User login
Class I recall for Medtronic’s HeartWare HVAD batteries
Medtronic is recalling a single lot of HeartWare Ventricular Assist Device (HVAD) System batteries because of welding defects that may cause separation of the two cell battery packs used to power the system, according to an alert on the Food and Drug Administration website.
“The welding defect may cause the battery to malfunction and no longer provide power or prevent the battery from holding a full charge or properly recharging,” the FDA said.
The agency has identified this as a class I recall, the most serious type because of the potential for serious injury or death.
Medtronic reports one death associated with this recall and two complaints in the affected lot.
Back in April, as reported by this news organization, Medtronic alerted providers that patients implanted with the Medtronic HVAD System who develop pump thrombosis could have a welding defect in the internal pump that causes the pump to malfunction.
The batteries from the recalled lot have a model number of 1650DE, were manufactured from April 13 to 19, 2021 and distributed from April 20 to July 19, 2021. The recall affects a total of 429 devices.
On May 5, 2022, Medtronic sent an urgent medical device correction notice to customers asking them to identify and quarantine all affected batteries and notify affected patients. The notice includes a patient template to help communicate directly with patients.
It also includes a customer confirmation form to initiate an exchange. The completed form should be returned to [email protected].
Medtronic is replacing the affected batteries with new product and has implemented actions to improve control of the welding process.
The Medtronic HVAD System was approved as a bridge to heart transplantation in 2012. Since then, it’s been fraught with problems.
Earlier in June, the company announced it was stopping all sales of the device and advised physicians to stop implanting it, as reported by this news organization.
Problems related to the Medtronic HVAD System should be reported to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
Medtronic is recalling a single lot of HeartWare Ventricular Assist Device (HVAD) System batteries because of welding defects that may cause separation of the two cell battery packs used to power the system, according to an alert on the Food and Drug Administration website.
“The welding defect may cause the battery to malfunction and no longer provide power or prevent the battery from holding a full charge or properly recharging,” the FDA said.
The agency has identified this as a class I recall, the most serious type because of the potential for serious injury or death.
Medtronic reports one death associated with this recall and two complaints in the affected lot.
Back in April, as reported by this news organization, Medtronic alerted providers that patients implanted with the Medtronic HVAD System who develop pump thrombosis could have a welding defect in the internal pump that causes the pump to malfunction.
The batteries from the recalled lot have a model number of 1650DE, were manufactured from April 13 to 19, 2021 and distributed from April 20 to July 19, 2021. The recall affects a total of 429 devices.
On May 5, 2022, Medtronic sent an urgent medical device correction notice to customers asking them to identify and quarantine all affected batteries and notify affected patients. The notice includes a patient template to help communicate directly with patients.
It also includes a customer confirmation form to initiate an exchange. The completed form should be returned to [email protected].
Medtronic is replacing the affected batteries with new product and has implemented actions to improve control of the welding process.
The Medtronic HVAD System was approved as a bridge to heart transplantation in 2012. Since then, it’s been fraught with problems.
Earlier in June, the company announced it was stopping all sales of the device and advised physicians to stop implanting it, as reported by this news organization.
Problems related to the Medtronic HVAD System should be reported to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
Medtronic is recalling a single lot of HeartWare Ventricular Assist Device (HVAD) System batteries because of welding defects that may cause separation of the two cell battery packs used to power the system, according to an alert on the Food and Drug Administration website.
“The welding defect may cause the battery to malfunction and no longer provide power or prevent the battery from holding a full charge or properly recharging,” the FDA said.
The agency has identified this as a class I recall, the most serious type because of the potential for serious injury or death.
Medtronic reports one death associated with this recall and two complaints in the affected lot.
Back in April, as reported by this news organization, Medtronic alerted providers that patients implanted with the Medtronic HVAD System who develop pump thrombosis could have a welding defect in the internal pump that causes the pump to malfunction.
The batteries from the recalled lot have a model number of 1650DE, were manufactured from April 13 to 19, 2021 and distributed from April 20 to July 19, 2021. The recall affects a total of 429 devices.
On May 5, 2022, Medtronic sent an urgent medical device correction notice to customers asking them to identify and quarantine all affected batteries and notify affected patients. The notice includes a patient template to help communicate directly with patients.
It also includes a customer confirmation form to initiate an exchange. The completed form should be returned to [email protected].
Medtronic is replacing the affected batteries with new product and has implemented actions to improve control of the welding process.
The Medtronic HVAD System was approved as a bridge to heart transplantation in 2012. Since then, it’s been fraught with problems.
Earlier in June, the company announced it was stopping all sales of the device and advised physicians to stop implanting it, as reported by this news organization.
Problems related to the Medtronic HVAD System should be reported to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
FDA okays cancer drugs faster than EMA. But at what cost?
Over the past decade, the U.S. Food and Drug Administration has approved new cancer drugs twice as fast as the European Medicines Agency (EMA), often using accelerated pathways, a new analysis shows.
Between 2010 and 2019, the FDA approved almost all oncology therapies ahead of the EMA. Drugs entered the United States market about 8 months (241 days) before European market authorization.
“The faster FDA approval process potentially provides earlier access to potentially life-prolonging medications for patients with cancer in the United States,” Ali Raza Khaki, MD, department of oncology, Stanford (Calif.) University School of Medicine, told this news organization. “On the surface, this is a good thing. However, it comes with limitations.”
Earlier drug approval often means greater uncertainty about an agent’s benefit – most notably, whether it will improve a patient’s survival or quality of life. Dr. Khaki pointed to a study published in JAMA Internal Medicine, which found that only 19 of 93 (20%) cancer drugs that had been recently approved through the FDA’s accelerated approval pathway demonstrated an improvement in overall survival.
In the new study, published online in JAMA Network Open, Dr. Khaki and colleagues found that among the 89 cancer drugs approved in the United States and Europe between January 2010 and December 2019, the FDA approved 85 (95%) before European authorization and four (5%) after.
The researchers found that the median FDA review time was half that of the EMA’s (200 vs. 426 days). Furthermore, 64 new drug applications (72%) were submitted to the FDA first, compared with 21 (23%) to the EMA.
Of the drugs approved through an accelerated pathway, three were ultimately pulled from the U.S. market, compared with one in Europe.
“These early drug approvals that later lead to withdrawal expose many more patients to toxicity, including financial toxicity, given the high cost of cancer medications,” Dr. Khaki commented.
In addition, 35 oncology therapies (39%) were approved by the FDA before trial results were published, compared with only eight (9%) by the EMA. Although FDA drug labels contain some information about efficacy and toxicity, scientific publications often have much more, including details about study populations and toxicities.
“Without this information, providers may be limited in their knowledge about patient selection, clinical benefit, and optimal toxicity management,” Dr. Khaki said.
Jeff Allen PhD, president and CEO of the nonprofit Friends of Cancer Research, who wasn’t involved in the study, believes that an FDA approval before publication shouldn’t be “particularly concerning.”
“Peer-reviewed publication is an important component of validating and communicating scientific findings, but the processes and time lines for individual journals can be highly variable,” he said. “I don’t think we would want to see a situation where potential beneficial treatments are held up due to unrelated publication processes.”
The author of an invited commentary in JAMA Network Open had a different take on the study findings.
“A tempting interpretation” of this study is that the FDA is a “superior agency for expedited review times that bring cancer drugs to patients earlier,” Kristina Jenei, BSN, MSc, with the University of British Columbia School of Population and Public Health, writes. In addition, the fact that more drugs were pulled from the market after approval in the United States than in Europe could be interpreted to mean that the system is working as it should.
Although the speed of FDA reviews and the number of subsequent approvals have increased over time, the proportion of cancer drugs that improve survival has declined. In addition, because the FDA’s follow-up of postmarketing studies has been “inconsistent,” a substantial number of cancer drugs that were approved through accelerated pathways have remained on the market for years without confirmation of their benefit.
Although regulatory agencies must balance earlier patient access to novel treatments with evidence that the therapies are effective and safe, “faster review times and approvals are not cause for celebration; better patient outcomes are,” Ms. Jenei writes. “In other words, quality over quantity.”
The study was supported by the National Cancer Institute. Dr. Khaki reported stock ownership from Merck and stock ownership from Sanofi outside the submitted work. Dr. Allen and Ms. Jenei have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Over the past decade, the U.S. Food and Drug Administration has approved new cancer drugs twice as fast as the European Medicines Agency (EMA), often using accelerated pathways, a new analysis shows.
Between 2010 and 2019, the FDA approved almost all oncology therapies ahead of the EMA. Drugs entered the United States market about 8 months (241 days) before European market authorization.
“The faster FDA approval process potentially provides earlier access to potentially life-prolonging medications for patients with cancer in the United States,” Ali Raza Khaki, MD, department of oncology, Stanford (Calif.) University School of Medicine, told this news organization. “On the surface, this is a good thing. However, it comes with limitations.”
Earlier drug approval often means greater uncertainty about an agent’s benefit – most notably, whether it will improve a patient’s survival or quality of life. Dr. Khaki pointed to a study published in JAMA Internal Medicine, which found that only 19 of 93 (20%) cancer drugs that had been recently approved through the FDA’s accelerated approval pathway demonstrated an improvement in overall survival.
In the new study, published online in JAMA Network Open, Dr. Khaki and colleagues found that among the 89 cancer drugs approved in the United States and Europe between January 2010 and December 2019, the FDA approved 85 (95%) before European authorization and four (5%) after.
The researchers found that the median FDA review time was half that of the EMA’s (200 vs. 426 days). Furthermore, 64 new drug applications (72%) were submitted to the FDA first, compared with 21 (23%) to the EMA.
Of the drugs approved through an accelerated pathway, three were ultimately pulled from the U.S. market, compared with one in Europe.
“These early drug approvals that later lead to withdrawal expose many more patients to toxicity, including financial toxicity, given the high cost of cancer medications,” Dr. Khaki commented.
In addition, 35 oncology therapies (39%) were approved by the FDA before trial results were published, compared with only eight (9%) by the EMA. Although FDA drug labels contain some information about efficacy and toxicity, scientific publications often have much more, including details about study populations and toxicities.
“Without this information, providers may be limited in their knowledge about patient selection, clinical benefit, and optimal toxicity management,” Dr. Khaki said.
Jeff Allen PhD, president and CEO of the nonprofit Friends of Cancer Research, who wasn’t involved in the study, believes that an FDA approval before publication shouldn’t be “particularly concerning.”
“Peer-reviewed publication is an important component of validating and communicating scientific findings, but the processes and time lines for individual journals can be highly variable,” he said. “I don’t think we would want to see a situation where potential beneficial treatments are held up due to unrelated publication processes.”
The author of an invited commentary in JAMA Network Open had a different take on the study findings.
“A tempting interpretation” of this study is that the FDA is a “superior agency for expedited review times that bring cancer drugs to patients earlier,” Kristina Jenei, BSN, MSc, with the University of British Columbia School of Population and Public Health, writes. In addition, the fact that more drugs were pulled from the market after approval in the United States than in Europe could be interpreted to mean that the system is working as it should.
Although the speed of FDA reviews and the number of subsequent approvals have increased over time, the proportion of cancer drugs that improve survival has declined. In addition, because the FDA’s follow-up of postmarketing studies has been “inconsistent,” a substantial number of cancer drugs that were approved through accelerated pathways have remained on the market for years without confirmation of their benefit.
Although regulatory agencies must balance earlier patient access to novel treatments with evidence that the therapies are effective and safe, “faster review times and approvals are not cause for celebration; better patient outcomes are,” Ms. Jenei writes. “In other words, quality over quantity.”
The study was supported by the National Cancer Institute. Dr. Khaki reported stock ownership from Merck and stock ownership from Sanofi outside the submitted work. Dr. Allen and Ms. Jenei have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Over the past decade, the U.S. Food and Drug Administration has approved new cancer drugs twice as fast as the European Medicines Agency (EMA), often using accelerated pathways, a new analysis shows.
Between 2010 and 2019, the FDA approved almost all oncology therapies ahead of the EMA. Drugs entered the United States market about 8 months (241 days) before European market authorization.
“The faster FDA approval process potentially provides earlier access to potentially life-prolonging medications for patients with cancer in the United States,” Ali Raza Khaki, MD, department of oncology, Stanford (Calif.) University School of Medicine, told this news organization. “On the surface, this is a good thing. However, it comes with limitations.”
Earlier drug approval often means greater uncertainty about an agent’s benefit – most notably, whether it will improve a patient’s survival or quality of life. Dr. Khaki pointed to a study published in JAMA Internal Medicine, which found that only 19 of 93 (20%) cancer drugs that had been recently approved through the FDA’s accelerated approval pathway demonstrated an improvement in overall survival.
In the new study, published online in JAMA Network Open, Dr. Khaki and colleagues found that among the 89 cancer drugs approved in the United States and Europe between January 2010 and December 2019, the FDA approved 85 (95%) before European authorization and four (5%) after.
The researchers found that the median FDA review time was half that of the EMA’s (200 vs. 426 days). Furthermore, 64 new drug applications (72%) were submitted to the FDA first, compared with 21 (23%) to the EMA.
Of the drugs approved through an accelerated pathway, three were ultimately pulled from the U.S. market, compared with one in Europe.
“These early drug approvals that later lead to withdrawal expose many more patients to toxicity, including financial toxicity, given the high cost of cancer medications,” Dr. Khaki commented.
In addition, 35 oncology therapies (39%) were approved by the FDA before trial results were published, compared with only eight (9%) by the EMA. Although FDA drug labels contain some information about efficacy and toxicity, scientific publications often have much more, including details about study populations and toxicities.
“Without this information, providers may be limited in their knowledge about patient selection, clinical benefit, and optimal toxicity management,” Dr. Khaki said.
Jeff Allen PhD, president and CEO of the nonprofit Friends of Cancer Research, who wasn’t involved in the study, believes that an FDA approval before publication shouldn’t be “particularly concerning.”
“Peer-reviewed publication is an important component of validating and communicating scientific findings, but the processes and time lines for individual journals can be highly variable,” he said. “I don’t think we would want to see a situation where potential beneficial treatments are held up due to unrelated publication processes.”
The author of an invited commentary in JAMA Network Open had a different take on the study findings.
“A tempting interpretation” of this study is that the FDA is a “superior agency for expedited review times that bring cancer drugs to patients earlier,” Kristina Jenei, BSN, MSc, with the University of British Columbia School of Population and Public Health, writes. In addition, the fact that more drugs were pulled from the market after approval in the United States than in Europe could be interpreted to mean that the system is working as it should.
Although the speed of FDA reviews and the number of subsequent approvals have increased over time, the proportion of cancer drugs that improve survival has declined. In addition, because the FDA’s follow-up of postmarketing studies has been “inconsistent,” a substantial number of cancer drugs that were approved through accelerated pathways have remained on the market for years without confirmation of their benefit.
Although regulatory agencies must balance earlier patient access to novel treatments with evidence that the therapies are effective and safe, “faster review times and approvals are not cause for celebration; better patient outcomes are,” Ms. Jenei writes. “In other words, quality over quantity.”
The study was supported by the National Cancer Institute. Dr. Khaki reported stock ownership from Merck and stock ownership from Sanofi outside the submitted work. Dr. Allen and Ms. Jenei have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
FDA approves risankizumab (Skyrizi) for Crohn’s disease
The U.S. Food and Drug Administration – making it the first specific anti–interleukin-23 monoclonal antibody indicated for Crohn’s disease.
The safety and efficacy of risankizumab in Crohn’s disease is supported by data from two induction clinical trials (ADVANCE and MOTIVATE) and one maintenance clinical trial (FORTIFY).
Results of the three studies were presented at the annual scientific meeting of the American College of Gastroenterology in 2021.
“In both the induction and maintenance clinical trials, a significantly greater number of adult patients saw few or no symptoms and a meaningful reduction of visible signs of intestinal inflammation, compared to placebo,” Marla Dubinsky, MD, gastroenterologist with the Mount Sinai Health System and codirector of the IBD Center at Mount Sinai, New York, said in a news release from AbbVie.
“This approval provides health care professionals with a greatly needed additional option for treating the disruptive symptoms of Crohn’s disease,” Dr. Dubinsky said.
For the treatment of Crohn’s disease, risankizumab is dosed at 600 mg administered by intravenous infusion over at least 1 hour at week 0, 4, and 8, followed by 360 mg self-administered by subcutaneous injection at week 12, and every 8 weeks thereafter.
Risankizumab is already approved in the United States for the treatment of adults with active psoriatic arthritis and moderate to severe plaque psoriasis.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration – making it the first specific anti–interleukin-23 monoclonal antibody indicated for Crohn’s disease.
The safety and efficacy of risankizumab in Crohn’s disease is supported by data from two induction clinical trials (ADVANCE and MOTIVATE) and one maintenance clinical trial (FORTIFY).
Results of the three studies were presented at the annual scientific meeting of the American College of Gastroenterology in 2021.
“In both the induction and maintenance clinical trials, a significantly greater number of adult patients saw few or no symptoms and a meaningful reduction of visible signs of intestinal inflammation, compared to placebo,” Marla Dubinsky, MD, gastroenterologist with the Mount Sinai Health System and codirector of the IBD Center at Mount Sinai, New York, said in a news release from AbbVie.
“This approval provides health care professionals with a greatly needed additional option for treating the disruptive symptoms of Crohn’s disease,” Dr. Dubinsky said.
For the treatment of Crohn’s disease, risankizumab is dosed at 600 mg administered by intravenous infusion over at least 1 hour at week 0, 4, and 8, followed by 360 mg self-administered by subcutaneous injection at week 12, and every 8 weeks thereafter.
Risankizumab is already approved in the United States for the treatment of adults with active psoriatic arthritis and moderate to severe plaque psoriasis.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration – making it the first specific anti–interleukin-23 monoclonal antibody indicated for Crohn’s disease.
The safety and efficacy of risankizumab in Crohn’s disease is supported by data from two induction clinical trials (ADVANCE and MOTIVATE) and one maintenance clinical trial (FORTIFY).
Results of the three studies were presented at the annual scientific meeting of the American College of Gastroenterology in 2021.
“In both the induction and maintenance clinical trials, a significantly greater number of adult patients saw few or no symptoms and a meaningful reduction of visible signs of intestinal inflammation, compared to placebo,” Marla Dubinsky, MD, gastroenterologist with the Mount Sinai Health System and codirector of the IBD Center at Mount Sinai, New York, said in a news release from AbbVie.
“This approval provides health care professionals with a greatly needed additional option for treating the disruptive symptoms of Crohn’s disease,” Dr. Dubinsky said.
For the treatment of Crohn’s disease, risankizumab is dosed at 600 mg administered by intravenous infusion over at least 1 hour at week 0, 4, and 8, followed by 360 mg self-administered by subcutaneous injection at week 12, and every 8 weeks thereafter.
Risankizumab is already approved in the United States for the treatment of adults with active psoriatic arthritis and moderate to severe plaque psoriasis.
A version of this article first appeared on Medscape.com.
Snoring may lead to a sedentary lifestyle
“People who snore are also likely to have sleep apnea, but those who snore and don’t have sleep apnea are a largely understudied group,” senior author Michael Grandner, PhD, told this news organization.
“We found that even just snoring alone can impact health and well-being,” said Dr. Grandner, director of the sleep and health research program at the University of Arizona, Tucson.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
A viscous cycle
Frequent snoring can signal sleep-disordered breathing, which is associated with a myriad of comorbidities, including increased risk for cardiovascular disease.
Prior studies have shown that sleep-disordered breathing is associated with less physical activity, but few studies have examined this at the population level or in relation to primary snoring.
Dr. Grandner and colleagues evaluated the relationship between snoring frequency and minutes of sedentary activity using 3 years’ worth of data from the National Health and Nutrition Examination Survey. Participants reported snoring frequency and sedentary activity.
After adjusting for sex, age, race, education level, and marital status, adults who were frequent snorers (5+ nights per week) spent about 36 more minutes per day sedentary, compared with peers who reported never snoring.
In addition, those individuals who were determined to be at increased risk of having sleep apnea had about 54 more minutes per day of sedentary time in the adjusted model.
“Snoring is very common, and it doesn’t just affect the nighttime,” said Dr. Grandner.
Snoring can lead to “more tiredness and less energy, which can impact everything from mood to stress to – as we saw – activity level,” he noted.
Commenting on the results for this news organization, Raman Malhotra, MD, of the Washington University Sleep Center in St. Louis, said this study clearly demonstrates how people who snore and people who are at risk for sleep apnea are more sedentary.
This could explain the “vicious cycle” that these patients suffer from, inasmuch as having obesity can lead to sleep apnea, and having sleep apnea can lead to further sedentary lifestyle and weight gain, owing to lack of energy and feeling tired, Dr. Malhotra told this news organization.
“It is important to intervene and treat the sleep disorder to hopefully make people more active,” he added.
The study had no specific funding. Dr. Grandner and Dr. Malhotra disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“People who snore are also likely to have sleep apnea, but those who snore and don’t have sleep apnea are a largely understudied group,” senior author Michael Grandner, PhD, told this news organization.
“We found that even just snoring alone can impact health and well-being,” said Dr. Grandner, director of the sleep and health research program at the University of Arizona, Tucson.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
A viscous cycle
Frequent snoring can signal sleep-disordered breathing, which is associated with a myriad of comorbidities, including increased risk for cardiovascular disease.
Prior studies have shown that sleep-disordered breathing is associated with less physical activity, but few studies have examined this at the population level or in relation to primary snoring.
Dr. Grandner and colleagues evaluated the relationship between snoring frequency and minutes of sedentary activity using 3 years’ worth of data from the National Health and Nutrition Examination Survey. Participants reported snoring frequency and sedentary activity.
After adjusting for sex, age, race, education level, and marital status, adults who were frequent snorers (5+ nights per week) spent about 36 more minutes per day sedentary, compared with peers who reported never snoring.
In addition, those individuals who were determined to be at increased risk of having sleep apnea had about 54 more minutes per day of sedentary time in the adjusted model.
“Snoring is very common, and it doesn’t just affect the nighttime,” said Dr. Grandner.
Snoring can lead to “more tiredness and less energy, which can impact everything from mood to stress to – as we saw – activity level,” he noted.
Commenting on the results for this news organization, Raman Malhotra, MD, of the Washington University Sleep Center in St. Louis, said this study clearly demonstrates how people who snore and people who are at risk for sleep apnea are more sedentary.
This could explain the “vicious cycle” that these patients suffer from, inasmuch as having obesity can lead to sleep apnea, and having sleep apnea can lead to further sedentary lifestyle and weight gain, owing to lack of energy and feeling tired, Dr. Malhotra told this news organization.
“It is important to intervene and treat the sleep disorder to hopefully make people more active,” he added.
The study had no specific funding. Dr. Grandner and Dr. Malhotra disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“People who snore are also likely to have sleep apnea, but those who snore and don’t have sleep apnea are a largely understudied group,” senior author Michael Grandner, PhD, told this news organization.
“We found that even just snoring alone can impact health and well-being,” said Dr. Grandner, director of the sleep and health research program at the University of Arizona, Tucson.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
A viscous cycle
Frequent snoring can signal sleep-disordered breathing, which is associated with a myriad of comorbidities, including increased risk for cardiovascular disease.
Prior studies have shown that sleep-disordered breathing is associated with less physical activity, but few studies have examined this at the population level or in relation to primary snoring.
Dr. Grandner and colleagues evaluated the relationship between snoring frequency and minutes of sedentary activity using 3 years’ worth of data from the National Health and Nutrition Examination Survey. Participants reported snoring frequency and sedentary activity.
After adjusting for sex, age, race, education level, and marital status, adults who were frequent snorers (5+ nights per week) spent about 36 more minutes per day sedentary, compared with peers who reported never snoring.
In addition, those individuals who were determined to be at increased risk of having sleep apnea had about 54 more minutes per day of sedentary time in the adjusted model.
“Snoring is very common, and it doesn’t just affect the nighttime,” said Dr. Grandner.
Snoring can lead to “more tiredness and less energy, which can impact everything from mood to stress to – as we saw – activity level,” he noted.
Commenting on the results for this news organization, Raman Malhotra, MD, of the Washington University Sleep Center in St. Louis, said this study clearly demonstrates how people who snore and people who are at risk for sleep apnea are more sedentary.
This could explain the “vicious cycle” that these patients suffer from, inasmuch as having obesity can lead to sleep apnea, and having sleep apnea can lead to further sedentary lifestyle and weight gain, owing to lack of energy and feeling tired, Dr. Malhotra told this news organization.
“It is important to intervene and treat the sleep disorder to hopefully make people more active,” he added.
The study had no specific funding. Dr. Grandner and Dr. Malhotra disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SLEEP 2022
Can too much sleep raise the risk of cancer?
The findings reveal that sleeping 10-plus hours may increase a woman’s risk of getting cancer and both men and women’s risk of dying from cancer.
The researchers say their findings may help refine sleep recommendations in Japan, which currently advise working, middle-aged adults to sleep “as long as they can.”
Based on the new findings, a sleep duration of 6-8 hours for men and 6-9 hours for women “may be the safest” regarding cancer incidence and mortality risk among Japanese adults, the authors conclude.
The findings were published online in the International Journal of Cancer.
The literature on sleep time and cancer risk is mixed. A trio of meta-analyses conducted between 2016 and 2019 found that long sleep duration, but not short, was associated with a slightly elevated risk of all cancer mortality in Asians.
A separate meta-analysis conducted in 2018 found that both short and long sleep durations were not related to cancer incidence. But in the stratified analysis, shorter sleep time was associated with 36% increased cancer risk among Asians.
To investigate further, the researchers pooled data from six population-based cohorts that included 271,694 adults – 126,930 men and 144,764 women – with 40,751 total incident cancer cases and 18,323 total cancer deaths during a follow-up lasting about 5.9 million person-years.
In the multivariable analysis, longer sleep duration was not associated with total cancer incidence in men. In women, however, sleeping 10 or more hours vs. 7 was associated with a 19% increased risk of cancer.
In addition, sleeping 10 or more hours was associated with an increased risk of dying from cancer in women (hazard ratio, 1.44) and men (HR, 1.18).
Sleeping for 5 hours or fewer, compared with 7, was not associated with cancer incidence and mortality. However, among postmenopausal women, shorter sleep durations did increase the risk of dying from cancer (HR, 1.15).
The authors highlight several strengths of the analysis, including a large sample size as well as stratification of the results by body mass index and menopause status, which has rarely been done in previous studies.
Limitations include self-reported sleep durations and lack of data on sleep quality. The researchers note that the mechanism by which sleep time may influence cancer incidence and mortality is unclear but likely to be complex and cancer site specific.
It’s also possible that reverse causation could explain associations between sleep duration and cancer occurrence and mortality – with pain from cancer, for instance, impairing sleep duration and quality. However, the sensitivity analysis found no evidence of reverse causality or other confounding factors.
Based on these findings, the researchers say sleep duration “may be an important variable to include in cancer incidence and mortality risk prediction models.”
The study had no specific funding. The authors declared no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The findings reveal that sleeping 10-plus hours may increase a woman’s risk of getting cancer and both men and women’s risk of dying from cancer.
The researchers say their findings may help refine sleep recommendations in Japan, which currently advise working, middle-aged adults to sleep “as long as they can.”
Based on the new findings, a sleep duration of 6-8 hours for men and 6-9 hours for women “may be the safest” regarding cancer incidence and mortality risk among Japanese adults, the authors conclude.
The findings were published online in the International Journal of Cancer.
The literature on sleep time and cancer risk is mixed. A trio of meta-analyses conducted between 2016 and 2019 found that long sleep duration, but not short, was associated with a slightly elevated risk of all cancer mortality in Asians.
A separate meta-analysis conducted in 2018 found that both short and long sleep durations were not related to cancer incidence. But in the stratified analysis, shorter sleep time was associated with 36% increased cancer risk among Asians.
To investigate further, the researchers pooled data from six population-based cohorts that included 271,694 adults – 126,930 men and 144,764 women – with 40,751 total incident cancer cases and 18,323 total cancer deaths during a follow-up lasting about 5.9 million person-years.
In the multivariable analysis, longer sleep duration was not associated with total cancer incidence in men. In women, however, sleeping 10 or more hours vs. 7 was associated with a 19% increased risk of cancer.
In addition, sleeping 10 or more hours was associated with an increased risk of dying from cancer in women (hazard ratio, 1.44) and men (HR, 1.18).
Sleeping for 5 hours or fewer, compared with 7, was not associated with cancer incidence and mortality. However, among postmenopausal women, shorter sleep durations did increase the risk of dying from cancer (HR, 1.15).
The authors highlight several strengths of the analysis, including a large sample size as well as stratification of the results by body mass index and menopause status, which has rarely been done in previous studies.
Limitations include self-reported sleep durations and lack of data on sleep quality. The researchers note that the mechanism by which sleep time may influence cancer incidence and mortality is unclear but likely to be complex and cancer site specific.
It’s also possible that reverse causation could explain associations between sleep duration and cancer occurrence and mortality – with pain from cancer, for instance, impairing sleep duration and quality. However, the sensitivity analysis found no evidence of reverse causality or other confounding factors.
Based on these findings, the researchers say sleep duration “may be an important variable to include in cancer incidence and mortality risk prediction models.”
The study had no specific funding. The authors declared no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The findings reveal that sleeping 10-plus hours may increase a woman’s risk of getting cancer and both men and women’s risk of dying from cancer.
The researchers say their findings may help refine sleep recommendations in Japan, which currently advise working, middle-aged adults to sleep “as long as they can.”
Based on the new findings, a sleep duration of 6-8 hours for men and 6-9 hours for women “may be the safest” regarding cancer incidence and mortality risk among Japanese adults, the authors conclude.
The findings were published online in the International Journal of Cancer.
The literature on sleep time and cancer risk is mixed. A trio of meta-analyses conducted between 2016 and 2019 found that long sleep duration, but not short, was associated with a slightly elevated risk of all cancer mortality in Asians.
A separate meta-analysis conducted in 2018 found that both short and long sleep durations were not related to cancer incidence. But in the stratified analysis, shorter sleep time was associated with 36% increased cancer risk among Asians.
To investigate further, the researchers pooled data from six population-based cohorts that included 271,694 adults – 126,930 men and 144,764 women – with 40,751 total incident cancer cases and 18,323 total cancer deaths during a follow-up lasting about 5.9 million person-years.
In the multivariable analysis, longer sleep duration was not associated with total cancer incidence in men. In women, however, sleeping 10 or more hours vs. 7 was associated with a 19% increased risk of cancer.
In addition, sleeping 10 or more hours was associated with an increased risk of dying from cancer in women (hazard ratio, 1.44) and men (HR, 1.18).
Sleeping for 5 hours or fewer, compared with 7, was not associated with cancer incidence and mortality. However, among postmenopausal women, shorter sleep durations did increase the risk of dying from cancer (HR, 1.15).
The authors highlight several strengths of the analysis, including a large sample size as well as stratification of the results by body mass index and menopause status, which has rarely been done in previous studies.
Limitations include self-reported sleep durations and lack of data on sleep quality. The researchers note that the mechanism by which sleep time may influence cancer incidence and mortality is unclear but likely to be complex and cancer site specific.
It’s also possible that reverse causation could explain associations between sleep duration and cancer occurrence and mortality – with pain from cancer, for instance, impairing sleep duration and quality. However, the sensitivity analysis found no evidence of reverse causality or other confounding factors.
Based on these findings, the researchers say sleep duration “may be an important variable to include in cancer incidence and mortality risk prediction models.”
The study had no specific funding. The authors declared no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM THE INTERNATIONAL JOURNAL OF CANCER
‘Forever chemicals’ linked to hypertension in middle-aged women
In a large, prospective study, researchers found an association between higher blood levels of PFAS and increased risk of hypertension in middle-aged women. Women in the highest tertile of overall PFAS concentrations had a 71% increased risk of developing hypertension.
“Our findings suggest that long-term cumulative exposure, even before midlife, may increase the risk of high blood pressure, and therefore, the benefit of reducing the population exposure to PFAS and potential prevention of high blood pressure and other health conditions would be enormous,” Sung Kyun Park, ScD, MPH, University of Michigan School of Public Health, Ann Arbor, said in an interview.
The study was published online in Hypertension.
Everywhere and forever
“PFAS are forever chemicals as well as everywhere chemicals,” Dr. Park noted.
Possible sources of PFAS exposure run the gamut from nonstick cookware, food wrappers, and waterproof fabrics to cosmetics and drinking water. They have been detected in the blood of most people and have been linked to a variety of health concerns.
“A few studies showed an association between PFAS and hypertension, but those were cross-sectional and examined prevalence of hypertension. It was unclear whether PFAS are associated with the development (incidence) of hypertension,” Dr. Park explained.
For their study, the researchers examined the association between serum concentrations of PFAS and risks of incident hypertension in 1,058 initially normotensive women participating in the Study of Women’s Health Across the Nation-Multi-Pollutant Study (SWAN-MPS). They were followed annually between 1999 and 2017.
During 11,722 person-years of follow-up, 470 of the women developed hypertension, at a rate of 40.1 cases per 1,000 person-years. Hypertension was defined as blood pressure of at least 140 mm Hg systolic or at least 90 mm Hg diastolic or receiving antihypertensive treatment.
Women in the highest tertile of baseline serum concentration of perfluorooctane sulfonate (PFOS) had a 42% higher risk of developing hypertension, compared with peers in the lowest tertile (adjusted hazard ratio, 1.42; 95% confidence interval, 1.19-1.68; P trend = .01).
Similar results were found for perfluorooctanoate (PFOA) and 2-N-ethyl-perfluorooctane sulfonamido acetate (EtFOSAA), with 47% (aHR, 1.47; 95% CI, 1.24-1.75; P trend = .01) and 42% (aHR, 1.42; 95% CI, 1.19-1.70; P trend = .01) higher risks of incident hypertension, comparing the highest to the lowest tertiles.
The risks persisted after adjusting for various factors, including race, study site, education, financial strain, smoking status, alcohol use, total calorie intake, and menopausal status.
In the PFAS “mixture” analysis, women in the highest tertile of overall PFAS concentrations were 71% more likely to develop hypertension during follow-up, compared with women in the lowest tertile (aHR, 1.71; 95% CI, 1.15-2.54; P trend = .008).
“These findings suggest that PFAS might be an underappreciated contributing factor to women’s cardiovascular disease risk,” the researchers write.
They caution that the study only included middle-aged women and that it is unclear whether the findings hold for middle-aged men.
“This is an important question, but the answer is that we do not know,” Dr. Park told this news organization.
“Women become more susceptible to metabolic changes and hypertension risk during the menopausal transition. Our findings suggest that PFAS may play a role in the development of hypertension in women during this critical life stage,” Dr. Park said.
The researchers say more research is needed to confirm and expand the findings and to find ways to reduce PFAS exposure.
“If confirmed in future studies, these findings suggest that understanding human exposure to PFAS and developing effective strategies to reduce PFAS exposure may help prevent the development of hypertension and thereby reduce the global burden of CVD,” the researchers write.
‘The more we learn, the worse it gets’
This is an “interesting” study and shows that “the more we learn about PFAS, the worse it seems to get,” Ankur Shah, MD, division of kidney disease and hypertension, Warren Alpert Medical School of Brown University, Providence, R.I., said in an interview.
“This multisite, multiracial and multiethnic, community-based longitudinal study establishes an association between PFAS and hypertension,” said Dr. Shah, who wasn’t involved in the study.
“This adds to a growing literature base of associations of PFAS with illnesses, including malignancy, thyroid disorders, diabetes, ulcerative colitis, hyperlipidemia, and pregnancy-induced hypertension,” he noted.
Dr. Shah also noted that the authors adjusted for race and ethnicity, study site, education, financial strain, smoking status, environmental tobacco smoke, alcohol consumption, total calorie intake, and menopausal status “and still found a strong association.”
“Still to be determined are both whether PFAS are the causative agent or if there is an unmeasured/unadjusted for entity which has resulted in both increased PFAS exposure and hypertension, as well as if PFAS are causative, if reduction in PFAS exposure would be result in blood pressure reduction,” Dr. Shah added.
The study had no sources of funding. Dr. Park and Dr. Shah have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a large, prospective study, researchers found an association between higher blood levels of PFAS and increased risk of hypertension in middle-aged women. Women in the highest tertile of overall PFAS concentrations had a 71% increased risk of developing hypertension.
“Our findings suggest that long-term cumulative exposure, even before midlife, may increase the risk of high blood pressure, and therefore, the benefit of reducing the population exposure to PFAS and potential prevention of high blood pressure and other health conditions would be enormous,” Sung Kyun Park, ScD, MPH, University of Michigan School of Public Health, Ann Arbor, said in an interview.
The study was published online in Hypertension.
Everywhere and forever
“PFAS are forever chemicals as well as everywhere chemicals,” Dr. Park noted.
Possible sources of PFAS exposure run the gamut from nonstick cookware, food wrappers, and waterproof fabrics to cosmetics and drinking water. They have been detected in the blood of most people and have been linked to a variety of health concerns.
“A few studies showed an association between PFAS and hypertension, but those were cross-sectional and examined prevalence of hypertension. It was unclear whether PFAS are associated with the development (incidence) of hypertension,” Dr. Park explained.
For their study, the researchers examined the association between serum concentrations of PFAS and risks of incident hypertension in 1,058 initially normotensive women participating in the Study of Women’s Health Across the Nation-Multi-Pollutant Study (SWAN-MPS). They were followed annually between 1999 and 2017.
During 11,722 person-years of follow-up, 470 of the women developed hypertension, at a rate of 40.1 cases per 1,000 person-years. Hypertension was defined as blood pressure of at least 140 mm Hg systolic or at least 90 mm Hg diastolic or receiving antihypertensive treatment.
Women in the highest tertile of baseline serum concentration of perfluorooctane sulfonate (PFOS) had a 42% higher risk of developing hypertension, compared with peers in the lowest tertile (adjusted hazard ratio, 1.42; 95% confidence interval, 1.19-1.68; P trend = .01).
Similar results were found for perfluorooctanoate (PFOA) and 2-N-ethyl-perfluorooctane sulfonamido acetate (EtFOSAA), with 47% (aHR, 1.47; 95% CI, 1.24-1.75; P trend = .01) and 42% (aHR, 1.42; 95% CI, 1.19-1.70; P trend = .01) higher risks of incident hypertension, comparing the highest to the lowest tertiles.
The risks persisted after adjusting for various factors, including race, study site, education, financial strain, smoking status, alcohol use, total calorie intake, and menopausal status.
In the PFAS “mixture” analysis, women in the highest tertile of overall PFAS concentrations were 71% more likely to develop hypertension during follow-up, compared with women in the lowest tertile (aHR, 1.71; 95% CI, 1.15-2.54; P trend = .008).
“These findings suggest that PFAS might be an underappreciated contributing factor to women’s cardiovascular disease risk,” the researchers write.
They caution that the study only included middle-aged women and that it is unclear whether the findings hold for middle-aged men.
“This is an important question, but the answer is that we do not know,” Dr. Park told this news organization.
“Women become more susceptible to metabolic changes and hypertension risk during the menopausal transition. Our findings suggest that PFAS may play a role in the development of hypertension in women during this critical life stage,” Dr. Park said.
The researchers say more research is needed to confirm and expand the findings and to find ways to reduce PFAS exposure.
“If confirmed in future studies, these findings suggest that understanding human exposure to PFAS and developing effective strategies to reduce PFAS exposure may help prevent the development of hypertension and thereby reduce the global burden of CVD,” the researchers write.
‘The more we learn, the worse it gets’
This is an “interesting” study and shows that “the more we learn about PFAS, the worse it seems to get,” Ankur Shah, MD, division of kidney disease and hypertension, Warren Alpert Medical School of Brown University, Providence, R.I., said in an interview.
“This multisite, multiracial and multiethnic, community-based longitudinal study establishes an association between PFAS and hypertension,” said Dr. Shah, who wasn’t involved in the study.
“This adds to a growing literature base of associations of PFAS with illnesses, including malignancy, thyroid disorders, diabetes, ulcerative colitis, hyperlipidemia, and pregnancy-induced hypertension,” he noted.
Dr. Shah also noted that the authors adjusted for race and ethnicity, study site, education, financial strain, smoking status, environmental tobacco smoke, alcohol consumption, total calorie intake, and menopausal status “and still found a strong association.”
“Still to be determined are both whether PFAS are the causative agent or if there is an unmeasured/unadjusted for entity which has resulted in both increased PFAS exposure and hypertension, as well as if PFAS are causative, if reduction in PFAS exposure would be result in blood pressure reduction,” Dr. Shah added.
The study had no sources of funding. Dr. Park and Dr. Shah have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a large, prospective study, researchers found an association between higher blood levels of PFAS and increased risk of hypertension in middle-aged women. Women in the highest tertile of overall PFAS concentrations had a 71% increased risk of developing hypertension.
“Our findings suggest that long-term cumulative exposure, even before midlife, may increase the risk of high blood pressure, and therefore, the benefit of reducing the population exposure to PFAS and potential prevention of high blood pressure and other health conditions would be enormous,” Sung Kyun Park, ScD, MPH, University of Michigan School of Public Health, Ann Arbor, said in an interview.
The study was published online in Hypertension.
Everywhere and forever
“PFAS are forever chemicals as well as everywhere chemicals,” Dr. Park noted.
Possible sources of PFAS exposure run the gamut from nonstick cookware, food wrappers, and waterproof fabrics to cosmetics and drinking water. They have been detected in the blood of most people and have been linked to a variety of health concerns.
“A few studies showed an association between PFAS and hypertension, but those were cross-sectional and examined prevalence of hypertension. It was unclear whether PFAS are associated with the development (incidence) of hypertension,” Dr. Park explained.
For their study, the researchers examined the association between serum concentrations of PFAS and risks of incident hypertension in 1,058 initially normotensive women participating in the Study of Women’s Health Across the Nation-Multi-Pollutant Study (SWAN-MPS). They were followed annually between 1999 and 2017.
During 11,722 person-years of follow-up, 470 of the women developed hypertension, at a rate of 40.1 cases per 1,000 person-years. Hypertension was defined as blood pressure of at least 140 mm Hg systolic or at least 90 mm Hg diastolic or receiving antihypertensive treatment.
Women in the highest tertile of baseline serum concentration of perfluorooctane sulfonate (PFOS) had a 42% higher risk of developing hypertension, compared with peers in the lowest tertile (adjusted hazard ratio, 1.42; 95% confidence interval, 1.19-1.68; P trend = .01).
Similar results were found for perfluorooctanoate (PFOA) and 2-N-ethyl-perfluorooctane sulfonamido acetate (EtFOSAA), with 47% (aHR, 1.47; 95% CI, 1.24-1.75; P trend = .01) and 42% (aHR, 1.42; 95% CI, 1.19-1.70; P trend = .01) higher risks of incident hypertension, comparing the highest to the lowest tertiles.
The risks persisted after adjusting for various factors, including race, study site, education, financial strain, smoking status, alcohol use, total calorie intake, and menopausal status.
In the PFAS “mixture” analysis, women in the highest tertile of overall PFAS concentrations were 71% more likely to develop hypertension during follow-up, compared with women in the lowest tertile (aHR, 1.71; 95% CI, 1.15-2.54; P trend = .008).
“These findings suggest that PFAS might be an underappreciated contributing factor to women’s cardiovascular disease risk,” the researchers write.
They caution that the study only included middle-aged women and that it is unclear whether the findings hold for middle-aged men.
“This is an important question, but the answer is that we do not know,” Dr. Park told this news organization.
“Women become more susceptible to metabolic changes and hypertension risk during the menopausal transition. Our findings suggest that PFAS may play a role in the development of hypertension in women during this critical life stage,” Dr. Park said.
The researchers say more research is needed to confirm and expand the findings and to find ways to reduce PFAS exposure.
“If confirmed in future studies, these findings suggest that understanding human exposure to PFAS and developing effective strategies to reduce PFAS exposure may help prevent the development of hypertension and thereby reduce the global burden of CVD,” the researchers write.
‘The more we learn, the worse it gets’
This is an “interesting” study and shows that “the more we learn about PFAS, the worse it seems to get,” Ankur Shah, MD, division of kidney disease and hypertension, Warren Alpert Medical School of Brown University, Providence, R.I., said in an interview.
“This multisite, multiracial and multiethnic, community-based longitudinal study establishes an association between PFAS and hypertension,” said Dr. Shah, who wasn’t involved in the study.
“This adds to a growing literature base of associations of PFAS with illnesses, including malignancy, thyroid disorders, diabetes, ulcerative colitis, hyperlipidemia, and pregnancy-induced hypertension,” he noted.
Dr. Shah also noted that the authors adjusted for race and ethnicity, study site, education, financial strain, smoking status, environmental tobacco smoke, alcohol consumption, total calorie intake, and menopausal status “and still found a strong association.”
“Still to be determined are both whether PFAS are the causative agent or if there is an unmeasured/unadjusted for entity which has resulted in both increased PFAS exposure and hypertension, as well as if PFAS are causative, if reduction in PFAS exposure would be result in blood pressure reduction,” Dr. Shah added.
The study had no sources of funding. Dr. Park and Dr. Shah have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HYPERTENSION
A ‘crisis’ of suicidal thoughts, attempts in transgender youth
Transgender youth are significantly more likely to consider suicide and attempt it, compared with their cisgender peers, new research shows.
In a large population-based study, investigators found the increased risk of suicidality is partly because of bullying and cyberbullying experienced by transgender teens.
The findings are “extremely concerning and should be a wake-up call,” Ian Colman, PhD, with the University of Ottawa School of Epidemiology and Public Health, said in an interview.
Young people who are exploring their sexual identities may suffer from depression and anxiety, both about the reactions of their peers and families, as well as their own sense of self.
“These youth are highly marginalized and stigmatized in many corners of our society, and these findings highlight just how distressing these experiences can be,” Dr. Colman said.
The study was published online in the Canadian Medical Association Journal.
Sevenfold increased risk of attempted suicide
The risk of suicidal thoughts and actions is not well studied in transgender and nonbinary youth.
To expand the evidence base, the researchers analyzed data for 6,800 adolescents aged 15-17 years from the 2019 Canadian Health Survey on Children and Youth.
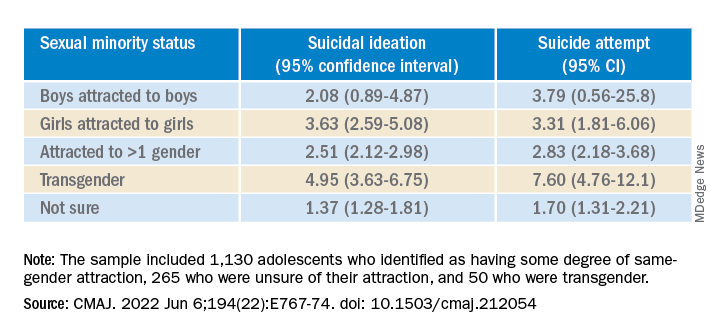
The sample included 1,130 (16.5%) adolescents who identified as having some degree of same-gender attraction, 265 (4.3%) who were unsure of their attraction (“questioning”), and 50 (0.6%) who were transgender, meaning they identified as being of a gender different from that assigned at birth.
Overall, 980 (14.0%) adolescents reported having thoughts of suicide in the prior year, and 480 (6.8%) had attempted suicide in their life.
Transgender youth were five times more likely to think about suicide and more than seven times more likely to have ever attempted suicide than cisgender, heterosexual peers.
Among cisgender adolescents, girls who were attracted to girls had 3.6 times the risk of suicidal ideation and 3.3 times the risk of having ever attempted suicide, compared with their heterosexual peers.
Teens attracted to multiple genders had more than twice the risk of suicidal ideation and suicide attempt. Youth who were questioning their sexual orientation had twice the risk of having attempted suicide in their lifetime.
A crisis – with reason for hope
“This is a crisis, and it shows just how much more needs to be done to support transgender young people,” co-author Fae Johnstone, MSW, executive director, Wisdom2Action, who is a trans woman herself, said in the news release.
“Suicide prevention programs specifically targeted to transgender, nonbinary, and sexual minority adolescents, as well as gender-affirming care for transgender adolescents, may help reduce the burden of suicidality among this group,” Ms. Johnstone added.
“The most important thing that parents, teachers, and health care providers can do is to be supportive of these youth,” Dr. Colman told this news organization.
“Providing a safe place where gender and sexual minorities can explore and express themselves is crucial. The first step is to listen and to be compassionate,” Dr. Colman added.
Reached for comment, Jess Ting, MD, director of surgery at the Mount Sinai Center for Transgender Medicine and Surgery, New York, said the data from this study on suicidal thoughts and actions among sexual minority and transgender adolescents “mirror what we see and what we know” about suicidality in trans and nonbinary adults.
“The reasons for this are complex, and it’s hard for someone who doesn’t have a lived experience as a trans or nonbinary person to understand the reasons for suicidality,” he told this news organization.
“But we also know that there are higher rates of anxiety and depression and self-image issues and posttraumatic stress disorder, not to mention outside factors – marginalization, discrimination, violence, abuse. When you add up all these intrinsic and extrinsic factors, it’s not hard to believe that there is a high rate of suicidality,” Dr. Ting said.
“There have been studies that have shown that in children who are supported in their gender identity, the rates of depression and anxiety decreased to almost the same levels as non-trans and nonbinary children, so I think that gives cause for hope,” Dr. Ting added.
The study was funded in part by the Research Council of Norway through its Centres of Excellence funding scheme and by a Frederick Banting and Charles Best Canada Graduate Scholarship Doctoral Award. Ms. Johnstone reports consulting fees from Spectrum Waterloo and volunteer participation with the Youth Suicide Prevention Leadership Committee of Ontario. No other competing interests were declared. Dr. Ting has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Transgender youth are significantly more likely to consider suicide and attempt it, compared with their cisgender peers, new research shows.
In a large population-based study, investigators found the increased risk of suicidality is partly because of bullying and cyberbullying experienced by transgender teens.
The findings are “extremely concerning and should be a wake-up call,” Ian Colman, PhD, with the University of Ottawa School of Epidemiology and Public Health, said in an interview.
Young people who are exploring their sexual identities may suffer from depression and anxiety, both about the reactions of their peers and families, as well as their own sense of self.
“These youth are highly marginalized and stigmatized in many corners of our society, and these findings highlight just how distressing these experiences can be,” Dr. Colman said.
The study was published online in the Canadian Medical Association Journal.
Sevenfold increased risk of attempted suicide
The risk of suicidal thoughts and actions is not well studied in transgender and nonbinary youth.
To expand the evidence base, the researchers analyzed data for 6,800 adolescents aged 15-17 years from the 2019 Canadian Health Survey on Children and Youth.
The sample included 1,130 (16.5%) adolescents who identified as having some degree of same-gender attraction, 265 (4.3%) who were unsure of their attraction (“questioning”), and 50 (0.6%) who were transgender, meaning they identified as being of a gender different from that assigned at birth.
Overall, 980 (14.0%) adolescents reported having thoughts of suicide in the prior year, and 480 (6.8%) had attempted suicide in their life.
Transgender youth were five times more likely to think about suicide and more than seven times more likely to have ever attempted suicide than cisgender, heterosexual peers.
Among cisgender adolescents, girls who were attracted to girls had 3.6 times the risk of suicidal ideation and 3.3 times the risk of having ever attempted suicide, compared with their heterosexual peers.
Teens attracted to multiple genders had more than twice the risk of suicidal ideation and suicide attempt. Youth who were questioning their sexual orientation had twice the risk of having attempted suicide in their lifetime.
A crisis – with reason for hope
“This is a crisis, and it shows just how much more needs to be done to support transgender young people,” co-author Fae Johnstone, MSW, executive director, Wisdom2Action, who is a trans woman herself, said in the news release.
“Suicide prevention programs specifically targeted to transgender, nonbinary, and sexual minority adolescents, as well as gender-affirming care for transgender adolescents, may help reduce the burden of suicidality among this group,” Ms. Johnstone added.
“The most important thing that parents, teachers, and health care providers can do is to be supportive of these youth,” Dr. Colman told this news organization.
“Providing a safe place where gender and sexual minorities can explore and express themselves is crucial. The first step is to listen and to be compassionate,” Dr. Colman added.
Reached for comment, Jess Ting, MD, director of surgery at the Mount Sinai Center for Transgender Medicine and Surgery, New York, said the data from this study on suicidal thoughts and actions among sexual minority and transgender adolescents “mirror what we see and what we know” about suicidality in trans and nonbinary adults.
“The reasons for this are complex, and it’s hard for someone who doesn’t have a lived experience as a trans or nonbinary person to understand the reasons for suicidality,” he told this news organization.
“But we also know that there are higher rates of anxiety and depression and self-image issues and posttraumatic stress disorder, not to mention outside factors – marginalization, discrimination, violence, abuse. When you add up all these intrinsic and extrinsic factors, it’s not hard to believe that there is a high rate of suicidality,” Dr. Ting said.
“There have been studies that have shown that in children who are supported in their gender identity, the rates of depression and anxiety decreased to almost the same levels as non-trans and nonbinary children, so I think that gives cause for hope,” Dr. Ting added.
The study was funded in part by the Research Council of Norway through its Centres of Excellence funding scheme and by a Frederick Banting and Charles Best Canada Graduate Scholarship Doctoral Award. Ms. Johnstone reports consulting fees from Spectrum Waterloo and volunteer participation with the Youth Suicide Prevention Leadership Committee of Ontario. No other competing interests were declared. Dr. Ting has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Transgender youth are significantly more likely to consider suicide and attempt it, compared with their cisgender peers, new research shows.
In a large population-based study, investigators found the increased risk of suicidality is partly because of bullying and cyberbullying experienced by transgender teens.
The findings are “extremely concerning and should be a wake-up call,” Ian Colman, PhD, with the University of Ottawa School of Epidemiology and Public Health, said in an interview.
Young people who are exploring their sexual identities may suffer from depression and anxiety, both about the reactions of their peers and families, as well as their own sense of self.
“These youth are highly marginalized and stigmatized in many corners of our society, and these findings highlight just how distressing these experiences can be,” Dr. Colman said.
The study was published online in the Canadian Medical Association Journal.
Sevenfold increased risk of attempted suicide
The risk of suicidal thoughts and actions is not well studied in transgender and nonbinary youth.
To expand the evidence base, the researchers analyzed data for 6,800 adolescents aged 15-17 years from the 2019 Canadian Health Survey on Children and Youth.
The sample included 1,130 (16.5%) adolescents who identified as having some degree of same-gender attraction, 265 (4.3%) who were unsure of their attraction (“questioning”), and 50 (0.6%) who were transgender, meaning they identified as being of a gender different from that assigned at birth.
Overall, 980 (14.0%) adolescents reported having thoughts of suicide in the prior year, and 480 (6.8%) had attempted suicide in their life.
Transgender youth were five times more likely to think about suicide and more than seven times more likely to have ever attempted suicide than cisgender, heterosexual peers.
Among cisgender adolescents, girls who were attracted to girls had 3.6 times the risk of suicidal ideation and 3.3 times the risk of having ever attempted suicide, compared with their heterosexual peers.
Teens attracted to multiple genders had more than twice the risk of suicidal ideation and suicide attempt. Youth who were questioning their sexual orientation had twice the risk of having attempted suicide in their lifetime.
A crisis – with reason for hope
“This is a crisis, and it shows just how much more needs to be done to support transgender young people,” co-author Fae Johnstone, MSW, executive director, Wisdom2Action, who is a trans woman herself, said in the news release.
“Suicide prevention programs specifically targeted to transgender, nonbinary, and sexual minority adolescents, as well as gender-affirming care for transgender adolescents, may help reduce the burden of suicidality among this group,” Ms. Johnstone added.
“The most important thing that parents, teachers, and health care providers can do is to be supportive of these youth,” Dr. Colman told this news organization.
“Providing a safe place where gender and sexual minorities can explore and express themselves is crucial. The first step is to listen and to be compassionate,” Dr. Colman added.
Reached for comment, Jess Ting, MD, director of surgery at the Mount Sinai Center for Transgender Medicine and Surgery, New York, said the data from this study on suicidal thoughts and actions among sexual minority and transgender adolescents “mirror what we see and what we know” about suicidality in trans and nonbinary adults.
“The reasons for this are complex, and it’s hard for someone who doesn’t have a lived experience as a trans or nonbinary person to understand the reasons for suicidality,” he told this news organization.
“But we also know that there are higher rates of anxiety and depression and self-image issues and posttraumatic stress disorder, not to mention outside factors – marginalization, discrimination, violence, abuse. When you add up all these intrinsic and extrinsic factors, it’s not hard to believe that there is a high rate of suicidality,” Dr. Ting said.
“There have been studies that have shown that in children who are supported in their gender identity, the rates of depression and anxiety decreased to almost the same levels as non-trans and nonbinary children, so I think that gives cause for hope,” Dr. Ting added.
The study was funded in part by the Research Council of Norway through its Centres of Excellence funding scheme and by a Frederick Banting and Charles Best Canada Graduate Scholarship Doctoral Award. Ms. Johnstone reports consulting fees from Spectrum Waterloo and volunteer participation with the Youth Suicide Prevention Leadership Committee of Ontario. No other competing interests were declared. Dr. Ting has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE CANADIAN MEDICAL ASSOCIATION JOURNAL
In utero COVID exposure tied to neurodevelopmental disorders at 1 year
Infants exposed to SARS-CoV-2 in utero are at increased risk for neurodevelopmental disorders in the first year of life, new research suggests.
But whether it is exposure to the pandemic or maternal exposure to the virus itself that may harm early childhood neurodevelopment is unclear, caution investigators, led by Roy Perlis, MD, MSc, with Massachusetts General Hospital, Boston.
“In this analysis of 222 offspring of mothers infected with SARS-CoV-2, compared with the offspring of 7,550 mothers in the control group (not infected) delivered during the same period, we observed neurodevelopmental diagnoses to be significantly more common among exposed offspring, particularly those exposed to third-trimester maternal infection,” they write.
The study was published online in JAMA Network Open.
Speech and language disorders
The study included 7,772 mostly singleton live births across six hospitals in Massachusetts between March and September 2020, including 222 (2.9%) births to mothers with SARS-CoV-2 infection confirmed by polymerase chain reaction testing during pregnancy.
In all, 14 of 222 children born to SARS-CoV-2–infected mothers (6.3%) were diagnosed with a neurodevelopmental disorder in the first year of life versus 227 of 7,550 unexposed offspring (3%) (unadjusted odds ratio, 2.17; 95% confidence interval, 1.24-3.79; P = .006).
In models adjusted for preterm delivery, as well as race, ethnicity, insurance status, child sex, and maternal age, COVID-exposed offspring were significantly more likely to receive a neurodevelopmental diagnosis in the first year of life (adjusted OR, 1.86; 95% CI, 1.03-3.36; P = .04).
The magnitude of the association with neurodevelopmental disorders was greater with third-trimester SARS-CoV-2 infection (aOR, 2.34; 95% CI, 1.23-4.44; P = .01).
The majority of these diagnoses reflected developmental disorders of motor function or speech and language.
The researchers noted that the finding of an association between prenatal SARS-CoV-2 exposure and neurodevelopmental diagnoses at 12 months is in line with a “large body of literature” linking maternal viral infection and maternal immune activation with offspring neurodevelopmental disorders later in life.
They cautioned, however, that whether a definitive connection exists between prenatal SARS-CoV-2 exposure and adverse neurodevelopment in offspring is not yet known, in part because children born to women infected in the first wave of the pandemic haven’t reached their second birthday – a time when neurodevelopment disorders such as autism are typically diagnosed.
There is also the risk for ascertainment bias arising from greater concern for offspring of infected mothers who were ill during pregnancy. These parents may be more inclined to seek evaluation, and clinicians may be more inclined to diagnose or refer for evaluation, the researchers noted.
Nonetheless, as reported by this news organization, the study results support those of research released at the European Psychiatric Association 2022 Congress; those results also showed an association between maternal SARS-CoV-2 infection and impaired neurodevelopment in 6-week-old infants.
Hypothesis generating
In an accompanying commentary, Torri D. Metz, MD, MS, with University of Utah Health, Salt Lake City, said the preliminary findings of Dr. Perlis and colleagues are “critically important, yet many questions remain.”
“Essentially all of what we know now about the effects of in utero exposure to maternal SARS-CoV-2 infection is from children who were exposed to the early and Alpha variants of SARS-CoV-2, as those are the only children now old enough to undergo rigorous neurodevelopmental assessments,” Dr. Metz pointed out.
Ultimately, Dr. Metz said it’s not surprising that the pandemic and in utero exposure to maternal SARS-CoV-2 infection may adversely affect neurodevelopmental outcomes in young children.
Yet, as a retrospective cohort study, the study can only demonstrate associations, not causality.
“This type of work is intended to be hypothesis generating, and that goal has been accomplished as these preliminary findings generate numerous additional research questions to explore,” Dr. Metz wrote.
Among them: Are there genetic predispositions to adverse outcomes? Will we observe differential effects by SARS-CoV-2 variant, by severity of infection, and by trimester of infection? Is it the virus itself or all of the societal changes that occurred during this period, including differences in how those changes were experienced among those with and without SARS-CoV-2?
“Perhaps the most important question is how do we intervene to help mitigate the adverse effects of the pandemic on young children,” Dr. Metz noted.
“Prospective studies to validate these findings, tease out some of the nuance, and identify those at highest risk will help health care practitioners appropriately dedicate resources to improve outcomes as we follow the life course of this generation of children born during the COVID-19 pandemic,” she added.
The study was supported by the National Institute of Mental Health and the National Institute of Child Health and Human Development. Dr. Perlis is an associate editor for JAMA Network Open but was not involved in the editorial review or decision for the study. Dr. Metz reported receiving personal fees and grants from Pfizer and grants from GestVision.
A version of this article first appeared on Medscape.com.
Infants exposed to SARS-CoV-2 in utero are at increased risk for neurodevelopmental disorders in the first year of life, new research suggests.
But whether it is exposure to the pandemic or maternal exposure to the virus itself that may harm early childhood neurodevelopment is unclear, caution investigators, led by Roy Perlis, MD, MSc, with Massachusetts General Hospital, Boston.
“In this analysis of 222 offspring of mothers infected with SARS-CoV-2, compared with the offspring of 7,550 mothers in the control group (not infected) delivered during the same period, we observed neurodevelopmental diagnoses to be significantly more common among exposed offspring, particularly those exposed to third-trimester maternal infection,” they write.
The study was published online in JAMA Network Open.
Speech and language disorders
The study included 7,772 mostly singleton live births across six hospitals in Massachusetts between March and September 2020, including 222 (2.9%) births to mothers with SARS-CoV-2 infection confirmed by polymerase chain reaction testing during pregnancy.
In all, 14 of 222 children born to SARS-CoV-2–infected mothers (6.3%) were diagnosed with a neurodevelopmental disorder in the first year of life versus 227 of 7,550 unexposed offspring (3%) (unadjusted odds ratio, 2.17; 95% confidence interval, 1.24-3.79; P = .006).
In models adjusted for preterm delivery, as well as race, ethnicity, insurance status, child sex, and maternal age, COVID-exposed offspring were significantly more likely to receive a neurodevelopmental diagnosis in the first year of life (adjusted OR, 1.86; 95% CI, 1.03-3.36; P = .04).
The magnitude of the association with neurodevelopmental disorders was greater with third-trimester SARS-CoV-2 infection (aOR, 2.34; 95% CI, 1.23-4.44; P = .01).
The majority of these diagnoses reflected developmental disorders of motor function or speech and language.
The researchers noted that the finding of an association between prenatal SARS-CoV-2 exposure and neurodevelopmental diagnoses at 12 months is in line with a “large body of literature” linking maternal viral infection and maternal immune activation with offspring neurodevelopmental disorders later in life.
They cautioned, however, that whether a definitive connection exists between prenatal SARS-CoV-2 exposure and adverse neurodevelopment in offspring is not yet known, in part because children born to women infected in the first wave of the pandemic haven’t reached their second birthday – a time when neurodevelopment disorders such as autism are typically diagnosed.
There is also the risk for ascertainment bias arising from greater concern for offspring of infected mothers who were ill during pregnancy. These parents may be more inclined to seek evaluation, and clinicians may be more inclined to diagnose or refer for evaluation, the researchers noted.
Nonetheless, as reported by this news organization, the study results support those of research released at the European Psychiatric Association 2022 Congress; those results also showed an association between maternal SARS-CoV-2 infection and impaired neurodevelopment in 6-week-old infants.
Hypothesis generating
In an accompanying commentary, Torri D. Metz, MD, MS, with University of Utah Health, Salt Lake City, said the preliminary findings of Dr. Perlis and colleagues are “critically important, yet many questions remain.”
“Essentially all of what we know now about the effects of in utero exposure to maternal SARS-CoV-2 infection is from children who were exposed to the early and Alpha variants of SARS-CoV-2, as those are the only children now old enough to undergo rigorous neurodevelopmental assessments,” Dr. Metz pointed out.
Ultimately, Dr. Metz said it’s not surprising that the pandemic and in utero exposure to maternal SARS-CoV-2 infection may adversely affect neurodevelopmental outcomes in young children.
Yet, as a retrospective cohort study, the study can only demonstrate associations, not causality.
“This type of work is intended to be hypothesis generating, and that goal has been accomplished as these preliminary findings generate numerous additional research questions to explore,” Dr. Metz wrote.
Among them: Are there genetic predispositions to adverse outcomes? Will we observe differential effects by SARS-CoV-2 variant, by severity of infection, and by trimester of infection? Is it the virus itself or all of the societal changes that occurred during this period, including differences in how those changes were experienced among those with and without SARS-CoV-2?
“Perhaps the most important question is how do we intervene to help mitigate the adverse effects of the pandemic on young children,” Dr. Metz noted.
“Prospective studies to validate these findings, tease out some of the nuance, and identify those at highest risk will help health care practitioners appropriately dedicate resources to improve outcomes as we follow the life course of this generation of children born during the COVID-19 pandemic,” she added.
The study was supported by the National Institute of Mental Health and the National Institute of Child Health and Human Development. Dr. Perlis is an associate editor for JAMA Network Open but was not involved in the editorial review or decision for the study. Dr. Metz reported receiving personal fees and grants from Pfizer and grants from GestVision.
A version of this article first appeared on Medscape.com.
Infants exposed to SARS-CoV-2 in utero are at increased risk for neurodevelopmental disorders in the first year of life, new research suggests.
But whether it is exposure to the pandemic or maternal exposure to the virus itself that may harm early childhood neurodevelopment is unclear, caution investigators, led by Roy Perlis, MD, MSc, with Massachusetts General Hospital, Boston.
“In this analysis of 222 offspring of mothers infected with SARS-CoV-2, compared with the offspring of 7,550 mothers in the control group (not infected) delivered during the same period, we observed neurodevelopmental diagnoses to be significantly more common among exposed offspring, particularly those exposed to third-trimester maternal infection,” they write.
The study was published online in JAMA Network Open.
Speech and language disorders
The study included 7,772 mostly singleton live births across six hospitals in Massachusetts between March and September 2020, including 222 (2.9%) births to mothers with SARS-CoV-2 infection confirmed by polymerase chain reaction testing during pregnancy.
In all, 14 of 222 children born to SARS-CoV-2–infected mothers (6.3%) were diagnosed with a neurodevelopmental disorder in the first year of life versus 227 of 7,550 unexposed offspring (3%) (unadjusted odds ratio, 2.17; 95% confidence interval, 1.24-3.79; P = .006).
In models adjusted for preterm delivery, as well as race, ethnicity, insurance status, child sex, and maternal age, COVID-exposed offspring were significantly more likely to receive a neurodevelopmental diagnosis in the first year of life (adjusted OR, 1.86; 95% CI, 1.03-3.36; P = .04).
The magnitude of the association with neurodevelopmental disorders was greater with third-trimester SARS-CoV-2 infection (aOR, 2.34; 95% CI, 1.23-4.44; P = .01).
The majority of these diagnoses reflected developmental disorders of motor function or speech and language.
The researchers noted that the finding of an association between prenatal SARS-CoV-2 exposure and neurodevelopmental diagnoses at 12 months is in line with a “large body of literature” linking maternal viral infection and maternal immune activation with offspring neurodevelopmental disorders later in life.
They cautioned, however, that whether a definitive connection exists between prenatal SARS-CoV-2 exposure and adverse neurodevelopment in offspring is not yet known, in part because children born to women infected in the first wave of the pandemic haven’t reached their second birthday – a time when neurodevelopment disorders such as autism are typically diagnosed.
There is also the risk for ascertainment bias arising from greater concern for offspring of infected mothers who were ill during pregnancy. These parents may be more inclined to seek evaluation, and clinicians may be more inclined to diagnose or refer for evaluation, the researchers noted.
Nonetheless, as reported by this news organization, the study results support those of research released at the European Psychiatric Association 2022 Congress; those results also showed an association between maternal SARS-CoV-2 infection and impaired neurodevelopment in 6-week-old infants.
Hypothesis generating
In an accompanying commentary, Torri D. Metz, MD, MS, with University of Utah Health, Salt Lake City, said the preliminary findings of Dr. Perlis and colleagues are “critically important, yet many questions remain.”
“Essentially all of what we know now about the effects of in utero exposure to maternal SARS-CoV-2 infection is from children who were exposed to the early and Alpha variants of SARS-CoV-2, as those are the only children now old enough to undergo rigorous neurodevelopmental assessments,” Dr. Metz pointed out.
Ultimately, Dr. Metz said it’s not surprising that the pandemic and in utero exposure to maternal SARS-CoV-2 infection may adversely affect neurodevelopmental outcomes in young children.
Yet, as a retrospective cohort study, the study can only demonstrate associations, not causality.
“This type of work is intended to be hypothesis generating, and that goal has been accomplished as these preliminary findings generate numerous additional research questions to explore,” Dr. Metz wrote.
Among them: Are there genetic predispositions to adverse outcomes? Will we observe differential effects by SARS-CoV-2 variant, by severity of infection, and by trimester of infection? Is it the virus itself or all of the societal changes that occurred during this period, including differences in how those changes were experienced among those with and without SARS-CoV-2?
“Perhaps the most important question is how do we intervene to help mitigate the adverse effects of the pandemic on young children,” Dr. Metz noted.
“Prospective studies to validate these findings, tease out some of the nuance, and identify those at highest risk will help health care practitioners appropriately dedicate resources to improve outcomes as we follow the life course of this generation of children born during the COVID-19 pandemic,” she added.
The study was supported by the National Institute of Mental Health and the National Institute of Child Health and Human Development. Dr. Perlis is an associate editor for JAMA Network Open but was not involved in the editorial review or decision for the study. Dr. Metz reported receiving personal fees and grants from Pfizer and grants from GestVision.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Surprising link between herpes zoster and dementia
Herpes zoster does not appear to increase dementia risk – on the contrary, the viral infection may offer some protection, a large population-based study suggests.
“We were surprised by these results [and] the reasons for the decreased risk are unclear,” study author Sigrun Alba Johannesdottir Schmidt, MD, PhD, with Aarhus (Denmark) University Hospital, said in a news release.
The study was published online in Neurology.
Conflicting findings
Herpes zoster (HZ) is an acute, cutaneous viral infection caused by the reactivation of varicella-zoster virus (VZV). Previous population-based studies have reported both decreased and increased risks of dementia after having HZ.
It’s thought that HZ may contribute to the development of dementia through neuroinflammation, cerebral vasculopathy, or direct neural damage, but epidemiologic evidence is limited.
To investigate further, Dr. Schmidt and colleagues used Danish medical registries to identify 247,305 people who had visited a hospital for HZ or were prescribed antiviral medication for HZ over a 20-year period and matched them to 1,235,890 people who did not have HZ. For both cohorts, the median age was 64 years, and 61% were women.
Dementia was diagnosed in 9.7% of zoster patients and 10.3% of matched control persons during up to 21 years of follow-up.
Contrary to the researchers’ expectation, HZ was associated with a small (7%) decreased relative risk of all-cause dementia during follow-up (hazard ratio, 0.93; 95% confidence interval, 0.90-0.95).
There was no increased long-term risk of dementia in subgroup analyses, except possibly among those with HZ that involved the central nervous system (HR, 1.94; 95% CI, 0.78-4.80), which has been shown before.
However, the population attributable fraction of dementia caused by this rare complication is low (< 1%), suggesting that universal vaccination against VZV in the elderly has limited potential to reduce dementia risk, the investigators noted.
Nonetheless, Dr. Schmidt said shingles vaccination should be encouraged in older people because it can prevent complications from the disease.
The research team admitted that the slightly decreased long-term risk of dementia, including Alzheimer’s disease, was “unexpected.” The reasons for this decreased risk are unclear, they say, and could be explained by missed diagnoses of shingles in people with undiagnosed dementia.
They were not able to examine whether antiviral treatment modifies the association between HZ and dementia and said that this topic merits further research.
The study was supported by the Edel and Wilhelm Daubenmerkls Charitable Foundation. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Herpes zoster does not appear to increase dementia risk – on the contrary, the viral infection may offer some protection, a large population-based study suggests.
“We were surprised by these results [and] the reasons for the decreased risk are unclear,” study author Sigrun Alba Johannesdottir Schmidt, MD, PhD, with Aarhus (Denmark) University Hospital, said in a news release.
The study was published online in Neurology.
Conflicting findings
Herpes zoster (HZ) is an acute, cutaneous viral infection caused by the reactivation of varicella-zoster virus (VZV). Previous population-based studies have reported both decreased and increased risks of dementia after having HZ.
It’s thought that HZ may contribute to the development of dementia through neuroinflammation, cerebral vasculopathy, or direct neural damage, but epidemiologic evidence is limited.
To investigate further, Dr. Schmidt and colleagues used Danish medical registries to identify 247,305 people who had visited a hospital for HZ or were prescribed antiviral medication for HZ over a 20-year period and matched them to 1,235,890 people who did not have HZ. For both cohorts, the median age was 64 years, and 61% were women.
Dementia was diagnosed in 9.7% of zoster patients and 10.3% of matched control persons during up to 21 years of follow-up.
Contrary to the researchers’ expectation, HZ was associated with a small (7%) decreased relative risk of all-cause dementia during follow-up (hazard ratio, 0.93; 95% confidence interval, 0.90-0.95).
There was no increased long-term risk of dementia in subgroup analyses, except possibly among those with HZ that involved the central nervous system (HR, 1.94; 95% CI, 0.78-4.80), which has been shown before.
However, the population attributable fraction of dementia caused by this rare complication is low (< 1%), suggesting that universal vaccination against VZV in the elderly has limited potential to reduce dementia risk, the investigators noted.
Nonetheless, Dr. Schmidt said shingles vaccination should be encouraged in older people because it can prevent complications from the disease.
The research team admitted that the slightly decreased long-term risk of dementia, including Alzheimer’s disease, was “unexpected.” The reasons for this decreased risk are unclear, they say, and could be explained by missed diagnoses of shingles in people with undiagnosed dementia.
They were not able to examine whether antiviral treatment modifies the association between HZ and dementia and said that this topic merits further research.
The study was supported by the Edel and Wilhelm Daubenmerkls Charitable Foundation. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Herpes zoster does not appear to increase dementia risk – on the contrary, the viral infection may offer some protection, a large population-based study suggests.
“We were surprised by these results [and] the reasons for the decreased risk are unclear,” study author Sigrun Alba Johannesdottir Schmidt, MD, PhD, with Aarhus (Denmark) University Hospital, said in a news release.
The study was published online in Neurology.
Conflicting findings
Herpes zoster (HZ) is an acute, cutaneous viral infection caused by the reactivation of varicella-zoster virus (VZV). Previous population-based studies have reported both decreased and increased risks of dementia after having HZ.
It’s thought that HZ may contribute to the development of dementia through neuroinflammation, cerebral vasculopathy, or direct neural damage, but epidemiologic evidence is limited.
To investigate further, Dr. Schmidt and colleagues used Danish medical registries to identify 247,305 people who had visited a hospital for HZ or were prescribed antiviral medication for HZ over a 20-year period and matched them to 1,235,890 people who did not have HZ. For both cohorts, the median age was 64 years, and 61% were women.
Dementia was diagnosed in 9.7% of zoster patients and 10.3% of matched control persons during up to 21 years of follow-up.
Contrary to the researchers’ expectation, HZ was associated with a small (7%) decreased relative risk of all-cause dementia during follow-up (hazard ratio, 0.93; 95% confidence interval, 0.90-0.95).
There was no increased long-term risk of dementia in subgroup analyses, except possibly among those with HZ that involved the central nervous system (HR, 1.94; 95% CI, 0.78-4.80), which has been shown before.
However, the population attributable fraction of dementia caused by this rare complication is low (< 1%), suggesting that universal vaccination against VZV in the elderly has limited potential to reduce dementia risk, the investigators noted.
Nonetheless, Dr. Schmidt said shingles vaccination should be encouraged in older people because it can prevent complications from the disease.
The research team admitted that the slightly decreased long-term risk of dementia, including Alzheimer’s disease, was “unexpected.” The reasons for this decreased risk are unclear, they say, and could be explained by missed diagnoses of shingles in people with undiagnosed dementia.
They were not able to examine whether antiviral treatment modifies the association between HZ and dementia and said that this topic merits further research.
The study was supported by the Edel and Wilhelm Daubenmerkls Charitable Foundation. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID tied to a profound impact on children’s sleep
During the first year of the pandemic, profound changes in screen use and sleep timing occurred among U.S. adolescents as a result of spending more time using electronic devices, going to bed later, and getting up later, compared with before the pandemic, new research indicates.
The excessive screen time negatively affected sleep, said lead investigator Orsolya Kiss, PhD, with the Center for Health Sciences at SRI International, Menlo Park, Calif.
And what’s “concerning,” she told this news organization, is that there is no indication of any spontaneous decline in screen use in 2021, when there were fewer restrictions.
Dr. Kiss said she is “very much interested to see what future studies will show.”
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Sleep takes a pandemic hit
“Adolescents and families have turned to online activities and social platforms more than ever before to maintain wellbeing, [to] connect with friends and family, and for online schooling,” Dr. Kiss said in a conference statement.
She and her colleagues examined longitudinal data from 5,027 adolescents aged 11-14 years who are participating in the ongoing Adolescent Brain Cognitive Development (ABCD) study.
As part of the study, participants reported sleep and daily screen time use prior to and at six time points during the first year of the pandemic (May 2020 to March 2021).
During the first year of the pandemic, relative to before the pandemic, recreational screen time was dramatically higher, with adolescents spending about 45 minutes more on social media and 20 minutes more playing video games, Dr. Kiss reported.
The jump in screen time was coupled with changes in sleep patterns.
Adolescents’ wake up times were delayed about 1.5 hours during May and August 2020, relative to prepandemic levels. The delay was partly due to summer break; wake-up times returned to earlier times in the fall of 2020.
During all pandemic assessments, bedtimes were delayed by about 1 hour, even when the new school year started. This was particularly the case in older adolescents and girls.
The findings highlight the need to promote “balanced and informed use of social media platforms, video games, and other digital technology to ensure adequate opportunity to sleep and maintain other healthy behaviors during this critical period of developmental change,” the authors wrote in their conference abstract.
Mental illness risk
In an interview, Ruth Benca, MD, PhD, co-chair of the Alliance for Sleep, noted that “during adolescence, the tendency to become more of a night owl naturally worsens, and when kids have no sleep schedule imposed on them, these patterns become exacerbated.”
Dr. Benca, who was not involved in the study, also noted that altered sleep patterns are risk factors for psychiatric illness.
“Adolescence, in particular, is so critical for brain development, and it really raises the question of whether sleep disturbances in adolescence or poor sleep patterns are contributing to the increase psychiatric epidemic we’re seeing in adolescents and children these days,” said Dr. Benca, with Wake Forest University School of Medicine and Atrium Health Wake Forest Baptist, Winston-Salem, N.C.
Also weighing in on the study, journalist and author Lisa Lewis, MS, based in Southern California, said, “It’s not surprising that tech use and social media – which is such an important part of their social worlds – went up during the pandemic.”
Ms. Lewis, a parent of two teenagers, played a key role in California’s new healthy school start times law, the first of its kind in the nation, and is the author of the newly released book, The Sleep-Deprived Teen (Mango Publishing).
“Far too many adolescents aren’t getting anywhere close to the 8-10 hours of nightly sleep they need,” Ms. Lewis said in an interview.
She noted that the the American Academy of Pediatrics recommends no tech use an hour before bed.
“And there are other house rules parents can implement, such as charging all devices in a central location, like the kitchen. Making sleep a priority helps teens, but it helps parents too: No one functions well when they’re sleep-deprived,” Ms. Lewis added.
Support for the study was provided by the National Institutes of Health. The authors have disclosed no relevant financial relationships. Dr. Benca is a consultant for Idorsia Pharmaceuticals. Ms. Lewis has no relevant disclosures.
A version of this article first appeared on Medscape.com.
During the first year of the pandemic, profound changes in screen use and sleep timing occurred among U.S. adolescents as a result of spending more time using electronic devices, going to bed later, and getting up later, compared with before the pandemic, new research indicates.
The excessive screen time negatively affected sleep, said lead investigator Orsolya Kiss, PhD, with the Center for Health Sciences at SRI International, Menlo Park, Calif.
And what’s “concerning,” she told this news organization, is that there is no indication of any spontaneous decline in screen use in 2021, when there were fewer restrictions.
Dr. Kiss said she is “very much interested to see what future studies will show.”
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Sleep takes a pandemic hit
“Adolescents and families have turned to online activities and social platforms more than ever before to maintain wellbeing, [to] connect with friends and family, and for online schooling,” Dr. Kiss said in a conference statement.
She and her colleagues examined longitudinal data from 5,027 adolescents aged 11-14 years who are participating in the ongoing Adolescent Brain Cognitive Development (ABCD) study.
As part of the study, participants reported sleep and daily screen time use prior to and at six time points during the first year of the pandemic (May 2020 to March 2021).
During the first year of the pandemic, relative to before the pandemic, recreational screen time was dramatically higher, with adolescents spending about 45 minutes more on social media and 20 minutes more playing video games, Dr. Kiss reported.
The jump in screen time was coupled with changes in sleep patterns.
Adolescents’ wake up times were delayed about 1.5 hours during May and August 2020, relative to prepandemic levels. The delay was partly due to summer break; wake-up times returned to earlier times in the fall of 2020.
During all pandemic assessments, bedtimes were delayed by about 1 hour, even when the new school year started. This was particularly the case in older adolescents and girls.
The findings highlight the need to promote “balanced and informed use of social media platforms, video games, and other digital technology to ensure adequate opportunity to sleep and maintain other healthy behaviors during this critical period of developmental change,” the authors wrote in their conference abstract.
Mental illness risk
In an interview, Ruth Benca, MD, PhD, co-chair of the Alliance for Sleep, noted that “during adolescence, the tendency to become more of a night owl naturally worsens, and when kids have no sleep schedule imposed on them, these patterns become exacerbated.”
Dr. Benca, who was not involved in the study, also noted that altered sleep patterns are risk factors for psychiatric illness.
“Adolescence, in particular, is so critical for brain development, and it really raises the question of whether sleep disturbances in adolescence or poor sleep patterns are contributing to the increase psychiatric epidemic we’re seeing in adolescents and children these days,” said Dr. Benca, with Wake Forest University School of Medicine and Atrium Health Wake Forest Baptist, Winston-Salem, N.C.
Also weighing in on the study, journalist and author Lisa Lewis, MS, based in Southern California, said, “It’s not surprising that tech use and social media – which is such an important part of their social worlds – went up during the pandemic.”
Ms. Lewis, a parent of two teenagers, played a key role in California’s new healthy school start times law, the first of its kind in the nation, and is the author of the newly released book, The Sleep-Deprived Teen (Mango Publishing).
“Far too many adolescents aren’t getting anywhere close to the 8-10 hours of nightly sleep they need,” Ms. Lewis said in an interview.
She noted that the the American Academy of Pediatrics recommends no tech use an hour before bed.
“And there are other house rules parents can implement, such as charging all devices in a central location, like the kitchen. Making sleep a priority helps teens, but it helps parents too: No one functions well when they’re sleep-deprived,” Ms. Lewis added.
Support for the study was provided by the National Institutes of Health. The authors have disclosed no relevant financial relationships. Dr. Benca is a consultant for Idorsia Pharmaceuticals. Ms. Lewis has no relevant disclosures.
A version of this article first appeared on Medscape.com.
During the first year of the pandemic, profound changes in screen use and sleep timing occurred among U.S. adolescents as a result of spending more time using electronic devices, going to bed later, and getting up later, compared with before the pandemic, new research indicates.
The excessive screen time negatively affected sleep, said lead investigator Orsolya Kiss, PhD, with the Center for Health Sciences at SRI International, Menlo Park, Calif.
And what’s “concerning,” she told this news organization, is that there is no indication of any spontaneous decline in screen use in 2021, when there were fewer restrictions.
Dr. Kiss said she is “very much interested to see what future studies will show.”
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Sleep takes a pandemic hit
“Adolescents and families have turned to online activities and social platforms more than ever before to maintain wellbeing, [to] connect with friends and family, and for online schooling,” Dr. Kiss said in a conference statement.
She and her colleagues examined longitudinal data from 5,027 adolescents aged 11-14 years who are participating in the ongoing Adolescent Brain Cognitive Development (ABCD) study.
As part of the study, participants reported sleep and daily screen time use prior to and at six time points during the first year of the pandemic (May 2020 to March 2021).
During the first year of the pandemic, relative to before the pandemic, recreational screen time was dramatically higher, with adolescents spending about 45 minutes more on social media and 20 minutes more playing video games, Dr. Kiss reported.
The jump in screen time was coupled with changes in sleep patterns.
Adolescents’ wake up times were delayed about 1.5 hours during May and August 2020, relative to prepandemic levels. The delay was partly due to summer break; wake-up times returned to earlier times in the fall of 2020.
During all pandemic assessments, bedtimes were delayed by about 1 hour, even when the new school year started. This was particularly the case in older adolescents and girls.
The findings highlight the need to promote “balanced and informed use of social media platforms, video games, and other digital technology to ensure adequate opportunity to sleep and maintain other healthy behaviors during this critical period of developmental change,” the authors wrote in their conference abstract.
Mental illness risk
In an interview, Ruth Benca, MD, PhD, co-chair of the Alliance for Sleep, noted that “during adolescence, the tendency to become more of a night owl naturally worsens, and when kids have no sleep schedule imposed on them, these patterns become exacerbated.”
Dr. Benca, who was not involved in the study, also noted that altered sleep patterns are risk factors for psychiatric illness.
“Adolescence, in particular, is so critical for brain development, and it really raises the question of whether sleep disturbances in adolescence or poor sleep patterns are contributing to the increase psychiatric epidemic we’re seeing in adolescents and children these days,” said Dr. Benca, with Wake Forest University School of Medicine and Atrium Health Wake Forest Baptist, Winston-Salem, N.C.
Also weighing in on the study, journalist and author Lisa Lewis, MS, based in Southern California, said, “It’s not surprising that tech use and social media – which is such an important part of their social worlds – went up during the pandemic.”
Ms. Lewis, a parent of two teenagers, played a key role in California’s new healthy school start times law, the first of its kind in the nation, and is the author of the newly released book, The Sleep-Deprived Teen (Mango Publishing).
“Far too many adolescents aren’t getting anywhere close to the 8-10 hours of nightly sleep they need,” Ms. Lewis said in an interview.
She noted that the the American Academy of Pediatrics recommends no tech use an hour before bed.
“And there are other house rules parents can implement, such as charging all devices in a central location, like the kitchen. Making sleep a priority helps teens, but it helps parents too: No one functions well when they’re sleep-deprived,” Ms. Lewis added.
Support for the study was provided by the National Institutes of Health. The authors have disclosed no relevant financial relationships. Dr. Benca is a consultant for Idorsia Pharmaceuticals. Ms. Lewis has no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SLEEP 2022