User login
CBT may improve comorbid posttraumatic headache, PTSD
Results from a randomized clinical trial of almost 200 military veterans showed that, compared with usual care, CBT for headache led to significant improvement in both headache disability and PTSD symptoms. Cognitive-processing therapy (CPT) also led to significant improvement in PTSD symptoms, but it did not improve headache disability.

Lead author Donald McGeary, PhD, department of rehabilitation medicine, the University of Texas Health Science Center,San Antonio, noted the improvements shown in headache disability after CBT were likely caused by its building of patients’ confidence that they could control or manage their headaches themselves.
That sense of control was key to helping patients “get their lives back. If you can improve a person’s belief that they can control their headache, they function better,” Dr. McGeary said in a news release.
The findings were published online in JAMA Neurology.
Signature wounds
Both mild traumatic brain injury (TBI) and PTSD are signature wounds of post-9/11 military conflicts. The two conditions commonly occur together and can harm quality of life and functioning, the investigators noted. Following mild TBI, many veterans experience persistent posttraumatic headache, which often co-occurs with PTSD.
To gauge the impact of CBTs for this patient population, researchers recruited 193 post-9/11 combat veterans (mean age, 39.7 years) with clinically significant PTSD symptoms and posttraumatic headache that had persisted more than 3 months after TBI. Of these, 167 were men.
All participants were receiving care at the Polytrauma Rehabilitation Center of the South Texas Veterans Health Care System in Houston.
They were randomly allocated to undergo 8 sessions of manualized CBT for headache, 12 sessions of manualized CPT for PTSD, or usual headache treatment.
CBT for headache uses CBT concepts to reduce headache disability and improve mood – and includes key components, such as relaxation, setting goals for activities patients want to resume, and planning for those situations.
CPT is a leading psychotherapy for PTSD. It teaches patients how to evaluate and change upsetting and maladaptive thoughts related to their trauma. The idea is that, by changing thoughts, patients can change the way they feel.
Treatment as usual was consistent with multidisciplinary treatment in a large Veterans Affairs multiple-trauma center and could include pharmacotherapies, physical and occupational therapies, pain medications, acupuncture, and massage.
The coprimary outcomes were headache-related disability on the six-item Headache Impact Test (HIT-6) and PTSD symptom severity on the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (PCL-5), assessed from end of treatment to 6 months post treatment.
At baseline, all participants reported severe headache-related disability (mean HIT-6 score, 65.8 points) and severe PTSD symptoms (mean PCL-5 score, 48.4 points).
Significant improvement
Compared with usual care, CBT for headache led to significant improvement in headache disability (posttreatment mean change in HIT-6 score, –3.4 points; P < .01) and PTSD symptoms (posttreatment change in PCL-5, –6.5 points; P = .04).
CPT also led to significant improvement in PTSD symptoms (8.9 points lower on the PCL-5 after treatment; P = .01), but it had only a modest effect on headache disability (1.4 points lower after treatment; P = .21).
“This was a surprise,” Dr. McGeary said. “If theories about PTSD driving posttraumatic headache are correct, you’d expect CPT to help both PTSD and headache. Our findings call that into question.”
Despite improvements in headache disability, CBT for headache did not significantly reduce headache frequency or intensity.
The researchers are now hoping to replicate their findings in a larger trial at multiple military and VA sites around the United States.
“We need more women, more racial and ethnic diversity, veterans as well as active military of different branches with varying comorbidities in different geographic regions attached to different hospitals and medical systems, because we’re comparing to usual care,” Dr. McGeary said.
A step forward
Commenting on the study, retired Col. Elspeth Cameron Ritchie, MD, chair of psychiatry, MedStar Washington Hospital Center, Washington, said she was “pleased” to see that this study was conducted and that she was pleased with the results.

“It’s been 20 years since 9/11, and wars are pretty much forgotten, but people are still suffering from the effects of traumatic brain injury and posttraumatic stress disorder. These are not conditions that go away quickly or lightly. They do take work,” said Dr. Ritchie, who was not involved with the research.
Finding therapies besides medication that are helpful is “good and is a step forward. The more alternatives we have, the better,” she concluded.
The study was supported in part by the Department of Defense and the Department of Veterans Affairs. Dr. McGeary and Dr. Ritchie have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Results from a randomized clinical trial of almost 200 military veterans showed that, compared with usual care, CBT for headache led to significant improvement in both headache disability and PTSD symptoms. Cognitive-processing therapy (CPT) also led to significant improvement in PTSD symptoms, but it did not improve headache disability.
Lead author Donald McGeary, PhD, department of rehabilitation medicine, the University of Texas Health Science Center,San Antonio, noted the improvements shown in headache disability after CBT were likely caused by its building of patients’ confidence that they could control or manage their headaches themselves.
That sense of control was key to helping patients “get their lives back. If you can improve a person’s belief that they can control their headache, they function better,” Dr. McGeary said in a news release.
The findings were published online in JAMA Neurology.
Signature wounds
Both mild traumatic brain injury (TBI) and PTSD are signature wounds of post-9/11 military conflicts. The two conditions commonly occur together and can harm quality of life and functioning, the investigators noted. Following mild TBI, many veterans experience persistent posttraumatic headache, which often co-occurs with PTSD.
To gauge the impact of CBTs for this patient population, researchers recruited 193 post-9/11 combat veterans (mean age, 39.7 years) with clinically significant PTSD symptoms and posttraumatic headache that had persisted more than 3 months after TBI. Of these, 167 were men.
All participants were receiving care at the Polytrauma Rehabilitation Center of the South Texas Veterans Health Care System in Houston.
They were randomly allocated to undergo 8 sessions of manualized CBT for headache, 12 sessions of manualized CPT for PTSD, or usual headache treatment.
CBT for headache uses CBT concepts to reduce headache disability and improve mood – and includes key components, such as relaxation, setting goals for activities patients want to resume, and planning for those situations.
CPT is a leading psychotherapy for PTSD. It teaches patients how to evaluate and change upsetting and maladaptive thoughts related to their trauma. The idea is that, by changing thoughts, patients can change the way they feel.
Treatment as usual was consistent with multidisciplinary treatment in a large Veterans Affairs multiple-trauma center and could include pharmacotherapies, physical and occupational therapies, pain medications, acupuncture, and massage.
The coprimary outcomes were headache-related disability on the six-item Headache Impact Test (HIT-6) and PTSD symptom severity on the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (PCL-5), assessed from end of treatment to 6 months post treatment.
At baseline, all participants reported severe headache-related disability (mean HIT-6 score, 65.8 points) and severe PTSD symptoms (mean PCL-5 score, 48.4 points).
Significant improvement
Compared with usual care, CBT for headache led to significant improvement in headache disability (posttreatment mean change in HIT-6 score, –3.4 points; P < .01) and PTSD symptoms (posttreatment change in PCL-5, –6.5 points; P = .04).
CPT also led to significant improvement in PTSD symptoms (8.9 points lower on the PCL-5 after treatment; P = .01), but it had only a modest effect on headache disability (1.4 points lower after treatment; P = .21).
“This was a surprise,” Dr. McGeary said. “If theories about PTSD driving posttraumatic headache are correct, you’d expect CPT to help both PTSD and headache. Our findings call that into question.”
Despite improvements in headache disability, CBT for headache did not significantly reduce headache frequency or intensity.
The researchers are now hoping to replicate their findings in a larger trial at multiple military and VA sites around the United States.
“We need more women, more racial and ethnic diversity, veterans as well as active military of different branches with varying comorbidities in different geographic regions attached to different hospitals and medical systems, because we’re comparing to usual care,” Dr. McGeary said.
A step forward
Commenting on the study, retired Col. Elspeth Cameron Ritchie, MD, chair of psychiatry, MedStar Washington Hospital Center, Washington, said she was “pleased” to see that this study was conducted and that she was pleased with the results.
“It’s been 20 years since 9/11, and wars are pretty much forgotten, but people are still suffering from the effects of traumatic brain injury and posttraumatic stress disorder. These are not conditions that go away quickly or lightly. They do take work,” said Dr. Ritchie, who was not involved with the research.
Finding therapies besides medication that are helpful is “good and is a step forward. The more alternatives we have, the better,” she concluded.
The study was supported in part by the Department of Defense and the Department of Veterans Affairs. Dr. McGeary and Dr. Ritchie have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Results from a randomized clinical trial of almost 200 military veterans showed that, compared with usual care, CBT for headache led to significant improvement in both headache disability and PTSD symptoms. Cognitive-processing therapy (CPT) also led to significant improvement in PTSD symptoms, but it did not improve headache disability.
Lead author Donald McGeary, PhD, department of rehabilitation medicine, the University of Texas Health Science Center,San Antonio, noted the improvements shown in headache disability after CBT were likely caused by its building of patients’ confidence that they could control or manage their headaches themselves.
That sense of control was key to helping patients “get their lives back. If you can improve a person’s belief that they can control their headache, they function better,” Dr. McGeary said in a news release.
The findings were published online in JAMA Neurology.
Signature wounds
Both mild traumatic brain injury (TBI) and PTSD are signature wounds of post-9/11 military conflicts. The two conditions commonly occur together and can harm quality of life and functioning, the investigators noted. Following mild TBI, many veterans experience persistent posttraumatic headache, which often co-occurs with PTSD.
To gauge the impact of CBTs for this patient population, researchers recruited 193 post-9/11 combat veterans (mean age, 39.7 years) with clinically significant PTSD symptoms and posttraumatic headache that had persisted more than 3 months after TBI. Of these, 167 were men.
All participants were receiving care at the Polytrauma Rehabilitation Center of the South Texas Veterans Health Care System in Houston.
They were randomly allocated to undergo 8 sessions of manualized CBT for headache, 12 sessions of manualized CPT for PTSD, or usual headache treatment.
CBT for headache uses CBT concepts to reduce headache disability and improve mood – and includes key components, such as relaxation, setting goals for activities patients want to resume, and planning for those situations.
CPT is a leading psychotherapy for PTSD. It teaches patients how to evaluate and change upsetting and maladaptive thoughts related to their trauma. The idea is that, by changing thoughts, patients can change the way they feel.
Treatment as usual was consistent with multidisciplinary treatment in a large Veterans Affairs multiple-trauma center and could include pharmacotherapies, physical and occupational therapies, pain medications, acupuncture, and massage.
The coprimary outcomes were headache-related disability on the six-item Headache Impact Test (HIT-6) and PTSD symptom severity on the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (PCL-5), assessed from end of treatment to 6 months post treatment.
At baseline, all participants reported severe headache-related disability (mean HIT-6 score, 65.8 points) and severe PTSD symptoms (mean PCL-5 score, 48.4 points).
Significant improvement
Compared with usual care, CBT for headache led to significant improvement in headache disability (posttreatment mean change in HIT-6 score, –3.4 points; P < .01) and PTSD symptoms (posttreatment change in PCL-5, –6.5 points; P = .04).
CPT also led to significant improvement in PTSD symptoms (8.9 points lower on the PCL-5 after treatment; P = .01), but it had only a modest effect on headache disability (1.4 points lower after treatment; P = .21).
“This was a surprise,” Dr. McGeary said. “If theories about PTSD driving posttraumatic headache are correct, you’d expect CPT to help both PTSD and headache. Our findings call that into question.”
Despite improvements in headache disability, CBT for headache did not significantly reduce headache frequency or intensity.
The researchers are now hoping to replicate their findings in a larger trial at multiple military and VA sites around the United States.
“We need more women, more racial and ethnic diversity, veterans as well as active military of different branches with varying comorbidities in different geographic regions attached to different hospitals and medical systems, because we’re comparing to usual care,” Dr. McGeary said.
A step forward
Commenting on the study, retired Col. Elspeth Cameron Ritchie, MD, chair of psychiatry, MedStar Washington Hospital Center, Washington, said she was “pleased” to see that this study was conducted and that she was pleased with the results.
“It’s been 20 years since 9/11, and wars are pretty much forgotten, but people are still suffering from the effects of traumatic brain injury and posttraumatic stress disorder. These are not conditions that go away quickly or lightly. They do take work,” said Dr. Ritchie, who was not involved with the research.
Finding therapies besides medication that are helpful is “good and is a step forward. The more alternatives we have, the better,” she concluded.
The study was supported in part by the Department of Defense and the Department of Veterans Affairs. Dr. McGeary and Dr. Ritchie have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NEUROLOGY
Benign Pneumatosis Intestinalis: A Case Report and Review of the Literature
Pneumatosis intestinalis (PI) is the finding of gas within the walls of the intestine on imaging. It is most commonly detected via radiograph or computed tomography (CT). The diseases leading to the accumulation of gas within the submucosal space of the gastrointestinal (GI) tract are heterogenous, and the finding of PI itself has a wide range of clinical implications from impending clinical deterioration to an incidental finding of minimal consequence.
We present the case of a veteran who had sustained a remote anoxic brain injury resulting in chronic dependence on a gastrostomy tube for enteral nutrition, found incidentally to have PI without signs of intra-abdominal catastrophe. An exclusion of other, more lifethreatening causes of PI led to a diagnosis of benign PI secondary to the presence of his gastrostomy tube. This case highlights the importance of interpreting the finding of PI in the clinical context of the specific patient and how conservative management may be appropriate in some cases.
Case Presentation
A 61-year-old male patient was admitted for fever. The patient had a remote history of cardiac arrest complicated by anoxic brain injury requiring tracheostomy, gastrostomy tube, and a suprapubic catheter with recurrent catheter-associated urinary tract infections (CAUTI), secondary seizure disorder, atrial fibrillation off anticoagulation due to recurrent GI bleeding, and treatment naive chronic hepatitis C virus. His ability to provide a clinical history was limited by his nonverbal status. He had no prior surgical history but had presented a month earlier for a high-grade small bowel obstruction (SBO) with pneumobilia that was managed conservatively as the surgical team deemed him a poor candidate for surgical intervention with his extensive comorbidities. A bioethics consultation at the time supported minimizing potential surgical risk in favor of conservative medical management; this was discussed with the patient’s surrogate decision maker, who also wished to avoid surgery. The SBO resolved with conservative management. He had been residing in a nursing home and doing well until 24 hours prior to admission when he developed fevers.
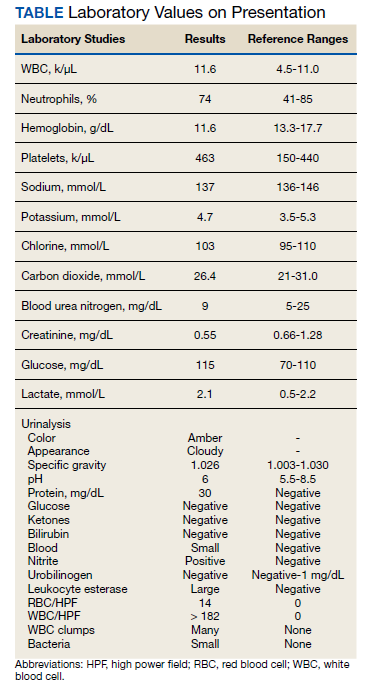
Vital signs on admission showed a temperature of 100.8 °F, heart rate 100 beats per minute, blood pressure 116/85, respiratory rate 22 per minute, and oxygen saturation of 100% on 6 L of oxygen via tracheostomy collar. His initial examination was notable for clear lung sounds, a nondistended nonrigid abdomen with an indwelling percutaneous gastrostomy tube, and absence of areas of skin breakdown or erythema. Notable laboratory studies showed a leukocytosis and urinalysis suggestive of CAUTI (Table). His urinary catheter was exchanged, he was fluid resuscitated and started on empiric vancomycin and piperacillin-tazobactam for management of sepsis due to CAUTI.
For the first 3 days of his hospitalization, he demonstrated clinical improvement on vancomycin and piperacillin-tazobactam while awaiting results from his urine bacterial culture. On hospital day 3, hedeveloped recurrent nonbloody, nonbilious emesis despite no change in the rate or formulation of his enteral nutrition. He also had 3 watery brown bowel movements. His vital signs remained within normal limits. His abdominal examination at this point showed mild distention and was hypertympanic to percussion, but there was no rigidity or involuntary guarding. On hospital day 4, he continued to have emesis with an unchanged abdominal examination. The differential diagnosis included recurrence of prior SBO, ileus, intestinal ischemia, enteral nutrition intolerance, Clostridioides difficile (C difficile) colitis, and GI dysmotility because of his anoxic brain injury.
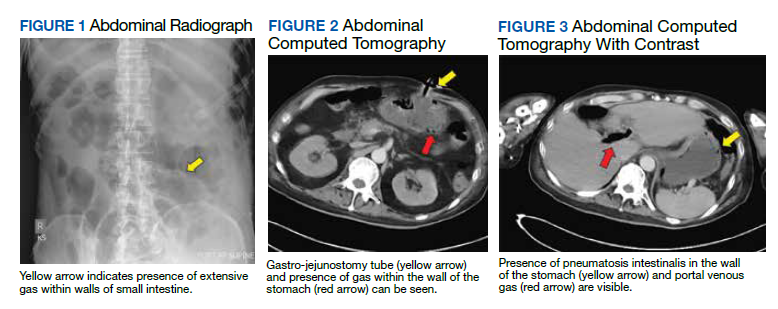
Testing for C difficile was negative. An abdominal radiograph was obtained and revealed no bowel obstruction but, alarmingly, showed extensive intramural bowel gas, suggestive of PI (Figure 1). His leukocyte count, serum bicarbonate, and serum lactate levels remained within normal limits. A CT with contrast of the abdomen and pelvis demonstrated no vascular obstruction but confirmed the presence of diffuse intramural gas in his stomach and proximal small bowel, as well as the presence of mesenteric and portal venous gas (Figures 2 and 3). Although his abdominal examination had not changed and did not suggest peritonitis, general surgery was consulted to discuss the need for surgical intervention. Given his overall clinical stability and high surgical risk due to his many comorbidities, surgery recommended a conservative approach.
Through the following hospital days, his enteral nutrition was held and serial abdominal examinations were performed without change. Serial laboratory studies, including serum lactate and leukocyte count, remained reassuringly within normal limits. His urine culture eventually revealed multidrugresistant Pseudomonas aeruginosa. Antimicrobial therapy was narrowed to piperacillintazobactam for a complete course. Enteral nutrition was gradually reintroduced at a low rate, ultimately reaching goal rate with return of bowel function by hospital day 9. Despite extensive workup, the etiology of his transient enteral nutrition intolerance remained uncertain, though an adverse effect of antibiotic therapy was thought possible. Follow-up abdominal radiographs demonstrated interval improvement of PI. He was discharged back to his skilled nursing facility on hospital day 11 without incident.
Discussion
PI is an incompletely understood condition seen in multiple diseases. Patients may present with highly variable symptoms, often more attributable to the underlying disease causing the PI than the presence of PI, as patients may be entirely asymptomatic. When symptoms are attributed to PI, those most reported are abdominal pain, bloody stools, and diarrhea.1 It is often detected on abdominal plain films. Alternative methods of diagnosis include ultrasonography, barium enema, and endoscopy although the last method has been known to occasionally lead to bowel perforation.2-6 The most sensitive method of detection is CT, which also provides additional information about abdominal pathology and may identify the underlying process responsible for the PI.7
While not fully understood, much information about PI and its pathogenesis is known. Understanding the mechanisms of PI is vital to direct the clinician’s evaluation of the patient for reversible conditions that may cause PI. Early descriptions of PI in the literature documented an association with pyloric stenosis, leading to the theory that gas from the intestinal lumen is driven into the submucosal space during episodes of forceful vomiting with increased intraluminal pressure.8 As PI was subsequently described in multiple other disease states not typically associated with increased intraluminal pressure such as inflammatory bowel disease, GI malignancy, cryptosporidiosis and CMV infection, additional theories about the pathogenesis of PI have arisen.9-24 There is now experimental data to support multiple mechanisms of intramural gas accumulation. It has become accepted that PI represents a common pathway shared across various pathologic states and results from multifactorial mechanisms of gas entry into the intestinal wall.25-29
Factors leading to the development of PI include bacterial production of gas, intraluminal GI gas compositions, increased intraluminal pressure, pulmonary gas tracking through vessels communicating with the thorax, and mucosal disruption. PI has been linked to bacterial infections of the GI tract in humans including C difficile, Klebsiella, and Whipple disease.14-18 In animal models, C difficile within the walls of rat intestine results in the appearance of pneumocysts, or discrete collections of submucosal gas, which are the hallmark feature of PI.30 It is thought that direct invasion of bacteria into intramural spaces can cause PI in humans, although bacteria have yet to be directly isolated from the pneumocysts. Translocation of luminal gas into pneumocysts found in PI is theorized to be driven by differences in partial pressures.31 The concentration of hydrogen within the intestinal lumen is high due to bacterial production. Hydrogen, diffusing along its partial pressure gradient between the lumen and blood, accumulates within the intestinal wall and causes the formation of pneumocysts. This phenomenon has been hypothesized to explain the tendency for pneumocysts to form around the mesenteric vasculature.
Gas from the lumen can also be forced into the intestinal wall during an abrupt increase in intra-abdominal pressure, such as that seen with forceful vomiting. The final possible origin of the gas is the lungs, as PI has been associated with lung disease. It was previously thought that gas from ruptured alveoli tracks along mediastinal vessels, below the diaphragm, and into the mesentery.30 Newer theories argue that increased intra-abdominal pressure, typical of patients with obstructive lung disease and frequent coughing, is the driver of PI by the mechanism previously described.32-34 Additionally, mucosal disruption leads to increased permeability and allows accumulation of gas within the intestinal walls. Mucosal abnormalities have been described in histopathologic studies of patients with PI and associated with conditions known to compromise mucosal integrity, such as immunodeficiencies, inflammatory bowel disease, and the receipt of cytotoxic chemotherapy.10,12,19-23
Our patient likely had mucosal disruption due to his gastrostomy tube as well as increased intraluminal pressure from recurrent vomiting, contributing to translocation of otherwise normal intraluminal gas. The presence of portal venous gas, as seen in this case, has historically portended a worse prognosis, with 37% mortality in one series.7,35,36 However, portal venous gas as well as pneumoperitoneum occur in benign etiologies of PI as well. It is thought that this occurs due to rupture of the submucosal pneumocysts through the wall opposite the intestinal lumen and thus does not result in a direct communication between the intestinal lumen and the peritoneal cavity.12
PI is not a diagnosis but a manifestation of an underlying disease. As such, the treatment of PI is targeted toward the underlying condition. Of note, the pattern and extent of PI seen on imaging has not been shown to correlate with the severity of the underlying pathologic process.35,37 Instead, assessment of the patient and their clinical trajectory should determine the appropriate treatment. The decision facing the clinician when PI is discovered is whether urgent surgery is indicated, as is the case in mesenteric ischemia, bowel necrosis, or intestinal perforation, conditions known to be associated with PI. Otherwise, there is no definitive treatment for PI. Bowel rest is almost universally pursued. There are reports of treating with supranormal levels of supplemental oxygen, maintaining arterial partial pressure of oxygen above 300 mm Hg, with a face mask and 8 L/min flow rate.38,39 The proposed mechanisms of benefit include establishing a favorable diffusion gradient for intramural gas to exit the pneumocysts as well as creating an inhospitable, aerobic environment for hydrogenproducing anaerobic enteric bacteria. A prudent approach for most cases of PI is conservative management with bowel rest and supplemental oxygen unless there is a definitive indication for urgent surgical intervention, such as peritonitis, abdominal sepsis, or perforation.40,41 Management recommendations suggest that up to 50% of cases can be successfully managed nonoperatively.42
Conclusions
PI is the radiographic finding of gas within the walls of the intestinal tract and has variable clinical significance. It can represent a benign incidental finding or a sequela of intraabdominal emergencies such as mesenteric ischemia or bowel necrosis. Because PI is seen in a variety of disorders, several proposed mechanisms are supported in the medical literature. These include bacterial production of gas, gas pressure gradients between the intestinal lumen and the blood, increased intraluminal pressure, pulmonary gas tracking from intrathoracic vessels, and mucosal disruption. The evaluation of a patient with PI must begin with an assessment for the need for urgent surgical intervention. Additional management measures include bowel rest, IV hydration, and supplemental oxygen administration. Because of its wide variety of etiologies of varying clinical urgency, placing the finding of PI in the context of the patient is paramount to selecting an appropriate management strategy.
1. Jamart J. Pneumatosis cystoides intestinalis. A statistical study of 919 cases. Acta Hepatogastroenterol (Stuttg). 1979;26(5):419-422.
2. Lafortune M, Trinh BC, Burns PN, et al. Air in the portal vein: sonographic and Doppler manifestations. Radiology. 1991;180(3):667-670. doi:10.1148/radiology.180.3.1871276
3. Kriegshauser JS, Reading CC, King BF, Welch TJ. Combined systemic and portal venous gas: sonographic and CT detection in two cases. AJR Am J Roentgenol. 1990;154(6):1219-1221. doi:10.2214/ajr.154.6.2110731
4. Goske MJ, Goldblum JR, Applegate KE, Mitchell CS, Bardo D. The “circle sign”: a new sonographic sign of pneumatosis intestinalis - clinical, pathologic and experimental findings. Pediatr Radiol. 1999;29(7):530-535. doi:10.1007/s002470050638
5. Marshak RH, Lindner AE, Maklansky D. Pneumatosis cystoides coli. Gastrointest Radiol. 1977;2(2):85-89. doi:10.1007/BF02256475
6. Jensen R, Gutnik SH. Pneumatosis cystoides intestinalis: a complication of colonoscopic polypectomy. S D J Med. 1991;44(7):177-179.
7. Knechtle SJ, Davidoff AM, Rice RP. Pneumatosis intestinalis. Surgical management and clinical outcome. Ann Surg. 1990;212(2):160-165. doi:10.1097/00000658-199008000-00008
8. Koss LG. Abdominal gas cysts (Pneumatosis cystoides intestinorum hominis); an analysis with a report of a case and a critical review of the literature. AMA Arch Pathol. 1952;53(6):523-549.
9. Jona JZ. Benign pneumatosis intestinalis coli after blunt trauma to the abdomen in a child. J Pediatr Surg. 2000;35(7):1109-1111. doi:10.1053/jpsu.2000.7837
10. Gagliardi G, Thompson IW, Hershman MJ, Forbes A, Hawley PR, Talbot IC. Pneumatosis coli: a proposed pathogenesis based on study of 25 cases and review of the literature. Int J Colorectal Dis. 1996;11(3):111-118. doi:10.1007/s003840050031
11. Seto T, Koide N, Taniuchi N, Yamada T, Hamaguchi M, Goto S. Pneumatosis cystoides intestinalis complicating carcinoma of the small intestine. Am J Surg. 2001;182(3):287-288. doi:10.1016/S0002-9610(01)00710-3
12. Galandiuk S, Fazio VW, Petras RE. Pneumatosis cystoides intestinalis in Crohn’s disease. Report of two cases. Dis Colon Rectum. 1985;28(12):951-956. doi:10.1007/BF02554315
13. Parra JA, Acinas O, Bueno J, Madrazo C, Fariñas C. An unusual form of pneumatosis intestinalis associated with appendicitis. Br J Radiol. 1998;71(843):326-328. doi:10.1259/bjr.71.843.9616245
14. Schenk P, Madl C, Kramer L, et al. Pneumatosis intestinalis with Clostridium difficile colitis as a cause of acute abdomen after lung transplantation. Dig Dis Sci. 1998;43(11):2455-2458. doi:10.1023/a:1026682131847
15. Kreiss C, Forohar F, Smithline AE, Brandt LJ. Pneumatosis intestinalis complicating C. difficile pseudomembranous colitis. Am J Gastroenterol. 1999;94(9):2560-2561. doi:10.1111/j.1572-0241.1999.01397.x
16. Day DL, Ramsay NK, Letourneau JG. Pneumatosis intestinalis after bone marrow transplantation. AJR Am J Roentgenol. 1988;151(1):85-87. doi:10.2214/ajr.151.1.85
17. Tahara S, Sakai Y, Katsuno H, Urano M, Kuroda M, Tsukamoto T. Pneumatosis intestinalis and hepatic portal venous gas associated with gas-forming bacterial translocation due to postoperative paralytic ileus: A case report. Medicine (Baltimore). 2019;98(2):e14079. doi:10.1097/MD.0000000000014079
18. Klochan C, Anderson TA, Rose D, Dimitrov RK, Johnson RM. Nearly fatal case of whipple’s disease in a patient mistakenly on anti-tnf therapy. ACG Case Rep J. 2013;1(1):25- 28. Published 2013 Oct 8. doi:10.14309/crj.2013.11
19. Burton EM, Mercado-Deane MG, Patel K. Pneumatosis intestinalis in a child with AIDS and pseudomembranous colitis. Pediatr Radiol. 1994;24(8):609-610. doi:10.1007/BF02012750
20. Berk RN, Wall SD, McArdle CB, et al. Cryptosporidiosis of the stomach and small intestine in patients with AIDS. AJR Am J Roentgenol. 1984;143(3):549-554. doi:10.2214/ajr.143.3.549
21. Samson VE, Brown WR. Pneumatosis cystoides intestinalis in AIDS-associated cryptosporidiosis. More than an incidental finding? J Clin Gastroenterol. 1996;22(4):311-312.doi:10.1097/00004836-199606000-00015
22. Tjon A Tham RT, Vlasveld LT, Willemze R. Gastrointestinal complications of cytosine-arabinoside chemotherapy: findings on plain abdominal radiographs. AJR Am J Roentgenol. 1990;154(1):95-98. doi:10.2214/ajr.154.1.2104733
23. Hashimoto S, Saitoh H, Wada K, et al. Pneumatosis cystoides intestinalis after chemotherapy for hematological malignancies: report of 4 cases. Intern Med. 1995;34(3):212-215. doi:10.2169/internalmedicine.34.212
24. Gelman SF, Brandt LJ. Pneumatosis intestinalis and AIDS: a case report and review of the literature. Am J Gastroenterol. 1998;93(4):646-650. doi:10.1111/j.1572-0241.1998.183_b.x
25. Gillon J, Tadesse K, Logan RF, Holt S, Sircus W. Breath hydrogen in pneumatosis cystoides intestinalis. Gut. 1979;20(11):1008-1011. doi:10.1136/gut.20.11.1008
26. Hughes DT, Gordon KC, Swann JC, Bolt GL. Pneumatosis cystoides intestinalis. Gut. 1966;7(5):553-557. doi:10.1136/gut.7.5.553
27. Read NW, Al-Janabi MN, Cann PA. Is raised breath hydrogen related to the pathogenesis of pneumatosis coli? Gut. 1984;25(8):839-845. doi:10.1136/gut.25.8.839
28. van der Linden W, Marsell R. Pneumatosis cystoides coli associated with high H2 excretion. Treatment with an elemental diet. Scand J Gastroenterol. 1979;14(2):173-174. doi:10.3109/00365527909179864
29. Christl SU, Gibson GR, Murgatroyd PR, Scheppach W, Cummings JH. Impaired hydrogen metabolism in pneumatosis cystoides intestinalis. Gastroenterology. 1993;104(2):392-397. doi:10.1016/0016-5085(93)90406-3
30. Keyting WS, Mccarver RR, Kovarik JL, Daywitt AL. Pneumatosis intestinalis: a new concept. Radiology. 1961;76:733-741. doi:10.1148/76.5.733
31. Florin TH, Hills BA. Does counterperfusion supersaturation cause gas cysts in pneumatosis cystoides coli, and can breathing heliox reduce them? Lancet. 1995;345(8959):1220-1222. doi:10.1016/S0140-6736(95)91996-1
32. Grieve DA, Unsworth IP. Pneumatosis cystoides intestinalis: an experience with hyperbaric oxygen treatment. Aust N Z J Surg. 1991;61(6):423-426.
33. Micklefield GH, Kuntz HD, May B. Pneumatosis cystoides intestinalis: case reports and review of the literature. Mater Med Pol. 1990;22(2):70-72.
34. Yale CE, Balish E, Wu JP. The bacterial etiology of pneumatosis cystoides intestinalis. Arch Surg. 1974;109(1):89- 94. doi:10.1001/archsurg.1974.01360010067017
35. Fenton LZ, Buonomo C. Benign pneumatosis in children. Pediatr Radiol. 2000;30(11):786-793. doi:10.1007/s002470000303
36. Tobias R, Coleman S, Helman CA. Pneumatosis coli simulating hepatomegaly. Am J Gastroenterol. 1985;80(2):146-149.
37. Feczko PJ, Mezwa DG, Farah MC, White BD. Clinical significance of pneumatosis of the bowel w a l l . Radiographics. 1992;12(6):1069-1078. doi:10.1148/radiographics.12.6.1439012
38. Masterson JS, Fratkin LB, Osler TR, Trapp WG. Treatment of pneumatosis cystoides intestinalis with hyperbaric oxygen. Ann Surg. 1978;187(3):245-247. doi:10.1097/00000658-197803000-00005
39. Höflin F, Linden W van der. Pneumatosis cystoides intestinalis treated by oxygen breathing. Scandinavian J Gastroenterol . 1974;9(5) :427-430. doi:10.1080/00365521.1974.12096852
40. St Peter SD, Abbas MA, Kelly KA. The spectrum of pneumatosis intestinalis. Arch Surg. 2003;138(1):68-75. doi:10.1001/archsurg.138.1.68
41. Ling F, Guo D, Zhu L. Pneumatosis cystoides intestinalis: a case report and literature review. BMC Gastroenterol. 2019;19(1):176. Published 2019 Nov 6. doi:10.1186/s12876-019-1087-9
42. Morris MS, Gee AC, Cho SD, et al. Management and outcome of pneumatosis intestinalis. Am J Surg. 2008;195(5):679-682. doi:10.1016/j.amjsurg.2008.01.011
Pneumatosis intestinalis (PI) is the finding of gas within the walls of the intestine on imaging. It is most commonly detected via radiograph or computed tomography (CT). The diseases leading to the accumulation of gas within the submucosal space of the gastrointestinal (GI) tract are heterogenous, and the finding of PI itself has a wide range of clinical implications from impending clinical deterioration to an incidental finding of minimal consequence.
We present the case of a veteran who had sustained a remote anoxic brain injury resulting in chronic dependence on a gastrostomy tube for enteral nutrition, found incidentally to have PI without signs of intra-abdominal catastrophe. An exclusion of other, more lifethreatening causes of PI led to a diagnosis of benign PI secondary to the presence of his gastrostomy tube. This case highlights the importance of interpreting the finding of PI in the clinical context of the specific patient and how conservative management may be appropriate in some cases.
Case Presentation
A 61-year-old male patient was admitted for fever. The patient had a remote history of cardiac arrest complicated by anoxic brain injury requiring tracheostomy, gastrostomy tube, and a suprapubic catheter with recurrent catheter-associated urinary tract infections (CAUTI), secondary seizure disorder, atrial fibrillation off anticoagulation due to recurrent GI bleeding, and treatment naive chronic hepatitis C virus. His ability to provide a clinical history was limited by his nonverbal status. He had no prior surgical history but had presented a month earlier for a high-grade small bowel obstruction (SBO) with pneumobilia that was managed conservatively as the surgical team deemed him a poor candidate for surgical intervention with his extensive comorbidities. A bioethics consultation at the time supported minimizing potential surgical risk in favor of conservative medical management; this was discussed with the patient’s surrogate decision maker, who also wished to avoid surgery. The SBO resolved with conservative management. He had been residing in a nursing home and doing well until 24 hours prior to admission when he developed fevers.
Vital signs on admission showed a temperature of 100.8 °F, heart rate 100 beats per minute, blood pressure 116/85, respiratory rate 22 per minute, and oxygen saturation of 100% on 6 L of oxygen via tracheostomy collar. His initial examination was notable for clear lung sounds, a nondistended nonrigid abdomen with an indwelling percutaneous gastrostomy tube, and absence of areas of skin breakdown or erythema. Notable laboratory studies showed a leukocytosis and urinalysis suggestive of CAUTI (Table). His urinary catheter was exchanged, he was fluid resuscitated and started on empiric vancomycin and piperacillin-tazobactam for management of sepsis due to CAUTI.
For the first 3 days of his hospitalization, he demonstrated clinical improvement on vancomycin and piperacillin-tazobactam while awaiting results from his urine bacterial culture. On hospital day 3, hedeveloped recurrent nonbloody, nonbilious emesis despite no change in the rate or formulation of his enteral nutrition. He also had 3 watery brown bowel movements. His vital signs remained within normal limits. His abdominal examination at this point showed mild distention and was hypertympanic to percussion, but there was no rigidity or involuntary guarding. On hospital day 4, he continued to have emesis with an unchanged abdominal examination. The differential diagnosis included recurrence of prior SBO, ileus, intestinal ischemia, enteral nutrition intolerance, Clostridioides difficile (C difficile) colitis, and GI dysmotility because of his anoxic brain injury.
Testing for C difficile was negative. An abdominal radiograph was obtained and revealed no bowel obstruction but, alarmingly, showed extensive intramural bowel gas, suggestive of PI (Figure 1). His leukocyte count, serum bicarbonate, and serum lactate levels remained within normal limits. A CT with contrast of the abdomen and pelvis demonstrated no vascular obstruction but confirmed the presence of diffuse intramural gas in his stomach and proximal small bowel, as well as the presence of mesenteric and portal venous gas (Figures 2 and 3). Although his abdominal examination had not changed and did not suggest peritonitis, general surgery was consulted to discuss the need for surgical intervention. Given his overall clinical stability and high surgical risk due to his many comorbidities, surgery recommended a conservative approach.
Through the following hospital days, his enteral nutrition was held and serial abdominal examinations were performed without change. Serial laboratory studies, including serum lactate and leukocyte count, remained reassuringly within normal limits. His urine culture eventually revealed multidrugresistant Pseudomonas aeruginosa. Antimicrobial therapy was narrowed to piperacillintazobactam for a complete course. Enteral nutrition was gradually reintroduced at a low rate, ultimately reaching goal rate with return of bowel function by hospital day 9. Despite extensive workup, the etiology of his transient enteral nutrition intolerance remained uncertain, though an adverse effect of antibiotic therapy was thought possible. Follow-up abdominal radiographs demonstrated interval improvement of PI. He was discharged back to his skilled nursing facility on hospital day 11 without incident.
Discussion
PI is an incompletely understood condition seen in multiple diseases. Patients may present with highly variable symptoms, often more attributable to the underlying disease causing the PI than the presence of PI, as patients may be entirely asymptomatic. When symptoms are attributed to PI, those most reported are abdominal pain, bloody stools, and diarrhea.1 It is often detected on abdominal plain films. Alternative methods of diagnosis include ultrasonography, barium enema, and endoscopy although the last method has been known to occasionally lead to bowel perforation.2-6 The most sensitive method of detection is CT, which also provides additional information about abdominal pathology and may identify the underlying process responsible for the PI.7
While not fully understood, much information about PI and its pathogenesis is known. Understanding the mechanisms of PI is vital to direct the clinician’s evaluation of the patient for reversible conditions that may cause PI. Early descriptions of PI in the literature documented an association with pyloric stenosis, leading to the theory that gas from the intestinal lumen is driven into the submucosal space during episodes of forceful vomiting with increased intraluminal pressure.8 As PI was subsequently described in multiple other disease states not typically associated with increased intraluminal pressure such as inflammatory bowel disease, GI malignancy, cryptosporidiosis and CMV infection, additional theories about the pathogenesis of PI have arisen.9-24 There is now experimental data to support multiple mechanisms of intramural gas accumulation. It has become accepted that PI represents a common pathway shared across various pathologic states and results from multifactorial mechanisms of gas entry into the intestinal wall.25-29
Factors leading to the development of PI include bacterial production of gas, intraluminal GI gas compositions, increased intraluminal pressure, pulmonary gas tracking through vessels communicating with the thorax, and mucosal disruption. PI has been linked to bacterial infections of the GI tract in humans including C difficile, Klebsiella, and Whipple disease.14-18 In animal models, C difficile within the walls of rat intestine results in the appearance of pneumocysts, or discrete collections of submucosal gas, which are the hallmark feature of PI.30 It is thought that direct invasion of bacteria into intramural spaces can cause PI in humans, although bacteria have yet to be directly isolated from the pneumocysts. Translocation of luminal gas into pneumocysts found in PI is theorized to be driven by differences in partial pressures.31 The concentration of hydrogen within the intestinal lumen is high due to bacterial production. Hydrogen, diffusing along its partial pressure gradient between the lumen and blood, accumulates within the intestinal wall and causes the formation of pneumocysts. This phenomenon has been hypothesized to explain the tendency for pneumocysts to form around the mesenteric vasculature.
Gas from the lumen can also be forced into the intestinal wall during an abrupt increase in intra-abdominal pressure, such as that seen with forceful vomiting. The final possible origin of the gas is the lungs, as PI has been associated with lung disease. It was previously thought that gas from ruptured alveoli tracks along mediastinal vessels, below the diaphragm, and into the mesentery.30 Newer theories argue that increased intra-abdominal pressure, typical of patients with obstructive lung disease and frequent coughing, is the driver of PI by the mechanism previously described.32-34 Additionally, mucosal disruption leads to increased permeability and allows accumulation of gas within the intestinal walls. Mucosal abnormalities have been described in histopathologic studies of patients with PI and associated with conditions known to compromise mucosal integrity, such as immunodeficiencies, inflammatory bowel disease, and the receipt of cytotoxic chemotherapy.10,12,19-23
Our patient likely had mucosal disruption due to his gastrostomy tube as well as increased intraluminal pressure from recurrent vomiting, contributing to translocation of otherwise normal intraluminal gas. The presence of portal venous gas, as seen in this case, has historically portended a worse prognosis, with 37% mortality in one series.7,35,36 However, portal venous gas as well as pneumoperitoneum occur in benign etiologies of PI as well. It is thought that this occurs due to rupture of the submucosal pneumocysts through the wall opposite the intestinal lumen and thus does not result in a direct communication between the intestinal lumen and the peritoneal cavity.12
PI is not a diagnosis but a manifestation of an underlying disease. As such, the treatment of PI is targeted toward the underlying condition. Of note, the pattern and extent of PI seen on imaging has not been shown to correlate with the severity of the underlying pathologic process.35,37 Instead, assessment of the patient and their clinical trajectory should determine the appropriate treatment. The decision facing the clinician when PI is discovered is whether urgent surgery is indicated, as is the case in mesenteric ischemia, bowel necrosis, or intestinal perforation, conditions known to be associated with PI. Otherwise, there is no definitive treatment for PI. Bowel rest is almost universally pursued. There are reports of treating with supranormal levels of supplemental oxygen, maintaining arterial partial pressure of oxygen above 300 mm Hg, with a face mask and 8 L/min flow rate.38,39 The proposed mechanisms of benefit include establishing a favorable diffusion gradient for intramural gas to exit the pneumocysts as well as creating an inhospitable, aerobic environment for hydrogenproducing anaerobic enteric bacteria. A prudent approach for most cases of PI is conservative management with bowel rest and supplemental oxygen unless there is a definitive indication for urgent surgical intervention, such as peritonitis, abdominal sepsis, or perforation.40,41 Management recommendations suggest that up to 50% of cases can be successfully managed nonoperatively.42
Conclusions
PI is the radiographic finding of gas within the walls of the intestinal tract and has variable clinical significance. It can represent a benign incidental finding or a sequela of intraabdominal emergencies such as mesenteric ischemia or bowel necrosis. Because PI is seen in a variety of disorders, several proposed mechanisms are supported in the medical literature. These include bacterial production of gas, gas pressure gradients between the intestinal lumen and the blood, increased intraluminal pressure, pulmonary gas tracking from intrathoracic vessels, and mucosal disruption. The evaluation of a patient with PI must begin with an assessment for the need for urgent surgical intervention. Additional management measures include bowel rest, IV hydration, and supplemental oxygen administration. Because of its wide variety of etiologies of varying clinical urgency, placing the finding of PI in the context of the patient is paramount to selecting an appropriate management strategy.
Pneumatosis intestinalis (PI) is the finding of gas within the walls of the intestine on imaging. It is most commonly detected via radiograph or computed tomography (CT). The diseases leading to the accumulation of gas within the submucosal space of the gastrointestinal (GI) tract are heterogenous, and the finding of PI itself has a wide range of clinical implications from impending clinical deterioration to an incidental finding of minimal consequence.
We present the case of a veteran who had sustained a remote anoxic brain injury resulting in chronic dependence on a gastrostomy tube for enteral nutrition, found incidentally to have PI without signs of intra-abdominal catastrophe. An exclusion of other, more lifethreatening causes of PI led to a diagnosis of benign PI secondary to the presence of his gastrostomy tube. This case highlights the importance of interpreting the finding of PI in the clinical context of the specific patient and how conservative management may be appropriate in some cases.
Case Presentation
A 61-year-old male patient was admitted for fever. The patient had a remote history of cardiac arrest complicated by anoxic brain injury requiring tracheostomy, gastrostomy tube, and a suprapubic catheter with recurrent catheter-associated urinary tract infections (CAUTI), secondary seizure disorder, atrial fibrillation off anticoagulation due to recurrent GI bleeding, and treatment naive chronic hepatitis C virus. His ability to provide a clinical history was limited by his nonverbal status. He had no prior surgical history but had presented a month earlier for a high-grade small bowel obstruction (SBO) with pneumobilia that was managed conservatively as the surgical team deemed him a poor candidate for surgical intervention with his extensive comorbidities. A bioethics consultation at the time supported minimizing potential surgical risk in favor of conservative medical management; this was discussed with the patient’s surrogate decision maker, who also wished to avoid surgery. The SBO resolved with conservative management. He had been residing in a nursing home and doing well until 24 hours prior to admission when he developed fevers.
Vital signs on admission showed a temperature of 100.8 °F, heart rate 100 beats per minute, blood pressure 116/85, respiratory rate 22 per minute, and oxygen saturation of 100% on 6 L of oxygen via tracheostomy collar. His initial examination was notable for clear lung sounds, a nondistended nonrigid abdomen with an indwelling percutaneous gastrostomy tube, and absence of areas of skin breakdown or erythema. Notable laboratory studies showed a leukocytosis and urinalysis suggestive of CAUTI (Table). His urinary catheter was exchanged, he was fluid resuscitated and started on empiric vancomycin and piperacillin-tazobactam for management of sepsis due to CAUTI.
For the first 3 days of his hospitalization, he demonstrated clinical improvement on vancomycin and piperacillin-tazobactam while awaiting results from his urine bacterial culture. On hospital day 3, hedeveloped recurrent nonbloody, nonbilious emesis despite no change in the rate or formulation of his enteral nutrition. He also had 3 watery brown bowel movements. His vital signs remained within normal limits. His abdominal examination at this point showed mild distention and was hypertympanic to percussion, but there was no rigidity or involuntary guarding. On hospital day 4, he continued to have emesis with an unchanged abdominal examination. The differential diagnosis included recurrence of prior SBO, ileus, intestinal ischemia, enteral nutrition intolerance, Clostridioides difficile (C difficile) colitis, and GI dysmotility because of his anoxic brain injury.
Testing for C difficile was negative. An abdominal radiograph was obtained and revealed no bowel obstruction but, alarmingly, showed extensive intramural bowel gas, suggestive of PI (Figure 1). His leukocyte count, serum bicarbonate, and serum lactate levels remained within normal limits. A CT with contrast of the abdomen and pelvis demonstrated no vascular obstruction but confirmed the presence of diffuse intramural gas in his stomach and proximal small bowel, as well as the presence of mesenteric and portal venous gas (Figures 2 and 3). Although his abdominal examination had not changed and did not suggest peritonitis, general surgery was consulted to discuss the need for surgical intervention. Given his overall clinical stability and high surgical risk due to his many comorbidities, surgery recommended a conservative approach.
Through the following hospital days, his enteral nutrition was held and serial abdominal examinations were performed without change. Serial laboratory studies, including serum lactate and leukocyte count, remained reassuringly within normal limits. His urine culture eventually revealed multidrugresistant Pseudomonas aeruginosa. Antimicrobial therapy was narrowed to piperacillintazobactam for a complete course. Enteral nutrition was gradually reintroduced at a low rate, ultimately reaching goal rate with return of bowel function by hospital day 9. Despite extensive workup, the etiology of his transient enteral nutrition intolerance remained uncertain, though an adverse effect of antibiotic therapy was thought possible. Follow-up abdominal radiographs demonstrated interval improvement of PI. He was discharged back to his skilled nursing facility on hospital day 11 without incident.
Discussion
PI is an incompletely understood condition seen in multiple diseases. Patients may present with highly variable symptoms, often more attributable to the underlying disease causing the PI than the presence of PI, as patients may be entirely asymptomatic. When symptoms are attributed to PI, those most reported are abdominal pain, bloody stools, and diarrhea.1 It is often detected on abdominal plain films. Alternative methods of diagnosis include ultrasonography, barium enema, and endoscopy although the last method has been known to occasionally lead to bowel perforation.2-6 The most sensitive method of detection is CT, which also provides additional information about abdominal pathology and may identify the underlying process responsible for the PI.7
While not fully understood, much information about PI and its pathogenesis is known. Understanding the mechanisms of PI is vital to direct the clinician’s evaluation of the patient for reversible conditions that may cause PI. Early descriptions of PI in the literature documented an association with pyloric stenosis, leading to the theory that gas from the intestinal lumen is driven into the submucosal space during episodes of forceful vomiting with increased intraluminal pressure.8 As PI was subsequently described in multiple other disease states not typically associated with increased intraluminal pressure such as inflammatory bowel disease, GI malignancy, cryptosporidiosis and CMV infection, additional theories about the pathogenesis of PI have arisen.9-24 There is now experimental data to support multiple mechanisms of intramural gas accumulation. It has become accepted that PI represents a common pathway shared across various pathologic states and results from multifactorial mechanisms of gas entry into the intestinal wall.25-29
Factors leading to the development of PI include bacterial production of gas, intraluminal GI gas compositions, increased intraluminal pressure, pulmonary gas tracking through vessels communicating with the thorax, and mucosal disruption. PI has been linked to bacterial infections of the GI tract in humans including C difficile, Klebsiella, and Whipple disease.14-18 In animal models, C difficile within the walls of rat intestine results in the appearance of pneumocysts, or discrete collections of submucosal gas, which are the hallmark feature of PI.30 It is thought that direct invasion of bacteria into intramural spaces can cause PI in humans, although bacteria have yet to be directly isolated from the pneumocysts. Translocation of luminal gas into pneumocysts found in PI is theorized to be driven by differences in partial pressures.31 The concentration of hydrogen within the intestinal lumen is high due to bacterial production. Hydrogen, diffusing along its partial pressure gradient between the lumen and blood, accumulates within the intestinal wall and causes the formation of pneumocysts. This phenomenon has been hypothesized to explain the tendency for pneumocysts to form around the mesenteric vasculature.
Gas from the lumen can also be forced into the intestinal wall during an abrupt increase in intra-abdominal pressure, such as that seen with forceful vomiting. The final possible origin of the gas is the lungs, as PI has been associated with lung disease. It was previously thought that gas from ruptured alveoli tracks along mediastinal vessels, below the diaphragm, and into the mesentery.30 Newer theories argue that increased intra-abdominal pressure, typical of patients with obstructive lung disease and frequent coughing, is the driver of PI by the mechanism previously described.32-34 Additionally, mucosal disruption leads to increased permeability and allows accumulation of gas within the intestinal walls. Mucosal abnormalities have been described in histopathologic studies of patients with PI and associated with conditions known to compromise mucosal integrity, such as immunodeficiencies, inflammatory bowel disease, and the receipt of cytotoxic chemotherapy.10,12,19-23
Our patient likely had mucosal disruption due to his gastrostomy tube as well as increased intraluminal pressure from recurrent vomiting, contributing to translocation of otherwise normal intraluminal gas. The presence of portal venous gas, as seen in this case, has historically portended a worse prognosis, with 37% mortality in one series.7,35,36 However, portal venous gas as well as pneumoperitoneum occur in benign etiologies of PI as well. It is thought that this occurs due to rupture of the submucosal pneumocysts through the wall opposite the intestinal lumen and thus does not result in a direct communication between the intestinal lumen and the peritoneal cavity.12
PI is not a diagnosis but a manifestation of an underlying disease. As such, the treatment of PI is targeted toward the underlying condition. Of note, the pattern and extent of PI seen on imaging has not been shown to correlate with the severity of the underlying pathologic process.35,37 Instead, assessment of the patient and their clinical trajectory should determine the appropriate treatment. The decision facing the clinician when PI is discovered is whether urgent surgery is indicated, as is the case in mesenteric ischemia, bowel necrosis, or intestinal perforation, conditions known to be associated with PI. Otherwise, there is no definitive treatment for PI. Bowel rest is almost universally pursued. There are reports of treating with supranormal levels of supplemental oxygen, maintaining arterial partial pressure of oxygen above 300 mm Hg, with a face mask and 8 L/min flow rate.38,39 The proposed mechanisms of benefit include establishing a favorable diffusion gradient for intramural gas to exit the pneumocysts as well as creating an inhospitable, aerobic environment for hydrogenproducing anaerobic enteric bacteria. A prudent approach for most cases of PI is conservative management with bowel rest and supplemental oxygen unless there is a definitive indication for urgent surgical intervention, such as peritonitis, abdominal sepsis, or perforation.40,41 Management recommendations suggest that up to 50% of cases can be successfully managed nonoperatively.42
Conclusions
PI is the radiographic finding of gas within the walls of the intestinal tract and has variable clinical significance. It can represent a benign incidental finding or a sequela of intraabdominal emergencies such as mesenteric ischemia or bowel necrosis. Because PI is seen in a variety of disorders, several proposed mechanisms are supported in the medical literature. These include bacterial production of gas, gas pressure gradients between the intestinal lumen and the blood, increased intraluminal pressure, pulmonary gas tracking from intrathoracic vessels, and mucosal disruption. The evaluation of a patient with PI must begin with an assessment for the need for urgent surgical intervention. Additional management measures include bowel rest, IV hydration, and supplemental oxygen administration. Because of its wide variety of etiologies of varying clinical urgency, placing the finding of PI in the context of the patient is paramount to selecting an appropriate management strategy.
1. Jamart J. Pneumatosis cystoides intestinalis. A statistical study of 919 cases. Acta Hepatogastroenterol (Stuttg). 1979;26(5):419-422.
2. Lafortune M, Trinh BC, Burns PN, et al. Air in the portal vein: sonographic and Doppler manifestations. Radiology. 1991;180(3):667-670. doi:10.1148/radiology.180.3.1871276
3. Kriegshauser JS, Reading CC, King BF, Welch TJ. Combined systemic and portal venous gas: sonographic and CT detection in two cases. AJR Am J Roentgenol. 1990;154(6):1219-1221. doi:10.2214/ajr.154.6.2110731
4. Goske MJ, Goldblum JR, Applegate KE, Mitchell CS, Bardo D. The “circle sign”: a new sonographic sign of pneumatosis intestinalis - clinical, pathologic and experimental findings. Pediatr Radiol. 1999;29(7):530-535. doi:10.1007/s002470050638
5. Marshak RH, Lindner AE, Maklansky D. Pneumatosis cystoides coli. Gastrointest Radiol. 1977;2(2):85-89. doi:10.1007/BF02256475
6. Jensen R, Gutnik SH. Pneumatosis cystoides intestinalis: a complication of colonoscopic polypectomy. S D J Med. 1991;44(7):177-179.
7. Knechtle SJ, Davidoff AM, Rice RP. Pneumatosis intestinalis. Surgical management and clinical outcome. Ann Surg. 1990;212(2):160-165. doi:10.1097/00000658-199008000-00008
8. Koss LG. Abdominal gas cysts (Pneumatosis cystoides intestinorum hominis); an analysis with a report of a case and a critical review of the literature. AMA Arch Pathol. 1952;53(6):523-549.
9. Jona JZ. Benign pneumatosis intestinalis coli after blunt trauma to the abdomen in a child. J Pediatr Surg. 2000;35(7):1109-1111. doi:10.1053/jpsu.2000.7837
10. Gagliardi G, Thompson IW, Hershman MJ, Forbes A, Hawley PR, Talbot IC. Pneumatosis coli: a proposed pathogenesis based on study of 25 cases and review of the literature. Int J Colorectal Dis. 1996;11(3):111-118. doi:10.1007/s003840050031
11. Seto T, Koide N, Taniuchi N, Yamada T, Hamaguchi M, Goto S. Pneumatosis cystoides intestinalis complicating carcinoma of the small intestine. Am J Surg. 2001;182(3):287-288. doi:10.1016/S0002-9610(01)00710-3
12. Galandiuk S, Fazio VW, Petras RE. Pneumatosis cystoides intestinalis in Crohn’s disease. Report of two cases. Dis Colon Rectum. 1985;28(12):951-956. doi:10.1007/BF02554315
13. Parra JA, Acinas O, Bueno J, Madrazo C, Fariñas C. An unusual form of pneumatosis intestinalis associated with appendicitis. Br J Radiol. 1998;71(843):326-328. doi:10.1259/bjr.71.843.9616245
14. Schenk P, Madl C, Kramer L, et al. Pneumatosis intestinalis with Clostridium difficile colitis as a cause of acute abdomen after lung transplantation. Dig Dis Sci. 1998;43(11):2455-2458. doi:10.1023/a:1026682131847
15. Kreiss C, Forohar F, Smithline AE, Brandt LJ. Pneumatosis intestinalis complicating C. difficile pseudomembranous colitis. Am J Gastroenterol. 1999;94(9):2560-2561. doi:10.1111/j.1572-0241.1999.01397.x
16. Day DL, Ramsay NK, Letourneau JG. Pneumatosis intestinalis after bone marrow transplantation. AJR Am J Roentgenol. 1988;151(1):85-87. doi:10.2214/ajr.151.1.85
17. Tahara S, Sakai Y, Katsuno H, Urano M, Kuroda M, Tsukamoto T. Pneumatosis intestinalis and hepatic portal venous gas associated with gas-forming bacterial translocation due to postoperative paralytic ileus: A case report. Medicine (Baltimore). 2019;98(2):e14079. doi:10.1097/MD.0000000000014079
18. Klochan C, Anderson TA, Rose D, Dimitrov RK, Johnson RM. Nearly fatal case of whipple’s disease in a patient mistakenly on anti-tnf therapy. ACG Case Rep J. 2013;1(1):25- 28. Published 2013 Oct 8. doi:10.14309/crj.2013.11
19. Burton EM, Mercado-Deane MG, Patel K. Pneumatosis intestinalis in a child with AIDS and pseudomembranous colitis. Pediatr Radiol. 1994;24(8):609-610. doi:10.1007/BF02012750
20. Berk RN, Wall SD, McArdle CB, et al. Cryptosporidiosis of the stomach and small intestine in patients with AIDS. AJR Am J Roentgenol. 1984;143(3):549-554. doi:10.2214/ajr.143.3.549
21. Samson VE, Brown WR. Pneumatosis cystoides intestinalis in AIDS-associated cryptosporidiosis. More than an incidental finding? J Clin Gastroenterol. 1996;22(4):311-312.doi:10.1097/00004836-199606000-00015
22. Tjon A Tham RT, Vlasveld LT, Willemze R. Gastrointestinal complications of cytosine-arabinoside chemotherapy: findings on plain abdominal radiographs. AJR Am J Roentgenol. 1990;154(1):95-98. doi:10.2214/ajr.154.1.2104733
23. Hashimoto S, Saitoh H, Wada K, et al. Pneumatosis cystoides intestinalis after chemotherapy for hematological malignancies: report of 4 cases. Intern Med. 1995;34(3):212-215. doi:10.2169/internalmedicine.34.212
24. Gelman SF, Brandt LJ. Pneumatosis intestinalis and AIDS: a case report and review of the literature. Am J Gastroenterol. 1998;93(4):646-650. doi:10.1111/j.1572-0241.1998.183_b.x
25. Gillon J, Tadesse K, Logan RF, Holt S, Sircus W. Breath hydrogen in pneumatosis cystoides intestinalis. Gut. 1979;20(11):1008-1011. doi:10.1136/gut.20.11.1008
26. Hughes DT, Gordon KC, Swann JC, Bolt GL. Pneumatosis cystoides intestinalis. Gut. 1966;7(5):553-557. doi:10.1136/gut.7.5.553
27. Read NW, Al-Janabi MN, Cann PA. Is raised breath hydrogen related to the pathogenesis of pneumatosis coli? Gut. 1984;25(8):839-845. doi:10.1136/gut.25.8.839
28. van der Linden W, Marsell R. Pneumatosis cystoides coli associated with high H2 excretion. Treatment with an elemental diet. Scand J Gastroenterol. 1979;14(2):173-174. doi:10.3109/00365527909179864
29. Christl SU, Gibson GR, Murgatroyd PR, Scheppach W, Cummings JH. Impaired hydrogen metabolism in pneumatosis cystoides intestinalis. Gastroenterology. 1993;104(2):392-397. doi:10.1016/0016-5085(93)90406-3
30. Keyting WS, Mccarver RR, Kovarik JL, Daywitt AL. Pneumatosis intestinalis: a new concept. Radiology. 1961;76:733-741. doi:10.1148/76.5.733
31. Florin TH, Hills BA. Does counterperfusion supersaturation cause gas cysts in pneumatosis cystoides coli, and can breathing heliox reduce them? Lancet. 1995;345(8959):1220-1222. doi:10.1016/S0140-6736(95)91996-1
32. Grieve DA, Unsworth IP. Pneumatosis cystoides intestinalis: an experience with hyperbaric oxygen treatment. Aust N Z J Surg. 1991;61(6):423-426.
33. Micklefield GH, Kuntz HD, May B. Pneumatosis cystoides intestinalis: case reports and review of the literature. Mater Med Pol. 1990;22(2):70-72.
34. Yale CE, Balish E, Wu JP. The bacterial etiology of pneumatosis cystoides intestinalis. Arch Surg. 1974;109(1):89- 94. doi:10.1001/archsurg.1974.01360010067017
35. Fenton LZ, Buonomo C. Benign pneumatosis in children. Pediatr Radiol. 2000;30(11):786-793. doi:10.1007/s002470000303
36. Tobias R, Coleman S, Helman CA. Pneumatosis coli simulating hepatomegaly. Am J Gastroenterol. 1985;80(2):146-149.
37. Feczko PJ, Mezwa DG, Farah MC, White BD. Clinical significance of pneumatosis of the bowel w a l l . Radiographics. 1992;12(6):1069-1078. doi:10.1148/radiographics.12.6.1439012
38. Masterson JS, Fratkin LB, Osler TR, Trapp WG. Treatment of pneumatosis cystoides intestinalis with hyperbaric oxygen. Ann Surg. 1978;187(3):245-247. doi:10.1097/00000658-197803000-00005
39. Höflin F, Linden W van der. Pneumatosis cystoides intestinalis treated by oxygen breathing. Scandinavian J Gastroenterol . 1974;9(5) :427-430. doi:10.1080/00365521.1974.12096852
40. St Peter SD, Abbas MA, Kelly KA. The spectrum of pneumatosis intestinalis. Arch Surg. 2003;138(1):68-75. doi:10.1001/archsurg.138.1.68
41. Ling F, Guo D, Zhu L. Pneumatosis cystoides intestinalis: a case report and literature review. BMC Gastroenterol. 2019;19(1):176. Published 2019 Nov 6. doi:10.1186/s12876-019-1087-9
42. Morris MS, Gee AC, Cho SD, et al. Management and outcome of pneumatosis intestinalis. Am J Surg. 2008;195(5):679-682. doi:10.1016/j.amjsurg.2008.01.011
1. Jamart J. Pneumatosis cystoides intestinalis. A statistical study of 919 cases. Acta Hepatogastroenterol (Stuttg). 1979;26(5):419-422.
2. Lafortune M, Trinh BC, Burns PN, et al. Air in the portal vein: sonographic and Doppler manifestations. Radiology. 1991;180(3):667-670. doi:10.1148/radiology.180.3.1871276
3. Kriegshauser JS, Reading CC, King BF, Welch TJ. Combined systemic and portal venous gas: sonographic and CT detection in two cases. AJR Am J Roentgenol. 1990;154(6):1219-1221. doi:10.2214/ajr.154.6.2110731
4. Goske MJ, Goldblum JR, Applegate KE, Mitchell CS, Bardo D. The “circle sign”: a new sonographic sign of pneumatosis intestinalis - clinical, pathologic and experimental findings. Pediatr Radiol. 1999;29(7):530-535. doi:10.1007/s002470050638
5. Marshak RH, Lindner AE, Maklansky D. Pneumatosis cystoides coli. Gastrointest Radiol. 1977;2(2):85-89. doi:10.1007/BF02256475
6. Jensen R, Gutnik SH. Pneumatosis cystoides intestinalis: a complication of colonoscopic polypectomy. S D J Med. 1991;44(7):177-179.
7. Knechtle SJ, Davidoff AM, Rice RP. Pneumatosis intestinalis. Surgical management and clinical outcome. Ann Surg. 1990;212(2):160-165. doi:10.1097/00000658-199008000-00008
8. Koss LG. Abdominal gas cysts (Pneumatosis cystoides intestinorum hominis); an analysis with a report of a case and a critical review of the literature. AMA Arch Pathol. 1952;53(6):523-549.
9. Jona JZ. Benign pneumatosis intestinalis coli after blunt trauma to the abdomen in a child. J Pediatr Surg. 2000;35(7):1109-1111. doi:10.1053/jpsu.2000.7837
10. Gagliardi G, Thompson IW, Hershman MJ, Forbes A, Hawley PR, Talbot IC. Pneumatosis coli: a proposed pathogenesis based on study of 25 cases and review of the literature. Int J Colorectal Dis. 1996;11(3):111-118. doi:10.1007/s003840050031
11. Seto T, Koide N, Taniuchi N, Yamada T, Hamaguchi M, Goto S. Pneumatosis cystoides intestinalis complicating carcinoma of the small intestine. Am J Surg. 2001;182(3):287-288. doi:10.1016/S0002-9610(01)00710-3
12. Galandiuk S, Fazio VW, Petras RE. Pneumatosis cystoides intestinalis in Crohn’s disease. Report of two cases. Dis Colon Rectum. 1985;28(12):951-956. doi:10.1007/BF02554315
13. Parra JA, Acinas O, Bueno J, Madrazo C, Fariñas C. An unusual form of pneumatosis intestinalis associated with appendicitis. Br J Radiol. 1998;71(843):326-328. doi:10.1259/bjr.71.843.9616245
14. Schenk P, Madl C, Kramer L, et al. Pneumatosis intestinalis with Clostridium difficile colitis as a cause of acute abdomen after lung transplantation. Dig Dis Sci. 1998;43(11):2455-2458. doi:10.1023/a:1026682131847
15. Kreiss C, Forohar F, Smithline AE, Brandt LJ. Pneumatosis intestinalis complicating C. difficile pseudomembranous colitis. Am J Gastroenterol. 1999;94(9):2560-2561. doi:10.1111/j.1572-0241.1999.01397.x
16. Day DL, Ramsay NK, Letourneau JG. Pneumatosis intestinalis after bone marrow transplantation. AJR Am J Roentgenol. 1988;151(1):85-87. doi:10.2214/ajr.151.1.85
17. Tahara S, Sakai Y, Katsuno H, Urano M, Kuroda M, Tsukamoto T. Pneumatosis intestinalis and hepatic portal venous gas associated with gas-forming bacterial translocation due to postoperative paralytic ileus: A case report. Medicine (Baltimore). 2019;98(2):e14079. doi:10.1097/MD.0000000000014079
18. Klochan C, Anderson TA, Rose D, Dimitrov RK, Johnson RM. Nearly fatal case of whipple’s disease in a patient mistakenly on anti-tnf therapy. ACG Case Rep J. 2013;1(1):25- 28. Published 2013 Oct 8. doi:10.14309/crj.2013.11
19. Burton EM, Mercado-Deane MG, Patel K. Pneumatosis intestinalis in a child with AIDS and pseudomembranous colitis. Pediatr Radiol. 1994;24(8):609-610. doi:10.1007/BF02012750
20. Berk RN, Wall SD, McArdle CB, et al. Cryptosporidiosis of the stomach and small intestine in patients with AIDS. AJR Am J Roentgenol. 1984;143(3):549-554. doi:10.2214/ajr.143.3.549
21. Samson VE, Brown WR. Pneumatosis cystoides intestinalis in AIDS-associated cryptosporidiosis. More than an incidental finding? J Clin Gastroenterol. 1996;22(4):311-312.doi:10.1097/00004836-199606000-00015
22. Tjon A Tham RT, Vlasveld LT, Willemze R. Gastrointestinal complications of cytosine-arabinoside chemotherapy: findings on plain abdominal radiographs. AJR Am J Roentgenol. 1990;154(1):95-98. doi:10.2214/ajr.154.1.2104733
23. Hashimoto S, Saitoh H, Wada K, et al. Pneumatosis cystoides intestinalis after chemotherapy for hematological malignancies: report of 4 cases. Intern Med. 1995;34(3):212-215. doi:10.2169/internalmedicine.34.212
24. Gelman SF, Brandt LJ. Pneumatosis intestinalis and AIDS: a case report and review of the literature. Am J Gastroenterol. 1998;93(4):646-650. doi:10.1111/j.1572-0241.1998.183_b.x
25. Gillon J, Tadesse K, Logan RF, Holt S, Sircus W. Breath hydrogen in pneumatosis cystoides intestinalis. Gut. 1979;20(11):1008-1011. doi:10.1136/gut.20.11.1008
26. Hughes DT, Gordon KC, Swann JC, Bolt GL. Pneumatosis cystoides intestinalis. Gut. 1966;7(5):553-557. doi:10.1136/gut.7.5.553
27. Read NW, Al-Janabi MN, Cann PA. Is raised breath hydrogen related to the pathogenesis of pneumatosis coli? Gut. 1984;25(8):839-845. doi:10.1136/gut.25.8.839
28. van der Linden W, Marsell R. Pneumatosis cystoides coli associated with high H2 excretion. Treatment with an elemental diet. Scand J Gastroenterol. 1979;14(2):173-174. doi:10.3109/00365527909179864
29. Christl SU, Gibson GR, Murgatroyd PR, Scheppach W, Cummings JH. Impaired hydrogen metabolism in pneumatosis cystoides intestinalis. Gastroenterology. 1993;104(2):392-397. doi:10.1016/0016-5085(93)90406-3
30. Keyting WS, Mccarver RR, Kovarik JL, Daywitt AL. Pneumatosis intestinalis: a new concept. Radiology. 1961;76:733-741. doi:10.1148/76.5.733
31. Florin TH, Hills BA. Does counterperfusion supersaturation cause gas cysts in pneumatosis cystoides coli, and can breathing heliox reduce them? Lancet. 1995;345(8959):1220-1222. doi:10.1016/S0140-6736(95)91996-1
32. Grieve DA, Unsworth IP. Pneumatosis cystoides intestinalis: an experience with hyperbaric oxygen treatment. Aust N Z J Surg. 1991;61(6):423-426.
33. Micklefield GH, Kuntz HD, May B. Pneumatosis cystoides intestinalis: case reports and review of the literature. Mater Med Pol. 1990;22(2):70-72.
34. Yale CE, Balish E, Wu JP. The bacterial etiology of pneumatosis cystoides intestinalis. Arch Surg. 1974;109(1):89- 94. doi:10.1001/archsurg.1974.01360010067017
35. Fenton LZ, Buonomo C. Benign pneumatosis in children. Pediatr Radiol. 2000;30(11):786-793. doi:10.1007/s002470000303
36. Tobias R, Coleman S, Helman CA. Pneumatosis coli simulating hepatomegaly. Am J Gastroenterol. 1985;80(2):146-149.
37. Feczko PJ, Mezwa DG, Farah MC, White BD. Clinical significance of pneumatosis of the bowel w a l l . Radiographics. 1992;12(6):1069-1078. doi:10.1148/radiographics.12.6.1439012
38. Masterson JS, Fratkin LB, Osler TR, Trapp WG. Treatment of pneumatosis cystoides intestinalis with hyperbaric oxygen. Ann Surg. 1978;187(3):245-247. doi:10.1097/00000658-197803000-00005
39. Höflin F, Linden W van der. Pneumatosis cystoides intestinalis treated by oxygen breathing. Scandinavian J Gastroenterol . 1974;9(5) :427-430. doi:10.1080/00365521.1974.12096852
40. St Peter SD, Abbas MA, Kelly KA. The spectrum of pneumatosis intestinalis. Arch Surg. 2003;138(1):68-75. doi:10.1001/archsurg.138.1.68
41. Ling F, Guo D, Zhu L. Pneumatosis cystoides intestinalis: a case report and literature review. BMC Gastroenterol. 2019;19(1):176. Published 2019 Nov 6. doi:10.1186/s12876-019-1087-9
42. Morris MS, Gee AC, Cho SD, et al. Management and outcome of pneumatosis intestinalis. Am J Surg. 2008;195(5):679-682. doi:10.1016/j.amjsurg.2008.01.011
‘Double-edged’ impact of sparring on the brains of MMA fighters
, early research suggests.
Investigators found sparring, defined as strategically hitting opponents with kicks, punches, and other strikes during practice sessions, is linked to increased white matter hyperintensities in the brain, pointing to possible vascular damage from repeated head trauma. However, the study results also show sparring was associated with a larger bilateral caudate which, in theory, is neuroprotective.
“From our preliminary study, sparring practice in MMA fighters may have a ‘double-edged sword’ effect on the brain,” study investigator Aaron Esagoff, a second-year medical student at Johns Hopkins University School of Medicine, Baltimore, told this news organization.

“The combination of complex movements along with constant strategy and anticipation of your opponent’s next move may provide a neuroprotective effect on the caudate,” Mr. Esagoff said. However, he added, more research is needed into understanding this particular finding.
The study results were presented at the American Psychiatric Association (APA) 2022 Annual Meeting.
Growing popularity
MMA is a full-contact combat sport that has become increasingly popular over the past 15 years. It combines techniques from boxing, wrestling, karate, judo, and jujitsu.
To prepare for fights, MMA practitioners incorporate sparring and grappling, which use techniques such as chokes and locks to submit an opponent. Head protection is sometimes incorporated during practice, but is not the norm during a fight, said Mr. Esagoff.
The study investigated sparring during practice rather than fights because, he said, MMA competitors only fight a few times a year but spend hundreds of hours training. “So the health effects of training are going to be really important,” he said.
As with other combat sports, MMA involves hits to the head. Previous research has shown repetitive head trauma can lead to neurodegenerative diseases, including chronic traumatic encephalopathy (CTE) and Alzheimer’s disease, Mr. Esagoff noted.
Previous studies have also linked more professional fights and years of fighting to a decrease in brain volume among MMA fighters, he added.
The new analysis was conducted as part of the Professional Fighters Brain Health Study, a longitudinal cohort study of MMA professional fighters. It included 92 fighters with data available on MRI and habits regarding practicing. The mean age of the participants was 30 years, 62% were White, and 85% were men.
The study examined sparring but did not include grappling because of “several challenges” with the current data analysis, Mr. Esagoff said. Researchers adjusted for age, sex, education, race, number of fights, total intracranial volume, and type of MRI scanner used.
A ‘highly strategic’ sport
Results showed a strong association between the number of sparring rounds per week and increased white matter hyperintensity volume (mcL) on MRI (P = .039).
This suggests white matter damage, possibly a result of direct neuronal injury, vascular damage, or immune modulation, said Mr. Esagoff. However, another mechanism may be involved, he added.
There was also a significant association between sparring and increased size of the caudate nucleus, an area of the brain involved in movement, learning, and memory (P = .014 for right caudate volume, P = .012 for left caudate volume).
There are some theories that might explain this finding, said Mr. Esagoff. For example, individuals who spar more may get better at avoiding impacts and injuries during a fight, which might in turn affect the size of the caudate.
The controlled movements and techniques used during sparring could also affect the caudate. “Some research has shown that behavior, learning, and/or exercise may increase the size of certain brain regions,” Mr. Esagoff said.
He noted the “highly strategic” nature of combat sports – and used the example of Brazilian jiu-jitsu. That sport “is known as human chess because it takes a thoughtful approach to defeat a larger opponent with base, leverage, and technique,” he said.
However, Mr. Esagoff stressed that while it is possible movements involved in MMA increase caudate size, this is just a theory at this point.
A study limitation was that fighters volunteered to participate and may not represent all fighters. As well, the study was cross-sectional and looked at only one point in time, so it cannot infer causation.
Overall, the new findings should help inform fighters, governing bodies, and the public about the potential risks and benefits of different styles of MMA fighting and practice, although more research is needed, said Mr. Esagoff.
He and his team now plan to conduct a longer-term study and investigate effects of grappling on brain structure and function in addition to sparring.
Jury still out
Commenting on the study, Howard Liu, MD, chair of the University of Nebraska Medical Center department of psychiatry and incoming chair of the APA’s Council on Communications, said the jury “is clearly still out” when it comes to the investigation of brain impacts.

“We don’t know quite what these changes fully correlate to,” said Dr. Liu, who moderated a press briefing highlighting the study.
He underlined the importance of protecting athletes vulnerable to head trauma, be they professionals or those involved at the youth sports level.
Dr. Liu also noted the “extreme popularity” and rapid growth of MMA around the world, which he said provides an opportunity for researchers to study these professional fighters.
“This is a unique population that signed up in the midst of hundreds of hours of sparring to advance neuroscience, and that’s quite amazing,” he said.
A version of this article first appeared on Medscape.com.
, early research suggests.
Investigators found sparring, defined as strategically hitting opponents with kicks, punches, and other strikes during practice sessions, is linked to increased white matter hyperintensities in the brain, pointing to possible vascular damage from repeated head trauma. However, the study results also show sparring was associated with a larger bilateral caudate which, in theory, is neuroprotective.
“From our preliminary study, sparring practice in MMA fighters may have a ‘double-edged sword’ effect on the brain,” study investigator Aaron Esagoff, a second-year medical student at Johns Hopkins University School of Medicine, Baltimore, told this news organization.
“The combination of complex movements along with constant strategy and anticipation of your opponent’s next move may provide a neuroprotective effect on the caudate,” Mr. Esagoff said. However, he added, more research is needed into understanding this particular finding.
The study results were presented at the American Psychiatric Association (APA) 2022 Annual Meeting.
Growing popularity
MMA is a full-contact combat sport that has become increasingly popular over the past 15 years. It combines techniques from boxing, wrestling, karate, judo, and jujitsu.
To prepare for fights, MMA practitioners incorporate sparring and grappling, which use techniques such as chokes and locks to submit an opponent. Head protection is sometimes incorporated during practice, but is not the norm during a fight, said Mr. Esagoff.
The study investigated sparring during practice rather than fights because, he said, MMA competitors only fight a few times a year but spend hundreds of hours training. “So the health effects of training are going to be really important,” he said.
As with other combat sports, MMA involves hits to the head. Previous research has shown repetitive head trauma can lead to neurodegenerative diseases, including chronic traumatic encephalopathy (CTE) and Alzheimer’s disease, Mr. Esagoff noted.
Previous studies have also linked more professional fights and years of fighting to a decrease in brain volume among MMA fighters, he added.
The new analysis was conducted as part of the Professional Fighters Brain Health Study, a longitudinal cohort study of MMA professional fighters. It included 92 fighters with data available on MRI and habits regarding practicing. The mean age of the participants was 30 years, 62% were White, and 85% were men.
The study examined sparring but did not include grappling because of “several challenges” with the current data analysis, Mr. Esagoff said. Researchers adjusted for age, sex, education, race, number of fights, total intracranial volume, and type of MRI scanner used.
A ‘highly strategic’ sport
Results showed a strong association between the number of sparring rounds per week and increased white matter hyperintensity volume (mcL) on MRI (P = .039).
This suggests white matter damage, possibly a result of direct neuronal injury, vascular damage, or immune modulation, said Mr. Esagoff. However, another mechanism may be involved, he added.
There was also a significant association between sparring and increased size of the caudate nucleus, an area of the brain involved in movement, learning, and memory (P = .014 for right caudate volume, P = .012 for left caudate volume).
There are some theories that might explain this finding, said Mr. Esagoff. For example, individuals who spar more may get better at avoiding impacts and injuries during a fight, which might in turn affect the size of the caudate.
The controlled movements and techniques used during sparring could also affect the caudate. “Some research has shown that behavior, learning, and/or exercise may increase the size of certain brain regions,” Mr. Esagoff said.
He noted the “highly strategic” nature of combat sports – and used the example of Brazilian jiu-jitsu. That sport “is known as human chess because it takes a thoughtful approach to defeat a larger opponent with base, leverage, and technique,” he said.
However, Mr. Esagoff stressed that while it is possible movements involved in MMA increase caudate size, this is just a theory at this point.
A study limitation was that fighters volunteered to participate and may not represent all fighters. As well, the study was cross-sectional and looked at only one point in time, so it cannot infer causation.
Overall, the new findings should help inform fighters, governing bodies, and the public about the potential risks and benefits of different styles of MMA fighting and practice, although more research is needed, said Mr. Esagoff.
He and his team now plan to conduct a longer-term study and investigate effects of grappling on brain structure and function in addition to sparring.
Jury still out
Commenting on the study, Howard Liu, MD, chair of the University of Nebraska Medical Center department of psychiatry and incoming chair of the APA’s Council on Communications, said the jury “is clearly still out” when it comes to the investigation of brain impacts.
“We don’t know quite what these changes fully correlate to,” said Dr. Liu, who moderated a press briefing highlighting the study.
He underlined the importance of protecting athletes vulnerable to head trauma, be they professionals or those involved at the youth sports level.
Dr. Liu also noted the “extreme popularity” and rapid growth of MMA around the world, which he said provides an opportunity for researchers to study these professional fighters.
“This is a unique population that signed up in the midst of hundreds of hours of sparring to advance neuroscience, and that’s quite amazing,” he said.
A version of this article first appeared on Medscape.com.
, early research suggests.
Investigators found sparring, defined as strategically hitting opponents with kicks, punches, and other strikes during practice sessions, is linked to increased white matter hyperintensities in the brain, pointing to possible vascular damage from repeated head trauma. However, the study results also show sparring was associated with a larger bilateral caudate which, in theory, is neuroprotective.
“From our preliminary study, sparring practice in MMA fighters may have a ‘double-edged sword’ effect on the brain,” study investigator Aaron Esagoff, a second-year medical student at Johns Hopkins University School of Medicine, Baltimore, told this news organization.
“The combination of complex movements along with constant strategy and anticipation of your opponent’s next move may provide a neuroprotective effect on the caudate,” Mr. Esagoff said. However, he added, more research is needed into understanding this particular finding.
The study results were presented at the American Psychiatric Association (APA) 2022 Annual Meeting.
Growing popularity
MMA is a full-contact combat sport that has become increasingly popular over the past 15 years. It combines techniques from boxing, wrestling, karate, judo, and jujitsu.
To prepare for fights, MMA practitioners incorporate sparring and grappling, which use techniques such as chokes and locks to submit an opponent. Head protection is sometimes incorporated during practice, but is not the norm during a fight, said Mr. Esagoff.
The study investigated sparring during practice rather than fights because, he said, MMA competitors only fight a few times a year but spend hundreds of hours training. “So the health effects of training are going to be really important,” he said.
As with other combat sports, MMA involves hits to the head. Previous research has shown repetitive head trauma can lead to neurodegenerative diseases, including chronic traumatic encephalopathy (CTE) and Alzheimer’s disease, Mr. Esagoff noted.
Previous studies have also linked more professional fights and years of fighting to a decrease in brain volume among MMA fighters, he added.
The new analysis was conducted as part of the Professional Fighters Brain Health Study, a longitudinal cohort study of MMA professional fighters. It included 92 fighters with data available on MRI and habits regarding practicing. The mean age of the participants was 30 years, 62% were White, and 85% were men.
The study examined sparring but did not include grappling because of “several challenges” with the current data analysis, Mr. Esagoff said. Researchers adjusted for age, sex, education, race, number of fights, total intracranial volume, and type of MRI scanner used.
A ‘highly strategic’ sport
Results showed a strong association between the number of sparring rounds per week and increased white matter hyperintensity volume (mcL) on MRI (P = .039).
This suggests white matter damage, possibly a result of direct neuronal injury, vascular damage, or immune modulation, said Mr. Esagoff. However, another mechanism may be involved, he added.
There was also a significant association between sparring and increased size of the caudate nucleus, an area of the brain involved in movement, learning, and memory (P = .014 for right caudate volume, P = .012 for left caudate volume).
There are some theories that might explain this finding, said Mr. Esagoff. For example, individuals who spar more may get better at avoiding impacts and injuries during a fight, which might in turn affect the size of the caudate.
The controlled movements and techniques used during sparring could also affect the caudate. “Some research has shown that behavior, learning, and/or exercise may increase the size of certain brain regions,” Mr. Esagoff said.
He noted the “highly strategic” nature of combat sports – and used the example of Brazilian jiu-jitsu. That sport “is known as human chess because it takes a thoughtful approach to defeat a larger opponent with base, leverage, and technique,” he said.
However, Mr. Esagoff stressed that while it is possible movements involved in MMA increase caudate size, this is just a theory at this point.
A study limitation was that fighters volunteered to participate and may not represent all fighters. As well, the study was cross-sectional and looked at only one point in time, so it cannot infer causation.
Overall, the new findings should help inform fighters, governing bodies, and the public about the potential risks and benefits of different styles of MMA fighting and practice, although more research is needed, said Mr. Esagoff.
He and his team now plan to conduct a longer-term study and investigate effects of grappling on brain structure and function in addition to sparring.
Jury still out
Commenting on the study, Howard Liu, MD, chair of the University of Nebraska Medical Center department of psychiatry and incoming chair of the APA’s Council on Communications, said the jury “is clearly still out” when it comes to the investigation of brain impacts.
“We don’t know quite what these changes fully correlate to,” said Dr. Liu, who moderated a press briefing highlighting the study.
He underlined the importance of protecting athletes vulnerable to head trauma, be they professionals or those involved at the youth sports level.
Dr. Liu also noted the “extreme popularity” and rapid growth of MMA around the world, which he said provides an opportunity for researchers to study these professional fighters.
“This is a unique population that signed up in the midst of hundreds of hours of sparring to advance neuroscience, and that’s quite amazing,” he said.
A version of this article first appeared on Medscape.com.
FROM APA 2022
Premature return to play after concussion has decreased
, according to a recent chart review. Rates of premature return to learn (RTL) are essentially unchanged, however.
“Delay in recovery is the major reason why it’s important not to RTL or RTP prematurely,” said James Carson, MD, associate professor of family and community medicine, University of Toronto.
“That delay in recovery only sets students further back in terms of the stress they get from being delayed with their schoolwork – they could lose their year in school, lose all their social contacts. So, there are a number of psychosocial issues that come into play if recovery is delayed, and that is what premature RTL and premature RTP will do – they delay the student’s recovery,” he emphasized.
The study was published in Canadian Family Physician.
Differences by sex
The study involved 241 students who had 258 distinct cases of SRC. The researchers defined premature RTP and RTL as chart records documenting the relapse, recurrence, or worsening of concussion symptoms that accompanied the patient’s RTP or RTL. Between 2011 and 2016, 26.7% of students had evidence of premature RTP, while 42.6% of them had evidence of premature RTL, the authors noted.
Compared with findings from an earlier survey of data from 2006 to 2011, the incidence of premature RTP dropped by 38.6% (P = .0003). In contrast, symptoms associated with premature RTL dropped by only 4.7% from the previous survey. This change was not statistically significant.
There was also a significant difference between males and females in the proportion of SRC cases with relapse of symptoms. Relapse occurred in 43.4% of female athletes with SRC versus 29.7% of male athletes with SRC (P = .023).
Female athletes also had significantly longer times before being cleared for RTP. The mean time was 74.5 days for females, compared with a mean of 42.3 days for male athletes (P < .001). “The median time to RTP clearance was nearly double [for female athletes] at 49 days versus 25 days [for male athletes],” wrote the authors.
The rate of premature RTL was also higher among secondary school students (48.8%), compared with 28% among elementary students and 42% among postsecondary students.
More concussions coming?
Before the first consensus conference, organized by the Concussion in Sport Group in 2001, management of concussion was based on rating and grading scales that had no medical evidence to support them, said Dr. Carson. After the consensus conference, it was recommended that physicians manage each concussion individually and, when it came to RTP, recommendations were based upon symptom resolution.
In contrast, there was nothing in the literature regarding how student athletes who sustain a concussion should RTL. Some schools made generous accommodations, and others none. This situation changed around 2011, when experts started publishing data about how better to accommodate student athletes who have a temporary disability for which schools need to introduce temporary accommodations to help them recover.
“Recommendations for RTP essentially had a 12-year head-start,” Dr. Carson emphasized, “and RTL had a much slower start.” Unfortunately, Dr. Carson foresees more athletes sustaining concussions as pandemic restrictions ease over the next few months. “As athletes RTP after the pandemic, they just will not be in game shape,” he said.
“In other words, athletes may not have the neuromuscular control to avoid these injuries as easily,” he added. Worse, athletes may not realize they are not quite ready to return to the expected level of participation so quickly. “I believe this scenario will lead to more concussions that will be difficult to manage in the context of an already strained health care system,” said Dr. Carson.
A limitation of the study was that it was difficult to assess whether all patients followed medical advice consistently.
“Very positive shifts”
Commenting on the findings, Nick Reed, PhD, Canada research chair in pediatric concussion and associate professor of occupational science and occupational therapy, University of Toronto, said that sports medicine physicians are seeing “very positive shifts” in concussion awareness and related behaviors such as providing education, support, and accommodations to students within the school environment. “More and more teachers are seeking education to learn what a concussion is and what to do to best support their students with concussion,” he said. Dr. Reed was not involved in the current study.
Indeed, this increasing awareness led to the development of a concussion education tool for teachers – SCHOOLFirst – although Dr. Reed did acknowledge that not all teachers have either the knowledge or the resources they need to optimally support their students with concussion. In the meantime, to reduce the risk of injury, Dr. Reed stressed that it is important for students to wear equipment appropriate for the game being played and to play by the rules.
“It is key to play sports in a way that is fair and respectful and not [engage] in behaviors with the intent of injuring an opponent,” he stressed. It is also important for athletes themselves to know the signs and symptoms of concussion and, if they think they have a concussion, to immediately stop playing, report how they are feeling to a coach, teacher, or parent, and to seek medical assessment to determine if they have a concussion or not.
“The key here is to focus on what the athlete can do after a concussion rather than what they can’t do,” Dr. Reed said. After even a few days of complete rest, students with a concussion can gradually introduce low levels of physical and cognitive activity that won’t make their symptoms worse. This activity can include going back to school with temporary accommodations in place, such as shorter school days and increased rest breaks. “When returning to school and to sport after a concussion, it is important to follow a stepwise and gradual return to activities so that you aren’t doing too much too fast,” Dr. Reed emphasized.
The study was conducted without external funding. Dr. Carson and Dr. Reed reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
, according to a recent chart review. Rates of premature return to learn (RTL) are essentially unchanged, however.
“Delay in recovery is the major reason why it’s important not to RTL or RTP prematurely,” said James Carson, MD, associate professor of family and community medicine, University of Toronto.
“That delay in recovery only sets students further back in terms of the stress they get from being delayed with their schoolwork – they could lose their year in school, lose all their social contacts. So, there are a number of psychosocial issues that come into play if recovery is delayed, and that is what premature RTL and premature RTP will do – they delay the student’s recovery,” he emphasized.
The study was published in Canadian Family Physician.
Differences by sex
The study involved 241 students who had 258 distinct cases of SRC. The researchers defined premature RTP and RTL as chart records documenting the relapse, recurrence, or worsening of concussion symptoms that accompanied the patient’s RTP or RTL. Between 2011 and 2016, 26.7% of students had evidence of premature RTP, while 42.6% of them had evidence of premature RTL, the authors noted.
Compared with findings from an earlier survey of data from 2006 to 2011, the incidence of premature RTP dropped by 38.6% (P = .0003). In contrast, symptoms associated with premature RTL dropped by only 4.7% from the previous survey. This change was not statistically significant.
There was also a significant difference between males and females in the proportion of SRC cases with relapse of symptoms. Relapse occurred in 43.4% of female athletes with SRC versus 29.7% of male athletes with SRC (P = .023).
Female athletes also had significantly longer times before being cleared for RTP. The mean time was 74.5 days for females, compared with a mean of 42.3 days for male athletes (P < .001). “The median time to RTP clearance was nearly double [for female athletes] at 49 days versus 25 days [for male athletes],” wrote the authors.
The rate of premature RTL was also higher among secondary school students (48.8%), compared with 28% among elementary students and 42% among postsecondary students.
More concussions coming?
Before the first consensus conference, organized by the Concussion in Sport Group in 2001, management of concussion was based on rating and grading scales that had no medical evidence to support them, said Dr. Carson. After the consensus conference, it was recommended that physicians manage each concussion individually and, when it came to RTP, recommendations were based upon symptom resolution.
In contrast, there was nothing in the literature regarding how student athletes who sustain a concussion should RTL. Some schools made generous accommodations, and others none. This situation changed around 2011, when experts started publishing data about how better to accommodate student athletes who have a temporary disability for which schools need to introduce temporary accommodations to help them recover.
“Recommendations for RTP essentially had a 12-year head-start,” Dr. Carson emphasized, “and RTL had a much slower start.” Unfortunately, Dr. Carson foresees more athletes sustaining concussions as pandemic restrictions ease over the next few months. “As athletes RTP after the pandemic, they just will not be in game shape,” he said.
“In other words, athletes may not have the neuromuscular control to avoid these injuries as easily,” he added. Worse, athletes may not realize they are not quite ready to return to the expected level of participation so quickly. “I believe this scenario will lead to more concussions that will be difficult to manage in the context of an already strained health care system,” said Dr. Carson.
A limitation of the study was that it was difficult to assess whether all patients followed medical advice consistently.
“Very positive shifts”
Commenting on the findings, Nick Reed, PhD, Canada research chair in pediatric concussion and associate professor of occupational science and occupational therapy, University of Toronto, said that sports medicine physicians are seeing “very positive shifts” in concussion awareness and related behaviors such as providing education, support, and accommodations to students within the school environment. “More and more teachers are seeking education to learn what a concussion is and what to do to best support their students with concussion,” he said. Dr. Reed was not involved in the current study.
Indeed, this increasing awareness led to the development of a concussion education tool for teachers – SCHOOLFirst – although Dr. Reed did acknowledge that not all teachers have either the knowledge or the resources they need to optimally support their students with concussion. In the meantime, to reduce the risk of injury, Dr. Reed stressed that it is important for students to wear equipment appropriate for the game being played and to play by the rules.
“It is key to play sports in a way that is fair and respectful and not [engage] in behaviors with the intent of injuring an opponent,” he stressed. It is also important for athletes themselves to know the signs and symptoms of concussion and, if they think they have a concussion, to immediately stop playing, report how they are feeling to a coach, teacher, or parent, and to seek medical assessment to determine if they have a concussion or not.
“The key here is to focus on what the athlete can do after a concussion rather than what they can’t do,” Dr. Reed said. After even a few days of complete rest, students with a concussion can gradually introduce low levels of physical and cognitive activity that won’t make their symptoms worse. This activity can include going back to school with temporary accommodations in place, such as shorter school days and increased rest breaks. “When returning to school and to sport after a concussion, it is important to follow a stepwise and gradual return to activities so that you aren’t doing too much too fast,” Dr. Reed emphasized.
The study was conducted without external funding. Dr. Carson and Dr. Reed reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
, according to a recent chart review. Rates of premature return to learn (RTL) are essentially unchanged, however.
“Delay in recovery is the major reason why it’s important not to RTL or RTP prematurely,” said James Carson, MD, associate professor of family and community medicine, University of Toronto.
“That delay in recovery only sets students further back in terms of the stress they get from being delayed with their schoolwork – they could lose their year in school, lose all their social contacts. So, there are a number of psychosocial issues that come into play if recovery is delayed, and that is what premature RTL and premature RTP will do – they delay the student’s recovery,” he emphasized.
The study was published in Canadian Family Physician.
Differences by sex
The study involved 241 students who had 258 distinct cases of SRC. The researchers defined premature RTP and RTL as chart records documenting the relapse, recurrence, or worsening of concussion symptoms that accompanied the patient’s RTP or RTL. Between 2011 and 2016, 26.7% of students had evidence of premature RTP, while 42.6% of them had evidence of premature RTL, the authors noted.
Compared with findings from an earlier survey of data from 2006 to 2011, the incidence of premature RTP dropped by 38.6% (P = .0003). In contrast, symptoms associated with premature RTL dropped by only 4.7% from the previous survey. This change was not statistically significant.
There was also a significant difference between males and females in the proportion of SRC cases with relapse of symptoms. Relapse occurred in 43.4% of female athletes with SRC versus 29.7% of male athletes with SRC (P = .023).
Female athletes also had significantly longer times before being cleared for RTP. The mean time was 74.5 days for females, compared with a mean of 42.3 days for male athletes (P < .001). “The median time to RTP clearance was nearly double [for female athletes] at 49 days versus 25 days [for male athletes],” wrote the authors.
The rate of premature RTL was also higher among secondary school students (48.8%), compared with 28% among elementary students and 42% among postsecondary students.
More concussions coming?
Before the first consensus conference, organized by the Concussion in Sport Group in 2001, management of concussion was based on rating and grading scales that had no medical evidence to support them, said Dr. Carson. After the consensus conference, it was recommended that physicians manage each concussion individually and, when it came to RTP, recommendations were based upon symptom resolution.
In contrast, there was nothing in the literature regarding how student athletes who sustain a concussion should RTL. Some schools made generous accommodations, and others none. This situation changed around 2011, when experts started publishing data about how better to accommodate student athletes who have a temporary disability for which schools need to introduce temporary accommodations to help them recover.
“Recommendations for RTP essentially had a 12-year head-start,” Dr. Carson emphasized, “and RTL had a much slower start.” Unfortunately, Dr. Carson foresees more athletes sustaining concussions as pandemic restrictions ease over the next few months. “As athletes RTP after the pandemic, they just will not be in game shape,” he said.
“In other words, athletes may not have the neuromuscular control to avoid these injuries as easily,” he added. Worse, athletes may not realize they are not quite ready to return to the expected level of participation so quickly. “I believe this scenario will lead to more concussions that will be difficult to manage in the context of an already strained health care system,” said Dr. Carson.
A limitation of the study was that it was difficult to assess whether all patients followed medical advice consistently.
“Very positive shifts”
Commenting on the findings, Nick Reed, PhD, Canada research chair in pediatric concussion and associate professor of occupational science and occupational therapy, University of Toronto, said that sports medicine physicians are seeing “very positive shifts” in concussion awareness and related behaviors such as providing education, support, and accommodations to students within the school environment. “More and more teachers are seeking education to learn what a concussion is and what to do to best support their students with concussion,” he said. Dr. Reed was not involved in the current study.
Indeed, this increasing awareness led to the development of a concussion education tool for teachers – SCHOOLFirst – although Dr. Reed did acknowledge that not all teachers have either the knowledge or the resources they need to optimally support their students with concussion. In the meantime, to reduce the risk of injury, Dr. Reed stressed that it is important for students to wear equipment appropriate for the game being played and to play by the rules.
“It is key to play sports in a way that is fair and respectful and not [engage] in behaviors with the intent of injuring an opponent,” he stressed. It is also important for athletes themselves to know the signs and symptoms of concussion and, if they think they have a concussion, to immediately stop playing, report how they are feeling to a coach, teacher, or parent, and to seek medical assessment to determine if they have a concussion or not.
“The key here is to focus on what the athlete can do after a concussion rather than what they can’t do,” Dr. Reed said. After even a few days of complete rest, students with a concussion can gradually introduce low levels of physical and cognitive activity that won’t make their symptoms worse. This activity can include going back to school with temporary accommodations in place, such as shorter school days and increased rest breaks. “When returning to school and to sport after a concussion, it is important to follow a stepwise and gradual return to activities so that you aren’t doing too much too fast,” Dr. Reed emphasized.
The study was conducted without external funding. Dr. Carson and Dr. Reed reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Traumatic brain injury linked to ‘striking’ risk for CVD, diabetes, brain disorders
Mild traumatic brain injury (TBI) is linked to a significantly increased risk for a host of subsequent cardiovascular, endocrine, neurologic, and psychiatric disorders, new research shows.
Incidence of hypertension, coronary heart disease, diabetes, stroke, depression, and dementia all began to increase soon after the brain injury and persisted over a decade in both mild and moderate to severe TBI.
Researchers found the multisystem comorbidities in all age groups, including in patients as young as 18. They also found that patients who developed multiple postinjury problems had higher mortality during the decade-long follow-up.
The findings suggest patients with TBI may require longer follow-up and proactive screening for multisystem disease, regardless of age or injury severity.
“The fact that both patients with mild and moderate to severe injuries both had long-term ongoing associations with comorbidities that continued over time and that they are cardiovascular, endocrine, neurologic, and behavioral health oriented was pretty striking,” study author Ross Zafonte, DO, PhD, president of Spaulding Rehab Hospital and professor and chair of physical medicine and rehab at Harvard Medical School, both in Boston, told this news organization.
The study was published online in JAMA Network Open.
Injury severity not a factor
An estimated 2.8 million individuals in the United States experience TBI every year. Worldwide, the figure may be as high as 74 million.
Studies have long suggested a link between brain injury and subsequent neurologic disorders, but research suggesting a possible link to cardiovascular and endocrine problems has recently gained attention.
Building on a 2021 study that showed increased incidence of cardiovascular issues following a concussion, the researchers examined medical records of previously healthy patients treated for TBI between 2000 and 2015 who also had at least 1 follow-up visit between 6 months and 10 years after the initial injury.
Researchers analyzed data from 13,053 individuals – 4,351 with mild injury (mTBI), 4351 with moderate to severe injury (msTBI), and 4351 with no TBI. The most common cause of injury was a fall. Patients with sports-related injuries were excluded.
Incidence of hypertension was significantly higher among patients with mTBI (hazard ratio, 2.5; 95% confidence interval, 2.1-2.9) and msTBI (HR, 2.4; 95% CI, 2.0-2.9), compared with the unaffected group. Risk for other cardiovascular problems, including hyperlipidemia, obesity, and coronary artery disease, were also higher in the affected groups.
TBI patients also reported higher incidence of endocrine diseases, including diabetes (mTBI: HR, 1.9; 95% CI, 1.4-2.7; msTBI: HR, 1.9; 95% CI, 1.4-2.6). Elevated risk for ischemic stroke or transient ischemic attack was also increased (mTBI: HR, 2.2; 95% CI, 1.4-3.3; msTBI: HR, 3.6; 95% CI, 2.4-5.3).
Regardless of injury severity, patients with TBI had a higher risk for neurologic and psychiatric diseases, particularly depression, dementia, and psychotic disorders. “This tells us that mild TBI is not clean of events,” Dr. Zafonte said.
Surprising rate of comorbidity in youth
Investigators found increased risk for posttrauma comorbidities in all age groups, but researchers were struck by the high rates in younger patients, aged 18-40. Compared with age-matched individuals with no TBI history, hypertension risk was nearly six times higher in those with mTBI (HR, 5.9; 95% CI, 3.9-9.1) and nearly four times higher in patients with msTBI (HR, 3.9; 95% CI, 2.5-6.1).
Rates of hyperlipidemia and diabetes were also higher in younger patients in the mTBI group and posttraumatic seizures and psychiatric disorders were elevated regardless of TBI severity.
Overall, patients with msTBI, but not those with mTBI, were at higher risk for mortality, compared with the unexposed group (432 deaths [9.9%] vs. 250 deaths [5.7%]; P < .001).
“It’s clear that what we may be dealing with is that it holds up even for the younger people,” Dr. Zafonte said. “We used to think brain injury risk is worse in the severe cases, which it is, and it’s worse later on among those who are older, which it is. But our younger folks don’t get away either.”
While the study offers associations between TBI and multisystem health problems, Dr. Zafonte said it’s impossible to say at this point whether the brain injury caused the increased risk for cardiovascular or endocrine problems. Other organ injuries sustained in the trauma may be a contributing factor.
“Further data is needed to elucidate the mechanism and the causative relationships, which we do not have here,” he said.
Many of the postinjury comorbidities emerged a median of 3.5 years after TBI, regardless of severity. But some of the cardiovascular and psychiatric conditions emerged far sooner than that.
That’s important because research suggests less than half of patients with TBI receive follow-up care.
“It does make sense for folks who are interacting with people who’ve had a TBI to be suspicious of medical comorbidities relatively early on, within the first couple of years,” Dr. Zafonte said.
In an invited commentary, Vijay Krishnamoorthy, MD, MPH, PhD, Duke University, Durham, N.C., and Monica S. Vavilala, MD, University of Washington, Seattle, highlight some of the study’s limitations, including a lack of information on comorbidity severity and the lack of a matched group of patients who experienced non-head trauma.
Despite those limitations, the study offers important information on how TBI may affect organs beyond the brain, they noted.
“These observations, if replicated in future studies, raise intriguing implications in the future care of patients with TBI, including heightened chronic disease-screening measures and possibly enhanced guidelines for chronic extracranial organ system care for patients who experience TBI,” Dr. Krishnamoorthy and Dr. Vavilala wrote.
The study received no specific funding. Dr. Zafonte reported having received personal fees from Springer/Demos, serving on scientific advisory boards for Myomo and OnCare and has received funding from the Football Players Health Study at Harvard, funded in part by the National Football League Players Association. Dr. Krishnamoorthy and Dr. Vavilala disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Mild traumatic brain injury (TBI) is linked to a significantly increased risk for a host of subsequent cardiovascular, endocrine, neurologic, and psychiatric disorders, new research shows.
Incidence of hypertension, coronary heart disease, diabetes, stroke, depression, and dementia all began to increase soon after the brain injury and persisted over a decade in both mild and moderate to severe TBI.
Researchers found the multisystem comorbidities in all age groups, including in patients as young as 18. They also found that patients who developed multiple postinjury problems had higher mortality during the decade-long follow-up.
The findings suggest patients with TBI may require longer follow-up and proactive screening for multisystem disease, regardless of age or injury severity.
“The fact that both patients with mild and moderate to severe injuries both had long-term ongoing associations with comorbidities that continued over time and that they are cardiovascular, endocrine, neurologic, and behavioral health oriented was pretty striking,” study author Ross Zafonte, DO, PhD, president of Spaulding Rehab Hospital and professor and chair of physical medicine and rehab at Harvard Medical School, both in Boston, told this news organization.
The study was published online in JAMA Network Open.
Injury severity not a factor
An estimated 2.8 million individuals in the United States experience TBI every year. Worldwide, the figure may be as high as 74 million.
Studies have long suggested a link between brain injury and subsequent neurologic disorders, but research suggesting a possible link to cardiovascular and endocrine problems has recently gained attention.
Building on a 2021 study that showed increased incidence of cardiovascular issues following a concussion, the researchers examined medical records of previously healthy patients treated for TBI between 2000 and 2015 who also had at least 1 follow-up visit between 6 months and 10 years after the initial injury.
Researchers analyzed data from 13,053 individuals – 4,351 with mild injury (mTBI), 4351 with moderate to severe injury (msTBI), and 4351 with no TBI. The most common cause of injury was a fall. Patients with sports-related injuries were excluded.
Incidence of hypertension was significantly higher among patients with mTBI (hazard ratio, 2.5; 95% confidence interval, 2.1-2.9) and msTBI (HR, 2.4; 95% CI, 2.0-2.9), compared with the unaffected group. Risk for other cardiovascular problems, including hyperlipidemia, obesity, and coronary artery disease, were also higher in the affected groups.
TBI patients also reported higher incidence of endocrine diseases, including diabetes (mTBI: HR, 1.9; 95% CI, 1.4-2.7; msTBI: HR, 1.9; 95% CI, 1.4-2.6). Elevated risk for ischemic stroke or transient ischemic attack was also increased (mTBI: HR, 2.2; 95% CI, 1.4-3.3; msTBI: HR, 3.6; 95% CI, 2.4-5.3).
Regardless of injury severity, patients with TBI had a higher risk for neurologic and psychiatric diseases, particularly depression, dementia, and psychotic disorders. “This tells us that mild TBI is not clean of events,” Dr. Zafonte said.
Surprising rate of comorbidity in youth
Investigators found increased risk for posttrauma comorbidities in all age groups, but researchers were struck by the high rates in younger patients, aged 18-40. Compared with age-matched individuals with no TBI history, hypertension risk was nearly six times higher in those with mTBI (HR, 5.9; 95% CI, 3.9-9.1) and nearly four times higher in patients with msTBI (HR, 3.9; 95% CI, 2.5-6.1).
Rates of hyperlipidemia and diabetes were also higher in younger patients in the mTBI group and posttraumatic seizures and psychiatric disorders were elevated regardless of TBI severity.
Overall, patients with msTBI, but not those with mTBI, were at higher risk for mortality, compared with the unexposed group (432 deaths [9.9%] vs. 250 deaths [5.7%]; P < .001).
“It’s clear that what we may be dealing with is that it holds up even for the younger people,” Dr. Zafonte said. “We used to think brain injury risk is worse in the severe cases, which it is, and it’s worse later on among those who are older, which it is. But our younger folks don’t get away either.”
While the study offers associations between TBI and multisystem health problems, Dr. Zafonte said it’s impossible to say at this point whether the brain injury caused the increased risk for cardiovascular or endocrine problems. Other organ injuries sustained in the trauma may be a contributing factor.
“Further data is needed to elucidate the mechanism and the causative relationships, which we do not have here,” he said.
Many of the postinjury comorbidities emerged a median of 3.5 years after TBI, regardless of severity. But some of the cardiovascular and psychiatric conditions emerged far sooner than that.
That’s important because research suggests less than half of patients with TBI receive follow-up care.
“It does make sense for folks who are interacting with people who’ve had a TBI to be suspicious of medical comorbidities relatively early on, within the first couple of years,” Dr. Zafonte said.
In an invited commentary, Vijay Krishnamoorthy, MD, MPH, PhD, Duke University, Durham, N.C., and Monica S. Vavilala, MD, University of Washington, Seattle, highlight some of the study’s limitations, including a lack of information on comorbidity severity and the lack of a matched group of patients who experienced non-head trauma.
Despite those limitations, the study offers important information on how TBI may affect organs beyond the brain, they noted.
“These observations, if replicated in future studies, raise intriguing implications in the future care of patients with TBI, including heightened chronic disease-screening measures and possibly enhanced guidelines for chronic extracranial organ system care for patients who experience TBI,” Dr. Krishnamoorthy and Dr. Vavilala wrote.
The study received no specific funding. Dr. Zafonte reported having received personal fees from Springer/Demos, serving on scientific advisory boards for Myomo and OnCare and has received funding from the Football Players Health Study at Harvard, funded in part by the National Football League Players Association. Dr. Krishnamoorthy and Dr. Vavilala disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Mild traumatic brain injury (TBI) is linked to a significantly increased risk for a host of subsequent cardiovascular, endocrine, neurologic, and psychiatric disorders, new research shows.
Incidence of hypertension, coronary heart disease, diabetes, stroke, depression, and dementia all began to increase soon after the brain injury and persisted over a decade in both mild and moderate to severe TBI.
Researchers found the multisystem comorbidities in all age groups, including in patients as young as 18. They also found that patients who developed multiple postinjury problems had higher mortality during the decade-long follow-up.
The findings suggest patients with TBI may require longer follow-up and proactive screening for multisystem disease, regardless of age or injury severity.
“The fact that both patients with mild and moderate to severe injuries both had long-term ongoing associations with comorbidities that continued over time and that they are cardiovascular, endocrine, neurologic, and behavioral health oriented was pretty striking,” study author Ross Zafonte, DO, PhD, president of Spaulding Rehab Hospital and professor and chair of physical medicine and rehab at Harvard Medical School, both in Boston, told this news organization.
The study was published online in JAMA Network Open.
Injury severity not a factor
An estimated 2.8 million individuals in the United States experience TBI every year. Worldwide, the figure may be as high as 74 million.
Studies have long suggested a link between brain injury and subsequent neurologic disorders, but research suggesting a possible link to cardiovascular and endocrine problems has recently gained attention.
Building on a 2021 study that showed increased incidence of cardiovascular issues following a concussion, the researchers examined medical records of previously healthy patients treated for TBI between 2000 and 2015 who also had at least 1 follow-up visit between 6 months and 10 years after the initial injury.
Researchers analyzed data from 13,053 individuals – 4,351 with mild injury (mTBI), 4351 with moderate to severe injury (msTBI), and 4351 with no TBI. The most common cause of injury was a fall. Patients with sports-related injuries were excluded.
Incidence of hypertension was significantly higher among patients with mTBI (hazard ratio, 2.5; 95% confidence interval, 2.1-2.9) and msTBI (HR, 2.4; 95% CI, 2.0-2.9), compared with the unaffected group. Risk for other cardiovascular problems, including hyperlipidemia, obesity, and coronary artery disease, were also higher in the affected groups.
TBI patients also reported higher incidence of endocrine diseases, including diabetes (mTBI: HR, 1.9; 95% CI, 1.4-2.7; msTBI: HR, 1.9; 95% CI, 1.4-2.6). Elevated risk for ischemic stroke or transient ischemic attack was also increased (mTBI: HR, 2.2; 95% CI, 1.4-3.3; msTBI: HR, 3.6; 95% CI, 2.4-5.3).
Regardless of injury severity, patients with TBI had a higher risk for neurologic and psychiatric diseases, particularly depression, dementia, and psychotic disorders. “This tells us that mild TBI is not clean of events,” Dr. Zafonte said.
Surprising rate of comorbidity in youth
Investigators found increased risk for posttrauma comorbidities in all age groups, but researchers were struck by the high rates in younger patients, aged 18-40. Compared with age-matched individuals with no TBI history, hypertension risk was nearly six times higher in those with mTBI (HR, 5.9; 95% CI, 3.9-9.1) and nearly four times higher in patients with msTBI (HR, 3.9; 95% CI, 2.5-6.1).
Rates of hyperlipidemia and diabetes were also higher in younger patients in the mTBI group and posttraumatic seizures and psychiatric disorders were elevated regardless of TBI severity.
Overall, patients with msTBI, but not those with mTBI, were at higher risk for mortality, compared with the unexposed group (432 deaths [9.9%] vs. 250 deaths [5.7%]; P < .001).
“It’s clear that what we may be dealing with is that it holds up even for the younger people,” Dr. Zafonte said. “We used to think brain injury risk is worse in the severe cases, which it is, and it’s worse later on among those who are older, which it is. But our younger folks don’t get away either.”
While the study offers associations between TBI and multisystem health problems, Dr. Zafonte said it’s impossible to say at this point whether the brain injury caused the increased risk for cardiovascular or endocrine problems. Other organ injuries sustained in the trauma may be a contributing factor.
“Further data is needed to elucidate the mechanism and the causative relationships, which we do not have here,” he said.
Many of the postinjury comorbidities emerged a median of 3.5 years after TBI, regardless of severity. But some of the cardiovascular and psychiatric conditions emerged far sooner than that.
That’s important because research suggests less than half of patients with TBI receive follow-up care.
“It does make sense for folks who are interacting with people who’ve had a TBI to be suspicious of medical comorbidities relatively early on, within the first couple of years,” Dr. Zafonte said.
In an invited commentary, Vijay Krishnamoorthy, MD, MPH, PhD, Duke University, Durham, N.C., and Monica S. Vavilala, MD, University of Washington, Seattle, highlight some of the study’s limitations, including a lack of information on comorbidity severity and the lack of a matched group of patients who experienced non-head trauma.
Despite those limitations, the study offers important information on how TBI may affect organs beyond the brain, they noted.
“These observations, if replicated in future studies, raise intriguing implications in the future care of patients with TBI, including heightened chronic disease-screening measures and possibly enhanced guidelines for chronic extracranial organ system care for patients who experience TBI,” Dr. Krishnamoorthy and Dr. Vavilala wrote.
The study received no specific funding. Dr. Zafonte reported having received personal fees from Springer/Demos, serving on scientific advisory boards for Myomo and OnCare and has received funding from the Football Players Health Study at Harvard, funded in part by the National Football League Players Association. Dr. Krishnamoorthy and Dr. Vavilala disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Stem cells restore lost function after traumatic brain injury
, results from a phase 2 trial indicate. “We proved for the first time that we can affect outcomes in moderately to severely disabled patients with TBI using stem cells,” said study investigator Peter McAllister, MD, cofounder and medical director of the New England Center for Neurology and Headache, Stamford, Conn.
“I think the potential of regenerative medicine was always out there, but we are now getting to the point where we’re living up to that potential,” said Dr. McAllister, associate professor of neurology at Yale University, New Haven, Conn.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
No effective treatment to date
TBI can lead to motor deficits and chronic disability and currently there are no effective drugs to treat these deficits.
Researchers are increasingly focused on using somatic stem cells to restore lost function. Stem cells can differentiate or proliferate into different types of cells and are thought to promote repair and regeneration of tissues or organs damaged due to illness or injury.
The study included 61 patients with TBI with an average age of 34 years (70% were male and 69% were White). The mean time from injury was 8 years and Glasgow Outcome Scale Extended (GOS-E) ranged from 3 to 6.
Forty-six participants were randomly assigned to receive the stem cell therapy and 15 a sham procedure. In the treatment group, there were three different doses of cells (2.5 x 106, 5 x 106, and 10 x 106).
The treatment involved an investigational regenerative cell medicine comprised of bone marrow-derived mesenchymal stem cells (SB623). The allogeneic cells came from a male donor.
For the 20-minute procedure, a neurosurgeon drilled a tiny hole in the skull and, guided by MRI, injected the stem cells into the area of the lesion.
Patients receiving a surgical sham procedure were brought to the operating room, anesthetized, and had a hole drilled into the head over the area of the lesion. However, the surgeon went only halfway through the skull bone.
Participants were instructed to do specific physiotherapy exercises at home every morning and afternoon for the first 6 months of the study.
The primary efficacy endpoint was change in the Fugl-Meyer Motor Scale score (FMMS). This scale is widely used for clinical assessment of motor function, including range of motion, walking, lower limb movement, and dexterity.
At 24 weeks, the change in FMMS score for SB623-treated patients (least square [LS] mean increase 8.3) compared with controls (LS increase 2.3) was significant (P = .04).
“When we looked at all the data at 6 months, the folks who got the stem cells did statistically significantly better than the group that got the sham,” and that improvement began within the first week or two, said Dr. McAllister.
‘A real impact’
The treatment had a real impact on people’s lives, he said. “Some who couldn’t move their arm at all were able to put a nut on a bolt or brush their teeth, and some were able to button and unbutton where they couldn’t do that before.”
One teenager who was previously completely aphasic spoke an entire sentence.
The middle dose (5 x 106) had “by far” the best outcome, said Dr. McAllister. It’s not yet known whether the improvements will be permanent, he added.
At 48 weeks, treated patients experienced improvement over controls in secondary endpoints of the Action Research Arm Test (ARAT), which assesses grasp, grip, pinch, and gross movements; Gait Velocity (walking 10 meters); and NeuroQOL, a self-report measure of ability to carry out various activities.
However, although these endpoints were all numerically better in the stem cell groups, none reached statistical significance. This is likely because of the small study size and the fact the control group improved so much, said Dr. McAllister.
The exact mechanism of stem cell therapy is unclear, but researchers believe it “establishes a milieu of growth” for cells in the brain and promotes anti-inflammatory properties, said Dr. McAllister.
By 48 weeks, all study subjects had experienced at least one adverse event, with no differences between groups and no patient withdrawing as a result of adverse events. “There was no safety signal at all related to the stem cells,” said Dr. McAllister.
A larger phase 3 study of SB623 is planned.
The treatment may be useful in other conditions. A study of stroke survivors “just barely missed statistical significance” likely for methodological reasons and an older, sicker population, but the company plans to do another study in patients who were affected by stroke, said Dr. McAllister.
In addition, there may be potential for this approach with brain hemorrhage, Parkinson’s disease, multiple sclerosis, and other brain-related disorders, he said.
‘Modern-day holy grail’
Reached for a comment, TBI specialist Frank Conidi, MD, director of the Florida Center for Headache and Sports Neurology, said stem cell therapy is the most promising potential treatment for brain injury. “It’s the modern-day ‘holy grail.’ “
In this study, “to see a modest improvement in gait in the primary outcome is impressive,” he said.
In addition, the fact the study didn’t have any significant or severe adverse outcomes “is promising,” he added.
Studies like this “are going to help to lay the groundwork for future studies and hopefully one day result in a safe, noninvasive treatment” for Parkinson’s disease, Alzheimer’s disease, and disorders that affect the central nervous system such as spinal cord injury, Dr. Conidi said.
This therapy involves an invasive procedure requiring implantation directly into the brain, he noted. “At present, there’s no way to get stem cells to cross the blood-brain barrier.”
In addition, although motor impairment is definitely a component of TBI, it’s not as prevalent as cognitive impairment, said Dr. Conidi.
The study was supported by SanBio Co Ltd. Dr. McAllister and Dr. Conidi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, results from a phase 2 trial indicate. “We proved for the first time that we can affect outcomes in moderately to severely disabled patients with TBI using stem cells,” said study investigator Peter McAllister, MD, cofounder and medical director of the New England Center for Neurology and Headache, Stamford, Conn.
“I think the potential of regenerative medicine was always out there, but we are now getting to the point where we’re living up to that potential,” said Dr. McAllister, associate professor of neurology at Yale University, New Haven, Conn.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
No effective treatment to date
TBI can lead to motor deficits and chronic disability and currently there are no effective drugs to treat these deficits.
Researchers are increasingly focused on using somatic stem cells to restore lost function. Stem cells can differentiate or proliferate into different types of cells and are thought to promote repair and regeneration of tissues or organs damaged due to illness or injury.
The study included 61 patients with TBI with an average age of 34 years (70% were male and 69% were White). The mean time from injury was 8 years and Glasgow Outcome Scale Extended (GOS-E) ranged from 3 to 6.
Forty-six participants were randomly assigned to receive the stem cell therapy and 15 a sham procedure. In the treatment group, there were three different doses of cells (2.5 x 106, 5 x 106, and 10 x 106).
The treatment involved an investigational regenerative cell medicine comprised of bone marrow-derived mesenchymal stem cells (SB623). The allogeneic cells came from a male donor.
For the 20-minute procedure, a neurosurgeon drilled a tiny hole in the skull and, guided by MRI, injected the stem cells into the area of the lesion.
Patients receiving a surgical sham procedure were brought to the operating room, anesthetized, and had a hole drilled into the head over the area of the lesion. However, the surgeon went only halfway through the skull bone.
Participants were instructed to do specific physiotherapy exercises at home every morning and afternoon for the first 6 months of the study.
The primary efficacy endpoint was change in the Fugl-Meyer Motor Scale score (FMMS). This scale is widely used for clinical assessment of motor function, including range of motion, walking, lower limb movement, and dexterity.
At 24 weeks, the change in FMMS score for SB623-treated patients (least square [LS] mean increase 8.3) compared with controls (LS increase 2.3) was significant (P = .04).
“When we looked at all the data at 6 months, the folks who got the stem cells did statistically significantly better than the group that got the sham,” and that improvement began within the first week or two, said Dr. McAllister.
‘A real impact’
The treatment had a real impact on people’s lives, he said. “Some who couldn’t move their arm at all were able to put a nut on a bolt or brush their teeth, and some were able to button and unbutton where they couldn’t do that before.”
One teenager who was previously completely aphasic spoke an entire sentence.
The middle dose (5 x 106) had “by far” the best outcome, said Dr. McAllister. It’s not yet known whether the improvements will be permanent, he added.
At 48 weeks, treated patients experienced improvement over controls in secondary endpoints of the Action Research Arm Test (ARAT), which assesses grasp, grip, pinch, and gross movements; Gait Velocity (walking 10 meters); and NeuroQOL, a self-report measure of ability to carry out various activities.
However, although these endpoints were all numerically better in the stem cell groups, none reached statistical significance. This is likely because of the small study size and the fact the control group improved so much, said Dr. McAllister.
The exact mechanism of stem cell therapy is unclear, but researchers believe it “establishes a milieu of growth” for cells in the brain and promotes anti-inflammatory properties, said Dr. McAllister.
By 48 weeks, all study subjects had experienced at least one adverse event, with no differences between groups and no patient withdrawing as a result of adverse events. “There was no safety signal at all related to the stem cells,” said Dr. McAllister.
A larger phase 3 study of SB623 is planned.
The treatment may be useful in other conditions. A study of stroke survivors “just barely missed statistical significance” likely for methodological reasons and an older, sicker population, but the company plans to do another study in patients who were affected by stroke, said Dr. McAllister.
In addition, there may be potential for this approach with brain hemorrhage, Parkinson’s disease, multiple sclerosis, and other brain-related disorders, he said.
‘Modern-day holy grail’
Reached for a comment, TBI specialist Frank Conidi, MD, director of the Florida Center for Headache and Sports Neurology, said stem cell therapy is the most promising potential treatment for brain injury. “It’s the modern-day ‘holy grail.’ “
In this study, “to see a modest improvement in gait in the primary outcome is impressive,” he said.
In addition, the fact the study didn’t have any significant or severe adverse outcomes “is promising,” he added.
Studies like this “are going to help to lay the groundwork for future studies and hopefully one day result in a safe, noninvasive treatment” for Parkinson’s disease, Alzheimer’s disease, and disorders that affect the central nervous system such as spinal cord injury, Dr. Conidi said.
This therapy involves an invasive procedure requiring implantation directly into the brain, he noted. “At present, there’s no way to get stem cells to cross the blood-brain barrier.”
In addition, although motor impairment is definitely a component of TBI, it’s not as prevalent as cognitive impairment, said Dr. Conidi.
The study was supported by SanBio Co Ltd. Dr. McAllister and Dr. Conidi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, results from a phase 2 trial indicate. “We proved for the first time that we can affect outcomes in moderately to severely disabled patients with TBI using stem cells,” said study investigator Peter McAllister, MD, cofounder and medical director of the New England Center for Neurology and Headache, Stamford, Conn.
“I think the potential of regenerative medicine was always out there, but we are now getting to the point where we’re living up to that potential,” said Dr. McAllister, associate professor of neurology at Yale University, New Haven, Conn.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
No effective treatment to date
TBI can lead to motor deficits and chronic disability and currently there are no effective drugs to treat these deficits.
Researchers are increasingly focused on using somatic stem cells to restore lost function. Stem cells can differentiate or proliferate into different types of cells and are thought to promote repair and regeneration of tissues or organs damaged due to illness or injury.
The study included 61 patients with TBI with an average age of 34 years (70% were male and 69% were White). The mean time from injury was 8 years and Glasgow Outcome Scale Extended (GOS-E) ranged from 3 to 6.
Forty-six participants were randomly assigned to receive the stem cell therapy and 15 a sham procedure. In the treatment group, there were three different doses of cells (2.5 x 106, 5 x 106, and 10 x 106).
The treatment involved an investigational regenerative cell medicine comprised of bone marrow-derived mesenchymal stem cells (SB623). The allogeneic cells came from a male donor.
For the 20-minute procedure, a neurosurgeon drilled a tiny hole in the skull and, guided by MRI, injected the stem cells into the area of the lesion.
Patients receiving a surgical sham procedure were brought to the operating room, anesthetized, and had a hole drilled into the head over the area of the lesion. However, the surgeon went only halfway through the skull bone.
Participants were instructed to do specific physiotherapy exercises at home every morning and afternoon for the first 6 months of the study.
The primary efficacy endpoint was change in the Fugl-Meyer Motor Scale score (FMMS). This scale is widely used for clinical assessment of motor function, including range of motion, walking, lower limb movement, and dexterity.
At 24 weeks, the change in FMMS score for SB623-treated patients (least square [LS] mean increase 8.3) compared with controls (LS increase 2.3) was significant (P = .04).
“When we looked at all the data at 6 months, the folks who got the stem cells did statistically significantly better than the group that got the sham,” and that improvement began within the first week or two, said Dr. McAllister.
‘A real impact’
The treatment had a real impact on people’s lives, he said. “Some who couldn’t move their arm at all were able to put a nut on a bolt or brush their teeth, and some were able to button and unbutton where they couldn’t do that before.”
One teenager who was previously completely aphasic spoke an entire sentence.
The middle dose (5 x 106) had “by far” the best outcome, said Dr. McAllister. It’s not yet known whether the improvements will be permanent, he added.
At 48 weeks, treated patients experienced improvement over controls in secondary endpoints of the Action Research Arm Test (ARAT), which assesses grasp, grip, pinch, and gross movements; Gait Velocity (walking 10 meters); and NeuroQOL, a self-report measure of ability to carry out various activities.
However, although these endpoints were all numerically better in the stem cell groups, none reached statistical significance. This is likely because of the small study size and the fact the control group improved so much, said Dr. McAllister.
The exact mechanism of stem cell therapy is unclear, but researchers believe it “establishes a milieu of growth” for cells in the brain and promotes anti-inflammatory properties, said Dr. McAllister.
By 48 weeks, all study subjects had experienced at least one adverse event, with no differences between groups and no patient withdrawing as a result of adverse events. “There was no safety signal at all related to the stem cells,” said Dr. McAllister.
A larger phase 3 study of SB623 is planned.
The treatment may be useful in other conditions. A study of stroke survivors “just barely missed statistical significance” likely for methodological reasons and an older, sicker population, but the company plans to do another study in patients who were affected by stroke, said Dr. McAllister.
In addition, there may be potential for this approach with brain hemorrhage, Parkinson’s disease, multiple sclerosis, and other brain-related disorders, he said.
‘Modern-day holy grail’
Reached for a comment, TBI specialist Frank Conidi, MD, director of the Florida Center for Headache and Sports Neurology, said stem cell therapy is the most promising potential treatment for brain injury. “It’s the modern-day ‘holy grail.’ “
In this study, “to see a modest improvement in gait in the primary outcome is impressive,” he said.
In addition, the fact the study didn’t have any significant or severe adverse outcomes “is promising,” he added.
Studies like this “are going to help to lay the groundwork for future studies and hopefully one day result in a safe, noninvasive treatment” for Parkinson’s disease, Alzheimer’s disease, and disorders that affect the central nervous system such as spinal cord injury, Dr. Conidi said.
This therapy involves an invasive procedure requiring implantation directly into the brain, he noted. “At present, there’s no way to get stem cells to cross the blood-brain barrier.”
In addition, although motor impairment is definitely a component of TBI, it’s not as prevalent as cognitive impairment, said Dr. Conidi.
The study was supported by SanBio Co Ltd. Dr. McAllister and Dr. Conidi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
More years of ice hockey play tied to higher CTE risk
new research suggests. Early results from a study that examined donor brains showed that each additional year of ice hockey play increased the risk for CTE by 23%.
This information should be on the “radar” of all clinicians, said coinvestigator Jesse Mez, MD, associate professor of neurology at Boston University. “When they’re talking to kids and families and parents about playing contact sports, they should discuss the benefits as well as the risks so all that information can be taken into consideration.”
Dr. Mez noted that clinicians should also consider the amount of hockey played when assessing patients for thinking and memory trouble later in life. “CTE could be in the differential diagnosis,” he said.
The study findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Football data
CTE is a neurodegenerative disease associated with repetitive hits to the head. In previous research, the investigators showed that the more that athletes play American football, the more likely they are to develop CTE.
“Hockey, like football, involves repetitive head impacts as part of the game,” said Dr. Mez. “So we hypothesized that we would see a similar type of dose-response relationship in hockey.”
From two brain banks – the Veterans Affairs–Boston University–Concussion Legacy Foundation and the Framingham Heart Study – the researchers accessed 74 consecutive brains from donors who had played ice hockey. They collected information about hockey play during “pretty comprehensive” interviews with next of kin, Dr. Mez reported.
The study participants ranged in age from 13 to 91 years. The cause of death varied; most died with end-stage dementia and neurodegenerative disease, but some died of cardiovascular disease, and others from accidents.
For 9% of the individuals, the highest level of play was a youth league; 34% had reached the high school level, 30% reached the juniors/college level, and 26% played professionally. In addition, 46% played another contact sport – including 43% who played American football.
Primary outcomes included evidence of CTE from stage 0 (no CTE) to stage IV and severity of CTE, which was defined by the amount of neurofibrillary tangle (NFT) burden in 11 brain regions. For this burden, the score ranged from 0 (absent) to 3 (severe) in each region for a total range of 0-33.
Dr. Mez noted that, in CTE, tau protein accumulates abnormally. “It typically begins in the cortex in the frontal lobe and then spreads to other parts of the brain, including to the medial temporal structures, and is widespread by stage IV.”
The researchers estimated the association of duration of ice hockey play in years with each neuropathologic outcome and adjusted for age at death and duration of football play.
Consistent findings
Results showed that, of the 74 donors, 40 (54%) had CTE. Each additional year of hockey play corresponded to increased chances for having CTE (odds ratio, 1.23; 95% confidence interval, 11%-36%; P < .01). This increase in risk is similar to that which was found with football players, Dr. Mez noted. This was somewhat surprising, as hockey involves fewer “hits” than football.
“Hits are not as quintessential to the game of hockey as they are in football, where contacts occur with nearly every play,” he said. “In football, you have several hundred impacts over the course of a season.”
Researchers also found a 15% increase in odds for increasing one CTE stage (95% CI, 8%-22%; P < .01), and a .03 standard deviation increase in cumulative NFT burden (95% CI, 0.01-0.05; P < .01).
Dr. Mez noted that the fact that the results were consistent across different outcomes “improves the validity” of the findings.
In a sensitivity analysis that excluded participants who also played football, estimates “were pretty similar” to those in the full analysis, said Dr. Mez.
The investigators have not yet examined the effect of level of hockey play, such as professionally or at the college level, on CTE risk. However, in football players, they found that level of play is another “valuable predictor of CTE pathology,” Dr. Mez said, adding that level of play, position played, and years of play “are all probably contributing” to CTE risk.
Asking about years of play is useful in a clinical setting. “It’s very easy for a clinician to ask patients how many years of hockey they played,” said Dr. Mez.
Overall, the new results are important, as “millions of individuals” play contact sports, whether that is hockey, football, or European soccer, he added. “And for all sports, there seems to be this relationship between more play and risk of this disease.”
‘Skewed’ population?
Commenting on the findings, Frank Conidi, MD, director, Florida Center for Health and Sports Neurology, Port St. Lucie, said he was surprised the investigators found a 23% per year increase in risk for CTE among hockey players.
Dr. Conidi has played hockey himself and works with the Florida Panthers of the National Hockey League. In his practice, he treats retired professional football players who have neurodegenerative disorders. From his experience, the number of repetitive direct head impacts in football is significantly higher than in hockey. “Most of the forces seen in hockey are from hits to the body, where the force is transferred to the head,” said Dr. Conidi, who was not involved with the research.
He noted differences in the way hockey is played around the world. In European countries, for example, the ice surface is relatively large and the emphasis tends to be more on skill than hitting.
“It would have been interesting to have the study group analyze the data based on where the athlete grew up,” he said. Dr. Conidi would also like to know when the participants played hockey. “The game is vastly different now than it was in the 1970s, ‘80s, and early ‘90s, when there was more fighting, less protective gear, and more hitting in general.”
As is the case for most studies of CTE in athletes, the study population is “skewed” because the participants likely had neurocognitive and other problems that led to their decision to donate their brain, said Dr. Conidi.
He also doesn’t believe the study should be the sole factor in a decision to continue or stop playing hockey. “We are still in the infancy stages of understanding the effects of high-impact sports on athletes’ brains.”
The study received funding from the National Institute of Neurological Diseases and Stroke and the National Institute on Aging. Dr. Mez and Dr. Conidi have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests. Early results from a study that examined donor brains showed that each additional year of ice hockey play increased the risk for CTE by 23%.
This information should be on the “radar” of all clinicians, said coinvestigator Jesse Mez, MD, associate professor of neurology at Boston University. “When they’re talking to kids and families and parents about playing contact sports, they should discuss the benefits as well as the risks so all that information can be taken into consideration.”
Dr. Mez noted that clinicians should also consider the amount of hockey played when assessing patients for thinking and memory trouble later in life. “CTE could be in the differential diagnosis,” he said.
The study findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Football data
CTE is a neurodegenerative disease associated with repetitive hits to the head. In previous research, the investigators showed that the more that athletes play American football, the more likely they are to develop CTE.
“Hockey, like football, involves repetitive head impacts as part of the game,” said Dr. Mez. “So we hypothesized that we would see a similar type of dose-response relationship in hockey.”
From two brain banks – the Veterans Affairs–Boston University–Concussion Legacy Foundation and the Framingham Heart Study – the researchers accessed 74 consecutive brains from donors who had played ice hockey. They collected information about hockey play during “pretty comprehensive” interviews with next of kin, Dr. Mez reported.
The study participants ranged in age from 13 to 91 years. The cause of death varied; most died with end-stage dementia and neurodegenerative disease, but some died of cardiovascular disease, and others from accidents.
For 9% of the individuals, the highest level of play was a youth league; 34% had reached the high school level, 30% reached the juniors/college level, and 26% played professionally. In addition, 46% played another contact sport – including 43% who played American football.
Primary outcomes included evidence of CTE from stage 0 (no CTE) to stage IV and severity of CTE, which was defined by the amount of neurofibrillary tangle (NFT) burden in 11 brain regions. For this burden, the score ranged from 0 (absent) to 3 (severe) in each region for a total range of 0-33.
Dr. Mez noted that, in CTE, tau protein accumulates abnormally. “It typically begins in the cortex in the frontal lobe and then spreads to other parts of the brain, including to the medial temporal structures, and is widespread by stage IV.”
The researchers estimated the association of duration of ice hockey play in years with each neuropathologic outcome and adjusted for age at death and duration of football play.
Consistent findings
Results showed that, of the 74 donors, 40 (54%) had CTE. Each additional year of hockey play corresponded to increased chances for having CTE (odds ratio, 1.23; 95% confidence interval, 11%-36%; P < .01). This increase in risk is similar to that which was found with football players, Dr. Mez noted. This was somewhat surprising, as hockey involves fewer “hits” than football.
“Hits are not as quintessential to the game of hockey as they are in football, where contacts occur with nearly every play,” he said. “In football, you have several hundred impacts over the course of a season.”
Researchers also found a 15% increase in odds for increasing one CTE stage (95% CI, 8%-22%; P < .01), and a .03 standard deviation increase in cumulative NFT burden (95% CI, 0.01-0.05; P < .01).
Dr. Mez noted that the fact that the results were consistent across different outcomes “improves the validity” of the findings.
In a sensitivity analysis that excluded participants who also played football, estimates “were pretty similar” to those in the full analysis, said Dr. Mez.
The investigators have not yet examined the effect of level of hockey play, such as professionally or at the college level, on CTE risk. However, in football players, they found that level of play is another “valuable predictor of CTE pathology,” Dr. Mez said, adding that level of play, position played, and years of play “are all probably contributing” to CTE risk.
Asking about years of play is useful in a clinical setting. “It’s very easy for a clinician to ask patients how many years of hockey they played,” said Dr. Mez.
Overall, the new results are important, as “millions of individuals” play contact sports, whether that is hockey, football, or European soccer, he added. “And for all sports, there seems to be this relationship between more play and risk of this disease.”
‘Skewed’ population?
Commenting on the findings, Frank Conidi, MD, director, Florida Center for Health and Sports Neurology, Port St. Lucie, said he was surprised the investigators found a 23% per year increase in risk for CTE among hockey players.
Dr. Conidi has played hockey himself and works with the Florida Panthers of the National Hockey League. In his practice, he treats retired professional football players who have neurodegenerative disorders. From his experience, the number of repetitive direct head impacts in football is significantly higher than in hockey. “Most of the forces seen in hockey are from hits to the body, where the force is transferred to the head,” said Dr. Conidi, who was not involved with the research.
He noted differences in the way hockey is played around the world. In European countries, for example, the ice surface is relatively large and the emphasis tends to be more on skill than hitting.
“It would have been interesting to have the study group analyze the data based on where the athlete grew up,” he said. Dr. Conidi would also like to know when the participants played hockey. “The game is vastly different now than it was in the 1970s, ‘80s, and early ‘90s, when there was more fighting, less protective gear, and more hitting in general.”
As is the case for most studies of CTE in athletes, the study population is “skewed” because the participants likely had neurocognitive and other problems that led to their decision to donate their brain, said Dr. Conidi.
He also doesn’t believe the study should be the sole factor in a decision to continue or stop playing hockey. “We are still in the infancy stages of understanding the effects of high-impact sports on athletes’ brains.”
The study received funding from the National Institute of Neurological Diseases and Stroke and the National Institute on Aging. Dr. Mez and Dr. Conidi have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests. Early results from a study that examined donor brains showed that each additional year of ice hockey play increased the risk for CTE by 23%.
This information should be on the “radar” of all clinicians, said coinvestigator Jesse Mez, MD, associate professor of neurology at Boston University. “When they’re talking to kids and families and parents about playing contact sports, they should discuss the benefits as well as the risks so all that information can be taken into consideration.”
Dr. Mez noted that clinicians should also consider the amount of hockey played when assessing patients for thinking and memory trouble later in life. “CTE could be in the differential diagnosis,” he said.
The study findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Football data
CTE is a neurodegenerative disease associated with repetitive hits to the head. In previous research, the investigators showed that the more that athletes play American football, the more likely they are to develop CTE.
“Hockey, like football, involves repetitive head impacts as part of the game,” said Dr. Mez. “So we hypothesized that we would see a similar type of dose-response relationship in hockey.”
From two brain banks – the Veterans Affairs–Boston University–Concussion Legacy Foundation and the Framingham Heart Study – the researchers accessed 74 consecutive brains from donors who had played ice hockey. They collected information about hockey play during “pretty comprehensive” interviews with next of kin, Dr. Mez reported.
The study participants ranged in age from 13 to 91 years. The cause of death varied; most died with end-stage dementia and neurodegenerative disease, but some died of cardiovascular disease, and others from accidents.
For 9% of the individuals, the highest level of play was a youth league; 34% had reached the high school level, 30% reached the juniors/college level, and 26% played professionally. In addition, 46% played another contact sport – including 43% who played American football.
Primary outcomes included evidence of CTE from stage 0 (no CTE) to stage IV and severity of CTE, which was defined by the amount of neurofibrillary tangle (NFT) burden in 11 brain regions. For this burden, the score ranged from 0 (absent) to 3 (severe) in each region for a total range of 0-33.
Dr. Mez noted that, in CTE, tau protein accumulates abnormally. “It typically begins in the cortex in the frontal lobe and then spreads to other parts of the brain, including to the medial temporal structures, and is widespread by stage IV.”
The researchers estimated the association of duration of ice hockey play in years with each neuropathologic outcome and adjusted for age at death and duration of football play.
Consistent findings
Results showed that, of the 74 donors, 40 (54%) had CTE. Each additional year of hockey play corresponded to increased chances for having CTE (odds ratio, 1.23; 95% confidence interval, 11%-36%; P < .01). This increase in risk is similar to that which was found with football players, Dr. Mez noted. This was somewhat surprising, as hockey involves fewer “hits” than football.
“Hits are not as quintessential to the game of hockey as they are in football, where contacts occur with nearly every play,” he said. “In football, you have several hundred impacts over the course of a season.”
Researchers also found a 15% increase in odds for increasing one CTE stage (95% CI, 8%-22%; P < .01), and a .03 standard deviation increase in cumulative NFT burden (95% CI, 0.01-0.05; P < .01).
Dr. Mez noted that the fact that the results were consistent across different outcomes “improves the validity” of the findings.
In a sensitivity analysis that excluded participants who also played football, estimates “were pretty similar” to those in the full analysis, said Dr. Mez.
The investigators have not yet examined the effect of level of hockey play, such as professionally or at the college level, on CTE risk. However, in football players, they found that level of play is another “valuable predictor of CTE pathology,” Dr. Mez said, adding that level of play, position played, and years of play “are all probably contributing” to CTE risk.
Asking about years of play is useful in a clinical setting. “It’s very easy for a clinician to ask patients how many years of hockey they played,” said Dr. Mez.
Overall, the new results are important, as “millions of individuals” play contact sports, whether that is hockey, football, or European soccer, he added. “And for all sports, there seems to be this relationship between more play and risk of this disease.”
‘Skewed’ population?
Commenting on the findings, Frank Conidi, MD, director, Florida Center for Health and Sports Neurology, Port St. Lucie, said he was surprised the investigators found a 23% per year increase in risk for CTE among hockey players.
Dr. Conidi has played hockey himself and works with the Florida Panthers of the National Hockey League. In his practice, he treats retired professional football players who have neurodegenerative disorders. From his experience, the number of repetitive direct head impacts in football is significantly higher than in hockey. “Most of the forces seen in hockey are from hits to the body, where the force is transferred to the head,” said Dr. Conidi, who was not involved with the research.
He noted differences in the way hockey is played around the world. In European countries, for example, the ice surface is relatively large and the emphasis tends to be more on skill than hitting.
“It would have been interesting to have the study group analyze the data based on where the athlete grew up,” he said. Dr. Conidi would also like to know when the participants played hockey. “The game is vastly different now than it was in the 1970s, ‘80s, and early ‘90s, when there was more fighting, less protective gear, and more hitting in general.”
As is the case for most studies of CTE in athletes, the study population is “skewed” because the participants likely had neurocognitive and other problems that led to their decision to donate their brain, said Dr. Conidi.
He also doesn’t believe the study should be the sole factor in a decision to continue or stop playing hockey. “We are still in the infancy stages of understanding the effects of high-impact sports on athletes’ brains.”
The study received funding from the National Institute of Neurological Diseases and Stroke and the National Institute on Aging. Dr. Mez and Dr. Conidi have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
Concussion increases risk of mental health issues in children
Among children and adolescents aged 5-18 years, concussion was associated with a higher risk of mental health problems, compared with age- and sex-matched children and adolescents with an orthopedic injury, according to a cohort study published in JAMA Network Open.
While concussions are one of the most common head injuries in the pediatric population, the extent to which they increase the risk of new onset psychiatric disorders or subsequent psychopathology is unclear, lead author Andrée-Anne Ledoux, PhD, of the Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and colleagues explained.

The researchers conducted a population-based retrospective cohort study to evaluate associations between concussion and risk of subsequent mental health issues, psychiatric hospitalizations, self-harm, or suicides in children and adolescents, with follow-up ranging from 1 month to 10 years.
The data were obtained from province-wide health administrative databases. Participants with concussion were included in an exposed group, while those with an orthopedic injury were included in a 1:2 age- and sex-matched comparison group.
Results
The study cohort comprised 448,803 participants, including 152,321 and 296,482 children and adolescents with concussion and orthopedic injury, respectively.
The incidence rates of any mental health problem were 11,141 per 100,000 person-years in the exposed group and 7,960 per 100,000 person-years in the unexposed group (difference, 3,181; 95% confidence interval, 3,073-3,291 per 100,000 person-years).
After concussion, the exposed group had a greater risk of developing a mental health issue (adjusted hazard ratio, 1.39; 95% CI, 1.37-1.40), psychiatric hospitalization (aHR, 1.47; 95% CI, 1.41-1.53), and self-harm (aHR, 1.49; 95% CI, 1.42-1.56). In addition, there was no significant difference in death by suicide between the exposed and unexposed groups (HR, 1.54; 95% CI, 0.90-2.61).
“Our results suggest that clinicians should assess for preexisting and new mental health symptoms throughout concussion recovery and treat mental health conditions or symptoms or refer the patient to a specialist in pediatric mental health,” wrote Dr. Ledoux and colleagues. “[Clinicians should also] assess suicidal ideation and self-harm behaviors during evaluation and follow-up visits for concussion.”
The researchers acknowledged that a key limitation of the study was the retrospective observational design. In addition, the identification of exposures using diagnostic billing codes could have introduced exposure or outcome misclassification.
Expert-recommended resources
“For more information, I’d recommend ‘Pedsconcussion,’ which are evidence-based living guidelines for pediatric concussion care,” Dr. Ledoux said in an interview. “Within domain 8, there are specific guidelines related to the management of mental health issues post concussion.”

Neuropsychology expert Talin Babikian, PhD, of the University of California, Los Angeles, commented: “Studies have shown that even a single psychoeducational session early after a concussion can minimize prolonged recoveries. Ensuring all stakeholders (family, clinicians, school, coach, peers) are on the same page and providing the same information is important to build trust and a sense of safety and agency.
“We want to provide psychoeducation early in the process to avoid unnecessary fear and avoidance. We also want to curtail misattribution of everyday symptoms or symptoms related to an unrelated condition to a brain injury, which are easier to do when caught early,” Dr. Babikian added.
This study was supported by the Institute for Clinical Evaluative Sciences, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-term Care. One author reported financial relationships with the University of Ottawa, the National Football League, Parachute Canada, and 360 Concussion Care, an interdisciplinary concussion clinic; no other conflicts of interest were reported.
Among children and adolescents aged 5-18 years, concussion was associated with a higher risk of mental health problems, compared with age- and sex-matched children and adolescents with an orthopedic injury, according to a cohort study published in JAMA Network Open.
While concussions are one of the most common head injuries in the pediatric population, the extent to which they increase the risk of new onset psychiatric disorders or subsequent psychopathology is unclear, lead author Andrée-Anne Ledoux, PhD, of the Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and colleagues explained.
The researchers conducted a population-based retrospective cohort study to evaluate associations between concussion and risk of subsequent mental health issues, psychiatric hospitalizations, self-harm, or suicides in children and adolescents, with follow-up ranging from 1 month to 10 years.
The data were obtained from province-wide health administrative databases. Participants with concussion were included in an exposed group, while those with an orthopedic injury were included in a 1:2 age- and sex-matched comparison group.
Results
The study cohort comprised 448,803 participants, including 152,321 and 296,482 children and adolescents with concussion and orthopedic injury, respectively.
The incidence rates of any mental health problem were 11,141 per 100,000 person-years in the exposed group and 7,960 per 100,000 person-years in the unexposed group (difference, 3,181; 95% confidence interval, 3,073-3,291 per 100,000 person-years).
After concussion, the exposed group had a greater risk of developing a mental health issue (adjusted hazard ratio, 1.39; 95% CI, 1.37-1.40), psychiatric hospitalization (aHR, 1.47; 95% CI, 1.41-1.53), and self-harm (aHR, 1.49; 95% CI, 1.42-1.56). In addition, there was no significant difference in death by suicide between the exposed and unexposed groups (HR, 1.54; 95% CI, 0.90-2.61).
“Our results suggest that clinicians should assess for preexisting and new mental health symptoms throughout concussion recovery and treat mental health conditions or symptoms or refer the patient to a specialist in pediatric mental health,” wrote Dr. Ledoux and colleagues. “[Clinicians should also] assess suicidal ideation and self-harm behaviors during evaluation and follow-up visits for concussion.”
The researchers acknowledged that a key limitation of the study was the retrospective observational design. In addition, the identification of exposures using diagnostic billing codes could have introduced exposure or outcome misclassification.
Expert-recommended resources
“For more information, I’d recommend ‘Pedsconcussion,’ which are evidence-based living guidelines for pediatric concussion care,” Dr. Ledoux said in an interview. “Within domain 8, there are specific guidelines related to the management of mental health issues post concussion.”
Neuropsychology expert Talin Babikian, PhD, of the University of California, Los Angeles, commented: “Studies have shown that even a single psychoeducational session early after a concussion can minimize prolonged recoveries. Ensuring all stakeholders (family, clinicians, school, coach, peers) are on the same page and providing the same information is important to build trust and a sense of safety and agency.
“We want to provide psychoeducation early in the process to avoid unnecessary fear and avoidance. We also want to curtail misattribution of everyday symptoms or symptoms related to an unrelated condition to a brain injury, which are easier to do when caught early,” Dr. Babikian added.
This study was supported by the Institute for Clinical Evaluative Sciences, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-term Care. One author reported financial relationships with the University of Ottawa, the National Football League, Parachute Canada, and 360 Concussion Care, an interdisciplinary concussion clinic; no other conflicts of interest were reported.
Among children and adolescents aged 5-18 years, concussion was associated with a higher risk of mental health problems, compared with age- and sex-matched children and adolescents with an orthopedic injury, according to a cohort study published in JAMA Network Open.
While concussions are one of the most common head injuries in the pediatric population, the extent to which they increase the risk of new onset psychiatric disorders or subsequent psychopathology is unclear, lead author Andrée-Anne Ledoux, PhD, of the Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and colleagues explained.
The researchers conducted a population-based retrospective cohort study to evaluate associations between concussion and risk of subsequent mental health issues, psychiatric hospitalizations, self-harm, or suicides in children and adolescents, with follow-up ranging from 1 month to 10 years.
The data were obtained from province-wide health administrative databases. Participants with concussion were included in an exposed group, while those with an orthopedic injury were included in a 1:2 age- and sex-matched comparison group.
Results
The study cohort comprised 448,803 participants, including 152,321 and 296,482 children and adolescents with concussion and orthopedic injury, respectively.
The incidence rates of any mental health problem were 11,141 per 100,000 person-years in the exposed group and 7,960 per 100,000 person-years in the unexposed group (difference, 3,181; 95% confidence interval, 3,073-3,291 per 100,000 person-years).
After concussion, the exposed group had a greater risk of developing a mental health issue (adjusted hazard ratio, 1.39; 95% CI, 1.37-1.40), psychiatric hospitalization (aHR, 1.47; 95% CI, 1.41-1.53), and self-harm (aHR, 1.49; 95% CI, 1.42-1.56). In addition, there was no significant difference in death by suicide between the exposed and unexposed groups (HR, 1.54; 95% CI, 0.90-2.61).
“Our results suggest that clinicians should assess for preexisting and new mental health symptoms throughout concussion recovery and treat mental health conditions or symptoms or refer the patient to a specialist in pediatric mental health,” wrote Dr. Ledoux and colleagues. “[Clinicians should also] assess suicidal ideation and self-harm behaviors during evaluation and follow-up visits for concussion.”
The researchers acknowledged that a key limitation of the study was the retrospective observational design. In addition, the identification of exposures using diagnostic billing codes could have introduced exposure or outcome misclassification.
Expert-recommended resources
“For more information, I’d recommend ‘Pedsconcussion,’ which are evidence-based living guidelines for pediatric concussion care,” Dr. Ledoux said in an interview. “Within domain 8, there are specific guidelines related to the management of mental health issues post concussion.”
Neuropsychology expert Talin Babikian, PhD, of the University of California, Los Angeles, commented: “Studies have shown that even a single psychoeducational session early after a concussion can minimize prolonged recoveries. Ensuring all stakeholders (family, clinicians, school, coach, peers) are on the same page and providing the same information is important to build trust and a sense of safety and agency.
“We want to provide psychoeducation early in the process to avoid unnecessary fear and avoidance. We also want to curtail misattribution of everyday symptoms or symptoms related to an unrelated condition to a brain injury, which are easier to do when caught early,” Dr. Babikian added.
This study was supported by the Institute for Clinical Evaluative Sciences, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-term Care. One author reported financial relationships with the University of Ottawa, the National Football League, Parachute Canada, and 360 Concussion Care, an interdisciplinary concussion clinic; no other conflicts of interest were reported.
FROM JAMA NETWORK OPEN
MRI is key to diagnosing CTE in living patients?
, new research suggests.
“These new results offer some hope for clinicians who are really struggling to confidently diagnose or detect CTE during life,” said lead author Michael L. Alosco, PhD, associate professor of neurology, codirector of the Boston University Alzheimer’s Disease Research Center, and investigator at the Boston University CTE Center.
The findings were published online Dec. 7, 2021, in Alzheimer’s Research & Therapy.
A new way to diagnose?
CTE is a neurodegenerative disease associated with exposure to repetitive blows to the head, such as those sustained playing contact sports. Currently, the condition can only be reliably diagnosed at autopsy using neuropathological diagnostic criteria.
There are four pathological stages of CTE, ranging from mild to severe. Each progressive stage reflects mounting accumulation of hyperphosphorylated tau (p-tau).
The study included 55 male brain donors with confirmed CTE, all with a history of repetitive head injury. Most (n = 52) played football, but two played ice hockey and one had military and combat exposure. The analysis also included 31 men with normal cognition (NC). Of these, some were living and some were deceased.
The study sample was restricted to participants age 60 and older and to those who had an MRI obtained through a medical record request.
Most referrals for MRI in the CTE group were related to dementia or neurodegenerative disease (65%). In the NC group, MRI indications were mostly related to cerebrovascular causes (22.6%), memory complaints (16.1%), or vertigo (9.7%).
From MRIs, neuroradiologists visually rated patterns of shrinkage in the brain, microvascular disease, and presence of cavum septum pellucidum (CSP) – a large hole in the tissue separating ventricles of the brain.
More atrophy
Results showed that compared with the NC group, the CTE group had significantly greater atrophy in several brain regions, including the orbital-frontal cortex, dorsolateral frontal cortex, superior frontal cortex, anterior temporal lobes, and medial temporal lobe.
The dorsolateral frontal cortex showed the largest group difference (estimated marginal mean difference, 1.31; 95% confidence interval, .42-2.19; false discovery rate-adjusted P = .01).
Previous research has shown early p-tau involvement in this area among CTE patients. Although the hippocampus is also affected in CTE, this occurs later in the disease course, the investigators noted.
The unique pattern, type, and distribution of p-tau pathology in CTE is different from Alzheimer’s disease. CTE is also distinct from Alzheimer’s disease in that there is no accumulation of beta-amyloid plaque.
The new results add to “converging evidence” for frontotemporal and medial temporal lobe atrophy in CTE “that might be able to be visualized on MRI,” the investigators noted.
Almost two-thirds of the CTE group had an additional neurodegenerative disease. Furthermore, the effect sizes remained similar in analyses that excluded CTE donors with frontotemporal lobar degeneration or Alzheimer’s disease.
“This suggests to us that these other diseases were not accounting for the atrophy,” Dr. Alosco said.
Individuals with CTE were 6.7 times more likely to have a CSP versus those with NC (odds ratio, 6.7; 95% CI, 1.5-50.1; P = .049).
Although previous research suggested an association between CSP and repetitive concussion, CSP is also frequently found in the general adult population. However, when combined with data on frontal lobe shrinkage, it may be a supportive differential diagnostic feature for CTE, Dr. Alosco said.
An important first step
The investigators also examined ventricle size. The lateral ventricles in the CTE group were significantly larger (mean difference, 1.72; 95% CI, .62-2.82; P = .01), as was the third ventricle (mean difference, .80; 95% CI, .26-1.35; P = .01).
When neuropathologists rated tau severity and atrophy at autopsy, they found that more severe p-tau pathology was associated with greater atrophy among those with CTE (beta = .68; P < .01).
Dr. Alosco called the finding “exciting,” noting that it suggests “this tau is a precipitant for neurodegeneration.”
He noted that, although some researchers have used positron emission tomography (PET) tau tracers to uncover a CTE pattern, MRI is relatively inexpensive and routinely used as part of dementia assessment.
While the new study is “an important first step” in using MRI to diagnose CTE, larger sample sizes are needed, Dr. Alosco said. “We also need to look at other disease groups and really nail down the difference with CTE in terms of patterns” (vs. Alzheimer’s disease and vs. frontotemporal lobar degeneration), he added.
“Once those differences are cleared, we will be ready to be more confident when we interpret these images.”.
‘Not unexpected’
Commenting on the research, neurologist and concussion expert Francis X. Conidi, DO, director, Florida Center for Headache and Sports Neurology, Port St. Lucie, said that, although the study was “well thought out and interesting,” the results were “not completely unexpected.”
Frontal and anterior temporal lobe atrophy and prominent third ventricles are very common in patients with traumatic brain injury (TBI), which is “a prerequisite to develop CTE,” said Dr. Conidi, who was not involved with the research.
The current study’s findings mirror observations found in a National Football League cohort he and his colleagues are following – and in his patients with TBI in general.
Dr. Conidi noted that there is a “significant subjective component” to the study results because they relied on the opinion of neuroradiologists. He is not convinced MRI findings of frontotemporal and medial temporal lobe atrophy necessarily represent CTE and not TBI. In fact, he noted that patients with TBI have a significantly greater chance of not developing a neurodegenerative disorder.
Dr. Conidi added that he doesn’t think MRI will ever be the gold standard for diagnosing or even assessing risk of developing CTE. “That lies in tau PET imaging,” he said.
Overstated conclusion?
Also commenting on the research findings, Kristen Dams-O’Connor, PhD, professor, vice chair of research, and director, Brain Injury Research Center, Department of Rehabilitation Medicine, Icahn School of Medicine at Mount Sinai in New York, said the sensitivity analyses, particularly those designed to clarify contributions of Alzheimer’s disease and other neuropathological contributions to associations between p-tau and atrophy, “increase our confidence” in the findings.
“What’s exciting about this paper is that it provides very preliminary support for adding another tool to our arsenal as we try to establish a constellation of in vivo diagnostic markers that, together, will help us rule in a post-traumatic neurodegenerative process and rule out other brain diseases.”
A possible study limitation is that the MRI scans were from low-field strength magnets, although that makes the study more “ecologically valid”, said Dr. Dams-O’Connor. “Many clinical scanners are built around a 1.5T magnet, so what the researchers see in this study is what a radiologist may see in the clinic.”
The conclusion that frontal-temporal atrophy is an MRI marker of CTE is “an overstatement” as this pattern of atrophy is not specific to CTE, said Dr. Dams-O’Connor. “The association of p-tau with atrophy is unsurprising and doesn’t bring us much closer to understanding how, or whether, the patterns of p-tau accumulation observed in CTE contribute to the clinical expression of symptoms.”
Dr. Alosco and Dr. Conidi report no relevant financial relationships. Disclosures for the other study authors are listed in the original journal article. The study was funded by grants from the National Institute on Aging, the National Institute on Neurological Disorders and Stroke, National Institute of Aging Boston University AD Center, Department of Veterans Affairs Merit Award, the Nick and Lynn Buoniconti Foundation, and BU-CTSI.
A version of this article first appeared on Medscape.com.
, new research suggests.
“These new results offer some hope for clinicians who are really struggling to confidently diagnose or detect CTE during life,” said lead author Michael L. Alosco, PhD, associate professor of neurology, codirector of the Boston University Alzheimer’s Disease Research Center, and investigator at the Boston University CTE Center.
The findings were published online Dec. 7, 2021, in Alzheimer’s Research & Therapy.
A new way to diagnose?
CTE is a neurodegenerative disease associated with exposure to repetitive blows to the head, such as those sustained playing contact sports. Currently, the condition can only be reliably diagnosed at autopsy using neuropathological diagnostic criteria.
There are four pathological stages of CTE, ranging from mild to severe. Each progressive stage reflects mounting accumulation of hyperphosphorylated tau (p-tau).
The study included 55 male brain donors with confirmed CTE, all with a history of repetitive head injury. Most (n = 52) played football, but two played ice hockey and one had military and combat exposure. The analysis also included 31 men with normal cognition (NC). Of these, some were living and some were deceased.
The study sample was restricted to participants age 60 and older and to those who had an MRI obtained through a medical record request.
Most referrals for MRI in the CTE group were related to dementia or neurodegenerative disease (65%). In the NC group, MRI indications were mostly related to cerebrovascular causes (22.6%), memory complaints (16.1%), or vertigo (9.7%).
From MRIs, neuroradiologists visually rated patterns of shrinkage in the brain, microvascular disease, and presence of cavum septum pellucidum (CSP) – a large hole in the tissue separating ventricles of the brain.
More atrophy
Results showed that compared with the NC group, the CTE group had significantly greater atrophy in several brain regions, including the orbital-frontal cortex, dorsolateral frontal cortex, superior frontal cortex, anterior temporal lobes, and medial temporal lobe.
The dorsolateral frontal cortex showed the largest group difference (estimated marginal mean difference, 1.31; 95% confidence interval, .42-2.19; false discovery rate-adjusted P = .01).
Previous research has shown early p-tau involvement in this area among CTE patients. Although the hippocampus is also affected in CTE, this occurs later in the disease course, the investigators noted.
The unique pattern, type, and distribution of p-tau pathology in CTE is different from Alzheimer’s disease. CTE is also distinct from Alzheimer’s disease in that there is no accumulation of beta-amyloid plaque.
The new results add to “converging evidence” for frontotemporal and medial temporal lobe atrophy in CTE “that might be able to be visualized on MRI,” the investigators noted.
Almost two-thirds of the CTE group had an additional neurodegenerative disease. Furthermore, the effect sizes remained similar in analyses that excluded CTE donors with frontotemporal lobar degeneration or Alzheimer’s disease.
“This suggests to us that these other diseases were not accounting for the atrophy,” Dr. Alosco said.
Individuals with CTE were 6.7 times more likely to have a CSP versus those with NC (odds ratio, 6.7; 95% CI, 1.5-50.1; P = .049).
Although previous research suggested an association between CSP and repetitive concussion, CSP is also frequently found in the general adult population. However, when combined with data on frontal lobe shrinkage, it may be a supportive differential diagnostic feature for CTE, Dr. Alosco said.
An important first step
The investigators also examined ventricle size. The lateral ventricles in the CTE group were significantly larger (mean difference, 1.72; 95% CI, .62-2.82; P = .01), as was the third ventricle (mean difference, .80; 95% CI, .26-1.35; P = .01).
When neuropathologists rated tau severity and atrophy at autopsy, they found that more severe p-tau pathology was associated with greater atrophy among those with CTE (beta = .68; P < .01).
Dr. Alosco called the finding “exciting,” noting that it suggests “this tau is a precipitant for neurodegeneration.”
He noted that, although some researchers have used positron emission tomography (PET) tau tracers to uncover a CTE pattern, MRI is relatively inexpensive and routinely used as part of dementia assessment.
While the new study is “an important first step” in using MRI to diagnose CTE, larger sample sizes are needed, Dr. Alosco said. “We also need to look at other disease groups and really nail down the difference with CTE in terms of patterns” (vs. Alzheimer’s disease and vs. frontotemporal lobar degeneration), he added.
“Once those differences are cleared, we will be ready to be more confident when we interpret these images.”.
‘Not unexpected’
Commenting on the research, neurologist and concussion expert Francis X. Conidi, DO, director, Florida Center for Headache and Sports Neurology, Port St. Lucie, said that, although the study was “well thought out and interesting,” the results were “not completely unexpected.”
Frontal and anterior temporal lobe atrophy and prominent third ventricles are very common in patients with traumatic brain injury (TBI), which is “a prerequisite to develop CTE,” said Dr. Conidi, who was not involved with the research.
The current study’s findings mirror observations found in a National Football League cohort he and his colleagues are following – and in his patients with TBI in general.
Dr. Conidi noted that there is a “significant subjective component” to the study results because they relied on the opinion of neuroradiologists. He is not convinced MRI findings of frontotemporal and medial temporal lobe atrophy necessarily represent CTE and not TBI. In fact, he noted that patients with TBI have a significantly greater chance of not developing a neurodegenerative disorder.
Dr. Conidi added that he doesn’t think MRI will ever be the gold standard for diagnosing or even assessing risk of developing CTE. “That lies in tau PET imaging,” he said.
Overstated conclusion?
Also commenting on the research findings, Kristen Dams-O’Connor, PhD, professor, vice chair of research, and director, Brain Injury Research Center, Department of Rehabilitation Medicine, Icahn School of Medicine at Mount Sinai in New York, said the sensitivity analyses, particularly those designed to clarify contributions of Alzheimer’s disease and other neuropathological contributions to associations between p-tau and atrophy, “increase our confidence” in the findings.
“What’s exciting about this paper is that it provides very preliminary support for adding another tool to our arsenal as we try to establish a constellation of in vivo diagnostic markers that, together, will help us rule in a post-traumatic neurodegenerative process and rule out other brain diseases.”
A possible study limitation is that the MRI scans were from low-field strength magnets, although that makes the study more “ecologically valid”, said Dr. Dams-O’Connor. “Many clinical scanners are built around a 1.5T magnet, so what the researchers see in this study is what a radiologist may see in the clinic.”
The conclusion that frontal-temporal atrophy is an MRI marker of CTE is “an overstatement” as this pattern of atrophy is not specific to CTE, said Dr. Dams-O’Connor. “The association of p-tau with atrophy is unsurprising and doesn’t bring us much closer to understanding how, or whether, the patterns of p-tau accumulation observed in CTE contribute to the clinical expression of symptoms.”
Dr. Alosco and Dr. Conidi report no relevant financial relationships. Disclosures for the other study authors are listed in the original journal article. The study was funded by grants from the National Institute on Aging, the National Institute on Neurological Disorders and Stroke, National Institute of Aging Boston University AD Center, Department of Veterans Affairs Merit Award, the Nick and Lynn Buoniconti Foundation, and BU-CTSI.
A version of this article first appeared on Medscape.com.
, new research suggests.
“These new results offer some hope for clinicians who are really struggling to confidently diagnose or detect CTE during life,” said lead author Michael L. Alosco, PhD, associate professor of neurology, codirector of the Boston University Alzheimer’s Disease Research Center, and investigator at the Boston University CTE Center.
The findings were published online Dec. 7, 2021, in Alzheimer’s Research & Therapy.
A new way to diagnose?
CTE is a neurodegenerative disease associated with exposure to repetitive blows to the head, such as those sustained playing contact sports. Currently, the condition can only be reliably diagnosed at autopsy using neuropathological diagnostic criteria.
There are four pathological stages of CTE, ranging from mild to severe. Each progressive stage reflects mounting accumulation of hyperphosphorylated tau (p-tau).
The study included 55 male brain donors with confirmed CTE, all with a history of repetitive head injury. Most (n = 52) played football, but two played ice hockey and one had military and combat exposure. The analysis also included 31 men with normal cognition (NC). Of these, some were living and some were deceased.
The study sample was restricted to participants age 60 and older and to those who had an MRI obtained through a medical record request.
Most referrals for MRI in the CTE group were related to dementia or neurodegenerative disease (65%). In the NC group, MRI indications were mostly related to cerebrovascular causes (22.6%), memory complaints (16.1%), or vertigo (9.7%).
From MRIs, neuroradiologists visually rated patterns of shrinkage in the brain, microvascular disease, and presence of cavum septum pellucidum (CSP) – a large hole in the tissue separating ventricles of the brain.
More atrophy
Results showed that compared with the NC group, the CTE group had significantly greater atrophy in several brain regions, including the orbital-frontal cortex, dorsolateral frontal cortex, superior frontal cortex, anterior temporal lobes, and medial temporal lobe.
The dorsolateral frontal cortex showed the largest group difference (estimated marginal mean difference, 1.31; 95% confidence interval, .42-2.19; false discovery rate-adjusted P = .01).
Previous research has shown early p-tau involvement in this area among CTE patients. Although the hippocampus is also affected in CTE, this occurs later in the disease course, the investigators noted.
The unique pattern, type, and distribution of p-tau pathology in CTE is different from Alzheimer’s disease. CTE is also distinct from Alzheimer’s disease in that there is no accumulation of beta-amyloid plaque.
The new results add to “converging evidence” for frontotemporal and medial temporal lobe atrophy in CTE “that might be able to be visualized on MRI,” the investigators noted.
Almost two-thirds of the CTE group had an additional neurodegenerative disease. Furthermore, the effect sizes remained similar in analyses that excluded CTE donors with frontotemporal lobar degeneration or Alzheimer’s disease.
“This suggests to us that these other diseases were not accounting for the atrophy,” Dr. Alosco said.
Individuals with CTE were 6.7 times more likely to have a CSP versus those with NC (odds ratio, 6.7; 95% CI, 1.5-50.1; P = .049).
Although previous research suggested an association between CSP and repetitive concussion, CSP is also frequently found in the general adult population. However, when combined with data on frontal lobe shrinkage, it may be a supportive differential diagnostic feature for CTE, Dr. Alosco said.
An important first step
The investigators also examined ventricle size. The lateral ventricles in the CTE group were significantly larger (mean difference, 1.72; 95% CI, .62-2.82; P = .01), as was the third ventricle (mean difference, .80; 95% CI, .26-1.35; P = .01).
When neuropathologists rated tau severity and atrophy at autopsy, they found that more severe p-tau pathology was associated with greater atrophy among those with CTE (beta = .68; P < .01).
Dr. Alosco called the finding “exciting,” noting that it suggests “this tau is a precipitant for neurodegeneration.”
He noted that, although some researchers have used positron emission tomography (PET) tau tracers to uncover a CTE pattern, MRI is relatively inexpensive and routinely used as part of dementia assessment.
While the new study is “an important first step” in using MRI to diagnose CTE, larger sample sizes are needed, Dr. Alosco said. “We also need to look at other disease groups and really nail down the difference with CTE in terms of patterns” (vs. Alzheimer’s disease and vs. frontotemporal lobar degeneration), he added.
“Once those differences are cleared, we will be ready to be more confident when we interpret these images.”.
‘Not unexpected’
Commenting on the research, neurologist and concussion expert Francis X. Conidi, DO, director, Florida Center for Headache and Sports Neurology, Port St. Lucie, said that, although the study was “well thought out and interesting,” the results were “not completely unexpected.”
Frontal and anterior temporal lobe atrophy and prominent third ventricles are very common in patients with traumatic brain injury (TBI), which is “a prerequisite to develop CTE,” said Dr. Conidi, who was not involved with the research.
The current study’s findings mirror observations found in a National Football League cohort he and his colleagues are following – and in his patients with TBI in general.
Dr. Conidi noted that there is a “significant subjective component” to the study results because they relied on the opinion of neuroradiologists. He is not convinced MRI findings of frontotemporal and medial temporal lobe atrophy necessarily represent CTE and not TBI. In fact, he noted that patients with TBI have a significantly greater chance of not developing a neurodegenerative disorder.
Dr. Conidi added that he doesn’t think MRI will ever be the gold standard for diagnosing or even assessing risk of developing CTE. “That lies in tau PET imaging,” he said.
Overstated conclusion?
Also commenting on the research findings, Kristen Dams-O’Connor, PhD, professor, vice chair of research, and director, Brain Injury Research Center, Department of Rehabilitation Medicine, Icahn School of Medicine at Mount Sinai in New York, said the sensitivity analyses, particularly those designed to clarify contributions of Alzheimer’s disease and other neuropathological contributions to associations between p-tau and atrophy, “increase our confidence” in the findings.
“What’s exciting about this paper is that it provides very preliminary support for adding another tool to our arsenal as we try to establish a constellation of in vivo diagnostic markers that, together, will help us rule in a post-traumatic neurodegenerative process and rule out other brain diseases.”
A possible study limitation is that the MRI scans were from low-field strength magnets, although that makes the study more “ecologically valid”, said Dr. Dams-O’Connor. “Many clinical scanners are built around a 1.5T magnet, so what the researchers see in this study is what a radiologist may see in the clinic.”
The conclusion that frontal-temporal atrophy is an MRI marker of CTE is “an overstatement” as this pattern of atrophy is not specific to CTE, said Dr. Dams-O’Connor. “The association of p-tau with atrophy is unsurprising and doesn’t bring us much closer to understanding how, or whether, the patterns of p-tau accumulation observed in CTE contribute to the clinical expression of symptoms.”
Dr. Alosco and Dr. Conidi report no relevant financial relationships. Disclosures for the other study authors are listed in the original journal article. The study was funded by grants from the National Institute on Aging, the National Institute on Neurological Disorders and Stroke, National Institute of Aging Boston University AD Center, Department of Veterans Affairs Merit Award, the Nick and Lynn Buoniconti Foundation, and BU-CTSI.
A version of this article first appeared on Medscape.com.
Posttraumatic epilepsy is common, even after ‘mild’ TBI
, new research suggests.
Results from a multicenter, prospective cohort study showed 2.7% of nearly 1,500 participants with TBI reported also having posttraumatic epilepsy, and these patients had significantly worse outcomes than those without posttraumatic epilepsy.
“Posttraumatic epilepsy is common even in so-called mild TBI, and we should be on the lookout for patients reporting these kinds of spells,” said coinvestigator Ramon Diaz-Arrastia, MD, PhD, professor of neurology and director of the TBI Clinical Research Center, University of Pennsylvania, Philadelphia.
Dr. Diaz-Arrastia said he dislikes the term “mild TBI” because many of these injuries have “pretty substantial consequences.”
The findings were published online Dec. 29 in JAMA Network Open.
Novel study
Seizures can occur after TBI, most commonly after a severe brain injury, such as those leading to coma or bleeding in the brain or requiring surgical intervention. However, there have been “hints” that some patients with milder brain injuries are also at increased risk for epilepsy, said Dr. Diaz-Arrastia.
To investigate, the researchers assessed data from the large, multicenter Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) database. Participants with TBI, defined as a Glasgow Coma Scale (GCS) score of 3-15, had presented to a level I trauma center within 24 hours of a head trauma needing evaluation with a CT scan.
The study included patients with relatively mild TBI (GCS score, 13-15), which is a “novel feature” of the study, the authors noted. Most prior studies of posttraumatic epilepsy focused on moderate to severe TBI.
The researchers included two sex- and age-matched control groups. The orthopedic trauma control (OTC) group consisted of patients with isolated trauma to the limbs, pelvis, and/or ribs. The “friend” or peer control group had backgrounds and lifestyles similar to those with TBI but had no history of TBI, concussion, or traumatic injury in the previous year.
The analysis included 1,885 participants (mean age, 41.3 years; 65.8% men). Of these, 1,493 had TBI, 182 were in the OTC group, and 210 were in the friends group. At 6- and 12-month follow-ups, investigators administered the Epilepsy Screening Questionnaire (ESQ), developed by the National Institute of Neurological Disorders and Stroke (NINDS).
Confirmatory data
Participants were asked about experiencing uncontrolled movements, unexplained changes in mental state, and repeated unusual attacks or convulsions, and whether they had been told they had epilepsy or seizures. If they answered yes to any of these questions, they received second-level screening, which asked about seizures.
Patients were deemed to have posttraumatic epilepsy if they answered affirmatively to any first-level screening item, experienced seizures 7 days after injury, and were diagnosed with epilepsy.
The primary outcome was rate of positive posttraumatic epilepsy diagnoses. At 12 months, 2.7% of those with TBI reported a posttraumatic epilepsy diagnosis compared with none of either of the control groups (P < .001).
This rate is consistent with prior literature and is “pretty close to what we expected,” said Dr. Diaz-Arrastia.
Among those with TBI and posttraumatic epilepsy, 12.2% had GCS scores of 3-8 (severe), 5.3% had scores of 9-12 (moderate), and 0.9% had scores of 13-15 (mild). That figure for mild TBI is not insignificant, said Dr. Diaz-Arrastia.
“Probably 90% of all those coming to the emergency room with a brain injury are diagnosed with mild TBI not requiring admission,” he noted.
The risk for posttraumatic epilepsy was higher the more severe the head injury, and among those with hemorrhage on head CT imaging. In patients with mild TBI, hemorrhage was associated with a two- to threefold risk of developing posttraumatic epilepsy.
“This prospective observational study confirms the epidemiologic data that even after mild brain injury, there is an increased risk for epilepsy,” said Dr. Diaz-Arrastia.
Universal screening?
The researchers also looked at whether seizures worsen other outcomes. Compared with those who had TBI but not posttraumatic epilepsy, those with posttraumatic epilepsy had significantly lower Glasgow Outcome Scale Extended (GOSE) scores (mean, 4.7 vs. 6.1; P < .001), higher Brief Symptom Inventory (BSI) scores (58.6 vs. 50.2; P = .02), and higher Rivermead Cognitive Metric (RCM) scores (5.3 vs. 3.1; P = .002) at 12 months after adjustment for age, initial GCS score, and imaging findings.
Higher GOSE and RCM scores reflect better outcomes, but a higher score on the BSI, which assesses overall mood, reflects a worse outcome, the investigators noted.
Previous evidence suggests prophylactic use of antiepileptic drugs in patients with TBI does not reduce risks. These drugs “are neither 100% safe nor 100% effective,” said Dr. Diaz-Arrastia. Some studies showed that certain agents actually worsen outcomes, he added.
What the field needs instead are antiepileptogenic drugs – those that interfere with the maladaptive synaptic plasticity that ends up in an epileptic circuit, he noted.
The new results suggest screening for posttraumatic epilepsy using the NINDS-ESQ “should be done pretty much routinely as a follow-up for all brain injuries,” Dr. Diaz-Arrastia said.
The investigators plan to have study participants assessed by an epileptologist later. A significant number of people with TBI, he noted, won’t develop posttraumatic epilepsy until 1-5 years after their injury – and even later in some cases.
A limitation of the study was that some patients reporting posttraumatic epilepsy may have had psychogenic nonepileptiform seizures, which are common in TBI patients, the investigators noted.
The study was supported by grants from One Mind, National Institutes of Health (NIH), National Institute of Neurological Disorders and Stroke (NINDS, and Department of Defence. Dr. Diaz-Arrastia reported receiving grants from the NIH, NINDS, and DOD during the conduct of the study.
A version of this article first appeared on Medscape.com.
, new research suggests.
Results from a multicenter, prospective cohort study showed 2.7% of nearly 1,500 participants with TBI reported also having posttraumatic epilepsy, and these patients had significantly worse outcomes than those without posttraumatic epilepsy.
“Posttraumatic epilepsy is common even in so-called mild TBI, and we should be on the lookout for patients reporting these kinds of spells,” said coinvestigator Ramon Diaz-Arrastia, MD, PhD, professor of neurology and director of the TBI Clinical Research Center, University of Pennsylvania, Philadelphia.
Dr. Diaz-Arrastia said he dislikes the term “mild TBI” because many of these injuries have “pretty substantial consequences.”
The findings were published online Dec. 29 in JAMA Network Open.
Novel study
Seizures can occur after TBI, most commonly after a severe brain injury, such as those leading to coma or bleeding in the brain or requiring surgical intervention. However, there have been “hints” that some patients with milder brain injuries are also at increased risk for epilepsy, said Dr. Diaz-Arrastia.
To investigate, the researchers assessed data from the large, multicenter Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) database. Participants with TBI, defined as a Glasgow Coma Scale (GCS) score of 3-15, had presented to a level I trauma center within 24 hours of a head trauma needing evaluation with a CT scan.
The study included patients with relatively mild TBI (GCS score, 13-15), which is a “novel feature” of the study, the authors noted. Most prior studies of posttraumatic epilepsy focused on moderate to severe TBI.
The researchers included two sex- and age-matched control groups. The orthopedic trauma control (OTC) group consisted of patients with isolated trauma to the limbs, pelvis, and/or ribs. The “friend” or peer control group had backgrounds and lifestyles similar to those with TBI but had no history of TBI, concussion, or traumatic injury in the previous year.
The analysis included 1,885 participants (mean age, 41.3 years; 65.8% men). Of these, 1,493 had TBI, 182 were in the OTC group, and 210 were in the friends group. At 6- and 12-month follow-ups, investigators administered the Epilepsy Screening Questionnaire (ESQ), developed by the National Institute of Neurological Disorders and Stroke (NINDS).
Confirmatory data
Participants were asked about experiencing uncontrolled movements, unexplained changes in mental state, and repeated unusual attacks or convulsions, and whether they had been told they had epilepsy or seizures. If they answered yes to any of these questions, they received second-level screening, which asked about seizures.
Patients were deemed to have posttraumatic epilepsy if they answered affirmatively to any first-level screening item, experienced seizures 7 days after injury, and were diagnosed with epilepsy.
The primary outcome was rate of positive posttraumatic epilepsy diagnoses. At 12 months, 2.7% of those with TBI reported a posttraumatic epilepsy diagnosis compared with none of either of the control groups (P < .001).
This rate is consistent with prior literature and is “pretty close to what we expected,” said Dr. Diaz-Arrastia.
Among those with TBI and posttraumatic epilepsy, 12.2% had GCS scores of 3-8 (severe), 5.3% had scores of 9-12 (moderate), and 0.9% had scores of 13-15 (mild). That figure for mild TBI is not insignificant, said Dr. Diaz-Arrastia.
“Probably 90% of all those coming to the emergency room with a brain injury are diagnosed with mild TBI not requiring admission,” he noted.
The risk for posttraumatic epilepsy was higher the more severe the head injury, and among those with hemorrhage on head CT imaging. In patients with mild TBI, hemorrhage was associated with a two- to threefold risk of developing posttraumatic epilepsy.
“This prospective observational study confirms the epidemiologic data that even after mild brain injury, there is an increased risk for epilepsy,” said Dr. Diaz-Arrastia.
Universal screening?
The researchers also looked at whether seizures worsen other outcomes. Compared with those who had TBI but not posttraumatic epilepsy, those with posttraumatic epilepsy had significantly lower Glasgow Outcome Scale Extended (GOSE) scores (mean, 4.7 vs. 6.1; P < .001), higher Brief Symptom Inventory (BSI) scores (58.6 vs. 50.2; P = .02), and higher Rivermead Cognitive Metric (RCM) scores (5.3 vs. 3.1; P = .002) at 12 months after adjustment for age, initial GCS score, and imaging findings.
Higher GOSE and RCM scores reflect better outcomes, but a higher score on the BSI, which assesses overall mood, reflects a worse outcome, the investigators noted.
Previous evidence suggests prophylactic use of antiepileptic drugs in patients with TBI does not reduce risks. These drugs “are neither 100% safe nor 100% effective,” said Dr. Diaz-Arrastia. Some studies showed that certain agents actually worsen outcomes, he added.
What the field needs instead are antiepileptogenic drugs – those that interfere with the maladaptive synaptic plasticity that ends up in an epileptic circuit, he noted.
The new results suggest screening for posttraumatic epilepsy using the NINDS-ESQ “should be done pretty much routinely as a follow-up for all brain injuries,” Dr. Diaz-Arrastia said.
The investigators plan to have study participants assessed by an epileptologist later. A significant number of people with TBI, he noted, won’t develop posttraumatic epilepsy until 1-5 years after their injury – and even later in some cases.
A limitation of the study was that some patients reporting posttraumatic epilepsy may have had psychogenic nonepileptiform seizures, which are common in TBI patients, the investigators noted.
The study was supported by grants from One Mind, National Institutes of Health (NIH), National Institute of Neurological Disorders and Stroke (NINDS, and Department of Defence. Dr. Diaz-Arrastia reported receiving grants from the NIH, NINDS, and DOD during the conduct of the study.
A version of this article first appeared on Medscape.com.
, new research suggests.
Results from a multicenter, prospective cohort study showed 2.7% of nearly 1,500 participants with TBI reported also having posttraumatic epilepsy, and these patients had significantly worse outcomes than those without posttraumatic epilepsy.
“Posttraumatic epilepsy is common even in so-called mild TBI, and we should be on the lookout for patients reporting these kinds of spells,” said coinvestigator Ramon Diaz-Arrastia, MD, PhD, professor of neurology and director of the TBI Clinical Research Center, University of Pennsylvania, Philadelphia.
Dr. Diaz-Arrastia said he dislikes the term “mild TBI” because many of these injuries have “pretty substantial consequences.”
The findings were published online Dec. 29 in JAMA Network Open.
Novel study
Seizures can occur after TBI, most commonly after a severe brain injury, such as those leading to coma or bleeding in the brain or requiring surgical intervention. However, there have been “hints” that some patients with milder brain injuries are also at increased risk for epilepsy, said Dr. Diaz-Arrastia.
To investigate, the researchers assessed data from the large, multicenter Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) database. Participants with TBI, defined as a Glasgow Coma Scale (GCS) score of 3-15, had presented to a level I trauma center within 24 hours of a head trauma needing evaluation with a CT scan.
The study included patients with relatively mild TBI (GCS score, 13-15), which is a “novel feature” of the study, the authors noted. Most prior studies of posttraumatic epilepsy focused on moderate to severe TBI.
The researchers included two sex- and age-matched control groups. The orthopedic trauma control (OTC) group consisted of patients with isolated trauma to the limbs, pelvis, and/or ribs. The “friend” or peer control group had backgrounds and lifestyles similar to those with TBI but had no history of TBI, concussion, or traumatic injury in the previous year.
The analysis included 1,885 participants (mean age, 41.3 years; 65.8% men). Of these, 1,493 had TBI, 182 were in the OTC group, and 210 were in the friends group. At 6- and 12-month follow-ups, investigators administered the Epilepsy Screening Questionnaire (ESQ), developed by the National Institute of Neurological Disorders and Stroke (NINDS).
Confirmatory data
Participants were asked about experiencing uncontrolled movements, unexplained changes in mental state, and repeated unusual attacks or convulsions, and whether they had been told they had epilepsy or seizures. If they answered yes to any of these questions, they received second-level screening, which asked about seizures.
Patients were deemed to have posttraumatic epilepsy if they answered affirmatively to any first-level screening item, experienced seizures 7 days after injury, and were diagnosed with epilepsy.
The primary outcome was rate of positive posttraumatic epilepsy diagnoses. At 12 months, 2.7% of those with TBI reported a posttraumatic epilepsy diagnosis compared with none of either of the control groups (P < .001).
This rate is consistent with prior literature and is “pretty close to what we expected,” said Dr. Diaz-Arrastia.
Among those with TBI and posttraumatic epilepsy, 12.2% had GCS scores of 3-8 (severe), 5.3% had scores of 9-12 (moderate), and 0.9% had scores of 13-15 (mild). That figure for mild TBI is not insignificant, said Dr. Diaz-Arrastia.
“Probably 90% of all those coming to the emergency room with a brain injury are diagnosed with mild TBI not requiring admission,” he noted.
The risk for posttraumatic epilepsy was higher the more severe the head injury, and among those with hemorrhage on head CT imaging. In patients with mild TBI, hemorrhage was associated with a two- to threefold risk of developing posttraumatic epilepsy.
“This prospective observational study confirms the epidemiologic data that even after mild brain injury, there is an increased risk for epilepsy,” said Dr. Diaz-Arrastia.
Universal screening?
The researchers also looked at whether seizures worsen other outcomes. Compared with those who had TBI but not posttraumatic epilepsy, those with posttraumatic epilepsy had significantly lower Glasgow Outcome Scale Extended (GOSE) scores (mean, 4.7 vs. 6.1; P < .001), higher Brief Symptom Inventory (BSI) scores (58.6 vs. 50.2; P = .02), and higher Rivermead Cognitive Metric (RCM) scores (5.3 vs. 3.1; P = .002) at 12 months after adjustment for age, initial GCS score, and imaging findings.
Higher GOSE and RCM scores reflect better outcomes, but a higher score on the BSI, which assesses overall mood, reflects a worse outcome, the investigators noted.
Previous evidence suggests prophylactic use of antiepileptic drugs in patients with TBI does not reduce risks. These drugs “are neither 100% safe nor 100% effective,” said Dr. Diaz-Arrastia. Some studies showed that certain agents actually worsen outcomes, he added.
What the field needs instead are antiepileptogenic drugs – those that interfere with the maladaptive synaptic plasticity that ends up in an epileptic circuit, he noted.
The new results suggest screening for posttraumatic epilepsy using the NINDS-ESQ “should be done pretty much routinely as a follow-up for all brain injuries,” Dr. Diaz-Arrastia said.
The investigators plan to have study participants assessed by an epileptologist later. A significant number of people with TBI, he noted, won’t develop posttraumatic epilepsy until 1-5 years after their injury – and even later in some cases.
A limitation of the study was that some patients reporting posttraumatic epilepsy may have had psychogenic nonepileptiform seizures, which are common in TBI patients, the investigators noted.
The study was supported by grants from One Mind, National Institutes of Health (NIH), National Institute of Neurological Disorders and Stroke (NINDS, and Department of Defence. Dr. Diaz-Arrastia reported receiving grants from the NIH, NINDS, and DOD during the conduct of the study.
A version of this article first appeared on Medscape.com.