User login
Official Newspaper of the American College of Surgeons
Post-TORS neck dissections extend hospital stay
SEATTLE – Oncologic transoral robotic surgery patients spend less time in the hospital if they have neck dissections at the same time, instead of later, according to a review of 441 patients by Stony Brook (N.Y.) University.
The average hospital length of stay (LOS) was 6 days for the 349 patients (79.1%) who had lymphadenectomy neck dissections at the same time as transoral robotic surgery (TORS). The 92 patients (20.9%) who had staged procedures - neck dissections and TORS about a month apart, with TORS usually done first - stayed in the hospital an average of 8 days (P less than .0001). After risk adjustment, LOS was 43% shorter for concurrent dissections.
Cardiac arrhythmias were also more common in staged patients, perhaps because they had general anesthesia twice in a short period or maybe because staged patients were more likely to be obese (18.5% vs. 7.5%; P less than .01).
However, there were no statistically significant outcome differences otherwise, and the investigators concluded that “concurrent and staged procedures are equally safe. It is therefore reasonable to allow operator preference and patient factors to determine surgical logistics.”
Neck dissection timing has been controversial since the advent of TORS several years ago, when surgeons and administrators realized they could fit more cases into the schedule by doing neck dissections, which can take a few hours, at a different time.
Proponents of the staged approach argue, among other things, that it reduces the risk of fistulas and tracheotomies, and allows surgeons a second go at positive margins. Advocates of concurrent procedures counter that fistulas, if found, can be repaired right away, and that same-time surgery saves money, allows for earlier adjuvant therapy, and cuts anesthesia risks.
There hasn’t been much data to settle the debate, and no one has compared LOS before, so it was “important” to look into the matter, lead investigator Catherine Frenkel, MD, a Stony Brook general surgery resident, said at the American Head and Neck Society International Conference on Head and Neck Cancer.
German investigators also recently concluded that it’s pretty much a draw between concurrent and staged dissections. In a study of 41 TORS cases, “the timing of neck dissection did not make a significant difference in the outcomes. We suggest, therefore, that aspiring and established TORS teams do not restrict their appropriate indications due to robotic slot and theatre time constraints, but perform each indicated TORS case as soon as possible within their given systems, even if the neck dissections cannot be done on the same day,” they said (Eur J Surg Oncol. 2015 Jun;41[6]:773-8).
In addition to obese patients, those who had tongue or tonsil lesions were more likely to be staged in the Stony Brook analysis. About half of the surgeons in the study stuck solely to concurrent procedures, while a handful opted for the staged approach, and the rest did both. Perhaps not surprisingly, high-volume surgeons – those who did five or more TORS cases per year – were more likely to stage.
Almost two-thirds of patients had at least one complication, most commonly renal failure, heart problems, extended ventilation, and surgical errors, which included accidental punctures, postop fistulas, hemorrhages, and wound complications. A total of 13% of patients had at least one postop readmission. Apart from arrhythmias, there were no statistically significant differences in complication or 30-day readmission rates between concurrent and staged patients. High-volume surgeons were less likely to have complications.
Postop bleeding was another common problem, and more likely with staged surgeries (12% vs. 7%). Concurrent procedures had a slightly higher rate of new tracheotomies and gastrostomies, but again the differences were not statistically significant, even with pedicle and free-flap reconstruction. There was no outside funding for the work, and the investigators had no relevant conflicts of interest.
SEATTLE – Oncologic transoral robotic surgery patients spend less time in the hospital if they have neck dissections at the same time, instead of later, according to a review of 441 patients by Stony Brook (N.Y.) University.
The average hospital length of stay (LOS) was 6 days for the 349 patients (79.1%) who had lymphadenectomy neck dissections at the same time as transoral robotic surgery (TORS). The 92 patients (20.9%) who had staged procedures - neck dissections and TORS about a month apart, with TORS usually done first - stayed in the hospital an average of 8 days (P less than .0001). After risk adjustment, LOS was 43% shorter for concurrent dissections.
Cardiac arrhythmias were also more common in staged patients, perhaps because they had general anesthesia twice in a short period or maybe because staged patients were more likely to be obese (18.5% vs. 7.5%; P less than .01).
However, there were no statistically significant outcome differences otherwise, and the investigators concluded that “concurrent and staged procedures are equally safe. It is therefore reasonable to allow operator preference and patient factors to determine surgical logistics.”
Neck dissection timing has been controversial since the advent of TORS several years ago, when surgeons and administrators realized they could fit more cases into the schedule by doing neck dissections, which can take a few hours, at a different time.
Proponents of the staged approach argue, among other things, that it reduces the risk of fistulas and tracheotomies, and allows surgeons a second go at positive margins. Advocates of concurrent procedures counter that fistulas, if found, can be repaired right away, and that same-time surgery saves money, allows for earlier adjuvant therapy, and cuts anesthesia risks.
There hasn’t been much data to settle the debate, and no one has compared LOS before, so it was “important” to look into the matter, lead investigator Catherine Frenkel, MD, a Stony Brook general surgery resident, said at the American Head and Neck Society International Conference on Head and Neck Cancer.
German investigators also recently concluded that it’s pretty much a draw between concurrent and staged dissections. In a study of 41 TORS cases, “the timing of neck dissection did not make a significant difference in the outcomes. We suggest, therefore, that aspiring and established TORS teams do not restrict their appropriate indications due to robotic slot and theatre time constraints, but perform each indicated TORS case as soon as possible within their given systems, even if the neck dissections cannot be done on the same day,” they said (Eur J Surg Oncol. 2015 Jun;41[6]:773-8).
In addition to obese patients, those who had tongue or tonsil lesions were more likely to be staged in the Stony Brook analysis. About half of the surgeons in the study stuck solely to concurrent procedures, while a handful opted for the staged approach, and the rest did both. Perhaps not surprisingly, high-volume surgeons – those who did five or more TORS cases per year – were more likely to stage.
Almost two-thirds of patients had at least one complication, most commonly renal failure, heart problems, extended ventilation, and surgical errors, which included accidental punctures, postop fistulas, hemorrhages, and wound complications. A total of 13% of patients had at least one postop readmission. Apart from arrhythmias, there were no statistically significant differences in complication or 30-day readmission rates between concurrent and staged patients. High-volume surgeons were less likely to have complications.
Postop bleeding was another common problem, and more likely with staged surgeries (12% vs. 7%). Concurrent procedures had a slightly higher rate of new tracheotomies and gastrostomies, but again the differences were not statistically significant, even with pedicle and free-flap reconstruction. There was no outside funding for the work, and the investigators had no relevant conflicts of interest.
SEATTLE – Oncologic transoral robotic surgery patients spend less time in the hospital if they have neck dissections at the same time, instead of later, according to a review of 441 patients by Stony Brook (N.Y.) University.
The average hospital length of stay (LOS) was 6 days for the 349 patients (79.1%) who had lymphadenectomy neck dissections at the same time as transoral robotic surgery (TORS). The 92 patients (20.9%) who had staged procedures - neck dissections and TORS about a month apart, with TORS usually done first - stayed in the hospital an average of 8 days (P less than .0001). After risk adjustment, LOS was 43% shorter for concurrent dissections.
Cardiac arrhythmias were also more common in staged patients, perhaps because they had general anesthesia twice in a short period or maybe because staged patients were more likely to be obese (18.5% vs. 7.5%; P less than .01).
However, there were no statistically significant outcome differences otherwise, and the investigators concluded that “concurrent and staged procedures are equally safe. It is therefore reasonable to allow operator preference and patient factors to determine surgical logistics.”
Neck dissection timing has been controversial since the advent of TORS several years ago, when surgeons and administrators realized they could fit more cases into the schedule by doing neck dissections, which can take a few hours, at a different time.
Proponents of the staged approach argue, among other things, that it reduces the risk of fistulas and tracheotomies, and allows surgeons a second go at positive margins. Advocates of concurrent procedures counter that fistulas, if found, can be repaired right away, and that same-time surgery saves money, allows for earlier adjuvant therapy, and cuts anesthesia risks.
There hasn’t been much data to settle the debate, and no one has compared LOS before, so it was “important” to look into the matter, lead investigator Catherine Frenkel, MD, a Stony Brook general surgery resident, said at the American Head and Neck Society International Conference on Head and Neck Cancer.
German investigators also recently concluded that it’s pretty much a draw between concurrent and staged dissections. In a study of 41 TORS cases, “the timing of neck dissection did not make a significant difference in the outcomes. We suggest, therefore, that aspiring and established TORS teams do not restrict their appropriate indications due to robotic slot and theatre time constraints, but perform each indicated TORS case as soon as possible within their given systems, even if the neck dissections cannot be done on the same day,” they said (Eur J Surg Oncol. 2015 Jun;41[6]:773-8).
In addition to obese patients, those who had tongue or tonsil lesions were more likely to be staged in the Stony Brook analysis. About half of the surgeons in the study stuck solely to concurrent procedures, while a handful opted for the staged approach, and the rest did both. Perhaps not surprisingly, high-volume surgeons – those who did five or more TORS cases per year – were more likely to stage.
Almost two-thirds of patients had at least one complication, most commonly renal failure, heart problems, extended ventilation, and surgical errors, which included accidental punctures, postop fistulas, hemorrhages, and wound complications. A total of 13% of patients had at least one postop readmission. Apart from arrhythmias, there were no statistically significant differences in complication or 30-day readmission rates between concurrent and staged patients. High-volume surgeons were less likely to have complications.
Postop bleeding was another common problem, and more likely with staged surgeries (12% vs. 7%). Concurrent procedures had a slightly higher rate of new tracheotomies and gastrostomies, but again the differences were not statistically significant, even with pedicle and free-flap reconstruction. There was no outside funding for the work, and the investigators had no relevant conflicts of interest.
AT THE INTERNATIONAL CONFERENCE ON HEAD AND NECK CANCER
Key clinical point: Oncologic transoral robotic surgery patients spend less time in the hospital if they have neck dissections at the same time, instead of later.
Major finding: The average hospital length of stay was 6 days for the 349 patients (79.1%) who had lymphadenectomy neck dissections at the same time as TORS. The 92 patients (20.9%) who had staged procedures – neck dissections and TORS about a month apart, with TORS usually done first – stayed in the hospital an average of 8 days (P less than .0001).
Data source: Review of 441 TORS patients.
Disclosures: There was no outside funding for the work, and the investigators had no relevant conflicts of interest.
Thymectomy improves clinical outcomes for myasthenia gravis
Thymectomy improved 3-year clinical outcomes and proved superior to medical therapy for mild to severe nonthymomatous myasthenia gravis, according to a report published online Aug. 11 in the New England Journal of Medicine.
Compared with standard prednisone therapy, thymectomy plus prednisone decreased the number and severity of symptoms, allowed the lowering of steroid doses, decreased the number and length of hospitalizations for disease exacerbations, reduced the need for immunosuppressive agents, and improved health-related quality of life in an international, randomized clinical trial, said Gil I. Wolfe, MD, of the department of neurology, State University of New York at Buffalo and his associates.
Until now, thymectomy was known to be beneficial in some cases of myasthenia gravis “but with widely varying rates of clinical improvement or remission.” And the success of immunotherapy has raised the question of whether an invasive surgery is necessary. Data from randomized, controlled studies have been sparse.
Moreover, thymectomy rarely causes adverse effects, but “the procedure can cost up to $80,000 and can be associated with operative complications that need to be weighed against benefits.” In comparison, medical therapy with glucocorticoids and other immunosuppressive agents is less invasive but is definitely associated with adverse events, including some that are life threatening, and negatively impacts quality of life, the investigators said.
To address the lack of randomized controlled trial data, they assessed 3-year outcomes in 126 patients treated at 67 medical centers in 18 countries during a 6-year period. The study participants were aged 18-65 years, had a disease duration of less than 5 years at enrollment (median duration, 1 year), and had class II (mild generalized disease) to class IV (severe generalized disease) myasthenia gravis. These patients were randomly assigned to undergo thymectomy and receive standard prednisone therapy (66 participants) or to receive standard prednisone alone (60 participants).
Thymectomy was performed using a median sternotomy “with the goal of an en bloc resection of all mediastinal tissue that could anatomically contain gross or microscopic thymus.”
At follow-up, time-weighted average scores on the Quantitative Myasthenia Gravis scale were significantly lower by 2.85 points, indicating improved clinical status, in the thymectomy group than in the control group. Time-weighted average prednisone dose also was significantly lower, at an average alternate-day dose of 44 mg in the thymectomy group and 60 mg in the control group, Dr. Wolfe and his associates said (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMoa1602489).
On a measure of treatment-related complications, scores favored thymectomy with regard to the number of patients with symptoms, the total number of symptoms, and the distress level related to symptoms throughout the study period. Fewer patients in the thymectomy group required hospitalization for exacerbations of myasthenia gravis (9% vs. 37%), and the mean cumulative number of hospital days was lower with thymectomy (8.4 vs. 19.2).
In addition, scores on the Myasthenia Gravis Activities of Daily Living scale favored thymectomy (2.24 vs. 3.41). Fewer patients in the thymectomy group required azathioprine (17% vs. 0.48%). And the percentage of patients who reported having minimal manifestations of the disease at 3 years was significantly higher with thymectomy (67%) than with prednisone alone (47%).
This study was supported by the National Institute of Neurological Disorders and Stroke, the Muscular Dystrophy Association, and the Myasthenia Gravis Foundation of America and received no commercial support. Dr. Wolfe reported ties to Alexion Pharmaceuticals, Alpha Cancer Technologies, Argenx, Baxalta, CSL Behring, Grifols, and UCB, and his associates reported ties to numerous industry sources.
Landmark trial establishes effectiveness of thymectomy in myasthenia gravis
One of the many challenges of treating patients with myasthenia gravis (MG) is the fluctuating nature of symptoms and deficits. The neurologist or neuromuscular specialist must decide whether the disease is truly worsening, whether the patient is experiencing more pronounced symptoms from intercurrent illness or the effects of a medication known to affect the neuromuscular junction adversely, or whether the patient is concerned that there might be worsening disease when all objective measures indicate stability. These factors make treatment decisions more difficult in MG than for many other neuromuscular disorders.
Similarly, researchers considering a trial investigating treatment efficacy in MG face the complex issues of disease fluctuation in cohorts of individuals with the disease, varying levels of corticosteroid and immunosuppressant doses in different MG patients, and thorny ethical dilemmas in providing accepted therapies but not withholding effective treatments from those in need.
Dr. Wolfe and his colleagues demonstrate that they have navigated these treacherous waters. They have succeeded in completing a landmark controlled clinical trial which establishes the effectiveness of transsternal thymectomy with adjuvant corticosteroid therapy in nonthymomatous MG vs. oral prednisone without surgery. While this international 36-center trial managed to recruit 126 subjects over a 6-year period, using sound inclusion and exclusion criteria and a meticulous trial design, the number of patients is not sufficient to allow for as robust a subgroup analysis for age, gender, and a variety of clinical variables reflecting severity of disease as would have been hoped for by the MG community.
Nonetheless, this paper sets the use of thymectomy in nonthymomatous MG on firmer ground going forward. The investigators will doubtless be presenting further data from the trial, including clinical-pathologic correlates and other relevant novel observations. In addition, Wolfe et al. have opened the door for future trials of thymectomy in MG to address such issues as the benefits vs. risks of performing the operation via the traditional transsternal vs. alternative non–sternal splitting approaches.
Benn E. Smith, MD, is an associate professor of neurology at the Mayo Clinic in Scottsdale, Ariz. and is the director of the sensory laboratory there. Dr. Smith is on the Editorial Advisory Board of Clinical Neurology News.
End to an 80-year controversy
These findings from Wolfe et al. end an 80-year controversy over the effectiveness of thymectomy for patients with myasthenia gravis.
Perhaps the most important benefit for patients is that even when they require prednisone following the surgery, they can take lower doses, endure fewer glucocorticoid-related symptoms, and experience less distress from those symptoms than patients who don’t undergo thymectomy.
Unfortunately, the study results cannot offer further clarity regarding patient selection for thymectomy. The patient population in this trial was so small that subgroup analyses couldn’t allow conclusions regarding the relative effectiveness of thymectomy in men vs. women or younger vs. older patients.
Allan H. Ropper, MD, is in the department of neurology at Brigham and Women’s Hospital and Harvard Medical School, both in Boston. His financial disclosures are available at NEJM.org. Dr. Ropper made these remarks in an editorial accompanying Dr. Wolfe’s report (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMe1607953).
Landmark trial establishes effectiveness of thymectomy in myasthenia gravis
One of the many challenges of treating patients with myasthenia gravis (MG) is the fluctuating nature of symptoms and deficits. The neurologist or neuromuscular specialist must decide whether the disease is truly worsening, whether the patient is experiencing more pronounced symptoms from intercurrent illness or the effects of a medication known to affect the neuromuscular junction adversely, or whether the patient is concerned that there might be worsening disease when all objective measures indicate stability. These factors make treatment decisions more difficult in MG than for many other neuromuscular disorders.
Similarly, researchers considering a trial investigating treatment efficacy in MG face the complex issues of disease fluctuation in cohorts of individuals with the disease, varying levels of corticosteroid and immunosuppressant doses in different MG patients, and thorny ethical dilemmas in providing accepted therapies but not withholding effective treatments from those in need.
Dr. Wolfe and his colleagues demonstrate that they have navigated these treacherous waters. They have succeeded in completing a landmark controlled clinical trial which establishes the effectiveness of transsternal thymectomy with adjuvant corticosteroid therapy in nonthymomatous MG vs. oral prednisone without surgery. While this international 36-center trial managed to recruit 126 subjects over a 6-year period, using sound inclusion and exclusion criteria and a meticulous trial design, the number of patients is not sufficient to allow for as robust a subgroup analysis for age, gender, and a variety of clinical variables reflecting severity of disease as would have been hoped for by the MG community.
Nonetheless, this paper sets the use of thymectomy in nonthymomatous MG on firmer ground going forward. The investigators will doubtless be presenting further data from the trial, including clinical-pathologic correlates and other relevant novel observations. In addition, Wolfe et al. have opened the door for future trials of thymectomy in MG to address such issues as the benefits vs. risks of performing the operation via the traditional transsternal vs. alternative non–sternal splitting approaches.
Benn E. Smith, MD, is an associate professor of neurology at the Mayo Clinic in Scottsdale, Ariz. and is the director of the sensory laboratory there. Dr. Smith is on the Editorial Advisory Board of Clinical Neurology News.
End to an 80-year controversy
These findings from Wolfe et al. end an 80-year controversy over the effectiveness of thymectomy for patients with myasthenia gravis.
Perhaps the most important benefit for patients is that even when they require prednisone following the surgery, they can take lower doses, endure fewer glucocorticoid-related symptoms, and experience less distress from those symptoms than patients who don’t undergo thymectomy.
Unfortunately, the study results cannot offer further clarity regarding patient selection for thymectomy. The patient population in this trial was so small that subgroup analyses couldn’t allow conclusions regarding the relative effectiveness of thymectomy in men vs. women or younger vs. older patients.
Allan H. Ropper, MD, is in the department of neurology at Brigham and Women’s Hospital and Harvard Medical School, both in Boston. His financial disclosures are available at NEJM.org. Dr. Ropper made these remarks in an editorial accompanying Dr. Wolfe’s report (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMe1607953).
Landmark trial establishes effectiveness of thymectomy in myasthenia gravis
One of the many challenges of treating patients with myasthenia gravis (MG) is the fluctuating nature of symptoms and deficits. The neurologist or neuromuscular specialist must decide whether the disease is truly worsening, whether the patient is experiencing more pronounced symptoms from intercurrent illness or the effects of a medication known to affect the neuromuscular junction adversely, or whether the patient is concerned that there might be worsening disease when all objective measures indicate stability. These factors make treatment decisions more difficult in MG than for many other neuromuscular disorders.
Similarly, researchers considering a trial investigating treatment efficacy in MG face the complex issues of disease fluctuation in cohorts of individuals with the disease, varying levels of corticosteroid and immunosuppressant doses in different MG patients, and thorny ethical dilemmas in providing accepted therapies but not withholding effective treatments from those in need.
Dr. Wolfe and his colleagues demonstrate that they have navigated these treacherous waters. They have succeeded in completing a landmark controlled clinical trial which establishes the effectiveness of transsternal thymectomy with adjuvant corticosteroid therapy in nonthymomatous MG vs. oral prednisone without surgery. While this international 36-center trial managed to recruit 126 subjects over a 6-year period, using sound inclusion and exclusion criteria and a meticulous trial design, the number of patients is not sufficient to allow for as robust a subgroup analysis for age, gender, and a variety of clinical variables reflecting severity of disease as would have been hoped for by the MG community.
Nonetheless, this paper sets the use of thymectomy in nonthymomatous MG on firmer ground going forward. The investigators will doubtless be presenting further data from the trial, including clinical-pathologic correlates and other relevant novel observations. In addition, Wolfe et al. have opened the door for future trials of thymectomy in MG to address such issues as the benefits vs. risks of performing the operation via the traditional transsternal vs. alternative non–sternal splitting approaches.
Benn E. Smith, MD, is an associate professor of neurology at the Mayo Clinic in Scottsdale, Ariz. and is the director of the sensory laboratory there. Dr. Smith is on the Editorial Advisory Board of Clinical Neurology News.
End to an 80-year controversy
These findings from Wolfe et al. end an 80-year controversy over the effectiveness of thymectomy for patients with myasthenia gravis.
Perhaps the most important benefit for patients is that even when they require prednisone following the surgery, they can take lower doses, endure fewer glucocorticoid-related symptoms, and experience less distress from those symptoms than patients who don’t undergo thymectomy.
Unfortunately, the study results cannot offer further clarity regarding patient selection for thymectomy. The patient population in this trial was so small that subgroup analyses couldn’t allow conclusions regarding the relative effectiveness of thymectomy in men vs. women or younger vs. older patients.
Allan H. Ropper, MD, is in the department of neurology at Brigham and Women’s Hospital and Harvard Medical School, both in Boston. His financial disclosures are available at NEJM.org. Dr. Ropper made these remarks in an editorial accompanying Dr. Wolfe’s report (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMe1607953).
Thymectomy improved 3-year clinical outcomes and proved superior to medical therapy for mild to severe nonthymomatous myasthenia gravis, according to a report published online Aug. 11 in the New England Journal of Medicine.
Compared with standard prednisone therapy, thymectomy plus prednisone decreased the number and severity of symptoms, allowed the lowering of steroid doses, decreased the number and length of hospitalizations for disease exacerbations, reduced the need for immunosuppressive agents, and improved health-related quality of life in an international, randomized clinical trial, said Gil I. Wolfe, MD, of the department of neurology, State University of New York at Buffalo and his associates.
Until now, thymectomy was known to be beneficial in some cases of myasthenia gravis “but with widely varying rates of clinical improvement or remission.” And the success of immunotherapy has raised the question of whether an invasive surgery is necessary. Data from randomized, controlled studies have been sparse.
Moreover, thymectomy rarely causes adverse effects, but “the procedure can cost up to $80,000 and can be associated with operative complications that need to be weighed against benefits.” In comparison, medical therapy with glucocorticoids and other immunosuppressive agents is less invasive but is definitely associated with adverse events, including some that are life threatening, and negatively impacts quality of life, the investigators said.
To address the lack of randomized controlled trial data, they assessed 3-year outcomes in 126 patients treated at 67 medical centers in 18 countries during a 6-year period. The study participants were aged 18-65 years, had a disease duration of less than 5 years at enrollment (median duration, 1 year), and had class II (mild generalized disease) to class IV (severe generalized disease) myasthenia gravis. These patients were randomly assigned to undergo thymectomy and receive standard prednisone therapy (66 participants) or to receive standard prednisone alone (60 participants).
Thymectomy was performed using a median sternotomy “with the goal of an en bloc resection of all mediastinal tissue that could anatomically contain gross or microscopic thymus.”
At follow-up, time-weighted average scores on the Quantitative Myasthenia Gravis scale were significantly lower by 2.85 points, indicating improved clinical status, in the thymectomy group than in the control group. Time-weighted average prednisone dose also was significantly lower, at an average alternate-day dose of 44 mg in the thymectomy group and 60 mg in the control group, Dr. Wolfe and his associates said (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMoa1602489).
On a measure of treatment-related complications, scores favored thymectomy with regard to the number of patients with symptoms, the total number of symptoms, and the distress level related to symptoms throughout the study period. Fewer patients in the thymectomy group required hospitalization for exacerbations of myasthenia gravis (9% vs. 37%), and the mean cumulative number of hospital days was lower with thymectomy (8.4 vs. 19.2).
In addition, scores on the Myasthenia Gravis Activities of Daily Living scale favored thymectomy (2.24 vs. 3.41). Fewer patients in the thymectomy group required azathioprine (17% vs. 0.48%). And the percentage of patients who reported having minimal manifestations of the disease at 3 years was significantly higher with thymectomy (67%) than with prednisone alone (47%).
This study was supported by the National Institute of Neurological Disorders and Stroke, the Muscular Dystrophy Association, and the Myasthenia Gravis Foundation of America and received no commercial support. Dr. Wolfe reported ties to Alexion Pharmaceuticals, Alpha Cancer Technologies, Argenx, Baxalta, CSL Behring, Grifols, and UCB, and his associates reported ties to numerous industry sources.
Thymectomy improved 3-year clinical outcomes and proved superior to medical therapy for mild to severe nonthymomatous myasthenia gravis, according to a report published online Aug. 11 in the New England Journal of Medicine.
Compared with standard prednisone therapy, thymectomy plus prednisone decreased the number and severity of symptoms, allowed the lowering of steroid doses, decreased the number and length of hospitalizations for disease exacerbations, reduced the need for immunosuppressive agents, and improved health-related quality of life in an international, randomized clinical trial, said Gil I. Wolfe, MD, of the department of neurology, State University of New York at Buffalo and his associates.
Until now, thymectomy was known to be beneficial in some cases of myasthenia gravis “but with widely varying rates of clinical improvement or remission.” And the success of immunotherapy has raised the question of whether an invasive surgery is necessary. Data from randomized, controlled studies have been sparse.
Moreover, thymectomy rarely causes adverse effects, but “the procedure can cost up to $80,000 and can be associated with operative complications that need to be weighed against benefits.” In comparison, medical therapy with glucocorticoids and other immunosuppressive agents is less invasive but is definitely associated with adverse events, including some that are life threatening, and negatively impacts quality of life, the investigators said.
To address the lack of randomized controlled trial data, they assessed 3-year outcomes in 126 patients treated at 67 medical centers in 18 countries during a 6-year period. The study participants were aged 18-65 years, had a disease duration of less than 5 years at enrollment (median duration, 1 year), and had class II (mild generalized disease) to class IV (severe generalized disease) myasthenia gravis. These patients were randomly assigned to undergo thymectomy and receive standard prednisone therapy (66 participants) or to receive standard prednisone alone (60 participants).
Thymectomy was performed using a median sternotomy “with the goal of an en bloc resection of all mediastinal tissue that could anatomically contain gross or microscopic thymus.”
At follow-up, time-weighted average scores on the Quantitative Myasthenia Gravis scale were significantly lower by 2.85 points, indicating improved clinical status, in the thymectomy group than in the control group. Time-weighted average prednisone dose also was significantly lower, at an average alternate-day dose of 44 mg in the thymectomy group and 60 mg in the control group, Dr. Wolfe and his associates said (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMoa1602489).
On a measure of treatment-related complications, scores favored thymectomy with regard to the number of patients with symptoms, the total number of symptoms, and the distress level related to symptoms throughout the study period. Fewer patients in the thymectomy group required hospitalization for exacerbations of myasthenia gravis (9% vs. 37%), and the mean cumulative number of hospital days was lower with thymectomy (8.4 vs. 19.2).
In addition, scores on the Myasthenia Gravis Activities of Daily Living scale favored thymectomy (2.24 vs. 3.41). Fewer patients in the thymectomy group required azathioprine (17% vs. 0.48%). And the percentage of patients who reported having minimal manifestations of the disease at 3 years was significantly higher with thymectomy (67%) than with prednisone alone (47%).
This study was supported by the National Institute of Neurological Disorders and Stroke, the Muscular Dystrophy Association, and the Myasthenia Gravis Foundation of America and received no commercial support. Dr. Wolfe reported ties to Alexion Pharmaceuticals, Alpha Cancer Technologies, Argenx, Baxalta, CSL Behring, Grifols, and UCB, and his associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Thymectomy improved 3-year clinical outcomes and was superior to medical therapy for mild to severe nonthymomatous myasthenia gravis.
Major finding: Scores on the Quantitative Myasthenia Gravis scale were significantly lower by 2.85 points, indicating improved clinical status, in the thymectomy group than in the control group.
Data source: An international, randomized, medication-controlled trial involving 126 patients at 67 medical centers.
Disclosures: This study was supported by the National Institute of Neurological Disorders and Stroke, the Muscular Dystrophy Association, and the Myasthenia Gravis Foundation of America and received no commercial support. Dr. Wolfe reported ties to Alexion Pharmaceuticals, Alpha Cancer Technologies, Argenx, Baxalta, CSL Behring, Grifols, and UCB, and his associates reported ties to numerous industry sources.
Hospitalist surgical comanagement program reduced complications, costs
The comanagement of surgical patients by a team of surgeons and hospitalists yielded improvements in rates of medical complications, 30-day readmissions, consultant involvement, length of hospital stay, and total cost of care per patient, according to a study published in the Annals of Surgery.
“Traditionally, hospitals have utilized a consultation model of care for surgical patients in which the medicine consultants are involved ‘as needed’ [but] this model, though common, may not be the best approach to care for surgical patients,” wrote the investigators, led by Nidhi Rohatgi, MD, MS, of Stanford (Calif.) University. “To address these limitations in the care of surgical patients, we transitioned from the consultation model to surgical comanagement (SCM) model in Orthopedic and Neurosurgery at our institution in August 2012.”

Dr. Rohatgi and her coinvestigators enrolled 16,930 patients admitted for orthopedic surgery or neurosurgery into the SCM intervention cohort, which was further divided into a preintervention cohort and a postintervention cohort. The former were admitted from January 2009 to July 2012, and the latter from September 2012 to September 2013. A further 3,695 patients were enrolled in a control group, also made up of orthopedic surgery and neurosurgery patients, which was divided into two cohorts of pre- and postcontrol over the same time periods. The two primary outcomes were the proportion of patients that had at least one medical complication – defined as sepsis, pneumonia, urinary tract infections, delirium, acute kidney injury, atrial fibrillation, or ileus – and the proportion of patients with a hospital stay of at least 5 days. Other outcomes included 30-day readmissions, costs, two or more medical consultants, and satisfaction of both patients and providers.
The findings
Overall, the SCM model was associated with a decrease in the proportion of patients with at least one complication (odds ratio, 0.86; 95% confidence interval, 0.74-0.96; P = .008) in the intervention group, compared with the control group. Similarly, there was a reduction in the proportion of patients with a hospital stay of at least 5 days (OR, 0.75; 95% CI, 0.67-0.84; P less than .001). In addition, the SCM model was associated with a reduction in 30-day readmission rates caused by medical complications (OR, 0.67; 95% CI, 0.52-0.81; P less than .001) and a drop in the proportion of patients with two or more medical consultants (OR, 0.55; 95% CI, 0.49-0.63; P less than .001).
The overall rate of provider satisfaction in the SCM cohort was 88.3%, but there was no significant change in patient satisfaction between the pre- and post-intervention cohorts (OR, 1.08; 95% CI, 0.87-1.33; P = .507). Furthermore, Dr. Rohatgi and her coinvestigators estimated that there was at least a $2,642 cost savings per patient, with that number also estimated as being as high as $4,303.
The SCM mode work flow
The SCM model consists of a structured work flow that hospitalists adhere to. On weekdays, an orthopedic and a neurosurgery hospitalist would screen all patients admitted for each respective specialty during the day and would consult with staff after hours to discuss any potential issues they were having with these patients. On weekends, one SCM hospitalist would remain on call to screen patients and consult for both specialities. If a medical intervention was deemed necessary, the SCM on call would formally see the patient to prevent medical complications from occurring.
The SCM would also go on rounds for select patients with the rest of the surgical team, making an effort to keep communication consistent throughout the day. These rounds would be in addition to the daily, multidisciplinary rounds that would include the “surgical team, case managers, social workers, unit nurses, physical and occupational therapists, pharmacist, [and] dietitian.” Additionally, while the surgical team would conduct the discharge summaries, the SCM hospitalists would be the ones response for discharge education, medication reconciliation, and tracking patients every 2 weeks via an electronic tracking system set up by the Stanford Health Care’s Quality and Patient Safety department.
“We postulate the effect of SCM on the quality of patient care has been underestimated due to methodological shortcomings of prior studies,” the authors noted, adding that while “the initial cost of setting up SCM might be perceived as a deterrent, [our] SCM model provided a meaningful return on investment with cost savings.”
No source of funding was provided for this study. Dr. Rohatgi and her coauthors did not report any relevant financial disclosures.
The comanagement of surgical patients by a team of surgeons and hospitalists yielded improvements in rates of medical complications, 30-day readmissions, consultant involvement, length of hospital stay, and total cost of care per patient, according to a study published in the Annals of Surgery.
“Traditionally, hospitals have utilized a consultation model of care for surgical patients in which the medicine consultants are involved ‘as needed’ [but] this model, though common, may not be the best approach to care for surgical patients,” wrote the investigators, led by Nidhi Rohatgi, MD, MS, of Stanford (Calif.) University. “To address these limitations in the care of surgical patients, we transitioned from the consultation model to surgical comanagement (SCM) model in Orthopedic and Neurosurgery at our institution in August 2012.”
Dr. Rohatgi and her coinvestigators enrolled 16,930 patients admitted for orthopedic surgery or neurosurgery into the SCM intervention cohort, which was further divided into a preintervention cohort and a postintervention cohort. The former were admitted from January 2009 to July 2012, and the latter from September 2012 to September 2013. A further 3,695 patients were enrolled in a control group, also made up of orthopedic surgery and neurosurgery patients, which was divided into two cohorts of pre- and postcontrol over the same time periods. The two primary outcomes were the proportion of patients that had at least one medical complication – defined as sepsis, pneumonia, urinary tract infections, delirium, acute kidney injury, atrial fibrillation, or ileus – and the proportion of patients with a hospital stay of at least 5 days. Other outcomes included 30-day readmissions, costs, two or more medical consultants, and satisfaction of both patients and providers.
The findings
Overall, the SCM model was associated with a decrease in the proportion of patients with at least one complication (odds ratio, 0.86; 95% confidence interval, 0.74-0.96; P = .008) in the intervention group, compared with the control group. Similarly, there was a reduction in the proportion of patients with a hospital stay of at least 5 days (OR, 0.75; 95% CI, 0.67-0.84; P less than .001). In addition, the SCM model was associated with a reduction in 30-day readmission rates caused by medical complications (OR, 0.67; 95% CI, 0.52-0.81; P less than .001) and a drop in the proportion of patients with two or more medical consultants (OR, 0.55; 95% CI, 0.49-0.63; P less than .001).
The overall rate of provider satisfaction in the SCM cohort was 88.3%, but there was no significant change in patient satisfaction between the pre- and post-intervention cohorts (OR, 1.08; 95% CI, 0.87-1.33; P = .507). Furthermore, Dr. Rohatgi and her coinvestigators estimated that there was at least a $2,642 cost savings per patient, with that number also estimated as being as high as $4,303.
The SCM mode work flow
The SCM model consists of a structured work flow that hospitalists adhere to. On weekdays, an orthopedic and a neurosurgery hospitalist would screen all patients admitted for each respective specialty during the day and would consult with staff after hours to discuss any potential issues they were having with these patients. On weekends, one SCM hospitalist would remain on call to screen patients and consult for both specialities. If a medical intervention was deemed necessary, the SCM on call would formally see the patient to prevent medical complications from occurring.
The SCM would also go on rounds for select patients with the rest of the surgical team, making an effort to keep communication consistent throughout the day. These rounds would be in addition to the daily, multidisciplinary rounds that would include the “surgical team, case managers, social workers, unit nurses, physical and occupational therapists, pharmacist, [and] dietitian.” Additionally, while the surgical team would conduct the discharge summaries, the SCM hospitalists would be the ones response for discharge education, medication reconciliation, and tracking patients every 2 weeks via an electronic tracking system set up by the Stanford Health Care’s Quality and Patient Safety department.
“We postulate the effect of SCM on the quality of patient care has been underestimated due to methodological shortcomings of prior studies,” the authors noted, adding that while “the initial cost of setting up SCM might be perceived as a deterrent, [our] SCM model provided a meaningful return on investment with cost savings.”
No source of funding was provided for this study. Dr. Rohatgi and her coauthors did not report any relevant financial disclosures.
The comanagement of surgical patients by a team of surgeons and hospitalists yielded improvements in rates of medical complications, 30-day readmissions, consultant involvement, length of hospital stay, and total cost of care per patient, according to a study published in the Annals of Surgery.
“Traditionally, hospitals have utilized a consultation model of care for surgical patients in which the medicine consultants are involved ‘as needed’ [but] this model, though common, may not be the best approach to care for surgical patients,” wrote the investigators, led by Nidhi Rohatgi, MD, MS, of Stanford (Calif.) University. “To address these limitations in the care of surgical patients, we transitioned from the consultation model to surgical comanagement (SCM) model in Orthopedic and Neurosurgery at our institution in August 2012.”
Dr. Rohatgi and her coinvestigators enrolled 16,930 patients admitted for orthopedic surgery or neurosurgery into the SCM intervention cohort, which was further divided into a preintervention cohort and a postintervention cohort. The former were admitted from January 2009 to July 2012, and the latter from September 2012 to September 2013. A further 3,695 patients were enrolled in a control group, also made up of orthopedic surgery and neurosurgery patients, which was divided into two cohorts of pre- and postcontrol over the same time periods. The two primary outcomes were the proportion of patients that had at least one medical complication – defined as sepsis, pneumonia, urinary tract infections, delirium, acute kidney injury, atrial fibrillation, or ileus – and the proportion of patients with a hospital stay of at least 5 days. Other outcomes included 30-day readmissions, costs, two or more medical consultants, and satisfaction of both patients and providers.
The findings
Overall, the SCM model was associated with a decrease in the proportion of patients with at least one complication (odds ratio, 0.86; 95% confidence interval, 0.74-0.96; P = .008) in the intervention group, compared with the control group. Similarly, there was a reduction in the proportion of patients with a hospital stay of at least 5 days (OR, 0.75; 95% CI, 0.67-0.84; P less than .001). In addition, the SCM model was associated with a reduction in 30-day readmission rates caused by medical complications (OR, 0.67; 95% CI, 0.52-0.81; P less than .001) and a drop in the proportion of patients with two or more medical consultants (OR, 0.55; 95% CI, 0.49-0.63; P less than .001).
The overall rate of provider satisfaction in the SCM cohort was 88.3%, but there was no significant change in patient satisfaction between the pre- and post-intervention cohorts (OR, 1.08; 95% CI, 0.87-1.33; P = .507). Furthermore, Dr. Rohatgi and her coinvestigators estimated that there was at least a $2,642 cost savings per patient, with that number also estimated as being as high as $4,303.
The SCM mode work flow
The SCM model consists of a structured work flow that hospitalists adhere to. On weekdays, an orthopedic and a neurosurgery hospitalist would screen all patients admitted for each respective specialty during the day and would consult with staff after hours to discuss any potential issues they were having with these patients. On weekends, one SCM hospitalist would remain on call to screen patients and consult for both specialities. If a medical intervention was deemed necessary, the SCM on call would formally see the patient to prevent medical complications from occurring.
The SCM would also go on rounds for select patients with the rest of the surgical team, making an effort to keep communication consistent throughout the day. These rounds would be in addition to the daily, multidisciplinary rounds that would include the “surgical team, case managers, social workers, unit nurses, physical and occupational therapists, pharmacist, [and] dietitian.” Additionally, while the surgical team would conduct the discharge summaries, the SCM hospitalists would be the ones response for discharge education, medication reconciliation, and tracking patients every 2 weeks via an electronic tracking system set up by the Stanford Health Care’s Quality and Patient Safety department.
“We postulate the effect of SCM on the quality of patient care has been underestimated due to methodological shortcomings of prior studies,” the authors noted, adding that while “the initial cost of setting up SCM might be perceived as a deterrent, [our] SCM model provided a meaningful return on investment with cost savings.”
No source of funding was provided for this study. Dr. Rohatgi and her coauthors did not report any relevant financial disclosures.
FROM THE ANNALS OF SURGERY
Key clinical point: Surgical comanagement (SCM) of hospital patients can mitigate medical complications, length of stay, and total cost of care.
Major finding: SCM was associated with a reduction of the proportion of patients with at least one medical complication, LOS of at least 5 days, 30-day readmissions, and those requiring at least two medical consultants.
Data source: A retrospective study of 16,930 patients receiving SCM intervention and 3,695 control patients between January 2009 and September 2013.
Disclosures: No funding source disclosed. Authors did not report any relevant financial disclosures.

Mayo Clinic tops hospital rankings for 2016-2017
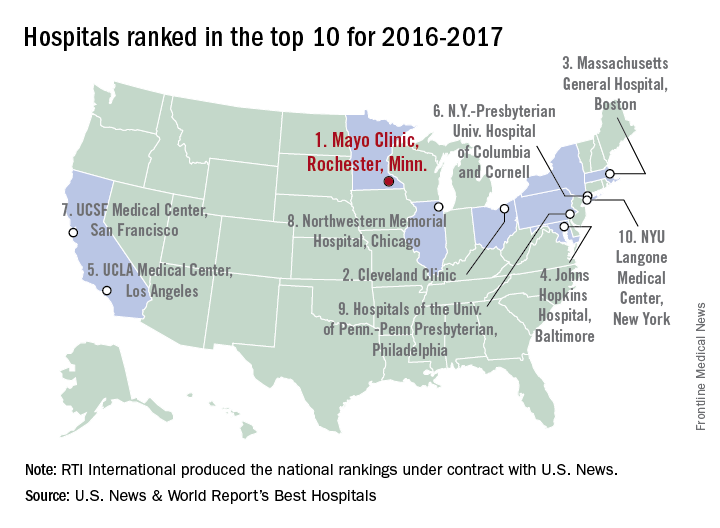
The Mayo Clinic in Rochester, Minn., was named the top hospital in the United States, according to the U.S. News & World Report Best Hospitals ranking for 2016-2017.
After finishing second to Massachusetts General Hospital in Boston last year, the Mayo Clinic regained the top spot it earned in 2014-2015. This year, the Cleveland Clinic finished second in the U.S. News Honor Roll, with Massachusetts General third, Johns Hopkins Hospital in Baltimore fourth, and the University of California, Los Angeles, Medical Center in fifth.

For 2016-2017, there were 20 hospitals in the Honor Roll, which is reserved for those institutions that finish at or near the top among the 16 specialties included in the U.S. News rankings. This year, 153 hospitals did well enough to be nationally ranked in one or more specialties, which is up from the 144 that were ranked nationally in at least one specialty last year.
The 16 specialties used in the analysis are cancer, cardiology and heart surgery, diabetes and endocrinology, otolaryngology, gastroenterology and gastrointestinal surgery, geriatrics, gynecology, nephrology, neurology and neurosurgery, ophthalmology, orthopedics, psychiatry, pulmonology, rehabilitation, rheumatology, and urology.
This year’s ranking process initially included 4,667 nonfederal community hospitals. The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News.
The Mayo Clinic in Rochester, Minn., was named the top hospital in the United States, according to the U.S. News & World Report Best Hospitals ranking for 2016-2017.
After finishing second to Massachusetts General Hospital in Boston last year, the Mayo Clinic regained the top spot it earned in 2014-2015. This year, the Cleveland Clinic finished second in the U.S. News Honor Roll, with Massachusetts General third, Johns Hopkins Hospital in Baltimore fourth, and the University of California, Los Angeles, Medical Center in fifth.
For 2016-2017, there were 20 hospitals in the Honor Roll, which is reserved for those institutions that finish at or near the top among the 16 specialties included in the U.S. News rankings. This year, 153 hospitals did well enough to be nationally ranked in one or more specialties, which is up from the 144 that were ranked nationally in at least one specialty last year.
The 16 specialties used in the analysis are cancer, cardiology and heart surgery, diabetes and endocrinology, otolaryngology, gastroenterology and gastrointestinal surgery, geriatrics, gynecology, nephrology, neurology and neurosurgery, ophthalmology, orthopedics, psychiatry, pulmonology, rehabilitation, rheumatology, and urology.
This year’s ranking process initially included 4,667 nonfederal community hospitals. The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News.
The Mayo Clinic in Rochester, Minn., was named the top hospital in the United States, according to the U.S. News & World Report Best Hospitals ranking for 2016-2017.
After finishing second to Massachusetts General Hospital in Boston last year, the Mayo Clinic regained the top spot it earned in 2014-2015. This year, the Cleveland Clinic finished second in the U.S. News Honor Roll, with Massachusetts General third, Johns Hopkins Hospital in Baltimore fourth, and the University of California, Los Angeles, Medical Center in fifth.
For 2016-2017, there were 20 hospitals in the Honor Roll, which is reserved for those institutions that finish at or near the top among the 16 specialties included in the U.S. News rankings. This year, 153 hospitals did well enough to be nationally ranked in one or more specialties, which is up from the 144 that were ranked nationally in at least one specialty last year.
The 16 specialties used in the analysis are cancer, cardiology and heart surgery, diabetes and endocrinology, otolaryngology, gastroenterology and gastrointestinal surgery, geriatrics, gynecology, nephrology, neurology and neurosurgery, ophthalmology, orthopedics, psychiatry, pulmonology, rehabilitation, rheumatology, and urology.
This year’s ranking process initially included 4,667 nonfederal community hospitals. The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News.
Preop G-tubes save money in head and neck cancer resections
SEATTLE – It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after, according to a review of 184 patients.
The 73 patients in the study who got preoperative gastrostomy tubes (G-tubes) were sicker than the 111 who had G-tubes placed after surgery, with significantly higher American Society of Anesthesiologists scores, lower body mass indexes, and greater likelihoods of having both prior radiation and more extensive resections requiring flap reconstructions. They were, overall, a higher-risk population with a greater potential for bad outcomes, which is why tubes were placed preemptively.

Even so, at 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postoperative group, a savings of $9,248 per patient. The difference was driven by inpatient savings; the preop group left the hospital an average of 3.2 days sooner than their postop G-tube peers (9.4 days versus 12.6 days; P less than .001). Readmissions and other postdischarge costs were similar between the two groups, as were wound and nonwound complications.
“This data suggests that preoperative placement of G-tubes is associated with lower total health care costs. It appears there’s a potential for health care cost savings if candidates for G-tubes can be identified” before surgery and the tubes placed preoperatively, said investigator Joshua Waltonen, MD, of Wake Forest University, Winston-Salem, N.C.
That’s exactly what Wake Forest is doing now. Physicians there use a scoring system to determine how likely patients are to need G-tubes after surgery. If the risk is high, patients are counseled that putting one in beforehand is a good idea, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The team previously found that risk factors include, among others, supracricoid laryngectomy, prior radiation, flap reconstruction, tracheostomy placement, and preop dysphagia and weight loss (JAMA Otolaryngol Head Neck Surg. 2014 Dec;140[12]:1198-206).
Two factors probably account for the shorter lengths of stay, Dr. Waltonen said. First, patients with preop feeding tubes go into surgery with a nutritional boost, which helps with recovery. Also, with a preop tube, patients don’t have to wait for general surgery to get around to placing one postoperatively.
Both groups were about 60 years old on average. The mean body mass index of the preop group was 23 kg/m2 and 26 kg/m2 in the postop group (P = .009). Almost two-thirds of preop patients had prior radiation versus a quarter of postop patients (P less than .001). Tumor and nodal stages were similar.
There was no outside funding for the work, and Dr. Waltonen had no disclosures.
SEATTLE – It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after, according to a review of 184 patients.
The 73 patients in the study who got preoperative gastrostomy tubes (G-tubes) were sicker than the 111 who had G-tubes placed after surgery, with significantly higher American Society of Anesthesiologists scores, lower body mass indexes, and greater likelihoods of having both prior radiation and more extensive resections requiring flap reconstructions. They were, overall, a higher-risk population with a greater potential for bad outcomes, which is why tubes were placed preemptively.
Even so, at 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postoperative group, a savings of $9,248 per patient. The difference was driven by inpatient savings; the preop group left the hospital an average of 3.2 days sooner than their postop G-tube peers (9.4 days versus 12.6 days; P less than .001). Readmissions and other postdischarge costs were similar between the two groups, as were wound and nonwound complications.
“This data suggests that preoperative placement of G-tubes is associated with lower total health care costs. It appears there’s a potential for health care cost savings if candidates for G-tubes can be identified” before surgery and the tubes placed preoperatively, said investigator Joshua Waltonen, MD, of Wake Forest University, Winston-Salem, N.C.
That’s exactly what Wake Forest is doing now. Physicians there use a scoring system to determine how likely patients are to need G-tubes after surgery. If the risk is high, patients are counseled that putting one in beforehand is a good idea, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The team previously found that risk factors include, among others, supracricoid laryngectomy, prior radiation, flap reconstruction, tracheostomy placement, and preop dysphagia and weight loss (JAMA Otolaryngol Head Neck Surg. 2014 Dec;140[12]:1198-206).
Two factors probably account for the shorter lengths of stay, Dr. Waltonen said. First, patients with preop feeding tubes go into surgery with a nutritional boost, which helps with recovery. Also, with a preop tube, patients don’t have to wait for general surgery to get around to placing one postoperatively.
Both groups were about 60 years old on average. The mean body mass index of the preop group was 23 kg/m2 and 26 kg/m2 in the postop group (P = .009). Almost two-thirds of preop patients had prior radiation versus a quarter of postop patients (P less than .001). Tumor and nodal stages were similar.
There was no outside funding for the work, and Dr. Waltonen had no disclosures.
SEATTLE – It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after, according to a review of 184 patients.
The 73 patients in the study who got preoperative gastrostomy tubes (G-tubes) were sicker than the 111 who had G-tubes placed after surgery, with significantly higher American Society of Anesthesiologists scores, lower body mass indexes, and greater likelihoods of having both prior radiation and more extensive resections requiring flap reconstructions. They were, overall, a higher-risk population with a greater potential for bad outcomes, which is why tubes were placed preemptively.
Even so, at 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postoperative group, a savings of $9,248 per patient. The difference was driven by inpatient savings; the preop group left the hospital an average of 3.2 days sooner than their postop G-tube peers (9.4 days versus 12.6 days; P less than .001). Readmissions and other postdischarge costs were similar between the two groups, as were wound and nonwound complications.
“This data suggests that preoperative placement of G-tubes is associated with lower total health care costs. It appears there’s a potential for health care cost savings if candidates for G-tubes can be identified” before surgery and the tubes placed preoperatively, said investigator Joshua Waltonen, MD, of Wake Forest University, Winston-Salem, N.C.
That’s exactly what Wake Forest is doing now. Physicians there use a scoring system to determine how likely patients are to need G-tubes after surgery. If the risk is high, patients are counseled that putting one in beforehand is a good idea, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The team previously found that risk factors include, among others, supracricoid laryngectomy, prior radiation, flap reconstruction, tracheostomy placement, and preop dysphagia and weight loss (JAMA Otolaryngol Head Neck Surg. 2014 Dec;140[12]:1198-206).
Two factors probably account for the shorter lengths of stay, Dr. Waltonen said. First, patients with preop feeding tubes go into surgery with a nutritional boost, which helps with recovery. Also, with a preop tube, patients don’t have to wait for general surgery to get around to placing one postoperatively.
Both groups were about 60 years old on average. The mean body mass index of the preop group was 23 kg/m2 and 26 kg/m2 in the postop group (P = .009). Almost two-thirds of preop patients had prior radiation versus a quarter of postop patients (P less than .001). Tumor and nodal stages were similar.
There was no outside funding for the work, and Dr. Waltonen had no disclosures.
AT AHNS 2016
Key clinical point: It’s better to place gastrostomy tubes before head and neck cancer surgery rather than after.
Major finding: At 6 months, the total average cost for the preop G-tube group was $39,751 versus $48,999 for the postop group, a savings of $9,248 per patient.
Data source: Review of 184 patients.
Disclosures: There was no outside funding for the work, and the presenter had no disclosures.

Medicaid expansion leads to better access to care
Low-income adults living in two states that expanded Medicaid enrollment are showing significant increases in outpatient utilization and preventive care, improved health care quality, and reductions in emergency department use, compared with those living in a state that did not expand Medicaid, according to a new study.
The study also found similar improvements in care whether a state expanded traditional Medicaid or increased coverage through a private insurance option.

Benjamin D. Sommers, MD, PhD, of Harvard University, Boston, and his colleagues examined outcomes for nearly 9,000 low-income Medicaid enrollees in Kentucky (where officials expanded traditional Medicaid), Arkansas (where the state used funds to purchase private insurance to expand coverage), and Texas (which did not expand Medicaid) in November and December of 2013, 2014, and 2015. They looked specifically at changes in use of healthcare services, preventive care, and self-reported health (JAMA Intern Med. 2016 Aug 8. doi: 10.1001/jamainternmed.2016.4419).
“By the end of 2015, we found marked increases in coverage and reduced cost-related barriers to care in the expansion states, with associated increases in preventive care, outpatient visits, annual checkups, and chronic disease care, as well as decreased reliance on the [emergency department],” the researchers wrote.
They found that by 2015 there was a 6 percentage point drop in the likelihood of ED visits (P = 0.04), an increase of 0.69 office visits per person in the outpatient setting (P = 0.04), and an increase likelihood of getting a checkup (16.1 percentage points, P less than .001) in Medicaid expansion states. In Medicaid expansion states the share of adults obtaining regular care for chronic conditions increased by 12 percentage points after expansion (P = .008), compared with Texas. Additionally, adults reporting fair or poor quality of care dropped by 7.1 percentage points (P = .03).
One significant difference between the expansion states was changes in glucose monitoring rates for patients with diabetes were lower in Arkansas than Kentucky (–11.6 percentage points, P = .04).
“Of note, we found improvements in receipt of checkups, care for chronic conditions, and quality of care even in areas with primary care shortages, suggesting that while clinician capacity is undoubtedly an important consideration, insurance expansion can have a demonstrable positive impact even in areas with relative shortages, perhaps partially due to increased use of safety net providers,” the researchers added.
The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.
Whether the premium assistance model proves to be durable and effective remains an open question. On the upside, the findings of Sommers et al suggest that the Arkansas initiative is living up to its promises. Moreover, the waiver seems to have increased the number of insurers participating in the marketplaces and contributed to lower premiums.
But other evidence concerning premium assistance waivers suggests the need for caution in assessing their effectiveness. The Government Accountability Office has questioned whether these waivers are budget neutral – a federal requirement. In this vein, the Congressional Budget Office has estimated that it will cost 50% more per enrollee to cover the expansion population on the exchanges than in the conventional Medicaid program. Nor are premium assistance waivers necessarily sustainable. In Pennsylvania, for instance, a newly elected Democratic governor worked to phase out that state’s existing alternative waiver, which had been negotiated by a prior Republican administration, in favor of a traditional expansion of the Medicaid entitlement.
Frank J. Thompson, PhD, and Joel C. Cantor, ScD, are both at Rutgers University in New Brunswick, N.J. They reported having no financial disclosures. Their comments were excerpted from a commentary in JAMA Internal Medicine (2016 Aug 8. doi: 10.1001/jamainternmed.2016.4422).
Whether the premium assistance model proves to be durable and effective remains an open question. On the upside, the findings of Sommers et al suggest that the Arkansas initiative is living up to its promises. Moreover, the waiver seems to have increased the number of insurers participating in the marketplaces and contributed to lower premiums.
But other evidence concerning premium assistance waivers suggests the need for caution in assessing their effectiveness. The Government Accountability Office has questioned whether these waivers are budget neutral – a federal requirement. In this vein, the Congressional Budget Office has estimated that it will cost 50% more per enrollee to cover the expansion population on the exchanges than in the conventional Medicaid program. Nor are premium assistance waivers necessarily sustainable. In Pennsylvania, for instance, a newly elected Democratic governor worked to phase out that state’s existing alternative waiver, which had been negotiated by a prior Republican administration, in favor of a traditional expansion of the Medicaid entitlement.
Frank J. Thompson, PhD, and Joel C. Cantor, ScD, are both at Rutgers University in New Brunswick, N.J. They reported having no financial disclosures. Their comments were excerpted from a commentary in JAMA Internal Medicine (2016 Aug 8. doi: 10.1001/jamainternmed.2016.4422).
Whether the premium assistance model proves to be durable and effective remains an open question. On the upside, the findings of Sommers et al suggest that the Arkansas initiative is living up to its promises. Moreover, the waiver seems to have increased the number of insurers participating in the marketplaces and contributed to lower premiums.
But other evidence concerning premium assistance waivers suggests the need for caution in assessing their effectiveness. The Government Accountability Office has questioned whether these waivers are budget neutral – a federal requirement. In this vein, the Congressional Budget Office has estimated that it will cost 50% more per enrollee to cover the expansion population on the exchanges than in the conventional Medicaid program. Nor are premium assistance waivers necessarily sustainable. In Pennsylvania, for instance, a newly elected Democratic governor worked to phase out that state’s existing alternative waiver, which had been negotiated by a prior Republican administration, in favor of a traditional expansion of the Medicaid entitlement.
Frank J. Thompson, PhD, and Joel C. Cantor, ScD, are both at Rutgers University in New Brunswick, N.J. They reported having no financial disclosures. Their comments were excerpted from a commentary in JAMA Internal Medicine (2016 Aug 8. doi: 10.1001/jamainternmed.2016.4422).
Low-income adults living in two states that expanded Medicaid enrollment are showing significant increases in outpatient utilization and preventive care, improved health care quality, and reductions in emergency department use, compared with those living in a state that did not expand Medicaid, according to a new study.
The study also found similar improvements in care whether a state expanded traditional Medicaid or increased coverage through a private insurance option.
Benjamin D. Sommers, MD, PhD, of Harvard University, Boston, and his colleagues examined outcomes for nearly 9,000 low-income Medicaid enrollees in Kentucky (where officials expanded traditional Medicaid), Arkansas (where the state used funds to purchase private insurance to expand coverage), and Texas (which did not expand Medicaid) in November and December of 2013, 2014, and 2015. They looked specifically at changes in use of healthcare services, preventive care, and self-reported health (JAMA Intern Med. 2016 Aug 8. doi: 10.1001/jamainternmed.2016.4419).
“By the end of 2015, we found marked increases in coverage and reduced cost-related barriers to care in the expansion states, with associated increases in preventive care, outpatient visits, annual checkups, and chronic disease care, as well as decreased reliance on the [emergency department],” the researchers wrote.
They found that by 2015 there was a 6 percentage point drop in the likelihood of ED visits (P = 0.04), an increase of 0.69 office visits per person in the outpatient setting (P = 0.04), and an increase likelihood of getting a checkup (16.1 percentage points, P less than .001) in Medicaid expansion states. In Medicaid expansion states the share of adults obtaining regular care for chronic conditions increased by 12 percentage points after expansion (P = .008), compared with Texas. Additionally, adults reporting fair or poor quality of care dropped by 7.1 percentage points (P = .03).
One significant difference between the expansion states was changes in glucose monitoring rates for patients with diabetes were lower in Arkansas than Kentucky (–11.6 percentage points, P = .04).
“Of note, we found improvements in receipt of checkups, care for chronic conditions, and quality of care even in areas with primary care shortages, suggesting that while clinician capacity is undoubtedly an important consideration, insurance expansion can have a demonstrable positive impact even in areas with relative shortages, perhaps partially due to increased use of safety net providers,” the researchers added.
The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.
Low-income adults living in two states that expanded Medicaid enrollment are showing significant increases in outpatient utilization and preventive care, improved health care quality, and reductions in emergency department use, compared with those living in a state that did not expand Medicaid, according to a new study.
The study also found similar improvements in care whether a state expanded traditional Medicaid or increased coverage through a private insurance option.
Benjamin D. Sommers, MD, PhD, of Harvard University, Boston, and his colleagues examined outcomes for nearly 9,000 low-income Medicaid enrollees in Kentucky (where officials expanded traditional Medicaid), Arkansas (where the state used funds to purchase private insurance to expand coverage), and Texas (which did not expand Medicaid) in November and December of 2013, 2014, and 2015. They looked specifically at changes in use of healthcare services, preventive care, and self-reported health (JAMA Intern Med. 2016 Aug 8. doi: 10.1001/jamainternmed.2016.4419).
“By the end of 2015, we found marked increases in coverage and reduced cost-related barriers to care in the expansion states, with associated increases in preventive care, outpatient visits, annual checkups, and chronic disease care, as well as decreased reliance on the [emergency department],” the researchers wrote.
They found that by 2015 there was a 6 percentage point drop in the likelihood of ED visits (P = 0.04), an increase of 0.69 office visits per person in the outpatient setting (P = 0.04), and an increase likelihood of getting a checkup (16.1 percentage points, P less than .001) in Medicaid expansion states. In Medicaid expansion states the share of adults obtaining regular care for chronic conditions increased by 12 percentage points after expansion (P = .008), compared with Texas. Additionally, adults reporting fair or poor quality of care dropped by 7.1 percentage points (P = .03).
One significant difference between the expansion states was changes in glucose monitoring rates for patients with diabetes were lower in Arkansas than Kentucky (–11.6 percentage points, P = .04).
“Of note, we found improvements in receipt of checkups, care for chronic conditions, and quality of care even in areas with primary care shortages, suggesting that while clinician capacity is undoubtedly an important consideration, insurance expansion can have a demonstrable positive impact even in areas with relative shortages, perhaps partially due to increased use of safety net providers,” the researchers added.
The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Medicaid expansion improved self-reported health outcomes and access to care.
Major finding: By 2015 there was a 6 percentage point drop in the likelihood of emergency department visits (P = .04) and an increase of 0.69 outpatient office visits per person (P = .04).
Data source: A differences-in-differences analysis of survey data from Nov. 2013 through Dec. 2015 of 8,676 low-income adults in Kentucky, Arkansas, and Texas.
Disclosures: The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.

Intraoperative nerve stimulation reduces risk of shoulder pain from neck dissection
SEATTLE – Direct, intraoperative electrical stimulation of the spinal accessory nerve reduced shoulder pain and dysfunction from oncologic neck dissection in a small, randomized trial.
Shoulder problems are common after neck dissection because of traction and compression of the spinal accessory nerve. Although brief electrical stimulation (BES) has been shown before to improve regeneration and recovery of injured peripheral nerves, it hasn’t been shown until now to help patients recover from neck surgery, said investigator Brittany Barber, MD, a fifth-year resident at the University of Alberta, Edmonton.

After neck dissection in 21 patients, the investigators wrapped a small electrode (Automatic Periodic Stimulation [APS] electrode, Medtronic) around the spinal accessory nerve at the base of the skull on the side of the neck with the most extensive nodal burden; the electrode delivered 100-msec pulses at 20 Hz and 3-5 V for an hour, and then the neck was closed. The team compared outcomes with 20 controls who had neck dissections without BES.
At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Outcome Score, while the controls lost a mean of 29.4 points. The Murley score measures shoulder pain, performance of daily tasks, range of motion, and strength; higher scores are better. Similarly, BES patients lost a mean of 16.2 points on the 50-point Neck Dissection Impairment Index, while controls lost 30.1 points, and controls performed markedly worse on nerve conduction studies. In short, BES patients “were less likely to have clinically significant shoulder dysfunction” after surgery, Dr. Barber said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The APS electrode is a tiny silicone cuff with a metal conductor. The device was originally designed to monitor recurrent laryngeal nerve function during thyroid surgery. “We had [Medtronic] write a software patch” so it could be used for stimulation, she said.
The team is planning a larger, multicenter trial to shore up their findings, and also plans to test the device for hypoglossal nerve preservation after resection.
Transcutaneous nerve stimulation is another option, but it’s a bit uncomfortable and patients often don’t complete their sessions. “Compliance is not as good as with a single intraoperative procedure,” and the results aren’t that great. “We thought this might be a better alternative,” Dr. Barber said.
The two groups were well matched: Mean age was about 60 years and most patients had advanced-stage tumors. There was no difference in preop shoulder problems or risks for poor postop shoulder outcomes, and no difference in the number of level 5 neck dissections or mean number of lymph nodes removed during surgery.
There was no outside funding for the work. Dr. Barber had no disclosures; a coinvestigator was a Medtronic consultant.
SEATTLE – Direct, intraoperative electrical stimulation of the spinal accessory nerve reduced shoulder pain and dysfunction from oncologic neck dissection in a small, randomized trial.
Shoulder problems are common after neck dissection because of traction and compression of the spinal accessory nerve. Although brief electrical stimulation (BES) has been shown before to improve regeneration and recovery of injured peripheral nerves, it hasn’t been shown until now to help patients recover from neck surgery, said investigator Brittany Barber, MD, a fifth-year resident at the University of Alberta, Edmonton.
After neck dissection in 21 patients, the investigators wrapped a small electrode (Automatic Periodic Stimulation [APS] electrode, Medtronic) around the spinal accessory nerve at the base of the skull on the side of the neck with the most extensive nodal burden; the electrode delivered 100-msec pulses at 20 Hz and 3-5 V for an hour, and then the neck was closed. The team compared outcomes with 20 controls who had neck dissections without BES.
At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Outcome Score, while the controls lost a mean of 29.4 points. The Murley score measures shoulder pain, performance of daily tasks, range of motion, and strength; higher scores are better. Similarly, BES patients lost a mean of 16.2 points on the 50-point Neck Dissection Impairment Index, while controls lost 30.1 points, and controls performed markedly worse on nerve conduction studies. In short, BES patients “were less likely to have clinically significant shoulder dysfunction” after surgery, Dr. Barber said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The APS electrode is a tiny silicone cuff with a metal conductor. The device was originally designed to monitor recurrent laryngeal nerve function during thyroid surgery. “We had [Medtronic] write a software patch” so it could be used for stimulation, she said.
The team is planning a larger, multicenter trial to shore up their findings, and also plans to test the device for hypoglossal nerve preservation after resection.
Transcutaneous nerve stimulation is another option, but it’s a bit uncomfortable and patients often don’t complete their sessions. “Compliance is not as good as with a single intraoperative procedure,” and the results aren’t that great. “We thought this might be a better alternative,” Dr. Barber said.
The two groups were well matched: Mean age was about 60 years and most patients had advanced-stage tumors. There was no difference in preop shoulder problems or risks for poor postop shoulder outcomes, and no difference in the number of level 5 neck dissections or mean number of lymph nodes removed during surgery.
There was no outside funding for the work. Dr. Barber had no disclosures; a coinvestigator was a Medtronic consultant.
SEATTLE – Direct, intraoperative electrical stimulation of the spinal accessory nerve reduced shoulder pain and dysfunction from oncologic neck dissection in a small, randomized trial.
Shoulder problems are common after neck dissection because of traction and compression of the spinal accessory nerve. Although brief electrical stimulation (BES) has been shown before to improve regeneration and recovery of injured peripheral nerves, it hasn’t been shown until now to help patients recover from neck surgery, said investigator Brittany Barber, MD, a fifth-year resident at the University of Alberta, Edmonton.
After neck dissection in 21 patients, the investigators wrapped a small electrode (Automatic Periodic Stimulation [APS] electrode, Medtronic) around the spinal accessory nerve at the base of the skull on the side of the neck with the most extensive nodal burden; the electrode delivered 100-msec pulses at 20 Hz and 3-5 V for an hour, and then the neck was closed. The team compared outcomes with 20 controls who had neck dissections without BES.
At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Outcome Score, while the controls lost a mean of 29.4 points. The Murley score measures shoulder pain, performance of daily tasks, range of motion, and strength; higher scores are better. Similarly, BES patients lost a mean of 16.2 points on the 50-point Neck Dissection Impairment Index, while controls lost 30.1 points, and controls performed markedly worse on nerve conduction studies. In short, BES patients “were less likely to have clinically significant shoulder dysfunction” after surgery, Dr. Barber said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
The APS electrode is a tiny silicone cuff with a metal conductor. The device was originally designed to monitor recurrent laryngeal nerve function during thyroid surgery. “We had [Medtronic] write a software patch” so it could be used for stimulation, she said.
The team is planning a larger, multicenter trial to shore up their findings, and also plans to test the device for hypoglossal nerve preservation after resection.
Transcutaneous nerve stimulation is another option, but it’s a bit uncomfortable and patients often don’t complete their sessions. “Compliance is not as good as with a single intraoperative procedure,” and the results aren’t that great. “We thought this might be a better alternative,” Dr. Barber said.
The two groups were well matched: Mean age was about 60 years and most patients had advanced-stage tumors. There was no difference in preop shoulder problems or risks for poor postop shoulder outcomes, and no difference in the number of level 5 neck dissections or mean number of lymph nodes removed during surgery.
There was no outside funding for the work. Dr. Barber had no disclosures; a coinvestigator was a Medtronic consultant.
AT AHNS 2016
Key clinical point: Direct, intraoperative electrical stimulation of the spinal accessory nerve reduces shoulder pain and dysfunction from oncologic neck dissection.
Major finding: At 12 months, the BES group had an 8.4 point drop from baseline on the 100-point Constant Murley Shoulder Score, while the controls lost a mean of 29.4 points.
Data source: Randomized trial with 41 patients.
Disclosures: There was no outside funding for the work. The presenter had no disclosures; a co-investigator was a Medtronic consultant.

Hospital safety culture may influence surgical outcomes
SAN DIEGO – Hospital safety culture may positively influence certain surgical patient outcomes, results from a study of 56 Illinois hospitals demonstrated.
“Efforts to improve awareness of safety and quality improvement principles should be encouraged at both the surgical system and hospital levels,” David D. Odell, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference. “Safety culture itself is a concept [that] is increasingly viewed as important in the delivery of high-quality care. Yet in the surgical world, very little is known about how hospital culture actually influences outcomes for our patients.”

Dr. Odell, a thoracic surgeon at Northwestern Memorial Hospital, Chicago, discussed results from a study by the Illinois Surgical Quality Improvement Collaborative, a group of Illinois hospitals working together to improve the quality of surgical care in the state. Participants in the Collaborative include 56 hospitals, including all academic medical centers in the state, as well as 11 rural hospitals. Combined, these facilities perform 60% of general surgery operations in the state and 80% of all complex operations, impacting more than 600,000 patients each year.
In an effort to evaluate the relationship between hospital safety culture and surgical patient outcomes, Dr. Odell and his associates invited staff of Collaborative members to complete the Safety Attitudes Questionnaire (SAQ), a 56-item validated tool for assessment of hospital culture. Domains focused on were teamwork, communication, engagement, and leadership. The SAQ was given to administrators, staff, and front-line providers “to measure safety culture across all levels of the hospital,” Dr. Odell said. Percent positive responses were calculated at the hospital level for each of the eight domains to calculate a composite measure of safety. The researchers measured the impact of safety culture by assessing positive SAQ response rates. Outcome variables of interest were morbidity, mortality, death or serious morbidity, and readmission. Hospital-level risk-adjusted event rates and linear regression models were used to assess the impact of safety culture while controlling for teaching status, rural location, trauma center designation, hospital control (management), and the annual surgical volume.
Of the 49 participating hospitals represented in the survey responses, 49% had an Accreditation Council for Graduate Medical Education (ACGME)-accredited residency program, 12% were rural, 61% provided trauma care, 35% had a religious affiliation, 57% were “other” not-for-profit, and the mean total surgical volume was 11,412 cases.
Dr. Odell reported that by domain, SAQ responses were most positive for operating room safety and lowest for hospital management. “That doesn’t necessarily reflect the management’s outcomes only, but the views of those who took the survey toward management,” he said.
When the researchers evaluated the impact of a more-positive safety culture on the risk-adjusted outcome measures, they observed a statistically significant impact on morbidity following surgery (P = .02). The trend was similar although not statistically significant for death/serious morbidity (P = .08), mortality (P =. 20), or readmission (P = .68).
Dr. Odell acknowledged certain limitations of the study, including its retrospective design and the fact that the SAQ is a subjective assessment tool. “Not all [staff invited] were surveyed,” he added. “We sent out just under 1,400 surveys and we had a response rate of 44%.”
Staff from participating institutions of the Collaborative meet on a semiannual basis to share ideas, celebrate successes and learn from each other’s experiences, Dr. Odell said. Ongoing efforts to improve safety culture include fostering opportunities for mentorship in quality improvement and process improvement endeavors, as well as the provision of educational materials targeted at all levels of hospital staff “so that we can get everyone thinking and speaking the same language when it comes to quality improvement,” he said.
The Collaborative is funded by Blue Cross Blue Shield of Illinois. Dr. Odell reported having no financial disclosures.
SAN DIEGO – Hospital safety culture may positively influence certain surgical patient outcomes, results from a study of 56 Illinois hospitals demonstrated.
“Efforts to improve awareness of safety and quality improvement principles should be encouraged at both the surgical system and hospital levels,” David D. Odell, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference. “Safety culture itself is a concept [that] is increasingly viewed as important in the delivery of high-quality care. Yet in the surgical world, very little is known about how hospital culture actually influences outcomes for our patients.”
Dr. Odell, a thoracic surgeon at Northwestern Memorial Hospital, Chicago, discussed results from a study by the Illinois Surgical Quality Improvement Collaborative, a group of Illinois hospitals working together to improve the quality of surgical care in the state. Participants in the Collaborative include 56 hospitals, including all academic medical centers in the state, as well as 11 rural hospitals. Combined, these facilities perform 60% of general surgery operations in the state and 80% of all complex operations, impacting more than 600,000 patients each year.
In an effort to evaluate the relationship between hospital safety culture and surgical patient outcomes, Dr. Odell and his associates invited staff of Collaborative members to complete the Safety Attitudes Questionnaire (SAQ), a 56-item validated tool for assessment of hospital culture. Domains focused on were teamwork, communication, engagement, and leadership. The SAQ was given to administrators, staff, and front-line providers “to measure safety culture across all levels of the hospital,” Dr. Odell said. Percent positive responses were calculated at the hospital level for each of the eight domains to calculate a composite measure of safety. The researchers measured the impact of safety culture by assessing positive SAQ response rates. Outcome variables of interest were morbidity, mortality, death or serious morbidity, and readmission. Hospital-level risk-adjusted event rates and linear regression models were used to assess the impact of safety culture while controlling for teaching status, rural location, trauma center designation, hospital control (management), and the annual surgical volume.
Of the 49 participating hospitals represented in the survey responses, 49% had an Accreditation Council for Graduate Medical Education (ACGME)-accredited residency program, 12% were rural, 61% provided trauma care, 35% had a religious affiliation, 57% were “other” not-for-profit, and the mean total surgical volume was 11,412 cases.
Dr. Odell reported that by domain, SAQ responses were most positive for operating room safety and lowest for hospital management. “That doesn’t necessarily reflect the management’s outcomes only, but the views of those who took the survey toward management,” he said.
When the researchers evaluated the impact of a more-positive safety culture on the risk-adjusted outcome measures, they observed a statistically significant impact on morbidity following surgery (P = .02). The trend was similar although not statistically significant for death/serious morbidity (P = .08), mortality (P =. 20), or readmission (P = .68).
Dr. Odell acknowledged certain limitations of the study, including its retrospective design and the fact that the SAQ is a subjective assessment tool. “Not all [staff invited] were surveyed,” he added. “We sent out just under 1,400 surveys and we had a response rate of 44%.”
Staff from participating institutions of the Collaborative meet on a semiannual basis to share ideas, celebrate successes and learn from each other’s experiences, Dr. Odell said. Ongoing efforts to improve safety culture include fostering opportunities for mentorship in quality improvement and process improvement endeavors, as well as the provision of educational materials targeted at all levels of hospital staff “so that we can get everyone thinking and speaking the same language when it comes to quality improvement,” he said.
The Collaborative is funded by Blue Cross Blue Shield of Illinois. Dr. Odell reported having no financial disclosures.
SAN DIEGO – Hospital safety culture may positively influence certain surgical patient outcomes, results from a study of 56 Illinois hospitals demonstrated.
“Efforts to improve awareness of safety and quality improvement principles should be encouraged at both the surgical system and hospital levels,” David D. Odell, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference. “Safety culture itself is a concept [that] is increasingly viewed as important in the delivery of high-quality care. Yet in the surgical world, very little is known about how hospital culture actually influences outcomes for our patients.”
Dr. Odell, a thoracic surgeon at Northwestern Memorial Hospital, Chicago, discussed results from a study by the Illinois Surgical Quality Improvement Collaborative, a group of Illinois hospitals working together to improve the quality of surgical care in the state. Participants in the Collaborative include 56 hospitals, including all academic medical centers in the state, as well as 11 rural hospitals. Combined, these facilities perform 60% of general surgery operations in the state and 80% of all complex operations, impacting more than 600,000 patients each year.
In an effort to evaluate the relationship between hospital safety culture and surgical patient outcomes, Dr. Odell and his associates invited staff of Collaborative members to complete the Safety Attitudes Questionnaire (SAQ), a 56-item validated tool for assessment of hospital culture. Domains focused on were teamwork, communication, engagement, and leadership. The SAQ was given to administrators, staff, and front-line providers “to measure safety culture across all levels of the hospital,” Dr. Odell said. Percent positive responses were calculated at the hospital level for each of the eight domains to calculate a composite measure of safety. The researchers measured the impact of safety culture by assessing positive SAQ response rates. Outcome variables of interest were morbidity, mortality, death or serious morbidity, and readmission. Hospital-level risk-adjusted event rates and linear regression models were used to assess the impact of safety culture while controlling for teaching status, rural location, trauma center designation, hospital control (management), and the annual surgical volume.
Of the 49 participating hospitals represented in the survey responses, 49% had an Accreditation Council for Graduate Medical Education (ACGME)-accredited residency program, 12% were rural, 61% provided trauma care, 35% had a religious affiliation, 57% were “other” not-for-profit, and the mean total surgical volume was 11,412 cases.
Dr. Odell reported that by domain, SAQ responses were most positive for operating room safety and lowest for hospital management. “That doesn’t necessarily reflect the management’s outcomes only, but the views of those who took the survey toward management,” he said.
When the researchers evaluated the impact of a more-positive safety culture on the risk-adjusted outcome measures, they observed a statistically significant impact on morbidity following surgery (P = .02). The trend was similar although not statistically significant for death/serious morbidity (P = .08), mortality (P =. 20), or readmission (P = .68).
Dr. Odell acknowledged certain limitations of the study, including its retrospective design and the fact that the SAQ is a subjective assessment tool. “Not all [staff invited] were surveyed,” he added. “We sent out just under 1,400 surveys and we had a response rate of 44%.”
Staff from participating institutions of the Collaborative meet on a semiannual basis to share ideas, celebrate successes and learn from each other’s experiences, Dr. Odell said. Ongoing efforts to improve safety culture include fostering opportunities for mentorship in quality improvement and process improvement endeavors, as well as the provision of educational materials targeted at all levels of hospital staff “so that we can get everyone thinking and speaking the same language when it comes to quality improvement,” he said.
The Collaborative is funded by Blue Cross Blue Shield of Illinois. Dr. Odell reported having no financial disclosures.
EXPERT ANALYSIS AT THE ACS NSQIP NATIONAL CONFERENCE
Key clinical point: A positive hospital safety culture significantly impacted morbidity following surgery.
Major finding: When the researchers evaluated the impact of a positive safety culture on risk-adjusted outcome measures, they observed a statistically significant impact on morbidity following surgery (P = .02).
Data source: A retrospective study by the Illinois Surgical Quality Improvement Collaborative, a group of 56 hospitals in the state.
Disclosures: The Collaborative is funded by Blue Cross Blue Shield of Illinois. Dr. Odell reported having no financial disclosures.

ACS NSQIP Geriatric Surgery Pilot Collaborative: Evaluating variables for inclusion
SAN DIEGO – A project to assess geriatric-specific variables for inclusion in the American College of Surgeons/National Surgical Quality Improvement Program National Conference is underway, according to Thomas N. Robinson, MD.
Dr. Robinson discussed results from the ACS-NSQIP Geriatric Surgery Pilot Collaborative, an effort launched in January 2014 with the ultimate goal of evaluating specific geriatric variables for incorporation into the ACS NSQIP set of essential variables collected by all participating hospitals.

Dr. Robinson, professor of surgery at the University of Colorado, Denver, said that 23 clinical sites in the United States are currently studying the following geriatric-specific variables in surgery patients aged 65 and older:
• Origin from home with support (to determine baseline functional status: lives alone at home, lives with support in home, origin status not from home).
• Discharge functional health status (ability to perform activities of daily living).
• Discharge with/without services (to capture care needs upon discharge).
• Preoperative use of a mobility aid.
• Preoperative history of prior falls.
• Postoperative history of pressure ulcer.
• Fall risk on discharge.
• New mobility aid on discharge.
• History of dementia.
• Competency status on admission.
• Postoperative delirium (yes or no).
• Hospice care on admission (yes or no).
• Do Not Resuscitate (DNR) order in place on admission (yes or no).
• DNR order during hospitalization (yes or no).
• Setting where DNR order was placed.
• Postoperative palliative care consult (yes or no).
• 30-day postoperative outcomes: functional health status (ability to perform activities of daily living), physical function compared with baseline, and living location.
The number of surgery cases in the collaborative grew from 7,235 in the first 6 months of 2014 to 24,835 cases in the last 6 months of 2015. The top 10 operations were total joint arthroplasty (29%), colectomy (12%), spine (8%), hip fracture (7%), carotid endarterectomy (4%), hysterectomy (4%), lung resection (2%), open lower extremity bypass (2%), laparoscopic cholecystectomy (2%), and pancreatectomy (2%).
Dr. Robinson reported that the rate of preoperative dementia among cases studied in the collaborative was 10%. “The incorporation of dementia into a surgical dataset represents an important step forward in providing quality surgical care for the elderly,” he said. “Dementia is a global public health concern.” He went on to note that patients with dementia have a 2.5-fold increased risk of developing postoperative delirium, making it “the perfect place to start a quality project. One in three cases of delirium is preventable. In our data set, delirium is associated with a hospital stay that’s 4 days longer, an increased chance of requiring discharge to an institutional care facility, an increased chance of a serious complication, and a higher 30-day mortality.”
Simple, low-tech bedside interventions such as ambulating in the hall three times a day, orienting the person, having the person sleep at night rather than sleep during the day, and avoiding medications with high risk for adverse events in older adults can prevent postoperative delirium, Dr. Robinson said.
One way that the Geriatric Surgery Pilot Collaborative can improve the surgical care of older adults is by fostering quality programs initiated at the participating local hospitals. “Preserving function after hospital stays is a first major goal,” he said. Another strategy involves creating a multidisciplinary frailty assessment to aid with decision making and risk assessment. “This takes into consideration NSQIP variables such as function, nutrition, comorbidity burden, cognition, social vulnerability, and mobility,” he said. The final and ultimate goal of the geriatric surgery collaborative is to establish a foundation of quality measurement for the Coalition for Quality in Geriatric Surgery, a project initiated by the American College of Surgeons to systematically improve the surgical care of older adults.
Dr. Robinson reported having no relevant financial disclosures.
SAN DIEGO – A project to assess geriatric-specific variables for inclusion in the American College of Surgeons/National Surgical Quality Improvement Program National Conference is underway, according to Thomas N. Robinson, MD.
Dr. Robinson discussed results from the ACS-NSQIP Geriatric Surgery Pilot Collaborative, an effort launched in January 2014 with the ultimate goal of evaluating specific geriatric variables for incorporation into the ACS NSQIP set of essential variables collected by all participating hospitals.
Dr. Robinson, professor of surgery at the University of Colorado, Denver, said that 23 clinical sites in the United States are currently studying the following geriatric-specific variables in surgery patients aged 65 and older:
• Origin from home with support (to determine baseline functional status: lives alone at home, lives with support in home, origin status not from home).
• Discharge functional health status (ability to perform activities of daily living).
• Discharge with/without services (to capture care needs upon discharge).
• Preoperative use of a mobility aid.
• Preoperative history of prior falls.
• Postoperative history of pressure ulcer.
• Fall risk on discharge.
• New mobility aid on discharge.
• History of dementia.
• Competency status on admission.
• Postoperative delirium (yes or no).
• Hospice care on admission (yes or no).
• Do Not Resuscitate (DNR) order in place on admission (yes or no).
• DNR order during hospitalization (yes or no).
• Setting where DNR order was placed.
• Postoperative palliative care consult (yes or no).
• 30-day postoperative outcomes: functional health status (ability to perform activities of daily living), physical function compared with baseline, and living location.
The number of surgery cases in the collaborative grew from 7,235 in the first 6 months of 2014 to 24,835 cases in the last 6 months of 2015. The top 10 operations were total joint arthroplasty (29%), colectomy (12%), spine (8%), hip fracture (7%), carotid endarterectomy (4%), hysterectomy (4%), lung resection (2%), open lower extremity bypass (2%), laparoscopic cholecystectomy (2%), and pancreatectomy (2%).
Dr. Robinson reported that the rate of preoperative dementia among cases studied in the collaborative was 10%. “The incorporation of dementia into a surgical dataset represents an important step forward in providing quality surgical care for the elderly,” he said. “Dementia is a global public health concern.” He went on to note that patients with dementia have a 2.5-fold increased risk of developing postoperative delirium, making it “the perfect place to start a quality project. One in three cases of delirium is preventable. In our data set, delirium is associated with a hospital stay that’s 4 days longer, an increased chance of requiring discharge to an institutional care facility, an increased chance of a serious complication, and a higher 30-day mortality.”
Simple, low-tech bedside interventions such as ambulating in the hall three times a day, orienting the person, having the person sleep at night rather than sleep during the day, and avoiding medications with high risk for adverse events in older adults can prevent postoperative delirium, Dr. Robinson said.
One way that the Geriatric Surgery Pilot Collaborative can improve the surgical care of older adults is by fostering quality programs initiated at the participating local hospitals. “Preserving function after hospital stays is a first major goal,” he said. Another strategy involves creating a multidisciplinary frailty assessment to aid with decision making and risk assessment. “This takes into consideration NSQIP variables such as function, nutrition, comorbidity burden, cognition, social vulnerability, and mobility,” he said. The final and ultimate goal of the geriatric surgery collaborative is to establish a foundation of quality measurement for the Coalition for Quality in Geriatric Surgery, a project initiated by the American College of Surgeons to systematically improve the surgical care of older adults.
Dr. Robinson reported having no relevant financial disclosures.
SAN DIEGO – A project to assess geriatric-specific variables for inclusion in the American College of Surgeons/National Surgical Quality Improvement Program National Conference is underway, according to Thomas N. Robinson, MD.
Dr. Robinson discussed results from the ACS-NSQIP Geriatric Surgery Pilot Collaborative, an effort launched in January 2014 with the ultimate goal of evaluating specific geriatric variables for incorporation into the ACS NSQIP set of essential variables collected by all participating hospitals.
Dr. Robinson, professor of surgery at the University of Colorado, Denver, said that 23 clinical sites in the United States are currently studying the following geriatric-specific variables in surgery patients aged 65 and older:
• Origin from home with support (to determine baseline functional status: lives alone at home, lives with support in home, origin status not from home).
• Discharge functional health status (ability to perform activities of daily living).
• Discharge with/without services (to capture care needs upon discharge).
• Preoperative use of a mobility aid.
• Preoperative history of prior falls.
• Postoperative history of pressure ulcer.
• Fall risk on discharge.
• New mobility aid on discharge.
• History of dementia.
• Competency status on admission.
• Postoperative delirium (yes or no).
• Hospice care on admission (yes or no).
• Do Not Resuscitate (DNR) order in place on admission (yes or no).
• DNR order during hospitalization (yes or no).
• Setting where DNR order was placed.
• Postoperative palliative care consult (yes or no).
• 30-day postoperative outcomes: functional health status (ability to perform activities of daily living), physical function compared with baseline, and living location.
The number of surgery cases in the collaborative grew from 7,235 in the first 6 months of 2014 to 24,835 cases in the last 6 months of 2015. The top 10 operations were total joint arthroplasty (29%), colectomy (12%), spine (8%), hip fracture (7%), carotid endarterectomy (4%), hysterectomy (4%), lung resection (2%), open lower extremity bypass (2%), laparoscopic cholecystectomy (2%), and pancreatectomy (2%).
Dr. Robinson reported that the rate of preoperative dementia among cases studied in the collaborative was 10%. “The incorporation of dementia into a surgical dataset represents an important step forward in providing quality surgical care for the elderly,” he said. “Dementia is a global public health concern.” He went on to note that patients with dementia have a 2.5-fold increased risk of developing postoperative delirium, making it “the perfect place to start a quality project. One in three cases of delirium is preventable. In our data set, delirium is associated with a hospital stay that’s 4 days longer, an increased chance of requiring discharge to an institutional care facility, an increased chance of a serious complication, and a higher 30-day mortality.”
Simple, low-tech bedside interventions such as ambulating in the hall three times a day, orienting the person, having the person sleep at night rather than sleep during the day, and avoiding medications with high risk for adverse events in older adults can prevent postoperative delirium, Dr. Robinson said.
One way that the Geriatric Surgery Pilot Collaborative can improve the surgical care of older adults is by fostering quality programs initiated at the participating local hospitals. “Preserving function after hospital stays is a first major goal,” he said. Another strategy involves creating a multidisciplinary frailty assessment to aid with decision making and risk assessment. “This takes into consideration NSQIP variables such as function, nutrition, comorbidity burden, cognition, social vulnerability, and mobility,” he said. The final and ultimate goal of the geriatric surgery collaborative is to establish a foundation of quality measurement for the Coalition for Quality in Geriatric Surgery, a project initiated by the American College of Surgeons to systematically improve the surgical care of older adults.
Dr. Robinson reported having no relevant financial disclosures.
EXPERT ANALYSIS AT THE ACS NSQIP NATIONAL CONFERENCE

Study aims to better understand readmissions in pediatric surgery
SAN DIEGO – Readmission rates and the underlying reasons for them vary between medical specialties following surgery in children, a study of national data suggests.
“Hospital readmission is a very hot topic, particularly in light of the Affordable Care Act,” Afif N. Kulaylat, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference. “Beyond economic costs there are very tangible costs to patients that we must consider. Readmissions have been associated with significant morbidity for patients. They often herald or implicate a postoperative complication. There are also indirect costs to patients and families such as time off from school or work.”

Dr. Kulaylat, of the division of pediatric surgery at Penn State Children’s Hospital, Hershey, Penn., presented findings from a retrospective analysis of NSQIP Pediatric (NSQIP-P), an ongoing collaboration between the ACS and the American Pediatric Surgical Association to improve the care of young patients. The researchers evaluated NSQIP-P data from 2013 and 2014 and focused on unplanned readmission within 30 days, including reasons for readmission based on NSQIP-P readmission categories and ICD-9 readmission codes as categorized by the AHRQ Clinical Classification Software. Multivariate logistic regression was used to evaluate factors associated with unplanned readmission.
Dr. Kulaylat reported results from a cohort of 129,849 patients cared for by 64 NSQIP-P participating hospitals. Among these, the all-cause readmission rate was 4.7%. After excluding patients with planned readmissions, the unplanned readmission rate was found to be 3.9%. From this cohort, 28% required reoperation within 30 days, and the median time from discharge to unplanned readmission was 8 days, with an interquartile range between 3 and 14 days.
Among the procedures captured in NSQIP-P, neurosurgery accounted for the highest readmission rate (10.8%), followed by general/thoracic surgery (5.2%), urology (2.6%), ENT (2%), orthopedic (1.9%), and plastic and reconstructive surgery (1.3%). The most common reason for readmission was surgical site infection at 23%, followed by GI complications such as ileus, obstruction, and constipation (17%); pulmonary-related complications (9%); device-related complications including shunt malfunction (8%); neurologic (7%); pain (6%); other medical diseases (6%); sepsis (5%); electrolytes/dehydration (5%); and urinary tract infection (UTI, 3%). It is estimated that at least two-thirds of unplanned readmissions (63%) were directly related to surgery. “These reasons for readmission and their frequency closely parallel what is seen in adults, with the exception of bleeding complications, which were rare in children compared to adults,” Dr. Kulaylat said.
The top five CPT codes associated with readmissions were laparoscopic appendectomy, laparoscopic gastrostomy tube placement, and three additional codes related to placement and replacement/revision of ventricular shunts/catheters.
Reasons for readmission varied among specialties. For example, among general and thoracic surgery, surgical-site infections (SSI) and GI-related issues dominated, while in neurosurgery SSI and device issues dominated. In urology, UTIs were the most frequent, while ENT had a greater proportion of pulmonary complications. Certain patient variables were also associated with an increased risk of hospital readmission, including comorbidities related to GI, CNS, renal, and immunosuppression and nutrition (P less than .001 for all). The strongest association was the occurrence of a postoperative complication, namely a post-discharge complication.
“The granularity of NSQIP-P can continue to be refined to help predict who is likely to get readmitted or if specific follow-up strategies might identify those headed to readmission,” remarked Robert E. Cilley, MD, a senior author and surgeon-in-chief at Penn State Children’s Hospital. Dr. Kulaylat acknowledged certain limitations of the study, including its retrospective design, the potential for data entry/data interpretation error, and that the researchers were unable to adjust for clustering at the hospital level. Directions of future research include a plan to study readmissions and predictive factors at the procedural level, establish risk-adjusted specialty/procedural-specific benchmarks for readmission rates, and refine the accuracy and reliability of the readmission data. “With these NSQIP-P data there is substantial opportunity for quality improvement as we strive to improve the care of children everywhere,” Dr. Kulaylat said. He reported having no relevant disclosures.
SAN DIEGO – Readmission rates and the underlying reasons for them vary between medical specialties following surgery in children, a study of national data suggests.
“Hospital readmission is a very hot topic, particularly in light of the Affordable Care Act,” Afif N. Kulaylat, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference. “Beyond economic costs there are very tangible costs to patients that we must consider. Readmissions have been associated with significant morbidity for patients. They often herald or implicate a postoperative complication. There are also indirect costs to patients and families such as time off from school or work.”
Dr. Kulaylat, of the division of pediatric surgery at Penn State Children’s Hospital, Hershey, Penn., presented findings from a retrospective analysis of NSQIP Pediatric (NSQIP-P), an ongoing collaboration between the ACS and the American Pediatric Surgical Association to improve the care of young patients. The researchers evaluated NSQIP-P data from 2013 and 2014 and focused on unplanned readmission within 30 days, including reasons for readmission based on NSQIP-P readmission categories and ICD-9 readmission codes as categorized by the AHRQ Clinical Classification Software. Multivariate logistic regression was used to evaluate factors associated with unplanned readmission.
Dr. Kulaylat reported results from a cohort of 129,849 patients cared for by 64 NSQIP-P participating hospitals. Among these, the all-cause readmission rate was 4.7%. After excluding patients with planned readmissions, the unplanned readmission rate was found to be 3.9%. From this cohort, 28% required reoperation within 30 days, and the median time from discharge to unplanned readmission was 8 days, with an interquartile range between 3 and 14 days.
Among the procedures captured in NSQIP-P, neurosurgery accounted for the highest readmission rate (10.8%), followed by general/thoracic surgery (5.2%), urology (2.6%), ENT (2%), orthopedic (1.9%), and plastic and reconstructive surgery (1.3%). The most common reason for readmission was surgical site infection at 23%, followed by GI complications such as ileus, obstruction, and constipation (17%); pulmonary-related complications (9%); device-related complications including shunt malfunction (8%); neurologic (7%); pain (6%); other medical diseases (6%); sepsis (5%); electrolytes/dehydration (5%); and urinary tract infection (UTI, 3%). It is estimated that at least two-thirds of unplanned readmissions (63%) were directly related to surgery. “These reasons for readmission and their frequency closely parallel what is seen in adults, with the exception of bleeding complications, which were rare in children compared to adults,” Dr. Kulaylat said.
The top five CPT codes associated with readmissions were laparoscopic appendectomy, laparoscopic gastrostomy tube placement, and three additional codes related to placement and replacement/revision of ventricular shunts/catheters.
Reasons for readmission varied among specialties. For example, among general and thoracic surgery, surgical-site infections (SSI) and GI-related issues dominated, while in neurosurgery SSI and device issues dominated. In urology, UTIs were the most frequent, while ENT had a greater proportion of pulmonary complications. Certain patient variables were also associated with an increased risk of hospital readmission, including comorbidities related to GI, CNS, renal, and immunosuppression and nutrition (P less than .001 for all). The strongest association was the occurrence of a postoperative complication, namely a post-discharge complication.
“The granularity of NSQIP-P can continue to be refined to help predict who is likely to get readmitted or if specific follow-up strategies might identify those headed to readmission,” remarked Robert E. Cilley, MD, a senior author and surgeon-in-chief at Penn State Children’s Hospital. Dr. Kulaylat acknowledged certain limitations of the study, including its retrospective design, the potential for data entry/data interpretation error, and that the researchers were unable to adjust for clustering at the hospital level. Directions of future research include a plan to study readmissions and predictive factors at the procedural level, establish risk-adjusted specialty/procedural-specific benchmarks for readmission rates, and refine the accuracy and reliability of the readmission data. “With these NSQIP-P data there is substantial opportunity for quality improvement as we strive to improve the care of children everywhere,” Dr. Kulaylat said. He reported having no relevant disclosures.
SAN DIEGO – Readmission rates and the underlying reasons for them vary between medical specialties following surgery in children, a study of national data suggests.
“Hospital readmission is a very hot topic, particularly in light of the Affordable Care Act,” Afif N. Kulaylat, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference. “Beyond economic costs there are very tangible costs to patients that we must consider. Readmissions have been associated with significant morbidity for patients. They often herald or implicate a postoperative complication. There are also indirect costs to patients and families such as time off from school or work.”
Dr. Kulaylat, of the division of pediatric surgery at Penn State Children’s Hospital, Hershey, Penn., presented findings from a retrospective analysis of NSQIP Pediatric (NSQIP-P), an ongoing collaboration between the ACS and the American Pediatric Surgical Association to improve the care of young patients. The researchers evaluated NSQIP-P data from 2013 and 2014 and focused on unplanned readmission within 30 days, including reasons for readmission based on NSQIP-P readmission categories and ICD-9 readmission codes as categorized by the AHRQ Clinical Classification Software. Multivariate logistic regression was used to evaluate factors associated with unplanned readmission.
Dr. Kulaylat reported results from a cohort of 129,849 patients cared for by 64 NSQIP-P participating hospitals. Among these, the all-cause readmission rate was 4.7%. After excluding patients with planned readmissions, the unplanned readmission rate was found to be 3.9%. From this cohort, 28% required reoperation within 30 days, and the median time from discharge to unplanned readmission was 8 days, with an interquartile range between 3 and 14 days.
Among the procedures captured in NSQIP-P, neurosurgery accounted for the highest readmission rate (10.8%), followed by general/thoracic surgery (5.2%), urology (2.6%), ENT (2%), orthopedic (1.9%), and plastic and reconstructive surgery (1.3%). The most common reason for readmission was surgical site infection at 23%, followed by GI complications such as ileus, obstruction, and constipation (17%); pulmonary-related complications (9%); device-related complications including shunt malfunction (8%); neurologic (7%); pain (6%); other medical diseases (6%); sepsis (5%); electrolytes/dehydration (5%); and urinary tract infection (UTI, 3%). It is estimated that at least two-thirds of unplanned readmissions (63%) were directly related to surgery. “These reasons for readmission and their frequency closely parallel what is seen in adults, with the exception of bleeding complications, which were rare in children compared to adults,” Dr. Kulaylat said.
The top five CPT codes associated with readmissions were laparoscopic appendectomy, laparoscopic gastrostomy tube placement, and three additional codes related to placement and replacement/revision of ventricular shunts/catheters.
Reasons for readmission varied among specialties. For example, among general and thoracic surgery, surgical-site infections (SSI) and GI-related issues dominated, while in neurosurgery SSI and device issues dominated. In urology, UTIs were the most frequent, while ENT had a greater proportion of pulmonary complications. Certain patient variables were also associated with an increased risk of hospital readmission, including comorbidities related to GI, CNS, renal, and immunosuppression and nutrition (P less than .001 for all). The strongest association was the occurrence of a postoperative complication, namely a post-discharge complication.
“The granularity of NSQIP-P can continue to be refined to help predict who is likely to get readmitted or if specific follow-up strategies might identify those headed to readmission,” remarked Robert E. Cilley, MD, a senior author and surgeon-in-chief at Penn State Children’s Hospital. Dr. Kulaylat acknowledged certain limitations of the study, including its retrospective design, the potential for data entry/data interpretation error, and that the researchers were unable to adjust for clustering at the hospital level. Directions of future research include a plan to study readmissions and predictive factors at the procedural level, establish risk-adjusted specialty/procedural-specific benchmarks for readmission rates, and refine the accuracy and reliability of the readmission data. “With these NSQIP-P data there is substantial opportunity for quality improvement as we strive to improve the care of children everywhere,” Dr. Kulaylat said. He reported having no relevant disclosures.
AT THE ACS NSQIP NATIONAL CONFERENCE
Key clinical point: Readmission rates following pediatric surgery vary between medical specialties.
Major finding: Among the procedures captured in ACS NSQIP Pediatric (NSQIP-P), neurosurgery accounted for the highest readmission rate (10.8%), followed by general/thoracic surgery (5.2%), urology (2.6%), ENT (2%), orthopedic (1.9%), and plastic and reconstructive surgery (1.3%).
Data source: An analysis of 129,849 pediatric patients cared for by 64 NSQIP-P participating hospitals.
Disclosures: Dr. Kulaylat reported having no financial disclosures.
