User login
Mitchel is a reporter for MDedge based in the Philadelphia area. He started with the company in 1992, when it was International Medical News Group (IMNG), and has since covered a range of medical specialties. Mitchel trained as a virologist at Roswell Park Memorial Institute in Buffalo, and then worked briefly as a researcher at Boston Children's Hospital before pivoting to journalism as a AAAS Mass Media Fellow in 1980. His first reporting job was with Science Digest magazine, and from the mid-1980s to early-1990s he was a reporter with Medical World News. @mitchelzoler
December 2017: Click for Credit
Here are 5 articles in the December issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. When Is It Really Recurrent Strep Throat?
To take the posttest, go to: http://bit.ly/2lHFh8i
Expires September 21, 2018
2. Revised Bethesda System Resets Thyroid Malignancy Risks
To take the posttest, go to: http://bit.ly/2iSLOvM
Expires August 10, 2018
3. Tips for Avoiding Potentially Dangerous Patients
To take the posttest, go to: http://bit.ly/2lH1Fi7
Expires August 10, 2018
4. Study Findings Support Uncapping MELD Score
To take the posttest, go to: http://bit.ly/2xOA7sI
Expires September 12, 2018
5. 'Motivational Pharmacotherapy' Engages Latino Patients With Depression
To take the posttest, go to: http://bit.ly/2zs2ly4
Expires August 14, 2018
Here are 5 articles in the December issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. When Is It Really Recurrent Strep Throat?
To take the posttest, go to: http://bit.ly/2lHFh8i
Expires September 21, 2018
2. Revised Bethesda System Resets Thyroid Malignancy Risks
To take the posttest, go to: http://bit.ly/2iSLOvM
Expires August 10, 2018
3. Tips for Avoiding Potentially Dangerous Patients
To take the posttest, go to: http://bit.ly/2lH1Fi7
Expires August 10, 2018
4. Study Findings Support Uncapping MELD Score
To take the posttest, go to: http://bit.ly/2xOA7sI
Expires September 12, 2018
5. 'Motivational Pharmacotherapy' Engages Latino Patients With Depression
To take the posttest, go to: http://bit.ly/2zs2ly4
Expires August 14, 2018
Here are 5 articles in the December issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. When Is It Really Recurrent Strep Throat?
To take the posttest, go to: http://bit.ly/2lHFh8i
Expires September 21, 2018
2. Revised Bethesda System Resets Thyroid Malignancy Risks
To take the posttest, go to: http://bit.ly/2iSLOvM
Expires August 10, 2018
3. Tips for Avoiding Potentially Dangerous Patients
To take the posttest, go to: http://bit.ly/2lH1Fi7
Expires August 10, 2018
4. Study Findings Support Uncapping MELD Score
To take the posttest, go to: http://bit.ly/2xOA7sI
Expires September 12, 2018
5. 'Motivational Pharmacotherapy' Engages Latino Patients With Depression
To take the posttest, go to: http://bit.ly/2zs2ly4
Expires August 14, 2018
VA, Kaiser lauded for hypertension control
At a time when the Department of Veterans Affairs is criticized for the care it delivers, and when some also see it threatened by privatization, it was refreshing to hear the VA praised for the quality of its hypertension care, a model for success in a new era of reduced blood pressure treatment targets and revised hypertension guidelines that classify millions more Americans as having hypertension.
“In systems of care, like the VA and Kaiser Permanente Northern California, we are doing much better with hypertension control, reaching control rates greater than 90%,” Paul Whelton, MD, said in November during a talk at the American Heart Association scientific sessions in Anaheim, Calif. In a separate report at the same meeting, Dr. Whelton, a professor of public health at Tulane University in New Orleans, first presented the new hypertension diagnosis and management guidelines, produced by the American College of Cardiology/American Heart Association panel that he chaired (J Am Coll Cardiol. 2017 Nov 13. doi: 10.1016/j.jacc.2017.11.006).

He again stressed that the VA and Kaiser are doing “remarkably well” when it came to controlling hypertension in the vast majority of their patients.
That assessment seems especially appropriate for Kaiser Permanente Northern California, Oakland, Calif. Data from an audit of Kaiser’s hypertension registry showed that during 2000-2013 the percentage of patients with hypertension at their goal blood pressure rose from 44% in 2000 to 90% in 2013 (J Clin Hypertension. 2016 April;18[4]:260-1). The two Kaiser researchers who reported these findings attributed the rise in control rates to a hypertension treatment program that Kaiser Permanente Northern California put into practice starting in 2000.
Current success in the VA Health System is harder to pin down and put in the Kaiser ballpark. The most up-to-date audit I could find was a 2012 report from a team of VA researchers who reviewed control rates of more than half a million hypertensive veterans at 15 VA medical centers during 2000-2010. They found that, during that 11-year period, the percentage of hypertensive patients with their blood pressure controlled to their target level had risen from 46% in 2000 to 76% in 2010 (Circulation. 2012 May 22;125[20]:2462-68).
While this 76% rate of control in 2010 is short of the 90% rate in Kaiser in 2013, it’s still not shabby. To put the 76% control rate in perspective, consider data reported at the AHA meeting from TargetBP, a national program begun in late 2015 to aid all U.S. health care programs in improving their hypertension control rates: This data showed that, among 310 participating programs that filed 2016 control-rate data with TargetBP, the average control rate was 66%. Specifically, of those 310 reporting programs, 191 (62%) had control rates that exceeded 70%, with an average control rate among these more successful programs of 76%.
As-yet-unpublished data collected by the VA show that other centers in the system beyond those 15 included in the study discussed above have also recently reached a similar control level of about 75%, said Vasilios Papademetriou, MD, a professor of medicine at Georgetown University and the director of the Interventional Hypertension and Vascular Medicine Program at the VA Medical Center in Washington. Plus, certain VA centers are now up to an 85% control rate, he added in an interview. “Blood pressure control rates have been exceptionally good in the VA medical system,” he declared. Dr. Papademetriou attributed the rising control rates to a concerted hypertension program the VA instituted starting in the early 2000s.
“The VA has had some physicians who have championed this issue, and they have built computer-based systems to identify patients with uncontrolled hypertension, and then they plug these patients into their care algorithms,” commented Donald M. Lloyd-Jones, MD, a professor and chairman of preventive medicine at Northwestern University in Chicago. “Often, when there are champions, things change,” he noted.
William C. Cushman, MD, a hypertension specialist who is chief of preventive medicine for the VA Medical Center in Memphis and professor of preventive medicine at the University of Tennessee, also in Memphis, highlighted several steps the VA took that have helped fuel the program’s success in controlling blood pressure.
Dr. Cushman couldn’t resist adding that this successful approach to hypertension management is now threatened by potential changes to the VA system that could take some patients out of the existing program and move them to privatized medical care. “If that happens, patients will not get the same comprehensive care” that until now has produced such high rates of hypertension control, he warned.
[email protected]
On Twitter @mitchelzoler
At a time when the Department of Veterans Affairs is criticized for the care it delivers, and when some also see it threatened by privatization, it was refreshing to hear the VA praised for the quality of its hypertension care, a model for success in a new era of reduced blood pressure treatment targets and revised hypertension guidelines that classify millions more Americans as having hypertension.
“In systems of care, like the VA and Kaiser Permanente Northern California, we are doing much better with hypertension control, reaching control rates greater than 90%,” Paul Whelton, MD, said in November during a talk at the American Heart Association scientific sessions in Anaheim, Calif. In a separate report at the same meeting, Dr. Whelton, a professor of public health at Tulane University in New Orleans, first presented the new hypertension diagnosis and management guidelines, produced by the American College of Cardiology/American Heart Association panel that he chaired (J Am Coll Cardiol. 2017 Nov 13. doi: 10.1016/j.jacc.2017.11.006).
He again stressed that the VA and Kaiser are doing “remarkably well” when it came to controlling hypertension in the vast majority of their patients.
That assessment seems especially appropriate for Kaiser Permanente Northern California, Oakland, Calif. Data from an audit of Kaiser’s hypertension registry showed that during 2000-2013 the percentage of patients with hypertension at their goal blood pressure rose from 44% in 2000 to 90% in 2013 (J Clin Hypertension. 2016 April;18[4]:260-1). The two Kaiser researchers who reported these findings attributed the rise in control rates to a hypertension treatment program that Kaiser Permanente Northern California put into practice starting in 2000.
Current success in the VA Health System is harder to pin down and put in the Kaiser ballpark. The most up-to-date audit I could find was a 2012 report from a team of VA researchers who reviewed control rates of more than half a million hypertensive veterans at 15 VA medical centers during 2000-2010. They found that, during that 11-year period, the percentage of hypertensive patients with their blood pressure controlled to their target level had risen from 46% in 2000 to 76% in 2010 (Circulation. 2012 May 22;125[20]:2462-68).
While this 76% rate of control in 2010 is short of the 90% rate in Kaiser in 2013, it’s still not shabby. To put the 76% control rate in perspective, consider data reported at the AHA meeting from TargetBP, a national program begun in late 2015 to aid all U.S. health care programs in improving their hypertension control rates: This data showed that, among 310 participating programs that filed 2016 control-rate data with TargetBP, the average control rate was 66%. Specifically, of those 310 reporting programs, 191 (62%) had control rates that exceeded 70%, with an average control rate among these more successful programs of 76%.
As-yet-unpublished data collected by the VA show that other centers in the system beyond those 15 included in the study discussed above have also recently reached a similar control level of about 75%, said Vasilios Papademetriou, MD, a professor of medicine at Georgetown University and the director of the Interventional Hypertension and Vascular Medicine Program at the VA Medical Center in Washington. Plus, certain VA centers are now up to an 85% control rate, he added in an interview. “Blood pressure control rates have been exceptionally good in the VA medical system,” he declared. Dr. Papademetriou attributed the rising control rates to a concerted hypertension program the VA instituted starting in the early 2000s.
“The VA has had some physicians who have championed this issue, and they have built computer-based systems to identify patients with uncontrolled hypertension, and then they plug these patients into their care algorithms,” commented Donald M. Lloyd-Jones, MD, a professor and chairman of preventive medicine at Northwestern University in Chicago. “Often, when there are champions, things change,” he noted.
William C. Cushman, MD, a hypertension specialist who is chief of preventive medicine for the VA Medical Center in Memphis and professor of preventive medicine at the University of Tennessee, also in Memphis, highlighted several steps the VA took that have helped fuel the program’s success in controlling blood pressure.
Dr. Cushman couldn’t resist adding that this successful approach to hypertension management is now threatened by potential changes to the VA system that could take some patients out of the existing program and move them to privatized medical care. “If that happens, patients will not get the same comprehensive care” that until now has produced such high rates of hypertension control, he warned.
[email protected]
On Twitter @mitchelzoler
At a time when the Department of Veterans Affairs is criticized for the care it delivers, and when some also see it threatened by privatization, it was refreshing to hear the VA praised for the quality of its hypertension care, a model for success in a new era of reduced blood pressure treatment targets and revised hypertension guidelines that classify millions more Americans as having hypertension.
“In systems of care, like the VA and Kaiser Permanente Northern California, we are doing much better with hypertension control, reaching control rates greater than 90%,” Paul Whelton, MD, said in November during a talk at the American Heart Association scientific sessions in Anaheim, Calif. In a separate report at the same meeting, Dr. Whelton, a professor of public health at Tulane University in New Orleans, first presented the new hypertension diagnosis and management guidelines, produced by the American College of Cardiology/American Heart Association panel that he chaired (J Am Coll Cardiol. 2017 Nov 13. doi: 10.1016/j.jacc.2017.11.006).
He again stressed that the VA and Kaiser are doing “remarkably well” when it came to controlling hypertension in the vast majority of their patients.
That assessment seems especially appropriate for Kaiser Permanente Northern California, Oakland, Calif. Data from an audit of Kaiser’s hypertension registry showed that during 2000-2013 the percentage of patients with hypertension at their goal blood pressure rose from 44% in 2000 to 90% in 2013 (J Clin Hypertension. 2016 April;18[4]:260-1). The two Kaiser researchers who reported these findings attributed the rise in control rates to a hypertension treatment program that Kaiser Permanente Northern California put into practice starting in 2000.
Current success in the VA Health System is harder to pin down and put in the Kaiser ballpark. The most up-to-date audit I could find was a 2012 report from a team of VA researchers who reviewed control rates of more than half a million hypertensive veterans at 15 VA medical centers during 2000-2010. They found that, during that 11-year period, the percentage of hypertensive patients with their blood pressure controlled to their target level had risen from 46% in 2000 to 76% in 2010 (Circulation. 2012 May 22;125[20]:2462-68).
While this 76% rate of control in 2010 is short of the 90% rate in Kaiser in 2013, it’s still not shabby. To put the 76% control rate in perspective, consider data reported at the AHA meeting from TargetBP, a national program begun in late 2015 to aid all U.S. health care programs in improving their hypertension control rates: This data showed that, among 310 participating programs that filed 2016 control-rate data with TargetBP, the average control rate was 66%. Specifically, of those 310 reporting programs, 191 (62%) had control rates that exceeded 70%, with an average control rate among these more successful programs of 76%.
As-yet-unpublished data collected by the VA show that other centers in the system beyond those 15 included in the study discussed above have also recently reached a similar control level of about 75%, said Vasilios Papademetriou, MD, a professor of medicine at Georgetown University and the director of the Interventional Hypertension and Vascular Medicine Program at the VA Medical Center in Washington. Plus, certain VA centers are now up to an 85% control rate, he added in an interview. “Blood pressure control rates have been exceptionally good in the VA medical system,” he declared. Dr. Papademetriou attributed the rising control rates to a concerted hypertension program the VA instituted starting in the early 2000s.
“The VA has had some physicians who have championed this issue, and they have built computer-based systems to identify patients with uncontrolled hypertension, and then they plug these patients into their care algorithms,” commented Donald M. Lloyd-Jones, MD, a professor and chairman of preventive medicine at Northwestern University in Chicago. “Often, when there are champions, things change,” he noted.
William C. Cushman, MD, a hypertension specialist who is chief of preventive medicine for the VA Medical Center in Memphis and professor of preventive medicine at the University of Tennessee, also in Memphis, highlighted several steps the VA took that have helped fuel the program’s success in controlling blood pressure.
Dr. Cushman couldn’t resist adding that this successful approach to hypertension management is now threatened by potential changes to the VA system that could take some patients out of the existing program and move them to privatized medical care. “If that happens, patients will not get the same comprehensive care” that until now has produced such high rates of hypertension control, he warned.
[email protected]
On Twitter @mitchelzoler
VIDEO: Team approach boosts effective blood pressure control
ANAHEIM, CALIF. – Using a multidisciplinary team of clinicians “could be one of the most effective measures we have to improve blood pressure control,” Tracy Y. Wang, MD, said in a video interview during the American Heart Association scientific sessions.
Speaking a day after the release of revised guidelines for the prevention, detection, evaluation, and management of high blood pressure in adults (J Am Coll Cardiol. 2017 Nov 13;doi: 10.1016/j.jacc.2017.11.006), Dr. Wang particularly highlighted the strong recommendation the guidelines made for a team-based approach for managing hypertension.
“I’m absolutely ecstatic that team management is embedded firmly in the new guidelines,” commented Dr. Wang, a cardiologist at Duke University in Durham, N.C. who has studied methods to optimize evidence-based treatment of cardiovascular diseases. “Endorsement of a team approach for blood pressure control was long overdue,” she said.
Dr. Wang discussed some approaches she believes would help better integrate team-based care into the routine management of patients with hypertension.
Dr. Wang has received honoraria from AstraZeneca, Eli Lilly, and Premier, and she has received research funding from several companies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Using a multidisciplinary team of clinicians “could be one of the most effective measures we have to improve blood pressure control,” Tracy Y. Wang, MD, said in a video interview during the American Heart Association scientific sessions.
Speaking a day after the release of revised guidelines for the prevention, detection, evaluation, and management of high blood pressure in adults (J Am Coll Cardiol. 2017 Nov 13;doi: 10.1016/j.jacc.2017.11.006), Dr. Wang particularly highlighted the strong recommendation the guidelines made for a team-based approach for managing hypertension.
“I’m absolutely ecstatic that team management is embedded firmly in the new guidelines,” commented Dr. Wang, a cardiologist at Duke University in Durham, N.C. who has studied methods to optimize evidence-based treatment of cardiovascular diseases. “Endorsement of a team approach for blood pressure control was long overdue,” she said.
Dr. Wang discussed some approaches she believes would help better integrate team-based care into the routine management of patients with hypertension.
Dr. Wang has received honoraria from AstraZeneca, Eli Lilly, and Premier, and she has received research funding from several companies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Using a multidisciplinary team of clinicians “could be one of the most effective measures we have to improve blood pressure control,” Tracy Y. Wang, MD, said in a video interview during the American Heart Association scientific sessions.
Speaking a day after the release of revised guidelines for the prevention, detection, evaluation, and management of high blood pressure in adults (J Am Coll Cardiol. 2017 Nov 13;doi: 10.1016/j.jacc.2017.11.006), Dr. Wang particularly highlighted the strong recommendation the guidelines made for a team-based approach for managing hypertension.
“I’m absolutely ecstatic that team management is embedded firmly in the new guidelines,” commented Dr. Wang, a cardiologist at Duke University in Durham, N.C. who has studied methods to optimize evidence-based treatment of cardiovascular diseases. “Endorsement of a team approach for blood pressure control was long overdue,” she said.
Dr. Wang discussed some approaches she believes would help better integrate team-based care into the routine management of patients with hypertension.
Dr. Wang has received honoraria from AstraZeneca, Eli Lilly, and Premier, and she has received research funding from several companies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE AHA SCIENTIFIC SESSIONS
Empagliflozin’s heart failure benefits linked to volume drop
ANAHEIM, CALIF. – When results from the EMPA-REG OUTCOME trial came out 2 years ago and showed a dramatic decrease in heart failure hospitalizations and deaths linked to treatment with the oral diabetes drug empagliflozin, some experts suggested that a completely hypothetical effect of empagliflozin on reducing fluid volume may have largely caused these unexpected clinical benefits.
New analyses of the trial results show this hypothesis may be at least partially correct.
Results from a post hoc analysis of data collected in Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) suggest that perhaps half the heart failure benefit was attributable to what appears to have been a roughly 7% drop in plasma volume in patients treated with empagliflozin (Jardiance), which began soon after treatment started and continued through the balance of the study, David Fitchett, MD, said at the American Heart Association scientific sessions.

“Markers of change in plasma volume were important mediators of the reduction in risk of hospitalization for heart failure or death from heart failure,” said Dr Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a coinvestigator of EMPA-REG OUTCOME (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
The analysis also showed that a “modest” effect from a reduction in uric acid might explain about 20%-25% of the observed heart failure benefit, he reported. In contrast, none of the traditional cardiovascular disease risk factors examined in the analysis – including lipids, blood pressure, obesity, and hemoglobin A1c – appeared to have any relationship to the heart failure effects of empagliflozin.
Dr. Fitchett and his associates assessed the possible impact of a list of potential mediators with a statistical method that performed an unadjusted, univariate analysis of the time-dependent change in each of several variables relative to the observed changes in heart failure outcomes.
This analysis showed that on-treatment changes in two markers of plasma volume, hematocrit and hemoglobin, each showed changes that appeared to mediate about half of the heart failure effects. A third marker of plasma volume, albumin level, appeared to mediate about a quarter of the heart failure effects.
The changes in both hematocrit and hemoglobin first appeared within a few weeks of treatment onset, and soon reached a plateau that remained sustained through the balance of the study. For example, during the first 12 weeks of treatment, the average hematocrit level rose from about 41% at baseline to about 44%. This 3% net rise corresponds to about a 7% drop in plasma volume, Dr. Fitchett said.
In addition to reflecting a potentially beneficial decrease in fluid volume, this effect would also boost the oxygen-carrying capacity of a patient’s blood that could be beneficial for patients with ischemic heart disease and those with reduced left ventricular function, he noted.
The EMPA-REG OUTCOME trial was sponsored by Boehringer Ingelheim and Eli Lilly, which jointly market empagliflozin (Jardiance). Dr. Fitchett has received honoraria from those companies and also from Amgen, AstraZeneca, Merck, and Sanofi.
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – When results from the EMPA-REG OUTCOME trial came out 2 years ago and showed a dramatic decrease in heart failure hospitalizations and deaths linked to treatment with the oral diabetes drug empagliflozin, some experts suggested that a completely hypothetical effect of empagliflozin on reducing fluid volume may have largely caused these unexpected clinical benefits.
New analyses of the trial results show this hypothesis may be at least partially correct.
Results from a post hoc analysis of data collected in Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) suggest that perhaps half the heart failure benefit was attributable to what appears to have been a roughly 7% drop in plasma volume in patients treated with empagliflozin (Jardiance), which began soon after treatment started and continued through the balance of the study, David Fitchett, MD, said at the American Heart Association scientific sessions.
“Markers of change in plasma volume were important mediators of the reduction in risk of hospitalization for heart failure or death from heart failure,” said Dr Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a coinvestigator of EMPA-REG OUTCOME (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
The analysis also showed that a “modest” effect from a reduction in uric acid might explain about 20%-25% of the observed heart failure benefit, he reported. In contrast, none of the traditional cardiovascular disease risk factors examined in the analysis – including lipids, blood pressure, obesity, and hemoglobin A1c – appeared to have any relationship to the heart failure effects of empagliflozin.
Dr. Fitchett and his associates assessed the possible impact of a list of potential mediators with a statistical method that performed an unadjusted, univariate analysis of the time-dependent change in each of several variables relative to the observed changes in heart failure outcomes.
This analysis showed that on-treatment changes in two markers of plasma volume, hematocrit and hemoglobin, each showed changes that appeared to mediate about half of the heart failure effects. A third marker of plasma volume, albumin level, appeared to mediate about a quarter of the heart failure effects.
The changes in both hematocrit and hemoglobin first appeared within a few weeks of treatment onset, and soon reached a plateau that remained sustained through the balance of the study. For example, during the first 12 weeks of treatment, the average hematocrit level rose from about 41% at baseline to about 44%. This 3% net rise corresponds to about a 7% drop in plasma volume, Dr. Fitchett said.
In addition to reflecting a potentially beneficial decrease in fluid volume, this effect would also boost the oxygen-carrying capacity of a patient’s blood that could be beneficial for patients with ischemic heart disease and those with reduced left ventricular function, he noted.
The EMPA-REG OUTCOME trial was sponsored by Boehringer Ingelheim and Eli Lilly, which jointly market empagliflozin (Jardiance). Dr. Fitchett has received honoraria from those companies and also from Amgen, AstraZeneca, Merck, and Sanofi.
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – When results from the EMPA-REG OUTCOME trial came out 2 years ago and showed a dramatic decrease in heart failure hospitalizations and deaths linked to treatment with the oral diabetes drug empagliflozin, some experts suggested that a completely hypothetical effect of empagliflozin on reducing fluid volume may have largely caused these unexpected clinical benefits.
New analyses of the trial results show this hypothesis may be at least partially correct.
Results from a post hoc analysis of data collected in Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) suggest that perhaps half the heart failure benefit was attributable to what appears to have been a roughly 7% drop in plasma volume in patients treated with empagliflozin (Jardiance), which began soon after treatment started and continued through the balance of the study, David Fitchett, MD, said at the American Heart Association scientific sessions.
“Markers of change in plasma volume were important mediators of the reduction in risk of hospitalization for heart failure or death from heart failure,” said Dr Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a coinvestigator of EMPA-REG OUTCOME (N Engl J Med. 2015 Nov 26;373[22]:2117-28).
The analysis also showed that a “modest” effect from a reduction in uric acid might explain about 20%-25% of the observed heart failure benefit, he reported. In contrast, none of the traditional cardiovascular disease risk factors examined in the analysis – including lipids, blood pressure, obesity, and hemoglobin A1c – appeared to have any relationship to the heart failure effects of empagliflozin.
Dr. Fitchett and his associates assessed the possible impact of a list of potential mediators with a statistical method that performed an unadjusted, univariate analysis of the time-dependent change in each of several variables relative to the observed changes in heart failure outcomes.
This analysis showed that on-treatment changes in two markers of plasma volume, hematocrit and hemoglobin, each showed changes that appeared to mediate about half of the heart failure effects. A third marker of plasma volume, albumin level, appeared to mediate about a quarter of the heart failure effects.
The changes in both hematocrit and hemoglobin first appeared within a few weeks of treatment onset, and soon reached a plateau that remained sustained through the balance of the study. For example, during the first 12 weeks of treatment, the average hematocrit level rose from about 41% at baseline to about 44%. This 3% net rise corresponds to about a 7% drop in plasma volume, Dr. Fitchett said.
In addition to reflecting a potentially beneficial decrease in fluid volume, this effect would also boost the oxygen-carrying capacity of a patient’s blood that could be beneficial for patients with ischemic heart disease and those with reduced left ventricular function, he noted.
The EMPA-REG OUTCOME trial was sponsored by Boehringer Ingelheim and Eli Lilly, which jointly market empagliflozin (Jardiance). Dr. Fitchett has received honoraria from those companies and also from Amgen, AstraZeneca, Merck, and Sanofi.
[email protected]
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: About according to post hoc analysis of the EMPA-REG OUTCOME study.
Major finding: About half of the observed heart failure benefit was tied to a roughly 3% rise in average hematocrit level.
Data source: Post hoc analysis of data from the 7,028 patients enrolled in the EMPA-REG OUTCOME trial.
Disclosures: The EMPA-REG OUTCOME trial was sponsored by Boehringer Ingelheim and Eli Lilly, the two companies that market empagliflozin (Jardiance). Dr. Fitchett has received honoraria from those companies and also from Amgen, AstraZeneca, Merck, and Sanofi.
VIDEO: Canakinumab’s cardiovascular benefits linked with hsCRP cuts
ANAHEIM, CALIF. – Targeting the anti-inflammatory drug canakinumab to cardiovascular disease patients with a robust response to a single dose may be an effective way to enhance the cost benefit of this novel treatment that is effective but also expensive.
A post hoc analysis of data collected in the ground-breaking CANTOS trial showed that among patients with a robust anti-inflammatory response to their first dose of canakinumab, the 4-year rate of major adverse cardiovascular events fell by 25% compared with patients who received placebo, a much higher relative risk reduction compared with all canakinumab recipients in the study. In this responsive subgroup, which constituted 55% of all patients assessed after their first dose, canakinumab also cut both cardiovascular death and all-cause death by 31% each relative to placebo, statistically significant reductions that had not been seen in the trial’s primary analysis that included all drug recipients, Paul M. Ridker, MD, said at the American Heart Association scientific sessions.
“The current analysis suggests that the magnitude of hsCRP [high sensitivity C-reactive protein] reduction following a single dose of canakinumab may provide a simple clinical method to identify individuals most likely to accrue the largest cardiovascular and cancer benefits from continued treatment.” The findings have importance “for patient selection, cost-effectiveness, and personalized medicine” as researchers and clinicians begin using anti-inflammatory drugs such as canakinumab to treat cardiovascular disease patients, said Dr. Ridker, professor of medicine at Harvard Medical School and director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital, both in Boston.
“The magnitude of the hsCRP reduction” after the first dose “is telling us who benefits most,” Dr. Ridker said in a video interview.
The Canakinumab Anti-inflammatory Thrombosis Outcome Study (CANTOS) enrolled patients with a history of a MI and a “residual” inflammatory risk based on having an hsCRP level above 2 mg/L at baseline despite receiving optimized standard treatments and having a median LDL cholesterol level of 82 mg/dL. Dr. Ridker and his associates reported the study’s primary outcome results in August at the European Society of Cardiology meeting and in a simultaneously-published article (N Engl J Med. 2017 Sept 21; 377[12]:1119-31).
For the current analyses they defined a robust anti-inflammatory response as CANTOS patients who maintained an hsCRP level below 2 mg/L when measured 3 months after their first canakinumab dose. When the researchers divided all canakinumab recipients into tertiles based on their achieved hsCRP level after one dose, those with the lowest level, less than 1.2 mg/L, also had the best outcome, with a 4-year rate of major adverse cardiovascular events that was 29% lower than the placebo patients. Patients in the middle tertile of achieved hsCRP, from 1.2 up to but not including 2.6 mg/L, showed a smaller but still statistically significant relative 17% reduction in events, while patients with the tertile with the highest hsCRP levels following one canakinumab dose had essentially no difference in their outcomes compared with placebo-treated control patients.
These findings suggest that for hsCRP, “lower is better,” Dr. Ridker noted. “It’s similar to where we were in 1994” when trial results showed how LDL levels related to cardiovascular disease events and the potential that statin treatment held had for reducing event rates.
The new analyses included three additional notable findings:
• The main serious adverse effect from canakinumab treatment, fatal infections, which occurred at a small but significantly higher rate than in control patients, had a similar incidence of about one episode/300 patient years regardless of whether the achieved hsCRP level fell below 2 mg/L or remained above that level. The placebo rate of fatal infections was about one for every 500 patient years.
• The substantially reduced incidence of lung cancer seen in the primary CANTOS results also tracked with achieved hsCRP. Patients with an achieved hsCRP that was below the median for all treated patients had a 71% cut in new-onset lung cancer compared with controls, while patients with hsCRP levels that fell above the median showed no significant difference compared with control patients.
• All three doses of canakinumab tested in CANTOS – 50 mg, 150 mg, and 300 mg administered by subcutaneous injection once every 3 months – produced a drop in hsCRP to below 2 mg/L in some patients, but the rate at which patients reached this level differed depending on dose: 44% among patients who received the lowest dose, 55% of those who received a 150-mg dose, and 65% among those on the highest dose.
But this “responder analysis” of patients who received canakinumab received a strong cautionary caveat from Robert M. Califf, MD, professor of medicine and vice chancellor for health data sciences at Duke University in Durham, N.C.
“Beware of responder analyses,” Dr. Califf said during a talk at the meeting in which he commented on the new CANTOS findings. “There is a long history in cardiology of being misled” by responder analyses, he said.
Dr. Ridker added that the mechanism that determines whether patients have a robust or modest response to canakinumab remains unclear, although it likely depends on genetic factors. He also noted that research being done by himself and others is investigating the efficacy of other anti-inflammatory drugs that could potentially cut cardiovascular disease rates, including methotrexate and colchicine.
Canakinumab (Ilaris) had Food and Drug Administration marketing approval to treat systemic juvenile idiopathic arthritis and pediatric fever syndromes. Concurrently with the meeting report, the results appeared in an article online (Lancet 2017 Nov 13. doi: 10.1016/S0140-6736[17]32814-3).
CANTOS was sponsored by Novartis, the company that markets canakinumab. Dr. Ridker has been a consultant to Novartis and was lead investigator of CANTOS. He also holds patents on using hsCRP to assess cardiovascular disease risk. Dr. Califf is an adviser to Verily Health Sciences.
[email protected]
On Twitter @mitchelzoler
CANTOS is a landmark trial for showing the importance of inflammation in causing cardiovascular disease events. The new analyses from CANTOS strengthen the biological premise of the study and better address some concerns about the magnitude of benefit raised following the first report of the CANTOS findings. We now see an increased effect on major cardiovascular disease events and, for the first time, an impact from treatment on cardiovascular death and all-cause death in the subgroup of patients with a robust anti-inflammatory response to the drug. This shows the possibility of an enhanced benefit-to-risk balance by focusing canakinumab treatment on responsive patients.
New anti-inflammatory agents now in development offer the prospect for oral drugs that could have similar benefits, and by targeting such treatments to selected patients we can envision using an anti-inflammatory strategy for primary prevention of cardiovascular disease events as well as for secondary prevention. We can also anticipate studies that will show how to better integrate anti-inflammatory interventions with lipid-lowering drugs, as well as selected drugs used to treat diabetes.
The data from CANTOS has opened a new world of possibilities related to anti-inflammatory treatments for preventing and treating cardiovascular diseases.
Ira Tabas, MD , is professor of medicine, cell biology, and physiology at Columbia University in New York. He had no disclosures. He made these comments as designated discussant for Dr. Ridker’s report.
CANTOS is a landmark trial for showing the importance of inflammation in causing cardiovascular disease events. The new analyses from CANTOS strengthen the biological premise of the study and better address some concerns about the magnitude of benefit raised following the first report of the CANTOS findings. We now see an increased effect on major cardiovascular disease events and, for the first time, an impact from treatment on cardiovascular death and all-cause death in the subgroup of patients with a robust anti-inflammatory response to the drug. This shows the possibility of an enhanced benefit-to-risk balance by focusing canakinumab treatment on responsive patients.
New anti-inflammatory agents now in development offer the prospect for oral drugs that could have similar benefits, and by targeting such treatments to selected patients we can envision using an anti-inflammatory strategy for primary prevention of cardiovascular disease events as well as for secondary prevention. We can also anticipate studies that will show how to better integrate anti-inflammatory interventions with lipid-lowering drugs, as well as selected drugs used to treat diabetes.
The data from CANTOS has opened a new world of possibilities related to anti-inflammatory treatments for preventing and treating cardiovascular diseases.
Ira Tabas, MD , is professor of medicine, cell biology, and physiology at Columbia University in New York. He had no disclosures. He made these comments as designated discussant for Dr. Ridker’s report.
CANTOS is a landmark trial for showing the importance of inflammation in causing cardiovascular disease events. The new analyses from CANTOS strengthen the biological premise of the study and better address some concerns about the magnitude of benefit raised following the first report of the CANTOS findings. We now see an increased effect on major cardiovascular disease events and, for the first time, an impact from treatment on cardiovascular death and all-cause death in the subgroup of patients with a robust anti-inflammatory response to the drug. This shows the possibility of an enhanced benefit-to-risk balance by focusing canakinumab treatment on responsive patients.
New anti-inflammatory agents now in development offer the prospect for oral drugs that could have similar benefits, and by targeting such treatments to selected patients we can envision using an anti-inflammatory strategy for primary prevention of cardiovascular disease events as well as for secondary prevention. We can also anticipate studies that will show how to better integrate anti-inflammatory interventions with lipid-lowering drugs, as well as selected drugs used to treat diabetes.
The data from CANTOS has opened a new world of possibilities related to anti-inflammatory treatments for preventing and treating cardiovascular diseases.
Ira Tabas, MD , is professor of medicine, cell biology, and physiology at Columbia University in New York. He had no disclosures. He made these comments as designated discussant for Dr. Ridker’s report.
ANAHEIM, CALIF. – Targeting the anti-inflammatory drug canakinumab to cardiovascular disease patients with a robust response to a single dose may be an effective way to enhance the cost benefit of this novel treatment that is effective but also expensive.
A post hoc analysis of data collected in the ground-breaking CANTOS trial showed that among patients with a robust anti-inflammatory response to their first dose of canakinumab, the 4-year rate of major adverse cardiovascular events fell by 25% compared with patients who received placebo, a much higher relative risk reduction compared with all canakinumab recipients in the study. In this responsive subgroup, which constituted 55% of all patients assessed after their first dose, canakinumab also cut both cardiovascular death and all-cause death by 31% each relative to placebo, statistically significant reductions that had not been seen in the trial’s primary analysis that included all drug recipients, Paul M. Ridker, MD, said at the American Heart Association scientific sessions.
“The current analysis suggests that the magnitude of hsCRP [high sensitivity C-reactive protein] reduction following a single dose of canakinumab may provide a simple clinical method to identify individuals most likely to accrue the largest cardiovascular and cancer benefits from continued treatment.” The findings have importance “for patient selection, cost-effectiveness, and personalized medicine” as researchers and clinicians begin using anti-inflammatory drugs such as canakinumab to treat cardiovascular disease patients, said Dr. Ridker, professor of medicine at Harvard Medical School and director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital, both in Boston.
“The magnitude of the hsCRP reduction” after the first dose “is telling us who benefits most,” Dr. Ridker said in a video interview.
The Canakinumab Anti-inflammatory Thrombosis Outcome Study (CANTOS) enrolled patients with a history of a MI and a “residual” inflammatory risk based on having an hsCRP level above 2 mg/L at baseline despite receiving optimized standard treatments and having a median LDL cholesterol level of 82 mg/dL. Dr. Ridker and his associates reported the study’s primary outcome results in August at the European Society of Cardiology meeting and in a simultaneously-published article (N Engl J Med. 2017 Sept 21; 377[12]:1119-31).
For the current analyses they defined a robust anti-inflammatory response as CANTOS patients who maintained an hsCRP level below 2 mg/L when measured 3 months after their first canakinumab dose. When the researchers divided all canakinumab recipients into tertiles based on their achieved hsCRP level after one dose, those with the lowest level, less than 1.2 mg/L, also had the best outcome, with a 4-year rate of major adverse cardiovascular events that was 29% lower than the placebo patients. Patients in the middle tertile of achieved hsCRP, from 1.2 up to but not including 2.6 mg/L, showed a smaller but still statistically significant relative 17% reduction in events, while patients with the tertile with the highest hsCRP levels following one canakinumab dose had essentially no difference in their outcomes compared with placebo-treated control patients.
These findings suggest that for hsCRP, “lower is better,” Dr. Ridker noted. “It’s similar to where we were in 1994” when trial results showed how LDL levels related to cardiovascular disease events and the potential that statin treatment held had for reducing event rates.
The new analyses included three additional notable findings:
• The main serious adverse effect from canakinumab treatment, fatal infections, which occurred at a small but significantly higher rate than in control patients, had a similar incidence of about one episode/300 patient years regardless of whether the achieved hsCRP level fell below 2 mg/L or remained above that level. The placebo rate of fatal infections was about one for every 500 patient years.
• The substantially reduced incidence of lung cancer seen in the primary CANTOS results also tracked with achieved hsCRP. Patients with an achieved hsCRP that was below the median for all treated patients had a 71% cut in new-onset lung cancer compared with controls, while patients with hsCRP levels that fell above the median showed no significant difference compared with control patients.
• All three doses of canakinumab tested in CANTOS – 50 mg, 150 mg, and 300 mg administered by subcutaneous injection once every 3 months – produced a drop in hsCRP to below 2 mg/L in some patients, but the rate at which patients reached this level differed depending on dose: 44% among patients who received the lowest dose, 55% of those who received a 150-mg dose, and 65% among those on the highest dose.
But this “responder analysis” of patients who received canakinumab received a strong cautionary caveat from Robert M. Califf, MD, professor of medicine and vice chancellor for health data sciences at Duke University in Durham, N.C.
“Beware of responder analyses,” Dr. Califf said during a talk at the meeting in which he commented on the new CANTOS findings. “There is a long history in cardiology of being misled” by responder analyses, he said.
Dr. Ridker added that the mechanism that determines whether patients have a robust or modest response to canakinumab remains unclear, although it likely depends on genetic factors. He also noted that research being done by himself and others is investigating the efficacy of other anti-inflammatory drugs that could potentially cut cardiovascular disease rates, including methotrexate and colchicine.
Canakinumab (Ilaris) had Food and Drug Administration marketing approval to treat systemic juvenile idiopathic arthritis and pediatric fever syndromes. Concurrently with the meeting report, the results appeared in an article online (Lancet 2017 Nov 13. doi: 10.1016/S0140-6736[17]32814-3).
CANTOS was sponsored by Novartis, the company that markets canakinumab. Dr. Ridker has been a consultant to Novartis and was lead investigator of CANTOS. He also holds patents on using hsCRP to assess cardiovascular disease risk. Dr. Califf is an adviser to Verily Health Sciences.
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Targeting the anti-inflammatory drug canakinumab to cardiovascular disease patients with a robust response to a single dose may be an effective way to enhance the cost benefit of this novel treatment that is effective but also expensive.
A post hoc analysis of data collected in the ground-breaking CANTOS trial showed that among patients with a robust anti-inflammatory response to their first dose of canakinumab, the 4-year rate of major adverse cardiovascular events fell by 25% compared with patients who received placebo, a much higher relative risk reduction compared with all canakinumab recipients in the study. In this responsive subgroup, which constituted 55% of all patients assessed after their first dose, canakinumab also cut both cardiovascular death and all-cause death by 31% each relative to placebo, statistically significant reductions that had not been seen in the trial’s primary analysis that included all drug recipients, Paul M. Ridker, MD, said at the American Heart Association scientific sessions.
“The current analysis suggests that the magnitude of hsCRP [high sensitivity C-reactive protein] reduction following a single dose of canakinumab may provide a simple clinical method to identify individuals most likely to accrue the largest cardiovascular and cancer benefits from continued treatment.” The findings have importance “for patient selection, cost-effectiveness, and personalized medicine” as researchers and clinicians begin using anti-inflammatory drugs such as canakinumab to treat cardiovascular disease patients, said Dr. Ridker, professor of medicine at Harvard Medical School and director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital, both in Boston.
“The magnitude of the hsCRP reduction” after the first dose “is telling us who benefits most,” Dr. Ridker said in a video interview.
The Canakinumab Anti-inflammatory Thrombosis Outcome Study (CANTOS) enrolled patients with a history of a MI and a “residual” inflammatory risk based on having an hsCRP level above 2 mg/L at baseline despite receiving optimized standard treatments and having a median LDL cholesterol level of 82 mg/dL. Dr. Ridker and his associates reported the study’s primary outcome results in August at the European Society of Cardiology meeting and in a simultaneously-published article (N Engl J Med. 2017 Sept 21; 377[12]:1119-31).
For the current analyses they defined a robust anti-inflammatory response as CANTOS patients who maintained an hsCRP level below 2 mg/L when measured 3 months after their first canakinumab dose. When the researchers divided all canakinumab recipients into tertiles based on their achieved hsCRP level after one dose, those with the lowest level, less than 1.2 mg/L, also had the best outcome, with a 4-year rate of major adverse cardiovascular events that was 29% lower than the placebo patients. Patients in the middle tertile of achieved hsCRP, from 1.2 up to but not including 2.6 mg/L, showed a smaller but still statistically significant relative 17% reduction in events, while patients with the tertile with the highest hsCRP levels following one canakinumab dose had essentially no difference in their outcomes compared with placebo-treated control patients.
These findings suggest that for hsCRP, “lower is better,” Dr. Ridker noted. “It’s similar to where we were in 1994” when trial results showed how LDL levels related to cardiovascular disease events and the potential that statin treatment held had for reducing event rates.
The new analyses included three additional notable findings:
• The main serious adverse effect from canakinumab treatment, fatal infections, which occurred at a small but significantly higher rate than in control patients, had a similar incidence of about one episode/300 patient years regardless of whether the achieved hsCRP level fell below 2 mg/L or remained above that level. The placebo rate of fatal infections was about one for every 500 patient years.
• The substantially reduced incidence of lung cancer seen in the primary CANTOS results also tracked with achieved hsCRP. Patients with an achieved hsCRP that was below the median for all treated patients had a 71% cut in new-onset lung cancer compared with controls, while patients with hsCRP levels that fell above the median showed no significant difference compared with control patients.
• All three doses of canakinumab tested in CANTOS – 50 mg, 150 mg, and 300 mg administered by subcutaneous injection once every 3 months – produced a drop in hsCRP to below 2 mg/L in some patients, but the rate at which patients reached this level differed depending on dose: 44% among patients who received the lowest dose, 55% of those who received a 150-mg dose, and 65% among those on the highest dose.
But this “responder analysis” of patients who received canakinumab received a strong cautionary caveat from Robert M. Califf, MD, professor of medicine and vice chancellor for health data sciences at Duke University in Durham, N.C.
“Beware of responder analyses,” Dr. Califf said during a talk at the meeting in which he commented on the new CANTOS findings. “There is a long history in cardiology of being misled” by responder analyses, he said.
Dr. Ridker added that the mechanism that determines whether patients have a robust or modest response to canakinumab remains unclear, although it likely depends on genetic factors. He also noted that research being done by himself and others is investigating the efficacy of other anti-inflammatory drugs that could potentially cut cardiovascular disease rates, including methotrexate and colchicine.
Canakinumab (Ilaris) had Food and Drug Administration marketing approval to treat systemic juvenile idiopathic arthritis and pediatric fever syndromes. Concurrently with the meeting report, the results appeared in an article online (Lancet 2017 Nov 13. doi: 10.1016/S0140-6736[17]32814-3).
CANTOS was sponsored by Novartis, the company that markets canakinumab. Dr. Ridker has been a consultant to Novartis and was lead investigator of CANTOS. He also holds patents on using hsCRP to assess cardiovascular disease risk. Dr. Califf is an adviser to Verily Health Sciences.
[email protected]
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Patients with a strong hsCRP canakinumab response had a 25% drop in cardiovascular disease events compared with controls.
Data source: Post hoc analyses of data collected in CANTOS, a multicenter trial with 10,061 patients.
Disclosures: CANTOS was sponsored by Novartis, the company that markets canakinumab (Ilaris). Dr. Ridker has been a consultant to Novartis and was lead investigator of CANTOS. He also holds patents on using hsCRP to assess cardiovascular disease risk. Dr. Califf is an adviser to Verily Health Sciences.

Heart failure readmission penalties linked with rise in deaths
ANAHEIM, CALIF. – Evidence continues to mount that Medicare’s penalization of hospitals with excess heart failure readmissions has cut readmissions but at the apparent price of more deaths.
During the penalty phase of the Hospital Readmission Reduction Program (HRRP), which started in Oct. 2012, 30-day all-cause mortality following a heart failure hospitalization was 18% higher compared with the adjusted rate during 2006-2010, based on Medicare data from 2006-2014 that underwent “extensive” risk adjustment using prospectively-collected clinical data, Gregg C. Fonarow, MD, and his associates reported in a poster at the American Heart Association scientific sessions. During the same 2012-2014 period with imposed penalties, 30-day all-cause readmissions following an index heart failure hospitalization fell by a risk-adjusted 9% compared to the era just before the HRRP. Both the drop in readmissions and rise in deaths were statistically significant.
A similar pattern existed for the risk-adjusted readmissions and mortality rates during the year following the index hospitalization: readmissions fell by 8% compared with the time before the program but deaths rose by a relative 10%, also statistically significant differences.
“This is urgent and alarming. The Centers for Medicare & Medicaid Services needs to revamp the program to exclude heart failure patients and take steps to mitigate the damage,” Dr. Fonarow said in an interview. He estimated that the uptick in mortality following heart failure hospitalizations is causing 5,000-10,000 excess annual deaths among U.S. heart failure patients that are directly attributable to the HRRP. Similar effects have not been seen for patients with an index hospitalization of pneumonia or acute MI, two other targets of the HRRP, he noted.
The HRRP “currently has penalties for readmissions that are 15-fold higher than for mortality. They need to penalize equally, and they need to get at the gaming that hospitals are doing” to shift outcomes away from readmissions even if it means more patients will die. Heart failure patients “who need hospitalization are being denied admission by hospitals out of fear of the readmissions penalty,” said Dr. Fonarow, professor and co-chief of cardiology at the University of California, Los Angeles. “Seeing increased mortality linked with implementation of the penalty is completely unacceptable.”
Although a prior report used similar Medicare data from 2008-2014 to initially find this inverse association, that analysis relied entirely on administrative data collected in Medicare records to perform risk adjustments (JAMA. 2017 July 17;318[3]:270-8). The new analysis reported by Dr. Fonarow and his associates combined the Medicare data with detailed clinical records for the same patients collected by the Get With the Guidelines--Heart Failure program. The extensive clinical data that the researchers used for risk-adjustment allowed for a more reliable attribution to the HRRP of readmission and mortality differences between the two time periods. Despite the extensive risk adjustment “we see exactly the same result” as initially reported, Dr. Fonarow said.
The findings “remind us that it is very important to look at the unintended consequences” of interventions that might initially seem reasonable, commented Lynne Warner Stevenson, MD, professor and director of cardiomyopathy at Vanderbilt University in Nashville, Tenn.
Concurrent with the presentation at the meeting the results also appeared in an article published online (JAMA Cardiol. 2017 Nov 12;doi:10.1001/jamacardio.2017.4265).
A separate analysis of data collected in the Get With the Guidelines--Heart Failure during 2005-2009 showed that within the past decade the 5-year survival of U.S. hospitalized heart failure patients has remained dismally low, and similar regardless of whether patients had heart failure with reduced ejection fraction (HFrEF, 46% of all heart failure patients in the analysis), heart failure with preserved ejection fraction (HFpEF, also 46% of patients), or the in-between patients who had heart failure with borderline ejection fraction (HFbEF, an ejection fraction of 41%-49%, in 8% of patients).
The results, from 39,982 patients, showed a 75% mortality rate during 5-years of follow-up, with similar mortality rates regardless of the patient’s ejection-fraction level, reported Dr. Fonarow and his associates in a separate poster. In every age group examined, patients with heart failure had dramatically reduced life expectancies compared with the general population. For example, among heart failure patients aged 65-69 years in the study, median survival was less than 4 years compared with a 19-year expected median survival for people in the general U.S. population in the same age range.
These very low survival rates of heart failure patients initially hospitalized for heart failure during the relatively recent era of 2005-2009 “is a call to action to prevent heart failure,” said Dr. Fonarow.
The poor prognosis most heart failure patients face should also spur aggressive treatment of HFrEF patients with all proven treatments, Dr. Fonarow said. It should also spur more effort to find effective treatments for HFpEF, which currently has no clearly-proven effective treatment.
These results also appeared in a report simultaneously published online (J Amer Coll Cardiol. 2017 Nov 12;doi: 10.1016/j.jacc.2017.08.074).
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Evidence continues to mount that Medicare’s penalization of hospitals with excess heart failure readmissions has cut readmissions but at the apparent price of more deaths.
During the penalty phase of the Hospital Readmission Reduction Program (HRRP), which started in Oct. 2012, 30-day all-cause mortality following a heart failure hospitalization was 18% higher compared with the adjusted rate during 2006-2010, based on Medicare data from 2006-2014 that underwent “extensive” risk adjustment using prospectively-collected clinical data, Gregg C. Fonarow, MD, and his associates reported in a poster at the American Heart Association scientific sessions. During the same 2012-2014 period with imposed penalties, 30-day all-cause readmissions following an index heart failure hospitalization fell by a risk-adjusted 9% compared to the era just before the HRRP. Both the drop in readmissions and rise in deaths were statistically significant.
A similar pattern existed for the risk-adjusted readmissions and mortality rates during the year following the index hospitalization: readmissions fell by 8% compared with the time before the program but deaths rose by a relative 10%, also statistically significant differences.
“This is urgent and alarming. The Centers for Medicare & Medicaid Services needs to revamp the program to exclude heart failure patients and take steps to mitigate the damage,” Dr. Fonarow said in an interview. He estimated that the uptick in mortality following heart failure hospitalizations is causing 5,000-10,000 excess annual deaths among U.S. heart failure patients that are directly attributable to the HRRP. Similar effects have not been seen for patients with an index hospitalization of pneumonia or acute MI, two other targets of the HRRP, he noted.
The HRRP “currently has penalties for readmissions that are 15-fold higher than for mortality. They need to penalize equally, and they need to get at the gaming that hospitals are doing” to shift outcomes away from readmissions even if it means more patients will die. Heart failure patients “who need hospitalization are being denied admission by hospitals out of fear of the readmissions penalty,” said Dr. Fonarow, professor and co-chief of cardiology at the University of California, Los Angeles. “Seeing increased mortality linked with implementation of the penalty is completely unacceptable.”
Although a prior report used similar Medicare data from 2008-2014 to initially find this inverse association, that analysis relied entirely on administrative data collected in Medicare records to perform risk adjustments (JAMA. 2017 July 17;318[3]:270-8). The new analysis reported by Dr. Fonarow and his associates combined the Medicare data with detailed clinical records for the same patients collected by the Get With the Guidelines--Heart Failure program. The extensive clinical data that the researchers used for risk-adjustment allowed for a more reliable attribution to the HRRP of readmission and mortality differences between the two time periods. Despite the extensive risk adjustment “we see exactly the same result” as initially reported, Dr. Fonarow said.
The findings “remind us that it is very important to look at the unintended consequences” of interventions that might initially seem reasonable, commented Lynne Warner Stevenson, MD, professor and director of cardiomyopathy at Vanderbilt University in Nashville, Tenn.
Concurrent with the presentation at the meeting the results also appeared in an article published online (JAMA Cardiol. 2017 Nov 12;doi:10.1001/jamacardio.2017.4265).
A separate analysis of data collected in the Get With the Guidelines--Heart Failure during 2005-2009 showed that within the past decade the 5-year survival of U.S. hospitalized heart failure patients has remained dismally low, and similar regardless of whether patients had heart failure with reduced ejection fraction (HFrEF, 46% of all heart failure patients in the analysis), heart failure with preserved ejection fraction (HFpEF, also 46% of patients), or the in-between patients who had heart failure with borderline ejection fraction (HFbEF, an ejection fraction of 41%-49%, in 8% of patients).
The results, from 39,982 patients, showed a 75% mortality rate during 5-years of follow-up, with similar mortality rates regardless of the patient’s ejection-fraction level, reported Dr. Fonarow and his associates in a separate poster. In every age group examined, patients with heart failure had dramatically reduced life expectancies compared with the general population. For example, among heart failure patients aged 65-69 years in the study, median survival was less than 4 years compared with a 19-year expected median survival for people in the general U.S. population in the same age range.
These very low survival rates of heart failure patients initially hospitalized for heart failure during the relatively recent era of 2005-2009 “is a call to action to prevent heart failure,” said Dr. Fonarow.
The poor prognosis most heart failure patients face should also spur aggressive treatment of HFrEF patients with all proven treatments, Dr. Fonarow said. It should also spur more effort to find effective treatments for HFpEF, which currently has no clearly-proven effective treatment.
These results also appeared in a report simultaneously published online (J Amer Coll Cardiol. 2017 Nov 12;doi: 10.1016/j.jacc.2017.08.074).
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Evidence continues to mount that Medicare’s penalization of hospitals with excess heart failure readmissions has cut readmissions but at the apparent price of more deaths.
During the penalty phase of the Hospital Readmission Reduction Program (HRRP), which started in Oct. 2012, 30-day all-cause mortality following a heart failure hospitalization was 18% higher compared with the adjusted rate during 2006-2010, based on Medicare data from 2006-2014 that underwent “extensive” risk adjustment using prospectively-collected clinical data, Gregg C. Fonarow, MD, and his associates reported in a poster at the American Heart Association scientific sessions. During the same 2012-2014 period with imposed penalties, 30-day all-cause readmissions following an index heart failure hospitalization fell by a risk-adjusted 9% compared to the era just before the HRRP. Both the drop in readmissions and rise in deaths were statistically significant.
A similar pattern existed for the risk-adjusted readmissions and mortality rates during the year following the index hospitalization: readmissions fell by 8% compared with the time before the program but deaths rose by a relative 10%, also statistically significant differences.
“This is urgent and alarming. The Centers for Medicare & Medicaid Services needs to revamp the program to exclude heart failure patients and take steps to mitigate the damage,” Dr. Fonarow said in an interview. He estimated that the uptick in mortality following heart failure hospitalizations is causing 5,000-10,000 excess annual deaths among U.S. heart failure patients that are directly attributable to the HRRP. Similar effects have not been seen for patients with an index hospitalization of pneumonia or acute MI, two other targets of the HRRP, he noted.
The HRRP “currently has penalties for readmissions that are 15-fold higher than for mortality. They need to penalize equally, and they need to get at the gaming that hospitals are doing” to shift outcomes away from readmissions even if it means more patients will die. Heart failure patients “who need hospitalization are being denied admission by hospitals out of fear of the readmissions penalty,” said Dr. Fonarow, professor and co-chief of cardiology at the University of California, Los Angeles. “Seeing increased mortality linked with implementation of the penalty is completely unacceptable.”
Although a prior report used similar Medicare data from 2008-2014 to initially find this inverse association, that analysis relied entirely on administrative data collected in Medicare records to perform risk adjustments (JAMA. 2017 July 17;318[3]:270-8). The new analysis reported by Dr. Fonarow and his associates combined the Medicare data with detailed clinical records for the same patients collected by the Get With the Guidelines--Heart Failure program. The extensive clinical data that the researchers used for risk-adjustment allowed for a more reliable attribution to the HRRP of readmission and mortality differences between the two time periods. Despite the extensive risk adjustment “we see exactly the same result” as initially reported, Dr. Fonarow said.
The findings “remind us that it is very important to look at the unintended consequences” of interventions that might initially seem reasonable, commented Lynne Warner Stevenson, MD, professor and director of cardiomyopathy at Vanderbilt University in Nashville, Tenn.
Concurrent with the presentation at the meeting the results also appeared in an article published online (JAMA Cardiol. 2017 Nov 12;doi:10.1001/jamacardio.2017.4265).
A separate analysis of data collected in the Get With the Guidelines--Heart Failure during 2005-2009 showed that within the past decade the 5-year survival of U.S. hospitalized heart failure patients has remained dismally low, and similar regardless of whether patients had heart failure with reduced ejection fraction (HFrEF, 46% of all heart failure patients in the analysis), heart failure with preserved ejection fraction (HFpEF, also 46% of patients), or the in-between patients who had heart failure with borderline ejection fraction (HFbEF, an ejection fraction of 41%-49%, in 8% of patients).
The results, from 39,982 patients, showed a 75% mortality rate during 5-years of follow-up, with similar mortality rates regardless of the patient’s ejection-fraction level, reported Dr. Fonarow and his associates in a separate poster. In every age group examined, patients with heart failure had dramatically reduced life expectancies compared with the general population. For example, among heart failure patients aged 65-69 years in the study, median survival was less than 4 years compared with a 19-year expected median survival for people in the general U.S. population in the same age range.
These very low survival rates of heart failure patients initially hospitalized for heart failure during the relatively recent era of 2005-2009 “is a call to action to prevent heart failure,” said Dr. Fonarow.
The poor prognosis most heart failure patients face should also spur aggressive treatment of HFrEF patients with all proven treatments, Dr. Fonarow said. It should also spur more effort to find effective treatments for HFpEF, which currently has no clearly-proven effective treatment.
These results also appeared in a report simultaneously published online (J Amer Coll Cardiol. 2017 Nov 12;doi: 10.1016/j.jacc.2017.08.074).
[email protected]
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Risk-adjusted 30-day readmissions fell by a relative 9% during the reduction program but relative mortality rose by 18%.
Data source: Review of 115,245 Medicare beneficiaries with heart failure treated at hospitals in the Get With the Guidelines--Heart Failure program.
Disclosures: Dr. Fonarow has been a consultant to Amgen, Janssen, Medtronic, Novartis, and St. Jude. Dr. Stevenson has been a consultant to Abbott, has received travel support from St. Jude, and has received research funding and food from Novartis.
Prescribers mostly ignore clopidogrel pharmacogenomic profiling
ANAHEIM, CALIF. – The boxed warning recommending pharmacogenomic testing of patients receiving clopidogrel to identify reduced metabolizers seems to be playing to a largely deaf audience.
Even when handed information on whether each clopidogrel-treated patient was a poor metabolizer of the drug, treating physicians usually did not switch them to a different antiplatelet drug, ticagrelor, that would be fully effective despite the patient’s reduced-metabolizer status. And clinicians who started patients on ticagrelor did not usually switch those with a good clopidogrel-metabolizing profile to the safer drug, clopidogrel, after learning that clopidogrel would be fully effective.
“Routine reporting of pharmacogenomics test results for acute coronary syndrome patients treated with P2Y12-inhibitor therapy had an uncertain yield and little impact on P2Y12-inhibitor switching,” E. Magnus Ohman, MBBS, said at the American Heart Association scientific sessions.
The study’s design gave each participating clinician free rein on whether to prescribe clopidogrel or ticagrelor (Brilinta) initially, and switching between the drugs was possible at any time after the initial prescription. At the trial’s start, 1,704 patients (56%) were on ticagrelor and 1,333 (44%) were on clopidogrel.
Pharmacogenomic testing showed that 34% of all patients were ultrametabolizers and 38% were extensive metabolizers. Patients in either of these categories metabolize enough clopidogrel into the active form to get full benefit from the drug and derive no additional efficacy benefit from switching to another P2Y12 inhibitor, such as ticagrelor or prasugrel (Effient) – drugs unaffected by metabolizer status. Testing also identified 25% of patients as intermediate metabolizers, who carry one loss-of-function allele for the CYP2C19 gene, and 3% were reduced metabolizers, who are homozygous for loss-of-function alleles. Standard practice is not to treat intermediate or reduced metabolizers with clopidogrel because they would not get an adequate antiplatelet effect; instead, these patients are usually treated with ticagrelor or with prasugrel when it’s an option.
After receiving the results regarding the clopidogrel-metabolizing status for each patient, attending physicians switched the drugs prescribed for only 7% of all patients: 9% of patients initially on ticagrelor and 4% of those initially on clopidogrel, reported Dr. Ohman, professor of medicine at Duke University in Durham, N.C. In addition, Dr. Ohman and his associates asked each participating physician who made a switch about his or her reasons for doing so. Of the patients who switched from clopidogrel to ticagrelor, only 23 were switched because of their pharmacogenomic results; this represents fewer than half of those who switched and only 2% of all patients who took clopidogrel. Only one patient changed from ticagrelor to clopidogrel based on pharmacogenomic results, representing 0.06% of all patients on ticagrelor.
“We believed the findings do not support the utility of mandatory testing in this context, as most did not act on the information,” Dr. Ohman said.

A major reason for the inertia, Dr. Gurbel suggested, may be the absence of any compelling data proving whether there’s any effect on clinical outcomes for switching reduced metabolizers off of clopidogrel or switching good metabolizers onto it.
“We have no large-scale, prospective data supporting pharmacogenomic-based personalization” of clopidogrel treatment leading to improved outcomes, but “we need to get over that,” he said. “It’s a challenge to get funding for this.” But “the answer is not to give ticagrelor or prasugrel to everyone because then the bleeding rate is too high.”
The findings Dr. Ohman reported came from the Study to Compare the Safety of Rivaroxaban Versus Acetylsalicylic Acid in Addition to Either Clopidogrel or Ticagrelor Therapy in Participants With Acute Coronary Syndrome (GEMINI-ACS-1), which had the primary goal of comparing the safety in acute coronary syndrome patients of a reduced dosage of rivaroxaban plus either clopidogrel or ticagrelor with the safety of aspirin plus one of these P2Y12 inhibitors. The primary endpoint was the rate of clinically significant bleeding events during a year of treatment. The study ran at 371 centers in 21 countries and showed similar bleeding rates in both treatment arms (Lancet. 2017 May 6; 389[10081]:1799-808).
The analysis also showed that patients identified as reduced metabolizers were fivefold more likely to be switched than patients identified as ultra metabolizers, and intermediate metabolizes had a 50% higher switching rate than ultra metabolizers. The rates of both ischemic and major bleeding outcomes were roughly similar across the spectrum of metabolizers, but Dr. Ohman cautioned that the trial was not designed to assess this. Dr. Gurbel urged the investigators to report on outcomes analyzed not just by metabolizer status but also by the treatment they received.
The boxed warning that clopidogrel received in 2010 regarding poor metabolizers led to “regulatory guidance” during design of the GEMINI-ACS-1 trial requiring routine pharmacogenomic testing for clopidogrel-metabolizing status, Dr. Ohman explained.
The trial was funded by Janssen and Bayer, the two companies that jointly market rivaroxaban (Xarelto). Dr. Ohman has been a consultant to Bayer and several other companies including AstraZeneca, the company that markets ticagrelor (Brilinta). He has also received research funding from Janssen, as well as Daiichi Sankyo and Gilead Sciences. Dr. Gurbel holds patents on platelet-function testing methods.
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – The boxed warning recommending pharmacogenomic testing of patients receiving clopidogrel to identify reduced metabolizers seems to be playing to a largely deaf audience.
Even when handed information on whether each clopidogrel-treated patient was a poor metabolizer of the drug, treating physicians usually did not switch them to a different antiplatelet drug, ticagrelor, that would be fully effective despite the patient’s reduced-metabolizer status. And clinicians who started patients on ticagrelor did not usually switch those with a good clopidogrel-metabolizing profile to the safer drug, clopidogrel, after learning that clopidogrel would be fully effective.
“Routine reporting of pharmacogenomics test results for acute coronary syndrome patients treated with P2Y12-inhibitor therapy had an uncertain yield and little impact on P2Y12-inhibitor switching,” E. Magnus Ohman, MBBS, said at the American Heart Association scientific sessions.
The study’s design gave each participating clinician free rein on whether to prescribe clopidogrel or ticagrelor (Brilinta) initially, and switching between the drugs was possible at any time after the initial prescription. At the trial’s start, 1,704 patients (56%) were on ticagrelor and 1,333 (44%) were on clopidogrel.
Pharmacogenomic testing showed that 34% of all patients were ultrametabolizers and 38% were extensive metabolizers. Patients in either of these categories metabolize enough clopidogrel into the active form to get full benefit from the drug and derive no additional efficacy benefit from switching to another P2Y12 inhibitor, such as ticagrelor or prasugrel (Effient) – drugs unaffected by metabolizer status. Testing also identified 25% of patients as intermediate metabolizers, who carry one loss-of-function allele for the CYP2C19 gene, and 3% were reduced metabolizers, who are homozygous for loss-of-function alleles. Standard practice is not to treat intermediate or reduced metabolizers with clopidogrel because they would not get an adequate antiplatelet effect; instead, these patients are usually treated with ticagrelor or with prasugrel when it’s an option.
After receiving the results regarding the clopidogrel-metabolizing status for each patient, attending physicians switched the drugs prescribed for only 7% of all patients: 9% of patients initially on ticagrelor and 4% of those initially on clopidogrel, reported Dr. Ohman, professor of medicine at Duke University in Durham, N.C. In addition, Dr. Ohman and his associates asked each participating physician who made a switch about his or her reasons for doing so. Of the patients who switched from clopidogrel to ticagrelor, only 23 were switched because of their pharmacogenomic results; this represents fewer than half of those who switched and only 2% of all patients who took clopidogrel. Only one patient changed from ticagrelor to clopidogrel based on pharmacogenomic results, representing 0.06% of all patients on ticagrelor.
“We believed the findings do not support the utility of mandatory testing in this context, as most did not act on the information,” Dr. Ohman said.
A major reason for the inertia, Dr. Gurbel suggested, may be the absence of any compelling data proving whether there’s any effect on clinical outcomes for switching reduced metabolizers off of clopidogrel or switching good metabolizers onto it.
“We have no large-scale, prospective data supporting pharmacogenomic-based personalization” of clopidogrel treatment leading to improved outcomes, but “we need to get over that,” he said. “It’s a challenge to get funding for this.” But “the answer is not to give ticagrelor or prasugrel to everyone because then the bleeding rate is too high.”
The findings Dr. Ohman reported came from the Study to Compare the Safety of Rivaroxaban Versus Acetylsalicylic Acid in Addition to Either Clopidogrel or Ticagrelor Therapy in Participants With Acute Coronary Syndrome (GEMINI-ACS-1), which had the primary goal of comparing the safety in acute coronary syndrome patients of a reduced dosage of rivaroxaban plus either clopidogrel or ticagrelor with the safety of aspirin plus one of these P2Y12 inhibitors. The primary endpoint was the rate of clinically significant bleeding events during a year of treatment. The study ran at 371 centers in 21 countries and showed similar bleeding rates in both treatment arms (Lancet. 2017 May 6; 389[10081]:1799-808).
The analysis also showed that patients identified as reduced metabolizers were fivefold more likely to be switched than patients identified as ultra metabolizers, and intermediate metabolizes had a 50% higher switching rate than ultra metabolizers. The rates of both ischemic and major bleeding outcomes were roughly similar across the spectrum of metabolizers, but Dr. Ohman cautioned that the trial was not designed to assess this. Dr. Gurbel urged the investigators to report on outcomes analyzed not just by metabolizer status but also by the treatment they received.
The boxed warning that clopidogrel received in 2010 regarding poor metabolizers led to “regulatory guidance” during design of the GEMINI-ACS-1 trial requiring routine pharmacogenomic testing for clopidogrel-metabolizing status, Dr. Ohman explained.
The trial was funded by Janssen and Bayer, the two companies that jointly market rivaroxaban (Xarelto). Dr. Ohman has been a consultant to Bayer and several other companies including AstraZeneca, the company that markets ticagrelor (Brilinta). He has also received research funding from Janssen, as well as Daiichi Sankyo and Gilead Sciences. Dr. Gurbel holds patents on platelet-function testing methods.
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – The boxed warning recommending pharmacogenomic testing of patients receiving clopidogrel to identify reduced metabolizers seems to be playing to a largely deaf audience.
Even when handed information on whether each clopidogrel-treated patient was a poor metabolizer of the drug, treating physicians usually did not switch them to a different antiplatelet drug, ticagrelor, that would be fully effective despite the patient’s reduced-metabolizer status. And clinicians who started patients on ticagrelor did not usually switch those with a good clopidogrel-metabolizing profile to the safer drug, clopidogrel, after learning that clopidogrel would be fully effective.
“Routine reporting of pharmacogenomics test results for acute coronary syndrome patients treated with P2Y12-inhibitor therapy had an uncertain yield and little impact on P2Y12-inhibitor switching,” E. Magnus Ohman, MBBS, said at the American Heart Association scientific sessions.
The study’s design gave each participating clinician free rein on whether to prescribe clopidogrel or ticagrelor (Brilinta) initially, and switching between the drugs was possible at any time after the initial prescription. At the trial’s start, 1,704 patients (56%) were on ticagrelor and 1,333 (44%) were on clopidogrel.
Pharmacogenomic testing showed that 34% of all patients were ultrametabolizers and 38% were extensive metabolizers. Patients in either of these categories metabolize enough clopidogrel into the active form to get full benefit from the drug and derive no additional efficacy benefit from switching to another P2Y12 inhibitor, such as ticagrelor or prasugrel (Effient) – drugs unaffected by metabolizer status. Testing also identified 25% of patients as intermediate metabolizers, who carry one loss-of-function allele for the CYP2C19 gene, and 3% were reduced metabolizers, who are homozygous for loss-of-function alleles. Standard practice is not to treat intermediate or reduced metabolizers with clopidogrel because they would not get an adequate antiplatelet effect; instead, these patients are usually treated with ticagrelor or with prasugrel when it’s an option.
After receiving the results regarding the clopidogrel-metabolizing status for each patient, attending physicians switched the drugs prescribed for only 7% of all patients: 9% of patients initially on ticagrelor and 4% of those initially on clopidogrel, reported Dr. Ohman, professor of medicine at Duke University in Durham, N.C. In addition, Dr. Ohman and his associates asked each participating physician who made a switch about his or her reasons for doing so. Of the patients who switched from clopidogrel to ticagrelor, only 23 were switched because of their pharmacogenomic results; this represents fewer than half of those who switched and only 2% of all patients who took clopidogrel. Only one patient changed from ticagrelor to clopidogrel based on pharmacogenomic results, representing 0.06% of all patients on ticagrelor.
“We believed the findings do not support the utility of mandatory testing in this context, as most did not act on the information,” Dr. Ohman said.
A major reason for the inertia, Dr. Gurbel suggested, may be the absence of any compelling data proving whether there’s any effect on clinical outcomes for switching reduced metabolizers off of clopidogrel or switching good metabolizers onto it.
“We have no large-scale, prospective data supporting pharmacogenomic-based personalization” of clopidogrel treatment leading to improved outcomes, but “we need to get over that,” he said. “It’s a challenge to get funding for this.” But “the answer is not to give ticagrelor or prasugrel to everyone because then the bleeding rate is too high.”
The findings Dr. Ohman reported came from the Study to Compare the Safety of Rivaroxaban Versus Acetylsalicylic Acid in Addition to Either Clopidogrel or Ticagrelor Therapy in Participants With Acute Coronary Syndrome (GEMINI-ACS-1), which had the primary goal of comparing the safety in acute coronary syndrome patients of a reduced dosage of rivaroxaban plus either clopidogrel or ticagrelor with the safety of aspirin plus one of these P2Y12 inhibitors. The primary endpoint was the rate of clinically significant bleeding events during a year of treatment. The study ran at 371 centers in 21 countries and showed similar bleeding rates in both treatment arms (Lancet. 2017 May 6; 389[10081]:1799-808).
The analysis also showed that patients identified as reduced metabolizers were fivefold more likely to be switched than patients identified as ultra metabolizers, and intermediate metabolizes had a 50% higher switching rate than ultra metabolizers. The rates of both ischemic and major bleeding outcomes were roughly similar across the spectrum of metabolizers, but Dr. Ohman cautioned that the trial was not designed to assess this. Dr. Gurbel urged the investigators to report on outcomes analyzed not just by metabolizer status but also by the treatment they received.
The boxed warning that clopidogrel received in 2010 regarding poor metabolizers led to “regulatory guidance” during design of the GEMINI-ACS-1 trial requiring routine pharmacogenomic testing for clopidogrel-metabolizing status, Dr. Ohman explained.
The trial was funded by Janssen and Bayer, the two companies that jointly market rivaroxaban (Xarelto). Dr. Ohman has been a consultant to Bayer and several other companies including AstraZeneca, the company that markets ticagrelor (Brilinta). He has also received research funding from Janssen, as well as Daiichi Sankyo and Gilead Sciences. Dr. Gurbel holds patents on platelet-function testing methods.
[email protected]
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Physicians switched P2Y12 inhibitors for only 2% of patients on clopidogrel and only 0.06% on ticagrelor on the basis of their pharmacogenomic results.
Data source: GEMINI-ACS-1, a multicenter, prospective trial with 3,037 patients.
Disclosures: The GEMINI-ACS-1 trial was funded by Janssen and Bayer, the two companies that jointly market rivaroxaban (Xarelto). Dr. Ohman has been a consultant to Bayer and several other companies, including AstraZeneca, the company that markets ticagrelor (Brilinta). He has also received research funding from Janssen, as well as Daiichi Sankyo and Gilead Sciences. Dr. Gurbel holds patents on platelet-function testing methods.
VIDEO: U.S. hypertension guidelines reset threshold to 130/80 mm Hg
ANAHEIM, CALIF. – Thirty million Americans became hypertensive overnight on Nov. 13 with the introduction of new high blood pressure guidelines from the American College of Cardiology and American Heart Association.
That happened by resetting the definition of adult hypertension from the long-standing threshold of 140/90 mm Hg to a blood pressure at or above 130/80 mm Hg, a change that jumps the U.S. adult prevalence of hypertension from roughly 32% to 46%. Nearly half of all U.S. adults now have hypertension, bringing the total national hypertensive population to a staggering 103 million.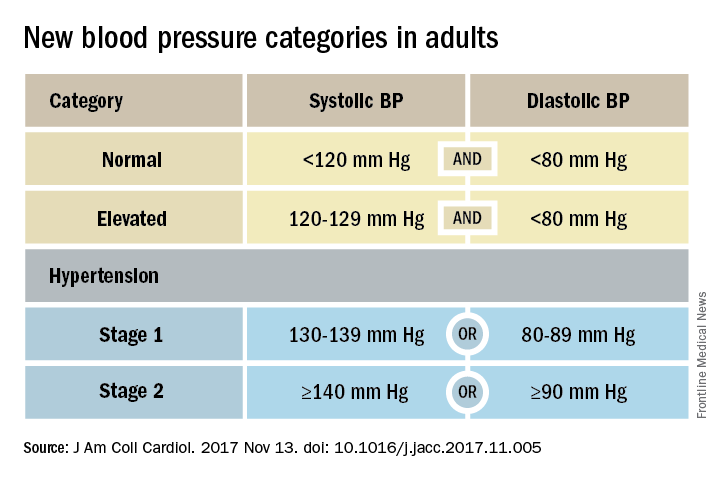
Goal is to transform care
But the new guidelines (J Am Coll Cardiol. 2017 Nov 13. doi: 10.1016/j.jacc.2017.11.005) for preventing, detecting, evaluating, and managing adult hypertension do lots more than just shake up the epidemiology of high blood pressure. With 106 total recommendations, the guidelines seek to transform every aspect of blood pressure in American medical practice, starting with how it’s measured and stretching to redefine applications of medical systems to try to ensure that every person with a blood pressure that truly falls outside the redefined limits gets a comprehensive package of interventions.
Many of these are “seismic changes,” said Lawrence J. Appel, MD. He particularly cited as seismic the new classification of stage 1 hypertension as a pressure at or above 130/80 mm Hg, the emphasis on using some form of out-of-office blood pressure measurement to confirm a diagnosis, the use of risk assessment when deciding whether to treat certain patients with drugs, and the same blood pressure goal of less than 130/80 mm Hg for all hypertensives, regardless of age, as long as they remain ambulatory and community dwelling.
One goal for all adults
“The systolic blood pressure goal for older people has gone from 140 mm Hg to 150 mm Hg and now to 130 mm Hg in the space of 2-3 years,” commented Dr. Appel, professor of epidemiology at Johns Hopkins University in Baltimore and not involved in the guideline-writing process.
In fact, the guidelines simplified the treatment goal all around, to less than 130/80 mm Hg for patients with diabetes, those with chronic kidney disease, and the elderly; that goal remains the same for all adults.
“It will be clearer and easier now that everyone should be less than 130/80 mm Hg. You won’t need to remember a second target,” said Sandra J. Taler, MD, a nephrologist and professor of medicine at the Mayo Clinic in Rochester, Minn., and a member of the guidelines task force.
“Some people may be upset that we changed the rules on them. They had normal blood pressure yesterday, and today it’s high. But it’s a good awakening, especially for using lifestyle interventions,” Dr. Taler said in an interview.
Preferred intervention: Lifestyle, not drugs
Lifestyle optimization is repeatedly cited as the cornerstone of intervention for everyone, including those with elevated blood pressure with a systolic pressure of 120-129 mm Hg, and as the only endorsed intervention for patients with hypertension of 130-139 mm Hg but below a 10% risk for a cardiovascular disease event during the next 10 years on the American College of Cardiology’s online risk calculator. The guidelines list six lifestyle goals: weight loss, following a DASH diet, reducing sodium, enhancing potassium, 90-150 min/wk of physical activity, and moderate alcohol intake.

Team-based care essential
The guidelines also put unprecedented emphasis on using a team-based management approach, which means having nurses, nurse practitioners, pharmacists, dietitians, and other clinicians, allowing for more frequent and focused care. Dr. Whelton and others cited in particular the VA Health System and Kaiser-Permanente as operating team-based and system-driven blood pressure management programs that have resulted in control rates for more than 90% of hypertensive patients. The team-based approach is also a key in the Target:BP program that the American Heart Association and American Medical Association founded. Target:BP will be instrumental in promoting implementation of the new guidelines, Dr. Carey said. Another systems recommendation is that every patient with hypertension should have a “clear, detailed, and current evidence-based plan of care.”
“Using nurse practitioners, physician assistants, and pharmacists has been shown to improve blood pressure levels,” and health systems that use this approach have had “great success,” commented Donald M. Lloyd-Jones, MD, professor and chairman of preventive medicine at Northwestern University in Chicago and not part of the guidelines task force. Some systems have used this approach to achieve high levels of blood pressure control. Now that financial penalties and incentives from payers also exist to push for higher levels of blood pressure control, the alignment of financial and health incentives should result in big changes, Dr. Lloyd-Jones predicted in a video interview.
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Thirty million Americans became hypertensive overnight on Nov. 13 with the introduction of new high blood pressure guidelines from the American College of Cardiology and American Heart Association.
That happened by resetting the definition of adult hypertension from the long-standing threshold of 140/90 mm Hg to a blood pressure at or above 130/80 mm Hg, a change that jumps the U.S. adult prevalence of hypertension from roughly 32% to 46%. Nearly half of all U.S. adults now have hypertension, bringing the total national hypertensive population to a staggering 103 million.
Goal is to transform care
But the new guidelines (J Am Coll Cardiol. 2017 Nov 13. doi: 10.1016/j.jacc.2017.11.005) for preventing, detecting, evaluating, and managing adult hypertension do lots more than just shake up the epidemiology of high blood pressure. With 106 total recommendations, the guidelines seek to transform every aspect of blood pressure in American medical practice, starting with how it’s measured and stretching to redefine applications of medical systems to try to ensure that every person with a blood pressure that truly falls outside the redefined limits gets a comprehensive package of interventions.
Many of these are “seismic changes,” said Lawrence J. Appel, MD. He particularly cited as seismic the new classification of stage 1 hypertension as a pressure at or above 130/80 mm Hg, the emphasis on using some form of out-of-office blood pressure measurement to confirm a diagnosis, the use of risk assessment when deciding whether to treat certain patients with drugs, and the same blood pressure goal of less than 130/80 mm Hg for all hypertensives, regardless of age, as long as they remain ambulatory and community dwelling.
One goal for all adults
“The systolic blood pressure goal for older people has gone from 140 mm Hg to 150 mm Hg and now to 130 mm Hg in the space of 2-3 years,” commented Dr. Appel, professor of epidemiology at Johns Hopkins University in Baltimore and not involved in the guideline-writing process.
In fact, the guidelines simplified the treatment goal all around, to less than 130/80 mm Hg for patients with diabetes, those with chronic kidney disease, and the elderly; that goal remains the same for all adults.
“It will be clearer and easier now that everyone should be less than 130/80 mm Hg. You won’t need to remember a second target,” said Sandra J. Taler, MD, a nephrologist and professor of medicine at the Mayo Clinic in Rochester, Minn., and a member of the guidelines task force.
“Some people may be upset that we changed the rules on them. They had normal blood pressure yesterday, and today it’s high. But it’s a good awakening, especially for using lifestyle interventions,” Dr. Taler said in an interview.
Preferred intervention: Lifestyle, not drugs
Lifestyle optimization is repeatedly cited as the cornerstone of intervention for everyone, including those with elevated blood pressure with a systolic pressure of 120-129 mm Hg, and as the only endorsed intervention for patients with hypertension of 130-139 mm Hg but below a 10% risk for a cardiovascular disease event during the next 10 years on the American College of Cardiology’s online risk calculator. The guidelines list six lifestyle goals: weight loss, following a DASH diet, reducing sodium, enhancing potassium, 90-150 min/wk of physical activity, and moderate alcohol intake.
Team-based care essential
The guidelines also put unprecedented emphasis on using a team-based management approach, which means having nurses, nurse practitioners, pharmacists, dietitians, and other clinicians, allowing for more frequent and focused care. Dr. Whelton and others cited in particular the VA Health System and Kaiser-Permanente as operating team-based and system-driven blood pressure management programs that have resulted in control rates for more than 90% of hypertensive patients. The team-based approach is also a key in the Target:BP program that the American Heart Association and American Medical Association founded. Target:BP will be instrumental in promoting implementation of the new guidelines, Dr. Carey said. Another systems recommendation is that every patient with hypertension should have a “clear, detailed, and current evidence-based plan of care.”
“Using nurse practitioners, physician assistants, and pharmacists has been shown to improve blood pressure levels,” and health systems that use this approach have had “great success,” commented Donald M. Lloyd-Jones, MD, professor and chairman of preventive medicine at Northwestern University in Chicago and not part of the guidelines task force. Some systems have used this approach to achieve high levels of blood pressure control. Now that financial penalties and incentives from payers also exist to push for higher levels of blood pressure control, the alignment of financial and health incentives should result in big changes, Dr. Lloyd-Jones predicted in a video interview.
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Thirty million Americans became hypertensive overnight on Nov. 13 with the introduction of new high blood pressure guidelines from the American College of Cardiology and American Heart Association.
That happened by resetting the definition of adult hypertension from the long-standing threshold of 140/90 mm Hg to a blood pressure at or above 130/80 mm Hg, a change that jumps the U.S. adult prevalence of hypertension from roughly 32% to 46%. Nearly half of all U.S. adults now have hypertension, bringing the total national hypertensive population to a staggering 103 million.
Goal is to transform care
But the new guidelines (J Am Coll Cardiol. 2017 Nov 13. doi: 10.1016/j.jacc.2017.11.005) for preventing, detecting, evaluating, and managing adult hypertension do lots more than just shake up the epidemiology of high blood pressure. With 106 total recommendations, the guidelines seek to transform every aspect of blood pressure in American medical practice, starting with how it’s measured and stretching to redefine applications of medical systems to try to ensure that every person with a blood pressure that truly falls outside the redefined limits gets a comprehensive package of interventions.
Many of these are “seismic changes,” said Lawrence J. Appel, MD. He particularly cited as seismic the new classification of stage 1 hypertension as a pressure at or above 130/80 mm Hg, the emphasis on using some form of out-of-office blood pressure measurement to confirm a diagnosis, the use of risk assessment when deciding whether to treat certain patients with drugs, and the same blood pressure goal of less than 130/80 mm Hg for all hypertensives, regardless of age, as long as they remain ambulatory and community dwelling.
One goal for all adults
“The systolic blood pressure goal for older people has gone from 140 mm Hg to 150 mm Hg and now to 130 mm Hg in the space of 2-3 years,” commented Dr. Appel, professor of epidemiology at Johns Hopkins University in Baltimore and not involved in the guideline-writing process.
In fact, the guidelines simplified the treatment goal all around, to less than 130/80 mm Hg for patients with diabetes, those with chronic kidney disease, and the elderly; that goal remains the same for all adults.
“It will be clearer and easier now that everyone should be less than 130/80 mm Hg. You won’t need to remember a second target,” said Sandra J. Taler, MD, a nephrologist and professor of medicine at the Mayo Clinic in Rochester, Minn., and a member of the guidelines task force.
“Some people may be upset that we changed the rules on them. They had normal blood pressure yesterday, and today it’s high. But it’s a good awakening, especially for using lifestyle interventions,” Dr. Taler said in an interview.
Preferred intervention: Lifestyle, not drugs
Lifestyle optimization is repeatedly cited as the cornerstone of intervention for everyone, including those with elevated blood pressure with a systolic pressure of 120-129 mm Hg, and as the only endorsed intervention for patients with hypertension of 130-139 mm Hg but below a 10% risk for a cardiovascular disease event during the next 10 years on the American College of Cardiology’s online risk calculator. The guidelines list six lifestyle goals: weight loss, following a DASH diet, reducing sodium, enhancing potassium, 90-150 min/wk of physical activity, and moderate alcohol intake.
Team-based care essential
The guidelines also put unprecedented emphasis on using a team-based management approach, which means having nurses, nurse practitioners, pharmacists, dietitians, and other clinicians, allowing for more frequent and focused care. Dr. Whelton and others cited in particular the VA Health System and Kaiser-Permanente as operating team-based and system-driven blood pressure management programs that have resulted in control rates for more than 90% of hypertensive patients. The team-based approach is also a key in the Target:BP program that the American Heart Association and American Medical Association founded. Target:BP will be instrumental in promoting implementation of the new guidelines, Dr. Carey said. Another systems recommendation is that every patient with hypertension should have a “clear, detailed, and current evidence-based plan of care.”
“Using nurse practitioners, physician assistants, and pharmacists has been shown to improve blood pressure levels,” and health systems that use this approach have had “great success,” commented Donald M. Lloyd-Jones, MD, professor and chairman of preventive medicine at Northwestern University in Chicago and not part of the guidelines task force. Some systems have used this approach to achieve high levels of blood pressure control. Now that financial penalties and incentives from payers also exist to push for higher levels of blood pressure control, the alignment of financial and health incentives should result in big changes, Dr. Lloyd-Jones predicted in a video interview.
[email protected]
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE AHA SCIENTIFIC SESSIONS
DAPT produces better CABG outcomes than aspirin alone
ANAHEIM, CALIF. – Treatment with dual-antiplatelet therapy following coronary artery bypass grafting with a saphenous vein maintained vein-graft patency better than aspirin alone in a randomized, multicenter trial with 500 patients.
After 1 year of dual-antiplatelet therapy (DAPT) with ticagrelor (Brilinta) and aspirin, 89% of saphenous-vein grafts remained patent, compared with a 77% patency rate in saphenous-vein grafts in patients treated with aspirin alone, a statistically significant difference for the study’s primary endpoint, Qiang Zhao, MD, said at the American Hart Association scientific sessions. The data, collected at six Chinese centers, also showed a nominal decrease in the combined rate of cardiovascular death, MI, and stroke: 2% with DAPT and 5% with aspirin alone. It further showed an increase in major or bypass-related bleeds: 2% with DAPT and none with aspirin alone, reported Dr. Zhao, professor and director of cardiac surgery at Ruijin Hospital in Shanghai, China.

“If this result were repeated in a larger study it would be important,” John H. Alexander, MD, professor of medicine at Duke University in Durham, N.C., commented in a video interview.
The Compare the Efficacy of Different Antiplatelet Therapy Strategy After Coronary Artery Bypass Graft Surgery (DACAB) trial randomized patients who underwent coronary artery bypass grafting (CABG). They averaged about 64 years of age, and received an average of nearly four grafts each including an average of nearly three saphenous vein grafts. The study assigned patients to one of three treatment arms starting within 24 hours after surgery: 168 received ticagrelor 90 mg twice daily plus aspirin 100 mg once daily, 166 got ticagrelor alone, and 166 received aspirin alone. Treatment continued for 1 year.
“Some surgeons and physicians currently prescribe DAPT to CABG patients, but there is not much evidence of its benefit. The DACAB trial is useful, but you need to show that it does not just improve patency but that patients also have better outcomes. The excess of major bleeds is a big deal. It gives one pause about adopting DAPT as standard treatment,” Dr. Gardner said.
DACAB received no commercial funding. Dr. Zhao has been a speaker on behalf of and has received research funding from AstraZeneca, the company that markets ticagrelor (Brilinta). He has also been a speaker for Johnson & Johnson and Medtronic and has received research funding from Bayer, Novartis, and Sanofi. Dr. Gardner had no disclosures.
[email protected]
On Twitter @mitchelzoler
Results from the DACAB trial showed that using aspirin and ticagrelor improved vein-graft patency, compared with using aspirin alone. It was a compelling result, but for the intermediate, imaging-based outcome of graft patency at 1 year after surgery. This finding is conclusive evidence that dual-antiplatelet therapy has some benefit.
But the findings from this trial, modestly sized with 500 patients, failed to prove that the clinical benefit from dual-antiplatelet therapy was worth the adverse effect of an increase in the rate of major and bypass-related bleeding. The study was underpowered to prove that dual-antiplatelet therapy had a clear beneficial impact on clinical outcomes such as cardiovascular death, MI, and stroke, although this combined rate went in the right direction with dual therapy, compared with aspirin alone. We need to see proof of a benefit for these clinical outcomes to justify using a treatment that causes an increase in major bleeds.
The DACAB results alone are not enough to justify a change in practice. It would be an important finding if the results could be replicated in a larger study. And if dual-antiplatelet therapy was proven to have a net clinical benefit for patients, we would still want to target it to patients with a higher ischemic risk and, in general, avoid using it in patients with a high bleeding risk.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
John H. Alexander, MD , is a cardiologist and professor of medicine at Duke University in Durham, N.C. He has been a consultant to and has received research funding from several companies, including AstraZeneca, the company that markets ticagrelor (Brilinta). He made these comments as designated discussant for the DACAB study and in a video interview .
Results from the DACAB trial showed that using aspirin and ticagrelor improved vein-graft patency, compared with using aspirin alone. It was a compelling result, but for the intermediate, imaging-based outcome of graft patency at 1 year after surgery. This finding is conclusive evidence that dual-antiplatelet therapy has some benefit.
But the findings from this trial, modestly sized with 500 patients, failed to prove that the clinical benefit from dual-antiplatelet therapy was worth the adverse effect of an increase in the rate of major and bypass-related bleeding. The study was underpowered to prove that dual-antiplatelet therapy had a clear beneficial impact on clinical outcomes such as cardiovascular death, MI, and stroke, although this combined rate went in the right direction with dual therapy, compared with aspirin alone. We need to see proof of a benefit for these clinical outcomes to justify using a treatment that causes an increase in major bleeds.
The DACAB results alone are not enough to justify a change in practice. It would be an important finding if the results could be replicated in a larger study. And if dual-antiplatelet therapy was proven to have a net clinical benefit for patients, we would still want to target it to patients with a higher ischemic risk and, in general, avoid using it in patients with a high bleeding risk.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
John H. Alexander, MD , is a cardiologist and professor of medicine at Duke University in Durham, N.C. He has been a consultant to and has received research funding from several companies, including AstraZeneca, the company that markets ticagrelor (Brilinta). He made these comments as designated discussant for the DACAB study and in a video interview .
Results from the DACAB trial showed that using aspirin and ticagrelor improved vein-graft patency, compared with using aspirin alone. It was a compelling result, but for the intermediate, imaging-based outcome of graft patency at 1 year after surgery. This finding is conclusive evidence that dual-antiplatelet therapy has some benefit.
But the findings from this trial, modestly sized with 500 patients, failed to prove that the clinical benefit from dual-antiplatelet therapy was worth the adverse effect of an increase in the rate of major and bypass-related bleeding. The study was underpowered to prove that dual-antiplatelet therapy had a clear beneficial impact on clinical outcomes such as cardiovascular death, MI, and stroke, although this combined rate went in the right direction with dual therapy, compared with aspirin alone. We need to see proof of a benefit for these clinical outcomes to justify using a treatment that causes an increase in major bleeds.
The DACAB results alone are not enough to justify a change in practice. It would be an important finding if the results could be replicated in a larger study. And if dual-antiplatelet therapy was proven to have a net clinical benefit for patients, we would still want to target it to patients with a higher ischemic risk and, in general, avoid using it in patients with a high bleeding risk.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
John H. Alexander, MD , is a cardiologist and professor of medicine at Duke University in Durham, N.C. He has been a consultant to and has received research funding from several companies, including AstraZeneca, the company that markets ticagrelor (Brilinta). He made these comments as designated discussant for the DACAB study and in a video interview .
ANAHEIM, CALIF. – Treatment with dual-antiplatelet therapy following coronary artery bypass grafting with a saphenous vein maintained vein-graft patency better than aspirin alone in a randomized, multicenter trial with 500 patients.
After 1 year of dual-antiplatelet therapy (DAPT) with ticagrelor (Brilinta) and aspirin, 89% of saphenous-vein grafts remained patent, compared with a 77% patency rate in saphenous-vein grafts in patients treated with aspirin alone, a statistically significant difference for the study’s primary endpoint, Qiang Zhao, MD, said at the American Hart Association scientific sessions. The data, collected at six Chinese centers, also showed a nominal decrease in the combined rate of cardiovascular death, MI, and stroke: 2% with DAPT and 5% with aspirin alone. It further showed an increase in major or bypass-related bleeds: 2% with DAPT and none with aspirin alone, reported Dr. Zhao, professor and director of cardiac surgery at Ruijin Hospital in Shanghai, China.
“If this result were repeated in a larger study it would be important,” John H. Alexander, MD, professor of medicine at Duke University in Durham, N.C., commented in a video interview.
The Compare the Efficacy of Different Antiplatelet Therapy Strategy After Coronary Artery Bypass Graft Surgery (DACAB) trial randomized patients who underwent coronary artery bypass grafting (CABG). They averaged about 64 years of age, and received an average of nearly four grafts each including an average of nearly three saphenous vein grafts. The study assigned patients to one of three treatment arms starting within 24 hours after surgery: 168 received ticagrelor 90 mg twice daily plus aspirin 100 mg once daily, 166 got ticagrelor alone, and 166 received aspirin alone. Treatment continued for 1 year.
“Some surgeons and physicians currently prescribe DAPT to CABG patients, but there is not much evidence of its benefit. The DACAB trial is useful, but you need to show that it does not just improve patency but that patients also have better outcomes. The excess of major bleeds is a big deal. It gives one pause about adopting DAPT as standard treatment,” Dr. Gardner said.
DACAB received no commercial funding. Dr. Zhao has been a speaker on behalf of and has received research funding from AstraZeneca, the company that markets ticagrelor (Brilinta). He has also been a speaker for Johnson & Johnson and Medtronic and has received research funding from Bayer, Novartis, and Sanofi. Dr. Gardner had no disclosures.
[email protected]
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Treatment with dual-antiplatelet therapy following coronary artery bypass grafting with a saphenous vein maintained vein-graft patency better than aspirin alone in a randomized, multicenter trial with 500 patients.
After 1 year of dual-antiplatelet therapy (DAPT) with ticagrelor (Brilinta) and aspirin, 89% of saphenous-vein grafts remained patent, compared with a 77% patency rate in saphenous-vein grafts in patients treated with aspirin alone, a statistically significant difference for the study’s primary endpoint, Qiang Zhao, MD, said at the American Hart Association scientific sessions. The data, collected at six Chinese centers, also showed a nominal decrease in the combined rate of cardiovascular death, MI, and stroke: 2% with DAPT and 5% with aspirin alone. It further showed an increase in major or bypass-related bleeds: 2% with DAPT and none with aspirin alone, reported Dr. Zhao, professor and director of cardiac surgery at Ruijin Hospital in Shanghai, China.
“If this result were repeated in a larger study it would be important,” John H. Alexander, MD, professor of medicine at Duke University in Durham, N.C., commented in a video interview.
The Compare the Efficacy of Different Antiplatelet Therapy Strategy After Coronary Artery Bypass Graft Surgery (DACAB) trial randomized patients who underwent coronary artery bypass grafting (CABG). They averaged about 64 years of age, and received an average of nearly four grafts each including an average of nearly three saphenous vein grafts. The study assigned patients to one of three treatment arms starting within 24 hours after surgery: 168 received ticagrelor 90 mg twice daily plus aspirin 100 mg once daily, 166 got ticagrelor alone, and 166 received aspirin alone. Treatment continued for 1 year.
“Some surgeons and physicians currently prescribe DAPT to CABG patients, but there is not much evidence of its benefit. The DACAB trial is useful, but you need to show that it does not just improve patency but that patients also have better outcomes. The excess of major bleeds is a big deal. It gives one pause about adopting DAPT as standard treatment,” Dr. Gardner said.
DACAB received no commercial funding. Dr. Zhao has been a speaker on behalf of and has received research funding from AstraZeneca, the company that markets ticagrelor (Brilinta). He has also been a speaker for Johnson & Johnson and Medtronic and has received research funding from Bayer, Novartis, and Sanofi. Dr. Gardner had no disclosures.
[email protected]
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The 1-year saphenous-vein graft patency rate was 89% with DAPT treatment and 77% with aspirin alone. Data source: DACAB, a multicenter, randomized trial with 500 Chinese patients.
Disclosures: DACAB received no commercial funding. Dr. Zhao has been a speaker on behalf of and has received research funding from AstraZeneca, the company that markets ticagrelor (Brilinta). He has also been a speaker for Johnson & Johnson and Medtronic and has received research funding from Bayer, Novartis, and Sanofi.
VIDEO: Evidence mounts for pulmonary embolism benefit from catheter thrombolysis
TORONTO – Catheter-directed thrombolysis of pulmonary embolism using an ultrasound-assisted device led to significantly better outcomes in patients hospitalized for pulmonary embolism, compared with conventional systemic thrombolytic treatment, in a propensity score–adjusted analysis of nearly 3,400 patients.
Catheter-directed thrombolysis (CDT) “represents an opportunity to locally treat pulmonary embolism with significant thrombus burden with lower bleeding complications,” Abhishek Mishra, MD, said at the CHEST annual meeting. “I think we are underusing CDT,” said Dr. Mishra, a cardiovascular disease physician at Guthrie Robert Packer Hospital in Sayre, Pa.
Although one CDT device, the EKOS endovascular system that uses ultrasound to facilitate pulmonary embolism (PE) thrombolysis, received Food & Drug Administration approval for U.S. marketing in 2014, the trials that have compared it with systemic thrombolysis have been small, noted Dr. Mishra, and none have looked at whether CDT improves patient survival, compared with standard treatments. The largest report on CDT treatment of PE came from a single-arm, uncontrolled study with 150 patients who received ultrasound-facilitated CDT (JACC Cardiovasc Interv. 2015 Aug;8[10]:1382-92).
To better document the incremental benefit from CDT, Dr. Mishra and his associates used data collected by the Nationwide Readmissions Database during 2013 and 2014, both before and after a CDT device became available for U.S. use. From among 4,426 patients hospitalized with a primary diagnosis of PE and treated with thrombolytic therapy, they used propensity score matching to compare 2,256 patients treated with systemic thrombolysis with 1,128 matched patients treated with CDT using tissue plasminogen activator.
The analysis showed that in-hospital death was 15% in the systemic patients and 6% in the CDT group, a relative risk reduction of 63%, and 30-day readmissions occurred in 11% of the systemic patients and in 8% of those treated with CDT, a 30% relative risk reduction. Both were statistically significant differences for the study’s two primary endpoints, Dr. Mishra reported at the meeting. Rates of intracerebral hemorrhage and gastrointestinal bleeds were both numerically lower with CDT, and significantly lower for gastrointestinal bleeds.
The researchers also ran a multivariate analysis on their data that showed CDT was linked with significant relative reductions of about 60% for both in-hospital death and 30-day readmissions, compared with patients on systemic therapy. The results Dr. Mishra reported also appeared in a published report (Am J Cardiol. 2017 Nov 1;120[9]:1653-61).
These findings help buttress the case for using CDT for at least some PE patients. “The key is which patients need it. What is the best way to stratify patients?” commented Victor F. Tapson, MD, a pulmonologist at Cedars-Sinai Medical Center in Los Angeles.
“Patients with PE and a normal right ventricle generally don’t need anything more aggressive than anticoagulation, and really sick patients with massive PE need systemic thrombolytics. Intermediate-risk patients” are best suited to CDT, but “the problem is that intermediate-risk patients are heterogeneous,” Dr. Tapson said in a video interview. Future studies should establish a more specific subgroup of intermediate-risk patients who benefit from routinely employed CDT, he suggested.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
BY MITCHEL L. ZOLER
Frontline Medical News
BY MITCHEL L. ZOLER
Frontline Medical News
BY MITCHEL L. ZOLER
Frontline Medical News
TORONTO – Catheter-directed thrombolysis of pulmonary embolism using an ultrasound-assisted device led to significantly better outcomes in patients hospitalized for pulmonary embolism, compared with conventional systemic thrombolytic treatment, in a propensity score–adjusted analysis of nearly 3,400 patients.
Catheter-directed thrombolysis (CDT) “represents an opportunity to locally treat pulmonary embolism with significant thrombus burden with lower bleeding complications,” Abhishek Mishra, MD, said at the CHEST annual meeting. “I think we are underusing CDT,” said Dr. Mishra, a cardiovascular disease physician at Guthrie Robert Packer Hospital in Sayre, Pa.
Although one CDT device, the EKOS endovascular system that uses ultrasound to facilitate pulmonary embolism (PE) thrombolysis, received Food & Drug Administration approval for U.S. marketing in 2014, the trials that have compared it with systemic thrombolysis have been small, noted Dr. Mishra, and none have looked at whether CDT improves patient survival, compared with standard treatments. The largest report on CDT treatment of PE came from a single-arm, uncontrolled study with 150 patients who received ultrasound-facilitated CDT (JACC Cardiovasc Interv. 2015 Aug;8[10]:1382-92).
To better document the incremental benefit from CDT, Dr. Mishra and his associates used data collected by the Nationwide Readmissions Database during 2013 and 2014, both before and after a CDT device became available for U.S. use. From among 4,426 patients hospitalized with a primary diagnosis of PE and treated with thrombolytic therapy, they used propensity score matching to compare 2,256 patients treated with systemic thrombolysis with 1,128 matched patients treated with CDT using tissue plasminogen activator.
The analysis showed that in-hospital death was 15% in the systemic patients and 6% in the CDT group, a relative risk reduction of 63%, and 30-day readmissions occurred in 11% of the systemic patients and in 8% of those treated with CDT, a 30% relative risk reduction. Both were statistically significant differences for the study’s two primary endpoints, Dr. Mishra reported at the meeting. Rates of intracerebral hemorrhage and gastrointestinal bleeds were both numerically lower with CDT, and significantly lower for gastrointestinal bleeds.
The researchers also ran a multivariate analysis on their data that showed CDT was linked with significant relative reductions of about 60% for both in-hospital death and 30-day readmissions, compared with patients on systemic therapy. The results Dr. Mishra reported also appeared in a published report (Am J Cardiol. 2017 Nov 1;120[9]:1653-61).
These findings help buttress the case for using CDT for at least some PE patients. “The key is which patients need it. What is the best way to stratify patients?” commented Victor F. Tapson, MD, a pulmonologist at Cedars-Sinai Medical Center in Los Angeles.
“Patients with PE and a normal right ventricle generally don’t need anything more aggressive than anticoagulation, and really sick patients with massive PE need systemic thrombolytics. Intermediate-risk patients” are best suited to CDT, but “the problem is that intermediate-risk patients are heterogeneous,” Dr. Tapson said in a video interview. Future studies should establish a more specific subgroup of intermediate-risk patients who benefit from routinely employed CDT, he suggested.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
TORONTO – Catheter-directed thrombolysis of pulmonary embolism using an ultrasound-assisted device led to significantly better outcomes in patients hospitalized for pulmonary embolism, compared with conventional systemic thrombolytic treatment, in a propensity score–adjusted analysis of nearly 3,400 patients.
Catheter-directed thrombolysis (CDT) “represents an opportunity to locally treat pulmonary embolism with significant thrombus burden with lower bleeding complications,” Abhishek Mishra, MD, said at the CHEST annual meeting. “I think we are underusing CDT,” said Dr. Mishra, a cardiovascular disease physician at Guthrie Robert Packer Hospital in Sayre, Pa.
Although one CDT device, the EKOS endovascular system that uses ultrasound to facilitate pulmonary embolism (PE) thrombolysis, received Food & Drug Administration approval for U.S. marketing in 2014, the trials that have compared it with systemic thrombolysis have been small, noted Dr. Mishra, and none have looked at whether CDT improves patient survival, compared with standard treatments. The largest report on CDT treatment of PE came from a single-arm, uncontrolled study with 150 patients who received ultrasound-facilitated CDT (JACC Cardiovasc Interv. 2015 Aug;8[10]:1382-92).
To better document the incremental benefit from CDT, Dr. Mishra and his associates used data collected by the Nationwide Readmissions Database during 2013 and 2014, both before and after a CDT device became available for U.S. use. From among 4,426 patients hospitalized with a primary diagnosis of PE and treated with thrombolytic therapy, they used propensity score matching to compare 2,256 patients treated with systemic thrombolysis with 1,128 matched patients treated with CDT using tissue plasminogen activator.
The analysis showed that in-hospital death was 15% in the systemic patients and 6% in the CDT group, a relative risk reduction of 63%, and 30-day readmissions occurred in 11% of the systemic patients and in 8% of those treated with CDT, a 30% relative risk reduction. Both were statistically significant differences for the study’s two primary endpoints, Dr. Mishra reported at the meeting. Rates of intracerebral hemorrhage and gastrointestinal bleeds were both numerically lower with CDT, and significantly lower for gastrointestinal bleeds.
The researchers also ran a multivariate analysis on their data that showed CDT was linked with significant relative reductions of about 60% for both in-hospital death and 30-day readmissions, compared with patients on systemic therapy. The results Dr. Mishra reported also appeared in a published report (Am J Cardiol. 2017 Nov 1;120[9]:1653-61).
These findings help buttress the case for using CDT for at least some PE patients. “The key is which patients need it. What is the best way to stratify patients?” commented Victor F. Tapson, MD, a pulmonologist at Cedars-Sinai Medical Center in Los Angeles.
“Patients with PE and a normal right ventricle generally don’t need anything more aggressive than anticoagulation, and really sick patients with massive PE need systemic thrombolytics. Intermediate-risk patients” are best suited to CDT, but “the problem is that intermediate-risk patients are heterogeneous,” Dr. Tapson said in a video interview. Future studies should establish a more specific subgroup of intermediate-risk patients who benefit from routinely employed CDT, he suggested.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
AT CHEST 2017
Key clinical point:
Major finding: Catheter-directed thrombolysis cut in-hospital mortality by 63%, compared with conventional systemic thrombolysis.
Data source: The National Readmission Database, which included 4,426 patients hospitalized during 2013 and 2014 with primary pulmonary embolism and treated with thrombolysis.
Disclosures: Dr. Mishra had no disclosures. Dr. Tapson has been a consultant to and had received research funding from Ekos/BTG, a company that markets a catheter-directed thrombolysis device. He has also ties to Daiichi Sankyo, Inari, Janssen, and Portola.
