User login
New insight into how brain stimulation eases major depression
For the first time, researchers understand what happens to the brain when patients with treatment-resistant depression receive repetitive transcranial magnetic stimulation (rTMS).
Using functional magnetic resonance imaging (fMRI), they showed that rTMS induces widespread alterations in functional connectivity in brain regions involved in emotion and motor control.
“‘How does rTMS work?’ is one of the most frequent questions I get in clinic. Providing an accurate explanation and narrative to patients is critical,” senior investigator Fidel Vila-Rodriguez, MD, PhD, director of the Non-Invasive Neurostimulation Therapies Laboratory, University of British Columbia, Vancouver, told this news organization.

“Our findings suggest that rTMS might rely on the brain’s capacity for change (neuroplasticity) to exert its effects and that rTMS effects on the brain are widespread beyond the focal area stimulated (functional network effects),” Dr. Vila-Rodriguez added.
The study was published online in the American Journal of Psychiatry.
Mechanistic insights
Although rTMS has proven efficacy for treatment-resistant depression, the mechanisms behind how it affects the brain are not well understood.
In the current study, researchers used fMRI to assess changes in functional connectivity induced by a single rTMS session in 26 women and 12 men with treatment-resistant depression.
They found that – from managing emotional responses to memory and motor control.
Following a 4-week course of rTMS, these connectivity changes predicted about 30% of the variance of improvement in scores on the Montgomery-Åsberg Depression Rating Scale after rTMS treatment.
The most robust predictive associations involved connections between prefrontal regions and motor, parietal, and insular cortices and between bilateral regions of the thalamus.
“By demonstrating this principle and identifying regions of the brain that are activated by rTMS, we can now try to understand whether this pattern can be used as a biomarker,” Dr. Vila-Rodriguez said in a news release.
“This work provides a mechanistic explanation of what rTMS does to treat depression and supports the notion that for rTMS to treat depressive symptoms a distributed change in brain activity (network or circuit base) is necessary,” he told this news organization.
With funding from the Canadian Institutes of Health Research (CIHR), the team will next see if they can use fMRI to guide rTMS at the individual level, with the ultimate goal of “personalizing” rTMS using individualized functional targets, Dr. Vila-Rodriguez said.
New generation of tms researchers
Reached for comment, Jonathan Downar, MD, PhD, department of psychiatry, University of Toronto, noted that TMS can be “very effective” for treatment-resistant depression, and it has a “very clean side effect profile compared to medications.”
What the field is trying to figure out now is “who it works for and how we can predict more effectively who’s going to benefit from it,” Dr. Downar said in an interview.
He noted that the study’s investigators are part of a “new generation of TMS researchers who are bringing new ideas into the fold and figuring out how to use brain imaging to personalize the treatment.” This study represents “a step” in that direction.
“A challenge for the field is that it’s often pretty easy to demonstrate a change at the group level, but the question is whether we can use that at the individual level. That’s a higher bar to meet, and we’re still not there yet,” Dr. Downar added.
Support for the study was provided by Brain Canada, the Michael Smith Foundation for Health Research and the Vancouver Coastal Health Research Institute. Dr. Vila-Rodriguez has received research support from CIHR, Brain Canada, the Michael Smith Foundation for Health Research, the Vancouver Coastal Health Research Institute, and the Weston Brain Institute for investigator-initiated research and philanthropic support from the Seedlings Foundation; he received in-kind equipment support from MagVenture for this investigator-initiated trial; and he has received honoraria for participation on an advisory board for Janssen. Dr. Downar has served as an adviser for BrainCheck, NeuroStim TMS, and Salience Neuro Health; received research grant from CIHR, National Institute for Mental Health, Brain Canada, Canadian Biomarker Integration Network in Depression, Ontario Brain Institute, Klarman Family Foundation, Arrell Family Foundation and the Edgestone Foundation; received travel stipends from Lundbeck and ANT Neuro; and received in-kind equipment support for investigator-initiated trials from MagVenture.
A version of this article first appeared on Medscape.com.
For the first time, researchers understand what happens to the brain when patients with treatment-resistant depression receive repetitive transcranial magnetic stimulation (rTMS).
Using functional magnetic resonance imaging (fMRI), they showed that rTMS induces widespread alterations in functional connectivity in brain regions involved in emotion and motor control.
“‘How does rTMS work?’ is one of the most frequent questions I get in clinic. Providing an accurate explanation and narrative to patients is critical,” senior investigator Fidel Vila-Rodriguez, MD, PhD, director of the Non-Invasive Neurostimulation Therapies Laboratory, University of British Columbia, Vancouver, told this news organization.
“Our findings suggest that rTMS might rely on the brain’s capacity for change (neuroplasticity) to exert its effects and that rTMS effects on the brain are widespread beyond the focal area stimulated (functional network effects),” Dr. Vila-Rodriguez added.
The study was published online in the American Journal of Psychiatry.
Mechanistic insights
Although rTMS has proven efficacy for treatment-resistant depression, the mechanisms behind how it affects the brain are not well understood.
In the current study, researchers used fMRI to assess changes in functional connectivity induced by a single rTMS session in 26 women and 12 men with treatment-resistant depression.
They found that – from managing emotional responses to memory and motor control.
Following a 4-week course of rTMS, these connectivity changes predicted about 30% of the variance of improvement in scores on the Montgomery-Åsberg Depression Rating Scale after rTMS treatment.
The most robust predictive associations involved connections between prefrontal regions and motor, parietal, and insular cortices and between bilateral regions of the thalamus.
“By demonstrating this principle and identifying regions of the brain that are activated by rTMS, we can now try to understand whether this pattern can be used as a biomarker,” Dr. Vila-Rodriguez said in a news release.
“This work provides a mechanistic explanation of what rTMS does to treat depression and supports the notion that for rTMS to treat depressive symptoms a distributed change in brain activity (network or circuit base) is necessary,” he told this news organization.
With funding from the Canadian Institutes of Health Research (CIHR), the team will next see if they can use fMRI to guide rTMS at the individual level, with the ultimate goal of “personalizing” rTMS using individualized functional targets, Dr. Vila-Rodriguez said.
New generation of tms researchers
Reached for comment, Jonathan Downar, MD, PhD, department of psychiatry, University of Toronto, noted that TMS can be “very effective” for treatment-resistant depression, and it has a “very clean side effect profile compared to medications.”
What the field is trying to figure out now is “who it works for and how we can predict more effectively who’s going to benefit from it,” Dr. Downar said in an interview.
He noted that the study’s investigators are part of a “new generation of TMS researchers who are bringing new ideas into the fold and figuring out how to use brain imaging to personalize the treatment.” This study represents “a step” in that direction.
“A challenge for the field is that it’s often pretty easy to demonstrate a change at the group level, but the question is whether we can use that at the individual level. That’s a higher bar to meet, and we’re still not there yet,” Dr. Downar added.
Support for the study was provided by Brain Canada, the Michael Smith Foundation for Health Research and the Vancouver Coastal Health Research Institute. Dr. Vila-Rodriguez has received research support from CIHR, Brain Canada, the Michael Smith Foundation for Health Research, the Vancouver Coastal Health Research Institute, and the Weston Brain Institute for investigator-initiated research and philanthropic support from the Seedlings Foundation; he received in-kind equipment support from MagVenture for this investigator-initiated trial; and he has received honoraria for participation on an advisory board for Janssen. Dr. Downar has served as an adviser for BrainCheck, NeuroStim TMS, and Salience Neuro Health; received research grant from CIHR, National Institute for Mental Health, Brain Canada, Canadian Biomarker Integration Network in Depression, Ontario Brain Institute, Klarman Family Foundation, Arrell Family Foundation and the Edgestone Foundation; received travel stipends from Lundbeck and ANT Neuro; and received in-kind equipment support for investigator-initiated trials from MagVenture.
A version of this article first appeared on Medscape.com.
For the first time, researchers understand what happens to the brain when patients with treatment-resistant depression receive repetitive transcranial magnetic stimulation (rTMS).
Using functional magnetic resonance imaging (fMRI), they showed that rTMS induces widespread alterations in functional connectivity in brain regions involved in emotion and motor control.
“‘How does rTMS work?’ is one of the most frequent questions I get in clinic. Providing an accurate explanation and narrative to patients is critical,” senior investigator Fidel Vila-Rodriguez, MD, PhD, director of the Non-Invasive Neurostimulation Therapies Laboratory, University of British Columbia, Vancouver, told this news organization.
“Our findings suggest that rTMS might rely on the brain’s capacity for change (neuroplasticity) to exert its effects and that rTMS effects on the brain are widespread beyond the focal area stimulated (functional network effects),” Dr. Vila-Rodriguez added.
The study was published online in the American Journal of Psychiatry.
Mechanistic insights
Although rTMS has proven efficacy for treatment-resistant depression, the mechanisms behind how it affects the brain are not well understood.
In the current study, researchers used fMRI to assess changes in functional connectivity induced by a single rTMS session in 26 women and 12 men with treatment-resistant depression.
They found that – from managing emotional responses to memory and motor control.
Following a 4-week course of rTMS, these connectivity changes predicted about 30% of the variance of improvement in scores on the Montgomery-Åsberg Depression Rating Scale after rTMS treatment.
The most robust predictive associations involved connections between prefrontal regions and motor, parietal, and insular cortices and between bilateral regions of the thalamus.
“By demonstrating this principle and identifying regions of the brain that are activated by rTMS, we can now try to understand whether this pattern can be used as a biomarker,” Dr. Vila-Rodriguez said in a news release.
“This work provides a mechanistic explanation of what rTMS does to treat depression and supports the notion that for rTMS to treat depressive symptoms a distributed change in brain activity (network or circuit base) is necessary,” he told this news organization.
With funding from the Canadian Institutes of Health Research (CIHR), the team will next see if they can use fMRI to guide rTMS at the individual level, with the ultimate goal of “personalizing” rTMS using individualized functional targets, Dr. Vila-Rodriguez said.
New generation of tms researchers
Reached for comment, Jonathan Downar, MD, PhD, department of psychiatry, University of Toronto, noted that TMS can be “very effective” for treatment-resistant depression, and it has a “very clean side effect profile compared to medications.”
What the field is trying to figure out now is “who it works for and how we can predict more effectively who’s going to benefit from it,” Dr. Downar said in an interview.
He noted that the study’s investigators are part of a “new generation of TMS researchers who are bringing new ideas into the fold and figuring out how to use brain imaging to personalize the treatment.” This study represents “a step” in that direction.
“A challenge for the field is that it’s often pretty easy to demonstrate a change at the group level, but the question is whether we can use that at the individual level. That’s a higher bar to meet, and we’re still not there yet,” Dr. Downar added.
Support for the study was provided by Brain Canada, the Michael Smith Foundation for Health Research and the Vancouver Coastal Health Research Institute. Dr. Vila-Rodriguez has received research support from CIHR, Brain Canada, the Michael Smith Foundation for Health Research, the Vancouver Coastal Health Research Institute, and the Weston Brain Institute for investigator-initiated research and philanthropic support from the Seedlings Foundation; he received in-kind equipment support from MagVenture for this investigator-initiated trial; and he has received honoraria for participation on an advisory board for Janssen. Dr. Downar has served as an adviser for BrainCheck, NeuroStim TMS, and Salience Neuro Health; received research grant from CIHR, National Institute for Mental Health, Brain Canada, Canadian Biomarker Integration Network in Depression, Ontario Brain Institute, Klarman Family Foundation, Arrell Family Foundation and the Edgestone Foundation; received travel stipends from Lundbeck and ANT Neuro; and received in-kind equipment support for investigator-initiated trials from MagVenture.
A version of this article first appeared on Medscape.com.
Anxiety in America: COVID ‘takes a backseat’ to global events
NEW ORLEANS – With 2 years of COVID-19 in the rearview mirror, anxiety among U.S. adults has turned instead toward global events, results from the annual Healthy Minds Poll from the American Psychiatric Association show.
“It’s not surprising that recent events, such as the war in Ukraine, racially motivated mass shootings, or the impacts of climate change, are weighing heavily on Americans’ minds,” APA president Vivian Pender, MD, said in a news release.

“COVID-19 in a way has taken a back seat, but the pandemic and its mental health effects are very much still with us. It’s important that we are cognizant of that and continue to work to ensure people who need psychiatric care, whether the causes are tied to the pandemic or to other issues, can access it,” Dr. Pender added.
Results from the 2022’s poll were released May 22 during the annual meeting of the APA.
Record low COVID anxiety
The poll was conducted by Morning Consult between April 23-24 and included 2,210 adult participants.
Results showed that This was down from 65% in 2021 and from 75% in 2020.
Instead, nearly three-quarters (73%) of adults are somewhat or extremely anxious about current events happening around the world, 64% are anxious about keeping themselves or their families safe, and 60% worry about their health in general.
Overall, about one-third (32%) reported being more anxious now than in 2021, 46% reported no change in their anxiety level, and 18% were less anxious.
About one-quarter (26%) have spoken with a mental health care professional in the past few years, which is down from 34% in 2021. In addition, Hispanic (36%) and Black (35%) adults were more likely to have reached out for help than White (25%) adults.
Despite the U.S. Surgeon General’s recent advisory on the mental health crisis among children, the poll results also showed that Americans are less concerned about their children’s mental health than in 2021. A total of 41% of parents expressed concern about this topic, which was down from 53% in 2021.
Still, 40% of parents said their children had received help from a mental health professional since the pandemic hit. Of that group, 36% sought help before the pandemic, whereas half said the pandemic had caused mental health issues for their children.

“While the overall level of concern has dropped, still 4 in 10 parents are worried about how their children are doing, and a third are having issues with access to care,” Saul Levin, MD, CEO and medical director of the APA, said in the release.
“This is unacceptable and as a nation, we need to invest in the kind of systems that will ensure any parent who’s worried about their child has access to lifesaving treatment,” Dr. Levin added.
Workplace mental health
In addition, the poll showed employees often have a tough time getting mental health support from employers, or are hesitant to ask for help.
“What’s troubling about the results of this poll is that, even as the pandemic has continued and its mental health effects wear on, fewer employees are reporting that they have access to mental health services,” Dr. Pender said.
“Workplaces need to ensure that they are paying attention to what their employees need, particularly now, and moving away from mental health benefits isn’t the right move,” she added.
About half (48%) of those polled said they can discuss mental health openly and honestly with their supervisor, down from 56% in 2021 and 62% in 2020.
Only about half (52%) said they feel comfortable using mental health services with their current employer, compared with 64% in 2021 and 67% in 2020.
In addition, fewer workers felt their employer is offering sufficient mental health resources and benefits. In 2022, 53% of workers thought resources and benefits were adequate, which was down from 65% in 2021 and 68% in 2020.
“It’s quite concerning to see that fewer people feel comfortable discussing mental health with a supervisor, at a time when people experiencing symptoms of anxiety, depression, and other conditions are on the rise and impact nearly every aspect of work, including productivity, performance, retention, and overall health care costs,” said Darcy Gruttadaro, JD, director of the APA Foundation’s Center for Workplace Mental Health.
“As rates of these conditions rise, we should see more employees knowing about available workplace mental health resources, not less,” Ms. Gruttadaro said.
Strong bipartisan support
Perhaps unexpectedly, the poll shows strong support among Democrats, Republicans, and Independents for three APA-backed approaches to improve timely access to mental health care and treatment.
Specifically, about three-quarters of those polled supported making it easier to see a mental health professional via telehealth, allowing patients to receive mental health care through a primary care provider, and funding mental health care professionals to work in rural or urban communities that are traditionally underserved.
“We’re in a moment when mental health is a big part of the national conversation, and clearly political party doesn’t matter as much on this issue,” Dr. Pender noted.
“It’s a rare thing in Washington these days to see such a resounding endorsement, but there is strong support for these practical workable solutions that mean more access to mental health care,” she said.
“What you see in this poll is agreement: It’s hard to access mental [health care] but we do have great solutions that could work across party lines,” Dr. Levin added.
“Many policy makers, in the administration and in Congress, are already putting these ideas into action, and they should feel encouraged that the public wants to see Congress act on them,” he said.
A version of this article first appeared on Medscape.com.
NEW ORLEANS – With 2 years of COVID-19 in the rearview mirror, anxiety among U.S. adults has turned instead toward global events, results from the annual Healthy Minds Poll from the American Psychiatric Association show.
“It’s not surprising that recent events, such as the war in Ukraine, racially motivated mass shootings, or the impacts of climate change, are weighing heavily on Americans’ minds,” APA president Vivian Pender, MD, said in a news release.
“COVID-19 in a way has taken a back seat, but the pandemic and its mental health effects are very much still with us. It’s important that we are cognizant of that and continue to work to ensure people who need psychiatric care, whether the causes are tied to the pandemic or to other issues, can access it,” Dr. Pender added.
Results from the 2022’s poll were released May 22 during the annual meeting of the APA.
Record low COVID anxiety
The poll was conducted by Morning Consult between April 23-24 and included 2,210 adult participants.
Results showed that This was down from 65% in 2021 and from 75% in 2020.
Instead, nearly three-quarters (73%) of adults are somewhat or extremely anxious about current events happening around the world, 64% are anxious about keeping themselves or their families safe, and 60% worry about their health in general.
Overall, about one-third (32%) reported being more anxious now than in 2021, 46% reported no change in their anxiety level, and 18% were less anxious.
About one-quarter (26%) have spoken with a mental health care professional in the past few years, which is down from 34% in 2021. In addition, Hispanic (36%) and Black (35%) adults were more likely to have reached out for help than White (25%) adults.
Despite the U.S. Surgeon General’s recent advisory on the mental health crisis among children, the poll results also showed that Americans are less concerned about their children’s mental health than in 2021. A total of 41% of parents expressed concern about this topic, which was down from 53% in 2021.
Still, 40% of parents said their children had received help from a mental health professional since the pandemic hit. Of that group, 36% sought help before the pandemic, whereas half said the pandemic had caused mental health issues for their children.
“While the overall level of concern has dropped, still 4 in 10 parents are worried about how their children are doing, and a third are having issues with access to care,” Saul Levin, MD, CEO and medical director of the APA, said in the release.
“This is unacceptable and as a nation, we need to invest in the kind of systems that will ensure any parent who’s worried about their child has access to lifesaving treatment,” Dr. Levin added.
Workplace mental health
In addition, the poll showed employees often have a tough time getting mental health support from employers, or are hesitant to ask for help.
“What’s troubling about the results of this poll is that, even as the pandemic has continued and its mental health effects wear on, fewer employees are reporting that they have access to mental health services,” Dr. Pender said.
“Workplaces need to ensure that they are paying attention to what their employees need, particularly now, and moving away from mental health benefits isn’t the right move,” she added.
About half (48%) of those polled said they can discuss mental health openly and honestly with their supervisor, down from 56% in 2021 and 62% in 2020.
Only about half (52%) said they feel comfortable using mental health services with their current employer, compared with 64% in 2021 and 67% in 2020.
In addition, fewer workers felt their employer is offering sufficient mental health resources and benefits. In 2022, 53% of workers thought resources and benefits were adequate, which was down from 65% in 2021 and 68% in 2020.
“It’s quite concerning to see that fewer people feel comfortable discussing mental health with a supervisor, at a time when people experiencing symptoms of anxiety, depression, and other conditions are on the rise and impact nearly every aspect of work, including productivity, performance, retention, and overall health care costs,” said Darcy Gruttadaro, JD, director of the APA Foundation’s Center for Workplace Mental Health.
“As rates of these conditions rise, we should see more employees knowing about available workplace mental health resources, not less,” Ms. Gruttadaro said.
Strong bipartisan support
Perhaps unexpectedly, the poll shows strong support among Democrats, Republicans, and Independents for three APA-backed approaches to improve timely access to mental health care and treatment.
Specifically, about three-quarters of those polled supported making it easier to see a mental health professional via telehealth, allowing patients to receive mental health care through a primary care provider, and funding mental health care professionals to work in rural or urban communities that are traditionally underserved.
“We’re in a moment when mental health is a big part of the national conversation, and clearly political party doesn’t matter as much on this issue,” Dr. Pender noted.
“It’s a rare thing in Washington these days to see such a resounding endorsement, but there is strong support for these practical workable solutions that mean more access to mental health care,” she said.
“What you see in this poll is agreement: It’s hard to access mental [health care] but we do have great solutions that could work across party lines,” Dr. Levin added.
“Many policy makers, in the administration and in Congress, are already putting these ideas into action, and they should feel encouraged that the public wants to see Congress act on them,” he said.
A version of this article first appeared on Medscape.com.
NEW ORLEANS – With 2 years of COVID-19 in the rearview mirror, anxiety among U.S. adults has turned instead toward global events, results from the annual Healthy Minds Poll from the American Psychiatric Association show.
“It’s not surprising that recent events, such as the war in Ukraine, racially motivated mass shootings, or the impacts of climate change, are weighing heavily on Americans’ minds,” APA president Vivian Pender, MD, said in a news release.
“COVID-19 in a way has taken a back seat, but the pandemic and its mental health effects are very much still with us. It’s important that we are cognizant of that and continue to work to ensure people who need psychiatric care, whether the causes are tied to the pandemic or to other issues, can access it,” Dr. Pender added.
Results from the 2022’s poll were released May 22 during the annual meeting of the APA.
Record low COVID anxiety
The poll was conducted by Morning Consult between April 23-24 and included 2,210 adult participants.
Results showed that This was down from 65% in 2021 and from 75% in 2020.
Instead, nearly three-quarters (73%) of adults are somewhat or extremely anxious about current events happening around the world, 64% are anxious about keeping themselves or their families safe, and 60% worry about their health in general.
Overall, about one-third (32%) reported being more anxious now than in 2021, 46% reported no change in their anxiety level, and 18% were less anxious.
About one-quarter (26%) have spoken with a mental health care professional in the past few years, which is down from 34% in 2021. In addition, Hispanic (36%) and Black (35%) adults were more likely to have reached out for help than White (25%) adults.
Despite the U.S. Surgeon General’s recent advisory on the mental health crisis among children, the poll results also showed that Americans are less concerned about their children’s mental health than in 2021. A total of 41% of parents expressed concern about this topic, which was down from 53% in 2021.
Still, 40% of parents said their children had received help from a mental health professional since the pandemic hit. Of that group, 36% sought help before the pandemic, whereas half said the pandemic had caused mental health issues for their children.
“While the overall level of concern has dropped, still 4 in 10 parents are worried about how their children are doing, and a third are having issues with access to care,” Saul Levin, MD, CEO and medical director of the APA, said in the release.
“This is unacceptable and as a nation, we need to invest in the kind of systems that will ensure any parent who’s worried about their child has access to lifesaving treatment,” Dr. Levin added.
Workplace mental health
In addition, the poll showed employees often have a tough time getting mental health support from employers, or are hesitant to ask for help.
“What’s troubling about the results of this poll is that, even as the pandemic has continued and its mental health effects wear on, fewer employees are reporting that they have access to mental health services,” Dr. Pender said.
“Workplaces need to ensure that they are paying attention to what their employees need, particularly now, and moving away from mental health benefits isn’t the right move,” she added.
About half (48%) of those polled said they can discuss mental health openly and honestly with their supervisor, down from 56% in 2021 and 62% in 2020.
Only about half (52%) said they feel comfortable using mental health services with their current employer, compared with 64% in 2021 and 67% in 2020.
In addition, fewer workers felt their employer is offering sufficient mental health resources and benefits. In 2022, 53% of workers thought resources and benefits were adequate, which was down from 65% in 2021 and 68% in 2020.
“It’s quite concerning to see that fewer people feel comfortable discussing mental health with a supervisor, at a time when people experiencing symptoms of anxiety, depression, and other conditions are on the rise and impact nearly every aspect of work, including productivity, performance, retention, and overall health care costs,” said Darcy Gruttadaro, JD, director of the APA Foundation’s Center for Workplace Mental Health.
“As rates of these conditions rise, we should see more employees knowing about available workplace mental health resources, not less,” Ms. Gruttadaro said.
Strong bipartisan support
Perhaps unexpectedly, the poll shows strong support among Democrats, Republicans, and Independents for three APA-backed approaches to improve timely access to mental health care and treatment.
Specifically, about three-quarters of those polled supported making it easier to see a mental health professional via telehealth, allowing patients to receive mental health care through a primary care provider, and funding mental health care professionals to work in rural or urban communities that are traditionally underserved.
“We’re in a moment when mental health is a big part of the national conversation, and clearly political party doesn’t matter as much on this issue,” Dr. Pender noted.
“It’s a rare thing in Washington these days to see such a resounding endorsement, but there is strong support for these practical workable solutions that mean more access to mental health care,” she said.
“What you see in this poll is agreement: It’s hard to access mental [health care] but we do have great solutions that could work across party lines,” Dr. Levin added.
“Many policy makers, in the administration and in Congress, are already putting these ideas into action, and they should feel encouraged that the public wants to see Congress act on them,” he said.
A version of this article first appeared on Medscape.com.
FROM APA 2022
FDA approves first drug for eosinophilic esophagitis
The U.S. Food and Drug Administration has approved dupilumab (Dupixent, Regeneron) to treat eosinophilic esophagitis (EoE) in adults and children aged 12 years and older weighing at least 40 kg.
EoE is a chronic inflammatory disorder driven by type 2 inflammation that damages the esophagus and causes difficulty swallowing and eating.
Dupilumab is a monoclonal antibody that acts to inhibit part of the inflammatory pathway. It’s the first drug to be approved by the FDA for EoE.
In a phase 3 trial, dupilumab 300 mg weekly significantly improved signs and symptoms of eosinophilic esophagitis, compared with placebo, underscoring the role of type 2 inflammation in this disease, Regeneron says in a news release.
According to the company, there are roughly 160,000 patients in the United States living with EoE who are currently using treatments not specifically approved for the disease. Of those patients, about 48,000 continue to experience symptoms despite multiple treatments.
“As researchers and clinicians have gained knowledge about eosinophilic esophagitis in recent years, more cases of the disorder have been recognized and diagnosed in the U.S.,” Jessica Lee, MD, director of the Division of Gastroenterology in the FDA’s Center for Drug Evaluation and Research, said in an FDA news release.
The approval of dupilumab will “fulfill an important unmet need for the increasing number of patients with eosinophilic esophagitis,” Dr. Lee said.
The efficacy and safety of dupilumab in EoE was demonstrated in a randomized, double-blind, parallel-group, multicenter, placebo-controlled trial that included two 24-week treatment periods (parts A and B) that were conducted independently in separate groups of patients.
In both part A and B, patients received dupilumab 300 mg or placebo every week.
In part A of the trial, 60% of the 42 patients who received dupilumab achieved the predetermined level of reduction of eosinophils in the esophagus, compared with 5% of the 39 patients who received placebo, the FDA said.
Patients who received dupilumab also experienced an average improvement of 22 points in the Dysphagia Symptom Questionnaire (DSQ) score, compared with 10 points for patients who received placebo.
In part B, 59% of the 80 patients who received dupilumab achieved the predetermined level of reduction of eosinophils in the esophagus, compared with 6% of the 79 patients who received placebo.
Patients who received dupilumab also experienced an average improvement of 24 points in their DSQ score, compared with 14 points for patients who received placebo.
“Assessments incorporating the perspectives from patients with EoE supported that the DSQ score improvement in patients who received Dupixent in the clinical trial was representative of clinically meaningful improvement in dysphagia,” the FDA noted.
“Treatment for patients with eosinophilic esophagitis can be challenging, particularly with no previously approved medications,” Evan Dellon, MD, principal investigator for the phase 3 trial, said in the company news release.
“Now, patients and their doctors have a treatment option available as part of their management plan that has the potential to control symptoms, improve inflammation, and heal the changes in the esophagus caused by this progressive and burdensome disease,” added Dr. Dellon, who is professor of medicine in the division of gastroenterology and hepatology at the University of North Carolina at Chapel Hill.
The FDA granted dupilumab priority review and breakthrough therapy designations for EoE.
Dupilumab is already approved in the United States for treatment of moderate to severe atopic dermatitis in adults and children aged 6 years and older whose disease is not adequately controlled by topical prescription therapies or for whom those therapies are not advisable.
The drug is also approved as an add-on maintenance treatment for adults and children aged 6 years and older with certain types of moderate to severe asthma and as an add-on maintenance treatment for adults with inadequately controlled chronic rhinosinusitis with nasal polyposis.
A version of this article first appeared on Medscape.com .
Eosinophilic esophagitis (EoE) is a chronic disease requiring long-term treatment for both induction and maintenance of response. For decades, however, Food and Drug Administration–approved therapies for EoE have not been available. Dupilumab is the first drug to receive FDA approval to treat EoE. This human monoclonal antibody directed against the interleukin (IL)4 receptor–alpha component of the type 2 receptor inhibits signaling of IL4 and IL13. Dupilumab has shown efficacy in similar diseases, such as atopic dermatitis and eosinophilic asthma. In 2017 dupilumab was granted Orphan Drug designation for the potential treatment of EoE and in 2020 the FDA granted Breakthrough Therapy designation for EoE. Recent data from the phase 3 trial of dupilumab 300 mg weekly enrolling patients aged 12 years and older demonstrated a significantly greater reduction in disease symptoms, normalization of esophageal eosinophilia, and reduction in endoscopic findings by week 24 compared with placebo.
The highly anticipated approval of dupilumab marks a paradigm shift toward biologic medications for treatment of EoE when historical treatments have relied on proton pump–inhibitor therapy or topical swallowed steroids. As we await updates about availability and access of dupilumab for our patients, we can rest assured that a highly efficacious treatment is now approved and will fill an important treatment gap in EoE, particularly for patients not deriving adequate response with traditionally used strategies. With multiple clinical trials underway, this milestone likely represents the beginning of additional effective therapies (nonbiologic and biologic) that will be available for EoE.
Rena Yadlapati, MD, MSHS, FACG, is associate professor of clinical medicine in the division of gastroenterology at the University of California, San Diego, medical director of the UCSD Center for Esophageal Diseases, and director of the GI Motility Lab. She has no relevant conflicts of interest.
Eosinophilic esophagitis (EoE) is a chronic disease requiring long-term treatment for both induction and maintenance of response. For decades, however, Food and Drug Administration–approved therapies for EoE have not been available. Dupilumab is the first drug to receive FDA approval to treat EoE. This human monoclonal antibody directed against the interleukin (IL)4 receptor–alpha component of the type 2 receptor inhibits signaling of IL4 and IL13. Dupilumab has shown efficacy in similar diseases, such as atopic dermatitis and eosinophilic asthma. In 2017 dupilumab was granted Orphan Drug designation for the potential treatment of EoE and in 2020 the FDA granted Breakthrough Therapy designation for EoE. Recent data from the phase 3 trial of dupilumab 300 mg weekly enrolling patients aged 12 years and older demonstrated a significantly greater reduction in disease symptoms, normalization of esophageal eosinophilia, and reduction in endoscopic findings by week 24 compared with placebo.
The highly anticipated approval of dupilumab marks a paradigm shift toward biologic medications for treatment of EoE when historical treatments have relied on proton pump–inhibitor therapy or topical swallowed steroids. As we await updates about availability and access of dupilumab for our patients, we can rest assured that a highly efficacious treatment is now approved and will fill an important treatment gap in EoE, particularly for patients not deriving adequate response with traditionally used strategies. With multiple clinical trials underway, this milestone likely represents the beginning of additional effective therapies (nonbiologic and biologic) that will be available for EoE.
Rena Yadlapati, MD, MSHS, FACG, is associate professor of clinical medicine in the division of gastroenterology at the University of California, San Diego, medical director of the UCSD Center for Esophageal Diseases, and director of the GI Motility Lab. She has no relevant conflicts of interest.
Eosinophilic esophagitis (EoE) is a chronic disease requiring long-term treatment for both induction and maintenance of response. For decades, however, Food and Drug Administration–approved therapies for EoE have not been available. Dupilumab is the first drug to receive FDA approval to treat EoE. This human monoclonal antibody directed against the interleukin (IL)4 receptor–alpha component of the type 2 receptor inhibits signaling of IL4 and IL13. Dupilumab has shown efficacy in similar diseases, such as atopic dermatitis and eosinophilic asthma. In 2017 dupilumab was granted Orphan Drug designation for the potential treatment of EoE and in 2020 the FDA granted Breakthrough Therapy designation for EoE. Recent data from the phase 3 trial of dupilumab 300 mg weekly enrolling patients aged 12 years and older demonstrated a significantly greater reduction in disease symptoms, normalization of esophageal eosinophilia, and reduction in endoscopic findings by week 24 compared with placebo.
The highly anticipated approval of dupilumab marks a paradigm shift toward biologic medications for treatment of EoE when historical treatments have relied on proton pump–inhibitor therapy or topical swallowed steroids. As we await updates about availability and access of dupilumab for our patients, we can rest assured that a highly efficacious treatment is now approved and will fill an important treatment gap in EoE, particularly for patients not deriving adequate response with traditionally used strategies. With multiple clinical trials underway, this milestone likely represents the beginning of additional effective therapies (nonbiologic and biologic) that will be available for EoE.
Rena Yadlapati, MD, MSHS, FACG, is associate professor of clinical medicine in the division of gastroenterology at the University of California, San Diego, medical director of the UCSD Center for Esophageal Diseases, and director of the GI Motility Lab. She has no relevant conflicts of interest.
The U.S. Food and Drug Administration has approved dupilumab (Dupixent, Regeneron) to treat eosinophilic esophagitis (EoE) in adults and children aged 12 years and older weighing at least 40 kg.
EoE is a chronic inflammatory disorder driven by type 2 inflammation that damages the esophagus and causes difficulty swallowing and eating.
Dupilumab is a monoclonal antibody that acts to inhibit part of the inflammatory pathway. It’s the first drug to be approved by the FDA for EoE.
In a phase 3 trial, dupilumab 300 mg weekly significantly improved signs and symptoms of eosinophilic esophagitis, compared with placebo, underscoring the role of type 2 inflammation in this disease, Regeneron says in a news release.
According to the company, there are roughly 160,000 patients in the United States living with EoE who are currently using treatments not specifically approved for the disease. Of those patients, about 48,000 continue to experience symptoms despite multiple treatments.
“As researchers and clinicians have gained knowledge about eosinophilic esophagitis in recent years, more cases of the disorder have been recognized and diagnosed in the U.S.,” Jessica Lee, MD, director of the Division of Gastroenterology in the FDA’s Center for Drug Evaluation and Research, said in an FDA news release.
The approval of dupilumab will “fulfill an important unmet need for the increasing number of patients with eosinophilic esophagitis,” Dr. Lee said.
The efficacy and safety of dupilumab in EoE was demonstrated in a randomized, double-blind, parallel-group, multicenter, placebo-controlled trial that included two 24-week treatment periods (parts A and B) that were conducted independently in separate groups of patients.
In both part A and B, patients received dupilumab 300 mg or placebo every week.
In part A of the trial, 60% of the 42 patients who received dupilumab achieved the predetermined level of reduction of eosinophils in the esophagus, compared with 5% of the 39 patients who received placebo, the FDA said.
Patients who received dupilumab also experienced an average improvement of 22 points in the Dysphagia Symptom Questionnaire (DSQ) score, compared with 10 points for patients who received placebo.
In part B, 59% of the 80 patients who received dupilumab achieved the predetermined level of reduction of eosinophils in the esophagus, compared with 6% of the 79 patients who received placebo.
Patients who received dupilumab also experienced an average improvement of 24 points in their DSQ score, compared with 14 points for patients who received placebo.
“Assessments incorporating the perspectives from patients with EoE supported that the DSQ score improvement in patients who received Dupixent in the clinical trial was representative of clinically meaningful improvement in dysphagia,” the FDA noted.
“Treatment for patients with eosinophilic esophagitis can be challenging, particularly with no previously approved medications,” Evan Dellon, MD, principal investigator for the phase 3 trial, said in the company news release.
“Now, patients and their doctors have a treatment option available as part of their management plan that has the potential to control symptoms, improve inflammation, and heal the changes in the esophagus caused by this progressive and burdensome disease,” added Dr. Dellon, who is professor of medicine in the division of gastroenterology and hepatology at the University of North Carolina at Chapel Hill.
The FDA granted dupilumab priority review and breakthrough therapy designations for EoE.
Dupilumab is already approved in the United States for treatment of moderate to severe atopic dermatitis in adults and children aged 6 years and older whose disease is not adequately controlled by topical prescription therapies or for whom those therapies are not advisable.
The drug is also approved as an add-on maintenance treatment for adults and children aged 6 years and older with certain types of moderate to severe asthma and as an add-on maintenance treatment for adults with inadequately controlled chronic rhinosinusitis with nasal polyposis.
A version of this article first appeared on Medscape.com .
The U.S. Food and Drug Administration has approved dupilumab (Dupixent, Regeneron) to treat eosinophilic esophagitis (EoE) in adults and children aged 12 years and older weighing at least 40 kg.
EoE is a chronic inflammatory disorder driven by type 2 inflammation that damages the esophagus and causes difficulty swallowing and eating.
Dupilumab is a monoclonal antibody that acts to inhibit part of the inflammatory pathway. It’s the first drug to be approved by the FDA for EoE.
In a phase 3 trial, dupilumab 300 mg weekly significantly improved signs and symptoms of eosinophilic esophagitis, compared with placebo, underscoring the role of type 2 inflammation in this disease, Regeneron says in a news release.
According to the company, there are roughly 160,000 patients in the United States living with EoE who are currently using treatments not specifically approved for the disease. Of those patients, about 48,000 continue to experience symptoms despite multiple treatments.
“As researchers and clinicians have gained knowledge about eosinophilic esophagitis in recent years, more cases of the disorder have been recognized and diagnosed in the U.S.,” Jessica Lee, MD, director of the Division of Gastroenterology in the FDA’s Center for Drug Evaluation and Research, said in an FDA news release.
The approval of dupilumab will “fulfill an important unmet need for the increasing number of patients with eosinophilic esophagitis,” Dr. Lee said.
The efficacy and safety of dupilumab in EoE was demonstrated in a randomized, double-blind, parallel-group, multicenter, placebo-controlled trial that included two 24-week treatment periods (parts A and B) that were conducted independently in separate groups of patients.
In both part A and B, patients received dupilumab 300 mg or placebo every week.
In part A of the trial, 60% of the 42 patients who received dupilumab achieved the predetermined level of reduction of eosinophils in the esophagus, compared with 5% of the 39 patients who received placebo, the FDA said.
Patients who received dupilumab also experienced an average improvement of 22 points in the Dysphagia Symptom Questionnaire (DSQ) score, compared with 10 points for patients who received placebo.
In part B, 59% of the 80 patients who received dupilumab achieved the predetermined level of reduction of eosinophils in the esophagus, compared with 6% of the 79 patients who received placebo.
Patients who received dupilumab also experienced an average improvement of 24 points in their DSQ score, compared with 14 points for patients who received placebo.
“Assessments incorporating the perspectives from patients with EoE supported that the DSQ score improvement in patients who received Dupixent in the clinical trial was representative of clinically meaningful improvement in dysphagia,” the FDA noted.
“Treatment for patients with eosinophilic esophagitis can be challenging, particularly with no previously approved medications,” Evan Dellon, MD, principal investigator for the phase 3 trial, said in the company news release.
“Now, patients and their doctors have a treatment option available as part of their management plan that has the potential to control symptoms, improve inflammation, and heal the changes in the esophagus caused by this progressive and burdensome disease,” added Dr. Dellon, who is professor of medicine in the division of gastroenterology and hepatology at the University of North Carolina at Chapel Hill.
The FDA granted dupilumab priority review and breakthrough therapy designations for EoE.
Dupilumab is already approved in the United States for treatment of moderate to severe atopic dermatitis in adults and children aged 6 years and older whose disease is not adequately controlled by topical prescription therapies or for whom those therapies are not advisable.
The drug is also approved as an add-on maintenance treatment for adults and children aged 6 years and older with certain types of moderate to severe asthma and as an add-on maintenance treatment for adults with inadequately controlled chronic rhinosinusitis with nasal polyposis.
A version of this article first appeared on Medscape.com .
Many Americans missing an opportunity to prevent dementia
(ADRD), including hypertension, low levels of physical activity, and obesity, new research shows.
Data from the Centers for Disease Control and Prevention reveal that among nearly 162,000 adults aged 45 and older who were surveyed in 2019 as part of the Behavioral Risk Factor Surveillance System (BRFSS), nearly half had high blood pressure and did not achieve aerobic physical activity recommendations. These were the two most common modifiable risk factors for ADRD.
In addition, more than one-third (35%) of adults were obese, 19% had diabetes, 18% had depression, 15% were smokers, 11% had hearing loss, and 10% were binge drinkers.
The findings were published online in the CDC’s Morbidity and Mortality Weekly Report.
A missed prevention opportunity
More than 1 in 10 (11.3%) adults surveyed reported subjective cognitive decline (SCD), an early indicator of possible future ADRD.
The prevalence of SCD increased from about 4% among adults with no modifiable risk factors for ADRD to 25% for those with four or more risk factors.
Adults with SCD were more apt to report having almost all modifiable risk factors and were more likely to report four or more risk factors (34%) than were peers without SCD (13%)
The prevalence of SCD ranged from a high of about 29% in those with depression and 25% in those with hearing loss to 11% in those who reported binge drinking.
In line with previous research, the findings indicate that American Indian or Alaska Native, Black or African American, and Hispanic populations were more likely to have modifiable risk factors for ADRD than other racial groups, the researchers reported.
The CDC’s National Healthy Brain Initiative supports culturally tailored interventions that address ADRD risk factors specifically in these populations.
In 2021, the federal government’s National Plan to Address Alzheimer’s Disease was updated to include a new goal to reduce risk factors for ADRD.
“Given the prevalence of modifiable risk factors for ADRD and anticipated growth of the older adult population and those with ADRD, this new goal has the potential to benefit a large proportion of U.S. adults,” the investigators wrote.
“In addition to helping patients discuss concerns about memory loss, health care professionals should also screen patients for modifiable risk factors, counsel patients with risk factors, and refer them to effective programs and interventions where recommended,” they advised.
A recent report from the Lancet Commission on Dementia Prevention, Intervention, and Care found that modifying 12 risk factors over the life course could delay or prevent 40% of dementia cases.
A version of this article first appeared on Medscape.com.
(ADRD), including hypertension, low levels of physical activity, and obesity, new research shows.
Data from the Centers for Disease Control and Prevention reveal that among nearly 162,000 adults aged 45 and older who were surveyed in 2019 as part of the Behavioral Risk Factor Surveillance System (BRFSS), nearly half had high blood pressure and did not achieve aerobic physical activity recommendations. These were the two most common modifiable risk factors for ADRD.
In addition, more than one-third (35%) of adults were obese, 19% had diabetes, 18% had depression, 15% were smokers, 11% had hearing loss, and 10% were binge drinkers.
The findings were published online in the CDC’s Morbidity and Mortality Weekly Report.
A missed prevention opportunity
More than 1 in 10 (11.3%) adults surveyed reported subjective cognitive decline (SCD), an early indicator of possible future ADRD.
The prevalence of SCD increased from about 4% among adults with no modifiable risk factors for ADRD to 25% for those with four or more risk factors.
Adults with SCD were more apt to report having almost all modifiable risk factors and were more likely to report four or more risk factors (34%) than were peers without SCD (13%)
The prevalence of SCD ranged from a high of about 29% in those with depression and 25% in those with hearing loss to 11% in those who reported binge drinking.
In line with previous research, the findings indicate that American Indian or Alaska Native, Black or African American, and Hispanic populations were more likely to have modifiable risk factors for ADRD than other racial groups, the researchers reported.
The CDC’s National Healthy Brain Initiative supports culturally tailored interventions that address ADRD risk factors specifically in these populations.
In 2021, the federal government’s National Plan to Address Alzheimer’s Disease was updated to include a new goal to reduce risk factors for ADRD.
“Given the prevalence of modifiable risk factors for ADRD and anticipated growth of the older adult population and those with ADRD, this new goal has the potential to benefit a large proportion of U.S. adults,” the investigators wrote.
“In addition to helping patients discuss concerns about memory loss, health care professionals should also screen patients for modifiable risk factors, counsel patients with risk factors, and refer them to effective programs and interventions where recommended,” they advised.
A recent report from the Lancet Commission on Dementia Prevention, Intervention, and Care found that modifying 12 risk factors over the life course could delay or prevent 40% of dementia cases.
A version of this article first appeared on Medscape.com.
(ADRD), including hypertension, low levels of physical activity, and obesity, new research shows.
Data from the Centers for Disease Control and Prevention reveal that among nearly 162,000 adults aged 45 and older who were surveyed in 2019 as part of the Behavioral Risk Factor Surveillance System (BRFSS), nearly half had high blood pressure and did not achieve aerobic physical activity recommendations. These were the two most common modifiable risk factors for ADRD.
In addition, more than one-third (35%) of adults were obese, 19% had diabetes, 18% had depression, 15% were smokers, 11% had hearing loss, and 10% were binge drinkers.
The findings were published online in the CDC’s Morbidity and Mortality Weekly Report.
A missed prevention opportunity
More than 1 in 10 (11.3%) adults surveyed reported subjective cognitive decline (SCD), an early indicator of possible future ADRD.
The prevalence of SCD increased from about 4% among adults with no modifiable risk factors for ADRD to 25% for those with four or more risk factors.
Adults with SCD were more apt to report having almost all modifiable risk factors and were more likely to report four or more risk factors (34%) than were peers without SCD (13%)
The prevalence of SCD ranged from a high of about 29% in those with depression and 25% in those with hearing loss to 11% in those who reported binge drinking.
In line with previous research, the findings indicate that American Indian or Alaska Native, Black or African American, and Hispanic populations were more likely to have modifiable risk factors for ADRD than other racial groups, the researchers reported.
The CDC’s National Healthy Brain Initiative supports culturally tailored interventions that address ADRD risk factors specifically in these populations.
In 2021, the federal government’s National Plan to Address Alzheimer’s Disease was updated to include a new goal to reduce risk factors for ADRD.
“Given the prevalence of modifiable risk factors for ADRD and anticipated growth of the older adult population and those with ADRD, this new goal has the potential to benefit a large proportion of U.S. adults,” the investigators wrote.
“In addition to helping patients discuss concerns about memory loss, health care professionals should also screen patients for modifiable risk factors, counsel patients with risk factors, and refer them to effective programs and interventions where recommended,” they advised.
A recent report from the Lancet Commission on Dementia Prevention, Intervention, and Care found that modifying 12 risk factors over the life course could delay or prevent 40% of dementia cases.
A version of this article first appeared on Medscape.com.
FROM MMWR
How social determinants of health impact disparities in IBD care, outcomes
The incidence of inflammatory bowel disease (IBD) is on the rise among racial and ethnic minority groups in the United States, and social determinants of health (SDOH) contribute to disparities in IBD care and outcome, say the authors of a new paper on the topic.
It’s an “overdue priority to acknowledge the weight and influence of the SDOH on health disparities in IBD care,” write Adjoa Anyane-Yeboa, MD, PhD, with Massachusetts General Hospital, Boston, and co-authors.
“Only after this acknowledgement can we begin to develop alternative systems that work to rectify the deleterious effects of our current policies in a more longitudinal and effective manner,” they say.
Their paper was published online in Clinical Gastroenterology and Hepatology.
Upstream factors propagate downstream outcomes
The authors found multiple examples in the literature of how upstream SDOH (for example, racism, poverty, neighborhood violence, and under-insurance) lead to midstream SDOH (for example, lack of social support, lack of access to specialized IBD care, poor housing conditions, and food insecurity) that result in poor downstream outcomes in IBD (for example, delayed diagnosis, increased disease activity, IBD flares, and suboptimal medical management).
The IBD literature shows that Black/African American adults with IBD often have worse outcomes across the IBD care continuum than White peers, with higher hospitalization rates, longer stays, increased hospitalization costs, higher readmission rates, and more complications after IBD surgery.
Unequal access to specialized IBD care is a factor, with Black/African American patients less likely to undergo annual visits to a gastroenterologist or IBD specialist, twice as likely than White patients to visit the emergency department over a 12-month period, and less likely to receive treatment with infliximab.
As has been shown for other chronic digestive diseases and cancers, disparities in outcomes related to IBD exist across race, ethnicity, differential insurance status and coverage, and socioeconomic status, the authors note.
Yet, they point out that, interestingly, a 2021 study of patients with Medicaid insurance from four states revealed no disparities in the use of IBD-specific medications between Black/African American and White patients, suggesting that when access to care is equal, disparities diminish.
Target multiple stakeholders to achieve IBD health equity
Achieving health equity in IBD will require strategies targeting medical trainees, providers, practices, and health systems, as well as community and industry leaders and policymakers, Dr. Anyane-Yeboa and colleagues say.
At the medical trainee level, racism and bias should be addressed early in medical student, resident, and fellow training and education. Curricula should move away from race-based training, where race is considered an independent risk factor for disease and often used to guide differential diagnoses and treatment, they suggest.
At the provider level, they say self-reflection around one’s own beliefs, biases, perceptions, and interactions with diverse and vulnerable patient groups is “paramount.” Individual self-reflection should be coupled with mandatory and effective implicit bias and anti-racism training.
At the practice or hospital system level, screening for SDOH at the point of care, addressing barriers to needed treatment, and connecting patients to appropriate resources are all important, they write.
The researchers also call for policy-level changes to increase funding for health equity research, which is historically undervalued and underfunded.
“Focusing on SDOH as the root cause of health inequity in IBD is essential to improve outcomes for marginalized patients,” they write.
Given that research describing specific interventions to address SDOH in IBD is currently nonexistent, “our paper serves as a call to action for more work to be done in this area,” they say.
“As medical providers and health care organizations, we all have a responsibility to address the SDOH when caring for our patients in order to provide each patient with IBD the opportunity to achieve the best health possible,” they conclude.
This research had no specific funding. The authors have disclosed no relevant financial relationships.
AGA applauds researchers who are working to raise our awareness of health disparities in digestive diseases. AGA is committed to addressing this important societal issue head on. Learn more about AGA’s commitment through the AGA Equity Project.
A version of this article first appeared on Medscape.com.
The incidence of inflammatory bowel disease (IBD) is on the rise among racial and ethnic minority groups in the United States, and social determinants of health (SDOH) contribute to disparities in IBD care and outcome, say the authors of a new paper on the topic.
It’s an “overdue priority to acknowledge the weight and influence of the SDOH on health disparities in IBD care,” write Adjoa Anyane-Yeboa, MD, PhD, with Massachusetts General Hospital, Boston, and co-authors.
“Only after this acknowledgement can we begin to develop alternative systems that work to rectify the deleterious effects of our current policies in a more longitudinal and effective manner,” they say.
Their paper was published online in Clinical Gastroenterology and Hepatology.
Upstream factors propagate downstream outcomes
The authors found multiple examples in the literature of how upstream SDOH (for example, racism, poverty, neighborhood violence, and under-insurance) lead to midstream SDOH (for example, lack of social support, lack of access to specialized IBD care, poor housing conditions, and food insecurity) that result in poor downstream outcomes in IBD (for example, delayed diagnosis, increased disease activity, IBD flares, and suboptimal medical management).
The IBD literature shows that Black/African American adults with IBD often have worse outcomes across the IBD care continuum than White peers, with higher hospitalization rates, longer stays, increased hospitalization costs, higher readmission rates, and more complications after IBD surgery.
Unequal access to specialized IBD care is a factor, with Black/African American patients less likely to undergo annual visits to a gastroenterologist or IBD specialist, twice as likely than White patients to visit the emergency department over a 12-month period, and less likely to receive treatment with infliximab.
As has been shown for other chronic digestive diseases and cancers, disparities in outcomes related to IBD exist across race, ethnicity, differential insurance status and coverage, and socioeconomic status, the authors note.
Yet, they point out that, interestingly, a 2021 study of patients with Medicaid insurance from four states revealed no disparities in the use of IBD-specific medications between Black/African American and White patients, suggesting that when access to care is equal, disparities diminish.
Target multiple stakeholders to achieve IBD health equity
Achieving health equity in IBD will require strategies targeting medical trainees, providers, practices, and health systems, as well as community and industry leaders and policymakers, Dr. Anyane-Yeboa and colleagues say.
At the medical trainee level, racism and bias should be addressed early in medical student, resident, and fellow training and education. Curricula should move away from race-based training, where race is considered an independent risk factor for disease and often used to guide differential diagnoses and treatment, they suggest.
At the provider level, they say self-reflection around one’s own beliefs, biases, perceptions, and interactions with diverse and vulnerable patient groups is “paramount.” Individual self-reflection should be coupled with mandatory and effective implicit bias and anti-racism training.
At the practice or hospital system level, screening for SDOH at the point of care, addressing barriers to needed treatment, and connecting patients to appropriate resources are all important, they write.
The researchers also call for policy-level changes to increase funding for health equity research, which is historically undervalued and underfunded.
“Focusing on SDOH as the root cause of health inequity in IBD is essential to improve outcomes for marginalized patients,” they write.
Given that research describing specific interventions to address SDOH in IBD is currently nonexistent, “our paper serves as a call to action for more work to be done in this area,” they say.
“As medical providers and health care organizations, we all have a responsibility to address the SDOH when caring for our patients in order to provide each patient with IBD the opportunity to achieve the best health possible,” they conclude.
This research had no specific funding. The authors have disclosed no relevant financial relationships.
AGA applauds researchers who are working to raise our awareness of health disparities in digestive diseases. AGA is committed to addressing this important societal issue head on. Learn more about AGA’s commitment through the AGA Equity Project.
A version of this article first appeared on Medscape.com.
The incidence of inflammatory bowel disease (IBD) is on the rise among racial and ethnic minority groups in the United States, and social determinants of health (SDOH) contribute to disparities in IBD care and outcome, say the authors of a new paper on the topic.
It’s an “overdue priority to acknowledge the weight and influence of the SDOH on health disparities in IBD care,” write Adjoa Anyane-Yeboa, MD, PhD, with Massachusetts General Hospital, Boston, and co-authors.
“Only after this acknowledgement can we begin to develop alternative systems that work to rectify the deleterious effects of our current policies in a more longitudinal and effective manner,” they say.
Their paper was published online in Clinical Gastroenterology and Hepatology.
Upstream factors propagate downstream outcomes
The authors found multiple examples in the literature of how upstream SDOH (for example, racism, poverty, neighborhood violence, and under-insurance) lead to midstream SDOH (for example, lack of social support, lack of access to specialized IBD care, poor housing conditions, and food insecurity) that result in poor downstream outcomes in IBD (for example, delayed diagnosis, increased disease activity, IBD flares, and suboptimal medical management).
The IBD literature shows that Black/African American adults with IBD often have worse outcomes across the IBD care continuum than White peers, with higher hospitalization rates, longer stays, increased hospitalization costs, higher readmission rates, and more complications after IBD surgery.
Unequal access to specialized IBD care is a factor, with Black/African American patients less likely to undergo annual visits to a gastroenterologist or IBD specialist, twice as likely than White patients to visit the emergency department over a 12-month period, and less likely to receive treatment with infliximab.
As has been shown for other chronic digestive diseases and cancers, disparities in outcomes related to IBD exist across race, ethnicity, differential insurance status and coverage, and socioeconomic status, the authors note.
Yet, they point out that, interestingly, a 2021 study of patients with Medicaid insurance from four states revealed no disparities in the use of IBD-specific medications between Black/African American and White patients, suggesting that when access to care is equal, disparities diminish.
Target multiple stakeholders to achieve IBD health equity
Achieving health equity in IBD will require strategies targeting medical trainees, providers, practices, and health systems, as well as community and industry leaders and policymakers, Dr. Anyane-Yeboa and colleagues say.
At the medical trainee level, racism and bias should be addressed early in medical student, resident, and fellow training and education. Curricula should move away from race-based training, where race is considered an independent risk factor for disease and often used to guide differential diagnoses and treatment, they suggest.
At the provider level, they say self-reflection around one’s own beliefs, biases, perceptions, and interactions with diverse and vulnerable patient groups is “paramount.” Individual self-reflection should be coupled with mandatory and effective implicit bias and anti-racism training.
At the practice or hospital system level, screening for SDOH at the point of care, addressing barriers to needed treatment, and connecting patients to appropriate resources are all important, they write.
The researchers also call for policy-level changes to increase funding for health equity research, which is historically undervalued and underfunded.
“Focusing on SDOH as the root cause of health inequity in IBD is essential to improve outcomes for marginalized patients,” they write.
Given that research describing specific interventions to address SDOH in IBD is currently nonexistent, “our paper serves as a call to action for more work to be done in this area,” they say.
“As medical providers and health care organizations, we all have a responsibility to address the SDOH when caring for our patients in order to provide each patient with IBD the opportunity to achieve the best health possible,” they conclude.
This research had no specific funding. The authors have disclosed no relevant financial relationships.
AGA applauds researchers who are working to raise our awareness of health disparities in digestive diseases. AGA is committed to addressing this important societal issue head on. Learn more about AGA’s commitment through the AGA Equity Project.
A version of this article first appeared on Medscape.com.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Updated AHA/ASA guideline changes care for spontaneous intracerebral hemorrhage
Many strategies widely considered “standard care” for managing spontaneous intracerebral hemorrhage (ICH) are not as effective as previously thought and are no longer recommended in updated guidelines from the American Heart Association/American Stroke Association (ASA).
Compression stockings, antiseizure medication, and steroid treatment are among the treatments with uncertain effectiveness, the writing group says.
The 2022 Guideline for the Management of Patients With Spontaneous ICH was published online in Stroke. The 80-page document contains major changes and refinements to the 2015 guideline on ICH management.
“Advances have been made in an array of fields related to ICH, including the organization of regional health care systems, reversal of the negative effects of blood thinners, minimally invasive surgical procedures, and the underlying disease in small blood vessels,” Steven M. Greenberg, MD, PhD, chair of the guideline writing group with Harvard Medical School and Massachusetts General Hospital, both in Boston, said in a news release.
“We’ve updated sections across the board. There’s probably no area that went untouched with some tweaking and new evidence added that led to some changes in level of evidence or strength of a recommendation,” Dr. Greenberg added in an interview with this news organization.
“Each section comes with knowledge gaps, and it wasn’t hard to come up with knowledge gaps in every section,” Dr. Greenberg acknowledged.
Time-honored treatments no more?
Among the key updates are changes to some “time-honored” treatments that continue to be used with some “regularity” for patients with ICH, yet appear to confer either no benefit or harm, Dr. Greenberg said.
For example, for emergency or critical care treatment of ICH, prophylactic corticosteroids or continuous hyperosmolar therapy is not recommended, because it appears to have no benefit for outcome, while use of platelet transfusions outside the setting of emergency surgery or severe thrombocytopenia appears to worsen outcome, the authors say.
Use of graduated knee- or thigh-high compression stockings alone is not an effective prophylactic therapy for prevention of deep vein thrombosis (DVT). Instead, intermittent pneumatic compression (IPC) starting on the day of diagnosis is now recommended for DVT prophylaxis.
“This is an area where we still have a lot of exploration to do. It is unclear whether even specialized compression devices reduce the risks of deep vein thrombosis or improve the overall health of people with a brain bleed,” Dr. Greenberg said in the release.
The new guidance advises against use of antiseizure or antidepressant medications for ICH patients in whom there is no evidence of seizures or depression.
In clinical trials, antiseizure medication did not contribute to improvements in functionality or long-term seizure control, and the use of antidepressants increased the chance of bone fractures, the authors say.
The guideline also provides updated recommendations for acute reversal of anticoagulation after ICH. It highlights the use of protein complex concentrate for reversal of vitamin K antagonists, such as warfarin; idarucizumab for reversal of the thrombin inhibitor dabigatran; and andexanet alfa for reversal of factor Xa inhibitors, such as rivaroxaban, apixaban, and edoxaban.
For acute blood pressure lowering after mild to moderate ICH, treatment regimens that limit blood pressure variability and achieve smooth, sustained blood pressure control appear to reduce hematoma expansion and yield better functional outcome, the guideline says.
It also notes that minimally invasive approaches for hematoma evacuation, compared with medical management alone‚ have been shown to reduce mortality.
For patients with cerebellar hemorrhage, indications for immediate surgical evacuation with or without an external ventricular drain to reduce mortality now include larger volume (> 15 mL) in addition to previously recommended indications of neurologic deterioration, brainstem compression, and hydrocephalus, the authors note.
However, a “major knowledge gap is whether we can improve functional outcome with hematoma evacuation,” Dr. Greenberg said.
Multidisciplinary care
For rehabilitation after ICH, the guideline reinforces the importance of having a multidisciplinary team to develop a comprehensive plan for recovery.
Starting rehabilitation activities such as stretching and functional task training may be considered 24 to 48 hours following mild or moderate ICH. However, early aggressive mobilization within the first 24 hours has been linked to an increased risk of death within 14 days after an ICH, the guideline says.
Knowledge gaps include how soon it’s safe to return to work, drive, and participate in other social engagements. Recommendations on sexual activity and exercise levels that are safe after a stroke are also needed.
“People need additional help with these lifestyle changes, whether it’s moving around more, curbing their alcohol use, or eating healthier foods. This all happens after they leave the hospital, and we need to be sure we are empowering families with the information they may need to be properly supportive,” Dr. Greenberg says in the release.
The guideline points to the patient’s home caregiver as a “key and sometimes overlooked” member of the care team. It recommends psychosocial education, practical support, and training for the caregiver to improve the patient’s balance, activity level, and overall quality of life.
Opportunity for prevention?
The guideline also suggests there may be an opportunity to prevent ICH in some people through neuroimaging markers.
While neuroimaging is not routinely performed as a part of risk stratification for primary ICH risk, damage to small blood vessels that is associated with ICH may be evident on MRI that could signal future ICH risk, the guideline says.
“We added to the guidelines for the first time a section on mostly imaging markers of risk for having a first-ever hemorrhage,” Dr. Greenberg said in an interview.
“We don’t make any recommendations as to how to act on these markers because there is a knowledge gap. The hope is that we’ll see growth in our ability to predict first-ever hemorrhage and be able to do things to prevent first-ever hemorrhage,” he said.
“We believe the wide range of knowledge set forth in the new guideline will translate into meaningful improvements in ICH care,” Dr. Greenberg adds in the release.
The updated guideline has been endorsed by the American Association of Neurological Surgeons and Congress of Neurological Surgeons, the Society of Vascular and Interventional Neurology, and the Neurocritical Care Society. The American Academy of Neurology has affirmed the value of this statement as an educational tool for neurologists.
This research had no commercial funding. Dr. Greenberg has disclosed no relevant financial relationships. A complete list of disclosures for the guideline group is available with the original article.
A version of this article first appeared on Medscape.com.
Many strategies widely considered “standard care” for managing spontaneous intracerebral hemorrhage (ICH) are not as effective as previously thought and are no longer recommended in updated guidelines from the American Heart Association/American Stroke Association (ASA).
Compression stockings, antiseizure medication, and steroid treatment are among the treatments with uncertain effectiveness, the writing group says.
The 2022 Guideline for the Management of Patients With Spontaneous ICH was published online in Stroke. The 80-page document contains major changes and refinements to the 2015 guideline on ICH management.
“Advances have been made in an array of fields related to ICH, including the organization of regional health care systems, reversal of the negative effects of blood thinners, minimally invasive surgical procedures, and the underlying disease in small blood vessels,” Steven M. Greenberg, MD, PhD, chair of the guideline writing group with Harvard Medical School and Massachusetts General Hospital, both in Boston, said in a news release.
“We’ve updated sections across the board. There’s probably no area that went untouched with some tweaking and new evidence added that led to some changes in level of evidence or strength of a recommendation,” Dr. Greenberg added in an interview with this news organization.
“Each section comes with knowledge gaps, and it wasn’t hard to come up with knowledge gaps in every section,” Dr. Greenberg acknowledged.
Time-honored treatments no more?
Among the key updates are changes to some “time-honored” treatments that continue to be used with some “regularity” for patients with ICH, yet appear to confer either no benefit or harm, Dr. Greenberg said.
For example, for emergency or critical care treatment of ICH, prophylactic corticosteroids or continuous hyperosmolar therapy is not recommended, because it appears to have no benefit for outcome, while use of platelet transfusions outside the setting of emergency surgery or severe thrombocytopenia appears to worsen outcome, the authors say.
Use of graduated knee- or thigh-high compression stockings alone is not an effective prophylactic therapy for prevention of deep vein thrombosis (DVT). Instead, intermittent pneumatic compression (IPC) starting on the day of diagnosis is now recommended for DVT prophylaxis.
“This is an area where we still have a lot of exploration to do. It is unclear whether even specialized compression devices reduce the risks of deep vein thrombosis or improve the overall health of people with a brain bleed,” Dr. Greenberg said in the release.
The new guidance advises against use of antiseizure or antidepressant medications for ICH patients in whom there is no evidence of seizures or depression.
In clinical trials, antiseizure medication did not contribute to improvements in functionality or long-term seizure control, and the use of antidepressants increased the chance of bone fractures, the authors say.
The guideline also provides updated recommendations for acute reversal of anticoagulation after ICH. It highlights the use of protein complex concentrate for reversal of vitamin K antagonists, such as warfarin; idarucizumab for reversal of the thrombin inhibitor dabigatran; and andexanet alfa for reversal of factor Xa inhibitors, such as rivaroxaban, apixaban, and edoxaban.
For acute blood pressure lowering after mild to moderate ICH, treatment regimens that limit blood pressure variability and achieve smooth, sustained blood pressure control appear to reduce hematoma expansion and yield better functional outcome, the guideline says.
It also notes that minimally invasive approaches for hematoma evacuation, compared with medical management alone‚ have been shown to reduce mortality.
For patients with cerebellar hemorrhage, indications for immediate surgical evacuation with or without an external ventricular drain to reduce mortality now include larger volume (> 15 mL) in addition to previously recommended indications of neurologic deterioration, brainstem compression, and hydrocephalus, the authors note.
However, a “major knowledge gap is whether we can improve functional outcome with hematoma evacuation,” Dr. Greenberg said.
Multidisciplinary care
For rehabilitation after ICH, the guideline reinforces the importance of having a multidisciplinary team to develop a comprehensive plan for recovery.
Starting rehabilitation activities such as stretching and functional task training may be considered 24 to 48 hours following mild or moderate ICH. However, early aggressive mobilization within the first 24 hours has been linked to an increased risk of death within 14 days after an ICH, the guideline says.
Knowledge gaps include how soon it’s safe to return to work, drive, and participate in other social engagements. Recommendations on sexual activity and exercise levels that are safe after a stroke are also needed.
“People need additional help with these lifestyle changes, whether it’s moving around more, curbing their alcohol use, or eating healthier foods. This all happens after they leave the hospital, and we need to be sure we are empowering families with the information they may need to be properly supportive,” Dr. Greenberg says in the release.
The guideline points to the patient’s home caregiver as a “key and sometimes overlooked” member of the care team. It recommends psychosocial education, practical support, and training for the caregiver to improve the patient’s balance, activity level, and overall quality of life.
Opportunity for prevention?
The guideline also suggests there may be an opportunity to prevent ICH in some people through neuroimaging markers.
While neuroimaging is not routinely performed as a part of risk stratification for primary ICH risk, damage to small blood vessels that is associated with ICH may be evident on MRI that could signal future ICH risk, the guideline says.
“We added to the guidelines for the first time a section on mostly imaging markers of risk for having a first-ever hemorrhage,” Dr. Greenberg said in an interview.
“We don’t make any recommendations as to how to act on these markers because there is a knowledge gap. The hope is that we’ll see growth in our ability to predict first-ever hemorrhage and be able to do things to prevent first-ever hemorrhage,” he said.
“We believe the wide range of knowledge set forth in the new guideline will translate into meaningful improvements in ICH care,” Dr. Greenberg adds in the release.
The updated guideline has been endorsed by the American Association of Neurological Surgeons and Congress of Neurological Surgeons, the Society of Vascular and Interventional Neurology, and the Neurocritical Care Society. The American Academy of Neurology has affirmed the value of this statement as an educational tool for neurologists.
This research had no commercial funding. Dr. Greenberg has disclosed no relevant financial relationships. A complete list of disclosures for the guideline group is available with the original article.
A version of this article first appeared on Medscape.com.
Many strategies widely considered “standard care” for managing spontaneous intracerebral hemorrhage (ICH) are not as effective as previously thought and are no longer recommended in updated guidelines from the American Heart Association/American Stroke Association (ASA).
Compression stockings, antiseizure medication, and steroid treatment are among the treatments with uncertain effectiveness, the writing group says.
The 2022 Guideline for the Management of Patients With Spontaneous ICH was published online in Stroke. The 80-page document contains major changes and refinements to the 2015 guideline on ICH management.
“Advances have been made in an array of fields related to ICH, including the organization of regional health care systems, reversal of the negative effects of blood thinners, minimally invasive surgical procedures, and the underlying disease in small blood vessels,” Steven M. Greenberg, MD, PhD, chair of the guideline writing group with Harvard Medical School and Massachusetts General Hospital, both in Boston, said in a news release.
“We’ve updated sections across the board. There’s probably no area that went untouched with some tweaking and new evidence added that led to some changes in level of evidence or strength of a recommendation,” Dr. Greenberg added in an interview with this news organization.
“Each section comes with knowledge gaps, and it wasn’t hard to come up with knowledge gaps in every section,” Dr. Greenberg acknowledged.
Time-honored treatments no more?
Among the key updates are changes to some “time-honored” treatments that continue to be used with some “regularity” for patients with ICH, yet appear to confer either no benefit or harm, Dr. Greenberg said.
For example, for emergency or critical care treatment of ICH, prophylactic corticosteroids or continuous hyperosmolar therapy is not recommended, because it appears to have no benefit for outcome, while use of platelet transfusions outside the setting of emergency surgery or severe thrombocytopenia appears to worsen outcome, the authors say.
Use of graduated knee- or thigh-high compression stockings alone is not an effective prophylactic therapy for prevention of deep vein thrombosis (DVT). Instead, intermittent pneumatic compression (IPC) starting on the day of diagnosis is now recommended for DVT prophylaxis.
“This is an area where we still have a lot of exploration to do. It is unclear whether even specialized compression devices reduce the risks of deep vein thrombosis or improve the overall health of people with a brain bleed,” Dr. Greenberg said in the release.
The new guidance advises against use of antiseizure or antidepressant medications for ICH patients in whom there is no evidence of seizures or depression.
In clinical trials, antiseizure medication did not contribute to improvements in functionality or long-term seizure control, and the use of antidepressants increased the chance of bone fractures, the authors say.
The guideline also provides updated recommendations for acute reversal of anticoagulation after ICH. It highlights the use of protein complex concentrate for reversal of vitamin K antagonists, such as warfarin; idarucizumab for reversal of the thrombin inhibitor dabigatran; and andexanet alfa for reversal of factor Xa inhibitors, such as rivaroxaban, apixaban, and edoxaban.
For acute blood pressure lowering after mild to moderate ICH, treatment regimens that limit blood pressure variability and achieve smooth, sustained blood pressure control appear to reduce hematoma expansion and yield better functional outcome, the guideline says.
It also notes that minimally invasive approaches for hematoma evacuation, compared with medical management alone‚ have been shown to reduce mortality.
For patients with cerebellar hemorrhage, indications for immediate surgical evacuation with or without an external ventricular drain to reduce mortality now include larger volume (> 15 mL) in addition to previously recommended indications of neurologic deterioration, brainstem compression, and hydrocephalus, the authors note.
However, a “major knowledge gap is whether we can improve functional outcome with hematoma evacuation,” Dr. Greenberg said.
Multidisciplinary care
For rehabilitation after ICH, the guideline reinforces the importance of having a multidisciplinary team to develop a comprehensive plan for recovery.
Starting rehabilitation activities such as stretching and functional task training may be considered 24 to 48 hours following mild or moderate ICH. However, early aggressive mobilization within the first 24 hours has been linked to an increased risk of death within 14 days after an ICH, the guideline says.
Knowledge gaps include how soon it’s safe to return to work, drive, and participate in other social engagements. Recommendations on sexual activity and exercise levels that are safe after a stroke are also needed.
“People need additional help with these lifestyle changes, whether it’s moving around more, curbing their alcohol use, or eating healthier foods. This all happens after they leave the hospital, and we need to be sure we are empowering families with the information they may need to be properly supportive,” Dr. Greenberg says in the release.
The guideline points to the patient’s home caregiver as a “key and sometimes overlooked” member of the care team. It recommends psychosocial education, practical support, and training for the caregiver to improve the patient’s balance, activity level, and overall quality of life.
Opportunity for prevention?
The guideline also suggests there may be an opportunity to prevent ICH in some people through neuroimaging markers.
While neuroimaging is not routinely performed as a part of risk stratification for primary ICH risk, damage to small blood vessels that is associated with ICH may be evident on MRI that could signal future ICH risk, the guideline says.
“We added to the guidelines for the first time a section on mostly imaging markers of risk for having a first-ever hemorrhage,” Dr. Greenberg said in an interview.
“We don’t make any recommendations as to how to act on these markers because there is a knowledge gap. The hope is that we’ll see growth in our ability to predict first-ever hemorrhage and be able to do things to prevent first-ever hemorrhage,” he said.
“We believe the wide range of knowledge set forth in the new guideline will translate into meaningful improvements in ICH care,” Dr. Greenberg adds in the release.
The updated guideline has been endorsed by the American Association of Neurological Surgeons and Congress of Neurological Surgeons, the Society of Vascular and Interventional Neurology, and the Neurocritical Care Society. The American Academy of Neurology has affirmed the value of this statement as an educational tool for neurologists.
This research had no commercial funding. Dr. Greenberg has disclosed no relevant financial relationships. A complete list of disclosures for the guideline group is available with the original article.
A version of this article first appeared on Medscape.com.
The psychopathic brain: New insight
Using MRI, researchers found that the striatum was about 10% larger on average in adults with psychopathic traits than in matched control persons and that this relationship was mediated by stimulation seeking and impulsivity.
The striatum is a subcortical region of the forebrain involved in the cognitive processing of reward-related information and motivational aspects of behavior.
“Our study’s results help advance our knowledge about what underlies antisocial behavior such as psychopathy,” co-author and neurocriminologist Olivia Choy, PhD, with Nanyang Technological University, Singapore, said in a news release.
“In addition to social environmental influences, it is important to consider that there can be differences in biology – in this case, the size of brain structures – between antisocial and non-antisocial individuals,” Dr. Choy added.
The study was published online in the Journal of Psychiatric Research.
Antisocial, egocentric
Individuals with psychopathic traits typically have an egocentric and antisocial personality. They generally lack remorse for their actions or empathy for others and often have criminal tendencies.
Some prior research suggests links between psychopathy and an overactive striatum, but it was unclear what role striatal volume plays in this behavior.
For the study, investigators assessed striatal volume using MRI in 120 adults living in the community, and they assessed psychopathy using the Psychopathy Checklist – Revised.
Correlational analyses showed that increased striatal volumes were associated with more psychopathic traits (P = .001) in both men and women.
Volumetric increases were found for all subregions of the striatum in psychopathic individuals, after controlling for age, substance dependence, substance abuse, antisocial personality disorder, attention-deficit/hyperactivity disorder, social adversity, and total brain volume.
An analysis of 18 psychopathic individuals showed that striatal volumes were increased 9.4%, compared with 18 propensity-matched control persons (P = .01).
Abnormal reward processing
Stimulation seeking and impulsivity partly mediated the striatal-psychopathy relationship, accounting for 49.4% of this association.
These findings “replicate and build on initial studies indicating striatal enlargement in adults with psychopathy, yielding an updated effect size of d = 0.48,” the researchers note.
The results are “consistent with the notion that striatal abnormalities in individuals with psychopathy partly reflect increased sensation-seeking and impulsivity and support the hypothesis of abnormal reward processing in psychopathy,” they add.

“We have always known that psychopaths go to extreme lengths to seek out rewards, including criminal activities that involve property, sex, and drugs,” co-author Adrian Raine, DPhil, department of criminology, psychiatry, and psychology, University of Pennsylvania, Philadelphia, said in a news release.
“We are now finding out a neurobiological underpinning of this impulsive and stimulating behavior in the form of enlargement to the striatum, a key brain area involved in rewards,” Dr. Raine added.
What causes striatal enlargement in individuals with psychopathy still needs to be determined.
In human development, the striatum typically becomes smaller as a child matures, suggesting that psychopathy is associated with differences in brain development, the researchers suggest.
“Because biological traits, such as the size of one’s striatum, can be inherited to child from parent, these findings give added support to neurodevelopmental perspectives of psychopathy – that the brains of these offenders do not develop normally throughout childhood and adolescence,” said Dr. Raine.
Larger studies needed
Commenting on the findings for this news organization, Terrie E. Moffitt, PhD, professor of psychology, Duke University, Durham, N.C., noted that there is “general consensus among brain-imaging researchers that testing brain-behavior relations requires very large samples in the thousands and also samples of research participants who represent the full extent of variation in the population as well as possible – from rich to poor, from well to unwell, from high IQ to low IQ, from strong mental health to mental illness, etc.
“It would be grand to see this study’s provocative finding replicated in a large, representative sampling design,” Dr. Moffitt said.
The study was supported in part by the National Institutes of Health. Dr. Choy, Dr. Raine, and Dr. Moffitt have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Using MRI, researchers found that the striatum was about 10% larger on average in adults with psychopathic traits than in matched control persons and that this relationship was mediated by stimulation seeking and impulsivity.
The striatum is a subcortical region of the forebrain involved in the cognitive processing of reward-related information and motivational aspects of behavior.
“Our study’s results help advance our knowledge about what underlies antisocial behavior such as psychopathy,” co-author and neurocriminologist Olivia Choy, PhD, with Nanyang Technological University, Singapore, said in a news release.
“In addition to social environmental influences, it is important to consider that there can be differences in biology – in this case, the size of brain structures – between antisocial and non-antisocial individuals,” Dr. Choy added.
The study was published online in the Journal of Psychiatric Research.
Antisocial, egocentric
Individuals with psychopathic traits typically have an egocentric and antisocial personality. They generally lack remorse for their actions or empathy for others and often have criminal tendencies.
Some prior research suggests links between psychopathy and an overactive striatum, but it was unclear what role striatal volume plays in this behavior.
For the study, investigators assessed striatal volume using MRI in 120 adults living in the community, and they assessed psychopathy using the Psychopathy Checklist – Revised.
Correlational analyses showed that increased striatal volumes were associated with more psychopathic traits (P = .001) in both men and women.
Volumetric increases were found for all subregions of the striatum in psychopathic individuals, after controlling for age, substance dependence, substance abuse, antisocial personality disorder, attention-deficit/hyperactivity disorder, social adversity, and total brain volume.
An analysis of 18 psychopathic individuals showed that striatal volumes were increased 9.4%, compared with 18 propensity-matched control persons (P = .01).
Abnormal reward processing
Stimulation seeking and impulsivity partly mediated the striatal-psychopathy relationship, accounting for 49.4% of this association.
These findings “replicate and build on initial studies indicating striatal enlargement in adults with psychopathy, yielding an updated effect size of d = 0.48,” the researchers note.
The results are “consistent with the notion that striatal abnormalities in individuals with psychopathy partly reflect increased sensation-seeking and impulsivity and support the hypothesis of abnormal reward processing in psychopathy,” they add.
“We have always known that psychopaths go to extreme lengths to seek out rewards, including criminal activities that involve property, sex, and drugs,” co-author Adrian Raine, DPhil, department of criminology, psychiatry, and psychology, University of Pennsylvania, Philadelphia, said in a news release.
“We are now finding out a neurobiological underpinning of this impulsive and stimulating behavior in the form of enlargement to the striatum, a key brain area involved in rewards,” Dr. Raine added.
What causes striatal enlargement in individuals with psychopathy still needs to be determined.
In human development, the striatum typically becomes smaller as a child matures, suggesting that psychopathy is associated with differences in brain development, the researchers suggest.
“Because biological traits, such as the size of one’s striatum, can be inherited to child from parent, these findings give added support to neurodevelopmental perspectives of psychopathy – that the brains of these offenders do not develop normally throughout childhood and adolescence,” said Dr. Raine.
Larger studies needed
Commenting on the findings for this news organization, Terrie E. Moffitt, PhD, professor of psychology, Duke University, Durham, N.C., noted that there is “general consensus among brain-imaging researchers that testing brain-behavior relations requires very large samples in the thousands and also samples of research participants who represent the full extent of variation in the population as well as possible – from rich to poor, from well to unwell, from high IQ to low IQ, from strong mental health to mental illness, etc.
“It would be grand to see this study’s provocative finding replicated in a large, representative sampling design,” Dr. Moffitt said.
The study was supported in part by the National Institutes of Health. Dr. Choy, Dr. Raine, and Dr. Moffitt have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Using MRI, researchers found that the striatum was about 10% larger on average in adults with psychopathic traits than in matched control persons and that this relationship was mediated by stimulation seeking and impulsivity.
The striatum is a subcortical region of the forebrain involved in the cognitive processing of reward-related information and motivational aspects of behavior.
“Our study’s results help advance our knowledge about what underlies antisocial behavior such as psychopathy,” co-author and neurocriminologist Olivia Choy, PhD, with Nanyang Technological University, Singapore, said in a news release.
“In addition to social environmental influences, it is important to consider that there can be differences in biology – in this case, the size of brain structures – between antisocial and non-antisocial individuals,” Dr. Choy added.
The study was published online in the Journal of Psychiatric Research.
Antisocial, egocentric
Individuals with psychopathic traits typically have an egocentric and antisocial personality. They generally lack remorse for their actions or empathy for others and often have criminal tendencies.
Some prior research suggests links between psychopathy and an overactive striatum, but it was unclear what role striatal volume plays in this behavior.
For the study, investigators assessed striatal volume using MRI in 120 adults living in the community, and they assessed psychopathy using the Psychopathy Checklist – Revised.
Correlational analyses showed that increased striatal volumes were associated with more psychopathic traits (P = .001) in both men and women.
Volumetric increases were found for all subregions of the striatum in psychopathic individuals, after controlling for age, substance dependence, substance abuse, antisocial personality disorder, attention-deficit/hyperactivity disorder, social adversity, and total brain volume.
An analysis of 18 psychopathic individuals showed that striatal volumes were increased 9.4%, compared with 18 propensity-matched control persons (P = .01).
Abnormal reward processing
Stimulation seeking and impulsivity partly mediated the striatal-psychopathy relationship, accounting for 49.4% of this association.
These findings “replicate and build on initial studies indicating striatal enlargement in adults with psychopathy, yielding an updated effect size of d = 0.48,” the researchers note.
The results are “consistent with the notion that striatal abnormalities in individuals with psychopathy partly reflect increased sensation-seeking and impulsivity and support the hypothesis of abnormal reward processing in psychopathy,” they add.
“We have always known that psychopaths go to extreme lengths to seek out rewards, including criminal activities that involve property, sex, and drugs,” co-author Adrian Raine, DPhil, department of criminology, psychiatry, and psychology, University of Pennsylvania, Philadelphia, said in a news release.
“We are now finding out a neurobiological underpinning of this impulsive and stimulating behavior in the form of enlargement to the striatum, a key brain area involved in rewards,” Dr. Raine added.
What causes striatal enlargement in individuals with psychopathy still needs to be determined.
In human development, the striatum typically becomes smaller as a child matures, suggesting that psychopathy is associated with differences in brain development, the researchers suggest.
“Because biological traits, such as the size of one’s striatum, can be inherited to child from parent, these findings give added support to neurodevelopmental perspectives of psychopathy – that the brains of these offenders do not develop normally throughout childhood and adolescence,” said Dr. Raine.
Larger studies needed
Commenting on the findings for this news organization, Terrie E. Moffitt, PhD, professor of psychology, Duke University, Durham, N.C., noted that there is “general consensus among brain-imaging researchers that testing brain-behavior relations requires very large samples in the thousands and also samples of research participants who represent the full extent of variation in the population as well as possible – from rich to poor, from well to unwell, from high IQ to low IQ, from strong mental health to mental illness, etc.
“It would be grand to see this study’s provocative finding replicated in a large, representative sampling design,” Dr. Moffitt said.
The study was supported in part by the National Institutes of Health. Dr. Choy, Dr. Raine, and Dr. Moffitt have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Doc faces U.S. federal charges for hacking, ransomware
According to a statement from the U.S. Department of Justice, 55-year-old Moises Luis Zagala Gonzalez, MD, is charged with creating and distributing ransomware with a “doomsday” clock and sharing in profits from ransomware attacks.
Dr. Zagala, also known as “Nosophoros,” “Aesculapius,” and “Nebuchadnezzar,” is a citizen of France and Venezuela who currently lives in Ciudad Bolivar, Venezuela.
Breon Peace, U.S. attorney for the Eastern District of New York, and Michael J. Driscoll, assistant director in charge of the Federal Bureau of Investigaton’s New York Field Office, announced the charges.
“As alleged, the multitasking doctor treated patients, created and named his cyber tool after death, profited from a global ransomware ecosystem in which he sold the tools for conducting ransomware attacks, trained the attackers about how to extort victims, and then boasted about successful attacks, including by malicious actors associated with the government of Iran,” Mr. Peace said in the news release from the DOJ.
“We allege Zagala not only created and sold ransomware products to hackers, but also trained them in their use. Our actions today will prevent Zagala from further victimizing users,” Mr. Driscoll said. “However, many other malicious criminals are searching for businesses and organizations that haven’t taken steps to protect their systems – which is an incredibly vital step in stopping the next ransomware attack.”
Ransomware tools are malicious software that cybercriminals use to extort money from companies, nonprofits, and other institutions by encrypting their files and then demanding a ransom for the decryption keys.
One of Dr. Zagala’s early ransomware tools, called “Jigsaw v. 2,” had what Dr. Zagala described as a doomsday counter that kept track of how many times the user tried to remove the ransomware. “If the user kills the ransomware too many times, then it’s clear he won’t pay so better erase the whole hard drive,” Dr. Zagala wrote.
According to the DOJ, beginning in late 2019, Dr. Zagala began advertising a new tool as a “private ransomware builder,” which he called Thanos. The name appears to be in reference to a fictional villain responsible for destroying half of all life in the universe and to “Thanatos” from Greek mythology, who is associated with death.
Dr. Zagala’s Thanos software allows users to create their own unique ransomware software for personal use or to rent to other cybercriminals.
Dr. Zagala allegedly not only sold or rented out his ransomware tools to cybercriminals, but he also taught users how to deploy the tools, steal passwords from victim computers, and set up a Bitcoin address for ransom payments.
Dr. Zagala’s customers were happy with his products, the DOJ release noted. In a message posted in July 2020, one user said the ransomware was “very powerful” and claimed that he had used it to infect a network of roughly 3,000 computers.
In December 2020, another user wrote a post in Russian: “We have been working with this product for over a month now, we have a good profit! Best support I’ve met.”
Earlier in May, law enforcement agents interviewed a relative of Dr. Zagala who lives in Florida and whose PayPal account was used by Dr. Zagala to receive illicit proceeds.
According to the DOJ, the relative confirmed that Dr. Zagala lives in Venezuela and had taught himself computer programming. The relative also showed agents contact information for Dr. Zagala that matched the registered email for malicious infrastructure associated with the Thanos ransomware.
Dr. Zagala, who remains in Venezuela, faces up to 10 years in prison for attempted computer intrusions and conspiracy charges if brought to justice in the United States.
A version of this article first appeared on Medscape.com.
According to a statement from the U.S. Department of Justice, 55-year-old Moises Luis Zagala Gonzalez, MD, is charged with creating and distributing ransomware with a “doomsday” clock and sharing in profits from ransomware attacks.
Dr. Zagala, also known as “Nosophoros,” “Aesculapius,” and “Nebuchadnezzar,” is a citizen of France and Venezuela who currently lives in Ciudad Bolivar, Venezuela.
Breon Peace, U.S. attorney for the Eastern District of New York, and Michael J. Driscoll, assistant director in charge of the Federal Bureau of Investigaton’s New York Field Office, announced the charges.
“As alleged, the multitasking doctor treated patients, created and named his cyber tool after death, profited from a global ransomware ecosystem in which he sold the tools for conducting ransomware attacks, trained the attackers about how to extort victims, and then boasted about successful attacks, including by malicious actors associated with the government of Iran,” Mr. Peace said in the news release from the DOJ.
“We allege Zagala not only created and sold ransomware products to hackers, but also trained them in their use. Our actions today will prevent Zagala from further victimizing users,” Mr. Driscoll said. “However, many other malicious criminals are searching for businesses and organizations that haven’t taken steps to protect their systems – which is an incredibly vital step in stopping the next ransomware attack.”
Ransomware tools are malicious software that cybercriminals use to extort money from companies, nonprofits, and other institutions by encrypting their files and then demanding a ransom for the decryption keys.
One of Dr. Zagala’s early ransomware tools, called “Jigsaw v. 2,” had what Dr. Zagala described as a doomsday counter that kept track of how many times the user tried to remove the ransomware. “If the user kills the ransomware too many times, then it’s clear he won’t pay so better erase the whole hard drive,” Dr. Zagala wrote.
According to the DOJ, beginning in late 2019, Dr. Zagala began advertising a new tool as a “private ransomware builder,” which he called Thanos. The name appears to be in reference to a fictional villain responsible for destroying half of all life in the universe and to “Thanatos” from Greek mythology, who is associated with death.
Dr. Zagala’s Thanos software allows users to create their own unique ransomware software for personal use or to rent to other cybercriminals.
Dr. Zagala allegedly not only sold or rented out his ransomware tools to cybercriminals, but he also taught users how to deploy the tools, steal passwords from victim computers, and set up a Bitcoin address for ransom payments.
Dr. Zagala’s customers were happy with his products, the DOJ release noted. In a message posted in July 2020, one user said the ransomware was “very powerful” and claimed that he had used it to infect a network of roughly 3,000 computers.
In December 2020, another user wrote a post in Russian: “We have been working with this product for over a month now, we have a good profit! Best support I’ve met.”
Earlier in May, law enforcement agents interviewed a relative of Dr. Zagala who lives in Florida and whose PayPal account was used by Dr. Zagala to receive illicit proceeds.
According to the DOJ, the relative confirmed that Dr. Zagala lives in Venezuela and had taught himself computer programming. The relative also showed agents contact information for Dr. Zagala that matched the registered email for malicious infrastructure associated with the Thanos ransomware.
Dr. Zagala, who remains in Venezuela, faces up to 10 years in prison for attempted computer intrusions and conspiracy charges if brought to justice in the United States.
A version of this article first appeared on Medscape.com.
According to a statement from the U.S. Department of Justice, 55-year-old Moises Luis Zagala Gonzalez, MD, is charged with creating and distributing ransomware with a “doomsday” clock and sharing in profits from ransomware attacks.
Dr. Zagala, also known as “Nosophoros,” “Aesculapius,” and “Nebuchadnezzar,” is a citizen of France and Venezuela who currently lives in Ciudad Bolivar, Venezuela.
Breon Peace, U.S. attorney for the Eastern District of New York, and Michael J. Driscoll, assistant director in charge of the Federal Bureau of Investigaton’s New York Field Office, announced the charges.
“As alleged, the multitasking doctor treated patients, created and named his cyber tool after death, profited from a global ransomware ecosystem in which he sold the tools for conducting ransomware attacks, trained the attackers about how to extort victims, and then boasted about successful attacks, including by malicious actors associated with the government of Iran,” Mr. Peace said in the news release from the DOJ.
“We allege Zagala not only created and sold ransomware products to hackers, but also trained them in their use. Our actions today will prevent Zagala from further victimizing users,” Mr. Driscoll said. “However, many other malicious criminals are searching for businesses and organizations that haven’t taken steps to protect their systems – which is an incredibly vital step in stopping the next ransomware attack.”
Ransomware tools are malicious software that cybercriminals use to extort money from companies, nonprofits, and other institutions by encrypting their files and then demanding a ransom for the decryption keys.
One of Dr. Zagala’s early ransomware tools, called “Jigsaw v. 2,” had what Dr. Zagala described as a doomsday counter that kept track of how many times the user tried to remove the ransomware. “If the user kills the ransomware too many times, then it’s clear he won’t pay so better erase the whole hard drive,” Dr. Zagala wrote.
According to the DOJ, beginning in late 2019, Dr. Zagala began advertising a new tool as a “private ransomware builder,” which he called Thanos. The name appears to be in reference to a fictional villain responsible for destroying half of all life in the universe and to “Thanatos” from Greek mythology, who is associated with death.
Dr. Zagala’s Thanos software allows users to create their own unique ransomware software for personal use or to rent to other cybercriminals.
Dr. Zagala allegedly not only sold or rented out his ransomware tools to cybercriminals, but he also taught users how to deploy the tools, steal passwords from victim computers, and set up a Bitcoin address for ransom payments.
Dr. Zagala’s customers were happy with his products, the DOJ release noted. In a message posted in July 2020, one user said the ransomware was “very powerful” and claimed that he had used it to infect a network of roughly 3,000 computers.
In December 2020, another user wrote a post in Russian: “We have been working with this product for over a month now, we have a good profit! Best support I’ve met.”
Earlier in May, law enforcement agents interviewed a relative of Dr. Zagala who lives in Florida and whose PayPal account was used by Dr. Zagala to receive illicit proceeds.
According to the DOJ, the relative confirmed that Dr. Zagala lives in Venezuela and had taught himself computer programming. The relative also showed agents contact information for Dr. Zagala that matched the registered email for malicious infrastructure associated with the Thanos ransomware.
Dr. Zagala, who remains in Venezuela, faces up to 10 years in prison for attempted computer intrusions and conspiracy charges if brought to justice in the United States.
A version of this article first appeared on Medscape.com.
Does suicide risk show up in the blood?
Investigators found patients with MDD who died by suicide had a gene expression signature in blood distinct from patients with MDD who died by other means.
The signature included genes involved in stress response changes, including polyamine metabolism, circadian rhythm, immune dysregulation, and telomere maintenance.
“These blood biomarkers are an important step toward developing blood tests to identify patients with imminent risk of ending their lives,” study investigator Adolfo Sequeira, PhD, associate researcher in the department of psychiatry and human behavior, University of California, Irvine, said in a news release.
“To our knowledge, this is the first study to analyze blood and brain samples in a well-defined population of MDDs demonstrating significant differences in gene expression associated with completed suicide,” Dr. Sequeira added.
The findings were published online in Translational Psychiatry.
A pressing challenge
Suicide rates in the United States have jumped by more than 35% over the past 2 decades, with more than 48,000 deaths by suicide occurring just last year. MDD is the most common diagnosis among completed suicides, and identifying individuals at the highest risk for suicide remains a “pressing challenge,” the researchers noted.
They looked for changes in gene expression associated with suicide in archived postmortem blood and brain samples from adults with MDD who died by suicide (MDD-S) or by other means (MDD-NS), as well as a group of controls with no psychiatric illness.
In total, there were blood and brain samples for 45 adults, including 53 blood samples and 69 dorsolateral prefrontal cortex (DLPFC) tissue samples.
In blood, investigators identified 14 genes that significantly differentiated MDD-S from MDD-NS. The top six genes differentially expressed in blood were PER3, MTPAP, SLC25A26, CD19, SOX9, and GAR1.
In addition, four genes showed significant changes in brain and blood between the MDD-S and MDD-NS groups. SOX9 was decreased and PER3 was increased in MDD-S in both blood and brain samples, while CD19 and TERF1 were increased in blood but decreased in DLPFC.
SOX9, an astrocytic marker in the brain and B-cell marker in blood, has been shown to be decreased in MDD-S compared with controls in the prefrontal cortex.
In the current study, researchers found that SOX9 expression was significantly reduced both in blood and brain in MDD-S compared with MDD-NS, “suggesting similar immune/astrocytic dysregulations in suicide that could be further investigated.”
Potential signatures, potential targets
PER3 is a circadian rhythm gene implicated in sleep disorders associated with shifts in circadian rhythms and is thought to increase susceptibility to MDD.
Mutations in PER3 have been shown previously to alter multiple systems, including response to antidepressants; and increased blood expression of PER1 has been linked to suicidality in women, the researchers noted.
There also were significantly higher levels of two inflammatory markers (CD19 and CD6 genes) in blood of MDD-S patients compared to MDD-NS patients.
Another “significant” finding was the involvement of several mitochondrial genes in suicide, the researchers said.
Two nuclear genes coding for mitochondria-located proteins MTPAP (a mitochondrial poly(A) polymerase) and the mitochondrial polyamine transporter SLC25A26 were increased in blood in MDD-S compared with MDD-NS and controls, suggesting that “mitochondrial alterations could be used as potential signatures to differentiate MDD-S from MDD-NS patients and also from controls.”
The researchers added that the genes found to be dysregulated in suicide represent potential targets for future drug therapies to prevent suicide and could also be used to develop a molecular test to identify individuals at high risk for suicide.
The study was funded by the National Institute of Mental Health, the American Society for Suicide Prevention, and the Pritzker Family Philanthropic Fund. The investigators have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators found patients with MDD who died by suicide had a gene expression signature in blood distinct from patients with MDD who died by other means.
The signature included genes involved in stress response changes, including polyamine metabolism, circadian rhythm, immune dysregulation, and telomere maintenance.
“These blood biomarkers are an important step toward developing blood tests to identify patients with imminent risk of ending their lives,” study investigator Adolfo Sequeira, PhD, associate researcher in the department of psychiatry and human behavior, University of California, Irvine, said in a news release.
“To our knowledge, this is the first study to analyze blood and brain samples in a well-defined population of MDDs demonstrating significant differences in gene expression associated with completed suicide,” Dr. Sequeira added.
The findings were published online in Translational Psychiatry.
A pressing challenge
Suicide rates in the United States have jumped by more than 35% over the past 2 decades, with more than 48,000 deaths by suicide occurring just last year. MDD is the most common diagnosis among completed suicides, and identifying individuals at the highest risk for suicide remains a “pressing challenge,” the researchers noted.
They looked for changes in gene expression associated with suicide in archived postmortem blood and brain samples from adults with MDD who died by suicide (MDD-S) or by other means (MDD-NS), as well as a group of controls with no psychiatric illness.
In total, there were blood and brain samples for 45 adults, including 53 blood samples and 69 dorsolateral prefrontal cortex (DLPFC) tissue samples.
In blood, investigators identified 14 genes that significantly differentiated MDD-S from MDD-NS. The top six genes differentially expressed in blood were PER3, MTPAP, SLC25A26, CD19, SOX9, and GAR1.
In addition, four genes showed significant changes in brain and blood between the MDD-S and MDD-NS groups. SOX9 was decreased and PER3 was increased in MDD-S in both blood and brain samples, while CD19 and TERF1 were increased in blood but decreased in DLPFC.
SOX9, an astrocytic marker in the brain and B-cell marker in blood, has been shown to be decreased in MDD-S compared with controls in the prefrontal cortex.
In the current study, researchers found that SOX9 expression was significantly reduced both in blood and brain in MDD-S compared with MDD-NS, “suggesting similar immune/astrocytic dysregulations in suicide that could be further investigated.”
Potential signatures, potential targets
PER3 is a circadian rhythm gene implicated in sleep disorders associated with shifts in circadian rhythms and is thought to increase susceptibility to MDD.
Mutations in PER3 have been shown previously to alter multiple systems, including response to antidepressants; and increased blood expression of PER1 has been linked to suicidality in women, the researchers noted.
There also were significantly higher levels of two inflammatory markers (CD19 and CD6 genes) in blood of MDD-S patients compared to MDD-NS patients.
Another “significant” finding was the involvement of several mitochondrial genes in suicide, the researchers said.
Two nuclear genes coding for mitochondria-located proteins MTPAP (a mitochondrial poly(A) polymerase) and the mitochondrial polyamine transporter SLC25A26 were increased in blood in MDD-S compared with MDD-NS and controls, suggesting that “mitochondrial alterations could be used as potential signatures to differentiate MDD-S from MDD-NS patients and also from controls.”
The researchers added that the genes found to be dysregulated in suicide represent potential targets for future drug therapies to prevent suicide and could also be used to develop a molecular test to identify individuals at high risk for suicide.
The study was funded by the National Institute of Mental Health, the American Society for Suicide Prevention, and the Pritzker Family Philanthropic Fund. The investigators have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators found patients with MDD who died by suicide had a gene expression signature in blood distinct from patients with MDD who died by other means.
The signature included genes involved in stress response changes, including polyamine metabolism, circadian rhythm, immune dysregulation, and telomere maintenance.
“These blood biomarkers are an important step toward developing blood tests to identify patients with imminent risk of ending their lives,” study investigator Adolfo Sequeira, PhD, associate researcher in the department of psychiatry and human behavior, University of California, Irvine, said in a news release.
“To our knowledge, this is the first study to analyze blood and brain samples in a well-defined population of MDDs demonstrating significant differences in gene expression associated with completed suicide,” Dr. Sequeira added.
The findings were published online in Translational Psychiatry.
A pressing challenge
Suicide rates in the United States have jumped by more than 35% over the past 2 decades, with more than 48,000 deaths by suicide occurring just last year. MDD is the most common diagnosis among completed suicides, and identifying individuals at the highest risk for suicide remains a “pressing challenge,” the researchers noted.
They looked for changes in gene expression associated with suicide in archived postmortem blood and brain samples from adults with MDD who died by suicide (MDD-S) or by other means (MDD-NS), as well as a group of controls with no psychiatric illness.
In total, there were blood and brain samples for 45 adults, including 53 blood samples and 69 dorsolateral prefrontal cortex (DLPFC) tissue samples.
In blood, investigators identified 14 genes that significantly differentiated MDD-S from MDD-NS. The top six genes differentially expressed in blood were PER3, MTPAP, SLC25A26, CD19, SOX9, and GAR1.
In addition, four genes showed significant changes in brain and blood between the MDD-S and MDD-NS groups. SOX9 was decreased and PER3 was increased in MDD-S in both blood and brain samples, while CD19 and TERF1 were increased in blood but decreased in DLPFC.
SOX9, an astrocytic marker in the brain and B-cell marker in blood, has been shown to be decreased in MDD-S compared with controls in the prefrontal cortex.
In the current study, researchers found that SOX9 expression was significantly reduced both in blood and brain in MDD-S compared with MDD-NS, “suggesting similar immune/astrocytic dysregulations in suicide that could be further investigated.”
Potential signatures, potential targets
PER3 is a circadian rhythm gene implicated in sleep disorders associated with shifts in circadian rhythms and is thought to increase susceptibility to MDD.
Mutations in PER3 have been shown previously to alter multiple systems, including response to antidepressants; and increased blood expression of PER1 has been linked to suicidality in women, the researchers noted.
There also were significantly higher levels of two inflammatory markers (CD19 and CD6 genes) in blood of MDD-S patients compared to MDD-NS patients.
Another “significant” finding was the involvement of several mitochondrial genes in suicide, the researchers said.
Two nuclear genes coding for mitochondria-located proteins MTPAP (a mitochondrial poly(A) polymerase) and the mitochondrial polyamine transporter SLC25A26 were increased in blood in MDD-S compared with MDD-NS and controls, suggesting that “mitochondrial alterations could be used as potential signatures to differentiate MDD-S from MDD-NS patients and also from controls.”
The researchers added that the genes found to be dysregulated in suicide represent potential targets for future drug therapies to prevent suicide and could also be used to develop a molecular test to identify individuals at high risk for suicide.
The study was funded by the National Institute of Mental Health, the American Society for Suicide Prevention, and the Pritzker Family Philanthropic Fund. The investigators have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM TRANSLATIONAL PSYCHIATRY
Neuropsychiatric risks of COVID-19: New data
The neuropsychiatric ramifications of severe COVID-19 infection appear to be no different than for other severe acute respiratory infections (SARI).
This suggests that disease severity, rather than pathogen, is the most relevant factor in new-onset neuropsychiatric illness, the investigators note.
The risk of new-onset neuropsychological illness after severe COVID-19 infection are “substantial, but similar to those after other severe respiratory infections,” study investigator Peter Watkinson, MD, Nuffield Department of Clinical Neurosciences, University of Oxford, and John Radcliffe Hospital, Oxford, England, told this news organization.

The study was published online in JAMA Psychiatry.
Significant mental health burden
Research has shown a significant burden of neuropsychological illness after severe COVID-19 infection. However, it’s unclear how this risk compares to SARI.
To investigate, Dr. Watkinson and colleagues evaluated electronic health record data on more than 8.3 million adults, including 16,679 (0.02%) who survived a hospital admission for SARI and 32,525 (0.03%) who survived a hospital stay for COVID-19.
Compared with the remaining population, risks of new anxiety disorder, dementia, psychotic disorder, depression, and bipolar disorder diagnoses were significantly and similarly increased in adults surviving hospitalization for either COVID-19 or SARI.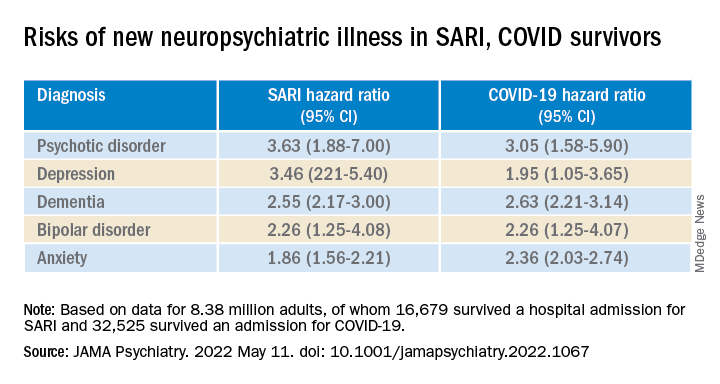
Compared with the wider population, survivors of severe SARI or COVID-19 were also at increased risk of starting treatment with antidepressants, hypnotics/anxiolytics, or antipsychotics.
When comparing survivors of SARI hospitalization to survivors of COVID-19 hospitalization, no significant differences were observed in the postdischarge rates of new-onset anxiety disorder, dementia, depression, or bipolar affective disorder.
The SARI and COVID groups also did not differ in terms of their postdischarge risks of antidepressant or hypnotic/anxiolytic use, but the COVID survivors had a 20% lower risk of starting an antipsychotic.
“In this cohort study, SARI were found to be associated with significant postacute neuropsychiatric morbidity, for which COVID-19 is not distinctly different,” Dr. Watkinson and colleagues write.
“These results may help refine our understanding of the post–severe COVID-19 phenotype and may inform post-discharge support for patients requiring hospital-based and intensive care for SARI regardless of causative pathogen,” they write.
Caveats, cautionary notes
Kevin McConway, PhD, emeritus professor of applied statistics at the Open University in Milton Keynes, England, described the study as “impressive.” However, he pointed out that the study’s observational design is a limitation.
“One can never be absolutely certain about the interpretation of findings of an observational study. What the research can’t tell us is what caused the increased psychiatric risks for people hospitalized with COVID-19 or some other serious respiratory disease,” Dr. McConway said.
“It can’t tell us what might happen in the future, when, we all hope, many fewer are being hospitalized with COVID-19 than was the case in those first two waves, and the current backlog of provision of some health services has decreased,” he added.
“So we can’t just say that, in general, serious COVID-19 has much the same neuropsychiatric consequences as other very serious respiratory illness. Maybe it does, maybe it doesn’t,” Dr. McConway cautioned.
Max Taquet, PhD, with the University of Oxford, noted that the study is limited to hospitalized adult patients, leaving open the question of risk in nonhospitalized individuals – which is the overwhelming majority of patients with COVID-19 – or in children.
Whether the neuropsychiatric risks have remained the same since the emergence of the Omicron variant also remains “an open question since all patients in this study were diagnosed before July 2021,” Dr. Taquet said in statement.
The study was funded by the Wellcome Trust, the John Fell Oxford University Press Research Fund, the Oxford Wellcome Institutional Strategic Support Fund and Cancer Research UK, through the Cancer Research UK Oxford Centre. Dr. Watkinson disclosed grants from the National Institute for Health Research and Sensyne Health outside the submitted work; and serving as chief medical officer for Sensyne Health prior to this work, as well as holding shares in the company. Dr. McConway is a trustee of the UK Science Media Centre and a member of its advisory committee. His comments were provided in his capacity as an independent professional statistician. Dr. Taquet has worked on similar studies trying to identify, quantify, and specify the neurological and psychiatric consequences of COVID-19.
A version of this article first appeared on Medscape.com.
The neuropsychiatric ramifications of severe COVID-19 infection appear to be no different than for other severe acute respiratory infections (SARI).
This suggests that disease severity, rather than pathogen, is the most relevant factor in new-onset neuropsychiatric illness, the investigators note.
The risk of new-onset neuropsychological illness after severe COVID-19 infection are “substantial, but similar to those after other severe respiratory infections,” study investigator Peter Watkinson, MD, Nuffield Department of Clinical Neurosciences, University of Oxford, and John Radcliffe Hospital, Oxford, England, told this news organization.
The study was published online in JAMA Psychiatry.
Significant mental health burden
Research has shown a significant burden of neuropsychological illness after severe COVID-19 infection. However, it’s unclear how this risk compares to SARI.
To investigate, Dr. Watkinson and colleagues evaluated electronic health record data on more than 8.3 million adults, including 16,679 (0.02%) who survived a hospital admission for SARI and 32,525 (0.03%) who survived a hospital stay for COVID-19.
Compared with the remaining population, risks of new anxiety disorder, dementia, psychotic disorder, depression, and bipolar disorder diagnoses were significantly and similarly increased in adults surviving hospitalization for either COVID-19 or SARI.
Compared with the wider population, survivors of severe SARI or COVID-19 were also at increased risk of starting treatment with antidepressants, hypnotics/anxiolytics, or antipsychotics.
When comparing survivors of SARI hospitalization to survivors of COVID-19 hospitalization, no significant differences were observed in the postdischarge rates of new-onset anxiety disorder, dementia, depression, or bipolar affective disorder.
The SARI and COVID groups also did not differ in terms of their postdischarge risks of antidepressant or hypnotic/anxiolytic use, but the COVID survivors had a 20% lower risk of starting an antipsychotic.
“In this cohort study, SARI were found to be associated with significant postacute neuropsychiatric morbidity, for which COVID-19 is not distinctly different,” Dr. Watkinson and colleagues write.
“These results may help refine our understanding of the post–severe COVID-19 phenotype and may inform post-discharge support for patients requiring hospital-based and intensive care for SARI regardless of causative pathogen,” they write.
Caveats, cautionary notes
Kevin McConway, PhD, emeritus professor of applied statistics at the Open University in Milton Keynes, England, described the study as “impressive.” However, he pointed out that the study’s observational design is a limitation.
“One can never be absolutely certain about the interpretation of findings of an observational study. What the research can’t tell us is what caused the increased psychiatric risks for people hospitalized with COVID-19 or some other serious respiratory disease,” Dr. McConway said.
“It can’t tell us what might happen in the future, when, we all hope, many fewer are being hospitalized with COVID-19 than was the case in those first two waves, and the current backlog of provision of some health services has decreased,” he added.
“So we can’t just say that, in general, serious COVID-19 has much the same neuropsychiatric consequences as other very serious respiratory illness. Maybe it does, maybe it doesn’t,” Dr. McConway cautioned.
Max Taquet, PhD, with the University of Oxford, noted that the study is limited to hospitalized adult patients, leaving open the question of risk in nonhospitalized individuals – which is the overwhelming majority of patients with COVID-19 – or in children.
Whether the neuropsychiatric risks have remained the same since the emergence of the Omicron variant also remains “an open question since all patients in this study were diagnosed before July 2021,” Dr. Taquet said in statement.
The study was funded by the Wellcome Trust, the John Fell Oxford University Press Research Fund, the Oxford Wellcome Institutional Strategic Support Fund and Cancer Research UK, through the Cancer Research UK Oxford Centre. Dr. Watkinson disclosed grants from the National Institute for Health Research and Sensyne Health outside the submitted work; and serving as chief medical officer for Sensyne Health prior to this work, as well as holding shares in the company. Dr. McConway is a trustee of the UK Science Media Centre and a member of its advisory committee. His comments were provided in his capacity as an independent professional statistician. Dr. Taquet has worked on similar studies trying to identify, quantify, and specify the neurological and psychiatric consequences of COVID-19.
A version of this article first appeared on Medscape.com.
The neuropsychiatric ramifications of severe COVID-19 infection appear to be no different than for other severe acute respiratory infections (SARI).
This suggests that disease severity, rather than pathogen, is the most relevant factor in new-onset neuropsychiatric illness, the investigators note.
The risk of new-onset neuropsychological illness after severe COVID-19 infection are “substantial, but similar to those after other severe respiratory infections,” study investigator Peter Watkinson, MD, Nuffield Department of Clinical Neurosciences, University of Oxford, and John Radcliffe Hospital, Oxford, England, told this news organization.
The study was published online in JAMA Psychiatry.
Significant mental health burden
Research has shown a significant burden of neuropsychological illness after severe COVID-19 infection. However, it’s unclear how this risk compares to SARI.
To investigate, Dr. Watkinson and colleagues evaluated electronic health record data on more than 8.3 million adults, including 16,679 (0.02%) who survived a hospital admission for SARI and 32,525 (0.03%) who survived a hospital stay for COVID-19.
Compared with the remaining population, risks of new anxiety disorder, dementia, psychotic disorder, depression, and bipolar disorder diagnoses were significantly and similarly increased in adults surviving hospitalization for either COVID-19 or SARI.
Compared with the wider population, survivors of severe SARI or COVID-19 were also at increased risk of starting treatment with antidepressants, hypnotics/anxiolytics, or antipsychotics.
When comparing survivors of SARI hospitalization to survivors of COVID-19 hospitalization, no significant differences were observed in the postdischarge rates of new-onset anxiety disorder, dementia, depression, or bipolar affective disorder.
The SARI and COVID groups also did not differ in terms of their postdischarge risks of antidepressant or hypnotic/anxiolytic use, but the COVID survivors had a 20% lower risk of starting an antipsychotic.
“In this cohort study, SARI were found to be associated with significant postacute neuropsychiatric morbidity, for which COVID-19 is not distinctly different,” Dr. Watkinson and colleagues write.
“These results may help refine our understanding of the post–severe COVID-19 phenotype and may inform post-discharge support for patients requiring hospital-based and intensive care for SARI regardless of causative pathogen,” they write.
Caveats, cautionary notes
Kevin McConway, PhD, emeritus professor of applied statistics at the Open University in Milton Keynes, England, described the study as “impressive.” However, he pointed out that the study’s observational design is a limitation.
“One can never be absolutely certain about the interpretation of findings of an observational study. What the research can’t tell us is what caused the increased psychiatric risks for people hospitalized with COVID-19 or some other serious respiratory disease,” Dr. McConway said.
“It can’t tell us what might happen in the future, when, we all hope, many fewer are being hospitalized with COVID-19 than was the case in those first two waves, and the current backlog of provision of some health services has decreased,” he added.
“So we can’t just say that, in general, serious COVID-19 has much the same neuropsychiatric consequences as other very serious respiratory illness. Maybe it does, maybe it doesn’t,” Dr. McConway cautioned.
Max Taquet, PhD, with the University of Oxford, noted that the study is limited to hospitalized adult patients, leaving open the question of risk in nonhospitalized individuals – which is the overwhelming majority of patients with COVID-19 – or in children.
Whether the neuropsychiatric risks have remained the same since the emergence of the Omicron variant also remains “an open question since all patients in this study were diagnosed before July 2021,” Dr. Taquet said in statement.
The study was funded by the Wellcome Trust, the John Fell Oxford University Press Research Fund, the Oxford Wellcome Institutional Strategic Support Fund and Cancer Research UK, through the Cancer Research UK Oxford Centre. Dr. Watkinson disclosed grants from the National Institute for Health Research and Sensyne Health outside the submitted work; and serving as chief medical officer for Sensyne Health prior to this work, as well as holding shares in the company. Dr. McConway is a trustee of the UK Science Media Centre and a member of its advisory committee. His comments were provided in his capacity as an independent professional statistician. Dr. Taquet has worked on similar studies trying to identify, quantify, and specify the neurological and psychiatric consequences of COVID-19.
A version of this article first appeared on Medscape.com.