User login
Official Newspaper of the American College of Surgeons
Can high hematocrit predict early shunt thrombosis?
Shunt occlusion has been a well-documented cause of shunt failure in newborns who have had systemic to pulmonary shunt placement, and little has been known about why shunts occlude. However, researchers have reported in a small retrospective study that higher postoperative hematocrit levels immediately after surgery may be predictors of shunt occlusion.
Reporting in the April 2017 issue of The Journal of Thoracic and Cardiovascular Surgery, Brett R. Anderson, MD, of New York-Presbyterian/Morgan Stanley Children’s Hospital, Columbia University Medical Center in New York, and coauthors, found that every 5-point increase in postoperative hematocrit more than doubled an infant’s odds of having early shunt occlusion (J Thorac Cardiovasc Surg. 2017;153:947-55).
“Beginning in the latter half of 2014, we noticed an increase in the incidence of early shunt occlusions in our neonatal cardiac intensive care unit,” Dr. Anderson and coauthors said. So they conducted a retrospective chart review of 80 infants who had undergone systemic to pulmonary shunt placement from January 2010 to July 2015, hypothesizing that increased hematocrit in the early postoperative period might have caused early shunt occlusion. They investigated the association between the first postoperative hematocrit and early shunt occlusion and in-hospital mortality in these patients.
Five patients (6.3%) experienced early shunt occlusion – that is, within 24 hours of placement (actually, within 10 hours of placement). Overall, 12 infants (15%) experienced shunt occlusion. The physicians at New York-Presbyterian do not administer anticoagulation in these patients during the first 12 hours after shunt placement.
The median initial postoperative hematocrit was 41.7%, with a range of 31.7%-55.8%. The survival analysis the researchers performed found that for every 5 additional percentage points, the hazard ratio for early shunt occlusion was 2.7 (P = .007) and 1.74 for any shunt occlusion (P less than .001). Incidentally, four cases of early shunt occlusion occurred in the later study period after 2014, during which the average first postoperative hematocrit was significantly higher than in the pre-2014 study period, 45.3% vs. 41.5% (P = .21), and the odds of early shunt occlusion were 16 times higher (P less than .001). Dr. Anderson and coauthors said the possible explanation for this variation was a switch to a new point-of-care analyzer in 2013.
With regard to mortality, six infants overall (7.4%) died before discharge, and four (5%) within 30 days of shunt placement. No infants with early shunt occlusion died, although two with late shunt occlusion died. Increased inotrope score and first postoperative arterial oxygen tension were the only factors associated with increased mortality. “No significant association was identified between hematocrit and 30-day mortality,” Dr. Anderson and coauthors said.
In the first 24 hours after surgery, 11 infants (13.8%) received packed red blood cell (PRBC) transfusions, seven (8.8%) received platelets, and four (5%) received fresh frozen plasma/cryoprecipitate. Higher postoperative PRBC transfusion volumes were associated with increased odds of mortality (P = .001), but none of these factors were significantly associated with early shunt occlusion.
Dr. Anderson and coauthors acknowledged that shunt occlusion is a “vexing problem” in infants with cyanotic heart disease. While other researchers studied postoperative hematocrit levels and possible associations with outcomes, including shunt occlusion and mortality, the New York-Presbyterian investigators said this is the first study of the first postoperative hematocrit.
Dr. Anderson and coauthors said their findings raise the question about the ideal perioperative prophylactic antithrombotic therapy in these patients. These researchers initiate aspirin therapy 12 hours after surgery if hemostasis is established.
As a result of this study, Dr. Anderson and coauthors instituted a number of practice changes at their center. They include:
• Cardiac anesthesiologists have been asked not to transfuse shunted neonates with hematocrit level of greater than or equal to 35%, and hematocrits are then immediately repeated when a patient returns to the cardiac ICU.
• Patients with hematocrits greater than or equal to 55% get partial exchange transfusions.
• An individualized approach for patients with lower hematocrits who are more cyanotic than expected. This includes a diagnostic echocardiogram, nitric oxide, oxygen and heparin, escalated inotropic support if necessary and sometimes a cautious approach to transfusions if symptoms do not resolve and an acute shunt occlusion if not likely.
Dr. Anderson and coauthors acknowledged limits to their study, most notably its retrospective nature and a small population at a single center, and that large investigations are needed to validate their findings.
Dr. Anderson disclosed receiving salary support from the National Center for Advancing Translational Sciences. Coauthor Jennifer M. Duchon, MDCM, MPH, receives salary support from the National Institute of Allergy and Infectious Disease. The remaining coauthors had no financial relationships to disclose.
In her invited commentary, Nancy S. Ghanayem, MD, of the Medical College of Wisconsin, gives credit to Dr. Anderson and coauthors for introducing the notion that high initial postoperative hematocrit may increase the risk of early shunt thrombosis in newborns, but with a caveat: “we remain somewhat hesitant regarding wholesale acceptance of the validity of the conclusions for several reasons” (J Thorac Cardiovasc Surg. 2017;153:956).
Those reasons include the low number of reported events, failure to list the actual hematocrits of the five patients who experienced early shunt occlusion and the lack of hemodynamic data – the latter of which she called “a significant limitation.”
A patient with low cardiac output, especially one who is cyanotic or has a single ventricle, is at higher risk for thrombosis and more likely to be transfused, “which in this case would potentially be masked by the method of comparing transfused volumes,” Dr. Ghanayem said. The inotrope score, while useful, is not a surrogate for actual cardiac output. She asks, “Accordingly, is early shunt occlusion due predominantly to passenger (corpuscular) overload or to a slow-moving train?”
Dr. Ghanayem had no financial relationships to disclose.
In her invited commentary, Nancy S. Ghanayem, MD, of the Medical College of Wisconsin, gives credit to Dr. Anderson and coauthors for introducing the notion that high initial postoperative hematocrit may increase the risk of early shunt thrombosis in newborns, but with a caveat: “we remain somewhat hesitant regarding wholesale acceptance of the validity of the conclusions for several reasons” (J Thorac Cardiovasc Surg. 2017;153:956).
Those reasons include the low number of reported events, failure to list the actual hematocrits of the five patients who experienced early shunt occlusion and the lack of hemodynamic data – the latter of which she called “a significant limitation.”
A patient with low cardiac output, especially one who is cyanotic or has a single ventricle, is at higher risk for thrombosis and more likely to be transfused, “which in this case would potentially be masked by the method of comparing transfused volumes,” Dr. Ghanayem said. The inotrope score, while useful, is not a surrogate for actual cardiac output. She asks, “Accordingly, is early shunt occlusion due predominantly to passenger (corpuscular) overload or to a slow-moving train?”
Dr. Ghanayem had no financial relationships to disclose.
In her invited commentary, Nancy S. Ghanayem, MD, of the Medical College of Wisconsin, gives credit to Dr. Anderson and coauthors for introducing the notion that high initial postoperative hematocrit may increase the risk of early shunt thrombosis in newborns, but with a caveat: “we remain somewhat hesitant regarding wholesale acceptance of the validity of the conclusions for several reasons” (J Thorac Cardiovasc Surg. 2017;153:956).
Those reasons include the low number of reported events, failure to list the actual hematocrits of the five patients who experienced early shunt occlusion and the lack of hemodynamic data – the latter of which she called “a significant limitation.”
A patient with low cardiac output, especially one who is cyanotic or has a single ventricle, is at higher risk for thrombosis and more likely to be transfused, “which in this case would potentially be masked by the method of comparing transfused volumes,” Dr. Ghanayem said. The inotrope score, while useful, is not a surrogate for actual cardiac output. She asks, “Accordingly, is early shunt occlusion due predominantly to passenger (corpuscular) overload or to a slow-moving train?”
Dr. Ghanayem had no financial relationships to disclose.
Shunt occlusion has been a well-documented cause of shunt failure in newborns who have had systemic to pulmonary shunt placement, and little has been known about why shunts occlude. However, researchers have reported in a small retrospective study that higher postoperative hematocrit levels immediately after surgery may be predictors of shunt occlusion.
Reporting in the April 2017 issue of The Journal of Thoracic and Cardiovascular Surgery, Brett R. Anderson, MD, of New York-Presbyterian/Morgan Stanley Children’s Hospital, Columbia University Medical Center in New York, and coauthors, found that every 5-point increase in postoperative hematocrit more than doubled an infant’s odds of having early shunt occlusion (J Thorac Cardiovasc Surg. 2017;153:947-55).
“Beginning in the latter half of 2014, we noticed an increase in the incidence of early shunt occlusions in our neonatal cardiac intensive care unit,” Dr. Anderson and coauthors said. So they conducted a retrospective chart review of 80 infants who had undergone systemic to pulmonary shunt placement from January 2010 to July 2015, hypothesizing that increased hematocrit in the early postoperative period might have caused early shunt occlusion. They investigated the association between the first postoperative hematocrit and early shunt occlusion and in-hospital mortality in these patients.
Five patients (6.3%) experienced early shunt occlusion – that is, within 24 hours of placement (actually, within 10 hours of placement). Overall, 12 infants (15%) experienced shunt occlusion. The physicians at New York-Presbyterian do not administer anticoagulation in these patients during the first 12 hours after shunt placement.
The median initial postoperative hematocrit was 41.7%, with a range of 31.7%-55.8%. The survival analysis the researchers performed found that for every 5 additional percentage points, the hazard ratio for early shunt occlusion was 2.7 (P = .007) and 1.74 for any shunt occlusion (P less than .001). Incidentally, four cases of early shunt occlusion occurred in the later study period after 2014, during which the average first postoperative hematocrit was significantly higher than in the pre-2014 study period, 45.3% vs. 41.5% (P = .21), and the odds of early shunt occlusion were 16 times higher (P less than .001). Dr. Anderson and coauthors said the possible explanation for this variation was a switch to a new point-of-care analyzer in 2013.
With regard to mortality, six infants overall (7.4%) died before discharge, and four (5%) within 30 days of shunt placement. No infants with early shunt occlusion died, although two with late shunt occlusion died. Increased inotrope score and first postoperative arterial oxygen tension were the only factors associated with increased mortality. “No significant association was identified between hematocrit and 30-day mortality,” Dr. Anderson and coauthors said.
In the first 24 hours after surgery, 11 infants (13.8%) received packed red blood cell (PRBC) transfusions, seven (8.8%) received platelets, and four (5%) received fresh frozen plasma/cryoprecipitate. Higher postoperative PRBC transfusion volumes were associated with increased odds of mortality (P = .001), but none of these factors were significantly associated with early shunt occlusion.
Dr. Anderson and coauthors acknowledged that shunt occlusion is a “vexing problem” in infants with cyanotic heart disease. While other researchers studied postoperative hematocrit levels and possible associations with outcomes, including shunt occlusion and mortality, the New York-Presbyterian investigators said this is the first study of the first postoperative hematocrit.
Dr. Anderson and coauthors said their findings raise the question about the ideal perioperative prophylactic antithrombotic therapy in these patients. These researchers initiate aspirin therapy 12 hours after surgery if hemostasis is established.
As a result of this study, Dr. Anderson and coauthors instituted a number of practice changes at their center. They include:
• Cardiac anesthesiologists have been asked not to transfuse shunted neonates with hematocrit level of greater than or equal to 35%, and hematocrits are then immediately repeated when a patient returns to the cardiac ICU.
• Patients with hematocrits greater than or equal to 55% get partial exchange transfusions.
• An individualized approach for patients with lower hematocrits who are more cyanotic than expected. This includes a diagnostic echocardiogram, nitric oxide, oxygen and heparin, escalated inotropic support if necessary and sometimes a cautious approach to transfusions if symptoms do not resolve and an acute shunt occlusion if not likely.
Dr. Anderson and coauthors acknowledged limits to their study, most notably its retrospective nature and a small population at a single center, and that large investigations are needed to validate their findings.
Dr. Anderson disclosed receiving salary support from the National Center for Advancing Translational Sciences. Coauthor Jennifer M. Duchon, MDCM, MPH, receives salary support from the National Institute of Allergy and Infectious Disease. The remaining coauthors had no financial relationships to disclose.
Shunt occlusion has been a well-documented cause of shunt failure in newborns who have had systemic to pulmonary shunt placement, and little has been known about why shunts occlude. However, researchers have reported in a small retrospective study that higher postoperative hematocrit levels immediately after surgery may be predictors of shunt occlusion.
Reporting in the April 2017 issue of The Journal of Thoracic and Cardiovascular Surgery, Brett R. Anderson, MD, of New York-Presbyterian/Morgan Stanley Children’s Hospital, Columbia University Medical Center in New York, and coauthors, found that every 5-point increase in postoperative hematocrit more than doubled an infant’s odds of having early shunt occlusion (J Thorac Cardiovasc Surg. 2017;153:947-55).
“Beginning in the latter half of 2014, we noticed an increase in the incidence of early shunt occlusions in our neonatal cardiac intensive care unit,” Dr. Anderson and coauthors said. So they conducted a retrospective chart review of 80 infants who had undergone systemic to pulmonary shunt placement from January 2010 to July 2015, hypothesizing that increased hematocrit in the early postoperative period might have caused early shunt occlusion. They investigated the association between the first postoperative hematocrit and early shunt occlusion and in-hospital mortality in these patients.
Five patients (6.3%) experienced early shunt occlusion – that is, within 24 hours of placement (actually, within 10 hours of placement). Overall, 12 infants (15%) experienced shunt occlusion. The physicians at New York-Presbyterian do not administer anticoagulation in these patients during the first 12 hours after shunt placement.
The median initial postoperative hematocrit was 41.7%, with a range of 31.7%-55.8%. The survival analysis the researchers performed found that for every 5 additional percentage points, the hazard ratio for early shunt occlusion was 2.7 (P = .007) and 1.74 for any shunt occlusion (P less than .001). Incidentally, four cases of early shunt occlusion occurred in the later study period after 2014, during which the average first postoperative hematocrit was significantly higher than in the pre-2014 study period, 45.3% vs. 41.5% (P = .21), and the odds of early shunt occlusion were 16 times higher (P less than .001). Dr. Anderson and coauthors said the possible explanation for this variation was a switch to a new point-of-care analyzer in 2013.
With regard to mortality, six infants overall (7.4%) died before discharge, and four (5%) within 30 days of shunt placement. No infants with early shunt occlusion died, although two with late shunt occlusion died. Increased inotrope score and first postoperative arterial oxygen tension were the only factors associated with increased mortality. “No significant association was identified between hematocrit and 30-day mortality,” Dr. Anderson and coauthors said.
In the first 24 hours after surgery, 11 infants (13.8%) received packed red blood cell (PRBC) transfusions, seven (8.8%) received platelets, and four (5%) received fresh frozen plasma/cryoprecipitate. Higher postoperative PRBC transfusion volumes were associated with increased odds of mortality (P = .001), but none of these factors were significantly associated with early shunt occlusion.
Dr. Anderson and coauthors acknowledged that shunt occlusion is a “vexing problem” in infants with cyanotic heart disease. While other researchers studied postoperative hematocrit levels and possible associations with outcomes, including shunt occlusion and mortality, the New York-Presbyterian investigators said this is the first study of the first postoperative hematocrit.
Dr. Anderson and coauthors said their findings raise the question about the ideal perioperative prophylactic antithrombotic therapy in these patients. These researchers initiate aspirin therapy 12 hours after surgery if hemostasis is established.
As a result of this study, Dr. Anderson and coauthors instituted a number of practice changes at their center. They include:
• Cardiac anesthesiologists have been asked not to transfuse shunted neonates with hematocrit level of greater than or equal to 35%, and hematocrits are then immediately repeated when a patient returns to the cardiac ICU.
• Patients with hematocrits greater than or equal to 55% get partial exchange transfusions.
• An individualized approach for patients with lower hematocrits who are more cyanotic than expected. This includes a diagnostic echocardiogram, nitric oxide, oxygen and heparin, escalated inotropic support if necessary and sometimes a cautious approach to transfusions if symptoms do not resolve and an acute shunt occlusion if not likely.
Dr. Anderson and coauthors acknowledged limits to their study, most notably its retrospective nature and a small population at a single center, and that large investigations are needed to validate their findings.
Dr. Anderson disclosed receiving salary support from the National Center for Advancing Translational Sciences. Coauthor Jennifer M. Duchon, MDCM, MPH, receives salary support from the National Institute of Allergy and Infectious Disease. The remaining coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Higher hematocrit levels have been associated with early shunt occlusion in newborns having systemic to pulmonary artery shunt placement.
Major finding: For every 5 additional percentage points of hematocrit, an infant’s odds of early shunt occlusion more than doubled (odds ratio, 2.70; P = .009).
Data source: Retrospective study of all newborns who underwent primary systemic to pulmonary artery shunt placement from January 2010 to July 2015 at a single center.
Disclosure: Dr. Anderson receives salary support from the National Center for Advancing Translational Sciences. Coauthor Jennifer M. Duchon, MDCM, MPH, receives salary support from the National Institute of Allergy and Infectious Disease. The remaining coauthors had no financial relationships to disclose.
Orbital, over rotational, atherectomy holds survival edge in elderly, obese
WASHINGTON – Orbital atherectomy (OA) was associated with a lower risk of in-hospital mortality than rotational atherectomy (RA) in female, obese, and elderly study groups, according to data from a prospective observational study.
Each procedure was employed to treat coronary artery calcifications (CAC) in the elderly and the obese prior to percutaneous interventions (PCI).
The data comparing OA with RA in these populations were drawn from the Clinical Outcomes of Atherectomy Prior to PCI (COAP) study, for which Perwaiz M. Meraj, MD, director of structural heart and peripheral vascular disease at the North Shore-LIJ Hospital, Manhasset, N.Y., served as the senior author.
Each set of data, as well as a third set of data comparing OA to RA in female patients, was presented separately at CRT 2017, sponsored by the Cardiovascular Research Institute at Washington Hospital Center.
In the comparison of OA to RA in the elderly, a substudy known as COAP-75, the focus was on patients 75 years of age or older who underwent either OA or RA to remove calcified coronary lesions within the context of PCI. As with the obese and female subgroups, the elderly patients in this study were drawn from 35,590 patients who underwent PCI at one of five tertiary care hospitals in a recent 5-year period.
Of the 310 elderly patients undergoing atherectomy, 117 were treated with OA and 193 with RA. The median lesion lengths and diameters were not significantly different between the two groups. Although OA was less likely to be performed through femoral access (53% vs. 68.9%; P = .005), no other measured differences in procedure were significant, with one exception: Fluoroscopy exposure was of shorter duration in the OA, versus the RA, arm (24.0 minutes vs. 29.4 minutes; P = .005).
On univariate analysis, the lower rate of in-hospital deaths for OA did not reach statistical significance (0% vs. 1.55%; P = .176), but the difference was significant on multivariate-adjusted analysis (P = .034).
There were also higher numerical rates of perforation, tamponade, heart failure, and red blood cell transfusion in the RA group, versus the OA group, but only the latter was significant (P = .002) on multivariate-adjusted analysis.
In contrast, there was a higher rate of MI among those treated with OA, rather than RA (17.1% vs. 13.5%), which was not significant on univariate analysis (P = .573) but did reach significance on adjusted-multivariate analysis (P = .008).
Overall, the authors suggested that both OA and RA are safe procedures, but the mortality reduction suggests a potential relative advantage for OA.
Similar conclusions were reached in the substudy of patients with obesity, called COAP-BMI. In that study, 222 patients were evaluated, of which 91 were treated with OA and 131 were treated with RA.
In-hospital mortality was 0% in the group treated with OA, compared with 3.05% in the group treated with RA (P = .004). The rate of in-hospital major adverse cardiovascular events was also significantly lower in the OA group (15.4% vs. 16.3%; P = .007).
“The rate of secondary outcomes for myocardial infarction and stroke were similar between groups, as were individual procedural safety endpoints, including dissection, perforation, tamponade, or heart failure,” reported Evan Shlofmitz, MD, a cardiology fellow at Northwell Health, Manhasset, N.Y., who collaborated with Dr. Meraj and presented the data at the meeting.
As with the study in the elderly, for which Dr. Shlofmitz was also a coauthor, the study in the obese is the first to compare OA and RA, he noted.
In a third substudy, called COAP-Female, OA and RA were compared in 247 women with CAC who were undergoing PCI.
Again, in-hospital mortality rates were higher in those treated with RA, compared with OA, but the difference was not significant (0.79% vs. 0%; P = .254). There were also no significant differences in any secondary outcomes, including MI, or in any procedural complications, such as rates of dissection, perforation, or major bleeding.
The only significant difference identified in the study was a lower fluoroscopy time in those treated with OA relative to RA (21.3 minutes vs. 27.6 minutes; P = .001).
Although fluoroscopy time was not a primary endpoint, “a reduction in radiation exposure has important ramifications for both patients and operators,” Dr. Shlofmitz noted. He suggested that objective data on outcomes in females is needed, because this group has been “severely underrepresented in atherectomy trials.”
Overall, the substudies reinforce a large body of evidence that atherectomy is safe and effective for achieving revascularization in patients undergoing PCI who have CAC, Dr. Shlofmitz concluded. However, the significant mortality advantage for OA relative to RA in the elderly and the obese suggests that the approaches may not be interchangeable.
Dr. Shlofmitz reported no financial relationships to disclose.
WASHINGTON – Orbital atherectomy (OA) was associated with a lower risk of in-hospital mortality than rotational atherectomy (RA) in female, obese, and elderly study groups, according to data from a prospective observational study.
Each procedure was employed to treat coronary artery calcifications (CAC) in the elderly and the obese prior to percutaneous interventions (PCI).
The data comparing OA with RA in these populations were drawn from the Clinical Outcomes of Atherectomy Prior to PCI (COAP) study, for which Perwaiz M. Meraj, MD, director of structural heart and peripheral vascular disease at the North Shore-LIJ Hospital, Manhasset, N.Y., served as the senior author.
Each set of data, as well as a third set of data comparing OA to RA in female patients, was presented separately at CRT 2017, sponsored by the Cardiovascular Research Institute at Washington Hospital Center.
In the comparison of OA to RA in the elderly, a substudy known as COAP-75, the focus was on patients 75 years of age or older who underwent either OA or RA to remove calcified coronary lesions within the context of PCI. As with the obese and female subgroups, the elderly patients in this study were drawn from 35,590 patients who underwent PCI at one of five tertiary care hospitals in a recent 5-year period.
Of the 310 elderly patients undergoing atherectomy, 117 were treated with OA and 193 with RA. The median lesion lengths and diameters were not significantly different between the two groups. Although OA was less likely to be performed through femoral access (53% vs. 68.9%; P = .005), no other measured differences in procedure were significant, with one exception: Fluoroscopy exposure was of shorter duration in the OA, versus the RA, arm (24.0 minutes vs. 29.4 minutes; P = .005).
On univariate analysis, the lower rate of in-hospital deaths for OA did not reach statistical significance (0% vs. 1.55%; P = .176), but the difference was significant on multivariate-adjusted analysis (P = .034).
There were also higher numerical rates of perforation, tamponade, heart failure, and red blood cell transfusion in the RA group, versus the OA group, but only the latter was significant (P = .002) on multivariate-adjusted analysis.
In contrast, there was a higher rate of MI among those treated with OA, rather than RA (17.1% vs. 13.5%), which was not significant on univariate analysis (P = .573) but did reach significance on adjusted-multivariate analysis (P = .008).
Overall, the authors suggested that both OA and RA are safe procedures, but the mortality reduction suggests a potential relative advantage for OA.
Similar conclusions were reached in the substudy of patients with obesity, called COAP-BMI. In that study, 222 patients were evaluated, of which 91 were treated with OA and 131 were treated with RA.
In-hospital mortality was 0% in the group treated with OA, compared with 3.05% in the group treated with RA (P = .004). The rate of in-hospital major adverse cardiovascular events was also significantly lower in the OA group (15.4% vs. 16.3%; P = .007).
“The rate of secondary outcomes for myocardial infarction and stroke were similar between groups, as were individual procedural safety endpoints, including dissection, perforation, tamponade, or heart failure,” reported Evan Shlofmitz, MD, a cardiology fellow at Northwell Health, Manhasset, N.Y., who collaborated with Dr. Meraj and presented the data at the meeting.
As with the study in the elderly, for which Dr. Shlofmitz was also a coauthor, the study in the obese is the first to compare OA and RA, he noted.
In a third substudy, called COAP-Female, OA and RA were compared in 247 women with CAC who were undergoing PCI.
Again, in-hospital mortality rates were higher in those treated with RA, compared with OA, but the difference was not significant (0.79% vs. 0%; P = .254). There were also no significant differences in any secondary outcomes, including MI, or in any procedural complications, such as rates of dissection, perforation, or major bleeding.
The only significant difference identified in the study was a lower fluoroscopy time in those treated with OA relative to RA (21.3 minutes vs. 27.6 minutes; P = .001).
Although fluoroscopy time was not a primary endpoint, “a reduction in radiation exposure has important ramifications for both patients and operators,” Dr. Shlofmitz noted. He suggested that objective data on outcomes in females is needed, because this group has been “severely underrepresented in atherectomy trials.”
Overall, the substudies reinforce a large body of evidence that atherectomy is safe and effective for achieving revascularization in patients undergoing PCI who have CAC, Dr. Shlofmitz concluded. However, the significant mortality advantage for OA relative to RA in the elderly and the obese suggests that the approaches may not be interchangeable.
Dr. Shlofmitz reported no financial relationships to disclose.
WASHINGTON – Orbital atherectomy (OA) was associated with a lower risk of in-hospital mortality than rotational atherectomy (RA) in female, obese, and elderly study groups, according to data from a prospective observational study.
Each procedure was employed to treat coronary artery calcifications (CAC) in the elderly and the obese prior to percutaneous interventions (PCI).
The data comparing OA with RA in these populations were drawn from the Clinical Outcomes of Atherectomy Prior to PCI (COAP) study, for which Perwaiz M. Meraj, MD, director of structural heart and peripheral vascular disease at the North Shore-LIJ Hospital, Manhasset, N.Y., served as the senior author.
Each set of data, as well as a third set of data comparing OA to RA in female patients, was presented separately at CRT 2017, sponsored by the Cardiovascular Research Institute at Washington Hospital Center.
In the comparison of OA to RA in the elderly, a substudy known as COAP-75, the focus was on patients 75 years of age or older who underwent either OA or RA to remove calcified coronary lesions within the context of PCI. As with the obese and female subgroups, the elderly patients in this study were drawn from 35,590 patients who underwent PCI at one of five tertiary care hospitals in a recent 5-year period.
Of the 310 elderly patients undergoing atherectomy, 117 were treated with OA and 193 with RA. The median lesion lengths and diameters were not significantly different between the two groups. Although OA was less likely to be performed through femoral access (53% vs. 68.9%; P = .005), no other measured differences in procedure were significant, with one exception: Fluoroscopy exposure was of shorter duration in the OA, versus the RA, arm (24.0 minutes vs. 29.4 minutes; P = .005).
On univariate analysis, the lower rate of in-hospital deaths for OA did not reach statistical significance (0% vs. 1.55%; P = .176), but the difference was significant on multivariate-adjusted analysis (P = .034).
There were also higher numerical rates of perforation, tamponade, heart failure, and red blood cell transfusion in the RA group, versus the OA group, but only the latter was significant (P = .002) on multivariate-adjusted analysis.
In contrast, there was a higher rate of MI among those treated with OA, rather than RA (17.1% vs. 13.5%), which was not significant on univariate analysis (P = .573) but did reach significance on adjusted-multivariate analysis (P = .008).
Overall, the authors suggested that both OA and RA are safe procedures, but the mortality reduction suggests a potential relative advantage for OA.
Similar conclusions were reached in the substudy of patients with obesity, called COAP-BMI. In that study, 222 patients were evaluated, of which 91 were treated with OA and 131 were treated with RA.
In-hospital mortality was 0% in the group treated with OA, compared with 3.05% in the group treated with RA (P = .004). The rate of in-hospital major adverse cardiovascular events was also significantly lower in the OA group (15.4% vs. 16.3%; P = .007).
“The rate of secondary outcomes for myocardial infarction and stroke were similar between groups, as were individual procedural safety endpoints, including dissection, perforation, tamponade, or heart failure,” reported Evan Shlofmitz, MD, a cardiology fellow at Northwell Health, Manhasset, N.Y., who collaborated with Dr. Meraj and presented the data at the meeting.
As with the study in the elderly, for which Dr. Shlofmitz was also a coauthor, the study in the obese is the first to compare OA and RA, he noted.
In a third substudy, called COAP-Female, OA and RA were compared in 247 women with CAC who were undergoing PCI.
Again, in-hospital mortality rates were higher in those treated with RA, compared with OA, but the difference was not significant (0.79% vs. 0%; P = .254). There were also no significant differences in any secondary outcomes, including MI, or in any procedural complications, such as rates of dissection, perforation, or major bleeding.
The only significant difference identified in the study was a lower fluoroscopy time in those treated with OA relative to RA (21.3 minutes vs. 27.6 minutes; P = .001).
Although fluoroscopy time was not a primary endpoint, “a reduction in radiation exposure has important ramifications for both patients and operators,” Dr. Shlofmitz noted. He suggested that objective data on outcomes in females is needed, because this group has been “severely underrepresented in atherectomy trials.”
Overall, the substudies reinforce a large body of evidence that atherectomy is safe and effective for achieving revascularization in patients undergoing PCI who have CAC, Dr. Shlofmitz concluded. However, the significant mortality advantage for OA relative to RA in the elderly and the obese suggests that the approaches may not be interchangeable.
Dr. Shlofmitz reported no financial relationships to disclose.
AT CRT 2017
Key clinical point: Orbital atherectomy was associated with better survival than rotational atherectomy in elderly and obese patients requiring percutaneous interventions.
Major finding: In-hospital mortality was significantly lower after orbital atherectomy, compared with rotational atherectomy, in both the elderly (0% vs. 1.55%; P = .034) and the obese (0% vs. 3.05%; P = .004).
Data source: A nonrandomized, prospective, multicenter study.
Disclosures: Dr. Shlofmitz reported no financial relationships to disclose.
Three-strategy combo reduces pancreatoduodenectomy fistula risk
MIAMI BEACH – Pancreaticojejunostomy reconstruction, use of stents, and avoidance of prophylactic octreotide, especially in combination, could reduce the fistula rate associated with pancreatoduodenectomy.
Failure of the anastomosis is “of greatest concern” to surgeons performing a pancreatoduodenectomy, said Brett L. Ecker, MD, a surgical resident at the University of Pennsylvania, Philadelphia.
“There is no shortage of high-quality data to help guide the use of [fistula reduction] strategies,” he added. However, “the utility of these strategies in patients most vulnerable to fistula … has rarely been particularly explored.”
Dr. Ecker and his colleagues conducted a study with 62 surgeons at 17 institutions to compare various fistula mitigation strategies in this higher-risk population. They assessed surgical reconstruction, dunking, tissue patches, intraperitoneal drains, stents, prophylactic octreotide, and use of tissue sealants.
“Ultimately, we want to know the best way to deal with this high-stakes situation, and whether outcomes might be optimized by bundling these proactive strategies,” Dr. Ecker explained.
“We found the combination of externalized stents and PJ [pancreaticojejunostomy] reconstruction with the omission of prophylactic octreotide was associated with significant improvements in fistula that exceeded the benefit of any individual mitigation approach or any other combination of strategies,” he said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“The mitigation of risk in real-life practice is often the result of multiple moving parts,” Dr. Ecker said. “The best outcomes [may result from] the synergistic effects of multiple strategies.”
Of the approximately 10% of patients with a Fistula Risk Score of 7-10, 152 ended up with clinically relevant postoperative pancreatic fistula (CR-POPF). “An FRS score of 7 or higher is associated with worse outcomes, including a fistula rate approaching 30%,” Dr. Ecker said. Grade B or C fistula based on International Study Group on Pancreatic Surgery criteria were considered clinically relevant. All patients had surgery from 2003 to 2016 in the retrospective, multinational study.
“This represents the only series of high-risk cases where current international standards were used to define both the risk and the outcome,” he noted.
“Almost all [of the 522] patients had a soft gland and a small duct, a median of 2 mm,” Dr. Ecker added. “High-risk pathology was common, in 86%.”
Surgeons contributing to the series were at high-volume centers and had performed more than 200 Whipple procedures in their careers. “Both institutional and surgeon volume were associated with improved fistula outcomes,” Dr. Ecker said. “We found that intraperitoneal drains were not associated with improved fistula outcomes, but that is limited by the fact that drains were rarely omitted in these cases.”
Four strategies compared
The investigators compared the outcomes of four fistula strategies among the patients considered high risk prior to surgery. When they combined pancreaticogastrostomy, prophylactic octreotide, and no stent, the CR-POPF rate was 47%. “This was associated with an alarming fistula rate approaching 50%,” Dr. Ecker said.
When surgeons combined pancreaticojejunostomy, octreotide, and no stent, the CR-POPF rate declined to 34%. Furthermore, pancreaticojejunostomy without octreotide or a stent yielded a 26% CR-POPF rate.
Ultimately, the most effective strategy to avoid clinically relevant fistula was pancreaticojejunostomy with an external stent and no octreotide.
“The use of PJ reconstruction with an external stent and omission of octreotide was associated with a fistula rate of about 13%, which was a greater than 50% risk reduction from the overall cohort,” Dr. Ecker said.
The researchers also performed propensity score matching to reduce bias associated with surgeon or patient factors. They matched 167 participants in the study with 155 controls. Dr. Ecker said, “Still, we observed that patients managed this way had significantly lower fistula rates.”
“This is an excellent paper and an important topic,” said study discussant Michael L. Kendrick, MD, a general surgeon at the Mayo Clinic in Rochester, Minn.
“At our institution, we’ve used the same Fistula Risk Score and found it very helpful for a mitigation strategy in a separate protocol, and we found that reduced our leak rates as well,” Dr. Kendrick noted.
Dr. Ecker and Dr. Kendrick had no relevant disclosures.
MIAMI BEACH – Pancreaticojejunostomy reconstruction, use of stents, and avoidance of prophylactic octreotide, especially in combination, could reduce the fistula rate associated with pancreatoduodenectomy.
Failure of the anastomosis is “of greatest concern” to surgeons performing a pancreatoduodenectomy, said Brett L. Ecker, MD, a surgical resident at the University of Pennsylvania, Philadelphia.
“There is no shortage of high-quality data to help guide the use of [fistula reduction] strategies,” he added. However, “the utility of these strategies in patients most vulnerable to fistula … has rarely been particularly explored.”
Dr. Ecker and his colleagues conducted a study with 62 surgeons at 17 institutions to compare various fistula mitigation strategies in this higher-risk population. They assessed surgical reconstruction, dunking, tissue patches, intraperitoneal drains, stents, prophylactic octreotide, and use of tissue sealants.
“Ultimately, we want to know the best way to deal with this high-stakes situation, and whether outcomes might be optimized by bundling these proactive strategies,” Dr. Ecker explained.
“We found the combination of externalized stents and PJ [pancreaticojejunostomy] reconstruction with the omission of prophylactic octreotide was associated with significant improvements in fistula that exceeded the benefit of any individual mitigation approach or any other combination of strategies,” he said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“The mitigation of risk in real-life practice is often the result of multiple moving parts,” Dr. Ecker said. “The best outcomes [may result from] the synergistic effects of multiple strategies.”
Of the approximately 10% of patients with a Fistula Risk Score of 7-10, 152 ended up with clinically relevant postoperative pancreatic fistula (CR-POPF). “An FRS score of 7 or higher is associated with worse outcomes, including a fistula rate approaching 30%,” Dr. Ecker said. Grade B or C fistula based on International Study Group on Pancreatic Surgery criteria were considered clinically relevant. All patients had surgery from 2003 to 2016 in the retrospective, multinational study.
“This represents the only series of high-risk cases where current international standards were used to define both the risk and the outcome,” he noted.
“Almost all [of the 522] patients had a soft gland and a small duct, a median of 2 mm,” Dr. Ecker added. “High-risk pathology was common, in 86%.”
Surgeons contributing to the series were at high-volume centers and had performed more than 200 Whipple procedures in their careers. “Both institutional and surgeon volume were associated with improved fistula outcomes,” Dr. Ecker said. “We found that intraperitoneal drains were not associated with improved fistula outcomes, but that is limited by the fact that drains were rarely omitted in these cases.”
Four strategies compared
The investigators compared the outcomes of four fistula strategies among the patients considered high risk prior to surgery. When they combined pancreaticogastrostomy, prophylactic octreotide, and no stent, the CR-POPF rate was 47%. “This was associated with an alarming fistula rate approaching 50%,” Dr. Ecker said.
When surgeons combined pancreaticojejunostomy, octreotide, and no stent, the CR-POPF rate declined to 34%. Furthermore, pancreaticojejunostomy without octreotide or a stent yielded a 26% CR-POPF rate.
Ultimately, the most effective strategy to avoid clinically relevant fistula was pancreaticojejunostomy with an external stent and no octreotide.
“The use of PJ reconstruction with an external stent and omission of octreotide was associated with a fistula rate of about 13%, which was a greater than 50% risk reduction from the overall cohort,” Dr. Ecker said.
The researchers also performed propensity score matching to reduce bias associated with surgeon or patient factors. They matched 167 participants in the study with 155 controls. Dr. Ecker said, “Still, we observed that patients managed this way had significantly lower fistula rates.”
“This is an excellent paper and an important topic,” said study discussant Michael L. Kendrick, MD, a general surgeon at the Mayo Clinic in Rochester, Minn.
“At our institution, we’ve used the same Fistula Risk Score and found it very helpful for a mitigation strategy in a separate protocol, and we found that reduced our leak rates as well,” Dr. Kendrick noted.
Dr. Ecker and Dr. Kendrick had no relevant disclosures.
MIAMI BEACH – Pancreaticojejunostomy reconstruction, use of stents, and avoidance of prophylactic octreotide, especially in combination, could reduce the fistula rate associated with pancreatoduodenectomy.
Failure of the anastomosis is “of greatest concern” to surgeons performing a pancreatoduodenectomy, said Brett L. Ecker, MD, a surgical resident at the University of Pennsylvania, Philadelphia.
“There is no shortage of high-quality data to help guide the use of [fistula reduction] strategies,” he added. However, “the utility of these strategies in patients most vulnerable to fistula … has rarely been particularly explored.”
Dr. Ecker and his colleagues conducted a study with 62 surgeons at 17 institutions to compare various fistula mitigation strategies in this higher-risk population. They assessed surgical reconstruction, dunking, tissue patches, intraperitoneal drains, stents, prophylactic octreotide, and use of tissue sealants.
“Ultimately, we want to know the best way to deal with this high-stakes situation, and whether outcomes might be optimized by bundling these proactive strategies,” Dr. Ecker explained.
“We found the combination of externalized stents and PJ [pancreaticojejunostomy] reconstruction with the omission of prophylactic octreotide was associated with significant improvements in fistula that exceeded the benefit of any individual mitigation approach or any other combination of strategies,” he said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“The mitigation of risk in real-life practice is often the result of multiple moving parts,” Dr. Ecker said. “The best outcomes [may result from] the synergistic effects of multiple strategies.”
Of the approximately 10% of patients with a Fistula Risk Score of 7-10, 152 ended up with clinically relevant postoperative pancreatic fistula (CR-POPF). “An FRS score of 7 or higher is associated with worse outcomes, including a fistula rate approaching 30%,” Dr. Ecker said. Grade B or C fistula based on International Study Group on Pancreatic Surgery criteria were considered clinically relevant. All patients had surgery from 2003 to 2016 in the retrospective, multinational study.
“This represents the only series of high-risk cases where current international standards were used to define both the risk and the outcome,” he noted.
“Almost all [of the 522] patients had a soft gland and a small duct, a median of 2 mm,” Dr. Ecker added. “High-risk pathology was common, in 86%.”
Surgeons contributing to the series were at high-volume centers and had performed more than 200 Whipple procedures in their careers. “Both institutional and surgeon volume were associated with improved fistula outcomes,” Dr. Ecker said. “We found that intraperitoneal drains were not associated with improved fistula outcomes, but that is limited by the fact that drains were rarely omitted in these cases.”
Four strategies compared
The investigators compared the outcomes of four fistula strategies among the patients considered high risk prior to surgery. When they combined pancreaticogastrostomy, prophylactic octreotide, and no stent, the CR-POPF rate was 47%. “This was associated with an alarming fistula rate approaching 50%,” Dr. Ecker said.
When surgeons combined pancreaticojejunostomy, octreotide, and no stent, the CR-POPF rate declined to 34%. Furthermore, pancreaticojejunostomy without octreotide or a stent yielded a 26% CR-POPF rate.
Ultimately, the most effective strategy to avoid clinically relevant fistula was pancreaticojejunostomy with an external stent and no octreotide.
“The use of PJ reconstruction with an external stent and omission of octreotide was associated with a fistula rate of about 13%, which was a greater than 50% risk reduction from the overall cohort,” Dr. Ecker said.
The researchers also performed propensity score matching to reduce bias associated with surgeon or patient factors. They matched 167 participants in the study with 155 controls. Dr. Ecker said, “Still, we observed that patients managed this way had significantly lower fistula rates.”
“This is an excellent paper and an important topic,” said study discussant Michael L. Kendrick, MD, a general surgeon at the Mayo Clinic in Rochester, Minn.
“At our institution, we’ve used the same Fistula Risk Score and found it very helpful for a mitigation strategy in a separate protocol, and we found that reduced our leak rates as well,” Dr. Kendrick noted.
Dr. Ecker and Dr. Kendrick had no relevant disclosures.
AT AHPBA 2017
Key clinical point: Reconstruction, use of stents, and avoidance of octreotide, especially in combination, could reduce the fistula rate associated with pancreatoduodenectomy.
Major finding: The incidence of fistula decreased from 33% to 13% by combining the three strategies.
Data source: Multicenter retrospective study from 2003 to 2016 with 522 patients undergoing pancreatoduodenectomy.
Disclosures: Dr. Ecker and Dr. Kendrick had no relevant disclosures.
Liposomal bupivacaine cut need for opioids after gyn surgery
SAN ANTONIO – Liposomal bupivacaine reduced pain after midurethral sling surgery, compared with placebo in a randomized trial, but because of its cost it may be best to keep it in reserve for women who can’t, or shouldn’t, take opioids, said lead investigator Donna Mazloomdoost, MD, a gynecologic surgeon at Good Samaritan Hospital, Cincinnati.
Fifty-four women were randomized to receive liposomal bupivacaine (Exparel) injected into the two trocar paths and the vaginal incision at the end of the procedure; 55 others were injected with normal saline as a placebo.

Fewer women in the liposomal bupivacaine group took narcotics on postop day 2 (12 versus 27, P = .006). However, there was no difference in overall satisfaction with pain control at 1 and 2 weeks follow-up.
Even so, “for this common outpatient surgery, liposomal bupivacaine may be a beneficial addition for pain control,” the investigators concluded.
Liposomal bupivacaine is a local anesthetic with slow release over 72 hours, approved for treatment of postsurgical pain in 2011. “The cost is about $300 at our institution; the charge to the patient is about $1,000,” Dr. Mazloomdoost said at the annual scientific meeting of the Society of Gynecologic Surgeons.
Because of the expense, liposomal bupivacaine is restricted in many hospitals, and gynecologic surgeons are trying to figure out what role it has, if any, in low-pain outpatient procedures like midurethral slings.
“I don’t know if you can justify” routine use for low-pain procedures, “but if you are concerned about opioid” use after surgery – intolerance or addiction – “I would use this,” Dr. Mazloomdoost said.
The investigators expanded 20 mL of liposomal bupivacaine with 10 mL of normal saline for a total of 30 mL. It was split evenly between the two trocar sites and the vaginal epithelium; 10 mL was injected in each of the three sites shortly before the intervention women were roused from anesthesia. The needle was inserted as deeply as possible, and liposomal bupivacaine was injected as the needle was drawn back. Because of the viscosity, it takes at least a 25-gauge needle.
Surgeons knew that they were injecting liposomal bupivacaine instead of saline because of the thickness and color, but they weren’t the ones collecting data, and the women were blinded to the treatment.
Patients were a mean age of 52 years. The mean body mass index was 29.2 kg/m2 in the liposomal bupivacaine group, and 31.6 kg/m2 in the placebo group; there were otherwise no significant demographic differences. Fifty-two women in the liposomal bupivacaine group received midazolam during anesthesia induction versus 44 women receiving placebo, but there were no significant differences in operating time or the number of women in each group who had concomitant anterior or urethrocele repairs, and no differences in urinary retention, time to first bowel movement – about 2 days – or adverse events. The most common adverse events in both groups were nausea/vomiting, headache, and itching.
Women in both groups received intravenous acetaminophen before anesthesia induction, and ketorolac before leaving the operating room; 10 mL of lidocaine with epinephrine was injected into the trocar paths and vaginal epithelium prior to the first incision.
The investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
SAN ANTONIO – Liposomal bupivacaine reduced pain after midurethral sling surgery, compared with placebo in a randomized trial, but because of its cost it may be best to keep it in reserve for women who can’t, or shouldn’t, take opioids, said lead investigator Donna Mazloomdoost, MD, a gynecologic surgeon at Good Samaritan Hospital, Cincinnati.
Fifty-four women were randomized to receive liposomal bupivacaine (Exparel) injected into the two trocar paths and the vaginal incision at the end of the procedure; 55 others were injected with normal saline as a placebo.
Fewer women in the liposomal bupivacaine group took narcotics on postop day 2 (12 versus 27, P = .006). However, there was no difference in overall satisfaction with pain control at 1 and 2 weeks follow-up.
Even so, “for this common outpatient surgery, liposomal bupivacaine may be a beneficial addition for pain control,” the investigators concluded.
Liposomal bupivacaine is a local anesthetic with slow release over 72 hours, approved for treatment of postsurgical pain in 2011. “The cost is about $300 at our institution; the charge to the patient is about $1,000,” Dr. Mazloomdoost said at the annual scientific meeting of the Society of Gynecologic Surgeons.
Because of the expense, liposomal bupivacaine is restricted in many hospitals, and gynecologic surgeons are trying to figure out what role it has, if any, in low-pain outpatient procedures like midurethral slings.
“I don’t know if you can justify” routine use for low-pain procedures, “but if you are concerned about opioid” use after surgery – intolerance or addiction – “I would use this,” Dr. Mazloomdoost said.
The investigators expanded 20 mL of liposomal bupivacaine with 10 mL of normal saline for a total of 30 mL. It was split evenly between the two trocar sites and the vaginal epithelium; 10 mL was injected in each of the three sites shortly before the intervention women were roused from anesthesia. The needle was inserted as deeply as possible, and liposomal bupivacaine was injected as the needle was drawn back. Because of the viscosity, it takes at least a 25-gauge needle.
Surgeons knew that they were injecting liposomal bupivacaine instead of saline because of the thickness and color, but they weren’t the ones collecting data, and the women were blinded to the treatment.
Patients were a mean age of 52 years. The mean body mass index was 29.2 kg/m2 in the liposomal bupivacaine group, and 31.6 kg/m2 in the placebo group; there were otherwise no significant demographic differences. Fifty-two women in the liposomal bupivacaine group received midazolam during anesthesia induction versus 44 women receiving placebo, but there were no significant differences in operating time or the number of women in each group who had concomitant anterior or urethrocele repairs, and no differences in urinary retention, time to first bowel movement – about 2 days – or adverse events. The most common adverse events in both groups were nausea/vomiting, headache, and itching.
Women in both groups received intravenous acetaminophen before anesthesia induction, and ketorolac before leaving the operating room; 10 mL of lidocaine with epinephrine was injected into the trocar paths and vaginal epithelium prior to the first incision.
The investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
SAN ANTONIO – Liposomal bupivacaine reduced pain after midurethral sling surgery, compared with placebo in a randomized trial, but because of its cost it may be best to keep it in reserve for women who can’t, or shouldn’t, take opioids, said lead investigator Donna Mazloomdoost, MD, a gynecologic surgeon at Good Samaritan Hospital, Cincinnati.
Fifty-four women were randomized to receive liposomal bupivacaine (Exparel) injected into the two trocar paths and the vaginal incision at the end of the procedure; 55 others were injected with normal saline as a placebo.
Fewer women in the liposomal bupivacaine group took narcotics on postop day 2 (12 versus 27, P = .006). However, there was no difference in overall satisfaction with pain control at 1 and 2 weeks follow-up.
Even so, “for this common outpatient surgery, liposomal bupivacaine may be a beneficial addition for pain control,” the investigators concluded.
Liposomal bupivacaine is a local anesthetic with slow release over 72 hours, approved for treatment of postsurgical pain in 2011. “The cost is about $300 at our institution; the charge to the patient is about $1,000,” Dr. Mazloomdoost said at the annual scientific meeting of the Society of Gynecologic Surgeons.
Because of the expense, liposomal bupivacaine is restricted in many hospitals, and gynecologic surgeons are trying to figure out what role it has, if any, in low-pain outpatient procedures like midurethral slings.
“I don’t know if you can justify” routine use for low-pain procedures, “but if you are concerned about opioid” use after surgery – intolerance or addiction – “I would use this,” Dr. Mazloomdoost said.
The investigators expanded 20 mL of liposomal bupivacaine with 10 mL of normal saline for a total of 30 mL. It was split evenly between the two trocar sites and the vaginal epithelium; 10 mL was injected in each of the three sites shortly before the intervention women were roused from anesthesia. The needle was inserted as deeply as possible, and liposomal bupivacaine was injected as the needle was drawn back. Because of the viscosity, it takes at least a 25-gauge needle.
Surgeons knew that they were injecting liposomal bupivacaine instead of saline because of the thickness and color, but they weren’t the ones collecting data, and the women were blinded to the treatment.
Patients were a mean age of 52 years. The mean body mass index was 29.2 kg/m2 in the liposomal bupivacaine group, and 31.6 kg/m2 in the placebo group; there were otherwise no significant demographic differences. Fifty-two women in the liposomal bupivacaine group received midazolam during anesthesia induction versus 44 women receiving placebo, but there were no significant differences in operating time or the number of women in each group who had concomitant anterior or urethrocele repairs, and no differences in urinary retention, time to first bowel movement – about 2 days – or adverse events. The most common adverse events in both groups were nausea/vomiting, headache, and itching.
Women in both groups received intravenous acetaminophen before anesthesia induction, and ketorolac before leaving the operating room; 10 mL of lidocaine with epinephrine was injected into the trocar paths and vaginal epithelium prior to the first incision.
The investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
AT SGS 2017
Key clinical point:
Major finding: Pain scores, assessed by diary, were lower in the liposomal bupivacaine group 4 hours after discharge on a 100-mm visual analogue scale (3.5 mm versus 13 mm, P = .014).
Data source: Randomized trial with 109 women at Good Samaritan Hospital, Cincinnati.
Disclosures: The investigators reported having no relevant financial disclosures.
Malpractice: Paid claims down, but average payment up
The rate of paid legal claims against physicians dropped by more than half between 1992 and 2014, but the average claim payment amount rose, according to an analysis of the National Practitioner Data Bank.
Adam C. Schaffer, MD, of Brigham and Women’s Hospital, Boston, and his colleagues examined paid claims from the National Practitioner Data Bank from Jan. 1, 1992, to Dec. 31, 2014, accounting for specialty. Dollar amounts were inflation-adjusted to 2014 dollars using the Consumer Price Index.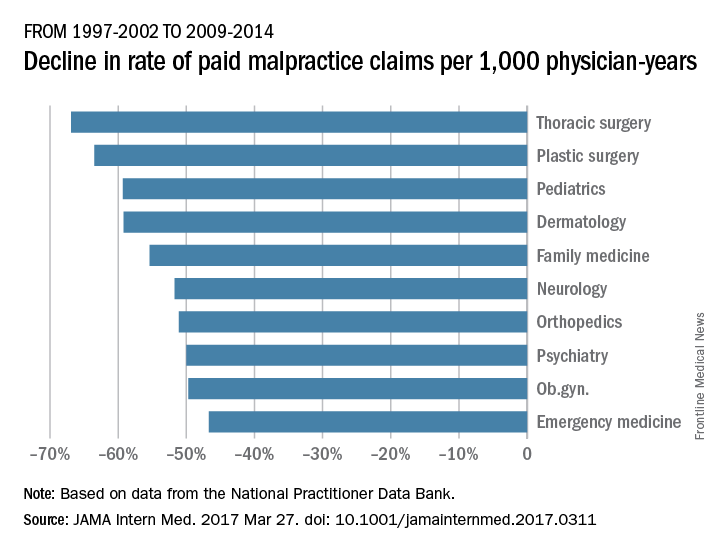
From 1992-1996 to 2009-2014, the rate of paid claims decreased by 56%, ranging from a 76% decrease in pediatrics to a 14% rate decrease in cardiology. The mean payment increased by 23% from $286,751 to $353,473 between 1992-1996 and 2009-2014. The increases ranged from $17,431 in general practice to $138,708 in pathology (JAMA Intern Med. 2017 Mar 27. doi: 10.1001/jamainternmed.2017.0311).
The most common allegation was diagnostic error, followed by surgical error and medication or treatment error. The proportion of paid claims attributable to diagnostic error varied widely and was highest in pathology and radiology. Plastic surgery had the highest percentage of paid claims related to surgical errors. Specialties with the highest percentage of paid claims related to medication/treatment errors were psychiatry, general practice, and pulmonology.
While prior data have shown the overall trend of declining paid malpractice claims and increasing average payments, this study is the first to examine such trends by medical specialty, said Dr. Schaffer.
“We think it is important to try to understand the reasons for the variation among specialties in characteristics of paid malpractice claims, as understanding the reasons for this variation may provide insights about how we can provide the safest care possible,” he said in an interview.
Dr. Schaffer said that he hopes the findings make physicians more aware of the malpractice landscape and aid their future practice decisions.
“Medical malpractice is an issue that concerns many physicians, and physicians’ perceptions of their liability risk can influence the decisions they make in caring for their patients,” he said. “By performing an analysis of a national database of paid medical malpractice claims broken down by specialty, we hope to provide physicians with data that give them an accurate picture of the medical malpractice environment in which they are practicing.”
[email protected]
On Twitter @legal_med
The rate of paid legal claims against physicians dropped by more than half between 1992 and 2014, but the average claim payment amount rose, according to an analysis of the National Practitioner Data Bank.
Adam C. Schaffer, MD, of Brigham and Women’s Hospital, Boston, and his colleagues examined paid claims from the National Practitioner Data Bank from Jan. 1, 1992, to Dec. 31, 2014, accounting for specialty. Dollar amounts were inflation-adjusted to 2014 dollars using the Consumer Price Index.
From 1992-1996 to 2009-2014, the rate of paid claims decreased by 56%, ranging from a 76% decrease in pediatrics to a 14% rate decrease in cardiology. The mean payment increased by 23% from $286,751 to $353,473 between 1992-1996 and 2009-2014. The increases ranged from $17,431 in general practice to $138,708 in pathology (JAMA Intern Med. 2017 Mar 27. doi: 10.1001/jamainternmed.2017.0311).
The most common allegation was diagnostic error, followed by surgical error and medication or treatment error. The proportion of paid claims attributable to diagnostic error varied widely and was highest in pathology and radiology. Plastic surgery had the highest percentage of paid claims related to surgical errors. Specialties with the highest percentage of paid claims related to medication/treatment errors were psychiatry, general practice, and pulmonology.
While prior data have shown the overall trend of declining paid malpractice claims and increasing average payments, this study is the first to examine such trends by medical specialty, said Dr. Schaffer.
“We think it is important to try to understand the reasons for the variation among specialties in characteristics of paid malpractice claims, as understanding the reasons for this variation may provide insights about how we can provide the safest care possible,” he said in an interview.
Dr. Schaffer said that he hopes the findings make physicians more aware of the malpractice landscape and aid their future practice decisions.
“Medical malpractice is an issue that concerns many physicians, and physicians’ perceptions of their liability risk can influence the decisions they make in caring for their patients,” he said. “By performing an analysis of a national database of paid medical malpractice claims broken down by specialty, we hope to provide physicians with data that give them an accurate picture of the medical malpractice environment in which they are practicing.”
[email protected]
On Twitter @legal_med
The rate of paid legal claims against physicians dropped by more than half between 1992 and 2014, but the average claim payment amount rose, according to an analysis of the National Practitioner Data Bank.
Adam C. Schaffer, MD, of Brigham and Women’s Hospital, Boston, and his colleagues examined paid claims from the National Practitioner Data Bank from Jan. 1, 1992, to Dec. 31, 2014, accounting for specialty. Dollar amounts were inflation-adjusted to 2014 dollars using the Consumer Price Index.
From 1992-1996 to 2009-2014, the rate of paid claims decreased by 56%, ranging from a 76% decrease in pediatrics to a 14% rate decrease in cardiology. The mean payment increased by 23% from $286,751 to $353,473 between 1992-1996 and 2009-2014. The increases ranged from $17,431 in general practice to $138,708 in pathology (JAMA Intern Med. 2017 Mar 27. doi: 10.1001/jamainternmed.2017.0311).
The most common allegation was diagnostic error, followed by surgical error and medication or treatment error. The proportion of paid claims attributable to diagnostic error varied widely and was highest in pathology and radiology. Plastic surgery had the highest percentage of paid claims related to surgical errors. Specialties with the highest percentage of paid claims related to medication/treatment errors were psychiatry, general practice, and pulmonology.
While prior data have shown the overall trend of declining paid malpractice claims and increasing average payments, this study is the first to examine such trends by medical specialty, said Dr. Schaffer.
“We think it is important to try to understand the reasons for the variation among specialties in characteristics of paid malpractice claims, as understanding the reasons for this variation may provide insights about how we can provide the safest care possible,” he said in an interview.
Dr. Schaffer said that he hopes the findings make physicians more aware of the malpractice landscape and aid their future practice decisions.
“Medical malpractice is an issue that concerns many physicians, and physicians’ perceptions of their liability risk can influence the decisions they make in caring for their patients,” he said. “By performing an analysis of a national database of paid medical malpractice claims broken down by specialty, we hope to provide physicians with data that give them an accurate picture of the medical malpractice environment in which they are practicing.”
[email protected]
On Twitter @legal_med
FROM JAMA INTERNAL MEDICINE
Apply By May 1 for International Scholarships for Surgical Education
Two international scholarships focused on surgical education and sponsored by the American College of Surgeons (ACS) Division of Education and the International Relations Committee will offer faculty members from countries outside the U.S. and Canada the opportunity to participate in a variety of faculty development activities. All application materials and supporting documents are due May 1.
The scholars will participate in the Surgical Education: Principles and Practice Course at the Clinical Congress 2017, October 22–26 in San Diego, CA. In addition, the scholars will attend plenary sessions and courses that address surgical education and training across the continuum of professional development. The scholars, in turn, will use the knowledge and skills they acquire to improve surgical education and training in their home institutions and countries. The scholarships include a stipend of $10,000 to cover travel, per diem expenses, and the cost of Clinical Congress courses. The registration cost for Clinical Congress and fees for the surgical education courses will be provided free to the scholars.
View the scholarship requirements and access the application on the ACS website at facs.org/member-services/scholarships/international/issurged. Direct questions to the ACS International Liaison at [email protected].
Two international scholarships focused on surgical education and sponsored by the American College of Surgeons (ACS) Division of Education and the International Relations Committee will offer faculty members from countries outside the U.S. and Canada the opportunity to participate in a variety of faculty development activities. All application materials and supporting documents are due May 1.
The scholars will participate in the Surgical Education: Principles and Practice Course at the Clinical Congress 2017, October 22–26 in San Diego, CA. In addition, the scholars will attend plenary sessions and courses that address surgical education and training across the continuum of professional development. The scholars, in turn, will use the knowledge and skills they acquire to improve surgical education and training in their home institutions and countries. The scholarships include a stipend of $10,000 to cover travel, per diem expenses, and the cost of Clinical Congress courses. The registration cost for Clinical Congress and fees for the surgical education courses will be provided free to the scholars.
View the scholarship requirements and access the application on the ACS website at facs.org/member-services/scholarships/international/issurged. Direct questions to the ACS International Liaison at [email protected].
Two international scholarships focused on surgical education and sponsored by the American College of Surgeons (ACS) Division of Education and the International Relations Committee will offer faculty members from countries outside the U.S. and Canada the opportunity to participate in a variety of faculty development activities. All application materials and supporting documents are due May 1.
The scholars will participate in the Surgical Education: Principles and Practice Course at the Clinical Congress 2017, October 22–26 in San Diego, CA. In addition, the scholars will attend plenary sessions and courses that address surgical education and training across the continuum of professional development. The scholars, in turn, will use the knowledge and skills they acquire to improve surgical education and training in their home institutions and countries. The scholarships include a stipend of $10,000 to cover travel, per diem expenses, and the cost of Clinical Congress courses. The registration cost for Clinical Congress and fees for the surgical education courses will be provided free to the scholars.
View the scholarship requirements and access the application on the ACS website at facs.org/member-services/scholarships/international/issurged. Direct questions to the ACS International Liaison at [email protected].
From the Washington Office: Advocacy in Action
Fellows frequently ask how they can get more involved in the advocacy efforts of the ACS. Whether you are new to the arena of policy and advocacy or an experienced veteran of innumerable efforts directed at ensuring access to quality surgical care, I can think of no better way to learn new skills and exercise old ones than by attending the ACS’ annual Leadership and Advocacy Summit.
The 2017 Leadership and Advocacy Summit will take place May 6–9 at the Renaissance Washington, DC Downtown Hotel. More than 300 individuals have already registered and you can join them by registering via the link found here: https://www.facs.org/advocacy/participate/summit-2017/register

The Advocacy Summit portion of the meeting will kick-off on the evening of May 7 with a reception and dinner featuring bestselling author, MSNBC political analyst, and former Communications Chief for President George W. Bush, Nicolle Wallace as the Keynote Speaker.
A robust agenda is planned for Monday, May 8. The morning will lead off with a panel entitled, Perspectives on 2017 Health Care Reform, featuring health policy experts from the Georgetown University Law Center, the George Washington University Milken Institute School of Public Health, the American Enterprise Institute, and the Heritage Foundation. The Monday agenda will also feature a panel of senior staffers from Capitol Hill discussing issues of particular interest to Fellows, a Medicare physician payment panel, and an address from a leading authority on effective communications strategies designed to make your interaction with legislators and their staff more effective.
The luncheon speaker for Monday will be Fox News contributor and Washington Examiner columnist, Lisa Boothe. The afternoon agenda will conclude with a series of issue briefings from ACS staff (in preparation for the Hill visits to legislator’s offices scheduled for Tuesday, May 9) and remarks from several United States Senators. ACSPA-SurgeonsPAC will host a reception on Monday evening, May 8 for all 2017 PAC contributors and a guest.
On Tuesday morning, May 9, attendees will be transported to Capitol Hill to visit the offices of their individual Member of Congress, Senators and staff with visits concluding in time to make flights out of Washington that afternoon.
I encourage all Fellows who are able to set aside time for the event to do so as I believe all will find the program educational and the experience rewarding.
For information about the Leadership Summit, contact Connie Bura at [email protected], or 312-919-5290. For information about the Advocacy Summit, contact Michael Carmody at [email protected], or 202-672-1511.
Until next month ….
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Fellows frequently ask how they can get more involved in the advocacy efforts of the ACS. Whether you are new to the arena of policy and advocacy or an experienced veteran of innumerable efforts directed at ensuring access to quality surgical care, I can think of no better way to learn new skills and exercise old ones than by attending the ACS’ annual Leadership and Advocacy Summit.
The 2017 Leadership and Advocacy Summit will take place May 6–9 at the Renaissance Washington, DC Downtown Hotel. More than 300 individuals have already registered and you can join them by registering via the link found here: https://www.facs.org/advocacy/participate/summit-2017/register
The Advocacy Summit portion of the meeting will kick-off on the evening of May 7 with a reception and dinner featuring bestselling author, MSNBC political analyst, and former Communications Chief for President George W. Bush, Nicolle Wallace as the Keynote Speaker.
A robust agenda is planned for Monday, May 8. The morning will lead off with a panel entitled, Perspectives on 2017 Health Care Reform, featuring health policy experts from the Georgetown University Law Center, the George Washington University Milken Institute School of Public Health, the American Enterprise Institute, and the Heritage Foundation. The Monday agenda will also feature a panel of senior staffers from Capitol Hill discussing issues of particular interest to Fellows, a Medicare physician payment panel, and an address from a leading authority on effective communications strategies designed to make your interaction with legislators and their staff more effective.
The luncheon speaker for Monday will be Fox News contributor and Washington Examiner columnist, Lisa Boothe. The afternoon agenda will conclude with a series of issue briefings from ACS staff (in preparation for the Hill visits to legislator’s offices scheduled for Tuesday, May 9) and remarks from several United States Senators. ACSPA-SurgeonsPAC will host a reception on Monday evening, May 8 for all 2017 PAC contributors and a guest.
On Tuesday morning, May 9, attendees will be transported to Capitol Hill to visit the offices of their individual Member of Congress, Senators and staff with visits concluding in time to make flights out of Washington that afternoon.
I encourage all Fellows who are able to set aside time for the event to do so as I believe all will find the program educational and the experience rewarding.
For information about the Leadership Summit, contact Connie Bura at [email protected], or 312-919-5290. For information about the Advocacy Summit, contact Michael Carmody at [email protected], or 202-672-1511.
Until next month ….
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Fellows frequently ask how they can get more involved in the advocacy efforts of the ACS. Whether you are new to the arena of policy and advocacy or an experienced veteran of innumerable efforts directed at ensuring access to quality surgical care, I can think of no better way to learn new skills and exercise old ones than by attending the ACS’ annual Leadership and Advocacy Summit.
The 2017 Leadership and Advocacy Summit will take place May 6–9 at the Renaissance Washington, DC Downtown Hotel. More than 300 individuals have already registered and you can join them by registering via the link found here: https://www.facs.org/advocacy/participate/summit-2017/register
The Advocacy Summit portion of the meeting will kick-off on the evening of May 7 with a reception and dinner featuring bestselling author, MSNBC political analyst, and former Communications Chief for President George W. Bush, Nicolle Wallace as the Keynote Speaker.
A robust agenda is planned for Monday, May 8. The morning will lead off with a panel entitled, Perspectives on 2017 Health Care Reform, featuring health policy experts from the Georgetown University Law Center, the George Washington University Milken Institute School of Public Health, the American Enterprise Institute, and the Heritage Foundation. The Monday agenda will also feature a panel of senior staffers from Capitol Hill discussing issues of particular interest to Fellows, a Medicare physician payment panel, and an address from a leading authority on effective communications strategies designed to make your interaction with legislators and their staff more effective.
The luncheon speaker for Monday will be Fox News contributor and Washington Examiner columnist, Lisa Boothe. The afternoon agenda will conclude with a series of issue briefings from ACS staff (in preparation for the Hill visits to legislator’s offices scheduled for Tuesday, May 9) and remarks from several United States Senators. ACSPA-SurgeonsPAC will host a reception on Monday evening, May 8 for all 2017 PAC contributors and a guest.
On Tuesday morning, May 9, attendees will be transported to Capitol Hill to visit the offices of their individual Member of Congress, Senators and staff with visits concluding in time to make flights out of Washington that afternoon.
I encourage all Fellows who are able to set aside time for the event to do so as I believe all will find the program educational and the experience rewarding.
For information about the Leadership Summit, contact Connie Bura at [email protected], or 312-919-5290. For information about the Advocacy Summit, contact Michael Carmody at [email protected], or 202-672-1511.
Until next month ….
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
2017 Claude H. Organ, Jr., MD, FACS Traveling Fellowship Applications due June 1
The family and friends of the late Dr. Claude H. Organ, Jr., established an endowment through the American College of Surgeons (ACS) Foundation to provide funding for an annual fellowship to be awarded to an outstanding young surgeon from the Society of Black Academic Surgeons, the Association of Women Surgeons, or the Surgical Section of the National Medical Association.
The fellowship, in the amount of $5,000, enables a U.S. or Canadian Fellow or Associate Fellow under age 45 who is a member of one of the above societies to attend an educational meeting or make an extended visit to an institution of his or her choice, tailored to his or her research interests.
Past awardees have used their fellowships to develop their careers in creative ways. The 2016 fellow, Stephanie Bonne, MD, is researching a successful hospital-based violence program in San Francisco in order to develop one at her home institution.
View the full requirements for the Claude H. Organ Traveling Fellowship at facs.org/member-services/scholarships/special/organ. The deadline for receipt of all application materials is June 1, with decisions to be made by August 2017. Questions and application materials should be submitted to the attention of the ACS Scholarships Administrator at [email protected].
The family and friends of the late Dr. Claude H. Organ, Jr., established an endowment through the American College of Surgeons (ACS) Foundation to provide funding for an annual fellowship to be awarded to an outstanding young surgeon from the Society of Black Academic Surgeons, the Association of Women Surgeons, or the Surgical Section of the National Medical Association.
The fellowship, in the amount of $5,000, enables a U.S. or Canadian Fellow or Associate Fellow under age 45 who is a member of one of the above societies to attend an educational meeting or make an extended visit to an institution of his or her choice, tailored to his or her research interests.
Past awardees have used their fellowships to develop their careers in creative ways. The 2016 fellow, Stephanie Bonne, MD, is researching a successful hospital-based violence program in San Francisco in order to develop one at her home institution.
View the full requirements for the Claude H. Organ Traveling Fellowship at facs.org/member-services/scholarships/special/organ. The deadline for receipt of all application materials is June 1, with decisions to be made by August 2017. Questions and application materials should be submitted to the attention of the ACS Scholarships Administrator at [email protected].
The family and friends of the late Dr. Claude H. Organ, Jr., established an endowment through the American College of Surgeons (ACS) Foundation to provide funding for an annual fellowship to be awarded to an outstanding young surgeon from the Society of Black Academic Surgeons, the Association of Women Surgeons, or the Surgical Section of the National Medical Association.
The fellowship, in the amount of $5,000, enables a U.S. or Canadian Fellow or Associate Fellow under age 45 who is a member of one of the above societies to attend an educational meeting or make an extended visit to an institution of his or her choice, tailored to his or her research interests.
Past awardees have used their fellowships to develop their careers in creative ways. The 2016 fellow, Stephanie Bonne, MD, is researching a successful hospital-based violence program in San Francisco in order to develop one at her home institution.
View the full requirements for the Claude H. Organ Traveling Fellowship at facs.org/member-services/scholarships/special/organ. The deadline for receipt of all application materials is June 1, with decisions to be made by August 2017. Questions and application materials should be submitted to the attention of the ACS Scholarships Administrator at [email protected].
Access new surgeon and resident well-being resources
Personal and professional well-being are vital to the success of members of the American College of Surgeons (ACS) and your patients. Many health care professionals experience periods of distress, yet few physicians seek help. In an effort to provide relief to interested surgeons, the ACS has compiled several resources to support surgeons and residents as they confront the challenges associated with surgical care.
Visit the ACS Surgeon Well-Being page at facs.org/burnout to learn more about the tool and how to access it, as well as to review other helpful resources.
Personal and professional well-being are vital to the success of members of the American College of Surgeons (ACS) and your patients. Many health care professionals experience periods of distress, yet few physicians seek help. In an effort to provide relief to interested surgeons, the ACS has compiled several resources to support surgeons and residents as they confront the challenges associated with surgical care.
Visit the ACS Surgeon Well-Being page at facs.org/burnout to learn more about the tool and how to access it, as well as to review other helpful resources.
Personal and professional well-being are vital to the success of members of the American College of Surgeons (ACS) and your patients. Many health care professionals experience periods of distress, yet few physicians seek help. In an effort to provide relief to interested surgeons, the ACS has compiled several resources to support surgeons and residents as they confront the challenges associated with surgical care.
Visit the ACS Surgeon Well-Being page at facs.org/burnout to learn more about the tool and how to access it, as well as to review other helpful resources.
Three days in the life of a surgeon
By sheer happenstance, I was visiting a surgery program on the day after “the Match.” As all of you know, four days before the official release of the placement of every new surgical trainee, both the medical students involved and the programs affected are informed as to whether they have been matched. Students don’t know where they are going, just that the last rung of training is now in place. They have a job and a relatively secure future. Those who have not been matched and those programs that did not fill all their slots now enter into a scramble (officially called SOAP) to find students for the remaining slots. This year, the scramble occurred on a Wednesday and was orchestrated by a set of rules I’d never been privy to before.
On Tuesday night, all the programs in need of students for their open slots, whether categorical or preliminary, looked over the list of candidates remaining and made their choices. So did the students now hoping to find a place. At 10 a.m., the offers went out to students in the first round. Next, in precisely timed order, the programs found out who had accepted the offers. And, if slots were left over, the programs had a short time to put up another set of offers – and so on throughout the day until all the slots were gone. Like a game of musical chairs, the music finally stopped and the Match was over for the entering class of residents for 2017.


Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and coeditor of ACS Surgery News.
By sheer happenstance, I was visiting a surgery program on the day after “the Match.” As all of you know, four days before the official release of the placement of every new surgical trainee, both the medical students involved and the programs affected are informed as to whether they have been matched. Students don’t know where they are going, just that the last rung of training is now in place. They have a job and a relatively secure future. Those who have not been matched and those programs that did not fill all their slots now enter into a scramble (officially called SOAP) to find students for the remaining slots. This year, the scramble occurred on a Wednesday and was orchestrated by a set of rules I’d never been privy to before.
On Tuesday night, all the programs in need of students for their open slots, whether categorical or preliminary, looked over the list of candidates remaining and made their choices. So did the students now hoping to find a place. At 10 a.m., the offers went out to students in the first round. Next, in precisely timed order, the programs found out who had accepted the offers. And, if slots were left over, the programs had a short time to put up another set of offers – and so on throughout the day until all the slots were gone. Like a game of musical chairs, the music finally stopped and the Match was over for the entering class of residents for 2017.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and coeditor of ACS Surgery News.
By sheer happenstance, I was visiting a surgery program on the day after “the Match.” As all of you know, four days before the official release of the placement of every new surgical trainee, both the medical students involved and the programs affected are informed as to whether they have been matched. Students don’t know where they are going, just that the last rung of training is now in place. They have a job and a relatively secure future. Those who have not been matched and those programs that did not fill all their slots now enter into a scramble (officially called SOAP) to find students for the remaining slots. This year, the scramble occurred on a Wednesday and was orchestrated by a set of rules I’d never been privy to before.
On Tuesday night, all the programs in need of students for their open slots, whether categorical or preliminary, looked over the list of candidates remaining and made their choices. So did the students now hoping to find a place. At 10 a.m., the offers went out to students in the first round. Next, in precisely timed order, the programs found out who had accepted the offers. And, if slots were left over, the programs had a short time to put up another set of offers – and so on throughout the day until all the slots were gone. Like a game of musical chairs, the music finally stopped and the Match was over for the entering class of residents for 2017.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and coeditor of ACS Surgery News.