User login
Official Newspaper of the American College of Surgeons
Preop atrial fib in CABG patients spells trouble
COLORADO SPRINGS – Preoperative atrial fibrillation is present in more than 10% of patients undergoing isolated coronary artery bypass graft (CABG) surgery, and if not subjected to concomitant surgical ablation it’s associated with increased perioperative and long-term major morbidity and mortality, S. Chris Malaisrie, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
The increased early and late risks posed by preoperative atrial fibrillation (AF) that go unaddressed remain significant even after adjusting for the numerous comorbid conditions more prevalent in CABG patients with preoperative AF than in those without the arrhythmia, added Dr. Malaisrie, a cardiac surgeon at Northwestern University in Chicago.

The unadjusted operative mortality rate was 1.8% in the no-AF group and 4.0% in patients with preoperative AF. Unadjusted in-hospital rates of permanent stroke, prolonged ventilation, reoperation, and new renal failure were also significantly higher in the preoperative AF group.
Not surprisingly, the preoperative AF group was older. They also had significantly higher baseline rates of numerous comorbid conditions, including diabetes, peripheral vascular disease, renal failure, and prior stroke, as well as a lower mean left ventricular ejection fraction. However, after adjustment for the many comorbidities in multivariate regression analysis, the risks of all in-hospital adverse outcomes remained significantly higher in the preoperative AF group. For example, their adjusted risk of operative mortality was 1.5-fold greater than in the no-AF patients.
In the long-term follow-up analysis, the unadjusted risk of mortality in the first 5 years after CABG was 2.5-fold greater in the preoperative AF group. Their 5-year risk of stroke or systemic embolization was 1.5-fold greater, too. Upon adjustment for potentially confounding comorbid conditions, preoperative AF was associated with a 1.5-fold increased 5-year risk of mortality and a 1.2-fold increase in stroke or systemic embolism.
In an effort to identify a particularly high-risk group of CABG patients with preoperative AF, Dr. Malaisrie and his coinvestigators stratified the group’s long-term stroke and mortality risks by their CHA2DS2-VASc score at the time of surgery. The results were revealing: the unadjusted 5-year risk of stroke or systemic embolization was 7.9% in those with a CHA2DS2-VASc score of 1-3, 12.2% with a score of 4-6, and 15.4% with a score of 7-9. The 5-year survival rate was 74.8% with a score of 1-3, 56.5% with a score of 4-6, and 41.2% with a score of 7-9.
“That’s really a striking finding,” Dr. Malaisrie observed. “When you consider a patient who’s, say, 72-75 years old, who is undergoing isolated CABG with preoperative atrial fibrillation and who has a high CHA2DS2-VASc score of 7-9, 5-year survival is only 41%, with a 15% risk of stroke or systemic embolization.”
Discussant William T. Caine, MD, found the study results unsettling.
“I was surprised to see that in this day and age, fully two-thirds of the patients who had preoperative atrial fibrillation had no attempt at any ablation procedure to treat their atrial fibrillation,” declared Dr. Caine of Intermountain Medical Center in Salt Lake City.
In reply, Dr. Malaisrie noted that other, smaller studies have also found that only about 30% of CABG patients with preoperative AF undergo surgical AF ablation through a maze procedure or some other method.
“Probably most of us in this room would go ahead and perform surgical ablation, but the STS database represents all isolated CABG procedures done throughout the United States,” Dr. Malaisrie said. “I think this dataset should help convince the other 70% of surgeons out there that there is a high cost for preoperative AF – in particular, in patients with very high CHA2DS2-VASc scores. If you can identify a group of patients at increased risk for stroke and mortality, you’d certainly want to bend their survival curve.”
The maze procedure has been convincingly shown to be very safe, with no associated increased risk of perioperative morbidity and mortality. The downside is cost. But while it’s true that adding surgical ablation to an isolated CABG procedure boosts OR time and procedural costs, a successful ablation is likely to pay dividends through reduced downstream rates of major morbidity and mortality.
“I look forward to the second part of our analysis, where we’ll look at the comparative data for the patients who did in fact have surgical ablation. That dataset is pending from the Duke Clinical Research Institute,” according to Dr. Malaisrie.
He cited as study limitations the inability to complete linkage to the Medicare database in about 37% of CABG patients in the STS database, or more than 200,000 people. Also, the Medicare database is an administrative dataset reliant upon medical record coding. The mortality data are probably quite accurate, but the stroke and systemic embolization rates cited in this analysis likely underestimate the true rates.
He reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
COLORADO SPRINGS – Preoperative atrial fibrillation is present in more than 10% of patients undergoing isolated coronary artery bypass graft (CABG) surgery, and if not subjected to concomitant surgical ablation it’s associated with increased perioperative and long-term major morbidity and mortality, S. Chris Malaisrie, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
The increased early and late risks posed by preoperative atrial fibrillation (AF) that go unaddressed remain significant even after adjusting for the numerous comorbid conditions more prevalent in CABG patients with preoperative AF than in those without the arrhythmia, added Dr. Malaisrie, a cardiac surgeon at Northwestern University in Chicago.
The unadjusted operative mortality rate was 1.8% in the no-AF group and 4.0% in patients with preoperative AF. Unadjusted in-hospital rates of permanent stroke, prolonged ventilation, reoperation, and new renal failure were also significantly higher in the preoperative AF group.
Not surprisingly, the preoperative AF group was older. They also had significantly higher baseline rates of numerous comorbid conditions, including diabetes, peripheral vascular disease, renal failure, and prior stroke, as well as a lower mean left ventricular ejection fraction. However, after adjustment for the many comorbidities in multivariate regression analysis, the risks of all in-hospital adverse outcomes remained significantly higher in the preoperative AF group. For example, their adjusted risk of operative mortality was 1.5-fold greater than in the no-AF patients.
In the long-term follow-up analysis, the unadjusted risk of mortality in the first 5 years after CABG was 2.5-fold greater in the preoperative AF group. Their 5-year risk of stroke or systemic embolization was 1.5-fold greater, too. Upon adjustment for potentially confounding comorbid conditions, preoperative AF was associated with a 1.5-fold increased 5-year risk of mortality and a 1.2-fold increase in stroke or systemic embolism.
In an effort to identify a particularly high-risk group of CABG patients with preoperative AF, Dr. Malaisrie and his coinvestigators stratified the group’s long-term stroke and mortality risks by their CHA2DS2-VASc score at the time of surgery. The results were revealing: the unadjusted 5-year risk of stroke or systemic embolization was 7.9% in those with a CHA2DS2-VASc score of 1-3, 12.2% with a score of 4-6, and 15.4% with a score of 7-9. The 5-year survival rate was 74.8% with a score of 1-3, 56.5% with a score of 4-6, and 41.2% with a score of 7-9.
“That’s really a striking finding,” Dr. Malaisrie observed. “When you consider a patient who’s, say, 72-75 years old, who is undergoing isolated CABG with preoperative atrial fibrillation and who has a high CHA2DS2-VASc score of 7-9, 5-year survival is only 41%, with a 15% risk of stroke or systemic embolization.”
Discussant William T. Caine, MD, found the study results unsettling.
“I was surprised to see that in this day and age, fully two-thirds of the patients who had preoperative atrial fibrillation had no attempt at any ablation procedure to treat their atrial fibrillation,” declared Dr. Caine of Intermountain Medical Center in Salt Lake City.
In reply, Dr. Malaisrie noted that other, smaller studies have also found that only about 30% of CABG patients with preoperative AF undergo surgical AF ablation through a maze procedure or some other method.
“Probably most of us in this room would go ahead and perform surgical ablation, but the STS database represents all isolated CABG procedures done throughout the United States,” Dr. Malaisrie said. “I think this dataset should help convince the other 70% of surgeons out there that there is a high cost for preoperative AF – in particular, in patients with very high CHA2DS2-VASc scores. If you can identify a group of patients at increased risk for stroke and mortality, you’d certainly want to bend their survival curve.”
The maze procedure has been convincingly shown to be very safe, with no associated increased risk of perioperative morbidity and mortality. The downside is cost. But while it’s true that adding surgical ablation to an isolated CABG procedure boosts OR time and procedural costs, a successful ablation is likely to pay dividends through reduced downstream rates of major morbidity and mortality.
“I look forward to the second part of our analysis, where we’ll look at the comparative data for the patients who did in fact have surgical ablation. That dataset is pending from the Duke Clinical Research Institute,” according to Dr. Malaisrie.
He cited as study limitations the inability to complete linkage to the Medicare database in about 37% of CABG patients in the STS database, or more than 200,000 people. Also, the Medicare database is an administrative dataset reliant upon medical record coding. The mortality data are probably quite accurate, but the stroke and systemic embolization rates cited in this analysis likely underestimate the true rates.
He reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
COLORADO SPRINGS – Preoperative atrial fibrillation is present in more than 10% of patients undergoing isolated coronary artery bypass graft (CABG) surgery, and if not subjected to concomitant surgical ablation it’s associated with increased perioperative and long-term major morbidity and mortality, S. Chris Malaisrie, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
The increased early and late risks posed by preoperative atrial fibrillation (AF) that go unaddressed remain significant even after adjusting for the numerous comorbid conditions more prevalent in CABG patients with preoperative AF than in those without the arrhythmia, added Dr. Malaisrie, a cardiac surgeon at Northwestern University in Chicago.
The unadjusted operative mortality rate was 1.8% in the no-AF group and 4.0% in patients with preoperative AF. Unadjusted in-hospital rates of permanent stroke, prolonged ventilation, reoperation, and new renal failure were also significantly higher in the preoperative AF group.
Not surprisingly, the preoperative AF group was older. They also had significantly higher baseline rates of numerous comorbid conditions, including diabetes, peripheral vascular disease, renal failure, and prior stroke, as well as a lower mean left ventricular ejection fraction. However, after adjustment for the many comorbidities in multivariate regression analysis, the risks of all in-hospital adverse outcomes remained significantly higher in the preoperative AF group. For example, their adjusted risk of operative mortality was 1.5-fold greater than in the no-AF patients.
In the long-term follow-up analysis, the unadjusted risk of mortality in the first 5 years after CABG was 2.5-fold greater in the preoperative AF group. Their 5-year risk of stroke or systemic embolization was 1.5-fold greater, too. Upon adjustment for potentially confounding comorbid conditions, preoperative AF was associated with a 1.5-fold increased 5-year risk of mortality and a 1.2-fold increase in stroke or systemic embolism.
In an effort to identify a particularly high-risk group of CABG patients with preoperative AF, Dr. Malaisrie and his coinvestigators stratified the group’s long-term stroke and mortality risks by their CHA2DS2-VASc score at the time of surgery. The results were revealing: the unadjusted 5-year risk of stroke or systemic embolization was 7.9% in those with a CHA2DS2-VASc score of 1-3, 12.2% with a score of 4-6, and 15.4% with a score of 7-9. The 5-year survival rate was 74.8% with a score of 1-3, 56.5% with a score of 4-6, and 41.2% with a score of 7-9.
“That’s really a striking finding,” Dr. Malaisrie observed. “When you consider a patient who’s, say, 72-75 years old, who is undergoing isolated CABG with preoperative atrial fibrillation and who has a high CHA2DS2-VASc score of 7-9, 5-year survival is only 41%, with a 15% risk of stroke or systemic embolization.”
Discussant William T. Caine, MD, found the study results unsettling.
“I was surprised to see that in this day and age, fully two-thirds of the patients who had preoperative atrial fibrillation had no attempt at any ablation procedure to treat their atrial fibrillation,” declared Dr. Caine of Intermountain Medical Center in Salt Lake City.
In reply, Dr. Malaisrie noted that other, smaller studies have also found that only about 30% of CABG patients with preoperative AF undergo surgical AF ablation through a maze procedure or some other method.
“Probably most of us in this room would go ahead and perform surgical ablation, but the STS database represents all isolated CABG procedures done throughout the United States,” Dr. Malaisrie said. “I think this dataset should help convince the other 70% of surgeons out there that there is a high cost for preoperative AF – in particular, in patients with very high CHA2DS2-VASc scores. If you can identify a group of patients at increased risk for stroke and mortality, you’d certainly want to bend their survival curve.”
The maze procedure has been convincingly shown to be very safe, with no associated increased risk of perioperative morbidity and mortality. The downside is cost. But while it’s true that adding surgical ablation to an isolated CABG procedure boosts OR time and procedural costs, a successful ablation is likely to pay dividends through reduced downstream rates of major morbidity and mortality.
“I look forward to the second part of our analysis, where we’ll look at the comparative data for the patients who did in fact have surgical ablation. That dataset is pending from the Duke Clinical Research Institute,” according to Dr. Malaisrie.
He cited as study limitations the inability to complete linkage to the Medicare database in about 37% of CABG patients in the STS database, or more than 200,000 people. Also, the Medicare database is an administrative dataset reliant upon medical record coding. The mortality data are probably quite accurate, but the stroke and systemic embolization rates cited in this analysis likely underestimate the true rates.
He reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
AT THE WTSA ANNUAL MEETING
Key clinical point:
Major finding: Preoperative AF in patients undergoing isolated CABG was tied to an adjusted 45% greater 5-year mortality and 25% increase in stroke and systemic embolization risk, compared with CABG patients without the preoperative arrhythmia.
Data source: This retrospective study compared perioperative and long-term morbidity and mortality in nearly 350,000 patients in the Society of Thoracic Surgeons database who underwent isolated CABG, including more than 24,000 who had preoperative atrial fibrillation that wasn’t addressed surgically.
Disclosures: The study presenter reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
From the Editors: Your call is important to us
There they were – dropping like a stone toward the lunar surface some 48 years ago. Buzz Aldrin looked at his onboard computer and it reported Error 1202, and alarms started going off in the Lunar Module. Fortunately for Neil Armstrong and Buzz Aldrin, they had a healthy relationship with their computer systems and IT support. Mission control was only 1.5 seconds away and had a huge team of experts that told them they could ignore the error message. The rest is, of course, history. Human beings, not computer software, landed the Eagle. They used their own judgment and experience and data provided by the computer to make their landing decisions.
At 25,000 feet Mission Control answers. Buzz describes the error code. Mission Control reports that his computer is made by Grumman and that Mission Control uses Lockheed-based software. He is advised to call the Grumman help line. At 15,000 feet Grumman responds. They report that Buzz’s password expired about the time the lunar descent burn occurred. He needs to put in a new password and confirm it. He will receive a confirmation email within the next 24 hours. Neil is getting increasingly restive despite his famously bland emotional responses in crises.
At 10,000 feet Buzz gets a new password confirmation, but Error 1202 remains on the display. The moon is enormous in the windshield. Grumman support responds that the error is likely because Buzz put in the wrong weight for the Lunar Module. Buzz begins again feeding in the data to the onboard computer. Grumman suggests that had Buzz simply created the right template, this problem would not have occurred. Buzz, through gritted teeth, asks how he was supposed to create a template for a problem that no one seemed to expect.
They are down to 150 feet now. Neil tells Buzz what he thinks of the computer systems and is told by Mission Control his microphone is hot and that such comments are not appropriate. At Mission Control, a notation is made on their system that Neil will need to discuss this pilot error with the astronaut office upon his return. Neil simply turns off the onboard computer and lands the Lunar Module with seconds of fuel left as he avoids a large boulder field and finds just the right spot. Tranquility Base reports in to Mission Control. Mankind has landed on the Moon.
The alternative history is what surgeons are experiencing every day because of the unhealthy relationship existing between American health care today and our institutional computer systems. Like Neil and Buzz, these surgeons are heroes who avoid boulder fields despite so many obstacles unrelated to their missions. No wonder burnout (a missile term) is so prevalent. We’ve gone from inconvenient to intolerable. Our health care computer systems must be interoperable to have any meaningful use. Our formats need to be understandable. Surgeons need computers to help them make judgments based on easily accessible data in real time. Surgeons need to “fly” the missions and computer systems need to be our servants, not our masters.

Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
There they were – dropping like a stone toward the lunar surface some 48 years ago. Buzz Aldrin looked at his onboard computer and it reported Error 1202, and alarms started going off in the Lunar Module. Fortunately for Neil Armstrong and Buzz Aldrin, they had a healthy relationship with their computer systems and IT support. Mission control was only 1.5 seconds away and had a huge team of experts that told them they could ignore the error message. The rest is, of course, history. Human beings, not computer software, landed the Eagle. They used their own judgment and experience and data provided by the computer to make their landing decisions.
At 25,000 feet Mission Control answers. Buzz describes the error code. Mission Control reports that his computer is made by Grumman and that Mission Control uses Lockheed-based software. He is advised to call the Grumman help line. At 15,000 feet Grumman responds. They report that Buzz’s password expired about the time the lunar descent burn occurred. He needs to put in a new password and confirm it. He will receive a confirmation email within the next 24 hours. Neil is getting increasingly restive despite his famously bland emotional responses in crises.
At 10,000 feet Buzz gets a new password confirmation, but Error 1202 remains on the display. The moon is enormous in the windshield. Grumman support responds that the error is likely because Buzz put in the wrong weight for the Lunar Module. Buzz begins again feeding in the data to the onboard computer. Grumman suggests that had Buzz simply created the right template, this problem would not have occurred. Buzz, through gritted teeth, asks how he was supposed to create a template for a problem that no one seemed to expect.
They are down to 150 feet now. Neil tells Buzz what he thinks of the computer systems and is told by Mission Control his microphone is hot and that such comments are not appropriate. At Mission Control, a notation is made on their system that Neil will need to discuss this pilot error with the astronaut office upon his return. Neil simply turns off the onboard computer and lands the Lunar Module with seconds of fuel left as he avoids a large boulder field and finds just the right spot. Tranquility Base reports in to Mission Control. Mankind has landed on the Moon.
The alternative history is what surgeons are experiencing every day because of the unhealthy relationship existing between American health care today and our institutional computer systems. Like Neil and Buzz, these surgeons are heroes who avoid boulder fields despite so many obstacles unrelated to their missions. No wonder burnout (a missile term) is so prevalent. We’ve gone from inconvenient to intolerable. Our health care computer systems must be interoperable to have any meaningful use. Our formats need to be understandable. Surgeons need computers to help them make judgments based on easily accessible data in real time. Surgeons need to “fly” the missions and computer systems need to be our servants, not our masters.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
There they were – dropping like a stone toward the lunar surface some 48 years ago. Buzz Aldrin looked at his onboard computer and it reported Error 1202, and alarms started going off in the Lunar Module. Fortunately for Neil Armstrong and Buzz Aldrin, they had a healthy relationship with their computer systems and IT support. Mission control was only 1.5 seconds away and had a huge team of experts that told them they could ignore the error message. The rest is, of course, history. Human beings, not computer software, landed the Eagle. They used their own judgment and experience and data provided by the computer to make their landing decisions.
At 25,000 feet Mission Control answers. Buzz describes the error code. Mission Control reports that his computer is made by Grumman and that Mission Control uses Lockheed-based software. He is advised to call the Grumman help line. At 15,000 feet Grumman responds. They report that Buzz’s password expired about the time the lunar descent burn occurred. He needs to put in a new password and confirm it. He will receive a confirmation email within the next 24 hours. Neil is getting increasingly restive despite his famously bland emotional responses in crises.
At 10,000 feet Buzz gets a new password confirmation, but Error 1202 remains on the display. The moon is enormous in the windshield. Grumman support responds that the error is likely because Buzz put in the wrong weight for the Lunar Module. Buzz begins again feeding in the data to the onboard computer. Grumman suggests that had Buzz simply created the right template, this problem would not have occurred. Buzz, through gritted teeth, asks how he was supposed to create a template for a problem that no one seemed to expect.
They are down to 150 feet now. Neil tells Buzz what he thinks of the computer systems and is told by Mission Control his microphone is hot and that such comments are not appropriate. At Mission Control, a notation is made on their system that Neil will need to discuss this pilot error with the astronaut office upon his return. Neil simply turns off the onboard computer and lands the Lunar Module with seconds of fuel left as he avoids a large boulder field and finds just the right spot. Tranquility Base reports in to Mission Control. Mankind has landed on the Moon.
The alternative history is what surgeons are experiencing every day because of the unhealthy relationship existing between American health care today and our institutional computer systems. Like Neil and Buzz, these surgeons are heroes who avoid boulder fields despite so many obstacles unrelated to their missions. No wonder burnout (a missile term) is so prevalent. We’ve gone from inconvenient to intolerable. Our health care computer systems must be interoperable to have any meaningful use. Our formats need to be understandable. Surgeons need computers to help them make judgments based on easily accessible data in real time. Surgeons need to “fly” the missions and computer systems need to be our servants, not our masters.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
ACS delegation influences AMA policy at HOD meeting
The American Medical Association (AMA) annual House of Delegates (HOD) meeting took place June 10–14, in Chicago, IL. The agenda included 62 reports from the AMA board and councils and 186 resolutions from state medical associations, specialty societies, and AMA sections.
The uncertain mood of the HOD was shaped by congressional activity on the Affordable Care Act and a competitive election for AMA president-elect. At the start of the meeting’s final day, the HOD paused to remember the lives lost and changed one year earlier at the Pulse nightclub in Orlando, FL. The HOD also noted the value of American College of Surgeons (ACS) Stop the Bleed® training in response to the shooting June 14 at the Republican congressional baseball team practice in Alexandria, VA.
In the AMA House of Delegates, which is composed of 545 members, the College was represented by its six-member delegation.
The meeting has eight reference committees that focus on the following issues: bylaws and medical ethics, health care system, legislation, medical education, public health, medical science and technology, governance, and medical practice. John H. Armstrong, MD, FACS, co-author of this article, chaired Reference Committee A, which reviewed items pertaining to the health care system. This article provides an overview of several issues of relevance to ACS members.
Medical education
The priority issue for the ACS at this meeting was protecting the profession’s autonomy in defining the standards of lifelong learning through Maintenance of Certification (MOC). Five items related to MOC and Continuing Medical Education (CME) resulted in considerable debate. Internists and medical specialists were particularly frustrated by their experiences with their certifying boards. While acknowledging opportunities to improve MOC, the College delegation took the lead in collaborating with other specialty and state societies to argue against referring MOC to the state legislatures and in creating a new solely CME-based certification system.
• Council on Medical Education Report 2, Update on Maintenance of Certification and Osteopathic Continuous Certification, provided an overview of board-specific MOC innovations that increase relevance and reduce cost. The report was amended to have the AMA advocate that physicians who participate in programs related to quality improvement and/or patient safety should receive credit for MOC Part IV.
• Resolution 302, Comprehensive Review of CME Process, directed the AMA, in collaboration with the Accreditation Council for Continuing Medical Education, to conduct a comprehensive review of the CME process on a national level, with the goal of decreasing costs and simplifying the process of providing CME.
• Resolution 316, Action Steps Regarding Maintenance of Certification, sponsored by the largest state delegations in the HOD (Arizona, California, Florida, Georgia, New York, Pennsylvania, and Texas), sought to extend AMA model state legislation against MOC by barring hospitals, health care insurers, and state licensing boards from linking nonparticipation in the American Board of Medical Specialties (ABMS) MOC process to exclusion from credentialing. Further, it sought to create AMA policy that would replace MOC with high-quality CME under the purview of a physician’s specialty society solely as the demonstration of lifelong learning in hospital, insurance, and licensing credentialing. The HOD conversation shifted from restricting how hospitals, licensing boards, and insurers can use MOC, to redefining MOC.
To address this challenge to professional autonomy while emphasizing the need for responsiveness to concerns across boards, the ACS Delegation applied a strategy that involved prepared talking points; caucus presentations by ACS Executive Director David B. Hoyt, MD, FACS, and Dr. Armstrong; reference committee testimony from Dr. Hoyt and Vice-Chair of the ACS Board of Regents Leigh A. Neumayer, MD, FACS, and ACS Regent James Denneny, MD, FACS, executive director, American Academy of Otolaryngology-Head and Neck Surgery; as well as hallway conversations and HOD floor discussion. As a result, the AMA affirmed that lifelong learning is a fundamental obligation of the profession and recognizes that, for a physician, it is best achieved through ongoing participation in a program of high-quality CME appropriate to the physician’s medical practice as determined by the relevant specialty society. The concept of the AMA lobbying hospital associations, health care insurers, and state licensing boards to not use the ABMS-sponsored MOC process with lifelong interval high stakes testing for credentialing, in addition to the idea of the AMA partnering with state medical associations and specialty societies to undertake a study to establish a separate program of certification by 2020, were referred for further consideration. The ACS will continue to emphasize that a core element of professionalism is self-regulation of lifelong learning through standard-setting.
• Resolution 318, Oppose Direct-to-Consumer Advertising of the ABMS MOC Product, asked the AMA to oppose direct-to-consumer marketing of the ABMS MOC product in print media, social media, apps, and websites that specifically target patients and their families, including but not limited to the promotion of false or misleading claims linking MOC participation with improved patient health outcomes and experiences where limited evidence exists. This item was referred for further study.
• Resolution 319, Public Access to Initial Board Certification Status of Time-Limited ABMS Diplomates, was adopted. The AMA now advocates that the initial certification status of time-limited diplomates be listed and publicly available on all ABMS and ABMS member board websites and physician certification databases and that the names and initial certification status of time-limited diplomates remain on ABMS and ABMS member board websites or physician certification databases, even if the diplomate opts out of MOC participation.
Health system
• Council on Medical Service Report 6, Expansion of U.S. Veterans’ Health Care Choices, was adopted with an amendment offered by the ACS delegation. The AMA will encourage the Veterans Health Administration (VHA) to engage with VHA physicians to explore and develop solutions to improve the health care choices of veterans. The AMA also will continue to support efforts to improve the Veterans Choice Program (VCP) and make it permanent, advocate for new funding to support expansion of the VCP, and encourage the acceleration of interoperability of electronic personal and health records and the exchange of medical records between VHA and non-VHA physicians.
• Substitute Resolution 115, Out-of-Network Care, combined four resolutions on the subject of greatest interest in the Reference Committee A hearing—surprise (unanticipated) billing for out-of-network care. It was adopted with eight AMA principles regarding unanticipated out-of-network care and AMA development of model state legislation addressing the coverage of and payment for unexpected unanticipated out-of-network care.
Public health
• Resolution 419, Improving Physicians’ Ability to Discuss Firearm Safety, was adopted with minor amendments. As a result, the AMA is working with appropriate stakeholders to develop state-specific guidance for physicians on how to counsel patients to reduce their risk for firearm-related injury or death by suicide, including guidance on when and how to ask sensitive questions about firearm ownership, access, and use; and clarification on the circumstances under which physicians are permitted or may be required to disclose the content of such conversations to family members, law enforcement, or other third parties.
Medical practice
• Substitute Resolution 706, Concurrent and Overlapping Surgery, was adopted. The AMA will work with interested national medical specialty societies on issues related to concurrent and overlapping surgery.
AMA elections
The June meeting is when AMA officers, trustees, and councilors are elected. Barbara McAneny, MD, an oncologist from New Mexico, was elected AMA president-elect. Three ACS-endorsed candidates were successful in their bids to serve on the Council on Medical Education. Liana Puscas, MD, MHS, FACS, associate professor of surgery, Duke University School of Medicine, Durham, NC, and Luke Selby, MD, a general surgery resident, University of Colorado School of Medicine, Denver, were reelected; Krystal Tomei, MD, assistant professor of neurosurgery, Case Western Reserve University School of Medicine, Cleveland, OH, was elected.
Surgical Caucus
The Surgical Caucus hosted a well-attended educational session, Cultivating and Protecting Your Digital Presence: Do’s and Don’ts of Social Media. Speakers included Deanna Attai, MD, FACS, a breast surgeon and assistant clinical professor of surgery, David Geffen School of Medicine, University of California, Los Angeles, and Ravi Goel, MD, an ophthalmologist in private practice in Cherry Hill, NJ, and delegate from the American Academy of Ophthalmology. Both presentations emphasized that surgeons need to manage their online reputation in practice reviews and other web content. Drs. Attai and Goel provided constructive ideas for personal and professional branding through social media, as well as practical ways for surgeons to build and protect their social media reputation. Both presentations are available on the Surgical Caucus web page at facs.org/advocacy/ama-house-of-delegates/surgical-caucus.
The ACS delegation successfully put forth the College’s priorities at the June AMA HOD meeting. The delegation is now working with the ACS Division of Advocacy and Health Policy, the Health Policy and Advocacy Group, and other committees to develop next steps in shaping AMA policy consistent with College principles.
The next AMA meeting is the Interim Meeting in Honolulu, HI, November 11–14. The College’s delegation welcomes input from Fellows regarding issues of importance to surgeons. Comments and questions should be directed to [email protected].
ACS delegation at the AMA HOD
John H. Armstrong, MD, FACS (Delegation Chair), acute care surgery, Ocala, FL
Brian J. Gavitt, MD, MPH (also Young Physicians Section delegate), general surgery, Cincinnati, OH
Jacob Moalem, MD, FACS, general surgery, Rochester, NY
Leigh A. Neumayer, MD, FACS, general surgery, Tucson, AZ; Vice-Chair, ACS Board of Regents
Naveen F. Sangji, MD, (also Resident and Fellow Section delegate), general surgery resident, Boston, MA
Patricia L. Turner, MD, FACS, general surgery, Chicago, IL; Director, ACS Division of Member Services; Chair, AMA Council on Medical Education
Dr. Armstrong is affiliate associate professor of surgery, University of South Florida Morsani College of Medicine, and former Florida Surgeon General and Secretary of Health (2012–2016). He is a member of the American College of Surgeons (ACS) Health Policy and Advocacy Group, and Past-Chair, ACS Professional Association political action committee (ACSPA-SurgeonsPAC).
Mr. Sutton is Manager, State Affairs, ACS Division of Advocacy and Health Policy.
The American Medical Association (AMA) annual House of Delegates (HOD) meeting took place June 10–14, in Chicago, IL. The agenda included 62 reports from the AMA board and councils and 186 resolutions from state medical associations, specialty societies, and AMA sections.
The uncertain mood of the HOD was shaped by congressional activity on the Affordable Care Act and a competitive election for AMA president-elect. At the start of the meeting’s final day, the HOD paused to remember the lives lost and changed one year earlier at the Pulse nightclub in Orlando, FL. The HOD also noted the value of American College of Surgeons (ACS) Stop the Bleed® training in response to the shooting June 14 at the Republican congressional baseball team practice in Alexandria, VA.
In the AMA House of Delegates, which is composed of 545 members, the College was represented by its six-member delegation.
The meeting has eight reference committees that focus on the following issues: bylaws and medical ethics, health care system, legislation, medical education, public health, medical science and technology, governance, and medical practice. John H. Armstrong, MD, FACS, co-author of this article, chaired Reference Committee A, which reviewed items pertaining to the health care system. This article provides an overview of several issues of relevance to ACS members.
Medical education
The priority issue for the ACS at this meeting was protecting the profession’s autonomy in defining the standards of lifelong learning through Maintenance of Certification (MOC). Five items related to MOC and Continuing Medical Education (CME) resulted in considerable debate. Internists and medical specialists were particularly frustrated by their experiences with their certifying boards. While acknowledging opportunities to improve MOC, the College delegation took the lead in collaborating with other specialty and state societies to argue against referring MOC to the state legislatures and in creating a new solely CME-based certification system.
• Council on Medical Education Report 2, Update on Maintenance of Certification and Osteopathic Continuous Certification, provided an overview of board-specific MOC innovations that increase relevance and reduce cost. The report was amended to have the AMA advocate that physicians who participate in programs related to quality improvement and/or patient safety should receive credit for MOC Part IV.
• Resolution 302, Comprehensive Review of CME Process, directed the AMA, in collaboration with the Accreditation Council for Continuing Medical Education, to conduct a comprehensive review of the CME process on a national level, with the goal of decreasing costs and simplifying the process of providing CME.
• Resolution 316, Action Steps Regarding Maintenance of Certification, sponsored by the largest state delegations in the HOD (Arizona, California, Florida, Georgia, New York, Pennsylvania, and Texas), sought to extend AMA model state legislation against MOC by barring hospitals, health care insurers, and state licensing boards from linking nonparticipation in the American Board of Medical Specialties (ABMS) MOC process to exclusion from credentialing. Further, it sought to create AMA policy that would replace MOC with high-quality CME under the purview of a physician’s specialty society solely as the demonstration of lifelong learning in hospital, insurance, and licensing credentialing. The HOD conversation shifted from restricting how hospitals, licensing boards, and insurers can use MOC, to redefining MOC.
To address this challenge to professional autonomy while emphasizing the need for responsiveness to concerns across boards, the ACS Delegation applied a strategy that involved prepared talking points; caucus presentations by ACS Executive Director David B. Hoyt, MD, FACS, and Dr. Armstrong; reference committee testimony from Dr. Hoyt and Vice-Chair of the ACS Board of Regents Leigh A. Neumayer, MD, FACS, and ACS Regent James Denneny, MD, FACS, executive director, American Academy of Otolaryngology-Head and Neck Surgery; as well as hallway conversations and HOD floor discussion. As a result, the AMA affirmed that lifelong learning is a fundamental obligation of the profession and recognizes that, for a physician, it is best achieved through ongoing participation in a program of high-quality CME appropriate to the physician’s medical practice as determined by the relevant specialty society. The concept of the AMA lobbying hospital associations, health care insurers, and state licensing boards to not use the ABMS-sponsored MOC process with lifelong interval high stakes testing for credentialing, in addition to the idea of the AMA partnering with state medical associations and specialty societies to undertake a study to establish a separate program of certification by 2020, were referred for further consideration. The ACS will continue to emphasize that a core element of professionalism is self-regulation of lifelong learning through standard-setting.
• Resolution 318, Oppose Direct-to-Consumer Advertising of the ABMS MOC Product, asked the AMA to oppose direct-to-consumer marketing of the ABMS MOC product in print media, social media, apps, and websites that specifically target patients and their families, including but not limited to the promotion of false or misleading claims linking MOC participation with improved patient health outcomes and experiences where limited evidence exists. This item was referred for further study.
• Resolution 319, Public Access to Initial Board Certification Status of Time-Limited ABMS Diplomates, was adopted. The AMA now advocates that the initial certification status of time-limited diplomates be listed and publicly available on all ABMS and ABMS member board websites and physician certification databases and that the names and initial certification status of time-limited diplomates remain on ABMS and ABMS member board websites or physician certification databases, even if the diplomate opts out of MOC participation.
Health system
• Council on Medical Service Report 6, Expansion of U.S. Veterans’ Health Care Choices, was adopted with an amendment offered by the ACS delegation. The AMA will encourage the Veterans Health Administration (VHA) to engage with VHA physicians to explore and develop solutions to improve the health care choices of veterans. The AMA also will continue to support efforts to improve the Veterans Choice Program (VCP) and make it permanent, advocate for new funding to support expansion of the VCP, and encourage the acceleration of interoperability of electronic personal and health records and the exchange of medical records between VHA and non-VHA physicians.
• Substitute Resolution 115, Out-of-Network Care, combined four resolutions on the subject of greatest interest in the Reference Committee A hearing—surprise (unanticipated) billing for out-of-network care. It was adopted with eight AMA principles regarding unanticipated out-of-network care and AMA development of model state legislation addressing the coverage of and payment for unexpected unanticipated out-of-network care.
Public health
• Resolution 419, Improving Physicians’ Ability to Discuss Firearm Safety, was adopted with minor amendments. As a result, the AMA is working with appropriate stakeholders to develop state-specific guidance for physicians on how to counsel patients to reduce their risk for firearm-related injury or death by suicide, including guidance on when and how to ask sensitive questions about firearm ownership, access, and use; and clarification on the circumstances under which physicians are permitted or may be required to disclose the content of such conversations to family members, law enforcement, or other third parties.
Medical practice
• Substitute Resolution 706, Concurrent and Overlapping Surgery, was adopted. The AMA will work with interested national medical specialty societies on issues related to concurrent and overlapping surgery.
AMA elections
The June meeting is when AMA officers, trustees, and councilors are elected. Barbara McAneny, MD, an oncologist from New Mexico, was elected AMA president-elect. Three ACS-endorsed candidates were successful in their bids to serve on the Council on Medical Education. Liana Puscas, MD, MHS, FACS, associate professor of surgery, Duke University School of Medicine, Durham, NC, and Luke Selby, MD, a general surgery resident, University of Colorado School of Medicine, Denver, were reelected; Krystal Tomei, MD, assistant professor of neurosurgery, Case Western Reserve University School of Medicine, Cleveland, OH, was elected.
Surgical Caucus
The Surgical Caucus hosted a well-attended educational session, Cultivating and Protecting Your Digital Presence: Do’s and Don’ts of Social Media. Speakers included Deanna Attai, MD, FACS, a breast surgeon and assistant clinical professor of surgery, David Geffen School of Medicine, University of California, Los Angeles, and Ravi Goel, MD, an ophthalmologist in private practice in Cherry Hill, NJ, and delegate from the American Academy of Ophthalmology. Both presentations emphasized that surgeons need to manage their online reputation in practice reviews and other web content. Drs. Attai and Goel provided constructive ideas for personal and professional branding through social media, as well as practical ways for surgeons to build and protect their social media reputation. Both presentations are available on the Surgical Caucus web page at facs.org/advocacy/ama-house-of-delegates/surgical-caucus.
The ACS delegation successfully put forth the College’s priorities at the June AMA HOD meeting. The delegation is now working with the ACS Division of Advocacy and Health Policy, the Health Policy and Advocacy Group, and other committees to develop next steps in shaping AMA policy consistent with College principles.
The next AMA meeting is the Interim Meeting in Honolulu, HI, November 11–14. The College’s delegation welcomes input from Fellows regarding issues of importance to surgeons. Comments and questions should be directed to [email protected].
ACS delegation at the AMA HOD
John H. Armstrong, MD, FACS (Delegation Chair), acute care surgery, Ocala, FL
Brian J. Gavitt, MD, MPH (also Young Physicians Section delegate), general surgery, Cincinnati, OH
Jacob Moalem, MD, FACS, general surgery, Rochester, NY
Leigh A. Neumayer, MD, FACS, general surgery, Tucson, AZ; Vice-Chair, ACS Board of Regents
Naveen F. Sangji, MD, (also Resident and Fellow Section delegate), general surgery resident, Boston, MA
Patricia L. Turner, MD, FACS, general surgery, Chicago, IL; Director, ACS Division of Member Services; Chair, AMA Council on Medical Education
Dr. Armstrong is affiliate associate professor of surgery, University of South Florida Morsani College of Medicine, and former Florida Surgeon General and Secretary of Health (2012–2016). He is a member of the American College of Surgeons (ACS) Health Policy and Advocacy Group, and Past-Chair, ACS Professional Association political action committee (ACSPA-SurgeonsPAC).
Mr. Sutton is Manager, State Affairs, ACS Division of Advocacy and Health Policy.
The American Medical Association (AMA) annual House of Delegates (HOD) meeting took place June 10–14, in Chicago, IL. The agenda included 62 reports from the AMA board and councils and 186 resolutions from state medical associations, specialty societies, and AMA sections.
The uncertain mood of the HOD was shaped by congressional activity on the Affordable Care Act and a competitive election for AMA president-elect. At the start of the meeting’s final day, the HOD paused to remember the lives lost and changed one year earlier at the Pulse nightclub in Orlando, FL. The HOD also noted the value of American College of Surgeons (ACS) Stop the Bleed® training in response to the shooting June 14 at the Republican congressional baseball team practice in Alexandria, VA.
In the AMA House of Delegates, which is composed of 545 members, the College was represented by its six-member delegation.
The meeting has eight reference committees that focus on the following issues: bylaws and medical ethics, health care system, legislation, medical education, public health, medical science and technology, governance, and medical practice. John H. Armstrong, MD, FACS, co-author of this article, chaired Reference Committee A, which reviewed items pertaining to the health care system. This article provides an overview of several issues of relevance to ACS members.
Medical education
The priority issue for the ACS at this meeting was protecting the profession’s autonomy in defining the standards of lifelong learning through Maintenance of Certification (MOC). Five items related to MOC and Continuing Medical Education (CME) resulted in considerable debate. Internists and medical specialists were particularly frustrated by their experiences with their certifying boards. While acknowledging opportunities to improve MOC, the College delegation took the lead in collaborating with other specialty and state societies to argue against referring MOC to the state legislatures and in creating a new solely CME-based certification system.
• Council on Medical Education Report 2, Update on Maintenance of Certification and Osteopathic Continuous Certification, provided an overview of board-specific MOC innovations that increase relevance and reduce cost. The report was amended to have the AMA advocate that physicians who participate in programs related to quality improvement and/or patient safety should receive credit for MOC Part IV.
• Resolution 302, Comprehensive Review of CME Process, directed the AMA, in collaboration with the Accreditation Council for Continuing Medical Education, to conduct a comprehensive review of the CME process on a national level, with the goal of decreasing costs and simplifying the process of providing CME.
• Resolution 316, Action Steps Regarding Maintenance of Certification, sponsored by the largest state delegations in the HOD (Arizona, California, Florida, Georgia, New York, Pennsylvania, and Texas), sought to extend AMA model state legislation against MOC by barring hospitals, health care insurers, and state licensing boards from linking nonparticipation in the American Board of Medical Specialties (ABMS) MOC process to exclusion from credentialing. Further, it sought to create AMA policy that would replace MOC with high-quality CME under the purview of a physician’s specialty society solely as the demonstration of lifelong learning in hospital, insurance, and licensing credentialing. The HOD conversation shifted from restricting how hospitals, licensing boards, and insurers can use MOC, to redefining MOC.
To address this challenge to professional autonomy while emphasizing the need for responsiveness to concerns across boards, the ACS Delegation applied a strategy that involved prepared talking points; caucus presentations by ACS Executive Director David B. Hoyt, MD, FACS, and Dr. Armstrong; reference committee testimony from Dr. Hoyt and Vice-Chair of the ACS Board of Regents Leigh A. Neumayer, MD, FACS, and ACS Regent James Denneny, MD, FACS, executive director, American Academy of Otolaryngology-Head and Neck Surgery; as well as hallway conversations and HOD floor discussion. As a result, the AMA affirmed that lifelong learning is a fundamental obligation of the profession and recognizes that, for a physician, it is best achieved through ongoing participation in a program of high-quality CME appropriate to the physician’s medical practice as determined by the relevant specialty society. The concept of the AMA lobbying hospital associations, health care insurers, and state licensing boards to not use the ABMS-sponsored MOC process with lifelong interval high stakes testing for credentialing, in addition to the idea of the AMA partnering with state medical associations and specialty societies to undertake a study to establish a separate program of certification by 2020, were referred for further consideration. The ACS will continue to emphasize that a core element of professionalism is self-regulation of lifelong learning through standard-setting.
• Resolution 318, Oppose Direct-to-Consumer Advertising of the ABMS MOC Product, asked the AMA to oppose direct-to-consumer marketing of the ABMS MOC product in print media, social media, apps, and websites that specifically target patients and their families, including but not limited to the promotion of false or misleading claims linking MOC participation with improved patient health outcomes and experiences where limited evidence exists. This item was referred for further study.
• Resolution 319, Public Access to Initial Board Certification Status of Time-Limited ABMS Diplomates, was adopted. The AMA now advocates that the initial certification status of time-limited diplomates be listed and publicly available on all ABMS and ABMS member board websites and physician certification databases and that the names and initial certification status of time-limited diplomates remain on ABMS and ABMS member board websites or physician certification databases, even if the diplomate opts out of MOC participation.
Health system
• Council on Medical Service Report 6, Expansion of U.S. Veterans’ Health Care Choices, was adopted with an amendment offered by the ACS delegation. The AMA will encourage the Veterans Health Administration (VHA) to engage with VHA physicians to explore and develop solutions to improve the health care choices of veterans. The AMA also will continue to support efforts to improve the Veterans Choice Program (VCP) and make it permanent, advocate for new funding to support expansion of the VCP, and encourage the acceleration of interoperability of electronic personal and health records and the exchange of medical records between VHA and non-VHA physicians.
• Substitute Resolution 115, Out-of-Network Care, combined four resolutions on the subject of greatest interest in the Reference Committee A hearing—surprise (unanticipated) billing for out-of-network care. It was adopted with eight AMA principles regarding unanticipated out-of-network care and AMA development of model state legislation addressing the coverage of and payment for unexpected unanticipated out-of-network care.
Public health
• Resolution 419, Improving Physicians’ Ability to Discuss Firearm Safety, was adopted with minor amendments. As a result, the AMA is working with appropriate stakeholders to develop state-specific guidance for physicians on how to counsel patients to reduce their risk for firearm-related injury or death by suicide, including guidance on when and how to ask sensitive questions about firearm ownership, access, and use; and clarification on the circumstances under which physicians are permitted or may be required to disclose the content of such conversations to family members, law enforcement, or other third parties.
Medical practice
• Substitute Resolution 706, Concurrent and Overlapping Surgery, was adopted. The AMA will work with interested national medical specialty societies on issues related to concurrent and overlapping surgery.
AMA elections
The June meeting is when AMA officers, trustees, and councilors are elected. Barbara McAneny, MD, an oncologist from New Mexico, was elected AMA president-elect. Three ACS-endorsed candidates were successful in their bids to serve on the Council on Medical Education. Liana Puscas, MD, MHS, FACS, associate professor of surgery, Duke University School of Medicine, Durham, NC, and Luke Selby, MD, a general surgery resident, University of Colorado School of Medicine, Denver, were reelected; Krystal Tomei, MD, assistant professor of neurosurgery, Case Western Reserve University School of Medicine, Cleveland, OH, was elected.
Surgical Caucus
The Surgical Caucus hosted a well-attended educational session, Cultivating and Protecting Your Digital Presence: Do’s and Don’ts of Social Media. Speakers included Deanna Attai, MD, FACS, a breast surgeon and assistant clinical professor of surgery, David Geffen School of Medicine, University of California, Los Angeles, and Ravi Goel, MD, an ophthalmologist in private practice in Cherry Hill, NJ, and delegate from the American Academy of Ophthalmology. Both presentations emphasized that surgeons need to manage their online reputation in practice reviews and other web content. Drs. Attai and Goel provided constructive ideas for personal and professional branding through social media, as well as practical ways for surgeons to build and protect their social media reputation. Both presentations are available on the Surgical Caucus web page at facs.org/advocacy/ama-house-of-delegates/surgical-caucus.
The ACS delegation successfully put forth the College’s priorities at the June AMA HOD meeting. The delegation is now working with the ACS Division of Advocacy and Health Policy, the Health Policy and Advocacy Group, and other committees to develop next steps in shaping AMA policy consistent with College principles.
The next AMA meeting is the Interim Meeting in Honolulu, HI, November 11–14. The College’s delegation welcomes input from Fellows regarding issues of importance to surgeons. Comments and questions should be directed to [email protected].
ACS delegation at the AMA HOD
John H. Armstrong, MD, FACS (Delegation Chair), acute care surgery, Ocala, FL
Brian J. Gavitt, MD, MPH (also Young Physicians Section delegate), general surgery, Cincinnati, OH
Jacob Moalem, MD, FACS, general surgery, Rochester, NY
Leigh A. Neumayer, MD, FACS, general surgery, Tucson, AZ; Vice-Chair, ACS Board of Regents
Naveen F. Sangji, MD, (also Resident and Fellow Section delegate), general surgery resident, Boston, MA
Patricia L. Turner, MD, FACS, general surgery, Chicago, IL; Director, ACS Division of Member Services; Chair, AMA Council on Medical Education
Dr. Armstrong is affiliate associate professor of surgery, University of South Florida Morsani College of Medicine, and former Florida Surgeon General and Secretary of Health (2012–2016). He is a member of the American College of Surgeons (ACS) Health Policy and Advocacy Group, and Past-Chair, ACS Professional Association political action committee (ACSPA-SurgeonsPAC).
Mr. Sutton is Manager, State Affairs, ACS Division of Advocacy and Health Policy.
Timothy A. M. Chuter, MD, FACS, receives 2017 ACS Jacobson Innovation Award
The American College of Surgeons (ACS) presented the 2017 Jacobson Innovation Award to Timothy A. M. Chuter, MB, BS, DM, FACS, at a dinner in his honor June 9 in Chicago. Dr. Chuter is professor of surgery at the University of California, San Francisco (UCSF), where he practices vascular surgery with a focus on the endovascular reconstruction of aneurysms involving the aortic arch and thoracoabdominal aorta.
The Jacobson Innovation Award honors living surgeons who have developed innovative devices or techniques in any field of surgery and is made possible through a gift from Julius H. Jacobson II, MD, FACS, and his wife Joan. Dr. Jacobson is a general vascular surgeon known for his pioneering work in the development of microsurgery.
Leading the way in endovascular aneurysm repair, Dr. Chuter was recognized for his role in the development of endovascular aneurysm repair. He was the first individual to design and implant bifurcated stent grafts to treat abdominal aortic aneurysms, based on the idea that if an aneurysm has branches—at the aortic arch or the bifurcation of the common iliac artery, for example—the endovascular prosthesis also should have branches. Because the most common site for aortic aneurysm involves the distal abdominal aorta, bifurcated endovascular repair has become the most accepted method of aneurysm repair worldwide.
In the years between 1993 and 2000, the scope of endovascular repair rapidly expanded, with several firsts in the field, such as the first bifurcated stent grafts in 1993, the first endovascular repair of a ruptured aortic aneurysm in 1994, the first fenestrated stent grafts for aneurysms of the pararenal aorta in 1998, and the first branched stent grafts for the thoracoabdominal aorta in 2000. Dr. Chuter played a role in many of these developments, though none was the work of a single inventor. Dr. Chuter has said that he is proud to have contributed to several advances in endovascular aneurysm repair, not only by inventing new forms of repair, but also by mentoring surgical residents, fellows, and faculty.
In addition to his noted surgical skill, Dr. Chuter has been lauded for inventing and patenting the stent grafts that facilitate his work. Dr. Chuter’s devices and surgical techniques allow aneurysm repair in patients who otherwise might have no other chance of receiving effective treatment. He holds more than 40 patents, including 23 related to endovascular aortic stent-graft devices, stents, attachment systems, delivery systems, and component junctions.
Worldwide recognition
Dr. Chuter is the author or co-author of at least 145 peer-reviewed articles and 23 books or book chapters in the field. Other organizations have recognized his role in the development of endovascular aneurysm repair as well, including the Royal College of Surgeons, through their Kinmonth Medal in 1995; the Society for Vascular Surgery, through their Medal for Innovation in Vascular Surgery in 2008; and the Society for Endovascular Therapy in 2009.
Read more about Dr. Chuter and the Jacobson Innovation Award in the ACS press release at facs.org/media/press-releases/2017/jacobson061217. For a list of previous Jacobson Innovation Award winners, visit the ACS website at facs.org/about-acs/governance/acs-committees/honors-committee/jacobson-list.
The American College of Surgeons (ACS) presented the 2017 Jacobson Innovation Award to Timothy A. M. Chuter, MB, BS, DM, FACS, at a dinner in his honor June 9 in Chicago. Dr. Chuter is professor of surgery at the University of California, San Francisco (UCSF), where he practices vascular surgery with a focus on the endovascular reconstruction of aneurysms involving the aortic arch and thoracoabdominal aorta.
The Jacobson Innovation Award honors living surgeons who have developed innovative devices or techniques in any field of surgery and is made possible through a gift from Julius H. Jacobson II, MD, FACS, and his wife Joan. Dr. Jacobson is a general vascular surgeon known for his pioneering work in the development of microsurgery.
Leading the way in endovascular aneurysm repair, Dr. Chuter was recognized for his role in the development of endovascular aneurysm repair. He was the first individual to design and implant bifurcated stent grafts to treat abdominal aortic aneurysms, based on the idea that if an aneurysm has branches—at the aortic arch or the bifurcation of the common iliac artery, for example—the endovascular prosthesis also should have branches. Because the most common site for aortic aneurysm involves the distal abdominal aorta, bifurcated endovascular repair has become the most accepted method of aneurysm repair worldwide.
In the years between 1993 and 2000, the scope of endovascular repair rapidly expanded, with several firsts in the field, such as the first bifurcated stent grafts in 1993, the first endovascular repair of a ruptured aortic aneurysm in 1994, the first fenestrated stent grafts for aneurysms of the pararenal aorta in 1998, and the first branched stent grafts for the thoracoabdominal aorta in 2000. Dr. Chuter played a role in many of these developments, though none was the work of a single inventor. Dr. Chuter has said that he is proud to have contributed to several advances in endovascular aneurysm repair, not only by inventing new forms of repair, but also by mentoring surgical residents, fellows, and faculty.
In addition to his noted surgical skill, Dr. Chuter has been lauded for inventing and patenting the stent grafts that facilitate his work. Dr. Chuter’s devices and surgical techniques allow aneurysm repair in patients who otherwise might have no other chance of receiving effective treatment. He holds more than 40 patents, including 23 related to endovascular aortic stent-graft devices, stents, attachment systems, delivery systems, and component junctions.
Worldwide recognition
Dr. Chuter is the author or co-author of at least 145 peer-reviewed articles and 23 books or book chapters in the field. Other organizations have recognized his role in the development of endovascular aneurysm repair as well, including the Royal College of Surgeons, through their Kinmonth Medal in 1995; the Society for Vascular Surgery, through their Medal for Innovation in Vascular Surgery in 2008; and the Society for Endovascular Therapy in 2009.
Read more about Dr. Chuter and the Jacobson Innovation Award in the ACS press release at facs.org/media/press-releases/2017/jacobson061217. For a list of previous Jacobson Innovation Award winners, visit the ACS website at facs.org/about-acs/governance/acs-committees/honors-committee/jacobson-list.
The American College of Surgeons (ACS) presented the 2017 Jacobson Innovation Award to Timothy A. M. Chuter, MB, BS, DM, FACS, at a dinner in his honor June 9 in Chicago. Dr. Chuter is professor of surgery at the University of California, San Francisco (UCSF), where he practices vascular surgery with a focus on the endovascular reconstruction of aneurysms involving the aortic arch and thoracoabdominal aorta.
The Jacobson Innovation Award honors living surgeons who have developed innovative devices or techniques in any field of surgery and is made possible through a gift from Julius H. Jacobson II, MD, FACS, and his wife Joan. Dr. Jacobson is a general vascular surgeon known for his pioneering work in the development of microsurgery.
Leading the way in endovascular aneurysm repair, Dr. Chuter was recognized for his role in the development of endovascular aneurysm repair. He was the first individual to design and implant bifurcated stent grafts to treat abdominal aortic aneurysms, based on the idea that if an aneurysm has branches—at the aortic arch or the bifurcation of the common iliac artery, for example—the endovascular prosthesis also should have branches. Because the most common site for aortic aneurysm involves the distal abdominal aorta, bifurcated endovascular repair has become the most accepted method of aneurysm repair worldwide.
In the years between 1993 and 2000, the scope of endovascular repair rapidly expanded, with several firsts in the field, such as the first bifurcated stent grafts in 1993, the first endovascular repair of a ruptured aortic aneurysm in 1994, the first fenestrated stent grafts for aneurysms of the pararenal aorta in 1998, and the first branched stent grafts for the thoracoabdominal aorta in 2000. Dr. Chuter played a role in many of these developments, though none was the work of a single inventor. Dr. Chuter has said that he is proud to have contributed to several advances in endovascular aneurysm repair, not only by inventing new forms of repair, but also by mentoring surgical residents, fellows, and faculty.
In addition to his noted surgical skill, Dr. Chuter has been lauded for inventing and patenting the stent grafts that facilitate his work. Dr. Chuter’s devices and surgical techniques allow aneurysm repair in patients who otherwise might have no other chance of receiving effective treatment. He holds more than 40 patents, including 23 related to endovascular aortic stent-graft devices, stents, attachment systems, delivery systems, and component junctions.
Worldwide recognition
Dr. Chuter is the author or co-author of at least 145 peer-reviewed articles and 23 books or book chapters in the field. Other organizations have recognized his role in the development of endovascular aneurysm repair as well, including the Royal College of Surgeons, through their Kinmonth Medal in 1995; the Society for Vascular Surgery, through their Medal for Innovation in Vascular Surgery in 2008; and the Society for Endovascular Therapy in 2009.
Read more about Dr. Chuter and the Jacobson Innovation Award in the ACS press release at facs.org/media/press-releases/2017/jacobson061217. For a list of previous Jacobson Innovation Award winners, visit the ACS website at facs.org/about-acs/governance/acs-committees/honors-committee/jacobson-list.
From the Washington Office: The Mission Zero Act
Surgeons are well familiar with the statistic from the Centers for Disease Control and Prevention (CDC) identifying trauma as the leading cause of death for children and adults under age 44. More Americans lose their lives each year to trauma than to AIDS and stroke combined. Unfortunately, nearly 45 million Americans live in areas more than an hour away from either a Level I or II trauma center. Ensuring access to trauma care requires many crucial components including trauma centers and appropriately trained physicians and nurses, all of which must dedicate extensive resources around the clock so that seriously injured patients have the best possible chance for survival.
It has long been a top legislative priority of the ACS to establish and maintain adequate funding for high-quality trauma systems throughout the United States, including those systems operated by our armed forces.The ACS was a sponsor of the National Academy of Medicine (NAM) report entitled, A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths After Injury. This report, released in June of 2016, outlines the steps necessary to secure a national trauma system and sets the goal of achieving zero preventable traumatic deaths.
In an effort to facilitate the achievement of the goals laid out in the report, The Mission Zero Act (H.R. 880) was introduced in the House of Representatives by Chairman of the House Energy and Commerce Health Subcommittee, Michael Burgess, MD (R-TX), Representatives Cathy Castor (D-FL), Gene Green (D-TX), and Richard Hudson (R-NC). Identical companion legislation was introduced in the Senate (S.1022) by Senators Johnny Isakson (R-GA), John Cornyn (R-TX), and Tammy Duckworth (D-IL). The Mission Zero Act creates a grant program to assist civilian trauma centers in partnering with military trauma professionals to establish a pathway to provide patients with the highest quality of trauma care in times of peace and war, thus taking a step in the direction of the NAM report recommendations.
Specifically, the legislation provides for:
• $40 million in grants to fund military trauma teams and providers to embed into civilian trauma facilities.
o Trauma centers are eligible for a $1 million grant to host military trauma teams at eligible high-acuity level 1 trauma centers
o Trauma centers are also eligible for grants to host individual providers ($100,000 for physician or $50,000 for non-physician providers) at eligible level I, II, or III trauma centers
As of today, the House and Senate versions of the Mission Zero Act have 25co-sponsors and 2 co-sponsors respectively. The ACS would very much like to build some momentum for the Mission Zero Act going into the fall when it is expected that there will be several large “must pass” pieces of legislation working their way through Congress to which the Mission Zero Act could potentially be attached. Accordingly, I respectfully ask all Fellows to take a few moments to visit the SurgeonsVoice website at www.surgeonsvoice.org, click on the Take Action tab on the right side of the page and send a message to their individual representatives and senators seeking support for this important legislation.
Until next month …

Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Surgeons are well familiar with the statistic from the Centers for Disease Control and Prevention (CDC) identifying trauma as the leading cause of death for children and adults under age 44. More Americans lose their lives each year to trauma than to AIDS and stroke combined. Unfortunately, nearly 45 million Americans live in areas more than an hour away from either a Level I or II trauma center. Ensuring access to trauma care requires many crucial components including trauma centers and appropriately trained physicians and nurses, all of which must dedicate extensive resources around the clock so that seriously injured patients have the best possible chance for survival.
It has long been a top legislative priority of the ACS to establish and maintain adequate funding for high-quality trauma systems throughout the United States, including those systems operated by our armed forces.The ACS was a sponsor of the National Academy of Medicine (NAM) report entitled, A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths After Injury. This report, released in June of 2016, outlines the steps necessary to secure a national trauma system and sets the goal of achieving zero preventable traumatic deaths.
In an effort to facilitate the achievement of the goals laid out in the report, The Mission Zero Act (H.R. 880) was introduced in the House of Representatives by Chairman of the House Energy and Commerce Health Subcommittee, Michael Burgess, MD (R-TX), Representatives Cathy Castor (D-FL), Gene Green (D-TX), and Richard Hudson (R-NC). Identical companion legislation was introduced in the Senate (S.1022) by Senators Johnny Isakson (R-GA), John Cornyn (R-TX), and Tammy Duckworth (D-IL). The Mission Zero Act creates a grant program to assist civilian trauma centers in partnering with military trauma professionals to establish a pathway to provide patients with the highest quality of trauma care in times of peace and war, thus taking a step in the direction of the NAM report recommendations.
Specifically, the legislation provides for:
• $40 million in grants to fund military trauma teams and providers to embed into civilian trauma facilities.
o Trauma centers are eligible for a $1 million grant to host military trauma teams at eligible high-acuity level 1 trauma centers
o Trauma centers are also eligible for grants to host individual providers ($100,000 for physician or $50,000 for non-physician providers) at eligible level I, II, or III trauma centers
As of today, the House and Senate versions of the Mission Zero Act have 25co-sponsors and 2 co-sponsors respectively. The ACS would very much like to build some momentum for the Mission Zero Act going into the fall when it is expected that there will be several large “must pass” pieces of legislation working their way through Congress to which the Mission Zero Act could potentially be attached. Accordingly, I respectfully ask all Fellows to take a few moments to visit the SurgeonsVoice website at www.surgeonsvoice.org, click on the Take Action tab on the right side of the page and send a message to their individual representatives and senators seeking support for this important legislation.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Surgeons are well familiar with the statistic from the Centers for Disease Control and Prevention (CDC) identifying trauma as the leading cause of death for children and adults under age 44. More Americans lose their lives each year to trauma than to AIDS and stroke combined. Unfortunately, nearly 45 million Americans live in areas more than an hour away from either a Level I or II trauma center. Ensuring access to trauma care requires many crucial components including trauma centers and appropriately trained physicians and nurses, all of which must dedicate extensive resources around the clock so that seriously injured patients have the best possible chance for survival.
It has long been a top legislative priority of the ACS to establish and maintain adequate funding for high-quality trauma systems throughout the United States, including those systems operated by our armed forces.The ACS was a sponsor of the National Academy of Medicine (NAM) report entitled, A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths After Injury. This report, released in June of 2016, outlines the steps necessary to secure a national trauma system and sets the goal of achieving zero preventable traumatic deaths.
In an effort to facilitate the achievement of the goals laid out in the report, The Mission Zero Act (H.R. 880) was introduced in the House of Representatives by Chairman of the House Energy and Commerce Health Subcommittee, Michael Burgess, MD (R-TX), Representatives Cathy Castor (D-FL), Gene Green (D-TX), and Richard Hudson (R-NC). Identical companion legislation was introduced in the Senate (S.1022) by Senators Johnny Isakson (R-GA), John Cornyn (R-TX), and Tammy Duckworth (D-IL). The Mission Zero Act creates a grant program to assist civilian trauma centers in partnering with military trauma professionals to establish a pathway to provide patients with the highest quality of trauma care in times of peace and war, thus taking a step in the direction of the NAM report recommendations.
Specifically, the legislation provides for:
• $40 million in grants to fund military trauma teams and providers to embed into civilian trauma facilities.
o Trauma centers are eligible for a $1 million grant to host military trauma teams at eligible high-acuity level 1 trauma centers
o Trauma centers are also eligible for grants to host individual providers ($100,000 for physician or $50,000 for non-physician providers) at eligible level I, II, or III trauma centers
As of today, the House and Senate versions of the Mission Zero Act have 25co-sponsors and 2 co-sponsors respectively. The ACS would very much like to build some momentum for the Mission Zero Act going into the fall when it is expected that there will be several large “must pass” pieces of legislation working their way through Congress to which the Mission Zero Act could potentially be attached. Accordingly, I respectfully ask all Fellows to take a few moments to visit the SurgeonsVoice website at www.surgeonsvoice.org, click on the Take Action tab on the right side of the page and send a message to their individual representatives and senators seeking support for this important legislation.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
ACS Committee on Trauma series highlights effort to complete nation’s trauma system
Today in America, more people survive serious injury than any time in the past. Yet trauma remains the leading killer of young people and military service members during combat. Trauma has been characterized as the “neglected epidemic of our time.”
A 2016 report by the National Academies of Science, Engineering and Medicine (NASEM) has added new momentum to the effort to complete the nation’s trauma system. It found one in five trauma deaths could be prevented through stronger Federal leadership, greater research funding to improve outcomes, strengthening prehospital care, distributing trauma centers based on need and integrating military and civilian trauma care into one national trauma system.
In a five-part series of stories, “Putting the Pieces Together: A National Effort to Complete the U.S. Trauma System,” the American College of Surgeons Committee on Trauma will share steps being taken to complete the nation’s trauma system. Stories will look at the history of trauma care and the trauma system in America, partnerships with the military to translate battlefield lessons to the home front and back again, the challenges facing America’s trauma systems, and the steps leading experts are taking to fill the gaps in the system and achieve the goal of zero preventable deaths and disability from injury.
Read the series online at www.facs.org/trauma or follow the ACS COT on Twitter @ACSTrauma.
Today in America, more people survive serious injury than any time in the past. Yet trauma remains the leading killer of young people and military service members during combat. Trauma has been characterized as the “neglected epidemic of our time.”
A 2016 report by the National Academies of Science, Engineering and Medicine (NASEM) has added new momentum to the effort to complete the nation’s trauma system. It found one in five trauma deaths could be prevented through stronger Federal leadership, greater research funding to improve outcomes, strengthening prehospital care, distributing trauma centers based on need and integrating military and civilian trauma care into one national trauma system.
In a five-part series of stories, “Putting the Pieces Together: A National Effort to Complete the U.S. Trauma System,” the American College of Surgeons Committee on Trauma will share steps being taken to complete the nation’s trauma system. Stories will look at the history of trauma care and the trauma system in America, partnerships with the military to translate battlefield lessons to the home front and back again, the challenges facing America’s trauma systems, and the steps leading experts are taking to fill the gaps in the system and achieve the goal of zero preventable deaths and disability from injury.
Read the series online at www.facs.org/trauma or follow the ACS COT on Twitter @ACSTrauma.
Today in America, more people survive serious injury than any time in the past. Yet trauma remains the leading killer of young people and military service members during combat. Trauma has been characterized as the “neglected epidemic of our time.”
A 2016 report by the National Academies of Science, Engineering and Medicine (NASEM) has added new momentum to the effort to complete the nation’s trauma system. It found one in five trauma deaths could be prevented through stronger Federal leadership, greater research funding to improve outcomes, strengthening prehospital care, distributing trauma centers based on need and integrating military and civilian trauma care into one national trauma system.
In a five-part series of stories, “Putting the Pieces Together: A National Effort to Complete the U.S. Trauma System,” the American College of Surgeons Committee on Trauma will share steps being taken to complete the nation’s trauma system. Stories will look at the history of trauma care and the trauma system in America, partnerships with the military to translate battlefield lessons to the home front and back again, the challenges facing America’s trauma systems, and the steps leading experts are taking to fill the gaps in the system and achieve the goal of zero preventable deaths and disability from injury.
Read the series online at www.facs.org/trauma or follow the ACS COT on Twitter @ACSTrauma.
Cancer the most common diagnosis in palliative care patients
More than a quarter of the patients in palliative care have a primary diagnosis of cancer, according to the Center to Advance Palliative Care.
A survey of 351 palliative care programs showed that 27% of their patients had been diagnosed with cancer in 2016, more than twice as many patients who had a cardiac (13%) or pulmonary (12%) diagnosis. The next most common primary diagnosis category in 2016 was neurologic at 8%, with a tie at 6% between diagnoses classified as infectious or complex chronic, followed by patients with dementia at 5%, Maggie Rogers and Tamara Dumanovsky, PhD, of the CAPC reported.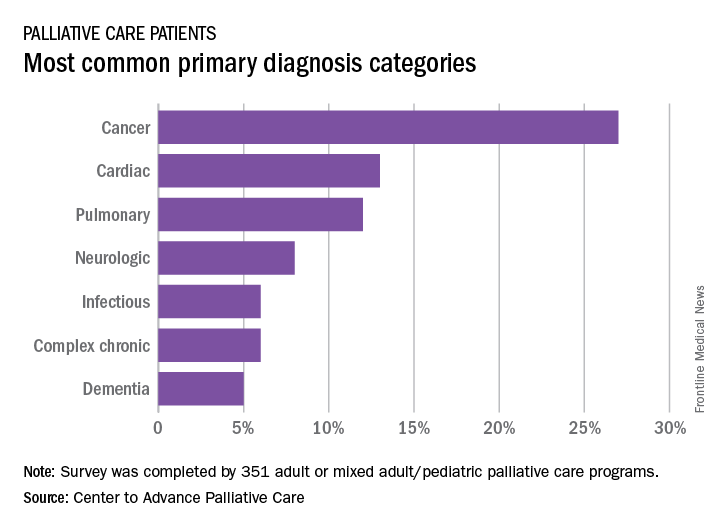
A medical/surgical unit was the referring site for 43% of palliative care referrals in 2016, with 26% of patients coming from an intensive care unit, 13% from a step-down unit, and 8% from an oncology unit, they noted.
More than a quarter of the patients in palliative care have a primary diagnosis of cancer, according to the Center to Advance Palliative Care.
A survey of 351 palliative care programs showed that 27% of their patients had been diagnosed with cancer in 2016, more than twice as many patients who had a cardiac (13%) or pulmonary (12%) diagnosis. The next most common primary diagnosis category in 2016 was neurologic at 8%, with a tie at 6% between diagnoses classified as infectious or complex chronic, followed by patients with dementia at 5%, Maggie Rogers and Tamara Dumanovsky, PhD, of the CAPC reported.
A medical/surgical unit was the referring site for 43% of palliative care referrals in 2016, with 26% of patients coming from an intensive care unit, 13% from a step-down unit, and 8% from an oncology unit, they noted.
More than a quarter of the patients in palliative care have a primary diagnosis of cancer, according to the Center to Advance Palliative Care.
A survey of 351 palliative care programs showed that 27% of their patients had been diagnosed with cancer in 2016, more than twice as many patients who had a cardiac (13%) or pulmonary (12%) diagnosis. The next most common primary diagnosis category in 2016 was neurologic at 8%, with a tie at 6% between diagnoses classified as infectious or complex chronic, followed by patients with dementia at 5%, Maggie Rogers and Tamara Dumanovsky, PhD, of the CAPC reported.
A medical/surgical unit was the referring site for 43% of palliative care referrals in 2016, with 26% of patients coming from an intensive care unit, 13% from a step-down unit, and 8% from an oncology unit, they noted.
Safety alert for intragastric balloon systems
The Food and Drug Administration announced a safety alert on Aug. 10, 2017, for liquid-filled intragastric balloon systems, as they have caused five reports of unanticipated deaths that occurred from 2016 to present in patients.
The cause or incidence of patient death is still unknown, and the FDA has not been able to definitively attribute the deaths to the devices or the insertion procedures for these devices. All five reports show that patient deaths occurred within a month or less of balloon placement. In three of the reports, death occurred as soon as 1-3 days after balloon placement. The FDA has also received two additional reports of deaths in the same time period related to potential complications associated with balloon treatment.
The FDA continues to recommend that health care providers closely monitor patients treated with these devices for complications. Any adverse events related to intragastric balloon systems should be reported through MedWatch. The FDA will keep the public informed as new information becomes available.
Read the full safety alert on the FDA’s website.
The Food and Drug Administration announced a safety alert on Aug. 10, 2017, for liquid-filled intragastric balloon systems, as they have caused five reports of unanticipated deaths that occurred from 2016 to present in patients.
The cause or incidence of patient death is still unknown, and the FDA has not been able to definitively attribute the deaths to the devices or the insertion procedures for these devices. All five reports show that patient deaths occurred within a month or less of balloon placement. In three of the reports, death occurred as soon as 1-3 days after balloon placement. The FDA has also received two additional reports of deaths in the same time period related to potential complications associated with balloon treatment.
The FDA continues to recommend that health care providers closely monitor patients treated with these devices for complications. Any adverse events related to intragastric balloon systems should be reported through MedWatch. The FDA will keep the public informed as new information becomes available.
Read the full safety alert on the FDA’s website.
The Food and Drug Administration announced a safety alert on Aug. 10, 2017, for liquid-filled intragastric balloon systems, as they have caused five reports of unanticipated deaths that occurred from 2016 to present in patients.
The cause or incidence of patient death is still unknown, and the FDA has not been able to definitively attribute the deaths to the devices or the insertion procedures for these devices. All five reports show that patient deaths occurred within a month or less of balloon placement. In three of the reports, death occurred as soon as 1-3 days after balloon placement. The FDA has also received two additional reports of deaths in the same time period related to potential complications associated with balloon treatment.
The FDA continues to recommend that health care providers closely monitor patients treated with these devices for complications. Any adverse events related to intragastric balloon systems should be reported through MedWatch. The FDA will keep the public informed as new information becomes available.
Read the full safety alert on the FDA’s website.
Contralateral nodal thyroid metastases show slow progression
BOSTON – More than a third of 63 patients with unilateral papillary thyroid carcinoma and ipsilateral lymph node metastases also had occult, contralateral, lateral-neck lymph nodes with metastases, but the low reported rate of contralateral neck recurrence has raised the question of whether routine resection of these contralateral lymph nodes benefits patients.
“Prophylactic contralateral lateral-neck dissection may not be relevant for patients with unilateral N1b tumors,” Dana Hartl, MD, PhD, said at the World Congress on Thyroid Cancer.

She envisioned a more targeted approach to using surgical resection of contralateral, lateral-neck lymph nodes. “We would still do this surgery for patients with lots of big, bulky nodules; it just takes an additional 10-20 minutes. It’s not that long or morbid. For patients with lots of [affected] nodes, you’ve got to clear it out. But for a patient with a small, level III node on one side I will no longer do [prophylactic, contralateral, lateral-neck lymph node removal].”
Dr. Hartl and her associates reviewed records for 63 patients with unilateral, unifocal papillary thyroid carcinoma who underwent prophylactic, contralateral, lymph node removal during 1997-2016. They ranged from 11-84 years old, and 60% had extrathyroidal extension of their primary tumor. The patients averaged having four lymph nodes with metastatic cells in the ipsilateral lateral neck, an average of five affected lymph nodes in the ipsilateral central neck, and an average of two affected lymph nodes in the contralateral central neck.
Among the 63 patients, 23 (37%) had metastases-containing lymph nodes at levels III and IV in the contralateral lateral neck, with a range of 1-17 metastases per node. All nodes were less than 1 cm in diameter. Extracapsular spread had occurred in 11 of the 23 cases.
The relatively frequent presence of metastases in the contralateral, lateral-neck lymph nodes contrasted with the reported low 5%-15% rate of recurrence in these lymph nodes in patients with N1b disease, Dr. Hartl said.
The analysis identified two factors that significantly linked with having contralateral, lateral-neck metastases: having a bilateral tumor with contralateral microcancer, or having at least four lymph nodes positive for metastases in the ipsilateral central compartment, she reported. When patients had fewer than five positive lymph nodes in the ipsilateral central neck, their risk for occult metastases in contralateral lymph nodes was 26%.
“It’s not very strong data; we were a little disappointed” with the results, Dr. Hartl said.
[email protected]
On Twitter @mitchelzoler
The finding reported by Dr. Hartl is consistent with recent experience with other tumor types, like prostate cancer, that often show low aggressiveness. The need to routinely resect what may be indolent microscopic metastases remains a big open question.
The dilemma for thyroid cancer was nicely summarized by Gilbert Welch, MD, and his associates who highlighted the risk of overdiagnosing thyroid cancer with aggressive screening. In South Korea, this resulted in a 15-fold increase in thyroid cancer diagnoses between 1993 and 2011, which led to substantial increases in the rates of thyroidectomy including patients with tumors too small to warrant surgery (N Engl J Med. 2014 Nov 6;371[19]:1765-7).

Pamela Hartzband, MD , is an endocrinologist at Beth Israel Deaconess Medical Center in Boston. She had no disclosures. She made these comments in an interview.
The finding reported by Dr. Hartl is consistent with recent experience with other tumor types, like prostate cancer, that often show low aggressiveness. The need to routinely resect what may be indolent microscopic metastases remains a big open question.
The dilemma for thyroid cancer was nicely summarized by Gilbert Welch, MD, and his associates who highlighted the risk of overdiagnosing thyroid cancer with aggressive screening. In South Korea, this resulted in a 15-fold increase in thyroid cancer diagnoses between 1993 and 2011, which led to substantial increases in the rates of thyroidectomy including patients with tumors too small to warrant surgery (N Engl J Med. 2014 Nov 6;371[19]:1765-7).
Pamela Hartzband, MD , is an endocrinologist at Beth Israel Deaconess Medical Center in Boston. She had no disclosures. She made these comments in an interview.
The finding reported by Dr. Hartl is consistent with recent experience with other tumor types, like prostate cancer, that often show low aggressiveness. The need to routinely resect what may be indolent microscopic metastases remains a big open question.
The dilemma for thyroid cancer was nicely summarized by Gilbert Welch, MD, and his associates who highlighted the risk of overdiagnosing thyroid cancer with aggressive screening. In South Korea, this resulted in a 15-fold increase in thyroid cancer diagnoses between 1993 and 2011, which led to substantial increases in the rates of thyroidectomy including patients with tumors too small to warrant surgery (N Engl J Med. 2014 Nov 6;371[19]:1765-7).
Pamela Hartzband, MD , is an endocrinologist at Beth Israel Deaconess Medical Center in Boston. She had no disclosures. She made these comments in an interview.
BOSTON – More than a third of 63 patients with unilateral papillary thyroid carcinoma and ipsilateral lymph node metastases also had occult, contralateral, lateral-neck lymph nodes with metastases, but the low reported rate of contralateral neck recurrence has raised the question of whether routine resection of these contralateral lymph nodes benefits patients.
“Prophylactic contralateral lateral-neck dissection may not be relevant for patients with unilateral N1b tumors,” Dana Hartl, MD, PhD, said at the World Congress on Thyroid Cancer.
She envisioned a more targeted approach to using surgical resection of contralateral, lateral-neck lymph nodes. “We would still do this surgery for patients with lots of big, bulky nodules; it just takes an additional 10-20 minutes. It’s not that long or morbid. For patients with lots of [affected] nodes, you’ve got to clear it out. But for a patient with a small, level III node on one side I will no longer do [prophylactic, contralateral, lateral-neck lymph node removal].”
Dr. Hartl and her associates reviewed records for 63 patients with unilateral, unifocal papillary thyroid carcinoma who underwent prophylactic, contralateral, lymph node removal during 1997-2016. They ranged from 11-84 years old, and 60% had extrathyroidal extension of their primary tumor. The patients averaged having four lymph nodes with metastatic cells in the ipsilateral lateral neck, an average of five affected lymph nodes in the ipsilateral central neck, and an average of two affected lymph nodes in the contralateral central neck.
Among the 63 patients, 23 (37%) had metastases-containing lymph nodes at levels III and IV in the contralateral lateral neck, with a range of 1-17 metastases per node. All nodes were less than 1 cm in diameter. Extracapsular spread had occurred in 11 of the 23 cases.
The relatively frequent presence of metastases in the contralateral, lateral-neck lymph nodes contrasted with the reported low 5%-15% rate of recurrence in these lymph nodes in patients with N1b disease, Dr. Hartl said.
The analysis identified two factors that significantly linked with having contralateral, lateral-neck metastases: having a bilateral tumor with contralateral microcancer, or having at least four lymph nodes positive for metastases in the ipsilateral central compartment, she reported. When patients had fewer than five positive lymph nodes in the ipsilateral central neck, their risk for occult metastases in contralateral lymph nodes was 26%.
“It’s not very strong data; we were a little disappointed” with the results, Dr. Hartl said.
[email protected]
On Twitter @mitchelzoler
BOSTON – More than a third of 63 patients with unilateral papillary thyroid carcinoma and ipsilateral lymph node metastases also had occult, contralateral, lateral-neck lymph nodes with metastases, but the low reported rate of contralateral neck recurrence has raised the question of whether routine resection of these contralateral lymph nodes benefits patients.
“Prophylactic contralateral lateral-neck dissection may not be relevant for patients with unilateral N1b tumors,” Dana Hartl, MD, PhD, said at the World Congress on Thyroid Cancer.
She envisioned a more targeted approach to using surgical resection of contralateral, lateral-neck lymph nodes. “We would still do this surgery for patients with lots of big, bulky nodules; it just takes an additional 10-20 minutes. It’s not that long or morbid. For patients with lots of [affected] nodes, you’ve got to clear it out. But for a patient with a small, level III node on one side I will no longer do [prophylactic, contralateral, lateral-neck lymph node removal].”
Dr. Hartl and her associates reviewed records for 63 patients with unilateral, unifocal papillary thyroid carcinoma who underwent prophylactic, contralateral, lymph node removal during 1997-2016. They ranged from 11-84 years old, and 60% had extrathyroidal extension of their primary tumor. The patients averaged having four lymph nodes with metastatic cells in the ipsilateral lateral neck, an average of five affected lymph nodes in the ipsilateral central neck, and an average of two affected lymph nodes in the contralateral central neck.
Among the 63 patients, 23 (37%) had metastases-containing lymph nodes at levels III and IV in the contralateral lateral neck, with a range of 1-17 metastases per node. All nodes were less than 1 cm in diameter. Extracapsular spread had occurred in 11 of the 23 cases.
The relatively frequent presence of metastases in the contralateral, lateral-neck lymph nodes contrasted with the reported low 5%-15% rate of recurrence in these lymph nodes in patients with N1b disease, Dr. Hartl said.
The analysis identified two factors that significantly linked with having contralateral, lateral-neck metastases: having a bilateral tumor with contralateral microcancer, or having at least four lymph nodes positive for metastases in the ipsilateral central compartment, she reported. When patients had fewer than five positive lymph nodes in the ipsilateral central neck, their risk for occult metastases in contralateral lymph nodes was 26%.
“It’s not very strong data; we were a little disappointed” with the results, Dr. Hartl said.
[email protected]
On Twitter @mitchelzoler
AT WCTC 2017
Key clinical point:
Major finding: Thirty-seven percent of patients with unilateral N1b thyroid tumors also had metastases in their contralateral lateral-neck lymph nodes.
Data source: Review of 63 patients treated at a single French center during a 20-year period.
Disclosures: Dr. Hartl had no disclosures.
Revised thyroid Bethesda System resets malignant risks
BOSTON – Under the newly revised Bethesda System for Reporting Thyroid Cytology, slated for official release in October 2017, the six cytology-based diagnostic categories for thyroid lesions stay exactly the same as in the 10-year-old first edition, but some associated malignancy risks have changed.
Important changes include molecular testing to further assess malignancy risk in thyroid nodules and the introduction of lobectomy as a treatment option, “which really wasn’t an option 10 years ago,” in the first iteration of the Bethesda System (New York: Springer US, 2010), its coauthor Edmund S. Cibas, MD, said at the World Congress on Thyroid Cancer.

An Endocrine Pathology Society working group created the NIFTP designation in 2016 to describe an encapsulated follicular variant of papillary thyroid carcinoma that is characterized by lack of invasion, a follicular growth pattern, and nuclear features of papillary thyroid carcinoma with a very low risk of an adverse outcome (JAMA Oncology. 2016 Aug;2[8]:1023-9) (Cancer Cytopathol. 2016 Sep;124[9]:616-20).
NIFTP is not an overt malignancy. The revised Bethesda System “limits malignancy to cases with features of classic malignant papillary thyroid carcinoma,” explained Dr. Cibas, professor of pathology at Harvard Medical School and director of cytopathology at Brigham and Women’s Hospital, both in Boston.
Because the Bethesda System categories link to specific management recommendations, the new edition orients patients toward more conservative management decisions, specifically lobectomies instead of total thyroidectomies, he said in an interview.
The International Cytology Congress held a symposium during its meeting in Yokohama, Japan, in 2016, which resulted in the second edition of the Bethesda System (ACTA Cytol. 2016 Sep-Oct; 60[5]:399-405).
The changes in risk of malignancy occurred primarily in two categories, either “atypia of undetermined significance” (AUS) or “follicular lesions of undetermined significance” (FLUS). The risk of malignancy jumped from 5%-15% in the Bethesda System first edition up to 10%-30% in the revision. A smaller bump-up hit the category of “follicular neoplasm” or “suspicious for follicular neoplasm,” in which the risk of malignancy increased from 20%-30% in the first edition to 25%-40% in the revision. And, in the suspicion of malignancy category, the risk of malignancy actually lowered modestly, easing from 60%-75% in the first edition to 50%-75% in the revision.
Dr. Cibas highlighted the AUS/FLUS category with further notable features. The limit on laboratories reporting this category increased to 10% of total reports, up from 7% in the first edition. Management changed from the single options of a repeat fine-needle aspiration specimen to either that or molecular testing. Also, “the first edition was not clear that AUS and FLUS are synonyms. That will be a lot clearer” in the second edition, Dr. Cibas promised. The revision “will encourage labs that currently use [the terms] AUS and FLUS to mean two different things to make a choice between them.”
Another quirk of the AUS and FLUS category is that the risk of malignancy estimates are based on what Dr. Cibas called “flawed” data from only the selected subset of AUS or FLUS patients who have their nodule resected. “The reality is that most of the nodules are not resected” from patients with AUS or FLUS, so conclusions about the risk of malignancy come from a subset with considerable selection bias.
The definition of “follicular neoplasm” or “suspicious for follicular neoplasm” category also added “mild nuclear changes,” which can include increased nuclear size, contour irregularity, or chromatin clearing. The “suspicious for malignancy” category made a modest tweak to the risk of malignancy. Plus, “some of these patients will now undergo lobectomy rather than total thyroidectomy, which has been usual management.
The “suspicious for malignant” and “malignant” categories had little change aside from wider use of lobectomy, now feasible for any patient except those with metastatic disease, Dr. Cibas said.
[email protected]
On Twitter @mitchelzoler
BOSTON – Under the newly revised Bethesda System for Reporting Thyroid Cytology, slated for official release in October 2017, the six cytology-based diagnostic categories for thyroid lesions stay exactly the same as in the 10-year-old first edition, but some associated malignancy risks have changed.
Important changes include molecular testing to further assess malignancy risk in thyroid nodules and the introduction of lobectomy as a treatment option, “which really wasn’t an option 10 years ago,” in the first iteration of the Bethesda System (New York: Springer US, 2010), its coauthor Edmund S. Cibas, MD, said at the World Congress on Thyroid Cancer.
An Endocrine Pathology Society working group created the NIFTP designation in 2016 to describe an encapsulated follicular variant of papillary thyroid carcinoma that is characterized by lack of invasion, a follicular growth pattern, and nuclear features of papillary thyroid carcinoma with a very low risk of an adverse outcome (JAMA Oncology. 2016 Aug;2[8]:1023-9) (Cancer Cytopathol. 2016 Sep;124[9]:616-20).
NIFTP is not an overt malignancy. The revised Bethesda System “limits malignancy to cases with features of classic malignant papillary thyroid carcinoma,” explained Dr. Cibas, professor of pathology at Harvard Medical School and director of cytopathology at Brigham and Women’s Hospital, both in Boston.
Because the Bethesda System categories link to specific management recommendations, the new edition orients patients toward more conservative management decisions, specifically lobectomies instead of total thyroidectomies, he said in an interview.
The International Cytology Congress held a symposium during its meeting in Yokohama, Japan, in 2016, which resulted in the second edition of the Bethesda System (ACTA Cytol. 2016 Sep-Oct; 60[5]:399-405).
The changes in risk of malignancy occurred primarily in two categories, either “atypia of undetermined significance” (AUS) or “follicular lesions of undetermined significance” (FLUS). The risk of malignancy jumped from 5%-15% in the Bethesda System first edition up to 10%-30% in the revision. A smaller bump-up hit the category of “follicular neoplasm” or “suspicious for follicular neoplasm,” in which the risk of malignancy increased from 20%-30% in the first edition to 25%-40% in the revision. And, in the suspicion of malignancy category, the risk of malignancy actually lowered modestly, easing from 60%-75% in the first edition to 50%-75% in the revision.
Dr. Cibas highlighted the AUS/FLUS category with further notable features. The limit on laboratories reporting this category increased to 10% of total reports, up from 7% in the first edition. Management changed from the single options of a repeat fine-needle aspiration specimen to either that or molecular testing. Also, “the first edition was not clear that AUS and FLUS are synonyms. That will be a lot clearer” in the second edition, Dr. Cibas promised. The revision “will encourage labs that currently use [the terms] AUS and FLUS to mean two different things to make a choice between them.”
Another quirk of the AUS and FLUS category is that the risk of malignancy estimates are based on what Dr. Cibas called “flawed” data from only the selected subset of AUS or FLUS patients who have their nodule resected. “The reality is that most of the nodules are not resected” from patients with AUS or FLUS, so conclusions about the risk of malignancy come from a subset with considerable selection bias.
The definition of “follicular neoplasm” or “suspicious for follicular neoplasm” category also added “mild nuclear changes,” which can include increased nuclear size, contour irregularity, or chromatin clearing. The “suspicious for malignancy” category made a modest tweak to the risk of malignancy. Plus, “some of these patients will now undergo lobectomy rather than total thyroidectomy, which has been usual management.
The “suspicious for malignant” and “malignant” categories had little change aside from wider use of lobectomy, now feasible for any patient except those with metastatic disease, Dr. Cibas said.
[email protected]
On Twitter @mitchelzoler
BOSTON – Under the newly revised Bethesda System for Reporting Thyroid Cytology, slated for official release in October 2017, the six cytology-based diagnostic categories for thyroid lesions stay exactly the same as in the 10-year-old first edition, but some associated malignancy risks have changed.
Important changes include molecular testing to further assess malignancy risk in thyroid nodules and the introduction of lobectomy as a treatment option, “which really wasn’t an option 10 years ago,” in the first iteration of the Bethesda System (New York: Springer US, 2010), its coauthor Edmund S. Cibas, MD, said at the World Congress on Thyroid Cancer.
An Endocrine Pathology Society working group created the NIFTP designation in 2016 to describe an encapsulated follicular variant of papillary thyroid carcinoma that is characterized by lack of invasion, a follicular growth pattern, and nuclear features of papillary thyroid carcinoma with a very low risk of an adverse outcome (JAMA Oncology. 2016 Aug;2[8]:1023-9) (Cancer Cytopathol. 2016 Sep;124[9]:616-20).
NIFTP is not an overt malignancy. The revised Bethesda System “limits malignancy to cases with features of classic malignant papillary thyroid carcinoma,” explained Dr. Cibas, professor of pathology at Harvard Medical School and director of cytopathology at Brigham and Women’s Hospital, both in Boston.
Because the Bethesda System categories link to specific management recommendations, the new edition orients patients toward more conservative management decisions, specifically lobectomies instead of total thyroidectomies, he said in an interview.
The International Cytology Congress held a symposium during its meeting in Yokohama, Japan, in 2016, which resulted in the second edition of the Bethesda System (ACTA Cytol. 2016 Sep-Oct; 60[5]:399-405).
The changes in risk of malignancy occurred primarily in two categories, either “atypia of undetermined significance” (AUS) or “follicular lesions of undetermined significance” (FLUS). The risk of malignancy jumped from 5%-15% in the Bethesda System first edition up to 10%-30% in the revision. A smaller bump-up hit the category of “follicular neoplasm” or “suspicious for follicular neoplasm,” in which the risk of malignancy increased from 20%-30% in the first edition to 25%-40% in the revision. And, in the suspicion of malignancy category, the risk of malignancy actually lowered modestly, easing from 60%-75% in the first edition to 50%-75% in the revision.
Dr. Cibas highlighted the AUS/FLUS category with further notable features. The limit on laboratories reporting this category increased to 10% of total reports, up from 7% in the first edition. Management changed from the single options of a repeat fine-needle aspiration specimen to either that or molecular testing. Also, “the first edition was not clear that AUS and FLUS are synonyms. That will be a lot clearer” in the second edition, Dr. Cibas promised. The revision “will encourage labs that currently use [the terms] AUS and FLUS to mean two different things to make a choice between them.”
Another quirk of the AUS and FLUS category is that the risk of malignancy estimates are based on what Dr. Cibas called “flawed” data from only the selected subset of AUS or FLUS patients who have their nodule resected. “The reality is that most of the nodules are not resected” from patients with AUS or FLUS, so conclusions about the risk of malignancy come from a subset with considerable selection bias.
The definition of “follicular neoplasm” or “suspicious for follicular neoplasm” category also added “mild nuclear changes,” which can include increased nuclear size, contour irregularity, or chromatin clearing. The “suspicious for malignancy” category made a modest tweak to the risk of malignancy. Plus, “some of these patients will now undergo lobectomy rather than total thyroidectomy, which has been usual management.
The “suspicious for malignant” and “malignant” categories had little change aside from wider use of lobectomy, now feasible for any patient except those with metastatic disease, Dr. Cibas said.
[email protected]
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM WCTC 2017