User login
Official Newspaper of the American College of Surgeons
NET can benefit breast cancer patients with delayed surgery
SEATTLE – A short course of neoadjuvant therapy could be considered in breast cancer patients with expected delays to resection, while they are awaiting surgery, according to study findings presented at the annual Society of Surgical Oncology Cancer Symposium.
More than half of breast cancer patients who undergo surgical resection as the initial modality will experience delays to surgery of more than 4 weeks. Of this group, more than half of patients receive shorter than standard courses of neoadjuvant therapy (NET), and the patients most likely to benefit were those older than 50 years, with ductal tumors, and the effect was seen in all T stages.

Recent reports show that NET is increasing. However, Dr. De Andrade pointed out, delays in receiving surgery remain a problem in breast cancer treatment and are associated with worse overall and cancer specific survival.
“Off-label use of NET is sometimes used in patients undergoing surgical delays,” he said.
NET use for 3 months has been associated with decreasing the size of tumors in patients with hormone receptor–positive (HR+) invasive breast cancer and allowing for breast conservation therapy. While short-term NET is sometimes used in women who are experiencing delay to surgery, the incidence and efficacy of this regimen remains undefined.
In the current study, Dr. De Andrade and his colleagues sought to answer three clinical questions:
• How long are patients with operable breast cancer waiting to undergo surgery?
• What is the pattern of use of short-course NET?
• What are the effects of short-course NET on outcomes?
The investigators used the National Cancer Database (NCDB) to identify women who had undergone surgery for stage 1-3 HR+ invasive breast cancer from 2004 to 2013. A total of 530,009 patients met inclusion criteria.
The primary outcomes of the study were time to surgery, the duration of NET, and if the pathologic stage at surgery was lower than clinical stage.
Among patients who did not receive NET, 49.3% underwent surgery within 30 days of diagnosis. More than a third (37.2%) underwent surgery within 60 days of diagnosis, and 13.5% did not have surgery until more than 60 days after their initial diagnosis. A total of 1.8% (9,664) patients underwent NET.
When looking at NET duration, 48% underwent NET for 12 or more weeks, while 52% received NET for less than 12 weeks; 27% received NET for less than 4 weeks, 17% for 4-8 weeks, and 9% for 8-12 weeks.
Downstaging from clinical stage to final pathology stage increased with longer duration of NET. It was 5.5% for less than 1 month on therapy, 9.7% for 1-2 months, and 17.2% for 2-3 months.
“For less than 4 weeks, there was no improvement in N or T downstaging,” said Dr. De Andrade. “As the amount of time on NET increased, it was associated with greater T downstaging. But for N downstaging, it was only at the standard of 12 or more weeks that a difference was seen in nodal downstaging.”
Standard NET of 12 or more weeks was associated with reduced mastectomy rates, but mastectomy rates were not lower in short-course NET.
Among patients undergoing breast conservation therapy, longer duration NET was also associated with a lower risk for re-excision (1-2 months: odds ratio, 0.82, P = .02; 2-3 months: OR, 0.40, P < .001). There was no reduction in re-excision for shorter courses of therapy.
Dr. De Andrade had no disclosures.
SEATTLE – A short course of neoadjuvant therapy could be considered in breast cancer patients with expected delays to resection, while they are awaiting surgery, according to study findings presented at the annual Society of Surgical Oncology Cancer Symposium.
More than half of breast cancer patients who undergo surgical resection as the initial modality will experience delays to surgery of more than 4 weeks. Of this group, more than half of patients receive shorter than standard courses of neoadjuvant therapy (NET), and the patients most likely to benefit were those older than 50 years, with ductal tumors, and the effect was seen in all T stages.
Recent reports show that NET is increasing. However, Dr. De Andrade pointed out, delays in receiving surgery remain a problem in breast cancer treatment and are associated with worse overall and cancer specific survival.
“Off-label use of NET is sometimes used in patients undergoing surgical delays,” he said.
NET use for 3 months has been associated with decreasing the size of tumors in patients with hormone receptor–positive (HR+) invasive breast cancer and allowing for breast conservation therapy. While short-term NET is sometimes used in women who are experiencing delay to surgery, the incidence and efficacy of this regimen remains undefined.
In the current study, Dr. De Andrade and his colleagues sought to answer three clinical questions:
• How long are patients with operable breast cancer waiting to undergo surgery?
• What is the pattern of use of short-course NET?
• What are the effects of short-course NET on outcomes?
The investigators used the National Cancer Database (NCDB) to identify women who had undergone surgery for stage 1-3 HR+ invasive breast cancer from 2004 to 2013. A total of 530,009 patients met inclusion criteria.
The primary outcomes of the study were time to surgery, the duration of NET, and if the pathologic stage at surgery was lower than clinical stage.
Among patients who did not receive NET, 49.3% underwent surgery within 30 days of diagnosis. More than a third (37.2%) underwent surgery within 60 days of diagnosis, and 13.5% did not have surgery until more than 60 days after their initial diagnosis. A total of 1.8% (9,664) patients underwent NET.
When looking at NET duration, 48% underwent NET for 12 or more weeks, while 52% received NET for less than 12 weeks; 27% received NET for less than 4 weeks, 17% for 4-8 weeks, and 9% for 8-12 weeks.
Downstaging from clinical stage to final pathology stage increased with longer duration of NET. It was 5.5% for less than 1 month on therapy, 9.7% for 1-2 months, and 17.2% for 2-3 months.
“For less than 4 weeks, there was no improvement in N or T downstaging,” said Dr. De Andrade. “As the amount of time on NET increased, it was associated with greater T downstaging. But for N downstaging, it was only at the standard of 12 or more weeks that a difference was seen in nodal downstaging.”
Standard NET of 12 or more weeks was associated with reduced mastectomy rates, but mastectomy rates were not lower in short-course NET.
Among patients undergoing breast conservation therapy, longer duration NET was also associated with a lower risk for re-excision (1-2 months: odds ratio, 0.82, P = .02; 2-3 months: OR, 0.40, P < .001). There was no reduction in re-excision for shorter courses of therapy.
Dr. De Andrade had no disclosures.
SEATTLE – A short course of neoadjuvant therapy could be considered in breast cancer patients with expected delays to resection, while they are awaiting surgery, according to study findings presented at the annual Society of Surgical Oncology Cancer Symposium.
More than half of breast cancer patients who undergo surgical resection as the initial modality will experience delays to surgery of more than 4 weeks. Of this group, more than half of patients receive shorter than standard courses of neoadjuvant therapy (NET), and the patients most likely to benefit were those older than 50 years, with ductal tumors, and the effect was seen in all T stages.
Recent reports show that NET is increasing. However, Dr. De Andrade pointed out, delays in receiving surgery remain a problem in breast cancer treatment and are associated with worse overall and cancer specific survival.
“Off-label use of NET is sometimes used in patients undergoing surgical delays,” he said.
NET use for 3 months has been associated with decreasing the size of tumors in patients with hormone receptor–positive (HR+) invasive breast cancer and allowing for breast conservation therapy. While short-term NET is sometimes used in women who are experiencing delay to surgery, the incidence and efficacy of this regimen remains undefined.
In the current study, Dr. De Andrade and his colleagues sought to answer three clinical questions:
• How long are patients with operable breast cancer waiting to undergo surgery?
• What is the pattern of use of short-course NET?
• What are the effects of short-course NET on outcomes?
The investigators used the National Cancer Database (NCDB) to identify women who had undergone surgery for stage 1-3 HR+ invasive breast cancer from 2004 to 2013. A total of 530,009 patients met inclusion criteria.
The primary outcomes of the study were time to surgery, the duration of NET, and if the pathologic stage at surgery was lower than clinical stage.
Among patients who did not receive NET, 49.3% underwent surgery within 30 days of diagnosis. More than a third (37.2%) underwent surgery within 60 days of diagnosis, and 13.5% did not have surgery until more than 60 days after their initial diagnosis. A total of 1.8% (9,664) patients underwent NET.
When looking at NET duration, 48% underwent NET for 12 or more weeks, while 52% received NET for less than 12 weeks; 27% received NET for less than 4 weeks, 17% for 4-8 weeks, and 9% for 8-12 weeks.
Downstaging from clinical stage to final pathology stage increased with longer duration of NET. It was 5.5% for less than 1 month on therapy, 9.7% for 1-2 months, and 17.2% for 2-3 months.
“For less than 4 weeks, there was no improvement in N or T downstaging,” said Dr. De Andrade. “As the amount of time on NET increased, it was associated with greater T downstaging. But for N downstaging, it was only at the standard of 12 or more weeks that a difference was seen in nodal downstaging.”
Standard NET of 12 or more weeks was associated with reduced mastectomy rates, but mastectomy rates were not lower in short-course NET.
Among patients undergoing breast conservation therapy, longer duration NET was also associated with a lower risk for re-excision (1-2 months: odds ratio, 0.82, P = .02; 2-3 months: OR, 0.40, P < .001). There was no reduction in re-excision for shorter courses of therapy.
Dr. De Andrade had no disclosures.
AT SSO 2017
Key clinical point: Short-course neoadjuvant therapy is an option for breast cancer patients with expected delays to surgery.
Major finding: Use of neoadjuvant therapy was associated with downstaging from clinical stage to final pathology stage and reducing re-excision in breast conservation surgery.
Data source: The National Cancer Database was used to identify 530,009 patients.
Disclosures: Dr. De Andrade had no disclosures.
Routine U.S. mitral clip use found reassuring
WASHINGTON – U.S. heart teams have used the mitral valve transcatheter clip repair device for fixing leaky mitral valves exactly the way it was designed to be used once the device hit the U.S. market in 2013.
In the first review of periprocedural and 1-year outcomes of U.S. patients treated with the MitraClip repair device and entered in the national device registry, the results showed “acute effectiveness and safety of transcatheter mitral valve repair,” Paul Sorajja, MD, said at the annual meeting of the American College of Cardiology.

“We need to be keenly aware of the impact of comorbidities on the prognosis of these patients. The data show that untreated comorbidities really impact prognosis,” said Dr. Sorajja, an interventional cardiologist and director of the Center of Valve and Structural Heart Disease of the Minneapolis Heart Institute.
“The clip is for the no-option patient, meaning patients at high risk who have no surgical option. The data show that these are the patients who are being treated” in routine U.S. practice. “The data show that, even for these patients, you can still get pretty good results,” Dr. Sorajja said in an interview. “These are the first data on clip use in routine U.S. practice, and they are really reassuring. The data show that the clip is being used in the correct way, without risk creep, on patients with prohibitive surgical risk based on their STS [Society of Thoracic Surgeons] predicted mortality and frailty scores.”
The data he and his associates reviewed came from the 2,952 U.S. patients who underwent a transcatheter mitral valve clip repair following the devices premarketing approval from the Food and Drug Administration in November 2013, and through September 2015 at any of 250 U.S. sites offering the procedure.
The data on patient demographics and clinical status came from the STS/American College of Cardiology Transcatheter Valve Therapy registry, and data on 1-year outcomes came from Medicare records for 1,867 (63%) of the patients.
The mitral valve repair patients averaged 82 years old, 85% had a New York Heart Association functional class of III or IV, 93% had a mitral valve regurgitation grade of 3 or 4, half were judged frail, and their STS predicted mortality risk from mitral valve repair was about 6% and from valve replacement about 9%.
Immediately after their procedure, 93% of patients had a valve regurgitation grade of 2 or less, the periprocedural mortality rate was just under 3%, and 86% of patients were discharged home following a median length of stay of 2 days. Acute procedural success occurred in 92% of patients, Dr. Sorajja reported.
At 1 year, the mortality rate among the patients followed through their Medicare records showed that 26% of patients had died, 20% had been hospitalized at least once for heart failure, and 38% had at least one of these two outcomes. In addition, 6% underwent a repeat procedure of transcatheter mitral repair, and 2% had mitral valve replacement surgery.
Although patients who had a successful repair with a residual regurgitation grade of 0 or 1 still had a substantial mortality rate of 22% during 1-year follow-up, survival was worse in patients with higher grades of residual mitral regurgitation. One-year mortality among those with residual grade 2 regurgitation was 29%, and for those with residual grade 3 or 4 regurgitation, 1-year mortality was 49%.
Many patients also had at least one comorbidity, and when these were present, 1-year survival was significantly worse. In a multivariate model, patients on dialysis had twofold greater mortality than did those not on dialysis, patients with severe tricuspid valve regurgitation had twice the mortality of those with lesser or no tricuspid regurgitation, and patients with moderate or severe lung disease had a 50% higher mortality, compared with those with milder or no lung disease.
The study was supported in part by Abbott Vascular, the company that markets the MitraClip. Dr. Sorajja has been a consultant to and speaker on behalf of Abbott Vascular. He has also been a consultant to Integer, Lake Region Medical, and Medtronic, and a speaker on behalf of Boston Scientific.
[email protected]
On Twitter @mitchelzoler
WASHINGTON – U.S. heart teams have used the mitral valve transcatheter clip repair device for fixing leaky mitral valves exactly the way it was designed to be used once the device hit the U.S. market in 2013.
In the first review of periprocedural and 1-year outcomes of U.S. patients treated with the MitraClip repair device and entered in the national device registry, the results showed “acute effectiveness and safety of transcatheter mitral valve repair,” Paul Sorajja, MD, said at the annual meeting of the American College of Cardiology.
“We need to be keenly aware of the impact of comorbidities on the prognosis of these patients. The data show that untreated comorbidities really impact prognosis,” said Dr. Sorajja, an interventional cardiologist and director of the Center of Valve and Structural Heart Disease of the Minneapolis Heart Institute.
“The clip is for the no-option patient, meaning patients at high risk who have no surgical option. The data show that these are the patients who are being treated” in routine U.S. practice. “The data show that, even for these patients, you can still get pretty good results,” Dr. Sorajja said in an interview. “These are the first data on clip use in routine U.S. practice, and they are really reassuring. The data show that the clip is being used in the correct way, without risk creep, on patients with prohibitive surgical risk based on their STS [Society of Thoracic Surgeons] predicted mortality and frailty scores.”
The data he and his associates reviewed came from the 2,952 U.S. patients who underwent a transcatheter mitral valve clip repair following the devices premarketing approval from the Food and Drug Administration in November 2013, and through September 2015 at any of 250 U.S. sites offering the procedure.
The data on patient demographics and clinical status came from the STS/American College of Cardiology Transcatheter Valve Therapy registry, and data on 1-year outcomes came from Medicare records for 1,867 (63%) of the patients.
The mitral valve repair patients averaged 82 years old, 85% had a New York Heart Association functional class of III or IV, 93% had a mitral valve regurgitation grade of 3 or 4, half were judged frail, and their STS predicted mortality risk from mitral valve repair was about 6% and from valve replacement about 9%.
Immediately after their procedure, 93% of patients had a valve regurgitation grade of 2 or less, the periprocedural mortality rate was just under 3%, and 86% of patients were discharged home following a median length of stay of 2 days. Acute procedural success occurred in 92% of patients, Dr. Sorajja reported.
At 1 year, the mortality rate among the patients followed through their Medicare records showed that 26% of patients had died, 20% had been hospitalized at least once for heart failure, and 38% had at least one of these two outcomes. In addition, 6% underwent a repeat procedure of transcatheter mitral repair, and 2% had mitral valve replacement surgery.
Although patients who had a successful repair with a residual regurgitation grade of 0 or 1 still had a substantial mortality rate of 22% during 1-year follow-up, survival was worse in patients with higher grades of residual mitral regurgitation. One-year mortality among those with residual grade 2 regurgitation was 29%, and for those with residual grade 3 or 4 regurgitation, 1-year mortality was 49%.
Many patients also had at least one comorbidity, and when these were present, 1-year survival was significantly worse. In a multivariate model, patients on dialysis had twofold greater mortality than did those not on dialysis, patients with severe tricuspid valve regurgitation had twice the mortality of those with lesser or no tricuspid regurgitation, and patients with moderate or severe lung disease had a 50% higher mortality, compared with those with milder or no lung disease.
The study was supported in part by Abbott Vascular, the company that markets the MitraClip. Dr. Sorajja has been a consultant to and speaker on behalf of Abbott Vascular. He has also been a consultant to Integer, Lake Region Medical, and Medtronic, and a speaker on behalf of Boston Scientific.
[email protected]
On Twitter @mitchelzoler
WASHINGTON – U.S. heart teams have used the mitral valve transcatheter clip repair device for fixing leaky mitral valves exactly the way it was designed to be used once the device hit the U.S. market in 2013.
In the first review of periprocedural and 1-year outcomes of U.S. patients treated with the MitraClip repair device and entered in the national device registry, the results showed “acute effectiveness and safety of transcatheter mitral valve repair,” Paul Sorajja, MD, said at the annual meeting of the American College of Cardiology.
“We need to be keenly aware of the impact of comorbidities on the prognosis of these patients. The data show that untreated comorbidities really impact prognosis,” said Dr. Sorajja, an interventional cardiologist and director of the Center of Valve and Structural Heart Disease of the Minneapolis Heart Institute.
“The clip is for the no-option patient, meaning patients at high risk who have no surgical option. The data show that these are the patients who are being treated” in routine U.S. practice. “The data show that, even for these patients, you can still get pretty good results,” Dr. Sorajja said in an interview. “These are the first data on clip use in routine U.S. practice, and they are really reassuring. The data show that the clip is being used in the correct way, without risk creep, on patients with prohibitive surgical risk based on their STS [Society of Thoracic Surgeons] predicted mortality and frailty scores.”
The data he and his associates reviewed came from the 2,952 U.S. patients who underwent a transcatheter mitral valve clip repair following the devices premarketing approval from the Food and Drug Administration in November 2013, and through September 2015 at any of 250 U.S. sites offering the procedure.
The data on patient demographics and clinical status came from the STS/American College of Cardiology Transcatheter Valve Therapy registry, and data on 1-year outcomes came from Medicare records for 1,867 (63%) of the patients.
The mitral valve repair patients averaged 82 years old, 85% had a New York Heart Association functional class of III or IV, 93% had a mitral valve regurgitation grade of 3 or 4, half were judged frail, and their STS predicted mortality risk from mitral valve repair was about 6% and from valve replacement about 9%.
Immediately after their procedure, 93% of patients had a valve regurgitation grade of 2 or less, the periprocedural mortality rate was just under 3%, and 86% of patients were discharged home following a median length of stay of 2 days. Acute procedural success occurred in 92% of patients, Dr. Sorajja reported.
At 1 year, the mortality rate among the patients followed through their Medicare records showed that 26% of patients had died, 20% had been hospitalized at least once for heart failure, and 38% had at least one of these two outcomes. In addition, 6% underwent a repeat procedure of transcatheter mitral repair, and 2% had mitral valve replacement surgery.
Although patients who had a successful repair with a residual regurgitation grade of 0 or 1 still had a substantial mortality rate of 22% during 1-year follow-up, survival was worse in patients with higher grades of residual mitral regurgitation. One-year mortality among those with residual grade 2 regurgitation was 29%, and for those with residual grade 3 or 4 regurgitation, 1-year mortality was 49%.
Many patients also had at least one comorbidity, and when these were present, 1-year survival was significantly worse. In a multivariate model, patients on dialysis had twofold greater mortality than did those not on dialysis, patients with severe tricuspid valve regurgitation had twice the mortality of those with lesser or no tricuspid regurgitation, and patients with moderate or severe lung disease had a 50% higher mortality, compared with those with milder or no lung disease.
The study was supported in part by Abbott Vascular, the company that markets the MitraClip. Dr. Sorajja has been a consultant to and speaker on behalf of Abbott Vascular. He has also been a consultant to Integer, Lake Region Medical, and Medtronic, and a speaker on behalf of Boston Scientific.
[email protected]
On Twitter @mitchelzoler
AT ACC 17
Key clinical point:
Major finding: U.S. mitral clip patients averaged 82 years of age, their acute success rate was 92%, and 1-year mortality was 26%.
Data source: A review of 2,952 U.S. patients who underwent transcatheter mitral clip repair and entered into the STS/ACC/TVT registry through September 2015.
Disclosures: The study was supported in part by Abbott Vascular, the company that markets the MitraClip. Dr. Sorajja has been a consultant to and speaker on behalf of Abbott Vascular. He has also been a consultant to Integer, Lake Region Medical, and Medtronic, and a speaker on behalf of Boston Scientific.

Lightweight mesh reduces erosion risk after sacrocolpopexy
SAN ANTONIO – Compared with heavier mesh types, ultralightweight polypropylene (Restorelle Y) did not increase the risk of mesh erosion after sacrocolpopexy in a retrospective, case-control study.
Delayed–absorbable monofilament polydioxanone suture (PDS) also decreased the risk, compared with nonabsorbable braided suture (Ethibond Excel) for vaginal mesh attachment.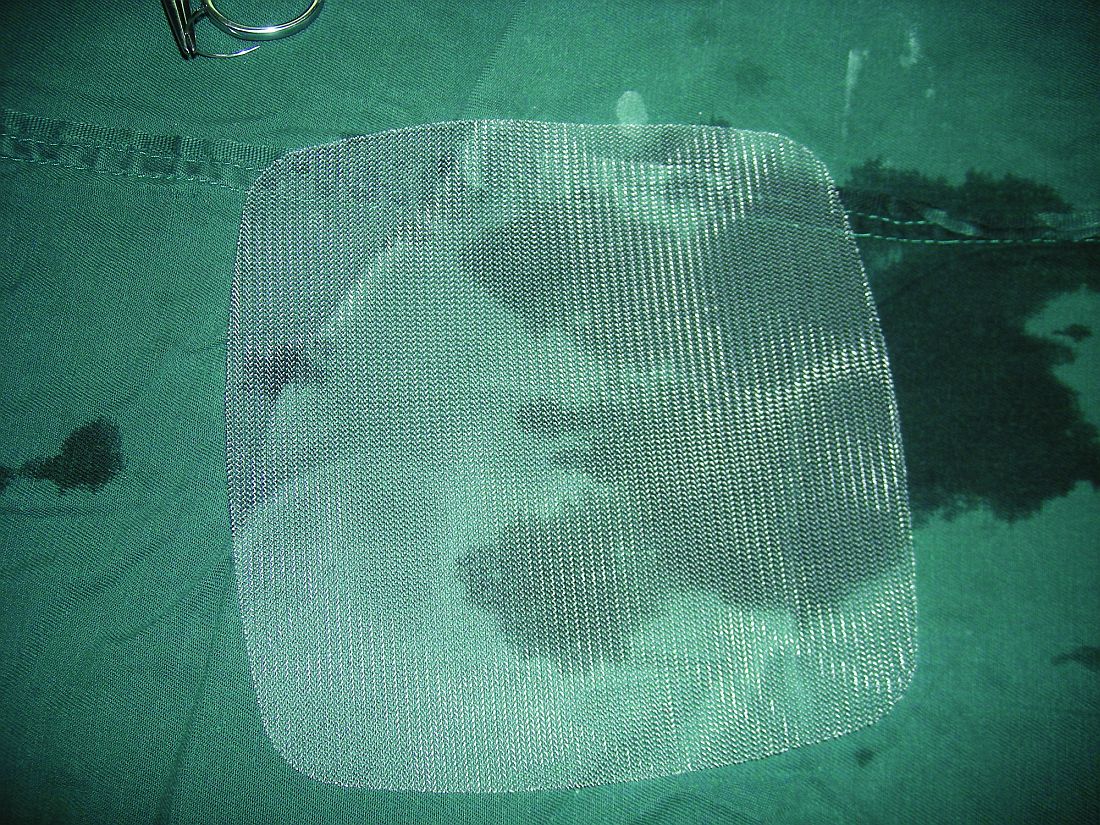
The odds ratio for the ultralightweight polypropylene mesh exposure, versus heavier mesh, was not statistically significant (odds ratio, 2.18; 95% confidence interval, 0.33-14.57), which led to the main study conclusion.
“Mesh choice and suture selection [are] important independent predictors of” erosion, she said at the annual scientific meeting of the Society of Gynecologic Surgeons. “Based on this study, surgeons should consider use of [PDS over nonabsorbable braided suture] to reduce the risk of mesh exposure when using ultralightweight mesh.”
The team also found that prior surgery for incontinence, as well as immediate postoperative complications, which likely impede healing, increase erosion risk. The findings are useful in counseling patients and perhaps guiding follow-up, at least early on. Most of the 133 erosions in the study – out of 1,247 sacrocolpopexies performed at the university from 2003 to2013 – occurred in the first year, usually in the first 3 months.
The 133 women with erosions were randomly matched with 261 women who did not have erosions after sacrocolpopexy. The erosion rate hovered around 9.5% for most years. They shot up to 19% in 2006, the first year of robot-assisted sacrocolpopexies and fell to about 6% in 2011, 4% in 2012, and 2% in 2013, when surgeons started using the ultralightweight mesh.
“Our study also confirmed several known risk factors,” Dr. Durst said, including smoking, stage IV prolapse, nonabsorbable braided suture, and heavyweight polypropylene mesh.
On multivariate regression, prior surgery for incontinence (OR, 2.87; 95% CI, 1.19-6.96), porcine acellular collagen matrix with soft polypropylene mesh (Pelvicol with soft Prolene, OR, 4.95; 95% CI, 1.70-14.42), other polypropylene mesh (OR, 6.73; 95% CI, 1.12-40.63); braided suture for vaginal mesh attachment (OR, 4.52; 95% CI, 1.53-13.37), and immediate perioperative complications (OR, 1.04; 95% CI, 1.58-8.43) all remained independent risk factors for mesh exposure, as did duration of follow-up (OR, 1.04; 95% CI, 1.03-1.06).
There was no industry funding for the study, and the investigators reported having no financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
SAN ANTONIO – Compared with heavier mesh types, ultralightweight polypropylene (Restorelle Y) did not increase the risk of mesh erosion after sacrocolpopexy in a retrospective, case-control study.
Delayed–absorbable monofilament polydioxanone suture (PDS) also decreased the risk, compared with nonabsorbable braided suture (Ethibond Excel) for vaginal mesh attachment.
The odds ratio for the ultralightweight polypropylene mesh exposure, versus heavier mesh, was not statistically significant (odds ratio, 2.18; 95% confidence interval, 0.33-14.57), which led to the main study conclusion.
“Mesh choice and suture selection [are] important independent predictors of” erosion, she said at the annual scientific meeting of the Society of Gynecologic Surgeons. “Based on this study, surgeons should consider use of [PDS over nonabsorbable braided suture] to reduce the risk of mesh exposure when using ultralightweight mesh.”
The team also found that prior surgery for incontinence, as well as immediate postoperative complications, which likely impede healing, increase erosion risk. The findings are useful in counseling patients and perhaps guiding follow-up, at least early on. Most of the 133 erosions in the study – out of 1,247 sacrocolpopexies performed at the university from 2003 to2013 – occurred in the first year, usually in the first 3 months.
The 133 women with erosions were randomly matched with 261 women who did not have erosions after sacrocolpopexy. The erosion rate hovered around 9.5% for most years. They shot up to 19% in 2006, the first year of robot-assisted sacrocolpopexies and fell to about 6% in 2011, 4% in 2012, and 2% in 2013, when surgeons started using the ultralightweight mesh.
“Our study also confirmed several known risk factors,” Dr. Durst said, including smoking, stage IV prolapse, nonabsorbable braided suture, and heavyweight polypropylene mesh.
On multivariate regression, prior surgery for incontinence (OR, 2.87; 95% CI, 1.19-6.96), porcine acellular collagen matrix with soft polypropylene mesh (Pelvicol with soft Prolene, OR, 4.95; 95% CI, 1.70-14.42), other polypropylene mesh (OR, 6.73; 95% CI, 1.12-40.63); braided suture for vaginal mesh attachment (OR, 4.52; 95% CI, 1.53-13.37), and immediate perioperative complications (OR, 1.04; 95% CI, 1.58-8.43) all remained independent risk factors for mesh exposure, as did duration of follow-up (OR, 1.04; 95% CI, 1.03-1.06).
There was no industry funding for the study, and the investigators reported having no financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
SAN ANTONIO – Compared with heavier mesh types, ultralightweight polypropylene (Restorelle Y) did not increase the risk of mesh erosion after sacrocolpopexy in a retrospective, case-control study.
Delayed–absorbable monofilament polydioxanone suture (PDS) also decreased the risk, compared with nonabsorbable braided suture (Ethibond Excel) for vaginal mesh attachment.
The odds ratio for the ultralightweight polypropylene mesh exposure, versus heavier mesh, was not statistically significant (odds ratio, 2.18; 95% confidence interval, 0.33-14.57), which led to the main study conclusion.
“Mesh choice and suture selection [are] important independent predictors of” erosion, she said at the annual scientific meeting of the Society of Gynecologic Surgeons. “Based on this study, surgeons should consider use of [PDS over nonabsorbable braided suture] to reduce the risk of mesh exposure when using ultralightweight mesh.”
The team also found that prior surgery for incontinence, as well as immediate postoperative complications, which likely impede healing, increase erosion risk. The findings are useful in counseling patients and perhaps guiding follow-up, at least early on. Most of the 133 erosions in the study – out of 1,247 sacrocolpopexies performed at the university from 2003 to2013 – occurred in the first year, usually in the first 3 months.
The 133 women with erosions were randomly matched with 261 women who did not have erosions after sacrocolpopexy. The erosion rate hovered around 9.5% for most years. They shot up to 19% in 2006, the first year of robot-assisted sacrocolpopexies and fell to about 6% in 2011, 4% in 2012, and 2% in 2013, when surgeons started using the ultralightweight mesh.
“Our study also confirmed several known risk factors,” Dr. Durst said, including smoking, stage IV prolapse, nonabsorbable braided suture, and heavyweight polypropylene mesh.
On multivariate regression, prior surgery for incontinence (OR, 2.87; 95% CI, 1.19-6.96), porcine acellular collagen matrix with soft polypropylene mesh (Pelvicol with soft Prolene, OR, 4.95; 95% CI, 1.70-14.42), other polypropylene mesh (OR, 6.73; 95% CI, 1.12-40.63); braided suture for vaginal mesh attachment (OR, 4.52; 95% CI, 1.53-13.37), and immediate perioperative complications (OR, 1.04; 95% CI, 1.58-8.43) all remained independent risk factors for mesh exposure, as did duration of follow-up (OR, 1.04; 95% CI, 1.03-1.06).
There was no industry funding for the study, and the investigators reported having no financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
AT SGS 2017
Key clinical point:
Major finding: The odds ratio for ultralightweight polypropylene (Restorelle Y) exposure, versus heavier polypropylene mesh, was not statistically significant (OR, 2.18; 95% CI, 0.33-14.57).
Data source: A single-center study matching 133 erosion cases to 261 controls.
Disclosures: There was no industry funding of the study, and the investigators reported no financial disclosures.
Transanal TME comparable to open, lap approaches to rectal cancer
HOUSTON – Transanal total mesorectal excision can consistently achieve good pathological results for obtaining specimens in rectal cancer, and overcome the shortcomings of the open and laparoscopic approaches to rectal cancer surgery, particularly in the distal part of the rectum where obtaining quality specimens can be technically challenging, researchers at the Hospital Clinic of Barcelona have found.
Reporting at the annual meeting of the Society of American Gastrointestinal and Endoscopic Surgeons, Jacqueline van Laarhoven, MD, PhD, said, “Pathologically, transanal total mesorectal excision [TME] provides good results on integrity of the mesorectum, negative circumferential and distal resection margins, and lymph nodes per specimen.” This study represents the first results of a relatively large, single-institution cohort, Dr. van Laarhoven said.

The study involved 187 patients with mid- or low-rectal cancer who had transanal TME from November 2011 to June 2016. Dr. van Laarhoven explained that obtaining high-quality specimens is an important prognostic factor for determining locoregional recurrence in rectal cancer. The study analyzed results of excised specimens in the mesorectum, circumferential and distal resected margins, and lymph nodes, and compared outcomes with those in two randomized clinical trials of both open and laparoscopic TME – the COLOR II (Lancet Oncol. 2013;14:210-8) and COREAN trials (Lancet Oncol. 2014;15:767-74) – where applicable.
In the Barcelona study population, 63.1% had tumors in the midrectum and 36.9% in the low rectum. Transanal TME yielded complete mesorectal quality in 95.7% of cases, almost-complete quality in 1.6% and incomplete in 1.1%, but comparison with COLOR II and COREAN trials was difficult because of differing inclusion criteria, Dr. van Laarhoven said.
Mean distal margin was 2.1 cm in midrectal cancer with a positive distal resection margin in 3.2%. In low-rectal cancer, the mean distal margin was 1.1 cm with a positive distal resection margin in 7.8%. Dr. van Laarhoven noted the overall circumferential resection margin (CRM) was 8.6% in this study, compared with 8.3% overall for the COREAN trial. As for COLOR II, the overall rate for positive CRM in mid- and low-rectal tumors was around 9%, Dr. van Laarhoven said, but in the open group the positive CRM was 3% in the midrectal excisions and 22% in low-rectal disease.
With regard to lymph nodes, the Barcelona study reported a median of 14 per specimen, with a range of 11 to 18, Dr. van Laarhoven said. However, in nonirradiated patients, the median was 15 per specimen. “This is consistent with the fact that neoadjuvant radiotherapy leads to a decrease in the lymph-node harvest,” she said. “These results are comparable to the COREAN and the COLOR II trials.”
Sixty-two percent of patients received neoadjuvant chemoradiotherapy, 3.2% received radiotherapy only, and 2.1% chemotherapy only.
On preoperative staging, 3.2% had T1 tumors, 20.3% T2, 67.9% T3, and 7.5% T4. The overall positive CRM (less than 1 mm) was 8.6% (including T4 tumors).
Postoperative pathological staging showed complete remission in 16% of patients, pT1 in 6.4%, pT2 in 28.9%, pT3 in 42.8%, pT4 in 2.7%, and pTis in 1.6%.
Dr. van Laarhoven commented, “As the quality of the surgical treatment is a surrogate marker for survival, transanal TME can be regarded as an oncologically safe method to treat patients with rectal cancer.”
Dr. van Laarhoven reported having no financial disclosures.
HOUSTON – Transanal total mesorectal excision can consistently achieve good pathological results for obtaining specimens in rectal cancer, and overcome the shortcomings of the open and laparoscopic approaches to rectal cancer surgery, particularly in the distal part of the rectum where obtaining quality specimens can be technically challenging, researchers at the Hospital Clinic of Barcelona have found.
Reporting at the annual meeting of the Society of American Gastrointestinal and Endoscopic Surgeons, Jacqueline van Laarhoven, MD, PhD, said, “Pathologically, transanal total mesorectal excision [TME] provides good results on integrity of the mesorectum, negative circumferential and distal resection margins, and lymph nodes per specimen.” This study represents the first results of a relatively large, single-institution cohort, Dr. van Laarhoven said.
The study involved 187 patients with mid- or low-rectal cancer who had transanal TME from November 2011 to June 2016. Dr. van Laarhoven explained that obtaining high-quality specimens is an important prognostic factor for determining locoregional recurrence in rectal cancer. The study analyzed results of excised specimens in the mesorectum, circumferential and distal resected margins, and lymph nodes, and compared outcomes with those in two randomized clinical trials of both open and laparoscopic TME – the COLOR II (Lancet Oncol. 2013;14:210-8) and COREAN trials (Lancet Oncol. 2014;15:767-74) – where applicable.
In the Barcelona study population, 63.1% had tumors in the midrectum and 36.9% in the low rectum. Transanal TME yielded complete mesorectal quality in 95.7% of cases, almost-complete quality in 1.6% and incomplete in 1.1%, but comparison with COLOR II and COREAN trials was difficult because of differing inclusion criteria, Dr. van Laarhoven said.
Mean distal margin was 2.1 cm in midrectal cancer with a positive distal resection margin in 3.2%. In low-rectal cancer, the mean distal margin was 1.1 cm with a positive distal resection margin in 7.8%. Dr. van Laarhoven noted the overall circumferential resection margin (CRM) was 8.6% in this study, compared with 8.3% overall for the COREAN trial. As for COLOR II, the overall rate for positive CRM in mid- and low-rectal tumors was around 9%, Dr. van Laarhoven said, but in the open group the positive CRM was 3% in the midrectal excisions and 22% in low-rectal disease.
With regard to lymph nodes, the Barcelona study reported a median of 14 per specimen, with a range of 11 to 18, Dr. van Laarhoven said. However, in nonirradiated patients, the median was 15 per specimen. “This is consistent with the fact that neoadjuvant radiotherapy leads to a decrease in the lymph-node harvest,” she said. “These results are comparable to the COREAN and the COLOR II trials.”
Sixty-two percent of patients received neoadjuvant chemoradiotherapy, 3.2% received radiotherapy only, and 2.1% chemotherapy only.
On preoperative staging, 3.2% had T1 tumors, 20.3% T2, 67.9% T3, and 7.5% T4. The overall positive CRM (less than 1 mm) was 8.6% (including T4 tumors).
Postoperative pathological staging showed complete remission in 16% of patients, pT1 in 6.4%, pT2 in 28.9%, pT3 in 42.8%, pT4 in 2.7%, and pTis in 1.6%.
Dr. van Laarhoven commented, “As the quality of the surgical treatment is a surrogate marker for survival, transanal TME can be regarded as an oncologically safe method to treat patients with rectal cancer.”
Dr. van Laarhoven reported having no financial disclosures.
HOUSTON – Transanal total mesorectal excision can consistently achieve good pathological results for obtaining specimens in rectal cancer, and overcome the shortcomings of the open and laparoscopic approaches to rectal cancer surgery, particularly in the distal part of the rectum where obtaining quality specimens can be technically challenging, researchers at the Hospital Clinic of Barcelona have found.
Reporting at the annual meeting of the Society of American Gastrointestinal and Endoscopic Surgeons, Jacqueline van Laarhoven, MD, PhD, said, “Pathologically, transanal total mesorectal excision [TME] provides good results on integrity of the mesorectum, negative circumferential and distal resection margins, and lymph nodes per specimen.” This study represents the first results of a relatively large, single-institution cohort, Dr. van Laarhoven said.
The study involved 187 patients with mid- or low-rectal cancer who had transanal TME from November 2011 to June 2016. Dr. van Laarhoven explained that obtaining high-quality specimens is an important prognostic factor for determining locoregional recurrence in rectal cancer. The study analyzed results of excised specimens in the mesorectum, circumferential and distal resected margins, and lymph nodes, and compared outcomes with those in two randomized clinical trials of both open and laparoscopic TME – the COLOR II (Lancet Oncol. 2013;14:210-8) and COREAN trials (Lancet Oncol. 2014;15:767-74) – where applicable.
In the Barcelona study population, 63.1% had tumors in the midrectum and 36.9% in the low rectum. Transanal TME yielded complete mesorectal quality in 95.7% of cases, almost-complete quality in 1.6% and incomplete in 1.1%, but comparison with COLOR II and COREAN trials was difficult because of differing inclusion criteria, Dr. van Laarhoven said.
Mean distal margin was 2.1 cm in midrectal cancer with a positive distal resection margin in 3.2%. In low-rectal cancer, the mean distal margin was 1.1 cm with a positive distal resection margin in 7.8%. Dr. van Laarhoven noted the overall circumferential resection margin (CRM) was 8.6% in this study, compared with 8.3% overall for the COREAN trial. As for COLOR II, the overall rate for positive CRM in mid- and low-rectal tumors was around 9%, Dr. van Laarhoven said, but in the open group the positive CRM was 3% in the midrectal excisions and 22% in low-rectal disease.
With regard to lymph nodes, the Barcelona study reported a median of 14 per specimen, with a range of 11 to 18, Dr. van Laarhoven said. However, in nonirradiated patients, the median was 15 per specimen. “This is consistent with the fact that neoadjuvant radiotherapy leads to a decrease in the lymph-node harvest,” she said. “These results are comparable to the COREAN and the COLOR II trials.”
Sixty-two percent of patients received neoadjuvant chemoradiotherapy, 3.2% received radiotherapy only, and 2.1% chemotherapy only.
On preoperative staging, 3.2% had T1 tumors, 20.3% T2, 67.9% T3, and 7.5% T4. The overall positive CRM (less than 1 mm) was 8.6% (including T4 tumors).
Postoperative pathological staging showed complete remission in 16% of patients, pT1 in 6.4%, pT2 in 28.9%, pT3 in 42.8%, pT4 in 2.7%, and pTis in 1.6%.
Dr. van Laarhoven commented, “As the quality of the surgical treatment is a surrogate marker for survival, transanal TME can be regarded as an oncologically safe method to treat patients with rectal cancer.”
Dr. van Laarhoven reported having no financial disclosures.
AT SAGES 2017
Key clinical point: Transanal total mesorectal excision (TME) is a viable alternative to open or laparoscopic TME in cancers of the low and midrectum.
Major finding: Postoperative pathological staging showed complete remission in 16%, with pT1 in 6.4%, pT2 in 28.9%, pT3 in 42.8%, pT4 in 2.7%, and pTis in 1.6%.
Data source: Analysis of 187 patients prospectively enrolled in a standardized database who had transanal TME from November 2011 to June 2016 at a single center.
Disclosures: Dr. van Laarhoven reported having no financial disclosures.
Neoadjuvant chemoradiation may give transplant the edge over resection in biliary cancer
MIAMI BEACH – Survival for patients with hilar cholangiocarcinoma was similar between those who underwent transplantation and those who underwent resection, but neoadjuvant therapy may give transplant strategy the edge, findings of a study and meta-analysis suggest.
“Neoadjuvant chemoradiation therapy is clearly a factor that affects patient survival, and may be the only reason the patients who received transplantation had better overall survival than [did those who had] resection,” Michele Gage, MD, a general surgeon at Johns Hopkins Medicine in Baltimore, said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“We found survival in the group that received neoadjuvant chemoradiation therapy and transplant had a statistically significantly better outcome compared to a control group of resection,” Dr. Gage said. More importantly, patients who received a transplant without neoadjuvant therapy had a statistically significant worse outcome than patients who got resection alone.”
The investigators noted that patient selection for neoadjuvant therapy might also be a factor contributing to superior overall survival. In a multicenter study of 147 patients undergoing liver transplantation for hilar cholangiocarcinoma, a subgroup of patients who met the selection criteria of the Mayo Clinic protocol but had not undergone neoadjuvant therapy had a 59% 5-year survival rate (PLoS One. 2016:11:e0156127).
Study discussant Maria B. Majella Doyle, MD, a general surgeon at Washington University in St. Louis, agreed that patient selection for transplantation is a likely factor.
Dr. Doyle then asked Dr. Gage how she accounts for the heterogeneity among studies performed over a 20-year period.
“That is why we did subgroup analysis of neoadjuvant versus no neoadjuvant therapy,” Dr. Gage replied.
In the future, an intent-to-treat analysis might be more accurate, Dr. Majella Doyle said, because more patients are placed on a liver transplant list than typically have the procedure.
Dr. Gage noted that 28%-48% of patients started on neoadjuvant therapy in the two studies that offered both neoadjuvant therapy and a transplant in the meta-analysis never made it to transplantation. When they were included, overall survival dropped to approximately 35% in one study and 44% in the other.
In the primary meta-analysis (before the subanalysis looking at neoadjuvant therapy), 398 patients underwent resection and another 200 underwent liver transplantation between 1996 and 2106. Patient demographics were similar between groups, including more men than women, except the average age in the resection group was older, Dr. Gage said.
Overall survival favored the transplant group at each time point: 78% versus 70% with resection at 1 year; 56% versus 42% at 3 years; and 46% versus 29% at 5 years. The odds ratios, respectively, were 1.27, 1.49 and 1.83, but the findings were not statistically significant at a 95% confidence interval.
Margin involvement was 9% in the transplant patients versus 32% in the resection patients, Dr. Gage said. The best chance of cure is R0 resection, but half of patients with hilar cholangiocarcinoma, the most common cancer of the biliary tract, are unresectable, she added.
Six of the nine studies in the meta-analysis reported margin status. Of the 344 patients in these studies, 79% achieved R0 status overall.
“The goal of treatment is R0 resection,” Dr. Gage said in response to a question about when neoadjuvant therapy is warranted. “In the patients who are resectable, I think the correct answer would be to proceed with resection. However, for those patients who are borderline resectable, it would be reasonable to consider neoadjuvant therapy.”
“One of the major things that is undervalued is neoadjuvant therapy allows better patient selection,” said session moderator Eric Jensen, MD, FACS, of University of Minnesota Health in Minneapolis. “When you say an obviously resectable tumor, when you look at the data – we’re wrong 30% of the time. So I’m in favor of neoadjuvant therapy for everybody, but that is just my bias.”
The small number of studies is a limitation of the study, Dr. Gage said. Also, all the studies were nonrandomized and retrospective, and some research spanned many years, which could introduce bias because of changes in practice over time, she added.
Based on their findings, the investigators proposed that future studies explore routine administration of neoadjuvant therapy prior to resection.
Dr. Gage and Dr. Majella Doyle had no relevant financial disclosures.
MIAMI BEACH – Survival for patients with hilar cholangiocarcinoma was similar between those who underwent transplantation and those who underwent resection, but neoadjuvant therapy may give transplant strategy the edge, findings of a study and meta-analysis suggest.
“Neoadjuvant chemoradiation therapy is clearly a factor that affects patient survival, and may be the only reason the patients who received transplantation had better overall survival than [did those who had] resection,” Michele Gage, MD, a general surgeon at Johns Hopkins Medicine in Baltimore, said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“We found survival in the group that received neoadjuvant chemoradiation therapy and transplant had a statistically significantly better outcome compared to a control group of resection,” Dr. Gage said. More importantly, patients who received a transplant without neoadjuvant therapy had a statistically significant worse outcome than patients who got resection alone.”
The investigators noted that patient selection for neoadjuvant therapy might also be a factor contributing to superior overall survival. In a multicenter study of 147 patients undergoing liver transplantation for hilar cholangiocarcinoma, a subgroup of patients who met the selection criteria of the Mayo Clinic protocol but had not undergone neoadjuvant therapy had a 59% 5-year survival rate (PLoS One. 2016:11:e0156127).
Study discussant Maria B. Majella Doyle, MD, a general surgeon at Washington University in St. Louis, agreed that patient selection for transplantation is a likely factor.
Dr. Doyle then asked Dr. Gage how she accounts for the heterogeneity among studies performed over a 20-year period.
“That is why we did subgroup analysis of neoadjuvant versus no neoadjuvant therapy,” Dr. Gage replied.
In the future, an intent-to-treat analysis might be more accurate, Dr. Majella Doyle said, because more patients are placed on a liver transplant list than typically have the procedure.
Dr. Gage noted that 28%-48% of patients started on neoadjuvant therapy in the two studies that offered both neoadjuvant therapy and a transplant in the meta-analysis never made it to transplantation. When they were included, overall survival dropped to approximately 35% in one study and 44% in the other.
In the primary meta-analysis (before the subanalysis looking at neoadjuvant therapy), 398 patients underwent resection and another 200 underwent liver transplantation between 1996 and 2106. Patient demographics were similar between groups, including more men than women, except the average age in the resection group was older, Dr. Gage said.
Overall survival favored the transplant group at each time point: 78% versus 70% with resection at 1 year; 56% versus 42% at 3 years; and 46% versus 29% at 5 years. The odds ratios, respectively, were 1.27, 1.49 and 1.83, but the findings were not statistically significant at a 95% confidence interval.
Margin involvement was 9% in the transplant patients versus 32% in the resection patients, Dr. Gage said. The best chance of cure is R0 resection, but half of patients with hilar cholangiocarcinoma, the most common cancer of the biliary tract, are unresectable, she added.
Six of the nine studies in the meta-analysis reported margin status. Of the 344 patients in these studies, 79% achieved R0 status overall.
“The goal of treatment is R0 resection,” Dr. Gage said in response to a question about when neoadjuvant therapy is warranted. “In the patients who are resectable, I think the correct answer would be to proceed with resection. However, for those patients who are borderline resectable, it would be reasonable to consider neoadjuvant therapy.”
“One of the major things that is undervalued is neoadjuvant therapy allows better patient selection,” said session moderator Eric Jensen, MD, FACS, of University of Minnesota Health in Minneapolis. “When you say an obviously resectable tumor, when you look at the data – we’re wrong 30% of the time. So I’m in favor of neoadjuvant therapy for everybody, but that is just my bias.”
The small number of studies is a limitation of the study, Dr. Gage said. Also, all the studies were nonrandomized and retrospective, and some research spanned many years, which could introduce bias because of changes in practice over time, she added.
Based on their findings, the investigators proposed that future studies explore routine administration of neoadjuvant therapy prior to resection.
Dr. Gage and Dr. Majella Doyle had no relevant financial disclosures.
MIAMI BEACH – Survival for patients with hilar cholangiocarcinoma was similar between those who underwent transplantation and those who underwent resection, but neoadjuvant therapy may give transplant strategy the edge, findings of a study and meta-analysis suggest.
“Neoadjuvant chemoradiation therapy is clearly a factor that affects patient survival, and may be the only reason the patients who received transplantation had better overall survival than [did those who had] resection,” Michele Gage, MD, a general surgeon at Johns Hopkins Medicine in Baltimore, said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“We found survival in the group that received neoadjuvant chemoradiation therapy and transplant had a statistically significantly better outcome compared to a control group of resection,” Dr. Gage said. More importantly, patients who received a transplant without neoadjuvant therapy had a statistically significant worse outcome than patients who got resection alone.”
The investigators noted that patient selection for neoadjuvant therapy might also be a factor contributing to superior overall survival. In a multicenter study of 147 patients undergoing liver transplantation for hilar cholangiocarcinoma, a subgroup of patients who met the selection criteria of the Mayo Clinic protocol but had not undergone neoadjuvant therapy had a 59% 5-year survival rate (PLoS One. 2016:11:e0156127).
Study discussant Maria B. Majella Doyle, MD, a general surgeon at Washington University in St. Louis, agreed that patient selection for transplantation is a likely factor.
Dr. Doyle then asked Dr. Gage how she accounts for the heterogeneity among studies performed over a 20-year period.
“That is why we did subgroup analysis of neoadjuvant versus no neoadjuvant therapy,” Dr. Gage replied.
In the future, an intent-to-treat analysis might be more accurate, Dr. Majella Doyle said, because more patients are placed on a liver transplant list than typically have the procedure.
Dr. Gage noted that 28%-48% of patients started on neoadjuvant therapy in the two studies that offered both neoadjuvant therapy and a transplant in the meta-analysis never made it to transplantation. When they were included, overall survival dropped to approximately 35% in one study and 44% in the other.
In the primary meta-analysis (before the subanalysis looking at neoadjuvant therapy), 398 patients underwent resection and another 200 underwent liver transplantation between 1996 and 2106. Patient demographics were similar between groups, including more men than women, except the average age in the resection group was older, Dr. Gage said.
Overall survival favored the transplant group at each time point: 78% versus 70% with resection at 1 year; 56% versus 42% at 3 years; and 46% versus 29% at 5 years. The odds ratios, respectively, were 1.27, 1.49 and 1.83, but the findings were not statistically significant at a 95% confidence interval.
Margin involvement was 9% in the transplant patients versus 32% in the resection patients, Dr. Gage said. The best chance of cure is R0 resection, but half of patients with hilar cholangiocarcinoma, the most common cancer of the biliary tract, are unresectable, she added.
Six of the nine studies in the meta-analysis reported margin status. Of the 344 patients in these studies, 79% achieved R0 status overall.
“The goal of treatment is R0 resection,” Dr. Gage said in response to a question about when neoadjuvant therapy is warranted. “In the patients who are resectable, I think the correct answer would be to proceed with resection. However, for those patients who are borderline resectable, it would be reasonable to consider neoadjuvant therapy.”
“One of the major things that is undervalued is neoadjuvant therapy allows better patient selection,” said session moderator Eric Jensen, MD, FACS, of University of Minnesota Health in Minneapolis. “When you say an obviously resectable tumor, when you look at the data – we’re wrong 30% of the time. So I’m in favor of neoadjuvant therapy for everybody, but that is just my bias.”
The small number of studies is a limitation of the study, Dr. Gage said. Also, all the studies were nonrandomized and retrospective, and some research spanned many years, which could introduce bias because of changes in practice over time, she added.
Based on their findings, the investigators proposed that future studies explore routine administration of neoadjuvant therapy prior to resection.
Dr. Gage and Dr. Majella Doyle had no relevant financial disclosures.
AT AHPBA 2017
Predicting extraction of an intact uterus in robotic-assisted laparoscopic hysterectomy
SAN ANTONIO – Investigators at the University of Tennessee, Chattanooga, have come up with a simple scoring system to predict if an intact uterus can be delivered vaginally during laparoscopic hysterectomy.
Age greater than 50 years counts as 1 point and uterine length greater than 11 cm, height greater than 8 cm, and width greater than 6.9 cm each count for 3 points. A score of 4 or higher suggests the need for an alternative to vaginal extraction, they reported at the annual scientific meeting of the Society of Gynecologic Surgeons.

The team reviewed 367 robotic-assisted total laparoscopic hysterectomies. An intact uterus was able to be extracted vaginally in 265 cases (72%); minilaparotomy was used for the rest. Uterine length, height, and width were documented from pathology reports. The scoring system correctly classified 94.6% of the cases. Sensitivity was 85.3%, specificity was 98.1%, positive predictive value was 94.57%, and negative predictive value was 94.55%.
Factoring in parity, uterine weight, body mass index, procedure indications, tobacco use, and comorbidities did not statistically influence the predictive power.
Gynecologic surgeons “are trying to get specimens out intact” and want to know ahead of time if it’s possible, Dr. Mohling said. “I wanted to create a model that was very reproducible.”
The general benchmark for vaginal delivery of an intact uterus is size below 12 weeks pregnancy, but the University of Tennessee model is more precise, according to Dr. Mohling. “I’ve added this to my counseling,” she said.
There was no external funding for the work and the investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
SAN ANTONIO – Investigators at the University of Tennessee, Chattanooga, have come up with a simple scoring system to predict if an intact uterus can be delivered vaginally during laparoscopic hysterectomy.
Age greater than 50 years counts as 1 point and uterine length greater than 11 cm, height greater than 8 cm, and width greater than 6.9 cm each count for 3 points. A score of 4 or higher suggests the need for an alternative to vaginal extraction, they reported at the annual scientific meeting of the Society of Gynecologic Surgeons.
The team reviewed 367 robotic-assisted total laparoscopic hysterectomies. An intact uterus was able to be extracted vaginally in 265 cases (72%); minilaparotomy was used for the rest. Uterine length, height, and width were documented from pathology reports. The scoring system correctly classified 94.6% of the cases. Sensitivity was 85.3%, specificity was 98.1%, positive predictive value was 94.57%, and negative predictive value was 94.55%.
Factoring in parity, uterine weight, body mass index, procedure indications, tobacco use, and comorbidities did not statistically influence the predictive power.
Gynecologic surgeons “are trying to get specimens out intact” and want to know ahead of time if it’s possible, Dr. Mohling said. “I wanted to create a model that was very reproducible.”
The general benchmark for vaginal delivery of an intact uterus is size below 12 weeks pregnancy, but the University of Tennessee model is more precise, according to Dr. Mohling. “I’ve added this to my counseling,” she said.
There was no external funding for the work and the investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
SAN ANTONIO – Investigators at the University of Tennessee, Chattanooga, have come up with a simple scoring system to predict if an intact uterus can be delivered vaginally during laparoscopic hysterectomy.
Age greater than 50 years counts as 1 point and uterine length greater than 11 cm, height greater than 8 cm, and width greater than 6.9 cm each count for 3 points. A score of 4 or higher suggests the need for an alternative to vaginal extraction, they reported at the annual scientific meeting of the Society of Gynecologic Surgeons.
The team reviewed 367 robotic-assisted total laparoscopic hysterectomies. An intact uterus was able to be extracted vaginally in 265 cases (72%); minilaparotomy was used for the rest. Uterine length, height, and width were documented from pathology reports. The scoring system correctly classified 94.6% of the cases. Sensitivity was 85.3%, specificity was 98.1%, positive predictive value was 94.57%, and negative predictive value was 94.55%.
Factoring in parity, uterine weight, body mass index, procedure indications, tobacco use, and comorbidities did not statistically influence the predictive power.
Gynecologic surgeons “are trying to get specimens out intact” and want to know ahead of time if it’s possible, Dr. Mohling said. “I wanted to create a model that was very reproducible.”
The general benchmark for vaginal delivery of an intact uterus is size below 12 weeks pregnancy, but the University of Tennessee model is more precise, according to Dr. Mohling. “I’ve added this to my counseling,” she said.
There was no external funding for the work and the investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
AT SGS 2017
Key clinical point:
Major finding: The sensitivity of the scoring system was 85.3%, specificity was 98.1%, positive predictive value was 94.57%, and negative predictive value was 94.55%.
Data source: Single-center review of 367 robotic total laparoscopic hysterectomies during 2012-2015.
Disclosures: There was no external funding for the work, and the investigators reported having no relevant financial disclosures.
BRCA2 mutations linked to greater risk for pancreatic cancer
MIAMI BEACH – Although population-wide screening for pancreatic cancer is considered unfeasible and costly, new evidence suggests a benefit to screening a select population: people who test positive for BRCA2 genetic mutations.
Cross-sectional imaging of 117 people with BRCA2 mutations revealed pancreatic abnormalities in 10 patients, including a patient with pancreatic cancer whose only symptom was unexplained weight loss.
Pancreatic cancer is not as common as are some other malignancies, with an incidence estimated between 1% and 3%. However, it is a particularly deadly form of cancer, with only 7.7% of people living to 5 years after diagnosis, according to data from the National Cancer Institute.
A relatively low incidence is a good thing, but it also limits widespread screening. “There is a low predictive value of screening the population at large, and it is not considered cost effective,” said Eugene P. Ceppa, MD, a general surgeon at IU Health University Hospital, Indianapolis. However, patients at high risk for pancreatic adenocarcinoma might be worth targeting for screening, he added.

“This represents a 21% increase in the chance of pancreatic cancer in these patients,” Dr. Ceppa said.
Buoyed by these and other findings, Dr. Ceppa and his colleagues launched a study of their own. “Our hypothesis is that screening all BRCA2s would identify more patients with pancreatic cancer,” he said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
Dr. Ceppa and coinvestigators reviewed electronic medical records at their institution from 2005 to 2015. They identified 204 BRCA mutation carriers, and after excluding 87 BRCA1 positive patients, further assessed the 117 with documented BRCA2 mutations. A total 47 people (40%) of this group had undergone cross-sectional imaging. The images were initially reviewed, and then re-reviewed for the study, by radiologists with specific expertise in pancreatology.
The cross-sectional imaging revealed pancreatic abnormalities in 10 people, including 1 patient with a pancreatic ductal adenocarcinoma located in the head of the pancreas. Another nine patients had intraductal papillary mucinous neoplasms (IPMNs). There were no significant demographic or clinical differences between the groups of patients with and without the imaging abnormalities, Dr. Ceppa said.
The investigators also compared the patients with BRCA2 mutations against a historical cohort representing the general population. They found 21% of patients with BRCA2 had a defined pancreatic abnormality, compared with 8% in the general population. The difference was statistically significant (P = .007).
Interestingly, the same comparison also revealed a rate of IPMN of 19%, versus 1%, respectively (P less than .001). “BRCA2 mutation carriers have significantly higher incidence of IPMN than the general population,” Dr. Ceppa said.
The study results support a high-risk screening protocol in asymptomatic BRCA patients regardless of family history, he said. In fact, a high-risk screening protocol implemented at his institution in 2013 led to a 14% detection rate of pancreatic cancer among BRCA2-positive patients, compared with a 3% rate in the general population.
“Your most significant finding might be the more IPMN patients – but how do we follow them, and will it be cost effective?” asked invited discussant Matthew J. Weiss, MD, of Johns Hopkins Medicine in Baltimore.
One of the most notable impacts of instituting the high-risk screening protocol has been an increase in patient referrals from other specialists at Dr. Ceppa’s institution. “I’ve looked at every single breast surgeon in our department, and I know how each of them are referring,” he explained.
Following initial screening of BRCA2 mutation patients, Dr. Ceppa repeats screening at 6 months, 1 year, and then annually. “However, some insurers may balk at our recommendations for frequency of screening,” he noted.
Dr. Ceppa and Dr. Weiss had no relevant financial disclosures.
MIAMI BEACH – Although population-wide screening for pancreatic cancer is considered unfeasible and costly, new evidence suggests a benefit to screening a select population: people who test positive for BRCA2 genetic mutations.
Cross-sectional imaging of 117 people with BRCA2 mutations revealed pancreatic abnormalities in 10 patients, including a patient with pancreatic cancer whose only symptom was unexplained weight loss.
Pancreatic cancer is not as common as are some other malignancies, with an incidence estimated between 1% and 3%. However, it is a particularly deadly form of cancer, with only 7.7% of people living to 5 years after diagnosis, according to data from the National Cancer Institute.
A relatively low incidence is a good thing, but it also limits widespread screening. “There is a low predictive value of screening the population at large, and it is not considered cost effective,” said Eugene P. Ceppa, MD, a general surgeon at IU Health University Hospital, Indianapolis. However, patients at high risk for pancreatic adenocarcinoma might be worth targeting for screening, he added.
“This represents a 21% increase in the chance of pancreatic cancer in these patients,” Dr. Ceppa said.
Buoyed by these and other findings, Dr. Ceppa and his colleagues launched a study of their own. “Our hypothesis is that screening all BRCA2s would identify more patients with pancreatic cancer,” he said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
Dr. Ceppa and coinvestigators reviewed electronic medical records at their institution from 2005 to 2015. They identified 204 BRCA mutation carriers, and after excluding 87 BRCA1 positive patients, further assessed the 117 with documented BRCA2 mutations. A total 47 people (40%) of this group had undergone cross-sectional imaging. The images were initially reviewed, and then re-reviewed for the study, by radiologists with specific expertise in pancreatology.
The cross-sectional imaging revealed pancreatic abnormalities in 10 people, including 1 patient with a pancreatic ductal adenocarcinoma located in the head of the pancreas. Another nine patients had intraductal papillary mucinous neoplasms (IPMNs). There were no significant demographic or clinical differences between the groups of patients with and without the imaging abnormalities, Dr. Ceppa said.
The investigators also compared the patients with BRCA2 mutations against a historical cohort representing the general population. They found 21% of patients with BRCA2 had a defined pancreatic abnormality, compared with 8% in the general population. The difference was statistically significant (P = .007).
Interestingly, the same comparison also revealed a rate of IPMN of 19%, versus 1%, respectively (P less than .001). “BRCA2 mutation carriers have significantly higher incidence of IPMN than the general population,” Dr. Ceppa said.
The study results support a high-risk screening protocol in asymptomatic BRCA patients regardless of family history, he said. In fact, a high-risk screening protocol implemented at his institution in 2013 led to a 14% detection rate of pancreatic cancer among BRCA2-positive patients, compared with a 3% rate in the general population.
“Your most significant finding might be the more IPMN patients – but how do we follow them, and will it be cost effective?” asked invited discussant Matthew J. Weiss, MD, of Johns Hopkins Medicine in Baltimore.
One of the most notable impacts of instituting the high-risk screening protocol has been an increase in patient referrals from other specialists at Dr. Ceppa’s institution. “I’ve looked at every single breast surgeon in our department, and I know how each of them are referring,” he explained.
Following initial screening of BRCA2 mutation patients, Dr. Ceppa repeats screening at 6 months, 1 year, and then annually. “However, some insurers may balk at our recommendations for frequency of screening,” he noted.
Dr. Ceppa and Dr. Weiss had no relevant financial disclosures.
MIAMI BEACH – Although population-wide screening for pancreatic cancer is considered unfeasible and costly, new evidence suggests a benefit to screening a select population: people who test positive for BRCA2 genetic mutations.
Cross-sectional imaging of 117 people with BRCA2 mutations revealed pancreatic abnormalities in 10 patients, including a patient with pancreatic cancer whose only symptom was unexplained weight loss.
Pancreatic cancer is not as common as are some other malignancies, with an incidence estimated between 1% and 3%. However, it is a particularly deadly form of cancer, with only 7.7% of people living to 5 years after diagnosis, according to data from the National Cancer Institute.
A relatively low incidence is a good thing, but it also limits widespread screening. “There is a low predictive value of screening the population at large, and it is not considered cost effective,” said Eugene P. Ceppa, MD, a general surgeon at IU Health University Hospital, Indianapolis. However, patients at high risk for pancreatic adenocarcinoma might be worth targeting for screening, he added.
“This represents a 21% increase in the chance of pancreatic cancer in these patients,” Dr. Ceppa said.
Buoyed by these and other findings, Dr. Ceppa and his colleagues launched a study of their own. “Our hypothesis is that screening all BRCA2s would identify more patients with pancreatic cancer,” he said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
Dr. Ceppa and coinvestigators reviewed electronic medical records at their institution from 2005 to 2015. They identified 204 BRCA mutation carriers, and after excluding 87 BRCA1 positive patients, further assessed the 117 with documented BRCA2 mutations. A total 47 people (40%) of this group had undergone cross-sectional imaging. The images were initially reviewed, and then re-reviewed for the study, by radiologists with specific expertise in pancreatology.
The cross-sectional imaging revealed pancreatic abnormalities in 10 people, including 1 patient with a pancreatic ductal adenocarcinoma located in the head of the pancreas. Another nine patients had intraductal papillary mucinous neoplasms (IPMNs). There were no significant demographic or clinical differences between the groups of patients with and without the imaging abnormalities, Dr. Ceppa said.
The investigators also compared the patients with BRCA2 mutations against a historical cohort representing the general population. They found 21% of patients with BRCA2 had a defined pancreatic abnormality, compared with 8% in the general population. The difference was statistically significant (P = .007).
Interestingly, the same comparison also revealed a rate of IPMN of 19%, versus 1%, respectively (P less than .001). “BRCA2 mutation carriers have significantly higher incidence of IPMN than the general population,” Dr. Ceppa said.
The study results support a high-risk screening protocol in asymptomatic BRCA patients regardless of family history, he said. In fact, a high-risk screening protocol implemented at his institution in 2013 led to a 14% detection rate of pancreatic cancer among BRCA2-positive patients, compared with a 3% rate in the general population.
“Your most significant finding might be the more IPMN patients – but how do we follow them, and will it be cost effective?” asked invited discussant Matthew J. Weiss, MD, of Johns Hopkins Medicine in Baltimore.
One of the most notable impacts of instituting the high-risk screening protocol has been an increase in patient referrals from other specialists at Dr. Ceppa’s institution. “I’ve looked at every single breast surgeon in our department, and I know how each of them are referring,” he explained.
Following initial screening of BRCA2 mutation patients, Dr. Ceppa repeats screening at 6 months, 1 year, and then annually. “However, some insurers may balk at our recommendations for frequency of screening,” he noted.
Dr. Ceppa and Dr. Weiss had no relevant financial disclosures.
Key clinical point: Although general population screening for pancreatic cancer is considered costly, with a low predictive value, targeting screening to patients with BRCA2 mutations could detect more cases of this deadly disease.
Major finding: People with BRCA2 mutations had a significantly greater incidence of intraductal papillary mucinous neoplasms, 19%, versus 1% in the general population (P less than .001).
Data source: Retrospective study of electronic medical records of 117 patients with BRCA2 mutations at a single academic institution.
Disclosures: Dr. Ceppa and Dr. Weiss had no relevant financial disclosures.
Does laparoscopy have an advantage for emergency VHR?
HOUSTON – The benefits of elective laparoscopic ventral hernia repair over the open approach have been well documented, but, when presented with emergency cases, surgeons still are about 10 times more likely to employ open surgery, possibly exposing patients to greater risk of complications, as well as longer hospital stays, according to an analysis of a national database.
“Despite the benefits of laparoscopic surgery, its utilization in ventral hernia repair (VHR) remains low,” said David Pechman, MD, MBA, of Mount Sinai Beth Israel Medical Center, New York, at the annual meeting of the American Society of Gastrointestinal and Endoscopic Surgeons. “This study suggests that utilization is further decreased in emergency cases. Relative to elective cases, emergency VHR is associated with markedly increased rates of morbidity, giving us more room to improve patient outcomes with the use of laparoscopy in these cases.”

The study analyzed 330 emergency VHR operations in the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database for 2012 and 2013. Thirty-two (9.3%) of those operations were performed laparoscopically, and the remainder were open. Because the sample size of laparoscopic operations was so small, drawing statistically significant conclusions from the findings is difficult without a larger, higher-powered study, Dr. Pechman said. “We do think that further research is warranted and believe that analysis of a larger sample would display that increased utilization of laparoscopy in emergency VHR could significantly improve outcomes.”
The analysis found significant differences in outcomes between the laparoscopic and the open operations for emergency VHR. Average hospital stay after laparoscopic emergency VHR was 2.8 days vs. 5.9 days for open VHR (P = .02). Surgical site infection rates were 0% vs. 7.7% (P = .15). Demographics between both laparoscopic and open groups were similar, Dr. Pechman said.
Session moderator E. Matthew Ritter, MD, of Walter Reed National Military Medical Center, Bethesda, Md., noted that the study conclusion is in line with the goals of SAGES’s minimally invasive surgery initiative to increase utilization of laparoscopy. When referring to the findings Dr. Pechman reported, Dr. Ritter said, “This is a remarkably low complication rate for a procedure that could seemingly have some benefit.”
Dr. Pechman’s response acknowledged the concerns of the surgeons doing the procedures: “A lot of this has to do with surgeon comfort and the preoperative decision-making, especially in an emergency setting.”
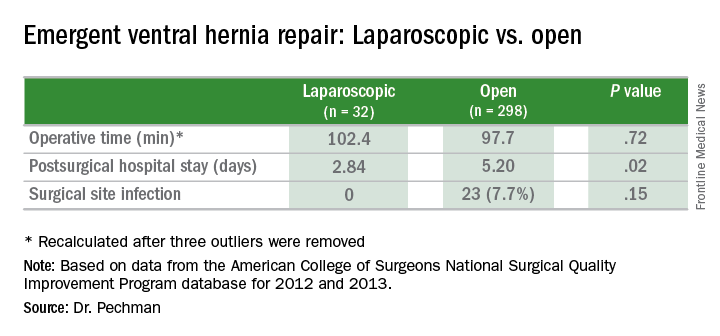
HOUSTON – The benefits of elective laparoscopic ventral hernia repair over the open approach have been well documented, but, when presented with emergency cases, surgeons still are about 10 times more likely to employ open surgery, possibly exposing patients to greater risk of complications, as well as longer hospital stays, according to an analysis of a national database.
“Despite the benefits of laparoscopic surgery, its utilization in ventral hernia repair (VHR) remains low,” said David Pechman, MD, MBA, of Mount Sinai Beth Israel Medical Center, New York, at the annual meeting of the American Society of Gastrointestinal and Endoscopic Surgeons. “This study suggests that utilization is further decreased in emergency cases. Relative to elective cases, emergency VHR is associated with markedly increased rates of morbidity, giving us more room to improve patient outcomes with the use of laparoscopy in these cases.”
The study analyzed 330 emergency VHR operations in the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database for 2012 and 2013. Thirty-two (9.3%) of those operations were performed laparoscopically, and the remainder were open. Because the sample size of laparoscopic operations was so small, drawing statistically significant conclusions from the findings is difficult without a larger, higher-powered study, Dr. Pechman said. “We do think that further research is warranted and believe that analysis of a larger sample would display that increased utilization of laparoscopy in emergency VHR could significantly improve outcomes.”
The analysis found significant differences in outcomes between the laparoscopic and the open operations for emergency VHR. Average hospital stay after laparoscopic emergency VHR was 2.8 days vs. 5.9 days for open VHR (P = .02). Surgical site infection rates were 0% vs. 7.7% (P = .15). Demographics between both laparoscopic and open groups were similar, Dr. Pechman said.
Session moderator E. Matthew Ritter, MD, of Walter Reed National Military Medical Center, Bethesda, Md., noted that the study conclusion is in line with the goals of SAGES’s minimally invasive surgery initiative to increase utilization of laparoscopy. When referring to the findings Dr. Pechman reported, Dr. Ritter said, “This is a remarkably low complication rate for a procedure that could seemingly have some benefit.”
Dr. Pechman’s response acknowledged the concerns of the surgeons doing the procedures: “A lot of this has to do with surgeon comfort and the preoperative decision-making, especially in an emergency setting.”
HOUSTON – The benefits of elective laparoscopic ventral hernia repair over the open approach have been well documented, but, when presented with emergency cases, surgeons still are about 10 times more likely to employ open surgery, possibly exposing patients to greater risk of complications, as well as longer hospital stays, according to an analysis of a national database.
“Despite the benefits of laparoscopic surgery, its utilization in ventral hernia repair (VHR) remains low,” said David Pechman, MD, MBA, of Mount Sinai Beth Israel Medical Center, New York, at the annual meeting of the American Society of Gastrointestinal and Endoscopic Surgeons. “This study suggests that utilization is further decreased in emergency cases. Relative to elective cases, emergency VHR is associated with markedly increased rates of morbidity, giving us more room to improve patient outcomes with the use of laparoscopy in these cases.”
The study analyzed 330 emergency VHR operations in the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database for 2012 and 2013. Thirty-two (9.3%) of those operations were performed laparoscopically, and the remainder were open. Because the sample size of laparoscopic operations was so small, drawing statistically significant conclusions from the findings is difficult without a larger, higher-powered study, Dr. Pechman said. “We do think that further research is warranted and believe that analysis of a larger sample would display that increased utilization of laparoscopy in emergency VHR could significantly improve outcomes.”
The analysis found significant differences in outcomes between the laparoscopic and the open operations for emergency VHR. Average hospital stay after laparoscopic emergency VHR was 2.8 days vs. 5.9 days for open VHR (P = .02). Surgical site infection rates were 0% vs. 7.7% (P = .15). Demographics between both laparoscopic and open groups were similar, Dr. Pechman said.
Session moderator E. Matthew Ritter, MD, of Walter Reed National Military Medical Center, Bethesda, Md., noted that the study conclusion is in line with the goals of SAGES’s minimally invasive surgery initiative to increase utilization of laparoscopy. When referring to the findings Dr. Pechman reported, Dr. Ritter said, “This is a remarkably low complication rate for a procedure that could seemingly have some benefit.”
Dr. Pechman’s response acknowledged the concerns of the surgeons doing the procedures: “A lot of this has to do with surgeon comfort and the preoperative decision-making, especially in an emergency setting.”
Key clinical point: Outcomes of laparoscopic ventral hernia repair (VHR) may be superior to those for open surgery in the emergency setting.
Major finding: Average hospital stay after laparoscopic emergency VHR was 2.8 days vs. 5.9 days for open surgery, and surgical site infection rates were 0% vs. 7.7%.
Data source: Analysis of 329 cases of emergency VHR enrolled in the American College of Surgeons National Surgical Quality Improvement Program in 2012 and 2013.
Disclosures: Dr. Pechman reported no financial disclosures.
Confirmatory blood typing unnecessary for closed prolapse repairs
SAN ANTONIO – It was safe to skip preoperative blood type and antibody screening before vaginal and robotic apical prolapse surgeries at the University of North Carolina, Chapel Hill, so long as the women didn’t have hemorrhage risk factors.
The rate of blood transfusions was 0.5% for both the 204 women who had vaginal repairs and the 203 women who underwent robotic repairs; the rate of positive antibody tests was 1.6%. Given the 0.4% risk of transfusion reactions in unscreened women, the investigators calculated that the risk of serious transfusion reactions was 1 in 50,000 with closed vaginal prolapse repairs.
“The bottom line for us is that the risk in this situation is very low, even if preop type and screens are not performed, and women hemorrhage. This information provides insight to answer our key clinical question, which was if we should continue to order preop type and screens,” lead investigator Taylor Brueseke, MD, an ob.gyn. fellow at the University of North Carolina, Chapel Hill, said at the annual scientific meeting of the Society of Gynecologic Surgeons.

That question has been on the minds of gynecologic surgeons, and it’s probably never been parsed out before by route of surgery. The American College of Pathologists recommends two blood type and antibody screens from separate venipunctures before surgery. Often, the second, confirmatory test means that women have to come in even earlier on the morning of surgery and deal with another painful blood draw. It also adds a few hundred dollars to the bill.
Every surgeon needs to draw their own line between risks and benefits, Dr. Brueseke said, but it seems reasonable in many cases to skip the second screening for closed repairs. Even if a woman has a transfusion reaction, “it doesn’t mean that the patient is going to die. It’s something that you can deal with,” he said.
However, the team reached a different conclusion for women who undergo open abdominal repairs. Among the 201 cases they reviewed, 10.5% had a transfusion, which translated to a transfusion reaction risk of 1 in 2,645 for unscreened women undergoing open apical prolapse surgery. The higher hemorrhage rate was probably due to concomitant Burch procedures and other open incontinence operations.
For abdominal cases, and for women who have had prior transfusions, surgeries, or anticoagulation, “consider type and screen,” Dr. Brueseke said at the meeting.
In a separate study presented at the conference, more than 50,000 pelvic floor disorder surgeries in the National Surgery Quality Improvement Program database further defined the hemorrhage risk.
Investigators at Ohio State University, Columbus, found that the overall incidence of blood transfusions was low at 1.26%, but open abdominal procedures again increased the risk. Other factors associated with an increased risk of blood transfusion included preoperative hematocrit less than 30%, an American Society of Anesthesiologists physical status score of 3 or higher, concomitant hysterectomy, body mass index below 18.5 kg/m2, age less than 30 and over 65 years, and a history of bleeding disorders.
In the UNC study, the median Pelvic Organ Prolapse Quantification was stage III. Patients with bleeding disorders, anticoagulant use, or combined surgery with other services were excluded.
There was no industry funding for the two studies, and the investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
A lot of people automatically order type and screen for vaginal prolapse repairs, but we really need to rethink that if there aren’t risk factors that warrant it. I defer to the anesthesiologists because they are the ones who usually want this, but most of the time we screen but don’t use the results. There’s room to improve clinical practice here.
Robert Gutman, MD, is a gynecologic surgeon in Washington, D.C., and the program chair for the 2017 Society of Gynecologic Surgeons annual scientific meeting. He wasn’t involved in the studies presented.
A lot of people automatically order type and screen for vaginal prolapse repairs, but we really need to rethink that if there aren’t risk factors that warrant it. I defer to the anesthesiologists because they are the ones who usually want this, but most of the time we screen but don’t use the results. There’s room to improve clinical practice here.
Robert Gutman, MD, is a gynecologic surgeon in Washington, D.C., and the program chair for the 2017 Society of Gynecologic Surgeons annual scientific meeting. He wasn’t involved in the studies presented.
A lot of people automatically order type and screen for vaginal prolapse repairs, but we really need to rethink that if there aren’t risk factors that warrant it. I defer to the anesthesiologists because they are the ones who usually want this, but most of the time we screen but don’t use the results. There’s room to improve clinical practice here.
Robert Gutman, MD, is a gynecologic surgeon in Washington, D.C., and the program chair for the 2017 Society of Gynecologic Surgeons annual scientific meeting. He wasn’t involved in the studies presented.
SAN ANTONIO – It was safe to skip preoperative blood type and antibody screening before vaginal and robotic apical prolapse surgeries at the University of North Carolina, Chapel Hill, so long as the women didn’t have hemorrhage risk factors.
The rate of blood transfusions was 0.5% for both the 204 women who had vaginal repairs and the 203 women who underwent robotic repairs; the rate of positive antibody tests was 1.6%. Given the 0.4% risk of transfusion reactions in unscreened women, the investigators calculated that the risk of serious transfusion reactions was 1 in 50,000 with closed vaginal prolapse repairs.
“The bottom line for us is that the risk in this situation is very low, even if preop type and screens are not performed, and women hemorrhage. This information provides insight to answer our key clinical question, which was if we should continue to order preop type and screens,” lead investigator Taylor Brueseke, MD, an ob.gyn. fellow at the University of North Carolina, Chapel Hill, said at the annual scientific meeting of the Society of Gynecologic Surgeons.
That question has been on the minds of gynecologic surgeons, and it’s probably never been parsed out before by route of surgery. The American College of Pathologists recommends two blood type and antibody screens from separate venipunctures before surgery. Often, the second, confirmatory test means that women have to come in even earlier on the morning of surgery and deal with another painful blood draw. It also adds a few hundred dollars to the bill.
Every surgeon needs to draw their own line between risks and benefits, Dr. Brueseke said, but it seems reasonable in many cases to skip the second screening for closed repairs. Even if a woman has a transfusion reaction, “it doesn’t mean that the patient is going to die. It’s something that you can deal with,” he said.
However, the team reached a different conclusion for women who undergo open abdominal repairs. Among the 201 cases they reviewed, 10.5% had a transfusion, which translated to a transfusion reaction risk of 1 in 2,645 for unscreened women undergoing open apical prolapse surgery. The higher hemorrhage rate was probably due to concomitant Burch procedures and other open incontinence operations.
For abdominal cases, and for women who have had prior transfusions, surgeries, or anticoagulation, “consider type and screen,” Dr. Brueseke said at the meeting.
In a separate study presented at the conference, more than 50,000 pelvic floor disorder surgeries in the National Surgery Quality Improvement Program database further defined the hemorrhage risk.
Investigators at Ohio State University, Columbus, found that the overall incidence of blood transfusions was low at 1.26%, but open abdominal procedures again increased the risk. Other factors associated with an increased risk of blood transfusion included preoperative hematocrit less than 30%, an American Society of Anesthesiologists physical status score of 3 or higher, concomitant hysterectomy, body mass index below 18.5 kg/m2, age less than 30 and over 65 years, and a history of bleeding disorders.
In the UNC study, the median Pelvic Organ Prolapse Quantification was stage III. Patients with bleeding disorders, anticoagulant use, or combined surgery with other services were excluded.
There was no industry funding for the two studies, and the investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
SAN ANTONIO – It was safe to skip preoperative blood type and antibody screening before vaginal and robotic apical prolapse surgeries at the University of North Carolina, Chapel Hill, so long as the women didn’t have hemorrhage risk factors.
The rate of blood transfusions was 0.5% for both the 204 women who had vaginal repairs and the 203 women who underwent robotic repairs; the rate of positive antibody tests was 1.6%. Given the 0.4% risk of transfusion reactions in unscreened women, the investigators calculated that the risk of serious transfusion reactions was 1 in 50,000 with closed vaginal prolapse repairs.
“The bottom line for us is that the risk in this situation is very low, even if preop type and screens are not performed, and women hemorrhage. This information provides insight to answer our key clinical question, which was if we should continue to order preop type and screens,” lead investigator Taylor Brueseke, MD, an ob.gyn. fellow at the University of North Carolina, Chapel Hill, said at the annual scientific meeting of the Society of Gynecologic Surgeons.
That question has been on the minds of gynecologic surgeons, and it’s probably never been parsed out before by route of surgery. The American College of Pathologists recommends two blood type and antibody screens from separate venipunctures before surgery. Often, the second, confirmatory test means that women have to come in even earlier on the morning of surgery and deal with another painful blood draw. It also adds a few hundred dollars to the bill.
Every surgeon needs to draw their own line between risks and benefits, Dr. Brueseke said, but it seems reasonable in many cases to skip the second screening for closed repairs. Even if a woman has a transfusion reaction, “it doesn’t mean that the patient is going to die. It’s something that you can deal with,” he said.
However, the team reached a different conclusion for women who undergo open abdominal repairs. Among the 201 cases they reviewed, 10.5% had a transfusion, which translated to a transfusion reaction risk of 1 in 2,645 for unscreened women undergoing open apical prolapse surgery. The higher hemorrhage rate was probably due to concomitant Burch procedures and other open incontinence operations.
For abdominal cases, and for women who have had prior transfusions, surgeries, or anticoagulation, “consider type and screen,” Dr. Brueseke said at the meeting.
In a separate study presented at the conference, more than 50,000 pelvic floor disorder surgeries in the National Surgery Quality Improvement Program database further defined the hemorrhage risk.
Investigators at Ohio State University, Columbus, found that the overall incidence of blood transfusions was low at 1.26%, but open abdominal procedures again increased the risk. Other factors associated with an increased risk of blood transfusion included preoperative hematocrit less than 30%, an American Society of Anesthesiologists physical status score of 3 or higher, concomitant hysterectomy, body mass index below 18.5 kg/m2, age less than 30 and over 65 years, and a history of bleeding disorders.
In the UNC study, the median Pelvic Organ Prolapse Quantification was stage III. Patients with bleeding disorders, anticoagulant use, or combined surgery with other services were excluded.
There was no industry funding for the two studies, and the investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
Key clinical point:
Major finding: Given the 0.4% risk of transfusion reactions in unscreened women, the risk of serious transfusion reactions was 1 in 50,000 women with closed apical prolapse repairs.
Data source: A review of more than 600 cases of apical prolapse surgery at a single center.
Disclosures: There was no industry funding, and the investigators reported having no relevant financial disclosures.