User login
ABIM sued over maintenance of certification
Also today, drug test results should not dictate treatment, duodenoscopes contain more bacteria than expected, and weight-loss medications may have a role following bariatric surgery.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, drug test results should not dictate treatment, duodenoscopes contain more bacteria than expected, and weight-loss medications may have a role following bariatric surgery.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, drug test results should not dictate treatment, duodenoscopes contain more bacteria than expected, and weight-loss medications may have a role following bariatric surgery.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

CABG surpasses PCI for diabetics out to 7.5 years
CHICAGO – Patients with diabetes who underwent coronary artery bypass grafting had significantly better survival than patients with diabetes who underwent percutaneous coronary intervention after a median 7.5 years of follow-up.

Those patients comprised about half the patients enrolled in the FREEDOM randomized trial.
Long-term follow-up was only possible for just under half the 1,900 patients with diabetes and multivessel coronary disease originally enrolled in FREEDOM, but when researchers combined the long-term results with the data collected in the original study that had a median 3.8-year follow-up, they found all-cause mortality occurred in 18.3% of the patients who underwent coronary artery bypass grafting (CABG) and in 24.3% of patients treated with percutaneous coronary intervention (PCI), a 6% absolute between-group difference that was statistically significant, Valentin Fuster, MD, said at the American Heart Association scientific sessions. This fully jibed with the primary FREEDOM results, which found after 5 years a statistically significant reduction in all-cause death with CABG, compared with PCI, and also a significant reduction in the study’s primary endpoint (a combination of all-cause death, MI, and stroke), which occurred in 18.7% of patients randomized to CABG and in 26.6% of those randomized to PCI (N Engl J Med. 2012 Dec 20;367[25]:2375-84).
The extended follow-up finding lent additional support to existing society recommendations that CABG is the preferred revascularization strategy for patients with diabetes and multivessel coronary disease, most recently from the European Society of Cardiology (Eur Heart J. 2018 Aug 25. doi: 10.1093/eurheartj/ehy394), said Dr. Fuster, professor of medicine at the Icahn School of Medicine at Mount Sinai and director of Mount Sinai Heart in New York. A subgroup analysis of the extended follow-up also suggested that the survival benefit from CABG, compared with PCI, was especially strong among patients at or below the study’s median age of 63 years. In the younger subgroup survival among patients treated with CABG was twice as good as it was among patients treated with PCI.
Dr. Fuster noted that few data have been previously reported for survival rates beyond 5 years after revascularization. “This was a difficult study. Following patients for more than 5 years is hard,” he said. Concurrently with his report at the meeting the results also appeared online (J Am Coll Cardiol. 2018 Nov 11. doi: 10.1016/j.jacc.2018.11.001).
The FREEDOM (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) trial enrolled patients at 140 participating centers during 2005-2010. A total of 25 sites agreed to participate in the extended follow-up and could track 943 patients, 50% of the starting cohort of 1,900 and 89% of the patients originally enrolled at these 25 centers. Dr. Fuster stressed that the 957 patients not included in the follow-up had not been lost, but rather had been managed at sites that declined to participate in this additional study.
Dr. Fuster acknowledged that methods and hardware for PCI have changed since the study ran a decade ago, as have options for medical management. He also highlighted that the long-term follow-up results had no data on rates of MIs and strokes.
FREEDOM had no commercial funding. Dr. Fuster reported no relevant disclosures.
SOURCE: Fuster V et al. AHA 2018, Abstract 18609.
These extended results from the FREEDOM trial that followed many patients for 10 years or longer add to the consistent evidence base that supports coronary artery bypass grafting (CABG) as the preferred revascularization strategy for patients with diabetes and multivessel coronary disease. The new findings support existing society guidelines that recommend CABG over percutaneous coronary intervention in these patients, most recently in the revascularization guidelines from the European Society of Cardiology (Eur Heart J. 2018 Aug 25. doi: 10.1093/eurheartj/ehy394). An update to the U.S. guidelines should appear in 2019.

Continued improvement of revascularization techniques, hardware, and medical management of patients with diabetes and multivessel coronary artery disease makes it challenging to apply the results of studies run in earlier eras to today’s practice. It is possible that continued evolution of coronary stent technology may reduce the differences in outcomes between bypass surgery and percutaneous coronary interventions, although this is less likely if much of CABG’s success relates to the protection it gives against new disease. Future comparisons of different approaches with revascularization will need to take into account the potential contribution of other procedures, other adverse outcomes aside from mortality during long-term follow-up, the consequences of incomplete revascularization, and the impact of new medications for treating diabetes that have been recently shown to also have cardiovascular disease effects. All these factors in concert will define the optimal approach to managing these patients.
Alice K. Jacobs, MD , is director of the cardiac catheterization laboratory at Boston Medical Center and a professor of medicine at Boston University. She has received research support from Abbott Vascular. She made these comments as designated discussant for the study.
These extended results from the FREEDOM trial that followed many patients for 10 years or longer add to the consistent evidence base that supports coronary artery bypass grafting (CABG) as the preferred revascularization strategy for patients with diabetes and multivessel coronary disease. The new findings support existing society guidelines that recommend CABG over percutaneous coronary intervention in these patients, most recently in the revascularization guidelines from the European Society of Cardiology (Eur Heart J. 2018 Aug 25. doi: 10.1093/eurheartj/ehy394). An update to the U.S. guidelines should appear in 2019.
Continued improvement of revascularization techniques, hardware, and medical management of patients with diabetes and multivessel coronary artery disease makes it challenging to apply the results of studies run in earlier eras to today’s practice. It is possible that continued evolution of coronary stent technology may reduce the differences in outcomes between bypass surgery and percutaneous coronary interventions, although this is less likely if much of CABG’s success relates to the protection it gives against new disease. Future comparisons of different approaches with revascularization will need to take into account the potential contribution of other procedures, other adverse outcomes aside from mortality during long-term follow-up, the consequences of incomplete revascularization, and the impact of new medications for treating diabetes that have been recently shown to also have cardiovascular disease effects. All these factors in concert will define the optimal approach to managing these patients.
Alice K. Jacobs, MD , is director of the cardiac catheterization laboratory at Boston Medical Center and a professor of medicine at Boston University. She has received research support from Abbott Vascular. She made these comments as designated discussant for the study.
These extended results from the FREEDOM trial that followed many patients for 10 years or longer add to the consistent evidence base that supports coronary artery bypass grafting (CABG) as the preferred revascularization strategy for patients with diabetes and multivessel coronary disease. The new findings support existing society guidelines that recommend CABG over percutaneous coronary intervention in these patients, most recently in the revascularization guidelines from the European Society of Cardiology (Eur Heart J. 2018 Aug 25. doi: 10.1093/eurheartj/ehy394). An update to the U.S. guidelines should appear in 2019.
Continued improvement of revascularization techniques, hardware, and medical management of patients with diabetes and multivessel coronary artery disease makes it challenging to apply the results of studies run in earlier eras to today’s practice. It is possible that continued evolution of coronary stent technology may reduce the differences in outcomes between bypass surgery and percutaneous coronary interventions, although this is less likely if much of CABG’s success relates to the protection it gives against new disease. Future comparisons of different approaches with revascularization will need to take into account the potential contribution of other procedures, other adverse outcomes aside from mortality during long-term follow-up, the consequences of incomplete revascularization, and the impact of new medications for treating diabetes that have been recently shown to also have cardiovascular disease effects. All these factors in concert will define the optimal approach to managing these patients.
Alice K. Jacobs, MD , is director of the cardiac catheterization laboratory at Boston Medical Center and a professor of medicine at Boston University. She has received research support from Abbott Vascular. She made these comments as designated discussant for the study.
CHICAGO – Patients with diabetes who underwent coronary artery bypass grafting had significantly better survival than patients with diabetes who underwent percutaneous coronary intervention after a median 7.5 years of follow-up.
Those patients comprised about half the patients enrolled in the FREEDOM randomized trial.
Long-term follow-up was only possible for just under half the 1,900 patients with diabetes and multivessel coronary disease originally enrolled in FREEDOM, but when researchers combined the long-term results with the data collected in the original study that had a median 3.8-year follow-up, they found all-cause mortality occurred in 18.3% of the patients who underwent coronary artery bypass grafting (CABG) and in 24.3% of patients treated with percutaneous coronary intervention (PCI), a 6% absolute between-group difference that was statistically significant, Valentin Fuster, MD, said at the American Heart Association scientific sessions. This fully jibed with the primary FREEDOM results, which found after 5 years a statistically significant reduction in all-cause death with CABG, compared with PCI, and also a significant reduction in the study’s primary endpoint (a combination of all-cause death, MI, and stroke), which occurred in 18.7% of patients randomized to CABG and in 26.6% of those randomized to PCI (N Engl J Med. 2012 Dec 20;367[25]:2375-84).
The extended follow-up finding lent additional support to existing society recommendations that CABG is the preferred revascularization strategy for patients with diabetes and multivessel coronary disease, most recently from the European Society of Cardiology (Eur Heart J. 2018 Aug 25. doi: 10.1093/eurheartj/ehy394), said Dr. Fuster, professor of medicine at the Icahn School of Medicine at Mount Sinai and director of Mount Sinai Heart in New York. A subgroup analysis of the extended follow-up also suggested that the survival benefit from CABG, compared with PCI, was especially strong among patients at or below the study’s median age of 63 years. In the younger subgroup survival among patients treated with CABG was twice as good as it was among patients treated with PCI.
Dr. Fuster noted that few data have been previously reported for survival rates beyond 5 years after revascularization. “This was a difficult study. Following patients for more than 5 years is hard,” he said. Concurrently with his report at the meeting the results also appeared online (J Am Coll Cardiol. 2018 Nov 11. doi: 10.1016/j.jacc.2018.11.001).
The FREEDOM (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) trial enrolled patients at 140 participating centers during 2005-2010. A total of 25 sites agreed to participate in the extended follow-up and could track 943 patients, 50% of the starting cohort of 1,900 and 89% of the patients originally enrolled at these 25 centers. Dr. Fuster stressed that the 957 patients not included in the follow-up had not been lost, but rather had been managed at sites that declined to participate in this additional study.
Dr. Fuster acknowledged that methods and hardware for PCI have changed since the study ran a decade ago, as have options for medical management. He also highlighted that the long-term follow-up results had no data on rates of MIs and strokes.
FREEDOM had no commercial funding. Dr. Fuster reported no relevant disclosures.
SOURCE: Fuster V et al. AHA 2018, Abstract 18609.
CHICAGO – Patients with diabetes who underwent coronary artery bypass grafting had significantly better survival than patients with diabetes who underwent percutaneous coronary intervention after a median 7.5 years of follow-up.
Those patients comprised about half the patients enrolled in the FREEDOM randomized trial.
Long-term follow-up was only possible for just under half the 1,900 patients with diabetes and multivessel coronary disease originally enrolled in FREEDOM, but when researchers combined the long-term results with the data collected in the original study that had a median 3.8-year follow-up, they found all-cause mortality occurred in 18.3% of the patients who underwent coronary artery bypass grafting (CABG) and in 24.3% of patients treated with percutaneous coronary intervention (PCI), a 6% absolute between-group difference that was statistically significant, Valentin Fuster, MD, said at the American Heart Association scientific sessions. This fully jibed with the primary FREEDOM results, which found after 5 years a statistically significant reduction in all-cause death with CABG, compared with PCI, and also a significant reduction in the study’s primary endpoint (a combination of all-cause death, MI, and stroke), which occurred in 18.7% of patients randomized to CABG and in 26.6% of those randomized to PCI (N Engl J Med. 2012 Dec 20;367[25]:2375-84).
The extended follow-up finding lent additional support to existing society recommendations that CABG is the preferred revascularization strategy for patients with diabetes and multivessel coronary disease, most recently from the European Society of Cardiology (Eur Heart J. 2018 Aug 25. doi: 10.1093/eurheartj/ehy394), said Dr. Fuster, professor of medicine at the Icahn School of Medicine at Mount Sinai and director of Mount Sinai Heart in New York. A subgroup analysis of the extended follow-up also suggested that the survival benefit from CABG, compared with PCI, was especially strong among patients at or below the study’s median age of 63 years. In the younger subgroup survival among patients treated with CABG was twice as good as it was among patients treated with PCI.
Dr. Fuster noted that few data have been previously reported for survival rates beyond 5 years after revascularization. “This was a difficult study. Following patients for more than 5 years is hard,” he said. Concurrently with his report at the meeting the results also appeared online (J Am Coll Cardiol. 2018 Nov 11. doi: 10.1016/j.jacc.2018.11.001).
The FREEDOM (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) trial enrolled patients at 140 participating centers during 2005-2010. A total of 25 sites agreed to participate in the extended follow-up and could track 943 patients, 50% of the starting cohort of 1,900 and 89% of the patients originally enrolled at these 25 centers. Dr. Fuster stressed that the 957 patients not included in the follow-up had not been lost, but rather had been managed at sites that declined to participate in this additional study.
Dr. Fuster acknowledged that methods and hardware for PCI have changed since the study ran a decade ago, as have options for medical management. He also highlighted that the long-term follow-up results had no data on rates of MIs and strokes.
FREEDOM had no commercial funding. Dr. Fuster reported no relevant disclosures.
SOURCE: Fuster V et al. AHA 2018, Abstract 18609.
REPORTING FROM THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: After 7.5 years, mortality in the full FREEDOM cohort was 18% after coronary artery bypass grafting and 24% after percutaneous coronary intervention.
Study details: An extended follow-up of 943 of patients enrolled in FREEDOM, a randomized, multicenter trial.
Disclosures: FREEDOM had no commercial funding. Dr. Fuster reported no relevant disclosures.
Source: Fuster V et al. AHA 2018, Abstract 18609.
Decreased insulin clearance may be first step on path to insulin resistance
LOS ANGELES – As obese, nondiabetic individuals become more insulin resistant, a decrease in insulin clearance is the first change to occur, according to Sun H. Kim, MD.

“You will often hear about how insulin resistance enhances demand on beta cells to increase insulin secretion, which leads to hyperinsulinemia,” Dr. Kim said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease. “While well accepted, this model ignores the role of insulin clearance rate in maintaining hyperinsulinemia in insulin resistance states.”
In an effort to understand the physiologic adaptation to insulin resistance prior to the development of type 2 diabetes mellitus, Dr. Kim, an associate professor of endocrinology at Stanford (Calif) University, Stanford, and her colleagues enrolled 91 adults who had a body mass index of at least 30 kg/m2. The study was published in the March 2018 issue of Diabetologia. Each subject underwent a 75-g oral glucose tolerance test as well as the insulin suppression test to measure insulin resistance and the graded glucose infusion test to determine each subject’s insulin secretion rate and insulin clearance rate. For the graded glucose infusion test, the researchers increased the glucose infusion rate every 40 minutes, from 1 mg/kg per minute up to 8 mg/kg per minute. Next, they divided the cohort of obese individuals into tertiles of insulin resistance as quantified by the steady-state plasma glucose (SSPG): less than 9.7 mmol/L (tertile 1), 9.7-12.7 mmol/L (tertile 2), and 12.8 mmol/L or greater (tertile 3).
The mean age of subjects was 54 years. The mean SSPG level was 7.2 mmol/L among subjects in tertile 1, 11.3 mmol/L among those in tertile 2, and 14.3 mmol/L among those in tertile 3. The remainder of the demographics was similar. “Most importantly, body mass index among tertiles was nearly identical,” Dr. Kim said. “The only biomarker that was different was ALT, which increased with increasing tertiles. The individuals who were more insulin resistant likely had more fatty liver. We didn’t do imaging in this particular study.”
When the researchers evaluated oral glucose tolerance test data, they observed that subjects who were most insulin resistant had slightly higher glucose levels, “which we often see,” she said. “The body does try to keep glucose in a narrow range. What was dramatic were the insulin levels. The most insulin-resistant subjects had insulin levels that were double those of the least insulin-resistant subjects in tertile 1 during the oral glucose tolerance test.”
During the intravenous glucose infusion test, glucose levels rose similarly in the three groups, but those in tertile 3 had slightly higher glucose levels (P = .04). The insulin secretion rate, meanwhile, was similar among subjects in tertiles 1 and 2 but was increased significantly among subjects in tertile 3 (P less than .001). In contrast, the researchers observed a stepwise decline in insulin clearance rate from tertiles 1 to 3. Thus the insulin clearance rate was significantly different between subjects in tertile 1 and tertile 2 (P = .04) as well as between subjects in tertile 2 and those in tertile 3 (P less than .001).
“We propose that insulin resistance leads to an increase in intrahepatic fat, which decreases the insulin clearance rate and helps maintain euglycemia,” Dr. Kim concluded. “In the most insulin-resistant tertile, a decrease in insulin clearance rate is not sufficient, and an increase in the insulin secretion rate is also required. If you look at the relationship between insulin resistance and insulin clearance rate, there is a negative correlation, so the more insulin resistant you are, the lower your insulin clearance rate. However, there are insulin-resistant individuals who perhaps have higher insulin clearance rates than we think they should have. Could those individuals be at the highest risk to develop diabetes? That’s the story to which I don’t yet have an ending.” She reported having no financial disclosures.
SOURCE: Jung SH et al. Diabetologia. 2018;61(3):681-7.
LOS ANGELES – As obese, nondiabetic individuals become more insulin resistant, a decrease in insulin clearance is the first change to occur, according to Sun H. Kim, MD.
“You will often hear about how insulin resistance enhances demand on beta cells to increase insulin secretion, which leads to hyperinsulinemia,” Dr. Kim said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease. “While well accepted, this model ignores the role of insulin clearance rate in maintaining hyperinsulinemia in insulin resistance states.”
In an effort to understand the physiologic adaptation to insulin resistance prior to the development of type 2 diabetes mellitus, Dr. Kim, an associate professor of endocrinology at Stanford (Calif) University, Stanford, and her colleagues enrolled 91 adults who had a body mass index of at least 30 kg/m2. The study was published in the March 2018 issue of Diabetologia. Each subject underwent a 75-g oral glucose tolerance test as well as the insulin suppression test to measure insulin resistance and the graded glucose infusion test to determine each subject’s insulin secretion rate and insulin clearance rate. For the graded glucose infusion test, the researchers increased the glucose infusion rate every 40 minutes, from 1 mg/kg per minute up to 8 mg/kg per minute. Next, they divided the cohort of obese individuals into tertiles of insulin resistance as quantified by the steady-state plasma glucose (SSPG): less than 9.7 mmol/L (tertile 1), 9.7-12.7 mmol/L (tertile 2), and 12.8 mmol/L or greater (tertile 3).
The mean age of subjects was 54 years. The mean SSPG level was 7.2 mmol/L among subjects in tertile 1, 11.3 mmol/L among those in tertile 2, and 14.3 mmol/L among those in tertile 3. The remainder of the demographics was similar. “Most importantly, body mass index among tertiles was nearly identical,” Dr. Kim said. “The only biomarker that was different was ALT, which increased with increasing tertiles. The individuals who were more insulin resistant likely had more fatty liver. We didn’t do imaging in this particular study.”
When the researchers evaluated oral glucose tolerance test data, they observed that subjects who were most insulin resistant had slightly higher glucose levels, “which we often see,” she said. “The body does try to keep glucose in a narrow range. What was dramatic were the insulin levels. The most insulin-resistant subjects had insulin levels that were double those of the least insulin-resistant subjects in tertile 1 during the oral glucose tolerance test.”
During the intravenous glucose infusion test, glucose levels rose similarly in the three groups, but those in tertile 3 had slightly higher glucose levels (P = .04). The insulin secretion rate, meanwhile, was similar among subjects in tertiles 1 and 2 but was increased significantly among subjects in tertile 3 (P less than .001). In contrast, the researchers observed a stepwise decline in insulin clearance rate from tertiles 1 to 3. Thus the insulin clearance rate was significantly different between subjects in tertile 1 and tertile 2 (P = .04) as well as between subjects in tertile 2 and those in tertile 3 (P less than .001).
“We propose that insulin resistance leads to an increase in intrahepatic fat, which decreases the insulin clearance rate and helps maintain euglycemia,” Dr. Kim concluded. “In the most insulin-resistant tertile, a decrease in insulin clearance rate is not sufficient, and an increase in the insulin secretion rate is also required. If you look at the relationship between insulin resistance and insulin clearance rate, there is a negative correlation, so the more insulin resistant you are, the lower your insulin clearance rate. However, there are insulin-resistant individuals who perhaps have higher insulin clearance rates than we think they should have. Could those individuals be at the highest risk to develop diabetes? That’s the story to which I don’t yet have an ending.” She reported having no financial disclosures.
SOURCE: Jung SH et al. Diabetologia. 2018;61(3):681-7.
LOS ANGELES – As obese, nondiabetic individuals become more insulin resistant, a decrease in insulin clearance is the first change to occur, according to Sun H. Kim, MD.
“You will often hear about how insulin resistance enhances demand on beta cells to increase insulin secretion, which leads to hyperinsulinemia,” Dr. Kim said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease. “While well accepted, this model ignores the role of insulin clearance rate in maintaining hyperinsulinemia in insulin resistance states.”
In an effort to understand the physiologic adaptation to insulin resistance prior to the development of type 2 diabetes mellitus, Dr. Kim, an associate professor of endocrinology at Stanford (Calif) University, Stanford, and her colleagues enrolled 91 adults who had a body mass index of at least 30 kg/m2. The study was published in the March 2018 issue of Diabetologia. Each subject underwent a 75-g oral glucose tolerance test as well as the insulin suppression test to measure insulin resistance and the graded glucose infusion test to determine each subject’s insulin secretion rate and insulin clearance rate. For the graded glucose infusion test, the researchers increased the glucose infusion rate every 40 minutes, from 1 mg/kg per minute up to 8 mg/kg per minute. Next, they divided the cohort of obese individuals into tertiles of insulin resistance as quantified by the steady-state plasma glucose (SSPG): less than 9.7 mmol/L (tertile 1), 9.7-12.7 mmol/L (tertile 2), and 12.8 mmol/L or greater (tertile 3).
The mean age of subjects was 54 years. The mean SSPG level was 7.2 mmol/L among subjects in tertile 1, 11.3 mmol/L among those in tertile 2, and 14.3 mmol/L among those in tertile 3. The remainder of the demographics was similar. “Most importantly, body mass index among tertiles was nearly identical,” Dr. Kim said. “The only biomarker that was different was ALT, which increased with increasing tertiles. The individuals who were more insulin resistant likely had more fatty liver. We didn’t do imaging in this particular study.”
When the researchers evaluated oral glucose tolerance test data, they observed that subjects who were most insulin resistant had slightly higher glucose levels, “which we often see,” she said. “The body does try to keep glucose in a narrow range. What was dramatic were the insulin levels. The most insulin-resistant subjects had insulin levels that were double those of the least insulin-resistant subjects in tertile 1 during the oral glucose tolerance test.”
During the intravenous glucose infusion test, glucose levels rose similarly in the three groups, but those in tertile 3 had slightly higher glucose levels (P = .04). The insulin secretion rate, meanwhile, was similar among subjects in tertiles 1 and 2 but was increased significantly among subjects in tertile 3 (P less than .001). In contrast, the researchers observed a stepwise decline in insulin clearance rate from tertiles 1 to 3. Thus the insulin clearance rate was significantly different between subjects in tertile 1 and tertile 2 (P = .04) as well as between subjects in tertile 2 and those in tertile 3 (P less than .001).
“We propose that insulin resistance leads to an increase in intrahepatic fat, which decreases the insulin clearance rate and helps maintain euglycemia,” Dr. Kim concluded. “In the most insulin-resistant tertile, a decrease in insulin clearance rate is not sufficient, and an increase in the insulin secretion rate is also required. If you look at the relationship between insulin resistance and insulin clearance rate, there is a negative correlation, so the more insulin resistant you are, the lower your insulin clearance rate. However, there are insulin-resistant individuals who perhaps have higher insulin clearance rates than we think they should have. Could those individuals be at the highest risk to develop diabetes? That’s the story to which I don’t yet have an ending.” She reported having no financial disclosures.
SOURCE: Jung SH et al. Diabetologia. 2018;61(3):681-7.
REPORTING FROM WCIRDC 2018
Key clinical point:
Major finding: In the most insulin-resistant subgroup, the insulin secretion rate increases and the insulin clearance rate decreases to compensate for insulin resistance.
Study details: A study of 91 obese adults without diabetes.
Disclosures: Dr. Kim reported having no disclosures.
Source: Jung SH et al. Diabetologia. 2018;61(3):681-7.
Study investigates statin-diabetes link
LOS ANGELES – On any given day, type “statins” in the subject line of your favorite search engine and many results are likely to focus on risks: some based on science, others not so much.

“There is all kind of misinformation that are preventing people from taking statins,” Joshua W. Knowles, MD, said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease. “The most important side effects of statins are the increased lifespan and decreased risk of heart attacks, but that’s not what our patients are telling us. One of the things that is true is that .”
In 2016, Dr. Knowles, a cardiologist at the Stanford (Calif.) Center for Inherited Cardiovascular Disease, coauthored a retrospective analysis of data from subjects without diabetes in the Treating to New Targets (TNT) and the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) randomized controlled trials (Am J Cardiol 2016;118[9]:1275-81). The authors found that statins particularly increase the risk of type 2 diabetes in those with prediabetes and insulin resistance. “That’s a risk group that we are all treating,” he said. “But that still doesn’t answer the question as to why this happens. Is this because statins increase insulin resistance, because they decrease beta cell function, or because they increase insulin clearance rate?”
In an effort to find out, Dr. Knowles and his colleagues have launched a clinical trial entitled “Relationship Between Insulin Resistance and Statin Induced Type 2 Diabetes, and Integrative Personal Omics Profiling” (NCT 02437084). Candidates do not have diabetes, yet qualify for statin therapy because they have a greater than 7.5% risk of cardiovascular disease over 10 years. To date, the researchers have enrolled 74 patients: 42 to the insulin-sensitive group (defined as having an LDL above 130 mg/dL and a triglyceride level below 150 mg/dL) and 11 to the insulin-resistant group (defined as having an LDL of 130 mg/dL or greater and a triglyceride level of 150 mg/dL or greater). Dr. Knowles said that about two-thirds of patients have been recruited and that full results are expected in late 2019.
At baseline, subjects underwent the insulin suppression test, the graded glucose infusion test, metabolic characterization, and integrated personal omics profiling (iPOP), a monitoring method. After 3 months of atorvastatin therapy 40 mg/day, the researchers repeated these measures and compared the results between groups. “Basically we were looking for changes in insulin resistance, secretion, and clearance between those groups over time,” said Dr. Knowles, who is the study’s principal investigator.
Of the 74 subjects, 13 decided that they did not want to participate and 6 are still undergoing baseline tests. In all, 55 started statin therapy, and 2 have dropped out. This left 42 in the low-triglyceride group and 11 in the high-triglyceride group.
The average age of the 52 individuals who have completed the study so far is 61 years, 30 are male, 35 are non-Hispanic white, their mean body mass index was 27.9 kg/m2, and their mean blood pressure was 127/79 mm Hg. By the end of statin therapy, body mass index did not change, but total cholesterol fell from a median of 234 mg/dL to a median of 150 mg/dL, triglycerides fell from a median of 109 mg/dL to a median of 78 mg/dL, LDL cholesterol fell from a median of 153 mg/dL to a median of 71 mg/dL, and mean high-sensitivity C-reactive protein dropped from a median of 1.2 mg/L to a median of 0.8 mg/L. All differences were statistically significant.
Fasting glucose levels have been completed on only 35 patients. “Two-hour glucose is going up, but it’s not yet significant, and on the oral glucose tolerance test, the curves are separating slightly but are not yet significant,” Dr. Knowles said.
On average, insulin resistance among the 35 patients worsened slightly, from 156 mg/dL before statin therapy to 170 mg/dL after initiation. “This is nominally significant (P = 0.03), and we’ll have to see if this holds up over time,” he said. The researchers also observed that statin use was associated with slight decreases in insulin secretion and clearance. Dr. Knowles emphasized that these are preliminary results and need to be further validated.
The study is funded by the Doris Duke Charitable Foundation. Dr. Knowles reported having no disclosures.
LOS ANGELES – On any given day, type “statins” in the subject line of your favorite search engine and many results are likely to focus on risks: some based on science, others not so much.
“There is all kind of misinformation that are preventing people from taking statins,” Joshua W. Knowles, MD, said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease. “The most important side effects of statins are the increased lifespan and decreased risk of heart attacks, but that’s not what our patients are telling us. One of the things that is true is that .”
In 2016, Dr. Knowles, a cardiologist at the Stanford (Calif.) Center for Inherited Cardiovascular Disease, coauthored a retrospective analysis of data from subjects without diabetes in the Treating to New Targets (TNT) and the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) randomized controlled trials (Am J Cardiol 2016;118[9]:1275-81). The authors found that statins particularly increase the risk of type 2 diabetes in those with prediabetes and insulin resistance. “That’s a risk group that we are all treating,” he said. “But that still doesn’t answer the question as to why this happens. Is this because statins increase insulin resistance, because they decrease beta cell function, or because they increase insulin clearance rate?”
In an effort to find out, Dr. Knowles and his colleagues have launched a clinical trial entitled “Relationship Between Insulin Resistance and Statin Induced Type 2 Diabetes, and Integrative Personal Omics Profiling” (NCT 02437084). Candidates do not have diabetes, yet qualify for statin therapy because they have a greater than 7.5% risk of cardiovascular disease over 10 years. To date, the researchers have enrolled 74 patients: 42 to the insulin-sensitive group (defined as having an LDL above 130 mg/dL and a triglyceride level below 150 mg/dL) and 11 to the insulin-resistant group (defined as having an LDL of 130 mg/dL or greater and a triglyceride level of 150 mg/dL or greater). Dr. Knowles said that about two-thirds of patients have been recruited and that full results are expected in late 2019.
At baseline, subjects underwent the insulin suppression test, the graded glucose infusion test, metabolic characterization, and integrated personal omics profiling (iPOP), a monitoring method. After 3 months of atorvastatin therapy 40 mg/day, the researchers repeated these measures and compared the results between groups. “Basically we were looking for changes in insulin resistance, secretion, and clearance between those groups over time,” said Dr. Knowles, who is the study’s principal investigator.
Of the 74 subjects, 13 decided that they did not want to participate and 6 are still undergoing baseline tests. In all, 55 started statin therapy, and 2 have dropped out. This left 42 in the low-triglyceride group and 11 in the high-triglyceride group.
The average age of the 52 individuals who have completed the study so far is 61 years, 30 are male, 35 are non-Hispanic white, their mean body mass index was 27.9 kg/m2, and their mean blood pressure was 127/79 mm Hg. By the end of statin therapy, body mass index did not change, but total cholesterol fell from a median of 234 mg/dL to a median of 150 mg/dL, triglycerides fell from a median of 109 mg/dL to a median of 78 mg/dL, LDL cholesterol fell from a median of 153 mg/dL to a median of 71 mg/dL, and mean high-sensitivity C-reactive protein dropped from a median of 1.2 mg/L to a median of 0.8 mg/L. All differences were statistically significant.
Fasting glucose levels have been completed on only 35 patients. “Two-hour glucose is going up, but it’s not yet significant, and on the oral glucose tolerance test, the curves are separating slightly but are not yet significant,” Dr. Knowles said.
On average, insulin resistance among the 35 patients worsened slightly, from 156 mg/dL before statin therapy to 170 mg/dL after initiation. “This is nominally significant (P = 0.03), and we’ll have to see if this holds up over time,” he said. The researchers also observed that statin use was associated with slight decreases in insulin secretion and clearance. Dr. Knowles emphasized that these are preliminary results and need to be further validated.
The study is funded by the Doris Duke Charitable Foundation. Dr. Knowles reported having no disclosures.
LOS ANGELES – On any given day, type “statins” in the subject line of your favorite search engine and many results are likely to focus on risks: some based on science, others not so much.
“There is all kind of misinformation that are preventing people from taking statins,” Joshua W. Knowles, MD, said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease. “The most important side effects of statins are the increased lifespan and decreased risk of heart attacks, but that’s not what our patients are telling us. One of the things that is true is that .”
In 2016, Dr. Knowles, a cardiologist at the Stanford (Calif.) Center for Inherited Cardiovascular Disease, coauthored a retrospective analysis of data from subjects without diabetes in the Treating to New Targets (TNT) and the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) randomized controlled trials (Am J Cardiol 2016;118[9]:1275-81). The authors found that statins particularly increase the risk of type 2 diabetes in those with prediabetes and insulin resistance. “That’s a risk group that we are all treating,” he said. “But that still doesn’t answer the question as to why this happens. Is this because statins increase insulin resistance, because they decrease beta cell function, or because they increase insulin clearance rate?”
In an effort to find out, Dr. Knowles and his colleagues have launched a clinical trial entitled “Relationship Between Insulin Resistance and Statin Induced Type 2 Diabetes, and Integrative Personal Omics Profiling” (NCT 02437084). Candidates do not have diabetes, yet qualify for statin therapy because they have a greater than 7.5% risk of cardiovascular disease over 10 years. To date, the researchers have enrolled 74 patients: 42 to the insulin-sensitive group (defined as having an LDL above 130 mg/dL and a triglyceride level below 150 mg/dL) and 11 to the insulin-resistant group (defined as having an LDL of 130 mg/dL or greater and a triglyceride level of 150 mg/dL or greater). Dr. Knowles said that about two-thirds of patients have been recruited and that full results are expected in late 2019.
At baseline, subjects underwent the insulin suppression test, the graded glucose infusion test, metabolic characterization, and integrated personal omics profiling (iPOP), a monitoring method. After 3 months of atorvastatin therapy 40 mg/day, the researchers repeated these measures and compared the results between groups. “Basically we were looking for changes in insulin resistance, secretion, and clearance between those groups over time,” said Dr. Knowles, who is the study’s principal investigator.
Of the 74 subjects, 13 decided that they did not want to participate and 6 are still undergoing baseline tests. In all, 55 started statin therapy, and 2 have dropped out. This left 42 in the low-triglyceride group and 11 in the high-triglyceride group.
The average age of the 52 individuals who have completed the study so far is 61 years, 30 are male, 35 are non-Hispanic white, their mean body mass index was 27.9 kg/m2, and their mean blood pressure was 127/79 mm Hg. By the end of statin therapy, body mass index did not change, but total cholesterol fell from a median of 234 mg/dL to a median of 150 mg/dL, triglycerides fell from a median of 109 mg/dL to a median of 78 mg/dL, LDL cholesterol fell from a median of 153 mg/dL to a median of 71 mg/dL, and mean high-sensitivity C-reactive protein dropped from a median of 1.2 mg/L to a median of 0.8 mg/L. All differences were statistically significant.
Fasting glucose levels have been completed on only 35 patients. “Two-hour glucose is going up, but it’s not yet significant, and on the oral glucose tolerance test, the curves are separating slightly but are not yet significant,” Dr. Knowles said.
On average, insulin resistance among the 35 patients worsened slightly, from 156 mg/dL before statin therapy to 170 mg/dL after initiation. “This is nominally significant (P = 0.03), and we’ll have to see if this holds up over time,” he said. The researchers also observed that statin use was associated with slight decreases in insulin secretion and clearance. Dr. Knowles emphasized that these are preliminary results and need to be further validated.
The study is funded by the Doris Duke Charitable Foundation. Dr. Knowles reported having no disclosures.
REPORTING FROM WCIRDC 2018
Should metabolic syndrome be renamed circadian syndrome?
LOS ANGELES – In the opinion of Paul Zimmet, MD, PhD, the
This scenario created the “perfect storm” for rising rates of metabolic syndrome, which is related to low HDL cholesterol levels, central obesity, hypertension, hyperglycemia, and high triglyceride levels, Dr. Zimmet said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease. These cardiometabolic risk factors “all seem to cluster together in relation to the changes in our society,” he said. “It’s on that basis and research findings that I think we should understand that most of them, if not all, have been demonstrated to relate to circadian rhythm disturbance.”
In fact, the associated comorbidities sleep apnea, depression, and fatty liver disease should be included in the metabolic syndrome cluster and should be renamed the “circadian syndrome,” according to Dr. Zimmet, professor of diabetes at Monash University, Melbourne.
The term metabolic syndrome is anathema, he said. “There have been numerous different definitions, which finally led to an effort to come up with a harmonized definition” by the International Diabetes Federation Task Force on Epidemiology and Prevention, with involvement from the American Heart Association (Circulation 2009;120[16]:1640-5).
In the early 1970s, Dr. Zimmet and his colleagues at Guys Hospital in London reported on diurnal variation in glucose tolerance. “If you did a glucose tolerance test in the afternoon it could be diabetic, whereas in the morning it was normal,” he noted. “Other researchers reported similar findings. That created in my own mind interest in this area of circadian rhythm. However, I had neglected this until recently, when I was doing background research while trying to find an answer to the elusive question of a central uniting explanation for the cardiometabolic cluster constituting the metabolic syndrome.” So decades later, Dr. Zimmet extended his research to include epigenetics in the quest. Described as the study of heritable changes in gene function that occur without a change in the sequence of the DNA, epigenetic changes “are closely linked to the circadian rhythm, otherwise known as ‘the body clock,’ ” said Dr. Zimmet, who also is codirector with Naftali Stern, MD, of the Sagol Center for Epigenetics of Metabolism and Aging at Tel Aviv Medical Center. “Many aspects of human behavior and metabolism are closely linked to the circadian clock and affected by its rhythm disturbance. We decided that we wanted to further investigate this area: To what extent is circadian rhythm the central feature to explain the clustering of all of these cardiovascular and metabolic risk factors of the metabolic syndrome.”
In recent years, he has been collaborating with Noga Kronfeld-Schor, PhD, of the department of zoology at Tel Aviv (Israel) University. The research focuses on a gerbil from the Negev: Psammomys obesus (otherwise known as the Israeli fat sand rat), which develops elevated blood sugar, obesity, depression, sleep disturbance, fatty liver, and circadian dysrhythmia when removed from the desert environment to the laboratory. “These are all key features of type 2 diabetes in humans,” he said. “This is probably the best animal model of type 2 diabetes, and we felt that it was worth looking more closely to see if there was a similar relationship in humans as to whether circadian dysrhythmia would be causing all or most of these features in humans including obesity.” An epigenetic study of the gerbil in the laboratory of Prof. Sam El-Osta at Monash has shown that parental diet during early life regulated expression of genes associated with DNA methylation in the key FTO gene associated with obesity (Int J Obesity 2016;40:1079-88). It suggests that diet-induced metabolic changes can be transmitted from parent to offspring by mechanisms under epigenetic control.
Published studies from other research groups support the link between other of the cardiometabolic metabolic syndrome characteristics, epigenetic modifications, and circadian dysrhythmia including cardiovascular regulation and disease (Eur Heart J 2018;39[14]:2326-9), sleep loss and alterations in DNA methylation (Science Advances 2018;4[8]:eaar8590), and circadian dysrhythmia and fatty liver (Cell Metab 2012;15[6]:848-60). “In 2009, the FDA approved bromocriptine mesylate, a drug which has effects on circadian rhythm, for treatment of type 2 diabetes, suggesting its use in diabetes may have some role through the alteration of circadian rhythm,” continued Dr. Zimmet, who also is honorary president of the International Diabetes Federation. “Depression is also clearly linked to circadian rhythm and there is evidence from research and human studies that light therapy may be an effective treatment for type 2 diabetes and depression.”
Dr. Zimmet ended his presentation with a strong call for adding sleep apnea, fatty liver, and depression to the existing features of the metabolic syndrome “to encourage clinicians and researchers look at the picture of cardiometabolic risk much more broadly than as just a group of metabolic abnormalities,” he said. “We propose that these comorbidities be embraced within the definition of the cardiometabolic cluster and be renamed the ‘circadian syndrome.’ This cluster is now the main driver of the global chronic disease epidemic and its health burden. This is a disease of civilization – the result of the way we live.”
Dr. Zimmet reported having no disclosures.
LOS ANGELES – In the opinion of Paul Zimmet, MD, PhD, the
This scenario created the “perfect storm” for rising rates of metabolic syndrome, which is related to low HDL cholesterol levels, central obesity, hypertension, hyperglycemia, and high triglyceride levels, Dr. Zimmet said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease. These cardiometabolic risk factors “all seem to cluster together in relation to the changes in our society,” he said. “It’s on that basis and research findings that I think we should understand that most of them, if not all, have been demonstrated to relate to circadian rhythm disturbance.”
In fact, the associated comorbidities sleep apnea, depression, and fatty liver disease should be included in the metabolic syndrome cluster and should be renamed the “circadian syndrome,” according to Dr. Zimmet, professor of diabetes at Monash University, Melbourne.
The term metabolic syndrome is anathema, he said. “There have been numerous different definitions, which finally led to an effort to come up with a harmonized definition” by the International Diabetes Federation Task Force on Epidemiology and Prevention, with involvement from the American Heart Association (Circulation 2009;120[16]:1640-5).
In the early 1970s, Dr. Zimmet and his colleagues at Guys Hospital in London reported on diurnal variation in glucose tolerance. “If you did a glucose tolerance test in the afternoon it could be diabetic, whereas in the morning it was normal,” he noted. “Other researchers reported similar findings. That created in my own mind interest in this area of circadian rhythm. However, I had neglected this until recently, when I was doing background research while trying to find an answer to the elusive question of a central uniting explanation for the cardiometabolic cluster constituting the metabolic syndrome.” So decades later, Dr. Zimmet extended his research to include epigenetics in the quest. Described as the study of heritable changes in gene function that occur without a change in the sequence of the DNA, epigenetic changes “are closely linked to the circadian rhythm, otherwise known as ‘the body clock,’ ” said Dr. Zimmet, who also is codirector with Naftali Stern, MD, of the Sagol Center for Epigenetics of Metabolism and Aging at Tel Aviv Medical Center. “Many aspects of human behavior and metabolism are closely linked to the circadian clock and affected by its rhythm disturbance. We decided that we wanted to further investigate this area: To what extent is circadian rhythm the central feature to explain the clustering of all of these cardiovascular and metabolic risk factors of the metabolic syndrome.”
In recent years, he has been collaborating with Noga Kronfeld-Schor, PhD, of the department of zoology at Tel Aviv (Israel) University. The research focuses on a gerbil from the Negev: Psammomys obesus (otherwise known as the Israeli fat sand rat), which develops elevated blood sugar, obesity, depression, sleep disturbance, fatty liver, and circadian dysrhythmia when removed from the desert environment to the laboratory. “These are all key features of type 2 diabetes in humans,” he said. “This is probably the best animal model of type 2 diabetes, and we felt that it was worth looking more closely to see if there was a similar relationship in humans as to whether circadian dysrhythmia would be causing all or most of these features in humans including obesity.” An epigenetic study of the gerbil in the laboratory of Prof. Sam El-Osta at Monash has shown that parental diet during early life regulated expression of genes associated with DNA methylation in the key FTO gene associated with obesity (Int J Obesity 2016;40:1079-88). It suggests that diet-induced metabolic changes can be transmitted from parent to offspring by mechanisms under epigenetic control.
Published studies from other research groups support the link between other of the cardiometabolic metabolic syndrome characteristics, epigenetic modifications, and circadian dysrhythmia including cardiovascular regulation and disease (Eur Heart J 2018;39[14]:2326-9), sleep loss and alterations in DNA methylation (Science Advances 2018;4[8]:eaar8590), and circadian dysrhythmia and fatty liver (Cell Metab 2012;15[6]:848-60). “In 2009, the FDA approved bromocriptine mesylate, a drug which has effects on circadian rhythm, for treatment of type 2 diabetes, suggesting its use in diabetes may have some role through the alteration of circadian rhythm,” continued Dr. Zimmet, who also is honorary president of the International Diabetes Federation. “Depression is also clearly linked to circadian rhythm and there is evidence from research and human studies that light therapy may be an effective treatment for type 2 diabetes and depression.”
Dr. Zimmet ended his presentation with a strong call for adding sleep apnea, fatty liver, and depression to the existing features of the metabolic syndrome “to encourage clinicians and researchers look at the picture of cardiometabolic risk much more broadly than as just a group of metabolic abnormalities,” he said. “We propose that these comorbidities be embraced within the definition of the cardiometabolic cluster and be renamed the ‘circadian syndrome.’ This cluster is now the main driver of the global chronic disease epidemic and its health burden. This is a disease of civilization – the result of the way we live.”
Dr. Zimmet reported having no disclosures.
LOS ANGELES – In the opinion of Paul Zimmet, MD, PhD, the
This scenario created the “perfect storm” for rising rates of metabolic syndrome, which is related to low HDL cholesterol levels, central obesity, hypertension, hyperglycemia, and high triglyceride levels, Dr. Zimmet said at the World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease. These cardiometabolic risk factors “all seem to cluster together in relation to the changes in our society,” he said. “It’s on that basis and research findings that I think we should understand that most of them, if not all, have been demonstrated to relate to circadian rhythm disturbance.”
In fact, the associated comorbidities sleep apnea, depression, and fatty liver disease should be included in the metabolic syndrome cluster and should be renamed the “circadian syndrome,” according to Dr. Zimmet, professor of diabetes at Monash University, Melbourne.
The term metabolic syndrome is anathema, he said. “There have been numerous different definitions, which finally led to an effort to come up with a harmonized definition” by the International Diabetes Federation Task Force on Epidemiology and Prevention, with involvement from the American Heart Association (Circulation 2009;120[16]:1640-5).
In the early 1970s, Dr. Zimmet and his colleagues at Guys Hospital in London reported on diurnal variation in glucose tolerance. “If you did a glucose tolerance test in the afternoon it could be diabetic, whereas in the morning it was normal,” he noted. “Other researchers reported similar findings. That created in my own mind interest in this area of circadian rhythm. However, I had neglected this until recently, when I was doing background research while trying to find an answer to the elusive question of a central uniting explanation for the cardiometabolic cluster constituting the metabolic syndrome.” So decades later, Dr. Zimmet extended his research to include epigenetics in the quest. Described as the study of heritable changes in gene function that occur without a change in the sequence of the DNA, epigenetic changes “are closely linked to the circadian rhythm, otherwise known as ‘the body clock,’ ” said Dr. Zimmet, who also is codirector with Naftali Stern, MD, of the Sagol Center for Epigenetics of Metabolism and Aging at Tel Aviv Medical Center. “Many aspects of human behavior and metabolism are closely linked to the circadian clock and affected by its rhythm disturbance. We decided that we wanted to further investigate this area: To what extent is circadian rhythm the central feature to explain the clustering of all of these cardiovascular and metabolic risk factors of the metabolic syndrome.”
In recent years, he has been collaborating with Noga Kronfeld-Schor, PhD, of the department of zoology at Tel Aviv (Israel) University. The research focuses on a gerbil from the Negev: Psammomys obesus (otherwise known as the Israeli fat sand rat), which develops elevated blood sugar, obesity, depression, sleep disturbance, fatty liver, and circadian dysrhythmia when removed from the desert environment to the laboratory. “These are all key features of type 2 diabetes in humans,” he said. “This is probably the best animal model of type 2 diabetes, and we felt that it was worth looking more closely to see if there was a similar relationship in humans as to whether circadian dysrhythmia would be causing all or most of these features in humans including obesity.” An epigenetic study of the gerbil in the laboratory of Prof. Sam El-Osta at Monash has shown that parental diet during early life regulated expression of genes associated with DNA methylation in the key FTO gene associated with obesity (Int J Obesity 2016;40:1079-88). It suggests that diet-induced metabolic changes can be transmitted from parent to offspring by mechanisms under epigenetic control.
Published studies from other research groups support the link between other of the cardiometabolic metabolic syndrome characteristics, epigenetic modifications, and circadian dysrhythmia including cardiovascular regulation and disease (Eur Heart J 2018;39[14]:2326-9), sleep loss and alterations in DNA methylation (Science Advances 2018;4[8]:eaar8590), and circadian dysrhythmia and fatty liver (Cell Metab 2012;15[6]:848-60). “In 2009, the FDA approved bromocriptine mesylate, a drug which has effects on circadian rhythm, for treatment of type 2 diabetes, suggesting its use in diabetes may have some role through the alteration of circadian rhythm,” continued Dr. Zimmet, who also is honorary president of the International Diabetes Federation. “Depression is also clearly linked to circadian rhythm and there is evidence from research and human studies that light therapy may be an effective treatment for type 2 diabetes and depression.”
Dr. Zimmet ended his presentation with a strong call for adding sleep apnea, fatty liver, and depression to the existing features of the metabolic syndrome “to encourage clinicians and researchers look at the picture of cardiometabolic risk much more broadly than as just a group of metabolic abnormalities,” he said. “We propose that these comorbidities be embraced within the definition of the cardiometabolic cluster and be renamed the ‘circadian syndrome.’ This cluster is now the main driver of the global chronic disease epidemic and its health burden. This is a disease of civilization – the result of the way we live.”
Dr. Zimmet reported having no disclosures.
EXPERT ANALYSIS FROM THE WCIRDC 2018
Diuretics linked to diabetic amputations in T2DM
BERLIN – presented at the annual meeting of the European Association for the Study of Diabetes.

A significant and independent increase in the risk of lower limb events, predominantly lower-extremity amputations was seen among patients with type 2 diabetes mellitus (T2DM) who were treated with diuretics versus those who were not. The adjusted hazard ratios in a propensity-matched cohort was 1.60 (95% confidence interval, 1.06-2.42; P = .027) for lower limb events, 2.13 (95% CI, 1.17-3.87; P = .013) for lower limb amputations, and 1.12 (95% CI, 0.70-1.79; P = .6443) for lower limb revascularizations.
“We know diabetes is a leading cause of nontraumatic lower limb amputations in the world,” and thus a very important public health issue, said study investigator Ronan Roussel, MD, PhD, of Hôpital Bichat, Assistance Publique Hôpitaux de Paris. “Many contributing factors are identified, susceptibility to infection, impaired wound healing, peripheral neuropathy; but the most important is the presence of peripheral arterial disease.”
The risk of diabetic amputations is of specific interest because of the recent findings from CANVAS, where treatment with canagliflozin, a sodium-glucose cotransporter 2 (SGLT2) inhibitor, was linked to an almost doubled rate of amputations versus placebo (HR, 1.97; 95% CI, 1.41-2.75) in patients with T2DM.
Conflicting results have been seen in observational studies with other SGLT2 inhibitors, however, and it’s not clear if the risk of amputations is just seen with canagliflozin or if it may be a class effect. The underlying mechanism is unknown, but one theory is that hypovolemia may be involved. If this is the case, Dr. Roussel explained, then diuretics would have a similar safety profile as SGLT2 inhibitors in terms of increasing the risk of amputations.
The aim of the present study was to look at the association between lower limb events and diuretic usage in patients with T2DM. Data on 1,459 subjects with T2DM treated with diuretics and data on lower limb events and amputations were obtained from the single-center SURDIAGENE study. Of these, 670 were and 789 were not taking diuretics.
Baseline differences between diuretic and nondiuretic users were seen, such as diuretic users being older (67 vs. 63 years), having longer diabetes duration (16 vs. 13 years), and being more likely to have cardiovascular disease (32.5% vs. 23.4%). A propensity-score approach was used to even out these differences, leaving a population of 1,074 subjects in the final matched cohort.
Over a median follow-up of 7.2 years, 12.7% of diuretic and 7.2% of nondiuretic users experienced lower limb events (P = .001). In multivariate and sensitivity analyses, lower limb amputations remained significantly higher in patients who had been treated with a diuretic than in those who had not.
These are “hypothesis-generating” data, Dr. Roussel pointed out and “we don’t want to be overconclusive, of course.” However, they may explain the risk signal seen with SGLT2 inhibitors in the CANVAS study. Further studies are needed to explore the role of drug-induced hypovolemia in the association between the use of diuretics and lower limb events.

EASD delegate Prashanth Vas, MBBS, MRCP, PhD, noted during the discussion that the use of diuretics was ubiquitous. “Nearly everyone uses diuretics,” he said. The potential risk of lower limb amputation and treatment with SGLT2 inhibitors had “been vexing us for some time since the data from CANVAS came out.”
Dr. Vas, who is a consultant diabetologist and diabetic foot specialist at King’s College Hospital NHS Foundation in London, went on to ask why only canagliflozin was found to be associated with amputations and not the other SGLT2 drugs.
Dr. Roussel responded that data were still needed on the other drugs in this class and that they needed to be treated with caution. The literature is not so clear, he admitted.
“It’s important that you noted it’s a single-center study,” Dr. Vas countered. “It’s very important to have multicenter data. An amputation is a decision made by someone. An amputation in one center may not be an amputation in another center.”
The SURDIAGENE study was supported by grants from the French Ministry of Health, the Association Française des Diabétiques, and the Groupement pour l’Etude des Maladies Métaboliques et Systémiques. Dr. Roussel reported relationships with Janssen, Merck, Sanofi-Aventis, AstraZeneca, and Boehringer Ingelheim. Dr. Vas was not involved in the study or analysis.
SOURCE: Roussel R et al. EASD 2018, Abstract 12.
BERLIN – presented at the annual meeting of the European Association for the Study of Diabetes.
A significant and independent increase in the risk of lower limb events, predominantly lower-extremity amputations was seen among patients with type 2 diabetes mellitus (T2DM) who were treated with diuretics versus those who were not. The adjusted hazard ratios in a propensity-matched cohort was 1.60 (95% confidence interval, 1.06-2.42; P = .027) for lower limb events, 2.13 (95% CI, 1.17-3.87; P = .013) for lower limb amputations, and 1.12 (95% CI, 0.70-1.79; P = .6443) for lower limb revascularizations.
“We know diabetes is a leading cause of nontraumatic lower limb amputations in the world,” and thus a very important public health issue, said study investigator Ronan Roussel, MD, PhD, of Hôpital Bichat, Assistance Publique Hôpitaux de Paris. “Many contributing factors are identified, susceptibility to infection, impaired wound healing, peripheral neuropathy; but the most important is the presence of peripheral arterial disease.”
The risk of diabetic amputations is of specific interest because of the recent findings from CANVAS, where treatment with canagliflozin, a sodium-glucose cotransporter 2 (SGLT2) inhibitor, was linked to an almost doubled rate of amputations versus placebo (HR, 1.97; 95% CI, 1.41-2.75) in patients with T2DM.
Conflicting results have been seen in observational studies with other SGLT2 inhibitors, however, and it’s not clear if the risk of amputations is just seen with canagliflozin or if it may be a class effect. The underlying mechanism is unknown, but one theory is that hypovolemia may be involved. If this is the case, Dr. Roussel explained, then diuretics would have a similar safety profile as SGLT2 inhibitors in terms of increasing the risk of amputations.
The aim of the present study was to look at the association between lower limb events and diuretic usage in patients with T2DM. Data on 1,459 subjects with T2DM treated with diuretics and data on lower limb events and amputations were obtained from the single-center SURDIAGENE study. Of these, 670 were and 789 were not taking diuretics.
Baseline differences between diuretic and nondiuretic users were seen, such as diuretic users being older (67 vs. 63 years), having longer diabetes duration (16 vs. 13 years), and being more likely to have cardiovascular disease (32.5% vs. 23.4%). A propensity-score approach was used to even out these differences, leaving a population of 1,074 subjects in the final matched cohort.
Over a median follow-up of 7.2 years, 12.7% of diuretic and 7.2% of nondiuretic users experienced lower limb events (P = .001). In multivariate and sensitivity analyses, lower limb amputations remained significantly higher in patients who had been treated with a diuretic than in those who had not.
These are “hypothesis-generating” data, Dr. Roussel pointed out and “we don’t want to be overconclusive, of course.” However, they may explain the risk signal seen with SGLT2 inhibitors in the CANVAS study. Further studies are needed to explore the role of drug-induced hypovolemia in the association between the use of diuretics and lower limb events.
EASD delegate Prashanth Vas, MBBS, MRCP, PhD, noted during the discussion that the use of diuretics was ubiquitous. “Nearly everyone uses diuretics,” he said. The potential risk of lower limb amputation and treatment with SGLT2 inhibitors had “been vexing us for some time since the data from CANVAS came out.”
Dr. Vas, who is a consultant diabetologist and diabetic foot specialist at King’s College Hospital NHS Foundation in London, went on to ask why only canagliflozin was found to be associated with amputations and not the other SGLT2 drugs.
Dr. Roussel responded that data were still needed on the other drugs in this class and that they needed to be treated with caution. The literature is not so clear, he admitted.
“It’s important that you noted it’s a single-center study,” Dr. Vas countered. “It’s very important to have multicenter data. An amputation is a decision made by someone. An amputation in one center may not be an amputation in another center.”
The SURDIAGENE study was supported by grants from the French Ministry of Health, the Association Française des Diabétiques, and the Groupement pour l’Etude des Maladies Métaboliques et Systémiques. Dr. Roussel reported relationships with Janssen, Merck, Sanofi-Aventis, AstraZeneca, and Boehringer Ingelheim. Dr. Vas was not involved in the study or analysis.
SOURCE: Roussel R et al. EASD 2018, Abstract 12.
BERLIN – presented at the annual meeting of the European Association for the Study of Diabetes.
A significant and independent increase in the risk of lower limb events, predominantly lower-extremity amputations was seen among patients with type 2 diabetes mellitus (T2DM) who were treated with diuretics versus those who were not. The adjusted hazard ratios in a propensity-matched cohort was 1.60 (95% confidence interval, 1.06-2.42; P = .027) for lower limb events, 2.13 (95% CI, 1.17-3.87; P = .013) for lower limb amputations, and 1.12 (95% CI, 0.70-1.79; P = .6443) for lower limb revascularizations.
“We know diabetes is a leading cause of nontraumatic lower limb amputations in the world,” and thus a very important public health issue, said study investigator Ronan Roussel, MD, PhD, of Hôpital Bichat, Assistance Publique Hôpitaux de Paris. “Many contributing factors are identified, susceptibility to infection, impaired wound healing, peripheral neuropathy; but the most important is the presence of peripheral arterial disease.”
The risk of diabetic amputations is of specific interest because of the recent findings from CANVAS, where treatment with canagliflozin, a sodium-glucose cotransporter 2 (SGLT2) inhibitor, was linked to an almost doubled rate of amputations versus placebo (HR, 1.97; 95% CI, 1.41-2.75) in patients with T2DM.
Conflicting results have been seen in observational studies with other SGLT2 inhibitors, however, and it’s not clear if the risk of amputations is just seen with canagliflozin or if it may be a class effect. The underlying mechanism is unknown, but one theory is that hypovolemia may be involved. If this is the case, Dr. Roussel explained, then diuretics would have a similar safety profile as SGLT2 inhibitors in terms of increasing the risk of amputations.
The aim of the present study was to look at the association between lower limb events and diuretic usage in patients with T2DM. Data on 1,459 subjects with T2DM treated with diuretics and data on lower limb events and amputations were obtained from the single-center SURDIAGENE study. Of these, 670 were and 789 were not taking diuretics.
Baseline differences between diuretic and nondiuretic users were seen, such as diuretic users being older (67 vs. 63 years), having longer diabetes duration (16 vs. 13 years), and being more likely to have cardiovascular disease (32.5% vs. 23.4%). A propensity-score approach was used to even out these differences, leaving a population of 1,074 subjects in the final matched cohort.
Over a median follow-up of 7.2 years, 12.7% of diuretic and 7.2% of nondiuretic users experienced lower limb events (P = .001). In multivariate and sensitivity analyses, lower limb amputations remained significantly higher in patients who had been treated with a diuretic than in those who had not.
These are “hypothesis-generating” data, Dr. Roussel pointed out and “we don’t want to be overconclusive, of course.” However, they may explain the risk signal seen with SGLT2 inhibitors in the CANVAS study. Further studies are needed to explore the role of drug-induced hypovolemia in the association between the use of diuretics and lower limb events.
EASD delegate Prashanth Vas, MBBS, MRCP, PhD, noted during the discussion that the use of diuretics was ubiquitous. “Nearly everyone uses diuretics,” he said. The potential risk of lower limb amputation and treatment with SGLT2 inhibitors had “been vexing us for some time since the data from CANVAS came out.”
Dr. Vas, who is a consultant diabetologist and diabetic foot specialist at King’s College Hospital NHS Foundation in London, went on to ask why only canagliflozin was found to be associated with amputations and not the other SGLT2 drugs.
Dr. Roussel responded that data were still needed on the other drugs in this class and that they needed to be treated with caution. The literature is not so clear, he admitted.
“It’s important that you noted it’s a single-center study,” Dr. Vas countered. “It’s very important to have multicenter data. An amputation is a decision made by someone. An amputation in one center may not be an amputation in another center.”
The SURDIAGENE study was supported by grants from the French Ministry of Health, the Association Française des Diabétiques, and the Groupement pour l’Etude des Maladies Métaboliques et Systémiques. Dr. Roussel reported relationships with Janssen, Merck, Sanofi-Aventis, AstraZeneca, and Boehringer Ingelheim. Dr. Vas was not involved in the study or analysis.
SOURCE: Roussel R et al. EASD 2018, Abstract 12.
REPORTING FROM EASD 2018
Key clinical point: Diuretics may need to be used cautiously in patients with type 2 diabetes at risk of amputations.
Major finding: The adjusted hazard ratio for lower limb amputations with diuretic versus no diuretic use was 2.13 (95% confidence interval, 1.17-3.87; P = .013).
Study details: The SURDIAGENE trial, a single-center, prospective, observational study including almost 1,500 type 2 diabetes mellitus patients enrolled from 2002 to 2012.
Disclosures: The SURDIAGENE study was supported by grants from the French Ministry of Health, the Association Française des Diabétiques, and the Groupement pour l’Etude des Maladies Métaboliques et Systémiques. Dr. Roussel reported relationships with Janssen, Merck, Sanofi-Aventis, AstraZeneca, and Boehringer Ingelheim. Dr. Vas was not involved in the study or analysis.
Source: Roussel R et al. EASD 2018, Abstract 12.
High prices driving insulin underuse
One in four patients at an urban diabetes center reported underusing insulin because of concerns about cost, according to a survey of patients with type 1 or type 2 diabetes mellitus who were recently prescribed the drug.
“These results highlight an urgent need to address affordability of insulin,” lead author Darby Herkert of Yale College in New Haven, Conn., and her coauthors wrote in a study published online in JAMA Internal Medicine.
In the survey of 199 diabetes patients who had an outpatient visit at the Yale Diabetes Center between June and August 2017, 25.5% reported cost-related insulin underuse. Only 60.8% of those patients discussed the prohibitive costs with their clinician, and 29.4% changed insulin types because of high prices. Patients who reported insulin underuse were also more likely to have poorer glycemic control than patients who did not, at a rate of 43.1% versus 28.1% (odds ratio, 2.96; 95% confidence interval, 1.14-8.16; P = .03).
The authors noted potential limitations in their study, including focusing on patients of just one treatment center and the inability to establish a causal relationship between cost-related underuse and poor glycemic control. Nonetheless, they strongly encouraged asking diabetes patients about potential cost issues; they also stressed the need for larger forces to step in and guarantee insulin’s availability. “Insulin is a life-saving, essential medicine, and most patients cannot act as price-sensitive buyers. Regulators and the medical community need to intervene to ensure that insulin is affordable to patients who need it,” they wrote.
This study was supported by the Global Health Field Experiences Award, the Yale College Fellowship for Research in Global Health Studies, and the Global Health Field Experiences Seed Funding Award. The corresponding author reported receiving funding from the Centers of Medicare and Medicaid Services to develop publicly reported quality measures. Another author reported receiving support from Health Action International and Alosa Health. No other disclosures were reported.
SOURCE: Herkert D et al. JAMA Internal Medicine. 2018 Dec 3. doi: 10.1001/jamainternmed.2018.5008.
This study by Herkert and colleagues reinforces that American drug makers, device manufacturers, and insurers are willing to sacrifice human lives in their quest for profit, according to Elisabeth Rosenthal, MD, of Kaiser Health News.
Diabetes is a disease that starts in childhood, she noted, which means young Americans who are often low-earning and uninsured must start managing it with insulin before they are financially stable. And if drug prices keep going up – and if competitors are sued out of the market – then that means people with chronic disease will suffer, including the 25.5% that Herkert et al. found underuse insulin because of cost.
“As drug costs have generally increased in the United States, we know that many patients are skimping on medicines, taking less than prescribed, and cutting pills in half to make every fill last longer. This is terrible, but for many diseases, it is not catastrophic,” she wrote.
“But skimping on insulin,” she added, “can be rapidly deadly in people whose bodies make none of their own and can result in a life-threatening metabolic disturbance.”
Dr. Rosenthal shared the story of a 29-year-old diabetes patient in Missouri who would consider only doctoral programs outside the United States. “My one goal in life has been to move to Europe so I don’t have to pay these staggering prices just to survive,” the patient revealed.
But others – that 25% – will quietly skimp on their insulin, taking less than they need but more, perhaps, than they can really afford. Some of them will die.
Dr. Rosenthal is the author of “An American Sickness: How Healthcare Became Big Business and How You Can Take It Back.” These comments are adapted from an accompanying editorial (JAMA Internal Med. 2018 Dec 3. doi: 10.1001/jamainternmed.2018.5007).
This study by Herkert and colleagues reinforces that American drug makers, device manufacturers, and insurers are willing to sacrifice human lives in their quest for profit, according to Elisabeth Rosenthal, MD, of Kaiser Health News.
Diabetes is a disease that starts in childhood, she noted, which means young Americans who are often low-earning and uninsured must start managing it with insulin before they are financially stable. And if drug prices keep going up – and if competitors are sued out of the market – then that means people with chronic disease will suffer, including the 25.5% that Herkert et al. found underuse insulin because of cost.
“As drug costs have generally increased in the United States, we know that many patients are skimping on medicines, taking less than prescribed, and cutting pills in half to make every fill last longer. This is terrible, but for many diseases, it is not catastrophic,” she wrote.
“But skimping on insulin,” she added, “can be rapidly deadly in people whose bodies make none of their own and can result in a life-threatening metabolic disturbance.”
Dr. Rosenthal shared the story of a 29-year-old diabetes patient in Missouri who would consider only doctoral programs outside the United States. “My one goal in life has been to move to Europe so I don’t have to pay these staggering prices just to survive,” the patient revealed.
But others – that 25% – will quietly skimp on their insulin, taking less than they need but more, perhaps, than they can really afford. Some of them will die.
Dr. Rosenthal is the author of “An American Sickness: How Healthcare Became Big Business and How You Can Take It Back.” These comments are adapted from an accompanying editorial (JAMA Internal Med. 2018 Dec 3. doi: 10.1001/jamainternmed.2018.5007).
This study by Herkert and colleagues reinforces that American drug makers, device manufacturers, and insurers are willing to sacrifice human lives in their quest for profit, according to Elisabeth Rosenthal, MD, of Kaiser Health News.
Diabetes is a disease that starts in childhood, she noted, which means young Americans who are often low-earning and uninsured must start managing it with insulin before they are financially stable. And if drug prices keep going up – and if competitors are sued out of the market – then that means people with chronic disease will suffer, including the 25.5% that Herkert et al. found underuse insulin because of cost.
“As drug costs have generally increased in the United States, we know that many patients are skimping on medicines, taking less than prescribed, and cutting pills in half to make every fill last longer. This is terrible, but for many diseases, it is not catastrophic,” she wrote.
“But skimping on insulin,” she added, “can be rapidly deadly in people whose bodies make none of their own and can result in a life-threatening metabolic disturbance.”
Dr. Rosenthal shared the story of a 29-year-old diabetes patient in Missouri who would consider only doctoral programs outside the United States. “My one goal in life has been to move to Europe so I don’t have to pay these staggering prices just to survive,” the patient revealed.
But others – that 25% – will quietly skimp on their insulin, taking less than they need but more, perhaps, than they can really afford. Some of them will die.
Dr. Rosenthal is the author of “An American Sickness: How Healthcare Became Big Business and How You Can Take It Back.” These comments are adapted from an accompanying editorial (JAMA Internal Med. 2018 Dec 3. doi: 10.1001/jamainternmed.2018.5007).
One in four patients at an urban diabetes center reported underusing insulin because of concerns about cost, according to a survey of patients with type 1 or type 2 diabetes mellitus who were recently prescribed the drug.
“These results highlight an urgent need to address affordability of insulin,” lead author Darby Herkert of Yale College in New Haven, Conn., and her coauthors wrote in a study published online in JAMA Internal Medicine.
In the survey of 199 diabetes patients who had an outpatient visit at the Yale Diabetes Center between June and August 2017, 25.5% reported cost-related insulin underuse. Only 60.8% of those patients discussed the prohibitive costs with their clinician, and 29.4% changed insulin types because of high prices. Patients who reported insulin underuse were also more likely to have poorer glycemic control than patients who did not, at a rate of 43.1% versus 28.1% (odds ratio, 2.96; 95% confidence interval, 1.14-8.16; P = .03).
The authors noted potential limitations in their study, including focusing on patients of just one treatment center and the inability to establish a causal relationship between cost-related underuse and poor glycemic control. Nonetheless, they strongly encouraged asking diabetes patients about potential cost issues; they also stressed the need for larger forces to step in and guarantee insulin’s availability. “Insulin is a life-saving, essential medicine, and most patients cannot act as price-sensitive buyers. Regulators and the medical community need to intervene to ensure that insulin is affordable to patients who need it,” they wrote.
This study was supported by the Global Health Field Experiences Award, the Yale College Fellowship for Research in Global Health Studies, and the Global Health Field Experiences Seed Funding Award. The corresponding author reported receiving funding from the Centers of Medicare and Medicaid Services to develop publicly reported quality measures. Another author reported receiving support from Health Action International and Alosa Health. No other disclosures were reported.
SOURCE: Herkert D et al. JAMA Internal Medicine. 2018 Dec 3. doi: 10.1001/jamainternmed.2018.5008.
One in four patients at an urban diabetes center reported underusing insulin because of concerns about cost, according to a survey of patients with type 1 or type 2 diabetes mellitus who were recently prescribed the drug.
“These results highlight an urgent need to address affordability of insulin,” lead author Darby Herkert of Yale College in New Haven, Conn., and her coauthors wrote in a study published online in JAMA Internal Medicine.
In the survey of 199 diabetes patients who had an outpatient visit at the Yale Diabetes Center between June and August 2017, 25.5% reported cost-related insulin underuse. Only 60.8% of those patients discussed the prohibitive costs with their clinician, and 29.4% changed insulin types because of high prices. Patients who reported insulin underuse were also more likely to have poorer glycemic control than patients who did not, at a rate of 43.1% versus 28.1% (odds ratio, 2.96; 95% confidence interval, 1.14-8.16; P = .03).
The authors noted potential limitations in their study, including focusing on patients of just one treatment center and the inability to establish a causal relationship between cost-related underuse and poor glycemic control. Nonetheless, they strongly encouraged asking diabetes patients about potential cost issues; they also stressed the need for larger forces to step in and guarantee insulin’s availability. “Insulin is a life-saving, essential medicine, and most patients cannot act as price-sensitive buyers. Regulators and the medical community need to intervene to ensure that insulin is affordable to patients who need it,” they wrote.
This study was supported by the Global Health Field Experiences Award, the Yale College Fellowship for Research in Global Health Studies, and the Global Health Field Experiences Seed Funding Award. The corresponding author reported receiving funding from the Centers of Medicare and Medicaid Services to develop publicly reported quality measures. Another author reported receiving support from Health Action International and Alosa Health. No other disclosures were reported.
SOURCE: Herkert D et al. JAMA Internal Medicine. 2018 Dec 3. doi: 10.1001/jamainternmed.2018.5008.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Patients who reported cost-related insulin underuse were more likely to have poorer glycemic control than those who were able to afford the drug.
Major finding: Insulin cost accounted for its underuse by 25.5% of diabetic patients surveyed.
Study details: A survey of 199 patients with type 1 or type 2 diabetes mellitus who were prescribed insulin in the last 6 months and had an outpatient visit at the Yale Diabetes Center between June and August 2017.
Disclosures: This study was supported by the Global Health Field Experiences Award, the Yale College Fellowship for Research in Global Health Studies, and the Global Health Field Experiences Seed Funding Award. The corresponding author reported receiving funding from the Centers of Medicare and Medicaid Services to develop publicly reported quality measures. Another author reported receiving support from Health Action International and Alosa Health. No other disclosures were reported.
Source: Herkert D et al. JAMA Inter Med. 2018 Dec 3. doi: 10.1001/jamainternmed.2018.5008.
Our missing microbes: Short-term antibiotic courses have long-term consequences
Recent years have seen dramatic increases in the prevalences of chronic diseases such as type 1 diabetes,1 gastroesophageal reflux disease,2 asthma,3 inflammatory bowel disease,4 and, notably, obesity.5 I propose the hypothesis that much of this increase may be due to loss of diversity in the bacteria that make our guts their home.6 While multiple causes contribute, much of the blame may be attributed to the use—and overuse—of antibiotics.
FAT AND GETTING FATTER
Today, nearly 40% of US adults are obese, and nearly three-fourths are either obese or overweight.7 More alarming, the prevalence of obesity is also high and getting higher in children and adolescents,8 having increased from 10.0% in 1988–1994 to 17.8% in 2013–2016.
And not just in the United States. Trends in weight have been going up around the world, with a lag of about 30 years between developing countries and industrialized countries.5
OUR BACTERIA, OURSELVES
I believe that the bacteria we carry are not random, but rather have coevolved along with us, passed down from generation to generation in a state of dynamic equilibrium between microbes and host. Evidence supporting this comes from a study by Ochman et al,9 who analyzed the DNA from fecal samples from different hominid species (including Homo sapiens) and found that the phylogenic relationships among the bacteria mirrored those among the apes.
Interacting with each other and with us in complex ways, our bacteria are a diverse community to which we can apply the term microbiome. They are acquired in a standard, choreographed process,10 and their composition comes to resemble that of adults by the age of 3.11
Before modern times, microbes were transferred from mother to child during vaginal birth, from the mother’s breast during nursing, through skin-to-skin contact, and from the mother’s mouth by kissing. Now, widespread cesarean delivery, bottle-feeding, extensive bathing (especially with antibacterial soaps), and especially the use of antibiotics have changed the human ecology and altered transmission and maintenance of ancestral microbes, which affects the composition of the microbiota. The microbes, both good and bad, that are usually acquired early in life are especially important, since they affect a developmentally critical stage.12
Loss of microbial diversity in the mother appears to be cumulative over succeeding generations.13 For example, in a study in Japanese families, Urita et al14 found a decline in the prevalence of Helicobacter pylori colonization from 68.7% in the first generation to 43.4% in the second generation and 12.5% in the third. Clemente et al15 studied the intestinal microbiota in a previously uncontacted group of Yanomami people in the Amazon jungle and found they had the highest diversity of bacteria ever reported in a human group. By comparison, the research team calculated that we in the United States have already lost 50% of our microbial diversity, and 2 other groups, the Guahibo (another Amerindian group) and rural Malawians, were in between. More recent studies are confirming these observations.16,17
USE AND OVERUSE OF ANTIBIOTICS
More than 73 billion antibiotic doses are prescribed worldwide yearly,18 or about 10 doses for every man, woman, and child on Earth, and the numbers are rising. In the United States 262 million courses were prescribed in 2011, or 842 per 1,000 population.19 Children receive a mean of 2.7 courses by age 2, and 10.9 by age 10. More than 50% of women receive antibiotics during pregnancy or perinatally. This is in addition to an unknown level of exposure from agricultural use of antibiotics.
Repeated antibiotic exposure is common in early life, varies widely by country, and is often not medically justified.20 In the United States, antibiotic use varies by region, with the heaviest use in the South.19,21 It also varies widely among prescribers.22 Jones et al23 examined antibiotic prescribing for acute respiratory infections in US veterans and found that the top 10% of physicians gave an antibiotic more than 90% of the time. Physicians in Sweden prescribe about 60% fewer antibiotics than we do in the United States.21,24
Observational data indicate that people who receive antibiotics have a higher risk of chronic diseases later in life, eg:
- Type 2 diabetes (odds ratio 1.21, 95% confidence interval 1.19–1.23 with 2 to 4 courses, and odds ratio 1.53 (1.50–1.55) with 5 or more courses, up to 15 years after25
- Obesity: US states with the highest prevalence of antibiotic use also have the highest prevalence of obesity26
- Kidney stones: prior antibiotic exposure in a large UK study was associated with increased kidney stone risk, for exposures up to 5 years earlier.27
The meat industry has exploited the weight effect for decades, adding subtherapeutic doses of antibiotics to animals’ feed to make them gain weight.28
FINDINGS FROM STUDIES IN MICE
Laboratory studies of the relationship between antibiotic exposure and disease phenotypes in mice have yielded interesting findings.
Mice exposed to antibiotics had more body fat at 10 weeks (32.0%) than control mice (22.9%).29
Low-dose penicillin, started at birth, induces long-lasting effects on the expression of genes involved in immunity and enhances the effect of a high-fat diet in terms of weight gain.30 If the antibiotic exposure is limited to early life, the effect on the microbiota is transient, but the mice still gain weight. If the microbiota from the mice who received penicillin is transferred to germ-free mice, the recipients also become fat, indicating that the bacteria, not the antibiotics per se, cause the weight gain.
In other experiments,31 a series of short, therapeutic doses of antibiotics early in life modeled after those given to children to treat their acute infections caused long-term changes in the composition of the microbiome and in metabolism.
A single course of a macrolide antibiotic also had long-term effects on the microbial population and on the host’s ileal gene expression, T-cell populations, and secretory immunoglobulin A expression.32 These effects were seen only in mice that had a microbiome to begin with, not in germ-free mice, indicating that the antibiotics had their effect through the changes in the microbiome, not directly. But when germ-free mice received a fecal transplant of an impaired microbiome, it was sufficient to affect immunity.
In nonobese diabetic mice, treatment with antibiotics early in life altered the gut microbiome and its metabolic capacities, intestinal gene expression, and T-cell populations, accelerating the onset of type 1 diabetes.33
In a study in Danish children,34 the likelihood of inflammatory bowel disease increased with early-life antibiotic exposure: the more courses the child received, the greater the likelihood of disease. This observation led researchers to wonder if an antibiotic-altered microbiome affects the outcome of inflammatory bowel disease in the next generation.35 Germ-free female mice who received microbiota from mice who had received antibiotics passed the altered microbiome to their pups. Mice lacking the gene for interleukin 10 are genetically susceptible to colitis, and when this experiment was done in mice lacking this gene, the offspring developed markedly more colitis. This indicated the mothers could pass down their altered microbiome to the next generation and that it would affect their risk of disease.
WHAT CAN WE DO?
All physicians must adhere to the principles of antibiotic stewardship,36 not only to prevent the development of resistant strains of pathogens and the overgrowth of potentially dangerous species such as Clostridium difficile, but also, possibly, to prevent the loss of diversity in the human microbiome and thus discourage the development of chronic diseases.
In the future, as we discover more about the microbiome and the optimal mix of bacteria to carry, this information may find practical application in medicine. A pediatrician, for example, may want to analyze a child’s microbiome and, if it is abnormal, administer specific organisms to reshape it.
- TEDDY Study Group. The Environmental Determinants of Diabetes in the Young (TEDDY) study. Ann NY Acad Sci 2008; 1150:1–13. doi:10.1196/annals.1447.062
- El-Serag HB, Sonnenberg A. Associations between different forms of gastro-oesophageal reflux disease. Gut 1997; 41(5):594–599. pmid:9414963
- Eder W, Ege MJ, von Mutius E. The asthma epidemic. N Engl J Med 2006; 355(21):2226–2235. doi:10.1056/NEJMra054308
- Kaplan GG, Ng SC. Understanding and preventing the global increase of inflammatory bowel disease. Gastroenterology 2017; 152(2):313–321. doi:10.1053/j.gastro.2016.10.020
- de Onis M, Blossner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr 2010; 92(5):1257–1264. doi:10.3945/ajcn.2010.29786
- Blaser MJ. The theory of disappearing microbiota and the epidemics of chronic disease. Nat Rev Immunol 2017; 17(8):461–463. doi:10.1038/nri.2017.77
- Centers for Disease Control and Prevention. National Center for Health Statistics. Obesity and overweight. www.cdc.gov/nchs/fastats/obesity-overweight.htm. Accessed November 6, 2018.
- Centers for Disease Control and Prevention. National Center for Health Statistics. Table 59. Obesity among children and adolescents aged 2-19 years, by selected characteristics: United States, selected years 1988–1994 through 2013–2016. www.cdc.gov/nchs/data/hus/2017/059.pdf. Accessed November 6, 2018.
- Ochman H, Worobey M, Kuo CH, et al. Evolutionary relationships of wild hominids recapitulated by gut microbial communities. PLoS Biology 2010; 8(11):e1000546. doi:10.1371/journal.pbio.1000546
- Bokulich NA, Chung J, Battaglia T, et al. Antibiotics, birth mode, and diet shape microbiome maturation during early life. Sci Trans Med 2016; 8(343):343ra82. doi:10.1126/scitranslmed.aad7121
- Yatsunenko T, Rey FE, Manary MJ, et al. Human gut microbiome viewed across age and geography. Nature 2012; 486(7402):222–227. doi:10.1038/nature11053
- Blaser MJ. The past and future biology of the human microbiome in an age of extinctions. Cell 2018; 172(6):1173–1177. doi:10.1016/j.cell.2018.02.040
- Blaser MJ, Falkow S. What are the consequences of the disappearing human microbiota? Nat Rev Microbiol 2009; 7(12):887–894. doi:10.1038/nrmicro2245
- Urita Y, Watanabe T, Kawagoe N, et al. Role of infected grandmothers in transmission of Helicobacter pylori to children in a Japanese rural town. J Ped Child Health 2013; 49(5):394–398. doi:10.1111/jpc.12191
- Clemente JC, Pehrsson EC, Blaser MJ, et al. The microbiome of uncontacted Amerindians. Sci Adv 2015; 1(3). Pii:e1500183. doi:10.1126/sciadv.1500183
- Smits SA, Leach J, Sonnenburg ED, et al. Seasonal cycling in the gut microbiome of the Hadza hunter-gatherers of Tanzania. Science 2017; 357(6353):802-806. doi:10.1126/science.aan4834
- Vangay P, Johnson AJ, Ward TL, et al. US immigration westernizes the human gut microbiome. Cell 2018; 175(4):962–972. doi:10.1016/j.cell.2018.10.029
- Van Broeckel TP, Gandra S, Ashok A, et al. Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. Lancet Infect Dis 2014; 14(8):742–750. doi:10.1016/S1473-3099(14)70780-7
- Hicks LA, Bartoces MG, Roberts RM, et al. US outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clin Infect Dis 2015; 60(9):1308–1316. doi:10.1093/cid/civ076
- Rogawski ET, Platts-Mills JA, Seidman JC, et al. Use of antibiotics in children younger than two years in eight countries: a prospective cohort study. Bull World Health Organ 2017; 95(1):49–61. doi:10.2471/BLT.16.176123
- Hicks LA, Taylor TH Jr, Hunkler RJ. U.S. outpatient antibiotic prescribing, 2010; N Engl J Med 2013; 368(15):1461–1462. doi:10.1056/NEJMc1212055
- Gerber JS, Prasad PA, Russell LA, et al. Variation in antibiotic prescribing across a pediatric primary care network. J Pediatric Infect Dis Soc 2015; 4(4):297–304. doi:10.1093/jpids/piu086
- Jones BE, Sauer B, Jones MM, et al. Variation in outpatient antibiotic prescribing for acute respiratory infections in the veteran population: a cross-sectional study. Ann Intern Med 2015; 163(2):73–80. doi:10.7326/M14-1933
- Ternhag A, Hellman J. More on U.S. outpatient antibiotic prescribing, 2010. N Engl J Med 2013; 369(12):1175. doi:10.1056/NEJMc1306863
- Mikkelsen KH, Knop FK, Frost M, Hallas J, Pottegard A. Use of antibiotics and risk of type 2 diabetes: a population-based case-control study. J Clin Endocrinol Metab 2015; 100(10):3633–3640. doi:10.1210/jc.2015-2696
- Petschow B, Dore J, Hibbert P, et al. Probiotics, prebiotics, and the host microbiome: the science of translation. Ann NY Acad Sci 2013; 1306:1–17. doi:10.1111/nyas.12303
- Tasian GE, Jemielita T, Goldfarb DS, et al. Oral antibiotic exposure and kidney stone disease. J Am Soc Nephrol 2018; 29(6):1731–1740. doi:10.1681/ASN.2017111213
- Zimmerman DR. Role of subtherapeutic levels of antimicrobials in pig production. J Anim Sci 1986; 62(suppl 3):6–16.
- Cho I, Yamanishi S, Cox L, et al. Antibiotics in early life alter the murine colonic microbiome and adiposity. Nature 2012; 488(7413):621–626. doi:10.1038/nature11400
- Cox LM, Yamanishi S, Sohn J, et al. Altering the intestinal microbiota during a critical developmental window has lasting metabolic consequences. Cell 2014; 158(4):705–721. doi:10.1016/j.cell.2014.05.052
- Nobel YR, Cox LM, Kirigin FF, et al. Metabolic and metagenomics outcomes from early-life pulsed antibiotic treatment. Nat Commun 2015; 6:7486. doi:10.1038/ncomms8486
- Ruiz VE, Battaglia T, Kurtz ZD, et al. A single early-in-life macrolide course has lasting effects on murine microbial network topology and immunity. Nat Commun 2017; 8(1):518. doi:10.1038/s41467-017-00531-6
- Livanos AE, Greiner TU, Vangay P, et al. Antibiotic-mediated gut microbiome perturbation accelerates development of type 1 diabetes in mice. Nat Microbiol 2016; 1(11):16149. doi:10.1038/nmicrobiol.2016.140
- Hvilid A, Svanström H, Frish M. Antibiotic use and inflammatory bowel disease in childhood. Gut 2011; 60(1):49–54. doi:10.1136/gut.2010.219683
- Schulfer AF, Battaglia T, Alvarez Y, et al. Intergenerational transfer of antibiotic-perturbed microbiota enhances colitis in susceptible mice. Nat Microbiol 2018; 3(2):234–242. doi:10.1038/s41564-017-0075-5
- Srinivasan A. Antibiotic stewardship: why we must, how we can. Cleve Clin J Med 2017; 84(9):673–679. doi:10.3949/ccjm.84gr.17003
Recent years have seen dramatic increases in the prevalences of chronic diseases such as type 1 diabetes,1 gastroesophageal reflux disease,2 asthma,3 inflammatory bowel disease,4 and, notably, obesity.5 I propose the hypothesis that much of this increase may be due to loss of diversity in the bacteria that make our guts their home.6 While multiple causes contribute, much of the blame may be attributed to the use—and overuse—of antibiotics.
FAT AND GETTING FATTER
Today, nearly 40% of US adults are obese, and nearly three-fourths are either obese or overweight.7 More alarming, the prevalence of obesity is also high and getting higher in children and adolescents,8 having increased from 10.0% in 1988–1994 to 17.8% in 2013–2016.
And not just in the United States. Trends in weight have been going up around the world, with a lag of about 30 years between developing countries and industrialized countries.5
OUR BACTERIA, OURSELVES
I believe that the bacteria we carry are not random, but rather have coevolved along with us, passed down from generation to generation in a state of dynamic equilibrium between microbes and host. Evidence supporting this comes from a study by Ochman et al,9 who analyzed the DNA from fecal samples from different hominid species (including Homo sapiens) and found that the phylogenic relationships among the bacteria mirrored those among the apes.
Interacting with each other and with us in complex ways, our bacteria are a diverse community to which we can apply the term microbiome. They are acquired in a standard, choreographed process,10 and their composition comes to resemble that of adults by the age of 3.11
Before modern times, microbes were transferred from mother to child during vaginal birth, from the mother’s breast during nursing, through skin-to-skin contact, and from the mother’s mouth by kissing. Now, widespread cesarean delivery, bottle-feeding, extensive bathing (especially with antibacterial soaps), and especially the use of antibiotics have changed the human ecology and altered transmission and maintenance of ancestral microbes, which affects the composition of the microbiota. The microbes, both good and bad, that are usually acquired early in life are especially important, since they affect a developmentally critical stage.12
Loss of microbial diversity in the mother appears to be cumulative over succeeding generations.13 For example, in a study in Japanese families, Urita et al14 found a decline in the prevalence of Helicobacter pylori colonization from 68.7% in the first generation to 43.4% in the second generation and 12.5% in the third. Clemente et al15 studied the intestinal microbiota in a previously uncontacted group of Yanomami people in the Amazon jungle and found they had the highest diversity of bacteria ever reported in a human group. By comparison, the research team calculated that we in the United States have already lost 50% of our microbial diversity, and 2 other groups, the Guahibo (another Amerindian group) and rural Malawians, were in between. More recent studies are confirming these observations.16,17
USE AND OVERUSE OF ANTIBIOTICS
More than 73 billion antibiotic doses are prescribed worldwide yearly,18 or about 10 doses for every man, woman, and child on Earth, and the numbers are rising. In the United States 262 million courses were prescribed in 2011, or 842 per 1,000 population.19 Children receive a mean of 2.7 courses by age 2, and 10.9 by age 10. More than 50% of women receive antibiotics during pregnancy or perinatally. This is in addition to an unknown level of exposure from agricultural use of antibiotics.
Repeated antibiotic exposure is common in early life, varies widely by country, and is often not medically justified.20 In the United States, antibiotic use varies by region, with the heaviest use in the South.19,21 It also varies widely among prescribers.22 Jones et al23 examined antibiotic prescribing for acute respiratory infections in US veterans and found that the top 10% of physicians gave an antibiotic more than 90% of the time. Physicians in Sweden prescribe about 60% fewer antibiotics than we do in the United States.21,24
Observational data indicate that people who receive antibiotics have a higher risk of chronic diseases later in life, eg:
- Type 2 diabetes (odds ratio 1.21, 95% confidence interval 1.19–1.23 with 2 to 4 courses, and odds ratio 1.53 (1.50–1.55) with 5 or more courses, up to 15 years after25
- Obesity: US states with the highest prevalence of antibiotic use also have the highest prevalence of obesity26
- Kidney stones: prior antibiotic exposure in a large UK study was associated with increased kidney stone risk, for exposures up to 5 years earlier.27
The meat industry has exploited the weight effect for decades, adding subtherapeutic doses of antibiotics to animals’ feed to make them gain weight.28
FINDINGS FROM STUDIES IN MICE
Laboratory studies of the relationship between antibiotic exposure and disease phenotypes in mice have yielded interesting findings.
Mice exposed to antibiotics had more body fat at 10 weeks (32.0%) than control mice (22.9%).29
Low-dose penicillin, started at birth, induces long-lasting effects on the expression of genes involved in immunity and enhances the effect of a high-fat diet in terms of weight gain.30 If the antibiotic exposure is limited to early life, the effect on the microbiota is transient, but the mice still gain weight. If the microbiota from the mice who received penicillin is transferred to germ-free mice, the recipients also become fat, indicating that the bacteria, not the antibiotics per se, cause the weight gain.
In other experiments,31 a series of short, therapeutic doses of antibiotics early in life modeled after those given to children to treat their acute infections caused long-term changes in the composition of the microbiome and in metabolism.
A single course of a macrolide antibiotic also had long-term effects on the microbial population and on the host’s ileal gene expression, T-cell populations, and secretory immunoglobulin A expression.32 These effects were seen only in mice that had a microbiome to begin with, not in germ-free mice, indicating that the antibiotics had their effect through the changes in the microbiome, not directly. But when germ-free mice received a fecal transplant of an impaired microbiome, it was sufficient to affect immunity.
In nonobese diabetic mice, treatment with antibiotics early in life altered the gut microbiome and its metabolic capacities, intestinal gene expression, and T-cell populations, accelerating the onset of type 1 diabetes.33
In a study in Danish children,34 the likelihood of inflammatory bowel disease increased with early-life antibiotic exposure: the more courses the child received, the greater the likelihood of disease. This observation led researchers to wonder if an antibiotic-altered microbiome affects the outcome of inflammatory bowel disease in the next generation.35 Germ-free female mice who received microbiota from mice who had received antibiotics passed the altered microbiome to their pups. Mice lacking the gene for interleukin 10 are genetically susceptible to colitis, and when this experiment was done in mice lacking this gene, the offspring developed markedly more colitis. This indicated the mothers could pass down their altered microbiome to the next generation and that it would affect their risk of disease.
WHAT CAN WE DO?
All physicians must adhere to the principles of antibiotic stewardship,36 not only to prevent the development of resistant strains of pathogens and the overgrowth of potentially dangerous species such as Clostridium difficile, but also, possibly, to prevent the loss of diversity in the human microbiome and thus discourage the development of chronic diseases.
In the future, as we discover more about the microbiome and the optimal mix of bacteria to carry, this information may find practical application in medicine. A pediatrician, for example, may want to analyze a child’s microbiome and, if it is abnormal, administer specific organisms to reshape it.
Recent years have seen dramatic increases in the prevalences of chronic diseases such as type 1 diabetes,1 gastroesophageal reflux disease,2 asthma,3 inflammatory bowel disease,4 and, notably, obesity.5 I propose the hypothesis that much of this increase may be due to loss of diversity in the bacteria that make our guts their home.6 While multiple causes contribute, much of the blame may be attributed to the use—and overuse—of antibiotics.
FAT AND GETTING FATTER
Today, nearly 40% of US adults are obese, and nearly three-fourths are either obese or overweight.7 More alarming, the prevalence of obesity is also high and getting higher in children and adolescents,8 having increased from 10.0% in 1988–1994 to 17.8% in 2013–2016.
And not just in the United States. Trends in weight have been going up around the world, with a lag of about 30 years between developing countries and industrialized countries.5
OUR BACTERIA, OURSELVES
I believe that the bacteria we carry are not random, but rather have coevolved along with us, passed down from generation to generation in a state of dynamic equilibrium between microbes and host. Evidence supporting this comes from a study by Ochman et al,9 who analyzed the DNA from fecal samples from different hominid species (including Homo sapiens) and found that the phylogenic relationships among the bacteria mirrored those among the apes.
Interacting with each other and with us in complex ways, our bacteria are a diverse community to which we can apply the term microbiome. They are acquired in a standard, choreographed process,10 and their composition comes to resemble that of adults by the age of 3.11
Before modern times, microbes were transferred from mother to child during vaginal birth, from the mother’s breast during nursing, through skin-to-skin contact, and from the mother’s mouth by kissing. Now, widespread cesarean delivery, bottle-feeding, extensive bathing (especially with antibacterial soaps), and especially the use of antibiotics have changed the human ecology and altered transmission and maintenance of ancestral microbes, which affects the composition of the microbiota. The microbes, both good and bad, that are usually acquired early in life are especially important, since they affect a developmentally critical stage.12
Loss of microbial diversity in the mother appears to be cumulative over succeeding generations.13 For example, in a study in Japanese families, Urita et al14 found a decline in the prevalence of Helicobacter pylori colonization from 68.7% in the first generation to 43.4% in the second generation and 12.5% in the third. Clemente et al15 studied the intestinal microbiota in a previously uncontacted group of Yanomami people in the Amazon jungle and found they had the highest diversity of bacteria ever reported in a human group. By comparison, the research team calculated that we in the United States have already lost 50% of our microbial diversity, and 2 other groups, the Guahibo (another Amerindian group) and rural Malawians, were in between. More recent studies are confirming these observations.16,17
USE AND OVERUSE OF ANTIBIOTICS
More than 73 billion antibiotic doses are prescribed worldwide yearly,18 or about 10 doses for every man, woman, and child on Earth, and the numbers are rising. In the United States 262 million courses were prescribed in 2011, or 842 per 1,000 population.19 Children receive a mean of 2.7 courses by age 2, and 10.9 by age 10. More than 50% of women receive antibiotics during pregnancy or perinatally. This is in addition to an unknown level of exposure from agricultural use of antibiotics.
Repeated antibiotic exposure is common in early life, varies widely by country, and is often not medically justified.20 In the United States, antibiotic use varies by region, with the heaviest use in the South.19,21 It also varies widely among prescribers.22 Jones et al23 examined antibiotic prescribing for acute respiratory infections in US veterans and found that the top 10% of physicians gave an antibiotic more than 90% of the time. Physicians in Sweden prescribe about 60% fewer antibiotics than we do in the United States.21,24
Observational data indicate that people who receive antibiotics have a higher risk of chronic diseases later in life, eg:
- Type 2 diabetes (odds ratio 1.21, 95% confidence interval 1.19–1.23 with 2 to 4 courses, and odds ratio 1.53 (1.50–1.55) with 5 or more courses, up to 15 years after25
- Obesity: US states with the highest prevalence of antibiotic use also have the highest prevalence of obesity26
- Kidney stones: prior antibiotic exposure in a large UK study was associated with increased kidney stone risk, for exposures up to 5 years earlier.27
The meat industry has exploited the weight effect for decades, adding subtherapeutic doses of antibiotics to animals’ feed to make them gain weight.28
FINDINGS FROM STUDIES IN MICE
Laboratory studies of the relationship between antibiotic exposure and disease phenotypes in mice have yielded interesting findings.
Mice exposed to antibiotics had more body fat at 10 weeks (32.0%) than control mice (22.9%).29
Low-dose penicillin, started at birth, induces long-lasting effects on the expression of genes involved in immunity and enhances the effect of a high-fat diet in terms of weight gain.30 If the antibiotic exposure is limited to early life, the effect on the microbiota is transient, but the mice still gain weight. If the microbiota from the mice who received penicillin is transferred to germ-free mice, the recipients also become fat, indicating that the bacteria, not the antibiotics per se, cause the weight gain.
In other experiments,31 a series of short, therapeutic doses of antibiotics early in life modeled after those given to children to treat their acute infections caused long-term changes in the composition of the microbiome and in metabolism.
A single course of a macrolide antibiotic also had long-term effects on the microbial population and on the host’s ileal gene expression, T-cell populations, and secretory immunoglobulin A expression.32 These effects were seen only in mice that had a microbiome to begin with, not in germ-free mice, indicating that the antibiotics had their effect through the changes in the microbiome, not directly. But when germ-free mice received a fecal transplant of an impaired microbiome, it was sufficient to affect immunity.
In nonobese diabetic mice, treatment with antibiotics early in life altered the gut microbiome and its metabolic capacities, intestinal gene expression, and T-cell populations, accelerating the onset of type 1 diabetes.33
In a study in Danish children,34 the likelihood of inflammatory bowel disease increased with early-life antibiotic exposure: the more courses the child received, the greater the likelihood of disease. This observation led researchers to wonder if an antibiotic-altered microbiome affects the outcome of inflammatory bowel disease in the next generation.35 Germ-free female mice who received microbiota from mice who had received antibiotics passed the altered microbiome to their pups. Mice lacking the gene for interleukin 10 are genetically susceptible to colitis, and when this experiment was done in mice lacking this gene, the offspring developed markedly more colitis. This indicated the mothers could pass down their altered microbiome to the next generation and that it would affect their risk of disease.
WHAT CAN WE DO?
All physicians must adhere to the principles of antibiotic stewardship,36 not only to prevent the development of resistant strains of pathogens and the overgrowth of potentially dangerous species such as Clostridium difficile, but also, possibly, to prevent the loss of diversity in the human microbiome and thus discourage the development of chronic diseases.
In the future, as we discover more about the microbiome and the optimal mix of bacteria to carry, this information may find practical application in medicine. A pediatrician, for example, may want to analyze a child’s microbiome and, if it is abnormal, administer specific organisms to reshape it.
- TEDDY Study Group. The Environmental Determinants of Diabetes in the Young (TEDDY) study. Ann NY Acad Sci 2008; 1150:1–13. doi:10.1196/annals.1447.062
- El-Serag HB, Sonnenberg A. Associations between different forms of gastro-oesophageal reflux disease. Gut 1997; 41(5):594–599. pmid:9414963
- Eder W, Ege MJ, von Mutius E. The asthma epidemic. N Engl J Med 2006; 355(21):2226–2235. doi:10.1056/NEJMra054308
- Kaplan GG, Ng SC. Understanding and preventing the global increase of inflammatory bowel disease. Gastroenterology 2017; 152(2):313–321. doi:10.1053/j.gastro.2016.10.020
- de Onis M, Blossner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr 2010; 92(5):1257–1264. doi:10.3945/ajcn.2010.29786
- Blaser MJ. The theory of disappearing microbiota and the epidemics of chronic disease. Nat Rev Immunol 2017; 17(8):461–463. doi:10.1038/nri.2017.77
- Centers for Disease Control and Prevention. National Center for Health Statistics. Obesity and overweight. www.cdc.gov/nchs/fastats/obesity-overweight.htm. Accessed November 6, 2018.
- Centers for Disease Control and Prevention. National Center for Health Statistics. Table 59. Obesity among children and adolescents aged 2-19 years, by selected characteristics: United States, selected years 1988–1994 through 2013–2016. www.cdc.gov/nchs/data/hus/2017/059.pdf. Accessed November 6, 2018.
- Ochman H, Worobey M, Kuo CH, et al. Evolutionary relationships of wild hominids recapitulated by gut microbial communities. PLoS Biology 2010; 8(11):e1000546. doi:10.1371/journal.pbio.1000546
- Bokulich NA, Chung J, Battaglia T, et al. Antibiotics, birth mode, and diet shape microbiome maturation during early life. Sci Trans Med 2016; 8(343):343ra82. doi:10.1126/scitranslmed.aad7121
- Yatsunenko T, Rey FE, Manary MJ, et al. Human gut microbiome viewed across age and geography. Nature 2012; 486(7402):222–227. doi:10.1038/nature11053
- Blaser MJ. The past and future biology of the human microbiome in an age of extinctions. Cell 2018; 172(6):1173–1177. doi:10.1016/j.cell.2018.02.040
- Blaser MJ, Falkow S. What are the consequences of the disappearing human microbiota? Nat Rev Microbiol 2009; 7(12):887–894. doi:10.1038/nrmicro2245
- Urita Y, Watanabe T, Kawagoe N, et al. Role of infected grandmothers in transmission of Helicobacter pylori to children in a Japanese rural town. J Ped Child Health 2013; 49(5):394–398. doi:10.1111/jpc.12191
- Clemente JC, Pehrsson EC, Blaser MJ, et al. The microbiome of uncontacted Amerindians. Sci Adv 2015; 1(3). Pii:e1500183. doi:10.1126/sciadv.1500183
- Smits SA, Leach J, Sonnenburg ED, et al. Seasonal cycling in the gut microbiome of the Hadza hunter-gatherers of Tanzania. Science 2017; 357(6353):802-806. doi:10.1126/science.aan4834
- Vangay P, Johnson AJ, Ward TL, et al. US immigration westernizes the human gut microbiome. Cell 2018; 175(4):962–972. doi:10.1016/j.cell.2018.10.029
- Van Broeckel TP, Gandra S, Ashok A, et al. Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. Lancet Infect Dis 2014; 14(8):742–750. doi:10.1016/S1473-3099(14)70780-7
- Hicks LA, Bartoces MG, Roberts RM, et al. US outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clin Infect Dis 2015; 60(9):1308–1316. doi:10.1093/cid/civ076
- Rogawski ET, Platts-Mills JA, Seidman JC, et al. Use of antibiotics in children younger than two years in eight countries: a prospective cohort study. Bull World Health Organ 2017; 95(1):49–61. doi:10.2471/BLT.16.176123
- Hicks LA, Taylor TH Jr, Hunkler RJ. U.S. outpatient antibiotic prescribing, 2010; N Engl J Med 2013; 368(15):1461–1462. doi:10.1056/NEJMc1212055
- Gerber JS, Prasad PA, Russell LA, et al. Variation in antibiotic prescribing across a pediatric primary care network. J Pediatric Infect Dis Soc 2015; 4(4):297–304. doi:10.1093/jpids/piu086
- Jones BE, Sauer B, Jones MM, et al. Variation in outpatient antibiotic prescribing for acute respiratory infections in the veteran population: a cross-sectional study. Ann Intern Med 2015; 163(2):73–80. doi:10.7326/M14-1933
- Ternhag A, Hellman J. More on U.S. outpatient antibiotic prescribing, 2010. N Engl J Med 2013; 369(12):1175. doi:10.1056/NEJMc1306863
- Mikkelsen KH, Knop FK, Frost M, Hallas J, Pottegard A. Use of antibiotics and risk of type 2 diabetes: a population-based case-control study. J Clin Endocrinol Metab 2015; 100(10):3633–3640. doi:10.1210/jc.2015-2696
- Petschow B, Dore J, Hibbert P, et al. Probiotics, prebiotics, and the host microbiome: the science of translation. Ann NY Acad Sci 2013; 1306:1–17. doi:10.1111/nyas.12303
- Tasian GE, Jemielita T, Goldfarb DS, et al. Oral antibiotic exposure and kidney stone disease. J Am Soc Nephrol 2018; 29(6):1731–1740. doi:10.1681/ASN.2017111213
- Zimmerman DR. Role of subtherapeutic levels of antimicrobials in pig production. J Anim Sci 1986; 62(suppl 3):6–16.
- Cho I, Yamanishi S, Cox L, et al. Antibiotics in early life alter the murine colonic microbiome and adiposity. Nature 2012; 488(7413):621–626. doi:10.1038/nature11400
- Cox LM, Yamanishi S, Sohn J, et al. Altering the intestinal microbiota during a critical developmental window has lasting metabolic consequences. Cell 2014; 158(4):705–721. doi:10.1016/j.cell.2014.05.052
- Nobel YR, Cox LM, Kirigin FF, et al. Metabolic and metagenomics outcomes from early-life pulsed antibiotic treatment. Nat Commun 2015; 6:7486. doi:10.1038/ncomms8486
- Ruiz VE, Battaglia T, Kurtz ZD, et al. A single early-in-life macrolide course has lasting effects on murine microbial network topology and immunity. Nat Commun 2017; 8(1):518. doi:10.1038/s41467-017-00531-6
- Livanos AE, Greiner TU, Vangay P, et al. Antibiotic-mediated gut microbiome perturbation accelerates development of type 1 diabetes in mice. Nat Microbiol 2016; 1(11):16149. doi:10.1038/nmicrobiol.2016.140
- Hvilid A, Svanström H, Frish M. Antibiotic use and inflammatory bowel disease in childhood. Gut 2011; 60(1):49–54. doi:10.1136/gut.2010.219683
- Schulfer AF, Battaglia T, Alvarez Y, et al. Intergenerational transfer of antibiotic-perturbed microbiota enhances colitis in susceptible mice. Nat Microbiol 2018; 3(2):234–242. doi:10.1038/s41564-017-0075-5
- Srinivasan A. Antibiotic stewardship: why we must, how we can. Cleve Clin J Med 2017; 84(9):673–679. doi:10.3949/ccjm.84gr.17003
- TEDDY Study Group. The Environmental Determinants of Diabetes in the Young (TEDDY) study. Ann NY Acad Sci 2008; 1150:1–13. doi:10.1196/annals.1447.062
- El-Serag HB, Sonnenberg A. Associations between different forms of gastro-oesophageal reflux disease. Gut 1997; 41(5):594–599. pmid:9414963
- Eder W, Ege MJ, von Mutius E. The asthma epidemic. N Engl J Med 2006; 355(21):2226–2235. doi:10.1056/NEJMra054308
- Kaplan GG, Ng SC. Understanding and preventing the global increase of inflammatory bowel disease. Gastroenterology 2017; 152(2):313–321. doi:10.1053/j.gastro.2016.10.020
- de Onis M, Blossner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr 2010; 92(5):1257–1264. doi:10.3945/ajcn.2010.29786
- Blaser MJ. The theory of disappearing microbiota and the epidemics of chronic disease. Nat Rev Immunol 2017; 17(8):461–463. doi:10.1038/nri.2017.77
- Centers for Disease Control and Prevention. National Center for Health Statistics. Obesity and overweight. www.cdc.gov/nchs/fastats/obesity-overweight.htm. Accessed November 6, 2018.
- Centers for Disease Control and Prevention. National Center for Health Statistics. Table 59. Obesity among children and adolescents aged 2-19 years, by selected characteristics: United States, selected years 1988–1994 through 2013–2016. www.cdc.gov/nchs/data/hus/2017/059.pdf. Accessed November 6, 2018.
- Ochman H, Worobey M, Kuo CH, et al. Evolutionary relationships of wild hominids recapitulated by gut microbial communities. PLoS Biology 2010; 8(11):e1000546. doi:10.1371/journal.pbio.1000546
- Bokulich NA, Chung J, Battaglia T, et al. Antibiotics, birth mode, and diet shape microbiome maturation during early life. Sci Trans Med 2016; 8(343):343ra82. doi:10.1126/scitranslmed.aad7121
- Yatsunenko T, Rey FE, Manary MJ, et al. Human gut microbiome viewed across age and geography. Nature 2012; 486(7402):222–227. doi:10.1038/nature11053
- Blaser MJ. The past and future biology of the human microbiome in an age of extinctions. Cell 2018; 172(6):1173–1177. doi:10.1016/j.cell.2018.02.040
- Blaser MJ, Falkow S. What are the consequences of the disappearing human microbiota? Nat Rev Microbiol 2009; 7(12):887–894. doi:10.1038/nrmicro2245
- Urita Y, Watanabe T, Kawagoe N, et al. Role of infected grandmothers in transmission of Helicobacter pylori to children in a Japanese rural town. J Ped Child Health 2013; 49(5):394–398. doi:10.1111/jpc.12191
- Clemente JC, Pehrsson EC, Blaser MJ, et al. The microbiome of uncontacted Amerindians. Sci Adv 2015; 1(3). Pii:e1500183. doi:10.1126/sciadv.1500183
- Smits SA, Leach J, Sonnenburg ED, et al. Seasonal cycling in the gut microbiome of the Hadza hunter-gatherers of Tanzania. Science 2017; 357(6353):802-806. doi:10.1126/science.aan4834
- Vangay P, Johnson AJ, Ward TL, et al. US immigration westernizes the human gut microbiome. Cell 2018; 175(4):962–972. doi:10.1016/j.cell.2018.10.029
- Van Broeckel TP, Gandra S, Ashok A, et al. Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. Lancet Infect Dis 2014; 14(8):742–750. doi:10.1016/S1473-3099(14)70780-7
- Hicks LA, Bartoces MG, Roberts RM, et al. US outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clin Infect Dis 2015; 60(9):1308–1316. doi:10.1093/cid/civ076
- Rogawski ET, Platts-Mills JA, Seidman JC, et al. Use of antibiotics in children younger than two years in eight countries: a prospective cohort study. Bull World Health Organ 2017; 95(1):49–61. doi:10.2471/BLT.16.176123
- Hicks LA, Taylor TH Jr, Hunkler RJ. U.S. outpatient antibiotic prescribing, 2010; N Engl J Med 2013; 368(15):1461–1462. doi:10.1056/NEJMc1212055
- Gerber JS, Prasad PA, Russell LA, et al. Variation in antibiotic prescribing across a pediatric primary care network. J Pediatric Infect Dis Soc 2015; 4(4):297–304. doi:10.1093/jpids/piu086
- Jones BE, Sauer B, Jones MM, et al. Variation in outpatient antibiotic prescribing for acute respiratory infections in the veteran population: a cross-sectional study. Ann Intern Med 2015; 163(2):73–80. doi:10.7326/M14-1933
- Ternhag A, Hellman J. More on U.S. outpatient antibiotic prescribing, 2010. N Engl J Med 2013; 369(12):1175. doi:10.1056/NEJMc1306863
- Mikkelsen KH, Knop FK, Frost M, Hallas J, Pottegard A. Use of antibiotics and risk of type 2 diabetes: a population-based case-control study. J Clin Endocrinol Metab 2015; 100(10):3633–3640. doi:10.1210/jc.2015-2696
- Petschow B, Dore J, Hibbert P, et al. Probiotics, prebiotics, and the host microbiome: the science of translation. Ann NY Acad Sci 2013; 1306:1–17. doi:10.1111/nyas.12303
- Tasian GE, Jemielita T, Goldfarb DS, et al. Oral antibiotic exposure and kidney stone disease. J Am Soc Nephrol 2018; 29(6):1731–1740. doi:10.1681/ASN.2017111213
- Zimmerman DR. Role of subtherapeutic levels of antimicrobials in pig production. J Anim Sci 1986; 62(suppl 3):6–16.
- Cho I, Yamanishi S, Cox L, et al. Antibiotics in early life alter the murine colonic microbiome and adiposity. Nature 2012; 488(7413):621–626. doi:10.1038/nature11400
- Cox LM, Yamanishi S, Sohn J, et al. Altering the intestinal microbiota during a critical developmental window has lasting metabolic consequences. Cell 2014; 158(4):705–721. doi:10.1016/j.cell.2014.05.052
- Nobel YR, Cox LM, Kirigin FF, et al. Metabolic and metagenomics outcomes from early-life pulsed antibiotic treatment. Nat Commun 2015; 6:7486. doi:10.1038/ncomms8486
- Ruiz VE, Battaglia T, Kurtz ZD, et al. A single early-in-life macrolide course has lasting effects on murine microbial network topology and immunity. Nat Commun 2017; 8(1):518. doi:10.1038/s41467-017-00531-6
- Livanos AE, Greiner TU, Vangay P, et al. Antibiotic-mediated gut microbiome perturbation accelerates development of type 1 diabetes in mice. Nat Microbiol 2016; 1(11):16149. doi:10.1038/nmicrobiol.2016.140
- Hvilid A, Svanström H, Frish M. Antibiotic use and inflammatory bowel disease in childhood. Gut 2011; 60(1):49–54. doi:10.1136/gut.2010.219683
- Schulfer AF, Battaglia T, Alvarez Y, et al. Intergenerational transfer of antibiotic-perturbed microbiota enhances colitis in susceptible mice. Nat Microbiol 2018; 3(2):234–242. doi:10.1038/s41564-017-0075-5
- Srinivasan A. Antibiotic stewardship: why we must, how we can. Cleve Clin J Med 2017; 84(9):673–679. doi:10.3949/ccjm.84gr.17003

Beta-cell therapies for type 1 diabetes: Transplants and bionics
With intensive insulin regimens and home blood glucose monitoring, patients with type 1 diabetes are controlling their blood glucose better than in the past. Nevertheless, glucose regulation is still imperfect and tedious, and striving for tight glycemic control poses the risk of hypoglycemia.

Prominent among the challenges are the sheer numbers involved. Some 1.25 million Americans have type 1 diabetes, and another 30 million have type 2, but only about 7,000 to 8,000 pancreases are available for transplant each year.1 While awaiting a breakthrough—perhaps involving stem cells, perhaps involving organs obtained from animals—an insulin pump may offer better diabetes control for many. Another possibility is a closed-loop system with a continuous glucose monitor that drives a dual-infusion pump, delivering insulin when glucose levels rise too high, and glucagon when they dip too low.
DIABETES WAS KNOWN IN ANCIENT TIMES
About 3,000 years ago, Egyptians described the syndrome of thirst, emaciation, and sweet urine that attracted ants. The term diabetes (Greek for siphon) was first recorded in 1425; mellitus (Latin for sweet with honey) was not added until 1675.
In 1857, Bernard hypothesized that diabetes was caused by overproduction of glucose in the liver. This idea was replaced in 1889, when Mering and Minkowski proposed the dysfunctional pancreas theory that eventually led to the discovery of the beta cell.2
In 1921, Banting and Best isolated insulin, and for the past 100 years subcutaneous insulin replacement has been the mainstay of treatment. But starting about 50 years ago, researchers have been looking for safe and long-lasting ways to replace beta cells and eliminate the need for exogenous insulin replacement.
TRANSPLANTING THE WHOLE PANCREAS
The first whole-pancreas transplant was performed in 1966 by Kelly et al,3 followed by 13 more by 1973.4 These first transplant grafts were short-lived, with only 1 graft surviving longer than 1 year. Since then, more than 12,000 pancreases have been transplanted worldwide, as refinements in surgical techniques and immunosuppressive therapies have improved patient and graft survival rates.4
Today, most pancreas transplants are in patients who have both type 1 diabetes and end-stage renal disease due to diabetic nephropathy, and most receive both a kidney and a pancreas at the same time. Far fewer patients receive a pancreas after previously receiving a kidney, or receive a pancreas alone.
The bile duct of the transplanted pancreas is usually routed into the patient’s small intestine, as nature intended, and less often into the bladder. Although bladder drainage is associated with urinary complications, it has the advantage of allowing measurement of pancreatic amylase levels in the urine to monitor for graft rejection. With simultaneous pancreas and kidney transplant, the serum creatinine concentration can also be monitored for rejection of the kidney graft.
Current immunosuppressive regimens vary but generally consist of anti-T-cell antibodies at the time of surgery, followed by lifelong treatment with the combination of a calcineurin inhibitor (cyclosporine or tacrolimus) and an antimetabolite (mycophenolate mofetil or azathioprine).
Outcomes are good. The rates of patient and graft survival are highest with simultaneous pancreas-kidney transplant, and somewhat lower with pancreas-after-kidney and pancreas-alone transplant.
Benefits of pancreas transplant
Most recipients can stop taking insulin immediately after the procedure, and their hemoglobin A1c levels normalize and stay low for the life of the graft. Lipid levels also decrease, although this has not been directly correlated with lower risk of vascular disease.4
Transplant also reduces or eliminates some complications of diabetes, including retinopathy, nephropathy, cardiomyopathy, and gastropathy.
For example, in patients undergoing simultaneous pancreas-kidney transplant, diabetic nephropathy does not recur in the new kidney. Fioretto et al5 reported that nephropathy lesions reversed during the 10 years after pancreas transplant.
Kennedy et al6,7 found that preexisting diabetic neuropathy improved slightly (although neurologic status did not completely return to normal) over a period of up to 42 months in a group of patients who received a pancreas transplant, whereas it tended to worsen in a control group. Both groups were assessed at baseline and at 12 and 24 months, with a subgroup followed through 42 months, and they underwent testing of motor, sensory, and autonomic function.6,7
Disadvantages of pancreas transplant
Disadvantages of whole-pancreas transplant include hypoglycemia (usually mild), adverse effects of immunosuppression, potential for surgical complications including an increased rate of death in the first 90 days after the procedure, and cost.
In an analysis comparing the 5-year estimated costs of dialysis, kidney transplant alone from cadavers or live donors, or simultaneous pancreas-kidney transplant for diabetic patients with end-stage renal disease, the least expensive option was kidney transplant from a live donor.8 The most expensive option was simultaneous pancreas-kidney transplant, but quality of life was better with this option. The analysis did not consider the potential cost of long-term treatments for complications related to diabetes that could be saved with a pancreas transplant.
Data conflict regarding the risk of death with different types of pancreas transplants. A retrospective cohort study of data from 124 US transplant centers reported in 2003 found higher mortality rates in pancreas-alone transplant recipients than in patients on a transplant waiting list receiving conventional therapy.9 In contrast, a 2004 study reported that after the first 90 days, when the risk of death was clearly higher, mortality rates were lower after simultaneous pancreas-kidney transplant and pancreas-after-kidney transplant.10 After pancreas-alone transplant, however, mortality rates were higher than with exogenous insulin therapy.
Although outcomes have improved, fewer patients with type 1 diabetes are undergoing pancreas transplant in recent years.
Interestingly, more simultaneous pancreas-kidney transplants are being successfully performed in patients with type 2 diabetes, who now account for 8% of all simultaneous pancreas-kidney transplant recipients.11 Outcomes of pancreas transplant appear to be similar regardless of diabetes type.
Bottom line
Pancreas transplant is a viable option for certain cases of complicated diabetes.
TRANSPLANTING ISLET CELLS
Despite its successes, pancreas transplant is major surgery and requires lifetime immunosuppression. Research is ongoing into a less-invasive procedure that, it is hoped, would require less immunosuppression: transplanting islets by themselves.
Islet autotransplant after pancreatectomy
For some patients with chronic pancreatitis, the only option to relieve chronic pain, narcotic dependence, and poor quality of life is to remove the pancreas. In the past, this desperate measure would instantly and inevitably cause diabetes, but not anymore.

Alpha cells and glucagon are a different story; a complication of islet transplant is hypoglycemia. In 2016, Lin et al12 reported spontaneous hypoglycemia in 6 of 12 patients who maintained insulin independence after autotransplant of islets. Although the transplanted islets had functional alpha cells that could in theory produce glucagon, as well as beta cells that produce insulin and C-peptide, apparently the alpha cells were not secreting glucagon in response to the hypoglycemia.
Location may matter. Gupta et al,13 in a 1997 study in dogs, found that more hypoglycemia occurs if islets are autotransplanted into the liver than if they are transplanted into the peritoneal cavity. A possible explanation may have to do with the glycemic environment of the liver.
Islet allotransplant
Islets can also be taken from cadaver donors and transplanted into patients with type 1 diabetes, who do not have enough working beta cells.
Success of allotransplant increased after the publication of observational data from the program in Edmonton in Canada, in which 7 consecutive patients with type 1 diabetes achieved initial insulin independence after islet allotransplant using steroid-free immunosuppression.14 Six recipients required islets from 2 donors, and 1 required islets from 4 donors, so they all received large volumes of at least 11,000 islet equivalents (IEQ) per kilogram of body weight.
In a subsequent report from the same team,15 16 (44%) of 36 patients remained insulin-free at 1 year, and C-peptide secretion was detectable in 70% at 2 years. But despite the elevated C-peptide levels, only 5 patients remained insulin-independent by 2 years. Lower hemoglobin A1c levels and decreases in hypoglycemic events from baseline also were noted.
The Clinical Islet Transplantation Consortium (CITC)16 and Collaborative Islet Transplant Registry (CITR)17 were established in 2004 to combine data and resources from centers around the world, including several that specialize in islet isolation and purification. Currently, more than 80 studies are being conducted.
The CITC and CITR now have data on more than 1,000 allogeneic islet transplant recipients (islet transplant alone, after kidney transplant, or simultaneous with it). The primary outcomes are hemoglobin A1c levels below 7% fasting C-peptide levels 0.3 ng/mL or higher, and fasting blood glucose of 60 to 140 mg/dL with no severe hypoglycemic events. The best results for islet-alone transplant have been in recipients over age 35 who received at least 325,000 IEQs with use of tumor necrosis factor antagonists for induction and calcineurin inhibitors or mammalian target of rapamycin (mTOR) inhibitors for maintenance.17
The best success for islet-after-kidney transplant was achieved with the same protocol but with insulin given to the donor during hospitalization before pancreas procurement. For participants with favorable factors, a hemoglobin A1c at or below 6.5% was achieved in about 80% at 1 year after last infusion, with more than 80% maintaining their fasting blood glucose level goals. About 70% of these patients were insulin-independent at 1 year. Hypoglycemia unawareness resolved in these patients even 5 years after infusion. Although there were no deaths or disabilities related to these transplants, bleeding occurred in 1 of 15 procedures. There was also a notable decline in estimated glomerular filtration rates with calcineurin inhibitor-based immunosuppression.17
Making islets go farther
One of the greatest challenges to islet transplant is the need for multiple donors to provide enough islet cells to overcome the loss of cells during transplant. Pancreases are already in short supply, and if each recipient needs more than 1, this makes the shortage worse. Some centers have achieved transplant with fewer donors,18,19 possibly by selecting pancreases from young donors who had a high body mass index and more islet cells, and harvesting and using them with a shorter cold ischemic time.
The number of viable, functioning islet cells drastically decreases after transplant, especially when transplanted into the portal system. This phenomenon is linked to an instant, blood-mediated inflammatory reaction involving antibody binding, complement and coagulation cascade activation, and platelet aggregation. The reaction, part of the innate immune system, damages the islet cells and leads to insulin dumping and early graft loss in studies in vitro and in vivo. Another factor affecting the survival of the graft cells is the low oxygen tension in the portal system.
For this reason, sites such as the pancreas, gastric submucosa, genitourinary tract, muscle, omentum, bone marrow, kidney capsule, peritoneum, anterior eye chamber, testis, and thymus are being explored.20
To create a more supportive environment for the transplanted cells, biotechnicians are trying to encapsulate islets in a semipermeable membrane that would protect them from the immune system while still allowing oxygen, nutrients, waste products, and, critically, insulin to diffuse in and out. Currently, no site or encapsulated product has been more successful than the current practice of implanting naked islets in the portal system.20
Bottom line
Without advances in transplant sites or increasing the yield of islet cells to allow single-donor transplants, islet cell allotransplant will not be feasible for most patients with type 1 diabetes.
Xenotransplant: Can pig cells make up the shortage?
Use of animal kidneys (xenotransplant) is a potential solution to the shortage of human organs for transplant.
In theory, pigs could be a source. Porcine insulin is similar to human insulin (differing by only 1 amino acid), and it should be possible to breed “knockout” pigs that lack the antigens responsible for acute humoral rejection.21
On the other hand, transplant of porcine islets poses several immunologic, physiologic, ethical, legal, and infectious concerns. For example, porcine tissue could carry pig viruses, such as porcine endogenous retroviruses.21 And even if the pigs are genetically modified, patients will still require immunosuppressive therapy.
A review of 17 studies of pig islet xenotransplant into nonhuman primates found that in 5 of the studies (4 using diabetic primates) the grafts survived at least 3 months.22 Of these, 1 study used encapsulation, and the rest used intensive and toxic immunosuppression.
More research is needed to make xenotransplant a clinical option.
Transplanting stem cells or beta cells grown from stem cells
Stem cells provide an exciting potential alternative to the limited donor pool. During the past decade, several studies have shown success using human pluripotent stem cells (embryonic stem cells and human-induced pluripotent stem cells), mesenchymal stem cells isolated from adult tissues, and directly programmed somatic cells. Researchers have created stable cultures of pluripotent stem cells from embryonic stem cells, which could possibly be produced on a large scale and banked.23
Human pluripotent stem cells derived from pancreatic progenitors have been shown to mature into more functional, islet-like structures in vivo. They transform into subtypes of islet cells including alpha, beta, and delta cells, ghrelin-producing cells, and pancreatic polypeptide hormone-producing cells. This process takes 2 to 6 weeks. In mice, these cells have been shown to maintain glucose homeostasis.24 Phase 1 and 2 trials in humans are now being conducted.
Pagliuca et al25 generated functional human pancreatic beta cells in vitro from embryonic stem cells. Rezania et al24 reversed diabetes with insulin-producing cells derived in vitro from human pluripotent stem cells. The techniques used in these studies contributed to the success of a study by Vegas et al,26 who achieved successful long-term glycemic control in mice using polymer-encapsulated human stem cell-derived beta cells.
Reversal of autoimmunity is an important step that needs to be overcome in stem cell transplant for type 1 diabetes. Nikolic et al27 have achieved mixed allogeneic chimerism across major histocompatibility complex barriers with nonmyeloablative conditioning in advanced-diabetic nonobese diabetic mice. However, conditioning alone (ie, without bone marrow transplant) does not permit acceptance of allogeneic islets and does not reverse autoimmunity or allow islet regeneration.28 Adding allogeneic bone marrow transplant to conditioned nonobese diabetic mice leads to tolerance to the donor and reverses autoimmunity.
THE ‘BIONIC’ PANCREAS
While we wait for advances in islet cell transplant, improved insulin pumps hold promise.
One such experimental device, the iLet (Beta Bionics, Boston, MA), designed by Damiano et al, consists of 2 infusion pumps (1 for insulin, 1 for glucagon) linked to a continuous glucose monitor via a smartphone app.
The monitor measures the glucose level every 5 minutes and transmits the information wirelessly to the phone app, which calculates the amount of insulin and glucagon required to stabilize the blood glucose: more insulin if too high, more glucagon if too low. The phone transmits this information to the pumps.
Dubbed the “bionic” pancreas, this closed-loop system frees patients from the tasks of measuring their glucose multiple times a day, calculating the appropriate dose, and giving multiple insulin injections.
The 2016 summer camp study29 followed 19 preteens wearing the bionic pancreas for 5 days. During this time, the patients had lower mean glucose levels and less hypoglycemia than during control periods. No episodes of severe hypoglycemia were recorded.
El-Khatib et al30 randomly assigned 43 patients to treatment with either the bihormonal bionic pancreas or usual care (a conventional insulin pump or a sensor-augmented insulin pump) for 11 days, followed by 11 days of the opposite treatment. All participants continued their normal activities. The bionic pancreas system was superior to the insulin pump in terms of the mean glucose concentration and mean time in the hypoglycemic range (P < .0001 for both results).
Bottom line
As the search continues for better solutions, advances in technology such as the bionic pancreas could provide a safer (ie, less hypoglycemic) and more successful alternative for insulin replacement in the near future.
- American Diabetes Association. Statistics about diabetes: overall numbers, diabetes and prediabetes. www.diabetes.org/diabetes-basics/statistics/. Accessed November 6, 2018.
- Ahmed AM. History of diabetes mellitus. Saudi Med J 2002; 23(4):373–378. pmid:11953758
- Kelly WD, Lillehei RC, Merkel FK, Idezuki Y, Goetz FC. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery 1967; 61:827–837. pmid: 5338113
- Sutherland DE, Gruessner RW, Dunn DL, et al. Lessons learned from more than 1,000 pancreas transplants at a single institution. Ann Surg 2001; 233(4):463–501. pmid:11303130
- Fioretto P, Steffes MW, Sutherland DE, Goetz FC, Mauer M. Reversal of lesions of diabetic nephropathy after pancreas transplantation. N Engl J Med 1998; 339(2):69–75. doi:10.1056/NEJM199807093390202
- Kennedy WR, Navarro X, Goetz FC, Sutherland DE, Najarian JS. Effects of pancreatic transplantation on diabetic neuropathy. N Engl J Med 1990; 322(15):1031–1037. doi:10.1056/NEJM199004123221503
- Kennedy WR, Navarro X, Sutherland DER. Neuropathy profile of diabetic patients in a pancreas transplantation program. Neurology 1995; 45(4):773–780. pmid:7723969
- Douzdjian V, Ferrara D, Silvestri G. Treatment strategies for insulin-dependent diabetics with ESRD: a cost-effectiveness decision analysis model. Am J Kidney Dis 1998; 31(5):794–802. pmid:9590189
- Venstrom JM, McBride MA, Rother KI, Hirshberg B, Orchard TJ, Harlan DM. Survival after pancreas transplantation in patients with diabetes and preserved kidney function. JAMA 2003; 290(21):2817–2823. doi:10.1001/jama.290.21.2817
- Gruessner RW, Sutherland DE, Gruessner AC. Mortality assessment for pancreas transplants. Am J Transplant 2004; 4(12):2018–2026. doi:10.1111/j.1600-6143.2004.00667.x
- Redfield RR, Scalea JR, Odorico JS. Simultaneous pancreas and kidney transplantation: current trends and future directions. Curr Opin Organ Transplant 2015; 20(1):94-102. doi:10.1097/MOT.0000000000000146
- Lin YK, Faiman C, Johnston PC, et al. Spontaneous hypoglycemia after islet autotransplantation for chronic pancreatitis. J Clin Endocrinol Metab 2016; 101(10):3669–3675. doi:10.1210/jc.2016-2111
- Gupta V, Wahoff DC, Rooney DP, et al. The defective glucagon response from transplanted intrahepatic pancreatic islets during hypoglycemia is transplantation site-determined. Diabetes 1997; 46(1):28–33. pmid:8971077
- Shapiro AM, Lakey JR, Ryan EA, et al. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med 2000; 343(4):230–238. doi:10.1056/NEJM200007273430401
- Shapiro AM, Ricordi C, Hering BJ, et al. International trial of the Edmonton protocol for islet transplantation. N Engl J Med 2006; 355(13):1318–1330. doi:10.1056/NEJMoa061267
- Clinical Islet Transplantation (CIT) Consortium. www.citisletstudy.org. Accessed November 6, 2018.
- Collaborative Islet Transplantation Registry (CITR). CITR 10th Annual Report. https://citregistry.org/system/files/10th_AR.pdf. Accessed November 6, 2018.
- Hering BJ, Kandaswamy R, Harmon JV, et al. Transplantation of cultured islets from two-layer preserved pancreases in type 1 diabetes with anti-CD3 antibody. Am J Transplant 2004; 4(3):390–401. pmid:14961992
- Posselt AM, Bellin MD, Tavakol M, et al. Islet transplantation in type 1 diabetics using an immunosuppressive protocol based on the anti-LFA-1 antibody efalizumab. Am J Transplant 2010; 10(8):1870–1880. doi:10.1111/j.1600-6143.2010.03073.x
- Cantarelli E, Piemonti L. Alternative transplantation sites for pancreatic islet grafts. Curr Diab Rep 2011; 11(5):364–374. doi:10.1007/s11892-011-0216-9
- Cooper DK, Gollackner B, Knosalla C, Teranishi K. Xenotransplantation—how far have we come? Transpl Immunol 2002; 9(2–4):251–256. pmid:12180839
- Marigliano M, Bertera S, Grupillo M, Trucco M, Bottino R. Pig-to-nonhuman primates pancreatic islet xenotransplantation: an overview. Curr Diab Rep 2011; 11(5):402–412. doi:10.1007/s11892-011-0213-z
- Bartlett ST, Markmann JF, Johnson P, et al. Report from IPITA-TTS opinion leaders meeting on the future of beta-cell replacement. Transplantation 2016; 100(suppl 2):S1–S44. doi:10.1097/TP.0000000000001055
- Rezania A, Bruin JE, Arora P, et al. Reversal of diabetes with insulin-producing cells derived in vitro from human pluripotent stem cells. Nat Biotechnol 2014; 32(11):1121–1133. doi:10.1038/nbt.3033
- Pagliuca FW, Millman JR, Gurtler M, et al. Generation of functional human pancreatic beta cells in vitro. Cell 2014; 159(2):428–439. doi:10.1016/j.cell.2014.09.040
- Vegas AJ, Veiseh O, Gurtler M, et al. Long-term glycemic control using polymer-encapsulated human stem cell-derived beta cells in immune-competent mice. Nat Med 2016; 22(3):306–311. doi:10.1038/nm.4030
- Nikolic B, Takeuchi Y, Leykin I, Fudaba Y, Smith RN, Sykes M. Mixed hematopoietic chimerism allows cure of autoimmune tolerance and reversal of autoimmunity. Diabetes 2004; 53(2):376–383. pmid:14747288
- Li HW, Sykes M. Emerging concepts in haematopoietic cell transplantation. Nat Rev Immunol 2012; 12(6):403–416. doi:10.1038/nri3226
- Russell SJ, Hillard MA, Balliro C, et al. Day and night glycaemic control with a bionic pancreas versus conventional insulin pump therapy in preadolescent children with type 1 diabetes: a randomised crossover trial. Lancet Diabetes Endocrinol 2016; 4(3):233–243. doi:10.1016/S2213-8587(15)00489-1
- El-Khatib FH, Balliro C, Hillard MA, et al. Home use of a bihormonal bionic pancreas versus insulin pump therapy in adults with type 1 diabetes: a multicenter randomized crossover trial. Lancet 2017; 389(10067):369–380. doi:10.1016/S0140-6736(16)32567-3
With intensive insulin regimens and home blood glucose monitoring, patients with type 1 diabetes are controlling their blood glucose better than in the past. Nevertheless, glucose regulation is still imperfect and tedious, and striving for tight glycemic control poses the risk of hypoglycemia.
Prominent among the challenges are the sheer numbers involved. Some 1.25 million Americans have type 1 diabetes, and another 30 million have type 2, but only about 7,000 to 8,000 pancreases are available for transplant each year.1 While awaiting a breakthrough—perhaps involving stem cells, perhaps involving organs obtained from animals—an insulin pump may offer better diabetes control for many. Another possibility is a closed-loop system with a continuous glucose monitor that drives a dual-infusion pump, delivering insulin when glucose levels rise too high, and glucagon when they dip too low.
DIABETES WAS KNOWN IN ANCIENT TIMES
About 3,000 years ago, Egyptians described the syndrome of thirst, emaciation, and sweet urine that attracted ants. The term diabetes (Greek for siphon) was first recorded in 1425; mellitus (Latin for sweet with honey) was not added until 1675.
In 1857, Bernard hypothesized that diabetes was caused by overproduction of glucose in the liver. This idea was replaced in 1889, when Mering and Minkowski proposed the dysfunctional pancreas theory that eventually led to the discovery of the beta cell.2
In 1921, Banting and Best isolated insulin, and for the past 100 years subcutaneous insulin replacement has been the mainstay of treatment. But starting about 50 years ago, researchers have been looking for safe and long-lasting ways to replace beta cells and eliminate the need for exogenous insulin replacement.
TRANSPLANTING THE WHOLE PANCREAS
The first whole-pancreas transplant was performed in 1966 by Kelly et al,3 followed by 13 more by 1973.4 These first transplant grafts were short-lived, with only 1 graft surviving longer than 1 year. Since then, more than 12,000 pancreases have been transplanted worldwide, as refinements in surgical techniques and immunosuppressive therapies have improved patient and graft survival rates.4
Today, most pancreas transplants are in patients who have both type 1 diabetes and end-stage renal disease due to diabetic nephropathy, and most receive both a kidney and a pancreas at the same time. Far fewer patients receive a pancreas after previously receiving a kidney, or receive a pancreas alone.
The bile duct of the transplanted pancreas is usually routed into the patient’s small intestine, as nature intended, and less often into the bladder. Although bladder drainage is associated with urinary complications, it has the advantage of allowing measurement of pancreatic amylase levels in the urine to monitor for graft rejection. With simultaneous pancreas and kidney transplant, the serum creatinine concentration can also be monitored for rejection of the kidney graft.
Current immunosuppressive regimens vary but generally consist of anti-T-cell antibodies at the time of surgery, followed by lifelong treatment with the combination of a calcineurin inhibitor (cyclosporine or tacrolimus) and an antimetabolite (mycophenolate mofetil or azathioprine).
Outcomes are good. The rates of patient and graft survival are highest with simultaneous pancreas-kidney transplant, and somewhat lower with pancreas-after-kidney and pancreas-alone transplant.
Benefits of pancreas transplant
Most recipients can stop taking insulin immediately after the procedure, and their hemoglobin A1c levels normalize and stay low for the life of the graft. Lipid levels also decrease, although this has not been directly correlated with lower risk of vascular disease.4
Transplant also reduces or eliminates some complications of diabetes, including retinopathy, nephropathy, cardiomyopathy, and gastropathy.
For example, in patients undergoing simultaneous pancreas-kidney transplant, diabetic nephropathy does not recur in the new kidney. Fioretto et al5 reported that nephropathy lesions reversed during the 10 years after pancreas transplant.
Kennedy et al6,7 found that preexisting diabetic neuropathy improved slightly (although neurologic status did not completely return to normal) over a period of up to 42 months in a group of patients who received a pancreas transplant, whereas it tended to worsen in a control group. Both groups were assessed at baseline and at 12 and 24 months, with a subgroup followed through 42 months, and they underwent testing of motor, sensory, and autonomic function.6,7
Disadvantages of pancreas transplant
Disadvantages of whole-pancreas transplant include hypoglycemia (usually mild), adverse effects of immunosuppression, potential for surgical complications including an increased rate of death in the first 90 days after the procedure, and cost.
In an analysis comparing the 5-year estimated costs of dialysis, kidney transplant alone from cadavers or live donors, or simultaneous pancreas-kidney transplant for diabetic patients with end-stage renal disease, the least expensive option was kidney transplant from a live donor.8 The most expensive option was simultaneous pancreas-kidney transplant, but quality of life was better with this option. The analysis did not consider the potential cost of long-term treatments for complications related to diabetes that could be saved with a pancreas transplant.
Data conflict regarding the risk of death with different types of pancreas transplants. A retrospective cohort study of data from 124 US transplant centers reported in 2003 found higher mortality rates in pancreas-alone transplant recipients than in patients on a transplant waiting list receiving conventional therapy.9 In contrast, a 2004 study reported that after the first 90 days, when the risk of death was clearly higher, mortality rates were lower after simultaneous pancreas-kidney transplant and pancreas-after-kidney transplant.10 After pancreas-alone transplant, however, mortality rates were higher than with exogenous insulin therapy.
Although outcomes have improved, fewer patients with type 1 diabetes are undergoing pancreas transplant in recent years.
Interestingly, more simultaneous pancreas-kidney transplants are being successfully performed in patients with type 2 diabetes, who now account for 8% of all simultaneous pancreas-kidney transplant recipients.11 Outcomes of pancreas transplant appear to be similar regardless of diabetes type.
Bottom line
Pancreas transplant is a viable option for certain cases of complicated diabetes.
TRANSPLANTING ISLET CELLS
Despite its successes, pancreas transplant is major surgery and requires lifetime immunosuppression. Research is ongoing into a less-invasive procedure that, it is hoped, would require less immunosuppression: transplanting islets by themselves.
Islet autotransplant after pancreatectomy
For some patients with chronic pancreatitis, the only option to relieve chronic pain, narcotic dependence, and poor quality of life is to remove the pancreas. In the past, this desperate measure would instantly and inevitably cause diabetes, but not anymore.
Alpha cells and glucagon are a different story; a complication of islet transplant is hypoglycemia. In 2016, Lin et al12 reported spontaneous hypoglycemia in 6 of 12 patients who maintained insulin independence after autotransplant of islets. Although the transplanted islets had functional alpha cells that could in theory produce glucagon, as well as beta cells that produce insulin and C-peptide, apparently the alpha cells were not secreting glucagon in response to the hypoglycemia.
Location may matter. Gupta et al,13 in a 1997 study in dogs, found that more hypoglycemia occurs if islets are autotransplanted into the liver than if they are transplanted into the peritoneal cavity. A possible explanation may have to do with the glycemic environment of the liver.
Islet allotransplant
Islets can also be taken from cadaver donors and transplanted into patients with type 1 diabetes, who do not have enough working beta cells.
Success of allotransplant increased after the publication of observational data from the program in Edmonton in Canada, in which 7 consecutive patients with type 1 diabetes achieved initial insulin independence after islet allotransplant using steroid-free immunosuppression.14 Six recipients required islets from 2 donors, and 1 required islets from 4 donors, so they all received large volumes of at least 11,000 islet equivalents (IEQ) per kilogram of body weight.
In a subsequent report from the same team,15 16 (44%) of 36 patients remained insulin-free at 1 year, and C-peptide secretion was detectable in 70% at 2 years. But despite the elevated C-peptide levels, only 5 patients remained insulin-independent by 2 years. Lower hemoglobin A1c levels and decreases in hypoglycemic events from baseline also were noted.
The Clinical Islet Transplantation Consortium (CITC)16 and Collaborative Islet Transplant Registry (CITR)17 were established in 2004 to combine data and resources from centers around the world, including several that specialize in islet isolation and purification. Currently, more than 80 studies are being conducted.
The CITC and CITR now have data on more than 1,000 allogeneic islet transplant recipients (islet transplant alone, after kidney transplant, or simultaneous with it). The primary outcomes are hemoglobin A1c levels below 7% fasting C-peptide levels 0.3 ng/mL or higher, and fasting blood glucose of 60 to 140 mg/dL with no severe hypoglycemic events. The best results for islet-alone transplant have been in recipients over age 35 who received at least 325,000 IEQs with use of tumor necrosis factor antagonists for induction and calcineurin inhibitors or mammalian target of rapamycin (mTOR) inhibitors for maintenance.17
The best success for islet-after-kidney transplant was achieved with the same protocol but with insulin given to the donor during hospitalization before pancreas procurement. For participants with favorable factors, a hemoglobin A1c at or below 6.5% was achieved in about 80% at 1 year after last infusion, with more than 80% maintaining their fasting blood glucose level goals. About 70% of these patients were insulin-independent at 1 year. Hypoglycemia unawareness resolved in these patients even 5 years after infusion. Although there were no deaths or disabilities related to these transplants, bleeding occurred in 1 of 15 procedures. There was also a notable decline in estimated glomerular filtration rates with calcineurin inhibitor-based immunosuppression.17
Making islets go farther
One of the greatest challenges to islet transplant is the need for multiple donors to provide enough islet cells to overcome the loss of cells during transplant. Pancreases are already in short supply, and if each recipient needs more than 1, this makes the shortage worse. Some centers have achieved transplant with fewer donors,18,19 possibly by selecting pancreases from young donors who had a high body mass index and more islet cells, and harvesting and using them with a shorter cold ischemic time.
The number of viable, functioning islet cells drastically decreases after transplant, especially when transplanted into the portal system. This phenomenon is linked to an instant, blood-mediated inflammatory reaction involving antibody binding, complement and coagulation cascade activation, and platelet aggregation. The reaction, part of the innate immune system, damages the islet cells and leads to insulin dumping and early graft loss in studies in vitro and in vivo. Another factor affecting the survival of the graft cells is the low oxygen tension in the portal system.
For this reason, sites such as the pancreas, gastric submucosa, genitourinary tract, muscle, omentum, bone marrow, kidney capsule, peritoneum, anterior eye chamber, testis, and thymus are being explored.20
To create a more supportive environment for the transplanted cells, biotechnicians are trying to encapsulate islets in a semipermeable membrane that would protect them from the immune system while still allowing oxygen, nutrients, waste products, and, critically, insulin to diffuse in and out. Currently, no site or encapsulated product has been more successful than the current practice of implanting naked islets in the portal system.20
Bottom line
Without advances in transplant sites or increasing the yield of islet cells to allow single-donor transplants, islet cell allotransplant will not be feasible for most patients with type 1 diabetes.
Xenotransplant: Can pig cells make up the shortage?
Use of animal kidneys (xenotransplant) is a potential solution to the shortage of human organs for transplant.
In theory, pigs could be a source. Porcine insulin is similar to human insulin (differing by only 1 amino acid), and it should be possible to breed “knockout” pigs that lack the antigens responsible for acute humoral rejection.21
On the other hand, transplant of porcine islets poses several immunologic, physiologic, ethical, legal, and infectious concerns. For example, porcine tissue could carry pig viruses, such as porcine endogenous retroviruses.21 And even if the pigs are genetically modified, patients will still require immunosuppressive therapy.
A review of 17 studies of pig islet xenotransplant into nonhuman primates found that in 5 of the studies (4 using diabetic primates) the grafts survived at least 3 months.22 Of these, 1 study used encapsulation, and the rest used intensive and toxic immunosuppression.
More research is needed to make xenotransplant a clinical option.
Transplanting stem cells or beta cells grown from stem cells
Stem cells provide an exciting potential alternative to the limited donor pool. During the past decade, several studies have shown success using human pluripotent stem cells (embryonic stem cells and human-induced pluripotent stem cells), mesenchymal stem cells isolated from adult tissues, and directly programmed somatic cells. Researchers have created stable cultures of pluripotent stem cells from embryonic stem cells, which could possibly be produced on a large scale and banked.23
Human pluripotent stem cells derived from pancreatic progenitors have been shown to mature into more functional, islet-like structures in vivo. They transform into subtypes of islet cells including alpha, beta, and delta cells, ghrelin-producing cells, and pancreatic polypeptide hormone-producing cells. This process takes 2 to 6 weeks. In mice, these cells have been shown to maintain glucose homeostasis.24 Phase 1 and 2 trials in humans are now being conducted.
Pagliuca et al25 generated functional human pancreatic beta cells in vitro from embryonic stem cells. Rezania et al24 reversed diabetes with insulin-producing cells derived in vitro from human pluripotent stem cells. The techniques used in these studies contributed to the success of a study by Vegas et al,26 who achieved successful long-term glycemic control in mice using polymer-encapsulated human stem cell-derived beta cells.
Reversal of autoimmunity is an important step that needs to be overcome in stem cell transplant for type 1 diabetes. Nikolic et al27 have achieved mixed allogeneic chimerism across major histocompatibility complex barriers with nonmyeloablative conditioning in advanced-diabetic nonobese diabetic mice. However, conditioning alone (ie, without bone marrow transplant) does not permit acceptance of allogeneic islets and does not reverse autoimmunity or allow islet regeneration.28 Adding allogeneic bone marrow transplant to conditioned nonobese diabetic mice leads to tolerance to the donor and reverses autoimmunity.
THE ‘BIONIC’ PANCREAS
While we wait for advances in islet cell transplant, improved insulin pumps hold promise.
One such experimental device, the iLet (Beta Bionics, Boston, MA), designed by Damiano et al, consists of 2 infusion pumps (1 for insulin, 1 for glucagon) linked to a continuous glucose monitor via a smartphone app.
The monitor measures the glucose level every 5 minutes and transmits the information wirelessly to the phone app, which calculates the amount of insulin and glucagon required to stabilize the blood glucose: more insulin if too high, more glucagon if too low. The phone transmits this information to the pumps.
Dubbed the “bionic” pancreas, this closed-loop system frees patients from the tasks of measuring their glucose multiple times a day, calculating the appropriate dose, and giving multiple insulin injections.
The 2016 summer camp study29 followed 19 preteens wearing the bionic pancreas for 5 days. During this time, the patients had lower mean glucose levels and less hypoglycemia than during control periods. No episodes of severe hypoglycemia were recorded.
El-Khatib et al30 randomly assigned 43 patients to treatment with either the bihormonal bionic pancreas or usual care (a conventional insulin pump or a sensor-augmented insulin pump) for 11 days, followed by 11 days of the opposite treatment. All participants continued their normal activities. The bionic pancreas system was superior to the insulin pump in terms of the mean glucose concentration and mean time in the hypoglycemic range (P < .0001 for both results).
Bottom line
As the search continues for better solutions, advances in technology such as the bionic pancreas could provide a safer (ie, less hypoglycemic) and more successful alternative for insulin replacement in the near future.
With intensive insulin regimens and home blood glucose monitoring, patients with type 1 diabetes are controlling their blood glucose better than in the past. Nevertheless, glucose regulation is still imperfect and tedious, and striving for tight glycemic control poses the risk of hypoglycemia.
Prominent among the challenges are the sheer numbers involved. Some 1.25 million Americans have type 1 diabetes, and another 30 million have type 2, but only about 7,000 to 8,000 pancreases are available for transplant each year.1 While awaiting a breakthrough—perhaps involving stem cells, perhaps involving organs obtained from animals—an insulin pump may offer better diabetes control for many. Another possibility is a closed-loop system with a continuous glucose monitor that drives a dual-infusion pump, delivering insulin when glucose levels rise too high, and glucagon when they dip too low.
DIABETES WAS KNOWN IN ANCIENT TIMES
About 3,000 years ago, Egyptians described the syndrome of thirst, emaciation, and sweet urine that attracted ants. The term diabetes (Greek for siphon) was first recorded in 1425; mellitus (Latin for sweet with honey) was not added until 1675.
In 1857, Bernard hypothesized that diabetes was caused by overproduction of glucose in the liver. This idea was replaced in 1889, when Mering and Minkowski proposed the dysfunctional pancreas theory that eventually led to the discovery of the beta cell.2
In 1921, Banting and Best isolated insulin, and for the past 100 years subcutaneous insulin replacement has been the mainstay of treatment. But starting about 50 years ago, researchers have been looking for safe and long-lasting ways to replace beta cells and eliminate the need for exogenous insulin replacement.
TRANSPLANTING THE WHOLE PANCREAS
The first whole-pancreas transplant was performed in 1966 by Kelly et al,3 followed by 13 more by 1973.4 These first transplant grafts were short-lived, with only 1 graft surviving longer than 1 year. Since then, more than 12,000 pancreases have been transplanted worldwide, as refinements in surgical techniques and immunosuppressive therapies have improved patient and graft survival rates.4
Today, most pancreas transplants are in patients who have both type 1 diabetes and end-stage renal disease due to diabetic nephropathy, and most receive both a kidney and a pancreas at the same time. Far fewer patients receive a pancreas after previously receiving a kidney, or receive a pancreas alone.
The bile duct of the transplanted pancreas is usually routed into the patient’s small intestine, as nature intended, and less often into the bladder. Although bladder drainage is associated with urinary complications, it has the advantage of allowing measurement of pancreatic amylase levels in the urine to monitor for graft rejection. With simultaneous pancreas and kidney transplant, the serum creatinine concentration can also be monitored for rejection of the kidney graft.
Current immunosuppressive regimens vary but generally consist of anti-T-cell antibodies at the time of surgery, followed by lifelong treatment with the combination of a calcineurin inhibitor (cyclosporine or tacrolimus) and an antimetabolite (mycophenolate mofetil or azathioprine).
Outcomes are good. The rates of patient and graft survival are highest with simultaneous pancreas-kidney transplant, and somewhat lower with pancreas-after-kidney and pancreas-alone transplant.
Benefits of pancreas transplant
Most recipients can stop taking insulin immediately after the procedure, and their hemoglobin A1c levels normalize and stay low for the life of the graft. Lipid levels also decrease, although this has not been directly correlated with lower risk of vascular disease.4
Transplant also reduces or eliminates some complications of diabetes, including retinopathy, nephropathy, cardiomyopathy, and gastropathy.
For example, in patients undergoing simultaneous pancreas-kidney transplant, diabetic nephropathy does not recur in the new kidney. Fioretto et al5 reported that nephropathy lesions reversed during the 10 years after pancreas transplant.
Kennedy et al6,7 found that preexisting diabetic neuropathy improved slightly (although neurologic status did not completely return to normal) over a period of up to 42 months in a group of patients who received a pancreas transplant, whereas it tended to worsen in a control group. Both groups were assessed at baseline and at 12 and 24 months, with a subgroup followed through 42 months, and they underwent testing of motor, sensory, and autonomic function.6,7
Disadvantages of pancreas transplant
Disadvantages of whole-pancreas transplant include hypoglycemia (usually mild), adverse effects of immunosuppression, potential for surgical complications including an increased rate of death in the first 90 days after the procedure, and cost.
In an analysis comparing the 5-year estimated costs of dialysis, kidney transplant alone from cadavers or live donors, or simultaneous pancreas-kidney transplant for diabetic patients with end-stage renal disease, the least expensive option was kidney transplant from a live donor.8 The most expensive option was simultaneous pancreas-kidney transplant, but quality of life was better with this option. The analysis did not consider the potential cost of long-term treatments for complications related to diabetes that could be saved with a pancreas transplant.
Data conflict regarding the risk of death with different types of pancreas transplants. A retrospective cohort study of data from 124 US transplant centers reported in 2003 found higher mortality rates in pancreas-alone transplant recipients than in patients on a transplant waiting list receiving conventional therapy.9 In contrast, a 2004 study reported that after the first 90 days, when the risk of death was clearly higher, mortality rates were lower after simultaneous pancreas-kidney transplant and pancreas-after-kidney transplant.10 After pancreas-alone transplant, however, mortality rates were higher than with exogenous insulin therapy.
Although outcomes have improved, fewer patients with type 1 diabetes are undergoing pancreas transplant in recent years.
Interestingly, more simultaneous pancreas-kidney transplants are being successfully performed in patients with type 2 diabetes, who now account for 8% of all simultaneous pancreas-kidney transplant recipients.11 Outcomes of pancreas transplant appear to be similar regardless of diabetes type.
Bottom line
Pancreas transplant is a viable option for certain cases of complicated diabetes.
TRANSPLANTING ISLET CELLS
Despite its successes, pancreas transplant is major surgery and requires lifetime immunosuppression. Research is ongoing into a less-invasive procedure that, it is hoped, would require less immunosuppression: transplanting islets by themselves.
Islet autotransplant after pancreatectomy
For some patients with chronic pancreatitis, the only option to relieve chronic pain, narcotic dependence, and poor quality of life is to remove the pancreas. In the past, this desperate measure would instantly and inevitably cause diabetes, but not anymore.
Alpha cells and glucagon are a different story; a complication of islet transplant is hypoglycemia. In 2016, Lin et al12 reported spontaneous hypoglycemia in 6 of 12 patients who maintained insulin independence after autotransplant of islets. Although the transplanted islets had functional alpha cells that could in theory produce glucagon, as well as beta cells that produce insulin and C-peptide, apparently the alpha cells were not secreting glucagon in response to the hypoglycemia.
Location may matter. Gupta et al,13 in a 1997 study in dogs, found that more hypoglycemia occurs if islets are autotransplanted into the liver than if they are transplanted into the peritoneal cavity. A possible explanation may have to do with the glycemic environment of the liver.
Islet allotransplant
Islets can also be taken from cadaver donors and transplanted into patients with type 1 diabetes, who do not have enough working beta cells.
Success of allotransplant increased after the publication of observational data from the program in Edmonton in Canada, in which 7 consecutive patients with type 1 diabetes achieved initial insulin independence after islet allotransplant using steroid-free immunosuppression.14 Six recipients required islets from 2 donors, and 1 required islets from 4 donors, so they all received large volumes of at least 11,000 islet equivalents (IEQ) per kilogram of body weight.
In a subsequent report from the same team,15 16 (44%) of 36 patients remained insulin-free at 1 year, and C-peptide secretion was detectable in 70% at 2 years. But despite the elevated C-peptide levels, only 5 patients remained insulin-independent by 2 years. Lower hemoglobin A1c levels and decreases in hypoglycemic events from baseline also were noted.
The Clinical Islet Transplantation Consortium (CITC)16 and Collaborative Islet Transplant Registry (CITR)17 were established in 2004 to combine data and resources from centers around the world, including several that specialize in islet isolation and purification. Currently, more than 80 studies are being conducted.
The CITC and CITR now have data on more than 1,000 allogeneic islet transplant recipients (islet transplant alone, after kidney transplant, or simultaneous with it). The primary outcomes are hemoglobin A1c levels below 7% fasting C-peptide levels 0.3 ng/mL or higher, and fasting blood glucose of 60 to 140 mg/dL with no severe hypoglycemic events. The best results for islet-alone transplant have been in recipients over age 35 who received at least 325,000 IEQs with use of tumor necrosis factor antagonists for induction and calcineurin inhibitors or mammalian target of rapamycin (mTOR) inhibitors for maintenance.17
The best success for islet-after-kidney transplant was achieved with the same protocol but with insulin given to the donor during hospitalization before pancreas procurement. For participants with favorable factors, a hemoglobin A1c at or below 6.5% was achieved in about 80% at 1 year after last infusion, with more than 80% maintaining their fasting blood glucose level goals. About 70% of these patients were insulin-independent at 1 year. Hypoglycemia unawareness resolved in these patients even 5 years after infusion. Although there were no deaths or disabilities related to these transplants, bleeding occurred in 1 of 15 procedures. There was also a notable decline in estimated glomerular filtration rates with calcineurin inhibitor-based immunosuppression.17
Making islets go farther
One of the greatest challenges to islet transplant is the need for multiple donors to provide enough islet cells to overcome the loss of cells during transplant. Pancreases are already in short supply, and if each recipient needs more than 1, this makes the shortage worse. Some centers have achieved transplant with fewer donors,18,19 possibly by selecting pancreases from young donors who had a high body mass index and more islet cells, and harvesting and using them with a shorter cold ischemic time.
The number of viable, functioning islet cells drastically decreases after transplant, especially when transplanted into the portal system. This phenomenon is linked to an instant, blood-mediated inflammatory reaction involving antibody binding, complement and coagulation cascade activation, and platelet aggregation. The reaction, part of the innate immune system, damages the islet cells and leads to insulin dumping and early graft loss in studies in vitro and in vivo. Another factor affecting the survival of the graft cells is the low oxygen tension in the portal system.
For this reason, sites such as the pancreas, gastric submucosa, genitourinary tract, muscle, omentum, bone marrow, kidney capsule, peritoneum, anterior eye chamber, testis, and thymus are being explored.20
To create a more supportive environment for the transplanted cells, biotechnicians are trying to encapsulate islets in a semipermeable membrane that would protect them from the immune system while still allowing oxygen, nutrients, waste products, and, critically, insulin to diffuse in and out. Currently, no site or encapsulated product has been more successful than the current practice of implanting naked islets in the portal system.20
Bottom line
Without advances in transplant sites or increasing the yield of islet cells to allow single-donor transplants, islet cell allotransplant will not be feasible for most patients with type 1 diabetes.
Xenotransplant: Can pig cells make up the shortage?
Use of animal kidneys (xenotransplant) is a potential solution to the shortage of human organs for transplant.
In theory, pigs could be a source. Porcine insulin is similar to human insulin (differing by only 1 amino acid), and it should be possible to breed “knockout” pigs that lack the antigens responsible for acute humoral rejection.21
On the other hand, transplant of porcine islets poses several immunologic, physiologic, ethical, legal, and infectious concerns. For example, porcine tissue could carry pig viruses, such as porcine endogenous retroviruses.21 And even if the pigs are genetically modified, patients will still require immunosuppressive therapy.
A review of 17 studies of pig islet xenotransplant into nonhuman primates found that in 5 of the studies (4 using diabetic primates) the grafts survived at least 3 months.22 Of these, 1 study used encapsulation, and the rest used intensive and toxic immunosuppression.
More research is needed to make xenotransplant a clinical option.
Transplanting stem cells or beta cells grown from stem cells
Stem cells provide an exciting potential alternative to the limited donor pool. During the past decade, several studies have shown success using human pluripotent stem cells (embryonic stem cells and human-induced pluripotent stem cells), mesenchymal stem cells isolated from adult tissues, and directly programmed somatic cells. Researchers have created stable cultures of pluripotent stem cells from embryonic stem cells, which could possibly be produced on a large scale and banked.23
Human pluripotent stem cells derived from pancreatic progenitors have been shown to mature into more functional, islet-like structures in vivo. They transform into subtypes of islet cells including alpha, beta, and delta cells, ghrelin-producing cells, and pancreatic polypeptide hormone-producing cells. This process takes 2 to 6 weeks. In mice, these cells have been shown to maintain glucose homeostasis.24 Phase 1 and 2 trials in humans are now being conducted.
Pagliuca et al25 generated functional human pancreatic beta cells in vitro from embryonic stem cells. Rezania et al24 reversed diabetes with insulin-producing cells derived in vitro from human pluripotent stem cells. The techniques used in these studies contributed to the success of a study by Vegas et al,26 who achieved successful long-term glycemic control in mice using polymer-encapsulated human stem cell-derived beta cells.
Reversal of autoimmunity is an important step that needs to be overcome in stem cell transplant for type 1 diabetes. Nikolic et al27 have achieved mixed allogeneic chimerism across major histocompatibility complex barriers with nonmyeloablative conditioning in advanced-diabetic nonobese diabetic mice. However, conditioning alone (ie, without bone marrow transplant) does not permit acceptance of allogeneic islets and does not reverse autoimmunity or allow islet regeneration.28 Adding allogeneic bone marrow transplant to conditioned nonobese diabetic mice leads to tolerance to the donor and reverses autoimmunity.
THE ‘BIONIC’ PANCREAS
While we wait for advances in islet cell transplant, improved insulin pumps hold promise.
One such experimental device, the iLet (Beta Bionics, Boston, MA), designed by Damiano et al, consists of 2 infusion pumps (1 for insulin, 1 for glucagon) linked to a continuous glucose monitor via a smartphone app.
The monitor measures the glucose level every 5 minutes and transmits the information wirelessly to the phone app, which calculates the amount of insulin and glucagon required to stabilize the blood glucose: more insulin if too high, more glucagon if too low. The phone transmits this information to the pumps.
Dubbed the “bionic” pancreas, this closed-loop system frees patients from the tasks of measuring their glucose multiple times a day, calculating the appropriate dose, and giving multiple insulin injections.
The 2016 summer camp study29 followed 19 preteens wearing the bionic pancreas for 5 days. During this time, the patients had lower mean glucose levels and less hypoglycemia than during control periods. No episodes of severe hypoglycemia were recorded.
El-Khatib et al30 randomly assigned 43 patients to treatment with either the bihormonal bionic pancreas or usual care (a conventional insulin pump or a sensor-augmented insulin pump) for 11 days, followed by 11 days of the opposite treatment. All participants continued their normal activities. The bionic pancreas system was superior to the insulin pump in terms of the mean glucose concentration and mean time in the hypoglycemic range (P < .0001 for both results).
Bottom line
As the search continues for better solutions, advances in technology such as the bionic pancreas could provide a safer (ie, less hypoglycemic) and more successful alternative for insulin replacement in the near future.
- American Diabetes Association. Statistics about diabetes: overall numbers, diabetes and prediabetes. www.diabetes.org/diabetes-basics/statistics/. Accessed November 6, 2018.
- Ahmed AM. History of diabetes mellitus. Saudi Med J 2002; 23(4):373–378. pmid:11953758
- Kelly WD, Lillehei RC, Merkel FK, Idezuki Y, Goetz FC. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery 1967; 61:827–837. pmid: 5338113
- Sutherland DE, Gruessner RW, Dunn DL, et al. Lessons learned from more than 1,000 pancreas transplants at a single institution. Ann Surg 2001; 233(4):463–501. pmid:11303130
- Fioretto P, Steffes MW, Sutherland DE, Goetz FC, Mauer M. Reversal of lesions of diabetic nephropathy after pancreas transplantation. N Engl J Med 1998; 339(2):69–75. doi:10.1056/NEJM199807093390202
- Kennedy WR, Navarro X, Goetz FC, Sutherland DE, Najarian JS. Effects of pancreatic transplantation on diabetic neuropathy. N Engl J Med 1990; 322(15):1031–1037. doi:10.1056/NEJM199004123221503
- Kennedy WR, Navarro X, Sutherland DER. Neuropathy profile of diabetic patients in a pancreas transplantation program. Neurology 1995; 45(4):773–780. pmid:7723969
- Douzdjian V, Ferrara D, Silvestri G. Treatment strategies for insulin-dependent diabetics with ESRD: a cost-effectiveness decision analysis model. Am J Kidney Dis 1998; 31(5):794–802. pmid:9590189
- Venstrom JM, McBride MA, Rother KI, Hirshberg B, Orchard TJ, Harlan DM. Survival after pancreas transplantation in patients with diabetes and preserved kidney function. JAMA 2003; 290(21):2817–2823. doi:10.1001/jama.290.21.2817
- Gruessner RW, Sutherland DE, Gruessner AC. Mortality assessment for pancreas transplants. Am J Transplant 2004; 4(12):2018–2026. doi:10.1111/j.1600-6143.2004.00667.x
- Redfield RR, Scalea JR, Odorico JS. Simultaneous pancreas and kidney transplantation: current trends and future directions. Curr Opin Organ Transplant 2015; 20(1):94-102. doi:10.1097/MOT.0000000000000146
- Lin YK, Faiman C, Johnston PC, et al. Spontaneous hypoglycemia after islet autotransplantation for chronic pancreatitis. J Clin Endocrinol Metab 2016; 101(10):3669–3675. doi:10.1210/jc.2016-2111
- Gupta V, Wahoff DC, Rooney DP, et al. The defective glucagon response from transplanted intrahepatic pancreatic islets during hypoglycemia is transplantation site-determined. Diabetes 1997; 46(1):28–33. pmid:8971077
- Shapiro AM, Lakey JR, Ryan EA, et al. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med 2000; 343(4):230–238. doi:10.1056/NEJM200007273430401
- Shapiro AM, Ricordi C, Hering BJ, et al. International trial of the Edmonton protocol for islet transplantation. N Engl J Med 2006; 355(13):1318–1330. doi:10.1056/NEJMoa061267
- Clinical Islet Transplantation (CIT) Consortium. www.citisletstudy.org. Accessed November 6, 2018.
- Collaborative Islet Transplantation Registry (CITR). CITR 10th Annual Report. https://citregistry.org/system/files/10th_AR.pdf. Accessed November 6, 2018.
- Hering BJ, Kandaswamy R, Harmon JV, et al. Transplantation of cultured islets from two-layer preserved pancreases in type 1 diabetes with anti-CD3 antibody. Am J Transplant 2004; 4(3):390–401. pmid:14961992
- Posselt AM, Bellin MD, Tavakol M, et al. Islet transplantation in type 1 diabetics using an immunosuppressive protocol based on the anti-LFA-1 antibody efalizumab. Am J Transplant 2010; 10(8):1870–1880. doi:10.1111/j.1600-6143.2010.03073.x
- Cantarelli E, Piemonti L. Alternative transplantation sites for pancreatic islet grafts. Curr Diab Rep 2011; 11(5):364–374. doi:10.1007/s11892-011-0216-9
- Cooper DK, Gollackner B, Knosalla C, Teranishi K. Xenotransplantation—how far have we come? Transpl Immunol 2002; 9(2–4):251–256. pmid:12180839
- Marigliano M, Bertera S, Grupillo M, Trucco M, Bottino R. Pig-to-nonhuman primates pancreatic islet xenotransplantation: an overview. Curr Diab Rep 2011; 11(5):402–412. doi:10.1007/s11892-011-0213-z
- Bartlett ST, Markmann JF, Johnson P, et al. Report from IPITA-TTS opinion leaders meeting on the future of beta-cell replacement. Transplantation 2016; 100(suppl 2):S1–S44. doi:10.1097/TP.0000000000001055
- Rezania A, Bruin JE, Arora P, et al. Reversal of diabetes with insulin-producing cells derived in vitro from human pluripotent stem cells. Nat Biotechnol 2014; 32(11):1121–1133. doi:10.1038/nbt.3033
- Pagliuca FW, Millman JR, Gurtler M, et al. Generation of functional human pancreatic beta cells in vitro. Cell 2014; 159(2):428–439. doi:10.1016/j.cell.2014.09.040
- Vegas AJ, Veiseh O, Gurtler M, et al. Long-term glycemic control using polymer-encapsulated human stem cell-derived beta cells in immune-competent mice. Nat Med 2016; 22(3):306–311. doi:10.1038/nm.4030
- Nikolic B, Takeuchi Y, Leykin I, Fudaba Y, Smith RN, Sykes M. Mixed hematopoietic chimerism allows cure of autoimmune tolerance and reversal of autoimmunity. Diabetes 2004; 53(2):376–383. pmid:14747288
- Li HW, Sykes M. Emerging concepts in haematopoietic cell transplantation. Nat Rev Immunol 2012; 12(6):403–416. doi:10.1038/nri3226
- Russell SJ, Hillard MA, Balliro C, et al. Day and night glycaemic control with a bionic pancreas versus conventional insulin pump therapy in preadolescent children with type 1 diabetes: a randomised crossover trial. Lancet Diabetes Endocrinol 2016; 4(3):233–243. doi:10.1016/S2213-8587(15)00489-1
- El-Khatib FH, Balliro C, Hillard MA, et al. Home use of a bihormonal bionic pancreas versus insulin pump therapy in adults with type 1 diabetes: a multicenter randomized crossover trial. Lancet 2017; 389(10067):369–380. doi:10.1016/S0140-6736(16)32567-3
- American Diabetes Association. Statistics about diabetes: overall numbers, diabetes and prediabetes. www.diabetes.org/diabetes-basics/statistics/. Accessed November 6, 2018.
- Ahmed AM. History of diabetes mellitus. Saudi Med J 2002; 23(4):373–378. pmid:11953758
- Kelly WD, Lillehei RC, Merkel FK, Idezuki Y, Goetz FC. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery 1967; 61:827–837. pmid: 5338113
- Sutherland DE, Gruessner RW, Dunn DL, et al. Lessons learned from more than 1,000 pancreas transplants at a single institution. Ann Surg 2001; 233(4):463–501. pmid:11303130
- Fioretto P, Steffes MW, Sutherland DE, Goetz FC, Mauer M. Reversal of lesions of diabetic nephropathy after pancreas transplantation. N Engl J Med 1998; 339(2):69–75. doi:10.1056/NEJM199807093390202
- Kennedy WR, Navarro X, Goetz FC, Sutherland DE, Najarian JS. Effects of pancreatic transplantation on diabetic neuropathy. N Engl J Med 1990; 322(15):1031–1037. doi:10.1056/NEJM199004123221503
- Kennedy WR, Navarro X, Sutherland DER. Neuropathy profile of diabetic patients in a pancreas transplantation program. Neurology 1995; 45(4):773–780. pmid:7723969
- Douzdjian V, Ferrara D, Silvestri G. Treatment strategies for insulin-dependent diabetics with ESRD: a cost-effectiveness decision analysis model. Am J Kidney Dis 1998; 31(5):794–802. pmid:9590189
- Venstrom JM, McBride MA, Rother KI, Hirshberg B, Orchard TJ, Harlan DM. Survival after pancreas transplantation in patients with diabetes and preserved kidney function. JAMA 2003; 290(21):2817–2823. doi:10.1001/jama.290.21.2817
- Gruessner RW, Sutherland DE, Gruessner AC. Mortality assessment for pancreas transplants. Am J Transplant 2004; 4(12):2018–2026. doi:10.1111/j.1600-6143.2004.00667.x
- Redfield RR, Scalea JR, Odorico JS. Simultaneous pancreas and kidney transplantation: current trends and future directions. Curr Opin Organ Transplant 2015; 20(1):94-102. doi:10.1097/MOT.0000000000000146
- Lin YK, Faiman C, Johnston PC, et al. Spontaneous hypoglycemia after islet autotransplantation for chronic pancreatitis. J Clin Endocrinol Metab 2016; 101(10):3669–3675. doi:10.1210/jc.2016-2111
- Gupta V, Wahoff DC, Rooney DP, et al. The defective glucagon response from transplanted intrahepatic pancreatic islets during hypoglycemia is transplantation site-determined. Diabetes 1997; 46(1):28–33. pmid:8971077
- Shapiro AM, Lakey JR, Ryan EA, et al. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med 2000; 343(4):230–238. doi:10.1056/NEJM200007273430401
- Shapiro AM, Ricordi C, Hering BJ, et al. International trial of the Edmonton protocol for islet transplantation. N Engl J Med 2006; 355(13):1318–1330. doi:10.1056/NEJMoa061267
- Clinical Islet Transplantation (CIT) Consortium. www.citisletstudy.org. Accessed November 6, 2018.
- Collaborative Islet Transplantation Registry (CITR). CITR 10th Annual Report. https://citregistry.org/system/files/10th_AR.pdf. Accessed November 6, 2018.
- Hering BJ, Kandaswamy R, Harmon JV, et al. Transplantation of cultured islets from two-layer preserved pancreases in type 1 diabetes with anti-CD3 antibody. Am J Transplant 2004; 4(3):390–401. pmid:14961992
- Posselt AM, Bellin MD, Tavakol M, et al. Islet transplantation in type 1 diabetics using an immunosuppressive protocol based on the anti-LFA-1 antibody efalizumab. Am J Transplant 2010; 10(8):1870–1880. doi:10.1111/j.1600-6143.2010.03073.x
- Cantarelli E, Piemonti L. Alternative transplantation sites for pancreatic islet grafts. Curr Diab Rep 2011; 11(5):364–374. doi:10.1007/s11892-011-0216-9
- Cooper DK, Gollackner B, Knosalla C, Teranishi K. Xenotransplantation—how far have we come? Transpl Immunol 2002; 9(2–4):251–256. pmid:12180839
- Marigliano M, Bertera S, Grupillo M, Trucco M, Bottino R. Pig-to-nonhuman primates pancreatic islet xenotransplantation: an overview. Curr Diab Rep 2011; 11(5):402–412. doi:10.1007/s11892-011-0213-z
- Bartlett ST, Markmann JF, Johnson P, et al. Report from IPITA-TTS opinion leaders meeting on the future of beta-cell replacement. Transplantation 2016; 100(suppl 2):S1–S44. doi:10.1097/TP.0000000000001055
- Rezania A, Bruin JE, Arora P, et al. Reversal of diabetes with insulin-producing cells derived in vitro from human pluripotent stem cells. Nat Biotechnol 2014; 32(11):1121–1133. doi:10.1038/nbt.3033
- Pagliuca FW, Millman JR, Gurtler M, et al. Generation of functional human pancreatic beta cells in vitro. Cell 2014; 159(2):428–439. doi:10.1016/j.cell.2014.09.040
- Vegas AJ, Veiseh O, Gurtler M, et al. Long-term glycemic control using polymer-encapsulated human stem cell-derived beta cells in immune-competent mice. Nat Med 2016; 22(3):306–311. doi:10.1038/nm.4030
- Nikolic B, Takeuchi Y, Leykin I, Fudaba Y, Smith RN, Sykes M. Mixed hematopoietic chimerism allows cure of autoimmune tolerance and reversal of autoimmunity. Diabetes 2004; 53(2):376–383. pmid:14747288
- Li HW, Sykes M. Emerging concepts in haematopoietic cell transplantation. Nat Rev Immunol 2012; 12(6):403–416. doi:10.1038/nri3226
- Russell SJ, Hillard MA, Balliro C, et al. Day and night glycaemic control with a bionic pancreas versus conventional insulin pump therapy in preadolescent children with type 1 diabetes: a randomised crossover trial. Lancet Diabetes Endocrinol 2016; 4(3):233–243. doi:10.1016/S2213-8587(15)00489-1
- El-Khatib FH, Balliro C, Hillard MA, et al. Home use of a bihormonal bionic pancreas versus insulin pump therapy in adults with type 1 diabetes: a multicenter randomized crossover trial. Lancet 2017; 389(10067):369–380. doi:10.1016/S0140-6736(16)32567-3
KEY POINTS
- Most pancreas transplant recipients become insulin-independent immediately.
- A key drawback to islet transplant is the need for multiple donors to provide enough islet cells to achieve insulin independence.
- As with other organs for transplant, the need for donor pancreases far outnumbers the supply. Stem cells or beta cells grown from stem cells may avoid this problem. Another potential solution is to use organs from animals, possibly pigs, but much more work is needed to make these procedures viable.
- While we await a breakthrough in beta-cell therapy, a bionic pancreas may be the answer for a number of patients.
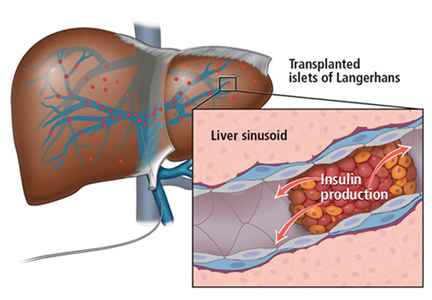
Cannabis for peripheral neuropathy: The good, the bad, and the unknown
Marijuana, which is still illegal under federal law but legal in 30 states for medical purposes as of this writing, has shown promising results for treating peripheral neuropathy. Studies suggest that cannabis may be an option for patients whose pain responds poorly to standard treatments; however, its use may be restricted by cognitive and psychiatric adverse effects, particularly at high doses.1
In this article, we discuss the basic pharmacology of cannabis and how it may affect neuropathic pain. We review clinical trials on its use for peripheral neuropathy and provide guidance for its use.
PERIPHERAL NEUROPATHY IS COMMON AND COMPLEX
An estimated 20 million people in the United States suffer from neuropathic pain. The prevalence is higher in certain populations, with 26% of people over age 65 and 30% of patients with diabetes mellitus affected.2–4
Peripheral neuropathy is a complex, chronic state that occurs when nerve fibers are damaged, dysfunctional, or injured, sending incorrect signals to pain centers in the central nervous system.5 It is characterized by weakness, pain, and paresthesias that typically begin in the hands or feet and progress proximally.4 Symptoms depend on the number and types of nerves affected.
In many cases, peripheral neuropathy is idiopathic, but common causes include diabetes, alcoholism, human immunodeficiency virus (HIV) infection, and autoimmune disease. Others include toxicity from chemotherapy and heavy metals.
Peripheral neuropathy significantly worsens quality of life and function. Many patients experience emotional, cognitive, and functional problems, resulting in high rates of medical and psychiatric comorbidities and occupational impairment.4,6,7 Yet despite its clinical and epidemiologic significance, it is often undertreated.8
STANDARD TREATMENTS INADEQUATE
Peripheral neuropathy occurs in patients with a wide range of comorbidities and is especially difficult to treat. Mainstays of therapy include anticonvulsants, tricyclic antidepressants, and serotonin-norepinephrine reuptake inhibitors.9 A more invasive option is spinal cord stimulation.
These treatments can have considerable adverse effects, and response rates remain suboptimal, with pain relief insufficient to improve quality of life for many patients.9,10 Better treatments are needed to improve clinical outcomes and patient experience.11
CANNABIS: A MIX OF COMPOUNDS
Cannabis sativa has been used as an analgesic for centuries. The plant contains more than 400 chemical compounds and is often used for its euphoric properties. Long-term use may lead to addiction and cognitive impairment.12,13
Tetrahydrocannabinol (THC) and cannabidiol (CBD) are the main components and the 2 best-studied cannabinoids with analgesic effects.
THC is the primary psychoactive component of cannabis. Its effects include relaxation, altered perception, heightened sensations, increased libido, and perceptual distortions of time and space. Temporary effects may include decreased short-term memory, dry mouth, impaired motor function, conjunctival injection, paranoia, and anxiety.
CBD is nonpsychoactive and has anti-inflammatory and antioxidant properties. It has been shown to reduce pain and inflammation without the effects of THC.14
Other compounds in the cannabis plant include phytocannabinoids, flavonoids, and tapenoids, which may produce individual, interactive, or synergistic effects.15 Different strains of cannabis have varying amounts of the individual components, making comparisons among clinical studies difficult.
THE ENDOCANNABINOID SYSTEM
The endogenous mammalian cannabinoid system plays a regulatory role in the development, homeostasis, and neuroplasticity of the central nervous system. It is also involved in modulating pain transmission in the nociceptive pathway.
Two of the most abundant cannabinoid endogenous ligands are anandamide and 2-arachidonylglycerol.9 These endocannabinoids are produced on demand in the central nervous system to reduce pain by acting as a circuit breaker.16–18 They target the G protein-coupled cannabinoid receptors CB1 and CB2, located throughout the central and peripheral nervous system and in organs and tissues.12
CB1 receptors are found primarily in the central nervous system, specifically in areas involved in movement, such as the basal ganglia and cerebellum, as well as in areas involved in memory, such as the hippocampus.12 They are also abundant in brain regions implicated in conducting and modulating pain signals, including the periaqueductal gray and the dorsal horn of the spinal cord.16–20
CB2 receptors are mostly found in peripheral tissues and organs, mainly those involved in the immune system, including splenic, tonsillar, and hematopoietic cells.12 They help regulate inflammation, allodynia, and hyperalgesia.17
Modifying response to injury
Following a nerve injury, neurons along the nociceptive pathway may become more reactive and responsive in a process known as sensitization.21 The process involves a cascade of cellular events that result in sprouting of pain-sensitive nerve endings.21,22
Cannabinoids are thought to reduce pain by modifying these cellular events. They also inhibit nociceptive conduction in the dorsal horn of the spinal cord and in the ascending spinothalamic tract.20 CB1 receptors found in nociceptive terminals along the peripheral nervous system impede pain conduction, while activation of CB2 receptors in immune cells decreases the release of nociceptive agents.
STUDIES OF CANNABIS FOR NEUROPATHIC PAIN
A number of studies have evaluated cannabis for treating neuropathic pain. Overall, available data support the efficacy of smoked or inhaled cannabis in its flower form when used as monotherapy or adjunctive therapy for relief of neuropathic pain of various etiologies. Many studies also report secondary benefits, including better sleep and functional improvement.23,24
However, adverse effects are common, especially at high doses, and include difficulty concentrating, lightheadedness, fatigue, and tachycardia. More serious reported adverse effects include anxiety, paranoia, and psychosis.
Wilsey et al, 2008: Neuropathic pain reduced
Wilsey et al25 conducted a double-blind, placebo-controlled crossover study that assessed the effects of smoking cannabis in 38 patients with central or peripheral neuropathic pain. Participants were assigned to smoke either high- or low-dose cannabis (7% or 3.5% delta-9-THC) or placebo cigarettes. Cigarettes were smoked during treatment sessions using the following regimen: 2 puffs at 60 minutes from baseline, 3 puffs at 120 minutes, and 4 puffs at 180 minutes. Patients were assessed after each set of puffs and for 2 hours afterwards. The primary outcome was spontaneous relief of pain as measured by a visual analog scale.
Pain intensity was comparable and significantly reduced in both treatment groups compared with placebo. At the high dose, some participants experienced neurocognitive impairment in attention, learning, memory, and psychomotor speed; only learning and memory declined at the low dose.
Ellis et al, 2009: Pain reduction in HIV neuropathy
Ellis et al23 conducted a double-blind, placebo-controlled crossover trial in patients with HIV neuropathy that was unresponsive to at least 2 analgesics with different modes of action. During each treatment week, participants were randomly assigned to smoke either active cannabis or placebo, while continuing their standard therapy. Titration started at 4% THC and was adjusted based on tolerability and efficacy. Twenty-eight of the 34 enrolled patients completed both cannabis and placebo treatments. The principal outcome was change in pain intensity from baseline at the end of each week, using the Descriptor Differential Scale of Pain Intensity.
Of the 28 patients, 46% achieved an average pain reduction of 3.3 points (30%). One patient experienced cannabis-induced psychosis, and another developed an intractable cough, which resolved with smoking cessation.
Ware et al, 2010: Reduced posttraumatic or postsurgical neuropathic pain
Ware et al24 performed a randomized crossover trial in 21 patients with posttraumatic or postsurgical neuropathic pain. Participants inhaled 4 different formulations of cannabis (containing 0%, 2.5%, 6.0%, and 9.4% THC) during 4 14-day periods. They inhaled a 25-mg dose through a pipe 3 times a day for the first 5 days of each cycle, followed by a 9-day washout period. Daily average pain intensity was measured using a numeric rating scale. The investigators also assessed mood, sleep, quality of life, and adverse effects.
Patients in the 9.4% THC group reported significantly less pain and better sleep, with average pain scores decreasing from 6.1 to 5.4 on an 11-point scale. Although the benefit was modest, the authors noted that the pain had been refractory to standard treatments.
The number of reported adverse events increased with greater potency and were most commonly throat irritation, burning sensation, headache, dizziness, and fatigue. This study suggests that THC potency affects tolerability, with higher doses eliciting clinically important adverse effects, some of which may reduce the ability to perform activities of daily living, such as driving.
Wilsey et al, 2013: Use in resistant neuropathic pain
Wilsey et al26 conducted another double-blind, placebo-controlled crossover study assessing the effect of vaporized cannabis on central and peripheral neuropathic pain resistant to first-line pharmacotherapies. Dose-effect relationships were explored using medium-dose (3.5%), low-dose (1.3%), and placebo cannabis. The primary outcome measure was a 30% reduction in pain intensity based on a visual analog scale.
In the placebo group, 26% of patients achieved this vs 57% of the low-dose cannabis group and 61% of those receiving the medium dose. No significant difference was found between the 2 active doses in reducing neuropathic pain, and both were more effective than placebo. The number needed to treat to achieve a 30% reduction in pain was about 3 for both cannabis groups compared with placebo. Psychoactive effects were minimal, of short duration, and reversible.
Wallace et al, 2015: Use in diabetic peripheral neuropathy
Wallace et al27 conducted a randomized, double-blind, placebo-controlled crossover study evaluating cannabis for diabetic peripheral neuropathy in 16 patients. Each had experienced at least 6 months of neuropathic pain in their feet. The participants inhaled a single dose of 1%, 4%, or 7% THC cannabis or placebo. Spontaneous pain was reported with a visual analog scale and also tested with a foam brush and von Frey filament at intervals until 4 hours after treatment.
Pain scores were lower with treatment compared with placebo, with high-dose cannabis having the greatest analgesic effect. Pain reduction lasted for the full duration of the test. Cannabis recipients had declines in attention and working memory, with the high-dose group experiencing the greatest impact 15 minutes after treatment. High-dose recipients also had poorer scores on testing of quick task-switching, with the greatest effect at 2 hours.27
Research and market cannabis are not equal
Results of US studies must be qualified. Most have used cannabis provided by the National Institute of Drug Abuse (NIDA),23–26 which differs in potency from commercially available preparations. This limits the clinical usefulness of the analysis of benefits and risks.
Vergara et al28 found that NIDA varieties contained much lower THC levels and as much as 23 times the cannabinol content as cannabis in state-legalized markets.
Studies based on NIDA varieties likely underestimate the risks of consumer-purchased cannabis, as THC is believed to be most responsible for the risk of psychosis and impaired driving and cognition.24,28
CBD MAY PROTECT AGAINST ADVERSE EFFECTS
Studies of CBD alone are limited to preclinical data.29 Evidence suggests that CBD alone or combined with THC can suppress chronic neuropathic pain, and that CBD may have a protective effect after nerve injury.30
Nabiximols, an oromucosal spray preparation with equal amounts of THC and CBD, has been approved in Canada as well as in European countries including the United Kingdom. Although its use has not been associated with many of the adverse effects of inhaled cannabis,30–32 evidence of efficacy from clinical trials has been mixed.
Lynch et al,31 in a 2014 randomized, double-blind, placebo-controlled crossover pilot study31 evaluated nabiximols in 16 patients with neuropathic pain related to chemotherapy. No statistically significant difference was found between treatment and placebo. However, the trial was underpowered.
Serpell et al,32 in a 2014 European randomized, placebo-controlled parallel-group study, evaluated 246 patients with peripheral neuropathy with allodynia, with 128 receiving active treatment (THC-CBD oromucosal spray) and 118 receiving placebo. Over the 15-week study, participants continued their current analgesic treatments.
Pain was reduced in the treatment group, but the difference from placebo was not statistically significant. However, the treatment group reported significantly better sleep quality and Patient Global Impression of Change measures (reflecting a patient’s belief of treatment efficacy).
META-ANALYSES CONFIRM EFFECT
Three meta-analyses of available studies of the effects of cannabis on neuropathic pain have been completed.
Andreae et al, 2015: 5 trials, 178 patients
Andreae et al1 evaluated 5 randomized controlled trials in 178 patients in North America. All had had neuropathy for at least 3 months, with a pain level of at least about 3 on a scale of 10. Two studies had patients with HIV-related neuropathy; the other 3 involved patients with neuropathy related to trauma, diabetes, complex regional pain syndrome, or spinal cord injury. All trials used whole cannabis plant provided by NIDA, and the main outcomes were patient-reported pain scales. No study evaluated pain beyond 2 weeks after trial termination.
They found that 1 of every 5 to 6 patients treated with cannabis had at least a 30% pain reduction.
Nugent et al, 2017: 13 trials, 246 patients
Nugent et al33 reviewed 13 trials in 246 patients that evaluated the effects of different cannabis-based preparations on either central or peripheral neuropathic pain from various conditions. Actively treated patients were more likely to report a 30% improvement in neuropathic pain. Again, studies tended to be small and brief.
Cochrane review, 2018: 16 trials, 1,750 patients
A Cochrane review34 analyzed 16 trials (in 1,750 patients) lasting 2 to 26 weeks. Treatments included an oromucosal spray with a plant-derived combination of THC and CBD, nabilone, inhaled herbal cannabis, and plant-derived THC.
With cannabis-based treatments, significantly more people achieved 50% or greater pain relief than with placebo (21% vs 17%, number needed to treat 20); 30% pain reduction was achieved in 39% of treated patients vs 33% of patients taking placebo (number needed to treat 11).
On the other hand, significantly more participants withdrew from studies because of adverse events with cannabis-based treatments than placebo (10% vs 5%), with psychiatric disorders occurring in 17% of patients receiving active treatment vs 5% of those receiving placebo (number needed to harm 10).
The primary studies suffered from methodologic limitations including small size, short duration, and inconsistency of formulations and study designs. Further evaluation of long-term efficacy, tolerability, and addiction potential is critical to determine the risk-benefit ratio.
RISKS OF CANNABIS USE
Like any drug therapy, cannabis has effects that may limit its use. Cannabis can affect a person’s psyche, physiology, and lifestyle.
Impaired attention, task speed
Neurocognitive changes associated with cannabis use—especially dizziness, fatigue, and slowed task-switching—could affect driving and other complex tasks. Evidence indicates that such activities should be avoided in the hours after treatment.26,27,32,33
Concern over brain development
Most worrisome is the effect of long-term cannabis use on brain development in young adults. Regular use of cannabis at an early age is associated with lower IQ, decline in school performance, and lower rates of high school graduation.35
Avoid in psychiatric patients
It is unlikely that cannabis can be safely used in patients with psychiatric illnesses. Anxiety, depression, and psychotic disorders can be exacerbated by the regular use of cannabis, and the risk of developing these conditions is increased while using cannabis.36,37
High concentrations of THC (the highest concentration used in the above studies was 9.5%) can cause anxiety, paranoia, and psychosis.
Respiratory effects
Long-term cannabis smoking may cause wheezing, cough, dyspnea, and exacerbations of chronic bronchitis. There is some evidence that symptoms improve after stopping smoking.33,38
SHOULD WE RECOMMEND CANNABIS?
Where cannabis can be legally used, doctors should be familiar with the literature and its limitations so that they can counsel patients on the best use and potential risks and benefits of cannabis treatment.
A recent conceptualization of pain suggests that a pain score reflects a composite of sensory factors (eg, tissue damage), cognitive factors (eg, beliefs about pain), and affective factors (eg, anxiety, depression).39 Physicians should keep this in mind when evaluating patients to better assess the risks and benefits of cannabis. While pharmacotherapy may address sensory factors, cognitive behavioral therapy may help alter beliefs about the pain as well as anxiety and depressive symptoms that might influence subjective reports.
Ideally, patients being considered for cannabis treatment would have a type of neuropathic pain proven to respond to cannabis in randomized, controlled studies, as well as evidence of failed first-line treatments.
Relative contraindications include depression, anxiety, substance use, psychotic disorders, and respiratory conditions, and these should also be considered.
Although current research shows an analgesic benefit of cannabis on neuropathic pain comparable to that of gabapentin,40 further investigation is needed to better evaluate long-term safety, efficacy, and interactions with standard therapies. Until we have a more complete picture, we should use the current literature, along with a thorough knowledge of each patient, to determine if the benefits of cannabis therapy outweigh the risks.
Acknowledgments: We thank Camillo Ferrari, BS, and Christina McMahon, BA, for their helpful comments.
- Andreae MH, Carter GM, Shaparin N, et al. Inhaled cannabis for chronic neuropathic pain: a meta-analysis of individual patient data. J Pain 2015; 16(12):1221–1232. doi:10.1016/j.jpain.2015.07.009
- National Institute of Neurological Disorders and Stroke. Peripheral Neuropathy Fact Sheet. www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Peripheral-Neuropathy-Fact-Sheet. Accessed November 14, 2018.
- Mold JW, Vesely SK, Keyl BA, Schenk JB, Roberts M. The prevalence, predictors, and consequences of peripheral sensory neuropathy in older adults. J Am Board Fam Med 2004; 17(5):308–318. doi:10.3122/jabfm.17.5.309
- Bansal D, Gudala K, Muthyala H, Esam HP, Nayakallu R, Bhansali A. Prevalence and risk factors of developing peripheral diabetic neuropathy in type 2 diabetes mellitus in a tertiary care setting. J Diabetes Investig 2014; 5(6):714–721. doi:10.1111/jdi.12223
- Finnerup NB, Haroutounian S, Kamerman P, et al. Neuropathic pain: an updated grading system for research and clinical practice. Pain 2016; 157(8):1599–1606. doi:10.1097/j.pain.0000000000000492
- Maldonado R, Banos JE, Cabanero D. The endocannabinoid system and neuropathic pain. Pain 2016; 157(suppl 1):S23–S32. doi:10.1097/j.pain.0000000000000428
- Zeng L, Alongkronrusmee D, van Rijn RM. An integrated perspective on diabetic, alcoholic, and drug-induced neuropathy, etiology, and treatment in the US. J Pain Res 2017; 10:219–228. doi:10.2147/JPR.S125987
- Callaghan BC, Price RS, Feldman EL. Distal symmetric polyneuropathy: a review. JAMA 2015; 314(20):2172–2181. doi:10.1001/jama.2015.13611
- Adams AS, Callaghan B, Grant RW. Overcoming barriers to diabetic polyneuropathy management in primary care. Healthc (Amst) 2017; 5(4):171–173. doi:10.1016/j.hjdsi.2016.10.003
- Gwak YS, Kim HY, Lee BH, Yang CH. Combined approaches for the relief of spinal cord injury-induced neuropathic pain. Complement Ther Med 2016; 25:27–33. doi:10.1016/j.ctim.2015.12.021
- Majithia N, Loprinzi CL, Smith TJ. New practical approaches to chemotherapy-induced neuropathic pain: prevention, assessment, and treatment. Oncology 2016; 30(11):1020–1029. pmid:27854104
- Grotenhermen F. Cannabinoids and the endocannabinoid system. Cannabinoids 2006; 1(1):10–14.
- Hill KP. Medical marijuana for treatment of chronic pain and other medical and psychiatric problems: a clinical review. JAMA 2015; 313(24):2474–2483. doi:10.1001/jama.2015.6199
- Campos AC, Fogaça MV, Scarante FF, et al. Plastic and neuroprotective mechanisms involved in the therapeutic effects of cannabidiol in psychiatric disorders. Front Pharmacol 2017; 8:269. doi:10.3389/fphar.2017.00269
- Russo EB. Taming THC: potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br J Pharmacol 2011; 163(7):1344–1364. doi:10.1111/j.1476-5381.2011.01238.x
- Freitas HR, Isaac AR, Malcher-Lopes R, Diaz BL, Trevenzoli IH, De Melo Reis RA. Polyunsaturated fatty acids and endocannabinoids in health and disease. Nutr Neurosci 2017; Jul 7: 1–20. doi:10.1080/1028415X.2017.1347373
- Hillard CJ. Circulating endocannabinoids: from whence do they come and where are they going? Neuropsychopharmacology 2018; 43(1):155–172. doi:10.1038/npp.2017.130
- Herkenham M, Lynn AB, Johnson MR, Melvin LS, de Costa BR, Rice KC. Characterization and localization of cannabinoid receptors in rat brain: a quantitative in vitro autoradiographic study. J Neurosci 1991; 11(2):563–583. pmid:1992016
- Tsou K, Brown S, Sañudo-Peña MC, Mackie K, Walker JM. Immunohistochemical distribution of cannabinoid CB1 receptors in the rat central nervous system. Neuroscience1998; 83(2):393–411. pmid:9460749
- Russo EB, Hohmann AG. Role of cannabinoids in pain management. In: Deer TR, Leong MS, ed. Comprehensve Treatment of Chronic Pain by Medical, Interventional, and Integrative Approaches. New York, NY: Springer; 2013:181–193.
- Vranken JH. Elucidation of pathophysiology and treatment of neuropathic pain. Cent Nerv Syst Agents Med Chem 2012; 12(4):304–314. pmid:23033930
- Yamanaka H, Noguchi K. Pathophysiology of neuropathic pain: molecular mechanisms underlying central sensitization in the dorsal horn in neuropathic pain. Brain Nerve 2012; 64(11):1255–1265. Japanese. pmid:23131736
- Ellis RJ, Toperoff W, Vaida F, et al. Smoked medicinal cannabis for neuropathic pain in HIV: a randomized, crossover clinical trial. Neuropsychopharmacology 2009; 34(3):672–680. doi:10.1038/npp.2008.120
- Ware MA, Wang T, Shapiro S, et al. Smoked cannabis for chronic neuropathic pain: a randomized controlled trial. CMAJ 2010; 182(14):E694–E701. doi:10.1503/cmaj.091414
- Wilsey B, Marcotte T, Tsodikov A, et al. A randomized, placebo-controlled, crossover trial of cannabis cigarettes in neuropathic pain. J Pain 2008; 9(6):506–521. doi:10.1016/j.jpain.2007.12.010
- Wilsey B, Marcotte T, Deutsch R, Gouaux B, Sakai S, Donaghe H. Low-dose vaporized cannabis significantly improves neuropathic pain. J Pain 2013; 14(2):136–148. doi:10.1016/j.jpain.2012.10.009
- Wallace MS, Marcotte TD, Umlauf A, Gouaux B, Atkinson JH. Efficacy of inhaled cannabis on painful diabetic neuropathy. J Pain 2015; 16(7):616–627. doi:10.1016/j.jpain.2015.03.008
- Vergara D, Bidwell LC, Gaudino R, et al. Compromised external validity: federally produced cannabis does not reflect legal markets. Scientific Reports. 2017; 7(1):1-8. doi:10.1038/srep46528
- Nurmikko TJ, Serpell MG, Hoggart B, Toomey PJ, Morlion BJ, Haines D. Sativex successfully treats neuropathic pain characterized by allodynia: a randomized, double-blind, placebo-controlled clinical trial. Pain 2007; 133(1–3):210–220. doi:10.1016/j.pain.2007.08.028
- Philpott HT, O’Brien M, McDougall JJ. Attenuation of early phase inflammation by cannabidiol prevents pain and nerve damage in rat osteoarthritis. Pain 2017; 158(12):2442–2451. doi:10.1097/j.pain.0000000000001052
- Lynch ME, Cesar-Rittenberg P, Hohmann AG. A double-blind, placebo-controlled, crossover pilot trial with extension using an oral mucosal cannabinoid extract for treatment of chemotherapy-induced neuropathic pain. J Pain Symptom Manage 2014; 47(1):166–173. doi:10.1016/j.jpainsymman.2013.02.018
- Serpell M, Ratcliffe S, Hovorka J, et al. A double-blind, randomized, placebo-controlled, parallel group study of THC/CBD spray in peripheral neuropathic pain treatment. Eur J Pain 2014; 18(7):999–1012. doi:10.1002/j.1532-2149.2013.00445.x
- Nugent SM, Morasco BJ, O’Neil ME, et al. The effects of cannabis among adults with chronic pain and an overview of general harms: a systematic review. Ann Intern Med 2017; 167(5):319–331. doi:10.7326/M17-0155
- Mücke M, Phillips T, Radbruch L, Petzke F, Häuser W. Cannabis-based medicines for chronic neuropathic pain in adults. Cochrane Database Syst Rev 2018; 3:CD012182. doi:10.1002/14651858.CD012182.pub2
- Castellanos-Ryan N, Pingault JB, Parent S, Vitaro F, Tremblay RE, Seguin JR. Adolescent cannabis use, change in neurocognitive function, and high-school graduation: a longitudinal study from early adolescence to young adulthood. Dev Psychopathol 2017; 29(4):1253–1266. doi:10.1017/S0954579416001280
- Karila L, Roux P, Benyamina A, et al. Acute and long-term effects of cannabis use: a review. Curr Pharm Des 2014; 20(25):4112–4118. pmid:24001294
- Johns A. Psychiatric effects of cannabis. Br J Psychiatry 2001; 178:116–122. pmid:11157424
- National Academies of Science, Engineering, and Medicine. The health effects of cannabis and cannabinoids: the current state of evidence and recommendations for research. Washington, DC: The National Academy Press; 2017. doi:10.17226/24625
- Modesto-Lowe V, Griard L, Chaplin M. Cancer pain in the opioid-addicted patient: can we treat it right? J Opioid Manag 2012; 8(3):167–175. doi:10.5055/jom.2012.0113
- Grant I. Medicinal cannabis and painful sensory neuropathy. Virtual Mentor 2013; 15(5):466–469. doi:10.1001/virtualmentor.2013.15.5.oped1-1305
Marijuana, which is still illegal under federal law but legal in 30 states for medical purposes as of this writing, has shown promising results for treating peripheral neuropathy. Studies suggest that cannabis may be an option for patients whose pain responds poorly to standard treatments; however, its use may be restricted by cognitive and psychiatric adverse effects, particularly at high doses.1
In this article, we discuss the basic pharmacology of cannabis and how it may affect neuropathic pain. We review clinical trials on its use for peripheral neuropathy and provide guidance for its use.
PERIPHERAL NEUROPATHY IS COMMON AND COMPLEX
An estimated 20 million people in the United States suffer from neuropathic pain. The prevalence is higher in certain populations, with 26% of people over age 65 and 30% of patients with diabetes mellitus affected.2–4
Peripheral neuropathy is a complex, chronic state that occurs when nerve fibers are damaged, dysfunctional, or injured, sending incorrect signals to pain centers in the central nervous system.5 It is characterized by weakness, pain, and paresthesias that typically begin in the hands or feet and progress proximally.4 Symptoms depend on the number and types of nerves affected.
In many cases, peripheral neuropathy is idiopathic, but common causes include diabetes, alcoholism, human immunodeficiency virus (HIV) infection, and autoimmune disease. Others include toxicity from chemotherapy and heavy metals.
Peripheral neuropathy significantly worsens quality of life and function. Many patients experience emotional, cognitive, and functional problems, resulting in high rates of medical and psychiatric comorbidities and occupational impairment.4,6,7 Yet despite its clinical and epidemiologic significance, it is often undertreated.8
STANDARD TREATMENTS INADEQUATE
Peripheral neuropathy occurs in patients with a wide range of comorbidities and is especially difficult to treat. Mainstays of therapy include anticonvulsants, tricyclic antidepressants, and serotonin-norepinephrine reuptake inhibitors.9 A more invasive option is spinal cord stimulation.
These treatments can have considerable adverse effects, and response rates remain suboptimal, with pain relief insufficient to improve quality of life for many patients.9,10 Better treatments are needed to improve clinical outcomes and patient experience.11
CANNABIS: A MIX OF COMPOUNDS
Cannabis sativa has been used as an analgesic for centuries. The plant contains more than 400 chemical compounds and is often used for its euphoric properties. Long-term use may lead to addiction and cognitive impairment.12,13
Tetrahydrocannabinol (THC) and cannabidiol (CBD) are the main components and the 2 best-studied cannabinoids with analgesic effects.
THC is the primary psychoactive component of cannabis. Its effects include relaxation, altered perception, heightened sensations, increased libido, and perceptual distortions of time and space. Temporary effects may include decreased short-term memory, dry mouth, impaired motor function, conjunctival injection, paranoia, and anxiety.
CBD is nonpsychoactive and has anti-inflammatory and antioxidant properties. It has been shown to reduce pain and inflammation without the effects of THC.14
Other compounds in the cannabis plant include phytocannabinoids, flavonoids, and tapenoids, which may produce individual, interactive, or synergistic effects.15 Different strains of cannabis have varying amounts of the individual components, making comparisons among clinical studies difficult.
THE ENDOCANNABINOID SYSTEM
The endogenous mammalian cannabinoid system plays a regulatory role in the development, homeostasis, and neuroplasticity of the central nervous system. It is also involved in modulating pain transmission in the nociceptive pathway.
Two of the most abundant cannabinoid endogenous ligands are anandamide and 2-arachidonylglycerol.9 These endocannabinoids are produced on demand in the central nervous system to reduce pain by acting as a circuit breaker.16–18 They target the G protein-coupled cannabinoid receptors CB1 and CB2, located throughout the central and peripheral nervous system and in organs and tissues.12
CB1 receptors are found primarily in the central nervous system, specifically in areas involved in movement, such as the basal ganglia and cerebellum, as well as in areas involved in memory, such as the hippocampus.12 They are also abundant in brain regions implicated in conducting and modulating pain signals, including the periaqueductal gray and the dorsal horn of the spinal cord.16–20
CB2 receptors are mostly found in peripheral tissues and organs, mainly those involved in the immune system, including splenic, tonsillar, and hematopoietic cells.12 They help regulate inflammation, allodynia, and hyperalgesia.17
Modifying response to injury
Following a nerve injury, neurons along the nociceptive pathway may become more reactive and responsive in a process known as sensitization.21 The process involves a cascade of cellular events that result in sprouting of pain-sensitive nerve endings.21,22
Cannabinoids are thought to reduce pain by modifying these cellular events. They also inhibit nociceptive conduction in the dorsal horn of the spinal cord and in the ascending spinothalamic tract.20 CB1 receptors found in nociceptive terminals along the peripheral nervous system impede pain conduction, while activation of CB2 receptors in immune cells decreases the release of nociceptive agents.
STUDIES OF CANNABIS FOR NEUROPATHIC PAIN
A number of studies have evaluated cannabis for treating neuropathic pain. Overall, available data support the efficacy of smoked or inhaled cannabis in its flower form when used as monotherapy or adjunctive therapy for relief of neuropathic pain of various etiologies. Many studies also report secondary benefits, including better sleep and functional improvement.23,24
However, adverse effects are common, especially at high doses, and include difficulty concentrating, lightheadedness, fatigue, and tachycardia. More serious reported adverse effects include anxiety, paranoia, and psychosis.
Wilsey et al, 2008: Neuropathic pain reduced
Wilsey et al25 conducted a double-blind, placebo-controlled crossover study that assessed the effects of smoking cannabis in 38 patients with central or peripheral neuropathic pain. Participants were assigned to smoke either high- or low-dose cannabis (7% or 3.5% delta-9-THC) or placebo cigarettes. Cigarettes were smoked during treatment sessions using the following regimen: 2 puffs at 60 minutes from baseline, 3 puffs at 120 minutes, and 4 puffs at 180 minutes. Patients were assessed after each set of puffs and for 2 hours afterwards. The primary outcome was spontaneous relief of pain as measured by a visual analog scale.
Pain intensity was comparable and significantly reduced in both treatment groups compared with placebo. At the high dose, some participants experienced neurocognitive impairment in attention, learning, memory, and psychomotor speed; only learning and memory declined at the low dose.
Ellis et al, 2009: Pain reduction in HIV neuropathy
Ellis et al23 conducted a double-blind, placebo-controlled crossover trial in patients with HIV neuropathy that was unresponsive to at least 2 analgesics with different modes of action. During each treatment week, participants were randomly assigned to smoke either active cannabis or placebo, while continuing their standard therapy. Titration started at 4% THC and was adjusted based on tolerability and efficacy. Twenty-eight of the 34 enrolled patients completed both cannabis and placebo treatments. The principal outcome was change in pain intensity from baseline at the end of each week, using the Descriptor Differential Scale of Pain Intensity.
Of the 28 patients, 46% achieved an average pain reduction of 3.3 points (30%). One patient experienced cannabis-induced psychosis, and another developed an intractable cough, which resolved with smoking cessation.
Ware et al, 2010: Reduced posttraumatic or postsurgical neuropathic pain
Ware et al24 performed a randomized crossover trial in 21 patients with posttraumatic or postsurgical neuropathic pain. Participants inhaled 4 different formulations of cannabis (containing 0%, 2.5%, 6.0%, and 9.4% THC) during 4 14-day periods. They inhaled a 25-mg dose through a pipe 3 times a day for the first 5 days of each cycle, followed by a 9-day washout period. Daily average pain intensity was measured using a numeric rating scale. The investigators also assessed mood, sleep, quality of life, and adverse effects.
Patients in the 9.4% THC group reported significantly less pain and better sleep, with average pain scores decreasing from 6.1 to 5.4 on an 11-point scale. Although the benefit was modest, the authors noted that the pain had been refractory to standard treatments.
The number of reported adverse events increased with greater potency and were most commonly throat irritation, burning sensation, headache, dizziness, and fatigue. This study suggests that THC potency affects tolerability, with higher doses eliciting clinically important adverse effects, some of which may reduce the ability to perform activities of daily living, such as driving.
Wilsey et al, 2013: Use in resistant neuropathic pain
Wilsey et al26 conducted another double-blind, placebo-controlled crossover study assessing the effect of vaporized cannabis on central and peripheral neuropathic pain resistant to first-line pharmacotherapies. Dose-effect relationships were explored using medium-dose (3.5%), low-dose (1.3%), and placebo cannabis. The primary outcome measure was a 30% reduction in pain intensity based on a visual analog scale.
In the placebo group, 26% of patients achieved this vs 57% of the low-dose cannabis group and 61% of those receiving the medium dose. No significant difference was found between the 2 active doses in reducing neuropathic pain, and both were more effective than placebo. The number needed to treat to achieve a 30% reduction in pain was about 3 for both cannabis groups compared with placebo. Psychoactive effects were minimal, of short duration, and reversible.
Wallace et al, 2015: Use in diabetic peripheral neuropathy
Wallace et al27 conducted a randomized, double-blind, placebo-controlled crossover study evaluating cannabis for diabetic peripheral neuropathy in 16 patients. Each had experienced at least 6 months of neuropathic pain in their feet. The participants inhaled a single dose of 1%, 4%, or 7% THC cannabis or placebo. Spontaneous pain was reported with a visual analog scale and also tested with a foam brush and von Frey filament at intervals until 4 hours after treatment.
Pain scores were lower with treatment compared with placebo, with high-dose cannabis having the greatest analgesic effect. Pain reduction lasted for the full duration of the test. Cannabis recipients had declines in attention and working memory, with the high-dose group experiencing the greatest impact 15 minutes after treatment. High-dose recipients also had poorer scores on testing of quick task-switching, with the greatest effect at 2 hours.27
Research and market cannabis are not equal
Results of US studies must be qualified. Most have used cannabis provided by the National Institute of Drug Abuse (NIDA),23–26 which differs in potency from commercially available preparations. This limits the clinical usefulness of the analysis of benefits and risks.
Vergara et al28 found that NIDA varieties contained much lower THC levels and as much as 23 times the cannabinol content as cannabis in state-legalized markets.
Studies based on NIDA varieties likely underestimate the risks of consumer-purchased cannabis, as THC is believed to be most responsible for the risk of psychosis and impaired driving and cognition.24,28
CBD MAY PROTECT AGAINST ADVERSE EFFECTS
Studies of CBD alone are limited to preclinical data.29 Evidence suggests that CBD alone or combined with THC can suppress chronic neuropathic pain, and that CBD may have a protective effect after nerve injury.30
Nabiximols, an oromucosal spray preparation with equal amounts of THC and CBD, has been approved in Canada as well as in European countries including the United Kingdom. Although its use has not been associated with many of the adverse effects of inhaled cannabis,30–32 evidence of efficacy from clinical trials has been mixed.
Lynch et al,31 in a 2014 randomized, double-blind, placebo-controlled crossover pilot study31 evaluated nabiximols in 16 patients with neuropathic pain related to chemotherapy. No statistically significant difference was found between treatment and placebo. However, the trial was underpowered.
Serpell et al,32 in a 2014 European randomized, placebo-controlled parallel-group study, evaluated 246 patients with peripheral neuropathy with allodynia, with 128 receiving active treatment (THC-CBD oromucosal spray) and 118 receiving placebo. Over the 15-week study, participants continued their current analgesic treatments.
Pain was reduced in the treatment group, but the difference from placebo was not statistically significant. However, the treatment group reported significantly better sleep quality and Patient Global Impression of Change measures (reflecting a patient’s belief of treatment efficacy).
META-ANALYSES CONFIRM EFFECT
Three meta-analyses of available studies of the effects of cannabis on neuropathic pain have been completed.
Andreae et al, 2015: 5 trials, 178 patients
Andreae et al1 evaluated 5 randomized controlled trials in 178 patients in North America. All had had neuropathy for at least 3 months, with a pain level of at least about 3 on a scale of 10. Two studies had patients with HIV-related neuropathy; the other 3 involved patients with neuropathy related to trauma, diabetes, complex regional pain syndrome, or spinal cord injury. All trials used whole cannabis plant provided by NIDA, and the main outcomes were patient-reported pain scales. No study evaluated pain beyond 2 weeks after trial termination.
They found that 1 of every 5 to 6 patients treated with cannabis had at least a 30% pain reduction.
Nugent et al, 2017: 13 trials, 246 patients
Nugent et al33 reviewed 13 trials in 246 patients that evaluated the effects of different cannabis-based preparations on either central or peripheral neuropathic pain from various conditions. Actively treated patients were more likely to report a 30% improvement in neuropathic pain. Again, studies tended to be small and brief.
Cochrane review, 2018: 16 trials, 1,750 patients
A Cochrane review34 analyzed 16 trials (in 1,750 patients) lasting 2 to 26 weeks. Treatments included an oromucosal spray with a plant-derived combination of THC and CBD, nabilone, inhaled herbal cannabis, and plant-derived THC.
With cannabis-based treatments, significantly more people achieved 50% or greater pain relief than with placebo (21% vs 17%, number needed to treat 20); 30% pain reduction was achieved in 39% of treated patients vs 33% of patients taking placebo (number needed to treat 11).
On the other hand, significantly more participants withdrew from studies because of adverse events with cannabis-based treatments than placebo (10% vs 5%), with psychiatric disorders occurring in 17% of patients receiving active treatment vs 5% of those receiving placebo (number needed to harm 10).
The primary studies suffered from methodologic limitations including small size, short duration, and inconsistency of formulations and study designs. Further evaluation of long-term efficacy, tolerability, and addiction potential is critical to determine the risk-benefit ratio.
RISKS OF CANNABIS USE
Like any drug therapy, cannabis has effects that may limit its use. Cannabis can affect a person’s psyche, physiology, and lifestyle.
Impaired attention, task speed
Neurocognitive changes associated with cannabis use—especially dizziness, fatigue, and slowed task-switching—could affect driving and other complex tasks. Evidence indicates that such activities should be avoided in the hours after treatment.26,27,32,33
Concern over brain development
Most worrisome is the effect of long-term cannabis use on brain development in young adults. Regular use of cannabis at an early age is associated with lower IQ, decline in school performance, and lower rates of high school graduation.35
Avoid in psychiatric patients
It is unlikely that cannabis can be safely used in patients with psychiatric illnesses. Anxiety, depression, and psychotic disorders can be exacerbated by the regular use of cannabis, and the risk of developing these conditions is increased while using cannabis.36,37
High concentrations of THC (the highest concentration used in the above studies was 9.5%) can cause anxiety, paranoia, and psychosis.
Respiratory effects
Long-term cannabis smoking may cause wheezing, cough, dyspnea, and exacerbations of chronic bronchitis. There is some evidence that symptoms improve after stopping smoking.33,38
SHOULD WE RECOMMEND CANNABIS?
Where cannabis can be legally used, doctors should be familiar with the literature and its limitations so that they can counsel patients on the best use and potential risks and benefits of cannabis treatment.
A recent conceptualization of pain suggests that a pain score reflects a composite of sensory factors (eg, tissue damage), cognitive factors (eg, beliefs about pain), and affective factors (eg, anxiety, depression).39 Physicians should keep this in mind when evaluating patients to better assess the risks and benefits of cannabis. While pharmacotherapy may address sensory factors, cognitive behavioral therapy may help alter beliefs about the pain as well as anxiety and depressive symptoms that might influence subjective reports.
Ideally, patients being considered for cannabis treatment would have a type of neuropathic pain proven to respond to cannabis in randomized, controlled studies, as well as evidence of failed first-line treatments.
Relative contraindications include depression, anxiety, substance use, psychotic disorders, and respiratory conditions, and these should also be considered.
Although current research shows an analgesic benefit of cannabis on neuropathic pain comparable to that of gabapentin,40 further investigation is needed to better evaluate long-term safety, efficacy, and interactions with standard therapies. Until we have a more complete picture, we should use the current literature, along with a thorough knowledge of each patient, to determine if the benefits of cannabis therapy outweigh the risks.
Acknowledgments: We thank Camillo Ferrari, BS, and Christina McMahon, BA, for their helpful comments.
Marijuana, which is still illegal under federal law but legal in 30 states for medical purposes as of this writing, has shown promising results for treating peripheral neuropathy. Studies suggest that cannabis may be an option for patients whose pain responds poorly to standard treatments; however, its use may be restricted by cognitive and psychiatric adverse effects, particularly at high doses.1
In this article, we discuss the basic pharmacology of cannabis and how it may affect neuropathic pain. We review clinical trials on its use for peripheral neuropathy and provide guidance for its use.
PERIPHERAL NEUROPATHY IS COMMON AND COMPLEX
An estimated 20 million people in the United States suffer from neuropathic pain. The prevalence is higher in certain populations, with 26% of people over age 65 and 30% of patients with diabetes mellitus affected.2–4
Peripheral neuropathy is a complex, chronic state that occurs when nerve fibers are damaged, dysfunctional, or injured, sending incorrect signals to pain centers in the central nervous system.5 It is characterized by weakness, pain, and paresthesias that typically begin in the hands or feet and progress proximally.4 Symptoms depend on the number and types of nerves affected.
In many cases, peripheral neuropathy is idiopathic, but common causes include diabetes, alcoholism, human immunodeficiency virus (HIV) infection, and autoimmune disease. Others include toxicity from chemotherapy and heavy metals.
Peripheral neuropathy significantly worsens quality of life and function. Many patients experience emotional, cognitive, and functional problems, resulting in high rates of medical and psychiatric comorbidities and occupational impairment.4,6,7 Yet despite its clinical and epidemiologic significance, it is often undertreated.8
STANDARD TREATMENTS INADEQUATE
Peripheral neuropathy occurs in patients with a wide range of comorbidities and is especially difficult to treat. Mainstays of therapy include anticonvulsants, tricyclic antidepressants, and serotonin-norepinephrine reuptake inhibitors.9 A more invasive option is spinal cord stimulation.
These treatments can have considerable adverse effects, and response rates remain suboptimal, with pain relief insufficient to improve quality of life for many patients.9,10 Better treatments are needed to improve clinical outcomes and patient experience.11
CANNABIS: A MIX OF COMPOUNDS
Cannabis sativa has been used as an analgesic for centuries. The plant contains more than 400 chemical compounds and is often used for its euphoric properties. Long-term use may lead to addiction and cognitive impairment.12,13
Tetrahydrocannabinol (THC) and cannabidiol (CBD) are the main components and the 2 best-studied cannabinoids with analgesic effects.
THC is the primary psychoactive component of cannabis. Its effects include relaxation, altered perception, heightened sensations, increased libido, and perceptual distortions of time and space. Temporary effects may include decreased short-term memory, dry mouth, impaired motor function, conjunctival injection, paranoia, and anxiety.
CBD is nonpsychoactive and has anti-inflammatory and antioxidant properties. It has been shown to reduce pain and inflammation without the effects of THC.14
Other compounds in the cannabis plant include phytocannabinoids, flavonoids, and tapenoids, which may produce individual, interactive, or synergistic effects.15 Different strains of cannabis have varying amounts of the individual components, making comparisons among clinical studies difficult.
THE ENDOCANNABINOID SYSTEM
The endogenous mammalian cannabinoid system plays a regulatory role in the development, homeostasis, and neuroplasticity of the central nervous system. It is also involved in modulating pain transmission in the nociceptive pathway.
Two of the most abundant cannabinoid endogenous ligands are anandamide and 2-arachidonylglycerol.9 These endocannabinoids are produced on demand in the central nervous system to reduce pain by acting as a circuit breaker.16–18 They target the G protein-coupled cannabinoid receptors CB1 and CB2, located throughout the central and peripheral nervous system and in organs and tissues.12
CB1 receptors are found primarily in the central nervous system, specifically in areas involved in movement, such as the basal ganglia and cerebellum, as well as in areas involved in memory, such as the hippocampus.12 They are also abundant in brain regions implicated in conducting and modulating pain signals, including the periaqueductal gray and the dorsal horn of the spinal cord.16–20
CB2 receptors are mostly found in peripheral tissues and organs, mainly those involved in the immune system, including splenic, tonsillar, and hematopoietic cells.12 They help regulate inflammation, allodynia, and hyperalgesia.17
Modifying response to injury
Following a nerve injury, neurons along the nociceptive pathway may become more reactive and responsive in a process known as sensitization.21 The process involves a cascade of cellular events that result in sprouting of pain-sensitive nerve endings.21,22
Cannabinoids are thought to reduce pain by modifying these cellular events. They also inhibit nociceptive conduction in the dorsal horn of the spinal cord and in the ascending spinothalamic tract.20 CB1 receptors found in nociceptive terminals along the peripheral nervous system impede pain conduction, while activation of CB2 receptors in immune cells decreases the release of nociceptive agents.
STUDIES OF CANNABIS FOR NEUROPATHIC PAIN
A number of studies have evaluated cannabis for treating neuropathic pain. Overall, available data support the efficacy of smoked or inhaled cannabis in its flower form when used as monotherapy or adjunctive therapy for relief of neuropathic pain of various etiologies. Many studies also report secondary benefits, including better sleep and functional improvement.23,24
However, adverse effects are common, especially at high doses, and include difficulty concentrating, lightheadedness, fatigue, and tachycardia. More serious reported adverse effects include anxiety, paranoia, and psychosis.
Wilsey et al, 2008: Neuropathic pain reduced
Wilsey et al25 conducted a double-blind, placebo-controlled crossover study that assessed the effects of smoking cannabis in 38 patients with central or peripheral neuropathic pain. Participants were assigned to smoke either high- or low-dose cannabis (7% or 3.5% delta-9-THC) or placebo cigarettes. Cigarettes were smoked during treatment sessions using the following regimen: 2 puffs at 60 minutes from baseline, 3 puffs at 120 minutes, and 4 puffs at 180 minutes. Patients were assessed after each set of puffs and for 2 hours afterwards. The primary outcome was spontaneous relief of pain as measured by a visual analog scale.
Pain intensity was comparable and significantly reduced in both treatment groups compared with placebo. At the high dose, some participants experienced neurocognitive impairment in attention, learning, memory, and psychomotor speed; only learning and memory declined at the low dose.
Ellis et al, 2009: Pain reduction in HIV neuropathy
Ellis et al23 conducted a double-blind, placebo-controlled crossover trial in patients with HIV neuropathy that was unresponsive to at least 2 analgesics with different modes of action. During each treatment week, participants were randomly assigned to smoke either active cannabis or placebo, while continuing their standard therapy. Titration started at 4% THC and was adjusted based on tolerability and efficacy. Twenty-eight of the 34 enrolled patients completed both cannabis and placebo treatments. The principal outcome was change in pain intensity from baseline at the end of each week, using the Descriptor Differential Scale of Pain Intensity.
Of the 28 patients, 46% achieved an average pain reduction of 3.3 points (30%). One patient experienced cannabis-induced psychosis, and another developed an intractable cough, which resolved with smoking cessation.
Ware et al, 2010: Reduced posttraumatic or postsurgical neuropathic pain
Ware et al24 performed a randomized crossover trial in 21 patients with posttraumatic or postsurgical neuropathic pain. Participants inhaled 4 different formulations of cannabis (containing 0%, 2.5%, 6.0%, and 9.4% THC) during 4 14-day periods. They inhaled a 25-mg dose through a pipe 3 times a day for the first 5 days of each cycle, followed by a 9-day washout period. Daily average pain intensity was measured using a numeric rating scale. The investigators also assessed mood, sleep, quality of life, and adverse effects.
Patients in the 9.4% THC group reported significantly less pain and better sleep, with average pain scores decreasing from 6.1 to 5.4 on an 11-point scale. Although the benefit was modest, the authors noted that the pain had been refractory to standard treatments.
The number of reported adverse events increased with greater potency and were most commonly throat irritation, burning sensation, headache, dizziness, and fatigue. This study suggests that THC potency affects tolerability, with higher doses eliciting clinically important adverse effects, some of which may reduce the ability to perform activities of daily living, such as driving.
Wilsey et al, 2013: Use in resistant neuropathic pain
Wilsey et al26 conducted another double-blind, placebo-controlled crossover study assessing the effect of vaporized cannabis on central and peripheral neuropathic pain resistant to first-line pharmacotherapies. Dose-effect relationships were explored using medium-dose (3.5%), low-dose (1.3%), and placebo cannabis. The primary outcome measure was a 30% reduction in pain intensity based on a visual analog scale.
In the placebo group, 26% of patients achieved this vs 57% of the low-dose cannabis group and 61% of those receiving the medium dose. No significant difference was found between the 2 active doses in reducing neuropathic pain, and both were more effective than placebo. The number needed to treat to achieve a 30% reduction in pain was about 3 for both cannabis groups compared with placebo. Psychoactive effects were minimal, of short duration, and reversible.
Wallace et al, 2015: Use in diabetic peripheral neuropathy
Wallace et al27 conducted a randomized, double-blind, placebo-controlled crossover study evaluating cannabis for diabetic peripheral neuropathy in 16 patients. Each had experienced at least 6 months of neuropathic pain in their feet. The participants inhaled a single dose of 1%, 4%, or 7% THC cannabis or placebo. Spontaneous pain was reported with a visual analog scale and also tested with a foam brush and von Frey filament at intervals until 4 hours after treatment.
Pain scores were lower with treatment compared with placebo, with high-dose cannabis having the greatest analgesic effect. Pain reduction lasted for the full duration of the test. Cannabis recipients had declines in attention and working memory, with the high-dose group experiencing the greatest impact 15 minutes after treatment. High-dose recipients also had poorer scores on testing of quick task-switching, with the greatest effect at 2 hours.27
Research and market cannabis are not equal
Results of US studies must be qualified. Most have used cannabis provided by the National Institute of Drug Abuse (NIDA),23–26 which differs in potency from commercially available preparations. This limits the clinical usefulness of the analysis of benefits and risks.
Vergara et al28 found that NIDA varieties contained much lower THC levels and as much as 23 times the cannabinol content as cannabis in state-legalized markets.
Studies based on NIDA varieties likely underestimate the risks of consumer-purchased cannabis, as THC is believed to be most responsible for the risk of psychosis and impaired driving and cognition.24,28
CBD MAY PROTECT AGAINST ADVERSE EFFECTS
Studies of CBD alone are limited to preclinical data.29 Evidence suggests that CBD alone or combined with THC can suppress chronic neuropathic pain, and that CBD may have a protective effect after nerve injury.30
Nabiximols, an oromucosal spray preparation with equal amounts of THC and CBD, has been approved in Canada as well as in European countries including the United Kingdom. Although its use has not been associated with many of the adverse effects of inhaled cannabis,30–32 evidence of efficacy from clinical trials has been mixed.
Lynch et al,31 in a 2014 randomized, double-blind, placebo-controlled crossover pilot study31 evaluated nabiximols in 16 patients with neuropathic pain related to chemotherapy. No statistically significant difference was found between treatment and placebo. However, the trial was underpowered.
Serpell et al,32 in a 2014 European randomized, placebo-controlled parallel-group study, evaluated 246 patients with peripheral neuropathy with allodynia, with 128 receiving active treatment (THC-CBD oromucosal spray) and 118 receiving placebo. Over the 15-week study, participants continued their current analgesic treatments.
Pain was reduced in the treatment group, but the difference from placebo was not statistically significant. However, the treatment group reported significantly better sleep quality and Patient Global Impression of Change measures (reflecting a patient’s belief of treatment efficacy).
META-ANALYSES CONFIRM EFFECT
Three meta-analyses of available studies of the effects of cannabis on neuropathic pain have been completed.
Andreae et al, 2015: 5 trials, 178 patients
Andreae et al1 evaluated 5 randomized controlled trials in 178 patients in North America. All had had neuropathy for at least 3 months, with a pain level of at least about 3 on a scale of 10. Two studies had patients with HIV-related neuropathy; the other 3 involved patients with neuropathy related to trauma, diabetes, complex regional pain syndrome, or spinal cord injury. All trials used whole cannabis plant provided by NIDA, and the main outcomes were patient-reported pain scales. No study evaluated pain beyond 2 weeks after trial termination.
They found that 1 of every 5 to 6 patients treated with cannabis had at least a 30% pain reduction.
Nugent et al, 2017: 13 trials, 246 patients
Nugent et al33 reviewed 13 trials in 246 patients that evaluated the effects of different cannabis-based preparations on either central or peripheral neuropathic pain from various conditions. Actively treated patients were more likely to report a 30% improvement in neuropathic pain. Again, studies tended to be small and brief.
Cochrane review, 2018: 16 trials, 1,750 patients
A Cochrane review34 analyzed 16 trials (in 1,750 patients) lasting 2 to 26 weeks. Treatments included an oromucosal spray with a plant-derived combination of THC and CBD, nabilone, inhaled herbal cannabis, and plant-derived THC.
With cannabis-based treatments, significantly more people achieved 50% or greater pain relief than with placebo (21% vs 17%, number needed to treat 20); 30% pain reduction was achieved in 39% of treated patients vs 33% of patients taking placebo (number needed to treat 11).
On the other hand, significantly more participants withdrew from studies because of adverse events with cannabis-based treatments than placebo (10% vs 5%), with psychiatric disorders occurring in 17% of patients receiving active treatment vs 5% of those receiving placebo (number needed to harm 10).
The primary studies suffered from methodologic limitations including small size, short duration, and inconsistency of formulations and study designs. Further evaluation of long-term efficacy, tolerability, and addiction potential is critical to determine the risk-benefit ratio.
RISKS OF CANNABIS USE
Like any drug therapy, cannabis has effects that may limit its use. Cannabis can affect a person’s psyche, physiology, and lifestyle.
Impaired attention, task speed
Neurocognitive changes associated with cannabis use—especially dizziness, fatigue, and slowed task-switching—could affect driving and other complex tasks. Evidence indicates that such activities should be avoided in the hours after treatment.26,27,32,33
Concern over brain development
Most worrisome is the effect of long-term cannabis use on brain development in young adults. Regular use of cannabis at an early age is associated with lower IQ, decline in school performance, and lower rates of high school graduation.35
Avoid in psychiatric patients
It is unlikely that cannabis can be safely used in patients with psychiatric illnesses. Anxiety, depression, and psychotic disorders can be exacerbated by the regular use of cannabis, and the risk of developing these conditions is increased while using cannabis.36,37
High concentrations of THC (the highest concentration used in the above studies was 9.5%) can cause anxiety, paranoia, and psychosis.
Respiratory effects
Long-term cannabis smoking may cause wheezing, cough, dyspnea, and exacerbations of chronic bronchitis. There is some evidence that symptoms improve after stopping smoking.33,38
SHOULD WE RECOMMEND CANNABIS?
Where cannabis can be legally used, doctors should be familiar with the literature and its limitations so that they can counsel patients on the best use and potential risks and benefits of cannabis treatment.
A recent conceptualization of pain suggests that a pain score reflects a composite of sensory factors (eg, tissue damage), cognitive factors (eg, beliefs about pain), and affective factors (eg, anxiety, depression).39 Physicians should keep this in mind when evaluating patients to better assess the risks and benefits of cannabis. While pharmacotherapy may address sensory factors, cognitive behavioral therapy may help alter beliefs about the pain as well as anxiety and depressive symptoms that might influence subjective reports.
Ideally, patients being considered for cannabis treatment would have a type of neuropathic pain proven to respond to cannabis in randomized, controlled studies, as well as evidence of failed first-line treatments.
Relative contraindications include depression, anxiety, substance use, psychotic disorders, and respiratory conditions, and these should also be considered.
Although current research shows an analgesic benefit of cannabis on neuropathic pain comparable to that of gabapentin,40 further investigation is needed to better evaluate long-term safety, efficacy, and interactions with standard therapies. Until we have a more complete picture, we should use the current literature, along with a thorough knowledge of each patient, to determine if the benefits of cannabis therapy outweigh the risks.
Acknowledgments: We thank Camillo Ferrari, BS, and Christina McMahon, BA, for their helpful comments.
- Andreae MH, Carter GM, Shaparin N, et al. Inhaled cannabis for chronic neuropathic pain: a meta-analysis of individual patient data. J Pain 2015; 16(12):1221–1232. doi:10.1016/j.jpain.2015.07.009
- National Institute of Neurological Disorders and Stroke. Peripheral Neuropathy Fact Sheet. www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Peripheral-Neuropathy-Fact-Sheet. Accessed November 14, 2018.
- Mold JW, Vesely SK, Keyl BA, Schenk JB, Roberts M. The prevalence, predictors, and consequences of peripheral sensory neuropathy in older adults. J Am Board Fam Med 2004; 17(5):308–318. doi:10.3122/jabfm.17.5.309
- Bansal D, Gudala K, Muthyala H, Esam HP, Nayakallu R, Bhansali A. Prevalence and risk factors of developing peripheral diabetic neuropathy in type 2 diabetes mellitus in a tertiary care setting. J Diabetes Investig 2014; 5(6):714–721. doi:10.1111/jdi.12223
- Finnerup NB, Haroutounian S, Kamerman P, et al. Neuropathic pain: an updated grading system for research and clinical practice. Pain 2016; 157(8):1599–1606. doi:10.1097/j.pain.0000000000000492
- Maldonado R, Banos JE, Cabanero D. The endocannabinoid system and neuropathic pain. Pain 2016; 157(suppl 1):S23–S32. doi:10.1097/j.pain.0000000000000428
- Zeng L, Alongkronrusmee D, van Rijn RM. An integrated perspective on diabetic, alcoholic, and drug-induced neuropathy, etiology, and treatment in the US. J Pain Res 2017; 10:219–228. doi:10.2147/JPR.S125987
- Callaghan BC, Price RS, Feldman EL. Distal symmetric polyneuropathy: a review. JAMA 2015; 314(20):2172–2181. doi:10.1001/jama.2015.13611
- Adams AS, Callaghan B, Grant RW. Overcoming barriers to diabetic polyneuropathy management in primary care. Healthc (Amst) 2017; 5(4):171–173. doi:10.1016/j.hjdsi.2016.10.003
- Gwak YS, Kim HY, Lee BH, Yang CH. Combined approaches for the relief of spinal cord injury-induced neuropathic pain. Complement Ther Med 2016; 25:27–33. doi:10.1016/j.ctim.2015.12.021
- Majithia N, Loprinzi CL, Smith TJ. New practical approaches to chemotherapy-induced neuropathic pain: prevention, assessment, and treatment. Oncology 2016; 30(11):1020–1029. pmid:27854104
- Grotenhermen F. Cannabinoids and the endocannabinoid system. Cannabinoids 2006; 1(1):10–14.
- Hill KP. Medical marijuana for treatment of chronic pain and other medical and psychiatric problems: a clinical review. JAMA 2015; 313(24):2474–2483. doi:10.1001/jama.2015.6199
- Campos AC, Fogaça MV, Scarante FF, et al. Plastic and neuroprotective mechanisms involved in the therapeutic effects of cannabidiol in psychiatric disorders. Front Pharmacol 2017; 8:269. doi:10.3389/fphar.2017.00269
- Russo EB. Taming THC: potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br J Pharmacol 2011; 163(7):1344–1364. doi:10.1111/j.1476-5381.2011.01238.x
- Freitas HR, Isaac AR, Malcher-Lopes R, Diaz BL, Trevenzoli IH, De Melo Reis RA. Polyunsaturated fatty acids and endocannabinoids in health and disease. Nutr Neurosci 2017; Jul 7: 1–20. doi:10.1080/1028415X.2017.1347373
- Hillard CJ. Circulating endocannabinoids: from whence do they come and where are they going? Neuropsychopharmacology 2018; 43(1):155–172. doi:10.1038/npp.2017.130
- Herkenham M, Lynn AB, Johnson MR, Melvin LS, de Costa BR, Rice KC. Characterization and localization of cannabinoid receptors in rat brain: a quantitative in vitro autoradiographic study. J Neurosci 1991; 11(2):563–583. pmid:1992016
- Tsou K, Brown S, Sañudo-Peña MC, Mackie K, Walker JM. Immunohistochemical distribution of cannabinoid CB1 receptors in the rat central nervous system. Neuroscience1998; 83(2):393–411. pmid:9460749
- Russo EB, Hohmann AG. Role of cannabinoids in pain management. In: Deer TR, Leong MS, ed. Comprehensve Treatment of Chronic Pain by Medical, Interventional, and Integrative Approaches. New York, NY: Springer; 2013:181–193.
- Vranken JH. Elucidation of pathophysiology and treatment of neuropathic pain. Cent Nerv Syst Agents Med Chem 2012; 12(4):304–314. pmid:23033930
- Yamanaka H, Noguchi K. Pathophysiology of neuropathic pain: molecular mechanisms underlying central sensitization in the dorsal horn in neuropathic pain. Brain Nerve 2012; 64(11):1255–1265. Japanese. pmid:23131736
- Ellis RJ, Toperoff W, Vaida F, et al. Smoked medicinal cannabis for neuropathic pain in HIV: a randomized, crossover clinical trial. Neuropsychopharmacology 2009; 34(3):672–680. doi:10.1038/npp.2008.120
- Ware MA, Wang T, Shapiro S, et al. Smoked cannabis for chronic neuropathic pain: a randomized controlled trial. CMAJ 2010; 182(14):E694–E701. doi:10.1503/cmaj.091414
- Wilsey B, Marcotte T, Tsodikov A, et al. A randomized, placebo-controlled, crossover trial of cannabis cigarettes in neuropathic pain. J Pain 2008; 9(6):506–521. doi:10.1016/j.jpain.2007.12.010
- Wilsey B, Marcotte T, Deutsch R, Gouaux B, Sakai S, Donaghe H. Low-dose vaporized cannabis significantly improves neuropathic pain. J Pain 2013; 14(2):136–148. doi:10.1016/j.jpain.2012.10.009
- Wallace MS, Marcotte TD, Umlauf A, Gouaux B, Atkinson JH. Efficacy of inhaled cannabis on painful diabetic neuropathy. J Pain 2015; 16(7):616–627. doi:10.1016/j.jpain.2015.03.008
- Vergara D, Bidwell LC, Gaudino R, et al. Compromised external validity: federally produced cannabis does not reflect legal markets. Scientific Reports. 2017; 7(1):1-8. doi:10.1038/srep46528
- Nurmikko TJ, Serpell MG, Hoggart B, Toomey PJ, Morlion BJ, Haines D. Sativex successfully treats neuropathic pain characterized by allodynia: a randomized, double-blind, placebo-controlled clinical trial. Pain 2007; 133(1–3):210–220. doi:10.1016/j.pain.2007.08.028
- Philpott HT, O’Brien M, McDougall JJ. Attenuation of early phase inflammation by cannabidiol prevents pain and nerve damage in rat osteoarthritis. Pain 2017; 158(12):2442–2451. doi:10.1097/j.pain.0000000000001052
- Lynch ME, Cesar-Rittenberg P, Hohmann AG. A double-blind, placebo-controlled, crossover pilot trial with extension using an oral mucosal cannabinoid extract for treatment of chemotherapy-induced neuropathic pain. J Pain Symptom Manage 2014; 47(1):166–173. doi:10.1016/j.jpainsymman.2013.02.018
- Serpell M, Ratcliffe S, Hovorka J, et al. A double-blind, randomized, placebo-controlled, parallel group study of THC/CBD spray in peripheral neuropathic pain treatment. Eur J Pain 2014; 18(7):999–1012. doi:10.1002/j.1532-2149.2013.00445.x
- Nugent SM, Morasco BJ, O’Neil ME, et al. The effects of cannabis among adults with chronic pain and an overview of general harms: a systematic review. Ann Intern Med 2017; 167(5):319–331. doi:10.7326/M17-0155
- Mücke M, Phillips T, Radbruch L, Petzke F, Häuser W. Cannabis-based medicines for chronic neuropathic pain in adults. Cochrane Database Syst Rev 2018; 3:CD012182. doi:10.1002/14651858.CD012182.pub2
- Castellanos-Ryan N, Pingault JB, Parent S, Vitaro F, Tremblay RE, Seguin JR. Adolescent cannabis use, change in neurocognitive function, and high-school graduation: a longitudinal study from early adolescence to young adulthood. Dev Psychopathol 2017; 29(4):1253–1266. doi:10.1017/S0954579416001280
- Karila L, Roux P, Benyamina A, et al. Acute and long-term effects of cannabis use: a review. Curr Pharm Des 2014; 20(25):4112–4118. pmid:24001294
- Johns A. Psychiatric effects of cannabis. Br J Psychiatry 2001; 178:116–122. pmid:11157424
- National Academies of Science, Engineering, and Medicine. The health effects of cannabis and cannabinoids: the current state of evidence and recommendations for research. Washington, DC: The National Academy Press; 2017. doi:10.17226/24625
- Modesto-Lowe V, Griard L, Chaplin M. Cancer pain in the opioid-addicted patient: can we treat it right? J Opioid Manag 2012; 8(3):167–175. doi:10.5055/jom.2012.0113
- Grant I. Medicinal cannabis and painful sensory neuropathy. Virtual Mentor 2013; 15(5):466–469. doi:10.1001/virtualmentor.2013.15.5.oped1-1305
- Andreae MH, Carter GM, Shaparin N, et al. Inhaled cannabis for chronic neuropathic pain: a meta-analysis of individual patient data. J Pain 2015; 16(12):1221–1232. doi:10.1016/j.jpain.2015.07.009
- National Institute of Neurological Disorders and Stroke. Peripheral Neuropathy Fact Sheet. www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Peripheral-Neuropathy-Fact-Sheet. Accessed November 14, 2018.
- Mold JW, Vesely SK, Keyl BA, Schenk JB, Roberts M. The prevalence, predictors, and consequences of peripheral sensory neuropathy in older adults. J Am Board Fam Med 2004; 17(5):308–318. doi:10.3122/jabfm.17.5.309
- Bansal D, Gudala K, Muthyala H, Esam HP, Nayakallu R, Bhansali A. Prevalence and risk factors of developing peripheral diabetic neuropathy in type 2 diabetes mellitus in a tertiary care setting. J Diabetes Investig 2014; 5(6):714–721. doi:10.1111/jdi.12223
- Finnerup NB, Haroutounian S, Kamerman P, et al. Neuropathic pain: an updated grading system for research and clinical practice. Pain 2016; 157(8):1599–1606. doi:10.1097/j.pain.0000000000000492
- Maldonado R, Banos JE, Cabanero D. The endocannabinoid system and neuropathic pain. Pain 2016; 157(suppl 1):S23–S32. doi:10.1097/j.pain.0000000000000428
- Zeng L, Alongkronrusmee D, van Rijn RM. An integrated perspective on diabetic, alcoholic, and drug-induced neuropathy, etiology, and treatment in the US. J Pain Res 2017; 10:219–228. doi:10.2147/JPR.S125987
- Callaghan BC, Price RS, Feldman EL. Distal symmetric polyneuropathy: a review. JAMA 2015; 314(20):2172–2181. doi:10.1001/jama.2015.13611
- Adams AS, Callaghan B, Grant RW. Overcoming barriers to diabetic polyneuropathy management in primary care. Healthc (Amst) 2017; 5(4):171–173. doi:10.1016/j.hjdsi.2016.10.003
- Gwak YS, Kim HY, Lee BH, Yang CH. Combined approaches for the relief of spinal cord injury-induced neuropathic pain. Complement Ther Med 2016; 25:27–33. doi:10.1016/j.ctim.2015.12.021
- Majithia N, Loprinzi CL, Smith TJ. New practical approaches to chemotherapy-induced neuropathic pain: prevention, assessment, and treatment. Oncology 2016; 30(11):1020–1029. pmid:27854104
- Grotenhermen F. Cannabinoids and the endocannabinoid system. Cannabinoids 2006; 1(1):10–14.
- Hill KP. Medical marijuana for treatment of chronic pain and other medical and psychiatric problems: a clinical review. JAMA 2015; 313(24):2474–2483. doi:10.1001/jama.2015.6199
- Campos AC, Fogaça MV, Scarante FF, et al. Plastic and neuroprotective mechanisms involved in the therapeutic effects of cannabidiol in psychiatric disorders. Front Pharmacol 2017; 8:269. doi:10.3389/fphar.2017.00269
- Russo EB. Taming THC: potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br J Pharmacol 2011; 163(7):1344–1364. doi:10.1111/j.1476-5381.2011.01238.x
- Freitas HR, Isaac AR, Malcher-Lopes R, Diaz BL, Trevenzoli IH, De Melo Reis RA. Polyunsaturated fatty acids and endocannabinoids in health and disease. Nutr Neurosci 2017; Jul 7: 1–20. doi:10.1080/1028415X.2017.1347373
- Hillard CJ. Circulating endocannabinoids: from whence do they come and where are they going? Neuropsychopharmacology 2018; 43(1):155–172. doi:10.1038/npp.2017.130
- Herkenham M, Lynn AB, Johnson MR, Melvin LS, de Costa BR, Rice KC. Characterization and localization of cannabinoid receptors in rat brain: a quantitative in vitro autoradiographic study. J Neurosci 1991; 11(2):563–583. pmid:1992016
- Tsou K, Brown S, Sañudo-Peña MC, Mackie K, Walker JM. Immunohistochemical distribution of cannabinoid CB1 receptors in the rat central nervous system. Neuroscience1998; 83(2):393–411. pmid:9460749
- Russo EB, Hohmann AG. Role of cannabinoids in pain management. In: Deer TR, Leong MS, ed. Comprehensve Treatment of Chronic Pain by Medical, Interventional, and Integrative Approaches. New York, NY: Springer; 2013:181–193.
- Vranken JH. Elucidation of pathophysiology and treatment of neuropathic pain. Cent Nerv Syst Agents Med Chem 2012; 12(4):304–314. pmid:23033930
- Yamanaka H, Noguchi K. Pathophysiology of neuropathic pain: molecular mechanisms underlying central sensitization in the dorsal horn in neuropathic pain. Brain Nerve 2012; 64(11):1255–1265. Japanese. pmid:23131736
- Ellis RJ, Toperoff W, Vaida F, et al. Smoked medicinal cannabis for neuropathic pain in HIV: a randomized, crossover clinical trial. Neuropsychopharmacology 2009; 34(3):672–680. doi:10.1038/npp.2008.120
- Ware MA, Wang T, Shapiro S, et al. Smoked cannabis for chronic neuropathic pain: a randomized controlled trial. CMAJ 2010; 182(14):E694–E701. doi:10.1503/cmaj.091414
- Wilsey B, Marcotte T, Tsodikov A, et al. A randomized, placebo-controlled, crossover trial of cannabis cigarettes in neuropathic pain. J Pain 2008; 9(6):506–521. doi:10.1016/j.jpain.2007.12.010
- Wilsey B, Marcotte T, Deutsch R, Gouaux B, Sakai S, Donaghe H. Low-dose vaporized cannabis significantly improves neuropathic pain. J Pain 2013; 14(2):136–148. doi:10.1016/j.jpain.2012.10.009
- Wallace MS, Marcotte TD, Umlauf A, Gouaux B, Atkinson JH. Efficacy of inhaled cannabis on painful diabetic neuropathy. J Pain 2015; 16(7):616–627. doi:10.1016/j.jpain.2015.03.008
- Vergara D, Bidwell LC, Gaudino R, et al. Compromised external validity: federally produced cannabis does not reflect legal markets. Scientific Reports. 2017; 7(1):1-8. doi:10.1038/srep46528
- Nurmikko TJ, Serpell MG, Hoggart B, Toomey PJ, Morlion BJ, Haines D. Sativex successfully treats neuropathic pain characterized by allodynia: a randomized, double-blind, placebo-controlled clinical trial. Pain 2007; 133(1–3):210–220. doi:10.1016/j.pain.2007.08.028
- Philpott HT, O’Brien M, McDougall JJ. Attenuation of early phase inflammation by cannabidiol prevents pain and nerve damage in rat osteoarthritis. Pain 2017; 158(12):2442–2451. doi:10.1097/j.pain.0000000000001052
- Lynch ME, Cesar-Rittenberg P, Hohmann AG. A double-blind, placebo-controlled, crossover pilot trial with extension using an oral mucosal cannabinoid extract for treatment of chemotherapy-induced neuropathic pain. J Pain Symptom Manage 2014; 47(1):166–173. doi:10.1016/j.jpainsymman.2013.02.018
- Serpell M, Ratcliffe S, Hovorka J, et al. A double-blind, randomized, placebo-controlled, parallel group study of THC/CBD spray in peripheral neuropathic pain treatment. Eur J Pain 2014; 18(7):999–1012. doi:10.1002/j.1532-2149.2013.00445.x
- Nugent SM, Morasco BJ, O’Neil ME, et al. The effects of cannabis among adults with chronic pain and an overview of general harms: a systematic review. Ann Intern Med 2017; 167(5):319–331. doi:10.7326/M17-0155
- Mücke M, Phillips T, Radbruch L, Petzke F, Häuser W. Cannabis-based medicines for chronic neuropathic pain in adults. Cochrane Database Syst Rev 2018; 3:CD012182. doi:10.1002/14651858.CD012182.pub2
- Castellanos-Ryan N, Pingault JB, Parent S, Vitaro F, Tremblay RE, Seguin JR. Adolescent cannabis use, change in neurocognitive function, and high-school graduation: a longitudinal study from early adolescence to young adulthood. Dev Psychopathol 2017; 29(4):1253–1266. doi:10.1017/S0954579416001280
- Karila L, Roux P, Benyamina A, et al. Acute and long-term effects of cannabis use: a review. Curr Pharm Des 2014; 20(25):4112–4118. pmid:24001294
- Johns A. Psychiatric effects of cannabis. Br J Psychiatry 2001; 178:116–122. pmid:11157424
- National Academies of Science, Engineering, and Medicine. The health effects of cannabis and cannabinoids: the current state of evidence and recommendations for research. Washington, DC: The National Academy Press; 2017. doi:10.17226/24625
- Modesto-Lowe V, Griard L, Chaplin M. Cancer pain in the opioid-addicted patient: can we treat it right? J Opioid Manag 2012; 8(3):167–175. doi:10.5055/jom.2012.0113
- Grant I. Medicinal cannabis and painful sensory neuropathy. Virtual Mentor 2013; 15(5):466–469. doi:10.1001/virtualmentor.2013.15.5.oped1-1305
KEY POINTS
- Small clinical studies have found that cannabis provides benefits for peripheral neuropathy, including pain reduction, better sleep, and improved function, even in patients with symptoms refractory to standard therapies.
- Adverse effects such as throat irritation, headache, and dizziness are common, and serious neuropsychiatric effects can occur at high doses.
- Safety may not be adequately assessed in US trials because cannabis supplied by the National Institute of Drug Abuse is less potent than commercially available products.
