User login
Official Newspaper of the American College of Surgeons
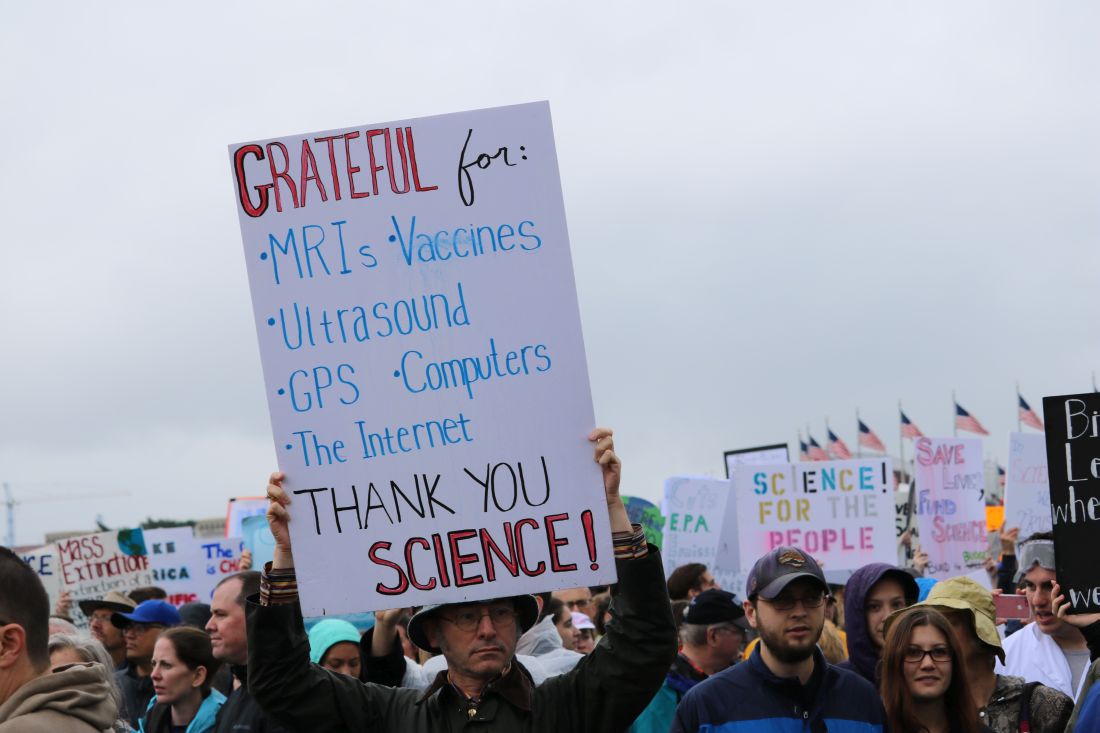
Science advocates take to D.C. streets in March for Science
WASHINGTON – Crowds of protesters packed the Washington’s National Mall for the March for Science, joining participants in 600 cities across the world on Saturday, April 22.
Advocates came in droves, braving the rain armed with homemade signs, chants, and a passion for peer review, to champion the scientific method and the importance of its role in society and policy making.
The event, organized by March for Science, Earth Day Network, and a robust list of advocacy groups and think tanks, started with learning sessions hosted in tents located beyond the Washington Monument, where experts in topics from physics to environmental science informed attendees about the importance of their subjects.
To the left of the tents, directly across from the White House, scores gathered around a large stage, where 56 science professionals from different fields came together to promote the importance of scientific research and science-based policy.
The main stage event was emceed by musician Questlove and Tyler DeWitt, PhD, host of the YouTube science education show “Science with Tyler DeWitt.”
“You cannot criticize a public that doesn’t understand science if we can’t explain it,” said Dr. DeWitt.

“A strong commitment to research is absolutely essential to crafting evidence-based policies to protect us from serious health threats,” said Georges C. Benjamin, MD, executive director of the America Public Health Association. “A nation that ignores science, that denies science, that underfunds science, does so at its own peril.”
Speakers like Kellan Baker, senior fellow with the LGBT Research and Communications Project at the Center for American Progress, promoted political action, echoing organizers’ intentions of being bipartisan but not shying away from promoting political action.
“Advocacy is not a dirty word” said Mr. Baker. “Science is objective, but it is not neutral.”
Other speakers included Mona Hanna-Attisha, MD, the pediatrician who helped expose the lead poisoning situation in Flint, Mich., and Bill Nye, CEO of the Planetary Society and host of the Netflix series “Bill Nye Saves the World.”
After speeches, protesters marched from the Washington Monument to the U.S. Capitol, chanting loudly and waving signs.
March for Science and its partners are continuing to promote advocacy through a “week of action” scheduled to run through April 29.
*This article was updated May 2, 2017.
[email protected]
On Twitter @eaztweets
WASHINGTON – Crowds of protesters packed the Washington’s National Mall for the March for Science, joining participants in 600 cities across the world on Saturday, April 22.
Advocates came in droves, braving the rain armed with homemade signs, chants, and a passion for peer review, to champion the scientific method and the importance of its role in society and policy making.
The event, organized by March for Science, Earth Day Network, and a robust list of advocacy groups and think tanks, started with learning sessions hosted in tents located beyond the Washington Monument, where experts in topics from physics to environmental science informed attendees about the importance of their subjects.
To the left of the tents, directly across from the White House, scores gathered around a large stage, where 56 science professionals from different fields came together to promote the importance of scientific research and science-based policy.
The main stage event was emceed by musician Questlove and Tyler DeWitt, PhD, host of the YouTube science education show “Science with Tyler DeWitt.”
“You cannot criticize a public that doesn’t understand science if we can’t explain it,” said Dr. DeWitt.
“A strong commitment to research is absolutely essential to crafting evidence-based policies to protect us from serious health threats,” said Georges C. Benjamin, MD, executive director of the America Public Health Association. “A nation that ignores science, that denies science, that underfunds science, does so at its own peril.”
Speakers like Kellan Baker, senior fellow with the LGBT Research and Communications Project at the Center for American Progress, promoted political action, echoing organizers’ intentions of being bipartisan but not shying away from promoting political action.
“Advocacy is not a dirty word” said Mr. Baker. “Science is objective, but it is not neutral.”
Other speakers included Mona Hanna-Attisha, MD, the pediatrician who helped expose the lead poisoning situation in Flint, Mich., and Bill Nye, CEO of the Planetary Society and host of the Netflix series “Bill Nye Saves the World.”
After speeches, protesters marched from the Washington Monument to the U.S. Capitol, chanting loudly and waving signs.
March for Science and its partners are continuing to promote advocacy through a “week of action” scheduled to run through April 29.
*This article was updated May 2, 2017.
[email protected]
On Twitter @eaztweets
WASHINGTON – Crowds of protesters packed the Washington’s National Mall for the March for Science, joining participants in 600 cities across the world on Saturday, April 22.
Advocates came in droves, braving the rain armed with homemade signs, chants, and a passion for peer review, to champion the scientific method and the importance of its role in society and policy making.
The event, organized by March for Science, Earth Day Network, and a robust list of advocacy groups and think tanks, started with learning sessions hosted in tents located beyond the Washington Monument, where experts in topics from physics to environmental science informed attendees about the importance of their subjects.
To the left of the tents, directly across from the White House, scores gathered around a large stage, where 56 science professionals from different fields came together to promote the importance of scientific research and science-based policy.
The main stage event was emceed by musician Questlove and Tyler DeWitt, PhD, host of the YouTube science education show “Science with Tyler DeWitt.”
“You cannot criticize a public that doesn’t understand science if we can’t explain it,” said Dr. DeWitt.
“A strong commitment to research is absolutely essential to crafting evidence-based policies to protect us from serious health threats,” said Georges C. Benjamin, MD, executive director of the America Public Health Association. “A nation that ignores science, that denies science, that underfunds science, does so at its own peril.”
Speakers like Kellan Baker, senior fellow with the LGBT Research and Communications Project at the Center for American Progress, promoted political action, echoing organizers’ intentions of being bipartisan but not shying away from promoting political action.
“Advocacy is not a dirty word” said Mr. Baker. “Science is objective, but it is not neutral.”
Other speakers included Mona Hanna-Attisha, MD, the pediatrician who helped expose the lead poisoning situation in Flint, Mich., and Bill Nye, CEO of the Planetary Society and host of the Netflix series “Bill Nye Saves the World.”
After speeches, protesters marched from the Washington Monument to the U.S. Capitol, chanting loudly and waving signs.
March for Science and its partners are continuing to promote advocacy through a “week of action” scheduled to run through April 29.
*This article was updated May 2, 2017.
[email protected]
On Twitter @eaztweets
VIDEO: Geeks brave rain to March for Science
WASHINGTON – Peaceful protesters in hundreds of cities around the globe gathered on Earth Day, April 22, to voice their support for evidence-based policies and funding for scientific research at the March for Science.
In Washington, thousands of participants gathered on the rainy National Mall for teach-ins and speeches, then marched from the Washington Monument to Capitol Hill. A key concern for marchers here was cuts in science agency funding in the Trump administration’s budget proposal for fiscal year 2018.
Organizers now are calling on supporters to participate in a week of action to continue to demonstrate widespread support for their positions.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @denisefulton
WASHINGTON – Peaceful protesters in hundreds of cities around the globe gathered on Earth Day, April 22, to voice their support for evidence-based policies and funding for scientific research at the March for Science.
In Washington, thousands of participants gathered on the rainy National Mall for teach-ins and speeches, then marched from the Washington Monument to Capitol Hill. A key concern for marchers here was cuts in science agency funding in the Trump administration’s budget proposal for fiscal year 2018.
Organizers now are calling on supporters to participate in a week of action to continue to demonstrate widespread support for their positions.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @denisefulton
WASHINGTON – Peaceful protesters in hundreds of cities around the globe gathered on Earth Day, April 22, to voice their support for evidence-based policies and funding for scientific research at the March for Science.
In Washington, thousands of participants gathered on the rainy National Mall for teach-ins and speeches, then marched from the Washington Monument to Capitol Hill. A key concern for marchers here was cuts in science agency funding in the Trump administration’s budget proposal for fiscal year 2018.
Organizers now are calling on supporters to participate in a week of action to continue to demonstrate widespread support for their positions.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @denisefulton
Plazomicin beats gold standard antibiotics in complex, gram-negative bacterial infections
VIENNA – An investigational antibiotic effective against several types of gram-negative antibiotic-resistant bacteria has proved its mettle against serious infections of the urinary tract, respiratory tract, and bloodstream.
Plazomicin (Achaogen, San Francisco) posted good results in two phase III studies, handily besting comparator drugs considered gold standard for treating complicated urinary tract infections and pyelonephritis, as well as bloodstream infections and hospital- and ventilator-associated bacterial pneumonia.
Both the EPIC (Evaluating Plazomicin In cUTI) and CARE (Combating Antibiotic Resistant Enterobacteriaceae) trials have provided enough positive data for the company to move forward with a new drug application later this year. The company also plans to seek European Medicines Agency approval in 2018.
Plazomicin is an aminoglycoside that has been modified with several side chains that block aminoglycoside-modifying enzymes, Daniel Cloutier, PhD, principal clinical scientist of Achaogen said at the European Society of Clinical Microbiology and Infectious Disease annual congress.
“Aminoglycoside enzymes tend to travel along with beta-lactamases and carbapenemases as well, so this drug retains potent bactericidal activity against extended spectrum beta-lactamase producing Enterobacteriaceae, carbapenem-resistant Enterobacteriaceae, and aminoglycoside-resistant Enterobacteriaceae,” said Dr. Cloutier, who presented the results of the EPIC trial. The drug is given once-daily as a 30-minute intravenous infusion.
EPIC enrolled 609 adult patients with complicated urinary tract infections or acute pyelonephritis; Dr. Cloutier presented a modified intent-to-treat analysis comprising 388 of these. They were randomized to plazomicin 15 mg/kg every 25 hours or to IV meropenem 1 gram every 24 hours. Treatment proceeded for 4-7 days, after which patients could step down to oral therapy (levofloxacin 500 m/day), for a total of 7-10 days of treatment. About 80% of patients had both IV and oral therapy. At 15-19 days from the first dose, patients had a test of cure; at 24-32 days from first dose, they returned for a safety follow-up.
Patients were a mean of 60 years old. About 60% had a complicated UTI; the rest had acute pyelonephritis. About 35% had a mean creatinine clearance of more than 30-60 mL/min; the rest had a mean clearance of more than 60-90 mL/min.
The primary efficacy endpoint was microbial eradication. Plazomicin performed significantly better than meropenem in this measure (87% vs.72%), a mean difference of about 15%. Patients with pyelonephritis responded marginally better than those with complicated UTI, both groups favoring plazomicin (mean treatment differences of 17.5% and 13.7%, respectively).
The results were similar when the investigators examined groups by whether they needed oral step-down treatment. In the IV-only groups, plazomicin bested meropenem in microbiological eradication by almost 19% (84% vs. 65%). In the IV plus oral therapy group, the mean difference was 14%, also in favor of plazomicin (88% vs. 74%).
Plazomicin was significantly more effective then meropenem in all of the resistant Enterobacteriaceae groups (ESBL-positive, and levofloxacin- and aminoglycoside-resistant). It was also significantly more effective against E. coli (17% treatment difference), Klebsiella pneumonia (9%), and Proteus mirabilis (25%). However, it was 20% less effective than meropenem against E. cloacae.
At late follow-up, 2% of the plazomicin group and 8% of the meropenem group had relapsed – a significant difference.
Plazomicin and meropenem had similar safety profiles. Diarrhea and hypertension were the most common adverse events (about 2% in each group). Headache occurred in 3% of the meropenem patients and 1% of the plazomicin patients. Nausea, vomiting, and anemia occurred in about 1% of each group.
More patients taking plazomicin experienced a serum creatinine clearance increase of at least 0.5 mg/dL during treatment (7% vs. 4%). All but two patients taking plazomicin experienced a full recovery by the last follow-up visit.
The CARE trial was much smaller, comprised of 39 patients who had either bloodstream infections, or hospital-acquired or ventilator-associated bacterial pneumonia caused by carbapenem-resistant Enterobacteriaceae. Lynn Connolly, MD, senior medical director and head of late development at Achaogen, presented the data. Recruitment for such a narrow diagnosis was difficult, and hampered patient accrual, she noted.
CARE’s primary endpoints were a combination of all-cause mortality and significant disease-related complications, and all-cause mortality only, both at 28 days.
Patients were randomized 1:1 to either plazomicin 15 mg/kg every 24 hours, or colistin in a 300-mg loading dose, followed by daily infusions of 5 mg/kg. Everyone, regardless of treatment group, could also receive meropenem or tigecycline if deemed necessary. Treatment lasted 7-14 days. There was a test of cure at 7 days from the last IV dose, a safety assessment at 28 days, and a long-term follow-up at 60 days.
The patients’ mean age was about 65 years. Most (about 80%) had a bloodstream infection; bacterial pneumonias were present in the remainder. Most infections (85%) were monomicrobial, with polymicrobial infections making up the balance. Tigecycline was the favored adjunctive therapy (60%), followed by meropenem.
At day 28, plazomicin was associated with significantly better overall outcomes than colistin. It reduced the combination mortality/significant disease complications endpoint by 26% (23% vs. 50% meropenem). This translated to a 53% relative reduction in the risk of death.
Plazomicin also reduced all-cause mortality only by 28% (12% vs. 40% meropenem). This translated to a relative risk reduction of 70.5%.
The study drug performed well in the subgroup of patients with bloodstream infections, reducing the occurrence of the composite endpoint by 39% (14% vs. 53%), and of the mortality-only endpoint by 33% (7% vs. 40%). This translated to a 63% increased chance of 60-day survival in the plazomicin group.
Almost all patients in each group experienced at least one adverse event; 28% were deemed related to plazomicin and 43% to colistin. Many of these events were related to renal function (33% plazomicin, 52% colistin). Serum creatinine increases of at least 0.5 mg/dL during IV treatment occurred in fewer taking plazomicin (1 vs. 6 taking colistin). Full renal recovery occurred in the patient taking plazomicin, but only in three taking colistin.
“These data suggest that plazomicin could offer an important new treatment option for patients with serious infections due to carbapenem-resistant Enterobacteriaceae,” Dr. Connolly said.
[email protected]
On Twitter @Alz_gal
VIENNA – An investigational antibiotic effective against several types of gram-negative antibiotic-resistant bacteria has proved its mettle against serious infections of the urinary tract, respiratory tract, and bloodstream.
Plazomicin (Achaogen, San Francisco) posted good results in two phase III studies, handily besting comparator drugs considered gold standard for treating complicated urinary tract infections and pyelonephritis, as well as bloodstream infections and hospital- and ventilator-associated bacterial pneumonia.
Both the EPIC (Evaluating Plazomicin In cUTI) and CARE (Combating Antibiotic Resistant Enterobacteriaceae) trials have provided enough positive data for the company to move forward with a new drug application later this year. The company also plans to seek European Medicines Agency approval in 2018.
Plazomicin is an aminoglycoside that has been modified with several side chains that block aminoglycoside-modifying enzymes, Daniel Cloutier, PhD, principal clinical scientist of Achaogen said at the European Society of Clinical Microbiology and Infectious Disease annual congress.
“Aminoglycoside enzymes tend to travel along with beta-lactamases and carbapenemases as well, so this drug retains potent bactericidal activity against extended spectrum beta-lactamase producing Enterobacteriaceae, carbapenem-resistant Enterobacteriaceae, and aminoglycoside-resistant Enterobacteriaceae,” said Dr. Cloutier, who presented the results of the EPIC trial. The drug is given once-daily as a 30-minute intravenous infusion.
EPIC enrolled 609 adult patients with complicated urinary tract infections or acute pyelonephritis; Dr. Cloutier presented a modified intent-to-treat analysis comprising 388 of these. They were randomized to plazomicin 15 mg/kg every 25 hours or to IV meropenem 1 gram every 24 hours. Treatment proceeded for 4-7 days, after which patients could step down to oral therapy (levofloxacin 500 m/day), for a total of 7-10 days of treatment. About 80% of patients had both IV and oral therapy. At 15-19 days from the first dose, patients had a test of cure; at 24-32 days from first dose, they returned for a safety follow-up.
Patients were a mean of 60 years old. About 60% had a complicated UTI; the rest had acute pyelonephritis. About 35% had a mean creatinine clearance of more than 30-60 mL/min; the rest had a mean clearance of more than 60-90 mL/min.
The primary efficacy endpoint was microbial eradication. Plazomicin performed significantly better than meropenem in this measure (87% vs.72%), a mean difference of about 15%. Patients with pyelonephritis responded marginally better than those with complicated UTI, both groups favoring plazomicin (mean treatment differences of 17.5% and 13.7%, respectively).
The results were similar when the investigators examined groups by whether they needed oral step-down treatment. In the IV-only groups, plazomicin bested meropenem in microbiological eradication by almost 19% (84% vs. 65%). In the IV plus oral therapy group, the mean difference was 14%, also in favor of plazomicin (88% vs. 74%).
Plazomicin was significantly more effective then meropenem in all of the resistant Enterobacteriaceae groups (ESBL-positive, and levofloxacin- and aminoglycoside-resistant). It was also significantly more effective against E. coli (17% treatment difference), Klebsiella pneumonia (9%), and Proteus mirabilis (25%). However, it was 20% less effective than meropenem against E. cloacae.
At late follow-up, 2% of the plazomicin group and 8% of the meropenem group had relapsed – a significant difference.
Plazomicin and meropenem had similar safety profiles. Diarrhea and hypertension were the most common adverse events (about 2% in each group). Headache occurred in 3% of the meropenem patients and 1% of the plazomicin patients. Nausea, vomiting, and anemia occurred in about 1% of each group.
More patients taking plazomicin experienced a serum creatinine clearance increase of at least 0.5 mg/dL during treatment (7% vs. 4%). All but two patients taking plazomicin experienced a full recovery by the last follow-up visit.
The CARE trial was much smaller, comprised of 39 patients who had either bloodstream infections, or hospital-acquired or ventilator-associated bacterial pneumonia caused by carbapenem-resistant Enterobacteriaceae. Lynn Connolly, MD, senior medical director and head of late development at Achaogen, presented the data. Recruitment for such a narrow diagnosis was difficult, and hampered patient accrual, she noted.
CARE’s primary endpoints were a combination of all-cause mortality and significant disease-related complications, and all-cause mortality only, both at 28 days.
Patients were randomized 1:1 to either plazomicin 15 mg/kg every 24 hours, or colistin in a 300-mg loading dose, followed by daily infusions of 5 mg/kg. Everyone, regardless of treatment group, could also receive meropenem or tigecycline if deemed necessary. Treatment lasted 7-14 days. There was a test of cure at 7 days from the last IV dose, a safety assessment at 28 days, and a long-term follow-up at 60 days.
The patients’ mean age was about 65 years. Most (about 80%) had a bloodstream infection; bacterial pneumonias were present in the remainder. Most infections (85%) were monomicrobial, with polymicrobial infections making up the balance. Tigecycline was the favored adjunctive therapy (60%), followed by meropenem.
At day 28, plazomicin was associated with significantly better overall outcomes than colistin. It reduced the combination mortality/significant disease complications endpoint by 26% (23% vs. 50% meropenem). This translated to a 53% relative reduction in the risk of death.
Plazomicin also reduced all-cause mortality only by 28% (12% vs. 40% meropenem). This translated to a relative risk reduction of 70.5%.
The study drug performed well in the subgroup of patients with bloodstream infections, reducing the occurrence of the composite endpoint by 39% (14% vs. 53%), and of the mortality-only endpoint by 33% (7% vs. 40%). This translated to a 63% increased chance of 60-day survival in the plazomicin group.
Almost all patients in each group experienced at least one adverse event; 28% were deemed related to plazomicin and 43% to colistin. Many of these events were related to renal function (33% plazomicin, 52% colistin). Serum creatinine increases of at least 0.5 mg/dL during IV treatment occurred in fewer taking plazomicin (1 vs. 6 taking colistin). Full renal recovery occurred in the patient taking plazomicin, but only in three taking colistin.
“These data suggest that plazomicin could offer an important new treatment option for patients with serious infections due to carbapenem-resistant Enterobacteriaceae,” Dr. Connolly said.
[email protected]
On Twitter @Alz_gal
VIENNA – An investigational antibiotic effective against several types of gram-negative antibiotic-resistant bacteria has proved its mettle against serious infections of the urinary tract, respiratory tract, and bloodstream.
Plazomicin (Achaogen, San Francisco) posted good results in two phase III studies, handily besting comparator drugs considered gold standard for treating complicated urinary tract infections and pyelonephritis, as well as bloodstream infections and hospital- and ventilator-associated bacterial pneumonia.
Both the EPIC (Evaluating Plazomicin In cUTI) and CARE (Combating Antibiotic Resistant Enterobacteriaceae) trials have provided enough positive data for the company to move forward with a new drug application later this year. The company also plans to seek European Medicines Agency approval in 2018.
Plazomicin is an aminoglycoside that has been modified with several side chains that block aminoglycoside-modifying enzymes, Daniel Cloutier, PhD, principal clinical scientist of Achaogen said at the European Society of Clinical Microbiology and Infectious Disease annual congress.
“Aminoglycoside enzymes tend to travel along with beta-lactamases and carbapenemases as well, so this drug retains potent bactericidal activity against extended spectrum beta-lactamase producing Enterobacteriaceae, carbapenem-resistant Enterobacteriaceae, and aminoglycoside-resistant Enterobacteriaceae,” said Dr. Cloutier, who presented the results of the EPIC trial. The drug is given once-daily as a 30-minute intravenous infusion.
EPIC enrolled 609 adult patients with complicated urinary tract infections or acute pyelonephritis; Dr. Cloutier presented a modified intent-to-treat analysis comprising 388 of these. They were randomized to plazomicin 15 mg/kg every 25 hours or to IV meropenem 1 gram every 24 hours. Treatment proceeded for 4-7 days, after which patients could step down to oral therapy (levofloxacin 500 m/day), for a total of 7-10 days of treatment. About 80% of patients had both IV and oral therapy. At 15-19 days from the first dose, patients had a test of cure; at 24-32 days from first dose, they returned for a safety follow-up.
Patients were a mean of 60 years old. About 60% had a complicated UTI; the rest had acute pyelonephritis. About 35% had a mean creatinine clearance of more than 30-60 mL/min; the rest had a mean clearance of more than 60-90 mL/min.
The primary efficacy endpoint was microbial eradication. Plazomicin performed significantly better than meropenem in this measure (87% vs.72%), a mean difference of about 15%. Patients with pyelonephritis responded marginally better than those with complicated UTI, both groups favoring plazomicin (mean treatment differences of 17.5% and 13.7%, respectively).
The results were similar when the investigators examined groups by whether they needed oral step-down treatment. In the IV-only groups, plazomicin bested meropenem in microbiological eradication by almost 19% (84% vs. 65%). In the IV plus oral therapy group, the mean difference was 14%, also in favor of plazomicin (88% vs. 74%).
Plazomicin was significantly more effective then meropenem in all of the resistant Enterobacteriaceae groups (ESBL-positive, and levofloxacin- and aminoglycoside-resistant). It was also significantly more effective against E. coli (17% treatment difference), Klebsiella pneumonia (9%), and Proteus mirabilis (25%). However, it was 20% less effective than meropenem against E. cloacae.
At late follow-up, 2% of the plazomicin group and 8% of the meropenem group had relapsed – a significant difference.
Plazomicin and meropenem had similar safety profiles. Diarrhea and hypertension were the most common adverse events (about 2% in each group). Headache occurred in 3% of the meropenem patients and 1% of the plazomicin patients. Nausea, vomiting, and anemia occurred in about 1% of each group.
More patients taking plazomicin experienced a serum creatinine clearance increase of at least 0.5 mg/dL during treatment (7% vs. 4%). All but two patients taking plazomicin experienced a full recovery by the last follow-up visit.
The CARE trial was much smaller, comprised of 39 patients who had either bloodstream infections, or hospital-acquired or ventilator-associated bacterial pneumonia caused by carbapenem-resistant Enterobacteriaceae. Lynn Connolly, MD, senior medical director and head of late development at Achaogen, presented the data. Recruitment for such a narrow diagnosis was difficult, and hampered patient accrual, she noted.
CARE’s primary endpoints were a combination of all-cause mortality and significant disease-related complications, and all-cause mortality only, both at 28 days.
Patients were randomized 1:1 to either plazomicin 15 mg/kg every 24 hours, or colistin in a 300-mg loading dose, followed by daily infusions of 5 mg/kg. Everyone, regardless of treatment group, could also receive meropenem or tigecycline if deemed necessary. Treatment lasted 7-14 days. There was a test of cure at 7 days from the last IV dose, a safety assessment at 28 days, and a long-term follow-up at 60 days.
The patients’ mean age was about 65 years. Most (about 80%) had a bloodstream infection; bacterial pneumonias were present in the remainder. Most infections (85%) were monomicrobial, with polymicrobial infections making up the balance. Tigecycline was the favored adjunctive therapy (60%), followed by meropenem.
At day 28, plazomicin was associated with significantly better overall outcomes than colistin. It reduced the combination mortality/significant disease complications endpoint by 26% (23% vs. 50% meropenem). This translated to a 53% relative reduction in the risk of death.
Plazomicin also reduced all-cause mortality only by 28% (12% vs. 40% meropenem). This translated to a relative risk reduction of 70.5%.
The study drug performed well in the subgroup of patients with bloodstream infections, reducing the occurrence of the composite endpoint by 39% (14% vs. 53%), and of the mortality-only endpoint by 33% (7% vs. 40%). This translated to a 63% increased chance of 60-day survival in the plazomicin group.
Almost all patients in each group experienced at least one adverse event; 28% were deemed related to plazomicin and 43% to colistin. Many of these events were related to renal function (33% plazomicin, 52% colistin). Serum creatinine increases of at least 0.5 mg/dL during IV treatment occurred in fewer taking plazomicin (1 vs. 6 taking colistin). Full renal recovery occurred in the patient taking plazomicin, but only in three taking colistin.
“These data suggest that plazomicin could offer an important new treatment option for patients with serious infections due to carbapenem-resistant Enterobacteriaceae,” Dr. Connolly said.
[email protected]
On Twitter @Alz_gal
Study underscores antipsoriatic effect of gastric bypass surgery
Gastric bypass surgery was associated with more than a 50% drop in baseline rates of psoriasis, and with about a 70% decrease in the incidence of psoriatic arthritis, investigators reported.
In contrast, gastric banding did not appear to affect baselines rates of either of these autoimmune conditions, Alexander Egeberg, MD, of Herlev and Gentofte Hospital, Hellerup, Denmark, and associates reported in JAMA Surgery. “Although speculative, these findings may be the result of post-operative differences in weight loss and nutrient uptake, as well as differences in the postsurgical secretion of a number of gut hormones, including [glucagon-like peptide-1],” they wrote.
Psoriasis strongly correlates with obesity, and weight loss appears to mitigate psoriatic symptoms, the investigators noted. Previously, small studies and case series indicated that bariatric surgery might induce remission of psoriasis. To further investigate this possibility, Dr. Egeberg and his associates conducted a longitudinal cohort study of all 12,364 patients who underwent gastric bypass surgery and all 1,071 patients who underwent gastric banding in Denmark between 1997 and 2012 (JAMA Surg. 2017;152:344-349). No patient had psoriasis symptoms at the start of the study. A total of 272 (2%) gastric bypass patients developed psoriasis before their surgery, while only 0.5% did so afterward. In contrast, gastric banding was not tied to a significant change in the incidence of psoriasis – the preoperative rate was 0.5%, and the postoperative rate was 0.4%. Similarly, respective rates of psoriatic arthritis were 0.5% and 0.1% before and after gastric bypass, but were 0.3% and 0.6% before and after gastric banding. Additionally, respective rates of severe psoriasis were 0.8% and 0% before and after gastric bypass, but were about 0.2% and 0.5% before and after gastric banding.
After adjusting for age, sex, alcohol abuse, socioeconomic status, smoking, and diabetes status, gastric bypass was associated with about a 48% drop in the incidence of any type of psoriasis (P = .004), with about a 56% drop in the rate of severe psoriasis (P = .02), and with about a 71% drop in the rate of psoriatic arthritis (P = .01). In contrast, neither crude nor adjusted models linked gastric banding to a decrease in the incidence of psoriasis, severe psoriasis, or psoriatic arthritis, the researchers said.
Gastric banding is “a purely restrictive procedure,” while gastric bypass – especially Roux-en-Y bypass – diverts nutrients to the distal small intestine, where enteroendocrine cells secrete GLP-1, the researchers wrote.
“These postoperative hormonal changes may, in addition to the weight loss, be important for the antipsoriatic effect of gastric bypass,” they added. “Both gastric bypass and gastric banding have been shown to lead to sustained weight loss, suggesting that the observed differences in our study might be caused by factors other than weight loss.”
An unrestricted research grant from the Novo Nordisk Foundation funded the work. Dr. Egeberg disclosed ties to Pfizer and Eli Lilly. One coinvestigator disclosed ties to these and several other pharmaceutical companies.
Gastric bypass surgery was associated with more than a 50% drop in baseline rates of psoriasis, and with about a 70% decrease in the incidence of psoriatic arthritis, investigators reported.
In contrast, gastric banding did not appear to affect baselines rates of either of these autoimmune conditions, Alexander Egeberg, MD, of Herlev and Gentofte Hospital, Hellerup, Denmark, and associates reported in JAMA Surgery. “Although speculative, these findings may be the result of post-operative differences in weight loss and nutrient uptake, as well as differences in the postsurgical secretion of a number of gut hormones, including [glucagon-like peptide-1],” they wrote.
Psoriasis strongly correlates with obesity, and weight loss appears to mitigate psoriatic symptoms, the investigators noted. Previously, small studies and case series indicated that bariatric surgery might induce remission of psoriasis. To further investigate this possibility, Dr. Egeberg and his associates conducted a longitudinal cohort study of all 12,364 patients who underwent gastric bypass surgery and all 1,071 patients who underwent gastric banding in Denmark between 1997 and 2012 (JAMA Surg. 2017;152:344-349). No patient had psoriasis symptoms at the start of the study. A total of 272 (2%) gastric bypass patients developed psoriasis before their surgery, while only 0.5% did so afterward. In contrast, gastric banding was not tied to a significant change in the incidence of psoriasis – the preoperative rate was 0.5%, and the postoperative rate was 0.4%. Similarly, respective rates of psoriatic arthritis were 0.5% and 0.1% before and after gastric bypass, but were 0.3% and 0.6% before and after gastric banding. Additionally, respective rates of severe psoriasis were 0.8% and 0% before and after gastric bypass, but were about 0.2% and 0.5% before and after gastric banding.
After adjusting for age, sex, alcohol abuse, socioeconomic status, smoking, and diabetes status, gastric bypass was associated with about a 48% drop in the incidence of any type of psoriasis (P = .004), with about a 56% drop in the rate of severe psoriasis (P = .02), and with about a 71% drop in the rate of psoriatic arthritis (P = .01). In contrast, neither crude nor adjusted models linked gastric banding to a decrease in the incidence of psoriasis, severe psoriasis, or psoriatic arthritis, the researchers said.
Gastric banding is “a purely restrictive procedure,” while gastric bypass – especially Roux-en-Y bypass – diverts nutrients to the distal small intestine, where enteroendocrine cells secrete GLP-1, the researchers wrote.
“These postoperative hormonal changes may, in addition to the weight loss, be important for the antipsoriatic effect of gastric bypass,” they added. “Both gastric bypass and gastric banding have been shown to lead to sustained weight loss, suggesting that the observed differences in our study might be caused by factors other than weight loss.”
An unrestricted research grant from the Novo Nordisk Foundation funded the work. Dr. Egeberg disclosed ties to Pfizer and Eli Lilly. One coinvestigator disclosed ties to these and several other pharmaceutical companies.
Gastric bypass surgery was associated with more than a 50% drop in baseline rates of psoriasis, and with about a 70% decrease in the incidence of psoriatic arthritis, investigators reported.
In contrast, gastric banding did not appear to affect baselines rates of either of these autoimmune conditions, Alexander Egeberg, MD, of Herlev and Gentofte Hospital, Hellerup, Denmark, and associates reported in JAMA Surgery. “Although speculative, these findings may be the result of post-operative differences in weight loss and nutrient uptake, as well as differences in the postsurgical secretion of a number of gut hormones, including [glucagon-like peptide-1],” they wrote.
Psoriasis strongly correlates with obesity, and weight loss appears to mitigate psoriatic symptoms, the investigators noted. Previously, small studies and case series indicated that bariatric surgery might induce remission of psoriasis. To further investigate this possibility, Dr. Egeberg and his associates conducted a longitudinal cohort study of all 12,364 patients who underwent gastric bypass surgery and all 1,071 patients who underwent gastric banding in Denmark between 1997 and 2012 (JAMA Surg. 2017;152:344-349). No patient had psoriasis symptoms at the start of the study. A total of 272 (2%) gastric bypass patients developed psoriasis before their surgery, while only 0.5% did so afterward. In contrast, gastric banding was not tied to a significant change in the incidence of psoriasis – the preoperative rate was 0.5%, and the postoperative rate was 0.4%. Similarly, respective rates of psoriatic arthritis were 0.5% and 0.1% before and after gastric bypass, but were 0.3% and 0.6% before and after gastric banding. Additionally, respective rates of severe psoriasis were 0.8% and 0% before and after gastric bypass, but were about 0.2% and 0.5% before and after gastric banding.
After adjusting for age, sex, alcohol abuse, socioeconomic status, smoking, and diabetes status, gastric bypass was associated with about a 48% drop in the incidence of any type of psoriasis (P = .004), with about a 56% drop in the rate of severe psoriasis (P = .02), and with about a 71% drop in the rate of psoriatic arthritis (P = .01). In contrast, neither crude nor adjusted models linked gastric banding to a decrease in the incidence of psoriasis, severe psoriasis, or psoriatic arthritis, the researchers said.
Gastric banding is “a purely restrictive procedure,” while gastric bypass – especially Roux-en-Y bypass – diverts nutrients to the distal small intestine, where enteroendocrine cells secrete GLP-1, the researchers wrote.
“These postoperative hormonal changes may, in addition to the weight loss, be important for the antipsoriatic effect of gastric bypass,” they added. “Both gastric bypass and gastric banding have been shown to lead to sustained weight loss, suggesting that the observed differences in our study might be caused by factors other than weight loss.”
An unrestricted research grant from the Novo Nordisk Foundation funded the work. Dr. Egeberg disclosed ties to Pfizer and Eli Lilly. One coinvestigator disclosed ties to these and several other pharmaceutical companies.
Key clinical point: Gastric bypass, but not gastric banding, was associated with significant drops in rates of psoriasis and psoriatic arthritis.
Major finding: In an adjusted model, gastric bypass was associated with about a 48% drop in the incidence of any type of psoriasis, with a 56% drop in the rate of severe psoriasis, and with a 71% drop in the rate of psoriatic arthritis.
Data source: A population-based cohort study of 12,364 gastric bypass patients and 1,071 gastric banding patients.
Disclosures: An unrestricted research grant from the Novo Nordisk Foundation funded the work. Dr. Egeberg disclosed ties to Pfizer and Eli Lilly. One coinvestigator disclosed ties to these and several other pharmaceutical companies. The other coinvestigators reported having no ties to industry.
EHR price alert doesn’t reduce lab orders
Displaying Medicare allowable fees in the electronic health record at the time of order entry did not significantly reduce the number of inpatient lab tests at three Philadelphia hospitals.
In a study involving 98,529 patients and 142,921 admissions, Medicare payment information popped up randomly in the EHR when standard tests including complete blood cell counts, metabolic panels, and liver function tests were ordered. The costs of the labs varied depending on their extent. The message mentioned that “the dollar amount represents Medicare reimbursement for the test. Actual costs to the consumer may vary by patient insurance status.” Just over a third of the patients were actually on Medicare; most had private insurance.
The idea of the study was to see if cost information would curb unnecessary testing, and save money. “There is growing interest in using price transparency to influence medical decision-making toward higher value care,” Mina Sedrak, MD, and her colleagues said in a paper presented at the annual meeting of the Society of General Internal Medicine.
It didn’t work out that way. Four tests ordered per patient day when the messages appeared, and 2.34 when they did not. With messaging, the mean lab fee per patient day was $38.85, versus $27.59 without it. In an adjusted analyses comparing the intervention to the control group, there were no significant changes in overall test ordering (0.05 tests ordered per patient day, P = .06) or associated fees when pricing information was displayed ($0.24 per patient day; P = .47).
In a subset analysis, the investigators did find a small decrease orders for the most expensive labs and a small but significant increase in orders for the least expensive ones when physicians aware of cost (top quartile of tests based on fee value: -0.01; P = .04; bottom quartile: 0.03, P = .04).
Despite the overall negative results, there’s still a likely role for cost information in value improvement programs; what the study shows is that there’s a better way to use it, according to Dr. Sedrak, currently of the City of Hope Comprehensive Cancer Center in Duarte, Calif., and colleagues.
The investigators made several suggestions when reviewing their work.
“First, the price transparency intervention in this study was always displayed regardless of the clinical scenario. The presence of this information for appropriate tests may have diminished its impact when tests were inappropriate. Future efforts may consider more selective targeting of price transparency.” It might also be a good idea to price out different testing options for providers, and use actual charges and other more on-point forms of cost estimates, they said, instead of Medicare fees that have little to do with what many patients are actually charged. Targeting only the most expensive tests might also help (JAMA Intern Med. 2017 April 21. doi: 10.1001/jamainternmed.2017.1144).
The investigators also noticed a problem when labs are ordered to repeat automatically; clinicians did not see the price information every day, and so missed cost information “when it would be most salient.”
The mean age in the study was 54.7 years; 52% of the patients were white, 39% black, and 57% women. The mean length of stay was about 6 days, and over 80% of the patients were discharged home.
The authors evaluated what happens when one randomizes which tests have price information; other studies examine what happens when one randomizes which physicians have price information. All contemporary studies conclude the same – no effect of price information on physician ordering behavior.
One possible conclusion is that making health care prices available at the point of care is not an effective strategy to decrease wasteful spending, yet we believe this is not the case.

The disconnect suggests that current price transparency initiatives are not enough to infuse clinical care with price information and encourage consumers and physicians to consider the value of health care decisions. This does not mean we should give up on increased price transparency in health care. Rather, a more thoughtful approach to the design, point of delivery, and context for health care price information is needed to achieve the promise of price transparency.
Little has been done to deliver [out-of-pocket cost] information to patients at the time when patients are making health care decisions. Also, if both patients and physicians could see prices for episodes or bundles of care, then it could allow them to assess value together. Future interventions need to deliver price and quality information together.
Anna Sinaiko, PhD, is a research scientist at the Harvard School of Public Health, Boston. Alyna Chien, MD, is an assistant professor of pediatrics at the Harvard Medical School and a healthcare quality researcher. They made their comments in an editorial, and had no relevant disclosures (JAMA Intern Med. 2017 April 21. doi: 10.1001/jamainternmed.2017.1676 ).
The authors evaluated what happens when one randomizes which tests have price information; other studies examine what happens when one randomizes which physicians have price information. All contemporary studies conclude the same – no effect of price information on physician ordering behavior.
One possible conclusion is that making health care prices available at the point of care is not an effective strategy to decrease wasteful spending, yet we believe this is not the case.
The disconnect suggests that current price transparency initiatives are not enough to infuse clinical care with price information and encourage consumers and physicians to consider the value of health care decisions. This does not mean we should give up on increased price transparency in health care. Rather, a more thoughtful approach to the design, point of delivery, and context for health care price information is needed to achieve the promise of price transparency.
Little has been done to deliver [out-of-pocket cost] information to patients at the time when patients are making health care decisions. Also, if both patients and physicians could see prices for episodes or bundles of care, then it could allow them to assess value together. Future interventions need to deliver price and quality information together.
Anna Sinaiko, PhD, is a research scientist at the Harvard School of Public Health, Boston. Alyna Chien, MD, is an assistant professor of pediatrics at the Harvard Medical School and a healthcare quality researcher. They made their comments in an editorial, and had no relevant disclosures (JAMA Intern Med. 2017 April 21. doi: 10.1001/jamainternmed.2017.1676 ).
The authors evaluated what happens when one randomizes which tests have price information; other studies examine what happens when one randomizes which physicians have price information. All contemporary studies conclude the same – no effect of price information on physician ordering behavior.
One possible conclusion is that making health care prices available at the point of care is not an effective strategy to decrease wasteful spending, yet we believe this is not the case.
The disconnect suggests that current price transparency initiatives are not enough to infuse clinical care with price information and encourage consumers and physicians to consider the value of health care decisions. This does not mean we should give up on increased price transparency in health care. Rather, a more thoughtful approach to the design, point of delivery, and context for health care price information is needed to achieve the promise of price transparency.
Little has been done to deliver [out-of-pocket cost] information to patients at the time when patients are making health care decisions. Also, if both patients and physicians could see prices for episodes or bundles of care, then it could allow them to assess value together. Future interventions need to deliver price and quality information together.
Anna Sinaiko, PhD, is a research scientist at the Harvard School of Public Health, Boston. Alyna Chien, MD, is an assistant professor of pediatrics at the Harvard Medical School and a healthcare quality researcher. They made their comments in an editorial, and had no relevant disclosures (JAMA Intern Med. 2017 April 21. doi: 10.1001/jamainternmed.2017.1676 ).
Displaying Medicare allowable fees in the electronic health record at the time of order entry did not significantly reduce the number of inpatient lab tests at three Philadelphia hospitals.
In a study involving 98,529 patients and 142,921 admissions, Medicare payment information popped up randomly in the EHR when standard tests including complete blood cell counts, metabolic panels, and liver function tests were ordered. The costs of the labs varied depending on their extent. The message mentioned that “the dollar amount represents Medicare reimbursement for the test. Actual costs to the consumer may vary by patient insurance status.” Just over a third of the patients were actually on Medicare; most had private insurance.
The idea of the study was to see if cost information would curb unnecessary testing, and save money. “There is growing interest in using price transparency to influence medical decision-making toward higher value care,” Mina Sedrak, MD, and her colleagues said in a paper presented at the annual meeting of the Society of General Internal Medicine.
It didn’t work out that way. Four tests ordered per patient day when the messages appeared, and 2.34 when they did not. With messaging, the mean lab fee per patient day was $38.85, versus $27.59 without it. In an adjusted analyses comparing the intervention to the control group, there were no significant changes in overall test ordering (0.05 tests ordered per patient day, P = .06) or associated fees when pricing information was displayed ($0.24 per patient day; P = .47).
In a subset analysis, the investigators did find a small decrease orders for the most expensive labs and a small but significant increase in orders for the least expensive ones when physicians aware of cost (top quartile of tests based on fee value: -0.01; P = .04; bottom quartile: 0.03, P = .04).
Despite the overall negative results, there’s still a likely role for cost information in value improvement programs; what the study shows is that there’s a better way to use it, according to Dr. Sedrak, currently of the City of Hope Comprehensive Cancer Center in Duarte, Calif., and colleagues.
The investigators made several suggestions when reviewing their work.
“First, the price transparency intervention in this study was always displayed regardless of the clinical scenario. The presence of this information for appropriate tests may have diminished its impact when tests were inappropriate. Future efforts may consider more selective targeting of price transparency.” It might also be a good idea to price out different testing options for providers, and use actual charges and other more on-point forms of cost estimates, they said, instead of Medicare fees that have little to do with what many patients are actually charged. Targeting only the most expensive tests might also help (JAMA Intern Med. 2017 April 21. doi: 10.1001/jamainternmed.2017.1144).
The investigators also noticed a problem when labs are ordered to repeat automatically; clinicians did not see the price information every day, and so missed cost information “when it would be most salient.”
The mean age in the study was 54.7 years; 52% of the patients were white, 39% black, and 57% women. The mean length of stay was about 6 days, and over 80% of the patients were discharged home.
Displaying Medicare allowable fees in the electronic health record at the time of order entry did not significantly reduce the number of inpatient lab tests at three Philadelphia hospitals.
In a study involving 98,529 patients and 142,921 admissions, Medicare payment information popped up randomly in the EHR when standard tests including complete blood cell counts, metabolic panels, and liver function tests were ordered. The costs of the labs varied depending on their extent. The message mentioned that “the dollar amount represents Medicare reimbursement for the test. Actual costs to the consumer may vary by patient insurance status.” Just over a third of the patients were actually on Medicare; most had private insurance.
The idea of the study was to see if cost information would curb unnecessary testing, and save money. “There is growing interest in using price transparency to influence medical decision-making toward higher value care,” Mina Sedrak, MD, and her colleagues said in a paper presented at the annual meeting of the Society of General Internal Medicine.
It didn’t work out that way. Four tests ordered per patient day when the messages appeared, and 2.34 when they did not. With messaging, the mean lab fee per patient day was $38.85, versus $27.59 without it. In an adjusted analyses comparing the intervention to the control group, there were no significant changes in overall test ordering (0.05 tests ordered per patient day, P = .06) or associated fees when pricing information was displayed ($0.24 per patient day; P = .47).
In a subset analysis, the investigators did find a small decrease orders for the most expensive labs and a small but significant increase in orders for the least expensive ones when physicians aware of cost (top quartile of tests based on fee value: -0.01; P = .04; bottom quartile: 0.03, P = .04).
Despite the overall negative results, there’s still a likely role for cost information in value improvement programs; what the study shows is that there’s a better way to use it, according to Dr. Sedrak, currently of the City of Hope Comprehensive Cancer Center in Duarte, Calif., and colleagues.
The investigators made several suggestions when reviewing their work.
“First, the price transparency intervention in this study was always displayed regardless of the clinical scenario. The presence of this information for appropriate tests may have diminished its impact when tests were inappropriate. Future efforts may consider more selective targeting of price transparency.” It might also be a good idea to price out different testing options for providers, and use actual charges and other more on-point forms of cost estimates, they said, instead of Medicare fees that have little to do with what many patients are actually charged. Targeting only the most expensive tests might also help (JAMA Intern Med. 2017 April 21. doi: 10.1001/jamainternmed.2017.1144).
The investigators also noticed a problem when labs are ordered to repeat automatically; clinicians did not see the price information every day, and so missed cost information “when it would be most salient.”
The mean age in the study was 54.7 years; 52% of the patients were white, 39% black, and 57% women. The mean length of stay was about 6 days, and over 80% of the patients were discharged home.
Key clinical point:
Major finding: There were no significant changes in overall test ordering (0.05 tests ordered per patient day, P = .06) or associated fees when pricing information was displayed ($0.24 per patient day; P = .47).
Data source: Analysis involving 98,529 patients and 142,921 admissions of the effect of Medicare reimbursement information on lab test ordering
Disclosures: This study was funded by the University of Pennsylvania Health System. The senior investigator Mitesh Patel, MD, an assistant professor of medicine at the University of Pennsylvania, Philadelphia, is a principal at Catalyst Health, a technology and behavioral change consulting firm. The authors had no other disclosures.
For doctors, a clampdown on visas could have an uneven effect in the U.S.
Limiting the number of foreign doctors who can get visas to practice in the United States could have a significant impact on certain hospitals and states that rely on them, according to a new study.
The research, published online in JAMA this week, found that more than 2,100 U.S. employers were certified to fill nearly 10,500 physician jobs nationwide, in 2016. That represents 1.4% of the physician workforce overall. There were wide variations by state and employer, however (JAMA. 2017 Apr 17. doi: 10.1001/jama.2017.4877).
Employers in New York, Michigan and Illinois accounted for the most H-1B visa applications for foreign physicians, nearly a third of the total. North Dakota, however, had the most applicants as a percentage of its physician workforce: 4.7%.
The top three employers that submitted applications for the most doctors through the visa program were William Beaumont Hospital in Royal Oak, Mich., with 470 physician applications, Bronx-Lebanon (N.Y.) Hospital Center, with 213, and Cleveland Clinic Foundation, with 180.
“People underestimate the fragility of certain hospitals and their reliance on certain physicians for their functioning,” said study coauthor Peter Kahn, who graduates from Albert Einstein College of Medicine, New York, this spring.
The H-1B visa program allows employers to hire highly skilled professionals from abroad to fill employment gaps in the United States, typically in high-tech, science, engineering, and math jobs. But hospitals use the program as well, often to recruit doctors to serve in rural or underserved urban areas. The number of visas is capped at 85,000 annually.
That could change. On Tuesday, President Donald Trump signed an executive order reiterating his administration’s priority to buy American goods and hire American workers. Among other things, it requires federal agencies to suggest reforms to the H-1B visa program to ensure the visas are awarded appropriately.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Limiting the number of foreign doctors who can get visas to practice in the United States could have a significant impact on certain hospitals and states that rely on them, according to a new study.
The research, published online in JAMA this week, found that more than 2,100 U.S. employers were certified to fill nearly 10,500 physician jobs nationwide, in 2016. That represents 1.4% of the physician workforce overall. There were wide variations by state and employer, however (JAMA. 2017 Apr 17. doi: 10.1001/jama.2017.4877).
Employers in New York, Michigan and Illinois accounted for the most H-1B visa applications for foreign physicians, nearly a third of the total. North Dakota, however, had the most applicants as a percentage of its physician workforce: 4.7%.
The top three employers that submitted applications for the most doctors through the visa program were William Beaumont Hospital in Royal Oak, Mich., with 470 physician applications, Bronx-Lebanon (N.Y.) Hospital Center, with 213, and Cleveland Clinic Foundation, with 180.
“People underestimate the fragility of certain hospitals and their reliance on certain physicians for their functioning,” said study coauthor Peter Kahn, who graduates from Albert Einstein College of Medicine, New York, this spring.
The H-1B visa program allows employers to hire highly skilled professionals from abroad to fill employment gaps in the United States, typically in high-tech, science, engineering, and math jobs. But hospitals use the program as well, often to recruit doctors to serve in rural or underserved urban areas. The number of visas is capped at 85,000 annually.
That could change. On Tuesday, President Donald Trump signed an executive order reiterating his administration’s priority to buy American goods and hire American workers. Among other things, it requires federal agencies to suggest reforms to the H-1B visa program to ensure the visas are awarded appropriately.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Limiting the number of foreign doctors who can get visas to practice in the United States could have a significant impact on certain hospitals and states that rely on them, according to a new study.
The research, published online in JAMA this week, found that more than 2,100 U.S. employers were certified to fill nearly 10,500 physician jobs nationwide, in 2016. That represents 1.4% of the physician workforce overall. There were wide variations by state and employer, however (JAMA. 2017 Apr 17. doi: 10.1001/jama.2017.4877).
Employers in New York, Michigan and Illinois accounted for the most H-1B visa applications for foreign physicians, nearly a third of the total. North Dakota, however, had the most applicants as a percentage of its physician workforce: 4.7%.
The top three employers that submitted applications for the most doctors through the visa program were William Beaumont Hospital in Royal Oak, Mich., with 470 physician applications, Bronx-Lebanon (N.Y.) Hospital Center, with 213, and Cleveland Clinic Foundation, with 180.
“People underestimate the fragility of certain hospitals and their reliance on certain physicians for their functioning,” said study coauthor Peter Kahn, who graduates from Albert Einstein College of Medicine, New York, this spring.
The H-1B visa program allows employers to hire highly skilled professionals from abroad to fill employment gaps in the United States, typically in high-tech, science, engineering, and math jobs. But hospitals use the program as well, often to recruit doctors to serve in rural or underserved urban areas. The number of visas is capped at 85,000 annually.
That could change. On Tuesday, President Donald Trump signed an executive order reiterating his administration’s priority to buy American goods and hire American workers. Among other things, it requires federal agencies to suggest reforms to the H-1B visa program to ensure the visas are awarded appropriately.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
ASBS annual meeting to explore treatment controversies
ACS Surgery News will be in Las Vegas this week at the annual meeting of the American Society of Breast Surgeons reporting on the latest in multidisciplinary management of benign and not-so-benign breast disease. Our reporters will cover controversies in neoadjuvant therapy, including managing axilla and skipping surgery with biopsy proven pathological complete response (pCR), as well as the use of axillary ultrasound on a clinically negative axilla, and what to do for in situ carcinoma and borderline cases. Coverage will also include the latest updates in high-risk and genetic predisposition, breast cancer subtypes, lymphedema, and recurrent and metastatic breast cancer, and guidance for coding and reimbursement.
Highly anticipated presentations include:
• Many Women are Choosing Unnecessarily Radical Surgeries for Early-Stage Cancer
• Debunking the Myth of Lymphedema Risk
• Aggressive Inflammatory Breast Cancer Treatment Yields Low Local/Regional Recurrence
Our team will provide daily coverage, beginning Thursday, April 27.
ACS Surgery News will be in Las Vegas this week at the annual meeting of the American Society of Breast Surgeons reporting on the latest in multidisciplinary management of benign and not-so-benign breast disease. Our reporters will cover controversies in neoadjuvant therapy, including managing axilla and skipping surgery with biopsy proven pathological complete response (pCR), as well as the use of axillary ultrasound on a clinically negative axilla, and what to do for in situ carcinoma and borderline cases. Coverage will also include the latest updates in high-risk and genetic predisposition, breast cancer subtypes, lymphedema, and recurrent and metastatic breast cancer, and guidance for coding and reimbursement.
Highly anticipated presentations include:
• Many Women are Choosing Unnecessarily Radical Surgeries for Early-Stage Cancer
• Debunking the Myth of Lymphedema Risk
• Aggressive Inflammatory Breast Cancer Treatment Yields Low Local/Regional Recurrence
Our team will provide daily coverage, beginning Thursday, April 27.
ACS Surgery News will be in Las Vegas this week at the annual meeting of the American Society of Breast Surgeons reporting on the latest in multidisciplinary management of benign and not-so-benign breast disease. Our reporters will cover controversies in neoadjuvant therapy, including managing axilla and skipping surgery with biopsy proven pathological complete response (pCR), as well as the use of axillary ultrasound on a clinically negative axilla, and what to do for in situ carcinoma and borderline cases. Coverage will also include the latest updates in high-risk and genetic predisposition, breast cancer subtypes, lymphedema, and recurrent and metastatic breast cancer, and guidance for coding and reimbursement.
Highly anticipated presentations include:
• Many Women are Choosing Unnecessarily Radical Surgeries for Early-Stage Cancer
• Debunking the Myth of Lymphedema Risk
• Aggressive Inflammatory Breast Cancer Treatment Yields Low Local/Regional Recurrence
Our team will provide daily coverage, beginning Thursday, April 27.
FROM ASBS 2017
Can public reporting improve pediatric heart surgery?
Public reporting of cardiac surgery outcomes has been a disruptive force in cardiology, and especially daunting in pediatric cardiac surgery because of low case volumes and rare mortality. To ensure that public reporting achieves its original goals – providing transparency to the patient care process, holding providers accountable, informing decision making for health care consumers, reducing costs, encouraging more efficient use of health system resources, and improving patient care and outcomes – further study that includes use of appropriate risk adjustment is needed, according to commentaries in the April issue of the Journal of Thoracic and Cardiovascular Surgery.
The journal asked two groups to provide perspective on a study Adam D. DeVore, MD, of Duke University in Durham, N.C., and his coauthors published last year (J Am Coll Cardiol. 2016 Mar 1;67:963-72). The study analyzed Medicare claims data from 2006 to 2012 for 37,829 hospitalizations for heart attack, 100,189 for heart failure (HF), and 79,076 for pneumonia. Dr. DeVore and his colleagues found readmission rates for the three conditions did not significantly improve after public reporting protocols were implemented in 2009. However, the study did show a significant decrease in ED visits and observation stays for those with HF: from 2.3% to –0.8% for the former (P = .007); and from 15% to 4% for the latter (P = .04).
• The metrics must be accurate, reliably discern hospital quality, and account for high-risk cases without penalizing hospitals. “In pediatric cardiac surgery, this can be particularly challenging, owing to the very wide heterogeneity of disease and variability in case mix and volumes across centers,” Dr. Gaynor and his coauthors wrote. While methodology for case mix and patient characteristics have improved in recent years, further improvement is needed.
• Metrics must be clearly reported and easy for stakeholders to interpret. “This is critical if the data are to be used to steer patients toward higher-performing centers and/or to provide incentives for hospitals with lower performance to make improvements,” the researchers said.
• Regional reporting or a methodology that indicates where a hospital ranks within larger categories deserve further investigation as tools to help families choose a high-performing center, “ideally based on geography and on the particular type and complexity of disease,” Dr. Gaynor and his coauthors stated (J Thorac Cardiovasc Surg. 2017 Apr;153:904-7).
• Indirect standardization, a statistical methodology used to calculate risk-adjusted performance, could help consumers to interpret hospital performance more easily. This methodology might help classify a hospital with a low-complexity population as a high performer. “Developing better methods to convey this information to consumers is vital,” according to the researchers.
The perspective acknowledged several reports of an unintended consequence of public reporting: surgeons and centers avoiding higher-risk cases to skew their performance scores higher, thus restricting access to care. However, in a separate perspective on Dr. DeVore’s study, James S. Tweddell, MD, of Cincinnati Children’s Hospital Medical Center, and his coauthors, questioned the quality of the evidence on which Dr. Gaynor and his colleagues based their conclusion of risk aversion and limited access to care: a newspaper report from the United Kingdom.

Dr. Tweddell and his coauthors noted, “The predominance of data suggest an overall beneficial impact of public reporting.” They cited a trial that showed a decrease in heart attack–related deaths after public reporting had been implemented (JAMA. 2009 Dec 2;302:2330-7); a 2012 Agency for Healthcare Research and Quality systemic review (Evidence Report No. 208) that showed that research on harm is limited, and most studies do not confirm potential harm; and a meta-analysis that found a 15% reduction in adverse events associated with public reporting (BMC Health Serv Res. 2016;16:296).
“Appropriate risk adjustment is critical to achieve effective and fair transparency, but there is little objective data of harm associated with public reporting,” Dr. Tweddell and his coauthors concluded. While examination of public reporting must continue, they said, “these efforts are likely to result in minor course changes and the effort to inform and educate our patients and their families must continue.”
Ds. Gaynor, Dr. Tweddell, and their coauthors reported having no financial disclosures.
Public reporting of cardiac surgery outcomes has been a disruptive force in cardiology, and especially daunting in pediatric cardiac surgery because of low case volumes and rare mortality. To ensure that public reporting achieves its original goals – providing transparency to the patient care process, holding providers accountable, informing decision making for health care consumers, reducing costs, encouraging more efficient use of health system resources, and improving patient care and outcomes – further study that includes use of appropriate risk adjustment is needed, according to commentaries in the April issue of the Journal of Thoracic and Cardiovascular Surgery.
The journal asked two groups to provide perspective on a study Adam D. DeVore, MD, of Duke University in Durham, N.C., and his coauthors published last year (J Am Coll Cardiol. 2016 Mar 1;67:963-72). The study analyzed Medicare claims data from 2006 to 2012 for 37,829 hospitalizations for heart attack, 100,189 for heart failure (HF), and 79,076 for pneumonia. Dr. DeVore and his colleagues found readmission rates for the three conditions did not significantly improve after public reporting protocols were implemented in 2009. However, the study did show a significant decrease in ED visits and observation stays for those with HF: from 2.3% to –0.8% for the former (P = .007); and from 15% to 4% for the latter (P = .04).
• The metrics must be accurate, reliably discern hospital quality, and account for high-risk cases without penalizing hospitals. “In pediatric cardiac surgery, this can be particularly challenging, owing to the very wide heterogeneity of disease and variability in case mix and volumes across centers,” Dr. Gaynor and his coauthors wrote. While methodology for case mix and patient characteristics have improved in recent years, further improvement is needed.
• Metrics must be clearly reported and easy for stakeholders to interpret. “This is critical if the data are to be used to steer patients toward higher-performing centers and/or to provide incentives for hospitals with lower performance to make improvements,” the researchers said.
• Regional reporting or a methodology that indicates where a hospital ranks within larger categories deserve further investigation as tools to help families choose a high-performing center, “ideally based on geography and on the particular type and complexity of disease,” Dr. Gaynor and his coauthors stated (J Thorac Cardiovasc Surg. 2017 Apr;153:904-7).
• Indirect standardization, a statistical methodology used to calculate risk-adjusted performance, could help consumers to interpret hospital performance more easily. This methodology might help classify a hospital with a low-complexity population as a high performer. “Developing better methods to convey this information to consumers is vital,” according to the researchers.
The perspective acknowledged several reports of an unintended consequence of public reporting: surgeons and centers avoiding higher-risk cases to skew their performance scores higher, thus restricting access to care. However, in a separate perspective on Dr. DeVore’s study, James S. Tweddell, MD, of Cincinnati Children’s Hospital Medical Center, and his coauthors, questioned the quality of the evidence on which Dr. Gaynor and his colleagues based their conclusion of risk aversion and limited access to care: a newspaper report from the United Kingdom.
Dr. Tweddell and his coauthors noted, “The predominance of data suggest an overall beneficial impact of public reporting.” They cited a trial that showed a decrease in heart attack–related deaths after public reporting had been implemented (JAMA. 2009 Dec 2;302:2330-7); a 2012 Agency for Healthcare Research and Quality systemic review (Evidence Report No. 208) that showed that research on harm is limited, and most studies do not confirm potential harm; and a meta-analysis that found a 15% reduction in adverse events associated with public reporting (BMC Health Serv Res. 2016;16:296).
“Appropriate risk adjustment is critical to achieve effective and fair transparency, but there is little objective data of harm associated with public reporting,” Dr. Tweddell and his coauthors concluded. While examination of public reporting must continue, they said, “these efforts are likely to result in minor course changes and the effort to inform and educate our patients and their families must continue.”
Ds. Gaynor, Dr. Tweddell, and their coauthors reported having no financial disclosures.
Public reporting of cardiac surgery outcomes has been a disruptive force in cardiology, and especially daunting in pediatric cardiac surgery because of low case volumes and rare mortality. To ensure that public reporting achieves its original goals – providing transparency to the patient care process, holding providers accountable, informing decision making for health care consumers, reducing costs, encouraging more efficient use of health system resources, and improving patient care and outcomes – further study that includes use of appropriate risk adjustment is needed, according to commentaries in the April issue of the Journal of Thoracic and Cardiovascular Surgery.
The journal asked two groups to provide perspective on a study Adam D. DeVore, MD, of Duke University in Durham, N.C., and his coauthors published last year (J Am Coll Cardiol. 2016 Mar 1;67:963-72). The study analyzed Medicare claims data from 2006 to 2012 for 37,829 hospitalizations for heart attack, 100,189 for heart failure (HF), and 79,076 for pneumonia. Dr. DeVore and his colleagues found readmission rates for the three conditions did not significantly improve after public reporting protocols were implemented in 2009. However, the study did show a significant decrease in ED visits and observation stays for those with HF: from 2.3% to –0.8% for the former (P = .007); and from 15% to 4% for the latter (P = .04).
• The metrics must be accurate, reliably discern hospital quality, and account for high-risk cases without penalizing hospitals. “In pediatric cardiac surgery, this can be particularly challenging, owing to the very wide heterogeneity of disease and variability in case mix and volumes across centers,” Dr. Gaynor and his coauthors wrote. While methodology for case mix and patient characteristics have improved in recent years, further improvement is needed.
• Metrics must be clearly reported and easy for stakeholders to interpret. “This is critical if the data are to be used to steer patients toward higher-performing centers and/or to provide incentives for hospitals with lower performance to make improvements,” the researchers said.
• Regional reporting or a methodology that indicates where a hospital ranks within larger categories deserve further investigation as tools to help families choose a high-performing center, “ideally based on geography and on the particular type and complexity of disease,” Dr. Gaynor and his coauthors stated (J Thorac Cardiovasc Surg. 2017 Apr;153:904-7).
• Indirect standardization, a statistical methodology used to calculate risk-adjusted performance, could help consumers to interpret hospital performance more easily. This methodology might help classify a hospital with a low-complexity population as a high performer. “Developing better methods to convey this information to consumers is vital,” according to the researchers.
The perspective acknowledged several reports of an unintended consequence of public reporting: surgeons and centers avoiding higher-risk cases to skew their performance scores higher, thus restricting access to care. However, in a separate perspective on Dr. DeVore’s study, James S. Tweddell, MD, of Cincinnati Children’s Hospital Medical Center, and his coauthors, questioned the quality of the evidence on which Dr. Gaynor and his colleagues based their conclusion of risk aversion and limited access to care: a newspaper report from the United Kingdom.
Dr. Tweddell and his coauthors noted, “The predominance of data suggest an overall beneficial impact of public reporting.” They cited a trial that showed a decrease in heart attack–related deaths after public reporting had been implemented (JAMA. 2009 Dec 2;302:2330-7); a 2012 Agency for Healthcare Research and Quality systemic review (Evidence Report No. 208) that showed that research on harm is limited, and most studies do not confirm potential harm; and a meta-analysis that found a 15% reduction in adverse events associated with public reporting (BMC Health Serv Res. 2016;16:296).
“Appropriate risk adjustment is critical to achieve effective and fair transparency, but there is little objective data of harm associated with public reporting,” Dr. Tweddell and his coauthors concluded. While examination of public reporting must continue, they said, “these efforts are likely to result in minor course changes and the effort to inform and educate our patients and their families must continue.”
Ds. Gaynor, Dr. Tweddell, and their coauthors reported having no financial disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Public reporting of outcomes in cardiac surgery in children requires further investigation but has also been associated with improved outcomes.
Major finding: Emergency department visits for patients with heart failure declined from 2.3% before public reporting to –0.8% after implementation, and observation stays declined from 15.1% to 4.1%.
Data source: Analysis of Medicare claims data from 2006 to 2012 for 271,094 patients discharged after hospitalization for heart attack, heart failure or pneumonia.
Disclosures: Dr. Gaynor and Dr. Tweddell had no financial relationships to disclose.
As some holdout states revisit Medicaid expansion, new data show it pays off
Although the GOP-controlled Congress is pledging its continued interest – despite stalls and snags – in dismantling Obamacare, some “red state” legislatures are changing course and showing a newfound interest in embracing the health law’s Medicaid expansion.
And a study published April 12 in Health Affairs adds to these discussions, percolating in places such as Kansas, Georgia, Virginia, North Carolina, and Maine. Thirty-one states plus the District of Columbia already opted to pursue the expansion, which provided federal funding to broaden eligibility to include most low-income adults with incomes up to 138 percent of the federal poverty level (about $16,000 for an individual).
Researchers analyzed data from the National Association of State Budget Officers for fiscal years 2010-2015 to assess the fiscal effects of expansion’s first 2 years.
Their findings address arguments put forth by some GOP lawmakers, who say the expansion will add to the nation’s budget deficit and saddle states with additional coverage costs, forcing them to skimp on other budget priorities like education or transportation.
The researchers concluded that when states expanded eligibility for the low-income health insurance program they did see larger health care expenditures – but those costs were covered with federal funding. In addition, expansion states didn’t have to skimp on other policy priorities – such as environment, housing, and other public health initiatives – to make ends meet.
“This is a potential big benefit, not only to people who get coverage, but to state economies,” said Benjamin Sommers, MD, PhD, an associate professor of health policy and economics at Harvard University’s public health school, and the study’s first author.
This finding – that states expanding Medicaid didn’t encounter unforeseen budget problems – shouldn’t be surprising.
“Expansion is basically free” to the states, agreed Massachusetts Institute of Technology economist Jonathan Gruber, PhD, one of Obamacare’s architects who worked with Dr. Sommers to systematically compare the budgets of all 50 states to examine Medicaid expansion’s impact. “That’s the big insight,” he said. “There’s no sort of hidden downside.”
And that may be part of what’s fueling this renewed interest, said Edwin Park, vice president for health policy at the left-leaning Center for Budget and Policy Priorities. These states are seeing the federal windfall their neighbors received while trying to navigate public health concerns like opioid addiction, he said. They “are looking at how their neighbors or expansion states have done and see the benefits,” Mr. Park said. “The primary argument against the expansion on the state level has been it’s going to break the bank. The research demonstrates that’s not the case.”
But a caveat: The data used in this analysis reflected only years during which the federal government picked up 100% of the tab for expanding Medicaid eligibility and therefore could overestimate the benefit to state budgets. That’s because in 2017 that federal support begins to taper off, and by 2020 states have to pay 10 percent of the expansion costs themselves.
That means policymakers should exert caution in reading too much into this study, said Tom Miller, a resident fellow at the conservative American Enterprise Institute. Because states will eventually shoulder more of the cost, he said, studies that assess its budgetary impact are preliminary at best. Plus, Miller said, other factors such as relative economic growth could have padded state budgets in the years studied – masking any unintended costs with a bigger Medicaid program. It’s unclear whether in times of downturn Medicaid would take a bigger bite out of state budgets.
“It’s just the beginning of this – it’s an early snapshot,” he said.
Dr. Sommers argued the limited data set means researchers should continue to track how state budgets compare between expansion and nonexpansion states. But even when states do take on more of Medicaid’s cost, that may not pose such a burden, suggested Sara Rosenbaum, a professor of health law and policy at George Washington University. Expanding Medicaid brings in other potential economic benefits that this paper doesn’t account for – less uncompensated care in hospitals, for instance – that could offset the expenditures states ultimately take up.
A bigger concern, some experts say, is that – even without the Obamacare repeal – some GOP health proposals would change the federal government’s Medicaid funding mechanism from being an open-ended match to a block grant or per-capita cap in an effort to curb national spending. Those proposals would take away at least some of the federal dollars that have insulated state budgets.
“Ironically, all the arguments that have been made against expansion for years – like creating a hole in the state budget or breaking the bank – that’s exactly what a per-capita grant or block grant does,” Park said.
As more states take on the Medicaid debate, those consequences matter, both Dr. Sommers and Dr. Gruber said. And not just for state budgets – for consumers, too.
“The main lesson is there’s no sort of big hidden cost of expanding Medicaid. What you see is what you get,” Dr. Gruber said. “You get free health insurance for your citizens.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Although the GOP-controlled Congress is pledging its continued interest – despite stalls and snags – in dismantling Obamacare, some “red state” legislatures are changing course and showing a newfound interest in embracing the health law’s Medicaid expansion.
And a study published April 12 in Health Affairs adds to these discussions, percolating in places such as Kansas, Georgia, Virginia, North Carolina, and Maine. Thirty-one states plus the District of Columbia already opted to pursue the expansion, which provided federal funding to broaden eligibility to include most low-income adults with incomes up to 138 percent of the federal poverty level (about $16,000 for an individual).
Researchers analyzed data from the National Association of State Budget Officers for fiscal years 2010-2015 to assess the fiscal effects of expansion’s first 2 years.
Their findings address arguments put forth by some GOP lawmakers, who say the expansion will add to the nation’s budget deficit and saddle states with additional coverage costs, forcing them to skimp on other budget priorities like education or transportation.
The researchers concluded that when states expanded eligibility for the low-income health insurance program they did see larger health care expenditures – but those costs were covered with federal funding. In addition, expansion states didn’t have to skimp on other policy priorities – such as environment, housing, and other public health initiatives – to make ends meet.
“This is a potential big benefit, not only to people who get coverage, but to state economies,” said Benjamin Sommers, MD, PhD, an associate professor of health policy and economics at Harvard University’s public health school, and the study’s first author.
This finding – that states expanding Medicaid didn’t encounter unforeseen budget problems – shouldn’t be surprising.
“Expansion is basically free” to the states, agreed Massachusetts Institute of Technology economist Jonathan Gruber, PhD, one of Obamacare’s architects who worked with Dr. Sommers to systematically compare the budgets of all 50 states to examine Medicaid expansion’s impact. “That’s the big insight,” he said. “There’s no sort of hidden downside.”
And that may be part of what’s fueling this renewed interest, said Edwin Park, vice president for health policy at the left-leaning Center for Budget and Policy Priorities. These states are seeing the federal windfall their neighbors received while trying to navigate public health concerns like opioid addiction, he said. They “are looking at how their neighbors or expansion states have done and see the benefits,” Mr. Park said. “The primary argument against the expansion on the state level has been it’s going to break the bank. The research demonstrates that’s not the case.”
But a caveat: The data used in this analysis reflected only years during which the federal government picked up 100% of the tab for expanding Medicaid eligibility and therefore could overestimate the benefit to state budgets. That’s because in 2017 that federal support begins to taper off, and by 2020 states have to pay 10 percent of the expansion costs themselves.
That means policymakers should exert caution in reading too much into this study, said Tom Miller, a resident fellow at the conservative American Enterprise Institute. Because states will eventually shoulder more of the cost, he said, studies that assess its budgetary impact are preliminary at best. Plus, Miller said, other factors such as relative economic growth could have padded state budgets in the years studied – masking any unintended costs with a bigger Medicaid program. It’s unclear whether in times of downturn Medicaid would take a bigger bite out of state budgets.
“It’s just the beginning of this – it’s an early snapshot,” he said.
Dr. Sommers argued the limited data set means researchers should continue to track how state budgets compare between expansion and nonexpansion states. But even when states do take on more of Medicaid’s cost, that may not pose such a burden, suggested Sara Rosenbaum, a professor of health law and policy at George Washington University. Expanding Medicaid brings in other potential economic benefits that this paper doesn’t account for – less uncompensated care in hospitals, for instance – that could offset the expenditures states ultimately take up.
A bigger concern, some experts say, is that – even without the Obamacare repeal – some GOP health proposals would change the federal government’s Medicaid funding mechanism from being an open-ended match to a block grant or per-capita cap in an effort to curb national spending. Those proposals would take away at least some of the federal dollars that have insulated state budgets.
“Ironically, all the arguments that have been made against expansion for years – like creating a hole in the state budget or breaking the bank – that’s exactly what a per-capita grant or block grant does,” Park said.
As more states take on the Medicaid debate, those consequences matter, both Dr. Sommers and Dr. Gruber said. And not just for state budgets – for consumers, too.
“The main lesson is there’s no sort of big hidden cost of expanding Medicaid. What you see is what you get,” Dr. Gruber said. “You get free health insurance for your citizens.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Although the GOP-controlled Congress is pledging its continued interest – despite stalls and snags – in dismantling Obamacare, some “red state” legislatures are changing course and showing a newfound interest in embracing the health law’s Medicaid expansion.
And a study published April 12 in Health Affairs adds to these discussions, percolating in places such as Kansas, Georgia, Virginia, North Carolina, and Maine. Thirty-one states plus the District of Columbia already opted to pursue the expansion, which provided federal funding to broaden eligibility to include most low-income adults with incomes up to 138 percent of the federal poverty level (about $16,000 for an individual).
Researchers analyzed data from the National Association of State Budget Officers for fiscal years 2010-2015 to assess the fiscal effects of expansion’s first 2 years.
Their findings address arguments put forth by some GOP lawmakers, who say the expansion will add to the nation’s budget deficit and saddle states with additional coverage costs, forcing them to skimp on other budget priorities like education or transportation.
The researchers concluded that when states expanded eligibility for the low-income health insurance program they did see larger health care expenditures – but those costs were covered with federal funding. In addition, expansion states didn’t have to skimp on other policy priorities – such as environment, housing, and other public health initiatives – to make ends meet.
“This is a potential big benefit, not only to people who get coverage, but to state economies,” said Benjamin Sommers, MD, PhD, an associate professor of health policy and economics at Harvard University’s public health school, and the study’s first author.
This finding – that states expanding Medicaid didn’t encounter unforeseen budget problems – shouldn’t be surprising.
“Expansion is basically free” to the states, agreed Massachusetts Institute of Technology economist Jonathan Gruber, PhD, one of Obamacare’s architects who worked with Dr. Sommers to systematically compare the budgets of all 50 states to examine Medicaid expansion’s impact. “That’s the big insight,” he said. “There’s no sort of hidden downside.”
And that may be part of what’s fueling this renewed interest, said Edwin Park, vice president for health policy at the left-leaning Center for Budget and Policy Priorities. These states are seeing the federal windfall their neighbors received while trying to navigate public health concerns like opioid addiction, he said. They “are looking at how their neighbors or expansion states have done and see the benefits,” Mr. Park said. “The primary argument against the expansion on the state level has been it’s going to break the bank. The research demonstrates that’s not the case.”
But a caveat: The data used in this analysis reflected only years during which the federal government picked up 100% of the tab for expanding Medicaid eligibility and therefore could overestimate the benefit to state budgets. That’s because in 2017 that federal support begins to taper off, and by 2020 states have to pay 10 percent of the expansion costs themselves.
That means policymakers should exert caution in reading too much into this study, said Tom Miller, a resident fellow at the conservative American Enterprise Institute. Because states will eventually shoulder more of the cost, he said, studies that assess its budgetary impact are preliminary at best. Plus, Miller said, other factors such as relative economic growth could have padded state budgets in the years studied – masking any unintended costs with a bigger Medicaid program. It’s unclear whether in times of downturn Medicaid would take a bigger bite out of state budgets.
“It’s just the beginning of this – it’s an early snapshot,” he said.
Dr. Sommers argued the limited data set means researchers should continue to track how state budgets compare between expansion and nonexpansion states. But even when states do take on more of Medicaid’s cost, that may not pose such a burden, suggested Sara Rosenbaum, a professor of health law and policy at George Washington University. Expanding Medicaid brings in other potential economic benefits that this paper doesn’t account for – less uncompensated care in hospitals, for instance – that could offset the expenditures states ultimately take up.
A bigger concern, some experts say, is that – even without the Obamacare repeal – some GOP health proposals would change the federal government’s Medicaid funding mechanism from being an open-ended match to a block grant or per-capita cap in an effort to curb national spending. Those proposals would take away at least some of the federal dollars that have insulated state budgets.
“Ironically, all the arguments that have been made against expansion for years – like creating a hole in the state budget or breaking the bank – that’s exactly what a per-capita grant or block grant does,” Park said.
As more states take on the Medicaid debate, those consequences matter, both Dr. Sommers and Dr. Gruber said. And not just for state budgets – for consumers, too.
“The main lesson is there’s no sort of big hidden cost of expanding Medicaid. What you see is what you get,” Dr. Gruber said. “You get free health insurance for your citizens.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Time to reexamine surgery for nonlocalized bronchiectasis
Nonlocalized bronchiectasis is becoming more common in developing countries and has been difficult to treat. While surgery for localized bronchiectasis has been proven, its role in nonlocalized disease is less established; researchers from China are advocating for a reexamination of surgical resection in this disease based on results of a small cohort study at their academic center.
“Lobectomy for the predominant lesion is a safe procedure in the surgical treatment of nonlocalized bronchiectasis and leads to significant relief of symptoms with good rates of satisfaction,” Jie Dai, PhD, of Shanghai (China) Pulmonary Hospital Tongji University and his coauthors reported in the Journal of Thoracic and Cardiovascular Surgery (2017 Apr;153:979-85).
The researchers reviewed the medical records of 37 consecutive patients – 10 men and 27 women – with nonlocalized bronchiectasis who had lobectomies via thoracotomies during 2010-2013. Twenty-three patients (62.2%) were symptom free after surgery and 10 (27%) reported that their symptoms had improved. Four (10.8%) said their symptoms either did not improve or worsened, but three of them also had chronic occlusive pulmonary disease. There were no deaths, and the morbidity rate was 21.6%.
The researchers used three criteria to select candidates for surgery: persistent symptoms despite medical treatment; an identifiable predominant lesion; and cardiopulmonary function compatible with anesthetic risk. Average age was 54.5 years and more than half (19) had no smoking history.
The surgical technique involved a posterolateral thoracotomy and a double-lumen endotracheal tube to avoid contamination of the opposite side of the lung during surgery. Surgery avoided excessive bronchial dissection and preserved peribronchial tissues. Extrapleural dissection avoided spillage of lung contents into the pleural space.
Treatment of the hilum followed an order from the pulmonary artery to the pulmonary vein and then to the bronchus. An ultrasonic device helped isolate and then ligate or sever distorted bronchial arteries. A mechanical stapler was used to close the bronchial stump. Reinforcement involved an intercostal muscle flap in 16 cases and a pedicled parietal pleural flap in 21. If any sign of pleural infection appeared after hemostasis, pleural space irrigation with 0.5% neomycin (500 mg/L) was initiated. Two chest drains were placed at the bronchial stump, and the bronchial suture checked with bronchoscopy. Airway secretions were removed, and pathology confirmed bronchiectasis all specimens.
The frequency of acute infection and hemoptysis decreased significantly at 1 year postoperatively, from 5.3% to 1.8% and 4.9% to 1.1%, respectively, (P less than .01 for both). Daily sputum volume decreased an average of 26.3 mL (P less than .01) and sputum cultures became sterile in 13 (35%) of patients (P less than .01).
Previously, surgery for nonlocalized bronchiectasis had been reserved for life-threatening symptoms only, but Dr. Dai and his coauthors fashioned their study on previous studies of lobectomy that included patients with nonlocalized bronchiectasis (Br J Surg. 2005;92:836-9; Ann Thorac Surg. 2003;75:382-7).
Two major complications occurred in the Shanghai cohort: empyema and persistent air leak, both of which were managed without a reoperation and had been reported in previous series. Dr. Dai and his coauthors have adopted protocols to reduce complications, among them, requiring that patients have sputum output greater than 20 mL/day with little purulence and no engorgement or edema in the tunica mucosa bronchiorum on bronchoscopy.
But the researchers are not ready to extend surgery as a blanket indication for nonlocalized bronchiectasis. “It is worth mentioning that the surgical benefit is limited to patients who have only one predominant area of bronchiectatic disease that can be localized by CT instead of those with diffuse bronchiectasis,” they wrote. “The ideal surgical candidate has a heterogeneous distribution of diseased areas.”
The investigators pointed out that the study was limited by its small size and lack of information on etiologies of disease.
Dr. Dai and his coauthors had no financial relationships to disclose.
The study by Dr. Dai and his coauthors “is an important contribution to the literature” despite its limitations, Steven Milman, MD, and Thomas Ng, MD, of Brown University, Providence, R.I., said in their invited commentary (J Thorac Cardiovasc Surg. 2017 Apr;153:986). However, they added, “Several important points need to be stressed.”
Among those points: The researchers studied a “highly selected group” of young patients with good pulmonary functions; mean follow-up was short (15 months); the etiology of bronchiectasis was unknown; and lobectomy was not the optimal treatment for nonlocalized bronchiectasis. “It must be remembered that these patients first failed medical therapy and that the study population received lobectomy due to the extent of the dominant disease and not as routine treatment,” Dr. Milman and Dr. Ng wrote.
To validate the findings, Dr. Milman and Dr. Ng said, not only do more patients need to be studied with longer follow-up but future investigators also should study minimally invasive approaches to see if that would improve the outcomes.
Dr. Milman and Dr. Ng had no financial relationships to disclose.
The study by Dr. Dai and his coauthors “is an important contribution to the literature” despite its limitations, Steven Milman, MD, and Thomas Ng, MD, of Brown University, Providence, R.I., said in their invited commentary (J Thorac Cardiovasc Surg. 2017 Apr;153:986). However, they added, “Several important points need to be stressed.”
Among those points: The researchers studied a “highly selected group” of young patients with good pulmonary functions; mean follow-up was short (15 months); the etiology of bronchiectasis was unknown; and lobectomy was not the optimal treatment for nonlocalized bronchiectasis. “It must be remembered that these patients first failed medical therapy and that the study population received lobectomy due to the extent of the dominant disease and not as routine treatment,” Dr. Milman and Dr. Ng wrote.
To validate the findings, Dr. Milman and Dr. Ng said, not only do more patients need to be studied with longer follow-up but future investigators also should study minimally invasive approaches to see if that would improve the outcomes.
Dr. Milman and Dr. Ng had no financial relationships to disclose.
The study by Dr. Dai and his coauthors “is an important contribution to the literature” despite its limitations, Steven Milman, MD, and Thomas Ng, MD, of Brown University, Providence, R.I., said in their invited commentary (J Thorac Cardiovasc Surg. 2017 Apr;153:986). However, they added, “Several important points need to be stressed.”
Among those points: The researchers studied a “highly selected group” of young patients with good pulmonary functions; mean follow-up was short (15 months); the etiology of bronchiectasis was unknown; and lobectomy was not the optimal treatment for nonlocalized bronchiectasis. “It must be remembered that these patients first failed medical therapy and that the study population received lobectomy due to the extent of the dominant disease and not as routine treatment,” Dr. Milman and Dr. Ng wrote.
To validate the findings, Dr. Milman and Dr. Ng said, not only do more patients need to be studied with longer follow-up but future investigators also should study minimally invasive approaches to see if that would improve the outcomes.
Dr. Milman and Dr. Ng had no financial relationships to disclose.
Nonlocalized bronchiectasis is becoming more common in developing countries and has been difficult to treat. While surgery for localized bronchiectasis has been proven, its role in nonlocalized disease is less established; researchers from China are advocating for a reexamination of surgical resection in this disease based on results of a small cohort study at their academic center.
“Lobectomy for the predominant lesion is a safe procedure in the surgical treatment of nonlocalized bronchiectasis and leads to significant relief of symptoms with good rates of satisfaction,” Jie Dai, PhD, of Shanghai (China) Pulmonary Hospital Tongji University and his coauthors reported in the Journal of Thoracic and Cardiovascular Surgery (2017 Apr;153:979-85).
The researchers reviewed the medical records of 37 consecutive patients – 10 men and 27 women – with nonlocalized bronchiectasis who had lobectomies via thoracotomies during 2010-2013. Twenty-three patients (62.2%) were symptom free after surgery and 10 (27%) reported that their symptoms had improved. Four (10.8%) said their symptoms either did not improve or worsened, but three of them also had chronic occlusive pulmonary disease. There were no deaths, and the morbidity rate was 21.6%.
The researchers used three criteria to select candidates for surgery: persistent symptoms despite medical treatment; an identifiable predominant lesion; and cardiopulmonary function compatible with anesthetic risk. Average age was 54.5 years and more than half (19) had no smoking history.
The surgical technique involved a posterolateral thoracotomy and a double-lumen endotracheal tube to avoid contamination of the opposite side of the lung during surgery. Surgery avoided excessive bronchial dissection and preserved peribronchial tissues. Extrapleural dissection avoided spillage of lung contents into the pleural space.
Treatment of the hilum followed an order from the pulmonary artery to the pulmonary vein and then to the bronchus. An ultrasonic device helped isolate and then ligate or sever distorted bronchial arteries. A mechanical stapler was used to close the bronchial stump. Reinforcement involved an intercostal muscle flap in 16 cases and a pedicled parietal pleural flap in 21. If any sign of pleural infection appeared after hemostasis, pleural space irrigation with 0.5% neomycin (500 mg/L) was initiated. Two chest drains were placed at the bronchial stump, and the bronchial suture checked with bronchoscopy. Airway secretions were removed, and pathology confirmed bronchiectasis all specimens.
The frequency of acute infection and hemoptysis decreased significantly at 1 year postoperatively, from 5.3% to 1.8% and 4.9% to 1.1%, respectively, (P less than .01 for both). Daily sputum volume decreased an average of 26.3 mL (P less than .01) and sputum cultures became sterile in 13 (35%) of patients (P less than .01).
Previously, surgery for nonlocalized bronchiectasis had been reserved for life-threatening symptoms only, but Dr. Dai and his coauthors fashioned their study on previous studies of lobectomy that included patients with nonlocalized bronchiectasis (Br J Surg. 2005;92:836-9; Ann Thorac Surg. 2003;75:382-7).
Two major complications occurred in the Shanghai cohort: empyema and persistent air leak, both of which were managed without a reoperation and had been reported in previous series. Dr. Dai and his coauthors have adopted protocols to reduce complications, among them, requiring that patients have sputum output greater than 20 mL/day with little purulence and no engorgement or edema in the tunica mucosa bronchiorum on bronchoscopy.
But the researchers are not ready to extend surgery as a blanket indication for nonlocalized bronchiectasis. “It is worth mentioning that the surgical benefit is limited to patients who have only one predominant area of bronchiectatic disease that can be localized by CT instead of those with diffuse bronchiectasis,” they wrote. “The ideal surgical candidate has a heterogeneous distribution of diseased areas.”
The investigators pointed out that the study was limited by its small size and lack of information on etiologies of disease.
Dr. Dai and his coauthors had no financial relationships to disclose.
Nonlocalized bronchiectasis is becoming more common in developing countries and has been difficult to treat. While surgery for localized bronchiectasis has been proven, its role in nonlocalized disease is less established; researchers from China are advocating for a reexamination of surgical resection in this disease based on results of a small cohort study at their academic center.
“Lobectomy for the predominant lesion is a safe procedure in the surgical treatment of nonlocalized bronchiectasis and leads to significant relief of symptoms with good rates of satisfaction,” Jie Dai, PhD, of Shanghai (China) Pulmonary Hospital Tongji University and his coauthors reported in the Journal of Thoracic and Cardiovascular Surgery (2017 Apr;153:979-85).
The researchers reviewed the medical records of 37 consecutive patients – 10 men and 27 women – with nonlocalized bronchiectasis who had lobectomies via thoracotomies during 2010-2013. Twenty-three patients (62.2%) were symptom free after surgery and 10 (27%) reported that their symptoms had improved. Four (10.8%) said their symptoms either did not improve or worsened, but three of them also had chronic occlusive pulmonary disease. There were no deaths, and the morbidity rate was 21.6%.
The researchers used three criteria to select candidates for surgery: persistent symptoms despite medical treatment; an identifiable predominant lesion; and cardiopulmonary function compatible with anesthetic risk. Average age was 54.5 years and more than half (19) had no smoking history.
The surgical technique involved a posterolateral thoracotomy and a double-lumen endotracheal tube to avoid contamination of the opposite side of the lung during surgery. Surgery avoided excessive bronchial dissection and preserved peribronchial tissues. Extrapleural dissection avoided spillage of lung contents into the pleural space.
Treatment of the hilum followed an order from the pulmonary artery to the pulmonary vein and then to the bronchus. An ultrasonic device helped isolate and then ligate or sever distorted bronchial arteries. A mechanical stapler was used to close the bronchial stump. Reinforcement involved an intercostal muscle flap in 16 cases and a pedicled parietal pleural flap in 21. If any sign of pleural infection appeared after hemostasis, pleural space irrigation with 0.5% neomycin (500 mg/L) was initiated. Two chest drains were placed at the bronchial stump, and the bronchial suture checked with bronchoscopy. Airway secretions were removed, and pathology confirmed bronchiectasis all specimens.
The frequency of acute infection and hemoptysis decreased significantly at 1 year postoperatively, from 5.3% to 1.8% and 4.9% to 1.1%, respectively, (P less than .01 for both). Daily sputum volume decreased an average of 26.3 mL (P less than .01) and sputum cultures became sterile in 13 (35%) of patients (P less than .01).
Previously, surgery for nonlocalized bronchiectasis had been reserved for life-threatening symptoms only, but Dr. Dai and his coauthors fashioned their study on previous studies of lobectomy that included patients with nonlocalized bronchiectasis (Br J Surg. 2005;92:836-9; Ann Thorac Surg. 2003;75:382-7).
Two major complications occurred in the Shanghai cohort: empyema and persistent air leak, both of which were managed without a reoperation and had been reported in previous series. Dr. Dai and his coauthors have adopted protocols to reduce complications, among them, requiring that patients have sputum output greater than 20 mL/day with little purulence and no engorgement or edema in the tunica mucosa bronchiorum on bronchoscopy.
But the researchers are not ready to extend surgery as a blanket indication for nonlocalized bronchiectasis. “It is worth mentioning that the surgical benefit is limited to patients who have only one predominant area of bronchiectatic disease that can be localized by CT instead of those with diffuse bronchiectasis,” they wrote. “The ideal surgical candidate has a heterogeneous distribution of diseased areas.”
The investigators pointed out that the study was limited by its small size and lack of information on etiologies of disease.
Dr. Dai and his coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Lobectomy for nonlocalized bronchiectasis can improve symptoms significantly.
Major finding: Among 37 patients who had lobectomy, 62.2% were asymptomatic after surgery.
Data source: Single-center retrospective review of 37 patients who had lobectomy for nonlocalized bronchiectasis from January 2010 to December 2013.
Disclosure: Dr. Dai and his coauthors had no financial relationships to disclose.