematic review in the March issue of the Journal of Thoracic and Cardiovascular Surgery reported (2016 Mar;151:708-15).
A team of investigators from McGill University in Montreal performed a systematic review of six studies that evaluated patient outcomes of both traditional and enhanced-recovery pathways (ERPs) in elective lung resection. They concluded that ERPs may reduce the length of hospital stays and hospital costs but that well-designed trials are needed to overcome limitations of existing studies.
“The influence of ERPs on postoperative outcomes after lung resection has not been extensively studied in comparative studies involving a control group receiving traditional care,” lead author Julio F. Fiore Jr., Ph.D., and his colleagues said. One of the six studies they reviewed was a randomized clinical trial. The six studies involved a total of 1,612 participants (821 ERP, 791 control).
The researchers also reported that the studies they analyzed shared a significant limitation. “Risk of bias favoring enhanced-recovery pathways was high,” Dr. Fiore and his colleagues wrote. The studies were unclear if patient selection may have factored into the results.
Five studies reported shorter hospital length of stay (LOS) for the ERP group. “The majority of the studies reported that LOS was significantly shorter when patients undergoing lung resection were treated within an ERP, which corroborates the results observed in other surgical populations,” Dr. Fiore and his colleagues said.
Three nonrandomized studies also evaluated costs per patient. Two reported significantly lower costs for ERP patients: $13,093 vs. $14,439 for controls; and $13,432 vs. $17,103 for controls (Jpn. J. Thorac. Cardiovasc. Surg. 2006 Sep;54:387-90; Ann. Thorac. Surg. 1998 Sep;66:914-9). The third showed what the authors said was no statistically significant cost differential between the two groups: $14,792 for ERP vs. $16,063 for controls (Ann. Thorac. Surg. 1997 Aug;64:299-302).
Three studies evaluated readmission rates, but only one showed measurably lower rates for the ERP group: 3% vs. 10% for controls (Lung Cancer. 2012 Dec;78:270-5). Three studies measured complication rates in both groups. Two reported cardiopulmonary complication rates of 18% and 17% in the ERP group vs. 16% and 14% in the control group, respectively (Eur. J. Cardiothorac. Surg. 2012 May;41:1083-7; Lung Cancer. 2012 Dec;78:270-5). One reported rates of pulmonary complications of 7% for ERP vs. 36% for controls (Eur. J. Cardiothorac. Surg. 2008 Jul;34:174-80).
Dr. Fiore and his colleagues pointed out that some of the studies they reviewed were completed before video-assisted thoracic surgery became routine for lung resection. But they acknowledged that research in other surgical specialties have validated the role of ERP, along with minimally invasive surgery, to improve outcomes. “Future research should investigate whether this holds true for patients undergoing lung resection,” they said.
The study authors had no financial relationships to disclose.
A host of medical specialties have adopted strategies to speed recovery of surgical patients, reduce length of hospital stays, and cut costs, known as fast-track or enhanced-recovery pathways, but when it comes to elective lung resection, the medical evidence has yet to establish if patients in expedited recovery protocols fare any better than do those in a conventional recovery course, a systematic review in the March issue of the Journal of Thoracic and Cardiovascular Surgery reported (2016 Mar;151:708-15).
A team of investigators from McGill University in Montreal performed a systematic review of six studies that evaluated patient outcomes of both traditional and enhanced-recovery pathways (ERPs) in elective lung resection. They concluded that ERPs may reduce the length of hospital stays and hospital costs but that well-designed trials are needed to overcome limitations of existing studies.
“The influence of ERPs on postoperative outcomes after lung resection has not been extensively studied in comparative studies involving a control group receiving traditional care,” lead author Julio F. Fiore Jr., Ph.D., and his colleagues said. One of the six studies they reviewed was a randomized clinical trial. The six studies involved a total of 1,612 participants (821 ERP, 791 control).
The researchers also reported that the studies they analyzed shared a significant limitation. “Risk of bias favoring enhanced-recovery pathways was high,” Dr. Fiore and his colleagues wrote. The studies were unclear if patient selection may have factored into the results.
Five studies reported shorter hospital length of stay (LOS) for the ERP group. “The majority of the studies reported that LOS was significantly shorter when patients undergoing lung resection were treated within an ERP, which corroborates the results observed in other surgical populations,” Dr. Fiore and his colleagues said.
Three nonrandomized studies also evaluated costs per patient. Two reported significantly lower costs for ERP patients: $13,093 vs. $14,439 for controls; and $13,432 vs. $17,103 for controls (Jpn. J. Thorac. Cardiovasc. Surg. 2006 Sep;54:387-90; Ann. Thorac. Surg. 1998 Sep;66:914-9). The third showed what the authors said was no statistically significant cost differential between the two groups: $14,792 for ERP vs. $16,063 for controls (Ann. Thorac. Surg. 1997 Aug;64:299-302).
Three studies evaluated readmission rates, but only one showed measurably lower rates for the ERP group: 3% vs. 10% for controls (Lung Cancer. 2012 Dec;78:270-5). Three studies measured complication rates in both groups. Two reported cardiopulmonary complication rates of 18% and 17% in the ERP group vs. 16% and 14% in the control group, respectively (Eur. J. Cardiothorac. Surg. 2012 May;41:1083-7; Lung Cancer. 2012 Dec;78:270-5). One reported rates of pulmonary complications of 7% for ERP vs. 36% for controls (Eur. J. Cardiothorac. Surg. 2008 Jul;34:174-80).
Dr. Fiore and his colleagues pointed out that some of the studies they reviewed were completed before video-assisted thoracic surgery became routine for lung resection. But they acknowledged that research in other surgical specialties have validated the role of ERP, along with minimally invasive surgery, to improve outcomes. “Future research should investigate whether this holds true for patients undergoing lung resection,” they said.
The study authors had no financial relationships to disclose.
Key clinical point: Well-designed clinical trials are needed to determine the effectiveness of fast-track recovery pathways in lung resection.
Major finding: Fast-track lung resection patients showed no differences in readmissions, overall complication and death rates compared to patients subjected to a traditional recovery course.
Data source: Systematic review of six studies published from 1997 to 2012 that involved 1,612 individuals who had lung resection.
Disclosures: The study authors had no financial relationships to disclose.
