User login
The importance of family acceptance for LGBTQ youth
It is well established that LGBTQ individuals experience more health disparities compared with their cisgender, heterosexual counterparts. In general, LGBTQ adolescents and young adults have higher levels of depression, suicide attempts, and substance use than those of their heterosexual peers. However, a key protective factor is family acceptance and support. By encouraging families to modify and change behaviors that are experienced by their LGBTQ children as rejecting and to engage in supportive and affirming behaviors, providers can help families to decrease risk and promote healthy outcomes for LGBTQ youth and young adults. 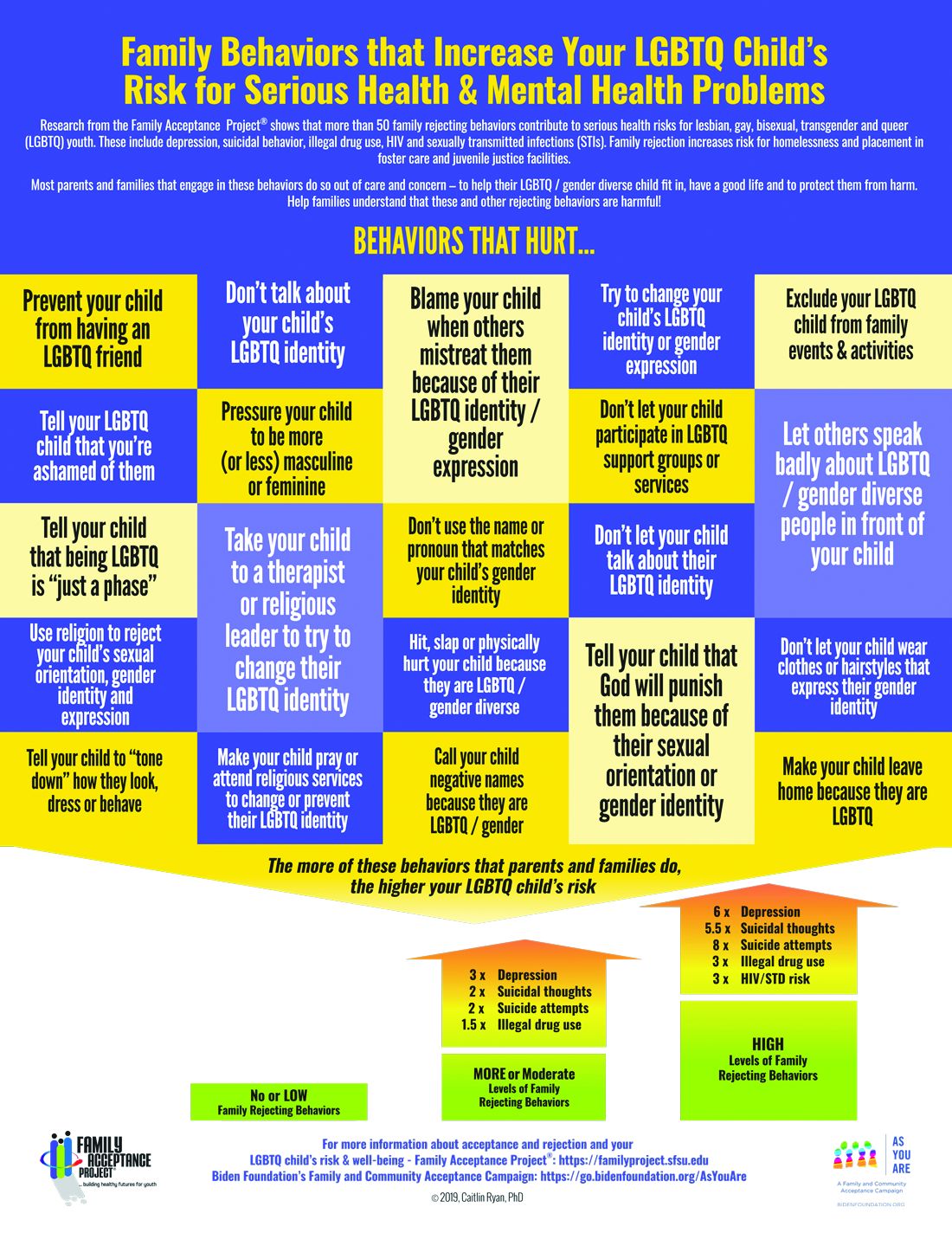
We all know that a supportive family can make a difference for any child, but this is especially true for LGBTQ youth and is critical during a pandemic when young people are confined with families and separated from peers and supportive adults outside the home. Several research studies show that family support can improve outcomes related to suicide, depression, homelessness, drug use, and HIV in LGBTQ young people. Family acceptance improves health outcomes, while rejection undermines family relationships and worsens both health and other serious outcomes such as homelessness and placement in custodial care. Pediatricians can help their patients by educating parents and caregivers with LGBTQ children about the critical role of family support – both those who see themselves as accepting and those who believe that being gay or transgender is wrong and are struggling with parenting a child who identifies as LGBTQ or who is gender diverse.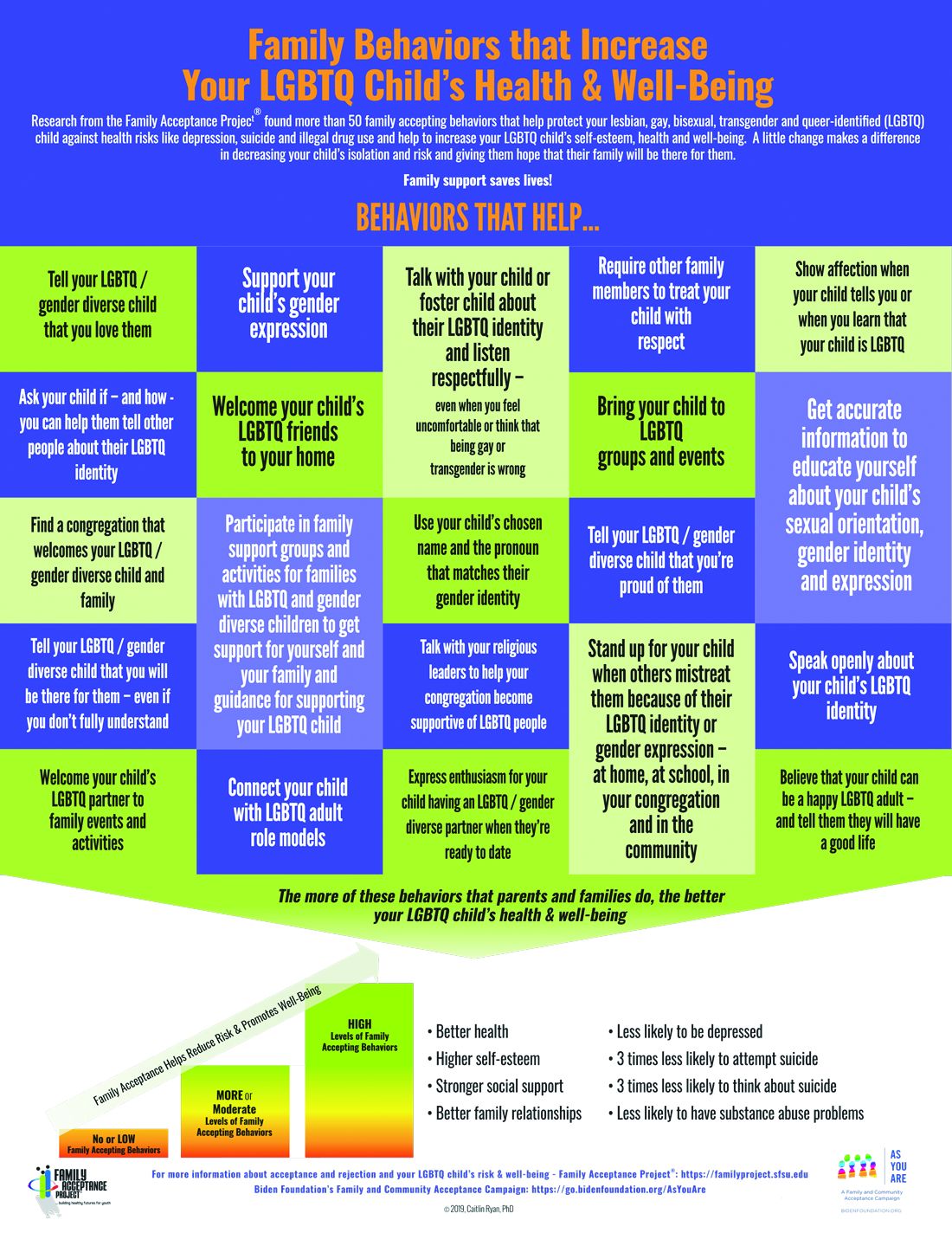
The Family Acceptance Project (FAP) at San Francisco State University conducted the first research on LGBTQ youth and families, developed the first evidence-informed family support model, and has published a range of studies and evidence-based resources that demonstrate the harm caused by family rejection, validate the importance of family acceptance, and provide guidance to increase family support. FAP’s research found that parents and caregivers that engage in rejecting behaviors are typically motivated by care and concern and by trying to protect their children from harm. They believe such behaviors will help their LGBTQ children fit in, have a good life, meet cultural and religious expectations, and be respected by others.1 FAP’s research identified and measured more than 50 rejecting behaviors that parents and caregivers use to respond to their LGBTQ children. Some of these commonly expressed rejecting behaviors include ridiculing and making disparaging comments about their child and other LGBTQ people; excluding them from family activities; blaming their child when others mistreat them because they are LGBTQ; blocking access to LGBTQ resources including friends, support groups, and activities; and trying to change their child’s sexual orientation and gender identity.2 LGBTQ youth experience these and other such behaviors as hurtful, harmful, and traumatic and may feel that they need to hide or repress their identity which can affect their self-esteem, increase isolation, depression, and risky behaviors.3 Providers working with families of LGBTQ youth should focus on shared goals, such as reducing risk and having a happy, healthy child. Most parents love their children and fear for their well-being. However, many are uninformed about their child’s gender identity and sexual orientation and don’t know how to nurture and support them.
In FAP’s initial study, LGB young people who reported higher levels of family rejection had substantially higher rates of attempted suicide, depression, illegal drug use, and unprotected sex.4 These rates were even more significant among Latino gay and bisexual men.4 Those who are rejected by family are less likely to want to have a family or to be parents themselves5 and have lower educational and income levels.6

To reduce risk, pediatricians should ask LGBTQ patients about family rejecting behaviors and help parents and caregivers to identify and understand the effect of such behaviors to reduce health risks and conflict that can lead to running away, expulsion, and removal from the home. Even decreasing rejecting behaviors to moderate levels can significantly improve negative outcomes.5
Caitlin Ryan, PhD, and her team also identified and measured more than 50 family accepting behaviors that help protect against risk and promote well-being. They found that young adults who experience high levels of family acceptance during adolescence report significantly higher levels of self-esteem, social support, and general health with much lower levels of depression, suicidality, and substance abuse.7 Family accepting and supportive behaviors include talking with the child about their LGBTQ identity; advocating for their LGBTQ child when others mistreat them; requiring other family members to treat their LGBTQ child with respect; and supporting their child’s gender identity.5 FAP has developed an evidence-informed family support model and multilingual educational resources for families, providers, youth and religious leaders to decrease rejection and increase family support. These are available in print copies and for download at familyproject.sfsu.edu.
In addition, Dr. Ryan and colleagues1,4,8 recommend the following guidance for providers:
- Ask LGBTQ adolescents about family reactions to their sexual orientation, gender identity, and expression, and refer to LGBTQ community support programs and for supportive counseling, as needed.
- Identify LGBTQ community support programs and online resources to educate parents about how to help their children. Parents need culturally relevant peer support to help decrease rejection and increase family support.
- Advise parents that negative reactions to their adolescent’s LGBTQ identity may negatively impact their child’s health and mental health while supportive and affirming reactions promote well-being.
- Advise parents and caregivers to modify and change family rejecting behaviors that increase their child’s risk for suicide, depression, substance abuse ,and risky sexual behaviors.
- Expand anticipatory guidance to include information on the need for support and the link between family rejection and negative health problems.
- Provide guidance on sexual orientation and gender identity as part of normative child development during well-baby and early childhood care.
- Use FAP’s multilingual family education booklets and Healthy Futures poster series in family and patient education and provide these materials in clinical and community settings. FAP’s Healthy Futures posters include a poster guidance, a version on family acceptance, a version on family rejection and a family acceptance version for conservative families and settings. They are available in camera-ready art in four sizes in English and Spanish and are forthcoming in five Asian languages: familyproject.sfsu.edu/poster.
Dr. Lawlis is assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures.
Resources
• Family Acceptance Project – consultation and training; evidence-based educational materials for families, providers, religious leaders and youth.
• PFLAG – peer support for parents and friends with LGBTQ children in all states and several other countries.
References
1. Ryan C. Generating a revolution in prevention, wellness & care for LGBT children & youth. Temple Political & Civil Rights Law Review. 2014;23(2):331-44.
2. Ryan C. Healthy Futures Poster Series – Family Accepting & Rejecting Behaviors That Impact LGBTQ Children’s Health & Well-Being. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2019.
3. Ryan C. Family Acceptance Project: Culturally grounded framework for supporting LGBTQ children and youth. J Am Acad Child Adolesc Psychiatr. 2019;58(10):S58-9.
4. Ryan C et al. Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123(1):346-52.
5. Ryan C. Supportive families, healthy children: Helping families with lesbian, gay, bisexual & transgender children. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2009.
6. Ryan C et al. Parent-initiated sexual orientation change efforts with LGBT adolescents: Implications for young adult mental health and adjustment. J Homosexuality. 2020;67(2):159-73.
7. Ryan C et al. Family acceptance in adolescence and the health of LGBT young adults. J Child Adolesc Psychiatr Nursing. 2010;23(4):205-13. 8. Substance Abuse and Mental Health Services Administration. A Practitioner’s Guide: Helping Families to Support Their LGBT Children. In: Administration SAaMhS, ed. Vol PEP14-LGBTKIDS. Rockville, MD: HHS Publication; 2014.
It is well established that LGBTQ individuals experience more health disparities compared with their cisgender, heterosexual counterparts. In general, LGBTQ adolescents and young adults have higher levels of depression, suicide attempts, and substance use than those of their heterosexual peers. However, a key protective factor is family acceptance and support. By encouraging families to modify and change behaviors that are experienced by their LGBTQ children as rejecting and to engage in supportive and affirming behaviors, providers can help families to decrease risk and promote healthy outcomes for LGBTQ youth and young adults.
We all know that a supportive family can make a difference for any child, but this is especially true for LGBTQ youth and is critical during a pandemic when young people are confined with families and separated from peers and supportive adults outside the home. Several research studies show that family support can improve outcomes related to suicide, depression, homelessness, drug use, and HIV in LGBTQ young people. Family acceptance improves health outcomes, while rejection undermines family relationships and worsens both health and other serious outcomes such as homelessness and placement in custodial care. Pediatricians can help their patients by educating parents and caregivers with LGBTQ children about the critical role of family support – both those who see themselves as accepting and those who believe that being gay or transgender is wrong and are struggling with parenting a child who identifies as LGBTQ or who is gender diverse.
The Family Acceptance Project (FAP) at San Francisco State University conducted the first research on LGBTQ youth and families, developed the first evidence-informed family support model, and has published a range of studies and evidence-based resources that demonstrate the harm caused by family rejection, validate the importance of family acceptance, and provide guidance to increase family support. FAP’s research found that parents and caregivers that engage in rejecting behaviors are typically motivated by care and concern and by trying to protect their children from harm. They believe such behaviors will help their LGBTQ children fit in, have a good life, meet cultural and religious expectations, and be respected by others.1 FAP’s research identified and measured more than 50 rejecting behaviors that parents and caregivers use to respond to their LGBTQ children. Some of these commonly expressed rejecting behaviors include ridiculing and making disparaging comments about their child and other LGBTQ people; excluding them from family activities; blaming their child when others mistreat them because they are LGBTQ; blocking access to LGBTQ resources including friends, support groups, and activities; and trying to change their child’s sexual orientation and gender identity.2 LGBTQ youth experience these and other such behaviors as hurtful, harmful, and traumatic and may feel that they need to hide or repress their identity which can affect their self-esteem, increase isolation, depression, and risky behaviors.3 Providers working with families of LGBTQ youth should focus on shared goals, such as reducing risk and having a happy, healthy child. Most parents love their children and fear for their well-being. However, many are uninformed about their child’s gender identity and sexual orientation and don’t know how to nurture and support them.
In FAP’s initial study, LGB young people who reported higher levels of family rejection had substantially higher rates of attempted suicide, depression, illegal drug use, and unprotected sex.4 These rates were even more significant among Latino gay and bisexual men.4 Those who are rejected by family are less likely to want to have a family or to be parents themselves5 and have lower educational and income levels.6
To reduce risk, pediatricians should ask LGBTQ patients about family rejecting behaviors and help parents and caregivers to identify and understand the effect of such behaviors to reduce health risks and conflict that can lead to running away, expulsion, and removal from the home. Even decreasing rejecting behaviors to moderate levels can significantly improve negative outcomes.5
Caitlin Ryan, PhD, and her team also identified and measured more than 50 family accepting behaviors that help protect against risk and promote well-being. They found that young adults who experience high levels of family acceptance during adolescence report significantly higher levels of self-esteem, social support, and general health with much lower levels of depression, suicidality, and substance abuse.7 Family accepting and supportive behaviors include talking with the child about their LGBTQ identity; advocating for their LGBTQ child when others mistreat them; requiring other family members to treat their LGBTQ child with respect; and supporting their child’s gender identity.5 FAP has developed an evidence-informed family support model and multilingual educational resources for families, providers, youth and religious leaders to decrease rejection and increase family support. These are available in print copies and for download at familyproject.sfsu.edu.
In addition, Dr. Ryan and colleagues1,4,8 recommend the following guidance for providers:
- Ask LGBTQ adolescents about family reactions to their sexual orientation, gender identity, and expression, and refer to LGBTQ community support programs and for supportive counseling, as needed.
- Identify LGBTQ community support programs and online resources to educate parents about how to help their children. Parents need culturally relevant peer support to help decrease rejection and increase family support.
- Advise parents that negative reactions to their adolescent’s LGBTQ identity may negatively impact their child’s health and mental health while supportive and affirming reactions promote well-being.
- Advise parents and caregivers to modify and change family rejecting behaviors that increase their child’s risk for suicide, depression, substance abuse ,and risky sexual behaviors.
- Expand anticipatory guidance to include information on the need for support and the link between family rejection and negative health problems.
- Provide guidance on sexual orientation and gender identity as part of normative child development during well-baby and early childhood care.
- Use FAP’s multilingual family education booklets and Healthy Futures poster series in family and patient education and provide these materials in clinical and community settings. FAP’s Healthy Futures posters include a poster guidance, a version on family acceptance, a version on family rejection and a family acceptance version for conservative families and settings. They are available in camera-ready art in four sizes in English and Spanish and are forthcoming in five Asian languages: familyproject.sfsu.edu/poster.
Dr. Lawlis is assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures.
Resources
• Family Acceptance Project – consultation and training; evidence-based educational materials for families, providers, religious leaders and youth.
• PFLAG – peer support for parents and friends with LGBTQ children in all states and several other countries.
References
1. Ryan C. Generating a revolution in prevention, wellness & care for LGBT children & youth. Temple Political & Civil Rights Law Review. 2014;23(2):331-44.
2. Ryan C. Healthy Futures Poster Series – Family Accepting & Rejecting Behaviors That Impact LGBTQ Children’s Health & Well-Being. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2019.
3. Ryan C. Family Acceptance Project: Culturally grounded framework for supporting LGBTQ children and youth. J Am Acad Child Adolesc Psychiatr. 2019;58(10):S58-9.
4. Ryan C et al. Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123(1):346-52.
5. Ryan C. Supportive families, healthy children: Helping families with lesbian, gay, bisexual & transgender children. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2009.
6. Ryan C et al. Parent-initiated sexual orientation change efforts with LGBT adolescents: Implications for young adult mental health and adjustment. J Homosexuality. 2020;67(2):159-73.
7. Ryan C et al. Family acceptance in adolescence and the health of LGBT young adults. J Child Adolesc Psychiatr Nursing. 2010;23(4):205-13. 8. Substance Abuse and Mental Health Services Administration. A Practitioner’s Guide: Helping Families to Support Their LGBT Children. In: Administration SAaMhS, ed. Vol PEP14-LGBTKIDS. Rockville, MD: HHS Publication; 2014.
It is well established that LGBTQ individuals experience more health disparities compared with their cisgender, heterosexual counterparts. In general, LGBTQ adolescents and young adults have higher levels of depression, suicide attempts, and substance use than those of their heterosexual peers. However, a key protective factor is family acceptance and support. By encouraging families to modify and change behaviors that are experienced by their LGBTQ children as rejecting and to engage in supportive and affirming behaviors, providers can help families to decrease risk and promote healthy outcomes for LGBTQ youth and young adults.
We all know that a supportive family can make a difference for any child, but this is especially true for LGBTQ youth and is critical during a pandemic when young people are confined with families and separated from peers and supportive adults outside the home. Several research studies show that family support can improve outcomes related to suicide, depression, homelessness, drug use, and HIV in LGBTQ young people. Family acceptance improves health outcomes, while rejection undermines family relationships and worsens both health and other serious outcomes such as homelessness and placement in custodial care. Pediatricians can help their patients by educating parents and caregivers with LGBTQ children about the critical role of family support – both those who see themselves as accepting and those who believe that being gay or transgender is wrong and are struggling with parenting a child who identifies as LGBTQ or who is gender diverse.
The Family Acceptance Project (FAP) at San Francisco State University conducted the first research on LGBTQ youth and families, developed the first evidence-informed family support model, and has published a range of studies and evidence-based resources that demonstrate the harm caused by family rejection, validate the importance of family acceptance, and provide guidance to increase family support. FAP’s research found that parents and caregivers that engage in rejecting behaviors are typically motivated by care and concern and by trying to protect their children from harm. They believe such behaviors will help their LGBTQ children fit in, have a good life, meet cultural and religious expectations, and be respected by others.1 FAP’s research identified and measured more than 50 rejecting behaviors that parents and caregivers use to respond to their LGBTQ children. Some of these commonly expressed rejecting behaviors include ridiculing and making disparaging comments about their child and other LGBTQ people; excluding them from family activities; blaming their child when others mistreat them because they are LGBTQ; blocking access to LGBTQ resources including friends, support groups, and activities; and trying to change their child’s sexual orientation and gender identity.2 LGBTQ youth experience these and other such behaviors as hurtful, harmful, and traumatic and may feel that they need to hide or repress their identity which can affect their self-esteem, increase isolation, depression, and risky behaviors.3 Providers working with families of LGBTQ youth should focus on shared goals, such as reducing risk and having a happy, healthy child. Most parents love their children and fear for their well-being. However, many are uninformed about their child’s gender identity and sexual orientation and don’t know how to nurture and support them.
In FAP’s initial study, LGB young people who reported higher levels of family rejection had substantially higher rates of attempted suicide, depression, illegal drug use, and unprotected sex.4 These rates were even more significant among Latino gay and bisexual men.4 Those who are rejected by family are less likely to want to have a family or to be parents themselves5 and have lower educational and income levels.6
To reduce risk, pediatricians should ask LGBTQ patients about family rejecting behaviors and help parents and caregivers to identify and understand the effect of such behaviors to reduce health risks and conflict that can lead to running away, expulsion, and removal from the home. Even decreasing rejecting behaviors to moderate levels can significantly improve negative outcomes.5
Caitlin Ryan, PhD, and her team also identified and measured more than 50 family accepting behaviors that help protect against risk and promote well-being. They found that young adults who experience high levels of family acceptance during adolescence report significantly higher levels of self-esteem, social support, and general health with much lower levels of depression, suicidality, and substance abuse.7 Family accepting and supportive behaviors include talking with the child about their LGBTQ identity; advocating for their LGBTQ child when others mistreat them; requiring other family members to treat their LGBTQ child with respect; and supporting their child’s gender identity.5 FAP has developed an evidence-informed family support model and multilingual educational resources for families, providers, youth and religious leaders to decrease rejection and increase family support. These are available in print copies and for download at familyproject.sfsu.edu.
In addition, Dr. Ryan and colleagues1,4,8 recommend the following guidance for providers:
- Ask LGBTQ adolescents about family reactions to their sexual orientation, gender identity, and expression, and refer to LGBTQ community support programs and for supportive counseling, as needed.
- Identify LGBTQ community support programs and online resources to educate parents about how to help their children. Parents need culturally relevant peer support to help decrease rejection and increase family support.
- Advise parents that negative reactions to their adolescent’s LGBTQ identity may negatively impact their child’s health and mental health while supportive and affirming reactions promote well-being.
- Advise parents and caregivers to modify and change family rejecting behaviors that increase their child’s risk for suicide, depression, substance abuse ,and risky sexual behaviors.
- Expand anticipatory guidance to include information on the need for support and the link between family rejection and negative health problems.
- Provide guidance on sexual orientation and gender identity as part of normative child development during well-baby and early childhood care.
- Use FAP’s multilingual family education booklets and Healthy Futures poster series in family and patient education and provide these materials in clinical and community settings. FAP’s Healthy Futures posters include a poster guidance, a version on family acceptance, a version on family rejection and a family acceptance version for conservative families and settings. They are available in camera-ready art in four sizes in English and Spanish and are forthcoming in five Asian languages: familyproject.sfsu.edu/poster.
Dr. Lawlis is assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures.
Resources
• Family Acceptance Project – consultation and training; evidence-based educational materials for families, providers, religious leaders and youth.
• PFLAG – peer support for parents and friends with LGBTQ children in all states and several other countries.
References
1. Ryan C. Generating a revolution in prevention, wellness & care for LGBT children & youth. Temple Political & Civil Rights Law Review. 2014;23(2):331-44.
2. Ryan C. Healthy Futures Poster Series – Family Accepting & Rejecting Behaviors That Impact LGBTQ Children’s Health & Well-Being. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2019.
3. Ryan C. Family Acceptance Project: Culturally grounded framework for supporting LGBTQ children and youth. J Am Acad Child Adolesc Psychiatr. 2019;58(10):S58-9.
4. Ryan C et al. Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123(1):346-52.
5. Ryan C. Supportive families, healthy children: Helping families with lesbian, gay, bisexual & transgender children. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2009.
6. Ryan C et al. Parent-initiated sexual orientation change efforts with LGBT adolescents: Implications for young adult mental health and adjustment. J Homosexuality. 2020;67(2):159-73.
7. Ryan C et al. Family acceptance in adolescence and the health of LGBT young adults. J Child Adolesc Psychiatr Nursing. 2010;23(4):205-13. 8. Substance Abuse and Mental Health Services Administration. A Practitioner’s Guide: Helping Families to Support Their LGBT Children. In: Administration SAaMhS, ed. Vol PEP14-LGBTKIDS. Rockville, MD: HHS Publication; 2014.
Child ‘Mis’behavior – What’s ‘mis’ing?
“What kind of parent are you? Why don’t you straighten him out!” rants the woman being jostled in the grocery store by your patient. “Easy for you to say,” thinks your patient’s frazzled and now insulted parent.

Blaming the parent for an out-of-control child has historically been a common refrain of neighbors, relatives, and even strangers. But considering child behavior as resulting from both parent and child factors is central to the current transactional model of child development. In this model, mismatch of the parent’s and child’s response patterns is seen as setting them up for chronically rough interactions around parent requests/demands. A parent escalating quickly from a briefly stated request to a tirade may create more tension paired with an anxious child who takes time to act, for example. Once a parent (and ultimately the child) recognize patterns in what leads to conflict, they can become more proactive in predicting and negotiating these situations. Ross Greene, PhD, explains this in his book “The Explosive Child,” calling the method Collaborative Problem Solving (now Collaborative & Proactive Solutions or CPS).
While there are general principles parents can use to modify what they consider “mis”behaviors, these methods often do not account for the “missing” skills of the individual child (and parent) predisposing to those “mis”takes. Thinking of misbehaviors as being because of a kind of “learning disability” in the child rather than willful defiance can help cool off interactions by instead focusing on solving the underlying problem.
What kinds of “gaps in skills” set a child up for defiant or explosive reactions? If you think about what features of children, and parent-child relationships are associated with harmonious interactions this becomes evident. Children over 3 who are patient, easygoing, flexible or adaptable, and good at transitions and problem-solving can delay gratification and tolerate frustration, regulate their emotions, explain their desires, and multitask. They are better at reading the parent’s needs and intent and tend to interpret requests as positive or at least neutral and are more likely to comply with parent requests without a fuss.
What? No kid you know is great at all of these? These skills, at best variable, develop with maturation. Some are part of temperament, considered normal variation in personality. For example, so-called difficult temperament includes low adaptability, high-intensity reactions, low regularity, tendency to withdraw, and negative mood. But in the extreme, weaknesses in these skills are core to or comorbid with diagnosable mental health disorders. Defiance and irritable responses are criteria for oppositional defiant disorder (ODD), and less severe categories called aggressive/oppositional problem or variation. ODD is often found in children diagnosed with ADHD (65%), Tourette’s (15%-65%), depression (70% if severe), bipolar disorder (85%), OCD, anxiety (45%), autism, and language-processing disorders (55%), or trauma. These conditions variably include lower emotion regulation, poorer executive functioning including poor task shifting and impulsivity, obsessiveness, lower expressive and receptive communication skills, and less social awareness that facilitates harmonious problem solving.
The basic components of the CPS approach to addressing parent-child conflict sound intuitive but defining them clearly is important when families are stuck. There are three levels of plans. If the problem is an emergency or nonnegotiable, e.g., child hurting the cat, it may call for Plan A – parent-imposed solutions, sometimes with consequences or rewards. As children mature, Plan A should be used less frequently. If solving the problem is not a top life priority, Plan C – postponing action, may be appropriate. Plan C highlights that behavior change is a long-term project and “picking your fights” is important.
The biggest value of CPS for resolving behavior problems comes from intermediate Plan B. In Plan B the first step of problem solving for parents facing child defiance or upset is to empathically and nonjudgmentally figure out the child’s concern. Questions such as “I’ve noticed that when I remind you that it is trash night you start shouting. What’s up with that?” then patiently asking about the who, what, where, and when of their concern and checking to ensure understanding. Specificity is important as well as noting times when the reaction occurs or not.
Once the child’s concern is clear, e.g., feeling that the demand to take out the trash now interrupts his games during the only time his friends are online, the parents should echo the child’s concern then express their own concern about how the behavior is affecting them and others, potentially including the child; e.g., mother is so upset by the shouting that she can’t sleep, and worry that the child is not learning responsibility, and then checking for child understanding.
Finally, the parent invites brainstorming for a solution that addresses both of their concerns, first asking the child for suggestions, aiming for a strategy that is realistic and specific. Children reluctant to make suggestions may need more time and the parent may be wondering “if there is a way for both of our concerns to be addressed.” Solutions chosen are then tried for several weeks, success tracked, and needed changes negotiated.
For parents, using a collaborative approach to dealing with their child’s behavior takes skills they may not have at the moment, or ever. Especially under the stresses of COVID-19 lockdown, taking a step back from an encounter to consider lack of a skill to turn off the video game promptly when a Zoom meeting starts is challenging. Parents may also genetically share the child’s predisposing ADHD, anxiety, depression, OCD, or weakness in communication or social sensitivity.
Sometimes part of the solution for a conflict is for the parent to reduce expectations. This requires understanding and accepting the child’s cognitive or emotional limitations. Reducing expectations is ideally done before a request rather than by giving in after it, which reinforces protests. For authoritarian adults rigid in their belief that parents are boss, changing expectations can be tough and can feel like losing control or failing as a leader. One benefit of working with a CPS coach (see livesinthebalance.org or ThinkKids.org) is to help parents identify their own limitations.
Predicting the types of demands that tend to create conflict, such as to act immediately or be flexible about options, allows parents to prioritize those requests for calmer moments or when there is more time for discussion. Reviewing a checklist of common gaps in skills and creating a list of expectations and triggers that are difficult for the child helps the family be more proactive in developing solutions. Authors of CPS have validated a checklist of skill deficits, “Thinking Skills Inventory,” to facilitate detection of gaps that is educational plus useful for planning specific solutions.
CPS has been shown in randomized trials with both parent groups and in home counseling to be as effective as Parent Training in reducing oppositional behavior and reducing maternal stress, with effects lasting even longer.
CPS Plan B notably has no reward or punishment components as it assumes the child wants to behave acceptably but can’t; has the “will but not the skill.” When skill deficits are worked around the child is satisfied with complying and pleasing the parents. The idea of a “function” of the misbehavior for the child of gaining attention or reward or avoiding consequences is reinterpreted as serving to communicate the problem the child is having trouble in meeting the parent’s demand. When the parent understands and helps the child solve the problem his/her misbehavior is no longer needed. A benefit of the communication and mutual problem solving used in CPS is on not only improving behavior but empowering parents and children, building parental empathy, and improving child skills.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She has no other relevant disclosures. Dr. Howard’s contribution to this publication is as a paid expert to MDedge News. Email her at [email protected].
Reference
Greene RW et al. A transactional model of oppositional behavior: Underpinnings of the Collaborative Problem Solving approach. J Psychosom Res. 2003;55(1):67-75.
“What kind of parent are you? Why don’t you straighten him out!” rants the woman being jostled in the grocery store by your patient. “Easy for you to say,” thinks your patient’s frazzled and now insulted parent.
Blaming the parent for an out-of-control child has historically been a common refrain of neighbors, relatives, and even strangers. But considering child behavior as resulting from both parent and child factors is central to the current transactional model of child development. In this model, mismatch of the parent’s and child’s response patterns is seen as setting them up for chronically rough interactions around parent requests/demands. A parent escalating quickly from a briefly stated request to a tirade may create more tension paired with an anxious child who takes time to act, for example. Once a parent (and ultimately the child) recognize patterns in what leads to conflict, they can become more proactive in predicting and negotiating these situations. Ross Greene, PhD, explains this in his book “The Explosive Child,” calling the method Collaborative Problem Solving (now Collaborative & Proactive Solutions or CPS).
While there are general principles parents can use to modify what they consider “mis”behaviors, these methods often do not account for the “missing” skills of the individual child (and parent) predisposing to those “mis”takes. Thinking of misbehaviors as being because of a kind of “learning disability” in the child rather than willful defiance can help cool off interactions by instead focusing on solving the underlying problem.
What kinds of “gaps in skills” set a child up for defiant or explosive reactions? If you think about what features of children, and parent-child relationships are associated with harmonious interactions this becomes evident. Children over 3 who are patient, easygoing, flexible or adaptable, and good at transitions and problem-solving can delay gratification and tolerate frustration, regulate their emotions, explain their desires, and multitask. They are better at reading the parent’s needs and intent and tend to interpret requests as positive or at least neutral and are more likely to comply with parent requests without a fuss.
What? No kid you know is great at all of these? These skills, at best variable, develop with maturation. Some are part of temperament, considered normal variation in personality. For example, so-called difficult temperament includes low adaptability, high-intensity reactions, low regularity, tendency to withdraw, and negative mood. But in the extreme, weaknesses in these skills are core to or comorbid with diagnosable mental health disorders. Defiance and irritable responses are criteria for oppositional defiant disorder (ODD), and less severe categories called aggressive/oppositional problem or variation. ODD is often found in children diagnosed with ADHD (65%), Tourette’s (15%-65%), depression (70% if severe), bipolar disorder (85%), OCD, anxiety (45%), autism, and language-processing disorders (55%), or trauma. These conditions variably include lower emotion regulation, poorer executive functioning including poor task shifting and impulsivity, obsessiveness, lower expressive and receptive communication skills, and less social awareness that facilitates harmonious problem solving.
The basic components of the CPS approach to addressing parent-child conflict sound intuitive but defining them clearly is important when families are stuck. There are three levels of plans. If the problem is an emergency or nonnegotiable, e.g., child hurting the cat, it may call for Plan A – parent-imposed solutions, sometimes with consequences or rewards. As children mature, Plan A should be used less frequently. If solving the problem is not a top life priority, Plan C – postponing action, may be appropriate. Plan C highlights that behavior change is a long-term project and “picking your fights” is important.
The biggest value of CPS for resolving behavior problems comes from intermediate Plan B. In Plan B the first step of problem solving for parents facing child defiance or upset is to empathically and nonjudgmentally figure out the child’s concern. Questions such as “I’ve noticed that when I remind you that it is trash night you start shouting. What’s up with that?” then patiently asking about the who, what, where, and when of their concern and checking to ensure understanding. Specificity is important as well as noting times when the reaction occurs or not.
Once the child’s concern is clear, e.g., feeling that the demand to take out the trash now interrupts his games during the only time his friends are online, the parents should echo the child’s concern then express their own concern about how the behavior is affecting them and others, potentially including the child; e.g., mother is so upset by the shouting that she can’t sleep, and worry that the child is not learning responsibility, and then checking for child understanding.
Finally, the parent invites brainstorming for a solution that addresses both of their concerns, first asking the child for suggestions, aiming for a strategy that is realistic and specific. Children reluctant to make suggestions may need more time and the parent may be wondering “if there is a way for both of our concerns to be addressed.” Solutions chosen are then tried for several weeks, success tracked, and needed changes negotiated.
For parents, using a collaborative approach to dealing with their child’s behavior takes skills they may not have at the moment, or ever. Especially under the stresses of COVID-19 lockdown, taking a step back from an encounter to consider lack of a skill to turn off the video game promptly when a Zoom meeting starts is challenging. Parents may also genetically share the child’s predisposing ADHD, anxiety, depression, OCD, or weakness in communication or social sensitivity.
Sometimes part of the solution for a conflict is for the parent to reduce expectations. This requires understanding and accepting the child’s cognitive or emotional limitations. Reducing expectations is ideally done before a request rather than by giving in after it, which reinforces protests. For authoritarian adults rigid in their belief that parents are boss, changing expectations can be tough and can feel like losing control or failing as a leader. One benefit of working with a CPS coach (see livesinthebalance.org or ThinkKids.org) is to help parents identify their own limitations.
Predicting the types of demands that tend to create conflict, such as to act immediately or be flexible about options, allows parents to prioritize those requests for calmer moments or when there is more time for discussion. Reviewing a checklist of common gaps in skills and creating a list of expectations and triggers that are difficult for the child helps the family be more proactive in developing solutions. Authors of CPS have validated a checklist of skill deficits, “Thinking Skills Inventory,” to facilitate detection of gaps that is educational plus useful for planning specific solutions.
CPS has been shown in randomized trials with both parent groups and in home counseling to be as effective as Parent Training in reducing oppositional behavior and reducing maternal stress, with effects lasting even longer.
CPS Plan B notably has no reward or punishment components as it assumes the child wants to behave acceptably but can’t; has the “will but not the skill.” When skill deficits are worked around the child is satisfied with complying and pleasing the parents. The idea of a “function” of the misbehavior for the child of gaining attention or reward or avoiding consequences is reinterpreted as serving to communicate the problem the child is having trouble in meeting the parent’s demand. When the parent understands and helps the child solve the problem his/her misbehavior is no longer needed. A benefit of the communication and mutual problem solving used in CPS is on not only improving behavior but empowering parents and children, building parental empathy, and improving child skills.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She has no other relevant disclosures. Dr. Howard’s contribution to this publication is as a paid expert to MDedge News. Email her at [email protected].
Reference
Greene RW et al. A transactional model of oppositional behavior: Underpinnings of the Collaborative Problem Solving approach. J Psychosom Res. 2003;55(1):67-75.
“What kind of parent are you? Why don’t you straighten him out!” rants the woman being jostled in the grocery store by your patient. “Easy for you to say,” thinks your patient’s frazzled and now insulted parent.
Blaming the parent for an out-of-control child has historically been a common refrain of neighbors, relatives, and even strangers. But considering child behavior as resulting from both parent and child factors is central to the current transactional model of child development. In this model, mismatch of the parent’s and child’s response patterns is seen as setting them up for chronically rough interactions around parent requests/demands. A parent escalating quickly from a briefly stated request to a tirade may create more tension paired with an anxious child who takes time to act, for example. Once a parent (and ultimately the child) recognize patterns in what leads to conflict, they can become more proactive in predicting and negotiating these situations. Ross Greene, PhD, explains this in his book “The Explosive Child,” calling the method Collaborative Problem Solving (now Collaborative & Proactive Solutions or CPS).
While there are general principles parents can use to modify what they consider “mis”behaviors, these methods often do not account for the “missing” skills of the individual child (and parent) predisposing to those “mis”takes. Thinking of misbehaviors as being because of a kind of “learning disability” in the child rather than willful defiance can help cool off interactions by instead focusing on solving the underlying problem.
What kinds of “gaps in skills” set a child up for defiant or explosive reactions? If you think about what features of children, and parent-child relationships are associated with harmonious interactions this becomes evident. Children over 3 who are patient, easygoing, flexible or adaptable, and good at transitions and problem-solving can delay gratification and tolerate frustration, regulate their emotions, explain their desires, and multitask. They are better at reading the parent’s needs and intent and tend to interpret requests as positive or at least neutral and are more likely to comply with parent requests without a fuss.
What? No kid you know is great at all of these? These skills, at best variable, develop with maturation. Some are part of temperament, considered normal variation in personality. For example, so-called difficult temperament includes low adaptability, high-intensity reactions, low regularity, tendency to withdraw, and negative mood. But in the extreme, weaknesses in these skills are core to or comorbid with diagnosable mental health disorders. Defiance and irritable responses are criteria for oppositional defiant disorder (ODD), and less severe categories called aggressive/oppositional problem or variation. ODD is often found in children diagnosed with ADHD (65%), Tourette’s (15%-65%), depression (70% if severe), bipolar disorder (85%), OCD, anxiety (45%), autism, and language-processing disorders (55%), or trauma. These conditions variably include lower emotion regulation, poorer executive functioning including poor task shifting and impulsivity, obsessiveness, lower expressive and receptive communication skills, and less social awareness that facilitates harmonious problem solving.
The basic components of the CPS approach to addressing parent-child conflict sound intuitive but defining them clearly is important when families are stuck. There are three levels of plans. If the problem is an emergency or nonnegotiable, e.g., child hurting the cat, it may call for Plan A – parent-imposed solutions, sometimes with consequences or rewards. As children mature, Plan A should be used less frequently. If solving the problem is not a top life priority, Plan C – postponing action, may be appropriate. Plan C highlights that behavior change is a long-term project and “picking your fights” is important.
The biggest value of CPS for resolving behavior problems comes from intermediate Plan B. In Plan B the first step of problem solving for parents facing child defiance or upset is to empathically and nonjudgmentally figure out the child’s concern. Questions such as “I’ve noticed that when I remind you that it is trash night you start shouting. What’s up with that?” then patiently asking about the who, what, where, and when of their concern and checking to ensure understanding. Specificity is important as well as noting times when the reaction occurs or not.
Once the child’s concern is clear, e.g., feeling that the demand to take out the trash now interrupts his games during the only time his friends are online, the parents should echo the child’s concern then express their own concern about how the behavior is affecting them and others, potentially including the child; e.g., mother is so upset by the shouting that she can’t sleep, and worry that the child is not learning responsibility, and then checking for child understanding.
Finally, the parent invites brainstorming for a solution that addresses both of their concerns, first asking the child for suggestions, aiming for a strategy that is realistic and specific. Children reluctant to make suggestions may need more time and the parent may be wondering “if there is a way for both of our concerns to be addressed.” Solutions chosen are then tried for several weeks, success tracked, and needed changes negotiated.
For parents, using a collaborative approach to dealing with their child’s behavior takes skills they may not have at the moment, or ever. Especially under the stresses of COVID-19 lockdown, taking a step back from an encounter to consider lack of a skill to turn off the video game promptly when a Zoom meeting starts is challenging. Parents may also genetically share the child’s predisposing ADHD, anxiety, depression, OCD, or weakness in communication or social sensitivity.
Sometimes part of the solution for a conflict is for the parent to reduce expectations. This requires understanding and accepting the child’s cognitive or emotional limitations. Reducing expectations is ideally done before a request rather than by giving in after it, which reinforces protests. For authoritarian adults rigid in their belief that parents are boss, changing expectations can be tough and can feel like losing control or failing as a leader. One benefit of working with a CPS coach (see livesinthebalance.org or ThinkKids.org) is to help parents identify their own limitations.
Predicting the types of demands that tend to create conflict, such as to act immediately or be flexible about options, allows parents to prioritize those requests for calmer moments or when there is more time for discussion. Reviewing a checklist of common gaps in skills and creating a list of expectations and triggers that are difficult for the child helps the family be more proactive in developing solutions. Authors of CPS have validated a checklist of skill deficits, “Thinking Skills Inventory,” to facilitate detection of gaps that is educational plus useful for planning specific solutions.
CPS has been shown in randomized trials with both parent groups and in home counseling to be as effective as Parent Training in reducing oppositional behavior and reducing maternal stress, with effects lasting even longer.
CPS Plan B notably has no reward or punishment components as it assumes the child wants to behave acceptably but can’t; has the “will but not the skill.” When skill deficits are worked around the child is satisfied with complying and pleasing the parents. The idea of a “function” of the misbehavior for the child of gaining attention or reward or avoiding consequences is reinterpreted as serving to communicate the problem the child is having trouble in meeting the parent’s demand. When the parent understands and helps the child solve the problem his/her misbehavior is no longer needed. A benefit of the communication and mutual problem solving used in CPS is on not only improving behavior but empowering parents and children, building parental empathy, and improving child skills.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She has no other relevant disclosures. Dr. Howard’s contribution to this publication is as a paid expert to MDedge News. Email her at [email protected].
Reference
Greene RW et al. A transactional model of oppositional behavior: Underpinnings of the Collaborative Problem Solving approach. J Psychosom Res. 2003;55(1):67-75.
COVID-19: Helping patients overcome what might feel like an existential crisis
Way back in the spring of last year, I wrote about a pandemic of posttraumatic stress disorder that would descend upon us because of COVID-19. At the time, we were told that, by summer – June or July 2020 – all the steps we needed to take to stay ahead of the virus, including remaining socially distant, and yes, even wearing masks, would be over. Life would get back to normal.

Little did we know that a national plan for our safety, including making sure that we had enough masks and PPE, would not be forthcoming, and that so many thousands of Americans would perish, leaving millions of distraught families and friends.
So many people are suffering. Mothers, for example, are struggling to balance remote schooling with additional child care and domestic work. More than 2 million women left the U.S. workforce last year between February 2020 and October 2020, according to a report by the National Women’s Law Center. Even before COVID-19, loneliness among young adults was considered a domestic epidemic – and the social isolation forced by the pandemic has worsened those trends, research shows. These trends are creating so much more anxiety, depression, despair, and yes, even PTSD. As mental health professionals, we have a lot of work to do in educating people about coping skills and in providing treatments when appropriate.
Experiences take on new meaning
One day a friend and professional colleague called me, and he sounded quite distraught. He had not been able to reach his primary care physician and thought that, as a physician, I might have some insights about his symptoms. He began telling me that something really strange was happening whenever he walked around outside with his mask on. He couldn’t breathe with it on, he told me. In addition, his eyes teared up, his nose started running, and his eyeglasses fogged up so much that he couldn’t see where he was going. He was really anxious, nervous, and felt a great sense of despair – and disorientation. He did not fully understand what was happening and didn’t know whether those disorienting symptoms were mask-related or whether he was incubating some yet undiagnosed illness.
I addressed his concerns in the moment by assuring him that I, too, had been experiencing similar challenges with fogged-up glasses and a runny nose; many people were experiencing some of the same things. I explained that even I had called an allergist to find out whether I might be allergic to some component in the mask and whether he had seen those symptoms in his practice.
Albeit, those issues tied to masks are relatively minor, compared with the enormous psychological toll this pandemic has taken on some people. But it’s clear that different people suffer different effects in light of the marked changes in life and lifestyles caused by the pandemic.
‘It’s something else’
Two people I know, both professionals, recently told me that in their social lives they constantly feel tired and anxious, and that their concentration has diminished. They worry more about their futures, they told me separately. (They don’t know each other.) They reported going through daily life “like being on automatic.” Both said they were far too irritable and reported feeling that social isolation had dulled their thinking.
They said they were not depressed; “it’s something else.” I reassured them both that this would pass with time and suggested that they work at not socially isolating – to the extent that they can – during the pandemic. I also encouraged them to get vaccinated and to talk with a professional if their malaise was altering their level of functioning.
So far, more than 475,000 people in the United States have died of COVID-19, and thousands continue to suffer. People are saying goodbye to loved ones on iPads, and watching news stories about hospitals at overcapacity and refrigeration units storing bodies. Meanwhile, health care workers, many of whom are putting their lives and those of their families at risk, are reporting increased levels of burnout – and moral injury.
Value of relaxation techniques
We know that the latest mitigation measures advised by the Centers for Disease Control and Prevention must continue during the COVID-19 vaccination process. The new CDC guidelines on the value of double masking make sense and should be followed. However, even as we learn more about the virus and how to stop its spread, we must recognize that social distancing is not the same as social isolation. We must continue to do what we can to maintain social relationships and keep open the lines of communication, including the use of virtual tools. I am pleased to see the growth of telemedicine during the pandemic. When applicable, telemedicine allows greater medical and mental health care without the stress of travel and the risk of exposure to more people than necessary.
, whether it’s hypnosis, mindfulness, transcendental meditation, or deep breathing exercises. For the more advanced therapies, guided imagery can help patients develop a sense of calm and equanimity.
For those who are not skilled in relaxation techniques, YouTube offers some excellent programs that teach relaxation and mindfulness. Another thing I do is talk regularly with people I know and sometimes with people I know I’ll disagree with – just to keep my brain active. I also try to learn new things in my spare time to establish new brain pathways and stay mentally active.
The pain and grief tied to the pandemic are unlike anything we’ve ever experienced. Our training as psychiatrists, psychologists, and other mental health care professionals makes us all uniquely suited to assist patients as they process these traumatic times. We must step forward and do so.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (Kettlehole Publishing, 2019). He has no conflicts of interest.
Way back in the spring of last year, I wrote about a pandemic of posttraumatic stress disorder that would descend upon us because of COVID-19. At the time, we were told that, by summer – June or July 2020 – all the steps we needed to take to stay ahead of the virus, including remaining socially distant, and yes, even wearing masks, would be over. Life would get back to normal.
Little did we know that a national plan for our safety, including making sure that we had enough masks and PPE, would not be forthcoming, and that so many thousands of Americans would perish, leaving millions of distraught families and friends.
So many people are suffering. Mothers, for example, are struggling to balance remote schooling with additional child care and domestic work. More than 2 million women left the U.S. workforce last year between February 2020 and October 2020, according to a report by the National Women’s Law Center. Even before COVID-19, loneliness among young adults was considered a domestic epidemic – and the social isolation forced by the pandemic has worsened those trends, research shows. These trends are creating so much more anxiety, depression, despair, and yes, even PTSD. As mental health professionals, we have a lot of work to do in educating people about coping skills and in providing treatments when appropriate.
Experiences take on new meaning
One day a friend and professional colleague called me, and he sounded quite distraught. He had not been able to reach his primary care physician and thought that, as a physician, I might have some insights about his symptoms. He began telling me that something really strange was happening whenever he walked around outside with his mask on. He couldn’t breathe with it on, he told me. In addition, his eyes teared up, his nose started running, and his eyeglasses fogged up so much that he couldn’t see where he was going. He was really anxious, nervous, and felt a great sense of despair – and disorientation. He did not fully understand what was happening and didn’t know whether those disorienting symptoms were mask-related or whether he was incubating some yet undiagnosed illness.
I addressed his concerns in the moment by assuring him that I, too, had been experiencing similar challenges with fogged-up glasses and a runny nose; many people were experiencing some of the same things. I explained that even I had called an allergist to find out whether I might be allergic to some component in the mask and whether he had seen those symptoms in his practice.
Albeit, those issues tied to masks are relatively minor, compared with the enormous psychological toll this pandemic has taken on some people. But it’s clear that different people suffer different effects in light of the marked changes in life and lifestyles caused by the pandemic.
‘It’s something else’
Two people I know, both professionals, recently told me that in their social lives they constantly feel tired and anxious, and that their concentration has diminished. They worry more about their futures, they told me separately. (They don’t know each other.) They reported going through daily life “like being on automatic.” Both said they were far too irritable and reported feeling that social isolation had dulled their thinking.
They said they were not depressed; “it’s something else.” I reassured them both that this would pass with time and suggested that they work at not socially isolating – to the extent that they can – during the pandemic. I also encouraged them to get vaccinated and to talk with a professional if their malaise was altering their level of functioning.
So far, more than 475,000 people in the United States have died of COVID-19, and thousands continue to suffer. People are saying goodbye to loved ones on iPads, and watching news stories about hospitals at overcapacity and refrigeration units storing bodies. Meanwhile, health care workers, many of whom are putting their lives and those of their families at risk, are reporting increased levels of burnout – and moral injury.
Value of relaxation techniques
We know that the latest mitigation measures advised by the Centers for Disease Control and Prevention must continue during the COVID-19 vaccination process. The new CDC guidelines on the value of double masking make sense and should be followed. However, even as we learn more about the virus and how to stop its spread, we must recognize that social distancing is not the same as social isolation. We must continue to do what we can to maintain social relationships and keep open the lines of communication, including the use of virtual tools. I am pleased to see the growth of telemedicine during the pandemic. When applicable, telemedicine allows greater medical and mental health care without the stress of travel and the risk of exposure to more people than necessary.
, whether it’s hypnosis, mindfulness, transcendental meditation, or deep breathing exercises. For the more advanced therapies, guided imagery can help patients develop a sense of calm and equanimity.
For those who are not skilled in relaxation techniques, YouTube offers some excellent programs that teach relaxation and mindfulness. Another thing I do is talk regularly with people I know and sometimes with people I know I’ll disagree with – just to keep my brain active. I also try to learn new things in my spare time to establish new brain pathways and stay mentally active.
The pain and grief tied to the pandemic are unlike anything we’ve ever experienced. Our training as psychiatrists, psychologists, and other mental health care professionals makes us all uniquely suited to assist patients as they process these traumatic times. We must step forward and do so.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (Kettlehole Publishing, 2019). He has no conflicts of interest.
Way back in the spring of last year, I wrote about a pandemic of posttraumatic stress disorder that would descend upon us because of COVID-19. At the time, we were told that, by summer – June or July 2020 – all the steps we needed to take to stay ahead of the virus, including remaining socially distant, and yes, even wearing masks, would be over. Life would get back to normal.
Little did we know that a national plan for our safety, including making sure that we had enough masks and PPE, would not be forthcoming, and that so many thousands of Americans would perish, leaving millions of distraught families and friends.
So many people are suffering. Mothers, for example, are struggling to balance remote schooling with additional child care and domestic work. More than 2 million women left the U.S. workforce last year between February 2020 and October 2020, according to a report by the National Women’s Law Center. Even before COVID-19, loneliness among young adults was considered a domestic epidemic – and the social isolation forced by the pandemic has worsened those trends, research shows. These trends are creating so much more anxiety, depression, despair, and yes, even PTSD. As mental health professionals, we have a lot of work to do in educating people about coping skills and in providing treatments when appropriate.
Experiences take on new meaning
One day a friend and professional colleague called me, and he sounded quite distraught. He had not been able to reach his primary care physician and thought that, as a physician, I might have some insights about his symptoms. He began telling me that something really strange was happening whenever he walked around outside with his mask on. He couldn’t breathe with it on, he told me. In addition, his eyes teared up, his nose started running, and his eyeglasses fogged up so much that he couldn’t see where he was going. He was really anxious, nervous, and felt a great sense of despair – and disorientation. He did not fully understand what was happening and didn’t know whether those disorienting symptoms were mask-related or whether he was incubating some yet undiagnosed illness.
I addressed his concerns in the moment by assuring him that I, too, had been experiencing similar challenges with fogged-up glasses and a runny nose; many people were experiencing some of the same things. I explained that even I had called an allergist to find out whether I might be allergic to some component in the mask and whether he had seen those symptoms in his practice.
Albeit, those issues tied to masks are relatively minor, compared with the enormous psychological toll this pandemic has taken on some people. But it’s clear that different people suffer different effects in light of the marked changes in life and lifestyles caused by the pandemic.
‘It’s something else’
Two people I know, both professionals, recently told me that in their social lives they constantly feel tired and anxious, and that their concentration has diminished. They worry more about their futures, they told me separately. (They don’t know each other.) They reported going through daily life “like being on automatic.” Both said they were far too irritable and reported feeling that social isolation had dulled their thinking.
They said they were not depressed; “it’s something else.” I reassured them both that this would pass with time and suggested that they work at not socially isolating – to the extent that they can – during the pandemic. I also encouraged them to get vaccinated and to talk with a professional if their malaise was altering their level of functioning.
So far, more than 475,000 people in the United States have died of COVID-19, and thousands continue to suffer. People are saying goodbye to loved ones on iPads, and watching news stories about hospitals at overcapacity and refrigeration units storing bodies. Meanwhile, health care workers, many of whom are putting their lives and those of their families at risk, are reporting increased levels of burnout – and moral injury.
Value of relaxation techniques
We know that the latest mitigation measures advised by the Centers for Disease Control and Prevention must continue during the COVID-19 vaccination process. The new CDC guidelines on the value of double masking make sense and should be followed. However, even as we learn more about the virus and how to stop its spread, we must recognize that social distancing is not the same as social isolation. We must continue to do what we can to maintain social relationships and keep open the lines of communication, including the use of virtual tools. I am pleased to see the growth of telemedicine during the pandemic. When applicable, telemedicine allows greater medical and mental health care without the stress of travel and the risk of exposure to more people than necessary.
, whether it’s hypnosis, mindfulness, transcendental meditation, or deep breathing exercises. For the more advanced therapies, guided imagery can help patients develop a sense of calm and equanimity.
For those who are not skilled in relaxation techniques, YouTube offers some excellent programs that teach relaxation and mindfulness. Another thing I do is talk regularly with people I know and sometimes with people I know I’ll disagree with – just to keep my brain active. I also try to learn new things in my spare time to establish new brain pathways and stay mentally active.
The pain and grief tied to the pandemic are unlike anything we’ve ever experienced. Our training as psychiatrists, psychologists, and other mental health care professionals makes us all uniquely suited to assist patients as they process these traumatic times. We must step forward and do so.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (Kettlehole Publishing, 2019). He has no conflicts of interest.
State of the evidence: Treatment-resistant depression in children and adolescents
Case
Max was a 17-year-old boy and avid video gamer who, predating COVID-19, was within a major depressive episode and continued to meet criteria through the duration of COVID-19 quarantine. He lives with his mother, who is a single mom and is working hard in a variety of jobs through the pandemic. Max had little motivation to engage in sports or other activities, and despite doing well enough in school, he spent much of his days escaping into video games and social media, where his friends communicated and bonded the most. He has had very little response to complete trials of two different selective serotonin reuptake inhibitors (SSRIs), and the off-label attempts at a serotonin-norepinephrine reuptake inhibitor and bupropion augmentation of an SSRI, as extrapolated by his pediatrician from adult data on treatment-resistant depression. He had ongoing supportive psychotherapy and his mother and pediatrician were wary of changing that relationship, as they were just happy he would engage at all. His shy nature made him very wary of attending any programs or groups. He had no other diagnosis including anxiety, substance abuse disorder, or learning disorder.
Case discussion
As a child and adolescent psychiatrist embedded in primary care practices, I (like you) am seeing more and more parents, children, and families struggling with depression through the course of this unprecedented and challenging year.

Max presented to me with his mother at the request of his primary care physician because within the course of many medication trials, it had been over 6 months of persistent symptoms without an end in sight for him, his family, or his primary care provider (PCP).
His diagnosis was treatment-resistant depression and his PCP was grasping at adult strategies to manage this all with additional psychopharmacology. As a consulting child-and-adolescent psychiatrist in primary care, how could I help the PCP? I too worry if there is anything that I can do to shift depression once standard treatments fail, and when the idea of engaging in behavioral activation or other pro-health activities is just too much for a depressed adolescent to bear. I weigh that with what is known about the evidence, and the good data driving us beyond medication solutions. I often find that it can be helpful to reiterate the following points to providers and families.
First, what to know about depression in kids
Depression looks different at different ages in children. In school-aged children, it’s widely known that irritability or psychosomatic symptoms (frequent headaches and stomach aches) can be the first preverbal signs of an emerging anxiety and depressive disorder in children. In adolescents, one would maybe expect more typical melancholic adult-like symptoms of depression; however, there is mounting evidence that adolescents actually present with more classically “atypical symptoms” of depression (low motivation, weight gain, escapism to sleep or video games, as with Max) with less persistence across setting (home, work, school) compared with adults (“Diagnosing Depression in Children and Adolescents” by Glen R. Elliott, PhD, MD, from The Carlat Child Psychiatry Report, November 2015, Antidepressant Use in Children).In addition, major life stressors (the breakup of a romantic relationship, failing a class, bullying) can be perceived as more permanent, and suicidal thinking can be acute and lethal in these contexts. With Max, it was accepted by all who were supporting him that he was struggling with depression, which is the first step in managing this well.
The idea of the designated patient
Often left out in a discussion of pediatric patients is the family. As a designated patient, much of our focus is on improving the symptoms of the patient in front of us. Parents direct their gaze at the child as the one with the condition who needs support. First following identification of depression, I find that a reframe of a diagnosis can be useful. Family systems theory approaches a child with a depression diagnosis, and says, that if one family member changes, even in a small way, a family as a system is forced to change. With a sense of an external locus of control, we often are left with a patient and parent feeling stuck. To provide a reorientation to the parents, ask how they are feeling. Can they get treatment for depression knowing the biology of the condition or consider making behavioral changes of their own and as a family? Can they consider family psychotherapy so they can cope better and break some cycles of maladaptive engagement shared across a family? These kinds of reorientations can be useful to shift the idea of treatment from the designated patient (the child) and medication options (limited data for kids who aren’t responding to them) to a family approach. Making the depression management strategy a family affair can help the entire family shift from seeing the only option as medications or interventions exclusively directed at a child. The Vermont Center for Children, Youth, and Families at the University of Vermont Medical Center has many pioneering developments in addressing family-based approaches to mental health concerns in the pediatric population, and can serve as a source of inspiration for this shift in discussing depression.
Practical strategies for the pediatrician
Medications can be useful for treating child and adolescent depression, but there is also strong evidence for psychotherapy, working with the child’s school and family, and different forms of behavioral activation (exercise, mindfulness, yoga, and other positive activities). Medications, if one is looking at standard of care treatment and Food and Drug Administration approval exclusively, is limited in scope and should not be the only intervention considered, as described in the case above.
In “The Use of Medication in Treating Childhood and Adolescent Depression: Information for Patients and Families,” which is a practical guide prepared by the American Psychiatric Association and the American Academy of Child and Adolescent Psychiatry, it is noted that Prozac and Lexapro are approved medications, as follows:
- Antidepressant medications can be effective in relieving the symptoms of depression for some children and adolescents. One antidepressant – fluoxetine, or Prozac – a medicine in the category of SSRIs, has been approved by the FDA for treating depression in children 8 years of age and older. Escitalopram, or Lexapro, has also been approved by the FDA for treating adolescents 12 years of age and older.
- About “60 percent of children and adolescents will respond to initial treatment with medication,” which leaves many children needing further interventions. “Of those who don’t [respond], a significant number may respond to another medication but also may respond to the addition of a form of psychotherapy called cognitive behavioral therapy (CBT).”
It is common, as in the case above, that a connection with a therapist or support is valued over the specific modality even if it’s not showing improvement or outcomes. It is important to consider CBT as a form of evidence-based treatment for children with depression and to cite the famous “Treatment for Adolescents with Depression Study (TADS)” funded by the National Institute of Mental Health, published in 2004, that shows the following findings: “After 12 weeks of treatment, 71 percent of the patients who received the combination of medication and CBT were much improved.” In looking at the group that does not improve with medications alone, adolescents in particular can have more gains with the addition of CBT.
Tracking progress, little by little
Often we reflexively ask parents of depressed children: Are they better? And we ask the child: How do you feel? It can be difficult for parents to reflect on that, or see progress or gains from appointment to appointment. I suggest trying to use structured measures and tools to frame a discussion with progress on medication and treatment such as what is available at the Mood Treatment Center website.I also suggest apps such as Mood Kit,which is for mood tracking with some CBT exercises in addition to behavioral activation strategies for children and parents. It can be useful to have families take some ownership of tracking their moods and what may be playing into them. In particular with the pandemic, we can reflect on how much isolation or socialization, activities, sleep, eating habits, and exercise can affect us and make corresponding behavioral changes as a family to improve our own coping. Depression itself can be like glasses clouding one’s vision in gray, and that can also cloud one’s review of progress. When we hear comments such as “nothing gets better” from a child or parent, it may be helpful to try to track any contributing factors to a persistent low mood and acknowledge any slow and steady progress.
In summary, we can strive as providers to maximize our approach to depression in children and adolescents beyond the limited FDA-approved medications, or extrapolating adult data to children. If we emphasize the evidence-based practice of CBT and other interventions in addition to encouraging a tracking and review of outcomes measures with parents and families, we can empower them to make meaningful change in both perspectives and behaviors that can perpetuate depressive states.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and assistant professor of psychiatry at the Larner College of Medicine at UVM in Burlington.
Case
Max was a 17-year-old boy and avid video gamer who, predating COVID-19, was within a major depressive episode and continued to meet criteria through the duration of COVID-19 quarantine. He lives with his mother, who is a single mom and is working hard in a variety of jobs through the pandemic. Max had little motivation to engage in sports or other activities, and despite doing well enough in school, he spent much of his days escaping into video games and social media, where his friends communicated and bonded the most. He has had very little response to complete trials of two different selective serotonin reuptake inhibitors (SSRIs), and the off-label attempts at a serotonin-norepinephrine reuptake inhibitor and bupropion augmentation of an SSRI, as extrapolated by his pediatrician from adult data on treatment-resistant depression. He had ongoing supportive psychotherapy and his mother and pediatrician were wary of changing that relationship, as they were just happy he would engage at all. His shy nature made him very wary of attending any programs or groups. He had no other diagnosis including anxiety, substance abuse disorder, or learning disorder.
Case discussion
As a child and adolescent psychiatrist embedded in primary care practices, I (like you) am seeing more and more parents, children, and families struggling with depression through the course of this unprecedented and challenging year.
Max presented to me with his mother at the request of his primary care physician because within the course of many medication trials, it had been over 6 months of persistent symptoms without an end in sight for him, his family, or his primary care provider (PCP).
His diagnosis was treatment-resistant depression and his PCP was grasping at adult strategies to manage this all with additional psychopharmacology. As a consulting child-and-adolescent psychiatrist in primary care, how could I help the PCP? I too worry if there is anything that I can do to shift depression once standard treatments fail, and when the idea of engaging in behavioral activation or other pro-health activities is just too much for a depressed adolescent to bear. I weigh that with what is known about the evidence, and the good data driving us beyond medication solutions. I often find that it can be helpful to reiterate the following points to providers and families.
First, what to know about depression in kids
Depression looks different at different ages in children. In school-aged children, it’s widely known that irritability or psychosomatic symptoms (frequent headaches and stomach aches) can be the first preverbal signs of an emerging anxiety and depressive disorder in children. In adolescents, one would maybe expect more typical melancholic adult-like symptoms of depression; however, there is mounting evidence that adolescents actually present with more classically “atypical symptoms” of depression (low motivation, weight gain, escapism to sleep or video games, as with Max) with less persistence across setting (home, work, school) compared with adults (“Diagnosing Depression in Children and Adolescents” by Glen R. Elliott, PhD, MD, from The Carlat Child Psychiatry Report, November 2015, Antidepressant Use in Children).In addition, major life stressors (the breakup of a romantic relationship, failing a class, bullying) can be perceived as more permanent, and suicidal thinking can be acute and lethal in these contexts. With Max, it was accepted by all who were supporting him that he was struggling with depression, which is the first step in managing this well.
The idea of the designated patient
Often left out in a discussion of pediatric patients is the family. As a designated patient, much of our focus is on improving the symptoms of the patient in front of us. Parents direct their gaze at the child as the one with the condition who needs support. First following identification of depression, I find that a reframe of a diagnosis can be useful. Family systems theory approaches a child with a depression diagnosis, and says, that if one family member changes, even in a small way, a family as a system is forced to change. With a sense of an external locus of control, we often are left with a patient and parent feeling stuck. To provide a reorientation to the parents, ask how they are feeling. Can they get treatment for depression knowing the biology of the condition or consider making behavioral changes of their own and as a family? Can they consider family psychotherapy so they can cope better and break some cycles of maladaptive engagement shared across a family? These kinds of reorientations can be useful to shift the idea of treatment from the designated patient (the child) and medication options (limited data for kids who aren’t responding to them) to a family approach. Making the depression management strategy a family affair can help the entire family shift from seeing the only option as medications or interventions exclusively directed at a child. The Vermont Center for Children, Youth, and Families at the University of Vermont Medical Center has many pioneering developments in addressing family-based approaches to mental health concerns in the pediatric population, and can serve as a source of inspiration for this shift in discussing depression.
Practical strategies for the pediatrician
Medications can be useful for treating child and adolescent depression, but there is also strong evidence for psychotherapy, working with the child’s school and family, and different forms of behavioral activation (exercise, mindfulness, yoga, and other positive activities). Medications, if one is looking at standard of care treatment and Food and Drug Administration approval exclusively, is limited in scope and should not be the only intervention considered, as described in the case above.
In “The Use of Medication in Treating Childhood and Adolescent Depression: Information for Patients and Families,” which is a practical guide prepared by the American Psychiatric Association and the American Academy of Child and Adolescent Psychiatry, it is noted that Prozac and Lexapro are approved medications, as follows:
- Antidepressant medications can be effective in relieving the symptoms of depression for some children and adolescents. One antidepressant – fluoxetine, or Prozac – a medicine in the category of SSRIs, has been approved by the FDA for treating depression in children 8 years of age and older. Escitalopram, or Lexapro, has also been approved by the FDA for treating adolescents 12 years of age and older.
- About “60 percent of children and adolescents will respond to initial treatment with medication,” which leaves many children needing further interventions. “Of those who don’t [respond], a significant number may respond to another medication but also may respond to the addition of a form of psychotherapy called cognitive behavioral therapy (CBT).”
It is common, as in the case above, that a connection with a therapist or support is valued over the specific modality even if it’s not showing improvement or outcomes. It is important to consider CBT as a form of evidence-based treatment for children with depression and to cite the famous “Treatment for Adolescents with Depression Study (TADS)” funded by the National Institute of Mental Health, published in 2004, that shows the following findings: “After 12 weeks of treatment, 71 percent of the patients who received the combination of medication and CBT were much improved.” In looking at the group that does not improve with medications alone, adolescents in particular can have more gains with the addition of CBT.
Tracking progress, little by little
Often we reflexively ask parents of depressed children: Are they better? And we ask the child: How do you feel? It can be difficult for parents to reflect on that, or see progress or gains from appointment to appointment. I suggest trying to use structured measures and tools to frame a discussion with progress on medication and treatment such as what is available at the Mood Treatment Center website.I also suggest apps such as Mood Kit,which is for mood tracking with some CBT exercises in addition to behavioral activation strategies for children and parents. It can be useful to have families take some ownership of tracking their moods and what may be playing into them. In particular with the pandemic, we can reflect on how much isolation or socialization, activities, sleep, eating habits, and exercise can affect us and make corresponding behavioral changes as a family to improve our own coping. Depression itself can be like glasses clouding one’s vision in gray, and that can also cloud one’s review of progress. When we hear comments such as “nothing gets better” from a child or parent, it may be helpful to try to track any contributing factors to a persistent low mood and acknowledge any slow and steady progress.
In summary, we can strive as providers to maximize our approach to depression in children and adolescents beyond the limited FDA-approved medications, or extrapolating adult data to children. If we emphasize the evidence-based practice of CBT and other interventions in addition to encouraging a tracking and review of outcomes measures with parents and families, we can empower them to make meaningful change in both perspectives and behaviors that can perpetuate depressive states.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and assistant professor of psychiatry at the Larner College of Medicine at UVM in Burlington.
Case
Max was a 17-year-old boy and avid video gamer who, predating COVID-19, was within a major depressive episode and continued to meet criteria through the duration of COVID-19 quarantine. He lives with his mother, who is a single mom and is working hard in a variety of jobs through the pandemic. Max had little motivation to engage in sports or other activities, and despite doing well enough in school, he spent much of his days escaping into video games and social media, where his friends communicated and bonded the most. He has had very little response to complete trials of two different selective serotonin reuptake inhibitors (SSRIs), and the off-label attempts at a serotonin-norepinephrine reuptake inhibitor and bupropion augmentation of an SSRI, as extrapolated by his pediatrician from adult data on treatment-resistant depression. He had ongoing supportive psychotherapy and his mother and pediatrician were wary of changing that relationship, as they were just happy he would engage at all. His shy nature made him very wary of attending any programs or groups. He had no other diagnosis including anxiety, substance abuse disorder, or learning disorder.
Case discussion
As a child and adolescent psychiatrist embedded in primary care practices, I (like you) am seeing more and more parents, children, and families struggling with depression through the course of this unprecedented and challenging year.
Max presented to me with his mother at the request of his primary care physician because within the course of many medication trials, it had been over 6 months of persistent symptoms without an end in sight for him, his family, or his primary care provider (PCP).
His diagnosis was treatment-resistant depression and his PCP was grasping at adult strategies to manage this all with additional psychopharmacology. As a consulting child-and-adolescent psychiatrist in primary care, how could I help the PCP? I too worry if there is anything that I can do to shift depression once standard treatments fail, and when the idea of engaging in behavioral activation or other pro-health activities is just too much for a depressed adolescent to bear. I weigh that with what is known about the evidence, and the good data driving us beyond medication solutions. I often find that it can be helpful to reiterate the following points to providers and families.
First, what to know about depression in kids
Depression looks different at different ages in children. In school-aged children, it’s widely known that irritability or psychosomatic symptoms (frequent headaches and stomach aches) can be the first preverbal signs of an emerging anxiety and depressive disorder in children. In adolescents, one would maybe expect more typical melancholic adult-like symptoms of depression; however, there is mounting evidence that adolescents actually present with more classically “atypical symptoms” of depression (low motivation, weight gain, escapism to sleep or video games, as with Max) with less persistence across setting (home, work, school) compared with adults (“Diagnosing Depression in Children and Adolescents” by Glen R. Elliott, PhD, MD, from The Carlat Child Psychiatry Report, November 2015, Antidepressant Use in Children).In addition, major life stressors (the breakup of a romantic relationship, failing a class, bullying) can be perceived as more permanent, and suicidal thinking can be acute and lethal in these contexts. With Max, it was accepted by all who were supporting him that he was struggling with depression, which is the first step in managing this well.
The idea of the designated patient
Often left out in a discussion of pediatric patients is the family. As a designated patient, much of our focus is on improving the symptoms of the patient in front of us. Parents direct their gaze at the child as the one with the condition who needs support. First following identification of depression, I find that a reframe of a diagnosis can be useful. Family systems theory approaches a child with a depression diagnosis, and says, that if one family member changes, even in a small way, a family as a system is forced to change. With a sense of an external locus of control, we often are left with a patient and parent feeling stuck. To provide a reorientation to the parents, ask how they are feeling. Can they get treatment for depression knowing the biology of the condition or consider making behavioral changes of their own and as a family? Can they consider family psychotherapy so they can cope better and break some cycles of maladaptive engagement shared across a family? These kinds of reorientations can be useful to shift the idea of treatment from the designated patient (the child) and medication options (limited data for kids who aren’t responding to them) to a family approach. Making the depression management strategy a family affair can help the entire family shift from seeing the only option as medications or interventions exclusively directed at a child. The Vermont Center for Children, Youth, and Families at the University of Vermont Medical Center has many pioneering developments in addressing family-based approaches to mental health concerns in the pediatric population, and can serve as a source of inspiration for this shift in discussing depression.
Practical strategies for the pediatrician
Medications can be useful for treating child and adolescent depression, but there is also strong evidence for psychotherapy, working with the child’s school and family, and different forms of behavioral activation (exercise, mindfulness, yoga, and other positive activities). Medications, if one is looking at standard of care treatment and Food and Drug Administration approval exclusively, is limited in scope and should not be the only intervention considered, as described in the case above.
In “The Use of Medication in Treating Childhood and Adolescent Depression: Information for Patients and Families,” which is a practical guide prepared by the American Psychiatric Association and the American Academy of Child and Adolescent Psychiatry, it is noted that Prozac and Lexapro are approved medications, as follows:
- Antidepressant medications can be effective in relieving the symptoms of depression for some children and adolescents. One antidepressant – fluoxetine, or Prozac – a medicine in the category of SSRIs, has been approved by the FDA for treating depression in children 8 years of age and older. Escitalopram, or Lexapro, has also been approved by the FDA for treating adolescents 12 years of age and older.
- About “60 percent of children and adolescents will respond to initial treatment with medication,” which leaves many children needing further interventions. “Of those who don’t [respond], a significant number may respond to another medication but also may respond to the addition of a form of psychotherapy called cognitive behavioral therapy (CBT).”
It is common, as in the case above, that a connection with a therapist or support is valued over the specific modality even if it’s not showing improvement or outcomes. It is important to consider CBT as a form of evidence-based treatment for children with depression and to cite the famous “Treatment for Adolescents with Depression Study (TADS)” funded by the National Institute of Mental Health, published in 2004, that shows the following findings: “After 12 weeks of treatment, 71 percent of the patients who received the combination of medication and CBT were much improved.” In looking at the group that does not improve with medications alone, adolescents in particular can have more gains with the addition of CBT.
Tracking progress, little by little
Often we reflexively ask parents of depressed children: Are they better? And we ask the child: How do you feel? It can be difficult for parents to reflect on that, or see progress or gains from appointment to appointment. I suggest trying to use structured measures and tools to frame a discussion with progress on medication and treatment such as what is available at the Mood Treatment Center website.I also suggest apps such as Mood Kit,which is for mood tracking with some CBT exercises in addition to behavioral activation strategies for children and parents. It can be useful to have families take some ownership of tracking their moods and what may be playing into them. In particular with the pandemic, we can reflect on how much isolation or socialization, activities, sleep, eating habits, and exercise can affect us and make corresponding behavioral changes as a family to improve our own coping. Depression itself can be like glasses clouding one’s vision in gray, and that can also cloud one’s review of progress. When we hear comments such as “nothing gets better” from a child or parent, it may be helpful to try to track any contributing factors to a persistent low mood and acknowledge any slow and steady progress.
In summary, we can strive as providers to maximize our approach to depression in children and adolescents beyond the limited FDA-approved medications, or extrapolating adult data to children. If we emphasize the evidence-based practice of CBT and other interventions in addition to encouraging a tracking and review of outcomes measures with parents and families, we can empower them to make meaningful change in both perspectives and behaviors that can perpetuate depressive states.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and assistant professor of psychiatry at the Larner College of Medicine at UVM in Burlington.
Inpatient psychiatrist? Maybe I’ll be a vaccinator instead
Now that completion of residency is fast approaching, I am asked regularly what I plan to do when I become a Real Doctor on July 1. It feels like it wasn’t so long ago I was trying to decide if I should even go to medical school, then later, if I should go into psychiatry, family medicine, or emergency medicine. And here I am at another decision point, another of the regular, 4-year milestones in my journey to full physicianhood.

A surprising thing happened to me during my psychiatry training: I fell in love with acute care. Instead of outpatient care, I preferred the longer hours with patients who insist they are Jesus Christ, believe deeply they are being actively pursued by the FBI, and sometimes eat their own feces. I was in awe of the remarkable capacity of the human brain to convince a graduate-school educated man with bipolar disorder that it is acceptable to call in bomb threats to a hospital. To lead a patient on a conservatorship to believe that I am not a doctor but, instead, a seamstress or leave socks full of feces as presents for Santa Claus (lots of feces in inpatient psychiatry). To believe their spouses are not humans or hear voices telling them they should jump off a bridge, sustaining near-lethal injuries. I was hooked.
Psychiatry as a field is not for those requiring instant gratification. Other than Ativan challenges and the remarkably quick response some patients have to ECT, outcomes of our treatments are usually modest, and they take time. We often delude ourselves into thinking that bumping a patient’s fluoxetine from 10 mg to 20 mg will be The Thing that changes a patient’s life. We address our own sense of helplessness as much as that of our patients, who are desperate for something, for someone, to do something that will alter the course of their lives.
Of course, what I can offer my patients usually falls short of their lofty expectations of my prowess. I offer them compassion, validation, empathy. I offer them medications for which we usually have meager data and meager results. I cannot find them shelter but for a few nights, perhaps a week. I rarely, in settings in which primary diagnoses of substance use and personality disorders are forbidden by insurance companies, can help them with their addiction to methamphetamine. I cannot cure their maladaptive characterological pathology stemming from childhood attachment trauma. To address my own sense of failure as a healer, I resort to the bottom of Maslow’s hierarchy of needs, providing their choice of juice box, more blankets. I slow-roll their discharges overnight so that they can stay in the ER hallway instead of spending the night outside in the rare Southern California rain.
In my 3rd year of residency, we were thrown into a pandemic. I felt both terrified of getting COVID-19 in the hospital and inadequate as a physician. I did not want to be intubating patients, but even more, I dreaded the potential “psychiatry-friendly” assignment of calling the family members of those who had perished from the disease. Rumors circulated that certain versions of surge planning had the inpatient psychiatry unit transitioned to a COVID unit and psychiatry residents “redeployed” to cover medicine floors. Fortunately, we did not have to (or have not yet had to) endure this apocalyptic episode of worst-case scenario. I remained a psychiatrist-in-training, seeing occasional COVID patients but with full personal protective equipment and the ability to maintain some physical distance to complete my examinations. Coming home to my apartment building in scrubs, now acceptable attire on inpatient units – it always should have been since, as we have established, our units are filled with feces – I early on felt like a leper. Later on, I was treated with dignity and respect, like a hero.
My position as a non–frontline-physician was personally challenging. I wanted to help, felt like I should and could help. I am a helper-in-recovery who has spent years learning to achieve a balance of service and loyalty to others and my own desires. The initial guilt I felt at feeling appreciated during the nightly celebration of health care workers downtown ultimately dissipated. I was no hero, nor did I claim to be one. I made peace with my pandemic hobbies of sourdough bread-baking, Moscow mule-making, jigsaw-puzzling, and, briefly, running (before a calcaneal stress fracture reminded me that I am not built for land exercise). I went to work; I came home. My cat was happy.
Then, in rapid succession, vaccines were approved and distributed. My hospital had partnered with the county to administer them at a new superstation, and they were in desperate need of licensed humans to be vaccinators. They cared not that I had given very few (n = 3) injections and only during medical school. I watched the YouTube videos on the Z-track technique for IMs, learned about needle gauges, and went off to the baseball stadium.
I loved this new gig, disproportionately. The 8+ hours flew by, 100 vaccines given to occupants of cars who had eagerly waited hours for the privilege of being vaccinated by an almost-psychiatrist. It was not the technical expertise of sticking a needle into someone’s arm that gave me a dopamine rush, nor the microstress of preparing the syringes with a flimsy needle and a slight caffeine-induced tremor while trying to flick air bubbles out of the syringe without dropping the precious vaccine vial. It was not the travel nurse asking me why anyone – especially an overworked resident – would volunteer to do this for free, while she and others were making “stupid amounts of money” to do the same job.
What drove me to keep volunteering for no pay, only Cheez-Its available as sustenance, minimal gratitude from my employer, long hours on my feet doing a task that was rote and at which I probably would never completely excel? On my second shift, I realized why I found it so gratifying to be a vaccinator: There was a perfect 1:1 correspondence in what patients wanted at that moment and in what I had to offer them. They did not want me to fix their lives, secure them housing, or go back in time and remove them from abusive homes so they could grow up to be more functional, happier adults. They merely wanted a shot. They were profusely grateful, hopeful that this was the Beginning of the End. Nobody spat on me; nobody called me obscene names. Nobody was upset with me for involuntarily holding them against their will. My services were welcome, appreciated. I had lovely, superficial conversations with dozens of people. I felt connected to strangers in a way that has been sorely lacking since March 2020. Understandably mistaken for a nurse throughout the day, I felt more like a bona fide physician than I had in over a year.
I know the adrenaline rush will fade, that volunteer-vaccinating in my free time will eventually become less exciting to me. I know I won’t be able to convince my colleagues indefinitely that volunteering together is a great, institution-sanctioned bonding opportunity. I know the initial enthusiasm over vaccine distribution will fade as the pandemic continues to transform our everyday lives and threaten the health of millions, the economy, and the sanctity of normal human interactions. The gratitude and hopefulness may well be replaced with frustration over waiting hours in a car to get an injection from a psychiatrist, with fear that this promised panacea may not restore normalcy anytime soon. But right now, 11 months into a pandemic that has left our profession exhausted and jaded, the coprophilia and catatonia have temporarily lost their allure. So, I’m adding “vaccinator” to my list of pandemic hobbies.
Dr. Stone is a chief resident in psychiatry at the University of California, San Diego. Before deciding to become a physician, she obtained a master’s degree in public health and worked in health policy research studying empathy and patient-doctor interactions. She has a passion for public psychiatry and acute care, and she dabbles in physician wellness, medical education, and the interface of psychiatry and primary care. Dr. Stone has no disclosures.
Now that completion of residency is fast approaching, I am asked regularly what I plan to do when I become a Real Doctor on July 1. It feels like it wasn’t so long ago I was trying to decide if I should even go to medical school, then later, if I should go into psychiatry, family medicine, or emergency medicine. And here I am at another decision point, another of the regular, 4-year milestones in my journey to full physicianhood.
A surprising thing happened to me during my psychiatry training: I fell in love with acute care. Instead of outpatient care, I preferred the longer hours with patients who insist they are Jesus Christ, believe deeply they are being actively pursued by the FBI, and sometimes eat their own feces. I was in awe of the remarkable capacity of the human brain to convince a graduate-school educated man with bipolar disorder that it is acceptable to call in bomb threats to a hospital. To lead a patient on a conservatorship to believe that I am not a doctor but, instead, a seamstress or leave socks full of feces as presents for Santa Claus (lots of feces in inpatient psychiatry). To believe their spouses are not humans or hear voices telling them they should jump off a bridge, sustaining near-lethal injuries. I was hooked.
Psychiatry as a field is not for those requiring instant gratification. Other than Ativan challenges and the remarkably quick response some patients have to ECT, outcomes of our treatments are usually modest, and they take time. We often delude ourselves into thinking that bumping a patient’s fluoxetine from 10 mg to 20 mg will be The Thing that changes a patient’s life. We address our own sense of helplessness as much as that of our patients, who are desperate for something, for someone, to do something that will alter the course of their lives.
Of course, what I can offer my patients usually falls short of their lofty expectations of my prowess. I offer them compassion, validation, empathy. I offer them medications for which we usually have meager data and meager results. I cannot find them shelter but for a few nights, perhaps a week. I rarely, in settings in which primary diagnoses of substance use and personality disorders are forbidden by insurance companies, can help them with their addiction to methamphetamine. I cannot cure their maladaptive characterological pathology stemming from childhood attachment trauma. To address my own sense of failure as a healer, I resort to the bottom of Maslow’s hierarchy of needs, providing their choice of juice box, more blankets. I slow-roll their discharges overnight so that they can stay in the ER hallway instead of spending the night outside in the rare Southern California rain.
In my 3rd year of residency, we were thrown into a pandemic. I felt both terrified of getting COVID-19 in the hospital and inadequate as a physician. I did not want to be intubating patients, but even more, I dreaded the potential “psychiatry-friendly” assignment of calling the family members of those who had perished from the disease. Rumors circulated that certain versions of surge planning had the inpatient psychiatry unit transitioned to a COVID unit and psychiatry residents “redeployed” to cover medicine floors. Fortunately, we did not have to (or have not yet had to) endure this apocalyptic episode of worst-case scenario. I remained a psychiatrist-in-training, seeing occasional COVID patients but with full personal protective equipment and the ability to maintain some physical distance to complete my examinations. Coming home to my apartment building in scrubs, now acceptable attire on inpatient units – it always should have been since, as we have established, our units are filled with feces – I early on felt like a leper. Later on, I was treated with dignity and respect, like a hero.
My position as a non–frontline-physician was personally challenging. I wanted to help, felt like I should and could help. I am a helper-in-recovery who has spent years learning to achieve a balance of service and loyalty to others and my own desires. The initial guilt I felt at feeling appreciated during the nightly celebration of health care workers downtown ultimately dissipated. I was no hero, nor did I claim to be one. I made peace with my pandemic hobbies of sourdough bread-baking, Moscow mule-making, jigsaw-puzzling, and, briefly, running (before a calcaneal stress fracture reminded me that I am not built for land exercise). I went to work; I came home. My cat was happy.
Then, in rapid succession, vaccines were approved and distributed. My hospital had partnered with the county to administer them at a new superstation, and they were in desperate need of licensed humans to be vaccinators. They cared not that I had given very few (n = 3) injections and only during medical school. I watched the YouTube videos on the Z-track technique for IMs, learned about needle gauges, and went off to the baseball stadium.
I loved this new gig, disproportionately. The 8+ hours flew by, 100 vaccines given to occupants of cars who had eagerly waited hours for the privilege of being vaccinated by an almost-psychiatrist. It was not the technical expertise of sticking a needle into someone’s arm that gave me a dopamine rush, nor the microstress of preparing the syringes with a flimsy needle and a slight caffeine-induced tremor while trying to flick air bubbles out of the syringe without dropping the precious vaccine vial. It was not the travel nurse asking me why anyone – especially an overworked resident – would volunteer to do this for free, while she and others were making “stupid amounts of money” to do the same job.
What drove me to keep volunteering for no pay, only Cheez-Its available as sustenance, minimal gratitude from my employer, long hours on my feet doing a task that was rote and at which I probably would never completely excel? On my second shift, I realized why I found it so gratifying to be a vaccinator: There was a perfect 1:1 correspondence in what patients wanted at that moment and in what I had to offer them. They did not want me to fix their lives, secure them housing, or go back in time and remove them from abusive homes so they could grow up to be more functional, happier adults. They merely wanted a shot. They were profusely grateful, hopeful that this was the Beginning of the End. Nobody spat on me; nobody called me obscene names. Nobody was upset with me for involuntarily holding them against their will. My services were welcome, appreciated. I had lovely, superficial conversations with dozens of people. I felt connected to strangers in a way that has been sorely lacking since March 2020. Understandably mistaken for a nurse throughout the day, I felt more like a bona fide physician than I had in over a year.
I know the adrenaline rush will fade, that volunteer-vaccinating in my free time will eventually become less exciting to me. I know I won’t be able to convince my colleagues indefinitely that volunteering together is a great, institution-sanctioned bonding opportunity. I know the initial enthusiasm over vaccine distribution will fade as the pandemic continues to transform our everyday lives and threaten the health of millions, the economy, and the sanctity of normal human interactions. The gratitude and hopefulness may well be replaced with frustration over waiting hours in a car to get an injection from a psychiatrist, with fear that this promised panacea may not restore normalcy anytime soon. But right now, 11 months into a pandemic that has left our profession exhausted and jaded, the coprophilia and catatonia have temporarily lost their allure. So, I’m adding “vaccinator” to my list of pandemic hobbies.
Dr. Stone is a chief resident in psychiatry at the University of California, San Diego. Before deciding to become a physician, she obtained a master’s degree in public health and worked in health policy research studying empathy and patient-doctor interactions. She has a passion for public psychiatry and acute care, and she dabbles in physician wellness, medical education, and the interface of psychiatry and primary care. Dr. Stone has no disclosures.
Now that completion of residency is fast approaching, I am asked regularly what I plan to do when I become a Real Doctor on July 1. It feels like it wasn’t so long ago I was trying to decide if I should even go to medical school, then later, if I should go into psychiatry, family medicine, or emergency medicine. And here I am at another decision point, another of the regular, 4-year milestones in my journey to full physicianhood.
A surprising thing happened to me during my psychiatry training: I fell in love with acute care. Instead of outpatient care, I preferred the longer hours with patients who insist they are Jesus Christ, believe deeply they are being actively pursued by the FBI, and sometimes eat their own feces. I was in awe of the remarkable capacity of the human brain to convince a graduate-school educated man with bipolar disorder that it is acceptable to call in bomb threats to a hospital. To lead a patient on a conservatorship to believe that I am not a doctor but, instead, a seamstress or leave socks full of feces as presents for Santa Claus (lots of feces in inpatient psychiatry). To believe their spouses are not humans or hear voices telling them they should jump off a bridge, sustaining near-lethal injuries. I was hooked.
Psychiatry as a field is not for those requiring instant gratification. Other than Ativan challenges and the remarkably quick response some patients have to ECT, outcomes of our treatments are usually modest, and they take time. We often delude ourselves into thinking that bumping a patient’s fluoxetine from 10 mg to 20 mg will be The Thing that changes a patient’s life. We address our own sense of helplessness as much as that of our patients, who are desperate for something, for someone, to do something that will alter the course of their lives.
Of course, what I can offer my patients usually falls short of their lofty expectations of my prowess. I offer them compassion, validation, empathy. I offer them medications for which we usually have meager data and meager results. I cannot find them shelter but for a few nights, perhaps a week. I rarely, in settings in which primary diagnoses of substance use and personality disorders are forbidden by insurance companies, can help them with their addiction to methamphetamine. I cannot cure their maladaptive characterological pathology stemming from childhood attachment trauma. To address my own sense of failure as a healer, I resort to the bottom of Maslow’s hierarchy of needs, providing their choice of juice box, more blankets. I slow-roll their discharges overnight so that they can stay in the ER hallway instead of spending the night outside in the rare Southern California rain.
In my 3rd year of residency, we were thrown into a pandemic. I felt both terrified of getting COVID-19 in the hospital and inadequate as a physician. I did not want to be intubating patients, but even more, I dreaded the potential “psychiatry-friendly” assignment of calling the family members of those who had perished from the disease. Rumors circulated that certain versions of surge planning had the inpatient psychiatry unit transitioned to a COVID unit and psychiatry residents “redeployed” to cover medicine floors. Fortunately, we did not have to (or have not yet had to) endure this apocalyptic episode of worst-case scenario. I remained a psychiatrist-in-training, seeing occasional COVID patients but with full personal protective equipment and the ability to maintain some physical distance to complete my examinations. Coming home to my apartment building in scrubs, now acceptable attire on inpatient units – it always should have been since, as we have established, our units are filled with feces – I early on felt like a leper. Later on, I was treated with dignity and respect, like a hero.
My position as a non–frontline-physician was personally challenging. I wanted to help, felt like I should and could help. I am a helper-in-recovery who has spent years learning to achieve a balance of service and loyalty to others and my own desires. The initial guilt I felt at feeling appreciated during the nightly celebration of health care workers downtown ultimately dissipated. I was no hero, nor did I claim to be one. I made peace with my pandemic hobbies of sourdough bread-baking, Moscow mule-making, jigsaw-puzzling, and, briefly, running (before a calcaneal stress fracture reminded me that I am not built for land exercise). I went to work; I came home. My cat was happy.
Then, in rapid succession, vaccines were approved and distributed. My hospital had partnered with the county to administer them at a new superstation, and they were in desperate need of licensed humans to be vaccinators. They cared not that I had given very few (n = 3) injections and only during medical school. I watched the YouTube videos on the Z-track technique for IMs, learned about needle gauges, and went off to the baseball stadium.
I loved this new gig, disproportionately. The 8+ hours flew by, 100 vaccines given to occupants of cars who had eagerly waited hours for the privilege of being vaccinated by an almost-psychiatrist. It was not the technical expertise of sticking a needle into someone’s arm that gave me a dopamine rush, nor the microstress of preparing the syringes with a flimsy needle and a slight caffeine-induced tremor while trying to flick air bubbles out of the syringe without dropping the precious vaccine vial. It was not the travel nurse asking me why anyone – especially an overworked resident – would volunteer to do this for free, while she and others were making “stupid amounts of money” to do the same job.
What drove me to keep volunteering for no pay, only Cheez-Its available as sustenance, minimal gratitude from my employer, long hours on my feet doing a task that was rote and at which I probably would never completely excel? On my second shift, I realized why I found it so gratifying to be a vaccinator: There was a perfect 1:1 correspondence in what patients wanted at that moment and in what I had to offer them. They did not want me to fix their lives, secure them housing, or go back in time and remove them from abusive homes so they could grow up to be more functional, happier adults. They merely wanted a shot. They were profusely grateful, hopeful that this was the Beginning of the End. Nobody spat on me; nobody called me obscene names. Nobody was upset with me for involuntarily holding them against their will. My services were welcome, appreciated. I had lovely, superficial conversations with dozens of people. I felt connected to strangers in a way that has been sorely lacking since March 2020. Understandably mistaken for a nurse throughout the day, I felt more like a bona fide physician than I had in over a year.
I know the adrenaline rush will fade, that volunteer-vaccinating in my free time will eventually become less exciting to me. I know I won’t be able to convince my colleagues indefinitely that volunteering together is a great, institution-sanctioned bonding opportunity. I know the initial enthusiasm over vaccine distribution will fade as the pandemic continues to transform our everyday lives and threaten the health of millions, the economy, and the sanctity of normal human interactions. The gratitude and hopefulness may well be replaced with frustration over waiting hours in a car to get an injection from a psychiatrist, with fear that this promised panacea may not restore normalcy anytime soon. But right now, 11 months into a pandemic that has left our profession exhausted and jaded, the coprophilia and catatonia have temporarily lost their allure. So, I’m adding “vaccinator” to my list of pandemic hobbies.
Dr. Stone is a chief resident in psychiatry at the University of California, San Diego. Before deciding to become a physician, she obtained a master’s degree in public health and worked in health policy research studying empathy and patient-doctor interactions. She has a passion for public psychiatry and acute care, and she dabbles in physician wellness, medical education, and the interface of psychiatry and primary care. Dr. Stone has no disclosures.
Treatment of horizontal neck lines
The interplay of the neck subunits, as outlined in the recent article by Friedman and colleagues, requires multiple combination treatments, including fat removal, augmentation of deficient bony prominences, relaxation of hyperkinetic muscles, tissue tightening, suture anchoring, skin resurfacing, and treatment of dyschromia.

Horizontal neck lines are linear etched lines or furrows that commonly appear at a young age and are not caused by the aging process. The anatomy of the neck and the manner in which it bends contributes to their development at an early age. It is hypothesized that variable adipose tissue thickness and fibromuscular bands contribute to deepening of these lines in overweight patients. The widespread use of cell phones, laptops, and tablets has increased their prevalence and this has become one of the most common concerns of patients aged under 30 years in my clinic.
Various treatments have been recommended for neck rejuvenation, including hyaluronic acid and dilute calcium hydroxylapatite. In my experience, neither of these treatments adequately resolves the horizontal neck lines, and more importantly, prevents them from reoccurring. In addition, given the variability in skin and adipose thickness in the anterior neck, side effects including lumps, irregular correction, and the Tyndall effect, are common, particularly with incorrect choice of filler and injection depth.

The fibromuscular bands along the transverse neck lines pose one of the complexities in treatment with injectable filler. I have had significant improvement in the aesthetic outcome of my patients by using subcision along the transverse bands extensively prior to injection with hyaluronic acid fillers. The subcision is done with a 27-gauge needle to release the fibrous bands that tether the tissue down. If a patient has excess adipose tissue on either side of the bands, injectable fillers often do not improve the appearance of the lines and can make the neck appear heavier. The use of subcision followed by one to six treatments of deoxycholic acid in the adjacent adipose tissue prior to injection with a filler will help even out the contour of the neck, decrease adipose tissue bulges, release the fibrous bands, and fill the lines properly.
Working from home and on handheld devices has increased the appearance of neck lines in young populations. Despite the vast array of treatments in the aging neck, none have been very successful for this particular problem in the young. We need an improved understanding of these lines and better studies to investigate treatment options and long-term correction.

References:
Friedman O et al. J Cosmet Dermatol. 2021 Feb;20(2):569-76.
Brandt FS and Boker A. Dermatol Clin. 2004 Apr;22(2):159-66.
Tseng F and Yu H. Plast Reconstr Surg Glob Open. 2019 Aug 19;7(8):e2366.
Dibernardo BE. J Cosmet Laser Ther. 2013 Apr;15(2):56-64.
Jones D et al. Dermatol Surg. 2016 Oct;4 Suppl 1(Suppl 1):S235-42.
Lee SK and Kim HS. J Cosmet Dermatol. 2018 Aug;17(4):590-5.
Chao YY et al. Dermatol Surg. 2011 Oct;37(10):1542-5.
Han TY et al. Dermatol Surg. 2011 Sep;37(9):1291-6.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
The interplay of the neck subunits, as outlined in the recent article by Friedman and colleagues, requires multiple combination treatments, including fat removal, augmentation of deficient bony prominences, relaxation of hyperkinetic muscles, tissue tightening, suture anchoring, skin resurfacing, and treatment of dyschromia.
Horizontal neck lines are linear etched lines or furrows that commonly appear at a young age and are not caused by the aging process. The anatomy of the neck and the manner in which it bends contributes to their development at an early age. It is hypothesized that variable adipose tissue thickness and fibromuscular bands contribute to deepening of these lines in overweight patients. The widespread use of cell phones, laptops, and tablets has increased their prevalence and this has become one of the most common concerns of patients aged under 30 years in my clinic.
Various treatments have been recommended for neck rejuvenation, including hyaluronic acid and dilute calcium hydroxylapatite. In my experience, neither of these treatments adequately resolves the horizontal neck lines, and more importantly, prevents them from reoccurring. In addition, given the variability in skin and adipose thickness in the anterior neck, side effects including lumps, irregular correction, and the Tyndall effect, are common, particularly with incorrect choice of filler and injection depth.
The fibromuscular bands along the transverse neck lines pose one of the complexities in treatment with injectable filler. I have had significant improvement in the aesthetic outcome of my patients by using subcision along the transverse bands extensively prior to injection with hyaluronic acid fillers. The subcision is done with a 27-gauge needle to release the fibrous bands that tether the tissue down. If a patient has excess adipose tissue on either side of the bands, injectable fillers often do not improve the appearance of the lines and can make the neck appear heavier. The use of subcision followed by one to six treatments of deoxycholic acid in the adjacent adipose tissue prior to injection with a filler will help even out the contour of the neck, decrease adipose tissue bulges, release the fibrous bands, and fill the lines properly.
Working from home and on handheld devices has increased the appearance of neck lines in young populations. Despite the vast array of treatments in the aging neck, none have been very successful for this particular problem in the young. We need an improved understanding of these lines and better studies to investigate treatment options and long-term correction.
References:
Friedman O et al. J Cosmet Dermatol. 2021 Feb;20(2):569-76.
Brandt FS and Boker A. Dermatol Clin. 2004 Apr;22(2):159-66.
Tseng F and Yu H. Plast Reconstr Surg Glob Open. 2019 Aug 19;7(8):e2366.
Dibernardo BE. J Cosmet Laser Ther. 2013 Apr;15(2):56-64.
Jones D et al. Dermatol Surg. 2016 Oct;4 Suppl 1(Suppl 1):S235-42.
Lee SK and Kim HS. J Cosmet Dermatol. 2018 Aug;17(4):590-5.
Chao YY et al. Dermatol Surg. 2011 Oct;37(10):1542-5.
Han TY et al. Dermatol Surg. 2011 Sep;37(9):1291-6.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
The interplay of the neck subunits, as outlined in the recent article by Friedman and colleagues, requires multiple combination treatments, including fat removal, augmentation of deficient bony prominences, relaxation of hyperkinetic muscles, tissue tightening, suture anchoring, skin resurfacing, and treatment of dyschromia.
Horizontal neck lines are linear etched lines or furrows that commonly appear at a young age and are not caused by the aging process. The anatomy of the neck and the manner in which it bends contributes to their development at an early age. It is hypothesized that variable adipose tissue thickness and fibromuscular bands contribute to deepening of these lines in overweight patients. The widespread use of cell phones, laptops, and tablets has increased their prevalence and this has become one of the most common concerns of patients aged under 30 years in my clinic.
Various treatments have been recommended for neck rejuvenation, including hyaluronic acid and dilute calcium hydroxylapatite. In my experience, neither of these treatments adequately resolves the horizontal neck lines, and more importantly, prevents them from reoccurring. In addition, given the variability in skin and adipose thickness in the anterior neck, side effects including lumps, irregular correction, and the Tyndall effect, are common, particularly with incorrect choice of filler and injection depth.
The fibromuscular bands along the transverse neck lines pose one of the complexities in treatment with injectable filler. I have had significant improvement in the aesthetic outcome of my patients by using subcision along the transverse bands extensively prior to injection with hyaluronic acid fillers. The subcision is done with a 27-gauge needle to release the fibrous bands that tether the tissue down. If a patient has excess adipose tissue on either side of the bands, injectable fillers often do not improve the appearance of the lines and can make the neck appear heavier. The use of subcision followed by one to six treatments of deoxycholic acid in the adjacent adipose tissue prior to injection with a filler will help even out the contour of the neck, decrease adipose tissue bulges, release the fibrous bands, and fill the lines properly.
Working from home and on handheld devices has increased the appearance of neck lines in young populations. Despite the vast array of treatments in the aging neck, none have been very successful for this particular problem in the young. We need an improved understanding of these lines and better studies to investigate treatment options and long-term correction.
References:
Friedman O et al. J Cosmet Dermatol. 2021 Feb;20(2):569-76.
Brandt FS and Boker A. Dermatol Clin. 2004 Apr;22(2):159-66.
Tseng F and Yu H. Plast Reconstr Surg Glob Open. 2019 Aug 19;7(8):e2366.
Dibernardo BE. J Cosmet Laser Ther. 2013 Apr;15(2):56-64.
Jones D et al. Dermatol Surg. 2016 Oct;4 Suppl 1(Suppl 1):S235-42.
Lee SK and Kim HS. J Cosmet Dermatol. 2018 Aug;17(4):590-5.
Chao YY et al. Dermatol Surg. 2011 Oct;37(10):1542-5.
Han TY et al. Dermatol Surg. 2011 Sep;37(9):1291-6.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
Reminders of our mortality can come when physicians least expect it
This time of year I spend weekend afternoons in my hot tub, catching up on medical journals, CME, paperbacks, and generally anything worth reading that shows up in my mailbox.

One of those items was the alumni news from my medical school. As usual, I leafed through it, reading articles of interest and glancing at updates on any classmates that were featured.
Then I stopped.
There, in the back of the magazine, was an obituary on the first of my classmates to pass (that I’m aware of).
I reread it a few times in disbelief. Maybe it was on her taking a new job or being promoted, and was in the wrong section. Nope.
I put the magazine down. She was 1 year younger than me and had gone into internal medicine. Not someone I’d kept in touch with, but certainly was friendly with during those 4 years and frequently chatted with in hallways or between classes. I remember meeting her during the first week of school, when I got her name mixed up with another girl’s in our class. I saw her at parties, meetings, and I think even played doubles tennis with her once, though who we played against I have no idea anymore.
She was at our 20th reunion, and we’d talked for a few minutes. We caught up on our lives since graduation and, as people do at these things, moved on to chat with others.
No details were given as to her death, and it really doesn’t matter.
. For most of each day it’s a fact in the back of our minds, behind the daily activities of working, shopping, doing laundry, commuting, and cooking dinner. After all, it’s really what we do while here that matters, no matter how mundane it may seem.
But sometimes something will push that realization to the front, and make us remember how important every minute really is.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
This time of year I spend weekend afternoons in my hot tub, catching up on medical journals, CME, paperbacks, and generally anything worth reading that shows up in my mailbox.
One of those items was the alumni news from my medical school. As usual, I leafed through it, reading articles of interest and glancing at updates on any classmates that were featured.
Then I stopped.
There, in the back of the magazine, was an obituary on the first of my classmates to pass (that I’m aware of).
I reread it a few times in disbelief. Maybe it was on her taking a new job or being promoted, and was in the wrong section. Nope.
I put the magazine down. She was 1 year younger than me and had gone into internal medicine. Not someone I’d kept in touch with, but certainly was friendly with during those 4 years and frequently chatted with in hallways or between classes. I remember meeting her during the first week of school, when I got her name mixed up with another girl’s in our class. I saw her at parties, meetings, and I think even played doubles tennis with her once, though who we played against I have no idea anymore.
She was at our 20th reunion, and we’d talked for a few minutes. We caught up on our lives since graduation and, as people do at these things, moved on to chat with others.
No details were given as to her death, and it really doesn’t matter.
. For most of each day it’s a fact in the back of our minds, behind the daily activities of working, shopping, doing laundry, commuting, and cooking dinner. After all, it’s really what we do while here that matters, no matter how mundane it may seem.
But sometimes something will push that realization to the front, and make us remember how important every minute really is.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
This time of year I spend weekend afternoons in my hot tub, catching up on medical journals, CME, paperbacks, and generally anything worth reading that shows up in my mailbox.
One of those items was the alumni news from my medical school. As usual, I leafed through it, reading articles of interest and glancing at updates on any classmates that were featured.
Then I stopped.
There, in the back of the magazine, was an obituary on the first of my classmates to pass (that I’m aware of).
I reread it a few times in disbelief. Maybe it was on her taking a new job or being promoted, and was in the wrong section. Nope.
I put the magazine down. She was 1 year younger than me and had gone into internal medicine. Not someone I’d kept in touch with, but certainly was friendly with during those 4 years and frequently chatted with in hallways or between classes. I remember meeting her during the first week of school, when I got her name mixed up with another girl’s in our class. I saw her at parties, meetings, and I think even played doubles tennis with her once, though who we played against I have no idea anymore.
She was at our 20th reunion, and we’d talked for a few minutes. We caught up on our lives since graduation and, as people do at these things, moved on to chat with others.
No details were given as to her death, and it really doesn’t matter.
. For most of each day it’s a fact in the back of our minds, behind the daily activities of working, shopping, doing laundry, commuting, and cooking dinner. After all, it’s really what we do while here that matters, no matter how mundane it may seem.
But sometimes something will push that realization to the front, and make us remember how important every minute really is.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Is COVID-19 accelerating progress toward high-value care?
As Rachna Rawal, MD, was donning her personal protective equipment (PPE), a process that has become deeply ingrained into her muscle memory, a nurse approached her to ask, “Hey, for Mr. Smith, any chance we can time these labs to be done together with his medication administration? We’ve been in and out of that room a few times already.”
As someone who embraces high-value care, this simple suggestion surprised her. What an easy strategy to minimize room entry with full PPE, lab testing, and patient interruptions. That same day, someone else asked, “Do we need overnight vitals?”

COVID-19 has forced hospitalists to reconsider almost every aspect of care. It feels like every decision we make including things we do routinely – labs, vital signs, imaging – needs to be reassessed to determine the actual benefit to the patient balanced against concerns about staff safety, dwindling PPE supplies, and medication reserves. We are all faced with frequently answering the question, “How will this intervention help the patient?” This question lies at the heart of delivering high-value care.
High-value care is providing the best care possible through efficient use of resources, achieving optimal results for each patient. While high-value care has become a prominent focus over the past decade, COVID-19’s high transmissibility without a cure – and associated scarcity of health care resources – have sparked additional discussions on the front lines about promoting patient outcomes while avoiding waste. Clinicians may not have realized that these were high-value care conversations.

The United States’ health care quality and cost crises, worsened in the face of the current pandemic, have been glaringly apparent for years. Our country is spending more money on health care than anywhere else in the world without desired improvements in patient outcomes. A 2019 JAMA study found that 25% of all health care spending, an estimated $760 to $935 billion, is considered waste, and a significant proportion of this waste is due to repetitive care, overuse and unnecessary care in the U.S.1
Examples of low-value care tests include ordering daily labs in stable medicine inpatients, routine urine electrolytes in acute kidney injury, and folate testing in anemia. The Choosing Wisely® national campaign, Journal of Hospital Medicine’s “Things We Do For No Reason,” and JAMA Internal Medicine’s “Teachable Moment” series have provided guidance on areas where common testing or interventions may not benefit patient outcomes.

The COVID-19 pandemic has raised questions related to other widely-utilized practices: Can medication times be readjusted to allow only one entry into the room? Will these labs or imaging studies actually change management? Are vital checks every 4 hours needed?
Why did it take the COVID-19 threat to our medical system to force many of us to have these discussions? Despite prior efforts to integrate high-value care into hospital practices, long-standing habits and deep-seeded culture are challenging to overcome. Once clinicians develop practice habits, these behaviors tend to persist throughout their careers.2 In many ways, COVID-19 was like hitting a “reset button” as health care professionals were forced to rapidly confront their deeply-ingrained hospital practices and habits. From new protocols for patient rounding to universal masking and social distancing to ground-breaking strategies like awake proning, the response to COVID-19 has represented an unprecedented rapid shift in practice. Previously, consequences of overuse were too downstream or too abstract for clinicians to see in real-time. However, now the ramifications of these choices hit closer to home with obvious potential consequences – like spreading a terrifying virus.
There are three interventions that hospitalists should consider implementing immediately in the COVID-19 era that accelerate us toward high-value care. Routine lab tests, imaging, and overnight vitals represent opportunities to provide patient-centered care while also remaining cognizant of resource utilization.
One area in hospital medicine that has proven challenging to significantly change practice has been routine daily labs. Patients on a general medical inpatient service who are clinically stable generally do not benefit from routine lab work.3 Avoiding these tests does not increase mortality or length of stay in clinically stable patients.3 However, despite this evidence, many patients with COVID-19 and other conditions experience lab draws that are not timed together and are done each morning out of “routine.” Choosing Wisely® recommendations from the Society of Hospital Medicine encourage clinicians to question routine lab work for COVID-19 patients and to consider batching them, if possible.3,4 In COVID-19 patients, the risks of not batching tests are magnified, both in terms of the patient-centered experience and for clinician safety. In essence, COVID-19 has pushed us to consider the elements of safety, PPE conservation and other factors, rather than making decisions based solely on their own comfort, convenience, or historical practice.
Clinicians are also reconsidering the necessity of imaging during the pandemic. The “Things We Do For No Reason” article on “Choosing Wisely® in the COVID-19 era” highlights this well.4 It is more important now than ever to decide whether the timing and type of imaging will change management for your patient. Questions to ask include: Can a portable x-ray be used to avoid patient travel and will that CT scan help your patient? A posterior-anterior/lateral x-ray can potentially provide more information depending on the clinical scenario. However, we now need to assess if that extra information is going to impact patient management. Downstream consequences of these decisions include not only risks to the patient but also infectious exposures for staff and others during patient travel.
Lastly, overnight vital sign checks are another intervention we should analyze through this high-value care lens. The Journal of Hospital Medicine released a “Things We Do For No Reason” article about minimizing overnight vitals to promote uninterrupted sleep at night.5 Deleterious effects of interrupting the sleep of our patients include delirium and patient dissatisfaction.5 Studies have shown the benefits of this approach, yet the shift away from routine overnight vitals has not yet widely occurred.
COVID-19 has pressed us to save PPE and minimize exposure risk; hence, some centers are coordinating the timing of vitals with medication administration times, when feasible. In the stable patient recovering from COVID-19, overnight vitals may not be necessary, particularly if remote monitoring is available. This accomplishes multiple goals: Providing high quality patient care, reducing resource utilization, and minimizing patient nighttime interruptions – all culminating in high-value care.
Even though the COVID-19 pandemic has brought unforeseen emotional, physical, and financial challenges for the health care system and its workers, there may be a silver lining. The pandemic has sparked high-value care discussions, and the urgency of the crisis may be instilling new practices in our daily work. This virus has indeed left a terrible wake of destruction, but may also be a nudge to permanently change our culture of overuse to help us shape the habits of all trainees during this tumultuous time. This experience will hopefully culminate in a culture in which clinicians routinely ask, “How will this intervention help the patient?”
Dr. Rawal is clinical assistant professor of medicine, University of Pittsburgh. Dr. Linker is assistant professor of medicine, Mount Sinai Hospital, Icahn School of Medicine at Mount Sinai, New York. Dr. Moriates is associate professor of internal medicine, Dell Medical School at the University of Texas at Austin.
References
1. Shrank W et al. Waste in The US healthcare system. JAMA. 2019;322(15):1501-9.
2. Chen C et al. Spending patterns in region of residency training and subsequent expenditures for care provided by practicing physicians for Medicare beneficiaries. JAMA. 2014;312(22):2385-93.
3. Eaton KP et al. Evidence-based guidelines to eliminate repetitive laboratory testing. JAMA Intern Med. 2017;177(12):1833-9.
4. Cho H et al. Choosing Wisely in the COVID-19 Era: Preventing harm to healthcare workers. J Hosp Med. 2020;15(6):360-2.
5. Orlov N and Arora V. Things we do for no reason: Routine overnight vital sign checks. J Hosp Med. 2020;15(5):272-27.
As Rachna Rawal, MD, was donning her personal protective equipment (PPE), a process that has become deeply ingrained into her muscle memory, a nurse approached her to ask, “Hey, for Mr. Smith, any chance we can time these labs to be done together with his medication administration? We’ve been in and out of that room a few times already.”
As someone who embraces high-value care, this simple suggestion surprised her. What an easy strategy to minimize room entry with full PPE, lab testing, and patient interruptions. That same day, someone else asked, “Do we need overnight vitals?”
COVID-19 has forced hospitalists to reconsider almost every aspect of care. It feels like every decision we make including things we do routinely – labs, vital signs, imaging – needs to be reassessed to determine the actual benefit to the patient balanced against concerns about staff safety, dwindling PPE supplies, and medication reserves. We are all faced with frequently answering the question, “How will this intervention help the patient?” This question lies at the heart of delivering high-value care.
High-value care is providing the best care possible through efficient use of resources, achieving optimal results for each patient. While high-value care has become a prominent focus over the past decade, COVID-19’s high transmissibility without a cure – and associated scarcity of health care resources – have sparked additional discussions on the front lines about promoting patient outcomes while avoiding waste. Clinicians may not have realized that these were high-value care conversations.
The United States’ health care quality and cost crises, worsened in the face of the current pandemic, have been glaringly apparent for years. Our country is spending more money on health care than anywhere else in the world without desired improvements in patient outcomes. A 2019 JAMA study found that 25% of all health care spending, an estimated $760 to $935 billion, is considered waste, and a significant proportion of this waste is due to repetitive care, overuse and unnecessary care in the U.S.1
Examples of low-value care tests include ordering daily labs in stable medicine inpatients, routine urine electrolytes in acute kidney injury, and folate testing in anemia. The Choosing Wisely® national campaign, Journal of Hospital Medicine’s “Things We Do For No Reason,” and JAMA Internal Medicine’s “Teachable Moment” series have provided guidance on areas where common testing or interventions may not benefit patient outcomes.
The COVID-19 pandemic has raised questions related to other widely-utilized practices: Can medication times be readjusted to allow only one entry into the room? Will these labs or imaging studies actually change management? Are vital checks every 4 hours needed?
Why did it take the COVID-19 threat to our medical system to force many of us to have these discussions? Despite prior efforts to integrate high-value care into hospital practices, long-standing habits and deep-seeded culture are challenging to overcome. Once clinicians develop practice habits, these behaviors tend to persist throughout their careers.2 In many ways, COVID-19 was like hitting a “reset button” as health care professionals were forced to rapidly confront their deeply-ingrained hospital practices and habits. From new protocols for patient rounding to universal masking and social distancing to ground-breaking strategies like awake proning, the response to COVID-19 has represented an unprecedented rapid shift in practice. Previously, consequences of overuse were too downstream or too abstract for clinicians to see in real-time. However, now the ramifications of these choices hit closer to home with obvious potential consequences – like spreading a terrifying virus.
There are three interventions that hospitalists should consider implementing immediately in the COVID-19 era that accelerate us toward high-value care. Routine lab tests, imaging, and overnight vitals represent opportunities to provide patient-centered care while also remaining cognizant of resource utilization.
One area in hospital medicine that has proven challenging to significantly change practice has been routine daily labs. Patients on a general medical inpatient service who are clinically stable generally do not benefit from routine lab work.3 Avoiding these tests does not increase mortality or length of stay in clinically stable patients.3 However, despite this evidence, many patients with COVID-19 and other conditions experience lab draws that are not timed together and are done each morning out of “routine.” Choosing Wisely® recommendations from the Society of Hospital Medicine encourage clinicians to question routine lab work for COVID-19 patients and to consider batching them, if possible.3,4 In COVID-19 patients, the risks of not batching tests are magnified, both in terms of the patient-centered experience and for clinician safety. In essence, COVID-19 has pushed us to consider the elements of safety, PPE conservation and other factors, rather than making decisions based solely on their own comfort, convenience, or historical practice.
Clinicians are also reconsidering the necessity of imaging during the pandemic. The “Things We Do For No Reason” article on “Choosing Wisely® in the COVID-19 era” highlights this well.4 It is more important now than ever to decide whether the timing and type of imaging will change management for your patient. Questions to ask include: Can a portable x-ray be used to avoid patient travel and will that CT scan help your patient? A posterior-anterior/lateral x-ray can potentially provide more information depending on the clinical scenario. However, we now need to assess if that extra information is going to impact patient management. Downstream consequences of these decisions include not only risks to the patient but also infectious exposures for staff and others during patient travel.
Lastly, overnight vital sign checks are another intervention we should analyze through this high-value care lens. The Journal of Hospital Medicine released a “Things We Do For No Reason” article about minimizing overnight vitals to promote uninterrupted sleep at night.5 Deleterious effects of interrupting the sleep of our patients include delirium and patient dissatisfaction.5 Studies have shown the benefits of this approach, yet the shift away from routine overnight vitals has not yet widely occurred.
COVID-19 has pressed us to save PPE and minimize exposure risk; hence, some centers are coordinating the timing of vitals with medication administration times, when feasible. In the stable patient recovering from COVID-19, overnight vitals may not be necessary, particularly if remote monitoring is available. This accomplishes multiple goals: Providing high quality patient care, reducing resource utilization, and minimizing patient nighttime interruptions – all culminating in high-value care.
Even though the COVID-19 pandemic has brought unforeseen emotional, physical, and financial challenges for the health care system and its workers, there may be a silver lining. The pandemic has sparked high-value care discussions, and the urgency of the crisis may be instilling new practices in our daily work. This virus has indeed left a terrible wake of destruction, but may also be a nudge to permanently change our culture of overuse to help us shape the habits of all trainees during this tumultuous time. This experience will hopefully culminate in a culture in which clinicians routinely ask, “How will this intervention help the patient?”
Dr. Rawal is clinical assistant professor of medicine, University of Pittsburgh. Dr. Linker is assistant professor of medicine, Mount Sinai Hospital, Icahn School of Medicine at Mount Sinai, New York. Dr. Moriates is associate professor of internal medicine, Dell Medical School at the University of Texas at Austin.
References
1. Shrank W et al. Waste in The US healthcare system. JAMA. 2019;322(15):1501-9.
2. Chen C et al. Spending patterns in region of residency training and subsequent expenditures for care provided by practicing physicians for Medicare beneficiaries. JAMA. 2014;312(22):2385-93.
3. Eaton KP et al. Evidence-based guidelines to eliminate repetitive laboratory testing. JAMA Intern Med. 2017;177(12):1833-9.
4. Cho H et al. Choosing Wisely in the COVID-19 Era: Preventing harm to healthcare workers. J Hosp Med. 2020;15(6):360-2.
5. Orlov N and Arora V. Things we do for no reason: Routine overnight vital sign checks. J Hosp Med. 2020;15(5):272-27.
As Rachna Rawal, MD, was donning her personal protective equipment (PPE), a process that has become deeply ingrained into her muscle memory, a nurse approached her to ask, “Hey, for Mr. Smith, any chance we can time these labs to be done together with his medication administration? We’ve been in and out of that room a few times already.”
As someone who embraces high-value care, this simple suggestion surprised her. What an easy strategy to minimize room entry with full PPE, lab testing, and patient interruptions. That same day, someone else asked, “Do we need overnight vitals?”
COVID-19 has forced hospitalists to reconsider almost every aspect of care. It feels like every decision we make including things we do routinely – labs, vital signs, imaging – needs to be reassessed to determine the actual benefit to the patient balanced against concerns about staff safety, dwindling PPE supplies, and medication reserves. We are all faced with frequently answering the question, “How will this intervention help the patient?” This question lies at the heart of delivering high-value care.
High-value care is providing the best care possible through efficient use of resources, achieving optimal results for each patient. While high-value care has become a prominent focus over the past decade, COVID-19’s high transmissibility without a cure – and associated scarcity of health care resources – have sparked additional discussions on the front lines about promoting patient outcomes while avoiding waste. Clinicians may not have realized that these were high-value care conversations.
The United States’ health care quality and cost crises, worsened in the face of the current pandemic, have been glaringly apparent for years. Our country is spending more money on health care than anywhere else in the world without desired improvements in patient outcomes. A 2019 JAMA study found that 25% of all health care spending, an estimated $760 to $935 billion, is considered waste, and a significant proportion of this waste is due to repetitive care, overuse and unnecessary care in the U.S.1
Examples of low-value care tests include ordering daily labs in stable medicine inpatients, routine urine electrolytes in acute kidney injury, and folate testing in anemia. The Choosing Wisely® national campaign, Journal of Hospital Medicine’s “Things We Do For No Reason,” and JAMA Internal Medicine’s “Teachable Moment” series have provided guidance on areas where common testing or interventions may not benefit patient outcomes.
The COVID-19 pandemic has raised questions related to other widely-utilized practices: Can medication times be readjusted to allow only one entry into the room? Will these labs or imaging studies actually change management? Are vital checks every 4 hours needed?
Why did it take the COVID-19 threat to our medical system to force many of us to have these discussions? Despite prior efforts to integrate high-value care into hospital practices, long-standing habits and deep-seeded culture are challenging to overcome. Once clinicians develop practice habits, these behaviors tend to persist throughout their careers.2 In many ways, COVID-19 was like hitting a “reset button” as health care professionals were forced to rapidly confront their deeply-ingrained hospital practices and habits. From new protocols for patient rounding to universal masking and social distancing to ground-breaking strategies like awake proning, the response to COVID-19 has represented an unprecedented rapid shift in practice. Previously, consequences of overuse were too downstream or too abstract for clinicians to see in real-time. However, now the ramifications of these choices hit closer to home with obvious potential consequences – like spreading a terrifying virus.
There are three interventions that hospitalists should consider implementing immediately in the COVID-19 era that accelerate us toward high-value care. Routine lab tests, imaging, and overnight vitals represent opportunities to provide patient-centered care while also remaining cognizant of resource utilization.
One area in hospital medicine that has proven challenging to significantly change practice has been routine daily labs. Patients on a general medical inpatient service who are clinically stable generally do not benefit from routine lab work.3 Avoiding these tests does not increase mortality or length of stay in clinically stable patients.3 However, despite this evidence, many patients with COVID-19 and other conditions experience lab draws that are not timed together and are done each morning out of “routine.” Choosing Wisely® recommendations from the Society of Hospital Medicine encourage clinicians to question routine lab work for COVID-19 patients and to consider batching them, if possible.3,4 In COVID-19 patients, the risks of not batching tests are magnified, both in terms of the patient-centered experience and for clinician safety. In essence, COVID-19 has pushed us to consider the elements of safety, PPE conservation and other factors, rather than making decisions based solely on their own comfort, convenience, or historical practice.
Clinicians are also reconsidering the necessity of imaging during the pandemic. The “Things We Do For No Reason” article on “Choosing Wisely® in the COVID-19 era” highlights this well.4 It is more important now than ever to decide whether the timing and type of imaging will change management for your patient. Questions to ask include: Can a portable x-ray be used to avoid patient travel and will that CT scan help your patient? A posterior-anterior/lateral x-ray can potentially provide more information depending on the clinical scenario. However, we now need to assess if that extra information is going to impact patient management. Downstream consequences of these decisions include not only risks to the patient but also infectious exposures for staff and others during patient travel.
Lastly, overnight vital sign checks are another intervention we should analyze through this high-value care lens. The Journal of Hospital Medicine released a “Things We Do For No Reason” article about minimizing overnight vitals to promote uninterrupted sleep at night.5 Deleterious effects of interrupting the sleep of our patients include delirium and patient dissatisfaction.5 Studies have shown the benefits of this approach, yet the shift away from routine overnight vitals has not yet widely occurred.
COVID-19 has pressed us to save PPE and minimize exposure risk; hence, some centers are coordinating the timing of vitals with medication administration times, when feasible. In the stable patient recovering from COVID-19, overnight vitals may not be necessary, particularly if remote monitoring is available. This accomplishes multiple goals: Providing high quality patient care, reducing resource utilization, and minimizing patient nighttime interruptions – all culminating in high-value care.
Even though the COVID-19 pandemic has brought unforeseen emotional, physical, and financial challenges for the health care system and its workers, there may be a silver lining. The pandemic has sparked high-value care discussions, and the urgency of the crisis may be instilling new practices in our daily work. This virus has indeed left a terrible wake of destruction, but may also be a nudge to permanently change our culture of overuse to help us shape the habits of all trainees during this tumultuous time. This experience will hopefully culminate in a culture in which clinicians routinely ask, “How will this intervention help the patient?”
Dr. Rawal is clinical assistant professor of medicine, University of Pittsburgh. Dr. Linker is assistant professor of medicine, Mount Sinai Hospital, Icahn School of Medicine at Mount Sinai, New York. Dr. Moriates is associate professor of internal medicine, Dell Medical School at the University of Texas at Austin.
References
1. Shrank W et al. Waste in The US healthcare system. JAMA. 2019;322(15):1501-9.
2. Chen C et al. Spending patterns in region of residency training and subsequent expenditures for care provided by practicing physicians for Medicare beneficiaries. JAMA. 2014;312(22):2385-93.
3. Eaton KP et al. Evidence-based guidelines to eliminate repetitive laboratory testing. JAMA Intern Med. 2017;177(12):1833-9.
4. Cho H et al. Choosing Wisely in the COVID-19 Era: Preventing harm to healthcare workers. J Hosp Med. 2020;15(6):360-2.
5. Orlov N and Arora V. Things we do for no reason: Routine overnight vital sign checks. J Hosp Med. 2020;15(5):272-27.
The cutaneous benefits of bee venom, Part I: Atopic dermatitis and acne
Honeybees, Apis mellifera, play an important role in the web of life. We rely on bees for pollinating approximately one-third of our crops, including multiple fruits, vegetables, nuts, and seeds.1,2 Bees are also instrumental in the propagation of other plants, flower nectar, and flower pollen. A. mellifera, the European honeybee, is the main pollinator in Europe and North America, but other species, including A. cerana, A. dorsata, A. floria, A. andreniformis, A. koschevnikov, and A. laboriosa, yield honey.3 Honey, propolis, and royal jelly, along with beeswax and bee pollen, are among some of the celebrated bee products that have been found to confer health benefits to human beings.4,5 Bee venom, a toxin bees use for protection, is a convoluted combination of peptides and toxic proteins such as phospholipase A2 (PLA2) and melittin that has garnered significant scientific attention of late and is used to treat various inflammatory conditions.6-8 This column will focus on the investigation of the use of bee venom to treat atopic dermatitis (AD) and acne.

Atopic dermatitis
In 2013, Kim et al. assessed the impact of bee venom on AD-related symptoms in mice, finding that it attenuated the effects of AD-simulating compounds in 48 of 80 patients injected subcutaneously. They concluded that bee venom acted by suppressing mast cell degranulation and proinflammatory cytokine expression.9 Three years later, You et al. conducted a double-blind, randomized, base-controlled multicenter study of 136 patients with AD to ascertain the effects of a bee venom emollient. For 4 weeks, patients applied an emollient with bee venom and silk protein or a vehicle lacking bee venom twice daily. Eczema area and severity index (EASI) scores were significantly lower in the bee venom group, as were the visual analogue scale (VAS) scores. The investigators concluded that bee venom is an effective and safe therapeutic choice for treating patients with AD.10 Further, in 2018, Shin et al. demonstrated that PLA2 derived from bee venom mitigates atopic skin inflammation via the CD206 mannose receptor. They had previously shown in a mouse model that PLA2 from bee venom exerts such activity against AD-like lesions induced by 2,4-dinitrochlorobenzene (DNCB) and house dust mite (Dermatophagoides farinae) extract.11 Gu et al. observed later that year that intraperitoneal administration of bee venom eased the symptoms of ovalbumin-induced AD-like skin lesions in an experimental mouse model. Bee venom also lowered serum immunoglobulin E levels and suppressed infiltration of eosinophils and mast cells. They concluded that bee venom is a viable alternative for attenuating the allergic skin inflammation characteristic of AD.12 At the end of 2018, An et al. reported on the use of an in vivo female Balb/c mouse AD model in which 1-chloro-DNCB acted as inducer in cultures of human keratinocytes, stimulated by TNF-alpha/IFN-gamma. The investigators found that bee venom and melittin displayed robust antiatopic effects as evidenced by reduced lesions. The bee products were also found to have hindered elevated expression of various chemokines and proinflammatory cytokines. The authors suggested that bee venom and melittin appear to warrant consideration as a topical treatment for AD.13 In 2019, Kim et al. demonstrated in mice that bee venom eases the symptoms of AD by inactivating the complement system, particularly through CD55 induction, which might account for its effectiveness in AD treatment in humans, they suggested.6 Early in 2020, Lee et al. demonstrated in a Balb/c mouse model that bee venom appears to be a possible therapeutic macromolecule for treating phthalic anhydride-induced AD.7
Acne
In 2013, in vitro experiments by Han et al. showed that purified bee venom exhibited antimicrobial activity, in a concentration-dependent manner, against Cutibacterium acnes (or Propionibacterium acnes). They followed up with a small randomized, double-blind, controlled trial with 12 subjects who were treated with cosmetics with pure bee venom or cosmetics without it for two weeks. The group receiving bee venom experienced significantly fewer inflammatory and noninflammatory lesions, and a significant decline in adenosine triphosphate levels (a 57.5% reduction) was noted in subjects in the bee venom group, with a nonsignificant decrease of 4.7% observed in the control group. The investigators concluded the purified bee venom may be suitable as an antiacne agent.14 Using a mouse model, An et al. studied the therapeutic effects of bee venom against C. acnes–induced skin inflammation. They found that bee venom significantly diminished the volume of infiltrated inflammatory cells in the treated mice, compared with untreated mice. Bee venom also decreased expression levels of tumor necrosis factor (TNF)-α, and interleukin (IL)-1beta and suppressed Toll-like receptor (TLR)2 and CD14 expression in C. acnes–injected tissue. The investigators concluded that bee venom imparts notable anti-inflammatory activity and has potential for use in treating acne and as an anti-inflammatory agent in skin care.15

In 2015, Kim et al. studied the influence of bee venom against C. acnes–induced inflammation in human keratinocytes (HaCaT) and monocytes (THP-1). They found that bee venom successfully suppressed the secretion of interferon-gamma, IL-1beta, IL-8, and TNF-alpha. It also galvanized the expression of IL-8 and TLR2 in HaCaT cells but hampered their expression in heat-killed C. acnes. The researchers concluded that bee venom displays considerable anti-inflammatory activity against C. acnes and warrants consideration as an alternative to antibiotic acne treatment.16 It is worth noting that early that year, in a comprehensive database review to evaluate the effects and safety of a wide range of complementary treatments for acne, Cao et al. found, among 35 studies including parallel-group randomized controlled trials, that one trial indicated bee venom was superior to control in lowering the number of acne lesions.17
Conclusion
More research, in the form of randomized, controlled trials, is required before bee venom can be incorporated into the dermatologic armamentarium as a first-line therapy for common and vexing cutaneous conditions. Nevertheless, .
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at [email protected].
References
1. Walsh B. The plight of the honeybee: Mass deaths in bee colonies may mean disaster for farmers – and your favorite Foods. Time Magazine, 2013 Aug 19.
2. Klein AM et al. Proc Biol Sci. 2007 Feb 7;274(1608):303-13. doi: 10.1098/rspb.2006.3721.
3. Ediriweera ER and Premarathna NY. AYU. 2012 Apr;33(2):178-82. doi: 10.4103/0974-8520.105233.
4. Baumann, L. Honey/Propolis/Royal Jelly. In Cosmeceuticals and Cosmetic Ingredients. New York:McGraw-Hill; 2014:203-212.
5. Cornara L et al. Front Pharmacol. 2017 Jun 28;8:412. doi: 10.3389/fphar.2017.00412.
6. Kim Y et al. Toxins (Basel). 2019 Apr 26;11(5):239. doi: 10.3390/toxins11050239.
7. Lee YJ et al. Inflammopharmacology. 2020 Feb;28(1):253-63. doi: 10.1007/s10787-019-00646-w.
8. Lee G and Bae H. Molecules. 2016 May 11;21(5):616. doi: 10.3390/molecules21050616.
9. Kim KH et al. Int J Clin Exp Pathol. 2013 Nov 15;6(12):2896-903.
10. You CE et al. Ann Dermatol. 2016 Oct;28(5):593-9. doi: 10.5021/ad.2016.28.5.593.
11. Shin D et al. Toxins (Basel). 2018 Apr 2;10(4):146. doi: 10.3390/toxins10040146.
12. Gu H et al. Mol Med Rep. 2018 Oct;18(4):3711-8. doi: 10.3892/mmr.2018.9398.
13. An HJ et al. Br J Pharmacol. 2018 Dec;175(23):4310-24. doi: 10.1111/bph.14487.
14. Han SM et al. J Integr Med. 2013 Sep;11(5):320-6. doi: 10.3736/jintegrmed2013043.
15. An HJ et al. Int J Mol Med. 2014 Nov;34(5):1341-8. doi: 10.3892/ijmm.2014.1933.
16. Kim JY et al. Int J Mol Med. 2015 Jun;35(6):1651-6. doi: 10.3892/ijmm.2015.2180.
17. Cao H et al. Cochrane Database Syst Rev. 2015 Jan 19;1:CD009436. doi: 10.1002/14651858.CD009436.pub2.
Honeybees, Apis mellifera, play an important role in the web of life. We rely on bees for pollinating approximately one-third of our crops, including multiple fruits, vegetables, nuts, and seeds.1,2 Bees are also instrumental in the propagation of other plants, flower nectar, and flower pollen. A. mellifera, the European honeybee, is the main pollinator in Europe and North America, but other species, including A. cerana, A. dorsata, A. floria, A. andreniformis, A. koschevnikov, and A. laboriosa, yield honey.3 Honey, propolis, and royal jelly, along with beeswax and bee pollen, are among some of the celebrated bee products that have been found to confer health benefits to human beings.4,5 Bee venom, a toxin bees use for protection, is a convoluted combination of peptides and toxic proteins such as phospholipase A2 (PLA2) and melittin that has garnered significant scientific attention of late and is used to treat various inflammatory conditions.6-8 This column will focus on the investigation of the use of bee venom to treat atopic dermatitis (AD) and acne.
Atopic dermatitis
In 2013, Kim et al. assessed the impact of bee venom on AD-related symptoms in mice, finding that it attenuated the effects of AD-simulating compounds in 48 of 80 patients injected subcutaneously. They concluded that bee venom acted by suppressing mast cell degranulation and proinflammatory cytokine expression.9 Three years later, You et al. conducted a double-blind, randomized, base-controlled multicenter study of 136 patients with AD to ascertain the effects of a bee venom emollient. For 4 weeks, patients applied an emollient with bee venom and silk protein or a vehicle lacking bee venom twice daily. Eczema area and severity index (EASI) scores were significantly lower in the bee venom group, as were the visual analogue scale (VAS) scores. The investigators concluded that bee venom is an effective and safe therapeutic choice for treating patients with AD.10 Further, in 2018, Shin et al. demonstrated that PLA2 derived from bee venom mitigates atopic skin inflammation via the CD206 mannose receptor. They had previously shown in a mouse model that PLA2 from bee venom exerts such activity against AD-like lesions induced by 2,4-dinitrochlorobenzene (DNCB) and house dust mite (Dermatophagoides farinae) extract.11 Gu et al. observed later that year that intraperitoneal administration of bee venom eased the symptoms of ovalbumin-induced AD-like skin lesions in an experimental mouse model. Bee venom also lowered serum immunoglobulin E levels and suppressed infiltration of eosinophils and mast cells. They concluded that bee venom is a viable alternative for attenuating the allergic skin inflammation characteristic of AD.12 At the end of 2018, An et al. reported on the use of an in vivo female Balb/c mouse AD model in which 1-chloro-DNCB acted as inducer in cultures of human keratinocytes, stimulated by TNF-alpha/IFN-gamma. The investigators found that bee venom and melittin displayed robust antiatopic effects as evidenced by reduced lesions. The bee products were also found to have hindered elevated expression of various chemokines and proinflammatory cytokines. The authors suggested that bee venom and melittin appear to warrant consideration as a topical treatment for AD.13 In 2019, Kim et al. demonstrated in mice that bee venom eases the symptoms of AD by inactivating the complement system, particularly through CD55 induction, which might account for its effectiveness in AD treatment in humans, they suggested.6 Early in 2020, Lee et al. demonstrated in a Balb/c mouse model that bee venom appears to be a possible therapeutic macromolecule for treating phthalic anhydride-induced AD.7
Acne
In 2013, in vitro experiments by Han et al. showed that purified bee venom exhibited antimicrobial activity, in a concentration-dependent manner, against Cutibacterium acnes (or Propionibacterium acnes). They followed up with a small randomized, double-blind, controlled trial with 12 subjects who were treated with cosmetics with pure bee venom or cosmetics without it for two weeks. The group receiving bee venom experienced significantly fewer inflammatory and noninflammatory lesions, and a significant decline in adenosine triphosphate levels (a 57.5% reduction) was noted in subjects in the bee venom group, with a nonsignificant decrease of 4.7% observed in the control group. The investigators concluded the purified bee venom may be suitable as an antiacne agent.14 Using a mouse model, An et al. studied the therapeutic effects of bee venom against C. acnes–induced skin inflammation. They found that bee venom significantly diminished the volume of infiltrated inflammatory cells in the treated mice, compared with untreated mice. Bee venom also decreased expression levels of tumor necrosis factor (TNF)-α, and interleukin (IL)-1beta and suppressed Toll-like receptor (TLR)2 and CD14 expression in C. acnes–injected tissue. The investigators concluded that bee venom imparts notable anti-inflammatory activity and has potential for use in treating acne and as an anti-inflammatory agent in skin care.15
In 2015, Kim et al. studied the influence of bee venom against C. acnes–induced inflammation in human keratinocytes (HaCaT) and monocytes (THP-1). They found that bee venom successfully suppressed the secretion of interferon-gamma, IL-1beta, IL-8, and TNF-alpha. It also galvanized the expression of IL-8 and TLR2 in HaCaT cells but hampered their expression in heat-killed C. acnes. The researchers concluded that bee venom displays considerable anti-inflammatory activity against C. acnes and warrants consideration as an alternative to antibiotic acne treatment.16 It is worth noting that early that year, in a comprehensive database review to evaluate the effects and safety of a wide range of complementary treatments for acne, Cao et al. found, among 35 studies including parallel-group randomized controlled trials, that one trial indicated bee venom was superior to control in lowering the number of acne lesions.17
Conclusion
More research, in the form of randomized, controlled trials, is required before bee venom can be incorporated into the dermatologic armamentarium as a first-line therapy for common and vexing cutaneous conditions. Nevertheless, .
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at [email protected].
References
1. Walsh B. The plight of the honeybee: Mass deaths in bee colonies may mean disaster for farmers – and your favorite Foods. Time Magazine, 2013 Aug 19.
2. Klein AM et al. Proc Biol Sci. 2007 Feb 7;274(1608):303-13. doi: 10.1098/rspb.2006.3721.
3. Ediriweera ER and Premarathna NY. AYU. 2012 Apr;33(2):178-82. doi: 10.4103/0974-8520.105233.
4. Baumann, L. Honey/Propolis/Royal Jelly. In Cosmeceuticals and Cosmetic Ingredients. New York:McGraw-Hill; 2014:203-212.
5. Cornara L et al. Front Pharmacol. 2017 Jun 28;8:412. doi: 10.3389/fphar.2017.00412.
6. Kim Y et al. Toxins (Basel). 2019 Apr 26;11(5):239. doi: 10.3390/toxins11050239.
7. Lee YJ et al. Inflammopharmacology. 2020 Feb;28(1):253-63. doi: 10.1007/s10787-019-00646-w.
8. Lee G and Bae H. Molecules. 2016 May 11;21(5):616. doi: 10.3390/molecules21050616.
9. Kim KH et al. Int J Clin Exp Pathol. 2013 Nov 15;6(12):2896-903.
10. You CE et al. Ann Dermatol. 2016 Oct;28(5):593-9. doi: 10.5021/ad.2016.28.5.593.
11. Shin D et al. Toxins (Basel). 2018 Apr 2;10(4):146. doi: 10.3390/toxins10040146.
12. Gu H et al. Mol Med Rep. 2018 Oct;18(4):3711-8. doi: 10.3892/mmr.2018.9398.
13. An HJ et al. Br J Pharmacol. 2018 Dec;175(23):4310-24. doi: 10.1111/bph.14487.
14. Han SM et al. J Integr Med. 2013 Sep;11(5):320-6. doi: 10.3736/jintegrmed2013043.
15. An HJ et al. Int J Mol Med. 2014 Nov;34(5):1341-8. doi: 10.3892/ijmm.2014.1933.
16. Kim JY et al. Int J Mol Med. 2015 Jun;35(6):1651-6. doi: 10.3892/ijmm.2015.2180.
17. Cao H et al. Cochrane Database Syst Rev. 2015 Jan 19;1:CD009436. doi: 10.1002/14651858.CD009436.pub2.
Honeybees, Apis mellifera, play an important role in the web of life. We rely on bees for pollinating approximately one-third of our crops, including multiple fruits, vegetables, nuts, and seeds.1,2 Bees are also instrumental in the propagation of other plants, flower nectar, and flower pollen. A. mellifera, the European honeybee, is the main pollinator in Europe and North America, but other species, including A. cerana, A. dorsata, A. floria, A. andreniformis, A. koschevnikov, and A. laboriosa, yield honey.3 Honey, propolis, and royal jelly, along with beeswax and bee pollen, are among some of the celebrated bee products that have been found to confer health benefits to human beings.4,5 Bee venom, a toxin bees use for protection, is a convoluted combination of peptides and toxic proteins such as phospholipase A2 (PLA2) and melittin that has garnered significant scientific attention of late and is used to treat various inflammatory conditions.6-8 This column will focus on the investigation of the use of bee venom to treat atopic dermatitis (AD) and acne.
Atopic dermatitis
In 2013, Kim et al. assessed the impact of bee venom on AD-related symptoms in mice, finding that it attenuated the effects of AD-simulating compounds in 48 of 80 patients injected subcutaneously. They concluded that bee venom acted by suppressing mast cell degranulation and proinflammatory cytokine expression.9 Three years later, You et al. conducted a double-blind, randomized, base-controlled multicenter study of 136 patients with AD to ascertain the effects of a bee venom emollient. For 4 weeks, patients applied an emollient with bee venom and silk protein or a vehicle lacking bee venom twice daily. Eczema area and severity index (EASI) scores were significantly lower in the bee venom group, as were the visual analogue scale (VAS) scores. The investigators concluded that bee venom is an effective and safe therapeutic choice for treating patients with AD.10 Further, in 2018, Shin et al. demonstrated that PLA2 derived from bee venom mitigates atopic skin inflammation via the CD206 mannose receptor. They had previously shown in a mouse model that PLA2 from bee venom exerts such activity against AD-like lesions induced by 2,4-dinitrochlorobenzene (DNCB) and house dust mite (Dermatophagoides farinae) extract.11 Gu et al. observed later that year that intraperitoneal administration of bee venom eased the symptoms of ovalbumin-induced AD-like skin lesions in an experimental mouse model. Bee venom also lowered serum immunoglobulin E levels and suppressed infiltration of eosinophils and mast cells. They concluded that bee venom is a viable alternative for attenuating the allergic skin inflammation characteristic of AD.12 At the end of 2018, An et al. reported on the use of an in vivo female Balb/c mouse AD model in which 1-chloro-DNCB acted as inducer in cultures of human keratinocytes, stimulated by TNF-alpha/IFN-gamma. The investigators found that bee venom and melittin displayed robust antiatopic effects as evidenced by reduced lesions. The bee products were also found to have hindered elevated expression of various chemokines and proinflammatory cytokines. The authors suggested that bee venom and melittin appear to warrant consideration as a topical treatment for AD.13 In 2019, Kim et al. demonstrated in mice that bee venom eases the symptoms of AD by inactivating the complement system, particularly through CD55 induction, which might account for its effectiveness in AD treatment in humans, they suggested.6 Early in 2020, Lee et al. demonstrated in a Balb/c mouse model that bee venom appears to be a possible therapeutic macromolecule for treating phthalic anhydride-induced AD.7
Acne
In 2013, in vitro experiments by Han et al. showed that purified bee venom exhibited antimicrobial activity, in a concentration-dependent manner, against Cutibacterium acnes (or Propionibacterium acnes). They followed up with a small randomized, double-blind, controlled trial with 12 subjects who were treated with cosmetics with pure bee venom or cosmetics without it for two weeks. The group receiving bee venom experienced significantly fewer inflammatory and noninflammatory lesions, and a significant decline in adenosine triphosphate levels (a 57.5% reduction) was noted in subjects in the bee venom group, with a nonsignificant decrease of 4.7% observed in the control group. The investigators concluded the purified bee venom may be suitable as an antiacne agent.14 Using a mouse model, An et al. studied the therapeutic effects of bee venom against C. acnes–induced skin inflammation. They found that bee venom significantly diminished the volume of infiltrated inflammatory cells in the treated mice, compared with untreated mice. Bee venom also decreased expression levels of tumor necrosis factor (TNF)-α, and interleukin (IL)-1beta and suppressed Toll-like receptor (TLR)2 and CD14 expression in C. acnes–injected tissue. The investigators concluded that bee venom imparts notable anti-inflammatory activity and has potential for use in treating acne and as an anti-inflammatory agent in skin care.15
In 2015, Kim et al. studied the influence of bee venom against C. acnes–induced inflammation in human keratinocytes (HaCaT) and monocytes (THP-1). They found that bee venom successfully suppressed the secretion of interferon-gamma, IL-1beta, IL-8, and TNF-alpha. It also galvanized the expression of IL-8 and TLR2 in HaCaT cells but hampered their expression in heat-killed C. acnes. The researchers concluded that bee venom displays considerable anti-inflammatory activity against C. acnes and warrants consideration as an alternative to antibiotic acne treatment.16 It is worth noting that early that year, in a comprehensive database review to evaluate the effects and safety of a wide range of complementary treatments for acne, Cao et al. found, among 35 studies including parallel-group randomized controlled trials, that one trial indicated bee venom was superior to control in lowering the number of acne lesions.17
Conclusion
More research, in the form of randomized, controlled trials, is required before bee venom can be incorporated into the dermatologic armamentarium as a first-line therapy for common and vexing cutaneous conditions. Nevertheless, .
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at [email protected].
References
1. Walsh B. The plight of the honeybee: Mass deaths in bee colonies may mean disaster for farmers – and your favorite Foods. Time Magazine, 2013 Aug 19.
2. Klein AM et al. Proc Biol Sci. 2007 Feb 7;274(1608):303-13. doi: 10.1098/rspb.2006.3721.
3. Ediriweera ER and Premarathna NY. AYU. 2012 Apr;33(2):178-82. doi: 10.4103/0974-8520.105233.
4. Baumann, L. Honey/Propolis/Royal Jelly. In Cosmeceuticals and Cosmetic Ingredients. New York:McGraw-Hill; 2014:203-212.
5. Cornara L et al. Front Pharmacol. 2017 Jun 28;8:412. doi: 10.3389/fphar.2017.00412.
6. Kim Y et al. Toxins (Basel). 2019 Apr 26;11(5):239. doi: 10.3390/toxins11050239.
7. Lee YJ et al. Inflammopharmacology. 2020 Feb;28(1):253-63. doi: 10.1007/s10787-019-00646-w.
8. Lee G and Bae H. Molecules. 2016 May 11;21(5):616. doi: 10.3390/molecules21050616.
9. Kim KH et al. Int J Clin Exp Pathol. 2013 Nov 15;6(12):2896-903.
10. You CE et al. Ann Dermatol. 2016 Oct;28(5):593-9. doi: 10.5021/ad.2016.28.5.593.
11. Shin D et al. Toxins (Basel). 2018 Apr 2;10(4):146. doi: 10.3390/toxins10040146.
12. Gu H et al. Mol Med Rep. 2018 Oct;18(4):3711-8. doi: 10.3892/mmr.2018.9398.
13. An HJ et al. Br J Pharmacol. 2018 Dec;175(23):4310-24. doi: 10.1111/bph.14487.
14. Han SM et al. J Integr Med. 2013 Sep;11(5):320-6. doi: 10.3736/jintegrmed2013043.
15. An HJ et al. Int J Mol Med. 2014 Nov;34(5):1341-8. doi: 10.3892/ijmm.2014.1933.
16. Kim JY et al. Int J Mol Med. 2015 Jun;35(6):1651-6. doi: 10.3892/ijmm.2015.2180.
17. Cao H et al. Cochrane Database Syst Rev. 2015 Jan 19;1:CD009436. doi: 10.1002/14651858.CD009436.pub2.
The journey from burnout to wellbeing
A check-in for you and your peers
COVID-19 did not discriminate when it came to the impact it imposed on our hospitalist community. As the nomenclature moves away from the negative connotations of ‘burnout’ to ‘wellbeing,’ the pandemic has taught us something important about being intentional about our personal health: we must secure our own oxygen masks before helping others.

In February 2020, the Society of Hospital Medicine’s Wellbeing Taskforce efforts quickly changed focus from addressing general wellbeing, to wellbeing during COVID-19. Our Taskforce was commissioned by SHM’s Board with a new charge: Address immediate and ongoing needs of well-being and resiliency support for hospitalists during the COVID-19 pandemic. In this essay, I will discuss how our SHM Wellbeing Taskforce approached the overall topic of wellbeing for hospitalists during the COVID-19 pandemic, including some of our Taskforce group experiences.
The Taskforce started with a framework to aide in cultivating open and authentic conversations within hospital medicine groups. Creating spaces for honest sharing around how providers are doing is a crucial first step to reducing stigma, building mutual support within a group, and elevating issues of wellbeing to the level where structural change can take place. The Taskforce established two objectives for normalizing and mitigating stressors we face as hospitalists during the COVID-19 pandemic:
- Provide a framework for hospitalists to take their own emotional pulse
- Provide an approach to reduce stigma of hospitalists who are suffering from pandemic stress
While a more typical approach to fix stress and burnout is using formal institutional interventions, we used the value and insight provided by SHM’s 7 Drivers of Burnout in Hospital Medicine to help guide the creation of SHM resources in addressing the severe emotional strain being felt across the country by hospitalists. The 7 Drivers support the idea that the social role peers and hospital leaders can make a crucial difference in mitigating stress and burnout. Two examples of social support come to mind from the Wellbeing Taskforce experience:
- Participate in your meetings. One example comes from a member of our group who had underestimated the “healing power” that our group meetings had provided to his psyche. The simple act of participating in our Taskforce meeting and being in the presence of our group had provided such a positive impact that he was better able to face the “death and misery” in his unit with a smile on his face.
- Share what is stressful. The second example of social support comes from an hour of Zoom-based facilitation meetings between the SHM’s Wellbeing Taskforce members and Chapter Leaders in late October. During our Taskforce debrief after the meeting, we came to realize the enormous burden of grief our peers were carrying as one hospitalist had lost a group colleague the previous week due to suicide. Our member who led this meeting was moved – as were we – at how this had impacted his small team, and he was reminded he was not alone.
To form meaningful relationships that foster support, there needs to be a space where people can safely come together at times that initially might feel awkward. After taking steps toward your peers, these conversations can become normalized and contribute to meaningful relationships, providing the opportunity for healthy exchanges on vulnerable topics like emotional and psychological wellbeing. A printable guide for this specific purpose (“HM COVID-19 Check-In Guide for Self and Peers”) was designed to help hospitalists move into safe and supportive conversations with each other. While it is difficult to place a value on the importance these types of conversations have on individual wellbeing, it is known that the quality of a positive work environment where people feel supported can moderate stress, morale, and depression. In other words, hospitalist groups can positively contribute to their social environment during stressful times by sharing meaningful and difficult experiences with one another.
Second, the Taskforce created a social media campaign to provide a public social space for sharing hospitalists’ COVID-19 experiences. We believed that sharing collective experiences with the theme of #YouAreNotAlone and a complementary social media campaign, SHM Cares, on SHM’s social media channels, would further connect the national hospitalist community and provide a different communication pathway to decrease a sense of isolation. This idea came from the second social support idea mentioned earlier to share what is stressful with others in a safe space. We understood that some hospitalists would be more comfortable sharing publicly their comments, photos, and videos in achieving a sense of hospitalist unity.
Using our shared experiences, we identified three pillars for the final structure of the HM COVID-19 Check-In Guide for Self and Peers:
- Pillar 1. Recognize your issues. Recall our oxygen mask metaphor and this is what we mean by recognizing symptoms of new stressors (e.g., sleeplessness, irritability, forgetfulness).
- Pillar 2. Know what to say. A simple open-ended question about how the other person is working through the pandemic is an easy way to start a connection. We learned from a mental health perspective that it is unlikely that you could say anything to make a situation worse by offering a listening ear.
- Pillar 3. Check in with others. Listen to others without trying to fix the person or the situation. When appropriate, offer humorous reflections without diminishing the problem. Be a partner and commit to check in regularly with the other person.
Cultivating human connections outside of your immediate peer group can be valuable and offer additional perspective to stressful situations. For instance, one of my roles as a hospitalist administrator has been offering support by regularly listening as my physicians ‘talk out’ their day confidentially for as long as they needed. Offering open conversation in a safe and confidential way can have a healing effect. As one of my former hospitalists used to say, if issues are not addressed, they will “ooze out somewhere else.”
The HM COVID-19 Check-In Guide for Self and Peers and the SHM Cares social media campaign was the result of the Taskforce’s collective observations to help others normalize the feeling that ‘it’s OK not to be OK.’ Using the pandemic as context, the 7 Drivers of Hospitalist Burnout reminded us that the increased burnout issues we face will require continued attention past the pandemic. The value in cultivating human connections has never been more important. The SHM Wellbeing Taskforce is committed to provide continued resources. Checking in with others and listening to peers are all part of a personal wellbeing and resilience strategy. On behalf of the SHM Wellbeing Taskforce, we hope the information in this article will highlight the importance of continued attention to personal wellbeing during and after the pandemic.
Dr. Robinson received her PhD in organizational learning, performance and change from Colorado State University in 2019. Her dissertation topic was exploring hospitalist burnout, engagement, and social support. She is administrative director of inpatient medicine at St. Mary’s Medical Center in Grand Junction, Colo., a part of SCL Health. She has volunteered in numerous SHM committees, and currently serves on the SHM Wellbeing Taskforce.
A check-in for you and your peers
A check-in for you and your peers
COVID-19 did not discriminate when it came to the impact it imposed on our hospitalist community. As the nomenclature moves away from the negative connotations of ‘burnout’ to ‘wellbeing,’ the pandemic has taught us something important about being intentional about our personal health: we must secure our own oxygen masks before helping others.
In February 2020, the Society of Hospital Medicine’s Wellbeing Taskforce efforts quickly changed focus from addressing general wellbeing, to wellbeing during COVID-19. Our Taskforce was commissioned by SHM’s Board with a new charge: Address immediate and ongoing needs of well-being and resiliency support for hospitalists during the COVID-19 pandemic. In this essay, I will discuss how our SHM Wellbeing Taskforce approached the overall topic of wellbeing for hospitalists during the COVID-19 pandemic, including some of our Taskforce group experiences.
The Taskforce started with a framework to aide in cultivating open and authentic conversations within hospital medicine groups. Creating spaces for honest sharing around how providers are doing is a crucial first step to reducing stigma, building mutual support within a group, and elevating issues of wellbeing to the level where structural change can take place. The Taskforce established two objectives for normalizing and mitigating stressors we face as hospitalists during the COVID-19 pandemic:
- Provide a framework for hospitalists to take their own emotional pulse
- Provide an approach to reduce stigma of hospitalists who are suffering from pandemic stress
While a more typical approach to fix stress and burnout is using formal institutional interventions, we used the value and insight provided by SHM’s 7 Drivers of Burnout in Hospital Medicine to help guide the creation of SHM resources in addressing the severe emotional strain being felt across the country by hospitalists. The 7 Drivers support the idea that the social role peers and hospital leaders can make a crucial difference in mitigating stress and burnout. Two examples of social support come to mind from the Wellbeing Taskforce experience:
- Participate in your meetings. One example comes from a member of our group who had underestimated the “healing power” that our group meetings had provided to his psyche. The simple act of participating in our Taskforce meeting and being in the presence of our group had provided such a positive impact that he was better able to face the “death and misery” in his unit with a smile on his face.
- Share what is stressful. The second example of social support comes from an hour of Zoom-based facilitation meetings between the SHM’s Wellbeing Taskforce members and Chapter Leaders in late October. During our Taskforce debrief after the meeting, we came to realize the enormous burden of grief our peers were carrying as one hospitalist had lost a group colleague the previous week due to suicide. Our member who led this meeting was moved – as were we – at how this had impacted his small team, and he was reminded he was not alone.
To form meaningful relationships that foster support, there needs to be a space where people can safely come together at times that initially might feel awkward. After taking steps toward your peers, these conversations can become normalized and contribute to meaningful relationships, providing the opportunity for healthy exchanges on vulnerable topics like emotional and psychological wellbeing. A printable guide for this specific purpose (“HM COVID-19 Check-In Guide for Self and Peers”) was designed to help hospitalists move into safe and supportive conversations with each other. While it is difficult to place a value on the importance these types of conversations have on individual wellbeing, it is known that the quality of a positive work environment where people feel supported can moderate stress, morale, and depression. In other words, hospitalist groups can positively contribute to their social environment during stressful times by sharing meaningful and difficult experiences with one another.
Second, the Taskforce created a social media campaign to provide a public social space for sharing hospitalists’ COVID-19 experiences. We believed that sharing collective experiences with the theme of #YouAreNotAlone and a complementary social media campaign, SHM Cares, on SHM’s social media channels, would further connect the national hospitalist community and provide a different communication pathway to decrease a sense of isolation. This idea came from the second social support idea mentioned earlier to share what is stressful with others in a safe space. We understood that some hospitalists would be more comfortable sharing publicly their comments, photos, and videos in achieving a sense of hospitalist unity.
Using our shared experiences, we identified three pillars for the final structure of the HM COVID-19 Check-In Guide for Self and Peers:
- Pillar 1. Recognize your issues. Recall our oxygen mask metaphor and this is what we mean by recognizing symptoms of new stressors (e.g., sleeplessness, irritability, forgetfulness).
- Pillar 2. Know what to say. A simple open-ended question about how the other person is working through the pandemic is an easy way to start a connection. We learned from a mental health perspective that it is unlikely that you could say anything to make a situation worse by offering a listening ear.
- Pillar 3. Check in with others. Listen to others without trying to fix the person or the situation. When appropriate, offer humorous reflections without diminishing the problem. Be a partner and commit to check in regularly with the other person.
Cultivating human connections outside of your immediate peer group can be valuable and offer additional perspective to stressful situations. For instance, one of my roles as a hospitalist administrator has been offering support by regularly listening as my physicians ‘talk out’ their day confidentially for as long as they needed. Offering open conversation in a safe and confidential way can have a healing effect. As one of my former hospitalists used to say, if issues are not addressed, they will “ooze out somewhere else.”
The HM COVID-19 Check-In Guide for Self and Peers and the SHM Cares social media campaign was the result of the Taskforce’s collective observations to help others normalize the feeling that ‘it’s OK not to be OK.’ Using the pandemic as context, the 7 Drivers of Hospitalist Burnout reminded us that the increased burnout issues we face will require continued attention past the pandemic. The value in cultivating human connections has never been more important. The SHM Wellbeing Taskforce is committed to provide continued resources. Checking in with others and listening to peers are all part of a personal wellbeing and resilience strategy. On behalf of the SHM Wellbeing Taskforce, we hope the information in this article will highlight the importance of continued attention to personal wellbeing during and after the pandemic.
Dr. Robinson received her PhD in organizational learning, performance and change from Colorado State University in 2019. Her dissertation topic was exploring hospitalist burnout, engagement, and social support. She is administrative director of inpatient medicine at St. Mary’s Medical Center in Grand Junction, Colo., a part of SCL Health. She has volunteered in numerous SHM committees, and currently serves on the SHM Wellbeing Taskforce.
COVID-19 did not discriminate when it came to the impact it imposed on our hospitalist community. As the nomenclature moves away from the negative connotations of ‘burnout’ to ‘wellbeing,’ the pandemic has taught us something important about being intentional about our personal health: we must secure our own oxygen masks before helping others.
In February 2020, the Society of Hospital Medicine’s Wellbeing Taskforce efforts quickly changed focus from addressing general wellbeing, to wellbeing during COVID-19. Our Taskforce was commissioned by SHM’s Board with a new charge: Address immediate and ongoing needs of well-being and resiliency support for hospitalists during the COVID-19 pandemic. In this essay, I will discuss how our SHM Wellbeing Taskforce approached the overall topic of wellbeing for hospitalists during the COVID-19 pandemic, including some of our Taskforce group experiences.
The Taskforce started with a framework to aide in cultivating open and authentic conversations within hospital medicine groups. Creating spaces for honest sharing around how providers are doing is a crucial first step to reducing stigma, building mutual support within a group, and elevating issues of wellbeing to the level where structural change can take place. The Taskforce established two objectives for normalizing and mitigating stressors we face as hospitalists during the COVID-19 pandemic:
- Provide a framework for hospitalists to take their own emotional pulse
- Provide an approach to reduce stigma of hospitalists who are suffering from pandemic stress
While a more typical approach to fix stress and burnout is using formal institutional interventions, we used the value and insight provided by SHM’s 7 Drivers of Burnout in Hospital Medicine to help guide the creation of SHM resources in addressing the severe emotional strain being felt across the country by hospitalists. The 7 Drivers support the idea that the social role peers and hospital leaders can make a crucial difference in mitigating stress and burnout. Two examples of social support come to mind from the Wellbeing Taskforce experience:
- Participate in your meetings. One example comes from a member of our group who had underestimated the “healing power” that our group meetings had provided to his psyche. The simple act of participating in our Taskforce meeting and being in the presence of our group had provided such a positive impact that he was better able to face the “death and misery” in his unit with a smile on his face.
- Share what is stressful. The second example of social support comes from an hour of Zoom-based facilitation meetings between the SHM’s Wellbeing Taskforce members and Chapter Leaders in late October. During our Taskforce debrief after the meeting, we came to realize the enormous burden of grief our peers were carrying as one hospitalist had lost a group colleague the previous week due to suicide. Our member who led this meeting was moved – as were we – at how this had impacted his small team, and he was reminded he was not alone.
To form meaningful relationships that foster support, there needs to be a space where people can safely come together at times that initially might feel awkward. After taking steps toward your peers, these conversations can become normalized and contribute to meaningful relationships, providing the opportunity for healthy exchanges on vulnerable topics like emotional and psychological wellbeing. A printable guide for this specific purpose (“HM COVID-19 Check-In Guide for Self and Peers”) was designed to help hospitalists move into safe and supportive conversations with each other. While it is difficult to place a value on the importance these types of conversations have on individual wellbeing, it is known that the quality of a positive work environment where people feel supported can moderate stress, morale, and depression. In other words, hospitalist groups can positively contribute to their social environment during stressful times by sharing meaningful and difficult experiences with one another.
Second, the Taskforce created a social media campaign to provide a public social space for sharing hospitalists’ COVID-19 experiences. We believed that sharing collective experiences with the theme of #YouAreNotAlone and a complementary social media campaign, SHM Cares, on SHM’s social media channels, would further connect the national hospitalist community and provide a different communication pathway to decrease a sense of isolation. This idea came from the second social support idea mentioned earlier to share what is stressful with others in a safe space. We understood that some hospitalists would be more comfortable sharing publicly their comments, photos, and videos in achieving a sense of hospitalist unity.
Using our shared experiences, we identified three pillars for the final structure of the HM COVID-19 Check-In Guide for Self and Peers:
- Pillar 1. Recognize your issues. Recall our oxygen mask metaphor and this is what we mean by recognizing symptoms of new stressors (e.g., sleeplessness, irritability, forgetfulness).
- Pillar 2. Know what to say. A simple open-ended question about how the other person is working through the pandemic is an easy way to start a connection. We learned from a mental health perspective that it is unlikely that you could say anything to make a situation worse by offering a listening ear.
- Pillar 3. Check in with others. Listen to others without trying to fix the person or the situation. When appropriate, offer humorous reflections without diminishing the problem. Be a partner and commit to check in regularly with the other person.
Cultivating human connections outside of your immediate peer group can be valuable and offer additional perspective to stressful situations. For instance, one of my roles as a hospitalist administrator has been offering support by regularly listening as my physicians ‘talk out’ their day confidentially for as long as they needed. Offering open conversation in a safe and confidential way can have a healing effect. As one of my former hospitalists used to say, if issues are not addressed, they will “ooze out somewhere else.”
The HM COVID-19 Check-In Guide for Self and Peers and the SHM Cares social media campaign was the result of the Taskforce’s collective observations to help others normalize the feeling that ‘it’s OK not to be OK.’ Using the pandemic as context, the 7 Drivers of Hospitalist Burnout reminded us that the increased burnout issues we face will require continued attention past the pandemic. The value in cultivating human connections has never been more important. The SHM Wellbeing Taskforce is committed to provide continued resources. Checking in with others and listening to peers are all part of a personal wellbeing and resilience strategy. On behalf of the SHM Wellbeing Taskforce, we hope the information in this article will highlight the importance of continued attention to personal wellbeing during and after the pandemic.
Dr. Robinson received her PhD in organizational learning, performance and change from Colorado State University in 2019. Her dissertation topic was exploring hospitalist burnout, engagement, and social support. She is administrative director of inpatient medicine at St. Mary’s Medical Center in Grand Junction, Colo., a part of SCL Health. She has volunteered in numerous SHM committees, and currently serves on the SHM Wellbeing Taskforce.