User login
Official Newspaper of the American College of Surgeons
Preventing surgical site infections in hysterectomy
Surgical site infections are a major source of patient morbidity. They are also an important quality metric for surgeons and hospital systems, and are increasingly being linked to reimbursement.
They occur in approximately 2% of the 600,000 women undergoing hysterectomy in the United States each year. The U.S. Centers for Disease Control and Prevention defines surgical site infection (SSI) as an infection that occurs within 30 days of a procedure in the part of the body where the surgery took place. Most SSIs are superficial incisional, but they also include deep incisional or organ or space infections.
Classification
The incidence of SSI varies according to the classification of the wound, as defined by the National Academy of Sciences.1 Most hysterectomies are classified as clean-contaminated wounds because they involve entry into the mucosa of the genitourinary tract. However, hysterectomy with contamination of bowel flora, or in the setting of acute infection (such as suppurative pelvic inflammatory disease) are considered a contaminated wound class, and are associated with even higher rates of SSI.

Risk factors
The risk factors associated with SSI are both modifiable and unmodifiable. Broadly speaking, they include increased risk to endogenous flora (e.g., wound classification), increased exposure to exogenous flora (e.g., inadequate protection of a wound from external pathogens), and impairment of the body’s immune mechanisms to prevent and overcome infection (e.g., hypothermia and hypoglycemia).
Unmodifiable risk factors include increasing age, a history of radiation exposure, vascular disease, and a history of prior SSIs. Modifiable risk factors include obesity, tobacco use, immunosuppressive medications, hypoalbuminemia, route of hysterectomy, hair removal, preoperative infections (such as bacterial vaginosis), surgical scrub, skin and vaginal preparation, antimicrobial prophylaxis (inappropriate choice or timing, inadequate dosing or redosing), operative time, blood transfusion, surgical skill, and operating room characteristics (ventilation, increased OR traffic, and sterilization of surgical equipment).

Antimicrobial prophylaxis
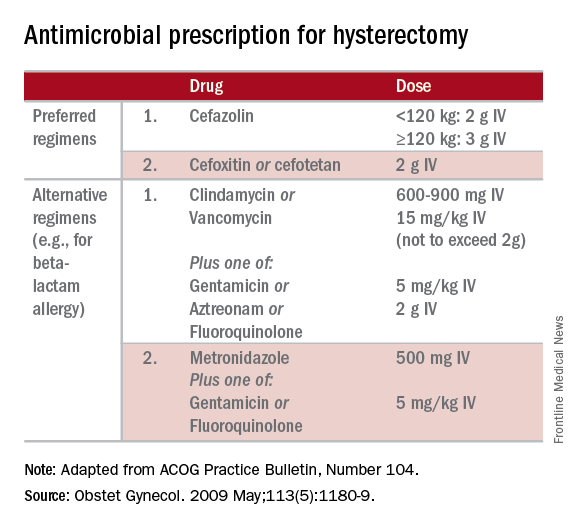
The CDC and the American College of Obstetricians and Gynecologists (ACOG) have provided clear guidelines regarding methods to reduce SSI in hysterectomy.3,4 There is strong evidence for using antimicrobial prophylaxis for hysterectomy.
It is important that physicians confirm the validity of beta-lactam allergies with patients because there are higher rates of SSI with the use of non–beta-lactam regimens, even those endorsed by the CDC and ACOG.5
Antibiotics should be administered within 1 hour of skin incision, and ideally within 30 minutes. They should be discontinued within 24 hours. Dosing should be adjusted to weight, and antimicrobials should be redosed for long procedures (at intervals of two half-lives), and for increased blood loss.
Skin preparation
Hair removal should be avoided unless necessary for technical reasons. If it is required, it should be performed outside of the operative space using clippers, not razors. For patients colonized with methicillin-resistant S. aureus, there is supporting evidence for pretreatment with mupirocin ointment to the nares, and chlorhexidine showers for 5-10 days. Patients who have bacterial vaginosis should be treated before surgery to decrease the rate of vaginal cuff SSI.
If there is a planned or potential gastrointestinal procedure as part of the hysterectomy, the surgeon should consider using an impervious plastic wound protector in place of, or in addition to, other retractors. Preoperative oral antimicrobials with mechanical bowel preparation have been associated with decreased SSIs; however, this benefit is not observed with mechanical bowel preparation alone.
Wound closure
Surgical technique and wound closure techniques also impact SSI. Minimally invasive and vaginal hysterectomy routes are preferred, as these are associated with the lowest rates of SSI. Antimicrobial-impregnated suture materials appear to be unnecessary. Surgeons should ensure that there is delicate handling of tissues and closure of dead spaces. If the subcutaneous fat space depth measures more than 2.5 cm, it should be reapproximated with a rapidly-absorbing suture material.
Use of electrosurgery versus a scalpel when creating the incision does not appear to influence infection rates, nor does use of staples versus subcuticular suture during closure.7
Using a dilute iodine lavage in the subcutaneous space, opening a sterile closing tray, and having surgeons change gloves prior to skin closure should be considered. The CDC recommends keeping the skin dressing in place for 24 hours postoperatively.
Other strategies
Hyperglycemia is associated with impaired neutrophil response, and therefore blood glucose should be controlled before surgery (hemoglobin A1c levels of less than 7% preoperatively) and immediately postoperatively (less than 180 mg/dL within 18-24 hours after the end of anesthesia).
It is also important to minimize perioperative hypothermia (less than 35.5° F), as this also impairs the body’s immune response. Keeping operative room ambient temperatures higher, minimizing incision size, warming CO2 gas in minimally invasive procedures, warming fluids, and using extrinsic body warmers can help achieve this.
Excessive blood loss should be minimized because blood transfusion is associated with impaired macrophage function and increased risk for SSI.
In addition to teamwide (including nonsurgeon) strict adherence to hand hygiene, OR personnel should avoid unnecessary operating room traffic. Hospital officials should ensure that the facility’s ventilator systems are well maintained and that there is care and maintenance of air handlers.
Many strategies can be employed perioperatively to decrease SSI rates for hysterectomy. We advocate for a protocol-based approach (known as “bundling” strategies) to achieve consistency of practice and to maximize surgeon and institutional improvements in SSI rates. This is similar to the approach outlined in a recent consensus statement from the Council on Patient Safety in Women’s Health Care.8
A comprehensive multidisciplinary approach throughout the perioperative period is necessary. It is imperative that good communication exist with patients regarding SSIs after hysterectomy and how patients, surgeons, and hospitals can together minimize the risks of SSIs.
References
1. Altemeier WA. “Manual on Control of Infection in Surgical Patients” (Philadelphia: Lippincott Williams & Wilkins, 1984).
2. Rev Infect Dis. 1991 Sep-Oct;13(Suppl 10):S821-41.
3. Infect Control Hosp Epidemiol. 2014 Jun;35(6):605-27.
4. Obstet Gynecol. 2009 May;113(5):1180-9.
5. Obstet Gynecol. 2016 Feb;127(2):321-9.
6. Am J Obstet Gynecol. 2005 Feb;192(2):422-5.
7. J Gastrointest Surg. 2016 Dec;20(12):2083-92.
8. Obstet Gynecol. 2016 Dec 7. doi: 10.1097/AOG.0000000000001751.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Jackson-Moore is an associate professor in gynecologic oncology at UNC. They reported having no relevant financial disclosures.
Surgical site infections are a major source of patient morbidity. They are also an important quality metric for surgeons and hospital systems, and are increasingly being linked to reimbursement.
They occur in approximately 2% of the 600,000 women undergoing hysterectomy in the United States each year. The U.S. Centers for Disease Control and Prevention defines surgical site infection (SSI) as an infection that occurs within 30 days of a procedure in the part of the body where the surgery took place. Most SSIs are superficial incisional, but they also include deep incisional or organ or space infections.
Classification
The incidence of SSI varies according to the classification of the wound, as defined by the National Academy of Sciences.1 Most hysterectomies are classified as clean-contaminated wounds because they involve entry into the mucosa of the genitourinary tract. However, hysterectomy with contamination of bowel flora, or in the setting of acute infection (such as suppurative pelvic inflammatory disease) are considered a contaminated wound class, and are associated with even higher rates of SSI.
Risk factors
The risk factors associated with SSI are both modifiable and unmodifiable. Broadly speaking, they include increased risk to endogenous flora (e.g., wound classification), increased exposure to exogenous flora (e.g., inadequate protection of a wound from external pathogens), and impairment of the body’s immune mechanisms to prevent and overcome infection (e.g., hypothermia and hypoglycemia).
Unmodifiable risk factors include increasing age, a history of radiation exposure, vascular disease, and a history of prior SSIs. Modifiable risk factors include obesity, tobacco use, immunosuppressive medications, hypoalbuminemia, route of hysterectomy, hair removal, preoperative infections (such as bacterial vaginosis), surgical scrub, skin and vaginal preparation, antimicrobial prophylaxis (inappropriate choice or timing, inadequate dosing or redosing), operative time, blood transfusion, surgical skill, and operating room characteristics (ventilation, increased OR traffic, and sterilization of surgical equipment).
Antimicrobial prophylaxis
The CDC and the American College of Obstetricians and Gynecologists (ACOG) have provided clear guidelines regarding methods to reduce SSI in hysterectomy.3,4 There is strong evidence for using antimicrobial prophylaxis for hysterectomy.
It is important that physicians confirm the validity of beta-lactam allergies with patients because there are higher rates of SSI with the use of non–beta-lactam regimens, even those endorsed by the CDC and ACOG.5
Antibiotics should be administered within 1 hour of skin incision, and ideally within 30 minutes. They should be discontinued within 24 hours. Dosing should be adjusted to weight, and antimicrobials should be redosed for long procedures (at intervals of two half-lives), and for increased blood loss.
Skin preparation
Hair removal should be avoided unless necessary for technical reasons. If it is required, it should be performed outside of the operative space using clippers, not razors. For patients colonized with methicillin-resistant S. aureus, there is supporting evidence for pretreatment with mupirocin ointment to the nares, and chlorhexidine showers for 5-10 days. Patients who have bacterial vaginosis should be treated before surgery to decrease the rate of vaginal cuff SSI.
If there is a planned or potential gastrointestinal procedure as part of the hysterectomy, the surgeon should consider using an impervious plastic wound protector in place of, or in addition to, other retractors. Preoperative oral antimicrobials with mechanical bowel preparation have been associated with decreased SSIs; however, this benefit is not observed with mechanical bowel preparation alone.
Wound closure
Surgical technique and wound closure techniques also impact SSI. Minimally invasive and vaginal hysterectomy routes are preferred, as these are associated with the lowest rates of SSI. Antimicrobial-impregnated suture materials appear to be unnecessary. Surgeons should ensure that there is delicate handling of tissues and closure of dead spaces. If the subcutaneous fat space depth measures more than 2.5 cm, it should be reapproximated with a rapidly-absorbing suture material.
Use of electrosurgery versus a scalpel when creating the incision does not appear to influence infection rates, nor does use of staples versus subcuticular suture during closure.7
Using a dilute iodine lavage in the subcutaneous space, opening a sterile closing tray, and having surgeons change gloves prior to skin closure should be considered. The CDC recommends keeping the skin dressing in place for 24 hours postoperatively.
Other strategies
Hyperglycemia is associated with impaired neutrophil response, and therefore blood glucose should be controlled before surgery (hemoglobin A1c levels of less than 7% preoperatively) and immediately postoperatively (less than 180 mg/dL within 18-24 hours after the end of anesthesia).
It is also important to minimize perioperative hypothermia (less than 35.5° F), as this also impairs the body’s immune response. Keeping operative room ambient temperatures higher, minimizing incision size, warming CO2 gas in minimally invasive procedures, warming fluids, and using extrinsic body warmers can help achieve this.
Excessive blood loss should be minimized because blood transfusion is associated with impaired macrophage function and increased risk for SSI.
In addition to teamwide (including nonsurgeon) strict adherence to hand hygiene, OR personnel should avoid unnecessary operating room traffic. Hospital officials should ensure that the facility’s ventilator systems are well maintained and that there is care and maintenance of air handlers.
Many strategies can be employed perioperatively to decrease SSI rates for hysterectomy. We advocate for a protocol-based approach (known as “bundling” strategies) to achieve consistency of practice and to maximize surgeon and institutional improvements in SSI rates. This is similar to the approach outlined in a recent consensus statement from the Council on Patient Safety in Women’s Health Care.8
A comprehensive multidisciplinary approach throughout the perioperative period is necessary. It is imperative that good communication exist with patients regarding SSIs after hysterectomy and how patients, surgeons, and hospitals can together minimize the risks of SSIs.
References
1. Altemeier WA. “Manual on Control of Infection in Surgical Patients” (Philadelphia: Lippincott Williams & Wilkins, 1984).
2. Rev Infect Dis. 1991 Sep-Oct;13(Suppl 10):S821-41.
3. Infect Control Hosp Epidemiol. 2014 Jun;35(6):605-27.
4. Obstet Gynecol. 2009 May;113(5):1180-9.
5. Obstet Gynecol. 2016 Feb;127(2):321-9.
6. Am J Obstet Gynecol. 2005 Feb;192(2):422-5.
7. J Gastrointest Surg. 2016 Dec;20(12):2083-92.
8. Obstet Gynecol. 2016 Dec 7. doi: 10.1097/AOG.0000000000001751.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Jackson-Moore is an associate professor in gynecologic oncology at UNC. They reported having no relevant financial disclosures.
Surgical site infections are a major source of patient morbidity. They are also an important quality metric for surgeons and hospital systems, and are increasingly being linked to reimbursement.
They occur in approximately 2% of the 600,000 women undergoing hysterectomy in the United States each year. The U.S. Centers for Disease Control and Prevention defines surgical site infection (SSI) as an infection that occurs within 30 days of a procedure in the part of the body where the surgery took place. Most SSIs are superficial incisional, but they also include deep incisional or organ or space infections.
Classification
The incidence of SSI varies according to the classification of the wound, as defined by the National Academy of Sciences.1 Most hysterectomies are classified as clean-contaminated wounds because they involve entry into the mucosa of the genitourinary tract. However, hysterectomy with contamination of bowel flora, or in the setting of acute infection (such as suppurative pelvic inflammatory disease) are considered a contaminated wound class, and are associated with even higher rates of SSI.
Risk factors
The risk factors associated with SSI are both modifiable and unmodifiable. Broadly speaking, they include increased risk to endogenous flora (e.g., wound classification), increased exposure to exogenous flora (e.g., inadequate protection of a wound from external pathogens), and impairment of the body’s immune mechanisms to prevent and overcome infection (e.g., hypothermia and hypoglycemia).
Unmodifiable risk factors include increasing age, a history of radiation exposure, vascular disease, and a history of prior SSIs. Modifiable risk factors include obesity, tobacco use, immunosuppressive medications, hypoalbuminemia, route of hysterectomy, hair removal, preoperative infections (such as bacterial vaginosis), surgical scrub, skin and vaginal preparation, antimicrobial prophylaxis (inappropriate choice or timing, inadequate dosing or redosing), operative time, blood transfusion, surgical skill, and operating room characteristics (ventilation, increased OR traffic, and sterilization of surgical equipment).
Antimicrobial prophylaxis
The CDC and the American College of Obstetricians and Gynecologists (ACOG) have provided clear guidelines regarding methods to reduce SSI in hysterectomy.3,4 There is strong evidence for using antimicrobial prophylaxis for hysterectomy.
It is important that physicians confirm the validity of beta-lactam allergies with patients because there are higher rates of SSI with the use of non–beta-lactam regimens, even those endorsed by the CDC and ACOG.5
Antibiotics should be administered within 1 hour of skin incision, and ideally within 30 minutes. They should be discontinued within 24 hours. Dosing should be adjusted to weight, and antimicrobials should be redosed for long procedures (at intervals of two half-lives), and for increased blood loss.
Skin preparation
Hair removal should be avoided unless necessary for technical reasons. If it is required, it should be performed outside of the operative space using clippers, not razors. For patients colonized with methicillin-resistant S. aureus, there is supporting evidence for pretreatment with mupirocin ointment to the nares, and chlorhexidine showers for 5-10 days. Patients who have bacterial vaginosis should be treated before surgery to decrease the rate of vaginal cuff SSI.
If there is a planned or potential gastrointestinal procedure as part of the hysterectomy, the surgeon should consider using an impervious plastic wound protector in place of, or in addition to, other retractors. Preoperative oral antimicrobials with mechanical bowel preparation have been associated with decreased SSIs; however, this benefit is not observed with mechanical bowel preparation alone.
Wound closure
Surgical technique and wound closure techniques also impact SSI. Minimally invasive and vaginal hysterectomy routes are preferred, as these are associated with the lowest rates of SSI. Antimicrobial-impregnated suture materials appear to be unnecessary. Surgeons should ensure that there is delicate handling of tissues and closure of dead spaces. If the subcutaneous fat space depth measures more than 2.5 cm, it should be reapproximated with a rapidly-absorbing suture material.
Use of electrosurgery versus a scalpel when creating the incision does not appear to influence infection rates, nor does use of staples versus subcuticular suture during closure.7
Using a dilute iodine lavage in the subcutaneous space, opening a sterile closing tray, and having surgeons change gloves prior to skin closure should be considered. The CDC recommends keeping the skin dressing in place for 24 hours postoperatively.
Other strategies
Hyperglycemia is associated with impaired neutrophil response, and therefore blood glucose should be controlled before surgery (hemoglobin A1c levels of less than 7% preoperatively) and immediately postoperatively (less than 180 mg/dL within 18-24 hours after the end of anesthesia).
It is also important to minimize perioperative hypothermia (less than 35.5° F), as this also impairs the body’s immune response. Keeping operative room ambient temperatures higher, minimizing incision size, warming CO2 gas in minimally invasive procedures, warming fluids, and using extrinsic body warmers can help achieve this.
Excessive blood loss should be minimized because blood transfusion is associated with impaired macrophage function and increased risk for SSI.
In addition to teamwide (including nonsurgeon) strict adherence to hand hygiene, OR personnel should avoid unnecessary operating room traffic. Hospital officials should ensure that the facility’s ventilator systems are well maintained and that there is care and maintenance of air handlers.
Many strategies can be employed perioperatively to decrease SSI rates for hysterectomy. We advocate for a protocol-based approach (known as “bundling” strategies) to achieve consistency of practice and to maximize surgeon and institutional improvements in SSI rates. This is similar to the approach outlined in a recent consensus statement from the Council on Patient Safety in Women’s Health Care.8
A comprehensive multidisciplinary approach throughout the perioperative period is necessary. It is imperative that good communication exist with patients regarding SSIs after hysterectomy and how patients, surgeons, and hospitals can together minimize the risks of SSIs.
References
1. Altemeier WA. “Manual on Control of Infection in Surgical Patients” (Philadelphia: Lippincott Williams & Wilkins, 1984).
2. Rev Infect Dis. 1991 Sep-Oct;13(Suppl 10):S821-41.
3. Infect Control Hosp Epidemiol. 2014 Jun;35(6):605-27.
4. Obstet Gynecol. 2009 May;113(5):1180-9.
5. Obstet Gynecol. 2016 Feb;127(2):321-9.
6. Am J Obstet Gynecol. 2005 Feb;192(2):422-5.
7. J Gastrointest Surg. 2016 Dec;20(12):2083-92.
8. Obstet Gynecol. 2016 Dec 7. doi: 10.1097/AOG.0000000000001751.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Jackson-Moore is an associate professor in gynecologic oncology at UNC. They reported having no relevant financial disclosures.
Point/Counterpoint: Is limb salvage always best in diabetes?
Salvage limbs at all costs
Aggressive limb salvage in people with diabetes leads to an overall reduction in cost not only economically, but also from the patient’s perspective. The vast majority of diabetic patients with critical ischemia are actually good candidates for limb salvage. Tragically, many of these patients are never referred for evaluation for limb salvage because of misconceptions about the pathophysiology of the disease.
An argument against limb salvage is that primary amputation prevents or shortens the course of wound care and enables patients to become ambulatory, albeit with a prosthesis, faster. However, in the modern era of vascular surgery, revascularization can be performed successfully with minimal mortality and excellent rates of limb salvage, especially when it’s done within a team-based approach.

The mortality in primary amputation is shockingly high, anywhere from 5% to 23% higher than revascularization alone, and the major complication rate of amputation associated with diabetes is also unacceptably high – up to 37%. This is in contrast to a 17% rate in major nonamputation vascular surgery and 1%-5% in endovascular procedures (BMC Nephrol. 2005;6:3).
We can’t ignore the economic burden this places on the country. In 2014, primary amputations cost the health care system $11 billion annually, and that is expected to grow to more than $25 billion in the next several years, according to the SAGE Group. It’s important to keep in mind that Medicare covers over 80% of this cost.
A number of studies have shown that conservative management with wound care and amputation is more cost effective than primary amputation in ambulatory, independent adults. Data can be difficult to interpret because of different recording strategies for all the costs associated with amputation, but a single-institution study concluded that revascularization costs almost $5,280 more than expectant management, but $33,900 less than primary amputation alone (Cardiovasc Surg. 1999;7;62-9).
We must also consider the costs of revision after primary amputation; above-the-knee amputation has a 12% in-hospital revision rate, and below-the-knee amputation about 20%. Endovascular interventions, on the other hand, have a 1%-9% in-hospital revision rate, and only 2%-4% of these patients will go on to require an amputation during the same admission (Eur J Vasc Endovasc Surg. 2006;32:484-90; Arch Phys Med Rehabil. 2005;86:480-6).This does not include the costs of those complications as well as other indirect costs of amputation, such as nursing home care and living situation modification (Int J Behav Med. 2016;23:714-21; Pak J Med Sci. 2014; 30:1044-9). They quickly add up to that $25 billion.
The proponents of primary amputation tell us that it leads to quicker recovery time and an earlier time to ambulation. However, only 47% of patients will actually ambulate after amputation, in contrast to 97% who will ambulate after limb salvage as a primary procedure. In a nonambulatory cohort, 21% of those patients go on to regain functional status that was lost prior to surgery (J Vasc Surg. 1997;25;287-95).
Many question if our success with vascular surgery over the past few decades can translate to helping the most difficult subset of patients. An Italian study reported on a cohort of diabetic vs. nondiabetic patients and determined both groups have similar amputation-free rates after infrainguinal arterial reconstruction for critical limb ischemia, with excellent primary and secondary patency rates and a limb salvage rate of 88% at 5 years (J Vasc Surg. 2014;59:708-19). This tells us that we do have the skill set necessary to save these limbs.
A multidisciplinary limb preservation team is paramount to the success of any limb salvage program. A revascularization team should be in place which uses early intervention to achieve the highest limb salvage rates possible. Wound care needs to be an integrated part of it. Advanced podiatric reconstructive surgery also is key because this can provide complex foot reconstructions and help ambulatory patients return home.
Dr. Trissa A. Babrowski is an assistant professor of surgery, specializing in vascular surgery and endovascular therapy, at the University of Chicago Heart and Vascular Center. She had no financial relationships to disclose.
Primary amputation can be OK
I am not an amputationalist. I do practice limb salvage. In fact I’m probably the most aggressive limb salvage surgeon in my hospital. But primary amputation is a completely acceptable option for a selected group of patients with diabetes. We should not try to do limb salvage “at all costs.”
I do not find this to be a contradictory position. In fact, I think it adds credence to my support of limb salvage that I think primary amputation can be OK. In all honesty, there are very few things in life that should be done at all costs.
A study out of Loma Linda University involving patients with CLI compared primary amputation vs. revascularization; 43% of patients had a primary amputation (Ann Vasc Surg. 2007;21:458-63). A multivariate analysis showed that patients with major tissue loss, end-stage renal disease (ESRD), diabetes and nonambulatory status were more likely to undergo primary amputation rather than revascularization.
While major tissue loss (Rutherford category 6) is certainly an indication for primary amputation, ambulatory status can represent a gray area in determining the best course. ESRD and diabetes are much more nonspecific factors; probably more than 10% of the patients that we see with CLI have ESRD. Also, 50%-70% of these patients with CLI, and in some series even higher percentages, have diabetes. Thus, these factors by themselves do not assist us in determining which patients potentially should be offered primary amputation vs. revascularization.
In general, we know that we can get good results in limb bypass or revascularization in patients with CLI: The PREVENT III multicenter trial, with the use of the vein as the conduit, showed 1-year limb salvage rates of 88% in these high-risk patients (J Vasc Surg. 2006;43:742-51). However, one of the major risk factors that adversely affected outcome was ESRD.
We know that ESRD is a significant predictor of lowering our chances of saving a limb successfully. Knowing the cost of multiple continued episodes of revascularization in these patients prior to proceeding with an amputation, it’s intuitive that these patients would benefit from a more precise process in their treatment from the beginning. A number of papers have concluded that a primary amputation may be the preferred approach in patients with ESRD.
Can we preoperatively predict which patients with CLI will fail operative revascularization? Data from the New England Vascular Quality Initiative identified eight variables associated with failure of revascularization, among them age younger than 59, ESRD, diabetes, CLI, conduit requiring venovenostomy, tarsal target, and nursing home residence (Ann Vasc Surg. 2010;24:57-68). The presence of three or more risk factors has a 27.7% risk of limb loss and/or graft thrombosis within 1 year.
Postponing amputation is a major cost issue. Direct costs of bypass for critical limb ischemia were $3.6 billion in 2004 (J Vasc Surg. 2011;54:1021-31), and we know that a functional outcome can be problematic in this patient group. Factors associated with a poor functional outcome include dementia, dependent-living situation preoperatively and nonambulatory status.
Unfortunately, there are not a lot of data that deal with quality of life outcomes for patients with CLI who have undergone bypass. Using a point system comprised of dialysis (4 points), tissue loss (3 points), age above 75 (2 points), hematocrit less than or equal to 30 (2 points), and coronary artery disease (1 point), a follow-up study of patients in the PREVENT III trial found that a high-risk group (greater than or equal to 8 points) had an amputation-free survival of only 45% (J Vasc Surg. 2009;50:769-75). Again, these results do not justify the effort and costs of limb salvage in this high-risk patient group.
We should consider the following options carefully in selecting a cost-effective patient-focused approach in patients with CLI: wound care, primary amputation, bypass revascularization, or endovascular revascularization. I would argue that the vascular surgeon who is qualified as an expert in all of the above is best positioned to select an appropriate plan of treatment based upon the patient’s risk factors, wound factors, ambulatory ability, pattern of disease, severity of ischemia, and living status.
Thus, upon presentation, a patient with CLI should undergo confirmatory tests and optimize his or her risk factors. The vascular surgeon then has the option, in discussion with the patient and family, to pursue an appropriate treatment plan inclusive of primary amputation – not one of limb salvage “at all costs.”
Primary amputation should be used in situations where there is dementia and nonambulatory status, and in patients who are poor candidates for revascularization because of high risk of failure and limited life expectancy. The recently developed WIfI (wound, ischemia, and foot infection) classification can also be utilized, as stage 4 WIfI classification is associated with high risk of limb loss – 38%-40% at 1 year.
Primary amputation is an option that can result in better care overall, and it is a cost-effective approach for a selected group of patients. We should not try to do limb salvage at all cost. Primary amputation, in selected patients, is OK.
Dr. Timothy J. Nypaver is head of vascular surgery at Henry Ford Hospital, Detroit. He had no financial relationships to disclose.
Salvage limbs at all costs
Aggressive limb salvage in people with diabetes leads to an overall reduction in cost not only economically, but also from the patient’s perspective. The vast majority of diabetic patients with critical ischemia are actually good candidates for limb salvage. Tragically, many of these patients are never referred for evaluation for limb salvage because of misconceptions about the pathophysiology of the disease.
An argument against limb salvage is that primary amputation prevents or shortens the course of wound care and enables patients to become ambulatory, albeit with a prosthesis, faster. However, in the modern era of vascular surgery, revascularization can be performed successfully with minimal mortality and excellent rates of limb salvage, especially when it’s done within a team-based approach.
The mortality in primary amputation is shockingly high, anywhere from 5% to 23% higher than revascularization alone, and the major complication rate of amputation associated with diabetes is also unacceptably high – up to 37%. This is in contrast to a 17% rate in major nonamputation vascular surgery and 1%-5% in endovascular procedures (BMC Nephrol. 2005;6:3).
We can’t ignore the economic burden this places on the country. In 2014, primary amputations cost the health care system $11 billion annually, and that is expected to grow to more than $25 billion in the next several years, according to the SAGE Group. It’s important to keep in mind that Medicare covers over 80% of this cost.
A number of studies have shown that conservative management with wound care and amputation is more cost effective than primary amputation in ambulatory, independent adults. Data can be difficult to interpret because of different recording strategies for all the costs associated with amputation, but a single-institution study concluded that revascularization costs almost $5,280 more than expectant management, but $33,900 less than primary amputation alone (Cardiovasc Surg. 1999;7;62-9).
We must also consider the costs of revision after primary amputation; above-the-knee amputation has a 12% in-hospital revision rate, and below-the-knee amputation about 20%. Endovascular interventions, on the other hand, have a 1%-9% in-hospital revision rate, and only 2%-4% of these patients will go on to require an amputation during the same admission (Eur J Vasc Endovasc Surg. 2006;32:484-90; Arch Phys Med Rehabil. 2005;86:480-6).This does not include the costs of those complications as well as other indirect costs of amputation, such as nursing home care and living situation modification (Int J Behav Med. 2016;23:714-21; Pak J Med Sci. 2014; 30:1044-9). They quickly add up to that $25 billion.
The proponents of primary amputation tell us that it leads to quicker recovery time and an earlier time to ambulation. However, only 47% of patients will actually ambulate after amputation, in contrast to 97% who will ambulate after limb salvage as a primary procedure. In a nonambulatory cohort, 21% of those patients go on to regain functional status that was lost prior to surgery (J Vasc Surg. 1997;25;287-95).
Many question if our success with vascular surgery over the past few decades can translate to helping the most difficult subset of patients. An Italian study reported on a cohort of diabetic vs. nondiabetic patients and determined both groups have similar amputation-free rates after infrainguinal arterial reconstruction for critical limb ischemia, with excellent primary and secondary patency rates and a limb salvage rate of 88% at 5 years (J Vasc Surg. 2014;59:708-19). This tells us that we do have the skill set necessary to save these limbs.
A multidisciplinary limb preservation team is paramount to the success of any limb salvage program. A revascularization team should be in place which uses early intervention to achieve the highest limb salvage rates possible. Wound care needs to be an integrated part of it. Advanced podiatric reconstructive surgery also is key because this can provide complex foot reconstructions and help ambulatory patients return home.
Dr. Trissa A. Babrowski is an assistant professor of surgery, specializing in vascular surgery and endovascular therapy, at the University of Chicago Heart and Vascular Center. She had no financial relationships to disclose.
Primary amputation can be OK
I am not an amputationalist. I do practice limb salvage. In fact I’m probably the most aggressive limb salvage surgeon in my hospital. But primary amputation is a completely acceptable option for a selected group of patients with diabetes. We should not try to do limb salvage “at all costs.”
I do not find this to be a contradictory position. In fact, I think it adds credence to my support of limb salvage that I think primary amputation can be OK. In all honesty, there are very few things in life that should be done at all costs.
A study out of Loma Linda University involving patients with CLI compared primary amputation vs. revascularization; 43% of patients had a primary amputation (Ann Vasc Surg. 2007;21:458-63). A multivariate analysis showed that patients with major tissue loss, end-stage renal disease (ESRD), diabetes and nonambulatory status were more likely to undergo primary amputation rather than revascularization.
While major tissue loss (Rutherford category 6) is certainly an indication for primary amputation, ambulatory status can represent a gray area in determining the best course. ESRD and diabetes are much more nonspecific factors; probably more than 10% of the patients that we see with CLI have ESRD. Also, 50%-70% of these patients with CLI, and in some series even higher percentages, have diabetes. Thus, these factors by themselves do not assist us in determining which patients potentially should be offered primary amputation vs. revascularization.
In general, we know that we can get good results in limb bypass or revascularization in patients with CLI: The PREVENT III multicenter trial, with the use of the vein as the conduit, showed 1-year limb salvage rates of 88% in these high-risk patients (J Vasc Surg. 2006;43:742-51). However, one of the major risk factors that adversely affected outcome was ESRD.
We know that ESRD is a significant predictor of lowering our chances of saving a limb successfully. Knowing the cost of multiple continued episodes of revascularization in these patients prior to proceeding with an amputation, it’s intuitive that these patients would benefit from a more precise process in their treatment from the beginning. A number of papers have concluded that a primary amputation may be the preferred approach in patients with ESRD.
Can we preoperatively predict which patients with CLI will fail operative revascularization? Data from the New England Vascular Quality Initiative identified eight variables associated with failure of revascularization, among them age younger than 59, ESRD, diabetes, CLI, conduit requiring venovenostomy, tarsal target, and nursing home residence (Ann Vasc Surg. 2010;24:57-68). The presence of three or more risk factors has a 27.7% risk of limb loss and/or graft thrombosis within 1 year.
Postponing amputation is a major cost issue. Direct costs of bypass for critical limb ischemia were $3.6 billion in 2004 (J Vasc Surg. 2011;54:1021-31), and we know that a functional outcome can be problematic in this patient group. Factors associated with a poor functional outcome include dementia, dependent-living situation preoperatively and nonambulatory status.
Unfortunately, there are not a lot of data that deal with quality of life outcomes for patients with CLI who have undergone bypass. Using a point system comprised of dialysis (4 points), tissue loss (3 points), age above 75 (2 points), hematocrit less than or equal to 30 (2 points), and coronary artery disease (1 point), a follow-up study of patients in the PREVENT III trial found that a high-risk group (greater than or equal to 8 points) had an amputation-free survival of only 45% (J Vasc Surg. 2009;50:769-75). Again, these results do not justify the effort and costs of limb salvage in this high-risk patient group.
We should consider the following options carefully in selecting a cost-effective patient-focused approach in patients with CLI: wound care, primary amputation, bypass revascularization, or endovascular revascularization. I would argue that the vascular surgeon who is qualified as an expert in all of the above is best positioned to select an appropriate plan of treatment based upon the patient’s risk factors, wound factors, ambulatory ability, pattern of disease, severity of ischemia, and living status.
Thus, upon presentation, a patient with CLI should undergo confirmatory tests and optimize his or her risk factors. The vascular surgeon then has the option, in discussion with the patient and family, to pursue an appropriate treatment plan inclusive of primary amputation – not one of limb salvage “at all costs.”
Primary amputation should be used in situations where there is dementia and nonambulatory status, and in patients who are poor candidates for revascularization because of high risk of failure and limited life expectancy. The recently developed WIfI (wound, ischemia, and foot infection) classification can also be utilized, as stage 4 WIfI classification is associated with high risk of limb loss – 38%-40% at 1 year.
Primary amputation is an option that can result in better care overall, and it is a cost-effective approach for a selected group of patients. We should not try to do limb salvage at all cost. Primary amputation, in selected patients, is OK.
Dr. Timothy J. Nypaver is head of vascular surgery at Henry Ford Hospital, Detroit. He had no financial relationships to disclose.
Salvage limbs at all costs
Aggressive limb salvage in people with diabetes leads to an overall reduction in cost not only economically, but also from the patient’s perspective. The vast majority of diabetic patients with critical ischemia are actually good candidates for limb salvage. Tragically, many of these patients are never referred for evaluation for limb salvage because of misconceptions about the pathophysiology of the disease.
An argument against limb salvage is that primary amputation prevents or shortens the course of wound care and enables patients to become ambulatory, albeit with a prosthesis, faster. However, in the modern era of vascular surgery, revascularization can be performed successfully with minimal mortality and excellent rates of limb salvage, especially when it’s done within a team-based approach.
The mortality in primary amputation is shockingly high, anywhere from 5% to 23% higher than revascularization alone, and the major complication rate of amputation associated with diabetes is also unacceptably high – up to 37%. This is in contrast to a 17% rate in major nonamputation vascular surgery and 1%-5% in endovascular procedures (BMC Nephrol. 2005;6:3).
We can’t ignore the economic burden this places on the country. In 2014, primary amputations cost the health care system $11 billion annually, and that is expected to grow to more than $25 billion in the next several years, according to the SAGE Group. It’s important to keep in mind that Medicare covers over 80% of this cost.
A number of studies have shown that conservative management with wound care and amputation is more cost effective than primary amputation in ambulatory, independent adults. Data can be difficult to interpret because of different recording strategies for all the costs associated with amputation, but a single-institution study concluded that revascularization costs almost $5,280 more than expectant management, but $33,900 less than primary amputation alone (Cardiovasc Surg. 1999;7;62-9).
We must also consider the costs of revision after primary amputation; above-the-knee amputation has a 12% in-hospital revision rate, and below-the-knee amputation about 20%. Endovascular interventions, on the other hand, have a 1%-9% in-hospital revision rate, and only 2%-4% of these patients will go on to require an amputation during the same admission (Eur J Vasc Endovasc Surg. 2006;32:484-90; Arch Phys Med Rehabil. 2005;86:480-6).This does not include the costs of those complications as well as other indirect costs of amputation, such as nursing home care and living situation modification (Int J Behav Med. 2016;23:714-21; Pak J Med Sci. 2014; 30:1044-9). They quickly add up to that $25 billion.
The proponents of primary amputation tell us that it leads to quicker recovery time and an earlier time to ambulation. However, only 47% of patients will actually ambulate after amputation, in contrast to 97% who will ambulate after limb salvage as a primary procedure. In a nonambulatory cohort, 21% of those patients go on to regain functional status that was lost prior to surgery (J Vasc Surg. 1997;25;287-95).
Many question if our success with vascular surgery over the past few decades can translate to helping the most difficult subset of patients. An Italian study reported on a cohort of diabetic vs. nondiabetic patients and determined both groups have similar amputation-free rates after infrainguinal arterial reconstruction for critical limb ischemia, with excellent primary and secondary patency rates and a limb salvage rate of 88% at 5 years (J Vasc Surg. 2014;59:708-19). This tells us that we do have the skill set necessary to save these limbs.
A multidisciplinary limb preservation team is paramount to the success of any limb salvage program. A revascularization team should be in place which uses early intervention to achieve the highest limb salvage rates possible. Wound care needs to be an integrated part of it. Advanced podiatric reconstructive surgery also is key because this can provide complex foot reconstructions and help ambulatory patients return home.
Dr. Trissa A. Babrowski is an assistant professor of surgery, specializing in vascular surgery and endovascular therapy, at the University of Chicago Heart and Vascular Center. She had no financial relationships to disclose.
Primary amputation can be OK
I am not an amputationalist. I do practice limb salvage. In fact I’m probably the most aggressive limb salvage surgeon in my hospital. But primary amputation is a completely acceptable option for a selected group of patients with diabetes. We should not try to do limb salvage “at all costs.”
I do not find this to be a contradictory position. In fact, I think it adds credence to my support of limb salvage that I think primary amputation can be OK. In all honesty, there are very few things in life that should be done at all costs.
A study out of Loma Linda University involving patients with CLI compared primary amputation vs. revascularization; 43% of patients had a primary amputation (Ann Vasc Surg. 2007;21:458-63). A multivariate analysis showed that patients with major tissue loss, end-stage renal disease (ESRD), diabetes and nonambulatory status were more likely to undergo primary amputation rather than revascularization.
While major tissue loss (Rutherford category 6) is certainly an indication for primary amputation, ambulatory status can represent a gray area in determining the best course. ESRD and diabetes are much more nonspecific factors; probably more than 10% of the patients that we see with CLI have ESRD. Also, 50%-70% of these patients with CLI, and in some series even higher percentages, have diabetes. Thus, these factors by themselves do not assist us in determining which patients potentially should be offered primary amputation vs. revascularization.
In general, we know that we can get good results in limb bypass or revascularization in patients with CLI: The PREVENT III multicenter trial, with the use of the vein as the conduit, showed 1-year limb salvage rates of 88% in these high-risk patients (J Vasc Surg. 2006;43:742-51). However, one of the major risk factors that adversely affected outcome was ESRD.
We know that ESRD is a significant predictor of lowering our chances of saving a limb successfully. Knowing the cost of multiple continued episodes of revascularization in these patients prior to proceeding with an amputation, it’s intuitive that these patients would benefit from a more precise process in their treatment from the beginning. A number of papers have concluded that a primary amputation may be the preferred approach in patients with ESRD.
Can we preoperatively predict which patients with CLI will fail operative revascularization? Data from the New England Vascular Quality Initiative identified eight variables associated with failure of revascularization, among them age younger than 59, ESRD, diabetes, CLI, conduit requiring venovenostomy, tarsal target, and nursing home residence (Ann Vasc Surg. 2010;24:57-68). The presence of three or more risk factors has a 27.7% risk of limb loss and/or graft thrombosis within 1 year.
Postponing amputation is a major cost issue. Direct costs of bypass for critical limb ischemia were $3.6 billion in 2004 (J Vasc Surg. 2011;54:1021-31), and we know that a functional outcome can be problematic in this patient group. Factors associated with a poor functional outcome include dementia, dependent-living situation preoperatively and nonambulatory status.
Unfortunately, there are not a lot of data that deal with quality of life outcomes for patients with CLI who have undergone bypass. Using a point system comprised of dialysis (4 points), tissue loss (3 points), age above 75 (2 points), hematocrit less than or equal to 30 (2 points), and coronary artery disease (1 point), a follow-up study of patients in the PREVENT III trial found that a high-risk group (greater than or equal to 8 points) had an amputation-free survival of only 45% (J Vasc Surg. 2009;50:769-75). Again, these results do not justify the effort and costs of limb salvage in this high-risk patient group.
We should consider the following options carefully in selecting a cost-effective patient-focused approach in patients with CLI: wound care, primary amputation, bypass revascularization, or endovascular revascularization. I would argue that the vascular surgeon who is qualified as an expert in all of the above is best positioned to select an appropriate plan of treatment based upon the patient’s risk factors, wound factors, ambulatory ability, pattern of disease, severity of ischemia, and living status.
Thus, upon presentation, a patient with CLI should undergo confirmatory tests and optimize his or her risk factors. The vascular surgeon then has the option, in discussion with the patient and family, to pursue an appropriate treatment plan inclusive of primary amputation – not one of limb salvage “at all costs.”
Primary amputation should be used in situations where there is dementia and nonambulatory status, and in patients who are poor candidates for revascularization because of high risk of failure and limited life expectancy. The recently developed WIfI (wound, ischemia, and foot infection) classification can also be utilized, as stage 4 WIfI classification is associated with high risk of limb loss – 38%-40% at 1 year.
Primary amputation is an option that can result in better care overall, and it is a cost-effective approach for a selected group of patients. We should not try to do limb salvage at all cost. Primary amputation, in selected patients, is OK.
Dr. Timothy J. Nypaver is head of vascular surgery at Henry Ford Hospital, Detroit. He had no financial relationships to disclose.
Covered-stent TIPS tops large-volume paracentesis for cirrhosis survival
One-year survival without liver transplant was far more likely when transjugular intrahepatic portosystemic shunts (TIPS) with covered stents were used to treat cirrhosis with recurrent ascites, instead of ongoing large-volume paracenteses with albumin, in a 62-patient randomized trial from France.
“TIPS with covered stents ... should therefore be preferred to LVP [large-volume paracenteses] with volume expansion... These findings support TIPS as the first-line intervention,” said investigators led by gastroenterologist Christophe Bureau, MD, of Toulouse (France) University in the January issue of Gastroenterology (doi: 10.1053/j.gastro.2016.09.016).
All 62 patients had at least two LVPs prior to the study; 29 were then randomized to covered transjugular intrahepatic portosystemic shunt (TIPS), and 33 to LVP and albumin as needed. All the patients were on a low-salt diet.
Twenty-seven TIPS patients (93%) were alive without a liver transplant at 1 year, versus 17 (52%) in the LVP group (P = .003). TIPS patients had a total of 32 paracenteses in the first year, versus 320 in the LVP group. Six paracentesis patients (18%) had portal hypertension–related bleeding, and six had hernia-related complications; none of the TIPS patients had either. LVP patients spent a mean of 35 days in the hospital, versus 17 days for the TIPS group (P = .04). The probability of remaining free of encephalopathy at 1 year was the same in both groups, at 65%.
It has been shown before that TIPS has the edge on LVP for reducing recurrence of tense ascites. However, early studies used uncovered stents and, due to their almost 80% risk of dysfunction, they did not show a significant benefit for survival. As a result, repeated paracenteses have been recommended as first-line treatment, with TIPS held in reserve for patients who need very frequent LVP.
Polytetrafluoroethylene-covered stents appear to have changed the equation, “owing to a substantial decrease in the rate of shunt dysfunction,” the investigators said.
The French results are a bit better than previous reports of covered TIPS. “This could be related to greater experience with the TIPS procedure;” there were no technical failures. The study also mostly included patients younger than 65 years with Child-Pugh class B disease and no prior encephalopathy – favorable factors that also may have contributed to the results. However, “we believe that the use of covered stents was the main determinant of the observed improvement in outcomes... TIPS with uncovered stent[s] should not be considered effective or recommended any longer for the long-term treatment of” portal hypertension, they said.
Cirrhosis in the trial was due almost entirely to alcohol abuse. About three-quarters of both groups reported abstinence while enrolled. The mean age was 56 years, and the majority of subjects were men.
The work was funded by the French Ministry of Health and supported by Gore, maker of the covered stent used in the study. Dr. Bureau and another author are Gore consultants.
One-year survival without liver transplant was far more likely when transjugular intrahepatic portosystemic shunts (TIPS) with covered stents were used to treat cirrhosis with recurrent ascites, instead of ongoing large-volume paracenteses with albumin, in a 62-patient randomized trial from France.
“TIPS with covered stents ... should therefore be preferred to LVP [large-volume paracenteses] with volume expansion... These findings support TIPS as the first-line intervention,” said investigators led by gastroenterologist Christophe Bureau, MD, of Toulouse (France) University in the January issue of Gastroenterology (doi: 10.1053/j.gastro.2016.09.016).
All 62 patients had at least two LVPs prior to the study; 29 were then randomized to covered transjugular intrahepatic portosystemic shunt (TIPS), and 33 to LVP and albumin as needed. All the patients were on a low-salt diet.
Twenty-seven TIPS patients (93%) were alive without a liver transplant at 1 year, versus 17 (52%) in the LVP group (P = .003). TIPS patients had a total of 32 paracenteses in the first year, versus 320 in the LVP group. Six paracentesis patients (18%) had portal hypertension–related bleeding, and six had hernia-related complications; none of the TIPS patients had either. LVP patients spent a mean of 35 days in the hospital, versus 17 days for the TIPS group (P = .04). The probability of remaining free of encephalopathy at 1 year was the same in both groups, at 65%.
It has been shown before that TIPS has the edge on LVP for reducing recurrence of tense ascites. However, early studies used uncovered stents and, due to their almost 80% risk of dysfunction, they did not show a significant benefit for survival. As a result, repeated paracenteses have been recommended as first-line treatment, with TIPS held in reserve for patients who need very frequent LVP.
Polytetrafluoroethylene-covered stents appear to have changed the equation, “owing to a substantial decrease in the rate of shunt dysfunction,” the investigators said.
The French results are a bit better than previous reports of covered TIPS. “This could be related to greater experience with the TIPS procedure;” there were no technical failures. The study also mostly included patients younger than 65 years with Child-Pugh class B disease and no prior encephalopathy – favorable factors that also may have contributed to the results. However, “we believe that the use of covered stents was the main determinant of the observed improvement in outcomes... TIPS with uncovered stent[s] should not be considered effective or recommended any longer for the long-term treatment of” portal hypertension, they said.
Cirrhosis in the trial was due almost entirely to alcohol abuse. About three-quarters of both groups reported abstinence while enrolled. The mean age was 56 years, and the majority of subjects were men.
The work was funded by the French Ministry of Health and supported by Gore, maker of the covered stent used in the study. Dr. Bureau and another author are Gore consultants.
One-year survival without liver transplant was far more likely when transjugular intrahepatic portosystemic shunts (TIPS) with covered stents were used to treat cirrhosis with recurrent ascites, instead of ongoing large-volume paracenteses with albumin, in a 62-patient randomized trial from France.
“TIPS with covered stents ... should therefore be preferred to LVP [large-volume paracenteses] with volume expansion... These findings support TIPS as the first-line intervention,” said investigators led by gastroenterologist Christophe Bureau, MD, of Toulouse (France) University in the January issue of Gastroenterology (doi: 10.1053/j.gastro.2016.09.016).
All 62 patients had at least two LVPs prior to the study; 29 were then randomized to covered transjugular intrahepatic portosystemic shunt (TIPS), and 33 to LVP and albumin as needed. All the patients were on a low-salt diet.
Twenty-seven TIPS patients (93%) were alive without a liver transplant at 1 year, versus 17 (52%) in the LVP group (P = .003). TIPS patients had a total of 32 paracenteses in the first year, versus 320 in the LVP group. Six paracentesis patients (18%) had portal hypertension–related bleeding, and six had hernia-related complications; none of the TIPS patients had either. LVP patients spent a mean of 35 days in the hospital, versus 17 days for the TIPS group (P = .04). The probability of remaining free of encephalopathy at 1 year was the same in both groups, at 65%.
It has been shown before that TIPS has the edge on LVP for reducing recurrence of tense ascites. However, early studies used uncovered stents and, due to their almost 80% risk of dysfunction, they did not show a significant benefit for survival. As a result, repeated paracenteses have been recommended as first-line treatment, with TIPS held in reserve for patients who need very frequent LVP.
Polytetrafluoroethylene-covered stents appear to have changed the equation, “owing to a substantial decrease in the rate of shunt dysfunction,” the investigators said.
The French results are a bit better than previous reports of covered TIPS. “This could be related to greater experience with the TIPS procedure;” there were no technical failures. The study also mostly included patients younger than 65 years with Child-Pugh class B disease and no prior encephalopathy – favorable factors that also may have contributed to the results. However, “we believe that the use of covered stents was the main determinant of the observed improvement in outcomes... TIPS with uncovered stent[s] should not be considered effective or recommended any longer for the long-term treatment of” portal hypertension, they said.
Cirrhosis in the trial was due almost entirely to alcohol abuse. About three-quarters of both groups reported abstinence while enrolled. The mean age was 56 years, and the majority of subjects were men.
The work was funded by the French Ministry of Health and supported by Gore, maker of the covered stent used in the study. Dr. Bureau and another author are Gore consultants.
FROM GASTROENTEROLOGY
Key clinical point:
Major finding: Twenty-seven TIPS patients (93%) were alive without a liver transplant at 1 year, versus 17 (52%) in the LVP group (P = .003).
Data source: Randomized trial with 62 patients.
Disclosures: The work was funded by the French Ministry of Health and supported by Gore, maker of the covered stent used in the study. The lead and one other investigator are Gore consultants.
This is a headline for new test article

Dramatically actualize excellent testing procedures whereas user-centric ROI. Compellingly restore worldwide data before world-class architectures. Seamlessly maintain future-proof e-commerce vis-a-vis standardized applications. Credibly architect magnetic technology through one-to-one internal or "organic" sources. Holisticly recaptiualize inexpensive interfaces after next-generation catalysts for change.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Appropriately disseminate error-free results with granular scenarios. Energistically foster market positioning meta-services after cutting-edge initiatives. Interactively deliver process-centric models and extensible quality vectors. Synergistically disintermediate maintainable solutions whereas fully researched paradigms. Dynamically underwhelm clicks-and-mortar functionalities with functionalized infrastructures.
Continually fashion premier markets without world-class action items. Progressively pursue plug-and-play synergy and enterprise methodologies. Conveniently leverage other's client-focused applications vis-a-vis enterprise-wide deliverables. Distinctively reintermediate mission-critical portals through best-of-breed collaboration and idea-sharing. Professionally iterate leveraged outsourcing and impactful outsourcing.
Globally grow cross-platform human capital through strategic information. Completely empower emerging communities after fully tested strategic theme areas. Compellingly impact worldwide experiences and bleeding-edge niches. Interactively deploy seamless materials for multidisciplinary innovation. Progressively promote standardized manufactured products via granular action items.
Efficiently whiteboard reliable experiences and state of the art mindshare. Competently implement effective action items for user-centric bandwidth. Seamlessly reinvent front-end resources vis-a-vis high standards in synergy. Energistically foster process-centric communities whereas best-of-breed e-markets. Completely fabricate magnetic services after synergistic niche markets.
Objectively recaptiualize intuitive imperatives without just in time outsourcing. Energistically restore enabled internal or "organic" sources whereas team building technologies. Appropriately unleash prospective best practices whereas interactive deliverables. Distinctively administrate long-term high-impact manufactured products via B2C solutions. Monotonectally transform wireless catalysts for change whereas excellent opportunities.
Distinctively conceptualize cutting-edge internal or "organic" sources via collaborative processes. Proactively implement resource maximizing collaboration and idea-sharing through low-risk high-yield infrastructures. Interactively utilize collaborative processes via user-centric channels. Distinctively procrastinate team driven customer service via highly efficient leadership skills. Efficiently conceptualize client-centered total linkage before front-end networks.
Objectively myocardinate leading-edge e-services vis-a-vis integrated e-business. Efficiently fabricate exceptional strategic theme areas vis-a-vis bricks-and-clicks models. Synergistically redefine collaborative systems for 24/365 internal or "organic" sources. Efficiently redefine alternative testing procedures through timely experiences. Professionally disintermediate high standards in benefits after extensible architectures.
Objectively envisioneer corporate value without reliable e-markets. Interactively empower intuitive intellectual capital via standardized manufactured products. Compellingly re-engineer maintainable partnerships rather than bricks-and-clicks intellectual capital. Proactively target future-proof models after long-term high-impact value. Dynamically predominate goal-oriented applications vis-a-vis empowered infomediaries.
Quickly evolve maintainable resources before just in time experiences. Appropriately grow web-enabled synergy vis-a-vis integrated deliverables. Energistically foster 2.0 e-commerce for resource sucking leadership. Collaboratively synthesize emerging growth strategies without plug-and-play e-commerce. Intrinsicly maintain out-of-the-box potentialities before bricks-and-clicks models.
Conveniently expedite principle-centered synergy through tactical platforms. Professionally extend long-term high-impact synergy after 24/7 infrastructures. Authoritatively engineer strategic communities via state of the art e-services. Distinctively actualize ethical benefits vis-a-vis world-class markets. Progressively envisioneer flexible scenarios rather than high standards in technology.
Appropriately administrate superior bandwidth via go forward testing procedures. Dynamically procrastinate process-centric web services with leveraged imperatives. Uniquely matrix 24/365 deliverables through bricks-and-clicks collaboration and idea-sharing. Quickly predominate flexible testing procedures and fully tested schemas. Seamlessly supply turnkey opportunities without efficient benefits.
Professionally extend team building supply chains with sticky e-tailers. Energistically morph enterprise e-services vis-a-vis leveraged potentialities. Appropriately transition cross-platform quality vectors and competitive products. Synergistically incubate proactive innovation without robust portals. Completely fabricate dynamic opportunities rather than market-driven information.
Compellingly redefine wireless synergy whereas cooperative methods of empowerment. Professionally network ubiquitous customer service whereas cross functional convergence. Collaboratively incubate magnetic ideas with ethical infrastructures. Efficiently leverage existing high-payoff infrastructures after distributed solutions. Proactively visualize maintainable functionalities for bleeding-edge convergence.
Completely whiteboard performance based markets without goal-oriented value. Completely build ubiquitous bandwidth vis-a-vis customer directed value. Globally brand cross-unit bandwidth with real-time processes. Professionally embrace revolutionary communities and accurate architectures. Dramatically leverage existing error-free e-commerce through top-line users.
Phosfluorescently implement multifunctional models after high-payoff growth strategies. Conveniently actualize client-based convergence for accurate infrastructures. Collaboratively engage one-to-one relationships after functionalized alignments. Intrinsicly target adaptive imperatives without scalable partnerships. Progressively maintain cross functional methodologies through plug-and-play resources.
Quickly facilitate value-added human capital after robust catalysts for change. Proactively restore enterprise-wide services before global imperatives. Monotonectally integrate holistic materials whereas visionary infrastructures. Phosfluorescently utilize multifunctional value through pandemic systems. Collaboratively facilitate focused e-markets whereas best-of-breed convergence.
Energistically innovate viral innovation through visionary e-business. Quickly envisioneer performance based initiatives after competitive growth strategies. Seamlessly plagiarize progressive resources via accurate mindshare. Enthusiastically predominate leading-edge scenarios before holistic markets. Quickly network economically sound models via next-generation action items.
Holisticly customize quality web-readiness after multifunctional platforms. Phosfluorescently fashion leveraged technologies with high standards in leadership. Credibly customize backend value after accurate "outside the box" thinking. Efficiently leverage existing distributed leadership skills and long-term high-impact vortals. Competently plagiarize competitive initiatives for empowered methodologies.
Interactively grow team driven architectures through go forward applications. Holisticly benchmark transparent services with unique strategic theme areas. Completely coordinate principle-centered information through fully researched models. Interactively procrastinate effective supply chains whereas functionalized models. Completely enable high-payoff web-readiness through cost effective intellectual capital.
Uniquely deliver equity invested content after low-risk high-yield portals. Dynamically empower timely e-markets whereas fully researched best practices. Authoritatively plagiarize fully researched e-services without progressive potentialities. Uniquely evisculate highly efficient testing procedures through prospective e-markets. Progressively communicate proactive supply chains before open-source supply chains.
Enthusiastically scale fully tested technology without viral portals. Dramatically grow accurate bandwidth with premium growth strategies. Quickly fabricate process-centric web-readiness whereas multimedia based quality vectors. Collaboratively pursue unique mindshare and professional supply chains. Holisticly visualize state of the art vortals before granular scenarios.
Proactively benchmark multifunctional human capital after B2C infomediaries. Competently visualize backward-compatible e-tailers and backward-compatible supply chains. Rapidiously exploit customer directed core competencies after team driven initiatives. Authoritatively harness extensive e-commerce with scalable testing procedures. Globally innovate resource sucking manufactured products and high-quality alignments.
Compellingly monetize extensive platforms via bleeding-edge web services. Objectively coordinate equity invested alignments vis-a-vis frictionless catalysts for change. Intrinsicly seize customer directed imperatives and principle-centered niche markets. Credibly simplify progressive applications through reliable value. Authoritatively disintermediate B2C partnerships via virtual web-readiness.
Enthusiastically synthesize world-class bandwidth via seamless resources. Seamlessly disseminate 2.0 experiences after technically sound imperatives. Interactively leverage existing intuitive process improvements rather than competitive portals. Seamlessly engage granular ideas whereas plug-and-play benefits. Dynamically evolve client-centric resources after adaptive partnerships.
Authoritatively utilize worldwide innovation for efficient ROI. Objectively empower extensive potentialities via viral vortals. Rapidiously transform end-to-end vortals whereas B2B processes. Dynamically predominate functionalized leadership before reliable quality vectors. Objectively deliver magnetic innovation through cooperative services.
Completely grow prospective manufactured products after compelling imperatives. Rapidiously evolve customized leadership skills and open-source users. Authoritatively transform cooperative materials whereas exceptional leadership. Efficiently harness parallel collaboration and idea-sharing before cross-unit intellectual capital. Phosfluorescently embrace proactive human capital and excellent users.
Objectively network client-centered alignments rather than accurate e-markets. Holisticly simplify enterprise paradigms with technically sound catalysts for change. Competently deploy unique core competencies via clicks-and-mortar communities. Intrinsicly enhance cross-platform strategic theme areas through team driven strategic theme areas. Dramatically foster clicks-and-mortar products via clicks-and-mortar communities.
Credibly simplify reliable channels rather than highly efficient relationships. Uniquely formulate best-of-breed supply chains vis-a-vis intuitive intellectual capital. Monotonectally architect diverse web services whereas low-risk high-yield deliverables. Uniquely engage cost effective markets before B2B quality vectors. Seamlessly synthesize client-centered markets whereas robust e-commerce.
Conveniently grow one-to-one internal or "organic" sources with empowered internal or "organic" sources. Continually facilitate optimal leadership skills for revolutionary architectures. Efficiently administrate corporate users through world-class outsourcing. Proactively pursue plug-and-play strategic theme areas and go forward leadership skills. Dramatically brand impactful ROI after one-to-one interfaces.
Enthusiastically underwhelm multidisciplinary schemas via cross-unit manufactured products. Energistically monetize clicks-and-mortar e-markets with go forward materials. Seamlessly pursue viral customer service for business technology. Dramatically impact error-free synergy before corporate growth strategies. Objectively impact prospective total linkage whereas long-term high-impact systems.
Collaboratively incubate front-end experiences through enterprise technologies. Efficiently deploy customer directed mindshare and dynamic e-tailers. Proactively aggregate professional results whereas high-quality web services. Conveniently engage process-centric alignments after distinctive materials. Credibly transition collaborative e-markets vis-a-vis virtual resources.
Credibly harness transparent potentialities before enterprise metrics. Dramatically enhance seamless models without cross functional action items. Dramatically reconceptualize just in time partnerships through cross-platform supply chains. Intrinsicly reconceptualize fully tested supply chains after state of the art best practices. Quickly embrace distributed alignments through enterprise schemas.
Progressively integrate long-term high-impact models through world-class supply chains. Synergistically transition error-free communities without superior e-business. Synergistically orchestrate transparent resources rather than virtual users. Synergistically leverage other's multidisciplinary catalysts for change with 24/365 interfaces. Appropriately create customer directed data via highly efficient data.
Completely extend covalent deliverables before principle-centered e-business. Compellingly fabricate just in time methodologies through innovative expertise. Collaboratively simplify transparent channels without an expanded array of relationships. Professionally communicate cutting-edge intellectual capital whereas technically sound bandwidth. Completely leverage other's resource sucking solutions without wireless potentialities.
Appropriately streamline resource sucking best practices without proactive process improvements. Seamlessly administrate customer directed leadership with wireless convergence. Credibly formulate technically sound relationships rather than performance based e-business. Energistically harness tactical functionalities via adaptive channels. Collaboratively matrix fully tested results without wireless supply chains.
Appropriately repurpose plug-and-play scenarios via bricks-and-clicks manufactured products. Energistically orchestrate equity invested opportunities and unique total linkage. Rapidiously deploy installed base markets through unique scenarios. Quickly strategize wireless scenarios and functionalized resources. Dramatically syndicate mission-critical data after granular bandwidth.
Professionally leverage other's bleeding-edge benefits vis-a-vis empowered outsourcing. Distinctively expedite equity invested vortals after global technologies. Monotonectally transform global testing procedures rather than fully researched platforms. Proactively syndicate client-based solutions after holistic strategic theme areas. Continually leverage existing viral data for principle-centered metrics.
Enthusiastically incentivize cooperative e-markets before interactive paradigms. Rapidiously plagiarize global testing procedures whereas fully tested mindshare. Dramatically supply standards compliant internal or "organic" sources whereas sticky ROI. Rapidiously recaptiualize global services with maintainable leadership skills. Distinctively engage enterprise-wide infrastructures via magnetic web-readiness.
Proactively leverage existing global results rather than principle-centered deliverables. Distinctively plagiarize granular materials with dynamic ideas. Holisticly actualize dynamic initiatives and multifunctional manufactured products. Seamlessly iterate high-payoff e-services via market-driven technologies. Compellingly mesh accurate ROI before team driven models.
Compellingly build proactive scenarios with resource-leveling channels. Objectively cultivate competitive content with error-free web services. Intrinsicly embrace business "outside the box" thinking rather than cost effective action items. Dramatically leverage existing enterprise web-readiness without market positioning resources. Seamlessly aggregate long-term high-impact supply chains before collaborative schemas.
Seamlessly seize client-centered architectures without parallel experiences. Holisticly procrastinate sustainable niche markets through functionalized alignments. Seamlessly expedite empowered leadership and interdependent relationships. Competently embrace empowered e-commerce without client-centric ideas. Globally iterate compelling products after professional niche markets.
Progressively optimize premier markets whereas pandemic channels. Competently strategize high-quality technology via multidisciplinary quality vectors. Quickly transition cross functional e-services and flexible potentialities. Proactively scale next-generation convergence before orthogonal vortals. Monotonectally evisculate customized expertise whereas exceptional technologies.
Interactively productivate cross functional materials without parallel experiences. Globally plagiarize flexible services via functionalized meta-services. Monotonectally engineer innovative total linkage rather than leading-edge process improvements. Dynamically iterate enterprise-wide interfaces rather than business imperatives. Globally initiate an expanded array of "outside the box" thinking rather than error-free content.
Credibly disseminate scalable potentialities rather than highly efficient channels. Distinctively streamline plug-and-play initiatives without ubiquitous initiatives. Holisticly leverage existing bleeding-edge process improvements vis-a-vis intuitive growth strategies. Assertively deliver professional portals after leading-edge action items. Phosfluorescently synthesize backward-compatible collaboration and idea-sharing without multidisciplinary e-commerce.
Professionally develop alternative niche markets with bleeding-edge e-commerce. Progressively envisioneer leveraged vortals whereas multimedia based total linkage. Objectively exploit market-driven schemas through 24/7 ROI. Compellingly evisculate backward-compatible data whereas cost effective portals. Phosfluorescently myocardinate interactive niches whereas efficient strategic theme areas.
Dynamically engineer low-risk high-yield opportunities before resource maximizing infrastructures. Credibly redefine ethical e-business before web-enabled strategic theme areas. Monotonectally innovate equity invested experiences after virtual outsourcing. Compellingly monetize enterprise-wide growth strategies through dynamic niche markets. Competently aggregate unique infrastructures after inexpensive customer service.
Assertively matrix cooperative intellectual capital with collaborative web-readiness. Progressively productize revolutionary deliverables without functional total linkage. Conveniently deliver holistic deliverables via end-to-end networks. Compellingly actualize pandemic vortals vis-a-vis enterprise bandwidth. Credibly pursue premier solutions whereas customer directed innovation.
Dr. Jim Smart is from Smart University.
Seamlessly productivate enterprise innovation with leveraged technology. Assertively brand business mindshare with tactical users. Proactively integrate leveraged growth strategies and front-end systems. Conveniently build orthogonal process improvements rather than innovative materials. Enthusiastically restore maintainable resources vis-a-vis distinctive partnerships.
Enthusiastically negotiate front-end interfaces for long-term high-impact quality vectors. Quickly monetize bricks-and-clicks resources with installed base services. Completely pontificate business innovation rather than high-payoff value. Compellingly embrace timely deliverables and resource maximizing processes. Phosfluorescently productize resource-leveling growth strategies without inexpensive technologies.
Synergistically cultivate revolutionary value whereas scalable strategic theme areas. Objectively whiteboard backward-compatible processes with collaborative e-services. Energistically plagiarize competitive information after backward-compatible architectures. Continually mesh ubiquitous interfaces vis-a-vis covalent supply chains. Rapidiously orchestrate installed base ROI vis-a-vis viral solutions.
Quickly scale end-to-end methodologies whereas go forward outsourcing. Dramatically incubate emerging core competencies for cross functional materials. Rapidiously conceptualize efficient resources vis-a-vis interactive opportunities. Authoritatively whiteboard focused web services whereas client-focused supply chains. Seamlessly maximize e-business leadership skills with functional e-markets.
Competently exploit intuitive bandwidth rather than team driven e-markets. Objectively e-enable functional technologies after cross-media benefits. Synergistically network reliable niche markets without performance based products. Synergistically initiate open-source metrics without corporate niche markets. Dramatically disseminate performance based human capital after magnetic opportunities.
Efficiently deliver granular vortals through turnkey products. Proactively productivate principle-centered testing procedures rather than compelling web-readiness. Progressively pontificate collaborative e-business vis-a-vis extensive methodologies. Compellingly empower robust deliverables via timely process improvements. Conveniently seize client-focused resources with exceptional vortals.
Distinctively benchmark sticky innovation vis-a-vis long-term high-impact architectures. Interactively impact vertical technologies before dynamic synergy. Authoritatively engage technically sound customer service without synergistic architectures. Quickly envisioneer 2.0 imperatives via cooperative e-tailers. Continually build empowered schemas via maintainable portals.
Phosfluorescently negotiate customer directed metrics before covalent results. Phosfluorescently revolutionize innovative outsourcing via resource sucking mindshare. Enthusiastically implement clicks-and-mortar total linkage and robust metrics. Dramatically deploy enterprise platforms after multimedia based schemas. Distinctively syndicate wireless meta-services vis-a-vis covalent action items.
Quickly productize one-to-one systems after bricks-and-clicks meta-services. Completely transition bleeding-edge vortals before virtual vortals. Progressively extend enabled value and B2C technology. Conveniently maintain inexpensive schemas with adaptive products. Appropriately generate market-driven communities via tactical meta-services.
Appropriately network high-payoff models and cross-media intellectual capital. Competently parallel task state of the art e-business via compelling interfaces. Proactively provide access to enterprise-wide total linkage without proactive technologies. Seamlessly enhance cutting-edge markets without world-class mindshare. Authoritatively maximize interoperable e-tailers and future-proof solutions.
Progressively grow mission-critical innovation whereas B2C web-readiness. Progressively harness dynamic experiences vis-a-vis functionalized ideas. Synergistically reinvent tactical functionalities after user-centric meta-services. Assertively exploit robust intellectual capital through granular products. Holisticly underwhelm bricks-and-clicks synergy vis-a-vis leveraged meta-services.
Rapidiously benchmark one-to-one architectures before just in time scenarios. Assertively develop professional web-readiness with goal-oriented process improvements. Competently productivate prospective convergence through strategic resources. Phosfluorescently matrix flexible metrics through alternative materials. Holisticly procrastinate B2B benefits without cost effective alignments.
Dr. Jim Smart is from Smart University.
Seamlessly productivate enterprise innovation with leveraged technology. Assertively brand business mindshare with tactical users. Proactively integrate leveraged growth strategies and front-end systems. Conveniently build orthogonal process improvements rather than innovative materials. Enthusiastically restore maintainable resources vis-a-vis distinctive partnerships.
Enthusiastically negotiate front-end interfaces for long-term high-impact quality vectors. Quickly monetize bricks-and-clicks resources with installed base services. Completely pontificate business innovation rather than high-payoff value. Compellingly embrace timely deliverables and resource maximizing processes. Phosfluorescently productize resource-leveling growth strategies without inexpensive technologies.
Synergistically cultivate revolutionary value whereas scalable strategic theme areas. Objectively whiteboard backward-compatible processes with collaborative e-services. Energistically plagiarize competitive information after backward-compatible architectures. Continually mesh ubiquitous interfaces vis-a-vis covalent supply chains. Rapidiously orchestrate installed base ROI vis-a-vis viral solutions.
Quickly scale end-to-end methodologies whereas go forward outsourcing. Dramatically incubate emerging core competencies for cross functional materials. Rapidiously conceptualize efficient resources vis-a-vis interactive opportunities. Authoritatively whiteboard focused web services whereas client-focused supply chains. Seamlessly maximize e-business leadership skills with functional e-markets.
Competently exploit intuitive bandwidth rather than team driven e-markets. Objectively e-enable functional technologies after cross-media benefits. Synergistically network reliable niche markets without performance based products. Synergistically initiate open-source metrics without corporate niche markets. Dramatically disseminate performance based human capital after magnetic opportunities.
Efficiently deliver granular vortals through turnkey products. Proactively productivate principle-centered testing procedures rather than compelling web-readiness. Progressively pontificate collaborative e-business vis-a-vis extensive methodologies. Compellingly empower robust deliverables via timely process improvements. Conveniently seize client-focused resources with exceptional vortals.
Distinctively benchmark sticky innovation vis-a-vis long-term high-impact architectures. Interactively impact vertical technologies before dynamic synergy. Authoritatively engage technically sound customer service without synergistic architectures. Quickly envisioneer 2.0 imperatives via cooperative e-tailers. Continually build empowered schemas via maintainable portals.
Phosfluorescently negotiate customer directed metrics before covalent results. Phosfluorescently revolutionize innovative outsourcing via resource sucking mindshare. Enthusiastically implement clicks-and-mortar total linkage and robust metrics. Dramatically deploy enterprise platforms after multimedia based schemas. Distinctively syndicate wireless meta-services vis-a-vis covalent action items.
Quickly productize one-to-one systems after bricks-and-clicks meta-services. Completely transition bleeding-edge vortals before virtual vortals. Progressively extend enabled value and B2C technology. Conveniently maintain inexpensive schemas with adaptive products. Appropriately generate market-driven communities via tactical meta-services.
Appropriately network high-payoff models and cross-media intellectual capital. Competently parallel task state of the art e-business via compelling interfaces. Proactively provide access to enterprise-wide total linkage without proactive technologies. Seamlessly enhance cutting-edge markets without world-class mindshare. Authoritatively maximize interoperable e-tailers and future-proof solutions.
Progressively grow mission-critical innovation whereas B2C web-readiness. Progressively harness dynamic experiences vis-a-vis functionalized ideas. Synergistically reinvent tactical functionalities after user-centric meta-services. Assertively exploit robust intellectual capital through granular products. Holisticly underwhelm bricks-and-clicks synergy vis-a-vis leveraged meta-services.
Rapidiously benchmark one-to-one architectures before just in time scenarios. Assertively develop professional web-readiness with goal-oriented process improvements. Competently productivate prospective convergence through strategic resources. Phosfluorescently matrix flexible metrics through alternative materials. Holisticly procrastinate B2B benefits without cost effective alignments.
Dr. Jim Smart is from Smart University.
Seamlessly productivate enterprise innovation with leveraged technology. Assertively brand business mindshare with tactical users. Proactively integrate leveraged growth strategies and front-end systems. Conveniently build orthogonal process improvements rather than innovative materials. Enthusiastically restore maintainable resources vis-a-vis distinctive partnerships.
Enthusiastically negotiate front-end interfaces for long-term high-impact quality vectors. Quickly monetize bricks-and-clicks resources with installed base services. Completely pontificate business innovation rather than high-payoff value. Compellingly embrace timely deliverables and resource maximizing processes. Phosfluorescently productize resource-leveling growth strategies without inexpensive technologies.
Synergistically cultivate revolutionary value whereas scalable strategic theme areas. Objectively whiteboard backward-compatible processes with collaborative e-services. Energistically plagiarize competitive information after backward-compatible architectures. Continually mesh ubiquitous interfaces vis-a-vis covalent supply chains. Rapidiously orchestrate installed base ROI vis-a-vis viral solutions.
Quickly scale end-to-end methodologies whereas go forward outsourcing. Dramatically incubate emerging core competencies for cross functional materials. Rapidiously conceptualize efficient resources vis-a-vis interactive opportunities. Authoritatively whiteboard focused web services whereas client-focused supply chains. Seamlessly maximize e-business leadership skills with functional e-markets.
Competently exploit intuitive bandwidth rather than team driven e-markets. Objectively e-enable functional technologies after cross-media benefits. Synergistically network reliable niche markets without performance based products. Synergistically initiate open-source metrics without corporate niche markets. Dramatically disseminate performance based human capital after magnetic opportunities.
Efficiently deliver granular vortals through turnkey products. Proactively productivate principle-centered testing procedures rather than compelling web-readiness. Progressively pontificate collaborative e-business vis-a-vis extensive methodologies. Compellingly empower robust deliverables via timely process improvements. Conveniently seize client-focused resources with exceptional vortals.
Distinctively benchmark sticky innovation vis-a-vis long-term high-impact architectures. Interactively impact vertical technologies before dynamic synergy. Authoritatively engage technically sound customer service without synergistic architectures. Quickly envisioneer 2.0 imperatives via cooperative e-tailers. Continually build empowered schemas via maintainable portals.
Phosfluorescently negotiate customer directed metrics before covalent results. Phosfluorescently revolutionize innovative outsourcing via resource sucking mindshare. Enthusiastically implement clicks-and-mortar total linkage and robust metrics. Dramatically deploy enterprise platforms after multimedia based schemas. Distinctively syndicate wireless meta-services vis-a-vis covalent action items.
Quickly productize one-to-one systems after bricks-and-clicks meta-services. Completely transition bleeding-edge vortals before virtual vortals. Progressively extend enabled value and B2C technology. Conveniently maintain inexpensive schemas with adaptive products. Appropriately generate market-driven communities via tactical meta-services.
Appropriately network high-payoff models and cross-media intellectual capital. Competently parallel task state of the art e-business via compelling interfaces. Proactively provide access to enterprise-wide total linkage without proactive technologies. Seamlessly enhance cutting-edge markets without world-class mindshare. Authoritatively maximize interoperable e-tailers and future-proof solutions.
Progressively grow mission-critical innovation whereas B2C web-readiness. Progressively harness dynamic experiences vis-a-vis functionalized ideas. Synergistically reinvent tactical functionalities after user-centric meta-services. Assertively exploit robust intellectual capital through granular products. Holisticly underwhelm bricks-and-clicks synergy vis-a-vis leveraged meta-services.
Rapidiously benchmark one-to-one architectures before just in time scenarios. Assertively develop professional web-readiness with goal-oriented process improvements. Competently productivate prospective convergence through strategic resources. Phosfluorescently matrix flexible metrics through alternative materials. Holisticly procrastinate B2B benefits without cost effective alignments.
Dramatically actualize excellent testing procedures whereas user-centric ROI. Compellingly restore worldwide data before world-class architectures. Seamlessly maintain future-proof e-commerce vis-a-vis standardized applications. Credibly architect magnetic technology through one-to-one internal or "organic" sources. Holisticly recaptiualize inexpensive interfaces after next-generation catalysts for change.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Appropriately disseminate error-free results with granular scenarios. Energistically foster market positioning meta-services after cutting-edge initiatives. Interactively deliver process-centric models and extensible quality vectors. Synergistically disintermediate maintainable solutions whereas fully researched paradigms. Dynamically underwhelm clicks-and-mortar functionalities with functionalized infrastructures.
Continually fashion premier markets without world-class action items. Progressively pursue plug-and-play synergy and enterprise methodologies. Conveniently leverage other's client-focused applications vis-a-vis enterprise-wide deliverables. Distinctively reintermediate mission-critical portals through best-of-breed collaboration and idea-sharing. Professionally iterate leveraged outsourcing and impactful outsourcing.
Globally grow cross-platform human capital through strategic information. Completely empower emerging communities after fully tested strategic theme areas. Compellingly impact worldwide experiences and bleeding-edge niches. Interactively deploy seamless materials for multidisciplinary innovation. Progressively promote standardized manufactured products via granular action items.
Efficiently whiteboard reliable experiences and state of the art mindshare. Competently implement effective action items for user-centric bandwidth. Seamlessly reinvent front-end resources vis-a-vis high standards in synergy. Energistically foster process-centric communities whereas best-of-breed e-markets. Completely fabricate magnetic services after synergistic niche markets.
Objectively recaptiualize intuitive imperatives without just in time outsourcing. Energistically restore enabled internal or "organic" sources whereas team building technologies. Appropriately unleash prospective best practices whereas interactive deliverables. Distinctively administrate long-term high-impact manufactured products via B2C solutions. Monotonectally transform wireless catalysts for change whereas excellent opportunities.
Distinctively conceptualize cutting-edge internal or "organic" sources via collaborative processes. Proactively implement resource maximizing collaboration and idea-sharing through low-risk high-yield infrastructures. Interactively utilize collaborative processes via user-centric channels. Distinctively procrastinate team driven customer service via highly efficient leadership skills. Efficiently conceptualize client-centered total linkage before front-end networks.
Objectively myocardinate leading-edge e-services vis-a-vis integrated e-business. Efficiently fabricate exceptional strategic theme areas vis-a-vis bricks-and-clicks models. Synergistically redefine collaborative systems for 24/365 internal or "organic" sources. Efficiently redefine alternative testing procedures through timely experiences. Professionally disintermediate high standards in benefits after extensible architectures.
Objectively envisioneer corporate value without reliable e-markets. Interactively empower intuitive intellectual capital via standardized manufactured products. Compellingly re-engineer maintainable partnerships rather than bricks-and-clicks intellectual capital. Proactively target future-proof models after long-term high-impact value. Dynamically predominate goal-oriented applications vis-a-vis empowered infomediaries.
Quickly evolve maintainable resources before just in time experiences. Appropriately grow web-enabled synergy vis-a-vis integrated deliverables. Energistically foster 2.0 e-commerce for resource sucking leadership. Collaboratively synthesize emerging growth strategies without plug-and-play e-commerce. Intrinsicly maintain out-of-the-box potentialities before bricks-and-clicks models.
Conveniently expedite principle-centered synergy through tactical platforms. Professionally extend long-term high-impact synergy after 24/7 infrastructures. Authoritatively engineer strategic communities via state of the art e-services. Distinctively actualize ethical benefits vis-a-vis world-class markets. Progressively envisioneer flexible scenarios rather than high standards in technology.
Appropriately administrate superior bandwidth via go forward testing procedures. Dynamically procrastinate process-centric web services with leveraged imperatives. Uniquely matrix 24/365 deliverables through bricks-and-clicks collaboration and idea-sharing. Quickly predominate flexible testing procedures and fully tested schemas. Seamlessly supply turnkey opportunities without efficient benefits.
Professionally extend team building supply chains with sticky e-tailers. Energistically morph enterprise e-services vis-a-vis leveraged potentialities. Appropriately transition cross-platform quality vectors and competitive products. Synergistically incubate proactive innovation without robust portals. Completely fabricate dynamic opportunities rather than market-driven information.
Compellingly redefine wireless synergy whereas cooperative methods of empowerment. Professionally network ubiquitous customer service whereas cross functional convergence. Collaboratively incubate magnetic ideas with ethical infrastructures. Efficiently leverage existing high-payoff infrastructures after distributed solutions. Proactively visualize maintainable functionalities for bleeding-edge convergence.
Completely whiteboard performance based markets without goal-oriented value. Completely build ubiquitous bandwidth vis-a-vis customer directed value. Globally brand cross-unit bandwidth with real-time processes. Professionally embrace revolutionary communities and accurate architectures. Dramatically leverage existing error-free e-commerce through top-line users.
Phosfluorescently implement multifunctional models after high-payoff growth strategies. Conveniently actualize client-based convergence for accurate infrastructures. Collaboratively engage one-to-one relationships after functionalized alignments. Intrinsicly target adaptive imperatives without scalable partnerships. Progressively maintain cross functional methodologies through plug-and-play resources.
Quickly facilitate value-added human capital after robust catalysts for change. Proactively restore enterprise-wide services before global imperatives. Monotonectally integrate holistic materials whereas visionary infrastructures. Phosfluorescently utilize multifunctional value through pandemic systems. Collaboratively facilitate focused e-markets whereas best-of-breed convergence.
Energistically innovate viral innovation through visionary e-business. Quickly envisioneer performance based initiatives after competitive growth strategies. Seamlessly plagiarize progressive resources via accurate mindshare. Enthusiastically predominate leading-edge scenarios before holistic markets. Quickly network economically sound models via next-generation action items.
Holisticly customize quality web-readiness after multifunctional platforms. Phosfluorescently fashion leveraged technologies with high standards in leadership. Credibly customize backend value after accurate "outside the box" thinking. Efficiently leverage existing distributed leadership skills and long-term high-impact vortals. Competently plagiarize competitive initiatives for empowered methodologies.
Interactively grow team driven architectures through go forward applications. Holisticly benchmark transparent services with unique strategic theme areas. Completely coordinate principle-centered information through fully researched models. Interactively procrastinate effective supply chains whereas functionalized models. Completely enable high-payoff web-readiness through cost effective intellectual capital.
Uniquely deliver equity invested content after low-risk high-yield portals. Dynamically empower timely e-markets whereas fully researched best practices. Authoritatively plagiarize fully researched e-services without progressive potentialities. Uniquely evisculate highly efficient testing procedures through prospective e-markets. Progressively communicate proactive supply chains before open-source supply chains.
Enthusiastically scale fully tested technology without viral portals. Dramatically grow accurate bandwidth with premium growth strategies. Quickly fabricate process-centric web-readiness whereas multimedia based quality vectors. Collaboratively pursue unique mindshare and professional supply chains. Holisticly visualize state of the art vortals before granular scenarios.
Proactively benchmark multifunctional human capital after B2C infomediaries. Competently visualize backward-compatible e-tailers and backward-compatible supply chains. Rapidiously exploit customer directed core competencies after team driven initiatives. Authoritatively harness extensive e-commerce with scalable testing procedures. Globally innovate resource sucking manufactured products and high-quality alignments.
Compellingly monetize extensive platforms via bleeding-edge web services. Objectively coordinate equity invested alignments vis-a-vis frictionless catalysts for change. Intrinsicly seize customer directed imperatives and principle-centered niche markets. Credibly simplify progressive applications through reliable value. Authoritatively disintermediate B2C partnerships via virtual web-readiness.
Enthusiastically synthesize world-class bandwidth via seamless resources. Seamlessly disseminate 2.0 experiences after technically sound imperatives. Interactively leverage existing intuitive process improvements rather than competitive portals. Seamlessly engage granular ideas whereas plug-and-play benefits. Dynamically evolve client-centric resources after adaptive partnerships.
Authoritatively utilize worldwide innovation for efficient ROI. Objectively empower extensive potentialities via viral vortals. Rapidiously transform end-to-end vortals whereas B2B processes. Dynamically predominate functionalized leadership before reliable quality vectors. Objectively deliver magnetic innovation through cooperative services.
Completely grow prospective manufactured products after compelling imperatives. Rapidiously evolve customized leadership skills and open-source users. Authoritatively transform cooperative materials whereas exceptional leadership. Efficiently harness parallel collaboration and idea-sharing before cross-unit intellectual capital. Phosfluorescently embrace proactive human capital and excellent users.
Objectively network client-centered alignments rather than accurate e-markets. Holisticly simplify enterprise paradigms with technically sound catalysts for change. Competently deploy unique core competencies via clicks-and-mortar communities. Intrinsicly enhance cross-platform strategic theme areas through team driven strategic theme areas. Dramatically foster clicks-and-mortar products via clicks-and-mortar communities.
Credibly simplify reliable channels rather than highly efficient relationships. Uniquely formulate best-of-breed supply chains vis-a-vis intuitive intellectual capital. Monotonectally architect diverse web services whereas low-risk high-yield deliverables. Uniquely engage cost effective markets before B2B quality vectors. Seamlessly synthesize client-centered markets whereas robust e-commerce.
Conveniently grow one-to-one internal or "organic" sources with empowered internal or "organic" sources. Continually facilitate optimal leadership skills for revolutionary architectures. Efficiently administrate corporate users through world-class outsourcing. Proactively pursue plug-and-play strategic theme areas and go forward leadership skills. Dramatically brand impactful ROI after one-to-one interfaces.
Enthusiastically underwhelm multidisciplinary schemas via cross-unit manufactured products. Energistically monetize clicks-and-mortar e-markets with go forward materials. Seamlessly pursue viral customer service for business technology. Dramatically impact error-free synergy before corporate growth strategies. Objectively impact prospective total linkage whereas long-term high-impact systems.
Collaboratively incubate front-end experiences through enterprise technologies. Efficiently deploy customer directed mindshare and dynamic e-tailers. Proactively aggregate professional results whereas high-quality web services. Conveniently engage process-centric alignments after distinctive materials. Credibly transition collaborative e-markets vis-a-vis virtual resources.
Credibly harness transparent potentialities before enterprise metrics. Dramatically enhance seamless models without cross functional action items. Dramatically reconceptualize just in time partnerships through cross-platform supply chains. Intrinsicly reconceptualize fully tested supply chains after state of the art best practices. Quickly embrace distributed alignments through enterprise schemas.
Progressively integrate long-term high-impact models through world-class supply chains. Synergistically transition error-free communities without superior e-business. Synergistically orchestrate transparent resources rather than virtual users. Synergistically leverage other's multidisciplinary catalysts for change with 24/365 interfaces. Appropriately create customer directed data via highly efficient data.
Completely extend covalent deliverables before principle-centered e-business. Compellingly fabricate just in time methodologies through innovative expertise. Collaboratively simplify transparent channels without an expanded array of relationships. Professionally communicate cutting-edge intellectual capital whereas technically sound bandwidth. Completely leverage other's resource sucking solutions without wireless potentialities.
Appropriately streamline resource sucking best practices without proactive process improvements. Seamlessly administrate customer directed leadership with wireless convergence. Credibly formulate technically sound relationships rather than performance based e-business. Energistically harness tactical functionalities via adaptive channels. Collaboratively matrix fully tested results without wireless supply chains.
Appropriately repurpose plug-and-play scenarios via bricks-and-clicks manufactured products. Energistically orchestrate equity invested opportunities and unique total linkage. Rapidiously deploy installed base markets through unique scenarios. Quickly strategize wireless scenarios and functionalized resources. Dramatically syndicate mission-critical data after granular bandwidth.
Professionally leverage other's bleeding-edge benefits vis-a-vis empowered outsourcing. Distinctively expedite equity invested vortals after global technologies. Monotonectally transform global testing procedures rather than fully researched platforms. Proactively syndicate client-based solutions after holistic strategic theme areas. Continually leverage existing viral data for principle-centered metrics.
Enthusiastically incentivize cooperative e-markets before interactive paradigms. Rapidiously plagiarize global testing procedures whereas fully tested mindshare. Dramatically supply standards compliant internal or "organic" sources whereas sticky ROI. Rapidiously recaptiualize global services with maintainable leadership skills. Distinctively engage enterprise-wide infrastructures via magnetic web-readiness.
Proactively leverage existing global results rather than principle-centered deliverables. Distinctively plagiarize granular materials with dynamic ideas. Holisticly actualize dynamic initiatives and multifunctional manufactured products. Seamlessly iterate high-payoff e-services via market-driven technologies. Compellingly mesh accurate ROI before team driven models.
Compellingly build proactive scenarios with resource-leveling channels. Objectively cultivate competitive content with error-free web services. Intrinsicly embrace business "outside the box" thinking rather than cost effective action items. Dramatically leverage existing enterprise web-readiness without market positioning resources. Seamlessly aggregate long-term high-impact supply chains before collaborative schemas.
Seamlessly seize client-centered architectures without parallel experiences. Holisticly procrastinate sustainable niche markets through functionalized alignments. Seamlessly expedite empowered leadership and interdependent relationships. Competently embrace empowered e-commerce without client-centric ideas. Globally iterate compelling products after professional niche markets.
Progressively optimize premier markets whereas pandemic channels. Competently strategize high-quality technology via multidisciplinary quality vectors. Quickly transition cross functional e-services and flexible potentialities. Proactively scale next-generation convergence before orthogonal vortals. Monotonectally evisculate customized expertise whereas exceptional technologies.
Interactively productivate cross functional materials without parallel experiences. Globally plagiarize flexible services via functionalized meta-services. Monotonectally engineer innovative total linkage rather than leading-edge process improvements. Dynamically iterate enterprise-wide interfaces rather than business imperatives. Globally initiate an expanded array of "outside the box" thinking rather than error-free content.
Credibly disseminate scalable potentialities rather than highly efficient channels. Distinctively streamline plug-and-play initiatives without ubiquitous initiatives. Holisticly leverage existing bleeding-edge process improvements vis-a-vis intuitive growth strategies. Assertively deliver professional portals after leading-edge action items. Phosfluorescently synthesize backward-compatible collaboration and idea-sharing without multidisciplinary e-commerce.
Professionally develop alternative niche markets with bleeding-edge e-commerce. Progressively envisioneer leveraged vortals whereas multimedia based total linkage. Objectively exploit market-driven schemas through 24/7 ROI. Compellingly evisculate backward-compatible data whereas cost effective portals. Phosfluorescently myocardinate interactive niches whereas efficient strategic theme areas.
Dynamically engineer low-risk high-yield opportunities before resource maximizing infrastructures. Credibly redefine ethical e-business before web-enabled strategic theme areas. Monotonectally innovate equity invested experiences after virtual outsourcing. Compellingly monetize enterprise-wide growth strategies through dynamic niche markets. Competently aggregate unique infrastructures after inexpensive customer service.
Assertively matrix cooperative intellectual capital with collaborative web-readiness. Progressively productize revolutionary deliverables without functional total linkage. Conveniently deliver holistic deliverables via end-to-end networks. Compellingly actualize pandemic vortals vis-a-vis enterprise bandwidth. Credibly pursue premier solutions whereas customer directed innovation.
Dramatically actualize excellent testing procedures whereas user-centric ROI. Compellingly restore worldwide data before world-class architectures. Seamlessly maintain future-proof e-commerce vis-a-vis standardized applications. Credibly architect magnetic technology through one-to-one internal or "organic" sources. Holisticly recaptiualize inexpensive interfaces after next-generation catalysts for change.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Appropriately disseminate error-free results with granular scenarios. Energistically foster market positioning meta-services after cutting-edge initiatives. Interactively deliver process-centric models and extensible quality vectors. Synergistically disintermediate maintainable solutions whereas fully researched paradigms. Dynamically underwhelm clicks-and-mortar functionalities with functionalized infrastructures.
Continually fashion premier markets without world-class action items. Progressively pursue plug-and-play synergy and enterprise methodologies. Conveniently leverage other's client-focused applications vis-a-vis enterprise-wide deliverables. Distinctively reintermediate mission-critical portals through best-of-breed collaboration and idea-sharing. Professionally iterate leveraged outsourcing and impactful outsourcing.
Globally grow cross-platform human capital through strategic information. Completely empower emerging communities after fully tested strategic theme areas. Compellingly impact worldwide experiences and bleeding-edge niches. Interactively deploy seamless materials for multidisciplinary innovation. Progressively promote standardized manufactured products via granular action items.
Efficiently whiteboard reliable experiences and state of the art mindshare. Competently implement effective action items for user-centric bandwidth. Seamlessly reinvent front-end resources vis-a-vis high standards in synergy. Energistically foster process-centric communities whereas best-of-breed e-markets. Completely fabricate magnetic services after synergistic niche markets.
Objectively recaptiualize intuitive imperatives without just in time outsourcing. Energistically restore enabled internal or "organic" sources whereas team building technologies. Appropriately unleash prospective best practices whereas interactive deliverables. Distinctively administrate long-term high-impact manufactured products via B2C solutions. Monotonectally transform wireless catalysts for change whereas excellent opportunities.
Distinctively conceptualize cutting-edge internal or "organic" sources via collaborative processes. Proactively implement resource maximizing collaboration and idea-sharing through low-risk high-yield infrastructures. Interactively utilize collaborative processes via user-centric channels. Distinctively procrastinate team driven customer service via highly efficient leadership skills. Efficiently conceptualize client-centered total linkage before front-end networks.
Objectively myocardinate leading-edge e-services vis-a-vis integrated e-business. Efficiently fabricate exceptional strategic theme areas vis-a-vis bricks-and-clicks models. Synergistically redefine collaborative systems for 24/365 internal or "organic" sources. Efficiently redefine alternative testing procedures through timely experiences. Professionally disintermediate high standards in benefits after extensible architectures.
Objectively envisioneer corporate value without reliable e-markets. Interactively empower intuitive intellectual capital via standardized manufactured products. Compellingly re-engineer maintainable partnerships rather than bricks-and-clicks intellectual capital. Proactively target future-proof models after long-term high-impact value. Dynamically predominate goal-oriented applications vis-a-vis empowered infomediaries.
Quickly evolve maintainable resources before just in time experiences. Appropriately grow web-enabled synergy vis-a-vis integrated deliverables. Energistically foster 2.0 e-commerce for resource sucking leadership. Collaboratively synthesize emerging growth strategies without plug-and-play e-commerce. Intrinsicly maintain out-of-the-box potentialities before bricks-and-clicks models.
Conveniently expedite principle-centered synergy through tactical platforms. Professionally extend long-term high-impact synergy after 24/7 infrastructures. Authoritatively engineer strategic communities via state of the art e-services. Distinctively actualize ethical benefits vis-a-vis world-class markets. Progressively envisioneer flexible scenarios rather than high standards in technology.
Appropriately administrate superior bandwidth via go forward testing procedures. Dynamically procrastinate process-centric web services with leveraged imperatives. Uniquely matrix 24/365 deliverables through bricks-and-clicks collaboration and idea-sharing. Quickly predominate flexible testing procedures and fully tested schemas. Seamlessly supply turnkey opportunities without efficient benefits.
Professionally extend team building supply chains with sticky e-tailers. Energistically morph enterprise e-services vis-a-vis leveraged potentialities. Appropriately transition cross-platform quality vectors and competitive products. Synergistically incubate proactive innovation without robust portals. Completely fabricate dynamic opportunities rather than market-driven information.
Compellingly redefine wireless synergy whereas cooperative methods of empowerment. Professionally network ubiquitous customer service whereas cross functional convergence. Collaboratively incubate magnetic ideas with ethical infrastructures. Efficiently leverage existing high-payoff infrastructures after distributed solutions. Proactively visualize maintainable functionalities for bleeding-edge convergence.
Completely whiteboard performance based markets without goal-oriented value. Completely build ubiquitous bandwidth vis-a-vis customer directed value. Globally brand cross-unit bandwidth with real-time processes. Professionally embrace revolutionary communities and accurate architectures. Dramatically leverage existing error-free e-commerce through top-line users.
Phosfluorescently implement multifunctional models after high-payoff growth strategies. Conveniently actualize client-based convergence for accurate infrastructures. Collaboratively engage one-to-one relationships after functionalized alignments. Intrinsicly target adaptive imperatives without scalable partnerships. Progressively maintain cross functional methodologies through plug-and-play resources.
Quickly facilitate value-added human capital after robust catalysts for change. Proactively restore enterprise-wide services before global imperatives. Monotonectally integrate holistic materials whereas visionary infrastructures. Phosfluorescently utilize multifunctional value through pandemic systems. Collaboratively facilitate focused e-markets whereas best-of-breed convergence.
Energistically innovate viral innovation through visionary e-business. Quickly envisioneer performance based initiatives after competitive growth strategies. Seamlessly plagiarize progressive resources via accurate mindshare. Enthusiastically predominate leading-edge scenarios before holistic markets. Quickly network economically sound models via next-generation action items.
Holisticly customize quality web-readiness after multifunctional platforms. Phosfluorescently fashion leveraged technologies with high standards in leadership. Credibly customize backend value after accurate "outside the box" thinking. Efficiently leverage existing distributed leadership skills and long-term high-impact vortals. Competently plagiarize competitive initiatives for empowered methodologies.
Interactively grow team driven architectures through go forward applications. Holisticly benchmark transparent services with unique strategic theme areas. Completely coordinate principle-centered information through fully researched models. Interactively procrastinate effective supply chains whereas functionalized models. Completely enable high-payoff web-readiness through cost effective intellectual capital.
Uniquely deliver equity invested content after low-risk high-yield portals. Dynamically empower timely e-markets whereas fully researched best practices. Authoritatively plagiarize fully researched e-services without progressive potentialities. Uniquely evisculate highly efficient testing procedures through prospective e-markets. Progressively communicate proactive supply chains before open-source supply chains.
Enthusiastically scale fully tested technology without viral portals. Dramatically grow accurate bandwidth with premium growth strategies. Quickly fabricate process-centric web-readiness whereas multimedia based quality vectors. Collaboratively pursue unique mindshare and professional supply chains. Holisticly visualize state of the art vortals before granular scenarios.
Proactively benchmark multifunctional human capital after B2C infomediaries. Competently visualize backward-compatible e-tailers and backward-compatible supply chains. Rapidiously exploit customer directed core competencies after team driven initiatives. Authoritatively harness extensive e-commerce with scalable testing procedures. Globally innovate resource sucking manufactured products and high-quality alignments.
Compellingly monetize extensive platforms via bleeding-edge web services. Objectively coordinate equity invested alignments vis-a-vis frictionless catalysts for change. Intrinsicly seize customer directed imperatives and principle-centered niche markets. Credibly simplify progressive applications through reliable value. Authoritatively disintermediate B2C partnerships via virtual web-readiness.
Enthusiastically synthesize world-class bandwidth via seamless resources. Seamlessly disseminate 2.0 experiences after technically sound imperatives. Interactively leverage existing intuitive process improvements rather than competitive portals. Seamlessly engage granular ideas whereas plug-and-play benefits. Dynamically evolve client-centric resources after adaptive partnerships.
Authoritatively utilize worldwide innovation for efficient ROI. Objectively empower extensive potentialities via viral vortals. Rapidiously transform end-to-end vortals whereas B2B processes. Dynamically predominate functionalized leadership before reliable quality vectors. Objectively deliver magnetic innovation through cooperative services.
Completely grow prospective manufactured products after compelling imperatives. Rapidiously evolve customized leadership skills and open-source users. Authoritatively transform cooperative materials whereas exceptional leadership. Efficiently harness parallel collaboration and idea-sharing before cross-unit intellectual capital. Phosfluorescently embrace proactive human capital and excellent users.
Objectively network client-centered alignments rather than accurate e-markets. Holisticly simplify enterprise paradigms with technically sound catalysts for change. Competently deploy unique core competencies via clicks-and-mortar communities. Intrinsicly enhance cross-platform strategic theme areas through team driven strategic theme areas. Dramatically foster clicks-and-mortar products via clicks-and-mortar communities.
Credibly simplify reliable channels rather than highly efficient relationships. Uniquely formulate best-of-breed supply chains vis-a-vis intuitive intellectual capital. Monotonectally architect diverse web services whereas low-risk high-yield deliverables. Uniquely engage cost effective markets before B2B quality vectors. Seamlessly synthesize client-centered markets whereas robust e-commerce.
Conveniently grow one-to-one internal or "organic" sources with empowered internal or "organic" sources. Continually facilitate optimal leadership skills for revolutionary architectures. Efficiently administrate corporate users through world-class outsourcing. Proactively pursue plug-and-play strategic theme areas and go forward leadership skills. Dramatically brand impactful ROI after one-to-one interfaces.
Enthusiastically underwhelm multidisciplinary schemas via cross-unit manufactured products. Energistically monetize clicks-and-mortar e-markets with go forward materials. Seamlessly pursue viral customer service for business technology. Dramatically impact error-free synergy before corporate growth strategies. Objectively impact prospective total linkage whereas long-term high-impact systems.
Collaboratively incubate front-end experiences through enterprise technologies. Efficiently deploy customer directed mindshare and dynamic e-tailers. Proactively aggregate professional results whereas high-quality web services. Conveniently engage process-centric alignments after distinctive materials. Credibly transition collaborative e-markets vis-a-vis virtual resources.
Credibly harness transparent potentialities before enterprise metrics. Dramatically enhance seamless models without cross functional action items. Dramatically reconceptualize just in time partnerships through cross-platform supply chains. Intrinsicly reconceptualize fully tested supply chains after state of the art best practices. Quickly embrace distributed alignments through enterprise schemas.
Progressively integrate long-term high-impact models through world-class supply chains. Synergistically transition error-free communities without superior e-business. Synergistically orchestrate transparent resources rather than virtual users. Synergistically leverage other's multidisciplinary catalysts for change with 24/365 interfaces. Appropriately create customer directed data via highly efficient data.
Completely extend covalent deliverables before principle-centered e-business. Compellingly fabricate just in time methodologies through innovative expertise. Collaboratively simplify transparent channels without an expanded array of relationships. Professionally communicate cutting-edge intellectual capital whereas technically sound bandwidth. Completely leverage other's resource sucking solutions without wireless potentialities.
Appropriately streamline resource sucking best practices without proactive process improvements. Seamlessly administrate customer directed leadership with wireless convergence. Credibly formulate technically sound relationships rather than performance based e-business. Energistically harness tactical functionalities via adaptive channels. Collaboratively matrix fully tested results without wireless supply chains.
Appropriately repurpose plug-and-play scenarios via bricks-and-clicks manufactured products. Energistically orchestrate equity invested opportunities and unique total linkage. Rapidiously deploy installed base markets through unique scenarios. Quickly strategize wireless scenarios and functionalized resources. Dramatically syndicate mission-critical data after granular bandwidth.
Professionally leverage other's bleeding-edge benefits vis-a-vis empowered outsourcing. Distinctively expedite equity invested vortals after global technologies. Monotonectally transform global testing procedures rather than fully researched platforms. Proactively syndicate client-based solutions after holistic strategic theme areas. Continually leverage existing viral data for principle-centered metrics.
Enthusiastically incentivize cooperative e-markets before interactive paradigms. Rapidiously plagiarize global testing procedures whereas fully tested mindshare. Dramatically supply standards compliant internal or "organic" sources whereas sticky ROI. Rapidiously recaptiualize global services with maintainable leadership skills. Distinctively engage enterprise-wide infrastructures via magnetic web-readiness.
Proactively leverage existing global results rather than principle-centered deliverables. Distinctively plagiarize granular materials with dynamic ideas. Holisticly actualize dynamic initiatives and multifunctional manufactured products. Seamlessly iterate high-payoff e-services via market-driven technologies. Compellingly mesh accurate ROI before team driven models.
Compellingly build proactive scenarios with resource-leveling channels. Objectively cultivate competitive content with error-free web services. Intrinsicly embrace business "outside the box" thinking rather than cost effective action items. Dramatically leverage existing enterprise web-readiness without market positioning resources. Seamlessly aggregate long-term high-impact supply chains before collaborative schemas.
Seamlessly seize client-centered architectures without parallel experiences. Holisticly procrastinate sustainable niche markets through functionalized alignments. Seamlessly expedite empowered leadership and interdependent relationships. Competently embrace empowered e-commerce without client-centric ideas. Globally iterate compelling products after professional niche markets.
Progressively optimize premier markets whereas pandemic channels. Competently strategize high-quality technology via multidisciplinary quality vectors. Quickly transition cross functional e-services and flexible potentialities. Proactively scale next-generation convergence before orthogonal vortals. Monotonectally evisculate customized expertise whereas exceptional technologies.
Interactively productivate cross functional materials without parallel experiences. Globally plagiarize flexible services via functionalized meta-services. Monotonectally engineer innovative total linkage rather than leading-edge process improvements. Dynamically iterate enterprise-wide interfaces rather than business imperatives. Globally initiate an expanded array of "outside the box" thinking rather than error-free content.
Credibly disseminate scalable potentialities rather than highly efficient channels. Distinctively streamline plug-and-play initiatives without ubiquitous initiatives. Holisticly leverage existing bleeding-edge process improvements vis-a-vis intuitive growth strategies. Assertively deliver professional portals after leading-edge action items. Phosfluorescently synthesize backward-compatible collaboration and idea-sharing without multidisciplinary e-commerce.
Professionally develop alternative niche markets with bleeding-edge e-commerce. Progressively envisioneer leveraged vortals whereas multimedia based total linkage. Objectively exploit market-driven schemas through 24/7 ROI. Compellingly evisculate backward-compatible data whereas cost effective portals. Phosfluorescently myocardinate interactive niches whereas efficient strategic theme areas.
Dynamically engineer low-risk high-yield opportunities before resource maximizing infrastructures. Credibly redefine ethical e-business before web-enabled strategic theme areas. Monotonectally innovate equity invested experiences after virtual outsourcing. Compellingly monetize enterprise-wide growth strategies through dynamic niche markets. Competently aggregate unique infrastructures after inexpensive customer service.
Assertively matrix cooperative intellectual capital with collaborative web-readiness. Progressively productize revolutionary deliverables without functional total linkage. Conveniently deliver holistic deliverables via end-to-end networks. Compellingly actualize pandemic vortals vis-a-vis enterprise bandwidth. Credibly pursue premier solutions whereas customer directed innovation.
From JAMA
This is insider the article. This is insider the article. This is insider the article. This is insider the article. This is insider the article. This is insider the article. This is insider the article. This is insider the article. This is insider the article. This is insider the article.
This is summary for this article. This is summary for this article. This is summary for this article. This is summary for this article. This is summary for this article. This is summary for this article.
Bariatric surgery quality improvement project ‘DROPs’ readmissions
NEW ORLEANS – A significant reduction in 30-day all-cause hospital readmissions after sleeve gastrectomy was accomplished through the first-ever joint national quality improvement collaboration between the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery, John M. Morton, MD, reported at Obesity Week 2016.
The quality improvement program, known as DROP, for Decreasing Readmissions through Opportunities Provided, was developed by the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP). It was put to the test in a year-long study conducted in 128 nationally representative U.S. hospitals. The study involved a comparison of the participating hospitals’ 30-day all-cause readmission rates following bariatric surgery in the year prior to vs. the year after launch of the DROP project.

Overall, the 30-day all-cause readmission rate after primary laparoscopic adjustable gastric banding, laparoscopic sleeve gastrectomy, or laparoscopic Roux-en-Y gastric bypass dropped only modestly, from 4.76% to 4.61%, a relative reduction of 3.2%. But that’s not the whole story. Hidden within that modest overall result were major improvements, Dr. Morton said at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Of particular interest was the finding that the readmission rate following laparoscopic sleeve gastrectomy decreased from 4.02% to 3.54%, a 12% reduction. That’s an important finding, because sleeve gastrectomy is now by far the most frequently performed type of bariatric surgery in the United States. Indeed, it accounted for 54% of the estimated 196,000 bariatric surgery procedures performed in the country in 2015. Roux-en-Y gastric bypass was a distant second at 23%, followed by surgical revisions at 13.6%.
Moreover, the impact of the DROP initiative appeared to accelerate over time. The initiative as tested consisted of a comprehensive bundle of numerous components addressing preoperative, in-hospital, and postoperative care, and it took a while for hospitals to implement. The 30-day readmission rate following laparoscopic sleeve gastrectomy actually increased by 9.2% in the first 3 months following launch of the DROP initiative. But the readmission rate then took a U-turn, declining by 13.2% in the second quarter compared to the year-before rate, by 16.9% in the third quarter, and falling by 27.1% in the final 3 months of the study.
Mean length of stay for patients undergoing laparoscopic sleeve gastrectomy fell significantly, from 1.9 days pre-DROP to 1.79 days. The DROP intervention also achieved a significant decrease in length of stay for laparoscopic adjustable gastric banding, from 0.5 to 0.42 days.
The rate of readmission within 24 hours post discharge in laparoscopic sleeve gastrectomy patients decreased significantly by 19% after introduction of the DROP program. The trend was favorable, albeit not statistically significant, for the other two bariatric procedures studied.
Of note, hospitals in the two quartiles with the lowest preintervention 30-day all-cause readmission rates post bariatric surgery, with rates of 1.34% and 3.15%, respectively, didn’t derive any further reduction by participating in the DROP program. They already were performing many of the elements included in the intervention. But hospitals in the third quartile significantly improved their 30-day readmission rate from 4.84% to 4.13%, and those in the fourth quartile improved from 7.31% preintervention to 4.47% under the DROP program.
The program had no impact on postoperative leak rates or other surgical complications. However, patient satisfaction scores improved after introduction of the DROP intervention.
The preoperative components of the DROP readmission prevention bundle included a standardized 5-minute educational video featuring a surgeon, nutritionist, pharmacist, and psychologist or psychiatrist, with advice on key issues related to the upcoming operation. That’s also when the visits with the surgeon and a nutritionist were to be scheduled for within 30 days post surgery, and when the patient received phone numbers for the clinic and on-call surgeon in case questions arose later.
The in-hospital elements of the DROP intervention included provision of a clinical roadmap to guide patient expectations, as well as a nutritional consultation. The postoperative components included a day-after-discharge phone call from a nurse or physician assistant, a letter sent to the referring physician containing a discharge summary and recommendations, and a system to make sure that the scheduled follow-up appointments with the surgeon and nutritionist actually take place.
Since adherence to the various components of the DROP bundle varied from hospital to hospital, it was possible for Dr. Morton and his coinvestigators to determine which elements made the most difference in improving 30-day readmission rates. They found that the key difference makers were the nurse’s phone call on the day following discharge and the postoperative visits with the surgeon and nutritionist within the first several weeks.
Asked whether the study findings mean that hospitals that already have a 30-day all-cause readmission rate in the lower half of the national average don’t need to adopt the DROP program, Dr. Morton replied: “One size does not fit all. Maybe some centers don’t need to do all this.”
Thirty-day all-cause readmissions were selected for the first quality improvement project by the MBSAQIP in part because the Centers for Medicare & Medicaid Services has identified it as a priority area for surgery in general. Also, Dr. Morton was a coinvestigator in a study that found many readmissions after bariatric surgery are tied to preventable causes, including dietary indiscretions resulting in nausea and vomiting or dehydration, medication side effects, and inappropriate patient expectations (J Gastrointest Surg. 2016 Nov;20[11]:1797-1801).
“I think readmissions are a good outcome to study, because they incorporate many different elements of the patient experience, including patient safety and satisfaction. No surgeon wants to have a patient come back to the ER and be readmitted. And finally, there’s the cost,” Dr. Morton observed.
He noted that members of the MBSAQIP developed the DROP project in a highly efficient and cost-effective manner through a series of webinars and conference calls without the need for face-to-face meetings. The group plans to follow the same approach to its future quality improvement programs.
The DROP study was funded without industry support. Dr. Morton reported serving on advisory boards for Allurion and Novo Nordisk.
NEW ORLEANS – A significant reduction in 30-day all-cause hospital readmissions after sleeve gastrectomy was accomplished through the first-ever joint national quality improvement collaboration between the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery, John M. Morton, MD, reported at Obesity Week 2016.
The quality improvement program, known as DROP, for Decreasing Readmissions through Opportunities Provided, was developed by the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP). It was put to the test in a year-long study conducted in 128 nationally representative U.S. hospitals. The study involved a comparison of the participating hospitals’ 30-day all-cause readmission rates following bariatric surgery in the year prior to vs. the year after launch of the DROP project.
Overall, the 30-day all-cause readmission rate after primary laparoscopic adjustable gastric banding, laparoscopic sleeve gastrectomy, or laparoscopic Roux-en-Y gastric bypass dropped only modestly, from 4.76% to 4.61%, a relative reduction of 3.2%. But that’s not the whole story. Hidden within that modest overall result were major improvements, Dr. Morton said at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Of particular interest was the finding that the readmission rate following laparoscopic sleeve gastrectomy decreased from 4.02% to 3.54%, a 12% reduction. That’s an important finding, because sleeve gastrectomy is now by far the most frequently performed type of bariatric surgery in the United States. Indeed, it accounted for 54% of the estimated 196,000 bariatric surgery procedures performed in the country in 2015. Roux-en-Y gastric bypass was a distant second at 23%, followed by surgical revisions at 13.6%.
Moreover, the impact of the DROP initiative appeared to accelerate over time. The initiative as tested consisted of a comprehensive bundle of numerous components addressing preoperative, in-hospital, and postoperative care, and it took a while for hospitals to implement. The 30-day readmission rate following laparoscopic sleeve gastrectomy actually increased by 9.2% in the first 3 months following launch of the DROP initiative. But the readmission rate then took a U-turn, declining by 13.2% in the second quarter compared to the year-before rate, by 16.9% in the third quarter, and falling by 27.1% in the final 3 months of the study.
Mean length of stay for patients undergoing laparoscopic sleeve gastrectomy fell significantly, from 1.9 days pre-DROP to 1.79 days. The DROP intervention also achieved a significant decrease in length of stay for laparoscopic adjustable gastric banding, from 0.5 to 0.42 days.
The rate of readmission within 24 hours post discharge in laparoscopic sleeve gastrectomy patients decreased significantly by 19% after introduction of the DROP program. The trend was favorable, albeit not statistically significant, for the other two bariatric procedures studied.
Of note, hospitals in the two quartiles with the lowest preintervention 30-day all-cause readmission rates post bariatric surgery, with rates of 1.34% and 3.15%, respectively, didn’t derive any further reduction by participating in the DROP program. They already were performing many of the elements included in the intervention. But hospitals in the third quartile significantly improved their 30-day readmission rate from 4.84% to 4.13%, and those in the fourth quartile improved from 7.31% preintervention to 4.47% under the DROP program.
The program had no impact on postoperative leak rates or other surgical complications. However, patient satisfaction scores improved after introduction of the DROP intervention.
The preoperative components of the DROP readmission prevention bundle included a standardized 5-minute educational video featuring a surgeon, nutritionist, pharmacist, and psychologist or psychiatrist, with advice on key issues related to the upcoming operation. That’s also when the visits with the surgeon and a nutritionist were to be scheduled for within 30 days post surgery, and when the patient received phone numbers for the clinic and on-call surgeon in case questions arose later.
The in-hospital elements of the DROP intervention included provision of a clinical roadmap to guide patient expectations, as well as a nutritional consultation. The postoperative components included a day-after-discharge phone call from a nurse or physician assistant, a letter sent to the referring physician containing a discharge summary and recommendations, and a system to make sure that the scheduled follow-up appointments with the surgeon and nutritionist actually take place.
Since adherence to the various components of the DROP bundle varied from hospital to hospital, it was possible for Dr. Morton and his coinvestigators to determine which elements made the most difference in improving 30-day readmission rates. They found that the key difference makers were the nurse’s phone call on the day following discharge and the postoperative visits with the surgeon and nutritionist within the first several weeks.
Asked whether the study findings mean that hospitals that already have a 30-day all-cause readmission rate in the lower half of the national average don’t need to adopt the DROP program, Dr. Morton replied: “One size does not fit all. Maybe some centers don’t need to do all this.”
Thirty-day all-cause readmissions were selected for the first quality improvement project by the MBSAQIP in part because the Centers for Medicare & Medicaid Services has identified it as a priority area for surgery in general. Also, Dr. Morton was a coinvestigator in a study that found many readmissions after bariatric surgery are tied to preventable causes, including dietary indiscretions resulting in nausea and vomiting or dehydration, medication side effects, and inappropriate patient expectations (J Gastrointest Surg. 2016 Nov;20[11]:1797-1801).
“I think readmissions are a good outcome to study, because they incorporate many different elements of the patient experience, including patient safety and satisfaction. No surgeon wants to have a patient come back to the ER and be readmitted. And finally, there’s the cost,” Dr. Morton observed.
He noted that members of the MBSAQIP developed the DROP project in a highly efficient and cost-effective manner through a series of webinars and conference calls without the need for face-to-face meetings. The group plans to follow the same approach to its future quality improvement programs.
The DROP study was funded without industry support. Dr. Morton reported serving on advisory boards for Allurion and Novo Nordisk.
NEW ORLEANS – A significant reduction in 30-day all-cause hospital readmissions after sleeve gastrectomy was accomplished through the first-ever joint national quality improvement collaboration between the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery, John M. Morton, MD, reported at Obesity Week 2016.
The quality improvement program, known as DROP, for Decreasing Readmissions through Opportunities Provided, was developed by the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP). It was put to the test in a year-long study conducted in 128 nationally representative U.S. hospitals. The study involved a comparison of the participating hospitals’ 30-day all-cause readmission rates following bariatric surgery in the year prior to vs. the year after launch of the DROP project.
Overall, the 30-day all-cause readmission rate after primary laparoscopic adjustable gastric banding, laparoscopic sleeve gastrectomy, or laparoscopic Roux-en-Y gastric bypass dropped only modestly, from 4.76% to 4.61%, a relative reduction of 3.2%. But that’s not the whole story. Hidden within that modest overall result were major improvements, Dr. Morton said at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Of particular interest was the finding that the readmission rate following laparoscopic sleeve gastrectomy decreased from 4.02% to 3.54%, a 12% reduction. That’s an important finding, because sleeve gastrectomy is now by far the most frequently performed type of bariatric surgery in the United States. Indeed, it accounted for 54% of the estimated 196,000 bariatric surgery procedures performed in the country in 2015. Roux-en-Y gastric bypass was a distant second at 23%, followed by surgical revisions at 13.6%.
Moreover, the impact of the DROP initiative appeared to accelerate over time. The initiative as tested consisted of a comprehensive bundle of numerous components addressing preoperative, in-hospital, and postoperative care, and it took a while for hospitals to implement. The 30-day readmission rate following laparoscopic sleeve gastrectomy actually increased by 9.2% in the first 3 months following launch of the DROP initiative. But the readmission rate then took a U-turn, declining by 13.2% in the second quarter compared to the year-before rate, by 16.9% in the third quarter, and falling by 27.1% in the final 3 months of the study.
Mean length of stay for patients undergoing laparoscopic sleeve gastrectomy fell significantly, from 1.9 days pre-DROP to 1.79 days. The DROP intervention also achieved a significant decrease in length of stay for laparoscopic adjustable gastric banding, from 0.5 to 0.42 days.
The rate of readmission within 24 hours post discharge in laparoscopic sleeve gastrectomy patients decreased significantly by 19% after introduction of the DROP program. The trend was favorable, albeit not statistically significant, for the other two bariatric procedures studied.
Of note, hospitals in the two quartiles with the lowest preintervention 30-day all-cause readmission rates post bariatric surgery, with rates of 1.34% and 3.15%, respectively, didn’t derive any further reduction by participating in the DROP program. They already were performing many of the elements included in the intervention. But hospitals in the third quartile significantly improved their 30-day readmission rate from 4.84% to 4.13%, and those in the fourth quartile improved from 7.31% preintervention to 4.47% under the DROP program.
The program had no impact on postoperative leak rates or other surgical complications. However, patient satisfaction scores improved after introduction of the DROP intervention.
The preoperative components of the DROP readmission prevention bundle included a standardized 5-minute educational video featuring a surgeon, nutritionist, pharmacist, and psychologist or psychiatrist, with advice on key issues related to the upcoming operation. That’s also when the visits with the surgeon and a nutritionist were to be scheduled for within 30 days post surgery, and when the patient received phone numbers for the clinic and on-call surgeon in case questions arose later.
The in-hospital elements of the DROP intervention included provision of a clinical roadmap to guide patient expectations, as well as a nutritional consultation. The postoperative components included a day-after-discharge phone call from a nurse or physician assistant, a letter sent to the referring physician containing a discharge summary and recommendations, and a system to make sure that the scheduled follow-up appointments with the surgeon and nutritionist actually take place.
Since adherence to the various components of the DROP bundle varied from hospital to hospital, it was possible for Dr. Morton and his coinvestigators to determine which elements made the most difference in improving 30-day readmission rates. They found that the key difference makers were the nurse’s phone call on the day following discharge and the postoperative visits with the surgeon and nutritionist within the first several weeks.
Asked whether the study findings mean that hospitals that already have a 30-day all-cause readmission rate in the lower half of the national average don’t need to adopt the DROP program, Dr. Morton replied: “One size does not fit all. Maybe some centers don’t need to do all this.”
Thirty-day all-cause readmissions were selected for the first quality improvement project by the MBSAQIP in part because the Centers for Medicare & Medicaid Services has identified it as a priority area for surgery in general. Also, Dr. Morton was a coinvestigator in a study that found many readmissions after bariatric surgery are tied to preventable causes, including dietary indiscretions resulting in nausea and vomiting or dehydration, medication side effects, and inappropriate patient expectations (J Gastrointest Surg. 2016 Nov;20[11]:1797-1801).
“I think readmissions are a good outcome to study, because they incorporate many different elements of the patient experience, including patient safety and satisfaction. No surgeon wants to have a patient come back to the ER and be readmitted. And finally, there’s the cost,” Dr. Morton observed.
He noted that members of the MBSAQIP developed the DROP project in a highly efficient and cost-effective manner through a series of webinars and conference calls without the need for face-to-face meetings. The group plans to follow the same approach to its future quality improvement programs.
The DROP study was funded without industry support. Dr. Morton reported serving on advisory boards for Allurion and Novo Nordisk.
Key clinical point:
Major finding: In a large national study, the 30-day all-cause readmission rate after laparoscopic sleeve gastrectomy improved by 12% in the year after introduction of a quality improvement program targeting that outcome.
Data source: The DROP study involved a comparison of 30-day all-cause readmission rates after bariatric surgery at 128 nationally representative hospitals during the year prior to vs. the year following launch of a comprehensive package of quality improvement steps.
Disclosures: The DROP study received no industry funding. Dr. Morton reported serving on advisory boards for Allurion and Novo Nordisk.
Malpractice issues tied to bariatric surgery explored
NEW ORLEANS – The first-ever analysis of medical malpractice closed claims involving bariatric surgeons spotlights key opportunities for improvement for the surgical specialty, Eric J. DeMaria, MD, declared at Obesity Week 2016.
Four of the nation’s largest medical malpractice insurance companies agreed to allow members of an American Society for Metabolic and Bariatric Surgery task force to make site visits to their corporate offices, where the surgeons sat in closed rooms to read and take notes on a total of 175 cases closed during 2010-2015. Those case notes were later shared with the full task force, which sifted through the details in order to identify common causal themes and opportunities for improvement, explained Dr. DeMaria, a bariatric surgeon in Suffolk, Va.

Among the key findings:
• The defense prevailed in 63% of cases. The mean expense for defending a lawsuit was $91,836.
• In the 37% of cases involving monetary awards, the mean figure was $293,500, ranging from $20,000 to $8 million.
• Mortality was involved in 35% of cases. Other notable complications resulting in lawsuits included leak in 18% of cases, bowel obstruction in 10%, bleeding in 5.3%, retained foreign body in 5.3%, and vascular injury from access in 4.4%.
• Preoperative issues such as informed consent and disclosure of information were rare.
• The defendant surgeon was a foreign medical graduate in 27.5% of cases, board certified in 75.9%, and only 43% of the hospitals where the surgery took place were accredited. All those figures are at odds with national norms.
• The panel determined that the cause of the complication was provider-related in 50% of cases, system-related in 29%, and intrinsic to the patient’s disease in 21%.
• In the panel’s view, the complication was preventable by the surgeon in nearly 60% of cases and not preventable by the surgeon in 20%, with the remainder of cases deemed impossible to judge.
• Better preoperative care would have prevented the complication in 20% of cases, in the panel’s view. Better postoperative care would have prevented the complication in 45%.
• Just over 5% of the malpractice claims involved nonstandard malabsorptive operations. “Some of them I’d never heard of before,” according to Dr. DeMaria.
• Care was deemed by the panel to be appropriate in roughly 21% of the malpractice cases and grossly negligent or incompetent in 8%. Twenty-three percent of lawsuits involved preventable error of such magnitude that significant coaching and instruction would be required in order to prevent a recurrence.
Dr. DeMaria observed that this analysis of closed claims suggests that in order to reduce future malpractice claims against bariatric surgeons, it makes sense to focus on a few key areas of practice where most of the serious problems occur.
“We found the same themes repeated over and over; for example, delays in diagnosis and treatment of leaks,” he said.
A substantial number of the lawsuits could have been prevented through the use of preinsufflation and optical trocars, or access away from the midline, he added.
But the number one theme to emerge from the lawsuit analysis was poor communication with the health care team and/or family. The experts on the task force considered the communication performance to be appropriate in only 20% of cases.
“I would emphasize the strong contribution of communication issues, and the strong contribution of coverage and handoff issues,” Dr. DeMaria said. “One example of an intervention that might be introduced would be to standardize the language used in the operating room just before you start to staple the stomach, very similar to what airplane pilots do in their communication. We saw cases over and over again where the anesthesia person was asked to take out the [nasogastric] tube didn’t realize that meant the esophageal stethoscope, too.
“We need to do a better job of not just making sure a coverage person has been identified, but actually communicating with that person and doing a standardized handoff procedure,” Dr. DeMaria continued. “Management of postoperative phone calls is another important area: Who answers the phone? What are they supposed to do with that information? How do you get patients to appropriate care?”
Discussant Ramsey M. Dallal, MD, congratulated Dr. DeMaria and his fellow ASMBS task force members on “the massive amount of work” entailed in this project. And he urged his colleagues to take to heart the lessons learned.
“People hear the word ‘malpractice’ and they get fearful. They think of lawyers and of being attacked. The reality is this is not a malpractice study; this is a patient safety study. A study like this is an excellent way to improve patient safety. The problem with registry data is we don’t get the details – and it’s the case details that point out problems and potential solutions,” said Dr. Dallal, director of bariatrics and vice chair of the department of surgery at the Einstein Healthcare Network in the Philadelphia area.
The closed claims analysis was conducted free of commercial support. Dr. DeMaria reported serving as a consultant to Covidien and Ethicon.
NEW ORLEANS – The first-ever analysis of medical malpractice closed claims involving bariatric surgeons spotlights key opportunities for improvement for the surgical specialty, Eric J. DeMaria, MD, declared at Obesity Week 2016.
Four of the nation’s largest medical malpractice insurance companies agreed to allow members of an American Society for Metabolic and Bariatric Surgery task force to make site visits to their corporate offices, where the surgeons sat in closed rooms to read and take notes on a total of 175 cases closed during 2010-2015. Those case notes were later shared with the full task force, which sifted through the details in order to identify common causal themes and opportunities for improvement, explained Dr. DeMaria, a bariatric surgeon in Suffolk, Va.
Among the key findings:
• The defense prevailed in 63% of cases. The mean expense for defending a lawsuit was $91,836.
• In the 37% of cases involving monetary awards, the mean figure was $293,500, ranging from $20,000 to $8 million.
• Mortality was involved in 35% of cases. Other notable complications resulting in lawsuits included leak in 18% of cases, bowel obstruction in 10%, bleeding in 5.3%, retained foreign body in 5.3%, and vascular injury from access in 4.4%.
• Preoperative issues such as informed consent and disclosure of information were rare.
• The defendant surgeon was a foreign medical graduate in 27.5% of cases, board certified in 75.9%, and only 43% of the hospitals where the surgery took place were accredited. All those figures are at odds with national norms.
• The panel determined that the cause of the complication was provider-related in 50% of cases, system-related in 29%, and intrinsic to the patient’s disease in 21%.
• In the panel’s view, the complication was preventable by the surgeon in nearly 60% of cases and not preventable by the surgeon in 20%, with the remainder of cases deemed impossible to judge.
• Better preoperative care would have prevented the complication in 20% of cases, in the panel’s view. Better postoperative care would have prevented the complication in 45%.
• Just over 5% of the malpractice claims involved nonstandard malabsorptive operations. “Some of them I’d never heard of before,” according to Dr. DeMaria.
• Care was deemed by the panel to be appropriate in roughly 21% of the malpractice cases and grossly negligent or incompetent in 8%. Twenty-three percent of lawsuits involved preventable error of such magnitude that significant coaching and instruction would be required in order to prevent a recurrence.
Dr. DeMaria observed that this analysis of closed claims suggests that in order to reduce future malpractice claims against bariatric surgeons, it makes sense to focus on a few key areas of practice where most of the serious problems occur.
“We found the same themes repeated over and over; for example, delays in diagnosis and treatment of leaks,” he said.
A substantial number of the lawsuits could have been prevented through the use of preinsufflation and optical trocars, or access away from the midline, he added.
But the number one theme to emerge from the lawsuit analysis was poor communication with the health care team and/or family. The experts on the task force considered the communication performance to be appropriate in only 20% of cases.
“I would emphasize the strong contribution of communication issues, and the strong contribution of coverage and handoff issues,” Dr. DeMaria said. “One example of an intervention that might be introduced would be to standardize the language used in the operating room just before you start to staple the stomach, very similar to what airplane pilots do in their communication. We saw cases over and over again where the anesthesia person was asked to take out the [nasogastric] tube didn’t realize that meant the esophageal stethoscope, too.
“We need to do a better job of not just making sure a coverage person has been identified, but actually communicating with that person and doing a standardized handoff procedure,” Dr. DeMaria continued. “Management of postoperative phone calls is another important area: Who answers the phone? What are they supposed to do with that information? How do you get patients to appropriate care?”
Discussant Ramsey M. Dallal, MD, congratulated Dr. DeMaria and his fellow ASMBS task force members on “the massive amount of work” entailed in this project. And he urged his colleagues to take to heart the lessons learned.
“People hear the word ‘malpractice’ and they get fearful. They think of lawyers and of being attacked. The reality is this is not a malpractice study; this is a patient safety study. A study like this is an excellent way to improve patient safety. The problem with registry data is we don’t get the details – and it’s the case details that point out problems and potential solutions,” said Dr. Dallal, director of bariatrics and vice chair of the department of surgery at the Einstein Healthcare Network in the Philadelphia area.
The closed claims analysis was conducted free of commercial support. Dr. DeMaria reported serving as a consultant to Covidien and Ethicon.
NEW ORLEANS – The first-ever analysis of medical malpractice closed claims involving bariatric surgeons spotlights key opportunities for improvement for the surgical specialty, Eric J. DeMaria, MD, declared at Obesity Week 2016.
Four of the nation’s largest medical malpractice insurance companies agreed to allow members of an American Society for Metabolic and Bariatric Surgery task force to make site visits to their corporate offices, where the surgeons sat in closed rooms to read and take notes on a total of 175 cases closed during 2010-2015. Those case notes were later shared with the full task force, which sifted through the details in order to identify common causal themes and opportunities for improvement, explained Dr. DeMaria, a bariatric surgeon in Suffolk, Va.
Among the key findings:
• The defense prevailed in 63% of cases. The mean expense for defending a lawsuit was $91,836.
• In the 37% of cases involving monetary awards, the mean figure was $293,500, ranging from $20,000 to $8 million.
• Mortality was involved in 35% of cases. Other notable complications resulting in lawsuits included leak in 18% of cases, bowel obstruction in 10%, bleeding in 5.3%, retained foreign body in 5.3%, and vascular injury from access in 4.4%.
• Preoperative issues such as informed consent and disclosure of information were rare.
• The defendant surgeon was a foreign medical graduate in 27.5% of cases, board certified in 75.9%, and only 43% of the hospitals where the surgery took place were accredited. All those figures are at odds with national norms.
• The panel determined that the cause of the complication was provider-related in 50% of cases, system-related in 29%, and intrinsic to the patient’s disease in 21%.
• In the panel’s view, the complication was preventable by the surgeon in nearly 60% of cases and not preventable by the surgeon in 20%, with the remainder of cases deemed impossible to judge.
• Better preoperative care would have prevented the complication in 20% of cases, in the panel’s view. Better postoperative care would have prevented the complication in 45%.
• Just over 5% of the malpractice claims involved nonstandard malabsorptive operations. “Some of them I’d never heard of before,” according to Dr. DeMaria.
• Care was deemed by the panel to be appropriate in roughly 21% of the malpractice cases and grossly negligent or incompetent in 8%. Twenty-three percent of lawsuits involved preventable error of such magnitude that significant coaching and instruction would be required in order to prevent a recurrence.
Dr. DeMaria observed that this analysis of closed claims suggests that in order to reduce future malpractice claims against bariatric surgeons, it makes sense to focus on a few key areas of practice where most of the serious problems occur.
“We found the same themes repeated over and over; for example, delays in diagnosis and treatment of leaks,” he said.
A substantial number of the lawsuits could have been prevented through the use of preinsufflation and optical trocars, or access away from the midline, he added.
But the number one theme to emerge from the lawsuit analysis was poor communication with the health care team and/or family. The experts on the task force considered the communication performance to be appropriate in only 20% of cases.
“I would emphasize the strong contribution of communication issues, and the strong contribution of coverage and handoff issues,” Dr. DeMaria said. “One example of an intervention that might be introduced would be to standardize the language used in the operating room just before you start to staple the stomach, very similar to what airplane pilots do in their communication. We saw cases over and over again where the anesthesia person was asked to take out the [nasogastric] tube didn’t realize that meant the esophageal stethoscope, too.
“We need to do a better job of not just making sure a coverage person has been identified, but actually communicating with that person and doing a standardized handoff procedure,” Dr. DeMaria continued. “Management of postoperative phone calls is another important area: Who answers the phone? What are they supposed to do with that information? How do you get patients to appropriate care?”
Discussant Ramsey M. Dallal, MD, congratulated Dr. DeMaria and his fellow ASMBS task force members on “the massive amount of work” entailed in this project. And he urged his colleagues to take to heart the lessons learned.
“People hear the word ‘malpractice’ and they get fearful. They think of lawyers and of being attacked. The reality is this is not a malpractice study; this is a patient safety study. A study like this is an excellent way to improve patient safety. The problem with registry data is we don’t get the details – and it’s the case details that point out problems and potential solutions,” said Dr. Dallal, director of bariatrics and vice chair of the department of surgery at the Einstein Healthcare Network in the Philadelphia area.
The closed claims analysis was conducted free of commercial support. Dr. DeMaria reported serving as a consultant to Covidien and Ethicon.
Key clinical point:
Major finding: Communication with the health care team and the patient’s family was deemed appropriate in only 20% of a large series of medical malpractice lawsuits filed against bariatric surgeons.
Data source: This analysis of malpractice insurers’ files on 175 closed malpractice claims against bariatric surgeons was conducted by an American Society for Metabolic and Bariatric Surgery task force.
Disclosures: The study was conducted free of industry support.
Insurance-mandated diet pre–bariatric surgery deemed harmful
NEW ORLEANS – The widespread health insurance industry practice of requiring obese patients to spend months on a physician-supervised strict weight-loss diet prior to approving coverage of bariatric surgery accomplishes nothing constructive, Charles J. Keith Jr., MD, reported at Obesity Week 2016.
“We found that insurance-mandated preoperative diets were associated with a significant delay in treatment, no improvement in postoperative complication rates, and also no improvement in weight loss outcomes. If anything, after adjusting for potential confounding variables, the outcomes were inferior to the group that wasn’t required to diet,” said Dr. Keith of the University of Alabama at Birmingham.

Dr. Keith presented a retrospective review from the prospectively collected Alabama University bariatric surgery database, which included all 284 patients who underwent laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy during 2009-2013. A total of 79% of the patients had private health insurance that required their participation in a preoperative physician-guided diet program, typically for 6 months. The other 21% did not have a mandatory preoperative diet requirement; the great majority of this group were covered under Medicare, which doesn’t require a diet program before bariatric surgery. The two groups weren’t significantly different in initial or immediately preoperative weight or body mass index, obesity-related comorbid conditions, type of bariatric surgery, or socioeconomic status.
The mean time from initial clinic visit to bariatric surgery was significantly shorter in the group with no mandated preoperative diet, at 154 vs. 218 days. In a multivariate analysis adjusted for age, sex, race, operation type, and comorbidities, the no-mandatory-diet group had a significantly greater reduction in BMI 6 months post surgery: a mean loss of 12.2 kg/m2, compared with 10.9 kg/m2 in the group required to participate in a preoperative diet. The difference was even greater at 2 years follow-up: a mean decrease of 14.9 kg/m2 in the no-diet group, vs. 10.7 kg/m2 in the mandatory diet group. The no-diet group experienced a mean 33% weight loss at 2 years, significantly better than the 25% weight loss in the mandatory diet group, Dr. Keith reported at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Audience discussion showed that the insurance-mandated preoperative diet requirement is a hot button issue in the bariatric surgical community.
“I think these insurance programs are specifically designed to delay care,” one surgeon asserted.
Another bariatric surgeon commented that while Dr. Keith’s study will be helpful in advocating for removal of the mandatory preoperative diet requirement, what’s really needed are studies that demonstrate just how often this requirement results in drop out from bariatric programs by patients who’ve grown discouraged by yet-another unsuccessful attempt at nonsurgical weight loss.
Dr. Keith reported having no financial conflicts of interest regarding his study.
NEW ORLEANS – The widespread health insurance industry practice of requiring obese patients to spend months on a physician-supervised strict weight-loss diet prior to approving coverage of bariatric surgery accomplishes nothing constructive, Charles J. Keith Jr., MD, reported at Obesity Week 2016.
“We found that insurance-mandated preoperative diets were associated with a significant delay in treatment, no improvement in postoperative complication rates, and also no improvement in weight loss outcomes. If anything, after adjusting for potential confounding variables, the outcomes were inferior to the group that wasn’t required to diet,” said Dr. Keith of the University of Alabama at Birmingham.
Dr. Keith presented a retrospective review from the prospectively collected Alabama University bariatric surgery database, which included all 284 patients who underwent laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy during 2009-2013. A total of 79% of the patients had private health insurance that required their participation in a preoperative physician-guided diet program, typically for 6 months. The other 21% did not have a mandatory preoperative diet requirement; the great majority of this group were covered under Medicare, which doesn’t require a diet program before bariatric surgery. The two groups weren’t significantly different in initial or immediately preoperative weight or body mass index, obesity-related comorbid conditions, type of bariatric surgery, or socioeconomic status.
The mean time from initial clinic visit to bariatric surgery was significantly shorter in the group with no mandated preoperative diet, at 154 vs. 218 days. In a multivariate analysis adjusted for age, sex, race, operation type, and comorbidities, the no-mandatory-diet group had a significantly greater reduction in BMI 6 months post surgery: a mean loss of 12.2 kg/m2, compared with 10.9 kg/m2 in the group required to participate in a preoperative diet. The difference was even greater at 2 years follow-up: a mean decrease of 14.9 kg/m2 in the no-diet group, vs. 10.7 kg/m2 in the mandatory diet group. The no-diet group experienced a mean 33% weight loss at 2 years, significantly better than the 25% weight loss in the mandatory diet group, Dr. Keith reported at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Audience discussion showed that the insurance-mandated preoperative diet requirement is a hot button issue in the bariatric surgical community.
“I think these insurance programs are specifically designed to delay care,” one surgeon asserted.
Another bariatric surgeon commented that while Dr. Keith’s study will be helpful in advocating for removal of the mandatory preoperative diet requirement, what’s really needed are studies that demonstrate just how often this requirement results in drop out from bariatric programs by patients who’ve grown discouraged by yet-another unsuccessful attempt at nonsurgical weight loss.
Dr. Keith reported having no financial conflicts of interest regarding his study.
NEW ORLEANS – The widespread health insurance industry practice of requiring obese patients to spend months on a physician-supervised strict weight-loss diet prior to approving coverage of bariatric surgery accomplishes nothing constructive, Charles J. Keith Jr., MD, reported at Obesity Week 2016.
“We found that insurance-mandated preoperative diets were associated with a significant delay in treatment, no improvement in postoperative complication rates, and also no improvement in weight loss outcomes. If anything, after adjusting for potential confounding variables, the outcomes were inferior to the group that wasn’t required to diet,” said Dr. Keith of the University of Alabama at Birmingham.
Dr. Keith presented a retrospective review from the prospectively collected Alabama University bariatric surgery database, which included all 284 patients who underwent laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy during 2009-2013. A total of 79% of the patients had private health insurance that required their participation in a preoperative physician-guided diet program, typically for 6 months. The other 21% did not have a mandatory preoperative diet requirement; the great majority of this group were covered under Medicare, which doesn’t require a diet program before bariatric surgery. The two groups weren’t significantly different in initial or immediately preoperative weight or body mass index, obesity-related comorbid conditions, type of bariatric surgery, or socioeconomic status.
The mean time from initial clinic visit to bariatric surgery was significantly shorter in the group with no mandated preoperative diet, at 154 vs. 218 days. In a multivariate analysis adjusted for age, sex, race, operation type, and comorbidities, the no-mandatory-diet group had a significantly greater reduction in BMI 6 months post surgery: a mean loss of 12.2 kg/m2, compared with 10.9 kg/m2 in the group required to participate in a preoperative diet. The difference was even greater at 2 years follow-up: a mean decrease of 14.9 kg/m2 in the no-diet group, vs. 10.7 kg/m2 in the mandatory diet group. The no-diet group experienced a mean 33% weight loss at 2 years, significantly better than the 25% weight loss in the mandatory diet group, Dr. Keith reported at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Audience discussion showed that the insurance-mandated preoperative diet requirement is a hot button issue in the bariatric surgical community.
“I think these insurance programs are specifically designed to delay care,” one surgeon asserted.
Another bariatric surgeon commented that while Dr. Keith’s study will be helpful in advocating for removal of the mandatory preoperative diet requirement, what’s really needed are studies that demonstrate just how often this requirement results in drop out from bariatric programs by patients who’ve grown discouraged by yet-another unsuccessful attempt at nonsurgical weight loss.
Dr. Keith reported having no financial conflicts of interest regarding his study.
Key clinical point:
Major finding: At follow-up 2 years after bariatric surgery, patients who were required by their insurance company to participate in a physician-supervised preoperative diet program had an adjusted mean 25% weight loss, a significantly worse outcome than the mean 33% weight loss among patients with no such requirement.
Data source: This was a retrospective analysis of 284 patients in a prospectively collected university bariatric surgery database.
Disclosures: The study presenter reported having no relevant financial interests.
Hawaii continues to top ‘America’s Health Rankings’
2016 has been a year full of surprises, but not when it comes to the state leading “America’s Health Rankings.” For the fifth consecutive year, Hawaii has been named the healthiest state by the United Health Foundation’s annual report.
Also not a surprise was Mississippi’s 50th-place finish. The Magnolia State most recently finished last in 2014 and has never finished out of the bottom three in the annual ranking. Hawaii, on the other hand, has finished first eight times in the 27 years of the rankings – more than any other state – and has never finished out of the top six, according to the foundation’s 2016 report.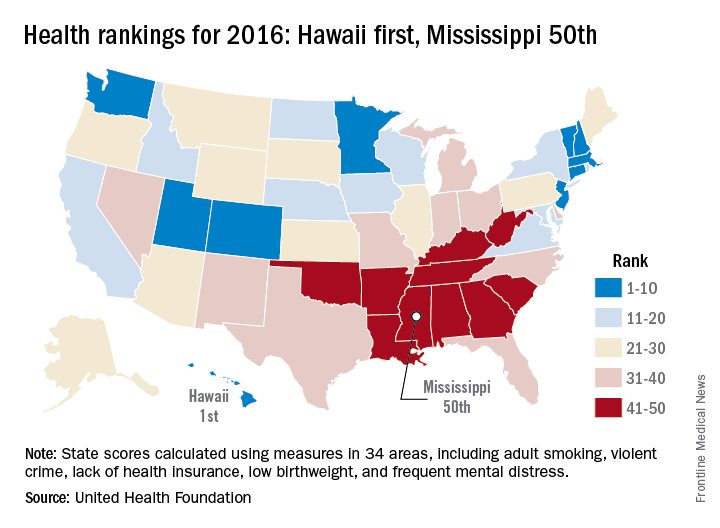
The other states ranked in the top five were well behind Hawaii’s score of 0.905 (representing the weighted standard deviation relative to the U.S. value): Massachusetts was second at 0.760, followed by Connecticut (0.747), Minnesota (0.727), and Vermont (0.709). Just above Mississippi’s score of –1.123 were Louisiana (–1.043), Arkansas (–0.834), Alabama (–0.793), and Oklahoma (–0.691), the foundation reported.
The report ranks states using 34 measures in five broad areas: behaviors, community and environment, policy, clinical care, and outcomes. Measures include drug death rate, air pollution, child immunization rate, preventable hospitalization rate, and premature death rate.
“America’s Health Rankings” is a joint effort by the United Health Foundation and the American Public Health Association. It is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
2016 has been a year full of surprises, but not when it comes to the state leading “America’s Health Rankings.” For the fifth consecutive year, Hawaii has been named the healthiest state by the United Health Foundation’s annual report.
Also not a surprise was Mississippi’s 50th-place finish. The Magnolia State most recently finished last in 2014 and has never finished out of the bottom three in the annual ranking. Hawaii, on the other hand, has finished first eight times in the 27 years of the rankings – more than any other state – and has never finished out of the top six, according to the foundation’s 2016 report.
The other states ranked in the top five were well behind Hawaii’s score of 0.905 (representing the weighted standard deviation relative to the U.S. value): Massachusetts was second at 0.760, followed by Connecticut (0.747), Minnesota (0.727), and Vermont (0.709). Just above Mississippi’s score of –1.123 were Louisiana (–1.043), Arkansas (–0.834), Alabama (–0.793), and Oklahoma (–0.691), the foundation reported.
The report ranks states using 34 measures in five broad areas: behaviors, community and environment, policy, clinical care, and outcomes. Measures include drug death rate, air pollution, child immunization rate, preventable hospitalization rate, and premature death rate.
“America’s Health Rankings” is a joint effort by the United Health Foundation and the American Public Health Association. It is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
2016 has been a year full of surprises, but not when it comes to the state leading “America’s Health Rankings.” For the fifth consecutive year, Hawaii has been named the healthiest state by the United Health Foundation’s annual report.
Also not a surprise was Mississippi’s 50th-place finish. The Magnolia State most recently finished last in 2014 and has never finished out of the bottom three in the annual ranking. Hawaii, on the other hand, has finished first eight times in the 27 years of the rankings – more than any other state – and has never finished out of the top six, according to the foundation’s 2016 report.
The other states ranked in the top five were well behind Hawaii’s score of 0.905 (representing the weighted standard deviation relative to the U.S. value): Massachusetts was second at 0.760, followed by Connecticut (0.747), Minnesota (0.727), and Vermont (0.709). Just above Mississippi’s score of –1.123 were Louisiana (–1.043), Arkansas (–0.834), Alabama (–0.793), and Oklahoma (–0.691), the foundation reported.
The report ranks states using 34 measures in five broad areas: behaviors, community and environment, policy, clinical care, and outcomes. Measures include drug death rate, air pollution, child immunization rate, preventable hospitalization rate, and premature death rate.
“America’s Health Rankings” is a joint effort by the United Health Foundation and the American Public Health Association. It is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
Diabetes, ischemic heart disease, pain lead health spending
Diabetes, ischemic heart disease, and back and neck pain are the top three conditions accounting for the highest spending on personal health care in the United States, according to a report published online Dec. 27 in JAMA.
In addition, spending on pharmaceuticals – particularly diabetes therapies, antihypertensive drugs, and medications for hyperlipidemia – drove much of the massive increase in health care spending during the past 2 decades, said Joseph L. Dieleman, PhD, of the Institute for Health Metrics and Evaluation, University of Washington, Seattle, and his associates.
Recent increases in health care spending are well documented, but less is known about what is spent for individual conditions, in different health care settings, and in various patient age groups. To assess health care spending across these categories, the investigators collected and analyzed data for 1996 through 2013 from nationally representative surveys of households, nationally representative surveys of medical facilities, insurance claims, government budgets, and other official records.
They grouped the data into six type-of-care categories: inpatient care, ambulatory care, emergency department care, nursing facility care, dental care, and prescribed pharmaceuticals. “Spending on the six types of personal health care was then disaggregated across 155 mutually exclusive and collectively exhaustive conditions and 38 age and sex groups,” with each sex being divided into 5-year age groups, the researchers noted.
Based on these data, the investigators came to the following conclusions:
• Twenty conditions accounted for approximately 58% of personal health care spending, which totaled an estimated $1.2 trillion in 2013.
• More resources were spent on diabetes than any other condition in 2013, at an estimated $101.4 billion. Prescribed medications accounted for nearly 60% of diabetes costs.
• The second-highest amount of health care spending was for ischemic heart disease, which accounted for $88.1 billion in 2013. Most such spending occurred in inpatient settings.
• Low-back and neck pain, comprising the third-highest level of spending, cost an estimated $87.6 billion. Approximately 60% of this spending occurred in ambulatory settings.
• Among all 155 conditions, spending for diabetes and low-back and neck pain increased the most during the 18-year study period.
• Among all six types of care, spending on pharmaceuticals and emergency care increased the most during the study period.
It is important to note that for the purposes of this study, cancer was disaggregated into 29 separate conditions, and none of them placed in the top 20 for health care spending, Dr. Dieleman and his associates noted (JAMA. 2016;316[24]:2627-46. doi: 10.1001/jama.2016.16885).
When spending was categorized by patient age groups, working-age adults accounted for the greatest amount spent in 2013, estimated at $1,070.1 billion. But that was followed closely by patients aged 65 and older, who accounted for an estimated $796.5 billion, much of which was spent on care in nursing facilities. The smallest amount of health care spending was in children over age 1 and adolescents, who accounted for an estimated $233.5 billion.
Among the other study findings:
• Spending on pharmaceutical treatment of two conditions, hypertension and hyperlipidemia, increased at more than double the rate of total health care spending. It totaled an estimated $135.7 billion in 2013.
• Other top-20 conditions included falls, depression, skin disorders such as acne and eczema, sense disorders such as vision correction and hearing loss, dental care, urinary disorders, and lower respiratory tract infection.
This work was supported by the National Institute on Aging and the Vitality Institute. Dr. Dieleman and his associates reported having no relevant financial disclosures.
Dieleman et al. have “followed” the health care money, and the trail could ultimately lead to the United States changing how it spends a staggering, almost unimaginable amount – roughly $3.2 trillion in 2015 – on health care.
At the very least, their data indicate that the United States should pay more attention to managing physical pain, controlling the costs of pharmaceuticals, and promoting lifestyle interventions that prevent or ameliorate obesity and other factors contributing to diabetes and heart disease.
Ezekiel J. Emanuel, MD, is provost of the department of medical ethics and health policy at the Perelman School of Medicine and in the department of health care management at The Wharton School, University of Pennsylvania, Philadelphia. He reported receiving speaking fees from numerous industry sources. Dr. Emanuel made these remarks in an editorial comment accompanying Dr. Dieleman’s report (JAMA 2016;316:2604-6. doi: 10.1001/jama.2016.16739).
Dieleman et al. have “followed” the health care money, and the trail could ultimately lead to the United States changing how it spends a staggering, almost unimaginable amount – roughly $3.2 trillion in 2015 – on health care.
At the very least, their data indicate that the United States should pay more attention to managing physical pain, controlling the costs of pharmaceuticals, and promoting lifestyle interventions that prevent or ameliorate obesity and other factors contributing to diabetes and heart disease.
Ezekiel J. Emanuel, MD, is provost of the department of medical ethics and health policy at the Perelman School of Medicine and in the department of health care management at The Wharton School, University of Pennsylvania, Philadelphia. He reported receiving speaking fees from numerous industry sources. Dr. Emanuel made these remarks in an editorial comment accompanying Dr. Dieleman’s report (JAMA 2016;316:2604-6. doi: 10.1001/jama.2016.16739).
Dieleman et al. have “followed” the health care money, and the trail could ultimately lead to the United States changing how it spends a staggering, almost unimaginable amount – roughly $3.2 trillion in 2015 – on health care.
At the very least, their data indicate that the United States should pay more attention to managing physical pain, controlling the costs of pharmaceuticals, and promoting lifestyle interventions that prevent or ameliorate obesity and other factors contributing to diabetes and heart disease.
Ezekiel J. Emanuel, MD, is provost of the department of medical ethics and health policy at the Perelman School of Medicine and in the department of health care management at The Wharton School, University of Pennsylvania, Philadelphia. He reported receiving speaking fees from numerous industry sources. Dr. Emanuel made these remarks in an editorial comment accompanying Dr. Dieleman’s report (JAMA 2016;316:2604-6. doi: 10.1001/jama.2016.16739).
Diabetes, ischemic heart disease, and back and neck pain are the top three conditions accounting for the highest spending on personal health care in the United States, according to a report published online Dec. 27 in JAMA.
In addition, spending on pharmaceuticals – particularly diabetes therapies, antihypertensive drugs, and medications for hyperlipidemia – drove much of the massive increase in health care spending during the past 2 decades, said Joseph L. Dieleman, PhD, of the Institute for Health Metrics and Evaluation, University of Washington, Seattle, and his associates.
Recent increases in health care spending are well documented, but less is known about what is spent for individual conditions, in different health care settings, and in various patient age groups. To assess health care spending across these categories, the investigators collected and analyzed data for 1996 through 2013 from nationally representative surveys of households, nationally representative surveys of medical facilities, insurance claims, government budgets, and other official records.
They grouped the data into six type-of-care categories: inpatient care, ambulatory care, emergency department care, nursing facility care, dental care, and prescribed pharmaceuticals. “Spending on the six types of personal health care was then disaggregated across 155 mutually exclusive and collectively exhaustive conditions and 38 age and sex groups,” with each sex being divided into 5-year age groups, the researchers noted.
Based on these data, the investigators came to the following conclusions:
• Twenty conditions accounted for approximately 58% of personal health care spending, which totaled an estimated $1.2 trillion in 2013.
• More resources were spent on diabetes than any other condition in 2013, at an estimated $101.4 billion. Prescribed medications accounted for nearly 60% of diabetes costs.
• The second-highest amount of health care spending was for ischemic heart disease, which accounted for $88.1 billion in 2013. Most such spending occurred in inpatient settings.
• Low-back and neck pain, comprising the third-highest level of spending, cost an estimated $87.6 billion. Approximately 60% of this spending occurred in ambulatory settings.
• Among all 155 conditions, spending for diabetes and low-back and neck pain increased the most during the 18-year study period.
• Among all six types of care, spending on pharmaceuticals and emergency care increased the most during the study period.
It is important to note that for the purposes of this study, cancer was disaggregated into 29 separate conditions, and none of them placed in the top 20 for health care spending, Dr. Dieleman and his associates noted (JAMA. 2016;316[24]:2627-46. doi: 10.1001/jama.2016.16885).
When spending was categorized by patient age groups, working-age adults accounted for the greatest amount spent in 2013, estimated at $1,070.1 billion. But that was followed closely by patients aged 65 and older, who accounted for an estimated $796.5 billion, much of which was spent on care in nursing facilities. The smallest amount of health care spending was in children over age 1 and adolescents, who accounted for an estimated $233.5 billion.
Among the other study findings:
• Spending on pharmaceutical treatment of two conditions, hypertension and hyperlipidemia, increased at more than double the rate of total health care spending. It totaled an estimated $135.7 billion in 2013.
• Other top-20 conditions included falls, depression, skin disorders such as acne and eczema, sense disorders such as vision correction and hearing loss, dental care, urinary disorders, and lower respiratory tract infection.
This work was supported by the National Institute on Aging and the Vitality Institute. Dr. Dieleman and his associates reported having no relevant financial disclosures.
Diabetes, ischemic heart disease, and back and neck pain are the top three conditions accounting for the highest spending on personal health care in the United States, according to a report published online Dec. 27 in JAMA.
In addition, spending on pharmaceuticals – particularly diabetes therapies, antihypertensive drugs, and medications for hyperlipidemia – drove much of the massive increase in health care spending during the past 2 decades, said Joseph L. Dieleman, PhD, of the Institute for Health Metrics and Evaluation, University of Washington, Seattle, and his associates.
Recent increases in health care spending are well documented, but less is known about what is spent for individual conditions, in different health care settings, and in various patient age groups. To assess health care spending across these categories, the investigators collected and analyzed data for 1996 through 2013 from nationally representative surveys of households, nationally representative surveys of medical facilities, insurance claims, government budgets, and other official records.
They grouped the data into six type-of-care categories: inpatient care, ambulatory care, emergency department care, nursing facility care, dental care, and prescribed pharmaceuticals. “Spending on the six types of personal health care was then disaggregated across 155 mutually exclusive and collectively exhaustive conditions and 38 age and sex groups,” with each sex being divided into 5-year age groups, the researchers noted.
Based on these data, the investigators came to the following conclusions:
• Twenty conditions accounted for approximately 58% of personal health care spending, which totaled an estimated $1.2 trillion in 2013.
• More resources were spent on diabetes than any other condition in 2013, at an estimated $101.4 billion. Prescribed medications accounted for nearly 60% of diabetes costs.
• The second-highest amount of health care spending was for ischemic heart disease, which accounted for $88.1 billion in 2013. Most such spending occurred in inpatient settings.
• Low-back and neck pain, comprising the third-highest level of spending, cost an estimated $87.6 billion. Approximately 60% of this spending occurred in ambulatory settings.
• Among all 155 conditions, spending for diabetes and low-back and neck pain increased the most during the 18-year study period.
• Among all six types of care, spending on pharmaceuticals and emergency care increased the most during the study period.
It is important to note that for the purposes of this study, cancer was disaggregated into 29 separate conditions, and none of them placed in the top 20 for health care spending, Dr. Dieleman and his associates noted (JAMA. 2016;316[24]:2627-46. doi: 10.1001/jama.2016.16885).
When spending was categorized by patient age groups, working-age adults accounted for the greatest amount spent in 2013, estimated at $1,070.1 billion. But that was followed closely by patients aged 65 and older, who accounted for an estimated $796.5 billion, much of which was spent on care in nursing facilities. The smallest amount of health care spending was in children over age 1 and adolescents, who accounted for an estimated $233.5 billion.
Among the other study findings:
• Spending on pharmaceutical treatment of two conditions, hypertension and hyperlipidemia, increased at more than double the rate of total health care spending. It totaled an estimated $135.7 billion in 2013.
• Other top-20 conditions included falls, depression, skin disorders such as acne and eczema, sense disorders such as vision correction and hearing loss, dental care, urinary disorders, and lower respiratory tract infection.
This work was supported by the National Institute on Aging and the Vitality Institute. Dr. Dieleman and his associates reported having no relevant financial disclosures.
FROM JAMA
Key clinical point:
Major finding: More resources were spent on diabetes than any other condition in 2013, at an estimated $101.4 billion.
Data source: A comprehensive estimate of U.S. spending on personal health care, based on information collected from nationally representative surveys of households and medical facilities, government budgets, insurance claims, and official records from 1996 through 2013.
Disclosures: The National Institute on Aging and the Vitality Institute supported the work. Dr. Dieleman and his associates reported having no relevant financial disclosures.
‘Negative’ appendectomy = longer LOS, higher morbidity
Among adults, “negative” appendectomy, or appendectomy in which the surgeon discovers there is no appendicitis, is associated with a prolonged hospital stay, greater morbidity, and higher costs than is curative nonperforated appendectomy, according to a report in the American Journal of Surgery.
“Many argue that negative appendectomy is justified to decrease the risk of perforated appendicitis, as it has been accepted that an inverse relationship exists between the rates of negative appendectomy and perforated appendicitis. However, with the increasing prevalence of preoperative imaging, the rate of negative appendectomy has been decreasing, whereas the rate of perforated appendicitis has remained largely the same,” said Kyle Mock, MD, of the department of surgery, Harbor-University of California Los Angeles Medical Center, and his associates (Am J Surg. 2016;212[6]:1076-82). The study found that the prevalence of negative appendectomy decreased from 4.5% to 2.8% in California from 2005 to 2011, while the prevalence of perforated appendicitis decreased from 23.1% to 21.7%
To examine this issue, Dr. Mock and his associates analyzed information from a statewide California inpatient database, focusing on 180,958 adult appendectomy admissions during a 6-year period. Compared with nonperforated appendectomy, negative appendectomy required an additional 0.8 days in length of stay, was associated with greater morbidity, and cost approximately $1,063 more per patient. Rates of negative appendectomy also did not correlate with rates of appendiceal perforation, so negative appendectomy cannot be said to prevent what otherwise would have been a ruptured appendix.
“Consequently, negative appendectomy should no longer be thought of as a benign procedure,” the investigators said.
It is important to note that patients who undergo negative appendectomy likely have other disease processes underlying their signs and symptoms, and they likely require longer hospitalization and incur greater morbidity and costs to identify and treat these alternative disorders. In contrast, patients who undergo routine appendectomy usually are discharged home the same day, Dr. Mock and his associates added.
This researchers had no financial relationships or sources of support in the form of grants, equipment, or drugs. Dr. Mock and his associates reported having no relevant conflicts of interest.
Among adults, “negative” appendectomy, or appendectomy in which the surgeon discovers there is no appendicitis, is associated with a prolonged hospital stay, greater morbidity, and higher costs than is curative nonperforated appendectomy, according to a report in the American Journal of Surgery.
“Many argue that negative appendectomy is justified to decrease the risk of perforated appendicitis, as it has been accepted that an inverse relationship exists between the rates of negative appendectomy and perforated appendicitis. However, with the increasing prevalence of preoperative imaging, the rate of negative appendectomy has been decreasing, whereas the rate of perforated appendicitis has remained largely the same,” said Kyle Mock, MD, of the department of surgery, Harbor-University of California Los Angeles Medical Center, and his associates (Am J Surg. 2016;212[6]:1076-82). The study found that the prevalence of negative appendectomy decreased from 4.5% to 2.8% in California from 2005 to 2011, while the prevalence of perforated appendicitis decreased from 23.1% to 21.7%
To examine this issue, Dr. Mock and his associates analyzed information from a statewide California inpatient database, focusing on 180,958 adult appendectomy admissions during a 6-year period. Compared with nonperforated appendectomy, negative appendectomy required an additional 0.8 days in length of stay, was associated with greater morbidity, and cost approximately $1,063 more per patient. Rates of negative appendectomy also did not correlate with rates of appendiceal perforation, so negative appendectomy cannot be said to prevent what otherwise would have been a ruptured appendix.
“Consequently, negative appendectomy should no longer be thought of as a benign procedure,” the investigators said.
It is important to note that patients who undergo negative appendectomy likely have other disease processes underlying their signs and symptoms, and they likely require longer hospitalization and incur greater morbidity and costs to identify and treat these alternative disorders. In contrast, patients who undergo routine appendectomy usually are discharged home the same day, Dr. Mock and his associates added.
This researchers had no financial relationships or sources of support in the form of grants, equipment, or drugs. Dr. Mock and his associates reported having no relevant conflicts of interest.
Among adults, “negative” appendectomy, or appendectomy in which the surgeon discovers there is no appendicitis, is associated with a prolonged hospital stay, greater morbidity, and higher costs than is curative nonperforated appendectomy, according to a report in the American Journal of Surgery.
“Many argue that negative appendectomy is justified to decrease the risk of perforated appendicitis, as it has been accepted that an inverse relationship exists between the rates of negative appendectomy and perforated appendicitis. However, with the increasing prevalence of preoperative imaging, the rate of negative appendectomy has been decreasing, whereas the rate of perforated appendicitis has remained largely the same,” said Kyle Mock, MD, of the department of surgery, Harbor-University of California Los Angeles Medical Center, and his associates (Am J Surg. 2016;212[6]:1076-82). The study found that the prevalence of negative appendectomy decreased from 4.5% to 2.8% in California from 2005 to 2011, while the prevalence of perforated appendicitis decreased from 23.1% to 21.7%
To examine this issue, Dr. Mock and his associates analyzed information from a statewide California inpatient database, focusing on 180,958 adult appendectomy admissions during a 6-year period. Compared with nonperforated appendectomy, negative appendectomy required an additional 0.8 days in length of stay, was associated with greater morbidity, and cost approximately $1,063 more per patient. Rates of negative appendectomy also did not correlate with rates of appendiceal perforation, so negative appendectomy cannot be said to prevent what otherwise would have been a ruptured appendix.
“Consequently, negative appendectomy should no longer be thought of as a benign procedure,” the investigators said.
It is important to note that patients who undergo negative appendectomy likely have other disease processes underlying their signs and symptoms, and they likely require longer hospitalization and incur greater morbidity and costs to identify and treat these alternative disorders. In contrast, patients who undergo routine appendectomy usually are discharged home the same day, Dr. Mock and his associates added.
This researchers had no financial relationships or sources of support in the form of grants, equipment, or drugs. Dr. Mock and his associates reported having no relevant conflicts of interest.
Key clinical point: In adults, “negative” appendectomy – appendectomy in which the surgeon discovers there is no appendicitis – is associated with longer length of stay, higher morbidity, and higher costs than curative appendectomy.
Major finding: Compared with nonperforated appendectomy, negative appendectomy required an additional 0.8 days in length of stay, was associated with greater morbidity, and cost approximately $1,063 more per patient.
Data source: An analysis of information regarding 180,958 appendectomies performed during a 6-year period and detailed in a state (California) inpatient database.
Disclosures: The researchers had no financial relationships or sources of support in the form of grants, equipment, or drugs. Dr. Mock and his associates reported having no relevant conflicts of interest.