User login
Rising Cancer Rates Among Young People Spur New Fertility Preservation Options
Rising Cancer Rates Among Young People Spur New Fertility Preservation Options
ATLANTA —Jacqueline Lee, MD, a reproductive endocrinologist at Emory School of Medicine, frequently treats patients with cancer. Recently, she treated 4 women in their 30s with histories of colon cancer, acute lymphoblastic leukemia, lymphoma, and breast cancer. A young man in his 20s sought her care, to discuss his case of lymphoma.
All these patients sought guidance from Lee because they want to protect their ability to have children. At the annual meeting of the Association of VA Hematology/Oncology, Lee explained that plenty of patients are finding themselves in similar straits due in part to recent trends.
Cancer rates in the US have been rising among people aged 15 to 39 years, who now account for 4.2% of all cancer cases. An estimated 84,100 people in this age group are expected to be diagnosed with cancer this year. Meanwhile, women are having children later in life-birth rates are up among those aged 25 to 49 years-making it more likely that they have histories of cancer.
Although it's difficult to predict how cancer will affect fertility, Lee emphasized that many chemotherapy medications, including cisplatin and carboplatin, are cytotoxic. "It's hard to always predict what someone's arc of care is going to be," she said, "so I really have a low threshold for recommending fertility preservation in patients who have a strong desire to have future childbearing."
For women with cancer, egg preservation isn't the only strategy. Clinicians can also try to protect ovarian tissue from pelvic radiation through surgical reposition of the ovaries, Lee noted. In addition goserelin, a hormone-suppressing therapy, may protect the ovaries from chemotherapy, though its effectiveness in boosting pregnancy rates is still unclear.
"When I mentioned this option, it's usually for patients who can't preserve fertility via egg or embryo preservation, or we don't have the luxury of that kind of time," Lee said. "I say that if helps at all, it might help you resume menses after treatment. But infertility is still very common."
For some patients, freezing eggs is an easy decision. "They don't have a reproductive partner they're ready to make embryos with, so we proceed with egg preservation. It's no longer considered experimental and comes with lower upfront costs since the costs of actually making embryos are deferred until the future."
In addition, she said, freezing eggs also avoids the touchy topic of disposing of embryos. Lee cautions patients that retrieving eggs is a 2-week process that requires any initiation of cancer care to be delayed. However, the retrieval process can be adjusted in patients with special needs due to the type of cancer they have.
For prepubertal girls with cancer, ovarian tissue can be removed and frozen as a fertility preservation option. However, this is not considered standard of care. "We don't do it," she said. "We refer out if needed. Hopefully we'll develop a program in the future."
As for the 5 patients that Lee mentioned, with details changed to protect their privacy, their outcomes were as follows:
- The woman with colon cancer, who had undergone a hemicolectomy, chose to defer fertility preservation.
- The woman with acute lymphoblastic leukemia, who was taking depo-Lupron, had undetectable anti-Müllerian hormone (AMH) levels. Lee discussed the possibility of IVF with a donor egg.
- The woman with breast cancer, who was newly diagnosed, deferred fertility preservation.
- The man with lymphoma (Hodgkin's), who was awaiting chemotherapy, had his sperm frozen.
- The woman with lymphoma (new diagnosis) had 27 eggs frozen.
Lee had no disclosures to report.
ATLANTA —Jacqueline Lee, MD, a reproductive endocrinologist at Emory School of Medicine, frequently treats patients with cancer. Recently, she treated 4 women in their 30s with histories of colon cancer, acute lymphoblastic leukemia, lymphoma, and breast cancer. A young man in his 20s sought her care, to discuss his case of lymphoma.
All these patients sought guidance from Lee because they want to protect their ability to have children. At the annual meeting of the Association of VA Hematology/Oncology, Lee explained that plenty of patients are finding themselves in similar straits due in part to recent trends.
Cancer rates in the US have been rising among people aged 15 to 39 years, who now account for 4.2% of all cancer cases. An estimated 84,100 people in this age group are expected to be diagnosed with cancer this year. Meanwhile, women are having children later in life-birth rates are up among those aged 25 to 49 years-making it more likely that they have histories of cancer.
Although it's difficult to predict how cancer will affect fertility, Lee emphasized that many chemotherapy medications, including cisplatin and carboplatin, are cytotoxic. "It's hard to always predict what someone's arc of care is going to be," she said, "so I really have a low threshold for recommending fertility preservation in patients who have a strong desire to have future childbearing."
For women with cancer, egg preservation isn't the only strategy. Clinicians can also try to protect ovarian tissue from pelvic radiation through surgical reposition of the ovaries, Lee noted. In addition goserelin, a hormone-suppressing therapy, may protect the ovaries from chemotherapy, though its effectiveness in boosting pregnancy rates is still unclear.
"When I mentioned this option, it's usually for patients who can't preserve fertility via egg or embryo preservation, or we don't have the luxury of that kind of time," Lee said. "I say that if helps at all, it might help you resume menses after treatment. But infertility is still very common."
For some patients, freezing eggs is an easy decision. "They don't have a reproductive partner they're ready to make embryos with, so we proceed with egg preservation. It's no longer considered experimental and comes with lower upfront costs since the costs of actually making embryos are deferred until the future."
In addition, she said, freezing eggs also avoids the touchy topic of disposing of embryos. Lee cautions patients that retrieving eggs is a 2-week process that requires any initiation of cancer care to be delayed. However, the retrieval process can be adjusted in patients with special needs due to the type of cancer they have.
For prepubertal girls with cancer, ovarian tissue can be removed and frozen as a fertility preservation option. However, this is not considered standard of care. "We don't do it," she said. "We refer out if needed. Hopefully we'll develop a program in the future."
As for the 5 patients that Lee mentioned, with details changed to protect their privacy, their outcomes were as follows:
- The woman with colon cancer, who had undergone a hemicolectomy, chose to defer fertility preservation.
- The woman with acute lymphoblastic leukemia, who was taking depo-Lupron, had undetectable anti-Müllerian hormone (AMH) levels. Lee discussed the possibility of IVF with a donor egg.
- The woman with breast cancer, who was newly diagnosed, deferred fertility preservation.
- The man with lymphoma (Hodgkin's), who was awaiting chemotherapy, had his sperm frozen.
- The woman with lymphoma (new diagnosis) had 27 eggs frozen.
Lee had no disclosures to report.
ATLANTA —Jacqueline Lee, MD, a reproductive endocrinologist at Emory School of Medicine, frequently treats patients with cancer. Recently, she treated 4 women in their 30s with histories of colon cancer, acute lymphoblastic leukemia, lymphoma, and breast cancer. A young man in his 20s sought her care, to discuss his case of lymphoma.
All these patients sought guidance from Lee because they want to protect their ability to have children. At the annual meeting of the Association of VA Hematology/Oncology, Lee explained that plenty of patients are finding themselves in similar straits due in part to recent trends.
Cancer rates in the US have been rising among people aged 15 to 39 years, who now account for 4.2% of all cancer cases. An estimated 84,100 people in this age group are expected to be diagnosed with cancer this year. Meanwhile, women are having children later in life-birth rates are up among those aged 25 to 49 years-making it more likely that they have histories of cancer.
Although it's difficult to predict how cancer will affect fertility, Lee emphasized that many chemotherapy medications, including cisplatin and carboplatin, are cytotoxic. "It's hard to always predict what someone's arc of care is going to be," she said, "so I really have a low threshold for recommending fertility preservation in patients who have a strong desire to have future childbearing."
For women with cancer, egg preservation isn't the only strategy. Clinicians can also try to protect ovarian tissue from pelvic radiation through surgical reposition of the ovaries, Lee noted. In addition goserelin, a hormone-suppressing therapy, may protect the ovaries from chemotherapy, though its effectiveness in boosting pregnancy rates is still unclear.
"When I mentioned this option, it's usually for patients who can't preserve fertility via egg or embryo preservation, or we don't have the luxury of that kind of time," Lee said. "I say that if helps at all, it might help you resume menses after treatment. But infertility is still very common."
For some patients, freezing eggs is an easy decision. "They don't have a reproductive partner they're ready to make embryos with, so we proceed with egg preservation. It's no longer considered experimental and comes with lower upfront costs since the costs of actually making embryos are deferred until the future."
In addition, she said, freezing eggs also avoids the touchy topic of disposing of embryos. Lee cautions patients that retrieving eggs is a 2-week process that requires any initiation of cancer care to be delayed. However, the retrieval process can be adjusted in patients with special needs due to the type of cancer they have.
For prepubertal girls with cancer, ovarian tissue can be removed and frozen as a fertility preservation option. However, this is not considered standard of care. "We don't do it," she said. "We refer out if needed. Hopefully we'll develop a program in the future."
As for the 5 patients that Lee mentioned, with details changed to protect their privacy, their outcomes were as follows:
- The woman with colon cancer, who had undergone a hemicolectomy, chose to defer fertility preservation.
- The woman with acute lymphoblastic leukemia, who was taking depo-Lupron, had undetectable anti-Müllerian hormone (AMH) levels. Lee discussed the possibility of IVF with a donor egg.
- The woman with breast cancer, who was newly diagnosed, deferred fertility preservation.
- The man with lymphoma (Hodgkin's), who was awaiting chemotherapy, had his sperm frozen.
- The woman with lymphoma (new diagnosis) had 27 eggs frozen.
Lee had no disclosures to report.
Rising Cancer Rates Among Young People Spur New Fertility Preservation Options
Rising Cancer Rates Among Young People Spur New Fertility Preservation Options

VA Cancer Clinical Trials as a Strategy for Increasing Accrual of Racial and Ethnic Underrepresented Groups
Background
Cancer clinical trials (CCTs) are central to improving cancer care. However, generalizability of findings from CCTs is difficult due to the lack of diversity in most United States CCTs. Clinical trial accrual of underrepresented groups, is low throughout the United States and is approximately 4-5% in most CCTs. Reasons for low accrual in this population are multifactorial. Despite numerous factors related to accruing racial and ethnic underrepresented groups, many institutions have sought to address these barriers. We conducted a scoping review to identify evidence-based approaches to increase participation in cancer treatment clinical trials.
Methods
We reviewed the Salisbury VA Medical Center Oncology clinical trial database from October 2019 to June 2024. The participants in these clinical trials required consent. These clinical trials included treatment interventional as well as non-treatment interventional. Fifteen studies were included and over 260 Veterans participated.
Results
Key themes emerged that included a focus on patient education, cultural competency, and building capacity in the clinics to care for the Veteran population at three separate sites in the Salisbury VA system. The Black Veteran accrual rate of 29% was achieved. This accrual rate is representative of our VA catchment population of 33% for Black Veterans, and is five times the national average.
Conclusions
The research team’s success in enrolling Black Veterans in clinical trials is attributed to several factors. The demographic composition of Veterans served by the Salisbury, Charlotte, and Kernersville VA provided a diverse population that included a 33% Black group. The type of clinical trials focused on patients who were most impacted by the disease. The VA did afford less barriers to access to health care.
Background
Cancer clinical trials (CCTs) are central to improving cancer care. However, generalizability of findings from CCTs is difficult due to the lack of diversity in most United States CCTs. Clinical trial accrual of underrepresented groups, is low throughout the United States and is approximately 4-5% in most CCTs. Reasons for low accrual in this population are multifactorial. Despite numerous factors related to accruing racial and ethnic underrepresented groups, many institutions have sought to address these barriers. We conducted a scoping review to identify evidence-based approaches to increase participation in cancer treatment clinical trials.
Methods
We reviewed the Salisbury VA Medical Center Oncology clinical trial database from October 2019 to June 2024. The participants in these clinical trials required consent. These clinical trials included treatment interventional as well as non-treatment interventional. Fifteen studies were included and over 260 Veterans participated.
Results
Key themes emerged that included a focus on patient education, cultural competency, and building capacity in the clinics to care for the Veteran population at three separate sites in the Salisbury VA system. The Black Veteran accrual rate of 29% was achieved. This accrual rate is representative of our VA catchment population of 33% for Black Veterans, and is five times the national average.
Conclusions
The research team’s success in enrolling Black Veterans in clinical trials is attributed to several factors. The demographic composition of Veterans served by the Salisbury, Charlotte, and Kernersville VA provided a diverse population that included a 33% Black group. The type of clinical trials focused on patients who were most impacted by the disease. The VA did afford less barriers to access to health care.
Background
Cancer clinical trials (CCTs) are central to improving cancer care. However, generalizability of findings from CCTs is difficult due to the lack of diversity in most United States CCTs. Clinical trial accrual of underrepresented groups, is low throughout the United States and is approximately 4-5% in most CCTs. Reasons for low accrual in this population are multifactorial. Despite numerous factors related to accruing racial and ethnic underrepresented groups, many institutions have sought to address these barriers. We conducted a scoping review to identify evidence-based approaches to increase participation in cancer treatment clinical trials.
Methods
We reviewed the Salisbury VA Medical Center Oncology clinical trial database from October 2019 to June 2024. The participants in these clinical trials required consent. These clinical trials included treatment interventional as well as non-treatment interventional. Fifteen studies were included and over 260 Veterans participated.
Results
Key themes emerged that included a focus on patient education, cultural competency, and building capacity in the clinics to care for the Veteran population at three separate sites in the Salisbury VA system. The Black Veteran accrual rate of 29% was achieved. This accrual rate is representative of our VA catchment population of 33% for Black Veterans, and is five times the national average.
Conclusions
The research team’s success in enrolling Black Veterans in clinical trials is attributed to several factors. The demographic composition of Veterans served by the Salisbury, Charlotte, and Kernersville VA provided a diverse population that included a 33% Black group. The type of clinical trials focused on patients who were most impacted by the disease. The VA did afford less barriers to access to health care.
Improving Colorectal Cancer Screening via Mailed Fecal Immunochemical Testing in a Veterans Affairs Health System
Colorectal cancer (CRC) is among the most common cancers and causes of cancer-related deaths in the United States.1 Reflective of a nationwide trend, CRC screening rates at the Veterans Affairs Connecticut Healthcare System (VACHS) decreased during the COVID-19 pandemic.2-5 Contributing factors to this decrease included cancellations of elective colonoscopies during the initial phase of the pandemic and concurrent turnover of endoscopists. In 2021, the US Preventive Services Task Force lowered the recommended initial CRC screening age from 50 years to 45 years, further increasing the backlog of unscreened patients.6
Fecal immunochemical testing (FIT) is a noninvasive screening method in which antibodies are used to detect hemoglobin in the stool. The sensitivity and specificity of 1-time FIT are 79% to 80% and 94%, respectively, for the detection of CRC, with sensitivity improving with successive testing.7,8 Annual FIT is recognized as a tier 1 preferred screening method by the US Multi-Society Task Force on Colorectal Cancer.7,9 Programs that mail FIT kits to eligible patients outside of physician visits have been successfully implemented in health care systems.10,11
The VACHS designed and implemented a mailed FIT program using existing infrastructure and staffing.
Program Description
A team of local stakeholders comprised of VACHS leadership, primary care, nursing, and gastroenterology staff, as well as representatives from laboratory, informatics, mail services, and group practice management, was established to execute the project. The team met monthly to plan the project.
The team developed a dataset consisting of patients aged 45 to 75 years who were at average risk for CRC and due for CRC screening. Patients were defined as due for CRC screening if they had not had a colonoscopy in the previous 9 years or a FIT or fecal occult blood test in the previous 11 months. Average risk for CRC was defined by excluding patients with associated diagnosis codes for CRC, colectomy, inflammatory bowel disease, and anemia. The program also excluded patients with diagnosis codes associated with dementia, deferring discussions about cancer screening to their primary care practitioners (PCPs). Patients with invalid mailing addresses were also excluded, as well as those whose PCPs had indicated in the electronic health record that the patient received CRC screening outside the US Department of Veterans Affairs (VA) system.
Letter Templates
Two patient letter electronic health record templates were developed. The first was a primer letter, which was mailed to patients 2 to 3 weeks before the mailed FIT kit as an introduction to the program.12 The purpose of the primer letter was to give advance notice to patients that they could expect a FIT kit to arrive in the mail. The goal was to prepare patients to complete FIT when the kit arrived and prompt them to call the VA to opt out of the mailed FIT program if they were up to date with CRC screening or if they had a condition which made them at high risk for CRC.
The second FIT letter arrived with the FIT kit, introduced FIT and described the importance of CRC screening. The letter detailed instructions for completing FIT and automatically created a FIT order. It also included a list of common conditions that may exclude patients, with a recommendation for patients to contact their medical team if they felt they were not candidates for FIT.
Staff Education
A previous VACHS pilot project demonstrated the success of a mailed FIT program to increase FIT use. Implemented as part of the pilot program, staff education consisted of a session for clinicians about the role of FIT in CRC screening and an all-staff education session. An additional education session about CRC and FIT for all staff was repeated with the program launch.
Program Launch
The mailed FIT program was introduced during a VACHS primary care all-staff meeting. After the meeting, each patient aligned care team (PACT) received an encrypted email that included a list of the patients on their team who were candidates for the program, a patient-facing FIT instruction sheet, detailed instructions on how to send the FIT primer letter, and a FIT package consisting of the labeled FIT kit, FIT letter, and patient instruction sheet. A reminder letter was sent to each patient 3 weeks after the FIT package was mailed. The patient lists were populated into a shared, encrypted Microsoft Teams folder that was edited in real time by PACT teams and viewed by VACHS leadership to track progress.
Program Metrics
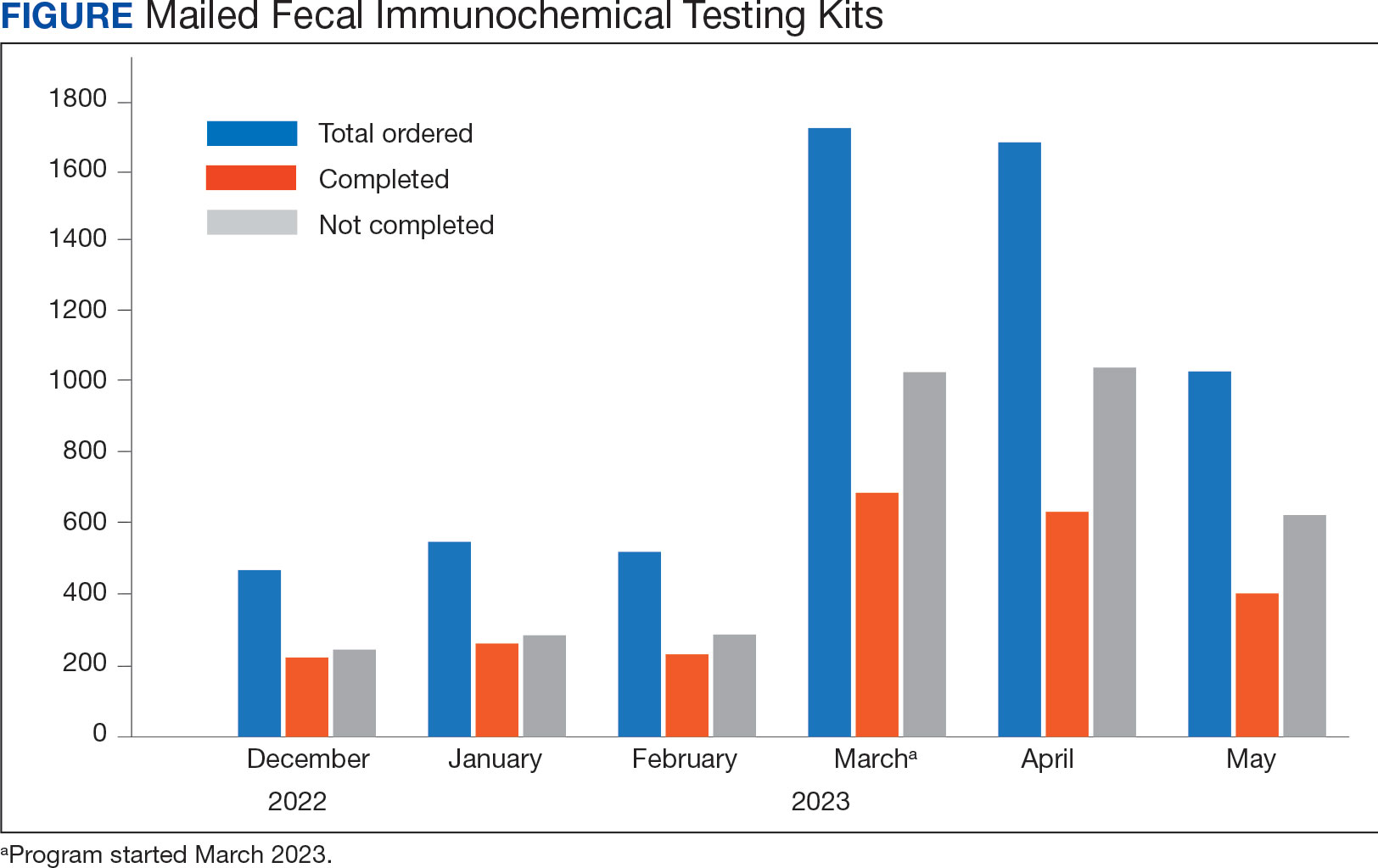
At program launch, the VACHS had 4642 patients due for CRC screening who were eligible for the mailed FIT program. On March 7, 2023, the data consisting of FIT tests ordered between December 2022 and May 2023—3 months before and after the launch of the program—were reviewed and categorized. In the 3 months before program launch, 1528 FIT were ordered and 714 were returned (46.7%). In the 3 months after the launch of the program, 4383 FIT were ordered and 1712 were returned (39.1%) (Figure). Test orders increased 287% from the preintervention to the postintervention period. The mean (SD) number of monthly FIT tests prelaunch was 509 (32.7), which increased to 1461 (331.6) postlaunch.
At the VACHS, 61.4% of patients aged 45 to 75 years were up to date with CRC screening before the program launch. In the 3 months after program launch, the rate increased to 63.8% among patients aged 45 to 75 years, the highest rate in our Veterans Integrated Services Network and exceeding the VA national average CRC screening rate, according to unpublished VA Monthly Management Report data.
In the 3 months following the program launch, 139 FIT kits tested positive for potential CRC. Of these, 79 (56.8%) patients had completed a diagnostic colonoscopy. PACT PCPs and nurses received reports on patients with positive FIT tests and those with no colonoscopy scheduled or completed and were asked to follow up.
Discussion
Through a proactive, population-based CRC screening program centered on mailed FIT kits outside of the traditional patient visit, the VACHS increased the use of FIT and rates of CRC screening. The numbers of FIT kits ordered and completed substantially increased in the 3 months after program launch.
Compared to mailed FIT programs described in the literature that rely on centralized processes in that a separate team operates the mailed FIT program for the entire organization, this program used existing PACT infrastructure and staff.10,11 This strategy allowed VACHS to design and implement the program in several months. Not needing to hire new staff or create a central team for the sole purpose of implementing the program allowed us to save on any organizational funding and efforts that would have accompanied the additional staff. The program described in this article may be more attainable for primary care practices or smaller health systems that do not have the capacity for the creation of a centralized process.
Limitations
Although the total number of FIT completions substantially increased during the program, the rate of FIT completion during the mailed FIT program was lower than the rate of completion prior to program launch. This decreased rate of FIT kit completion may be related to separation from a patient visit and potential loss of real-time education with a clinician. The program’s decentralized design increased the existing workload for primary care staff, and as a result, consideration must be given to local staffing levels. Additionally, the report of eligible patients depended on diagnosis codes and may have captured patients with higher-than-average risk of CRC, such as patients with prior history of adenomatous polyps, family history of CRC, or other medical or genetic conditions. We attempted to mitigate this by including a list of conditions that would exclude patients from FIT eligibility in the FIT letter and giving them the option to opt out.
Conclusions
CRC screening rates improved following implementation of a primary care team-centered quality improvement process to proactively identify patients appropriate for FIT and mail them FIT kits. This project highlights that population-health interventions around CRC screening via use of FIT can be successful within a primary care patient-centered medical home model, considering the increases in both CRC screening rates and increase in FIT tests ordered.
1. American Cancer Society. Key statistics for colorectal cancer. Revised January 29, 2024. Accessed June 11, 2024. https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html
2. Chen RC, Haynes K, Du S, Barron J, Katz AJ. Association of cancer screening deficit in the United States with the COVID-19 pandemic. JAMA Oncol. 2021;7(6):878-884. doi:10.1001/jamaoncol.2021.0884
3. Mazidimoradi A, Tiznobaik A, Salehiniya H. Impact of the COVID-19 pandemic on colorectal cancer screening: a systematic review. J Gastrointest Cancer. 2022;53(3):730-744. doi:10.1007/s12029-021-00679-x
4. Adams MA, Kurlander JE, Gao Y, Yankey N, Saini SD. Impact of coronavirus disease 2019 on screening colonoscopy utilization in a large integrated health system. Gastroenterology. 2022;162(7):2098-2100.e2. doi:10.1053/j.gastro.2022.02.034
5. Sundaram S, Olson S, Sharma P, Rajendra S. A review of the impact of the COVID-19 pandemic on colorectal cancer screening: implications and solutions. Pathogens. 2021;10(11):558. doi:10.3390/pathogens10111508
6. US Preventive Services Task Force. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965-1977. doi:10.1001/jama.2021.6238
7. Robertson DJ, Lee JK, Boland CR, et al. Recommendations on fecal immunochemical testing to screen for colorectal neoplasia: a consensus statement by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2017;85(1):2-21.e3. doi:10.1016/j.gie.2016.09.025
8. Lee JK, Liles EG, Bent S, Levin TR, Corley DA. Accuracy of fecal immunochemical tests for colorectal cancer: systematic review and meta-analysis. Ann Intern Med. 2014;160(3):171. doi:10.7326/M13-1484
9. Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2017;153(1):307-323. doi:10.1053/j.gastro.2017.05.013
10. Deeds SA, Moore CB, Gunnink EJ, et al. Implementation of a mailed faecal immunochemical test programme for colorectal cancer screening among veterans. BMJ Open Qual. 2022;11(4):e001927. doi:10.1136/bmjoq-2022-001927
11. Selby K, Jensen CD, Levin TR, et al. Program components and results from an organized colorectal cancer screening program using annual fecal immunochemical testing. Clin Gastroenterol Hepatol. 2022;20(1):145-152. doi:10.1016/j.cgh.2020.09.042
12. Deeds S, Liu T, Schuttner L, et al. A postcard primer prior to mailed fecal immunochemical test among veterans: a randomized controlled trial. J Gen Intern Med. 2023:38(14):3235-3241. doi:10.1007/s11606-023-08248-7
Colorectal cancer (CRC) is among the most common cancers and causes of cancer-related deaths in the United States.1 Reflective of a nationwide trend, CRC screening rates at the Veterans Affairs Connecticut Healthcare System (VACHS) decreased during the COVID-19 pandemic.2-5 Contributing factors to this decrease included cancellations of elective colonoscopies during the initial phase of the pandemic and concurrent turnover of endoscopists. In 2021, the US Preventive Services Task Force lowered the recommended initial CRC screening age from 50 years to 45 years, further increasing the backlog of unscreened patients.6
Fecal immunochemical testing (FIT) is a noninvasive screening method in which antibodies are used to detect hemoglobin in the stool. The sensitivity and specificity of 1-time FIT are 79% to 80% and 94%, respectively, for the detection of CRC, with sensitivity improving with successive testing.7,8 Annual FIT is recognized as a tier 1 preferred screening method by the US Multi-Society Task Force on Colorectal Cancer.7,9 Programs that mail FIT kits to eligible patients outside of physician visits have been successfully implemented in health care systems.10,11
The VACHS designed and implemented a mailed FIT program using existing infrastructure and staffing.
Program Description
A team of local stakeholders comprised of VACHS leadership, primary care, nursing, and gastroenterology staff, as well as representatives from laboratory, informatics, mail services, and group practice management, was established to execute the project. The team met monthly to plan the project.
The team developed a dataset consisting of patients aged 45 to 75 years who were at average risk for CRC and due for CRC screening. Patients were defined as due for CRC screening if they had not had a colonoscopy in the previous 9 years or a FIT or fecal occult blood test in the previous 11 months. Average risk for CRC was defined by excluding patients with associated diagnosis codes for CRC, colectomy, inflammatory bowel disease, and anemia. The program also excluded patients with diagnosis codes associated with dementia, deferring discussions about cancer screening to their primary care practitioners (PCPs). Patients with invalid mailing addresses were also excluded, as well as those whose PCPs had indicated in the electronic health record that the patient received CRC screening outside the US Department of Veterans Affairs (VA) system.
Letter Templates
Two patient letter electronic health record templates were developed. The first was a primer letter, which was mailed to patients 2 to 3 weeks before the mailed FIT kit as an introduction to the program.12 The purpose of the primer letter was to give advance notice to patients that they could expect a FIT kit to arrive in the mail. The goal was to prepare patients to complete FIT when the kit arrived and prompt them to call the VA to opt out of the mailed FIT program if they were up to date with CRC screening or if they had a condition which made them at high risk for CRC.
The second FIT letter arrived with the FIT kit, introduced FIT and described the importance of CRC screening. The letter detailed instructions for completing FIT and automatically created a FIT order. It also included a list of common conditions that may exclude patients, with a recommendation for patients to contact their medical team if they felt they were not candidates for FIT.
Staff Education
A previous VACHS pilot project demonstrated the success of a mailed FIT program to increase FIT use. Implemented as part of the pilot program, staff education consisted of a session for clinicians about the role of FIT in CRC screening and an all-staff education session. An additional education session about CRC and FIT for all staff was repeated with the program launch.
Program Launch
The mailed FIT program was introduced during a VACHS primary care all-staff meeting. After the meeting, each patient aligned care team (PACT) received an encrypted email that included a list of the patients on their team who were candidates for the program, a patient-facing FIT instruction sheet, detailed instructions on how to send the FIT primer letter, and a FIT package consisting of the labeled FIT kit, FIT letter, and patient instruction sheet. A reminder letter was sent to each patient 3 weeks after the FIT package was mailed. The patient lists were populated into a shared, encrypted Microsoft Teams folder that was edited in real time by PACT teams and viewed by VACHS leadership to track progress.
Program Metrics
At program launch, the VACHS had 4642 patients due for CRC screening who were eligible for the mailed FIT program. On March 7, 2023, the data consisting of FIT tests ordered between December 2022 and May 2023—3 months before and after the launch of the program—were reviewed and categorized. In the 3 months before program launch, 1528 FIT were ordered and 714 were returned (46.7%). In the 3 months after the launch of the program, 4383 FIT were ordered and 1712 were returned (39.1%) (Figure). Test orders increased 287% from the preintervention to the postintervention period. The mean (SD) number of monthly FIT tests prelaunch was 509 (32.7), which increased to 1461 (331.6) postlaunch.
At the VACHS, 61.4% of patients aged 45 to 75 years were up to date with CRC screening before the program launch. In the 3 months after program launch, the rate increased to 63.8% among patients aged 45 to 75 years, the highest rate in our Veterans Integrated Services Network and exceeding the VA national average CRC screening rate, according to unpublished VA Monthly Management Report data.
In the 3 months following the program launch, 139 FIT kits tested positive for potential CRC. Of these, 79 (56.8%) patients had completed a diagnostic colonoscopy. PACT PCPs and nurses received reports on patients with positive FIT tests and those with no colonoscopy scheduled or completed and were asked to follow up.
Discussion
Through a proactive, population-based CRC screening program centered on mailed FIT kits outside of the traditional patient visit, the VACHS increased the use of FIT and rates of CRC screening. The numbers of FIT kits ordered and completed substantially increased in the 3 months after program launch.
Compared to mailed FIT programs described in the literature that rely on centralized processes in that a separate team operates the mailed FIT program for the entire organization, this program used existing PACT infrastructure and staff.10,11 This strategy allowed VACHS to design and implement the program in several months. Not needing to hire new staff or create a central team for the sole purpose of implementing the program allowed us to save on any organizational funding and efforts that would have accompanied the additional staff. The program described in this article may be more attainable for primary care practices or smaller health systems that do not have the capacity for the creation of a centralized process.
Limitations
Although the total number of FIT completions substantially increased during the program, the rate of FIT completion during the mailed FIT program was lower than the rate of completion prior to program launch. This decreased rate of FIT kit completion may be related to separation from a patient visit and potential loss of real-time education with a clinician. The program’s decentralized design increased the existing workload for primary care staff, and as a result, consideration must be given to local staffing levels. Additionally, the report of eligible patients depended on diagnosis codes and may have captured patients with higher-than-average risk of CRC, such as patients with prior history of adenomatous polyps, family history of CRC, or other medical or genetic conditions. We attempted to mitigate this by including a list of conditions that would exclude patients from FIT eligibility in the FIT letter and giving them the option to opt out.
Conclusions
CRC screening rates improved following implementation of a primary care team-centered quality improvement process to proactively identify patients appropriate for FIT and mail them FIT kits. This project highlights that population-health interventions around CRC screening via use of FIT can be successful within a primary care patient-centered medical home model, considering the increases in both CRC screening rates and increase in FIT tests ordered.
Colorectal cancer (CRC) is among the most common cancers and causes of cancer-related deaths in the United States.1 Reflective of a nationwide trend, CRC screening rates at the Veterans Affairs Connecticut Healthcare System (VACHS) decreased during the COVID-19 pandemic.2-5 Contributing factors to this decrease included cancellations of elective colonoscopies during the initial phase of the pandemic and concurrent turnover of endoscopists. In 2021, the US Preventive Services Task Force lowered the recommended initial CRC screening age from 50 years to 45 years, further increasing the backlog of unscreened patients.6
Fecal immunochemical testing (FIT) is a noninvasive screening method in which antibodies are used to detect hemoglobin in the stool. The sensitivity and specificity of 1-time FIT are 79% to 80% and 94%, respectively, for the detection of CRC, with sensitivity improving with successive testing.7,8 Annual FIT is recognized as a tier 1 preferred screening method by the US Multi-Society Task Force on Colorectal Cancer.7,9 Programs that mail FIT kits to eligible patients outside of physician visits have been successfully implemented in health care systems.10,11
The VACHS designed and implemented a mailed FIT program using existing infrastructure and staffing.
Program Description
A team of local stakeholders comprised of VACHS leadership, primary care, nursing, and gastroenterology staff, as well as representatives from laboratory, informatics, mail services, and group practice management, was established to execute the project. The team met monthly to plan the project.
The team developed a dataset consisting of patients aged 45 to 75 years who were at average risk for CRC and due for CRC screening. Patients were defined as due for CRC screening if they had not had a colonoscopy in the previous 9 years or a FIT or fecal occult blood test in the previous 11 months. Average risk for CRC was defined by excluding patients with associated diagnosis codes for CRC, colectomy, inflammatory bowel disease, and anemia. The program also excluded patients with diagnosis codes associated with dementia, deferring discussions about cancer screening to their primary care practitioners (PCPs). Patients with invalid mailing addresses were also excluded, as well as those whose PCPs had indicated in the electronic health record that the patient received CRC screening outside the US Department of Veterans Affairs (VA) system.
Letter Templates
Two patient letter electronic health record templates were developed. The first was a primer letter, which was mailed to patients 2 to 3 weeks before the mailed FIT kit as an introduction to the program.12 The purpose of the primer letter was to give advance notice to patients that they could expect a FIT kit to arrive in the mail. The goal was to prepare patients to complete FIT when the kit arrived and prompt them to call the VA to opt out of the mailed FIT program if they were up to date with CRC screening or if they had a condition which made them at high risk for CRC.
The second FIT letter arrived with the FIT kit, introduced FIT and described the importance of CRC screening. The letter detailed instructions for completing FIT and automatically created a FIT order. It also included a list of common conditions that may exclude patients, with a recommendation for patients to contact their medical team if they felt they were not candidates for FIT.
Staff Education
A previous VACHS pilot project demonstrated the success of a mailed FIT program to increase FIT use. Implemented as part of the pilot program, staff education consisted of a session for clinicians about the role of FIT in CRC screening and an all-staff education session. An additional education session about CRC and FIT for all staff was repeated with the program launch.
Program Launch
The mailed FIT program was introduced during a VACHS primary care all-staff meeting. After the meeting, each patient aligned care team (PACT) received an encrypted email that included a list of the patients on their team who were candidates for the program, a patient-facing FIT instruction sheet, detailed instructions on how to send the FIT primer letter, and a FIT package consisting of the labeled FIT kit, FIT letter, and patient instruction sheet. A reminder letter was sent to each patient 3 weeks after the FIT package was mailed. The patient lists were populated into a shared, encrypted Microsoft Teams folder that was edited in real time by PACT teams and viewed by VACHS leadership to track progress.
Program Metrics
At program launch, the VACHS had 4642 patients due for CRC screening who were eligible for the mailed FIT program. On March 7, 2023, the data consisting of FIT tests ordered between December 2022 and May 2023—3 months before and after the launch of the program—were reviewed and categorized. In the 3 months before program launch, 1528 FIT were ordered and 714 were returned (46.7%). In the 3 months after the launch of the program, 4383 FIT were ordered and 1712 were returned (39.1%) (Figure). Test orders increased 287% from the preintervention to the postintervention period. The mean (SD) number of monthly FIT tests prelaunch was 509 (32.7), which increased to 1461 (331.6) postlaunch.
At the VACHS, 61.4% of patients aged 45 to 75 years were up to date with CRC screening before the program launch. In the 3 months after program launch, the rate increased to 63.8% among patients aged 45 to 75 years, the highest rate in our Veterans Integrated Services Network and exceeding the VA national average CRC screening rate, according to unpublished VA Monthly Management Report data.
In the 3 months following the program launch, 139 FIT kits tested positive for potential CRC. Of these, 79 (56.8%) patients had completed a diagnostic colonoscopy. PACT PCPs and nurses received reports on patients with positive FIT tests and those with no colonoscopy scheduled or completed and were asked to follow up.
Discussion
Through a proactive, population-based CRC screening program centered on mailed FIT kits outside of the traditional patient visit, the VACHS increased the use of FIT and rates of CRC screening. The numbers of FIT kits ordered and completed substantially increased in the 3 months after program launch.
Compared to mailed FIT programs described in the literature that rely on centralized processes in that a separate team operates the mailed FIT program for the entire organization, this program used existing PACT infrastructure and staff.10,11 This strategy allowed VACHS to design and implement the program in several months. Not needing to hire new staff or create a central team for the sole purpose of implementing the program allowed us to save on any organizational funding and efforts that would have accompanied the additional staff. The program described in this article may be more attainable for primary care practices or smaller health systems that do not have the capacity for the creation of a centralized process.
Limitations
Although the total number of FIT completions substantially increased during the program, the rate of FIT completion during the mailed FIT program was lower than the rate of completion prior to program launch. This decreased rate of FIT kit completion may be related to separation from a patient visit and potential loss of real-time education with a clinician. The program’s decentralized design increased the existing workload for primary care staff, and as a result, consideration must be given to local staffing levels. Additionally, the report of eligible patients depended on diagnosis codes and may have captured patients with higher-than-average risk of CRC, such as patients with prior history of adenomatous polyps, family history of CRC, or other medical or genetic conditions. We attempted to mitigate this by including a list of conditions that would exclude patients from FIT eligibility in the FIT letter and giving them the option to opt out.
Conclusions
CRC screening rates improved following implementation of a primary care team-centered quality improvement process to proactively identify patients appropriate for FIT and mail them FIT kits. This project highlights that population-health interventions around CRC screening via use of FIT can be successful within a primary care patient-centered medical home model, considering the increases in both CRC screening rates and increase in FIT tests ordered.
1. American Cancer Society. Key statistics for colorectal cancer. Revised January 29, 2024. Accessed June 11, 2024. https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html
2. Chen RC, Haynes K, Du S, Barron J, Katz AJ. Association of cancer screening deficit in the United States with the COVID-19 pandemic. JAMA Oncol. 2021;7(6):878-884. doi:10.1001/jamaoncol.2021.0884
3. Mazidimoradi A, Tiznobaik A, Salehiniya H. Impact of the COVID-19 pandemic on colorectal cancer screening: a systematic review. J Gastrointest Cancer. 2022;53(3):730-744. doi:10.1007/s12029-021-00679-x
4. Adams MA, Kurlander JE, Gao Y, Yankey N, Saini SD. Impact of coronavirus disease 2019 on screening colonoscopy utilization in a large integrated health system. Gastroenterology. 2022;162(7):2098-2100.e2. doi:10.1053/j.gastro.2022.02.034
5. Sundaram S, Olson S, Sharma P, Rajendra S. A review of the impact of the COVID-19 pandemic on colorectal cancer screening: implications and solutions. Pathogens. 2021;10(11):558. doi:10.3390/pathogens10111508
6. US Preventive Services Task Force. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965-1977. doi:10.1001/jama.2021.6238
7. Robertson DJ, Lee JK, Boland CR, et al. Recommendations on fecal immunochemical testing to screen for colorectal neoplasia: a consensus statement by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2017;85(1):2-21.e3. doi:10.1016/j.gie.2016.09.025
8. Lee JK, Liles EG, Bent S, Levin TR, Corley DA. Accuracy of fecal immunochemical tests for colorectal cancer: systematic review and meta-analysis. Ann Intern Med. 2014;160(3):171. doi:10.7326/M13-1484
9. Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2017;153(1):307-323. doi:10.1053/j.gastro.2017.05.013
10. Deeds SA, Moore CB, Gunnink EJ, et al. Implementation of a mailed faecal immunochemical test programme for colorectal cancer screening among veterans. BMJ Open Qual. 2022;11(4):e001927. doi:10.1136/bmjoq-2022-001927
11. Selby K, Jensen CD, Levin TR, et al. Program components and results from an organized colorectal cancer screening program using annual fecal immunochemical testing. Clin Gastroenterol Hepatol. 2022;20(1):145-152. doi:10.1016/j.cgh.2020.09.042
12. Deeds S, Liu T, Schuttner L, et al. A postcard primer prior to mailed fecal immunochemical test among veterans: a randomized controlled trial. J Gen Intern Med. 2023:38(14):3235-3241. doi:10.1007/s11606-023-08248-7
1. American Cancer Society. Key statistics for colorectal cancer. Revised January 29, 2024. Accessed June 11, 2024. https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html
2. Chen RC, Haynes K, Du S, Barron J, Katz AJ. Association of cancer screening deficit in the United States with the COVID-19 pandemic. JAMA Oncol. 2021;7(6):878-884. doi:10.1001/jamaoncol.2021.0884
3. Mazidimoradi A, Tiznobaik A, Salehiniya H. Impact of the COVID-19 pandemic on colorectal cancer screening: a systematic review. J Gastrointest Cancer. 2022;53(3):730-744. doi:10.1007/s12029-021-00679-x
4. Adams MA, Kurlander JE, Gao Y, Yankey N, Saini SD. Impact of coronavirus disease 2019 on screening colonoscopy utilization in a large integrated health system. Gastroenterology. 2022;162(7):2098-2100.e2. doi:10.1053/j.gastro.2022.02.034
5. Sundaram S, Olson S, Sharma P, Rajendra S. A review of the impact of the COVID-19 pandemic on colorectal cancer screening: implications and solutions. Pathogens. 2021;10(11):558. doi:10.3390/pathogens10111508
6. US Preventive Services Task Force. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965-1977. doi:10.1001/jama.2021.6238
7. Robertson DJ, Lee JK, Boland CR, et al. Recommendations on fecal immunochemical testing to screen for colorectal neoplasia: a consensus statement by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2017;85(1):2-21.e3. doi:10.1016/j.gie.2016.09.025
8. Lee JK, Liles EG, Bent S, Levin TR, Corley DA. Accuracy of fecal immunochemical tests for colorectal cancer: systematic review and meta-analysis. Ann Intern Med. 2014;160(3):171. doi:10.7326/M13-1484
9. Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2017;153(1):307-323. doi:10.1053/j.gastro.2017.05.013
10. Deeds SA, Moore CB, Gunnink EJ, et al. Implementation of a mailed faecal immunochemical test programme for colorectal cancer screening among veterans. BMJ Open Qual. 2022;11(4):e001927. doi:10.1136/bmjoq-2022-001927
11. Selby K, Jensen CD, Levin TR, et al. Program components and results from an organized colorectal cancer screening program using annual fecal immunochemical testing. Clin Gastroenterol Hepatol. 2022;20(1):145-152. doi:10.1016/j.cgh.2020.09.042
12. Deeds S, Liu T, Schuttner L, et al. A postcard primer prior to mailed fecal immunochemical test among veterans: a randomized controlled trial. J Gen Intern Med. 2023:38(14):3235-3241. doi:10.1007/s11606-023-08248-7
Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology
Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology
This transcript has been edited for clarity.
Coral Olazagasti, MD: Hi, everyone. Good afternoon. My name is Dr Coral Olazagasti, and I’m a medical oncologist from the University of Miami. I’m excited to be here with my colleague and my friend, Carolina. Dr Bernabe, Can you please introduce yourself?
Carolina Bernabe, MD: I am Dr Carolina Bernabe. I’m one of the gastrointestinal (GI) oncologists at Montefiore Einstein Comprehensive Cancer Center. Thank you for having me today.
Olazagasti: We’re excited because we know that there has been excitement and interest in GLP-1s in cancer. You would think, like, “Hmm, let’s just combine a GI oncologist with a thoracic oncologist to talk about GLP-1s.”
I wanted to bring the conversation to the GLP-1s because we know that it’s been becoming a boom. You see it in your home because your husband is an endocrinologist, and many people are on these drugs. It’s been remarkable, the use and the benefits that we’ve seen so far. Then to know that they might have a benefit in cancer, I think it’s wonderful and very interesting.
What are your thoughts?
Bernabe: When looking at the data on how many patients are using this medication, you’re talking about 12% of the whole US population, which is, like, 44 million people. That’s crazy. Looking at the abstracts that were presented here at ASCO, they looked at these numbers and looked at these patients with cancer, which is around 1000 patients, and then they were evaluating what is the benefit of GLP-1s. You had a chance to look at the abstract, I think?
Olazagasti: Yeah. We have a retrospective study where the authors review a database. There were around 1000 patients, like you said, on GLP-1s with a history of cancer, and the benefit was profound. They found at 24 months there was an overall survival benefit, not only for breast but also prostate cancer, in patients on GLP-1s. Granted, I know that we’re looking into retrospective studies, but I think it makes you wonder if we’re seeing these trends in a retrospective fashion in breast and prostate, where else are we seeing it? I think it’s just a matter of looking at the data.
Bernabe: Even though it was a retrospective analysis, they also did this propensity score where it’s like matching, and that tries to create kind of a randomized clinical trial.
Olazagasti: After adjusting, it was for age and other factors.
Bernabe: Correct.
Olazagasti: The benefits were sustained, so I think it’s wonderful.
What about the other abstract? There was also another abstract. This one was in patients that had a history of cancer and were on GLP-1s, but they also were on immune checkpoint inhibitors. This database covered more patients. I think it was around 3800 patients that were in this particular retrospective study. That study found that not only were the patients having benefits of survival those patients on immune checkpoint inhibitors and GLP-1s, but also we’re seeing that the patients had lower rates of immune-related adverse events. It’s just mind-blowing to me.
Bernabe: Completely agree with you. We are seeing the benefit not only in the survival, who knows, maybe some decrease in the inflammatory component on cancer and tumor microenvironment, but also we’re seeing less events related to immunotherapy and less immune toxicity, right, that we’re always worried about and the patients need to start using a steroid. Maybe in the future, this can be used as a steroid-sparing agent. It’s wonderful news.
Olazagasti: Yeah, I know. We’ve been seeing data from rheumatologic disorders that GLP-1s help with that inflammation, so you’re right. Sometimes autoimmune diseases are our limiting factor to be able to offer these patients immunotherapy, and oftentimes our only choices are chemotherapy.
Bernabe: It opens a window.
Olazagasti: It may be allowing them a possibility of controlling their autoimmune disease while also being able to challenge them. I’m so excited. I think we’re going to start seeing these studies planned and designed in a prospective fashion, so I wonder how these data are going to look in the long term.
Bernabe: I think this is just the tip of an iceberg and will open up the opportunities to further prospective studies and trials.
Olazagasti: There’s a large amount of excitement also for patients, at least in the thoracic space, where with many of these drugs — especially TKIs, like lorlatinib for ALK-positive lung cancer — you have a large amount of edema. Even in patients with docetaxel, too, you have some swelling. With that agent that I mentioned, lorlatinib, patients also had high cholesterol levels, and that’s really a challenge.
I’m interested to see what the role will be of GLP-1s in these cohorts of patients. Is this going to be something where not only do they hopefully derive a survival benefit, but also in the side effect profile and in quality of life?
I’m excited to see. It’s crazy to be an oncologist in 2026, and so it’s honestly such a pleasure for me to see science advancing. At the end of the day, we want to make sure that the studies and the discoveries that we have are applicable to our patients and are something that we can incorporate outside of clinical trials and into the real world.
Bernabe: Especially this drug that is already popular, right? Now we’re seeing an extra benefit on top of all the weight loss and decrease in inflammation in general.
Olazagasti: Thank you for this wonderful discussion, and thank you for watching our video. Have a great day.
Bernabe: Thank you for having me.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Coral Olazagasti, MD: Hi, everyone. Good afternoon. My name is Dr Coral Olazagasti, and I’m a medical oncologist from the University of Miami. I’m excited to be here with my colleague and my friend, Carolina. Dr Bernabe, Can you please introduce yourself?
Carolina Bernabe, MD: I am Dr Carolina Bernabe. I’m one of the gastrointestinal (GI) oncologists at Montefiore Einstein Comprehensive Cancer Center. Thank you for having me today.
Olazagasti: We’re excited because we know that there has been excitement and interest in GLP-1s in cancer. You would think, like, “Hmm, let’s just combine a GI oncologist with a thoracic oncologist to talk about GLP-1s.”
I wanted to bring the conversation to the GLP-1s because we know that it’s been becoming a boom. You see it in your home because your husband is an endocrinologist, and many people are on these drugs. It’s been remarkable, the use and the benefits that we’ve seen so far. Then to know that they might have a benefit in cancer, I think it’s wonderful and very interesting.
What are your thoughts?
Bernabe: When looking at the data on how many patients are using this medication, you’re talking about 12% of the whole US population, which is, like, 44 million people. That’s crazy. Looking at the abstracts that were presented here at ASCO, they looked at these numbers and looked at these patients with cancer, which is around 1000 patients, and then they were evaluating what is the benefit of GLP-1s. You had a chance to look at the abstract, I think?
Olazagasti: Yeah. We have a retrospective study where the authors review a database. There were around 1000 patients, like you said, on GLP-1s with a history of cancer, and the benefit was profound. They found at 24 months there was an overall survival benefit, not only for breast but also prostate cancer, in patients on GLP-1s. Granted, I know that we’re looking into retrospective studies, but I think it makes you wonder if we’re seeing these trends in a retrospective fashion in breast and prostate, where else are we seeing it? I think it’s just a matter of looking at the data.
Bernabe: Even though it was a retrospective analysis, they also did this propensity score where it’s like matching, and that tries to create kind of a randomized clinical trial.
Olazagasti: After adjusting, it was for age and other factors.
Bernabe: Correct.
Olazagasti: The benefits were sustained, so I think it’s wonderful.
What about the other abstract? There was also another abstract. This one was in patients that had a history of cancer and were on GLP-1s, but they also were on immune checkpoint inhibitors. This database covered more patients. I think it was around 3800 patients that were in this particular retrospective study. That study found that not only were the patients having benefits of survival those patients on immune checkpoint inhibitors and GLP-1s, but also we’re seeing that the patients had lower rates of immune-related adverse events. It’s just mind-blowing to me.
Bernabe: Completely agree with you. We are seeing the benefit not only in the survival, who knows, maybe some decrease in the inflammatory component on cancer and tumor microenvironment, but also we’re seeing less events related to immunotherapy and less immune toxicity, right, that we’re always worried about and the patients need to start using a steroid. Maybe in the future, this can be used as a steroid-sparing agent. It’s wonderful news.
Olazagasti: Yeah, I know. We’ve been seeing data from rheumatologic disorders that GLP-1s help with that inflammation, so you’re right. Sometimes autoimmune diseases are our limiting factor to be able to offer these patients immunotherapy, and oftentimes our only choices are chemotherapy.
Bernabe: It opens a window.
Olazagasti: It may be allowing them a possibility of controlling their autoimmune disease while also being able to challenge them. I’m so excited. I think we’re going to start seeing these studies planned and designed in a prospective fashion, so I wonder how these data are going to look in the long term.
Bernabe: I think this is just the tip of an iceberg and will open up the opportunities to further prospective studies and trials.
Olazagasti: There’s a large amount of excitement also for patients, at least in the thoracic space, where with many of these drugs — especially TKIs, like lorlatinib for ALK-positive lung cancer — you have a large amount of edema. Even in patients with docetaxel, too, you have some swelling. With that agent that I mentioned, lorlatinib, patients also had high cholesterol levels, and that’s really a challenge.
I’m interested to see what the role will be of GLP-1s in these cohorts of patients. Is this going to be something where not only do they hopefully derive a survival benefit, but also in the side effect profile and in quality of life?
I’m excited to see. It’s crazy to be an oncologist in 2026, and so it’s honestly such a pleasure for me to see science advancing. At the end of the day, we want to make sure that the studies and the discoveries that we have are applicable to our patients and are something that we can incorporate outside of clinical trials and into the real world.
Bernabe: Especially this drug that is already popular, right? Now we’re seeing an extra benefit on top of all the weight loss and decrease in inflammation in general.
Olazagasti: Thank you for this wonderful discussion, and thank you for watching our video. Have a great day.
Bernabe: Thank you for having me.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Coral Olazagasti, MD: Hi, everyone. Good afternoon. My name is Dr Coral Olazagasti, and I’m a medical oncologist from the University of Miami. I’m excited to be here with my colleague and my friend, Carolina. Dr Bernabe, Can you please introduce yourself?
Carolina Bernabe, MD: I am Dr Carolina Bernabe. I’m one of the gastrointestinal (GI) oncologists at Montefiore Einstein Comprehensive Cancer Center. Thank you for having me today.
Olazagasti: We’re excited because we know that there has been excitement and interest in GLP-1s in cancer. You would think, like, “Hmm, let’s just combine a GI oncologist with a thoracic oncologist to talk about GLP-1s.”
I wanted to bring the conversation to the GLP-1s because we know that it’s been becoming a boom. You see it in your home because your husband is an endocrinologist, and many people are on these drugs. It’s been remarkable, the use and the benefits that we’ve seen so far. Then to know that they might have a benefit in cancer, I think it’s wonderful and very interesting.
What are your thoughts?
Bernabe: When looking at the data on how many patients are using this medication, you’re talking about 12% of the whole US population, which is, like, 44 million people. That’s crazy. Looking at the abstracts that were presented here at ASCO, they looked at these numbers and looked at these patients with cancer, which is around 1000 patients, and then they were evaluating what is the benefit of GLP-1s. You had a chance to look at the abstract, I think?
Olazagasti: Yeah. We have a retrospective study where the authors review a database. There were around 1000 patients, like you said, on GLP-1s with a history of cancer, and the benefit was profound. They found at 24 months there was an overall survival benefit, not only for breast but also prostate cancer, in patients on GLP-1s. Granted, I know that we’re looking into retrospective studies, but I think it makes you wonder if we’re seeing these trends in a retrospective fashion in breast and prostate, where else are we seeing it? I think it’s just a matter of looking at the data.
Bernabe: Even though it was a retrospective analysis, they also did this propensity score where it’s like matching, and that tries to create kind of a randomized clinical trial.
Olazagasti: After adjusting, it was for age and other factors.
Bernabe: Correct.
Olazagasti: The benefits were sustained, so I think it’s wonderful.
What about the other abstract? There was also another abstract. This one was in patients that had a history of cancer and were on GLP-1s, but they also were on immune checkpoint inhibitors. This database covered more patients. I think it was around 3800 patients that were in this particular retrospective study. That study found that not only were the patients having benefits of survival those patients on immune checkpoint inhibitors and GLP-1s, but also we’re seeing that the patients had lower rates of immune-related adverse events. It’s just mind-blowing to me.
Bernabe: Completely agree with you. We are seeing the benefit not only in the survival, who knows, maybe some decrease in the inflammatory component on cancer and tumor microenvironment, but also we’re seeing less events related to immunotherapy and less immune toxicity, right, that we’re always worried about and the patients need to start using a steroid. Maybe in the future, this can be used as a steroid-sparing agent. It’s wonderful news.
Olazagasti: Yeah, I know. We’ve been seeing data from rheumatologic disorders that GLP-1s help with that inflammation, so you’re right. Sometimes autoimmune diseases are our limiting factor to be able to offer these patients immunotherapy, and oftentimes our only choices are chemotherapy.
Bernabe: It opens a window.
Olazagasti: It may be allowing them a possibility of controlling their autoimmune disease while also being able to challenge them. I’m so excited. I think we’re going to start seeing these studies planned and designed in a prospective fashion, so I wonder how these data are going to look in the long term.
Bernabe: I think this is just the tip of an iceberg and will open up the opportunities to further prospective studies and trials.
Olazagasti: There’s a large amount of excitement also for patients, at least in the thoracic space, where with many of these drugs — especially TKIs, like lorlatinib for ALK-positive lung cancer — you have a large amount of edema. Even in patients with docetaxel, too, you have some swelling. With that agent that I mentioned, lorlatinib, patients also had high cholesterol levels, and that’s really a challenge.
I’m interested to see what the role will be of GLP-1s in these cohorts of patients. Is this going to be something where not only do they hopefully derive a survival benefit, but also in the side effect profile and in quality of life?
I’m excited to see. It’s crazy to be an oncologist in 2026, and so it’s honestly such a pleasure for me to see science advancing. At the end of the day, we want to make sure that the studies and the discoveries that we have are applicable to our patients and are something that we can incorporate outside of clinical trials and into the real world.
Bernabe: Especially this drug that is already popular, right? Now we’re seeing an extra benefit on top of all the weight loss and decrease in inflammation in general.
Olazagasti: Thank you for this wonderful discussion, and thank you for watching our video. Have a great day.
Bernabe: Thank you for having me.
A version of this article first appeared on Medscape.com.
Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology
Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology

COVID-19 Pandemic Left Many Veteran Colon Cancers Undetected
Disruptions caused by the COVID-19 pandemic led to an estimated 619 missed cases of colorectal cancer (CRC) diagnoses among US veterans, and those whose cases were caught had larger tumors and more malignant bowel obstructions compared with a prepandemic period, a new longitudinal study finds.
The decline in diagnoses during the pandemic (March 2020-October 2023) represented a 5% decrease in anticipated cases compared with the prepandemic period (January 2017-February 2020) reported Veterans Health Administration (VHA) researchers in the Journal of Gastrointestinal Surgery.
Meanwhile, the percentage of cancers > 4 cm increased from 48.9% to 57.3% from the prepandemic to pandemic periods, and the percentage of patients with malignant bowel obstructions at presentation nearly doubled from 2.7% to 5.3%.
“The COVID-19 pandemic resulted in a significant initial decrease in rates of colon cancer diagnosis, with a slow return to baseline,” Louise Davies, MD, MS, a head-and-neck surgeon at the University of Wisconsin-Madison and senior author of the study told Federal Practitioner. “The length of time it took for things to return to normal surprised us. Patterns of detection did not return to more normal baselines until 2023.”
The Pandemic’s Toll on Colonoscopies
While mortality and diagnosis rates have fallen significantly over the past 3 decades, an estimated 158,850 colorectal cancer cases will be diagnosed in the US in 2026, and 55,230 patients will die. Within the VHA, an estimated 4000 new cases of colorectal cancer are diagnosed annually.
The pandemic disrupted medical care across the board, and colonoscopies were no exceptions. “There are various estimates that there were anywhere from 2 to 3 million missed exams,” said Timothy Pawlik, MD, PhD, MBA, MPH, a surgical oncologist and professor at The Ohio State University Wexner Medical Center, in an interview.
“At the height of the pandemic, all nonurgent procedures were put on hold,” explained Pawlik, who was not involved in the new study. “I suspect that a number of procedures were missed because different institutions and GI practices simply weren't providing that service at that time. In addition, I'm sure there was some reticence among patients to seek care even after the procedures were restarted and reoffered, especially at a hospital.”
Inside the VHA Data
The researchers found that 22,256 VHA patients were diagnosed with CRC during the study period (mean age, 71 years; 95.6% male; 72.1% White, 19.3% Black, and 6.4% Hispanic).
In a subset of 1087 patients, the percentage with an American Society of Anesthesiologists class ≥ 3 rose from 74.4% before the pandemic to 78.9% during it.
In light of the study findings, “clinicians should encourage their eligible patients to get screened for colon cancer, especially if they delayed screening as a result of the pandemic,” Davies said.
Why Colonoscopy Delays Matter
Pawlik, the Ohio State University Wexner Medical Center surgical oncologist, said even small delays in colonoscopies can be important.
“There are data suggesting that even a delay beyond 6 to 12 months can significantly increase the risk of advanced-stage cancer. Longer delays of a year, which were associated with the pandemic, definitely increase the risk of presenting with later stages of disease and potentially have a meaningful impact on your prognosis and survival.”
However, he noted that the study findings are limited because the results don’t clarify when patients were due for colonoscopies.
Still, in the big picture, the research “emphasizes the importance of timely colonoscopy compliance with national guidelines for screening of colon cancer,” he said.
Lessons About At-Home Tests
Pawlik added that the research also highlights that in times of limited access such as pandemics, there can be value to pivoting to home-based screening methods.
Study coauthor Douglas Robertson, MD, MPH, national deputy director of the Colorectal Cancer Screening Program with the US Department of Veterans Affairs National Gastroenterology and Hepatology Program, said the pandemic spurred a shift toward fecal immunochemical testing (FIT) via mail.
The VA is now mailing > 40,000 FIT tests per month to veterans. “This program was an outgrowth of and response to the pandemic and would enhance VA’s readiness to maintain CRC screening efforts should something similar occur in the future,” Robertson said in an interview.
The Department of Veterans Affairs funded the study. Davies, Robertson, and the other study authors have no disclosures. Pawlik is co-editor-in-chief of the Journal of Gastrointestinal Surgery and has no other disclosures.
Disruptions caused by the COVID-19 pandemic led to an estimated 619 missed cases of colorectal cancer (CRC) diagnoses among US veterans, and those whose cases were caught had larger tumors and more malignant bowel obstructions compared with a prepandemic period, a new longitudinal study finds.
The decline in diagnoses during the pandemic (March 2020-October 2023) represented a 5% decrease in anticipated cases compared with the prepandemic period (January 2017-February 2020) reported Veterans Health Administration (VHA) researchers in the Journal of Gastrointestinal Surgery.
Meanwhile, the percentage of cancers > 4 cm increased from 48.9% to 57.3% from the prepandemic to pandemic periods, and the percentage of patients with malignant bowel obstructions at presentation nearly doubled from 2.7% to 5.3%.
“The COVID-19 pandemic resulted in a significant initial decrease in rates of colon cancer diagnosis, with a slow return to baseline,” Louise Davies, MD, MS, a head-and-neck surgeon at the University of Wisconsin-Madison and senior author of the study told Federal Practitioner. “The length of time it took for things to return to normal surprised us. Patterns of detection did not return to more normal baselines until 2023.”
The Pandemic’s Toll on Colonoscopies
While mortality and diagnosis rates have fallen significantly over the past 3 decades, an estimated 158,850 colorectal cancer cases will be diagnosed in the US in 2026, and 55,230 patients will die. Within the VHA, an estimated 4000 new cases of colorectal cancer are diagnosed annually.
The pandemic disrupted medical care across the board, and colonoscopies were no exceptions. “There are various estimates that there were anywhere from 2 to 3 million missed exams,” said Timothy Pawlik, MD, PhD, MBA, MPH, a surgical oncologist and professor at The Ohio State University Wexner Medical Center, in an interview.
“At the height of the pandemic, all nonurgent procedures were put on hold,” explained Pawlik, who was not involved in the new study. “I suspect that a number of procedures were missed because different institutions and GI practices simply weren't providing that service at that time. In addition, I'm sure there was some reticence among patients to seek care even after the procedures were restarted and reoffered, especially at a hospital.”
Inside the VHA Data
The researchers found that 22,256 VHA patients were diagnosed with CRC during the study period (mean age, 71 years; 95.6% male; 72.1% White, 19.3% Black, and 6.4% Hispanic).
In a subset of 1087 patients, the percentage with an American Society of Anesthesiologists class ≥ 3 rose from 74.4% before the pandemic to 78.9% during it.
In light of the study findings, “clinicians should encourage their eligible patients to get screened for colon cancer, especially if they delayed screening as a result of the pandemic,” Davies said.
Why Colonoscopy Delays Matter
Pawlik, the Ohio State University Wexner Medical Center surgical oncologist, said even small delays in colonoscopies can be important.
“There are data suggesting that even a delay beyond 6 to 12 months can significantly increase the risk of advanced-stage cancer. Longer delays of a year, which were associated with the pandemic, definitely increase the risk of presenting with later stages of disease and potentially have a meaningful impact on your prognosis and survival.”
However, he noted that the study findings are limited because the results don’t clarify when patients were due for colonoscopies.
Still, in the big picture, the research “emphasizes the importance of timely colonoscopy compliance with national guidelines for screening of colon cancer,” he said.
Lessons About At-Home Tests
Pawlik added that the research also highlights that in times of limited access such as pandemics, there can be value to pivoting to home-based screening methods.
Study coauthor Douglas Robertson, MD, MPH, national deputy director of the Colorectal Cancer Screening Program with the US Department of Veterans Affairs National Gastroenterology and Hepatology Program, said the pandemic spurred a shift toward fecal immunochemical testing (FIT) via mail.
The VA is now mailing > 40,000 FIT tests per month to veterans. “This program was an outgrowth of and response to the pandemic and would enhance VA’s readiness to maintain CRC screening efforts should something similar occur in the future,” Robertson said in an interview.
The Department of Veterans Affairs funded the study. Davies, Robertson, and the other study authors have no disclosures. Pawlik is co-editor-in-chief of the Journal of Gastrointestinal Surgery and has no other disclosures.
Disruptions caused by the COVID-19 pandemic led to an estimated 619 missed cases of colorectal cancer (CRC) diagnoses among US veterans, and those whose cases were caught had larger tumors and more malignant bowel obstructions compared with a prepandemic period, a new longitudinal study finds.
The decline in diagnoses during the pandemic (March 2020-October 2023) represented a 5% decrease in anticipated cases compared with the prepandemic period (January 2017-February 2020) reported Veterans Health Administration (VHA) researchers in the Journal of Gastrointestinal Surgery.
Meanwhile, the percentage of cancers > 4 cm increased from 48.9% to 57.3% from the prepandemic to pandemic periods, and the percentage of patients with malignant bowel obstructions at presentation nearly doubled from 2.7% to 5.3%.
“The COVID-19 pandemic resulted in a significant initial decrease in rates of colon cancer diagnosis, with a slow return to baseline,” Louise Davies, MD, MS, a head-and-neck surgeon at the University of Wisconsin-Madison and senior author of the study told Federal Practitioner. “The length of time it took for things to return to normal surprised us. Patterns of detection did not return to more normal baselines until 2023.”
The Pandemic’s Toll on Colonoscopies
While mortality and diagnosis rates have fallen significantly over the past 3 decades, an estimated 158,850 colorectal cancer cases will be diagnosed in the US in 2026, and 55,230 patients will die. Within the VHA, an estimated 4000 new cases of colorectal cancer are diagnosed annually.
The pandemic disrupted medical care across the board, and colonoscopies were no exceptions. “There are various estimates that there were anywhere from 2 to 3 million missed exams,” said Timothy Pawlik, MD, PhD, MBA, MPH, a surgical oncologist and professor at The Ohio State University Wexner Medical Center, in an interview.
“At the height of the pandemic, all nonurgent procedures were put on hold,” explained Pawlik, who was not involved in the new study. “I suspect that a number of procedures were missed because different institutions and GI practices simply weren't providing that service at that time. In addition, I'm sure there was some reticence among patients to seek care even after the procedures were restarted and reoffered, especially at a hospital.”
Inside the VHA Data
The researchers found that 22,256 VHA patients were diagnosed with CRC during the study period (mean age, 71 years; 95.6% male; 72.1% White, 19.3% Black, and 6.4% Hispanic).
In a subset of 1087 patients, the percentage with an American Society of Anesthesiologists class ≥ 3 rose from 74.4% before the pandemic to 78.9% during it.
In light of the study findings, “clinicians should encourage their eligible patients to get screened for colon cancer, especially if they delayed screening as a result of the pandemic,” Davies said.
Why Colonoscopy Delays Matter
Pawlik, the Ohio State University Wexner Medical Center surgical oncologist, said even small delays in colonoscopies can be important.
“There are data suggesting that even a delay beyond 6 to 12 months can significantly increase the risk of advanced-stage cancer. Longer delays of a year, which were associated with the pandemic, definitely increase the risk of presenting with later stages of disease and potentially have a meaningful impact on your prognosis and survival.”
However, he noted that the study findings are limited because the results don’t clarify when patients were due for colonoscopies.
Still, in the big picture, the research “emphasizes the importance of timely colonoscopy compliance with national guidelines for screening of colon cancer,” he said.
Lessons About At-Home Tests
Pawlik added that the research also highlights that in times of limited access such as pandemics, there can be value to pivoting to home-based screening methods.
Study coauthor Douglas Robertson, MD, MPH, national deputy director of the Colorectal Cancer Screening Program with the US Department of Veterans Affairs National Gastroenterology and Hepatology Program, said the pandemic spurred a shift toward fecal immunochemical testing (FIT) via mail.
The VA is now mailing > 40,000 FIT tests per month to veterans. “This program was an outgrowth of and response to the pandemic and would enhance VA’s readiness to maintain CRC screening efforts should something similar occur in the future,” Robertson said in an interview.
The Department of Veterans Affairs funded the study. Davies, Robertson, and the other study authors have no disclosures. Pawlik is co-editor-in-chief of the Journal of Gastrointestinal Surgery and has no other disclosures.
Human Papillomavirus Vaccination Linked to Substantial Reduction in Cervical Cancer Deaths, Data Reveal
Human Papillomavirus Vaccination Linked to Substantial Reduction in Cervical Cancer Deaths, Data Reveal
TOPLINE:
In a population-based study, human papillomavirus (HPV) vaccination in England was associated with a 100% reduction in mortality due to cervical cancer between 2020 and 2024 among women aged 20-24 years who were mostly vaccinated at the age of 12-13 years.
METHODOLOGY:
- Researchers conducted a population-based study using cervical cancer mortality data of women aged 20-24, 25-29, and 30-34 years from the National Disease Registration Service and Office for National Statistics in England from 2000 to 2024.
- The analysis included women from the first eligible birth cohort (born from September 1990 to August 1991) who were targeted by England's school-based HPV vaccination programme introduced in September 2008 for girls aged 12-13 years, with a catch-up programme for girls aged 14-18 years implemented in 2008-2010.
- HPV vaccination coverage by birth cohort was obtained from annual reports of the UK Health Security Agency and used to estimate the proportion of women vaccinated for each age group and calendar year.
- The relative risk reduction (RRR) in mortality among vaccinated women compared with expected rates in the absence of vaccination, assuming no herd immunity, was evaluated.
TAKEAWAY:
- Among women aged 20-24 years between 2020 and 2024 with approximately 88%-91% vaccination coverage, no deaths occurred compared with 23.1 expected deaths on the basis of the observed average rate from 2000 to 2014, corresponding to a reduction in mortality of 100% (95% CI, 84%-100%).
- Among vaccinated women, the RRR in mortality due to cervical cancer was estimated at 100% (P = .0008) in those aged 20-24 years, 100% (P < .0001) in those aged 25-29 years, and 63% (P = .094) in those aged 30-34 years.
- Mortality reductions of 80% (95% CI, 51%-94%) were observed in women aged 20-24 years during 2015-2019 and 69% (95% CI, 55%-79%) were observed in those aged 25-29 years during 2020-2024.
- Up until the end of 2024, the HPV vaccination programme in England was associated with a reduction of approximately 199.6 deaths due to cervical cancer (95% CI, 125.0-274.2) among cohorts offered vaccination.
IN PRACTICE:
The authors concluded that "we found a substantial reduction in cervical cancer mortality in women aged 20-29 years that was associated with high uptake of HPV vaccination." "This observation further supports the benefit of HPV vaccination in reducing not only the incidence of but also the mortality from a cancer that is globally still the second most common cause of cancer death in women younger than 65 years," they added. SOURCE: The study was led by Peter Sasieni, PhD, Centre for Cancer Screening, Prevention and Early Diagnosis, Wolfson Institute of Population Health, Queen Mary University of London, London, England. It was published online on June 17, 2026, in The Lancet.
LIMITATIONS:
The analysis relied on population-level vaccination coverage data instead of individual-level status; the researchers had access to mortality data in 5-year age groups only rather than single-year cohorts, and the study assumed no herd protection among unvaccinated women within birth cohorts.
DISCLOSURES:
The study was funded by the Cancer Research UK. One author reported serving as a lead investigator of a trial examining the HPV vaccine Gardasil 9 that was partially supported by a research grant from the Investigator-Initiated Studies Program of Merck Sharp & Dohme. Additional disclosures are listed in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
In a population-based study, human papillomavirus (HPV) vaccination in England was associated with a 100% reduction in mortality due to cervical cancer between 2020 and 2024 among women aged 20-24 years who were mostly vaccinated at the age of 12-13 years.
METHODOLOGY:
- Researchers conducted a population-based study using cervical cancer mortality data of women aged 20-24, 25-29, and 30-34 years from the National Disease Registration Service and Office for National Statistics in England from 2000 to 2024.
- The analysis included women from the first eligible birth cohort (born from September 1990 to August 1991) who were targeted by England's school-based HPV vaccination programme introduced in September 2008 for girls aged 12-13 years, with a catch-up programme for girls aged 14-18 years implemented in 2008-2010.
- HPV vaccination coverage by birth cohort was obtained from annual reports of the UK Health Security Agency and used to estimate the proportion of women vaccinated for each age group and calendar year.
- The relative risk reduction (RRR) in mortality among vaccinated women compared with expected rates in the absence of vaccination, assuming no herd immunity, was evaluated.
TAKEAWAY:
- Among women aged 20-24 years between 2020 and 2024 with approximately 88%-91% vaccination coverage, no deaths occurred compared with 23.1 expected deaths on the basis of the observed average rate from 2000 to 2014, corresponding to a reduction in mortality of 100% (95% CI, 84%-100%).
- Among vaccinated women, the RRR in mortality due to cervical cancer was estimated at 100% (P = .0008) in those aged 20-24 years, 100% (P < .0001) in those aged 25-29 years, and 63% (P = .094) in those aged 30-34 years.
- Mortality reductions of 80% (95% CI, 51%-94%) were observed in women aged 20-24 years during 2015-2019 and 69% (95% CI, 55%-79%) were observed in those aged 25-29 years during 2020-2024.
- Up until the end of 2024, the HPV vaccination programme in England was associated with a reduction of approximately 199.6 deaths due to cervical cancer (95% CI, 125.0-274.2) among cohorts offered vaccination.
IN PRACTICE:
The authors concluded that "we found a substantial reduction in cervical cancer mortality in women aged 20-29 years that was associated with high uptake of HPV vaccination." "This observation further supports the benefit of HPV vaccination in reducing not only the incidence of but also the mortality from a cancer that is globally still the second most common cause of cancer death in women younger than 65 years," they added. SOURCE: The study was led by Peter Sasieni, PhD, Centre for Cancer Screening, Prevention and Early Diagnosis, Wolfson Institute of Population Health, Queen Mary University of London, London, England. It was published online on June 17, 2026, in The Lancet.
LIMITATIONS:
The analysis relied on population-level vaccination coverage data instead of individual-level status; the researchers had access to mortality data in 5-year age groups only rather than single-year cohorts, and the study assumed no herd protection among unvaccinated women within birth cohorts.
DISCLOSURES:
The study was funded by the Cancer Research UK. One author reported serving as a lead investigator of a trial examining the HPV vaccine Gardasil 9 that was partially supported by a research grant from the Investigator-Initiated Studies Program of Merck Sharp & Dohme. Additional disclosures are listed in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
In a population-based study, human papillomavirus (HPV) vaccination in England was associated with a 100% reduction in mortality due to cervical cancer between 2020 and 2024 among women aged 20-24 years who were mostly vaccinated at the age of 12-13 years.
METHODOLOGY:
- Researchers conducted a population-based study using cervical cancer mortality data of women aged 20-24, 25-29, and 30-34 years from the National Disease Registration Service and Office for National Statistics in England from 2000 to 2024.
- The analysis included women from the first eligible birth cohort (born from September 1990 to August 1991) who were targeted by England's school-based HPV vaccination programme introduced in September 2008 for girls aged 12-13 years, with a catch-up programme for girls aged 14-18 years implemented in 2008-2010.
- HPV vaccination coverage by birth cohort was obtained from annual reports of the UK Health Security Agency and used to estimate the proportion of women vaccinated for each age group and calendar year.
- The relative risk reduction (RRR) in mortality among vaccinated women compared with expected rates in the absence of vaccination, assuming no herd immunity, was evaluated.
TAKEAWAY:
- Among women aged 20-24 years between 2020 and 2024 with approximately 88%-91% vaccination coverage, no deaths occurred compared with 23.1 expected deaths on the basis of the observed average rate from 2000 to 2014, corresponding to a reduction in mortality of 100% (95% CI, 84%-100%).
- Among vaccinated women, the RRR in mortality due to cervical cancer was estimated at 100% (P = .0008) in those aged 20-24 years, 100% (P < .0001) in those aged 25-29 years, and 63% (P = .094) in those aged 30-34 years.
- Mortality reductions of 80% (95% CI, 51%-94%) were observed in women aged 20-24 years during 2015-2019 and 69% (95% CI, 55%-79%) were observed in those aged 25-29 years during 2020-2024.
- Up until the end of 2024, the HPV vaccination programme in England was associated with a reduction of approximately 199.6 deaths due to cervical cancer (95% CI, 125.0-274.2) among cohorts offered vaccination.
IN PRACTICE:
The authors concluded that "we found a substantial reduction in cervical cancer mortality in women aged 20-29 years that was associated with high uptake of HPV vaccination." "This observation further supports the benefit of HPV vaccination in reducing not only the incidence of but also the mortality from a cancer that is globally still the second most common cause of cancer death in women younger than 65 years," they added. SOURCE: The study was led by Peter Sasieni, PhD, Centre for Cancer Screening, Prevention and Early Diagnosis, Wolfson Institute of Population Health, Queen Mary University of London, London, England. It was published online on June 17, 2026, in The Lancet.
LIMITATIONS:
The analysis relied on population-level vaccination coverage data instead of individual-level status; the researchers had access to mortality data in 5-year age groups only rather than single-year cohorts, and the study assumed no herd protection among unvaccinated women within birth cohorts.
DISCLOSURES:
The study was funded by the Cancer Research UK. One author reported serving as a lead investigator of a trial examining the HPV vaccine Gardasil 9 that was partially supported by a research grant from the Investigator-Initiated Studies Program of Merck Sharp & Dohme. Additional disclosures are listed in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Human Papillomavirus Vaccination Linked to Substantial Reduction in Cervical Cancer Deaths, Data Reveal
Human Papillomavirus Vaccination Linked to Substantial Reduction in Cervical Cancer Deaths, Data Reveal
Why Does the Heart Rarely Develop Cancer?
Why Does the Heart Rarely Develop Cancer?
The heart is one of the organs least likely to develop cancer, a long-standing biologic puzzle that may now have an explanation. A study published in Science found that the mechanical load generated by the beating heart suppresses tumor cell proliferation through a molecular pathway that alters gene expression, raising the possibility of new therapeutic targets.
Mechanical Protection
Tumors that originate directly in the myocardium are exceptionally rare, occurring in < 1% of autopsies. Even cardiac metastases, which have been reported in up to 18% of autopsies, are often small, asymptomatic, and incidentally discovered. Although this phenomenon has long been recognized, its biologic basis remains unclear.
The heart is notable for its limited capacity for regeneration. After birth, cardiomyocytes stop dividing and subsequently renew at a rate of about 1% per year. However, when the mechanical load is reduced, such as in patients supported by left ventricular assist devices, cardiomyocytes once again show signs of proliferation.
This observation prompted researchers to investigate whether the same mechanical load that restrains normal cardiac cells might also suppress cancer growth.
More Load, Less Growth
To investigate this question, researchers introduced two genetic alterations commonly found in human cancers, activation of the KRAS oncogene and loss of the TP53, into the liver, skeletal muscle, and hearts of mice. Tumors developed in multiple organs, but not in the heart.
The researchers then used a heterotopic heart transplant model in which a donor mouse’s heart is surgically connected to the neck (cervical) or abdominal vessels of a recipient mouse. The transplanted heart remained perfused but lost its normal mechanical loading (constant beating).
When researchers injected lung adenocarcinoma cells into 2 different hearts of the same animal, they observed entirely different outcomes. The cancer cells did not grow in the native mechanically loaded heart. However, the same cells grew rapidly and extensively in the mechanically unloaded transplanted heart.
Tumor cells had replaced nearly all normal tissue in the unloaded heart, whereas they occupied only approximately 20% of the ventricle in the native heart in 14 days. This difference could not be explained by differences in the initial tumor engraftment or cell death. Instead, the findings pointed to substantial differences in tumor cell proliferation.
Similar results were observed in bioengineered cardiac tissues exposed to varying degrees of mechanical stress. Tumor cells proliferated under conditions of low mechanical load but ceased proliferating as the mechanical load increased. Tumor growth was lowest in regions exposed to the greatest mechanical stimulation of cardiomyocytes in vitro.
However, the possibility of metabolic competition between cardiac and tumor cells for nutrition was ruled out.
From Mechanics to Genes
Next, we examined the influence of mechanical forces on tumor cell behavior.
Gene expression analyses of both human cardiac metastases and mouse tumor cells showed that mechanical stimulation altered chromatin accessibility through the activation of genes involved in chromatin remodeling. These changes promoted the expression of genes that suppress cell division.
The study also identified Nesprin-2, a part of the linker of the nucleoskeleton and cytoskeleton complex, which acts as a physical bridge. It is a multitasking protein that connects the cell’s outer structural network (cytoskeleton) to its inner genetic storage (nucleus) and appears to play a significant role in converting mechanical signals into changes in gene expression.
When Nesprin-2 was inactivated, cancer cells resumed proliferation despite exposure to a mechanical load, both in engineered tissues and animal models.
“Collectively, these results shed light on the role of mechanical forces in protecting the heart from cancer and may pave the way to cancer therapies based on mechanical stimulation,” concluded the authors.
An Actively Protected Organ
Speaking with Univadis Italy, part of the Medscape Professional Network, Giorgio Scita, PhD, director of the Mechanisms of Tumor Cell Migration research unit at AIRC Institute of Molecular Oncology and professor of general pathology at the University of Milan in Milan, Italy, said, “The study addressed a simple but fundamental question: Why is the heart largely resistant to cancer despite being highly vascularized and continuously exposed to circulating tumor cells?
These findings suggest that the heartbeat itself creates a mechanical environment that is hostile to tumor growth. The compressive forces generated by rhythmic myocardial contraction are sensed by cancer cells and translated into biochemical signals that limit their proliferation.
In this view, the heart is not simply an organ that is unfavorable for cancer growth but a tissue actively protected by its own mechanical forces.”
Speaking with Univadis Italy, Serena Zacchigna, PhD, study coauthor and head of the Cardiovascular Biology Laboratory at the International Centre for Genetic Engineering and Biotechnology, Trieste, Italy, said, “Until now, however, attention had focused primarily on signals from the extracellular matrix, such as tissue stiffness. Our study adds a new element: even forces generated directly by the movement of an organ — in this case, cardiac contraction — can influence the growth of cancer cells.”
Beyond the Heart
Scita said the findings have implications that extend well beyond the heart.
“The most significant aspect is that this work identifies tissue mechanics as an active regulator of tumor behavior,” he said. Stiffness, compression, tension, and confinement are not merely consequences of tumor growth, but factors capable of influencing proliferation, invasion, and dormancy.
The concept may apply to many solid tumors. Scita noted that cancer cells growing in confined environments, such as ductal carcinoma in situ of the breast, are exposed to substantial mechanical constraints. Understanding why some tumor cells remain susceptible to these forces whereas others evade them and become invasive remains a major unanswered question in cancer biology.
Research on these mechanisms is expanding internationally and in Italy as well. One example is the AIRC “5 per mille” (5 per thousand) research programs on metastatic disease, which includes projects designed to clarify how the mechanical properties of tumor tissue influence cancer initiation, metastatic spread, and disease progression.
Therapeutic Potential
According to Zacchigna, these findings open 2 principal avenues for future research.
“The first focuses on mechanical stimulation itself. In collaboration with engineers at the University of Siena, including a group led by Domenico Prattichizzo, researchers are developing wearable robotic devices designed to mimic the heartbeat and deliver mechanical stimulation to superficial solid tumors such as certain skin cancers.
The second approach is pharmacology. Researchers are investigating whether epigenetic therapies capable of modifying chromatin remodeling can reproduce the effects of cardiac contraction and suppress tumor cell proliferation.
However, Zacchigna cautioned that this work remains at an early experimental phase.”
However, before therapeutic applications can be pursued, important mechanistic questions remain unanswered.
Zacchigna noted that although the linker of nucleoskeleton and cytoskeleton (LINC) complex and Nesprin-2 are involved in signal transduction leading to chromatin reorganization and activation of cell cycle inhibitory loci, the molecular intermediates involved have yet to be fully defined.
Researchers also need to determine which genes are most critical, whether the mechanism operates across different tumor types, and whether it can be safely manipulated for therapeutic purposes.
In an accompanying commentary published in Science, Wyatt G. Paltzer, PhD, and James F. Martin, MD, from the Department of Integrative Physiology at the Baylor College of Medicine in Houston, noted that the findings suggest enhancing LINC complex activity could potentially suppress tumor growth.
However, because the complex has broad biologic functions, it may prove difficult to target therapeutically. The authors suggested that future studies should focus on identifying proteins that interact with Nesprin-2 or other components of the LINC complex and play a more specific role in inhibiting cancer cell proliferation.
Looking Ahead
Despite these challenges, Scita said that the study’s conceptual significance is already clear.
“Even if therapeutic applications remain years away, the findings suggest that cancer may one day be targeted by altering how tumor cells perceive and interpret physical forces.”
Scita and Zacchigna reported having no relevant conflicts of interest.
This story was translated from Univadis Italy.
A version of this article first appeared on Medscape.com.
The heart is one of the organs least likely to develop cancer, a long-standing biologic puzzle that may now have an explanation. A study published in Science found that the mechanical load generated by the beating heart suppresses tumor cell proliferation through a molecular pathway that alters gene expression, raising the possibility of new therapeutic targets.
Mechanical Protection
Tumors that originate directly in the myocardium are exceptionally rare, occurring in < 1% of autopsies. Even cardiac metastases, which have been reported in up to 18% of autopsies, are often small, asymptomatic, and incidentally discovered. Although this phenomenon has long been recognized, its biologic basis remains unclear.
The heart is notable for its limited capacity for regeneration. After birth, cardiomyocytes stop dividing and subsequently renew at a rate of about 1% per year. However, when the mechanical load is reduced, such as in patients supported by left ventricular assist devices, cardiomyocytes once again show signs of proliferation.
This observation prompted researchers to investigate whether the same mechanical load that restrains normal cardiac cells might also suppress cancer growth.
More Load, Less Growth
To investigate this question, researchers introduced two genetic alterations commonly found in human cancers, activation of the KRAS oncogene and loss of the TP53, into the liver, skeletal muscle, and hearts of mice. Tumors developed in multiple organs, but not in the heart.
The researchers then used a heterotopic heart transplant model in which a donor mouse’s heart is surgically connected to the neck (cervical) or abdominal vessels of a recipient mouse. The transplanted heart remained perfused but lost its normal mechanical loading (constant beating).
When researchers injected lung adenocarcinoma cells into 2 different hearts of the same animal, they observed entirely different outcomes. The cancer cells did not grow in the native mechanically loaded heart. However, the same cells grew rapidly and extensively in the mechanically unloaded transplanted heart.
Tumor cells had replaced nearly all normal tissue in the unloaded heart, whereas they occupied only approximately 20% of the ventricle in the native heart in 14 days. This difference could not be explained by differences in the initial tumor engraftment or cell death. Instead, the findings pointed to substantial differences in tumor cell proliferation.
Similar results were observed in bioengineered cardiac tissues exposed to varying degrees of mechanical stress. Tumor cells proliferated under conditions of low mechanical load but ceased proliferating as the mechanical load increased. Tumor growth was lowest in regions exposed to the greatest mechanical stimulation of cardiomyocytes in vitro.
However, the possibility of metabolic competition between cardiac and tumor cells for nutrition was ruled out.
From Mechanics to Genes
Next, we examined the influence of mechanical forces on tumor cell behavior.
Gene expression analyses of both human cardiac metastases and mouse tumor cells showed that mechanical stimulation altered chromatin accessibility through the activation of genes involved in chromatin remodeling. These changes promoted the expression of genes that suppress cell division.
The study also identified Nesprin-2, a part of the linker of the nucleoskeleton and cytoskeleton complex, which acts as a physical bridge. It is a multitasking protein that connects the cell’s outer structural network (cytoskeleton) to its inner genetic storage (nucleus) and appears to play a significant role in converting mechanical signals into changes in gene expression.
When Nesprin-2 was inactivated, cancer cells resumed proliferation despite exposure to a mechanical load, both in engineered tissues and animal models.
“Collectively, these results shed light on the role of mechanical forces in protecting the heart from cancer and may pave the way to cancer therapies based on mechanical stimulation,” concluded the authors.
An Actively Protected Organ
Speaking with Univadis Italy, part of the Medscape Professional Network, Giorgio Scita, PhD, director of the Mechanisms of Tumor Cell Migration research unit at AIRC Institute of Molecular Oncology and professor of general pathology at the University of Milan in Milan, Italy, said, “The study addressed a simple but fundamental question: Why is the heart largely resistant to cancer despite being highly vascularized and continuously exposed to circulating tumor cells?
These findings suggest that the heartbeat itself creates a mechanical environment that is hostile to tumor growth. The compressive forces generated by rhythmic myocardial contraction are sensed by cancer cells and translated into biochemical signals that limit their proliferation.
In this view, the heart is not simply an organ that is unfavorable for cancer growth but a tissue actively protected by its own mechanical forces.”
Speaking with Univadis Italy, Serena Zacchigna, PhD, study coauthor and head of the Cardiovascular Biology Laboratory at the International Centre for Genetic Engineering and Biotechnology, Trieste, Italy, said, “Until now, however, attention had focused primarily on signals from the extracellular matrix, such as tissue stiffness. Our study adds a new element: even forces generated directly by the movement of an organ — in this case, cardiac contraction — can influence the growth of cancer cells.”
Beyond the Heart
Scita said the findings have implications that extend well beyond the heart.
“The most significant aspect is that this work identifies tissue mechanics as an active regulator of tumor behavior,” he said. Stiffness, compression, tension, and confinement are not merely consequences of tumor growth, but factors capable of influencing proliferation, invasion, and dormancy.
The concept may apply to many solid tumors. Scita noted that cancer cells growing in confined environments, such as ductal carcinoma in situ of the breast, are exposed to substantial mechanical constraints. Understanding why some tumor cells remain susceptible to these forces whereas others evade them and become invasive remains a major unanswered question in cancer biology.
Research on these mechanisms is expanding internationally and in Italy as well. One example is the AIRC “5 per mille” (5 per thousand) research programs on metastatic disease, which includes projects designed to clarify how the mechanical properties of tumor tissue influence cancer initiation, metastatic spread, and disease progression.
Therapeutic Potential
According to Zacchigna, these findings open 2 principal avenues for future research.
“The first focuses on mechanical stimulation itself. In collaboration with engineers at the University of Siena, including a group led by Domenico Prattichizzo, researchers are developing wearable robotic devices designed to mimic the heartbeat and deliver mechanical stimulation to superficial solid tumors such as certain skin cancers.
The second approach is pharmacology. Researchers are investigating whether epigenetic therapies capable of modifying chromatin remodeling can reproduce the effects of cardiac contraction and suppress tumor cell proliferation.
However, Zacchigna cautioned that this work remains at an early experimental phase.”
However, before therapeutic applications can be pursued, important mechanistic questions remain unanswered.
Zacchigna noted that although the linker of nucleoskeleton and cytoskeleton (LINC) complex and Nesprin-2 are involved in signal transduction leading to chromatin reorganization and activation of cell cycle inhibitory loci, the molecular intermediates involved have yet to be fully defined.
Researchers also need to determine which genes are most critical, whether the mechanism operates across different tumor types, and whether it can be safely manipulated for therapeutic purposes.
In an accompanying commentary published in Science, Wyatt G. Paltzer, PhD, and James F. Martin, MD, from the Department of Integrative Physiology at the Baylor College of Medicine in Houston, noted that the findings suggest enhancing LINC complex activity could potentially suppress tumor growth.
However, because the complex has broad biologic functions, it may prove difficult to target therapeutically. The authors suggested that future studies should focus on identifying proteins that interact with Nesprin-2 or other components of the LINC complex and play a more specific role in inhibiting cancer cell proliferation.
Looking Ahead
Despite these challenges, Scita said that the study’s conceptual significance is already clear.
“Even if therapeutic applications remain years away, the findings suggest that cancer may one day be targeted by altering how tumor cells perceive and interpret physical forces.”
Scita and Zacchigna reported having no relevant conflicts of interest.
This story was translated from Univadis Italy.
A version of this article first appeared on Medscape.com.
The heart is one of the organs least likely to develop cancer, a long-standing biologic puzzle that may now have an explanation. A study published in Science found that the mechanical load generated by the beating heart suppresses tumor cell proliferation through a molecular pathway that alters gene expression, raising the possibility of new therapeutic targets.
Mechanical Protection
Tumors that originate directly in the myocardium are exceptionally rare, occurring in < 1% of autopsies. Even cardiac metastases, which have been reported in up to 18% of autopsies, are often small, asymptomatic, and incidentally discovered. Although this phenomenon has long been recognized, its biologic basis remains unclear.
The heart is notable for its limited capacity for regeneration. After birth, cardiomyocytes stop dividing and subsequently renew at a rate of about 1% per year. However, when the mechanical load is reduced, such as in patients supported by left ventricular assist devices, cardiomyocytes once again show signs of proliferation.
This observation prompted researchers to investigate whether the same mechanical load that restrains normal cardiac cells might also suppress cancer growth.
More Load, Less Growth
To investigate this question, researchers introduced two genetic alterations commonly found in human cancers, activation of the KRAS oncogene and loss of the TP53, into the liver, skeletal muscle, and hearts of mice. Tumors developed in multiple organs, but not in the heart.
The researchers then used a heterotopic heart transplant model in which a donor mouse’s heart is surgically connected to the neck (cervical) or abdominal vessels of a recipient mouse. The transplanted heart remained perfused but lost its normal mechanical loading (constant beating).
When researchers injected lung adenocarcinoma cells into 2 different hearts of the same animal, they observed entirely different outcomes. The cancer cells did not grow in the native mechanically loaded heart. However, the same cells grew rapidly and extensively in the mechanically unloaded transplanted heart.
Tumor cells had replaced nearly all normal tissue in the unloaded heart, whereas they occupied only approximately 20% of the ventricle in the native heart in 14 days. This difference could not be explained by differences in the initial tumor engraftment or cell death. Instead, the findings pointed to substantial differences in tumor cell proliferation.
Similar results were observed in bioengineered cardiac tissues exposed to varying degrees of mechanical stress. Tumor cells proliferated under conditions of low mechanical load but ceased proliferating as the mechanical load increased. Tumor growth was lowest in regions exposed to the greatest mechanical stimulation of cardiomyocytes in vitro.
However, the possibility of metabolic competition between cardiac and tumor cells for nutrition was ruled out.
From Mechanics to Genes
Next, we examined the influence of mechanical forces on tumor cell behavior.
Gene expression analyses of both human cardiac metastases and mouse tumor cells showed that mechanical stimulation altered chromatin accessibility through the activation of genes involved in chromatin remodeling. These changes promoted the expression of genes that suppress cell division.
The study also identified Nesprin-2, a part of the linker of the nucleoskeleton and cytoskeleton complex, which acts as a physical bridge. It is a multitasking protein that connects the cell’s outer structural network (cytoskeleton) to its inner genetic storage (nucleus) and appears to play a significant role in converting mechanical signals into changes in gene expression.
When Nesprin-2 was inactivated, cancer cells resumed proliferation despite exposure to a mechanical load, both in engineered tissues and animal models.
“Collectively, these results shed light on the role of mechanical forces in protecting the heart from cancer and may pave the way to cancer therapies based on mechanical stimulation,” concluded the authors.
An Actively Protected Organ
Speaking with Univadis Italy, part of the Medscape Professional Network, Giorgio Scita, PhD, director of the Mechanisms of Tumor Cell Migration research unit at AIRC Institute of Molecular Oncology and professor of general pathology at the University of Milan in Milan, Italy, said, “The study addressed a simple but fundamental question: Why is the heart largely resistant to cancer despite being highly vascularized and continuously exposed to circulating tumor cells?
These findings suggest that the heartbeat itself creates a mechanical environment that is hostile to tumor growth. The compressive forces generated by rhythmic myocardial contraction are sensed by cancer cells and translated into biochemical signals that limit their proliferation.
In this view, the heart is not simply an organ that is unfavorable for cancer growth but a tissue actively protected by its own mechanical forces.”
Speaking with Univadis Italy, Serena Zacchigna, PhD, study coauthor and head of the Cardiovascular Biology Laboratory at the International Centre for Genetic Engineering and Biotechnology, Trieste, Italy, said, “Until now, however, attention had focused primarily on signals from the extracellular matrix, such as tissue stiffness. Our study adds a new element: even forces generated directly by the movement of an organ — in this case, cardiac contraction — can influence the growth of cancer cells.”
Beyond the Heart
Scita said the findings have implications that extend well beyond the heart.
“The most significant aspect is that this work identifies tissue mechanics as an active regulator of tumor behavior,” he said. Stiffness, compression, tension, and confinement are not merely consequences of tumor growth, but factors capable of influencing proliferation, invasion, and dormancy.
The concept may apply to many solid tumors. Scita noted that cancer cells growing in confined environments, such as ductal carcinoma in situ of the breast, are exposed to substantial mechanical constraints. Understanding why some tumor cells remain susceptible to these forces whereas others evade them and become invasive remains a major unanswered question in cancer biology.
Research on these mechanisms is expanding internationally and in Italy as well. One example is the AIRC “5 per mille” (5 per thousand) research programs on metastatic disease, which includes projects designed to clarify how the mechanical properties of tumor tissue influence cancer initiation, metastatic spread, and disease progression.
Therapeutic Potential
According to Zacchigna, these findings open 2 principal avenues for future research.
“The first focuses on mechanical stimulation itself. In collaboration with engineers at the University of Siena, including a group led by Domenico Prattichizzo, researchers are developing wearable robotic devices designed to mimic the heartbeat and deliver mechanical stimulation to superficial solid tumors such as certain skin cancers.
The second approach is pharmacology. Researchers are investigating whether epigenetic therapies capable of modifying chromatin remodeling can reproduce the effects of cardiac contraction and suppress tumor cell proliferation.
However, Zacchigna cautioned that this work remains at an early experimental phase.”
However, before therapeutic applications can be pursued, important mechanistic questions remain unanswered.
Zacchigna noted that although the linker of nucleoskeleton and cytoskeleton (LINC) complex and Nesprin-2 are involved in signal transduction leading to chromatin reorganization and activation of cell cycle inhibitory loci, the molecular intermediates involved have yet to be fully defined.
Researchers also need to determine which genes are most critical, whether the mechanism operates across different tumor types, and whether it can be safely manipulated for therapeutic purposes.
In an accompanying commentary published in Science, Wyatt G. Paltzer, PhD, and James F. Martin, MD, from the Department of Integrative Physiology at the Baylor College of Medicine in Houston, noted that the findings suggest enhancing LINC complex activity could potentially suppress tumor growth.
However, because the complex has broad biologic functions, it may prove difficult to target therapeutically. The authors suggested that future studies should focus on identifying proteins that interact with Nesprin-2 or other components of the LINC complex and play a more specific role in inhibiting cancer cell proliferation.
Looking Ahead
Despite these challenges, Scita said that the study’s conceptual significance is already clear.
“Even if therapeutic applications remain years away, the findings suggest that cancer may one day be targeted by altering how tumor cells perceive and interpret physical forces.”
Scita and Zacchigna reported having no relevant conflicts of interest.
This story was translated from Univadis Italy.
A version of this article first appeared on Medscape.com.
Why Does the Heart Rarely Develop Cancer?
Why Does the Heart Rarely Develop Cancer?
Simpler Screening Criteria Could Catch More Lung Cancers
Simpler Screening Criteria Could Catch More Lung Cancers
Offering lung cancer screening to everyone with a 20-year smoking history could expand access to screening, identify more cancers, and reduce disparities, new research suggests.
In an analysis of nearly 1 million US veterans, researchers estimated that a simplified approach to lung cancer screening — based on smoking duration rather than pack-years — would expand screening eligibility by nearly 30% and reduce potentially missed lung cancers by over 70%.
Those shifts would be especially pronounced among women and Black individuals — 2 groups that are underserved by current screening criteria.
The results, presented at the American Society of Clinical Oncology (ASCO) 2026, come at a time when some groups are revisiting their lung cancer screening guidelines.
And they support smoking duration as a “simpler, more sensitive, and more equitable metric for screening eligibility,” researcher Brendan T. Heiden, MD, MPHS, Washington University School of Medicine in St. Louis, St. Louis, told meeting attendees.
Toward a Better Metric
Current guidelines from the US Preventive Services Task Force (USPSTF) recommend annual lung cancer screening with low-dose CT for adults aged 50-80 years who have at least a 20 pack-year smoking history and either currently smoke or quit within the past 15 years.
The 20 pack-year metric is equivalent to smoking a pack of cigarettes per day for 20 years. Because it requires patients to remember their smoking intensity over decades, it can be challenging to calculate and translate into care, Heiden said.
As it stands, few Americans who are eligible under current USPSTF guidelines actually undergo lung cancer screening, at about 15%-20%, Heiden noted. Meanwhile, mounting evidence suggests that many lung cancers occur in individuals who never meet those eligibility criteria.
Boosting screening uptake, Heiden said, is not enough: There’s a need to revisit eligibility itself to reach more high-risk individuals.
Some groups are already taking steps in that direction. Recently updated guidelines from the National Comprehensive Cancer Network (NCCN) added a category 2B recommendation supporting screening for individuals with at least a 20-year smoking history, regardless of pack-years. (The guidelines also say former smokers are eligible no matter how long ago they quit.)
For their study, Heiden’s team sought to estimate the performance of that smoking-duration metric against current USPSTF pack-year criteria. They used Veterans Health Administration data on over 980,000 veterans whose smoking histories were prospectively collected; lung cancer diagnoses were identified through the Veterans Affairs Central Cancer Registry.
Most of the included veterans (67%) had a smoking history; their mean age was 64 years, and 21% were Black.
Overall, the researchers found that basing eligibility on 20-year smoking duration would substantially expand access to screening: Among veterans with a smoking history, 68% qualified for screening under current USPSTF criteria compared with 87% using the smoking-duration approach.
The gains were especially pronounced among women and Black individuals (who, based on prior research, typically smoke less intensely than White males). Under USPSTF criteria, only about 55% of female and Black veterans qualified for screening compared with 83% for both groups under the smoking-duration criterion.
Importantly, Heiden said, people meeting the smoking-duration threshold remained at substantially elevated risk for lung cancer, suggesting the broader screening criteria were not merely capturing low-risk smokers.
The 5-year lung cancer incidence among veterans eligible under the smoking-duration approach was 1.59% — 11 times the rate of 0.14% among never smokers.
Perhaps most striking, Heiden said, the proportion of potentially missed cancers dropped from 13% with the pack-year metric to just 4% using the smoking-duration metric — a relative reduction of more than 70%.
Again, women and Black individuals would see the largest gains: Among Black veterans, potentially missed cancers fell from 25% to 6%, whereas among female veterans they declined from 22% to 7%.
Optimal Approach Still Unclear
The analysis had limitations, including a predominantly male veteran population whose smoking exposure was far greater than that of the general US population, indicating high inherent lung cancer risk.
But the results support what the NCCN has already done, according to Mary Reid, PhD, MSPH, BSN, a member of the group’s lung cancer screening guideline panel and chief of cancer screening, survivorship and mentorship at Roswell Park Comprehensive Cancer Center in Buffalo, New York.
“Doing the calculation for pack-years can be difficult,” Reid told Medscape Medical News. “Smoking duration is easier to calculate and really the way to go.”
The USPSTF does not comment on individual studies outside of its recommendation development process.
At the meeting, study discussant Katharine A. Rendle, PhD, called the work “impressive,” citing the size of the cohort and strength of the data.
It’s particularly noteworthy that the simpler screening criteria improved sensitivity for all veterans, while largely eliminating disparities, according to Rendle, of the Abramson Cancer Center at the University of Pennsylvania in Philadelphia.
Still, she said, further research could better define the optimal screening strategy.
“Smoking duration is a promising approach, but in my opinion, guidelines likely need to account for the underlying risk in the population,” Rendle said, noting that current smoking prevalence in the US population is about 10%.
She suggested future studies consider other smoking-duration thresholds, such as 30 or 40 years, and look at other outcomes, including life-years gained.
“It’s critical that we prioritize strategies that maximize potential benefit from screening — not just identify those at lung cancer risk — given downstream costs and burden on populations and health care systems,” Rendle said.
The study had no commercial funding. Heiden, Rendle, and Reid had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Offering lung cancer screening to everyone with a 20-year smoking history could expand access to screening, identify more cancers, and reduce disparities, new research suggests.
In an analysis of nearly 1 million US veterans, researchers estimated that a simplified approach to lung cancer screening — based on smoking duration rather than pack-years — would expand screening eligibility by nearly 30% and reduce potentially missed lung cancers by over 70%.
Those shifts would be especially pronounced among women and Black individuals — 2 groups that are underserved by current screening criteria.
The results, presented at the American Society of Clinical Oncology (ASCO) 2026, come at a time when some groups are revisiting their lung cancer screening guidelines.
And they support smoking duration as a “simpler, more sensitive, and more equitable metric for screening eligibility,” researcher Brendan T. Heiden, MD, MPHS, Washington University School of Medicine in St. Louis, St. Louis, told meeting attendees.
Toward a Better Metric
Current guidelines from the US Preventive Services Task Force (USPSTF) recommend annual lung cancer screening with low-dose CT for adults aged 50-80 years who have at least a 20 pack-year smoking history and either currently smoke or quit within the past 15 years.
The 20 pack-year metric is equivalent to smoking a pack of cigarettes per day for 20 years. Because it requires patients to remember their smoking intensity over decades, it can be challenging to calculate and translate into care, Heiden said.
As it stands, few Americans who are eligible under current USPSTF guidelines actually undergo lung cancer screening, at about 15%-20%, Heiden noted. Meanwhile, mounting evidence suggests that many lung cancers occur in individuals who never meet those eligibility criteria.
Boosting screening uptake, Heiden said, is not enough: There’s a need to revisit eligibility itself to reach more high-risk individuals.
Some groups are already taking steps in that direction. Recently updated guidelines from the National Comprehensive Cancer Network (NCCN) added a category 2B recommendation supporting screening for individuals with at least a 20-year smoking history, regardless of pack-years. (The guidelines also say former smokers are eligible no matter how long ago they quit.)
For their study, Heiden’s team sought to estimate the performance of that smoking-duration metric against current USPSTF pack-year criteria. They used Veterans Health Administration data on over 980,000 veterans whose smoking histories were prospectively collected; lung cancer diagnoses were identified through the Veterans Affairs Central Cancer Registry.
Most of the included veterans (67%) had a smoking history; their mean age was 64 years, and 21% were Black.
Overall, the researchers found that basing eligibility on 20-year smoking duration would substantially expand access to screening: Among veterans with a smoking history, 68% qualified for screening under current USPSTF criteria compared with 87% using the smoking-duration approach.
The gains were especially pronounced among women and Black individuals (who, based on prior research, typically smoke less intensely than White males). Under USPSTF criteria, only about 55% of female and Black veterans qualified for screening compared with 83% for both groups under the smoking-duration criterion.
Importantly, Heiden said, people meeting the smoking-duration threshold remained at substantially elevated risk for lung cancer, suggesting the broader screening criteria were not merely capturing low-risk smokers.
The 5-year lung cancer incidence among veterans eligible under the smoking-duration approach was 1.59% — 11 times the rate of 0.14% among never smokers.
Perhaps most striking, Heiden said, the proportion of potentially missed cancers dropped from 13% with the pack-year metric to just 4% using the smoking-duration metric — a relative reduction of more than 70%.
Again, women and Black individuals would see the largest gains: Among Black veterans, potentially missed cancers fell from 25% to 6%, whereas among female veterans they declined from 22% to 7%.
Optimal Approach Still Unclear
The analysis had limitations, including a predominantly male veteran population whose smoking exposure was far greater than that of the general US population, indicating high inherent lung cancer risk.
But the results support what the NCCN has already done, according to Mary Reid, PhD, MSPH, BSN, a member of the group’s lung cancer screening guideline panel and chief of cancer screening, survivorship and mentorship at Roswell Park Comprehensive Cancer Center in Buffalo, New York.
“Doing the calculation for pack-years can be difficult,” Reid told Medscape Medical News. “Smoking duration is easier to calculate and really the way to go.”
The USPSTF does not comment on individual studies outside of its recommendation development process.
At the meeting, study discussant Katharine A. Rendle, PhD, called the work “impressive,” citing the size of the cohort and strength of the data.
It’s particularly noteworthy that the simpler screening criteria improved sensitivity for all veterans, while largely eliminating disparities, according to Rendle, of the Abramson Cancer Center at the University of Pennsylvania in Philadelphia.
Still, she said, further research could better define the optimal screening strategy.
“Smoking duration is a promising approach, but in my opinion, guidelines likely need to account for the underlying risk in the population,” Rendle said, noting that current smoking prevalence in the US population is about 10%.
She suggested future studies consider other smoking-duration thresholds, such as 30 or 40 years, and look at other outcomes, including life-years gained.
“It’s critical that we prioritize strategies that maximize potential benefit from screening — not just identify those at lung cancer risk — given downstream costs and burden on populations and health care systems,” Rendle said.
The study had no commercial funding. Heiden, Rendle, and Reid had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Offering lung cancer screening to everyone with a 20-year smoking history could expand access to screening, identify more cancers, and reduce disparities, new research suggests.
In an analysis of nearly 1 million US veterans, researchers estimated that a simplified approach to lung cancer screening — based on smoking duration rather than pack-years — would expand screening eligibility by nearly 30% and reduce potentially missed lung cancers by over 70%.
Those shifts would be especially pronounced among women and Black individuals — 2 groups that are underserved by current screening criteria.
The results, presented at the American Society of Clinical Oncology (ASCO) 2026, come at a time when some groups are revisiting their lung cancer screening guidelines.
And they support smoking duration as a “simpler, more sensitive, and more equitable metric for screening eligibility,” researcher Brendan T. Heiden, MD, MPHS, Washington University School of Medicine in St. Louis, St. Louis, told meeting attendees.
Toward a Better Metric
Current guidelines from the US Preventive Services Task Force (USPSTF) recommend annual lung cancer screening with low-dose CT for adults aged 50-80 years who have at least a 20 pack-year smoking history and either currently smoke or quit within the past 15 years.
The 20 pack-year metric is equivalent to smoking a pack of cigarettes per day for 20 years. Because it requires patients to remember their smoking intensity over decades, it can be challenging to calculate and translate into care, Heiden said.
As it stands, few Americans who are eligible under current USPSTF guidelines actually undergo lung cancer screening, at about 15%-20%, Heiden noted. Meanwhile, mounting evidence suggests that many lung cancers occur in individuals who never meet those eligibility criteria.
Boosting screening uptake, Heiden said, is not enough: There’s a need to revisit eligibility itself to reach more high-risk individuals.
Some groups are already taking steps in that direction. Recently updated guidelines from the National Comprehensive Cancer Network (NCCN) added a category 2B recommendation supporting screening for individuals with at least a 20-year smoking history, regardless of pack-years. (The guidelines also say former smokers are eligible no matter how long ago they quit.)
For their study, Heiden’s team sought to estimate the performance of that smoking-duration metric against current USPSTF pack-year criteria. They used Veterans Health Administration data on over 980,000 veterans whose smoking histories were prospectively collected; lung cancer diagnoses were identified through the Veterans Affairs Central Cancer Registry.
Most of the included veterans (67%) had a smoking history; their mean age was 64 years, and 21% were Black.
Overall, the researchers found that basing eligibility on 20-year smoking duration would substantially expand access to screening: Among veterans with a smoking history, 68% qualified for screening under current USPSTF criteria compared with 87% using the smoking-duration approach.
The gains were especially pronounced among women and Black individuals (who, based on prior research, typically smoke less intensely than White males). Under USPSTF criteria, only about 55% of female and Black veterans qualified for screening compared with 83% for both groups under the smoking-duration criterion.
Importantly, Heiden said, people meeting the smoking-duration threshold remained at substantially elevated risk for lung cancer, suggesting the broader screening criteria were not merely capturing low-risk smokers.
The 5-year lung cancer incidence among veterans eligible under the smoking-duration approach was 1.59% — 11 times the rate of 0.14% among never smokers.
Perhaps most striking, Heiden said, the proportion of potentially missed cancers dropped from 13% with the pack-year metric to just 4% using the smoking-duration metric — a relative reduction of more than 70%.
Again, women and Black individuals would see the largest gains: Among Black veterans, potentially missed cancers fell from 25% to 6%, whereas among female veterans they declined from 22% to 7%.
Optimal Approach Still Unclear
The analysis had limitations, including a predominantly male veteran population whose smoking exposure was far greater than that of the general US population, indicating high inherent lung cancer risk.
But the results support what the NCCN has already done, according to Mary Reid, PhD, MSPH, BSN, a member of the group’s lung cancer screening guideline panel and chief of cancer screening, survivorship and mentorship at Roswell Park Comprehensive Cancer Center in Buffalo, New York.
“Doing the calculation for pack-years can be difficult,” Reid told Medscape Medical News. “Smoking duration is easier to calculate and really the way to go.”
The USPSTF does not comment on individual studies outside of its recommendation development process.
At the meeting, study discussant Katharine A. Rendle, PhD, called the work “impressive,” citing the size of the cohort and strength of the data.
It’s particularly noteworthy that the simpler screening criteria improved sensitivity for all veterans, while largely eliminating disparities, according to Rendle, of the Abramson Cancer Center at the University of Pennsylvania in Philadelphia.
Still, she said, further research could better define the optimal screening strategy.
“Smoking duration is a promising approach, but in my opinion, guidelines likely need to account for the underlying risk in the population,” Rendle said, noting that current smoking prevalence in the US population is about 10%.
She suggested future studies consider other smoking-duration thresholds, such as 30 or 40 years, and look at other outcomes, including life-years gained.
“It’s critical that we prioritize strategies that maximize potential benefit from screening — not just identify those at lung cancer risk — given downstream costs and burden on populations and health care systems,” Rendle said.
The study had no commercial funding. Heiden, Rendle, and Reid had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Simpler Screening Criteria Could Catch More Lung Cancers
Simpler Screening Criteria Could Catch More Lung Cancers
Can PAK6 Transform Small Cell Lung Cancer Diagnosis?
TOPLINE: Serum P21 Activated Kinase 6 (PAK6) demonstrated diagnostic accuracy comparable to pro-gastrin-releasing peptide (ProGRP) for small cell lung cancer (SCLC), with area under the curve (AUC) values of 0.892 and 0.935, respectively, in a study of 109 patients with SCLC. Combining PAK6, ProGRP, and neuron-specific enolase (NSE) achieved diagnostic efficiency of 0.98. Elevated baseline PAK6 levels correlated with shorter progression-free survival and increased risk for disease progression.
METHODOLOGY:
Participants included 380 people in China: 109 with SCLC, 92 with non–small cell lung cancer (NSCLC), 85 with benign pulmonary nodules, and 94 healthy controls who received routine physical examinations.
Laboratory testing measured serum PAK6 by ELISA, while NSE, carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and ProGRP were quantified by chemiluminescence.
Pretreatment and posttreatment serum samples from 56 patients with SCLC were analyzed to evaluate changes in biomarker levels following 3 months of treatment.
Progression-free survival data were collected through case review and follow-up, defined as time from treatment initiation to radiographic disease progression per RECIST 1.1 criteria or death from any cause.
TAKEAWAY:
Median serum PAK6 is reported as 56.44 ng/L in SCLC vs 41.06 ng/L in NSCLC, 37.82 ng/L in pulmonary nodules, and 34.75 ng/L in healthy controls (P < .01).
PAK6 demonstrated diagnostic efficacy with and AUC of 0.892 (95% CI, 0.857-0.927), sensitivity of 0.82, and specificity of 0.86 at optimal cut-off value of 47.30 ng/L, comparable to ProGRP (AUC, 0.935) and superior to CEA (AUC, 0.676) and CA19-9 (AUC, 0.611).
In 56 paired SCLC samples, PAK6, NSE, and ProGRP decrease after 3 months of treatment (P < .001), while CEA and CA19-9 display no meaningful change.
Elevated baseline PAK6 expression correlated with shorter progression-free survival, with high-expression patients demonstrating median survival of 92 days vs 194 days in low-expression patients (HR, 2.02; 95% CI, 1.33-3.07; P = .001).
IN PRACTICE: “We identify PAK6 as a multi-faceted biomarker for SCLC with diagnostic, prognostic, and therapeutic monitoring value. Its cost-effective ELISA quantification facilitates clinical translation,” wrote the authors of the study. “Integrating PAK6 with emerging technologies could further refine SCLC management paradigms.”
SOURCE:The study was led by Simei Chen, Department of Blood Transfusion, the Second Affiliated Hospital, Jiangxi Medical College, Nanchang University in Nanchang, China. It was published online in PeerJ.
LIMITATIONS: A single-center design and modest sample size may limit generalizability of the diagnostic and prognostic estimates. The authors also note the absence of immunohistochemical validation, leaving tissue-level correlation of PAK6 unaddressed. Finally, insufficient overall survival data were reported, which constrains interpretation beyond PFS and supports the need for prospective follow-up and larger multi-center validation.
DISCLOSURES: Grant support came from the Science and Technology Program Project of Jiangxi Provincial Administration of Traditional Chinese Medicine (Grant 2024B1433). The authors stated the funders had no role in study design, data collection and analysis, the decision to publish, or manuscript preparation. No competing interests were disclosed.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Serum P21 Activated Kinase 6 (PAK6) demonstrated diagnostic accuracy comparable to pro-gastrin-releasing peptide (ProGRP) for small cell lung cancer (SCLC), with area under the curve (AUC) values of 0.892 and 0.935, respectively, in a study of 109 patients with SCLC. Combining PAK6, ProGRP, and neuron-specific enolase (NSE) achieved diagnostic efficiency of 0.98. Elevated baseline PAK6 levels correlated with shorter progression-free survival and increased risk for disease progression.
METHODOLOGY:
Participants included 380 people in China: 109 with SCLC, 92 with non–small cell lung cancer (NSCLC), 85 with benign pulmonary nodules, and 94 healthy controls who received routine physical examinations.
Laboratory testing measured serum PAK6 by ELISA, while NSE, carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and ProGRP were quantified by chemiluminescence.
Pretreatment and posttreatment serum samples from 56 patients with SCLC were analyzed to evaluate changes in biomarker levels following 3 months of treatment.
Progression-free survival data were collected through case review and follow-up, defined as time from treatment initiation to radiographic disease progression per RECIST 1.1 criteria or death from any cause.
TAKEAWAY:
Median serum PAK6 is reported as 56.44 ng/L in SCLC vs 41.06 ng/L in NSCLC, 37.82 ng/L in pulmonary nodules, and 34.75 ng/L in healthy controls (P < .01).
PAK6 demonstrated diagnostic efficacy with and AUC of 0.892 (95% CI, 0.857-0.927), sensitivity of 0.82, and specificity of 0.86 at optimal cut-off value of 47.30 ng/L, comparable to ProGRP (AUC, 0.935) and superior to CEA (AUC, 0.676) and CA19-9 (AUC, 0.611).
In 56 paired SCLC samples, PAK6, NSE, and ProGRP decrease after 3 months of treatment (P < .001), while CEA and CA19-9 display no meaningful change.
Elevated baseline PAK6 expression correlated with shorter progression-free survival, with high-expression patients demonstrating median survival of 92 days vs 194 days in low-expression patients (HR, 2.02; 95% CI, 1.33-3.07; P = .001).
IN PRACTICE: “We identify PAK6 as a multi-faceted biomarker for SCLC with diagnostic, prognostic, and therapeutic monitoring value. Its cost-effective ELISA quantification facilitates clinical translation,” wrote the authors of the study. “Integrating PAK6 with emerging technologies could further refine SCLC management paradigms.”
SOURCE:The study was led by Simei Chen, Department of Blood Transfusion, the Second Affiliated Hospital, Jiangxi Medical College, Nanchang University in Nanchang, China. It was published online in PeerJ.
LIMITATIONS: A single-center design and modest sample size may limit generalizability of the diagnostic and prognostic estimates. The authors also note the absence of immunohistochemical validation, leaving tissue-level correlation of PAK6 unaddressed. Finally, insufficient overall survival data were reported, which constrains interpretation beyond PFS and supports the need for prospective follow-up and larger multi-center validation.
DISCLOSURES: Grant support came from the Science and Technology Program Project of Jiangxi Provincial Administration of Traditional Chinese Medicine (Grant 2024B1433). The authors stated the funders had no role in study design, data collection and analysis, the decision to publish, or manuscript preparation. No competing interests were disclosed.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Serum P21 Activated Kinase 6 (PAK6) demonstrated diagnostic accuracy comparable to pro-gastrin-releasing peptide (ProGRP) for small cell lung cancer (SCLC), with area under the curve (AUC) values of 0.892 and 0.935, respectively, in a study of 109 patients with SCLC. Combining PAK6, ProGRP, and neuron-specific enolase (NSE) achieved diagnostic efficiency of 0.98. Elevated baseline PAK6 levels correlated with shorter progression-free survival and increased risk for disease progression.
METHODOLOGY:
Participants included 380 people in China: 109 with SCLC, 92 with non–small cell lung cancer (NSCLC), 85 with benign pulmonary nodules, and 94 healthy controls who received routine physical examinations.
Laboratory testing measured serum PAK6 by ELISA, while NSE, carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and ProGRP were quantified by chemiluminescence.
Pretreatment and posttreatment serum samples from 56 patients with SCLC were analyzed to evaluate changes in biomarker levels following 3 months of treatment.
Progression-free survival data were collected through case review and follow-up, defined as time from treatment initiation to radiographic disease progression per RECIST 1.1 criteria or death from any cause.
TAKEAWAY:
Median serum PAK6 is reported as 56.44 ng/L in SCLC vs 41.06 ng/L in NSCLC, 37.82 ng/L in pulmonary nodules, and 34.75 ng/L in healthy controls (P < .01).
PAK6 demonstrated diagnostic efficacy with and AUC of 0.892 (95% CI, 0.857-0.927), sensitivity of 0.82, and specificity of 0.86 at optimal cut-off value of 47.30 ng/L, comparable to ProGRP (AUC, 0.935) and superior to CEA (AUC, 0.676) and CA19-9 (AUC, 0.611).
In 56 paired SCLC samples, PAK6, NSE, and ProGRP decrease after 3 months of treatment (P < .001), while CEA and CA19-9 display no meaningful change.
Elevated baseline PAK6 expression correlated with shorter progression-free survival, with high-expression patients demonstrating median survival of 92 days vs 194 days in low-expression patients (HR, 2.02; 95% CI, 1.33-3.07; P = .001).
IN PRACTICE: “We identify PAK6 as a multi-faceted biomarker for SCLC with diagnostic, prognostic, and therapeutic monitoring value. Its cost-effective ELISA quantification facilitates clinical translation,” wrote the authors of the study. “Integrating PAK6 with emerging technologies could further refine SCLC management paradigms.”
SOURCE:The study was led by Simei Chen, Department of Blood Transfusion, the Second Affiliated Hospital, Jiangxi Medical College, Nanchang University in Nanchang, China. It was published online in PeerJ.
LIMITATIONS: A single-center design and modest sample size may limit generalizability of the diagnostic and prognostic estimates. The authors also note the absence of immunohistochemical validation, leaving tissue-level correlation of PAK6 unaddressed. Finally, insufficient overall survival data were reported, which constrains interpretation beyond PFS and supports the need for prospective follow-up and larger multi-center validation.
DISCLOSURES: Grant support came from the Science and Technology Program Project of Jiangxi Provincial Administration of Traditional Chinese Medicine (Grant 2024B1433). The authors stated the funders had no role in study design, data collection and analysis, the decision to publish, or manuscript preparation. No competing interests were disclosed.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
This transcript has been edited for clarity.
Hello, everyone. This is Dr Bishal Gyawali, from Queens University, Kingston, Canada. Today, I’m back with you to talk about some of the fallacies that I have seen in medicine, oncology, and the drug regulatory space. I wanted to clarify some of these fallacies.
In my last video, I talked about the FDA denying the approval of a new cancer drug. Let me start with one of the fallacies that is pertinent to that, which is that some people make an argument that patients are dying from a certain condition, such as cancer, or even any other disease besides cancer. That is an absolutely true statement, but that does not necessarily mean there should be a lower bar for drug approvals or we should be approving any drug that has a hint of benefit.
In fact, if we have increased mortality rates and our patients are dying from a certain condition, that means we actually need to have good drugs. We need to have drugs that prevent mortality. We need to have drugs that improve outcomes. Just having any drug out there, if we lower our threshold and are letting any drug be used in these patients because the argument is that people are dying, then in fact, it can have negative consequences.
First, there will be opportunity costs. If you can get any lousy drug into the market and make billions of dollars out of it, then there is no strong motivation to produce drugs that actually remarkably improve outcomes.
Second, patients will also be misled. It’s the patient’s opportunity cost in that they will use whatever time they have remaining to pursue these treatments that were not going to improve their outcomes anyway. This is time they could have better spent either in pursuing better treatments, if those treatments are out there, or to prioritize their time accordingly. This rather gives them a false hope, which can be harmful in the long term.
The first fallacy is that just because people are dying does not necessarily mean we should have more new drugs with a lower bar for approval.
The second fallacy I want to talk about, which is also related to this, is that if a certain cancer is rare, the bar for new drug approval should be quite low.
Of course, rare cancers are a special category, and rare cancers should be treated differently from a regulatory perspective. Absolutely. If the cancer is rare, we cannot have trials with large sample sizes to generate evidence. That problem is there, but that does not necessarily translate to the decision that we should approve anything, even something with a small hint of benefit.
There are other methods to make sure that, even in rare cancers, we can generate good-quality evidence. In fact, from an equity perspective, why should patients with rare cancer not deserve drugs that have good-quality evidence?
We can’t tell someone that, “Your cancer is rare, so you should get drugs that only have a benefit in terms of response rate whereas other cancers that are not rare will have drugs based on survival.”
Going back to the point about the difficulty in doing big trials in patients with rare cancers, that is absolutely true and there should be regulatory flexibility in this. I think accelerated approval is a pathway that allows for this regulatory flexibility, which allows access to these drugs early on based on earlier signals of benefit. You can continue to generate evidence in the future and confirm the clinical benefit.
There are also other nuances to this. One is that we should also make sure that this regulatory flexibility with rare cancers should not be misused. What do I mean by that? First, all rare cancers are not the same. There are some cancers that are ultra rare, and then there are some cancers that technically might fit the definition of rare, but trials are possible. Case in point: adrenocortical cancer. It is considered to be a very rare cancer, but there have been randomized trials in adrenocortical cancer.
Our efforts should be to maximize our collaboration globally so that a cancer that is rare locally will still not be so rare globally when we collect all these patients.
In certain situations, like let’s say, based on the molecular subtypes, any common cancer can be sliced and diced into a rare subtype: MSI-high, BRAF-negative, HER2-positive, right-sided colon cancer. If you start to slice cancers into these smaller and smaller molecular subtypes, you can consider anything as a rare cancer. That should not be misused as an excuse to get away from doing proper trials and generating adequate evidence for our patients.
The third fallacy I want to talk about is that increasing cancer incidence in a certain subgroup of population does not automatically translate into, “We should start screening this subgroup of population.”
A certain cancer — let’s say cancer X or cancer Y — is increasing in a young population, so therefore, we should lower the age of the screening of young populations. This cancer is increasing in this ethnic population, so therefore we should start screening this ethnic population more frequently. This cancer is increasing in this type of minority, so therefore, we should start screening this minority more.
No, it does not work like that. Increasing incidence will make us concerned, of course, but that does not necessarily translate into, “We should start screening them.” In order for a screening test to be useful, it has to fulfill a number of criteria.
The goal is not to detect cancers. The goal is to detect cancers that are not indolent enough that they would have never caused problems, nor speed up the diagnosis of aggressive cancers that are going to be lethal pretty soon anyway. The goal is to detect those cancers in the middle, so that by detecting early, we can intervene and improve the outcomes and improve the mortality from that cancer.
This type of intervention requires a thoughtful consideration of the increasing incidence of the cancer, of course, but also the utility of the screening test in that subgroup of population; the life expectancy of this subgroup of patients with and without cancer; the interventions available to address that increasing burden of cancer; and whether by intervening we are going to reduce the mortality rates.
Just because we can detect cancers does not mean we should detect cancers. That’s the third fallacy I wanted to talk about.
The fourth fallacy is related to when someone is asking for more evidence for anything. There is a new drug for this cancer,so what is the evidence? Or there is this new intervention that will detect ctDNA or whatever before the cancer relapses, or before the cancer even shows up as a screening test.
Whenever there is any treatment that is being promoted and someone asks for evidence, people sometimes try to make personal attacks by saying, “Oh, so, you’re okay with patients dying. You don’t want to save lives.”
Absolutely we want to save lives. That’s why we’re in this field, and that’s why we’re asking for more evidence. You should not consider someone who is asking for evidence as evil or that this person does not want this new drug, or this person does not want this innovation. No, that person actually wants to make sure that that innovation actually helps people. That’s why that person is asking for more evidence.
If we stop asking for evidence, then our whole practice becomes based on emotions, faith, and trust rather than science. You could extrapolate it to the other extreme, like if you are not asking for evidence. If it is interpreted as someone who is asking for evidence is evil, or someone who does not want patients to get new drugs, then you could extrapolate these to people also making claims about alternative medicines or ivermectin nowadays, and claiming that this cures cancer.
Science is science. You need to be the same no matter the circumstances. If you are asking for data for ivermectin, you should also be asking data for your cancer drug that you think is going to work. We should always ask for evidence.
Asking for evidence is not a sign that whoever is asking for evidence does not want the patient to have access to the drug. It is showing that the person who is asking for evidence actually wants to make sure that the patients who get this drug are actually being helped by the drug rather than being harmed.
I’m talking about 5 fallacies today. The final, fifth fallacy is that clinical expertise does not equal expertise in making public health decisions or even expertise in critical appraisal. Someone can be a fantastic breast cancer doctor, the best oncologist for breast cancer. That does not automatically make that person the best person to evaluate clinical trials of breast cancer drugs.
Someone can be a fantastic colon cancer doctor. That does not make that person automatically the best person to evaluate whether or not colonoscopy or colon cancer screening is indicated in a certain patient population.
These population-level decisions — including should this drug be approved, should this drug be funded, and should this screening test be made a public health measure, all of these public health decisions that are done at a population level — require different expertise in critical appraisal, clinical epidemiology, and public health.
Just because someone is a fantastic clinician does not make that person a fantastic public health expert. I see on social media often that a famous doctor with expertise in their domain, let’s say a famous neurosurgeon, might say, “I think brain tumors are increasing in incidence in young persons, so we should be targeting an MRI screening for everyone over the age of 30.”
I’m just making this up, but we see examples of things not dissimilar to this. Just because someone is a neurosurgeon does not make them an expert on brain tumor epidemiology, surveillance, or screening. We should separate clinical expertise from public health expertise.
Thank you.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello, everyone. This is Dr Bishal Gyawali, from Queens University, Kingston, Canada. Today, I’m back with you to talk about some of the fallacies that I have seen in medicine, oncology, and the drug regulatory space. I wanted to clarify some of these fallacies.
In my last video, I talked about the FDA denying the approval of a new cancer drug. Let me start with one of the fallacies that is pertinent to that, which is that some people make an argument that patients are dying from a certain condition, such as cancer, or even any other disease besides cancer. That is an absolutely true statement, but that does not necessarily mean there should be a lower bar for drug approvals or we should be approving any drug that has a hint of benefit.
In fact, if we have increased mortality rates and our patients are dying from a certain condition, that means we actually need to have good drugs. We need to have drugs that prevent mortality. We need to have drugs that improve outcomes. Just having any drug out there, if we lower our threshold and are letting any drug be used in these patients because the argument is that people are dying, then in fact, it can have negative consequences.
First, there will be opportunity costs. If you can get any lousy drug into the market and make billions of dollars out of it, then there is no strong motivation to produce drugs that actually remarkably improve outcomes.
Second, patients will also be misled. It’s the patient’s opportunity cost in that they will use whatever time they have remaining to pursue these treatments that were not going to improve their outcomes anyway. This is time they could have better spent either in pursuing better treatments, if those treatments are out there, or to prioritize their time accordingly. This rather gives them a false hope, which can be harmful in the long term.
The first fallacy is that just because people are dying does not necessarily mean we should have more new drugs with a lower bar for approval.
The second fallacy I want to talk about, which is also related to this, is that if a certain cancer is rare, the bar for new drug approval should be quite low.
Of course, rare cancers are a special category, and rare cancers should be treated differently from a regulatory perspective. Absolutely. If the cancer is rare, we cannot have trials with large sample sizes to generate evidence. That problem is there, but that does not necessarily translate to the decision that we should approve anything, even something with a small hint of benefit.
There are other methods to make sure that, even in rare cancers, we can generate good-quality evidence. In fact, from an equity perspective, why should patients with rare cancer not deserve drugs that have good-quality evidence?
We can’t tell someone that, “Your cancer is rare, so you should get drugs that only have a benefit in terms of response rate whereas other cancers that are not rare will have drugs based on survival.”
Going back to the point about the difficulty in doing big trials in patients with rare cancers, that is absolutely true and there should be regulatory flexibility in this. I think accelerated approval is a pathway that allows for this regulatory flexibility, which allows access to these drugs early on based on earlier signals of benefit. You can continue to generate evidence in the future and confirm the clinical benefit.
There are also other nuances to this. One is that we should also make sure that this regulatory flexibility with rare cancers should not be misused. What do I mean by that? First, all rare cancers are not the same. There are some cancers that are ultra rare, and then there are some cancers that technically might fit the definition of rare, but trials are possible. Case in point: adrenocortical cancer. It is considered to be a very rare cancer, but there have been randomized trials in adrenocortical cancer.
Our efforts should be to maximize our collaboration globally so that a cancer that is rare locally will still not be so rare globally when we collect all these patients.
In certain situations, like let’s say, based on the molecular subtypes, any common cancer can be sliced and diced into a rare subtype: MSI-high, BRAF-negative, HER2-positive, right-sided colon cancer. If you start to slice cancers into these smaller and smaller molecular subtypes, you can consider anything as a rare cancer. That should not be misused as an excuse to get away from doing proper trials and generating adequate evidence for our patients.
The third fallacy I want to talk about is that increasing cancer incidence in a certain subgroup of population does not automatically translate into, “We should start screening this subgroup of population.”
A certain cancer — let’s say cancer X or cancer Y — is increasing in a young population, so therefore, we should lower the age of the screening of young populations. This cancer is increasing in this ethnic population, so therefore we should start screening this ethnic population more frequently. This cancer is increasing in this type of minority, so therefore, we should start screening this minority more.
No, it does not work like that. Increasing incidence will make us concerned, of course, but that does not necessarily translate into, “We should start screening them.” In order for a screening test to be useful, it has to fulfill a number of criteria.
The goal is not to detect cancers. The goal is to detect cancers that are not indolent enough that they would have never caused problems, nor speed up the diagnosis of aggressive cancers that are going to be lethal pretty soon anyway. The goal is to detect those cancers in the middle, so that by detecting early, we can intervene and improve the outcomes and improve the mortality from that cancer.
This type of intervention requires a thoughtful consideration of the increasing incidence of the cancer, of course, but also the utility of the screening test in that subgroup of population; the life expectancy of this subgroup of patients with and without cancer; the interventions available to address that increasing burden of cancer; and whether by intervening we are going to reduce the mortality rates.
Just because we can detect cancers does not mean we should detect cancers. That’s the third fallacy I wanted to talk about.
The fourth fallacy is related to when someone is asking for more evidence for anything. There is a new drug for this cancer,so what is the evidence? Or there is this new intervention that will detect ctDNA or whatever before the cancer relapses, or before the cancer even shows up as a screening test.
Whenever there is any treatment that is being promoted and someone asks for evidence, people sometimes try to make personal attacks by saying, “Oh, so, you’re okay with patients dying. You don’t want to save lives.”
Absolutely we want to save lives. That’s why we’re in this field, and that’s why we’re asking for more evidence. You should not consider someone who is asking for evidence as evil or that this person does not want this new drug, or this person does not want this innovation. No, that person actually wants to make sure that that innovation actually helps people. That’s why that person is asking for more evidence.
If we stop asking for evidence, then our whole practice becomes based on emotions, faith, and trust rather than science. You could extrapolate it to the other extreme, like if you are not asking for evidence. If it is interpreted as someone who is asking for evidence is evil, or someone who does not want patients to get new drugs, then you could extrapolate these to people also making claims about alternative medicines or ivermectin nowadays, and claiming that this cures cancer.
Science is science. You need to be the same no matter the circumstances. If you are asking for data for ivermectin, you should also be asking data for your cancer drug that you think is going to work. We should always ask for evidence.
Asking for evidence is not a sign that whoever is asking for evidence does not want the patient to have access to the drug. It is showing that the person who is asking for evidence actually wants to make sure that the patients who get this drug are actually being helped by the drug rather than being harmed.
I’m talking about 5 fallacies today. The final, fifth fallacy is that clinical expertise does not equal expertise in making public health decisions or even expertise in critical appraisal. Someone can be a fantastic breast cancer doctor, the best oncologist for breast cancer. That does not automatically make that person the best person to evaluate clinical trials of breast cancer drugs.
Someone can be a fantastic colon cancer doctor. That does not make that person automatically the best person to evaluate whether or not colonoscopy or colon cancer screening is indicated in a certain patient population.
These population-level decisions — including should this drug be approved, should this drug be funded, and should this screening test be made a public health measure, all of these public health decisions that are done at a population level — require different expertise in critical appraisal, clinical epidemiology, and public health.
Just because someone is a fantastic clinician does not make that person a fantastic public health expert. I see on social media often that a famous doctor with expertise in their domain, let’s say a famous neurosurgeon, might say, “I think brain tumors are increasing in incidence in young persons, so we should be targeting an MRI screening for everyone over the age of 30.”
I’m just making this up, but we see examples of things not dissimilar to this. Just because someone is a neurosurgeon does not make them an expert on brain tumor epidemiology, surveillance, or screening. We should separate clinical expertise from public health expertise.
Thank you.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello, everyone. This is Dr Bishal Gyawali, from Queens University, Kingston, Canada. Today, I’m back with you to talk about some of the fallacies that I have seen in medicine, oncology, and the drug regulatory space. I wanted to clarify some of these fallacies.
In my last video, I talked about the FDA denying the approval of a new cancer drug. Let me start with one of the fallacies that is pertinent to that, which is that some people make an argument that patients are dying from a certain condition, such as cancer, or even any other disease besides cancer. That is an absolutely true statement, but that does not necessarily mean there should be a lower bar for drug approvals or we should be approving any drug that has a hint of benefit.
In fact, if we have increased mortality rates and our patients are dying from a certain condition, that means we actually need to have good drugs. We need to have drugs that prevent mortality. We need to have drugs that improve outcomes. Just having any drug out there, if we lower our threshold and are letting any drug be used in these patients because the argument is that people are dying, then in fact, it can have negative consequences.
First, there will be opportunity costs. If you can get any lousy drug into the market and make billions of dollars out of it, then there is no strong motivation to produce drugs that actually remarkably improve outcomes.
Second, patients will also be misled. It’s the patient’s opportunity cost in that they will use whatever time they have remaining to pursue these treatments that were not going to improve their outcomes anyway. This is time they could have better spent either in pursuing better treatments, if those treatments are out there, or to prioritize their time accordingly. This rather gives them a false hope, which can be harmful in the long term.
The first fallacy is that just because people are dying does not necessarily mean we should have more new drugs with a lower bar for approval.
The second fallacy I want to talk about, which is also related to this, is that if a certain cancer is rare, the bar for new drug approval should be quite low.
Of course, rare cancers are a special category, and rare cancers should be treated differently from a regulatory perspective. Absolutely. If the cancer is rare, we cannot have trials with large sample sizes to generate evidence. That problem is there, but that does not necessarily translate to the decision that we should approve anything, even something with a small hint of benefit.
There are other methods to make sure that, even in rare cancers, we can generate good-quality evidence. In fact, from an equity perspective, why should patients with rare cancer not deserve drugs that have good-quality evidence?
We can’t tell someone that, “Your cancer is rare, so you should get drugs that only have a benefit in terms of response rate whereas other cancers that are not rare will have drugs based on survival.”
Going back to the point about the difficulty in doing big trials in patients with rare cancers, that is absolutely true and there should be regulatory flexibility in this. I think accelerated approval is a pathway that allows for this regulatory flexibility, which allows access to these drugs early on based on earlier signals of benefit. You can continue to generate evidence in the future and confirm the clinical benefit.
There are also other nuances to this. One is that we should also make sure that this regulatory flexibility with rare cancers should not be misused. What do I mean by that? First, all rare cancers are not the same. There are some cancers that are ultra rare, and then there are some cancers that technically might fit the definition of rare, but trials are possible. Case in point: adrenocortical cancer. It is considered to be a very rare cancer, but there have been randomized trials in adrenocortical cancer.
Our efforts should be to maximize our collaboration globally so that a cancer that is rare locally will still not be so rare globally when we collect all these patients.
In certain situations, like let’s say, based on the molecular subtypes, any common cancer can be sliced and diced into a rare subtype: MSI-high, BRAF-negative, HER2-positive, right-sided colon cancer. If you start to slice cancers into these smaller and smaller molecular subtypes, you can consider anything as a rare cancer. That should not be misused as an excuse to get away from doing proper trials and generating adequate evidence for our patients.
The third fallacy I want to talk about is that increasing cancer incidence in a certain subgroup of population does not automatically translate into, “We should start screening this subgroup of population.”
A certain cancer — let’s say cancer X or cancer Y — is increasing in a young population, so therefore, we should lower the age of the screening of young populations. This cancer is increasing in this ethnic population, so therefore we should start screening this ethnic population more frequently. This cancer is increasing in this type of minority, so therefore, we should start screening this minority more.
No, it does not work like that. Increasing incidence will make us concerned, of course, but that does not necessarily translate into, “We should start screening them.” In order for a screening test to be useful, it has to fulfill a number of criteria.
The goal is not to detect cancers. The goal is to detect cancers that are not indolent enough that they would have never caused problems, nor speed up the diagnosis of aggressive cancers that are going to be lethal pretty soon anyway. The goal is to detect those cancers in the middle, so that by detecting early, we can intervene and improve the outcomes and improve the mortality from that cancer.
This type of intervention requires a thoughtful consideration of the increasing incidence of the cancer, of course, but also the utility of the screening test in that subgroup of population; the life expectancy of this subgroup of patients with and without cancer; the interventions available to address that increasing burden of cancer; and whether by intervening we are going to reduce the mortality rates.
Just because we can detect cancers does not mean we should detect cancers. That’s the third fallacy I wanted to talk about.
The fourth fallacy is related to when someone is asking for more evidence for anything. There is a new drug for this cancer,so what is the evidence? Or there is this new intervention that will detect ctDNA or whatever before the cancer relapses, or before the cancer even shows up as a screening test.
Whenever there is any treatment that is being promoted and someone asks for evidence, people sometimes try to make personal attacks by saying, “Oh, so, you’re okay with patients dying. You don’t want to save lives.”
Absolutely we want to save lives. That’s why we’re in this field, and that’s why we’re asking for more evidence. You should not consider someone who is asking for evidence as evil or that this person does not want this new drug, or this person does not want this innovation. No, that person actually wants to make sure that that innovation actually helps people. That’s why that person is asking for more evidence.
If we stop asking for evidence, then our whole practice becomes based on emotions, faith, and trust rather than science. You could extrapolate it to the other extreme, like if you are not asking for evidence. If it is interpreted as someone who is asking for evidence is evil, or someone who does not want patients to get new drugs, then you could extrapolate these to people also making claims about alternative medicines or ivermectin nowadays, and claiming that this cures cancer.
Science is science. You need to be the same no matter the circumstances. If you are asking for data for ivermectin, you should also be asking data for your cancer drug that you think is going to work. We should always ask for evidence.
Asking for evidence is not a sign that whoever is asking for evidence does not want the patient to have access to the drug. It is showing that the person who is asking for evidence actually wants to make sure that the patients who get this drug are actually being helped by the drug rather than being harmed.
I’m talking about 5 fallacies today. The final, fifth fallacy is that clinical expertise does not equal expertise in making public health decisions or even expertise in critical appraisal. Someone can be a fantastic breast cancer doctor, the best oncologist for breast cancer. That does not automatically make that person the best person to evaluate clinical trials of breast cancer drugs.
Someone can be a fantastic colon cancer doctor. That does not make that person automatically the best person to evaluate whether or not colonoscopy or colon cancer screening is indicated in a certain patient population.
These population-level decisions — including should this drug be approved, should this drug be funded, and should this screening test be made a public health measure, all of these public health decisions that are done at a population level — require different expertise in critical appraisal, clinical epidemiology, and public health.
Just because someone is a fantastic clinician does not make that person a fantastic public health expert. I see on social media often that a famous doctor with expertise in their domain, let’s say a famous neurosurgeon, might say, “I think brain tumors are increasing in incidence in young persons, so we should be targeting an MRI screening for everyone over the age of 30.”
I’m just making this up, but we see examples of things not dissimilar to this. Just because someone is a neurosurgeon does not make them an expert on brain tumor epidemiology, surveillance, or screening. We should separate clinical expertise from public health expertise.
Thank you.
A version of this article first appeared on Medscape.com.
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine
Fact vs Fallacy: Challenging the Norms of Cancer Care Fallacies in Medicine