User login
Official Newspaper of the American College of Surgeons
Acute cholecystitis guidelines need work
SCOTTSDALE, ARIZ. – In patients with right upper quadrant pain, the Tokyo Guidelines (TG13) failed to detect acute cholecystitis with adequate sensitivity, according to a single institution retrospective review.
Researchers at the University of Arizona, Tucson, also found that the Tokyo Guidelines’ advice to manage grade II and grade III cholecystitis patients conservatively may be unwarranted, because there were no differences in safety outcomes between grade I and grade II patients who underwent early cholecystectomy.

The Tokyo Guidelines were based on expert opinion rather than evidence, and may be limited by differences in practices in Japan and other countries. “There was no formal evaluation of the sensitivity and specificity in any other country,” Faisal Jehan, MD, a research fellow at the University of Arizona, said in an interview. Dr. Jehan presented the study at the annual meeting of the Western Surgical Association.
The study suggests there is additional work to be done before the guidelines are more generally applicable. They are being updated and the new version is slated to appear in 2018.
Cholecystectomy is one of the most common procedures in the United States, and hence represents a major source of health care expenditure. Useful guidelines will therefore be welcome to help standardize treatment, according to Dr. Riall. “I think while we’ve moved as a population toward earlier cholecystectomy, it isn’t uniformly practiced in the United States. So I think there is value in having guidelines that are relevant to our population and relevant to our practice,” she said.
But compared with the pathology report, the TG13 guidelines fared poorly in prediction of acute cholecystitis, with a sensitivity of just 53% (definitive 27%, suspected 26%, undiagnosed 53%). The underperformance of the guidelines may be due in part to recent changes in health-seeking behavior, as patients are likely to get to the hospital more quickly than in the past, and thus exhibit fewer clinical signs when first examined. “That could be decreasing the sensitivity,” said Dr. Jehan.
Suspicious that the guidelines were inadequate, the researchers analyzed their institution’s Emergency General Surgery registry, examining records from 952 patients who presented with right upper quadrant pain between 2013 and 2015. They compared diagnoses and severity assessed using the TG13 guidelines to the ensuing pathology reports, which were obtained from patient charts.
A total of 857 patients of the 952 had biliary disease. Of these, 779 patients went on to cholecystectomy, 15 had cholecystostomy-tube placement, and 63 were managed conservatively with no surgery. Among patients with biliary disease, the frequency of fever at presentation was just 4%, while 51.8% had leukocytosis. Right upper quadrant tenderness was the most sensitive predictor of acute cholecystitis (92%). Murphy’s sign occurred in 28.8% of patients and had a 72% sensitivity.
Following the TG13 guidelines resulted in classification of 414 patients as grade I, 400 as grade II, and 43 as grade III. A total of 92.5% of grade I patients underwent early cholecystectomy, as the TG-13 guidelines suggest. Nearly as many (89.3%) grade II patients also underwent early surgery, as did 50% of grade III patients. The complication rate was similar between grade I and grade II patients who underwent surgery (3.7% vs. 4.7%; P = .81). The rate of return to the operating room was also similar (0.6% vs. 0.7%; P = .95), as was mortality (0.3% vs. 0%; P = .96).
SCOTTSDALE, ARIZ. – In patients with right upper quadrant pain, the Tokyo Guidelines (TG13) failed to detect acute cholecystitis with adequate sensitivity, according to a single institution retrospective review.
Researchers at the University of Arizona, Tucson, also found that the Tokyo Guidelines’ advice to manage grade II and grade III cholecystitis patients conservatively may be unwarranted, because there were no differences in safety outcomes between grade I and grade II patients who underwent early cholecystectomy.
The Tokyo Guidelines were based on expert opinion rather than evidence, and may be limited by differences in practices in Japan and other countries. “There was no formal evaluation of the sensitivity and specificity in any other country,” Faisal Jehan, MD, a research fellow at the University of Arizona, said in an interview. Dr. Jehan presented the study at the annual meeting of the Western Surgical Association.
The study suggests there is additional work to be done before the guidelines are more generally applicable. They are being updated and the new version is slated to appear in 2018.
Cholecystectomy is one of the most common procedures in the United States, and hence represents a major source of health care expenditure. Useful guidelines will therefore be welcome to help standardize treatment, according to Dr. Riall. “I think while we’ve moved as a population toward earlier cholecystectomy, it isn’t uniformly practiced in the United States. So I think there is value in having guidelines that are relevant to our population and relevant to our practice,” she said.
But compared with the pathology report, the TG13 guidelines fared poorly in prediction of acute cholecystitis, with a sensitivity of just 53% (definitive 27%, suspected 26%, undiagnosed 53%). The underperformance of the guidelines may be due in part to recent changes in health-seeking behavior, as patients are likely to get to the hospital more quickly than in the past, and thus exhibit fewer clinical signs when first examined. “That could be decreasing the sensitivity,” said Dr. Jehan.
Suspicious that the guidelines were inadequate, the researchers analyzed their institution’s Emergency General Surgery registry, examining records from 952 patients who presented with right upper quadrant pain between 2013 and 2015. They compared diagnoses and severity assessed using the TG13 guidelines to the ensuing pathology reports, which were obtained from patient charts.
A total of 857 patients of the 952 had biliary disease. Of these, 779 patients went on to cholecystectomy, 15 had cholecystostomy-tube placement, and 63 were managed conservatively with no surgery. Among patients with biliary disease, the frequency of fever at presentation was just 4%, while 51.8% had leukocytosis. Right upper quadrant tenderness was the most sensitive predictor of acute cholecystitis (92%). Murphy’s sign occurred in 28.8% of patients and had a 72% sensitivity.
Following the TG13 guidelines resulted in classification of 414 patients as grade I, 400 as grade II, and 43 as grade III. A total of 92.5% of grade I patients underwent early cholecystectomy, as the TG-13 guidelines suggest. Nearly as many (89.3%) grade II patients also underwent early surgery, as did 50% of grade III patients. The complication rate was similar between grade I and grade II patients who underwent surgery (3.7% vs. 4.7%; P = .81). The rate of return to the operating room was also similar (0.6% vs. 0.7%; P = .95), as was mortality (0.3% vs. 0%; P = .96).
SCOTTSDALE, ARIZ. – In patients with right upper quadrant pain, the Tokyo Guidelines (TG13) failed to detect acute cholecystitis with adequate sensitivity, according to a single institution retrospective review.
Researchers at the University of Arizona, Tucson, also found that the Tokyo Guidelines’ advice to manage grade II and grade III cholecystitis patients conservatively may be unwarranted, because there were no differences in safety outcomes between grade I and grade II patients who underwent early cholecystectomy.
The Tokyo Guidelines were based on expert opinion rather than evidence, and may be limited by differences in practices in Japan and other countries. “There was no formal evaluation of the sensitivity and specificity in any other country,” Faisal Jehan, MD, a research fellow at the University of Arizona, said in an interview. Dr. Jehan presented the study at the annual meeting of the Western Surgical Association.
The study suggests there is additional work to be done before the guidelines are more generally applicable. They are being updated and the new version is slated to appear in 2018.
Cholecystectomy is one of the most common procedures in the United States, and hence represents a major source of health care expenditure. Useful guidelines will therefore be welcome to help standardize treatment, according to Dr. Riall. “I think while we’ve moved as a population toward earlier cholecystectomy, it isn’t uniformly practiced in the United States. So I think there is value in having guidelines that are relevant to our population and relevant to our practice,” she said.
But compared with the pathology report, the TG13 guidelines fared poorly in prediction of acute cholecystitis, with a sensitivity of just 53% (definitive 27%, suspected 26%, undiagnosed 53%). The underperformance of the guidelines may be due in part to recent changes in health-seeking behavior, as patients are likely to get to the hospital more quickly than in the past, and thus exhibit fewer clinical signs when first examined. “That could be decreasing the sensitivity,” said Dr. Jehan.
Suspicious that the guidelines were inadequate, the researchers analyzed their institution’s Emergency General Surgery registry, examining records from 952 patients who presented with right upper quadrant pain between 2013 and 2015. They compared diagnoses and severity assessed using the TG13 guidelines to the ensuing pathology reports, which were obtained from patient charts.
A total of 857 patients of the 952 had biliary disease. Of these, 779 patients went on to cholecystectomy, 15 had cholecystostomy-tube placement, and 63 were managed conservatively with no surgery. Among patients with biliary disease, the frequency of fever at presentation was just 4%, while 51.8% had leukocytosis. Right upper quadrant tenderness was the most sensitive predictor of acute cholecystitis (92%). Murphy’s sign occurred in 28.8% of patients and had a 72% sensitivity.
Following the TG13 guidelines resulted in classification of 414 patients as grade I, 400 as grade II, and 43 as grade III. A total of 92.5% of grade I patients underwent early cholecystectomy, as the TG-13 guidelines suggest. Nearly as many (89.3%) grade II patients also underwent early surgery, as did 50% of grade III patients. The complication rate was similar between grade I and grade II patients who underwent surgery (3.7% vs. 4.7%; P = .81). The rate of return to the operating room was also similar (0.6% vs. 0.7%; P = .95), as was mortality (0.3% vs. 0%; P = .96).
AT WSA 2017
Key clinical point: Early surgery for acute cholecystitis appears safe in well selected patients.
Major finding: TG13 guidelines predicted acute cholecystitis with a sensitivity of 53%.
Data source: Analysis of a prospectively collected data on 952 patients at a single institution.
Disclosures: The study received no outside funding. Dr. Jehan and Dr. Riall reported having no financial disclosures.
Breast cancer margin guidelines reduced re-excisions, cost
SCOTTSDALE, ARIZ. – In breast conservation surgery with whole-breast radiation, costs and the number of re-excisions performed at a single institution dropped after the implementation of 2014 consensus guidelines on excision margins.
The guidelines, created by a multidisciplinary margins panel convened by the Society of Surgical Oncology and the American Society for Radiation Oncology recommend “no ink on tumor” as an adequate margin in cases of invasive carcinoma.
The guidelines sought to reduce costs and re-excision rates and improve cosmetic outcomes. The results of the study carried out at the University of Louisville suggest that the guidelines may be successful in achieving these goals. The reduced need for re-excision is a key point. “That’s very traumatic for the patient. With this consensus, we were able to decrease that, improve patient satisfaction, and decrease the cost,” lead author Nicolás Ajkay, MD, assistant professor of surgery at the University of Louisville School of Medicine, said in an interview.
Dr. Ajkay presented the results of the study at the annual meeting of the Western Surgical Association.
“Surgeons need to be aware of the guidelines, and if the margin is close, they need to be in multidisciplinary discussions with other breast cancer experts to determine which patients would benefit from going back to the operating room,” he said.
The researchers examined the experiences of 237 patients with stage I or stage II invasive carcinoma who had a partial mastectomy. Of these patients, 126 underwent the procedure before the university incorporated the guidelines in March 2014 (PRE), while 111 were seen after that date (POST). The study excluded those who were diagnosed by excisional biopsy and those who were treated with neoadjuvant chemotherapy.
Per-patient operative costs went down on average after the guidelines were implemented ($4,247 vs. $5,465; difference, $1,218; P less than .001). The estimated savings for the entire POST cohort of 111 patients was approximately $135,000.
Patient satisfaction improved as measured by the breast satisfaction domain of the BREAST-Q survey tool (77/100 vs. 61/100; P = .03).
A multivariate analysis showed that the implementation of the consensus statement predicted lower re-excision rates (odds ratio, 0.17; 95% confidence interval, 0.08-0.38; P less than .001) as well as lower operative cost per patient (cost greater than $5,465 OR, 0.14; 95% CI, 0.07-0.30; P less than .001). Guideline implementation did not, however, predict decreased total resection volume, or probability of conversion to mastectomy.
Perhaps because diagnostic methods have improved over time, there were some significant differences between the two populations. The PRE group had a larger median tumor size (1.5 cm vs. 1.1 cm; P less than .001), and a lower proportion of the PRE group was diagnosed as stage I (62% vs. 77%; P = .005). The PRE group also had significantly larger initial resection volume (69.3 cm3 versus 47.1 cm3; P = .02), higher selective margin volume (50.0 cm3 vs. 11.3 cm3; P less than .001), and a larger final resection volume (81.0 cm3 vs. 51.5 cm3; P = .05). Additional selective margin resection was less frequent in the PRE group (76% vs. 41%; P less than .001).
Those differences may confound the findings, since outcomes might have been expected to improve anyway due to improvements in care.
One member of the audience asked whether the guidelines might boost rates of cancer recurrence. It’s too soon to tell, according to Dr. Ajkay, who said that researchers will need at least 4 or 5 years of clinical experience to make that determination. But he is optimistic. “Even though we’re excising less, I would predict we will not see an increase in recurrence, because adjuvant therapy is getting significantly better, and adjuvant therapy reduces the risk of recurrence just as margin re-excisions do,” he said.
The study received no external funding. Dr. Ajkay reported having no financial disclosures.
SCOTTSDALE, ARIZ. – In breast conservation surgery with whole-breast radiation, costs and the number of re-excisions performed at a single institution dropped after the implementation of 2014 consensus guidelines on excision margins.
The guidelines, created by a multidisciplinary margins panel convened by the Society of Surgical Oncology and the American Society for Radiation Oncology recommend “no ink on tumor” as an adequate margin in cases of invasive carcinoma.
The guidelines sought to reduce costs and re-excision rates and improve cosmetic outcomes. The results of the study carried out at the University of Louisville suggest that the guidelines may be successful in achieving these goals. The reduced need for re-excision is a key point. “That’s very traumatic for the patient. With this consensus, we were able to decrease that, improve patient satisfaction, and decrease the cost,” lead author Nicolás Ajkay, MD, assistant professor of surgery at the University of Louisville School of Medicine, said in an interview.
Dr. Ajkay presented the results of the study at the annual meeting of the Western Surgical Association.
“Surgeons need to be aware of the guidelines, and if the margin is close, they need to be in multidisciplinary discussions with other breast cancer experts to determine which patients would benefit from going back to the operating room,” he said.
The researchers examined the experiences of 237 patients with stage I or stage II invasive carcinoma who had a partial mastectomy. Of these patients, 126 underwent the procedure before the university incorporated the guidelines in March 2014 (PRE), while 111 were seen after that date (POST). The study excluded those who were diagnosed by excisional biopsy and those who were treated with neoadjuvant chemotherapy.
Per-patient operative costs went down on average after the guidelines were implemented ($4,247 vs. $5,465; difference, $1,218; P less than .001). The estimated savings for the entire POST cohort of 111 patients was approximately $135,000.
Patient satisfaction improved as measured by the breast satisfaction domain of the BREAST-Q survey tool (77/100 vs. 61/100; P = .03).
A multivariate analysis showed that the implementation of the consensus statement predicted lower re-excision rates (odds ratio, 0.17; 95% confidence interval, 0.08-0.38; P less than .001) as well as lower operative cost per patient (cost greater than $5,465 OR, 0.14; 95% CI, 0.07-0.30; P less than .001). Guideline implementation did not, however, predict decreased total resection volume, or probability of conversion to mastectomy.
Perhaps because diagnostic methods have improved over time, there were some significant differences between the two populations. The PRE group had a larger median tumor size (1.5 cm vs. 1.1 cm; P less than .001), and a lower proportion of the PRE group was diagnosed as stage I (62% vs. 77%; P = .005). The PRE group also had significantly larger initial resection volume (69.3 cm3 versus 47.1 cm3; P = .02), higher selective margin volume (50.0 cm3 vs. 11.3 cm3; P less than .001), and a larger final resection volume (81.0 cm3 vs. 51.5 cm3; P = .05). Additional selective margin resection was less frequent in the PRE group (76% vs. 41%; P less than .001).
Those differences may confound the findings, since outcomes might have been expected to improve anyway due to improvements in care.
One member of the audience asked whether the guidelines might boost rates of cancer recurrence. It’s too soon to tell, according to Dr. Ajkay, who said that researchers will need at least 4 or 5 years of clinical experience to make that determination. But he is optimistic. “Even though we’re excising less, I would predict we will not see an increase in recurrence, because adjuvant therapy is getting significantly better, and adjuvant therapy reduces the risk of recurrence just as margin re-excisions do,” he said.
The study received no external funding. Dr. Ajkay reported having no financial disclosures.
SCOTTSDALE, ARIZ. – In breast conservation surgery with whole-breast radiation, costs and the number of re-excisions performed at a single institution dropped after the implementation of 2014 consensus guidelines on excision margins.
The guidelines, created by a multidisciplinary margins panel convened by the Society of Surgical Oncology and the American Society for Radiation Oncology recommend “no ink on tumor” as an adequate margin in cases of invasive carcinoma.
The guidelines sought to reduce costs and re-excision rates and improve cosmetic outcomes. The results of the study carried out at the University of Louisville suggest that the guidelines may be successful in achieving these goals. The reduced need for re-excision is a key point. “That’s very traumatic for the patient. With this consensus, we were able to decrease that, improve patient satisfaction, and decrease the cost,” lead author Nicolás Ajkay, MD, assistant professor of surgery at the University of Louisville School of Medicine, said in an interview.
Dr. Ajkay presented the results of the study at the annual meeting of the Western Surgical Association.
“Surgeons need to be aware of the guidelines, and if the margin is close, they need to be in multidisciplinary discussions with other breast cancer experts to determine which patients would benefit from going back to the operating room,” he said.
The researchers examined the experiences of 237 patients with stage I or stage II invasive carcinoma who had a partial mastectomy. Of these patients, 126 underwent the procedure before the university incorporated the guidelines in March 2014 (PRE), while 111 were seen after that date (POST). The study excluded those who were diagnosed by excisional biopsy and those who were treated with neoadjuvant chemotherapy.
Per-patient operative costs went down on average after the guidelines were implemented ($4,247 vs. $5,465; difference, $1,218; P less than .001). The estimated savings for the entire POST cohort of 111 patients was approximately $135,000.
Patient satisfaction improved as measured by the breast satisfaction domain of the BREAST-Q survey tool (77/100 vs. 61/100; P = .03).
A multivariate analysis showed that the implementation of the consensus statement predicted lower re-excision rates (odds ratio, 0.17; 95% confidence interval, 0.08-0.38; P less than .001) as well as lower operative cost per patient (cost greater than $5,465 OR, 0.14; 95% CI, 0.07-0.30; P less than .001). Guideline implementation did not, however, predict decreased total resection volume, or probability of conversion to mastectomy.
Perhaps because diagnostic methods have improved over time, there were some significant differences between the two populations. The PRE group had a larger median tumor size (1.5 cm vs. 1.1 cm; P less than .001), and a lower proportion of the PRE group was diagnosed as stage I (62% vs. 77%; P = .005). The PRE group also had significantly larger initial resection volume (69.3 cm3 versus 47.1 cm3; P = .02), higher selective margin volume (50.0 cm3 vs. 11.3 cm3; P less than .001), and a larger final resection volume (81.0 cm3 vs. 51.5 cm3; P = .05). Additional selective margin resection was less frequent in the PRE group (76% vs. 41%; P less than .001).
Those differences may confound the findings, since outcomes might have been expected to improve anyway due to improvements in care.
One member of the audience asked whether the guidelines might boost rates of cancer recurrence. It’s too soon to tell, according to Dr. Ajkay, who said that researchers will need at least 4 or 5 years of clinical experience to make that determination. But he is optimistic. “Even though we’re excising less, I would predict we will not see an increase in recurrence, because adjuvant therapy is getting significantly better, and adjuvant therapy reduces the risk of recurrence just as margin re-excisions do,” he said.
The study received no external funding. Dr. Ajkay reported having no financial disclosures.
AT WSA 2017
Key clinical point: Breast cancer margin guidelines may help reduce re-excisions and lower costs.
Major finding: Operative costs per patient fell by $1,218 after the adoption of the “no ink on tumor” guidelines.
Data source: Retrospective analysis of 237 patients undergoing breast conservation surgery.
Disclosures: The study received no external funding. Dr. Ajkay reported having no financial disclosures.
VIDEO: MBSAQIP data looks at sleeve gastrectomy outcomes
Surgeon Matthew A. Hutter, MD, FACS, discusses the first report from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP) focused on laparoscopic sleeve gastrectomy. The study (Ann Surg. 2016;264[3]:464-73) looked at outcomes, methods, and complications of this procedure based on a database of nearly 190,000 patients, more than 1,600 surgeons, and 720 centers. Dr. Hutter said that is high-quality data that offers surgeons good information on the procedure.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Surgeon Matthew A. Hutter, MD, FACS, discusses the first report from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP) focused on laparoscopic sleeve gastrectomy. The study (Ann Surg. 2016;264[3]:464-73) looked at outcomes, methods, and complications of this procedure based on a database of nearly 190,000 patients, more than 1,600 surgeons, and 720 centers. Dr. Hutter said that is high-quality data that offers surgeons good information on the procedure.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Surgeon Matthew A. Hutter, MD, FACS, discusses the first report from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP) focused on laparoscopic sleeve gastrectomy. The study (Ann Surg. 2016;264[3]:464-73) looked at outcomes, methods, and complications of this procedure based on a database of nearly 190,000 patients, more than 1,600 surgeons, and 720 centers. Dr. Hutter said that is high-quality data that offers surgeons good information on the procedure.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Gastrectomy mortality risk increased fivefold with same-day discharge
NATIONAL HARBOR, MD. – Laparoscopic sleeve gastrectomy has been associated with low mortality, but the mortality is even lower when it includes overnight observation, according to a national database evaluation.
Among patients discharged on the same day, 30-day mortality was 0.1%, but it fell to 0.02% among patients discharged the following day, according to Colette Inaba, MD, a surgery resident at the University of California, Irvine.*

“Surgeons who are considering same-day discharge in sleeve gastrectomy patients should have a low threshold to admit these patients for overnight observation given our findings,” Dr. Inaba reported at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society.
Same-day discharge has been associated with an increased mortality risk in previously published descriptive institutional reviews, but this is the first study to evaluate this question through analysis of a national database, according to Dr. Inaba. It was based on 37,301 laparoscopic sleeve gastrectomy cases performed in 2015 and submitted to the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database. All participants in this database are accredited bariatric centers.
There were baseline differences between same-day and next-day discharges, but many of these differences conferred the next-day group with higher risk. In particular, the next-day group had significantly higher rates of hypertension, diabetes mellitus, hypercholesterolemia, chronic obstructive pulmonary disease, and sleep apnea. On average, the procedure time was 13 minutes longer in the next-day versus the same-day discharge groups.
In addition to mortality, 30-day morbidity and need for revisions were compared between the two groups, but there were no significant differences between groups in the rates of these outcomes.
Overall, the baseline demographics of the patients in same-day and next-day groups were comparable, according to Dr. Inaba. She described the population as predominantly female and white with an average body mass index of 45 kg/m2. In this analysis, only primary procedures (excluding redos and revisions) were included.
Relative to the next-day discharge cases, a significantly higher percentage of same-day discharge procedures were performed with a surgical tech or another provider rather than a designated first-assist surgeon, according to Dr. Inaba. For next-day cases, a higher percentage was performed with the participation of fellows or surgical residents. There were fewer swallow studies performed before discharge in the same-day discharge group.
Very similar results were generated by a study evaluating same-day discharge after laparoscopic Roux-en-Y gastric bypass, according to John M. Morton, MD, chief of bariatric and minimally invasive surgery, Stanford (Calif.) University. Dr. Morton, first author of the study and moderator of the session in which Dr. Inaba presented the LSG data, reported that same-day discharge in that study was also associated with a trend for an increased risk of serious complications (Ann Surg. 2014;259:286-92).
“Same-day discharge is often reimbursed at a lower rate, so there is less pay and patients are at greater risk of harm,” Dr. Morton said.
The reasons that same-day discharge is associated with higher mortality cannot be derived from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database, but, Dr. Inaba said, “Our thought is it is a function of failure to rescue patients from respiratory complications.” She acknowledged that this is a speculative assessment not supported by data, but she suggested that history of sleep apnea might be a particular indication to consider next-day discharge.
Dr. Inaba reports no financial relationships relevant to this topic.
Correction, 12/4/17: An earlier version of this article misstated the 30-day mortality among patients discharged the next day.
NATIONAL HARBOR, MD. – Laparoscopic sleeve gastrectomy has been associated with low mortality, but the mortality is even lower when it includes overnight observation, according to a national database evaluation.
Among patients discharged on the same day, 30-day mortality was 0.1%, but it fell to 0.02% among patients discharged the following day, according to Colette Inaba, MD, a surgery resident at the University of California, Irvine.*
“Surgeons who are considering same-day discharge in sleeve gastrectomy patients should have a low threshold to admit these patients for overnight observation given our findings,” Dr. Inaba reported at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society.
Same-day discharge has been associated with an increased mortality risk in previously published descriptive institutional reviews, but this is the first study to evaluate this question through analysis of a national database, according to Dr. Inaba. It was based on 37,301 laparoscopic sleeve gastrectomy cases performed in 2015 and submitted to the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database. All participants in this database are accredited bariatric centers.
There were baseline differences between same-day and next-day discharges, but many of these differences conferred the next-day group with higher risk. In particular, the next-day group had significantly higher rates of hypertension, diabetes mellitus, hypercholesterolemia, chronic obstructive pulmonary disease, and sleep apnea. On average, the procedure time was 13 minutes longer in the next-day versus the same-day discharge groups.
In addition to mortality, 30-day morbidity and need for revisions were compared between the two groups, but there were no significant differences between groups in the rates of these outcomes.
Overall, the baseline demographics of the patients in same-day and next-day groups were comparable, according to Dr. Inaba. She described the population as predominantly female and white with an average body mass index of 45 kg/m2. In this analysis, only primary procedures (excluding redos and revisions) were included.
Relative to the next-day discharge cases, a significantly higher percentage of same-day discharge procedures were performed with a surgical tech or another provider rather than a designated first-assist surgeon, according to Dr. Inaba. For next-day cases, a higher percentage was performed with the participation of fellows or surgical residents. There were fewer swallow studies performed before discharge in the same-day discharge group.
Very similar results were generated by a study evaluating same-day discharge after laparoscopic Roux-en-Y gastric bypass, according to John M. Morton, MD, chief of bariatric and minimally invasive surgery, Stanford (Calif.) University. Dr. Morton, first author of the study and moderator of the session in which Dr. Inaba presented the LSG data, reported that same-day discharge in that study was also associated with a trend for an increased risk of serious complications (Ann Surg. 2014;259:286-92).
“Same-day discharge is often reimbursed at a lower rate, so there is less pay and patients are at greater risk of harm,” Dr. Morton said.
The reasons that same-day discharge is associated with higher mortality cannot be derived from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database, but, Dr. Inaba said, “Our thought is it is a function of failure to rescue patients from respiratory complications.” She acknowledged that this is a speculative assessment not supported by data, but she suggested that history of sleep apnea might be a particular indication to consider next-day discharge.
Dr. Inaba reports no financial relationships relevant to this topic.
Correction, 12/4/17: An earlier version of this article misstated the 30-day mortality among patients discharged the next day.
NATIONAL HARBOR, MD. – Laparoscopic sleeve gastrectomy has been associated with low mortality, but the mortality is even lower when it includes overnight observation, according to a national database evaluation.
Among patients discharged on the same day, 30-day mortality was 0.1%, but it fell to 0.02% among patients discharged the following day, according to Colette Inaba, MD, a surgery resident at the University of California, Irvine.*
“Surgeons who are considering same-day discharge in sleeve gastrectomy patients should have a low threshold to admit these patients for overnight observation given our findings,” Dr. Inaba reported at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society.
Same-day discharge has been associated with an increased mortality risk in previously published descriptive institutional reviews, but this is the first study to evaluate this question through analysis of a national database, according to Dr. Inaba. It was based on 37,301 laparoscopic sleeve gastrectomy cases performed in 2015 and submitted to the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database. All participants in this database are accredited bariatric centers.
There were baseline differences between same-day and next-day discharges, but many of these differences conferred the next-day group with higher risk. In particular, the next-day group had significantly higher rates of hypertension, diabetes mellitus, hypercholesterolemia, chronic obstructive pulmonary disease, and sleep apnea. On average, the procedure time was 13 minutes longer in the next-day versus the same-day discharge groups.
In addition to mortality, 30-day morbidity and need for revisions were compared between the two groups, but there were no significant differences between groups in the rates of these outcomes.
Overall, the baseline demographics of the patients in same-day and next-day groups were comparable, according to Dr. Inaba. She described the population as predominantly female and white with an average body mass index of 45 kg/m2. In this analysis, only primary procedures (excluding redos and revisions) were included.
Relative to the next-day discharge cases, a significantly higher percentage of same-day discharge procedures were performed with a surgical tech or another provider rather than a designated first-assist surgeon, according to Dr. Inaba. For next-day cases, a higher percentage was performed with the participation of fellows or surgical residents. There were fewer swallow studies performed before discharge in the same-day discharge group.
Very similar results were generated by a study evaluating same-day discharge after laparoscopic Roux-en-Y gastric bypass, according to John M. Morton, MD, chief of bariatric and minimally invasive surgery, Stanford (Calif.) University. Dr. Morton, first author of the study and moderator of the session in which Dr. Inaba presented the LSG data, reported that same-day discharge in that study was also associated with a trend for an increased risk of serious complications (Ann Surg. 2014;259:286-92).
“Same-day discharge is often reimbursed at a lower rate, so there is less pay and patients are at greater risk of harm,” Dr. Morton said.
The reasons that same-day discharge is associated with higher mortality cannot be derived from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database, but, Dr. Inaba said, “Our thought is it is a function of failure to rescue patients from respiratory complications.” She acknowledged that this is a speculative assessment not supported by data, but she suggested that history of sleep apnea might be a particular indication to consider next-day discharge.
Dr. Inaba reports no financial relationships relevant to this topic.
Correction, 12/4/17: An earlier version of this article misstated the 30-day mortality among patients discharged the next day.
AT OBESITY WEEK 2017
Key clinical point: Thirty-day mortality after laparoscopic sleeve gastrectomy is several times higher with same-day discharge relative to an overnight stay.
Major finding: In an analysis of a national database with more than 35,000 cases, the mortality odds ratio for same-day discharge was 5.7 (P = .032) relative to next-day discharge.
Data source: Retrospective database analysis.
Disclosures: Dr. Inaba reports no financial relationships relevant to this topic.
ED visits after bariatric surgery may be difficult to reduce
NATIONAL HARBOR, MD. – In an evaluation of 633 emergency department visits following bariatric surgery in Michigan over a 1-year period, the vast majority were for complaints amenable to a phone call consultation or treatment in a lower-acuity setting, but few patients would have been satisfied with this type of management, according to an evaluation based on patient interviews presented at Obesity Week 2017.
“Unfortunately, 91% of the patients said that there was nothing the surgical team could have done that would have helped avoid the ED visit,” reported Haley Stevens, quality improvement coordinator at the Michigan Bariatric Surgery Collaborative, University of Michigan, Ann Arbor.

The 633 ED visits followed 7,617 bariatric surgeries for a rate of 8.3%. According to Ms. Stevens, this is consistent with the rates of 5%-11% reported previously. Based on clinically abstracted data and patient interviews conducted by trained nurses in a sample of patients involved in these ED visits, it was estimated that 62% were made without any attempt to first contact the surgical team, she reported at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society.
In the interviews, a variety of reasons were offered for not first contacting the surgical team, according to Ms. Stevens. Most commonly, patients reported that a sense of urgency drove them to the ED. In 18% of cases, the complaint occurred after office hours, leading the patient to believe that the ED was the only option. Another 16% of patients reported that calling the surgeon simply did not occur to them.
“When interviewed, many patients considered the visit necessary and unavoidable even after learning subsequently that the symptoms were not serious,” Ms. Stevens reported.
The primary reasons for the ED visit were nausea, vomiting, or abdominal pain, which accounted for 50% of the visits. The next most common reasons were chest pain (8%) and concerns regarding the incision (7%). Only 30% of the ED visits ultimately resulted in a hospital admission, but 60% of the visits resulted in administration of intravenous fluids. Thirty-eight percent of ED visits resulted in oral or intravenous therapy for pain.
Based on the interviews, most patients reported that they visited the ED because they wanted an immediate evaluation of their symptoms, according to Ms. Stevens. She said that the goal in most cases was simply obtaining reassurance. While better patient education about symptoms and recovery might have circumvented patient concerns about nonurgent complaints, Ms. Stevens also suggested that visits to a lower-acuity center, such as an urgent care facility, might provide a lower-cost alternative for reassurance or simple treatments.
As this study represents the first in a series to guide a quality improvement initiative, Ms. Stevens acknowledged that the best solution to reducing unnecessary ED visits is unclear, but she did suggest that multiple strategies might be needed. Based on this and previously published studies evaluating this issue “there is no silver bullet” for reducing ED visits, Ms. Stevens said.
In an animated discussion that followed presentation of these results, others recounting efforts to reduce ED visits following bariatric surgery emphasized the importance of follow-up phone calls or home visits within 2 or 3 days of surgery. According to several of those who commented, these steps allow early identification of problems while providing the type of reassurance that can prevent unnecessary ED visits.
The average cost of an ED visit following bariatric surgery is approximately $1,300, according to Ms. Stevens. For this and other reasons, strategies to reduce ED visits are needed, but Ms. Stevens cautioned that the solutions might not be simple. Based on data from this study, the key may be providing patients with a clear route to the reassurance they need to avoid seeking care for nonurgent issues.
Ms. Stevens reports no financial relationships relevant to this topic.
NATIONAL HARBOR, MD. – In an evaluation of 633 emergency department visits following bariatric surgery in Michigan over a 1-year period, the vast majority were for complaints amenable to a phone call consultation or treatment in a lower-acuity setting, but few patients would have been satisfied with this type of management, according to an evaluation based on patient interviews presented at Obesity Week 2017.
“Unfortunately, 91% of the patients said that there was nothing the surgical team could have done that would have helped avoid the ED visit,” reported Haley Stevens, quality improvement coordinator at the Michigan Bariatric Surgery Collaborative, University of Michigan, Ann Arbor.
The 633 ED visits followed 7,617 bariatric surgeries for a rate of 8.3%. According to Ms. Stevens, this is consistent with the rates of 5%-11% reported previously. Based on clinically abstracted data and patient interviews conducted by trained nurses in a sample of patients involved in these ED visits, it was estimated that 62% were made without any attempt to first contact the surgical team, she reported at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society.
In the interviews, a variety of reasons were offered for not first contacting the surgical team, according to Ms. Stevens. Most commonly, patients reported that a sense of urgency drove them to the ED. In 18% of cases, the complaint occurred after office hours, leading the patient to believe that the ED was the only option. Another 16% of patients reported that calling the surgeon simply did not occur to them.
“When interviewed, many patients considered the visit necessary and unavoidable even after learning subsequently that the symptoms were not serious,” Ms. Stevens reported.
The primary reasons for the ED visit were nausea, vomiting, or abdominal pain, which accounted for 50% of the visits. The next most common reasons were chest pain (8%) and concerns regarding the incision (7%). Only 30% of the ED visits ultimately resulted in a hospital admission, but 60% of the visits resulted in administration of intravenous fluids. Thirty-eight percent of ED visits resulted in oral or intravenous therapy for pain.
Based on the interviews, most patients reported that they visited the ED because they wanted an immediate evaluation of their symptoms, according to Ms. Stevens. She said that the goal in most cases was simply obtaining reassurance. While better patient education about symptoms and recovery might have circumvented patient concerns about nonurgent complaints, Ms. Stevens also suggested that visits to a lower-acuity center, such as an urgent care facility, might provide a lower-cost alternative for reassurance or simple treatments.
As this study represents the first in a series to guide a quality improvement initiative, Ms. Stevens acknowledged that the best solution to reducing unnecessary ED visits is unclear, but she did suggest that multiple strategies might be needed. Based on this and previously published studies evaluating this issue “there is no silver bullet” for reducing ED visits, Ms. Stevens said.
In an animated discussion that followed presentation of these results, others recounting efforts to reduce ED visits following bariatric surgery emphasized the importance of follow-up phone calls or home visits within 2 or 3 days of surgery. According to several of those who commented, these steps allow early identification of problems while providing the type of reassurance that can prevent unnecessary ED visits.
The average cost of an ED visit following bariatric surgery is approximately $1,300, according to Ms. Stevens. For this and other reasons, strategies to reduce ED visits are needed, but Ms. Stevens cautioned that the solutions might not be simple. Based on data from this study, the key may be providing patients with a clear route to the reassurance they need to avoid seeking care for nonurgent issues.
Ms. Stevens reports no financial relationships relevant to this topic.
NATIONAL HARBOR, MD. – In an evaluation of 633 emergency department visits following bariatric surgery in Michigan over a 1-year period, the vast majority were for complaints amenable to a phone call consultation or treatment in a lower-acuity setting, but few patients would have been satisfied with this type of management, according to an evaluation based on patient interviews presented at Obesity Week 2017.
“Unfortunately, 91% of the patients said that there was nothing the surgical team could have done that would have helped avoid the ED visit,” reported Haley Stevens, quality improvement coordinator at the Michigan Bariatric Surgery Collaborative, University of Michigan, Ann Arbor.
The 633 ED visits followed 7,617 bariatric surgeries for a rate of 8.3%. According to Ms. Stevens, this is consistent with the rates of 5%-11% reported previously. Based on clinically abstracted data and patient interviews conducted by trained nurses in a sample of patients involved in these ED visits, it was estimated that 62% were made without any attempt to first contact the surgical team, she reported at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society.
In the interviews, a variety of reasons were offered for not first contacting the surgical team, according to Ms. Stevens. Most commonly, patients reported that a sense of urgency drove them to the ED. In 18% of cases, the complaint occurred after office hours, leading the patient to believe that the ED was the only option. Another 16% of patients reported that calling the surgeon simply did not occur to them.
“When interviewed, many patients considered the visit necessary and unavoidable even after learning subsequently that the symptoms were not serious,” Ms. Stevens reported.
The primary reasons for the ED visit were nausea, vomiting, or abdominal pain, which accounted for 50% of the visits. The next most common reasons were chest pain (8%) and concerns regarding the incision (7%). Only 30% of the ED visits ultimately resulted in a hospital admission, but 60% of the visits resulted in administration of intravenous fluids. Thirty-eight percent of ED visits resulted in oral or intravenous therapy for pain.
Based on the interviews, most patients reported that they visited the ED because they wanted an immediate evaluation of their symptoms, according to Ms. Stevens. She said that the goal in most cases was simply obtaining reassurance. While better patient education about symptoms and recovery might have circumvented patient concerns about nonurgent complaints, Ms. Stevens also suggested that visits to a lower-acuity center, such as an urgent care facility, might provide a lower-cost alternative for reassurance or simple treatments.
As this study represents the first in a series to guide a quality improvement initiative, Ms. Stevens acknowledged that the best solution to reducing unnecessary ED visits is unclear, but she did suggest that multiple strategies might be needed. Based on this and previously published studies evaluating this issue “there is no silver bullet” for reducing ED visits, Ms. Stevens said.
In an animated discussion that followed presentation of these results, others recounting efforts to reduce ED visits following bariatric surgery emphasized the importance of follow-up phone calls or home visits within 2 or 3 days of surgery. According to several of those who commented, these steps allow early identification of problems while providing the type of reassurance that can prevent unnecessary ED visits.
The average cost of an ED visit following bariatric surgery is approximately $1,300, according to Ms. Stevens. For this and other reasons, strategies to reduce ED visits are needed, but Ms. Stevens cautioned that the solutions might not be simple. Based on data from this study, the key may be providing patients with a clear route to the reassurance they need to avoid seeking care for nonurgent issues.
Ms. Stevens reports no financial relationships relevant to this topic.
AT OBESITY WEEK 2017
Key clinical point:
Major finding: In interviews after their ED visit, 91% of bariatric patients insisted the visit was needed, even when informed it was nonurgent.
Data source: Retrospective review and patient interview.
Disclosures: Ms. Stevens reports no financial relationships relevant to this topic.
Psych evaluation identifies bariatric surgery patients who do less well
NATIONAL HARBOR, MD. – Psychological screening prior to bariatric surgery is not effective for identifying who will do poorly after the procedure, but it can identify patients who are at risk for less weight loss and likely to benefit from additional support, according to one of the largest studies designed to evaluate the predictive accuracy of this screening. The results were presented at Obesity Week 2017.
“Psychological evaluations should not be used to exclude patients, because we do not appear to be very good at predicting who does well,” said Nina E. Boulard, PhD, a psychologist who currently performs preoperative psychological screening of bariatric surgery candidates at Eastern Maine Medical Center, Bangor. Rather, “our evaluations identify those who need to be followed more closely so we can intervene early when patients struggle,” she said at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society.

The two primary outcomes of interest were the ability to predict postsurgical mental health issues and the ability to predict difficulty in complying with behavioral changes. Percent excess weight loss (EWL) was also monitored. For mental health screening, the protocol included clinical interviews augmented with standardized testing, such as the Minnesota Multiphasic Personality Inventory-2-Restuctured Form (MMPI-2-RF). Patients were placed into five risk categories: low, low-moderate, moderate, moderate-high, and high.
For compliance, the patient evaluation was based primarily on interviews capturing self-reports of adherence to presurgical dietary and other lifestyle recommendations. Patients were also asked about eating behaviors, such as binge eating, and history of sexual abuse and attention-deficit/hyperactivity disorder and other neurodevelopmental issues.
The psychological screening report is provided to the surgeon, who ultimately decides whether patients go on to surgery. In this analysis, relatively few high-risk patients were included because these patients, such as those with active psychosis, uncontrolled binge eating, or severe depression, were excluded from surgery and therefore did not generate postsurgical follow-up data.
As has been reported by others, Dr. Boulard reported that no single standardized test or clinical variable was an effective predictor of “who will and will not struggle” psychologically after surgery. However, after adjusting for age, gender, presurgery weight, diabetes history, and surgery type, several variables were associated with reduced proportion EWL. These included anxiety (P = .02), ADHD (P = .01), and prior hospitalization of a psychological indication (P less than .05). History of sexual abuse was predictive of reduced percentage EWL 1 year but not 2 years after surgery.
“So, what this tells us is the clinical interpretation of the big picture might be important,” Dr. Boulard commented.
The presurgical psychological screening was not predictive of compliance, a result that Dr. Boulard labeled as “surprising.” She speculated that because weight loss in the first 2 years after bariatric surgery is relatively uniform, longer follow-up, such as 5 years, might be needed to capture the impact of patients predicted to have poor compliance.
Importantly, percent EWL remained high even among patients with risk factors associated with mental health challenges after surgery, according to Dr. Boulard. She stressed that even those with less weight loss “did not do poorly.” Rather, the relative differences in postsurgical weight loss for those who were predicted to struggle versus those who were not was “a matter of degrees.”
While Dr. Boulard acknowledged a prospective study using a standardized psychological screening protocol would be appropriate to validate the findings of this study, the study results have already changed practice at her institution.
“We are following the at-risk patients more closely, so we can intervene quickly if there are issues after surgery,” Dr. Boulard explained. The question raised by this study is, “can we bring them [patients at higher risk] to a higher level of response so they are just as successful” as those without risk factors identified in psychological screening.
Dr. Boulard reports no financial relationships relevant to this topic.
NATIONAL HARBOR, MD. – Psychological screening prior to bariatric surgery is not effective for identifying who will do poorly after the procedure, but it can identify patients who are at risk for less weight loss and likely to benefit from additional support, according to one of the largest studies designed to evaluate the predictive accuracy of this screening. The results were presented at Obesity Week 2017.
“Psychological evaluations should not be used to exclude patients, because we do not appear to be very good at predicting who does well,” said Nina E. Boulard, PhD, a psychologist who currently performs preoperative psychological screening of bariatric surgery candidates at Eastern Maine Medical Center, Bangor. Rather, “our evaluations identify those who need to be followed more closely so we can intervene early when patients struggle,” she said at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society.
The two primary outcomes of interest were the ability to predict postsurgical mental health issues and the ability to predict difficulty in complying with behavioral changes. Percent excess weight loss (EWL) was also monitored. For mental health screening, the protocol included clinical interviews augmented with standardized testing, such as the Minnesota Multiphasic Personality Inventory-2-Restuctured Form (MMPI-2-RF). Patients were placed into five risk categories: low, low-moderate, moderate, moderate-high, and high.
For compliance, the patient evaluation was based primarily on interviews capturing self-reports of adherence to presurgical dietary and other lifestyle recommendations. Patients were also asked about eating behaviors, such as binge eating, and history of sexual abuse and attention-deficit/hyperactivity disorder and other neurodevelopmental issues.
The psychological screening report is provided to the surgeon, who ultimately decides whether patients go on to surgery. In this analysis, relatively few high-risk patients were included because these patients, such as those with active psychosis, uncontrolled binge eating, or severe depression, were excluded from surgery and therefore did not generate postsurgical follow-up data.
As has been reported by others, Dr. Boulard reported that no single standardized test or clinical variable was an effective predictor of “who will and will not struggle” psychologically after surgery. However, after adjusting for age, gender, presurgery weight, diabetes history, and surgery type, several variables were associated with reduced proportion EWL. These included anxiety (P = .02), ADHD (P = .01), and prior hospitalization of a psychological indication (P less than .05). History of sexual abuse was predictive of reduced percentage EWL 1 year but not 2 years after surgery.
“So, what this tells us is the clinical interpretation of the big picture might be important,” Dr. Boulard commented.
The presurgical psychological screening was not predictive of compliance, a result that Dr. Boulard labeled as “surprising.” She speculated that because weight loss in the first 2 years after bariatric surgery is relatively uniform, longer follow-up, such as 5 years, might be needed to capture the impact of patients predicted to have poor compliance.
Importantly, percent EWL remained high even among patients with risk factors associated with mental health challenges after surgery, according to Dr. Boulard. She stressed that even those with less weight loss “did not do poorly.” Rather, the relative differences in postsurgical weight loss for those who were predicted to struggle versus those who were not was “a matter of degrees.”
While Dr. Boulard acknowledged a prospective study using a standardized psychological screening protocol would be appropriate to validate the findings of this study, the study results have already changed practice at her institution.
“We are following the at-risk patients more closely, so we can intervene quickly if there are issues after surgery,” Dr. Boulard explained. The question raised by this study is, “can we bring them [patients at higher risk] to a higher level of response so they are just as successful” as those without risk factors identified in psychological screening.
Dr. Boulard reports no financial relationships relevant to this topic.
NATIONAL HARBOR, MD. – Psychological screening prior to bariatric surgery is not effective for identifying who will do poorly after the procedure, but it can identify patients who are at risk for less weight loss and likely to benefit from additional support, according to one of the largest studies designed to evaluate the predictive accuracy of this screening. The results were presented at Obesity Week 2017.
“Psychological evaluations should not be used to exclude patients, because we do not appear to be very good at predicting who does well,” said Nina E. Boulard, PhD, a psychologist who currently performs preoperative psychological screening of bariatric surgery candidates at Eastern Maine Medical Center, Bangor. Rather, “our evaluations identify those who need to be followed more closely so we can intervene early when patients struggle,” she said at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society.
The two primary outcomes of interest were the ability to predict postsurgical mental health issues and the ability to predict difficulty in complying with behavioral changes. Percent excess weight loss (EWL) was also monitored. For mental health screening, the protocol included clinical interviews augmented with standardized testing, such as the Minnesota Multiphasic Personality Inventory-2-Restuctured Form (MMPI-2-RF). Patients were placed into five risk categories: low, low-moderate, moderate, moderate-high, and high.
For compliance, the patient evaluation was based primarily on interviews capturing self-reports of adherence to presurgical dietary and other lifestyle recommendations. Patients were also asked about eating behaviors, such as binge eating, and history of sexual abuse and attention-deficit/hyperactivity disorder and other neurodevelopmental issues.
The psychological screening report is provided to the surgeon, who ultimately decides whether patients go on to surgery. In this analysis, relatively few high-risk patients were included because these patients, such as those with active psychosis, uncontrolled binge eating, or severe depression, were excluded from surgery and therefore did not generate postsurgical follow-up data.
As has been reported by others, Dr. Boulard reported that no single standardized test or clinical variable was an effective predictor of “who will and will not struggle” psychologically after surgery. However, after adjusting for age, gender, presurgery weight, diabetes history, and surgery type, several variables were associated with reduced proportion EWL. These included anxiety (P = .02), ADHD (P = .01), and prior hospitalization of a psychological indication (P less than .05). History of sexual abuse was predictive of reduced percentage EWL 1 year but not 2 years after surgery.
“So, what this tells us is the clinical interpretation of the big picture might be important,” Dr. Boulard commented.
The presurgical psychological screening was not predictive of compliance, a result that Dr. Boulard labeled as “surprising.” She speculated that because weight loss in the first 2 years after bariatric surgery is relatively uniform, longer follow-up, such as 5 years, might be needed to capture the impact of patients predicted to have poor compliance.
Importantly, percent EWL remained high even among patients with risk factors associated with mental health challenges after surgery, according to Dr. Boulard. She stressed that even those with less weight loss “did not do poorly.” Rather, the relative differences in postsurgical weight loss for those who were predicted to struggle versus those who were not was “a matter of degrees.”
While Dr. Boulard acknowledged a prospective study using a standardized psychological screening protocol would be appropriate to validate the findings of this study, the study results have already changed practice at her institution.
“We are following the at-risk patients more closely, so we can intervene quickly if there are issues after surgery,” Dr. Boulard explained. The question raised by this study is, “can we bring them [patients at higher risk] to a higher level of response so they are just as successful” as those without risk factors identified in psychological screening.
Dr. Boulard reports no financial relationships relevant to this topic.
AT OBESITY WEEK 2017
Key clinical point: Psychological screening prior to bariatric surgery selects patients at risk for reduced postoperative weight loss.
Major finding: Prior psychological hospitalization (P less than .05) and number of previous psychological diagnoses (P = .04) are among markers of less postop weight loss.
Data source: Retrospective analysis.
Disclosures: Dr. Boulard reports no financial relationships relevant to this topic.
Chronicity of obesity provides rationale for physician-surgeon collaboration
NATIONAL HARBOR, MD. – When combined with bariatric surgery, adjunctive therapies for obesity should be individualized for specific drivers of weight gain, which can differ among obesity phenotypes, according to an expert view presented at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society .
“Surgery is the most effective therapy we have, but it is only one of multiple treatments that should be considered in a treatment paradigm,” suggested Robert F. Kushner, MD, a professor of endocrinology and specialist in obesity at the Northwestern University, Chicago.
“It is very useful to take a narrative approach to understand the patients in front of us and to understand who they are and how they got to where they are now,” Dr. Kushner explained. Dr. Kushner often asks patients to graph weight history over time. This can connect social, biological, and psychological events with significant weight gains, and these connections can generate insight into the underlying obesity phenotype.
“It is a like a fingerprint. Everyone has his or her own story to tell,” Dr. Kushner explained. A clinical picture of patients’ phenotypes can be developed from observing large jumps in weight connected to such factors as a stressful life event, a period of sustained inactivity, or a pregnancy. Over a weight history, several events may be identified that provide insight into each patient’s “unique weight journey.”
This understanding provides the basis for a systematic approach to combining strategies that may include lifestyle changes, surgery, and pharmacologic management, all tailored for the specific triggers and needs of the patient. Dr. Kushner advised that, even for those who are candidates for surgery, bariatric procedures are just one component of the treatment and must be integrated in a team approach with other modalities.
This approach may include pharmacologic therapy both before and after surgery; Dr. Kushner noted that the availability of drug options has expanded in recent years with approval of such therapies as lorcaserin and liraglutide. According to Dr. Kushner, drug therapy can be used for preoperative weight loss and may be useful for preventing postoperative weight gain in certain patients.
“There are no randomized trials demonstrating efficacy for prevention of postoperative weight gain, but there is supportive evidence from a retrospective study,” said Dr. Kushner, referring to a recently published two-center evaluation (Surg Obes Relat Dis. 2017;13:491-500).
In that study, 258 patients underwent Roux-en-Y gastric bypass, and 61 patients underwent sleeve gastrectomy. Those who received adjunctive drug support, particularly in the RYGB group, had greater sustained weight loss than those who did not, leading to the conclusion that postoperative pharmacotherapy “is a useful adjunct.” The advantage for drug therapy was observed even though patients did not receive the most recently approved and potentially more effective drugs, according to Dr. Kushner. However, he cautioned that information about the optimal timing of treatment after surgery remains “limited.”
The variability in weight loss and weight regain after bariatric procedures is one reason to consider bariatric surgery as only one component in a continuum of care, according to Dr. Kushner. He emphasized that obesity is a chronic condition that requires ongoing and perhaps indefinite treatment. While surgeons may already work with a team that manages preoperative and postoperative lifestyle changes to improve immediate surgical outcomes, Dr. Kushner believes that surgeons and physicians should work more collaboratively toward long-term management plans. By also appreciating obesity phenotypes and the specific mix of treatments that are most likely to help individual patients achieve durable weight loss, surgeons and physicians working together are likely to improve outcomes beyond those that could be expected from either working alone.
Dr. Kushner reports he has financial relationships with Novo Nordisk, Retrofit, Takeda Pharmaceuticals, and Vivus.
NATIONAL HARBOR, MD. – When combined with bariatric surgery, adjunctive therapies for obesity should be individualized for specific drivers of weight gain, which can differ among obesity phenotypes, according to an expert view presented at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society .
“Surgery is the most effective therapy we have, but it is only one of multiple treatments that should be considered in a treatment paradigm,” suggested Robert F. Kushner, MD, a professor of endocrinology and specialist in obesity at the Northwestern University, Chicago.
“It is very useful to take a narrative approach to understand the patients in front of us and to understand who they are and how they got to where they are now,” Dr. Kushner explained. Dr. Kushner often asks patients to graph weight history over time. This can connect social, biological, and psychological events with significant weight gains, and these connections can generate insight into the underlying obesity phenotype.
“It is a like a fingerprint. Everyone has his or her own story to tell,” Dr. Kushner explained. A clinical picture of patients’ phenotypes can be developed from observing large jumps in weight connected to such factors as a stressful life event, a period of sustained inactivity, or a pregnancy. Over a weight history, several events may be identified that provide insight into each patient’s “unique weight journey.”
This understanding provides the basis for a systematic approach to combining strategies that may include lifestyle changes, surgery, and pharmacologic management, all tailored for the specific triggers and needs of the patient. Dr. Kushner advised that, even for those who are candidates for surgery, bariatric procedures are just one component of the treatment and must be integrated in a team approach with other modalities.
This approach may include pharmacologic therapy both before and after surgery; Dr. Kushner noted that the availability of drug options has expanded in recent years with approval of such therapies as lorcaserin and liraglutide. According to Dr. Kushner, drug therapy can be used for preoperative weight loss and may be useful for preventing postoperative weight gain in certain patients.
“There are no randomized trials demonstrating efficacy for prevention of postoperative weight gain, but there is supportive evidence from a retrospective study,” said Dr. Kushner, referring to a recently published two-center evaluation (Surg Obes Relat Dis. 2017;13:491-500).
In that study, 258 patients underwent Roux-en-Y gastric bypass, and 61 patients underwent sleeve gastrectomy. Those who received adjunctive drug support, particularly in the RYGB group, had greater sustained weight loss than those who did not, leading to the conclusion that postoperative pharmacotherapy “is a useful adjunct.” The advantage for drug therapy was observed even though patients did not receive the most recently approved and potentially more effective drugs, according to Dr. Kushner. However, he cautioned that information about the optimal timing of treatment after surgery remains “limited.”
The variability in weight loss and weight regain after bariatric procedures is one reason to consider bariatric surgery as only one component in a continuum of care, according to Dr. Kushner. He emphasized that obesity is a chronic condition that requires ongoing and perhaps indefinite treatment. While surgeons may already work with a team that manages preoperative and postoperative lifestyle changes to improve immediate surgical outcomes, Dr. Kushner believes that surgeons and physicians should work more collaboratively toward long-term management plans. By also appreciating obesity phenotypes and the specific mix of treatments that are most likely to help individual patients achieve durable weight loss, surgeons and physicians working together are likely to improve outcomes beyond those that could be expected from either working alone.
Dr. Kushner reports he has financial relationships with Novo Nordisk, Retrofit, Takeda Pharmaceuticals, and Vivus.
NATIONAL HARBOR, MD. – When combined with bariatric surgery, adjunctive therapies for obesity should be individualized for specific drivers of weight gain, which can differ among obesity phenotypes, according to an expert view presented at an annual meeting presented by the American Society for Metabolic and Bariatric Surgery and The Obesity Society .
“Surgery is the most effective therapy we have, but it is only one of multiple treatments that should be considered in a treatment paradigm,” suggested Robert F. Kushner, MD, a professor of endocrinology and specialist in obesity at the Northwestern University, Chicago.
“It is very useful to take a narrative approach to understand the patients in front of us and to understand who they are and how they got to where they are now,” Dr. Kushner explained. Dr. Kushner often asks patients to graph weight history over time. This can connect social, biological, and psychological events with significant weight gains, and these connections can generate insight into the underlying obesity phenotype.
“It is a like a fingerprint. Everyone has his or her own story to tell,” Dr. Kushner explained. A clinical picture of patients’ phenotypes can be developed from observing large jumps in weight connected to such factors as a stressful life event, a period of sustained inactivity, or a pregnancy. Over a weight history, several events may be identified that provide insight into each patient’s “unique weight journey.”
This understanding provides the basis for a systematic approach to combining strategies that may include lifestyle changes, surgery, and pharmacologic management, all tailored for the specific triggers and needs of the patient. Dr. Kushner advised that, even for those who are candidates for surgery, bariatric procedures are just one component of the treatment and must be integrated in a team approach with other modalities.
This approach may include pharmacologic therapy both before and after surgery; Dr. Kushner noted that the availability of drug options has expanded in recent years with approval of such therapies as lorcaserin and liraglutide. According to Dr. Kushner, drug therapy can be used for preoperative weight loss and may be useful for preventing postoperative weight gain in certain patients.
“There are no randomized trials demonstrating efficacy for prevention of postoperative weight gain, but there is supportive evidence from a retrospective study,” said Dr. Kushner, referring to a recently published two-center evaluation (Surg Obes Relat Dis. 2017;13:491-500).
In that study, 258 patients underwent Roux-en-Y gastric bypass, and 61 patients underwent sleeve gastrectomy. Those who received adjunctive drug support, particularly in the RYGB group, had greater sustained weight loss than those who did not, leading to the conclusion that postoperative pharmacotherapy “is a useful adjunct.” The advantage for drug therapy was observed even though patients did not receive the most recently approved and potentially more effective drugs, according to Dr. Kushner. However, he cautioned that information about the optimal timing of treatment after surgery remains “limited.”
The variability in weight loss and weight regain after bariatric procedures is one reason to consider bariatric surgery as only one component in a continuum of care, according to Dr. Kushner. He emphasized that obesity is a chronic condition that requires ongoing and perhaps indefinite treatment. While surgeons may already work with a team that manages preoperative and postoperative lifestyle changes to improve immediate surgical outcomes, Dr. Kushner believes that surgeons and physicians should work more collaboratively toward long-term management plans. By also appreciating obesity phenotypes and the specific mix of treatments that are most likely to help individual patients achieve durable weight loss, surgeons and physicians working together are likely to improve outcomes beyond those that could be expected from either working alone.
Dr. Kushner reports he has financial relationships with Novo Nordisk, Retrofit, Takeda Pharmaceuticals, and Vivus.
AT OBESITY WEEK 2017
Key clinical point: For treatment of obesity as a chronic disease, bariatric surgery must be incorporated into a continuum of therapies.
Major finding: Obesity phenotypes differ, requiring individualized adjunctive therapies to surgery in order to ensure durable benefit.
Data source: Expert interpretation of published studies.
Disclosures: Dr. Kushner reports he has financial relationships with Novo Nordisk, Retrofit, Takeda Pharmaceuticals, and Vivus.
Public health hazard: Bring your flu to work day
Slightly more than 41% of health care personnel who had the flu during the 2014-2015 influenza season went to work while they were ill, according to an annual survey.
Physicians, however, were well above this average, with 63% reporting they had worked with an influenza-like illness (ILI); they were not quite as far above average as pharmacists, though, who had a 67% rate of “presenteeism” – the highest among all of the health care occupations included in the survey, said Sophia Chiu, MD, MPH, of the Centers for Disease Control and Prevention’s National Institute for Occupational Safety and Health, and her associates.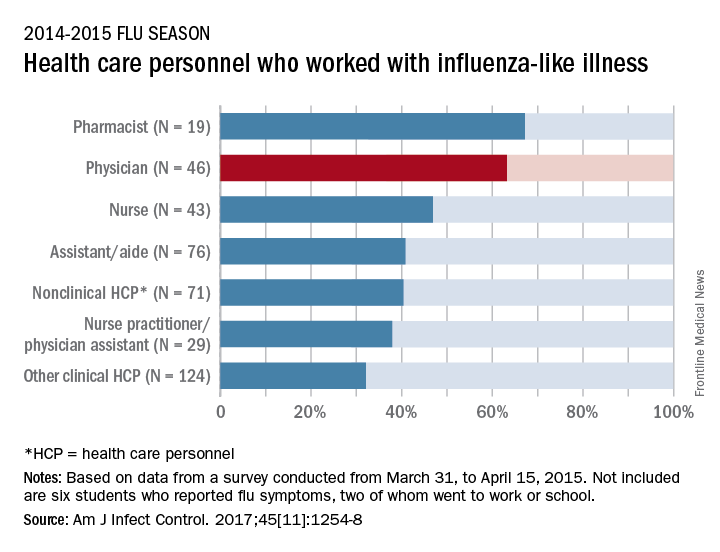
“The statistics are alarming. At least one earlier study has shown that patients who are exposed to a health care worker who is sick are five times more likely to get a health care–associated infection,” Dr. Chiu said in a separate written statement.
For the study, ILI was defined as “fever (without a specified temperature cutoff) and sore throat or cough.” The “nonclinical personnel” category included managers, food service workers, and janitors, while the “other clinical personnel” category included technicians and technologists. The annual Internet panel survey was conducted from March 31, 2015, to April 15, 2015, and 414 of its 1,914 respondents self-reported having an ILI, of whom 183 said that they worked during their illness, Dr. Chiu and her associates said.
The investigators are all CDC employees. The respondents were recruited from Internet panels operated by Survey Sampling International through a contract with Abt Associates.
Slightly more than 41% of health care personnel who had the flu during the 2014-2015 influenza season went to work while they were ill, according to an annual survey.
Physicians, however, were well above this average, with 63% reporting they had worked with an influenza-like illness (ILI); they were not quite as far above average as pharmacists, though, who had a 67% rate of “presenteeism” – the highest among all of the health care occupations included in the survey, said Sophia Chiu, MD, MPH, of the Centers for Disease Control and Prevention’s National Institute for Occupational Safety and Health, and her associates.
“The statistics are alarming. At least one earlier study has shown that patients who are exposed to a health care worker who is sick are five times more likely to get a health care–associated infection,” Dr. Chiu said in a separate written statement.
For the study, ILI was defined as “fever (without a specified temperature cutoff) and sore throat or cough.” The “nonclinical personnel” category included managers, food service workers, and janitors, while the “other clinical personnel” category included technicians and technologists. The annual Internet panel survey was conducted from March 31, 2015, to April 15, 2015, and 414 of its 1,914 respondents self-reported having an ILI, of whom 183 said that they worked during their illness, Dr. Chiu and her associates said.
The investigators are all CDC employees. The respondents were recruited from Internet panels operated by Survey Sampling International through a contract with Abt Associates.
Slightly more than 41% of health care personnel who had the flu during the 2014-2015 influenza season went to work while they were ill, according to an annual survey.
Physicians, however, were well above this average, with 63% reporting they had worked with an influenza-like illness (ILI); they were not quite as far above average as pharmacists, though, who had a 67% rate of “presenteeism” – the highest among all of the health care occupations included in the survey, said Sophia Chiu, MD, MPH, of the Centers for Disease Control and Prevention’s National Institute for Occupational Safety and Health, and her associates.
“The statistics are alarming. At least one earlier study has shown that patients who are exposed to a health care worker who is sick are five times more likely to get a health care–associated infection,” Dr. Chiu said in a separate written statement.
For the study, ILI was defined as “fever (without a specified temperature cutoff) and sore throat or cough.” The “nonclinical personnel” category included managers, food service workers, and janitors, while the “other clinical personnel” category included technicians and technologists. The annual Internet panel survey was conducted from March 31, 2015, to April 15, 2015, and 414 of its 1,914 respondents self-reported having an ILI, of whom 183 said that they worked during their illness, Dr. Chiu and her associates said.
The investigators are all CDC employees. The respondents were recruited from Internet panels operated by Survey Sampling International through a contract with Abt Associates.
FROM THE AMERICAN JOURNAL OF INFECTION CONTROL
MedPAC offers more details of MIPS replacement
WASHINGTON – The Medicare Payment Advisory Commission continues to mull the specifics of its proposed recommendation to scrap the Quality Payment Program’s MIPS component.
The basics of the MIPS (Merit-based Incentive Payment System) replacement have not changed. The proposal calls for creation of a voluntary value program (VVP) that would withhold a percentage – currently 2% – of Medicare payments for physicians who are not part of an advanced alternative payment model (APM) under the Quality Payment Program of the Medicare Access and CHIP Reauthorization Act of 2015.
There would be two ways to recapture the withheld pay. The first would be to join an APM. The second would be to participate in a VVP by entering a voluntary reporting group. Under the proposal, VVPs would be at least 10 providers who would report together on population-based measures, patient experience, and cost measures, according to staff presentations given Nov. 2 at a meeting of the Medicare Payment Advisory Commission (MedPAC).
Proposed measures would be patient oriented, would encourage coordination across all providers, would promote positive change in the delivery system, and would be less burdensome to providers. Measures would be more in line with those employed by APMs – important because the overall goal would be encouraging participation in an APM rather than permanently lingering in the VVP.
To that end, MedPAC staff member Kate Bloniarz noted during the presentation of the VVP proposal that the total payments in the program “should be capped to be less attractive than joining an [advanced] APM. This comes from a general sense among commissioners that clinicians should not be able to receive large bonuses” for remaining in Medicare fee-for-service.
MedPAC staff recommended that the Centers for Medicare & Medicaid Services offer a fallback group that would provide an option to providers that would otherwise not have access to other groups to join.
Commission member Kathy Buto, former vice president of global health policy at Johnson & Johnson, suggested withholding be increased to perhaps 3%, with providers able to recoup 2% in the VVP and 3% in an APM, to further incentivize APM participation.
Staff noted that certain quality measures and process measures would be lost if MIPS were to go away, but they could be accounted for in other channels, such as through electronic health records and registries.
Most commissioners expressed support for both the repeal of MIPS and the conceptual framework for the new VVP, although many sought more details, particularly in the handling of specialists.
“I don’t know that we want to try to make the VVP do too much, especially when you get into the specialties that are very, very episodic,” said commission member Brian DeBusk, PhD, CEO of DeRoyal Industries. “The classic example would be a joint replacement. … I hope to see some specialist APMs developed in parallel and I think that is going to take some pressure off to try to make the VVP be all things to all people.”
Commission member Pat Wang, CEO of Healthfirst, offered a possible solution.
“I would suggest that we try to think about doing that in the context of something that is a little bit, perhaps, not full bore APM, but a VVP for specialists with their own metrics that are not big, gigantic readmissions,” she said. “Those are very broad population health metrics [that may not work for specialists].”
But at least two commission members voiced their dissent to the proposal as presented, with one going so far as to saying that MIPS should not be repealed.
David Nerenz, PhD, of the Henry Ford Health System, said that he had “very serious concerns about the VVP part of this proposal [and] they are such that if it comes to us as a recommendation in more or less its current form I will not support it.”
He called it “pretty significant social engineering in the structure of medical practice and I think we are doing it in the absence of what to me would be compelling evidence that this large group structure we are talking about is good.
“I also don’t see any evidence that beneficiaries find value in the set of measures we are talking about,” Dr. Nerenz added. He is on the record as supporting the repeal of MIPS.
Commission member Alice Coombs, MD, of Weymouth, Mass., was the lone voice speaking in support of MIPS: “I think MIPS has a lot of problems … but there are some things that are coming out of MIPS that are actually good.”
She called the VVP proposal “inadequate” and took issue with the measures. As a practicing physician, she said that she favors more population health measures that will affect patient outcomes.
MedPAC staff expect to have a draft recommendation prepared for discussion at the December meeting, with a final vote on what will be presented to Congress coming as soon as January.
WASHINGTON – The Medicare Payment Advisory Commission continues to mull the specifics of its proposed recommendation to scrap the Quality Payment Program’s MIPS component.
The basics of the MIPS (Merit-based Incentive Payment System) replacement have not changed. The proposal calls for creation of a voluntary value program (VVP) that would withhold a percentage – currently 2% – of Medicare payments for physicians who are not part of an advanced alternative payment model (APM) under the Quality Payment Program of the Medicare Access and CHIP Reauthorization Act of 2015.
There would be two ways to recapture the withheld pay. The first would be to join an APM. The second would be to participate in a VVP by entering a voluntary reporting group. Under the proposal, VVPs would be at least 10 providers who would report together on population-based measures, patient experience, and cost measures, according to staff presentations given Nov. 2 at a meeting of the Medicare Payment Advisory Commission (MedPAC).
Proposed measures would be patient oriented, would encourage coordination across all providers, would promote positive change in the delivery system, and would be less burdensome to providers. Measures would be more in line with those employed by APMs – important because the overall goal would be encouraging participation in an APM rather than permanently lingering in the VVP.
To that end, MedPAC staff member Kate Bloniarz noted during the presentation of the VVP proposal that the total payments in the program “should be capped to be less attractive than joining an [advanced] APM. This comes from a general sense among commissioners that clinicians should not be able to receive large bonuses” for remaining in Medicare fee-for-service.
MedPAC staff recommended that the Centers for Medicare & Medicaid Services offer a fallback group that would provide an option to providers that would otherwise not have access to other groups to join.
Commission member Kathy Buto, former vice president of global health policy at Johnson & Johnson, suggested withholding be increased to perhaps 3%, with providers able to recoup 2% in the VVP and 3% in an APM, to further incentivize APM participation.
Staff noted that certain quality measures and process measures would be lost if MIPS were to go away, but they could be accounted for in other channels, such as through electronic health records and registries.
Most commissioners expressed support for both the repeal of MIPS and the conceptual framework for the new VVP, although many sought more details, particularly in the handling of specialists.
“I don’t know that we want to try to make the VVP do too much, especially when you get into the specialties that are very, very episodic,” said commission member Brian DeBusk, PhD, CEO of DeRoyal Industries. “The classic example would be a joint replacement. … I hope to see some specialist APMs developed in parallel and I think that is going to take some pressure off to try to make the VVP be all things to all people.”
Commission member Pat Wang, CEO of Healthfirst, offered a possible solution.
“I would suggest that we try to think about doing that in the context of something that is a little bit, perhaps, not full bore APM, but a VVP for specialists with their own metrics that are not big, gigantic readmissions,” she said. “Those are very broad population health metrics [that may not work for specialists].”
But at least two commission members voiced their dissent to the proposal as presented, with one going so far as to saying that MIPS should not be repealed.
David Nerenz, PhD, of the Henry Ford Health System, said that he had “very serious concerns about the VVP part of this proposal [and] they are such that if it comes to us as a recommendation in more or less its current form I will not support it.”
He called it “pretty significant social engineering in the structure of medical practice and I think we are doing it in the absence of what to me would be compelling evidence that this large group structure we are talking about is good.
“I also don’t see any evidence that beneficiaries find value in the set of measures we are talking about,” Dr. Nerenz added. He is on the record as supporting the repeal of MIPS.
Commission member Alice Coombs, MD, of Weymouth, Mass., was the lone voice speaking in support of MIPS: “I think MIPS has a lot of problems … but there are some things that are coming out of MIPS that are actually good.”
She called the VVP proposal “inadequate” and took issue with the measures. As a practicing physician, she said that she favors more population health measures that will affect patient outcomes.
MedPAC staff expect to have a draft recommendation prepared for discussion at the December meeting, with a final vote on what will be presented to Congress coming as soon as January.
WASHINGTON – The Medicare Payment Advisory Commission continues to mull the specifics of its proposed recommendation to scrap the Quality Payment Program’s MIPS component.
The basics of the MIPS (Merit-based Incentive Payment System) replacement have not changed. The proposal calls for creation of a voluntary value program (VVP) that would withhold a percentage – currently 2% – of Medicare payments for physicians who are not part of an advanced alternative payment model (APM) under the Quality Payment Program of the Medicare Access and CHIP Reauthorization Act of 2015.
There would be two ways to recapture the withheld pay. The first would be to join an APM. The second would be to participate in a VVP by entering a voluntary reporting group. Under the proposal, VVPs would be at least 10 providers who would report together on population-based measures, patient experience, and cost measures, according to staff presentations given Nov. 2 at a meeting of the Medicare Payment Advisory Commission (MedPAC).
Proposed measures would be patient oriented, would encourage coordination across all providers, would promote positive change in the delivery system, and would be less burdensome to providers. Measures would be more in line with those employed by APMs – important because the overall goal would be encouraging participation in an APM rather than permanently lingering in the VVP.
To that end, MedPAC staff member Kate Bloniarz noted during the presentation of the VVP proposal that the total payments in the program “should be capped to be less attractive than joining an [advanced] APM. This comes from a general sense among commissioners that clinicians should not be able to receive large bonuses” for remaining in Medicare fee-for-service.
MedPAC staff recommended that the Centers for Medicare & Medicaid Services offer a fallback group that would provide an option to providers that would otherwise not have access to other groups to join.
Commission member Kathy Buto, former vice president of global health policy at Johnson & Johnson, suggested withholding be increased to perhaps 3%, with providers able to recoup 2% in the VVP and 3% in an APM, to further incentivize APM participation.
Staff noted that certain quality measures and process measures would be lost if MIPS were to go away, but they could be accounted for in other channels, such as through electronic health records and registries.
Most commissioners expressed support for both the repeal of MIPS and the conceptual framework for the new VVP, although many sought more details, particularly in the handling of specialists.
“I don’t know that we want to try to make the VVP do too much, especially when you get into the specialties that are very, very episodic,” said commission member Brian DeBusk, PhD, CEO of DeRoyal Industries. “The classic example would be a joint replacement. … I hope to see some specialist APMs developed in parallel and I think that is going to take some pressure off to try to make the VVP be all things to all people.”
Commission member Pat Wang, CEO of Healthfirst, offered a possible solution.
“I would suggest that we try to think about doing that in the context of something that is a little bit, perhaps, not full bore APM, but a VVP for specialists with their own metrics that are not big, gigantic readmissions,” she said. “Those are very broad population health metrics [that may not work for specialists].”
But at least two commission members voiced their dissent to the proposal as presented, with one going so far as to saying that MIPS should not be repealed.
David Nerenz, PhD, of the Henry Ford Health System, said that he had “very serious concerns about the VVP part of this proposal [and] they are such that if it comes to us as a recommendation in more or less its current form I will not support it.”
He called it “pretty significant social engineering in the structure of medical practice and I think we are doing it in the absence of what to me would be compelling evidence that this large group structure we are talking about is good.
“I also don’t see any evidence that beneficiaries find value in the set of measures we are talking about,” Dr. Nerenz added. He is on the record as supporting the repeal of MIPS.
Commission member Alice Coombs, MD, of Weymouth, Mass., was the lone voice speaking in support of MIPS: “I think MIPS has a lot of problems … but there are some things that are coming out of MIPS that are actually good.”
She called the VVP proposal “inadequate” and took issue with the measures. As a practicing physician, she said that she favors more population health measures that will affect patient outcomes.
MedPAC staff expect to have a draft recommendation prepared for discussion at the December meeting, with a final vote on what will be presented to Congress coming as soon as January.
AT A PUBLIC MEETING OF MEDPAC
Most hyperparathyroidism cases can be considered cured after surgery
SCOTTSDALE, ARIZ. – Patients with hyperparathyroidism and single-gland disease can be considered cured if their intraoperative parathyroid hormone (PTH) level drops by 50% or more, or to normal or near-normal levels (15-65 pg/mL), and don’t require immediate follow-up for lab work, according to a retrospective review of patients who underwent parathyroidectomy at Mayo Clinic, Rochester, Minn.
These findings applied only to patients in the study whose preoperative sestamibi scans were concordant with intraoperative findings. Single-gland disease represented about 85% of cases, Melanie L. Lyden, MD, reported at the annual meeting of the Western Surgical Association.

Her team conducted a retrospective analysis of 214 patients who underwent parathyroidectomy at Mayo Clinic, Rochester, between January 2012 and March 2014. The investigators excluded patients with a history of multiple endocrine neoplasia syndrome, as well as patients with secondary or tertiary hyperparathyroidism. All patients received instructions at discharge for completing calcium testing, as well as a follow-up letter and phone call.
The overall cure rate at 6 months was 94% (202 cured, 12 not cured). In 205 of 214 cases (96%), the patients had an intraoperative drop in PTH level by 50% to normal or near-normal levels, and were therefore considered cured immediately.
The cured and not cured rate groups had no significant differences in age, gland weight, or preoperative PTH levels. Final intraoperative PTH levels were lower in patients who were cured (37 pg/mL vs. 55 pg/mL, P = .008), and the percentage decrease in PTH was greater (69% vs. 43%, P less than .0001).
A subgroup analysis found that concordant sestamibi imaging, single adenoma pathology, and an intraoperative cure combined to correlate with a 6-month cure rate of 97%.
In addition to identifying cures early, the findings suggest that patients whose PTH levels don’t drop adequately during surgery, and those with multiglandular disease should be aggressively targeted for follow-up – an important concern because many patients fail to complete calcium testing. “We were very aggressive in terms of follow-up recommendations, a follow-up letter, and a follow-up phone call, and still close to 30% of them we were not able to get to come in and get their blood checked,” said Dr. Lyden.
The study received no external funding. Dr. Lyden reported having no relevant financial disclosures.
SCOTTSDALE, ARIZ. – Patients with hyperparathyroidism and single-gland disease can be considered cured if their intraoperative parathyroid hormone (PTH) level drops by 50% or more, or to normal or near-normal levels (15-65 pg/mL), and don’t require immediate follow-up for lab work, according to a retrospective review of patients who underwent parathyroidectomy at Mayo Clinic, Rochester, Minn.
These findings applied only to patients in the study whose preoperative sestamibi scans were concordant with intraoperative findings. Single-gland disease represented about 85% of cases, Melanie L. Lyden, MD, reported at the annual meeting of the Western Surgical Association.
Her team conducted a retrospective analysis of 214 patients who underwent parathyroidectomy at Mayo Clinic, Rochester, between January 2012 and March 2014. The investigators excluded patients with a history of multiple endocrine neoplasia syndrome, as well as patients with secondary or tertiary hyperparathyroidism. All patients received instructions at discharge for completing calcium testing, as well as a follow-up letter and phone call.
The overall cure rate at 6 months was 94% (202 cured, 12 not cured). In 205 of 214 cases (96%), the patients had an intraoperative drop in PTH level by 50% to normal or near-normal levels, and were therefore considered cured immediately.
The cured and not cured rate groups had no significant differences in age, gland weight, or preoperative PTH levels. Final intraoperative PTH levels were lower in patients who were cured (37 pg/mL vs. 55 pg/mL, P = .008), and the percentage decrease in PTH was greater (69% vs. 43%, P less than .0001).
A subgroup analysis found that concordant sestamibi imaging, single adenoma pathology, and an intraoperative cure combined to correlate with a 6-month cure rate of 97%.
In addition to identifying cures early, the findings suggest that patients whose PTH levels don’t drop adequately during surgery, and those with multiglandular disease should be aggressively targeted for follow-up – an important concern because many patients fail to complete calcium testing. “We were very aggressive in terms of follow-up recommendations, a follow-up letter, and a follow-up phone call, and still close to 30% of them we were not able to get to come in and get their blood checked,” said Dr. Lyden.
The study received no external funding. Dr. Lyden reported having no relevant financial disclosures.
SCOTTSDALE, ARIZ. – Patients with hyperparathyroidism and single-gland disease can be considered cured if their intraoperative parathyroid hormone (PTH) level drops by 50% or more, or to normal or near-normal levels (15-65 pg/mL), and don’t require immediate follow-up for lab work, according to a retrospective review of patients who underwent parathyroidectomy at Mayo Clinic, Rochester, Minn.
These findings applied only to patients in the study whose preoperative sestamibi scans were concordant with intraoperative findings. Single-gland disease represented about 85% of cases, Melanie L. Lyden, MD, reported at the annual meeting of the Western Surgical Association.
Her team conducted a retrospective analysis of 214 patients who underwent parathyroidectomy at Mayo Clinic, Rochester, between January 2012 and March 2014. The investigators excluded patients with a history of multiple endocrine neoplasia syndrome, as well as patients with secondary or tertiary hyperparathyroidism. All patients received instructions at discharge for completing calcium testing, as well as a follow-up letter and phone call.
The overall cure rate at 6 months was 94% (202 cured, 12 not cured). In 205 of 214 cases (96%), the patients had an intraoperative drop in PTH level by 50% to normal or near-normal levels, and were therefore considered cured immediately.
The cured and not cured rate groups had no significant differences in age, gland weight, or preoperative PTH levels. Final intraoperative PTH levels were lower in patients who were cured (37 pg/mL vs. 55 pg/mL, P = .008), and the percentage decrease in PTH was greater (69% vs. 43%, P less than .0001).
A subgroup analysis found that concordant sestamibi imaging, single adenoma pathology, and an intraoperative cure combined to correlate with a 6-month cure rate of 97%.
In addition to identifying cures early, the findings suggest that patients whose PTH levels don’t drop adequately during surgery, and those with multiglandular disease should be aggressively targeted for follow-up – an important concern because many patients fail to complete calcium testing. “We were very aggressive in terms of follow-up recommendations, a follow-up letter, and a follow-up phone call, and still close to 30% of them we were not able to get to come in and get their blood checked,” said Dr. Lyden.
The study received no external funding. Dr. Lyden reported having no relevant financial disclosures.
AT WSA 2017
Key clinical point: The vast majority of cures could be identified during surgery, reducing the need for costly follow-up to monitor calcium levels.
Major finding: Concordant sestamibi imaging, single adenoma pathology, and an intraoperative cure combined to correlate with a 6-month cure rate of 97%.
Data source: A retrospective analysis of 214 patients at a single center.
Disclosures: The study received no external funding. Dr. Lyden reported having no relevant financial disclosures.