User login
Official Newspaper of the American College of Surgeons
Core curriculum for opioid prescribing preempts certification
LAKE BUENA VISTA, FLA. – If the Food and Drug Administration moves to require some form of certification to prescribe opioids, an educational program based on the FDA’s own risk evaluation and mitigation strategy (REMS) report of 2012 is already in place to fulfill that purpose, according to a pain specialist who explained the principles of this program at Pain Care for Primary Care.
Some form of certification process for opioid prescribing has been discussed for many years, explained David E. J. Bazzo, MD, clinical professor of family medicine at the University of California, San Diego, but “there has been renewed interest as a result of the continuing public health crisis regarding opioid overdoses.”

The core curriculum provided by the Collaborative for REMS Education (CO*RE) curriculum is based on clinical competencies to meet the requirements of the FDA REMS blueprint, which was issued in July 2012. The focus of REMS is on opioids with an extended-release (ER) or long-acting (LA) formulation. It is not the only such program available, but Dr. Bazzo noted that CO*RE was actually initiated in 2010 and provided some of the basis for the FDA REMS that followed 2 years later.
The CO*RE program, which can be completed at no cost, is available online. Those who complete the program are provided with a completer certificate, which Dr. Bazzo expects to be honored by the FDA if it does decide to require proof of competency. The program involves the participation of 13 organizations, such as the American Pain Society (APS), the American Society of Addiction Medicine (ASAM), and the American College of Emergency Physicians (ACEP).
There is a substantial possibility that the FDA will move to require competency for opioid prescribers. At a recent joint meeting of the FDA’s Drug Safety and Risk Management Advisory Committee and the Anesthetic and Analgesic Drug Products Advisory Committee in which modifications in the REMS were discussed, the majority of those on both advisory committees endorsed mandatory training.
“Why is education so important? It is because we are in a super tough position,” Dr. Bazzo explained. He suggested that physicians need effective agents for controlling pain, but the mortality and morbidity associated with opioids has steadily increased despite the FDA REMS.
“Deaths due to drug abuse or poisoning are just the beginning. For every death, there are 10 treatment admissions for abuse, and 130 people who are addicted,” said Dr. Bazzo, citing data from the Centers for Disease Control and Prevention (CDC).
In addition to an introduction, which outlines the goals of appropriate opioid prescribing, the CO*RE curriculum consists of six units. The first focuses on assessing candidates for opioid therapy, which includes instructions on history taking and documenting the findings. Tools for assessing risks posed by opioids, particularly for abuse, are also outlined.
The second unit describes best practices for initiating therapy, modifying doses, and discontinuing opioids, the third unit provides information on monitoring adherence and aberrant behavior in patients, and the fourth unit provides information about how to counsel patients about what constitutes appropriate use of opioids and the risks of inappropriate use. The fifth unit is largely an overview of key information in the previous four units and the sixth unit outlines the specific features of currently available opioids.
“The bottom line for the program overall is learning how to balance risks and benefits,” Dr. Bazzo explained. He suggested that many clinicians do not fully grasp that opioids are not stand-alone medications but a tool within a more comprehensive strategy for improving function.
“When we give analgesics for chronic pain, the goal is not to eliminate pain. If this is your goal, you will fail 99.9999% of the time. The goal is to improve function,” Dr. Bazzo said. He characterized treatment of chronic pain “as a team sport” that involves a collaboration between specialists and patients to achieve specific endpoints.
“It is a little like treating hypertension. You adjust medications until you get to the goal,” Dr. Bazzo said. This involves defining the goal before the treatment is initiated and then documenting progress toward that goal to guide treatment strategies.
The CO*RE REMS program is consistent with the CDC Guideline for Prescribing Opioids for Chronic Pain (MMWR. 65[1];1–49). It is part of a nationwide effort to reduce deaths related to opioid use.
“The problems with opioids can be greatly reduced if clinicians recognize and adhere to best practices,” Dr. Bazzo maintained.
Dr. Bazzo reports no potential financial conflicts of interest. The meeting was held by the APS and Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
LAKE BUENA VISTA, FLA. – If the Food and Drug Administration moves to require some form of certification to prescribe opioids, an educational program based on the FDA’s own risk evaluation and mitigation strategy (REMS) report of 2012 is already in place to fulfill that purpose, according to a pain specialist who explained the principles of this program at Pain Care for Primary Care.
Some form of certification process for opioid prescribing has been discussed for many years, explained David E. J. Bazzo, MD, clinical professor of family medicine at the University of California, San Diego, but “there has been renewed interest as a result of the continuing public health crisis regarding opioid overdoses.”
The core curriculum provided by the Collaborative for REMS Education (CO*RE) curriculum is based on clinical competencies to meet the requirements of the FDA REMS blueprint, which was issued in July 2012. The focus of REMS is on opioids with an extended-release (ER) or long-acting (LA) formulation. It is not the only such program available, but Dr. Bazzo noted that CO*RE was actually initiated in 2010 and provided some of the basis for the FDA REMS that followed 2 years later.
The CO*RE program, which can be completed at no cost, is available online. Those who complete the program are provided with a completer certificate, which Dr. Bazzo expects to be honored by the FDA if it does decide to require proof of competency. The program involves the participation of 13 organizations, such as the American Pain Society (APS), the American Society of Addiction Medicine (ASAM), and the American College of Emergency Physicians (ACEP).
There is a substantial possibility that the FDA will move to require competency for opioid prescribers. At a recent joint meeting of the FDA’s Drug Safety and Risk Management Advisory Committee and the Anesthetic and Analgesic Drug Products Advisory Committee in which modifications in the REMS were discussed, the majority of those on both advisory committees endorsed mandatory training.
“Why is education so important? It is because we are in a super tough position,” Dr. Bazzo explained. He suggested that physicians need effective agents for controlling pain, but the mortality and morbidity associated with opioids has steadily increased despite the FDA REMS.
“Deaths due to drug abuse or poisoning are just the beginning. For every death, there are 10 treatment admissions for abuse, and 130 people who are addicted,” said Dr. Bazzo, citing data from the Centers for Disease Control and Prevention (CDC).
In addition to an introduction, which outlines the goals of appropriate opioid prescribing, the CO*RE curriculum consists of six units. The first focuses on assessing candidates for opioid therapy, which includes instructions on history taking and documenting the findings. Tools for assessing risks posed by opioids, particularly for abuse, are also outlined.
The second unit describes best practices for initiating therapy, modifying doses, and discontinuing opioids, the third unit provides information on monitoring adherence and aberrant behavior in patients, and the fourth unit provides information about how to counsel patients about what constitutes appropriate use of opioids and the risks of inappropriate use. The fifth unit is largely an overview of key information in the previous four units and the sixth unit outlines the specific features of currently available opioids.
“The bottom line for the program overall is learning how to balance risks and benefits,” Dr. Bazzo explained. He suggested that many clinicians do not fully grasp that opioids are not stand-alone medications but a tool within a more comprehensive strategy for improving function.
“When we give analgesics for chronic pain, the goal is not to eliminate pain. If this is your goal, you will fail 99.9999% of the time. The goal is to improve function,” Dr. Bazzo said. He characterized treatment of chronic pain “as a team sport” that involves a collaboration between specialists and patients to achieve specific endpoints.
“It is a little like treating hypertension. You adjust medications until you get to the goal,” Dr. Bazzo said. This involves defining the goal before the treatment is initiated and then documenting progress toward that goal to guide treatment strategies.
The CO*RE REMS program is consistent with the CDC Guideline for Prescribing Opioids for Chronic Pain (MMWR. 65[1];1–49). It is part of a nationwide effort to reduce deaths related to opioid use.
“The problems with opioids can be greatly reduced if clinicians recognize and adhere to best practices,” Dr. Bazzo maintained.
Dr. Bazzo reports no potential financial conflicts of interest. The meeting was held by the APS and Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
LAKE BUENA VISTA, FLA. – If the Food and Drug Administration moves to require some form of certification to prescribe opioids, an educational program based on the FDA’s own risk evaluation and mitigation strategy (REMS) report of 2012 is already in place to fulfill that purpose, according to a pain specialist who explained the principles of this program at Pain Care for Primary Care.
Some form of certification process for opioid prescribing has been discussed for many years, explained David E. J. Bazzo, MD, clinical professor of family medicine at the University of California, San Diego, but “there has been renewed interest as a result of the continuing public health crisis regarding opioid overdoses.”
The core curriculum provided by the Collaborative for REMS Education (CO*RE) curriculum is based on clinical competencies to meet the requirements of the FDA REMS blueprint, which was issued in July 2012. The focus of REMS is on opioids with an extended-release (ER) or long-acting (LA) formulation. It is not the only such program available, but Dr. Bazzo noted that CO*RE was actually initiated in 2010 and provided some of the basis for the FDA REMS that followed 2 years later.
The CO*RE program, which can be completed at no cost, is available online. Those who complete the program are provided with a completer certificate, which Dr. Bazzo expects to be honored by the FDA if it does decide to require proof of competency. The program involves the participation of 13 organizations, such as the American Pain Society (APS), the American Society of Addiction Medicine (ASAM), and the American College of Emergency Physicians (ACEP).
There is a substantial possibility that the FDA will move to require competency for opioid prescribers. At a recent joint meeting of the FDA’s Drug Safety and Risk Management Advisory Committee and the Anesthetic and Analgesic Drug Products Advisory Committee in which modifications in the REMS were discussed, the majority of those on both advisory committees endorsed mandatory training.
“Why is education so important? It is because we are in a super tough position,” Dr. Bazzo explained. He suggested that physicians need effective agents for controlling pain, but the mortality and morbidity associated with opioids has steadily increased despite the FDA REMS.
“Deaths due to drug abuse or poisoning are just the beginning. For every death, there are 10 treatment admissions for abuse, and 130 people who are addicted,” said Dr. Bazzo, citing data from the Centers for Disease Control and Prevention (CDC).
In addition to an introduction, which outlines the goals of appropriate opioid prescribing, the CO*RE curriculum consists of six units. The first focuses on assessing candidates for opioid therapy, which includes instructions on history taking and documenting the findings. Tools for assessing risks posed by opioids, particularly for abuse, are also outlined.
The second unit describes best practices for initiating therapy, modifying doses, and discontinuing opioids, the third unit provides information on monitoring adherence and aberrant behavior in patients, and the fourth unit provides information about how to counsel patients about what constitutes appropriate use of opioids and the risks of inappropriate use. The fifth unit is largely an overview of key information in the previous four units and the sixth unit outlines the specific features of currently available opioids.
“The bottom line for the program overall is learning how to balance risks and benefits,” Dr. Bazzo explained. He suggested that many clinicians do not fully grasp that opioids are not stand-alone medications but a tool within a more comprehensive strategy for improving function.
“When we give analgesics for chronic pain, the goal is not to eliminate pain. If this is your goal, you will fail 99.9999% of the time. The goal is to improve function,” Dr. Bazzo said. He characterized treatment of chronic pain “as a team sport” that involves a collaboration between specialists and patients to achieve specific endpoints.
“It is a little like treating hypertension. You adjust medications until you get to the goal,” Dr. Bazzo said. This involves defining the goal before the treatment is initiated and then documenting progress toward that goal to guide treatment strategies.
The CO*RE REMS program is consistent with the CDC Guideline for Prescribing Opioids for Chronic Pain (MMWR. 65[1];1–49). It is part of a nationwide effort to reduce deaths related to opioid use.
“The problems with opioids can be greatly reduced if clinicians recognize and adhere to best practices,” Dr. Bazzo maintained.
Dr. Bazzo reports no potential financial conflicts of interest. The meeting was held by the APS and Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
EXPERT ANALYSIS FROM PAIN CARE FOR PRIMARY CARE

Enhanced recovery protocol for colectomy patients reduced hospital stay
SAN DIEGO – Multihospital collaboration and implementation of enhanced recovery have the potential to improve outcomes, in particular, length of hospital stay, results from a pilot study showed.
“Given the importance of patient engagement, enhanced recovery has the potential to improve patient experience and provide high-value health care,” Julia R. Berian, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference.

Dr. Berian, the James C. Thompson Geriatric Surgery Research Fellow at the University of Chicago Medical Center, presented findings from the Enhanced Recovery in NSQIP (ERIN) Pilot, a collaborative effort by 16 ACS-NSQIP hospitals to improve length of stay in patients who undergo colectomy, a procedure that has been shown to have an adverse event rate of 28.9% and an average length of stay of 9.8 days for those who experience an adverse event (J Am Coll Surg. 2008; 207[5]:698-704).
Implementation of the ERIN Pilot showed reductions in length of hospital stay and morbidity among colectomy patients. The average length of stay decreased by 1.2 days (from a mean of 6.6 among preimplementation cases to 5.4 days among post implementation cases; P less than .0001). Morbidity also decreased from 14% to 11% (P = .01), but the rate of readmission was 11% for both pre- and postimplementation cases. In the adjusted model, the enhanced recovery protocol decreased the risk of prolonged length of stay by 40% (odds ratio, 0.6; 95% confidence interval, 0.5-0.8).
For the ERIN Pilot, she and her associates participated in monthly conference calls for collaborative experience and expert guidance from project leaders Julie Thacker, MD, and Liane Feldman, MD. Enhanced recovery protocols were tailored to each individual hospital. Data were collected before and after implementation using 14 novel ERIN variables, including preoperative elements such as defining expectations and minimizing starvation, intraoperative variables such as optimizing fluid management and minimizing surgical trauma, and postoperative elements such as aggressive adherence to best practices including feeding, early ambulation, and minimizing the use of tethers such as urinary catheters.
The researchers evaluated procedure-targeted colectomy cases performed between July 2013 and June 2015, and excluded emergency cases or those with preoperative sepsis. They used bivariate analysis and multivariate logistic regression with forward selection, and the outcome of interest, prolonged hospital length of stay, was specified by the standard ACS NSQIP definition: greater than the 75th percentile of uncomplicated cases.
Dr. Berian reported results from 2,523 colectomies performed prior to implementation of the ERIN Pilot process and 823 colectomies performed after implementation of the process. The researchers observed no differences between the preimplementation and postimplementation cases in terms of sex, preoperative functional status, hypertension, renal failure, ascites, diabetes, disseminated cancer, or use of steroids for inflammatory bowel disease. However, compared with preimplementation colectomies, a significantly higher proportion of postimplementation cases were white (77% vs. 68%, respectively), had heart failure (2.8% vs. 1.2%), had chronic obstructive pulmonary disease (7.8% vs. 5.3%), were American Society of Anesthesiologists (ASA) class 1 and 2 ( 50.2% vs. 44.7%), were smokers (21.6% vs. 16.7%), had unintentional weight loss (7.7% vs. 5.7%), had used mechanical bowel prep (77% vs. 53%), and used more oral antibiotics (68% vs. 33%).
On the other hand, compared with preimplementation cases, there were significantly fewer bleeding disorders in the postimplementation colectomies (3.9% vs. 6.4%), as well as fewer cases with preoperative systemic inflammatory response syndrome (2.9% vs. 5.4%) and open surgery approaches (31.7% vs. 42.3%).
Dr. Berian disclosed that her fellowship position is funded by the John A. Hartford Foundation.
SAN DIEGO – Multihospital collaboration and implementation of enhanced recovery have the potential to improve outcomes, in particular, length of hospital stay, results from a pilot study showed.
“Given the importance of patient engagement, enhanced recovery has the potential to improve patient experience and provide high-value health care,” Julia R. Berian, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference.
Dr. Berian, the James C. Thompson Geriatric Surgery Research Fellow at the University of Chicago Medical Center, presented findings from the Enhanced Recovery in NSQIP (ERIN) Pilot, a collaborative effort by 16 ACS-NSQIP hospitals to improve length of stay in patients who undergo colectomy, a procedure that has been shown to have an adverse event rate of 28.9% and an average length of stay of 9.8 days for those who experience an adverse event (J Am Coll Surg. 2008; 207[5]:698-704).
Implementation of the ERIN Pilot showed reductions in length of hospital stay and morbidity among colectomy patients. The average length of stay decreased by 1.2 days (from a mean of 6.6 among preimplementation cases to 5.4 days among post implementation cases; P less than .0001). Morbidity also decreased from 14% to 11% (P = .01), but the rate of readmission was 11% for both pre- and postimplementation cases. In the adjusted model, the enhanced recovery protocol decreased the risk of prolonged length of stay by 40% (odds ratio, 0.6; 95% confidence interval, 0.5-0.8).
For the ERIN Pilot, she and her associates participated in monthly conference calls for collaborative experience and expert guidance from project leaders Julie Thacker, MD, and Liane Feldman, MD. Enhanced recovery protocols were tailored to each individual hospital. Data were collected before and after implementation using 14 novel ERIN variables, including preoperative elements such as defining expectations and minimizing starvation, intraoperative variables such as optimizing fluid management and minimizing surgical trauma, and postoperative elements such as aggressive adherence to best practices including feeding, early ambulation, and minimizing the use of tethers such as urinary catheters.
The researchers evaluated procedure-targeted colectomy cases performed between July 2013 and June 2015, and excluded emergency cases or those with preoperative sepsis. They used bivariate analysis and multivariate logistic regression with forward selection, and the outcome of interest, prolonged hospital length of stay, was specified by the standard ACS NSQIP definition: greater than the 75th percentile of uncomplicated cases.
Dr. Berian reported results from 2,523 colectomies performed prior to implementation of the ERIN Pilot process and 823 colectomies performed after implementation of the process. The researchers observed no differences between the preimplementation and postimplementation cases in terms of sex, preoperative functional status, hypertension, renal failure, ascites, diabetes, disseminated cancer, or use of steroids for inflammatory bowel disease. However, compared with preimplementation colectomies, a significantly higher proportion of postimplementation cases were white (77% vs. 68%, respectively), had heart failure (2.8% vs. 1.2%), had chronic obstructive pulmonary disease (7.8% vs. 5.3%), were American Society of Anesthesiologists (ASA) class 1 and 2 ( 50.2% vs. 44.7%), were smokers (21.6% vs. 16.7%), had unintentional weight loss (7.7% vs. 5.7%), had used mechanical bowel prep (77% vs. 53%), and used more oral antibiotics (68% vs. 33%).
On the other hand, compared with preimplementation cases, there were significantly fewer bleeding disorders in the postimplementation colectomies (3.9% vs. 6.4%), as well as fewer cases with preoperative systemic inflammatory response syndrome (2.9% vs. 5.4%) and open surgery approaches (31.7% vs. 42.3%).
Dr. Berian disclosed that her fellowship position is funded by the John A. Hartford Foundation.
SAN DIEGO – Multihospital collaboration and implementation of enhanced recovery have the potential to improve outcomes, in particular, length of hospital stay, results from a pilot study showed.
“Given the importance of patient engagement, enhanced recovery has the potential to improve patient experience and provide high-value health care,” Julia R. Berian, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference.
Dr. Berian, the James C. Thompson Geriatric Surgery Research Fellow at the University of Chicago Medical Center, presented findings from the Enhanced Recovery in NSQIP (ERIN) Pilot, a collaborative effort by 16 ACS-NSQIP hospitals to improve length of stay in patients who undergo colectomy, a procedure that has been shown to have an adverse event rate of 28.9% and an average length of stay of 9.8 days for those who experience an adverse event (J Am Coll Surg. 2008; 207[5]:698-704).
Implementation of the ERIN Pilot showed reductions in length of hospital stay and morbidity among colectomy patients. The average length of stay decreased by 1.2 days (from a mean of 6.6 among preimplementation cases to 5.4 days among post implementation cases; P less than .0001). Morbidity also decreased from 14% to 11% (P = .01), but the rate of readmission was 11% for both pre- and postimplementation cases. In the adjusted model, the enhanced recovery protocol decreased the risk of prolonged length of stay by 40% (odds ratio, 0.6; 95% confidence interval, 0.5-0.8).
For the ERIN Pilot, she and her associates participated in monthly conference calls for collaborative experience and expert guidance from project leaders Julie Thacker, MD, and Liane Feldman, MD. Enhanced recovery protocols were tailored to each individual hospital. Data were collected before and after implementation using 14 novel ERIN variables, including preoperative elements such as defining expectations and minimizing starvation, intraoperative variables such as optimizing fluid management and minimizing surgical trauma, and postoperative elements such as aggressive adherence to best practices including feeding, early ambulation, and minimizing the use of tethers such as urinary catheters.
The researchers evaluated procedure-targeted colectomy cases performed between July 2013 and June 2015, and excluded emergency cases or those with preoperative sepsis. They used bivariate analysis and multivariate logistic regression with forward selection, and the outcome of interest, prolonged hospital length of stay, was specified by the standard ACS NSQIP definition: greater than the 75th percentile of uncomplicated cases.
Dr. Berian reported results from 2,523 colectomies performed prior to implementation of the ERIN Pilot process and 823 colectomies performed after implementation of the process. The researchers observed no differences between the preimplementation and postimplementation cases in terms of sex, preoperative functional status, hypertension, renal failure, ascites, diabetes, disseminated cancer, or use of steroids for inflammatory bowel disease. However, compared with preimplementation colectomies, a significantly higher proportion of postimplementation cases were white (77% vs. 68%, respectively), had heart failure (2.8% vs. 1.2%), had chronic obstructive pulmonary disease (7.8% vs. 5.3%), were American Society of Anesthesiologists (ASA) class 1 and 2 ( 50.2% vs. 44.7%), were smokers (21.6% vs. 16.7%), had unintentional weight loss (7.7% vs. 5.7%), had used mechanical bowel prep (77% vs. 53%), and used more oral antibiotics (68% vs. 33%).
On the other hand, compared with preimplementation cases, there were significantly fewer bleeding disorders in the postimplementation colectomies (3.9% vs. 6.4%), as well as fewer cases with preoperative systemic inflammatory response syndrome (2.9% vs. 5.4%) and open surgery approaches (31.7% vs. 42.3%).
Dr. Berian disclosed that her fellowship position is funded by the John A. Hartford Foundation.
AT THE ACS NSQIP NATIONAL CONFERENCE
Key clinical point: A multihospital enhanced recovery process for colectomy patients decreased length of stay and morbidity.
Major finding: After implementation of an enhanced recovery protocol in colectomy patients, the average hospital length of stay decreased by 1.2 days (from a mean of 6.6 days among preimplementation cases to 5.4 days among post implementation cases; P less than .0001). Morbidity also decreased from 14% to 11% (P = .01).
Data source: An analysis of 2,523 colectomies performed prior to implementation of the Enhanced Recovery in NSQIP (ERIN) Pilot process and 823 colectomies performed after implementation of the process.
Disclosures: Dr. Berian disclosed that her fellowship position is funded by the John A. Hartford Foundation.

Testosterone might counteract chemotherapy heart damage
SEATTLE – Adjunct testosterone improved short-term cardiac function in head, neck, and cervical cancer patients undergoing standard treatment in a small randomized trial from the University of Texas Medical Branch, Galveston.
The finding suggests that testosterone might counteract the cardiotoxic effects of chemotherapy, reducing “the incidence of chemotherapy-induced remodeling. It might also have rehabilitation implications and make patients better surgical candidates. Further investigation is warranted,” said investigator Albert Chamberlain, MD, an endocrine research fellow at the university. Although the results were positive, follow-up was short; years-long data are needed to know if testosterone really protects the heart from chemotherapy damage.

Dr. Chamberlain’s team looked into the issue because “many current chemotherapy drug classes have cardiotoxicity that progresses subclinically for a long time” before problems emerge. “Testosterone is known to cause vasodilation in both large and resistance arteries,” which might help prevent damage. “With that in mind, we decided to” investigate testosterone’s impact on cardiac performance during chemotherapy, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Five women and one man were randomized to weekly intramuscular 100 mg testosterone injections for 7 weeks; six men and four women were randomized to placebo injections. They were all recently diagnosed with stage IIIB, IV, or recurrent head and neck cancer, or cervical cancer, and were undergoing concomitant standard-of-care chemotherapy or chemoradiation. Cardiac function was measured blindly by transthoracic echocardiogram at baseline and the end of the study.
The testosterone group had significantly improved stroke volumes (+18.2% versus –2.6%, P = 0.01), ejection fractions (+6.2% versus –1.8%, P = 0.02), and cardiac output (+1402.2 mL/min versus –16.8mL/min, P = 0.011). Heart rate, arterial pressure, end-diastolic volume, and end-systolic volume remained unchanged in both groups, so the improved systolic function was attributed to reduced vascular resistance in the testosterone group (–26.5% versus +3.9% in the placebo group, P = 0.001).
Systolic improvements remained as cardiac index increased 27.6% in the testosterone group versus 2.8% in the placebo group. Testosterone didn’t seem to have any negative impacts on diastolic function. A placebo patient had a stroke, but there were no other adverse events in the study.
Although improved stroke volume is likely due to the reduced afterload, “increased contractility cannot be eliminated as a potential contributing factor. End diastolic volume remained unchanged in both groups, [suggesting] that preload is unlikely to be the mechanism for increased stroke volume,” Dr. Chamberlain said.
This study was funded by the National Cancer Institute. Dr. Chamberlain reported having no relevant disclosures.

|
Dr. Benjamin Judson |
The data are promising but preliminary for a problem we see a lot, chemotherapy-induced cardiotoxicity that presents years after treatment. We have to be really careful before we give testosterone to anyone who is under active treatment for cancer, because I don’t think we really know if it’s safe.
Benjamin Judson, MD, is an associate professor of otolaryngologic surgery at Yale Medical School in New Haven, Conn. He moderated Dr. Chamberlain’s talk and was not involved in the study.
|
|
Dr. Benjamin Judson |
The data are promising but preliminary for a problem we see a lot, chemotherapy-induced cardiotoxicity that presents years after treatment. We have to be really careful before we give testosterone to anyone who is under active treatment for cancer, because I don’t think we really know if it’s safe.
Benjamin Judson, MD, is an associate professor of otolaryngologic surgery at Yale Medical School in New Haven, Conn. He moderated Dr. Chamberlain’s talk and was not involved in the study.
|
|
Dr. Benjamin Judson |
The data are promising but preliminary for a problem we see a lot, chemotherapy-induced cardiotoxicity that presents years after treatment. We have to be really careful before we give testosterone to anyone who is under active treatment for cancer, because I don’t think we really know if it’s safe.
Benjamin Judson, MD, is an associate professor of otolaryngologic surgery at Yale Medical School in New Haven, Conn. He moderated Dr. Chamberlain’s talk and was not involved in the study.
SEATTLE – Adjunct testosterone improved short-term cardiac function in head, neck, and cervical cancer patients undergoing standard treatment in a small randomized trial from the University of Texas Medical Branch, Galveston.
The finding suggests that testosterone might counteract the cardiotoxic effects of chemotherapy, reducing “the incidence of chemotherapy-induced remodeling. It might also have rehabilitation implications and make patients better surgical candidates. Further investigation is warranted,” said investigator Albert Chamberlain, MD, an endocrine research fellow at the university. Although the results were positive, follow-up was short; years-long data are needed to know if testosterone really protects the heart from chemotherapy damage.
Dr. Chamberlain’s team looked into the issue because “many current chemotherapy drug classes have cardiotoxicity that progresses subclinically for a long time” before problems emerge. “Testosterone is known to cause vasodilation in both large and resistance arteries,” which might help prevent damage. “With that in mind, we decided to” investigate testosterone’s impact on cardiac performance during chemotherapy, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Five women and one man were randomized to weekly intramuscular 100 mg testosterone injections for 7 weeks; six men and four women were randomized to placebo injections. They were all recently diagnosed with stage IIIB, IV, or recurrent head and neck cancer, or cervical cancer, and were undergoing concomitant standard-of-care chemotherapy or chemoradiation. Cardiac function was measured blindly by transthoracic echocardiogram at baseline and the end of the study.
The testosterone group had significantly improved stroke volumes (+18.2% versus –2.6%, P = 0.01), ejection fractions (+6.2% versus –1.8%, P = 0.02), and cardiac output (+1402.2 mL/min versus –16.8mL/min, P = 0.011). Heart rate, arterial pressure, end-diastolic volume, and end-systolic volume remained unchanged in both groups, so the improved systolic function was attributed to reduced vascular resistance in the testosterone group (–26.5% versus +3.9% in the placebo group, P = 0.001).
Systolic improvements remained as cardiac index increased 27.6% in the testosterone group versus 2.8% in the placebo group. Testosterone didn’t seem to have any negative impacts on diastolic function. A placebo patient had a stroke, but there were no other adverse events in the study.
Although improved stroke volume is likely due to the reduced afterload, “increased contractility cannot be eliminated as a potential contributing factor. End diastolic volume remained unchanged in both groups, [suggesting] that preload is unlikely to be the mechanism for increased stroke volume,” Dr. Chamberlain said.
This study was funded by the National Cancer Institute. Dr. Chamberlain reported having no relevant disclosures.
SEATTLE – Adjunct testosterone improved short-term cardiac function in head, neck, and cervical cancer patients undergoing standard treatment in a small randomized trial from the University of Texas Medical Branch, Galveston.
The finding suggests that testosterone might counteract the cardiotoxic effects of chemotherapy, reducing “the incidence of chemotherapy-induced remodeling. It might also have rehabilitation implications and make patients better surgical candidates. Further investigation is warranted,” said investigator Albert Chamberlain, MD, an endocrine research fellow at the university. Although the results were positive, follow-up was short; years-long data are needed to know if testosterone really protects the heart from chemotherapy damage.
Dr. Chamberlain’s team looked into the issue because “many current chemotherapy drug classes have cardiotoxicity that progresses subclinically for a long time” before problems emerge. “Testosterone is known to cause vasodilation in both large and resistance arteries,” which might help prevent damage. “With that in mind, we decided to” investigate testosterone’s impact on cardiac performance during chemotherapy, he said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Five women and one man were randomized to weekly intramuscular 100 mg testosterone injections for 7 weeks; six men and four women were randomized to placebo injections. They were all recently diagnosed with stage IIIB, IV, or recurrent head and neck cancer, or cervical cancer, and were undergoing concomitant standard-of-care chemotherapy or chemoradiation. Cardiac function was measured blindly by transthoracic echocardiogram at baseline and the end of the study.
The testosterone group had significantly improved stroke volumes (+18.2% versus –2.6%, P = 0.01), ejection fractions (+6.2% versus –1.8%, P = 0.02), and cardiac output (+1402.2 mL/min versus –16.8mL/min, P = 0.011). Heart rate, arterial pressure, end-diastolic volume, and end-systolic volume remained unchanged in both groups, so the improved systolic function was attributed to reduced vascular resistance in the testosterone group (–26.5% versus +3.9% in the placebo group, P = 0.001).
Systolic improvements remained as cardiac index increased 27.6% in the testosterone group versus 2.8% in the placebo group. Testosterone didn’t seem to have any negative impacts on diastolic function. A placebo patient had a stroke, but there were no other adverse events in the study.
Although improved stroke volume is likely due to the reduced afterload, “increased contractility cannot be eliminated as a potential contributing factor. End diastolic volume remained unchanged in both groups, [suggesting] that preload is unlikely to be the mechanism for increased stroke volume,” Dr. Chamberlain said.
This study was funded by the National Cancer Institute. Dr. Chamberlain reported having no relevant disclosures.
AT AHNS 2016
Key clinical point: Adjunct testosterone improved cardiac function in head, neck, and cervical cancer patients undergoing standard treatment in a small randomized trial.
Major finding: The testosterone group had significantly improved stroke volumes (+18.2% versus –2.6%, P = 0.01), ejection fractions (+6.2% versus –1.8%, P = 0.02), and cardiac output (+1402.2 mL/min versus –16.8mL/min, P = 0.011), but there was no years-long follow-up to show lasting cardiac benefit.
Data source: Randomized trial with 16 patients.
Disclosures: The National Cancer Institute funded the work. The lead investigator had no disclosures.

Simple colon surgery bundle accelerated outcomes improvement
SAN DIEGO – Implementation of a simple colon bundle decreased the rate of colonic and enteric resections faster, compared with improvements seen for other procedures, according to a study that involved 23 hospitals in Tennessee.
At the American College of Surgeons/National Surgical Quality Improvement Program National Conference, Brian J. Daley, MD, discussed findings from an analysis conducted by members of the Tennessee Surgical Quality Collaborative (TSQC), which he described as “a collection of surgeons who put aside their hospital and regional affiliations to work together to help each other and to help our fellow Tennesseans.” Established in 2008 with member hospitals, the TSQC has grown to 23 member hospitals, including 18 community hospitals and 5 academic medical centers. It provides data on nearly 600 surgeons across the state. “While this only represents about half of the surgical procedures in the state, there is sufficient statistical power to make comments about our surgical performance,” said Dr. Daley of the department of surgery at the University of Tennessee Medical Center, Knoxville.

To quantify TSQC’s impact on surgical outcomes, surgeons at the member hospitals evaluated the TSQC colon bundle, which was developed in 2012 and implemented in 2013. It bundles four processes of care: maintaining intraoperative oxygen delivery, maintaining a temperature of 36° C, making sure the patient’s blood glucose is normal, and choosing the appropriate antibiotics. “We kept it simple: easy, not expensive, and hopefully helpful,” Dr. Daley said.
With other procedures as a baseline, they used statistical analyses to determine if implementation of the bundle led to an incremental acceleration of reduced complications, compared with other improvements observed in other procedures. “To understand our outcomes, we needed to prove three points: that the trend improved [a negative trend in the resection rate], that this negative trend was more negative than trends for other comparator procedures, and that the trend for intercept was not equal to the comparator in any way,” Dr. Daley explained.
Following adoption of the bundle, he and his associates observed that the rate of decrease in postoperative recurrences was greater in colectomy, compared with that for all other surgical procedures (P less than .001 for both the trend and the intercept statistical models). Adoption of the bundle also positively impacted decreases in postoperative recurrences among enterectomy cases (P less than .001 for both the trend and the intercept statistical models).
“We were able to demonstrate that our TSQC bundle paid dividends in improving colectomy outcomes,” Dr. Daley concluded. “We have seen these efforts spill over into enterectomy. From this we can also infer that participation in the collaborative improves outcomes and is imperative to maintain the acceleration in surgical improvement.”
Dr. Daley reported that he and his coauthors had no relevant financial disclosures.
SAN DIEGO – Implementation of a simple colon bundle decreased the rate of colonic and enteric resections faster, compared with improvements seen for other procedures, according to a study that involved 23 hospitals in Tennessee.
At the American College of Surgeons/National Surgical Quality Improvement Program National Conference, Brian J. Daley, MD, discussed findings from an analysis conducted by members of the Tennessee Surgical Quality Collaborative (TSQC), which he described as “a collection of surgeons who put aside their hospital and regional affiliations to work together to help each other and to help our fellow Tennesseans.” Established in 2008 with member hospitals, the TSQC has grown to 23 member hospitals, including 18 community hospitals and 5 academic medical centers. It provides data on nearly 600 surgeons across the state. “While this only represents about half of the surgical procedures in the state, there is sufficient statistical power to make comments about our surgical performance,” said Dr. Daley of the department of surgery at the University of Tennessee Medical Center, Knoxville.
To quantify TSQC’s impact on surgical outcomes, surgeons at the member hospitals evaluated the TSQC colon bundle, which was developed in 2012 and implemented in 2013. It bundles four processes of care: maintaining intraoperative oxygen delivery, maintaining a temperature of 36° C, making sure the patient’s blood glucose is normal, and choosing the appropriate antibiotics. “We kept it simple: easy, not expensive, and hopefully helpful,” Dr. Daley said.
With other procedures as a baseline, they used statistical analyses to determine if implementation of the bundle led to an incremental acceleration of reduced complications, compared with other improvements observed in other procedures. “To understand our outcomes, we needed to prove three points: that the trend improved [a negative trend in the resection rate], that this negative trend was more negative than trends for other comparator procedures, and that the trend for intercept was not equal to the comparator in any way,” Dr. Daley explained.
Following adoption of the bundle, he and his associates observed that the rate of decrease in postoperative recurrences was greater in colectomy, compared with that for all other surgical procedures (P less than .001 for both the trend and the intercept statistical models). Adoption of the bundle also positively impacted decreases in postoperative recurrences among enterectomy cases (P less than .001 for both the trend and the intercept statistical models).
“We were able to demonstrate that our TSQC bundle paid dividends in improving colectomy outcomes,” Dr. Daley concluded. “We have seen these efforts spill over into enterectomy. From this we can also infer that participation in the collaborative improves outcomes and is imperative to maintain the acceleration in surgical improvement.”
Dr. Daley reported that he and his coauthors had no relevant financial disclosures.
SAN DIEGO – Implementation of a simple colon bundle decreased the rate of colonic and enteric resections faster, compared with improvements seen for other procedures, according to a study that involved 23 hospitals in Tennessee.
At the American College of Surgeons/National Surgical Quality Improvement Program National Conference, Brian J. Daley, MD, discussed findings from an analysis conducted by members of the Tennessee Surgical Quality Collaborative (TSQC), which he described as “a collection of surgeons who put aside their hospital and regional affiliations to work together to help each other and to help our fellow Tennesseans.” Established in 2008 with member hospitals, the TSQC has grown to 23 member hospitals, including 18 community hospitals and 5 academic medical centers. It provides data on nearly 600 surgeons across the state. “While this only represents about half of the surgical procedures in the state, there is sufficient statistical power to make comments about our surgical performance,” said Dr. Daley of the department of surgery at the University of Tennessee Medical Center, Knoxville.
To quantify TSQC’s impact on surgical outcomes, surgeons at the member hospitals evaluated the TSQC colon bundle, which was developed in 2012 and implemented in 2013. It bundles four processes of care: maintaining intraoperative oxygen delivery, maintaining a temperature of 36° C, making sure the patient’s blood glucose is normal, and choosing the appropriate antibiotics. “We kept it simple: easy, not expensive, and hopefully helpful,” Dr. Daley said.
With other procedures as a baseline, they used statistical analyses to determine if implementation of the bundle led to an incremental acceleration of reduced complications, compared with other improvements observed in other procedures. “To understand our outcomes, we needed to prove three points: that the trend improved [a negative trend in the resection rate], that this negative trend was more negative than trends for other comparator procedures, and that the trend for intercept was not equal to the comparator in any way,” Dr. Daley explained.
Following adoption of the bundle, he and his associates observed that the rate of decrease in postoperative recurrences was greater in colectomy, compared with that for all other surgical procedures (P less than .001 for both the trend and the intercept statistical models). Adoption of the bundle also positively impacted decreases in postoperative recurrences among enterectomy cases (P less than .001 for both the trend and the intercept statistical models).
“We were able to demonstrate that our TSQC bundle paid dividends in improving colectomy outcomes,” Dr. Daley concluded. “We have seen these efforts spill over into enterectomy. From this we can also infer that participation in the collaborative improves outcomes and is imperative to maintain the acceleration in surgical improvement.”
Dr. Daley reported that he and his coauthors had no relevant financial disclosures.
AT THE ACS NSQIP NATIONAL CONFERENCE
Key clinical point: Adoption of a colon bundle by a collaborative of Tennessee hospitals improved certain colectomy outcomes.
Major finding: Following adoption of a colon bundle, the rate of decrease in postoperative recurrences was greater in colectomy than for all other surgical procedures (P less than .001 for both the trend and the intercept statistical models).
Data source: An analysis conducted by members of the Tennessee Surgical Quality Collaborative, which included 23 hospitals in the state.
Disclosures: The researchers reported having no relevant financial disclosures.

Oxaliplatin boosts pCR in patients with locally advanced rectal cancer
Adding oxaliplatin to perioperative fluorouracil and radiotherapy was associated with a higher rate of pathologic complete response (pCR) in advanced rectal cancer patients, compared with single-agent fluorouracil plus radiotherapy, investigators report in the Journal of Clinical Oncology.
For the Neoadjuvant FOLFOX6 Chemotherapy With or Without Radiation in Rectal Cancer (FOWARC) study, 495 patients with locally advanced rectal cancer (LARC) who were undergoing total mesorectal excision were randomly assigned to one of three preoperative treatment arms: neoadjuvant therapy with fluorouracil plus radiotherapy (fluorouracil-radiotherapy group), fluorouracil chemotherapy with perioperative fluorouracil and oxaliplatin plus radiotherapy (mFOLFOX6-radiotherapy group), or fluorouracil chemotherapy with perioperative fluorouracil and oxaliplatin without radiotherapy (mFOLFOX6 group).The rates of pCR were 14.0%, 27.5%, and 6.6% for patients in the fluorouracil-radiotherapy, mFOLFOX6-radiotherapy, and mFOLFOX6 groups, respectively, Dr. Yanhong Deng of the Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou City, China, and her associates reported (J Clin Oncol. 2016. doi: 10.1200/JCO.2016.66.6198).
No patients died during neoadjuvant treatment. Grade 3 or 4 toxicities occurred in 55.5% (n = 86), 88% (n = 139), and 24.5% (n = 40) of patients in the fluorouracil-radiotherapy group, mFOLFOX6-radiotherapy, and mFOLFOX6 groups, respectively. The most common grade 3 to 4 toxicities were leukopenia, radiodermatitis, and radiation proctitis.
Initial analysis of this study showed that “compared with the single-agent fluorouracil, mFOLFOX6 concurrent with radiotherapy preoperatively results in a higher rate of pCR (14.0% vs. 27.5%), a higher good response rate, good compliance, and acceptable toxicity for patients with stage II/III rectal cancer,” the investigators wrote.
“These preliminary results suggest that a strategy of combining full-dose chemotherapy with radiation over chemosensitizing radiation may be a new option for neoadjuvant treatment in LARC,” they added.
Sun Yat-sen University funded this study. Dr. Deng and her associates did not have any disclosures to report.
On Twitter @jessnicolecraig
Adding oxaliplatin to perioperative fluorouracil and radiotherapy was associated with a higher rate of pathologic complete response (pCR) in advanced rectal cancer patients, compared with single-agent fluorouracil plus radiotherapy, investigators report in the Journal of Clinical Oncology.
For the Neoadjuvant FOLFOX6 Chemotherapy With or Without Radiation in Rectal Cancer (FOWARC) study, 495 patients with locally advanced rectal cancer (LARC) who were undergoing total mesorectal excision were randomly assigned to one of three preoperative treatment arms: neoadjuvant therapy with fluorouracil plus radiotherapy (fluorouracil-radiotherapy group), fluorouracil chemotherapy with perioperative fluorouracil and oxaliplatin plus radiotherapy (mFOLFOX6-radiotherapy group), or fluorouracil chemotherapy with perioperative fluorouracil and oxaliplatin without radiotherapy (mFOLFOX6 group).The rates of pCR were 14.0%, 27.5%, and 6.6% for patients in the fluorouracil-radiotherapy, mFOLFOX6-radiotherapy, and mFOLFOX6 groups, respectively, Dr. Yanhong Deng of the Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou City, China, and her associates reported (J Clin Oncol. 2016. doi: 10.1200/JCO.2016.66.6198).
No patients died during neoadjuvant treatment. Grade 3 or 4 toxicities occurred in 55.5% (n = 86), 88% (n = 139), and 24.5% (n = 40) of patients in the fluorouracil-radiotherapy group, mFOLFOX6-radiotherapy, and mFOLFOX6 groups, respectively. The most common grade 3 to 4 toxicities were leukopenia, radiodermatitis, and radiation proctitis.
Initial analysis of this study showed that “compared with the single-agent fluorouracil, mFOLFOX6 concurrent with radiotherapy preoperatively results in a higher rate of pCR (14.0% vs. 27.5%), a higher good response rate, good compliance, and acceptable toxicity for patients with stage II/III rectal cancer,” the investigators wrote.
“These preliminary results suggest that a strategy of combining full-dose chemotherapy with radiation over chemosensitizing radiation may be a new option for neoadjuvant treatment in LARC,” they added.
Sun Yat-sen University funded this study. Dr. Deng and her associates did not have any disclosures to report.
On Twitter @jessnicolecraig
Adding oxaliplatin to perioperative fluorouracil and radiotherapy was associated with a higher rate of pathologic complete response (pCR) in advanced rectal cancer patients, compared with single-agent fluorouracil plus radiotherapy, investigators report in the Journal of Clinical Oncology.
For the Neoadjuvant FOLFOX6 Chemotherapy With or Without Radiation in Rectal Cancer (FOWARC) study, 495 patients with locally advanced rectal cancer (LARC) who were undergoing total mesorectal excision were randomly assigned to one of three preoperative treatment arms: neoadjuvant therapy with fluorouracil plus radiotherapy (fluorouracil-radiotherapy group), fluorouracil chemotherapy with perioperative fluorouracil and oxaliplatin plus radiotherapy (mFOLFOX6-radiotherapy group), or fluorouracil chemotherapy with perioperative fluorouracil and oxaliplatin without radiotherapy (mFOLFOX6 group).The rates of pCR were 14.0%, 27.5%, and 6.6% for patients in the fluorouracil-radiotherapy, mFOLFOX6-radiotherapy, and mFOLFOX6 groups, respectively, Dr. Yanhong Deng of the Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou City, China, and her associates reported (J Clin Oncol. 2016. doi: 10.1200/JCO.2016.66.6198).
No patients died during neoadjuvant treatment. Grade 3 or 4 toxicities occurred in 55.5% (n = 86), 88% (n = 139), and 24.5% (n = 40) of patients in the fluorouracil-radiotherapy group, mFOLFOX6-radiotherapy, and mFOLFOX6 groups, respectively. The most common grade 3 to 4 toxicities were leukopenia, radiodermatitis, and radiation proctitis.
Initial analysis of this study showed that “compared with the single-agent fluorouracil, mFOLFOX6 concurrent with radiotherapy preoperatively results in a higher rate of pCR (14.0% vs. 27.5%), a higher good response rate, good compliance, and acceptable toxicity for patients with stage II/III rectal cancer,” the investigators wrote.
“These preliminary results suggest that a strategy of combining full-dose chemotherapy with radiation over chemosensitizing radiation may be a new option for neoadjuvant treatment in LARC,” they added.
Sun Yat-sen University funded this study. Dr. Deng and her associates did not have any disclosures to report.
On Twitter @jessnicolecraig
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Perioperative oxaliplatin administered in combination with fluorouracil and radiotherapy was associated with a higher rate of pathologic complete response in advanced rectal cancer patients compared with single-agent fluorouracil and radiotherapy.
Major finding: The rate of pathologic complete response was 27.5% for patients receiving oxaliplatin, fluorouracil, and radiotherapy vs. 14.0% for patients receiving single-agent fluorouracil and radiotherapy.
Data source: A multicenter, open-label, phase III trial involving 495 patients with locally advanced stage II/III rectal cancer.
Disclosures: Sun Yat-sen University funded this study. Dr. Deng and her associates did not have any disclosures to report.
NSQIP Study: Symptomatic AAAs have a twofold increased periop mortality risk over asymptomatic
A recent small study suggested that, in the age of endovascular aortic aneurysm repair (EVAR), the mortality rates between symptomatic and asymptomatic abdominal aortic aneurysm (AAA) repair have become similar, according to Peter A. Soden, MD, of Beth Deaconess Medical Center, Boston, and his colleagues. However, in their large database study, Dr. Soden and his colleagues found that outcomes for the repair of abdominal aortic aneurysms were increasingly worse from asymptomatic to symptomatic to ruptured AAA.
The researchers assessed all patients undergoing endovascular and open AAA repair in the 2011-2013 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data set, according to a report published in the August issue of the Journal of Vascular Surgery.
Symptomatic AAA was defined as lack of evidence of rupture but with the presence of abdominal or back pain or symptoms from local compression by the aneurysm causing early satiety, hydronephrosis, or deep vein thrombosis. Ruptured aneurysms were divided into two categories: hypotensive (defined as systolic blood pressure less than 90 mmm Hg or drop of greater than 40 mm HG from baseline) and nonhypotensive (J Vasc Surg. 2016;64:297-305).
There were numerous demographic and comorbidity differences between asymptomatic and symptomatic patients and between symptomatic and ruptured patients, with a general trend of increasing of commodities and factors influencing operative risk.
The final study included 5,502 patients undergoing repair of infrarenal (85%; 92% EVAR) or juxtarenal (15%;20% EVAR) aneurysms. These differences in the use of EVAR were statistically significant.
This population comprised 4,495 asymptomatic patients (82% EVAR), 455 symptomatic patients (69% EVAR), and 552 ruptured patients (52% EVAR).
The overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (5.1% vs. 1.9%; P less than .001).Similarly, for EVAR, the overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (3.8% vs. 1.4%; P less than .001). For open repair, there was no significant difference in mortality (7.7% vs. 4.3%) between symptomatic and asymptomatic patients, respectively.
Multivariate analysis showed that symptomatic patients had twice the operative mortality as asymptomatic patients (odds ratio, 2.1). A symptomatic aneurysm was also predictive of a major adverse event (OR, 1.5). Ruptured aneurysms had a significant nearly sevenfold increase in mortality risk vs. symptomatic aneurysms (OR, 6.5) and a fivefold increase of risk of a major adverse event (OR 5.1), with all ORs within their 95% confidence interval levels).
“In this large contemporary study of symptomatic AAA patients, in which the majority were treated with EVAR, we found that symptomatic patients have twice the perioperative mortality compared with asymptomatic patients. Despite this, we also find a reduction in perioperative mortality for symptomatic aneurysms compared with prior reports in which the majority were treated with open repair, and we believe this supports an EVAR-first approach for symptomatic aneurysms with suitable anatomy,” the researchers concluded.
The authors reported that they had no relevant disclosures.
A recent small study suggested that, in the age of endovascular aortic aneurysm repair (EVAR), the mortality rates between symptomatic and asymptomatic abdominal aortic aneurysm (AAA) repair have become similar, according to Peter A. Soden, MD, of Beth Deaconess Medical Center, Boston, and his colleagues. However, in their large database study, Dr. Soden and his colleagues found that outcomes for the repair of abdominal aortic aneurysms were increasingly worse from asymptomatic to symptomatic to ruptured AAA.
The researchers assessed all patients undergoing endovascular and open AAA repair in the 2011-2013 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data set, according to a report published in the August issue of the Journal of Vascular Surgery.
Symptomatic AAA was defined as lack of evidence of rupture but with the presence of abdominal or back pain or symptoms from local compression by the aneurysm causing early satiety, hydronephrosis, or deep vein thrombosis. Ruptured aneurysms were divided into two categories: hypotensive (defined as systolic blood pressure less than 90 mmm Hg or drop of greater than 40 mm HG from baseline) and nonhypotensive (J Vasc Surg. 2016;64:297-305).
There were numerous demographic and comorbidity differences between asymptomatic and symptomatic patients and between symptomatic and ruptured patients, with a general trend of increasing of commodities and factors influencing operative risk.
The final study included 5,502 patients undergoing repair of infrarenal (85%; 92% EVAR) or juxtarenal (15%;20% EVAR) aneurysms. These differences in the use of EVAR were statistically significant.
This population comprised 4,495 asymptomatic patients (82% EVAR), 455 symptomatic patients (69% EVAR), and 552 ruptured patients (52% EVAR).
The overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (5.1% vs. 1.9%; P less than .001).Similarly, for EVAR, the overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (3.8% vs. 1.4%; P less than .001). For open repair, there was no significant difference in mortality (7.7% vs. 4.3%) between symptomatic and asymptomatic patients, respectively.
Multivariate analysis showed that symptomatic patients had twice the operative mortality as asymptomatic patients (odds ratio, 2.1). A symptomatic aneurysm was also predictive of a major adverse event (OR, 1.5). Ruptured aneurysms had a significant nearly sevenfold increase in mortality risk vs. symptomatic aneurysms (OR, 6.5) and a fivefold increase of risk of a major adverse event (OR 5.1), with all ORs within their 95% confidence interval levels).
“In this large contemporary study of symptomatic AAA patients, in which the majority were treated with EVAR, we found that symptomatic patients have twice the perioperative mortality compared with asymptomatic patients. Despite this, we also find a reduction in perioperative mortality for symptomatic aneurysms compared with prior reports in which the majority were treated with open repair, and we believe this supports an EVAR-first approach for symptomatic aneurysms with suitable anatomy,” the researchers concluded.
The authors reported that they had no relevant disclosures.
A recent small study suggested that, in the age of endovascular aortic aneurysm repair (EVAR), the mortality rates between symptomatic and asymptomatic abdominal aortic aneurysm (AAA) repair have become similar, according to Peter A. Soden, MD, of Beth Deaconess Medical Center, Boston, and his colleagues. However, in their large database study, Dr. Soden and his colleagues found that outcomes for the repair of abdominal aortic aneurysms were increasingly worse from asymptomatic to symptomatic to ruptured AAA.
The researchers assessed all patients undergoing endovascular and open AAA repair in the 2011-2013 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) data set, according to a report published in the August issue of the Journal of Vascular Surgery.
Symptomatic AAA was defined as lack of evidence of rupture but with the presence of abdominal or back pain or symptoms from local compression by the aneurysm causing early satiety, hydronephrosis, or deep vein thrombosis. Ruptured aneurysms were divided into two categories: hypotensive (defined as systolic blood pressure less than 90 mmm Hg or drop of greater than 40 mm HG from baseline) and nonhypotensive (J Vasc Surg. 2016;64:297-305).
There were numerous demographic and comorbidity differences between asymptomatic and symptomatic patients and between symptomatic and ruptured patients, with a general trend of increasing of commodities and factors influencing operative risk.
The final study included 5,502 patients undergoing repair of infrarenal (85%; 92% EVAR) or juxtarenal (15%;20% EVAR) aneurysms. These differences in the use of EVAR were statistically significant.
This population comprised 4,495 asymptomatic patients (82% EVAR), 455 symptomatic patients (69% EVAR), and 552 ruptured patients (52% EVAR).
The overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (5.1% vs. 1.9%; P less than .001).Similarly, for EVAR, the overall 30-day mortality rate was significantly higher in symptomatic over asymptomatic patients (3.8% vs. 1.4%; P less than .001). For open repair, there was no significant difference in mortality (7.7% vs. 4.3%) between symptomatic and asymptomatic patients, respectively.
Multivariate analysis showed that symptomatic patients had twice the operative mortality as asymptomatic patients (odds ratio, 2.1). A symptomatic aneurysm was also predictive of a major adverse event (OR, 1.5). Ruptured aneurysms had a significant nearly sevenfold increase in mortality risk vs. symptomatic aneurysms (OR, 6.5) and a fivefold increase of risk of a major adverse event (OR 5.1), with all ORs within their 95% confidence interval levels).
“In this large contemporary study of symptomatic AAA patients, in which the majority were treated with EVAR, we found that symptomatic patients have twice the perioperative mortality compared with asymptomatic patients. Despite this, we also find a reduction in perioperative mortality for symptomatic aneurysms compared with prior reports in which the majority were treated with open repair, and we believe this supports an EVAR-first approach for symptomatic aneurysms with suitable anatomy,” the researchers concluded.
The authors reported that they had no relevant disclosures.
FROM THE JOURNAL OF VASCULAR SURGERY
Key clinical point: Outcomes for repair of abdominal aortic aneurysm repair were increasingly worse from asymptomatic to symptomatic to ruptured AAA.
Major finding: Patients with symptomatic AAA had a twofold increased risk of perioperative mortality, compared with patients with asymptomatic AAA undergoing repair.
Data source: The study assessed all patients undergoing AAA repair in the 2011-2013 American College of Surgeons NSQIP data set.
Disclosures: The authors reported that they had no relevant disclosures.

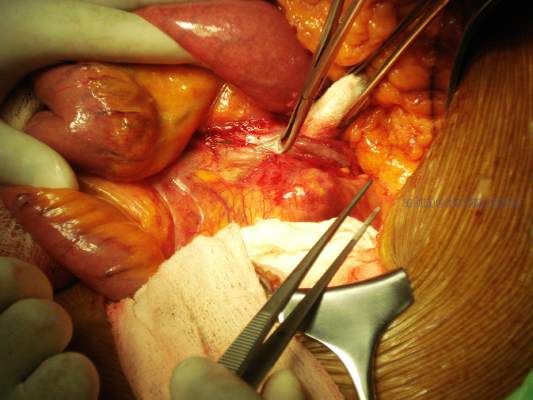
Abdominal compartment syndrome – a common adverse event after rAAA repair
Abdominal compartment syndrome (ACS) was common after ruptured abdominal aortic aneurysm (AAA) repair, with a similar incidence for both open surgical and endovascular repair (EVAR), according to a report published in the European Journal of Vascular and Endovascular Surgery.
Samuel Ersryd, a doctoral student, and his colleagues at Uppsala (Sweden) University performed their study to determine the contemporary incidence, treatment, and outcomes of ACS after AAA repair.
The analysis included 6,634 patients in the Swedish vascular registry who were treated for abdominal aortic aneurysm repair at 31 institutions from May 2008 to December 2013. The mean patient age was 72.8 years, and 16.6% were women. There were 5,271 intact AAA (iAAA) repairs and 1,341 ruptured AAA (rAAA repairs). A total of 41.9% of iAAA repairs were open, as were 72.0% of the rAAA repairs (Eur J Vasc Endovasc Surg. 2016;52:158-65).The study found an incidence of ACS in the rAAA group of 6.8% after open surgery and 6.9% after EVAR.
The morbidity and mortality rates for iAAA and rAAA with ACS were “devastating” in both groups, according to the authors.
Mortality at 90 days for patients with ACS after rAAA was 58.7%, twice that of patients without ACS. In patients with iAAA repair with ACS, the 90-day mortality was 19.2%, six times higher than for those without ACS.
Prophylactic open abdomen treatment was performed in 10.7% of open-surgery patients.
The researchers found no differences in mortality among patients in either group that developed ACS, whether they were treated with decompression laparotomy or not.
Age, sex, and perioperative comorbidities were not associated with ACS, Mr. Ersryd and his associates said. Within the rAAA group, however, ACS was associated with the lowest measured preoperative blood pressure and with preoperative unconsciousness. In addition, ACS was more common in both the iAAA and rAAA groups after perioperative bleeding greater than 5 L, in the iAAA group after reimplantation of a renal artery, and in the rAAA group after the use of balloon occlusion after EVAR. In those patients operated on for iAAA, the risk of developing ACS was 8.1% in patients who had perioperative bleeding greater than 5 L, compared with only 0.8% if bleeding was less than 5 L (P less than .001).
“With such poor results among patients who developed ACS, prevention is the obvious key to success. Massive transfusion protocols and permissive hypotension in patients with ongoing bleeding are important, as well as being restrictive with crystalloids,” the authors said. In addition, they recommended a proactive strategy treating intra-abdominal hypertension with medical therapy, effective pain relief, and neuromuscular blockade as important preventive measures.
“ACS is associated with a devastating effect on outcome after surgery for both ruptured and intact AAA. There was no difference in outcome among those who developed ACS, depending on whether the primary treatment had been performed with an open or endovascular technique,” the researchers concluded.
The authors reported they had no conflicts of interest and the study was funded by the Swedish Research Council and Uppsala University.
On Twitter @VascularTweets
The authors of this paper provide compelling data demonstrating the seriousness of abdominal compartment syndrome developing following abdominal aortic surgery. Recognition of this complication is therefore mandatory and techniques to relieve it should be instituted immediately. In my practice, I have successfully used the Wittmann patch, but recently I switched to the VAC (vacuum-assisted closure) device. Following an endovascular approach for a ruptured AAA, patients may require concomitant exploration for retrograde bleeding sources, such as an inferior mesenteric artery or large lumbars that will continue to bleed unless ligated.
Dr. Russell Samson is the medical editor of Vascular Specialist.
The authors of this paper provide compelling data demonstrating the seriousness of abdominal compartment syndrome developing following abdominal aortic surgery. Recognition of this complication is therefore mandatory and techniques to relieve it should be instituted immediately. In my practice, I have successfully used the Wittmann patch, but recently I switched to the VAC (vacuum-assisted closure) device. Following an endovascular approach for a ruptured AAA, patients may require concomitant exploration for retrograde bleeding sources, such as an inferior mesenteric artery or large lumbars that will continue to bleed unless ligated.
Dr. Russell Samson is the medical editor of Vascular Specialist.
The authors of this paper provide compelling data demonstrating the seriousness of abdominal compartment syndrome developing following abdominal aortic surgery. Recognition of this complication is therefore mandatory and techniques to relieve it should be instituted immediately. In my practice, I have successfully used the Wittmann patch, but recently I switched to the VAC (vacuum-assisted closure) device. Following an endovascular approach for a ruptured AAA, patients may require concomitant exploration for retrograde bleeding sources, such as an inferior mesenteric artery or large lumbars that will continue to bleed unless ligated.
Dr. Russell Samson is the medical editor of Vascular Specialist.
Abdominal compartment syndrome (ACS) was common after ruptured abdominal aortic aneurysm (AAA) repair, with a similar incidence for both open surgical and endovascular repair (EVAR), according to a report published in the European Journal of Vascular and Endovascular Surgery.
Samuel Ersryd, a doctoral student, and his colleagues at Uppsala (Sweden) University performed their study to determine the contemporary incidence, treatment, and outcomes of ACS after AAA repair.
The analysis included 6,634 patients in the Swedish vascular registry who were treated for abdominal aortic aneurysm repair at 31 institutions from May 2008 to December 2013. The mean patient age was 72.8 years, and 16.6% were women. There were 5,271 intact AAA (iAAA) repairs and 1,341 ruptured AAA (rAAA repairs). A total of 41.9% of iAAA repairs were open, as were 72.0% of the rAAA repairs (Eur J Vasc Endovasc Surg. 2016;52:158-65).The study found an incidence of ACS in the rAAA group of 6.8% after open surgery and 6.9% after EVAR.
The morbidity and mortality rates for iAAA and rAAA with ACS were “devastating” in both groups, according to the authors.
Mortality at 90 days for patients with ACS after rAAA was 58.7%, twice that of patients without ACS. In patients with iAAA repair with ACS, the 90-day mortality was 19.2%, six times higher than for those without ACS.
Prophylactic open abdomen treatment was performed in 10.7% of open-surgery patients.
The researchers found no differences in mortality among patients in either group that developed ACS, whether they were treated with decompression laparotomy or not.
Age, sex, and perioperative comorbidities were not associated with ACS, Mr. Ersryd and his associates said. Within the rAAA group, however, ACS was associated with the lowest measured preoperative blood pressure and with preoperative unconsciousness. In addition, ACS was more common in both the iAAA and rAAA groups after perioperative bleeding greater than 5 L, in the iAAA group after reimplantation of a renal artery, and in the rAAA group after the use of balloon occlusion after EVAR. In those patients operated on for iAAA, the risk of developing ACS was 8.1% in patients who had perioperative bleeding greater than 5 L, compared with only 0.8% if bleeding was less than 5 L (P less than .001).
“With such poor results among patients who developed ACS, prevention is the obvious key to success. Massive transfusion protocols and permissive hypotension in patients with ongoing bleeding are important, as well as being restrictive with crystalloids,” the authors said. In addition, they recommended a proactive strategy treating intra-abdominal hypertension with medical therapy, effective pain relief, and neuromuscular blockade as important preventive measures.
“ACS is associated with a devastating effect on outcome after surgery for both ruptured and intact AAA. There was no difference in outcome among those who developed ACS, depending on whether the primary treatment had been performed with an open or endovascular technique,” the researchers concluded.
The authors reported they had no conflicts of interest and the study was funded by the Swedish Research Council and Uppsala University.
On Twitter @VascularTweets
Abdominal compartment syndrome (ACS) was common after ruptured abdominal aortic aneurysm (AAA) repair, with a similar incidence for both open surgical and endovascular repair (EVAR), according to a report published in the European Journal of Vascular and Endovascular Surgery.
Samuel Ersryd, a doctoral student, and his colleagues at Uppsala (Sweden) University performed their study to determine the contemporary incidence, treatment, and outcomes of ACS after AAA repair.
The analysis included 6,634 patients in the Swedish vascular registry who were treated for abdominal aortic aneurysm repair at 31 institutions from May 2008 to December 2013. The mean patient age was 72.8 years, and 16.6% were women. There were 5,271 intact AAA (iAAA) repairs and 1,341 ruptured AAA (rAAA repairs). A total of 41.9% of iAAA repairs were open, as were 72.0% of the rAAA repairs (Eur J Vasc Endovasc Surg. 2016;52:158-65).The study found an incidence of ACS in the rAAA group of 6.8% after open surgery and 6.9% after EVAR.
The morbidity and mortality rates for iAAA and rAAA with ACS were “devastating” in both groups, according to the authors.
Mortality at 90 days for patients with ACS after rAAA was 58.7%, twice that of patients without ACS. In patients with iAAA repair with ACS, the 90-day mortality was 19.2%, six times higher than for those without ACS.
Prophylactic open abdomen treatment was performed in 10.7% of open-surgery patients.
The researchers found no differences in mortality among patients in either group that developed ACS, whether they were treated with decompression laparotomy or not.
Age, sex, and perioperative comorbidities were not associated with ACS, Mr. Ersryd and his associates said. Within the rAAA group, however, ACS was associated with the lowest measured preoperative blood pressure and with preoperative unconsciousness. In addition, ACS was more common in both the iAAA and rAAA groups after perioperative bleeding greater than 5 L, in the iAAA group after reimplantation of a renal artery, and in the rAAA group after the use of balloon occlusion after EVAR. In those patients operated on for iAAA, the risk of developing ACS was 8.1% in patients who had perioperative bleeding greater than 5 L, compared with only 0.8% if bleeding was less than 5 L (P less than .001).
“With such poor results among patients who developed ACS, prevention is the obvious key to success. Massive transfusion protocols and permissive hypotension in patients with ongoing bleeding are important, as well as being restrictive with crystalloids,” the authors said. In addition, they recommended a proactive strategy treating intra-abdominal hypertension with medical therapy, effective pain relief, and neuromuscular blockade as important preventive measures.
“ACS is associated with a devastating effect on outcome after surgery for both ruptured and intact AAA. There was no difference in outcome among those who developed ACS, depending on whether the primary treatment had been performed with an open or endovascular technique,” the researchers concluded.
The authors reported they had no conflicts of interest and the study was funded by the Swedish Research Council and Uppsala University.
On Twitter @VascularTweets
FROM THE EUROPEAN JOURNAL OF VASCULAR AND ENDOVASCULAR SURGERY
Key clinical point: Abdominal compartment syndrome is a dangerous and frequent complication after treatment of ruptured abdominal aortic aneurysms.
Major finding: After ruptured AAA repair, ACS developed in 6.8% of patients with open repair and 6.9% of patients with EVAR.
Data source: Researchers performed a population-based study using the Swedish vascular registry and the Swedish national population registry.
Disclosures: The authors reported they had no conflicts of interest and the study was funded by the Swedish Research Council and Uppsala University.
Postop delirium linked to greater long-term cognitive decline
Patients with postoperative delirium have significantly worse preoperative short-term cognitive performance and significantly greater long-term cognitive decline, compared with patients without delirium, according to Sharon K. Inouye, MD, and her associates.
In a prospective cohort study of 560 patients aged 70 years and older, 134 patients were selected for the delirium group and 426 for the nondelirium group. The delirium group had a significantly greater decline (–1.03 points) at 1 month, compared with those without delirium (P = .003). After cognitive function had recovered at 2 months, there were no significant differences between groups (P = 0.99). After 2 months, both groups decline on average; however, the delirium group declined significantly more (–1.07) in adjusted mean scores at 36 months (P =.02).

From baseline to 36 months, there was a significant change for the delirium group (–1.30, P less than .01) and no significant change for the group without delirium (–0.23, P = .30). Researchers noted that the effect of delirium remains undiminished after consecutive rehospitalizations, intercurrent illnesses, and major postoperative complications were controlled for.
The patients underwent major noncardiac surgery, such as total hip or knee replacement, open abdominal aortic aneurysm repair, colectomy, and lower-extremity arterial bypass.
“This study provides a novel presentation of the biphasic relationship of delirium and cognitive trajectory, both its well-recognized acute effects but also long-term effects,” the researchers wrote. “Our results suggest that after a period of initial recovery, patients with delirium experience a substantially accelerated trajectory of cognitive aging.”
Read the full study in Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association (doi:10.1016/j.jalz.2016.03.005).
Patients with postoperative delirium have significantly worse preoperative short-term cognitive performance and significantly greater long-term cognitive decline, compared with patients without delirium, according to Sharon K. Inouye, MD, and her associates.
In a prospective cohort study of 560 patients aged 70 years and older, 134 patients were selected for the delirium group and 426 for the nondelirium group. The delirium group had a significantly greater decline (–1.03 points) at 1 month, compared with those without delirium (P = .003). After cognitive function had recovered at 2 months, there were no significant differences between groups (P = 0.99). After 2 months, both groups decline on average; however, the delirium group declined significantly more (–1.07) in adjusted mean scores at 36 months (P =.02).
From baseline to 36 months, there was a significant change for the delirium group (–1.30, P less than .01) and no significant change for the group without delirium (–0.23, P = .30). Researchers noted that the effect of delirium remains undiminished after consecutive rehospitalizations, intercurrent illnesses, and major postoperative complications were controlled for.
The patients underwent major noncardiac surgery, such as total hip or knee replacement, open abdominal aortic aneurysm repair, colectomy, and lower-extremity arterial bypass.
“This study provides a novel presentation of the biphasic relationship of delirium and cognitive trajectory, both its well-recognized acute effects but also long-term effects,” the researchers wrote. “Our results suggest that after a period of initial recovery, patients with delirium experience a substantially accelerated trajectory of cognitive aging.”
Read the full study in Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association (doi:10.1016/j.jalz.2016.03.005).
Patients with postoperative delirium have significantly worse preoperative short-term cognitive performance and significantly greater long-term cognitive decline, compared with patients without delirium, according to Sharon K. Inouye, MD, and her associates.
In a prospective cohort study of 560 patients aged 70 years and older, 134 patients were selected for the delirium group and 426 for the nondelirium group. The delirium group had a significantly greater decline (–1.03 points) at 1 month, compared with those without delirium (P = .003). After cognitive function had recovered at 2 months, there were no significant differences between groups (P = 0.99). After 2 months, both groups decline on average; however, the delirium group declined significantly more (–1.07) in adjusted mean scores at 36 months (P =.02).
From baseline to 36 months, there was a significant change for the delirium group (–1.30, P less than .01) and no significant change for the group without delirium (–0.23, P = .30). Researchers noted that the effect of delirium remains undiminished after consecutive rehospitalizations, intercurrent illnesses, and major postoperative complications were controlled for.
The patients underwent major noncardiac surgery, such as total hip or knee replacement, open abdominal aortic aneurysm repair, colectomy, and lower-extremity arterial bypass.
“This study provides a novel presentation of the biphasic relationship of delirium and cognitive trajectory, both its well-recognized acute effects but also long-term effects,” the researchers wrote. “Our results suggest that after a period of initial recovery, patients with delirium experience a substantially accelerated trajectory of cognitive aging.”
Read the full study in Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association (doi:10.1016/j.jalz.2016.03.005).
FROM ALZHEIMER’S & DEMENTIA

Surgeons raise red flag on proposed 2017 physician fee schedule
The physician fee schedule for 2017 proposed by the Centers for Medicare & Medicaid Services has raised a red flag for the American College of Surgeons (ACS).
A proposal related to data collection on the transition of all 10- and 90- day global codes to 0-day codes in the proposed physician fee schedule 2017 is the area of greatest concern to the ACS. The provision would require all surgeons and other physicians who receive payment from these codes to devote many hours to collecting and reporting these data.

Two years ago, the CMS had pushed this exact transition through in regulation. However, Congress halted that transition in the Medicare Access and CHIP Reauthorization Act (MACRA), instead directing the CMS to study the effects of the transition by collecting data from a “representative sample” of physicians who receive payment from these codes.
For most surgical procedures, Medicare pays surgeons for either 10 or 90 days of care that include the procedure itself and postoperative care. Most global codes are 90-day codes. The CMS would have debundled the global payments 2 years ago had Congress not intervened.
However, in the proposed physician fee schedule update for 2017, the CMS would require all physicians to report data on these codes, something the ACS believes is overly burdensome.
“ACS believes that this proposal does not align with the MACRA requirement that CMS only collect data from a representative sample of physicians performing 10- or 90-day global codes,” ACS Regulatory Affairs Manager Vinita Ollapally told ACS Surgery News. “ACS is currently pursuing a legislative strategy that urges CMS to not finalize the proposal to collect data from all practitioners who perform 10- and 90-day global services, and instead revise the policy to collect data on 10- and 90-day global services from a ‘representative sample’ of practitioners.”
The college is developing a definition for what it believes that representative sample should include and expects to have that ready when the ACS files its comments on the physician fee schedule update proposal. Comments on the proposal are due Sept. 6.
The proposed update, published July 15 in the Federal Register, brings in several new policies aimed at improving physician payment for caring for patients with multiple chronic conditions; mental and behavioral health issues; and cognitive impairment or mobility-related issues.
Among the provisions in the 800+ page proposal are revised billing codes that would more accurately recognize the work of primary care and other cognitive specialties. The changes, according to the CMS, will help “better identify and value primary care, care management, and cognitive services.”
The agency is proposing several coding changes that “could improve health care delivery for all types of services holding the most promise for healthier people and smarter spending, and advance our health equity goals,” according to a CMS fact sheet.
The proposed fee schedule also would update how quality is measured and reported by accountable care organizations in the Medicare Shared Savings Program, align Accountable Care Organization reporting with the Physician Quality Reporting System, and change how beneficiaries are assigned to an ACO. Potentially misvalued services also would continue to be reviewed under the proposal.
The agency is also proposing a code to allow for the payment of advanced care planning services furnished via telehealth.
The physician fee schedule for 2017 proposed by the Centers for Medicare & Medicaid Services has raised a red flag for the American College of Surgeons (ACS).
A proposal related to data collection on the transition of all 10- and 90- day global codes to 0-day codes in the proposed physician fee schedule 2017 is the area of greatest concern to the ACS. The provision would require all surgeons and other physicians who receive payment from these codes to devote many hours to collecting and reporting these data.
Two years ago, the CMS had pushed this exact transition through in regulation. However, Congress halted that transition in the Medicare Access and CHIP Reauthorization Act (MACRA), instead directing the CMS to study the effects of the transition by collecting data from a “representative sample” of physicians who receive payment from these codes.
For most surgical procedures, Medicare pays surgeons for either 10 or 90 days of care that include the procedure itself and postoperative care. Most global codes are 90-day codes. The CMS would have debundled the global payments 2 years ago had Congress not intervened.
However, in the proposed physician fee schedule update for 2017, the CMS would require all physicians to report data on these codes, something the ACS believes is overly burdensome.
“ACS believes that this proposal does not align with the MACRA requirement that CMS only collect data from a representative sample of physicians performing 10- or 90-day global codes,” ACS Regulatory Affairs Manager Vinita Ollapally told ACS Surgery News. “ACS is currently pursuing a legislative strategy that urges CMS to not finalize the proposal to collect data from all practitioners who perform 10- and 90-day global services, and instead revise the policy to collect data on 10- and 90-day global services from a ‘representative sample’ of practitioners.”
The college is developing a definition for what it believes that representative sample should include and expects to have that ready when the ACS files its comments on the physician fee schedule update proposal. Comments on the proposal are due Sept. 6.
The proposed update, published July 15 in the Federal Register, brings in several new policies aimed at improving physician payment for caring for patients with multiple chronic conditions; mental and behavioral health issues; and cognitive impairment or mobility-related issues.
Among the provisions in the 800+ page proposal are revised billing codes that would more accurately recognize the work of primary care and other cognitive specialties. The changes, according to the CMS, will help “better identify and value primary care, care management, and cognitive services.”
The agency is proposing several coding changes that “could improve health care delivery for all types of services holding the most promise for healthier people and smarter spending, and advance our health equity goals,” according to a CMS fact sheet.
The proposed fee schedule also would update how quality is measured and reported by accountable care organizations in the Medicare Shared Savings Program, align Accountable Care Organization reporting with the Physician Quality Reporting System, and change how beneficiaries are assigned to an ACO. Potentially misvalued services also would continue to be reviewed under the proposal.
The agency is also proposing a code to allow for the payment of advanced care planning services furnished via telehealth.
The physician fee schedule for 2017 proposed by the Centers for Medicare & Medicaid Services has raised a red flag for the American College of Surgeons (ACS).
A proposal related to data collection on the transition of all 10- and 90- day global codes to 0-day codes in the proposed physician fee schedule 2017 is the area of greatest concern to the ACS. The provision would require all surgeons and other physicians who receive payment from these codes to devote many hours to collecting and reporting these data.
Two years ago, the CMS had pushed this exact transition through in regulation. However, Congress halted that transition in the Medicare Access and CHIP Reauthorization Act (MACRA), instead directing the CMS to study the effects of the transition by collecting data from a “representative sample” of physicians who receive payment from these codes.
For most surgical procedures, Medicare pays surgeons for either 10 or 90 days of care that include the procedure itself and postoperative care. Most global codes are 90-day codes. The CMS would have debundled the global payments 2 years ago had Congress not intervened.
However, in the proposed physician fee schedule update for 2017, the CMS would require all physicians to report data on these codes, something the ACS believes is overly burdensome.
“ACS believes that this proposal does not align with the MACRA requirement that CMS only collect data from a representative sample of physicians performing 10- or 90-day global codes,” ACS Regulatory Affairs Manager Vinita Ollapally told ACS Surgery News. “ACS is currently pursuing a legislative strategy that urges CMS to not finalize the proposal to collect data from all practitioners who perform 10- and 90-day global services, and instead revise the policy to collect data on 10- and 90-day global services from a ‘representative sample’ of practitioners.”
The college is developing a definition for what it believes that representative sample should include and expects to have that ready when the ACS files its comments on the physician fee schedule update proposal. Comments on the proposal are due Sept. 6.
The proposed update, published July 15 in the Federal Register, brings in several new policies aimed at improving physician payment for caring for patients with multiple chronic conditions; mental and behavioral health issues; and cognitive impairment or mobility-related issues.
Among the provisions in the 800+ page proposal are revised billing codes that would more accurately recognize the work of primary care and other cognitive specialties. The changes, according to the CMS, will help “better identify and value primary care, care management, and cognitive services.”
The agency is proposing several coding changes that “could improve health care delivery for all types of services holding the most promise for healthier people and smarter spending, and advance our health equity goals,” according to a CMS fact sheet.
The proposed fee schedule also would update how quality is measured and reported by accountable care organizations in the Medicare Shared Savings Program, align Accountable Care Organization reporting with the Physician Quality Reporting System, and change how beneficiaries are assigned to an ACO. Potentially misvalued services also would continue to be reviewed under the proposal.
The agency is also proposing a code to allow for the payment of advanced care planning services furnished via telehealth.

Transfers to tertiary acute care surgery service point to shortage of rural general surgeons
Nearly half of all transfer patients admitted to a tertiary facility’s acute care surgery service over a 12-month period underwent only basic surgical procedures or required no intervention after the transfer, according to a retrospective chart review.
The 161 patients transferred through the acute care surgery system during the 2014 study period were in need of the services for which they were transferred; thus, the findings highlight a “concerning lack of general surgery resources” in the community, Brittany Misercola, MD, and her colleagues at Maine Medical Center, Portland, reported in the Journal of Surgical Research.
Acute care surgery (ACS) is a relatively new paradigm – borne in part out of a heavy call burden for trauma and general surgeons – for managing patients in need of non–trauma-related emergency surgery, the investigators explained.
“At the same time as the ACS paradigm has developed, rural areas are suffering worsening shortages of physicians, especially specialists like surgeons. Another change has been regionalization of sick, complex, and resource-intensive patients to larger hospitals with more specialized care.

However, no one has yet examined the effect of an ACS service in a predominantly rural area, given these changes in health care,” they wrote (J Surg Res. 2016. [doi:10.106/j.jss.2016.06.090]).
Patients included all adults aged 18 and older admitted between Jan. 1 and Dec. 31, 2014, excluding elective surgical and trauma patients. Transfer patients were admitted from 29 different institutions. The hospital is the largest in Maine, with a wide and rural catchment area. Transfer patients came from every county in the state, with a few from outside the state; 18% were transferred from a Maine Critical Access Hospital.
Compared with 611 local patients admitted through the emergency department or from local long-term care facilities, the transfer patients were older (61.2 years vs. 54.7 years), had more comorbidities (Charlson Comorbidity Index, or CCI, of 4 vs. 3.1), and required more resources (length of stay, 8.2 vs. 3.4 days; intensive care unit admission, 24% vs. 6%), the investigators reported.
Stratification by CCI showed that the difference in length of stay between transfer and local patients was largest in those with a low CCI (0-3), compared with those with a higher CCI.
The admission diagnosis was similar in the transferred and local patients, with pancreaticobiliary and small bowel complaints being the most common (29% and 30%, and 25% and 23%, respectively, for the two diagnoses). The most common interventions were laparoscopic cholecystectomy in both groups (29% and 25%, respectively). Subspecialty interventions were also similar in the groups, and were performed in 10% and 8%, respectively.
However, the transfer patients were more likely than the local patients to not require any intervention, including subspecialty care (32% vs. 23%), they said, noting that the most common reason for admission without operative intervention was “small bowel obstruction, followed by diverticulitis without drainable abscess and mesenteric ischemia.”
The transfer patients also were more likely to have Medicare (55% vs. 24%) and less likely to be privately insured (26% vs. 45%).
The discharge destination differed significantly between the groups, with local patients being more likely to be discharged directly to home (76% vs. 46%), and transfer patients more often discharged home with services (46% vs. 12%) or to acute rehabilitation or skilled nursing facilities (12% vs. 9%). In-hospital mortality and discharge to hospice care also were more likely among transfer patients (6% vs. 2%).
“If changes are not made to support rural hospitals in caring for these patients, tertiary centers in larger cities will see increasing volume of basic surgical emergencies. As such, investing in community hospitals is important to improve patient outcomes not only locally but also after transfer to tertiary referral centers,” they wrote, adding that additional research on the populations most affected is needed.
The authors reported having no relevant financial disclosures.
Nearly half of all transfer patients admitted to a tertiary facility’s acute care surgery service over a 12-month period underwent only basic surgical procedures or required no intervention after the transfer, according to a retrospective chart review.
The 161 patients transferred through the acute care surgery system during the 2014 study period were in need of the services for which they were transferred; thus, the findings highlight a “concerning lack of general surgery resources” in the community, Brittany Misercola, MD, and her colleagues at Maine Medical Center, Portland, reported in the Journal of Surgical Research.
Acute care surgery (ACS) is a relatively new paradigm – borne in part out of a heavy call burden for trauma and general surgeons – for managing patients in need of non–trauma-related emergency surgery, the investigators explained.
“At the same time as the ACS paradigm has developed, rural areas are suffering worsening shortages of physicians, especially specialists like surgeons. Another change has been regionalization of sick, complex, and resource-intensive patients to larger hospitals with more specialized care.
However, no one has yet examined the effect of an ACS service in a predominantly rural area, given these changes in health care,” they wrote (J Surg Res. 2016. [doi:10.106/j.jss.2016.06.090]).
Patients included all adults aged 18 and older admitted between Jan. 1 and Dec. 31, 2014, excluding elective surgical and trauma patients. Transfer patients were admitted from 29 different institutions. The hospital is the largest in Maine, with a wide and rural catchment area. Transfer patients came from every county in the state, with a few from outside the state; 18% were transferred from a Maine Critical Access Hospital.
Compared with 611 local patients admitted through the emergency department or from local long-term care facilities, the transfer patients were older (61.2 years vs. 54.7 years), had more comorbidities (Charlson Comorbidity Index, or CCI, of 4 vs. 3.1), and required more resources (length of stay, 8.2 vs. 3.4 days; intensive care unit admission, 24% vs. 6%), the investigators reported.
Stratification by CCI showed that the difference in length of stay between transfer and local patients was largest in those with a low CCI (0-3), compared with those with a higher CCI.
The admission diagnosis was similar in the transferred and local patients, with pancreaticobiliary and small bowel complaints being the most common (29% and 30%, and 25% and 23%, respectively, for the two diagnoses). The most common interventions were laparoscopic cholecystectomy in both groups (29% and 25%, respectively). Subspecialty interventions were also similar in the groups, and were performed in 10% and 8%, respectively.
However, the transfer patients were more likely than the local patients to not require any intervention, including subspecialty care (32% vs. 23%), they said, noting that the most common reason for admission without operative intervention was “small bowel obstruction, followed by diverticulitis without drainable abscess and mesenteric ischemia.”
The transfer patients also were more likely to have Medicare (55% vs. 24%) and less likely to be privately insured (26% vs. 45%).
The discharge destination differed significantly between the groups, with local patients being more likely to be discharged directly to home (76% vs. 46%), and transfer patients more often discharged home with services (46% vs. 12%) or to acute rehabilitation or skilled nursing facilities (12% vs. 9%). In-hospital mortality and discharge to hospice care also were more likely among transfer patients (6% vs. 2%).
“If changes are not made to support rural hospitals in caring for these patients, tertiary centers in larger cities will see increasing volume of basic surgical emergencies. As such, investing in community hospitals is important to improve patient outcomes not only locally but also after transfer to tertiary referral centers,” they wrote, adding that additional research on the populations most affected is needed.
The authors reported having no relevant financial disclosures.
Nearly half of all transfer patients admitted to a tertiary facility’s acute care surgery service over a 12-month period underwent only basic surgical procedures or required no intervention after the transfer, according to a retrospective chart review.
The 161 patients transferred through the acute care surgery system during the 2014 study period were in need of the services for which they were transferred; thus, the findings highlight a “concerning lack of general surgery resources” in the community, Brittany Misercola, MD, and her colleagues at Maine Medical Center, Portland, reported in the Journal of Surgical Research.
Acute care surgery (ACS) is a relatively new paradigm – borne in part out of a heavy call burden for trauma and general surgeons – for managing patients in need of non–trauma-related emergency surgery, the investigators explained.
“At the same time as the ACS paradigm has developed, rural areas are suffering worsening shortages of physicians, especially specialists like surgeons. Another change has been regionalization of sick, complex, and resource-intensive patients to larger hospitals with more specialized care.
However, no one has yet examined the effect of an ACS service in a predominantly rural area, given these changes in health care,” they wrote (J Surg Res. 2016. [doi:10.106/j.jss.2016.06.090]).
Patients included all adults aged 18 and older admitted between Jan. 1 and Dec. 31, 2014, excluding elective surgical and trauma patients. Transfer patients were admitted from 29 different institutions. The hospital is the largest in Maine, with a wide and rural catchment area. Transfer patients came from every county in the state, with a few from outside the state; 18% were transferred from a Maine Critical Access Hospital.
Compared with 611 local patients admitted through the emergency department or from local long-term care facilities, the transfer patients were older (61.2 years vs. 54.7 years), had more comorbidities (Charlson Comorbidity Index, or CCI, of 4 vs. 3.1), and required more resources (length of stay, 8.2 vs. 3.4 days; intensive care unit admission, 24% vs. 6%), the investigators reported.
Stratification by CCI showed that the difference in length of stay between transfer and local patients was largest in those with a low CCI (0-3), compared with those with a higher CCI.
The admission diagnosis was similar in the transferred and local patients, with pancreaticobiliary and small bowel complaints being the most common (29% and 30%, and 25% and 23%, respectively, for the two diagnoses). The most common interventions were laparoscopic cholecystectomy in both groups (29% and 25%, respectively). Subspecialty interventions were also similar in the groups, and were performed in 10% and 8%, respectively.
However, the transfer patients were more likely than the local patients to not require any intervention, including subspecialty care (32% vs. 23%), they said, noting that the most common reason for admission without operative intervention was “small bowel obstruction, followed by diverticulitis without drainable abscess and mesenteric ischemia.”
The transfer patients also were more likely to have Medicare (55% vs. 24%) and less likely to be privately insured (26% vs. 45%).
The discharge destination differed significantly between the groups, with local patients being more likely to be discharged directly to home (76% vs. 46%), and transfer patients more often discharged home with services (46% vs. 12%) or to acute rehabilitation or skilled nursing facilities (12% vs. 9%). In-hospital mortality and discharge to hospice care also were more likely among transfer patients (6% vs. 2%).
“If changes are not made to support rural hospitals in caring for these patients, tertiary centers in larger cities will see increasing volume of basic surgical emergencies. As such, investing in community hospitals is important to improve patient outcomes not only locally but also after transfer to tertiary referral centers,” they wrote, adding that additional research on the populations most affected is needed.
The authors reported having no relevant financial disclosures.
FROM THE JOURNAL OF SURGICAL RESEARCH
Key clinical point: Transfer of patients to a tertiary facility and acute care surgery service who require basic surgical procedures or no intervention points to a shortage of general surgery capability in the rural areas.
Major finding: Transfer patients were more likely than local patients to not require any intervention, including subspecialty care (32% vs. 23%).
Data source: A retrospective review of 772 patient charts.
Disclosures: The authors reported having no relevant financial disclosures.
