User login
What I want people to know about the Chauvin verdict
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.

There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.
There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.
There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Is common courtesy no longer contagious?
The other day, in a fairly common occurrence, I needed to fax a records request over to another office.

Not having memorized all the fax numbers in my area, I turned to the internet and quickly had their website and the needed information in front of me.
But at the top of the page, before you got to phone numbers and directions, was this statement in bold print (caps as seen):
“NOTICE TO ALL PATIENTS:
“Please show RESPECT AND KINDNESS to other patients and staff.
“We have a ZERO TOLERANCE policy for aggressive behavior, vulgar language, and violence, whether in person, on the phone, or online.”
A veterinarian I know recently put something similar up, saying: “We DO NOT TOLERATE physically or verbally abusive behavior by clients. We are compassionate and understand you are under stress, but we are also human and deserve respect. Thank you.”
I absolutely agree with this. Hell, I’m the same way.
But what is wrong with people that we actually need to have notices like that up?
Realistically, the vast majority of patients don’t need the reminder. They treat each other, and my staff, with politeness and respect, and we do the same. To me that’s part of the whole sandbox thing. Personally, I prefer my office to have the same atmosphere as a library, and am known to “shhhh” people who are too loud.
But the real point here is that we shouldn’t have to remind anyone else to behave with common courtesy. If you’re an adult, I’m going to assume your parents and teachers taught you the importance of manners and the Golden Rule.
I’ve been in practice for 23 years now, and I’ve never had to deal with this sort of behavior, this frequently, before. Is it that the pandemic, and its economic and social consequences, has gotten on everyone’s nerves? If so, hopefully it will gradually fade away as the crisis does. I’m vaccinated. My family and the majority of my patients are vaccinated. I encourage pretty much everyone who asks me about it to get vaccinated.
But I’m more concerned that isn’t really the issue. Maybe our polarized, divided society is moving in that direction. Common good is now often reduced to us against them, and the conditions of the times have just aggravated a problem that was festering.
The majority of people, of all beliefs, remain decent people. But
Decency and manners, unfortunately, can’t be legislated. If you’ve forgotten yours, though, don’t think others will put up with you.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The other day, in a fairly common occurrence, I needed to fax a records request over to another office.
Not having memorized all the fax numbers in my area, I turned to the internet and quickly had their website and the needed information in front of me.
But at the top of the page, before you got to phone numbers and directions, was this statement in bold print (caps as seen):
“NOTICE TO ALL PATIENTS:
“Please show RESPECT AND KINDNESS to other patients and staff.
“We have a ZERO TOLERANCE policy for aggressive behavior, vulgar language, and violence, whether in person, on the phone, or online.”
A veterinarian I know recently put something similar up, saying: “We DO NOT TOLERATE physically or verbally abusive behavior by clients. We are compassionate and understand you are under stress, but we are also human and deserve respect. Thank you.”
I absolutely agree with this. Hell, I’m the same way.
But what is wrong with people that we actually need to have notices like that up?
Realistically, the vast majority of patients don’t need the reminder. They treat each other, and my staff, with politeness and respect, and we do the same. To me that’s part of the whole sandbox thing. Personally, I prefer my office to have the same atmosphere as a library, and am known to “shhhh” people who are too loud.
But the real point here is that we shouldn’t have to remind anyone else to behave with common courtesy. If you’re an adult, I’m going to assume your parents and teachers taught you the importance of manners and the Golden Rule.
I’ve been in practice for 23 years now, and I’ve never had to deal with this sort of behavior, this frequently, before. Is it that the pandemic, and its economic and social consequences, has gotten on everyone’s nerves? If so, hopefully it will gradually fade away as the crisis does. I’m vaccinated. My family and the majority of my patients are vaccinated. I encourage pretty much everyone who asks me about it to get vaccinated.
But I’m more concerned that isn’t really the issue. Maybe our polarized, divided society is moving in that direction. Common good is now often reduced to us against them, and the conditions of the times have just aggravated a problem that was festering.
The majority of people, of all beliefs, remain decent people. But
Decency and manners, unfortunately, can’t be legislated. If you’ve forgotten yours, though, don’t think others will put up with you.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The other day, in a fairly common occurrence, I needed to fax a records request over to another office.
Not having memorized all the fax numbers in my area, I turned to the internet and quickly had their website and the needed information in front of me.
But at the top of the page, before you got to phone numbers and directions, was this statement in bold print (caps as seen):
“NOTICE TO ALL PATIENTS:
“Please show RESPECT AND KINDNESS to other patients and staff.
“We have a ZERO TOLERANCE policy for aggressive behavior, vulgar language, and violence, whether in person, on the phone, or online.”
A veterinarian I know recently put something similar up, saying: “We DO NOT TOLERATE physically or verbally abusive behavior by clients. We are compassionate and understand you are under stress, but we are also human and deserve respect. Thank you.”
I absolutely agree with this. Hell, I’m the same way.
But what is wrong with people that we actually need to have notices like that up?
Realistically, the vast majority of patients don’t need the reminder. They treat each other, and my staff, with politeness and respect, and we do the same. To me that’s part of the whole sandbox thing. Personally, I prefer my office to have the same atmosphere as a library, and am known to “shhhh” people who are too loud.
But the real point here is that we shouldn’t have to remind anyone else to behave with common courtesy. If you’re an adult, I’m going to assume your parents and teachers taught you the importance of manners and the Golden Rule.
I’ve been in practice for 23 years now, and I’ve never had to deal with this sort of behavior, this frequently, before. Is it that the pandemic, and its economic and social consequences, has gotten on everyone’s nerves? If so, hopefully it will gradually fade away as the crisis does. I’m vaccinated. My family and the majority of my patients are vaccinated. I encourage pretty much everyone who asks me about it to get vaccinated.
But I’m more concerned that isn’t really the issue. Maybe our polarized, divided society is moving in that direction. Common good is now often reduced to us against them, and the conditions of the times have just aggravated a problem that was festering.
The majority of people, of all beliefs, remain decent people. But
Decency and manners, unfortunately, can’t be legislated. If you’ve forgotten yours, though, don’t think others will put up with you.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Commentary: Functional assessment developed for older adults with sickle cell disease
As individuals with sickle cell disease (SCD) are living longer than ever before there is a greater need to focus on maintaining and improving function and independence in this growing population. In the general population, impairments in functional measures such as usual gait speed, grip strength, Timed Up and Go, and cognition are associated with adverse health outcomes such as falls, fractures, loss of independence, and death.

Adults with SCD experience multiple complications such as avascular necrosis of the joints, retinopathy, and strokes that lead to functional limitations similar to those experienced by geriatric populations. However, functional assessments are not routinely performed during clinic visits with older adults with SCD.
In order to address this gap in care, my colleagues and I developed the first functional assessment for older adults with SCD, called the Sickle Cell Disease Functional Assessment (SCD-FA). This assessment will allow providers to evaluate the capabilities and vulnerabilities of older adults with SCD.
We assessed the feasibility of administering the SCD-FA in a prospective cohort pilot study. We enrolled 40 adults with SCD (20 older adults aged at least 50 years and 20 younger adults aged 18-49 years as a comparison group). All participants were assessed at steady-state.
For the SCD-FA, we selected geriatric assessment measures across seven domains: functional status, comorbid medical conditions, psychological state, social support, nutritional status, cognition, and medications. Several of these measures were previously validated in an oncology geriatric assessment and enriched with additional physical and cognitive measures to evaluate conditions at the intersection of SCD and geriatrics.
In September 2020, we published a protocol describing the methods and rationale for selecting measures for the SCD-FA in Pilot and Feasibility Studies.1 The preliminary data was presented at the annual meeting of the American Society of Hematology in December 2020 and was included in the annual Hematology and Aging Poster Walk.
The results of this pilot study showed that the SCD-FA is feasible (91% of participants who consented completed the SCD-FA), acceptable (95% reported the length as appropriate and had no difficulty understanding the measures), and safe with no adverse events.2 On physical performance testing, both younger and older participants had results consistent with accelerated aging with a functional age at least 20-30 years older than their chronological age.2
The majority of the participants (63%) had a usual gait speed slower than the speed required to safely cross the street at an intersection, and 25% had a gait speed slower than 1 m/s, which has been associated with increased mortality in the general population.3,4
Benefits to management
The SCD-FA can improve management of adults with SCD by:
- Characterizing their capabilities and physiological age, identifying individuals at high risk for functional decline and death early identifying targets for interventions that have been successful in geriatrics,5 assessing risk of toxicity from curative therapies, and evaluating functional response to SCD-specific therapies.
The SCD-FA provides a framework for developing exercise interventions to target functional impairments. This work supports our goal of improving the quality of life and longevity for people with SCD.
Dr. Oyedeji is a senior hematology Fellow at the department of medicine, division of hematology, Duke University, Durham, N.C. She reported that she has no conflicts of interest.
References
1. Pilot Feasibility Stud. 2020;6:131.
2. Blood. 2020;136(Supplement 1):26-7.
3. J Rehabil Res Dev. 2005;42(4):535-46.
4. JAMA. 2011;305(1):50-8.
5. South Med J. 1994;87(5):S83-7.
As individuals with sickle cell disease (SCD) are living longer than ever before there is a greater need to focus on maintaining and improving function and independence in this growing population. In the general population, impairments in functional measures such as usual gait speed, grip strength, Timed Up and Go, and cognition are associated with adverse health outcomes such as falls, fractures, loss of independence, and death.
Adults with SCD experience multiple complications such as avascular necrosis of the joints, retinopathy, and strokes that lead to functional limitations similar to those experienced by geriatric populations. However, functional assessments are not routinely performed during clinic visits with older adults with SCD.
In order to address this gap in care, my colleagues and I developed the first functional assessment for older adults with SCD, called the Sickle Cell Disease Functional Assessment (SCD-FA). This assessment will allow providers to evaluate the capabilities and vulnerabilities of older adults with SCD.
We assessed the feasibility of administering the SCD-FA in a prospective cohort pilot study. We enrolled 40 adults with SCD (20 older adults aged at least 50 years and 20 younger adults aged 18-49 years as a comparison group). All participants were assessed at steady-state.
For the SCD-FA, we selected geriatric assessment measures across seven domains: functional status, comorbid medical conditions, psychological state, social support, nutritional status, cognition, and medications. Several of these measures were previously validated in an oncology geriatric assessment and enriched with additional physical and cognitive measures to evaluate conditions at the intersection of SCD and geriatrics.
In September 2020, we published a protocol describing the methods and rationale for selecting measures for the SCD-FA in Pilot and Feasibility Studies.1 The preliminary data was presented at the annual meeting of the American Society of Hematology in December 2020 and was included in the annual Hematology and Aging Poster Walk.
The results of this pilot study showed that the SCD-FA is feasible (91% of participants who consented completed the SCD-FA), acceptable (95% reported the length as appropriate and had no difficulty understanding the measures), and safe with no adverse events.2 On physical performance testing, both younger and older participants had results consistent with accelerated aging with a functional age at least 20-30 years older than their chronological age.2
The majority of the participants (63%) had a usual gait speed slower than the speed required to safely cross the street at an intersection, and 25% had a gait speed slower than 1 m/s, which has been associated with increased mortality in the general population.3,4
Benefits to management
The SCD-FA can improve management of adults with SCD by:
- Characterizing their capabilities and physiological age, identifying individuals at high risk for functional decline and death early identifying targets for interventions that have been successful in geriatrics,5 assessing risk of toxicity from curative therapies, and evaluating functional response to SCD-specific therapies.
The SCD-FA provides a framework for developing exercise interventions to target functional impairments. This work supports our goal of improving the quality of life and longevity for people with SCD.
Dr. Oyedeji is a senior hematology Fellow at the department of medicine, division of hematology, Duke University, Durham, N.C. She reported that she has no conflicts of interest.
References
1. Pilot Feasibility Stud. 2020;6:131.
2. Blood. 2020;136(Supplement 1):26-7.
3. J Rehabil Res Dev. 2005;42(4):535-46.
4. JAMA. 2011;305(1):50-8.
5. South Med J. 1994;87(5):S83-7.
As individuals with sickle cell disease (SCD) are living longer than ever before there is a greater need to focus on maintaining and improving function and independence in this growing population. In the general population, impairments in functional measures such as usual gait speed, grip strength, Timed Up and Go, and cognition are associated with adverse health outcomes such as falls, fractures, loss of independence, and death.
Adults with SCD experience multiple complications such as avascular necrosis of the joints, retinopathy, and strokes that lead to functional limitations similar to those experienced by geriatric populations. However, functional assessments are not routinely performed during clinic visits with older adults with SCD.
In order to address this gap in care, my colleagues and I developed the first functional assessment for older adults with SCD, called the Sickle Cell Disease Functional Assessment (SCD-FA). This assessment will allow providers to evaluate the capabilities and vulnerabilities of older adults with SCD.
We assessed the feasibility of administering the SCD-FA in a prospective cohort pilot study. We enrolled 40 adults with SCD (20 older adults aged at least 50 years and 20 younger adults aged 18-49 years as a comparison group). All participants were assessed at steady-state.
For the SCD-FA, we selected geriatric assessment measures across seven domains: functional status, comorbid medical conditions, psychological state, social support, nutritional status, cognition, and medications. Several of these measures were previously validated in an oncology geriatric assessment and enriched with additional physical and cognitive measures to evaluate conditions at the intersection of SCD and geriatrics.
In September 2020, we published a protocol describing the methods and rationale for selecting measures for the SCD-FA in Pilot and Feasibility Studies.1 The preliminary data was presented at the annual meeting of the American Society of Hematology in December 2020 and was included in the annual Hematology and Aging Poster Walk.
The results of this pilot study showed that the SCD-FA is feasible (91% of participants who consented completed the SCD-FA), acceptable (95% reported the length as appropriate and had no difficulty understanding the measures), and safe with no adverse events.2 On physical performance testing, both younger and older participants had results consistent with accelerated aging with a functional age at least 20-30 years older than their chronological age.2
The majority of the participants (63%) had a usual gait speed slower than the speed required to safely cross the street at an intersection, and 25% had a gait speed slower than 1 m/s, which has been associated with increased mortality in the general population.3,4
Benefits to management
The SCD-FA can improve management of adults with SCD by:
- Characterizing their capabilities and physiological age, identifying individuals at high risk for functional decline and death early identifying targets for interventions that have been successful in geriatrics,5 assessing risk of toxicity from curative therapies, and evaluating functional response to SCD-specific therapies.
The SCD-FA provides a framework for developing exercise interventions to target functional impairments. This work supports our goal of improving the quality of life and longevity for people with SCD.
Dr. Oyedeji is a senior hematology Fellow at the department of medicine, division of hematology, Duke University, Durham, N.C. She reported that she has no conflicts of interest.
References
1. Pilot Feasibility Stud. 2020;6:131.
2. Blood. 2020;136(Supplement 1):26-7.
3. J Rehabil Res Dev. 2005;42(4):535-46.
4. JAMA. 2011;305(1):50-8.
5. South Med J. 1994;87(5):S83-7.
How about contraceptives for men?
With the introduction of new technology to vaccinate the world with the Pfizer and Moderna mRNA vaccines, I considered other health conditions that could benefit from new modalities. Unplanned pregnancies are a public health crisis, yet the burden falls solely on women to solve, burdening them with contraceptive practices to prevent unplanned pregnancy. With the insurrection of Row v. Wade and the new bills being pushed through states that are limiting abortion, perhaps the time has come for males to accept the responsibility for contraception to prevent unplanned pregnancy. The methods that currently exist for males are condoms and vasectomy. Other options are being explored – both nonhormonal and reversible contraception including daily pills, gels, and long-acting injections.

The pill for men has been under preliminary trials with promising results. This contraceptive pill contains dimethandrolone undecanoate, which is an androgen anabolic steroid progesterone once-daily pill that suppresses FSH and LH, causing a decrease in the production of testosterone and consequently sperm production.1 (Long, Lee, & Blithe, 2019). This pill is in long-term trials to determine the efficacy and side effects, including the impact on libido, liver, and kidney disease.
The injectable male contraceptive in trials now includes two different options. The first was a long-acting progestin, testosterone, and androgen combination. The male participants received an intramuscular injection every 8 weeks. Although the results of the study were promising – sperm production was effectively reduced, the side effects were too severe for participants to continue use. Side effects much like those of the female Depo-Provera injections included acne and mood disorders. Men experienced erectile dysfunction while at the same time having an increase in sex drive.2 (Em, 2018).
Recently, researchers in India have studied a nonhormonal injectable with promising outcomes. It prevented pregnancy in more than 97% of participants. This injectable polymer gel is placed into the male’s vas deferens to block sperm from leaving the body. This product inactivates sperm, essentially creating temporary sterilization for men. The benefit of this product, called RISUG (reversible inhibition of sperm under guidance), is a single injection that can be effective for 13 years. It can be reversed earlier if needed by injecting a dissolving gel into the male’s vas deferens.1,2 In the United States, there is an identical product called Vasalgel – a polymer injected into the vas deferens – also being studied for temporary infertility.
Another synthetic implanted androgen product being studied is 7 alpha-methyl-19-nortestosterone (MENT), a synthetic steroid that resembles testosterone but does not convert into testosterone and, consequently, does not stimulate prostate growth. It is administered via two subdermal implants and is effective for 12 months. The first subdermal implant releases the synthetic androgen, which is more potent than testosterone, and the other emits LH-releasing hormone.3 Studies demonstrate that MENT suppresses sperm production.1
Finally, studies are underway using transdermal gel applications to suppress sperm concentrations. The daily gel is absorbed through the skin after application to two different areas of the man’s body: the shoulders and upper arms. The daily application of the progestin product, Nestorone, and testosterone gel has been found to reduce sperm concentrations to < 1 x 106/mL. Studies measured gonadal concentrations after 4 weeks.1 Users were happy with the use of a topical gel, with minimal side effects such as lower libido, weight gain, and changes in cholesterol, yet inconsistent use of the product resulted in lower than anticipated results.4
Male contraceptive options are long overdue to dramatically reduce the rate of unplanned pregnancies and the burden of contraception placed on women. Getting these products to market will be half the battle – getting men to commit to using these options and women to trust male compliance may further impede acceptance. Men have not had to carry the burden and economics of single parenting. Men interested in casual sex may now need to accept more responsibility for unplanned pregnancy and be proactive with prevention, particularly as abortion laws are being challenged.
Ms. Thew is medical director of the department of pediatrics division of adolescent medicine at the Medical College of Wisconsin in Milwaukee. She is a member of the editorial board for Pediatric News and has no relevant disclosures.
References
1. Long J E et al. Clin Chem. 2019;65(1):153-60.
2. Male birth control: Current options and new breakthroughs, SingleCare: Health Education. Aug. 6, 2018.
3. Sundaram K et al. Ann Med. 1993;25(2):199-205.
4. Anawalt BD et al. Andrology. 2019;7(6):878-87.
With the introduction of new technology to vaccinate the world with the Pfizer and Moderna mRNA vaccines, I considered other health conditions that could benefit from new modalities. Unplanned pregnancies are a public health crisis, yet the burden falls solely on women to solve, burdening them with contraceptive practices to prevent unplanned pregnancy. With the insurrection of Row v. Wade and the new bills being pushed through states that are limiting abortion, perhaps the time has come for males to accept the responsibility for contraception to prevent unplanned pregnancy. The methods that currently exist for males are condoms and vasectomy. Other options are being explored – both nonhormonal and reversible contraception including daily pills, gels, and long-acting injections.
The pill for men has been under preliminary trials with promising results. This contraceptive pill contains dimethandrolone undecanoate, which is an androgen anabolic steroid progesterone once-daily pill that suppresses FSH and LH, causing a decrease in the production of testosterone and consequently sperm production.1 (Long, Lee, & Blithe, 2019). This pill is in long-term trials to determine the efficacy and side effects, including the impact on libido, liver, and kidney disease.
The injectable male contraceptive in trials now includes two different options. The first was a long-acting progestin, testosterone, and androgen combination. The male participants received an intramuscular injection every 8 weeks. Although the results of the study were promising – sperm production was effectively reduced, the side effects were too severe for participants to continue use. Side effects much like those of the female Depo-Provera injections included acne and mood disorders. Men experienced erectile dysfunction while at the same time having an increase in sex drive.2 (Em, 2018).
Recently, researchers in India have studied a nonhormonal injectable with promising outcomes. It prevented pregnancy in more than 97% of participants. This injectable polymer gel is placed into the male’s vas deferens to block sperm from leaving the body. This product inactivates sperm, essentially creating temporary sterilization for men. The benefit of this product, called RISUG (reversible inhibition of sperm under guidance), is a single injection that can be effective for 13 years. It can be reversed earlier if needed by injecting a dissolving gel into the male’s vas deferens.1,2 In the United States, there is an identical product called Vasalgel – a polymer injected into the vas deferens – also being studied for temporary infertility.
Another synthetic implanted androgen product being studied is 7 alpha-methyl-19-nortestosterone (MENT), a synthetic steroid that resembles testosterone but does not convert into testosterone and, consequently, does not stimulate prostate growth. It is administered via two subdermal implants and is effective for 12 months. The first subdermal implant releases the synthetic androgen, which is more potent than testosterone, and the other emits LH-releasing hormone.3 Studies demonstrate that MENT suppresses sperm production.1
Finally, studies are underway using transdermal gel applications to suppress sperm concentrations. The daily gel is absorbed through the skin after application to two different areas of the man’s body: the shoulders and upper arms. The daily application of the progestin product, Nestorone, and testosterone gel has been found to reduce sperm concentrations to < 1 x 106/mL. Studies measured gonadal concentrations after 4 weeks.1 Users were happy with the use of a topical gel, with minimal side effects such as lower libido, weight gain, and changes in cholesterol, yet inconsistent use of the product resulted in lower than anticipated results.4
Male contraceptive options are long overdue to dramatically reduce the rate of unplanned pregnancies and the burden of contraception placed on women. Getting these products to market will be half the battle – getting men to commit to using these options and women to trust male compliance may further impede acceptance. Men have not had to carry the burden and economics of single parenting. Men interested in casual sex may now need to accept more responsibility for unplanned pregnancy and be proactive with prevention, particularly as abortion laws are being challenged.
Ms. Thew is medical director of the department of pediatrics division of adolescent medicine at the Medical College of Wisconsin in Milwaukee. She is a member of the editorial board for Pediatric News and has no relevant disclosures.
References
1. Long J E et al. Clin Chem. 2019;65(1):153-60.
2. Male birth control: Current options and new breakthroughs, SingleCare: Health Education. Aug. 6, 2018.
3. Sundaram K et al. Ann Med. 1993;25(2):199-205.
4. Anawalt BD et al. Andrology. 2019;7(6):878-87.
With the introduction of new technology to vaccinate the world with the Pfizer and Moderna mRNA vaccines, I considered other health conditions that could benefit from new modalities. Unplanned pregnancies are a public health crisis, yet the burden falls solely on women to solve, burdening them with contraceptive practices to prevent unplanned pregnancy. With the insurrection of Row v. Wade and the new bills being pushed through states that are limiting abortion, perhaps the time has come for males to accept the responsibility for contraception to prevent unplanned pregnancy. The methods that currently exist for males are condoms and vasectomy. Other options are being explored – both nonhormonal and reversible contraception including daily pills, gels, and long-acting injections.
The pill for men has been under preliminary trials with promising results. This contraceptive pill contains dimethandrolone undecanoate, which is an androgen anabolic steroid progesterone once-daily pill that suppresses FSH and LH, causing a decrease in the production of testosterone and consequently sperm production.1 (Long, Lee, & Blithe, 2019). This pill is in long-term trials to determine the efficacy and side effects, including the impact on libido, liver, and kidney disease.
The injectable male contraceptive in trials now includes two different options. The first was a long-acting progestin, testosterone, and androgen combination. The male participants received an intramuscular injection every 8 weeks. Although the results of the study were promising – sperm production was effectively reduced, the side effects were too severe for participants to continue use. Side effects much like those of the female Depo-Provera injections included acne and mood disorders. Men experienced erectile dysfunction while at the same time having an increase in sex drive.2 (Em, 2018).
Recently, researchers in India have studied a nonhormonal injectable with promising outcomes. It prevented pregnancy in more than 97% of participants. This injectable polymer gel is placed into the male’s vas deferens to block sperm from leaving the body. This product inactivates sperm, essentially creating temporary sterilization for men. The benefit of this product, called RISUG (reversible inhibition of sperm under guidance), is a single injection that can be effective for 13 years. It can be reversed earlier if needed by injecting a dissolving gel into the male’s vas deferens.1,2 In the United States, there is an identical product called Vasalgel – a polymer injected into the vas deferens – also being studied for temporary infertility.
Another synthetic implanted androgen product being studied is 7 alpha-methyl-19-nortestosterone (MENT), a synthetic steroid that resembles testosterone but does not convert into testosterone and, consequently, does not stimulate prostate growth. It is administered via two subdermal implants and is effective for 12 months. The first subdermal implant releases the synthetic androgen, which is more potent than testosterone, and the other emits LH-releasing hormone.3 Studies demonstrate that MENT suppresses sperm production.1
Finally, studies are underway using transdermal gel applications to suppress sperm concentrations. The daily gel is absorbed through the skin after application to two different areas of the man’s body: the shoulders and upper arms. The daily application of the progestin product, Nestorone, and testosterone gel has been found to reduce sperm concentrations to < 1 x 106/mL. Studies measured gonadal concentrations after 4 weeks.1 Users were happy with the use of a topical gel, with minimal side effects such as lower libido, weight gain, and changes in cholesterol, yet inconsistent use of the product resulted in lower than anticipated results.4
Male contraceptive options are long overdue to dramatically reduce the rate of unplanned pregnancies and the burden of contraception placed on women. Getting these products to market will be half the battle – getting men to commit to using these options and women to trust male compliance may further impede acceptance. Men have not had to carry the burden and economics of single parenting. Men interested in casual sex may now need to accept more responsibility for unplanned pregnancy and be proactive with prevention, particularly as abortion laws are being challenged.
Ms. Thew is medical director of the department of pediatrics division of adolescent medicine at the Medical College of Wisconsin in Milwaukee. She is a member of the editorial board for Pediatric News and has no relevant disclosures.
References
1. Long J E et al. Clin Chem. 2019;65(1):153-60.
2. Male birth control: Current options and new breakthroughs, SingleCare: Health Education. Aug. 6, 2018.
3. Sundaram K et al. Ann Med. 1993;25(2):199-205.
4. Anawalt BD et al. Andrology. 2019;7(6):878-87.
Surgery for early-stage cervical cancer: Are we still too radical?
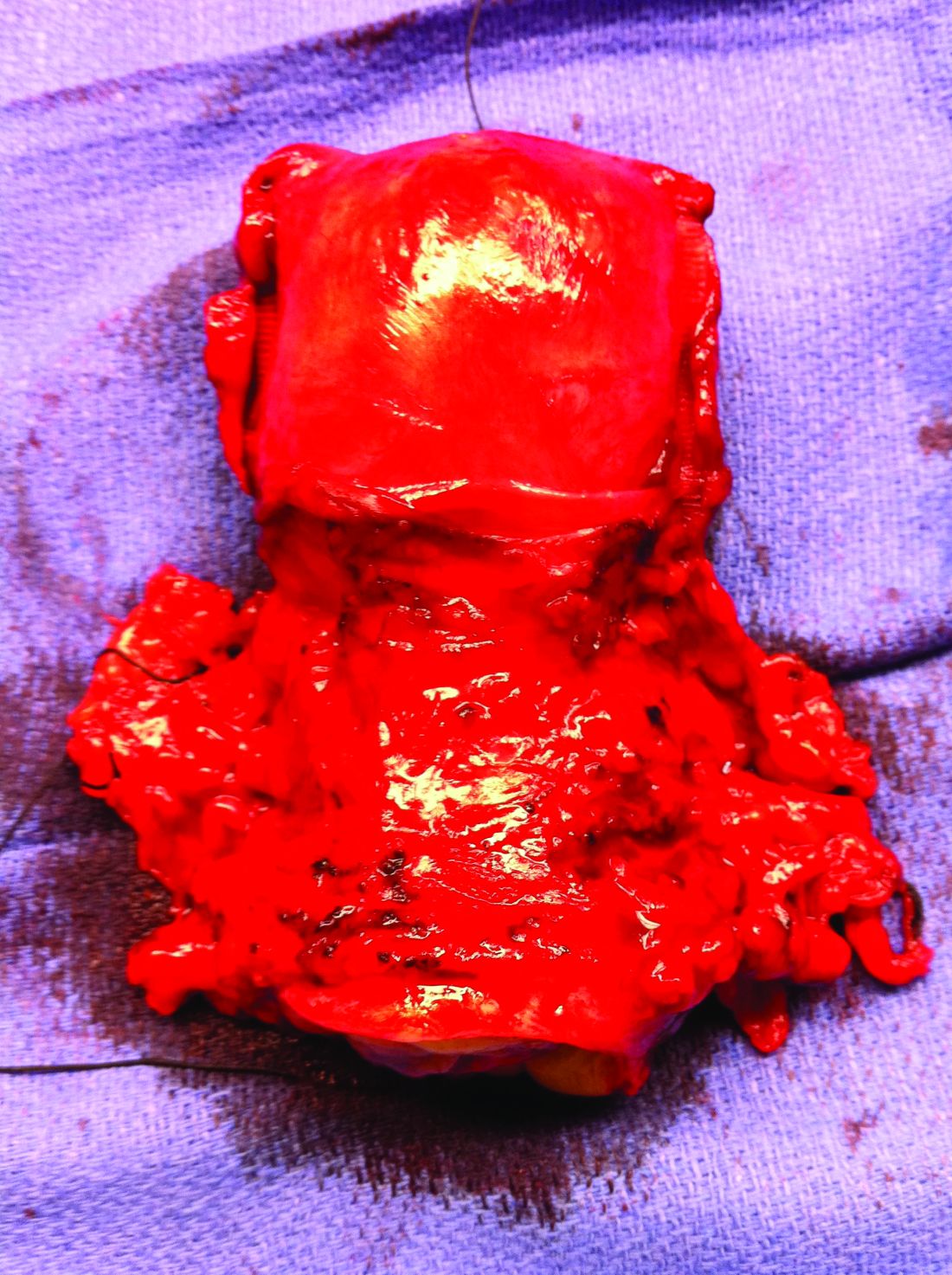
It has been more than 120 years since Ernst Wertheim, a Viennese surgeon, performed and described what is considered to have been the first radical total hysterectomy with lymphadenectomy for early-stage cervical cancer, yet this morbid procedure remains the standard of care for most early-stage cervical cancers. The rationale for this procedure, which included removal of the parametrial tissue, uterosacral and cardinal ligaments, and upper vagina en bloc with the cervix and uterus, was to obtain margins around a cancer that has a dominant radial growth pattern. The morbidity associated with this procedure is substantial. The parametrium houses important vascular, neural, and urologic structures. Unlike extrafascial hysterectomy, often referred to as “simple” hysterectomy, in which surgeons follow a fascial plane, and therefore a relatively avascular dissection, surgeons performing radical hysterectomy must venture outside of these embryologic fusion planes into less well–defined anatomy. Therefore, surgical complications are relatively common including hemorrhage, ureteral and bladder injury, as well as late-onset devastating complications such as fistula, urinary retention, or incontinence, and sexual dysfunction.1 More recently, variations of the Wertheim-Meigs radical hysterectomy have been described, and objective classifications created, which include modified radical procedures (removing less parametria) and nerve-sparing procedures to facilitate standardized nomenclature for tailoring the most appropriate procedure for any given tumor.2
The trend, and a positive one at that, over the course of the past century, has been a move away from routine radical surgical procedures for most clinical stage 1 cancers. No better example exists than breast cancer, in which the Halsted radical mastectomy has been largely replaced by less morbid breast-conserving or nonradical procedures with adjunct medical and radiation therapies offered to achieve high rates of cure with far more acceptable patient-centered outcomes.3 And so why is it that radical hysterectomy is still considered the standard of care for all but the smallest of microscopic cervical cancers?
The risk of lymph node metastases or recurrence is exceptionally low for women with microscopic (stage IA1) cervical cancers that are less than 3 mm in depth. Therefore, the National Comprehensive Cancer Network guidelines recommend nonradical surgical remedies (such as extrafascial hysterectomy, or cone biopsy or trachelectomy if fertility preservation is desired) for this earlier stage of disease.4 If there is lymphovascular space invasion (an indicator of poor prognosis and potential lymphatic involvement), a lymphadenectomy or sentinel lymph node biopsy is also recommended. For women with stage IA2 or IB lesions, radical excisions (either trachelectomy or hysterectomy) are considered the standard of care. However, this “gold standard” was achieved largely through legacy, and not a result of randomized trials comparing its outcomes with nonradical procedures.
Initial strides away from radical cervical cancer surgery focused on the goal of fertility preservation via radical trachelectomy which allowed women to preserve an intact uterine fundus. This was initially met with skepticism and concern that surgeons could be sacrificing oncologic outcomes in order to preserve a woman’s fertility. Thanks to pioneering work, including prospective research studies by surgeon innovators it has been shown that, in appropriately selected candidates with tumors less than 2 cm, it is an accepted standard of care.4 Radical vaginal or abdominal trachelectomy is associated with cancer recurrence rates of less than 5% and successful pregnancy in approximately three-quarters of patients in whom this is desired.5,6 However, full-term pregnancy is achieved in 50%-75% of cases, reflecting increased obstetric risk, and radical trachelectomy still subjects patients to the morbidity of a radical parametrial resection, despite the fact that many of them will have no residual carcinoma in their final pathological specimens.

Therefore, can we be even more conservative in our surgery for these patients? Are simple hysterectomy or conization potentially adequate treatments for small (<2 cm) stage IA2 and IB1 lesions that have favorable histology (<10 mm stromal invasion, low-risk histology, no lymphovascular space involvement, negative margins on conization and no lymph node metastases)? In patients whose tumor exhibits these histologic features, the likelihood of parametrial involvement is approximately 1%, calling into question the virtue of parametrial resection.7 Observational studies have identified mixed results on the safety of conservative surgical techniques in early-stage cervical cancer. In a study of the National Cancer Database, the outcomes of 2,543 radical hysterectomies and 1,388 extrafascial hysterectomies for women with stage IB1 disease were evaluated and observed a difference in 5-year survival (92.4% vs. 95.3%) favoring the radical procedure.8 Unfortunately, database analyses such as these are limited by potential confounders and discordance between the groups such as rates of lymphadenectomy, known involvement of oncologic surgeon specialists, and margin status. An alternative evaluation of the Surveillance, Epidemiology, and End Results database including 2,571 patients with stage IB1 disease, all of whom had lymphadenectomy performed, showed no difference in 10-year disease-specific survival between the two surgical approaches.9
Ultimately, whether conservative procedures (such as conization or extrafascial hysterectomy) can be offered to women with small, low-risk IB1 or IA2 cervical cancers will be best determined by prospective single-arm or randomized trials. Fortunately, these are underway. Preliminary results from the ConCerv trial in which 100 women with early-stage, low-risk stage IA2 and IB1 cervical cancer were treated with either repeat conization or extrafascial hysterectomy with sentinel lymph node biopsy showed acceptably low rates of recurrence (3%) with this approach.10 If the mature data supports this finding, it seems that, for appropriately selected and well-counseled patients, conservative surgery may become more broadly accepted as a reasonable option for treatment that spares women not only loss of fertility, but also the early and late surgical morbidity from radical procedures.
In the meantime, until more is known about the oncologic safety of nonradical procedures for stage IA2 and IB1 cervical cancer, this option should not be considered standard of care, and only offered to patients with favorable tumor factors who are well counseled regarding the uncertainty of this approach. It is critical that patients with early-stage cervical cancer be evaluated by a gynecologic cancer specialist prior to definitive surgical treatment as they are best equipped to evaluate risk profiles and counsel about her options for surgery, its known and unknown consequences, and the appropriateness of fertility preservation or radicality of surgery. We eagerly await the results of trials evaluating the safety of conservative cervical cancer surgery, which promise to advance us from 19th-century practices, preserving not only fertility, but also quality of life.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no disclosures and can be contacted at [email protected].
References
1. Trimbos JB et al. Eur J Cancer. 2004;40(3):375-8.
2. Querleu D and Morrow CP. Lancet Oncol. 2008;9:297-303.
3. Sakorafas GH and Safioleas M. Eur J Cancer Care. 2010 Mar;19(2):145-66.
4. National Comprehensive Cancer Network. Cervical Cancer (Version 1.2021). https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf. Accessed 2021 Apr 21.
5. Plante M et al. Gynecol Oncol. 2011;121:290-7.
6. Wethington SL et al. Int J Gynecol Cancer. 2012;22:1251-7.
7. Domgue J and Schmeler K. Best Pract Res Clin Obstet Gynaecol. 2019 Feb;55:79-92.
8. Sia TY et al. Obstet Gyenecol. 2019;134(6):1132.
9. Tseng J et al. Gynecol Oncol. 2018;150(1):44.
10. Schmeler K et al. Int J Gynecol Cancer. 2019;29:A14-5.
It has been more than 120 years since Ernst Wertheim, a Viennese surgeon, performed and described what is considered to have been the first radical total hysterectomy with lymphadenectomy for early-stage cervical cancer, yet this morbid procedure remains the standard of care for most early-stage cervical cancers. The rationale for this procedure, which included removal of the parametrial tissue, uterosacral and cardinal ligaments, and upper vagina en bloc with the cervix and uterus, was to obtain margins around a cancer that has a dominant radial growth pattern. The morbidity associated with this procedure is substantial. The parametrium houses important vascular, neural, and urologic structures. Unlike extrafascial hysterectomy, often referred to as “simple” hysterectomy, in which surgeons follow a fascial plane, and therefore a relatively avascular dissection, surgeons performing radical hysterectomy must venture outside of these embryologic fusion planes into less well–defined anatomy. Therefore, surgical complications are relatively common including hemorrhage, ureteral and bladder injury, as well as late-onset devastating complications such as fistula, urinary retention, or incontinence, and sexual dysfunction.1 More recently, variations of the Wertheim-Meigs radical hysterectomy have been described, and objective classifications created, which include modified radical procedures (removing less parametria) and nerve-sparing procedures to facilitate standardized nomenclature for tailoring the most appropriate procedure for any given tumor.2
The trend, and a positive one at that, over the course of the past century, has been a move away from routine radical surgical procedures for most clinical stage 1 cancers. No better example exists than breast cancer, in which the Halsted radical mastectomy has been largely replaced by less morbid breast-conserving or nonradical procedures with adjunct medical and radiation therapies offered to achieve high rates of cure with far more acceptable patient-centered outcomes.3 And so why is it that radical hysterectomy is still considered the standard of care for all but the smallest of microscopic cervical cancers?
The risk of lymph node metastases or recurrence is exceptionally low for women with microscopic (stage IA1) cervical cancers that are less than 3 mm in depth. Therefore, the National Comprehensive Cancer Network guidelines recommend nonradical surgical remedies (such as extrafascial hysterectomy, or cone biopsy or trachelectomy if fertility preservation is desired) for this earlier stage of disease.4 If there is lymphovascular space invasion (an indicator of poor prognosis and potential lymphatic involvement), a lymphadenectomy or sentinel lymph node biopsy is also recommended. For women with stage IA2 or IB lesions, radical excisions (either trachelectomy or hysterectomy) are considered the standard of care. However, this “gold standard” was achieved largely through legacy, and not a result of randomized trials comparing its outcomes with nonradical procedures.
Initial strides away from radical cervical cancer surgery focused on the goal of fertility preservation via radical trachelectomy which allowed women to preserve an intact uterine fundus. This was initially met with skepticism and concern that surgeons could be sacrificing oncologic outcomes in order to preserve a woman’s fertility. Thanks to pioneering work, including prospective research studies by surgeon innovators it has been shown that, in appropriately selected candidates with tumors less than 2 cm, it is an accepted standard of care.4 Radical vaginal or abdominal trachelectomy is associated with cancer recurrence rates of less than 5% and successful pregnancy in approximately three-quarters of patients in whom this is desired.5,6 However, full-term pregnancy is achieved in 50%-75% of cases, reflecting increased obstetric risk, and radical trachelectomy still subjects patients to the morbidity of a radical parametrial resection, despite the fact that many of them will have no residual carcinoma in their final pathological specimens.
Therefore, can we be even more conservative in our surgery for these patients? Are simple hysterectomy or conization potentially adequate treatments for small (<2 cm) stage IA2 and IB1 lesions that have favorable histology (<10 mm stromal invasion, low-risk histology, no lymphovascular space involvement, negative margins on conization and no lymph node metastases)? In patients whose tumor exhibits these histologic features, the likelihood of parametrial involvement is approximately 1%, calling into question the virtue of parametrial resection.7 Observational studies have identified mixed results on the safety of conservative surgical techniques in early-stage cervical cancer. In a study of the National Cancer Database, the outcomes of 2,543 radical hysterectomies and 1,388 extrafascial hysterectomies for women with stage IB1 disease were evaluated and observed a difference in 5-year survival (92.4% vs. 95.3%) favoring the radical procedure.8 Unfortunately, database analyses such as these are limited by potential confounders and discordance between the groups such as rates of lymphadenectomy, known involvement of oncologic surgeon specialists, and margin status. An alternative evaluation of the Surveillance, Epidemiology, and End Results database including 2,571 patients with stage IB1 disease, all of whom had lymphadenectomy performed, showed no difference in 10-year disease-specific survival between the two surgical approaches.9
Ultimately, whether conservative procedures (such as conization or extrafascial hysterectomy) can be offered to women with small, low-risk IB1 or IA2 cervical cancers will be best determined by prospective single-arm or randomized trials. Fortunately, these are underway. Preliminary results from the ConCerv trial in which 100 women with early-stage, low-risk stage IA2 and IB1 cervical cancer were treated with either repeat conization or extrafascial hysterectomy with sentinel lymph node biopsy showed acceptably low rates of recurrence (3%) with this approach.10 If the mature data supports this finding, it seems that, for appropriately selected and well-counseled patients, conservative surgery may become more broadly accepted as a reasonable option for treatment that spares women not only loss of fertility, but also the early and late surgical morbidity from radical procedures.
In the meantime, until more is known about the oncologic safety of nonradical procedures for stage IA2 and IB1 cervical cancer, this option should not be considered standard of care, and only offered to patients with favorable tumor factors who are well counseled regarding the uncertainty of this approach. It is critical that patients with early-stage cervical cancer be evaluated by a gynecologic cancer specialist prior to definitive surgical treatment as they are best equipped to evaluate risk profiles and counsel about her options for surgery, its known and unknown consequences, and the appropriateness of fertility preservation or radicality of surgery. We eagerly await the results of trials evaluating the safety of conservative cervical cancer surgery, which promise to advance us from 19th-century practices, preserving not only fertility, but also quality of life.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no disclosures and can be contacted at [email protected].
References
1. Trimbos JB et al. Eur J Cancer. 2004;40(3):375-8.
2. Querleu D and Morrow CP. Lancet Oncol. 2008;9:297-303.
3. Sakorafas GH and Safioleas M. Eur J Cancer Care. 2010 Mar;19(2):145-66.
4. National Comprehensive Cancer Network. Cervical Cancer (Version 1.2021). https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf. Accessed 2021 Apr 21.
5. Plante M et al. Gynecol Oncol. 2011;121:290-7.
6. Wethington SL et al. Int J Gynecol Cancer. 2012;22:1251-7.
7. Domgue J and Schmeler K. Best Pract Res Clin Obstet Gynaecol. 2019 Feb;55:79-92.
8. Sia TY et al. Obstet Gyenecol. 2019;134(6):1132.
9. Tseng J et al. Gynecol Oncol. 2018;150(1):44.
10. Schmeler K et al. Int J Gynecol Cancer. 2019;29:A14-5.
It has been more than 120 years since Ernst Wertheim, a Viennese surgeon, performed and described what is considered to have been the first radical total hysterectomy with lymphadenectomy for early-stage cervical cancer, yet this morbid procedure remains the standard of care for most early-stage cervical cancers. The rationale for this procedure, which included removal of the parametrial tissue, uterosacral and cardinal ligaments, and upper vagina en bloc with the cervix and uterus, was to obtain margins around a cancer that has a dominant radial growth pattern. The morbidity associated with this procedure is substantial. The parametrium houses important vascular, neural, and urologic structures. Unlike extrafascial hysterectomy, often referred to as “simple” hysterectomy, in which surgeons follow a fascial plane, and therefore a relatively avascular dissection, surgeons performing radical hysterectomy must venture outside of these embryologic fusion planes into less well–defined anatomy. Therefore, surgical complications are relatively common including hemorrhage, ureteral and bladder injury, as well as late-onset devastating complications such as fistula, urinary retention, or incontinence, and sexual dysfunction.1 More recently, variations of the Wertheim-Meigs radical hysterectomy have been described, and objective classifications created, which include modified radical procedures (removing less parametria) and nerve-sparing procedures to facilitate standardized nomenclature for tailoring the most appropriate procedure for any given tumor.2
The trend, and a positive one at that, over the course of the past century, has been a move away from routine radical surgical procedures for most clinical stage 1 cancers. No better example exists than breast cancer, in which the Halsted radical mastectomy has been largely replaced by less morbid breast-conserving or nonradical procedures with adjunct medical and radiation therapies offered to achieve high rates of cure with far more acceptable patient-centered outcomes.3 And so why is it that radical hysterectomy is still considered the standard of care for all but the smallest of microscopic cervical cancers?
The risk of lymph node metastases or recurrence is exceptionally low for women with microscopic (stage IA1) cervical cancers that are less than 3 mm in depth. Therefore, the National Comprehensive Cancer Network guidelines recommend nonradical surgical remedies (such as extrafascial hysterectomy, or cone biopsy or trachelectomy if fertility preservation is desired) for this earlier stage of disease.4 If there is lymphovascular space invasion (an indicator of poor prognosis and potential lymphatic involvement), a lymphadenectomy or sentinel lymph node biopsy is also recommended. For women with stage IA2 or IB lesions, radical excisions (either trachelectomy or hysterectomy) are considered the standard of care. However, this “gold standard” was achieved largely through legacy, and not a result of randomized trials comparing its outcomes with nonradical procedures.
Initial strides away from radical cervical cancer surgery focused on the goal of fertility preservation via radical trachelectomy which allowed women to preserve an intact uterine fundus. This was initially met with skepticism and concern that surgeons could be sacrificing oncologic outcomes in order to preserve a woman’s fertility. Thanks to pioneering work, including prospective research studies by surgeon innovators it has been shown that, in appropriately selected candidates with tumors less than 2 cm, it is an accepted standard of care.4 Radical vaginal or abdominal trachelectomy is associated with cancer recurrence rates of less than 5% and successful pregnancy in approximately three-quarters of patients in whom this is desired.5,6 However, full-term pregnancy is achieved in 50%-75% of cases, reflecting increased obstetric risk, and radical trachelectomy still subjects patients to the morbidity of a radical parametrial resection, despite the fact that many of them will have no residual carcinoma in their final pathological specimens.
Therefore, can we be even more conservative in our surgery for these patients? Are simple hysterectomy or conization potentially adequate treatments for small (<2 cm) stage IA2 and IB1 lesions that have favorable histology (<10 mm stromal invasion, low-risk histology, no lymphovascular space involvement, negative margins on conization and no lymph node metastases)? In patients whose tumor exhibits these histologic features, the likelihood of parametrial involvement is approximately 1%, calling into question the virtue of parametrial resection.7 Observational studies have identified mixed results on the safety of conservative surgical techniques in early-stage cervical cancer. In a study of the National Cancer Database, the outcomes of 2,543 radical hysterectomies and 1,388 extrafascial hysterectomies for women with stage IB1 disease were evaluated and observed a difference in 5-year survival (92.4% vs. 95.3%) favoring the radical procedure.8 Unfortunately, database analyses such as these are limited by potential confounders and discordance between the groups such as rates of lymphadenectomy, known involvement of oncologic surgeon specialists, and margin status. An alternative evaluation of the Surveillance, Epidemiology, and End Results database including 2,571 patients with stage IB1 disease, all of whom had lymphadenectomy performed, showed no difference in 10-year disease-specific survival between the two surgical approaches.9
Ultimately, whether conservative procedures (such as conization or extrafascial hysterectomy) can be offered to women with small, low-risk IB1 or IA2 cervical cancers will be best determined by prospective single-arm or randomized trials. Fortunately, these are underway. Preliminary results from the ConCerv trial in which 100 women with early-stage, low-risk stage IA2 and IB1 cervical cancer were treated with either repeat conization or extrafascial hysterectomy with sentinel lymph node biopsy showed acceptably low rates of recurrence (3%) with this approach.10 If the mature data supports this finding, it seems that, for appropriately selected and well-counseled patients, conservative surgery may become more broadly accepted as a reasonable option for treatment that spares women not only loss of fertility, but also the early and late surgical morbidity from radical procedures.
In the meantime, until more is known about the oncologic safety of nonradical procedures for stage IA2 and IB1 cervical cancer, this option should not be considered standard of care, and only offered to patients with favorable tumor factors who are well counseled regarding the uncertainty of this approach. It is critical that patients with early-stage cervical cancer be evaluated by a gynecologic cancer specialist prior to definitive surgical treatment as they are best equipped to evaluate risk profiles and counsel about her options for surgery, its known and unknown consequences, and the appropriateness of fertility preservation or radicality of surgery. We eagerly await the results of trials evaluating the safety of conservative cervical cancer surgery, which promise to advance us from 19th-century practices, preserving not only fertility, but also quality of life.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no disclosures and can be contacted at [email protected].
References
1. Trimbos JB et al. Eur J Cancer. 2004;40(3):375-8.
2. Querleu D and Morrow CP. Lancet Oncol. 2008;9:297-303.
3. Sakorafas GH and Safioleas M. Eur J Cancer Care. 2010 Mar;19(2):145-66.
4. National Comprehensive Cancer Network. Cervical Cancer (Version 1.2021). https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf. Accessed 2021 Apr 21.
5. Plante M et al. Gynecol Oncol. 2011;121:290-7.
6. Wethington SL et al. Int J Gynecol Cancer. 2012;22:1251-7.
7. Domgue J and Schmeler K. Best Pract Res Clin Obstet Gynaecol. 2019 Feb;55:79-92.
8. Sia TY et al. Obstet Gyenecol. 2019;134(6):1132.
9. Tseng J et al. Gynecol Oncol. 2018;150(1):44.
10. Schmeler K et al. Int J Gynecol Cancer. 2019;29:A14-5.
When should antibiotics be used in acute uncomplicated diverticulitis?
Dear colleagues and friends,
The Perspectives series returns, this time with an exciting discussion about antibiotic use in acute uncomplicated diverticulitis. It has been fascinating to witness this field evolve from an era where not using antibiotics was inconceivable! Dr. Anne F. Peery and Dr. Neil Stollman, both recognized experts in the matter, provide arguments to both sides of the debate, as well as much-needed nuance. As always, I welcome your comments and suggestions for future topics at [email protected]. Thank you for your support, and I hope you will enjoy the reading and learning from this as much as I did.

Charles J. Kahi, MD, MS, AGAF, is a professor of medicine at Indiana University, Indianapolis. He is also an associate editor for GI & Hepatology News.
Think carefully about when to withhold
For decades, it was standard practice to give antibiotics to all patients with acute uncomplicated diverticulitis (AUD). While most patients with a first diagnosis of AUD recover within a few weeks, a small proportion will develop a complication.1 Among generally healthy patients with an initial diagnosis of AUD, about 3% will progress to complicated diverticulitis, and about 1% will require emergency surgery within 6 months. Around another 6% of cases will develop chronic diverticulitis with ongoing diverticular inflammation that persists for weeks to months.
Because the complications are uncommon, we don’t know if antibiotics reduce the risk of progression to complicated diverticulitis, emergency surgery, or the development of chronic diverticulitis. Investigating these patient-centered and morbid outcomes would require trials enrolling thousands of patients and to following these patients for months. This trial hasn’t happened yet.

To date, only small studies have compared the use of antibiotics with no antibiotics in patients with AUD. A review sponsored by the Agency for Healthcare Research and Quality published last year concluded that the current evidence was too sparse or too inconsistent to make strong conclusions about the use of antibiotics for patients with uncomplicated diverticulitis.2
With little evidence for or against antibiotics, recent guidelines have begun to recommend that antibiotics be used selectively, rather than routinely, in patients with diverticulitis.3 “Selectively” clearly means that there are some patients who should receive antibiotics, but the guidelines are vague about who those patients are. To this end, it is safest to refer to those small, underpowered trials to identify which patients are at the greatest risk of developing a complication.1,4 The authors of those trials considered a number of groups high risk and therefore excluded them from those trials. In the absence of further definitive research, it seems clear that those groups, listed below, should therefore be selected for antibiotic treatment:
- Patients with complicated diverticulitis including paracolic extraluminal air on CT scan.
- Patients who are immunocompromised.
- Patients with a high fever, affected general condition, or clinical suspicion of sepsis.
- Patients with inflammatory bowel disease.
- Patients who are pregnant or breast feeding.
As with most clinical trials, participants in these smaller trials were younger (median age, late 50s) and healthier (63% normal, healthy patient; 34% mild systemic disease; 4% severe systemic disease) than the general population. In secondary analyses, however, several factors were independently associated with a complicated disease course after an initial diagnosis of acute uncomplicated diverticulitis. As with the first list above, the following high-risk patients should also be treated with antibiotics at diagnosis:
- Patients with American Society of Anesthesiologists scores III or IV were 4.4 times more likely to have a poor outcome, compared with those with ASA score I.
- Patients with ASA score II were 2.0 times more likely to have a poor outcome, compared with ASA score I.
- Patients with symptoms for more than 5 days at diagnosis were 3.3 times more likely to have a poor outcome, compared with those with symptoms for 5 days or less.
- Patients with vomiting at diagnosis were 3.9 times more likely to have a poor outcome, compared with those who were not vomiting.
- Patients with C-reactive protein levels higher than 140 mg/L at diagnosis were 2.9 times more likely to have a poor outcome, compared with C-reactive protein level of 140 mg/L or less.
- Patients with white blood cell count greater than 15 x 109 cells/L at diagnosis were 3.7 times more likely to have a poor outcome, compared with those with 15 x 109 cells/L.
- Patients with a longer segment (>86mm) of inflamed colon on CT scan were more likely to have a poor outcome, compared those who had a shorter segment (<65mm).
To help clinicians think about antibiotic treatment in patients with AUD, a recent American Gastroenterological Association clinical practice update provided the following advice: First, antibiotic treatment is advised in patients with uncomplicated diverticulitis who have comorbidities or are frail, who present with refractory symptoms or vomiting, or who have a C-reactive protein level greater than 140 mg/L, or baseline white blood cell count greater than 15 x 109 cells/L.5 Also, antibiotic treatment is advised in patients with complicated diverticulitis or uncomplicated diverticulitis with a fluid collection or longer segment of inflammation on CT scan. Finally, patients with uncomplicated diverticulitis who are immunosuppressed are high risk for progression to complicated diverticulitis or sepsis and should be treated with antibiotics.
The lists above clearly leave some patients with AUD who may be managed without antibiotics. These patients are otherwise healthy, have good social support, access to health care, and are experiencing a mild, self-limited episode. Avoiding antibiotics requires shared decision-making with a well-informed patient. I have patients who have embraced this approach, while others found this unacceptable. Given the current level of uncertainty in the literature, I make it my practice to offer antibiotics to any patient who feels strongly about receiving them.
As with many issues in modern medicine, the use of antibiotics in AUD is an unsettled question. Given the known harms of progression of diverticulitis, it is clearly safest to treat patients who were excluded from the small studies we have or flagged by those same studies as being at increased risk of progression. Our uncertainty also demands a shared decision-making model, filling in our patients on what we can and cannot say with confidence. As is often the case, further research is desperately needed. Until that happens, antibiotics for AUD will remain a regular part of my practice.
Anne F. Peery, MD, MSCR, is with the center for gastrointestinal biology and disease at the University of North Carolina at Chapel Hill. She has no conflicts to disclose.
References
1. Daniels L et al. Br J Surg. 2017 Jan;104(1):52-61.
2. Balk EM et al. Management of Colonic Diverticulitis. Comparative Effectiveness Review No. 233. Agency for Healthcare Research and Quality. 2020 Oct. doi: 10.23970/AHRQEPCCER233.
3. Stollman N et al. Gastroenterology. 2015 Dec;149(7):1944-9.
4. Chabok A et al. Br J Surg. 2012 Jan 30;99(4):532-9.
5. Peery AF et al. Gastroenterology. 2021 Feb;160(3):906-11.e1.
The data are robust for withholding more often
That we are engaged in a legitimate debate about the role of antibiotics in acute uncomplicated diverticulitis (AUD) is itself quite notable. In the 1999 American College of Gastroenterology Practice Guidelines,1 we did not even entertain the concept of withholding antibiotics; the only discussion points were intravenous versus oral. Fast forward 15 years, and in the 2015 American Gastroenterological Association practice guidelines (which the other contributor for this installment of Perspectives, Anne F. Peery, MD, and I worked on together) our first recommendation was that antibiotics should be used “selectively,” rather than routinely.2 This did generate some raised eyebrows and hand-wringing in the community, but our position was the result of a rigorous data analysis process and we stood by it.

In fact, Dr. Peery and I also coauthored an accompanying editorial that concluded with an important endorsement “allowing the clinician to consider withholding antibiotics from select uncomplicated patients with mild disease.” I suspect, then, that Dr. Peery and I are very much coincident in our overall thoughts here, and I’m pretty sure that neither of us would defend an “always” or “never” stance on this issue, so for this educational debate, we’re really talking about where in the middle to draw the line (that is, how to define “selectively”). To that end, I will defend the supposition that the subsequent data in support of withholding antibiotics remains robust and even more supportive of this practice in many (but certainly not all) patients with acute, uncomplicated diverticulitis.
The logic underlying selective use was based on two drivers over the past decade, one being an emerging concept that diverticular pathology was often inflammatory rather than solely infectious, coupled with a timely and very important worldwide push toward restraint of antibiotic use. A recent retrospective claims analysis of outpatient antibiotic use for immunocompetent patients with AUD did reported that the dominant antibiotic combination used, metronidazole plus a fluoroquinolone, was associated with an increased risk of Clostridioides difficile infection, compared with the far less frequently used amoxicillin/clavulanate regimen, which highlights that routine antibiotics are not without risk.3
Recently, the U.S. Agency for Healthcare Research and Quality performed a rigorous meta-analysis of this body of evidence, and summarized that “antibiotic treatment may not affect pain symptoms, length of hospital stay, recurrence risk, quality of life, or need for surgery, compared to no antibiotic treatment,” with an admitted low strength of evidence (based on four randomized, controlled trials).4
Finally, I’ll close my evidence-based case with a quote from a Clinical Practice Update just published in February 2021 in Gastroenterology: “Antibiotic treatment can be used selectively, rather than routinely, in immunocompetent patients with mild uncomplicated diverticulitis. ... Antibiotic treatment is advised in patients with uncomplicated diverticulitis who have comorbidities or are frail, who present with refractory symptoms or vomiting, or who have a [C-reactive protein] >140 mg/L or baseline [white blood cell count] > 15 x 109. Antibiotic treatment is advised in patients with complicated diverticulitis or uncomplicated diverticulitis with a fluid collection or longer segment of inflammation on CT scan.”5 I think this is most excellent advice, providing a practical and clinically useful framework for those in whom antibiotics absolutely should be used, but permitting a fairly large group to avoid antibiotics, which may carry significant harm, based on strong consistent data that does not support a benefit.
So, practically speaking, things are a bit harder for us now when our patient shows up in the ED and if found to have AUD on CT. In the “old days” (that is, the early 2000s), a patient with either clinically suspected or CT-confirmed AUD was simply given antibiotics, mostly a fluoroquinolone, and this was community standard. The only real decision tree was inpatient or outpatient. But now, I would respectfully suggest, we need to invest a bit more time on a nuanced discussion with the potential “no antibiotics” patient (for example, one without immunosuppression, severe comorbidities, or lab or imaging markers of aggressive disease). It is now appropriate to inform such a patient that the data suggest that a conservative approach will not increase their risk of complications and may well spare them antibiotic-related morbidity.
In the context of that informed discussion, factually framed by the practitioner, many patients should (and will, in my experience, although the San Francisco Bay Area may not entirely reflect the country as a whole) choose a strategy of observation. Of course, close follow-up with such patients is required, as is clear reassurance that if things “turn bad” that we’re available and antibiotics remain a salvage option. The “write a script and be done” days are over, and while withholding antibiotics may still feel dangerous or uncomfortable to the patient (or to us), the data is the data, and our patients deserve to at least be offered that option.
Neil Stollman, MD, AGAF, FACG, is chairman of the division of gastroenterology at Alta Bates Summit Medical Center in Oakland, Calif., and an associate clinical professor of medicine in the division of gastroenterology at the University of California, San Francisco. He discloses being a consultant for Cosmo Pharmaceuticals, which has a potential future diverticulitis study of a rifampin-class antibiotic.
References
1. Stollman N and Raskin JB. Am J Gastroenterol. 1999 Nov;94(11):3110-21.
2. Peery AF and Stollman N. Gastroenterology. 2015 Dec;149(7):1944-9.
3. Gaber CE et al. Ann Intern Med. 2021 Feb 23. doi: 10.7326/M20-6315.
4. Balk EM et al. Management of Colonic Diverticulitis. Comparative Effectiveness Review No. 233. Agency for Healthcare Research and Quality. October 2020. doi: 10.23970/AHRQEPCCER233.
5. Peery AF et al. Gastroenterology. 2021 Feb;160(3):906-11.e1.
Dear colleagues and friends,
The Perspectives series returns, this time with an exciting discussion about antibiotic use in acute uncomplicated diverticulitis. It has been fascinating to witness this field evolve from an era where not using antibiotics was inconceivable! Dr. Anne F. Peery and Dr. Neil Stollman, both recognized experts in the matter, provide arguments to both sides of the debate, as well as much-needed nuance. As always, I welcome your comments and suggestions for future topics at [email protected]. Thank you for your support, and I hope you will enjoy the reading and learning from this as much as I did.
Charles J. Kahi, MD, MS, AGAF, is a professor of medicine at Indiana University, Indianapolis. He is also an associate editor for GI & Hepatology News.
Think carefully about when to withhold
For decades, it was standard practice to give antibiotics to all patients with acute uncomplicated diverticulitis (AUD). While most patients with a first diagnosis of AUD recover within a few weeks, a small proportion will develop a complication.1 Among generally healthy patients with an initial diagnosis of AUD, about 3% will progress to complicated diverticulitis, and about 1% will require emergency surgery within 6 months. Around another 6% of cases will develop chronic diverticulitis with ongoing diverticular inflammation that persists for weeks to months.
Because the complications are uncommon, we don’t know if antibiotics reduce the risk of progression to complicated diverticulitis, emergency surgery, or the development of chronic diverticulitis. Investigating these patient-centered and morbid outcomes would require trials enrolling thousands of patients and to following these patients for months. This trial hasn’t happened yet.
To date, only small studies have compared the use of antibiotics with no antibiotics in patients with AUD. A review sponsored by the Agency for Healthcare Research and Quality published last year concluded that the current evidence was too sparse or too inconsistent to make strong conclusions about the use of antibiotics for patients with uncomplicated diverticulitis.2
With little evidence for or against antibiotics, recent guidelines have begun to recommend that antibiotics be used selectively, rather than routinely, in patients with diverticulitis.3 “Selectively” clearly means that there are some patients who should receive antibiotics, but the guidelines are vague about who those patients are. To this end, it is safest to refer to those small, underpowered trials to identify which patients are at the greatest risk of developing a complication.1,4 The authors of those trials considered a number of groups high risk and therefore excluded them from those trials. In the absence of further definitive research, it seems clear that those groups, listed below, should therefore be selected for antibiotic treatment:
- Patients with complicated diverticulitis including paracolic extraluminal air on CT scan.
- Patients who are immunocompromised.
- Patients with a high fever, affected general condition, or clinical suspicion of sepsis.
- Patients with inflammatory bowel disease.
- Patients who are pregnant or breast feeding.
As with most clinical trials, participants in these smaller trials were younger (median age, late 50s) and healthier (63% normal, healthy patient; 34% mild systemic disease; 4% severe systemic disease) than the general population. In secondary analyses, however, several factors were independently associated with a complicated disease course after an initial diagnosis of acute uncomplicated diverticulitis. As with the first list above, the following high-risk patients should also be treated with antibiotics at diagnosis:
- Patients with American Society of Anesthesiologists scores III or IV were 4.4 times more likely to have a poor outcome, compared with those with ASA score I.
- Patients with ASA score II were 2.0 times more likely to have a poor outcome, compared with ASA score I.
- Patients with symptoms for more than 5 days at diagnosis were 3.3 times more likely to have a poor outcome, compared with those with symptoms for 5 days or less.
- Patients with vomiting at diagnosis were 3.9 times more likely to have a poor outcome, compared with those who were not vomiting.
- Patients with C-reactive protein levels higher than 140 mg/L at diagnosis were 2.9 times more likely to have a poor outcome, compared with C-reactive protein level of 140 mg/L or less.
- Patients with white blood cell count greater than 15 x 109 cells/L at diagnosis were 3.7 times more likely to have a poor outcome, compared with those with 15 x 109 cells/L.
- Patients with a longer segment (>86mm) of inflamed colon on CT scan were more likely to have a poor outcome, compared those who had a shorter segment (<65mm).
To help clinicians think about antibiotic treatment in patients with AUD, a recent American Gastroenterological Association clinical practice update provided the following advice: First, antibiotic treatment is advised in patients with uncomplicated diverticulitis who have comorbidities or are frail, who present with refractory symptoms or vomiting, or who have a C-reactive protein level greater than 140 mg/L, or baseline white blood cell count greater than 15 x 109 cells/L.5 Also, antibiotic treatment is advised in patients with complicated diverticulitis or uncomplicated diverticulitis with a fluid collection or longer segment of inflammation on CT scan. Finally, patients with uncomplicated diverticulitis who are immunosuppressed are high risk for progression to complicated diverticulitis or sepsis and should be treated with antibiotics.
The lists above clearly leave some patients with AUD who may be managed without antibiotics. These patients are otherwise healthy, have good social support, access to health care, and are experiencing a mild, self-limited episode. Avoiding antibiotics requires shared decision-making with a well-informed patient. I have patients who have embraced this approach, while others found this unacceptable. Given the current level of uncertainty in the literature, I make it my practice to offer antibiotics to any patient who feels strongly about receiving them.
As with many issues in modern medicine, the use of antibiotics in AUD is an unsettled question. Given the known harms of progression of diverticulitis, it is clearly safest to treat patients who were excluded from the small studies we have or flagged by those same studies as being at increased risk of progression. Our uncertainty also demands a shared decision-making model, filling in our patients on what we can and cannot say with confidence. As is often the case, further research is desperately needed. Until that happens, antibiotics for AUD will remain a regular part of my practice.
Anne F. Peery, MD, MSCR, is with the center for gastrointestinal biology and disease at the University of North Carolina at Chapel Hill. She has no conflicts to disclose.
References
1. Daniels L et al. Br J Surg. 2017 Jan;104(1):52-61.
2. Balk EM et al. Management of Colonic Diverticulitis. Comparative Effectiveness Review No. 233. Agency for Healthcare Research and Quality. 2020 Oct. doi: 10.23970/AHRQEPCCER233.
3. Stollman N et al. Gastroenterology. 2015 Dec;149(7):1944-9.
4. Chabok A et al. Br J Surg. 2012 Jan 30;99(4):532-9.
5. Peery AF et al. Gastroenterology. 2021 Feb;160(3):906-11.e1.
The data are robust for withholding more often
That we are engaged in a legitimate debate about the role of antibiotics in acute uncomplicated diverticulitis (AUD) is itself quite notable. In the 1999 American College of Gastroenterology Practice Guidelines,1 we did not even entertain the concept of withholding antibiotics; the only discussion points were intravenous versus oral. Fast forward 15 years, and in the 2015 American Gastroenterological Association practice guidelines (which the other contributor for this installment of Perspectives, Anne F. Peery, MD, and I worked on together) our first recommendation was that antibiotics should be used “selectively,” rather than routinely.2 This did generate some raised eyebrows and hand-wringing in the community, but our position was the result of a rigorous data analysis process and we stood by it.
In fact, Dr. Peery and I also coauthored an accompanying editorial that concluded with an important endorsement “allowing the clinician to consider withholding antibiotics from select uncomplicated patients with mild disease.” I suspect, then, that Dr. Peery and I are very much coincident in our overall thoughts here, and I’m pretty sure that neither of us would defend an “always” or “never” stance on this issue, so for this educational debate, we’re really talking about where in the middle to draw the line (that is, how to define “selectively”). To that end, I will defend the supposition that the subsequent data in support of withholding antibiotics remains robust and even more supportive of this practice in many (but certainly not all) patients with acute, uncomplicated diverticulitis.
The logic underlying selective use was based on two drivers over the past decade, one being an emerging concept that diverticular pathology was often inflammatory rather than solely infectious, coupled with a timely and very important worldwide push toward restraint of antibiotic use. A recent retrospective claims analysis of outpatient antibiotic use for immunocompetent patients with AUD did reported that the dominant antibiotic combination used, metronidazole plus a fluoroquinolone, was associated with an increased risk of Clostridioides difficile infection, compared with the far less frequently used amoxicillin/clavulanate regimen, which highlights that routine antibiotics are not without risk.3
Recently, the U.S. Agency for Healthcare Research and Quality performed a rigorous meta-analysis of this body of evidence, and summarized that “antibiotic treatment may not affect pain symptoms, length of hospital stay, recurrence risk, quality of life, or need for surgery, compared to no antibiotic treatment,” with an admitted low strength of evidence (based on four randomized, controlled trials).4
Finally, I’ll close my evidence-based case with a quote from a Clinical Practice Update just published in February 2021 in Gastroenterology: “Antibiotic treatment can be used selectively, rather than routinely, in immunocompetent patients with mild uncomplicated diverticulitis. ... Antibiotic treatment is advised in patients with uncomplicated diverticulitis who have comorbidities or are frail, who present with refractory symptoms or vomiting, or who have a [C-reactive protein] >140 mg/L or baseline [white blood cell count] > 15 x 109. Antibiotic treatment is advised in patients with complicated diverticulitis or uncomplicated diverticulitis with a fluid collection or longer segment of inflammation on CT scan.”5 I think this is most excellent advice, providing a practical and clinically useful framework for those in whom antibiotics absolutely should be used, but permitting a fairly large group to avoid antibiotics, which may carry significant harm, based on strong consistent data that does not support a benefit.
So, practically speaking, things are a bit harder for us now when our patient shows up in the ED and if found to have AUD on CT. In the “old days” (that is, the early 2000s), a patient with either clinically suspected or CT-confirmed AUD was simply given antibiotics, mostly a fluoroquinolone, and this was community standard. The only real decision tree was inpatient or outpatient. But now, I would respectfully suggest, we need to invest a bit more time on a nuanced discussion with the potential “no antibiotics” patient (for example, one without immunosuppression, severe comorbidities, or lab or imaging markers of aggressive disease). It is now appropriate to inform such a patient that the data suggest that a conservative approach will not increase their risk of complications and may well spare them antibiotic-related morbidity.
In the context of that informed discussion, factually framed by the practitioner, many patients should (and will, in my experience, although the San Francisco Bay Area may not entirely reflect the country as a whole) choose a strategy of observation. Of course, close follow-up with such patients is required, as is clear reassurance that if things “turn bad” that we’re available and antibiotics remain a salvage option. The “write a script and be done” days are over, and while withholding antibiotics may still feel dangerous or uncomfortable to the patient (or to us), the data is the data, and our patients deserve to at least be offered that option.
Neil Stollman, MD, AGAF, FACG, is chairman of the division of gastroenterology at Alta Bates Summit Medical Center in Oakland, Calif., and an associate clinical professor of medicine in the division of gastroenterology at the University of California, San Francisco. He discloses being a consultant for Cosmo Pharmaceuticals, which has a potential future diverticulitis study of a rifampin-class antibiotic.
References
1. Stollman N and Raskin JB. Am J Gastroenterol. 1999 Nov;94(11):3110-21.
2. Peery AF and Stollman N. Gastroenterology. 2015 Dec;149(7):1944-9.
3. Gaber CE et al. Ann Intern Med. 2021 Feb 23. doi: 10.7326/M20-6315.
4. Balk EM et al. Management of Colonic Diverticulitis. Comparative Effectiveness Review No. 233. Agency for Healthcare Research and Quality. October 2020. doi: 10.23970/AHRQEPCCER233.
5. Peery AF et al. Gastroenterology. 2021 Feb;160(3):906-11.e1.
Dear colleagues and friends,
The Perspectives series returns, this time with an exciting discussion about antibiotic use in acute uncomplicated diverticulitis. It has been fascinating to witness this field evolve from an era where not using antibiotics was inconceivable! Dr. Anne F. Peery and Dr. Neil Stollman, both recognized experts in the matter, provide arguments to both sides of the debate, as well as much-needed nuance. As always, I welcome your comments and suggestions for future topics at [email protected]. Thank you for your support, and I hope you will enjoy the reading and learning from this as much as I did.
Charles J. Kahi, MD, MS, AGAF, is a professor of medicine at Indiana University, Indianapolis. He is also an associate editor for GI & Hepatology News.
Think carefully about when to withhold
For decades, it was standard practice to give antibiotics to all patients with acute uncomplicated diverticulitis (AUD). While most patients with a first diagnosis of AUD recover within a few weeks, a small proportion will develop a complication.1 Among generally healthy patients with an initial diagnosis of AUD, about 3% will progress to complicated diverticulitis, and about 1% will require emergency surgery within 6 months. Around another 6% of cases will develop chronic diverticulitis with ongoing diverticular inflammation that persists for weeks to months.
Because the complications are uncommon, we don’t know if antibiotics reduce the risk of progression to complicated diverticulitis, emergency surgery, or the development of chronic diverticulitis. Investigating these patient-centered and morbid outcomes would require trials enrolling thousands of patients and to following these patients for months. This trial hasn’t happened yet.
To date, only small studies have compared the use of antibiotics with no antibiotics in patients with AUD. A review sponsored by the Agency for Healthcare Research and Quality published last year concluded that the current evidence was too sparse or too inconsistent to make strong conclusions about the use of antibiotics for patients with uncomplicated diverticulitis.2
With little evidence for or against antibiotics, recent guidelines have begun to recommend that antibiotics be used selectively, rather than routinely, in patients with diverticulitis.3 “Selectively” clearly means that there are some patients who should receive antibiotics, but the guidelines are vague about who those patients are. To this end, it is safest to refer to those small, underpowered trials to identify which patients are at the greatest risk of developing a complication.1,4 The authors of those trials considered a number of groups high risk and therefore excluded them from those trials. In the absence of further definitive research, it seems clear that those groups, listed below, should therefore be selected for antibiotic treatment:
- Patients with complicated diverticulitis including paracolic extraluminal air on CT scan.
- Patients who are immunocompromised.
- Patients with a high fever, affected general condition, or clinical suspicion of sepsis.
- Patients with inflammatory bowel disease.
- Patients who are pregnant or breast feeding.
As with most clinical trials, participants in these smaller trials were younger (median age, late 50s) and healthier (63% normal, healthy patient; 34% mild systemic disease; 4% severe systemic disease) than the general population. In secondary analyses, however, several factors were independently associated with a complicated disease course after an initial diagnosis of acute uncomplicated diverticulitis. As with the first list above, the following high-risk patients should also be treated with antibiotics at diagnosis:
- Patients with American Society of Anesthesiologists scores III or IV were 4.4 times more likely to have a poor outcome, compared with those with ASA score I.
- Patients with ASA score II were 2.0 times more likely to have a poor outcome, compared with ASA score I.
- Patients with symptoms for more than 5 days at diagnosis were 3.3 times more likely to have a poor outcome, compared with those with symptoms for 5 days or less.
- Patients with vomiting at diagnosis were 3.9 times more likely to have a poor outcome, compared with those who were not vomiting.
- Patients with C-reactive protein levels higher than 140 mg/L at diagnosis were 2.9 times more likely to have a poor outcome, compared with C-reactive protein level of 140 mg/L or less.
- Patients with white blood cell count greater than 15 x 109 cells/L at diagnosis were 3.7 times more likely to have a poor outcome, compared with those with 15 x 109 cells/L.
- Patients with a longer segment (>86mm) of inflamed colon on CT scan were more likely to have a poor outcome, compared those who had a shorter segment (<65mm).
To help clinicians think about antibiotic treatment in patients with AUD, a recent American Gastroenterological Association clinical practice update provided the following advice: First, antibiotic treatment is advised in patients with uncomplicated diverticulitis who have comorbidities or are frail, who present with refractory symptoms or vomiting, or who have a C-reactive protein level greater than 140 mg/L, or baseline white blood cell count greater than 15 x 109 cells/L.5 Also, antibiotic treatment is advised in patients with complicated diverticulitis or uncomplicated diverticulitis with a fluid collection or longer segment of inflammation on CT scan. Finally, patients with uncomplicated diverticulitis who are immunosuppressed are high risk for progression to complicated diverticulitis or sepsis and should be treated with antibiotics.
The lists above clearly leave some patients with AUD who may be managed without antibiotics. These patients are otherwise healthy, have good social support, access to health care, and are experiencing a mild, self-limited episode. Avoiding antibiotics requires shared decision-making with a well-informed patient. I have patients who have embraced this approach, while others found this unacceptable. Given the current level of uncertainty in the literature, I make it my practice to offer antibiotics to any patient who feels strongly about receiving them.
As with many issues in modern medicine, the use of antibiotics in AUD is an unsettled question. Given the known harms of progression of diverticulitis, it is clearly safest to treat patients who were excluded from the small studies we have or flagged by those same studies as being at increased risk of progression. Our uncertainty also demands a shared decision-making model, filling in our patients on what we can and cannot say with confidence. As is often the case, further research is desperately needed. Until that happens, antibiotics for AUD will remain a regular part of my practice.
Anne F. Peery, MD, MSCR, is with the center for gastrointestinal biology and disease at the University of North Carolina at Chapel Hill. She has no conflicts to disclose.
References
1. Daniels L et al. Br J Surg. 2017 Jan;104(1):52-61.
2. Balk EM et al. Management of Colonic Diverticulitis. Comparative Effectiveness Review No. 233. Agency for Healthcare Research and Quality. 2020 Oct. doi: 10.23970/AHRQEPCCER233.
3. Stollman N et al. Gastroenterology. 2015 Dec;149(7):1944-9.
4. Chabok A et al. Br J Surg. 2012 Jan 30;99(4):532-9.
5. Peery AF et al. Gastroenterology. 2021 Feb;160(3):906-11.e1.
The data are robust for withholding more often
That we are engaged in a legitimate debate about the role of antibiotics in acute uncomplicated diverticulitis (AUD) is itself quite notable. In the 1999 American College of Gastroenterology Practice Guidelines,1 we did not even entertain the concept of withholding antibiotics; the only discussion points were intravenous versus oral. Fast forward 15 years, and in the 2015 American Gastroenterological Association practice guidelines (which the other contributor for this installment of Perspectives, Anne F. Peery, MD, and I worked on together) our first recommendation was that antibiotics should be used “selectively,” rather than routinely.2 This did generate some raised eyebrows and hand-wringing in the community, but our position was the result of a rigorous data analysis process and we stood by it.
In fact, Dr. Peery and I also coauthored an accompanying editorial that concluded with an important endorsement “allowing the clinician to consider withholding antibiotics from select uncomplicated patients with mild disease.” I suspect, then, that Dr. Peery and I are very much coincident in our overall thoughts here, and I’m pretty sure that neither of us would defend an “always” or “never” stance on this issue, so for this educational debate, we’re really talking about where in the middle to draw the line (that is, how to define “selectively”). To that end, I will defend the supposition that the subsequent data in support of withholding antibiotics remains robust and even more supportive of this practice in many (but certainly not all) patients with acute, uncomplicated diverticulitis.
The logic underlying selective use was based on two drivers over the past decade, one being an emerging concept that diverticular pathology was often inflammatory rather than solely infectious, coupled with a timely and very important worldwide push toward restraint of antibiotic use. A recent retrospective claims analysis of outpatient antibiotic use for immunocompetent patients with AUD did reported that the dominant antibiotic combination used, metronidazole plus a fluoroquinolone, was associated with an increased risk of Clostridioides difficile infection, compared with the far less frequently used amoxicillin/clavulanate regimen, which highlights that routine antibiotics are not without risk.3
Recently, the U.S. Agency for Healthcare Research and Quality performed a rigorous meta-analysis of this body of evidence, and summarized that “antibiotic treatment may not affect pain symptoms, length of hospital stay, recurrence risk, quality of life, or need for surgery, compared to no antibiotic treatment,” with an admitted low strength of evidence (based on four randomized, controlled trials).4
Finally, I’ll close my evidence-based case with a quote from a Clinical Practice Update just published in February 2021 in Gastroenterology: “Antibiotic treatment can be used selectively, rather than routinely, in immunocompetent patients with mild uncomplicated diverticulitis. ... Antibiotic treatment is advised in patients with uncomplicated diverticulitis who have comorbidities or are frail, who present with refractory symptoms or vomiting, or who have a [C-reactive protein] >140 mg/L or baseline [white blood cell count] > 15 x 109. Antibiotic treatment is advised in patients with complicated diverticulitis or uncomplicated diverticulitis with a fluid collection or longer segment of inflammation on CT scan.”5 I think this is most excellent advice, providing a practical and clinically useful framework for those in whom antibiotics absolutely should be used, but permitting a fairly large group to avoid antibiotics, which may carry significant harm, based on strong consistent data that does not support a benefit.
So, practically speaking, things are a bit harder for us now when our patient shows up in the ED and if found to have AUD on CT. In the “old days” (that is, the early 2000s), a patient with either clinically suspected or CT-confirmed AUD was simply given antibiotics, mostly a fluoroquinolone, and this was community standard. The only real decision tree was inpatient or outpatient. But now, I would respectfully suggest, we need to invest a bit more time on a nuanced discussion with the potential “no antibiotics” patient (for example, one without immunosuppression, severe comorbidities, or lab or imaging markers of aggressive disease). It is now appropriate to inform such a patient that the data suggest that a conservative approach will not increase their risk of complications and may well spare them antibiotic-related morbidity.
In the context of that informed discussion, factually framed by the practitioner, many patients should (and will, in my experience, although the San Francisco Bay Area may not entirely reflect the country as a whole) choose a strategy of observation. Of course, close follow-up with such patients is required, as is clear reassurance that if things “turn bad” that we’re available and antibiotics remain a salvage option. The “write a script and be done” days are over, and while withholding antibiotics may still feel dangerous or uncomfortable to the patient (or to us), the data is the data, and our patients deserve to at least be offered that option.
Neil Stollman, MD, AGAF, FACG, is chairman of the division of gastroenterology at Alta Bates Summit Medical Center in Oakland, Calif., and an associate clinical professor of medicine in the division of gastroenterology at the University of California, San Francisco. He discloses being a consultant for Cosmo Pharmaceuticals, which has a potential future diverticulitis study of a rifampin-class antibiotic.
References
1. Stollman N and Raskin JB. Am J Gastroenterol. 1999 Nov;94(11):3110-21.
2. Peery AF and Stollman N. Gastroenterology. 2015 Dec;149(7):1944-9.
3. Gaber CE et al. Ann Intern Med. 2021 Feb 23. doi: 10.7326/M20-6315.
4. Balk EM et al. Management of Colonic Diverticulitis. Comparative Effectiveness Review No. 233. Agency for Healthcare Research and Quality. October 2020. doi: 10.23970/AHRQEPCCER233.
5. Peery AF et al. Gastroenterology. 2021 Feb;160(3):906-11.e1.
Preimplantation genetic testing for aneuploidy
Why does the debate linger after 30 years?
The holy grail of assisted reproductive technology (ART) is the delivery of a healthy child. From the world’s first successful ART cycle of in vitro fertilization in 1978 (3 years later in the United States), the goal of every cycle is to provide the woman with an embryo that has the highest potential for implantation and, ultimately, a single live birth.

Embryo aneuploidy is a major factor in the success of human reproduction. As women age, aneuploidy is reported in less than 30% of women aged younger than 35 years but rises to 90% for those in their mid-40s. Intuitively and through randomized, controlled trials, chromosome testing of embryos is a reasonable approach toward improved cycle outcomes and allows for the transfer of a single euploid embryo.
Recently, the phrase “add-ons” has entered the vernacular of editorials on IVF. These additional procedures are offered to patients with the expectation of improving results, yet many have not been supported by rigorous scientifically controlled research trials, e.g., endometrial scratch, embryo glue, and time-lapse imaging of embryos. Where does preimplantation genetic testing (PGT) belong in the IVF armamentarium and why, after 30 years, are there two diametrically opposed views on its benefit? (We will not address testing for single gene defects or chromosome structural rearrangements.)
How did we get here?
The first iteration of PGT used fluorescence in situ hybridization to not only identify X-linked recessive diseases (Hum Genet. 1992;89:18-22) but also the most common chromosome disorders (13, 18, 21, X, Y) by removing one to two blastomere cells from a day 3 embryo (six- to eight-cell stage). Despite wide enthusiasm, the technique was eventually determined to reduce implantation by nearly 40% and was abandoned; presumably impairing the embryo by removing up to one-third of its make-up.
Because of extended embryo culture to the blastocyst stage along with the improved cryopreservation process of vitrification, the next generation of embryo analysis surfaced, what we now refer to as PGT 2.0. Currently, approximately five to six cells from the outer embryo trophectoderm are removed and sent to a specialized laboratory for 24-chromosome screening while the biopsied embryos are cryopreserved. Outcome data (aneuploidy rates, mosaicism) have been influenced by the evolution of genetic platforms – from array comparative genome hybridization to single-nucleotide polymorphism array, to quantitative polymerase chain reaction, to next-generation sequencing (NGS). The newest platform, NGS with high resolution, provides the most extensive degree of analysis by detecting unbalanced translocations and a low cut-off percentage for mosaicism (20%). The clinical error rate is approximately 1%-2%, improved from the 2%-4% of earlier techniques.
The phenomenon of mosaicism describes two distinct cell lines in one embryo (typically one normal and one abnormal) and is defined based on the percentage of mosaicism – currently, the lower limit is 20%. Embryos with less than 20%-30% mosaicism are considered euploid and those greater than 70%-80% are aneuploid. Of note, clinics that do not request the reporting of mosaicism can result in the potential discarding of embryos labeled as aneuploid that would otherwise have potentially resulted in a live birth. The higher the cut-off value for designating mosaicism, the lower the false-positive rate (declaring an embryo aneuploid when euploid). While there is no safe degree of mosaicism, most transfers have resulted in chromosomally normal infants despite a lower implantation rate and higher miscarriage rate.
Current status
The greatest advantage of PGT for aneuploidy (PGT-A) is its increase in promoting a single embryo transfer. Medical evidence supports pregnancy outcomes equivalent from a single euploid embryo transfer versus a double “untested” embryo transfer.
Only a handful of randomized, controlled trials have evaluated the efficacy of PGT-A. Outcomes have favored improved live birth rates; however, criticism exists for enrolling only good prognosis patients given their high likelihood of developing blastocyst embryos to biopsy. The only trial that used an “intention to treat” protocol (rather than randomization at the time of biopsy) did not demonstrate any difference in live birth or miscarriage comparing embryo selection by PGT-A versus embryo morphology alone. However, post hoc analysis did show a benefit with PGT-A in the 35- to 40-year-old age group, not in the less than 35-year-old group. All other trials demonstrated a reduction in miscarriage with PGT-A but only as a secondary outcome.
The medical literature does not support PGT-A to manage patients with recurrent pregnancy loss and there is no evidence for improvement in women aged less than 35 years or egg donors (F&S Reports. 2021;2:36-42). PGT-A has been effective in patients wishing family balancing.
Controversy
Enthusiasm for PGT-A is countered by lingering concerns. Trophectoderm cells are not in 100% concordance with the inner cell mass, which presumably explains the reports of chromosomally normal live births from the transfer of aneuploid embryos. Biopsy techniques among embryologists are not standardized. As a result, damage to the embryo has been raised as a possible explanation for equivalent pregnancy rates in studies showing no superiority of PGT-A in pregnancy outcome, although this point has recently been refuted.
PGT-A also embraces the “blast-or-bust” credo whereby no embryo transfer occurs unless a blastocyst embryo develops. This continues to beg the unanswerable question – would a woman who did not develop a blastocyst embryo for potential biopsy still conceive if she underwent a day 3 cleavage stage embryo transfer?
Future
Exciting iterations are encroaching for PGT 3.0. One method is blastocyst fluid aspiration to obtain DNA suitable for analysis by molecular genetic methods. Another is noninvasive PGT whereby spent media from the embryo is analyzed using cell-free DNA. Concordance with inner cell mass is reasonably good (approximately 85%) but needs to improve. A major advantage is the biopsy skill set among embryologists is eliminated. A criticism of noninvasive PGT is the risk of false-positive results from contamination of aneuploid cell secretion by physiologic apoptotic cells. Confined placental mosaicism can also increase aneuploidy in cell-free DNA thereby contributing to false positives.
Conclusion
PGT-A is robust technology that appears to benefit women aged above 35 years but not the general infertile population. Error rates must be consistent among laboratories and be lowered. Regarding mosaic embryos, the American Society for Reproductive Medicine guidelines recommend offering another egg retrieval if only mosaic embryos are available and to only consider mosaic embryo transfer following extensive genetic counseling. Long-term effects of PGT-A on children are lacking. The Cochrane Database concluded there was insufficient evidence to make PGT-A routine.
So, the debate is clear and ongoing – universal versus discretionary use of PGT-A? As in all things of life, one size does not fit all, and PGT-A is no exception.
Dr. Trolice is director of Fertility CARE – The IVF Center in Winter Park, Fla., and professor of obstetrics and gynecology at the University of Central Florida, Orlando. Contact him at [email protected].
Why does the debate linger after 30 years?
Why does the debate linger after 30 years?
The holy grail of assisted reproductive technology (ART) is the delivery of a healthy child. From the world’s first successful ART cycle of in vitro fertilization in 1978 (3 years later in the United States), the goal of every cycle is to provide the woman with an embryo that has the highest potential for implantation and, ultimately, a single live birth.
Embryo aneuploidy is a major factor in the success of human reproduction. As women age, aneuploidy is reported in less than 30% of women aged younger than 35 years but rises to 90% for those in their mid-40s. Intuitively and through randomized, controlled trials, chromosome testing of embryos is a reasonable approach toward improved cycle outcomes and allows for the transfer of a single euploid embryo.
Recently, the phrase “add-ons” has entered the vernacular of editorials on IVF. These additional procedures are offered to patients with the expectation of improving results, yet many have not been supported by rigorous scientifically controlled research trials, e.g., endometrial scratch, embryo glue, and time-lapse imaging of embryos. Where does preimplantation genetic testing (PGT) belong in the IVF armamentarium and why, after 30 years, are there two diametrically opposed views on its benefit? (We will not address testing for single gene defects or chromosome structural rearrangements.)
How did we get here?
The first iteration of PGT used fluorescence in situ hybridization to not only identify X-linked recessive diseases (Hum Genet. 1992;89:18-22) but also the most common chromosome disorders (13, 18, 21, X, Y) by removing one to two blastomere cells from a day 3 embryo (six- to eight-cell stage). Despite wide enthusiasm, the technique was eventually determined to reduce implantation by nearly 40% and was abandoned; presumably impairing the embryo by removing up to one-third of its make-up.
Because of extended embryo culture to the blastocyst stage along with the improved cryopreservation process of vitrification, the next generation of embryo analysis surfaced, what we now refer to as PGT 2.0. Currently, approximately five to six cells from the outer embryo trophectoderm are removed and sent to a specialized laboratory for 24-chromosome screening while the biopsied embryos are cryopreserved. Outcome data (aneuploidy rates, mosaicism) have been influenced by the evolution of genetic platforms – from array comparative genome hybridization to single-nucleotide polymorphism array, to quantitative polymerase chain reaction, to next-generation sequencing (NGS). The newest platform, NGS with high resolution, provides the most extensive degree of analysis by detecting unbalanced translocations and a low cut-off percentage for mosaicism (20%). The clinical error rate is approximately 1%-2%, improved from the 2%-4% of earlier techniques.
The phenomenon of mosaicism describes two distinct cell lines in one embryo (typically one normal and one abnormal) and is defined based on the percentage of mosaicism – currently, the lower limit is 20%. Embryos with less than 20%-30% mosaicism are considered euploid and those greater than 70%-80% are aneuploid. Of note, clinics that do not request the reporting of mosaicism can result in the potential discarding of embryos labeled as aneuploid that would otherwise have potentially resulted in a live birth. The higher the cut-off value for designating mosaicism, the lower the false-positive rate (declaring an embryo aneuploid when euploid). While there is no safe degree of mosaicism, most transfers have resulted in chromosomally normal infants despite a lower implantation rate and higher miscarriage rate.
Current status
The greatest advantage of PGT for aneuploidy (PGT-A) is its increase in promoting a single embryo transfer. Medical evidence supports pregnancy outcomes equivalent from a single euploid embryo transfer versus a double “untested” embryo transfer.
Only a handful of randomized, controlled trials have evaluated the efficacy of PGT-A. Outcomes have favored improved live birth rates; however, criticism exists for enrolling only good prognosis patients given their high likelihood of developing blastocyst embryos to biopsy. The only trial that used an “intention to treat” protocol (rather than randomization at the time of biopsy) did not demonstrate any difference in live birth or miscarriage comparing embryo selection by PGT-A versus embryo morphology alone. However, post hoc analysis did show a benefit with PGT-A in the 35- to 40-year-old age group, not in the less than 35-year-old group. All other trials demonstrated a reduction in miscarriage with PGT-A but only as a secondary outcome.
The medical literature does not support PGT-A to manage patients with recurrent pregnancy loss and there is no evidence for improvement in women aged less than 35 years or egg donors (F&S Reports. 2021;2:36-42). PGT-A has been effective in patients wishing family balancing.
Controversy
Enthusiasm for PGT-A is countered by lingering concerns. Trophectoderm cells are not in 100% concordance with the inner cell mass, which presumably explains the reports of chromosomally normal live births from the transfer of aneuploid embryos. Biopsy techniques among embryologists are not standardized. As a result, damage to the embryo has been raised as a possible explanation for equivalent pregnancy rates in studies showing no superiority of PGT-A in pregnancy outcome, although this point has recently been refuted.
PGT-A also embraces the “blast-or-bust” credo whereby no embryo transfer occurs unless a blastocyst embryo develops. This continues to beg the unanswerable question – would a woman who did not develop a blastocyst embryo for potential biopsy still conceive if she underwent a day 3 cleavage stage embryo transfer?
Future
Exciting iterations are encroaching for PGT 3.0. One method is blastocyst fluid aspiration to obtain DNA suitable for analysis by molecular genetic methods. Another is noninvasive PGT whereby spent media from the embryo is analyzed using cell-free DNA. Concordance with inner cell mass is reasonably good (approximately 85%) but needs to improve. A major advantage is the biopsy skill set among embryologists is eliminated. A criticism of noninvasive PGT is the risk of false-positive results from contamination of aneuploid cell secretion by physiologic apoptotic cells. Confined placental mosaicism can also increase aneuploidy in cell-free DNA thereby contributing to false positives.
Conclusion
PGT-A is robust technology that appears to benefit women aged above 35 years but not the general infertile population. Error rates must be consistent among laboratories and be lowered. Regarding mosaic embryos, the American Society for Reproductive Medicine guidelines recommend offering another egg retrieval if only mosaic embryos are available and to only consider mosaic embryo transfer following extensive genetic counseling. Long-term effects of PGT-A on children are lacking. The Cochrane Database concluded there was insufficient evidence to make PGT-A routine.
So, the debate is clear and ongoing – universal versus discretionary use of PGT-A? As in all things of life, one size does not fit all, and PGT-A is no exception.
Dr. Trolice is director of Fertility CARE – The IVF Center in Winter Park, Fla., and professor of obstetrics and gynecology at the University of Central Florida, Orlando. Contact him at [email protected].
The holy grail of assisted reproductive technology (ART) is the delivery of a healthy child. From the world’s first successful ART cycle of in vitro fertilization in 1978 (3 years later in the United States), the goal of every cycle is to provide the woman with an embryo that has the highest potential for implantation and, ultimately, a single live birth.
Embryo aneuploidy is a major factor in the success of human reproduction. As women age, aneuploidy is reported in less than 30% of women aged younger than 35 years but rises to 90% for those in their mid-40s. Intuitively and through randomized, controlled trials, chromosome testing of embryos is a reasonable approach toward improved cycle outcomes and allows for the transfer of a single euploid embryo.
Recently, the phrase “add-ons” has entered the vernacular of editorials on IVF. These additional procedures are offered to patients with the expectation of improving results, yet many have not been supported by rigorous scientifically controlled research trials, e.g., endometrial scratch, embryo glue, and time-lapse imaging of embryos. Where does preimplantation genetic testing (PGT) belong in the IVF armamentarium and why, after 30 years, are there two diametrically opposed views on its benefit? (We will not address testing for single gene defects or chromosome structural rearrangements.)
How did we get here?
The first iteration of PGT used fluorescence in situ hybridization to not only identify X-linked recessive diseases (Hum Genet. 1992;89:18-22) but also the most common chromosome disorders (13, 18, 21, X, Y) by removing one to two blastomere cells from a day 3 embryo (six- to eight-cell stage). Despite wide enthusiasm, the technique was eventually determined to reduce implantation by nearly 40% and was abandoned; presumably impairing the embryo by removing up to one-third of its make-up.
Because of extended embryo culture to the blastocyst stage along with the improved cryopreservation process of vitrification, the next generation of embryo analysis surfaced, what we now refer to as PGT 2.0. Currently, approximately five to six cells from the outer embryo trophectoderm are removed and sent to a specialized laboratory for 24-chromosome screening while the biopsied embryos are cryopreserved. Outcome data (aneuploidy rates, mosaicism) have been influenced by the evolution of genetic platforms – from array comparative genome hybridization to single-nucleotide polymorphism array, to quantitative polymerase chain reaction, to next-generation sequencing (NGS). The newest platform, NGS with high resolution, provides the most extensive degree of analysis by detecting unbalanced translocations and a low cut-off percentage for mosaicism (20%). The clinical error rate is approximately 1%-2%, improved from the 2%-4% of earlier techniques.
The phenomenon of mosaicism describes two distinct cell lines in one embryo (typically one normal and one abnormal) and is defined based on the percentage of mosaicism – currently, the lower limit is 20%. Embryos with less than 20%-30% mosaicism are considered euploid and those greater than 70%-80% are aneuploid. Of note, clinics that do not request the reporting of mosaicism can result in the potential discarding of embryos labeled as aneuploid that would otherwise have potentially resulted in a live birth. The higher the cut-off value for designating mosaicism, the lower the false-positive rate (declaring an embryo aneuploid when euploid). While there is no safe degree of mosaicism, most transfers have resulted in chromosomally normal infants despite a lower implantation rate and higher miscarriage rate.
Current status
The greatest advantage of PGT for aneuploidy (PGT-A) is its increase in promoting a single embryo transfer. Medical evidence supports pregnancy outcomes equivalent from a single euploid embryo transfer versus a double “untested” embryo transfer.
Only a handful of randomized, controlled trials have evaluated the efficacy of PGT-A. Outcomes have favored improved live birth rates; however, criticism exists for enrolling only good prognosis patients given their high likelihood of developing blastocyst embryos to biopsy. The only trial that used an “intention to treat” protocol (rather than randomization at the time of biopsy) did not demonstrate any difference in live birth or miscarriage comparing embryo selection by PGT-A versus embryo morphology alone. However, post hoc analysis did show a benefit with PGT-A in the 35- to 40-year-old age group, not in the less than 35-year-old group. All other trials demonstrated a reduction in miscarriage with PGT-A but only as a secondary outcome.
The medical literature does not support PGT-A to manage patients with recurrent pregnancy loss and there is no evidence for improvement in women aged less than 35 years or egg donors (F&S Reports. 2021;2:36-42). PGT-A has been effective in patients wishing family balancing.
Controversy
Enthusiasm for PGT-A is countered by lingering concerns. Trophectoderm cells are not in 100% concordance with the inner cell mass, which presumably explains the reports of chromosomally normal live births from the transfer of aneuploid embryos. Biopsy techniques among embryologists are not standardized. As a result, damage to the embryo has been raised as a possible explanation for equivalent pregnancy rates in studies showing no superiority of PGT-A in pregnancy outcome, although this point has recently been refuted.
PGT-A also embraces the “blast-or-bust” credo whereby no embryo transfer occurs unless a blastocyst embryo develops. This continues to beg the unanswerable question – would a woman who did not develop a blastocyst embryo for potential biopsy still conceive if she underwent a day 3 cleavage stage embryo transfer?
Future
Exciting iterations are encroaching for PGT 3.0. One method is blastocyst fluid aspiration to obtain DNA suitable for analysis by molecular genetic methods. Another is noninvasive PGT whereby spent media from the embryo is analyzed using cell-free DNA. Concordance with inner cell mass is reasonably good (approximately 85%) but needs to improve. A major advantage is the biopsy skill set among embryologists is eliminated. A criticism of noninvasive PGT is the risk of false-positive results from contamination of aneuploid cell secretion by physiologic apoptotic cells. Confined placental mosaicism can also increase aneuploidy in cell-free DNA thereby contributing to false positives.
Conclusion
PGT-A is robust technology that appears to benefit women aged above 35 years but not the general infertile population. Error rates must be consistent among laboratories and be lowered. Regarding mosaic embryos, the American Society for Reproductive Medicine guidelines recommend offering another egg retrieval if only mosaic embryos are available and to only consider mosaic embryo transfer following extensive genetic counseling. Long-term effects of PGT-A on children are lacking. The Cochrane Database concluded there was insufficient evidence to make PGT-A routine.
So, the debate is clear and ongoing – universal versus discretionary use of PGT-A? As in all things of life, one size does not fit all, and PGT-A is no exception.
Dr. Trolice is director of Fertility CARE – The IVF Center in Winter Park, Fla., and professor of obstetrics and gynecology at the University of Central Florida, Orlando. Contact him at [email protected].
Chauvin guilty verdict: Now it’s time to get to work
On Tuesday, April 20, the country braced for the impact of the trial verdict in death of George Floyd. Despite the case having what many would consider an overwhelming amount of evidence pointing toward conviction, if we’re completely honest, the country – and particularly the African American community – had significant doubts that the jury would render a guilty verdict.

In the hour leading up to the announcement, people and images dominated my thoughts; Tamir Rice, Breonna Taylor, Eric Garner, Rashard Brooks, and most recently, Daunte Wright. With the deaths of these Black Americans and many others as historical context, I took a stoic stance and held my breath as the verdict was read. Former Minneapolis Police Officer Derek Chauvin was found guilty of second-degree murder, third-degree murder, and second-degree manslaughter.
As Mr. Chauvin was remanded to custody and led away in handcuffs, it was clear there were no “winners” in this verdict. Mr. Floyd is still dead, and violent encounters experienced by Black Americans continue at a vastly disproportionate rate. The result is far from true justice, but what we as a country do have is a moment of accountability – and perhaps an opportunity for true system-level reform.
The final report of the President’s Task Force on 21st Century Policing, released in May 2015, recommended major policy changes at the federal level and developed key pillars aimed at promoting effective crime reduction while building public trust. Based on this report, four key takeaways are relevant to any discussion of police reform. All are vitally important, but two stand out as particularly relevant in the aftermath of the verdict. One of the key recommendations was “embracing a guardian – rather than a warrior mindset” in an effort to build trust and legitimacy. Another was ensuring that “peace officer and standards training (POST) boards include mandatory Crisis Intervention Training.”
As health professionals, we know that the ultimate effectiveness of any intervention is based upon the amount of shared trust and collaboration in the patient-physician relationship. As a consultation-liaison psychiatrist, I’ve been trained to recognize that, when requested to consult on a case, I’m frequently not making a medical diagnosis or delivering an intervention; I’m helping the team and patient reestablish trust in each other. Communication skills and techniques help start a dialogue, but you will ultimately fall short of shared understanding without trust. The underpinning of trust could begin with a commitment to procedural justice. Procedural justice, as described in The Justice Collaboratory of Yale Law School, “speaks to the idea of fair processes and how the quality of their experiences strongly impacts people’s perception of fairness.” There are four central tenets of procedural justice:
- Whether they were treated with dignity and respect.
- Whether they were given voice.
- Whether the decision-maker was neutral and transparent.
- Whether the decision-maker conveyed trustworthy motives.
These four tenets have been researched and shown to improve the trust and confidence a community has in police, and lay the foundation for creating a standard set of shared interests and values.

As health professionals, there are many aspects of procedural justice that we can and should embrace, particularly as we come to our reckoning with the use of restraints in medical settings.
Building on the work of the Task Force on 21st Century Policing, the National Initiative for Building Community Trust and Justice, from January 2015 through December 2018, implemented a six-city intervention aimed at generating measurable improvements in officer behavior, public safety, and community trust in police. The National Initiative was organized around three principal ideas: procedural justice, implicit bias training, and reconciliation and candid conversations about law enforcement’s historic role in racial tensions.
In addition to the recommendations of the federal government and independent institutions, national-level health policy organizations have made clear statements regarding police brutality and the need for systemic reform to address police brutality and systemic racism. In 2018, the American Psychiatric Association released a position statement on Police Brutality and Black Males. This was then followed in 2020 with a joint statement from the National Medical Association and the APA condemning systemic racism and police violence against Black Americans. Other health policy associations, including the American Medical Association and the American Association of Medical Colleges, have made clear statements condemning systemic racism and police brutality.
In the aftermath of the verdict, we also saw something very different. In our partisan country, there appeared to be uniform common ground. Statements were made acknowledging the importance of this historic moment, from police unions, and both political parties, and various invested grassroots organizations. In short, we may have true agreement and motivation to take the next hard steps in police reform for this country. There will be policy discussions and new mandates for training, and certainly a push to ban the use of lethal techniques, such as choke holds. While helpful, these will ultimately fall short unless we hold ourselves accountable for a true culture change.
The challenge of implementing procedural justice shouldn’t be just a law enforcement challenge, and it shouldn’t fall on the shoulders of communities with high crime areas. In other words, no single racial group should own it. Ultimately, procedural justice will need to be embraced by all of us.
On April 20, as I watched the verdict, my oldest daughter watched with me, and she asked, “What do you think, Dad?” I responded: “It’s accountability and an opportunity.” She nodded her head with resolve. She then grabbed her smartphone and jumped into social media and proclaimed in her very knowledgeable teenage voice, “See Dad, one voice is cool, but many voices in unison is better; time to get to work!” To Darnella Frazier, who captured the crime on video at age 17, and all in your generation who dare to hold us accountable, I salute you. I thank you for forcing us to look even when it was painful and not ignore the humanity of our fellow man. It is indeed time to get to work.
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.
On Tuesday, April 20, the country braced for the impact of the trial verdict in death of George Floyd. Despite the case having what many would consider an overwhelming amount of evidence pointing toward conviction, if we’re completely honest, the country – and particularly the African American community – had significant doubts that the jury would render a guilty verdict.
In the hour leading up to the announcement, people and images dominated my thoughts; Tamir Rice, Breonna Taylor, Eric Garner, Rashard Brooks, and most recently, Daunte Wright. With the deaths of these Black Americans and many others as historical context, I took a stoic stance and held my breath as the verdict was read. Former Minneapolis Police Officer Derek Chauvin was found guilty of second-degree murder, third-degree murder, and second-degree manslaughter.
As Mr. Chauvin was remanded to custody and led away in handcuffs, it was clear there were no “winners” in this verdict. Mr. Floyd is still dead, and violent encounters experienced by Black Americans continue at a vastly disproportionate rate. The result is far from true justice, but what we as a country do have is a moment of accountability – and perhaps an opportunity for true system-level reform.
The final report of the President’s Task Force on 21st Century Policing, released in May 2015, recommended major policy changes at the federal level and developed key pillars aimed at promoting effective crime reduction while building public trust. Based on this report, four key takeaways are relevant to any discussion of police reform. All are vitally important, but two stand out as particularly relevant in the aftermath of the verdict. One of the key recommendations was “embracing a guardian – rather than a warrior mindset” in an effort to build trust and legitimacy. Another was ensuring that “peace officer and standards training (POST) boards include mandatory Crisis Intervention Training.”
As health professionals, we know that the ultimate effectiveness of any intervention is based upon the amount of shared trust and collaboration in the patient-physician relationship. As a consultation-liaison psychiatrist, I’ve been trained to recognize that, when requested to consult on a case, I’m frequently not making a medical diagnosis or delivering an intervention; I’m helping the team and patient reestablish trust in each other. Communication skills and techniques help start a dialogue, but you will ultimately fall short of shared understanding without trust. The underpinning of trust could begin with a commitment to procedural justice. Procedural justice, as described in The Justice Collaboratory of Yale Law School, “speaks to the idea of fair processes and how the quality of their experiences strongly impacts people’s perception of fairness.” There are four central tenets of procedural justice:
- Whether they were treated with dignity and respect.
- Whether they were given voice.
- Whether the decision-maker was neutral and transparent.
- Whether the decision-maker conveyed trustworthy motives.
These four tenets have been researched and shown to improve the trust and confidence a community has in police, and lay the foundation for creating a standard set of shared interests and values.
As health professionals, there are many aspects of procedural justice that we can and should embrace, particularly as we come to our reckoning with the use of restraints in medical settings.
Building on the work of the Task Force on 21st Century Policing, the National Initiative for Building Community Trust and Justice, from January 2015 through December 2018, implemented a six-city intervention aimed at generating measurable improvements in officer behavior, public safety, and community trust in police. The National Initiative was organized around three principal ideas: procedural justice, implicit bias training, and reconciliation and candid conversations about law enforcement’s historic role in racial tensions.
In addition to the recommendations of the federal government and independent institutions, national-level health policy organizations have made clear statements regarding police brutality and the need for systemic reform to address police brutality and systemic racism. In 2018, the American Psychiatric Association released a position statement on Police Brutality and Black Males. This was then followed in 2020 with a joint statement from the National Medical Association and the APA condemning systemic racism and police violence against Black Americans. Other health policy associations, including the American Medical Association and the American Association of Medical Colleges, have made clear statements condemning systemic racism and police brutality.
In the aftermath of the verdict, we also saw something very different. In our partisan country, there appeared to be uniform common ground. Statements were made acknowledging the importance of this historic moment, from police unions, and both political parties, and various invested grassroots organizations. In short, we may have true agreement and motivation to take the next hard steps in police reform for this country. There will be policy discussions and new mandates for training, and certainly a push to ban the use of lethal techniques, such as choke holds. While helpful, these will ultimately fall short unless we hold ourselves accountable for a true culture change.
The challenge of implementing procedural justice shouldn’t be just a law enforcement challenge, and it shouldn’t fall on the shoulders of communities with high crime areas. In other words, no single racial group should own it. Ultimately, procedural justice will need to be embraced by all of us.
On April 20, as I watched the verdict, my oldest daughter watched with me, and she asked, “What do you think, Dad?” I responded: “It’s accountability and an opportunity.” She nodded her head with resolve. She then grabbed her smartphone and jumped into social media and proclaimed in her very knowledgeable teenage voice, “See Dad, one voice is cool, but many voices in unison is better; time to get to work!” To Darnella Frazier, who captured the crime on video at age 17, and all in your generation who dare to hold us accountable, I salute you. I thank you for forcing us to look even when it was painful and not ignore the humanity of our fellow man. It is indeed time to get to work.
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.
On Tuesday, April 20, the country braced for the impact of the trial verdict in death of George Floyd. Despite the case having what many would consider an overwhelming amount of evidence pointing toward conviction, if we’re completely honest, the country – and particularly the African American community – had significant doubts that the jury would render a guilty verdict.
In the hour leading up to the announcement, people and images dominated my thoughts; Tamir Rice, Breonna Taylor, Eric Garner, Rashard Brooks, and most recently, Daunte Wright. With the deaths of these Black Americans and many others as historical context, I took a stoic stance and held my breath as the verdict was read. Former Minneapolis Police Officer Derek Chauvin was found guilty of second-degree murder, third-degree murder, and second-degree manslaughter.
As Mr. Chauvin was remanded to custody and led away in handcuffs, it was clear there were no “winners” in this verdict. Mr. Floyd is still dead, and violent encounters experienced by Black Americans continue at a vastly disproportionate rate. The result is far from true justice, but what we as a country do have is a moment of accountability – and perhaps an opportunity for true system-level reform.
The final report of the President’s Task Force on 21st Century Policing, released in May 2015, recommended major policy changes at the federal level and developed key pillars aimed at promoting effective crime reduction while building public trust. Based on this report, four key takeaways are relevant to any discussion of police reform. All are vitally important, but two stand out as particularly relevant in the aftermath of the verdict. One of the key recommendations was “embracing a guardian – rather than a warrior mindset” in an effort to build trust and legitimacy. Another was ensuring that “peace officer and standards training (POST) boards include mandatory Crisis Intervention Training.”
As health professionals, we know that the ultimate effectiveness of any intervention is based upon the amount of shared trust and collaboration in the patient-physician relationship. As a consultation-liaison psychiatrist, I’ve been trained to recognize that, when requested to consult on a case, I’m frequently not making a medical diagnosis or delivering an intervention; I’m helping the team and patient reestablish trust in each other. Communication skills and techniques help start a dialogue, but you will ultimately fall short of shared understanding without trust. The underpinning of trust could begin with a commitment to procedural justice. Procedural justice, as described in The Justice Collaboratory of Yale Law School, “speaks to the idea of fair processes and how the quality of their experiences strongly impacts people’s perception of fairness.” There are four central tenets of procedural justice:
- Whether they were treated with dignity and respect.
- Whether they were given voice.
- Whether the decision-maker was neutral and transparent.
- Whether the decision-maker conveyed trustworthy motives.
These four tenets have been researched and shown to improve the trust and confidence a community has in police, and lay the foundation for creating a standard set of shared interests and values.
As health professionals, there are many aspects of procedural justice that we can and should embrace, particularly as we come to our reckoning with the use of restraints in medical settings.
Building on the work of the Task Force on 21st Century Policing, the National Initiative for Building Community Trust and Justice, from January 2015 through December 2018, implemented a six-city intervention aimed at generating measurable improvements in officer behavior, public safety, and community trust in police. The National Initiative was organized around three principal ideas: procedural justice, implicit bias training, and reconciliation and candid conversations about law enforcement’s historic role in racial tensions.
In addition to the recommendations of the federal government and independent institutions, national-level health policy organizations have made clear statements regarding police brutality and the need for systemic reform to address police brutality and systemic racism. In 2018, the American Psychiatric Association released a position statement on Police Brutality and Black Males. This was then followed in 2020 with a joint statement from the National Medical Association and the APA condemning systemic racism and police violence against Black Americans. Other health policy associations, including the American Medical Association and the American Association of Medical Colleges, have made clear statements condemning systemic racism and police brutality.
In the aftermath of the verdict, we also saw something very different. In our partisan country, there appeared to be uniform common ground. Statements were made acknowledging the importance of this historic moment, from police unions, and both political parties, and various invested grassroots organizations. In short, we may have true agreement and motivation to take the next hard steps in police reform for this country. There will be policy discussions and new mandates for training, and certainly a push to ban the use of lethal techniques, such as choke holds. While helpful, these will ultimately fall short unless we hold ourselves accountable for a true culture change.
The challenge of implementing procedural justice shouldn’t be just a law enforcement challenge, and it shouldn’t fall on the shoulders of communities with high crime areas. In other words, no single racial group should own it. Ultimately, procedural justice will need to be embraced by all of us.
On April 20, as I watched the verdict, my oldest daughter watched with me, and she asked, “What do you think, Dad?” I responded: “It’s accountability and an opportunity.” She nodded her head with resolve. She then grabbed her smartphone and jumped into social media and proclaimed in her very knowledgeable teenage voice, “See Dad, one voice is cool, but many voices in unison is better; time to get to work!” To Darnella Frazier, who captured the crime on video at age 17, and all in your generation who dare to hold us accountable, I salute you. I thank you for forcing us to look even when it was painful and not ignore the humanity of our fellow man. It is indeed time to get to work.
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.

Antifungals during pregnancy and breastfeeding
There are three general classes of antifungal agents (number of agents): azole antifungals (9), echinocandins (3), and polyenes (5). The azole antifungals contain an azole ring and inhibit a wide range of fungi. Echinocandins target the fungal cell wall and the polyenes increase the fungal membrane permeability and lead to cell death.

Pregnancy
Azole antifungals inhibit the growth of fungi. Their trade names and molecular weights:
- Clotrimazole (Mycelex), an over-the-counter product, is available as a topical cream. Several studies have found no association between the drug and birth defects.
- Fluconazole (Diflucan) is a teratogen when doses of ≥400 mg/day are used during the first trimester. Smaller doses do not appear to cause embryo/fetal harm.
- Isavuconazonium (Cresemba) if used in pregnancy, exposure of the embryo/fetus would probably be low based on the >99% plasma protein binding, but the plasma half-life is 130 hours. Moreover, the drug is a potent animal teratogen and is best avoided in pregnancy.
- Itraconazole (Onmel, Sporanox, Tolsura), has a low risk, if any, of structural defects, according to what reported human experience suggests.
- Ketoconazole (Xolegel, Extina, Nizoral; 531) does not appear to adversely effect embryos and fetuses, but the human data are very limited. As with any drug, avoiding organogenesis is the best recommendation.
- Miconazole (Oravig) is usually used topically. Small amounts are absorbed from the vagina. The available evidence suggests that the drug does not increase the risk of congenital malformations.
- Posaconazole (Noxafil) does not have reported use in human pregnancy. The animal reproduction data suggest risk. Based on its molecular weight (about 701), the drug will most likely cross the placenta to the embryo/fetus. Thus, the best course is to avoid the drug during pregnancy, especially in the first trimester.
- Voriconazole (Vfend) has one human report of the drug use in pregnancy. The drug was started at about 19 weeks and continued until the woman gave birth at 35 weeks to a healthy male baby. At 6 months of age, the baby remained normal.
Echinocandin antifungals target the fungal cell wall by inhibiting its synthesis. Their trade names and molecular weights:
- Anidulafungin (Eraxis; 1,140) has no published human data. It is indicated for the treatment of candidemia and other forms of Candida infections. The animal data suggest low risk.
- Caspofungin (Cancidas; 1,213) has no published human data. It is indicated for presumed fungal infections in febrile, neutropenic patients. The animal data are suggestive of human risk, especially if exposure occurs in the first trimester. If possible, maternal treatment should be avoided in the first trimester.
- Micafungin (Mycamine; 1,292) has no published human data. It is indicated for the treatment of patients with esophageal candidiasis and for the prophylaxis of Candida infections in patients undergoing hematopoietic stem cell transplantation. The animal data in one species suggest high risk. If possible, maternal treatment should be avoided in the first trimester.
Polyene antifungals cause depolarization of the fungal cell membrane to increase the membrane permeability, which leads to cell death. Their trade names and molecular weights:
- Amphotericin b (Amphocin; Fungizone; 924) There are three other amphotericin agents: amphotericin b cholesteryl sulfate (Amphotec); amphotericin b lipid complex (Abelcet); amphotericin b liposomal (AmBisome). No reports linking amphotericin b with congenital defects have been found. The drug does cross the human placenta. Although there was a higher rate of spontaneous abortions in rabbits given amphotericin b, there was no fetal harm in rats and rabbits when given amphotericin b lipid complex.
- Nystatin (Bio-Statin; Mycostatin; Nilstat; 926). The drug does not appear to cause embryo-fetal harm. Based on published data, the drug can be used at any time in pregnancy.
Breastfeeding
Small amounts of all the above drugs are probably excreted into breast milk if they are used close to breastfeeding. Most can probably be used during breastfeeding, but there are no data for any of these agents. The safest decision is to not use these drugs when breastfeeding.
Mr. Briggs is clinical professor of pharmacy at the University of California, San Francisco, and adjunct professor of pharmacy at the University of Southern California, Los Angeles, as well as at Washington State University, Spokane. Mr. Briggs said he had no relevant financial disclosures. Email him at [email protected].
There are three general classes of antifungal agents (number of agents): azole antifungals (9), echinocandins (3), and polyenes (5). The azole antifungals contain an azole ring and inhibit a wide range of fungi. Echinocandins target the fungal cell wall and the polyenes increase the fungal membrane permeability and lead to cell death.
Pregnancy
Azole antifungals inhibit the growth of fungi. Their trade names and molecular weights:
- Clotrimazole (Mycelex), an over-the-counter product, is available as a topical cream. Several studies have found no association between the drug and birth defects.
- Fluconazole (Diflucan) is a teratogen when doses of ≥400 mg/day are used during the first trimester. Smaller doses do not appear to cause embryo/fetal harm.
- Isavuconazonium (Cresemba) if used in pregnancy, exposure of the embryo/fetus would probably be low based on the >99% plasma protein binding, but the plasma half-life is 130 hours. Moreover, the drug is a potent animal teratogen and is best avoided in pregnancy.
- Itraconazole (Onmel, Sporanox, Tolsura), has a low risk, if any, of structural defects, according to what reported human experience suggests.
- Ketoconazole (Xolegel, Extina, Nizoral; 531) does not appear to adversely effect embryos and fetuses, but the human data are very limited. As with any drug, avoiding organogenesis is the best recommendation.
- Miconazole (Oravig) is usually used topically. Small amounts are absorbed from the vagina. The available evidence suggests that the drug does not increase the risk of congenital malformations.
- Posaconazole (Noxafil) does not have reported use in human pregnancy. The animal reproduction data suggest risk. Based on its molecular weight (about 701), the drug will most likely cross the placenta to the embryo/fetus. Thus, the best course is to avoid the drug during pregnancy, especially in the first trimester.
- Voriconazole (Vfend) has one human report of the drug use in pregnancy. The drug was started at about 19 weeks and continued until the woman gave birth at 35 weeks to a healthy male baby. At 6 months of age, the baby remained normal.
Echinocandin antifungals target the fungal cell wall by inhibiting its synthesis. Their trade names and molecular weights:
- Anidulafungin (Eraxis; 1,140) has no published human data. It is indicated for the treatment of candidemia and other forms of Candida infections. The animal data suggest low risk.
- Caspofungin (Cancidas; 1,213) has no published human data. It is indicated for presumed fungal infections in febrile, neutropenic patients. The animal data are suggestive of human risk, especially if exposure occurs in the first trimester. If possible, maternal treatment should be avoided in the first trimester.
- Micafungin (Mycamine; 1,292) has no published human data. It is indicated for the treatment of patients with esophageal candidiasis and for the prophylaxis of Candida infections in patients undergoing hematopoietic stem cell transplantation. The animal data in one species suggest high risk. If possible, maternal treatment should be avoided in the first trimester.
Polyene antifungals cause depolarization of the fungal cell membrane to increase the membrane permeability, which leads to cell death. Their trade names and molecular weights:
- Amphotericin b (Amphocin; Fungizone; 924) There are three other amphotericin agents: amphotericin b cholesteryl sulfate (Amphotec); amphotericin b lipid complex (Abelcet); amphotericin b liposomal (AmBisome). No reports linking amphotericin b with congenital defects have been found. The drug does cross the human placenta. Although there was a higher rate of spontaneous abortions in rabbits given amphotericin b, there was no fetal harm in rats and rabbits when given amphotericin b lipid complex.
- Nystatin (Bio-Statin; Mycostatin; Nilstat; 926). The drug does not appear to cause embryo-fetal harm. Based on published data, the drug can be used at any time in pregnancy.
Breastfeeding
Small amounts of all the above drugs are probably excreted into breast milk if they are used close to breastfeeding. Most can probably be used during breastfeeding, but there are no data for any of these agents. The safest decision is to not use these drugs when breastfeeding.
Mr. Briggs is clinical professor of pharmacy at the University of California, San Francisco, and adjunct professor of pharmacy at the University of Southern California, Los Angeles, as well as at Washington State University, Spokane. Mr. Briggs said he had no relevant financial disclosures. Email him at [email protected].
There are three general classes of antifungal agents (number of agents): azole antifungals (9), echinocandins (3), and polyenes (5). The azole antifungals contain an azole ring and inhibit a wide range of fungi. Echinocandins target the fungal cell wall and the polyenes increase the fungal membrane permeability and lead to cell death.
Pregnancy
Azole antifungals inhibit the growth of fungi. Their trade names and molecular weights:
- Clotrimazole (Mycelex), an over-the-counter product, is available as a topical cream. Several studies have found no association between the drug and birth defects.
- Fluconazole (Diflucan) is a teratogen when doses of ≥400 mg/day are used during the first trimester. Smaller doses do not appear to cause embryo/fetal harm.
- Isavuconazonium (Cresemba) if used in pregnancy, exposure of the embryo/fetus would probably be low based on the >99% plasma protein binding, but the plasma half-life is 130 hours. Moreover, the drug is a potent animal teratogen and is best avoided in pregnancy.
- Itraconazole (Onmel, Sporanox, Tolsura), has a low risk, if any, of structural defects, according to what reported human experience suggests.
- Ketoconazole (Xolegel, Extina, Nizoral; 531) does not appear to adversely effect embryos and fetuses, but the human data are very limited. As with any drug, avoiding organogenesis is the best recommendation.
- Miconazole (Oravig) is usually used topically. Small amounts are absorbed from the vagina. The available evidence suggests that the drug does not increase the risk of congenital malformations.
- Posaconazole (Noxafil) does not have reported use in human pregnancy. The animal reproduction data suggest risk. Based on its molecular weight (about 701), the drug will most likely cross the placenta to the embryo/fetus. Thus, the best course is to avoid the drug during pregnancy, especially in the first trimester.
- Voriconazole (Vfend) has one human report of the drug use in pregnancy. The drug was started at about 19 weeks and continued until the woman gave birth at 35 weeks to a healthy male baby. At 6 months of age, the baby remained normal.
Echinocandin antifungals target the fungal cell wall by inhibiting its synthesis. Their trade names and molecular weights:
- Anidulafungin (Eraxis; 1,140) has no published human data. It is indicated for the treatment of candidemia and other forms of Candida infections. The animal data suggest low risk.
- Caspofungin (Cancidas; 1,213) has no published human data. It is indicated for presumed fungal infections in febrile, neutropenic patients. The animal data are suggestive of human risk, especially if exposure occurs in the first trimester. If possible, maternal treatment should be avoided in the first trimester.
- Micafungin (Mycamine; 1,292) has no published human data. It is indicated for the treatment of patients with esophageal candidiasis and for the prophylaxis of Candida infections in patients undergoing hematopoietic stem cell transplantation. The animal data in one species suggest high risk. If possible, maternal treatment should be avoided in the first trimester.
Polyene antifungals cause depolarization of the fungal cell membrane to increase the membrane permeability, which leads to cell death. Their trade names and molecular weights:
- Amphotericin b (Amphocin; Fungizone; 924) There are three other amphotericin agents: amphotericin b cholesteryl sulfate (Amphotec); amphotericin b lipid complex (Abelcet); amphotericin b liposomal (AmBisome). No reports linking amphotericin b with congenital defects have been found. The drug does cross the human placenta. Although there was a higher rate of spontaneous abortions in rabbits given amphotericin b, there was no fetal harm in rats and rabbits when given amphotericin b lipid complex.
- Nystatin (Bio-Statin; Mycostatin; Nilstat; 926). The drug does not appear to cause embryo-fetal harm. Based on published data, the drug can be used at any time in pregnancy.
Breastfeeding
Small amounts of all the above drugs are probably excreted into breast milk if they are used close to breastfeeding. Most can probably be used during breastfeeding, but there are no data for any of these agents. The safest decision is to not use these drugs when breastfeeding.
Mr. Briggs is clinical professor of pharmacy at the University of California, San Francisco, and adjunct professor of pharmacy at the University of Southern California, Los Angeles, as well as at Washington State University, Spokane. Mr. Briggs said he had no relevant financial disclosures. Email him at [email protected].
VEXAS syndrome: Implications for dermatologists
When I was a medical student, I always found it gratifying when there was a unifying mechanism that explained the symptoms of a disease. Part of the reason I chose dermatology as a specialty was how frequently we are able to “see” these mechanisms in the skin, both clinically and histologically. What’s even more interesting is that this condition is caused by a postzygotic somatic mutation, an apparently underrecognized cause of disease that we are just now beginning to understand. An example of a postzygotic somatic mutation causing a disease that we all learned about in medical school is paroxysmal nocturnal hemoglobinuria.

Using a “bottom-up” approach, researchers at the National Institutes of Health and in the United Kingdom identified 25 patients with somatic UBA1 mutations and noticed that they had strikingly similar autoinflammatory syndromes. UBA1 encodes ubiquitin E1, which is part of the pathway the breaks down proteins as part of the normal cellular machine. It is localized to the X chromosome, so all 25 affected patients were males, and most were aged between 40 and 70 years. These patients had an autoinflammatory syndrome characterized by fever, chondritis (similar to relapsing polychondritis), vasculitis, and neutrophilic dermatoses. Many patients also had features of myelodysplastic syndrome and plasma cell dyscrasia. The inflammatory pattern in this condition seems to show elevations in tumor necrosis factor, interleukin-6, and interferon-gamma.
So why is this syndrome relevant to dermatology? We are often asked to evaluate patients for neutrophilic dermatosis and vasculitis, and many affected patients had clinical and histologic findings compatible with polyarteritis nodosa and Sweet syndrome. When confronted with a neutrophilic dermatosis, we’ve all been taught to evaluate for myelodysplastic syndrome, which many of these patients appeared to have, at least on the surface. When bone marrow biopsies were done, the myeloid cell precursors that give rise to neutrophils were noted to have prominent cytoplasmic vacuoles, hence the “V” in VEXAS.
In reading the article describing 25 patients with this syndrome, which was published in the New England Journal of Medicine, I was struck by how refractory they were to treatment. Most patients had been treated with systemic steroids, multiple biologics, and several nonbiologic medications that are mainstays of treatment for neutrophilic dermatosis like dapsone and colchicine. I was fortunate enough to speak to Amanda Ombrello, MD, of the National Human Genome Research Institute, one of the lead authors of the paper, who drew my attention to the supplementary appendix, which showed the marked injection-site reactions some patients had to anakinra – yet another reason why a patient might end up in a dermatology clinic. In my mind, all of these features could be a clue to a diagnosis of VEXAS syndrome.
Many patients seemed to fare poorly, with 40% of patients dying before the completion of the study. When it comes to extremely rare diseases, it seems that the more physicians who are aware of the existence of a particular syndrome, the more likely it is a patient will come under our care and be correctly diagnosed.
Dr. Saardi is a dermatologist and internist, and is director of the inpatient dermatology service at the George Washington University Hospital, Washington. He has no disclosures.
When I was a medical student, I always found it gratifying when there was a unifying mechanism that explained the symptoms of a disease. Part of the reason I chose dermatology as a specialty was how frequently we are able to “see” these mechanisms in the skin, both clinically and histologically. What’s even more interesting is that this condition is caused by a postzygotic somatic mutation, an apparently underrecognized cause of disease that we are just now beginning to understand. An example of a postzygotic somatic mutation causing a disease that we all learned about in medical school is paroxysmal nocturnal hemoglobinuria.
Using a “bottom-up” approach, researchers at the National Institutes of Health and in the United Kingdom identified 25 patients with somatic UBA1 mutations and noticed that they had strikingly similar autoinflammatory syndromes. UBA1 encodes ubiquitin E1, which is part of the pathway the breaks down proteins as part of the normal cellular machine. It is localized to the X chromosome, so all 25 affected patients were males, and most were aged between 40 and 70 years. These patients had an autoinflammatory syndrome characterized by fever, chondritis (similar to relapsing polychondritis), vasculitis, and neutrophilic dermatoses. Many patients also had features of myelodysplastic syndrome and plasma cell dyscrasia. The inflammatory pattern in this condition seems to show elevations in tumor necrosis factor, interleukin-6, and interferon-gamma.
So why is this syndrome relevant to dermatology? We are often asked to evaluate patients for neutrophilic dermatosis and vasculitis, and many affected patients had clinical and histologic findings compatible with polyarteritis nodosa and Sweet syndrome. When confronted with a neutrophilic dermatosis, we’ve all been taught to evaluate for myelodysplastic syndrome, which many of these patients appeared to have, at least on the surface. When bone marrow biopsies were done, the myeloid cell precursors that give rise to neutrophils were noted to have prominent cytoplasmic vacuoles, hence the “V” in VEXAS.
In reading the article describing 25 patients with this syndrome, which was published in the New England Journal of Medicine, I was struck by how refractory they were to treatment. Most patients had been treated with systemic steroids, multiple biologics, and several nonbiologic medications that are mainstays of treatment for neutrophilic dermatosis like dapsone and colchicine. I was fortunate enough to speak to Amanda Ombrello, MD, of the National Human Genome Research Institute, one of the lead authors of the paper, who drew my attention to the supplementary appendix, which showed the marked injection-site reactions some patients had to anakinra – yet another reason why a patient might end up in a dermatology clinic. In my mind, all of these features could be a clue to a diagnosis of VEXAS syndrome.
Many patients seemed to fare poorly, with 40% of patients dying before the completion of the study. When it comes to extremely rare diseases, it seems that the more physicians who are aware of the existence of a particular syndrome, the more likely it is a patient will come under our care and be correctly diagnosed.
Dr. Saardi is a dermatologist and internist, and is director of the inpatient dermatology service at the George Washington University Hospital, Washington. He has no disclosures.
When I was a medical student, I always found it gratifying when there was a unifying mechanism that explained the symptoms of a disease. Part of the reason I chose dermatology as a specialty was how frequently we are able to “see” these mechanisms in the skin, both clinically and histologically. What’s even more interesting is that this condition is caused by a postzygotic somatic mutation, an apparently underrecognized cause of disease that we are just now beginning to understand. An example of a postzygotic somatic mutation causing a disease that we all learned about in medical school is paroxysmal nocturnal hemoglobinuria.
Using a “bottom-up” approach, researchers at the National Institutes of Health and in the United Kingdom identified 25 patients with somatic UBA1 mutations and noticed that they had strikingly similar autoinflammatory syndromes. UBA1 encodes ubiquitin E1, which is part of the pathway the breaks down proteins as part of the normal cellular machine. It is localized to the X chromosome, so all 25 affected patients were males, and most were aged between 40 and 70 years. These patients had an autoinflammatory syndrome characterized by fever, chondritis (similar to relapsing polychondritis), vasculitis, and neutrophilic dermatoses. Many patients also had features of myelodysplastic syndrome and plasma cell dyscrasia. The inflammatory pattern in this condition seems to show elevations in tumor necrosis factor, interleukin-6, and interferon-gamma.
So why is this syndrome relevant to dermatology? We are often asked to evaluate patients for neutrophilic dermatosis and vasculitis, and many affected patients had clinical and histologic findings compatible with polyarteritis nodosa and Sweet syndrome. When confronted with a neutrophilic dermatosis, we’ve all been taught to evaluate for myelodysplastic syndrome, which many of these patients appeared to have, at least on the surface. When bone marrow biopsies were done, the myeloid cell precursors that give rise to neutrophils were noted to have prominent cytoplasmic vacuoles, hence the “V” in VEXAS.
In reading the article describing 25 patients with this syndrome, which was published in the New England Journal of Medicine, I was struck by how refractory they were to treatment. Most patients had been treated with systemic steroids, multiple biologics, and several nonbiologic medications that are mainstays of treatment for neutrophilic dermatosis like dapsone and colchicine. I was fortunate enough to speak to Amanda Ombrello, MD, of the National Human Genome Research Institute, one of the lead authors of the paper, who drew my attention to the supplementary appendix, which showed the marked injection-site reactions some patients had to anakinra – yet another reason why a patient might end up in a dermatology clinic. In my mind, all of these features could be a clue to a diagnosis of VEXAS syndrome.
Many patients seemed to fare poorly, with 40% of patients dying before the completion of the study. When it comes to extremely rare diseases, it seems that the more physicians who are aware of the existence of a particular syndrome, the more likely it is a patient will come under our care and be correctly diagnosed.
Dr. Saardi is a dermatologist and internist, and is director of the inpatient dermatology service at the George Washington University Hospital, Washington. He has no disclosures.