User login
Who is my neighbor? The ethics of sharing medical resources in the world
India is in a crisis as the burden of COVID-19 has collapsed parts of the health care system. There are not enough beds, not enough oxygen, and not enough crematoria to handle the pandemic. India is also a major supplier of vaccines for itself and many other countries. That production capacity has also been affected by the local events, further worsening the response to the pandemic over the next few months.

This collapse is the specter that, in April 2020, placed a hospital ship next to Manhattan and rows of beds in its convention center. Fortunately, the lockdown in March 2020 sufficiently flattened the curve. The city avoided utilizing that disaster capacity, though many New Yorkers died out of sight in nursing homes. When the third and largest wave of cases in the United States peaked in January 2021, hospitals throughout California reached capacity but avoided bursting. In April 2021, localized outbreaks in Michigan, Arizona, and Ontario again tested the maximum capacity for providing modern medical treatments. Great Britain used a second lockdown in October 2020 and a third in January 2021 to control the pandemic, with Prime Minister Boris Johnson emphasizing that it was these social interventions, and not vaccines, which provided the mitigating effects. Other European Union nations adopted similar strategies. Prudent choices by government guided by science, combined with the cooperation of the public, have been and still are crucial to mollify the pandemic.
There is hope that soon vaccines will return daily life to a new normal. In the United States, the Centers for Disease Control and Prevention has loosened restrictions on social gathering. An increase in daily new cases of COVID-19 in April 2021 has turned into just a blip before continuing to recede. Perhaps that is the first sign of vaccination working at the level of public health. However, the May 2021 lockdown in highly vaccinated Seychelles is a warning that the danger remains. A single match can start a huge forest fire. The first 150 million cases of COVID-19 worldwide have, through natural rates of mutation, produced several variants that might partially evade current vaccines. The danger of newer variants persists with the next 150 million cases as the pandemic continues to rage in many nations which are just one airplane ride away. All human inhabitants of this blue-covered third rock from the sun are interconnected.
The benefits of scientific advancement have been extolled for centuries. This includes both individual discoveries as well as a mindset that favors rationalism over fatalism. On the whole, the benefits of scientific progress outweigh the negatives. Negative environmental impacts include pollution and climate change. Economic impacts include raising the mean economic standard of living but with greater inequity. Historically, governmental and social institutions have attempted to mitigate these negative consequences. Those efforts have attempted to provide guidance and a moral compass to direct the progress of scientific advancement, particularly in fields like gene therapy. Those efforts have called upon developed nations to share the bounties of progress with other nations.
Modern medicine has provided the fruit of these scientific advancements to a limited fraction of the world’s population during the 20th century. The improvements in life expectancy and infant mortality have come primarily from civil engineers getting running water into cities and sewage out. A smaller portion of the benefits are from public health measures that reduced tuberculosis, smallpox, polio, and measles. Agriculture became more reliable, productive, and nutritious. In the 21st century, medical care (control of hypertension, diabetes, and clotting) aimed at reducing heart disease and strokes have added another 2-3 years to the life expectancy in the United States, with much of that benefit erased by the epidemics of obesity and opioid abuse.
Modern medical technology has created treatments that cost $10,000 a month to add a few extra months of life to geriatric patients with terminal cancer. Meanwhile, in more mundane care, efforts like Choosing Wisely seek to save money wasted on low-value, useless, and even harmful tests and therapies. There is no single person or agency managing this chaotic process of inventing expensive new technologies while inadequately addressing the widespread shortages of mental health care, disparities in education, and other social determinants of health. The pandemic has highlighted these preexisting weaknesses in the social fabric.
The cries from India have been accompanied by voices of anger from India and other nations accusing the United States of hoarding vaccines and the raw materials needed to produce them. This has been called vaccine apartheid. The United States is not alone in its political decision to prioritize domestic interests over international ones; India’s recent government is similarly nationalistic. Scientists warn that no one is safe locally as long as the pandemic rages in other countries. The Biden administration, in a delayed response to the crisis in India, finally announced plans to share some unused vaccines (of a brand not yet Food and Drug Administration approved) as well as some vaccine raw materials whose export was forbidden by a regulation under the Defense Production Act. Reading below the headlines, the promised response won’t be implemented for weeks or months. We must do better.
The logistics of sharing the benefits of advanced science are complicated. The ethics are not. Who is my neighbor? If you didn’t learn the answer to that in Sunday school, there isn’t much more I can say.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no financial disclosures, Email him at [email protected]
India is in a crisis as the burden of COVID-19 has collapsed parts of the health care system. There are not enough beds, not enough oxygen, and not enough crematoria to handle the pandemic. India is also a major supplier of vaccines for itself and many other countries. That production capacity has also been affected by the local events, further worsening the response to the pandemic over the next few months.
This collapse is the specter that, in April 2020, placed a hospital ship next to Manhattan and rows of beds in its convention center. Fortunately, the lockdown in March 2020 sufficiently flattened the curve. The city avoided utilizing that disaster capacity, though many New Yorkers died out of sight in nursing homes. When the third and largest wave of cases in the United States peaked in January 2021, hospitals throughout California reached capacity but avoided bursting. In April 2021, localized outbreaks in Michigan, Arizona, and Ontario again tested the maximum capacity for providing modern medical treatments. Great Britain used a second lockdown in October 2020 and a third in January 2021 to control the pandemic, with Prime Minister Boris Johnson emphasizing that it was these social interventions, and not vaccines, which provided the mitigating effects. Other European Union nations adopted similar strategies. Prudent choices by government guided by science, combined with the cooperation of the public, have been and still are crucial to mollify the pandemic.
There is hope that soon vaccines will return daily life to a new normal. In the United States, the Centers for Disease Control and Prevention has loosened restrictions on social gathering. An increase in daily new cases of COVID-19 in April 2021 has turned into just a blip before continuing to recede. Perhaps that is the first sign of vaccination working at the level of public health. However, the May 2021 lockdown in highly vaccinated Seychelles is a warning that the danger remains. A single match can start a huge forest fire. The first 150 million cases of COVID-19 worldwide have, through natural rates of mutation, produced several variants that might partially evade current vaccines. The danger of newer variants persists with the next 150 million cases as the pandemic continues to rage in many nations which are just one airplane ride away. All human inhabitants of this blue-covered third rock from the sun are interconnected.
The benefits of scientific advancement have been extolled for centuries. This includes both individual discoveries as well as a mindset that favors rationalism over fatalism. On the whole, the benefits of scientific progress outweigh the negatives. Negative environmental impacts include pollution and climate change. Economic impacts include raising the mean economic standard of living but with greater inequity. Historically, governmental and social institutions have attempted to mitigate these negative consequences. Those efforts have attempted to provide guidance and a moral compass to direct the progress of scientific advancement, particularly in fields like gene therapy. Those efforts have called upon developed nations to share the bounties of progress with other nations.
Modern medicine has provided the fruit of these scientific advancements to a limited fraction of the world’s population during the 20th century. The improvements in life expectancy and infant mortality have come primarily from civil engineers getting running water into cities and sewage out. A smaller portion of the benefits are from public health measures that reduced tuberculosis, smallpox, polio, and measles. Agriculture became more reliable, productive, and nutritious. In the 21st century, medical care (control of hypertension, diabetes, and clotting) aimed at reducing heart disease and strokes have added another 2-3 years to the life expectancy in the United States, with much of that benefit erased by the epidemics of obesity and opioid abuse.
Modern medical technology has created treatments that cost $10,000 a month to add a few extra months of life to geriatric patients with terminal cancer. Meanwhile, in more mundane care, efforts like Choosing Wisely seek to save money wasted on low-value, useless, and even harmful tests and therapies. There is no single person or agency managing this chaotic process of inventing expensive new technologies while inadequately addressing the widespread shortages of mental health care, disparities in education, and other social determinants of health. The pandemic has highlighted these preexisting weaknesses in the social fabric.
The cries from India have been accompanied by voices of anger from India and other nations accusing the United States of hoarding vaccines and the raw materials needed to produce them. This has been called vaccine apartheid. The United States is not alone in its political decision to prioritize domestic interests over international ones; India’s recent government is similarly nationalistic. Scientists warn that no one is safe locally as long as the pandemic rages in other countries. The Biden administration, in a delayed response to the crisis in India, finally announced plans to share some unused vaccines (of a brand not yet Food and Drug Administration approved) as well as some vaccine raw materials whose export was forbidden by a regulation under the Defense Production Act. Reading below the headlines, the promised response won’t be implemented for weeks or months. We must do better.
The logistics of sharing the benefits of advanced science are complicated. The ethics are not. Who is my neighbor? If you didn’t learn the answer to that in Sunday school, there isn’t much more I can say.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no financial disclosures, Email him at [email protected]
India is in a crisis as the burden of COVID-19 has collapsed parts of the health care system. There are not enough beds, not enough oxygen, and not enough crematoria to handle the pandemic. India is also a major supplier of vaccines for itself and many other countries. That production capacity has also been affected by the local events, further worsening the response to the pandemic over the next few months.
This collapse is the specter that, in April 2020, placed a hospital ship next to Manhattan and rows of beds in its convention center. Fortunately, the lockdown in March 2020 sufficiently flattened the curve. The city avoided utilizing that disaster capacity, though many New Yorkers died out of sight in nursing homes. When the third and largest wave of cases in the United States peaked in January 2021, hospitals throughout California reached capacity but avoided bursting. In April 2021, localized outbreaks in Michigan, Arizona, and Ontario again tested the maximum capacity for providing modern medical treatments. Great Britain used a second lockdown in October 2020 and a third in January 2021 to control the pandemic, with Prime Minister Boris Johnson emphasizing that it was these social interventions, and not vaccines, which provided the mitigating effects. Other European Union nations adopted similar strategies. Prudent choices by government guided by science, combined with the cooperation of the public, have been and still are crucial to mollify the pandemic.
There is hope that soon vaccines will return daily life to a new normal. In the United States, the Centers for Disease Control and Prevention has loosened restrictions on social gathering. An increase in daily new cases of COVID-19 in April 2021 has turned into just a blip before continuing to recede. Perhaps that is the first sign of vaccination working at the level of public health. However, the May 2021 lockdown in highly vaccinated Seychelles is a warning that the danger remains. A single match can start a huge forest fire. The first 150 million cases of COVID-19 worldwide have, through natural rates of mutation, produced several variants that might partially evade current vaccines. The danger of newer variants persists with the next 150 million cases as the pandemic continues to rage in many nations which are just one airplane ride away. All human inhabitants of this blue-covered third rock from the sun are interconnected.
The benefits of scientific advancement have been extolled for centuries. This includes both individual discoveries as well as a mindset that favors rationalism over fatalism. On the whole, the benefits of scientific progress outweigh the negatives. Negative environmental impacts include pollution and climate change. Economic impacts include raising the mean economic standard of living but with greater inequity. Historically, governmental and social institutions have attempted to mitigate these negative consequences. Those efforts have attempted to provide guidance and a moral compass to direct the progress of scientific advancement, particularly in fields like gene therapy. Those efforts have called upon developed nations to share the bounties of progress with other nations.
Modern medicine has provided the fruit of these scientific advancements to a limited fraction of the world’s population during the 20th century. The improvements in life expectancy and infant mortality have come primarily from civil engineers getting running water into cities and sewage out. A smaller portion of the benefits are from public health measures that reduced tuberculosis, smallpox, polio, and measles. Agriculture became more reliable, productive, and nutritious. In the 21st century, medical care (control of hypertension, diabetes, and clotting) aimed at reducing heart disease and strokes have added another 2-3 years to the life expectancy in the United States, with much of that benefit erased by the epidemics of obesity and opioid abuse.
Modern medical technology has created treatments that cost $10,000 a month to add a few extra months of life to geriatric patients with terminal cancer. Meanwhile, in more mundane care, efforts like Choosing Wisely seek to save money wasted on low-value, useless, and even harmful tests and therapies. There is no single person or agency managing this chaotic process of inventing expensive new technologies while inadequately addressing the widespread shortages of mental health care, disparities in education, and other social determinants of health. The pandemic has highlighted these preexisting weaknesses in the social fabric.
The cries from India have been accompanied by voices of anger from India and other nations accusing the United States of hoarding vaccines and the raw materials needed to produce them. This has been called vaccine apartheid. The United States is not alone in its political decision to prioritize domestic interests over international ones; India’s recent government is similarly nationalistic. Scientists warn that no one is safe locally as long as the pandemic rages in other countries. The Biden administration, in a delayed response to the crisis in India, finally announced plans to share some unused vaccines (of a brand not yet Food and Drug Administration approved) as well as some vaccine raw materials whose export was forbidden by a regulation under the Defense Production Act. Reading below the headlines, the promised response won’t be implemented for weeks or months. We must do better.
The logistics of sharing the benefits of advanced science are complicated. The ethics are not. Who is my neighbor? If you didn’t learn the answer to that in Sunday school, there isn’t much more I can say.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no financial disclosures, Email him at [email protected]
Perinatal depression and the pediatrician’s role
Postpartum depression (PPD) is a common and treatable problem affecting over 10% of all pregnant women. Without routine use of a screening questionnaire, many women go undiagnosed and without treatment. The risks of untreated PPD in a new mother are the risks of depression tripled: to her health and to the health of her new infant and their whole family. Although pediatricians treat children, they take care of the whole family. They appreciate their role in offering support and guidance to new parents, and in the case of PPD, they are in a unique position. The American Academy of Pediatrics recognized this when they issued their policy statement, “Incorporating Recognition and Management of Perinatal Depression into Pediatric Practice,” in January 2019. By screening, tracking, and connecting affected mothers to care and services, you can truly provide “two-generational care” for your youngest patients.

PPD affects an estimated one in seven women (13%) globally. In one large retrospective study that looked at the 39 weeks before and after delivery, 15.4% of mothers received a diagnosis of PPD and a second study indicated that 22% of new mothers had depressive symptoms that were persistent for 6 months.1 The pathways to PPD include prior personal or family history of depression, stressors in the family (connected to social determinants of health), previous miscarriage or serious complications in a previous pregnancy, and sensitivity to hormonal changes. Indeed, PPD is the most common complication of childbirth.2 Although as many as half of all women eventually diagnosed with PPD had symptoms during their pregnancy, the misperception that PPD is only post partum leads to it being mistaken for the normal process of adjustment to parenthood. PPD is particularly insidious as new mothers are likely to be silent if they feel shame for not enjoying what they have been told will be a special and happy time, and those around them may mistake symptoms for the normal “baby blues” that will resolve quickly and with routine supports.
Untreated PPD, creates risks for mother, infant, and family as she manages needless suffering during a critical period for her new baby. While depression may remit over months without treatment, suicide is a real risk, and accounts for 20% of postpartum deaths.3 Infants face serious developmental consequences when their mothers are withdrawn and disconnected from them during the first months of life, including impaired social development, physical growth, and cognitive development. This impairment persists. Exposure to maternal depression during infancy is associated with lower IQ, attentional problems, and special educational needs by elementary school,4 and is a risk factor for psychiatric illnesses in childhood and adolescence.5,6 PPD has a broad range of severity, including psychosis that may include paranoia with the rare risk of infanticide. And maternal depression can add to the strains in a vulnerable caregiver relationship that can raise the risk for neglect or abuse of the mother, children, or both.
It is important to note that anxiety is often the presenting problem in perinatal mood disorders, with mothers experiencing intense morbid worries about their infant’s safety and health, and fear of inadequacy, criticism, and even infant removal. These fears may reinforce silence and isolation. But pediatricians are one group that these mothers are most likely to share their anxieties with as they look for reassurance. It can be challenging to distinguish PPD from obsessive-compulsive disorder or PTSD. The critical work of the pediatrician is not specific diagnosis and treatment. Instead, your task is to provide screening and support, to create a safe place to overcome silence and shame.

There are many reliable and valid screening instruments available for depression, but the Edinburgh Postnatal Depression Scale (EDPS) has been specially developed for and tested in this population. It is a 10-item scale that is easy to complete and to score. Scores range from 0 to 30 and a score of 10 is considered a cutoff for depression. It can be used to track symptoms and is free and widely available online and in multiple languages. Ideally, this scale can be administered as part of a previsit, automatically entered into an electronic medical record and given at regular intervals during the infant’s first year of primary care. Some new mothers, especially if they are suffering from depression, may feel anxious about filling this out. It is important that your staff tell them that you screen all new mothers in your practice, and that PPD is common and treatable and the pediatrician’s office is committed to the health of the whole family.
If a new mother screens positive, you might consider yourself to have three tasks: Reassure her that she is a wonderful mother and this is a treatable illness, not a cause for guilt, shame, or alarm; expand her support and decrease her isolation by helping her to communicate with her family; and identify treatment resources for her. Start by being curious about some of her specific worries or feelings, her energy level, feelings of isolation or trouble with sleep. Offer compassion and validation around the pain of these experiences in the midst of so much transition. Only after hearing a little detail about her experience, then you may offer that such feelings are common, but when they are persistent or severe, they often indicate PPD, and that her screening test suggests they do for her. Offer that this form of depression is very treatable, with both pharmacologic and psychotherapy interventions. And if she is resistant, gently offer that treatment will be very protective of her new infant’s physical, social, and cognitive growth and development. Hearing this from a pediatrician is powerful for a new mother, even if depressed. Finally, ask if you might help her bring other important adults in her family into an understanding of this. Could she tell her spouse? Her sister? Her best friend? Perhaps she could bring one of them to the next weekly visit, so you can all speak together. This intervention greatly improves the likelihood of her engaging in treatment, and strong interpersonal connections are therapeutic in and of themselves.
For treatment, the easier your office can make it, the more likely she is to follow up. Identify local resources, perhaps through connected community organizations such as Jewish Family and Children’s Services or through a public program like California’s First Five. Connect with the local obstetric practice, which may already have a referral process in place. If you can connect with her primary care provider, they may take on the referral process or may even have integrated capacity for treatment. Identify strategies that may support her restful sleep, including realistic daily exercise, sharing infant care, and being cautious with caffeine and screen time. Identify ways for her to meet other new mothers or reconnect with friends. Reassure her that easy attachment activities, such as reading a book or singing to her baby can be good for both of them without requiring much energy. This may sound like a daunting task, but the conversation will only take a few minutes. Helping an isolated new parent recognize that their feelings of fear, inadequacy, and guilt are not facts, offering some simple immediate strategies and facilitating a referral can be lifesaving.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected]
References
1. Dietz PM et al. Am J Psychiatry. 2007;164(10):1515-20.
2. Hanusa BH et al. J Women’s Health (Larchmt) 2008;17(4):585-96.
3. Lindahl V et al. Arch Womens Ment Health. 2005;8(2):77-87.
4. Hay DF et al. J Child Psychol Psychiatry. 2001;42(7):871-89.
5. Tully EC et al. Am J Psychiatry. 2008:165(9):1148-54.
6. Maternal depression and child development. Paediatr. Child Health 2004;9(8):575-98.
Postpartum depression (PPD) is a common and treatable problem affecting over 10% of all pregnant women. Without routine use of a screening questionnaire, many women go undiagnosed and without treatment. The risks of untreated PPD in a new mother are the risks of depression tripled: to her health and to the health of her new infant and their whole family. Although pediatricians treat children, they take care of the whole family. They appreciate their role in offering support and guidance to new parents, and in the case of PPD, they are in a unique position. The American Academy of Pediatrics recognized this when they issued their policy statement, “Incorporating Recognition and Management of Perinatal Depression into Pediatric Practice,” in January 2019. By screening, tracking, and connecting affected mothers to care and services, you can truly provide “two-generational care” for your youngest patients.
PPD affects an estimated one in seven women (13%) globally. In one large retrospective study that looked at the 39 weeks before and after delivery, 15.4% of mothers received a diagnosis of PPD and a second study indicated that 22% of new mothers had depressive symptoms that were persistent for 6 months.1 The pathways to PPD include prior personal or family history of depression, stressors in the family (connected to social determinants of health), previous miscarriage or serious complications in a previous pregnancy, and sensitivity to hormonal changes. Indeed, PPD is the most common complication of childbirth.2 Although as many as half of all women eventually diagnosed with PPD had symptoms during their pregnancy, the misperception that PPD is only post partum leads to it being mistaken for the normal process of adjustment to parenthood. PPD is particularly insidious as new mothers are likely to be silent if they feel shame for not enjoying what they have been told will be a special and happy time, and those around them may mistake symptoms for the normal “baby blues” that will resolve quickly and with routine supports.
Untreated PPD, creates risks for mother, infant, and family as she manages needless suffering during a critical period for her new baby. While depression may remit over months without treatment, suicide is a real risk, and accounts for 20% of postpartum deaths.3 Infants face serious developmental consequences when their mothers are withdrawn and disconnected from them during the first months of life, including impaired social development, physical growth, and cognitive development. This impairment persists. Exposure to maternal depression during infancy is associated with lower IQ, attentional problems, and special educational needs by elementary school,4 and is a risk factor for psychiatric illnesses in childhood and adolescence.5,6 PPD has a broad range of severity, including psychosis that may include paranoia with the rare risk of infanticide. And maternal depression can add to the strains in a vulnerable caregiver relationship that can raise the risk for neglect or abuse of the mother, children, or both.
It is important to note that anxiety is often the presenting problem in perinatal mood disorders, with mothers experiencing intense morbid worries about their infant’s safety and health, and fear of inadequacy, criticism, and even infant removal. These fears may reinforce silence and isolation. But pediatricians are one group that these mothers are most likely to share their anxieties with as they look for reassurance. It can be challenging to distinguish PPD from obsessive-compulsive disorder or PTSD. The critical work of the pediatrician is not specific diagnosis and treatment. Instead, your task is to provide screening and support, to create a safe place to overcome silence and shame.
There are many reliable and valid screening instruments available for depression, but the Edinburgh Postnatal Depression Scale (EDPS) has been specially developed for and tested in this population. It is a 10-item scale that is easy to complete and to score. Scores range from 0 to 30 and a score of 10 is considered a cutoff for depression. It can be used to track symptoms and is free and widely available online and in multiple languages. Ideally, this scale can be administered as part of a previsit, automatically entered into an electronic medical record and given at regular intervals during the infant’s first year of primary care. Some new mothers, especially if they are suffering from depression, may feel anxious about filling this out. It is important that your staff tell them that you screen all new mothers in your practice, and that PPD is common and treatable and the pediatrician’s office is committed to the health of the whole family.
If a new mother screens positive, you might consider yourself to have three tasks: Reassure her that she is a wonderful mother and this is a treatable illness, not a cause for guilt, shame, or alarm; expand her support and decrease her isolation by helping her to communicate with her family; and identify treatment resources for her. Start by being curious about some of her specific worries or feelings, her energy level, feelings of isolation or trouble with sleep. Offer compassion and validation around the pain of these experiences in the midst of so much transition. Only after hearing a little detail about her experience, then you may offer that such feelings are common, but when they are persistent or severe, they often indicate PPD, and that her screening test suggests they do for her. Offer that this form of depression is very treatable, with both pharmacologic and psychotherapy interventions. And if she is resistant, gently offer that treatment will be very protective of her new infant’s physical, social, and cognitive growth and development. Hearing this from a pediatrician is powerful for a new mother, even if depressed. Finally, ask if you might help her bring other important adults in her family into an understanding of this. Could she tell her spouse? Her sister? Her best friend? Perhaps she could bring one of them to the next weekly visit, so you can all speak together. This intervention greatly improves the likelihood of her engaging in treatment, and strong interpersonal connections are therapeutic in and of themselves.
For treatment, the easier your office can make it, the more likely she is to follow up. Identify local resources, perhaps through connected community organizations such as Jewish Family and Children’s Services or through a public program like California’s First Five. Connect with the local obstetric practice, which may already have a referral process in place. If you can connect with her primary care provider, they may take on the referral process or may even have integrated capacity for treatment. Identify strategies that may support her restful sleep, including realistic daily exercise, sharing infant care, and being cautious with caffeine and screen time. Identify ways for her to meet other new mothers or reconnect with friends. Reassure her that easy attachment activities, such as reading a book or singing to her baby can be good for both of them without requiring much energy. This may sound like a daunting task, but the conversation will only take a few minutes. Helping an isolated new parent recognize that their feelings of fear, inadequacy, and guilt are not facts, offering some simple immediate strategies and facilitating a referral can be lifesaving.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected]
References
1. Dietz PM et al. Am J Psychiatry. 2007;164(10):1515-20.
2. Hanusa BH et al. J Women’s Health (Larchmt) 2008;17(4):585-96.
3. Lindahl V et al. Arch Womens Ment Health. 2005;8(2):77-87.
4. Hay DF et al. J Child Psychol Psychiatry. 2001;42(7):871-89.
5. Tully EC et al. Am J Psychiatry. 2008:165(9):1148-54.
6. Maternal depression and child development. Paediatr. Child Health 2004;9(8):575-98.
Postpartum depression (PPD) is a common and treatable problem affecting over 10% of all pregnant women. Without routine use of a screening questionnaire, many women go undiagnosed and without treatment. The risks of untreated PPD in a new mother are the risks of depression tripled: to her health and to the health of her new infant and their whole family. Although pediatricians treat children, they take care of the whole family. They appreciate their role in offering support and guidance to new parents, and in the case of PPD, they are in a unique position. The American Academy of Pediatrics recognized this when they issued their policy statement, “Incorporating Recognition and Management of Perinatal Depression into Pediatric Practice,” in January 2019. By screening, tracking, and connecting affected mothers to care and services, you can truly provide “two-generational care” for your youngest patients.
PPD affects an estimated one in seven women (13%) globally. In one large retrospective study that looked at the 39 weeks before and after delivery, 15.4% of mothers received a diagnosis of PPD and a second study indicated that 22% of new mothers had depressive symptoms that were persistent for 6 months.1 The pathways to PPD include prior personal or family history of depression, stressors in the family (connected to social determinants of health), previous miscarriage or serious complications in a previous pregnancy, and sensitivity to hormonal changes. Indeed, PPD is the most common complication of childbirth.2 Although as many as half of all women eventually diagnosed with PPD had symptoms during their pregnancy, the misperception that PPD is only post partum leads to it being mistaken for the normal process of adjustment to parenthood. PPD is particularly insidious as new mothers are likely to be silent if they feel shame for not enjoying what they have been told will be a special and happy time, and those around them may mistake symptoms for the normal “baby blues” that will resolve quickly and with routine supports.
Untreated PPD, creates risks for mother, infant, and family as she manages needless suffering during a critical period for her new baby. While depression may remit over months without treatment, suicide is a real risk, and accounts for 20% of postpartum deaths.3 Infants face serious developmental consequences when their mothers are withdrawn and disconnected from them during the first months of life, including impaired social development, physical growth, and cognitive development. This impairment persists. Exposure to maternal depression during infancy is associated with lower IQ, attentional problems, and special educational needs by elementary school,4 and is a risk factor for psychiatric illnesses in childhood and adolescence.5,6 PPD has a broad range of severity, including psychosis that may include paranoia with the rare risk of infanticide. And maternal depression can add to the strains in a vulnerable caregiver relationship that can raise the risk for neglect or abuse of the mother, children, or both.
It is important to note that anxiety is often the presenting problem in perinatal mood disorders, with mothers experiencing intense morbid worries about their infant’s safety and health, and fear of inadequacy, criticism, and even infant removal. These fears may reinforce silence and isolation. But pediatricians are one group that these mothers are most likely to share their anxieties with as they look for reassurance. It can be challenging to distinguish PPD from obsessive-compulsive disorder or PTSD. The critical work of the pediatrician is not specific diagnosis and treatment. Instead, your task is to provide screening and support, to create a safe place to overcome silence and shame.
There are many reliable and valid screening instruments available for depression, but the Edinburgh Postnatal Depression Scale (EDPS) has been specially developed for and tested in this population. It is a 10-item scale that is easy to complete and to score. Scores range from 0 to 30 and a score of 10 is considered a cutoff for depression. It can be used to track symptoms and is free and widely available online and in multiple languages. Ideally, this scale can be administered as part of a previsit, automatically entered into an electronic medical record and given at regular intervals during the infant’s first year of primary care. Some new mothers, especially if they are suffering from depression, may feel anxious about filling this out. It is important that your staff tell them that you screen all new mothers in your practice, and that PPD is common and treatable and the pediatrician’s office is committed to the health of the whole family.
If a new mother screens positive, you might consider yourself to have three tasks: Reassure her that she is a wonderful mother and this is a treatable illness, not a cause for guilt, shame, or alarm; expand her support and decrease her isolation by helping her to communicate with her family; and identify treatment resources for her. Start by being curious about some of her specific worries or feelings, her energy level, feelings of isolation or trouble with sleep. Offer compassion and validation around the pain of these experiences in the midst of so much transition. Only after hearing a little detail about her experience, then you may offer that such feelings are common, but when they are persistent or severe, they often indicate PPD, and that her screening test suggests they do for her. Offer that this form of depression is very treatable, with both pharmacologic and psychotherapy interventions. And if she is resistant, gently offer that treatment will be very protective of her new infant’s physical, social, and cognitive growth and development. Hearing this from a pediatrician is powerful for a new mother, even if depressed. Finally, ask if you might help her bring other important adults in her family into an understanding of this. Could she tell her spouse? Her sister? Her best friend? Perhaps she could bring one of them to the next weekly visit, so you can all speak together. This intervention greatly improves the likelihood of her engaging in treatment, and strong interpersonal connections are therapeutic in and of themselves.
For treatment, the easier your office can make it, the more likely she is to follow up. Identify local resources, perhaps through connected community organizations such as Jewish Family and Children’s Services or through a public program like California’s First Five. Connect with the local obstetric practice, which may already have a referral process in place. If you can connect with her primary care provider, they may take on the referral process or may even have integrated capacity for treatment. Identify strategies that may support her restful sleep, including realistic daily exercise, sharing infant care, and being cautious with caffeine and screen time. Identify ways for her to meet other new mothers or reconnect with friends. Reassure her that easy attachment activities, such as reading a book or singing to her baby can be good for both of them without requiring much energy. This may sound like a daunting task, but the conversation will only take a few minutes. Helping an isolated new parent recognize that their feelings of fear, inadequacy, and guilt are not facts, offering some simple immediate strategies and facilitating a referral can be lifesaving.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected]
References
1. Dietz PM et al. Am J Psychiatry. 2007;164(10):1515-20.
2. Hanusa BH et al. J Women’s Health (Larchmt) 2008;17(4):585-96.
3. Lindahl V et al. Arch Womens Ment Health. 2005;8(2):77-87.
4. Hay DF et al. J Child Psychol Psychiatry. 2001;42(7):871-89.
5. Tully EC et al. Am J Psychiatry. 2008:165(9):1148-54.
6. Maternal depression and child development. Paediatr. Child Health 2004;9(8):575-98.
COVID-19 in children and adolescents: Disease burden and severity
My first thought on this column was maybe Pediatric News has written sufficiently about SARS-CoV-2 infection, and it is time to move on. However, the agenda for the May 12th Advisory Committee on Immunization Practice includes a review of the Pfizer-BioNTech COVID-19 vaccine safety and immunogenicity data for the 12- to 15-year-old age cohort that suggests the potential for vaccine availability and roll out for early adolescents in the near future and the need for up-to-date knowledge about the incidence, severity, and long-term outcome of COVID-19 in the pediatric population.

Updating and summarizing the pediatric experience for the pediatric community on what children and adolescents have experienced because of SARS-CoV-2 infection is critical to address the myriad of questions that will come from colleagues, parents, and adolescents themselves. A great resource, published weekly, is the joint report from the American Academy of Pediatrics and the Children’s Hospital Association.1 As of April 29, 2021, 3,782,724 total child COVID-19 cases have been reported from 49 states, New York City (NYC), the District of Columbia, Guam, and Puerto Rico. Children represent approximately 14% of cases in the United States and not surprisingly are an increasing proportion of total cases as vaccine impact reduces cases among older age groups. Nearly 5% of the pediatric population has already been infected with SARS-CoV-2. Fortunately, compared with adults, hospitalization, severe disease, and mortality remain far lower both in number and proportion than in the adult population. Cumulative hospitalizations from 24 states and NYC total 15,456 (0.8%) among those infected, with 303 deaths reported (from 43 states, NYC, Guam, and Puerto Rico). Case fatality rate approximates 0.01% in the most recent summary of state reports. One of the limitations of this report is that each state decides how to report the age distribution of COVID-19 cases resulting in variation in age range; another is the data are limited to those details individual states chose to make publicly available.
Although children do not commonly develop severe disease, and the case fatality is low, there are still insights to be learned from understanding risk features for severe disease. Preston et al. reviewed discharge data from 869 medical facilities to describe patients 18 years or younger who had an inpatient or emergency department encounter with a primary or secondary COVID-19 discharge diagnosis from March 1 through October 31, 2020.2 They reported that approximately 2,430 (11.7%) children were hospitalized and 746, nearly 31% of those hospitalized, had severe COVID disease. Those at greatest risk for severe disease were children with comorbid conditions and those less than 12 years, compared with the 12- to 18-year age group. They did not identify race as a risk for severe disease in this study. Moreira et al. described risk factors for morbidity and death from COVID in children less than 18 years of age3 using CDC COVID-NET, the Centers for Disease Control and Prevention COVID-19–associated hospitalization surveillance network. They reported a hospitalization rate of 4.7% among 27,045 cases. They identified three risk factors for hospitalization – age, race/ethnicity, and comorbid conditions. Thirty-nine children (0.19%) died; children who were black, non-Hispanic, and those with an underlying medical condition had a significantly increased risk of death. Thirty-three (85%) children who died had a comorbidity, and 27 (69%) were African American or Hispanic/Latino. The U.S. experience in children is also consistent with reports from the United Kingdom, Italy, Spain, Germany, France, and South Korea.4 Deaths from COVID-19 were uncommon but relatively more frequent in older children, compared with younger age groups among children less than 18 years of age in these countries.
Acute COVID-19 and multisystem inflammatory syndrome in children (MIS-C) do not predominantly target the neurologic systems; however, neurologic complications have been reported, some of which appear to result in long-lasting disability. LaRovere et al. identified 354 (22%) of 1,695 patients less than 21 years of age with acute COVID or MIS-C who had neurologic signs or symptoms during their illness. Among those with neurologic involvement, most children had prior neurologic deficits, mild symptoms, that resolved by the time of discharge. Forty-three (12%) were considered life threatening and included severe encephalopathy, stroke, central nervous system infection/demyelination, Guillain-Barre syndrome or variant, or acute cerebral edema. Several children, including some who were previously healthy prior to COVID, had persistent neurologic deficits at discharge. In addition to neurologic morbidity, long COVID – a syndrome of persistent symptoms following acute COVID that lasts for more than 12 weeks without alternative diagnosis – has also been described in children. Buonsenso et al. assessed 129 children diagnosed with COVID-19 between March and November 2020 in Rome, Italy.5 Persisting symptoms after 120 days were reported by more than 50%. Symptoms like fatigue, muscle and joint pain, headache, insomnia, respiratory problems, and palpitations were most common. Clearly, further follow-up of the long-term outcomes is necessary to understand the full spectrum of morbidity resulting from COVID-19 disease in children and its natural history.
The current picture of COVID infection in children younger than 18 reinforces that children are part of the pandemic. Although deaths in children have now exceeded 300 cases, severe disease remains uncommon in both the United States and western Europe. Risk factors for severe disease include comorbid illness and race/ethnicity with a disproportionate number of severe cases in children with underlying comorbidity and in African American and Hispanic/Latino children. Ongoing surveillance is critical as changes are likely to be observed over time as viral evolution affects disease burden and characteristics.
Dr. Pelton is professor of pediatrics and epidemiology at Boston University schools of medicine and public health and senior attending physician in pediatric infectious diseases, Boston Medical Center. Email him at [email protected].
References
1. Children and COVID-19: State-Level Data Report. Services AAP.org.
2. Preston LE et al. JAMA Network Open. 2021;4(4):e215298. doi:10.1001/jamanetworkopen.2021.5298
3. Moreira A et al. Eur J Pediatr. 2021;180:1659-63.
4. SS Bhopal et al. Lancet 2021. doi: 10.1016/ S2352-4642(21)00066-3.
5. Buonsenso D et al. medRxiv preprint. doi: 10.1101/2021.01.23.21250375.
My first thought on this column was maybe Pediatric News has written sufficiently about SARS-CoV-2 infection, and it is time to move on. However, the agenda for the May 12th Advisory Committee on Immunization Practice includes a review of the Pfizer-BioNTech COVID-19 vaccine safety and immunogenicity data for the 12- to 15-year-old age cohort that suggests the potential for vaccine availability and roll out for early adolescents in the near future and the need for up-to-date knowledge about the incidence, severity, and long-term outcome of COVID-19 in the pediatric population.
Updating and summarizing the pediatric experience for the pediatric community on what children and adolescents have experienced because of SARS-CoV-2 infection is critical to address the myriad of questions that will come from colleagues, parents, and adolescents themselves. A great resource, published weekly, is the joint report from the American Academy of Pediatrics and the Children’s Hospital Association.1 As of April 29, 2021, 3,782,724 total child COVID-19 cases have been reported from 49 states, New York City (NYC), the District of Columbia, Guam, and Puerto Rico. Children represent approximately 14% of cases in the United States and not surprisingly are an increasing proportion of total cases as vaccine impact reduces cases among older age groups. Nearly 5% of the pediatric population has already been infected with SARS-CoV-2. Fortunately, compared with adults, hospitalization, severe disease, and mortality remain far lower both in number and proportion than in the adult population. Cumulative hospitalizations from 24 states and NYC total 15,456 (0.8%) among those infected, with 303 deaths reported (from 43 states, NYC, Guam, and Puerto Rico). Case fatality rate approximates 0.01% in the most recent summary of state reports. One of the limitations of this report is that each state decides how to report the age distribution of COVID-19 cases resulting in variation in age range; another is the data are limited to those details individual states chose to make publicly available.
Although children do not commonly develop severe disease, and the case fatality is low, there are still insights to be learned from understanding risk features for severe disease. Preston et al. reviewed discharge data from 869 medical facilities to describe patients 18 years or younger who had an inpatient or emergency department encounter with a primary or secondary COVID-19 discharge diagnosis from March 1 through October 31, 2020.2 They reported that approximately 2,430 (11.7%) children were hospitalized and 746, nearly 31% of those hospitalized, had severe COVID disease. Those at greatest risk for severe disease were children with comorbid conditions and those less than 12 years, compared with the 12- to 18-year age group. They did not identify race as a risk for severe disease in this study. Moreira et al. described risk factors for morbidity and death from COVID in children less than 18 years of age3 using CDC COVID-NET, the Centers for Disease Control and Prevention COVID-19–associated hospitalization surveillance network. They reported a hospitalization rate of 4.7% among 27,045 cases. They identified three risk factors for hospitalization – age, race/ethnicity, and comorbid conditions. Thirty-nine children (0.19%) died; children who were black, non-Hispanic, and those with an underlying medical condition had a significantly increased risk of death. Thirty-three (85%) children who died had a comorbidity, and 27 (69%) were African American or Hispanic/Latino. The U.S. experience in children is also consistent with reports from the United Kingdom, Italy, Spain, Germany, France, and South Korea.4 Deaths from COVID-19 were uncommon but relatively more frequent in older children, compared with younger age groups among children less than 18 years of age in these countries.
Acute COVID-19 and multisystem inflammatory syndrome in children (MIS-C) do not predominantly target the neurologic systems; however, neurologic complications have been reported, some of which appear to result in long-lasting disability. LaRovere et al. identified 354 (22%) of 1,695 patients less than 21 years of age with acute COVID or MIS-C who had neurologic signs or symptoms during their illness. Among those with neurologic involvement, most children had prior neurologic deficits, mild symptoms, that resolved by the time of discharge. Forty-three (12%) were considered life threatening and included severe encephalopathy, stroke, central nervous system infection/demyelination, Guillain-Barre syndrome or variant, or acute cerebral edema. Several children, including some who were previously healthy prior to COVID, had persistent neurologic deficits at discharge. In addition to neurologic morbidity, long COVID – a syndrome of persistent symptoms following acute COVID that lasts for more than 12 weeks without alternative diagnosis – has also been described in children. Buonsenso et al. assessed 129 children diagnosed with COVID-19 between March and November 2020 in Rome, Italy.5 Persisting symptoms after 120 days were reported by more than 50%. Symptoms like fatigue, muscle and joint pain, headache, insomnia, respiratory problems, and palpitations were most common. Clearly, further follow-up of the long-term outcomes is necessary to understand the full spectrum of morbidity resulting from COVID-19 disease in children and its natural history.
The current picture of COVID infection in children younger than 18 reinforces that children are part of the pandemic. Although deaths in children have now exceeded 300 cases, severe disease remains uncommon in both the United States and western Europe. Risk factors for severe disease include comorbid illness and race/ethnicity with a disproportionate number of severe cases in children with underlying comorbidity and in African American and Hispanic/Latino children. Ongoing surveillance is critical as changes are likely to be observed over time as viral evolution affects disease burden and characteristics.
Dr. Pelton is professor of pediatrics and epidemiology at Boston University schools of medicine and public health and senior attending physician in pediatric infectious diseases, Boston Medical Center. Email him at [email protected].
References
1. Children and COVID-19: State-Level Data Report. Services AAP.org.
2. Preston LE et al. JAMA Network Open. 2021;4(4):e215298. doi:10.1001/jamanetworkopen.2021.5298
3. Moreira A et al. Eur J Pediatr. 2021;180:1659-63.
4. SS Bhopal et al. Lancet 2021. doi: 10.1016/ S2352-4642(21)00066-3.
5. Buonsenso D et al. medRxiv preprint. doi: 10.1101/2021.01.23.21250375.
My first thought on this column was maybe Pediatric News has written sufficiently about SARS-CoV-2 infection, and it is time to move on. However, the agenda for the May 12th Advisory Committee on Immunization Practice includes a review of the Pfizer-BioNTech COVID-19 vaccine safety and immunogenicity data for the 12- to 15-year-old age cohort that suggests the potential for vaccine availability and roll out for early adolescents in the near future and the need for up-to-date knowledge about the incidence, severity, and long-term outcome of COVID-19 in the pediatric population.
Updating and summarizing the pediatric experience for the pediatric community on what children and adolescents have experienced because of SARS-CoV-2 infection is critical to address the myriad of questions that will come from colleagues, parents, and adolescents themselves. A great resource, published weekly, is the joint report from the American Academy of Pediatrics and the Children’s Hospital Association.1 As of April 29, 2021, 3,782,724 total child COVID-19 cases have been reported from 49 states, New York City (NYC), the District of Columbia, Guam, and Puerto Rico. Children represent approximately 14% of cases in the United States and not surprisingly are an increasing proportion of total cases as vaccine impact reduces cases among older age groups. Nearly 5% of the pediatric population has already been infected with SARS-CoV-2. Fortunately, compared with adults, hospitalization, severe disease, and mortality remain far lower both in number and proportion than in the adult population. Cumulative hospitalizations from 24 states and NYC total 15,456 (0.8%) among those infected, with 303 deaths reported (from 43 states, NYC, Guam, and Puerto Rico). Case fatality rate approximates 0.01% in the most recent summary of state reports. One of the limitations of this report is that each state decides how to report the age distribution of COVID-19 cases resulting in variation in age range; another is the data are limited to those details individual states chose to make publicly available.
Although children do not commonly develop severe disease, and the case fatality is low, there are still insights to be learned from understanding risk features for severe disease. Preston et al. reviewed discharge data from 869 medical facilities to describe patients 18 years or younger who had an inpatient or emergency department encounter with a primary or secondary COVID-19 discharge diagnosis from March 1 through October 31, 2020.2 They reported that approximately 2,430 (11.7%) children were hospitalized and 746, nearly 31% of those hospitalized, had severe COVID disease. Those at greatest risk for severe disease were children with comorbid conditions and those less than 12 years, compared with the 12- to 18-year age group. They did not identify race as a risk for severe disease in this study. Moreira et al. described risk factors for morbidity and death from COVID in children less than 18 years of age3 using CDC COVID-NET, the Centers for Disease Control and Prevention COVID-19–associated hospitalization surveillance network. They reported a hospitalization rate of 4.7% among 27,045 cases. They identified three risk factors for hospitalization – age, race/ethnicity, and comorbid conditions. Thirty-nine children (0.19%) died; children who were black, non-Hispanic, and those with an underlying medical condition had a significantly increased risk of death. Thirty-three (85%) children who died had a comorbidity, and 27 (69%) were African American or Hispanic/Latino. The U.S. experience in children is also consistent with reports from the United Kingdom, Italy, Spain, Germany, France, and South Korea.4 Deaths from COVID-19 were uncommon but relatively more frequent in older children, compared with younger age groups among children less than 18 years of age in these countries.
Acute COVID-19 and multisystem inflammatory syndrome in children (MIS-C) do not predominantly target the neurologic systems; however, neurologic complications have been reported, some of which appear to result in long-lasting disability. LaRovere et al. identified 354 (22%) of 1,695 patients less than 21 years of age with acute COVID or MIS-C who had neurologic signs or symptoms during their illness. Among those with neurologic involvement, most children had prior neurologic deficits, mild symptoms, that resolved by the time of discharge. Forty-three (12%) were considered life threatening and included severe encephalopathy, stroke, central nervous system infection/demyelination, Guillain-Barre syndrome or variant, or acute cerebral edema. Several children, including some who were previously healthy prior to COVID, had persistent neurologic deficits at discharge. In addition to neurologic morbidity, long COVID – a syndrome of persistent symptoms following acute COVID that lasts for more than 12 weeks without alternative diagnosis – has also been described in children. Buonsenso et al. assessed 129 children diagnosed with COVID-19 between March and November 2020 in Rome, Italy.5 Persisting symptoms after 120 days were reported by more than 50%. Symptoms like fatigue, muscle and joint pain, headache, insomnia, respiratory problems, and palpitations were most common. Clearly, further follow-up of the long-term outcomes is necessary to understand the full spectrum of morbidity resulting from COVID-19 disease in children and its natural history.
The current picture of COVID infection in children younger than 18 reinforces that children are part of the pandemic. Although deaths in children have now exceeded 300 cases, severe disease remains uncommon in both the United States and western Europe. Risk factors for severe disease include comorbid illness and race/ethnicity with a disproportionate number of severe cases in children with underlying comorbidity and in African American and Hispanic/Latino children. Ongoing surveillance is critical as changes are likely to be observed over time as viral evolution affects disease burden and characteristics.
Dr. Pelton is professor of pediatrics and epidemiology at Boston University schools of medicine and public health and senior attending physician in pediatric infectious diseases, Boston Medical Center. Email him at [email protected].
References
1. Children and COVID-19: State-Level Data Report. Services AAP.org.
2. Preston LE et al. JAMA Network Open. 2021;4(4):e215298. doi:10.1001/jamanetworkopen.2021.5298
3. Moreira A et al. Eur J Pediatr. 2021;180:1659-63.
4. SS Bhopal et al. Lancet 2021. doi: 10.1016/ S2352-4642(21)00066-3.
5. Buonsenso D et al. medRxiv preprint. doi: 10.1101/2021.01.23.21250375.
An infant girl presents with a growing pink-red leg nodule
The history of a brownish to pink patch with color change and rapid growth within the first year combined with the exam findings, are suggestive of a tufted angioma, though the findings presented may be nonspecific.

A tufted angioma is a rare vascular tumor of infancy or early childhood, that is present at birth in approximately half of cases. It may initially present as a faint pink to brown plaque, but develops as a firm, red to violaceous nodule or plaque, usually with “lumpiness” or nodularity.1-3 Lesions usually are infiltrative with indistinct borders. They are named for their histologic appearance, with lobules of capillaries which appear as “tufts” in the dermis and subdermis with “cannonball” appearance, and are considered to be on a spectrum with another vascular tumor called kaposiform hemangioendothelioma (KHE).4 These vascular tumors can trigger Kasabach-Merritt syndrome, a disease process in which vascular tumors trap platelets and clotting factors, resulting in a life-threatening thrombocytopenia and consumptive coagulopathy with a high risk of bleeding and high-output heart failure.5
What’s the differential diagnosis?
The differential diagnosis of tufted angioma includes other potentially large vascular lesions including infantile hemangioma, congenital hemangioma, port-wine birth marks (capillary malformations), hemangioendotheliomas, and rhabdomyosarcomas.

Infantile hemangiomas (IH) are common vascular tumors of infancy seen in 4%-5% of infants that are characterized by a growth and involution phase. Classically, lesions can be absent or minimally evident at birth, becoming noticeable within the first months of life with a rapid growth phase and typical progression to bright red papules, nodules, or plaques. Deeper hemangiomas may appear more skin colored on the surface with a bluish coloration underneath. They are usually more discreet, with relatively defined borders. Diagnosis is typically clinical and many IHs self-resolve, albeit with residual findings including skin atrophy, scarring, and telangiectasia. Observation or topical timolol are first-line treatment options for more superficial lesions while systemic propranolol is the treatment of choice for deeper IHs or those resulting in possible airway or vision compromise.
Congenital hemangiomas (CH) are another type of vascular growth characterized by a solitary erythematous to violaceous plaque or nodule present at birth with overlying telangiectasia. CHs can be subdivided into categories including rapidly involuting (RICH), partially involuting (PICH), and noninvoluting (NICH). Diagnosis is usually clinical and, depending on the subtype, treatment can involve watchful waiting (for RICHs) or more active intervention such as pulse dye laser or surgical resection (for PICHs or NICHs). The growing nature of this patient’s mass makes a diagnosis of CH unlikely.
Port-wine birth mark, also known as nevus flammeus, is a vascular malformation that appears at birth as a nonpalpable irregular erythematous to violaceous macular plaque. Port-wine stains may be isolated birthmarks, or associated with Sturge-Weber syndrome, complex vascular malformations, or soft-tissue overgrowth. Klippel-Trenauny syndrome (KTS) describes capillary-venous malformations with limb overgrowth, with or without lymphatic malformations, and many are associated with somatic mutations in the PIK3CA gene. While KTS could be considered in this patient, the nodular appearance with lumpy texture and rapid growth makes a vascular tumor more likely.
Rhabdomyosarcoma is a malignancy of skeletal muscle lineage and the most common soft tissue tumor in pediatrics. Cutaneous rhabdomyosarcomas present as erythematous nodules, markedly firm, often “fixed” to deep tissue. A rapidly growing atypical, firm tumor of infancy should raise the consideration of rhabdomyosarcoma and imaging and biopsy are appropriate for evaluation.
What should the evaluation and management of this patient be?
Initial workup should include a complete blood count with platelet count as well as coagulation studies including D-dimer, fibrinogen, prothrombin time, and activated partial thromboplastin time, to assess for any thrombocytopenia or coagulopathy.6 Ultrasound and/or MRI may also be performed to determine lesion extent. While typical MRI findings might be suggestive of a tufted angioma or hemangioendothelioma, biopsy for histologic examination is usually the approach to diagnosis, which will demonstrate stereotypic round lobules of capillaries in a “tufted” distribution.2,7 Biopsy may be performed by a surgeon or dermatologist but bleeding at time of biopsy needs to be considered before moving forward with the procedure.

Tufted angiomas of early life may regress spontaneously, though lesions with symptoms, with functional significance, or associated with KHE may require therapy. Surgical excision is one option, but it may be difficult to execute given that these lesions often have poorly defined margins.1 Other treatment choices include but are not limited to aspirin, systemic corticosteroids, vincristine, interferon-alpha, embolization, and sirolimus.8 No specific expert-directed consensus guidelines exist for these lesions, and suspicion of this lesion should prompt urgent referral to a pediatric dermatologist. Concern for Kasabach-Merritt syndrome should trigger immediate referral for rapid evaluation and management.
Complete blood count with platelet count and coagulation studies were normal in our patient. This infant underwent biopsy to confirm the diagnosis of tufted angioma and MRI to determine lesion extent. The lesion slowly involuted spontaneously without recurrence.
Mr. Haft is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital, San Diego. He is MS4 at the University of Rochester, N.Y. Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Neither Mr. Haft nor Dr. Eichenfield have any relevant financial disclosures.
References
1. Herron MD et al. Pediatr Dermatol. 2002;19(5):394-401.
2. Jones EW and Orkin M. J Am Acad Dermatol. 1989;20(2 Pt 1):214-25.
3. Wong SN and Tay YK. Pediatr Dermatol. 2002;19(5):388-93.
4. Croteau SE and Gupta D. Semin Cutan Med Surg. 2016;35(3):147-52.
5. Kelly M. Pediatr Clin North Am. 2010;57(5):1085-9.
6. Osio A et al. Arch Dermatol. 2010;146(7):758-63.
7. Padilla RS et al. Am J Dermatopathol. 1987;9(4):292-300.
8. Liu XH et al. Int J Cancer. 2016;139(7):1658-66.
The history of a brownish to pink patch with color change and rapid growth within the first year combined with the exam findings, are suggestive of a tufted angioma, though the findings presented may be nonspecific.
A tufted angioma is a rare vascular tumor of infancy or early childhood, that is present at birth in approximately half of cases. It may initially present as a faint pink to brown plaque, but develops as a firm, red to violaceous nodule or plaque, usually with “lumpiness” or nodularity.1-3 Lesions usually are infiltrative with indistinct borders. They are named for their histologic appearance, with lobules of capillaries which appear as “tufts” in the dermis and subdermis with “cannonball” appearance, and are considered to be on a spectrum with another vascular tumor called kaposiform hemangioendothelioma (KHE).4 These vascular tumors can trigger Kasabach-Merritt syndrome, a disease process in which vascular tumors trap platelets and clotting factors, resulting in a life-threatening thrombocytopenia and consumptive coagulopathy with a high risk of bleeding and high-output heart failure.5
What’s the differential diagnosis?
The differential diagnosis of tufted angioma includes other potentially large vascular lesions including infantile hemangioma, congenital hemangioma, port-wine birth marks (capillary malformations), hemangioendotheliomas, and rhabdomyosarcomas.
Infantile hemangiomas (IH) are common vascular tumors of infancy seen in 4%-5% of infants that are characterized by a growth and involution phase. Classically, lesions can be absent or minimally evident at birth, becoming noticeable within the first months of life with a rapid growth phase and typical progression to bright red papules, nodules, or plaques. Deeper hemangiomas may appear more skin colored on the surface with a bluish coloration underneath. They are usually more discreet, with relatively defined borders. Diagnosis is typically clinical and many IHs self-resolve, albeit with residual findings including skin atrophy, scarring, and telangiectasia. Observation or topical timolol are first-line treatment options for more superficial lesions while systemic propranolol is the treatment of choice for deeper IHs or those resulting in possible airway or vision compromise.
Congenital hemangiomas (CH) are another type of vascular growth characterized by a solitary erythematous to violaceous plaque or nodule present at birth with overlying telangiectasia. CHs can be subdivided into categories including rapidly involuting (RICH), partially involuting (PICH), and noninvoluting (NICH). Diagnosis is usually clinical and, depending on the subtype, treatment can involve watchful waiting (for RICHs) or more active intervention such as pulse dye laser or surgical resection (for PICHs or NICHs). The growing nature of this patient’s mass makes a diagnosis of CH unlikely.
Port-wine birth mark, also known as nevus flammeus, is a vascular malformation that appears at birth as a nonpalpable irregular erythematous to violaceous macular plaque. Port-wine stains may be isolated birthmarks, or associated with Sturge-Weber syndrome, complex vascular malformations, or soft-tissue overgrowth. Klippel-Trenauny syndrome (KTS) describes capillary-venous malformations with limb overgrowth, with or without lymphatic malformations, and many are associated with somatic mutations in the PIK3CA gene. While KTS could be considered in this patient, the nodular appearance with lumpy texture and rapid growth makes a vascular tumor more likely.
Rhabdomyosarcoma is a malignancy of skeletal muscle lineage and the most common soft tissue tumor in pediatrics. Cutaneous rhabdomyosarcomas present as erythematous nodules, markedly firm, often “fixed” to deep tissue. A rapidly growing atypical, firm tumor of infancy should raise the consideration of rhabdomyosarcoma and imaging and biopsy are appropriate for evaluation.
What should the evaluation and management of this patient be?
Initial workup should include a complete blood count with platelet count as well as coagulation studies including D-dimer, fibrinogen, prothrombin time, and activated partial thromboplastin time, to assess for any thrombocytopenia or coagulopathy.6 Ultrasound and/or MRI may also be performed to determine lesion extent. While typical MRI findings might be suggestive of a tufted angioma or hemangioendothelioma, biopsy for histologic examination is usually the approach to diagnosis, which will demonstrate stereotypic round lobules of capillaries in a “tufted” distribution.2,7 Biopsy may be performed by a surgeon or dermatologist but bleeding at time of biopsy needs to be considered before moving forward with the procedure.
Tufted angiomas of early life may regress spontaneously, though lesions with symptoms, with functional significance, or associated with KHE may require therapy. Surgical excision is one option, but it may be difficult to execute given that these lesions often have poorly defined margins.1 Other treatment choices include but are not limited to aspirin, systemic corticosteroids, vincristine, interferon-alpha, embolization, and sirolimus.8 No specific expert-directed consensus guidelines exist for these lesions, and suspicion of this lesion should prompt urgent referral to a pediatric dermatologist. Concern for Kasabach-Merritt syndrome should trigger immediate referral for rapid evaluation and management.
Complete blood count with platelet count and coagulation studies were normal in our patient. This infant underwent biopsy to confirm the diagnosis of tufted angioma and MRI to determine lesion extent. The lesion slowly involuted spontaneously without recurrence.
Mr. Haft is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital, San Diego. He is MS4 at the University of Rochester, N.Y. Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Neither Mr. Haft nor Dr. Eichenfield have any relevant financial disclosures.
References
1. Herron MD et al. Pediatr Dermatol. 2002;19(5):394-401.
2. Jones EW and Orkin M. J Am Acad Dermatol. 1989;20(2 Pt 1):214-25.
3. Wong SN and Tay YK. Pediatr Dermatol. 2002;19(5):388-93.
4. Croteau SE and Gupta D. Semin Cutan Med Surg. 2016;35(3):147-52.
5. Kelly M. Pediatr Clin North Am. 2010;57(5):1085-9.
6. Osio A et al. Arch Dermatol. 2010;146(7):758-63.
7. Padilla RS et al. Am J Dermatopathol. 1987;9(4):292-300.
8. Liu XH et al. Int J Cancer. 2016;139(7):1658-66.
The history of a brownish to pink patch with color change and rapid growth within the first year combined with the exam findings, are suggestive of a tufted angioma, though the findings presented may be nonspecific.
A tufted angioma is a rare vascular tumor of infancy or early childhood, that is present at birth in approximately half of cases. It may initially present as a faint pink to brown plaque, but develops as a firm, red to violaceous nodule or plaque, usually with “lumpiness” or nodularity.1-3 Lesions usually are infiltrative with indistinct borders. They are named for their histologic appearance, with lobules of capillaries which appear as “tufts” in the dermis and subdermis with “cannonball” appearance, and are considered to be on a spectrum with another vascular tumor called kaposiform hemangioendothelioma (KHE).4 These vascular tumors can trigger Kasabach-Merritt syndrome, a disease process in which vascular tumors trap platelets and clotting factors, resulting in a life-threatening thrombocytopenia and consumptive coagulopathy with a high risk of bleeding and high-output heart failure.5
What’s the differential diagnosis?
The differential diagnosis of tufted angioma includes other potentially large vascular lesions including infantile hemangioma, congenital hemangioma, port-wine birth marks (capillary malformations), hemangioendotheliomas, and rhabdomyosarcomas.
Infantile hemangiomas (IH) are common vascular tumors of infancy seen in 4%-5% of infants that are characterized by a growth and involution phase. Classically, lesions can be absent or minimally evident at birth, becoming noticeable within the first months of life with a rapid growth phase and typical progression to bright red papules, nodules, or plaques. Deeper hemangiomas may appear more skin colored on the surface with a bluish coloration underneath. They are usually more discreet, with relatively defined borders. Diagnosis is typically clinical and many IHs self-resolve, albeit with residual findings including skin atrophy, scarring, and telangiectasia. Observation or topical timolol are first-line treatment options for more superficial lesions while systemic propranolol is the treatment of choice for deeper IHs or those resulting in possible airway or vision compromise.
Congenital hemangiomas (CH) are another type of vascular growth characterized by a solitary erythematous to violaceous plaque or nodule present at birth with overlying telangiectasia. CHs can be subdivided into categories including rapidly involuting (RICH), partially involuting (PICH), and noninvoluting (NICH). Diagnosis is usually clinical and, depending on the subtype, treatment can involve watchful waiting (for RICHs) or more active intervention such as pulse dye laser or surgical resection (for PICHs or NICHs). The growing nature of this patient’s mass makes a diagnosis of CH unlikely.
Port-wine birth mark, also known as nevus flammeus, is a vascular malformation that appears at birth as a nonpalpable irregular erythematous to violaceous macular plaque. Port-wine stains may be isolated birthmarks, or associated with Sturge-Weber syndrome, complex vascular malformations, or soft-tissue overgrowth. Klippel-Trenauny syndrome (KTS) describes capillary-venous malformations with limb overgrowth, with or without lymphatic malformations, and many are associated with somatic mutations in the PIK3CA gene. While KTS could be considered in this patient, the nodular appearance with lumpy texture and rapid growth makes a vascular tumor more likely.
Rhabdomyosarcoma is a malignancy of skeletal muscle lineage and the most common soft tissue tumor in pediatrics. Cutaneous rhabdomyosarcomas present as erythematous nodules, markedly firm, often “fixed” to deep tissue. A rapidly growing atypical, firm tumor of infancy should raise the consideration of rhabdomyosarcoma and imaging and biopsy are appropriate for evaluation.
What should the evaluation and management of this patient be?
Initial workup should include a complete blood count with platelet count as well as coagulation studies including D-dimer, fibrinogen, prothrombin time, and activated partial thromboplastin time, to assess for any thrombocytopenia or coagulopathy.6 Ultrasound and/or MRI may also be performed to determine lesion extent. While typical MRI findings might be suggestive of a tufted angioma or hemangioendothelioma, biopsy for histologic examination is usually the approach to diagnosis, which will demonstrate stereotypic round lobules of capillaries in a “tufted” distribution.2,7 Biopsy may be performed by a surgeon or dermatologist but bleeding at time of biopsy needs to be considered before moving forward with the procedure.
Tufted angiomas of early life may regress spontaneously, though lesions with symptoms, with functional significance, or associated with KHE may require therapy. Surgical excision is one option, but it may be difficult to execute given that these lesions often have poorly defined margins.1 Other treatment choices include but are not limited to aspirin, systemic corticosteroids, vincristine, interferon-alpha, embolization, and sirolimus.8 No specific expert-directed consensus guidelines exist for these lesions, and suspicion of this lesion should prompt urgent referral to a pediatric dermatologist. Concern for Kasabach-Merritt syndrome should trigger immediate referral for rapid evaluation and management.
Complete blood count with platelet count and coagulation studies were normal in our patient. This infant underwent biopsy to confirm the diagnosis of tufted angioma and MRI to determine lesion extent. The lesion slowly involuted spontaneously without recurrence.
Mr. Haft is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital, San Diego. He is MS4 at the University of Rochester, N.Y. Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Neither Mr. Haft nor Dr. Eichenfield have any relevant financial disclosures.
References
1. Herron MD et al. Pediatr Dermatol. 2002;19(5):394-401.
2. Jones EW and Orkin M. J Am Acad Dermatol. 1989;20(2 Pt 1):214-25.
3. Wong SN and Tay YK. Pediatr Dermatol. 2002;19(5):388-93.
4. Croteau SE and Gupta D. Semin Cutan Med Surg. 2016;35(3):147-52.
5. Kelly M. Pediatr Clin North Am. 2010;57(5):1085-9.
6. Osio A et al. Arch Dermatol. 2010;146(7):758-63.
7. Padilla RS et al. Am J Dermatopathol. 1987;9(4):292-300.
8. Liu XH et al. Int J Cancer. 2016;139(7):1658-66.
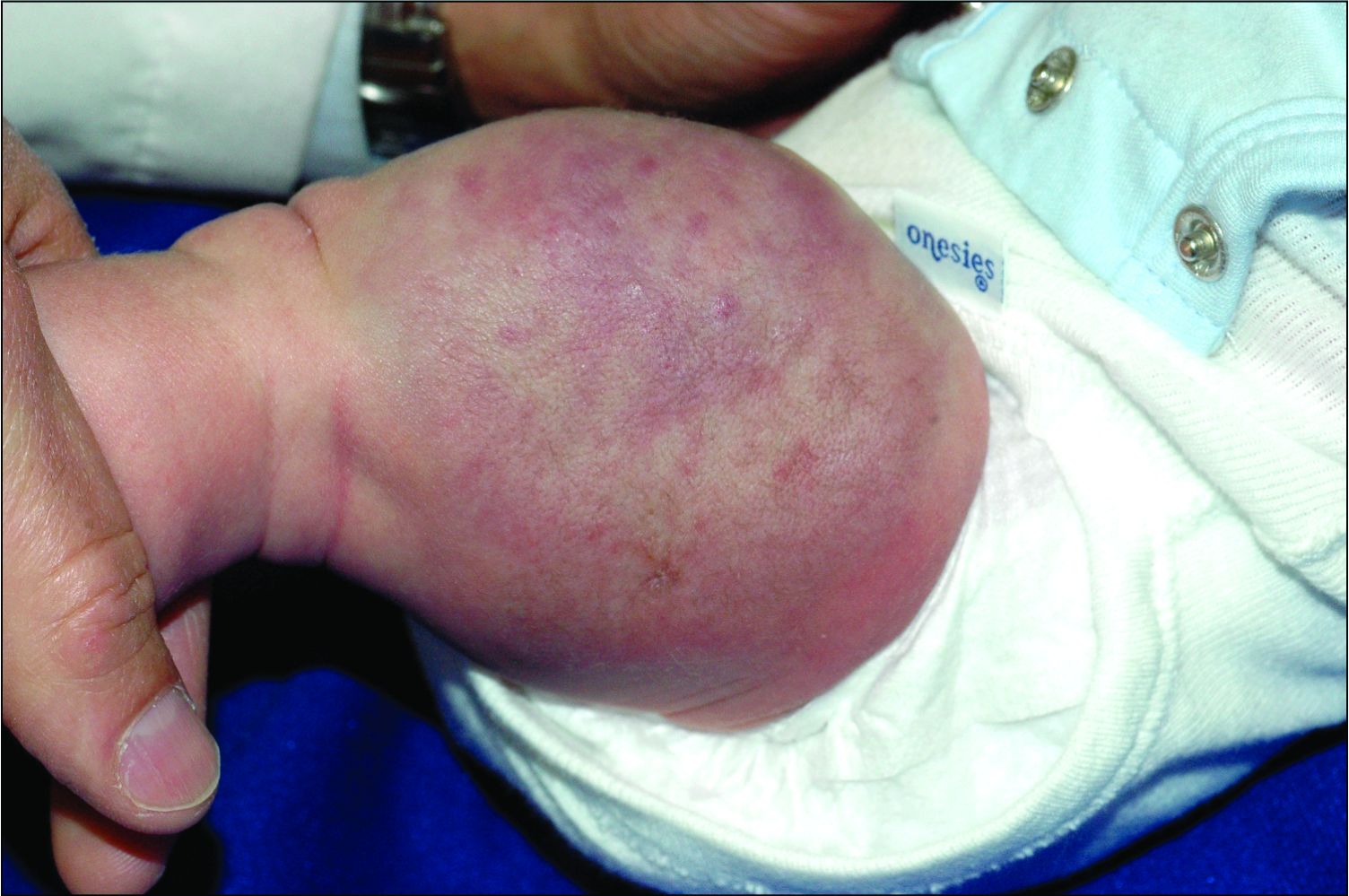
On physical exam, you see an infant with a mass of the left lower extremity. Close examination reveals an approximately 7 cm x 8 cm poorly defined mass with overlying central erythematous to violaceous color of the left anterior upper leg with a lumpy texture. The lesion is moderately firm and mildly tender on palpation.
Trends in hospital medicine program operations during COVID-19
Staffing was a challenge for most groups
What a year it has been in the world of hospital medicine with all the changes, challenges, and uncertainties surrounding the COVID-19 pandemic. Some hospitalist programs were hit hard early on with an early surge, when little was known about COVID-19, and other programs have had more time to plan and adapt to later surges.

As many readers of The Hospitalist know, the Society of Hospital Medicine publishes a biennial State of Hospital Medicine (SoHM) Report – last published in September 2020 using data from 2019. The SoHM Report contains a wealth of information that many groups find useful in evaluating their programs, with topics ranging from compensation to staffing to scheduling. As some prior months’ Survey Insights columns have alluded to, with the rapid pace of change in 2020 because of the COVID-19 pandemic, the Society of Hospital Medicine made the decision to publish an addendum highlighting the myriad of adjustments and adaptations that have occurred in such a short period of time. The COVID-19 Addendum is available to all purchasers of the SoHM Report and contains data from survey responses submitted in September 2020.
Let’s take a look at what transpired in 2020, starting with staffing – no doubt a challenge for many groups. During some periods of time, patient volumes may have fallen below historical averages with stay-at-home orders, canceled procedures, and a reluctance by patients to seek medical care. In contrast, for many groups, other parts of the year were all-hands-on-deck scenarios to care for extraordinary surges in patient volume. To compound this, many hospitalist groups had physicians and staff facing quarantine or isolation requirements because of exposures or contracting COVID-19, and locums positions may have been difficult to fill because of travel restrictions and extreme demand.
What operational changes were made in response to these staffing challenges? Perhaps one notable finding from the COVID-19 Addendum was the need for contingency planning and backup systems. From the 2020 SoHM, prior to the pandemic, 47.4% of adult hospital medicine groups had backup systems in place. In our recently published addendum, we found that 61.9% of groups instituted a backup system where none previously existed. In addition, 54.2% of groups modified their existing backup system. Some 39.6% of hospital medicine groups also utilized clinicians from other service lines to help cover service needs.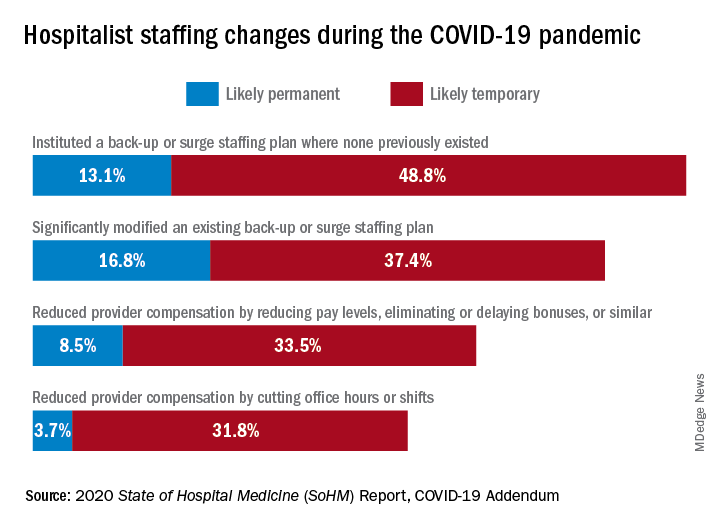
Aside from staffing, hospitals faced unprecedented financial challenges, and these effects rippled through to hospitalists. Our addendum found that 42.0% of hospitalist groups faced reductions in salary or bonuses, and 35.5% of hospital medicine groups reduced provider compensation by a reduction of work hours or shifts. I’ve personally been struck by these findings – that many hospitalists at the front-lines of COVID-19 received salary reductions, albeit temporary for many groups, during one of the most challenging years of their professional careers. Our addendum, interestingly, also found that a smaller 10.7% of groups instituted hazard pay for clinicians caring for COVID-19 patients.
So, are the changes and challenges your group faced similar to what was experienced by other hospital medicine programs? These findings and many more interesting and useful pieces of data are available in the full COVID-19 Addendum. Perhaps my biggest takeaway is that hospitalists have been perhaps the most uniquely positioned specialty to tackle the challenges of the COVID-19 pandemic. We have always been a dynamic, changing field, ready to lead and tackle change – and while change may have happened more quickly and in ways that were unforeseen just a year ago, hospitalists have undoubtedly demonstrated their strengths as leaders ready to adapt and rise to the occasion.
I am optimistic that, as we move beyond the pandemic in the coming months and years, the value that hospitalists have proven yet again will yield long-term recognition and benefits to our programs and our specialty.
Dr. Huang is a physician adviser and clinical professor of medicine in the division of hospital medicine at the University of California, San Diego. He is a member of SHM’s Practice Analysis Committee.
Staffing was a challenge for most groups
Staffing was a challenge for most groups
What a year it has been in the world of hospital medicine with all the changes, challenges, and uncertainties surrounding the COVID-19 pandemic. Some hospitalist programs were hit hard early on with an early surge, when little was known about COVID-19, and other programs have had more time to plan and adapt to later surges.
As many readers of The Hospitalist know, the Society of Hospital Medicine publishes a biennial State of Hospital Medicine (SoHM) Report – last published in September 2020 using data from 2019. The SoHM Report contains a wealth of information that many groups find useful in evaluating their programs, with topics ranging from compensation to staffing to scheduling. As some prior months’ Survey Insights columns have alluded to, with the rapid pace of change in 2020 because of the COVID-19 pandemic, the Society of Hospital Medicine made the decision to publish an addendum highlighting the myriad of adjustments and adaptations that have occurred in such a short period of time. The COVID-19 Addendum is available to all purchasers of the SoHM Report and contains data from survey responses submitted in September 2020.
Let’s take a look at what transpired in 2020, starting with staffing – no doubt a challenge for many groups. During some periods of time, patient volumes may have fallen below historical averages with stay-at-home orders, canceled procedures, and a reluctance by patients to seek medical care. In contrast, for many groups, other parts of the year were all-hands-on-deck scenarios to care for extraordinary surges in patient volume. To compound this, many hospitalist groups had physicians and staff facing quarantine or isolation requirements because of exposures or contracting COVID-19, and locums positions may have been difficult to fill because of travel restrictions and extreme demand.
What operational changes were made in response to these staffing challenges? Perhaps one notable finding from the COVID-19 Addendum was the need for contingency planning and backup systems. From the 2020 SoHM, prior to the pandemic, 47.4% of adult hospital medicine groups had backup systems in place. In our recently published addendum, we found that 61.9% of groups instituted a backup system where none previously existed. In addition, 54.2% of groups modified their existing backup system. Some 39.6% of hospital medicine groups also utilized clinicians from other service lines to help cover service needs.
Aside from staffing, hospitals faced unprecedented financial challenges, and these effects rippled through to hospitalists. Our addendum found that 42.0% of hospitalist groups faced reductions in salary or bonuses, and 35.5% of hospital medicine groups reduced provider compensation by a reduction of work hours or shifts. I’ve personally been struck by these findings – that many hospitalists at the front-lines of COVID-19 received salary reductions, albeit temporary for many groups, during one of the most challenging years of their professional careers. Our addendum, interestingly, also found that a smaller 10.7% of groups instituted hazard pay for clinicians caring for COVID-19 patients.
So, are the changes and challenges your group faced similar to what was experienced by other hospital medicine programs? These findings and many more interesting and useful pieces of data are available in the full COVID-19 Addendum. Perhaps my biggest takeaway is that hospitalists have been perhaps the most uniquely positioned specialty to tackle the challenges of the COVID-19 pandemic. We have always been a dynamic, changing field, ready to lead and tackle change – and while change may have happened more quickly and in ways that were unforeseen just a year ago, hospitalists have undoubtedly demonstrated their strengths as leaders ready to adapt and rise to the occasion.
I am optimistic that, as we move beyond the pandemic in the coming months and years, the value that hospitalists have proven yet again will yield long-term recognition and benefits to our programs and our specialty.
Dr. Huang is a physician adviser and clinical professor of medicine in the division of hospital medicine at the University of California, San Diego. He is a member of SHM’s Practice Analysis Committee.
What a year it has been in the world of hospital medicine with all the changes, challenges, and uncertainties surrounding the COVID-19 pandemic. Some hospitalist programs were hit hard early on with an early surge, when little was known about COVID-19, and other programs have had more time to plan and adapt to later surges.
As many readers of The Hospitalist know, the Society of Hospital Medicine publishes a biennial State of Hospital Medicine (SoHM) Report – last published in September 2020 using data from 2019. The SoHM Report contains a wealth of information that many groups find useful in evaluating their programs, with topics ranging from compensation to staffing to scheduling. As some prior months’ Survey Insights columns have alluded to, with the rapid pace of change in 2020 because of the COVID-19 pandemic, the Society of Hospital Medicine made the decision to publish an addendum highlighting the myriad of adjustments and adaptations that have occurred in such a short period of time. The COVID-19 Addendum is available to all purchasers of the SoHM Report and contains data from survey responses submitted in September 2020.
Let’s take a look at what transpired in 2020, starting with staffing – no doubt a challenge for many groups. During some periods of time, patient volumes may have fallen below historical averages with stay-at-home orders, canceled procedures, and a reluctance by patients to seek medical care. In contrast, for many groups, other parts of the year were all-hands-on-deck scenarios to care for extraordinary surges in patient volume. To compound this, many hospitalist groups had physicians and staff facing quarantine or isolation requirements because of exposures or contracting COVID-19, and locums positions may have been difficult to fill because of travel restrictions and extreme demand.
What operational changes were made in response to these staffing challenges? Perhaps one notable finding from the COVID-19 Addendum was the need for contingency planning and backup systems. From the 2020 SoHM, prior to the pandemic, 47.4% of adult hospital medicine groups had backup systems in place. In our recently published addendum, we found that 61.9% of groups instituted a backup system where none previously existed. In addition, 54.2% of groups modified their existing backup system. Some 39.6% of hospital medicine groups also utilized clinicians from other service lines to help cover service needs.
Aside from staffing, hospitals faced unprecedented financial challenges, and these effects rippled through to hospitalists. Our addendum found that 42.0% of hospitalist groups faced reductions in salary or bonuses, and 35.5% of hospital medicine groups reduced provider compensation by a reduction of work hours or shifts. I’ve personally been struck by these findings – that many hospitalists at the front-lines of COVID-19 received salary reductions, albeit temporary for many groups, during one of the most challenging years of their professional careers. Our addendum, interestingly, also found that a smaller 10.7% of groups instituted hazard pay for clinicians caring for COVID-19 patients.
So, are the changes and challenges your group faced similar to what was experienced by other hospital medicine programs? These findings and many more interesting and useful pieces of data are available in the full COVID-19 Addendum. Perhaps my biggest takeaway is that hospitalists have been perhaps the most uniquely positioned specialty to tackle the challenges of the COVID-19 pandemic. We have always been a dynamic, changing field, ready to lead and tackle change – and while change may have happened more quickly and in ways that were unforeseen just a year ago, hospitalists have undoubtedly demonstrated their strengths as leaders ready to adapt and rise to the occasion.
I am optimistic that, as we move beyond the pandemic in the coming months and years, the value that hospitalists have proven yet again will yield long-term recognition and benefits to our programs and our specialty.
Dr. Huang is a physician adviser and clinical professor of medicine in the division of hospital medicine at the University of California, San Diego. He is a member of SHM’s Practice Analysis Committee.
How I got started in advocacy
Rheumatology News and the Coalition of State Rheumatology Organizations have partnered together to keep rheumatologists regularly informed on the advocacy issues of the day and perhaps inspire those who may be on the fence about finding “room” in their lives for action. This inaugural piece tells how CSRO President Dr. Madelaine (Mattie) A. Feldman views advocacy and how she found her way to action.
As a rheumatologist in private practice for 30 years, with husband and kids (and now grandkids), an active social life, and an exercise regimen, I realized if I were to become active in advocacy I would have to make room for it in my busy schedule. We all come up against the question of where will we find the time for a new hobby, exercise, joining a new organization, or even just eating right? Next comes the priority list discussion. How important is advocacy for my patients, my specialty, and my profession? Ultimately, how important is it for me? Where did that desire to get involved even come from? Why have I become so passionate about the issues?

For me, the answer to these questions goes back to the 1960s when I was growing up in New Orleans. My mom participated in civil rights protests, which did not make our family popular in the neighborhood, back when the KKK put flyers on everyone’s screen door. My mother didn’t care and told me that, no matter what people said, it was our duty to stand up for what was right. That was a long time ago and sadly my mom passed away just a year after I was old enough to vote. Her words have stayed with me and are more important now than ever.
Striving for justice despite how formidable the foe is requires an inner knowing that what you are doing is meaningful and will make a difference maybe not now, maybe not next year. At some point you must believe that your efforts will create a change for the better, small as it may be. My “saying” on Twitter (@MattieRheumMD) is “I’ll keep doing what I’m doing until my cynicism catches up to my passion.”
The story about my mom is just one of the many stories in my life taking me to where I am today. We all have them. I think the reason many of us go into rheumatology may be similar to the reasoning that leads one to advocacy efforts. At this point in time we can’t yet offer a cure, but we can point to a path that leads to improvements in the lives of our patients. I have to remind myself of that, every time there is an advocacy battle ahead, whether with insurance companies or the government ... increments are important.
The four Ps of advocacy
Living with compromise is hard, particularly when working within a system that needs a complete overhaul. Still, compromise is the key to getting anything done. Compromise is one of the four Ps of advocacy. I realize that compromise doesn’t start with a P, but it is such an integral part of advocacy, I am making allowances for it. The other Ps include patience, persistence/perseverance, and passion. I’m sure there are many others that could be part of the P family, like planning and performance, but let’s stick with these.
You don’t need to have all of these qualities when you start on the road to action in advocacy. For example, my passion came first. It developed when my patients could not get access to the treatments they needed. For many reasons, the medications were either unavailable (i.e., not on formulary, tiered very high) or unaffordable (i.e., copay too high, deductible too high). My passion deepened when I saw the hypocrisy within the drug-supply channel and the mistruths being told by those who profit from this channel. It wasn’t the “profit” part that bothered me, as I’m a believer in the free market. But this was not free market, and the companies were actually profiteering on the backs of my patients and justifying it by claiming they were saving the health care system billions of dollars. The fallacy of that claim and the players in this broken system are stories for another day.
Persistence came next for me. If you let up on the message, things might not only stay the same but could get worse. Perseverance is part of persistence because you need it to keep knocking on the same door even after that door is metaphorically (hopefully not literally) slammed in your face. Often, I will feel like a broken record and think that everyone has already heard the issues, not only from me but also from my fellow advocates. But never underestimate how many times a message, particularly on a difficult issue to understand, needs to be heard before it is fully comprehended.
Patience is one of the more difficult attributes to practice when you want action. I want things to happen yesterday – not tomorrow and definitely not next year. I have learned that the wheels of change turn quite slowly in this arena, sometimes pausing for inordinately long periods of time. I realize now that during the long wait, new facts can arise, allowing me to shape a different advocacy approach, one that ultimately bolsters my case. It still is very difficult to hear that a piece of legislation that seemed to be moving forward suddenly died and won’t be heard again until the next session. With patience you move forward with a smile, maybe a half-hearted one, but a smile nonetheless. This just makes life better.
Then there is compromise. This took me the longest to understand, particularly on the issues where my passion ran the deepest. Here is where passion could potentially get in the way of action. Feeling very strongly about an issue makes it difficult to let any piece of your ideal end result fall by the wayside. Here is where the saying “the perfect is the enemy of the good” comes into play. Just because you can’t have it all, doesn’t mean you can’t do good by achieving just part of what you have been striving for. Remember if you seek perfection, without compromise, you may lose the entire battle. Is there such a thing as compromising too much? I think so, but that may just be my passion speaking.
Rheumatology News and the Coalition of State Rheumatology Organizations started this column to keep you informed about current advocacy issues in rheumatology and perhaps inspire those who may be on the fence about finding “room” in their lives for action.
Advocacy doesn’t have to take up much room in your life. It can be as simple as clicking on CSRO.info/map, finding your state, and taking action by writing a letter to your representative on an important piece of legislation, like an accumulator adjustment ban (lots more on that in future columns). Or maybe just finding the time to read this column is all the action you have room for. We all have different amounts of space for any particular activity in our busy lives. It seems one of my stories from childhood created that space for advocacy in my life. I guess you could say it created a “Rheum” for Action.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is President of the CSRO, chair of the Alliance for Safe Biologic Medicines, and a past member of the American College of Rheumatology insurance subcommittee. You can reach her at [email protected].
Rheumatology News and the Coalition of State Rheumatology Organizations have partnered together to keep rheumatologists regularly informed on the advocacy issues of the day and perhaps inspire those who may be on the fence about finding “room” in their lives for action. This inaugural piece tells how CSRO President Dr. Madelaine (Mattie) A. Feldman views advocacy and how she found her way to action.
As a rheumatologist in private practice for 30 years, with husband and kids (and now grandkids), an active social life, and an exercise regimen, I realized if I were to become active in advocacy I would have to make room for it in my busy schedule. We all come up against the question of where will we find the time for a new hobby, exercise, joining a new organization, or even just eating right? Next comes the priority list discussion. How important is advocacy for my patients, my specialty, and my profession? Ultimately, how important is it for me? Where did that desire to get involved even come from? Why have I become so passionate about the issues?
For me, the answer to these questions goes back to the 1960s when I was growing up in New Orleans. My mom participated in civil rights protests, which did not make our family popular in the neighborhood, back when the KKK put flyers on everyone’s screen door. My mother didn’t care and told me that, no matter what people said, it was our duty to stand up for what was right. That was a long time ago and sadly my mom passed away just a year after I was old enough to vote. Her words have stayed with me and are more important now than ever.
Striving for justice despite how formidable the foe is requires an inner knowing that what you are doing is meaningful and will make a difference maybe not now, maybe not next year. At some point you must believe that your efforts will create a change for the better, small as it may be. My “saying” on Twitter (@MattieRheumMD) is “I’ll keep doing what I’m doing until my cynicism catches up to my passion.”
The story about my mom is just one of the many stories in my life taking me to where I am today. We all have them. I think the reason many of us go into rheumatology may be similar to the reasoning that leads one to advocacy efforts. At this point in time we can’t yet offer a cure, but we can point to a path that leads to improvements in the lives of our patients. I have to remind myself of that, every time there is an advocacy battle ahead, whether with insurance companies or the government ... increments are important.
The four Ps of advocacy
Living with compromise is hard, particularly when working within a system that needs a complete overhaul. Still, compromise is the key to getting anything done. Compromise is one of the four Ps of advocacy. I realize that compromise doesn’t start with a P, but it is such an integral part of advocacy, I am making allowances for it. The other Ps include patience, persistence/perseverance, and passion. I’m sure there are many others that could be part of the P family, like planning and performance, but let’s stick with these.
You don’t need to have all of these qualities when you start on the road to action in advocacy. For example, my passion came first. It developed when my patients could not get access to the treatments they needed. For many reasons, the medications were either unavailable (i.e., not on formulary, tiered very high) or unaffordable (i.e., copay too high, deductible too high). My passion deepened when I saw the hypocrisy within the drug-supply channel and the mistruths being told by those who profit from this channel. It wasn’t the “profit” part that bothered me, as I’m a believer in the free market. But this was not free market, and the companies were actually profiteering on the backs of my patients and justifying it by claiming they were saving the health care system billions of dollars. The fallacy of that claim and the players in this broken system are stories for another day.
Persistence came next for me. If you let up on the message, things might not only stay the same but could get worse. Perseverance is part of persistence because you need it to keep knocking on the same door even after that door is metaphorically (hopefully not literally) slammed in your face. Often, I will feel like a broken record and think that everyone has already heard the issues, not only from me but also from my fellow advocates. But never underestimate how many times a message, particularly on a difficult issue to understand, needs to be heard before it is fully comprehended.
Patience is one of the more difficult attributes to practice when you want action. I want things to happen yesterday – not tomorrow and definitely not next year. I have learned that the wheels of change turn quite slowly in this arena, sometimes pausing for inordinately long periods of time. I realize now that during the long wait, new facts can arise, allowing me to shape a different advocacy approach, one that ultimately bolsters my case. It still is very difficult to hear that a piece of legislation that seemed to be moving forward suddenly died and won’t be heard again until the next session. With patience you move forward with a smile, maybe a half-hearted one, but a smile nonetheless. This just makes life better.
Then there is compromise. This took me the longest to understand, particularly on the issues where my passion ran the deepest. Here is where passion could potentially get in the way of action. Feeling very strongly about an issue makes it difficult to let any piece of your ideal end result fall by the wayside. Here is where the saying “the perfect is the enemy of the good” comes into play. Just because you can’t have it all, doesn’t mean you can’t do good by achieving just part of what you have been striving for. Remember if you seek perfection, without compromise, you may lose the entire battle. Is there such a thing as compromising too much? I think so, but that may just be my passion speaking.
Rheumatology News and the Coalition of State Rheumatology Organizations started this column to keep you informed about current advocacy issues in rheumatology and perhaps inspire those who may be on the fence about finding “room” in their lives for action.
Advocacy doesn’t have to take up much room in your life. It can be as simple as clicking on CSRO.info/map, finding your state, and taking action by writing a letter to your representative on an important piece of legislation, like an accumulator adjustment ban (lots more on that in future columns). Or maybe just finding the time to read this column is all the action you have room for. We all have different amounts of space for any particular activity in our busy lives. It seems one of my stories from childhood created that space for advocacy in my life. I guess you could say it created a “Rheum” for Action.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is President of the CSRO, chair of the Alliance for Safe Biologic Medicines, and a past member of the American College of Rheumatology insurance subcommittee. You can reach her at [email protected].
Rheumatology News and the Coalition of State Rheumatology Organizations have partnered together to keep rheumatologists regularly informed on the advocacy issues of the day and perhaps inspire those who may be on the fence about finding “room” in their lives for action. This inaugural piece tells how CSRO President Dr. Madelaine (Mattie) A. Feldman views advocacy and how she found her way to action.
As a rheumatologist in private practice for 30 years, with husband and kids (and now grandkids), an active social life, and an exercise regimen, I realized if I were to become active in advocacy I would have to make room for it in my busy schedule. We all come up against the question of where will we find the time for a new hobby, exercise, joining a new organization, or even just eating right? Next comes the priority list discussion. How important is advocacy for my patients, my specialty, and my profession? Ultimately, how important is it for me? Where did that desire to get involved even come from? Why have I become so passionate about the issues?
For me, the answer to these questions goes back to the 1960s when I was growing up in New Orleans. My mom participated in civil rights protests, which did not make our family popular in the neighborhood, back when the KKK put flyers on everyone’s screen door. My mother didn’t care and told me that, no matter what people said, it was our duty to stand up for what was right. That was a long time ago and sadly my mom passed away just a year after I was old enough to vote. Her words have stayed with me and are more important now than ever.
Striving for justice despite how formidable the foe is requires an inner knowing that what you are doing is meaningful and will make a difference maybe not now, maybe not next year. At some point you must believe that your efforts will create a change for the better, small as it may be. My “saying” on Twitter (@MattieRheumMD) is “I’ll keep doing what I’m doing until my cynicism catches up to my passion.”
The story about my mom is just one of the many stories in my life taking me to where I am today. We all have them. I think the reason many of us go into rheumatology may be similar to the reasoning that leads one to advocacy efforts. At this point in time we can’t yet offer a cure, but we can point to a path that leads to improvements in the lives of our patients. I have to remind myself of that, every time there is an advocacy battle ahead, whether with insurance companies or the government ... increments are important.
The four Ps of advocacy
Living with compromise is hard, particularly when working within a system that needs a complete overhaul. Still, compromise is the key to getting anything done. Compromise is one of the four Ps of advocacy. I realize that compromise doesn’t start with a P, but it is such an integral part of advocacy, I am making allowances for it. The other Ps include patience, persistence/perseverance, and passion. I’m sure there are many others that could be part of the P family, like planning and performance, but let’s stick with these.
You don’t need to have all of these qualities when you start on the road to action in advocacy. For example, my passion came first. It developed when my patients could not get access to the treatments they needed. For many reasons, the medications were either unavailable (i.e., not on formulary, tiered very high) or unaffordable (i.e., copay too high, deductible too high). My passion deepened when I saw the hypocrisy within the drug-supply channel and the mistruths being told by those who profit from this channel. It wasn’t the “profit” part that bothered me, as I’m a believer in the free market. But this was not free market, and the companies were actually profiteering on the backs of my patients and justifying it by claiming they were saving the health care system billions of dollars. The fallacy of that claim and the players in this broken system are stories for another day.
Persistence came next for me. If you let up on the message, things might not only stay the same but could get worse. Perseverance is part of persistence because you need it to keep knocking on the same door even after that door is metaphorically (hopefully not literally) slammed in your face. Often, I will feel like a broken record and think that everyone has already heard the issues, not only from me but also from my fellow advocates. But never underestimate how many times a message, particularly on a difficult issue to understand, needs to be heard before it is fully comprehended.
Patience is one of the more difficult attributes to practice when you want action. I want things to happen yesterday – not tomorrow and definitely not next year. I have learned that the wheels of change turn quite slowly in this arena, sometimes pausing for inordinately long periods of time. I realize now that during the long wait, new facts can arise, allowing me to shape a different advocacy approach, one that ultimately bolsters my case. It still is very difficult to hear that a piece of legislation that seemed to be moving forward suddenly died and won’t be heard again until the next session. With patience you move forward with a smile, maybe a half-hearted one, but a smile nonetheless. This just makes life better.
Then there is compromise. This took me the longest to understand, particularly on the issues where my passion ran the deepest. Here is where passion could potentially get in the way of action. Feeling very strongly about an issue makes it difficult to let any piece of your ideal end result fall by the wayside. Here is where the saying “the perfect is the enemy of the good” comes into play. Just because you can’t have it all, doesn’t mean you can’t do good by achieving just part of what you have been striving for. Remember if you seek perfection, without compromise, you may lose the entire battle. Is there such a thing as compromising too much? I think so, but that may just be my passion speaking.
Rheumatology News and the Coalition of State Rheumatology Organizations started this column to keep you informed about current advocacy issues in rheumatology and perhaps inspire those who may be on the fence about finding “room” in their lives for action.
Advocacy doesn’t have to take up much room in your life. It can be as simple as clicking on CSRO.info/map, finding your state, and taking action by writing a letter to your representative on an important piece of legislation, like an accumulator adjustment ban (lots more on that in future columns). Or maybe just finding the time to read this column is all the action you have room for. We all have different amounts of space for any particular activity in our busy lives. It seems one of my stories from childhood created that space for advocacy in my life. I guess you could say it created a “Rheum” for Action.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is President of the CSRO, chair of the Alliance for Safe Biologic Medicines, and a past member of the American College of Rheumatology insurance subcommittee. You can reach her at [email protected].
Is empathy the limit to sociopathy?
Society is having a moment of reflection about the role of law enforcement and correctional facilities in addressing societal problems. During this moment, psychiatry is being asked by courts to arbitrate who qualifies and ultimately deserves certain judgments.

In particular, we are asked to assess how dangerous an individual may be using violent risk assessment tools and measures of antisocial disorders. As such, we are tasked with pointing out the negative factors of defendants. Alternatively, psychiatry is also asked to explain, using biopsychosocial determinants, what led an individual to act in a deviant manner. As such, we are tasked with pointing out mitigating factors of defendants. In this article, we attempt to look at limitations in both paradigms to encourage a more prudent forensic approach.
Negative factors
The criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM) are not composed of rigid rules with validity markers to measure their veracity but leave room for clinical judgment, variance across individuals, and future research and treatment needs.

There are some benefits to having room for clinical judgment, but it can also lead to overdiagnosis.1 This problem is particularly reflected in the diagnosis of antisocial personality disorder (ASPD), the criteria of which includes failure to conform to social norms, deceitfulness, impulsivity, irritability, recklessness, irresponsibility, and lack of remorse. Each of these criteria is ripe for subjectivity by an inexperienced or biased reviewer.
For example, it is common in our practice to see only two discrete events interpreted as a “pattern of behavior.” Such events could include two lapses in judgment to demonstrate a pattern of behavior meeting the criteria for ASPD. Using this logic, however, most Americans would meet those criteria. According to the National Survey of Drug Use and Health, the majority of Americans have tried illicit substances.2 We presume that many have tried illicit substances at least two times in their lives – in theory creating a pattern – and that subsequently they omitted that information on standard employment application forms. In doing so, they could easily be interpreted in court to have demonstrated failure to follow rules, deceitfulness in wrongfully filing an employment application, impulsivity in deciding to use drugs, recklessness in choosing to use drugs, irresponsibility for using drugs, and a lack of remorse by not acknowledging the use on an employment application, thereby meeting criteria for antisocial personality disorder.
The well-respected Hare Psychopathy Checklist contains similar opportunities for subjective interpretation by a biased evaluator. Conning, glibness, lack of guilt, lack of realistic goals, and irresponsibility are easily diverted to pathologize an individual into an exaggerated sense of menace. Journalist Jon Ronson famously challenged those concepts in his book, “The Psychopath Test: A Journey Through the Madness Industry,” a New York Times bestseller. It is common in our practice to see evaluators list dozens of scales allegedly proving someone’s dangerousness, without realizing the recurrent subjectivity involved in all those assessments.
Forensic evaluators arguing for conviction often rely on violence risk assessments to establish defendants’ propensity for future violence and to predict recidivism. There are numerous violence risk assessment tools, including: the Violence Risk Scale,3 the HCR-20 version 3 (HCR-20 v3),4 and Correctional Offender Management Profiling for Alternative Sanctions (COMPAS). Yet, despite their perceived rigor and reliability from being established assessments, their usefulness continues to be challenged.5Julia Dressel and Hany Farid, PhD, showed in 2018 how people with little to no criminal justice expertise and given only the sex, age, and previous criminal history of defendants were no less accurate than COMPAS.6 Those findings are concerning and should give us pause when we are tempted to rely on seemingly objective measures that can lead us astray. Not only can such reliance result in injudicious court decisions, but it can saddle defendants with a documented report of their perceived elevated risk for violence.
In the forensic setting, ASPD is often treated like a lifelong diagnosis. This is in part because of personality disorders being defined since the DSM-III as “enduring patterns ... [that] continue throughout most of adult life.” Even if a defendant who is diagnosed with ASPD no longer behaves antisocially, a historical ASPD diagnosis is difficult to escape. Historical behavior is part of the diagnosis, and there are no guidelines to determine at what point a person can be rid of it or what redeeming qualities or circumstances make a prior diagnosis inappropriate.
Yet, some evidence suggests that ASPD is one of the least reliable psychiatric diagnoses and that the agreement between providers of such a diagnosis was “questionable.”7Robert D. Hare, PhD, himself has been described as believing that “an awful lot of people misuse his checklist.”8 And a recent study found no “evidence for the claim that [Hare Psychopathy Checklist] psychopaths are untreatable ... on the contrary, there was replicated evidence of positive treatment outcomes.”9 Unfortunately, legal structures often help enshrine an erroneous ASPD diagnosis by imposing more punishing sentences to those diagnosed. Instead, we should recognize that ASPD can also be the culmination of biological as well as changing social and environmental circumstances.
Mitigating factors
On the other side, the defense expert also faces significant challenges, though the tools are different. Contrary to the prosecuting expert who loads an arsenal of subjective assessment tools, the defense expert will point to childhood trauma and mental illness as extenuating explanations for a crime. Having suffered abuse as a child is advanced to justify someone’s subsequent violence. This problem is reflected in the diagnosis of posttraumatic stress disorder (PTSD). An unscrupulous expert may simply allow an evaluee to endorse symptoms without clinical correlates or rigorous validation to advance this narrative.
For example, psychiatrists commonly ascribe the DSM criteria A for PTSD, “directly experiencing the traumatic event(s),” to a smaller slight in life. Some experts suggest that a medical diagnosis, even if not life-threatening but perceived as such, could warrant the diagnosis.10 This would expand our understanding of trauma and its consequences significantly. Yet already, a survey of Detroit area residents in 1998 found that 89.6% of the interviewees reported having experienced a significant trauma and that the average number of traumatic experiences was 4.8.11 The meaning of a diagnosis that can be applied to almost 90% of a population has unclear usefulness, especially if meant to diminish guilt and responsibility.
More recently, citing Adverse Childhood Experiences (ACEs) has been a common method of supporting mitigating evaluations. Using the ACEs questionnaires, researchers have supported the idea that social programs are a key player in an improved criminal justice system. The ACEs study identified 10 forms of childhood trauma in 17,000 patients, including abuse, neglect, abandonment, household dysfunction, and exposure to violence, that were strongly associated with negative psychological outcomes, engagement in high-risk behaviors, significant medical consequences, and even early death.12 However, similarly to past trauma, the prevalence of ACEs in the forensic population is the norm, not the exception.
Additional thoughts
Of particular concern is when diagnostic criteria intersect or seemingly contradict one another. For example, acts such as an outburst of anger may be interpreted by one evaluator as a sign of deviance, irritability, or recklessness – and meeting antisocial personality disorder criteria. Whereas another evaluator may interpret the same incident as hypervigilance, exaggerated startle response, or self-destructive behavior in PTSD.
An incident of not assisting someone in need may be interpreted as lack of remorse and glibness from antisocial characteristics or avoidance and detachment from others as a reaction to past trauma. Flashbacks from trauma can be interpreted by some as violent fantasies. Even the experience of trauma can be viewed as a risk factor for future violence. In some ways, our perspectives are influenced by our examination of someone’s history through the lens of sociopathy or empathy.
In summary
Psychiatry is entrusted by courts to comment on negative and mitigating factors. Negative factors hinge in part on our subjective impression of sociopathy, and mitigating factors hinge, in part, on our empathy for a defendant’s trauma. Psychiatry should recognize the limitations of both sides and humble itself in providing balanced evaluations to courts.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Amendolara is a first-year psychiatry resident at University of California, San Diego. He spent years advocating for survivors of rape and domestic violence at the Crime Victims Treatment Center in New York and conducted public health research at Lourdes Center for Public Health in Camden, N.J. Dr. Amendolara has no disclosures. Dr. Ngo is a second-year child neurology resident at University of California, Los Angeles. She received a master’s degree in narrative medicine from Columbia University, New York. She has no disclosures.
References
1. Frances A. Saving Normal: An Insider’s Revolt Against Out-of-Control Psychiatric Diagnosis, DSM-5, Big Pharma and the Medicalization of Ordinary Life. Harper Collins, 2013.
2. Key Substance Use and Mental Health Indicators in the United States. National Survey on Drug Use and Health. 2018.
3. Wong SCP and Gordon A. Psychol Public Policy Law. 2006;12(3):279-309.
4. Douglas KS et al. Mental Health Law & Policy Institute. About the Historical Clinical Risk Management-20, Version 3.
5. Angwin J et al. ProPublica. 2016 May 23.
6. Dressel J and Farid H. Sci Adv. 2018;4(1). doi: 10.1126/sciady.aao5580.
7. Freedman R et al. Am J Psychiatry. 2013 Jan;170(1):1-5.
8. Lillie B. The complexities of the psychopath test: A Q&A with Ron Jonson. TEDBlog. 2012 Aug 15.
9. Larsen RR et al. Psychol Public Policy Law. 2020;26(3):297-311.
10. Cordova MJ. Psychiatric Times. 2020 Jul 31;37(7).
11. Breslau N et al. Arch Gen Psychiatry. 1998;55(7):626-32.
12. Reavis JA et al. Perm J. 2013 Spring;17(2):44-8.
Society is having a moment of reflection about the role of law enforcement and correctional facilities in addressing societal problems. During this moment, psychiatry is being asked by courts to arbitrate who qualifies and ultimately deserves certain judgments.
In particular, we are asked to assess how dangerous an individual may be using violent risk assessment tools and measures of antisocial disorders. As such, we are tasked with pointing out the negative factors of defendants. Alternatively, psychiatry is also asked to explain, using biopsychosocial determinants, what led an individual to act in a deviant manner. As such, we are tasked with pointing out mitigating factors of defendants. In this article, we attempt to look at limitations in both paradigms to encourage a more prudent forensic approach.
Negative factors
The criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM) are not composed of rigid rules with validity markers to measure their veracity but leave room for clinical judgment, variance across individuals, and future research and treatment needs.
There are some benefits to having room for clinical judgment, but it can also lead to overdiagnosis.1 This problem is particularly reflected in the diagnosis of antisocial personality disorder (ASPD), the criteria of which includes failure to conform to social norms, deceitfulness, impulsivity, irritability, recklessness, irresponsibility, and lack of remorse. Each of these criteria is ripe for subjectivity by an inexperienced or biased reviewer.
For example, it is common in our practice to see only two discrete events interpreted as a “pattern of behavior.” Such events could include two lapses in judgment to demonstrate a pattern of behavior meeting the criteria for ASPD. Using this logic, however, most Americans would meet those criteria. According to the National Survey of Drug Use and Health, the majority of Americans have tried illicit substances.2 We presume that many have tried illicit substances at least two times in their lives – in theory creating a pattern – and that subsequently they omitted that information on standard employment application forms. In doing so, they could easily be interpreted in court to have demonstrated failure to follow rules, deceitfulness in wrongfully filing an employment application, impulsivity in deciding to use drugs, recklessness in choosing to use drugs, irresponsibility for using drugs, and a lack of remorse by not acknowledging the use on an employment application, thereby meeting criteria for antisocial personality disorder.
The well-respected Hare Psychopathy Checklist contains similar opportunities for subjective interpretation by a biased evaluator. Conning, glibness, lack of guilt, lack of realistic goals, and irresponsibility are easily diverted to pathologize an individual into an exaggerated sense of menace. Journalist Jon Ronson famously challenged those concepts in his book, “The Psychopath Test: A Journey Through the Madness Industry,” a New York Times bestseller. It is common in our practice to see evaluators list dozens of scales allegedly proving someone’s dangerousness, without realizing the recurrent subjectivity involved in all those assessments.
Forensic evaluators arguing for conviction often rely on violence risk assessments to establish defendants’ propensity for future violence and to predict recidivism. There are numerous violence risk assessment tools, including: the Violence Risk Scale,3 the HCR-20 version 3 (HCR-20 v3),4 and Correctional Offender Management Profiling for Alternative Sanctions (COMPAS). Yet, despite their perceived rigor and reliability from being established assessments, their usefulness continues to be challenged.5Julia Dressel and Hany Farid, PhD, showed in 2018 how people with little to no criminal justice expertise and given only the sex, age, and previous criminal history of defendants were no less accurate than COMPAS.6 Those findings are concerning and should give us pause when we are tempted to rely on seemingly objective measures that can lead us astray. Not only can such reliance result in injudicious court decisions, but it can saddle defendants with a documented report of their perceived elevated risk for violence.
In the forensic setting, ASPD is often treated like a lifelong diagnosis. This is in part because of personality disorders being defined since the DSM-III as “enduring patterns ... [that] continue throughout most of adult life.” Even if a defendant who is diagnosed with ASPD no longer behaves antisocially, a historical ASPD diagnosis is difficult to escape. Historical behavior is part of the diagnosis, and there are no guidelines to determine at what point a person can be rid of it or what redeeming qualities or circumstances make a prior diagnosis inappropriate.
Yet, some evidence suggests that ASPD is one of the least reliable psychiatric diagnoses and that the agreement between providers of such a diagnosis was “questionable.”7Robert D. Hare, PhD, himself has been described as believing that “an awful lot of people misuse his checklist.”8 And a recent study found no “evidence for the claim that [Hare Psychopathy Checklist] psychopaths are untreatable ... on the contrary, there was replicated evidence of positive treatment outcomes.”9 Unfortunately, legal structures often help enshrine an erroneous ASPD diagnosis by imposing more punishing sentences to those diagnosed. Instead, we should recognize that ASPD can also be the culmination of biological as well as changing social and environmental circumstances.
Mitigating factors
On the other side, the defense expert also faces significant challenges, though the tools are different. Contrary to the prosecuting expert who loads an arsenal of subjective assessment tools, the defense expert will point to childhood trauma and mental illness as extenuating explanations for a crime. Having suffered abuse as a child is advanced to justify someone’s subsequent violence. This problem is reflected in the diagnosis of posttraumatic stress disorder (PTSD). An unscrupulous expert may simply allow an evaluee to endorse symptoms without clinical correlates or rigorous validation to advance this narrative.
For example, psychiatrists commonly ascribe the DSM criteria A for PTSD, “directly experiencing the traumatic event(s),” to a smaller slight in life. Some experts suggest that a medical diagnosis, even if not life-threatening but perceived as such, could warrant the diagnosis.10 This would expand our understanding of trauma and its consequences significantly. Yet already, a survey of Detroit area residents in 1998 found that 89.6% of the interviewees reported having experienced a significant trauma and that the average number of traumatic experiences was 4.8.11 The meaning of a diagnosis that can be applied to almost 90% of a population has unclear usefulness, especially if meant to diminish guilt and responsibility.
More recently, citing Adverse Childhood Experiences (ACEs) has been a common method of supporting mitigating evaluations. Using the ACEs questionnaires, researchers have supported the idea that social programs are a key player in an improved criminal justice system. The ACEs study identified 10 forms of childhood trauma in 17,000 patients, including abuse, neglect, abandonment, household dysfunction, and exposure to violence, that were strongly associated with negative psychological outcomes, engagement in high-risk behaviors, significant medical consequences, and even early death.12 However, similarly to past trauma, the prevalence of ACEs in the forensic population is the norm, not the exception.
Additional thoughts
Of particular concern is when diagnostic criteria intersect or seemingly contradict one another. For example, acts such as an outburst of anger may be interpreted by one evaluator as a sign of deviance, irritability, or recklessness – and meeting antisocial personality disorder criteria. Whereas another evaluator may interpret the same incident as hypervigilance, exaggerated startle response, or self-destructive behavior in PTSD.
An incident of not assisting someone in need may be interpreted as lack of remorse and glibness from antisocial characteristics or avoidance and detachment from others as a reaction to past trauma. Flashbacks from trauma can be interpreted by some as violent fantasies. Even the experience of trauma can be viewed as a risk factor for future violence. In some ways, our perspectives are influenced by our examination of someone’s history through the lens of sociopathy or empathy.
In summary
Psychiatry is entrusted by courts to comment on negative and mitigating factors. Negative factors hinge in part on our subjective impression of sociopathy, and mitigating factors hinge, in part, on our empathy for a defendant’s trauma. Psychiatry should recognize the limitations of both sides and humble itself in providing balanced evaluations to courts.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Amendolara is a first-year psychiatry resident at University of California, San Diego. He spent years advocating for survivors of rape and domestic violence at the Crime Victims Treatment Center in New York and conducted public health research at Lourdes Center for Public Health in Camden, N.J. Dr. Amendolara has no disclosures. Dr. Ngo is a second-year child neurology resident at University of California, Los Angeles. She received a master’s degree in narrative medicine from Columbia University, New York. She has no disclosures.
References
1. Frances A. Saving Normal: An Insider’s Revolt Against Out-of-Control Psychiatric Diagnosis, DSM-5, Big Pharma and the Medicalization of Ordinary Life. Harper Collins, 2013.
2. Key Substance Use and Mental Health Indicators in the United States. National Survey on Drug Use and Health. 2018.
3. Wong SCP and Gordon A. Psychol Public Policy Law. 2006;12(3):279-309.
4. Douglas KS et al. Mental Health Law & Policy Institute. About the Historical Clinical Risk Management-20, Version 3.
5. Angwin J et al. ProPublica. 2016 May 23.
6. Dressel J and Farid H. Sci Adv. 2018;4(1). doi: 10.1126/sciady.aao5580.
7. Freedman R et al. Am J Psychiatry. 2013 Jan;170(1):1-5.
8. Lillie B. The complexities of the psychopath test: A Q&A with Ron Jonson. TEDBlog. 2012 Aug 15.
9. Larsen RR et al. Psychol Public Policy Law. 2020;26(3):297-311.
10. Cordova MJ. Psychiatric Times. 2020 Jul 31;37(7).
11. Breslau N et al. Arch Gen Psychiatry. 1998;55(7):626-32.
12. Reavis JA et al. Perm J. 2013 Spring;17(2):44-8.
Society is having a moment of reflection about the role of law enforcement and correctional facilities in addressing societal problems. During this moment, psychiatry is being asked by courts to arbitrate who qualifies and ultimately deserves certain judgments.
In particular, we are asked to assess how dangerous an individual may be using violent risk assessment tools and measures of antisocial disorders. As such, we are tasked with pointing out the negative factors of defendants. Alternatively, psychiatry is also asked to explain, using biopsychosocial determinants, what led an individual to act in a deviant manner. As such, we are tasked with pointing out mitigating factors of defendants. In this article, we attempt to look at limitations in both paradigms to encourage a more prudent forensic approach.
Negative factors
The criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM) are not composed of rigid rules with validity markers to measure their veracity but leave room for clinical judgment, variance across individuals, and future research and treatment needs.
There are some benefits to having room for clinical judgment, but it can also lead to overdiagnosis.1 This problem is particularly reflected in the diagnosis of antisocial personality disorder (ASPD), the criteria of which includes failure to conform to social norms, deceitfulness, impulsivity, irritability, recklessness, irresponsibility, and lack of remorse. Each of these criteria is ripe for subjectivity by an inexperienced or biased reviewer.
For example, it is common in our practice to see only two discrete events interpreted as a “pattern of behavior.” Such events could include two lapses in judgment to demonstrate a pattern of behavior meeting the criteria for ASPD. Using this logic, however, most Americans would meet those criteria. According to the National Survey of Drug Use and Health, the majority of Americans have tried illicit substances.2 We presume that many have tried illicit substances at least two times in their lives – in theory creating a pattern – and that subsequently they omitted that information on standard employment application forms. In doing so, they could easily be interpreted in court to have demonstrated failure to follow rules, deceitfulness in wrongfully filing an employment application, impulsivity in deciding to use drugs, recklessness in choosing to use drugs, irresponsibility for using drugs, and a lack of remorse by not acknowledging the use on an employment application, thereby meeting criteria for antisocial personality disorder.
The well-respected Hare Psychopathy Checklist contains similar opportunities for subjective interpretation by a biased evaluator. Conning, glibness, lack of guilt, lack of realistic goals, and irresponsibility are easily diverted to pathologize an individual into an exaggerated sense of menace. Journalist Jon Ronson famously challenged those concepts in his book, “The Psychopath Test: A Journey Through the Madness Industry,” a New York Times bestseller. It is common in our practice to see evaluators list dozens of scales allegedly proving someone’s dangerousness, without realizing the recurrent subjectivity involved in all those assessments.
Forensic evaluators arguing for conviction often rely on violence risk assessments to establish defendants’ propensity for future violence and to predict recidivism. There are numerous violence risk assessment tools, including: the Violence Risk Scale,3 the HCR-20 version 3 (HCR-20 v3),4 and Correctional Offender Management Profiling for Alternative Sanctions (COMPAS). Yet, despite their perceived rigor and reliability from being established assessments, their usefulness continues to be challenged.5Julia Dressel and Hany Farid, PhD, showed in 2018 how people with little to no criminal justice expertise and given only the sex, age, and previous criminal history of defendants were no less accurate than COMPAS.6 Those findings are concerning and should give us pause when we are tempted to rely on seemingly objective measures that can lead us astray. Not only can such reliance result in injudicious court decisions, but it can saddle defendants with a documented report of their perceived elevated risk for violence.
In the forensic setting, ASPD is often treated like a lifelong diagnosis. This is in part because of personality disorders being defined since the DSM-III as “enduring patterns ... [that] continue throughout most of adult life.” Even if a defendant who is diagnosed with ASPD no longer behaves antisocially, a historical ASPD diagnosis is difficult to escape. Historical behavior is part of the diagnosis, and there are no guidelines to determine at what point a person can be rid of it or what redeeming qualities or circumstances make a prior diagnosis inappropriate.
Yet, some evidence suggests that ASPD is one of the least reliable psychiatric diagnoses and that the agreement between providers of such a diagnosis was “questionable.”7Robert D. Hare, PhD, himself has been described as believing that “an awful lot of people misuse his checklist.”8 And a recent study found no “evidence for the claim that [Hare Psychopathy Checklist] psychopaths are untreatable ... on the contrary, there was replicated evidence of positive treatment outcomes.”9 Unfortunately, legal structures often help enshrine an erroneous ASPD diagnosis by imposing more punishing sentences to those diagnosed. Instead, we should recognize that ASPD can also be the culmination of biological as well as changing social and environmental circumstances.
Mitigating factors
On the other side, the defense expert also faces significant challenges, though the tools are different. Contrary to the prosecuting expert who loads an arsenal of subjective assessment tools, the defense expert will point to childhood trauma and mental illness as extenuating explanations for a crime. Having suffered abuse as a child is advanced to justify someone’s subsequent violence. This problem is reflected in the diagnosis of posttraumatic stress disorder (PTSD). An unscrupulous expert may simply allow an evaluee to endorse symptoms without clinical correlates or rigorous validation to advance this narrative.
For example, psychiatrists commonly ascribe the DSM criteria A for PTSD, “directly experiencing the traumatic event(s),” to a smaller slight in life. Some experts suggest that a medical diagnosis, even if not life-threatening but perceived as such, could warrant the diagnosis.10 This would expand our understanding of trauma and its consequences significantly. Yet already, a survey of Detroit area residents in 1998 found that 89.6% of the interviewees reported having experienced a significant trauma and that the average number of traumatic experiences was 4.8.11 The meaning of a diagnosis that can be applied to almost 90% of a population has unclear usefulness, especially if meant to diminish guilt and responsibility.
More recently, citing Adverse Childhood Experiences (ACEs) has been a common method of supporting mitigating evaluations. Using the ACEs questionnaires, researchers have supported the idea that social programs are a key player in an improved criminal justice system. The ACEs study identified 10 forms of childhood trauma in 17,000 patients, including abuse, neglect, abandonment, household dysfunction, and exposure to violence, that were strongly associated with negative psychological outcomes, engagement in high-risk behaviors, significant medical consequences, and even early death.12 However, similarly to past trauma, the prevalence of ACEs in the forensic population is the norm, not the exception.
Additional thoughts
Of particular concern is when diagnostic criteria intersect or seemingly contradict one another. For example, acts such as an outburst of anger may be interpreted by one evaluator as a sign of deviance, irritability, or recklessness – and meeting antisocial personality disorder criteria. Whereas another evaluator may interpret the same incident as hypervigilance, exaggerated startle response, or self-destructive behavior in PTSD.
An incident of not assisting someone in need may be interpreted as lack of remorse and glibness from antisocial characteristics or avoidance and detachment from others as a reaction to past trauma. Flashbacks from trauma can be interpreted by some as violent fantasies. Even the experience of trauma can be viewed as a risk factor for future violence. In some ways, our perspectives are influenced by our examination of someone’s history through the lens of sociopathy or empathy.
In summary
Psychiatry is entrusted by courts to comment on negative and mitigating factors. Negative factors hinge in part on our subjective impression of sociopathy, and mitigating factors hinge, in part, on our empathy for a defendant’s trauma. Psychiatry should recognize the limitations of both sides and humble itself in providing balanced evaluations to courts.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Amendolara is a first-year psychiatry resident at University of California, San Diego. He spent years advocating for survivors of rape and domestic violence at the Crime Victims Treatment Center in New York and conducted public health research at Lourdes Center for Public Health in Camden, N.J. Dr. Amendolara has no disclosures. Dr. Ngo is a second-year child neurology resident at University of California, Los Angeles. She received a master’s degree in narrative medicine from Columbia University, New York. She has no disclosures.
References
1. Frances A. Saving Normal: An Insider’s Revolt Against Out-of-Control Psychiatric Diagnosis, DSM-5, Big Pharma and the Medicalization of Ordinary Life. Harper Collins, 2013.
2. Key Substance Use and Mental Health Indicators in the United States. National Survey on Drug Use and Health. 2018.
3. Wong SCP and Gordon A. Psychol Public Policy Law. 2006;12(3):279-309.
4. Douglas KS et al. Mental Health Law & Policy Institute. About the Historical Clinical Risk Management-20, Version 3.
5. Angwin J et al. ProPublica. 2016 May 23.
6. Dressel J and Farid H. Sci Adv. 2018;4(1). doi: 10.1126/sciady.aao5580.
7. Freedman R et al. Am J Psychiatry. 2013 Jan;170(1):1-5.
8. Lillie B. The complexities of the psychopath test: A Q&A with Ron Jonson. TEDBlog. 2012 Aug 15.
9. Larsen RR et al. Psychol Public Policy Law. 2020;26(3):297-311.
10. Cordova MJ. Psychiatric Times. 2020 Jul 31;37(7).
11. Breslau N et al. Arch Gen Psychiatry. 1998;55(7):626-32.
12. Reavis JA et al. Perm J. 2013 Spring;17(2):44-8.
A tumultuous and unforgettable year
SHM president bids farewell
As my SHM presidency wraps up, it is a good time to reflect on the past year in hospital medicine. Dominated by COVID-19 preparedness, mitigation, and (now) recovery efforts, the impacts of COVID-19 throughout the medical industry have been profound. For hospital medicine, although we have endured work and home stress unlike anything in recent memory, fortunately a few notably good changes have come about as a result of COVID-19.

Hospitalists have proven that we are extremely capable of adapting to rapidly changing evidence-based practice. The old adage of evidence taking 7 years to become mainstream clinical practice certainly has not been the paradigm during COVID-19. In many cases, clinical care pathways were changing by the week, or even by the day. Usage of SHM’s website, HMX, and educational platforms rose exponentially to keep pace with the changing landscape. Information exchange between and among hospital medicine groups was efficient and effective. This is exactly how it should be, with SHM serving as the catalyst for such information exchange.
Hospitalists were able to shift to telehealth care as the need arose. The use of telehealth is now becoming a core competency for hospitalists around the country, and we are leading the way for other specialists in adoption. COVID-19 enabled not only rapid transformation, but also better payer coverage for the use of all types of telehealth services. SHM will remain a source of training and education in telehealth best practices going forward.
Related, hospitalists also found their programs were being asked to become purveyors for remote monitoring and hospital-at-home programs. Because CMS has allowed some reimbursement for these programs, at least during the public health emergency, hospital medicine programs can more feasibly pursue building and sustaining such programs, and SHM can serve as the hub for best practice exchanges in the field.
The pandemic also created a sizable shift in the mindset of the need and enthusiasm for mainstream maintenance of certification. Although there were already questions about the value of high-stakes exams before the pandemic, both within and outside the medical industry, the pandemic created an immediate need to shift away from such exams. Now, the entire pipeline is questioning the value of these high-stakes exams, such as SATs and ACTs for college admissions, Step 1 exams for medical students, and certification exams for physicians. The pandemic has made us question these milestone exams with more scrutiny and has created a sense of urgency for a change to more adult-learner–focused alternatives. SHM will continue to be at the centerpiece of the discussion, as well as the leader in cultivating educational venues for continuous learning.
So where do we go from here?
I am confident that SHM will continue to pay deep attention to the activities that bring value to hospitalists and support changing practice patterns such as telehealth and hospital-at-home work. Not only will SHM serve as a center for best practices and a conduit for networking and information sharing at the national level – there will be significantly more focus on the support and growth of local chapters. SHM realizes that local chapters are a vital source of networking, education, and pipeline development and will continue to increase the resources to make the chapter programs dynamic and inviting for everyone interested in hospital medicine.
While this presidency year was far different than expected, I have continuously been amazed and delighted with the resiliency and endurance of our hospitalists around the country. We stood out at the front lines of the pandemic, with a mission toward service and a relentless commitment to our patients. Although we still have a long way to go before the pandemic is behind us, I firmly believe we are emerging from the haze stronger and more agile than ever. Thank you for allowing me to serve this incredible organization during such a tumultuous and unforgettable year.
Yours in service.
Dr. Scheurer is a hospitalist and chief quality officer, MUSC Health System, Medical University of South Carolina, Charleston. She is the outgoing president of SHM.
SHM president bids farewell
SHM president bids farewell
As my SHM presidency wraps up, it is a good time to reflect on the past year in hospital medicine. Dominated by COVID-19 preparedness, mitigation, and (now) recovery efforts, the impacts of COVID-19 throughout the medical industry have been profound. For hospital medicine, although we have endured work and home stress unlike anything in recent memory, fortunately a few notably good changes have come about as a result of COVID-19.
Hospitalists have proven that we are extremely capable of adapting to rapidly changing evidence-based practice. The old adage of evidence taking 7 years to become mainstream clinical practice certainly has not been the paradigm during COVID-19. In many cases, clinical care pathways were changing by the week, or even by the day. Usage of SHM’s website, HMX, and educational platforms rose exponentially to keep pace with the changing landscape. Information exchange between and among hospital medicine groups was efficient and effective. This is exactly how it should be, with SHM serving as the catalyst for such information exchange.
Hospitalists were able to shift to telehealth care as the need arose. The use of telehealth is now becoming a core competency for hospitalists around the country, and we are leading the way for other specialists in adoption. COVID-19 enabled not only rapid transformation, but also better payer coverage for the use of all types of telehealth services. SHM will remain a source of training and education in telehealth best practices going forward.
Related, hospitalists also found their programs were being asked to become purveyors for remote monitoring and hospital-at-home programs. Because CMS has allowed some reimbursement for these programs, at least during the public health emergency, hospital medicine programs can more feasibly pursue building and sustaining such programs, and SHM can serve as the hub for best practice exchanges in the field.
The pandemic also created a sizable shift in the mindset of the need and enthusiasm for mainstream maintenance of certification. Although there were already questions about the value of high-stakes exams before the pandemic, both within and outside the medical industry, the pandemic created an immediate need to shift away from such exams. Now, the entire pipeline is questioning the value of these high-stakes exams, such as SATs and ACTs for college admissions, Step 1 exams for medical students, and certification exams for physicians. The pandemic has made us question these milestone exams with more scrutiny and has created a sense of urgency for a change to more adult-learner–focused alternatives. SHM will continue to be at the centerpiece of the discussion, as well as the leader in cultivating educational venues for continuous learning.
So where do we go from here?
I am confident that SHM will continue to pay deep attention to the activities that bring value to hospitalists and support changing practice patterns such as telehealth and hospital-at-home work. Not only will SHM serve as a center for best practices and a conduit for networking and information sharing at the national level – there will be significantly more focus on the support and growth of local chapters. SHM realizes that local chapters are a vital source of networking, education, and pipeline development and will continue to increase the resources to make the chapter programs dynamic and inviting for everyone interested in hospital medicine.
While this presidency year was far different than expected, I have continuously been amazed and delighted with the resiliency and endurance of our hospitalists around the country. We stood out at the front lines of the pandemic, with a mission toward service and a relentless commitment to our patients. Although we still have a long way to go before the pandemic is behind us, I firmly believe we are emerging from the haze stronger and more agile than ever. Thank you for allowing me to serve this incredible organization during such a tumultuous and unforgettable year.
Yours in service.
Dr. Scheurer is a hospitalist and chief quality officer, MUSC Health System, Medical University of South Carolina, Charleston. She is the outgoing president of SHM.
As my SHM presidency wraps up, it is a good time to reflect on the past year in hospital medicine. Dominated by COVID-19 preparedness, mitigation, and (now) recovery efforts, the impacts of COVID-19 throughout the medical industry have been profound. For hospital medicine, although we have endured work and home stress unlike anything in recent memory, fortunately a few notably good changes have come about as a result of COVID-19.
Hospitalists have proven that we are extremely capable of adapting to rapidly changing evidence-based practice. The old adage of evidence taking 7 years to become mainstream clinical practice certainly has not been the paradigm during COVID-19. In many cases, clinical care pathways were changing by the week, or even by the day. Usage of SHM’s website, HMX, and educational platforms rose exponentially to keep pace with the changing landscape. Information exchange between and among hospital medicine groups was efficient and effective. This is exactly how it should be, with SHM serving as the catalyst for such information exchange.
Hospitalists were able to shift to telehealth care as the need arose. The use of telehealth is now becoming a core competency for hospitalists around the country, and we are leading the way for other specialists in adoption. COVID-19 enabled not only rapid transformation, but also better payer coverage for the use of all types of telehealth services. SHM will remain a source of training and education in telehealth best practices going forward.
Related, hospitalists also found their programs were being asked to become purveyors for remote monitoring and hospital-at-home programs. Because CMS has allowed some reimbursement for these programs, at least during the public health emergency, hospital medicine programs can more feasibly pursue building and sustaining such programs, and SHM can serve as the hub for best practice exchanges in the field.
The pandemic also created a sizable shift in the mindset of the need and enthusiasm for mainstream maintenance of certification. Although there were already questions about the value of high-stakes exams before the pandemic, both within and outside the medical industry, the pandemic created an immediate need to shift away from such exams. Now, the entire pipeline is questioning the value of these high-stakes exams, such as SATs and ACTs for college admissions, Step 1 exams for medical students, and certification exams for physicians. The pandemic has made us question these milestone exams with more scrutiny and has created a sense of urgency for a change to more adult-learner–focused alternatives. SHM will continue to be at the centerpiece of the discussion, as well as the leader in cultivating educational venues for continuous learning.
So where do we go from here?
I am confident that SHM will continue to pay deep attention to the activities that bring value to hospitalists and support changing practice patterns such as telehealth and hospital-at-home work. Not only will SHM serve as a center for best practices and a conduit for networking and information sharing at the national level – there will be significantly more focus on the support and growth of local chapters. SHM realizes that local chapters are a vital source of networking, education, and pipeline development and will continue to increase the resources to make the chapter programs dynamic and inviting for everyone interested in hospital medicine.
While this presidency year was far different than expected, I have continuously been amazed and delighted with the resiliency and endurance of our hospitalists around the country. We stood out at the front lines of the pandemic, with a mission toward service and a relentless commitment to our patients. Although we still have a long way to go before the pandemic is behind us, I firmly believe we are emerging from the haze stronger and more agile than ever. Thank you for allowing me to serve this incredible organization during such a tumultuous and unforgettable year.
Yours in service.
Dr. Scheurer is a hospitalist and chief quality officer, MUSC Health System, Medical University of South Carolina, Charleston. She is the outgoing president of SHM.
TIPP the scales in managing stress
The past year presented unprecedented challenges for many. In addition, mental health services have also been stretched to capacity. Anecdotally, some hospitals and emergency departments note that more youth have been presenting in mental health crises, and the severity of symptoms has also been higher. Safety planning is important, including working with patients to identify skills they can use in distress. Even those who do not experience suicidal thoughts may struggle with dysregulation or may use coping strategies that may not be the healthiest in the long term.

Within my practice, I see some families who are still waiting for an available therapist, or some may not wish to participate in therapy despite its being recommended. For these families, supporting them in using strategies that they may be willing and able to use in the moment to help them get through the moment of crisis can been helpful:
Case example (identifying details have been changed)
Emily is a 17-year-old girl who has a history of generalized anxiety disorder and obsessive-compulsive disorder. She has had multiple medication trials and a course of cognitive behavioral therapy when younger, with significant improvement in symptoms. She returns to clinic because of increased anxiety related to stressors of the pandemic. She wishes to not return to therapy because of feeling that she received maximal benefit and that further sessions would not be fruitful. However, she struggles with identifying what skills she can use, and her anxiety heightens significantly to near-panic and hyperventilating with even cursory exploration of triggers for her symptoms. Medications are also discussed during this appointment, and it is noted that it may take some time to see therapeutic effect. Of note, she reports no acute safety concerns. She has engaged in skin picking. No reported substance use. As she hyperventilates, she was asked to identify items in the room matching the colors of the rainbow in order. She was able to quickly do this, and then was asked to do it again. Afterward, she noted feeling much less anxious because it distracted her from her thoughts.
Distress tolerance skills can be very helpful to navigate getting through a crisis. When under stress, some may be more likely to engage in behaviors that are not helpful in the long term such as using avoidance; procrastinating; consuming tobacco, alcohol, or other substances; spending too much time on screens; or engaging in self-harm behaviors. While some of these activities may be okay in moderation, others are always harmful. At times, when encouraging patients to use skills with which they may be more familiar, e.g., deep breathing, progressive muscle relaxation, the response may be, “these don’t work!” It can be important to distinguish that the function of these skills is not to make someone feel good or to eliminate the stressor, but to “take some of the edge off” so they are less likely to slide into problematic behaviors. It can be beneficial to have multiple tools at one’s disposal because not all skills will always be effective or available.
TIPP skills (temperature, intense exercise, paced breathing, progressive muscle relaxation) are distress tolerance skills from dialectical behavioral therapy (DBT),1 which was initially developed to treat individuals with borderline personality disorder. More recently, the therapy modality has been applied to individuals who may struggle with emotion regulation for a variety of reasons. TIPP skills work quickly (within seconds to minutes) with the aim to decrease physiological arousal. They do not require a lot of thinking, and many are portable or easy to use. Given the speed of effect, these skills can also be used in lieu of p.r.n. medications or patients can be counseled about trying these instead of turning to substance use. The effect is brief (5-20 minutes), although this may lower the affective temperature sufficiently for someone to get through the intense moment or to be able to then utilize other skills that may require more cognitive reserves.
T – Temperature
Holding one’s breath and placing one’s face in cold water (above 50°) for 10-20 seconds to stimulate the diving response and decrease heart rate. Patients can repeat this up to 3 times. Alternatively, cold compresses or gel eye masks can be used.
I – Intense exercise
Aerobic exercise for 10-20 minutes. This can include running, jumping jacks, dancing to loud music in a way that feels intense. The parasympathetic nervous system (PNS) is activated for approximately 20 minutes after cessation of intense exercise.
P – Paced breathing
Decreasing rate of breathing, with each inhalation/exhalation cycle lasting 10-12 seconds and the exhale being longer than the inhale also activates the PNS.
P – Progressive muscle relaxation (PMR)
Sequentially tensing and relaxing muscles from head to toes. Having at least 5-10 minutes to perform this exercise is preferred.2 Children’s Hospital of Philadelphia offerssample PMR recordings.
Body scans can also be helpful. This practice differs from PMR in that it is a mindfulness practice noting body sensations without trying to change them. The University of Vermont offers some sample exercises.3
These skills were described to Emily. She noted that dunking her face in cold water was effective and it was reassuring knowing she had a tool to help her anxiety. She started to push herself to go outside to exercise. We additionally incorporated other distraction techniques such as identifying items from colors of the rainbow that were around her. She appreciated that she could even do this discreetly while at school. At times she had to do a couple of rounds, but this could help stop her repetitive thoughts so she could use other skills.
Helping patients identify skills that can help in the moment can help them feel supported and gain traction in other areas.
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures
References
1. Rathus JH, Miller AL. DBT® Skills manual for adolescents. 2015. Guilford Press.
2. Guided Relaxation Exercises, Children’s Hospital of Philadelphia.
3. Vermont Center for Children, Youth, and Families: Staying Close While Keeping Your Distance.
The past year presented unprecedented challenges for many. In addition, mental health services have also been stretched to capacity. Anecdotally, some hospitals and emergency departments note that more youth have been presenting in mental health crises, and the severity of symptoms has also been higher. Safety planning is important, including working with patients to identify skills they can use in distress. Even those who do not experience suicidal thoughts may struggle with dysregulation or may use coping strategies that may not be the healthiest in the long term.
Within my practice, I see some families who are still waiting for an available therapist, or some may not wish to participate in therapy despite its being recommended. For these families, supporting them in using strategies that they may be willing and able to use in the moment to help them get through the moment of crisis can been helpful:
Case example (identifying details have been changed)
Emily is a 17-year-old girl who has a history of generalized anxiety disorder and obsessive-compulsive disorder. She has had multiple medication trials and a course of cognitive behavioral therapy when younger, with significant improvement in symptoms. She returns to clinic because of increased anxiety related to stressors of the pandemic. She wishes to not return to therapy because of feeling that she received maximal benefit and that further sessions would not be fruitful. However, she struggles with identifying what skills she can use, and her anxiety heightens significantly to near-panic and hyperventilating with even cursory exploration of triggers for her symptoms. Medications are also discussed during this appointment, and it is noted that it may take some time to see therapeutic effect. Of note, she reports no acute safety concerns. She has engaged in skin picking. No reported substance use. As she hyperventilates, she was asked to identify items in the room matching the colors of the rainbow in order. She was able to quickly do this, and then was asked to do it again. Afterward, she noted feeling much less anxious because it distracted her from her thoughts.
Distress tolerance skills can be very helpful to navigate getting through a crisis. When under stress, some may be more likely to engage in behaviors that are not helpful in the long term such as using avoidance; procrastinating; consuming tobacco, alcohol, or other substances; spending too much time on screens; or engaging in self-harm behaviors. While some of these activities may be okay in moderation, others are always harmful. At times, when encouraging patients to use skills with which they may be more familiar, e.g., deep breathing, progressive muscle relaxation, the response may be, “these don’t work!” It can be important to distinguish that the function of these skills is not to make someone feel good or to eliminate the stressor, but to “take some of the edge off” so they are less likely to slide into problematic behaviors. It can be beneficial to have multiple tools at one’s disposal because not all skills will always be effective or available.
TIPP skills (temperature, intense exercise, paced breathing, progressive muscle relaxation) are distress tolerance skills from dialectical behavioral therapy (DBT),1 which was initially developed to treat individuals with borderline personality disorder. More recently, the therapy modality has been applied to individuals who may struggle with emotion regulation for a variety of reasons. TIPP skills work quickly (within seconds to minutes) with the aim to decrease physiological arousal. They do not require a lot of thinking, and many are portable or easy to use. Given the speed of effect, these skills can also be used in lieu of p.r.n. medications or patients can be counseled about trying these instead of turning to substance use. The effect is brief (5-20 minutes), although this may lower the affective temperature sufficiently for someone to get through the intense moment or to be able to then utilize other skills that may require more cognitive reserves.
T – Temperature
Holding one’s breath and placing one’s face in cold water (above 50°) for 10-20 seconds to stimulate the diving response and decrease heart rate. Patients can repeat this up to 3 times. Alternatively, cold compresses or gel eye masks can be used.
I – Intense exercise
Aerobic exercise for 10-20 minutes. This can include running, jumping jacks, dancing to loud music in a way that feels intense. The parasympathetic nervous system (PNS) is activated for approximately 20 minutes after cessation of intense exercise.
P – Paced breathing
Decreasing rate of breathing, with each inhalation/exhalation cycle lasting 10-12 seconds and the exhale being longer than the inhale also activates the PNS.
P – Progressive muscle relaxation (PMR)
Sequentially tensing and relaxing muscles from head to toes. Having at least 5-10 minutes to perform this exercise is preferred.2 Children’s Hospital of Philadelphia offerssample PMR recordings.
Body scans can also be helpful. This practice differs from PMR in that it is a mindfulness practice noting body sensations without trying to change them. The University of Vermont offers some sample exercises.3
These skills were described to Emily. She noted that dunking her face in cold water was effective and it was reassuring knowing she had a tool to help her anxiety. She started to push herself to go outside to exercise. We additionally incorporated other distraction techniques such as identifying items from colors of the rainbow that were around her. She appreciated that she could even do this discreetly while at school. At times she had to do a couple of rounds, but this could help stop her repetitive thoughts so she could use other skills.
Helping patients identify skills that can help in the moment can help them feel supported and gain traction in other areas.
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures
References
1. Rathus JH, Miller AL. DBT® Skills manual for adolescents. 2015. Guilford Press.
2. Guided Relaxation Exercises, Children’s Hospital of Philadelphia.
3. Vermont Center for Children, Youth, and Families: Staying Close While Keeping Your Distance.
The past year presented unprecedented challenges for many. In addition, mental health services have also been stretched to capacity. Anecdotally, some hospitals and emergency departments note that more youth have been presenting in mental health crises, and the severity of symptoms has also been higher. Safety planning is important, including working with patients to identify skills they can use in distress. Even those who do not experience suicidal thoughts may struggle with dysregulation or may use coping strategies that may not be the healthiest in the long term.
Within my practice, I see some families who are still waiting for an available therapist, or some may not wish to participate in therapy despite its being recommended. For these families, supporting them in using strategies that they may be willing and able to use in the moment to help them get through the moment of crisis can been helpful:
Case example (identifying details have been changed)
Emily is a 17-year-old girl who has a history of generalized anxiety disorder and obsessive-compulsive disorder. She has had multiple medication trials and a course of cognitive behavioral therapy when younger, with significant improvement in symptoms. She returns to clinic because of increased anxiety related to stressors of the pandemic. She wishes to not return to therapy because of feeling that she received maximal benefit and that further sessions would not be fruitful. However, she struggles with identifying what skills she can use, and her anxiety heightens significantly to near-panic and hyperventilating with even cursory exploration of triggers for her symptoms. Medications are also discussed during this appointment, and it is noted that it may take some time to see therapeutic effect. Of note, she reports no acute safety concerns. She has engaged in skin picking. No reported substance use. As she hyperventilates, she was asked to identify items in the room matching the colors of the rainbow in order. She was able to quickly do this, and then was asked to do it again. Afterward, she noted feeling much less anxious because it distracted her from her thoughts.
Distress tolerance skills can be very helpful to navigate getting through a crisis. When under stress, some may be more likely to engage in behaviors that are not helpful in the long term such as using avoidance; procrastinating; consuming tobacco, alcohol, or other substances; spending too much time on screens; or engaging in self-harm behaviors. While some of these activities may be okay in moderation, others are always harmful. At times, when encouraging patients to use skills with which they may be more familiar, e.g., deep breathing, progressive muscle relaxation, the response may be, “these don’t work!” It can be important to distinguish that the function of these skills is not to make someone feel good or to eliminate the stressor, but to “take some of the edge off” so they are less likely to slide into problematic behaviors. It can be beneficial to have multiple tools at one’s disposal because not all skills will always be effective or available.
TIPP skills (temperature, intense exercise, paced breathing, progressive muscle relaxation) are distress tolerance skills from dialectical behavioral therapy (DBT),1 which was initially developed to treat individuals with borderline personality disorder. More recently, the therapy modality has been applied to individuals who may struggle with emotion regulation for a variety of reasons. TIPP skills work quickly (within seconds to minutes) with the aim to decrease physiological arousal. They do not require a lot of thinking, and many are portable or easy to use. Given the speed of effect, these skills can also be used in lieu of p.r.n. medications or patients can be counseled about trying these instead of turning to substance use. The effect is brief (5-20 minutes), although this may lower the affective temperature sufficiently for someone to get through the intense moment or to be able to then utilize other skills that may require more cognitive reserves.
T – Temperature
Holding one’s breath and placing one’s face in cold water (above 50°) for 10-20 seconds to stimulate the diving response and decrease heart rate. Patients can repeat this up to 3 times. Alternatively, cold compresses or gel eye masks can be used.
I – Intense exercise
Aerobic exercise for 10-20 minutes. This can include running, jumping jacks, dancing to loud music in a way that feels intense. The parasympathetic nervous system (PNS) is activated for approximately 20 minutes after cessation of intense exercise.
P – Paced breathing
Decreasing rate of breathing, with each inhalation/exhalation cycle lasting 10-12 seconds and the exhale being longer than the inhale also activates the PNS.
P – Progressive muscle relaxation (PMR)
Sequentially tensing and relaxing muscles from head to toes. Having at least 5-10 minutes to perform this exercise is preferred.2 Children’s Hospital of Philadelphia offerssample PMR recordings.
Body scans can also be helpful. This practice differs from PMR in that it is a mindfulness practice noting body sensations without trying to change them. The University of Vermont offers some sample exercises.3
These skills were described to Emily. She noted that dunking her face in cold water was effective and it was reassuring knowing she had a tool to help her anxiety. She started to push herself to go outside to exercise. We additionally incorporated other distraction techniques such as identifying items from colors of the rainbow that were around her. She appreciated that she could even do this discreetly while at school. At times she had to do a couple of rounds, but this could help stop her repetitive thoughts so she could use other skills.
Helping patients identify skills that can help in the moment can help them feel supported and gain traction in other areas.
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures
References
1. Rathus JH, Miller AL. DBT® Skills manual for adolescents. 2015. Guilford Press.
2. Guided Relaxation Exercises, Children’s Hospital of Philadelphia.
3. Vermont Center for Children, Youth, and Families: Staying Close While Keeping Your Distance.
The problem with samples
Ubrelvy and Nurtec are the latest in acute migraine treatment, both with solid data to back them up.

As with the triptans 25 years ago, my sample cabinet (and probably everyone else’s) is loaded with them, and friendly sales reps bringing coupon cards are a frequent occurrence.
Unfortunately, samples also bring up the same conundrum I faced with the triptans earlier in my career. It’s one thing to give patients samples to see if they work. It’s quite another to get them covered if they do.
This is an ongoing issue in modern medicine. It’s hard to resist the temptation to just hand something out when it’s conveniently at hand. It saves the patient a trip to the pharmacy and a medication copay up front, which is great.
But if it works, you have a whole new set of issues. The patient wants a real prescription now. So you call it in, then get a denial back saying it isn’t covered. It tells you to call a number, or try CoverMyMeds.
You do that, but the patient has to have failed three triptans, two NSAIDs, and a partridge in a pear tree to get it approved. The “copay assistance cards” don’t help if the medication isn’t covered at all. Each of these new medications is currently listed at roughly $900/month on GoodRx.com. Inevitably, your staff gets an earful when a patient with sticker shock calls your office.
One manufacturer is now eating the cost of the first script, so the patient leaves the pharmacy with a 1-month supply, under the impression that it was covered by insurance. This only kicks the can down the road 4-6 weeks, until they call for a refill.
To the chagrin of my sales reps (who are certainly going to read this), I’ve been burned on this and similar issues many times in my career, so I don’t even bother playing the game.
Certainly, there are cases where handing out a sample of Ubrelvy or Nurtec is indicated – some patients have already failed other agents, or have medical contraindications to them – but most don’t. So I start with triptans, currently going for $15/month. That doesn’t mean I’m not open to a newer agent at some point, but leaping directly to them quickly becomes an exercise in frustration.
Which brings up another issue I’ve encountered. While I try to be aware of this sort of thing, many other docs aren’t. Especially my already overburdened colleagues in primary care, who have enough on their plate with COVID-19, insurance regulations, paperwork, and an insanely busy schedule. In the controlled chaos of a general practice, it’s often easier for the staff to just hand out a sample at the same time they refer to a neurologist. So when the patient comes to me, they’re expecting I’ll be able to get it covered. After all, I’m the specialist. Getting expensive tests and medications covered seem to be something that’s expected for the higher copay to see me.
It doesn’t work that way, either.
I have nothing against new drugs. It’s the breakthroughs that keep medicine moving forward (like the COVID-19 vaccines). Nor do I have anything against samples or sales reps.
But in many cases, the time you save handing out samples isn’t worth the time you have to spend on them down the line.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Ubrelvy and Nurtec are the latest in acute migraine treatment, both with solid data to back them up.
As with the triptans 25 years ago, my sample cabinet (and probably everyone else’s) is loaded with them, and friendly sales reps bringing coupon cards are a frequent occurrence.
Unfortunately, samples also bring up the same conundrum I faced with the triptans earlier in my career. It’s one thing to give patients samples to see if they work. It’s quite another to get them covered if they do.
This is an ongoing issue in modern medicine. It’s hard to resist the temptation to just hand something out when it’s conveniently at hand. It saves the patient a trip to the pharmacy and a medication copay up front, which is great.
But if it works, you have a whole new set of issues. The patient wants a real prescription now. So you call it in, then get a denial back saying it isn’t covered. It tells you to call a number, or try CoverMyMeds.
You do that, but the patient has to have failed three triptans, two NSAIDs, and a partridge in a pear tree to get it approved. The “copay assistance cards” don’t help if the medication isn’t covered at all. Each of these new medications is currently listed at roughly $900/month on GoodRx.com. Inevitably, your staff gets an earful when a patient with sticker shock calls your office.
One manufacturer is now eating the cost of the first script, so the patient leaves the pharmacy with a 1-month supply, under the impression that it was covered by insurance. This only kicks the can down the road 4-6 weeks, until they call for a refill.
To the chagrin of my sales reps (who are certainly going to read this), I’ve been burned on this and similar issues many times in my career, so I don’t even bother playing the game.
Certainly, there are cases where handing out a sample of Ubrelvy or Nurtec is indicated – some patients have already failed other agents, or have medical contraindications to them – but most don’t. So I start with triptans, currently going for $15/month. That doesn’t mean I’m not open to a newer agent at some point, but leaping directly to them quickly becomes an exercise in frustration.
Which brings up another issue I’ve encountered. While I try to be aware of this sort of thing, many other docs aren’t. Especially my already overburdened colleagues in primary care, who have enough on their plate with COVID-19, insurance regulations, paperwork, and an insanely busy schedule. In the controlled chaos of a general practice, it’s often easier for the staff to just hand out a sample at the same time they refer to a neurologist. So when the patient comes to me, they’re expecting I’ll be able to get it covered. After all, I’m the specialist. Getting expensive tests and medications covered seem to be something that’s expected for the higher copay to see me.
It doesn’t work that way, either.
I have nothing against new drugs. It’s the breakthroughs that keep medicine moving forward (like the COVID-19 vaccines). Nor do I have anything against samples or sales reps.
But in many cases, the time you save handing out samples isn’t worth the time you have to spend on them down the line.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Ubrelvy and Nurtec are the latest in acute migraine treatment, both with solid data to back them up.
As with the triptans 25 years ago, my sample cabinet (and probably everyone else’s) is loaded with them, and friendly sales reps bringing coupon cards are a frequent occurrence.
Unfortunately, samples also bring up the same conundrum I faced with the triptans earlier in my career. It’s one thing to give patients samples to see if they work. It’s quite another to get them covered if they do.
This is an ongoing issue in modern medicine. It’s hard to resist the temptation to just hand something out when it’s conveniently at hand. It saves the patient a trip to the pharmacy and a medication copay up front, which is great.
But if it works, you have a whole new set of issues. The patient wants a real prescription now. So you call it in, then get a denial back saying it isn’t covered. It tells you to call a number, or try CoverMyMeds.
You do that, but the patient has to have failed three triptans, two NSAIDs, and a partridge in a pear tree to get it approved. The “copay assistance cards” don’t help if the medication isn’t covered at all. Each of these new medications is currently listed at roughly $900/month on GoodRx.com. Inevitably, your staff gets an earful when a patient with sticker shock calls your office.
One manufacturer is now eating the cost of the first script, so the patient leaves the pharmacy with a 1-month supply, under the impression that it was covered by insurance. This only kicks the can down the road 4-6 weeks, until they call for a refill.
To the chagrin of my sales reps (who are certainly going to read this), I’ve been burned on this and similar issues many times in my career, so I don’t even bother playing the game.
Certainly, there are cases where handing out a sample of Ubrelvy or Nurtec is indicated – some patients have already failed other agents, or have medical contraindications to them – but most don’t. So I start with triptans, currently going for $15/month. That doesn’t mean I’m not open to a newer agent at some point, but leaping directly to them quickly becomes an exercise in frustration.
Which brings up another issue I’ve encountered. While I try to be aware of this sort of thing, many other docs aren’t. Especially my already overburdened colleagues in primary care, who have enough on their plate with COVID-19, insurance regulations, paperwork, and an insanely busy schedule. In the controlled chaos of a general practice, it’s often easier for the staff to just hand out a sample at the same time they refer to a neurologist. So when the patient comes to me, they’re expecting I’ll be able to get it covered. After all, I’m the specialist. Getting expensive tests and medications covered seem to be something that’s expected for the higher copay to see me.
It doesn’t work that way, either.
I have nothing against new drugs. It’s the breakthroughs that keep medicine moving forward (like the COVID-19 vaccines). Nor do I have anything against samples or sales reps.
But in many cases, the time you save handing out samples isn’t worth the time you have to spend on them down the line.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.