User login
Shades of gray
If you were born in or after the 1970s, it is very likely that you have never watched a television show on a black and white set. Although the roots of its technology extend well back into the early 20th century, the first color broadcast on a national television network didn’t occur until 1954 with NBC’s coverage of the Tournament of Roses Parade.
When we compare the popularization of color television with the rapid pace at which we adopt new technology today, the popularization of color TV was glacial. In large part because of their expense, sales of color sets did not surpass black and white sets until 1972. Our family lagged behind the curve and finally caved in and junked our black and white television around 1977.
The observable change in our viewing behavior was dramatic. While programming in black and white was interesting, the color images were magnetic. We were drawn by the visual excitement and stimulation that color offered, and our family’s viewing standards took a precipitous dip. We seemed to watch anything that was colorful and moved. The quality of the content took a back seat. Viewing in color seemed to require much less cognitive effort. Ironically what attracted our attention allowed us to invest less energy in paying attention.
As a regular reader of Letters From Maine, you know that I am convinced that sleep deprivation is a major contributor to the emergence of the ADHD phenomenon. However, I can make a similar argument that the introduction of color television is an equally potent coconspirator or confounder. The magnetism inherent in a moving color image can tempt even the most health conscious among us to stay well past a brain-friendly bedtime. The invention of the electric light may have gotten the ball rolling, but the ubiquity of moving electronic color images has certainly greased what was already a very slippery slope into an abyss of unhealthy sleep habits.
There are those who argue that smartphones and tablets can open a world of creative opportunities for even very young children. And, it is obvious that parents are struggling to find a balance as they try to decide when, where, and how often to allow their infants and toddlers access to handheld electronic devices.
Recently there has been much finger-pointing at the developers and manufacturers of smartphones and tablets. How can any company with a social conscience sell a product with such dangerous attractive potential for children without providing safeguards? Isn’t it like selling a swimming pool without a gated fence?
Of course the answer to this question goes to the heart of how our society views its responsibility to protect its children. Regardless of who makes the rules and how the responsibility is assigned, it is still the child’s parents who must make sure that the gate is locked.

Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
If you were born in or after the 1970s, it is very likely that you have never watched a television show on a black and white set. Although the roots of its technology extend well back into the early 20th century, the first color broadcast on a national television network didn’t occur until 1954 with NBC’s coverage of the Tournament of Roses Parade.
When we compare the popularization of color television with the rapid pace at which we adopt new technology today, the popularization of color TV was glacial. In large part because of their expense, sales of color sets did not surpass black and white sets until 1972. Our family lagged behind the curve and finally caved in and junked our black and white television around 1977.
The observable change in our viewing behavior was dramatic. While programming in black and white was interesting, the color images were magnetic. We were drawn by the visual excitement and stimulation that color offered, and our family’s viewing standards took a precipitous dip. We seemed to watch anything that was colorful and moved. The quality of the content took a back seat. Viewing in color seemed to require much less cognitive effort. Ironically what attracted our attention allowed us to invest less energy in paying attention.
As a regular reader of Letters From Maine, you know that I am convinced that sleep deprivation is a major contributor to the emergence of the ADHD phenomenon. However, I can make a similar argument that the introduction of color television is an equally potent coconspirator or confounder. The magnetism inherent in a moving color image can tempt even the most health conscious among us to stay well past a brain-friendly bedtime. The invention of the electric light may have gotten the ball rolling, but the ubiquity of moving electronic color images has certainly greased what was already a very slippery slope into an abyss of unhealthy sleep habits.
There are those who argue that smartphones and tablets can open a world of creative opportunities for even very young children. And, it is obvious that parents are struggling to find a balance as they try to decide when, where, and how often to allow their infants and toddlers access to handheld electronic devices.
Recently there has been much finger-pointing at the developers and manufacturers of smartphones and tablets. How can any company with a social conscience sell a product with such dangerous attractive potential for children without providing safeguards? Isn’t it like selling a swimming pool without a gated fence?
Of course the answer to this question goes to the heart of how our society views its responsibility to protect its children. Regardless of who makes the rules and how the responsibility is assigned, it is still the child’s parents who must make sure that the gate is locked.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
If you were born in or after the 1970s, it is very likely that you have never watched a television show on a black and white set. Although the roots of its technology extend well back into the early 20th century, the first color broadcast on a national television network didn’t occur until 1954 with NBC’s coverage of the Tournament of Roses Parade.
When we compare the popularization of color television with the rapid pace at which we adopt new technology today, the popularization of color TV was glacial. In large part because of their expense, sales of color sets did not surpass black and white sets until 1972. Our family lagged behind the curve and finally caved in and junked our black and white television around 1977.
The observable change in our viewing behavior was dramatic. While programming in black and white was interesting, the color images were magnetic. We were drawn by the visual excitement and stimulation that color offered, and our family’s viewing standards took a precipitous dip. We seemed to watch anything that was colorful and moved. The quality of the content took a back seat. Viewing in color seemed to require much less cognitive effort. Ironically what attracted our attention allowed us to invest less energy in paying attention.
As a regular reader of Letters From Maine, you know that I am convinced that sleep deprivation is a major contributor to the emergence of the ADHD phenomenon. However, I can make a similar argument that the introduction of color television is an equally potent coconspirator or confounder. The magnetism inherent in a moving color image can tempt even the most health conscious among us to stay well past a brain-friendly bedtime. The invention of the electric light may have gotten the ball rolling, but the ubiquity of moving electronic color images has certainly greased what was already a very slippery slope into an abyss of unhealthy sleep habits.
There are those who argue that smartphones and tablets can open a world of creative opportunities for even very young children. And, it is obvious that parents are struggling to find a balance as they try to decide when, where, and how often to allow their infants and toddlers access to handheld electronic devices.
Recently there has been much finger-pointing at the developers and manufacturers of smartphones and tablets. How can any company with a social conscience sell a product with such dangerous attractive potential for children without providing safeguards? Isn’t it like selling a swimming pool without a gated fence?
Of course the answer to this question goes to the heart of how our society views its responsibility to protect its children. Regardless of who makes the rules and how the responsibility is assigned, it is still the child’s parents who must make sure that the gate is locked.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Integrating behavioral health into primary care
This is the sixth in a series of articles from the National Center for Excellence in Primary Care Research in the Agency for Healthcare Research and Quality. This series introduces sets of tools and resources designed to help your practice.
Primary care practice is under increasing pressure to evolve. As highlighted in this series, topics such as shared decision making, team-based care, integration of behavioral health into primary care practice, and practice facilitation all offer the potential to enhance your primary care practice. On the other hand, quality of care must remain a top priority during this transformation. While much of the Agency for Healthcare Research and Quality’s (AHRQ) work in quality of care focuses on the inpatient setting, AHRQ offers many tools and resources to evaluate quality of care and to implement quality improvement into your primary care practice.

The NQMC mission is to provide an accessible mechanism for obtaining detailed information on quality measures and to further the dissemination, implementation, and use of these measures to inform health care decisions. NQMC is designed for practitioners, health care providers, health plans, integrated delivery systems, purchasers, and others interested in health care quality measurement. Funding for the NQMC is in question, and the future of this resource is not certain.
Confidential feedback reporting is widely considered to be a precursor to and a foundation for performance improvement. However, to enable change, the clinician responsible for and capable of change must receive, understand, and act on the information. The following publications from the National Center for Excellence in Primary Care Research offer some guidance from the on ways to best do so:
- Confidential Physician Feedback Reports: Designing for Optimal Impact on Performance is a guide that informs developers of feedback reports about evidence-based strategies to consider when they develop or refine a feedback reporting system.
- Will It Work Here? A Decisionmaker’s Guide to Adopting Innovations can help you determine if an innovation would be a good fit – or an appropriate stretch – for your practice or health care organization by asking a series of questions. It links users to actionable Web-based tools and presents case studies that illustrate how other organizations have addressed these questions.
- Improving Your Office Testing Process: A Toolkit for Rapid-Cycle Patient Safety and Quality Improvement provides information and resources to help physicians’ offices, clinics, and other ambulatory care facilities assess and improve the testing process in their offices.
These and other tools can be found at the AHRQ website.
Dr. Ganiats is the director for the National Center for Excellence in Primary Care Research at AHRQ.
This is the sixth in a series of articles from the National Center for Excellence in Primary Care Research in the Agency for Healthcare Research and Quality. This series introduces sets of tools and resources designed to help your practice.
Primary care practice is under increasing pressure to evolve. As highlighted in this series, topics such as shared decision making, team-based care, integration of behavioral health into primary care practice, and practice facilitation all offer the potential to enhance your primary care practice. On the other hand, quality of care must remain a top priority during this transformation. While much of the Agency for Healthcare Research and Quality’s (AHRQ) work in quality of care focuses on the inpatient setting, AHRQ offers many tools and resources to evaluate quality of care and to implement quality improvement into your primary care practice.
The NQMC mission is to provide an accessible mechanism for obtaining detailed information on quality measures and to further the dissemination, implementation, and use of these measures to inform health care decisions. NQMC is designed for practitioners, health care providers, health plans, integrated delivery systems, purchasers, and others interested in health care quality measurement. Funding for the NQMC is in question, and the future of this resource is not certain.
Confidential feedback reporting is widely considered to be a precursor to and a foundation for performance improvement. However, to enable change, the clinician responsible for and capable of change must receive, understand, and act on the information. The following publications from the National Center for Excellence in Primary Care Research offer some guidance from the on ways to best do so:
- Confidential Physician Feedback Reports: Designing for Optimal Impact on Performance is a guide that informs developers of feedback reports about evidence-based strategies to consider when they develop or refine a feedback reporting system.
- Will It Work Here? A Decisionmaker’s Guide to Adopting Innovations can help you determine if an innovation would be a good fit – or an appropriate stretch – for your practice or health care organization by asking a series of questions. It links users to actionable Web-based tools and presents case studies that illustrate how other organizations have addressed these questions.
- Improving Your Office Testing Process: A Toolkit for Rapid-Cycle Patient Safety and Quality Improvement provides information and resources to help physicians’ offices, clinics, and other ambulatory care facilities assess and improve the testing process in their offices.
These and other tools can be found at the AHRQ website.
Dr. Ganiats is the director for the National Center for Excellence in Primary Care Research at AHRQ.
This is the sixth in a series of articles from the National Center for Excellence in Primary Care Research in the Agency for Healthcare Research and Quality. This series introduces sets of tools and resources designed to help your practice.
Primary care practice is under increasing pressure to evolve. As highlighted in this series, topics such as shared decision making, team-based care, integration of behavioral health into primary care practice, and practice facilitation all offer the potential to enhance your primary care practice. On the other hand, quality of care must remain a top priority during this transformation. While much of the Agency for Healthcare Research and Quality’s (AHRQ) work in quality of care focuses on the inpatient setting, AHRQ offers many tools and resources to evaluate quality of care and to implement quality improvement into your primary care practice.
The NQMC mission is to provide an accessible mechanism for obtaining detailed information on quality measures and to further the dissemination, implementation, and use of these measures to inform health care decisions. NQMC is designed for practitioners, health care providers, health plans, integrated delivery systems, purchasers, and others interested in health care quality measurement. Funding for the NQMC is in question, and the future of this resource is not certain.
Confidential feedback reporting is widely considered to be a precursor to and a foundation for performance improvement. However, to enable change, the clinician responsible for and capable of change must receive, understand, and act on the information. The following publications from the National Center for Excellence in Primary Care Research offer some guidance from the on ways to best do so:
- Confidential Physician Feedback Reports: Designing for Optimal Impact on Performance is a guide that informs developers of feedback reports about evidence-based strategies to consider when they develop or refine a feedback reporting system.
- Will It Work Here? A Decisionmaker’s Guide to Adopting Innovations can help you determine if an innovation would be a good fit – or an appropriate stretch – for your practice or health care organization by asking a series of questions. It links users to actionable Web-based tools and presents case studies that illustrate how other organizations have addressed these questions.
- Improving Your Office Testing Process: A Toolkit for Rapid-Cycle Patient Safety and Quality Improvement provides information and resources to help physicians’ offices, clinics, and other ambulatory care facilities assess and improve the testing process in their offices.
These and other tools can be found at the AHRQ website.
Dr. Ganiats is the director for the National Center for Excellence in Primary Care Research at AHRQ.
Making hospital medicine a lifelong, enjoyable, and engaging career
Editor’s note: Each month, the Society of Hospital Medicine puts the spotlight on some of our most active members who are making substantial contributions to hospital medicine. Visit www.hospitalmedicine.org for more information on how you can lend your expertise to help SHM improve the care of hospitalized patients.
This month, The Hospitalist spotlights Amith Skandhan, MD, FHM, a hospitalist, a director/physician liaison for clinical documentation improvement and core faculty member in the Internal Medicine Residency Program at Southeast Alabama Medical Center in Dothan, Ala., and clinical faculty member at the Alabama College of Osteopathic Medicine also in Dothan. Dr. Skandhan is the cofounder and current president of the SHM Wiregrass Chapter and is an active member of SHM’s Annual Conference and Performance Measurement Reporting committees.
When did you join SHM, and what prompted you to apply for your current committee roles?
There were many things that were not sufficiently taught during clinical training that were required in my day-to-day practice, like clinical documentation improvement, practice management, billing, coding, and so forth. I also quickly understood how vast and dynamic hospital medicine really was. While looking for an outlet to voice my questions, concerns, and curiosity, I decided to join SHM, which has helped me find and apply the techniques I’d been looking for to further my career as a hospitalist.
I’m now fortunate to be a part of SHM’s national committees, which involve hospitalists of various backgrounds and experiences, who work together to improve the overall quality of inpatient medicine. I currently serve on the Performance Reporting Measurement Committee and the Annual Conference Committee. My interests in reviewing the ever-evolving policies of health care made me apply to be a part of the Performance Reporting Measurement Committee. We work very closely with the Public Policy Committee, analyzing written policies and subsequently offering our recommendations. It’s been fulfilling to be a part of a committee that works towards developing policies that support a good quality of care on such a large scale.
My penchant for organizing events and bringing people together based on common ground led me to apply for the Annual Conference Committee. We meet every week to discuss various topics, choose and invite speakers, and help organize the entire event, which will host close to 5,000 hospitalists later this year. It has made me appreciate being a member of an organization that provides hospitalists with opportunities for education and growth. I’m hopeful that the attendees next year will find the conference to be a worthwhile experience!
As the president of SHM’s Wiregrass Chapter, how has the chapter grown since its establishment in May 2015?
Our chapter is based in Dothan, a small, rural Alabama town where Southeast Alabama Medical Center is located. The chapter covers the counties of lower Alabama and the panhandle of Florida. We named the chapter after a special species of grass that grows in this region.
When we started the chapter, our goal was to bring the best and brightest of hospital medicine to our region to give talks on hot topics in the field and also to use their expertise to guide inpatient care in our hospital system. We aggressively marketed the events to bring in large crowds of medical professionals, and we consistently average around 70-80 attendees in our meetings. Bringing in leaders from the field helped create an atmosphere of learning and inspired us to grow and develop our hospitalist program. We now closely work with hospital medicine groups in surrounding rural areas toward improving inpatient hospital care.
During these past years, we also realized that, for the further growth of our chapter, we would need to nurture an interest in hospital medicine among future generations of doctors, and this realization led to the creation of our medical student and resident wing. So far, the students have been very enthusiastic about participating in SHM-related events, and I hope that continues. We also developed a mentor-mentee program, in which we paired selected medical students with hospitalists to help guide future careers in acute care medicine. This year, we have also been helping the hospital medicine division at Southeast Alabama Medical Center create a clinical research track for medical students. To that end, we have just completed our second annual poster competition where we presented around 50 posters in the areas of clinical vignettes, quality improvement, and original research.
In addition, the chapter is very active with community activities. We took notice of the fact that many of our patients and community members were unaware of what hospitalists did because they could not understand how our work was different from that of primary care physicians. Our members have therefore participated in TV, radio, and newspaper interviews to help elucidate the role of hospitalists in patient care. We have also periodically visited primary care physician offices, nursing homes, senior citizen groups, and cancer support groups to educate these patients on various facets of health care and how hospitalists influence these areas.
In 2014, we organized a “walk with a hospitalist” event, for which we set up a half-mile “admission to discharge” scenario explaining the role of hospitalists and other departments involved in patient care. This year, in hopes of improving patient literacy in our region, we held a “shop with a doc” event, where the Southeast Alabama Medical Center hospitalists teamed up with dietitians and taught patients how food and lifestyle influenced their chronic medical illnesses. This was followed by physicians and dietitians shopping with patients in the grocery store, educating them on healthy choices and label reading.
We’re incredibly grateful for the support that we’ve received from our medical and patient communities; they’ve been critical in helping our chapter grow as much as it has, and they motivate us to work harder and do more with the chapter. We were honored to receive the SHM’s Rising Star Award at the Hospital Medicine 2017 conference in Las Vegas. We never thought that our little chapter in the American countryside would be chosen, but we’re very thankful to have our efforts recognized on the national stage!
Which SHM conferences have you attended? Tell TH about your most memorable highlights or takeaways.
When I started out as a hospitalist in 2014, I decided to attend the annual conference in Las Vegas, and I can honestly say that conference changed the course of my career. I can still remember listening to the opening speech and realizing that I was surrounded by more than 3,000 hospitalists who understood the power we had to influence inpatient care. I’ve attended all the national conferences since then and am grateful that I now get to help organize the Hospital Medicine 2018 annual conference, also known as HM18.
I had been working to find a way to improve documentation within my group, as well as change the culture and perception towards billing and coding practices, which prompted me to attend the Quality and Safety Educators Academy. During one of the problem-solving sessions, I explained the challenges that I faced to my conference group. The exercise required me to explain the problem at hand, and the players of my group then discussed their thoughts while I took notes. It was a fantastic experience, as the participants at my table offered strong solutions to my problems within a matter of minutes. Their advice led to meaningful changes in our group’s hospital documentation practices, and in turn, I’ve been promoted to physician advisor in Southeast Alabama Medical Center.
After such a great experience at Quality and Safety Educators Academy, I went on to attend SHM’s Leadership Academy, where I had the opportunity to meet some of the top leaders and pioneers in the field of hospital medicine. It’s empowering to be mentored by the very people you look up to and aspire to be like. Not only was I able to bring ideas home to my institution, but I was able to reflect and improve my own professional and personal growth. I’m happy to say that I’ve completed all three levels of Leadership Academy.
As I’ve become involved with the medical student and residency programs at my medical center, I recently attended the Academic Hospitalist Academy to help my transition into academic hospital medicine. Meeting and spending time with the faculty at Academic Hospitalist Academy made me further realize the roles that academic hospitalists play in the education of future physicians, emphasizing the idea that we can all be champions in quality and patient safety.
If you’re looking to advance your career as a hospitalist, take advantage of the conferences that SHM offers. I’ve gained so much from each experience, and I’m looking forward to returning to these conferences as a potential facilitator, in hopes of offering what I’ve learned to hospitalists looking to bring about change in their fields and careers.
What can attendees at HM18 expect to see in the area of career development, and how is this different than previous years?
Hospital medicine is only about 2 decades old, making it one of the youngest branches in medicine today. Given this fact, the Annual Conference Committee feels that it is paramount to focus on career development for both new and midcareer hospitalists alike.
One question that we wish to explore and answer this year is: “How do you make hospital medicine a life-long, enjoyable, and engaging career?” In turn, our committee has created several new additions to HM18. This includes a “Seasoning Your Career” track, which will provide ideas on how to advance in leadership, use emotional intelligence to achieve success, change your roles midcareer, and change hospitalist schedules. Another unique addition this year are career development workshops, which will aim to developing various aspects of a hospitalist’s career, such as working on leadership skills, refining presentation and communication skills, providing constructive feedback, promoting women in hospital medicine, preventing burnout, and turning ideas into clinical research. We also plan to incorporate an education track, which will focus on how hospitalists can expand their careers towards educational leadership.
Given your involvement in SHM at both the local and national levels, do you have any advice for young hospital medicine professionals looking to build their professional profiles?
I’ve frequently noticed that young hospitalists don’t realize the potential influence they hold within their own institutions or the power they have to elicit change in health care at the national level.
Though we don’t often admit it, some hospitalists feel like they are glorified residents, which definitely is not the case. As a provider on the front lines, you have the unique opportunity to implement changes pertaining to issues of cost, utilization of resources, process management, quality and patient safety, and bottlenecks in care, to name a few. These are issues that keep the administrators of your organization and leaders of hospital medicine up at night. Don’t sit around and complain about how things could be or should be; look toward creating change. Bring up possible solutions to these problems with your leaders. They will appreciate the effort, and hopefully together you can find ways to tackle these problems.
I will conclude by saying this: Hospital medicine is such a unique specialty in that it’s constantly evolving, and the pioneers of this field are still alive and practicing medicine. You can meet and interact with them during the SHM conferences and look to them as sources of inspiration or guidance. Meeting people you look up to and having them as your mentors can take you places.
Ms. Steele is the marketing communications specialist at the Society of Hospital Medicine.
Editor’s note: Each month, the Society of Hospital Medicine puts the spotlight on some of our most active members who are making substantial contributions to hospital medicine. Visit www.hospitalmedicine.org for more information on how you can lend your expertise to help SHM improve the care of hospitalized patients.
This month, The Hospitalist spotlights Amith Skandhan, MD, FHM, a hospitalist, a director/physician liaison for clinical documentation improvement and core faculty member in the Internal Medicine Residency Program at Southeast Alabama Medical Center in Dothan, Ala., and clinical faculty member at the Alabama College of Osteopathic Medicine also in Dothan. Dr. Skandhan is the cofounder and current president of the SHM Wiregrass Chapter and is an active member of SHM’s Annual Conference and Performance Measurement Reporting committees.
When did you join SHM, and what prompted you to apply for your current committee roles?
There were many things that were not sufficiently taught during clinical training that were required in my day-to-day practice, like clinical documentation improvement, practice management, billing, coding, and so forth. I also quickly understood how vast and dynamic hospital medicine really was. While looking for an outlet to voice my questions, concerns, and curiosity, I decided to join SHM, which has helped me find and apply the techniques I’d been looking for to further my career as a hospitalist.
I’m now fortunate to be a part of SHM’s national committees, which involve hospitalists of various backgrounds and experiences, who work together to improve the overall quality of inpatient medicine. I currently serve on the Performance Reporting Measurement Committee and the Annual Conference Committee. My interests in reviewing the ever-evolving policies of health care made me apply to be a part of the Performance Reporting Measurement Committee. We work very closely with the Public Policy Committee, analyzing written policies and subsequently offering our recommendations. It’s been fulfilling to be a part of a committee that works towards developing policies that support a good quality of care on such a large scale.
My penchant for organizing events and bringing people together based on common ground led me to apply for the Annual Conference Committee. We meet every week to discuss various topics, choose and invite speakers, and help organize the entire event, which will host close to 5,000 hospitalists later this year. It has made me appreciate being a member of an organization that provides hospitalists with opportunities for education and growth. I’m hopeful that the attendees next year will find the conference to be a worthwhile experience!
As the president of SHM’s Wiregrass Chapter, how has the chapter grown since its establishment in May 2015?
Our chapter is based in Dothan, a small, rural Alabama town where Southeast Alabama Medical Center is located. The chapter covers the counties of lower Alabama and the panhandle of Florida. We named the chapter after a special species of grass that grows in this region.
When we started the chapter, our goal was to bring the best and brightest of hospital medicine to our region to give talks on hot topics in the field and also to use their expertise to guide inpatient care in our hospital system. We aggressively marketed the events to bring in large crowds of medical professionals, and we consistently average around 70-80 attendees in our meetings. Bringing in leaders from the field helped create an atmosphere of learning and inspired us to grow and develop our hospitalist program. We now closely work with hospital medicine groups in surrounding rural areas toward improving inpatient hospital care.
During these past years, we also realized that, for the further growth of our chapter, we would need to nurture an interest in hospital medicine among future generations of doctors, and this realization led to the creation of our medical student and resident wing. So far, the students have been very enthusiastic about participating in SHM-related events, and I hope that continues. We also developed a mentor-mentee program, in which we paired selected medical students with hospitalists to help guide future careers in acute care medicine. This year, we have also been helping the hospital medicine division at Southeast Alabama Medical Center create a clinical research track for medical students. To that end, we have just completed our second annual poster competition where we presented around 50 posters in the areas of clinical vignettes, quality improvement, and original research.
In addition, the chapter is very active with community activities. We took notice of the fact that many of our patients and community members were unaware of what hospitalists did because they could not understand how our work was different from that of primary care physicians. Our members have therefore participated in TV, radio, and newspaper interviews to help elucidate the role of hospitalists in patient care. We have also periodically visited primary care physician offices, nursing homes, senior citizen groups, and cancer support groups to educate these patients on various facets of health care and how hospitalists influence these areas.
In 2014, we organized a “walk with a hospitalist” event, for which we set up a half-mile “admission to discharge” scenario explaining the role of hospitalists and other departments involved in patient care. This year, in hopes of improving patient literacy in our region, we held a “shop with a doc” event, where the Southeast Alabama Medical Center hospitalists teamed up with dietitians and taught patients how food and lifestyle influenced their chronic medical illnesses. This was followed by physicians and dietitians shopping with patients in the grocery store, educating them on healthy choices and label reading.
We’re incredibly grateful for the support that we’ve received from our medical and patient communities; they’ve been critical in helping our chapter grow as much as it has, and they motivate us to work harder and do more with the chapter. We were honored to receive the SHM’s Rising Star Award at the Hospital Medicine 2017 conference in Las Vegas. We never thought that our little chapter in the American countryside would be chosen, but we’re very thankful to have our efforts recognized on the national stage!
Which SHM conferences have you attended? Tell TH about your most memorable highlights or takeaways.
When I started out as a hospitalist in 2014, I decided to attend the annual conference in Las Vegas, and I can honestly say that conference changed the course of my career. I can still remember listening to the opening speech and realizing that I was surrounded by more than 3,000 hospitalists who understood the power we had to influence inpatient care. I’ve attended all the national conferences since then and am grateful that I now get to help organize the Hospital Medicine 2018 annual conference, also known as HM18.
I had been working to find a way to improve documentation within my group, as well as change the culture and perception towards billing and coding practices, which prompted me to attend the Quality and Safety Educators Academy. During one of the problem-solving sessions, I explained the challenges that I faced to my conference group. The exercise required me to explain the problem at hand, and the players of my group then discussed their thoughts while I took notes. It was a fantastic experience, as the participants at my table offered strong solutions to my problems within a matter of minutes. Their advice led to meaningful changes in our group’s hospital documentation practices, and in turn, I’ve been promoted to physician advisor in Southeast Alabama Medical Center.
After such a great experience at Quality and Safety Educators Academy, I went on to attend SHM’s Leadership Academy, where I had the opportunity to meet some of the top leaders and pioneers in the field of hospital medicine. It’s empowering to be mentored by the very people you look up to and aspire to be like. Not only was I able to bring ideas home to my institution, but I was able to reflect and improve my own professional and personal growth. I’m happy to say that I’ve completed all three levels of Leadership Academy.
As I’ve become involved with the medical student and residency programs at my medical center, I recently attended the Academic Hospitalist Academy to help my transition into academic hospital medicine. Meeting and spending time with the faculty at Academic Hospitalist Academy made me further realize the roles that academic hospitalists play in the education of future physicians, emphasizing the idea that we can all be champions in quality and patient safety.
If you’re looking to advance your career as a hospitalist, take advantage of the conferences that SHM offers. I’ve gained so much from each experience, and I’m looking forward to returning to these conferences as a potential facilitator, in hopes of offering what I’ve learned to hospitalists looking to bring about change in their fields and careers.
What can attendees at HM18 expect to see in the area of career development, and how is this different than previous years?
Hospital medicine is only about 2 decades old, making it one of the youngest branches in medicine today. Given this fact, the Annual Conference Committee feels that it is paramount to focus on career development for both new and midcareer hospitalists alike.
One question that we wish to explore and answer this year is: “How do you make hospital medicine a life-long, enjoyable, and engaging career?” In turn, our committee has created several new additions to HM18. This includes a “Seasoning Your Career” track, which will provide ideas on how to advance in leadership, use emotional intelligence to achieve success, change your roles midcareer, and change hospitalist schedules. Another unique addition this year are career development workshops, which will aim to developing various aspects of a hospitalist’s career, such as working on leadership skills, refining presentation and communication skills, providing constructive feedback, promoting women in hospital medicine, preventing burnout, and turning ideas into clinical research. We also plan to incorporate an education track, which will focus on how hospitalists can expand their careers towards educational leadership.
Given your involvement in SHM at both the local and national levels, do you have any advice for young hospital medicine professionals looking to build their professional profiles?
I’ve frequently noticed that young hospitalists don’t realize the potential influence they hold within their own institutions or the power they have to elicit change in health care at the national level.
Though we don’t often admit it, some hospitalists feel like they are glorified residents, which definitely is not the case. As a provider on the front lines, you have the unique opportunity to implement changes pertaining to issues of cost, utilization of resources, process management, quality and patient safety, and bottlenecks in care, to name a few. These are issues that keep the administrators of your organization and leaders of hospital medicine up at night. Don’t sit around and complain about how things could be or should be; look toward creating change. Bring up possible solutions to these problems with your leaders. They will appreciate the effort, and hopefully together you can find ways to tackle these problems.
I will conclude by saying this: Hospital medicine is such a unique specialty in that it’s constantly evolving, and the pioneers of this field are still alive and practicing medicine. You can meet and interact with them during the SHM conferences and look to them as sources of inspiration or guidance. Meeting people you look up to and having them as your mentors can take you places.
Ms. Steele is the marketing communications specialist at the Society of Hospital Medicine.
Editor’s note: Each month, the Society of Hospital Medicine puts the spotlight on some of our most active members who are making substantial contributions to hospital medicine. Visit www.hospitalmedicine.org for more information on how you can lend your expertise to help SHM improve the care of hospitalized patients.
This month, The Hospitalist spotlights Amith Skandhan, MD, FHM, a hospitalist, a director/physician liaison for clinical documentation improvement and core faculty member in the Internal Medicine Residency Program at Southeast Alabama Medical Center in Dothan, Ala., and clinical faculty member at the Alabama College of Osteopathic Medicine also in Dothan. Dr. Skandhan is the cofounder and current president of the SHM Wiregrass Chapter and is an active member of SHM’s Annual Conference and Performance Measurement Reporting committees.
When did you join SHM, and what prompted you to apply for your current committee roles?
There were many things that were not sufficiently taught during clinical training that were required in my day-to-day practice, like clinical documentation improvement, practice management, billing, coding, and so forth. I also quickly understood how vast and dynamic hospital medicine really was. While looking for an outlet to voice my questions, concerns, and curiosity, I decided to join SHM, which has helped me find and apply the techniques I’d been looking for to further my career as a hospitalist.
I’m now fortunate to be a part of SHM’s national committees, which involve hospitalists of various backgrounds and experiences, who work together to improve the overall quality of inpatient medicine. I currently serve on the Performance Reporting Measurement Committee and the Annual Conference Committee. My interests in reviewing the ever-evolving policies of health care made me apply to be a part of the Performance Reporting Measurement Committee. We work very closely with the Public Policy Committee, analyzing written policies and subsequently offering our recommendations. It’s been fulfilling to be a part of a committee that works towards developing policies that support a good quality of care on such a large scale.
My penchant for organizing events and bringing people together based on common ground led me to apply for the Annual Conference Committee. We meet every week to discuss various topics, choose and invite speakers, and help organize the entire event, which will host close to 5,000 hospitalists later this year. It has made me appreciate being a member of an organization that provides hospitalists with opportunities for education and growth. I’m hopeful that the attendees next year will find the conference to be a worthwhile experience!
As the president of SHM’s Wiregrass Chapter, how has the chapter grown since its establishment in May 2015?
Our chapter is based in Dothan, a small, rural Alabama town where Southeast Alabama Medical Center is located. The chapter covers the counties of lower Alabama and the panhandle of Florida. We named the chapter after a special species of grass that grows in this region.
When we started the chapter, our goal was to bring the best and brightest of hospital medicine to our region to give talks on hot topics in the field and also to use their expertise to guide inpatient care in our hospital system. We aggressively marketed the events to bring in large crowds of medical professionals, and we consistently average around 70-80 attendees in our meetings. Bringing in leaders from the field helped create an atmosphere of learning and inspired us to grow and develop our hospitalist program. We now closely work with hospital medicine groups in surrounding rural areas toward improving inpatient hospital care.
During these past years, we also realized that, for the further growth of our chapter, we would need to nurture an interest in hospital medicine among future generations of doctors, and this realization led to the creation of our medical student and resident wing. So far, the students have been very enthusiastic about participating in SHM-related events, and I hope that continues. We also developed a mentor-mentee program, in which we paired selected medical students with hospitalists to help guide future careers in acute care medicine. This year, we have also been helping the hospital medicine division at Southeast Alabama Medical Center create a clinical research track for medical students. To that end, we have just completed our second annual poster competition where we presented around 50 posters in the areas of clinical vignettes, quality improvement, and original research.
In addition, the chapter is very active with community activities. We took notice of the fact that many of our patients and community members were unaware of what hospitalists did because they could not understand how our work was different from that of primary care physicians. Our members have therefore participated in TV, radio, and newspaper interviews to help elucidate the role of hospitalists in patient care. We have also periodically visited primary care physician offices, nursing homes, senior citizen groups, and cancer support groups to educate these patients on various facets of health care and how hospitalists influence these areas.
In 2014, we organized a “walk with a hospitalist” event, for which we set up a half-mile “admission to discharge” scenario explaining the role of hospitalists and other departments involved in patient care. This year, in hopes of improving patient literacy in our region, we held a “shop with a doc” event, where the Southeast Alabama Medical Center hospitalists teamed up with dietitians and taught patients how food and lifestyle influenced their chronic medical illnesses. This was followed by physicians and dietitians shopping with patients in the grocery store, educating them on healthy choices and label reading.
We’re incredibly grateful for the support that we’ve received from our medical and patient communities; they’ve been critical in helping our chapter grow as much as it has, and they motivate us to work harder and do more with the chapter. We were honored to receive the SHM’s Rising Star Award at the Hospital Medicine 2017 conference in Las Vegas. We never thought that our little chapter in the American countryside would be chosen, but we’re very thankful to have our efforts recognized on the national stage!
Which SHM conferences have you attended? Tell TH about your most memorable highlights or takeaways.
When I started out as a hospitalist in 2014, I decided to attend the annual conference in Las Vegas, and I can honestly say that conference changed the course of my career. I can still remember listening to the opening speech and realizing that I was surrounded by more than 3,000 hospitalists who understood the power we had to influence inpatient care. I’ve attended all the national conferences since then and am grateful that I now get to help organize the Hospital Medicine 2018 annual conference, also known as HM18.
I had been working to find a way to improve documentation within my group, as well as change the culture and perception towards billing and coding practices, which prompted me to attend the Quality and Safety Educators Academy. During one of the problem-solving sessions, I explained the challenges that I faced to my conference group. The exercise required me to explain the problem at hand, and the players of my group then discussed their thoughts while I took notes. It was a fantastic experience, as the participants at my table offered strong solutions to my problems within a matter of minutes. Their advice led to meaningful changes in our group’s hospital documentation practices, and in turn, I’ve been promoted to physician advisor in Southeast Alabama Medical Center.
After such a great experience at Quality and Safety Educators Academy, I went on to attend SHM’s Leadership Academy, where I had the opportunity to meet some of the top leaders and pioneers in the field of hospital medicine. It’s empowering to be mentored by the very people you look up to and aspire to be like. Not only was I able to bring ideas home to my institution, but I was able to reflect and improve my own professional and personal growth. I’m happy to say that I’ve completed all three levels of Leadership Academy.
As I’ve become involved with the medical student and residency programs at my medical center, I recently attended the Academic Hospitalist Academy to help my transition into academic hospital medicine. Meeting and spending time with the faculty at Academic Hospitalist Academy made me further realize the roles that academic hospitalists play in the education of future physicians, emphasizing the idea that we can all be champions in quality and patient safety.
If you’re looking to advance your career as a hospitalist, take advantage of the conferences that SHM offers. I’ve gained so much from each experience, and I’m looking forward to returning to these conferences as a potential facilitator, in hopes of offering what I’ve learned to hospitalists looking to bring about change in their fields and careers.
What can attendees at HM18 expect to see in the area of career development, and how is this different than previous years?
Hospital medicine is only about 2 decades old, making it one of the youngest branches in medicine today. Given this fact, the Annual Conference Committee feels that it is paramount to focus on career development for both new and midcareer hospitalists alike.
One question that we wish to explore and answer this year is: “How do you make hospital medicine a life-long, enjoyable, and engaging career?” In turn, our committee has created several new additions to HM18. This includes a “Seasoning Your Career” track, which will provide ideas on how to advance in leadership, use emotional intelligence to achieve success, change your roles midcareer, and change hospitalist schedules. Another unique addition this year are career development workshops, which will aim to developing various aspects of a hospitalist’s career, such as working on leadership skills, refining presentation and communication skills, providing constructive feedback, promoting women in hospital medicine, preventing burnout, and turning ideas into clinical research. We also plan to incorporate an education track, which will focus on how hospitalists can expand their careers towards educational leadership.
Given your involvement in SHM at both the local and national levels, do you have any advice for young hospital medicine professionals looking to build their professional profiles?
I’ve frequently noticed that young hospitalists don’t realize the potential influence they hold within their own institutions or the power they have to elicit change in health care at the national level.
Though we don’t often admit it, some hospitalists feel like they are glorified residents, which definitely is not the case. As a provider on the front lines, you have the unique opportunity to implement changes pertaining to issues of cost, utilization of resources, process management, quality and patient safety, and bottlenecks in care, to name a few. These are issues that keep the administrators of your organization and leaders of hospital medicine up at night. Don’t sit around and complain about how things could be or should be; look toward creating change. Bring up possible solutions to these problems with your leaders. They will appreciate the effort, and hopefully together you can find ways to tackle these problems.
I will conclude by saying this: Hospital medicine is such a unique specialty in that it’s constantly evolving, and the pioneers of this field are still alive and practicing medicine. You can meet and interact with them during the SHM conferences and look to them as sources of inspiration or guidance. Meeting people you look up to and having them as your mentors can take you places.
Ms. Steele is the marketing communications specialist at the Society of Hospital Medicine.

Medication pricing: So this is how it works
This is the second part in a series on medication pricing.
In my last column, I looked at the tremendous variation in prices among pharmacies for two psychotropic medications, aripiprazole and modafinil. The cash price variation could be as much as 45 times more from one pharmacy to the next, which I found to be both outrageous and incomprehensible.
To learn more about pharmaceutical pricing, I contacted Doug Hirsch, the cofounder of GoodRx, a firm based in Santa Monica, Calif., that offers deep discounts on some medications. The company sends discount cards to physicians’ offices – call me if you need some, I have many boxes of GoodRx cards – and has a website (www.GoodRx.com) and an app. It advertises that it is about transparency, and if you’ve ever tried the company’s site or app, the service it offers is remarkable and simple to use.
I approached Mr. Hirsch with two simple questions. The company offers “up to 90% discount” on the cash price of medications through its app, website, or discount card – all of which can be gotten for free. I wanted to know 1) Who pays for this difference in the medication cost, and 2) How does the company, with 95 employees, make any money? Mr. Hirsch was gracious enough (and patient enough!) to spend the next hour walking me through the steps of medication pricing. It was a lively conversation, so let me share with you what I have learned.
Medications are made by a pharmaceutical company or, for generics, there may be many manufacturers. The medications are sent to a pharmaceutical distributor, such as McKesson, and it, in turn, sells and delivers the products to pharmacy chains, as well as to smaller, independent pharmacies. The pharmacies pay an acquisition cost for medications then set a price for these medications that are considerably – or even astronomically – higher than the acquisition price. This is the cash retail price, or in medicine, what is called the Usual & Customary (U&C) cost of the medication. The price may be neither usual, customary, nor reasonable, and it’s not the price the pharmacy expects to recoup on sales.
Every major insurance company contracts with a pharmacy benefits manager (for example, Caremark, Express Scripts, and Optum) to negotiate the cost of medications with each major pharmacy chain. Physicians are familiar with PBMs, who intercede by requiring preauthorization procedures for certain medications or by instituting stepwise, fail-first, requirements before they will allow pharmacy benefits toward the purchase of medications. When the PBMs negotiate with the pharmacies, they will negotiate for a discount off the pharmacy’s U&C charge for medication, perhaps a discount as much as 75% or 80%. Mr. Hirsch noted, “The discount is not negotiated on a per-medication basis but as an across-the-board average, so for one medication, the insurance price may be 2% discount from the U&C cost, and on another medicine it may be 95%. There is a dramatic variation, more than you’d ever expect.”
GoodRx gathers prices from many places, including partnerships with a number of PBMs. In addition to providing discounted prices for insured customers, the PBMs also include in their negotiations a slightly less-discounted price for cash-paying patients who present with a GoodRx card or coupon. You might be surprised to learn that discounted prices can often be less than the typical patient copay. For patients with a high deductible, for medications that are not covered at all, or for times when the copay is higher than the cost of the medication, it will often be less expensive for patients to use a GoodRx discount instead of their insurance. And whether patients uses either their insurance or a GoodRx discount, part of the cost of the prescription includes an administrative fee that goes to the PBM. When GoodRx cards are used, the PBM pays GoodRx part of that fee. I hope you are still with me, because this is the part of the conversation where I started telling Mr. Hirsch that I was getting a headache.
I went back to the enormous cost discrepancy that I had discovered a couple of years ago with Provigil (modafinil). Thirty pills cost just under $35 at Costco, while all other pharmacies were charging close to $1,000. Mr. Hirsch explained, “From what I’ve been told, Costco bases their prices on their acquisition costs and then raises them a certain percent. It’s one way to provide a fair price, but that doesn’t mean they always have the lowest price. They are also the only major pharmacy that lists their drug prices on their website.”
I wanted to know what was in it for the PBMs. Why would Express Scripts be motivated to negotiate a discount in price for cash-paying customers outside of the insurance networks, and how did partnering with GoodRx benefit them? The answer, in part, lies with the fact that the website and app allow patients to comparison shop and go to pharmacies with lower prices. If patients use their insurance, the insurance company is paying less; if they don’t use their insurance because they learned the cash cost is less, then the cost burden has shifted from the insurance company entirely to the patient.
What’s in it for the pharmacies? Why would they be willing to accept less money from a patient bearing a discount card? Mr. Hirsch explained, “Pharmacies want to honor their contracts with PBMs, and the U&C prices are set high to enable negotiation so that they still make some profit. Most people couldn’t afford to pay the high U&C, but they can’t lower them for individual cash-pay customers because that would violate their agreements with PBMs, and Medicare and Medicaid, which is a felony. With the GoodRx price, they still make a profit, and people in drugstores buy other items as well.

GoodRx has 95 employees, and I was still left wondering how they generate income. Mr. Hirsch pinned it down to three sources: the portion of the administration fees the PBMs pay GoodRx, a small amount of advertising, and finally, GoodRx provides technology for the PBMs and charges for this service.
“We started asking how we could gather prices in this bizarre marketplace and address the pricing inefficiencies,” Mr. Hirsch said, “and now I get emails every day expressing gratitude.”
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016).
This is the second part in a series on medication pricing.
In my last column, I looked at the tremendous variation in prices among pharmacies for two psychotropic medications, aripiprazole and modafinil. The cash price variation could be as much as 45 times more from one pharmacy to the next, which I found to be both outrageous and incomprehensible.
To learn more about pharmaceutical pricing, I contacted Doug Hirsch, the cofounder of GoodRx, a firm based in Santa Monica, Calif., that offers deep discounts on some medications. The company sends discount cards to physicians’ offices – call me if you need some, I have many boxes of GoodRx cards – and has a website (www.GoodRx.com) and an app. It advertises that it is about transparency, and if you’ve ever tried the company’s site or app, the service it offers is remarkable and simple to use.
I approached Mr. Hirsch with two simple questions. The company offers “up to 90% discount” on the cash price of medications through its app, website, or discount card – all of which can be gotten for free. I wanted to know 1) Who pays for this difference in the medication cost, and 2) How does the company, with 95 employees, make any money? Mr. Hirsch was gracious enough (and patient enough!) to spend the next hour walking me through the steps of medication pricing. It was a lively conversation, so let me share with you what I have learned.
Medications are made by a pharmaceutical company or, for generics, there may be many manufacturers. The medications are sent to a pharmaceutical distributor, such as McKesson, and it, in turn, sells and delivers the products to pharmacy chains, as well as to smaller, independent pharmacies. The pharmacies pay an acquisition cost for medications then set a price for these medications that are considerably – or even astronomically – higher than the acquisition price. This is the cash retail price, or in medicine, what is called the Usual & Customary (U&C) cost of the medication. The price may be neither usual, customary, nor reasonable, and it’s not the price the pharmacy expects to recoup on sales.
Every major insurance company contracts with a pharmacy benefits manager (for example, Caremark, Express Scripts, and Optum) to negotiate the cost of medications with each major pharmacy chain. Physicians are familiar with PBMs, who intercede by requiring preauthorization procedures for certain medications or by instituting stepwise, fail-first, requirements before they will allow pharmacy benefits toward the purchase of medications. When the PBMs negotiate with the pharmacies, they will negotiate for a discount off the pharmacy’s U&C charge for medication, perhaps a discount as much as 75% or 80%. Mr. Hirsch noted, “The discount is not negotiated on a per-medication basis but as an across-the-board average, so for one medication, the insurance price may be 2% discount from the U&C cost, and on another medicine it may be 95%. There is a dramatic variation, more than you’d ever expect.”
GoodRx gathers prices from many places, including partnerships with a number of PBMs. In addition to providing discounted prices for insured customers, the PBMs also include in their negotiations a slightly less-discounted price for cash-paying patients who present with a GoodRx card or coupon. You might be surprised to learn that discounted prices can often be less than the typical patient copay. For patients with a high deductible, for medications that are not covered at all, or for times when the copay is higher than the cost of the medication, it will often be less expensive for patients to use a GoodRx discount instead of their insurance. And whether patients uses either their insurance or a GoodRx discount, part of the cost of the prescription includes an administrative fee that goes to the PBM. When GoodRx cards are used, the PBM pays GoodRx part of that fee. I hope you are still with me, because this is the part of the conversation where I started telling Mr. Hirsch that I was getting a headache.
I went back to the enormous cost discrepancy that I had discovered a couple of years ago with Provigil (modafinil). Thirty pills cost just under $35 at Costco, while all other pharmacies were charging close to $1,000. Mr. Hirsch explained, “From what I’ve been told, Costco bases their prices on their acquisition costs and then raises them a certain percent. It’s one way to provide a fair price, but that doesn’t mean they always have the lowest price. They are also the only major pharmacy that lists their drug prices on their website.”
I wanted to know what was in it for the PBMs. Why would Express Scripts be motivated to negotiate a discount in price for cash-paying customers outside of the insurance networks, and how did partnering with GoodRx benefit them? The answer, in part, lies with the fact that the website and app allow patients to comparison shop and go to pharmacies with lower prices. If patients use their insurance, the insurance company is paying less; if they don’t use their insurance because they learned the cash cost is less, then the cost burden has shifted from the insurance company entirely to the patient.
What’s in it for the pharmacies? Why would they be willing to accept less money from a patient bearing a discount card? Mr. Hirsch explained, “Pharmacies want to honor their contracts with PBMs, and the U&C prices are set high to enable negotiation so that they still make some profit. Most people couldn’t afford to pay the high U&C, but they can’t lower them for individual cash-pay customers because that would violate their agreements with PBMs, and Medicare and Medicaid, which is a felony. With the GoodRx price, they still make a profit, and people in drugstores buy other items as well.
GoodRx has 95 employees, and I was still left wondering how they generate income. Mr. Hirsch pinned it down to three sources: the portion of the administration fees the PBMs pay GoodRx, a small amount of advertising, and finally, GoodRx provides technology for the PBMs and charges for this service.
“We started asking how we could gather prices in this bizarre marketplace and address the pricing inefficiencies,” Mr. Hirsch said, “and now I get emails every day expressing gratitude.”
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016).
This is the second part in a series on medication pricing.
In my last column, I looked at the tremendous variation in prices among pharmacies for two psychotropic medications, aripiprazole and modafinil. The cash price variation could be as much as 45 times more from one pharmacy to the next, which I found to be both outrageous and incomprehensible.
To learn more about pharmaceutical pricing, I contacted Doug Hirsch, the cofounder of GoodRx, a firm based in Santa Monica, Calif., that offers deep discounts on some medications. The company sends discount cards to physicians’ offices – call me if you need some, I have many boxes of GoodRx cards – and has a website (www.GoodRx.com) and an app. It advertises that it is about transparency, and if you’ve ever tried the company’s site or app, the service it offers is remarkable and simple to use.
I approached Mr. Hirsch with two simple questions. The company offers “up to 90% discount” on the cash price of medications through its app, website, or discount card – all of which can be gotten for free. I wanted to know 1) Who pays for this difference in the medication cost, and 2) How does the company, with 95 employees, make any money? Mr. Hirsch was gracious enough (and patient enough!) to spend the next hour walking me through the steps of medication pricing. It was a lively conversation, so let me share with you what I have learned.
Medications are made by a pharmaceutical company or, for generics, there may be many manufacturers. The medications are sent to a pharmaceutical distributor, such as McKesson, and it, in turn, sells and delivers the products to pharmacy chains, as well as to smaller, independent pharmacies. The pharmacies pay an acquisition cost for medications then set a price for these medications that are considerably – or even astronomically – higher than the acquisition price. This is the cash retail price, or in medicine, what is called the Usual & Customary (U&C) cost of the medication. The price may be neither usual, customary, nor reasonable, and it’s not the price the pharmacy expects to recoup on sales.
Every major insurance company contracts with a pharmacy benefits manager (for example, Caremark, Express Scripts, and Optum) to negotiate the cost of medications with each major pharmacy chain. Physicians are familiar with PBMs, who intercede by requiring preauthorization procedures for certain medications or by instituting stepwise, fail-first, requirements before they will allow pharmacy benefits toward the purchase of medications. When the PBMs negotiate with the pharmacies, they will negotiate for a discount off the pharmacy’s U&C charge for medication, perhaps a discount as much as 75% or 80%. Mr. Hirsch noted, “The discount is not negotiated on a per-medication basis but as an across-the-board average, so for one medication, the insurance price may be 2% discount from the U&C cost, and on another medicine it may be 95%. There is a dramatic variation, more than you’d ever expect.”
GoodRx gathers prices from many places, including partnerships with a number of PBMs. In addition to providing discounted prices for insured customers, the PBMs also include in their negotiations a slightly less-discounted price for cash-paying patients who present with a GoodRx card or coupon. You might be surprised to learn that discounted prices can often be less than the typical patient copay. For patients with a high deductible, for medications that are not covered at all, or for times when the copay is higher than the cost of the medication, it will often be less expensive for patients to use a GoodRx discount instead of their insurance. And whether patients uses either their insurance or a GoodRx discount, part of the cost of the prescription includes an administrative fee that goes to the PBM. When GoodRx cards are used, the PBM pays GoodRx part of that fee. I hope you are still with me, because this is the part of the conversation where I started telling Mr. Hirsch that I was getting a headache.
I went back to the enormous cost discrepancy that I had discovered a couple of years ago with Provigil (modafinil). Thirty pills cost just under $35 at Costco, while all other pharmacies were charging close to $1,000. Mr. Hirsch explained, “From what I’ve been told, Costco bases their prices on their acquisition costs and then raises them a certain percent. It’s one way to provide a fair price, but that doesn’t mean they always have the lowest price. They are also the only major pharmacy that lists their drug prices on their website.”
I wanted to know what was in it for the PBMs. Why would Express Scripts be motivated to negotiate a discount in price for cash-paying customers outside of the insurance networks, and how did partnering with GoodRx benefit them? The answer, in part, lies with the fact that the website and app allow patients to comparison shop and go to pharmacies with lower prices. If patients use their insurance, the insurance company is paying less; if they don’t use their insurance because they learned the cash cost is less, then the cost burden has shifted from the insurance company entirely to the patient.
What’s in it for the pharmacies? Why would they be willing to accept less money from a patient bearing a discount card? Mr. Hirsch explained, “Pharmacies want to honor their contracts with PBMs, and the U&C prices are set high to enable negotiation so that they still make some profit. Most people couldn’t afford to pay the high U&C, but they can’t lower them for individual cash-pay customers because that would violate their agreements with PBMs, and Medicare and Medicaid, which is a felony. With the GoodRx price, they still make a profit, and people in drugstores buy other items as well.
GoodRx has 95 employees, and I was still left wondering how they generate income. Mr. Hirsch pinned it down to three sources: the portion of the administration fees the PBMs pay GoodRx, a small amount of advertising, and finally, GoodRx provides technology for the PBMs and charges for this service.
“We started asking how we could gather prices in this bizarre marketplace and address the pricing inefficiencies,” Mr. Hirsch said, “and now I get emails every day expressing gratitude.”
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016).
Mental health stressors still loom for Puerto Ricans after Maria
The physical and mental health needs of the people of Puerto Rico cannot be underestimated. Just think of what they have been through over the last few months.
When Hurricane Maria barreled onto the island on Sept. 20, 2017 – just 2 weeks after Hurricane Irma reportedly left more than 1 million residents without power – it ripped off roofs and left behind massive flooding, roads washed out, and utility poles and transmission lines knocked down. Whole forests were defoliated, a massive loss of flora and fauna occurred, and 80% of the crop value was destroyed, along with massive loss of stray dogs and cats, dairy cows, industrial chicken coops, and tropical birds, including endangered species. Beloved pets were displaced.

The official death toll as a result of Maria was 64 in December, but according to reporting by The New York Times, that number could be as high as 1,052. Most of the people who died reportedly were men and women over age 50 in hospitals and nursing homes suffering from illnesses such as diabetes, Alzheimer’s, kidney disease, hypertension, pneumonia, and other respiratory diseases.
One grassroots organization that mobilized to provide supplies and medical assistance was Doctoras Boricuas, a group of all-female doctors in the United States and Puerto Rico that formed after the hurricanes to coordinate the delivery and distribution of supplies directly to Puerto Rico and the Virgin Islands. Two groups affiliated with the University of Missouri at Columbia joined forces to help: Global First Responder or GFR, a nonprofit, secular international medical relief organization founded in 2011 by Adam Beckett, MD, and the International Center for Psychosocial Trauma, or ICPT, a group established in 1995 by Syed Arshad Husain, MD, to help war-traumatized children in Bosnia. I joined Dr. Husain’s group of professionals – Kathryn Dewein, PhD; Andra Ferguson, PhD; and Cathy Grigg, PsyD, – all of whom have traveled broadly in the field of disaster psychiatry – to see how we could help the people of Puerto Rico in Maria’s aftermath.
What we did
ICPT and GFR were a combined team, but we served different functions. As part of ICPT, I focused on the mental health component and helped to train doctors, psychologists, social workers, and other mental health workers in both San Juan and Ponce. All told, we worked with about 50 people using the model of “Training the Trainers.” Many of our students were participants in the outreach teams. Our hope is that they will be able to train their peers to recognize and alleviate symptoms of acute and chronic stress disorders. Some of the techniques taught include patient education, relaxation training, breath work, visualization techniques, mindfulness training, narrative therapy, art therapy, and other expressive techniques.
What the PMSF did
Before Maria, the Ponce Medical School Foundation was in the process of facilitating the transfer of medical records into an electronic format. After the hurricane hit, however, PMSF’s program director, Antonio Fernandez, led a shift to disaster recovery work. PMSF got involved in airlifting dialysis patients off the island to safety, provided health care, and also collaborated with the Primary Care Psychology Program at Ponce Health Services University to assist in locating patients, identifying their health needs – including mental health – and providing for those needs to the extent possible.
At the time of our visit, Puerto Rico’s network of more than 90 largely rural federally funded primary care clinics mostly had reopened, but nearly half remained on back-up generators. Even with the medical centers open, patients were not coming in for one reason or another. People had medical problems, but the daily reality of survival, obtaining food and water, took precedence. Some patients were not showing up because they had left the country, or they were in shelters without transportation. Some people did not have fuel. Some could not keep track of their appointments without cell phones and electricity allowing them to access electronic planners. Some, having been without their medications since the storms, were too sick to travel. Outreach teams were necessary to locate patients, identify their needs, and provide medical and psychological care.
Community outreach
Nydia M. Cappas, PsyD, director of the Primary Care Psychology Program, told us that the outreach teams – consisting of doctors or other medical professionals, social workers, and psychologists, were being sent out to communities once a week. They visited homes for the elderly, orphans’ homes, and children in foster care, as well as individual patients. A similar service was provided by Vargas Medicine (VARMED) in the San Juan area.
Team members found that many people were suffering symptoms of posttraumatic stress disorder, even people who did not have prior psychiatric symptoms. They were having flashbacks and nightmares. Those flashbacks and nightmares were being triggered by clouds, by rain, by supplies beginning to run out.

Another trend we observed is that terrain changes prompted by Maria triggered PTSD symptoms among many veterans. The defoliated trees and brown earth were causing them to have flashbacks to the deserts of Afghanistan and Iraq. Children were showing regressive behaviors, loss of developmental milestones, and symptoms of separation anxiety such as wanting to sleep with their parents. In severe cases, they were having psychotic symptoms and auditory hallucinations. The children were grieving the loss of their homes, toys, pets, and family members, in some cases. , including medications, food, toiletries, and other household goods.
Puerto Rico’s future
Two and a half months after Maria, we learned from our students that things gradually had begun to improve. For example, the public schools had just reopened, and that change was expected to have a stabilizing effect on the children. We also learned that, of the 80 shelters that had been set up housing about 12,500 people, 40 shelters had closed. The five medical shelters that had been set up and funded by FEMA also were in the process of closing, and private donations were beginning to slow down. People were slowly returning to their tarped or otherwise repaired homes, albeit all too often without power.
During the storm, nearly 500,000* homes were destroyed. FEMA offered to airlift about 3,000 people who had no home 2 months past Maria to the U.S. mainland – either Florida or New York.
According to our students, people living in the mountains, mainly coffee growers and retired people and comprising about one-third of the population, remain in acute crisis. Part of the challenge is being able to reach this population: Some roads are still impassable, and supplies – such as drinking water – can be delivered only by helicopter. Despite current conditions, FEMA reportedly has announced that it would end emergency operations on the island.
Our team is currently involved in applying for grant funding that will enable us to return to provide additional training to physicians’ and teachers’ groups. Over the course of the next year, we would like to make six trips to Puerto Rico and focus each trip on a different region and different group of professionals so that the entire island has resources. In addition, we will offer follow-up consultations to professionals we trained previously. The regions to be trained would be San Juan, Ponce, Utuado, Mayagüez, Guayama, and a sixth to be determined upon need. We also would like to address the needs of any ongoing relief workers so that they will be more effective in their ongoing role. Meanwhile, financial assistance from the mainland remains uneven.
Many months after Maria (and Irma), the physical and mental health needs of the Puerto Rican people remain great. However, as mental health professionals, we have the tools to help them move forward.
Judith R. Milner, MD, MEd, SpecEd, is a general, child, and adolescent psychiatrist in private practice in Everett, Wash. She has traveled with various groups over the years in an effort to alleviate some of the suffering caused by war and natural disaster. Her predominant association has been with the International Center for Psychosocial Trauma. She also has worked with Step Up Rwanda Women and Pygmy Survival Alliance, as well as on the Committee for Women at the American Psychiatric Association and the Consumer Issues Committee and Membership Committee for the American Academy of Child and Adolescent Psychiatry.
*Correction, 2/12/2018: An earlier version of this story misstated the number of homes reportedly destroyed by Hurricane Maria.
The physical and mental health needs of the people of Puerto Rico cannot be underestimated. Just think of what they have been through over the last few months.
When Hurricane Maria barreled onto the island on Sept. 20, 2017 – just 2 weeks after Hurricane Irma reportedly left more than 1 million residents without power – it ripped off roofs and left behind massive flooding, roads washed out, and utility poles and transmission lines knocked down. Whole forests were defoliated, a massive loss of flora and fauna occurred, and 80% of the crop value was destroyed, along with massive loss of stray dogs and cats, dairy cows, industrial chicken coops, and tropical birds, including endangered species. Beloved pets were displaced.
The official death toll as a result of Maria was 64 in December, but according to reporting by The New York Times, that number could be as high as 1,052. Most of the people who died reportedly were men and women over age 50 in hospitals and nursing homes suffering from illnesses such as diabetes, Alzheimer’s, kidney disease, hypertension, pneumonia, and other respiratory diseases.
One grassroots organization that mobilized to provide supplies and medical assistance was Doctoras Boricuas, a group of all-female doctors in the United States and Puerto Rico that formed after the hurricanes to coordinate the delivery and distribution of supplies directly to Puerto Rico and the Virgin Islands. Two groups affiliated with the University of Missouri at Columbia joined forces to help: Global First Responder or GFR, a nonprofit, secular international medical relief organization founded in 2011 by Adam Beckett, MD, and the International Center for Psychosocial Trauma, or ICPT, a group established in 1995 by Syed Arshad Husain, MD, to help war-traumatized children in Bosnia. I joined Dr. Husain’s group of professionals – Kathryn Dewein, PhD; Andra Ferguson, PhD; and Cathy Grigg, PsyD, – all of whom have traveled broadly in the field of disaster psychiatry – to see how we could help the people of Puerto Rico in Maria’s aftermath.
What we did
ICPT and GFR were a combined team, but we served different functions. As part of ICPT, I focused on the mental health component and helped to train doctors, psychologists, social workers, and other mental health workers in both San Juan and Ponce. All told, we worked with about 50 people using the model of “Training the Trainers.” Many of our students were participants in the outreach teams. Our hope is that they will be able to train their peers to recognize and alleviate symptoms of acute and chronic stress disorders. Some of the techniques taught include patient education, relaxation training, breath work, visualization techniques, mindfulness training, narrative therapy, art therapy, and other expressive techniques.
What the PMSF did
Before Maria, the Ponce Medical School Foundation was in the process of facilitating the transfer of medical records into an electronic format. After the hurricane hit, however, PMSF’s program director, Antonio Fernandez, led a shift to disaster recovery work. PMSF got involved in airlifting dialysis patients off the island to safety, provided health care, and also collaborated with the Primary Care Psychology Program at Ponce Health Services University to assist in locating patients, identifying their health needs – including mental health – and providing for those needs to the extent possible.
At the time of our visit, Puerto Rico’s network of more than 90 largely rural federally funded primary care clinics mostly had reopened, but nearly half remained on back-up generators. Even with the medical centers open, patients were not coming in for one reason or another. People had medical problems, but the daily reality of survival, obtaining food and water, took precedence. Some patients were not showing up because they had left the country, or they were in shelters without transportation. Some people did not have fuel. Some could not keep track of their appointments without cell phones and electricity allowing them to access electronic planners. Some, having been without their medications since the storms, were too sick to travel. Outreach teams were necessary to locate patients, identify their needs, and provide medical and psychological care.
Community outreach
Nydia M. Cappas, PsyD, director of the Primary Care Psychology Program, told us that the outreach teams – consisting of doctors or other medical professionals, social workers, and psychologists, were being sent out to communities once a week. They visited homes for the elderly, orphans’ homes, and children in foster care, as well as individual patients. A similar service was provided by Vargas Medicine (VARMED) in the San Juan area.
Team members found that many people were suffering symptoms of posttraumatic stress disorder, even people who did not have prior psychiatric symptoms. They were having flashbacks and nightmares. Those flashbacks and nightmares were being triggered by clouds, by rain, by supplies beginning to run out.
Another trend we observed is that terrain changes prompted by Maria triggered PTSD symptoms among many veterans. The defoliated trees and brown earth were causing them to have flashbacks to the deserts of Afghanistan and Iraq. Children were showing regressive behaviors, loss of developmental milestones, and symptoms of separation anxiety such as wanting to sleep with their parents. In severe cases, they were having psychotic symptoms and auditory hallucinations. The children were grieving the loss of their homes, toys, pets, and family members, in some cases. , including medications, food, toiletries, and other household goods.
Puerto Rico’s future
Two and a half months after Maria, we learned from our students that things gradually had begun to improve. For example, the public schools had just reopened, and that change was expected to have a stabilizing effect on the children. We also learned that, of the 80 shelters that had been set up housing about 12,500 people, 40 shelters had closed. The five medical shelters that had been set up and funded by FEMA also were in the process of closing, and private donations were beginning to slow down. People were slowly returning to their tarped or otherwise repaired homes, albeit all too often without power.
During the storm, nearly 500,000* homes were destroyed. FEMA offered to airlift about 3,000 people who had no home 2 months past Maria to the U.S. mainland – either Florida or New York.
According to our students, people living in the mountains, mainly coffee growers and retired people and comprising about one-third of the population, remain in acute crisis. Part of the challenge is being able to reach this population: Some roads are still impassable, and supplies – such as drinking water – can be delivered only by helicopter. Despite current conditions, FEMA reportedly has announced that it would end emergency operations on the island.
Our team is currently involved in applying for grant funding that will enable us to return to provide additional training to physicians’ and teachers’ groups. Over the course of the next year, we would like to make six trips to Puerto Rico and focus each trip on a different region and different group of professionals so that the entire island has resources. In addition, we will offer follow-up consultations to professionals we trained previously. The regions to be trained would be San Juan, Ponce, Utuado, Mayagüez, Guayama, and a sixth to be determined upon need. We also would like to address the needs of any ongoing relief workers so that they will be more effective in their ongoing role. Meanwhile, financial assistance from the mainland remains uneven.
Many months after Maria (and Irma), the physical and mental health needs of the Puerto Rican people remain great. However, as mental health professionals, we have the tools to help them move forward.
Judith R. Milner, MD, MEd, SpecEd, is a general, child, and adolescent psychiatrist in private practice in Everett, Wash. She has traveled with various groups over the years in an effort to alleviate some of the suffering caused by war and natural disaster. Her predominant association has been with the International Center for Psychosocial Trauma. She also has worked with Step Up Rwanda Women and Pygmy Survival Alliance, as well as on the Committee for Women at the American Psychiatric Association and the Consumer Issues Committee and Membership Committee for the American Academy of Child and Adolescent Psychiatry.
*Correction, 2/12/2018: An earlier version of this story misstated the number of homes reportedly destroyed by Hurricane Maria.
The physical and mental health needs of the people of Puerto Rico cannot be underestimated. Just think of what they have been through over the last few months.
When Hurricane Maria barreled onto the island on Sept. 20, 2017 – just 2 weeks after Hurricane Irma reportedly left more than 1 million residents without power – it ripped off roofs and left behind massive flooding, roads washed out, and utility poles and transmission lines knocked down. Whole forests were defoliated, a massive loss of flora and fauna occurred, and 80% of the crop value was destroyed, along with massive loss of stray dogs and cats, dairy cows, industrial chicken coops, and tropical birds, including endangered species. Beloved pets were displaced.
The official death toll as a result of Maria was 64 in December, but according to reporting by The New York Times, that number could be as high as 1,052. Most of the people who died reportedly were men and women over age 50 in hospitals and nursing homes suffering from illnesses such as diabetes, Alzheimer’s, kidney disease, hypertension, pneumonia, and other respiratory diseases.
One grassroots organization that mobilized to provide supplies and medical assistance was Doctoras Boricuas, a group of all-female doctors in the United States and Puerto Rico that formed after the hurricanes to coordinate the delivery and distribution of supplies directly to Puerto Rico and the Virgin Islands. Two groups affiliated with the University of Missouri at Columbia joined forces to help: Global First Responder or GFR, a nonprofit, secular international medical relief organization founded in 2011 by Adam Beckett, MD, and the International Center for Psychosocial Trauma, or ICPT, a group established in 1995 by Syed Arshad Husain, MD, to help war-traumatized children in Bosnia. I joined Dr. Husain’s group of professionals – Kathryn Dewein, PhD; Andra Ferguson, PhD; and Cathy Grigg, PsyD, – all of whom have traveled broadly in the field of disaster psychiatry – to see how we could help the people of Puerto Rico in Maria’s aftermath.
What we did
ICPT and GFR were a combined team, but we served different functions. As part of ICPT, I focused on the mental health component and helped to train doctors, psychologists, social workers, and other mental health workers in both San Juan and Ponce. All told, we worked with about 50 people using the model of “Training the Trainers.” Many of our students were participants in the outreach teams. Our hope is that they will be able to train their peers to recognize and alleviate symptoms of acute and chronic stress disorders. Some of the techniques taught include patient education, relaxation training, breath work, visualization techniques, mindfulness training, narrative therapy, art therapy, and other expressive techniques.
What the PMSF did
Before Maria, the Ponce Medical School Foundation was in the process of facilitating the transfer of medical records into an electronic format. After the hurricane hit, however, PMSF’s program director, Antonio Fernandez, led a shift to disaster recovery work. PMSF got involved in airlifting dialysis patients off the island to safety, provided health care, and also collaborated with the Primary Care Psychology Program at Ponce Health Services University to assist in locating patients, identifying their health needs – including mental health – and providing for those needs to the extent possible.
At the time of our visit, Puerto Rico’s network of more than 90 largely rural federally funded primary care clinics mostly had reopened, but nearly half remained on back-up generators. Even with the medical centers open, patients were not coming in for one reason or another. People had medical problems, but the daily reality of survival, obtaining food and water, took precedence. Some patients were not showing up because they had left the country, or they were in shelters without transportation. Some people did not have fuel. Some could not keep track of their appointments without cell phones and electricity allowing them to access electronic planners. Some, having been without their medications since the storms, were too sick to travel. Outreach teams were necessary to locate patients, identify their needs, and provide medical and psychological care.
Community outreach
Nydia M. Cappas, PsyD, director of the Primary Care Psychology Program, told us that the outreach teams – consisting of doctors or other medical professionals, social workers, and psychologists, were being sent out to communities once a week. They visited homes for the elderly, orphans’ homes, and children in foster care, as well as individual patients. A similar service was provided by Vargas Medicine (VARMED) in the San Juan area.
Team members found that many people were suffering symptoms of posttraumatic stress disorder, even people who did not have prior psychiatric symptoms. They were having flashbacks and nightmares. Those flashbacks and nightmares were being triggered by clouds, by rain, by supplies beginning to run out.
Another trend we observed is that terrain changes prompted by Maria triggered PTSD symptoms among many veterans. The defoliated trees and brown earth were causing them to have flashbacks to the deserts of Afghanistan and Iraq. Children were showing regressive behaviors, loss of developmental milestones, and symptoms of separation anxiety such as wanting to sleep with their parents. In severe cases, they were having psychotic symptoms and auditory hallucinations. The children were grieving the loss of their homes, toys, pets, and family members, in some cases. , including medications, food, toiletries, and other household goods.
Puerto Rico’s future
Two and a half months after Maria, we learned from our students that things gradually had begun to improve. For example, the public schools had just reopened, and that change was expected to have a stabilizing effect on the children. We also learned that, of the 80 shelters that had been set up housing about 12,500 people, 40 shelters had closed. The five medical shelters that had been set up and funded by FEMA also were in the process of closing, and private donations were beginning to slow down. People were slowly returning to their tarped or otherwise repaired homes, albeit all too often without power.
During the storm, nearly 500,000* homes were destroyed. FEMA offered to airlift about 3,000 people who had no home 2 months past Maria to the U.S. mainland – either Florida or New York.
According to our students, people living in the mountains, mainly coffee growers and retired people and comprising about one-third of the population, remain in acute crisis. Part of the challenge is being able to reach this population: Some roads are still impassable, and supplies – such as drinking water – can be delivered only by helicopter. Despite current conditions, FEMA reportedly has announced that it would end emergency operations on the island.
Our team is currently involved in applying for grant funding that will enable us to return to provide additional training to physicians’ and teachers’ groups. Over the course of the next year, we would like to make six trips to Puerto Rico and focus each trip on a different region and different group of professionals so that the entire island has resources. In addition, we will offer follow-up consultations to professionals we trained previously. The regions to be trained would be San Juan, Ponce, Utuado, Mayagüez, Guayama, and a sixth to be determined upon need. We also would like to address the needs of any ongoing relief workers so that they will be more effective in their ongoing role. Meanwhile, financial assistance from the mainland remains uneven.
Many months after Maria (and Irma), the physical and mental health needs of the Puerto Rican people remain great. However, as mental health professionals, we have the tools to help them move forward.
Judith R. Milner, MD, MEd, SpecEd, is a general, child, and adolescent psychiatrist in private practice in Everett, Wash. She has traveled with various groups over the years in an effort to alleviate some of the suffering caused by war and natural disaster. Her predominant association has been with the International Center for Psychosocial Trauma. She also has worked with Step Up Rwanda Women and Pygmy Survival Alliance, as well as on the Committee for Women at the American Psychiatric Association and the Consumer Issues Committee and Membership Committee for the American Academy of Child and Adolescent Psychiatry.
*Correction, 2/12/2018: An earlier version of this story misstated the number of homes reportedly destroyed by Hurricane Maria.
A fantasy
The day had gone very well. The vascular surgeon woke early excited for a morning in the OR and then an afternoon in the office. Driving to the hospital, he had planned out his day. A patient with a fempop at 7:30, an AV fistula at 10:30 am, a quick bite in the doctor’s lounge, and then to the office for two phlebectomies, a few new consults, as well as some returning patients.

Fortunately, he had purchased an advanced electronic medical record so that reviewing old records and inputting new data went smoothly. He had been on call for the local hospital’s ER, but he received no calls, so his day was not impacted. After a dinner with his wife, also a surgeon, he helped put their youngest baby to sleep, played with his older children, took the dog out for a walk, read the latest JVS and went to sleep. Despite being on call, the phone never rang, and he had an uninterrupted sleep.
Now, what really happened!
The vascular surgeon woke early in preparation for a day in the OR and office. Traffic slowed him down, but he still arrived at the hospital just before his 7:30 start time. He expected his patient to be on the table prepped and ready for the procedure. But the OR supervisor informed him that new regulations required him to personally mark the site of surgery, update the H&P, and date and time the consent.
He was nonplussed. He had marked the patient last night and had signed the consent too. His PA had dictated a three-page H&P that was in the chart. However, the patient was still in the holding room. The surgeon rushed over, marked the leg again, and completed the required documentation.
“Well,” he thought, “I’ll run upstairs, discharge my carotid from yesterday, and by the time that’s done and I’ve changed into scrubs, my patient will be ready.” Impatiently he waited 5 minutes for the elevator, but it never arrived. So he elected to run up 10 floors and across to the other side of the hospital where the administrators had inconveniently placed the postop vascular patients. The patient was eager to leave. The vascular surgeon dictated the discharge note and signed into the hospital electronic medical record.
But the software insisted that he had to comply with numerous “safety” regulations before signing off. These required reviewing every medication and all discharge instructions. The patient was on 15 drugs, and the surgeon was unfamiliar with most. After 10 minutes of unsuccessfully trying to enter the relevant orders, he called a medical student over to help.
The patient was going to a skilled nursing facility. This required completing two more electronic forms. The software stubbornly refused to close the discharge section till he assigned the appropriate ICD-10 codes. After a few more frustrating minutes he finally clicked the proper boxes and completed the discharge.
It was 8:15 by the time he made the skin incision. The case went smoothly. He relaxed a little knowing that he probably would not run too late for the rest of his day. Finishing ahead of schedule, he dictated the note, spoke to the patient’s family, and went to preop his AV fistula scheduled for 10:30. Then back to the wards to complete rounds.
The first two patients were uncomplicated. The third had a fever requiring multiple orders in the EMR. Then heated conversations with the pharmacist and head of infection control, since the EMR would not allow him to prescribe the antibiotic of his choice. Back across the entire length of the hospital to see a patient with renal failure. But she was in dialysis at another distant location in the hospital.
At 10:30 he ran down to the OR ready to scrub. Again, this patient was still in the holding area. The patient’s potassium was 5.6, and the anesthesiologist wanted to run another blood test. Then the nurse had to go on break. Now there was confusion about whether a room would be available as another surgeon had a bump case.
Ultimately, he started at 11:30. During the procedure, his beeper went off constantly. There were already two consults in the ER. The fistula took a mere 30 minutes, but he had waited 90 minutes since finishing the fempop.
“Medicare should pay me for the time between cases, and I’ll do the procedure for free” he complained to a colleague as he passed her on the way to the ER to see the consults.
He sent the patient with the DVT home, but the patient with the infected foot would require later debridement. He admitted her and booked the OR for after office hours.
By the time he got to the doctors’ lounge all that was left was a half-eaten pack of Doritos and burned coffee.
He thought he would have a brief respite driving to the office. Then his surgeon wife called him in the car asking him to field a call from their son’s school since she was stuck in the OR.
He arrived late to the office. The waiting room was filled with hostile-looking patients one of whom made a point of holding up her watch as if to reinforce his tardiness. There were already three additions to his schedule. Further, his nurse told him that there was some issue with the internet connection to the server. Thus, despite his expensive EMR, no records were available. She had informed the patients that there would be a “little” delay.
While they were waiting she brought in reams of documents that had come in the prior day and needed his signatures. He also used the time “productively” to answer emails. When the EMR was back online, he returned to his patients who by now were seething.
A patient brought in a CD of a CTA. He loaded it up on a computer, but the disc kept spinning relentlessly. Cursing, he loaded it on a second computer. The instructions were indecipherable. He could get a picture up but could not scroll through the images. The program froze. By the time he had evaluated the disc, he had wasted over 20 minutes. He was running even further behind.
The next patient was a second opinion from a physician in another state. She brought in over 200 pages of medical records describing a multitude of prior procedures. Politely he explained he would need to read them first and rescheduled her.
The ER called again with a patient with a cold leg. He canceled the rest of the office and snuck out through a back door, afraid to witness the consternation in the waiting room.
At the hospital, he argued briefly with the anesthesiologist who was reluctant to anesthetize the patient who had eaten 5 hours before. So the harried surgeon read some vascular labs, and visited a few less stable patients. Then back to the OR to revascularize the ER patient’s leg and later to debride the earlier patient’s foot.
He got home at 8:30 pm. His wife had also been delayed by a long surgery. They put the baby to bed. There was no time to play with the other children. The surgical couple barely had the energy left to microwave leftovers for dinner. He was too tired to take the dog out for its nocturnal pee. He went to his study, picked up the JVS, and fell asleep in his chair. He woke up with a start as he felt the dog urinate on his leg.
Exhausted he climbed into bed. It had been a good day, he told himself. After all the ER had not been too disruptive. He drifted off into a deep sleep. And then the phone rang. Ruptured AAA in the ER.
The day had gone very well. The vascular surgeon woke early excited for a morning in the OR and then an afternoon in the office. Driving to the hospital, he had planned out his day. A patient with a fempop at 7:30, an AV fistula at 10:30 am, a quick bite in the doctor’s lounge, and then to the office for two phlebectomies, a few new consults, as well as some returning patients.
Fortunately, he had purchased an advanced electronic medical record so that reviewing old records and inputting new data went smoothly. He had been on call for the local hospital’s ER, but he received no calls, so his day was not impacted. After a dinner with his wife, also a surgeon, he helped put their youngest baby to sleep, played with his older children, took the dog out for a walk, read the latest JVS and went to sleep. Despite being on call, the phone never rang, and he had an uninterrupted sleep.
Now, what really happened!
The vascular surgeon woke early in preparation for a day in the OR and office. Traffic slowed him down, but he still arrived at the hospital just before his 7:30 start time. He expected his patient to be on the table prepped and ready for the procedure. But the OR supervisor informed him that new regulations required him to personally mark the site of surgery, update the H&P, and date and time the consent.
He was nonplussed. He had marked the patient last night and had signed the consent too. His PA had dictated a three-page H&P that was in the chart. However, the patient was still in the holding room. The surgeon rushed over, marked the leg again, and completed the required documentation.
“Well,” he thought, “I’ll run upstairs, discharge my carotid from yesterday, and by the time that’s done and I’ve changed into scrubs, my patient will be ready.” Impatiently he waited 5 minutes for the elevator, but it never arrived. So he elected to run up 10 floors and across to the other side of the hospital where the administrators had inconveniently placed the postop vascular patients. The patient was eager to leave. The vascular surgeon dictated the discharge note and signed into the hospital electronic medical record.
But the software insisted that he had to comply with numerous “safety” regulations before signing off. These required reviewing every medication and all discharge instructions. The patient was on 15 drugs, and the surgeon was unfamiliar with most. After 10 minutes of unsuccessfully trying to enter the relevant orders, he called a medical student over to help.
The patient was going to a skilled nursing facility. This required completing two more electronic forms. The software stubbornly refused to close the discharge section till he assigned the appropriate ICD-10 codes. After a few more frustrating minutes he finally clicked the proper boxes and completed the discharge.
It was 8:15 by the time he made the skin incision. The case went smoothly. He relaxed a little knowing that he probably would not run too late for the rest of his day. Finishing ahead of schedule, he dictated the note, spoke to the patient’s family, and went to preop his AV fistula scheduled for 10:30. Then back to the wards to complete rounds.
The first two patients were uncomplicated. The third had a fever requiring multiple orders in the EMR. Then heated conversations with the pharmacist and head of infection control, since the EMR would not allow him to prescribe the antibiotic of his choice. Back across the entire length of the hospital to see a patient with renal failure. But she was in dialysis at another distant location in the hospital.
At 10:30 he ran down to the OR ready to scrub. Again, this patient was still in the holding area. The patient’s potassium was 5.6, and the anesthesiologist wanted to run another blood test. Then the nurse had to go on break. Now there was confusion about whether a room would be available as another surgeon had a bump case.
Ultimately, he started at 11:30. During the procedure, his beeper went off constantly. There were already two consults in the ER. The fistula took a mere 30 minutes, but he had waited 90 minutes since finishing the fempop.
“Medicare should pay me for the time between cases, and I’ll do the procedure for free” he complained to a colleague as he passed her on the way to the ER to see the consults.
He sent the patient with the DVT home, but the patient with the infected foot would require later debridement. He admitted her and booked the OR for after office hours.
By the time he got to the doctors’ lounge all that was left was a half-eaten pack of Doritos and burned coffee.
He thought he would have a brief respite driving to the office. Then his surgeon wife called him in the car asking him to field a call from their son’s school since she was stuck in the OR.
He arrived late to the office. The waiting room was filled with hostile-looking patients one of whom made a point of holding up her watch as if to reinforce his tardiness. There were already three additions to his schedule. Further, his nurse told him that there was some issue with the internet connection to the server. Thus, despite his expensive EMR, no records were available. She had informed the patients that there would be a “little” delay.
While they were waiting she brought in reams of documents that had come in the prior day and needed his signatures. He also used the time “productively” to answer emails. When the EMR was back online, he returned to his patients who by now were seething.
A patient brought in a CD of a CTA. He loaded it up on a computer, but the disc kept spinning relentlessly. Cursing, he loaded it on a second computer. The instructions were indecipherable. He could get a picture up but could not scroll through the images. The program froze. By the time he had evaluated the disc, he had wasted over 20 minutes. He was running even further behind.
The next patient was a second opinion from a physician in another state. She brought in over 200 pages of medical records describing a multitude of prior procedures. Politely he explained he would need to read them first and rescheduled her.
The ER called again with a patient with a cold leg. He canceled the rest of the office and snuck out through a back door, afraid to witness the consternation in the waiting room.
At the hospital, he argued briefly with the anesthesiologist who was reluctant to anesthetize the patient who had eaten 5 hours before. So the harried surgeon read some vascular labs, and visited a few less stable patients. Then back to the OR to revascularize the ER patient’s leg and later to debride the earlier patient’s foot.
He got home at 8:30 pm. His wife had also been delayed by a long surgery. They put the baby to bed. There was no time to play with the other children. The surgical couple barely had the energy left to microwave leftovers for dinner. He was too tired to take the dog out for its nocturnal pee. He went to his study, picked up the JVS, and fell asleep in his chair. He woke up with a start as he felt the dog urinate on his leg.
Exhausted he climbed into bed. It had been a good day, he told himself. After all the ER had not been too disruptive. He drifted off into a deep sleep. And then the phone rang. Ruptured AAA in the ER.
The day had gone very well. The vascular surgeon woke early excited for a morning in the OR and then an afternoon in the office. Driving to the hospital, he had planned out his day. A patient with a fempop at 7:30, an AV fistula at 10:30 am, a quick bite in the doctor’s lounge, and then to the office for two phlebectomies, a few new consults, as well as some returning patients.
Fortunately, he had purchased an advanced electronic medical record so that reviewing old records and inputting new data went smoothly. He had been on call for the local hospital’s ER, but he received no calls, so his day was not impacted. After a dinner with his wife, also a surgeon, he helped put their youngest baby to sleep, played with his older children, took the dog out for a walk, read the latest JVS and went to sleep. Despite being on call, the phone never rang, and he had an uninterrupted sleep.
Now, what really happened!
The vascular surgeon woke early in preparation for a day in the OR and office. Traffic slowed him down, but he still arrived at the hospital just before his 7:30 start time. He expected his patient to be on the table prepped and ready for the procedure. But the OR supervisor informed him that new regulations required him to personally mark the site of surgery, update the H&P, and date and time the consent.
He was nonplussed. He had marked the patient last night and had signed the consent too. His PA had dictated a three-page H&P that was in the chart. However, the patient was still in the holding room. The surgeon rushed over, marked the leg again, and completed the required documentation.
“Well,” he thought, “I’ll run upstairs, discharge my carotid from yesterday, and by the time that’s done and I’ve changed into scrubs, my patient will be ready.” Impatiently he waited 5 minutes for the elevator, but it never arrived. So he elected to run up 10 floors and across to the other side of the hospital where the administrators had inconveniently placed the postop vascular patients. The patient was eager to leave. The vascular surgeon dictated the discharge note and signed into the hospital electronic medical record.
But the software insisted that he had to comply with numerous “safety” regulations before signing off. These required reviewing every medication and all discharge instructions. The patient was on 15 drugs, and the surgeon was unfamiliar with most. After 10 minutes of unsuccessfully trying to enter the relevant orders, he called a medical student over to help.
The patient was going to a skilled nursing facility. This required completing two more electronic forms. The software stubbornly refused to close the discharge section till he assigned the appropriate ICD-10 codes. After a few more frustrating minutes he finally clicked the proper boxes and completed the discharge.
It was 8:15 by the time he made the skin incision. The case went smoothly. He relaxed a little knowing that he probably would not run too late for the rest of his day. Finishing ahead of schedule, he dictated the note, spoke to the patient’s family, and went to preop his AV fistula scheduled for 10:30. Then back to the wards to complete rounds.
The first two patients were uncomplicated. The third had a fever requiring multiple orders in the EMR. Then heated conversations with the pharmacist and head of infection control, since the EMR would not allow him to prescribe the antibiotic of his choice. Back across the entire length of the hospital to see a patient with renal failure. But she was in dialysis at another distant location in the hospital.
At 10:30 he ran down to the OR ready to scrub. Again, this patient was still in the holding area. The patient’s potassium was 5.6, and the anesthesiologist wanted to run another blood test. Then the nurse had to go on break. Now there was confusion about whether a room would be available as another surgeon had a bump case.
Ultimately, he started at 11:30. During the procedure, his beeper went off constantly. There were already two consults in the ER. The fistula took a mere 30 minutes, but he had waited 90 minutes since finishing the fempop.
“Medicare should pay me for the time between cases, and I’ll do the procedure for free” he complained to a colleague as he passed her on the way to the ER to see the consults.
He sent the patient with the DVT home, but the patient with the infected foot would require later debridement. He admitted her and booked the OR for after office hours.
By the time he got to the doctors’ lounge all that was left was a half-eaten pack of Doritos and burned coffee.
He thought he would have a brief respite driving to the office. Then his surgeon wife called him in the car asking him to field a call from their son’s school since she was stuck in the OR.
He arrived late to the office. The waiting room was filled with hostile-looking patients one of whom made a point of holding up her watch as if to reinforce his tardiness. There were already three additions to his schedule. Further, his nurse told him that there was some issue with the internet connection to the server. Thus, despite his expensive EMR, no records were available. She had informed the patients that there would be a “little” delay.
While they were waiting she brought in reams of documents that had come in the prior day and needed his signatures. He also used the time “productively” to answer emails. When the EMR was back online, he returned to his patients who by now were seething.
A patient brought in a CD of a CTA. He loaded it up on a computer, but the disc kept spinning relentlessly. Cursing, he loaded it on a second computer. The instructions were indecipherable. He could get a picture up but could not scroll through the images. The program froze. By the time he had evaluated the disc, he had wasted over 20 minutes. He was running even further behind.
The next patient was a second opinion from a physician in another state. She brought in over 200 pages of medical records describing a multitude of prior procedures. Politely he explained he would need to read them first and rescheduled her.
The ER called again with a patient with a cold leg. He canceled the rest of the office and snuck out through a back door, afraid to witness the consternation in the waiting room.
At the hospital, he argued briefly with the anesthesiologist who was reluctant to anesthetize the patient who had eaten 5 hours before. So the harried surgeon read some vascular labs, and visited a few less stable patients. Then back to the OR to revascularize the ER patient’s leg and later to debride the earlier patient’s foot.
He got home at 8:30 pm. His wife had also been delayed by a long surgery. They put the baby to bed. There was no time to play with the other children. The surgical couple barely had the energy left to microwave leftovers for dinner. He was too tired to take the dog out for its nocturnal pee. He went to his study, picked up the JVS, and fell asleep in his chair. He woke up with a start as he felt the dog urinate on his leg.
Exhausted he climbed into bed. It had been a good day, he told himself. After all the ER had not been too disruptive. He drifted off into a deep sleep. And then the phone rang. Ruptured AAA in the ER.
Make the Diagnosis - February 2018
Neurofibromatosis (NF) is an autosomal dominant genetic neurocutaneous disorder. There are eight subtypes of NF: NF type 1-7 and NF-NOS, or not otherwise specified. Neurofibromatosis type 1 (NF-1), or von Recklinghausen disease, is the most common and is a result of a genetic mutation on chromosome 17 that is involved in producing a protein called neurofibromin. Neurofibromin is a tumor suppressor that suppresses products of ras proto-oncogenes. When it is absent, tumor progression may occur.
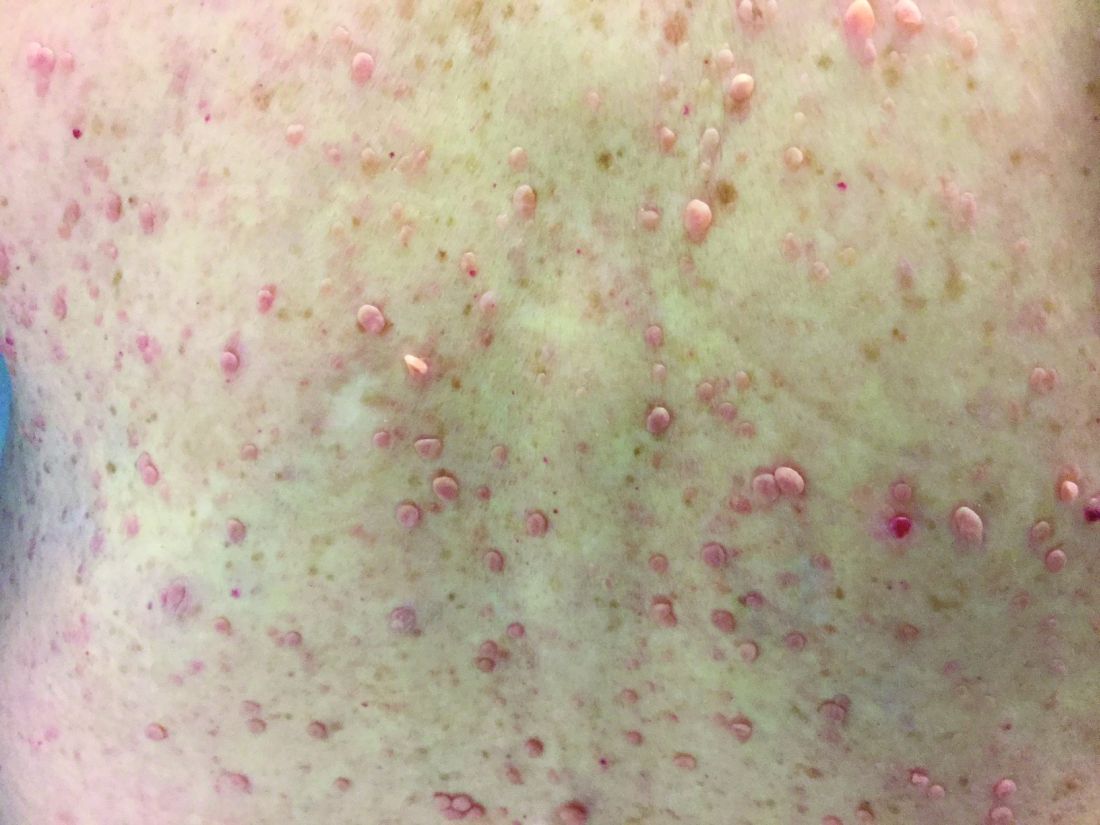
Von Recklinghausen NF-1 appears in childhood, usually by age 10. Diagnosis requires the presence of at least 2 of the following 7 criteria:
•Six or more café au lait macules measuring 5 mm in diameter or greater in prepubertal children and measuring greater than 15 mm in postpubertal children.
•Axillary or inguinal freckling (Crowe’s sign).
•Two or more neurofibromas or one plexiform neurofibroma.
•Optic nerve glioma.
•Two or more iris hamartomas (Lisch nodules).
•Sphenoid dysplasia or long-bone abnormalities, such as pseudoarthrosis.
•First degree relative with NF-1.
The diagnosis is usually made via physical examination. Supportive tests include an ophthalmologic exam to detect Lisch nodules and cataracts. A neurological evaluation is essential. Imaging examinations can identify bony abnormalities and tumor growths. Also, genetic testing to identify genetic mutations can be performed.

Neurofibromatosis type 2 results from a genetic mutation located on chromosome 22 that produces a protein called merlin and occurs in adolescence. Acoustic or vestibular neuromas may occur; these interfere with the transmission of sound and maintaining balance. Symptoms include gradual hearing loss, tinnitus, poor balance, and headaches. Radiosurgery and cochlear implants have shown a role for symptomatic treatment in patients with NF-2.
This case and photo were submitted by Parteek Singla, MD, of the division of dermatology at Washington University and Barnes Jewish Hospital, both in St. Louis, and by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
Neurofibromatosis (NF) is an autosomal dominant genetic neurocutaneous disorder. There are eight subtypes of NF: NF type 1-7 and NF-NOS, or not otherwise specified. Neurofibromatosis type 1 (NF-1), or von Recklinghausen disease, is the most common and is a result of a genetic mutation on chromosome 17 that is involved in producing a protein called neurofibromin. Neurofibromin is a tumor suppressor that suppresses products of ras proto-oncogenes. When it is absent, tumor progression may occur.
Von Recklinghausen NF-1 appears in childhood, usually by age 10. Diagnosis requires the presence of at least 2 of the following 7 criteria:
•Six or more café au lait macules measuring 5 mm in diameter or greater in prepubertal children and measuring greater than 15 mm in postpubertal children.
•Axillary or inguinal freckling (Crowe’s sign).
•Two or more neurofibromas or one plexiform neurofibroma.
•Optic nerve glioma.
•Two or more iris hamartomas (Lisch nodules).
•Sphenoid dysplasia or long-bone abnormalities, such as pseudoarthrosis.
•First degree relative with NF-1.
The diagnosis is usually made via physical examination. Supportive tests include an ophthalmologic exam to detect Lisch nodules and cataracts. A neurological evaluation is essential. Imaging examinations can identify bony abnormalities and tumor growths. Also, genetic testing to identify genetic mutations can be performed.
Neurofibromatosis type 2 results from a genetic mutation located on chromosome 22 that produces a protein called merlin and occurs in adolescence. Acoustic or vestibular neuromas may occur; these interfere with the transmission of sound and maintaining balance. Symptoms include gradual hearing loss, tinnitus, poor balance, and headaches. Radiosurgery and cochlear implants have shown a role for symptomatic treatment in patients with NF-2.
This case and photo were submitted by Parteek Singla, MD, of the division of dermatology at Washington University and Barnes Jewish Hospital, both in St. Louis, and by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
Neurofibromatosis (NF) is an autosomal dominant genetic neurocutaneous disorder. There are eight subtypes of NF: NF type 1-7 and NF-NOS, or not otherwise specified. Neurofibromatosis type 1 (NF-1), or von Recklinghausen disease, is the most common and is a result of a genetic mutation on chromosome 17 that is involved in producing a protein called neurofibromin. Neurofibromin is a tumor suppressor that suppresses products of ras proto-oncogenes. When it is absent, tumor progression may occur.
Von Recklinghausen NF-1 appears in childhood, usually by age 10. Diagnosis requires the presence of at least 2 of the following 7 criteria:
•Six or more café au lait macules measuring 5 mm in diameter or greater in prepubertal children and measuring greater than 15 mm in postpubertal children.
•Axillary or inguinal freckling (Crowe’s sign).
•Two or more neurofibromas or one plexiform neurofibroma.
•Optic nerve glioma.
•Two or more iris hamartomas (Lisch nodules).
•Sphenoid dysplasia or long-bone abnormalities, such as pseudoarthrosis.
•First degree relative with NF-1.
The diagnosis is usually made via physical examination. Supportive tests include an ophthalmologic exam to detect Lisch nodules and cataracts. A neurological evaluation is essential. Imaging examinations can identify bony abnormalities and tumor growths. Also, genetic testing to identify genetic mutations can be performed.
Neurofibromatosis type 2 results from a genetic mutation located on chromosome 22 that produces a protein called merlin and occurs in adolescence. Acoustic or vestibular neuromas may occur; these interfere with the transmission of sound and maintaining balance. Symptoms include gradual hearing loss, tinnitus, poor balance, and headaches. Radiosurgery and cochlear implants have shown a role for symptomatic treatment in patients with NF-2.
This case and photo were submitted by Parteek Singla, MD, of the division of dermatology at Washington University and Barnes Jewish Hospital, both in St. Louis, and by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
Using oral and topical cosmeceuticals to prevent and treat skin aging, Part II
This month’s column resumes my review of prevention and treatment strategies for aging skin using oral and topical cosmeceutical agents.
Preventing and treating inflammation
Skin aging can result from inflammation through several mechanisms, including the formation of reactive oxygen species. Inflammation itself arises from myriad etiologic pathways, with multiple inflammatory mediators potentially involved, including histamines, cytokines, eicosanoids (for example, prostaglandins, thromboxanes, and leukotrienes), complement cascade components, kinins, fibrinopeptide enzymes, nuclear factor–kappa B, and free radicals.

Topically applied argan oil, caffeine, chamomile, feverfew, green tea, licorice extract, aloe, linoleic acid (found in high concentrations in argan oil and safflower oil), and niacinamide are among the anti-inflammatory ingredients that have been used successfully in topical skin care to reduce inflammation. The Food and Drug Administration does not allow cosmetics to make “anti-inflammatory” claims. For this reason, these products will state they have “soothing” effects or imply they improve of redness.
Oral polypodium leucotomos has been demonstrated to suppress the effect of UV radiation on COX-2 expression.2 Also, glycolic acid has exhibited the capacity to inhibit COX-2 signaling and other inflammatory mediators.3
Preventing and treating glycation
Glycation is produced by the Maillard reaction, a chemical reaction – particularly well known in cooking – between an amino acid and a sugar molecule that typically requires heat. This reaction was first described by Louis Camille Maillard in 1912 when he noted that amino acids can react with sugar to yield brown or golden-brown substances. It took until the 1980s for scientists to understand the importance of glycation in health.
When glycation occurs, sugar molecules attach to proteins, creating cross-linked proteins known as advanced glycation end products (or AGEs) and causing a series of chemical reactions. Glycation occurs in collagen fibers and results in the formation of cross-links that bind collagen fibers to each other, which leaves the skin stiffer. Glycosylated collagen is believed to be a factor in the appearance of aged skin.4 Glycation also can affect elastin: Recent research suggests that glycation can engender elastosis, which is elastin that is abnormally clumped together and presents more frequently in aged skin.
Several antiaging skin care products claim to treat glycation, but – unfortunately – glycation is not a reversible reaction. It must be prevented in the first place. Some studies suggest that antioxidants can prevent glycation, but it is more likely that they just divert the process down a different pathway that still leads to glycation. Reducing serum glucose levels is the optimum method of preventing glycation.5 Dietary intervention and oral metformin are recommended for lowering glycation.
REVERSING SKIN CELL AGING
Epidermal keratinocytes in aging
Young basal stem cells synthesize a plethora of new keratinocytes at a pace that leads to fast cell turnover and vigorous production of protective epidermal constituents. Old keratinocytes display less energy, show reduced responsiveness to cellular signals, and do not synthesize these protective components.6,7 Keratinocyte stem cell function declines over time while damage accumulates, as seen in a diminished response to growth factors, decreased keratinization, and impaired function.8
Dermal fibroblasts in cutaneous aging
Young fibroblasts produce key cellular constituents, including collagen, elastin, hyaluronic acid, and heparan sulfate. This production declines in older fibroblasts. Like aging keratinocytes, old fibroblasts lose energy and responsiveness to growth factors and other cellular signals.6,7
Rejuvenating aged skin with cosmeceuticals
Gene expression, growth factors, cytokines, chemokines, and receptor activation guide the function of keratinocytes and fibroblasts. To reverse or slow cellular skin aging, old keratinocytes and fibroblasts must be galvanized to respond to such signals or the signals must be enhanced.
Stimulating old keratinocytes and fibroblasts
Essential steps in stimulating aged keratinocytes and fibroblasts include: activating gene expression, adding growth factors, activating cytokines and chemokines, turning on receptors, and making cells more responsive to signals.
Influencing gene expression
Retinoids are known to affect collagen genes and increase activity of procollagen genes, thereby reducing the production of collagenase. Many studies have shown the efficacy of retinoids in treating aged skin and preventing cutaneous aging in both areas frequently exposed to the sun but also those that aren’t.9,10 Prescription retinoids (tretinoin, adapalene, tazarotene) and over-the-counter retinoids (retinol) are first-line options to treat and prevent aging by stimulating old keratinocytes and fibroblasts.10,11 However, exposing retinoic acid receptors to retinoids almost invariably leads to erythema and flaking in the first few weeks. Therefore, retinoids should be titrated slowly. Note that retinoid esters, such as retinyl palmitate and retinyl linoleate, do not penetrate well into the dermis;12 they also are not as effective as retinol, tretinoin, adapalene, and tazarotene. Compliance with retinoids is always an issue with patients. They should receive printed educational material about how to begin use and why it is important to use these products consistently.

Growth factors
The use of cosmetic formulations that contain growth factors can contribute to skin rejuvenation. There are various types of growth factors that have the capacity to stimulate old keratinocytes and fibroblasts to enhance function.17 Growth factors, which are inactive or vulnerable to degradation in their native, soluble form, can directly energize genes or act as a signaling mechanism. To exert their quintessential functions, growth factors must be transferred to the correct receptor site in order for the cell to respond to their signal.18
Heparan sulfate
Heparan sulfate (HS) plays a primary role in cell-to-cell communications. It increases cellular response to growth factors by facilitating the response of old, lazy fibroblasts to the cellular signals.18 HS binds, stores, and protects growth factors, which allows them to complete movement to their targets, and then presents them to the appropriate binding site.18,19 A topically applied analogue of HS has been demonstrated to rejuvenate aged skin.20
Stem cells
Stem cells included and pointedly marketed in cosmeceutical products are usually plant derived, are too large to penetrate the stratum corneum, display short shelf lives, and do not behave as human stem cells would. As a result, stem cells in cosmeceutical agents are essentially useless.
However, novel technologies have revealed ingredients that can incite native stem cells to repopulate the epidermis and dermis with young cells. Stem cells in skin include basal stem cells and 10 varieties of hair follicle stem cells. The LGR6+ hair follicle cells play a pivotal role in repopulating the epidermis after wounding has occurred.21,22 Aesthetic physicians have known for several years that inducing skin wounding with lasers, needles, and acidic peels leads to improvement in its appearance. Researchers have provided new data showing that wounding the skin prompts LGR6+ stem cells to repopulate the epidermis. Once wounding occurs, neutrophils release the peptide defensin, which stimulates the LGR6+ stem cells to repopulate the epidermis.23 Topical defensin that has been formulated to penetrate into hair follicles, where the LGR6+ stem cells reside, has been demonstrated to render a smoother, more youthful appearance to the skin.
Conclusion
It is important for practitioners to identify patients at risk for premature skin aging as early as possible and start them on an appropriate and consistent skin care regimen. This typically will include at least a daily sunscreen with an SPF 15 or higher, a nightly topical retinoid, and oral and topical antioxidants. The patient’s additional skin type proclivities (for example, dryness, inflammation, melanocyte activity) should guide the physician as to how to combine these baseline product types with cleansers, moisturizers, and formulations with hydroxy acids, growth factors, heparan sulfate, and defensin.
Several studies have revealed that patients exhibit poor compliance with recommended regimens.24 Informing patients about the need for skin protection and providing printed instructions can help to improve compliance.25 This can promote healthy lifestyle habits and compliance with scientifically proven antiaging therapies.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
1. Arch Dermatol Res. 2010 Jan;302(1):5-17.
2. Am J Pathol. 2009 Nov;175(5):1952-61.
3. J Dermatol Sci. 2017 Jun;86(3):238-48.
4. Eur J Dermatol. 2007 Jan-Feb;17(1):12-20.
5. “Advanced Glycation End Products (AGEs): Emerging Mediators of Skin Aging,” in Textbook of Aging Skin (Berlin: Springer, 2017, pp. 1675-86).
6. Mech Ageing Dev. 1986 Jul;35(2):185-98.
7. Exp Cell Res. 1996 Sep 15;227(2):252-5.
8. J Cutan Pathol. 2003 Jul;30(6):351-7.
9. PLoS One. 2015 Feb 6;10(2):e0117491.
10. Arch Dermatol. 2007 May;143(5):606-12.
11. JAMA. 1988 Jan 22-29;259(4):527-32.
12. J Invest Dermatol. 1997 Sep;109(3):301-5.
13. J Am Acad Dermatol. 1996 Feb;34(2 Pt 1):187-95.
14. J Am Acad Dermatol. 1996 Sep;35(3 Pt 1):388-91.
15. Dermatol Surg. 2001 May;27(5):429-33.
16. J Invest Dermatol. 1994 Aug;103(2):228-32.
17. Clin Cosmet Investig Dermatol. 2016 Nov 9;9:411-9.
18. Chem Biol Drug Des. 2008 Dec;72(6):455-82.
19. Front Immunol. 2013 Dec 18;4:470.
20. J Drugs Dermatol. 2015 Jul;14(7):669-74.
21. Science. 2010 Mar 12;327(5971):1385-9.
22. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
23. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
24. J Am Acad Dermatol. 2008 Jul;59(1):27-33.
25. J Am Acad Dermatol. 2013 Mar;68(3):364.e1-10.
This month’s column resumes my review of prevention and treatment strategies for aging skin using oral and topical cosmeceutical agents.
Preventing and treating inflammation
Skin aging can result from inflammation through several mechanisms, including the formation of reactive oxygen species. Inflammation itself arises from myriad etiologic pathways, with multiple inflammatory mediators potentially involved, including histamines, cytokines, eicosanoids (for example, prostaglandins, thromboxanes, and leukotrienes), complement cascade components, kinins, fibrinopeptide enzymes, nuclear factor–kappa B, and free radicals.
Topically applied argan oil, caffeine, chamomile, feverfew, green tea, licorice extract, aloe, linoleic acid (found in high concentrations in argan oil and safflower oil), and niacinamide are among the anti-inflammatory ingredients that have been used successfully in topical skin care to reduce inflammation. The Food and Drug Administration does not allow cosmetics to make “anti-inflammatory” claims. For this reason, these products will state they have “soothing” effects or imply they improve of redness.
Oral polypodium leucotomos has been demonstrated to suppress the effect of UV radiation on COX-2 expression.2 Also, glycolic acid has exhibited the capacity to inhibit COX-2 signaling and other inflammatory mediators.3
Preventing and treating glycation
Glycation is produced by the Maillard reaction, a chemical reaction – particularly well known in cooking – between an amino acid and a sugar molecule that typically requires heat. This reaction was first described by Louis Camille Maillard in 1912 when he noted that amino acids can react with sugar to yield brown or golden-brown substances. It took until the 1980s for scientists to understand the importance of glycation in health.
When glycation occurs, sugar molecules attach to proteins, creating cross-linked proteins known as advanced glycation end products (or AGEs) and causing a series of chemical reactions. Glycation occurs in collagen fibers and results in the formation of cross-links that bind collagen fibers to each other, which leaves the skin stiffer. Glycosylated collagen is believed to be a factor in the appearance of aged skin.4 Glycation also can affect elastin: Recent research suggests that glycation can engender elastosis, which is elastin that is abnormally clumped together and presents more frequently in aged skin.
Several antiaging skin care products claim to treat glycation, but – unfortunately – glycation is not a reversible reaction. It must be prevented in the first place. Some studies suggest that antioxidants can prevent glycation, but it is more likely that they just divert the process down a different pathway that still leads to glycation. Reducing serum glucose levels is the optimum method of preventing glycation.5 Dietary intervention and oral metformin are recommended for lowering glycation.
REVERSING SKIN CELL AGING
Epidermal keratinocytes in aging
Young basal stem cells synthesize a plethora of new keratinocytes at a pace that leads to fast cell turnover and vigorous production of protective epidermal constituents. Old keratinocytes display less energy, show reduced responsiveness to cellular signals, and do not synthesize these protective components.6,7 Keratinocyte stem cell function declines over time while damage accumulates, as seen in a diminished response to growth factors, decreased keratinization, and impaired function.8
Dermal fibroblasts in cutaneous aging
Young fibroblasts produce key cellular constituents, including collagen, elastin, hyaluronic acid, and heparan sulfate. This production declines in older fibroblasts. Like aging keratinocytes, old fibroblasts lose energy and responsiveness to growth factors and other cellular signals.6,7
Rejuvenating aged skin with cosmeceuticals
Gene expression, growth factors, cytokines, chemokines, and receptor activation guide the function of keratinocytes and fibroblasts. To reverse or slow cellular skin aging, old keratinocytes and fibroblasts must be galvanized to respond to such signals or the signals must be enhanced.
Stimulating old keratinocytes and fibroblasts
Essential steps in stimulating aged keratinocytes and fibroblasts include: activating gene expression, adding growth factors, activating cytokines and chemokines, turning on receptors, and making cells more responsive to signals.
Influencing gene expression
Retinoids are known to affect collagen genes and increase activity of procollagen genes, thereby reducing the production of collagenase. Many studies have shown the efficacy of retinoids in treating aged skin and preventing cutaneous aging in both areas frequently exposed to the sun but also those that aren’t.9,10 Prescription retinoids (tretinoin, adapalene, tazarotene) and over-the-counter retinoids (retinol) are first-line options to treat and prevent aging by stimulating old keratinocytes and fibroblasts.10,11 However, exposing retinoic acid receptors to retinoids almost invariably leads to erythema and flaking in the first few weeks. Therefore, retinoids should be titrated slowly. Note that retinoid esters, such as retinyl palmitate and retinyl linoleate, do not penetrate well into the dermis;12 they also are not as effective as retinol, tretinoin, adapalene, and tazarotene. Compliance with retinoids is always an issue with patients. They should receive printed educational material about how to begin use and why it is important to use these products consistently.
Growth factors
The use of cosmetic formulations that contain growth factors can contribute to skin rejuvenation. There are various types of growth factors that have the capacity to stimulate old keratinocytes and fibroblasts to enhance function.17 Growth factors, which are inactive or vulnerable to degradation in their native, soluble form, can directly energize genes or act as a signaling mechanism. To exert their quintessential functions, growth factors must be transferred to the correct receptor site in order for the cell to respond to their signal.18
Heparan sulfate
Heparan sulfate (HS) plays a primary role in cell-to-cell communications. It increases cellular response to growth factors by facilitating the response of old, lazy fibroblasts to the cellular signals.18 HS binds, stores, and protects growth factors, which allows them to complete movement to their targets, and then presents them to the appropriate binding site.18,19 A topically applied analogue of HS has been demonstrated to rejuvenate aged skin.20
Stem cells
Stem cells included and pointedly marketed in cosmeceutical products are usually plant derived, are too large to penetrate the stratum corneum, display short shelf lives, and do not behave as human stem cells would. As a result, stem cells in cosmeceutical agents are essentially useless.
However, novel technologies have revealed ingredients that can incite native stem cells to repopulate the epidermis and dermis with young cells. Stem cells in skin include basal stem cells and 10 varieties of hair follicle stem cells. The LGR6+ hair follicle cells play a pivotal role in repopulating the epidermis after wounding has occurred.21,22 Aesthetic physicians have known for several years that inducing skin wounding with lasers, needles, and acidic peels leads to improvement in its appearance. Researchers have provided new data showing that wounding the skin prompts LGR6+ stem cells to repopulate the epidermis. Once wounding occurs, neutrophils release the peptide defensin, which stimulates the LGR6+ stem cells to repopulate the epidermis.23 Topical defensin that has been formulated to penetrate into hair follicles, where the LGR6+ stem cells reside, has been demonstrated to render a smoother, more youthful appearance to the skin.
Conclusion
It is important for practitioners to identify patients at risk for premature skin aging as early as possible and start them on an appropriate and consistent skin care regimen. This typically will include at least a daily sunscreen with an SPF 15 or higher, a nightly topical retinoid, and oral and topical antioxidants. The patient’s additional skin type proclivities (for example, dryness, inflammation, melanocyte activity) should guide the physician as to how to combine these baseline product types with cleansers, moisturizers, and formulations with hydroxy acids, growth factors, heparan sulfate, and defensin.
Several studies have revealed that patients exhibit poor compliance with recommended regimens.24 Informing patients about the need for skin protection and providing printed instructions can help to improve compliance.25 This can promote healthy lifestyle habits and compliance with scientifically proven antiaging therapies.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
1. Arch Dermatol Res. 2010 Jan;302(1):5-17.
2. Am J Pathol. 2009 Nov;175(5):1952-61.
3. J Dermatol Sci. 2017 Jun;86(3):238-48.
4. Eur J Dermatol. 2007 Jan-Feb;17(1):12-20.
5. “Advanced Glycation End Products (AGEs): Emerging Mediators of Skin Aging,” in Textbook of Aging Skin (Berlin: Springer, 2017, pp. 1675-86).
6. Mech Ageing Dev. 1986 Jul;35(2):185-98.
7. Exp Cell Res. 1996 Sep 15;227(2):252-5.
8. J Cutan Pathol. 2003 Jul;30(6):351-7.
9. PLoS One. 2015 Feb 6;10(2):e0117491.
10. Arch Dermatol. 2007 May;143(5):606-12.
11. JAMA. 1988 Jan 22-29;259(4):527-32.
12. J Invest Dermatol. 1997 Sep;109(3):301-5.
13. J Am Acad Dermatol. 1996 Feb;34(2 Pt 1):187-95.
14. J Am Acad Dermatol. 1996 Sep;35(3 Pt 1):388-91.
15. Dermatol Surg. 2001 May;27(5):429-33.
16. J Invest Dermatol. 1994 Aug;103(2):228-32.
17. Clin Cosmet Investig Dermatol. 2016 Nov 9;9:411-9.
18. Chem Biol Drug Des. 2008 Dec;72(6):455-82.
19. Front Immunol. 2013 Dec 18;4:470.
20. J Drugs Dermatol. 2015 Jul;14(7):669-74.
21. Science. 2010 Mar 12;327(5971):1385-9.
22. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
23. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
24. J Am Acad Dermatol. 2008 Jul;59(1):27-33.
25. J Am Acad Dermatol. 2013 Mar;68(3):364.e1-10.
This month’s column resumes my review of prevention and treatment strategies for aging skin using oral and topical cosmeceutical agents.
Preventing and treating inflammation
Skin aging can result from inflammation through several mechanisms, including the formation of reactive oxygen species. Inflammation itself arises from myriad etiologic pathways, with multiple inflammatory mediators potentially involved, including histamines, cytokines, eicosanoids (for example, prostaglandins, thromboxanes, and leukotrienes), complement cascade components, kinins, fibrinopeptide enzymes, nuclear factor–kappa B, and free radicals.
Topically applied argan oil, caffeine, chamomile, feverfew, green tea, licorice extract, aloe, linoleic acid (found in high concentrations in argan oil and safflower oil), and niacinamide are among the anti-inflammatory ingredients that have been used successfully in topical skin care to reduce inflammation. The Food and Drug Administration does not allow cosmetics to make “anti-inflammatory” claims. For this reason, these products will state they have “soothing” effects or imply they improve of redness.
Oral polypodium leucotomos has been demonstrated to suppress the effect of UV radiation on COX-2 expression.2 Also, glycolic acid has exhibited the capacity to inhibit COX-2 signaling and other inflammatory mediators.3
Preventing and treating glycation
Glycation is produced by the Maillard reaction, a chemical reaction – particularly well known in cooking – between an amino acid and a sugar molecule that typically requires heat. This reaction was first described by Louis Camille Maillard in 1912 when he noted that amino acids can react with sugar to yield brown or golden-brown substances. It took until the 1980s for scientists to understand the importance of glycation in health.
When glycation occurs, sugar molecules attach to proteins, creating cross-linked proteins known as advanced glycation end products (or AGEs) and causing a series of chemical reactions. Glycation occurs in collagen fibers and results in the formation of cross-links that bind collagen fibers to each other, which leaves the skin stiffer. Glycosylated collagen is believed to be a factor in the appearance of aged skin.4 Glycation also can affect elastin: Recent research suggests that glycation can engender elastosis, which is elastin that is abnormally clumped together and presents more frequently in aged skin.
Several antiaging skin care products claim to treat glycation, but – unfortunately – glycation is not a reversible reaction. It must be prevented in the first place. Some studies suggest that antioxidants can prevent glycation, but it is more likely that they just divert the process down a different pathway that still leads to glycation. Reducing serum glucose levels is the optimum method of preventing glycation.5 Dietary intervention and oral metformin are recommended for lowering glycation.
REVERSING SKIN CELL AGING
Epidermal keratinocytes in aging
Young basal stem cells synthesize a plethora of new keratinocytes at a pace that leads to fast cell turnover and vigorous production of protective epidermal constituents. Old keratinocytes display less energy, show reduced responsiveness to cellular signals, and do not synthesize these protective components.6,7 Keratinocyte stem cell function declines over time while damage accumulates, as seen in a diminished response to growth factors, decreased keratinization, and impaired function.8
Dermal fibroblasts in cutaneous aging
Young fibroblasts produce key cellular constituents, including collagen, elastin, hyaluronic acid, and heparan sulfate. This production declines in older fibroblasts. Like aging keratinocytes, old fibroblasts lose energy and responsiveness to growth factors and other cellular signals.6,7
Rejuvenating aged skin with cosmeceuticals
Gene expression, growth factors, cytokines, chemokines, and receptor activation guide the function of keratinocytes and fibroblasts. To reverse or slow cellular skin aging, old keratinocytes and fibroblasts must be galvanized to respond to such signals or the signals must be enhanced.
Stimulating old keratinocytes and fibroblasts
Essential steps in stimulating aged keratinocytes and fibroblasts include: activating gene expression, adding growth factors, activating cytokines and chemokines, turning on receptors, and making cells more responsive to signals.
Influencing gene expression
Retinoids are known to affect collagen genes and increase activity of procollagen genes, thereby reducing the production of collagenase. Many studies have shown the efficacy of retinoids in treating aged skin and preventing cutaneous aging in both areas frequently exposed to the sun but also those that aren’t.9,10 Prescription retinoids (tretinoin, adapalene, tazarotene) and over-the-counter retinoids (retinol) are first-line options to treat and prevent aging by stimulating old keratinocytes and fibroblasts.10,11 However, exposing retinoic acid receptors to retinoids almost invariably leads to erythema and flaking in the first few weeks. Therefore, retinoids should be titrated slowly. Note that retinoid esters, such as retinyl palmitate and retinyl linoleate, do not penetrate well into the dermis;12 they also are not as effective as retinol, tretinoin, adapalene, and tazarotene. Compliance with retinoids is always an issue with patients. They should receive printed educational material about how to begin use and why it is important to use these products consistently.
Growth factors
The use of cosmetic formulations that contain growth factors can contribute to skin rejuvenation. There are various types of growth factors that have the capacity to stimulate old keratinocytes and fibroblasts to enhance function.17 Growth factors, which are inactive or vulnerable to degradation in their native, soluble form, can directly energize genes or act as a signaling mechanism. To exert their quintessential functions, growth factors must be transferred to the correct receptor site in order for the cell to respond to their signal.18
Heparan sulfate
Heparan sulfate (HS) plays a primary role in cell-to-cell communications. It increases cellular response to growth factors by facilitating the response of old, lazy fibroblasts to the cellular signals.18 HS binds, stores, and protects growth factors, which allows them to complete movement to their targets, and then presents them to the appropriate binding site.18,19 A topically applied analogue of HS has been demonstrated to rejuvenate aged skin.20
Stem cells
Stem cells included and pointedly marketed in cosmeceutical products are usually plant derived, are too large to penetrate the stratum corneum, display short shelf lives, and do not behave as human stem cells would. As a result, stem cells in cosmeceutical agents are essentially useless.
However, novel technologies have revealed ingredients that can incite native stem cells to repopulate the epidermis and dermis with young cells. Stem cells in skin include basal stem cells and 10 varieties of hair follicle stem cells. The LGR6+ hair follicle cells play a pivotal role in repopulating the epidermis after wounding has occurred.21,22 Aesthetic physicians have known for several years that inducing skin wounding with lasers, needles, and acidic peels leads to improvement in its appearance. Researchers have provided new data showing that wounding the skin prompts LGR6+ stem cells to repopulate the epidermis. Once wounding occurs, neutrophils release the peptide defensin, which stimulates the LGR6+ stem cells to repopulate the epidermis.23 Topical defensin that has been formulated to penetrate into hair follicles, where the LGR6+ stem cells reside, has been demonstrated to render a smoother, more youthful appearance to the skin.
Conclusion
It is important for practitioners to identify patients at risk for premature skin aging as early as possible and start them on an appropriate and consistent skin care regimen. This typically will include at least a daily sunscreen with an SPF 15 or higher, a nightly topical retinoid, and oral and topical antioxidants. The patient’s additional skin type proclivities (for example, dryness, inflammation, melanocyte activity) should guide the physician as to how to combine these baseline product types with cleansers, moisturizers, and formulations with hydroxy acids, growth factors, heparan sulfate, and defensin.
Several studies have revealed that patients exhibit poor compliance with recommended regimens.24 Informing patients about the need for skin protection and providing printed instructions can help to improve compliance.25 This can promote healthy lifestyle habits and compliance with scientifically proven antiaging therapies.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
1. Arch Dermatol Res. 2010 Jan;302(1):5-17.
2. Am J Pathol. 2009 Nov;175(5):1952-61.
3. J Dermatol Sci. 2017 Jun;86(3):238-48.
4. Eur J Dermatol. 2007 Jan-Feb;17(1):12-20.
5. “Advanced Glycation End Products (AGEs): Emerging Mediators of Skin Aging,” in Textbook of Aging Skin (Berlin: Springer, 2017, pp. 1675-86).
6. Mech Ageing Dev. 1986 Jul;35(2):185-98.
7. Exp Cell Res. 1996 Sep 15;227(2):252-5.
8. J Cutan Pathol. 2003 Jul;30(6):351-7.
9. PLoS One. 2015 Feb 6;10(2):e0117491.
10. Arch Dermatol. 2007 May;143(5):606-12.
11. JAMA. 1988 Jan 22-29;259(4):527-32.
12. J Invest Dermatol. 1997 Sep;109(3):301-5.
13. J Am Acad Dermatol. 1996 Feb;34(2 Pt 1):187-95.
14. J Am Acad Dermatol. 1996 Sep;35(3 Pt 1):388-91.
15. Dermatol Surg. 2001 May;27(5):429-33.
16. J Invest Dermatol. 1994 Aug;103(2):228-32.
17. Clin Cosmet Investig Dermatol. 2016 Nov 9;9:411-9.
18. Chem Biol Drug Des. 2008 Dec;72(6):455-82.
19. Front Immunol. 2013 Dec 18;4:470.
20. J Drugs Dermatol. 2015 Jul;14(7):669-74.
21. Science. 2010 Mar 12;327(5971):1385-9.
22. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
23. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
24. J Am Acad Dermatol. 2008 Jul;59(1):27-33.
25. J Am Acad Dermatol. 2013 Mar;68(3):364.e1-10.
Welcome to The New Gastroenterologist online!
Dear Colleagues,
It is with great excitement that I introduce the first e-newsletter version of The New Gastroenterologist! As more content in medicine, and life in general, is moving toward digital platforms, we at the AGA believe this transition will improve both content dissemination and accessibility to all our readers. In this new format, we will continue to provide articles on topics of importance to the early-career community, expand our offerings by including the new “In Focus” articles (concise overviews of GI topics) both digitally and in GI & Hepatology News print issues, as well as increase the use of multimedia resources, such as videos, to further enhance our content.
In this issue of The New Gastroenterologist, our In Focus article provides a practical overview of the management of chronic constipation. This article, written by Nitin Ahuja and James Reynolds from the Neurogastroenterology and Motility Program at the University of Pennsylvania, Philadelphia, addresses a common topic in our field, and can also be found in the February print issue of GI & Hepatology News. To complement this article, there is a corresponding video abstract that can be viewed.
Also in this issue, Richard Peek (Vanderbilt University, Nashville, Tenn.) – one of the Coeditors in Chief of Gastroenterology – provides a summary of the newly created 1-year editorial fellowship for the AGA’s flagship journal. This is a fantastic new opportunity and you can learn firsthand about the experience of the inaugural editorial fellow, Eric Shah (University of Michigan, Ann Arbor), in an accompanying video. Additionally, as helping patients make a successful transition from a pediatric GI practice to an adult GI practice can be very challenging, in this issue Manreet Kaur and Allyson Wyatt (Baylor College of Medicine, Houston) provide a primer on how to successfully aid in this transition.
Are you considering a career in hospital administration? If so, you will enjoy reading about pursuing a career in hospital administration from Brijen Shah, who is the chief medical officer of Mount Sinai Queens (Icahn School of Medicine at Mount Sinai, New York). Have you been to one of the AGA’s Regional Practice Skills Workshops? These workshops are sponsored by the AGA Trainee and Early Career Committee and held in a growing number of cities across the country. In this issue, Munish Ashat (University of Iowa, Iowa City) provides a recap of the workshop he attended, complete with many useful career pearls.
I hope that you also enjoy the other features in the new e-newsletter format of The New Gastroenterologist. I especially want to point out one of our new sections entitled “In Case You Missed It.” As we all undoubtedly experience information overload with so many new articles released each month, this section collects relevant articles from the numerous AGA publications and consolidates them to ensure you don’t miss any of this great content.
If you are interested in contributing to future issues of The New Gastroenterologist or if there are topics that would interest you, please let us know. You can contact me ([email protected]) or the managing editor of The New Gastroenterologist, Ryan Farrell ([email protected]).
Sincerely,
Bryson W. Katona, MD, PhD
Editor in Chief
Dr. Katona is an instructor of medicine in the division of gastroenterology at the University of Pennsylvania, Philadelphia.
Dear Colleagues,
It is with great excitement that I introduce the first e-newsletter version of The New Gastroenterologist! As more content in medicine, and life in general, is moving toward digital platforms, we at the AGA believe this transition will improve both content dissemination and accessibility to all our readers. In this new format, we will continue to provide articles on topics of importance to the early-career community, expand our offerings by including the new “In Focus” articles (concise overviews of GI topics) both digitally and in GI & Hepatology News print issues, as well as increase the use of multimedia resources, such as videos, to further enhance our content.
In this issue of The New Gastroenterologist, our In Focus article provides a practical overview of the management of chronic constipation. This article, written by Nitin Ahuja and James Reynolds from the Neurogastroenterology and Motility Program at the University of Pennsylvania, Philadelphia, addresses a common topic in our field, and can also be found in the February print issue of GI & Hepatology News. To complement this article, there is a corresponding video abstract that can be viewed.
Also in this issue, Richard Peek (Vanderbilt University, Nashville, Tenn.) – one of the Coeditors in Chief of Gastroenterology – provides a summary of the newly created 1-year editorial fellowship for the AGA’s flagship journal. This is a fantastic new opportunity and you can learn firsthand about the experience of the inaugural editorial fellow, Eric Shah (University of Michigan, Ann Arbor), in an accompanying video. Additionally, as helping patients make a successful transition from a pediatric GI practice to an adult GI practice can be very challenging, in this issue Manreet Kaur and Allyson Wyatt (Baylor College of Medicine, Houston) provide a primer on how to successfully aid in this transition.
Are you considering a career in hospital administration? If so, you will enjoy reading about pursuing a career in hospital administration from Brijen Shah, who is the chief medical officer of Mount Sinai Queens (Icahn School of Medicine at Mount Sinai, New York). Have you been to one of the AGA’s Regional Practice Skills Workshops? These workshops are sponsored by the AGA Trainee and Early Career Committee and held in a growing number of cities across the country. In this issue, Munish Ashat (University of Iowa, Iowa City) provides a recap of the workshop he attended, complete with many useful career pearls.
I hope that you also enjoy the other features in the new e-newsletter format of The New Gastroenterologist. I especially want to point out one of our new sections entitled “In Case You Missed It.” As we all undoubtedly experience information overload with so many new articles released each month, this section collects relevant articles from the numerous AGA publications and consolidates them to ensure you don’t miss any of this great content.
If you are interested in contributing to future issues of The New Gastroenterologist or if there are topics that would interest you, please let us know. You can contact me ([email protected]) or the managing editor of The New Gastroenterologist, Ryan Farrell ([email protected]).
Sincerely,
Bryson W. Katona, MD, PhD
Editor in Chief
Dr. Katona is an instructor of medicine in the division of gastroenterology at the University of Pennsylvania, Philadelphia.
Dear Colleagues,
It is with great excitement that I introduce the first e-newsletter version of The New Gastroenterologist! As more content in medicine, and life in general, is moving toward digital platforms, we at the AGA believe this transition will improve both content dissemination and accessibility to all our readers. In this new format, we will continue to provide articles on topics of importance to the early-career community, expand our offerings by including the new “In Focus” articles (concise overviews of GI topics) both digitally and in GI & Hepatology News print issues, as well as increase the use of multimedia resources, such as videos, to further enhance our content.
In this issue of The New Gastroenterologist, our In Focus article provides a practical overview of the management of chronic constipation. This article, written by Nitin Ahuja and James Reynolds from the Neurogastroenterology and Motility Program at the University of Pennsylvania, Philadelphia, addresses a common topic in our field, and can also be found in the February print issue of GI & Hepatology News. To complement this article, there is a corresponding video abstract that can be viewed.
Also in this issue, Richard Peek (Vanderbilt University, Nashville, Tenn.) – one of the Coeditors in Chief of Gastroenterology – provides a summary of the newly created 1-year editorial fellowship for the AGA’s flagship journal. This is a fantastic new opportunity and you can learn firsthand about the experience of the inaugural editorial fellow, Eric Shah (University of Michigan, Ann Arbor), in an accompanying video. Additionally, as helping patients make a successful transition from a pediatric GI practice to an adult GI practice can be very challenging, in this issue Manreet Kaur and Allyson Wyatt (Baylor College of Medicine, Houston) provide a primer on how to successfully aid in this transition.
Are you considering a career in hospital administration? If so, you will enjoy reading about pursuing a career in hospital administration from Brijen Shah, who is the chief medical officer of Mount Sinai Queens (Icahn School of Medicine at Mount Sinai, New York). Have you been to one of the AGA’s Regional Practice Skills Workshops? These workshops are sponsored by the AGA Trainee and Early Career Committee and held in a growing number of cities across the country. In this issue, Munish Ashat (University of Iowa, Iowa City) provides a recap of the workshop he attended, complete with many useful career pearls.
I hope that you also enjoy the other features in the new e-newsletter format of The New Gastroenterologist. I especially want to point out one of our new sections entitled “In Case You Missed It.” As we all undoubtedly experience information overload with so many new articles released each month, this section collects relevant articles from the numerous AGA publications and consolidates them to ensure you don’t miss any of this great content.
If you are interested in contributing to future issues of The New Gastroenterologist or if there are topics that would interest you, please let us know. You can contact me ([email protected]) or the managing editor of The New Gastroenterologist, Ryan Farrell ([email protected]).
Sincerely,
Bryson W. Katona, MD, PhD
Editor in Chief
Dr. Katona is an instructor of medicine in the division of gastroenterology at the University of Pennsylvania, Philadelphia.
Preventive health: Getting rid of the middleman (uh-oh, that’s us!)
As physicians, we find that preventive health is, frankly, really difficult. It requires thinking about a changing list of recommendations unprompted by the symptoms for which patients present. Compounding that challenge is that, in doing preventive health well, we need to have personalized discussions with our patients and this requires they come into the office, which doesn’t always happen on a regular basis. Furthermore, when patients do come in, they usually are presenting for an acute care visit, so there is little time set aside to discuss preventive health.

For all these reasons and many others, the data suggest that we are not particularly good at performing preventive health maintenance. We are much better at figuring out diagnostic dilemmas and choosing among competing medications or procedures to most effectively address acute and chronic medical problems. Let’s examine the data to see if there is a shred of truth in what we are saying; then let’s look at a potential solution to the dilemma of preventive health that we all believe in and that we carry out less frequently than any of us would like.
First, let’s look at recent data on cancer screening reported by the CDC1:
- Mammography: 72% of women aged 50–74 years reported having had a mammogram within the past 2 years.
- Pap test: 83% of women reported being up to date with cervical cancer screening.
- Colorectal cancer screening: 62% of men and women reported colorectal cancer screening test use consistent with USPSTF recommendations.
Of note, colorectal cancer screening has improved dramatically over he last 15 years, while screening for breast and cervical cancer has largely plateaued.1
Our success with cancer screening – or lack thereof depending upon one’s perspective – looks quite good next to national vaccination rates for adults. The immunization rate for commonly recommended vaccines are as follows2:
- The Tdap vaccination rate is 20%.
- The tetanus-diphtheria vaccination rate is 62%.
- The herpes zoster vaccination rate is 28%.
- The influenza vaccination rate is 43%.
- The pneumococcal vaccination rate among high-risk persons aged 19-64 years is 20% and among adults aged greater than or equal to 65 years is 61%.
Of adults who had health insurance and at least 10 physician contacts within the past year, 23.8%-88.8% reported not having received vaccinations that were recommended.
In the business literature there is a great deal of disagreement about the value of the “middleman.” The term middleman describes someone who brings the product from the producer, or factory, to the consumer. On the one hand, if the factory can sell the product directly to the consumer, the consumer can save money and the factory can make more money. On the other hand, if the middleman can help the consumer make a better choice among the variety of products available, then the middleman provides value and the consumer benefits.3
Traditionally, clinicians have served the role of the middleman for preventive health activities, knowing what to recommend to patients and informing them of the correct preventive health choices that fit their needs. The problem with this concept is that preventive health recommendations are largely demographically based, are tied to population-based risk assessment, and usually require very little individual judgment.
We as physicians are good at – and I believe truly enjoy – exercising judgment. We love thinking things through and helping the person in front of us. We are not as good at remembering unprompted information in the middle of busy visits that are often made for unrelated reasons. Most of the people who have not had a colonoscopy or pneumococcal vaccine have not decided against the procedure after a detailed discussion with their physician. On the contrary, the service was never recommended, or it was recommended, but the patient did not follow up to have the procedure performed.
Let’s now imagine another approach. You’re a patient and once a year you click on an email that shows up in your inbox from your doctor with the words “Preventive Health” in the subject line. The EHR – based on your gender, age, and a query of what has been documented in your chart – has determined the preventive health activities that are recommended for you. You can choose to pursue, opt out, or get more information for each of the recommended preventive services as you read through them.
If you choose to have more information, it is provided in a structured format that allows you to drill down to the level of detail that you desire. In all probability, you will find a greater level of detail and accuracy of information about each preventive service than could possibly be provided during a routine office visit. Specifics about the risks and benefits of the procedure will also be more extensive, as it is unlikely your care providers are able to keep all of the details and risk ratios in their heads. If desired, you as a patient can take your time to read and digest the information, sleep on it, and come back to it to make an informed decision. This is not something you can do during a routine office visit.
If you choose to opt out of the procedure, just click the “declined” box. Otherwise, when you’ve made all of your decisions and indicate that you’re done, the necessary prescriptions for blood work and x-rays, as well as referrals to the appropriate specialists, will print out. An entry will also be made in the electronic record showing you’ve been provided preventive health recommendations that are appropriate for your age and sex and made your preferred choices. At any point, if you feel you’d like further discussion with your physician, you can make an appointment electronically through the interface.
The hurdles for implementing such a system are real, but they are solvable, and the development of such an approach is inevitable, enviable, and will ultimately be good for both patients and their providers. Patients will get more predictable and complete recommendations for preventive care and providers will have more time to do what we enjoy and are most skilled at – talking with patients to clarify diagnoses, decide upon treatment, and clarify questions that come up about preventive health recommendations.
Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records.
References
1. White A et al. Cancer screening test use – United States, 2015. MMWR Morb Mortal Wkly Rep. 2017 Mar 3;66(8):201-6.
2. Williams WW et al. Surveillance of vaccination coverage among adult populations – United States, 2014. MMWR Surveill Summ. 2016 Feb 5;65(1):1-36.
3. Conerly B. Don’t eliminate the middleman – He’s much too valuable. Forbes. Oct 28, 2015.
As physicians, we find that preventive health is, frankly, really difficult. It requires thinking about a changing list of recommendations unprompted by the symptoms for which patients present. Compounding that challenge is that, in doing preventive health well, we need to have personalized discussions with our patients and this requires they come into the office, which doesn’t always happen on a regular basis. Furthermore, when patients do come in, they usually are presenting for an acute care visit, so there is little time set aside to discuss preventive health.
For all these reasons and many others, the data suggest that we are not particularly good at performing preventive health maintenance. We are much better at figuring out diagnostic dilemmas and choosing among competing medications or procedures to most effectively address acute and chronic medical problems. Let’s examine the data to see if there is a shred of truth in what we are saying; then let’s look at a potential solution to the dilemma of preventive health that we all believe in and that we carry out less frequently than any of us would like.
First, let’s look at recent data on cancer screening reported by the CDC1:
- Mammography: 72% of women aged 50–74 years reported having had a mammogram within the past 2 years.
- Pap test: 83% of women reported being up to date with cervical cancer screening.
- Colorectal cancer screening: 62% of men and women reported colorectal cancer screening test use consistent with USPSTF recommendations.
Of note, colorectal cancer screening has improved dramatically over he last 15 years, while screening for breast and cervical cancer has largely plateaued.1
Our success with cancer screening – or lack thereof depending upon one’s perspective – looks quite good next to national vaccination rates for adults. The immunization rate for commonly recommended vaccines are as follows2:
- The Tdap vaccination rate is 20%.
- The tetanus-diphtheria vaccination rate is 62%.
- The herpes zoster vaccination rate is 28%.
- The influenza vaccination rate is 43%.
- The pneumococcal vaccination rate among high-risk persons aged 19-64 years is 20% and among adults aged greater than or equal to 65 years is 61%.
Of adults who had health insurance and at least 10 physician contacts within the past year, 23.8%-88.8% reported not having received vaccinations that were recommended.
In the business literature there is a great deal of disagreement about the value of the “middleman.” The term middleman describes someone who brings the product from the producer, or factory, to the consumer. On the one hand, if the factory can sell the product directly to the consumer, the consumer can save money and the factory can make more money. On the other hand, if the middleman can help the consumer make a better choice among the variety of products available, then the middleman provides value and the consumer benefits.3
Traditionally, clinicians have served the role of the middleman for preventive health activities, knowing what to recommend to patients and informing them of the correct preventive health choices that fit their needs. The problem with this concept is that preventive health recommendations are largely demographically based, are tied to population-based risk assessment, and usually require very little individual judgment.
We as physicians are good at – and I believe truly enjoy – exercising judgment. We love thinking things through and helping the person in front of us. We are not as good at remembering unprompted information in the middle of busy visits that are often made for unrelated reasons. Most of the people who have not had a colonoscopy or pneumococcal vaccine have not decided against the procedure after a detailed discussion with their physician. On the contrary, the service was never recommended, or it was recommended, but the patient did not follow up to have the procedure performed.
Let’s now imagine another approach. You’re a patient and once a year you click on an email that shows up in your inbox from your doctor with the words “Preventive Health” in the subject line. The EHR – based on your gender, age, and a query of what has been documented in your chart – has determined the preventive health activities that are recommended for you. You can choose to pursue, opt out, or get more information for each of the recommended preventive services as you read through them.
If you choose to have more information, it is provided in a structured format that allows you to drill down to the level of detail that you desire. In all probability, you will find a greater level of detail and accuracy of information about each preventive service than could possibly be provided during a routine office visit. Specifics about the risks and benefits of the procedure will also be more extensive, as it is unlikely your care providers are able to keep all of the details and risk ratios in their heads. If desired, you as a patient can take your time to read and digest the information, sleep on it, and come back to it to make an informed decision. This is not something you can do during a routine office visit.
If you choose to opt out of the procedure, just click the “declined” box. Otherwise, when you’ve made all of your decisions and indicate that you’re done, the necessary prescriptions for blood work and x-rays, as well as referrals to the appropriate specialists, will print out. An entry will also be made in the electronic record showing you’ve been provided preventive health recommendations that are appropriate for your age and sex and made your preferred choices. At any point, if you feel you’d like further discussion with your physician, you can make an appointment electronically through the interface.
The hurdles for implementing such a system are real, but they are solvable, and the development of such an approach is inevitable, enviable, and will ultimately be good for both patients and their providers. Patients will get more predictable and complete recommendations for preventive care and providers will have more time to do what we enjoy and are most skilled at – talking with patients to clarify diagnoses, decide upon treatment, and clarify questions that come up about preventive health recommendations.
Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records.
References
1. White A et al. Cancer screening test use – United States, 2015. MMWR Morb Mortal Wkly Rep. 2017 Mar 3;66(8):201-6.
2. Williams WW et al. Surveillance of vaccination coverage among adult populations – United States, 2014. MMWR Surveill Summ. 2016 Feb 5;65(1):1-36.
3. Conerly B. Don’t eliminate the middleman – He’s much too valuable. Forbes. Oct 28, 2015.
As physicians, we find that preventive health is, frankly, really difficult. It requires thinking about a changing list of recommendations unprompted by the symptoms for which patients present. Compounding that challenge is that, in doing preventive health well, we need to have personalized discussions with our patients and this requires they come into the office, which doesn’t always happen on a regular basis. Furthermore, when patients do come in, they usually are presenting for an acute care visit, so there is little time set aside to discuss preventive health.
For all these reasons and many others, the data suggest that we are not particularly good at performing preventive health maintenance. We are much better at figuring out diagnostic dilemmas and choosing among competing medications or procedures to most effectively address acute and chronic medical problems. Let’s examine the data to see if there is a shred of truth in what we are saying; then let’s look at a potential solution to the dilemma of preventive health that we all believe in and that we carry out less frequently than any of us would like.
First, let’s look at recent data on cancer screening reported by the CDC1:
- Mammography: 72% of women aged 50–74 years reported having had a mammogram within the past 2 years.
- Pap test: 83% of women reported being up to date with cervical cancer screening.
- Colorectal cancer screening: 62% of men and women reported colorectal cancer screening test use consistent with USPSTF recommendations.
Of note, colorectal cancer screening has improved dramatically over he last 15 years, while screening for breast and cervical cancer has largely plateaued.1
Our success with cancer screening – or lack thereof depending upon one’s perspective – looks quite good next to national vaccination rates for adults. The immunization rate for commonly recommended vaccines are as follows2:
- The Tdap vaccination rate is 20%.
- The tetanus-diphtheria vaccination rate is 62%.
- The herpes zoster vaccination rate is 28%.
- The influenza vaccination rate is 43%.
- The pneumococcal vaccination rate among high-risk persons aged 19-64 years is 20% and among adults aged greater than or equal to 65 years is 61%.
Of adults who had health insurance and at least 10 physician contacts within the past year, 23.8%-88.8% reported not having received vaccinations that were recommended.
In the business literature there is a great deal of disagreement about the value of the “middleman.” The term middleman describes someone who brings the product from the producer, or factory, to the consumer. On the one hand, if the factory can sell the product directly to the consumer, the consumer can save money and the factory can make more money. On the other hand, if the middleman can help the consumer make a better choice among the variety of products available, then the middleman provides value and the consumer benefits.3
Traditionally, clinicians have served the role of the middleman for preventive health activities, knowing what to recommend to patients and informing them of the correct preventive health choices that fit their needs. The problem with this concept is that preventive health recommendations are largely demographically based, are tied to population-based risk assessment, and usually require very little individual judgment.
We as physicians are good at – and I believe truly enjoy – exercising judgment. We love thinking things through and helping the person in front of us. We are not as good at remembering unprompted information in the middle of busy visits that are often made for unrelated reasons. Most of the people who have not had a colonoscopy or pneumococcal vaccine have not decided against the procedure after a detailed discussion with their physician. On the contrary, the service was never recommended, or it was recommended, but the patient did not follow up to have the procedure performed.
Let’s now imagine another approach. You’re a patient and once a year you click on an email that shows up in your inbox from your doctor with the words “Preventive Health” in the subject line. The EHR – based on your gender, age, and a query of what has been documented in your chart – has determined the preventive health activities that are recommended for you. You can choose to pursue, opt out, or get more information for each of the recommended preventive services as you read through them.
If you choose to have more information, it is provided in a structured format that allows you to drill down to the level of detail that you desire. In all probability, you will find a greater level of detail and accuracy of information about each preventive service than could possibly be provided during a routine office visit. Specifics about the risks and benefits of the procedure will also be more extensive, as it is unlikely your care providers are able to keep all of the details and risk ratios in their heads. If desired, you as a patient can take your time to read and digest the information, sleep on it, and come back to it to make an informed decision. This is not something you can do during a routine office visit.
If you choose to opt out of the procedure, just click the “declined” box. Otherwise, when you’ve made all of your decisions and indicate that you’re done, the necessary prescriptions for blood work and x-rays, as well as referrals to the appropriate specialists, will print out. An entry will also be made in the electronic record showing you’ve been provided preventive health recommendations that are appropriate for your age and sex and made your preferred choices. At any point, if you feel you’d like further discussion with your physician, you can make an appointment electronically through the interface.
The hurdles for implementing such a system are real, but they are solvable, and the development of such an approach is inevitable, enviable, and will ultimately be good for both patients and their providers. Patients will get more predictable and complete recommendations for preventive care and providers will have more time to do what we enjoy and are most skilled at – talking with patients to clarify diagnoses, decide upon treatment, and clarify questions that come up about preventive health recommendations.
Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records.
References
1. White A et al. Cancer screening test use – United States, 2015. MMWR Morb Mortal Wkly Rep. 2017 Mar 3;66(8):201-6.
2. Williams WW et al. Surveillance of vaccination coverage among adult populations – United States, 2014. MMWR Surveill Summ. 2016 Feb 5;65(1):1-36.
3. Conerly B. Don’t eliminate the middleman – He’s much too valuable. Forbes. Oct 28, 2015.