User login
Obstetric units place twice as many wrong-patient orders as medical-surgical units
Clinicians in obstetric units place nearly twice as many wrong-patient orders as their medical-surgical counterparts, based on a retrospective look at more than 1.3 million orders.
These findings suggest that obstetric patients are at particular risk for this type of medical error, and that steps are needed to address obstetric clinical culture, work flow, and electronic medical record interfaces, reported lead author Adina R. Kern-Goldberger, MD, of the department of obstetrics and gynecology at the University of Pennsylvania, Philadelphia, and colleagues.
The root of the issue may come from the very nature of obstetrics, and the homogeneity of the patient population, they wrote in Obstetrics & Gynecology.
“Obstetrics is a unique clinical environment because all patients are admitted with a common diagnosis – pregnancy – and have much more overlap in demographic characteristics than a typical inpatient unit given that they are all females of reproductive age,” the investigators wrote. “The labor and delivery environment also is distinct in the hospital given its dynamic tempo and unpredictable work flow. There also is the added risk of neonates typically being registered in the hospital record under the mother’s name after birth. This generates abundant opportunity for errors in order placement, both between obstetric patients and between postpartum patients and their newborns.”
To determine the relative magnitude of this risk, Dr. Kern-Goldberger and colleagues analyzed EMRs from 45,436 obstetric patients and 12,915 medical-surgical patients at “a large, urban, integrated health system in New York City,” including 1,329,463 order sessions placed between 2016 and 2018.
The primary outcome was near-miss wrong-patient orders, which were identified by the Wrong-Patient Retract-and-Reorder measure.
“The measure uses an electronic query to detect retract-and-reorder events, defined as one or more orders placed for patient A, canceled by the same clinician within 10 minutes, and reordered by the same clinician for patient B within the next 10 minutes,” the investigators wrote.In obstetric units, 79.5 wrong-patient orders were placed per 100,000 order sessions, which was 98% higher than the rate of 42.3 wrong-patient orders per 100,000 order sessions in medical-surgical units (odds ratio, 1.98; 95% confidence interval, 1.64-2.39), a disparity that was observed across clinician types and times of day.Advanced practice clinicians in obstetrics placed 47.3 wrong-patient orders per 100,000 order sessions, which was significantly lower than that of their colleagues: attending physicians (127.0 per 100,000) and house staff (119.9 per 100,000).
Wrong-patient orders in obstetrics most often involved medication (73.2 per 100,000), particularly nifedipine, antibiotics, tocolytics, and nonoxytocin uterotonics. The “other” category, including but not limited to lab studies and nursing orders, was associated with 51.0 wrong-patient orders per 100,000 order sessions, while errors in diagnostic imaging orders followed distantly behind, at a rate of 5.7 per 1000,000.
“Although the obstetric clinical environment – particularly labor and delivery – is vibrant and frequently chaotic, it is critical to establish a calm, orderly, and safe culture around order entry,” the investigators wrote. “This, combined with efforts to improve house staff work flow and to optimize EMR interfaces, is likely to help mitigate the threat of wrong order errors to patient care and ultimately improve maternal health and safety.”
According to Catherine D. Cansino, MD, associate clinical professor of obstetrics and gynecology at UC Davis (Calif.) Health, the findings highlight the value of medical informatics while revealing a need to improve EMR interfaces.
“Medical informatics is a growing field and expertise among ob.gyns. is very important,” Dr. Cansino said in an interview. “This study by Kern-Goldberger and colleagues highlights the vulnerability of our EMR systems (and our patients, indirectly) when medical informatics systems are not optimized. The investigators present a study that advocates for greater emphasis on optimizing such systems in obstetrics units, especially in the context of high acuity settings such as obstetrics, compared to medical-surgical units. Appropriately, the study highlights the avoided harm when correcting medical errors for obstetric patients since such errors potentially affect both the delivering patient and the newborn.”
The study was funded by AHRQ. One coauthor disclosed funding from the Icahn School of Medicine at Mount Sinai, Georgetown University, the National Institutes of Health – Office of Scientific Review, and the Social Science Research Council. Another reported funding from Roche.
Clinicians in obstetric units place nearly twice as many wrong-patient orders as their medical-surgical counterparts, based on a retrospective look at more than 1.3 million orders.
These findings suggest that obstetric patients are at particular risk for this type of medical error, and that steps are needed to address obstetric clinical culture, work flow, and electronic medical record interfaces, reported lead author Adina R. Kern-Goldberger, MD, of the department of obstetrics and gynecology at the University of Pennsylvania, Philadelphia, and colleagues.
The root of the issue may come from the very nature of obstetrics, and the homogeneity of the patient population, they wrote in Obstetrics & Gynecology.
“Obstetrics is a unique clinical environment because all patients are admitted with a common diagnosis – pregnancy – and have much more overlap in demographic characteristics than a typical inpatient unit given that they are all females of reproductive age,” the investigators wrote. “The labor and delivery environment also is distinct in the hospital given its dynamic tempo and unpredictable work flow. There also is the added risk of neonates typically being registered in the hospital record under the mother’s name after birth. This generates abundant opportunity for errors in order placement, both between obstetric patients and between postpartum patients and their newborns.”
To determine the relative magnitude of this risk, Dr. Kern-Goldberger and colleagues analyzed EMRs from 45,436 obstetric patients and 12,915 medical-surgical patients at “a large, urban, integrated health system in New York City,” including 1,329,463 order sessions placed between 2016 and 2018.
The primary outcome was near-miss wrong-patient orders, which were identified by the Wrong-Patient Retract-and-Reorder measure.
“The measure uses an electronic query to detect retract-and-reorder events, defined as one or more orders placed for patient A, canceled by the same clinician within 10 minutes, and reordered by the same clinician for patient B within the next 10 minutes,” the investigators wrote.In obstetric units, 79.5 wrong-patient orders were placed per 100,000 order sessions, which was 98% higher than the rate of 42.3 wrong-patient orders per 100,000 order sessions in medical-surgical units (odds ratio, 1.98; 95% confidence interval, 1.64-2.39), a disparity that was observed across clinician types and times of day.Advanced practice clinicians in obstetrics placed 47.3 wrong-patient orders per 100,000 order sessions, which was significantly lower than that of their colleagues: attending physicians (127.0 per 100,000) and house staff (119.9 per 100,000).
Wrong-patient orders in obstetrics most often involved medication (73.2 per 100,000), particularly nifedipine, antibiotics, tocolytics, and nonoxytocin uterotonics. The “other” category, including but not limited to lab studies and nursing orders, was associated with 51.0 wrong-patient orders per 100,000 order sessions, while errors in diagnostic imaging orders followed distantly behind, at a rate of 5.7 per 1000,000.
“Although the obstetric clinical environment – particularly labor and delivery – is vibrant and frequently chaotic, it is critical to establish a calm, orderly, and safe culture around order entry,” the investigators wrote. “This, combined with efforts to improve house staff work flow and to optimize EMR interfaces, is likely to help mitigate the threat of wrong order errors to patient care and ultimately improve maternal health and safety.”
According to Catherine D. Cansino, MD, associate clinical professor of obstetrics and gynecology at UC Davis (Calif.) Health, the findings highlight the value of medical informatics while revealing a need to improve EMR interfaces.
“Medical informatics is a growing field and expertise among ob.gyns. is very important,” Dr. Cansino said in an interview. “This study by Kern-Goldberger and colleagues highlights the vulnerability of our EMR systems (and our patients, indirectly) when medical informatics systems are not optimized. The investigators present a study that advocates for greater emphasis on optimizing such systems in obstetrics units, especially in the context of high acuity settings such as obstetrics, compared to medical-surgical units. Appropriately, the study highlights the avoided harm when correcting medical errors for obstetric patients since such errors potentially affect both the delivering patient and the newborn.”
The study was funded by AHRQ. One coauthor disclosed funding from the Icahn School of Medicine at Mount Sinai, Georgetown University, the National Institutes of Health – Office of Scientific Review, and the Social Science Research Council. Another reported funding from Roche.
Clinicians in obstetric units place nearly twice as many wrong-patient orders as their medical-surgical counterparts, based on a retrospective look at more than 1.3 million orders.
These findings suggest that obstetric patients are at particular risk for this type of medical error, and that steps are needed to address obstetric clinical culture, work flow, and electronic medical record interfaces, reported lead author Adina R. Kern-Goldberger, MD, of the department of obstetrics and gynecology at the University of Pennsylvania, Philadelphia, and colleagues.
The root of the issue may come from the very nature of obstetrics, and the homogeneity of the patient population, they wrote in Obstetrics & Gynecology.
“Obstetrics is a unique clinical environment because all patients are admitted with a common diagnosis – pregnancy – and have much more overlap in demographic characteristics than a typical inpatient unit given that they are all females of reproductive age,” the investigators wrote. “The labor and delivery environment also is distinct in the hospital given its dynamic tempo and unpredictable work flow. There also is the added risk of neonates typically being registered in the hospital record under the mother’s name after birth. This generates abundant opportunity for errors in order placement, both between obstetric patients and between postpartum patients and their newborns.”
To determine the relative magnitude of this risk, Dr. Kern-Goldberger and colleagues analyzed EMRs from 45,436 obstetric patients and 12,915 medical-surgical patients at “a large, urban, integrated health system in New York City,” including 1,329,463 order sessions placed between 2016 and 2018.
The primary outcome was near-miss wrong-patient orders, which were identified by the Wrong-Patient Retract-and-Reorder measure.
“The measure uses an electronic query to detect retract-and-reorder events, defined as one or more orders placed for patient A, canceled by the same clinician within 10 minutes, and reordered by the same clinician for patient B within the next 10 minutes,” the investigators wrote.In obstetric units, 79.5 wrong-patient orders were placed per 100,000 order sessions, which was 98% higher than the rate of 42.3 wrong-patient orders per 100,000 order sessions in medical-surgical units (odds ratio, 1.98; 95% confidence interval, 1.64-2.39), a disparity that was observed across clinician types and times of day.Advanced practice clinicians in obstetrics placed 47.3 wrong-patient orders per 100,000 order sessions, which was significantly lower than that of their colleagues: attending physicians (127.0 per 100,000) and house staff (119.9 per 100,000).
Wrong-patient orders in obstetrics most often involved medication (73.2 per 100,000), particularly nifedipine, antibiotics, tocolytics, and nonoxytocin uterotonics. The “other” category, including but not limited to lab studies and nursing orders, was associated with 51.0 wrong-patient orders per 100,000 order sessions, while errors in diagnostic imaging orders followed distantly behind, at a rate of 5.7 per 1000,000.
“Although the obstetric clinical environment – particularly labor and delivery – is vibrant and frequently chaotic, it is critical to establish a calm, orderly, and safe culture around order entry,” the investigators wrote. “This, combined with efforts to improve house staff work flow and to optimize EMR interfaces, is likely to help mitigate the threat of wrong order errors to patient care and ultimately improve maternal health and safety.”
According to Catherine D. Cansino, MD, associate clinical professor of obstetrics and gynecology at UC Davis (Calif.) Health, the findings highlight the value of medical informatics while revealing a need to improve EMR interfaces.
“Medical informatics is a growing field and expertise among ob.gyns. is very important,” Dr. Cansino said in an interview. “This study by Kern-Goldberger and colleagues highlights the vulnerability of our EMR systems (and our patients, indirectly) when medical informatics systems are not optimized. The investigators present a study that advocates for greater emphasis on optimizing such systems in obstetrics units, especially in the context of high acuity settings such as obstetrics, compared to medical-surgical units. Appropriately, the study highlights the avoided harm when correcting medical errors for obstetric patients since such errors potentially affect both the delivering patient and the newborn.”
The study was funded by AHRQ. One coauthor disclosed funding from the Icahn School of Medicine at Mount Sinai, Georgetown University, the National Institutes of Health – Office of Scientific Review, and the Social Science Research Council. Another reported funding from Roche.
FROM OBSTETRICS & GYNECOLOGY
Does optimal iron absorption include vitamin C?
Her blood work shows a hematocrit level of 32, a mean corpuscular volume of 77, a platelet count of 390,000, and a ferritin level of 5.

What would you recommend for iron replacement?
A. FeSO4 325 mg three times a day with vitamin C
B. FeSO4 325 mg daily with vitamin C
C. FeSO4 325 mg every other day
Recommendations and supporting research
I think I would start with choice C, FeSO4 every other day.
Treatment of iron deficiency with oral iron has traditionally been done by giving 150-200 mg of elemental iron (which is equal to three 325 mg tablets of iron sulfate).1 This dosing regimen has considerable gastrointestinal side effects. Recent evidence has shown that iron absorption is diminished the more frequently it is given.
Stoffel and colleagues found that fractional iron absorption was higher in iron-deficient women who were given iron every other day, compared with those who received daily iron.2 They also found that the more frequently iron was administered, the higher the hepcidin levels were, and the lower the iron absorption.
Karacok and colleagues studied every other day iron versus daily iron for the treatment of iron-deficiency anemia of pregnancy.3 A total of 217 women completed randomization and participated in the study, with all women receiving 100 mg of elemental iron, either daily (111) or every other day (106). There was no significant difference in increase in ferritin levels, or hemoglobin increase between the groups. The daily iron group had more gastrointestinal symptoms (41.4%) than the every other day iron group (15.1%) (P < .0057).
Düzen Oflas and colleagues looked at the same question in nonpregnant women with iron deficiency anemia.4 Study patients either received 80 mg iron sulfate twice a day, 80 mg once a day, or 80 mg every other day. There was no statistically significant difference in hemoglobin improvement between groups, but the group that received twice a day dosing of iron had statistically significantly higher ferritin levels than the daily or every other day iron groups. This improvement in ferritin levels came at a cost, though, as 68% of patients in the twice daily iron group had gastrointestinal symptoms, compared with only 10% in the every other day iron group (P < .01).
Vitamin C is often recommended to be taken with iron to promote absorption. The evidence for this practice is scant, and dates back almost 50 years.5,6
Cook and Reddy found there was no significant difference in mean iron absorption among the three dietary periods studied in 12 patients despite a range of mean daily intakes of dietary vitamin C of 51-247 mg/d.7
Hunt and colleagues studied 25 non pregnant, healthy women with low ferritin levels.8 The women’s meals were supplemented with vitamin C (500 mg, three times a day) for 5 of the 10 weeks, in a double-blind, crossover design. Vitamin C supplementation did not lead to a difference in iron absorption, lab indices of iron deficiency, or the biological half-life of iron.
Li and colleagues looked at the effect of vitamin C supplementation on iron levels in women with iron deficiency anemia.9 A total of 440 women were recruited, with 432 completing the trial. Women were randomized to receive iron supplements plus vitamin C or iron supplements only. Their findings were that oral iron supplements alone were equivalent to oral iron supplements plus vitamin C in improving hemoglobin recovery and iron absorption.
Bottom line
Less frequent administration of iron supplements (every other day) is as effective as more frequent administration, with less GI symptoms. Also, adding vitamin C does not appear to improve absorption of iron supplements.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. 1. Fairbanks VF and Beutler E. Iron deficiency, in “Williams Textbook of Hematology, 6th ed.” (New York: McGraw-Hill, 2001).
2. Stoffel N et al. Lancet Haematology. 2017;4: e524-33.
3. Karakoc G et al. J Matern Fetal Neonatal Med. 2021 Apr 18:1-5
4. Düzen Oflas N et al. Intern Med J. 2020 Jul;50(7):854-8
5. Cook JD and Monsen ER. Am J Clin Nutr. 1977;30:235-41.
6. Hallberg L etal. Hum Nutr Appl Nutr. 1986;40: 97-113.
7. Cook JD and Reddy M. Am J Clin Nutr. 2001;73:93-8.
8. Hunt JR et al. Am J Clin Nutr. 1994 Jun;59(6):1381-5.
9. Li N et al. JAMA Netw Open. 2020 Nov 2;3(11):e2023644.
Her blood work shows a hematocrit level of 32, a mean corpuscular volume of 77, a platelet count of 390,000, and a ferritin level of 5.
What would you recommend for iron replacement?
A. FeSO4 325 mg three times a day with vitamin C
B. FeSO4 325 mg daily with vitamin C
C. FeSO4 325 mg every other day
Recommendations and supporting research
I think I would start with choice C, FeSO4 every other day.
Treatment of iron deficiency with oral iron has traditionally been done by giving 150-200 mg of elemental iron (which is equal to three 325 mg tablets of iron sulfate).1 This dosing regimen has considerable gastrointestinal side effects. Recent evidence has shown that iron absorption is diminished the more frequently it is given.
Stoffel and colleagues found that fractional iron absorption was higher in iron-deficient women who were given iron every other day, compared with those who received daily iron.2 They also found that the more frequently iron was administered, the higher the hepcidin levels were, and the lower the iron absorption.
Karacok and colleagues studied every other day iron versus daily iron for the treatment of iron-deficiency anemia of pregnancy.3 A total of 217 women completed randomization and participated in the study, with all women receiving 100 mg of elemental iron, either daily (111) or every other day (106). There was no significant difference in increase in ferritin levels, or hemoglobin increase between the groups. The daily iron group had more gastrointestinal symptoms (41.4%) than the every other day iron group (15.1%) (P < .0057).
Düzen Oflas and colleagues looked at the same question in nonpregnant women with iron deficiency anemia.4 Study patients either received 80 mg iron sulfate twice a day, 80 mg once a day, or 80 mg every other day. There was no statistically significant difference in hemoglobin improvement between groups, but the group that received twice a day dosing of iron had statistically significantly higher ferritin levels than the daily or every other day iron groups. This improvement in ferritin levels came at a cost, though, as 68% of patients in the twice daily iron group had gastrointestinal symptoms, compared with only 10% in the every other day iron group (P < .01).
Vitamin C is often recommended to be taken with iron to promote absorption. The evidence for this practice is scant, and dates back almost 50 years.5,6
Cook and Reddy found there was no significant difference in mean iron absorption among the three dietary periods studied in 12 patients despite a range of mean daily intakes of dietary vitamin C of 51-247 mg/d.7
Hunt and colleagues studied 25 non pregnant, healthy women with low ferritin levels.8 The women’s meals were supplemented with vitamin C (500 mg, three times a day) for 5 of the 10 weeks, in a double-blind, crossover design. Vitamin C supplementation did not lead to a difference in iron absorption, lab indices of iron deficiency, or the biological half-life of iron.
Li and colleagues looked at the effect of vitamin C supplementation on iron levels in women with iron deficiency anemia.9 A total of 440 women were recruited, with 432 completing the trial. Women were randomized to receive iron supplements plus vitamin C or iron supplements only. Their findings were that oral iron supplements alone were equivalent to oral iron supplements plus vitamin C in improving hemoglobin recovery and iron absorption.
Bottom line
Less frequent administration of iron supplements (every other day) is as effective as more frequent administration, with less GI symptoms. Also, adding vitamin C does not appear to improve absorption of iron supplements.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. 1. Fairbanks VF and Beutler E. Iron deficiency, in “Williams Textbook of Hematology, 6th ed.” (New York: McGraw-Hill, 2001).
2. Stoffel N et al. Lancet Haematology. 2017;4: e524-33.
3. Karakoc G et al. J Matern Fetal Neonatal Med. 2021 Apr 18:1-5
4. Düzen Oflas N et al. Intern Med J. 2020 Jul;50(7):854-8
5. Cook JD and Monsen ER. Am J Clin Nutr. 1977;30:235-41.
6. Hallberg L etal. Hum Nutr Appl Nutr. 1986;40: 97-113.
7. Cook JD and Reddy M. Am J Clin Nutr. 2001;73:93-8.
8. Hunt JR et al. Am J Clin Nutr. 1994 Jun;59(6):1381-5.
9. Li N et al. JAMA Netw Open. 2020 Nov 2;3(11):e2023644.
Her blood work shows a hematocrit level of 32, a mean corpuscular volume of 77, a platelet count of 390,000, and a ferritin level of 5.
What would you recommend for iron replacement?
A. FeSO4 325 mg three times a day with vitamin C
B. FeSO4 325 mg daily with vitamin C
C. FeSO4 325 mg every other day
Recommendations and supporting research
I think I would start with choice C, FeSO4 every other day.
Treatment of iron deficiency with oral iron has traditionally been done by giving 150-200 mg of elemental iron (which is equal to three 325 mg tablets of iron sulfate).1 This dosing regimen has considerable gastrointestinal side effects. Recent evidence has shown that iron absorption is diminished the more frequently it is given.
Stoffel and colleagues found that fractional iron absorption was higher in iron-deficient women who were given iron every other day, compared with those who received daily iron.2 They also found that the more frequently iron was administered, the higher the hepcidin levels were, and the lower the iron absorption.
Karacok and colleagues studied every other day iron versus daily iron for the treatment of iron-deficiency anemia of pregnancy.3 A total of 217 women completed randomization and participated in the study, with all women receiving 100 mg of elemental iron, either daily (111) or every other day (106). There was no significant difference in increase in ferritin levels, or hemoglobin increase between the groups. The daily iron group had more gastrointestinal symptoms (41.4%) than the every other day iron group (15.1%) (P < .0057).
Düzen Oflas and colleagues looked at the same question in nonpregnant women with iron deficiency anemia.4 Study patients either received 80 mg iron sulfate twice a day, 80 mg once a day, or 80 mg every other day. There was no statistically significant difference in hemoglobin improvement between groups, but the group that received twice a day dosing of iron had statistically significantly higher ferritin levels than the daily or every other day iron groups. This improvement in ferritin levels came at a cost, though, as 68% of patients in the twice daily iron group had gastrointestinal symptoms, compared with only 10% in the every other day iron group (P < .01).
Vitamin C is often recommended to be taken with iron to promote absorption. The evidence for this practice is scant, and dates back almost 50 years.5,6
Cook and Reddy found there was no significant difference in mean iron absorption among the three dietary periods studied in 12 patients despite a range of mean daily intakes of dietary vitamin C of 51-247 mg/d.7
Hunt and colleagues studied 25 non pregnant, healthy women with low ferritin levels.8 The women’s meals were supplemented with vitamin C (500 mg, three times a day) for 5 of the 10 weeks, in a double-blind, crossover design. Vitamin C supplementation did not lead to a difference in iron absorption, lab indices of iron deficiency, or the biological half-life of iron.
Li and colleagues looked at the effect of vitamin C supplementation on iron levels in women with iron deficiency anemia.9 A total of 440 women were recruited, with 432 completing the trial. Women were randomized to receive iron supplements plus vitamin C or iron supplements only. Their findings were that oral iron supplements alone were equivalent to oral iron supplements plus vitamin C in improving hemoglobin recovery and iron absorption.
Bottom line
Less frequent administration of iron supplements (every other day) is as effective as more frequent administration, with less GI symptoms. Also, adding vitamin C does not appear to improve absorption of iron supplements.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. 1. Fairbanks VF and Beutler E. Iron deficiency, in “Williams Textbook of Hematology, 6th ed.” (New York: McGraw-Hill, 2001).
2. Stoffel N et al. Lancet Haematology. 2017;4: e524-33.
3. Karakoc G et al. J Matern Fetal Neonatal Med. 2021 Apr 18:1-5
4. Düzen Oflas N et al. Intern Med J. 2020 Jul;50(7):854-8
5. Cook JD and Monsen ER. Am J Clin Nutr. 1977;30:235-41.
6. Hallberg L etal. Hum Nutr Appl Nutr. 1986;40: 97-113.
7. Cook JD and Reddy M. Am J Clin Nutr. 2001;73:93-8.
8. Hunt JR et al. Am J Clin Nutr. 1994 Jun;59(6):1381-5.
9. Li N et al. JAMA Netw Open. 2020 Nov 2;3(11):e2023644.
Pregnant women no longer detained by ICE
Immigration and Customs Enforcement will no longer detain most migrant women who are pregnant, postpartum, or nursing for deportation. This reverses the policy previously put in place by the Trump administration.
Under the new directive, ICE officials generally will not detain or arrest women who are pregnant or nursing, or who have given birth within the previous year. In a July 1 memo signed by ICE Acting Director Tae Johnson, ICE officers are directed to house women in “an appropriate facility to manage their care.”
The memo goes on to state that “generally ICE should not detain, arrest, or take into custody for an administrative violation of the immigration laws individuals known to be pregnant, post partum, or nursing unless release is prohibited by law or exceptional circumstances exist.”
In addition, ICE is also required to evaluate those individuals who are already in custody “to determine if continued detention is appropriate.”
During the Obama administration, pregnant women were generally not detained except under extraordinary circumstances. However, these policies were reversed after Donald Trump took office, and there was an 80% increase in the number of times ICE detained pregnant women in the year that followed implementation of the new directive – from 1,160 in 2017 to 2,097 in 2018.
The new guidance now goes even further than the directive issued under President Obama as it also includes women who are nursing and the 1-year postpartum period.
This policy stems from the Biden-Harris administration’s plan to reform the immigration system, part of which was to create a more humane asylum system. In a statement released early in February 2021, the White House stated that the “Trump administration’s policies at the border have caused chaos, cruelty, and confusion,” and that they will now “begin to roll back the most damaging policies adopted by the prior administration, while taking effective action to manage migration across the region.” After migrant women are taken into custody, pregnancy tests are administered as part of regular health screenings. If women are found to be pregnant, the new ICE policy states that they “generally” should be released from detention.
However, there will still be circumstances when pregnant and postpartum women may be detained, such as when there is a high risk that the individual is violent or a national security concern. In these cases, a field office director must approve the arrest and detention as well as making sure that the women receive appropriate medical care.
“The harmful consequences of immigration detention have been documented for years,” said Rebekah Wolf, JD, staff attorney with the American Immigration Council. “Our 2017 joint complaint urging a thorough investigation into the increasing numbers of pregnant women facing harm in detention, illustrated the disturbing practice of detaining pregnant women and the lack of quality medical care provided to these women.”
She added that the “federal government should not be in the business of detaining pregnant or nursing individuals, and it’s good to see the Biden administration directing ICE to finally take meaningful steps to limit enforcement activities in this manner. We are hopeful that this announcement is an indication of a broader shift on detention policy.”
There are currently 13 pregnant women in ICE custody, and they are being considered for release under the new policy.
Immigration and Customs Enforcement will no longer detain most migrant women who are pregnant, postpartum, or nursing for deportation. This reverses the policy previously put in place by the Trump administration.
Under the new directive, ICE officials generally will not detain or arrest women who are pregnant or nursing, or who have given birth within the previous year. In a July 1 memo signed by ICE Acting Director Tae Johnson, ICE officers are directed to house women in “an appropriate facility to manage their care.”
The memo goes on to state that “generally ICE should not detain, arrest, or take into custody for an administrative violation of the immigration laws individuals known to be pregnant, post partum, or nursing unless release is prohibited by law or exceptional circumstances exist.”
In addition, ICE is also required to evaluate those individuals who are already in custody “to determine if continued detention is appropriate.”
During the Obama administration, pregnant women were generally not detained except under extraordinary circumstances. However, these policies were reversed after Donald Trump took office, and there was an 80% increase in the number of times ICE detained pregnant women in the year that followed implementation of the new directive – from 1,160 in 2017 to 2,097 in 2018.
The new guidance now goes even further than the directive issued under President Obama as it also includes women who are nursing and the 1-year postpartum period.
This policy stems from the Biden-Harris administration’s plan to reform the immigration system, part of which was to create a more humane asylum system. In a statement released early in February 2021, the White House stated that the “Trump administration’s policies at the border have caused chaos, cruelty, and confusion,” and that they will now “begin to roll back the most damaging policies adopted by the prior administration, while taking effective action to manage migration across the region.” After migrant women are taken into custody, pregnancy tests are administered as part of regular health screenings. If women are found to be pregnant, the new ICE policy states that they “generally” should be released from detention.
However, there will still be circumstances when pregnant and postpartum women may be detained, such as when there is a high risk that the individual is violent or a national security concern. In these cases, a field office director must approve the arrest and detention as well as making sure that the women receive appropriate medical care.
“The harmful consequences of immigration detention have been documented for years,” said Rebekah Wolf, JD, staff attorney with the American Immigration Council. “Our 2017 joint complaint urging a thorough investigation into the increasing numbers of pregnant women facing harm in detention, illustrated the disturbing practice of detaining pregnant women and the lack of quality medical care provided to these women.”
She added that the “federal government should not be in the business of detaining pregnant or nursing individuals, and it’s good to see the Biden administration directing ICE to finally take meaningful steps to limit enforcement activities in this manner. We are hopeful that this announcement is an indication of a broader shift on detention policy.”
There are currently 13 pregnant women in ICE custody, and they are being considered for release under the new policy.
Immigration and Customs Enforcement will no longer detain most migrant women who are pregnant, postpartum, or nursing for deportation. This reverses the policy previously put in place by the Trump administration.
Under the new directive, ICE officials generally will not detain or arrest women who are pregnant or nursing, or who have given birth within the previous year. In a July 1 memo signed by ICE Acting Director Tae Johnson, ICE officers are directed to house women in “an appropriate facility to manage their care.”
The memo goes on to state that “generally ICE should not detain, arrest, or take into custody for an administrative violation of the immigration laws individuals known to be pregnant, post partum, or nursing unless release is prohibited by law or exceptional circumstances exist.”
In addition, ICE is also required to evaluate those individuals who are already in custody “to determine if continued detention is appropriate.”
During the Obama administration, pregnant women were generally not detained except under extraordinary circumstances. However, these policies were reversed after Donald Trump took office, and there was an 80% increase in the number of times ICE detained pregnant women in the year that followed implementation of the new directive – from 1,160 in 2017 to 2,097 in 2018.
The new guidance now goes even further than the directive issued under President Obama as it also includes women who are nursing and the 1-year postpartum period.
This policy stems from the Biden-Harris administration’s plan to reform the immigration system, part of which was to create a more humane asylum system. In a statement released early in February 2021, the White House stated that the “Trump administration’s policies at the border have caused chaos, cruelty, and confusion,” and that they will now “begin to roll back the most damaging policies adopted by the prior administration, while taking effective action to manage migration across the region.” After migrant women are taken into custody, pregnancy tests are administered as part of regular health screenings. If women are found to be pregnant, the new ICE policy states that they “generally” should be released from detention.
However, there will still be circumstances when pregnant and postpartum women may be detained, such as when there is a high risk that the individual is violent or a national security concern. In these cases, a field office director must approve the arrest and detention as well as making sure that the women receive appropriate medical care.
“The harmful consequences of immigration detention have been documented for years,” said Rebekah Wolf, JD, staff attorney with the American Immigration Council. “Our 2017 joint complaint urging a thorough investigation into the increasing numbers of pregnant women facing harm in detention, illustrated the disturbing practice of detaining pregnant women and the lack of quality medical care provided to these women.”
She added that the “federal government should not be in the business of detaining pregnant or nursing individuals, and it’s good to see the Biden administration directing ICE to finally take meaningful steps to limit enforcement activities in this manner. We are hopeful that this announcement is an indication of a broader shift on detention policy.”
There are currently 13 pregnant women in ICE custody, and they are being considered for release under the new policy.
Postpartum depression affects dads, too
Michael W., a 38-year-old New Jersey–based attorney, and his wife had been excitedly planning for the birth of their baby and were overjoyed when she was born.
But after that, “I found that parenting a newborn was shockingly exhausting. I felt unprepared for the task, overwhelmed by the burden of the 24-hour-schedule and lack of sleep, and I struggled with feelings of inadequacy,” he said in an interview.
Michael never thought he had postpartum depression (PPD), perhaps because the condition is more commonly associated with women. But a study published in the American Journal of Men’s Health suggests that PPD also affects men.
A team of Danish investigators led by researcher Sarah Pedersen, of the department of public health, Aarhus University, extensively interviewed eight fathers with PPD and found their primary experiences involved feelings of being overwhelmed and powerless or inadequate, which sometimes turned into anger and frustration.
“I think one of the most important take-home messages is that practicing clinicians working with new parents should invite fathers to your consultations and engage the fathers as much as possible,” Ms. Pedersen said in an interview.
The findings also contained a message for parents, she says.
“I hope you will support each other and talk about your feelings and how you experience the transition to parenthood – know that it will take time to adjust to your new role,” she said.
Not enough attention
There’s been too little focus on fathers when it comes to PPD, according to Ms. Pedersen.
“During the last decade, several studies have examined the prevalence of PPD in men, and there is rising evidence that paternal PPD is associated with increased risk of long-term adverse behavioral and emotional outcomes in children,” she said.
Nevertheless, only three studies have been based on interviews with fathers who had personal experience with PPD.
“The purpose of our study was, first of all, to explore the lived experience of fathers who had PPD and, secondly, to gain deeper understanding of their help-seeking behavior – barriers to seeking help and facilitators of help-seeking,” Ms. Pedersen said.
The study was based on “semistructured” interviews with eight Danish fathers (ages 29-38 years) who had had PPD, none of whom had a previous history of depression.
All of them had received a formal diagnosis of PPD by a general practitioner or psychologist, and all had sought or received mental health care and considered themselves recovered from depression at the time of the interview.
The researchers used a technique called interpretative phenomenological analysis to analyze the interviews.
This method “aims to produce in-depth examinations of certain phenomena by examining how individuals make meaning of their own life experiences,” the authors wrote.
A ‘radical change’
Of the fathers, five described the period of pregnancy as a “time of happiness, full of positive expectations about fatherhood.”
But “the fathers’ great expectations were later replaced by a very different reality of fatherhood,” the authors wrote, noting that the transition to fatherhood was, in the words of one participant, a “radical change that you just can’t imagine.”
Most fathers expressed a feeling of being overwhelmed, and three felt unready for the task, which added to their depression.
“The participants wanted to be emotionally and physically present in their child’s life, but during the time of their depression, these kind-hearted intentions changed into feelings of guilt and inadequacy, as the participants did not feel they had enough energy and mental strength to become the kind of fathers they wanted to be,” the authors wrote.
The fathers mentioned stressors they believed contributed to their PPD, including complications during their partners’ pregnancies, unplanned cesarean birth (three fathers), the partners’ difficulties with breastfeeding (five fathers), and employment-related concerns. Five reported that their partners had postpartum emotional distress.
‘Masculine norms’
A second focus of the research was to examine fathers’ help-seeking behaviors, Ms. Pedersen said.
Ultimately, all the men sought formal help, either from their general practitioners or from a health visitor, with two seeking help right after birth.
Although the men were able to recognize changes in mood and behavior in retrospect, many did not regard them as signs of depression before their diagnosis.
Most had heard of PPD, but primarily as it affects women. Three sought information online about paternal PPD but couldn’t find any.
Four participants described experiencing PPD as “taboo,” based on a “combination of false beliefs, stigma, and masculine norms,” the authors stated, since men “are supposed to be big and strong and take care of everything, and suddenly you can’t.”
The authors reported that seven participants were screened for PPD or depression by a health care professional.
“The screening was an important part of the help-seeking process, as this was the first time two of the fathers were introduced to PPD,” the authors noted.
Although the screening “had the potential to spark conversation” about PPD, it was geared toward women, and some participants did not feel it was relevant to them.
“Future research should focus on identification of educational needs about paternal PPD among both parents, health care professionals, and other professionals taking care of new families,” Ms. Pedersen said.
Michael W. says it would have been helpful if someone had prepared him and his wife for what to expect, or if there had been some type of screening. Also, he advises expectant parents to “get some real-life experience by spending time around a newborn to see what’s involved.”
Different symptoms
“We often talk about mothers suffering from PPD, so it is more normalized for mothers to bring it up or for loved ones to ask mothers about how they are doing physically and psychologically after the birth,” Craig Garfield, MD, an attending physician and founder/director of Family and Child Health innovations at Ann and Robert H. Lurie Children’s Hospital, Chicago, said in an interview.
For fathers, “it is not discussed as commonly, so friends and families don’t often ask dads, and dads don’t know where to turn,” said Dr. Garfield, professor of pediatrics and medical social sciences at Northwestern University, Chicago. He was not involved with the study.
He noted that symptoms in fathers might differ from those of mothers.
“I have seen fathers who are anxious or more moody than they had been prior, or more angry, and I have seen fathers who throw themselves into work or begin drinking more – all related to changes in mood and depressive symptoms in the postnatal period,” he said.
Symptoms in men may last longer than in women. Dr. Garfield’s group published a study in which they surveyed 400 mothers and fathers of premature infants in the neonatal intensive care unit (NICU) about depressive symptoms around the time of NICU admission, at discharge home, and then after 30 days at home.
Roughly one-third of mothers screened positive for depressive symptoms around NICU admission, as did 17% of fathers. But the mothers’ depression scores improved by discharge and 30 days after being home, while the fathers’ remained “essentially unchanged,” he said.
“Further, we found that if doctors were to screen mothers and fathers during the NICU stay – at admission or even at discharge – that would greatly improve their ability to predict who would still have depressive symptoms 1 month after going home.”
Ms. Pedersen agrees that clinicians should incorporate screening for PPD into their practices and be proactive in encouraging fathers to get help.
“Keep pushing,” she advised, as “men rarely seek help, compared to women, in matters of mental health.”
A version of this article first appeared on WebMD.com.
Michael W., a 38-year-old New Jersey–based attorney, and his wife had been excitedly planning for the birth of their baby and were overjoyed when she was born.
But after that, “I found that parenting a newborn was shockingly exhausting. I felt unprepared for the task, overwhelmed by the burden of the 24-hour-schedule and lack of sleep, and I struggled with feelings of inadequacy,” he said in an interview.
Michael never thought he had postpartum depression (PPD), perhaps because the condition is more commonly associated with women. But a study published in the American Journal of Men’s Health suggests that PPD also affects men.
A team of Danish investigators led by researcher Sarah Pedersen, of the department of public health, Aarhus University, extensively interviewed eight fathers with PPD and found their primary experiences involved feelings of being overwhelmed and powerless or inadequate, which sometimes turned into anger and frustration.
“I think one of the most important take-home messages is that practicing clinicians working with new parents should invite fathers to your consultations and engage the fathers as much as possible,” Ms. Pedersen said in an interview.
The findings also contained a message for parents, she says.
“I hope you will support each other and talk about your feelings and how you experience the transition to parenthood – know that it will take time to adjust to your new role,” she said.
Not enough attention
There’s been too little focus on fathers when it comes to PPD, according to Ms. Pedersen.
“During the last decade, several studies have examined the prevalence of PPD in men, and there is rising evidence that paternal PPD is associated with increased risk of long-term adverse behavioral and emotional outcomes in children,” she said.
Nevertheless, only three studies have been based on interviews with fathers who had personal experience with PPD.
“The purpose of our study was, first of all, to explore the lived experience of fathers who had PPD and, secondly, to gain deeper understanding of their help-seeking behavior – barriers to seeking help and facilitators of help-seeking,” Ms. Pedersen said.
The study was based on “semistructured” interviews with eight Danish fathers (ages 29-38 years) who had had PPD, none of whom had a previous history of depression.
All of them had received a formal diagnosis of PPD by a general practitioner or psychologist, and all had sought or received mental health care and considered themselves recovered from depression at the time of the interview.
The researchers used a technique called interpretative phenomenological analysis to analyze the interviews.
This method “aims to produce in-depth examinations of certain phenomena by examining how individuals make meaning of their own life experiences,” the authors wrote.
A ‘radical change’
Of the fathers, five described the period of pregnancy as a “time of happiness, full of positive expectations about fatherhood.”
But “the fathers’ great expectations were later replaced by a very different reality of fatherhood,” the authors wrote, noting that the transition to fatherhood was, in the words of one participant, a “radical change that you just can’t imagine.”
Most fathers expressed a feeling of being overwhelmed, and three felt unready for the task, which added to their depression.
“The participants wanted to be emotionally and physically present in their child’s life, but during the time of their depression, these kind-hearted intentions changed into feelings of guilt and inadequacy, as the participants did not feel they had enough energy and mental strength to become the kind of fathers they wanted to be,” the authors wrote.
The fathers mentioned stressors they believed contributed to their PPD, including complications during their partners’ pregnancies, unplanned cesarean birth (three fathers), the partners’ difficulties with breastfeeding (five fathers), and employment-related concerns. Five reported that their partners had postpartum emotional distress.
‘Masculine norms’
A second focus of the research was to examine fathers’ help-seeking behaviors, Ms. Pedersen said.
Ultimately, all the men sought formal help, either from their general practitioners or from a health visitor, with two seeking help right after birth.
Although the men were able to recognize changes in mood and behavior in retrospect, many did not regard them as signs of depression before their diagnosis.
Most had heard of PPD, but primarily as it affects women. Three sought information online about paternal PPD but couldn’t find any.
Four participants described experiencing PPD as “taboo,” based on a “combination of false beliefs, stigma, and masculine norms,” the authors stated, since men “are supposed to be big and strong and take care of everything, and suddenly you can’t.”
The authors reported that seven participants were screened for PPD or depression by a health care professional.
“The screening was an important part of the help-seeking process, as this was the first time two of the fathers were introduced to PPD,” the authors noted.
Although the screening “had the potential to spark conversation” about PPD, it was geared toward women, and some participants did not feel it was relevant to them.
“Future research should focus on identification of educational needs about paternal PPD among both parents, health care professionals, and other professionals taking care of new families,” Ms. Pedersen said.
Michael W. says it would have been helpful if someone had prepared him and his wife for what to expect, or if there had been some type of screening. Also, he advises expectant parents to “get some real-life experience by spending time around a newborn to see what’s involved.”
Different symptoms
“We often talk about mothers suffering from PPD, so it is more normalized for mothers to bring it up or for loved ones to ask mothers about how they are doing physically and psychologically after the birth,” Craig Garfield, MD, an attending physician and founder/director of Family and Child Health innovations at Ann and Robert H. Lurie Children’s Hospital, Chicago, said in an interview.
For fathers, “it is not discussed as commonly, so friends and families don’t often ask dads, and dads don’t know where to turn,” said Dr. Garfield, professor of pediatrics and medical social sciences at Northwestern University, Chicago. He was not involved with the study.
He noted that symptoms in fathers might differ from those of mothers.
“I have seen fathers who are anxious or more moody than they had been prior, or more angry, and I have seen fathers who throw themselves into work or begin drinking more – all related to changes in mood and depressive symptoms in the postnatal period,” he said.
Symptoms in men may last longer than in women. Dr. Garfield’s group published a study in which they surveyed 400 mothers and fathers of premature infants in the neonatal intensive care unit (NICU) about depressive symptoms around the time of NICU admission, at discharge home, and then after 30 days at home.
Roughly one-third of mothers screened positive for depressive symptoms around NICU admission, as did 17% of fathers. But the mothers’ depression scores improved by discharge and 30 days after being home, while the fathers’ remained “essentially unchanged,” he said.
“Further, we found that if doctors were to screen mothers and fathers during the NICU stay – at admission or even at discharge – that would greatly improve their ability to predict who would still have depressive symptoms 1 month after going home.”
Ms. Pedersen agrees that clinicians should incorporate screening for PPD into their practices and be proactive in encouraging fathers to get help.
“Keep pushing,” she advised, as “men rarely seek help, compared to women, in matters of mental health.”
A version of this article first appeared on WebMD.com.
Michael W., a 38-year-old New Jersey–based attorney, and his wife had been excitedly planning for the birth of their baby and were overjoyed when she was born.
But after that, “I found that parenting a newborn was shockingly exhausting. I felt unprepared for the task, overwhelmed by the burden of the 24-hour-schedule and lack of sleep, and I struggled with feelings of inadequacy,” he said in an interview.
Michael never thought he had postpartum depression (PPD), perhaps because the condition is more commonly associated with women. But a study published in the American Journal of Men’s Health suggests that PPD also affects men.
A team of Danish investigators led by researcher Sarah Pedersen, of the department of public health, Aarhus University, extensively interviewed eight fathers with PPD and found their primary experiences involved feelings of being overwhelmed and powerless or inadequate, which sometimes turned into anger and frustration.
“I think one of the most important take-home messages is that practicing clinicians working with new parents should invite fathers to your consultations and engage the fathers as much as possible,” Ms. Pedersen said in an interview.
The findings also contained a message for parents, she says.
“I hope you will support each other and talk about your feelings and how you experience the transition to parenthood – know that it will take time to adjust to your new role,” she said.
Not enough attention
There’s been too little focus on fathers when it comes to PPD, according to Ms. Pedersen.
“During the last decade, several studies have examined the prevalence of PPD in men, and there is rising evidence that paternal PPD is associated with increased risk of long-term adverse behavioral and emotional outcomes in children,” she said.
Nevertheless, only three studies have been based on interviews with fathers who had personal experience with PPD.
“The purpose of our study was, first of all, to explore the lived experience of fathers who had PPD and, secondly, to gain deeper understanding of their help-seeking behavior – barriers to seeking help and facilitators of help-seeking,” Ms. Pedersen said.
The study was based on “semistructured” interviews with eight Danish fathers (ages 29-38 years) who had had PPD, none of whom had a previous history of depression.
All of them had received a formal diagnosis of PPD by a general practitioner or psychologist, and all had sought or received mental health care and considered themselves recovered from depression at the time of the interview.
The researchers used a technique called interpretative phenomenological analysis to analyze the interviews.
This method “aims to produce in-depth examinations of certain phenomena by examining how individuals make meaning of their own life experiences,” the authors wrote.
A ‘radical change’
Of the fathers, five described the period of pregnancy as a “time of happiness, full of positive expectations about fatherhood.”
But “the fathers’ great expectations were later replaced by a very different reality of fatherhood,” the authors wrote, noting that the transition to fatherhood was, in the words of one participant, a “radical change that you just can’t imagine.”
Most fathers expressed a feeling of being overwhelmed, and three felt unready for the task, which added to their depression.
“The participants wanted to be emotionally and physically present in their child’s life, but during the time of their depression, these kind-hearted intentions changed into feelings of guilt and inadequacy, as the participants did not feel they had enough energy and mental strength to become the kind of fathers they wanted to be,” the authors wrote.
The fathers mentioned stressors they believed contributed to their PPD, including complications during their partners’ pregnancies, unplanned cesarean birth (three fathers), the partners’ difficulties with breastfeeding (five fathers), and employment-related concerns. Five reported that their partners had postpartum emotional distress.
‘Masculine norms’
A second focus of the research was to examine fathers’ help-seeking behaviors, Ms. Pedersen said.
Ultimately, all the men sought formal help, either from their general practitioners or from a health visitor, with two seeking help right after birth.
Although the men were able to recognize changes in mood and behavior in retrospect, many did not regard them as signs of depression before their diagnosis.
Most had heard of PPD, but primarily as it affects women. Three sought information online about paternal PPD but couldn’t find any.
Four participants described experiencing PPD as “taboo,” based on a “combination of false beliefs, stigma, and masculine norms,” the authors stated, since men “are supposed to be big and strong and take care of everything, and suddenly you can’t.”
The authors reported that seven participants were screened for PPD or depression by a health care professional.
“The screening was an important part of the help-seeking process, as this was the first time two of the fathers were introduced to PPD,” the authors noted.
Although the screening “had the potential to spark conversation” about PPD, it was geared toward women, and some participants did not feel it was relevant to them.
“Future research should focus on identification of educational needs about paternal PPD among both parents, health care professionals, and other professionals taking care of new families,” Ms. Pedersen said.
Michael W. says it would have been helpful if someone had prepared him and his wife for what to expect, or if there had been some type of screening. Also, he advises expectant parents to “get some real-life experience by spending time around a newborn to see what’s involved.”
Different symptoms
“We often talk about mothers suffering from PPD, so it is more normalized for mothers to bring it up or for loved ones to ask mothers about how they are doing physically and psychologically after the birth,” Craig Garfield, MD, an attending physician and founder/director of Family and Child Health innovations at Ann and Robert H. Lurie Children’s Hospital, Chicago, said in an interview.
For fathers, “it is not discussed as commonly, so friends and families don’t often ask dads, and dads don’t know where to turn,” said Dr. Garfield, professor of pediatrics and medical social sciences at Northwestern University, Chicago. He was not involved with the study.
He noted that symptoms in fathers might differ from those of mothers.
“I have seen fathers who are anxious or more moody than they had been prior, or more angry, and I have seen fathers who throw themselves into work or begin drinking more – all related to changes in mood and depressive symptoms in the postnatal period,” he said.
Symptoms in men may last longer than in women. Dr. Garfield’s group published a study in which they surveyed 400 mothers and fathers of premature infants in the neonatal intensive care unit (NICU) about depressive symptoms around the time of NICU admission, at discharge home, and then after 30 days at home.
Roughly one-third of mothers screened positive for depressive symptoms around NICU admission, as did 17% of fathers. But the mothers’ depression scores improved by discharge and 30 days after being home, while the fathers’ remained “essentially unchanged,” he said.
“Further, we found that if doctors were to screen mothers and fathers during the NICU stay – at admission or even at discharge – that would greatly improve their ability to predict who would still have depressive symptoms 1 month after going home.”
Ms. Pedersen agrees that clinicians should incorporate screening for PPD into their practices and be proactive in encouraging fathers to get help.
“Keep pushing,” she advised, as “men rarely seek help, compared to women, in matters of mental health.”
A version of this article first appeared on WebMD.com.
Placental allograft, cytology processor, cell-free RNA testing, and male infertility
Human placental allograft

For case reports involving Revita and for more information, visit https://www.stimlabs.com/revita.
FDA approval for cytology processor
For more information, visit: https://www.hologic.com/.
Cell-free RNA testing for pregnancy complications

Currently, Mirvie is recruiting for their Miracle of Life study, which requests that single gestation pregnant mothers who are not scheduled for cesarean delivery provide a blood sample during their second trimester. Women can see if they are eligible for study participation by visiting https://www.curebase.com/study/miracle/home.
For more information, visit: https://mirvie.com/.
Male fertility platform
![]()
For more information, visit: https://posterityhealth.com/.
Human placental allograft
For case reports involving Revita and for more information, visit https://www.stimlabs.com/revita.
FDA approval for cytology processor
For more information, visit: https://www.hologic.com/.
Cell-free RNA testing for pregnancy complications
Currently, Mirvie is recruiting for their Miracle of Life study, which requests that single gestation pregnant mothers who are not scheduled for cesarean delivery provide a blood sample during their second trimester. Women can see if they are eligible for study participation by visiting https://www.curebase.com/study/miracle/home.
For more information, visit: https://mirvie.com/.
Male fertility platform
![]()
For more information, visit: https://posterityhealth.com/.
Human placental allograft
For case reports involving Revita and for more information, visit https://www.stimlabs.com/revita.
FDA approval for cytology processor
For more information, visit: https://www.hologic.com/.
Cell-free RNA testing for pregnancy complications
Currently, Mirvie is recruiting for their Miracle of Life study, which requests that single gestation pregnant mothers who are not scheduled for cesarean delivery provide a blood sample during their second trimester. Women can see if they are eligible for study participation by visiting https://www.curebase.com/study/miracle/home.
For more information, visit: https://mirvie.com/.
Male fertility platform
![]()
For more information, visit: https://posterityhealth.com/.
VTE prevention: Patient selection and treatment planning throughout pregnancy
Pregnancy and the postpartum period are times of increased risk for venous thromboembolism (VTE). While VTE is a rare event overall, it is responsible for more than 9% of maternal deaths in the United States.1 The increased risk of VTE exists throughout pregnancy, rising in the third trimester.2 The highest-risk period is the first 6 weeks postpartum, likely peaking in the first 2 to 3 weeks and returning to baseline at about 12 weeks postpartum.2,3
To reduce this source of maternal harm, the National Partnership for Maternal Safety and the Council on Patient Safety in Women’s Health Care recommend the use of VTE prevention bundles. Bundles include standard assessment of risk during prenatal care, any admission to the hospital, and postpartum coupled with standard recommendations for treatment.4-6 Multiple published guidelines are available for prevention of VTE in pregnancy, and they provide varying recommendations on patient selection and treatment. Many of these recommendations are based on low quality of evidence, making the choice of standard practice difficult.
In this article, I attempt to simplify patient selection and treatment based on currently published guidelines from the American College of Obstetricians and Gynecologists (ACOG), Royal College of Obstetricians and Gynaecologists (RCOG), American College of Chest Physicians (CHEST), American Society of Hematology (ASH), and expert opinion.
Determining VTE risk and need for prophylaxis
CASE 1 Woman with factor V Leiden
A 25-year-old woman (G1P0) presents for her initial prenatal visit. She says she is a carrier for factor V Leiden but has never had a clot. She was tested after her sister had a VTE. She asks, does she need VTE prophylaxis before her delivery?
What are the considerations and options for this patient?
Options for VTE prophylaxis
Before considering patients at risk for VTE, it is helpful to review the options for prophylaxis. Patients can undergo clinical surveillance or routine care with attention to VTE symptoms and a low threshold for workup.
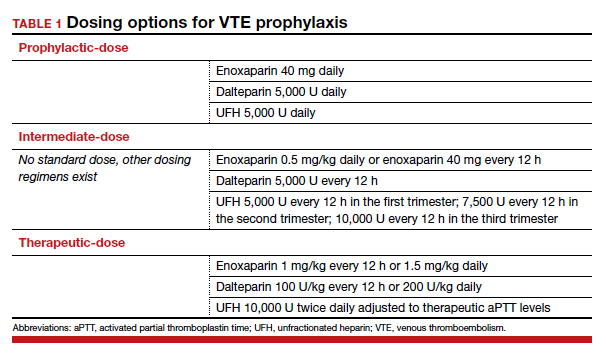
There are 3 categories of chemoprophylaxis for prevention of VTE. (TABLE 1 offers examples of dosing regimens.) No strategy has been proven optimal over another:
- prophylactic-dose: the lowest, fixed dose.
- intermediate-dose: lacks a standard definition and is any dose higher than prophylactic-dose but lower than therapeutic-dose. This includes fixed twice-daily doses, weight-based doses, and incrementally increasing doses.
- therapeutic-dose: typically used for treatment but mentioned here since patients with high-risk conditions may use it for prevention of VTE.
The preferred agent for VTE chemoprophylaxis is low molecular weight heparin (LMWH; dalteparin, enoxaparin). LMWH has a lower risk of complications than unfractionated heparin (UFH) and can be injected once daily. LMWH and UFH do not cross the placenta. LMWH and UFH are safe in breastfeeding. Oral direct thrombin inhibitors and anti-Xa inhibitors are not recommended in pregnancy or lactation at this time. Warfarin is avoided in pregnancy except in situations with mechanical heart valves, which will not be addressed here. Patients taking warfarin for long-term anticoagulation can transition back while breastfeeding with appropriate bridging.
Expert opinion recommends antepartum chemoprophylaxis when there is a 2% to 3% risk of VTE in pregnancy.7-9 This is balanced against an approximately 2% overall risk of bleeding, with less than 1% risk of bleeding antepartum.9
Continue to: Risk factors for VTE...
Risk factors for VTE
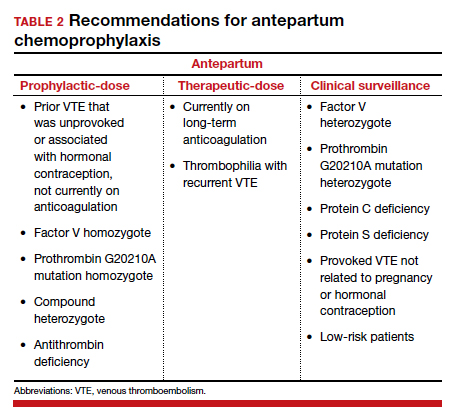
History of VTE. The most important risk factor for VTE is a personal history of prior VTE.6 Recurrence risks have been widely reported and depend on the factors surrounding the initial event. For patients with a prior provoked deep vein thrombosis (DVT; associated with trauma or surgery), the antepartum VTE risk likely is less than 1%, and VTE chemoprophylaxis is not recommended antepartum.7
For patients with a prior VTE that was not associated with surgery or trauma (unprovoked), the risk is approximately 3%; for prior VTE related to pregnancy or hormonal contraception, the risk is approximately 6%.7 For both of these groups, prophylactic-dose antepartum is recommended. Patients with recurrent VTE are often taking long-term anticoagulation. Anyone on long-term anticoagulation should be placed on therapeutic-dose antepartum. For patients not receiving long-term anticoagulation, consider a hematology consultation when available, and begin an intermediate-dose or therapeutic-dose regimen after assessing other risk factors and the risk of bleeding and discussing treatment with the patient.
Thrombophilias. The next most important risk factor is the presence of inherited thrombophilias.6 Factor V homozygote, prothrombin G20210A mutation homozygote, antithrombin deficiency, and combined factor V heterozygote and prothrombin G20210A heterozygote (also called compound heterozygote) have the strongest association with VTE in pregnancy.8 It is recommended that patients with these high-risk thrombophilias receive prophylactic-dose antepartum.8
Factor V heterozygote, prothrombin G20210A mutation heterozygote, and protein C or protein S deficiency are considered low-risk thrombophilias. Patients with low-risk thrombophilias and no personal history of VTE or first-degree relative with VTE can be monitored with clinical surveillance antepartum. However, if a family history of VTE or other risk factors for VTE are present, antepartum prophylactic-dose is recommended. Clinical factors to consider antepartum include obesity, age older than 35 years, parity of 3 or higher, varicose veins, immobility, smoking, assisted reproductive technology use, multiple gestation, and preeclampsia.10
Antiphospholipid syndrome (APS) is another high-risk condition. For patients not taking long-term anticoagulation antepartum, prophylactic-dose is recommended. For patients on long-term anticoagulation, therapeutic-dose is recommended.
Other medical conditions. Patients with medical conditions that place them at high risk for VTE may warrant prophylactic-dose antepartum. These include active cancer, active systemic lupus erythematosus, sickle cell disease, nephropathy, and inflammatory bowel disease.10 This decision can be made in conjunction with other specialists caring for the patient.
Antepartum prophylactic-dose is not recommended for low-risk patients as there is less than 1% risk of VTE.7 (TABLE 2 summarizes antepartum chemoprophylaxis recommendations.)
CASE 1 continued Patient develops another VTE risk factor
The patient is being followed with clinical surveillance. At 19 weeks’ gestation, she presents to the emergency department with shortness of breath and fever. She is diagnosed with COVID-19 and is admitted by a medicine service. They call the OB team to ask for recommendations regarding anticoagulation.
What should the next steps include?
Hospitalization and nonobstetric surgery are risk factors for VTE. Many hospitals use a standardized assessment for all inpatients, such as the Padua or Caprini VTE risk assessment scores. These can be modified for use in pregnant patients, although neither scoring system is currently validated for use in pregnancy.5 For any pregnant patient admitted to the hospital, mechanical prophylaxis is recommended.
COVID-19. Infection with the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and its associated clinical syndrome, COVID-19, is associated with increased rates of VTE. Recommendations for pregnant patients with COVID-19 are the same as for the general population. During hospitalization for COVID-19, pregnant patients should be placed on prophylactic-dose chemoprophylaxis. Patients should not be discharged home on chemoprophylaxis, and patients managed as outpatients for their disease do not need chemoprophylaxis.11
Management approach. Prophylactic-dose administration is recommended during hospital stay for all patients admitted with anticipated length of stay of 3 days or longer and who are not at high risk for bleeding or delivery.10 Both LMWH and UFH are options for inpatients. For any nonobstetric surgery or admission, LMWH may be most appropriate. However, as most obstetrics admissions are at increased risk for delivery, UFH 5,000 U twice daily to 3 times daily is the best option to increase the chances for neuraxial anesthesia. (I review anesthesia considerations for delivery later in this article.) For patients at high risk for bleeding or delivery, mechanical prophylaxis alone, with elastic stockings or pneumatic compression devices, can be used.
Continue to: CASE 1 continued Patient is discharged home...
CASE 1 continued Patient is discharged home
The patient received enoxaparin while she was in the hospital. She is now discharged and doing well. She asks, will she need anticoagulation prophylaxis after delivery?
How would you counsel her?
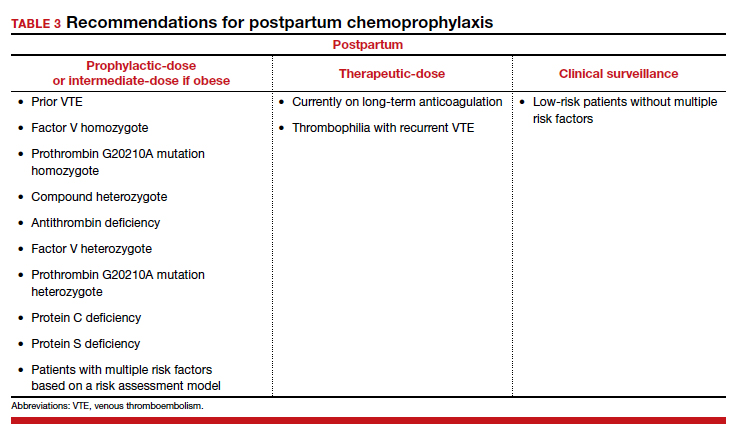
Chemoprophylaxis in the postpartum period
With no risk of fetal harm and a higher risk of VTE per day, the threshold for chemoprophylaxis is lower in the postpartum period. The risk of postpartum bleeding is less than 1%, with the most common complication being wound hematomas (0.61%).9 For this case patient, the COVID-19 diagnosis does not alter the recommendations for postpartum chemoprophylaxis. Additionally, as the need for neuraxial anesthesia has passed, the use of intermediate-dose chemoprophylaxis over prophylactic-dose is advocated in the postpartum period, especially in obese patients.12
As mentioned previously, there is no standard definition of intermediate-dose. Data suggest that a weight-based intermediate-dose is most likely to achieve therapeutic levels of anti-Xa in this high-risk population compared with a fixed dose.13,14 For example, enoxaparin 0.5 mg/kg twice daily is recommended for patients with class 3 obesity or higher by the Society for Maternal-Fetal Medicine.12
As a rule, anyone who was on chemoprophylaxis antepartum should be continued on at least an equivalent dose for 6 weeks postpartum. Postpartum, patients with any prior DVT should take prophylactic-dose or intermediate-dose chemoprophylaxis for 6 weeks. Patients with a known high-risk thrombophilia should receive prophylactic-dose or intermediate-dose chemoprophylaxis postpartum for 6 weeks. For patients with a low-risk thrombophilia, prophylactic-dose or intermediate-dose chemoprophylaxis is recommended for 6 weeks.
For low-risk patients without prior VTE or thrombophilia, standardized risk assessment is recommended.
Cesarean delivery
Cesarean delivery (CD) is a risk factor for postpartum VTE.9 A universal chemoprophylaxis strategy has not been proven in this patient population. Mechanical prophylaxis with sequential compression devices is recommended for all patients undergoing CD pre-procedure and until patients are fully ambulatory.8,9 Early ambulation also should be encouraged.
Many risk assessment models are available for postoperative VTE prevention, and they have widely different chemoprophylaxis rates. Studies have shown chemoprophylaxis rates of 85% by RCOG, 1% by ACOG, 35% by CHEST, 94% by Caprini, and less than 1% by Padua.15,16 In addition to the antepartum patient-specific risk factors mentioned, postpartum risk factors include infection, postpartum hemorrhage, and transfusion. Based on data extrapolated from the nonobstetric literature, chemoprophylaxis is recommended until discharge from the hospital unless risk factors are expected to continue.9
Neuraxial anesthesia
For patients who require postpartum chemoprophylaxis, the Society for Obstetric Anesthesia and Perinatology (SOAP) offers evidence-based guidelines for use after neuraxial anesthesia. UFH can be initiated 1 hour or longer after a neuraxial procedure and 1 hour or longer after catheter removal. Prophylactic-dose LMWH can be restarted at 12 hours or longer after a neuraxial procedure and at 4 to 6 hours or longer after catheter removal. For patients restarting intermediate-dose or therapeutic-dose, the recommendations are to wait 24 hours or longer after a neuraxial procedure and 4 hours or longer after catheter removal.17 Timing can be individualized based on the patient’s risk of hemorrhage and surgical bleeding. Although it may be tempting to delay chemoprophylaxis in the setting of bleeding, postpartum hemorrhage and transfusion increase the risks of VTE. In this setting, it is best to consider the use of UFH, which safely can be started earlier than LMWH.
For patients without neuraxial anesthesia, ACOG recommends chemoprophylaxis 4 to 6 hours after vaginal delivery and 6 to 12 hours after CD.8 (TABLE 3 summarizes recommendations for postpartum chemoprophylaxis.)
Continue to: Adjusting the anticoagulation regimen...
Adjusting the anticoagulation regimen
CASE 2 Pregnant woman with prior VTE
A 36-year-old woman (G1P0) with prior VTE is taking enoxaparin 40 mg daily. She asks, does she need any blood work for her anticoagulation?
What would you test for?
Increased renal clearance of LMWH and increased volume of distribution during pregnancy has led to the consideration of monitoring anti-Xa levels. There are no published standards or recommendations for dose adjustment. At this time, anti-Xa level monitoring antepartum is not recommended, but it may be considered when a patient is at the extremes of weight. With a weight-based strategy in the postpartum period, monitoring is not recommended as studies show a higher likelihood of therapeutic anti-Xa levels with this approach.13,14 This is an active area of research, and these recommendations may change.
For prophylactic-dose or intermediate-dose anticoagulation, a peak anti-Xa level of 0.2 to 0.6 U/mL is generally accepted as the target. For therapeutic-dose, a peak anti-Xa level of 0.6 to 1.2 U/mL is generally accepted as the therapeutic range. This blood draw must be collected 4 hours after the third dose.
CASE 2 continued Anticoagulation considerations nearing delivery
The patient is now at 36 weeks’ gestation, and she asks, what should be done regarding her anticoagulation prior to delivery?
What would be an appropriate approach?
Traditionally, patients were transitioned to UFH at 36 weeks and allowed to present in spontaneous labor to increase the likelihood of neuraxial anesthesia. The alternative is to continue prophylactic-dose LMWH until a scheduled delivery. While the SOAP guidelines establish the timeframe that is safe to proceed with neuraxial anesthesia, there is variation in practice, so consider discussing this with your anesthesia providers.
SOAP considers prophylactic-dose UFH to be 5,000 U 2 to 3 times per day. In this setting, neuraxial anesthesia can be placed more than 4 to 6 hours from the last dose.17 But due to the pharmacokinetics of pregnancy, ACOG recommends 10,000 U in the third trimester.8 This dose is considered intermediate-dose by SOAP, and 12 hours or longer plus a normal activated partial thromboplastin time (aPTT) or undetectable anti-Xa level are required prior to neuraxial anesthesia. This is the same time allowed for prophylactic-dose LMWH without lab work. Prophylactic-dose LMWH is considered to be enoxaparin 40 mg or less daily or 30 mg twice daily, and dalteparin 5,000 U daily. For therapeutic-dose LMWH or UFH, 24 hours or more from last dose is recommended prior to neuraxial anesthesia. For intermediate-dose LMWH, data are limited to recommend anything between 12 and 24 hours.17
In my practice, we favor a shared decision-making approach with patients. We discuss the likelihood of labor prior to 39 weeks based on a patient’s history, the importance of neuraxial anesthesia to the patient, and the importance of the number of daily injections. Most patients continue enoxaparin until a scheduled induction, and they are instructed to skip their dose if labor symptoms begin. Patients at high risk for preterm delivery can be transitioned to heparin earlier than 36 weeks. ●
- Creanga AA, Syverson C, Seed K, et al. Pregnancy-related mortality in the United States, 2011-2013. Obstet Gynecol. 2017;130:366-373. doi: 10.1097/AOG.0000000000002114.
- Kourlaba G, Relakis J, Kontodimas S, et al. A systematic review and meta-analysis of the epidemiology and burden of venous thromboembolism among pregnant women. Int J Gynaecol Obstet. 2016;132:4-10. doi: 10.1016/j.ijgo.2015.06.054.
- Sultan AA, West J, Tata LJ, et al. Risk of first venous thromboembolism in and around pregnancy: a population-based cohort study. Br J Haematol. 2012;156:366-373. doi: 10.1111/j.1365-2141.2011.08956.x.
- American College of Obstetricians and Gynecologists. Council on Patient Safety in Women’s Health Care: maternal venous thromboembolism (+AIM). 2015. https://safehealthcareforeverywoman.org/council/patient-safety-bundles/maternal-safety-bundles/maternal-venous-thromboembolism-aim/. Accessed February 26, 2021.
- Urato AC, Abi-Jaoude E, Abramson J, et al. National Partnership for Maternal Safety: consensus bundle on venous thromboembolism. Obstet Gynecol. 2019;134:1115-1117. doi: 10.1097/AOG.0000000000003540.
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. ACOG practice bulletin no. 196: thromboembolism in pregnancy. Obstet Gynecol. 2018;132:e1-e17. doi: 10.1097/AOG.0000000000002706.
- Bates SM, Rajasekhar A, Middeldorp S, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: venous thromboembolism in the context of pregnancy. Blood Adv. 2018;2:3317-3359. doi: 10.1182/bloodadvances.2018024802.
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics. ACOG practice bulletin no. 197: inherited thrombophilias in pregnancy. Obstet Gynecol. 2018;132:e18-e34. doi: 10.1097/AOG.0000000000002703.
- Bates SM, Greer IA, Middeldorp S, et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2, suppl):e691S-e736S. doi: 10.1378/chest.11-2300.
- Lamont MC, McDermott C, Thomson AJ, et al. United Kingdom recommendations for obstetric venous thromboembolism prophylaxis: evidence and rationale. Semin Perinatol. 2019;43:222-228. doi: 10.1053/j.semperi.2019.03.008.
- National Institutes of Health. COVID-19 Treatment Guidelines Panel. Coronavirus disease 2019 (COVID-19) treatment guidelines. https://www.covid19treatmentguidelines.nih.gov/. Accessed February 26, 2021.
- Society for Maternal-Fetal Medicine (SMFM); Pacheco LD, Saade G, Metz TD. Society for Maternal-Fetal Medicine Consult Series #51: thromboembolism prophylaxis for cesarean delivery. Am J Obstet Gynecol. 2020;223:B11-B17. doi: 10.1016/j.ajog.2020.04.032.
- Overcash RT, Somers AT, LaCoursiere DY. Enoxaparin dosing after cesarean delivery in morbidly obese women. Obstet Gynecol. 2015;125:1371-1376. doi: 10.1097/AOG.0000000000000873.
- Hiscock RJ, Casey E, Simmons SW, et al. Peak plasma anti-Xa levels after first and third doses of enoxaparin in women receiving weight-based thromboprophylaxis following caesarean section: a prospective cohort study. Int J Obstet Anesth. 2013;22:280-288. doi: 10.1016/j.ijoa.2013.05.008.
- Palmerola KL, D’Alton ME, Brock CO, et al. A comparison of recommendations for pharmacologic thromboembolism prophylaxis after caesarean delivery from three major guidelines. BJOG. 2016;123:2157-2162. doi: 10.1111/1471-0528.13706.
- Tran JP, Stribling SS, Ibezim UC, et al. Performance of risk assessment models for peripartum thromboprophylaxis. Reprod Sci. 2019;26:1243-1248. doi: 10.1177/1933719118813197.
- Leffert L, Butwick A, Carvalho B, et al; members of the SOAP VTE Taskforce. The Society for Obstetric Anesthesia and Perinatology consensus statement on the anesthetic management of pregnant and postpartum women receiving thromboprophylaxis or higher dose anticoagulants. Anesth Analg. 2018;126:928-944. doi: 10.1213/ANE.0000000000002530.

Dr. Lauring is Assistant Professor, Division
of Maternal Fetal Medicine, Department
of Obstetrics and Gynecology, University
of Massachusetts Medical School,
and Maternity Center Medical Director,
UMass Memorial Health, Worcester.
The author reports no financial relationships relevant to this article.
Dr. Lauring is Assistant Professor, Division
of Maternal Fetal Medicine, Department
of Obstetrics and Gynecology, University
of Massachusetts Medical School,
and Maternity Center Medical Director,
UMass Memorial Health, Worcester.
The author reports no financial relationships relevant to this article.
Dr. Lauring is Assistant Professor, Division
of Maternal Fetal Medicine, Department
of Obstetrics and Gynecology, University
of Massachusetts Medical School,
and Maternity Center Medical Director,
UMass Memorial Health, Worcester.
The author reports no financial relationships relevant to this article.
Pregnancy and the postpartum period are times of increased risk for venous thromboembolism (VTE). While VTE is a rare event overall, it is responsible for more than 9% of maternal deaths in the United States.1 The increased risk of VTE exists throughout pregnancy, rising in the third trimester.2 The highest-risk period is the first 6 weeks postpartum, likely peaking in the first 2 to 3 weeks and returning to baseline at about 12 weeks postpartum.2,3
To reduce this source of maternal harm, the National Partnership for Maternal Safety and the Council on Patient Safety in Women’s Health Care recommend the use of VTE prevention bundles. Bundles include standard assessment of risk during prenatal care, any admission to the hospital, and postpartum coupled with standard recommendations for treatment.4-6 Multiple published guidelines are available for prevention of VTE in pregnancy, and they provide varying recommendations on patient selection and treatment. Many of these recommendations are based on low quality of evidence, making the choice of standard practice difficult.
In this article, I attempt to simplify patient selection and treatment based on currently published guidelines from the American College of Obstetricians and Gynecologists (ACOG), Royal College of Obstetricians and Gynaecologists (RCOG), American College of Chest Physicians (CHEST), American Society of Hematology (ASH), and expert opinion.
Determining VTE risk and need for prophylaxis
CASE 1 Woman with factor V Leiden
A 25-year-old woman (G1P0) presents for her initial prenatal visit. She says she is a carrier for factor V Leiden but has never had a clot. She was tested after her sister had a VTE. She asks, does she need VTE prophylaxis before her delivery?
What are the considerations and options for this patient?
Options for VTE prophylaxis
Before considering patients at risk for VTE, it is helpful to review the options for prophylaxis. Patients can undergo clinical surveillance or routine care with attention to VTE symptoms and a low threshold for workup.
There are 3 categories of chemoprophylaxis for prevention of VTE. (TABLE 1 offers examples of dosing regimens.) No strategy has been proven optimal over another:
- prophylactic-dose: the lowest, fixed dose.
- intermediate-dose: lacks a standard definition and is any dose higher than prophylactic-dose but lower than therapeutic-dose. This includes fixed twice-daily doses, weight-based doses, and incrementally increasing doses.
- therapeutic-dose: typically used for treatment but mentioned here since patients with high-risk conditions may use it for prevention of VTE.
The preferred agent for VTE chemoprophylaxis is low molecular weight heparin (LMWH; dalteparin, enoxaparin). LMWH has a lower risk of complications than unfractionated heparin (UFH) and can be injected once daily. LMWH and UFH do not cross the placenta. LMWH and UFH are safe in breastfeeding. Oral direct thrombin inhibitors and anti-Xa inhibitors are not recommended in pregnancy or lactation at this time. Warfarin is avoided in pregnancy except in situations with mechanical heart valves, which will not be addressed here. Patients taking warfarin for long-term anticoagulation can transition back while breastfeeding with appropriate bridging.
Expert opinion recommends antepartum chemoprophylaxis when there is a 2% to 3% risk of VTE in pregnancy.7-9 This is balanced against an approximately 2% overall risk of bleeding, with less than 1% risk of bleeding antepartum.9
Continue to: Risk factors for VTE...
Risk factors for VTE
History of VTE. The most important risk factor for VTE is a personal history of prior VTE.6 Recurrence risks have been widely reported and depend on the factors surrounding the initial event. For patients with a prior provoked deep vein thrombosis (DVT; associated with trauma or surgery), the antepartum VTE risk likely is less than 1%, and VTE chemoprophylaxis is not recommended antepartum.7
For patients with a prior VTE that was not associated with surgery or trauma (unprovoked), the risk is approximately 3%; for prior VTE related to pregnancy or hormonal contraception, the risk is approximately 6%.7 For both of these groups, prophylactic-dose antepartum is recommended. Patients with recurrent VTE are often taking long-term anticoagulation. Anyone on long-term anticoagulation should be placed on therapeutic-dose antepartum. For patients not receiving long-term anticoagulation, consider a hematology consultation when available, and begin an intermediate-dose or therapeutic-dose regimen after assessing other risk factors and the risk of bleeding and discussing treatment with the patient.
Thrombophilias. The next most important risk factor is the presence of inherited thrombophilias.6 Factor V homozygote, prothrombin G20210A mutation homozygote, antithrombin deficiency, and combined factor V heterozygote and prothrombin G20210A heterozygote (also called compound heterozygote) have the strongest association with VTE in pregnancy.8 It is recommended that patients with these high-risk thrombophilias receive prophylactic-dose antepartum.8
Factor V heterozygote, prothrombin G20210A mutation heterozygote, and protein C or protein S deficiency are considered low-risk thrombophilias. Patients with low-risk thrombophilias and no personal history of VTE or first-degree relative with VTE can be monitored with clinical surveillance antepartum. However, if a family history of VTE or other risk factors for VTE are present, antepartum prophylactic-dose is recommended. Clinical factors to consider antepartum include obesity, age older than 35 years, parity of 3 or higher, varicose veins, immobility, smoking, assisted reproductive technology use, multiple gestation, and preeclampsia.10
Antiphospholipid syndrome (APS) is another high-risk condition. For patients not taking long-term anticoagulation antepartum, prophylactic-dose is recommended. For patients on long-term anticoagulation, therapeutic-dose is recommended.
Other medical conditions. Patients with medical conditions that place them at high risk for VTE may warrant prophylactic-dose antepartum. These include active cancer, active systemic lupus erythematosus, sickle cell disease, nephropathy, and inflammatory bowel disease.10 This decision can be made in conjunction with other specialists caring for the patient.
Antepartum prophylactic-dose is not recommended for low-risk patients as there is less than 1% risk of VTE.7 (TABLE 2 summarizes antepartum chemoprophylaxis recommendations.)
CASE 1 continued Patient develops another VTE risk factor
The patient is being followed with clinical surveillance. At 19 weeks’ gestation, she presents to the emergency department with shortness of breath and fever. She is diagnosed with COVID-19 and is admitted by a medicine service. They call the OB team to ask for recommendations regarding anticoagulation.
What should the next steps include?
Hospitalization and nonobstetric surgery are risk factors for VTE. Many hospitals use a standardized assessment for all inpatients, such as the Padua or Caprini VTE risk assessment scores. These can be modified for use in pregnant patients, although neither scoring system is currently validated for use in pregnancy.5 For any pregnant patient admitted to the hospital, mechanical prophylaxis is recommended.
COVID-19. Infection with the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and its associated clinical syndrome, COVID-19, is associated with increased rates of VTE. Recommendations for pregnant patients with COVID-19 are the same as for the general population. During hospitalization for COVID-19, pregnant patients should be placed on prophylactic-dose chemoprophylaxis. Patients should not be discharged home on chemoprophylaxis, and patients managed as outpatients for their disease do not need chemoprophylaxis.11
Management approach. Prophylactic-dose administration is recommended during hospital stay for all patients admitted with anticipated length of stay of 3 days or longer and who are not at high risk for bleeding or delivery.10 Both LMWH and UFH are options for inpatients. For any nonobstetric surgery or admission, LMWH may be most appropriate. However, as most obstetrics admissions are at increased risk for delivery, UFH 5,000 U twice daily to 3 times daily is the best option to increase the chances for neuraxial anesthesia. (I review anesthesia considerations for delivery later in this article.) For patients at high risk for bleeding or delivery, mechanical prophylaxis alone, with elastic stockings or pneumatic compression devices, can be used.
Continue to: CASE 1 continued Patient is discharged home...
CASE 1 continued Patient is discharged home
The patient received enoxaparin while she was in the hospital. She is now discharged and doing well. She asks, will she need anticoagulation prophylaxis after delivery?
How would you counsel her?
Chemoprophylaxis in the postpartum period
With no risk of fetal harm and a higher risk of VTE per day, the threshold for chemoprophylaxis is lower in the postpartum period. The risk of postpartum bleeding is less than 1%, with the most common complication being wound hematomas (0.61%).9 For this case patient, the COVID-19 diagnosis does not alter the recommendations for postpartum chemoprophylaxis. Additionally, as the need for neuraxial anesthesia has passed, the use of intermediate-dose chemoprophylaxis over prophylactic-dose is advocated in the postpartum period, especially in obese patients.12
As mentioned previously, there is no standard definition of intermediate-dose. Data suggest that a weight-based intermediate-dose is most likely to achieve therapeutic levels of anti-Xa in this high-risk population compared with a fixed dose.13,14 For example, enoxaparin 0.5 mg/kg twice daily is recommended for patients with class 3 obesity or higher by the Society for Maternal-Fetal Medicine.12
As a rule, anyone who was on chemoprophylaxis antepartum should be continued on at least an equivalent dose for 6 weeks postpartum. Postpartum, patients with any prior DVT should take prophylactic-dose or intermediate-dose chemoprophylaxis for 6 weeks. Patients with a known high-risk thrombophilia should receive prophylactic-dose or intermediate-dose chemoprophylaxis postpartum for 6 weeks. For patients with a low-risk thrombophilia, prophylactic-dose or intermediate-dose chemoprophylaxis is recommended for 6 weeks.
For low-risk patients without prior VTE or thrombophilia, standardized risk assessment is recommended.
Cesarean delivery
Cesarean delivery (CD) is a risk factor for postpartum VTE.9 A universal chemoprophylaxis strategy has not been proven in this patient population. Mechanical prophylaxis with sequential compression devices is recommended for all patients undergoing CD pre-procedure and until patients are fully ambulatory.8,9 Early ambulation also should be encouraged.
Many risk assessment models are available for postoperative VTE prevention, and they have widely different chemoprophylaxis rates. Studies have shown chemoprophylaxis rates of 85% by RCOG, 1% by ACOG, 35% by CHEST, 94% by Caprini, and less than 1% by Padua.15,16 In addition to the antepartum patient-specific risk factors mentioned, postpartum risk factors include infection, postpartum hemorrhage, and transfusion. Based on data extrapolated from the nonobstetric literature, chemoprophylaxis is recommended until discharge from the hospital unless risk factors are expected to continue.9
Neuraxial anesthesia
For patients who require postpartum chemoprophylaxis, the Society for Obstetric Anesthesia and Perinatology (SOAP) offers evidence-based guidelines for use after neuraxial anesthesia. UFH can be initiated 1 hour or longer after a neuraxial procedure and 1 hour or longer after catheter removal. Prophylactic-dose LMWH can be restarted at 12 hours or longer after a neuraxial procedure and at 4 to 6 hours or longer after catheter removal. For patients restarting intermediate-dose or therapeutic-dose, the recommendations are to wait 24 hours or longer after a neuraxial procedure and 4 hours or longer after catheter removal.17 Timing can be individualized based on the patient’s risk of hemorrhage and surgical bleeding. Although it may be tempting to delay chemoprophylaxis in the setting of bleeding, postpartum hemorrhage and transfusion increase the risks of VTE. In this setting, it is best to consider the use of UFH, which safely can be started earlier than LMWH.
For patients without neuraxial anesthesia, ACOG recommends chemoprophylaxis 4 to 6 hours after vaginal delivery and 6 to 12 hours after CD.8 (TABLE 3 summarizes recommendations for postpartum chemoprophylaxis.)
Continue to: Adjusting the anticoagulation regimen...
Adjusting the anticoagulation regimen
CASE 2 Pregnant woman with prior VTE
A 36-year-old woman (G1P0) with prior VTE is taking enoxaparin 40 mg daily. She asks, does she need any blood work for her anticoagulation?
What would you test for?
Increased renal clearance of LMWH and increased volume of distribution during pregnancy has led to the consideration of monitoring anti-Xa levels. There are no published standards or recommendations for dose adjustment. At this time, anti-Xa level monitoring antepartum is not recommended, but it may be considered when a patient is at the extremes of weight. With a weight-based strategy in the postpartum period, monitoring is not recommended as studies show a higher likelihood of therapeutic anti-Xa levels with this approach.13,14 This is an active area of research, and these recommendations may change.
For prophylactic-dose or intermediate-dose anticoagulation, a peak anti-Xa level of 0.2 to 0.6 U/mL is generally accepted as the target. For therapeutic-dose, a peak anti-Xa level of 0.6 to 1.2 U/mL is generally accepted as the therapeutic range. This blood draw must be collected 4 hours after the third dose.
CASE 2 continued Anticoagulation considerations nearing delivery
The patient is now at 36 weeks’ gestation, and she asks, what should be done regarding her anticoagulation prior to delivery?
What would be an appropriate approach?
Traditionally, patients were transitioned to UFH at 36 weeks and allowed to present in spontaneous labor to increase the likelihood of neuraxial anesthesia. The alternative is to continue prophylactic-dose LMWH until a scheduled delivery. While the SOAP guidelines establish the timeframe that is safe to proceed with neuraxial anesthesia, there is variation in practice, so consider discussing this with your anesthesia providers.
SOAP considers prophylactic-dose UFH to be 5,000 U 2 to 3 times per day. In this setting, neuraxial anesthesia can be placed more than 4 to 6 hours from the last dose.17 But due to the pharmacokinetics of pregnancy, ACOG recommends 10,000 U in the third trimester.8 This dose is considered intermediate-dose by SOAP, and 12 hours or longer plus a normal activated partial thromboplastin time (aPTT) or undetectable anti-Xa level are required prior to neuraxial anesthesia. This is the same time allowed for prophylactic-dose LMWH without lab work. Prophylactic-dose LMWH is considered to be enoxaparin 40 mg or less daily or 30 mg twice daily, and dalteparin 5,000 U daily. For therapeutic-dose LMWH or UFH, 24 hours or more from last dose is recommended prior to neuraxial anesthesia. For intermediate-dose LMWH, data are limited to recommend anything between 12 and 24 hours.17
In my practice, we favor a shared decision-making approach with patients. We discuss the likelihood of labor prior to 39 weeks based on a patient’s history, the importance of neuraxial anesthesia to the patient, and the importance of the number of daily injections. Most patients continue enoxaparin until a scheduled induction, and they are instructed to skip their dose if labor symptoms begin. Patients at high risk for preterm delivery can be transitioned to heparin earlier than 36 weeks. ●
Pregnancy and the postpartum period are times of increased risk for venous thromboembolism (VTE). While VTE is a rare event overall, it is responsible for more than 9% of maternal deaths in the United States.1 The increased risk of VTE exists throughout pregnancy, rising in the third trimester.2 The highest-risk period is the first 6 weeks postpartum, likely peaking in the first 2 to 3 weeks and returning to baseline at about 12 weeks postpartum.2,3
To reduce this source of maternal harm, the National Partnership for Maternal Safety and the Council on Patient Safety in Women’s Health Care recommend the use of VTE prevention bundles. Bundles include standard assessment of risk during prenatal care, any admission to the hospital, and postpartum coupled with standard recommendations for treatment.4-6 Multiple published guidelines are available for prevention of VTE in pregnancy, and they provide varying recommendations on patient selection and treatment. Many of these recommendations are based on low quality of evidence, making the choice of standard practice difficult.
In this article, I attempt to simplify patient selection and treatment based on currently published guidelines from the American College of Obstetricians and Gynecologists (ACOG), Royal College of Obstetricians and Gynaecologists (RCOG), American College of Chest Physicians (CHEST), American Society of Hematology (ASH), and expert opinion.
Determining VTE risk and need for prophylaxis
CASE 1 Woman with factor V Leiden
A 25-year-old woman (G1P0) presents for her initial prenatal visit. She says she is a carrier for factor V Leiden but has never had a clot. She was tested after her sister had a VTE. She asks, does she need VTE prophylaxis before her delivery?
What are the considerations and options for this patient?
Options for VTE prophylaxis
Before considering patients at risk for VTE, it is helpful to review the options for prophylaxis. Patients can undergo clinical surveillance or routine care with attention to VTE symptoms and a low threshold for workup.
There are 3 categories of chemoprophylaxis for prevention of VTE. (TABLE 1 offers examples of dosing regimens.) No strategy has been proven optimal over another:
- prophylactic-dose: the lowest, fixed dose.
- intermediate-dose: lacks a standard definition and is any dose higher than prophylactic-dose but lower than therapeutic-dose. This includes fixed twice-daily doses, weight-based doses, and incrementally increasing doses.
- therapeutic-dose: typically used for treatment but mentioned here since patients with high-risk conditions may use it for prevention of VTE.
The preferred agent for VTE chemoprophylaxis is low molecular weight heparin (LMWH; dalteparin, enoxaparin). LMWH has a lower risk of complications than unfractionated heparin (UFH) and can be injected once daily. LMWH and UFH do not cross the placenta. LMWH and UFH are safe in breastfeeding. Oral direct thrombin inhibitors and anti-Xa inhibitors are not recommended in pregnancy or lactation at this time. Warfarin is avoided in pregnancy except in situations with mechanical heart valves, which will not be addressed here. Patients taking warfarin for long-term anticoagulation can transition back while breastfeeding with appropriate bridging.
Expert opinion recommends antepartum chemoprophylaxis when there is a 2% to 3% risk of VTE in pregnancy.7-9 This is balanced against an approximately 2% overall risk of bleeding, with less than 1% risk of bleeding antepartum.9
Continue to: Risk factors for VTE...
Risk factors for VTE
History of VTE. The most important risk factor for VTE is a personal history of prior VTE.6 Recurrence risks have been widely reported and depend on the factors surrounding the initial event. For patients with a prior provoked deep vein thrombosis (DVT; associated with trauma or surgery), the antepartum VTE risk likely is less than 1%, and VTE chemoprophylaxis is not recommended antepartum.7
For patients with a prior VTE that was not associated with surgery or trauma (unprovoked), the risk is approximately 3%; for prior VTE related to pregnancy or hormonal contraception, the risk is approximately 6%.7 For both of these groups, prophylactic-dose antepartum is recommended. Patients with recurrent VTE are often taking long-term anticoagulation. Anyone on long-term anticoagulation should be placed on therapeutic-dose antepartum. For patients not receiving long-term anticoagulation, consider a hematology consultation when available, and begin an intermediate-dose or therapeutic-dose regimen after assessing other risk factors and the risk of bleeding and discussing treatment with the patient.
Thrombophilias. The next most important risk factor is the presence of inherited thrombophilias.6 Factor V homozygote, prothrombin G20210A mutation homozygote, antithrombin deficiency, and combined factor V heterozygote and prothrombin G20210A heterozygote (also called compound heterozygote) have the strongest association with VTE in pregnancy.8 It is recommended that patients with these high-risk thrombophilias receive prophylactic-dose antepartum.8
Factor V heterozygote, prothrombin G20210A mutation heterozygote, and protein C or protein S deficiency are considered low-risk thrombophilias. Patients with low-risk thrombophilias and no personal history of VTE or first-degree relative with VTE can be monitored with clinical surveillance antepartum. However, if a family history of VTE or other risk factors for VTE are present, antepartum prophylactic-dose is recommended. Clinical factors to consider antepartum include obesity, age older than 35 years, parity of 3 or higher, varicose veins, immobility, smoking, assisted reproductive technology use, multiple gestation, and preeclampsia.10
Antiphospholipid syndrome (APS) is another high-risk condition. For patients not taking long-term anticoagulation antepartum, prophylactic-dose is recommended. For patients on long-term anticoagulation, therapeutic-dose is recommended.
Other medical conditions. Patients with medical conditions that place them at high risk for VTE may warrant prophylactic-dose antepartum. These include active cancer, active systemic lupus erythematosus, sickle cell disease, nephropathy, and inflammatory bowel disease.10 This decision can be made in conjunction with other specialists caring for the patient.
Antepartum prophylactic-dose is not recommended for low-risk patients as there is less than 1% risk of VTE.7 (TABLE 2 summarizes antepartum chemoprophylaxis recommendations.)
CASE 1 continued Patient develops another VTE risk factor
The patient is being followed with clinical surveillance. At 19 weeks’ gestation, she presents to the emergency department with shortness of breath and fever. She is diagnosed with COVID-19 and is admitted by a medicine service. They call the OB team to ask for recommendations regarding anticoagulation.
What should the next steps include?
Hospitalization and nonobstetric surgery are risk factors for VTE. Many hospitals use a standardized assessment for all inpatients, such as the Padua or Caprini VTE risk assessment scores. These can be modified for use in pregnant patients, although neither scoring system is currently validated for use in pregnancy.5 For any pregnant patient admitted to the hospital, mechanical prophylaxis is recommended.
COVID-19. Infection with the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and its associated clinical syndrome, COVID-19, is associated with increased rates of VTE. Recommendations for pregnant patients with COVID-19 are the same as for the general population. During hospitalization for COVID-19, pregnant patients should be placed on prophylactic-dose chemoprophylaxis. Patients should not be discharged home on chemoprophylaxis, and patients managed as outpatients for their disease do not need chemoprophylaxis.11
Management approach. Prophylactic-dose administration is recommended during hospital stay for all patients admitted with anticipated length of stay of 3 days or longer and who are not at high risk for bleeding or delivery.10 Both LMWH and UFH are options for inpatients. For any nonobstetric surgery or admission, LMWH may be most appropriate. However, as most obstetrics admissions are at increased risk for delivery, UFH 5,000 U twice daily to 3 times daily is the best option to increase the chances for neuraxial anesthesia. (I review anesthesia considerations for delivery later in this article.) For patients at high risk for bleeding or delivery, mechanical prophylaxis alone, with elastic stockings or pneumatic compression devices, can be used.
Continue to: CASE 1 continued Patient is discharged home...
CASE 1 continued Patient is discharged home
The patient received enoxaparin while she was in the hospital. She is now discharged and doing well. She asks, will she need anticoagulation prophylaxis after delivery?
How would you counsel her?
Chemoprophylaxis in the postpartum period
With no risk of fetal harm and a higher risk of VTE per day, the threshold for chemoprophylaxis is lower in the postpartum period. The risk of postpartum bleeding is less than 1%, with the most common complication being wound hematomas (0.61%).9 For this case patient, the COVID-19 diagnosis does not alter the recommendations for postpartum chemoprophylaxis. Additionally, as the need for neuraxial anesthesia has passed, the use of intermediate-dose chemoprophylaxis over prophylactic-dose is advocated in the postpartum period, especially in obese patients.12
As mentioned previously, there is no standard definition of intermediate-dose. Data suggest that a weight-based intermediate-dose is most likely to achieve therapeutic levels of anti-Xa in this high-risk population compared with a fixed dose.13,14 For example, enoxaparin 0.5 mg/kg twice daily is recommended for patients with class 3 obesity or higher by the Society for Maternal-Fetal Medicine.12
As a rule, anyone who was on chemoprophylaxis antepartum should be continued on at least an equivalent dose for 6 weeks postpartum. Postpartum, patients with any prior DVT should take prophylactic-dose or intermediate-dose chemoprophylaxis for 6 weeks. Patients with a known high-risk thrombophilia should receive prophylactic-dose or intermediate-dose chemoprophylaxis postpartum for 6 weeks. For patients with a low-risk thrombophilia, prophylactic-dose or intermediate-dose chemoprophylaxis is recommended for 6 weeks.
For low-risk patients without prior VTE or thrombophilia, standardized risk assessment is recommended.
Cesarean delivery
Cesarean delivery (CD) is a risk factor for postpartum VTE.9 A universal chemoprophylaxis strategy has not been proven in this patient population. Mechanical prophylaxis with sequential compression devices is recommended for all patients undergoing CD pre-procedure and until patients are fully ambulatory.8,9 Early ambulation also should be encouraged.
Many risk assessment models are available for postoperative VTE prevention, and they have widely different chemoprophylaxis rates. Studies have shown chemoprophylaxis rates of 85% by RCOG, 1% by ACOG, 35% by CHEST, 94% by Caprini, and less than 1% by Padua.15,16 In addition to the antepartum patient-specific risk factors mentioned, postpartum risk factors include infection, postpartum hemorrhage, and transfusion. Based on data extrapolated from the nonobstetric literature, chemoprophylaxis is recommended until discharge from the hospital unless risk factors are expected to continue.9
Neuraxial anesthesia
For patients who require postpartum chemoprophylaxis, the Society for Obstetric Anesthesia and Perinatology (SOAP) offers evidence-based guidelines for use after neuraxial anesthesia. UFH can be initiated 1 hour or longer after a neuraxial procedure and 1 hour or longer after catheter removal. Prophylactic-dose LMWH can be restarted at 12 hours or longer after a neuraxial procedure and at 4 to 6 hours or longer after catheter removal. For patients restarting intermediate-dose or therapeutic-dose, the recommendations are to wait 24 hours or longer after a neuraxial procedure and 4 hours or longer after catheter removal.17 Timing can be individualized based on the patient’s risk of hemorrhage and surgical bleeding. Although it may be tempting to delay chemoprophylaxis in the setting of bleeding, postpartum hemorrhage and transfusion increase the risks of VTE. In this setting, it is best to consider the use of UFH, which safely can be started earlier than LMWH.
For patients without neuraxial anesthesia, ACOG recommends chemoprophylaxis 4 to 6 hours after vaginal delivery and 6 to 12 hours after CD.8 (TABLE 3 summarizes recommendations for postpartum chemoprophylaxis.)
Continue to: Adjusting the anticoagulation regimen...
Adjusting the anticoagulation regimen
CASE 2 Pregnant woman with prior VTE
A 36-year-old woman (G1P0) with prior VTE is taking enoxaparin 40 mg daily. She asks, does she need any blood work for her anticoagulation?
What would you test for?
Increased renal clearance of LMWH and increased volume of distribution during pregnancy has led to the consideration of monitoring anti-Xa levels. There are no published standards or recommendations for dose adjustment. At this time, anti-Xa level monitoring antepartum is not recommended, but it may be considered when a patient is at the extremes of weight. With a weight-based strategy in the postpartum period, monitoring is not recommended as studies show a higher likelihood of therapeutic anti-Xa levels with this approach.13,14 This is an active area of research, and these recommendations may change.
For prophylactic-dose or intermediate-dose anticoagulation, a peak anti-Xa level of 0.2 to 0.6 U/mL is generally accepted as the target. For therapeutic-dose, a peak anti-Xa level of 0.6 to 1.2 U/mL is generally accepted as the therapeutic range. This blood draw must be collected 4 hours after the third dose.
CASE 2 continued Anticoagulation considerations nearing delivery
The patient is now at 36 weeks’ gestation, and she asks, what should be done regarding her anticoagulation prior to delivery?
What would be an appropriate approach?
Traditionally, patients were transitioned to UFH at 36 weeks and allowed to present in spontaneous labor to increase the likelihood of neuraxial anesthesia. The alternative is to continue prophylactic-dose LMWH until a scheduled delivery. While the SOAP guidelines establish the timeframe that is safe to proceed with neuraxial anesthesia, there is variation in practice, so consider discussing this with your anesthesia providers.
SOAP considers prophylactic-dose UFH to be 5,000 U 2 to 3 times per day. In this setting, neuraxial anesthesia can be placed more than 4 to 6 hours from the last dose.17 But due to the pharmacokinetics of pregnancy, ACOG recommends 10,000 U in the third trimester.8 This dose is considered intermediate-dose by SOAP, and 12 hours or longer plus a normal activated partial thromboplastin time (aPTT) or undetectable anti-Xa level are required prior to neuraxial anesthesia. This is the same time allowed for prophylactic-dose LMWH without lab work. Prophylactic-dose LMWH is considered to be enoxaparin 40 mg or less daily or 30 mg twice daily, and dalteparin 5,000 U daily. For therapeutic-dose LMWH or UFH, 24 hours or more from last dose is recommended prior to neuraxial anesthesia. For intermediate-dose LMWH, data are limited to recommend anything between 12 and 24 hours.17
In my practice, we favor a shared decision-making approach with patients. We discuss the likelihood of labor prior to 39 weeks based on a patient’s history, the importance of neuraxial anesthesia to the patient, and the importance of the number of daily injections. Most patients continue enoxaparin until a scheduled induction, and they are instructed to skip their dose if labor symptoms begin. Patients at high risk for preterm delivery can be transitioned to heparin earlier than 36 weeks. ●
- Creanga AA, Syverson C, Seed K, et al. Pregnancy-related mortality in the United States, 2011-2013. Obstet Gynecol. 2017;130:366-373. doi: 10.1097/AOG.0000000000002114.
- Kourlaba G, Relakis J, Kontodimas S, et al. A systematic review and meta-analysis of the epidemiology and burden of venous thromboembolism among pregnant women. Int J Gynaecol Obstet. 2016;132:4-10. doi: 10.1016/j.ijgo.2015.06.054.
- Sultan AA, West J, Tata LJ, et al. Risk of first venous thromboembolism in and around pregnancy: a population-based cohort study. Br J Haematol. 2012;156:366-373. doi: 10.1111/j.1365-2141.2011.08956.x.
- American College of Obstetricians and Gynecologists. Council on Patient Safety in Women’s Health Care: maternal venous thromboembolism (+AIM). 2015. https://safehealthcareforeverywoman.org/council/patient-safety-bundles/maternal-safety-bundles/maternal-venous-thromboembolism-aim/. Accessed February 26, 2021.
- Urato AC, Abi-Jaoude E, Abramson J, et al. National Partnership for Maternal Safety: consensus bundle on venous thromboembolism. Obstet Gynecol. 2019;134:1115-1117. doi: 10.1097/AOG.0000000000003540.
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. ACOG practice bulletin no. 196: thromboembolism in pregnancy. Obstet Gynecol. 2018;132:e1-e17. doi: 10.1097/AOG.0000000000002706.
- Bates SM, Rajasekhar A, Middeldorp S, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: venous thromboembolism in the context of pregnancy. Blood Adv. 2018;2:3317-3359. doi: 10.1182/bloodadvances.2018024802.
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics. ACOG practice bulletin no. 197: inherited thrombophilias in pregnancy. Obstet Gynecol. 2018;132:e18-e34. doi: 10.1097/AOG.0000000000002703.
- Bates SM, Greer IA, Middeldorp S, et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2, suppl):e691S-e736S. doi: 10.1378/chest.11-2300.
- Lamont MC, McDermott C, Thomson AJ, et al. United Kingdom recommendations for obstetric venous thromboembolism prophylaxis: evidence and rationale. Semin Perinatol. 2019;43:222-228. doi: 10.1053/j.semperi.2019.03.008.
- National Institutes of Health. COVID-19 Treatment Guidelines Panel. Coronavirus disease 2019 (COVID-19) treatment guidelines. https://www.covid19treatmentguidelines.nih.gov/. Accessed February 26, 2021.
- Society for Maternal-Fetal Medicine (SMFM); Pacheco LD, Saade G, Metz TD. Society for Maternal-Fetal Medicine Consult Series #51: thromboembolism prophylaxis for cesarean delivery. Am J Obstet Gynecol. 2020;223:B11-B17. doi: 10.1016/j.ajog.2020.04.032.
- Overcash RT, Somers AT, LaCoursiere DY. Enoxaparin dosing after cesarean delivery in morbidly obese women. Obstet Gynecol. 2015;125:1371-1376. doi: 10.1097/AOG.0000000000000873.
- Hiscock RJ, Casey E, Simmons SW, et al. Peak plasma anti-Xa levels after first and third doses of enoxaparin in women receiving weight-based thromboprophylaxis following caesarean section: a prospective cohort study. Int J Obstet Anesth. 2013;22:280-288. doi: 10.1016/j.ijoa.2013.05.008.
- Palmerola KL, D’Alton ME, Brock CO, et al. A comparison of recommendations for pharmacologic thromboembolism prophylaxis after caesarean delivery from three major guidelines. BJOG. 2016;123:2157-2162. doi: 10.1111/1471-0528.13706.
- Tran JP, Stribling SS, Ibezim UC, et al. Performance of risk assessment models for peripartum thromboprophylaxis. Reprod Sci. 2019;26:1243-1248. doi: 10.1177/1933719118813197.
- Leffert L, Butwick A, Carvalho B, et al; members of the SOAP VTE Taskforce. The Society for Obstetric Anesthesia and Perinatology consensus statement on the anesthetic management of pregnant and postpartum women receiving thromboprophylaxis or higher dose anticoagulants. Anesth Analg. 2018;126:928-944. doi: 10.1213/ANE.0000000000002530.
- Creanga AA, Syverson C, Seed K, et al. Pregnancy-related mortality in the United States, 2011-2013. Obstet Gynecol. 2017;130:366-373. doi: 10.1097/AOG.0000000000002114.
- Kourlaba G, Relakis J, Kontodimas S, et al. A systematic review and meta-analysis of the epidemiology and burden of venous thromboembolism among pregnant women. Int J Gynaecol Obstet. 2016;132:4-10. doi: 10.1016/j.ijgo.2015.06.054.
- Sultan AA, West J, Tata LJ, et al. Risk of first venous thromboembolism in and around pregnancy: a population-based cohort study. Br J Haematol. 2012;156:366-373. doi: 10.1111/j.1365-2141.2011.08956.x.
- American College of Obstetricians and Gynecologists. Council on Patient Safety in Women’s Health Care: maternal venous thromboembolism (+AIM). 2015. https://safehealthcareforeverywoman.org/council/patient-safety-bundles/maternal-safety-bundles/maternal-venous-thromboembolism-aim/. Accessed February 26, 2021.
- Urato AC, Abi-Jaoude E, Abramson J, et al. National Partnership for Maternal Safety: consensus bundle on venous thromboembolism. Obstet Gynecol. 2019;134:1115-1117. doi: 10.1097/AOG.0000000000003540.
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. ACOG practice bulletin no. 196: thromboembolism in pregnancy. Obstet Gynecol. 2018;132:e1-e17. doi: 10.1097/AOG.0000000000002706.
- Bates SM, Rajasekhar A, Middeldorp S, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: venous thromboembolism in the context of pregnancy. Blood Adv. 2018;2:3317-3359. doi: 10.1182/bloodadvances.2018024802.
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics. ACOG practice bulletin no. 197: inherited thrombophilias in pregnancy. Obstet Gynecol. 2018;132:e18-e34. doi: 10.1097/AOG.0000000000002703.
- Bates SM, Greer IA, Middeldorp S, et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2, suppl):e691S-e736S. doi: 10.1378/chest.11-2300.
- Lamont MC, McDermott C, Thomson AJ, et al. United Kingdom recommendations for obstetric venous thromboembolism prophylaxis: evidence and rationale. Semin Perinatol. 2019;43:222-228. doi: 10.1053/j.semperi.2019.03.008.
- National Institutes of Health. COVID-19 Treatment Guidelines Panel. Coronavirus disease 2019 (COVID-19) treatment guidelines. https://www.covid19treatmentguidelines.nih.gov/. Accessed February 26, 2021.
- Society for Maternal-Fetal Medicine (SMFM); Pacheco LD, Saade G, Metz TD. Society for Maternal-Fetal Medicine Consult Series #51: thromboembolism prophylaxis for cesarean delivery. Am J Obstet Gynecol. 2020;223:B11-B17. doi: 10.1016/j.ajog.2020.04.032.
- Overcash RT, Somers AT, LaCoursiere DY. Enoxaparin dosing after cesarean delivery in morbidly obese women. Obstet Gynecol. 2015;125:1371-1376. doi: 10.1097/AOG.0000000000000873.
- Hiscock RJ, Casey E, Simmons SW, et al. Peak plasma anti-Xa levels after first and third doses of enoxaparin in women receiving weight-based thromboprophylaxis following caesarean section: a prospective cohort study. Int J Obstet Anesth. 2013;22:280-288. doi: 10.1016/j.ijoa.2013.05.008.
- Palmerola KL, D’Alton ME, Brock CO, et al. A comparison of recommendations for pharmacologic thromboembolism prophylaxis after caesarean delivery from three major guidelines. BJOG. 2016;123:2157-2162. doi: 10.1111/1471-0528.13706.
- Tran JP, Stribling SS, Ibezim UC, et al. Performance of risk assessment models for peripartum thromboprophylaxis. Reprod Sci. 2019;26:1243-1248. doi: 10.1177/1933719118813197.
- Leffert L, Butwick A, Carvalho B, et al; members of the SOAP VTE Taskforce. The Society for Obstetric Anesthesia and Perinatology consensus statement on the anesthetic management of pregnant and postpartum women receiving thromboprophylaxis or higher dose anticoagulants. Anesth Analg. 2018;126:928-944. doi: 10.1213/ANE.0000000000002530.
Hepatitis in pregnancy: Sorting through the alphabet
A 27-year-old primigravida at 9 weeks 3 days of gestation tests positive for the hepatitis B surface antigen at her first prenatal appointment. She is completely asymptomatic.
- What additional tests are indicated?
- Does she pose a risk to her sexual partner, and is her newborn at risk for acquiring hepatitis B?
- Can anything be done to protect her partner and newborn from infection?
Meet our perpetrator
Hepatitis is one of the more common viral infections that may occur during pregnancy. Two forms of hepatitis, notably hepatitis A and E, pose a primary threat to the mother. Three forms (B, C, and D) present dangers for the mother, fetus, and newborn. This article will review the epidemiology, clinical manifestations, perinatal implications, and management of the various forms of viral hepatitis. (TABLE 1).
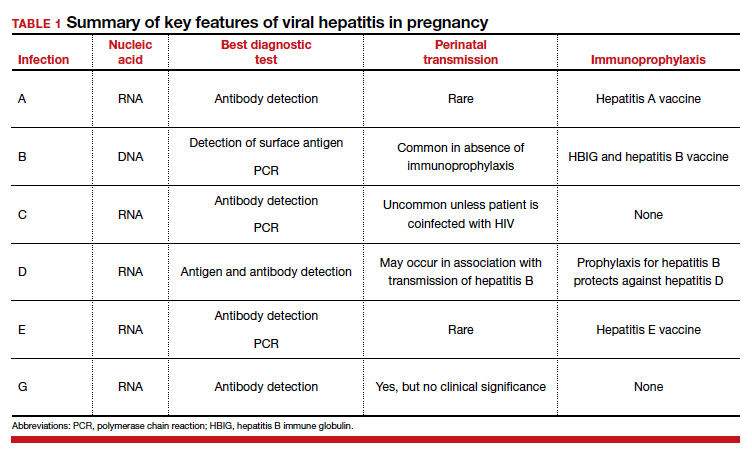
Hepatitis A
Hepatitis A is caused by an RNA virus that is transmitted by fecal-oral contact. The disease is most prevalent in areas with poor sanitation and close living conditions. The incubation period ranges from 15 to 50 days. Most children who acquire this disease are asymptomatic. By contrast, most infected adults are acutely symptomatic. Clinical manifestations typically include low-grade fever, malaise, anorexia, right upper quadrant pain and tenderness, jaundice, and claycolored stools.1,2
The diagnosis of acute hepatitis A infection is best confirmed by detection of immunoglobulin M (IgM)-specific antibodies. The serum transaminase concentrations and the serum bilirubin concentrations usually are significantly elevated. The international normalized ratio, prothrombin time, and partial thromboplastin time also may be elevated.1,2
The treatment for acute hepatitis A largely is supportive care: maintaining hydration, optimizing nutrition, and correcting coagulation abnormalities. The appropriate measures for prevention of hepatitis A are adoption of sound sanitation practices, particularly water purification; minimizing overcrowded living conditions; and administering the hepatitis A vaccine for both pre and postexposure prophylaxis.3,4 The hepatitis A vaccine is preferred over administration of immune globulin because it provides lifelong immunity.
The hepatitis A vaccine is produced in 2 monovalent formulations: Havrix (GlaxoSmithKline) and Vaqta (Merck & Co, Inc). The vaccine should be administered intramuscularly in 2 doses 6 to 12 months apart. The wholesale cost of the vaccine varies from $66 to $119 (according to http://www.goodrx.com). The vaccine also is available in a bivalent form, with recombinant hepatitis B vaccine (Twinrix, GlaxoSmithKline). When used in this form, 3 vaccine administrations are given—at 0, 1, and 6 months apart. The cost of the vaccine is approximately $150 (according to http://www.goodrx.com). TABLE 2 lists the individuals who are appropriate candidates for the hepatitis A vaccine.3,4
Hepatitis B
Hepatitis B is caused by a DNA virus that is transmitted parenterally or perinatally or through
Acute hepatitis B affects 1 to 2 of 1,000 pregnancies in the United States. Approximately 6 to 10 patients per 1,000 pregnancies are asymptomatic but chronically infected.4 The natural history of hepatitis B infection is shown in the FIGURE. The diagnosis of acute and chronic hepatitis B is best established by serology and polymerase chain reaction (PCR; TABLE 3).
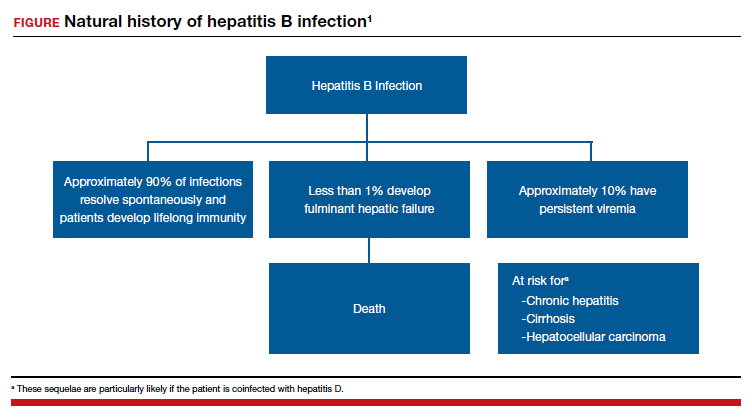

All pregnant women should be routinely screened for the hepatitis B surface antigen.5,6 If they are seropositive for the surface antigen alone and receive no immunoprophylaxis, they have a 20% to 30% risk of transmitting infection to their neonate. Subsequently, if they also test positive for the hepatitis Be antigen, the risk of perinatal transmission increases to approximately 90%. Fortunately, 2 forms of immunoprophylaxis are highly effective in preventing perinatal transmission. Infants delivered to seropositive mothers should receive hepatitis B immune globulin within 12 hours of birth. Prior to discharge, the infant also should receive the first dose of the hepatitis B vaccine. Subsequent doses should be administered at 1 and 6 months of age. Infants delivered to seronegative mothers require only the vaccine series.1
Although immunoprophylaxis is highly effective, some neonates still acquire infection perinatally. Pan and colleagues7 and Jourdain et al8 demonstrated that administration of tenofovir 200 mg orally each day from 32 weeks’ gestation until delivery provided further protection against perinatal transmission in patients with a high viral load (defined as >1 million copies/mL). In 2016, the Society for Maternal-Fetal Medicine endorsed the use of tenofovir in women with a high viral load.6
Following delivery, women with chronic hepatitis B infection should be referred to a hepatology specialist for consideration of direct antiviral treatment. Multiple drugs are now available that are highly active against this micro-organism. These drugs include several forms of interferon, lamivudine, adefovir, entecavir, telbivudine, and tenofovir.1
Continue to: Hepatitis C...
Hepatitis C
Hepatitis C is caused by an RNA virus that has 6 genotypes. The most common genotype is HCV1, which affects 79% of patients; approximately 13% of patients have HCV2, and 6% have HCV3.9 Of note, the 3 individuals who discovered this virus—Drs. Harvey Alter, Michael Houghton, and Charles Rice—received the 2020 Nobel Prize in Medicine.10
Hepatitis C is transmitted via sexual contact, parenterally, and perinatally. In many patient populations in the United States, hepatitis C is now more prevalent than hepatitis B. Only about half of all infected persons are aware of their infection. If patients go untreated, approximately 15% to 30% eventually develop cirrhosis. Of these individuals, 1% to 3% develop hepatocellular cancer. Chronic hepatitis C is now the most common indication for liver transplantation in the United States.1,9
In the initial stages of infection, hepatitis C usually is asymptomatic. The best screening test is detection of hepatitis C antibody. Because of the increasing prevalence of this disease, the seriousness of the infection, and the recent availability of remarkably effective treatment, routine screening, rather than screening on the basis of risk factors, for hepatitis C in pregnancy is now indicated.11,12
The best tests for confirmation of infection are detection of antibody by enzyme immunoassay and recombinant immuno-blot assay and detection of viral RNA in serum by PCR. Seroconversion may not occur for up to 16 weeks after infection. Therefore, in at-risk patients who initially test negative, retesting is advisable. Patients with positive test results should have tests to identify the specific genotype, determine the viral load, and assess liver function.1
In patients who have undetectable viral loads and who do not have coexisting HIV infection, the risk of perinatal transmission of hepatitis C is less than 5%. If HIV infection is present, the risk of perinatal transmission approaches 20%.1,13,14
If the patient is coinfected with HIV, a scheduled cesarean delivery should be performed at 38 weeks’ gestation.1 If the viral load is undetectable, vaginal delivery is appropriate. If the viral load is high, however (arbitrarily defined as >2.5 millioncopies/mL), the optimal method of delivery is controversial. Several small, nonrandomized noncontrolled cohort studies support elective cesarean delivery in such patients.14
There is no contraindication to breastfeeding in women with hepatitis C unless they are coinfected with HIV. In such a circumstance, formula feeding should be chosen. After delivery, patients with hepatitis C should be referred to a gastroenterology specialist to receive antiviral treatment. Multiple new single-agent and combination regimens have produced cures in more than 90% of patients. These regimens usually require 8 to 12 weeks of treatment, and they are very expensive. They have not been widely tested in pregnant women.1
Hepatitis D
Hepatitis D, or delta hepatitis, is caused by an RNA virus. This virus is unique because it is incapable of independent replication. It must be present in association with hepatitis B to replicate and cause clinical infection. Therefore, the epidemiology of hepatitis D closely mirrors that of hepatitis B.1,2
Patients with hepatitis D typically present in one of two ways. Some individuals are acutely infected with hepatitis D at the same time that they acquire hepatitis B (coinfection). The natural history of this infection usually is spontaneous resolution without sequelae. Other patients have chronic hepatitis D superimposed on chronic hepatitis B (superinfection). Unfortunately, patients with the latter condition are at a notably increased risk for developing severe persistent liver disease.1,2
The diagnosis of hepatitis D may be confirmed by identifying the delta antigen in serum or in liver tissue obtained by biopsy or by identifying IgM- and IgG-specific antibodies in serum. In conjunction with hepatitis B, the delta virus can cause a chronic carrier state. Perinatal transmission is possible but uncommon. Of greatest importance, the immunoprophylaxis described for hepatitis B is almost perfectly protective against perinatal transmission of hepatitis D.1,2
Continue to: Hepatitis E...
Hepatitis E
Hepatitis E is an RNA virus that has 1 serotype and 4 genotypes. Its epidemiology is similar to that of hepatitis A. It is the most common waterborne illness in the world. The incubation period varies from 21 to 56 days. This disease is quite rare in the United States but is endemic in developing nations. In those countries, maternal infection has an alarmingly high mortality rate (5%–25%). For example, in Bangladesh, hepatitis E is responsible for more than 1,000 deaths per year in pregnant women. When hepatitis E is identified in more affluent countries, the individual cases and small outbreaks usually are linked to consumption of undercooked pork or wild game.1,15-17
The clinical presentation of acute hepatitis E also is similar to that of hepatitis A. The usual manifestations are fever, malaise, anorexia, nausea, right upper quadrant pain and tenderness, jaundice, darkened urine, and clay-colored stools. The most useful diagnostic tests are serologic detection of viral-specific antibodies (positive IgM or a 4-fold increase in the prior IgG titer) and PCR-RNA.1,17
Hepatitis E usually does not cause a chronic carrier state, and perinatal transmission is rare. Fortunately, a highly effective vaccine was recently developed (Hecolin, Xiamen Innovax Biotech). This recombinant vaccine is specifically directed against the hepatitis E genotype 1. In the initial efficacy study, healthy adults aged 16 to 65 years were randomly assigned to receive either the hepatitis E vaccine or the hepatitis B vaccine. The vaccine was administered at time point 0, and 1 and 6 months later. Patients were followed for up to 4.5 years to assess efficacy, immunogenicity, and safety. During the study period, 7 cases of hepatitis E occurred in the vaccine group, compared with 53 in the control group. Approximately 56,000 patients were included in each group. The efficacy of the vaccine was 86.8% (P<.001).18
Hepatitis G
Hepatitis G is caused by 2 single-stranded RNA viruses that are virtually identical—hepatitis G virus and GB virus type C. The viruses share approximately 30% homology with hepatitis C virus. The organism is present throughout the world and infects approximately 1.5% to 2.0% of the population. The virus is transmitted by blood and sexual contact. It replicates preferentially in mononuclear cells and the bone marrow rather than in the liver.19-21
Hepatitis G is much less virulent than hepatitis C. Hepatitis G often coexists with hepatitis A, B, and C, as well as with HIV. Coinfection with hepatitis G does not adversely affect the clinical course of the other conditions.22,23
Most patients with hepatitis G are asymptomatic, and no treatment is indicated. The virus can cause a chronic carrier state. Perinatal transmission is distinctly uncommon. When it does occur, however, injury to mother, fetus, or neonate is unlikely.1,24
The diagnosis of hepatitis G can be established by detection of virus with PCR and by the identification of antibody by enzyme immunoassay. Routine screening for this infection in pregnancy is not indicated.1,2
Hepatitis B is highly contagious and can be transmitted from the patient to her sexual partner and neonate. Testing for hepatitis B surface antigen and antibody is indicated in her partner. If these tests are negative, the partner should immediately receive hepatitis B immune globulin and then be started on the 3-dose hepatitis B vaccination series. The patient’s newborn also should receive hepatitis B immune globulin within 12 hours of delivery and should receive the first dose of the hepatitis B vaccine prior to discharge from the hospital. The second and third doses should be administered 1 and 6 months after delivery.
The patient also should have the following tests:
• liver function tests
-serum transaminases
-direct and indirect bilirubin
-coagulation profile
• hepatitis D antigen
• hepatitis B genotype
• hepatitis B viral load
• HIV serology.
If the hepatitis B viral load exceeds 1 million copies/mL, the patient should be treated with tenofovir 200 mg daily from 28 weeks’ gestation until delivery. In addition, she should be referred to a liver disease specialist after delivery for consideration of treatment with directly-acting antiviral agents. ●
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TB, et al, eds. Creasy & Resnik’s MaternalFetal Medicine Principles and Practice. 8th ed. Elsevier; 2019:862-919.
- Duff P. Hepatitis in pregnancy. In: Queenan JR, Spong CY, Lockwood CJ, eds. Management of HighRisk Pregnancy. An EvidenceBased Approach. 5th ed. Blackwell; 2007:238-241.
- Duff B, Duff P. Hepatitis A vaccine: ready for prime time. Obstet Gynecol. 1998;91:468-471.
- Victor JC, Monto AS, Surdina TY, et al. Hepatitis A vaccine versus immune globulin for postexposure prophylaxis. N Engl J Med. 2007;367:1685-1694.
- Dienstag JL. Hepatitis B virus infection. N Engl J Med. 2008;359:1486-1500.
- Society for MaternalFetal Medicine (SMFM); Dionne-Odom J, Tita ATN, Silverman NS. #38. Hepatitis B in pregnancy: screening, treatment, and prevention of vertical transmission. Am J Obstet Gynecol. 2016;214:6-14.
- Pan CQ, Duan Z, Dai E, et al. Tenofovir to prevent hepatitis B transmission in mothers with high viral load. N Engl J Med. 2016;374:2324-2334.
- Jourdain G, Huong N, Harrison L, et al. Tenofovir versus placebo to prevent perinatal transmission of hepatitis B. N Engl J Med. 2018;378:911-923.
- Rosen HR. Chronic hepatitis C infection. N Engl J Med. 2011;364:2429-2438.
- Hoofnagle JH, Feinstore SM. The discovery of hepatitis C—the 2020 Nobel Prize in Physiology or Medicine. N Engl J Med. 2020;384:2297-2299.
- Hughes BL, Page CM, Juller JA. Hepatitis C in pregnancy: screening, treatment, and management. Am J Obstet Gynecol. 2017;217:B2-B12.
- Saab S, Kullar R, Gounder P. The urgent need for hepatitis C screening in pregnant women: a call to action. Obstet Gynecol. 2020;135:773-777.
- Berkley EMF, Leslie KK, Arora S, et al. Chronic hepatitis C in pregnancy. Obstet Gynecol. 2008;112:304-310.
- Brazel M, Duff P. Considerations on the mode of delivery for pregnant women with hepatitis C infection [published online November 22, 2019]. OBG Manag. 2020;32:39-44.
- Emerson SU, Purcell RH. Hepatitis E virus. Rev Med Virol. 2003;13:145-154.
- Khuroo MS, Teli MR, Skidmore S, et al. Incidence and severity of viral hepatitis in pregnancy. Am J Med. 1981;70:252-255.
- Hoofnangle JH, Nelson KE, Purcell RH. Hepatitis E. N Engl J Med. 2012;367:1237-1244.
- Zhang J, Zhang XF, Huang SJ, et al. Longterm efficacy of a hepatitis E vaccine. N Engl J Med. 2015;372:914-922.
- Pickering L, ed. Red Book 2000 Report of Committee on Infectious Diseases. 25th ed. American Academy of Pediatrics; 2000.
- Chopra S. GB virus C (hepatitis G) infection. UpToDate website. Updated January 16, 2020. Accessed June 3, 2021. https://www.uptodate.com/contents/gb-virus-c-hepatitis-g-infection.
- Reshetnyak VI, Karlovich TI, Ilchenko LU. Hepatitis G virus. World J Gastroenterol. 2008;14:4725-4734.
- Kew MC, Kassianides C. HGV: hepatitis G virus or harmless G virus. Lancet. 1996;348(suppl II):10.
- Jarvis LM, Davidson F, Hanley JP, et al. Infection with hepatitis G virus among recipients of plasma products. Lancet. 1996;348;1352-1355.
- Feucht HH, Zollner B, Polywka S, et al. Vertical transmission of hepatitis G. Lancet. 1996;347;615-616.

Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine.
The author reports no financial relationships relevant to this article.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine.
The author reports no financial relationships relevant to this article.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine.
The author reports no financial relationships relevant to this article.
A 27-year-old primigravida at 9 weeks 3 days of gestation tests positive for the hepatitis B surface antigen at her first prenatal appointment. She is completely asymptomatic.
- What additional tests are indicated?
- Does she pose a risk to her sexual partner, and is her newborn at risk for acquiring hepatitis B?
- Can anything be done to protect her partner and newborn from infection?
Meet our perpetrator
Hepatitis is one of the more common viral infections that may occur during pregnancy. Two forms of hepatitis, notably hepatitis A and E, pose a primary threat to the mother. Three forms (B, C, and D) present dangers for the mother, fetus, and newborn. This article will review the epidemiology, clinical manifestations, perinatal implications, and management of the various forms of viral hepatitis. (TABLE 1).
Hepatitis A
Hepatitis A is caused by an RNA virus that is transmitted by fecal-oral contact. The disease is most prevalent in areas with poor sanitation and close living conditions. The incubation period ranges from 15 to 50 days. Most children who acquire this disease are asymptomatic. By contrast, most infected adults are acutely symptomatic. Clinical manifestations typically include low-grade fever, malaise, anorexia, right upper quadrant pain and tenderness, jaundice, and claycolored stools.1,2
The diagnosis of acute hepatitis A infection is best confirmed by detection of immunoglobulin M (IgM)-specific antibodies. The serum transaminase concentrations and the serum bilirubin concentrations usually are significantly elevated. The international normalized ratio, prothrombin time, and partial thromboplastin time also may be elevated.1,2
The treatment for acute hepatitis A largely is supportive care: maintaining hydration, optimizing nutrition, and correcting coagulation abnormalities. The appropriate measures for prevention of hepatitis A are adoption of sound sanitation practices, particularly water purification; minimizing overcrowded living conditions; and administering the hepatitis A vaccine for both pre and postexposure prophylaxis.3,4 The hepatitis A vaccine is preferred over administration of immune globulin because it provides lifelong immunity.
The hepatitis A vaccine is produced in 2 monovalent formulations: Havrix (GlaxoSmithKline) and Vaqta (Merck & Co, Inc). The vaccine should be administered intramuscularly in 2 doses 6 to 12 months apart. The wholesale cost of the vaccine varies from $66 to $119 (according to http://www.goodrx.com). The vaccine also is available in a bivalent form, with recombinant hepatitis B vaccine (Twinrix, GlaxoSmithKline). When used in this form, 3 vaccine administrations are given—at 0, 1, and 6 months apart. The cost of the vaccine is approximately $150 (according to http://www.goodrx.com). TABLE 2 lists the individuals who are appropriate candidates for the hepatitis A vaccine.3,4
Hepatitis B
Hepatitis B is caused by a DNA virus that is transmitted parenterally or perinatally or through
Acute hepatitis B affects 1 to 2 of 1,000 pregnancies in the United States. Approximately 6 to 10 patients per 1,000 pregnancies are asymptomatic but chronically infected.4 The natural history of hepatitis B infection is shown in the FIGURE. The diagnosis of acute and chronic hepatitis B is best established by serology and polymerase chain reaction (PCR; TABLE 3).
All pregnant women should be routinely screened for the hepatitis B surface antigen.5,6 If they are seropositive for the surface antigen alone and receive no immunoprophylaxis, they have a 20% to 30% risk of transmitting infection to their neonate. Subsequently, if they also test positive for the hepatitis Be antigen, the risk of perinatal transmission increases to approximately 90%. Fortunately, 2 forms of immunoprophylaxis are highly effective in preventing perinatal transmission. Infants delivered to seropositive mothers should receive hepatitis B immune globulin within 12 hours of birth. Prior to discharge, the infant also should receive the first dose of the hepatitis B vaccine. Subsequent doses should be administered at 1 and 6 months of age. Infants delivered to seronegative mothers require only the vaccine series.1
Although immunoprophylaxis is highly effective, some neonates still acquire infection perinatally. Pan and colleagues7 and Jourdain et al8 demonstrated that administration of tenofovir 200 mg orally each day from 32 weeks’ gestation until delivery provided further protection against perinatal transmission in patients with a high viral load (defined as >1 million copies/mL). In 2016, the Society for Maternal-Fetal Medicine endorsed the use of tenofovir in women with a high viral load.6
Following delivery, women with chronic hepatitis B infection should be referred to a hepatology specialist for consideration of direct antiviral treatment. Multiple drugs are now available that are highly active against this micro-organism. These drugs include several forms of interferon, lamivudine, adefovir, entecavir, telbivudine, and tenofovir.1
Continue to: Hepatitis C...
Hepatitis C
Hepatitis C is caused by an RNA virus that has 6 genotypes. The most common genotype is HCV1, which affects 79% of patients; approximately 13% of patients have HCV2, and 6% have HCV3.9 Of note, the 3 individuals who discovered this virus—Drs. Harvey Alter, Michael Houghton, and Charles Rice—received the 2020 Nobel Prize in Medicine.10
Hepatitis C is transmitted via sexual contact, parenterally, and perinatally. In many patient populations in the United States, hepatitis C is now more prevalent than hepatitis B. Only about half of all infected persons are aware of their infection. If patients go untreated, approximately 15% to 30% eventually develop cirrhosis. Of these individuals, 1% to 3% develop hepatocellular cancer. Chronic hepatitis C is now the most common indication for liver transplantation in the United States.1,9
In the initial stages of infection, hepatitis C usually is asymptomatic. The best screening test is detection of hepatitis C antibody. Because of the increasing prevalence of this disease, the seriousness of the infection, and the recent availability of remarkably effective treatment, routine screening, rather than screening on the basis of risk factors, for hepatitis C in pregnancy is now indicated.11,12
The best tests for confirmation of infection are detection of antibody by enzyme immunoassay and recombinant immuno-blot assay and detection of viral RNA in serum by PCR. Seroconversion may not occur for up to 16 weeks after infection. Therefore, in at-risk patients who initially test negative, retesting is advisable. Patients with positive test results should have tests to identify the specific genotype, determine the viral load, and assess liver function.1
In patients who have undetectable viral loads and who do not have coexisting HIV infection, the risk of perinatal transmission of hepatitis C is less than 5%. If HIV infection is present, the risk of perinatal transmission approaches 20%.1,13,14
If the patient is coinfected with HIV, a scheduled cesarean delivery should be performed at 38 weeks’ gestation.1 If the viral load is undetectable, vaginal delivery is appropriate. If the viral load is high, however (arbitrarily defined as >2.5 millioncopies/mL), the optimal method of delivery is controversial. Several small, nonrandomized noncontrolled cohort studies support elective cesarean delivery in such patients.14
There is no contraindication to breastfeeding in women with hepatitis C unless they are coinfected with HIV. In such a circumstance, formula feeding should be chosen. After delivery, patients with hepatitis C should be referred to a gastroenterology specialist to receive antiviral treatment. Multiple new single-agent and combination regimens have produced cures in more than 90% of patients. These regimens usually require 8 to 12 weeks of treatment, and they are very expensive. They have not been widely tested in pregnant women.1
Hepatitis D
Hepatitis D, or delta hepatitis, is caused by an RNA virus. This virus is unique because it is incapable of independent replication. It must be present in association with hepatitis B to replicate and cause clinical infection. Therefore, the epidemiology of hepatitis D closely mirrors that of hepatitis B.1,2
Patients with hepatitis D typically present in one of two ways. Some individuals are acutely infected with hepatitis D at the same time that they acquire hepatitis B (coinfection). The natural history of this infection usually is spontaneous resolution without sequelae. Other patients have chronic hepatitis D superimposed on chronic hepatitis B (superinfection). Unfortunately, patients with the latter condition are at a notably increased risk for developing severe persistent liver disease.1,2
The diagnosis of hepatitis D may be confirmed by identifying the delta antigen in serum or in liver tissue obtained by biopsy or by identifying IgM- and IgG-specific antibodies in serum. In conjunction with hepatitis B, the delta virus can cause a chronic carrier state. Perinatal transmission is possible but uncommon. Of greatest importance, the immunoprophylaxis described for hepatitis B is almost perfectly protective against perinatal transmission of hepatitis D.1,2
Continue to: Hepatitis E...
Hepatitis E
Hepatitis E is an RNA virus that has 1 serotype and 4 genotypes. Its epidemiology is similar to that of hepatitis A. It is the most common waterborne illness in the world. The incubation period varies from 21 to 56 days. This disease is quite rare in the United States but is endemic in developing nations. In those countries, maternal infection has an alarmingly high mortality rate (5%–25%). For example, in Bangladesh, hepatitis E is responsible for more than 1,000 deaths per year in pregnant women. When hepatitis E is identified in more affluent countries, the individual cases and small outbreaks usually are linked to consumption of undercooked pork or wild game.1,15-17
The clinical presentation of acute hepatitis E also is similar to that of hepatitis A. The usual manifestations are fever, malaise, anorexia, nausea, right upper quadrant pain and tenderness, jaundice, darkened urine, and clay-colored stools. The most useful diagnostic tests are serologic detection of viral-specific antibodies (positive IgM or a 4-fold increase in the prior IgG titer) and PCR-RNA.1,17
Hepatitis E usually does not cause a chronic carrier state, and perinatal transmission is rare. Fortunately, a highly effective vaccine was recently developed (Hecolin, Xiamen Innovax Biotech). This recombinant vaccine is specifically directed against the hepatitis E genotype 1. In the initial efficacy study, healthy adults aged 16 to 65 years were randomly assigned to receive either the hepatitis E vaccine or the hepatitis B vaccine. The vaccine was administered at time point 0, and 1 and 6 months later. Patients were followed for up to 4.5 years to assess efficacy, immunogenicity, and safety. During the study period, 7 cases of hepatitis E occurred in the vaccine group, compared with 53 in the control group. Approximately 56,000 patients were included in each group. The efficacy of the vaccine was 86.8% (P<.001).18
Hepatitis G
Hepatitis G is caused by 2 single-stranded RNA viruses that are virtually identical—hepatitis G virus and GB virus type C. The viruses share approximately 30% homology with hepatitis C virus. The organism is present throughout the world and infects approximately 1.5% to 2.0% of the population. The virus is transmitted by blood and sexual contact. It replicates preferentially in mononuclear cells and the bone marrow rather than in the liver.19-21
Hepatitis G is much less virulent than hepatitis C. Hepatitis G often coexists with hepatitis A, B, and C, as well as with HIV. Coinfection with hepatitis G does not adversely affect the clinical course of the other conditions.22,23
Most patients with hepatitis G are asymptomatic, and no treatment is indicated. The virus can cause a chronic carrier state. Perinatal transmission is distinctly uncommon. When it does occur, however, injury to mother, fetus, or neonate is unlikely.1,24
The diagnosis of hepatitis G can be established by detection of virus with PCR and by the identification of antibody by enzyme immunoassay. Routine screening for this infection in pregnancy is not indicated.1,2
Hepatitis B is highly contagious and can be transmitted from the patient to her sexual partner and neonate. Testing for hepatitis B surface antigen and antibody is indicated in her partner. If these tests are negative, the partner should immediately receive hepatitis B immune globulin and then be started on the 3-dose hepatitis B vaccination series. The patient’s newborn also should receive hepatitis B immune globulin within 12 hours of delivery and should receive the first dose of the hepatitis B vaccine prior to discharge from the hospital. The second and third doses should be administered 1 and 6 months after delivery.
The patient also should have the following tests:
• liver function tests
-serum transaminases
-direct and indirect bilirubin
-coagulation profile
• hepatitis D antigen
• hepatitis B genotype
• hepatitis B viral load
• HIV serology.
If the hepatitis B viral load exceeds 1 million copies/mL, the patient should be treated with tenofovir 200 mg daily from 28 weeks’ gestation until delivery. In addition, she should be referred to a liver disease specialist after delivery for consideration of treatment with directly-acting antiviral agents. ●
A 27-year-old primigravida at 9 weeks 3 days of gestation tests positive for the hepatitis B surface antigen at her first prenatal appointment. She is completely asymptomatic.
- What additional tests are indicated?
- Does she pose a risk to her sexual partner, and is her newborn at risk for acquiring hepatitis B?
- Can anything be done to protect her partner and newborn from infection?
Meet our perpetrator
Hepatitis is one of the more common viral infections that may occur during pregnancy. Two forms of hepatitis, notably hepatitis A and E, pose a primary threat to the mother. Three forms (B, C, and D) present dangers for the mother, fetus, and newborn. This article will review the epidemiology, clinical manifestations, perinatal implications, and management of the various forms of viral hepatitis. (TABLE 1).
Hepatitis A
Hepatitis A is caused by an RNA virus that is transmitted by fecal-oral contact. The disease is most prevalent in areas with poor sanitation and close living conditions. The incubation period ranges from 15 to 50 days. Most children who acquire this disease are asymptomatic. By contrast, most infected adults are acutely symptomatic. Clinical manifestations typically include low-grade fever, malaise, anorexia, right upper quadrant pain and tenderness, jaundice, and claycolored stools.1,2
The diagnosis of acute hepatitis A infection is best confirmed by detection of immunoglobulin M (IgM)-specific antibodies. The serum transaminase concentrations and the serum bilirubin concentrations usually are significantly elevated. The international normalized ratio, prothrombin time, and partial thromboplastin time also may be elevated.1,2
The treatment for acute hepatitis A largely is supportive care: maintaining hydration, optimizing nutrition, and correcting coagulation abnormalities. The appropriate measures for prevention of hepatitis A are adoption of sound sanitation practices, particularly water purification; minimizing overcrowded living conditions; and administering the hepatitis A vaccine for both pre and postexposure prophylaxis.3,4 The hepatitis A vaccine is preferred over administration of immune globulin because it provides lifelong immunity.
The hepatitis A vaccine is produced in 2 monovalent formulations: Havrix (GlaxoSmithKline) and Vaqta (Merck & Co, Inc). The vaccine should be administered intramuscularly in 2 doses 6 to 12 months apart. The wholesale cost of the vaccine varies from $66 to $119 (according to http://www.goodrx.com). The vaccine also is available in a bivalent form, with recombinant hepatitis B vaccine (Twinrix, GlaxoSmithKline). When used in this form, 3 vaccine administrations are given—at 0, 1, and 6 months apart. The cost of the vaccine is approximately $150 (according to http://www.goodrx.com). TABLE 2 lists the individuals who are appropriate candidates for the hepatitis A vaccine.3,4
Hepatitis B
Hepatitis B is caused by a DNA virus that is transmitted parenterally or perinatally or through
Acute hepatitis B affects 1 to 2 of 1,000 pregnancies in the United States. Approximately 6 to 10 patients per 1,000 pregnancies are asymptomatic but chronically infected.4 The natural history of hepatitis B infection is shown in the FIGURE. The diagnosis of acute and chronic hepatitis B is best established by serology and polymerase chain reaction (PCR; TABLE 3).
All pregnant women should be routinely screened for the hepatitis B surface antigen.5,6 If they are seropositive for the surface antigen alone and receive no immunoprophylaxis, they have a 20% to 30% risk of transmitting infection to their neonate. Subsequently, if they also test positive for the hepatitis Be antigen, the risk of perinatal transmission increases to approximately 90%. Fortunately, 2 forms of immunoprophylaxis are highly effective in preventing perinatal transmission. Infants delivered to seropositive mothers should receive hepatitis B immune globulin within 12 hours of birth. Prior to discharge, the infant also should receive the first dose of the hepatitis B vaccine. Subsequent doses should be administered at 1 and 6 months of age. Infants delivered to seronegative mothers require only the vaccine series.1
Although immunoprophylaxis is highly effective, some neonates still acquire infection perinatally. Pan and colleagues7 and Jourdain et al8 demonstrated that administration of tenofovir 200 mg orally each day from 32 weeks’ gestation until delivery provided further protection against perinatal transmission in patients with a high viral load (defined as >1 million copies/mL). In 2016, the Society for Maternal-Fetal Medicine endorsed the use of tenofovir in women with a high viral load.6
Following delivery, women with chronic hepatitis B infection should be referred to a hepatology specialist for consideration of direct antiviral treatment. Multiple drugs are now available that are highly active against this micro-organism. These drugs include several forms of interferon, lamivudine, adefovir, entecavir, telbivudine, and tenofovir.1
Continue to: Hepatitis C...
Hepatitis C
Hepatitis C is caused by an RNA virus that has 6 genotypes. The most common genotype is HCV1, which affects 79% of patients; approximately 13% of patients have HCV2, and 6% have HCV3.9 Of note, the 3 individuals who discovered this virus—Drs. Harvey Alter, Michael Houghton, and Charles Rice—received the 2020 Nobel Prize in Medicine.10
Hepatitis C is transmitted via sexual contact, parenterally, and perinatally. In many patient populations in the United States, hepatitis C is now more prevalent than hepatitis B. Only about half of all infected persons are aware of their infection. If patients go untreated, approximately 15% to 30% eventually develop cirrhosis. Of these individuals, 1% to 3% develop hepatocellular cancer. Chronic hepatitis C is now the most common indication for liver transplantation in the United States.1,9
In the initial stages of infection, hepatitis C usually is asymptomatic. The best screening test is detection of hepatitis C antibody. Because of the increasing prevalence of this disease, the seriousness of the infection, and the recent availability of remarkably effective treatment, routine screening, rather than screening on the basis of risk factors, for hepatitis C in pregnancy is now indicated.11,12
The best tests for confirmation of infection are detection of antibody by enzyme immunoassay and recombinant immuno-blot assay and detection of viral RNA in serum by PCR. Seroconversion may not occur for up to 16 weeks after infection. Therefore, in at-risk patients who initially test negative, retesting is advisable. Patients with positive test results should have tests to identify the specific genotype, determine the viral load, and assess liver function.1
In patients who have undetectable viral loads and who do not have coexisting HIV infection, the risk of perinatal transmission of hepatitis C is less than 5%. If HIV infection is present, the risk of perinatal transmission approaches 20%.1,13,14
If the patient is coinfected with HIV, a scheduled cesarean delivery should be performed at 38 weeks’ gestation.1 If the viral load is undetectable, vaginal delivery is appropriate. If the viral load is high, however (arbitrarily defined as >2.5 millioncopies/mL), the optimal method of delivery is controversial. Several small, nonrandomized noncontrolled cohort studies support elective cesarean delivery in such patients.14
There is no contraindication to breastfeeding in women with hepatitis C unless they are coinfected with HIV. In such a circumstance, formula feeding should be chosen. After delivery, patients with hepatitis C should be referred to a gastroenterology specialist to receive antiviral treatment. Multiple new single-agent and combination regimens have produced cures in more than 90% of patients. These regimens usually require 8 to 12 weeks of treatment, and they are very expensive. They have not been widely tested in pregnant women.1
Hepatitis D
Hepatitis D, or delta hepatitis, is caused by an RNA virus. This virus is unique because it is incapable of independent replication. It must be present in association with hepatitis B to replicate and cause clinical infection. Therefore, the epidemiology of hepatitis D closely mirrors that of hepatitis B.1,2
Patients with hepatitis D typically present in one of two ways. Some individuals are acutely infected with hepatitis D at the same time that they acquire hepatitis B (coinfection). The natural history of this infection usually is spontaneous resolution without sequelae. Other patients have chronic hepatitis D superimposed on chronic hepatitis B (superinfection). Unfortunately, patients with the latter condition are at a notably increased risk for developing severe persistent liver disease.1,2
The diagnosis of hepatitis D may be confirmed by identifying the delta antigen in serum or in liver tissue obtained by biopsy or by identifying IgM- and IgG-specific antibodies in serum. In conjunction with hepatitis B, the delta virus can cause a chronic carrier state. Perinatal transmission is possible but uncommon. Of greatest importance, the immunoprophylaxis described for hepatitis B is almost perfectly protective against perinatal transmission of hepatitis D.1,2
Continue to: Hepatitis E...
Hepatitis E
Hepatitis E is an RNA virus that has 1 serotype and 4 genotypes. Its epidemiology is similar to that of hepatitis A. It is the most common waterborne illness in the world. The incubation period varies from 21 to 56 days. This disease is quite rare in the United States but is endemic in developing nations. In those countries, maternal infection has an alarmingly high mortality rate (5%–25%). For example, in Bangladesh, hepatitis E is responsible for more than 1,000 deaths per year in pregnant women. When hepatitis E is identified in more affluent countries, the individual cases and small outbreaks usually are linked to consumption of undercooked pork or wild game.1,15-17
The clinical presentation of acute hepatitis E also is similar to that of hepatitis A. The usual manifestations are fever, malaise, anorexia, nausea, right upper quadrant pain and tenderness, jaundice, darkened urine, and clay-colored stools. The most useful diagnostic tests are serologic detection of viral-specific antibodies (positive IgM or a 4-fold increase in the prior IgG titer) and PCR-RNA.1,17
Hepatitis E usually does not cause a chronic carrier state, and perinatal transmission is rare. Fortunately, a highly effective vaccine was recently developed (Hecolin, Xiamen Innovax Biotech). This recombinant vaccine is specifically directed against the hepatitis E genotype 1. In the initial efficacy study, healthy adults aged 16 to 65 years were randomly assigned to receive either the hepatitis E vaccine or the hepatitis B vaccine. The vaccine was administered at time point 0, and 1 and 6 months later. Patients were followed for up to 4.5 years to assess efficacy, immunogenicity, and safety. During the study period, 7 cases of hepatitis E occurred in the vaccine group, compared with 53 in the control group. Approximately 56,000 patients were included in each group. The efficacy of the vaccine was 86.8% (P<.001).18
Hepatitis G
Hepatitis G is caused by 2 single-stranded RNA viruses that are virtually identical—hepatitis G virus and GB virus type C. The viruses share approximately 30% homology with hepatitis C virus. The organism is present throughout the world and infects approximately 1.5% to 2.0% of the population. The virus is transmitted by blood and sexual contact. It replicates preferentially in mononuclear cells and the bone marrow rather than in the liver.19-21
Hepatitis G is much less virulent than hepatitis C. Hepatitis G often coexists with hepatitis A, B, and C, as well as with HIV. Coinfection with hepatitis G does not adversely affect the clinical course of the other conditions.22,23
Most patients with hepatitis G are asymptomatic, and no treatment is indicated. The virus can cause a chronic carrier state. Perinatal transmission is distinctly uncommon. When it does occur, however, injury to mother, fetus, or neonate is unlikely.1,24
The diagnosis of hepatitis G can be established by detection of virus with PCR and by the identification of antibody by enzyme immunoassay. Routine screening for this infection in pregnancy is not indicated.1,2
Hepatitis B is highly contagious and can be transmitted from the patient to her sexual partner and neonate. Testing for hepatitis B surface antigen and antibody is indicated in her partner. If these tests are negative, the partner should immediately receive hepatitis B immune globulin and then be started on the 3-dose hepatitis B vaccination series. The patient’s newborn also should receive hepatitis B immune globulin within 12 hours of delivery and should receive the first dose of the hepatitis B vaccine prior to discharge from the hospital. The second and third doses should be administered 1 and 6 months after delivery.
The patient also should have the following tests:
• liver function tests
-serum transaminases
-direct and indirect bilirubin
-coagulation profile
• hepatitis D antigen
• hepatitis B genotype
• hepatitis B viral load
• HIV serology.
If the hepatitis B viral load exceeds 1 million copies/mL, the patient should be treated with tenofovir 200 mg daily from 28 weeks’ gestation until delivery. In addition, she should be referred to a liver disease specialist after delivery for consideration of treatment with directly-acting antiviral agents. ●
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TB, et al, eds. Creasy & Resnik’s MaternalFetal Medicine Principles and Practice. 8th ed. Elsevier; 2019:862-919.
- Duff P. Hepatitis in pregnancy. In: Queenan JR, Spong CY, Lockwood CJ, eds. Management of HighRisk Pregnancy. An EvidenceBased Approach. 5th ed. Blackwell; 2007:238-241.
- Duff B, Duff P. Hepatitis A vaccine: ready for prime time. Obstet Gynecol. 1998;91:468-471.
- Victor JC, Monto AS, Surdina TY, et al. Hepatitis A vaccine versus immune globulin for postexposure prophylaxis. N Engl J Med. 2007;367:1685-1694.
- Dienstag JL. Hepatitis B virus infection. N Engl J Med. 2008;359:1486-1500.
- Society for MaternalFetal Medicine (SMFM); Dionne-Odom J, Tita ATN, Silverman NS. #38. Hepatitis B in pregnancy: screening, treatment, and prevention of vertical transmission. Am J Obstet Gynecol. 2016;214:6-14.
- Pan CQ, Duan Z, Dai E, et al. Tenofovir to prevent hepatitis B transmission in mothers with high viral load. N Engl J Med. 2016;374:2324-2334.
- Jourdain G, Huong N, Harrison L, et al. Tenofovir versus placebo to prevent perinatal transmission of hepatitis B. N Engl J Med. 2018;378:911-923.
- Rosen HR. Chronic hepatitis C infection. N Engl J Med. 2011;364:2429-2438.
- Hoofnagle JH, Feinstore SM. The discovery of hepatitis C—the 2020 Nobel Prize in Physiology or Medicine. N Engl J Med. 2020;384:2297-2299.
- Hughes BL, Page CM, Juller JA. Hepatitis C in pregnancy: screening, treatment, and management. Am J Obstet Gynecol. 2017;217:B2-B12.
- Saab S, Kullar R, Gounder P. The urgent need for hepatitis C screening in pregnant women: a call to action. Obstet Gynecol. 2020;135:773-777.
- Berkley EMF, Leslie KK, Arora S, et al. Chronic hepatitis C in pregnancy. Obstet Gynecol. 2008;112:304-310.
- Brazel M, Duff P. Considerations on the mode of delivery for pregnant women with hepatitis C infection [published online November 22, 2019]. OBG Manag. 2020;32:39-44.
- Emerson SU, Purcell RH. Hepatitis E virus. Rev Med Virol. 2003;13:145-154.
- Khuroo MS, Teli MR, Skidmore S, et al. Incidence and severity of viral hepatitis in pregnancy. Am J Med. 1981;70:252-255.
- Hoofnangle JH, Nelson KE, Purcell RH. Hepatitis E. N Engl J Med. 2012;367:1237-1244.
- Zhang J, Zhang XF, Huang SJ, et al. Longterm efficacy of a hepatitis E vaccine. N Engl J Med. 2015;372:914-922.
- Pickering L, ed. Red Book 2000 Report of Committee on Infectious Diseases. 25th ed. American Academy of Pediatrics; 2000.
- Chopra S. GB virus C (hepatitis G) infection. UpToDate website. Updated January 16, 2020. Accessed June 3, 2021. https://www.uptodate.com/contents/gb-virus-c-hepatitis-g-infection.
- Reshetnyak VI, Karlovich TI, Ilchenko LU. Hepatitis G virus. World J Gastroenterol. 2008;14:4725-4734.
- Kew MC, Kassianides C. HGV: hepatitis G virus or harmless G virus. Lancet. 1996;348(suppl II):10.
- Jarvis LM, Davidson F, Hanley JP, et al. Infection with hepatitis G virus among recipients of plasma products. Lancet. 1996;348;1352-1355.
- Feucht HH, Zollner B, Polywka S, et al. Vertical transmission of hepatitis G. Lancet. 1996;347;615-616.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TB, et al, eds. Creasy & Resnik’s MaternalFetal Medicine Principles and Practice. 8th ed. Elsevier; 2019:862-919.
- Duff P. Hepatitis in pregnancy. In: Queenan JR, Spong CY, Lockwood CJ, eds. Management of HighRisk Pregnancy. An EvidenceBased Approach. 5th ed. Blackwell; 2007:238-241.
- Duff B, Duff P. Hepatitis A vaccine: ready for prime time. Obstet Gynecol. 1998;91:468-471.
- Victor JC, Monto AS, Surdina TY, et al. Hepatitis A vaccine versus immune globulin for postexposure prophylaxis. N Engl J Med. 2007;367:1685-1694.
- Dienstag JL. Hepatitis B virus infection. N Engl J Med. 2008;359:1486-1500.
- Society for MaternalFetal Medicine (SMFM); Dionne-Odom J, Tita ATN, Silverman NS. #38. Hepatitis B in pregnancy: screening, treatment, and prevention of vertical transmission. Am J Obstet Gynecol. 2016;214:6-14.
- Pan CQ, Duan Z, Dai E, et al. Tenofovir to prevent hepatitis B transmission in mothers with high viral load. N Engl J Med. 2016;374:2324-2334.
- Jourdain G, Huong N, Harrison L, et al. Tenofovir versus placebo to prevent perinatal transmission of hepatitis B. N Engl J Med. 2018;378:911-923.
- Rosen HR. Chronic hepatitis C infection. N Engl J Med. 2011;364:2429-2438.
- Hoofnagle JH, Feinstore SM. The discovery of hepatitis C—the 2020 Nobel Prize in Physiology or Medicine. N Engl J Med. 2020;384:2297-2299.
- Hughes BL, Page CM, Juller JA. Hepatitis C in pregnancy: screening, treatment, and management. Am J Obstet Gynecol. 2017;217:B2-B12.
- Saab S, Kullar R, Gounder P. The urgent need for hepatitis C screening in pregnant women: a call to action. Obstet Gynecol. 2020;135:773-777.
- Berkley EMF, Leslie KK, Arora S, et al. Chronic hepatitis C in pregnancy. Obstet Gynecol. 2008;112:304-310.
- Brazel M, Duff P. Considerations on the mode of delivery for pregnant women with hepatitis C infection [published online November 22, 2019]. OBG Manag. 2020;32:39-44.
- Emerson SU, Purcell RH. Hepatitis E virus. Rev Med Virol. 2003;13:145-154.
- Khuroo MS, Teli MR, Skidmore S, et al. Incidence and severity of viral hepatitis in pregnancy. Am J Med. 1981;70:252-255.
- Hoofnangle JH, Nelson KE, Purcell RH. Hepatitis E. N Engl J Med. 2012;367:1237-1244.
- Zhang J, Zhang XF, Huang SJ, et al. Longterm efficacy of a hepatitis E vaccine. N Engl J Med. 2015;372:914-922.
- Pickering L, ed. Red Book 2000 Report of Committee on Infectious Diseases. 25th ed. American Academy of Pediatrics; 2000.
- Chopra S. GB virus C (hepatitis G) infection. UpToDate website. Updated January 16, 2020. Accessed June 3, 2021. https://www.uptodate.com/contents/gb-virus-c-hepatitis-g-infection.
- Reshetnyak VI, Karlovich TI, Ilchenko LU. Hepatitis G virus. World J Gastroenterol. 2008;14:4725-4734.
- Kew MC, Kassianides C. HGV: hepatitis G virus or harmless G virus. Lancet. 1996;348(suppl II):10.
- Jarvis LM, Davidson F, Hanley JP, et al. Infection with hepatitis G virus among recipients of plasma products. Lancet. 1996;348;1352-1355.
- Feucht HH, Zollner B, Polywka S, et al. Vertical transmission of hepatitis G. Lancet. 1996;347;615-616.
Does prophylactic use of tranexamic acid reduce PPH from cesarean delivery when coupled with uterotonics?
Sentilhes L, Senat MV, Le Lous M, et al; Groupe de Recherche en Obstetrique et Gynecologie. Tranexamic acid for the prevention of blood loss after cesarean delivery. N Engl J Med. 2021;384:1623-1634. doi: 10.1056/NEJMoa2028788.
EXPERT COMMENTARY
Postpartum hemorrhage is the leading cause of maternal mortality worldwide.1 Many preventive strategies, including tranexamic acid administration, have been studied in an attempt to reduce the risk of PPH. Tranexamic acid prevents the conversion of plasminogen to plasmin, preventing the breakdown of fibrin, and ultimately stabilizing the fibrin matrix of clot.2 It has been shown to be an effective approach to treating hemorrhage in patients after trauma as well as cardiac surgery.3,4 The use of tranexamic acid in obstetric hemorrhage has reduced mortality in previous trials,5 but its prophylactic use has had mixed results in preventing obstetric hemorrhage.6-8
Recently, Sentilhes and colleagues published the largest prospective study to date addressing the efficacy of tranexamic acid for the primary prevention of PPH.
Details of the study
Multiple hospitals throughout France participated in the investigators’ double-blind randomized, placebo-controlled trial. Women undergoing CD at 34 or more weeks’ gestation (N = 4,551) were randomly assigned to receive 1 g of intravenous (IV) tranexamic acid or placebo after cord clamping. Both groups received IV prophylactic uterotonics. The primary outcome was PPH, defined by estimated blood loss (EBL) greater than 1 L or receipt of red blood cell transfusion within the first 2 days after surgery.
Results. The rate of PPH was significantly lower in women who received tranexamic acid compared with those who received placebo. Yet, the mean EBL between the 2 groups differed by only 100 mL. The rates of blood transfusions, additional uterotonic administration, arterial embolization, and hysterectomy did not differ between groups.
The clinicians responsible for the care of these patients did not observe a difference in the rate of “clinically significant” PPH between those who received tranexamic acid and those who received placebo. Women who received tranexamic acid were more likely to experience nausea and vomiting, but they did not have any increased risk of venous thromboembolic disease.
Study strengths and limitations
Sentilhes and colleagues’ study findings contradict those of an earlier meta-analysis on the topic.9 This may be due to the effect of publication bias on meta-analyses, which makes them prone to supporting the findings of published positive trials while missing data from negative trials that did not reach publication. The gold standard for addressing a research question such as this is a randomized controlled trial (RCT). The study reviewed here is an excellent example of a well-designed and executed RCT.
There may be a benefit to prophylactic tranexamic acid in certain populations not well captured among these study participants. The inclusion criteria were broad, including both prelabor and intrapartum CDs, making the results generalizable. However, the population studied, with a mean body mass index of 26 kg/m2 and age of 33, may not resemble some readers’ patient population. Prespecified subgroup analyses did not find a benefit to tranexamic acid in patients considered at high risk for PPH or in those undergoing intrapartum CD. ●
Prevention of PPH would reduce the burden of maternal morbidity and mortality dramatically. Unfortunately, the addition of tranexamic acid as a prophylactic agent at CD does not appear to have a clinically significant impact on the outcomes that matter to patients or providers. While tranexamic acid certainly has a role in the treatment of PPH, its benefit as a preventive agent has yet to be demonstrated.
JONATHAN S. HIRSHBERG, MD,
AND ALISON G. CAHILL, MD, MSCI
- Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2:e323-e333.
- Chauncey JM, Wieters JS. Tranexamic Acid. StatPearls Publishing LLC [internet]; 2021.
- Karski JM, Teasdale SJ, Norman P, et al. Prevention of bleeding after cardiopulmonary bypass with high-dose tranexamic acid. Double-blind, randomized clinical trial. J Thorac Cardiovasc Surg. 1995;110:835-842.
- Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess. 2013;17:1-79.
- WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet. 2017;389:2105-2116.
- Sentilhes L, Winer N, Azria E, et al; Groupe de Recherche en Obstetrique et Gynecologie. Tranexamic acid for the prevention of blood loss after vaginal delivery. N Engl J Med. 2018;379:731-742.
- Shahid A, Khan A. Tranexamic acid in decreasing blood loss during and after caesarean section. J Coll Physicians Surg Pak. 2013;23;459-462.
- Simonazzi G, Bisulli M, Saccone G, et al. Tranexamic acid for preventing postpartum blood loss after cesarean delivery: a systematic review and meta-analysis of randomized controlled trials. Acta Obstet Gynecol Scand. 2016;95:28-37.
- Wang Y, Liu S, He L. Prophylactic use of tranexamic acid reduces blood loss and transfusion requirements in patients undergoing cesarean section: a meta-analysis. J Obstet Gynaecol Res. 2019;45:1562-1575.
Sentilhes L, Senat MV, Le Lous M, et al; Groupe de Recherche en Obstetrique et Gynecologie. Tranexamic acid for the prevention of blood loss after cesarean delivery. N Engl J Med. 2021;384:1623-1634. doi: 10.1056/NEJMoa2028788.
EXPERT COMMENTARY
Postpartum hemorrhage is the leading cause of maternal mortality worldwide.1 Many preventive strategies, including tranexamic acid administration, have been studied in an attempt to reduce the risk of PPH. Tranexamic acid prevents the conversion of plasminogen to plasmin, preventing the breakdown of fibrin, and ultimately stabilizing the fibrin matrix of clot.2 It has been shown to be an effective approach to treating hemorrhage in patients after trauma as well as cardiac surgery.3,4 The use of tranexamic acid in obstetric hemorrhage has reduced mortality in previous trials,5 but its prophylactic use has had mixed results in preventing obstetric hemorrhage.6-8
Recently, Sentilhes and colleagues published the largest prospective study to date addressing the efficacy of tranexamic acid for the primary prevention of PPH.
Details of the study
Multiple hospitals throughout France participated in the investigators’ double-blind randomized, placebo-controlled trial. Women undergoing CD at 34 or more weeks’ gestation (N = 4,551) were randomly assigned to receive 1 g of intravenous (IV) tranexamic acid or placebo after cord clamping. Both groups received IV prophylactic uterotonics. The primary outcome was PPH, defined by estimated blood loss (EBL) greater than 1 L or receipt of red blood cell transfusion within the first 2 days after surgery.
Results. The rate of PPH was significantly lower in women who received tranexamic acid compared with those who received placebo. Yet, the mean EBL between the 2 groups differed by only 100 mL. The rates of blood transfusions, additional uterotonic administration, arterial embolization, and hysterectomy did not differ between groups.
The clinicians responsible for the care of these patients did not observe a difference in the rate of “clinically significant” PPH between those who received tranexamic acid and those who received placebo. Women who received tranexamic acid were more likely to experience nausea and vomiting, but they did not have any increased risk of venous thromboembolic disease.
Study strengths and limitations
Sentilhes and colleagues’ study findings contradict those of an earlier meta-analysis on the topic.9 This may be due to the effect of publication bias on meta-analyses, which makes them prone to supporting the findings of published positive trials while missing data from negative trials that did not reach publication. The gold standard for addressing a research question such as this is a randomized controlled trial (RCT). The study reviewed here is an excellent example of a well-designed and executed RCT.
There may be a benefit to prophylactic tranexamic acid in certain populations not well captured among these study participants. The inclusion criteria were broad, including both prelabor and intrapartum CDs, making the results generalizable. However, the population studied, with a mean body mass index of 26 kg/m2 and age of 33, may not resemble some readers’ patient population. Prespecified subgroup analyses did not find a benefit to tranexamic acid in patients considered at high risk for PPH or in those undergoing intrapartum CD. ●
Prevention of PPH would reduce the burden of maternal morbidity and mortality dramatically. Unfortunately, the addition of tranexamic acid as a prophylactic agent at CD does not appear to have a clinically significant impact on the outcomes that matter to patients or providers. While tranexamic acid certainly has a role in the treatment of PPH, its benefit as a preventive agent has yet to be demonstrated.
JONATHAN S. HIRSHBERG, MD,
AND ALISON G. CAHILL, MD, MSCI
Sentilhes L, Senat MV, Le Lous M, et al; Groupe de Recherche en Obstetrique et Gynecologie. Tranexamic acid for the prevention of blood loss after cesarean delivery. N Engl J Med. 2021;384:1623-1634. doi: 10.1056/NEJMoa2028788.
EXPERT COMMENTARY
Postpartum hemorrhage is the leading cause of maternal mortality worldwide.1 Many preventive strategies, including tranexamic acid administration, have been studied in an attempt to reduce the risk of PPH. Tranexamic acid prevents the conversion of plasminogen to plasmin, preventing the breakdown of fibrin, and ultimately stabilizing the fibrin matrix of clot.2 It has been shown to be an effective approach to treating hemorrhage in patients after trauma as well as cardiac surgery.3,4 The use of tranexamic acid in obstetric hemorrhage has reduced mortality in previous trials,5 but its prophylactic use has had mixed results in preventing obstetric hemorrhage.6-8
Recently, Sentilhes and colleagues published the largest prospective study to date addressing the efficacy of tranexamic acid for the primary prevention of PPH.
Details of the study
Multiple hospitals throughout France participated in the investigators’ double-blind randomized, placebo-controlled trial. Women undergoing CD at 34 or more weeks’ gestation (N = 4,551) were randomly assigned to receive 1 g of intravenous (IV) tranexamic acid or placebo after cord clamping. Both groups received IV prophylactic uterotonics. The primary outcome was PPH, defined by estimated blood loss (EBL) greater than 1 L or receipt of red blood cell transfusion within the first 2 days after surgery.
Results. The rate of PPH was significantly lower in women who received tranexamic acid compared with those who received placebo. Yet, the mean EBL between the 2 groups differed by only 100 mL. The rates of blood transfusions, additional uterotonic administration, arterial embolization, and hysterectomy did not differ between groups.
The clinicians responsible for the care of these patients did not observe a difference in the rate of “clinically significant” PPH between those who received tranexamic acid and those who received placebo. Women who received tranexamic acid were more likely to experience nausea and vomiting, but they did not have any increased risk of venous thromboembolic disease.
Study strengths and limitations
Sentilhes and colleagues’ study findings contradict those of an earlier meta-analysis on the topic.9 This may be due to the effect of publication bias on meta-analyses, which makes them prone to supporting the findings of published positive trials while missing data from negative trials that did not reach publication. The gold standard for addressing a research question such as this is a randomized controlled trial (RCT). The study reviewed here is an excellent example of a well-designed and executed RCT.
There may be a benefit to prophylactic tranexamic acid in certain populations not well captured among these study participants. The inclusion criteria were broad, including both prelabor and intrapartum CDs, making the results generalizable. However, the population studied, with a mean body mass index of 26 kg/m2 and age of 33, may not resemble some readers’ patient population. Prespecified subgroup analyses did not find a benefit to tranexamic acid in patients considered at high risk for PPH or in those undergoing intrapartum CD. ●
Prevention of PPH would reduce the burden of maternal morbidity and mortality dramatically. Unfortunately, the addition of tranexamic acid as a prophylactic agent at CD does not appear to have a clinically significant impact on the outcomes that matter to patients or providers. While tranexamic acid certainly has a role in the treatment of PPH, its benefit as a preventive agent has yet to be demonstrated.
JONATHAN S. HIRSHBERG, MD,
AND ALISON G. CAHILL, MD, MSCI
- Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2:e323-e333.
- Chauncey JM, Wieters JS. Tranexamic Acid. StatPearls Publishing LLC [internet]; 2021.
- Karski JM, Teasdale SJ, Norman P, et al. Prevention of bleeding after cardiopulmonary bypass with high-dose tranexamic acid. Double-blind, randomized clinical trial. J Thorac Cardiovasc Surg. 1995;110:835-842.
- Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess. 2013;17:1-79.
- WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet. 2017;389:2105-2116.
- Sentilhes L, Winer N, Azria E, et al; Groupe de Recherche en Obstetrique et Gynecologie. Tranexamic acid for the prevention of blood loss after vaginal delivery. N Engl J Med. 2018;379:731-742.
- Shahid A, Khan A. Tranexamic acid in decreasing blood loss during and after caesarean section. J Coll Physicians Surg Pak. 2013;23;459-462.
- Simonazzi G, Bisulli M, Saccone G, et al. Tranexamic acid for preventing postpartum blood loss after cesarean delivery: a systematic review and meta-analysis of randomized controlled trials. Acta Obstet Gynecol Scand. 2016;95:28-37.
- Wang Y, Liu S, He L. Prophylactic use of tranexamic acid reduces blood loss and transfusion requirements in patients undergoing cesarean section: a meta-analysis. J Obstet Gynaecol Res. 2019;45:1562-1575.
- Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2:e323-e333.
- Chauncey JM, Wieters JS. Tranexamic Acid. StatPearls Publishing LLC [internet]; 2021.
- Karski JM, Teasdale SJ, Norman P, et al. Prevention of bleeding after cardiopulmonary bypass with high-dose tranexamic acid. Double-blind, randomized clinical trial. J Thorac Cardiovasc Surg. 1995;110:835-842.
- Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess. 2013;17:1-79.
- WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet. 2017;389:2105-2116.
- Sentilhes L, Winer N, Azria E, et al; Groupe de Recherche en Obstetrique et Gynecologie. Tranexamic acid for the prevention of blood loss after vaginal delivery. N Engl J Med. 2018;379:731-742.
- Shahid A, Khan A. Tranexamic acid in decreasing blood loss during and after caesarean section. J Coll Physicians Surg Pak. 2013;23;459-462.
- Simonazzi G, Bisulli M, Saccone G, et al. Tranexamic acid for preventing postpartum blood loss after cesarean delivery: a systematic review and meta-analysis of randomized controlled trials. Acta Obstet Gynecol Scand. 2016;95:28-37.
- Wang Y, Liu S, He L. Prophylactic use of tranexamic acid reduces blood loss and transfusion requirements in patients undergoing cesarean section: a meta-analysis. J Obstet Gynaecol Res. 2019;45:1562-1575.
Screen pregnant women for OSA, given known risks
Pregnant women who have even mild sleep apnea should be treated for their sleep-disordered breathing given what is known about associated risks for hypertensive disorders of pregnancy and gestational diabetes, Carolyn M. D’Ambrosio, MS, MD, FCCP, said at the virtual annual meeting of the Associated Professional Sleep Societies.
“This is the current standard of care,” Dr. D’Ambrosio said. “Although guidelines on this issue are not hard and fast, I’d say that knowing what we know about the risk of adverse [maternal] outcomes, we should all try to treat these problems as soon as they’re identified” and then repeat polysomnography or home sleep testing 3-6 months post partum to “be sure the sleep-disordered breathing has resolved.”
Estimates of obstructive sleep apnea (OSA) prevalence range from approximately 9% in the first trimester to 20% in the third trimester. Yet recognizing the significance of OSA in pregnant women and identifying women for testing remains a major challenge. “Most women won’t [report sleep problems] because it’s pretty much common folklore that you don’t sleep well when you’re pregnant,” said Dr. D’Ambrosio, associate professor of medicine at Harvard Medical School, Boston, and current past-chair of the Women’s Lung Health Network for CHEST.
Many obstetricians and obstetrics providers, meanwhile, do not adequately screen. Typical screening tools like the Epworth Sleepiness Scale have low sensitivity and specificity during pregnancy, which means that inquiries about sleepiness, snoring, and disruptions in sleep are important, as is attention to potential risks for OSA posed by obesity, chronic hypertension, and neck circumference.
Only about a quarter of women in the United States snore during pregnancy, she noted. Snoring prevalence does increase as pregnancy progresses, reaching up to almost 50% in during the third trimester in some studies.
A four-variable screening tool reported almost 10 years ago for pregnant women is reliable for gauging risk, Dr. D’Ambrosio said. The model considers self-reported frequent snoring (more than three times/week), chronic hypertension, advanced maternal age, and a pregestational body mass index of at least 30 kg/m2. “If these [factors] are present, the patient is at significant risk for OSA and should be strongly considered for testing,” she said.
Home sleep apnea testing (HSAT) is validated for pregnant women but “it can underestimate,” she said. “If you get a negative result and [have clinical suspicion], then don’t stop there.”
And considering that the prevalence of OSA – at all levels of severity – increases as pregnancy progresses, it’s important to continue talking about sleep with patients who have frequent snoring, for instance, but negative sleep test results early in pregnancy. “They could develop [OSA] as time goes on,” she said.
Associated risk factors
Independent associations between sleep-disordered breathing and adverse maternal outcomes were demonstrated in a prospective cohort study published several years ago of 3,705 women who underwent HSAT in early and mid-pregnancy. The adjusted odds ratios for preeclampsia when sleep-disordered breathing (an apnea-hypopnea index of ≥5) was present early in pregnancy and in mid-pregnancy were 1.94 and 1.95, respectively.
For hypertensive disorders of pregnancy more broadly, the ORs were 1.46 and 1.73, and for gestational diabetes, the ORs were 3.47 and 2.79.
“Faced with the question about why it’s important to diagnosis and treat OSA [during pregnancy] since the pregnancy will be over in a few months, I go to this study,” Dr. D’Ambrosio said. “Waiting until the end of pregnancy is not safe. There are increased risks of very serious conditions if sleep apnea is there and it’s not treated.”
Another study demonstrating a link between OSA and maternal outcomes looked over 1.5 million deliveries in the United States and found a significantly higher prevalence of gestational diabetes (OR, 2.08), gestational hypertension (OR, 1.77), preeclampsia (OR, 2.07), and eclampsia (OR, 2.70) in pregnant women with OSA than without, after adjusting for maternal obesity. Associations remained significant after adjusting for a more comprehensive list of covariates.
Multiple potential casual pathways are at play, Dr. D’Ambrosio said. Short sleep duration decreases leptin and increases ghrelin levels, for instance, and sleep fragmentation activates the HPA axis and increases cortisol. Intermittent hypoxemia affects sympathetic activity, and intrathoracic pressure swings cause increased oxidative stress and systemic inflammation.
The resulting endothelial dysfunction, glucose dysfunction, and dyslipidemia can drive the adverse maternal outcomes documented in these studies, she said, noting that the adverse outcomes can have long-term cardiovascular consequences.
Continuous positive airway pressure therapy is well tolerated in pregnancy, and given pregnancy’s continual weight change, auto-titrating CPAP may be the best option, she said.
There is “some limited data that treatment improves maternal outcomes, and we’re still working on trying to get better data and more solid recommendations,” Dr. D’Ambrosio said. There currently are no guidelines covering the diagnosis and management of OSA during pregnancy.
“We’ve come a long way ... but we still have more to do,” she said. “We have a long way to go to getting [OSA in pregnant women] well recognized, with screening techniques and diagnosis.”
Asked after the meeting about Dr. D’Ambrosio’s messages, Anita Rajagopal, MD, said that OSA screening during pregnancy needs to be improved through more collaboration “with our ob.gyn. and primary care colleagues.”
Too often, she said, “the signs and symptoms of OSA in pregnancy are written off as ‘just harmless snoring’ while in fact the patient has treatable sleep disordered breathing with potential adverse effects.” Dr. Rajagopal is department medical director for sleep medicine at Community Physician Network and medical director of the Community Health Network Sleep-Wake Disorders Center, both in Indianapolis.
Dr. D’Ambrosio reported that she has no potential conflicts of interest related to the material she presented, and Dr. Rajagopal stated she has no potential conflicts of interest.
Pregnant women who have even mild sleep apnea should be treated for their sleep-disordered breathing given what is known about associated risks for hypertensive disorders of pregnancy and gestational diabetes, Carolyn M. D’Ambrosio, MS, MD, FCCP, said at the virtual annual meeting of the Associated Professional Sleep Societies.
“This is the current standard of care,” Dr. D’Ambrosio said. “Although guidelines on this issue are not hard and fast, I’d say that knowing what we know about the risk of adverse [maternal] outcomes, we should all try to treat these problems as soon as they’re identified” and then repeat polysomnography or home sleep testing 3-6 months post partum to “be sure the sleep-disordered breathing has resolved.”
Estimates of obstructive sleep apnea (OSA) prevalence range from approximately 9% in the first trimester to 20% in the third trimester. Yet recognizing the significance of OSA in pregnant women and identifying women for testing remains a major challenge. “Most women won’t [report sleep problems] because it’s pretty much common folklore that you don’t sleep well when you’re pregnant,” said Dr. D’Ambrosio, associate professor of medicine at Harvard Medical School, Boston, and current past-chair of the Women’s Lung Health Network for CHEST.
Many obstetricians and obstetrics providers, meanwhile, do not adequately screen. Typical screening tools like the Epworth Sleepiness Scale have low sensitivity and specificity during pregnancy, which means that inquiries about sleepiness, snoring, and disruptions in sleep are important, as is attention to potential risks for OSA posed by obesity, chronic hypertension, and neck circumference.
Only about a quarter of women in the United States snore during pregnancy, she noted. Snoring prevalence does increase as pregnancy progresses, reaching up to almost 50% in during the third trimester in some studies.
A four-variable screening tool reported almost 10 years ago for pregnant women is reliable for gauging risk, Dr. D’Ambrosio said. The model considers self-reported frequent snoring (more than three times/week), chronic hypertension, advanced maternal age, and a pregestational body mass index of at least 30 kg/m2. “If these [factors] are present, the patient is at significant risk for OSA and should be strongly considered for testing,” she said.
Home sleep apnea testing (HSAT) is validated for pregnant women but “it can underestimate,” she said. “If you get a negative result and [have clinical suspicion], then don’t stop there.”
And considering that the prevalence of OSA – at all levels of severity – increases as pregnancy progresses, it’s important to continue talking about sleep with patients who have frequent snoring, for instance, but negative sleep test results early in pregnancy. “They could develop [OSA] as time goes on,” she said.
Associated risk factors
Independent associations between sleep-disordered breathing and adverse maternal outcomes were demonstrated in a prospective cohort study published several years ago of 3,705 women who underwent HSAT in early and mid-pregnancy. The adjusted odds ratios for preeclampsia when sleep-disordered breathing (an apnea-hypopnea index of ≥5) was present early in pregnancy and in mid-pregnancy were 1.94 and 1.95, respectively.
For hypertensive disorders of pregnancy more broadly, the ORs were 1.46 and 1.73, and for gestational diabetes, the ORs were 3.47 and 2.79.
“Faced with the question about why it’s important to diagnosis and treat OSA [during pregnancy] since the pregnancy will be over in a few months, I go to this study,” Dr. D’Ambrosio said. “Waiting until the end of pregnancy is not safe. There are increased risks of very serious conditions if sleep apnea is there and it’s not treated.”
Another study demonstrating a link between OSA and maternal outcomes looked over 1.5 million deliveries in the United States and found a significantly higher prevalence of gestational diabetes (OR, 2.08), gestational hypertension (OR, 1.77), preeclampsia (OR, 2.07), and eclampsia (OR, 2.70) in pregnant women with OSA than without, after adjusting for maternal obesity. Associations remained significant after adjusting for a more comprehensive list of covariates.
Multiple potential casual pathways are at play, Dr. D’Ambrosio said. Short sleep duration decreases leptin and increases ghrelin levels, for instance, and sleep fragmentation activates the HPA axis and increases cortisol. Intermittent hypoxemia affects sympathetic activity, and intrathoracic pressure swings cause increased oxidative stress and systemic inflammation.
The resulting endothelial dysfunction, glucose dysfunction, and dyslipidemia can drive the adverse maternal outcomes documented in these studies, she said, noting that the adverse outcomes can have long-term cardiovascular consequences.
Continuous positive airway pressure therapy is well tolerated in pregnancy, and given pregnancy’s continual weight change, auto-titrating CPAP may be the best option, she said.
There is “some limited data that treatment improves maternal outcomes, and we’re still working on trying to get better data and more solid recommendations,” Dr. D’Ambrosio said. There currently are no guidelines covering the diagnosis and management of OSA during pregnancy.
“We’ve come a long way ... but we still have more to do,” she said. “We have a long way to go to getting [OSA in pregnant women] well recognized, with screening techniques and diagnosis.”
Asked after the meeting about Dr. D’Ambrosio’s messages, Anita Rajagopal, MD, said that OSA screening during pregnancy needs to be improved through more collaboration “with our ob.gyn. and primary care colleagues.”
Too often, she said, “the signs and symptoms of OSA in pregnancy are written off as ‘just harmless snoring’ while in fact the patient has treatable sleep disordered breathing with potential adverse effects.” Dr. Rajagopal is department medical director for sleep medicine at Community Physician Network and medical director of the Community Health Network Sleep-Wake Disorders Center, both in Indianapolis.
Dr. D’Ambrosio reported that she has no potential conflicts of interest related to the material she presented, and Dr. Rajagopal stated she has no potential conflicts of interest.
Pregnant women who have even mild sleep apnea should be treated for their sleep-disordered breathing given what is known about associated risks for hypertensive disorders of pregnancy and gestational diabetes, Carolyn M. D’Ambrosio, MS, MD, FCCP, said at the virtual annual meeting of the Associated Professional Sleep Societies.
“This is the current standard of care,” Dr. D’Ambrosio said. “Although guidelines on this issue are not hard and fast, I’d say that knowing what we know about the risk of adverse [maternal] outcomes, we should all try to treat these problems as soon as they’re identified” and then repeat polysomnography or home sleep testing 3-6 months post partum to “be sure the sleep-disordered breathing has resolved.”
Estimates of obstructive sleep apnea (OSA) prevalence range from approximately 9% in the first trimester to 20% in the third trimester. Yet recognizing the significance of OSA in pregnant women and identifying women for testing remains a major challenge. “Most women won’t [report sleep problems] because it’s pretty much common folklore that you don’t sleep well when you’re pregnant,” said Dr. D’Ambrosio, associate professor of medicine at Harvard Medical School, Boston, and current past-chair of the Women’s Lung Health Network for CHEST.
Many obstetricians and obstetrics providers, meanwhile, do not adequately screen. Typical screening tools like the Epworth Sleepiness Scale have low sensitivity and specificity during pregnancy, which means that inquiries about sleepiness, snoring, and disruptions in sleep are important, as is attention to potential risks for OSA posed by obesity, chronic hypertension, and neck circumference.
Only about a quarter of women in the United States snore during pregnancy, she noted. Snoring prevalence does increase as pregnancy progresses, reaching up to almost 50% in during the third trimester in some studies.
A four-variable screening tool reported almost 10 years ago for pregnant women is reliable for gauging risk, Dr. D’Ambrosio said. The model considers self-reported frequent snoring (more than three times/week), chronic hypertension, advanced maternal age, and a pregestational body mass index of at least 30 kg/m2. “If these [factors] are present, the patient is at significant risk for OSA and should be strongly considered for testing,” she said.
Home sleep apnea testing (HSAT) is validated for pregnant women but “it can underestimate,” she said. “If you get a negative result and [have clinical suspicion], then don’t stop there.”
And considering that the prevalence of OSA – at all levels of severity – increases as pregnancy progresses, it’s important to continue talking about sleep with patients who have frequent snoring, for instance, but negative sleep test results early in pregnancy. “They could develop [OSA] as time goes on,” she said.
Associated risk factors
Independent associations between sleep-disordered breathing and adverse maternal outcomes were demonstrated in a prospective cohort study published several years ago of 3,705 women who underwent HSAT in early and mid-pregnancy. The adjusted odds ratios for preeclampsia when sleep-disordered breathing (an apnea-hypopnea index of ≥5) was present early in pregnancy and in mid-pregnancy were 1.94 and 1.95, respectively.
For hypertensive disorders of pregnancy more broadly, the ORs were 1.46 and 1.73, and for gestational diabetes, the ORs were 3.47 and 2.79.
“Faced with the question about why it’s important to diagnosis and treat OSA [during pregnancy] since the pregnancy will be over in a few months, I go to this study,” Dr. D’Ambrosio said. “Waiting until the end of pregnancy is not safe. There are increased risks of very serious conditions if sleep apnea is there and it’s not treated.”
Another study demonstrating a link between OSA and maternal outcomes looked over 1.5 million deliveries in the United States and found a significantly higher prevalence of gestational diabetes (OR, 2.08), gestational hypertension (OR, 1.77), preeclampsia (OR, 2.07), and eclampsia (OR, 2.70) in pregnant women with OSA than without, after adjusting for maternal obesity. Associations remained significant after adjusting for a more comprehensive list of covariates.
Multiple potential casual pathways are at play, Dr. D’Ambrosio said. Short sleep duration decreases leptin and increases ghrelin levels, for instance, and sleep fragmentation activates the HPA axis and increases cortisol. Intermittent hypoxemia affects sympathetic activity, and intrathoracic pressure swings cause increased oxidative stress and systemic inflammation.
The resulting endothelial dysfunction, glucose dysfunction, and dyslipidemia can drive the adverse maternal outcomes documented in these studies, she said, noting that the adverse outcomes can have long-term cardiovascular consequences.
Continuous positive airway pressure therapy is well tolerated in pregnancy, and given pregnancy’s continual weight change, auto-titrating CPAP may be the best option, she said.
There is “some limited data that treatment improves maternal outcomes, and we’re still working on trying to get better data and more solid recommendations,” Dr. D’Ambrosio said. There currently are no guidelines covering the diagnosis and management of OSA during pregnancy.
“We’ve come a long way ... but we still have more to do,” she said. “We have a long way to go to getting [OSA in pregnant women] well recognized, with screening techniques and diagnosis.”
Asked after the meeting about Dr. D’Ambrosio’s messages, Anita Rajagopal, MD, said that OSA screening during pregnancy needs to be improved through more collaboration “with our ob.gyn. and primary care colleagues.”
Too often, she said, “the signs and symptoms of OSA in pregnancy are written off as ‘just harmless snoring’ while in fact the patient has treatable sleep disordered breathing with potential adverse effects.” Dr. Rajagopal is department medical director for sleep medicine at Community Physician Network and medical director of the Community Health Network Sleep-Wake Disorders Center, both in Indianapolis.
Dr. D’Ambrosio reported that she has no potential conflicts of interest related to the material she presented, and Dr. Rajagopal stated she has no potential conflicts of interest.
FROM SLEEP 2021
Average childbirth costs more than $3,000 out of pocket with private insurance
Families with private health insurance pay around $3,000 for newborn delivery and hospitalization, while adding neonatal intensive care can push the bill closer to $5,000, based on a retrospective look at almost 400,000 episodes.
The findings suggest that privately insured families need prenatal financial counseling, as well as screening for financial hardship after delivery, reported lead author Kao-Ping Chua, MD, PhD, assistant professor and health policy researcher in the department of pediatrics and the Susan B. Meister Child Health Evaluation and Research Center at the University of Michigan, Ann Arbor, and colleagues.
“Concern is growing regarding the high and rising financial burden of childbirth for privately insured families,” the investigators wrote in Pediatrics. “Previous studies assessing this burden have focused on out-of-pocket spending for maternal care, including hospitalizations for delivery. However, there are no recent national data on out-of-pocket spending across the childbirth episode, including both deliveries and newborn hospitalizations.”
To address this knowledge gap, Dr. Chua and colleagues turned to Optum’s deidentified Clinformatics Data Mart, comprising 12 million privately insured individuals across the United States. The investigators identified 398,410 childbirth episodes occurring between 2016 and 2019. Each episode was defined as one delivery and at least one newborn hospitalization under the same family plan.
Out-of-pocket cost included copayment plus coinsurance and deductibles. Primary outcomes included mean total out-of-pocket spending and proportion of episodes exceeding $5,000 or $10,000. Subgroup analyses compared differences in spending between episodes involving neonatal intensive care or cesarean birth.
The mean out-of-pocket spending was $2,281 for delivery and $788 for newborn hospitalization, giving a total of $3,068 per childbirth episode. Coinsurance and deductibles accounted for much of that cost, at 55.8% and 42.1%, respectively, whereas copayments accounted for a relatively minor portion (2.2%).
Almost all episodes (95%) cost more than zero dollars, while 17.1% cost more than $5,000 and 1.0% cost more than $10,000. Total mean out-of-pocket spending was higher for episodes involving cesarean birth ($3,389) or neonatal intensive care ($4,969), the latter of which cost more than $10,000 in 8.8% of episodes.
“Because details on plan benefit design were unavailable, the generalizability of findings to all privately insured Americans is unclear,” the investigators noted. “However, the proportion of childbirth episodes covered by high-deductible health plans in this study is consistent with the prevalence of such plans among Americans with employer-sponsored insurance.”
The findings suggest that financial reform is needed, Dr. Chua and colleagues concluded.
“To avoid imposing undue financial burden on families, private insurers should improve childbirth coverage,” they wrote. “An incremental step would be providing first-dollar coverage of deliveries and newborn hospitalizations before deductibles are met. Ideally, however, insurers would waive most or all cost-sharing for these hospitalizations, consistent with the approach taken by Medicaid programs and many developed countries.”

According to Madeline Sutton, MD, assistant professor of obstetrics and gynecology at Morehouse School of Medicine, Atlanta, the size of the study is commendable, but some details are lacking.
“Although the overall sample size allows for a robust analysis, deciding to not report the confidence intervals in this report does not allow for understanding of [the findings with] smaller sample sizes,” Dr. Sutton said in an interview.
(Dr. Chua and colleagues noted that they did not report confidence intervals because “all differences between subgroups were significant owing to large sample sizes.”)
“Still,” Dr. Sutton went on, “this is an important study that has implications for financial counseling that may need to be a part of preconceptional, prenatal, and postnatal visits for privately insured families to help with planning and to decrease the chances of childbirth-related financial hardships. Additionally, policy-level changes that decrease or eliminate these private insurance–related childbirth-episode costs that may negatively impact some families with lower incomes, are warranted.”
The study was funded by the National Institutes of Health. Dr. Chua disclosed a grant from the National Institute on Drug Abuse, while Dr. Moniz is supported by the Agency for Healthcare Research and Quality. Dr. Sutton had no relevant disclosures.
Families with private health insurance pay around $3,000 for newborn delivery and hospitalization, while adding neonatal intensive care can push the bill closer to $5,000, based on a retrospective look at almost 400,000 episodes.
The findings suggest that privately insured families need prenatal financial counseling, as well as screening for financial hardship after delivery, reported lead author Kao-Ping Chua, MD, PhD, assistant professor and health policy researcher in the department of pediatrics and the Susan B. Meister Child Health Evaluation and Research Center at the University of Michigan, Ann Arbor, and colleagues.
“Concern is growing regarding the high and rising financial burden of childbirth for privately insured families,” the investigators wrote in Pediatrics. “Previous studies assessing this burden have focused on out-of-pocket spending for maternal care, including hospitalizations for delivery. However, there are no recent national data on out-of-pocket spending across the childbirth episode, including both deliveries and newborn hospitalizations.”
To address this knowledge gap, Dr. Chua and colleagues turned to Optum’s deidentified Clinformatics Data Mart, comprising 12 million privately insured individuals across the United States. The investigators identified 398,410 childbirth episodes occurring between 2016 and 2019. Each episode was defined as one delivery and at least one newborn hospitalization under the same family plan.
Out-of-pocket cost included copayment plus coinsurance and deductibles. Primary outcomes included mean total out-of-pocket spending and proportion of episodes exceeding $5,000 or $10,000. Subgroup analyses compared differences in spending between episodes involving neonatal intensive care or cesarean birth.
The mean out-of-pocket spending was $2,281 for delivery and $788 for newborn hospitalization, giving a total of $3,068 per childbirth episode. Coinsurance and deductibles accounted for much of that cost, at 55.8% and 42.1%, respectively, whereas copayments accounted for a relatively minor portion (2.2%).
Almost all episodes (95%) cost more than zero dollars, while 17.1% cost more than $5,000 and 1.0% cost more than $10,000. Total mean out-of-pocket spending was higher for episodes involving cesarean birth ($3,389) or neonatal intensive care ($4,969), the latter of which cost more than $10,000 in 8.8% of episodes.
“Because details on plan benefit design were unavailable, the generalizability of findings to all privately insured Americans is unclear,” the investigators noted. “However, the proportion of childbirth episodes covered by high-deductible health plans in this study is consistent with the prevalence of such plans among Americans with employer-sponsored insurance.”
The findings suggest that financial reform is needed, Dr. Chua and colleagues concluded.
“To avoid imposing undue financial burden on families, private insurers should improve childbirth coverage,” they wrote. “An incremental step would be providing first-dollar coverage of deliveries and newborn hospitalizations before deductibles are met. Ideally, however, insurers would waive most or all cost-sharing for these hospitalizations, consistent with the approach taken by Medicaid programs and many developed countries.”
According to Madeline Sutton, MD, assistant professor of obstetrics and gynecology at Morehouse School of Medicine, Atlanta, the size of the study is commendable, but some details are lacking.
“Although the overall sample size allows for a robust analysis, deciding to not report the confidence intervals in this report does not allow for understanding of [the findings with] smaller sample sizes,” Dr. Sutton said in an interview.
(Dr. Chua and colleagues noted that they did not report confidence intervals because “all differences between subgroups were significant owing to large sample sizes.”)
“Still,” Dr. Sutton went on, “this is an important study that has implications for financial counseling that may need to be a part of preconceptional, prenatal, and postnatal visits for privately insured families to help with planning and to decrease the chances of childbirth-related financial hardships. Additionally, policy-level changes that decrease or eliminate these private insurance–related childbirth-episode costs that may negatively impact some families with lower incomes, are warranted.”
The study was funded by the National Institutes of Health. Dr. Chua disclosed a grant from the National Institute on Drug Abuse, while Dr. Moniz is supported by the Agency for Healthcare Research and Quality. Dr. Sutton had no relevant disclosures.
Families with private health insurance pay around $3,000 for newborn delivery and hospitalization, while adding neonatal intensive care can push the bill closer to $5,000, based on a retrospective look at almost 400,000 episodes.
The findings suggest that privately insured families need prenatal financial counseling, as well as screening for financial hardship after delivery, reported lead author Kao-Ping Chua, MD, PhD, assistant professor and health policy researcher in the department of pediatrics and the Susan B. Meister Child Health Evaluation and Research Center at the University of Michigan, Ann Arbor, and colleagues.
“Concern is growing regarding the high and rising financial burden of childbirth for privately insured families,” the investigators wrote in Pediatrics. “Previous studies assessing this burden have focused on out-of-pocket spending for maternal care, including hospitalizations for delivery. However, there are no recent national data on out-of-pocket spending across the childbirth episode, including both deliveries and newborn hospitalizations.”
To address this knowledge gap, Dr. Chua and colleagues turned to Optum’s deidentified Clinformatics Data Mart, comprising 12 million privately insured individuals across the United States. The investigators identified 398,410 childbirth episodes occurring between 2016 and 2019. Each episode was defined as one delivery and at least one newborn hospitalization under the same family plan.
Out-of-pocket cost included copayment plus coinsurance and deductibles. Primary outcomes included mean total out-of-pocket spending and proportion of episodes exceeding $5,000 or $10,000. Subgroup analyses compared differences in spending between episodes involving neonatal intensive care or cesarean birth.
The mean out-of-pocket spending was $2,281 for delivery and $788 for newborn hospitalization, giving a total of $3,068 per childbirth episode. Coinsurance and deductibles accounted for much of that cost, at 55.8% and 42.1%, respectively, whereas copayments accounted for a relatively minor portion (2.2%).
Almost all episodes (95%) cost more than zero dollars, while 17.1% cost more than $5,000 and 1.0% cost more than $10,000. Total mean out-of-pocket spending was higher for episodes involving cesarean birth ($3,389) or neonatal intensive care ($4,969), the latter of which cost more than $10,000 in 8.8% of episodes.
“Because details on plan benefit design were unavailable, the generalizability of findings to all privately insured Americans is unclear,” the investigators noted. “However, the proportion of childbirth episodes covered by high-deductible health plans in this study is consistent with the prevalence of such plans among Americans with employer-sponsored insurance.”
The findings suggest that financial reform is needed, Dr. Chua and colleagues concluded.
“To avoid imposing undue financial burden on families, private insurers should improve childbirth coverage,” they wrote. “An incremental step would be providing first-dollar coverage of deliveries and newborn hospitalizations before deductibles are met. Ideally, however, insurers would waive most or all cost-sharing for these hospitalizations, consistent with the approach taken by Medicaid programs and many developed countries.”
According to Madeline Sutton, MD, assistant professor of obstetrics and gynecology at Morehouse School of Medicine, Atlanta, the size of the study is commendable, but some details are lacking.
“Although the overall sample size allows for a robust analysis, deciding to not report the confidence intervals in this report does not allow for understanding of [the findings with] smaller sample sizes,” Dr. Sutton said in an interview.
(Dr. Chua and colleagues noted that they did not report confidence intervals because “all differences between subgroups were significant owing to large sample sizes.”)
“Still,” Dr. Sutton went on, “this is an important study that has implications for financial counseling that may need to be a part of preconceptional, prenatal, and postnatal visits for privately insured families to help with planning and to decrease the chances of childbirth-related financial hardships. Additionally, policy-level changes that decrease or eliminate these private insurance–related childbirth-episode costs that may negatively impact some families with lower incomes, are warranted.”
The study was funded by the National Institutes of Health. Dr. Chua disclosed a grant from the National Institute on Drug Abuse, while Dr. Moniz is supported by the Agency for Healthcare Research and Quality. Dr. Sutton had no relevant disclosures.
FROM PEDIATRICS