User login
Diabetes prevalence increases, but so does diabetes control
The prevalence of diagnosed diabetes in the United States rose significantly from 1988 to 2010, jumping from 6% to 10%.
Prediabetes doubled in prevalence over the same time period, from 6% to 12%, Elizabeth Selvin, Ph.D., and her colleagues reported in the April 14 issue of the Annals of Internal Medicine (2014 [doi=10.7326/M13-2411]).
But while the prevalence of confirmed cases increased sharply, the prevalence of undiagnosed diabetes actually decreased slightly over the same time – meaning that almost all cases of diabetes in the United States are now being identified, wrote Dr. Selvin of Johns Hopkins University, Baltimore, and her coinvestigators. "At present, approximately 89% of all diabetes cases are diagnosed," the team wrote. "Furthermore, glycemic control among persons with diagnosed diabetes has improved, probably reflecting a combination of improvements in diagnosis, screening, and care."

The researchers mined their data from two epochs of the National Health and Nutrition Examination Survey (1988-1994 and 1999-2010), comprising a total of almost 43,500 people. They assessed diabetes and prediabetes prevalence by both fasting plasma glucose and hemoglobin A1c (HbA1c) levels. They also looked at glucose control parameters and medication type in diagnosed patients. To investigate any association between diabetes and weight, they evaluated body mass index in the survey populations.
The mean prevalence of obesity in U.S. adults without diabetes jumped from 21% in the first epoch to 32% in the second. The change was similar among those with diabetes. The increases in both prediabetes and diabetes tracked the jump in obesity, leading the authors to conclude that obesity was a direct cause of disease.
Overall, the mean HbA1c level rose from 5.25% in the earliest years to 5.36% in 2010 – a small but significant increase. But the level was entirely stable in a subset of young adults who had normal body weight, blood pressure, and lipid levels (5%).
The prevalence of diabetes as measured by an HbA1c of at least 6.5% increased over the two epochs, from a low of 6% in the earliest years to 10% by the latest. The prevalence of prediabetes doubled (from 6% to 12%). "When applied to the 2010 U.S. Census, the total number of adults aged 20 [years] or older with total confirmed diabetes was 20.6 million," the authors wrote.
When the team used HbA1c levels to identify undiagnosed cases, they determined that 16% of cases in the earlier epoch were undiagnosed, compared with 11% in the later years – meaning that by 2010, 89% of U.S. cases were being identified.
As measured by an HbA1c of less than 7%, glycemic control improved from 51% to 59% over the study period. Among those who reported that they were taking diabetes medications, control increased from 40% to 55%.
Blacks and Hispanics shouldered a larger disease burden than did whites, the researchers wrote. "The prevalence ... in blacks was nearly double the prevalence in whites (15% vs. almost 9%). Mexican-Americans also had a greater prevalence of diabetes than whites (15.4% vs. 8.6%). Both ethnic minority groups had a greater prevalence of undiagnosed diabetes."
Control was also poorer, they said: Only 52% of blacks and 43% of Mexican-Americans had a calibrated HbA1c level less than 7%, compared with 57% of whites.
"The substantially greater prevalence of diabetes and prediabetes and poor rates of glycemic control (even among persons with medication-treated diabetes) in ethnic minority populations ... is particularly concerning because blacks and Mexican-Americans are also at greater risk for complications of diabetes, particularly retinopathy and kidney disease," the team noted.
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Neither Dr. Selvin nor any of her coauthors had any financial declarations.
On Twitter @alz_gal
Yes, diabetes control has improved over the past decades. But not everyone is benefiting and, with the disease still on the rise, more needs to be done to stop it before it even starts.
Nearly 40% of patients are not achieving their glycemic target – especially minority groups, which continue to suffer more, and have more-serious, long-term diabetes complications. The "alarming increase" in both obesity and diabetes should give society pause, and inspire a national effort to interrupt both.
"We know from the Diabetes Prevention Program that an intensive lifestyle change effectively prevents or delays the onset of diabetes. Public policy should focus on increasing physical activity and optimizing and improving access to healthy food choices for adults as well as children.
"Although the Centers for Disease Control and Prevention is actively engaged in adapting the Diabetes Prevention Program model for the community, we need to ensure that adequate resources are allocated to target these issues at the individual, societal, and environmental levels. Indeed, the public and private sectors need to work closely together to tackle this immense problem."
Dr. Martin J. Abrahamson and Dr. Roeland J.W. Middelbeek of the Joslin Diabetes Center and Harvard Medical School, Boston, made these remarks in an accompanying editorial (Ann. Int. Med. 2014;160:572-3). Dr. Abrahamson has received fees from several pharmaceutical companies. Dr. Middelbeek had no relevant disclosures.
Yes, diabetes control has improved over the past decades. But not everyone is benefiting and, with the disease still on the rise, more needs to be done to stop it before it even starts.
Nearly 40% of patients are not achieving their glycemic target – especially minority groups, which continue to suffer more, and have more-serious, long-term diabetes complications. The "alarming increase" in both obesity and diabetes should give society pause, and inspire a national effort to interrupt both.
"We know from the Diabetes Prevention Program that an intensive lifestyle change effectively prevents or delays the onset of diabetes. Public policy should focus on increasing physical activity and optimizing and improving access to healthy food choices for adults as well as children.
"Although the Centers for Disease Control and Prevention is actively engaged in adapting the Diabetes Prevention Program model for the community, we need to ensure that adequate resources are allocated to target these issues at the individual, societal, and environmental levels. Indeed, the public and private sectors need to work closely together to tackle this immense problem."
Dr. Martin J. Abrahamson and Dr. Roeland J.W. Middelbeek of the Joslin Diabetes Center and Harvard Medical School, Boston, made these remarks in an accompanying editorial (Ann. Int. Med. 2014;160:572-3). Dr. Abrahamson has received fees from several pharmaceutical companies. Dr. Middelbeek had no relevant disclosures.
Yes, diabetes control has improved over the past decades. But not everyone is benefiting and, with the disease still on the rise, more needs to be done to stop it before it even starts.
Nearly 40% of patients are not achieving their glycemic target – especially minority groups, which continue to suffer more, and have more-serious, long-term diabetes complications. The "alarming increase" in both obesity and diabetes should give society pause, and inspire a national effort to interrupt both.
"We know from the Diabetes Prevention Program that an intensive lifestyle change effectively prevents or delays the onset of diabetes. Public policy should focus on increasing physical activity and optimizing and improving access to healthy food choices for adults as well as children.
"Although the Centers for Disease Control and Prevention is actively engaged in adapting the Diabetes Prevention Program model for the community, we need to ensure that adequate resources are allocated to target these issues at the individual, societal, and environmental levels. Indeed, the public and private sectors need to work closely together to tackle this immense problem."
Dr. Martin J. Abrahamson and Dr. Roeland J.W. Middelbeek of the Joslin Diabetes Center and Harvard Medical School, Boston, made these remarks in an accompanying editorial (Ann. Int. Med. 2014;160:572-3). Dr. Abrahamson has received fees from several pharmaceutical companies. Dr. Middelbeek had no relevant disclosures.
The prevalence of diagnosed diabetes in the United States rose significantly from 1988 to 2010, jumping from 6% to 10%.
Prediabetes doubled in prevalence over the same time period, from 6% to 12%, Elizabeth Selvin, Ph.D., and her colleagues reported in the April 14 issue of the Annals of Internal Medicine (2014 [doi=10.7326/M13-2411]).
But while the prevalence of confirmed cases increased sharply, the prevalence of undiagnosed diabetes actually decreased slightly over the same time – meaning that almost all cases of diabetes in the United States are now being identified, wrote Dr. Selvin of Johns Hopkins University, Baltimore, and her coinvestigators. "At present, approximately 89% of all diabetes cases are diagnosed," the team wrote. "Furthermore, glycemic control among persons with diagnosed diabetes has improved, probably reflecting a combination of improvements in diagnosis, screening, and care."
The researchers mined their data from two epochs of the National Health and Nutrition Examination Survey (1988-1994 and 1999-2010), comprising a total of almost 43,500 people. They assessed diabetes and prediabetes prevalence by both fasting plasma glucose and hemoglobin A1c (HbA1c) levels. They also looked at glucose control parameters and medication type in diagnosed patients. To investigate any association between diabetes and weight, they evaluated body mass index in the survey populations.
The mean prevalence of obesity in U.S. adults without diabetes jumped from 21% in the first epoch to 32% in the second. The change was similar among those with diabetes. The increases in both prediabetes and diabetes tracked the jump in obesity, leading the authors to conclude that obesity was a direct cause of disease.
Overall, the mean HbA1c level rose from 5.25% in the earliest years to 5.36% in 2010 – a small but significant increase. But the level was entirely stable in a subset of young adults who had normal body weight, blood pressure, and lipid levels (5%).
The prevalence of diabetes as measured by an HbA1c of at least 6.5% increased over the two epochs, from a low of 6% in the earliest years to 10% by the latest. The prevalence of prediabetes doubled (from 6% to 12%). "When applied to the 2010 U.S. Census, the total number of adults aged 20 [years] or older with total confirmed diabetes was 20.6 million," the authors wrote.
When the team used HbA1c levels to identify undiagnosed cases, they determined that 16% of cases in the earlier epoch were undiagnosed, compared with 11% in the later years – meaning that by 2010, 89% of U.S. cases were being identified.
As measured by an HbA1c of less than 7%, glycemic control improved from 51% to 59% over the study period. Among those who reported that they were taking diabetes medications, control increased from 40% to 55%.
Blacks and Hispanics shouldered a larger disease burden than did whites, the researchers wrote. "The prevalence ... in blacks was nearly double the prevalence in whites (15% vs. almost 9%). Mexican-Americans also had a greater prevalence of diabetes than whites (15.4% vs. 8.6%). Both ethnic minority groups had a greater prevalence of undiagnosed diabetes."
Control was also poorer, they said: Only 52% of blacks and 43% of Mexican-Americans had a calibrated HbA1c level less than 7%, compared with 57% of whites.
"The substantially greater prevalence of diabetes and prediabetes and poor rates of glycemic control (even among persons with medication-treated diabetes) in ethnic minority populations ... is particularly concerning because blacks and Mexican-Americans are also at greater risk for complications of diabetes, particularly retinopathy and kidney disease," the team noted.
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Neither Dr. Selvin nor any of her coauthors had any financial declarations.
On Twitter @alz_gal
The prevalence of diagnosed diabetes in the United States rose significantly from 1988 to 2010, jumping from 6% to 10%.
Prediabetes doubled in prevalence over the same time period, from 6% to 12%, Elizabeth Selvin, Ph.D., and her colleagues reported in the April 14 issue of the Annals of Internal Medicine (2014 [doi=10.7326/M13-2411]).
But while the prevalence of confirmed cases increased sharply, the prevalence of undiagnosed diabetes actually decreased slightly over the same time – meaning that almost all cases of diabetes in the United States are now being identified, wrote Dr. Selvin of Johns Hopkins University, Baltimore, and her coinvestigators. "At present, approximately 89% of all diabetes cases are diagnosed," the team wrote. "Furthermore, glycemic control among persons with diagnosed diabetes has improved, probably reflecting a combination of improvements in diagnosis, screening, and care."
The researchers mined their data from two epochs of the National Health and Nutrition Examination Survey (1988-1994 and 1999-2010), comprising a total of almost 43,500 people. They assessed diabetes and prediabetes prevalence by both fasting plasma glucose and hemoglobin A1c (HbA1c) levels. They also looked at glucose control parameters and medication type in diagnosed patients. To investigate any association between diabetes and weight, they evaluated body mass index in the survey populations.
The mean prevalence of obesity in U.S. adults without diabetes jumped from 21% in the first epoch to 32% in the second. The change was similar among those with diabetes. The increases in both prediabetes and diabetes tracked the jump in obesity, leading the authors to conclude that obesity was a direct cause of disease.
Overall, the mean HbA1c level rose from 5.25% in the earliest years to 5.36% in 2010 – a small but significant increase. But the level was entirely stable in a subset of young adults who had normal body weight, blood pressure, and lipid levels (5%).
The prevalence of diabetes as measured by an HbA1c of at least 6.5% increased over the two epochs, from a low of 6% in the earliest years to 10% by the latest. The prevalence of prediabetes doubled (from 6% to 12%). "When applied to the 2010 U.S. Census, the total number of adults aged 20 [years] or older with total confirmed diabetes was 20.6 million," the authors wrote.
When the team used HbA1c levels to identify undiagnosed cases, they determined that 16% of cases in the earlier epoch were undiagnosed, compared with 11% in the later years – meaning that by 2010, 89% of U.S. cases were being identified.
As measured by an HbA1c of less than 7%, glycemic control improved from 51% to 59% over the study period. Among those who reported that they were taking diabetes medications, control increased from 40% to 55%.
Blacks and Hispanics shouldered a larger disease burden than did whites, the researchers wrote. "The prevalence ... in blacks was nearly double the prevalence in whites (15% vs. almost 9%). Mexican-Americans also had a greater prevalence of diabetes than whites (15.4% vs. 8.6%). Both ethnic minority groups had a greater prevalence of undiagnosed diabetes."
Control was also poorer, they said: Only 52% of blacks and 43% of Mexican-Americans had a calibrated HbA1c level less than 7%, compared with 57% of whites.
"The substantially greater prevalence of diabetes and prediabetes and poor rates of glycemic control (even among persons with medication-treated diabetes) in ethnic minority populations ... is particularly concerning because blacks and Mexican-Americans are also at greater risk for complications of diabetes, particularly retinopathy and kidney disease," the team noted.
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Neither Dr. Selvin nor any of her coauthors had any financial declarations.
On Twitter @alz_gal
FROM THE ANNALS OF INTERNAL MEDICINE
Major finding: The prevalence of diagnosed diabetes in the United States rose significantly, from 6%-10% from 1988-2010.
Data source: The findings were extracted from national data collected from 1988-2010.
Disclosures: Neither Dr. Selvin not her coauthors had any financial declarations.

Short CAM-S delirium scale predicted clinical outcomes
A new delirium scoring system has shown excellent correlation with clinical outcomes in hospitalized elderly patients, including length of stay, functional decline, and death, investigators report.
In both short and long form, the Confusion Assessment Methods-S (CAM-S) is designed to complement the existing CAM, Dr. Sharon Inouye and her colleagues reported in the April 14 issue of Annals of Internal Medicine (2014;160:526-33).
"The short form (5-minute completion and scoring time), which is based on the CAM diagnostic algorithm alone, is quicker and simpler to rate; however, the long form (10-minute completion and scoring time) provides a broader range of severity scores in delirium and no-delirium groups," wrote Dr. Inouye of the Institute for Aging Research, Boston, and her coauthors.
"Unlike the Delirium Rating Scale, a clinician rater is not required for the CAM-S. Instead, well-trained research assistants can reliably conduct the assessments," the researchers wrote.
Both the short-form and long-form CAM-S instruments were validated in a group of 919 patients aged 70 years or older, who were scheduled for major surgery. The cohort was drawn from two extant study groups: the ongoing SAGES (Successful Aging After Elective Surgery) study,and Project Recovery, which ran from 1995 to 1998. Delirium was first rated by the existing CAM, and then according to the two versions of CAM-S.
The short-form CAM-S rates patients on four features of the CAM: symptom fluctuation, inattention, disorganized thinking, and altered level of consciousness. The most severe score is a 7. The longer form is based on 10 features, which also include disorientation, memory impairment, perceptual disturbances, psychomotor agitation, and sleep-wake cycle disturbance. The most severe score is a 19.
The measures had excellent correlation with each other, and with several clinical outcomes, the investigators said.
Length of hospital stay increased with increasing delirium severity across both forms, with an adjusted mean stay of 6.5 days for no delirium to almost 13 days with high severity in the short form. In the long form, length of stay increased from about 6 days to 12 days.
Hospital costs also tracked severity, ranging from an adjusted mean of $5,100 for no delirium to $13,200 for severe delirium in the short form. A similar pattern emerged in the long form, ranging from $4,200 to $11,400.
Functional decline was also highly correlated with score. On the short form, it occurred in 36%-68% of patients, depending on severity. In the long form, the range was 25%-61%. Cognitive decline showed a similar pattern.
In the short form, the cumulative adjusted rates of death within 90 days ranged from 7% to 27%, depending on severity. In the long form, the range was 7%-22%.
In the composite outcome of death or nursing home placement, results on the short form ranged from 15% to 51%, depending on severity. In the long form, the range was 13%-48%
While the Project Recovery data are more than 16 years old, the researchers said that this time lapse is not an issue because their primary interest is in comparison of outcomes among severity groups, which minimizes the importance of the internal values.
Also, "there may be inherent dependencies between CAM-S score and adverse outcomes," investigators wrote. "For example, patients with longer lengths of stay may have had higher CAM-S scores because of more opportunities for measurement."
The CAM-S score requires validation in groups younger than the age 70-plus patients addressed in the current study, researchers noted.
The National Institute on Aging funded the study. None of the authors reported having any financial declarations.
On Twitter @alz_gal
A new delirium scoring system has shown excellent correlation with clinical outcomes in hospitalized elderly patients, including length of stay, functional decline, and death, investigators report.
In both short and long form, the Confusion Assessment Methods-S (CAM-S) is designed to complement the existing CAM, Dr. Sharon Inouye and her colleagues reported in the April 14 issue of Annals of Internal Medicine (2014;160:526-33).
"The short form (5-minute completion and scoring time), which is based on the CAM diagnostic algorithm alone, is quicker and simpler to rate; however, the long form (10-minute completion and scoring time) provides a broader range of severity scores in delirium and no-delirium groups," wrote Dr. Inouye of the Institute for Aging Research, Boston, and her coauthors.
"Unlike the Delirium Rating Scale, a clinician rater is not required for the CAM-S. Instead, well-trained research assistants can reliably conduct the assessments," the researchers wrote.
Both the short-form and long-form CAM-S instruments were validated in a group of 919 patients aged 70 years or older, who were scheduled for major surgery. The cohort was drawn from two extant study groups: the ongoing SAGES (Successful Aging After Elective Surgery) study,and Project Recovery, which ran from 1995 to 1998. Delirium was first rated by the existing CAM, and then according to the two versions of CAM-S.
The short-form CAM-S rates patients on four features of the CAM: symptom fluctuation, inattention, disorganized thinking, and altered level of consciousness. The most severe score is a 7. The longer form is based on 10 features, which also include disorientation, memory impairment, perceptual disturbances, psychomotor agitation, and sleep-wake cycle disturbance. The most severe score is a 19.
The measures had excellent correlation with each other, and with several clinical outcomes, the investigators said.
Length of hospital stay increased with increasing delirium severity across both forms, with an adjusted mean stay of 6.5 days for no delirium to almost 13 days with high severity in the short form. In the long form, length of stay increased from about 6 days to 12 days.
Hospital costs also tracked severity, ranging from an adjusted mean of $5,100 for no delirium to $13,200 for severe delirium in the short form. A similar pattern emerged in the long form, ranging from $4,200 to $11,400.
Functional decline was also highly correlated with score. On the short form, it occurred in 36%-68% of patients, depending on severity. In the long form, the range was 25%-61%. Cognitive decline showed a similar pattern.
In the short form, the cumulative adjusted rates of death within 90 days ranged from 7% to 27%, depending on severity. In the long form, the range was 7%-22%.
In the composite outcome of death or nursing home placement, results on the short form ranged from 15% to 51%, depending on severity. In the long form, the range was 13%-48%
While the Project Recovery data are more than 16 years old, the researchers said that this time lapse is not an issue because their primary interest is in comparison of outcomes among severity groups, which minimizes the importance of the internal values.
Also, "there may be inherent dependencies between CAM-S score and adverse outcomes," investigators wrote. "For example, patients with longer lengths of stay may have had higher CAM-S scores because of more opportunities for measurement."
The CAM-S score requires validation in groups younger than the age 70-plus patients addressed in the current study, researchers noted.
The National Institute on Aging funded the study. None of the authors reported having any financial declarations.
On Twitter @alz_gal
A new delirium scoring system has shown excellent correlation with clinical outcomes in hospitalized elderly patients, including length of stay, functional decline, and death, investigators report.
In both short and long form, the Confusion Assessment Methods-S (CAM-S) is designed to complement the existing CAM, Dr. Sharon Inouye and her colleagues reported in the April 14 issue of Annals of Internal Medicine (2014;160:526-33).
"The short form (5-minute completion and scoring time), which is based on the CAM diagnostic algorithm alone, is quicker and simpler to rate; however, the long form (10-minute completion and scoring time) provides a broader range of severity scores in delirium and no-delirium groups," wrote Dr. Inouye of the Institute for Aging Research, Boston, and her coauthors.
"Unlike the Delirium Rating Scale, a clinician rater is not required for the CAM-S. Instead, well-trained research assistants can reliably conduct the assessments," the researchers wrote.
Both the short-form and long-form CAM-S instruments were validated in a group of 919 patients aged 70 years or older, who were scheduled for major surgery. The cohort was drawn from two extant study groups: the ongoing SAGES (Successful Aging After Elective Surgery) study,and Project Recovery, which ran from 1995 to 1998. Delirium was first rated by the existing CAM, and then according to the two versions of CAM-S.
The short-form CAM-S rates patients on four features of the CAM: symptom fluctuation, inattention, disorganized thinking, and altered level of consciousness. The most severe score is a 7. The longer form is based on 10 features, which also include disorientation, memory impairment, perceptual disturbances, psychomotor agitation, and sleep-wake cycle disturbance. The most severe score is a 19.
The measures had excellent correlation with each other, and with several clinical outcomes, the investigators said.
Length of hospital stay increased with increasing delirium severity across both forms, with an adjusted mean stay of 6.5 days for no delirium to almost 13 days with high severity in the short form. In the long form, length of stay increased from about 6 days to 12 days.
Hospital costs also tracked severity, ranging from an adjusted mean of $5,100 for no delirium to $13,200 for severe delirium in the short form. A similar pattern emerged in the long form, ranging from $4,200 to $11,400.
Functional decline was also highly correlated with score. On the short form, it occurred in 36%-68% of patients, depending on severity. In the long form, the range was 25%-61%. Cognitive decline showed a similar pattern.
In the short form, the cumulative adjusted rates of death within 90 days ranged from 7% to 27%, depending on severity. In the long form, the range was 7%-22%.
In the composite outcome of death or nursing home placement, results on the short form ranged from 15% to 51%, depending on severity. In the long form, the range was 13%-48%
While the Project Recovery data are more than 16 years old, the researchers said that this time lapse is not an issue because their primary interest is in comparison of outcomes among severity groups, which minimizes the importance of the internal values.
Also, "there may be inherent dependencies between CAM-S score and adverse outcomes," investigators wrote. "For example, patients with longer lengths of stay may have had higher CAM-S scores because of more opportunities for measurement."
The CAM-S score requires validation in groups younger than the age 70-plus patients addressed in the current study, researchers noted.
The National Institute on Aging funded the study. None of the authors reported having any financial declarations.
On Twitter @alz_gal
FROM ANNALS OF INTERNAL MEDICINE
Major finding: Two versions of the CAM-S delirium scale were predictive of major clinical outcomes in the elderly, including death within 30 days of surgery (7%-27%, depending on severity scores).
Data source: CAM-S was validated in a group of 919 patients.
Disclosures: The National Institute on Aging funded the study. Neither Dr. Inouye nor any of the coauthors had any financial disclosures.
Monoclonal antibody pinpoints BRAF status in melanoma
DENVER - A murine monoclonal antibody had very high sensitivity and specificity for melanomas with the V600E BRAF mutation, and exhibited perfect concordance between the primary and metastatic tumors in individual patients.
In addition to being a valuable screening tool, VE1 (anti-BRAF V600E) could be an extremely useful adjunct to DNA analysis, Michelle Vernali said at the annual meeting of the American Academy of Dermatology.
"I think that the sequential use of immunohistochemistry and molecular analysis will dramatically improve sensitivity and specificity for the detection of BRAF mutations, which is essential for the effective use of BRAF inhibitors," said Ms. Vernali, a fourth-year medical student at the University of North Carolina, Chapel Hill.

According to Roche Diagnostics, the VE1 antibody has demonstrated 100% sensitivity and 99% specificity for BRAF mutations in colon cancer. In addition, it has shown high efficacy in detecting those mutations in thyroid cancer and hairy cell leukemia, and "shows promise" in non–small cell lung cancer and serous ovarian tumors.
According to the company, "The ... antibody has also been said to be a promising tool for patient stratification among individuals presenting with brain metastases."
Ms. Vernali and her colleagues examined the benefit of VE1 staining in 93 patients with metastatic melanoma. Of these, 76 had DNA pyrosequencing of either the primary (19) or metastatic lesion (57). Both primary and metastatic tumor samples were available for 17 patients.
Of the 76 patients with either primary or metastatic lesion samples, DNA pyrosequencing identified 26 that were positive for V600E and 40 that were negative. VE1 staining identified 22 positive samples and 44 negative samples, for a specificity of 100% and a sensitivity of 85%.
Sequencing also identified eight samples positive for V600K, and one each for V600R and V600Q. VE1 did not stain any of these samples.
Among the 17 patients with both primary and metastatic samples, VE1 was in 100% concordance with DNA sequencing, identifying three positive samples and 14 negative samples.
"There was little variability of strength or intensity of the staining, and very little intra-interpreter variance," Ms. Vernali said.
She proposed an algorithm for BRAF testing using VE1 with and without DNA sequencing.
· Insufficient tissue for initial DNA pyrosequencing:
– Stain with VE1.
– Identify BRAF V600E-positive or -negative patients.
· Sufficient tissue for DNA pyrosequencing:
– Stain with VE1.
– Stratify as VE1 positive or negative.
– If VE1 positive, conclude the patient is BRAF V600E positive.
– If VE1 negative, send sample for molecular sequencing to stratify into V600E positive, positive for another BRAF mutation, or BRAF negative.
This algorithm would identify V600E status in patients with tissue samples that would otherwise be insufficient for BRAF testing, she said. "If they had insufficient tissue for DNA sequencing, they could be stratified by immunohistochemistry and if positive, could be treated. Otherwise this is a population that now goes without BRAF-inhibiting therapy."
The algorithm is being tested in some sites already, she added, but needs additional validation before it can be broadly adopted.
Ms. Vernali had no financial disclosures.
DENVER - A murine monoclonal antibody had very high sensitivity and specificity for melanomas with the V600E BRAF mutation, and exhibited perfect concordance between the primary and metastatic tumors in individual patients.
In addition to being a valuable screening tool, VE1 (anti-BRAF V600E) could be an extremely useful adjunct to DNA analysis, Michelle Vernali said at the annual meeting of the American Academy of Dermatology.
"I think that the sequential use of immunohistochemistry and molecular analysis will dramatically improve sensitivity and specificity for the detection of BRAF mutations, which is essential for the effective use of BRAF inhibitors," said Ms. Vernali, a fourth-year medical student at the University of North Carolina, Chapel Hill.
According to Roche Diagnostics, the VE1 antibody has demonstrated 100% sensitivity and 99% specificity for BRAF mutations in colon cancer. In addition, it has shown high efficacy in detecting those mutations in thyroid cancer and hairy cell leukemia, and "shows promise" in non–small cell lung cancer and serous ovarian tumors.
According to the company, "The ... antibody has also been said to be a promising tool for patient stratification among individuals presenting with brain metastases."
Ms. Vernali and her colleagues examined the benefit of VE1 staining in 93 patients with metastatic melanoma. Of these, 76 had DNA pyrosequencing of either the primary (19) or metastatic lesion (57). Both primary and metastatic tumor samples were available for 17 patients.
Of the 76 patients with either primary or metastatic lesion samples, DNA pyrosequencing identified 26 that were positive for V600E and 40 that were negative. VE1 staining identified 22 positive samples and 44 negative samples, for a specificity of 100% and a sensitivity of 85%.
Sequencing also identified eight samples positive for V600K, and one each for V600R and V600Q. VE1 did not stain any of these samples.
Among the 17 patients with both primary and metastatic samples, VE1 was in 100% concordance with DNA sequencing, identifying three positive samples and 14 negative samples.
"There was little variability of strength or intensity of the staining, and very little intra-interpreter variance," Ms. Vernali said.
She proposed an algorithm for BRAF testing using VE1 with and without DNA sequencing.
· Insufficient tissue for initial DNA pyrosequencing:
– Stain with VE1.
– Identify BRAF V600E-positive or -negative patients.
· Sufficient tissue for DNA pyrosequencing:
– Stain with VE1.
– Stratify as VE1 positive or negative.
– If VE1 positive, conclude the patient is BRAF V600E positive.
– If VE1 negative, send sample for molecular sequencing to stratify into V600E positive, positive for another BRAF mutation, or BRAF negative.
This algorithm would identify V600E status in patients with tissue samples that would otherwise be insufficient for BRAF testing, she said. "If they had insufficient tissue for DNA sequencing, they could be stratified by immunohistochemistry and if positive, could be treated. Otherwise this is a population that now goes without BRAF-inhibiting therapy."
The algorithm is being tested in some sites already, she added, but needs additional validation before it can be broadly adopted.
Ms. Vernali had no financial disclosures.
DENVER - A murine monoclonal antibody had very high sensitivity and specificity for melanomas with the V600E BRAF mutation, and exhibited perfect concordance between the primary and metastatic tumors in individual patients.
In addition to being a valuable screening tool, VE1 (anti-BRAF V600E) could be an extremely useful adjunct to DNA analysis, Michelle Vernali said at the annual meeting of the American Academy of Dermatology.
"I think that the sequential use of immunohistochemistry and molecular analysis will dramatically improve sensitivity and specificity for the detection of BRAF mutations, which is essential for the effective use of BRAF inhibitors," said Ms. Vernali, a fourth-year medical student at the University of North Carolina, Chapel Hill.
According to Roche Diagnostics, the VE1 antibody has demonstrated 100% sensitivity and 99% specificity for BRAF mutations in colon cancer. In addition, it has shown high efficacy in detecting those mutations in thyroid cancer and hairy cell leukemia, and "shows promise" in non–small cell lung cancer and serous ovarian tumors.
According to the company, "The ... antibody has also been said to be a promising tool for patient stratification among individuals presenting with brain metastases."
Ms. Vernali and her colleagues examined the benefit of VE1 staining in 93 patients with metastatic melanoma. Of these, 76 had DNA pyrosequencing of either the primary (19) or metastatic lesion (57). Both primary and metastatic tumor samples were available for 17 patients.
Of the 76 patients with either primary or metastatic lesion samples, DNA pyrosequencing identified 26 that were positive for V600E and 40 that were negative. VE1 staining identified 22 positive samples and 44 negative samples, for a specificity of 100% and a sensitivity of 85%.
Sequencing also identified eight samples positive for V600K, and one each for V600R and V600Q. VE1 did not stain any of these samples.
Among the 17 patients with both primary and metastatic samples, VE1 was in 100% concordance with DNA sequencing, identifying three positive samples and 14 negative samples.
"There was little variability of strength or intensity of the staining, and very little intra-interpreter variance," Ms. Vernali said.
She proposed an algorithm for BRAF testing using VE1 with and without DNA sequencing.
· Insufficient tissue for initial DNA pyrosequencing:
– Stain with VE1.
– Identify BRAF V600E-positive or -negative patients.
· Sufficient tissue for DNA pyrosequencing:
– Stain with VE1.
– Stratify as VE1 positive or negative.
– If VE1 positive, conclude the patient is BRAF V600E positive.
– If VE1 negative, send sample for molecular sequencing to stratify into V600E positive, positive for another BRAF mutation, or BRAF negative.
This algorithm would identify V600E status in patients with tissue samples that would otherwise be insufficient for BRAF testing, she said. "If they had insufficient tissue for DNA sequencing, they could be stratified by immunohistochemistry and if positive, could be treated. Otherwise this is a population that now goes without BRAF-inhibiting therapy."
The algorithm is being tested in some sites already, she added, but needs additional validation before it can be broadly adopted.
Ms. Vernali had no financial disclosures.
AT THE AAD ANNUAL MEETING
Major finding: A monoclonal antibody showed 100% specificity and 85% sensitivity for identifying V600E BRAF mutations in metastatic melanoma.
Data source: The prospective study comprised 93 patients.
Disclosures: Ms. Vernali had no financial disclosures.

Try Tackling Cysts or Lipomas With Punch Tool Instead of Scalpel
DENVER – A little lidocaine and a punch biopsy tool allow physicians to tackle most cysts and lipomas in the office, providing effective treatment without interrupting patient flow.
The punch technique easily eliminates the contents of these annoying, sometimes painful, lesions, Dr. Robert T. Brodell said at the annual meeting of the American Academy of Dermatology. But more importantly, it allows the complete removal of the cyst wall, which is key to preventing recurrence, he said.
Despite dogma, it’s not really necessary deliver the entire cyst unbroken, a technique that requires a much larger incision, explained Dr Brodell, professor and chairman of dermatology and a professor of pathology at the University of Mississippi Medical Center, Jackson.

"When I was training, it was common for surgeons to excise cysts and hold them up ... to demonstrate that the entire cyst had been removed intact," he said. "But it doesn’t really matter if it is removed this way. What does matter is that the entire wall is removed. If you don’t, the remainder will keep making keratin and set up a foreign body reaction," or set the stage for cyst recurrence.
Pilar cysts and multiple painful lipomas on the forearms or legs seem to be the easiest to remove this way, Dr. Brodell said in an interview. Lesions on the back where the skin is quite thick are more difficult. But his early study on the technique found a recurrence rate of only 14% in these more difficult areas and an overall recurrence rate of 8% for all cysts.
Dr. Brodell’s preferred technique starts with an intradermal injection of 1% lidocaine plus epinephrine, enough to raise and blanch the overlying skin. "You don’t need any deep anesthesia," he said. "This seems to be enough to take care of the innervation of these structures."
A punch appropriate to the cyst size – usually 4-6 mm – is used to incise the lesion. A forceps is used to free the wall from the surrounding dermis. Dr. Brodell then manually expresses the contents with lateral finger pressure. Portions of the cyst wall will also be extruded. Looking through the punch excision defect, any remaining fragments of cyst wall are removed.
It most cases, it takes only a stitch or two to close the small wound.
Lipomas are slightly more complicated. After incising the lesion, Dr. Brodell again applies lateral pressure, and the contents will start to deliver. "If you grab the lipoma with forceps, a portion of the lipoma is incised and removed. Then more fat can be delivered through the punch incision hole and removed. The process continues until the entire contents are removed. "If I’m not getting all of it out, I’m getting at least 90%-95%, which seems to minimize the chance for recurrence," Dr. Brodell said.
He said that he finishes by making a bolster with gauze to place over the wound and wrapping it with a pressure bandage. This strategy prevents a hematoma from developing in the potential space where the lipoma was removed.
The technique also is appropriate for infected cysts, Dr. Brodell said, and in such cases it is accompanied by a standard course of systemic antibiotics.
"For most cysts, and for lipomas smaller than 2 cm, the process takes less than 5 minutes," Dr. Brodell said. "For a really big lipoma, maybe 15 minutes."
Punch excision carries benefits for both the provider and the patient. "You can do it in the office, without interrupting patient flow," said Dr. Brodell. "In some cases it saves the patient a trip to the surgery center. In this case it is certainly less expensive."
The charge is calculated according to lesion size, typically ranging from $130 to $350. "A trip to the surgery center is going to be at least $1,200," Dr. Brodell added.
Dr. Brodell began performing this procedure in the late 1980s. In 2002, he published a retrospective review of 299 patients who had undergone pilar or keratinous cyst removal via punch technique and who had complete follow-up data (Dermatol. Surg. 2002;28:673-7). Follow-up averaged 80 weeks.
Most of the patients (267) reported no recurrence. The recurrence rate was 9% for keratinous cysts, 5% for pilar cysts, and 8% overall. Recurrence was higher among back and ear lobe cysts (14% and 13%, respectively).
Most cysts (54%) recurred within 1 year of surgery; 24% recurred 1-2 years later.
Given the ease and convenience of this technique, and the excellent clinical results, Dr. Brodell encouraged physicians to reconsider their anti-cyst weaponry – and try putting down the scalpels and reaching for a punch.
Dr. Brodell had no financial disclosures relevant to this presentation.
On Twitter @alz_gal
DENVER – A little lidocaine and a punch biopsy tool allow physicians to tackle most cysts and lipomas in the office, providing effective treatment without interrupting patient flow.
The punch technique easily eliminates the contents of these annoying, sometimes painful, lesions, Dr. Robert T. Brodell said at the annual meeting of the American Academy of Dermatology. But more importantly, it allows the complete removal of the cyst wall, which is key to preventing recurrence, he said.
Despite dogma, it’s not really necessary deliver the entire cyst unbroken, a technique that requires a much larger incision, explained Dr Brodell, professor and chairman of dermatology and a professor of pathology at the University of Mississippi Medical Center, Jackson.
"When I was training, it was common for surgeons to excise cysts and hold them up ... to demonstrate that the entire cyst had been removed intact," he said. "But it doesn’t really matter if it is removed this way. What does matter is that the entire wall is removed. If you don’t, the remainder will keep making keratin and set up a foreign body reaction," or set the stage for cyst recurrence.
Pilar cysts and multiple painful lipomas on the forearms or legs seem to be the easiest to remove this way, Dr. Brodell said in an interview. Lesions on the back where the skin is quite thick are more difficult. But his early study on the technique found a recurrence rate of only 14% in these more difficult areas and an overall recurrence rate of 8% for all cysts.
Dr. Brodell’s preferred technique starts with an intradermal injection of 1% lidocaine plus epinephrine, enough to raise and blanch the overlying skin. "You don’t need any deep anesthesia," he said. "This seems to be enough to take care of the innervation of these structures."
A punch appropriate to the cyst size – usually 4-6 mm – is used to incise the lesion. A forceps is used to free the wall from the surrounding dermis. Dr. Brodell then manually expresses the contents with lateral finger pressure. Portions of the cyst wall will also be extruded. Looking through the punch excision defect, any remaining fragments of cyst wall are removed.
It most cases, it takes only a stitch or two to close the small wound.
Lipomas are slightly more complicated. After incising the lesion, Dr. Brodell again applies lateral pressure, and the contents will start to deliver. "If you grab the lipoma with forceps, a portion of the lipoma is incised and removed. Then more fat can be delivered through the punch incision hole and removed. The process continues until the entire contents are removed. "If I’m not getting all of it out, I’m getting at least 90%-95%, which seems to minimize the chance for recurrence," Dr. Brodell said.
He said that he finishes by making a bolster with gauze to place over the wound and wrapping it with a pressure bandage. This strategy prevents a hematoma from developing in the potential space where the lipoma was removed.
The technique also is appropriate for infected cysts, Dr. Brodell said, and in such cases it is accompanied by a standard course of systemic antibiotics.
"For most cysts, and for lipomas smaller than 2 cm, the process takes less than 5 minutes," Dr. Brodell said. "For a really big lipoma, maybe 15 minutes."
Punch excision carries benefits for both the provider and the patient. "You can do it in the office, without interrupting patient flow," said Dr. Brodell. "In some cases it saves the patient a trip to the surgery center. In this case it is certainly less expensive."
The charge is calculated according to lesion size, typically ranging from $130 to $350. "A trip to the surgery center is going to be at least $1,200," Dr. Brodell added.
Dr. Brodell began performing this procedure in the late 1980s. In 2002, he published a retrospective review of 299 patients who had undergone pilar or keratinous cyst removal via punch technique and who had complete follow-up data (Dermatol. Surg. 2002;28:673-7). Follow-up averaged 80 weeks.
Most of the patients (267) reported no recurrence. The recurrence rate was 9% for keratinous cysts, 5% for pilar cysts, and 8% overall. Recurrence was higher among back and ear lobe cysts (14% and 13%, respectively).
Most cysts (54%) recurred within 1 year of surgery; 24% recurred 1-2 years later.
Given the ease and convenience of this technique, and the excellent clinical results, Dr. Brodell encouraged physicians to reconsider their anti-cyst weaponry – and try putting down the scalpels and reaching for a punch.
Dr. Brodell had no financial disclosures relevant to this presentation.
On Twitter @alz_gal
DENVER – A little lidocaine and a punch biopsy tool allow physicians to tackle most cysts and lipomas in the office, providing effective treatment without interrupting patient flow.
The punch technique easily eliminates the contents of these annoying, sometimes painful, lesions, Dr. Robert T. Brodell said at the annual meeting of the American Academy of Dermatology. But more importantly, it allows the complete removal of the cyst wall, which is key to preventing recurrence, he said.
Despite dogma, it’s not really necessary deliver the entire cyst unbroken, a technique that requires a much larger incision, explained Dr Brodell, professor and chairman of dermatology and a professor of pathology at the University of Mississippi Medical Center, Jackson.
"When I was training, it was common for surgeons to excise cysts and hold them up ... to demonstrate that the entire cyst had been removed intact," he said. "But it doesn’t really matter if it is removed this way. What does matter is that the entire wall is removed. If you don’t, the remainder will keep making keratin and set up a foreign body reaction," or set the stage for cyst recurrence.
Pilar cysts and multiple painful lipomas on the forearms or legs seem to be the easiest to remove this way, Dr. Brodell said in an interview. Lesions on the back where the skin is quite thick are more difficult. But his early study on the technique found a recurrence rate of only 14% in these more difficult areas and an overall recurrence rate of 8% for all cysts.
Dr. Brodell’s preferred technique starts with an intradermal injection of 1% lidocaine plus epinephrine, enough to raise and blanch the overlying skin. "You don’t need any deep anesthesia," he said. "This seems to be enough to take care of the innervation of these structures."
A punch appropriate to the cyst size – usually 4-6 mm – is used to incise the lesion. A forceps is used to free the wall from the surrounding dermis. Dr. Brodell then manually expresses the contents with lateral finger pressure. Portions of the cyst wall will also be extruded. Looking through the punch excision defect, any remaining fragments of cyst wall are removed.
It most cases, it takes only a stitch or two to close the small wound.
Lipomas are slightly more complicated. After incising the lesion, Dr. Brodell again applies lateral pressure, and the contents will start to deliver. "If you grab the lipoma with forceps, a portion of the lipoma is incised and removed. Then more fat can be delivered through the punch incision hole and removed. The process continues until the entire contents are removed. "If I’m not getting all of it out, I’m getting at least 90%-95%, which seems to minimize the chance for recurrence," Dr. Brodell said.
He said that he finishes by making a bolster with gauze to place over the wound and wrapping it with a pressure bandage. This strategy prevents a hematoma from developing in the potential space where the lipoma was removed.
The technique also is appropriate for infected cysts, Dr. Brodell said, and in such cases it is accompanied by a standard course of systemic antibiotics.
"For most cysts, and for lipomas smaller than 2 cm, the process takes less than 5 minutes," Dr. Brodell said. "For a really big lipoma, maybe 15 minutes."
Punch excision carries benefits for both the provider and the patient. "You can do it in the office, without interrupting patient flow," said Dr. Brodell. "In some cases it saves the patient a trip to the surgery center. In this case it is certainly less expensive."
The charge is calculated according to lesion size, typically ranging from $130 to $350. "A trip to the surgery center is going to be at least $1,200," Dr. Brodell added.
Dr. Brodell began performing this procedure in the late 1980s. In 2002, he published a retrospective review of 299 patients who had undergone pilar or keratinous cyst removal via punch technique and who had complete follow-up data (Dermatol. Surg. 2002;28:673-7). Follow-up averaged 80 weeks.
Most of the patients (267) reported no recurrence. The recurrence rate was 9% for keratinous cysts, 5% for pilar cysts, and 8% overall. Recurrence was higher among back and ear lobe cysts (14% and 13%, respectively).
Most cysts (54%) recurred within 1 year of surgery; 24% recurred 1-2 years later.
Given the ease and convenience of this technique, and the excellent clinical results, Dr. Brodell encouraged physicians to reconsider their anti-cyst weaponry – and try putting down the scalpels and reaching for a punch.
Dr. Brodell had no financial disclosures relevant to this presentation.
On Twitter @alz_gal
EXPERT ANALYSIS FROM AAD 2014

Try tackling cysts or lipomas with punch tool instead of scalpel
DENVER – A little lidocaine and a punch biopsy tool allow physicians to tackle most cysts and lipomas in the office, providing effective treatment without interrupting patient flow.
The punch technique easily eliminates the contents of these annoying, sometimes painful, lesions, Dr. Robert T. Brodell said at the annual meeting of the American Academy of Dermatology. But more importantly, it allows the complete removal of the cyst wall, which is key to preventing recurrence, he said.
Despite dogma, it’s not really necessary deliver the entire cyst unbroken, a technique that requires a much larger incision, explained Dr Brodell, professor and chairman of dermatology and a professor of pathology at the University of Mississippi Medical Center, Jackson.

"When I was training, it was common for surgeons to excise cysts and hold them up ... to demonstrate that the entire cyst had been removed intact," he said. "But it doesn’t really matter if it is removed this way. What does matter is that the entire wall is removed. If you don’t, the remainder will keep making keratin and set up a foreign body reaction," or set the stage for cyst recurrence.
Pilar cysts and multiple painful lipomas on the forearms or legs seem to be the easiest to remove this way, Dr. Brodell said in an interview. Lesions on the back where the skin is quite thick are more difficult. But his early study on the technique found a recurrence rate of only 14% in these more difficult areas and an overall recurrence rate of 8% for all cysts.
Dr. Brodell’s preferred technique starts with an intradermal injection of 1% lidocaine plus epinephrine, enough to raise and blanch the overlying skin. "You don’t need any deep anesthesia," he said. "This seems to be enough to take care of the innervation of these structures."
A punch appropriate to the cyst size – usually 4-6 mm – is used to incise the lesion. A forceps is used to free the wall from the surrounding dermis. Dr. Brodell then manually expresses the contents with lateral finger pressure. Portions of the cyst wall will also be extruded. Looking through the punch excision defect, any remaining fragments of cyst wall are removed.
It most cases, it takes only a stitch or two to close the small wound.
Lipomas are slightly more complicated. After incising the lesion, Dr. Brodell again applies lateral pressure, and the contents will start to deliver. "If you grab the lipoma with forceps, a portion of the lipoma is incised and removed. Then more fat can be delivered through the punch incision hole and removed. The process continues until the entire contents are removed. "If I’m not getting all of it out, I’m getting at least 90%-95%, which seems to minimize the chance for recurrence," Dr. Brodell said.
He said that he finishes by making a bolster with gauze to place over the wound and wrapping it with a pressure bandage. This strategy prevents a hematoma from developing in the potential space where the lipoma was removed.
The technique also is appropriate for infected cysts, Dr. Brodell said, and in such cases it is accompanied by a standard course of systemic antibiotics.
"For most cysts, and for lipomas smaller than 2 cm, the process takes less than 5 minutes," Dr. Brodell said. "For a really big lipoma, maybe 15 minutes."
Punch excision carries benefits for both the provider and the patient. "You can do it in the office, without interrupting patient flow," said Dr. Brodell. "In some cases it saves the patient a trip to the surgery center. In this case it is certainly less expensive."
The charge is calculated according to lesion size, typically ranging from $130 to $350. "A trip to the surgery center is going to be at least $1,200," Dr. Brodell added.
Dr. Brodell began performing this procedure in the late 1980s. In 2002, he published a retrospective review of 299 patients who had undergone pilar or keratinous cyst removal via punch technique and who had complete follow-up data (Dermatol. Surg. 2002;28:673-7). Follow-up averaged 80 weeks.
Most of the patients (267) reported no recurrence. The recurrence rate was 9% for keratinous cysts, 5% for pilar cysts, and 8% overall. Recurrence was higher among back and ear lobe cysts (14% and 13%, respectively).
Most cysts (54%) recurred within 1 year of surgery; 24% recurred 1-2 years later.
Given the ease and convenience of this technique, and the excellent clinical results, Dr. Brodell encouraged physicians to reconsider their anti-cyst weaponry – and try putting down the scalpels and reaching for a punch.
Dr. Brodell had no financial disclosures relevant to this presentation.
On Twitter @alz_gal
DENVER – A little lidocaine and a punch biopsy tool allow physicians to tackle most cysts and lipomas in the office, providing effective treatment without interrupting patient flow.
The punch technique easily eliminates the contents of these annoying, sometimes painful, lesions, Dr. Robert T. Brodell said at the annual meeting of the American Academy of Dermatology. But more importantly, it allows the complete removal of the cyst wall, which is key to preventing recurrence, he said.
Despite dogma, it’s not really necessary deliver the entire cyst unbroken, a technique that requires a much larger incision, explained Dr Brodell, professor and chairman of dermatology and a professor of pathology at the University of Mississippi Medical Center, Jackson.
"When I was training, it was common for surgeons to excise cysts and hold them up ... to demonstrate that the entire cyst had been removed intact," he said. "But it doesn’t really matter if it is removed this way. What does matter is that the entire wall is removed. If you don’t, the remainder will keep making keratin and set up a foreign body reaction," or set the stage for cyst recurrence.
Pilar cysts and multiple painful lipomas on the forearms or legs seem to be the easiest to remove this way, Dr. Brodell said in an interview. Lesions on the back where the skin is quite thick are more difficult. But his early study on the technique found a recurrence rate of only 14% in these more difficult areas and an overall recurrence rate of 8% for all cysts.
Dr. Brodell’s preferred technique starts with an intradermal injection of 1% lidocaine plus epinephrine, enough to raise and blanch the overlying skin. "You don’t need any deep anesthesia," he said. "This seems to be enough to take care of the innervation of these structures."
A punch appropriate to the cyst size – usually 4-6 mm – is used to incise the lesion. A forceps is used to free the wall from the surrounding dermis. Dr. Brodell then manually expresses the contents with lateral finger pressure. Portions of the cyst wall will also be extruded. Looking through the punch excision defect, any remaining fragments of cyst wall are removed.
It most cases, it takes only a stitch or two to close the small wound.
Lipomas are slightly more complicated. After incising the lesion, Dr. Brodell again applies lateral pressure, and the contents will start to deliver. "If you grab the lipoma with forceps, a portion of the lipoma is incised and removed. Then more fat can be delivered through the punch incision hole and removed. The process continues until the entire contents are removed. "If I’m not getting all of it out, I’m getting at least 90%-95%, which seems to minimize the chance for recurrence," Dr. Brodell said.
He said that he finishes by making a bolster with gauze to place over the wound and wrapping it with a pressure bandage. This strategy prevents a hematoma from developing in the potential space where the lipoma was removed.
The technique also is appropriate for infected cysts, Dr. Brodell said, and in such cases it is accompanied by a standard course of systemic antibiotics.
"For most cysts, and for lipomas smaller than 2 cm, the process takes less than 5 minutes," Dr. Brodell said. "For a really big lipoma, maybe 15 minutes."
Punch excision carries benefits for both the provider and the patient. "You can do it in the office, without interrupting patient flow," said Dr. Brodell. "In some cases it saves the patient a trip to the surgery center. In this case it is certainly less expensive."
The charge is calculated according to lesion size, typically ranging from $130 to $350. "A trip to the surgery center is going to be at least $1,200," Dr. Brodell added.
Dr. Brodell began performing this procedure in the late 1980s. In 2002, he published a retrospective review of 299 patients who had undergone pilar or keratinous cyst removal via punch technique and who had complete follow-up data (Dermatol. Surg. 2002;28:673-7). Follow-up averaged 80 weeks.
Most of the patients (267) reported no recurrence. The recurrence rate was 9% for keratinous cysts, 5% for pilar cysts, and 8% overall. Recurrence was higher among back and ear lobe cysts (14% and 13%, respectively).
Most cysts (54%) recurred within 1 year of surgery; 24% recurred 1-2 years later.
Given the ease and convenience of this technique, and the excellent clinical results, Dr. Brodell encouraged physicians to reconsider their anti-cyst weaponry – and try putting down the scalpels and reaching for a punch.
Dr. Brodell had no financial disclosures relevant to this presentation.
On Twitter @alz_gal
DENVER – A little lidocaine and a punch biopsy tool allow physicians to tackle most cysts and lipomas in the office, providing effective treatment without interrupting patient flow.
The punch technique easily eliminates the contents of these annoying, sometimes painful, lesions, Dr. Robert T. Brodell said at the annual meeting of the American Academy of Dermatology. But more importantly, it allows the complete removal of the cyst wall, which is key to preventing recurrence, he said.
Despite dogma, it’s not really necessary deliver the entire cyst unbroken, a technique that requires a much larger incision, explained Dr Brodell, professor and chairman of dermatology and a professor of pathology at the University of Mississippi Medical Center, Jackson.
"When I was training, it was common for surgeons to excise cysts and hold them up ... to demonstrate that the entire cyst had been removed intact," he said. "But it doesn’t really matter if it is removed this way. What does matter is that the entire wall is removed. If you don’t, the remainder will keep making keratin and set up a foreign body reaction," or set the stage for cyst recurrence.
Pilar cysts and multiple painful lipomas on the forearms or legs seem to be the easiest to remove this way, Dr. Brodell said in an interview. Lesions on the back where the skin is quite thick are more difficult. But his early study on the technique found a recurrence rate of only 14% in these more difficult areas and an overall recurrence rate of 8% for all cysts.
Dr. Brodell’s preferred technique starts with an intradermal injection of 1% lidocaine plus epinephrine, enough to raise and blanch the overlying skin. "You don’t need any deep anesthesia," he said. "This seems to be enough to take care of the innervation of these structures."
A punch appropriate to the cyst size – usually 4-6 mm – is used to incise the lesion. A forceps is used to free the wall from the surrounding dermis. Dr. Brodell then manually expresses the contents with lateral finger pressure. Portions of the cyst wall will also be extruded. Looking through the punch excision defect, any remaining fragments of cyst wall are removed.
It most cases, it takes only a stitch or two to close the small wound.
Lipomas are slightly more complicated. After incising the lesion, Dr. Brodell again applies lateral pressure, and the contents will start to deliver. "If you grab the lipoma with forceps, a portion of the lipoma is incised and removed. Then more fat can be delivered through the punch incision hole and removed. The process continues until the entire contents are removed. "If I’m not getting all of it out, I’m getting at least 90%-95%, which seems to minimize the chance for recurrence," Dr. Brodell said.
He said that he finishes by making a bolster with gauze to place over the wound and wrapping it with a pressure bandage. This strategy prevents a hematoma from developing in the potential space where the lipoma was removed.
The technique also is appropriate for infected cysts, Dr. Brodell said, and in such cases it is accompanied by a standard course of systemic antibiotics.
"For most cysts, and for lipomas smaller than 2 cm, the process takes less than 5 minutes," Dr. Brodell said. "For a really big lipoma, maybe 15 minutes."
Punch excision carries benefits for both the provider and the patient. "You can do it in the office, without interrupting patient flow," said Dr. Brodell. "In some cases it saves the patient a trip to the surgery center. In this case it is certainly less expensive."
The charge is calculated according to lesion size, typically ranging from $130 to $350. "A trip to the surgery center is going to be at least $1,200," Dr. Brodell added.
Dr. Brodell began performing this procedure in the late 1980s. In 2002, he published a retrospective review of 299 patients who had undergone pilar or keratinous cyst removal via punch technique and who had complete follow-up data (Dermatol. Surg. 2002;28:673-7). Follow-up averaged 80 weeks.
Most of the patients (267) reported no recurrence. The recurrence rate was 9% for keratinous cysts, 5% for pilar cysts, and 8% overall. Recurrence was higher among back and ear lobe cysts (14% and 13%, respectively).
Most cysts (54%) recurred within 1 year of surgery; 24% recurred 1-2 years later.
Given the ease and convenience of this technique, and the excellent clinical results, Dr. Brodell encouraged physicians to reconsider their anti-cyst weaponry – and try putting down the scalpels and reaching for a punch.
Dr. Brodell had no financial disclosures relevant to this presentation.
On Twitter @alz_gal
EXPERT ANALYSIS FROM AAD 2014

Many late-life hospitalizations and ED visits could be avoidable
WASHINGTON – During the last year of life for community-dwelling elders, up to three-fourths of hospital visits might have been avoidable.
Nursing home residents also were susceptible to potentially unnecessary admissions, with about 50% experiencing at least one avoidable visit during the final months, Dr. Zhanlian Feng said at a briefing to unveil the April special issue of Health Affairs, "The Long Reach of Alzheimer’s Disease."
Dementia was a significant contributor to hospital and emergency department use: Those with dementia were 74% more likely to have a potentially avoidable hospitalization and 51% more likely to have had a potentially avoidable ED visit.
The researchers did not speculate on what care might have been more appropriate for these patients, said Dr. Feng, a senior research public health analyst in the Aging, Disability, and Long-Term Care program at RTI International, Waltham, Mass. It does, however, suggest a very high level of caregiver anxiety about dealing with a loved one’s acute health issues.
"It’s much more challenging to provide care and support for someone who is living at home," he said in an interview. "Whenever their loved one gets worse, the caregiver is worried about how to respond to the new crisis. Often they believe their only option is the emergency department."
At-home care "is probably a big driver of hospital utilization," among the elderly, and one to which policy makers may be blind, he said in an interview.
"There are many initiatives designed to reduce hospitalizations among the elderly, but they focus almost exclusively on nursing homes, and don’t target people with dementia in particular. In the community setting, there is very little discussion on how to accomplish this."
At the briefing, Dr. Feng discussed his study, which was published April 7 in Health Affairs (Health Aff. 2014;33:683-90). It looked at hospitalization and emergency department use among more than 12,000 Medicare beneficiaries who were included in the Health and Retirement Study during 2000-2008. The study included four outcomes: 5-year hospital/ED utilization among elders with and without dementia, and hospital/ED utilization among both groups within the last year of life.
Potentially avoidable conditions were considered to be those that could have been effectively dealt with in the patients’ out-of-hospital care setting with community-based resources or within a long-term care or nursing home facility.
Some of these problems included heart failure and chronic obstructive pulmonary disease, blood pressure complications, hyper- and hypoglycemia, diabetes, dehydration or diarrhea, electrolyte imbalances, constipation or fecal impaction, urinary and respiratory tract infections (including some pneumonias), and skin ulcers. Problems relating to malnutrition and asthma also were included.
There were some differences among these groups, however. "For example, acute, severe diarrhea due to gastroenteritis or food poisoning can often be managed in nursing homes without hospitalization, but patients with the same condition in the community may require hospitalization."
ED visits that resulted in admission weren’t included because the authors assumed that those represented unavoidable admissions. They conducted a multivariate analysis that controlled for age, gender, race/ethnicity, income, education, marital status, other insurance, chronic health problems, self-reported health, and the ability to perform activities of daily living.
Dementia was significantly more common among nursing home residents than among community residents (84% vs. 12%). Almost half (44%) of those who died had dementia in the last year of life.
Dr. Feng said that more than a quarter of community-dwelling elders with dementia (27%) were hospitalized each year, a rate significantly higher than that among those without dementia (19%). And, he said, significantly more of these admissions were considered potentially avoidable among dementia patients (8% vs. 5%).
Significantly more ED visits occurred among those with dementia (24% vs. 18%) with significantly more deemed potentially preventable among dementia patients (5% vs. 3%). And significantly more patients with dementia were admitted as a result of these visits (19% vs. 12%).
After adjustment for the variables, dementia was a significant contributor to all of these outcomes. Dementia patients were 74% more likely to have an avoidable hospitalization and 51% more likely to have an avoidable ED visit than were patients without dementia.
Nursing home residents also had high hospital and ED utilization each year, but there were no significant differences between those with and without dementia. Still, Dr. Feng said, "About half of these hospitalizations and ED visits might have been preventable."
Utilization skyrocketed in the last year of life, he said. About 80% of community dwellers, regardless of dementia status or living situation, had at least one hospitalization or ED visit during that time, and up to 75% of these might have been unnecessary.
Significantly more patients with dementia had an ED visit as well (50% vs. 44%). Among both groups, about 38% of hospitalizations and up to 14% of ED visits could have been unnecessary.
Among nursing home residents during the last year of life, there were no significant differences in utilization between dementia and non-dementia patients. But up to half of this utilization might have been dealt with in the facility, rather than through a hospital admission, he said.
"It is really striking to me how, in the last year of life, the rate jumps so high," Dr. Feng said. "This finding of so many potentially avoidable hospitalizations suggests that there is a lot of room for improvement in quality of care, which could very well lead to improvements in quality of life for our elderly."
The study was funded in part by the Office of the Assistant Secretary for Planning and Evaluation in the Department of Health and Human Services. Dr. Feng had no financial disclosures.
On Twitter @alz_gal
WASHINGTON – During the last year of life for community-dwelling elders, up to three-fourths of hospital visits might have been avoidable.
Nursing home residents also were susceptible to potentially unnecessary admissions, with about 50% experiencing at least one avoidable visit during the final months, Dr. Zhanlian Feng said at a briefing to unveil the April special issue of Health Affairs, "The Long Reach of Alzheimer’s Disease."
Dementia was a significant contributor to hospital and emergency department use: Those with dementia were 74% more likely to have a potentially avoidable hospitalization and 51% more likely to have had a potentially avoidable ED visit.
The researchers did not speculate on what care might have been more appropriate for these patients, said Dr. Feng, a senior research public health analyst in the Aging, Disability, and Long-Term Care program at RTI International, Waltham, Mass. It does, however, suggest a very high level of caregiver anxiety about dealing with a loved one’s acute health issues.
"It’s much more challenging to provide care and support for someone who is living at home," he said in an interview. "Whenever their loved one gets worse, the caregiver is worried about how to respond to the new crisis. Often they believe their only option is the emergency department."
At-home care "is probably a big driver of hospital utilization," among the elderly, and one to which policy makers may be blind, he said in an interview.
"There are many initiatives designed to reduce hospitalizations among the elderly, but they focus almost exclusively on nursing homes, and don’t target people with dementia in particular. In the community setting, there is very little discussion on how to accomplish this."
At the briefing, Dr. Feng discussed his study, which was published April 7 in Health Affairs (Health Aff. 2014;33:683-90). It looked at hospitalization and emergency department use among more than 12,000 Medicare beneficiaries who were included in the Health and Retirement Study during 2000-2008. The study included four outcomes: 5-year hospital/ED utilization among elders with and without dementia, and hospital/ED utilization among both groups within the last year of life.
Potentially avoidable conditions were considered to be those that could have been effectively dealt with in the patients’ out-of-hospital care setting with community-based resources or within a long-term care or nursing home facility.
Some of these problems included heart failure and chronic obstructive pulmonary disease, blood pressure complications, hyper- and hypoglycemia, diabetes, dehydration or diarrhea, electrolyte imbalances, constipation or fecal impaction, urinary and respiratory tract infections (including some pneumonias), and skin ulcers. Problems relating to malnutrition and asthma also were included.
There were some differences among these groups, however. "For example, acute, severe diarrhea due to gastroenteritis or food poisoning can often be managed in nursing homes without hospitalization, but patients with the same condition in the community may require hospitalization."
ED visits that resulted in admission weren’t included because the authors assumed that those represented unavoidable admissions. They conducted a multivariate analysis that controlled for age, gender, race/ethnicity, income, education, marital status, other insurance, chronic health problems, self-reported health, and the ability to perform activities of daily living.
Dementia was significantly more common among nursing home residents than among community residents (84% vs. 12%). Almost half (44%) of those who died had dementia in the last year of life.
Dr. Feng said that more than a quarter of community-dwelling elders with dementia (27%) were hospitalized each year, a rate significantly higher than that among those without dementia (19%). And, he said, significantly more of these admissions were considered potentially avoidable among dementia patients (8% vs. 5%).
Significantly more ED visits occurred among those with dementia (24% vs. 18%) with significantly more deemed potentially preventable among dementia patients (5% vs. 3%). And significantly more patients with dementia were admitted as a result of these visits (19% vs. 12%).
After adjustment for the variables, dementia was a significant contributor to all of these outcomes. Dementia patients were 74% more likely to have an avoidable hospitalization and 51% more likely to have an avoidable ED visit than were patients without dementia.
Nursing home residents also had high hospital and ED utilization each year, but there were no significant differences between those with and without dementia. Still, Dr. Feng said, "About half of these hospitalizations and ED visits might have been preventable."
Utilization skyrocketed in the last year of life, he said. About 80% of community dwellers, regardless of dementia status or living situation, had at least one hospitalization or ED visit during that time, and up to 75% of these might have been unnecessary.
Significantly more patients with dementia had an ED visit as well (50% vs. 44%). Among both groups, about 38% of hospitalizations and up to 14% of ED visits could have been unnecessary.
Among nursing home residents during the last year of life, there were no significant differences in utilization between dementia and non-dementia patients. But up to half of this utilization might have been dealt with in the facility, rather than through a hospital admission, he said.
"It is really striking to me how, in the last year of life, the rate jumps so high," Dr. Feng said. "This finding of so many potentially avoidable hospitalizations suggests that there is a lot of room for improvement in quality of care, which could very well lead to improvements in quality of life for our elderly."
The study was funded in part by the Office of the Assistant Secretary for Planning and Evaluation in the Department of Health and Human Services. Dr. Feng had no financial disclosures.
On Twitter @alz_gal
WASHINGTON – During the last year of life for community-dwelling elders, up to three-fourths of hospital visits might have been avoidable.
Nursing home residents also were susceptible to potentially unnecessary admissions, with about 50% experiencing at least one avoidable visit during the final months, Dr. Zhanlian Feng said at a briefing to unveil the April special issue of Health Affairs, "The Long Reach of Alzheimer’s Disease."
Dementia was a significant contributor to hospital and emergency department use: Those with dementia were 74% more likely to have a potentially avoidable hospitalization and 51% more likely to have had a potentially avoidable ED visit.
The researchers did not speculate on what care might have been more appropriate for these patients, said Dr. Feng, a senior research public health analyst in the Aging, Disability, and Long-Term Care program at RTI International, Waltham, Mass. It does, however, suggest a very high level of caregiver anxiety about dealing with a loved one’s acute health issues.
"It’s much more challenging to provide care and support for someone who is living at home," he said in an interview. "Whenever their loved one gets worse, the caregiver is worried about how to respond to the new crisis. Often they believe their only option is the emergency department."
At-home care "is probably a big driver of hospital utilization," among the elderly, and one to which policy makers may be blind, he said in an interview.
"There are many initiatives designed to reduce hospitalizations among the elderly, but they focus almost exclusively on nursing homes, and don’t target people with dementia in particular. In the community setting, there is very little discussion on how to accomplish this."
At the briefing, Dr. Feng discussed his study, which was published April 7 in Health Affairs (Health Aff. 2014;33:683-90). It looked at hospitalization and emergency department use among more than 12,000 Medicare beneficiaries who were included in the Health and Retirement Study during 2000-2008. The study included four outcomes: 5-year hospital/ED utilization among elders with and without dementia, and hospital/ED utilization among both groups within the last year of life.
Potentially avoidable conditions were considered to be those that could have been effectively dealt with in the patients’ out-of-hospital care setting with community-based resources or within a long-term care or nursing home facility.
Some of these problems included heart failure and chronic obstructive pulmonary disease, blood pressure complications, hyper- and hypoglycemia, diabetes, dehydration or diarrhea, electrolyte imbalances, constipation or fecal impaction, urinary and respiratory tract infections (including some pneumonias), and skin ulcers. Problems relating to malnutrition and asthma also were included.
There were some differences among these groups, however. "For example, acute, severe diarrhea due to gastroenteritis or food poisoning can often be managed in nursing homes without hospitalization, but patients with the same condition in the community may require hospitalization."
ED visits that resulted in admission weren’t included because the authors assumed that those represented unavoidable admissions. They conducted a multivariate analysis that controlled for age, gender, race/ethnicity, income, education, marital status, other insurance, chronic health problems, self-reported health, and the ability to perform activities of daily living.
Dementia was significantly more common among nursing home residents than among community residents (84% vs. 12%). Almost half (44%) of those who died had dementia in the last year of life.
Dr. Feng said that more than a quarter of community-dwelling elders with dementia (27%) were hospitalized each year, a rate significantly higher than that among those without dementia (19%). And, he said, significantly more of these admissions were considered potentially avoidable among dementia patients (8% vs. 5%).
Significantly more ED visits occurred among those with dementia (24% vs. 18%) with significantly more deemed potentially preventable among dementia patients (5% vs. 3%). And significantly more patients with dementia were admitted as a result of these visits (19% vs. 12%).
After adjustment for the variables, dementia was a significant contributor to all of these outcomes. Dementia patients were 74% more likely to have an avoidable hospitalization and 51% more likely to have an avoidable ED visit than were patients without dementia.
Nursing home residents also had high hospital and ED utilization each year, but there were no significant differences between those with and without dementia. Still, Dr. Feng said, "About half of these hospitalizations and ED visits might have been preventable."
Utilization skyrocketed in the last year of life, he said. About 80% of community dwellers, regardless of dementia status or living situation, had at least one hospitalization or ED visit during that time, and up to 75% of these might have been unnecessary.
Significantly more patients with dementia had an ED visit as well (50% vs. 44%). Among both groups, about 38% of hospitalizations and up to 14% of ED visits could have been unnecessary.
Among nursing home residents during the last year of life, there were no significant differences in utilization between dementia and non-dementia patients. But up to half of this utilization might have been dealt with in the facility, rather than through a hospital admission, he said.
"It is really striking to me how, in the last year of life, the rate jumps so high," Dr. Feng said. "This finding of so many potentially avoidable hospitalizations suggests that there is a lot of room for improvement in quality of care, which could very well lead to improvements in quality of life for our elderly."
The study was funded in part by the Office of the Assistant Secretary for Planning and Evaluation in the Department of Health and Human Services. Dr. Feng had no financial disclosures.
On Twitter @alz_gal
AT A HEALTH AFFAIRS BRIEFING
Major finding: Among community-dwelling elderly, up to 75% of hospital admissions and emergency department visits occurring during the last year of life might be avoidable.
Data source: A retrospective study of 12,000 Medicare beneficiaries.
Disclosures: The study was funded in part by the Office of the Assistant Secretary for Planning and Evaluation in the Department of Health and Human Services. Dr. Feng had no financial disclosures.
Substantial delay seen in melanoma surgery for Medicare patients
DENVER – As many as 25% of Medicare patients with melanoma will experience treatment delays of up to 1.5 months, and 18% may have treatment delays as long as 3 months after a lesion is biopsied, especially if a nondermatologist is performing the excision, based on data from a review of more than 32,000 patients.
Patients who saw dermatologists for their surgery were much less likely to experience a delay in treatment, Dr. Jason Lott said at the annual meeting of the American Academy of Dermatology.

"If a primary care provider was doing the surgery – and many still do their own surgery – patients were 1.6 times more likely to have a delay of more than 1.5 months, and twice as likely to have a delay of more than 3 months," said Dr. Lott of Yale University, New Haven, Conn. "I am making the argument that specialty matters."
Other factors significantly associated with treatment delay included older patient age, comorbidities, tumor stage, and lesion location.
To examine factors contributing to a surgical delay in the United States, Dr. Lott and his colleagues conducted a population-based study of treatment waiting times in more than 32,501 Medicare patients who had been diagnosed with melanoma from 2000 to 2009. The primary outcome was the time between biopsy and surgical treatment.
The most common lesion sites were the head and neck (40%), followed by the extremities and trunk. Compared with head/neck lesions, surgery on the trunk and extremities was significantly less likely to be delayed up to 1.5 months (odds ratio, 0.74).
Melanomas were about equally divided between in situ and localized disease (48% and 44%), with the remainder having distant occurrence. Compared with in situ disease, regional and distant disease were significantly more likely to be treated later, with odds ratios ranging from 1.31 for a delay of up to 1.5 months (regional disease) to 2.15 for a delay of more than 3 months (distant disease).
Older patients had greater delays than did younger patients, with the biggest disparities between those aged 80-84 years and those aged 70-74 years, In the younger group, 54% were treated within 1 month, compared with 50% of the older patients. A delay of up to 3 months occurred in 38% of the younger group and 41% of the older group.
Patients with no medical comorbidities received significantly prompter treatment, with 54% being treated within 1 month compared with 47% of those with three comorbidities.
Expeditious treatment is certainly important to patients, Dr. Lott said, and likely important for achieving optimal outcomes. "Patients don’t like walking around knowing they have a malignancy that’s not treated, with even a marginally increased chance that something bad will happen," he noted.
That risk is not unfounded, Dr. Lott said. The United Kingdom’s "2-week" rule, implemented in 2000, mandates an urgent consultation for suspected malignancies. Patients with suspected melanomas are seen in a special pigmented lesions clinic, and often treated on the same day. In 2007, this practice was shown to positively impact melanoma survival.
Dr. Lott described a retrospective study conducted in the United Kingdom that examined outcomes in 4,399 patients, all of whom were evaluated at a pigmented lesions clinic within 2 weeks of a primary care identification of a suspicious lesion. During the study period, 96 melanomas were identified, and 96% of those were treated within 2 weeks of the primary referral. Most (74%) were excised on the day of the clinic visit.
The authors compared these results with those of 78 melanoma patients who were diagnosed in the 2 years before urgent referral became standard. These patients waited up to 34 days for a referral and up to 74 days for treatment. Patients seen in the clinic had significantly thinner tumors (Breslow thickness 1.68 vs. 2.39 mm). In addition to melanomas, 748 nonmelanoma skin cancers were treated at the clinics.
Among the melanoma patients diagnosed in the clinics, the 5-year survival rate was 82%, compared with 62% in patients diagnosed before the urgent referral.
"Earlier treatment does matter," Dr. Lott said.
Dr. Lott said he had no relevant financial conflicts to disclose.
On Twitter @alz_gal
DENVER – As many as 25% of Medicare patients with melanoma will experience treatment delays of up to 1.5 months, and 18% may have treatment delays as long as 3 months after a lesion is biopsied, especially if a nondermatologist is performing the excision, based on data from a review of more than 32,000 patients.
Patients who saw dermatologists for their surgery were much less likely to experience a delay in treatment, Dr. Jason Lott said at the annual meeting of the American Academy of Dermatology.
"If a primary care provider was doing the surgery – and many still do their own surgery – patients were 1.6 times more likely to have a delay of more than 1.5 months, and twice as likely to have a delay of more than 3 months," said Dr. Lott of Yale University, New Haven, Conn. "I am making the argument that specialty matters."
Other factors significantly associated with treatment delay included older patient age, comorbidities, tumor stage, and lesion location.
To examine factors contributing to a surgical delay in the United States, Dr. Lott and his colleagues conducted a population-based study of treatment waiting times in more than 32,501 Medicare patients who had been diagnosed with melanoma from 2000 to 2009. The primary outcome was the time between biopsy and surgical treatment.
The most common lesion sites were the head and neck (40%), followed by the extremities and trunk. Compared with head/neck lesions, surgery on the trunk and extremities was significantly less likely to be delayed up to 1.5 months (odds ratio, 0.74).
Melanomas were about equally divided between in situ and localized disease (48% and 44%), with the remainder having distant occurrence. Compared with in situ disease, regional and distant disease were significantly more likely to be treated later, with odds ratios ranging from 1.31 for a delay of up to 1.5 months (regional disease) to 2.15 for a delay of more than 3 months (distant disease).
Older patients had greater delays than did younger patients, with the biggest disparities between those aged 80-84 years and those aged 70-74 years, In the younger group, 54% were treated within 1 month, compared with 50% of the older patients. A delay of up to 3 months occurred in 38% of the younger group and 41% of the older group.
Patients with no medical comorbidities received significantly prompter treatment, with 54% being treated within 1 month compared with 47% of those with three comorbidities.
Expeditious treatment is certainly important to patients, Dr. Lott said, and likely important for achieving optimal outcomes. "Patients don’t like walking around knowing they have a malignancy that’s not treated, with even a marginally increased chance that something bad will happen," he noted.
That risk is not unfounded, Dr. Lott said. The United Kingdom’s "2-week" rule, implemented in 2000, mandates an urgent consultation for suspected malignancies. Patients with suspected melanomas are seen in a special pigmented lesions clinic, and often treated on the same day. In 2007, this practice was shown to positively impact melanoma survival.
Dr. Lott described a retrospective study conducted in the United Kingdom that examined outcomes in 4,399 patients, all of whom were evaluated at a pigmented lesions clinic within 2 weeks of a primary care identification of a suspicious lesion. During the study period, 96 melanomas were identified, and 96% of those were treated within 2 weeks of the primary referral. Most (74%) were excised on the day of the clinic visit.
The authors compared these results with those of 78 melanoma patients who were diagnosed in the 2 years before urgent referral became standard. These patients waited up to 34 days for a referral and up to 74 days for treatment. Patients seen in the clinic had significantly thinner tumors (Breslow thickness 1.68 vs. 2.39 mm). In addition to melanomas, 748 nonmelanoma skin cancers were treated at the clinics.
Among the melanoma patients diagnosed in the clinics, the 5-year survival rate was 82%, compared with 62% in patients diagnosed before the urgent referral.
"Earlier treatment does matter," Dr. Lott said.
Dr. Lott said he had no relevant financial conflicts to disclose.
On Twitter @alz_gal
DENVER – As many as 25% of Medicare patients with melanoma will experience treatment delays of up to 1.5 months, and 18% may have treatment delays as long as 3 months after a lesion is biopsied, especially if a nondermatologist is performing the excision, based on data from a review of more than 32,000 patients.
Patients who saw dermatologists for their surgery were much less likely to experience a delay in treatment, Dr. Jason Lott said at the annual meeting of the American Academy of Dermatology.
"If a primary care provider was doing the surgery – and many still do their own surgery – patients were 1.6 times more likely to have a delay of more than 1.5 months, and twice as likely to have a delay of more than 3 months," said Dr. Lott of Yale University, New Haven, Conn. "I am making the argument that specialty matters."
Other factors significantly associated with treatment delay included older patient age, comorbidities, tumor stage, and lesion location.
To examine factors contributing to a surgical delay in the United States, Dr. Lott and his colleagues conducted a population-based study of treatment waiting times in more than 32,501 Medicare patients who had been diagnosed with melanoma from 2000 to 2009. The primary outcome was the time between biopsy and surgical treatment.
The most common lesion sites were the head and neck (40%), followed by the extremities and trunk. Compared with head/neck lesions, surgery on the trunk and extremities was significantly less likely to be delayed up to 1.5 months (odds ratio, 0.74).
Melanomas were about equally divided between in situ and localized disease (48% and 44%), with the remainder having distant occurrence. Compared with in situ disease, regional and distant disease were significantly more likely to be treated later, with odds ratios ranging from 1.31 for a delay of up to 1.5 months (regional disease) to 2.15 for a delay of more than 3 months (distant disease).
Older patients had greater delays than did younger patients, with the biggest disparities between those aged 80-84 years and those aged 70-74 years, In the younger group, 54% were treated within 1 month, compared with 50% of the older patients. A delay of up to 3 months occurred in 38% of the younger group and 41% of the older group.
Patients with no medical comorbidities received significantly prompter treatment, with 54% being treated within 1 month compared with 47% of those with three comorbidities.
Expeditious treatment is certainly important to patients, Dr. Lott said, and likely important for achieving optimal outcomes. "Patients don’t like walking around knowing they have a malignancy that’s not treated, with even a marginally increased chance that something bad will happen," he noted.
That risk is not unfounded, Dr. Lott said. The United Kingdom’s "2-week" rule, implemented in 2000, mandates an urgent consultation for suspected malignancies. Patients with suspected melanomas are seen in a special pigmented lesions clinic, and often treated on the same day. In 2007, this practice was shown to positively impact melanoma survival.
Dr. Lott described a retrospective study conducted in the United Kingdom that examined outcomes in 4,399 patients, all of whom were evaluated at a pigmented lesions clinic within 2 weeks of a primary care identification of a suspicious lesion. During the study period, 96 melanomas were identified, and 96% of those were treated within 2 weeks of the primary referral. Most (74%) were excised on the day of the clinic visit.
The authors compared these results with those of 78 melanoma patients who were diagnosed in the 2 years before urgent referral became standard. These patients waited up to 34 days for a referral and up to 74 days for treatment. Patients seen in the clinic had significantly thinner tumors (Breslow thickness 1.68 vs. 2.39 mm). In addition to melanomas, 748 nonmelanoma skin cancers were treated at the clinics.
Among the melanoma patients diagnosed in the clinics, the 5-year survival rate was 82%, compared with 62% in patients diagnosed before the urgent referral.
"Earlier treatment does matter," Dr. Lott said.
Dr. Lott said he had no relevant financial conflicts to disclose.
On Twitter @alz_gal
AT THE AAD ANNUAL MEETING
Major finding: Melanoma excision delays were significantly less common when the diagnostic physician was a dermatologist, rather than a nondermatologist (OR, 0.67 for more than 1.5 months; 0.58 for more than 3 months).
Data source: A Medicare database study involving more than 32,000 patients with melanoma.
Disclosures: Dr. Lott said he had no relevant financial disclosures.

Psoriatic pruritus improves with TrkA-blocking drug
An investigational topical drug that targets a nerve sensitization pathway showed good efficacy against chronic itch in patients with pruritic psoriasis.
CT327 works by inhibiting the kinase pathway of TrkA, a receptor that controls uptake of nerve growth factor, Dr. Gil Yosipovitch said at the annual meeting of the American Academy of Dermatology.
In a placebo-controlled trial of 160 patients with pruritic psoriasis, CT327 reduced itch by a mean of 60%, said Dr. Yosipovitch, chair of dermatology at the Temple University, Philadelphia.
"Sixty percent is not 90%," he said. "But when we consider that most of the antipruritic drugs have about a 15% efficacy in comparison to a vehicle, this is an effect we should consider. It’s well tolerated, and there were no application site reactions. I see potential in this drug."
CT327, developed by Creabilis, is a selective kinase inhibitor that targets TrkA, the receptor for nerve growth factor (NGF). NGF, which is overexpressed in atopic dermatitis and psoriatic skin, sensitizes neural networks that transmit the itch sensation to the brain, Dr. Yosipovitch said.

The phase IIb study comprised 160 adults with mild to moderate psoriasis, with at least a 10% body surface area involvement. Their mean score on the modified Psoriasis Area and Severity Index (mPASI) was about 9. Most (97%) had pruritus; 69% reported this as at least moderate, with a score of 40 on a 100-point visual analog scale (VAS). A third of the group reported severe pruritus, with a VAS of more than 70. They were randomized to four groups: an emollient placebo or CT327 in concentrations of 0.05%, 0.1%, or 0.5%.
The primary endpoint was reduction on a validated 100-point pruritus visual analog scale. The secondary endpoint was change on the mPASI.
By the end of 8 weeks, most patients (108) had experienced a significant reduction on the pruritus VAS. Reductions were about 35 points for the 0.1% group and 38 points for the 0.05% and 0.5% groups. These changes represented about a 60% decrease overall, Dr. Yosipovitch said.
Changes began early and continued along a steep trajectory, reaching a significant difference from baseline by week 2. However, he pointed out, by that point, the placebo group was similarly improved. This was probably because of the benefit of the daily emollient vehicle, he noted.
The curves began to separate shortly thereafter. By week 4, all of the treatment groups had experienced about a 30-point reduction on the VAS, while the placebo group had actually increased its score slightly. The active groups continued to improve over the next 4 weeks, while the placebo group plateaued at about a 20-point decrease from baseline.
The study concluded with 4 weeks of non–treatment follow-up. During that time, the placebo group stayed at about a 20-point decline and the active groups rebounded to about that level, "suggesting that there really is something going on here biologically," Dr. Yosipovitch said.
Patients using CT327 also experienced significant – although not overwhelming – benefit on the mPASI score. About 45% responded at the 50% level, compared with 23% of those using the emollient placebo. The active groups had similar improvements, with reductions on the mPASI of between 3 and 4 points. Those in the placebo group experienced about a 1-point improvement.
Dr. Yosipovitch said he was "not too impressed" with the mPASI changes. However, he noted, "Breaking the itch-scratch cycle at its source may have broader effects on other symptoms of psoriasis."
Based on the study results, Creabilis has decided to move forward into phase III testing with the 0.05% concentration. "Preparations are already underway," Dr. Yosipovitch said in an interview. "We also have a second phase IIb study ongoing that is investigating CT327 in patients with atopic dermatitis, which will be used to help finalize our phase III programs. This study should be completed in the middle of this year."
The NGF/TrkA pathway is implicated in other disorders as well, Dr. Yosipovitch said. CT327 might be investigated in some of these.
"These include disorders [in which] pruritus is important, such as pruritus with cutaneous T cell lymphoma, where NGF/TrkA has been shown to play a role. The pathway has also been shown to play an important role in chronic neuropathic and inflammatory pain. Molecules targeting NGF have already shown clinical efficacy."
Creabilis is investigating a related molecule, CT340, an inhibitor of both TrkA and MAP2K kinase, for treating those chronic pain conditions.
Creabilis funded the study. Dr. Yosipovitch is on the company’s scientific advisory board.
On Twitter @alz_gal
An investigational topical drug that targets a nerve sensitization pathway showed good efficacy against chronic itch in patients with pruritic psoriasis.
CT327 works by inhibiting the kinase pathway of TrkA, a receptor that controls uptake of nerve growth factor, Dr. Gil Yosipovitch said at the annual meeting of the American Academy of Dermatology.
In a placebo-controlled trial of 160 patients with pruritic psoriasis, CT327 reduced itch by a mean of 60%, said Dr. Yosipovitch, chair of dermatology at the Temple University, Philadelphia.
"Sixty percent is not 90%," he said. "But when we consider that most of the antipruritic drugs have about a 15% efficacy in comparison to a vehicle, this is an effect we should consider. It’s well tolerated, and there were no application site reactions. I see potential in this drug."
CT327, developed by Creabilis, is a selective kinase inhibitor that targets TrkA, the receptor for nerve growth factor (NGF). NGF, which is overexpressed in atopic dermatitis and psoriatic skin, sensitizes neural networks that transmit the itch sensation to the brain, Dr. Yosipovitch said.
The phase IIb study comprised 160 adults with mild to moderate psoriasis, with at least a 10% body surface area involvement. Their mean score on the modified Psoriasis Area and Severity Index (mPASI) was about 9. Most (97%) had pruritus; 69% reported this as at least moderate, with a score of 40 on a 100-point visual analog scale (VAS). A third of the group reported severe pruritus, with a VAS of more than 70. They were randomized to four groups: an emollient placebo or CT327 in concentrations of 0.05%, 0.1%, or 0.5%.
The primary endpoint was reduction on a validated 100-point pruritus visual analog scale. The secondary endpoint was change on the mPASI.
By the end of 8 weeks, most patients (108) had experienced a significant reduction on the pruritus VAS. Reductions were about 35 points for the 0.1% group and 38 points for the 0.05% and 0.5% groups. These changes represented about a 60% decrease overall, Dr. Yosipovitch said.
Changes began early and continued along a steep trajectory, reaching a significant difference from baseline by week 2. However, he pointed out, by that point, the placebo group was similarly improved. This was probably because of the benefit of the daily emollient vehicle, he noted.
The curves began to separate shortly thereafter. By week 4, all of the treatment groups had experienced about a 30-point reduction on the VAS, while the placebo group had actually increased its score slightly. The active groups continued to improve over the next 4 weeks, while the placebo group plateaued at about a 20-point decrease from baseline.
The study concluded with 4 weeks of non–treatment follow-up. During that time, the placebo group stayed at about a 20-point decline and the active groups rebounded to about that level, "suggesting that there really is something going on here biologically," Dr. Yosipovitch said.
Patients using CT327 also experienced significant – although not overwhelming – benefit on the mPASI score. About 45% responded at the 50% level, compared with 23% of those using the emollient placebo. The active groups had similar improvements, with reductions on the mPASI of between 3 and 4 points. Those in the placebo group experienced about a 1-point improvement.
Dr. Yosipovitch said he was "not too impressed" with the mPASI changes. However, he noted, "Breaking the itch-scratch cycle at its source may have broader effects on other symptoms of psoriasis."
Based on the study results, Creabilis has decided to move forward into phase III testing with the 0.05% concentration. "Preparations are already underway," Dr. Yosipovitch said in an interview. "We also have a second phase IIb study ongoing that is investigating CT327 in patients with atopic dermatitis, which will be used to help finalize our phase III programs. This study should be completed in the middle of this year."
The NGF/TrkA pathway is implicated in other disorders as well, Dr. Yosipovitch said. CT327 might be investigated in some of these.
"These include disorders [in which] pruritus is important, such as pruritus with cutaneous T cell lymphoma, where NGF/TrkA has been shown to play a role. The pathway has also been shown to play an important role in chronic neuropathic and inflammatory pain. Molecules targeting NGF have already shown clinical efficacy."
Creabilis is investigating a related molecule, CT340, an inhibitor of both TrkA and MAP2K kinase, for treating those chronic pain conditions.
Creabilis funded the study. Dr. Yosipovitch is on the company’s scientific advisory board.
On Twitter @alz_gal
An investigational topical drug that targets a nerve sensitization pathway showed good efficacy against chronic itch in patients with pruritic psoriasis.
CT327 works by inhibiting the kinase pathway of TrkA, a receptor that controls uptake of nerve growth factor, Dr. Gil Yosipovitch said at the annual meeting of the American Academy of Dermatology.
In a placebo-controlled trial of 160 patients with pruritic psoriasis, CT327 reduced itch by a mean of 60%, said Dr. Yosipovitch, chair of dermatology at the Temple University, Philadelphia.
"Sixty percent is not 90%," he said. "But when we consider that most of the antipruritic drugs have about a 15% efficacy in comparison to a vehicle, this is an effect we should consider. It’s well tolerated, and there were no application site reactions. I see potential in this drug."
CT327, developed by Creabilis, is a selective kinase inhibitor that targets TrkA, the receptor for nerve growth factor (NGF). NGF, which is overexpressed in atopic dermatitis and psoriatic skin, sensitizes neural networks that transmit the itch sensation to the brain, Dr. Yosipovitch said.
The phase IIb study comprised 160 adults with mild to moderate psoriasis, with at least a 10% body surface area involvement. Their mean score on the modified Psoriasis Area and Severity Index (mPASI) was about 9. Most (97%) had pruritus; 69% reported this as at least moderate, with a score of 40 on a 100-point visual analog scale (VAS). A third of the group reported severe pruritus, with a VAS of more than 70. They were randomized to four groups: an emollient placebo or CT327 in concentrations of 0.05%, 0.1%, or 0.5%.
The primary endpoint was reduction on a validated 100-point pruritus visual analog scale. The secondary endpoint was change on the mPASI.
By the end of 8 weeks, most patients (108) had experienced a significant reduction on the pruritus VAS. Reductions were about 35 points for the 0.1% group and 38 points for the 0.05% and 0.5% groups. These changes represented about a 60% decrease overall, Dr. Yosipovitch said.
Changes began early and continued along a steep trajectory, reaching a significant difference from baseline by week 2. However, he pointed out, by that point, the placebo group was similarly improved. This was probably because of the benefit of the daily emollient vehicle, he noted.
The curves began to separate shortly thereafter. By week 4, all of the treatment groups had experienced about a 30-point reduction on the VAS, while the placebo group had actually increased its score slightly. The active groups continued to improve over the next 4 weeks, while the placebo group plateaued at about a 20-point decrease from baseline.
The study concluded with 4 weeks of non–treatment follow-up. During that time, the placebo group stayed at about a 20-point decline and the active groups rebounded to about that level, "suggesting that there really is something going on here biologically," Dr. Yosipovitch said.
Patients using CT327 also experienced significant – although not overwhelming – benefit on the mPASI score. About 45% responded at the 50% level, compared with 23% of those using the emollient placebo. The active groups had similar improvements, with reductions on the mPASI of between 3 and 4 points. Those in the placebo group experienced about a 1-point improvement.
Dr. Yosipovitch said he was "not too impressed" with the mPASI changes. However, he noted, "Breaking the itch-scratch cycle at its source may have broader effects on other symptoms of psoriasis."
Based on the study results, Creabilis has decided to move forward into phase III testing with the 0.05% concentration. "Preparations are already underway," Dr. Yosipovitch said in an interview. "We also have a second phase IIb study ongoing that is investigating CT327 in patients with atopic dermatitis, which will be used to help finalize our phase III programs. This study should be completed in the middle of this year."
The NGF/TrkA pathway is implicated in other disorders as well, Dr. Yosipovitch said. CT327 might be investigated in some of these.
"These include disorders [in which] pruritus is important, such as pruritus with cutaneous T cell lymphoma, where NGF/TrkA has been shown to play a role. The pathway has also been shown to play an important role in chronic neuropathic and inflammatory pain. Molecules targeting NGF have already shown clinical efficacy."
Creabilis is investigating a related molecule, CT340, an inhibitor of both TrkA and MAP2K kinase, for treating those chronic pain conditions.
Creabilis funded the study. Dr. Yosipovitch is on the company’s scientific advisory board.
On Twitter @alz_gal
AT THE AAD ANNUAL MEETING
Major finding: The investigational drug CT327 reduced pruritus scores by 60% in a group of pruritic psoriatic patients.
Data source: The randomized, placebo-controlled trial of 160 patients.
Disclosures: Creabilis funded the study. Dr. Gil Yosipovitch is on the company’s scientific advisory board.

Revascularization saves limbs, costs in elderly
In older, frailer patients, limb revascularization appeared to preserve both limbs and ambulation longer ? and cost less ? than either amputation or a program of local wound care. Although these patients had worse clinical outcomes than did healthy patients who had revascularization, the benefits were still evident, Dr. Neal R. Barshes and his colleagues wrote in the January issue of Annals of Vascular Surgery.
"We believe that major amputation should be reserved for patients who develop life-threatening foot infections that cannot be controlled with foot drainage or minor amputations and subsequent palliative wound care," wrote Dr. Barshes of the Michael E. DeBakey Veterans Affairs Medical Center, Houston, and his coauthors.

They conducted a clinical outcomes and cost model that ran 1,000 simulated trials of 1,000 patients each. The parameters were drawn from the landmark MOVIE (Model to Optimize Healthcare Value in Ischemic Extremities) study. The study was modified to simulate a patient population older than 80 years, or who had undergone a prior major amputation of the contralateral lower limb, as these two groups have poorer postop outcomes than the usual population undergoing revascularization for lower limb ischemia. The analysis examined outcomes associated with six procedures:
? Primary amputation.
? Local wound care.
? Surgical revascularization followed if needed by surgical revision.
? Surgical revascularization followed if needed by endovascular revision.
? Initial endo revascularization followed if needed by surgical revision.
? Endo revascularization followed if needed by endovascular revision.
Primary amputation was the least clinically beneficial and the most expensive, with no limb salvage, a median ambulatory period of 1.5 years, and a total 10-year cost of $185,955. Much of the cost was for nursing and long-term care due to loss of independence.

Wound care also produced less desirable outcomes. The median 5-year limb salvage rate was 28%. See costs, salvage period, below.
Surgical bypass with either surgical or endo revision produced a limb salvage rate of 80%. Endo revascularization followed by surgical revision produced a 5-year limb salvage rate of 80%. Endo revascularization with endovascular revision produced a 5-year limb salvage rate of 80.5%, with a median salvage period of 3 years and a median ambulatory period of 2.5 years. This was the least expensive.
These outcomes were worse than those seen in the population of younger, healthier patients. The median 10-year cost for revascularization was up to $35,000 more. Clinical outcomes of the older population were also worse, with a 3-year period of limb preservation compared with more than 4 years in a healthier population, and about 2.5 ambulatory years compared with 4.6 years.
"In spite of these findings, revascularization still appears to be the most cost-effective alternative to wound care and primary amputation," the team noted.
The paper did not note any conflicts.
Dr. Barshes and colleagues suggest that an aggressive approach to limb revascularization, both endovascular and open bypass, may be appropriate and cost effective in older, frailer patients.
Certainly, in today?s era of cost-effective care, it is incumbent upon all of us, as health care providers, to further examine these types of issues. However, the studies necessary are not necessarily easy to perform. We must take into account not only the costs of the actual procedures and hospital stays, which are relatively easy to determine, but also the costs of rehabilitation, outpatient nursing care, wound care, and long-term care for those with loss of functional independence. Even this type of study does not assess all aspects that are important, including how much it is worth to maintain a limb and functional independence per year for each patient. What is not so easy to do is to put a value on limb salvage.
Hopefully we will be able to cull out the factors that may impact upon our decisions to re-intervene for critical limb ischemia, versus offering amputation when the patient presents with inadequate perfusion to the limb after initial attempts at limb salvage.
Dr. Linda Harris is an ACS Fellow and division chief, vascular surgery, State University of New York at Buffalo. She has no disclosures.
Dr. Barshes and colleagues suggest that an aggressive approach to limb revascularization, both endovascular and open bypass, may be appropriate and cost effective in older, frailer patients.
Certainly, in today?s era of cost-effective care, it is incumbent upon all of us, as health care providers, to further examine these types of issues. However, the studies necessary are not necessarily easy to perform. We must take into account not only the costs of the actual procedures and hospital stays, which are relatively easy to determine, but also the costs of rehabilitation, outpatient nursing care, wound care, and long-term care for those with loss of functional independence. Even this type of study does not assess all aspects that are important, including how much it is worth to maintain a limb and functional independence per year for each patient. What is not so easy to do is to put a value on limb salvage.
Hopefully we will be able to cull out the factors that may impact upon our decisions to re-intervene for critical limb ischemia, versus offering amputation when the patient presents with inadequate perfusion to the limb after initial attempts at limb salvage.
Dr. Linda Harris is an ACS Fellow and division chief, vascular surgery, State University of New York at Buffalo. She has no disclosures.
Dr. Barshes and colleagues suggest that an aggressive approach to limb revascularization, both endovascular and open bypass, may be appropriate and cost effective in older, frailer patients.
Certainly, in today?s era of cost-effective care, it is incumbent upon all of us, as health care providers, to further examine these types of issues. However, the studies necessary are not necessarily easy to perform. We must take into account not only the costs of the actual procedures and hospital stays, which are relatively easy to determine, but also the costs of rehabilitation, outpatient nursing care, wound care, and long-term care for those with loss of functional independence. Even this type of study does not assess all aspects that are important, including how much it is worth to maintain a limb and functional independence per year for each patient. What is not so easy to do is to put a value on limb salvage.
Hopefully we will be able to cull out the factors that may impact upon our decisions to re-intervene for critical limb ischemia, versus offering amputation when the patient presents with inadequate perfusion to the limb after initial attempts at limb salvage.
Dr. Linda Harris is an ACS Fellow and division chief, vascular surgery, State University of New York at Buffalo. She has no disclosures.
In older, frailer patients, limb revascularization appeared to preserve both limbs and ambulation longer ? and cost less ? than either amputation or a program of local wound care. Although these patients had worse clinical outcomes than did healthy patients who had revascularization, the benefits were still evident, Dr. Neal R. Barshes and his colleagues wrote in the January issue of Annals of Vascular Surgery.
"We believe that major amputation should be reserved for patients who develop life-threatening foot infections that cannot be controlled with foot drainage or minor amputations and subsequent palliative wound care," wrote Dr. Barshes of the Michael E. DeBakey Veterans Affairs Medical Center, Houston, and his coauthors.
They conducted a clinical outcomes and cost model that ran 1,000 simulated trials of 1,000 patients each. The parameters were drawn from the landmark MOVIE (Model to Optimize Healthcare Value in Ischemic Extremities) study. The study was modified to simulate a patient population older than 80 years, or who had undergone a prior major amputation of the contralateral lower limb, as these two groups have poorer postop outcomes than the usual population undergoing revascularization for lower limb ischemia. The analysis examined outcomes associated with six procedures:
? Primary amputation.
? Local wound care.
? Surgical revascularization followed if needed by surgical revision.
? Surgical revascularization followed if needed by endovascular revision.
? Initial endo revascularization followed if needed by surgical revision.
? Endo revascularization followed if needed by endovascular revision.
Primary amputation was the least clinically beneficial and the most expensive, with no limb salvage, a median ambulatory period of 1.5 years, and a total 10-year cost of $185,955. Much of the cost was for nursing and long-term care due to loss of independence.
Wound care also produced less desirable outcomes. The median 5-year limb salvage rate was 28%. See costs, salvage period, below.
Surgical bypass with either surgical or endo revision produced a limb salvage rate of 80%. Endo revascularization followed by surgical revision produced a 5-year limb salvage rate of 80%. Endo revascularization with endovascular revision produced a 5-year limb salvage rate of 80.5%, with a median salvage period of 3 years and a median ambulatory period of 2.5 years. This was the least expensive.
These outcomes were worse than those seen in the population of younger, healthier patients. The median 10-year cost for revascularization was up to $35,000 more. Clinical outcomes of the older population were also worse, with a 3-year period of limb preservation compared with more than 4 years in a healthier population, and about 2.5 ambulatory years compared with 4.6 years.
"In spite of these findings, revascularization still appears to be the most cost-effective alternative to wound care and primary amputation," the team noted.
The paper did not note any conflicts.
In older, frailer patients, limb revascularization appeared to preserve both limbs and ambulation longer ? and cost less ? than either amputation or a program of local wound care. Although these patients had worse clinical outcomes than did healthy patients who had revascularization, the benefits were still evident, Dr. Neal R. Barshes and his colleagues wrote in the January issue of Annals of Vascular Surgery.
"We believe that major amputation should be reserved for patients who develop life-threatening foot infections that cannot be controlled with foot drainage or minor amputations and subsequent palliative wound care," wrote Dr. Barshes of the Michael E. DeBakey Veterans Affairs Medical Center, Houston, and his coauthors.
They conducted a clinical outcomes and cost model that ran 1,000 simulated trials of 1,000 patients each. The parameters were drawn from the landmark MOVIE (Model to Optimize Healthcare Value in Ischemic Extremities) study. The study was modified to simulate a patient population older than 80 years, or who had undergone a prior major amputation of the contralateral lower limb, as these two groups have poorer postop outcomes than the usual population undergoing revascularization for lower limb ischemia. The analysis examined outcomes associated with six procedures:
? Primary amputation.
? Local wound care.
? Surgical revascularization followed if needed by surgical revision.
? Surgical revascularization followed if needed by endovascular revision.
? Initial endo revascularization followed if needed by surgical revision.
? Endo revascularization followed if needed by endovascular revision.
Primary amputation was the least clinically beneficial and the most expensive, with no limb salvage, a median ambulatory period of 1.5 years, and a total 10-year cost of $185,955. Much of the cost was for nursing and long-term care due to loss of independence.
Wound care also produced less desirable outcomes. The median 5-year limb salvage rate was 28%. See costs, salvage period, below.
Surgical bypass with either surgical or endo revision produced a limb salvage rate of 80%. Endo revascularization followed by surgical revision produced a 5-year limb salvage rate of 80%. Endo revascularization with endovascular revision produced a 5-year limb salvage rate of 80.5%, with a median salvage period of 3 years and a median ambulatory period of 2.5 years. This was the least expensive.
These outcomes were worse than those seen in the population of younger, healthier patients. The median 10-year cost for revascularization was up to $35,000 more. Clinical outcomes of the older population were also worse, with a 3-year period of limb preservation compared with more than 4 years in a healthier population, and about 2.5 ambulatory years compared with 4.6 years.
"In spite of these findings, revascularization still appears to be the most cost-effective alternative to wound care and primary amputation," the team noted.
The paper did not note any conflicts.
Major finding: In older, more frail patients, lower limb revascularization cost up to $90,000 less over 10 years, and yielded better clinical outcomes, than did primary amputation.
Data source: The clinical and cost outcomes model simulated 1,000 trials of 1,000 patients each.
Disclosures: The paper did not note any potential financial conflicts of interest or the study?s sponsor.
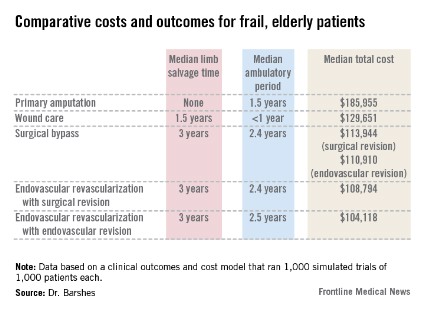
Postmastectomy radiotherapy improves survival with one to three positive nodes
Radiotherapy after mastectomy for women with one to three positive nodes significantly reduces the risk of recurrence and breast cancer mortality, researchers found in a meta-analysis.
With follow-up of 20 years for breast cancer mortality, a review of 22 randomized trials found that among women with one to three positive nodes after mastectomy and axillary dissection, radiotherapy reduced the rates of overall recurrence by almost a third (relative risk, 0.68; 95% confidence interval, 0.57-0.82; P = .00006) and breast cancer mortality by a fifth (RR, 0.80; 95% CI, 0.67-0.95; P = .01), investigators reported online March 19 in the Lancet.
This benefit from radiotherapy in women with one to three positive nodes held up when women also received chemotherapy and/or hormone treatment. The proportional reductions in the rates of any first recurrence and breast cancer mortality did not differ significantly according to whether or not systemic therapy was given, the investigators said.
The group analyzed outcomes for 8,135 women enrolled in 22 studies, randomized to receive radiotherapy to the chest wall and regional lymph nodes after mastectomy and axillary surgery, or to receive the same surgery with no radiotherapy. The median length of follow-up per woman was about 9 years, although many in the studies have now been followed for up to 20 years. Most had positive nodes at dissection (72%); 20% had node-negative disease, and nodal status was unknown for the remainder.
For women with no positive nodes, radiotherapy had no significant effect on locoregional recurrence, overall recurrence, or breast cancer morality, but did however increase overall mortality (RR, 1.23; 95% CI, 1.02-1.49; P = .03). For women with axillary dissection and four or more positive nodes, radiotherapy reduced overall recurrence (RR, 0.79; 95% CI, 0.69-0.90; P = .0003) and breast cancer mortality (RR, 0.87; 95% CI, 0.77-0.99; P = .04).
All of the studies were conducted between 1964 and 1986. Benefits could be even greater today, "... because radiotherapy planning has changed substantially and women today receive better coverage of target areas. Furthermore, doses to normal tissues are lower today, so the risks of radiotherapy are also likely to be lower," wrote the investigators with the Early Breast Cancer Trialists’ Collaborative Group, which conducted the analysis (Lancet 2014 March 19 [doi: 10.1016/S0140-6736(14)60488-8]).
"Breast cancer is a disease with a long natural history," the researchers wrote. "Many of the women in these trials have now been followed up for 20 years and therefore they provide information about the long-term benefits of radiotherapy. Radiotherapy techniques have improved in the past few decades, and so the proportional benefits of radiotherapy are likely to be larger than in these trials."
However, they added, "the absolute risks of breast cancer recurrence and mortality have [been] reduced in many countries because of advances in detection and treatment of breast cancer, so the absolute benefits from postmastectomy radiotherapy today are likely to be smaller than those reported here."
The study group is funded by Cancer Research UK, the British Heart Foundation, and the UK Medical Research Council. None of the members reported any financial disclosures.
Radiotherapy after mastectomy for women with one to three positive nodes significantly reduces the risk of recurrence and breast cancer mortality, researchers found in a meta-analysis.
With follow-up of 20 years for breast cancer mortality, a review of 22 randomized trials found that among women with one to three positive nodes after mastectomy and axillary dissection, radiotherapy reduced the rates of overall recurrence by almost a third (relative risk, 0.68; 95% confidence interval, 0.57-0.82; P = .00006) and breast cancer mortality by a fifth (RR, 0.80; 95% CI, 0.67-0.95; P = .01), investigators reported online March 19 in the Lancet.
This benefit from radiotherapy in women with one to three positive nodes held up when women also received chemotherapy and/or hormone treatment. The proportional reductions in the rates of any first recurrence and breast cancer mortality did not differ significantly according to whether or not systemic therapy was given, the investigators said.
The group analyzed outcomes for 8,135 women enrolled in 22 studies, randomized to receive radiotherapy to the chest wall and regional lymph nodes after mastectomy and axillary surgery, or to receive the same surgery with no radiotherapy. The median length of follow-up per woman was about 9 years, although many in the studies have now been followed for up to 20 years. Most had positive nodes at dissection (72%); 20% had node-negative disease, and nodal status was unknown for the remainder.
For women with no positive nodes, radiotherapy had no significant effect on locoregional recurrence, overall recurrence, or breast cancer morality, but did however increase overall mortality (RR, 1.23; 95% CI, 1.02-1.49; P = .03). For women with axillary dissection and four or more positive nodes, radiotherapy reduced overall recurrence (RR, 0.79; 95% CI, 0.69-0.90; P = .0003) and breast cancer mortality (RR, 0.87; 95% CI, 0.77-0.99; P = .04).
All of the studies were conducted between 1964 and 1986. Benefits could be even greater today, "... because radiotherapy planning has changed substantially and women today receive better coverage of target areas. Furthermore, doses to normal tissues are lower today, so the risks of radiotherapy are also likely to be lower," wrote the investigators with the Early Breast Cancer Trialists’ Collaborative Group, which conducted the analysis (Lancet 2014 March 19 [doi: 10.1016/S0140-6736(14)60488-8]).
"Breast cancer is a disease with a long natural history," the researchers wrote. "Many of the women in these trials have now been followed up for 20 years and therefore they provide information about the long-term benefits of radiotherapy. Radiotherapy techniques have improved in the past few decades, and so the proportional benefits of radiotherapy are likely to be larger than in these trials."
However, they added, "the absolute risks of breast cancer recurrence and mortality have [been] reduced in many countries because of advances in detection and treatment of breast cancer, so the absolute benefits from postmastectomy radiotherapy today are likely to be smaller than those reported here."
The study group is funded by Cancer Research UK, the British Heart Foundation, and the UK Medical Research Council. None of the members reported any financial disclosures.
Radiotherapy after mastectomy for women with one to three positive nodes significantly reduces the risk of recurrence and breast cancer mortality, researchers found in a meta-analysis.
With follow-up of 20 years for breast cancer mortality, a review of 22 randomized trials found that among women with one to three positive nodes after mastectomy and axillary dissection, radiotherapy reduced the rates of overall recurrence by almost a third (relative risk, 0.68; 95% confidence interval, 0.57-0.82; P = .00006) and breast cancer mortality by a fifth (RR, 0.80; 95% CI, 0.67-0.95; P = .01), investigators reported online March 19 in the Lancet.
This benefit from radiotherapy in women with one to three positive nodes held up when women also received chemotherapy and/or hormone treatment. The proportional reductions in the rates of any first recurrence and breast cancer mortality did not differ significantly according to whether or not systemic therapy was given, the investigators said.
The group analyzed outcomes for 8,135 women enrolled in 22 studies, randomized to receive radiotherapy to the chest wall and regional lymph nodes after mastectomy and axillary surgery, or to receive the same surgery with no radiotherapy. The median length of follow-up per woman was about 9 years, although many in the studies have now been followed for up to 20 years. Most had positive nodes at dissection (72%); 20% had node-negative disease, and nodal status was unknown for the remainder.
For women with no positive nodes, radiotherapy had no significant effect on locoregional recurrence, overall recurrence, or breast cancer morality, but did however increase overall mortality (RR, 1.23; 95% CI, 1.02-1.49; P = .03). For women with axillary dissection and four or more positive nodes, radiotherapy reduced overall recurrence (RR, 0.79; 95% CI, 0.69-0.90; P = .0003) and breast cancer mortality (RR, 0.87; 95% CI, 0.77-0.99; P = .04).
All of the studies were conducted between 1964 and 1986. Benefits could be even greater today, "... because radiotherapy planning has changed substantially and women today receive better coverage of target areas. Furthermore, doses to normal tissues are lower today, so the risks of radiotherapy are also likely to be lower," wrote the investigators with the Early Breast Cancer Trialists’ Collaborative Group, which conducted the analysis (Lancet 2014 March 19 [doi: 10.1016/S0140-6736(14)60488-8]).
"Breast cancer is a disease with a long natural history," the researchers wrote. "Many of the women in these trials have now been followed up for 20 years and therefore they provide information about the long-term benefits of radiotherapy. Radiotherapy techniques have improved in the past few decades, and so the proportional benefits of radiotherapy are likely to be larger than in these trials."
However, they added, "the absolute risks of breast cancer recurrence and mortality have [been] reduced in many countries because of advances in detection and treatment of breast cancer, so the absolute benefits from postmastectomy radiotherapy today are likely to be smaller than those reported here."
The study group is funded by Cancer Research UK, the British Heart Foundation, and the UK Medical Research Council. None of the members reported any financial disclosures.
FROM THE LANCET
Major finding: Among those with one to three positive nodes, radiotherapy significantly reduced locoregional recurrence (RR, 0.68) and breast cancer mortality (RR, 0.80).
Data source: A meta-analysis of 22 randomized trials evaluating radiotherapy after mastectomy in 8,135 women.
Disclosures: The study group is funded by Cancer Research UK, the British Heart Foundation, and the UK Medical Research Council. None of the members reported any financial disclosures.