User login
Risk alleles linked to thiopurine-induced pancreatitis
CHICAGO – A genomewide association study has identified specific alleles that may pinpoint those at risk for thiopurine-induced pancreatitis in inflammatory bowel disease.
Patients heterozygous at rs2647087 are 2.5 times more likely to get pancreatitis if treated with thiopurine (Imuran), while those with homozygous risk alleles were 5 times more likely to do so, Dr. Graham Heap reported at the annual Digestive Disease Week.
Pancreatitis is a well-recognized, idiosyncratic complication of thiopurine that occurs in 4%-7% of patients, independent of dose, and usually stops treatment in its tracks. Thiopurines are a mainstay treatment in inflammatory bowel disease (IBD), particularly as an adjunct to anti–tumor necrosis factor–alpha drugs.

Dr. Heap and his associates at 168 research sites recruited 314 IBD patients with pancreatitis that developed within 3 months of starting a thiopurine for the genomewide linkage study and another 119 IBD patients for a case-control cohort. Thiopurine-induced pancreatitis was adjudicated by four independent experts, and determined to be definite in 61 patients, probable in 274, possible in 28, and unlikely in 70.
Among the definite and probable cases, pancreatitis developed within an average of 24 days after starting a thiopurine. Most cases were mild, but 70% of patients were hospitalized for an average of 5.7 days, noted Dr. Heap of Royal Devon and Exeter Hospital, Devon, England.
Analyses performed on three different genotyping platforms for 177 samples identified a significant single-nucleotide polymorphism (SNP) association in chromosome 6 within the class II HLA region. All four SNPs – rs7745656, rs2647087, rs6935723, and rs2647089 – had odds ratios of 2.6, with P values of 2.2 x 10–16.
The investigators then looked in more detail at the HLA region, previously linked to celiac disease, and identified a strong association between thiopurine-induced pancreatitis and HLA-DRB1:07:01 (OR, 2.55; P = 1.17 x 10–14) and HLA-DQA1:02:01 (OR, 2.54; P = 1.68 x 10–14), he said.
The results were replicated in an independent cohort of 78 thiopurine-induced pancreatitis cases and 472 IBD controls who did not develop pancreatitis after at least a year of thiopurine therapy, and again there was a significant association with rs2647078 (OR, 2.21; P = 4 x 10–6), Dr. Heap said.
Interestingly, there was no significant association between rs2647078 and known risk factors such as smoking status at the time of pancreatitis, thiopurine methyltransferase (TPMT) status, or inosine triphosphate pyrophosphatase genotype, he said.
What all this means for clinicians is that for every 1,000 patients tested, 77 risk allele homozygotes will be identified, and these individuals will have a 17% risk of pancreatitis, Dr. Heap said. If azathioprine and 6-mercaptopurine are avoided in these individuals, the number needed to treat is 76 patients to prevent one case of pancreatitis.
Session cochair and gastroenterologist Barrett Levesque of the University of California, San Diego,said in an interview that further testing is needed, but that the study approach was very robust, especially to show a number needed to treat of 76.
"Compared to what we use, TPMT activity levels, where there’s a few patients in a thousand who might not have the activity at all, this is very promising," he said. "I thought it was a great study."
In a separate interview, Dr. Heap said, "We do not currently feel this test has clinical utility on its own, but we will investigate its utility in combination with other pharmacogenetic tests in the future."
The study was funded by the International Serious Adverse Events Consortium. The authors reported no financial disclosures.
CHICAGO – A genomewide association study has identified specific alleles that may pinpoint those at risk for thiopurine-induced pancreatitis in inflammatory bowel disease.
Patients heterozygous at rs2647087 are 2.5 times more likely to get pancreatitis if treated with thiopurine (Imuran), while those with homozygous risk alleles were 5 times more likely to do so, Dr. Graham Heap reported at the annual Digestive Disease Week.
Pancreatitis is a well-recognized, idiosyncratic complication of thiopurine that occurs in 4%-7% of patients, independent of dose, and usually stops treatment in its tracks. Thiopurines are a mainstay treatment in inflammatory bowel disease (IBD), particularly as an adjunct to anti–tumor necrosis factor–alpha drugs.
Dr. Heap and his associates at 168 research sites recruited 314 IBD patients with pancreatitis that developed within 3 months of starting a thiopurine for the genomewide linkage study and another 119 IBD patients for a case-control cohort. Thiopurine-induced pancreatitis was adjudicated by four independent experts, and determined to be definite in 61 patients, probable in 274, possible in 28, and unlikely in 70.
Among the definite and probable cases, pancreatitis developed within an average of 24 days after starting a thiopurine. Most cases were mild, but 70% of patients were hospitalized for an average of 5.7 days, noted Dr. Heap of Royal Devon and Exeter Hospital, Devon, England.
Analyses performed on three different genotyping platforms for 177 samples identified a significant single-nucleotide polymorphism (SNP) association in chromosome 6 within the class II HLA region. All four SNPs – rs7745656, rs2647087, rs6935723, and rs2647089 – had odds ratios of 2.6, with P values of 2.2 x 10–16.
The investigators then looked in more detail at the HLA region, previously linked to celiac disease, and identified a strong association between thiopurine-induced pancreatitis and HLA-DRB1:07:01 (OR, 2.55; P = 1.17 x 10–14) and HLA-DQA1:02:01 (OR, 2.54; P = 1.68 x 10–14), he said.
The results were replicated in an independent cohort of 78 thiopurine-induced pancreatitis cases and 472 IBD controls who did not develop pancreatitis after at least a year of thiopurine therapy, and again there was a significant association with rs2647078 (OR, 2.21; P = 4 x 10–6), Dr. Heap said.
Interestingly, there was no significant association between rs2647078 and known risk factors such as smoking status at the time of pancreatitis, thiopurine methyltransferase (TPMT) status, or inosine triphosphate pyrophosphatase genotype, he said.
What all this means for clinicians is that for every 1,000 patients tested, 77 risk allele homozygotes will be identified, and these individuals will have a 17% risk of pancreatitis, Dr. Heap said. If azathioprine and 6-mercaptopurine are avoided in these individuals, the number needed to treat is 76 patients to prevent one case of pancreatitis.
Session cochair and gastroenterologist Barrett Levesque of the University of California, San Diego,said in an interview that further testing is needed, but that the study approach was very robust, especially to show a number needed to treat of 76.
"Compared to what we use, TPMT activity levels, where there’s a few patients in a thousand who might not have the activity at all, this is very promising," he said. "I thought it was a great study."
In a separate interview, Dr. Heap said, "We do not currently feel this test has clinical utility on its own, but we will investigate its utility in combination with other pharmacogenetic tests in the future."
The study was funded by the International Serious Adverse Events Consortium. The authors reported no financial disclosures.
CHICAGO – A genomewide association study has identified specific alleles that may pinpoint those at risk for thiopurine-induced pancreatitis in inflammatory bowel disease.
Patients heterozygous at rs2647087 are 2.5 times more likely to get pancreatitis if treated with thiopurine (Imuran), while those with homozygous risk alleles were 5 times more likely to do so, Dr. Graham Heap reported at the annual Digestive Disease Week.
Pancreatitis is a well-recognized, idiosyncratic complication of thiopurine that occurs in 4%-7% of patients, independent of dose, and usually stops treatment in its tracks. Thiopurines are a mainstay treatment in inflammatory bowel disease (IBD), particularly as an adjunct to anti–tumor necrosis factor–alpha drugs.
Dr. Heap and his associates at 168 research sites recruited 314 IBD patients with pancreatitis that developed within 3 months of starting a thiopurine for the genomewide linkage study and another 119 IBD patients for a case-control cohort. Thiopurine-induced pancreatitis was adjudicated by four independent experts, and determined to be definite in 61 patients, probable in 274, possible in 28, and unlikely in 70.
Among the definite and probable cases, pancreatitis developed within an average of 24 days after starting a thiopurine. Most cases were mild, but 70% of patients were hospitalized for an average of 5.7 days, noted Dr. Heap of Royal Devon and Exeter Hospital, Devon, England.
Analyses performed on three different genotyping platforms for 177 samples identified a significant single-nucleotide polymorphism (SNP) association in chromosome 6 within the class II HLA region. All four SNPs – rs7745656, rs2647087, rs6935723, and rs2647089 – had odds ratios of 2.6, with P values of 2.2 x 10–16.
The investigators then looked in more detail at the HLA region, previously linked to celiac disease, and identified a strong association between thiopurine-induced pancreatitis and HLA-DRB1:07:01 (OR, 2.55; P = 1.17 x 10–14) and HLA-DQA1:02:01 (OR, 2.54; P = 1.68 x 10–14), he said.
The results were replicated in an independent cohort of 78 thiopurine-induced pancreatitis cases and 472 IBD controls who did not develop pancreatitis after at least a year of thiopurine therapy, and again there was a significant association with rs2647078 (OR, 2.21; P = 4 x 10–6), Dr. Heap said.
Interestingly, there was no significant association between rs2647078 and known risk factors such as smoking status at the time of pancreatitis, thiopurine methyltransferase (TPMT) status, or inosine triphosphate pyrophosphatase genotype, he said.
What all this means for clinicians is that for every 1,000 patients tested, 77 risk allele homozygotes will be identified, and these individuals will have a 17% risk of pancreatitis, Dr. Heap said. If azathioprine and 6-mercaptopurine are avoided in these individuals, the number needed to treat is 76 patients to prevent one case of pancreatitis.
Session cochair and gastroenterologist Barrett Levesque of the University of California, San Diego,said in an interview that further testing is needed, but that the study approach was very robust, especially to show a number needed to treat of 76.
"Compared to what we use, TPMT activity levels, where there’s a few patients in a thousand who might not have the activity at all, this is very promising," he said. "I thought it was a great study."
In a separate interview, Dr. Heap said, "We do not currently feel this test has clinical utility on its own, but we will investigate its utility in combination with other pharmacogenetic tests in the future."
The study was funded by the International Serious Adverse Events Consortium. The authors reported no financial disclosures.
AT DDW 2014
Key clinical point: Avoiding azathioprine/6-mercaptopurine in patients with the risk alleles results in a number needed to treat of 76 patients to prevent 1 case of pancreatitis.
Major finding: Four single-nucleotide polymorphisms on chromosome 6 were significantly associated with thiopurine-induced pancreatitis.
Data source: A genomewide association study and clinical chart review.
Disclosures: The study was funded by the International Serious Adverse Events Consortium. The authors reported no financial disclosures.

Study takes air out of pre–bypass intragastric balloon
CHICAGO – Treatment with an intragastric balloon before bariatric surgery produces significant weight loss in the morbidly obese, but at the cost of more surgical complications, according to the prospective randomized BIGPOM trial.
Preoperative weight loss is recommended, and in some cases mandated by third-party payer organizations, to improve comorbidities and postoperative outcomes in the morbidly obese. It’s also been suggested to be a predictive factor of postoperative weight loss, but overall the data are limited and methodological quality of prospective studies in this area poor, Dr. Benoit Coffin said at the annual Digestive Disease Week.
The prospective BIGPOM (Balloon Intra Gastrique Préopératoire Pour Obésité Morbide) study randomly assigned 60 patients to standard medical care and 55 to an air- or water-filled intragastric balloon (IGB) for 6 months before laparoscopic bypass surgery. Their average body mass index was 54.7 kg/m2 and 53.9 kg/m2, respectively. The average balloon insertion time was 17 minutes and average age in both groups was 40 years.
Weight loss in months 0-6 was significantly higher in the IGB group, compared with standard care (–10.3 kg vs. –3.0 kg; P less than .0001), but did not differ from months 6-12 (–30.4 kg vs. –35.1 kg) or overall from months 0-12 (–40.7 kg vs. –38.1 kg), said Dr. Coffin, of Hôpital Louis Mourier, Colombes, France.
There was no significant difference in weight loss between those treated with water- or air-filled balloons (P = .0.96).
"Preoperative weight loss is not a predictive factor of postoperative weight loss," he said.
Treatment with an IGB, compared with standard care, did not modify operative time (188 minutes vs. 175 minutes), ICU stays greater than 24 hours (71.4% vs. 76%), mean hospital stay (6.8 vs. 6.3 days), or need for laparotomy (2 vs. 1).
Surgical complications, however, were significantly higher with IGB (5 vs. 0; P = .02), and included digestive hemorrhage, intraperitoneal abscess, fistula, peritonitis, occlusion, and reintervention, Dr. Coffin said.
It is not possible to conclude if the increase in complications noted in the group of patients treated by intragastric balloon is the consequence of the balloon itself or the weight loss it induced, he said.
There were no deaths or medical complications in the IGB group, although two patients experienced complications during IGB removal and one patient required surgical removal of the balloon.
Dr. Coffin reported financial relationships with Shire Pharmaceuticals, Cephalon, Almirall, Gerson Lehrman Group, Mayoly-Spindler, and Mundipharma.
CHICAGO – Treatment with an intragastric balloon before bariatric surgery produces significant weight loss in the morbidly obese, but at the cost of more surgical complications, according to the prospective randomized BIGPOM trial.
Preoperative weight loss is recommended, and in some cases mandated by third-party payer organizations, to improve comorbidities and postoperative outcomes in the morbidly obese. It’s also been suggested to be a predictive factor of postoperative weight loss, but overall the data are limited and methodological quality of prospective studies in this area poor, Dr. Benoit Coffin said at the annual Digestive Disease Week.
The prospective BIGPOM (Balloon Intra Gastrique Préopératoire Pour Obésité Morbide) study randomly assigned 60 patients to standard medical care and 55 to an air- or water-filled intragastric balloon (IGB) for 6 months before laparoscopic bypass surgery. Their average body mass index was 54.7 kg/m2 and 53.9 kg/m2, respectively. The average balloon insertion time was 17 minutes and average age in both groups was 40 years.
Weight loss in months 0-6 was significantly higher in the IGB group, compared with standard care (–10.3 kg vs. –3.0 kg; P less than .0001), but did not differ from months 6-12 (–30.4 kg vs. –35.1 kg) or overall from months 0-12 (–40.7 kg vs. –38.1 kg), said Dr. Coffin, of Hôpital Louis Mourier, Colombes, France.
There was no significant difference in weight loss between those treated with water- or air-filled balloons (P = .0.96).
"Preoperative weight loss is not a predictive factor of postoperative weight loss," he said.
Treatment with an IGB, compared with standard care, did not modify operative time (188 minutes vs. 175 minutes), ICU stays greater than 24 hours (71.4% vs. 76%), mean hospital stay (6.8 vs. 6.3 days), or need for laparotomy (2 vs. 1).
Surgical complications, however, were significantly higher with IGB (5 vs. 0; P = .02), and included digestive hemorrhage, intraperitoneal abscess, fistula, peritonitis, occlusion, and reintervention, Dr. Coffin said.
It is not possible to conclude if the increase in complications noted in the group of patients treated by intragastric balloon is the consequence of the balloon itself or the weight loss it induced, he said.
There were no deaths or medical complications in the IGB group, although two patients experienced complications during IGB removal and one patient required surgical removal of the balloon.
Dr. Coffin reported financial relationships with Shire Pharmaceuticals, Cephalon, Almirall, Gerson Lehrman Group, Mayoly-Spindler, and Mundipharma.
CHICAGO – Treatment with an intragastric balloon before bariatric surgery produces significant weight loss in the morbidly obese, but at the cost of more surgical complications, according to the prospective randomized BIGPOM trial.
Preoperative weight loss is recommended, and in some cases mandated by third-party payer organizations, to improve comorbidities and postoperative outcomes in the morbidly obese. It’s also been suggested to be a predictive factor of postoperative weight loss, but overall the data are limited and methodological quality of prospective studies in this area poor, Dr. Benoit Coffin said at the annual Digestive Disease Week.
The prospective BIGPOM (Balloon Intra Gastrique Préopératoire Pour Obésité Morbide) study randomly assigned 60 patients to standard medical care and 55 to an air- or water-filled intragastric balloon (IGB) for 6 months before laparoscopic bypass surgery. Their average body mass index was 54.7 kg/m2 and 53.9 kg/m2, respectively. The average balloon insertion time was 17 minutes and average age in both groups was 40 years.
Weight loss in months 0-6 was significantly higher in the IGB group, compared with standard care (–10.3 kg vs. –3.0 kg; P less than .0001), but did not differ from months 6-12 (–30.4 kg vs. –35.1 kg) or overall from months 0-12 (–40.7 kg vs. –38.1 kg), said Dr. Coffin, of Hôpital Louis Mourier, Colombes, France.
There was no significant difference in weight loss between those treated with water- or air-filled balloons (P = .0.96).
"Preoperative weight loss is not a predictive factor of postoperative weight loss," he said.
Treatment with an IGB, compared with standard care, did not modify operative time (188 minutes vs. 175 minutes), ICU stays greater than 24 hours (71.4% vs. 76%), mean hospital stay (6.8 vs. 6.3 days), or need for laparotomy (2 vs. 1).
Surgical complications, however, were significantly higher with IGB (5 vs. 0; P = .02), and included digestive hemorrhage, intraperitoneal abscess, fistula, peritonitis, occlusion, and reintervention, Dr. Coffin said.
It is not possible to conclude if the increase in complications noted in the group of patients treated by intragastric balloon is the consequence of the balloon itself or the weight loss it induced, he said.
There were no deaths or medical complications in the IGB group, although two patients experienced complications during IGB removal and one patient required surgical removal of the balloon.
Dr. Coffin reported financial relationships with Shire Pharmaceuticals, Cephalon, Almirall, Gerson Lehrman Group, Mayoly-Spindler, and Mundipharma.
AT DDW 2014
Key clinical point: A temporary intragastric balloon helps reduce weight in the morbidly obese awaiting bypass surgery, but induces morbidity after surgery.
Major finding: IGB patients lost more weight in months 0-6 than did controls (–10.3 kg vs. –3.0 kg; P less than .0001), but had more surgical complications (5 vs. 0; P = .02).
Data source: A prospective study in 115 morbidly obese patients.
Disclosures: Dr. Coffin reported financial relationships with Shire Pharmaceuticals, Cephalon, Almirall, Gerson Lehrman Group, Mayoly-Spindler, and Mundipharma.
Early endoscopic follow-up nets dysplasia in 9.5% of Barrett’s
CHICAGO – Early endoscopic follow-up within 24 months detected dysplasia in nearly one in 10 patients with nondysplastic or low-grade Barrett’s esophagus in a retrospective study at the Mayo Clinic.
Initial endoscopy missed four cases of high-grade dysplasia or esophageal adenocarcinoma (1.9%) and 16 cases of low-grade dysplasia (7.6%) for an overall miss-rate of 9.5%.
Patients on proton pump inhibitors were less likely to have dysplasia missed than were those off PPIs (20% vs. 52.6%, P = .008).
Those with long- versus short-segment Barrett’s esophagus were more likely to have dysplasia overlooked (85% vs. 53.6%; P = .008; mean 6 mm vs. 4 mm; P = .006), Dr. Kavel Visrodia said at the annual Digestive Disease Week.

Current American College of Gastroenterology (ACG) guidelines recommend early repeat esophagogastroduodenoscopy (EGD) to exclude the presence of missed dysplasia in newly diagnosed nondysplastic Barrett’s esophagus (BE), while the ACG and American Society for Gastrointestinal Endoscopy call for repeat EGD within 6 months for those with low-grade dysplasia.
The yield for repeat EGD has not been established, and only one study exists in the literature, said Dr. Visrodia of the department of medicine, Mayo Clinic, Rochester, Minn.
That study (Dis. Esophagus 2012 Sept. 28. [doi:10.1111/j.1442-2050.2012.01431.x]) showed a miss-rate of 8.2% among 146 patients with newly diagnosed nondysplastic BE. Long-segment BE was the only significant predictor of dysplasia on follow-up (odds ratio, 9.18; P = .008).
The cohort was relatively small and had no long-term follow-up, and with an interval to follow-up of 36 months, "it’s possible that some of these were actually incident cases of dysplasia and not prevalent cases," he said.
To address these gaps, Dr. Visrodia and his colleagues identified 488 BE cases from 1977 to 2011 in the Rochester Epidemiology Project in Olmsted County, Minn. A total of 278 patients were excluded because of high-grade dysplasia (HGD) or esophageal cancer on index endoscopy or repeat endoscopy after 24 months, leaving 181 patients with nondysplastic BE and 29 with low-grade dysplasia (LGD).
Repeat endoscopy within 24 months revealed 2 cases of HGD or cancer and 16 cases of LGD in the nondysplastic BE group, and 2 cases of HGD or cancer in the LGD group, Dr. Visrodia said.
Three of the four HGD/cancer cases were in patients with long-segment BE, defined as at least 3 cm of columnar mucosa.
Biopsies were insufficient in 63% of patients with missed dysplasia, compared with 55% in the group without missed dysplasia. Biopsies were considered adequate if the number of biopsies divided by the BE length was at least 2, indicating that samples were taken every 2 cm in accordance with guidelines. This risk factor is noteworthy, although the difference between groups was not statistically significant, possibly because of the small sample size, he said.
Finally, after a median of 6.8 years of follow-up, 30 asymptomatic, prevalent HGDs or cancers were detected within 24 months, compared with 22 incident cases detected after 24 months. This suggests that "a greater number of high-grade dysplasias and cancers were detected up front rather than during long-term careful surveillance," Dr. Visrodia said.
During a discussion of the study, one attendee asked whether the results make a better case for aggressive ablation up front rather than for surveillance, while others expressed surprise at the high miss rate at an institution such as the Mayo Clinic.
Dr. Visrodia replied that the results do give them pause, and suggested that tighter early endoscopic surveillance may be warranted, particularly in those with long-segment BE.
Dr. Visrodia and his coauthors reported no financial disclosures.
CHICAGO – Early endoscopic follow-up within 24 months detected dysplasia in nearly one in 10 patients with nondysplastic or low-grade Barrett’s esophagus in a retrospective study at the Mayo Clinic.
Initial endoscopy missed four cases of high-grade dysplasia or esophageal adenocarcinoma (1.9%) and 16 cases of low-grade dysplasia (7.6%) for an overall miss-rate of 9.5%.
Patients on proton pump inhibitors were less likely to have dysplasia missed than were those off PPIs (20% vs. 52.6%, P = .008).
Those with long- versus short-segment Barrett’s esophagus were more likely to have dysplasia overlooked (85% vs. 53.6%; P = .008; mean 6 mm vs. 4 mm; P = .006), Dr. Kavel Visrodia said at the annual Digestive Disease Week.
Current American College of Gastroenterology (ACG) guidelines recommend early repeat esophagogastroduodenoscopy (EGD) to exclude the presence of missed dysplasia in newly diagnosed nondysplastic Barrett’s esophagus (BE), while the ACG and American Society for Gastrointestinal Endoscopy call for repeat EGD within 6 months for those with low-grade dysplasia.
The yield for repeat EGD has not been established, and only one study exists in the literature, said Dr. Visrodia of the department of medicine, Mayo Clinic, Rochester, Minn.
That study (Dis. Esophagus 2012 Sept. 28. [doi:10.1111/j.1442-2050.2012.01431.x]) showed a miss-rate of 8.2% among 146 patients with newly diagnosed nondysplastic BE. Long-segment BE was the only significant predictor of dysplasia on follow-up (odds ratio, 9.18; P = .008).
The cohort was relatively small and had no long-term follow-up, and with an interval to follow-up of 36 months, "it’s possible that some of these were actually incident cases of dysplasia and not prevalent cases," he said.
To address these gaps, Dr. Visrodia and his colleagues identified 488 BE cases from 1977 to 2011 in the Rochester Epidemiology Project in Olmsted County, Minn. A total of 278 patients were excluded because of high-grade dysplasia (HGD) or esophageal cancer on index endoscopy or repeat endoscopy after 24 months, leaving 181 patients with nondysplastic BE and 29 with low-grade dysplasia (LGD).
Repeat endoscopy within 24 months revealed 2 cases of HGD or cancer and 16 cases of LGD in the nondysplastic BE group, and 2 cases of HGD or cancer in the LGD group, Dr. Visrodia said.
Three of the four HGD/cancer cases were in patients with long-segment BE, defined as at least 3 cm of columnar mucosa.
Biopsies were insufficient in 63% of patients with missed dysplasia, compared with 55% in the group without missed dysplasia. Biopsies were considered adequate if the number of biopsies divided by the BE length was at least 2, indicating that samples were taken every 2 cm in accordance with guidelines. This risk factor is noteworthy, although the difference between groups was not statistically significant, possibly because of the small sample size, he said.
Finally, after a median of 6.8 years of follow-up, 30 asymptomatic, prevalent HGDs or cancers were detected within 24 months, compared with 22 incident cases detected after 24 months. This suggests that "a greater number of high-grade dysplasias and cancers were detected up front rather than during long-term careful surveillance," Dr. Visrodia said.
During a discussion of the study, one attendee asked whether the results make a better case for aggressive ablation up front rather than for surveillance, while others expressed surprise at the high miss rate at an institution such as the Mayo Clinic.
Dr. Visrodia replied that the results do give them pause, and suggested that tighter early endoscopic surveillance may be warranted, particularly in those with long-segment BE.
Dr. Visrodia and his coauthors reported no financial disclosures.
CHICAGO – Early endoscopic follow-up within 24 months detected dysplasia in nearly one in 10 patients with nondysplastic or low-grade Barrett’s esophagus in a retrospective study at the Mayo Clinic.
Initial endoscopy missed four cases of high-grade dysplasia or esophageal adenocarcinoma (1.9%) and 16 cases of low-grade dysplasia (7.6%) for an overall miss-rate of 9.5%.
Patients on proton pump inhibitors were less likely to have dysplasia missed than were those off PPIs (20% vs. 52.6%, P = .008).
Those with long- versus short-segment Barrett’s esophagus were more likely to have dysplasia overlooked (85% vs. 53.6%; P = .008; mean 6 mm vs. 4 mm; P = .006), Dr. Kavel Visrodia said at the annual Digestive Disease Week.
Current American College of Gastroenterology (ACG) guidelines recommend early repeat esophagogastroduodenoscopy (EGD) to exclude the presence of missed dysplasia in newly diagnosed nondysplastic Barrett’s esophagus (BE), while the ACG and American Society for Gastrointestinal Endoscopy call for repeat EGD within 6 months for those with low-grade dysplasia.
The yield for repeat EGD has not been established, and only one study exists in the literature, said Dr. Visrodia of the department of medicine, Mayo Clinic, Rochester, Minn.
That study (Dis. Esophagus 2012 Sept. 28. [doi:10.1111/j.1442-2050.2012.01431.x]) showed a miss-rate of 8.2% among 146 patients with newly diagnosed nondysplastic BE. Long-segment BE was the only significant predictor of dysplasia on follow-up (odds ratio, 9.18; P = .008).
The cohort was relatively small and had no long-term follow-up, and with an interval to follow-up of 36 months, "it’s possible that some of these were actually incident cases of dysplasia and not prevalent cases," he said.
To address these gaps, Dr. Visrodia and his colleagues identified 488 BE cases from 1977 to 2011 in the Rochester Epidemiology Project in Olmsted County, Minn. A total of 278 patients were excluded because of high-grade dysplasia (HGD) or esophageal cancer on index endoscopy or repeat endoscopy after 24 months, leaving 181 patients with nondysplastic BE and 29 with low-grade dysplasia (LGD).
Repeat endoscopy within 24 months revealed 2 cases of HGD or cancer and 16 cases of LGD in the nondysplastic BE group, and 2 cases of HGD or cancer in the LGD group, Dr. Visrodia said.
Three of the four HGD/cancer cases were in patients with long-segment BE, defined as at least 3 cm of columnar mucosa.
Biopsies were insufficient in 63% of patients with missed dysplasia, compared with 55% in the group without missed dysplasia. Biopsies were considered adequate if the number of biopsies divided by the BE length was at least 2, indicating that samples were taken every 2 cm in accordance with guidelines. This risk factor is noteworthy, although the difference between groups was not statistically significant, possibly because of the small sample size, he said.
Finally, after a median of 6.8 years of follow-up, 30 asymptomatic, prevalent HGDs or cancers were detected within 24 months, compared with 22 incident cases detected after 24 months. This suggests that "a greater number of high-grade dysplasias and cancers were detected up front rather than during long-term careful surveillance," Dr. Visrodia said.
During a discussion of the study, one attendee asked whether the results make a better case for aggressive ablation up front rather than for surveillance, while others expressed surprise at the high miss rate at an institution such as the Mayo Clinic.
Dr. Visrodia replied that the results do give them pause, and suggested that tighter early endoscopic surveillance may be warranted, particularly in those with long-segment BE.
Dr. Visrodia and his coauthors reported no financial disclosures.
AT DDW 2014
Key clinical point: Early endoscopic follow-up catches 9.5% of dysplasia missed on initial exam, but is not universally recommended by medical societies.
Major finding: Index endoscopy missed 1.9% of high-grade dysplasia or esophageal cancer and 7.6% of low-grade dysplasia.
Data source: A retrospective study in 181 patients with Barrett’s esophagus.
Disclosures: Dr. Visrodia and his coauthors reported no financial disclosures.

Fecal transplant falls short in UC, but may not be the end
CHICAGO – Results were negative from the first randomized placebo-controlled trial of fecal microbiota transplant in ulcerative colitis, but enthusiasm remains for this newly regulated and trendy therapy.
"We need to get more data and we need to understand how better to use this approach, but I don’t think this study is telling us we should stop exploring. I still think it is an interesting avenue that we need to evaluate," study author Dr. Paul Moayyedi said during a late-breaking abstract session at Digestive Disease Week.

Part of the enthusiasm for what was described as "the new kid on the block for altering gut flora," has been fueled by a roughly 90% success rate for fecal transplant in treating Clostridium difficile infection.
Dr. Moayyedi also showcased a success story from the trial that "typifies a few patients in this study." The patient had ulcerative colitis for almost 20 years that was unresponsive to steroids and 5-aminosalicylic acid for 2 years before the study and so severe it caused bloody diarrhea 10-20 times per day. No improvement was seen after 6 weeks of placebo therapy and his Mayo Clinic score was "about as bad as it can be" at 12.
After crossing over to 6 weeks of open-label fecal microbiota transplantation (FMT), symptoms were much improved and his Mayo score dropped to 5. After 20 weeks, mucosa healed throughout the colon, his Mayo score reached 0, and he was "fine" on no medication.
"What we’re finding is that 6 weeks is usually not enough and that if you continue longer, you can get remission in some patients," said Dr. Moayyedi, the Richard Hunt-Astra Zeneca Chair in Gastroenterology, McMaster University, Hamilton, Ontario.
He went on to say, "I’m a very big proponent of evidenced-based medicine, but cases like these make you think something must be going on in some patients, but we don’t have the funding to do the 500-patient trial you need to get that signal."
Dr. Moayyedi and his associates enrolled ambulatory patients with active ulcerative colitis, defined as a Mayo score of at least 4 and an endoscopic Mayo score of at least 1, who tested negative for the C. difficile gene. Patients could be on ulcerative colitis medications, if doses were stable for at least 12 weeks but had to be off antibiotics for 30 days.
Patients were randomly assigned to receive a 50-mL retention enema containing fecal microbiota from an anonymous donor or water, once per week for 6 weeks. The primary outcome was remission of ulcerative colitis, defined as a Mayo score of 2 or less and an endoscopic Mayo score of 0 at week 7. Patients, clinicians, and investigators were blinded to therapy.
The 31 FMT and 30 placebo patients were well matched at baseline, except for significantly more pancolitis in the FMT group (64% vs. 36%).
Remission was achieved by seven FMT patients (23%) and two placebo patients (7%), which was not significantly different (P = .15), Dr. Moayyedi said.
There also were no differences between the FMT and placebo groups in any of the secondary outcomes: 6-week Mayo score (6.36 vs. 6.30; P = .95), 6-week Inflammatory Bowel Disease Questionnaire (148.4 vs. 146.4; P = .85), and 6-week EQ-5D health questionnaire (61.0 vs. 66.2; P = .34).
Based on these findings, the study is being stopped for futility, he said.
There were no major adverse events, although the diagnosis changed to Crohn’s colitis for two patients given FMT and one on placebo.
This was "much bigger than you’d expect," Dr. Moayyedi said. "We’re not sure why, and of course the worry is that FMT may change the phenotype, which would not be good."
If FMT is to succeed in ulcerative colitis, he suggested more data will be needed on the fecal microbiome and the best approach to administer FMT, including donor selection, timing, preparation, and duration of treatment. The group has not done an analysis of enema dwell time and response, and no signal was seen that FMT is more effective in left-sided disease.
More detailed microbiome analyses of the patient highlighted during the talk, however, revealed the man had a "very diverse and unstable" microbiome at baseline that gradually became more stable, "with a loss of Ruminococcus that seems to be a feature of improvement and a movement toward the phenotype of the donor," Dr. Moayyedi said.
During a discussion of the results, some audience members expressed concern that FMT might change the phenotype, while others were more enthusiastic about the therapy.
Dr. Scott Harris, a gastroenterologist and professor of medicine, Georgetown University Medical Center, Washington, said the trial was likely underpowered, and that by including patients with less severe disease, it may have been more difficult to see a treatment effect. Other trials have also shown that 6 weeks of therapy may not be enough for refractory patients.
"I’m very optimistic, I wouldn’t stop at this point," he said.
Session cochair Dr. John M. Inadomi, professor of medicine and head of gastroenterology, University of Washington School of Medicine, Seattle, agreed that the length of treatment as well as the study’s use of anonymous donors could have affected results. One of the big questions is whether the donor feces actually grafted and thus affected the recipient.
"If you use the wrong donor stool, if the stool didn’t graft, these kinds of things can obviously make a negative result, even if the concept is potentially fine," he said in an interview.
Last year, the Food and Drug Administration moved to require an investigational new drug permit to treat C. difficile with fecal microbiota, but changed course within weeks citing public pressure. While researchers are studying the potential to deliver feces via capsule, Dr. Moayyedi observed that some enthusiasts are offering Internet advice on how to mix your own FMT at home.
Dr. Moayyedi reported financial ties with AstraZeneca Pharmaceuticals, Forest Laboratories, and Shire Canada. Dr. Harris reported no conflicting interests. Dr. Inadomi reported financial relationships with Given Imaging, ChemImage, Cernostics, and Epigenomics.
CHICAGO – Results were negative from the first randomized placebo-controlled trial of fecal microbiota transplant in ulcerative colitis, but enthusiasm remains for this newly regulated and trendy therapy.
"We need to get more data and we need to understand how better to use this approach, but I don’t think this study is telling us we should stop exploring. I still think it is an interesting avenue that we need to evaluate," study author Dr. Paul Moayyedi said during a late-breaking abstract session at Digestive Disease Week.
Part of the enthusiasm for what was described as "the new kid on the block for altering gut flora," has been fueled by a roughly 90% success rate for fecal transplant in treating Clostridium difficile infection.
Dr. Moayyedi also showcased a success story from the trial that "typifies a few patients in this study." The patient had ulcerative colitis for almost 20 years that was unresponsive to steroids and 5-aminosalicylic acid for 2 years before the study and so severe it caused bloody diarrhea 10-20 times per day. No improvement was seen after 6 weeks of placebo therapy and his Mayo Clinic score was "about as bad as it can be" at 12.
After crossing over to 6 weeks of open-label fecal microbiota transplantation (FMT), symptoms were much improved and his Mayo score dropped to 5. After 20 weeks, mucosa healed throughout the colon, his Mayo score reached 0, and he was "fine" on no medication.
"What we’re finding is that 6 weeks is usually not enough and that if you continue longer, you can get remission in some patients," said Dr. Moayyedi, the Richard Hunt-Astra Zeneca Chair in Gastroenterology, McMaster University, Hamilton, Ontario.
He went on to say, "I’m a very big proponent of evidenced-based medicine, but cases like these make you think something must be going on in some patients, but we don’t have the funding to do the 500-patient trial you need to get that signal."
Dr. Moayyedi and his associates enrolled ambulatory patients with active ulcerative colitis, defined as a Mayo score of at least 4 and an endoscopic Mayo score of at least 1, who tested negative for the C. difficile gene. Patients could be on ulcerative colitis medications, if doses were stable for at least 12 weeks but had to be off antibiotics for 30 days.
Patients were randomly assigned to receive a 50-mL retention enema containing fecal microbiota from an anonymous donor or water, once per week for 6 weeks. The primary outcome was remission of ulcerative colitis, defined as a Mayo score of 2 or less and an endoscopic Mayo score of 0 at week 7. Patients, clinicians, and investigators were blinded to therapy.
The 31 FMT and 30 placebo patients were well matched at baseline, except for significantly more pancolitis in the FMT group (64% vs. 36%).
Remission was achieved by seven FMT patients (23%) and two placebo patients (7%), which was not significantly different (P = .15), Dr. Moayyedi said.
There also were no differences between the FMT and placebo groups in any of the secondary outcomes: 6-week Mayo score (6.36 vs. 6.30; P = .95), 6-week Inflammatory Bowel Disease Questionnaire (148.4 vs. 146.4; P = .85), and 6-week EQ-5D health questionnaire (61.0 vs. 66.2; P = .34).
Based on these findings, the study is being stopped for futility, he said.
There were no major adverse events, although the diagnosis changed to Crohn’s colitis for two patients given FMT and one on placebo.
This was "much bigger than you’d expect," Dr. Moayyedi said. "We’re not sure why, and of course the worry is that FMT may change the phenotype, which would not be good."
If FMT is to succeed in ulcerative colitis, he suggested more data will be needed on the fecal microbiome and the best approach to administer FMT, including donor selection, timing, preparation, and duration of treatment. The group has not done an analysis of enema dwell time and response, and no signal was seen that FMT is more effective in left-sided disease.
More detailed microbiome analyses of the patient highlighted during the talk, however, revealed the man had a "very diverse and unstable" microbiome at baseline that gradually became more stable, "with a loss of Ruminococcus that seems to be a feature of improvement and a movement toward the phenotype of the donor," Dr. Moayyedi said.
During a discussion of the results, some audience members expressed concern that FMT might change the phenotype, while others were more enthusiastic about the therapy.
Dr. Scott Harris, a gastroenterologist and professor of medicine, Georgetown University Medical Center, Washington, said the trial was likely underpowered, and that by including patients with less severe disease, it may have been more difficult to see a treatment effect. Other trials have also shown that 6 weeks of therapy may not be enough for refractory patients.
"I’m very optimistic, I wouldn’t stop at this point," he said.
Session cochair Dr. John M. Inadomi, professor of medicine and head of gastroenterology, University of Washington School of Medicine, Seattle, agreed that the length of treatment as well as the study’s use of anonymous donors could have affected results. One of the big questions is whether the donor feces actually grafted and thus affected the recipient.
"If you use the wrong donor stool, if the stool didn’t graft, these kinds of things can obviously make a negative result, even if the concept is potentially fine," he said in an interview.
Last year, the Food and Drug Administration moved to require an investigational new drug permit to treat C. difficile with fecal microbiota, but changed course within weeks citing public pressure. While researchers are studying the potential to deliver feces via capsule, Dr. Moayyedi observed that some enthusiasts are offering Internet advice on how to mix your own FMT at home.
Dr. Moayyedi reported financial ties with AstraZeneca Pharmaceuticals, Forest Laboratories, and Shire Canada. Dr. Harris reported no conflicting interests. Dr. Inadomi reported financial relationships with Given Imaging, ChemImage, Cernostics, and Epigenomics.
CHICAGO – Results were negative from the first randomized placebo-controlled trial of fecal microbiota transplant in ulcerative colitis, but enthusiasm remains for this newly regulated and trendy therapy.
"We need to get more data and we need to understand how better to use this approach, but I don’t think this study is telling us we should stop exploring. I still think it is an interesting avenue that we need to evaluate," study author Dr. Paul Moayyedi said during a late-breaking abstract session at Digestive Disease Week.
Part of the enthusiasm for what was described as "the new kid on the block for altering gut flora," has been fueled by a roughly 90% success rate for fecal transplant in treating Clostridium difficile infection.
Dr. Moayyedi also showcased a success story from the trial that "typifies a few patients in this study." The patient had ulcerative colitis for almost 20 years that was unresponsive to steroids and 5-aminosalicylic acid for 2 years before the study and so severe it caused bloody diarrhea 10-20 times per day. No improvement was seen after 6 weeks of placebo therapy and his Mayo Clinic score was "about as bad as it can be" at 12.
After crossing over to 6 weeks of open-label fecal microbiota transplantation (FMT), symptoms were much improved and his Mayo score dropped to 5. After 20 weeks, mucosa healed throughout the colon, his Mayo score reached 0, and he was "fine" on no medication.
"What we’re finding is that 6 weeks is usually not enough and that if you continue longer, you can get remission in some patients," said Dr. Moayyedi, the Richard Hunt-Astra Zeneca Chair in Gastroenterology, McMaster University, Hamilton, Ontario.
He went on to say, "I’m a very big proponent of evidenced-based medicine, but cases like these make you think something must be going on in some patients, but we don’t have the funding to do the 500-patient trial you need to get that signal."
Dr. Moayyedi and his associates enrolled ambulatory patients with active ulcerative colitis, defined as a Mayo score of at least 4 and an endoscopic Mayo score of at least 1, who tested negative for the C. difficile gene. Patients could be on ulcerative colitis medications, if doses were stable for at least 12 weeks but had to be off antibiotics for 30 days.
Patients were randomly assigned to receive a 50-mL retention enema containing fecal microbiota from an anonymous donor or water, once per week for 6 weeks. The primary outcome was remission of ulcerative colitis, defined as a Mayo score of 2 or less and an endoscopic Mayo score of 0 at week 7. Patients, clinicians, and investigators were blinded to therapy.
The 31 FMT and 30 placebo patients were well matched at baseline, except for significantly more pancolitis in the FMT group (64% vs. 36%).
Remission was achieved by seven FMT patients (23%) and two placebo patients (7%), which was not significantly different (P = .15), Dr. Moayyedi said.
There also were no differences between the FMT and placebo groups in any of the secondary outcomes: 6-week Mayo score (6.36 vs. 6.30; P = .95), 6-week Inflammatory Bowel Disease Questionnaire (148.4 vs. 146.4; P = .85), and 6-week EQ-5D health questionnaire (61.0 vs. 66.2; P = .34).
Based on these findings, the study is being stopped for futility, he said.
There were no major adverse events, although the diagnosis changed to Crohn’s colitis for two patients given FMT and one on placebo.
This was "much bigger than you’d expect," Dr. Moayyedi said. "We’re not sure why, and of course the worry is that FMT may change the phenotype, which would not be good."
If FMT is to succeed in ulcerative colitis, he suggested more data will be needed on the fecal microbiome and the best approach to administer FMT, including donor selection, timing, preparation, and duration of treatment. The group has not done an analysis of enema dwell time and response, and no signal was seen that FMT is more effective in left-sided disease.
More detailed microbiome analyses of the patient highlighted during the talk, however, revealed the man had a "very diverse and unstable" microbiome at baseline that gradually became more stable, "with a loss of Ruminococcus that seems to be a feature of improvement and a movement toward the phenotype of the donor," Dr. Moayyedi said.
During a discussion of the results, some audience members expressed concern that FMT might change the phenotype, while others were more enthusiastic about the therapy.
Dr. Scott Harris, a gastroenterologist and professor of medicine, Georgetown University Medical Center, Washington, said the trial was likely underpowered, and that by including patients with less severe disease, it may have been more difficult to see a treatment effect. Other trials have also shown that 6 weeks of therapy may not be enough for refractory patients.
"I’m very optimistic, I wouldn’t stop at this point," he said.
Session cochair Dr. John M. Inadomi, professor of medicine and head of gastroenterology, University of Washington School of Medicine, Seattle, agreed that the length of treatment as well as the study’s use of anonymous donors could have affected results. One of the big questions is whether the donor feces actually grafted and thus affected the recipient.
"If you use the wrong donor stool, if the stool didn’t graft, these kinds of things can obviously make a negative result, even if the concept is potentially fine," he said in an interview.
Last year, the Food and Drug Administration moved to require an investigational new drug permit to treat C. difficile with fecal microbiota, but changed course within weeks citing public pressure. While researchers are studying the potential to deliver feces via capsule, Dr. Moayyedi observed that some enthusiasts are offering Internet advice on how to mix your own FMT at home.
Dr. Moayyedi reported financial ties with AstraZeneca Pharmaceuticals, Forest Laboratories, and Shire Canada. Dr. Harris reported no conflicting interests. Dr. Inadomi reported financial relationships with Given Imaging, ChemImage, Cernostics, and Epigenomics.
AT DDW 2014
Key clinical finding: Fecal microbiota transplant is not ready for ulcerative colitis yet.
Major finding: Remission was achieved by seven FMT patients (23%) and two placebo patients (7%) (P = .15).
Data source: A double-blind, prospective study of 61 patients with ulcerative colitis.
Disclosures: Dr. Moayyedi reported financial ties with AstraZeneca Pharmaceuticals, Forest Laboratories, and Shire Canada. Dr. Harris reported no conflicting interests. Dr. Inadomi reported financial relationships with Given Imaging, ChemImage, Cernostics, and Epigenomics.

Lobectomy suffices for surgery of small papillary thyroid cancers
BOSTON – Extensive surgery beyond lobectomy offers no survival advantage for small papillary thyroid cancers, according to a large database analysis.
Total thyroidectomy was not associated with an overall survival benefit over lobectomy for papillary thyroid cancers sized 1-2 cm (hazard ratio, 1.05; P = .61) or 2.1-4.0 cm (HR, 0.89; P = .21), even after adjusting for multiple patient and pathologic factors.
"Despite guidelines, our results call into question whether tumor size 1-4 cm should be an absolute determinant for extent of surgery," Dr. Mohamed Abdelgadir Adam said at the annual meeting of the American Surgical Association.
Current American Thyroid Association guidelines recommend lobectomy for tumors less than 1 cm in size and total thyroidectomy for those exceeding 1 cm.

"Using total thyroidectomy based on tumor size alone may unnecessarily subject patients to increased risks of complications without a survival benefit," he said. "In addition to tumor size up to 4 cm, other factors are important for determining extent of surgery such as nodal and distant metastases and patient preference."
The extent of surgery for papillary thyroid cancer, however, remains controversial. Recent analyses (Arch. Otolaryngol. Head Neck Surg. 2010;136:1055-61) have shown no survival difference between lobectomy and total thyroidectomy, while an earlier landmark study found improved overall survival with total thyroidectomy for tumors 1 cm or more (Ann. Surg. 2007;246;375-81). The latter study, however, has been criticized because it did not take into account patient comorbidities, multifocality, extrathyroidal extension, or completeness of resection, said Dr. Adam of Duke University School of Medicine, Durham, N.C.
The current analysis adjusted for age, gender, race, annual income, insurance status, hospital volume, patient comorbidities, tumor multifocality, extrathyroidal extension, lymph node involvement, metastases, surgical margins, and radioactive iodine ablation.
Discussant Dr. Blake Cady, professor emeritus of surgery at Harvard Medical School and Massachusetts General Hospital in Boston, said the current report is an important contribution to the controversy. It also supports his own bias against overtreatment of these mostly young patients with total thyroidectomy, which necessitates long-term medication and is accompanied by almost routine use of radioactive iodine, despite no evidence it improves outcomes in low-risk patients.
"In no other human cancer with a 99% 20-year survival is a policy of routine total primary organ removal practiced and routine systemic therapy used," he said. "Therefore, this report may help to scale back toward a more measured balance between treatment and morbidity."
Study coauthor Dr. Julie Ann Sosa, chief of endocrine surgery at Duke, challenged the audience to promote the growing body of evidence supporting equivalence in overall survival, such as a recent study described as coming the closest to a head-to-head comparison and having the longest follow-up at 18 years. It showed equivalence between lobectomy, without radioactive iodine, and total thyroidectomy for overall, progression-free, and disease-specific survival and risk of recurrence in tumors 40 mm or less (World J. Surg. 2014;38:68-79.
"In light of these data, I think it is probably high time for guidelines to potentially reconsider this issue," she said, noting that the American Thyroid Association will issue new guidelines later this spring or summer.
Dr. Sosa also advocated for "a more sophisticated approach" to preoperative evaluation and risk stratification for papillary thyroid cancer that distinguishes between low-, medium-, and high-risk tumors. The Duke study did not exclude most high-risk tumors, but rather adjusted for high-risk characteristics such as extrathyroidal extension, lymph node involvement, and distant metastases.
"When you adjust for these high-risk characteristics, the afforded overall survival benefit disappears," she said. "So what I think we would argue is that there is equivalence in outcome for the majority of patients for low- and medium-risk tumors. But for those patients who have high-risk tumors, as defined by some of these high-risk characteristics, then I think all of us would agree that total thyroidectomy, with or without radioactive iodine, would be indicated."
The study involved 61,775 patients in the National Cancer Database who underwent total thyroidectomy (n = 54,926) or lobectomy with or without isthmusectomy (n = 6,849) for papillary thyroid cancer from 1998 to 2006. Compared with the lobectomy group, the thyroidectomy group had more tumor multifocality (44% vs. 29%), positive surgical margins (27% vs. 7%), distant metastases (1% vs. 0.4%), and radioactive iodine (65% vs. 33%; P value less than .01 for all).
In multivariable analysis, nodal and distant metastases were associated with compromised survival, Dr. Adam said.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting, April 2014 in Boston, is anticipated to be published in the Annals of Surgery, pending editorial review.
The authors reported no conflicting interests
This excellent study by Adam et al. contributes to a growing body of literature supporting thyroid lobectomy for low risk, small, differentiated thyroid tumors. I should say this represents a shift back toward lobectomy. Total thyroidectomy became the procedure of choice for nearly all differentiated thyroid tumors over the last 2-3 decades in part because of the landmark study by Bilimoria et al. (Surgery 2007;142:906-14).
Now the tide is shifting back the other direction.
I do not mean to imply that passing trends drive how we treat thyroid cancer. Mortality rates from differentiated thyroid cancer remain extremely low. This makes measuring any differences in mortality challenging. The outcome can differ depending on the cohort and the other variables included in the modeling. Recurrence is the real driver of morbidity in thyroid cancer, with anywhere from 10%-30% of patients experiencing a recurrence. Unfortunately, large national cancer registries do not capture recurrence very well.
This study controlled for many tumor features that will also impact disease specific survival apart from just the treatment received. The follow-up time is also impressive. So, if we are to undertake a more nuanced and stratified approach to determining the extent of surgery, there are a few things to consider. The first is patient selection.
In this study and in a growing body of retrospective, single institution studies looking at lobectomy for low-risk cancers, one must remember that these patients are selected based on other tumor features (multifocality, extrathyroidal extension, etc.) and not just size alone. Remember that 30%-40% of patients with papillary thyroid cancer will have multifocal disease.
The second is that successfully treating thyroid cancer patients with lobectomy requires buy-in from all parties involved - surgeons, endocrinologists, and, most importantly, the patient. Everyone must be comfortable with omitting radioactive iodine, detectable thyroglobulin levels, and following the remaining lobe with ultrasound. Some patients will not be comfortable with this and may choose to undergo total thyroidectomy. Even if we surgeons agree to shift back toward less aggressive surgery, we cannot do so in isolation.
Dr. David F. Schneider is an associate professor and the director of endocrine surgery research in the department of surgery, University of Wisconsin, Madison. He has no conflicts to disclose.
This excellent study by Adam et al. contributes to a growing body of literature supporting thyroid lobectomy for low risk, small, differentiated thyroid tumors. I should say this represents a shift back toward lobectomy. Total thyroidectomy became the procedure of choice for nearly all differentiated thyroid tumors over the last 2-3 decades in part because of the landmark study by Bilimoria et al. (Surgery 2007;142:906-14).
Now the tide is shifting back the other direction.
I do not mean to imply that passing trends drive how we treat thyroid cancer. Mortality rates from differentiated thyroid cancer remain extremely low. This makes measuring any differences in mortality challenging. The outcome can differ depending on the cohort and the other variables included in the modeling. Recurrence is the real driver of morbidity in thyroid cancer, with anywhere from 10%-30% of patients experiencing a recurrence. Unfortunately, large national cancer registries do not capture recurrence very well.
This study controlled for many tumor features that will also impact disease specific survival apart from just the treatment received. The follow-up time is also impressive. So, if we are to undertake a more nuanced and stratified approach to determining the extent of surgery, there are a few things to consider. The first is patient selection.
In this study and in a growing body of retrospective, single institution studies looking at lobectomy for low-risk cancers, one must remember that these patients are selected based on other tumor features (multifocality, extrathyroidal extension, etc.) and not just size alone. Remember that 30%-40% of patients with papillary thyroid cancer will have multifocal disease.
The second is that successfully treating thyroid cancer patients with lobectomy requires buy-in from all parties involved - surgeons, endocrinologists, and, most importantly, the patient. Everyone must be comfortable with omitting radioactive iodine, detectable thyroglobulin levels, and following the remaining lobe with ultrasound. Some patients will not be comfortable with this and may choose to undergo total thyroidectomy. Even if we surgeons agree to shift back toward less aggressive surgery, we cannot do so in isolation.
Dr. David F. Schneider is an associate professor and the director of endocrine surgery research in the department of surgery, University of Wisconsin, Madison. He has no conflicts to disclose.
This excellent study by Adam et al. contributes to a growing body of literature supporting thyroid lobectomy for low risk, small, differentiated thyroid tumors. I should say this represents a shift back toward lobectomy. Total thyroidectomy became the procedure of choice for nearly all differentiated thyroid tumors over the last 2-3 decades in part because of the landmark study by Bilimoria et al. (Surgery 2007;142:906-14).
Now the tide is shifting back the other direction.
I do not mean to imply that passing trends drive how we treat thyroid cancer. Mortality rates from differentiated thyroid cancer remain extremely low. This makes measuring any differences in mortality challenging. The outcome can differ depending on the cohort and the other variables included in the modeling. Recurrence is the real driver of morbidity in thyroid cancer, with anywhere from 10%-30% of patients experiencing a recurrence. Unfortunately, large national cancer registries do not capture recurrence very well.
This study controlled for many tumor features that will also impact disease specific survival apart from just the treatment received. The follow-up time is also impressive. So, if we are to undertake a more nuanced and stratified approach to determining the extent of surgery, there are a few things to consider. The first is patient selection.
In this study and in a growing body of retrospective, single institution studies looking at lobectomy for low-risk cancers, one must remember that these patients are selected based on other tumor features (multifocality, extrathyroidal extension, etc.) and not just size alone. Remember that 30%-40% of patients with papillary thyroid cancer will have multifocal disease.
The second is that successfully treating thyroid cancer patients with lobectomy requires buy-in from all parties involved - surgeons, endocrinologists, and, most importantly, the patient. Everyone must be comfortable with omitting radioactive iodine, detectable thyroglobulin levels, and following the remaining lobe with ultrasound. Some patients will not be comfortable with this and may choose to undergo total thyroidectomy. Even if we surgeons agree to shift back toward less aggressive surgery, we cannot do so in isolation.
Dr. David F. Schneider is an associate professor and the director of endocrine surgery research in the department of surgery, University of Wisconsin, Madison. He has no conflicts to disclose.
BOSTON – Extensive surgery beyond lobectomy offers no survival advantage for small papillary thyroid cancers, according to a large database analysis.
Total thyroidectomy was not associated with an overall survival benefit over lobectomy for papillary thyroid cancers sized 1-2 cm (hazard ratio, 1.05; P = .61) or 2.1-4.0 cm (HR, 0.89; P = .21), even after adjusting for multiple patient and pathologic factors.
"Despite guidelines, our results call into question whether tumor size 1-4 cm should be an absolute determinant for extent of surgery," Dr. Mohamed Abdelgadir Adam said at the annual meeting of the American Surgical Association.
Current American Thyroid Association guidelines recommend lobectomy for tumors less than 1 cm in size and total thyroidectomy for those exceeding 1 cm.
"Using total thyroidectomy based on tumor size alone may unnecessarily subject patients to increased risks of complications without a survival benefit," he said. "In addition to tumor size up to 4 cm, other factors are important for determining extent of surgery such as nodal and distant metastases and patient preference."
The extent of surgery for papillary thyroid cancer, however, remains controversial. Recent analyses (Arch. Otolaryngol. Head Neck Surg. 2010;136:1055-61) have shown no survival difference between lobectomy and total thyroidectomy, while an earlier landmark study found improved overall survival with total thyroidectomy for tumors 1 cm or more (Ann. Surg. 2007;246;375-81). The latter study, however, has been criticized because it did not take into account patient comorbidities, multifocality, extrathyroidal extension, or completeness of resection, said Dr. Adam of Duke University School of Medicine, Durham, N.C.
The current analysis adjusted for age, gender, race, annual income, insurance status, hospital volume, patient comorbidities, tumor multifocality, extrathyroidal extension, lymph node involvement, metastases, surgical margins, and radioactive iodine ablation.
Discussant Dr. Blake Cady, professor emeritus of surgery at Harvard Medical School and Massachusetts General Hospital in Boston, said the current report is an important contribution to the controversy. It also supports his own bias against overtreatment of these mostly young patients with total thyroidectomy, which necessitates long-term medication and is accompanied by almost routine use of radioactive iodine, despite no evidence it improves outcomes in low-risk patients.
"In no other human cancer with a 99% 20-year survival is a policy of routine total primary organ removal practiced and routine systemic therapy used," he said. "Therefore, this report may help to scale back toward a more measured balance between treatment and morbidity."
Study coauthor Dr. Julie Ann Sosa, chief of endocrine surgery at Duke, challenged the audience to promote the growing body of evidence supporting equivalence in overall survival, such as a recent study described as coming the closest to a head-to-head comparison and having the longest follow-up at 18 years. It showed equivalence between lobectomy, without radioactive iodine, and total thyroidectomy for overall, progression-free, and disease-specific survival and risk of recurrence in tumors 40 mm or less (World J. Surg. 2014;38:68-79.
"In light of these data, I think it is probably high time for guidelines to potentially reconsider this issue," she said, noting that the American Thyroid Association will issue new guidelines later this spring or summer.
Dr. Sosa also advocated for "a more sophisticated approach" to preoperative evaluation and risk stratification for papillary thyroid cancer that distinguishes between low-, medium-, and high-risk tumors. The Duke study did not exclude most high-risk tumors, but rather adjusted for high-risk characteristics such as extrathyroidal extension, lymph node involvement, and distant metastases.
"When you adjust for these high-risk characteristics, the afforded overall survival benefit disappears," she said. "So what I think we would argue is that there is equivalence in outcome for the majority of patients for low- and medium-risk tumors. But for those patients who have high-risk tumors, as defined by some of these high-risk characteristics, then I think all of us would agree that total thyroidectomy, with or without radioactive iodine, would be indicated."
The study involved 61,775 patients in the National Cancer Database who underwent total thyroidectomy (n = 54,926) or lobectomy with or without isthmusectomy (n = 6,849) for papillary thyroid cancer from 1998 to 2006. Compared with the lobectomy group, the thyroidectomy group had more tumor multifocality (44% vs. 29%), positive surgical margins (27% vs. 7%), distant metastases (1% vs. 0.4%), and radioactive iodine (65% vs. 33%; P value less than .01 for all).
In multivariable analysis, nodal and distant metastases were associated with compromised survival, Dr. Adam said.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting, April 2014 in Boston, is anticipated to be published in the Annals of Surgery, pending editorial review.
The authors reported no conflicting interests
BOSTON – Extensive surgery beyond lobectomy offers no survival advantage for small papillary thyroid cancers, according to a large database analysis.
Total thyroidectomy was not associated with an overall survival benefit over lobectomy for papillary thyroid cancers sized 1-2 cm (hazard ratio, 1.05; P = .61) or 2.1-4.0 cm (HR, 0.89; P = .21), even after adjusting for multiple patient and pathologic factors.
"Despite guidelines, our results call into question whether tumor size 1-4 cm should be an absolute determinant for extent of surgery," Dr. Mohamed Abdelgadir Adam said at the annual meeting of the American Surgical Association.
Current American Thyroid Association guidelines recommend lobectomy for tumors less than 1 cm in size and total thyroidectomy for those exceeding 1 cm.
"Using total thyroidectomy based on tumor size alone may unnecessarily subject patients to increased risks of complications without a survival benefit," he said. "In addition to tumor size up to 4 cm, other factors are important for determining extent of surgery such as nodal and distant metastases and patient preference."
The extent of surgery for papillary thyroid cancer, however, remains controversial. Recent analyses (Arch. Otolaryngol. Head Neck Surg. 2010;136:1055-61) have shown no survival difference between lobectomy and total thyroidectomy, while an earlier landmark study found improved overall survival with total thyroidectomy for tumors 1 cm or more (Ann. Surg. 2007;246;375-81). The latter study, however, has been criticized because it did not take into account patient comorbidities, multifocality, extrathyroidal extension, or completeness of resection, said Dr. Adam of Duke University School of Medicine, Durham, N.C.
The current analysis adjusted for age, gender, race, annual income, insurance status, hospital volume, patient comorbidities, tumor multifocality, extrathyroidal extension, lymph node involvement, metastases, surgical margins, and radioactive iodine ablation.
Discussant Dr. Blake Cady, professor emeritus of surgery at Harvard Medical School and Massachusetts General Hospital in Boston, said the current report is an important contribution to the controversy. It also supports his own bias against overtreatment of these mostly young patients with total thyroidectomy, which necessitates long-term medication and is accompanied by almost routine use of radioactive iodine, despite no evidence it improves outcomes in low-risk patients.
"In no other human cancer with a 99% 20-year survival is a policy of routine total primary organ removal practiced and routine systemic therapy used," he said. "Therefore, this report may help to scale back toward a more measured balance between treatment and morbidity."
Study coauthor Dr. Julie Ann Sosa, chief of endocrine surgery at Duke, challenged the audience to promote the growing body of evidence supporting equivalence in overall survival, such as a recent study described as coming the closest to a head-to-head comparison and having the longest follow-up at 18 years. It showed equivalence between lobectomy, without radioactive iodine, and total thyroidectomy for overall, progression-free, and disease-specific survival and risk of recurrence in tumors 40 mm or less (World J. Surg. 2014;38:68-79.
"In light of these data, I think it is probably high time for guidelines to potentially reconsider this issue," she said, noting that the American Thyroid Association will issue new guidelines later this spring or summer.
Dr. Sosa also advocated for "a more sophisticated approach" to preoperative evaluation and risk stratification for papillary thyroid cancer that distinguishes between low-, medium-, and high-risk tumors. The Duke study did not exclude most high-risk tumors, but rather adjusted for high-risk characteristics such as extrathyroidal extension, lymph node involvement, and distant metastases.
"When you adjust for these high-risk characteristics, the afforded overall survival benefit disappears," she said. "So what I think we would argue is that there is equivalence in outcome for the majority of patients for low- and medium-risk tumors. But for those patients who have high-risk tumors, as defined by some of these high-risk characteristics, then I think all of us would agree that total thyroidectomy, with or without radioactive iodine, would be indicated."
The study involved 61,775 patients in the National Cancer Database who underwent total thyroidectomy (n = 54,926) or lobectomy with or without isthmusectomy (n = 6,849) for papillary thyroid cancer from 1998 to 2006. Compared with the lobectomy group, the thyroidectomy group had more tumor multifocality (44% vs. 29%), positive surgical margins (27% vs. 7%), distant metastases (1% vs. 0.4%), and radioactive iodine (65% vs. 33%; P value less than .01 for all).
In multivariable analysis, nodal and distant metastases were associated with compromised survival, Dr. Adam said.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting, April 2014 in Boston, is anticipated to be published in the Annals of Surgery, pending editorial review.
The authors reported no conflicting interests
AT THE ASA ANNUAL MEETING
Major finding: After adjustment, total thyroidectomy did not improve overall survival over lobectomy for tumors 1-2 cm (HR, 1.05; P = .61) or 2.1-4.0 cm (HR, 0.89; P = .21).
Data source: A retrospective database analysis of 61,775 papillary thyroid cancers.
Disclosures: The authors reported no conflicting interests.

Resident participation linked to more postsurgery complications
BOSTON – Resident participation in emergency general surgery cases was independently associated with a host of complications – pulmonary embolism, surgical site infections, and unplanned reoperation in a secondary analysis of the American College of Surgeons prospective National Surgical Quality Improvement database.
Adequate exposure of residents to emergency general surgery is crucial for surgical training, but academic operating teams should be mindful of this association, Dr. George Kasotakis said at the annual meeting of the American Surgical Association.

Three recent papers have shown resident participation modestly increases complications in elective surgery, but their impact is not well understood for emergency general surgery, where patient physiology is typically deranged and timely surgery is imperative.
To examine this, Dr. Kasotakis and his colleagues at Boston University identified 141,010 patients who underwent emergency general surgery procedures in the 2005-2010 American College of Surgeons prospective National Surgical Quality Improvement database. Due to the nonrandom assignment of more complex cases to resident participation, patients were matched 1:1 based on age; gender; use of alcohol, tobacco, and steroids; inpatient status; obesity; diabetes; renal failure; cardiopulmonary disease; and expected probability for morbidity and mortality. Regression models were fitted for each outcome and adjusted for the same risk factors and operative time.
The most common procedures in the matched cohort were appendectomy (40%), exploratory laparotomy (8.75%), bowel resection (9.2%), cholecystectomy (6%), and lysis of adhesions (6%).
Thirty-day mortality was similar with and without residents (3.25% vs. 2.96%; P = .082), but hospital length of stay was longer by about a half a day with residents (4.97 days vs. 4.59 days; P = .019), said Dr. Kasotakis, an acute care surgeon and intensivist.
More importantly, resident participation added about 20 minutes to operative (75 minutes vs. 59 minutes; P less than .001) and anesthesia times (122 minutes vs. 100 minutes; P less than .001).
Intraoperative transfusions were more common with residents (3.43% vs. 2.55%; P less than .001), perhaps because of longer operating room times, and, as a result, fewer postoperative transfusions were needed (1.12% vs. 1.28% P = .031), he said. Unplanned reoperations, however, were more common with residents, as well (4.22% vs. 3.80%; P = .002).
Postsurgical superficial wound infections (3.5% vs. 2.78%; P less than .001) and organ space surgical site infections (2.27% vs. 1.77%; P less than .001) were more common in the resident group, while wound dehiscence was not (0.63% vs. 0.69%; P = .266), Dr. Kasotakis noted.
Pulmonary complications were significantly more common in the resident group including postoperative pneumonia (1.85% vs. 1.67%; P = .04), reintubation (1.64% vs. 1.15%; P less than .001), and mechanical ventilation for more than 48 hours (2.87% vs. 2.06%; P less than .001).
The same was true for deep vein thrombosis (DVT) (0.80% vs. 0.62%; P = .002) and pulmonary embolism (PE) (0.43% vs. 0.28%; P less than .001).
Urinary tract infections (UTI) were higher with resident participation (1.45% vs. 1.14%; P less than .001), as was sepsis (2.42% vs. 2.13%; P = .005), likely because of the increase in surgical infections, Dr. Kasotakis said.
Thankfully, significant cardiac complications and septic shock were not more common with residents, he said.
Adjusted analyses
After adjusting for operative duration, case complexity and pre-existing comorbidities, residents did not increase length of stay (odds ratio, 0.07; P = .242) or septic events (OR, 1.07; P = .155), but their participation was still independently associated with about 20% more superficial surgical site infections (odds ratio, 1.23; P less than .001), organ space infections (OR, 1.21; P less than .001), UTIs (OR, 1.23; P = .001), and intraoperative transfusions (OR, 1.20; P = .001), he said.
Also, about 8% more patients required a return trip to the operating room when residents participated (OR, 1.08; P = .041).
"These outcomes can perhaps be attributed to their underdeveloped surgical skills," Dr. Kasotakis said.
The incidence of DVT and PE were also higher by about 25% (OR, 1.25; P = .011) and 40% (OR, 1.42; P = .005), respectively, perhaps because of delayed DVT prophylaxis initiation because of concerns of hemostasis or missed doses due to additional return trips to the emergency department, he suggested.
Interestingly, reintubation and prolonged mechanical ventilation rates were increased by about 40% (OR, 1.38; OR, 1.43; both P less than .001), perhaps due to prolonged operative times or greater resuscitation requirements, he added.
Dr. Kasotakis was quick to point out that this was a secondary analysis of a data set not originally intended to assess the effect of trainee participation, that no information was available on the degree of resident involvement during surgery or in perioperative care, and that participating institutions were skewed toward tertiary centers, which typically receive more complex cases.
"Staff surgeons should supervise as needed and minimize unnecessary [emergency department] time. And residents, for their part, should be well prepared for emergency procedures through simulation training and aim to maximize their operating room efficiency," he suggested.
The results sparked a flurry of rebuttals led off by discussant Dr. Julie Ann Sosa, chief of endocrine surgery and director of health sciences research at Duke University, Durham, N.C., who said they conflict with other analyses showing little to no impact from residents in elective cases.
"If not interpreted with care, policy makers, payers, and the public could construe that surgical care at academic health centers is compromised by trainees, which could have unfortunate ramifications for everyone in the room as well as the trainees and the patients," she said.
Dr. Sosa expressed concern about drawing causal inferences from an observational study in the setting of possible selection bias and said attempts to match for case complexity using CPT codes do not necessarily account for say, "the difference between a routine appendectomy that takes 15 to 30 minutes and a complex one that takes 3 hours for a perforation."
Some attendees questioned why the authors didn’t match the institutions in the analysis and chose to ascribe all of the outcomes to residents, with a round of applause following the suggestion that the paper should be entitled Academic centers increase emergency surgery complications. Other attendees questioned whether the poor outcomes are a reflection of resident training and supervision.
Finally, Dr. George Velmahos, chief of trauma, emergency surgery, and surgical critical care, Massachusetts General Hospital, Boston, questioned whether, based on these findings, hospitals have a responsibility from a medical/legal standpoint to inform emergency surgery patients that a resident is in the operating room and may impact outcomes.
Dr. Kasotakis responded that institutions may want to add a clause to consent paperwork stating that residents and trainees will be participating in the case.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting, April 2014, in Boston, is anticipated to be published in the Annals of Surgery, pending editorial review.
Dr. Kasotakis and his coauthors reported no conflicting interests.
surgical training, Dr. George Kasotakis, American Surgical Association, complications in elective surgery, American College of Surgeons prospective National Surgical Quality Improvement database,
BOSTON – Resident participation in emergency general surgery cases was independently associated with a host of complications – pulmonary embolism, surgical site infections, and unplanned reoperation in a secondary analysis of the American College of Surgeons prospective National Surgical Quality Improvement database.
Adequate exposure of residents to emergency general surgery is crucial for surgical training, but academic operating teams should be mindful of this association, Dr. George Kasotakis said at the annual meeting of the American Surgical Association.
Three recent papers have shown resident participation modestly increases complications in elective surgery, but their impact is not well understood for emergency general surgery, where patient physiology is typically deranged and timely surgery is imperative.
To examine this, Dr. Kasotakis and his colleagues at Boston University identified 141,010 patients who underwent emergency general surgery procedures in the 2005-2010 American College of Surgeons prospective National Surgical Quality Improvement database. Due to the nonrandom assignment of more complex cases to resident participation, patients were matched 1:1 based on age; gender; use of alcohol, tobacco, and steroids; inpatient status; obesity; diabetes; renal failure; cardiopulmonary disease; and expected probability for morbidity and mortality. Regression models were fitted for each outcome and adjusted for the same risk factors and operative time.
The most common procedures in the matched cohort were appendectomy (40%), exploratory laparotomy (8.75%), bowel resection (9.2%), cholecystectomy (6%), and lysis of adhesions (6%).
Thirty-day mortality was similar with and without residents (3.25% vs. 2.96%; P = .082), but hospital length of stay was longer by about a half a day with residents (4.97 days vs. 4.59 days; P = .019), said Dr. Kasotakis, an acute care surgeon and intensivist.
More importantly, resident participation added about 20 minutes to operative (75 minutes vs. 59 minutes; P less than .001) and anesthesia times (122 minutes vs. 100 minutes; P less than .001).
Intraoperative transfusions were more common with residents (3.43% vs. 2.55%; P less than .001), perhaps because of longer operating room times, and, as a result, fewer postoperative transfusions were needed (1.12% vs. 1.28% P = .031), he said. Unplanned reoperations, however, were more common with residents, as well (4.22% vs. 3.80%; P = .002).
Postsurgical superficial wound infections (3.5% vs. 2.78%; P less than .001) and organ space surgical site infections (2.27% vs. 1.77%; P less than .001) were more common in the resident group, while wound dehiscence was not (0.63% vs. 0.69%; P = .266), Dr. Kasotakis noted.
Pulmonary complications were significantly more common in the resident group including postoperative pneumonia (1.85% vs. 1.67%; P = .04), reintubation (1.64% vs. 1.15%; P less than .001), and mechanical ventilation for more than 48 hours (2.87% vs. 2.06%; P less than .001).
The same was true for deep vein thrombosis (DVT) (0.80% vs. 0.62%; P = .002) and pulmonary embolism (PE) (0.43% vs. 0.28%; P less than .001).
Urinary tract infections (UTI) were higher with resident participation (1.45% vs. 1.14%; P less than .001), as was sepsis (2.42% vs. 2.13%; P = .005), likely because of the increase in surgical infections, Dr. Kasotakis said.
Thankfully, significant cardiac complications and septic shock were not more common with residents, he said.
Adjusted analyses
After adjusting for operative duration, case complexity and pre-existing comorbidities, residents did not increase length of stay (odds ratio, 0.07; P = .242) or septic events (OR, 1.07; P = .155), but their participation was still independently associated with about 20% more superficial surgical site infections (odds ratio, 1.23; P less than .001), organ space infections (OR, 1.21; P less than .001), UTIs (OR, 1.23; P = .001), and intraoperative transfusions (OR, 1.20; P = .001), he said.
Also, about 8% more patients required a return trip to the operating room when residents participated (OR, 1.08; P = .041).
"These outcomes can perhaps be attributed to their underdeveloped surgical skills," Dr. Kasotakis said.
The incidence of DVT and PE were also higher by about 25% (OR, 1.25; P = .011) and 40% (OR, 1.42; P = .005), respectively, perhaps because of delayed DVT prophylaxis initiation because of concerns of hemostasis or missed doses due to additional return trips to the emergency department, he suggested.
Interestingly, reintubation and prolonged mechanical ventilation rates were increased by about 40% (OR, 1.38; OR, 1.43; both P less than .001), perhaps due to prolonged operative times or greater resuscitation requirements, he added.
Dr. Kasotakis was quick to point out that this was a secondary analysis of a data set not originally intended to assess the effect of trainee participation, that no information was available on the degree of resident involvement during surgery or in perioperative care, and that participating institutions were skewed toward tertiary centers, which typically receive more complex cases.
"Staff surgeons should supervise as needed and minimize unnecessary [emergency department] time. And residents, for their part, should be well prepared for emergency procedures through simulation training and aim to maximize their operating room efficiency," he suggested.
The results sparked a flurry of rebuttals led off by discussant Dr. Julie Ann Sosa, chief of endocrine surgery and director of health sciences research at Duke University, Durham, N.C., who said they conflict with other analyses showing little to no impact from residents in elective cases.
"If not interpreted with care, policy makers, payers, and the public could construe that surgical care at academic health centers is compromised by trainees, which could have unfortunate ramifications for everyone in the room as well as the trainees and the patients," she said.
Dr. Sosa expressed concern about drawing causal inferences from an observational study in the setting of possible selection bias and said attempts to match for case complexity using CPT codes do not necessarily account for say, "the difference between a routine appendectomy that takes 15 to 30 minutes and a complex one that takes 3 hours for a perforation."
Some attendees questioned why the authors didn’t match the institutions in the analysis and chose to ascribe all of the outcomes to residents, with a round of applause following the suggestion that the paper should be entitled Academic centers increase emergency surgery complications. Other attendees questioned whether the poor outcomes are a reflection of resident training and supervision.
Finally, Dr. George Velmahos, chief of trauma, emergency surgery, and surgical critical care, Massachusetts General Hospital, Boston, questioned whether, based on these findings, hospitals have a responsibility from a medical/legal standpoint to inform emergency surgery patients that a resident is in the operating room and may impact outcomes.
Dr. Kasotakis responded that institutions may want to add a clause to consent paperwork stating that residents and trainees will be participating in the case.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting, April 2014, in Boston, is anticipated to be published in the Annals of Surgery, pending editorial review.
Dr. Kasotakis and his coauthors reported no conflicting interests.
BOSTON – Resident participation in emergency general surgery cases was independently associated with a host of complications – pulmonary embolism, surgical site infections, and unplanned reoperation in a secondary analysis of the American College of Surgeons prospective National Surgical Quality Improvement database.
Adequate exposure of residents to emergency general surgery is crucial for surgical training, but academic operating teams should be mindful of this association, Dr. George Kasotakis said at the annual meeting of the American Surgical Association.
Three recent papers have shown resident participation modestly increases complications in elective surgery, but their impact is not well understood for emergency general surgery, where patient physiology is typically deranged and timely surgery is imperative.
To examine this, Dr. Kasotakis and his colleagues at Boston University identified 141,010 patients who underwent emergency general surgery procedures in the 2005-2010 American College of Surgeons prospective National Surgical Quality Improvement database. Due to the nonrandom assignment of more complex cases to resident participation, patients were matched 1:1 based on age; gender; use of alcohol, tobacco, and steroids; inpatient status; obesity; diabetes; renal failure; cardiopulmonary disease; and expected probability for morbidity and mortality. Regression models were fitted for each outcome and adjusted for the same risk factors and operative time.
The most common procedures in the matched cohort were appendectomy (40%), exploratory laparotomy (8.75%), bowel resection (9.2%), cholecystectomy (6%), and lysis of adhesions (6%).
Thirty-day mortality was similar with and without residents (3.25% vs. 2.96%; P = .082), but hospital length of stay was longer by about a half a day with residents (4.97 days vs. 4.59 days; P = .019), said Dr. Kasotakis, an acute care surgeon and intensivist.
More importantly, resident participation added about 20 minutes to operative (75 minutes vs. 59 minutes; P less than .001) and anesthesia times (122 minutes vs. 100 minutes; P less than .001).
Intraoperative transfusions were more common with residents (3.43% vs. 2.55%; P less than .001), perhaps because of longer operating room times, and, as a result, fewer postoperative transfusions were needed (1.12% vs. 1.28% P = .031), he said. Unplanned reoperations, however, were more common with residents, as well (4.22% vs. 3.80%; P = .002).
Postsurgical superficial wound infections (3.5% vs. 2.78%; P less than .001) and organ space surgical site infections (2.27% vs. 1.77%; P less than .001) were more common in the resident group, while wound dehiscence was not (0.63% vs. 0.69%; P = .266), Dr. Kasotakis noted.
Pulmonary complications were significantly more common in the resident group including postoperative pneumonia (1.85% vs. 1.67%; P = .04), reintubation (1.64% vs. 1.15%; P less than .001), and mechanical ventilation for more than 48 hours (2.87% vs. 2.06%; P less than .001).
The same was true for deep vein thrombosis (DVT) (0.80% vs. 0.62%; P = .002) and pulmonary embolism (PE) (0.43% vs. 0.28%; P less than .001).
Urinary tract infections (UTI) were higher with resident participation (1.45% vs. 1.14%; P less than .001), as was sepsis (2.42% vs. 2.13%; P = .005), likely because of the increase in surgical infections, Dr. Kasotakis said.
Thankfully, significant cardiac complications and septic shock were not more common with residents, he said.
Adjusted analyses
After adjusting for operative duration, case complexity and pre-existing comorbidities, residents did not increase length of stay (odds ratio, 0.07; P = .242) or septic events (OR, 1.07; P = .155), but their participation was still independently associated with about 20% more superficial surgical site infections (odds ratio, 1.23; P less than .001), organ space infections (OR, 1.21; P less than .001), UTIs (OR, 1.23; P = .001), and intraoperative transfusions (OR, 1.20; P = .001), he said.
Also, about 8% more patients required a return trip to the operating room when residents participated (OR, 1.08; P = .041).
"These outcomes can perhaps be attributed to their underdeveloped surgical skills," Dr. Kasotakis said.
The incidence of DVT and PE were also higher by about 25% (OR, 1.25; P = .011) and 40% (OR, 1.42; P = .005), respectively, perhaps because of delayed DVT prophylaxis initiation because of concerns of hemostasis or missed doses due to additional return trips to the emergency department, he suggested.
Interestingly, reintubation and prolonged mechanical ventilation rates were increased by about 40% (OR, 1.38; OR, 1.43; both P less than .001), perhaps due to prolonged operative times or greater resuscitation requirements, he added.
Dr. Kasotakis was quick to point out that this was a secondary analysis of a data set not originally intended to assess the effect of trainee participation, that no information was available on the degree of resident involvement during surgery or in perioperative care, and that participating institutions were skewed toward tertiary centers, which typically receive more complex cases.
"Staff surgeons should supervise as needed and minimize unnecessary [emergency department] time. And residents, for their part, should be well prepared for emergency procedures through simulation training and aim to maximize their operating room efficiency," he suggested.
The results sparked a flurry of rebuttals led off by discussant Dr. Julie Ann Sosa, chief of endocrine surgery and director of health sciences research at Duke University, Durham, N.C., who said they conflict with other analyses showing little to no impact from residents in elective cases.
"If not interpreted with care, policy makers, payers, and the public could construe that surgical care at academic health centers is compromised by trainees, which could have unfortunate ramifications for everyone in the room as well as the trainees and the patients," she said.
Dr. Sosa expressed concern about drawing causal inferences from an observational study in the setting of possible selection bias and said attempts to match for case complexity using CPT codes do not necessarily account for say, "the difference between a routine appendectomy that takes 15 to 30 minutes and a complex one that takes 3 hours for a perforation."
Some attendees questioned why the authors didn’t match the institutions in the analysis and chose to ascribe all of the outcomes to residents, with a round of applause following the suggestion that the paper should be entitled Academic centers increase emergency surgery complications. Other attendees questioned whether the poor outcomes are a reflection of resident training and supervision.
Finally, Dr. George Velmahos, chief of trauma, emergency surgery, and surgical critical care, Massachusetts General Hospital, Boston, questioned whether, based on these findings, hospitals have a responsibility from a medical/legal standpoint to inform emergency surgery patients that a resident is in the operating room and may impact outcomes.
Dr. Kasotakis responded that institutions may want to add a clause to consent paperwork stating that residents and trainees will be participating in the case.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting, April 2014, in Boston, is anticipated to be published in the Annals of Surgery, pending editorial review.
Dr. Kasotakis and his coauthors reported no conflicting interests.
surgical training, Dr. George Kasotakis, American Surgical Association, complications in elective surgery, American College of Surgeons prospective National Surgical Quality Improvement database,
surgical training, Dr. George Kasotakis, American Surgical Association, complications in elective surgery, American College of Surgeons prospective National Surgical Quality Improvement database,
At the ASA Annual Meeting
Major finding: Rates were significantly higher with resident participation than without for DVT (0.80% vs. 0.62%; P = .002) and PE (0.43% vs. 0.28%; P less than .001).
Data source: A secondary analysis of 141,010 emergency general surgery cases in the prospective ACS NSQIP database.
Disclosures: Dr. Kasotakis and his coauthors reported no conflicting interests.

Inflammatory ultrasound changes track with hand OA progression
PARIS – Inflammatory ultrasound features in hand osteoarthritis may point clinicians toward patients at higher risk for radiographic progression, a longitudinal study suggests.
"We found inflammatory ultrasound features are independently associated with both progressive joint space narrowing and progression of osteophytes in hand osteoarthritis. This is especially true with persistent inflammation," Dr. Marion Kortekaas said at the World Congress on Osteoarthritis.

She presented data on 56 consecutive hand OA patients who underwent baseline and 2.3-year follow-up radiographic and ultrasound assessment of all first carpometacarpal, distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and first interphalangeal joints.
Radiographs were scored for osteophytes and joint space narrowing using the OARSI Atlas grading system (0-3 scale). Ultrasound synovial thickening, effusion, and power Doppler signal (PDS) were scored on a validated 3-point scale, with 3 being severe. Progression was defined as at least one grade increase of either joint space narrowing or osteophytes, explained Dr. Kortekaas, a rheumatologist at Leiden (the Netherlands) University Medical Center.
Most patients were female (86%) and their average age was 61 years. Patients with rheumatic diseases, trauma/operation, and corticosteroid use were excluded.
Of 1,680 joints at baseline, 141 (8.4%) had synovial thickening, 332 (19.8%) effusion, and 146 (8.7%) PDS.
At follow-up, progression of osteophytes and joint space narrowing was present in 120 and 96 joints, respectively, she said.
PDS, synovial thickening, and effusion were "persistent," defined as present at baseline and follow-up, in 40, 118, and 232 joints, and were "fluctuating," or present only at baseline or follow-up, in 243, 641, and 636 joints, respectively.
Using generalized estimating equations analyses, progression was independently associated with ultrasound synovial thickening (odds ratio, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7) for grade 2-3 vs. grade 0, after adjustment for age, sex, body mass index, baseline osteophytes, and joint space narrowing scores, Dr. Kortekaas said.
Joint space narrowing was also independently associated with the ultrasound features of synovial thickening (OR, 3.4), effusion (OR, 3.3), and power Doppler signal (OR, 3.1), again after adjustment and comparing grade 2-3 vs. grade 0.
Persistent inflammation showed stronger associations with radiographic progression than did fluctuating inflammatory features in comparison with no inflammatory features at all, she said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, Dr. Kortekaas said inflammatory and synovial changes are loosely related to symptoms and pain, but that the group has yet to look at an association with C-reactive protein or inflammation in other joints.
Session comoderator Dr. Gillian Hawker, professor of medicine at the University of Toronto and physician in chief of medicine at Women’s College Hospital, Toronto, commented that until recently, ultrasound for hand OA has been far more common in clinical practice in Europe than in North America.
"I think that’s exactly where the radiology community is starting to go," she said in an interview. "Would we be doing a better job, picking things up earlier if we were ultrasounding? [There’s] definitely higher sensitivity. But, we haven’t quite gotten there yet. It’s going to cost money to get ultrasound machines into practices and train physicians."
Dr. Hawker observed that the American College of Radiology has added an ultrasound course and that residents at her institution are now going through ultrasound training as part of their residency.
Dr. Kortekaas and her coauthors reported no conflicting interests.
PARIS – Inflammatory ultrasound features in hand osteoarthritis may point clinicians toward patients at higher risk for radiographic progression, a longitudinal study suggests.
"We found inflammatory ultrasound features are independently associated with both progressive joint space narrowing and progression of osteophytes in hand osteoarthritis. This is especially true with persistent inflammation," Dr. Marion Kortekaas said at the World Congress on Osteoarthritis.
She presented data on 56 consecutive hand OA patients who underwent baseline and 2.3-year follow-up radiographic and ultrasound assessment of all first carpometacarpal, distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and first interphalangeal joints.
Radiographs were scored for osteophytes and joint space narrowing using the OARSI Atlas grading system (0-3 scale). Ultrasound synovial thickening, effusion, and power Doppler signal (PDS) were scored on a validated 3-point scale, with 3 being severe. Progression was defined as at least one grade increase of either joint space narrowing or osteophytes, explained Dr. Kortekaas, a rheumatologist at Leiden (the Netherlands) University Medical Center.
Most patients were female (86%) and their average age was 61 years. Patients with rheumatic diseases, trauma/operation, and corticosteroid use were excluded.
Of 1,680 joints at baseline, 141 (8.4%) had synovial thickening, 332 (19.8%) effusion, and 146 (8.7%) PDS.
At follow-up, progression of osteophytes and joint space narrowing was present in 120 and 96 joints, respectively, she said.
PDS, synovial thickening, and effusion were "persistent," defined as present at baseline and follow-up, in 40, 118, and 232 joints, and were "fluctuating," or present only at baseline or follow-up, in 243, 641, and 636 joints, respectively.
Using generalized estimating equations analyses, progression was independently associated with ultrasound synovial thickening (odds ratio, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7) for grade 2-3 vs. grade 0, after adjustment for age, sex, body mass index, baseline osteophytes, and joint space narrowing scores, Dr. Kortekaas said.
Joint space narrowing was also independently associated with the ultrasound features of synovial thickening (OR, 3.4), effusion (OR, 3.3), and power Doppler signal (OR, 3.1), again after adjustment and comparing grade 2-3 vs. grade 0.
Persistent inflammation showed stronger associations with radiographic progression than did fluctuating inflammatory features in comparison with no inflammatory features at all, she said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, Dr. Kortekaas said inflammatory and synovial changes are loosely related to symptoms and pain, but that the group has yet to look at an association with C-reactive protein or inflammation in other joints.
Session comoderator Dr. Gillian Hawker, professor of medicine at the University of Toronto and physician in chief of medicine at Women’s College Hospital, Toronto, commented that until recently, ultrasound for hand OA has been far more common in clinical practice in Europe than in North America.
"I think that’s exactly where the radiology community is starting to go," she said in an interview. "Would we be doing a better job, picking things up earlier if we were ultrasounding? [There’s] definitely higher sensitivity. But, we haven’t quite gotten there yet. It’s going to cost money to get ultrasound machines into practices and train physicians."
Dr. Hawker observed that the American College of Radiology has added an ultrasound course and that residents at her institution are now going through ultrasound training as part of their residency.
Dr. Kortekaas and her coauthors reported no conflicting interests.
PARIS – Inflammatory ultrasound features in hand osteoarthritis may point clinicians toward patients at higher risk for radiographic progression, a longitudinal study suggests.
"We found inflammatory ultrasound features are independently associated with both progressive joint space narrowing and progression of osteophytes in hand osteoarthritis. This is especially true with persistent inflammation," Dr. Marion Kortekaas said at the World Congress on Osteoarthritis.
She presented data on 56 consecutive hand OA patients who underwent baseline and 2.3-year follow-up radiographic and ultrasound assessment of all first carpometacarpal, distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and first interphalangeal joints.
Radiographs were scored for osteophytes and joint space narrowing using the OARSI Atlas grading system (0-3 scale). Ultrasound synovial thickening, effusion, and power Doppler signal (PDS) were scored on a validated 3-point scale, with 3 being severe. Progression was defined as at least one grade increase of either joint space narrowing or osteophytes, explained Dr. Kortekaas, a rheumatologist at Leiden (the Netherlands) University Medical Center.
Most patients were female (86%) and their average age was 61 years. Patients with rheumatic diseases, trauma/operation, and corticosteroid use were excluded.
Of 1,680 joints at baseline, 141 (8.4%) had synovial thickening, 332 (19.8%) effusion, and 146 (8.7%) PDS.
At follow-up, progression of osteophytes and joint space narrowing was present in 120 and 96 joints, respectively, she said.
PDS, synovial thickening, and effusion were "persistent," defined as present at baseline and follow-up, in 40, 118, and 232 joints, and were "fluctuating," or present only at baseline or follow-up, in 243, 641, and 636 joints, respectively.
Using generalized estimating equations analyses, progression was independently associated with ultrasound synovial thickening (odds ratio, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7) for grade 2-3 vs. grade 0, after adjustment for age, sex, body mass index, baseline osteophytes, and joint space narrowing scores, Dr. Kortekaas said.
Joint space narrowing was also independently associated with the ultrasound features of synovial thickening (OR, 3.4), effusion (OR, 3.3), and power Doppler signal (OR, 3.1), again after adjustment and comparing grade 2-3 vs. grade 0.
Persistent inflammation showed stronger associations with radiographic progression than did fluctuating inflammatory features in comparison with no inflammatory features at all, she said at the meeting, sponsored by the Osteoarthritis Research Society International.
During a discussion of the results, Dr. Kortekaas said inflammatory and synovial changes are loosely related to symptoms and pain, but that the group has yet to look at an association with C-reactive protein or inflammation in other joints.
Session comoderator Dr. Gillian Hawker, professor of medicine at the University of Toronto and physician in chief of medicine at Women’s College Hospital, Toronto, commented that until recently, ultrasound for hand OA has been far more common in clinical practice in Europe than in North America.
"I think that’s exactly where the radiology community is starting to go," she said in an interview. "Would we be doing a better job, picking things up earlier if we were ultrasounding? [There’s] definitely higher sensitivity. But, we haven’t quite gotten there yet. It’s going to cost money to get ultrasound machines into practices and train physicians."
Dr. Hawker observed that the American College of Radiology has added an ultrasound course and that residents at her institution are now going through ultrasound training as part of their residency.
Dr. Kortekaas and her coauthors reported no conflicting interests.
AT OARSI 2014
Key clinical point: Patients with inflammatory changes in hand OA on ultrasound during follow-up are at higher risk for radiographic progression.
Major finding: In adjusted analyses, hand OA progression was independently associated with ultrasound synovial thickening (OR, 2.6), effusion (OR, 3.5), and power Doppler signal (OR, 5.7).
Data source: A longitudinal study in 56 consecutive hand OA patients.
Disclosures: Dr. Kortekaas and her coauthors reported no conflicting interests.

Tapping office IT boosts orthopedic patient–reported outcomes
PARIS – Combining e-mail and office-based technology garnered patient-reported outcomes from more than 90% of patients receiving orthopedic care, in an analysis of 18,073 physician-patient encounters.
"Integrating [patient-reported outcomes] measurement into orthopedic standard of care without interrupting clinical practice is possible and currently in use," Xiang Zhou, Ph.D., reported at the World Congress on Osteoarthritis.
Patient-reported outcomes, or PROs, have taken center stage in recent years as a way to measure the safety and effectiveness of total joint arthroplasty, with respect to both technical and patient satisfaction.
New York University Langone Medical Center implemented an IT system in May 2012 for all nine adult orthopedic reconstructive surgeons at its Center for Musculoskeletal Care. Patients with e-mail addresses on file were sent a link to a PRO questionnaire, individualized to their clinical needs, 3 days before their appointment. A reminder e-mail was sent the day before their visit if the questionnaire was not completed. Tablets were also distributed in the waiting room for patients who did not complete via e-mail. Real-time and previous PRO scores were available in the electronic health record for physicians to review during the examination.
PRO records were captured for 83% of 8,864 patients seen in 20 months. Of those, 72% had multiple, longitudinal PRO scores recorded, according to Dr. Zhou, a research scientist in NYU Langone’s orthopedic surgery department.
Of the 18,073 physician-patient encounters, 71% included a completed PRO score. Monthly completion rates ranged from a high of 91% to a low of 56%.
"Reaching more than a 90% PRO collection rate is possible with the support of participating physicians," he noted.
Patients under age 65 had a significantly higher overall PRO completion rate than did older patients (76% vs. 65%; P less than .001), as did males vs. females (73% vs. 70%; P less than .001), Dr. Zhou reported at the meeting, sponsored by the Osteoarthritis Research Society International.
In all, 55% of patients who provided an e-mail address completed their PRO questionnaires via e-mail. In that subset, no significant differences were seen by age (55% both groups; P = .996) or gender (56% male vs. 55% female; P = .752).
PRO scores are now included in the electronic health record and routinely captured and used by physicians.
"Routine real-time and longitudinal PRO reports are a valuable tool to stimulate patient-physician communication and inform treatment decisions," the authors concluded in the poster presentation.
Dr. Zhou reported having no financial disclosures.
PARIS – Combining e-mail and office-based technology garnered patient-reported outcomes from more than 90% of patients receiving orthopedic care, in an analysis of 18,073 physician-patient encounters.
"Integrating [patient-reported outcomes] measurement into orthopedic standard of care without interrupting clinical practice is possible and currently in use," Xiang Zhou, Ph.D., reported at the World Congress on Osteoarthritis.
Patient-reported outcomes, or PROs, have taken center stage in recent years as a way to measure the safety and effectiveness of total joint arthroplasty, with respect to both technical and patient satisfaction.
New York University Langone Medical Center implemented an IT system in May 2012 for all nine adult orthopedic reconstructive surgeons at its Center for Musculoskeletal Care. Patients with e-mail addresses on file were sent a link to a PRO questionnaire, individualized to their clinical needs, 3 days before their appointment. A reminder e-mail was sent the day before their visit if the questionnaire was not completed. Tablets were also distributed in the waiting room for patients who did not complete via e-mail. Real-time and previous PRO scores were available in the electronic health record for physicians to review during the examination.
PRO records were captured for 83% of 8,864 patients seen in 20 months. Of those, 72% had multiple, longitudinal PRO scores recorded, according to Dr. Zhou, a research scientist in NYU Langone’s orthopedic surgery department.
Of the 18,073 physician-patient encounters, 71% included a completed PRO score. Monthly completion rates ranged from a high of 91% to a low of 56%.
"Reaching more than a 90% PRO collection rate is possible with the support of participating physicians," he noted.
Patients under age 65 had a significantly higher overall PRO completion rate than did older patients (76% vs. 65%; P less than .001), as did males vs. females (73% vs. 70%; P less than .001), Dr. Zhou reported at the meeting, sponsored by the Osteoarthritis Research Society International.
In all, 55% of patients who provided an e-mail address completed their PRO questionnaires via e-mail. In that subset, no significant differences were seen by age (55% both groups; P = .996) or gender (56% male vs. 55% female; P = .752).
PRO scores are now included in the electronic health record and routinely captured and used by physicians.
"Routine real-time and longitudinal PRO reports are a valuable tool to stimulate patient-physician communication and inform treatment decisions," the authors concluded in the poster presentation.
Dr. Zhou reported having no financial disclosures.
PARIS – Combining e-mail and office-based technology garnered patient-reported outcomes from more than 90% of patients receiving orthopedic care, in an analysis of 18,073 physician-patient encounters.
"Integrating [patient-reported outcomes] measurement into orthopedic standard of care without interrupting clinical practice is possible and currently in use," Xiang Zhou, Ph.D., reported at the World Congress on Osteoarthritis.
Patient-reported outcomes, or PROs, have taken center stage in recent years as a way to measure the safety and effectiveness of total joint arthroplasty, with respect to both technical and patient satisfaction.
New York University Langone Medical Center implemented an IT system in May 2012 for all nine adult orthopedic reconstructive surgeons at its Center for Musculoskeletal Care. Patients with e-mail addresses on file were sent a link to a PRO questionnaire, individualized to their clinical needs, 3 days before their appointment. A reminder e-mail was sent the day before their visit if the questionnaire was not completed. Tablets were also distributed in the waiting room for patients who did not complete via e-mail. Real-time and previous PRO scores were available in the electronic health record for physicians to review during the examination.
PRO records were captured for 83% of 8,864 patients seen in 20 months. Of those, 72% had multiple, longitudinal PRO scores recorded, according to Dr. Zhou, a research scientist in NYU Langone’s orthopedic surgery department.
Of the 18,073 physician-patient encounters, 71% included a completed PRO score. Monthly completion rates ranged from a high of 91% to a low of 56%.
"Reaching more than a 90% PRO collection rate is possible with the support of participating physicians," he noted.
Patients under age 65 had a significantly higher overall PRO completion rate than did older patients (76% vs. 65%; P less than .001), as did males vs. females (73% vs. 70%; P less than .001), Dr. Zhou reported at the meeting, sponsored by the Osteoarthritis Research Society International.
In all, 55% of patients who provided an e-mail address completed their PRO questionnaires via e-mail. In that subset, no significant differences were seen by age (55% both groups; P = .996) or gender (56% male vs. 55% female; P = .752).
PRO scores are now included in the electronic health record and routinely captured and used by physicians.
"Routine real-time and longitudinal PRO reports are a valuable tool to stimulate patient-physician communication and inform treatment decisions," the authors concluded in the poster presentation.
Dr. Zhou reported having no financial disclosures.
AT OARSI 2014
Major finding: Monthly completion rates of patient-reported outcomes questionnaires ranged from a high of 91% to a low of 56%.
Data source: An analysis of 18,073 orthopedic physician-patient encounters.
Disclosures: Dr. Zhou reported having no financial disclosures.
In obesity and knee OA, weight loss is a big win
PARIS – Weight loss of more than 5% produced clinically meaningful improvements in knee osteoarthritis, even when final body mass index remained high, a large, community-based study has shown.
For those patients who lost 10% body weight in the study, knee osteoarthritis symptoms improved by about 40%, consistent with the recent IDEA (Intensive Diet and Exercise for Arthritis) trial findings.
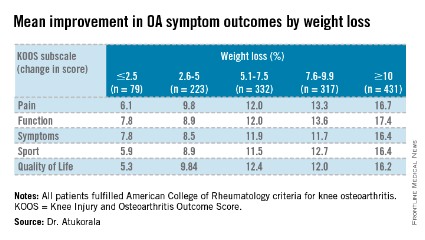
"There is a strong dose-response relationship between percentage weight loss and improvement in knee pain, function, symptoms, sport or recreation, and quality of life," Dr. Inoshi Atukorala said at the World Congress on Osteoarthritis.
Dr. Atukorala described the study as the first to examine the dose-response relationship between changes in body weight and knee osteoarthritis in a real-world, community setting.
The researchers evaluated 1,383 Australians who fulfilled the American College of Rheumatology criteria for knee osteoarthritis (OA) and were enrolled in the structured, remotely delivered "Healthy Weight for Life" knee and hip osteoarthritis management program. It integrates intensive weight loss as a component of tailored interventions, with the aim of achieving a 7%-10% body weight loss over 18 weeks, explained Dr. Atukorala, a consultant rheumatologist at the University of Colombo, Sri Lanka.
The program uses a partial very-low-calorie diet, portion management tools and devices, written healthy eating advice, and lifestyle education together with targeted telephone, e-mail, and text-message motivation and support. All participants were given the same strength, balance, and mobility exercise tools, instruction, and support.

At baseline, 81.7% of participants were obese, the average body mass index (BMI) was 34.3 kg/m2, and the mean Knee injury and Osteoarthritis Outcome Score (KOOS) pain and function subscale scores were 56.3 and 59.5. The cohort was 71% female and had an average age of 64 years.
At 18-weeks, there was a clear and significant incremental improvement in KOOS subscales across the weight-loss categories, with the greatest improvements in those losing at least 10% body weight, Dr. Atukorala said.
The weight-loss category cutoffs were chosen based on the IDEA trial (JAMA 2013;310:1263-73), as well as the weight-loss goal in the diet groups in the ADAPT study and the weight loss typically achieved in its exercise-only cohort of older adults with knee OA (Arthritis Rheum. 2004;50;1501-10), she explained.
Using repeated measures analysis of covariance, the investigators next examined the dose-response of weight loss, compared with differences in pain and function. For this analysis, the 2.5% or less weight-loss category was set as the reference.
The dose-relationship between weight loss and improvements in pain and function persisted, even after controlling for baseline age, gender, weight, height, and KOOS, Dr. Atukorala said at the meeting, sponsored by the Osteoarthritis Research Society International. The differences reached statistical significance on all KOOS subscales for the two highest weight-loss categories and on all but one subscale (KOOS sport) for those losing 5.1%-7.5% body weight.
"We are limited by the fact that the program did not assess the magnitude of exercise interventions in each weight-loss category, but it confirms the dose-response benefit of weight loss as a therapeutic intervention in knee osteoarthritis," Dr. Atukorala concluded. "And, it demonstrates the effectiveness of disseminating and implementing intensive weight-loss intervention in a community-based setting."
Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
PARIS – Weight loss of more than 5% produced clinically meaningful improvements in knee osteoarthritis, even when final body mass index remained high, a large, community-based study has shown.
For those patients who lost 10% body weight in the study, knee osteoarthritis symptoms improved by about 40%, consistent with the recent IDEA (Intensive Diet and Exercise for Arthritis) trial findings.
"There is a strong dose-response relationship between percentage weight loss and improvement in knee pain, function, symptoms, sport or recreation, and quality of life," Dr. Inoshi Atukorala said at the World Congress on Osteoarthritis.
Dr. Atukorala described the study as the first to examine the dose-response relationship between changes in body weight and knee osteoarthritis in a real-world, community setting.
The researchers evaluated 1,383 Australians who fulfilled the American College of Rheumatology criteria for knee osteoarthritis (OA) and were enrolled in the structured, remotely delivered "Healthy Weight for Life" knee and hip osteoarthritis management program. It integrates intensive weight loss as a component of tailored interventions, with the aim of achieving a 7%-10% body weight loss over 18 weeks, explained Dr. Atukorala, a consultant rheumatologist at the University of Colombo, Sri Lanka.
The program uses a partial very-low-calorie diet, portion management tools and devices, written healthy eating advice, and lifestyle education together with targeted telephone, e-mail, and text-message motivation and support. All participants were given the same strength, balance, and mobility exercise tools, instruction, and support.
At baseline, 81.7% of participants were obese, the average body mass index (BMI) was 34.3 kg/m2, and the mean Knee injury and Osteoarthritis Outcome Score (KOOS) pain and function subscale scores were 56.3 and 59.5. The cohort was 71% female and had an average age of 64 years.
At 18-weeks, there was a clear and significant incremental improvement in KOOS subscales across the weight-loss categories, with the greatest improvements in those losing at least 10% body weight, Dr. Atukorala said.
The weight-loss category cutoffs were chosen based on the IDEA trial (JAMA 2013;310:1263-73), as well as the weight-loss goal in the diet groups in the ADAPT study and the weight loss typically achieved in its exercise-only cohort of older adults with knee OA (Arthritis Rheum. 2004;50;1501-10), she explained.
Using repeated measures analysis of covariance, the investigators next examined the dose-response of weight loss, compared with differences in pain and function. For this analysis, the 2.5% or less weight-loss category was set as the reference.
The dose-relationship between weight loss and improvements in pain and function persisted, even after controlling for baseline age, gender, weight, height, and KOOS, Dr. Atukorala said at the meeting, sponsored by the Osteoarthritis Research Society International. The differences reached statistical significance on all KOOS subscales for the two highest weight-loss categories and on all but one subscale (KOOS sport) for those losing 5.1%-7.5% body weight.
"We are limited by the fact that the program did not assess the magnitude of exercise interventions in each weight-loss category, but it confirms the dose-response benefit of weight loss as a therapeutic intervention in knee osteoarthritis," Dr. Atukorala concluded. "And, it demonstrates the effectiveness of disseminating and implementing intensive weight-loss intervention in a community-based setting."
Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
PARIS – Weight loss of more than 5% produced clinically meaningful improvements in knee osteoarthritis, even when final body mass index remained high, a large, community-based study has shown.
For those patients who lost 10% body weight in the study, knee osteoarthritis symptoms improved by about 40%, consistent with the recent IDEA (Intensive Diet and Exercise for Arthritis) trial findings.
"There is a strong dose-response relationship between percentage weight loss and improvement in knee pain, function, symptoms, sport or recreation, and quality of life," Dr. Inoshi Atukorala said at the World Congress on Osteoarthritis.
Dr. Atukorala described the study as the first to examine the dose-response relationship between changes in body weight and knee osteoarthritis in a real-world, community setting.
The researchers evaluated 1,383 Australians who fulfilled the American College of Rheumatology criteria for knee osteoarthritis (OA) and were enrolled in the structured, remotely delivered "Healthy Weight for Life" knee and hip osteoarthritis management program. It integrates intensive weight loss as a component of tailored interventions, with the aim of achieving a 7%-10% body weight loss over 18 weeks, explained Dr. Atukorala, a consultant rheumatologist at the University of Colombo, Sri Lanka.
The program uses a partial very-low-calorie diet, portion management tools and devices, written healthy eating advice, and lifestyle education together with targeted telephone, e-mail, and text-message motivation and support. All participants were given the same strength, balance, and mobility exercise tools, instruction, and support.
At baseline, 81.7% of participants were obese, the average body mass index (BMI) was 34.3 kg/m2, and the mean Knee injury and Osteoarthritis Outcome Score (KOOS) pain and function subscale scores were 56.3 and 59.5. The cohort was 71% female and had an average age of 64 years.
At 18-weeks, there was a clear and significant incremental improvement in KOOS subscales across the weight-loss categories, with the greatest improvements in those losing at least 10% body weight, Dr. Atukorala said.
The weight-loss category cutoffs were chosen based on the IDEA trial (JAMA 2013;310:1263-73), as well as the weight-loss goal in the diet groups in the ADAPT study and the weight loss typically achieved in its exercise-only cohort of older adults with knee OA (Arthritis Rheum. 2004;50;1501-10), she explained.
Using repeated measures analysis of covariance, the investigators next examined the dose-response of weight loss, compared with differences in pain and function. For this analysis, the 2.5% or less weight-loss category was set as the reference.
The dose-relationship between weight loss and improvements in pain and function persisted, even after controlling for baseline age, gender, weight, height, and KOOS, Dr. Atukorala said at the meeting, sponsored by the Osteoarthritis Research Society International. The differences reached statistical significance on all KOOS subscales for the two highest weight-loss categories and on all but one subscale (KOOS sport) for those losing 5.1%-7.5% body weight.
"We are limited by the fact that the program did not assess the magnitude of exercise interventions in each weight-loss category, but it confirms the dose-response benefit of weight loss as a therapeutic intervention in knee osteoarthritis," Dr. Atukorala concluded. "And, it demonstrates the effectiveness of disseminating and implementing intensive weight-loss intervention in a community-based setting."
Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
AT OARSI 2014
Major finding: Participants who lost at least 10% body weight (mean 12.5%) had mean improvements on the KOOS pain, function, symptoms, sport, and quality of life subscales of 16.7, 17.4, 16.4, 16.4, and 16.2 points (P =.000).
Data source: Analysis of 1,383 consecutive knee OA participants in a knee and hip OA management program.
Disclosures: Dr. Atukorala reported no financial disclosures. One coauthor is the CEO and scientific director of Prima Health Solutions, and another is funded by the Australian Research Council future fellowships program.
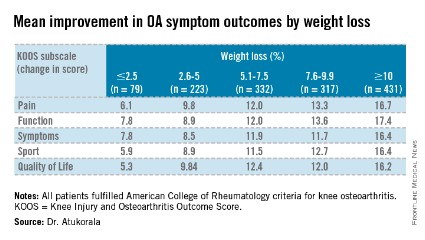
Poor vibratory sense contributes to OA knee instability
PARIS – Impaired vibratory sense and muscle strength may be important risk factors for knee instability in persons with or at risk for symptomatic knee osteoarthritis, according to an analysis of a large, longitudinal cohort.
"Buckling is commonly been thought of as a mechanical phenomenon, but no one really knows the risk factors," Dr. Najia Shakoor said in an interview at the World Congress on Osteoarthritis. "For many, sensory input may be important. If you have greater sensory input, in this case, greater vibratory sense, perhaps you can protect yourself from buckling."
Knee instability is common in persons with knee osteoarthritis (OA) and has been found in studies to be associated with muscle weakness. None have examined whether weakness predicts onset or worsening of knee instability, she said.

It is also unknown whether decreased vibratory sense, often seen in older adults with knee OA, may distort one’s sense of knee position and increase the risk of instability.
For the current analysis, unilateral knee extensor strength and bilateral vibratory perception thresholds (VPT) were evaluated in 2,212 participants with or at risk for knee OA in the Multicenter Osteoarthritis Study (MOST). VPT was measured using a biothesiometer, with the tip placed on the tibial tuberosity and the voltage increased by 1 volt/sec from 0 until the participant acknowledged sensation.
The mean age of study participants was 68 years, mean body mass index (BMI) was 31 kg/m2, and 60% were women.
At the 60-month visit, 17% of participants reported knee buckling in the past 3 months, 29% reported slipping or "shifting, slipping, or going to give way, but didn’t actually do so," and 37% reported instability (buckling and/or slipping), said Dr. Shakoor, a rheumatologist with Rush University Medical Center, Chicago.
During follow-up, 32% of patients developed incident instability, 20% incident buckling, 11% worsening instability, and 21% worsening buckling.
In Poisson regression person-based analyses, the risk of incident knee instability was significantly less in those with greater quadriceps strength (relative risk, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024), after adjustment for age, sex, BMI, race, clinic site, Kellgren-Lawrence OA grade, Western Ontario and McMaster Osteoarthritis Index knee pain, and both predictors.
Better vibratory sense also protected against worsening of both knee instability (RR, 0.42; P = .021) and buckling (RR, 0.67; P = .020), Dr. Shakoor reported in the poster presentation at the meeting, sponsored by the Osteoarthritis Research Society International.
Although it’s not known whether vibratory sense can be improved, muscle strength can be. "So these are potentially modifiable risk factors for a common problem," she said.
Prior work by the group has found that vibratory sense is impaired in hip as well as knee OA, compared with healthy controls.
The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
PARIS – Impaired vibratory sense and muscle strength may be important risk factors for knee instability in persons with or at risk for symptomatic knee osteoarthritis, according to an analysis of a large, longitudinal cohort.
"Buckling is commonly been thought of as a mechanical phenomenon, but no one really knows the risk factors," Dr. Najia Shakoor said in an interview at the World Congress on Osteoarthritis. "For many, sensory input may be important. If you have greater sensory input, in this case, greater vibratory sense, perhaps you can protect yourself from buckling."
Knee instability is common in persons with knee osteoarthritis (OA) and has been found in studies to be associated with muscle weakness. None have examined whether weakness predicts onset or worsening of knee instability, she said.
It is also unknown whether decreased vibratory sense, often seen in older adults with knee OA, may distort one’s sense of knee position and increase the risk of instability.
For the current analysis, unilateral knee extensor strength and bilateral vibratory perception thresholds (VPT) were evaluated in 2,212 participants with or at risk for knee OA in the Multicenter Osteoarthritis Study (MOST). VPT was measured using a biothesiometer, with the tip placed on the tibial tuberosity and the voltage increased by 1 volt/sec from 0 until the participant acknowledged sensation.
The mean age of study participants was 68 years, mean body mass index (BMI) was 31 kg/m2, and 60% were women.
At the 60-month visit, 17% of participants reported knee buckling in the past 3 months, 29% reported slipping or "shifting, slipping, or going to give way, but didn’t actually do so," and 37% reported instability (buckling and/or slipping), said Dr. Shakoor, a rheumatologist with Rush University Medical Center, Chicago.
During follow-up, 32% of patients developed incident instability, 20% incident buckling, 11% worsening instability, and 21% worsening buckling.
In Poisson regression person-based analyses, the risk of incident knee instability was significantly less in those with greater quadriceps strength (relative risk, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024), after adjustment for age, sex, BMI, race, clinic site, Kellgren-Lawrence OA grade, Western Ontario and McMaster Osteoarthritis Index knee pain, and both predictors.
Better vibratory sense also protected against worsening of both knee instability (RR, 0.42; P = .021) and buckling (RR, 0.67; P = .020), Dr. Shakoor reported in the poster presentation at the meeting, sponsored by the Osteoarthritis Research Society International.
Although it’s not known whether vibratory sense can be improved, muscle strength can be. "So these are potentially modifiable risk factors for a common problem," she said.
Prior work by the group has found that vibratory sense is impaired in hip as well as knee OA, compared with healthy controls.
The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
PARIS – Impaired vibratory sense and muscle strength may be important risk factors for knee instability in persons with or at risk for symptomatic knee osteoarthritis, according to an analysis of a large, longitudinal cohort.
"Buckling is commonly been thought of as a mechanical phenomenon, but no one really knows the risk factors," Dr. Najia Shakoor said in an interview at the World Congress on Osteoarthritis. "For many, sensory input may be important. If you have greater sensory input, in this case, greater vibratory sense, perhaps you can protect yourself from buckling."
Knee instability is common in persons with knee osteoarthritis (OA) and has been found in studies to be associated with muscle weakness. None have examined whether weakness predicts onset or worsening of knee instability, she said.
It is also unknown whether decreased vibratory sense, often seen in older adults with knee OA, may distort one’s sense of knee position and increase the risk of instability.
For the current analysis, unilateral knee extensor strength and bilateral vibratory perception thresholds (VPT) were evaluated in 2,212 participants with or at risk for knee OA in the Multicenter Osteoarthritis Study (MOST). VPT was measured using a biothesiometer, with the tip placed on the tibial tuberosity and the voltage increased by 1 volt/sec from 0 until the participant acknowledged sensation.
The mean age of study participants was 68 years, mean body mass index (BMI) was 31 kg/m2, and 60% were women.
At the 60-month visit, 17% of participants reported knee buckling in the past 3 months, 29% reported slipping or "shifting, slipping, or going to give way, but didn’t actually do so," and 37% reported instability (buckling and/or slipping), said Dr. Shakoor, a rheumatologist with Rush University Medical Center, Chicago.
During follow-up, 32% of patients developed incident instability, 20% incident buckling, 11% worsening instability, and 21% worsening buckling.
In Poisson regression person-based analyses, the risk of incident knee instability was significantly less in those with greater quadriceps strength (relative risk, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024), after adjustment for age, sex, BMI, race, clinic site, Kellgren-Lawrence OA grade, Western Ontario and McMaster Osteoarthritis Index knee pain, and both predictors.
Better vibratory sense also protected against worsening of both knee instability (RR, 0.42; P = .021) and buckling (RR, 0.67; P = .020), Dr. Shakoor reported in the poster presentation at the meeting, sponsored by the Osteoarthritis Research Society International.
Although it’s not known whether vibratory sense can be improved, muscle strength can be. "So these are potentially modifiable risk factors for a common problem," she said.
Prior work by the group has found that vibratory sense is impaired in hip as well as knee OA, compared with healthy controls.
The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
AT OARSI 2014
Key clinical point: Working to increase quadriceps strength may reduce knee instability in OA patients.
Major finding: The risk of incident knee instability was significantly less in those with greater quadriceps strength (RR, 0.60; P = .003) as well as in those with better vibratory sense (P value for linear trend of .024).
Data source: A longitudinal analysis of 2,212 patients with knee OA.
Disclosures: The study was supported by the National Institutes of Health. Dr. Shakoor reported no conflicting interests.
