User login
For MD-IQ use only
Match Day 2019: Another strong year for neurology
according to the National Resident Matching Program (NRMP).
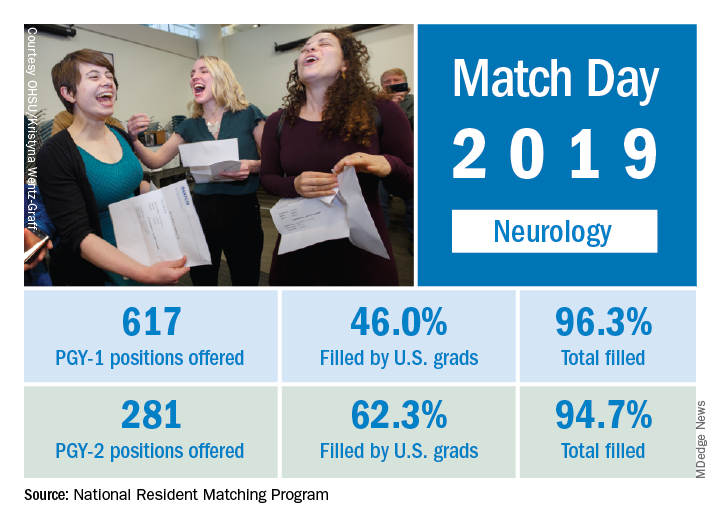
This year, 617 first-year (PGY-1) neurology slots were offered, an increase of 11.8% over the 552 offered in 2018 and well above the 6.5% gain recorded for the Match as whole. The 114 neurology programs participating this year filled 96.3% of those PGY-1 positions, compared with 94.7% for the 52 programs that offered PGY-2 positions, the NRMP reported.
“The results of the Match are closely watched because they can be predictors of future physician workforce supply. There also is significant interest in the competitiveness of specialties, as measured by the percentage of positions filled overall and the percentage filled by senior students in U.S. allopathic medical schools,” the NRMP said.
The proportion of PGY-1 neurology positions filled by U.S. seniors dropped to 46.0% from 50.7% last year, although the number of U.S. seniors filling spots actually went up from 280 in 2018 to 284. The PGY-2 positions saw declines in both cases: The 175 U.S. seniors represented 62.3% of the 2019 spots, compared with the 190 U.S. seniors who filled 66.2% of slots in 2018, the NRMP data show.
The total numbers of applicants (38,376) and positions offered (35,185) were both record highs for the Match, although they were affected, in part, by “increased numbers of osteopathic programs that joined the Main Residency Match as a result of the ongoing transition to a single accreditation system for graduate medical education programs,” the NRMP noted.
according to the National Resident Matching Program (NRMP).
This year, 617 first-year (PGY-1) neurology slots were offered, an increase of 11.8% over the 552 offered in 2018 and well above the 6.5% gain recorded for the Match as whole. The 114 neurology programs participating this year filled 96.3% of those PGY-1 positions, compared with 94.7% for the 52 programs that offered PGY-2 positions, the NRMP reported.
“The results of the Match are closely watched because they can be predictors of future physician workforce supply. There also is significant interest in the competitiveness of specialties, as measured by the percentage of positions filled overall and the percentage filled by senior students in U.S. allopathic medical schools,” the NRMP said.
The proportion of PGY-1 neurology positions filled by U.S. seniors dropped to 46.0% from 50.7% last year, although the number of U.S. seniors filling spots actually went up from 280 in 2018 to 284. The PGY-2 positions saw declines in both cases: The 175 U.S. seniors represented 62.3% of the 2019 spots, compared with the 190 U.S. seniors who filled 66.2% of slots in 2018, the NRMP data show.
The total numbers of applicants (38,376) and positions offered (35,185) were both record highs for the Match, although they were affected, in part, by “increased numbers of osteopathic programs that joined the Main Residency Match as a result of the ongoing transition to a single accreditation system for graduate medical education programs,” the NRMP noted.
according to the National Resident Matching Program (NRMP).
This year, 617 first-year (PGY-1) neurology slots were offered, an increase of 11.8% over the 552 offered in 2018 and well above the 6.5% gain recorded for the Match as whole. The 114 neurology programs participating this year filled 96.3% of those PGY-1 positions, compared with 94.7% for the 52 programs that offered PGY-2 positions, the NRMP reported.
“The results of the Match are closely watched because they can be predictors of future physician workforce supply. There also is significant interest in the competitiveness of specialties, as measured by the percentage of positions filled overall and the percentage filled by senior students in U.S. allopathic medical schools,” the NRMP said.
The proportion of PGY-1 neurology positions filled by U.S. seniors dropped to 46.0% from 50.7% last year, although the number of U.S. seniors filling spots actually went up from 280 in 2018 to 284. The PGY-2 positions saw declines in both cases: The 175 U.S. seniors represented 62.3% of the 2019 spots, compared with the 190 U.S. seniors who filled 66.2% of slots in 2018, the NRMP data show.
The total numbers of applicants (38,376) and positions offered (35,185) were both record highs for the Match, although they were affected, in part, by “increased numbers of osteopathic programs that joined the Main Residency Match as a result of the ongoing transition to a single accreditation system for graduate medical education programs,” the NRMP noted.
Bempedoic acid: funny name, serious LDL lowering
Recent trials advance axial spondyloarthritis therapy. Newer antihyperglycemic drugs have distinctive cardiovascular, kidney benefits. And doctors’ prior authorization burden is increasing.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Recent trials advance axial spondyloarthritis therapy. Newer antihyperglycemic drugs have distinctive cardiovascular, kidney benefits. And doctors’ prior authorization burden is increasing.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Recent trials advance axial spondyloarthritis therapy. Newer antihyperglycemic drugs have distinctive cardiovascular, kidney benefits. And doctors’ prior authorization burden is increasing.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Journal of Hospital Medicine launches new clinical guidelines series
The Journal of Hospital Medicine, the official peer-reviewed journal of the Society of Hospital Medicine, has launched its second new series this year, entitled Clinical Guideline Highlights for the Hospitalist. Alongside the new Leadership and Professional Development series, this addition plays a large role in the vision for the future of the journal, spearheaded by new editor in chief, Samir Shah, MD, MSCE, MHM.

“As a new deputy editor for reviews and perspectives, I’m thrilled to help execute Dr. Shah’s vision for a series of articles that aims to facilitate the rapid translation of the latest evidence-based guidelines into hospitalist practice,” said Erin Shaughnessy, MD. “My coeditor, Dr. Read Pierce, and I envision these reviews as tools to enable busy clinicians to quickly understand the latest research and apply it to practice.”
The March issue of JHM features an introduction to the series as well as the first two articles, “The Use of Intravenous Fluids in the Hospitalized Adult” and “Maintenance Intravenous Fluids in Infants and Children.” The introduction provides details on the formatting of the series and discusses a second format that will be introduced in 2019 called Progress Notes, which will be shorter than JHM’s traditional review format. Progress Notes will accept two types or articles, clinical and methodological, and will focus on diagnostics, therapeutics, or risk assessment and prevention of a clinical problem relevant to hospitalists.
“National guidelines and society position statements are important in informing care standards but can be time consuming to read, and only a small portion may be pertinent to the practice of hospital medicine,” Dr. Shah said. “Our Clinical Guideline Highlights for the Hospitalist series, under the leadership of Dr. Shaughnessy and Dr. Pierce, will distill the key elements of national guidelines with a focus on recommendations that are most relevant to the practicing hospitalist. Authors include a brief critique to ensure hospitalists understand the strength of evidence behind the guideline when making decisions.”
Along with this series comes another new feature for the journal, Hospital Medicine: The Year in Review. This annual feature “concisely compiles and critiques the top articles in both adult and pediatric hospital medicine in the past year” and “will serve as a written corollary to the popular ‘Updates in Hospital Medicine’ presentation at the SHM Annual Conference.”
With so many updates, “JHM’s overarching commitment remains unchanged: support clinicians, leaders, and scholars in our field in their pursuit of delivering evidence-based, high-value clinical care.” The journal will continue to accept traditional, long-form review on topics relevant to hospitalists.
Visit www.journalofhospitalmedicine.com for the Clinical Guideline Highlights for the Hospitalist series and additional research.
The Journal of Hospital Medicine, the official peer-reviewed journal of the Society of Hospital Medicine, has launched its second new series this year, entitled Clinical Guideline Highlights for the Hospitalist. Alongside the new Leadership and Professional Development series, this addition plays a large role in the vision for the future of the journal, spearheaded by new editor in chief, Samir Shah, MD, MSCE, MHM.
“As a new deputy editor for reviews and perspectives, I’m thrilled to help execute Dr. Shah’s vision for a series of articles that aims to facilitate the rapid translation of the latest evidence-based guidelines into hospitalist practice,” said Erin Shaughnessy, MD. “My coeditor, Dr. Read Pierce, and I envision these reviews as tools to enable busy clinicians to quickly understand the latest research and apply it to practice.”
The March issue of JHM features an introduction to the series as well as the first two articles, “The Use of Intravenous Fluids in the Hospitalized Adult” and “Maintenance Intravenous Fluids in Infants and Children.” The introduction provides details on the formatting of the series and discusses a second format that will be introduced in 2019 called Progress Notes, which will be shorter than JHM’s traditional review format. Progress Notes will accept two types or articles, clinical and methodological, and will focus on diagnostics, therapeutics, or risk assessment and prevention of a clinical problem relevant to hospitalists.
“National guidelines and society position statements are important in informing care standards but can be time consuming to read, and only a small portion may be pertinent to the practice of hospital medicine,” Dr. Shah said. “Our Clinical Guideline Highlights for the Hospitalist series, under the leadership of Dr. Shaughnessy and Dr. Pierce, will distill the key elements of national guidelines with a focus on recommendations that are most relevant to the practicing hospitalist. Authors include a brief critique to ensure hospitalists understand the strength of evidence behind the guideline when making decisions.”
Along with this series comes another new feature for the journal, Hospital Medicine: The Year in Review. This annual feature “concisely compiles and critiques the top articles in both adult and pediatric hospital medicine in the past year” and “will serve as a written corollary to the popular ‘Updates in Hospital Medicine’ presentation at the SHM Annual Conference.”
With so many updates, “JHM’s overarching commitment remains unchanged: support clinicians, leaders, and scholars in our field in their pursuit of delivering evidence-based, high-value clinical care.” The journal will continue to accept traditional, long-form review on topics relevant to hospitalists.
Visit www.journalofhospitalmedicine.com for the Clinical Guideline Highlights for the Hospitalist series and additional research.
The Journal of Hospital Medicine, the official peer-reviewed journal of the Society of Hospital Medicine, has launched its second new series this year, entitled Clinical Guideline Highlights for the Hospitalist. Alongside the new Leadership and Professional Development series, this addition plays a large role in the vision for the future of the journal, spearheaded by new editor in chief, Samir Shah, MD, MSCE, MHM.
“As a new deputy editor for reviews and perspectives, I’m thrilled to help execute Dr. Shah’s vision for a series of articles that aims to facilitate the rapid translation of the latest evidence-based guidelines into hospitalist practice,” said Erin Shaughnessy, MD. “My coeditor, Dr. Read Pierce, and I envision these reviews as tools to enable busy clinicians to quickly understand the latest research and apply it to practice.”
The March issue of JHM features an introduction to the series as well as the first two articles, “The Use of Intravenous Fluids in the Hospitalized Adult” and “Maintenance Intravenous Fluids in Infants and Children.” The introduction provides details on the formatting of the series and discusses a second format that will be introduced in 2019 called Progress Notes, which will be shorter than JHM’s traditional review format. Progress Notes will accept two types or articles, clinical and methodological, and will focus on diagnostics, therapeutics, or risk assessment and prevention of a clinical problem relevant to hospitalists.
“National guidelines and society position statements are important in informing care standards but can be time consuming to read, and only a small portion may be pertinent to the practice of hospital medicine,” Dr. Shah said. “Our Clinical Guideline Highlights for the Hospitalist series, under the leadership of Dr. Shaughnessy and Dr. Pierce, will distill the key elements of national guidelines with a focus on recommendations that are most relevant to the practicing hospitalist. Authors include a brief critique to ensure hospitalists understand the strength of evidence behind the guideline when making decisions.”
Along with this series comes another new feature for the journal, Hospital Medicine: The Year in Review. This annual feature “concisely compiles and critiques the top articles in both adult and pediatric hospital medicine in the past year” and “will serve as a written corollary to the popular ‘Updates in Hospital Medicine’ presentation at the SHM Annual Conference.”
With so many updates, “JHM’s overarching commitment remains unchanged: support clinicians, leaders, and scholars in our field in their pursuit of delivering evidence-based, high-value clinical care.” The journal will continue to accept traditional, long-form review on topics relevant to hospitalists.
Visit www.journalofhospitalmedicine.com for the Clinical Guideline Highlights for the Hospitalist series and additional research.
Learning from the history of hospitals
Storytelling can inform medical practice
Every year the Society of Hospital Medicine’s Annual Conference Committee examines prior attendee surveys, reviews the content presented the preceding year, and asks itself what new areas of learning are needed by hospitalists, said Dustin Smith, MD, SFHM, hospitalist and associate professor of medicine at Emory University School of Medicine in Atlanta, and HM19 course director.
“The conference’s schedule-at-a-glance of content can be overwhelming, so we have tried to use distinct educational tracks to provide focus and clarity for conference attendees,” he said. “Every year there are a few areas where questions often come up about complex clinical situations where established medical guidelines aren’t much help.”
As a result, for HM19 an educational mini-track called “Between the Guidelines” was developed to gather up several of these areas of clinical complexity where what’s available in established clinical practice guidelines doesn’t offer clear answers, Dr. Smith said. These include controversies around antithrombotic therapy in patients with major bleeds, and a debate on controversial aspects of guidelines to direct inpatient care.
Another planned session, “The History of Hospitals via Arts and Stories,” fits nicely into this mini-track, Dr. Smith noted.
“It’s a history lesson you can’t glean from medical guidelines, which maybe points us toward what to incorporate and what not to repeat from across the history of hospitals,” he said. “That could help us better appreciate the work hospitalists are doing today and into the future.”

Jordan Messler, MD, a hospitalist with the Morton Plant Hospitalist group in Clearwater, Fla., will lead the session and thinks that modern physicians can learn a lot from both the history of medicine and the evolution of hospitals, starting with the ancient Greek physician, Galen (129-200 AD), who directed the celebrated Asclepeion or hospital in Pergamon (present-day Bergama, Turkey). Dr. Messler said this ancient hospital’s treatment of disease also addressed the senses, the emotions, and the spirit – an early prototype for whole-person care – with an emphasis on self-therapy through rest, relaxation, exercise, and the promotion of healthy lifestyles.1
A different perspective on hospitals
“People used to travel to Pergamon for healing at the Asclepeion, next to the amphitheater, where plays and music were presented, and to be outdoors in the natural elements. Now we’re seeing hospitals being built with healing gardens, and a new emphasis on how artwork and music and environmental design can assist in healing,” Dr. Messler said.
Dr. Messler explained that his “History of Hospitals” presentation will also survey the advent of more recent hospitals in France in the 18th century, pioneering work done at Johns Hopkins Hospital in Baltimore and Bellevue Hospital in New York, and the influence on the modern hospital of nursing pioneer Florence Nightingale (1820-1910). Dr. Messler said she helped improve hospitals in her day, which still influences their modern design, and fundamentally changed the role of nursing in hospitals, introducing professional training standards for nurses.

He also noted that the portico of the beautiful 15th century Hospital of the Innocents in Florence, Italy, the first organic creation of Filippo Brunelleschi (1377-1446), marks the birth of Renaissance architecture in Florence. The Hospital of Santa Maria Nuova, founded in 1288, is the oldest hospital still active in Florence.
Part of the goal for this new annual conference session is to take a break from more clinically focused presentations, and to think about the hospital from a different perspective, Dr. Messler said. His session will emphasize the power of stories and storytelling to inform and inspire medical practice.
“This is not something that can be applied clinically the next day, but lessons from the past can inform the design of hospitals and how we manage patients,” he said. “We need to ask ourselves, ‘How can we analyze hospital history to inform what we do today?’ ”
References
“Asclepeion.” Wikipedia. Accessed Jan. 28, 2019: https://en.wikipedia.org/wiki/Asclepeion.
Storytelling can inform medical practice
Storytelling can inform medical practice
Every year the Society of Hospital Medicine’s Annual Conference Committee examines prior attendee surveys, reviews the content presented the preceding year, and asks itself what new areas of learning are needed by hospitalists, said Dustin Smith, MD, SFHM, hospitalist and associate professor of medicine at Emory University School of Medicine in Atlanta, and HM19 course director.
“The conference’s schedule-at-a-glance of content can be overwhelming, so we have tried to use distinct educational tracks to provide focus and clarity for conference attendees,” he said. “Every year there are a few areas where questions often come up about complex clinical situations where established medical guidelines aren’t much help.”
As a result, for HM19 an educational mini-track called “Between the Guidelines” was developed to gather up several of these areas of clinical complexity where what’s available in established clinical practice guidelines doesn’t offer clear answers, Dr. Smith said. These include controversies around antithrombotic therapy in patients with major bleeds, and a debate on controversial aspects of guidelines to direct inpatient care.
Another planned session, “The History of Hospitals via Arts and Stories,” fits nicely into this mini-track, Dr. Smith noted.
“It’s a history lesson you can’t glean from medical guidelines, which maybe points us toward what to incorporate and what not to repeat from across the history of hospitals,” he said. “That could help us better appreciate the work hospitalists are doing today and into the future.”
Jordan Messler, MD, a hospitalist with the Morton Plant Hospitalist group in Clearwater, Fla., will lead the session and thinks that modern physicians can learn a lot from both the history of medicine and the evolution of hospitals, starting with the ancient Greek physician, Galen (129-200 AD), who directed the celebrated Asclepeion or hospital in Pergamon (present-day Bergama, Turkey). Dr. Messler said this ancient hospital’s treatment of disease also addressed the senses, the emotions, and the spirit – an early prototype for whole-person care – with an emphasis on self-therapy through rest, relaxation, exercise, and the promotion of healthy lifestyles.1
A different perspective on hospitals
“People used to travel to Pergamon for healing at the Asclepeion, next to the amphitheater, where plays and music were presented, and to be outdoors in the natural elements. Now we’re seeing hospitals being built with healing gardens, and a new emphasis on how artwork and music and environmental design can assist in healing,” Dr. Messler said.
Dr. Messler explained that his “History of Hospitals” presentation will also survey the advent of more recent hospitals in France in the 18th century, pioneering work done at Johns Hopkins Hospital in Baltimore and Bellevue Hospital in New York, and the influence on the modern hospital of nursing pioneer Florence Nightingale (1820-1910). Dr. Messler said she helped improve hospitals in her day, which still influences their modern design, and fundamentally changed the role of nursing in hospitals, introducing professional training standards for nurses.
He also noted that the portico of the beautiful 15th century Hospital of the Innocents in Florence, Italy, the first organic creation of Filippo Brunelleschi (1377-1446), marks the birth of Renaissance architecture in Florence. The Hospital of Santa Maria Nuova, founded in 1288, is the oldest hospital still active in Florence.
Part of the goal for this new annual conference session is to take a break from more clinically focused presentations, and to think about the hospital from a different perspective, Dr. Messler said. His session will emphasize the power of stories and storytelling to inform and inspire medical practice.
“This is not something that can be applied clinically the next day, but lessons from the past can inform the design of hospitals and how we manage patients,” he said. “We need to ask ourselves, ‘How can we analyze hospital history to inform what we do today?’ ”
References
“Asclepeion.” Wikipedia. Accessed Jan. 28, 2019: https://en.wikipedia.org/wiki/Asclepeion.
Every year the Society of Hospital Medicine’s Annual Conference Committee examines prior attendee surveys, reviews the content presented the preceding year, and asks itself what new areas of learning are needed by hospitalists, said Dustin Smith, MD, SFHM, hospitalist and associate professor of medicine at Emory University School of Medicine in Atlanta, and HM19 course director.
“The conference’s schedule-at-a-glance of content can be overwhelming, so we have tried to use distinct educational tracks to provide focus and clarity for conference attendees,” he said. “Every year there are a few areas where questions often come up about complex clinical situations where established medical guidelines aren’t much help.”
As a result, for HM19 an educational mini-track called “Between the Guidelines” was developed to gather up several of these areas of clinical complexity where what’s available in established clinical practice guidelines doesn’t offer clear answers, Dr. Smith said. These include controversies around antithrombotic therapy in patients with major bleeds, and a debate on controversial aspects of guidelines to direct inpatient care.
Another planned session, “The History of Hospitals via Arts and Stories,” fits nicely into this mini-track, Dr. Smith noted.
“It’s a history lesson you can’t glean from medical guidelines, which maybe points us toward what to incorporate and what not to repeat from across the history of hospitals,” he said. “That could help us better appreciate the work hospitalists are doing today and into the future.”
Jordan Messler, MD, a hospitalist with the Morton Plant Hospitalist group in Clearwater, Fla., will lead the session and thinks that modern physicians can learn a lot from both the history of medicine and the evolution of hospitals, starting with the ancient Greek physician, Galen (129-200 AD), who directed the celebrated Asclepeion or hospital in Pergamon (present-day Bergama, Turkey). Dr. Messler said this ancient hospital’s treatment of disease also addressed the senses, the emotions, and the spirit – an early prototype for whole-person care – with an emphasis on self-therapy through rest, relaxation, exercise, and the promotion of healthy lifestyles.1
A different perspective on hospitals
“People used to travel to Pergamon for healing at the Asclepeion, next to the amphitheater, where plays and music were presented, and to be outdoors in the natural elements. Now we’re seeing hospitals being built with healing gardens, and a new emphasis on how artwork and music and environmental design can assist in healing,” Dr. Messler said.
Dr. Messler explained that his “History of Hospitals” presentation will also survey the advent of more recent hospitals in France in the 18th century, pioneering work done at Johns Hopkins Hospital in Baltimore and Bellevue Hospital in New York, and the influence on the modern hospital of nursing pioneer Florence Nightingale (1820-1910). Dr. Messler said she helped improve hospitals in her day, which still influences their modern design, and fundamentally changed the role of nursing in hospitals, introducing professional training standards for nurses.
He also noted that the portico of the beautiful 15th century Hospital of the Innocents in Florence, Italy, the first organic creation of Filippo Brunelleschi (1377-1446), marks the birth of Renaissance architecture in Florence. The Hospital of Santa Maria Nuova, founded in 1288, is the oldest hospital still active in Florence.
Part of the goal for this new annual conference session is to take a break from more clinically focused presentations, and to think about the hospital from a different perspective, Dr. Messler said. His session will emphasize the power of stories and storytelling to inform and inspire medical practice.
“This is not something that can be applied clinically the next day, but lessons from the past can inform the design of hospitals and how we manage patients,” he said. “We need to ask ourselves, ‘How can we analyze hospital history to inform what we do today?’ ”
References
“Asclepeion.” Wikipedia. Accessed Jan. 28, 2019: https://en.wikipedia.org/wiki/Asclepeion.
When a Public Health Alert Goes Wrong
At 8:07 am on January 13, 2018, people in Hawaii received an emergency alert advising them to seek shelter from an incoming ballistic missile.
A very long 38 minutes later, the message was retracted via the same systems that had sent it—the Wireless Emergency Alert system, which sends location-based warnings to wireless carrier systems, and the Emergency Alert System, which sends television and radio alerts.
The Federal Communications Commission report that covered the debacle noted that, among other errors, the employee responsible for triggering the false alert believed the missile threat was real. Moreover, the exercise plans did not document a process for disseminating an all-clear message. And on top of that, the established ballistic missile alert checklist did not include a step to notify the Hawaii Emergency Management Agency’s public information officer responsible for communicating with the public, media, other agencies, and other stakeholders during an incident.
Researchers from the CDC and Hawaii Department of Health analyzed tweets sent during 2 periods: early (8:07-8:45 am), the 38 minutes during which the alert circulated; and the late period (8:46-9:24 am), the same amount of elapsed time after the correction had been issued.
They found 4 themes dominated the early period: information processing, information sharing, authentication, and emotional reaction (shock, fear, panic, terror). Information processing was defined as any indication of initial mental processing of the alert. Many of the tweets dealt with coming to terms with the threat.
During the late period, information sharing and emotional reaction persisted, but they were joined by new themes that, according to the researchers, were “fundamentally different” from the early-period themes and reflected reactions to misinformation: denunciation, insufficient knowledge to act, and mistrust of authority. “Insufficient knowledge to act” involved reacting to the lack of a response plan, particularly not knowing how to properly take shelter. Denunciations blamed the emergency warning and response, especially the time it took to correct the mistake. Mistrust of authority involved doubting the emergency alert system or governmental response.
How can a situation like this be better handled? The researchers say public health messaging during an emergency is complicated. For instance, it is influenced by how messages are perceived and interpreted by different people, and by the fact that messages need to be sent over multiple platforms to ensure that the information is disseminated accurately and quickly.
Which is why social media is both a handicap and a boon in public health emergencies. Tweets spread misinformation as fast as information (if not faster), so the first messages are critical. In addition to conveying timely messages, the researchers advise, public health authorities need to address the reactions during each phase of a crisis. They also need to establish credibility to prevent the public from mistrusting the public health message and its issuers.
Most important, perhaps: Alerts should carry clear instructions for persons in the affected area to carry out during an emergency.
At 8:07 am on January 13, 2018, people in Hawaii received an emergency alert advising them to seek shelter from an incoming ballistic missile.
A very long 38 minutes later, the message was retracted via the same systems that had sent it—the Wireless Emergency Alert system, which sends location-based warnings to wireless carrier systems, and the Emergency Alert System, which sends television and radio alerts.
The Federal Communications Commission report that covered the debacle noted that, among other errors, the employee responsible for triggering the false alert believed the missile threat was real. Moreover, the exercise plans did not document a process for disseminating an all-clear message. And on top of that, the established ballistic missile alert checklist did not include a step to notify the Hawaii Emergency Management Agency’s public information officer responsible for communicating with the public, media, other agencies, and other stakeholders during an incident.
Researchers from the CDC and Hawaii Department of Health analyzed tweets sent during 2 periods: early (8:07-8:45 am), the 38 minutes during which the alert circulated; and the late period (8:46-9:24 am), the same amount of elapsed time after the correction had been issued.
They found 4 themes dominated the early period: information processing, information sharing, authentication, and emotional reaction (shock, fear, panic, terror). Information processing was defined as any indication of initial mental processing of the alert. Many of the tweets dealt with coming to terms with the threat.
During the late period, information sharing and emotional reaction persisted, but they were joined by new themes that, according to the researchers, were “fundamentally different” from the early-period themes and reflected reactions to misinformation: denunciation, insufficient knowledge to act, and mistrust of authority. “Insufficient knowledge to act” involved reacting to the lack of a response plan, particularly not knowing how to properly take shelter. Denunciations blamed the emergency warning and response, especially the time it took to correct the mistake. Mistrust of authority involved doubting the emergency alert system or governmental response.
How can a situation like this be better handled? The researchers say public health messaging during an emergency is complicated. For instance, it is influenced by how messages are perceived and interpreted by different people, and by the fact that messages need to be sent over multiple platforms to ensure that the information is disseminated accurately and quickly.
Which is why social media is both a handicap and a boon in public health emergencies. Tweets spread misinformation as fast as information (if not faster), so the first messages are critical. In addition to conveying timely messages, the researchers advise, public health authorities need to address the reactions during each phase of a crisis. They also need to establish credibility to prevent the public from mistrusting the public health message and its issuers.
Most important, perhaps: Alerts should carry clear instructions for persons in the affected area to carry out during an emergency.
At 8:07 am on January 13, 2018, people in Hawaii received an emergency alert advising them to seek shelter from an incoming ballistic missile.
A very long 38 minutes later, the message was retracted via the same systems that had sent it—the Wireless Emergency Alert system, which sends location-based warnings to wireless carrier systems, and the Emergency Alert System, which sends television and radio alerts.
The Federal Communications Commission report that covered the debacle noted that, among other errors, the employee responsible for triggering the false alert believed the missile threat was real. Moreover, the exercise plans did not document a process for disseminating an all-clear message. And on top of that, the established ballistic missile alert checklist did not include a step to notify the Hawaii Emergency Management Agency’s public information officer responsible for communicating with the public, media, other agencies, and other stakeholders during an incident.
Researchers from the CDC and Hawaii Department of Health analyzed tweets sent during 2 periods: early (8:07-8:45 am), the 38 minutes during which the alert circulated; and the late period (8:46-9:24 am), the same amount of elapsed time after the correction had been issued.
They found 4 themes dominated the early period: information processing, information sharing, authentication, and emotional reaction (shock, fear, panic, terror). Information processing was defined as any indication of initial mental processing of the alert. Many of the tweets dealt with coming to terms with the threat.
During the late period, information sharing and emotional reaction persisted, but they were joined by new themes that, according to the researchers, were “fundamentally different” from the early-period themes and reflected reactions to misinformation: denunciation, insufficient knowledge to act, and mistrust of authority. “Insufficient knowledge to act” involved reacting to the lack of a response plan, particularly not knowing how to properly take shelter. Denunciations blamed the emergency warning and response, especially the time it took to correct the mistake. Mistrust of authority involved doubting the emergency alert system or governmental response.
How can a situation like this be better handled? The researchers say public health messaging during an emergency is complicated. For instance, it is influenced by how messages are perceived and interpreted by different people, and by the fact that messages need to be sent over multiple platforms to ensure that the information is disseminated accurately and quickly.
Which is why social media is both a handicap and a boon in public health emergencies. Tweets spread misinformation as fast as information (if not faster), so the first messages are critical. In addition to conveying timely messages, the researchers advise, public health authorities need to address the reactions during each phase of a crisis. They also need to establish credibility to prevent the public from mistrusting the public health message and its issuers.
Most important, perhaps: Alerts should carry clear instructions for persons in the affected area to carry out during an emergency.
Semaglutide plus SGLT2 inhibitors for type 2 diabetes
Also today, patients with HIV may have a greater risk of opioid overdose, why Eisenmeyer syndrome can be a minefield for unwary physicians, and heart attacks and strokes spike in the month after cancer diagnosis.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, patients with HIV may have a greater risk of opioid overdose, why Eisenmeyer syndrome can be a minefield for unwary physicians, and heart attacks and strokes spike in the month after cancer diagnosis.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, patients with HIV may have a greater risk of opioid overdose, why Eisenmeyer syndrome can be a minefield for unwary physicians, and heart attacks and strokes spike in the month after cancer diagnosis.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Treating lymphoma in patients with HIV
In this episode, Stefan Barta, MD, of the University of Pennsylvania, joins David Henry, MD, to discuss the treatment and diagnosis of lymphoma in patients with HIV.
And in this week’s Clinical Correlation, Ilana Yurkiewicz, MD, has Part 2 of her discussion on informed consent in cancer. Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University and is also a columnist for Hematology News. More from Dr. Yurkiewicz here.
Subscribe to Blood & Cancer here:
Apple Podcasts
Google Podcasts
Show notes
By Emily Bryer, DO
Resident in the department of internal medicine, University of Pennsylvania Health System
Immunosuppression in patients with HIV, especially with low CD4 counts, is associated with the development of lymphomas.
Diffuse large B-cell lymphoma is the most common lymphoma in patients with HIV followed by Burkitt lymphoma and Hodgkin lymphoma.
Extra-nodal manifestations of lymphoma are more common in patients with HIV, especially with lower CD4 counts.
Following pathologic diagnosis, staging of lymphoma should include:
- CT scan, PET scan, evaluation of CNS (MRI brain and LP), bone marrow biopsy, and evaluation for hepatitis B and C co-infection.
- Fluorescence in situ hybridization (FISH) is a molecular technique that identifies portions of DNA and helps to identify translocations and rearrangements.
- cMYC, BCL2, and BCL6 are all pro-proliferative genes and commonly implicated in lymphoma.
- cMYC rearrangement poses higher risk of CNS involvement and CNS relapse.
- cMYC rearrangement (as opposed to cMYC translocation) requires therapy that is more aggressive therapy than R-CHOP.
Treatment of high grade diffuse large B-cell lymphoma:
- R-EPOCH
- Ibrutinib plus R-EPOCH
Resources:AIDS Malignancy ConsortiumBlood. 2004;103:275-82.
Blood. 2010 Apr 15; 115(15): 3008–16.
NCT03220022: Ibrutinib, Rituximab, Etoposide, Prednisone, Vincristine Sulfate, Cyclophosphamide, and Doxorubicin Hydrochloride in Treating Patients With HIV-Positive Stage II-IV Diffuse Large B-Cell Lymphomas
In this episode, Stefan Barta, MD, of the University of Pennsylvania, joins David Henry, MD, to discuss the treatment and diagnosis of lymphoma in patients with HIV.
And in this week’s Clinical Correlation, Ilana Yurkiewicz, MD, has Part 2 of her discussion on informed consent in cancer. Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University and is also a columnist for Hematology News. More from Dr. Yurkiewicz here.
Subscribe to Blood & Cancer here:
Apple Podcasts
Google Podcasts
Show notes
By Emily Bryer, DO
Resident in the department of internal medicine, University of Pennsylvania Health System
Immunosuppression in patients with HIV, especially with low CD4 counts, is associated with the development of lymphomas.
Diffuse large B-cell lymphoma is the most common lymphoma in patients with HIV followed by Burkitt lymphoma and Hodgkin lymphoma.
Extra-nodal manifestations of lymphoma are more common in patients with HIV, especially with lower CD4 counts.
Following pathologic diagnosis, staging of lymphoma should include:
- CT scan, PET scan, evaluation of CNS (MRI brain and LP), bone marrow biopsy, and evaluation for hepatitis B and C co-infection.
- Fluorescence in situ hybridization (FISH) is a molecular technique that identifies portions of DNA and helps to identify translocations and rearrangements.
- cMYC, BCL2, and BCL6 are all pro-proliferative genes and commonly implicated in lymphoma.
- cMYC rearrangement poses higher risk of CNS involvement and CNS relapse.
- cMYC rearrangement (as opposed to cMYC translocation) requires therapy that is more aggressive therapy than R-CHOP.
Treatment of high grade diffuse large B-cell lymphoma:
- R-EPOCH
- Ibrutinib plus R-EPOCH
Resources:AIDS Malignancy ConsortiumBlood. 2004;103:275-82.
Blood. 2010 Apr 15; 115(15): 3008–16.
NCT03220022: Ibrutinib, Rituximab, Etoposide, Prednisone, Vincristine Sulfate, Cyclophosphamide, and Doxorubicin Hydrochloride in Treating Patients With HIV-Positive Stage II-IV Diffuse Large B-Cell Lymphomas
In this episode, Stefan Barta, MD, of the University of Pennsylvania, joins David Henry, MD, to discuss the treatment and diagnosis of lymphoma in patients with HIV.
And in this week’s Clinical Correlation, Ilana Yurkiewicz, MD, has Part 2 of her discussion on informed consent in cancer. Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University and is also a columnist for Hematology News. More from Dr. Yurkiewicz here.
Subscribe to Blood & Cancer here:
Apple Podcasts
Google Podcasts
Show notes
By Emily Bryer, DO
Resident in the department of internal medicine, University of Pennsylvania Health System
Immunosuppression in patients with HIV, especially with low CD4 counts, is associated with the development of lymphomas.
Diffuse large B-cell lymphoma is the most common lymphoma in patients with HIV followed by Burkitt lymphoma and Hodgkin lymphoma.
Extra-nodal manifestations of lymphoma are more common in patients with HIV, especially with lower CD4 counts.
Following pathologic diagnosis, staging of lymphoma should include:
- CT scan, PET scan, evaluation of CNS (MRI brain and LP), bone marrow biopsy, and evaluation for hepatitis B and C co-infection.
- Fluorescence in situ hybridization (FISH) is a molecular technique that identifies portions of DNA and helps to identify translocations and rearrangements.
- cMYC, BCL2, and BCL6 are all pro-proliferative genes and commonly implicated in lymphoma.
- cMYC rearrangement poses higher risk of CNS involvement and CNS relapse.
- cMYC rearrangement (as opposed to cMYC translocation) requires therapy that is more aggressive therapy than R-CHOP.
Treatment of high grade diffuse large B-cell lymphoma:
- R-EPOCH
- Ibrutinib plus R-EPOCH
Resources:AIDS Malignancy ConsortiumBlood. 2004;103:275-82.
Blood. 2010 Apr 15; 115(15): 3008–16.
NCT03220022: Ibrutinib, Rituximab, Etoposide, Prednisone, Vincristine Sulfate, Cyclophosphamide, and Doxorubicin Hydrochloride in Treating Patients With HIV-Positive Stage II-IV Diffuse Large B-Cell Lymphomas
Aspirin and lower risk of COPD flare-up
Also today, how to handle patients who won’t believe negative drug-allergy results, which complications to watch for in black patients who undergo bariatric surgery, and the measles outbreak now affects a dozen U.S. states.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, how to handle patients who won’t believe negative drug-allergy results, which complications to watch for in black patients who undergo bariatric surgery, and the measles outbreak now affects a dozen U.S. states.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, how to handle patients who won’t believe negative drug-allergy results, which complications to watch for in black patients who undergo bariatric surgery, and the measles outbreak now affects a dozen U.S. states.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Funduscopy: Critical to the Right Diagnosis
It is always good to look the patient in the eye, say researchers from Texas Tech University in Odessa, Texas, and Centro Policlinico Valencia in Venezuela. They report on the case of a patient with atheroembolism, a “rare but feared complication of arteriography.” Most commonly, it affects small-diameter vessels in the skin and kidneys.
The patient, a 69-year-old man, had a history of hypertension, type 2 diabetes, and unstable angina; he had a drug-eluting stent placed in the left anterior descending coronary artery 10 days before he was admitted to the hospital. He arrived at the emergency department with intense abdominal pain, nausea, vomiting, oliguria, and pain in his legs and feet.
Physical examination revealed livedo reticularis (which is caused by small blood clots) in his left foot, and a tender abdomen. His creatinine and blood urea nitrogen levels were increased. Funduscopy showed a Hollenhorst crystal in the right inferotemporal quadrant.
He was treated with methylprednisolone, which improved the abdominal symptoms, renal function, and skin findings; then prednisone. His initial symptoms resolved over the next year.
The clinicians say the usual treatment for atheroembolism is supportive and depends on the affected organ. To their knowledge, they say, no formal studies have evaluated the use of anti-inflammatory therapies for this complication.
Funduscopy was an essential part of their examination, the researchers note, and spared the patient from invasive diagnostic studies such as biopsies. They also say that contrast-induced renal failure might have been the cause of the majority of his symptoms, but the combination of physical exam and differential diagnosis led them to the appropriate cause, as well as allowing for opportune treatment.
It is always good to look the patient in the eye, say researchers from Texas Tech University in Odessa, Texas, and Centro Policlinico Valencia in Venezuela. They report on the case of a patient with atheroembolism, a “rare but feared complication of arteriography.” Most commonly, it affects small-diameter vessels in the skin and kidneys.
The patient, a 69-year-old man, had a history of hypertension, type 2 diabetes, and unstable angina; he had a drug-eluting stent placed in the left anterior descending coronary artery 10 days before he was admitted to the hospital. He arrived at the emergency department with intense abdominal pain, nausea, vomiting, oliguria, and pain in his legs and feet.
Physical examination revealed livedo reticularis (which is caused by small blood clots) in his left foot, and a tender abdomen. His creatinine and blood urea nitrogen levels were increased. Funduscopy showed a Hollenhorst crystal in the right inferotemporal quadrant.
He was treated with methylprednisolone, which improved the abdominal symptoms, renal function, and skin findings; then prednisone. His initial symptoms resolved over the next year.
The clinicians say the usual treatment for atheroembolism is supportive and depends on the affected organ. To their knowledge, they say, no formal studies have evaluated the use of anti-inflammatory therapies for this complication.
Funduscopy was an essential part of their examination, the researchers note, and spared the patient from invasive diagnostic studies such as biopsies. They also say that contrast-induced renal failure might have been the cause of the majority of his symptoms, but the combination of physical exam and differential diagnosis led them to the appropriate cause, as well as allowing for opportune treatment.
It is always good to look the patient in the eye, say researchers from Texas Tech University in Odessa, Texas, and Centro Policlinico Valencia in Venezuela. They report on the case of a patient with atheroembolism, a “rare but feared complication of arteriography.” Most commonly, it affects small-diameter vessels in the skin and kidneys.
The patient, a 69-year-old man, had a history of hypertension, type 2 diabetes, and unstable angina; he had a drug-eluting stent placed in the left anterior descending coronary artery 10 days before he was admitted to the hospital. He arrived at the emergency department with intense abdominal pain, nausea, vomiting, oliguria, and pain in his legs and feet.
Physical examination revealed livedo reticularis (which is caused by small blood clots) in his left foot, and a tender abdomen. His creatinine and blood urea nitrogen levels were increased. Funduscopy showed a Hollenhorst crystal in the right inferotemporal quadrant.
He was treated with methylprednisolone, which improved the abdominal symptoms, renal function, and skin findings; then prednisone. His initial symptoms resolved over the next year.
The clinicians say the usual treatment for atheroembolism is supportive and depends on the affected organ. To their knowledge, they say, no formal studies have evaluated the use of anti-inflammatory therapies for this complication.
Funduscopy was an essential part of their examination, the researchers note, and spared the patient from invasive diagnostic studies such as biopsies. They also say that contrast-induced renal failure might have been the cause of the majority of his symptoms, but the combination of physical exam and differential diagnosis led them to the appropriate cause, as well as allowing for opportune treatment.
HHS Updates Decontamination Guidance With New Research
With help from researchers from the University of Hertfordshire in the United Kingdom, The US Department of Health and Human Services (HHS) has updated guidance on how best to decontaminate after mass chemical exposure. This second edition of Primary Response Incident Scene Management (PRISM) incorporates new scientific evidence on emergency self-decontamination, hair decontamination, and the interactions of chemicals with hair.
The goal of working with the University of Hertfordshire was to help emergency managers and first responders make “fundamental and fast decisions on how to save the greatest number of lives in chemical emergencies,” says Rick Bright, PhD, director of the Biomedical Advanced Research and Development Authority (BARDA).
The study included a large-scale exercise in which > 80 volunteers were dosed with a chemical warfare agent simulant to quantify the efficacy of different forms of decontamination.
Notably, the research demonstrates that immediate “dry” decontamination—wiping down the victim with any absorbent material (eg, toilet paper, paper towels, wound dressings) can be highly effective on its own and can be done by affected individuals themselves under the instruction of first responders. The dry decontamination step removes up to 99% of contamination and minimizes the accumulation of hazardous material in the subsequent steps.
The new guidance also expands on the effects of the “triple protocol,” a combined decontamination strategy. The 3 steps of that protocol—dry decontamination, wet decontamination using water deluges from fire trucks, and technical decontamination—have been shown to remove 99.9% of chemical contamination. Moreover, the latest clinical evidence indicates that the 3-step approach is faster and more effective than traditional methods for treating chemically contaminated patients.
The guideline also addresses how communities can prepare for chemical emergencies and what to do after the event, such as providing washcloths, towels, blankets, and temporary clothing.
Federal experts and the researchers devised the Algorithm Suggesting Proportionate Incident Response Engagement (ASPIRE), a decision-support tool to help emergency management planners and responders decide which decontamination approach suits a given situation. Using the algorithm, they can tailor plans and responses based on the chemical and type of exposure, how quickly the chemical evaporates, and the amount of time passed since exposure.
ASPIRE and the guidance are integrated into the Chemical Hazards Emergency Medical Management (CHEMM), a web-based resource and suite of preparedness and emergency response tools. The developers also plan to incorporate them into a mobile app.
PRISM is available at www.medicalcountermeasures.gov.
With help from researchers from the University of Hertfordshire in the United Kingdom, The US Department of Health and Human Services (HHS) has updated guidance on how best to decontaminate after mass chemical exposure. This second edition of Primary Response Incident Scene Management (PRISM) incorporates new scientific evidence on emergency self-decontamination, hair decontamination, and the interactions of chemicals with hair.
The goal of working with the University of Hertfordshire was to help emergency managers and first responders make “fundamental and fast decisions on how to save the greatest number of lives in chemical emergencies,” says Rick Bright, PhD, director of the Biomedical Advanced Research and Development Authority (BARDA).
The study included a large-scale exercise in which > 80 volunteers were dosed with a chemical warfare agent simulant to quantify the efficacy of different forms of decontamination.
Notably, the research demonstrates that immediate “dry” decontamination—wiping down the victim with any absorbent material (eg, toilet paper, paper towels, wound dressings) can be highly effective on its own and can be done by affected individuals themselves under the instruction of first responders. The dry decontamination step removes up to 99% of contamination and minimizes the accumulation of hazardous material in the subsequent steps.
The new guidance also expands on the effects of the “triple protocol,” a combined decontamination strategy. The 3 steps of that protocol—dry decontamination, wet decontamination using water deluges from fire trucks, and technical decontamination—have been shown to remove 99.9% of chemical contamination. Moreover, the latest clinical evidence indicates that the 3-step approach is faster and more effective than traditional methods for treating chemically contaminated patients.
The guideline also addresses how communities can prepare for chemical emergencies and what to do after the event, such as providing washcloths, towels, blankets, and temporary clothing.
Federal experts and the researchers devised the Algorithm Suggesting Proportionate Incident Response Engagement (ASPIRE), a decision-support tool to help emergency management planners and responders decide which decontamination approach suits a given situation. Using the algorithm, they can tailor plans and responses based on the chemical and type of exposure, how quickly the chemical evaporates, and the amount of time passed since exposure.
ASPIRE and the guidance are integrated into the Chemical Hazards Emergency Medical Management (CHEMM), a web-based resource and suite of preparedness and emergency response tools. The developers also plan to incorporate them into a mobile app.
PRISM is available at www.medicalcountermeasures.gov.
With help from researchers from the University of Hertfordshire in the United Kingdom, The US Department of Health and Human Services (HHS) has updated guidance on how best to decontaminate after mass chemical exposure. This second edition of Primary Response Incident Scene Management (PRISM) incorporates new scientific evidence on emergency self-decontamination, hair decontamination, and the interactions of chemicals with hair.
The goal of working with the University of Hertfordshire was to help emergency managers and first responders make “fundamental and fast decisions on how to save the greatest number of lives in chemical emergencies,” says Rick Bright, PhD, director of the Biomedical Advanced Research and Development Authority (BARDA).
The study included a large-scale exercise in which > 80 volunteers were dosed with a chemical warfare agent simulant to quantify the efficacy of different forms of decontamination.
Notably, the research demonstrates that immediate “dry” decontamination—wiping down the victim with any absorbent material (eg, toilet paper, paper towels, wound dressings) can be highly effective on its own and can be done by affected individuals themselves under the instruction of first responders. The dry decontamination step removes up to 99% of contamination and minimizes the accumulation of hazardous material in the subsequent steps.
The new guidance also expands on the effects of the “triple protocol,” a combined decontamination strategy. The 3 steps of that protocol—dry decontamination, wet decontamination using water deluges from fire trucks, and technical decontamination—have been shown to remove 99.9% of chemical contamination. Moreover, the latest clinical evidence indicates that the 3-step approach is faster and more effective than traditional methods for treating chemically contaminated patients.
The guideline also addresses how communities can prepare for chemical emergencies and what to do after the event, such as providing washcloths, towels, blankets, and temporary clothing.
Federal experts and the researchers devised the Algorithm Suggesting Proportionate Incident Response Engagement (ASPIRE), a decision-support tool to help emergency management planners and responders decide which decontamination approach suits a given situation. Using the algorithm, they can tailor plans and responses based on the chemical and type of exposure, how quickly the chemical evaporates, and the amount of time passed since exposure.
ASPIRE and the guidance are integrated into the Chemical Hazards Emergency Medical Management (CHEMM), a web-based resource and suite of preparedness and emergency response tools. The developers also plan to incorporate them into a mobile app.
PRISM is available at www.medicalcountermeasures.gov.