User login
Vigorous exercise hastens knee OA progression
PARIS – Vigorous, but not moderate, physical exercise was associated with a significantly greater risk of knee osteoarthritis progression over 1 year in a longitudinal analysis of 99 patients.
Engaging in vigorous activity was associated with a 1.38-times increased risk for progression (95% confidence intervals, 1.04-1.83; P = .025), defined as an increase in either cartilage or meniscus defect scores at 1 year.

The odds ratios were not significantly increased for moderate activity (OR, 0.78; 95% CI, 0.47-1.28; P = .322) but were close to significance for walking activity (OR, 1.50; 95% CI, 1-2.25; P = .052), lead author Deepak Kumar, Ph.D., said at the World Congress on Osteoarthritis.
The analyses adjusted for age, body mass index, sex, pain, Kellgren-Lawrence (KL) score, and modified Whole Organ Magnetic Resonance Scores for cartilage and meniscus in the first block, and International Physical Activity Questionnaire (IPAQ) scores in the second block.
"We did not see that moderate activity was associated with progression, and this indicates that we need to further investigate the optimal dosage of physical activity for someone with knee osteoarthritis," said Dr. Kumar, a postdoctoral scholar, radiology department, University of California, San Francisco.
Although greater physical activity has been shown to reduce pain and improve function, the results support more recent work suggesting that certain types of activity may be associated with disease progression. Walking 10,000 steps or more per day was found to increase the risk of meniscus and cartilage lesions on MRI in people with knee OA (Ann. Rheum. Dis. 2013;72:1170-5), while high and very low levels of self-reported activity were associated with greater cartilage relaxation times on 2T MRI at 4 years in data from the Osteoarthritis Initiative (Osteoarthritis Cartilage 2013;12:1558-66).
For the current analysis, 99 participants in the ongoing, longitudinal Cartilage Loading and Unloading (CLOC) knee OA study underwent 3T MRI of the knee using a sagittal, high-resolution 3D fast spin-echo Cube sequence at baseline, which was repeated 1 year later. Cartilage and meniscus defects were graded by experienced radiologists. Participants with OA had a baseline radiographic KL score of more than 1 and were symptomatic; controls had a KL of 0 or 1 and no knee symptoms.
By 1 year, 35 participants showed progression (14 with OA and 21 controls) and 64 did not. Surprisingly, there was greater progression in the lateral compartment (11 lateral menisci, 12 lateral tibiae) and, more expectedly, in the patella in 12 persons, Dr. Kumar said at the meeting, sponsored by the Osteoarthritis Research Society International.
No significant baseline differences existed between nonprogressors and progressors with respect to age (53.2 years vs. 50.8 years), body mass index (24.4 kg/m2 vs. 24.5 kg/m2), and sex (62.5% vs. 48.5% female), he said.
Knee injury and Osteoarthritis Outcome Score subscale scores were also similar for pain (85.7 vs. 82.4) and symptoms (84.5 vs. 83.4).
Progressors had engaged, however, in significantly more metabolic equivalent-minutes per week of vigorous exercise than did nonprogressors (2,410.6 vs. 1,413.1; P = .046), Dr. Kumar said. Metabolic equivalent-minutes per week were similar for moderate activity (1,094.1 vs. 858.7; P = .396) and walking (1,646.2 vs. 1,245.1; P = .151).
During the discussion following the formal presentation, an attendee said the study is potentially very valuable because it suggests that something all clinicians want to do is "dangerous" but questioned whether some of the MRI data were "overread" given the almost 40% rate of progression in a relatively fit cohort. A Danish attendee also remarked that her group has experienced so many problems with patients filling out the IPAQ questionnaire that they no longer trust the data.
Dr. Kumar responded that the MRI readings were performed by expert radiologists and were reliable, and that more stringent definitions of progression are being explored. His group is also working on a new questionnaire to better define physical activity levels.
Data are also being analyzed from the rest of the cohort (160 participants) and over a longer, 3-year follow-up, he said in an interview.
"We are also identifying quantitative MRI and biomechanical metrics that may be more sensitive to disease progression in knee OA. These will help us understand the factors that are related to worsening of knee OA and develop therapies."
The National Institutes of Health–National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the work. Dr. Kumar and his coauthors reported no conflicting interests.
PARIS – Vigorous, but not moderate, physical exercise was associated with a significantly greater risk of knee osteoarthritis progression over 1 year in a longitudinal analysis of 99 patients.
Engaging in vigorous activity was associated with a 1.38-times increased risk for progression (95% confidence intervals, 1.04-1.83; P = .025), defined as an increase in either cartilage or meniscus defect scores at 1 year.
The odds ratios were not significantly increased for moderate activity (OR, 0.78; 95% CI, 0.47-1.28; P = .322) but were close to significance for walking activity (OR, 1.50; 95% CI, 1-2.25; P = .052), lead author Deepak Kumar, Ph.D., said at the World Congress on Osteoarthritis.
The analyses adjusted for age, body mass index, sex, pain, Kellgren-Lawrence (KL) score, and modified Whole Organ Magnetic Resonance Scores for cartilage and meniscus in the first block, and International Physical Activity Questionnaire (IPAQ) scores in the second block.
"We did not see that moderate activity was associated with progression, and this indicates that we need to further investigate the optimal dosage of physical activity for someone with knee osteoarthritis," said Dr. Kumar, a postdoctoral scholar, radiology department, University of California, San Francisco.
Although greater physical activity has been shown to reduce pain and improve function, the results support more recent work suggesting that certain types of activity may be associated with disease progression. Walking 10,000 steps or more per day was found to increase the risk of meniscus and cartilage lesions on MRI in people with knee OA (Ann. Rheum. Dis. 2013;72:1170-5), while high and very low levels of self-reported activity were associated with greater cartilage relaxation times on 2T MRI at 4 years in data from the Osteoarthritis Initiative (Osteoarthritis Cartilage 2013;12:1558-66).
For the current analysis, 99 participants in the ongoing, longitudinal Cartilage Loading and Unloading (CLOC) knee OA study underwent 3T MRI of the knee using a sagittal, high-resolution 3D fast spin-echo Cube sequence at baseline, which was repeated 1 year later. Cartilage and meniscus defects were graded by experienced radiologists. Participants with OA had a baseline radiographic KL score of more than 1 and were symptomatic; controls had a KL of 0 or 1 and no knee symptoms.
By 1 year, 35 participants showed progression (14 with OA and 21 controls) and 64 did not. Surprisingly, there was greater progression in the lateral compartment (11 lateral menisci, 12 lateral tibiae) and, more expectedly, in the patella in 12 persons, Dr. Kumar said at the meeting, sponsored by the Osteoarthritis Research Society International.
No significant baseline differences existed between nonprogressors and progressors with respect to age (53.2 years vs. 50.8 years), body mass index (24.4 kg/m2 vs. 24.5 kg/m2), and sex (62.5% vs. 48.5% female), he said.
Knee injury and Osteoarthritis Outcome Score subscale scores were also similar for pain (85.7 vs. 82.4) and symptoms (84.5 vs. 83.4).
Progressors had engaged, however, in significantly more metabolic equivalent-minutes per week of vigorous exercise than did nonprogressors (2,410.6 vs. 1,413.1; P = .046), Dr. Kumar said. Metabolic equivalent-minutes per week were similar for moderate activity (1,094.1 vs. 858.7; P = .396) and walking (1,646.2 vs. 1,245.1; P = .151).
During the discussion following the formal presentation, an attendee said the study is potentially very valuable because it suggests that something all clinicians want to do is "dangerous" but questioned whether some of the MRI data were "overread" given the almost 40% rate of progression in a relatively fit cohort. A Danish attendee also remarked that her group has experienced so many problems with patients filling out the IPAQ questionnaire that they no longer trust the data.
Dr. Kumar responded that the MRI readings were performed by expert radiologists and were reliable, and that more stringent definitions of progression are being explored. His group is also working on a new questionnaire to better define physical activity levels.
Data are also being analyzed from the rest of the cohort (160 participants) and over a longer, 3-year follow-up, he said in an interview.
"We are also identifying quantitative MRI and biomechanical metrics that may be more sensitive to disease progression in knee OA. These will help us understand the factors that are related to worsening of knee OA and develop therapies."
The National Institutes of Health–National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the work. Dr. Kumar and his coauthors reported no conflicting interests.
PARIS – Vigorous, but not moderate, physical exercise was associated with a significantly greater risk of knee osteoarthritis progression over 1 year in a longitudinal analysis of 99 patients.
Engaging in vigorous activity was associated with a 1.38-times increased risk for progression (95% confidence intervals, 1.04-1.83; P = .025), defined as an increase in either cartilage or meniscus defect scores at 1 year.
The odds ratios were not significantly increased for moderate activity (OR, 0.78; 95% CI, 0.47-1.28; P = .322) but were close to significance for walking activity (OR, 1.50; 95% CI, 1-2.25; P = .052), lead author Deepak Kumar, Ph.D., said at the World Congress on Osteoarthritis.
The analyses adjusted for age, body mass index, sex, pain, Kellgren-Lawrence (KL) score, and modified Whole Organ Magnetic Resonance Scores for cartilage and meniscus in the first block, and International Physical Activity Questionnaire (IPAQ) scores in the second block.
"We did not see that moderate activity was associated with progression, and this indicates that we need to further investigate the optimal dosage of physical activity for someone with knee osteoarthritis," said Dr. Kumar, a postdoctoral scholar, radiology department, University of California, San Francisco.
Although greater physical activity has been shown to reduce pain and improve function, the results support more recent work suggesting that certain types of activity may be associated with disease progression. Walking 10,000 steps or more per day was found to increase the risk of meniscus and cartilage lesions on MRI in people with knee OA (Ann. Rheum. Dis. 2013;72:1170-5), while high and very low levels of self-reported activity were associated with greater cartilage relaxation times on 2T MRI at 4 years in data from the Osteoarthritis Initiative (Osteoarthritis Cartilage 2013;12:1558-66).
For the current analysis, 99 participants in the ongoing, longitudinal Cartilage Loading and Unloading (CLOC) knee OA study underwent 3T MRI of the knee using a sagittal, high-resolution 3D fast spin-echo Cube sequence at baseline, which was repeated 1 year later. Cartilage and meniscus defects were graded by experienced radiologists. Participants with OA had a baseline radiographic KL score of more than 1 and were symptomatic; controls had a KL of 0 or 1 and no knee symptoms.
By 1 year, 35 participants showed progression (14 with OA and 21 controls) and 64 did not. Surprisingly, there was greater progression in the lateral compartment (11 lateral menisci, 12 lateral tibiae) and, more expectedly, in the patella in 12 persons, Dr. Kumar said at the meeting, sponsored by the Osteoarthritis Research Society International.
No significant baseline differences existed between nonprogressors and progressors with respect to age (53.2 years vs. 50.8 years), body mass index (24.4 kg/m2 vs. 24.5 kg/m2), and sex (62.5% vs. 48.5% female), he said.
Knee injury and Osteoarthritis Outcome Score subscale scores were also similar for pain (85.7 vs. 82.4) and symptoms (84.5 vs. 83.4).
Progressors had engaged, however, in significantly more metabolic equivalent-minutes per week of vigorous exercise than did nonprogressors (2,410.6 vs. 1,413.1; P = .046), Dr. Kumar said. Metabolic equivalent-minutes per week were similar for moderate activity (1,094.1 vs. 858.7; P = .396) and walking (1,646.2 vs. 1,245.1; P = .151).
During the discussion following the formal presentation, an attendee said the study is potentially very valuable because it suggests that something all clinicians want to do is "dangerous" but questioned whether some of the MRI data were "overread" given the almost 40% rate of progression in a relatively fit cohort. A Danish attendee also remarked that her group has experienced so many problems with patients filling out the IPAQ questionnaire that they no longer trust the data.
Dr. Kumar responded that the MRI readings were performed by expert radiologists and were reliable, and that more stringent definitions of progression are being explored. His group is also working on a new questionnaire to better define physical activity levels.
Data are also being analyzed from the rest of the cohort (160 participants) and over a longer, 3-year follow-up, he said in an interview.
"We are also identifying quantitative MRI and biomechanical metrics that may be more sensitive to disease progression in knee OA. These will help us understand the factors that are related to worsening of knee OA and develop therapies."
The National Institutes of Health–National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the work. Dr. Kumar and his coauthors reported no conflicting interests.
AT OARSI 2014
Major finding: Vigorous activity was associated with a 1.38 times increased risk for progression (95% CI, 1.04-1.83; P = .025).
Data source: Longitudinal analysis of 99 participants in the ongoing CLOC knee OA study.
Disclosures: The National Institutes of Health–National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the work. Dr. Kumar and his coauthors reported no conflicting interests.

Bariatric surgery sliced asthma inhaler use
MADRID – Morbidly obese asthmatics may require less inhaler therapy after bariatric surgery, a retrospective chart review and longitudinal cohort study suggests.
Among patients who used any form of inhaler therapy prior to surgery, one or more classes of inhalers were discontinued in 30% (P less than .05), Dr. Randall Schwartz reported at the world congress of the American College of Chest Physicians.

Specifically, short-acting beta agonist (SABA) use decreased significantly by 13.1% from baseline (64.5% to 51.4%; P less than .0001) and long-acting beta agonist/inhaled corticosteroid (LABA/ICS) combinations by 8.1% (40.2% to 32.1%; P = .0034). Fewer patients were on short- or long-acting muscarinic antagonists (SAMA/LAMA), which declined 1.6% (9.4% to 7.8%; P = .305).
The corresponding number need to treat was 8 patients for SABA, 12 for LABA/ICS combinations, and 7 for SAMA/LAMA.
Prior studies have shown a decrease in asthma severity after gastric surgery but haven’t specifically looked at inhaler usage.
Though there was a 30% reduction among those using inhalers, 10% of patients actually required more inhaler therapy after surgery, said Dr. Schwartz, chief internal medicine resident, Cleveland Clinic Florida, Weston.
"Our supposition is that the overwhelming majority of these patients have obesity-related asthma – neutrophilic mediated inflammation; whereas some of those who ended up having to go up in their inhaler therapy might have had classic atopic eosinophilic-mediated asthma," he explained in an interview.
Unfortunately, only 203 of the 505 patients had formal pulmonary function tests (PFT) and only 9 had fractional exhaled nitric oxide measured. "I think nitric oxide would be a really non-invasive and simple thing we could do to follow-up with these patients because PFTs represent a bit of a challenge in this population because of body mechanics," Dr. Schwartz said. "I would bet we’re going to see a disproportionate amount of elevated phenotypes in those who actually had to increase their inhaler usage and probably not significant eosinophilic inflammation in the majority of patients, particularly those who decreased their inhaler usage."
Of those who started a LABA/ICS for the first time after surgery, 72% had already been on a SAMA/LAMA prior to surgery.
Of those starting a SAMA/LAMA for the first time after surgery, 100% were on a SABA or LABA/ICS prior to surgery.
Overall, there was a 20% reduction in postoperative inhaler use, with a number needed to treat of only seven patients, according to the poster presentation (Chest 2014;145:15A [doi:10.1378/chest.1824454]).
Because of the retrospective nature of the study, it was not possible to determine whether type of gastric surgery or amount of weight loss influenced postoperative inhaler use, he said. Other possible factors could be improved body mechanics and decreased inflammation from less adipose tissue.
The mean change in body mass index was –16.2 kg/m2, which occurred at an average of 19 months after surgery.
The review included 716 patients who underwent gastric bypass surgery or sleeve gastrectomy with an accompanying diagnosis of asthma. A total of 211 patients were excluded because of concomitant or suspected chronic obstructive pulmonary disease.
At baseline, the average BMI was 50.7 kg/m2, average forced expiratory volume in 1 second was 79%, and average FEV1/forced vital capacity was 91%.
Going forward, the investigators reported that they hope to perform follow-up testing in the existing cohort and prospectively study post–gastric bypass inhaler use, including asthma severity, fractional exhaled nitric oxide testing, and a cost-benefit analysis.
"Gastric surgery costs about $20,000 and it can cost $3,000-$6,000 a year depending on whether patients are using one or two inhalers to control their asthma," Dr. Schwartz said. "So over the course of a few years, you make up that difference with asthma alone, not to mention the cardiovascular benefits."
The investigators reported having nothing to disclose.
MADRID – Morbidly obese asthmatics may require less inhaler therapy after bariatric surgery, a retrospective chart review and longitudinal cohort study suggests.
Among patients who used any form of inhaler therapy prior to surgery, one or more classes of inhalers were discontinued in 30% (P less than .05), Dr. Randall Schwartz reported at the world congress of the American College of Chest Physicians.
Specifically, short-acting beta agonist (SABA) use decreased significantly by 13.1% from baseline (64.5% to 51.4%; P less than .0001) and long-acting beta agonist/inhaled corticosteroid (LABA/ICS) combinations by 8.1% (40.2% to 32.1%; P = .0034). Fewer patients were on short- or long-acting muscarinic antagonists (SAMA/LAMA), which declined 1.6% (9.4% to 7.8%; P = .305).
The corresponding number need to treat was 8 patients for SABA, 12 for LABA/ICS combinations, and 7 for SAMA/LAMA.
Prior studies have shown a decrease in asthma severity after gastric surgery but haven’t specifically looked at inhaler usage.
Though there was a 30% reduction among those using inhalers, 10% of patients actually required more inhaler therapy after surgery, said Dr. Schwartz, chief internal medicine resident, Cleveland Clinic Florida, Weston.
"Our supposition is that the overwhelming majority of these patients have obesity-related asthma – neutrophilic mediated inflammation; whereas some of those who ended up having to go up in their inhaler therapy might have had classic atopic eosinophilic-mediated asthma," he explained in an interview.
Unfortunately, only 203 of the 505 patients had formal pulmonary function tests (PFT) and only 9 had fractional exhaled nitric oxide measured. "I think nitric oxide would be a really non-invasive and simple thing we could do to follow-up with these patients because PFTs represent a bit of a challenge in this population because of body mechanics," Dr. Schwartz said. "I would bet we’re going to see a disproportionate amount of elevated phenotypes in those who actually had to increase their inhaler usage and probably not significant eosinophilic inflammation in the majority of patients, particularly those who decreased their inhaler usage."
Of those who started a LABA/ICS for the first time after surgery, 72% had already been on a SAMA/LAMA prior to surgery.
Of those starting a SAMA/LAMA for the first time after surgery, 100% were on a SABA or LABA/ICS prior to surgery.
Overall, there was a 20% reduction in postoperative inhaler use, with a number needed to treat of only seven patients, according to the poster presentation (Chest 2014;145:15A [doi:10.1378/chest.1824454]).
Because of the retrospective nature of the study, it was not possible to determine whether type of gastric surgery or amount of weight loss influenced postoperative inhaler use, he said. Other possible factors could be improved body mechanics and decreased inflammation from less adipose tissue.
The mean change in body mass index was –16.2 kg/m2, which occurred at an average of 19 months after surgery.
The review included 716 patients who underwent gastric bypass surgery or sleeve gastrectomy with an accompanying diagnosis of asthma. A total of 211 patients were excluded because of concomitant or suspected chronic obstructive pulmonary disease.
At baseline, the average BMI was 50.7 kg/m2, average forced expiratory volume in 1 second was 79%, and average FEV1/forced vital capacity was 91%.
Going forward, the investigators reported that they hope to perform follow-up testing in the existing cohort and prospectively study post–gastric bypass inhaler use, including asthma severity, fractional exhaled nitric oxide testing, and a cost-benefit analysis.
"Gastric surgery costs about $20,000 and it can cost $3,000-$6,000 a year depending on whether patients are using one or two inhalers to control their asthma," Dr. Schwartz said. "So over the course of a few years, you make up that difference with asthma alone, not to mention the cardiovascular benefits."
The investigators reported having nothing to disclose.
MADRID – Morbidly obese asthmatics may require less inhaler therapy after bariatric surgery, a retrospective chart review and longitudinal cohort study suggests.
Among patients who used any form of inhaler therapy prior to surgery, one or more classes of inhalers were discontinued in 30% (P less than .05), Dr. Randall Schwartz reported at the world congress of the American College of Chest Physicians.
Specifically, short-acting beta agonist (SABA) use decreased significantly by 13.1% from baseline (64.5% to 51.4%; P less than .0001) and long-acting beta agonist/inhaled corticosteroid (LABA/ICS) combinations by 8.1% (40.2% to 32.1%; P = .0034). Fewer patients were on short- or long-acting muscarinic antagonists (SAMA/LAMA), which declined 1.6% (9.4% to 7.8%; P = .305).
The corresponding number need to treat was 8 patients for SABA, 12 for LABA/ICS combinations, and 7 for SAMA/LAMA.
Prior studies have shown a decrease in asthma severity after gastric surgery but haven’t specifically looked at inhaler usage.
Though there was a 30% reduction among those using inhalers, 10% of patients actually required more inhaler therapy after surgery, said Dr. Schwartz, chief internal medicine resident, Cleveland Clinic Florida, Weston.
"Our supposition is that the overwhelming majority of these patients have obesity-related asthma – neutrophilic mediated inflammation; whereas some of those who ended up having to go up in their inhaler therapy might have had classic atopic eosinophilic-mediated asthma," he explained in an interview.
Unfortunately, only 203 of the 505 patients had formal pulmonary function tests (PFT) and only 9 had fractional exhaled nitric oxide measured. "I think nitric oxide would be a really non-invasive and simple thing we could do to follow-up with these patients because PFTs represent a bit of a challenge in this population because of body mechanics," Dr. Schwartz said. "I would bet we’re going to see a disproportionate amount of elevated phenotypes in those who actually had to increase their inhaler usage and probably not significant eosinophilic inflammation in the majority of patients, particularly those who decreased their inhaler usage."
Of those who started a LABA/ICS for the first time after surgery, 72% had already been on a SAMA/LAMA prior to surgery.
Of those starting a SAMA/LAMA for the first time after surgery, 100% were on a SABA or LABA/ICS prior to surgery.
Overall, there was a 20% reduction in postoperative inhaler use, with a number needed to treat of only seven patients, according to the poster presentation (Chest 2014;145:15A [doi:10.1378/chest.1824454]).
Because of the retrospective nature of the study, it was not possible to determine whether type of gastric surgery or amount of weight loss influenced postoperative inhaler use, he said. Other possible factors could be improved body mechanics and decreased inflammation from less adipose tissue.
The mean change in body mass index was –16.2 kg/m2, which occurred at an average of 19 months after surgery.
The review included 716 patients who underwent gastric bypass surgery or sleeve gastrectomy with an accompanying diagnosis of asthma. A total of 211 patients were excluded because of concomitant or suspected chronic obstructive pulmonary disease.
At baseline, the average BMI was 50.7 kg/m2, average forced expiratory volume in 1 second was 79%, and average FEV1/forced vital capacity was 91%.
Going forward, the investigators reported that they hope to perform follow-up testing in the existing cohort and prospectively study post–gastric bypass inhaler use, including asthma severity, fractional exhaled nitric oxide testing, and a cost-benefit analysis.
"Gastric surgery costs about $20,000 and it can cost $3,000-$6,000 a year depending on whether patients are using one or two inhalers to control their asthma," Dr. Schwartz said. "So over the course of a few years, you make up that difference with asthma alone, not to mention the cardiovascular benefits."
The investigators reported having nothing to disclose.
AT CHEST WORLD CONGRESS 2014
Major finding: Bariatric surgery cut use of SABA by 13.1% (P less than .0001), (LABA/ICS) by 8.1% (P = .0034), and SAMA/LAMA antagonists by 1.6% (P = .305).
Data source: A retrospective chart review and longitudinal cohort study of 505 asthmatics.
Disclosures: The investigators reported having nothing to disclose.

Be sure to keep mesenteric ischemia on your radar in your younger patients
CHICAGO – Early recognition of mesenteric ischemia in young adults and children is essential to prevent bowel loss and other serious consequences associated with this rare condition, Dr. Michael Dalsing said at a vascular surgery symposium.
Mesenteric ischemia is generally seen in the elderly as the result of atherosclerotic and embolic occlusive diseases. Because young adults and children typically don’t have any of the telltale associated comorbidities such as cardiac arrhythmia or coronary artery disease to point physicians in this direction, the diagnosis of mesenteric ischemia is often delayed or misinterpreted as appendicitis, cholecystitis, or intra-abdominal abscess, he said.

Among 26 young adults under age 40 years who presented with acute mesenteric ischemia, only 6 were properly diagnosed preoperatively (Wien. Med. Wochenschr. 2012;162:349-53). The postoperative complication and mortality rates reached 61.5% and 27%, which is typical in this population, despite their otherwise good health, said Dr. Dalsing, director of vascular surgery at Indiana University, Indianapolis.
The hallmarks of acute mesenteric ischemia are standard in both young and old patients and include abdominal pain out of proportion to the physical exam, nausea, vomiting, and/or diarrhea. Acidosis, acute renal failure, and septic shock/sepsis can develop in roughly half of patients with more extensive liver or bowel ischemia or necrosis. The signs and symptoms of chronic ischemia are weight loss, food fear, and postprandial abdominal pain.
"For chronic mesenteric ischemia, what’s the important message? Consider the diagnosis," Dr. Dalsing said. "Do the imaging, find out what you have, and then you can worry about ancillary testing because, in general, these aren’t going to be your typical etiologies. In fact, they’re not standard fare at all."
The broad and atypical list of etiologies to consider in those under age 40 years include congenital aortic anomalies, hypercoagulable states, inflammatory conditions, collagen vascular disorders, and environmental agents such as cocaine use, smoking, or trauma. While MI is often suspected in those using cocaine, the vasoconstrictive effects of the drug can also cause vasospasm of the smaller branches of the mesenteric vessels, leading to nonocclusive mesenteric ischemia, he explained.
Once a diagnosis of chronic mesenteric ischemia is made in a young patient, management consists of fluid resuscitation, broad spectrum antibiotics, bowel rest, and imaging, often with a CT angiogram. The need for additional work-up, including hypercoagulable and inflammatory marker panels, varies based on initial clinical symptoms.
If vascular compromise is identified, the overall management goals should be to remove frankly necrotic bowel, reperfuse ischemic bowel, limit the resection length when possible to prevent short-gut syndrome, and treat the underlying etiology, Dr. Dalsing advised. Anticoagulation is also integral to prevent thrombus propagation.
Just six cases of mesenteric ischemia have been diagnosed at Indiana University in young adults over the last 16 years, with Takayasu’s arteritis the most common etiology, he noted. This includes a 20-year-old woman with a 5-year history of Takayasu’s, who presented with worsening abdominal pain despite remission of her Takayasu’s, as indicated by a normal sedimentation rate.
Repeat CT imaging revealed more than 70% celiac artery stenosis and more than 50% stenosis of the superior mesenteric artery (SMA). A median arcuate ligament division and celiac and SMA bypass graft, both with reverse saphenous vein originating from bilateral iliac arteries, was performed. "She’s had dramatic improvement" in her symptoms and remains on clopidogrel (Plavix) and low-dose steroids, Dr. Dalsing said.

A second patient with Takayasu’s presented with a 4-month history of abdominal pain, a 50-pound weight loss, stenosis of all major mesenteric arteries, and bowel pneumatosis. Despite this, her sedimentation rate was only slightly elevated at 33 mm/hour, and all other coagulation and inflammatory tests were normal. She remains symptom free at 2 years on daily aspirin after undergoing an emergent right common iliac-to-SMA bypass graft with reversed saphenous vein and bowel resection.
In cases in which bypass grafting is necessary, the internal iliac artery is the preferred conduit in children since the saphenous vein is very thin walled and thus, more prone to aneurysmal degeneration, Dr. Dalsing observed. In grown patients, the saphenous vein may be the best conduit in terms of ease of harvest and adequate length for even bifurcated grafts or C-loop alignment.
During postoperative follow-up, special effort should be taken because of the young age of these patients to reduce the detrimental effects of radiation from recurrent CT angiograms, he said. Patients with symptomatic improvement are followed at 1 month postoperatively with a physical exam that includes their weight and a mesenteric duplex to evaluate graft or stent patency. This is repeated every 6 months for 1-2 years, and decreased to yearly visits, if no disease progression is detected. More aggressive imaging with CT angiography is reserved for patients with recurrent symptoms or if duplex ultrasound is insufficient or shows progressive disease, he said at the meeting, sponsored by Northwestern University.
Dr. Dalsing reported having no financial disclosures.
CHICAGO – Early recognition of mesenteric ischemia in young adults and children is essential to prevent bowel loss and other serious consequences associated with this rare condition, Dr. Michael Dalsing said at a vascular surgery symposium.
Mesenteric ischemia is generally seen in the elderly as the result of atherosclerotic and embolic occlusive diseases. Because young adults and children typically don’t have any of the telltale associated comorbidities such as cardiac arrhythmia or coronary artery disease to point physicians in this direction, the diagnosis of mesenteric ischemia is often delayed or misinterpreted as appendicitis, cholecystitis, or intra-abdominal abscess, he said.
Among 26 young adults under age 40 years who presented with acute mesenteric ischemia, only 6 were properly diagnosed preoperatively (Wien. Med. Wochenschr. 2012;162:349-53). The postoperative complication and mortality rates reached 61.5% and 27%, which is typical in this population, despite their otherwise good health, said Dr. Dalsing, director of vascular surgery at Indiana University, Indianapolis.
The hallmarks of acute mesenteric ischemia are standard in both young and old patients and include abdominal pain out of proportion to the physical exam, nausea, vomiting, and/or diarrhea. Acidosis, acute renal failure, and septic shock/sepsis can develop in roughly half of patients with more extensive liver or bowel ischemia or necrosis. The signs and symptoms of chronic ischemia are weight loss, food fear, and postprandial abdominal pain.
"For chronic mesenteric ischemia, what’s the important message? Consider the diagnosis," Dr. Dalsing said. "Do the imaging, find out what you have, and then you can worry about ancillary testing because, in general, these aren’t going to be your typical etiologies. In fact, they’re not standard fare at all."
The broad and atypical list of etiologies to consider in those under age 40 years include congenital aortic anomalies, hypercoagulable states, inflammatory conditions, collagen vascular disorders, and environmental agents such as cocaine use, smoking, or trauma. While MI is often suspected in those using cocaine, the vasoconstrictive effects of the drug can also cause vasospasm of the smaller branches of the mesenteric vessels, leading to nonocclusive mesenteric ischemia, he explained.
Once a diagnosis of chronic mesenteric ischemia is made in a young patient, management consists of fluid resuscitation, broad spectrum antibiotics, bowel rest, and imaging, often with a CT angiogram. The need for additional work-up, including hypercoagulable and inflammatory marker panels, varies based on initial clinical symptoms.
If vascular compromise is identified, the overall management goals should be to remove frankly necrotic bowel, reperfuse ischemic bowel, limit the resection length when possible to prevent short-gut syndrome, and treat the underlying etiology, Dr. Dalsing advised. Anticoagulation is also integral to prevent thrombus propagation.
Just six cases of mesenteric ischemia have been diagnosed at Indiana University in young adults over the last 16 years, with Takayasu’s arteritis the most common etiology, he noted. This includes a 20-year-old woman with a 5-year history of Takayasu’s, who presented with worsening abdominal pain despite remission of her Takayasu’s, as indicated by a normal sedimentation rate.
Repeat CT imaging revealed more than 70% celiac artery stenosis and more than 50% stenosis of the superior mesenteric artery (SMA). A median arcuate ligament division and celiac and SMA bypass graft, both with reverse saphenous vein originating from bilateral iliac arteries, was performed. "She’s had dramatic improvement" in her symptoms and remains on clopidogrel (Plavix) and low-dose steroids, Dr. Dalsing said.
A second patient with Takayasu’s presented with a 4-month history of abdominal pain, a 50-pound weight loss, stenosis of all major mesenteric arteries, and bowel pneumatosis. Despite this, her sedimentation rate was only slightly elevated at 33 mm/hour, and all other coagulation and inflammatory tests were normal. She remains symptom free at 2 years on daily aspirin after undergoing an emergent right common iliac-to-SMA bypass graft with reversed saphenous vein and bowel resection.
In cases in which bypass grafting is necessary, the internal iliac artery is the preferred conduit in children since the saphenous vein is very thin walled and thus, more prone to aneurysmal degeneration, Dr. Dalsing observed. In grown patients, the saphenous vein may be the best conduit in terms of ease of harvest and adequate length for even bifurcated grafts or C-loop alignment.
During postoperative follow-up, special effort should be taken because of the young age of these patients to reduce the detrimental effects of radiation from recurrent CT angiograms, he said. Patients with symptomatic improvement are followed at 1 month postoperatively with a physical exam that includes their weight and a mesenteric duplex to evaluate graft or stent patency. This is repeated every 6 months for 1-2 years, and decreased to yearly visits, if no disease progression is detected. More aggressive imaging with CT angiography is reserved for patients with recurrent symptoms or if duplex ultrasound is insufficient or shows progressive disease, he said at the meeting, sponsored by Northwestern University.
Dr. Dalsing reported having no financial disclosures.
CHICAGO – Early recognition of mesenteric ischemia in young adults and children is essential to prevent bowel loss and other serious consequences associated with this rare condition, Dr. Michael Dalsing said at a vascular surgery symposium.
Mesenteric ischemia is generally seen in the elderly as the result of atherosclerotic and embolic occlusive diseases. Because young adults and children typically don’t have any of the telltale associated comorbidities such as cardiac arrhythmia or coronary artery disease to point physicians in this direction, the diagnosis of mesenteric ischemia is often delayed or misinterpreted as appendicitis, cholecystitis, or intra-abdominal abscess, he said.
Among 26 young adults under age 40 years who presented with acute mesenteric ischemia, only 6 were properly diagnosed preoperatively (Wien. Med. Wochenschr. 2012;162:349-53). The postoperative complication and mortality rates reached 61.5% and 27%, which is typical in this population, despite their otherwise good health, said Dr. Dalsing, director of vascular surgery at Indiana University, Indianapolis.
The hallmarks of acute mesenteric ischemia are standard in both young and old patients and include abdominal pain out of proportion to the physical exam, nausea, vomiting, and/or diarrhea. Acidosis, acute renal failure, and septic shock/sepsis can develop in roughly half of patients with more extensive liver or bowel ischemia or necrosis. The signs and symptoms of chronic ischemia are weight loss, food fear, and postprandial abdominal pain.
"For chronic mesenteric ischemia, what’s the important message? Consider the diagnosis," Dr. Dalsing said. "Do the imaging, find out what you have, and then you can worry about ancillary testing because, in general, these aren’t going to be your typical etiologies. In fact, they’re not standard fare at all."
The broad and atypical list of etiologies to consider in those under age 40 years include congenital aortic anomalies, hypercoagulable states, inflammatory conditions, collagen vascular disorders, and environmental agents such as cocaine use, smoking, or trauma. While MI is often suspected in those using cocaine, the vasoconstrictive effects of the drug can also cause vasospasm of the smaller branches of the mesenteric vessels, leading to nonocclusive mesenteric ischemia, he explained.
Once a diagnosis of chronic mesenteric ischemia is made in a young patient, management consists of fluid resuscitation, broad spectrum antibiotics, bowel rest, and imaging, often with a CT angiogram. The need for additional work-up, including hypercoagulable and inflammatory marker panels, varies based on initial clinical symptoms.
If vascular compromise is identified, the overall management goals should be to remove frankly necrotic bowel, reperfuse ischemic bowel, limit the resection length when possible to prevent short-gut syndrome, and treat the underlying etiology, Dr. Dalsing advised. Anticoagulation is also integral to prevent thrombus propagation.
Just six cases of mesenteric ischemia have been diagnosed at Indiana University in young adults over the last 16 years, with Takayasu’s arteritis the most common etiology, he noted. This includes a 20-year-old woman with a 5-year history of Takayasu’s, who presented with worsening abdominal pain despite remission of her Takayasu’s, as indicated by a normal sedimentation rate.
Repeat CT imaging revealed more than 70% celiac artery stenosis and more than 50% stenosis of the superior mesenteric artery (SMA). A median arcuate ligament division and celiac and SMA bypass graft, both with reverse saphenous vein originating from bilateral iliac arteries, was performed. "She’s had dramatic improvement" in her symptoms and remains on clopidogrel (Plavix) and low-dose steroids, Dr. Dalsing said.
A second patient with Takayasu’s presented with a 4-month history of abdominal pain, a 50-pound weight loss, stenosis of all major mesenteric arteries, and bowel pneumatosis. Despite this, her sedimentation rate was only slightly elevated at 33 mm/hour, and all other coagulation and inflammatory tests were normal. She remains symptom free at 2 years on daily aspirin after undergoing an emergent right common iliac-to-SMA bypass graft with reversed saphenous vein and bowel resection.
In cases in which bypass grafting is necessary, the internal iliac artery is the preferred conduit in children since the saphenous vein is very thin walled and thus, more prone to aneurysmal degeneration, Dr. Dalsing observed. In grown patients, the saphenous vein may be the best conduit in terms of ease of harvest and adequate length for even bifurcated grafts or C-loop alignment.
During postoperative follow-up, special effort should be taken because of the young age of these patients to reduce the detrimental effects of radiation from recurrent CT angiograms, he said. Patients with symptomatic improvement are followed at 1 month postoperatively with a physical exam that includes their weight and a mesenteric duplex to evaluate graft or stent patency. This is repeated every 6 months for 1-2 years, and decreased to yearly visits, if no disease progression is detected. More aggressive imaging with CT angiography is reserved for patients with recurrent symptoms or if duplex ultrasound is insufficient or shows progressive disease, he said at the meeting, sponsored by Northwestern University.
Dr. Dalsing reported having no financial disclosures.

Recent knee injuries spark rapid cascade to joint failure
PARIS – Recent knee injuries are strongly associated with accelerated knee osteoarthritis, according to an analysis from the prospective, multicenter Osteoarthritis Initiative.
"Certain injuries may initiate or coincide with an accelerated cascade towards joint failure in as little as 12 months," Jeffrey Driban, Ph.D., said at the World Congress on Osteoarthritis. "In fact, 76% of individuals with an injury and accelerated knee osteoarthritis experienced their injury in the 12 months prior to the study outcome."
The study defined accelerated knee OA as progression from a Kellgren-Lawrence grade 0 or 1 on baseline bilateral radiographs to end-stage KL grade 3 or 4 within 48 months.
Although knee OA typically has been a slowly progressive disorder, 5%-17% of patients now experience accelerated forms of OA.
"If we can better characterize this phenomenon and its potential risk factors, we can provide more insights into the nature of progression in hopes of identifying an at-risk subset," said Dr. Driban of the division of rheumatology at Tufts Medical Center, Boston.
The study by Dr. Driban and his colleagues was published in Arthritis Care & Research (2014 April 29 [doi:10.1002/acr.22359]).
A total of 1,930 participants in the Osteoarthritis Initiative, all with a KL grade of 0 or 1 on baseline bilateral radiographs, were asked at baseline and at each annual visit whether they had ever been "injured enough to limit ability to walk for at least 2 days."
On follow-up, 1,325 had no knee OA, 54 had accelerated knee OA, and 187 had typical knee OA, defined as at least one knee increased in radiographic scoring within 48 months (excluding accelerated OA).
After exclusion of 12 patients with missing data, 30% of the accelerated OA group, 28% in the typical OA group, and 35% in the no OA group had a history of knee injury before baseline. A new knee injury was reported by 32%, 13%, and 11%, respectively, with data missing from 59 persons.
In univariate analyses, participants with accelerated knee OA were significantly older than were those with typical OA or no OA (61.8 years vs. 58 years vs. 59.2 years; P = .023) and had a greater body mass index (28.9 kg/m2 vs. 27.9 kg/m2 vs. 27.1 kg/m2; P = .002), Dr. Driban said.
In multinomial logistic regression analyses that adjusted for age, sex, BMI, presence of static knee malalignment, and systolic blood pressure, there was no association between prior knee injury and accelerated OA (odds ratio, 0.84) or typical OA (OR, 0.76).
However, when the investigators looked further, participants with accelerated OA were almost 3.5 times more likely to report a recent knee injury during the observation period (OR, 3.37; 95% confidence interval, 1.82-6.25) than were those with typical OA (OR, 0.99) or no OA (reference), he said.
Moreover, if a participant experienced a knee injury 1 year before the study outcome, the risk of accelerated OA increased ninefold (OR, 9.22; CI, 4.50-18.90) versus threefold for typical OA (OR, 3.04; CI, 1.66-5.58).
Despite the focus on injuries leading to accelerated OA, the analyses can’t rule out that accelerated OA may also cause an injury or that there could be a "vicious cycle," in which an injury can cause accelerated OA, associated with joint space loss, increased symptoms, and increased risk for subsequent injury, Dr. Driban said.
This line of thought helps explain why prior injury was not associated with accelerated knee OA, but recent injury was. As patients were free of radiographic OA at baseline, those with a history of a prior injury that could cause accelerated knee OA would already have been eliminated from the study, he explained in an interview.
Secondly, if accelerated knee OA can increase the risk of injury, knee injuries from years ago would not be related to accelerated knee OA because the disorder did not exist at the time of the injury.
Finally, there also could be a recall bias, as patients often have a hard time recalling injuries that may have happened years ago.
Despite the limitations of self-reported injuries and insufficient data regarding the type, severity, status of the meniscus, mechanism, or subsequent treatment of the knee injury, the findings represent an important "starting point" in understanding the association between injuries and accelerated osteoarthritis, Dr. Driban said.
"We need to monitor older adults who report an injury, as this may initiate accelerated OA or indicate an individual experiencing accelerated OA, and we need to determine which injuries may be related to accelerated osteoarthritis," he said at the meeting, sponsored by the Osteoarthritis Research Society International.
During the discussion following the formal presentation, Dr. David Felson, professor of medicine and epidemiology at Boston University, said, "I think what you are saying is exactly right," but suggested that the investigators exclude patients with spontaneous osteonecrosis of the knee and osteochondritis dissecans, as both conditions are more common than anticipated and can drive very rapid development of OA. Conversely, inclusion of patients with osteophyte-only knee OA would increase the number likely identified with accelerated OA, he said.
Dr. Driban reported no conflicting interests.
PARIS – Recent knee injuries are strongly associated with accelerated knee osteoarthritis, according to an analysis from the prospective, multicenter Osteoarthritis Initiative.
"Certain injuries may initiate or coincide with an accelerated cascade towards joint failure in as little as 12 months," Jeffrey Driban, Ph.D., said at the World Congress on Osteoarthritis. "In fact, 76% of individuals with an injury and accelerated knee osteoarthritis experienced their injury in the 12 months prior to the study outcome."
The study defined accelerated knee OA as progression from a Kellgren-Lawrence grade 0 or 1 on baseline bilateral radiographs to end-stage KL grade 3 or 4 within 48 months.
Although knee OA typically has been a slowly progressive disorder, 5%-17% of patients now experience accelerated forms of OA.
"If we can better characterize this phenomenon and its potential risk factors, we can provide more insights into the nature of progression in hopes of identifying an at-risk subset," said Dr. Driban of the division of rheumatology at Tufts Medical Center, Boston.
The study by Dr. Driban and his colleagues was published in Arthritis Care & Research (2014 April 29 [doi:10.1002/acr.22359]).
A total of 1,930 participants in the Osteoarthritis Initiative, all with a KL grade of 0 or 1 on baseline bilateral radiographs, were asked at baseline and at each annual visit whether they had ever been "injured enough to limit ability to walk for at least 2 days."
On follow-up, 1,325 had no knee OA, 54 had accelerated knee OA, and 187 had typical knee OA, defined as at least one knee increased in radiographic scoring within 48 months (excluding accelerated OA).
After exclusion of 12 patients with missing data, 30% of the accelerated OA group, 28% in the typical OA group, and 35% in the no OA group had a history of knee injury before baseline. A new knee injury was reported by 32%, 13%, and 11%, respectively, with data missing from 59 persons.
In univariate analyses, participants with accelerated knee OA were significantly older than were those with typical OA or no OA (61.8 years vs. 58 years vs. 59.2 years; P = .023) and had a greater body mass index (28.9 kg/m2 vs. 27.9 kg/m2 vs. 27.1 kg/m2; P = .002), Dr. Driban said.
In multinomial logistic regression analyses that adjusted for age, sex, BMI, presence of static knee malalignment, and systolic blood pressure, there was no association between prior knee injury and accelerated OA (odds ratio, 0.84) or typical OA (OR, 0.76).
However, when the investigators looked further, participants with accelerated OA were almost 3.5 times more likely to report a recent knee injury during the observation period (OR, 3.37; 95% confidence interval, 1.82-6.25) than were those with typical OA (OR, 0.99) or no OA (reference), he said.
Moreover, if a participant experienced a knee injury 1 year before the study outcome, the risk of accelerated OA increased ninefold (OR, 9.22; CI, 4.50-18.90) versus threefold for typical OA (OR, 3.04; CI, 1.66-5.58).
Despite the focus on injuries leading to accelerated OA, the analyses can’t rule out that accelerated OA may also cause an injury or that there could be a "vicious cycle," in which an injury can cause accelerated OA, associated with joint space loss, increased symptoms, and increased risk for subsequent injury, Dr. Driban said.
This line of thought helps explain why prior injury was not associated with accelerated knee OA, but recent injury was. As patients were free of radiographic OA at baseline, those with a history of a prior injury that could cause accelerated knee OA would already have been eliminated from the study, he explained in an interview.
Secondly, if accelerated knee OA can increase the risk of injury, knee injuries from years ago would not be related to accelerated knee OA because the disorder did not exist at the time of the injury.
Finally, there also could be a recall bias, as patients often have a hard time recalling injuries that may have happened years ago.
Despite the limitations of self-reported injuries and insufficient data regarding the type, severity, status of the meniscus, mechanism, or subsequent treatment of the knee injury, the findings represent an important "starting point" in understanding the association between injuries and accelerated osteoarthritis, Dr. Driban said.
"We need to monitor older adults who report an injury, as this may initiate accelerated OA or indicate an individual experiencing accelerated OA, and we need to determine which injuries may be related to accelerated osteoarthritis," he said at the meeting, sponsored by the Osteoarthritis Research Society International.
During the discussion following the formal presentation, Dr. David Felson, professor of medicine and epidemiology at Boston University, said, "I think what you are saying is exactly right," but suggested that the investigators exclude patients with spontaneous osteonecrosis of the knee and osteochondritis dissecans, as both conditions are more common than anticipated and can drive very rapid development of OA. Conversely, inclusion of patients with osteophyte-only knee OA would increase the number likely identified with accelerated OA, he said.
Dr. Driban reported no conflicting interests.
PARIS – Recent knee injuries are strongly associated with accelerated knee osteoarthritis, according to an analysis from the prospective, multicenter Osteoarthritis Initiative.
"Certain injuries may initiate or coincide with an accelerated cascade towards joint failure in as little as 12 months," Jeffrey Driban, Ph.D., said at the World Congress on Osteoarthritis. "In fact, 76% of individuals with an injury and accelerated knee osteoarthritis experienced their injury in the 12 months prior to the study outcome."
The study defined accelerated knee OA as progression from a Kellgren-Lawrence grade 0 or 1 on baseline bilateral radiographs to end-stage KL grade 3 or 4 within 48 months.
Although knee OA typically has been a slowly progressive disorder, 5%-17% of patients now experience accelerated forms of OA.
"If we can better characterize this phenomenon and its potential risk factors, we can provide more insights into the nature of progression in hopes of identifying an at-risk subset," said Dr. Driban of the division of rheumatology at Tufts Medical Center, Boston.
The study by Dr. Driban and his colleagues was published in Arthritis Care & Research (2014 April 29 [doi:10.1002/acr.22359]).
A total of 1,930 participants in the Osteoarthritis Initiative, all with a KL grade of 0 or 1 on baseline bilateral radiographs, were asked at baseline and at each annual visit whether they had ever been "injured enough to limit ability to walk for at least 2 days."
On follow-up, 1,325 had no knee OA, 54 had accelerated knee OA, and 187 had typical knee OA, defined as at least one knee increased in radiographic scoring within 48 months (excluding accelerated OA).
After exclusion of 12 patients with missing data, 30% of the accelerated OA group, 28% in the typical OA group, and 35% in the no OA group had a history of knee injury before baseline. A new knee injury was reported by 32%, 13%, and 11%, respectively, with data missing from 59 persons.
In univariate analyses, participants with accelerated knee OA were significantly older than were those with typical OA or no OA (61.8 years vs. 58 years vs. 59.2 years; P = .023) and had a greater body mass index (28.9 kg/m2 vs. 27.9 kg/m2 vs. 27.1 kg/m2; P = .002), Dr. Driban said.
In multinomial logistic regression analyses that adjusted for age, sex, BMI, presence of static knee malalignment, and systolic blood pressure, there was no association between prior knee injury and accelerated OA (odds ratio, 0.84) or typical OA (OR, 0.76).
However, when the investigators looked further, participants with accelerated OA were almost 3.5 times more likely to report a recent knee injury during the observation period (OR, 3.37; 95% confidence interval, 1.82-6.25) than were those with typical OA (OR, 0.99) or no OA (reference), he said.
Moreover, if a participant experienced a knee injury 1 year before the study outcome, the risk of accelerated OA increased ninefold (OR, 9.22; CI, 4.50-18.90) versus threefold for typical OA (OR, 3.04; CI, 1.66-5.58).
Despite the focus on injuries leading to accelerated OA, the analyses can’t rule out that accelerated OA may also cause an injury or that there could be a "vicious cycle," in which an injury can cause accelerated OA, associated with joint space loss, increased symptoms, and increased risk for subsequent injury, Dr. Driban said.
This line of thought helps explain why prior injury was not associated with accelerated knee OA, but recent injury was. As patients were free of radiographic OA at baseline, those with a history of a prior injury that could cause accelerated knee OA would already have been eliminated from the study, he explained in an interview.
Secondly, if accelerated knee OA can increase the risk of injury, knee injuries from years ago would not be related to accelerated knee OA because the disorder did not exist at the time of the injury.
Finally, there also could be a recall bias, as patients often have a hard time recalling injuries that may have happened years ago.
Despite the limitations of self-reported injuries and insufficient data regarding the type, severity, status of the meniscus, mechanism, or subsequent treatment of the knee injury, the findings represent an important "starting point" in understanding the association between injuries and accelerated osteoarthritis, Dr. Driban said.
"We need to monitor older adults who report an injury, as this may initiate accelerated OA or indicate an individual experiencing accelerated OA, and we need to determine which injuries may be related to accelerated osteoarthritis," he said at the meeting, sponsored by the Osteoarthritis Research Society International.
During the discussion following the formal presentation, Dr. David Felson, professor of medicine and epidemiology at Boston University, said, "I think what you are saying is exactly right," but suggested that the investigators exclude patients with spontaneous osteonecrosis of the knee and osteochondritis dissecans, as both conditions are more common than anticipated and can drive very rapid development of OA. Conversely, inclusion of patients with osteophyte-only knee OA would increase the number likely identified with accelerated OA, he said.
Dr. Driban reported no conflicting interests.
AT OARSI 2014
Key clinical point: Older adults who report a knee injury should be monitored for accelerated knee OA.
Major finding: Knee injury within 1 year of the study outcome increased the odds of accelerated OA ninefold (OR, 9.22; CI, 4.50-18.90).
Data source: Person-based analyses of 1,930 participants in the Osteoarthritis Initiative.
Disclosures: Dr. Driban reported no conflicting interests.
Childhood sports knee injuries carry heavy burden
PARIS – Knee trauma from a childhood sports injury can have serious consequences in young adults, judging from preliminary results from a historical cohort.
When assessed 3-10 years after the sports injury, at an average age of 22 years, young adults appear to be at higher risk of abnormalities visible on MRI that are consistent with future arthropathy and have poorer knee-related quality of life and more knee symptoms.
They are at higher risk of having structural asymmetry of the vastus medialis muscle and being categorized as being overweight or obese.
There also appears to be some trends for increased percent body fat and reduced participation in physical activity, Jackie L. Whittaker, Ph.D., said at the World Congress on Osteoarthritis.
She stressed that these are preliminary findings and that the group hopes to quadruple the size of the cohort this year in order to better understand the relationships they’ve identified.
"With that being said, if we are seeing what we think we’re seeing, there may be some clinical, structural, physiologic, and behavioral markers that can be used to identify individuals who are at risk and target them with secondary prevention strategies at an earlier age," said Dr. Whittaker, a postdoctoral fellow and physiotherapist, University of Calgary Sport Injury Prevention Research Centre, Alberta, Canada.
The historical cohort study involved 25 patients recruited from previous sports injury epidemiology studies who had an intra-articular knee injury in ice hockey (male and female), soccer, basketball, or other sports that required medical attention and time off play, and 25 uninjured controls matched on age, sex, and sport. The median age at injury was 15 years (range 9-18 years). Eight patients in the injured group had contralateral knee surgeries, in addition to surgery on the primary knee. The median age in both groups was 22 years.
Using the Knee injury and Osteoarthritis Outcome Scores (KOOS) outcome, injured participants scored significantly lower, indicating worse function, on all five, 100-point subscales: pain (mean 93 vs. 97), symptoms (mean 82.9 vs. 92.4), activities of daily living (mean 96.3 vs. 99.3), sport/recreation (mean 90.6 vs. 97.4), and knee-related quality of life (mean 89.7 vs. 97.7), Dr. Whittaker said.
Further, in a subsample of 10 matched pairs, injured participants were three times more likely to have an MRI Osteoarthritis Score (MOAKS) of one than were matched controls, according to the study, led by her colleague Carolyn Emery, Ph.D.
Although there was no difference in quadriceps strength between groups, injured participants were 3.8 times more likely to have a difference in the cross-sectional area of the vastus medialis muscle greater than 15%.
"We think that this may be clinically relevant, as there has been some recent prospective work (Arthritis Rheum. 2012;64:3917-25) that has shown a temporal relationship between a decrease in size of the vastus medialis muscle and progression or loss of tibial joint cartilage," she said.
Within 3-10 years after their knee trauma, injured participants have a significantly higher mean body mass index (BMI) than do uninjured participants (25.4 kg/m2 vs. 23.2 kg/m2) and a trend for more body fat (20.8% vs. 18.7%).
Not surprisingly, these troubling findings were coupled with a trend for injured participants to spend less time each week participating in moderate to strenuous activity (97.8 minutes vs. 101.4 minutes) and also fewer participated in sports in the previous year (4% vs. 16%).
"If we dichotomize BMI, what we see is that those individuals in the injured group are two times more likely to have a BMI that is [classified as] overweight or obese," Dr. Whittaker said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, the suggestion was made to stratify future data by age at injury, as puberty has an influence on response to injury.
Dr. Whittaker reported funding from the Alberta Children’s Hospital Foundation, Alberta Innovates Health Solutions Alberta Team Osteoarthritis, Canadian Institutes of Health Research, and the University of Calgary Sport Injury Prevention Research Centre.
PARIS – Knee trauma from a childhood sports injury can have serious consequences in young adults, judging from preliminary results from a historical cohort.
When assessed 3-10 years after the sports injury, at an average age of 22 years, young adults appear to be at higher risk of abnormalities visible on MRI that are consistent with future arthropathy and have poorer knee-related quality of life and more knee symptoms.
They are at higher risk of having structural asymmetry of the vastus medialis muscle and being categorized as being overweight or obese.
There also appears to be some trends for increased percent body fat and reduced participation in physical activity, Jackie L. Whittaker, Ph.D., said at the World Congress on Osteoarthritis.
She stressed that these are preliminary findings and that the group hopes to quadruple the size of the cohort this year in order to better understand the relationships they’ve identified.
"With that being said, if we are seeing what we think we’re seeing, there may be some clinical, structural, physiologic, and behavioral markers that can be used to identify individuals who are at risk and target them with secondary prevention strategies at an earlier age," said Dr. Whittaker, a postdoctoral fellow and physiotherapist, University of Calgary Sport Injury Prevention Research Centre, Alberta, Canada.
The historical cohort study involved 25 patients recruited from previous sports injury epidemiology studies who had an intra-articular knee injury in ice hockey (male and female), soccer, basketball, or other sports that required medical attention and time off play, and 25 uninjured controls matched on age, sex, and sport. The median age at injury was 15 years (range 9-18 years). Eight patients in the injured group had contralateral knee surgeries, in addition to surgery on the primary knee. The median age in both groups was 22 years.
Using the Knee injury and Osteoarthritis Outcome Scores (KOOS) outcome, injured participants scored significantly lower, indicating worse function, on all five, 100-point subscales: pain (mean 93 vs. 97), symptoms (mean 82.9 vs. 92.4), activities of daily living (mean 96.3 vs. 99.3), sport/recreation (mean 90.6 vs. 97.4), and knee-related quality of life (mean 89.7 vs. 97.7), Dr. Whittaker said.
Further, in a subsample of 10 matched pairs, injured participants were three times more likely to have an MRI Osteoarthritis Score (MOAKS) of one than were matched controls, according to the study, led by her colleague Carolyn Emery, Ph.D.
Although there was no difference in quadriceps strength between groups, injured participants were 3.8 times more likely to have a difference in the cross-sectional area of the vastus medialis muscle greater than 15%.
"We think that this may be clinically relevant, as there has been some recent prospective work (Arthritis Rheum. 2012;64:3917-25) that has shown a temporal relationship between a decrease in size of the vastus medialis muscle and progression or loss of tibial joint cartilage," she said.
Within 3-10 years after their knee trauma, injured participants have a significantly higher mean body mass index (BMI) than do uninjured participants (25.4 kg/m2 vs. 23.2 kg/m2) and a trend for more body fat (20.8% vs. 18.7%).
Not surprisingly, these troubling findings were coupled with a trend for injured participants to spend less time each week participating in moderate to strenuous activity (97.8 minutes vs. 101.4 minutes) and also fewer participated in sports in the previous year (4% vs. 16%).
"If we dichotomize BMI, what we see is that those individuals in the injured group are two times more likely to have a BMI that is [classified as] overweight or obese," Dr. Whittaker said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, the suggestion was made to stratify future data by age at injury, as puberty has an influence on response to injury.
Dr. Whittaker reported funding from the Alberta Children’s Hospital Foundation, Alberta Innovates Health Solutions Alberta Team Osteoarthritis, Canadian Institutes of Health Research, and the University of Calgary Sport Injury Prevention Research Centre.
PARIS – Knee trauma from a childhood sports injury can have serious consequences in young adults, judging from preliminary results from a historical cohort.
When assessed 3-10 years after the sports injury, at an average age of 22 years, young adults appear to be at higher risk of abnormalities visible on MRI that are consistent with future arthropathy and have poorer knee-related quality of life and more knee symptoms.
They are at higher risk of having structural asymmetry of the vastus medialis muscle and being categorized as being overweight or obese.
There also appears to be some trends for increased percent body fat and reduced participation in physical activity, Jackie L. Whittaker, Ph.D., said at the World Congress on Osteoarthritis.
She stressed that these are preliminary findings and that the group hopes to quadruple the size of the cohort this year in order to better understand the relationships they’ve identified.
"With that being said, if we are seeing what we think we’re seeing, there may be some clinical, structural, physiologic, and behavioral markers that can be used to identify individuals who are at risk and target them with secondary prevention strategies at an earlier age," said Dr. Whittaker, a postdoctoral fellow and physiotherapist, University of Calgary Sport Injury Prevention Research Centre, Alberta, Canada.
The historical cohort study involved 25 patients recruited from previous sports injury epidemiology studies who had an intra-articular knee injury in ice hockey (male and female), soccer, basketball, or other sports that required medical attention and time off play, and 25 uninjured controls matched on age, sex, and sport. The median age at injury was 15 years (range 9-18 years). Eight patients in the injured group had contralateral knee surgeries, in addition to surgery on the primary knee. The median age in both groups was 22 years.
Using the Knee injury and Osteoarthritis Outcome Scores (KOOS) outcome, injured participants scored significantly lower, indicating worse function, on all five, 100-point subscales: pain (mean 93 vs. 97), symptoms (mean 82.9 vs. 92.4), activities of daily living (mean 96.3 vs. 99.3), sport/recreation (mean 90.6 vs. 97.4), and knee-related quality of life (mean 89.7 vs. 97.7), Dr. Whittaker said.
Further, in a subsample of 10 matched pairs, injured participants were three times more likely to have an MRI Osteoarthritis Score (MOAKS) of one than were matched controls, according to the study, led by her colleague Carolyn Emery, Ph.D.
Although there was no difference in quadriceps strength between groups, injured participants were 3.8 times more likely to have a difference in the cross-sectional area of the vastus medialis muscle greater than 15%.
"We think that this may be clinically relevant, as there has been some recent prospective work (Arthritis Rheum. 2012;64:3917-25) that has shown a temporal relationship between a decrease in size of the vastus medialis muscle and progression or loss of tibial joint cartilage," she said.
Within 3-10 years after their knee trauma, injured participants have a significantly higher mean body mass index (BMI) than do uninjured participants (25.4 kg/m2 vs. 23.2 kg/m2) and a trend for more body fat (20.8% vs. 18.7%).
Not surprisingly, these troubling findings were coupled with a trend for injured participants to spend less time each week participating in moderate to strenuous activity (97.8 minutes vs. 101.4 minutes) and also fewer participated in sports in the previous year (4% vs. 16%).
"If we dichotomize BMI, what we see is that those individuals in the injured group are two times more likely to have a BMI that is [classified as] overweight or obese," Dr. Whittaker said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, the suggestion was made to stratify future data by age at injury, as puberty has an influence on response to injury.
Dr. Whittaker reported funding from the Alberta Children’s Hospital Foundation, Alberta Innovates Health Solutions Alberta Team Osteoarthritis, Canadian Institutes of Health Research, and the University of Calgary Sport Injury Prevention Research Centre.
AT OARSI 2014
Major finding: Preliminary evidence suggests that young adults with history of a sports-related knee injury differ in symptomatology, physiology, knee muscle morphology, and joint structure from uninjured controls 3-10 years post injury.
Data source: Historical cohort of 25 sport-related knee injured and 25 uninjured young adults.
Disclosures: Dr. Whittaker reported funding from the Alberta Children’s Hospital Foundation, Alberta Innovates Health Solutions Alberta Team Osteoarthritis, Canadian Institutes of Health Research, and the University of Calgary Sport Injury Prevention Research Centre.
Polyp, adenoma detection rises with Endocuff device
CHICAGO – German investigators reported on their experience using the disposable Endocuff device in a prospective, randomized two-center trial involving 498 patients undergoing colonoscopy. The flexible Endocuff attaches to the tip of the colonoscope and features two rows of small flexible, hinged wings, Dr. Tobias Meister said at the annual Digestive Disease Week.
The polyp detection rate was 56% for Endocuff-assisted colonoscopy and 42% for standard colonoscopy (P = .001), reported Dr. Meister of Helios Albert-Schweitzer-Klinik, Northeim, Germany.

Compared with standard colonoscopy, Endocuff-assisted colonoscopy detected significantly more polyps per patient (mean 1.58 vs. 0.97; P less than .0001), more sigmoid polyps less than 1 cm in size (120 vs. 42; P = .001), and more cecum polyps less than 1 cm (37 vs. 14; P = .002).
The adenoma detection rate was 36% with Endocuff colonoscopy and 28% with standard colonoscopy patients (P = .043).
The number of carcinomas detected was similar in the two groups (2 vs. 3; P = .68), but the Endocuff outperformed standard colonoscopy for low-grade adenomas (208 vs. 112; P = .008), mean adenomas per patient (0.91 vs. 0.49; P =.011), and hyperplastic polyps (33% vs. 21%; P = .003), Dr. Meister said.
Withdrawal time was not measured, although there was a slight increase in total procedure time in the Endocuff group (23.11 minutes vs. 21.51 minutes; P = .04).
Most patients (96%) had no complications, but minor mucosal lacerations were more common with the Endocuff (9 vs. 2; P = .028). The cuff was lost during six colonoscopies, but endoscopically retrieved.
"The Endocuff is feasible, safe, reliable, and easy to handle, and might have the potential to reduce the incidence of colorectal cancer," Dr. Meister concluded. The Endocuff is available in Europe and the United States; it was approved by the Food and Drug Administration in 2012.
The study was supported by Helios Albert-Schweitzer-Klinik. Dr. Meister reported no conflicting interests.
CHICAGO – German investigators reported on their experience using the disposable Endocuff device in a prospective, randomized two-center trial involving 498 patients undergoing colonoscopy. The flexible Endocuff attaches to the tip of the colonoscope and features two rows of small flexible, hinged wings, Dr. Tobias Meister said at the annual Digestive Disease Week.
The polyp detection rate was 56% for Endocuff-assisted colonoscopy and 42% for standard colonoscopy (P = .001), reported Dr. Meister of Helios Albert-Schweitzer-Klinik, Northeim, Germany.
Compared with standard colonoscopy, Endocuff-assisted colonoscopy detected significantly more polyps per patient (mean 1.58 vs. 0.97; P less than .0001), more sigmoid polyps less than 1 cm in size (120 vs. 42; P = .001), and more cecum polyps less than 1 cm (37 vs. 14; P = .002).
The adenoma detection rate was 36% with Endocuff colonoscopy and 28% with standard colonoscopy patients (P = .043).
The number of carcinomas detected was similar in the two groups (2 vs. 3; P = .68), but the Endocuff outperformed standard colonoscopy for low-grade adenomas (208 vs. 112; P = .008), mean adenomas per patient (0.91 vs. 0.49; P =.011), and hyperplastic polyps (33% vs. 21%; P = .003), Dr. Meister said.
Withdrawal time was not measured, although there was a slight increase in total procedure time in the Endocuff group (23.11 minutes vs. 21.51 minutes; P = .04).
Most patients (96%) had no complications, but minor mucosal lacerations were more common with the Endocuff (9 vs. 2; P = .028). The cuff was lost during six colonoscopies, but endoscopically retrieved.
"The Endocuff is feasible, safe, reliable, and easy to handle, and might have the potential to reduce the incidence of colorectal cancer," Dr. Meister concluded. The Endocuff is available in Europe and the United States; it was approved by the Food and Drug Administration in 2012.
The study was supported by Helios Albert-Schweitzer-Klinik. Dr. Meister reported no conflicting interests.
CHICAGO – German investigators reported on their experience using the disposable Endocuff device in a prospective, randomized two-center trial involving 498 patients undergoing colonoscopy. The flexible Endocuff attaches to the tip of the colonoscope and features two rows of small flexible, hinged wings, Dr. Tobias Meister said at the annual Digestive Disease Week.
The polyp detection rate was 56% for Endocuff-assisted colonoscopy and 42% for standard colonoscopy (P = .001), reported Dr. Meister of Helios Albert-Schweitzer-Klinik, Northeim, Germany.
Compared with standard colonoscopy, Endocuff-assisted colonoscopy detected significantly more polyps per patient (mean 1.58 vs. 0.97; P less than .0001), more sigmoid polyps less than 1 cm in size (120 vs. 42; P = .001), and more cecum polyps less than 1 cm (37 vs. 14; P = .002).
The adenoma detection rate was 36% with Endocuff colonoscopy and 28% with standard colonoscopy patients (P = .043).
The number of carcinomas detected was similar in the two groups (2 vs. 3; P = .68), but the Endocuff outperformed standard colonoscopy for low-grade adenomas (208 vs. 112; P = .008), mean adenomas per patient (0.91 vs. 0.49; P =.011), and hyperplastic polyps (33% vs. 21%; P = .003), Dr. Meister said.
Withdrawal time was not measured, although there was a slight increase in total procedure time in the Endocuff group (23.11 minutes vs. 21.51 minutes; P = .04).
Most patients (96%) had no complications, but minor mucosal lacerations were more common with the Endocuff (9 vs. 2; P = .028). The cuff was lost during six colonoscopies, but endoscopically retrieved.
"The Endocuff is feasible, safe, reliable, and easy to handle, and might have the potential to reduce the incidence of colorectal cancer," Dr. Meister concluded. The Endocuff is available in Europe and the United States; it was approved by the Food and Drug Administration in 2012.
The study was supported by Helios Albert-Schweitzer-Klinik. Dr. Meister reported no conflicting interests.
AT DDW 2014
Major finding: The polyp detection rate was 56% for Endocuff-assisted colonoscopy and 42% for standard colonoscopy (P = .001).
Data source: A prospective, two-center trial in 498 patients undergoing colonoscopy.
Disclosures: The study was supported by Helios Albert-Schweitzer-Klinik. Dr. Meister reported no conflicting interests.

PCPs all over the map in conservative OA therapy use
PARIS – Use of conservative, nonpharmacologic osteoarthritis therapies was relatively low and varied considerably across 10 primary care clinics within the same U.S. health care system.
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were currently using pain medications such as opioids or NSAIDs to treat their symptomatic hip and/or knee OA, according to the cross-sectional analysis.
Patients received care at 1 of 10 family and internal medicine Duke Primary Care clinics in North Carolina. All were overweight and not meeting physical activity recommendations. Patients had OA symptoms for an average of 10 years, their average WOMAC (Western Ontario and McMaster Osteoarthritis Index) score was 39, and average age was 63 years.
Four of the clinics were in a rural setting (population less than 20,000), one in a medium-size town (20,000-99,999), four in small cities (100,000-250,000), and one in a large city (more than 250,000). The clinics had an average of 6.4 physicians and one nurse practitioner or physician’s assistant.
Knee brace use of any type ranged from 40%-64% across clinics, Dr. Allen reported. Use of knee braces with metal supports was even lower at 0%-18%.
The relatively low use of PT and knee braces with metal supports "may signal a need for more specific treatment recommendations or guidance for consistent application," suggested Dr. Allen, a health services researcher and exercise physiologist, Duke University Medical Center and Durham VA Medical Center, both in Durham, N.C.
Knee injections were reported by 43%-70% of patients.
Intraclass correlation coefficients (ICCs) were calculated to measure between-clinic variation in treatment use, with an ICC of more than .01 indicating considerable variation.
ICCs were 0.01 for the proportion using any pain medications, 0 for opioids, NSAIDS, knee injections and knee braces, 0.02 for metal knee braces, 0.07 for knee PT, and 0.08 for hip PT, according to Dr. Allen.
Rural clinics were typically below the median for nonpharmacologic use, possibly because of fewer resources in these areas, according to the poster presentation.
Clinics with fewer patients reporting "fair" or "poor" general health, however, tended to have higher use across treatment categories.
"These OA therapies may be more highly utilized when patients have fewer competing health problems," she suggested at the meeting, sponsored by the Osteoarthritis Research Society International.
Overall, 20% of patients in the study reported having fair or poor health, but rates ranged from a low of 10% to a high of 35%.
The study was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Allen reported no conflicts of interest.
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were curre
PARIS – Use of conservative, nonpharmacologic osteoarthritis therapies was relatively low and varied considerably across 10 primary care clinics within the same U.S. health care system.
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were currently using pain medications such as opioids or NSAIDs to treat their symptomatic hip and/or knee OA, according to the cross-sectional analysis.
Patients received care at 1 of 10 family and internal medicine Duke Primary Care clinics in North Carolina. All were overweight and not meeting physical activity recommendations. Patients had OA symptoms for an average of 10 years, their average WOMAC (Western Ontario and McMaster Osteoarthritis Index) score was 39, and average age was 63 years.
Four of the clinics were in a rural setting (population less than 20,000), one in a medium-size town (20,000-99,999), four in small cities (100,000-250,000), and one in a large city (more than 250,000). The clinics had an average of 6.4 physicians and one nurse practitioner or physician’s assistant.
Knee brace use of any type ranged from 40%-64% across clinics, Dr. Allen reported. Use of knee braces with metal supports was even lower at 0%-18%.
The relatively low use of PT and knee braces with metal supports "may signal a need for more specific treatment recommendations or guidance for consistent application," suggested Dr. Allen, a health services researcher and exercise physiologist, Duke University Medical Center and Durham VA Medical Center, both in Durham, N.C.
Knee injections were reported by 43%-70% of patients.
Intraclass correlation coefficients (ICCs) were calculated to measure between-clinic variation in treatment use, with an ICC of more than .01 indicating considerable variation.
ICCs were 0.01 for the proportion using any pain medications, 0 for opioids, NSAIDS, knee injections and knee braces, 0.02 for metal knee braces, 0.07 for knee PT, and 0.08 for hip PT, according to Dr. Allen.
Rural clinics were typically below the median for nonpharmacologic use, possibly because of fewer resources in these areas, according to the poster presentation.
Clinics with fewer patients reporting "fair" or "poor" general health, however, tended to have higher use across treatment categories.
"These OA therapies may be more highly utilized when patients have fewer competing health problems," she suggested at the meeting, sponsored by the Osteoarthritis Research Society International.
Overall, 20% of patients in the study reported having fair or poor health, but rates ranged from a low of 10% to a high of 35%.
The study was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Allen reported no conflicts of interest.
PARIS – Use of conservative, nonpharmacologic osteoarthritis therapies was relatively low and varied considerably across 10 primary care clinics within the same U.S. health care system.
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were currently using pain medications such as opioids or NSAIDs to treat their symptomatic hip and/or knee OA, according to the cross-sectional analysis.
Patients received care at 1 of 10 family and internal medicine Duke Primary Care clinics in North Carolina. All were overweight and not meeting physical activity recommendations. Patients had OA symptoms for an average of 10 years, their average WOMAC (Western Ontario and McMaster Osteoarthritis Index) score was 39, and average age was 63 years.
Four of the clinics were in a rural setting (population less than 20,000), one in a medium-size town (20,000-99,999), four in small cities (100,000-250,000), and one in a large city (more than 250,000). The clinics had an average of 6.4 physicians and one nurse practitioner or physician’s assistant.
Knee brace use of any type ranged from 40%-64% across clinics, Dr. Allen reported. Use of knee braces with metal supports was even lower at 0%-18%.
The relatively low use of PT and knee braces with metal supports "may signal a need for more specific treatment recommendations or guidance for consistent application," suggested Dr. Allen, a health services researcher and exercise physiologist, Duke University Medical Center and Durham VA Medical Center, both in Durham, N.C.
Knee injections were reported by 43%-70% of patients.
Intraclass correlation coefficients (ICCs) were calculated to measure between-clinic variation in treatment use, with an ICC of more than .01 indicating considerable variation.
ICCs were 0.01 for the proportion using any pain medications, 0 for opioids, NSAIDS, knee injections and knee braces, 0.02 for metal knee braces, 0.07 for knee PT, and 0.08 for hip PT, according to Dr. Allen.
Rural clinics were typically below the median for nonpharmacologic use, possibly because of fewer resources in these areas, according to the poster presentation.
Clinics with fewer patients reporting "fair" or "poor" general health, however, tended to have higher use across treatment categories.
"These OA therapies may be more highly utilized when patients have fewer competing health problems," she suggested at the meeting, sponsored by the Osteoarthritis Research Society International.
Overall, 20% of patients in the study reported having fair or poor health, but rates ranged from a low of 10% to a high of 35%.
The study was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Allen reported no conflicts of interest.
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were curre
In seven of the clinics, for example, less than half of patients had ever received physical therapy for knee osteoarthritis, with a range of 24%-61%.
Physical therapy for hip OA was even less common, ranging from 0%-71%, Kelli D. Allen, Ph.D., reported at the World Congress on Osteoarthritis.
In contrast, 70%-88% of patients were curre
AT OARSI 2014
Data source: Cross-sectional analysis of 537 OA patients at 10 PCP clinics.
Disclosures: The study was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Allen reported no conflicting interests.
EndoRings-assisted colonoscopy hikes polyp, adenoma detection
CHICAGO – Adding a small rubber tip with flexible, circular rings to the end of a colonoscope dramatically improves polyp and adenoma detection during colonoscopy, according to interim results from a randomized, tandem study.
In a per lesion analysis, the adenoma miss rate was 13% when patients underwent an EndoRing colonoscopy followed by a standard colonoscopy and 53% when standard colonoscopy was done before the EndoRing colonoscopy (P less than .001).
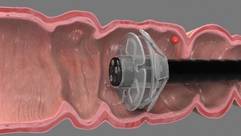
The miss rates for polyps were 11% and 58% (P less than .001), *Dr. Peter D. Siersema said in a late-breaking abstract session at the annual Digestive Disease Week.
Adenomas are missed in about 25% of tandem studies with standard colonoscopies, and the miss rate may be as high as 40% with new techniques. This is mainly due to inadequate visualization of proximal aspects of folds and inner curves of flexures. The flexible, circular rings of the EndoRings improve visualization by engaging and stretching colonic folds during withdrawal, explained Dr. Siersema of the University Medical Center Utrecht, the Netherlands. The EndoRings device is Food and Drug Administration and CE approved and available in the U.S. and Europe.

From July 2013 to April 2014, investigators in the Netherlands and Israel enrolled 106 patients, aged 40-75 years, with an indication for screening, surveillance, or diagnostic colonoscopy, to undergo same-day, back-to-back colonoscopies by the same endoscopist. Bowel preparation followed standard protocol at the centers (polyethylene glycol or sodium picosulfate). Conscious sedation (midazolam, fentanyl, propofol, or combination) was used in most patients. Polyps found during the first procedure were immediately removed.
The average time to the cecum and withdrawal times were similar in the two groups, although total procedure time was significantly longer with the EndoRings (mean 22 minutes vs. 18 minutes; P less than .001) due to the removal of more polyps, Dr. Siersema said.
Among 49 evaluable patients in the study group, 79 polyps were detected with EndoRings during the first procedure and 10 additional polyps during the subsequent standard colonoscopy.
Among 47 evaluable controls, 25 polyps were detected during the first pass with standard colonoscopy and 34 additional adenomas in the second pass with EndoRings.
There was no difference in the location, size, morphology, and histology of the missed polyps between groups, he said.
In the study group, 46 adenomas were found during the initial procedure with EndoRings and 7 more during the second pass using standard colonoscopy.
Among controls, 17 adenomas were detected during the first pass with standard colonoscopy and 19 more in the second pass with EndoRings.

Surveillance intervals were shortened for eight patients who underwent standard colonoscopy first and two patients who underwent EndoRings colonoscopy first, Dr. Siersema said. There were no adverse events in the study.
During a discussion of the results, Dr. Siersema said the single-use device "was very cheap" to purchase and has an additional advantage of stabilizing the scope in the center of the colon.
Session cochair Dr. Pankaj Pasricha, director of the Johns Hopkins Center for Neurogastroenterology, said some colonoscopes are incorporating expandable tips, and that there are four or five other add-on devices, one with streamers and another with a balloon.
"They are relatively inexpensive, simple approaches to solving a complex problem," he said in an interview. "It is a real problem looking behind folds, missed polyps, and if large-scale studies show that [this is improved], then this could be really something very easily incorporated into your practice, as opposed to buying a new scope for hundreds of thousands of dollars."
Dr. Siersema reported a travel grant to attend the meeting. Three coauthors reported consultancy for and one reported employment with the study sponsor, EndoAid. Dr. Pasricha reported relationships with Pentax, GI Supply, and Apollo Endosurgery.
Correction 5/20/14: A previous version of this story incorrectly identified Dr. Peter D. Siersema in both the photograph and in references throughout the text. This version has been corrected and updated.
CHICAGO – Adding a small rubber tip with flexible, circular rings to the end of a colonoscope dramatically improves polyp and adenoma detection during colonoscopy, according to interim results from a randomized, tandem study.
In a per lesion analysis, the adenoma miss rate was 13% when patients underwent an EndoRing colonoscopy followed by a standard colonoscopy and 53% when standard colonoscopy was done before the EndoRing colonoscopy (P less than .001).
The miss rates for polyps were 11% and 58% (P less than .001), *Dr. Peter D. Siersema said in a late-breaking abstract session at the annual Digestive Disease Week.
Adenomas are missed in about 25% of tandem studies with standard colonoscopies, and the miss rate may be as high as 40% with new techniques. This is mainly due to inadequate visualization of proximal aspects of folds and inner curves of flexures. The flexible, circular rings of the EndoRings improve visualization by engaging and stretching colonic folds during withdrawal, explained Dr. Siersema of the University Medical Center Utrecht, the Netherlands. The EndoRings device is Food and Drug Administration and CE approved and available in the U.S. and Europe.
From July 2013 to April 2014, investigators in the Netherlands and Israel enrolled 106 patients, aged 40-75 years, with an indication for screening, surveillance, or diagnostic colonoscopy, to undergo same-day, back-to-back colonoscopies by the same endoscopist. Bowel preparation followed standard protocol at the centers (polyethylene glycol or sodium picosulfate). Conscious sedation (midazolam, fentanyl, propofol, or combination) was used in most patients. Polyps found during the first procedure were immediately removed.
The average time to the cecum and withdrawal times were similar in the two groups, although total procedure time was significantly longer with the EndoRings (mean 22 minutes vs. 18 minutes; P less than .001) due to the removal of more polyps, Dr. Siersema said.
Among 49 evaluable patients in the study group, 79 polyps were detected with EndoRings during the first procedure and 10 additional polyps during the subsequent standard colonoscopy.
Among 47 evaluable controls, 25 polyps were detected during the first pass with standard colonoscopy and 34 additional adenomas in the second pass with EndoRings.
There was no difference in the location, size, morphology, and histology of the missed polyps between groups, he said.
In the study group, 46 adenomas were found during the initial procedure with EndoRings and 7 more during the second pass using standard colonoscopy.
Among controls, 17 adenomas were detected during the first pass with standard colonoscopy and 19 more in the second pass with EndoRings.
Surveillance intervals were shortened for eight patients who underwent standard colonoscopy first and two patients who underwent EndoRings colonoscopy first, Dr. Siersema said. There were no adverse events in the study.
During a discussion of the results, Dr. Siersema said the single-use device "was very cheap" to purchase and has an additional advantage of stabilizing the scope in the center of the colon.
Session cochair Dr. Pankaj Pasricha, director of the Johns Hopkins Center for Neurogastroenterology, said some colonoscopes are incorporating expandable tips, and that there are four or five other add-on devices, one with streamers and another with a balloon.
"They are relatively inexpensive, simple approaches to solving a complex problem," he said in an interview. "It is a real problem looking behind folds, missed polyps, and if large-scale studies show that [this is improved], then this could be really something very easily incorporated into your practice, as opposed to buying a new scope for hundreds of thousands of dollars."
Dr. Siersema reported a travel grant to attend the meeting. Three coauthors reported consultancy for and one reported employment with the study sponsor, EndoAid. Dr. Pasricha reported relationships with Pentax, GI Supply, and Apollo Endosurgery.
Correction 5/20/14: A previous version of this story incorrectly identified Dr. Peter D. Siersema in both the photograph and in references throughout the text. This version has been corrected and updated.
CHICAGO – Adding a small rubber tip with flexible, circular rings to the end of a colonoscope dramatically improves polyp and adenoma detection during colonoscopy, according to interim results from a randomized, tandem study.
In a per lesion analysis, the adenoma miss rate was 13% when patients underwent an EndoRing colonoscopy followed by a standard colonoscopy and 53% when standard colonoscopy was done before the EndoRing colonoscopy (P less than .001).
The miss rates for polyps were 11% and 58% (P less than .001), *Dr. Peter D. Siersema said in a late-breaking abstract session at the annual Digestive Disease Week.
Adenomas are missed in about 25% of tandem studies with standard colonoscopies, and the miss rate may be as high as 40% with new techniques. This is mainly due to inadequate visualization of proximal aspects of folds and inner curves of flexures. The flexible, circular rings of the EndoRings improve visualization by engaging and stretching colonic folds during withdrawal, explained Dr. Siersema of the University Medical Center Utrecht, the Netherlands. The EndoRings device is Food and Drug Administration and CE approved and available in the U.S. and Europe.
From July 2013 to April 2014, investigators in the Netherlands and Israel enrolled 106 patients, aged 40-75 years, with an indication for screening, surveillance, or diagnostic colonoscopy, to undergo same-day, back-to-back colonoscopies by the same endoscopist. Bowel preparation followed standard protocol at the centers (polyethylene glycol or sodium picosulfate). Conscious sedation (midazolam, fentanyl, propofol, or combination) was used in most patients. Polyps found during the first procedure were immediately removed.
The average time to the cecum and withdrawal times were similar in the two groups, although total procedure time was significantly longer with the EndoRings (mean 22 minutes vs. 18 minutes; P less than .001) due to the removal of more polyps, Dr. Siersema said.
Among 49 evaluable patients in the study group, 79 polyps were detected with EndoRings during the first procedure and 10 additional polyps during the subsequent standard colonoscopy.
Among 47 evaluable controls, 25 polyps were detected during the first pass with standard colonoscopy and 34 additional adenomas in the second pass with EndoRings.
There was no difference in the location, size, morphology, and histology of the missed polyps between groups, he said.
In the study group, 46 adenomas were found during the initial procedure with EndoRings and 7 more during the second pass using standard colonoscopy.
Among controls, 17 adenomas were detected during the first pass with standard colonoscopy and 19 more in the second pass with EndoRings.
Surveillance intervals were shortened for eight patients who underwent standard colonoscopy first and two patients who underwent EndoRings colonoscopy first, Dr. Siersema said. There were no adverse events in the study.
During a discussion of the results, Dr. Siersema said the single-use device "was very cheap" to purchase and has an additional advantage of stabilizing the scope in the center of the colon.
Session cochair Dr. Pankaj Pasricha, director of the Johns Hopkins Center for Neurogastroenterology, said some colonoscopes are incorporating expandable tips, and that there are four or five other add-on devices, one with streamers and another with a balloon.
"They are relatively inexpensive, simple approaches to solving a complex problem," he said in an interview. "It is a real problem looking behind folds, missed polyps, and if large-scale studies show that [this is improved], then this could be really something very easily incorporated into your practice, as opposed to buying a new scope for hundreds of thousands of dollars."
Dr. Siersema reported a travel grant to attend the meeting. Three coauthors reported consultancy for and one reported employment with the study sponsor, EndoAid. Dr. Pasricha reported relationships with Pentax, GI Supply, and Apollo Endosurgery.
Correction 5/20/14: A previous version of this story incorrectly identified Dr. Peter D. Siersema in both the photograph and in references throughout the text. This version has been corrected and updated.
AT DDW 2014
Major finding: In 49 study patients, 79 polyps were found with EndoRings, then 10 more were found with standard follow-up colonoscopy; in 47 control patients 25 polyps were found by standard colonoscopy, then 34 more adenomas were found with EndoRings device.
Data source: A prospective study in 96 patients with back-to-back colonoscopies.
Disclosures: Dr. Dik reported a travel grant to attend the meeting. Three coauthors reported consultancy for and one employment with the study sponsor, EndoAid. Dr. Pasricha reported relationships with Pentax, GI Supply, and Apollo Endosurgery.
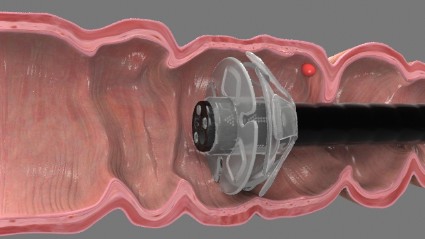
Negative moods tied to OA pain flares
PARIS – Patients with knee osteoarthritis are significantly more likely to experience a flare if they report a higher negative mood in the previous 10 days.
Passive coping strategies such as "I restrict my social activities" or "I focus on the location and intensity of pain" were also significantly associated with an increased risk of flares, while more active coping strategies were protective in a Web-based, case-crossover study.

"We really need to elaborate on this, replicate it, and elucidate this connection because psychosocial factors of mood and pain coping are modifiable and ultimately may improve our patients experience of this disease, osteoarthritis," Dr. David J. Hunter said at the World Congress on Osteoarthritis.
The investigators recruited 298 patients with symptomatic knee osteoarthritis (OA) and asked them to log on to the study website if they experienced a knee pain exacerbation over 3 months of follow-up.
Daily mood (negative/positive) in the previous 10 days was assessed using the Profile of Mood States (POMS) questionnaire. The Pain Coping Inventory (PCI) was used to assess daily pain coping in the previous 30 days.
Pain exacerbation during follow-up was defined as a 2-unit increase in the patient’s visual analog knee pain score (10-point scale) from his or her mildest pain score reported at the baseline visit, said Dr. Hunter, the Florance and Cope Chair of Rheumatology, Northern Clinical School, University of Sydney, Australia.
Most of the patients were female (61%) and white (92%), and their average body mass index was 29.4 kg/m2. Their average baseline Knee injury and Osteoarthritis Outcome Score (KOOS) symptoms subscale score was 44.5 and KOOS pain subscale score 55.6.
The average POMS positive mood score was 33.9 and average negative mood (for example, distressed, irritable, nervous) score 16.5, both on a 50-point scale. The average PCI passive coping score was 8.1 on a 24-point scale, and average PCI active coping score 12.2 on a 20-point scale.
In conditional logistic regression analyses, increasing negative affect scores were significantly associated with having a pain exacerbation (P less than .001) such that patients with a score of 13-17 were nearly three times more likely to experience a flare (odds ratio, 2.77) and those with a score of 18 or more were 6.5 times more likely to do so (OR, 6.5), Dr. Hunter said.
Patients with higher PCI passive coping scores were also significantly more likely to have a pain exacerbation (OR, 1.26; P = .01), while those with more active coping strategies such as "I stay busy or active," or "I clear my mind of bothersome thoughts" were less likely to have a pain flare (OR, 0.81; P = .03).
During a discussion of the results, Dr. Hunter said they have yet to look at trajectories to see whether patients returned to their prior pain level.
Session comoderator Aileen Davis, Ph.D., senior scientist with the Toronto Western Research Institute, said the general literature recognizes there is a psychosocial component to OA pain, but that this is the first study to make the direct link with OA pain flares.
If the results can be replicated, "It means there’s a lot more we can do in terms of coping strategies and in recognizing this a lot more often," she said in an interview at the meeting, sponsored by the Osteoarthritis Research Society International.
Since many OA patients are cared for by primary care physicians, Dr. Davis suggested they may want to have a psychosocial profile of their OA patients and push management strategies or referrals to psychologists or social workers skilled in coping strategies to patients who are "fluctuators," so they can "proactively change how they’re doing things."
Dr. Hunter reported support from the Australian National Health and Medical Research Council.
Passive coping strategies, pain, active coping strategies, psychosocial factors, mood, pain, Dr. David J. Hunter, World Congress on Osteoarthritis, symptomatic knee osteoarthritis, knee pain exacerbation, Profile of Mood States questionnaire, The Pain Coping Inventory, Knee injury and Osteoarthritis Outcome Score symptoms subscale score,
PARIS – Patients with knee osteoarthritis are significantly more likely to experience a flare if they report a higher negative mood in the previous 10 days.
Passive coping strategies such as "I restrict my social activities" or "I focus on the location and intensity of pain" were also significantly associated with an increased risk of flares, while more active coping strategies were protective in a Web-based, case-crossover study.
"We really need to elaborate on this, replicate it, and elucidate this connection because psychosocial factors of mood and pain coping are modifiable and ultimately may improve our patients experience of this disease, osteoarthritis," Dr. David J. Hunter said at the World Congress on Osteoarthritis.
The investigators recruited 298 patients with symptomatic knee osteoarthritis (OA) and asked them to log on to the study website if they experienced a knee pain exacerbation over 3 months of follow-up.
Daily mood (negative/positive) in the previous 10 days was assessed using the Profile of Mood States (POMS) questionnaire. The Pain Coping Inventory (PCI) was used to assess daily pain coping in the previous 30 days.
Pain exacerbation during follow-up was defined as a 2-unit increase in the patient’s visual analog knee pain score (10-point scale) from his or her mildest pain score reported at the baseline visit, said Dr. Hunter, the Florance and Cope Chair of Rheumatology, Northern Clinical School, University of Sydney, Australia.
Most of the patients were female (61%) and white (92%), and their average body mass index was 29.4 kg/m2. Their average baseline Knee injury and Osteoarthritis Outcome Score (KOOS) symptoms subscale score was 44.5 and KOOS pain subscale score 55.6.
The average POMS positive mood score was 33.9 and average negative mood (for example, distressed, irritable, nervous) score 16.5, both on a 50-point scale. The average PCI passive coping score was 8.1 on a 24-point scale, and average PCI active coping score 12.2 on a 20-point scale.
In conditional logistic regression analyses, increasing negative affect scores were significantly associated with having a pain exacerbation (P less than .001) such that patients with a score of 13-17 were nearly three times more likely to experience a flare (odds ratio, 2.77) and those with a score of 18 or more were 6.5 times more likely to do so (OR, 6.5), Dr. Hunter said.
Patients with higher PCI passive coping scores were also significantly more likely to have a pain exacerbation (OR, 1.26; P = .01), while those with more active coping strategies such as "I stay busy or active," or "I clear my mind of bothersome thoughts" were less likely to have a pain flare (OR, 0.81; P = .03).
During a discussion of the results, Dr. Hunter said they have yet to look at trajectories to see whether patients returned to their prior pain level.
Session comoderator Aileen Davis, Ph.D., senior scientist with the Toronto Western Research Institute, said the general literature recognizes there is a psychosocial component to OA pain, but that this is the first study to make the direct link with OA pain flares.
If the results can be replicated, "It means there’s a lot more we can do in terms of coping strategies and in recognizing this a lot more often," she said in an interview at the meeting, sponsored by the Osteoarthritis Research Society International.
Since many OA patients are cared for by primary care physicians, Dr. Davis suggested they may want to have a psychosocial profile of their OA patients and push management strategies or referrals to psychologists or social workers skilled in coping strategies to patients who are "fluctuators," so they can "proactively change how they’re doing things."
Dr. Hunter reported support from the Australian National Health and Medical Research Council.
PARIS – Patients with knee osteoarthritis are significantly more likely to experience a flare if they report a higher negative mood in the previous 10 days.
Passive coping strategies such as "I restrict my social activities" or "I focus on the location and intensity of pain" were also significantly associated with an increased risk of flares, while more active coping strategies were protective in a Web-based, case-crossover study.
"We really need to elaborate on this, replicate it, and elucidate this connection because psychosocial factors of mood and pain coping are modifiable and ultimately may improve our patients experience of this disease, osteoarthritis," Dr. David J. Hunter said at the World Congress on Osteoarthritis.
The investigators recruited 298 patients with symptomatic knee osteoarthritis (OA) and asked them to log on to the study website if they experienced a knee pain exacerbation over 3 months of follow-up.
Daily mood (negative/positive) in the previous 10 days was assessed using the Profile of Mood States (POMS) questionnaire. The Pain Coping Inventory (PCI) was used to assess daily pain coping in the previous 30 days.
Pain exacerbation during follow-up was defined as a 2-unit increase in the patient’s visual analog knee pain score (10-point scale) from his or her mildest pain score reported at the baseline visit, said Dr. Hunter, the Florance and Cope Chair of Rheumatology, Northern Clinical School, University of Sydney, Australia.
Most of the patients were female (61%) and white (92%), and their average body mass index was 29.4 kg/m2. Their average baseline Knee injury and Osteoarthritis Outcome Score (KOOS) symptoms subscale score was 44.5 and KOOS pain subscale score 55.6.
The average POMS positive mood score was 33.9 and average negative mood (for example, distressed, irritable, nervous) score 16.5, both on a 50-point scale. The average PCI passive coping score was 8.1 on a 24-point scale, and average PCI active coping score 12.2 on a 20-point scale.
In conditional logistic regression analyses, increasing negative affect scores were significantly associated with having a pain exacerbation (P less than .001) such that patients with a score of 13-17 were nearly three times more likely to experience a flare (odds ratio, 2.77) and those with a score of 18 or more were 6.5 times more likely to do so (OR, 6.5), Dr. Hunter said.
Patients with higher PCI passive coping scores were also significantly more likely to have a pain exacerbation (OR, 1.26; P = .01), while those with more active coping strategies such as "I stay busy or active," or "I clear my mind of bothersome thoughts" were less likely to have a pain flare (OR, 0.81; P = .03).
During a discussion of the results, Dr. Hunter said they have yet to look at trajectories to see whether patients returned to their prior pain level.
Session comoderator Aileen Davis, Ph.D., senior scientist with the Toronto Western Research Institute, said the general literature recognizes there is a psychosocial component to OA pain, but that this is the first study to make the direct link with OA pain flares.
If the results can be replicated, "It means there’s a lot more we can do in terms of coping strategies and in recognizing this a lot more often," she said in an interview at the meeting, sponsored by the Osteoarthritis Research Society International.
Since many OA patients are cared for by primary care physicians, Dr. Davis suggested they may want to have a psychosocial profile of their OA patients and push management strategies or referrals to psychologists or social workers skilled in coping strategies to patients who are "fluctuators," so they can "proactively change how they’re doing things."
Dr. Hunter reported support from the Australian National Health and Medical Research Council.
Passive coping strategies, pain, active coping strategies, psychosocial factors, mood, pain, Dr. David J. Hunter, World Congress on Osteoarthritis, symptomatic knee osteoarthritis, knee pain exacerbation, Profile of Mood States questionnaire, The Pain Coping Inventory, Knee injury and Osteoarthritis Outcome Score symptoms subscale score,
Passive coping strategies, pain, active coping strategies, psychosocial factors, mood, pain, Dr. David J. Hunter, World Congress on Osteoarthritis, symptomatic knee osteoarthritis, knee pain exacerbation, Profile of Mood States questionnaire, The Pain Coping Inventory, Knee injury and Osteoarthritis Outcome Score symptoms subscale score,
AT OARSI 2014
Key clinical point: Clinicians may want to help OA patients with coping strategies by requesting a psychosocial profile and tailoring management strategies to it or referral to psychologists or social workers skilled in coping strategies.
Major finding: Patients with a negative affect score of 18 or more were 6.5 times more likely to experience an OA pain flare (OR, 6.5).
Data source: A case-crossover study in 298 patients with knee OA.
Disclosures: Dr. Hunter reported support from the Australian National Health and Medical Research Council.

Menopause isn’t a culprit behind severe asthma
MADRID – Menopause is blamed for many things, but it’s unlikely to be the reason for the increased risk of severe asthma or worse quality of life in elderly asthmatic women, a study suggests.
"The increased unadjusted asthma severity and need for health care utilization in postmenopausal women are more likely due to other factors like age and other comorbidities rather than menopause per se," Dr. Joe Zein, FCCP, said at CHEST World Congress 2014.
The investigators used a propensity score matching method to analyze the effect of menopause on asthma severity, quality of life, and health care utilization in 166 menopausal and 538 premenopausal women enrolled in the Severe Asthma Research program from 2002 to 2011.

Subsequent multivariate logistic regression analyses were used to adjust for the covariates of age at enrollment, hypertension, gastroesophageal reflux disease (GERD), and hormone therapy, which was used in only 35 menopausal women.
Compared with premenopausal women, menopausal women were older and reported less atopy and more comorbidities, such as higher body mass index, diabetes mellitus, hypertension, GERD, obstructive sleep apnea, sinusitis, and nasal polyps, said Dr. Zein, a pulmonologist at Cleveland Clinic.
Menopausal women also had lower lung function and higher neutrophil percentage in both induced sputum and bronchoalveolar lavage fluid.
Severe asthma was present in 31% (167/538) of premenopausal and 72% (119/166) of menopausal women.
In unadjusted analysis, the risk of severe asthma was almost sixfold higher in menopausal women (odds ratio, 5.62; 95% confidence interval 3.83-8.26), but dropped dramatically in the adjusted analysis (OR, 1.46), 95% C.I. 0.50-4.22),he said.
Menopausal women also had lower average scores than did premenopausal women (4.06 vs. 4.56) on the 7-point Asthma Quality of Life Questionnaire, with 7 being "not impaired at all" and 1 being "severely impaired."
The mean difference between groups pointed to worse quality of life among menopausal women in unadjusted analysis (–0.5),; 95% C.I. -0.71 to -0.27), but again this faded after multivariate adjustment (0.31; 95% C.I. –0.-0.93).
Similar trends were observed for health care utilization including emergency department visits (unadjusted OR, 1.33; adjusted OR, 1.15) and hospitalization (unadjusted OR, 2.93; adjusted OR, 0.70), Dr. Zein said.
Finally, an analysis stratified by menopausal status that looked at the association between enrollment age and the probability of severe asthma suggested a rise in severe asthma among premenopausal women and those in early menopause, followed by a steady decline around age 55 years. Two possible hypotheses are that insulin resistance is higher during the period around menopause and thus may worsen asthma and that estrogen levels initially rise during early menopause before declining and also may increase asthma severity, Dr. Zein said.
"We don’t know exactly, but I think we should not look at menopause as one entity."
Several studies have tried to tease out the effects of menopause and aging on asthma severity, with conflicting results.
A recent study reported that menopausal women in their fifties and sixties are more than twice as likely to be hospitalized for asthma as men the same age (Ann. Allergy Asthma Immunol. 2013;111:176-81).
The Harvard Nurses Health Study, however, found that postmenopausal women who never used hormone therapy had a significantly lower age-adjusted risk of asthma than premenopausal women (Am. J. Respir. Crit. Care Med. 1995;152:1183-8).
The role of estrogen in asthma remains controversial, Dr. Zein observed. The incidence of asthma is twice as high among boys during childhood, but this switches during puberty when girls have a higher incidence of asthma as well as asthma-related hospitalizations and health care utilization, he noted.
Dr. Vera DePalo, FCCP, comments: Asthma severity changes over the spectrum of a lifetime with changing linkage to gender at different ages. During menopause, while there is an increased likelihood of severe asthma, there are several confounding factors, resulting in lower adjusted odds ratios. As we learn more about asthma and its associations, the complexity of its manifestations becomes more evident.
Dr. Vera DePalo, FCCP, comments: Asthma severity changes over the spectrum of a lifetime with changing linkage to gender at different ages. During menopause, while there is an increased likelihood of severe asthma, there are several confounding factors, resulting in lower adjusted odds ratios. As we learn more about asthma and its associations, the complexity of its manifestations becomes more evident.
Dr. Vera DePalo, FCCP, comments: Asthma severity changes over the spectrum of a lifetime with changing linkage to gender at different ages. During menopause, while there is an increased likelihood of severe asthma, there are several confounding factors, resulting in lower adjusted odds ratios. As we learn more about asthma and its associations, the complexity of its manifestations becomes more evident.
MADRID – Menopause is blamed for many things, but it’s unlikely to be the reason for the increased risk of severe asthma or worse quality of life in elderly asthmatic women, a study suggests.
"The increased unadjusted asthma severity and need for health care utilization in postmenopausal women are more likely due to other factors like age and other comorbidities rather than menopause per se," Dr. Joe Zein, FCCP, said at CHEST World Congress 2014.
The investigators used a propensity score matching method to analyze the effect of menopause on asthma severity, quality of life, and health care utilization in 166 menopausal and 538 premenopausal women enrolled in the Severe Asthma Research program from 2002 to 2011.
Subsequent multivariate logistic regression analyses were used to adjust for the covariates of age at enrollment, hypertension, gastroesophageal reflux disease (GERD), and hormone therapy, which was used in only 35 menopausal women.
Compared with premenopausal women, menopausal women were older and reported less atopy and more comorbidities, such as higher body mass index, diabetes mellitus, hypertension, GERD, obstructive sleep apnea, sinusitis, and nasal polyps, said Dr. Zein, a pulmonologist at Cleveland Clinic.
Menopausal women also had lower lung function and higher neutrophil percentage in both induced sputum and bronchoalveolar lavage fluid.
Severe asthma was present in 31% (167/538) of premenopausal and 72% (119/166) of menopausal women.
In unadjusted analysis, the risk of severe asthma was almost sixfold higher in menopausal women (odds ratio, 5.62; 95% confidence interval 3.83-8.26), but dropped dramatically in the adjusted analysis (OR, 1.46), 95% C.I. 0.50-4.22),he said.
Menopausal women also had lower average scores than did premenopausal women (4.06 vs. 4.56) on the 7-point Asthma Quality of Life Questionnaire, with 7 being "not impaired at all" and 1 being "severely impaired."
The mean difference between groups pointed to worse quality of life among menopausal women in unadjusted analysis (–0.5),; 95% C.I. -0.71 to -0.27), but again this faded after multivariate adjustment (0.31; 95% C.I. –0.-0.93).
Similar trends were observed for health care utilization including emergency department visits (unadjusted OR, 1.33; adjusted OR, 1.15) and hospitalization (unadjusted OR, 2.93; adjusted OR, 0.70), Dr. Zein said.
Finally, an analysis stratified by menopausal status that looked at the association between enrollment age and the probability of severe asthma suggested a rise in severe asthma among premenopausal women and those in early menopause, followed by a steady decline around age 55 years. Two possible hypotheses are that insulin resistance is higher during the period around menopause and thus may worsen asthma and that estrogen levels initially rise during early menopause before declining and also may increase asthma severity, Dr. Zein said.
"We don’t know exactly, but I think we should not look at menopause as one entity."
Several studies have tried to tease out the effects of menopause and aging on asthma severity, with conflicting results.
A recent study reported that menopausal women in their fifties and sixties are more than twice as likely to be hospitalized for asthma as men the same age (Ann. Allergy Asthma Immunol. 2013;111:176-81).
The Harvard Nurses Health Study, however, found that postmenopausal women who never used hormone therapy had a significantly lower age-adjusted risk of asthma than premenopausal women (Am. J. Respir. Crit. Care Med. 1995;152:1183-8).
The role of estrogen in asthma remains controversial, Dr. Zein observed. The incidence of asthma is twice as high among boys during childhood, but this switches during puberty when girls have a higher incidence of asthma as well as asthma-related hospitalizations and health care utilization, he noted.
MADRID – Menopause is blamed for many things, but it’s unlikely to be the reason for the increased risk of severe asthma or worse quality of life in elderly asthmatic women, a study suggests.
"The increased unadjusted asthma severity and need for health care utilization in postmenopausal women are more likely due to other factors like age and other comorbidities rather than menopause per se," Dr. Joe Zein, FCCP, said at CHEST World Congress 2014.
The investigators used a propensity score matching method to analyze the effect of menopause on asthma severity, quality of life, and health care utilization in 166 menopausal and 538 premenopausal women enrolled in the Severe Asthma Research program from 2002 to 2011.
Subsequent multivariate logistic regression analyses were used to adjust for the covariates of age at enrollment, hypertension, gastroesophageal reflux disease (GERD), and hormone therapy, which was used in only 35 menopausal women.
Compared with premenopausal women, menopausal women were older and reported less atopy and more comorbidities, such as higher body mass index, diabetes mellitus, hypertension, GERD, obstructive sleep apnea, sinusitis, and nasal polyps, said Dr. Zein, a pulmonologist at Cleveland Clinic.
Menopausal women also had lower lung function and higher neutrophil percentage in both induced sputum and bronchoalveolar lavage fluid.
Severe asthma was present in 31% (167/538) of premenopausal and 72% (119/166) of menopausal women.
In unadjusted analysis, the risk of severe asthma was almost sixfold higher in menopausal women (odds ratio, 5.62; 95% confidence interval 3.83-8.26), but dropped dramatically in the adjusted analysis (OR, 1.46), 95% C.I. 0.50-4.22),he said.
Menopausal women also had lower average scores than did premenopausal women (4.06 vs. 4.56) on the 7-point Asthma Quality of Life Questionnaire, with 7 being "not impaired at all" and 1 being "severely impaired."
The mean difference between groups pointed to worse quality of life among menopausal women in unadjusted analysis (–0.5),; 95% C.I. -0.71 to -0.27), but again this faded after multivariate adjustment (0.31; 95% C.I. –0.-0.93).
Similar trends were observed for health care utilization including emergency department visits (unadjusted OR, 1.33; adjusted OR, 1.15) and hospitalization (unadjusted OR, 2.93; adjusted OR, 0.70), Dr. Zein said.
Finally, an analysis stratified by menopausal status that looked at the association between enrollment age and the probability of severe asthma suggested a rise in severe asthma among premenopausal women and those in early menopause, followed by a steady decline around age 55 years. Two possible hypotheses are that insulin resistance is higher during the period around menopause and thus may worsen asthma and that estrogen levels initially rise during early menopause before declining and also may increase asthma severity, Dr. Zein said.
"We don’t know exactly, but I think we should not look at menopause as one entity."
Several studies have tried to tease out the effects of menopause and aging on asthma severity, with conflicting results.
A recent study reported that menopausal women in their fifties and sixties are more than twice as likely to be hospitalized for asthma as men the same age (Ann. Allergy Asthma Immunol. 2013;111:176-81).
The Harvard Nurses Health Study, however, found that postmenopausal women who never used hormone therapy had a significantly lower age-adjusted risk of asthma than premenopausal women (Am. J. Respir. Crit. Care Med. 1995;152:1183-8).
The role of estrogen in asthma remains controversial, Dr. Zein observed. The incidence of asthma is twice as high among boys during childhood, but this switches during puberty when girls have a higher incidence of asthma as well as asthma-related hospitalizations and health care utilization, he noted.
AT CHEST WORLD CONGRESS 2014
Major finding: The odds ratio for severe asthma was 5.62 for menopausal vs. premenopausal women in unadjusted analysis, but 1.46 after adjustment.
Data source: A retrospective analysis of 166 menopausal and 538 premenopausal asthmatic women.
Disclosures: Dr. Zein reported no financial disclosures; a coauthor reported grant monies from the National Institutes of Health.
