User login
We all struggle with the unwritten rules of medical culture
There is a two-lane bridge in my town. It is quaint and picturesque, and when we first moved here, I would gaze out at the water as I drove, letting my mind wander along with the seagulls drifting alongside the car. Until one day, crossing back over, I passed a school bus stopped in the other lane, and instead of waving back, the driver gave me such a fierce look of disapproval I felt like I’d been to the principal’s office. What had I done?
I started paying more attention to the pattern of the other cars on the bridge. Although it appeared to be a standard two-lane width, the lanes weren’t quite wide enough if a school bus or large truck needed to cross at the same time as a car coming from the opposite direction. They had to wait until the other lane was clear. It was an unwritten rule of the town that if you saw a school bus on the other side, you stopped your car and yielded the bridge to the bus. It took me weeks to figure this out. When I did, I felt like I finally belonged in the community. Before, I’d been an outsider.
This got me thinking about culture. Every place has its unwritten rules, whether a community or a workplace. But how do we know the culture of a place? It’s pretty much impossible until we experience it for ourselves.
When I did figure out the bridge, I had a little bit of anger, to be honest. How was I supposed to know about the lanes? There weren’t any signs. Geez.
Now, when I approach the bridge, I don’t even think about it. I know what to do if I see a bus coming.
But sometimes I remember that time of confusion before I deciphered the unwritten rule. I still have a twinge of guilt for having done something wrong, even though it hadn’t been my fault.
It reminded me of a memory from medical training. I was an MS4, and my ER rotation was in a busy county hospital with a level I trauma center. To say that the place was chaotic would be an understatement.
On the first morning, I was shown the chart rack (yes, this was back in the day of paper charts). Charts were placed in the order that patients arrived. Med students and residents were to take a chart in chronological order, go triage and assess the patient, and then find an attending. Once finished, you put the chart back on the rack and picked up the next one. This was the extent of my orientation to the ER.
The days and weeks of the rotation flew by. It was a busy and exciting time. By the end of the month, I’d come to feel a part of the team.
Until one day, after finishing discharging a patient, an attending asked me, “Where’s the billing sheet?”
I had no idea what she was talking about. No one had ever shown me a billing sheet. But by this point, as an MS4, I knew well that if an attending asked you something you didn’t know the answer to, you shouldn’t just say that you didn’t know. You should try to figure out if you could at least approximate an answer first.
As I scrambled in my mind to figure out what she was asking me, she took one look at the apprehension in my eyes and asked again, raising her voice, “You haven’t been doing the billing sheets?”
I thought back to the first day of the rotation. The cursory 30-second orientation. Chart rack. Take one. See the patient. Put it back. See the next patient. Nothing about billing sheets.
“No,” I said. “No one ever told me about – ”
But the attending didn’t care that I hadn’t been instructed on the billing sheets. She ripped into me, yelling about how she couldn’t believe I’d been working there the entire month and was not doing the billing sheets. She showed me what they were and where they were supposed to be going and, in front of the whole staff, treated me like not only the biggest idiot she’d ever worked with but that the hospital had ever seen.
As she berated me, I thought about all the patients I’d seen that month. All the billing sheets I hadn’t placed in the pile. All the attendings who hadn’t gotten credit for the patients they’d staffed with me.
But how could I have known? I wanted to ask. How could I have known if nobody showed me or told me?
It was like the bridge. I was in a new environment and somehow expected to know the rules without anyone telling me; and when I didn’t know, people treated me like I’d done it the wrong way on purpose.
I didn’t end up saying anything more to that attending. What could I have said? She had already unleashed a mountain of her pent-up anger at me.
What I did decide in that moment was that I would never be an attending like that.
Like the bridge, this memory years later can still make me feel guilt and shame for doing something wrong. Even though it wasn’t my fault.
I was thinking about this recently with the Match. Thousands of freshly graduated medical students embarking on their new positions as interns in teaching hospitals across the country.
If someone treats you poorly for not knowing something, you are not an idiot. You’ve worked incredibly hard to get where you are, and you deserve to be there.
For attendings and more senior trainees, remember what it was like to be starting in a new place. We all make mistakes, and often it’s simply because of a lack of information.
Trainees shouldn’t have to suffer and be made to feel like outsiders until they figure out the unwritten rules of the place. They belong.
Dr. Lycette is medical director of Providence Oncology and Hematology Care Clinic, Seaside, Ore. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
There is a two-lane bridge in my town. It is quaint and picturesque, and when we first moved here, I would gaze out at the water as I drove, letting my mind wander along with the seagulls drifting alongside the car. Until one day, crossing back over, I passed a school bus stopped in the other lane, and instead of waving back, the driver gave me such a fierce look of disapproval I felt like I’d been to the principal’s office. What had I done?
I started paying more attention to the pattern of the other cars on the bridge. Although it appeared to be a standard two-lane width, the lanes weren’t quite wide enough if a school bus or large truck needed to cross at the same time as a car coming from the opposite direction. They had to wait until the other lane was clear. It was an unwritten rule of the town that if you saw a school bus on the other side, you stopped your car and yielded the bridge to the bus. It took me weeks to figure this out. When I did, I felt like I finally belonged in the community. Before, I’d been an outsider.
This got me thinking about culture. Every place has its unwritten rules, whether a community or a workplace. But how do we know the culture of a place? It’s pretty much impossible until we experience it for ourselves.
When I did figure out the bridge, I had a little bit of anger, to be honest. How was I supposed to know about the lanes? There weren’t any signs. Geez.
Now, when I approach the bridge, I don’t even think about it. I know what to do if I see a bus coming.
But sometimes I remember that time of confusion before I deciphered the unwritten rule. I still have a twinge of guilt for having done something wrong, even though it hadn’t been my fault.
It reminded me of a memory from medical training. I was an MS4, and my ER rotation was in a busy county hospital with a level I trauma center. To say that the place was chaotic would be an understatement.
On the first morning, I was shown the chart rack (yes, this was back in the day of paper charts). Charts were placed in the order that patients arrived. Med students and residents were to take a chart in chronological order, go triage and assess the patient, and then find an attending. Once finished, you put the chart back on the rack and picked up the next one. This was the extent of my orientation to the ER.
The days and weeks of the rotation flew by. It was a busy and exciting time. By the end of the month, I’d come to feel a part of the team.
Until one day, after finishing discharging a patient, an attending asked me, “Where’s the billing sheet?”
I had no idea what she was talking about. No one had ever shown me a billing sheet. But by this point, as an MS4, I knew well that if an attending asked you something you didn’t know the answer to, you shouldn’t just say that you didn’t know. You should try to figure out if you could at least approximate an answer first.
As I scrambled in my mind to figure out what she was asking me, she took one look at the apprehension in my eyes and asked again, raising her voice, “You haven’t been doing the billing sheets?”
I thought back to the first day of the rotation. The cursory 30-second orientation. Chart rack. Take one. See the patient. Put it back. See the next patient. Nothing about billing sheets.
“No,” I said. “No one ever told me about – ”
But the attending didn’t care that I hadn’t been instructed on the billing sheets. She ripped into me, yelling about how she couldn’t believe I’d been working there the entire month and was not doing the billing sheets. She showed me what they were and where they were supposed to be going and, in front of the whole staff, treated me like not only the biggest idiot she’d ever worked with but that the hospital had ever seen.
As she berated me, I thought about all the patients I’d seen that month. All the billing sheets I hadn’t placed in the pile. All the attendings who hadn’t gotten credit for the patients they’d staffed with me.
But how could I have known? I wanted to ask. How could I have known if nobody showed me or told me?
It was like the bridge. I was in a new environment and somehow expected to know the rules without anyone telling me; and when I didn’t know, people treated me like I’d done it the wrong way on purpose.
I didn’t end up saying anything more to that attending. What could I have said? She had already unleashed a mountain of her pent-up anger at me.
What I did decide in that moment was that I would never be an attending like that.
Like the bridge, this memory years later can still make me feel guilt and shame for doing something wrong. Even though it wasn’t my fault.
I was thinking about this recently with the Match. Thousands of freshly graduated medical students embarking on their new positions as interns in teaching hospitals across the country.
If someone treats you poorly for not knowing something, you are not an idiot. You’ve worked incredibly hard to get where you are, and you deserve to be there.
For attendings and more senior trainees, remember what it was like to be starting in a new place. We all make mistakes, and often it’s simply because of a lack of information.
Trainees shouldn’t have to suffer and be made to feel like outsiders until they figure out the unwritten rules of the place. They belong.
Dr. Lycette is medical director of Providence Oncology and Hematology Care Clinic, Seaside, Ore. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
There is a two-lane bridge in my town. It is quaint and picturesque, and when we first moved here, I would gaze out at the water as I drove, letting my mind wander along with the seagulls drifting alongside the car. Until one day, crossing back over, I passed a school bus stopped in the other lane, and instead of waving back, the driver gave me such a fierce look of disapproval I felt like I’d been to the principal’s office. What had I done?
I started paying more attention to the pattern of the other cars on the bridge. Although it appeared to be a standard two-lane width, the lanes weren’t quite wide enough if a school bus or large truck needed to cross at the same time as a car coming from the opposite direction. They had to wait until the other lane was clear. It was an unwritten rule of the town that if you saw a school bus on the other side, you stopped your car and yielded the bridge to the bus. It took me weeks to figure this out. When I did, I felt like I finally belonged in the community. Before, I’d been an outsider.
This got me thinking about culture. Every place has its unwritten rules, whether a community or a workplace. But how do we know the culture of a place? It’s pretty much impossible until we experience it for ourselves.
When I did figure out the bridge, I had a little bit of anger, to be honest. How was I supposed to know about the lanes? There weren’t any signs. Geez.
Now, when I approach the bridge, I don’t even think about it. I know what to do if I see a bus coming.
But sometimes I remember that time of confusion before I deciphered the unwritten rule. I still have a twinge of guilt for having done something wrong, even though it hadn’t been my fault.
It reminded me of a memory from medical training. I was an MS4, and my ER rotation was in a busy county hospital with a level I trauma center. To say that the place was chaotic would be an understatement.
On the first morning, I was shown the chart rack (yes, this was back in the day of paper charts). Charts were placed in the order that patients arrived. Med students and residents were to take a chart in chronological order, go triage and assess the patient, and then find an attending. Once finished, you put the chart back on the rack and picked up the next one. This was the extent of my orientation to the ER.
The days and weeks of the rotation flew by. It was a busy and exciting time. By the end of the month, I’d come to feel a part of the team.
Until one day, after finishing discharging a patient, an attending asked me, “Where’s the billing sheet?”
I had no idea what she was talking about. No one had ever shown me a billing sheet. But by this point, as an MS4, I knew well that if an attending asked you something you didn’t know the answer to, you shouldn’t just say that you didn’t know. You should try to figure out if you could at least approximate an answer first.
As I scrambled in my mind to figure out what she was asking me, she took one look at the apprehension in my eyes and asked again, raising her voice, “You haven’t been doing the billing sheets?”
I thought back to the first day of the rotation. The cursory 30-second orientation. Chart rack. Take one. See the patient. Put it back. See the next patient. Nothing about billing sheets.
“No,” I said. “No one ever told me about – ”
But the attending didn’t care that I hadn’t been instructed on the billing sheets. She ripped into me, yelling about how she couldn’t believe I’d been working there the entire month and was not doing the billing sheets. She showed me what they were and where they were supposed to be going and, in front of the whole staff, treated me like not only the biggest idiot she’d ever worked with but that the hospital had ever seen.
As she berated me, I thought about all the patients I’d seen that month. All the billing sheets I hadn’t placed in the pile. All the attendings who hadn’t gotten credit for the patients they’d staffed with me.
But how could I have known? I wanted to ask. How could I have known if nobody showed me or told me?
It was like the bridge. I was in a new environment and somehow expected to know the rules without anyone telling me; and when I didn’t know, people treated me like I’d done it the wrong way on purpose.
I didn’t end up saying anything more to that attending. What could I have said? She had already unleashed a mountain of her pent-up anger at me.
What I did decide in that moment was that I would never be an attending like that.
Like the bridge, this memory years later can still make me feel guilt and shame for doing something wrong. Even though it wasn’t my fault.
I was thinking about this recently with the Match. Thousands of freshly graduated medical students embarking on their new positions as interns in teaching hospitals across the country.
If someone treats you poorly for not knowing something, you are not an idiot. You’ve worked incredibly hard to get where you are, and you deserve to be there.
For attendings and more senior trainees, remember what it was like to be starting in a new place. We all make mistakes, and often it’s simply because of a lack of information.
Trainees shouldn’t have to suffer and be made to feel like outsiders until they figure out the unwritten rules of the place. They belong.
Dr. Lycette is medical director of Providence Oncology and Hematology Care Clinic, Seaside, Ore. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
The importance of treating insomnia in psychiatric illness
Data suggests this symptom, defined as chronic sleep onset and/or sleep continuity problems associated with impaired daytime functioning, is common in psychiatric illnesses, and can worsen their course.2
The incidence of psychiatric illness in patients with insomnia is estimated at near 50%, with the highest rates found in mood disorders such as depression and bipolar disorder, as well as anxiety disorders.3 In patients with diagnosed major depressive disorder, insomnia rates can approach 90%.4-6

Insomnia has been identified as a risk factor for development of mental illness, including doubling the risk of major depressive disorder and tripling the risk of any depressive or anxiety disorder.7,8 It can also significantly increase the risk of alcohol abuse and psychosis.8
Sleep disturbances can worsen symptoms of diagnosed mental illness, including substance abuse, mood and psychotic disorders.9-10 In one study, nearly 75% of patients with a diagnosis of schizophrenia or bipolar spectrum disorder had at least one type of sleep disturbance (insomnia, hypersomnia, or delayed sleep phase).10 This was almost twice the rate in healthy controls. Importantly, compared with well-rested subjects with mental illness in this study, sleep-disordered participants had higher rates of negative and depressive symptoms on the Positive and Negative Syndrome Scale, as well as significantly lower function via the global assessment of functioning.11,12
Additional data suggests simply being awake during the night (00:00-05:59) elevates risk of suicide. The mean incident rate of completed suicide in one study was a striking four times the rate noted during daytime hours (06:00-23:59 ) (P < .001).13
Although insomnia symptoms can resolve after relief from a particular life stressor, as many as half of patients with more severe symptoms develop a chronic course.14 This then leads to an extended use of many types of sedative-hypnotics designed and studied primarily for short-term use.15 In a survey reviewing national use of prescription drugs for insomnia, as many as 20% of individuals use a medication to target insomnia in a given month.16
Fortunately, despite the many challenges posed by COVID-19, particularly for those with psychiatric illness and limited access to care, telehealth has become more readily available. Additionally, digital versions of evidence-based treatments specifically for sleep problems, such as cognitive-behavioral therapy for insomnia (CBT-I), are regularly being developed.
The benefits of CBT-I have been demonstrated repeatedly and it is recommended as the first line treatment for insomnia by the Clinical Guidelines of the American Academy of Sleep Medicine, the Centers for Disease Control and Prevention, and the National Institutes of Health.17-21 Studies suggest benefits persist long-term, even after completing the therapy sessions, which differ in durability from medication choices.18
One group that may be particularly suited for treatment with CBT-I is women with insomnia during pregnancy or the postpartum period. In these women, options for treatment may be limited by risk of medication during breastfeeding, as well as difficulty traveling to a physician’s or therapist’s office to receive psychotherapy. However, two recent studies evaluated the use of digital CBT-I to treat insomnia during pregnancy and in the postpartum period, respectively.22-23
In both studies,the same group of women with insomnia diagnosed during pregnancy were given six weekly 20-minute sessions of digital CBT-I or standard treatment for insomnia, including medication and psychotherapy per their usual provider.
By study end, the pregnant women receiving the CBT-I intervention not only had significantly improved severity of insomnia, they also experienced improved depression and anxiety symptoms, and a decrease in the use of prescription or over-the-counter sleep aides, compared with the standard treatment group, lowering the fetal exposure to medication during pregnancy.22
In the more recent study, the same group was followed for 6 months post partum.23 Results were again notable, with the women who received CBT-I reporting significantly less insomnia, as well as significantly lower rates of probable major depression at 3 and 6 months (18% vs. 4%, 10% vs. 0%, respectively.) They also exhibited lower rates of moderate to severe anxiety (17% vs. 4%) at 3 months, compared with those receiving standard care. With as many as one in seven women suffering from postpartum depression, these findings represent a substantial public health benefit.
In summary, insomnia is a critical area of focus for any provider diagnosing and treating psychiatric illness. Attempts to optimize sleep, whether through CBT-I or other psychotherapy approaches, or evidence-based medications dosed for appropriate lengths and at safe doses, should be a part of most, if not all, clinical encounters.
Dr. Reid is a board-certified psychiatrist and award-winning medical educator with a private practice in Philadelphia, as well as a clinical faculty role at the University of Pennsylvania, also in Philadelphia. She attended medical school at Columbia University, New York, and completed her psychiatry residency at the University of California, Los Angeles. Dr. Reid is a regular contributor to Psychology Today with her blog, “Think Like a Shrink,” and writes and podcasts as The Reflective Doc.
References
1. Voitsidis P et al. Psychiatry Res. 2020 Jul;289:113076. doi: 10.1016/j.psychres.2020.113076.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, Va.: American Psychiatric Publishing, 2013.
3. Ford DE and Kamerow DB. JAMA. 1989;262(11):1479-84. doi: 10.1001/jama.1989.03430110069030.
4. Ohayon MM and Roth T. J Psychiatr Res. Jan-Feb 2003;37(1):9-15. doi: 10.1016/s0022-3956(02)00052-3.
5. Seow LSE et al. J Ment Health. 2016 Dec;25(6):492-9. doi: 10.3109/09638237.2015.1124390.
6. Thase ME. J Clin Psychiatry. 1999;60 Suppl 17:28-31; discussion 46-8.
7. Baglioni C et al. J Affect Disord. 2011 Dec;135(1-3):10-9. doi: 10.1016/j.jad.2011.01.011.
8. Hertenstein E et al. Sleep Med Rev. 2019 Feb;43:96-105. doi: 10.1016/j.smrv.2018.10.006.
9. Brower KJ et al. Medical Hypotheses. 2010;74(5):928-33. doi: 10.1016/j.mehy.2009.10.020.
10. Laskemoen JF et al. Compr Psychiatry. 2019 May;91:6-12. doi: 10.1016/j.comppsych.2019.02.006.
11. Kay SR et al. Schizophr Bull. 1987;13(2):261-76. doi: 10.1093/schbul/13.2.261.
12. Hall R. Psychosomatics. May-Jun 1995;36(3):267-75. doi: 10.1016/S0033-3182(95)71666-8.
13. Perlis ML et al. J Clin Psychiatry. 2016 Jun;77(6):e726-33. doi: 10.4088/JCP.15m10131.
14. Morin CM et al. Arch Intern Med. 2009 Mar 9. doi: 10.1001/archinternmed.2008.610.
15. Cheung J et al. Sleep Med Clin. 2019 Jun;14(2):253-65. doi: 10.1016/j.jsmc.2019.01.006.
16. Bertisch SM et al. Sleep. 2014 Feb 1. doi: 10.5665/sleep.3410.
17. Okajima I et al. Sleep Biol Rhythms. 2010 Nov 28. doi: 10.1111/j.1479-8425.2010.00481.x.
18. Trauer JM et al. Ann Intern Med. 2015 Aug 4. doi: 10.7326/M14-2841.
19. Edinger J et al. J Clin Sleep Med. 2021 Feb 1. doi: 10.5664/jcsm.8986.
20. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/sleep/for-clinicians.html.
21. National Institutes of Health. Sleep Health. https://www.nhlbi.nih.gov/health-topics/education-and-awareness/sleep-health.
22. Felder JN et al. JAMA Psychiatry. 2020;77(5):484-92. doi:10.1001/jamapsychiatry.2019.4491.
23. Felder JN et al. Sleep. 2022 Feb 14. doi: 10.1093/sleep/zsab280.
Data suggests this symptom, defined as chronic sleep onset and/or sleep continuity problems associated with impaired daytime functioning, is common in psychiatric illnesses, and can worsen their course.2
The incidence of psychiatric illness in patients with insomnia is estimated at near 50%, with the highest rates found in mood disorders such as depression and bipolar disorder, as well as anxiety disorders.3 In patients with diagnosed major depressive disorder, insomnia rates can approach 90%.4-6
Insomnia has been identified as a risk factor for development of mental illness, including doubling the risk of major depressive disorder and tripling the risk of any depressive or anxiety disorder.7,8 It can also significantly increase the risk of alcohol abuse and psychosis.8
Sleep disturbances can worsen symptoms of diagnosed mental illness, including substance abuse, mood and psychotic disorders.9-10 In one study, nearly 75% of patients with a diagnosis of schizophrenia or bipolar spectrum disorder had at least one type of sleep disturbance (insomnia, hypersomnia, or delayed sleep phase).10 This was almost twice the rate in healthy controls. Importantly, compared with well-rested subjects with mental illness in this study, sleep-disordered participants had higher rates of negative and depressive symptoms on the Positive and Negative Syndrome Scale, as well as significantly lower function via the global assessment of functioning.11,12
Additional data suggests simply being awake during the night (00:00-05:59) elevates risk of suicide. The mean incident rate of completed suicide in one study was a striking four times the rate noted during daytime hours (06:00-23:59 ) (P < .001).13
Although insomnia symptoms can resolve after relief from a particular life stressor, as many as half of patients with more severe symptoms develop a chronic course.14 This then leads to an extended use of many types of sedative-hypnotics designed and studied primarily for short-term use.15 In a survey reviewing national use of prescription drugs for insomnia, as many as 20% of individuals use a medication to target insomnia in a given month.16
Fortunately, despite the many challenges posed by COVID-19, particularly for those with psychiatric illness and limited access to care, telehealth has become more readily available. Additionally, digital versions of evidence-based treatments specifically for sleep problems, such as cognitive-behavioral therapy for insomnia (CBT-I), are regularly being developed.
The benefits of CBT-I have been demonstrated repeatedly and it is recommended as the first line treatment for insomnia by the Clinical Guidelines of the American Academy of Sleep Medicine, the Centers for Disease Control and Prevention, and the National Institutes of Health.17-21 Studies suggest benefits persist long-term, even after completing the therapy sessions, which differ in durability from medication choices.18
One group that may be particularly suited for treatment with CBT-I is women with insomnia during pregnancy or the postpartum period. In these women, options for treatment may be limited by risk of medication during breastfeeding, as well as difficulty traveling to a physician’s or therapist’s office to receive psychotherapy. However, two recent studies evaluated the use of digital CBT-I to treat insomnia during pregnancy and in the postpartum period, respectively.22-23
In both studies,the same group of women with insomnia diagnosed during pregnancy were given six weekly 20-minute sessions of digital CBT-I or standard treatment for insomnia, including medication and psychotherapy per their usual provider.
By study end, the pregnant women receiving the CBT-I intervention not only had significantly improved severity of insomnia, they also experienced improved depression and anxiety symptoms, and a decrease in the use of prescription or over-the-counter sleep aides, compared with the standard treatment group, lowering the fetal exposure to medication during pregnancy.22
In the more recent study, the same group was followed for 6 months post partum.23 Results were again notable, with the women who received CBT-I reporting significantly less insomnia, as well as significantly lower rates of probable major depression at 3 and 6 months (18% vs. 4%, 10% vs. 0%, respectively.) They also exhibited lower rates of moderate to severe anxiety (17% vs. 4%) at 3 months, compared with those receiving standard care. With as many as one in seven women suffering from postpartum depression, these findings represent a substantial public health benefit.
In summary, insomnia is a critical area of focus for any provider diagnosing and treating psychiatric illness. Attempts to optimize sleep, whether through CBT-I or other psychotherapy approaches, or evidence-based medications dosed for appropriate lengths and at safe doses, should be a part of most, if not all, clinical encounters.
Dr. Reid is a board-certified psychiatrist and award-winning medical educator with a private practice in Philadelphia, as well as a clinical faculty role at the University of Pennsylvania, also in Philadelphia. She attended medical school at Columbia University, New York, and completed her psychiatry residency at the University of California, Los Angeles. Dr. Reid is a regular contributor to Psychology Today with her blog, “Think Like a Shrink,” and writes and podcasts as The Reflective Doc.
References
1. Voitsidis P et al. Psychiatry Res. 2020 Jul;289:113076. doi: 10.1016/j.psychres.2020.113076.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, Va.: American Psychiatric Publishing, 2013.
3. Ford DE and Kamerow DB. JAMA. 1989;262(11):1479-84. doi: 10.1001/jama.1989.03430110069030.
4. Ohayon MM and Roth T. J Psychiatr Res. Jan-Feb 2003;37(1):9-15. doi: 10.1016/s0022-3956(02)00052-3.
5. Seow LSE et al. J Ment Health. 2016 Dec;25(6):492-9. doi: 10.3109/09638237.2015.1124390.
6. Thase ME. J Clin Psychiatry. 1999;60 Suppl 17:28-31; discussion 46-8.
7. Baglioni C et al. J Affect Disord. 2011 Dec;135(1-3):10-9. doi: 10.1016/j.jad.2011.01.011.
8. Hertenstein E et al. Sleep Med Rev. 2019 Feb;43:96-105. doi: 10.1016/j.smrv.2018.10.006.
9. Brower KJ et al. Medical Hypotheses. 2010;74(5):928-33. doi: 10.1016/j.mehy.2009.10.020.
10. Laskemoen JF et al. Compr Psychiatry. 2019 May;91:6-12. doi: 10.1016/j.comppsych.2019.02.006.
11. Kay SR et al. Schizophr Bull. 1987;13(2):261-76. doi: 10.1093/schbul/13.2.261.
12. Hall R. Psychosomatics. May-Jun 1995;36(3):267-75. doi: 10.1016/S0033-3182(95)71666-8.
13. Perlis ML et al. J Clin Psychiatry. 2016 Jun;77(6):e726-33. doi: 10.4088/JCP.15m10131.
14. Morin CM et al. Arch Intern Med. 2009 Mar 9. doi: 10.1001/archinternmed.2008.610.
15. Cheung J et al. Sleep Med Clin. 2019 Jun;14(2):253-65. doi: 10.1016/j.jsmc.2019.01.006.
16. Bertisch SM et al. Sleep. 2014 Feb 1. doi: 10.5665/sleep.3410.
17. Okajima I et al. Sleep Biol Rhythms. 2010 Nov 28. doi: 10.1111/j.1479-8425.2010.00481.x.
18. Trauer JM et al. Ann Intern Med. 2015 Aug 4. doi: 10.7326/M14-2841.
19. Edinger J et al. J Clin Sleep Med. 2021 Feb 1. doi: 10.5664/jcsm.8986.
20. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/sleep/for-clinicians.html.
21. National Institutes of Health. Sleep Health. https://www.nhlbi.nih.gov/health-topics/education-and-awareness/sleep-health.
22. Felder JN et al. JAMA Psychiatry. 2020;77(5):484-92. doi:10.1001/jamapsychiatry.2019.4491.
23. Felder JN et al. Sleep. 2022 Feb 14. doi: 10.1093/sleep/zsab280.
Data suggests this symptom, defined as chronic sleep onset and/or sleep continuity problems associated with impaired daytime functioning, is common in psychiatric illnesses, and can worsen their course.2
The incidence of psychiatric illness in patients with insomnia is estimated at near 50%, with the highest rates found in mood disorders such as depression and bipolar disorder, as well as anxiety disorders.3 In patients with diagnosed major depressive disorder, insomnia rates can approach 90%.4-6
Insomnia has been identified as a risk factor for development of mental illness, including doubling the risk of major depressive disorder and tripling the risk of any depressive or anxiety disorder.7,8 It can also significantly increase the risk of alcohol abuse and psychosis.8
Sleep disturbances can worsen symptoms of diagnosed mental illness, including substance abuse, mood and psychotic disorders.9-10 In one study, nearly 75% of patients with a diagnosis of schizophrenia or bipolar spectrum disorder had at least one type of sleep disturbance (insomnia, hypersomnia, or delayed sleep phase).10 This was almost twice the rate in healthy controls. Importantly, compared with well-rested subjects with mental illness in this study, sleep-disordered participants had higher rates of negative and depressive symptoms on the Positive and Negative Syndrome Scale, as well as significantly lower function via the global assessment of functioning.11,12
Additional data suggests simply being awake during the night (00:00-05:59) elevates risk of suicide. The mean incident rate of completed suicide in one study was a striking four times the rate noted during daytime hours (06:00-23:59 ) (P < .001).13
Although insomnia symptoms can resolve after relief from a particular life stressor, as many as half of patients with more severe symptoms develop a chronic course.14 This then leads to an extended use of many types of sedative-hypnotics designed and studied primarily for short-term use.15 In a survey reviewing national use of prescription drugs for insomnia, as many as 20% of individuals use a medication to target insomnia in a given month.16
Fortunately, despite the many challenges posed by COVID-19, particularly for those with psychiatric illness and limited access to care, telehealth has become more readily available. Additionally, digital versions of evidence-based treatments specifically for sleep problems, such as cognitive-behavioral therapy for insomnia (CBT-I), are regularly being developed.
The benefits of CBT-I have been demonstrated repeatedly and it is recommended as the first line treatment for insomnia by the Clinical Guidelines of the American Academy of Sleep Medicine, the Centers for Disease Control and Prevention, and the National Institutes of Health.17-21 Studies suggest benefits persist long-term, even after completing the therapy sessions, which differ in durability from medication choices.18
One group that may be particularly suited for treatment with CBT-I is women with insomnia during pregnancy or the postpartum period. In these women, options for treatment may be limited by risk of medication during breastfeeding, as well as difficulty traveling to a physician’s or therapist’s office to receive psychotherapy. However, two recent studies evaluated the use of digital CBT-I to treat insomnia during pregnancy and in the postpartum period, respectively.22-23
In both studies,the same group of women with insomnia diagnosed during pregnancy were given six weekly 20-minute sessions of digital CBT-I or standard treatment for insomnia, including medication and psychotherapy per their usual provider.
By study end, the pregnant women receiving the CBT-I intervention not only had significantly improved severity of insomnia, they also experienced improved depression and anxiety symptoms, and a decrease in the use of prescription or over-the-counter sleep aides, compared with the standard treatment group, lowering the fetal exposure to medication during pregnancy.22
In the more recent study, the same group was followed for 6 months post partum.23 Results were again notable, with the women who received CBT-I reporting significantly less insomnia, as well as significantly lower rates of probable major depression at 3 and 6 months (18% vs. 4%, 10% vs. 0%, respectively.) They also exhibited lower rates of moderate to severe anxiety (17% vs. 4%) at 3 months, compared with those receiving standard care. With as many as one in seven women suffering from postpartum depression, these findings represent a substantial public health benefit.
In summary, insomnia is a critical area of focus for any provider diagnosing and treating psychiatric illness. Attempts to optimize sleep, whether through CBT-I or other psychotherapy approaches, or evidence-based medications dosed for appropriate lengths and at safe doses, should be a part of most, if not all, clinical encounters.
Dr. Reid is a board-certified psychiatrist and award-winning medical educator with a private practice in Philadelphia, as well as a clinical faculty role at the University of Pennsylvania, also in Philadelphia. She attended medical school at Columbia University, New York, and completed her psychiatry residency at the University of California, Los Angeles. Dr. Reid is a regular contributor to Psychology Today with her blog, “Think Like a Shrink,” and writes and podcasts as The Reflective Doc.
References
1. Voitsidis P et al. Psychiatry Res. 2020 Jul;289:113076. doi: 10.1016/j.psychres.2020.113076.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, Va.: American Psychiatric Publishing, 2013.
3. Ford DE and Kamerow DB. JAMA. 1989;262(11):1479-84. doi: 10.1001/jama.1989.03430110069030.
4. Ohayon MM and Roth T. J Psychiatr Res. Jan-Feb 2003;37(1):9-15. doi: 10.1016/s0022-3956(02)00052-3.
5. Seow LSE et al. J Ment Health. 2016 Dec;25(6):492-9. doi: 10.3109/09638237.2015.1124390.
6. Thase ME. J Clin Psychiatry. 1999;60 Suppl 17:28-31; discussion 46-8.
7. Baglioni C et al. J Affect Disord. 2011 Dec;135(1-3):10-9. doi: 10.1016/j.jad.2011.01.011.
8. Hertenstein E et al. Sleep Med Rev. 2019 Feb;43:96-105. doi: 10.1016/j.smrv.2018.10.006.
9. Brower KJ et al. Medical Hypotheses. 2010;74(5):928-33. doi: 10.1016/j.mehy.2009.10.020.
10. Laskemoen JF et al. Compr Psychiatry. 2019 May;91:6-12. doi: 10.1016/j.comppsych.2019.02.006.
11. Kay SR et al. Schizophr Bull. 1987;13(2):261-76. doi: 10.1093/schbul/13.2.261.
12. Hall R. Psychosomatics. May-Jun 1995;36(3):267-75. doi: 10.1016/S0033-3182(95)71666-8.
13. Perlis ML et al. J Clin Psychiatry. 2016 Jun;77(6):e726-33. doi: 10.4088/JCP.15m10131.
14. Morin CM et al. Arch Intern Med. 2009 Mar 9. doi: 10.1001/archinternmed.2008.610.
15. Cheung J et al. Sleep Med Clin. 2019 Jun;14(2):253-65. doi: 10.1016/j.jsmc.2019.01.006.
16. Bertisch SM et al. Sleep. 2014 Feb 1. doi: 10.5665/sleep.3410.
17. Okajima I et al. Sleep Biol Rhythms. 2010 Nov 28. doi: 10.1111/j.1479-8425.2010.00481.x.
18. Trauer JM et al. Ann Intern Med. 2015 Aug 4. doi: 10.7326/M14-2841.
19. Edinger J et al. J Clin Sleep Med. 2021 Feb 1. doi: 10.5664/jcsm.8986.
20. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/sleep/for-clinicians.html.
21. National Institutes of Health. Sleep Health. https://www.nhlbi.nih.gov/health-topics/education-and-awareness/sleep-health.
22. Felder JN et al. JAMA Psychiatry. 2020;77(5):484-92. doi:10.1001/jamapsychiatry.2019.4491.
23. Felder JN et al. Sleep. 2022 Feb 14. doi: 10.1093/sleep/zsab280.
It’s a gimmick
March 30 was National Doctor’s Day, which resulted in my getting all kinds of generic emails from pharmaceutical reps, market research places, insurance companies, and the two hospitals I’m on staff at.
They all had similar meaningless platitudes thanking me for what I do, reassuring me that I’m appreciated, that I make the world a better place, yadda yadda yadda. The hospital even said I could swing by the medical staff office and pick up an “appreciation bag,” which I’m told contained a T-shirt, bottle of hand sanitizer, and a few other trinkets.
Spare me.
I’m not looking for any of that. In fact, I really don’t care.

Wishing me a “Happy Doctors Day” after spending the other 364 days denying my claims, refusing to cover tests or medications for my patients who need them (I don’t order these things for the hell of it, you know), telling me that I’m bringing down your Press Ganey scores, complaining about the copay that I have no control over, yelling at my staff for doing their jobs ... is pretty damn hollow.
It’s kind of like Mother’s Day: If you’re a jackass to your mom most of the year, sending her flowers on a Sunday in May doesn’t make it all right.
People also seem to forget that, in a small practice, my awesome staff is an extension of myself. Mistreating them, then wishing me a “Happy Doctor’s Day,” is also worthless.
I still like what I do. All the hassles from insurance companies, various administrators, the occasional angry patient … after all these years, they put a dent in it, but I still have no regrets about the course I’ve chosen. They can’t take away the happiness I get from helping those who need me.
It’s a job I love that’s allowed me to support my family and work with two wonderful staff members I’d never have met otherwise.
And that’s all I need.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
March 30 was National Doctor’s Day, which resulted in my getting all kinds of generic emails from pharmaceutical reps, market research places, insurance companies, and the two hospitals I’m on staff at.
They all had similar meaningless platitudes thanking me for what I do, reassuring me that I’m appreciated, that I make the world a better place, yadda yadda yadda. The hospital even said I could swing by the medical staff office and pick up an “appreciation bag,” which I’m told contained a T-shirt, bottle of hand sanitizer, and a few other trinkets.
Spare me.
I’m not looking for any of that. In fact, I really don’t care.
Wishing me a “Happy Doctors Day” after spending the other 364 days denying my claims, refusing to cover tests or medications for my patients who need them (I don’t order these things for the hell of it, you know), telling me that I’m bringing down your Press Ganey scores, complaining about the copay that I have no control over, yelling at my staff for doing their jobs ... is pretty damn hollow.
It’s kind of like Mother’s Day: If you’re a jackass to your mom most of the year, sending her flowers on a Sunday in May doesn’t make it all right.
People also seem to forget that, in a small practice, my awesome staff is an extension of myself. Mistreating them, then wishing me a “Happy Doctor’s Day,” is also worthless.
I still like what I do. All the hassles from insurance companies, various administrators, the occasional angry patient … after all these years, they put a dent in it, but I still have no regrets about the course I’ve chosen. They can’t take away the happiness I get from helping those who need me.
It’s a job I love that’s allowed me to support my family and work with two wonderful staff members I’d never have met otherwise.
And that’s all I need.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
March 30 was National Doctor’s Day, which resulted in my getting all kinds of generic emails from pharmaceutical reps, market research places, insurance companies, and the two hospitals I’m on staff at.
They all had similar meaningless platitudes thanking me for what I do, reassuring me that I’m appreciated, that I make the world a better place, yadda yadda yadda. The hospital even said I could swing by the medical staff office and pick up an “appreciation bag,” which I’m told contained a T-shirt, bottle of hand sanitizer, and a few other trinkets.
Spare me.
I’m not looking for any of that. In fact, I really don’t care.
Wishing me a “Happy Doctors Day” after spending the other 364 days denying my claims, refusing to cover tests or medications for my patients who need them (I don’t order these things for the hell of it, you know), telling me that I’m bringing down your Press Ganey scores, complaining about the copay that I have no control over, yelling at my staff for doing their jobs ... is pretty damn hollow.
It’s kind of like Mother’s Day: If you’re a jackass to your mom most of the year, sending her flowers on a Sunday in May doesn’t make it all right.
People also seem to forget that, in a small practice, my awesome staff is an extension of myself. Mistreating them, then wishing me a “Happy Doctor’s Day,” is also worthless.
I still like what I do. All the hassles from insurance companies, various administrators, the occasional angry patient … after all these years, they put a dent in it, but I still have no regrets about the course I’ve chosen. They can’t take away the happiness I get from helping those who need me.
It’s a job I love that’s allowed me to support my family and work with two wonderful staff members I’d never have met otherwise.
And that’s all I need.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Give patients can’ts but also can do’s
On his last shift in the last hockey game of the regular season, our 14-year-old grandson broke his arm. Although this was his first fracture, the rest of the nuclear family has had ample experience with orthopedic trauma over the last year, both planned and unplanned.
As I drove Peter and my daughter-in-law to his first postsetting and casting appointment I told him how sorry I was that he had been told “no contact sports for the next 3 months.” This was a tough pill for a kid eager to begin his first high school lacrosse season. Then I asked him what the doctor had told him he could do in the way of activity.

Based on personal and professional experience I was not surprised when he told me that no one had suggested things he could be doing. In fact, being a cautious and thoughtful kid, he was concerned about what he should be doing around the house let alone any athletic activities. It turns out he wasn’t even lifting his laptop computer with two hands because some nurse had told him not to lift anything over 2 pounds.
I told him “Peter, even some of the most experienced doctors focus on the ‘can’ts’ and forget to tell you the ‘cans’ and ‘shoulds.’ While you’re in the waiting room make up a mental list of what you would like to be doing that you aren’t.”
As he climbed back in the car for the ride home I asked how the visit went. The x-ray showed good alignment and the doctor was pleased. But, as I predicted, they were already on the launch pad to the receptionist to make a follow-up appointment without the physician uttering a single word about what activities he could resume. Always a very coachable kid, Peter piped up with the list he had created in the waiting room and was relieved to hear that he could do anything as long as it didn’t hurt. In fact, the doctor encouraged him to use his fingers because it might speed the healing.
Not every patient, regardless of age, is as cautious as my grandson and in some circumstances the physician must err on the side of emphasizing the “don’ts.” However, in my experience, too many physicians forget to include a generous list of “can do’s” in their visit closing discussions. This oversight is a mistake for several reasons.
First, and maybe most importantly, even a brief discussion of “can do’s” can soften the depressing message that the patient will not be able to do things he or she enjoys. I can’t quote the references but I am sure there is plenty of evidence that depression slows the healing process.
Second, and this is particularly true in older patients with orthopedic problems – failure to include a plan for return to activity can hinder recovery. I can recall more than a few patients who were seen in the emergency department and diagnosed with sprains but not given even the simplest instructions on how to begin moving the injured joint. When they finally returned to see me we had to begin the painful and unnecessary project of thawing a frozen joint.
Fortunately, we have evolved past the era when best rest was near the top of the list of our recommended remedies. However, there still remains a bias against activity in some situations. The most recent example is the evolving strategies for the management of concussion. There is some evidence that involving the patient in a return to activity plan may shorten the time to recovery. The myth about brain rest has been slow to die.
Finally, providing the patient with a personalized list of “can do’s” makes good business sense because it can head off those time-gobbling call backs that tie up you and your office staff. As an experienced physician, you have probably learned the most frequently asked “Can Jason do ... ?” questions. Make your own list and give the patient your answers. An ounce of anticipatory guidance is worth hours on the telephone or sorting through the email inbox.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
On his last shift in the last hockey game of the regular season, our 14-year-old grandson broke his arm. Although this was his first fracture, the rest of the nuclear family has had ample experience with orthopedic trauma over the last year, both planned and unplanned.
As I drove Peter and my daughter-in-law to his first postsetting and casting appointment I told him how sorry I was that he had been told “no contact sports for the next 3 months.” This was a tough pill for a kid eager to begin his first high school lacrosse season. Then I asked him what the doctor had told him he could do in the way of activity.
Based on personal and professional experience I was not surprised when he told me that no one had suggested things he could be doing. In fact, being a cautious and thoughtful kid, he was concerned about what he should be doing around the house let alone any athletic activities. It turns out he wasn’t even lifting his laptop computer with two hands because some nurse had told him not to lift anything over 2 pounds.
I told him “Peter, even some of the most experienced doctors focus on the ‘can’ts’ and forget to tell you the ‘cans’ and ‘shoulds.’ While you’re in the waiting room make up a mental list of what you would like to be doing that you aren’t.”
As he climbed back in the car for the ride home I asked how the visit went. The x-ray showed good alignment and the doctor was pleased. But, as I predicted, they were already on the launch pad to the receptionist to make a follow-up appointment without the physician uttering a single word about what activities he could resume. Always a very coachable kid, Peter piped up with the list he had created in the waiting room and was relieved to hear that he could do anything as long as it didn’t hurt. In fact, the doctor encouraged him to use his fingers because it might speed the healing.
Not every patient, regardless of age, is as cautious as my grandson and in some circumstances the physician must err on the side of emphasizing the “don’ts.” However, in my experience, too many physicians forget to include a generous list of “can do’s” in their visit closing discussions. This oversight is a mistake for several reasons.
First, and maybe most importantly, even a brief discussion of “can do’s” can soften the depressing message that the patient will not be able to do things he or she enjoys. I can’t quote the references but I am sure there is plenty of evidence that depression slows the healing process.
Second, and this is particularly true in older patients with orthopedic problems – failure to include a plan for return to activity can hinder recovery. I can recall more than a few patients who were seen in the emergency department and diagnosed with sprains but not given even the simplest instructions on how to begin moving the injured joint. When they finally returned to see me we had to begin the painful and unnecessary project of thawing a frozen joint.
Fortunately, we have evolved past the era when best rest was near the top of the list of our recommended remedies. However, there still remains a bias against activity in some situations. The most recent example is the evolving strategies for the management of concussion. There is some evidence that involving the patient in a return to activity plan may shorten the time to recovery. The myth about brain rest has been slow to die.
Finally, providing the patient with a personalized list of “can do’s” makes good business sense because it can head off those time-gobbling call backs that tie up you and your office staff. As an experienced physician, you have probably learned the most frequently asked “Can Jason do ... ?” questions. Make your own list and give the patient your answers. An ounce of anticipatory guidance is worth hours on the telephone or sorting through the email inbox.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
On his last shift in the last hockey game of the regular season, our 14-year-old grandson broke his arm. Although this was his first fracture, the rest of the nuclear family has had ample experience with orthopedic trauma over the last year, both planned and unplanned.
As I drove Peter and my daughter-in-law to his first postsetting and casting appointment I told him how sorry I was that he had been told “no contact sports for the next 3 months.” This was a tough pill for a kid eager to begin his first high school lacrosse season. Then I asked him what the doctor had told him he could do in the way of activity.
Based on personal and professional experience I was not surprised when he told me that no one had suggested things he could be doing. In fact, being a cautious and thoughtful kid, he was concerned about what he should be doing around the house let alone any athletic activities. It turns out he wasn’t even lifting his laptop computer with two hands because some nurse had told him not to lift anything over 2 pounds.
I told him “Peter, even some of the most experienced doctors focus on the ‘can’ts’ and forget to tell you the ‘cans’ and ‘shoulds.’ While you’re in the waiting room make up a mental list of what you would like to be doing that you aren’t.”
As he climbed back in the car for the ride home I asked how the visit went. The x-ray showed good alignment and the doctor was pleased. But, as I predicted, they were already on the launch pad to the receptionist to make a follow-up appointment without the physician uttering a single word about what activities he could resume. Always a very coachable kid, Peter piped up with the list he had created in the waiting room and was relieved to hear that he could do anything as long as it didn’t hurt. In fact, the doctor encouraged him to use his fingers because it might speed the healing.
Not every patient, regardless of age, is as cautious as my grandson and in some circumstances the physician must err on the side of emphasizing the “don’ts.” However, in my experience, too many physicians forget to include a generous list of “can do’s” in their visit closing discussions. This oversight is a mistake for several reasons.
First, and maybe most importantly, even a brief discussion of “can do’s” can soften the depressing message that the patient will not be able to do things he or she enjoys. I can’t quote the references but I am sure there is plenty of evidence that depression slows the healing process.
Second, and this is particularly true in older patients with orthopedic problems – failure to include a plan for return to activity can hinder recovery. I can recall more than a few patients who were seen in the emergency department and diagnosed with sprains but not given even the simplest instructions on how to begin moving the injured joint. When they finally returned to see me we had to begin the painful and unnecessary project of thawing a frozen joint.
Fortunately, we have evolved past the era when best rest was near the top of the list of our recommended remedies. However, there still remains a bias against activity in some situations. The most recent example is the evolving strategies for the management of concussion. There is some evidence that involving the patient in a return to activity plan may shorten the time to recovery. The myth about brain rest has been slow to die.
Finally, providing the patient with a personalized list of “can do’s” makes good business sense because it can head off those time-gobbling call backs that tie up you and your office staff. As an experienced physician, you have probably learned the most frequently asked “Can Jason do ... ?” questions. Make your own list and give the patient your answers. An ounce of anticipatory guidance is worth hours on the telephone or sorting through the email inbox.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Celebrating our colleagues
several of whom I am privileged to work with on a daily basis. We also welcome the newest members of AGA’s Governing Board, Maria T. Abreu, MD, AGAF, who is an outstanding leader and representative of a much larger group of volunteer members who work tirelessly to advance AGA’s initiatives to enhance the clinical practice of gastroenterology and improve patient outcomes. The nominating committee also appointed the following slate of councilors, which is subject to membership vote: Kim Barrett, PhD, AGAF; Lawrence Kosinski, MD, MBA, AGAF; and Sheryl Pfeil, MD, AGAF.

This month’s issue also highlights two newly-developed clinical risk-prediction tools – one designed to assist clinicians in predicting alcoholic hepatitis mortality, and another designed to identify inflammatory bowel disease (IBD) patients at high-risk of developing venous thromboembolism (VTE) post-hospitalization. While no prediction model is perfect, these tools can positively impact clinical decision-making and contribute to improved patient outcomes. We also include recommendations on managing IBD in older patients, and report on a study suggesting an increase in late-stage cancer diagnoses in the wake of the COVID-19 pandemic. AGA’s new clinical guideline on systemic therapy for hepatocellular carcinoma and Clinical Practice Update on non-invasive colorectal cancer screening also are featured. Finally, in this month’s Practice Management Toolbox, Dr. Feuerstein, Dr. Sofia, Dr. Guha, and Dr. Streett offer timely recommendations regarding how to overcome existing barriers to achieve high-value IBD care.
Megan A. Adams, MD, JD, MSc
Editor in Chief
several of whom I am privileged to work with on a daily basis. We also welcome the newest members of AGA’s Governing Board, Maria T. Abreu, MD, AGAF, who is an outstanding leader and representative of a much larger group of volunteer members who work tirelessly to advance AGA’s initiatives to enhance the clinical practice of gastroenterology and improve patient outcomes. The nominating committee also appointed the following slate of councilors, which is subject to membership vote: Kim Barrett, PhD, AGAF; Lawrence Kosinski, MD, MBA, AGAF; and Sheryl Pfeil, MD, AGAF.
This month’s issue also highlights two newly-developed clinical risk-prediction tools – one designed to assist clinicians in predicting alcoholic hepatitis mortality, and another designed to identify inflammatory bowel disease (IBD) patients at high-risk of developing venous thromboembolism (VTE) post-hospitalization. While no prediction model is perfect, these tools can positively impact clinical decision-making and contribute to improved patient outcomes. We also include recommendations on managing IBD in older patients, and report on a study suggesting an increase in late-stage cancer diagnoses in the wake of the COVID-19 pandemic. AGA’s new clinical guideline on systemic therapy for hepatocellular carcinoma and Clinical Practice Update on non-invasive colorectal cancer screening also are featured. Finally, in this month’s Practice Management Toolbox, Dr. Feuerstein, Dr. Sofia, Dr. Guha, and Dr. Streett offer timely recommendations regarding how to overcome existing barriers to achieve high-value IBD care.
Megan A. Adams, MD, JD, MSc
Editor in Chief
several of whom I am privileged to work with on a daily basis. We also welcome the newest members of AGA’s Governing Board, Maria T. Abreu, MD, AGAF, who is an outstanding leader and representative of a much larger group of volunteer members who work tirelessly to advance AGA’s initiatives to enhance the clinical practice of gastroenterology and improve patient outcomes. The nominating committee also appointed the following slate of councilors, which is subject to membership vote: Kim Barrett, PhD, AGAF; Lawrence Kosinski, MD, MBA, AGAF; and Sheryl Pfeil, MD, AGAF.
This month’s issue also highlights two newly-developed clinical risk-prediction tools – one designed to assist clinicians in predicting alcoholic hepatitis mortality, and another designed to identify inflammatory bowel disease (IBD) patients at high-risk of developing venous thromboembolism (VTE) post-hospitalization. While no prediction model is perfect, these tools can positively impact clinical decision-making and contribute to improved patient outcomes. We also include recommendations on managing IBD in older patients, and report on a study suggesting an increase in late-stage cancer diagnoses in the wake of the COVID-19 pandemic. AGA’s new clinical guideline on systemic therapy for hepatocellular carcinoma and Clinical Practice Update on non-invasive colorectal cancer screening also are featured. Finally, in this month’s Practice Management Toolbox, Dr. Feuerstein, Dr. Sofia, Dr. Guha, and Dr. Streett offer timely recommendations regarding how to overcome existing barriers to achieve high-value IBD care.
Megan A. Adams, MD, JD, MSc
Editor in Chief
How and why the language of medicine must change
The United States has never achieved a single high standard of medical care equity for all of its people, and the trend line does not appear favorable. The closest we have reached is basic Medicare (Parts A and B), military medicine, the Veterans Health Administration, and large nonprofit groups like Kaiser Permanente. It seems that the nature of we individualistic Americans is to always try to seek an advantage.
But even achieving equity in medical care would not ensure equity in health. The social determinants of health (income level, education, politics, government, geography, neighborhood, country of origin, language spoken, literacy, gender, and yes – race and ethnicity) have far more influence on health equity than does medical care.
Narratives can both reflect and influence culture. Considering the harmful effects of the current political divisiveness in the United States, the timing is ideal for our three leading medical and health education organizations – the American Medical Association, the Association of American Medical Colleges (AAMC), and the Centers for Disease Control and Prevention – to publish a definitive position paper called “Advancing Health Equity: A Guide to Language, Narrative and Concepts.”
What’s in a word?
According to William Shakespeare, “A rose by any other name would smell as sweet” (Romeo and Juliet). Maybe. But if the word used were “thorn” or “thistle,” it just would not be the same.
Words comprise language and wield enormous power with human beings. Wars are fought over geographic boundaries often defined by the language spoken by the people: think 2022, Russian-speaking Ukrainians. Think Winston Churchill’s massive 1,500-page “A History of the English-Speaking Peoples.” Think about the political power of French in Quebec, Canada.
Thus, it should be no surprise that words, acronyms, and abbreviations become rallying cries for political activists of all stripes: PC, January 6, Woke, 1619, BLM, Critical Race Theory, 1776, Remember Pearl Harbor, Remember the Alamo, the Civil War or the War Between the States, the War for Southern Independence, the War of Northern Aggression, the War of the Rebellion, or simply “The Lost Cause.” How about Realpolitik?
Is “medical language” the language of the people or of the profession? Physicians must understand each other, and physicians also must communicate clearly with patients using words that convey neutral meanings and don’t interfere with objective understanding. Medical editors prefer the brevity of one or a few words to clearly convey meaning.
I consider this document from the AMA and AAMC to be both profound and profoundly important for the healing professions. The contributors frequently use words like “humility” as they describe their efforts and products, knowing full well that they (and their organizations) stand to be figuratively torn limb from limb by a host of critics – or worse, ignored and marginalized.
Part 1 of the Health Equity Guide is titled “Language for promoting health equity.”(the reader is referred to the Health Equity Guide for the reasoning and explanations for all).
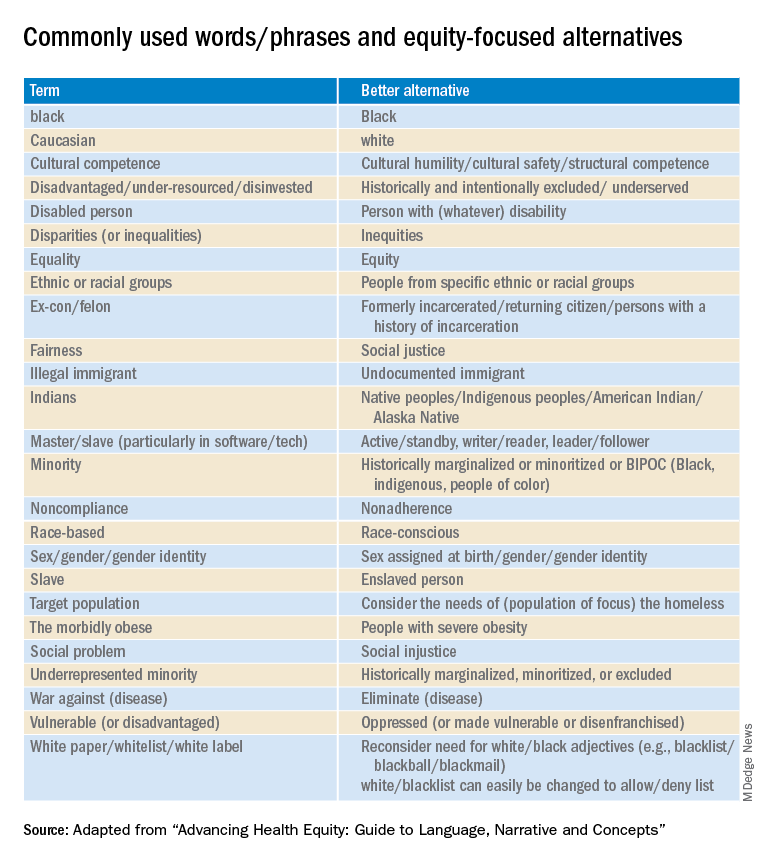
Part 2 of the Health Equity Guide is called “Why narratives matter.” It includes features of dominant narratives; a substantial section on the narrative of race and the narrative of individualism; the purpose of a health equity–based narrative; how to change the narrative; and how to see and think critically through dialogue.
Part 3 of the Health Equity Guide is a glossary of 138 key terms such as “class,” “discrimination,” “gender dysphoria,” “non-White,” “racial capitalism,” and “structural competency.”
The CDC also has a toolkit for inclusive communication, the “Health Equity Guiding Principles for Inclusive Communication.”
The substantive message of the Health Equity Guide could affect what you say, write, and do (even how you think) every day as well as how those with whom you interact view you. It can affect the entire communication milieu in which you live, whether or not you like it. Read it seriously, as though your professional life depended on it. It may.
Dr. Lundberg is consulting professor of health research policy and pathology at Stanford (Calif.) University. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The United States has never achieved a single high standard of medical care equity for all of its people, and the trend line does not appear favorable. The closest we have reached is basic Medicare (Parts A and B), military medicine, the Veterans Health Administration, and large nonprofit groups like Kaiser Permanente. It seems that the nature of we individualistic Americans is to always try to seek an advantage.
But even achieving equity in medical care would not ensure equity in health. The social determinants of health (income level, education, politics, government, geography, neighborhood, country of origin, language spoken, literacy, gender, and yes – race and ethnicity) have far more influence on health equity than does medical care.
Narratives can both reflect and influence culture. Considering the harmful effects of the current political divisiveness in the United States, the timing is ideal for our three leading medical and health education organizations – the American Medical Association, the Association of American Medical Colleges (AAMC), and the Centers for Disease Control and Prevention – to publish a definitive position paper called “Advancing Health Equity: A Guide to Language, Narrative and Concepts.”
What’s in a word?
According to William Shakespeare, “A rose by any other name would smell as sweet” (Romeo and Juliet). Maybe. But if the word used were “thorn” or “thistle,” it just would not be the same.
Words comprise language and wield enormous power with human beings. Wars are fought over geographic boundaries often defined by the language spoken by the people: think 2022, Russian-speaking Ukrainians. Think Winston Churchill’s massive 1,500-page “A History of the English-Speaking Peoples.” Think about the political power of French in Quebec, Canada.
Thus, it should be no surprise that words, acronyms, and abbreviations become rallying cries for political activists of all stripes: PC, January 6, Woke, 1619, BLM, Critical Race Theory, 1776, Remember Pearl Harbor, Remember the Alamo, the Civil War or the War Between the States, the War for Southern Independence, the War of Northern Aggression, the War of the Rebellion, or simply “The Lost Cause.” How about Realpolitik?
Is “medical language” the language of the people or of the profession? Physicians must understand each other, and physicians also must communicate clearly with patients using words that convey neutral meanings and don’t interfere with objective understanding. Medical editors prefer the brevity of one or a few words to clearly convey meaning.
I consider this document from the AMA and AAMC to be both profound and profoundly important for the healing professions. The contributors frequently use words like “humility” as they describe their efforts and products, knowing full well that they (and their organizations) stand to be figuratively torn limb from limb by a host of critics – or worse, ignored and marginalized.
Part 1 of the Health Equity Guide is titled “Language for promoting health equity.”(the reader is referred to the Health Equity Guide for the reasoning and explanations for all).
Part 2 of the Health Equity Guide is called “Why narratives matter.” It includes features of dominant narratives; a substantial section on the narrative of race and the narrative of individualism; the purpose of a health equity–based narrative; how to change the narrative; and how to see and think critically through dialogue.
Part 3 of the Health Equity Guide is a glossary of 138 key terms such as “class,” “discrimination,” “gender dysphoria,” “non-White,” “racial capitalism,” and “structural competency.”
The CDC also has a toolkit for inclusive communication, the “Health Equity Guiding Principles for Inclusive Communication.”
The substantive message of the Health Equity Guide could affect what you say, write, and do (even how you think) every day as well as how those with whom you interact view you. It can affect the entire communication milieu in which you live, whether or not you like it. Read it seriously, as though your professional life depended on it. It may.
Dr. Lundberg is consulting professor of health research policy and pathology at Stanford (Calif.) University. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The United States has never achieved a single high standard of medical care equity for all of its people, and the trend line does not appear favorable. The closest we have reached is basic Medicare (Parts A and B), military medicine, the Veterans Health Administration, and large nonprofit groups like Kaiser Permanente. It seems that the nature of we individualistic Americans is to always try to seek an advantage.
But even achieving equity in medical care would not ensure equity in health. The social determinants of health (income level, education, politics, government, geography, neighborhood, country of origin, language spoken, literacy, gender, and yes – race and ethnicity) have far more influence on health equity than does medical care.
Narratives can both reflect and influence culture. Considering the harmful effects of the current political divisiveness in the United States, the timing is ideal for our three leading medical and health education organizations – the American Medical Association, the Association of American Medical Colleges (AAMC), and the Centers for Disease Control and Prevention – to publish a definitive position paper called “Advancing Health Equity: A Guide to Language, Narrative and Concepts.”
What’s in a word?
According to William Shakespeare, “A rose by any other name would smell as sweet” (Romeo and Juliet). Maybe. But if the word used were “thorn” or “thistle,” it just would not be the same.
Words comprise language and wield enormous power with human beings. Wars are fought over geographic boundaries often defined by the language spoken by the people: think 2022, Russian-speaking Ukrainians. Think Winston Churchill’s massive 1,500-page “A History of the English-Speaking Peoples.” Think about the political power of French in Quebec, Canada.
Thus, it should be no surprise that words, acronyms, and abbreviations become rallying cries for political activists of all stripes: PC, January 6, Woke, 1619, BLM, Critical Race Theory, 1776, Remember Pearl Harbor, Remember the Alamo, the Civil War or the War Between the States, the War for Southern Independence, the War of Northern Aggression, the War of the Rebellion, or simply “The Lost Cause.” How about Realpolitik?
Is “medical language” the language of the people or of the profession? Physicians must understand each other, and physicians also must communicate clearly with patients using words that convey neutral meanings and don’t interfere with objective understanding. Medical editors prefer the brevity of one or a few words to clearly convey meaning.
I consider this document from the AMA and AAMC to be both profound and profoundly important for the healing professions. The contributors frequently use words like “humility” as they describe their efforts and products, knowing full well that they (and their organizations) stand to be figuratively torn limb from limb by a host of critics – or worse, ignored and marginalized.
Part 1 of the Health Equity Guide is titled “Language for promoting health equity.”(the reader is referred to the Health Equity Guide for the reasoning and explanations for all).
Part 2 of the Health Equity Guide is called “Why narratives matter.” It includes features of dominant narratives; a substantial section on the narrative of race and the narrative of individualism; the purpose of a health equity–based narrative; how to change the narrative; and how to see and think critically through dialogue.
Part 3 of the Health Equity Guide is a glossary of 138 key terms such as “class,” “discrimination,” “gender dysphoria,” “non-White,” “racial capitalism,” and “structural competency.”
The CDC also has a toolkit for inclusive communication, the “Health Equity Guiding Principles for Inclusive Communication.”
The substantive message of the Health Equity Guide could affect what you say, write, and do (even how you think) every day as well as how those with whom you interact view you. It can affect the entire communication milieu in which you live, whether or not you like it. Read it seriously, as though your professional life depended on it. It may.
Dr. Lundberg is consulting professor of health research policy and pathology at Stanford (Calif.) University. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
A little-known offshoot of hem/onc opens pathway for professional development
Only a small number of pediatric hematologist oncologists and even fewer of our adult counterparts feel comfortable evaluating and treating vascular anomalies.
While admittedly rare, these conditions are still common enough that clinicians in many disciplines encounter them. Hematologist/oncologists are most likely to see vascular malformations, which often present as mass lesions. Complications of these disorders occur across the hematology-oncology spectrum and include clots, pulmonary emboli, cancer predisposition, and an array of functional and psychosocial disorders.
Vascular anomalies are broadly categorized as vascular tumors or malformations. The tumors include hemangiomas, locally aggressive lesions, and true cancers. Malformations can be isolated disorders of one or more blood vessel types (veins, arteries, capillaries or lymphatics), or they can be one part of syndromic disorders. Lymphedema also falls under the heading of vascular anomalies. To make the terminology less confusing, in 2018 the International Society for the Study of Vascular Anomalies refined its classification scheme.
Vascular malformations are thought to be congenital. Although some are obvious at birth, others aren’t apparent until adulthood. In most cases, they grow with a child and may do so disproportionately at puberty and with pregnancies. The fact that vascular malformations persist into adulthood is one reason why their care should be integral to medical hematology-oncology.
Although the cause of a vascular malformation is not always known, a wide range of genetic mutations thought to be pathogenic have been reported. These mutations are usually somatic (only within the involved tissues, not in the blood or germ cells and therefore, not heritable) and tend to cluster in the VEGF-PIK3CA and RAS-MAP signaling pathways.
These genes and pathways will be familiar to any oncologist who cares for patients with solid tumors, notably breast cancer or melanoma. However, unlike the clonal expansion seen in cancers, most vascular malformations will express pathogenic mutations in less than 20% of vascular endothelium within a malformation.
Since 2008, medical management has been limited to sirolimus (rapamycin), a mammalian target of rapamycin inhibitor, which can be effective even when mTOR mutations aren’t apparent. In a seminal phase 2 trial of 57 patients with complex vascular anomalies who were aged 0-29 years, 47 patients had a partial response, 3 patients had stable disease, and 7 patients had progressive disease. None had complete responses. These data highlight the need for more effective treatments.
Recently, vascular anomalists have begun to repurpose drugs from adult oncology that specifically target pathogenic mutations. Some studies underway include Novartis’ international Alpelisib (Piqray) clinical trial for adults and children with PIK3CA-related overgrowth syndromes (NCT04589650) and Merck’s follow-up study of the AKT inhibitor miransertib for PROS and Proteus syndrome. Doses tend to be lower than those used to treat cancers. To date, these have been generally well-tolerated, with sometimes striking but preliminary evidence of efficacy.
During the past 2 years, symposia on vascular anomalies at the annual meeting of the American Society of Hematology have launched what we are hoping is just the start of a broader discussion. In 2020, Fran Blei, MD, chaired Vascular Anomalies 101: Case-Based Discussion on the Diagnosis, Treatment and Lifelong Care of These Patients, and in 2021, Adrienne Hammill, MD, PhD, and Dr. Raj Kasthuri, MBBS, MD, chaired a more specialized symposium: Hereditary Hemorrhagic Telangiectasia (HHT): A Practical Guide to Management.
Dr. Blatt is in the division of pediatric hematology oncology at the University of North Carolina at Chapel Hill. She disclosed no relevant financial relationships.
Only a small number of pediatric hematologist oncologists and even fewer of our adult counterparts feel comfortable evaluating and treating vascular anomalies.
While admittedly rare, these conditions are still common enough that clinicians in many disciplines encounter them. Hematologist/oncologists are most likely to see vascular malformations, which often present as mass lesions. Complications of these disorders occur across the hematology-oncology spectrum and include clots, pulmonary emboli, cancer predisposition, and an array of functional and psychosocial disorders.
Vascular anomalies are broadly categorized as vascular tumors or malformations. The tumors include hemangiomas, locally aggressive lesions, and true cancers. Malformations can be isolated disorders of one or more blood vessel types (veins, arteries, capillaries or lymphatics), or they can be one part of syndromic disorders. Lymphedema also falls under the heading of vascular anomalies. To make the terminology less confusing, in 2018 the International Society for the Study of Vascular Anomalies refined its classification scheme.
Vascular malformations are thought to be congenital. Although some are obvious at birth, others aren’t apparent until adulthood. In most cases, they grow with a child and may do so disproportionately at puberty and with pregnancies. The fact that vascular malformations persist into adulthood is one reason why their care should be integral to medical hematology-oncology.
Although the cause of a vascular malformation is not always known, a wide range of genetic mutations thought to be pathogenic have been reported. These mutations are usually somatic (only within the involved tissues, not in the blood or germ cells and therefore, not heritable) and tend to cluster in the VEGF-PIK3CA and RAS-MAP signaling pathways.
These genes and pathways will be familiar to any oncologist who cares for patients with solid tumors, notably breast cancer or melanoma. However, unlike the clonal expansion seen in cancers, most vascular malformations will express pathogenic mutations in less than 20% of vascular endothelium within a malformation.
Since 2008, medical management has been limited to sirolimus (rapamycin), a mammalian target of rapamycin inhibitor, which can be effective even when mTOR mutations aren’t apparent. In a seminal phase 2 trial of 57 patients with complex vascular anomalies who were aged 0-29 years, 47 patients had a partial response, 3 patients had stable disease, and 7 patients had progressive disease. None had complete responses. These data highlight the need for more effective treatments.
Recently, vascular anomalists have begun to repurpose drugs from adult oncology that specifically target pathogenic mutations. Some studies underway include Novartis’ international Alpelisib (Piqray) clinical trial for adults and children with PIK3CA-related overgrowth syndromes (NCT04589650) and Merck’s follow-up study of the AKT inhibitor miransertib for PROS and Proteus syndrome. Doses tend to be lower than those used to treat cancers. To date, these have been generally well-tolerated, with sometimes striking but preliminary evidence of efficacy.
During the past 2 years, symposia on vascular anomalies at the annual meeting of the American Society of Hematology have launched what we are hoping is just the start of a broader discussion. In 2020, Fran Blei, MD, chaired Vascular Anomalies 101: Case-Based Discussion on the Diagnosis, Treatment and Lifelong Care of These Patients, and in 2021, Adrienne Hammill, MD, PhD, and Dr. Raj Kasthuri, MBBS, MD, chaired a more specialized symposium: Hereditary Hemorrhagic Telangiectasia (HHT): A Practical Guide to Management.
Dr. Blatt is in the division of pediatric hematology oncology at the University of North Carolina at Chapel Hill. She disclosed no relevant financial relationships.
Only a small number of pediatric hematologist oncologists and even fewer of our adult counterparts feel comfortable evaluating and treating vascular anomalies.
While admittedly rare, these conditions are still common enough that clinicians in many disciplines encounter them. Hematologist/oncologists are most likely to see vascular malformations, which often present as mass lesions. Complications of these disorders occur across the hematology-oncology spectrum and include clots, pulmonary emboli, cancer predisposition, and an array of functional and psychosocial disorders.
Vascular anomalies are broadly categorized as vascular tumors or malformations. The tumors include hemangiomas, locally aggressive lesions, and true cancers. Malformations can be isolated disorders of one or more blood vessel types (veins, arteries, capillaries or lymphatics), or they can be one part of syndromic disorders. Lymphedema also falls under the heading of vascular anomalies. To make the terminology less confusing, in 2018 the International Society for the Study of Vascular Anomalies refined its classification scheme.
Vascular malformations are thought to be congenital. Although some are obvious at birth, others aren’t apparent until adulthood. In most cases, they grow with a child and may do so disproportionately at puberty and with pregnancies. The fact that vascular malformations persist into adulthood is one reason why their care should be integral to medical hematology-oncology.
Although the cause of a vascular malformation is not always known, a wide range of genetic mutations thought to be pathogenic have been reported. These mutations are usually somatic (only within the involved tissues, not in the blood or germ cells and therefore, not heritable) and tend to cluster in the VEGF-PIK3CA and RAS-MAP signaling pathways.
These genes and pathways will be familiar to any oncologist who cares for patients with solid tumors, notably breast cancer or melanoma. However, unlike the clonal expansion seen in cancers, most vascular malformations will express pathogenic mutations in less than 20% of vascular endothelium within a malformation.
Since 2008, medical management has been limited to sirolimus (rapamycin), a mammalian target of rapamycin inhibitor, which can be effective even when mTOR mutations aren’t apparent. In a seminal phase 2 trial of 57 patients with complex vascular anomalies who were aged 0-29 years, 47 patients had a partial response, 3 patients had stable disease, and 7 patients had progressive disease. None had complete responses. These data highlight the need for more effective treatments.
Recently, vascular anomalists have begun to repurpose drugs from adult oncology that specifically target pathogenic mutations. Some studies underway include Novartis’ international Alpelisib (Piqray) clinical trial for adults and children with PIK3CA-related overgrowth syndromes (NCT04589650) and Merck’s follow-up study of the AKT inhibitor miransertib for PROS and Proteus syndrome. Doses tend to be lower than those used to treat cancers. To date, these have been generally well-tolerated, with sometimes striking but preliminary evidence of efficacy.
During the past 2 years, symposia on vascular anomalies at the annual meeting of the American Society of Hematology have launched what we are hoping is just the start of a broader discussion. In 2020, Fran Blei, MD, chaired Vascular Anomalies 101: Case-Based Discussion on the Diagnosis, Treatment and Lifelong Care of These Patients, and in 2021, Adrienne Hammill, MD, PhD, and Dr. Raj Kasthuri, MBBS, MD, chaired a more specialized symposium: Hereditary Hemorrhagic Telangiectasia (HHT): A Practical Guide to Management.
Dr. Blatt is in the division of pediatric hematology oncology at the University of North Carolina at Chapel Hill. She disclosed no relevant financial relationships.
Removing barriers to high-value IBD care: Challenges and opportunities
Over the last several years, payer policies that dictate and restrict treatments for patients with inflammatory bowel diseases (IBD) have proliferated. The implementation of new coverage restrictions, expansion of services and procedures requiring prior authorization (PA), and dosing and access restriction to covered drugs, and the requirement of repeated treatment reviews including nonmedical switching for stable patients are widespread. The AGA administered a member needs assessment survey in December 2021 to determine the extent to which these policies harm patients and overburden gastroenterologists and their staff.
Survey findings
Most of the 100 surveyed members reported facing administrative burdens that prevented timely access to patient care. Utilization management practices such as PA, step therapy, and nonmedical switching and dosing restrictions create critical barriers to high quality GI care for patients with chronic conditions and jeopardize the physician-patient relationship. At a time when physicians have faced unprecedented challenges because of the public health emergency from the COVID-19 pandemic, these burdens also contribute to increasing physician burnout.
Prior authorization: Among AGA members, 96% of members said that PA is burdensome, with 61% indicating that it is significantly burdensome. Almost 99% of members indicated that PA has a negative impact on patients’ access to clinically appropriate treatments; 89% reported that the burden associated with PA has increased over the last 5 years in their practice.
Step therapy: Among members, 87% described the impact step therapy has on their practice as burdensome. Almost 90% of members said step therapy negatively impacted patients’ access to clinically appropriate treatments. Almost 90% of members felt that there was an overall negative impact on patient clinical outcomes for those patients who were required to follow a step therapy protocol.
Nonmedical switching and dosing restrictions: Out of all members, 86% reported an increase in nonmedical switching and dosing restrictions over the last 5 years; 79% of members noted that these restrictions had a negative impact on patient clinical outcomes.
An increasing number of insurance companies are restricting effective biologic therapy to Food and Drug Administration–labeled doses, in direct conflict with current established best practices. It is most concerning that many patients who had been stable on optimized dosing are suddenly notified that they will no longer be able to receive the dose or treatment frequency prescribed by their physician. The concept of optimizing drug therapy based on disease activity and therapeutic drug monitoring is well established, and artificial restrictions to FDA-labeled doses force unnecessary drug deescalation. This transparent effort to reduce costs lacks evidence for safety. Our sickest patients often require higher doses for induction in order to respond, given drug losses, yet some payers refuse to cover the doses these patients require. This new payer-centered effort prioritizes cost containment over the judgment of the treating physician. It causes direct patient harm risking efficacy or loss of response, and subsequent irreversible disease-related complications.
Medicare drug costs
Medicare patients receiving self-injectable or oral medications are not eligible for co-pay assistance programs through pharmaceutical companies because of federal rules. For non-Medicare patients, these programs reduce the co-pay costs to as low as $5 per month. Medicare patients are able to receive infusions like infliximab and vedolizumab at no cost. However, any self-injectable or oral agent can carry a co-pay of over $1,000. Other than for patients meeting income-based eligibility requirements (e.g., below the poverty line), these treatments become prohibitively expensive. Thousands of patients have had to discontinue their self-injectable and/or oral medications because of this cost or have been denied access to the therapy altogether because of cost.
Need for change

These recent changes in insurance policies have resulted in increased harm to our patients with IBD rather than improving the safety or quality of their care. These changes create barriers to disease treatment and have not improved quality of care, patient outcomes, or quality of life. The AGA and other societies have published multiple guidelines and literature on the management of patients with IBD that should serve as the foundation for insurers’ medication coverage policies. Additionally, insurance companies should seek input from panels of IBD experts when developing their medication coverage policies to ensure they are patient oriented and facilitate high-quality IBD care.
The following are opportunities for insurers to improve the IBD drug approval process:
- Simplify the appeal process.
- Guarantee rapid response/turnaround to appeal processes to avoid additional delays in care.
- Incorporate experienced expert review by a gastroenterologist.
- Ensure coverage of drug and disease monitoring.
- Integrate expert input in policy development.
Conclusion
Effective patient care in IBD, as well as in other chronic gastrointestinal diseases, requires a collaborative approach to maximize clinical outcomes. It is an exciting time in our field, with rapidly expanding therapeutic options to treat IBD that have the potential to modify the disease course and prevent long-term complications for patients. However, optimizing the use of these treatments to achieve disease remission is challenging and requires the ability to individualize the timely choice of medications at the right dose for each patient to capture and monitor response. The ability to provide individualized, data driven care is essential to improving the quality of life of our patients, as well as to reducing health care spending over time.

Achieving high-value care is a goal that benefits everyone involved in the health care system. Policies that interfere with the timely treatment of sick patients with the right therapies, optimized to achieve disease remission, hurt the very patients that our health care system exists to serve. We cannot stand by while impediments to treatment result in harm to our patients and worsen clinical outcomes. Collaboratively developing aligned incentives can lead us to patient-centered policies that fulfill a shared purpose to optimize the health of people with chronic digestive diseases.
The authors reported having no relevant conflicts of interest.
Dr. Feuerstein is with the Center for Inflammatory Bowel Disease at Beth Israel Deaconess Medical Center and is an associate professor of medicine Harvard Medical School, both in Boston. Dr. Sofia is an assistant professor of medicine with the division of gastroenterology and hepatology at Oregon Health and Science University, Portland. Dr. Guha is a professor of medicine at the division of gastroenterology, hepatology and nutrition and is codirector of the Center for Interventional Gastroenterology at UTHealth (iGUT) at UT Health Science Center, Houston. Dr. Streett is a clinical professor of medicine, gastroenterology, and hepatology and director of the IBD Education and Advanced IBD Fellowship at Stanford (Calif.) Medicine.
Over the last several years, payer policies that dictate and restrict treatments for patients with inflammatory bowel diseases (IBD) have proliferated. The implementation of new coverage restrictions, expansion of services and procedures requiring prior authorization (PA), and dosing and access restriction to covered drugs, and the requirement of repeated treatment reviews including nonmedical switching for stable patients are widespread. The AGA administered a member needs assessment survey in December 2021 to determine the extent to which these policies harm patients and overburden gastroenterologists and their staff.
Survey findings
Most of the 100 surveyed members reported facing administrative burdens that prevented timely access to patient care. Utilization management practices such as PA, step therapy, and nonmedical switching and dosing restrictions create critical barriers to high quality GI care for patients with chronic conditions and jeopardize the physician-patient relationship. At a time when physicians have faced unprecedented challenges because of the public health emergency from the COVID-19 pandemic, these burdens also contribute to increasing physician burnout.
Prior authorization: Among AGA members, 96% of members said that PA is burdensome, with 61% indicating that it is significantly burdensome. Almost 99% of members indicated that PA has a negative impact on patients’ access to clinically appropriate treatments; 89% reported that the burden associated with PA has increased over the last 5 years in their practice.
Step therapy: Among members, 87% described the impact step therapy has on their practice as burdensome. Almost 90% of members said step therapy negatively impacted patients’ access to clinically appropriate treatments. Almost 90% of members felt that there was an overall negative impact on patient clinical outcomes for those patients who were required to follow a step therapy protocol.
Nonmedical switching and dosing restrictions: Out of all members, 86% reported an increase in nonmedical switching and dosing restrictions over the last 5 years; 79% of members noted that these restrictions had a negative impact on patient clinical outcomes.
An increasing number of insurance companies are restricting effective biologic therapy to Food and Drug Administration–labeled doses, in direct conflict with current established best practices. It is most concerning that many patients who had been stable on optimized dosing are suddenly notified that they will no longer be able to receive the dose or treatment frequency prescribed by their physician. The concept of optimizing drug therapy based on disease activity and therapeutic drug monitoring is well established, and artificial restrictions to FDA-labeled doses force unnecessary drug deescalation. This transparent effort to reduce costs lacks evidence for safety. Our sickest patients often require higher doses for induction in order to respond, given drug losses, yet some payers refuse to cover the doses these patients require. This new payer-centered effort prioritizes cost containment over the judgment of the treating physician. It causes direct patient harm risking efficacy or loss of response, and subsequent irreversible disease-related complications.
Medicare drug costs
Medicare patients receiving self-injectable or oral medications are not eligible for co-pay assistance programs through pharmaceutical companies because of federal rules. For non-Medicare patients, these programs reduce the co-pay costs to as low as $5 per month. Medicare patients are able to receive infusions like infliximab and vedolizumab at no cost. However, any self-injectable or oral agent can carry a co-pay of over $1,000. Other than for patients meeting income-based eligibility requirements (e.g., below the poverty line), these treatments become prohibitively expensive. Thousands of patients have had to discontinue their self-injectable and/or oral medications because of this cost or have been denied access to the therapy altogether because of cost.
Need for change
These recent changes in insurance policies have resulted in increased harm to our patients with IBD rather than improving the safety or quality of their care. These changes create barriers to disease treatment and have not improved quality of care, patient outcomes, or quality of life. The AGA and other societies have published multiple guidelines and literature on the management of patients with IBD that should serve as the foundation for insurers’ medication coverage policies. Additionally, insurance companies should seek input from panels of IBD experts when developing their medication coverage policies to ensure they are patient oriented and facilitate high-quality IBD care.
The following are opportunities for insurers to improve the IBD drug approval process:
- Simplify the appeal process.
- Guarantee rapid response/turnaround to appeal processes to avoid additional delays in care.
- Incorporate experienced expert review by a gastroenterologist.
- Ensure coverage of drug and disease monitoring.
- Integrate expert input in policy development.
Conclusion
Effective patient care in IBD, as well as in other chronic gastrointestinal diseases, requires a collaborative approach to maximize clinical outcomes. It is an exciting time in our field, with rapidly expanding therapeutic options to treat IBD that have the potential to modify the disease course and prevent long-term complications for patients. However, optimizing the use of these treatments to achieve disease remission is challenging and requires the ability to individualize the timely choice of medications at the right dose for each patient to capture and monitor response. The ability to provide individualized, data driven care is essential to improving the quality of life of our patients, as well as to reducing health care spending over time.
Achieving high-value care is a goal that benefits everyone involved in the health care system. Policies that interfere with the timely treatment of sick patients with the right therapies, optimized to achieve disease remission, hurt the very patients that our health care system exists to serve. We cannot stand by while impediments to treatment result in harm to our patients and worsen clinical outcomes. Collaboratively developing aligned incentives can lead us to patient-centered policies that fulfill a shared purpose to optimize the health of people with chronic digestive diseases.
The authors reported having no relevant conflicts of interest.
Dr. Feuerstein is with the Center for Inflammatory Bowel Disease at Beth Israel Deaconess Medical Center and is an associate professor of medicine Harvard Medical School, both in Boston. Dr. Sofia is an assistant professor of medicine with the division of gastroenterology and hepatology at Oregon Health and Science University, Portland. Dr. Guha is a professor of medicine at the division of gastroenterology, hepatology and nutrition and is codirector of the Center for Interventional Gastroenterology at UTHealth (iGUT) at UT Health Science Center, Houston. Dr. Streett is a clinical professor of medicine, gastroenterology, and hepatology and director of the IBD Education and Advanced IBD Fellowship at Stanford (Calif.) Medicine.
Over the last several years, payer policies that dictate and restrict treatments for patients with inflammatory bowel diseases (IBD) have proliferated. The implementation of new coverage restrictions, expansion of services and procedures requiring prior authorization (PA), and dosing and access restriction to covered drugs, and the requirement of repeated treatment reviews including nonmedical switching for stable patients are widespread. The AGA administered a member needs assessment survey in December 2021 to determine the extent to which these policies harm patients and overburden gastroenterologists and their staff.
Survey findings
Most of the 100 surveyed members reported facing administrative burdens that prevented timely access to patient care. Utilization management practices such as PA, step therapy, and nonmedical switching and dosing restrictions create critical barriers to high quality GI care for patients with chronic conditions and jeopardize the physician-patient relationship. At a time when physicians have faced unprecedented challenges because of the public health emergency from the COVID-19 pandemic, these burdens also contribute to increasing physician burnout.
Prior authorization: Among AGA members, 96% of members said that PA is burdensome, with 61% indicating that it is significantly burdensome. Almost 99% of members indicated that PA has a negative impact on patients’ access to clinically appropriate treatments; 89% reported that the burden associated with PA has increased over the last 5 years in their practice.
Step therapy: Among members, 87% described the impact step therapy has on their practice as burdensome. Almost 90% of members said step therapy negatively impacted patients’ access to clinically appropriate treatments. Almost 90% of members felt that there was an overall negative impact on patient clinical outcomes for those patients who were required to follow a step therapy protocol.
Nonmedical switching and dosing restrictions: Out of all members, 86% reported an increase in nonmedical switching and dosing restrictions over the last 5 years; 79% of members noted that these restrictions had a negative impact on patient clinical outcomes.
An increasing number of insurance companies are restricting effective biologic therapy to Food and Drug Administration–labeled doses, in direct conflict with current established best practices. It is most concerning that many patients who had been stable on optimized dosing are suddenly notified that they will no longer be able to receive the dose or treatment frequency prescribed by their physician. The concept of optimizing drug therapy based on disease activity and therapeutic drug monitoring is well established, and artificial restrictions to FDA-labeled doses force unnecessary drug deescalation. This transparent effort to reduce costs lacks evidence for safety. Our sickest patients often require higher doses for induction in order to respond, given drug losses, yet some payers refuse to cover the doses these patients require. This new payer-centered effort prioritizes cost containment over the judgment of the treating physician. It causes direct patient harm risking efficacy or loss of response, and subsequent irreversible disease-related complications.
Medicare drug costs
Medicare patients receiving self-injectable or oral medications are not eligible for co-pay assistance programs through pharmaceutical companies because of federal rules. For non-Medicare patients, these programs reduce the co-pay costs to as low as $5 per month. Medicare patients are able to receive infusions like infliximab and vedolizumab at no cost. However, any self-injectable or oral agent can carry a co-pay of over $1,000. Other than for patients meeting income-based eligibility requirements (e.g., below the poverty line), these treatments become prohibitively expensive. Thousands of patients have had to discontinue their self-injectable and/or oral medications because of this cost or have been denied access to the therapy altogether because of cost.
Need for change
These recent changes in insurance policies have resulted in increased harm to our patients with IBD rather than improving the safety or quality of their care. These changes create barriers to disease treatment and have not improved quality of care, patient outcomes, or quality of life. The AGA and other societies have published multiple guidelines and literature on the management of patients with IBD that should serve as the foundation for insurers’ medication coverage policies. Additionally, insurance companies should seek input from panels of IBD experts when developing their medication coverage policies to ensure they are patient oriented and facilitate high-quality IBD care.
The following are opportunities for insurers to improve the IBD drug approval process:
- Simplify the appeal process.
- Guarantee rapid response/turnaround to appeal processes to avoid additional delays in care.
- Incorporate experienced expert review by a gastroenterologist.
- Ensure coverage of drug and disease monitoring.
- Integrate expert input in policy development.
Conclusion
Effective patient care in IBD, as well as in other chronic gastrointestinal diseases, requires a collaborative approach to maximize clinical outcomes. It is an exciting time in our field, with rapidly expanding therapeutic options to treat IBD that have the potential to modify the disease course and prevent long-term complications for patients. However, optimizing the use of these treatments to achieve disease remission is challenging and requires the ability to individualize the timely choice of medications at the right dose for each patient to capture and monitor response. The ability to provide individualized, data driven care is essential to improving the quality of life of our patients, as well as to reducing health care spending over time.
Achieving high-value care is a goal that benefits everyone involved in the health care system. Policies that interfere with the timely treatment of sick patients with the right therapies, optimized to achieve disease remission, hurt the very patients that our health care system exists to serve. We cannot stand by while impediments to treatment result in harm to our patients and worsen clinical outcomes. Collaboratively developing aligned incentives can lead us to patient-centered policies that fulfill a shared purpose to optimize the health of people with chronic digestive diseases.
The authors reported having no relevant conflicts of interest.
Dr. Feuerstein is with the Center for Inflammatory Bowel Disease at Beth Israel Deaconess Medical Center and is an associate professor of medicine Harvard Medical School, both in Boston. Dr. Sofia is an assistant professor of medicine with the division of gastroenterology and hepatology at Oregon Health and Science University, Portland. Dr. Guha is a professor of medicine at the division of gastroenterology, hepatology and nutrition and is codirector of the Center for Interventional Gastroenterology at UTHealth (iGUT) at UT Health Science Center, Houston. Dr. Streett is a clinical professor of medicine, gastroenterology, and hepatology and director of the IBD Education and Advanced IBD Fellowship at Stanford (Calif.) Medicine.
Late to the game: Parenting after 40
As they rolled me down the hallway to the OR, ceiling lights rhythmically passing above, I zoned out into a 1,000-mile stare. How did I get here? I started humming “Swing Low, Sweet Chariot,” praying for a miracle to happen. I thought back to my birth plan, meticulously crafted, a one-pager so that the no-nonsense labor and delivery nurses wouldn›t think me completely off my rocker. No C-section unless medically necessary. Those words laughed back at me – cackling, even. I’d planned out the whole birthing process and here we were, my team almost jogging me to the OR. I lay still, utterly gobsmacked and partially anesthetized.
If I squint my eyes and hallucinate just a bit, that is sort of what motherhood has been like.
It’s about knowing all the things that could go wrong and meeting the unplanned head-on. Motherhood has indeed been a whirlwind – so many physical, psychological, and emotional transformations. And to top it off, the added effort of giving birth in a pandemic. As an over-40 physician, you’d think I would have been better prepared.
I was, but in a sense, I was not. The knowledge, the wisdom, the experience of my medical training surrounded me, but even I panicked at times in the beginning: Am I feeding her correctly? Am I making enough food for her? Am I doing the best that I can for her? What more could I be doing for her?
Over time, I’ve learned to lighten up. Some. In those teachable moments with my daughter Gia, I’ve learned to not sugarcoat reality but encourage the hopeful. If Gia falls on the ground? “You’re okay, sweetie. Now get back up.” If Gia has a tantrum and starts hitting herself? “Honey, our hands are for hugs, not hurting ourselves. Let’s go play.” Eighty percent of motherhood right now is redirection and the other 20% is patience.
I remember this one time I was rushing out the door for work. After getting in the car with my keys, I realized I forgot my coffee back in the house. I left the car, went back in the house to grab the blessed joe, went back to the car, and couldn’t get in because it was locked. I panicked at that moment, went back inside the house, and found Gia playing with my extra key fob. My own daughter locked me out of my car. Of course, it wasn’t her fault. Deep breath and I offered her another kiss while simultaneously taking the key fob from her.
Before Gia could walk, she could climb the stairs in our home. Her father and I sometimes refer to her as “Lil Bamm-Bamm” because she is so strong. One day, Daddy was supposed to be watching her while Mommy was folding laundry upstairs. She was not allowed on the stairs, but what should I hear? Literally, the pitter-patter of little feet, running down the upstairs hallway. Her father had drifted off watching yet another episode of something Star Wars–related. My strong little girl made it up the stairs all by herself and Dad received a strong word. The Force was with me that day.
I would say that I feel like having a child ages you, but what does that really mean when you’re already old? I’ve become acutely aware of my lack of endurance, stamina, and bodily strength. My knees will creak when taking her upstairs to bed, an osseous dirge of a lullaby. Date nights become unintentionally less and less frequent. Friday night dress-up becomes Friday night dress-down. I’ve replaced stiletto heels with comfy sweats.
Once we put Gia down for the night, we are usually exhausted from the day, and the couch and TV are welcome respites. We exhale. As over-40 parents, we knew that having children late in life would bring its challenges. But I’d like to think that we are meeting them the best way that we can. Often I encourage my body to meet Gia at her eye level, see what she sees, play with her on her own terms, and match her energy. She absolutely loves it when I do this. I’m out of breath and my knees are sore by the end of our play session, but I wouldn’t have it any other way.
We are learning from each other. She has a bright and assertive personality, and I am protective of that innocence. Her innocence is without fear. I often wonder what she is thinking when I see her facial expressions. A side-eye, a fleeting giggle. Is she secretly contemplating the chronicity of the cosmos, or is it just gas? I look at her in stolen moments and still can’t believe that I grew a human inside me, and said human was extracted from me and is now walking around my house commanding her bidding. So surreal. The unromanticized, scientific ingredients that are at play from conception to delivery are nothing short of miraculous. And the miracles of parenting over 40 are present every day.
Dr. Tolliver is a family medicine physician at The Ohio State University Wexner Medical Center in Columbus. A version of this article first appeared on Medscape.com.
As they rolled me down the hallway to the OR, ceiling lights rhythmically passing above, I zoned out into a 1,000-mile stare. How did I get here? I started humming “Swing Low, Sweet Chariot,” praying for a miracle to happen. I thought back to my birth plan, meticulously crafted, a one-pager so that the no-nonsense labor and delivery nurses wouldn›t think me completely off my rocker. No C-section unless medically necessary. Those words laughed back at me – cackling, even. I’d planned out the whole birthing process and here we were, my team almost jogging me to the OR. I lay still, utterly gobsmacked and partially anesthetized.
If I squint my eyes and hallucinate just a bit, that is sort of what motherhood has been like.
It’s about knowing all the things that could go wrong and meeting the unplanned head-on. Motherhood has indeed been a whirlwind – so many physical, psychological, and emotional transformations. And to top it off, the added effort of giving birth in a pandemic. As an over-40 physician, you’d think I would have been better prepared.
I was, but in a sense, I was not. The knowledge, the wisdom, the experience of my medical training surrounded me, but even I panicked at times in the beginning: Am I feeding her correctly? Am I making enough food for her? Am I doing the best that I can for her? What more could I be doing for her?
Over time, I’ve learned to lighten up. Some. In those teachable moments with my daughter Gia, I’ve learned to not sugarcoat reality but encourage the hopeful. If Gia falls on the ground? “You’re okay, sweetie. Now get back up.” If Gia has a tantrum and starts hitting herself? “Honey, our hands are for hugs, not hurting ourselves. Let’s go play.” Eighty percent of motherhood right now is redirection and the other 20% is patience.
I remember this one time I was rushing out the door for work. After getting in the car with my keys, I realized I forgot my coffee back in the house. I left the car, went back in the house to grab the blessed joe, went back to the car, and couldn’t get in because it was locked. I panicked at that moment, went back inside the house, and found Gia playing with my extra key fob. My own daughter locked me out of my car. Of course, it wasn’t her fault. Deep breath and I offered her another kiss while simultaneously taking the key fob from her.
Before Gia could walk, she could climb the stairs in our home. Her father and I sometimes refer to her as “Lil Bamm-Bamm” because she is so strong. One day, Daddy was supposed to be watching her while Mommy was folding laundry upstairs. She was not allowed on the stairs, but what should I hear? Literally, the pitter-patter of little feet, running down the upstairs hallway. Her father had drifted off watching yet another episode of something Star Wars–related. My strong little girl made it up the stairs all by herself and Dad received a strong word. The Force was with me that day.
I would say that I feel like having a child ages you, but what does that really mean when you’re already old? I’ve become acutely aware of my lack of endurance, stamina, and bodily strength. My knees will creak when taking her upstairs to bed, an osseous dirge of a lullaby. Date nights become unintentionally less and less frequent. Friday night dress-up becomes Friday night dress-down. I’ve replaced stiletto heels with comfy sweats.
Once we put Gia down for the night, we are usually exhausted from the day, and the couch and TV are welcome respites. We exhale. As over-40 parents, we knew that having children late in life would bring its challenges. But I’d like to think that we are meeting them the best way that we can. Often I encourage my body to meet Gia at her eye level, see what she sees, play with her on her own terms, and match her energy. She absolutely loves it when I do this. I’m out of breath and my knees are sore by the end of our play session, but I wouldn’t have it any other way.
We are learning from each other. She has a bright and assertive personality, and I am protective of that innocence. Her innocence is without fear. I often wonder what she is thinking when I see her facial expressions. A side-eye, a fleeting giggle. Is she secretly contemplating the chronicity of the cosmos, or is it just gas? I look at her in stolen moments and still can’t believe that I grew a human inside me, and said human was extracted from me and is now walking around my house commanding her bidding. So surreal. The unromanticized, scientific ingredients that are at play from conception to delivery are nothing short of miraculous. And the miracles of parenting over 40 are present every day.
Dr. Tolliver is a family medicine physician at The Ohio State University Wexner Medical Center in Columbus. A version of this article first appeared on Medscape.com.
As they rolled me down the hallway to the OR, ceiling lights rhythmically passing above, I zoned out into a 1,000-mile stare. How did I get here? I started humming “Swing Low, Sweet Chariot,” praying for a miracle to happen. I thought back to my birth plan, meticulously crafted, a one-pager so that the no-nonsense labor and delivery nurses wouldn›t think me completely off my rocker. No C-section unless medically necessary. Those words laughed back at me – cackling, even. I’d planned out the whole birthing process and here we were, my team almost jogging me to the OR. I lay still, utterly gobsmacked and partially anesthetized.
If I squint my eyes and hallucinate just a bit, that is sort of what motherhood has been like.
It’s about knowing all the things that could go wrong and meeting the unplanned head-on. Motherhood has indeed been a whirlwind – so many physical, psychological, and emotional transformations. And to top it off, the added effort of giving birth in a pandemic. As an over-40 physician, you’d think I would have been better prepared.
I was, but in a sense, I was not. The knowledge, the wisdom, the experience of my medical training surrounded me, but even I panicked at times in the beginning: Am I feeding her correctly? Am I making enough food for her? Am I doing the best that I can for her? What more could I be doing for her?
Over time, I’ve learned to lighten up. Some. In those teachable moments with my daughter Gia, I’ve learned to not sugarcoat reality but encourage the hopeful. If Gia falls on the ground? “You’re okay, sweetie. Now get back up.” If Gia has a tantrum and starts hitting herself? “Honey, our hands are for hugs, not hurting ourselves. Let’s go play.” Eighty percent of motherhood right now is redirection and the other 20% is patience.
I remember this one time I was rushing out the door for work. After getting in the car with my keys, I realized I forgot my coffee back in the house. I left the car, went back in the house to grab the blessed joe, went back to the car, and couldn’t get in because it was locked. I panicked at that moment, went back inside the house, and found Gia playing with my extra key fob. My own daughter locked me out of my car. Of course, it wasn’t her fault. Deep breath and I offered her another kiss while simultaneously taking the key fob from her.
Before Gia could walk, she could climb the stairs in our home. Her father and I sometimes refer to her as “Lil Bamm-Bamm” because she is so strong. One day, Daddy was supposed to be watching her while Mommy was folding laundry upstairs. She was not allowed on the stairs, but what should I hear? Literally, the pitter-patter of little feet, running down the upstairs hallway. Her father had drifted off watching yet another episode of something Star Wars–related. My strong little girl made it up the stairs all by herself and Dad received a strong word. The Force was with me that day.
I would say that I feel like having a child ages you, but what does that really mean when you’re already old? I’ve become acutely aware of my lack of endurance, stamina, and bodily strength. My knees will creak when taking her upstairs to bed, an osseous dirge of a lullaby. Date nights become unintentionally less and less frequent. Friday night dress-up becomes Friday night dress-down. I’ve replaced stiletto heels with comfy sweats.
Once we put Gia down for the night, we are usually exhausted from the day, and the couch and TV are welcome respites. We exhale. As over-40 parents, we knew that having children late in life would bring its challenges. But I’d like to think that we are meeting them the best way that we can. Often I encourage my body to meet Gia at her eye level, see what she sees, play with her on her own terms, and match her energy. She absolutely loves it when I do this. I’m out of breath and my knees are sore by the end of our play session, but I wouldn’t have it any other way.
We are learning from each other. She has a bright and assertive personality, and I am protective of that innocence. Her innocence is without fear. I often wonder what she is thinking when I see her facial expressions. A side-eye, a fleeting giggle. Is she secretly contemplating the chronicity of the cosmos, or is it just gas? I look at her in stolen moments and still can’t believe that I grew a human inside me, and said human was extracted from me and is now walking around my house commanding her bidding. So surreal. The unromanticized, scientific ingredients that are at play from conception to delivery are nothing short of miraculous. And the miracles of parenting over 40 are present every day.
Dr. Tolliver is a family medicine physician at The Ohio State University Wexner Medical Center in Columbus. A version of this article first appeared on Medscape.com.
Will we ever outgrow the Goldwater rule?
Since it appeared in the first edition of the American Psychiatric Association’s Principles of Medical Ethics in 1973, the “Goldwater rule” – often referred to in terms of where in the APA’s guideline it can be found, Section 7.3 – has placed a stringent prohibition on psychiatrists offering professional opinions about public figures “unless he or she has conducted an examination and has been granted proper authorization for such a statement.”1
Some psychiatrists experienced the restrictive nature of Section 7.3 more acutely perhaps than ever during the Trump presidency. This spurred numerous articles criticizing the guideline as an outdated “gag rule”2 that harms the public image of psychiatry.3 Some psychiatrists violated the rule to warn the public of the dangers of a president with “incipient dementia”4 occupying the most powerful position on earth.

Following President Trump’s exit from the White House, the alarm bells surrounding his presidency have quieted. Criticisms of the Goldwater rule, on the other hand, have persisted. Many of these criticisms now call for the rule to be refined, allowing for psychiatrists to give their professional opinions about public figures, but with certain guidelines on how to do so.5 Few have yet to make a sober case for the outright abolition of Section 7.3.6
Self-regulating and internal policing are important factors in the continued independence of the medical profession, and we should continue to hold each other to high professional standards. That being said, do psychiatrists need training wheels to prevent us from devolving into unprofessional social commentators? Other medical specialties do not see the need to implement a rule preventing their colleagues from expressing expertise in fear of embarrassment. Do we not have faith in our ability to conduct ourselves professionally? Is the Goldwater rule an admission of a juvenile lack of self-control within our field?

Not only do other medical specialties not forcibly handhold their members in public settings, but other “providers” in the realm of mental health likewise do not implement such strict self-restraints. Psychiatry staying silent on the matter of public figures leaves a void filled by other, arguably less qualified, individuals. Subsequently, the public discord risks being flooded with pseudoscientific pontification and distorted views of psychiatric illness. The cycle of speculating on the mental fitness of the president has outlived President Trump, with concerns about Joe Biden’s incoherence and waning cognition.7 Therein is an important argument to be made for the public duty of psychiatrists, with their greater expertise and clinical acumen, to weigh in on matters of societal importance in an attempt to dispel dangerous misconceptions.
Practical limitations are often raised and serve as the cornerstone for the Goldwater rule. Specifically, the limitation being that a psychiatrist cannot provide a professional opinion about an individual without a proper in-person evaluation. The psychiatric interview could be considered the most in-depth and comprehensive evaluation in all of medicine. Even so, is a trained psychiatrist presented with grandiosity, flight-of-ideas, and pressured speech unable to comment on the possibility of mania without a lengthy and comprehensive evaluation? How much disorganization of behavior and dialogue does one need to observe to recognize psychosis? For the experienced psychiatrist, many of these behavioral hallmarks are akin to an ST elevation on an EKG representing a heart attack.
When considering less extreme examples of mental affliction, such as depression and anxiety, many signs – including demeanor, motor activity, manner of speaking, and other aspects of behavior – are apparent to the perceptive psychiatrist without needing an extensive interview that dives into the depths of a person’s social history and childhood. After all, our own criteria for depression and mania do not require the presence of social stressors or childhood trauma. Even personality disorders can be reasonably postulated when a person behaves in a particular fashion. The recognition of transitional objects, items used to provide psychological comfort, including the “teddy bear sign” are common and scientifically studied methods to recognize personality disorder.8
The necessity for an in-person evaluation has become less compelling over the years. In our modern age, important social moments are memorialized in countless videos that are arguably more relevant, more accurate, and less subjective than a psychiatric interview. Furthermore, forensic psychiatrists routinely comment on individuals they have not examined for a variety of reasons, from postmortem analysis to the refusal of the client to be interviewed. Moreover, and with significant contradiction, many leaders in the field of psychiatry view integrated care, the practice of psychiatrists advising primary care doctors, often without even seeing patients, to be the future of psychiatry.9
Some reading this may scoff at the above examples. Perhaps Section 7.3 speaks to an underlying insecurity in our field regarding our ability to accurately diagnose. That insecurity is not unfounded. In terms of the DSM-5, the bar for reliability has been lowered to a kappa of 0.2-0.4, from a previous standard of 0.6, in an attempt to avoid critiques of unreliability.10 Yet herein lies a powerful recognition of the necessity of the Goldwater rule. If psychiatrists cannot reliably agree on the presence of diagnoses in the controlled setting of scientific study, how can we expect to speak with coherence and consistency on highly mediatized and provoking topics?
The defense – that the difficulty psychiatrists have at providing an accurate diagnosis stems from the immense complexity of the system being evaluated, the human mind – is a valid one. Attempts to force such complex pathology, with all its many variables, into the check-box approach implemented in the DSM inevitably leads to problems with diagnostic reliability. Still, as psychiatrists we retain a level of expertise in assessing and treating complex disorders of the mind that no other field can claim.
The duty physicians have not only to work toward the health of their individual patients, but also to act in service of the public health and well-being of communities in which our patients live, is well established. How ethical is it then for psychiatry to absolve itself from duty when it comes to public figures at the center of shaping public opinion? There are numerous recent, high-profile instances where our expertise may have helped shine light in an otherwise murky public discussion filled with disinformation. The death of George Floyd and the year of turmoil that followed is a salient example. The conservatorship of Britney Spears and the resulting societal outcry is another. Even setting the matter of diagnosis aside, we can help illuminate the societal implications of conservatorship laws,11 in addition to providing input on how to safely and responsibly approach an individual who is in crisis, under the influence of multiple illicit substances, and possibly suffering from excited delirium.
Whether psychiatry has progressed enough as a medical specialty to trust ourselves with the option of providing professional opinions on public figures is an ongoing debate. The persistence of the Goldwater rule is a strong testament to the internal lack of confidence among psychiatrists regarding our ability to provide accurate diagnoses, act with integrity in the public space, and foster a positive public image. That lack of confidence may be well deserved. However, it is possible that our field will never go through the necessary pains of maturing as long as Section 7.3 remains in place.
Dr. Compton is a psychiatry resident at University of California, San Diego. His background includes medical education, mental health advocacy, work with underserved populations, and brain cancer research. Dr. Compton has no conflicts of interest. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. American Psychiatric Association. The principles of medical ethics with annotations especially applicable to psychiatry. Section 7. American Psychiatric Association; 2013 edition.
2. Glass LL. The Goldwater rule is broken. Here’s how to fix it. STAT News. 2018 June 18.
3. Plymyer D. The Goldwater rule paradox. 2020 Aug 7.
4. Lieberman JA. Trump’s brain and the 25th Amendment. Vice. 2017 Sep 8.
5. Blotcky AD et al. The Goldwater rule is fine, if refined. Here’s how to do it. Psychiatric Times. 2022 Jan 6;39(1).
6. Blotcky AD and Norrholm SD. After Trump, end the Goldwater rule once and for all. New York Daily News. 2020 Dec 22.
7. Stephens B. Biden should not run again – And he should say he won’t. New York Times. 2021 Dec 14.
8. Schmaling KB et al. The positive teddy bear sign: Transitional objects in the medical setting. J Nerv Ment Dis. 1994 Dec;182(12):725.
9. Badre N et al. Psychopharmacologic management in integrated care: Challenges for residency education. Acad Psychiatry. 2015; 39(4):466-9.
10. Kraemer HC et al. DSM-5: How reliable is reliable enough? Am J Psychiatry. 2012 Jan;169(1):13-5.
11. Badre N and Compton C. Britney Spears – Reflections on conservatorship. Clinical Psychiatry News. 2021 Nov 16.
Since it appeared in the first edition of the American Psychiatric Association’s Principles of Medical Ethics in 1973, the “Goldwater rule” – often referred to in terms of where in the APA’s guideline it can be found, Section 7.3 – has placed a stringent prohibition on psychiatrists offering professional opinions about public figures “unless he or she has conducted an examination and has been granted proper authorization for such a statement.”1
Some psychiatrists experienced the restrictive nature of Section 7.3 more acutely perhaps than ever during the Trump presidency. This spurred numerous articles criticizing the guideline as an outdated “gag rule”2 that harms the public image of psychiatry.3 Some psychiatrists violated the rule to warn the public of the dangers of a president with “incipient dementia”4 occupying the most powerful position on earth.
Following President Trump’s exit from the White House, the alarm bells surrounding his presidency have quieted. Criticisms of the Goldwater rule, on the other hand, have persisted. Many of these criticisms now call for the rule to be refined, allowing for psychiatrists to give their professional opinions about public figures, but with certain guidelines on how to do so.5 Few have yet to make a sober case for the outright abolition of Section 7.3.6
Self-regulating and internal policing are important factors in the continued independence of the medical profession, and we should continue to hold each other to high professional standards. That being said, do psychiatrists need training wheels to prevent us from devolving into unprofessional social commentators? Other medical specialties do not see the need to implement a rule preventing their colleagues from expressing expertise in fear of embarrassment. Do we not have faith in our ability to conduct ourselves professionally? Is the Goldwater rule an admission of a juvenile lack of self-control within our field?
Not only do other medical specialties not forcibly handhold their members in public settings, but other “providers” in the realm of mental health likewise do not implement such strict self-restraints. Psychiatry staying silent on the matter of public figures leaves a void filled by other, arguably less qualified, individuals. Subsequently, the public discord risks being flooded with pseudoscientific pontification and distorted views of psychiatric illness. The cycle of speculating on the mental fitness of the president has outlived President Trump, with concerns about Joe Biden’s incoherence and waning cognition.7 Therein is an important argument to be made for the public duty of psychiatrists, with their greater expertise and clinical acumen, to weigh in on matters of societal importance in an attempt to dispel dangerous misconceptions.
Practical limitations are often raised and serve as the cornerstone for the Goldwater rule. Specifically, the limitation being that a psychiatrist cannot provide a professional opinion about an individual without a proper in-person evaluation. The psychiatric interview could be considered the most in-depth and comprehensive evaluation in all of medicine. Even so, is a trained psychiatrist presented with grandiosity, flight-of-ideas, and pressured speech unable to comment on the possibility of mania without a lengthy and comprehensive evaluation? How much disorganization of behavior and dialogue does one need to observe to recognize psychosis? For the experienced psychiatrist, many of these behavioral hallmarks are akin to an ST elevation on an EKG representing a heart attack.
When considering less extreme examples of mental affliction, such as depression and anxiety, many signs – including demeanor, motor activity, manner of speaking, and other aspects of behavior – are apparent to the perceptive psychiatrist without needing an extensive interview that dives into the depths of a person’s social history and childhood. After all, our own criteria for depression and mania do not require the presence of social stressors or childhood trauma. Even personality disorders can be reasonably postulated when a person behaves in a particular fashion. The recognition of transitional objects, items used to provide psychological comfort, including the “teddy bear sign” are common and scientifically studied methods to recognize personality disorder.8
The necessity for an in-person evaluation has become less compelling over the years. In our modern age, important social moments are memorialized in countless videos that are arguably more relevant, more accurate, and less subjective than a psychiatric interview. Furthermore, forensic psychiatrists routinely comment on individuals they have not examined for a variety of reasons, from postmortem analysis to the refusal of the client to be interviewed. Moreover, and with significant contradiction, many leaders in the field of psychiatry view integrated care, the practice of psychiatrists advising primary care doctors, often without even seeing patients, to be the future of psychiatry.9
Some reading this may scoff at the above examples. Perhaps Section 7.3 speaks to an underlying insecurity in our field regarding our ability to accurately diagnose. That insecurity is not unfounded. In terms of the DSM-5, the bar for reliability has been lowered to a kappa of 0.2-0.4, from a previous standard of 0.6, in an attempt to avoid critiques of unreliability.10 Yet herein lies a powerful recognition of the necessity of the Goldwater rule. If psychiatrists cannot reliably agree on the presence of diagnoses in the controlled setting of scientific study, how can we expect to speak with coherence and consistency on highly mediatized and provoking topics?
The defense – that the difficulty psychiatrists have at providing an accurate diagnosis stems from the immense complexity of the system being evaluated, the human mind – is a valid one. Attempts to force such complex pathology, with all its many variables, into the check-box approach implemented in the DSM inevitably leads to problems with diagnostic reliability. Still, as psychiatrists we retain a level of expertise in assessing and treating complex disorders of the mind that no other field can claim.
The duty physicians have not only to work toward the health of their individual patients, but also to act in service of the public health and well-being of communities in which our patients live, is well established. How ethical is it then for psychiatry to absolve itself from duty when it comes to public figures at the center of shaping public opinion? There are numerous recent, high-profile instances where our expertise may have helped shine light in an otherwise murky public discussion filled with disinformation. The death of George Floyd and the year of turmoil that followed is a salient example. The conservatorship of Britney Spears and the resulting societal outcry is another. Even setting the matter of diagnosis aside, we can help illuminate the societal implications of conservatorship laws,11 in addition to providing input on how to safely and responsibly approach an individual who is in crisis, under the influence of multiple illicit substances, and possibly suffering from excited delirium.
Whether psychiatry has progressed enough as a medical specialty to trust ourselves with the option of providing professional opinions on public figures is an ongoing debate. The persistence of the Goldwater rule is a strong testament to the internal lack of confidence among psychiatrists regarding our ability to provide accurate diagnoses, act with integrity in the public space, and foster a positive public image. That lack of confidence may be well deserved. However, it is possible that our field will never go through the necessary pains of maturing as long as Section 7.3 remains in place.
Dr. Compton is a psychiatry resident at University of California, San Diego. His background includes medical education, mental health advocacy, work with underserved populations, and brain cancer research. Dr. Compton has no conflicts of interest. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. American Psychiatric Association. The principles of medical ethics with annotations especially applicable to psychiatry. Section 7. American Psychiatric Association; 2013 edition.
2. Glass LL. The Goldwater rule is broken. Here’s how to fix it. STAT News. 2018 June 18.
3. Plymyer D. The Goldwater rule paradox. 2020 Aug 7.
4. Lieberman JA. Trump’s brain and the 25th Amendment. Vice. 2017 Sep 8.
5. Blotcky AD et al. The Goldwater rule is fine, if refined. Here’s how to do it. Psychiatric Times. 2022 Jan 6;39(1).
6. Blotcky AD and Norrholm SD. After Trump, end the Goldwater rule once and for all. New York Daily News. 2020 Dec 22.
7. Stephens B. Biden should not run again – And he should say he won’t. New York Times. 2021 Dec 14.
8. Schmaling KB et al. The positive teddy bear sign: Transitional objects in the medical setting. J Nerv Ment Dis. 1994 Dec;182(12):725.
9. Badre N et al. Psychopharmacologic management in integrated care: Challenges for residency education. Acad Psychiatry. 2015; 39(4):466-9.
10. Kraemer HC et al. DSM-5: How reliable is reliable enough? Am J Psychiatry. 2012 Jan;169(1):13-5.
11. Badre N and Compton C. Britney Spears – Reflections on conservatorship. Clinical Psychiatry News. 2021 Nov 16.
Since it appeared in the first edition of the American Psychiatric Association’s Principles of Medical Ethics in 1973, the “Goldwater rule” – often referred to in terms of where in the APA’s guideline it can be found, Section 7.3 – has placed a stringent prohibition on psychiatrists offering professional opinions about public figures “unless he or she has conducted an examination and has been granted proper authorization for such a statement.”1
Some psychiatrists experienced the restrictive nature of Section 7.3 more acutely perhaps than ever during the Trump presidency. This spurred numerous articles criticizing the guideline as an outdated “gag rule”2 that harms the public image of psychiatry.3 Some psychiatrists violated the rule to warn the public of the dangers of a president with “incipient dementia”4 occupying the most powerful position on earth.
Following President Trump’s exit from the White House, the alarm bells surrounding his presidency have quieted. Criticisms of the Goldwater rule, on the other hand, have persisted. Many of these criticisms now call for the rule to be refined, allowing for psychiatrists to give their professional opinions about public figures, but with certain guidelines on how to do so.5 Few have yet to make a sober case for the outright abolition of Section 7.3.6
Self-regulating and internal policing are important factors in the continued independence of the medical profession, and we should continue to hold each other to high professional standards. That being said, do psychiatrists need training wheels to prevent us from devolving into unprofessional social commentators? Other medical specialties do not see the need to implement a rule preventing their colleagues from expressing expertise in fear of embarrassment. Do we not have faith in our ability to conduct ourselves professionally? Is the Goldwater rule an admission of a juvenile lack of self-control within our field?
Not only do other medical specialties not forcibly handhold their members in public settings, but other “providers” in the realm of mental health likewise do not implement such strict self-restraints. Psychiatry staying silent on the matter of public figures leaves a void filled by other, arguably less qualified, individuals. Subsequently, the public discord risks being flooded with pseudoscientific pontification and distorted views of psychiatric illness. The cycle of speculating on the mental fitness of the president has outlived President Trump, with concerns about Joe Biden’s incoherence and waning cognition.7 Therein is an important argument to be made for the public duty of psychiatrists, with their greater expertise and clinical acumen, to weigh in on matters of societal importance in an attempt to dispel dangerous misconceptions.
Practical limitations are often raised and serve as the cornerstone for the Goldwater rule. Specifically, the limitation being that a psychiatrist cannot provide a professional opinion about an individual without a proper in-person evaluation. The psychiatric interview could be considered the most in-depth and comprehensive evaluation in all of medicine. Even so, is a trained psychiatrist presented with grandiosity, flight-of-ideas, and pressured speech unable to comment on the possibility of mania without a lengthy and comprehensive evaluation? How much disorganization of behavior and dialogue does one need to observe to recognize psychosis? For the experienced psychiatrist, many of these behavioral hallmarks are akin to an ST elevation on an EKG representing a heart attack.
When considering less extreme examples of mental affliction, such as depression and anxiety, many signs – including demeanor, motor activity, manner of speaking, and other aspects of behavior – are apparent to the perceptive psychiatrist without needing an extensive interview that dives into the depths of a person’s social history and childhood. After all, our own criteria for depression and mania do not require the presence of social stressors or childhood trauma. Even personality disorders can be reasonably postulated when a person behaves in a particular fashion. The recognition of transitional objects, items used to provide psychological comfort, including the “teddy bear sign” are common and scientifically studied methods to recognize personality disorder.8
The necessity for an in-person evaluation has become less compelling over the years. In our modern age, important social moments are memorialized in countless videos that are arguably more relevant, more accurate, and less subjective than a psychiatric interview. Furthermore, forensic psychiatrists routinely comment on individuals they have not examined for a variety of reasons, from postmortem analysis to the refusal of the client to be interviewed. Moreover, and with significant contradiction, many leaders in the field of psychiatry view integrated care, the practice of psychiatrists advising primary care doctors, often without even seeing patients, to be the future of psychiatry.9
Some reading this may scoff at the above examples. Perhaps Section 7.3 speaks to an underlying insecurity in our field regarding our ability to accurately diagnose. That insecurity is not unfounded. In terms of the DSM-5, the bar for reliability has been lowered to a kappa of 0.2-0.4, from a previous standard of 0.6, in an attempt to avoid critiques of unreliability.10 Yet herein lies a powerful recognition of the necessity of the Goldwater rule. If psychiatrists cannot reliably agree on the presence of diagnoses in the controlled setting of scientific study, how can we expect to speak with coherence and consistency on highly mediatized and provoking topics?
The defense – that the difficulty psychiatrists have at providing an accurate diagnosis stems from the immense complexity of the system being evaluated, the human mind – is a valid one. Attempts to force such complex pathology, with all its many variables, into the check-box approach implemented in the DSM inevitably leads to problems with diagnostic reliability. Still, as psychiatrists we retain a level of expertise in assessing and treating complex disorders of the mind that no other field can claim.
The duty physicians have not only to work toward the health of their individual patients, but also to act in service of the public health and well-being of communities in which our patients live, is well established. How ethical is it then for psychiatry to absolve itself from duty when it comes to public figures at the center of shaping public opinion? There are numerous recent, high-profile instances where our expertise may have helped shine light in an otherwise murky public discussion filled with disinformation. The death of George Floyd and the year of turmoil that followed is a salient example. The conservatorship of Britney Spears and the resulting societal outcry is another. Even setting the matter of diagnosis aside, we can help illuminate the societal implications of conservatorship laws,11 in addition to providing input on how to safely and responsibly approach an individual who is in crisis, under the influence of multiple illicit substances, and possibly suffering from excited delirium.
Whether psychiatry has progressed enough as a medical specialty to trust ourselves with the option of providing professional opinions on public figures is an ongoing debate. The persistence of the Goldwater rule is a strong testament to the internal lack of confidence among psychiatrists regarding our ability to provide accurate diagnoses, act with integrity in the public space, and foster a positive public image. That lack of confidence may be well deserved. However, it is possible that our field will never go through the necessary pains of maturing as long as Section 7.3 remains in place.
Dr. Compton is a psychiatry resident at University of California, San Diego. His background includes medical education, mental health advocacy, work with underserved populations, and brain cancer research. Dr. Compton has no conflicts of interest. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. American Psychiatric Association. The principles of medical ethics with annotations especially applicable to psychiatry. Section 7. American Psychiatric Association; 2013 edition.
2. Glass LL. The Goldwater rule is broken. Here’s how to fix it. STAT News. 2018 June 18.
3. Plymyer D. The Goldwater rule paradox. 2020 Aug 7.
4. Lieberman JA. Trump’s brain and the 25th Amendment. Vice. 2017 Sep 8.
5. Blotcky AD et al. The Goldwater rule is fine, if refined. Here’s how to do it. Psychiatric Times. 2022 Jan 6;39(1).
6. Blotcky AD and Norrholm SD. After Trump, end the Goldwater rule once and for all. New York Daily News. 2020 Dec 22.
7. Stephens B. Biden should not run again – And he should say he won’t. New York Times. 2021 Dec 14.
8. Schmaling KB et al. The positive teddy bear sign: Transitional objects in the medical setting. J Nerv Ment Dis. 1994 Dec;182(12):725.
9. Badre N et al. Psychopharmacologic management in integrated care: Challenges for residency education. Acad Psychiatry. 2015; 39(4):466-9.
10. Kraemer HC et al. DSM-5: How reliable is reliable enough? Am J Psychiatry. 2012 Jan;169(1):13-5.
11. Badre N and Compton C. Britney Spears – Reflections on conservatorship. Clinical Psychiatry News. 2021 Nov 16.