User login
Psoriasis patients post above-average cancer rates
CHICAGO – Malignancy rates in patients with psoriasis outstrip those in the general population, based on data from a retrospective analysis of commercial claims.
Rates for all cancers were similar among patients undergoing different psoriasis treatments, with the exception of nonmelanoma skin cancer and lymphoma.

Rates for these two cancers were more variable across treatment groups, but were still above those in the general public, Dr. Alexa B. Kimball reported at the American Academy of Dermatology summer meeting.
The increased cancer risk may be associated with chronic inflammation, a hallmark of psoriasis, and exposure to some psoriasis therapies such as phototherapy with psoralen plus ultraviolet, cyclosporine, and methotrexate, she noted in the study’s background information.
Previous studies also have suggested that patients with psoriasis may be at increased risk for some cancers such as respiratory tract, urinary tract, and liver cancers, non-Hodgkin’s lymphoma, and skin cancers.
To evaluate the incidence of malignancy, the investigators obtained data from the MarketScan Commercial and Medicare Supplemental claims databases for patients with a diagnosis of psoriasis on or before Dec. 31, 2006, and at least one prescription claim for etanercept (Enbrel), adalimumab (Humira), infliximab (Remicade), ustekinumab (Stelara), nonbiologic therapies, or phototherapy.
The general population cohort included patients at least 18 years old as of 2005 or at enrollment in the health care plan. Both cohorts had 12 months’ continuous enrollment in the health care plan from Jan. 1, 2005, through Dec. 31, 2006.
Follow-up for a patient ended at the first cancer event, disenrollment from the health care plan, or after 5 years from the index date.
Patients with psoriasis had a 5-year malignancy rate of 115.5 cases/10,000 person-years, compared with 96/10,000 person-years for the general population, reported Dr. Kimball of Massachusetts General Hospital, Boston.
Excluding nonmelanoma skin cancer and lymphoma, incidence rates were similar across treatment groups: etanercept (100.2/10,000), adalimumab (94.6/10,000), infliximab (138.1/10,000), ustekinumab (100.6/10,000), nonbiologics (116.8/10,000), and phototherapy (117.3/10,000).
"These large database queries continue to be reassuring that most systemic therapies are not changing the risk for common cancers, excluding lymphoma and skin cancer, which we continue to examine separately," Dr. Kimball said in an interview.
Nonmelanoma skin cancer was far and away the most common malignancy in psoriasis patients, occurring at a rate of 147.2/10,000 person-years vs. 94.2/10,000 person-years among the general public. Rates were highest in patients treated with adalimumab (234.2/10,000 person-years) and ustekinumab (233.3/10,000) and lowest in those treated with etanercept (155.9/10,000).
"Even with the large size of the database, the number of skin cancers remains small, so making conclusions about specific therapies may be premature," she said.
Incidence rates of lymphoma were considerably lower, but again higher in psoriasis patients than the general public (11.1/10,000 vs. 6.6/10,000). Rates of this hematologic cancer were highest with ustekinumab (25.1/10,000) and, once again, lowest with etanercept (6.9/10,000), according to the poster.
In all, 5,857 patients received nonbiologic therapies, 6,856 received etanercept, 3,314 adalimumab, 1,044 infliximab, 526 ustekinumab, and 5,156 were treated with phototherapy.
Dr. Kimball is a consultant for several pharmaceutical companies including Amgen, the study sponsor.
CHICAGO – Malignancy rates in patients with psoriasis outstrip those in the general population, based on data from a retrospective analysis of commercial claims.
Rates for all cancers were similar among patients undergoing different psoriasis treatments, with the exception of nonmelanoma skin cancer and lymphoma.
Rates for these two cancers were more variable across treatment groups, but were still above those in the general public, Dr. Alexa B. Kimball reported at the American Academy of Dermatology summer meeting.
The increased cancer risk may be associated with chronic inflammation, a hallmark of psoriasis, and exposure to some psoriasis therapies such as phototherapy with psoralen plus ultraviolet, cyclosporine, and methotrexate, she noted in the study’s background information.
Previous studies also have suggested that patients with psoriasis may be at increased risk for some cancers such as respiratory tract, urinary tract, and liver cancers, non-Hodgkin’s lymphoma, and skin cancers.
To evaluate the incidence of malignancy, the investigators obtained data from the MarketScan Commercial and Medicare Supplemental claims databases for patients with a diagnosis of psoriasis on or before Dec. 31, 2006, and at least one prescription claim for etanercept (Enbrel), adalimumab (Humira), infliximab (Remicade), ustekinumab (Stelara), nonbiologic therapies, or phototherapy.
The general population cohort included patients at least 18 years old as of 2005 or at enrollment in the health care plan. Both cohorts had 12 months’ continuous enrollment in the health care plan from Jan. 1, 2005, through Dec. 31, 2006.
Follow-up for a patient ended at the first cancer event, disenrollment from the health care plan, or after 5 years from the index date.
Patients with psoriasis had a 5-year malignancy rate of 115.5 cases/10,000 person-years, compared with 96/10,000 person-years for the general population, reported Dr. Kimball of Massachusetts General Hospital, Boston.
Excluding nonmelanoma skin cancer and lymphoma, incidence rates were similar across treatment groups: etanercept (100.2/10,000), adalimumab (94.6/10,000), infliximab (138.1/10,000), ustekinumab (100.6/10,000), nonbiologics (116.8/10,000), and phototherapy (117.3/10,000).
"These large database queries continue to be reassuring that most systemic therapies are not changing the risk for common cancers, excluding lymphoma and skin cancer, which we continue to examine separately," Dr. Kimball said in an interview.
Nonmelanoma skin cancer was far and away the most common malignancy in psoriasis patients, occurring at a rate of 147.2/10,000 person-years vs. 94.2/10,000 person-years among the general public. Rates were highest in patients treated with adalimumab (234.2/10,000 person-years) and ustekinumab (233.3/10,000) and lowest in those treated with etanercept (155.9/10,000).
"Even with the large size of the database, the number of skin cancers remains small, so making conclusions about specific therapies may be premature," she said.
Incidence rates of lymphoma were considerably lower, but again higher in psoriasis patients than the general public (11.1/10,000 vs. 6.6/10,000). Rates of this hematologic cancer were highest with ustekinumab (25.1/10,000) and, once again, lowest with etanercept (6.9/10,000), according to the poster.
In all, 5,857 patients received nonbiologic therapies, 6,856 received etanercept, 3,314 adalimumab, 1,044 infliximab, 526 ustekinumab, and 5,156 were treated with phototherapy.
Dr. Kimball is a consultant for several pharmaceutical companies including Amgen, the study sponsor.
CHICAGO – Malignancy rates in patients with psoriasis outstrip those in the general population, based on data from a retrospective analysis of commercial claims.
Rates for all cancers were similar among patients undergoing different psoriasis treatments, with the exception of nonmelanoma skin cancer and lymphoma.
Rates for these two cancers were more variable across treatment groups, but were still above those in the general public, Dr. Alexa B. Kimball reported at the American Academy of Dermatology summer meeting.
The increased cancer risk may be associated with chronic inflammation, a hallmark of psoriasis, and exposure to some psoriasis therapies such as phototherapy with psoralen plus ultraviolet, cyclosporine, and methotrexate, she noted in the study’s background information.
Previous studies also have suggested that patients with psoriasis may be at increased risk for some cancers such as respiratory tract, urinary tract, and liver cancers, non-Hodgkin’s lymphoma, and skin cancers.
To evaluate the incidence of malignancy, the investigators obtained data from the MarketScan Commercial and Medicare Supplemental claims databases for patients with a diagnosis of psoriasis on or before Dec. 31, 2006, and at least one prescription claim for etanercept (Enbrel), adalimumab (Humira), infliximab (Remicade), ustekinumab (Stelara), nonbiologic therapies, or phototherapy.
The general population cohort included patients at least 18 years old as of 2005 or at enrollment in the health care plan. Both cohorts had 12 months’ continuous enrollment in the health care plan from Jan. 1, 2005, through Dec. 31, 2006.
Follow-up for a patient ended at the first cancer event, disenrollment from the health care plan, or after 5 years from the index date.
Patients with psoriasis had a 5-year malignancy rate of 115.5 cases/10,000 person-years, compared with 96/10,000 person-years for the general population, reported Dr. Kimball of Massachusetts General Hospital, Boston.
Excluding nonmelanoma skin cancer and lymphoma, incidence rates were similar across treatment groups: etanercept (100.2/10,000), adalimumab (94.6/10,000), infliximab (138.1/10,000), ustekinumab (100.6/10,000), nonbiologics (116.8/10,000), and phototherapy (117.3/10,000).
"These large database queries continue to be reassuring that most systemic therapies are not changing the risk for common cancers, excluding lymphoma and skin cancer, which we continue to examine separately," Dr. Kimball said in an interview.
Nonmelanoma skin cancer was far and away the most common malignancy in psoriasis patients, occurring at a rate of 147.2/10,000 person-years vs. 94.2/10,000 person-years among the general public. Rates were highest in patients treated with adalimumab (234.2/10,000 person-years) and ustekinumab (233.3/10,000) and lowest in those treated with etanercept (155.9/10,000).
"Even with the large size of the database, the number of skin cancers remains small, so making conclusions about specific therapies may be premature," she said.
Incidence rates of lymphoma were considerably lower, but again higher in psoriasis patients than the general public (11.1/10,000 vs. 6.6/10,000). Rates of this hematologic cancer were highest with ustekinumab (25.1/10,000) and, once again, lowest with etanercept (6.9/10,000), according to the poster.
In all, 5,857 patients received nonbiologic therapies, 6,856 received etanercept, 3,314 adalimumab, 1,044 infliximab, 526 ustekinumab, and 5,156 were treated with phototherapy.
Dr. Kimball is a consultant for several pharmaceutical companies including Amgen, the study sponsor.
AT THE AAD SUMMER ACADEMY 2014
Key clinical point: Rates of malignancy were higher among patients with psoriasis than in the general population.
Major finding: The 5-year malignancy rate in patients with psoriasis was 115.5 cases/10,000 person-years vs. 96/10,000 person-years in the general population.
Data source: Retrospective database analysis of 22,753 patients with psoriasis.
Disclosures: Dr. Kimball is a consultant for several pharmaceutical companies including Amgen, the study sponsor.

Don’t overlook anus, genitalia during total body skin exam
CHICAGO – The anus and genitalia are often overlooked during total body skin examinations, leaving mucosal diseases to go unchecked, especially in women, according to Dr. Bethanee Schlosser.
She acknowledged that there is no literature to quantify the issue but said that her experience suggests mucocutaneous exams may be getting short shrift.

When Dr. Schlosser queried some 300 dermatologists assembled earlier this year, almost all said that they examine the oral cavity during total body skin exams; three-fourths responded that they routinely examine male patients’ genitalia. When asked whether they do the same for their female patients, less than 20 hands went up in the crowd.
"I think there are a couple of reasons for it," Dr. Schlosser of Northwestern University, Chicago, said at the American Academy of Dermatology summer meeting.
First, dermatologists don’t often look at the genitalia, so they may not know what the normal variations are.
Second, many patients don’t expect a dermatologist to examine genitalia. "Patients may be like, ‘You want to look where? I just have a mole on my chest.’ So it’s a matter of patient education," she said.
Third is the added time involved, and finally, some dermatologists are hesitant because they may not be comfortable managing mucosal disease should they find it.
Most dermatologists assume that gynecologists are evaluating their patients’ vulvar skin, but some gynecologists view the vulva more as "the doorway to the cervix. They may simply walk through it, not looking at what is around them, and to that effect, I don’t think it’s necessarily their fault, but their training," Dr. Schlosser said. "While vulvar disease is on the ob.gyn. board exam, the senior ob.gyn. residents rotate through our clinic with me and they routinely say they don’t get that education anywhere else."
Dr. Schlosser offered pearls for managing a number of mucosal diseases, including vulvar lichen sclerosis (VLS).
VLS affects about 1 in 600 women and can carry significant morbidity, including complete obliteration of the clitoral hood and labia minora, narrowing of the vaginal introitus, sexual dysfunction, and potential urinary obstruction, she said.
The risk of developing squamous cell carcinoma (SCC) in patients with VLS is 300-fold higher than in the general patient population. The specific risk factors for vulvar SCC are not fully elucidated in VLS, but include localized hyperkeratosis and age over 75 years.
"It’s important to realize that these older patients ... often don’t see their gynecologists because they’re told the pelvic examination is not indicated anymore," Dr. Schlosser said. "It really behooves us as dermatologists to be doing a genital exam as part of our total body skin exam."
Researchers think, but don’t have the evidence to suggest, that treating VLS changes the risk of SCC, "which is one of the hardest things to discuss with our patients," she added.
Suspicion of SCC should be raised if the patient has hyperkeratotic lesions; ulceration, even pinpoint in size, that doesn’t improve with standard therapy; erythematous, indurated plaques; or if the patient reports a change in symptom quality – previously itchy and now painful, for example – or a change in symptom distribution, such as previously all over and now localized to one spot.
"That can really herald that something bad has occurred," Dr. Schlosser cautioned.
Superpotent topical corticosteroids such as clobetasol propionate are first-line therapy for VLS, with no rationale to support the old-school treatment of topical testosterone. Maintenance therapy is common, as up to 85% of women will relapse.
Dr. Schlosser also advised physicians to educate women on how much medication to use, to send them home with a diagram of the affected area, and to use a hand mirror during the exam.
"Patients don’t want to look, but I tell them you’re not going to get better if you don’t know where to put your medication," she said.
Dr. Schlosser reported no relevant conflicts of interest.
CHICAGO – The anus and genitalia are often overlooked during total body skin examinations, leaving mucosal diseases to go unchecked, especially in women, according to Dr. Bethanee Schlosser.
She acknowledged that there is no literature to quantify the issue but said that her experience suggests mucocutaneous exams may be getting short shrift.
When Dr. Schlosser queried some 300 dermatologists assembled earlier this year, almost all said that they examine the oral cavity during total body skin exams; three-fourths responded that they routinely examine male patients’ genitalia. When asked whether they do the same for their female patients, less than 20 hands went up in the crowd.
"I think there are a couple of reasons for it," Dr. Schlosser of Northwestern University, Chicago, said at the American Academy of Dermatology summer meeting.
First, dermatologists don’t often look at the genitalia, so they may not know what the normal variations are.
Second, many patients don’t expect a dermatologist to examine genitalia. "Patients may be like, ‘You want to look where? I just have a mole on my chest.’ So it’s a matter of patient education," she said.
Third is the added time involved, and finally, some dermatologists are hesitant because they may not be comfortable managing mucosal disease should they find it.
Most dermatologists assume that gynecologists are evaluating their patients’ vulvar skin, but some gynecologists view the vulva more as "the doorway to the cervix. They may simply walk through it, not looking at what is around them, and to that effect, I don’t think it’s necessarily their fault, but their training," Dr. Schlosser said. "While vulvar disease is on the ob.gyn. board exam, the senior ob.gyn. residents rotate through our clinic with me and they routinely say they don’t get that education anywhere else."
Dr. Schlosser offered pearls for managing a number of mucosal diseases, including vulvar lichen sclerosis (VLS).
VLS affects about 1 in 600 women and can carry significant morbidity, including complete obliteration of the clitoral hood and labia minora, narrowing of the vaginal introitus, sexual dysfunction, and potential urinary obstruction, she said.
The risk of developing squamous cell carcinoma (SCC) in patients with VLS is 300-fold higher than in the general patient population. The specific risk factors for vulvar SCC are not fully elucidated in VLS, but include localized hyperkeratosis and age over 75 years.
"It’s important to realize that these older patients ... often don’t see their gynecologists because they’re told the pelvic examination is not indicated anymore," Dr. Schlosser said. "It really behooves us as dermatologists to be doing a genital exam as part of our total body skin exam."
Researchers think, but don’t have the evidence to suggest, that treating VLS changes the risk of SCC, "which is one of the hardest things to discuss with our patients," she added.
Suspicion of SCC should be raised if the patient has hyperkeratotic lesions; ulceration, even pinpoint in size, that doesn’t improve with standard therapy; erythematous, indurated plaques; or if the patient reports a change in symptom quality – previously itchy and now painful, for example – or a change in symptom distribution, such as previously all over and now localized to one spot.
"That can really herald that something bad has occurred," Dr. Schlosser cautioned.
Superpotent topical corticosteroids such as clobetasol propionate are first-line therapy for VLS, with no rationale to support the old-school treatment of topical testosterone. Maintenance therapy is common, as up to 85% of women will relapse.
Dr. Schlosser also advised physicians to educate women on how much medication to use, to send them home with a diagram of the affected area, and to use a hand mirror during the exam.
"Patients don’t want to look, but I tell them you’re not going to get better if you don’t know where to put your medication," she said.
Dr. Schlosser reported no relevant conflicts of interest.
CHICAGO – The anus and genitalia are often overlooked during total body skin examinations, leaving mucosal diseases to go unchecked, especially in women, according to Dr. Bethanee Schlosser.
She acknowledged that there is no literature to quantify the issue but said that her experience suggests mucocutaneous exams may be getting short shrift.
When Dr. Schlosser queried some 300 dermatologists assembled earlier this year, almost all said that they examine the oral cavity during total body skin exams; three-fourths responded that they routinely examine male patients’ genitalia. When asked whether they do the same for their female patients, less than 20 hands went up in the crowd.
"I think there are a couple of reasons for it," Dr. Schlosser of Northwestern University, Chicago, said at the American Academy of Dermatology summer meeting.
First, dermatologists don’t often look at the genitalia, so they may not know what the normal variations are.
Second, many patients don’t expect a dermatologist to examine genitalia. "Patients may be like, ‘You want to look where? I just have a mole on my chest.’ So it’s a matter of patient education," she said.
Third is the added time involved, and finally, some dermatologists are hesitant because they may not be comfortable managing mucosal disease should they find it.
Most dermatologists assume that gynecologists are evaluating their patients’ vulvar skin, but some gynecologists view the vulva more as "the doorway to the cervix. They may simply walk through it, not looking at what is around them, and to that effect, I don’t think it’s necessarily their fault, but their training," Dr. Schlosser said. "While vulvar disease is on the ob.gyn. board exam, the senior ob.gyn. residents rotate through our clinic with me and they routinely say they don’t get that education anywhere else."
Dr. Schlosser offered pearls for managing a number of mucosal diseases, including vulvar lichen sclerosis (VLS).
VLS affects about 1 in 600 women and can carry significant morbidity, including complete obliteration of the clitoral hood and labia minora, narrowing of the vaginal introitus, sexual dysfunction, and potential urinary obstruction, she said.
The risk of developing squamous cell carcinoma (SCC) in patients with VLS is 300-fold higher than in the general patient population. The specific risk factors for vulvar SCC are not fully elucidated in VLS, but include localized hyperkeratosis and age over 75 years.
"It’s important to realize that these older patients ... often don’t see their gynecologists because they’re told the pelvic examination is not indicated anymore," Dr. Schlosser said. "It really behooves us as dermatologists to be doing a genital exam as part of our total body skin exam."
Researchers think, but don’t have the evidence to suggest, that treating VLS changes the risk of SCC, "which is one of the hardest things to discuss with our patients," she added.
Suspicion of SCC should be raised if the patient has hyperkeratotic lesions; ulceration, even pinpoint in size, that doesn’t improve with standard therapy; erythematous, indurated plaques; or if the patient reports a change in symptom quality – previously itchy and now painful, for example – or a change in symptom distribution, such as previously all over and now localized to one spot.
"That can really herald that something bad has occurred," Dr. Schlosser cautioned.
Superpotent topical corticosteroids such as clobetasol propionate are first-line therapy for VLS, with no rationale to support the old-school treatment of topical testosterone. Maintenance therapy is common, as up to 85% of women will relapse.
Dr. Schlosser also advised physicians to educate women on how much medication to use, to send them home with a diagram of the affected area, and to use a hand mirror during the exam.
"Patients don’t want to look, but I tell them you’re not going to get better if you don’t know where to put your medication," she said.
Dr. Schlosser reported no relevant conflicts of interest.
EXPERT ANALYSIS FROM THE AAD SUMMER ACADEMY 2014

AAD puts data mining atop its agenda
CHICAGO – The American Academy of Dermatology is establishing a clinical data registry in an effort to better benchmark physician performance through patient outcomes and advocate for the specialty.
"We’re now practicing in a data-driven world for better or worse, and without good data we’re defenseless in front of bureaucrats and insurance companies. And that’s not a good position for the future of our specialty," AAD president Dr. Brett Coldiron said in the president’s address at the AAD summer meeting.

The registry is expected to cost $2 million up front and another $5 million to $7 million over the next several years.
The investment in data gathering is needed to provide data for members to use and benchmark against in quality reporting, to demonstrate cost effectiveness, and to fight a half dozen or so legislative and regulatory issues in play, he said. Key among them was the decision by United HealthCare and Humana to delist or drop about half of the dermatologists from their networks in 20 states, many of which already have 4-month wait times to see a dermatologist.
To add insult to injury, the remaining rosters of dermatologists were found to be riddled with errors, as high as 69%, including quadruplicate listings and listings for dead or retired physicians, said Dr. Coldiron, a dermatologist in private practice in Cincinnati.
"This isn’t really about us, it’s about patients," he added. "Patients are going to be hurt, maybe die, but at a minimum, suffer much more because they don’t know their insurance policy is hollow. They don’t know they’re going to need to see a dermatologist because their wife hasn’t spotted that black mole on their back yet, and now it’s going to take them 4 months to have that mole looked at, if they get in [to see a dermatologist] at all."
Dr. Coldiron said he expects that patients in health insurance exchanges will be having the same problem of restricted access and called on individual dermatologists to help their patients register their complaints and concerns through the Centers for Medicare & Medicaid Services website and hotline and to lobby Congress.
To help pay for the data registry, AAD members will be asked to pony up $50 more in membership dues, with an annual cost of living increase to follow the urban consumer price index. Dues haven’t increased in 12 years and 30% inflation and are well below those of other specialties, such as plastic surgery and ophthalmology, he said. A similar request last year failed by a 55% to 45% vote.
"If you want to fight back against rapacious insurance companies and intrusive government bureaucrats, and you want to practice medicine, not paperwork, you need big data," Dr. Coldiron asserted.
CHICAGO – The American Academy of Dermatology is establishing a clinical data registry in an effort to better benchmark physician performance through patient outcomes and advocate for the specialty.
"We’re now practicing in a data-driven world for better or worse, and without good data we’re defenseless in front of bureaucrats and insurance companies. And that’s not a good position for the future of our specialty," AAD president Dr. Brett Coldiron said in the president’s address at the AAD summer meeting.
The registry is expected to cost $2 million up front and another $5 million to $7 million over the next several years.
The investment in data gathering is needed to provide data for members to use and benchmark against in quality reporting, to demonstrate cost effectiveness, and to fight a half dozen or so legislative and regulatory issues in play, he said. Key among them was the decision by United HealthCare and Humana to delist or drop about half of the dermatologists from their networks in 20 states, many of which already have 4-month wait times to see a dermatologist.
To add insult to injury, the remaining rosters of dermatologists were found to be riddled with errors, as high as 69%, including quadruplicate listings and listings for dead or retired physicians, said Dr. Coldiron, a dermatologist in private practice in Cincinnati.
"This isn’t really about us, it’s about patients," he added. "Patients are going to be hurt, maybe die, but at a minimum, suffer much more because they don’t know their insurance policy is hollow. They don’t know they’re going to need to see a dermatologist because their wife hasn’t spotted that black mole on their back yet, and now it’s going to take them 4 months to have that mole looked at, if they get in [to see a dermatologist] at all."
Dr. Coldiron said he expects that patients in health insurance exchanges will be having the same problem of restricted access and called on individual dermatologists to help their patients register their complaints and concerns through the Centers for Medicare & Medicaid Services website and hotline and to lobby Congress.
To help pay for the data registry, AAD members will be asked to pony up $50 more in membership dues, with an annual cost of living increase to follow the urban consumer price index. Dues haven’t increased in 12 years and 30% inflation and are well below those of other specialties, such as plastic surgery and ophthalmology, he said. A similar request last year failed by a 55% to 45% vote.
"If you want to fight back against rapacious insurance companies and intrusive government bureaucrats, and you want to practice medicine, not paperwork, you need big data," Dr. Coldiron asserted.
CHICAGO – The American Academy of Dermatology is establishing a clinical data registry in an effort to better benchmark physician performance through patient outcomes and advocate for the specialty.
"We’re now practicing in a data-driven world for better or worse, and without good data we’re defenseless in front of bureaucrats and insurance companies. And that’s not a good position for the future of our specialty," AAD president Dr. Brett Coldiron said in the president’s address at the AAD summer meeting.
The registry is expected to cost $2 million up front and another $5 million to $7 million over the next several years.
The investment in data gathering is needed to provide data for members to use and benchmark against in quality reporting, to demonstrate cost effectiveness, and to fight a half dozen or so legislative and regulatory issues in play, he said. Key among them was the decision by United HealthCare and Humana to delist or drop about half of the dermatologists from their networks in 20 states, many of which already have 4-month wait times to see a dermatologist.
To add insult to injury, the remaining rosters of dermatologists were found to be riddled with errors, as high as 69%, including quadruplicate listings and listings for dead or retired physicians, said Dr. Coldiron, a dermatologist in private practice in Cincinnati.
"This isn’t really about us, it’s about patients," he added. "Patients are going to be hurt, maybe die, but at a minimum, suffer much more because they don’t know their insurance policy is hollow. They don’t know they’re going to need to see a dermatologist because their wife hasn’t spotted that black mole on their back yet, and now it’s going to take them 4 months to have that mole looked at, if they get in [to see a dermatologist] at all."
Dr. Coldiron said he expects that patients in health insurance exchanges will be having the same problem of restricted access and called on individual dermatologists to help their patients register their complaints and concerns through the Centers for Medicare & Medicaid Services website and hotline and to lobby Congress.
To help pay for the data registry, AAD members will be asked to pony up $50 more in membership dues, with an annual cost of living increase to follow the urban consumer price index. Dues haven’t increased in 12 years and 30% inflation and are well below those of other specialties, such as plastic surgery and ophthalmology, he said. A similar request last year failed by a 55% to 45% vote.
"If you want to fight back against rapacious insurance companies and intrusive government bureaucrats, and you want to practice medicine, not paperwork, you need big data," Dr. Coldiron asserted.
EXPERT ANALYSIS FROM THE AAD SUMMER ACADEMY 2014

Novel antiviral therapy 100% protective against lethal Ebola-like Marburg virus
For the first time, a novel antiviral treatment has saved the lives of primates when given in the late stage of infection with the Marburg virus, a lethal filovirus closely related to the Ebola virus.
Seven daily doses of the lipid-encapsulated small interfering RNA (siRNA) treatment started 3 days after exposure to a lethal dose of Marburg virus–Angola hemorrhagic fever (MARV-Angola) resulted in 100% protection in 16 rhesus macaques already showing clinical signs of the disease.

All untreated animals died; most died early on day 8 after infection, according to results reported in the Aug. 20 issue of Science Translational Medicine.
Delaying treatment until day 3 is clinically significant because this is the earliest time at which viremia can be detected, "showing real-world utility of this technology," study coauthor Thomas Geisbert, Ph.D., professor of microbiology and immunology at the University of Texas Medical Branch, Galveston, said during a press briefing.
The anti-MARV nucleoprotein-targeting siRNAs have been designed to protect against all known strains of Marburg virus, but will not protect against the Ebola virus.
A previous study, however, showed that the same technology completely protected rhesus monkeys exposed to the Zaire Ebola virus, the same species involved in the current outbreak, he said. That study examined treatment given only shortly after exposure, not when the signs of illness were already present, which is crucial to outbreak control (Lancet 2010;375:1896-905).
Still, the siRNA Ebola treatment could be used on a compassionate-use basis in the current Ebola outbreak, he added.
Recently two cases of MARV were imported to the United States and Europe, raising concerns about the public health threat posed by this virus.
There are no approved vaccines or drugs for humans infected with MARV-Angola. It has been associated with the highest case fatality rates of any strain or species of filovirus, causing 90% mortality in man in the largest Marburg outbreak in 2005 in Angola, Dr. Geisbert observed.

A phase I human study has been started with the Ebola siRNA product, but funding is needed before a trial evaluating the Marburg siRNA product can be launched in humans.
The antiviral strategy is based on siRNAs or double-stranded molecules that cause messenger RNA to be broken down after transcription. Thus, there is no translation of the Marburg virus proteins. The siRNAs are packaged in a proprietary lipid nanoparticle that serves as the delivery vehicle (Tekmira Pharmaceuticals, Burnaby, British Columbia).
Future work will examine how much further out treatment can be delayed in MARV-Angola as well as in Ebola hemorrhagic fever, Dr. Geisbert said.
So far, only one other strategy combining monoclonal antibodies and adenovirus vector expressing interferon-alpha has been shown to confer complete protection to macaques when given 3 days after infection (Sci. Transl. Med. 2013 Oct 16;5:207ra143. doi: 10.1126/scitranslmed.3006605), he said.
The National Institutes of Health provided up to $26 million in grant funding this March to UTMB, Tekmira, Profectus, and Vanderbilt University to allow researchers to evaluate both strategies and whether combining antibodies and siRNAs will further enhance the benefits, he said.
Treatment dosing has yet to be optimized. So far, no serious safety concerns have been identified in primates given the Marburg siRNA product or in humans dosed with the siRNA Ebola product, he added.
For the first time, a novel antiviral treatment has saved the lives of primates when given in the late stage of infection with the Marburg virus, a lethal filovirus closely related to the Ebola virus.
Seven daily doses of the lipid-encapsulated small interfering RNA (siRNA) treatment started 3 days after exposure to a lethal dose of Marburg virus–Angola hemorrhagic fever (MARV-Angola) resulted in 100% protection in 16 rhesus macaques already showing clinical signs of the disease.
All untreated animals died; most died early on day 8 after infection, according to results reported in the Aug. 20 issue of Science Translational Medicine.
Delaying treatment until day 3 is clinically significant because this is the earliest time at which viremia can be detected, "showing real-world utility of this technology," study coauthor Thomas Geisbert, Ph.D., professor of microbiology and immunology at the University of Texas Medical Branch, Galveston, said during a press briefing.
The anti-MARV nucleoprotein-targeting siRNAs have been designed to protect against all known strains of Marburg virus, but will not protect against the Ebola virus.
A previous study, however, showed that the same technology completely protected rhesus monkeys exposed to the Zaire Ebola virus, the same species involved in the current outbreak, he said. That study examined treatment given only shortly after exposure, not when the signs of illness were already present, which is crucial to outbreak control (Lancet 2010;375:1896-905).
Still, the siRNA Ebola treatment could be used on a compassionate-use basis in the current Ebola outbreak, he added.
Recently two cases of MARV were imported to the United States and Europe, raising concerns about the public health threat posed by this virus.
There are no approved vaccines or drugs for humans infected with MARV-Angola. It has been associated with the highest case fatality rates of any strain or species of filovirus, causing 90% mortality in man in the largest Marburg outbreak in 2005 in Angola, Dr. Geisbert observed.
A phase I human study has been started with the Ebola siRNA product, but funding is needed before a trial evaluating the Marburg siRNA product can be launched in humans.
The antiviral strategy is based on siRNAs or double-stranded molecules that cause messenger RNA to be broken down after transcription. Thus, there is no translation of the Marburg virus proteins. The siRNAs are packaged in a proprietary lipid nanoparticle that serves as the delivery vehicle (Tekmira Pharmaceuticals, Burnaby, British Columbia).
Future work will examine how much further out treatment can be delayed in MARV-Angola as well as in Ebola hemorrhagic fever, Dr. Geisbert said.
So far, only one other strategy combining monoclonal antibodies and adenovirus vector expressing interferon-alpha has been shown to confer complete protection to macaques when given 3 days after infection (Sci. Transl. Med. 2013 Oct 16;5:207ra143. doi: 10.1126/scitranslmed.3006605), he said.
The National Institutes of Health provided up to $26 million in grant funding this March to UTMB, Tekmira, Profectus, and Vanderbilt University to allow researchers to evaluate both strategies and whether combining antibodies and siRNAs will further enhance the benefits, he said.
Treatment dosing has yet to be optimized. So far, no serious safety concerns have been identified in primates given the Marburg siRNA product or in humans dosed with the siRNA Ebola product, he added.
For the first time, a novel antiviral treatment has saved the lives of primates when given in the late stage of infection with the Marburg virus, a lethal filovirus closely related to the Ebola virus.
Seven daily doses of the lipid-encapsulated small interfering RNA (siRNA) treatment started 3 days after exposure to a lethal dose of Marburg virus–Angola hemorrhagic fever (MARV-Angola) resulted in 100% protection in 16 rhesus macaques already showing clinical signs of the disease.
All untreated animals died; most died early on day 8 after infection, according to results reported in the Aug. 20 issue of Science Translational Medicine.
Delaying treatment until day 3 is clinically significant because this is the earliest time at which viremia can be detected, "showing real-world utility of this technology," study coauthor Thomas Geisbert, Ph.D., professor of microbiology and immunology at the University of Texas Medical Branch, Galveston, said during a press briefing.
The anti-MARV nucleoprotein-targeting siRNAs have been designed to protect against all known strains of Marburg virus, but will not protect against the Ebola virus.
A previous study, however, showed that the same technology completely protected rhesus monkeys exposed to the Zaire Ebola virus, the same species involved in the current outbreak, he said. That study examined treatment given only shortly after exposure, not when the signs of illness were already present, which is crucial to outbreak control (Lancet 2010;375:1896-905).
Still, the siRNA Ebola treatment could be used on a compassionate-use basis in the current Ebola outbreak, he added.
Recently two cases of MARV were imported to the United States and Europe, raising concerns about the public health threat posed by this virus.
There are no approved vaccines or drugs for humans infected with MARV-Angola. It has been associated with the highest case fatality rates of any strain or species of filovirus, causing 90% mortality in man in the largest Marburg outbreak in 2005 in Angola, Dr. Geisbert observed.
A phase I human study has been started with the Ebola siRNA product, but funding is needed before a trial evaluating the Marburg siRNA product can be launched in humans.
The antiviral strategy is based on siRNAs or double-stranded molecules that cause messenger RNA to be broken down after transcription. Thus, there is no translation of the Marburg virus proteins. The siRNAs are packaged in a proprietary lipid nanoparticle that serves as the delivery vehicle (Tekmira Pharmaceuticals, Burnaby, British Columbia).
Future work will examine how much further out treatment can be delayed in MARV-Angola as well as in Ebola hemorrhagic fever, Dr. Geisbert said.
So far, only one other strategy combining monoclonal antibodies and adenovirus vector expressing interferon-alpha has been shown to confer complete protection to macaques when given 3 days after infection (Sci. Transl. Med. 2013 Oct 16;5:207ra143. doi: 10.1126/scitranslmed.3006605), he said.
The National Institutes of Health provided up to $26 million in grant funding this March to UTMB, Tekmira, Profectus, and Vanderbilt University to allow researchers to evaluate both strategies and whether combining antibodies and siRNAs will further enhance the benefits, he said.
Treatment dosing has yet to be optimized. So far, no serious safety concerns have been identified in primates given the Marburg siRNA product or in humans dosed with the siRNA Ebola product, he added.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point: Complete protection from Marburg virus–Angola hemorrhagic fever can be achieved in nonhuman primates, even when the treatment window is expanded to 72 hours post infection.
Major finding: A small interfering RNA treatment started 3 days after exposure to Marburg virus–Angola hemorrhagic fever resulted in 100% protection in 16 rhesus macaques.
Data source: Four randomized studies in 21 adult rhesus macaques infected with MARV-Angola.
Disclosures: The research was supported by the U.S. Department of Health & Human Services and the National Institutes of Health.

Infliximab may carry a higher infection rate in psoriasis patients
CHICAGO – Patients with psoriasis treated with infliximab had the highest incidence of serious infections in a retrospective analysis of commercial claims data.
After 5 years of follow-up among 22,753 patients, there were 554.7 hospitalized infectious events (HIEs) per 10,000 patient-years of exposure to infliximab (Remicade).
Among the other treatment groups, the incidence of HIEs varied within a comparatively narrow range of 261.2 for phototherapy to 341.4 per 10,000 patient-years of exposure to nonbiologic therapies, Dr. Alexa B. Kimball reported at the American Academy of Dermatology summer meeting.

The biologics etanercept (Enbrel), ustekinumab (Stelara), and adalimumab (Humira) fell somewhere in between with HIE incidence rates of 261.5, 287.1, and 321.9 per 10,000 patient years, respectively.
"It is reassuring that some of the rates we reported for patients on biologics were similar to that found in the phototherapy-treated population, which is not expected to have a reduced immune response to infection," Dr. Kimball of Massachusetts General Hospital, Boston, said in an interview. "Still, in any given patient, individual risk and benefits are important to assess when starting or continuing therapy."
In one other study evaluating the safety of anti–tumor necrosis factor agents, rates of serious infections and lymphoma were higher among patients with psoriasis and psoriatic arthritis treated with infliximab and adalimumab, compared with etanercept (Immunopharmacol. Immunotoxicol. 2012;34:548-60).
In the current analysis, hospitalizations for an infectious event were also higher in patients on concomitant corticosteroid therapy at baseline, Dr. Kimball reported.
Five-year HIE incidence rates were higher in patients with systemic corticosteroid exposure versus those without, regardless of treatment group: nonbiologics (649.2 vs. 251.6); etanercept (676.9 vs. 198.1); adalimumab (424.5 vs. 260.9); infliximab (990.2 vs. 443.3); ustekinumab (542.4 vs. 201.2); and phototherapy (320.3 vs. 235.3).
"This finding reinforces that combination therapy, especially with systemic steroids, may confer additional risk," Dr. Kimball said. "Patients on infliximab were also more likely to have psoriatic arthritis and may have a different underlying level of disease severity and risk, which we could not ascertain from these data."
The retrospective analysis was based on data obtained from the MarketScan Commercial Claims and Encounters and Medicare Supplemental and COB databases for patients with a diagnosis of psoriasis on or before Dec. 31, 2006, and at least one prescription claim for one of the above-mentioned therapies. Patients could belong to more than one treatment group.
A new HIE was defined as at least one overnight hospitalization with an ICD-9 infection code. Patients hospitalized in the previous 3 months for the same ICD-9 code were not eligible.
In all, there were 5,857 patients with any exposure to nonbiologics, 6,856 to etanercept, 3,314 to adalimumab, 1,044 to infliximab, 526 to ustekinumab, and 5,156 to phototherapy.
Unique exposures to these agents totaled 2,700; 3,433; 719; 301; 0; and 3,482, respectively, according to the poster.
Amgen sponsored the study. Dr. Kimball is a consultant for Amgen and several other pharmaceutical companies.
CHICAGO – Patients with psoriasis treated with infliximab had the highest incidence of serious infections in a retrospective analysis of commercial claims data.
After 5 years of follow-up among 22,753 patients, there were 554.7 hospitalized infectious events (HIEs) per 10,000 patient-years of exposure to infliximab (Remicade).
Among the other treatment groups, the incidence of HIEs varied within a comparatively narrow range of 261.2 for phototherapy to 341.4 per 10,000 patient-years of exposure to nonbiologic therapies, Dr. Alexa B. Kimball reported at the American Academy of Dermatology summer meeting.
The biologics etanercept (Enbrel), ustekinumab (Stelara), and adalimumab (Humira) fell somewhere in between with HIE incidence rates of 261.5, 287.1, and 321.9 per 10,000 patient years, respectively.
"It is reassuring that some of the rates we reported for patients on biologics were similar to that found in the phototherapy-treated population, which is not expected to have a reduced immune response to infection," Dr. Kimball of Massachusetts General Hospital, Boston, said in an interview. "Still, in any given patient, individual risk and benefits are important to assess when starting or continuing therapy."
In one other study evaluating the safety of anti–tumor necrosis factor agents, rates of serious infections and lymphoma were higher among patients with psoriasis and psoriatic arthritis treated with infliximab and adalimumab, compared with etanercept (Immunopharmacol. Immunotoxicol. 2012;34:548-60).
In the current analysis, hospitalizations for an infectious event were also higher in patients on concomitant corticosteroid therapy at baseline, Dr. Kimball reported.
Five-year HIE incidence rates were higher in patients with systemic corticosteroid exposure versus those without, regardless of treatment group: nonbiologics (649.2 vs. 251.6); etanercept (676.9 vs. 198.1); adalimumab (424.5 vs. 260.9); infliximab (990.2 vs. 443.3); ustekinumab (542.4 vs. 201.2); and phototherapy (320.3 vs. 235.3).
"This finding reinforces that combination therapy, especially with systemic steroids, may confer additional risk," Dr. Kimball said. "Patients on infliximab were also more likely to have psoriatic arthritis and may have a different underlying level of disease severity and risk, which we could not ascertain from these data."
The retrospective analysis was based on data obtained from the MarketScan Commercial Claims and Encounters and Medicare Supplemental and COB databases for patients with a diagnosis of psoriasis on or before Dec. 31, 2006, and at least one prescription claim for one of the above-mentioned therapies. Patients could belong to more than one treatment group.
A new HIE was defined as at least one overnight hospitalization with an ICD-9 infection code. Patients hospitalized in the previous 3 months for the same ICD-9 code were not eligible.
In all, there were 5,857 patients with any exposure to nonbiologics, 6,856 to etanercept, 3,314 to adalimumab, 1,044 to infliximab, 526 to ustekinumab, and 5,156 to phototherapy.
Unique exposures to these agents totaled 2,700; 3,433; 719; 301; 0; and 3,482, respectively, according to the poster.
Amgen sponsored the study. Dr. Kimball is a consultant for Amgen and several other pharmaceutical companies.
CHICAGO – Patients with psoriasis treated with infliximab had the highest incidence of serious infections in a retrospective analysis of commercial claims data.
After 5 years of follow-up among 22,753 patients, there were 554.7 hospitalized infectious events (HIEs) per 10,000 patient-years of exposure to infliximab (Remicade).
Among the other treatment groups, the incidence of HIEs varied within a comparatively narrow range of 261.2 for phototherapy to 341.4 per 10,000 patient-years of exposure to nonbiologic therapies, Dr. Alexa B. Kimball reported at the American Academy of Dermatology summer meeting.
The biologics etanercept (Enbrel), ustekinumab (Stelara), and adalimumab (Humira) fell somewhere in between with HIE incidence rates of 261.5, 287.1, and 321.9 per 10,000 patient years, respectively.
"It is reassuring that some of the rates we reported for patients on biologics were similar to that found in the phototherapy-treated population, which is not expected to have a reduced immune response to infection," Dr. Kimball of Massachusetts General Hospital, Boston, said in an interview. "Still, in any given patient, individual risk and benefits are important to assess when starting or continuing therapy."
In one other study evaluating the safety of anti–tumor necrosis factor agents, rates of serious infections and lymphoma were higher among patients with psoriasis and psoriatic arthritis treated with infliximab and adalimumab, compared with etanercept (Immunopharmacol. Immunotoxicol. 2012;34:548-60).
In the current analysis, hospitalizations for an infectious event were also higher in patients on concomitant corticosteroid therapy at baseline, Dr. Kimball reported.
Five-year HIE incidence rates were higher in patients with systemic corticosteroid exposure versus those without, regardless of treatment group: nonbiologics (649.2 vs. 251.6); etanercept (676.9 vs. 198.1); adalimumab (424.5 vs. 260.9); infliximab (990.2 vs. 443.3); ustekinumab (542.4 vs. 201.2); and phototherapy (320.3 vs. 235.3).
"This finding reinforces that combination therapy, especially with systemic steroids, may confer additional risk," Dr. Kimball said. "Patients on infliximab were also more likely to have psoriatic arthritis and may have a different underlying level of disease severity and risk, which we could not ascertain from these data."
The retrospective analysis was based on data obtained from the MarketScan Commercial Claims and Encounters and Medicare Supplemental and COB databases for patients with a diagnosis of psoriasis on or before Dec. 31, 2006, and at least one prescription claim for one of the above-mentioned therapies. Patients could belong to more than one treatment group.
A new HIE was defined as at least one overnight hospitalization with an ICD-9 infection code. Patients hospitalized in the previous 3 months for the same ICD-9 code were not eligible.
In all, there were 5,857 patients with any exposure to nonbiologics, 6,856 to etanercept, 3,314 to adalimumab, 1,044 to infliximab, 526 to ustekinumab, and 5,156 to phototherapy.
Unique exposures to these agents totaled 2,700; 3,433; 719; 301; 0; and 3,482, respectively, according to the poster.
Amgen sponsored the study. Dr. Kimball is a consultant for Amgen and several other pharmaceutical companies.
AT THE AAD SUMMER ACADEMY 2014
Key clinical point: The risk of being hospitalized for an infectious event was higher with exposure to infliximab.
Major finding: The incidence of hospitalized infectious events was 554.7 per 10,000 patient-years of exposure to infliximab, compared with 261.2-341.4 events per 10,000 patient-years of exposure to other therapies.
Data source: Retrospective database analysis of 22,753 patients with psoriasis.
Disclosures: Amgen sponsored the study. Dr. Kimball is a consultant for Amgen and several other pharmaceutical companies.

Thoracic radiotherapy backed for extensive SCLC
CHICAGO – Thoracic radiotherapy improved overall survival, progression-free survival, and intrathoracic control in patients with extensive small-cell lung cancer who responded to chemotherapy, according to results from the randomized CREST study.
"Thoracic radiotherapy should be offered in addition to PCI [prophylactic cranial irradiation] to all extensive-stage small-cell lung cancer patients responding to initial chemotherapy," Dr. Ben J. Slotman said at the annual meeting of the American Society of Clinical Oncology.

The rationale for CREST (Chest Radiotherapy Extensive Stage Trial) was based on an earlier trial by Dr. Slotman showing that prophylactic cranial irradiation not only lowered the risk of symptomatic brain metastases but also significantly improved 1-year overall survival compared with no additional therapy in patients with extensive small-cell lung cancer (SCLC) who had any response to chemotherapy (N. Engl. J. Med. 2007;357:664-72).
Most patients, however, had persistent intrathoracic disease after chemotherapy or intrathoracic progression, said Dr. Slotman, professor and head of radiation oncology, VU Medical Center, Amsterdam.
CREST investigators at 42 centers in the Netherlands, the United Kingdom, Norway, and Belgium randomly assigned 498 patients with any response after four to six cycles of initial platinum-based chemotherapy to thoracic radiotherapy (TRT) (30 Gy in 10 fractions) plus PCI or PCI only. Treatment began within 2-7 weeks of their last chemotherapy. Patients with brain or plural metastasis, pleuritis carcinomatosa, or prior radiotherapy (RT) to the brain or thorax were excluded.
About 70% of patients had a partial response to chemotherapy, and almost 90% still had persistent intrathoracic disease at the time of randomization. Their median age was 63 years.
Overall survival at 1 year was not statistically different between the TRT and no TRT arms (33% vs. 28%; hazard ratio, 0.84; P = .066). The survival curves began to diverge after 9 months, however, leading to a significant overall survival benefit favoring TRT at 18 months (P = .03) and 24 months (13% vs. 3%; P = .004), Dr. Slotman said.
A subgroup analysis found no influence on overall survival for treatment factors such as age, sex, response after chemotherapy, or presence of intrathoracic disease at randomization.
Discussant Dr. Walter J. Curran Jr., executive director of the Winship Cancer Institute of Emory University, Atlanta, said CREST was a well-executed and adequately powered trial, but argued that its conclusion that thoracic RT improves overall survival "is not supported by the presented data."
The hazard ratio of 0.84 failed to reach the HR goal of 0.76, and the comparison at 2 years was not the primary end point of the trial, he said.
Dr. Curran said there is a rationale for why sequential chemotherapy-radiation would work for patients with more extensive disease, even though every randomized limited disease small-cell trial has shown a benefit with concurrent vs. sequential chemotherapy-radiation therapy or early vs. delayed concurrent chemoradiation, and little to no benefit with sequential chemoradiation, compared with chemotherapy alone.
"The rationale behind it, and it’s a reasonable one, is that in the noncurative setting, which is what we’re dealing with if you remember the survival curves Dr. Slotman showed us, we really are probably talking about debulking chemoresistant disease," he said. "If one is able to do that with limited toxicity and without long-lasting morbidity, that might extend survival but certainly is not going to procure cure rates as thoracic radiation can do in limited disease."
Progression-free survival was significantly better in patients receiving TRT vs. no TRT (HR, 0.73; P = .001), Dr. Slotman said.
TRT-treated patients also had significantly less intrathoracic progression overall (43.7% vs. 80%; P less than .001), as the first site of relapse (41.7% vs. 78%; P less than .001), and as the only site of relapse (20% vs. 46%; P less than .001).
Going forward, Dr. Curran said it will be important to know whether patients with extensive-stage disease receiving TRT also have less progression of thoracic disease and to better understand quality of life and toxicity associated with the therapy.
Dr. Slotman said grade 3/4 toxicity was similar between groups, although those receiving radiation had a modest increased risk of grade 3 fatigue (11 vs. 8 events) and grade 3 esophagitis (4 events vs. 0 events).
CHICAGO – Thoracic radiotherapy improved overall survival, progression-free survival, and intrathoracic control in patients with extensive small-cell lung cancer who responded to chemotherapy, according to results from the randomized CREST study.
"Thoracic radiotherapy should be offered in addition to PCI [prophylactic cranial irradiation] to all extensive-stage small-cell lung cancer patients responding to initial chemotherapy," Dr. Ben J. Slotman said at the annual meeting of the American Society of Clinical Oncology.
The rationale for CREST (Chest Radiotherapy Extensive Stage Trial) was based on an earlier trial by Dr. Slotman showing that prophylactic cranial irradiation not only lowered the risk of symptomatic brain metastases but also significantly improved 1-year overall survival compared with no additional therapy in patients with extensive small-cell lung cancer (SCLC) who had any response to chemotherapy (N. Engl. J. Med. 2007;357:664-72).
Most patients, however, had persistent intrathoracic disease after chemotherapy or intrathoracic progression, said Dr. Slotman, professor and head of radiation oncology, VU Medical Center, Amsterdam.
CREST investigators at 42 centers in the Netherlands, the United Kingdom, Norway, and Belgium randomly assigned 498 patients with any response after four to six cycles of initial platinum-based chemotherapy to thoracic radiotherapy (TRT) (30 Gy in 10 fractions) plus PCI or PCI only. Treatment began within 2-7 weeks of their last chemotherapy. Patients with brain or plural metastasis, pleuritis carcinomatosa, or prior radiotherapy (RT) to the brain or thorax were excluded.
About 70% of patients had a partial response to chemotherapy, and almost 90% still had persistent intrathoracic disease at the time of randomization. Their median age was 63 years.
Overall survival at 1 year was not statistically different between the TRT and no TRT arms (33% vs. 28%; hazard ratio, 0.84; P = .066). The survival curves began to diverge after 9 months, however, leading to a significant overall survival benefit favoring TRT at 18 months (P = .03) and 24 months (13% vs. 3%; P = .004), Dr. Slotman said.
A subgroup analysis found no influence on overall survival for treatment factors such as age, sex, response after chemotherapy, or presence of intrathoracic disease at randomization.
Discussant Dr. Walter J. Curran Jr., executive director of the Winship Cancer Institute of Emory University, Atlanta, said CREST was a well-executed and adequately powered trial, but argued that its conclusion that thoracic RT improves overall survival "is not supported by the presented data."
The hazard ratio of 0.84 failed to reach the HR goal of 0.76, and the comparison at 2 years was not the primary end point of the trial, he said.
Dr. Curran said there is a rationale for why sequential chemotherapy-radiation would work for patients with more extensive disease, even though every randomized limited disease small-cell trial has shown a benefit with concurrent vs. sequential chemotherapy-radiation therapy or early vs. delayed concurrent chemoradiation, and little to no benefit with sequential chemoradiation, compared with chemotherapy alone.
"The rationale behind it, and it’s a reasonable one, is that in the noncurative setting, which is what we’re dealing with if you remember the survival curves Dr. Slotman showed us, we really are probably talking about debulking chemoresistant disease," he said. "If one is able to do that with limited toxicity and without long-lasting morbidity, that might extend survival but certainly is not going to procure cure rates as thoracic radiation can do in limited disease."
Progression-free survival was significantly better in patients receiving TRT vs. no TRT (HR, 0.73; P = .001), Dr. Slotman said.
TRT-treated patients also had significantly less intrathoracic progression overall (43.7% vs. 80%; P less than .001), as the first site of relapse (41.7% vs. 78%; P less than .001), and as the only site of relapse (20% vs. 46%; P less than .001).
Going forward, Dr. Curran said it will be important to know whether patients with extensive-stage disease receiving TRT also have less progression of thoracic disease and to better understand quality of life and toxicity associated with the therapy.
Dr. Slotman said grade 3/4 toxicity was similar between groups, although those receiving radiation had a modest increased risk of grade 3 fatigue (11 vs. 8 events) and grade 3 esophagitis (4 events vs. 0 events).
CHICAGO – Thoracic radiotherapy improved overall survival, progression-free survival, and intrathoracic control in patients with extensive small-cell lung cancer who responded to chemotherapy, according to results from the randomized CREST study.
"Thoracic radiotherapy should be offered in addition to PCI [prophylactic cranial irradiation] to all extensive-stage small-cell lung cancer patients responding to initial chemotherapy," Dr. Ben J. Slotman said at the annual meeting of the American Society of Clinical Oncology.
The rationale for CREST (Chest Radiotherapy Extensive Stage Trial) was based on an earlier trial by Dr. Slotman showing that prophylactic cranial irradiation not only lowered the risk of symptomatic brain metastases but also significantly improved 1-year overall survival compared with no additional therapy in patients with extensive small-cell lung cancer (SCLC) who had any response to chemotherapy (N. Engl. J. Med. 2007;357:664-72).
Most patients, however, had persistent intrathoracic disease after chemotherapy or intrathoracic progression, said Dr. Slotman, professor and head of radiation oncology, VU Medical Center, Amsterdam.
CREST investigators at 42 centers in the Netherlands, the United Kingdom, Norway, and Belgium randomly assigned 498 patients with any response after four to six cycles of initial platinum-based chemotherapy to thoracic radiotherapy (TRT) (30 Gy in 10 fractions) plus PCI or PCI only. Treatment began within 2-7 weeks of their last chemotherapy. Patients with brain or plural metastasis, pleuritis carcinomatosa, or prior radiotherapy (RT) to the brain or thorax were excluded.
About 70% of patients had a partial response to chemotherapy, and almost 90% still had persistent intrathoracic disease at the time of randomization. Their median age was 63 years.
Overall survival at 1 year was not statistically different between the TRT and no TRT arms (33% vs. 28%; hazard ratio, 0.84; P = .066). The survival curves began to diverge after 9 months, however, leading to a significant overall survival benefit favoring TRT at 18 months (P = .03) and 24 months (13% vs. 3%; P = .004), Dr. Slotman said.
A subgroup analysis found no influence on overall survival for treatment factors such as age, sex, response after chemotherapy, or presence of intrathoracic disease at randomization.
Discussant Dr. Walter J. Curran Jr., executive director of the Winship Cancer Institute of Emory University, Atlanta, said CREST was a well-executed and adequately powered trial, but argued that its conclusion that thoracic RT improves overall survival "is not supported by the presented data."
The hazard ratio of 0.84 failed to reach the HR goal of 0.76, and the comparison at 2 years was not the primary end point of the trial, he said.
Dr. Curran said there is a rationale for why sequential chemotherapy-radiation would work for patients with more extensive disease, even though every randomized limited disease small-cell trial has shown a benefit with concurrent vs. sequential chemotherapy-radiation therapy or early vs. delayed concurrent chemoradiation, and little to no benefit with sequential chemoradiation, compared with chemotherapy alone.
"The rationale behind it, and it’s a reasonable one, is that in the noncurative setting, which is what we’re dealing with if you remember the survival curves Dr. Slotman showed us, we really are probably talking about debulking chemoresistant disease," he said. "If one is able to do that with limited toxicity and without long-lasting morbidity, that might extend survival but certainly is not going to procure cure rates as thoracic radiation can do in limited disease."
Progression-free survival was significantly better in patients receiving TRT vs. no TRT (HR, 0.73; P = .001), Dr. Slotman said.
TRT-treated patients also had significantly less intrathoracic progression overall (43.7% vs. 80%; P less than .001), as the first site of relapse (41.7% vs. 78%; P less than .001), and as the only site of relapse (20% vs. 46%; P less than .001).
Going forward, Dr. Curran said it will be important to know whether patients with extensive-stage disease receiving TRT also have less progression of thoracic disease and to better understand quality of life and toxicity associated with the therapy.
Dr. Slotman said grade 3/4 toxicity was similar between groups, although those receiving radiation had a modest increased risk of grade 3 fatigue (11 vs. 8 events) and grade 3 esophagitis (4 events vs. 0 events).
AT THE ASCO ANNUAL MEETING 2014
Key clinical point: Thoracic radiotherapy may improve survival when delivered after chemotherapy in extensive-stage lung cancer responding to chemotherapy.
Major finding: Overall survival at 1 year was not statistically different between the TRT and no TRT arms (HR, 0.84; P = .066) but was significantly different at 18 months (P = .03) and 24 months (P = .004).
Data source: A randomized study of 498 patients with extensive-stage small-cell lung cancer responding to initial chemotherapy.
Disclosures: Dr. Slotman and his coauthors reported no financial disclosures.

RADIANT: Mixed results for adjuvant erlotinib in NSCLC
CHICAGO – The phase III RADIANT trial of adjuvant erlotinib failed to meet its primary endpoint in early-stage, resected non–small cell lung cancer, but shores up support for adjuvant EGFR tyrosine kinase inhibitors in patients with an EGFR mutation.
RADIANT sought to determine whether adjuvant erlotinib (Tarceva) 150 mg/day, with or without chemotherapy, would prolong disease-free survival (DFS) in patients with completely resected stage IB to IIIA epidermal growth factor receptor (EGFR)–positive non–small cell lung cancer (NSCLC).
Erlotinib, an EGFR tyrosine kinase inhibitor (TKI), has proven efficacy in advanced-stage NSCLC in several settings: as second- and third-line therapy in unselected patients, first-line maintenance therapy in unselected patients, and first-line therapy in patients with EGFR-activating mutations.
Among all 973 randomized patients, however, the study’s primary endpoint of median disease-free survival (DFS) was not significantly different at 48.2 months for placebo and 50.5 months for erlotinib (hazard ratio, 0.90; P = .32), Dr. Karen Kelly reported at the annual meeting of the American Society of Clinical Oncology.
The median duration of treatment was noticeably shorter with erlotinib (11.9 months vs. 21.9 months).
At a median follow-up of 47 months, overall survival (OS) data were immature, she said. At the time of the analysis, there were 95 events in the placebo arm and 182 events in the erlotinib arm (HR, 1.13; P = .33), with the median not yet reached.
It was hoped the results of RADIANT would also clarify the broader question of whether adjuvant treatment with EGFR TKIs improves outcomes for patients whose tumors harbor an EGFR mutation.
In a subset analysis of 161 patients with deletion 19 or L858R EGFR mutations, median DFS favored erlotinib at 46.4 months vs. 28.5 months for placebo (HR, 0.61; P = .0391).
This 18-month difference, however, was not statistically significant because the study’s hierarchical testing procedure dictated that if the primary endpoint was not met all subsequent endpoints would be deemed nonsignificant, explained Dr. Kelly of the University of California–Davis Comprehensive Cancer Center, Sacramento.
Exposure to erlotinib and placebo was similar in the EGFR-mutated subgroup (median 21.2 months vs. 21.9 months). Importantly, patients treated with placebo had more stage IIIA disease at baseline (30.5% vs. 17.6%), she noted.
Median OS in the mutation-positive subset was also not reached, with 13 events in the placebo arm and 22 in the erlotinib arm (HR, 1.09; P = .81).
Invited discussant Dr. Nasser Hanna of the Indiana University Melvin and Bren Simon Cancer Center, Indianapolis, called the data of adjuvant erlotinib in patients with an activating EGFR mutation "persuasive and compelling."
Enthusiasm for adjuvant EGFR TKI therapy for early-stage NSCLC has wavered in light of the consistent development of acquired resistance to EGFR TKIs in metastatic disease, and data from two randomized trials showing that the EGFR TKI gefitinib (Iressa) did not improve survival in advanced NSCLC and was potentially detrimental after chemoradiotherapy plus docetaxel in stage III disease.
The results prompted the premature closure of the Canadian phase III BR19 trial of adjuvant gefitinib in completely resected stage 1B-IIIA NSCLC, which reported no DFS or OS benefits from gefitinib in the total population or in the 15 patients with EGFR mutations (J. Clin. Oncol. 2013;31:3320-6).
To put the current subset analysis in perspective, however, Dr. Hanna pointed out that the magnitude of gain in DFS with adjuvant EGFR TKI therapy is now consistent across three datasets: RADIANT, the phase II SELECT trial, and an analysis by Memorial Sloan-Kettering Cancer Center (MSKCC), New York (J. Thorac. Oncol. 2011;6:569-75).
Two-year DFS with adjuvant erlotinib was 89% in patients with completely resected stage I-III NSCLC with EGFR exon 19 or 21 mutations treated at MSKCC, after controlling for stage, type of surgery, and adjuvant platinum chemotherapy.
Data reported from SELECT at this year’s ASCO ( Ab. 7514) showed 2-year DFS was also 89% with adjuvant erlotinib in EGFR mutation–positive NSCLC, and reached 96% in stage I and 91% in stage III disease, he said.
"We don’t have just one data point; we have three data points that are consistent," Dr. Hanna said. "This magnitude of gain is substantial and it is significant, and it appears potentially far more than with adjuvant chemotherapy."
He said the jury is still out on overall survival, but observed that the Food and Drug Aadministration granted accelerated approval for imatinib (Gleevec) in KIT-mutant gastrointestinal stromal tumors based on DFS alone.
In an interview, Dr. Hanna said he has never used an EGFR TKI in any disease setting except the metastatic setting, and though persuasive, the RADIANT, SELECT, and MSKCC data are not conclusive and that a phase III trial is planned.
"I know that other experts have been using erlotinib in the adjuvant setting, though, off of a clinical trial," he said. "I’ve struggled with the issue, but I don’t think I’m ready to go there yet."
Dr. Kelly said the safety profile of erlotinib was generally consistent with that observed in the advanced disease setting and that additional biomarker analyses are ongoing.
Dr. Kelly and Dr. Hanna reported no relevant disclosures. Several coauthors reported financial relationships with Astellas Pharma, Roche, OSI Pharmaceuticals, or Novella Clinical.
Dr. Lary Robinson, FCCP, comments: Adjuvant chemotherapy is generally recommended in resected Stage IB (>4 cm diameter), stage II and III NSCLC. The randomized phase III RADIANT trial sought to demonstrate whether adding the tyrosine kinase inhibitor erlotinib to adjuvant therapy for resected EGFR-positive patients would further improve disease-free survival.
Unfortunately, there was no difference in the entire 973 patients randomized to erlotinib versus placebo. But a subset analysis of patients with the more sensitizing EGFR mutations (deletion 19 or L858R) who represented 16% of the overall patients showed an impressive DFS advantage in the erlotinib group compared with placebo (46.4 mo. vs. 28.5 mo.).
Although the data are compelling, further planned trials will likely verify whether erlotinib is recommended routinely as adjuvant therapy in selected EGFR-positive resected NSCLC patients.
Dr. Lary Robinson, FCCP, comments: Adjuvant chemotherapy is generally recommended in resected Stage IB (>4 cm diameter), stage II and III NSCLC. The randomized phase III RADIANT trial sought to demonstrate whether adding the tyrosine kinase inhibitor erlotinib to adjuvant therapy for resected EGFR-positive patients would further improve disease-free survival.
Unfortunately, there was no difference in the entire 973 patients randomized to erlotinib versus placebo. But a subset analysis of patients with the more sensitizing EGFR mutations (deletion 19 or L858R) who represented 16% of the overall patients showed an impressive DFS advantage in the erlotinib group compared with placebo (46.4 mo. vs. 28.5 mo.).
Although the data are compelling, further planned trials will likely verify whether erlotinib is recommended routinely as adjuvant therapy in selected EGFR-positive resected NSCLC patients.
Dr. Lary Robinson, FCCP, comments: Adjuvant chemotherapy is generally recommended in resected Stage IB (>4 cm diameter), stage II and III NSCLC. The randomized phase III RADIANT trial sought to demonstrate whether adding the tyrosine kinase inhibitor erlotinib to adjuvant therapy for resected EGFR-positive patients would further improve disease-free survival.
Unfortunately, there was no difference in the entire 973 patients randomized to erlotinib versus placebo. But a subset analysis of patients with the more sensitizing EGFR mutations (deletion 19 or L858R) who represented 16% of the overall patients showed an impressive DFS advantage in the erlotinib group compared with placebo (46.4 mo. vs. 28.5 mo.).
Although the data are compelling, further planned trials will likely verify whether erlotinib is recommended routinely as adjuvant therapy in selected EGFR-positive resected NSCLC patients.
CHICAGO – The phase III RADIANT trial of adjuvant erlotinib failed to meet its primary endpoint in early-stage, resected non–small cell lung cancer, but shores up support for adjuvant EGFR tyrosine kinase inhibitors in patients with an EGFR mutation.
RADIANT sought to determine whether adjuvant erlotinib (Tarceva) 150 mg/day, with or without chemotherapy, would prolong disease-free survival (DFS) in patients with completely resected stage IB to IIIA epidermal growth factor receptor (EGFR)–positive non–small cell lung cancer (NSCLC).
Erlotinib, an EGFR tyrosine kinase inhibitor (TKI), has proven efficacy in advanced-stage NSCLC in several settings: as second- and third-line therapy in unselected patients, first-line maintenance therapy in unselected patients, and first-line therapy in patients with EGFR-activating mutations.
Among all 973 randomized patients, however, the study’s primary endpoint of median disease-free survival (DFS) was not significantly different at 48.2 months for placebo and 50.5 months for erlotinib (hazard ratio, 0.90; P = .32), Dr. Karen Kelly reported at the annual meeting of the American Society of Clinical Oncology.
The median duration of treatment was noticeably shorter with erlotinib (11.9 months vs. 21.9 months).
At a median follow-up of 47 months, overall survival (OS) data were immature, she said. At the time of the analysis, there were 95 events in the placebo arm and 182 events in the erlotinib arm (HR, 1.13; P = .33), with the median not yet reached.
It was hoped the results of RADIANT would also clarify the broader question of whether adjuvant treatment with EGFR TKIs improves outcomes for patients whose tumors harbor an EGFR mutation.
In a subset analysis of 161 patients with deletion 19 or L858R EGFR mutations, median DFS favored erlotinib at 46.4 months vs. 28.5 months for placebo (HR, 0.61; P = .0391).
This 18-month difference, however, was not statistically significant because the study’s hierarchical testing procedure dictated that if the primary endpoint was not met all subsequent endpoints would be deemed nonsignificant, explained Dr. Kelly of the University of California–Davis Comprehensive Cancer Center, Sacramento.
Exposure to erlotinib and placebo was similar in the EGFR-mutated subgroup (median 21.2 months vs. 21.9 months). Importantly, patients treated with placebo had more stage IIIA disease at baseline (30.5% vs. 17.6%), she noted.
Median OS in the mutation-positive subset was also not reached, with 13 events in the placebo arm and 22 in the erlotinib arm (HR, 1.09; P = .81).
Invited discussant Dr. Nasser Hanna of the Indiana University Melvin and Bren Simon Cancer Center, Indianapolis, called the data of adjuvant erlotinib in patients with an activating EGFR mutation "persuasive and compelling."
Enthusiasm for adjuvant EGFR TKI therapy for early-stage NSCLC has wavered in light of the consistent development of acquired resistance to EGFR TKIs in metastatic disease, and data from two randomized trials showing that the EGFR TKI gefitinib (Iressa) did not improve survival in advanced NSCLC and was potentially detrimental after chemoradiotherapy plus docetaxel in stage III disease.
The results prompted the premature closure of the Canadian phase III BR19 trial of adjuvant gefitinib in completely resected stage 1B-IIIA NSCLC, which reported no DFS or OS benefits from gefitinib in the total population or in the 15 patients with EGFR mutations (J. Clin. Oncol. 2013;31:3320-6).
To put the current subset analysis in perspective, however, Dr. Hanna pointed out that the magnitude of gain in DFS with adjuvant EGFR TKI therapy is now consistent across three datasets: RADIANT, the phase II SELECT trial, and an analysis by Memorial Sloan-Kettering Cancer Center (MSKCC), New York (J. Thorac. Oncol. 2011;6:569-75).
Two-year DFS with adjuvant erlotinib was 89% in patients with completely resected stage I-III NSCLC with EGFR exon 19 or 21 mutations treated at MSKCC, after controlling for stage, type of surgery, and adjuvant platinum chemotherapy.
Data reported from SELECT at this year’s ASCO ( Ab. 7514) showed 2-year DFS was also 89% with adjuvant erlotinib in EGFR mutation–positive NSCLC, and reached 96% in stage I and 91% in stage III disease, he said.
"We don’t have just one data point; we have three data points that are consistent," Dr. Hanna said. "This magnitude of gain is substantial and it is significant, and it appears potentially far more than with adjuvant chemotherapy."
He said the jury is still out on overall survival, but observed that the Food and Drug Aadministration granted accelerated approval for imatinib (Gleevec) in KIT-mutant gastrointestinal stromal tumors based on DFS alone.
In an interview, Dr. Hanna said he has never used an EGFR TKI in any disease setting except the metastatic setting, and though persuasive, the RADIANT, SELECT, and MSKCC data are not conclusive and that a phase III trial is planned.
"I know that other experts have been using erlotinib in the adjuvant setting, though, off of a clinical trial," he said. "I’ve struggled with the issue, but I don’t think I’m ready to go there yet."
Dr. Kelly said the safety profile of erlotinib was generally consistent with that observed in the advanced disease setting and that additional biomarker analyses are ongoing.
Dr. Kelly and Dr. Hanna reported no relevant disclosures. Several coauthors reported financial relationships with Astellas Pharma, Roche, OSI Pharmaceuticals, or Novella Clinical.
CHICAGO – The phase III RADIANT trial of adjuvant erlotinib failed to meet its primary endpoint in early-stage, resected non–small cell lung cancer, but shores up support for adjuvant EGFR tyrosine kinase inhibitors in patients with an EGFR mutation.
RADIANT sought to determine whether adjuvant erlotinib (Tarceva) 150 mg/day, with or without chemotherapy, would prolong disease-free survival (DFS) in patients with completely resected stage IB to IIIA epidermal growth factor receptor (EGFR)–positive non–small cell lung cancer (NSCLC).
Erlotinib, an EGFR tyrosine kinase inhibitor (TKI), has proven efficacy in advanced-stage NSCLC in several settings: as second- and third-line therapy in unselected patients, first-line maintenance therapy in unselected patients, and first-line therapy in patients with EGFR-activating mutations.
Among all 973 randomized patients, however, the study’s primary endpoint of median disease-free survival (DFS) was not significantly different at 48.2 months for placebo and 50.5 months for erlotinib (hazard ratio, 0.90; P = .32), Dr. Karen Kelly reported at the annual meeting of the American Society of Clinical Oncology.
The median duration of treatment was noticeably shorter with erlotinib (11.9 months vs. 21.9 months).
At a median follow-up of 47 months, overall survival (OS) data were immature, she said. At the time of the analysis, there were 95 events in the placebo arm and 182 events in the erlotinib arm (HR, 1.13; P = .33), with the median not yet reached.
It was hoped the results of RADIANT would also clarify the broader question of whether adjuvant treatment with EGFR TKIs improves outcomes for patients whose tumors harbor an EGFR mutation.
In a subset analysis of 161 patients with deletion 19 or L858R EGFR mutations, median DFS favored erlotinib at 46.4 months vs. 28.5 months for placebo (HR, 0.61; P = .0391).
This 18-month difference, however, was not statistically significant because the study’s hierarchical testing procedure dictated that if the primary endpoint was not met all subsequent endpoints would be deemed nonsignificant, explained Dr. Kelly of the University of California–Davis Comprehensive Cancer Center, Sacramento.
Exposure to erlotinib and placebo was similar in the EGFR-mutated subgroup (median 21.2 months vs. 21.9 months). Importantly, patients treated with placebo had more stage IIIA disease at baseline (30.5% vs. 17.6%), she noted.
Median OS in the mutation-positive subset was also not reached, with 13 events in the placebo arm and 22 in the erlotinib arm (HR, 1.09; P = .81).
Invited discussant Dr. Nasser Hanna of the Indiana University Melvin and Bren Simon Cancer Center, Indianapolis, called the data of adjuvant erlotinib in patients with an activating EGFR mutation "persuasive and compelling."
Enthusiasm for adjuvant EGFR TKI therapy for early-stage NSCLC has wavered in light of the consistent development of acquired resistance to EGFR TKIs in metastatic disease, and data from two randomized trials showing that the EGFR TKI gefitinib (Iressa) did not improve survival in advanced NSCLC and was potentially detrimental after chemoradiotherapy plus docetaxel in stage III disease.
The results prompted the premature closure of the Canadian phase III BR19 trial of adjuvant gefitinib in completely resected stage 1B-IIIA NSCLC, which reported no DFS or OS benefits from gefitinib in the total population or in the 15 patients with EGFR mutations (J. Clin. Oncol. 2013;31:3320-6).
To put the current subset analysis in perspective, however, Dr. Hanna pointed out that the magnitude of gain in DFS with adjuvant EGFR TKI therapy is now consistent across three datasets: RADIANT, the phase II SELECT trial, and an analysis by Memorial Sloan-Kettering Cancer Center (MSKCC), New York (J. Thorac. Oncol. 2011;6:569-75).
Two-year DFS with adjuvant erlotinib was 89% in patients with completely resected stage I-III NSCLC with EGFR exon 19 or 21 mutations treated at MSKCC, after controlling for stage, type of surgery, and adjuvant platinum chemotherapy.
Data reported from SELECT at this year’s ASCO ( Ab. 7514) showed 2-year DFS was also 89% with adjuvant erlotinib in EGFR mutation–positive NSCLC, and reached 96% in stage I and 91% in stage III disease, he said.
"We don’t have just one data point; we have three data points that are consistent," Dr. Hanna said. "This magnitude of gain is substantial and it is significant, and it appears potentially far more than with adjuvant chemotherapy."
He said the jury is still out on overall survival, but observed that the Food and Drug Aadministration granted accelerated approval for imatinib (Gleevec) in KIT-mutant gastrointestinal stromal tumors based on DFS alone.
In an interview, Dr. Hanna said he has never used an EGFR TKI in any disease setting except the metastatic setting, and though persuasive, the RADIANT, SELECT, and MSKCC data are not conclusive and that a phase III trial is planned.
"I know that other experts have been using erlotinib in the adjuvant setting, though, off of a clinical trial," he said. "I’ve struggled with the issue, but I don’t think I’m ready to go there yet."
Dr. Kelly said the safety profile of erlotinib was generally consistent with that observed in the advanced disease setting and that additional biomarker analyses are ongoing.
Dr. Kelly and Dr. Hanna reported no relevant disclosures. Several coauthors reported financial relationships with Astellas Pharma, Roche, OSI Pharmaceuticals, or Novella Clinical.
Key clinical point: Adjuvant EGFR TKI therapy may delay disease progression in NSCLC patients harboring an EGFR mutation.
Major finding: Median DFS in patients with EGFR-mutant NSCLC was 46.4 months with adjuvant erlotinib and 28.5 months with placebo (HR, 0.61; P = .0391).
Data source: A prospective study in 973 patients with stage IA-IIIA NSCLC.
Disclosures: Dr. Kelly and Dr. Hanna reported no relevant disclosures. Several coauthors reported financial relationships with Astellas Pharma, Roche, OSI Pharmaceuticals, or Novella Clinical.
Dermatologist biopsy rate undercut by digital device
CHICAGO – The number of skin lesions biopsied to rule out melanoma remains exceedingly high among U.S. dermatologists, compared with the MelaFind digital skin analysis device.
Dermatologists performed approximately 22 biopsies of histologically benign lesions for every one melanoma or severely dysplastic nevus removed, according to a dermatopathology review of 1,100 lesions from patients in approximately 500 practices nationwide.
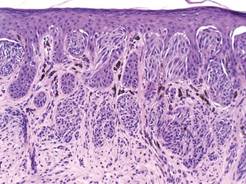
This compares with a biopsy ratio of 7.6:1 reported in a pivotal prospective study of the MelaFind device (Arch. Dermatol. 2011;147:188-94), Dr. Clay J. Cockerell reported at the American Academy of Dermatology summer meeting.
The noninvasive MelaFind device was designed to aid dermatologists in diagnosing melanoma and uses multispectral light to characterize the morphologic disorganization of clinically atypical pigmented lesions.
It is approved in the European Union and gained U.S. approval in November 2011, with a long list of indications and caveats regarding how the device should be used and by whom.
The 22:1 biopsy rate among dermatologists is "pretty high" and likely reflects several factors, according to past AAD president Dr. Cockerell, who is director of the division of dermatopathology at the University of Texas Southwestern Medical Center and in group practice in Dallas.
Overall, clinicians are conservative regarding pigmented lesions, particularly in litigious areas of the country, and the device may have made some clinicians "more of a student of pigmented lesions, pushing them to look more carefully, and heightening awareness," he said in an interview.
Biopsies also may have been conducted by physician assistants and nurse practitioners, who may have a lower threshold for biopsy than dermatologists.
Lesion data were collected at Dr. Cockerell’s facility over a 3-week period for 1,400 lesions, but information was not available on how many practices had a MelaFind device, who performed the biopsy, the level of that clinician’s expertise in pigmented lesion management, or the proportion of high-risk patients, a group for whom biopsy ratios can reach 33:1 to 53:1, he said.
A total of 300 lesions were excluded from analysis because they were ineligible for use with the MelaFind device based on its indications.
Still, the MelaFind biopsy ratio is better than that observed in the real-world and was seen in lesions that were more clinically difficult, Dr. Cockerell reported in a poster.
The proportion of lesions that were melanoma or high-grade dysplastic nevi was higher in the pivotal study than in the real world data (11% vs. 4%), as was the proportion of nevi that were low-grade dysplastic nevi (79.3% vs. 41%).
Invasive melanomas, however, were thicker in the real life review (1.1 vs. 0.36 mm), raising a red flag that patients are still not fully educated on the need for early evaluation of suspicious lesions, he said.
"Biopsies, at least in our part of the country and I think in other parts as well, are performed in a seasonal fashion," Dr. Cockerell said. "There are people who don’t go to the dermatologist and don’t get a skin biopsy done for the first 5-6 months of the year because they’re waiting to get their deductible met. If they had a melanoma and put off a biopsy until June, it’s had 6 months of growth time. The doubling time can be very rapid."
Although the MelaFind-computed scores are subjective and do not state whether a biopsy is warranted, the data would be useful if sent along with a specimen to aid dermatopathologists in rendering a more definitive diagnosis, he said. Optimally, the device is "handcrafted" for practices and clinics that follow patients with hundreds of dysplastic nevi where repeated biopsies are not practical, an avenue Dr. Cockerell said he hopes to pursue in the future.
Mela Sciences sponsored the study. Dr. Cockerell and his coauthors disclosed no conflicting financial interests.
CHICAGO – The number of skin lesions biopsied to rule out melanoma remains exceedingly high among U.S. dermatologists, compared with the MelaFind digital skin analysis device.
Dermatologists performed approximately 22 biopsies of histologically benign lesions for every one melanoma or severely dysplastic nevus removed, according to a dermatopathology review of 1,100 lesions from patients in approximately 500 practices nationwide.
This compares with a biopsy ratio of 7.6:1 reported in a pivotal prospective study of the MelaFind device (Arch. Dermatol. 2011;147:188-94), Dr. Clay J. Cockerell reported at the American Academy of Dermatology summer meeting.
The noninvasive MelaFind device was designed to aid dermatologists in diagnosing melanoma and uses multispectral light to characterize the morphologic disorganization of clinically atypical pigmented lesions.
It is approved in the European Union and gained U.S. approval in November 2011, with a long list of indications and caveats regarding how the device should be used and by whom.
The 22:1 biopsy rate among dermatologists is "pretty high" and likely reflects several factors, according to past AAD president Dr. Cockerell, who is director of the division of dermatopathology at the University of Texas Southwestern Medical Center and in group practice in Dallas.
Overall, clinicians are conservative regarding pigmented lesions, particularly in litigious areas of the country, and the device may have made some clinicians "more of a student of pigmented lesions, pushing them to look more carefully, and heightening awareness," he said in an interview.
Biopsies also may have been conducted by physician assistants and nurse practitioners, who may have a lower threshold for biopsy than dermatologists.
Lesion data were collected at Dr. Cockerell’s facility over a 3-week period for 1,400 lesions, but information was not available on how many practices had a MelaFind device, who performed the biopsy, the level of that clinician’s expertise in pigmented lesion management, or the proportion of high-risk patients, a group for whom biopsy ratios can reach 33:1 to 53:1, he said.
A total of 300 lesions were excluded from analysis because they were ineligible for use with the MelaFind device based on its indications.
Still, the MelaFind biopsy ratio is better than that observed in the real-world and was seen in lesions that were more clinically difficult, Dr. Cockerell reported in a poster.
The proportion of lesions that were melanoma or high-grade dysplastic nevi was higher in the pivotal study than in the real world data (11% vs. 4%), as was the proportion of nevi that were low-grade dysplastic nevi (79.3% vs. 41%).
Invasive melanomas, however, were thicker in the real life review (1.1 vs. 0.36 mm), raising a red flag that patients are still not fully educated on the need for early evaluation of suspicious lesions, he said.
"Biopsies, at least in our part of the country and I think in other parts as well, are performed in a seasonal fashion," Dr. Cockerell said. "There are people who don’t go to the dermatologist and don’t get a skin biopsy done for the first 5-6 months of the year because they’re waiting to get their deductible met. If they had a melanoma and put off a biopsy until June, it’s had 6 months of growth time. The doubling time can be very rapid."
Although the MelaFind-computed scores are subjective and do not state whether a biopsy is warranted, the data would be useful if sent along with a specimen to aid dermatopathologists in rendering a more definitive diagnosis, he said. Optimally, the device is "handcrafted" for practices and clinics that follow patients with hundreds of dysplastic nevi where repeated biopsies are not practical, an avenue Dr. Cockerell said he hopes to pursue in the future.
Mela Sciences sponsored the study. Dr. Cockerell and his coauthors disclosed no conflicting financial interests.
CHICAGO – The number of skin lesions biopsied to rule out melanoma remains exceedingly high among U.S. dermatologists, compared with the MelaFind digital skin analysis device.
Dermatologists performed approximately 22 biopsies of histologically benign lesions for every one melanoma or severely dysplastic nevus removed, according to a dermatopathology review of 1,100 lesions from patients in approximately 500 practices nationwide.
This compares with a biopsy ratio of 7.6:1 reported in a pivotal prospective study of the MelaFind device (Arch. Dermatol. 2011;147:188-94), Dr. Clay J. Cockerell reported at the American Academy of Dermatology summer meeting.
The noninvasive MelaFind device was designed to aid dermatologists in diagnosing melanoma and uses multispectral light to characterize the morphologic disorganization of clinically atypical pigmented lesions.
It is approved in the European Union and gained U.S. approval in November 2011, with a long list of indications and caveats regarding how the device should be used and by whom.
The 22:1 biopsy rate among dermatologists is "pretty high" and likely reflects several factors, according to past AAD president Dr. Cockerell, who is director of the division of dermatopathology at the University of Texas Southwestern Medical Center and in group practice in Dallas.
Overall, clinicians are conservative regarding pigmented lesions, particularly in litigious areas of the country, and the device may have made some clinicians "more of a student of pigmented lesions, pushing them to look more carefully, and heightening awareness," he said in an interview.
Biopsies also may have been conducted by physician assistants and nurse practitioners, who may have a lower threshold for biopsy than dermatologists.
Lesion data were collected at Dr. Cockerell’s facility over a 3-week period for 1,400 lesions, but information was not available on how many practices had a MelaFind device, who performed the biopsy, the level of that clinician’s expertise in pigmented lesion management, or the proportion of high-risk patients, a group for whom biopsy ratios can reach 33:1 to 53:1, he said.
A total of 300 lesions were excluded from analysis because they were ineligible for use with the MelaFind device based on its indications.
Still, the MelaFind biopsy ratio is better than that observed in the real-world and was seen in lesions that were more clinically difficult, Dr. Cockerell reported in a poster.
The proportion of lesions that were melanoma or high-grade dysplastic nevi was higher in the pivotal study than in the real world data (11% vs. 4%), as was the proportion of nevi that were low-grade dysplastic nevi (79.3% vs. 41%).
Invasive melanomas, however, were thicker in the real life review (1.1 vs. 0.36 mm), raising a red flag that patients are still not fully educated on the need for early evaluation of suspicious lesions, he said.
"Biopsies, at least in our part of the country and I think in other parts as well, are performed in a seasonal fashion," Dr. Cockerell said. "There are people who don’t go to the dermatologist and don’t get a skin biopsy done for the first 5-6 months of the year because they’re waiting to get their deductible met. If they had a melanoma and put off a biopsy until June, it’s had 6 months of growth time. The doubling time can be very rapid."
Although the MelaFind-computed scores are subjective and do not state whether a biopsy is warranted, the data would be useful if sent along with a specimen to aid dermatopathologists in rendering a more definitive diagnosis, he said. Optimally, the device is "handcrafted" for practices and clinics that follow patients with hundreds of dysplastic nevi where repeated biopsies are not practical, an avenue Dr. Cockerell said he hopes to pursue in the future.
Mela Sciences sponsored the study. Dr. Cockerell and his coauthors disclosed no conflicting financial interests.
AT THE AAD SUMMER ACADEMY 2014
Key clinical point: The MelaFind device may be helpful to dermatologists when deciding which clinically ambiguous lesions may be early melanoma.
Major finding: The biopsy rate for melanoma or severely dysplastic nevi was 22:1 among clinicians in the review and 7.6:1 with the MelaFind in a prior prospective study.
Data source: A retrospective analysis of 1,100 biopsied skin lesions from patients in 500 U.S. practices.
Disclosures: Mela Sciences sponsored the study. Dr. Cockerell and his coauthors disclosed no conflicting financial interests.
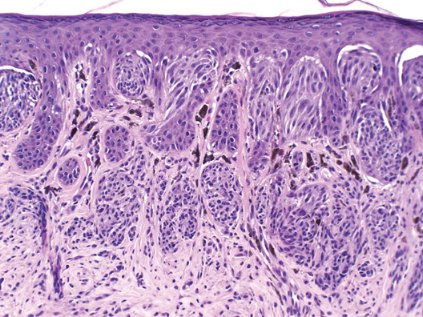
Depth of molecular response factors into safe TKI withdrawal in CML
MILAN – A full 61.5% of patients with chronic myeloid leukemia in deep molecular remission for more than 1 year on long-term tyrosine kinase inhibitor therapy remained alive and free of relapse 6 months after stopping their TKI in the EURO-SKI trial.
Molecular relapse-free survival at 9 months was 58% and 55% at 12 months.
The preplanned interim analysis after 200 patients allowed the trialists to discard the study’s null hypothesis that molecular relapse-free survival at 6 months would be 40% or less (P less than .0001).
"With less strict inclusion and relapse criteria than the A-STIM study and other trials, stopping is safe and we can continue with the trial," Dr. Susanne Saussele said in a late-breaking abstract session at the annual meeting of the European Hematology Association.
Importantly, interim results from the EURO-SKI (European Stop TKI) study also suggest that the level of molecular response (MR) achieved prior to TKI withdrawal affects molecular relapse-free survival.
Among 197 patients with molecular laboratory results available for exact classification, 49% of patients in MR4 relapsed, compared with 39% in MR4.5 and 39% in MR5.
"In the setting of standardized molecular testing within a CML [chronic myeloid leukemia] stopping trial, it seems that molecular remission has an impact on molecular free-survival," said Dr. Saussele of University Medical Centre Mannheim, Germany.
As no statistical test was performed and this was an interim analysis, MR4.5 or MR5 cannot yet be used as a criterion to select patients to withdraw from treatment, she said in an interview.
The findings do confirm results from the recent A-STIM (According to Stop Imatinib) study showing that loss of major molecular response can be used as a practical criterion for restarting imatinib (J. Clin. Oncol. 2014;32:424-30).
Several studies including the STIM (Stop Imatinib) trial and the STOP 2G-TKI (Stop Second Generation Tyrosine Kinase Inhibitors) study have shown that imatinib (Gleevec), dasatinib (Sprycel), and nilotinib (Tasigna) can be safely withdrawn in a substantial proportion of patients with CML in deep MR.
A number of questions remain open, however, such as which molecular level has to be reached before stopping TKI therapy, the minimal duration of TKI pretreatment or MR4 before stopping, and which prognostic factors influence molecular relapse-free survival, she said.
EURO-SKI was set up to define prognostic markers to increase the rate of patients in durable deep MR after stopping TKI treatment. Other aims are to evaluate methods of molecular monitoring, quality of life, and saved treatment costs per country.
Patients with chronic-phase CML from eight countries were eligible if they were on a TKI for at least 3 years and had a confirmed deep MR, defined as more than a 4 log reduction in BCR-ABL (breakpoint cluster region–Abelson) transcripts for more than 12 months confirmed by three consecutive polymerase chain reaction results.
MR4 status also had to be confirmed in an MR4-standardized laboratory according to criteria by Cross et al. (Leukemia 2012;26:2172-5)
Patients with previous or planned allogeneic stem cell transplantation or a prior TKI failure were excluded.
A total of 103 patients received pretreatment before TKI therapy, mostly with hydroxyurea alone (n = 71) or with interferon (n = 22). Their median age was 53 years.
First-line TKI was imatinib in 194 patients, nilotinib in 3, and dasatinib in 3.
The median duration of TKI therapy was 8 years and median MR4 duration before stopping TKI therapy was 5 years.
Dr. Saussele cautioned that adverse events and quality of life must be taken into account when considering TKI withdrawal in these patients.
A total of 222 adverse events were reported in 98 patients, with 57 events in 37 patients related to treatment stop. None were grade 4.
The most common adverse event was musculoskeletal or joint pain (39 events of all grades and 6 grade 3/4 events). This was first described in the Swedish EURO-SKI patients in 15-20% of patients after TKI withdrawal, prompting the investigators to send an advisory letter to all participating physicians, she remarked.
Other adverse events included sweating, skin disorders, folliculitis, depressive episodes, fatigue, urticaria, and weight loss.
The EURO-SKI trial was recently expanded to enroll 700 patients, with a quality of life analysis expected later this year. The next report on the primary endpoint is expected at the American Society of Hematology annual meeting, Dr. Saussele said.
Dr. Saussele reported honoraria and research and travel support from BMS, Novartis, and Pfizer.
MILAN – A full 61.5% of patients with chronic myeloid leukemia in deep molecular remission for more than 1 year on long-term tyrosine kinase inhibitor therapy remained alive and free of relapse 6 months after stopping their TKI in the EURO-SKI trial.
Molecular relapse-free survival at 9 months was 58% and 55% at 12 months.
The preplanned interim analysis after 200 patients allowed the trialists to discard the study’s null hypothesis that molecular relapse-free survival at 6 months would be 40% or less (P less than .0001).
"With less strict inclusion and relapse criteria than the A-STIM study and other trials, stopping is safe and we can continue with the trial," Dr. Susanne Saussele said in a late-breaking abstract session at the annual meeting of the European Hematology Association.
Importantly, interim results from the EURO-SKI (European Stop TKI) study also suggest that the level of molecular response (MR) achieved prior to TKI withdrawal affects molecular relapse-free survival.
Among 197 patients with molecular laboratory results available for exact classification, 49% of patients in MR4 relapsed, compared with 39% in MR4.5 and 39% in MR5.
"In the setting of standardized molecular testing within a CML [chronic myeloid leukemia] stopping trial, it seems that molecular remission has an impact on molecular free-survival," said Dr. Saussele of University Medical Centre Mannheim, Germany.
As no statistical test was performed and this was an interim analysis, MR4.5 or MR5 cannot yet be used as a criterion to select patients to withdraw from treatment, she said in an interview.
The findings do confirm results from the recent A-STIM (According to Stop Imatinib) study showing that loss of major molecular response can be used as a practical criterion for restarting imatinib (J. Clin. Oncol. 2014;32:424-30).
Several studies including the STIM (Stop Imatinib) trial and the STOP 2G-TKI (Stop Second Generation Tyrosine Kinase Inhibitors) study have shown that imatinib (Gleevec), dasatinib (Sprycel), and nilotinib (Tasigna) can be safely withdrawn in a substantial proportion of patients with CML in deep MR.
A number of questions remain open, however, such as which molecular level has to be reached before stopping TKI therapy, the minimal duration of TKI pretreatment or MR4 before stopping, and which prognostic factors influence molecular relapse-free survival, she said.
EURO-SKI was set up to define prognostic markers to increase the rate of patients in durable deep MR after stopping TKI treatment. Other aims are to evaluate methods of molecular monitoring, quality of life, and saved treatment costs per country.
Patients with chronic-phase CML from eight countries were eligible if they were on a TKI for at least 3 years and had a confirmed deep MR, defined as more than a 4 log reduction in BCR-ABL (breakpoint cluster region–Abelson) transcripts for more than 12 months confirmed by three consecutive polymerase chain reaction results.
MR4 status also had to be confirmed in an MR4-standardized laboratory according to criteria by Cross et al. (Leukemia 2012;26:2172-5)
Patients with previous or planned allogeneic stem cell transplantation or a prior TKI failure were excluded.
A total of 103 patients received pretreatment before TKI therapy, mostly with hydroxyurea alone (n = 71) or with interferon (n = 22). Their median age was 53 years.
First-line TKI was imatinib in 194 patients, nilotinib in 3, and dasatinib in 3.
The median duration of TKI therapy was 8 years and median MR4 duration before stopping TKI therapy was 5 years.
Dr. Saussele cautioned that adverse events and quality of life must be taken into account when considering TKI withdrawal in these patients.
A total of 222 adverse events were reported in 98 patients, with 57 events in 37 patients related to treatment stop. None were grade 4.
The most common adverse event was musculoskeletal or joint pain (39 events of all grades and 6 grade 3/4 events). This was first described in the Swedish EURO-SKI patients in 15-20% of patients after TKI withdrawal, prompting the investigators to send an advisory letter to all participating physicians, she remarked.
Other adverse events included sweating, skin disorders, folliculitis, depressive episodes, fatigue, urticaria, and weight loss.
The EURO-SKI trial was recently expanded to enroll 700 patients, with a quality of life analysis expected later this year. The next report on the primary endpoint is expected at the American Society of Hematology annual meeting, Dr. Saussele said.
Dr. Saussele reported honoraria and research and travel support from BMS, Novartis, and Pfizer.
MILAN – A full 61.5% of patients with chronic myeloid leukemia in deep molecular remission for more than 1 year on long-term tyrosine kinase inhibitor therapy remained alive and free of relapse 6 months after stopping their TKI in the EURO-SKI trial.
Molecular relapse-free survival at 9 months was 58% and 55% at 12 months.
The preplanned interim analysis after 200 patients allowed the trialists to discard the study’s null hypothesis that molecular relapse-free survival at 6 months would be 40% or less (P less than .0001).
"With less strict inclusion and relapse criteria than the A-STIM study and other trials, stopping is safe and we can continue with the trial," Dr. Susanne Saussele said in a late-breaking abstract session at the annual meeting of the European Hematology Association.
Importantly, interim results from the EURO-SKI (European Stop TKI) study also suggest that the level of molecular response (MR) achieved prior to TKI withdrawal affects molecular relapse-free survival.
Among 197 patients with molecular laboratory results available for exact classification, 49% of patients in MR4 relapsed, compared with 39% in MR4.5 and 39% in MR5.
"In the setting of standardized molecular testing within a CML [chronic myeloid leukemia] stopping trial, it seems that molecular remission has an impact on molecular free-survival," said Dr. Saussele of University Medical Centre Mannheim, Germany.
As no statistical test was performed and this was an interim analysis, MR4.5 or MR5 cannot yet be used as a criterion to select patients to withdraw from treatment, she said in an interview.
The findings do confirm results from the recent A-STIM (According to Stop Imatinib) study showing that loss of major molecular response can be used as a practical criterion for restarting imatinib (J. Clin. Oncol. 2014;32:424-30).
Several studies including the STIM (Stop Imatinib) trial and the STOP 2G-TKI (Stop Second Generation Tyrosine Kinase Inhibitors) study have shown that imatinib (Gleevec), dasatinib (Sprycel), and nilotinib (Tasigna) can be safely withdrawn in a substantial proportion of patients with CML in deep MR.
A number of questions remain open, however, such as which molecular level has to be reached before stopping TKI therapy, the minimal duration of TKI pretreatment or MR4 before stopping, and which prognostic factors influence molecular relapse-free survival, she said.
EURO-SKI was set up to define prognostic markers to increase the rate of patients in durable deep MR after stopping TKI treatment. Other aims are to evaluate methods of molecular monitoring, quality of life, and saved treatment costs per country.
Patients with chronic-phase CML from eight countries were eligible if they were on a TKI for at least 3 years and had a confirmed deep MR, defined as more than a 4 log reduction in BCR-ABL (breakpoint cluster region–Abelson) transcripts for more than 12 months confirmed by three consecutive polymerase chain reaction results.
MR4 status also had to be confirmed in an MR4-standardized laboratory according to criteria by Cross et al. (Leukemia 2012;26:2172-5)
Patients with previous or planned allogeneic stem cell transplantation or a prior TKI failure were excluded.
A total of 103 patients received pretreatment before TKI therapy, mostly with hydroxyurea alone (n = 71) or with interferon (n = 22). Their median age was 53 years.
First-line TKI was imatinib in 194 patients, nilotinib in 3, and dasatinib in 3.
The median duration of TKI therapy was 8 years and median MR4 duration before stopping TKI therapy was 5 years.
Dr. Saussele cautioned that adverse events and quality of life must be taken into account when considering TKI withdrawal in these patients.
A total of 222 adverse events were reported in 98 patients, with 57 events in 37 patients related to treatment stop. None were grade 4.
The most common adverse event was musculoskeletal or joint pain (39 events of all grades and 6 grade 3/4 events). This was first described in the Swedish EURO-SKI patients in 15-20% of patients after TKI withdrawal, prompting the investigators to send an advisory letter to all participating physicians, she remarked.
Other adverse events included sweating, skin disorders, folliculitis, depressive episodes, fatigue, urticaria, and weight loss.
The EURO-SKI trial was recently expanded to enroll 700 patients, with a quality of life analysis expected later this year. The next report on the primary endpoint is expected at the American Society of Hematology annual meeting, Dr. Saussele said.
Dr. Saussele reported honoraria and research and travel support from BMS, Novartis, and Pfizer.
AT THE EHA CONGRESS
Key clinical point: Long-time TKI therapy can be stopped in chronic myeloid leukemia in deep molecular remission. The level of molecular response prior to TKI withdrawal affects molecular relapse-free survival.
Major finding: After TKI withdrawal, 49% of patients in MR4 relapsed, compared with 39% in MR4.5 and 39% in MR5.
Data source: First interim analysis from a prospective study in 200 CML patients in deep molecular remission.
Disclosures: Dr. Saussele reported honoraria and research and travel support from BMS, Novartis, and Pfizer.
Depth of molecular response factors into safe TKI withdrawal in CML
MILAN – A full 61.5% of patients with chronic myeloid leukemia in deep molecular remission for more than 1 year on long-term tyrosine kinase inhibitor therapy remained alive and free of relapse 6 months after stopping their TKI in the EURO-SKI trial.
Molecular relapse-free survival at 9 months was 58% and 55% at 12 months.
The preplanned interim analysis after 200 patients allowed the trialists to discard the study’s null hypothesis that molecular relapse-free survival at 6 months would be 40% or less (P less than .0001).
"With less strict inclusion and relapse criteria than the A-STIM study and other trials, stopping is safe and we can continue with the trial," Dr. Susanne Saussele said in a late-breaking abstract session at the annual meeting of the European Hematology Association.
Importantly, interim results from the EURO-SKI (European Stop TKI) study also suggest that the level of molecular response (MR) achieved prior to TKI withdrawal affects molecular relapse-free survival.
Among 197 patients with molecular laboratory results available for exact classification, 49% of patients in MR4 relapsed, compared with 39% in MR4.5 and 39% in MR5.
"In the setting of standardized molecular testing within a CML [chronic myeloid leukemia] stopping trial, it seems that molecular remission has an impact on molecular free-survival," said Dr. Saussele of University Medical Centre Mannheim, Germany.
As no statistical test was performed and this was an interim analysis, MR4.5 or MR5 cannot yet be used as a criterion to select patients to withdraw from treatment, she said in an interview.
The findings do confirm results from the recent A-STIM (According to Stop Imatinib) study showing that loss of major molecular response can be used as a practical criterion for restarting imatinib (J. Clin. Oncol. 2014;32:424-30).
Several studies including the STIM (Stop Imatinib) trial and the STOP 2G-TKI (Stop Second Generation Tyrosine Kinase Inhibitors) study have shown that imatinib (Gleevec), dasatinib (Sprycel), and nilotinib (Tasigna) can be safely withdrawn in a substantial proportion of patients with CML in deep MR.
A number of questions remain open, however, such as which molecular level has to be reached before stopping TKI therapy, the minimal duration of TKI pretreatment or MR4 before stopping, and which prognostic factors influence molecular relapse-free survival, she said.
EURO-SKI was set up to define prognostic markers to increase the rate of patients in durable deep MR after stopping TKI treatment. Other aims are to evaluate methods of molecular monitoring, quality of life, and saved treatment costs per country.
Patients with chronic-phase CML from eight countries were eligible if they were on a TKI for at least 3 years and had a confirmed deep MR, defined as more than a 4 log reduction in BCR-ABL (breakpoint cluster region–Abelson) transcripts for more than 12 months confirmed by three consecutive polymerase chain reaction results.
MR4 status also had to be confirmed in an MR4-standardized laboratory according to criteria by Cross et al. (Leukemia 2012;26:2172-5)
Patients with previous or planned allogeneic stem cell transplantation or a prior TKI failure were excluded.
A total of 103 patients received pretreatment before TKI therapy, mostly with hydroxyurea alone (n = 71) or with interferon (n = 22). Their median age was 53 years.
First-line TKI was imatinib in 194 patients, nilotinib in 3, and dasatinib in 3.
The median duration of TKI therapy was 8 years and median MR4 duration before stopping TKI therapy was 5 years.
Dr. Saussele cautioned that adverse events and quality of life must be taken into account when considering TKI withdrawal in these patients.
A total of 222 adverse events were reported in 98 patients, with 57 events in 37 patients related to treatment stop. None were grade 4.
The most common adverse event was musculoskeletal or joint pain (39 events of all grades and 6 grade 3/4 events). This was first described in the Swedish EURO-SKI patients in 15-20% of patients after TKI withdrawal, prompting the investigators to send an advisory letter to all participating physicians, she remarked.
Other adverse events included sweating, skin disorders, folliculitis, depressive episodes, fatigue, urticaria, and weight loss.
The EURO-SKI trial was recently expanded to enroll 700 patients, with a quality of life analysis expected later this year. The next report on the primary endpoint is expected at the American Society of Hematology annual meeting, Dr. Saussele said.
Dr. Saussele reported honoraria and research and travel support from BMS, Novartis, and Pfizer.
MILAN – A full 61.5% of patients with chronic myeloid leukemia in deep molecular remission for more than 1 year on long-term tyrosine kinase inhibitor therapy remained alive and free of relapse 6 months after stopping their TKI in the EURO-SKI trial.
Molecular relapse-free survival at 9 months was 58% and 55% at 12 months.
The preplanned interim analysis after 200 patients allowed the trialists to discard the study’s null hypothesis that molecular relapse-free survival at 6 months would be 40% or less (P less than .0001).
"With less strict inclusion and relapse criteria than the A-STIM study and other trials, stopping is safe and we can continue with the trial," Dr. Susanne Saussele said in a late-breaking abstract session at the annual meeting of the European Hematology Association.
Importantly, interim results from the EURO-SKI (European Stop TKI) study also suggest that the level of molecular response (MR) achieved prior to TKI withdrawal affects molecular relapse-free survival.
Among 197 patients with molecular laboratory results available for exact classification, 49% of patients in MR4 relapsed, compared with 39% in MR4.5 and 39% in MR5.
"In the setting of standardized molecular testing within a CML [chronic myeloid leukemia] stopping trial, it seems that molecular remission has an impact on molecular free-survival," said Dr. Saussele of University Medical Centre Mannheim, Germany.
As no statistical test was performed and this was an interim analysis, MR4.5 or MR5 cannot yet be used as a criterion to select patients to withdraw from treatment, she said in an interview.
The findings do confirm results from the recent A-STIM (According to Stop Imatinib) study showing that loss of major molecular response can be used as a practical criterion for restarting imatinib (J. Clin. Oncol. 2014;32:424-30).
Several studies including the STIM (Stop Imatinib) trial and the STOP 2G-TKI (Stop Second Generation Tyrosine Kinase Inhibitors) study have shown that imatinib (Gleevec), dasatinib (Sprycel), and nilotinib (Tasigna) can be safely withdrawn in a substantial proportion of patients with CML in deep MR.
A number of questions remain open, however, such as which molecular level has to be reached before stopping TKI therapy, the minimal duration of TKI pretreatment or MR4 before stopping, and which prognostic factors influence molecular relapse-free survival, she said.
EURO-SKI was set up to define prognostic markers to increase the rate of patients in durable deep MR after stopping TKI treatment. Other aims are to evaluate methods of molecular monitoring, quality of life, and saved treatment costs per country.
Patients with chronic-phase CML from eight countries were eligible if they were on a TKI for at least 3 years and had a confirmed deep MR, defined as more than a 4 log reduction in BCR-ABL (breakpoint cluster region–Abelson) transcripts for more than 12 months confirmed by three consecutive polymerase chain reaction results.
MR4 status also had to be confirmed in an MR4-standardized laboratory according to criteria by Cross et al. (Leukemia 2012;26:2172-5)
Patients with previous or planned allogeneic stem cell transplantation or a prior TKI failure were excluded.
A total of 103 patients received pretreatment before TKI therapy, mostly with hydroxyurea alone (n = 71) or with interferon (n = 22). Their median age was 53 years.
First-line TKI was imatinib in 194 patients, nilotinib in 3, and dasatinib in 3.
The median duration of TKI therapy was 8 years and median MR4 duration before stopping TKI therapy was 5 years.
Dr. Saussele cautioned that adverse events and quality of life must be taken into account when considering TKI withdrawal in these patients.
A total of 222 adverse events were reported in 98 patients, with 57 events in 37 patients related to treatment stop. None were grade 4.
The most common adverse event was musculoskeletal or joint pain (39 events of all grades and 6 grade 3/4 events). This was first described in the Swedish EURO-SKI patients in 15-20% of patients after TKI withdrawal, prompting the investigators to send an advisory letter to all participating physicians, she remarked.
Other adverse events included sweating, skin disorders, folliculitis, depressive episodes, fatigue, urticaria, and weight loss.
The EURO-SKI trial was recently expanded to enroll 700 patients, with a quality of life analysis expected later this year. The next report on the primary endpoint is expected at the American Society of Hematology annual meeting, Dr. Saussele said.
Dr. Saussele reported honoraria and research and travel support from BMS, Novartis, and Pfizer.
MILAN – A full 61.5% of patients with chronic myeloid leukemia in deep molecular remission for more than 1 year on long-term tyrosine kinase inhibitor therapy remained alive and free of relapse 6 months after stopping their TKI in the EURO-SKI trial.
Molecular relapse-free survival at 9 months was 58% and 55% at 12 months.
The preplanned interim analysis after 200 patients allowed the trialists to discard the study’s null hypothesis that molecular relapse-free survival at 6 months would be 40% or less (P less than .0001).
"With less strict inclusion and relapse criteria than the A-STIM study and other trials, stopping is safe and we can continue with the trial," Dr. Susanne Saussele said in a late-breaking abstract session at the annual meeting of the European Hematology Association.
Importantly, interim results from the EURO-SKI (European Stop TKI) study also suggest that the level of molecular response (MR) achieved prior to TKI withdrawal affects molecular relapse-free survival.
Among 197 patients with molecular laboratory results available for exact classification, 49% of patients in MR4 relapsed, compared with 39% in MR4.5 and 39% in MR5.
"In the setting of standardized molecular testing within a CML [chronic myeloid leukemia] stopping trial, it seems that molecular remission has an impact on molecular free-survival," said Dr. Saussele of University Medical Centre Mannheim, Germany.
As no statistical test was performed and this was an interim analysis, MR4.5 or MR5 cannot yet be used as a criterion to select patients to withdraw from treatment, she said in an interview.
The findings do confirm results from the recent A-STIM (According to Stop Imatinib) study showing that loss of major molecular response can be used as a practical criterion for restarting imatinib (J. Clin. Oncol. 2014;32:424-30).
Several studies including the STIM (Stop Imatinib) trial and the STOP 2G-TKI (Stop Second Generation Tyrosine Kinase Inhibitors) study have shown that imatinib (Gleevec), dasatinib (Sprycel), and nilotinib (Tasigna) can be safely withdrawn in a substantial proportion of patients with CML in deep MR.
A number of questions remain open, however, such as which molecular level has to be reached before stopping TKI therapy, the minimal duration of TKI pretreatment or MR4 before stopping, and which prognostic factors influence molecular relapse-free survival, she said.
EURO-SKI was set up to define prognostic markers to increase the rate of patients in durable deep MR after stopping TKI treatment. Other aims are to evaluate methods of molecular monitoring, quality of life, and saved treatment costs per country.
Patients with chronic-phase CML from eight countries were eligible if they were on a TKI for at least 3 years and had a confirmed deep MR, defined as more than a 4 log reduction in BCR-ABL (breakpoint cluster region–Abelson) transcripts for more than 12 months confirmed by three consecutive polymerase chain reaction results.
MR4 status also had to be confirmed in an MR4-standardized laboratory according to criteria by Cross et al. (Leukemia 2012;26:2172-5)
Patients with previous or planned allogeneic stem cell transplantation or a prior TKI failure were excluded.
A total of 103 patients received pretreatment before TKI therapy, mostly with hydroxyurea alone (n = 71) or with interferon (n = 22). Their median age was 53 years.
First-line TKI was imatinib in 194 patients, nilotinib in 3, and dasatinib in 3.
The median duration of TKI therapy was 8 years and median MR4 duration before stopping TKI therapy was 5 years.
Dr. Saussele cautioned that adverse events and quality of life must be taken into account when considering TKI withdrawal in these patients.
A total of 222 adverse events were reported in 98 patients, with 57 events in 37 patients related to treatment stop. None were grade 4.
The most common adverse event was musculoskeletal or joint pain (39 events of all grades and 6 grade 3/4 events). This was first described in the Swedish EURO-SKI patients in 15-20% of patients after TKI withdrawal, prompting the investigators to send an advisory letter to all participating physicians, she remarked.
Other adverse events included sweating, skin disorders, folliculitis, depressive episodes, fatigue, urticaria, and weight loss.
The EURO-SKI trial was recently expanded to enroll 700 patients, with a quality of life analysis expected later this year. The next report on the primary endpoint is expected at the American Society of Hematology annual meeting, Dr. Saussele said.
Dr. Saussele reported honoraria and research and travel support from BMS, Novartis, and Pfizer.
AT THE EHA CONGRESS
Key clinical point: Long-time TKI therapy can be stopped in chronic myeloid leukemia in deep molecular remission. The level of molecular response prior to TKI withdrawal affects molecular relapse-free survival.
Major finding: After TKI withdrawal, 49% of patients in MR4 relapsed, compared with 39% in MR4.5 and 39% in MR5.
Data source: First interim analysis from a prospective study in 200 CML patients in deep molecular remission.
Disclosures: Dr. Saussele reported honoraria and research and travel support from BMS, Novartis, and Pfizer.