User login
CGRP-targeted migraine prevention drugs succeed in phase II
Two investigational migraine prevention drugs that target a vasodilating peptide significantly decreased the number of migraine days per month, compared with placebo, during a pair of phase II studies.
Both drugs reduced mean migraine headache days per month by more than 4 days overall, and one even eliminated migraine in up to 30% of patients.

Each is a monoclonal antibody that inhibits calcitonin gene–related peptide (CGRP). Activated trigeminal sensory nerves release the peptide, which dilates intra- and extracranial blood vessels and modulates vascular nociception.
The antibodies could be game changers for migraine patients, Dr. Peter Goadsby said in an interview.
"Here are the first mechanism-based preventive treatments for migraine," said Dr. Goadsby of the University of California, San Francisco. "They are easy to use, biweekly or even monthly injections, which are effective and well tolerated. For neurologists it means the first major addition to the preventive armamentarium for a generation or more, and for patients, a tangible advance that they can look forward to enjoying soon."
During the annual meeting of the American Academy of Neurology, Dr. Goadsby will present the findings on ALD403, developed by Alder Biopharmaceuticals. His colleague Dr. David W. Dodick of the Mayo Clinic, Rochester, Minn., will present findings on LY2951742, which is being developed by Arteaus Therapeutics in conjunction with Eli Lily. Both presentations are scheduled for May 1.
The trial of ALD403 comprised 163 patients who experienced 5-14 migraine headache days per month; 81 were randomized to receive a single infusion of 1,000 mg ALD403 and the rest received placebo. Patients were followed for 24 weeks. The primary outcome was the mean change in migraine days between weeks 5-8 and baseline.
Patients in the active treatment group fared significantly better than those in the placebo group, with a mean reduction in migraine headache days of –5.6, compared to –4.6 for the placebo group (66% vs. 52% decrease).
Most patients taking the study drug had at least a 50% reduction in migraine headache days at 12 weeks (60% vs. 30%); the proportions of those with at least a 75% reduction were 32% vs. 9%. A 100% reduction occurred in 16% of the active group and in none of the placebo group. These differences were all statistically significant.
There were no differences in the type or frequency of adverse events, vital signs, or laboratory safety data between the two treatment groups.
The LY2951742 study was similarly successful. It comprised 217 patients who experienced 4-14 migraine headache days per month, said Dr. Dodick. They were randomized to placebo or to biweekly subcutaneous injections of LY2951742 150 mg for 12 weeks. The primary end point was the mean change in number of migraine days per month. Secondary end points were the change in headache days, migraine attacks, and responder rate.

Patients in the active treatment group experienced a significantly greater reduction in migraine days than those taking placebo (–4.2 vs. –3 days; 63% vs. 42% decrease).
LY2951742 was significantly better than placebo in all secondary end points including headache days (–4.9 vs. –3.7), migraine attacks (–3 vs. –2.3), and overall response rate (70% vs. 45%).
In an exploratory analysis, 33% of those in the active treatment group were complete responders, with a 100% reduction in migraine headache days, compared with 17% of the placebo group,
Adverse events seen more frequently with LY2951742 than placebo included injection site pain, upper respiratory tract infections, and abdominal pain.
Both drugs will advance to phase III studies, Dr. Dodick said in an interview. "If they are ultimately confirmed to be effective and safe, this will represent a new era in mechanism-based migraine prevention – in other words, treatment directed at a molecule now known to be very important in generating a migraine attack. This would provide a highly effective treatment option that is delivered intermittently by subcutaneous injection or infusion rather than requiring patients to consume oral medications 1-3 times daily."
And, he said, because the antibodies act on the very specific target of CGRP, they exhibit a very favorable side effect profile.
"This would be a major advantage over currently available medications, which have a high rate of side effects [weight gain, sedation, altered concentration, fatigue, etc]. The lack of efficacy and the side effect profile of currently available preventive migraine medications account in large part for the lack of adherence to these medications. We recently showed that even in patients with chronic migraine who experience headaches every other day, about 86% have discontinued their oral migraine preventive drug within 1 year."
Drugs that hit CGRP may even help other headache types, Dr. Dodick added.
"There is some evidence that CGRP is also important in other serious headache disorders such as chronic migraine, medication overuse headache, and cluster headache – disorders that are currently very difficult to manage."
The ALD403 study was supported by Alder Biopharmaceuticals. The LY2951742 study was supported by Arteaus Therapeutics in conjunction with Eli Lily. Both Dr. Goadsby and Dr. Dodick have financial relationships with numerous pharmaceutical companies, including receiving research monies, and participating as officers or speakers.
Two investigational migraine prevention drugs that target a vasodilating peptide significantly decreased the number of migraine days per month, compared with placebo, during a pair of phase II studies.
Both drugs reduced mean migraine headache days per month by more than 4 days overall, and one even eliminated migraine in up to 30% of patients.
Each is a monoclonal antibody that inhibits calcitonin gene–related peptide (CGRP). Activated trigeminal sensory nerves release the peptide, which dilates intra- and extracranial blood vessels and modulates vascular nociception.
The antibodies could be game changers for migraine patients, Dr. Peter Goadsby said in an interview.
"Here are the first mechanism-based preventive treatments for migraine," said Dr. Goadsby of the University of California, San Francisco. "They are easy to use, biweekly or even monthly injections, which are effective and well tolerated. For neurologists it means the first major addition to the preventive armamentarium for a generation or more, and for patients, a tangible advance that they can look forward to enjoying soon."
During the annual meeting of the American Academy of Neurology, Dr. Goadsby will present the findings on ALD403, developed by Alder Biopharmaceuticals. His colleague Dr. David W. Dodick of the Mayo Clinic, Rochester, Minn., will present findings on LY2951742, which is being developed by Arteaus Therapeutics in conjunction with Eli Lily. Both presentations are scheduled for May 1.
The trial of ALD403 comprised 163 patients who experienced 5-14 migraine headache days per month; 81 were randomized to receive a single infusion of 1,000 mg ALD403 and the rest received placebo. Patients were followed for 24 weeks. The primary outcome was the mean change in migraine days between weeks 5-8 and baseline.
Patients in the active treatment group fared significantly better than those in the placebo group, with a mean reduction in migraine headache days of –5.6, compared to –4.6 for the placebo group (66% vs. 52% decrease).
Most patients taking the study drug had at least a 50% reduction in migraine headache days at 12 weeks (60% vs. 30%); the proportions of those with at least a 75% reduction were 32% vs. 9%. A 100% reduction occurred in 16% of the active group and in none of the placebo group. These differences were all statistically significant.
There were no differences in the type or frequency of adverse events, vital signs, or laboratory safety data between the two treatment groups.
The LY2951742 study was similarly successful. It comprised 217 patients who experienced 4-14 migraine headache days per month, said Dr. Dodick. They were randomized to placebo or to biweekly subcutaneous injections of LY2951742 150 mg for 12 weeks. The primary end point was the mean change in number of migraine days per month. Secondary end points were the change in headache days, migraine attacks, and responder rate.
Patients in the active treatment group experienced a significantly greater reduction in migraine days than those taking placebo (–4.2 vs. –3 days; 63% vs. 42% decrease).
LY2951742 was significantly better than placebo in all secondary end points including headache days (–4.9 vs. –3.7), migraine attacks (–3 vs. –2.3), and overall response rate (70% vs. 45%).
In an exploratory analysis, 33% of those in the active treatment group were complete responders, with a 100% reduction in migraine headache days, compared with 17% of the placebo group,
Adverse events seen more frequently with LY2951742 than placebo included injection site pain, upper respiratory tract infections, and abdominal pain.
Both drugs will advance to phase III studies, Dr. Dodick said in an interview. "If they are ultimately confirmed to be effective and safe, this will represent a new era in mechanism-based migraine prevention – in other words, treatment directed at a molecule now known to be very important in generating a migraine attack. This would provide a highly effective treatment option that is delivered intermittently by subcutaneous injection or infusion rather than requiring patients to consume oral medications 1-3 times daily."
And, he said, because the antibodies act on the very specific target of CGRP, they exhibit a very favorable side effect profile.
"This would be a major advantage over currently available medications, which have a high rate of side effects [weight gain, sedation, altered concentration, fatigue, etc]. The lack of efficacy and the side effect profile of currently available preventive migraine medications account in large part for the lack of adherence to these medications. We recently showed that even in patients with chronic migraine who experience headaches every other day, about 86% have discontinued their oral migraine preventive drug within 1 year."
Drugs that hit CGRP may even help other headache types, Dr. Dodick added.
"There is some evidence that CGRP is also important in other serious headache disorders such as chronic migraine, medication overuse headache, and cluster headache – disorders that are currently very difficult to manage."
The ALD403 study was supported by Alder Biopharmaceuticals. The LY2951742 study was supported by Arteaus Therapeutics in conjunction with Eli Lily. Both Dr. Goadsby and Dr. Dodick have financial relationships with numerous pharmaceutical companies, including receiving research monies, and participating as officers or speakers.
Two investigational migraine prevention drugs that target a vasodilating peptide significantly decreased the number of migraine days per month, compared with placebo, during a pair of phase II studies.
Both drugs reduced mean migraine headache days per month by more than 4 days overall, and one even eliminated migraine in up to 30% of patients.
Each is a monoclonal antibody that inhibits calcitonin gene–related peptide (CGRP). Activated trigeminal sensory nerves release the peptide, which dilates intra- and extracranial blood vessels and modulates vascular nociception.
The antibodies could be game changers for migraine patients, Dr. Peter Goadsby said in an interview.
"Here are the first mechanism-based preventive treatments for migraine," said Dr. Goadsby of the University of California, San Francisco. "They are easy to use, biweekly or even monthly injections, which are effective and well tolerated. For neurologists it means the first major addition to the preventive armamentarium for a generation or more, and for patients, a tangible advance that they can look forward to enjoying soon."
During the annual meeting of the American Academy of Neurology, Dr. Goadsby will present the findings on ALD403, developed by Alder Biopharmaceuticals. His colleague Dr. David W. Dodick of the Mayo Clinic, Rochester, Minn., will present findings on LY2951742, which is being developed by Arteaus Therapeutics in conjunction with Eli Lily. Both presentations are scheduled for May 1.
The trial of ALD403 comprised 163 patients who experienced 5-14 migraine headache days per month; 81 were randomized to receive a single infusion of 1,000 mg ALD403 and the rest received placebo. Patients were followed for 24 weeks. The primary outcome was the mean change in migraine days between weeks 5-8 and baseline.
Patients in the active treatment group fared significantly better than those in the placebo group, with a mean reduction in migraine headache days of –5.6, compared to –4.6 for the placebo group (66% vs. 52% decrease).
Most patients taking the study drug had at least a 50% reduction in migraine headache days at 12 weeks (60% vs. 30%); the proportions of those with at least a 75% reduction were 32% vs. 9%. A 100% reduction occurred in 16% of the active group and in none of the placebo group. These differences were all statistically significant.
There were no differences in the type or frequency of adverse events, vital signs, or laboratory safety data between the two treatment groups.
The LY2951742 study was similarly successful. It comprised 217 patients who experienced 4-14 migraine headache days per month, said Dr. Dodick. They were randomized to placebo or to biweekly subcutaneous injections of LY2951742 150 mg for 12 weeks. The primary end point was the mean change in number of migraine days per month. Secondary end points were the change in headache days, migraine attacks, and responder rate.
Patients in the active treatment group experienced a significantly greater reduction in migraine days than those taking placebo (–4.2 vs. –3 days; 63% vs. 42% decrease).
LY2951742 was significantly better than placebo in all secondary end points including headache days (–4.9 vs. –3.7), migraine attacks (–3 vs. –2.3), and overall response rate (70% vs. 45%).
In an exploratory analysis, 33% of those in the active treatment group were complete responders, with a 100% reduction in migraine headache days, compared with 17% of the placebo group,
Adverse events seen more frequently with LY2951742 than placebo included injection site pain, upper respiratory tract infections, and abdominal pain.
Both drugs will advance to phase III studies, Dr. Dodick said in an interview. "If they are ultimately confirmed to be effective and safe, this will represent a new era in mechanism-based migraine prevention – in other words, treatment directed at a molecule now known to be very important in generating a migraine attack. This would provide a highly effective treatment option that is delivered intermittently by subcutaneous injection or infusion rather than requiring patients to consume oral medications 1-3 times daily."
And, he said, because the antibodies act on the very specific target of CGRP, they exhibit a very favorable side effect profile.
"This would be a major advantage over currently available medications, which have a high rate of side effects [weight gain, sedation, altered concentration, fatigue, etc]. The lack of efficacy and the side effect profile of currently available preventive migraine medications account in large part for the lack of adherence to these medications. We recently showed that even in patients with chronic migraine who experience headaches every other day, about 86% have discontinued their oral migraine preventive drug within 1 year."
Drugs that hit CGRP may even help other headache types, Dr. Dodick added.
"There is some evidence that CGRP is also important in other serious headache disorders such as chronic migraine, medication overuse headache, and cluster headache – disorders that are currently very difficult to manage."
The ALD403 study was supported by Alder Biopharmaceuticals. The LY2951742 study was supported by Arteaus Therapeutics in conjunction with Eli Lily. Both Dr. Goadsby and Dr. Dodick have financial relationships with numerous pharmaceutical companies, including receiving research monies, and participating as officers or speakers.
FROM THE AAN 2014 ANNUAL MEETING
Key clinical point: These investigational drugs may be an improvement over currently available migraine prevention drugs in terms of side effects and dosing frequency.
Major finding: Both drugs significantly decreased the number of migraine headache days per month, compared with placebo.
Data source: Two randomized, double-blind phase II studies
Disclosures: The ALD403 study was supported by Alder Biopharmaceuticals. The LY2951742 study was supported by Arteaus Therapeutics in conjunction with Eli Lily. Both Dr. Goadsby and Dr. Dodick have financial relationships with numerous pharmaceutical companies

Asymptomatic stenosis could cause cognitive impairment
Asymptomatic carotid stenosis may not be asymptomatic after all.
Patients with a stenosis of 50% or more performed significantly worse on cognitive tests than did those without. Those cognitive issues were very likely clinically significant as well, according to a study to be presented April 30 at the annual meeting of the American Academy of Neurology.
The study is the first to definitively link asymptomatic carotid stenosis with symptomatic cognitive impairment, primary investigator Brajesh K. Lal said in an interview. But since the stenosis itself is not apparent, and the cognitive changes not profound, patients are not being treated for either, said Dr. Lal, chief of vascular surgery at the Baltimore Veterans Affairs Medical Center, and professor of vascular surgery at the University of Maryland.

"If the cognitive decline was severe, it probably would have been enough for the patient to be evaluated for dementia. Instead, this is floating beneath the radar. It’s not as severe as an obvious dementia that would be picked up on cursory evaluation, but it is significant enough to impact activities of daily living, or the patient’s ability to perform a job," he said.
Dr. Lal and his team conducted cognitive testing on 127 patients: 67 with ultrasound-confirmed asymptomatic carotid stenosis of 50% or more, and 60 controls. Although the control patients did not have carotid stenosis, they did have similar vascular comorbidities, including diabetes, hypertension, and coronary artery disease. The investigators used a Cohen’s d test to determine whether any statistically significant cognitive differences were likely to be clinically meaningful. They found that all the detected impairments were at least mild to moderate in severity, Dr. Lal said.
The stenotic group performed worse on the overall neurocognitive composite score, and the motor/processing speed and learning/memory domains. The Cohen’s measure of effect size showed that all of these differences would have a mild to moderate effect on cognitive function.
A trend of poorer performance for executive function and attention/working memory emerged also, although these differences were neither statistically nor clinically significant.
Extrapolating these results out to the number of people who probably have asymptomatic carotid stenosis presents a sobering picture, he added.
"There are probably somewhere between 8 and 13 million people in the U.S. who have an asymptomatic blockage of 50% or more. And while not every one of them is going to have cognitive decline, this does open the door to the idea that there may be a significant population that is affected."
Right now, the pathophysiologic link between stenosis and cognition remains unclear. It might be related to microemboli shedding from the vascular plaque and causing microinfarcts, or to decreased blood flow and oxygenation to the brain, Dr. Lal said.
Dr. Lal reported that he has several NIH and VA Merit grants focused on developing new methods of diagnosing and treating carotid occlusive disease. He reported having no other financial disclosures.
On Twitter @Alz_Gal
Asymptomatic carotid stenosis may not be asymptomatic after all.
Patients with a stenosis of 50% or more performed significantly worse on cognitive tests than did those without. Those cognitive issues were very likely clinically significant as well, according to a study to be presented April 30 at the annual meeting of the American Academy of Neurology.
The study is the first to definitively link asymptomatic carotid stenosis with symptomatic cognitive impairment, primary investigator Brajesh K. Lal said in an interview. But since the stenosis itself is not apparent, and the cognitive changes not profound, patients are not being treated for either, said Dr. Lal, chief of vascular surgery at the Baltimore Veterans Affairs Medical Center, and professor of vascular surgery at the University of Maryland.
"If the cognitive decline was severe, it probably would have been enough for the patient to be evaluated for dementia. Instead, this is floating beneath the radar. It’s not as severe as an obvious dementia that would be picked up on cursory evaluation, but it is significant enough to impact activities of daily living, or the patient’s ability to perform a job," he said.
Dr. Lal and his team conducted cognitive testing on 127 patients: 67 with ultrasound-confirmed asymptomatic carotid stenosis of 50% or more, and 60 controls. Although the control patients did not have carotid stenosis, they did have similar vascular comorbidities, including diabetes, hypertension, and coronary artery disease. The investigators used a Cohen’s d test to determine whether any statistically significant cognitive differences were likely to be clinically meaningful. They found that all the detected impairments were at least mild to moderate in severity, Dr. Lal said.
The stenotic group performed worse on the overall neurocognitive composite score, and the motor/processing speed and learning/memory domains. The Cohen’s measure of effect size showed that all of these differences would have a mild to moderate effect on cognitive function.
A trend of poorer performance for executive function and attention/working memory emerged also, although these differences were neither statistically nor clinically significant.
Extrapolating these results out to the number of people who probably have asymptomatic carotid stenosis presents a sobering picture, he added.
"There are probably somewhere between 8 and 13 million people in the U.S. who have an asymptomatic blockage of 50% or more. And while not every one of them is going to have cognitive decline, this does open the door to the idea that there may be a significant population that is affected."
Right now, the pathophysiologic link between stenosis and cognition remains unclear. It might be related to microemboli shedding from the vascular plaque and causing microinfarcts, or to decreased blood flow and oxygenation to the brain, Dr. Lal said.
Dr. Lal reported that he has several NIH and VA Merit grants focused on developing new methods of diagnosing and treating carotid occlusive disease. He reported having no other financial disclosures.
On Twitter @Alz_Gal
Asymptomatic carotid stenosis may not be asymptomatic after all.
Patients with a stenosis of 50% or more performed significantly worse on cognitive tests than did those without. Those cognitive issues were very likely clinically significant as well, according to a study to be presented April 30 at the annual meeting of the American Academy of Neurology.
The study is the first to definitively link asymptomatic carotid stenosis with symptomatic cognitive impairment, primary investigator Brajesh K. Lal said in an interview. But since the stenosis itself is not apparent, and the cognitive changes not profound, patients are not being treated for either, said Dr. Lal, chief of vascular surgery at the Baltimore Veterans Affairs Medical Center, and professor of vascular surgery at the University of Maryland.
"If the cognitive decline was severe, it probably would have been enough for the patient to be evaluated for dementia. Instead, this is floating beneath the radar. It’s not as severe as an obvious dementia that would be picked up on cursory evaluation, but it is significant enough to impact activities of daily living, or the patient’s ability to perform a job," he said.
Dr. Lal and his team conducted cognitive testing on 127 patients: 67 with ultrasound-confirmed asymptomatic carotid stenosis of 50% or more, and 60 controls. Although the control patients did not have carotid stenosis, they did have similar vascular comorbidities, including diabetes, hypertension, and coronary artery disease. The investigators used a Cohen’s d test to determine whether any statistically significant cognitive differences were likely to be clinically meaningful. They found that all the detected impairments were at least mild to moderate in severity, Dr. Lal said.
The stenotic group performed worse on the overall neurocognitive composite score, and the motor/processing speed and learning/memory domains. The Cohen’s measure of effect size showed that all of these differences would have a mild to moderate effect on cognitive function.
A trend of poorer performance for executive function and attention/working memory emerged also, although these differences were neither statistically nor clinically significant.
Extrapolating these results out to the number of people who probably have asymptomatic carotid stenosis presents a sobering picture, he added.
"There are probably somewhere between 8 and 13 million people in the U.S. who have an asymptomatic blockage of 50% or more. And while not every one of them is going to have cognitive decline, this does open the door to the idea that there may be a significant population that is affected."
Right now, the pathophysiologic link between stenosis and cognition remains unclear. It might be related to microemboli shedding from the vascular plaque and causing microinfarcts, or to decreased blood flow and oxygenation to the brain, Dr. Lal said.
Dr. Lal reported that he has several NIH and VA Merit grants focused on developing new methods of diagnosing and treating carotid occlusive disease. He reported having no other financial disclosures.
On Twitter @Alz_Gal
FROM THE AAN 2014 ANNUAL MEETING
Major finding: Patients with a stenosis of 50% or more performed significantly worse on cognitive tests than did those without stenosis but with similar vascular comorbidities.
Data source: Cognitive testing on 127 patients: 67 with ultrasound-confirmed asymptomatic carotid stenosis of 50% or more, and 60 controls.
Disclosures: Dr. Lal has several NIH and VA Merit grants focused on developing new methods of diagnosing and treating carotid occlusive disease. He reported having no other disclosures.

Childhood maltreatment raises risk of clinical, subclinical psychotic symptoms
Childhood maltreatment contributes to clinical and subclinical symptoms of psychosis in patients and healthy volunteers.
The intensity of symptoms was greater among patients, and the self-reported psychotic symptoms of the volunteers were considered to be subclinical. However, the strength of association between maltreatment and self-reported symptoms was found to be comparable in both groups, Pamela DeRosse, Ph.D., and her colleagues reported online April 7 in Schizophrenia Research.
The findings "provide strong support for the continuity of the relation between childhood maltreatment and severity of subclinical psychotic symptoms observed in the general population and the severity of psychotic symptoms observed in patients with schizophrenia and schizoaffective disorder," wrote Dr. DeRosse of the Feinstein Institute for Medical Research, Manhasset, N.Y., and her coauthors. "Elucidating the mechanisms that underlie this relationship may provide insight into the pathophysiology of risk and resilience to psychotic disorders," they said (Schizophr. Res. 2014 April 7 [doi: 10.1016/j.schres.2014.03.009]).
She and her coauthors examined the relationships between self-reported psychotic symptoms and several forms of childhood maltreatment (emotional, physical, and sexual abuse; and emotional and physical neglect). The study cohort included 447 healthy adults and 184 stable patients with schizophrenia or schizoaffective disorder. Controls were assessed by using several tools, including the Childhood Trauma Questionnaire. Participants in both groups were assessed with that tool and also with others typically used to identify clinically apparent symptoms.
All forms of childhood abuse were significantly more common among the patients than the controls. Among patients, severity of their clinical symptoms (positive, negative, and depressive) significantly correlated with the severity of abuse. The controls experienced that same significant association between abuse and subclinical symptoms.
For both groups, the associations were particularly strong between all categories of symptoms and childhood emotional abuse, the authors said. In fact, the strongest and most consistent relationships were among the CAPE (Community Assessment of Psychic Experiences) subscale scores and severity of childhood emotional abuse. All P values in that category were less than .001 among participants in both groups. All of the associations remained unchanged when the groups were broken down by gender and by race/ethnicity.
Because the associations affected all symptom categories, it’s tough to tease out specifics, they noted. "This overlap makes it difficult to draw conclusions regarding the relationship between specific forms of childhood maltreatment and specific types of subclinical/clinical psychotic symptoms."
The study was sponsored by the National Institute of Mental Health and several research centers. Dr. DeRosse had no financial declarations. One of her coauthors reported associations with numerous pharmaceutical companies.
Childhood maltreatment contributes to clinical and subclinical symptoms of psychosis in patients and healthy volunteers.
The intensity of symptoms was greater among patients, and the self-reported psychotic symptoms of the volunteers were considered to be subclinical. However, the strength of association between maltreatment and self-reported symptoms was found to be comparable in both groups, Pamela DeRosse, Ph.D., and her colleagues reported online April 7 in Schizophrenia Research.
The findings "provide strong support for the continuity of the relation between childhood maltreatment and severity of subclinical psychotic symptoms observed in the general population and the severity of psychotic symptoms observed in patients with schizophrenia and schizoaffective disorder," wrote Dr. DeRosse of the Feinstein Institute for Medical Research, Manhasset, N.Y., and her coauthors. "Elucidating the mechanisms that underlie this relationship may provide insight into the pathophysiology of risk and resilience to psychotic disorders," they said (Schizophr. Res. 2014 April 7 [doi: 10.1016/j.schres.2014.03.009]).
She and her coauthors examined the relationships between self-reported psychotic symptoms and several forms of childhood maltreatment (emotional, physical, and sexual abuse; and emotional and physical neglect). The study cohort included 447 healthy adults and 184 stable patients with schizophrenia or schizoaffective disorder. Controls were assessed by using several tools, including the Childhood Trauma Questionnaire. Participants in both groups were assessed with that tool and also with others typically used to identify clinically apparent symptoms.
All forms of childhood abuse were significantly more common among the patients than the controls. Among patients, severity of their clinical symptoms (positive, negative, and depressive) significantly correlated with the severity of abuse. The controls experienced that same significant association between abuse and subclinical symptoms.
For both groups, the associations were particularly strong between all categories of symptoms and childhood emotional abuse, the authors said. In fact, the strongest and most consistent relationships were among the CAPE (Community Assessment of Psychic Experiences) subscale scores and severity of childhood emotional abuse. All P values in that category were less than .001 among participants in both groups. All of the associations remained unchanged when the groups were broken down by gender and by race/ethnicity.
Because the associations affected all symptom categories, it’s tough to tease out specifics, they noted. "This overlap makes it difficult to draw conclusions regarding the relationship between specific forms of childhood maltreatment and specific types of subclinical/clinical psychotic symptoms."
The study was sponsored by the National Institute of Mental Health and several research centers. Dr. DeRosse had no financial declarations. One of her coauthors reported associations with numerous pharmaceutical companies.
Childhood maltreatment contributes to clinical and subclinical symptoms of psychosis in patients and healthy volunteers.
The intensity of symptoms was greater among patients, and the self-reported psychotic symptoms of the volunteers were considered to be subclinical. However, the strength of association between maltreatment and self-reported symptoms was found to be comparable in both groups, Pamela DeRosse, Ph.D., and her colleagues reported online April 7 in Schizophrenia Research.
The findings "provide strong support for the continuity of the relation between childhood maltreatment and severity of subclinical psychotic symptoms observed in the general population and the severity of psychotic symptoms observed in patients with schizophrenia and schizoaffective disorder," wrote Dr. DeRosse of the Feinstein Institute for Medical Research, Manhasset, N.Y., and her coauthors. "Elucidating the mechanisms that underlie this relationship may provide insight into the pathophysiology of risk and resilience to psychotic disorders," they said (Schizophr. Res. 2014 April 7 [doi: 10.1016/j.schres.2014.03.009]).
She and her coauthors examined the relationships between self-reported psychotic symptoms and several forms of childhood maltreatment (emotional, physical, and sexual abuse; and emotional and physical neglect). The study cohort included 447 healthy adults and 184 stable patients with schizophrenia or schizoaffective disorder. Controls were assessed by using several tools, including the Childhood Trauma Questionnaire. Participants in both groups were assessed with that tool and also with others typically used to identify clinically apparent symptoms.
All forms of childhood abuse were significantly more common among the patients than the controls. Among patients, severity of their clinical symptoms (positive, negative, and depressive) significantly correlated with the severity of abuse. The controls experienced that same significant association between abuse and subclinical symptoms.
For both groups, the associations were particularly strong between all categories of symptoms and childhood emotional abuse, the authors said. In fact, the strongest and most consistent relationships were among the CAPE (Community Assessment of Psychic Experiences) subscale scores and severity of childhood emotional abuse. All P values in that category were less than .001 among participants in both groups. All of the associations remained unchanged when the groups were broken down by gender and by race/ethnicity.
Because the associations affected all symptom categories, it’s tough to tease out specifics, they noted. "This overlap makes it difficult to draw conclusions regarding the relationship between specific forms of childhood maltreatment and specific types of subclinical/clinical psychotic symptoms."
The study was sponsored by the National Institute of Mental Health and several research centers. Dr. DeRosse had no financial declarations. One of her coauthors reported associations with numerous pharmaceutical companies.
FROM SCHIZOPHRENIA RESEARCH
Major finding: Childhood maltreatment was associated with symptoms of psychosis in patients with schizophrenia and schizoaffective disorder, and healthy controls. The strongest and most consistent relationships were among the CAPE (Community Assessment of Psychic Experiences) subscale scores and the severity of childhood emotional abuse. All P values in that category were less than .001 among participants in both groups.
Data source: A review of 447 healthy volunteers and 184 patients with stable schizophrenia or schizoaffective disorder.
Disclosures: The study was sponsored by the National Institute of Mental Health and several research centers. Dr. DeRosse had no financial disclosures. One of her coauthors reported financial relationships with several pharmaceutical companies.
Case report: Choroidal metastases after targeted treatment with crizotinib
A 31-year-old man presented to an ophthalmologist with a 2-week history of intermittent flashes in both eyes.
The source of the flashes turned out to be a partial retinal detachment secondary to choroidal metastases from a non–small cell lung cancer with an unusual genetic profile, Dr. Rajesh Rao and colleagues reported online in the April issue of the Journal of Clinical Oncology.
Retinal exams of both eyes had revealed yellow, subretinal masses; in the right eye, these showed blocked choroidal fluorescence in the laminar venous plane, consistent with exudative retinal detachment, reported Dr. Rao, an ophthalmologist at the University of Michigan, Ann Arbor, and his coauthors (J. Clin. Oncol. 2014 April 14 [doi:10.1200/JCO.2013.50.2740]).
Two years earlier, the nonsmoking patient had been diagnosed with a stage IV non–small cell lung tumor with regional nodal and rib metastasis. Platinum-based therapy and bevicizumab were ineffective. A genetic evaluation revealed a fusion gene that encodes for the oncogenic EML4-ALK tyrosine kinase.

The patient immediately started the then-investigational crizotinib, a newly developed small-molecule ALK kinase inhibitor. Although the patient’s lung lesions improved, he developed choroidal and brain metastases within 6 months. The eye lesions were treated with proton beam therapy with partial response. He subsequently died of a pulmonary embolism 1 year after the crizotinib treatment began.
Choroidal metastases are the most common intraocular tumor and often arise from a lung cancer. In this case, fluorescein angiography of the right eye showed early, blocked choroidal fluorescence corresponding to the locations of the subretinal masses. It is tempting to speculate that the vascular characteristics of the metastases found are characteristic of the non–small cell lung cancer EML4-ALK translocation, but larger studies are needed, the investigators said.
The EML4-ALK fusion mutation found in the patient’s lung tumor occurs in 5% of non–small cell lung cancer patients, but is detected six times more often in white nonsmokers or light smokers than in regular smokers. Therefore, any nonsmoking patient who presents with choroidal metastases – with or without a known primary lung tumor – should be tested for the translocation. However, future studies will be needed to demonstrate whether crizotinib represents a new tool to treat ophthalmic complications of ALK-positive cancers, such as neuroblastoma or lung-related orbital and intraocular metastases, exudative retinal detachment, and other pathologic effects, the investigators wrote.
The authors reported no financial conflicts of interest.
On Twitter @Alz_Gal
A 31-year-old man presented to an ophthalmologist with a 2-week history of intermittent flashes in both eyes.
The source of the flashes turned out to be a partial retinal detachment secondary to choroidal metastases from a non–small cell lung cancer with an unusual genetic profile, Dr. Rajesh Rao and colleagues reported online in the April issue of the Journal of Clinical Oncology.
Retinal exams of both eyes had revealed yellow, subretinal masses; in the right eye, these showed blocked choroidal fluorescence in the laminar venous plane, consistent with exudative retinal detachment, reported Dr. Rao, an ophthalmologist at the University of Michigan, Ann Arbor, and his coauthors (J. Clin. Oncol. 2014 April 14 [doi:10.1200/JCO.2013.50.2740]).
Two years earlier, the nonsmoking patient had been diagnosed with a stage IV non–small cell lung tumor with regional nodal and rib metastasis. Platinum-based therapy and bevicizumab were ineffective. A genetic evaluation revealed a fusion gene that encodes for the oncogenic EML4-ALK tyrosine kinase.
The patient immediately started the then-investigational crizotinib, a newly developed small-molecule ALK kinase inhibitor. Although the patient’s lung lesions improved, he developed choroidal and brain metastases within 6 months. The eye lesions were treated with proton beam therapy with partial response. He subsequently died of a pulmonary embolism 1 year after the crizotinib treatment began.
Choroidal metastases are the most common intraocular tumor and often arise from a lung cancer. In this case, fluorescein angiography of the right eye showed early, blocked choroidal fluorescence corresponding to the locations of the subretinal masses. It is tempting to speculate that the vascular characteristics of the metastases found are characteristic of the non–small cell lung cancer EML4-ALK translocation, but larger studies are needed, the investigators said.
The EML4-ALK fusion mutation found in the patient’s lung tumor occurs in 5% of non–small cell lung cancer patients, but is detected six times more often in white nonsmokers or light smokers than in regular smokers. Therefore, any nonsmoking patient who presents with choroidal metastases – with or without a known primary lung tumor – should be tested for the translocation. However, future studies will be needed to demonstrate whether crizotinib represents a new tool to treat ophthalmic complications of ALK-positive cancers, such as neuroblastoma or lung-related orbital and intraocular metastases, exudative retinal detachment, and other pathologic effects, the investigators wrote.
The authors reported no financial conflicts of interest.
On Twitter @Alz_Gal
A 31-year-old man presented to an ophthalmologist with a 2-week history of intermittent flashes in both eyes.
The source of the flashes turned out to be a partial retinal detachment secondary to choroidal metastases from a non–small cell lung cancer with an unusual genetic profile, Dr. Rajesh Rao and colleagues reported online in the April issue of the Journal of Clinical Oncology.
Retinal exams of both eyes had revealed yellow, subretinal masses; in the right eye, these showed blocked choroidal fluorescence in the laminar venous plane, consistent with exudative retinal detachment, reported Dr. Rao, an ophthalmologist at the University of Michigan, Ann Arbor, and his coauthors (J. Clin. Oncol. 2014 April 14 [doi:10.1200/JCO.2013.50.2740]).
Two years earlier, the nonsmoking patient had been diagnosed with a stage IV non–small cell lung tumor with regional nodal and rib metastasis. Platinum-based therapy and bevicizumab were ineffective. A genetic evaluation revealed a fusion gene that encodes for the oncogenic EML4-ALK tyrosine kinase.
The patient immediately started the then-investigational crizotinib, a newly developed small-molecule ALK kinase inhibitor. Although the patient’s lung lesions improved, he developed choroidal and brain metastases within 6 months. The eye lesions were treated with proton beam therapy with partial response. He subsequently died of a pulmonary embolism 1 year after the crizotinib treatment began.
Choroidal metastases are the most common intraocular tumor and often arise from a lung cancer. In this case, fluorescein angiography of the right eye showed early, blocked choroidal fluorescence corresponding to the locations of the subretinal masses. It is tempting to speculate that the vascular characteristics of the metastases found are characteristic of the non–small cell lung cancer EML4-ALK translocation, but larger studies are needed, the investigators said.
The EML4-ALK fusion mutation found in the patient’s lung tumor occurs in 5% of non–small cell lung cancer patients, but is detected six times more often in white nonsmokers or light smokers than in regular smokers. Therefore, any nonsmoking patient who presents with choroidal metastases – with or without a known primary lung tumor – should be tested for the translocation. However, future studies will be needed to demonstrate whether crizotinib represents a new tool to treat ophthalmic complications of ALK-positive cancers, such as neuroblastoma or lung-related orbital and intraocular metastases, exudative retinal detachment, and other pathologic effects, the investigators wrote.
The authors reported no financial conflicts of interest.
On Twitter @Alz_Gal
FROM JOURNAL OF CLINICAL ONCOLOGY

Auditory hallucinations in schizophrenia tied to decreased brain current
Abnormal electrical current in two brain regions might underlie the phenomenon of auditory verbal hallucinations in patients with schizophrenia.
An electroencephalographic study of patients with schizophrenia determined that their hallucination severity correlated negatively with amplitude in the frontal currents. Their negative symptom severity correlated negatively with the temporal current amplitude, according to research conducted by Dr. Jérôme Graux and his colleagues (Schizophr. Res. 2014 April 1 [doi.org/10.1016/j.schres.2014.03.007]).
Dr. Graux and his coauthors examined brainwave responses to a single spoken "A" in 13 patients with schizophrenia-related auditory hallucinations, 13 nonhallucinating patients, and 13 healthy controls. The researchers focused on waves associated with auditory processes in the frontal region (P1, N1, and P2), and current in the temporal sinks.
The overall response patterns were similar between groups, with P1 peaking first, followed by N1 and P2. But hallucinating patients showed lower-amplitude responses in the frontocentral regions. Current at the left and right temporal sinks also was reduced, reported Dr. Graux of UMR 930 Imagerie et Cerveau, INSERM, Université François Rabelais de Tours, France.
The amplitudes of both frontal and temporal current negatively correlated with symptom scores. The higher the severity of hallucinations, the smaller the amplitude of the frontal currents; the higher the PANSS (Positive and Negative Syndrome Scale) negative symptom score, the smaller the amplitude of the temporal currents, wrote Dr. Graux, who also is affiliated with CHRU de Tours Hospital, France.
"The small amplitude of the frontal current in the present study suggests the involvement of a deep source in the frontal lobe, which might correspond to the involvement of the anterior cingulate cortex in the perception of human speech," the authors wrote.
The study was supported by several French private foundations. None of the authors disclosed had any financial disclosures.
On Twitter @alz_gal
Abnormal electrical current in two brain regions might underlie the phenomenon of auditory verbal hallucinations in patients with schizophrenia.
An electroencephalographic study of patients with schizophrenia determined that their hallucination severity correlated negatively with amplitude in the frontal currents. Their negative symptom severity correlated negatively with the temporal current amplitude, according to research conducted by Dr. Jérôme Graux and his colleagues (Schizophr. Res. 2014 April 1 [doi.org/10.1016/j.schres.2014.03.007]).
Dr. Graux and his coauthors examined brainwave responses to a single spoken "A" in 13 patients with schizophrenia-related auditory hallucinations, 13 nonhallucinating patients, and 13 healthy controls. The researchers focused on waves associated with auditory processes in the frontal region (P1, N1, and P2), and current in the temporal sinks.
The overall response patterns were similar between groups, with P1 peaking first, followed by N1 and P2. But hallucinating patients showed lower-amplitude responses in the frontocentral regions. Current at the left and right temporal sinks also was reduced, reported Dr. Graux of UMR 930 Imagerie et Cerveau, INSERM, Université François Rabelais de Tours, France.
The amplitudes of both frontal and temporal current negatively correlated with symptom scores. The higher the severity of hallucinations, the smaller the amplitude of the frontal currents; the higher the PANSS (Positive and Negative Syndrome Scale) negative symptom score, the smaller the amplitude of the temporal currents, wrote Dr. Graux, who also is affiliated with CHRU de Tours Hospital, France.
"The small amplitude of the frontal current in the present study suggests the involvement of a deep source in the frontal lobe, which might correspond to the involvement of the anterior cingulate cortex in the perception of human speech," the authors wrote.
The study was supported by several French private foundations. None of the authors disclosed had any financial disclosures.
On Twitter @alz_gal
Abnormal electrical current in two brain regions might underlie the phenomenon of auditory verbal hallucinations in patients with schizophrenia.
An electroencephalographic study of patients with schizophrenia determined that their hallucination severity correlated negatively with amplitude in the frontal currents. Their negative symptom severity correlated negatively with the temporal current amplitude, according to research conducted by Dr. Jérôme Graux and his colleagues (Schizophr. Res. 2014 April 1 [doi.org/10.1016/j.schres.2014.03.007]).
Dr. Graux and his coauthors examined brainwave responses to a single spoken "A" in 13 patients with schizophrenia-related auditory hallucinations, 13 nonhallucinating patients, and 13 healthy controls. The researchers focused on waves associated with auditory processes in the frontal region (P1, N1, and P2), and current in the temporal sinks.
The overall response patterns were similar between groups, with P1 peaking first, followed by N1 and P2. But hallucinating patients showed lower-amplitude responses in the frontocentral regions. Current at the left and right temporal sinks also was reduced, reported Dr. Graux of UMR 930 Imagerie et Cerveau, INSERM, Université François Rabelais de Tours, France.
The amplitudes of both frontal and temporal current negatively correlated with symptom scores. The higher the severity of hallucinations, the smaller the amplitude of the frontal currents; the higher the PANSS (Positive and Negative Syndrome Scale) negative symptom score, the smaller the amplitude of the temporal currents, wrote Dr. Graux, who also is affiliated with CHRU de Tours Hospital, France.
"The small amplitude of the frontal current in the present study suggests the involvement of a deep source in the frontal lobe, which might correspond to the involvement of the anterior cingulate cortex in the perception of human speech," the authors wrote.
The study was supported by several French private foundations. None of the authors disclosed had any financial disclosures.
On Twitter @alz_gal
FROM SCHIZOPHRENIA RESEARCH
Major finding: Schizophrenia patients with auditory hallucinations showed decreased electrical activity in the frontal and temporal brain regions. But hallucinating patients showed lower-amplitude responses in the frontocentral regions.
Data source: The prospective study comprised 13 hallucinating schizophrenia patients, 13 nonhallucinating patients, and 13 healthy controls.
Disclosures: The study was supported by several private foundations in France. None of the authors disclosed had any financial disclosures.
Reduced risk of RA in schizophrenia may be bias, not biology
The observed reduced risk of rheumatoid arthritis and osteoarthritis in patients with schizophrenia might be tied to reporting bias rather than disease-specific biology, Dr. Carl Sellgren and colleagues reported.
Data on more than 6 million people contained in the Swedish Population Register showed significantly reduced risks of both disorders, and of other musculoskeletal diseases, among schizophrenia patients, wrote Dr. Sellgren of the Karolinksa Institute, Stockholm, and his associates. Conversely, no increased risks were found among patients with bipolar disorder, despite a shared polygenic component of 68% between the two mental illnesses (Schizophr. Bull. 2014 Apr. 8 [doi:10.1093/schbul/sbu054]).
"In light of the more severe loss of function in schizophrenia and schizoaffective disorder patients in comparison to bipolar disease patients, this is compatible with differential misclassification bias in the observed inverse association between schizophrenia and rheumatoid arthritis," the researchers wrote.
Dr. Sellgren and his team were not ready to entirely scrap the possibility of some biologic link, however.
"Interestingly, we observed a significantly decreased risk for seronegative RA in children and siblings of schizophrenia probands," he said in an interview. "Correspondingly, the lowest point estimate for schizophrenia was observed in relatives of seronegative RA patients, and the lowest point estimate among schizophrenia patients was also observed for seronegative RA. Genetic causation may be present regarding the specific association between schizophrenia and seronegative RA."
Whatever the link, the study points up the importance of looking at schizophrenia patients holistically, rather than only focusing on their mental illnesses. "It appears that the more severely affected the patient is of the psychiatric disorder, the less likely is the clinician to identify a comorbid musculoskeletal disease," he said. "These data emphasize the need of assessing and being aware of nonpsychiatric symptoms in schizophrenia."
The Swedish Medical Research Council funded the study. Dr. Sellgren made no financial disclosures.
On Twitter @Alz_Gal
The observed reduced risk of rheumatoid arthritis and osteoarthritis in patients with schizophrenia might be tied to reporting bias rather than disease-specific biology, Dr. Carl Sellgren and colleagues reported.
Data on more than 6 million people contained in the Swedish Population Register showed significantly reduced risks of both disorders, and of other musculoskeletal diseases, among schizophrenia patients, wrote Dr. Sellgren of the Karolinksa Institute, Stockholm, and his associates. Conversely, no increased risks were found among patients with bipolar disorder, despite a shared polygenic component of 68% between the two mental illnesses (Schizophr. Bull. 2014 Apr. 8 [doi:10.1093/schbul/sbu054]).
"In light of the more severe loss of function in schizophrenia and schizoaffective disorder patients in comparison to bipolar disease patients, this is compatible with differential misclassification bias in the observed inverse association between schizophrenia and rheumatoid arthritis," the researchers wrote.
Dr. Sellgren and his team were not ready to entirely scrap the possibility of some biologic link, however.
"Interestingly, we observed a significantly decreased risk for seronegative RA in children and siblings of schizophrenia probands," he said in an interview. "Correspondingly, the lowest point estimate for schizophrenia was observed in relatives of seronegative RA patients, and the lowest point estimate among schizophrenia patients was also observed for seronegative RA. Genetic causation may be present regarding the specific association between schizophrenia and seronegative RA."
Whatever the link, the study points up the importance of looking at schizophrenia patients holistically, rather than only focusing on their mental illnesses. "It appears that the more severely affected the patient is of the psychiatric disorder, the less likely is the clinician to identify a comorbid musculoskeletal disease," he said. "These data emphasize the need of assessing and being aware of nonpsychiatric symptoms in schizophrenia."
The Swedish Medical Research Council funded the study. Dr. Sellgren made no financial disclosures.
On Twitter @Alz_Gal
The observed reduced risk of rheumatoid arthritis and osteoarthritis in patients with schizophrenia might be tied to reporting bias rather than disease-specific biology, Dr. Carl Sellgren and colleagues reported.
Data on more than 6 million people contained in the Swedish Population Register showed significantly reduced risks of both disorders, and of other musculoskeletal diseases, among schizophrenia patients, wrote Dr. Sellgren of the Karolinksa Institute, Stockholm, and his associates. Conversely, no increased risks were found among patients with bipolar disorder, despite a shared polygenic component of 68% between the two mental illnesses (Schizophr. Bull. 2014 Apr. 8 [doi:10.1093/schbul/sbu054]).
"In light of the more severe loss of function in schizophrenia and schizoaffective disorder patients in comparison to bipolar disease patients, this is compatible with differential misclassification bias in the observed inverse association between schizophrenia and rheumatoid arthritis," the researchers wrote.
Dr. Sellgren and his team were not ready to entirely scrap the possibility of some biologic link, however.
"Interestingly, we observed a significantly decreased risk for seronegative RA in children and siblings of schizophrenia probands," he said in an interview. "Correspondingly, the lowest point estimate for schizophrenia was observed in relatives of seronegative RA patients, and the lowest point estimate among schizophrenia patients was also observed for seronegative RA. Genetic causation may be present regarding the specific association between schizophrenia and seronegative RA."
Whatever the link, the study points up the importance of looking at schizophrenia patients holistically, rather than only focusing on their mental illnesses. "It appears that the more severely affected the patient is of the psychiatric disorder, the less likely is the clinician to identify a comorbid musculoskeletal disease," he said. "These data emphasize the need of assessing and being aware of nonpsychiatric symptoms in schizophrenia."
The Swedish Medical Research Council funded the study. Dr. Sellgren made no financial disclosures.
On Twitter @Alz_Gal
FROM SCHIZOPHRENIA BULLETIN
Major finding: The risk for RA was decreased (hazard ratio, 0.69; 95% confidence interval, 0.59-0.80) in schizophrenia, but not in bipolar disorder. These findings suggest that the risk reduction could be attributable to reporting and misclassification bias.
Data source: The review included more than 6 million people in the Swedish Population Register.
Disclosures: The Swedish Medical Research Council funded the study. Dr. Sellgren had no financial disclosures.
Memory-disorder care program costs little but saves much
WASHINGTON – A collaborative care program that supports both Alzheimer’s patients and caregivers saved an Indiana health care system more than $1 million during its initial yearlong test period.
The Healthy Aging Brain Center (HABC) at Eskenazi Health in Indianapolis saved $2,856 per patient per year, while costing just $618 per patient to administer, Dr. Dustin French said at a briefing on Alzheimer’s disease hosted by Health Affairs. "The cost to administer the program comes to about $1.69 per patient per day – way less than the cost of a cup of coffee," Dr. French said.
The HABC creates individual care plans for patients with newly diagnosed memory disorders, including Alzheimer’s, mild cognitive impairment, and late-life depression. A team of physicians, social workers, and nurses works with the patient, caregiver, and family members. After the initial assessment, there is ongoing, unlimited support in the form of clinic visits and phone contact.

The individual care plans target a number of problem areas, including self-management, problem-solving, medication management, dealing with depression, managing cardiovascular risks, caregiver emotional and physical health support, transition of care across settings, and managing acute care issues.
The pilot ran from 2008 to 2009 with an initial cohort of 303 patients. A total of 1,453 patients did not enroll, mostly because the program was not being widely publicized at that point. If all eligible patients had enrolled, the annual cost savings would top $6 million, said Dr. French, the study’s primary investigator. He is a faculty member at the Center for Healthcare Studies at Northwestern University and a research scientist at Veterans Affairs Health Services Research and Development Service, both in Chicago.
The HABC patients were referred by primary care physician, self, or family member. The primary reasons for referral were memory problems (88%) or behavioral problems (12%), including wandering and agitation. The comparison group was similar in diagnosis and behavioral issues. Outcomes were cost and savings data extracted from Eskenazi Health’s accounting system and adjusted for comorbid illness, hospital charges and length of stay, and mortality (Health Aff. 2014;33:613-8).
The average risk-adjusted HABC patient cost savings was $3,474, compared with the control group. Half of that was in decreased inpatient expenses and the other half was in decreased emergency department and related outpatient costs. After subtraction of the $618-per-patient administration cost, the annual net per-patient savings was $2,865. This left an estimated net savings of $865,368 for the HABC cohort of 303 patients and $5,015,136 if all 1,756 patients had been enrolled.
The study could help lay a business foundation that might encourage payers to take notice of this kind of an intervention program, the authors noted. The current system does not encourage "the development of innovative health care delivery models" such as the one at the HABC, nor does it reimburse for caregiver support, such as telephone backup, unless it’s delivered in a remote locations.
"Reimbursement processes ... fail to address the complex needs of patients with dementia, which require multifaceted care. Unfortunately, these needs are often not fully addressed until the patient is institutionalized and the medical costs have begun to mount," the investigators wrote in their report.
The federal government may be waking up to the possibilities. The HABC program was awarded a grant from the Center for Medicare & Medicaid Innovation, which supported this study and allowed Eskenazi Health to expand the program to more than 2,000 Medicare beneficiaries with dementia or late-life depression.
"If we can do this in Indiana, anyone can do it anywhere," Dr. French said.
Dr. French had no disclosures. Several of his coauthors are employees of Eskenazi Health.
On Twitter @Alz_Gal
WASHINGTON – A collaborative care program that supports both Alzheimer’s patients and caregivers saved an Indiana health care system more than $1 million during its initial yearlong test period.
The Healthy Aging Brain Center (HABC) at Eskenazi Health in Indianapolis saved $2,856 per patient per year, while costing just $618 per patient to administer, Dr. Dustin French said at a briefing on Alzheimer’s disease hosted by Health Affairs. "The cost to administer the program comes to about $1.69 per patient per day – way less than the cost of a cup of coffee," Dr. French said.
The HABC creates individual care plans for patients with newly diagnosed memory disorders, including Alzheimer’s, mild cognitive impairment, and late-life depression. A team of physicians, social workers, and nurses works with the patient, caregiver, and family members. After the initial assessment, there is ongoing, unlimited support in the form of clinic visits and phone contact.
The individual care plans target a number of problem areas, including self-management, problem-solving, medication management, dealing with depression, managing cardiovascular risks, caregiver emotional and physical health support, transition of care across settings, and managing acute care issues.
The pilot ran from 2008 to 2009 with an initial cohort of 303 patients. A total of 1,453 patients did not enroll, mostly because the program was not being widely publicized at that point. If all eligible patients had enrolled, the annual cost savings would top $6 million, said Dr. French, the study’s primary investigator. He is a faculty member at the Center for Healthcare Studies at Northwestern University and a research scientist at Veterans Affairs Health Services Research and Development Service, both in Chicago.
The HABC patients were referred by primary care physician, self, or family member. The primary reasons for referral were memory problems (88%) or behavioral problems (12%), including wandering and agitation. The comparison group was similar in diagnosis and behavioral issues. Outcomes were cost and savings data extracted from Eskenazi Health’s accounting system and adjusted for comorbid illness, hospital charges and length of stay, and mortality (Health Aff. 2014;33:613-8).
The average risk-adjusted HABC patient cost savings was $3,474, compared with the control group. Half of that was in decreased inpatient expenses and the other half was in decreased emergency department and related outpatient costs. After subtraction of the $618-per-patient administration cost, the annual net per-patient savings was $2,865. This left an estimated net savings of $865,368 for the HABC cohort of 303 patients and $5,015,136 if all 1,756 patients had been enrolled.
The study could help lay a business foundation that might encourage payers to take notice of this kind of an intervention program, the authors noted. The current system does not encourage "the development of innovative health care delivery models" such as the one at the HABC, nor does it reimburse for caregiver support, such as telephone backup, unless it’s delivered in a remote locations.
"Reimbursement processes ... fail to address the complex needs of patients with dementia, which require multifaceted care. Unfortunately, these needs are often not fully addressed until the patient is institutionalized and the medical costs have begun to mount," the investigators wrote in their report.
The federal government may be waking up to the possibilities. The HABC program was awarded a grant from the Center for Medicare & Medicaid Innovation, which supported this study and allowed Eskenazi Health to expand the program to more than 2,000 Medicare beneficiaries with dementia or late-life depression.
"If we can do this in Indiana, anyone can do it anywhere," Dr. French said.
Dr. French had no disclosures. Several of his coauthors are employees of Eskenazi Health.
On Twitter @Alz_Gal
WASHINGTON – A collaborative care program that supports both Alzheimer’s patients and caregivers saved an Indiana health care system more than $1 million during its initial yearlong test period.
The Healthy Aging Brain Center (HABC) at Eskenazi Health in Indianapolis saved $2,856 per patient per year, while costing just $618 per patient to administer, Dr. Dustin French said at a briefing on Alzheimer’s disease hosted by Health Affairs. "The cost to administer the program comes to about $1.69 per patient per day – way less than the cost of a cup of coffee," Dr. French said.
The HABC creates individual care plans for patients with newly diagnosed memory disorders, including Alzheimer’s, mild cognitive impairment, and late-life depression. A team of physicians, social workers, and nurses works with the patient, caregiver, and family members. After the initial assessment, there is ongoing, unlimited support in the form of clinic visits and phone contact.
The individual care plans target a number of problem areas, including self-management, problem-solving, medication management, dealing with depression, managing cardiovascular risks, caregiver emotional and physical health support, transition of care across settings, and managing acute care issues.
The pilot ran from 2008 to 2009 with an initial cohort of 303 patients. A total of 1,453 patients did not enroll, mostly because the program was not being widely publicized at that point. If all eligible patients had enrolled, the annual cost savings would top $6 million, said Dr. French, the study’s primary investigator. He is a faculty member at the Center for Healthcare Studies at Northwestern University and a research scientist at Veterans Affairs Health Services Research and Development Service, both in Chicago.
The HABC patients were referred by primary care physician, self, or family member. The primary reasons for referral were memory problems (88%) or behavioral problems (12%), including wandering and agitation. The comparison group was similar in diagnosis and behavioral issues. Outcomes were cost and savings data extracted from Eskenazi Health’s accounting system and adjusted for comorbid illness, hospital charges and length of stay, and mortality (Health Aff. 2014;33:613-8).
The average risk-adjusted HABC patient cost savings was $3,474, compared with the control group. Half of that was in decreased inpatient expenses and the other half was in decreased emergency department and related outpatient costs. After subtraction of the $618-per-patient administration cost, the annual net per-patient savings was $2,865. This left an estimated net savings of $865,368 for the HABC cohort of 303 patients and $5,015,136 if all 1,756 patients had been enrolled.
The study could help lay a business foundation that might encourage payers to take notice of this kind of an intervention program, the authors noted. The current system does not encourage "the development of innovative health care delivery models" such as the one at the HABC, nor does it reimburse for caregiver support, such as telephone backup, unless it’s delivered in a remote locations.
"Reimbursement processes ... fail to address the complex needs of patients with dementia, which require multifaceted care. Unfortunately, these needs are often not fully addressed until the patient is institutionalized and the medical costs have begun to mount," the investigators wrote in their report.
The federal government may be waking up to the possibilities. The HABC program was awarded a grant from the Center for Medicare & Medicaid Innovation, which supported this study and allowed Eskenazi Health to expand the program to more than 2,000 Medicare beneficiaries with dementia or late-life depression.
"If we can do this in Indiana, anyone can do it anywhere," Dr. French said.
Dr. French had no disclosures. Several of his coauthors are employees of Eskenazi Health.
On Twitter @Alz_Gal
AT A HEALTH AFFAIRS BRIEFING
Major finding: The Healthy Aging Brain Center program saved $2,856 per patient each year.
Data source: A 1-year pilot program involving 303 patients and 1,453 controls.
Disclosures: The Center for Medicare and Medicaid Innovation supported the study. Dr. French had no disclosures. Several coauthors are employees of Eskenazi Health.

Some providers quicker to tube feed end-of-life elderly
Hospitalists who care for dementia patients near the end of life are much less likely to introduce a feeding tube than other physicians who follow such patients.
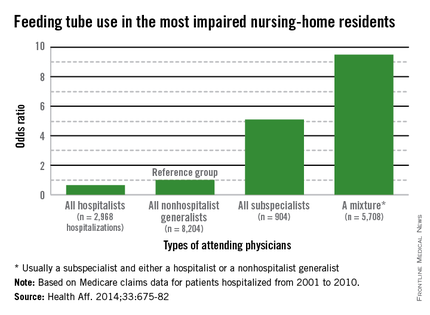
Compared with nonhospital generalists, hospitalists were 22% less likely to tube-feed hospitalized nursing home residents – and even less likely to tube-feed patients who were the most severely impaired (35%). In contrast, subspecialists were five times more likely to insert a tube. When a mixed group of physicians was on the case, rates were even higher, with a 9-fold increase overall and a 9.5-fold increase for severely demented patients.
The findings clearly illustrate that nonhospitalists could benefit from some education about the most appropriate interventions when patients near the end of life enter a hospital, Dr. Joan Teno and her associates reported in the April issue of Health Affairs (Health Aff. April 2014;33:675-82).
"It may be that subspecialists do not have adequate knowledge about the risks and benefits of using feeding tubes in people with advanced dementia," said Dr. Teno of Brown University, Providence, R.I., and her coauthors. "Hospitals should educate physicians about the lack of efficacy of PEG [percutaneous endoscopic gastrostomy] feeding tubes, compared with hand feeding, in prolonging survival and preventing aspiration pneumonias and pressure ulcers in people with advanced dementia. In addition, hospitals should examine how they staff the role of attending physician and ensure coordination of care when patient hand-offs are made between different types of attending physicians."
Such education would bring all physicians up to speed with position statements against tube feeding for this group of patients. The issue sits atop the Choosing Wisely lists of both the American Academy of Hospice and Palliative Medicine and the American Geriatrics Society. The American Academy of Hospice and Palliative Medicine states that "feeding tubes do not result in improved survival, prevention of aspiration pneumonia, or improved healing of pressure ulcers. Feeding tube use in such patients has actually been associated with pressure ulcer development, use of physical and pharmacological restraints, and patient distress about the tube itself."
Internal medicine physician Eric G. Tangalos of the Alzheimer’s Disease Research Center at Mayo Clinic, Rochester, Minn., works closely with hospitalists. He agrees with the concept that tube feeding can impose even more distress on both these patients and their families. "As a medical profession and a society, we have yet to accept some of the futility of our actions and continue to ignore the burdens tube feedings place on patients, families, and the health care system once a hospitalization has come to its conclusion," he said in an interview.
Dr. Teno and her team looked at the rate of feeding tube insertion in fee-for-service Medicare patients with advanced dementia who were within 90 days of death and hospitalized with a diagnosis of urinary tract infection, sepsis, pneumonia, or dehydration. The study examined decisions made by four groups of physicians who cared for these patients: hospitalists, nonhospitalist generalists (geriatricians, general practitioners, internists, and family physicians), subspecialists, and mixed groups that included a subspecialist and either a hospitalist or nonhospitalist generalist.
The cohort comprised 53,492 patients hospitalized from 2001 to 2010. The patients’ mean age was 85 years. About 60% had a do not resuscitate order, and 10% had an order against tube feeding.
The rate of hospitalists as attending physicians increased from 11% in 2001 to 28% in 2010. The portion of patients seen by a mixture of attending physicians increased from 29% in 2001 to 38% in 2010.

The rates of tube feeding were lowest when a hospitalist or nonhospitalist generalist was the attending physician (1.6% and 2.2%, respectively). Subspecialists had significantly higher rates (11%). The highest rate occurred when there were mixed groups of physicians involved in the patient’s care (15.6%).
Using the nonhospitalist generalists as a reference group, the researchers found that hospitalists were 22% less likely to insert a tube overall and 35% less likely to do so when the patient had very severe cognitive and physical impairment.
Conversely, subspecialists were five times more likely to commence tube feeding for all patients and for very severely impaired patients. The mixed groups were the most likely to begin tube feeding – almost 9 times more likely overall and 9.5 times more likely for the most severely impaired patients.
"Our finding that subspecialists had a higher rate of insertions of PEG feeding tubes might reflect their lack of experience in providing care for people with advanced dementia," the authors wrote.
The mixed-physician group could be seen as a proxy for discontinuity of care among the attending physicians, they noted. Prior studies have found that such discontinuity was associated with longer hospital stays.
"There may be a lack of care coordination during patient hand offs between attending physicians that begins a cascade of events, ending with the insertion of a PEG feeding tube."
Dr. Diane E. Meier, professor of geriatrics and palliative medicine at Icahn School of Medicine at Mount Sinai, New York, and director of the Center to Advance Palliative Care, agreed that group care without a leader creates confusion. "One of the hallmarks of modern medicine in the U.S. is fragmentation. It is typical for a person with dementia to have a different specialist for every organ system, a problem compounded in the hospital when a completely new group of specialists is brought into the care team. The problem with this abundance of doctors is that no one is really in charge of the whole patient and what makes the most sense for the patient as a person. Organ- and specialty-specific decision making leads to bad practices – including trying to ‘solve’ a feeding difficulty as if it is an isolated problem when the real issue is progressive brain failure – a terminal illness that cannot be fixed with a feeding tube."
The study not only questions the feeding tube issue, but also the wisdom of repeatedly hospitalizing elderly patients with severe dementia who could be in the last phase of life – especially for conditions that are expected complications of severe dementia. The authors suggested that there may be financial motives to admit fee-for-service patients.
"The fee-for-service system provides incentives to hospitalize nursing home residents with severe dementia because such hospitalizations qualify the patients for skilled nursing home services. Bundling of payments and institutional special needs plans that reverse these financial incentives may reduce health care expenditures and improve the quality of care for nursing home residents with advanced dementia by avoiding burdensome transitions between facilities and the stress of relocation."
The National Institute on Aging funded the study. Dr. Teno made no financial declarations.
Hospitalists who care for dementia patients near the end of life are much less likely to introduce a feeding tube than other physicians who follow such patients.
Compared with nonhospital generalists, hospitalists were 22% less likely to tube-feed hospitalized nursing home residents – and even less likely to tube-feed patients who were the most severely impaired (35%). In contrast, subspecialists were five times more likely to insert a tube. When a mixed group of physicians was on the case, rates were even higher, with a 9-fold increase overall and a 9.5-fold increase for severely demented patients.
The findings clearly illustrate that nonhospitalists could benefit from some education about the most appropriate interventions when patients near the end of life enter a hospital, Dr. Joan Teno and her associates reported in the April issue of Health Affairs (Health Aff. April 2014;33:675-82).
"It may be that subspecialists do not have adequate knowledge about the risks and benefits of using feeding tubes in people with advanced dementia," said Dr. Teno of Brown University, Providence, R.I., and her coauthors. "Hospitals should educate physicians about the lack of efficacy of PEG [percutaneous endoscopic gastrostomy] feeding tubes, compared with hand feeding, in prolonging survival and preventing aspiration pneumonias and pressure ulcers in people with advanced dementia. In addition, hospitals should examine how they staff the role of attending physician and ensure coordination of care when patient hand-offs are made between different types of attending physicians."
Such education would bring all physicians up to speed with position statements against tube feeding for this group of patients. The issue sits atop the Choosing Wisely lists of both the American Academy of Hospice and Palliative Medicine and the American Geriatrics Society. The American Academy of Hospice and Palliative Medicine states that "feeding tubes do not result in improved survival, prevention of aspiration pneumonia, or improved healing of pressure ulcers. Feeding tube use in such patients has actually been associated with pressure ulcer development, use of physical and pharmacological restraints, and patient distress about the tube itself."
Internal medicine physician Eric G. Tangalos of the Alzheimer’s Disease Research Center at Mayo Clinic, Rochester, Minn., works closely with hospitalists. He agrees with the concept that tube feeding can impose even more distress on both these patients and their families. "As a medical profession and a society, we have yet to accept some of the futility of our actions and continue to ignore the burdens tube feedings place on patients, families, and the health care system once a hospitalization has come to its conclusion," he said in an interview.
Dr. Teno and her team looked at the rate of feeding tube insertion in fee-for-service Medicare patients with advanced dementia who were within 90 days of death and hospitalized with a diagnosis of urinary tract infection, sepsis, pneumonia, or dehydration. The study examined decisions made by four groups of physicians who cared for these patients: hospitalists, nonhospitalist generalists (geriatricians, general practitioners, internists, and family physicians), subspecialists, and mixed groups that included a subspecialist and either a hospitalist or nonhospitalist generalist.
The cohort comprised 53,492 patients hospitalized from 2001 to 2010. The patients’ mean age was 85 years. About 60% had a do not resuscitate order, and 10% had an order against tube feeding.
The rate of hospitalists as attending physicians increased from 11% in 2001 to 28% in 2010. The portion of patients seen by a mixture of attending physicians increased from 29% in 2001 to 38% in 2010.
The rates of tube feeding were lowest when a hospitalist or nonhospitalist generalist was the attending physician (1.6% and 2.2%, respectively). Subspecialists had significantly higher rates (11%). The highest rate occurred when there were mixed groups of physicians involved in the patient’s care (15.6%).
Using the nonhospitalist generalists as a reference group, the researchers found that hospitalists were 22% less likely to insert a tube overall and 35% less likely to do so when the patient had very severe cognitive and physical impairment.
Conversely, subspecialists were five times more likely to commence tube feeding for all patients and for very severely impaired patients. The mixed groups were the most likely to begin tube feeding – almost 9 times more likely overall and 9.5 times more likely for the most severely impaired patients.
"Our finding that subspecialists had a higher rate of insertions of PEG feeding tubes might reflect their lack of experience in providing care for people with advanced dementia," the authors wrote.
The mixed-physician group could be seen as a proxy for discontinuity of care among the attending physicians, they noted. Prior studies have found that such discontinuity was associated with longer hospital stays.
"There may be a lack of care coordination during patient hand offs between attending physicians that begins a cascade of events, ending with the insertion of a PEG feeding tube."
Dr. Diane E. Meier, professor of geriatrics and palliative medicine at Icahn School of Medicine at Mount Sinai, New York, and director of the Center to Advance Palliative Care, agreed that group care without a leader creates confusion. "One of the hallmarks of modern medicine in the U.S. is fragmentation. It is typical for a person with dementia to have a different specialist for every organ system, a problem compounded in the hospital when a completely new group of specialists is brought into the care team. The problem with this abundance of doctors is that no one is really in charge of the whole patient and what makes the most sense for the patient as a person. Organ- and specialty-specific decision making leads to bad practices – including trying to ‘solve’ a feeding difficulty as if it is an isolated problem when the real issue is progressive brain failure – a terminal illness that cannot be fixed with a feeding tube."
The study not only questions the feeding tube issue, but also the wisdom of repeatedly hospitalizing elderly patients with severe dementia who could be in the last phase of life – especially for conditions that are expected complications of severe dementia. The authors suggested that there may be financial motives to admit fee-for-service patients.
"The fee-for-service system provides incentives to hospitalize nursing home residents with severe dementia because such hospitalizations qualify the patients for skilled nursing home services. Bundling of payments and institutional special needs plans that reverse these financial incentives may reduce health care expenditures and improve the quality of care for nursing home residents with advanced dementia by avoiding burdensome transitions between facilities and the stress of relocation."
The National Institute on Aging funded the study. Dr. Teno made no financial declarations.
Hospitalists who care for dementia patients near the end of life are much less likely to introduce a feeding tube than other physicians who follow such patients.
Compared with nonhospital generalists, hospitalists were 22% less likely to tube-feed hospitalized nursing home residents – and even less likely to tube-feed patients who were the most severely impaired (35%). In contrast, subspecialists were five times more likely to insert a tube. When a mixed group of physicians was on the case, rates were even higher, with a 9-fold increase overall and a 9.5-fold increase for severely demented patients.
The findings clearly illustrate that nonhospitalists could benefit from some education about the most appropriate interventions when patients near the end of life enter a hospital, Dr. Joan Teno and her associates reported in the April issue of Health Affairs (Health Aff. April 2014;33:675-82).
"It may be that subspecialists do not have adequate knowledge about the risks and benefits of using feeding tubes in people with advanced dementia," said Dr. Teno of Brown University, Providence, R.I., and her coauthors. "Hospitals should educate physicians about the lack of efficacy of PEG [percutaneous endoscopic gastrostomy] feeding tubes, compared with hand feeding, in prolonging survival and preventing aspiration pneumonias and pressure ulcers in people with advanced dementia. In addition, hospitals should examine how they staff the role of attending physician and ensure coordination of care when patient hand-offs are made between different types of attending physicians."
Such education would bring all physicians up to speed with position statements against tube feeding for this group of patients. The issue sits atop the Choosing Wisely lists of both the American Academy of Hospice and Palliative Medicine and the American Geriatrics Society. The American Academy of Hospice and Palliative Medicine states that "feeding tubes do not result in improved survival, prevention of aspiration pneumonia, or improved healing of pressure ulcers. Feeding tube use in such patients has actually been associated with pressure ulcer development, use of physical and pharmacological restraints, and patient distress about the tube itself."
Internal medicine physician Eric G. Tangalos of the Alzheimer’s Disease Research Center at Mayo Clinic, Rochester, Minn., works closely with hospitalists. He agrees with the concept that tube feeding can impose even more distress on both these patients and their families. "As a medical profession and a society, we have yet to accept some of the futility of our actions and continue to ignore the burdens tube feedings place on patients, families, and the health care system once a hospitalization has come to its conclusion," he said in an interview.
Dr. Teno and her team looked at the rate of feeding tube insertion in fee-for-service Medicare patients with advanced dementia who were within 90 days of death and hospitalized with a diagnosis of urinary tract infection, sepsis, pneumonia, or dehydration. The study examined decisions made by four groups of physicians who cared for these patients: hospitalists, nonhospitalist generalists (geriatricians, general practitioners, internists, and family physicians), subspecialists, and mixed groups that included a subspecialist and either a hospitalist or nonhospitalist generalist.
The cohort comprised 53,492 patients hospitalized from 2001 to 2010. The patients’ mean age was 85 years. About 60% had a do not resuscitate order, and 10% had an order against tube feeding.
The rate of hospitalists as attending physicians increased from 11% in 2001 to 28% in 2010. The portion of patients seen by a mixture of attending physicians increased from 29% in 2001 to 38% in 2010.
The rates of tube feeding were lowest when a hospitalist or nonhospitalist generalist was the attending physician (1.6% and 2.2%, respectively). Subspecialists had significantly higher rates (11%). The highest rate occurred when there were mixed groups of physicians involved in the patient’s care (15.6%).
Using the nonhospitalist generalists as a reference group, the researchers found that hospitalists were 22% less likely to insert a tube overall and 35% less likely to do so when the patient had very severe cognitive and physical impairment.
Conversely, subspecialists were five times more likely to commence tube feeding for all patients and for very severely impaired patients. The mixed groups were the most likely to begin tube feeding – almost 9 times more likely overall and 9.5 times more likely for the most severely impaired patients.
"Our finding that subspecialists had a higher rate of insertions of PEG feeding tubes might reflect their lack of experience in providing care for people with advanced dementia," the authors wrote.
The mixed-physician group could be seen as a proxy for discontinuity of care among the attending physicians, they noted. Prior studies have found that such discontinuity was associated with longer hospital stays.
"There may be a lack of care coordination during patient hand offs between attending physicians that begins a cascade of events, ending with the insertion of a PEG feeding tube."
Dr. Diane E. Meier, professor of geriatrics and palliative medicine at Icahn School of Medicine at Mount Sinai, New York, and director of the Center to Advance Palliative Care, agreed that group care without a leader creates confusion. "One of the hallmarks of modern medicine in the U.S. is fragmentation. It is typical for a person with dementia to have a different specialist for every organ system, a problem compounded in the hospital when a completely new group of specialists is brought into the care team. The problem with this abundance of doctors is that no one is really in charge of the whole patient and what makes the most sense for the patient as a person. Organ- and specialty-specific decision making leads to bad practices – including trying to ‘solve’ a feeding difficulty as if it is an isolated problem when the real issue is progressive brain failure – a terminal illness that cannot be fixed with a feeding tube."
The study not only questions the feeding tube issue, but also the wisdom of repeatedly hospitalizing elderly patients with severe dementia who could be in the last phase of life – especially for conditions that are expected complications of severe dementia. The authors suggested that there may be financial motives to admit fee-for-service patients.
"The fee-for-service system provides incentives to hospitalize nursing home residents with severe dementia because such hospitalizations qualify the patients for skilled nursing home services. Bundling of payments and institutional special needs plans that reverse these financial incentives may reduce health care expenditures and improve the quality of care for nursing home residents with advanced dementia by avoiding burdensome transitions between facilities and the stress of relocation."
The National Institute on Aging funded the study. Dr. Teno made no financial declarations.
FROM HEALTH AFFAIRS
Major finding: Primary care doctors and subspecialists were up to 9 times more likely to initiate tube feeding in hospitalized patients with severe dementia.
Data source: Data are from a review of more than 53,000 Medicare fee-for-service nursing home patients.
Disclosures: The National Institute on Aging sponsored the study. Dr. Teno had no financial disclosures.
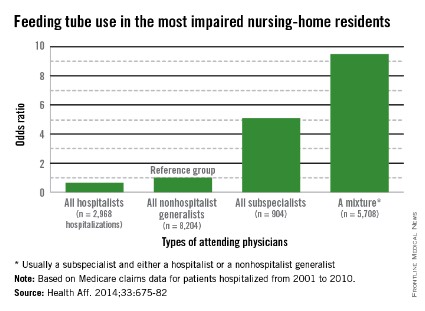
Short CAM-S delirium scale predicted clinical outcomes
A new delirium scoring system has shown excellent correlation with clinical outcomes in hospitalized elderly patients, including length of stay, functional decline, and death, investigators report.
In both short and long form, the Confusion Assessment Methods-S (CAM-S) is designed to complement the existing CAM, Dr. Sharon Inouye and her colleagues reported in the April 14 issue of Annals of Internal Medicine (2014;160:526-33).
"The short form (5-minute completion and scoring time), which is based on the CAM diagnostic algorithm alone, is quicker and simpler to rate; however, the long form (10-minute completion and scoring time) provides a broader range of severity scores in delirium and no-delirium groups," wrote Dr. Inouye of the Institute for Aging Research, Boston, and her coauthors.
"Unlike the Delirium Rating Scale, a clinician rater is not required for the CAM-S. Instead, well-trained research assistants can reliably conduct the assessments," the researchers wrote.
Both the short-form and long-form CAM-S instruments were validated in a group of 919 patients aged 70 years or older, who were scheduled for major surgery. The cohort was drawn from two extant study groups: the ongoing SAGES (Successful Aging After Elective Surgery) study,and Project Recovery, which ran from 1995 to 1998. Delirium was first rated by the existing CAM, and then according to the two versions of CAM-S.
The short-form CAM-S rates patients on four features of the CAM: symptom fluctuation, inattention, disorganized thinking, and altered level of consciousness. The most severe score is a 7. The longer form is based on 10 features, which also include disorientation, memory impairment, perceptual disturbances, psychomotor agitation, and sleep-wake cycle disturbance. The most severe score is a 19.
The measures had excellent correlation with each other, and with several clinical outcomes, the investigators said.
Length of hospital stay increased with increasing delirium severity across both forms, with an adjusted mean stay of 6.5 days for no delirium to almost 13 days with high severity in the short form. In the long form, length of stay increased from about 6 days to 12 days.
Hospital costs also tracked severity, ranging from an adjusted mean of $5,100 for no delirium to $13,200 for severe delirium in the short form. A similar pattern emerged in the long form, ranging from $4,200 to $11,400.
Functional decline was also highly correlated with score. On the short form, it occurred in 36%-68% of patients, depending on severity. In the long form, the range was 25%-61%. Cognitive decline showed a similar pattern.
In the short form, the cumulative adjusted rates of death within 90 days ranged from 7% to 27%, depending on severity. In the long form, the range was 7%-22%.
In the composite outcome of death or nursing home placement, results on the short form ranged from 15% to 51%, depending on severity. In the long form, the range was 13%-48%
While the Project Recovery data are more than 16 years old, the researchers said that this time lapse is not an issue because their primary interest is in comparison of outcomes among severity groups, which minimizes the importance of the internal values.
Also, "there may be inherent dependencies between CAM-S score and adverse outcomes," investigators wrote. "For example, patients with longer lengths of stay may have had higher CAM-S scores because of more opportunities for measurement."
The CAM-S score requires validation in groups younger than the age 70-plus patients addressed in the current study, researchers noted.
The National Institute on Aging funded the study. None of the authors reported having any financial declarations.
On Twitter @alz_gal
Dr. Jennifer Cox, FCCP, comments: The CAM-S delirium scoring system complements the original Confusion Assessment Method for evaluating outcomes in our elderly population. In the short or long form, they are a quick method to predict length of stay, functional decline, and death. These outcomes are of keen interest to patient's families, clinicians, and hospital administrations. Validation of the CAM-S over a broader age range of at-risk patients is needed.
Dr. Jennifer Cox, FCCP, comments: The CAM-S delirium scoring system complements the original Confusion Assessment Method for evaluating outcomes in our elderly population. In the short or long form, they are a quick method to predict length of stay, functional decline, and death. These outcomes are of keen interest to patient's families, clinicians, and hospital administrations. Validation of the CAM-S over a broader age range of at-risk patients is needed.
Dr. Jennifer Cox, FCCP, comments: The CAM-S delirium scoring system complements the original Confusion Assessment Method for evaluating outcomes in our elderly population. In the short or long form, they are a quick method to predict length of stay, functional decline, and death. These outcomes are of keen interest to patient's families, clinicians, and hospital administrations. Validation of the CAM-S over a broader age range of at-risk patients is needed.
A new delirium scoring system has shown excellent correlation with clinical outcomes in hospitalized elderly patients, including length of stay, functional decline, and death, investigators report.
In both short and long form, the Confusion Assessment Methods-S (CAM-S) is designed to complement the existing CAM, Dr. Sharon Inouye and her colleagues reported in the April 14 issue of Annals of Internal Medicine (2014;160:526-33).
"The short form (5-minute completion and scoring time), which is based on the CAM diagnostic algorithm alone, is quicker and simpler to rate; however, the long form (10-minute completion and scoring time) provides a broader range of severity scores in delirium and no-delirium groups," wrote Dr. Inouye of the Institute for Aging Research, Boston, and her coauthors.
"Unlike the Delirium Rating Scale, a clinician rater is not required for the CAM-S. Instead, well-trained research assistants can reliably conduct the assessments," the researchers wrote.
Both the short-form and long-form CAM-S instruments were validated in a group of 919 patients aged 70 years or older, who were scheduled for major surgery. The cohort was drawn from two extant study groups: the ongoing SAGES (Successful Aging After Elective Surgery) study,and Project Recovery, which ran from 1995 to 1998. Delirium was first rated by the existing CAM, and then according to the two versions of CAM-S.
The short-form CAM-S rates patients on four features of the CAM: symptom fluctuation, inattention, disorganized thinking, and altered level of consciousness. The most severe score is a 7. The longer form is based on 10 features, which also include disorientation, memory impairment, perceptual disturbances, psychomotor agitation, and sleep-wake cycle disturbance. The most severe score is a 19.
The measures had excellent correlation with each other, and with several clinical outcomes, the investigators said.
Length of hospital stay increased with increasing delirium severity across both forms, with an adjusted mean stay of 6.5 days for no delirium to almost 13 days with high severity in the short form. In the long form, length of stay increased from about 6 days to 12 days.
Hospital costs also tracked severity, ranging from an adjusted mean of $5,100 for no delirium to $13,200 for severe delirium in the short form. A similar pattern emerged in the long form, ranging from $4,200 to $11,400.
Functional decline was also highly correlated with score. On the short form, it occurred in 36%-68% of patients, depending on severity. In the long form, the range was 25%-61%. Cognitive decline showed a similar pattern.
In the short form, the cumulative adjusted rates of death within 90 days ranged from 7% to 27%, depending on severity. In the long form, the range was 7%-22%.
In the composite outcome of death or nursing home placement, results on the short form ranged from 15% to 51%, depending on severity. In the long form, the range was 13%-48%
While the Project Recovery data are more than 16 years old, the researchers said that this time lapse is not an issue because their primary interest is in comparison of outcomes among severity groups, which minimizes the importance of the internal values.
Also, "there may be inherent dependencies between CAM-S score and adverse outcomes," investigators wrote. "For example, patients with longer lengths of stay may have had higher CAM-S scores because of more opportunities for measurement."
The CAM-S score requires validation in groups younger than the age 70-plus patients addressed in the current study, researchers noted.
The National Institute on Aging funded the study. None of the authors reported having any financial declarations.
On Twitter @alz_gal
A new delirium scoring system has shown excellent correlation with clinical outcomes in hospitalized elderly patients, including length of stay, functional decline, and death, investigators report.
In both short and long form, the Confusion Assessment Methods-S (CAM-S) is designed to complement the existing CAM, Dr. Sharon Inouye and her colleagues reported in the April 14 issue of Annals of Internal Medicine (2014;160:526-33).
"The short form (5-minute completion and scoring time), which is based on the CAM diagnostic algorithm alone, is quicker and simpler to rate; however, the long form (10-minute completion and scoring time) provides a broader range of severity scores in delirium and no-delirium groups," wrote Dr. Inouye of the Institute for Aging Research, Boston, and her coauthors.
"Unlike the Delirium Rating Scale, a clinician rater is not required for the CAM-S. Instead, well-trained research assistants can reliably conduct the assessments," the researchers wrote.
Both the short-form and long-form CAM-S instruments were validated in a group of 919 patients aged 70 years or older, who were scheduled for major surgery. The cohort was drawn from two extant study groups: the ongoing SAGES (Successful Aging After Elective Surgery) study,and Project Recovery, which ran from 1995 to 1998. Delirium was first rated by the existing CAM, and then according to the two versions of CAM-S.
The short-form CAM-S rates patients on four features of the CAM: symptom fluctuation, inattention, disorganized thinking, and altered level of consciousness. The most severe score is a 7. The longer form is based on 10 features, which also include disorientation, memory impairment, perceptual disturbances, psychomotor agitation, and sleep-wake cycle disturbance. The most severe score is a 19.
The measures had excellent correlation with each other, and with several clinical outcomes, the investigators said.
Length of hospital stay increased with increasing delirium severity across both forms, with an adjusted mean stay of 6.5 days for no delirium to almost 13 days with high severity in the short form. In the long form, length of stay increased from about 6 days to 12 days.
Hospital costs also tracked severity, ranging from an adjusted mean of $5,100 for no delirium to $13,200 for severe delirium in the short form. A similar pattern emerged in the long form, ranging from $4,200 to $11,400.
Functional decline was also highly correlated with score. On the short form, it occurred in 36%-68% of patients, depending on severity. In the long form, the range was 25%-61%. Cognitive decline showed a similar pattern.
In the short form, the cumulative adjusted rates of death within 90 days ranged from 7% to 27%, depending on severity. In the long form, the range was 7%-22%.
In the composite outcome of death or nursing home placement, results on the short form ranged from 15% to 51%, depending on severity. In the long form, the range was 13%-48%
While the Project Recovery data are more than 16 years old, the researchers said that this time lapse is not an issue because their primary interest is in comparison of outcomes among severity groups, which minimizes the importance of the internal values.
Also, "there may be inherent dependencies between CAM-S score and adverse outcomes," investigators wrote. "For example, patients with longer lengths of stay may have had higher CAM-S scores because of more opportunities for measurement."
The CAM-S score requires validation in groups younger than the age 70-plus patients addressed in the current study, researchers noted.
The National Institute on Aging funded the study. None of the authors reported having any financial declarations.
On Twitter @alz_gal
FROM ANNALS OF INTERNAL MEDICINE
Major finding: Two versions of the CAM-S delirium scale were predictive of major clinical outcomes in the elderly, including death within 30 days of surgery (7%-27%, depending on severity scores).
Data source: CAM-S was validated in a group of 919 patients.
Disclosures: The National Institute on Aging funded the study. Neither Dr. Inouye nor any of the coauthors had any financial disclosures.
Diabetes Prevalence Increases, But so Does Diabetes Control
The prevalence of diagnosed diabetes in the United States rose significantly from 1988 to 2010, jumping from 6% to 10%.
Prediabetes doubled in prevalence over the same time period, from 6% to 12%, Elizabeth Selvin, Ph.D., and her colleagues reported in the April 14 issue of the Annals of Internal Medicine (2014 [doi=10.7326/M13-2411]).
But while the prevalence of confirmed cases increased sharply, the prevalence of undiagnosed diabetes actually decreased slightly over the same time – meaning that almost all cases of diabetes in the United States are now being identified, wrote Dr. Selvin of Johns Hopkins University, Baltimore, and her coinvestigators. "At present, approximately 89% of all diabetes cases are diagnosed," the team wrote. "Furthermore, glycemic control among persons with diagnosed diabetes has improved, probably reflecting a combination of improvements in diagnosis, screening, and care."
The researchers mined their data from two epochs of the National Health and Nutrition Examination Survey (1988-1994 and 1999-2010), comprising a total of almost 43,500 people. They assessed diabetes and prediabetes prevalence by both fasting plasma glucose and hemoglobin A1c (HbA1c) levels. They also looked at glucose control parameters and medication type in diagnosed patients. To investigate any association between diabetes and weight, they evaluated body mass index in the survey populations.
The mean prevalence of obesity in U.S. adults without diabetes jumped from 21% in the first epoch to 32% in the second. The change was similar among those with diabetes. The increases in both prediabetes and diabetes tracked the jump in obesity, leading the authors to conclude that obesity was a direct cause of disease.
Overall, the mean HbA1c level rose from 5.25% in the earliest years to 5.36% in 2010 – a small but significant increase. But the level was entirely stable in a subset of young adults who had normal body weight, blood pressure, and lipid levels (5%).
The prevalence of diabetes as measured by an HbA1c of at least 6.5% increased over the two epochs, from a low of 6% in the earliest years to 10% by the latest. The prevalence of prediabetes doubled (from 6% to 12%). "When applied to the 2010 U.S. Census, the total number of adults aged 20 [years] or older with total confirmed diabetes was 20.6 million," the authors wrote.
When the team used HbA1c levels to identify undiagnosed cases, they determined that 16% of cases in the earlier epoch were undiagnosed, compared with 11% in the later years – meaning that by 2010, 89% of U.S. cases were being identified.
As measured by an HbA1c of less than 7%, glycemic control improved from 51% to 59% over the study period. Among those who reported that they were taking diabetes medications, control increased from 40% to 55%.
Blacks and Hispanics shouldered a larger disease burden than did whites, the researchers wrote. "The prevalence ... in blacks was nearly double the prevalence in whites (15% vs. almost 9%). Mexican-Americans also had a greater prevalence of diabetes than whites (15.4% vs. 8.6%). Both ethnic minority groups had a greater prevalence of undiagnosed diabetes."
Control was also poorer, they said: Only 52% of blacks and 43% of Mexican-Americans had a calibrated HbA1c level less than 7%, compared with 57% of whites.
"The substantially greater prevalence of diabetes and prediabetes and poor rates of glycemic control (even among persons with medication-treated diabetes) in ethnic minority populations ... is particularly concerning because blacks and Mexican-Americans are also at greater risk for complications of diabetes, particularly retinopathy and kidney disease," the team noted.
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Neither Dr. Selvin nor any of her coauthors had any financial declarations.
On Twitter @alz_gal
Yes, diabetes control has improved over the past decades. But not everyone is benefiting and, with the disease still on the rise, more needs to be done to stop it before it even starts.
Nearly 40% of patients are not achieving their glycemic target – especially minority groups, which continue to suffer more, and have more-serious, long-term diabetes complications. The "alarming increase" in both obesity and diabetes should give society pause, and inspire a national effort to interrupt both.
"We know from the Diabetes Prevention Program that an intensive lifestyle change effectively prevents or delays the onset of diabetes. Public policy should focus on increasing physical activity and optimizing and improving access to healthy food choices for adults as well as children.
"Although the Centers for Disease Control and Prevention is actively engaged in adapting the Diabetes Prevention Program model for the community, we need to ensure that adequate resources are allocated to target these issues at the individual, societal, and environmental levels. Indeed, the public and private sectors need to work closely together to tackle this immense problem."
Dr. Martin J. Abrahamson and Dr. Roeland J.W. Middelbeek of the Joslin Diabetes Center and Harvard Medical School, Boston, made these remarks in an accompanying editorial (Ann. Int. Med. 2014;160:572-3). Dr. Abrahamson has received fees from several pharmaceutical companies. Dr. Middelbeek had no relevant disclosures.
Yes, diabetes control has improved over the past decades. But not everyone is benefiting and, with the disease still on the rise, more needs to be done to stop it before it even starts.
Nearly 40% of patients are not achieving their glycemic target – especially minority groups, which continue to suffer more, and have more-serious, long-term diabetes complications. The "alarming increase" in both obesity and diabetes should give society pause, and inspire a national effort to interrupt both.
"We know from the Diabetes Prevention Program that an intensive lifestyle change effectively prevents or delays the onset of diabetes. Public policy should focus on increasing physical activity and optimizing and improving access to healthy food choices for adults as well as children.
"Although the Centers for Disease Control and Prevention is actively engaged in adapting the Diabetes Prevention Program model for the community, we need to ensure that adequate resources are allocated to target these issues at the individual, societal, and environmental levels. Indeed, the public and private sectors need to work closely together to tackle this immense problem."
Dr. Martin J. Abrahamson and Dr. Roeland J.W. Middelbeek of the Joslin Diabetes Center and Harvard Medical School, Boston, made these remarks in an accompanying editorial (Ann. Int. Med. 2014;160:572-3). Dr. Abrahamson has received fees from several pharmaceutical companies. Dr. Middelbeek had no relevant disclosures.
Yes, diabetes control has improved over the past decades. But not everyone is benefiting and, with the disease still on the rise, more needs to be done to stop it before it even starts.
Nearly 40% of patients are not achieving their glycemic target – especially minority groups, which continue to suffer more, and have more-serious, long-term diabetes complications. The "alarming increase" in both obesity and diabetes should give society pause, and inspire a national effort to interrupt both.
"We know from the Diabetes Prevention Program that an intensive lifestyle change effectively prevents or delays the onset of diabetes. Public policy should focus on increasing physical activity and optimizing and improving access to healthy food choices for adults as well as children.
"Although the Centers for Disease Control and Prevention is actively engaged in adapting the Diabetes Prevention Program model for the community, we need to ensure that adequate resources are allocated to target these issues at the individual, societal, and environmental levels. Indeed, the public and private sectors need to work closely together to tackle this immense problem."
Dr. Martin J. Abrahamson and Dr. Roeland J.W. Middelbeek of the Joslin Diabetes Center and Harvard Medical School, Boston, made these remarks in an accompanying editorial (Ann. Int. Med. 2014;160:572-3). Dr. Abrahamson has received fees from several pharmaceutical companies. Dr. Middelbeek had no relevant disclosures.
The prevalence of diagnosed diabetes in the United States rose significantly from 1988 to 2010, jumping from 6% to 10%.
Prediabetes doubled in prevalence over the same time period, from 6% to 12%, Elizabeth Selvin, Ph.D., and her colleagues reported in the April 14 issue of the Annals of Internal Medicine (2014 [doi=10.7326/M13-2411]).
But while the prevalence of confirmed cases increased sharply, the prevalence of undiagnosed diabetes actually decreased slightly over the same time – meaning that almost all cases of diabetes in the United States are now being identified, wrote Dr. Selvin of Johns Hopkins University, Baltimore, and her coinvestigators. "At present, approximately 89% of all diabetes cases are diagnosed," the team wrote. "Furthermore, glycemic control among persons with diagnosed diabetes has improved, probably reflecting a combination of improvements in diagnosis, screening, and care."
The researchers mined their data from two epochs of the National Health and Nutrition Examination Survey (1988-1994 and 1999-2010), comprising a total of almost 43,500 people. They assessed diabetes and prediabetes prevalence by both fasting plasma glucose and hemoglobin A1c (HbA1c) levels. They also looked at glucose control parameters and medication type in diagnosed patients. To investigate any association between diabetes and weight, they evaluated body mass index in the survey populations.
The mean prevalence of obesity in U.S. adults without diabetes jumped from 21% in the first epoch to 32% in the second. The change was similar among those with diabetes. The increases in both prediabetes and diabetes tracked the jump in obesity, leading the authors to conclude that obesity was a direct cause of disease.
Overall, the mean HbA1c level rose from 5.25% in the earliest years to 5.36% in 2010 – a small but significant increase. But the level was entirely stable in a subset of young adults who had normal body weight, blood pressure, and lipid levels (5%).
The prevalence of diabetes as measured by an HbA1c of at least 6.5% increased over the two epochs, from a low of 6% in the earliest years to 10% by the latest. The prevalence of prediabetes doubled (from 6% to 12%). "When applied to the 2010 U.S. Census, the total number of adults aged 20 [years] or older with total confirmed diabetes was 20.6 million," the authors wrote.
When the team used HbA1c levels to identify undiagnosed cases, they determined that 16% of cases in the earlier epoch were undiagnosed, compared with 11% in the later years – meaning that by 2010, 89% of U.S. cases were being identified.
As measured by an HbA1c of less than 7%, glycemic control improved from 51% to 59% over the study period. Among those who reported that they were taking diabetes medications, control increased from 40% to 55%.
Blacks and Hispanics shouldered a larger disease burden than did whites, the researchers wrote. "The prevalence ... in blacks was nearly double the prevalence in whites (15% vs. almost 9%). Mexican-Americans also had a greater prevalence of diabetes than whites (15.4% vs. 8.6%). Both ethnic minority groups had a greater prevalence of undiagnosed diabetes."
Control was also poorer, they said: Only 52% of blacks and 43% of Mexican-Americans had a calibrated HbA1c level less than 7%, compared with 57% of whites.
"The substantially greater prevalence of diabetes and prediabetes and poor rates of glycemic control (even among persons with medication-treated diabetes) in ethnic minority populations ... is particularly concerning because blacks and Mexican-Americans are also at greater risk for complications of diabetes, particularly retinopathy and kidney disease," the team noted.
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Neither Dr. Selvin nor any of her coauthors had any financial declarations.
On Twitter @alz_gal
The prevalence of diagnosed diabetes in the United States rose significantly from 1988 to 2010, jumping from 6% to 10%.
Prediabetes doubled in prevalence over the same time period, from 6% to 12%, Elizabeth Selvin, Ph.D., and her colleagues reported in the April 14 issue of the Annals of Internal Medicine (2014 [doi=10.7326/M13-2411]).
But while the prevalence of confirmed cases increased sharply, the prevalence of undiagnosed diabetes actually decreased slightly over the same time – meaning that almost all cases of diabetes in the United States are now being identified, wrote Dr. Selvin of Johns Hopkins University, Baltimore, and her coinvestigators. "At present, approximately 89% of all diabetes cases are diagnosed," the team wrote. "Furthermore, glycemic control among persons with diagnosed diabetes has improved, probably reflecting a combination of improvements in diagnosis, screening, and care."
The researchers mined their data from two epochs of the National Health and Nutrition Examination Survey (1988-1994 and 1999-2010), comprising a total of almost 43,500 people. They assessed diabetes and prediabetes prevalence by both fasting plasma glucose and hemoglobin A1c (HbA1c) levels. They also looked at glucose control parameters and medication type in diagnosed patients. To investigate any association between diabetes and weight, they evaluated body mass index in the survey populations.
The mean prevalence of obesity in U.S. adults without diabetes jumped from 21% in the first epoch to 32% in the second. The change was similar among those with diabetes. The increases in both prediabetes and diabetes tracked the jump in obesity, leading the authors to conclude that obesity was a direct cause of disease.
Overall, the mean HbA1c level rose from 5.25% in the earliest years to 5.36% in 2010 – a small but significant increase. But the level was entirely stable in a subset of young adults who had normal body weight, blood pressure, and lipid levels (5%).
The prevalence of diabetes as measured by an HbA1c of at least 6.5% increased over the two epochs, from a low of 6% in the earliest years to 10% by the latest. The prevalence of prediabetes doubled (from 6% to 12%). "When applied to the 2010 U.S. Census, the total number of adults aged 20 [years] or older with total confirmed diabetes was 20.6 million," the authors wrote.
When the team used HbA1c levels to identify undiagnosed cases, they determined that 16% of cases in the earlier epoch were undiagnosed, compared with 11% in the later years – meaning that by 2010, 89% of U.S. cases were being identified.
As measured by an HbA1c of less than 7%, glycemic control improved from 51% to 59% over the study period. Among those who reported that they were taking diabetes medications, control increased from 40% to 55%.
Blacks and Hispanics shouldered a larger disease burden than did whites, the researchers wrote. "The prevalence ... in blacks was nearly double the prevalence in whites (15% vs. almost 9%). Mexican-Americans also had a greater prevalence of diabetes than whites (15.4% vs. 8.6%). Both ethnic minority groups had a greater prevalence of undiagnosed diabetes."
Control was also poorer, they said: Only 52% of blacks and 43% of Mexican-Americans had a calibrated HbA1c level less than 7%, compared with 57% of whites.
"The substantially greater prevalence of diabetes and prediabetes and poor rates of glycemic control (even among persons with medication-treated diabetes) in ethnic minority populations ... is particularly concerning because blacks and Mexican-Americans are also at greater risk for complications of diabetes, particularly retinopathy and kidney disease," the team noted.
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Neither Dr. Selvin nor any of her coauthors had any financial declarations.
On Twitter @alz_gal
FROM THE ANNALS OF INTERNAL MEDICINE
