User login
For MD-IQ use only
Nephrogenic Systemic Fibrosis in the Setting of Transient Renal Insufficiency
Nephrogenic systemic fibrosis (NSF) is a rare debilitating disorder characterized by dermal plaques, joint contractures, and fibrosis of the skin with possible involvement of muscles and internal organs.1-3 Originally identified in 1997 as nephrogenic fibrosing dermopathy to describe its characteristic cutaneous thickening and hardening, the name was changed to NSF to more accurately reflect the noncutaneous manifestations present in other organ tissues.2,4,5 Nephrogenic systemic fibrosis occurs in patients with a history of renal insufficiency and exposure to gadolinium-based contrast agents (GBCAs) used in magnetic resonance angiography and magnetic resonance imaging. There is no predilection for age, sex, or ethnicity.
Nephrogenic systemic fibrosis may develop over a period of days to several weeks. However, there have been cases of NSF developing 10 years after gadolinium exposure.2 In most cases, patients have a history of severe chronic renal disease requiring hemodialysis. There have been a few reported cases of NSF occurring in patients with resolved acute kidney injury or resolved acute on chronic renal disease.1,6-10 We present a case of NSF occurring in a patient with resolved transient renal insufficiency and no history of chronic renal disease.
Case Report
A 68-year-old woman presented with new dark, painless, pink plaques on the right thigh and calf. The patient stated the condition started and got worse after she was hospitalized 12 years prior for lower extremity cellulitis, sepsis, and acute renal failure. The patient developed complications during that hospital stay and underwent a renal biopsy and renal artery embolization requiring use of a GBCA. After the procedure, she noticed skin hardening in the extremities and decreased mobility in both legs while she was still in the hospital. It was thought that the lower leg changes were due to cellulitis. Therefore, when the renal issues resolved, she was discharged. Her skin and joint changes remained stable until 6 years later when she noticed new pink plaques appearing. Her medical history was positive for breast cancer, which was surgically and medically treated 16 years prior to presentation.
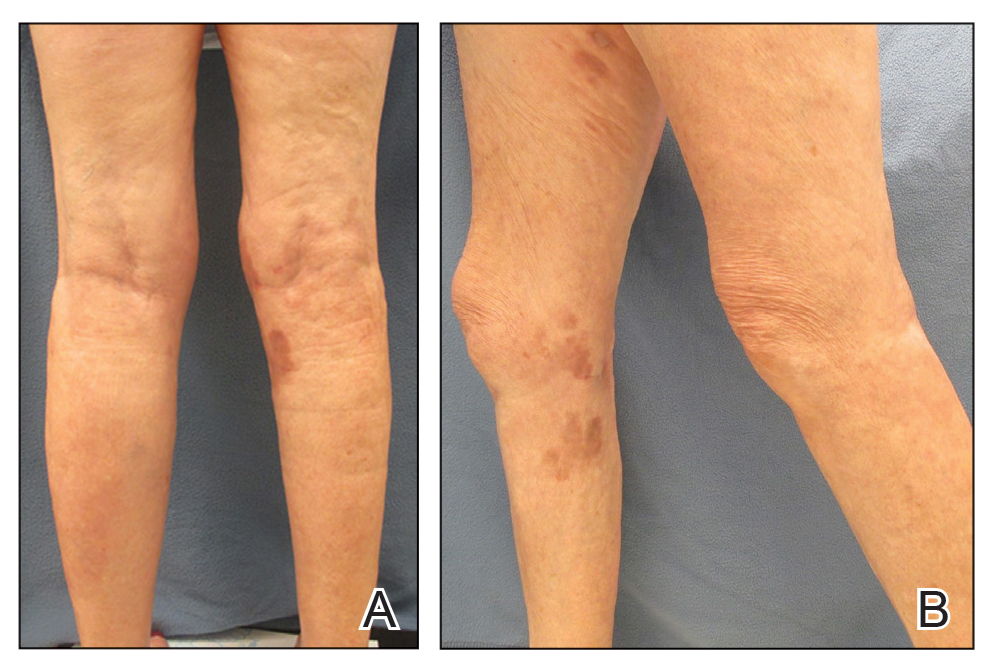
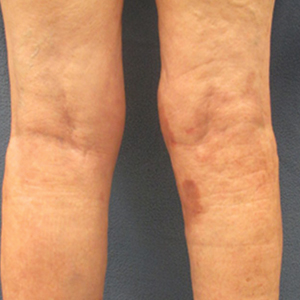
On presentation, physical examination revealed dark pink, hyperpigmented plaques on the right leg and a firm hypopigmented broad linear plaque on the right forearm. Palpation of the legs revealed thickened sclerotic plaques from the thighs down to the ankles (Figure 1). The plaques were not tender to palpation. She did have a decreased range of motion with eversion and inversion of the feet and ankles.
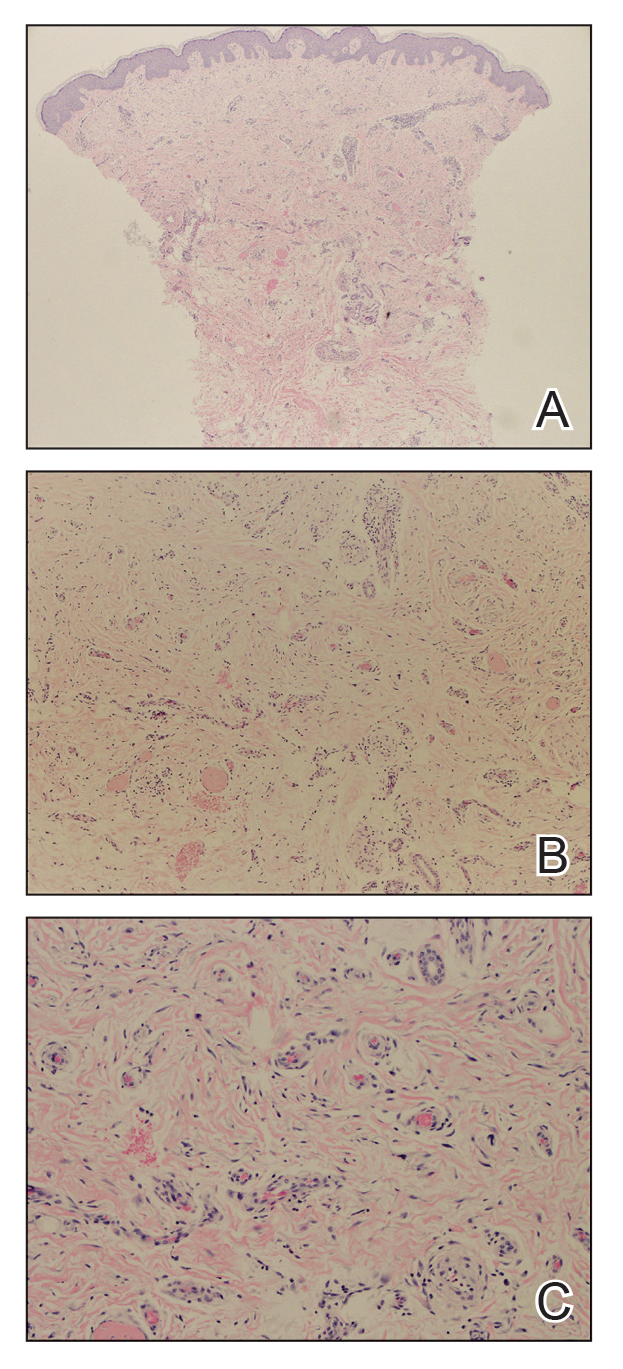
Biopsies from the right medial leg and right volar forearm showed increased bland dermal spindle cellularity associated with numerous round to ovoid osteoid aggregates encircling elastic fibers and surrounded by osteoblasts (Figure 2). CD34 immunohistochemistry showed general retention of staining within the dermal fibroblast population, and elastin stain showed general retention of elastic fiber bundles and thickening.
Laboratory workup included a complete blood cell count, comprehensive metabolic panel, thyroid-stimulating hormone level, and serum protein electrophoresis; results were all within reference range. The patient also had a urine element profile from an outside provider 1 month after presenting to our office that showed an elevated urine gadolinium level of 4.146 μg/g (reference range, 0–0.019 μg/g). The patient’s skin lesions have remained stable, and she is now working with physical therapy to help with her range of motion.
Comment
Gadolinium Causing Fibrosis—The incidence of NSF varies according to the severity of renal impairment, dosage level of GBCA used, and the history of GBCA use. In patients with normal renal function, gadolinium is excreted within 90 minutes. In patients with severe renal disease, the half-life can increase to up to 34.3 hours.11 Reduced renal clearance and increased half-life of gadolinium lead to prolonged excretion, causing the GBCA to become unstable and dissociate into its constituents, leading to tissue deposition of Gd3+ cations. This dissociation is thought to be due to differences in the stability of the various chelation complexes among the different formulations of GBCAs.12 The mechanism by which the dissociated gadolinium causes the fibrosis in the skin or other organs of the body is still unknown. Furthermore, even patients with normal renal function who undergo repeated administration of GBCA have been found to have higher levels of Gd3+ in their tissues, even in the absence of symptoms.13
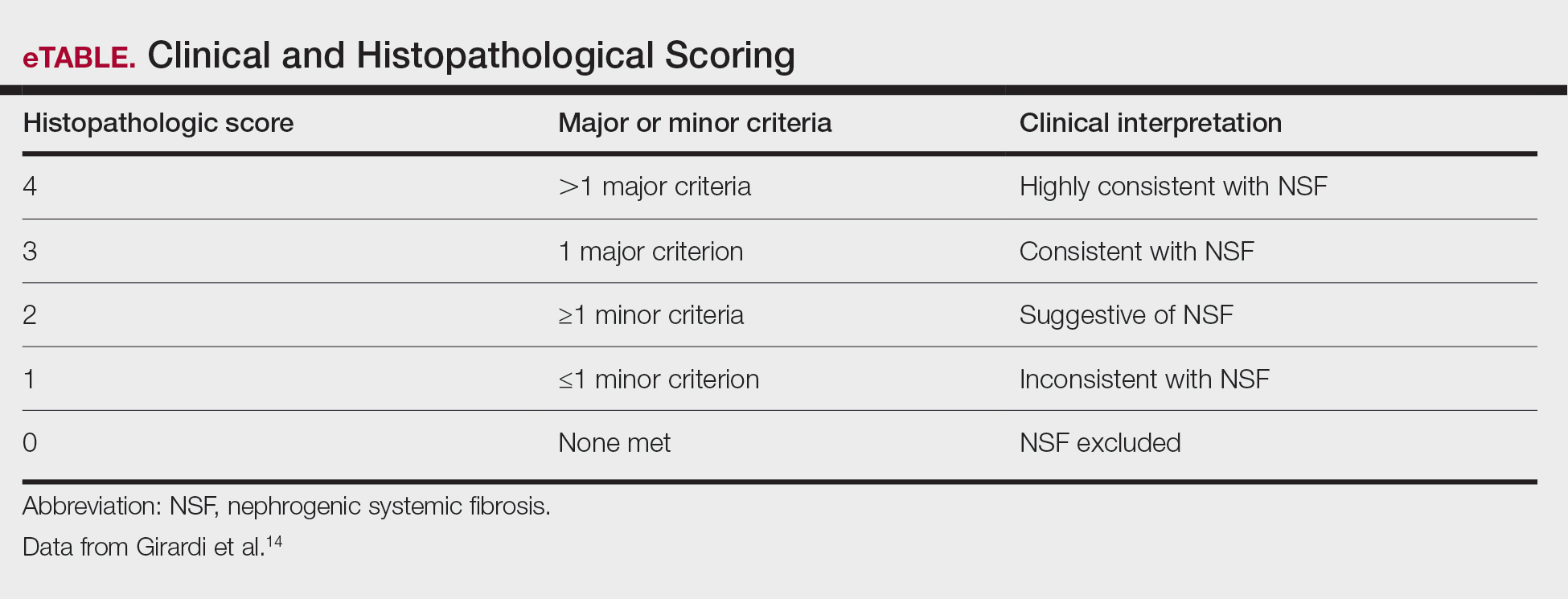
Diagnosing NSF—In 2011, Girardi et al14 created a clinical and histopathological scoring system to help diagnose NSF. Clinical findings can be broken down into major criteria and minor criteria. Major criteria consist of patterned plaques, joint contractures, cobblestoning, marked induration, or peau d’orange change. Minor criteria consist of puckering, linear banding, superficial plaques or patches, dermal papules, and scleral plaques. Histopathologic findings include increased dermal cellularity (score +1), CD34+ cells with tram tracking (score +1), thickened or thin collagen bundles (score +1), preserved elastic fibers (score −1), septal involvement (score +1), and osseous metaplasia (score +3)(eTable).14
Differential Diagnosis—The differential diagnosis of NSF includes scleromyxedema, scleroderma, eosinophilic fasciitis, eosinophilia-myalgia syndrome, lipodermatosclerosis, morphea, and chronic graft-vs-host disease. Histopathologic examination of scleromyxedema can look identical to NSF. Therefore, a review of the patient’s medical history, prior hospitalizations, and prior gadolinium exposure is important. Appropriate laboratory workups should be ordered to rule out the other differential diagnoses.
NSF and Kidney Injury—A PubMed search of articles indexed for MEDLINE using the terms NSF with kidney injury revealed 7 cases of NSF occurring in patients who either had resolved acute kidney injury or resolved acute on chronic kidney disease.1,6-10 Of those cases, 3 reported NSF occurring in patients with completely resolved acute kidney injury.6,7,10 One of those cases involved a 65-year-old man who developed acute renal failure due to acute tubular necrosis.7 He had no history of renal disease prior to hospitalization. His skin lesions continued to improve as his renal function normalized back to baseline after discharge.7 The second case involved a 42-year-old man who had repeated exposure to GBCAs during a brief period of acute kidney injury.6 Nephrogenic systemic fibrosis developed after his renal function normalized. The authors did not mention if there was clinical improvement.6 The third case involved a 22-year-old man who developed acute renal failure after ingestion of hair dye. He did not have a history of chronic renal disease, and as he recovered from the acute kidney injury, almost all of the skin lesions cleared after 1 year.10
Our patient did not have a history of chronic renal disease when she presented to the hospital for sepsis and acute tubular necrosis. Unlike 2 of the prior cases, she did not notice improvement of the skin lesions as the renal function returned to baseline. She continued to experience changes in the skin, even up to 5 years after, and then stabilized. Throughout that time, her renal function was normal. Interestingly, despite having a normal creatinine level, the patient had an elevated gadolinium level on the urine gadolinium test, which typically is not a standard test for NSF. However, the elevated value does shed light on the persistence of gadolinium in the patient despite her exposure having been more than 10 years earlier.
Treatment of NSF—There is no gold standard treatment of NSF, and reversing the fibrosis has proven to be difficult. Avoidance of GBCAs in acute kidney injury or chronic severe renal disease, as recommended by the US Food and Drug Administration, is key to preventing this debilitating disease.15 Restoration of renal function is essential for excreting the gadolinium and improvement in NSF.12 Physical and occupational therapy can improve joint mobility. Therapies such as extracorporeal photopheresis, sodium thiosulfate, pentoxifylline, glucocorticoids, plasmapheresis, intravenous immunoglobulin, cyclophosphamide, imatinib mesylate, intralesional interferon alfa, topical calcipotriene, corticosteroids, and UVA1 light therapy have been used with varying results.12 It has been suggested that renal transplantation can stop the progression of NSF. However, in the cases we reviewed, renal transplantation would not have benefited those patients because their renal function normalized.6,7,10 Additionally, even though our patient’s renal function normalized after discharge from the hospital, she continued to see more skin lesions developing, likely due to the accumulated gadolinium that was already in her tissue. The possibility of chelation therapy to remove the gadolinium has been proposed. In 1 case study involving deferoxamine injected intramuscularly in a patient with NSF, the urine excretion of gadolinium increased almost 2-fold, but there was no change in the serum concentration level of gadolinium or improvement in the patient’s clinical symptoms.16 We anticipate that our patient’s symptoms will slowly improve, as her body is still excreting the gadolinium. Our patient also was added to the International NSF Registry that was created by Dr. Shawn E. Cowper at the Yale School of Medicine (New Haven, Connecticut).
Conclusion
We report a rare case of NSF occurring in a patient with resolved acute kidney injury and no history of chronic renal disease. Our patient initially did not improve after her renal function normalized, as she continued to develop lesions 10 years after the exposure. Her elevated urine gadolinium excretion level also sheds light on the persistence of gadolinium in her body despite her normal renal function 10 years after her exposure. Although her clinical symptoms have stabilized, our case reiterates the complex pathology of this entity and challenge regarding treatment options. Physicians should be aware that NSF can still occur in healthy patients with no chronic renal disease who have had an episode of acute renal insufficiency along with exposure to a GBCA.
- Cowper SE, Su LD, Bhawan J, et al. Nephrogenic fibrosing dermopathy. Am J Dermatopathol. 2001;23:383-393.
- Grobner T. Gadolinium—a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant. 2006;21:1104-1108.
- Larson KN, Gagnon AL, Darling MD, et al. Nephrogenic systemic fibrosis manifesting a decade after exposure to gadolinium. JAMA Dermatol. 2015;151:1117-1120.
- Mendoza FA, Artlett CM, Sandorfi N, et al. Description of 12 cases of nephrogenic fibrosing dermopathy and review of the literature. Semin Arthritis Rheum. 2006;35:238-249.
- Ting WW, Stone MS, Madison KC, et al. Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol. 2003;139:903-906.
- Lu CF, Hsiao CH, Tjiu JW. Nephrogenic systemic fibrosis developed after recovery from acute renal failure: gadolinium as a possible aetiological factor. J Eur Acad Dermatol Venereol. 2009;23:339-340.
- Cassis TB, Jackson JM, Sonnier GB, et al. Nephrogenic fibrosing dermopathy in a patient with acute renal failure never requiring dialysis. Int J Dermatol. 2006;45:56-59.
- Swartz RD, Crofford LJ, Phan SH, et al. Nephrogenic fibrosing dermopathy: a novel cutaneous fibrosing disorder in patients with renal failure. Am J Med. 2003;114:563-572.
- Mackay-Wiggan JM, Cohen DJ, Hardy MA, et al. Nephrogenic fibrosing dermopathy (scleromyxedema-like illness of renal disease). J Am Acad Dermatol. 2003;48:55-60.
- Reddy IS, Somani VK, Swarnalata G, et al. Nephrogenic systemic fibrosis following hair-dye ingestion induced acute renal failure. Indian J Dermatol Venereol Leprol. 2006;76:400-403.
- Marckmann P, Skov L, Rossen K, et al. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. J Am Soc Nephrol. 2006;17:2359-2362.
- Cheong BYC, Muthupillai R. Nephrogenic systemic fibrosis: a concise review for cardiologists. Texas Heart Inst J. 2010;37:508-515.
- Rogosnitzky M, Branch S. Gadolinium-based contrast agent toxicity: a review of known and proposed mechanisms. BioMetals. 2016;29:365-376.
- Girardi M, Kay J, Elston DM, et al. Nephrogenic systemic fibrosis: clinicopathological definition and workup recommendations. J Am Acad Dermatol. 2011;65:1095-1106.
- US Food and Drug Administration. FDA Drug Safety Communication: new warnings for using gadolinium-based contrast agents in patients with kidney dysfunction. Updated February 6, 2018. Accessed November 22, 2021. http://www.fda.gov/Drugs/DrugSafety/ucm223966.htm
- Leung N, Pittelkow MR, Lee CU, et al. Chelation of gadolinium with deferoxamine in a patient with nephrogenic systemic fibrosis. NDT Plus. 2009;2:309-311.
Nephrogenic systemic fibrosis (NSF) is a rare debilitating disorder characterized by dermal plaques, joint contractures, and fibrosis of the skin with possible involvement of muscles and internal organs.1-3 Originally identified in 1997 as nephrogenic fibrosing dermopathy to describe its characteristic cutaneous thickening and hardening, the name was changed to NSF to more accurately reflect the noncutaneous manifestations present in other organ tissues.2,4,5 Nephrogenic systemic fibrosis occurs in patients with a history of renal insufficiency and exposure to gadolinium-based contrast agents (GBCAs) used in magnetic resonance angiography and magnetic resonance imaging. There is no predilection for age, sex, or ethnicity.
Nephrogenic systemic fibrosis may develop over a period of days to several weeks. However, there have been cases of NSF developing 10 years after gadolinium exposure.2 In most cases, patients have a history of severe chronic renal disease requiring hemodialysis. There have been a few reported cases of NSF occurring in patients with resolved acute kidney injury or resolved acute on chronic renal disease.1,6-10 We present a case of NSF occurring in a patient with resolved transient renal insufficiency and no history of chronic renal disease.
Case Report
A 68-year-old woman presented with new dark, painless, pink plaques on the right thigh and calf. The patient stated the condition started and got worse after she was hospitalized 12 years prior for lower extremity cellulitis, sepsis, and acute renal failure. The patient developed complications during that hospital stay and underwent a renal biopsy and renal artery embolization requiring use of a GBCA. After the procedure, she noticed skin hardening in the extremities and decreased mobility in both legs while she was still in the hospital. It was thought that the lower leg changes were due to cellulitis. Therefore, when the renal issues resolved, she was discharged. Her skin and joint changes remained stable until 6 years later when she noticed new pink plaques appearing. Her medical history was positive for breast cancer, which was surgically and medically treated 16 years prior to presentation.
On presentation, physical examination revealed dark pink, hyperpigmented plaques on the right leg and a firm hypopigmented broad linear plaque on the right forearm. Palpation of the legs revealed thickened sclerotic plaques from the thighs down to the ankles (Figure 1). The plaques were not tender to palpation. She did have a decreased range of motion with eversion and inversion of the feet and ankles.
Biopsies from the right medial leg and right volar forearm showed increased bland dermal spindle cellularity associated with numerous round to ovoid osteoid aggregates encircling elastic fibers and surrounded by osteoblasts (Figure 2). CD34 immunohistochemistry showed general retention of staining within the dermal fibroblast population, and elastin stain showed general retention of elastic fiber bundles and thickening.
Laboratory workup included a complete blood cell count, comprehensive metabolic panel, thyroid-stimulating hormone level, and serum protein electrophoresis; results were all within reference range. The patient also had a urine element profile from an outside provider 1 month after presenting to our office that showed an elevated urine gadolinium level of 4.146 μg/g (reference range, 0–0.019 μg/g). The patient’s skin lesions have remained stable, and she is now working with physical therapy to help with her range of motion.
Comment
Gadolinium Causing Fibrosis—The incidence of NSF varies according to the severity of renal impairment, dosage level of GBCA used, and the history of GBCA use. In patients with normal renal function, gadolinium is excreted within 90 minutes. In patients with severe renal disease, the half-life can increase to up to 34.3 hours.11 Reduced renal clearance and increased half-life of gadolinium lead to prolonged excretion, causing the GBCA to become unstable and dissociate into its constituents, leading to tissue deposition of Gd3+ cations. This dissociation is thought to be due to differences in the stability of the various chelation complexes among the different formulations of GBCAs.12 The mechanism by which the dissociated gadolinium causes the fibrosis in the skin or other organs of the body is still unknown. Furthermore, even patients with normal renal function who undergo repeated administration of GBCA have been found to have higher levels of Gd3+ in their tissues, even in the absence of symptoms.13
Diagnosing NSF—In 2011, Girardi et al14 created a clinical and histopathological scoring system to help diagnose NSF. Clinical findings can be broken down into major criteria and minor criteria. Major criteria consist of patterned plaques, joint contractures, cobblestoning, marked induration, or peau d’orange change. Minor criteria consist of puckering, linear banding, superficial plaques or patches, dermal papules, and scleral plaques. Histopathologic findings include increased dermal cellularity (score +1), CD34+ cells with tram tracking (score +1), thickened or thin collagen bundles (score +1), preserved elastic fibers (score −1), septal involvement (score +1), and osseous metaplasia (score +3)(eTable).14
Differential Diagnosis—The differential diagnosis of NSF includes scleromyxedema, scleroderma, eosinophilic fasciitis, eosinophilia-myalgia syndrome, lipodermatosclerosis, morphea, and chronic graft-vs-host disease. Histopathologic examination of scleromyxedema can look identical to NSF. Therefore, a review of the patient’s medical history, prior hospitalizations, and prior gadolinium exposure is important. Appropriate laboratory workups should be ordered to rule out the other differential diagnoses.
NSF and Kidney Injury—A PubMed search of articles indexed for MEDLINE using the terms NSF with kidney injury revealed 7 cases of NSF occurring in patients who either had resolved acute kidney injury or resolved acute on chronic kidney disease.1,6-10 Of those cases, 3 reported NSF occurring in patients with completely resolved acute kidney injury.6,7,10 One of those cases involved a 65-year-old man who developed acute renal failure due to acute tubular necrosis.7 He had no history of renal disease prior to hospitalization. His skin lesions continued to improve as his renal function normalized back to baseline after discharge.7 The second case involved a 42-year-old man who had repeated exposure to GBCAs during a brief period of acute kidney injury.6 Nephrogenic systemic fibrosis developed after his renal function normalized. The authors did not mention if there was clinical improvement.6 The third case involved a 22-year-old man who developed acute renal failure after ingestion of hair dye. He did not have a history of chronic renal disease, and as he recovered from the acute kidney injury, almost all of the skin lesions cleared after 1 year.10
Our patient did not have a history of chronic renal disease when she presented to the hospital for sepsis and acute tubular necrosis. Unlike 2 of the prior cases, she did not notice improvement of the skin lesions as the renal function returned to baseline. She continued to experience changes in the skin, even up to 5 years after, and then stabilized. Throughout that time, her renal function was normal. Interestingly, despite having a normal creatinine level, the patient had an elevated gadolinium level on the urine gadolinium test, which typically is not a standard test for NSF. However, the elevated value does shed light on the persistence of gadolinium in the patient despite her exposure having been more than 10 years earlier.
Treatment of NSF—There is no gold standard treatment of NSF, and reversing the fibrosis has proven to be difficult. Avoidance of GBCAs in acute kidney injury or chronic severe renal disease, as recommended by the US Food and Drug Administration, is key to preventing this debilitating disease.15 Restoration of renal function is essential for excreting the gadolinium and improvement in NSF.12 Physical and occupational therapy can improve joint mobility. Therapies such as extracorporeal photopheresis, sodium thiosulfate, pentoxifylline, glucocorticoids, plasmapheresis, intravenous immunoglobulin, cyclophosphamide, imatinib mesylate, intralesional interferon alfa, topical calcipotriene, corticosteroids, and UVA1 light therapy have been used with varying results.12 It has been suggested that renal transplantation can stop the progression of NSF. However, in the cases we reviewed, renal transplantation would not have benefited those patients because their renal function normalized.6,7,10 Additionally, even though our patient’s renal function normalized after discharge from the hospital, she continued to see more skin lesions developing, likely due to the accumulated gadolinium that was already in her tissue. The possibility of chelation therapy to remove the gadolinium has been proposed. In 1 case study involving deferoxamine injected intramuscularly in a patient with NSF, the urine excretion of gadolinium increased almost 2-fold, but there was no change in the serum concentration level of gadolinium or improvement in the patient’s clinical symptoms.16 We anticipate that our patient’s symptoms will slowly improve, as her body is still excreting the gadolinium. Our patient also was added to the International NSF Registry that was created by Dr. Shawn E. Cowper at the Yale School of Medicine (New Haven, Connecticut).
Conclusion
We report a rare case of NSF occurring in a patient with resolved acute kidney injury and no history of chronic renal disease. Our patient initially did not improve after her renal function normalized, as she continued to develop lesions 10 years after the exposure. Her elevated urine gadolinium excretion level also sheds light on the persistence of gadolinium in her body despite her normal renal function 10 years after her exposure. Although her clinical symptoms have stabilized, our case reiterates the complex pathology of this entity and challenge regarding treatment options. Physicians should be aware that NSF can still occur in healthy patients with no chronic renal disease who have had an episode of acute renal insufficiency along with exposure to a GBCA.
Nephrogenic systemic fibrosis (NSF) is a rare debilitating disorder characterized by dermal plaques, joint contractures, and fibrosis of the skin with possible involvement of muscles and internal organs.1-3 Originally identified in 1997 as nephrogenic fibrosing dermopathy to describe its characteristic cutaneous thickening and hardening, the name was changed to NSF to more accurately reflect the noncutaneous manifestations present in other organ tissues.2,4,5 Nephrogenic systemic fibrosis occurs in patients with a history of renal insufficiency and exposure to gadolinium-based contrast agents (GBCAs) used in magnetic resonance angiography and magnetic resonance imaging. There is no predilection for age, sex, or ethnicity.
Nephrogenic systemic fibrosis may develop over a period of days to several weeks. However, there have been cases of NSF developing 10 years after gadolinium exposure.2 In most cases, patients have a history of severe chronic renal disease requiring hemodialysis. There have been a few reported cases of NSF occurring in patients with resolved acute kidney injury or resolved acute on chronic renal disease.1,6-10 We present a case of NSF occurring in a patient with resolved transient renal insufficiency and no history of chronic renal disease.
Case Report
A 68-year-old woman presented with new dark, painless, pink plaques on the right thigh and calf. The patient stated the condition started and got worse after she was hospitalized 12 years prior for lower extremity cellulitis, sepsis, and acute renal failure. The patient developed complications during that hospital stay and underwent a renal biopsy and renal artery embolization requiring use of a GBCA. After the procedure, she noticed skin hardening in the extremities and decreased mobility in both legs while she was still in the hospital. It was thought that the lower leg changes were due to cellulitis. Therefore, when the renal issues resolved, she was discharged. Her skin and joint changes remained stable until 6 years later when she noticed new pink plaques appearing. Her medical history was positive for breast cancer, which was surgically and medically treated 16 years prior to presentation.
On presentation, physical examination revealed dark pink, hyperpigmented plaques on the right leg and a firm hypopigmented broad linear plaque on the right forearm. Palpation of the legs revealed thickened sclerotic plaques from the thighs down to the ankles (Figure 1). The plaques were not tender to palpation. She did have a decreased range of motion with eversion and inversion of the feet and ankles.
Biopsies from the right medial leg and right volar forearm showed increased bland dermal spindle cellularity associated with numerous round to ovoid osteoid aggregates encircling elastic fibers and surrounded by osteoblasts (Figure 2). CD34 immunohistochemistry showed general retention of staining within the dermal fibroblast population, and elastin stain showed general retention of elastic fiber bundles and thickening.
Laboratory workup included a complete blood cell count, comprehensive metabolic panel, thyroid-stimulating hormone level, and serum protein electrophoresis; results were all within reference range. The patient also had a urine element profile from an outside provider 1 month after presenting to our office that showed an elevated urine gadolinium level of 4.146 μg/g (reference range, 0–0.019 μg/g). The patient’s skin lesions have remained stable, and she is now working with physical therapy to help with her range of motion.
Comment
Gadolinium Causing Fibrosis—The incidence of NSF varies according to the severity of renal impairment, dosage level of GBCA used, and the history of GBCA use. In patients with normal renal function, gadolinium is excreted within 90 minutes. In patients with severe renal disease, the half-life can increase to up to 34.3 hours.11 Reduced renal clearance and increased half-life of gadolinium lead to prolonged excretion, causing the GBCA to become unstable and dissociate into its constituents, leading to tissue deposition of Gd3+ cations. This dissociation is thought to be due to differences in the stability of the various chelation complexes among the different formulations of GBCAs.12 The mechanism by which the dissociated gadolinium causes the fibrosis in the skin or other organs of the body is still unknown. Furthermore, even patients with normal renal function who undergo repeated administration of GBCA have been found to have higher levels of Gd3+ in their tissues, even in the absence of symptoms.13
Diagnosing NSF—In 2011, Girardi et al14 created a clinical and histopathological scoring system to help diagnose NSF. Clinical findings can be broken down into major criteria and minor criteria. Major criteria consist of patterned plaques, joint contractures, cobblestoning, marked induration, or peau d’orange change. Minor criteria consist of puckering, linear banding, superficial plaques or patches, dermal papules, and scleral plaques. Histopathologic findings include increased dermal cellularity (score +1), CD34+ cells with tram tracking (score +1), thickened or thin collagen bundles (score +1), preserved elastic fibers (score −1), septal involvement (score +1), and osseous metaplasia (score +3)(eTable).14
Differential Diagnosis—The differential diagnosis of NSF includes scleromyxedema, scleroderma, eosinophilic fasciitis, eosinophilia-myalgia syndrome, lipodermatosclerosis, morphea, and chronic graft-vs-host disease. Histopathologic examination of scleromyxedema can look identical to NSF. Therefore, a review of the patient’s medical history, prior hospitalizations, and prior gadolinium exposure is important. Appropriate laboratory workups should be ordered to rule out the other differential diagnoses.
NSF and Kidney Injury—A PubMed search of articles indexed for MEDLINE using the terms NSF with kidney injury revealed 7 cases of NSF occurring in patients who either had resolved acute kidney injury or resolved acute on chronic kidney disease.1,6-10 Of those cases, 3 reported NSF occurring in patients with completely resolved acute kidney injury.6,7,10 One of those cases involved a 65-year-old man who developed acute renal failure due to acute tubular necrosis.7 He had no history of renal disease prior to hospitalization. His skin lesions continued to improve as his renal function normalized back to baseline after discharge.7 The second case involved a 42-year-old man who had repeated exposure to GBCAs during a brief period of acute kidney injury.6 Nephrogenic systemic fibrosis developed after his renal function normalized. The authors did not mention if there was clinical improvement.6 The third case involved a 22-year-old man who developed acute renal failure after ingestion of hair dye. He did not have a history of chronic renal disease, and as he recovered from the acute kidney injury, almost all of the skin lesions cleared after 1 year.10
Our patient did not have a history of chronic renal disease when she presented to the hospital for sepsis and acute tubular necrosis. Unlike 2 of the prior cases, she did not notice improvement of the skin lesions as the renal function returned to baseline. She continued to experience changes in the skin, even up to 5 years after, and then stabilized. Throughout that time, her renal function was normal. Interestingly, despite having a normal creatinine level, the patient had an elevated gadolinium level on the urine gadolinium test, which typically is not a standard test for NSF. However, the elevated value does shed light on the persistence of gadolinium in the patient despite her exposure having been more than 10 years earlier.
Treatment of NSF—There is no gold standard treatment of NSF, and reversing the fibrosis has proven to be difficult. Avoidance of GBCAs in acute kidney injury or chronic severe renal disease, as recommended by the US Food and Drug Administration, is key to preventing this debilitating disease.15 Restoration of renal function is essential for excreting the gadolinium and improvement in NSF.12 Physical and occupational therapy can improve joint mobility. Therapies such as extracorporeal photopheresis, sodium thiosulfate, pentoxifylline, glucocorticoids, plasmapheresis, intravenous immunoglobulin, cyclophosphamide, imatinib mesylate, intralesional interferon alfa, topical calcipotriene, corticosteroids, and UVA1 light therapy have been used with varying results.12 It has been suggested that renal transplantation can stop the progression of NSF. However, in the cases we reviewed, renal transplantation would not have benefited those patients because their renal function normalized.6,7,10 Additionally, even though our patient’s renal function normalized after discharge from the hospital, she continued to see more skin lesions developing, likely due to the accumulated gadolinium that was already in her tissue. The possibility of chelation therapy to remove the gadolinium has been proposed. In 1 case study involving deferoxamine injected intramuscularly in a patient with NSF, the urine excretion of gadolinium increased almost 2-fold, but there was no change in the serum concentration level of gadolinium or improvement in the patient’s clinical symptoms.16 We anticipate that our patient’s symptoms will slowly improve, as her body is still excreting the gadolinium. Our patient also was added to the International NSF Registry that was created by Dr. Shawn E. Cowper at the Yale School of Medicine (New Haven, Connecticut).
Conclusion
We report a rare case of NSF occurring in a patient with resolved acute kidney injury and no history of chronic renal disease. Our patient initially did not improve after her renal function normalized, as she continued to develop lesions 10 years after the exposure. Her elevated urine gadolinium excretion level also sheds light on the persistence of gadolinium in her body despite her normal renal function 10 years after her exposure. Although her clinical symptoms have stabilized, our case reiterates the complex pathology of this entity and challenge regarding treatment options. Physicians should be aware that NSF can still occur in healthy patients with no chronic renal disease who have had an episode of acute renal insufficiency along with exposure to a GBCA.
- Cowper SE, Su LD, Bhawan J, et al. Nephrogenic fibrosing dermopathy. Am J Dermatopathol. 2001;23:383-393.
- Grobner T. Gadolinium—a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant. 2006;21:1104-1108.
- Larson KN, Gagnon AL, Darling MD, et al. Nephrogenic systemic fibrosis manifesting a decade after exposure to gadolinium. JAMA Dermatol. 2015;151:1117-1120.
- Mendoza FA, Artlett CM, Sandorfi N, et al. Description of 12 cases of nephrogenic fibrosing dermopathy and review of the literature. Semin Arthritis Rheum. 2006;35:238-249.
- Ting WW, Stone MS, Madison KC, et al. Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol. 2003;139:903-906.
- Lu CF, Hsiao CH, Tjiu JW. Nephrogenic systemic fibrosis developed after recovery from acute renal failure: gadolinium as a possible aetiological factor. J Eur Acad Dermatol Venereol. 2009;23:339-340.
- Cassis TB, Jackson JM, Sonnier GB, et al. Nephrogenic fibrosing dermopathy in a patient with acute renal failure never requiring dialysis. Int J Dermatol. 2006;45:56-59.
- Swartz RD, Crofford LJ, Phan SH, et al. Nephrogenic fibrosing dermopathy: a novel cutaneous fibrosing disorder in patients with renal failure. Am J Med. 2003;114:563-572.
- Mackay-Wiggan JM, Cohen DJ, Hardy MA, et al. Nephrogenic fibrosing dermopathy (scleromyxedema-like illness of renal disease). J Am Acad Dermatol. 2003;48:55-60.
- Reddy IS, Somani VK, Swarnalata G, et al. Nephrogenic systemic fibrosis following hair-dye ingestion induced acute renal failure. Indian J Dermatol Venereol Leprol. 2006;76:400-403.
- Marckmann P, Skov L, Rossen K, et al. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. J Am Soc Nephrol. 2006;17:2359-2362.
- Cheong BYC, Muthupillai R. Nephrogenic systemic fibrosis: a concise review for cardiologists. Texas Heart Inst J. 2010;37:508-515.
- Rogosnitzky M, Branch S. Gadolinium-based contrast agent toxicity: a review of known and proposed mechanisms. BioMetals. 2016;29:365-376.
- Girardi M, Kay J, Elston DM, et al. Nephrogenic systemic fibrosis: clinicopathological definition and workup recommendations. J Am Acad Dermatol. 2011;65:1095-1106.
- US Food and Drug Administration. FDA Drug Safety Communication: new warnings for using gadolinium-based contrast agents in patients with kidney dysfunction. Updated February 6, 2018. Accessed November 22, 2021. http://www.fda.gov/Drugs/DrugSafety/ucm223966.htm
- Leung N, Pittelkow MR, Lee CU, et al. Chelation of gadolinium with deferoxamine in a patient with nephrogenic systemic fibrosis. NDT Plus. 2009;2:309-311.
- Cowper SE, Su LD, Bhawan J, et al. Nephrogenic fibrosing dermopathy. Am J Dermatopathol. 2001;23:383-393.
- Grobner T. Gadolinium—a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant. 2006;21:1104-1108.
- Larson KN, Gagnon AL, Darling MD, et al. Nephrogenic systemic fibrosis manifesting a decade after exposure to gadolinium. JAMA Dermatol. 2015;151:1117-1120.
- Mendoza FA, Artlett CM, Sandorfi N, et al. Description of 12 cases of nephrogenic fibrosing dermopathy and review of the literature. Semin Arthritis Rheum. 2006;35:238-249.
- Ting WW, Stone MS, Madison KC, et al. Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol. 2003;139:903-906.
- Lu CF, Hsiao CH, Tjiu JW. Nephrogenic systemic fibrosis developed after recovery from acute renal failure: gadolinium as a possible aetiological factor. J Eur Acad Dermatol Venereol. 2009;23:339-340.
- Cassis TB, Jackson JM, Sonnier GB, et al. Nephrogenic fibrosing dermopathy in a patient with acute renal failure never requiring dialysis. Int J Dermatol. 2006;45:56-59.
- Swartz RD, Crofford LJ, Phan SH, et al. Nephrogenic fibrosing dermopathy: a novel cutaneous fibrosing disorder in patients with renal failure. Am J Med. 2003;114:563-572.
- Mackay-Wiggan JM, Cohen DJ, Hardy MA, et al. Nephrogenic fibrosing dermopathy (scleromyxedema-like illness of renal disease). J Am Acad Dermatol. 2003;48:55-60.
- Reddy IS, Somani VK, Swarnalata G, et al. Nephrogenic systemic fibrosis following hair-dye ingestion induced acute renal failure. Indian J Dermatol Venereol Leprol. 2006;76:400-403.
- Marckmann P, Skov L, Rossen K, et al. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. J Am Soc Nephrol. 2006;17:2359-2362.
- Cheong BYC, Muthupillai R. Nephrogenic systemic fibrosis: a concise review for cardiologists. Texas Heart Inst J. 2010;37:508-515.
- Rogosnitzky M, Branch S. Gadolinium-based contrast agent toxicity: a review of known and proposed mechanisms. BioMetals. 2016;29:365-376.
- Girardi M, Kay J, Elston DM, et al. Nephrogenic systemic fibrosis: clinicopathological definition and workup recommendations. J Am Acad Dermatol. 2011;65:1095-1106.
- US Food and Drug Administration. FDA Drug Safety Communication: new warnings for using gadolinium-based contrast agents in patients with kidney dysfunction. Updated February 6, 2018. Accessed November 22, 2021. http://www.fda.gov/Drugs/DrugSafety/ucm223966.htm
- Leung N, Pittelkow MR, Lee CU, et al. Chelation of gadolinium with deferoxamine in a patient with nephrogenic systemic fibrosis. NDT Plus. 2009;2:309-311.
Practice Points
- Nephrogenic systemic fibrosis may occur in patients with a history of renal insufficiency and exposure to gadolinium-based contrast agents.
- Nephrogenic systemic fibrosis may develop over a period of days to several years after exposure.
- Symptoms of this rare disease can progress and get worse even after renal function normalizes.
Sleep disorders and cancer: It’s complicated
Sleep apnea and other types of sleep disorders appear to elevate the risk for some types of cancer, specifically prostate cancer, more so than others. But the overall risk can be highly variable, and some sleep problems were found to be associated with a lower risk for cancer and cancer-related death, an analysis of a large observational cohort study of cardiovascular patients found.
Results of the analysis were published online in the journal Cancer Epidemiology. Investigators analyzed the presence of sleep apnea and insomnia and cancer risk in more than 8,500 patients in the Cardiovascular Health Study (CHS). “The fact that we observed certain sleep problems, like apneas, to be associated with elevated risk of some cancers but not others reflects the fact that cancer is a heterogeneous disease,” senior author Amanda Phipps, PhD, said in an interview. Dr. Phipps is an associate professor of epidemiology at the University of Washington and the Fred Hutchinson Cancer Research Center, both in Seattle.
Variable cancer links
The researchers assessed sleep problems in two groups in the CHS: an incident cancer group of 3,930 patients and a cancer mortality group of 4,580 patients. Within those respective groups, the investigators identified 885 first-incident cancers and 804 cancer deaths with a median follow-up of 12 and 14 years. The average age of the study population was 73 years, and 57% were women.
Sleep apnea symptoms (SAS) were associated with a lower risk for incident cancers – a 16% lower baseline risk and a 24% lower time-dependent risk. The study showed no association between cancer incidence and daytime sleepiness and apneas.
However, there was a significantly elevated risk relationship between sleep problems and prostate cancer. A time-dependent analysis of apnea showed more than double the risk (hazard ratio, 2.34), and baseline snoring carried a 69% greater risk. There was also a dose-response relationship for baseline cumulative SAS, compared with not having symptoms: an HR of 1.30 for one symptom, and 2.22 for two or more symptoms.
Risks for lymphatic or hematopoietic cancers were also associated with baseline daytime sleepiness (HR, 1.81), but not with insomnia (HR, 0.54).
With regard to cancer mortality, the study found no relationship between sleep problems and cancer death. In fact, it found an overall inverse relationship with snoring (time-dependent HR, 0.73; cumulative average HR, 0.67) and baseline apnea (HR, 0.69). Likewise, patients reporting SAS had lower risks than those having no SAS: an HR of 0.90 for one symptom and 0.75 for multiple symptoms. No relationships were found between any insomnia symptom and cancer death.
“We know the pathways that lead to prostate cancer can be very different than the pathways that lead to colorectal cancer,” Dr. Phipps said. “What we don’t yet understand is why these associations differ or what mechanisms are responsible for these cancer site-specific associations.”
Need for sleep assessment
The findings don’t change much for how clinicians should evaluate cancer risks in patients with sleep problems, Dr. Phipps said. “Other studies have clearly demonstrated the implications that sleep apnea has for a variety of other important health conditions – such as cardiovascular disease – so there are already plenty of good reasons for clinicians to ask their patients about their sleep and to connect patients with resources for the diagnosis and treatment of sleep apnea,” she added. “This study provides another possible reason.”
These findings provide context for future studies of the relationship between sleep problems and cancer. “But, given that sleep is something we all do and given that sleep problems are so pervasive, it’s important that we keep trying to better understand this relationship,” Dr. Phipps said.
“My hope is that future cancer studies will build in more detailed, longitudinal information on sleep patterns to help us fill current gaps in knowledge.”
Dr. Phipps has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Sleep apnea and other types of sleep disorders appear to elevate the risk for some types of cancer, specifically prostate cancer, more so than others. But the overall risk can be highly variable, and some sleep problems were found to be associated with a lower risk for cancer and cancer-related death, an analysis of a large observational cohort study of cardiovascular patients found.
Results of the analysis were published online in the journal Cancer Epidemiology. Investigators analyzed the presence of sleep apnea and insomnia and cancer risk in more than 8,500 patients in the Cardiovascular Health Study (CHS). “The fact that we observed certain sleep problems, like apneas, to be associated with elevated risk of some cancers but not others reflects the fact that cancer is a heterogeneous disease,” senior author Amanda Phipps, PhD, said in an interview. Dr. Phipps is an associate professor of epidemiology at the University of Washington and the Fred Hutchinson Cancer Research Center, both in Seattle.
Variable cancer links
The researchers assessed sleep problems in two groups in the CHS: an incident cancer group of 3,930 patients and a cancer mortality group of 4,580 patients. Within those respective groups, the investigators identified 885 first-incident cancers and 804 cancer deaths with a median follow-up of 12 and 14 years. The average age of the study population was 73 years, and 57% were women.
Sleep apnea symptoms (SAS) were associated with a lower risk for incident cancers – a 16% lower baseline risk and a 24% lower time-dependent risk. The study showed no association between cancer incidence and daytime sleepiness and apneas.
However, there was a significantly elevated risk relationship between sleep problems and prostate cancer. A time-dependent analysis of apnea showed more than double the risk (hazard ratio, 2.34), and baseline snoring carried a 69% greater risk. There was also a dose-response relationship for baseline cumulative SAS, compared with not having symptoms: an HR of 1.30 for one symptom, and 2.22 for two or more symptoms.
Risks for lymphatic or hematopoietic cancers were also associated with baseline daytime sleepiness (HR, 1.81), but not with insomnia (HR, 0.54).
With regard to cancer mortality, the study found no relationship between sleep problems and cancer death. In fact, it found an overall inverse relationship with snoring (time-dependent HR, 0.73; cumulative average HR, 0.67) and baseline apnea (HR, 0.69). Likewise, patients reporting SAS had lower risks than those having no SAS: an HR of 0.90 for one symptom and 0.75 for multiple symptoms. No relationships were found between any insomnia symptom and cancer death.
“We know the pathways that lead to prostate cancer can be very different than the pathways that lead to colorectal cancer,” Dr. Phipps said. “What we don’t yet understand is why these associations differ or what mechanisms are responsible for these cancer site-specific associations.”
Need for sleep assessment
The findings don’t change much for how clinicians should evaluate cancer risks in patients with sleep problems, Dr. Phipps said. “Other studies have clearly demonstrated the implications that sleep apnea has for a variety of other important health conditions – such as cardiovascular disease – so there are already plenty of good reasons for clinicians to ask their patients about their sleep and to connect patients with resources for the diagnosis and treatment of sleep apnea,” she added. “This study provides another possible reason.”
These findings provide context for future studies of the relationship between sleep problems and cancer. “But, given that sleep is something we all do and given that sleep problems are so pervasive, it’s important that we keep trying to better understand this relationship,” Dr. Phipps said.
“My hope is that future cancer studies will build in more detailed, longitudinal information on sleep patterns to help us fill current gaps in knowledge.”
Dr. Phipps has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Sleep apnea and other types of sleep disorders appear to elevate the risk for some types of cancer, specifically prostate cancer, more so than others. But the overall risk can be highly variable, and some sleep problems were found to be associated with a lower risk for cancer and cancer-related death, an analysis of a large observational cohort study of cardiovascular patients found.
Results of the analysis were published online in the journal Cancer Epidemiology. Investigators analyzed the presence of sleep apnea and insomnia and cancer risk in more than 8,500 patients in the Cardiovascular Health Study (CHS). “The fact that we observed certain sleep problems, like apneas, to be associated with elevated risk of some cancers but not others reflects the fact that cancer is a heterogeneous disease,” senior author Amanda Phipps, PhD, said in an interview. Dr. Phipps is an associate professor of epidemiology at the University of Washington and the Fred Hutchinson Cancer Research Center, both in Seattle.
Variable cancer links
The researchers assessed sleep problems in two groups in the CHS: an incident cancer group of 3,930 patients and a cancer mortality group of 4,580 patients. Within those respective groups, the investigators identified 885 first-incident cancers and 804 cancer deaths with a median follow-up of 12 and 14 years. The average age of the study population was 73 years, and 57% were women.
Sleep apnea symptoms (SAS) were associated with a lower risk for incident cancers – a 16% lower baseline risk and a 24% lower time-dependent risk. The study showed no association between cancer incidence and daytime sleepiness and apneas.
However, there was a significantly elevated risk relationship between sleep problems and prostate cancer. A time-dependent analysis of apnea showed more than double the risk (hazard ratio, 2.34), and baseline snoring carried a 69% greater risk. There was also a dose-response relationship for baseline cumulative SAS, compared with not having symptoms: an HR of 1.30 for one symptom, and 2.22 for two or more symptoms.
Risks for lymphatic or hematopoietic cancers were also associated with baseline daytime sleepiness (HR, 1.81), but not with insomnia (HR, 0.54).
With regard to cancer mortality, the study found no relationship between sleep problems and cancer death. In fact, it found an overall inverse relationship with snoring (time-dependent HR, 0.73; cumulative average HR, 0.67) and baseline apnea (HR, 0.69). Likewise, patients reporting SAS had lower risks than those having no SAS: an HR of 0.90 for one symptom and 0.75 for multiple symptoms. No relationships were found between any insomnia symptom and cancer death.
“We know the pathways that lead to prostate cancer can be very different than the pathways that lead to colorectal cancer,” Dr. Phipps said. “What we don’t yet understand is why these associations differ or what mechanisms are responsible for these cancer site-specific associations.”
Need for sleep assessment
The findings don’t change much for how clinicians should evaluate cancer risks in patients with sleep problems, Dr. Phipps said. “Other studies have clearly demonstrated the implications that sleep apnea has for a variety of other important health conditions – such as cardiovascular disease – so there are already plenty of good reasons for clinicians to ask their patients about their sleep and to connect patients with resources for the diagnosis and treatment of sleep apnea,” she added. “This study provides another possible reason.”
These findings provide context for future studies of the relationship between sleep problems and cancer. “But, given that sleep is something we all do and given that sleep problems are so pervasive, it’s important that we keep trying to better understand this relationship,” Dr. Phipps said.
“My hope is that future cancer studies will build in more detailed, longitudinal information on sleep patterns to help us fill current gaps in knowledge.”
Dr. Phipps has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CANCER EPIDEMIOLOGY
ASH meeting: Diversity, inclusion, immunotherapy, and COVID-19
In 2021, the American Society of Hematology will be hosting its annual meeting in a hybrid format. Content will be presented both live and in person at the Georgia World Congress Center in Atlanta and also online for those who can’t or don’t want to be there in person.
Inevitably during the ongoing pandemic, the meeting will contain key sessions on COVID-19 in hematology, including a plenary presentation outlining a biologic mechanism for the increased coagulopathy with SARS-CoV-2 infections.
In addition, there will be a scientific symposium on COVID-19 vaccination in immunocompromised patients and a special moderated session summarizing nine abstracts on the science of thrombosis in COVID-19, outcomes in patients with hematologic disease, and vaccine responses.
And speaking of COVID, lest anyone forget, annual meeting attendees will be required to be fully vaccinated and masked. Free COVID-19 testing will be available at stations situated throughout the convention center.
Diversifying care
chair of the ASH committee on communications and chief of the division of hematology at the Sylvester Comprehensive Cancer Center at the University of Miami.
For example, investigators at Massachusetts General Hospital in Boston will present new data on code-status transitions among patients with poor-prognosis high-risk acute myeloid leukemia (AML) who are approaching the end of life. Their findings suggest that physician-patient discussions about the goals of care may occur too late in the course of illness for many patients (abstract 109).
“While there have been many advances in the treatment of acute myeloid leukemia, and in fact there has been significant progress even among high-risk patients, addressing end-of-life issues is an often neglected area,” commented briefing participant Martin A. Tallman, MD, from Memorial Sloan Kettering Cancer Center, New York, who is also the current ASH president.
On a more upbeat note, Dr. Tallman also pointed to the results of the phase 3, randomized AGILE trial as an example of progress in AML, especially for patients with newly diagnosed high-risk disease who have mutations in IDH1. This trial investigated a new approach to treatment, with a combination of the combination of the IDH1 inhibitor ivosidenib (Tibsovo) and azacitidine, and compared it with azacitidine alone. The investigators assessed impact on event-free survival, overall survival, and clinical responses (abstract 697).
Dr. Tallman also highlighted abstracts touching on racial, social, and socioeconomic contributors to health care disparities among children with acute lymphoblastic leukemia (ALL; abstract 211) and on clinical trial enrollment characteristics and outcomes for Black and Hispanic adolescents and young adults with ALL (abstract 337).
Immunotherapy advances
Some of the most eagerly awaited abstracts will be highlighting advances in immunotherapy for hematologic malignancies, and these were previewed by Cynthia E. Dunbar, MD, ASH secretary and chief of the Translational Stem Cell Biology Branch within the Intramural Research Program of the National Heart, Lung, and Blood Institute in Bethesda, Md.
These abstracts include the primary analysis of the ZUMA-7 trial, a randomized, phase 3 study comparing the chimeric antigen receptor T-cell (CAR T) construct axicabtagene ciloleucel (axi-cel; Yescarta) with standard of care in patients with relapsed or refractory large B-cell lymphomas (LBCLs; abstract 2) and the interim analysis of the randomized, phase 3 Transform Study comparing the CAR T construct lisocabtagene maralecleucl (liso-cel; Breyanzi) with salvage chemotherapy in patients with relapsed/refractory LBCL (abstract 91).
“Over 500 patients were enrolled in the two studies, and both abstracts report significantly longer survival without relapse in the CAR T arm – for instance, fourfold higher in ZUMA-7, compared to standard of care,” Dr. Dunbar said at the briefing.
“These abstracts provide really critical information to patients, their treating physicians, and the payers who are trying to decide whether use of these expensive, complex, and potentially toxic CAR T-cell therapies are justified, compared to standard therapy,” she said.
Dr. Dunbar also highlighted an abstract on the addition of the anti-CD38 monoclonal antibody isatuximab (Sarclisa) to lenalidomide, bortezomib, and dexamethasone as induction therapy for patients with newly diagnosed multiple myeloma who are eligible for stem cell transplantation (abstract 463).
“The authors report that patients on the isatuximab arm had significantly fewer tumor cells following treatment,” Dr. Dunbar said. “We have come a long way beyond treating myeloma with a single drug, with remissions now measured in many years instead of 1 or 2 following initiation of treatment, and this abstract is another demonstration that novel combinations of multiple agents are really making a difference in this very debilitating disease.”
She also cited an abstract (abstract 127) on monotherapy with the novel bispecific T-cell–engaging monoclonal antibody mosunetuzumab for treatment of patients with follicular lymphoma that has relapsed or is refractory to at least two prior lines of therapy.
Old disorders, new insights
Other abstracts highlighted at the premeeting press briefing included a study that found a high prevalence of monoclonal gammopathy in persons at risk for multiple myeloma (abstract 152) and another with the surprising finding that clonal hematopoiesis, a risk factor myeloid malignancies, may be protective against Alzheimer’s disease (abstract 5).
In addition, a long-term follow-up study of patients with transfusion-dependent beta-thalassemia treated with gene therapy showed that some patients have become transfusion independent and iron homeostasis was restored (abstract 573).
Presentations from CDC and FDA
Dr. Sekeres highlighted other events of interest scheduled for ASH 2021, including a Grassroots Network Lunch featuring a discussion with Rochelle Walensky, MD, MPH, director of the Centers for Disease Control and Prevention in Atlanta, and a joint symposium between ASH and the Food and Drug Administration on newly approved drugs in hematology.
Dr. Sekeres has disclosed consulting/advising for Novartis, Takea/Millennium, and Bristol-Myers Squibb. Dr. Dunbar reported no relevant conflicts of interest. Dr. Tallman disclosed consulting/advising with and research funding from multiple entities.
A version of this article first appeared on Medscape.com.
In 2021, the American Society of Hematology will be hosting its annual meeting in a hybrid format. Content will be presented both live and in person at the Georgia World Congress Center in Atlanta and also online for those who can’t or don’t want to be there in person.
Inevitably during the ongoing pandemic, the meeting will contain key sessions on COVID-19 in hematology, including a plenary presentation outlining a biologic mechanism for the increased coagulopathy with SARS-CoV-2 infections.
In addition, there will be a scientific symposium on COVID-19 vaccination in immunocompromised patients and a special moderated session summarizing nine abstracts on the science of thrombosis in COVID-19, outcomes in patients with hematologic disease, and vaccine responses.
And speaking of COVID, lest anyone forget, annual meeting attendees will be required to be fully vaccinated and masked. Free COVID-19 testing will be available at stations situated throughout the convention center.
Diversifying care
chair of the ASH committee on communications and chief of the division of hematology at the Sylvester Comprehensive Cancer Center at the University of Miami.
For example, investigators at Massachusetts General Hospital in Boston will present new data on code-status transitions among patients with poor-prognosis high-risk acute myeloid leukemia (AML) who are approaching the end of life. Their findings suggest that physician-patient discussions about the goals of care may occur too late in the course of illness for many patients (abstract 109).
“While there have been many advances in the treatment of acute myeloid leukemia, and in fact there has been significant progress even among high-risk patients, addressing end-of-life issues is an often neglected area,” commented briefing participant Martin A. Tallman, MD, from Memorial Sloan Kettering Cancer Center, New York, who is also the current ASH president.
On a more upbeat note, Dr. Tallman also pointed to the results of the phase 3, randomized AGILE trial as an example of progress in AML, especially for patients with newly diagnosed high-risk disease who have mutations in IDH1. This trial investigated a new approach to treatment, with a combination of the combination of the IDH1 inhibitor ivosidenib (Tibsovo) and azacitidine, and compared it with azacitidine alone. The investigators assessed impact on event-free survival, overall survival, and clinical responses (abstract 697).
Dr. Tallman also highlighted abstracts touching on racial, social, and socioeconomic contributors to health care disparities among children with acute lymphoblastic leukemia (ALL; abstract 211) and on clinical trial enrollment characteristics and outcomes for Black and Hispanic adolescents and young adults with ALL (abstract 337).
Immunotherapy advances
Some of the most eagerly awaited abstracts will be highlighting advances in immunotherapy for hematologic malignancies, and these were previewed by Cynthia E. Dunbar, MD, ASH secretary and chief of the Translational Stem Cell Biology Branch within the Intramural Research Program of the National Heart, Lung, and Blood Institute in Bethesda, Md.
These abstracts include the primary analysis of the ZUMA-7 trial, a randomized, phase 3 study comparing the chimeric antigen receptor T-cell (CAR T) construct axicabtagene ciloleucel (axi-cel; Yescarta) with standard of care in patients with relapsed or refractory large B-cell lymphomas (LBCLs; abstract 2) and the interim analysis of the randomized, phase 3 Transform Study comparing the CAR T construct lisocabtagene maralecleucl (liso-cel; Breyanzi) with salvage chemotherapy in patients with relapsed/refractory LBCL (abstract 91).
“Over 500 patients were enrolled in the two studies, and both abstracts report significantly longer survival without relapse in the CAR T arm – for instance, fourfold higher in ZUMA-7, compared to standard of care,” Dr. Dunbar said at the briefing.
“These abstracts provide really critical information to patients, their treating physicians, and the payers who are trying to decide whether use of these expensive, complex, and potentially toxic CAR T-cell therapies are justified, compared to standard therapy,” she said.
Dr. Dunbar also highlighted an abstract on the addition of the anti-CD38 monoclonal antibody isatuximab (Sarclisa) to lenalidomide, bortezomib, and dexamethasone as induction therapy for patients with newly diagnosed multiple myeloma who are eligible for stem cell transplantation (abstract 463).
“The authors report that patients on the isatuximab arm had significantly fewer tumor cells following treatment,” Dr. Dunbar said. “We have come a long way beyond treating myeloma with a single drug, with remissions now measured in many years instead of 1 or 2 following initiation of treatment, and this abstract is another demonstration that novel combinations of multiple agents are really making a difference in this very debilitating disease.”
She also cited an abstract (abstract 127) on monotherapy with the novel bispecific T-cell–engaging monoclonal antibody mosunetuzumab for treatment of patients with follicular lymphoma that has relapsed or is refractory to at least two prior lines of therapy.
Old disorders, new insights
Other abstracts highlighted at the premeeting press briefing included a study that found a high prevalence of monoclonal gammopathy in persons at risk for multiple myeloma (abstract 152) and another with the surprising finding that clonal hematopoiesis, a risk factor myeloid malignancies, may be protective against Alzheimer’s disease (abstract 5).
In addition, a long-term follow-up study of patients with transfusion-dependent beta-thalassemia treated with gene therapy showed that some patients have become transfusion independent and iron homeostasis was restored (abstract 573).
Presentations from CDC and FDA
Dr. Sekeres highlighted other events of interest scheduled for ASH 2021, including a Grassroots Network Lunch featuring a discussion with Rochelle Walensky, MD, MPH, director of the Centers for Disease Control and Prevention in Atlanta, and a joint symposium between ASH and the Food and Drug Administration on newly approved drugs in hematology.
Dr. Sekeres has disclosed consulting/advising for Novartis, Takea/Millennium, and Bristol-Myers Squibb. Dr. Dunbar reported no relevant conflicts of interest. Dr. Tallman disclosed consulting/advising with and research funding from multiple entities.
A version of this article first appeared on Medscape.com.
In 2021, the American Society of Hematology will be hosting its annual meeting in a hybrid format. Content will be presented both live and in person at the Georgia World Congress Center in Atlanta and also online for those who can’t or don’t want to be there in person.
Inevitably during the ongoing pandemic, the meeting will contain key sessions on COVID-19 in hematology, including a plenary presentation outlining a biologic mechanism for the increased coagulopathy with SARS-CoV-2 infections.
In addition, there will be a scientific symposium on COVID-19 vaccination in immunocompromised patients and a special moderated session summarizing nine abstracts on the science of thrombosis in COVID-19, outcomes in patients with hematologic disease, and vaccine responses.
And speaking of COVID, lest anyone forget, annual meeting attendees will be required to be fully vaccinated and masked. Free COVID-19 testing will be available at stations situated throughout the convention center.
Diversifying care
chair of the ASH committee on communications and chief of the division of hematology at the Sylvester Comprehensive Cancer Center at the University of Miami.
For example, investigators at Massachusetts General Hospital in Boston will present new data on code-status transitions among patients with poor-prognosis high-risk acute myeloid leukemia (AML) who are approaching the end of life. Their findings suggest that physician-patient discussions about the goals of care may occur too late in the course of illness for many patients (abstract 109).
“While there have been many advances in the treatment of acute myeloid leukemia, and in fact there has been significant progress even among high-risk patients, addressing end-of-life issues is an often neglected area,” commented briefing participant Martin A. Tallman, MD, from Memorial Sloan Kettering Cancer Center, New York, who is also the current ASH president.
On a more upbeat note, Dr. Tallman also pointed to the results of the phase 3, randomized AGILE trial as an example of progress in AML, especially for patients with newly diagnosed high-risk disease who have mutations in IDH1. This trial investigated a new approach to treatment, with a combination of the combination of the IDH1 inhibitor ivosidenib (Tibsovo) and azacitidine, and compared it with azacitidine alone. The investigators assessed impact on event-free survival, overall survival, and clinical responses (abstract 697).
Dr. Tallman also highlighted abstracts touching on racial, social, and socioeconomic contributors to health care disparities among children with acute lymphoblastic leukemia (ALL; abstract 211) and on clinical trial enrollment characteristics and outcomes for Black and Hispanic adolescents and young adults with ALL (abstract 337).
Immunotherapy advances
Some of the most eagerly awaited abstracts will be highlighting advances in immunotherapy for hematologic malignancies, and these were previewed by Cynthia E. Dunbar, MD, ASH secretary and chief of the Translational Stem Cell Biology Branch within the Intramural Research Program of the National Heart, Lung, and Blood Institute in Bethesda, Md.
These abstracts include the primary analysis of the ZUMA-7 trial, a randomized, phase 3 study comparing the chimeric antigen receptor T-cell (CAR T) construct axicabtagene ciloleucel (axi-cel; Yescarta) with standard of care in patients with relapsed or refractory large B-cell lymphomas (LBCLs; abstract 2) and the interim analysis of the randomized, phase 3 Transform Study comparing the CAR T construct lisocabtagene maralecleucl (liso-cel; Breyanzi) with salvage chemotherapy in patients with relapsed/refractory LBCL (abstract 91).
“Over 500 patients were enrolled in the two studies, and both abstracts report significantly longer survival without relapse in the CAR T arm – for instance, fourfold higher in ZUMA-7, compared to standard of care,” Dr. Dunbar said at the briefing.
“These abstracts provide really critical information to patients, their treating physicians, and the payers who are trying to decide whether use of these expensive, complex, and potentially toxic CAR T-cell therapies are justified, compared to standard therapy,” she said.
Dr. Dunbar also highlighted an abstract on the addition of the anti-CD38 monoclonal antibody isatuximab (Sarclisa) to lenalidomide, bortezomib, and dexamethasone as induction therapy for patients with newly diagnosed multiple myeloma who are eligible for stem cell transplantation (abstract 463).
“The authors report that patients on the isatuximab arm had significantly fewer tumor cells following treatment,” Dr. Dunbar said. “We have come a long way beyond treating myeloma with a single drug, with remissions now measured in many years instead of 1 or 2 following initiation of treatment, and this abstract is another demonstration that novel combinations of multiple agents are really making a difference in this very debilitating disease.”
She also cited an abstract (abstract 127) on monotherapy with the novel bispecific T-cell–engaging monoclonal antibody mosunetuzumab for treatment of patients with follicular lymphoma that has relapsed or is refractory to at least two prior lines of therapy.
Old disorders, new insights
Other abstracts highlighted at the premeeting press briefing included a study that found a high prevalence of monoclonal gammopathy in persons at risk for multiple myeloma (abstract 152) and another with the surprising finding that clonal hematopoiesis, a risk factor myeloid malignancies, may be protective against Alzheimer’s disease (abstract 5).
In addition, a long-term follow-up study of patients with transfusion-dependent beta-thalassemia treated with gene therapy showed that some patients have become transfusion independent and iron homeostasis was restored (abstract 573).
Presentations from CDC and FDA
Dr. Sekeres highlighted other events of interest scheduled for ASH 2021, including a Grassroots Network Lunch featuring a discussion with Rochelle Walensky, MD, MPH, director of the Centers for Disease Control and Prevention in Atlanta, and a joint symposium between ASH and the Food and Drug Administration on newly approved drugs in hematology.
Dr. Sekeres has disclosed consulting/advising for Novartis, Takea/Millennium, and Bristol-Myers Squibb. Dr. Dunbar reported no relevant conflicts of interest. Dr. Tallman disclosed consulting/advising with and research funding from multiple entities.
A version of this article first appeared on Medscape.com.
Residency programs readjust during COVID
Hospitalist-honed agility proves invaluable
It could be argued that hospital medicine in the United States was made vital by a major infectious disease epidemic – the HIV/AIDS crisis – said Emily Gottenborg, MD, a hospitalist and program director of hospitalist training at the University of Colorado at Denver, Aurora. Certainly, it was born out of the need for change, for physicians who could coordinate complex patient care plans and serve as the “quarterbacks” of the hospital. “As a result, we have always been very nimble and ready to embrace change,” said Dr. Gottenborg.

That hospitalist-honed agility and penchant for innovation has proven to be invaluable during the current COVID-19 pandemic as hospital medicine–focused residency programs have been forced to pivot quickly and modify their agendas. From managing the pandemic’s impact on residents’ day-to-day experiences, to carefully balancing educational needs and goals, program leaders have worked tirelessly to ensure that residents continue to receive excellent training.
The overarching theme across U.S.-based residency programs is that the educational changes and challenges during the COVID-19 pandemic have often been one and the same.
Service versus education
At the beginning of the pandemic, trainees at the University of Pittsburgh Medical Center were limited in seeing COVID patients in order to curb exposure. But now that COVID appears to be the new normal, “I think the question becomes: ‘How do we incorporate our trainees to take care of COVID patients since it seems it will be staying around for a while?’ ” said Rachna Rawal, MD, a hospitalist and clinical assistant professor of medicine at UPMC.
This dilemma highlights the conflict between service and education. Residents have been motivated and eager to help, which has been beneficial whenever there is a surge. “At the same time, you want to preserve their education, and it’s a very difficult balance at times,” said Dr. Rawal. It’s also challenging to figure out the safest way for residents to see patients, as well as how to include medical students, since interns and residents serve as important educational resources for them.
Keeping trainees involved with daily virtual conferences rather than in-person interactions raises the question of whether or not the engagement is equivalent. “It’s harder to keep them accountable when they’re not in person, but it’s also not worth the risk given the COVID numbers at times,” Dr. Rawal said. The goal has become to make sure residents stay safe while still feeling that they are getting a good education.
A balancing act
“I think early on, there was a lot of pride in what we were doing, that we were on the front line managing this thing that was emerging,” said Daniel Ricotta, MD, a hospitalist and associate program director of the internal medicine residency at Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, both in Boston. “And now I think people are starting to feel a little bit weary.”

It has been demanding trying to manage ongoing educational needs through this time. “At the end of the day, residents are still trainees and have to be trained and educated. They’re not just worker bees taking care of patients,” Dr. Ricotta said. Residents need a well-rounded clinical experience – “they can’t just take care of COVID patients and then be able to graduate as general internists,” he said – but that becomes onerous when the hospital is full of patients with COVID.
Along with balancing residents’ clinical immersion, Dr. Ricotta said there has been the challenge of doing “the content-based teaching from didactics that occur in the context of clinical work, but are somewhat separated when you need to limit the number of people in the rooms and try to keep as many people at home as possible when they’re not taking care of patients in order to limit their level of risk.” Adjusting and readjusting both of these aspects has had a major impact on residents’ day-to-day education.
“A big part of residency is community,” noted Dr. Ricotta, but the sense of community has been disrupted because some of the bonding experiences residents used to do outside the hospital to build that community have necessarily gone by the wayside. This particularly affects interns from around the country who are meeting each other for the first time. “We actually had a normal intern orientation this year, but last year, when everything was virtual, we were trying to find ways to bridge relationships in a way that was safe and socially distanced,” he said.
Improving quality
UC Denver is unique in that they have a 3-year program specifically for hospital medicine residents, said Dr. Gottenborg. Right away, “our residents rose to the challenge and wanted to be part of the workforce that helps care for this critical population of [COVID] patients.” The residents were able to run the ICUs and take care of COVID patients, but in exchange, they had to give up some of their elective rotation time.
One aspect of the UC Denver hospital medicine residency program is participation in projects that focus on how to improve the health care system. Over the past year, the residents worked on one project in particular that focused on restructuring the guidelines for consulting physical therapists. Since many patients end up needing a physical therapist for a variety of reasons, a full hospital puts increased strain on their workload, making their time more precious.
“[The project] forced us to think about the right criteria to consult them,” explained Dr. Gottenborg. “We cut down essentially all the inappropriate consults to PT, opening their time. That project was driven by how the residents were experiencing the pandemic in the hospital.”
Learning to adapt
“The training environment during this pandemic has been tumultuous for both our residents and medical students,” said Alan M. Hall, MD, associate professor of internal medicine and pediatrics and assistant dean of curriculum integration at the University of Kentucky, Lexington. Along with treating patients with COVID-19, he said trainees have also had to cope with anxiety about getting the virus themselves or inadvertently bringing it home to their families.

Like most medical schools, University of Kentucky students were shifted away from clinical rotations and into alternative and online education for a time. When they returned to in-person education, the students were initially restricted from seeing patients with confirmed or suspected COVID-19 in order to reduce their personal risk and to conserve personal protective equipment.
This especially impacted certain rotations, such as pediatrics. Because respiratory symptoms are common in this population, students were greatly limited in the number of new patients they could see. Now they are given the option to see patients with COVID-19 if they want to.
“Our residents have had to adapt to seemingly endless changes during this pandemic,” Dr. Hall said. For example, at the beginning of the surge, the internal medicine residents trained for a completely new clinical model, though this ultimately never needed to be implemented. Then they had to adjust to extremely high census numbers that continue to have an effect on almost all of their rotations.
Conversely, the pediatrics residents saw far fewer inpatients last winter than they typically would. This made it more difficult for them to feel comfortable when census numbers increased with common diagnoses like bronchiolitis. “However, those respiratory viruses that were hibernating last winter caused an unusual and challenging summer surge,” Dr. Hall said.
The biggest challenge though “is knowing that there is not a perfect solution for this global pandemic’s effect on medical education,” said Dr. Hall. “We can’t possibly perfectly balance the safety of our learners and their families with the dangers of COVID-19.”
Leadership discussions
As a residency program leader, Dr. Ricotta said there are conversations about multiple topics, including maintaining a safe learning environment; providing important aspects of residency training; whether to go back to full in-person teaching, keep doing virtual teaching, or implement a hybrid model; and how to help residents understand the balance between their personal and professional lives, especially in terms of safety.
“They have to their lives outside of the hospital, but we also are trying to instill ... what their responsibility is to society, to their patients, and to each other,” said Dr. Ricotta.
A more recent discussion has been about how to manage the COVID vaccine boosters. “We can’t have everyone getting vaccines at the same time because they might have symptoms afterward, and then be out sick – you’re missing half your workforce,” Dr. Ricotta said. But staggering residents’ booster shots created yet another dilemma around deciding who received the booster sooner rather than later.
The biggest consideration for Dr. Gottenborg’s leadership team was deciding whether to use their residents to help with the COVID surges or keep them in a traditional residency experience. While the residents wanted to be part of the pandemic response, there were many factors to consider. Ultimately, they came up with a balance between the amount of time residents should spend taking care of COVID patients while also assuring that they leave the program with all the skills and experiences they need.
Though Dr. Hall works more closely with medical students than residents, he sees the challenges and effects as being similar. Creating harmony between a safe learning environment and students’ educational goals has been the topic of endless discussions. This includes decisions as to whether or not students should be involved in person in certain activities such as large classroom didactics, written exams, seeing patients in clinical settings, and small group discussions.
Recruitment effects
When it comes to recruiting during a global pandemic, the experiences and predictions are mixed. Dr. Hall believes virtual interviews are making recruitment easier, but in turn, the fact that they are virtual also makes it harder for the applicant to get a good feel for the program and the people involved in it.
Dr. Ricotta reported that recruitment numbers have been fairly steady at Beth Israel Deaconess over the last few years. “In addition to the critical care physicians, hospital medicine was really the front line of this pandemic and so in some ways, we gained some recognition that we may not have had otherwise,” said Dr. Ricotta. He believes this has the benefit of attracting some residents, but at the same time, it could potentially scare others away from what they perceive as a demanding, grueling job. “I think it has been mixed. It’s dependent on the person.”
At UC Denver, Dr. Gottenborg said they are seeing a rapid rise in the number of applications and interest in their programs. Still, “I think this could go both ways,” she acknowledged. With the focus on hospital medicine in the media, medical students are more aware of the specialty and what it involves. “I think the sense of mission is really exemplified and everyone is talking about it,” she said. This is evident in the arrival this summer of the first new class of interns since the pandemic. “They’re incredibly passionate about the work,” said Dr. Gottenborg.
However, there is also the notable increase in physician burnout since the pandemic started. That this has been regularly featured in the media leaves Dr. Gottenborg to wonder if prospective residents will shy away from hospital medicine because they believe it is an area that leads to burnout. “I hope that’s not the case,” she said.
“I would actually argue [recruitment] is easier,” said Dr. Rawal. Like Dr. Hall, she sees virtual interviews as a big benefit to prospective trainees because they don’t have to spend a large amount of money on travel, food, and other expenses like they did before, a welcome relief for residents with significant debt. “I think that is one very big positive from the pandemic,” she said. Her trainees were advised to make a final list and consider going to see the top two or three in person, but “at this point, there’s really no expectation to go see all 15 places that you look into.”
Dr. Rawal also pointed out that recruitment is affected by whether or not trainees are expected to see COVID patients. “I know in some places they aren’t and in some places they are, so it just depends on where you are and what you’re looking for,” she said.
Shifts in education
It remains to be seen if all the educational changes will be permanent, though it appears that many will remain. Dr. Hall hopes that virtual visits to provide care to patients who have difficulty getting to physical clinics will continue to be a focus for hospital medicine trainees. “For medical students, I think this will allow us to better assess what content can best be delivered in person, synchronously online, or asynchronously through recorded content,” he said.
Dr. Ricotta predicts that virtual conferences will become more pervasive as academic hospitals continue to acquire more community hospitals, especially for grand rounds. “The virtual teaching that occurred in the residency program because it’s required by the [Accreditation Council for Graduate Medical Education] has, I think, informed how academic centers do ongoing faculty development, professional development, and obviously education for the residents,” Dr. Ricotta said. “I think virtual teaching is here to stay.” This includes telehealth training, which had not been a widespread part of residency education before now.
Trainees have been given tools to handle high patient censuses and learned a whole new set of communication skills, thanks to the pandemic, said Dr. Rawal. There has been a focus on learning how to advocate for the vaccine, along with education on situations like how to have conversations with patients who don’t believe they have COVID, even when their tests are positive. “Learning to handle these situations and still be a physician and provide appropriate care regardless of the patient’s views is very important. This is not something I learned in my training because it never came up,” she said.
Dr. Gottenborg has been impressed by the resident workforce’s response across all specialties throughout these difficult days. “They were universally ready to dive in and work long hours and care for these very sick patients and ultimately share their experiences so that we could do it better as these patients continue to flow through our systems,” she said. “It has been very invigorating.”
The pandemic has also put a spotlight on the importance of being flexible, as well as various problems with how health care systems operate, “which, for people in our field, gets us both excited and gives us a lot of work to do,” said Dr. Gottenborg. “Our residents see that and feel that and will hopefully continue to hold that torch in hospital medicine.”
In spite of everything, Dr. Rawal believes this is an exhilarating time to be a trainee. “They’re getting an opportunity that none of us got. Usually, when policies are made, we really don’t see the immediate impact.” But with recent mandates like masks and social distancing, “the rate of change that they get to see things happen is exciting. They’re going to be a very exciting group of physicians.”
Hospitalist-honed agility proves invaluable
Hospitalist-honed agility proves invaluable
It could be argued that hospital medicine in the United States was made vital by a major infectious disease epidemic – the HIV/AIDS crisis – said Emily Gottenborg, MD, a hospitalist and program director of hospitalist training at the University of Colorado at Denver, Aurora. Certainly, it was born out of the need for change, for physicians who could coordinate complex patient care plans and serve as the “quarterbacks” of the hospital. “As a result, we have always been very nimble and ready to embrace change,” said Dr. Gottenborg.
That hospitalist-honed agility and penchant for innovation has proven to be invaluable during the current COVID-19 pandemic as hospital medicine–focused residency programs have been forced to pivot quickly and modify their agendas. From managing the pandemic’s impact on residents’ day-to-day experiences, to carefully balancing educational needs and goals, program leaders have worked tirelessly to ensure that residents continue to receive excellent training.
The overarching theme across U.S.-based residency programs is that the educational changes and challenges during the COVID-19 pandemic have often been one and the same.
Service versus education
At the beginning of the pandemic, trainees at the University of Pittsburgh Medical Center were limited in seeing COVID patients in order to curb exposure. But now that COVID appears to be the new normal, “I think the question becomes: ‘How do we incorporate our trainees to take care of COVID patients since it seems it will be staying around for a while?’ ” said Rachna Rawal, MD, a hospitalist and clinical assistant professor of medicine at UPMC.
This dilemma highlights the conflict between service and education. Residents have been motivated and eager to help, which has been beneficial whenever there is a surge. “At the same time, you want to preserve their education, and it’s a very difficult balance at times,” said Dr. Rawal. It’s also challenging to figure out the safest way for residents to see patients, as well as how to include medical students, since interns and residents serve as important educational resources for them.
Keeping trainees involved with daily virtual conferences rather than in-person interactions raises the question of whether or not the engagement is equivalent. “It’s harder to keep them accountable when they’re not in person, but it’s also not worth the risk given the COVID numbers at times,” Dr. Rawal said. The goal has become to make sure residents stay safe while still feeling that they are getting a good education.
A balancing act
“I think early on, there was a lot of pride in what we were doing, that we were on the front line managing this thing that was emerging,” said Daniel Ricotta, MD, a hospitalist and associate program director of the internal medicine residency at Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, both in Boston. “And now I think people are starting to feel a little bit weary.”
It has been demanding trying to manage ongoing educational needs through this time. “At the end of the day, residents are still trainees and have to be trained and educated. They’re not just worker bees taking care of patients,” Dr. Ricotta said. Residents need a well-rounded clinical experience – “they can’t just take care of COVID patients and then be able to graduate as general internists,” he said – but that becomes onerous when the hospital is full of patients with COVID.
Along with balancing residents’ clinical immersion, Dr. Ricotta said there has been the challenge of doing “the content-based teaching from didactics that occur in the context of clinical work, but are somewhat separated when you need to limit the number of people in the rooms and try to keep as many people at home as possible when they’re not taking care of patients in order to limit their level of risk.” Adjusting and readjusting both of these aspects has had a major impact on residents’ day-to-day education.
“A big part of residency is community,” noted Dr. Ricotta, but the sense of community has been disrupted because some of the bonding experiences residents used to do outside the hospital to build that community have necessarily gone by the wayside. This particularly affects interns from around the country who are meeting each other for the first time. “We actually had a normal intern orientation this year, but last year, when everything was virtual, we were trying to find ways to bridge relationships in a way that was safe and socially distanced,” he said.
Improving quality
UC Denver is unique in that they have a 3-year program specifically for hospital medicine residents, said Dr. Gottenborg. Right away, “our residents rose to the challenge and wanted to be part of the workforce that helps care for this critical population of [COVID] patients.” The residents were able to run the ICUs and take care of COVID patients, but in exchange, they had to give up some of their elective rotation time.
One aspect of the UC Denver hospital medicine residency program is participation in projects that focus on how to improve the health care system. Over the past year, the residents worked on one project in particular that focused on restructuring the guidelines for consulting physical therapists. Since many patients end up needing a physical therapist for a variety of reasons, a full hospital puts increased strain on their workload, making their time more precious.
“[The project] forced us to think about the right criteria to consult them,” explained Dr. Gottenborg. “We cut down essentially all the inappropriate consults to PT, opening their time. That project was driven by how the residents were experiencing the pandemic in the hospital.”
Learning to adapt
“The training environment during this pandemic has been tumultuous for both our residents and medical students,” said Alan M. Hall, MD, associate professor of internal medicine and pediatrics and assistant dean of curriculum integration at the University of Kentucky, Lexington. Along with treating patients with COVID-19, he said trainees have also had to cope with anxiety about getting the virus themselves or inadvertently bringing it home to their families.
Like most medical schools, University of Kentucky students were shifted away from clinical rotations and into alternative and online education for a time. When they returned to in-person education, the students were initially restricted from seeing patients with confirmed or suspected COVID-19 in order to reduce their personal risk and to conserve personal protective equipment.
This especially impacted certain rotations, such as pediatrics. Because respiratory symptoms are common in this population, students were greatly limited in the number of new patients they could see. Now they are given the option to see patients with COVID-19 if they want to.
“Our residents have had to adapt to seemingly endless changes during this pandemic,” Dr. Hall said. For example, at the beginning of the surge, the internal medicine residents trained for a completely new clinical model, though this ultimately never needed to be implemented. Then they had to adjust to extremely high census numbers that continue to have an effect on almost all of their rotations.
Conversely, the pediatrics residents saw far fewer inpatients last winter than they typically would. This made it more difficult for them to feel comfortable when census numbers increased with common diagnoses like bronchiolitis. “However, those respiratory viruses that were hibernating last winter caused an unusual and challenging summer surge,” Dr. Hall said.
The biggest challenge though “is knowing that there is not a perfect solution for this global pandemic’s effect on medical education,” said Dr. Hall. “We can’t possibly perfectly balance the safety of our learners and their families with the dangers of COVID-19.”
Leadership discussions
As a residency program leader, Dr. Ricotta said there are conversations about multiple topics, including maintaining a safe learning environment; providing important aspects of residency training; whether to go back to full in-person teaching, keep doing virtual teaching, or implement a hybrid model; and how to help residents understand the balance between their personal and professional lives, especially in terms of safety.
“They have to their lives outside of the hospital, but we also are trying to instill ... what their responsibility is to society, to their patients, and to each other,” said Dr. Ricotta.
A more recent discussion has been about how to manage the COVID vaccine boosters. “We can’t have everyone getting vaccines at the same time because they might have symptoms afterward, and then be out sick – you’re missing half your workforce,” Dr. Ricotta said. But staggering residents’ booster shots created yet another dilemma around deciding who received the booster sooner rather than later.
The biggest consideration for Dr. Gottenborg’s leadership team was deciding whether to use their residents to help with the COVID surges or keep them in a traditional residency experience. While the residents wanted to be part of the pandemic response, there were many factors to consider. Ultimately, they came up with a balance between the amount of time residents should spend taking care of COVID patients while also assuring that they leave the program with all the skills and experiences they need.
Though Dr. Hall works more closely with medical students than residents, he sees the challenges and effects as being similar. Creating harmony between a safe learning environment and students’ educational goals has been the topic of endless discussions. This includes decisions as to whether or not students should be involved in person in certain activities such as large classroom didactics, written exams, seeing patients in clinical settings, and small group discussions.
Recruitment effects
When it comes to recruiting during a global pandemic, the experiences and predictions are mixed. Dr. Hall believes virtual interviews are making recruitment easier, but in turn, the fact that they are virtual also makes it harder for the applicant to get a good feel for the program and the people involved in it.
Dr. Ricotta reported that recruitment numbers have been fairly steady at Beth Israel Deaconess over the last few years. “In addition to the critical care physicians, hospital medicine was really the front line of this pandemic and so in some ways, we gained some recognition that we may not have had otherwise,” said Dr. Ricotta. He believes this has the benefit of attracting some residents, but at the same time, it could potentially scare others away from what they perceive as a demanding, grueling job. “I think it has been mixed. It’s dependent on the person.”
At UC Denver, Dr. Gottenborg said they are seeing a rapid rise in the number of applications and interest in their programs. Still, “I think this could go both ways,” she acknowledged. With the focus on hospital medicine in the media, medical students are more aware of the specialty and what it involves. “I think the sense of mission is really exemplified and everyone is talking about it,” she said. This is evident in the arrival this summer of the first new class of interns since the pandemic. “They’re incredibly passionate about the work,” said Dr. Gottenborg.
However, there is also the notable increase in physician burnout since the pandemic started. That this has been regularly featured in the media leaves Dr. Gottenborg to wonder if prospective residents will shy away from hospital medicine because they believe it is an area that leads to burnout. “I hope that’s not the case,” she said.
“I would actually argue [recruitment] is easier,” said Dr. Rawal. Like Dr. Hall, she sees virtual interviews as a big benefit to prospective trainees because they don’t have to spend a large amount of money on travel, food, and other expenses like they did before, a welcome relief for residents with significant debt. “I think that is one very big positive from the pandemic,” she said. Her trainees were advised to make a final list and consider going to see the top two or three in person, but “at this point, there’s really no expectation to go see all 15 places that you look into.”
Dr. Rawal also pointed out that recruitment is affected by whether or not trainees are expected to see COVID patients. “I know in some places they aren’t and in some places they are, so it just depends on where you are and what you’re looking for,” she said.
Shifts in education
It remains to be seen if all the educational changes will be permanent, though it appears that many will remain. Dr. Hall hopes that virtual visits to provide care to patients who have difficulty getting to physical clinics will continue to be a focus for hospital medicine trainees. “For medical students, I think this will allow us to better assess what content can best be delivered in person, synchronously online, or asynchronously through recorded content,” he said.
Dr. Ricotta predicts that virtual conferences will become more pervasive as academic hospitals continue to acquire more community hospitals, especially for grand rounds. “The virtual teaching that occurred in the residency program because it’s required by the [Accreditation Council for Graduate Medical Education] has, I think, informed how academic centers do ongoing faculty development, professional development, and obviously education for the residents,” Dr. Ricotta said. “I think virtual teaching is here to stay.” This includes telehealth training, which had not been a widespread part of residency education before now.
Trainees have been given tools to handle high patient censuses and learned a whole new set of communication skills, thanks to the pandemic, said Dr. Rawal. There has been a focus on learning how to advocate for the vaccine, along with education on situations like how to have conversations with patients who don’t believe they have COVID, even when their tests are positive. “Learning to handle these situations and still be a physician and provide appropriate care regardless of the patient’s views is very important. This is not something I learned in my training because it never came up,” she said.
Dr. Gottenborg has been impressed by the resident workforce’s response across all specialties throughout these difficult days. “They were universally ready to dive in and work long hours and care for these very sick patients and ultimately share their experiences so that we could do it better as these patients continue to flow through our systems,” she said. “It has been very invigorating.”
The pandemic has also put a spotlight on the importance of being flexible, as well as various problems with how health care systems operate, “which, for people in our field, gets us both excited and gives us a lot of work to do,” said Dr. Gottenborg. “Our residents see that and feel that and will hopefully continue to hold that torch in hospital medicine.”
In spite of everything, Dr. Rawal believes this is an exhilarating time to be a trainee. “They’re getting an opportunity that none of us got. Usually, when policies are made, we really don’t see the immediate impact.” But with recent mandates like masks and social distancing, “the rate of change that they get to see things happen is exciting. They’re going to be a very exciting group of physicians.”
It could be argued that hospital medicine in the United States was made vital by a major infectious disease epidemic – the HIV/AIDS crisis – said Emily Gottenborg, MD, a hospitalist and program director of hospitalist training at the University of Colorado at Denver, Aurora. Certainly, it was born out of the need for change, for physicians who could coordinate complex patient care plans and serve as the “quarterbacks” of the hospital. “As a result, we have always been very nimble and ready to embrace change,” said Dr. Gottenborg.
That hospitalist-honed agility and penchant for innovation has proven to be invaluable during the current COVID-19 pandemic as hospital medicine–focused residency programs have been forced to pivot quickly and modify their agendas. From managing the pandemic’s impact on residents’ day-to-day experiences, to carefully balancing educational needs and goals, program leaders have worked tirelessly to ensure that residents continue to receive excellent training.
The overarching theme across U.S.-based residency programs is that the educational changes and challenges during the COVID-19 pandemic have often been one and the same.
Service versus education
At the beginning of the pandemic, trainees at the University of Pittsburgh Medical Center were limited in seeing COVID patients in order to curb exposure. But now that COVID appears to be the new normal, “I think the question becomes: ‘How do we incorporate our trainees to take care of COVID patients since it seems it will be staying around for a while?’ ” said Rachna Rawal, MD, a hospitalist and clinical assistant professor of medicine at UPMC.
This dilemma highlights the conflict between service and education. Residents have been motivated and eager to help, which has been beneficial whenever there is a surge. “At the same time, you want to preserve their education, and it’s a very difficult balance at times,” said Dr. Rawal. It’s also challenging to figure out the safest way for residents to see patients, as well as how to include medical students, since interns and residents serve as important educational resources for them.
Keeping trainees involved with daily virtual conferences rather than in-person interactions raises the question of whether or not the engagement is equivalent. “It’s harder to keep them accountable when they’re not in person, but it’s also not worth the risk given the COVID numbers at times,” Dr. Rawal said. The goal has become to make sure residents stay safe while still feeling that they are getting a good education.
A balancing act
“I think early on, there was a lot of pride in what we were doing, that we were on the front line managing this thing that was emerging,” said Daniel Ricotta, MD, a hospitalist and associate program director of the internal medicine residency at Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, both in Boston. “And now I think people are starting to feel a little bit weary.”
It has been demanding trying to manage ongoing educational needs through this time. “At the end of the day, residents are still trainees and have to be trained and educated. They’re not just worker bees taking care of patients,” Dr. Ricotta said. Residents need a well-rounded clinical experience – “they can’t just take care of COVID patients and then be able to graduate as general internists,” he said – but that becomes onerous when the hospital is full of patients with COVID.
Along with balancing residents’ clinical immersion, Dr. Ricotta said there has been the challenge of doing “the content-based teaching from didactics that occur in the context of clinical work, but are somewhat separated when you need to limit the number of people in the rooms and try to keep as many people at home as possible when they’re not taking care of patients in order to limit their level of risk.” Adjusting and readjusting both of these aspects has had a major impact on residents’ day-to-day education.
“A big part of residency is community,” noted Dr. Ricotta, but the sense of community has been disrupted because some of the bonding experiences residents used to do outside the hospital to build that community have necessarily gone by the wayside. This particularly affects interns from around the country who are meeting each other for the first time. “We actually had a normal intern orientation this year, but last year, when everything was virtual, we were trying to find ways to bridge relationships in a way that was safe and socially distanced,” he said.
Improving quality
UC Denver is unique in that they have a 3-year program specifically for hospital medicine residents, said Dr. Gottenborg. Right away, “our residents rose to the challenge and wanted to be part of the workforce that helps care for this critical population of [COVID] patients.” The residents were able to run the ICUs and take care of COVID patients, but in exchange, they had to give up some of their elective rotation time.
One aspect of the UC Denver hospital medicine residency program is participation in projects that focus on how to improve the health care system. Over the past year, the residents worked on one project in particular that focused on restructuring the guidelines for consulting physical therapists. Since many patients end up needing a physical therapist for a variety of reasons, a full hospital puts increased strain on their workload, making their time more precious.
“[The project] forced us to think about the right criteria to consult them,” explained Dr. Gottenborg. “We cut down essentially all the inappropriate consults to PT, opening their time. That project was driven by how the residents were experiencing the pandemic in the hospital.”
Learning to adapt
“The training environment during this pandemic has been tumultuous for both our residents and medical students,” said Alan M. Hall, MD, associate professor of internal medicine and pediatrics and assistant dean of curriculum integration at the University of Kentucky, Lexington. Along with treating patients with COVID-19, he said trainees have also had to cope with anxiety about getting the virus themselves or inadvertently bringing it home to their families.
Like most medical schools, University of Kentucky students were shifted away from clinical rotations and into alternative and online education for a time. When they returned to in-person education, the students were initially restricted from seeing patients with confirmed or suspected COVID-19 in order to reduce their personal risk and to conserve personal protective equipment.
This especially impacted certain rotations, such as pediatrics. Because respiratory symptoms are common in this population, students were greatly limited in the number of new patients they could see. Now they are given the option to see patients with COVID-19 if they want to.
“Our residents have had to adapt to seemingly endless changes during this pandemic,” Dr. Hall said. For example, at the beginning of the surge, the internal medicine residents trained for a completely new clinical model, though this ultimately never needed to be implemented. Then they had to adjust to extremely high census numbers that continue to have an effect on almost all of their rotations.
Conversely, the pediatrics residents saw far fewer inpatients last winter than they typically would. This made it more difficult for them to feel comfortable when census numbers increased with common diagnoses like bronchiolitis. “However, those respiratory viruses that were hibernating last winter caused an unusual and challenging summer surge,” Dr. Hall said.
The biggest challenge though “is knowing that there is not a perfect solution for this global pandemic’s effect on medical education,” said Dr. Hall. “We can’t possibly perfectly balance the safety of our learners and their families with the dangers of COVID-19.”
Leadership discussions
As a residency program leader, Dr. Ricotta said there are conversations about multiple topics, including maintaining a safe learning environment; providing important aspects of residency training; whether to go back to full in-person teaching, keep doing virtual teaching, or implement a hybrid model; and how to help residents understand the balance between their personal and professional lives, especially in terms of safety.
“They have to their lives outside of the hospital, but we also are trying to instill ... what their responsibility is to society, to their patients, and to each other,” said Dr. Ricotta.
A more recent discussion has been about how to manage the COVID vaccine boosters. “We can’t have everyone getting vaccines at the same time because they might have symptoms afterward, and then be out sick – you’re missing half your workforce,” Dr. Ricotta said. But staggering residents’ booster shots created yet another dilemma around deciding who received the booster sooner rather than later.
The biggest consideration for Dr. Gottenborg’s leadership team was deciding whether to use their residents to help with the COVID surges or keep them in a traditional residency experience. While the residents wanted to be part of the pandemic response, there were many factors to consider. Ultimately, they came up with a balance between the amount of time residents should spend taking care of COVID patients while also assuring that they leave the program with all the skills and experiences they need.
Though Dr. Hall works more closely with medical students than residents, he sees the challenges and effects as being similar. Creating harmony between a safe learning environment and students’ educational goals has been the topic of endless discussions. This includes decisions as to whether or not students should be involved in person in certain activities such as large classroom didactics, written exams, seeing patients in clinical settings, and small group discussions.
Recruitment effects
When it comes to recruiting during a global pandemic, the experiences and predictions are mixed. Dr. Hall believes virtual interviews are making recruitment easier, but in turn, the fact that they are virtual also makes it harder for the applicant to get a good feel for the program and the people involved in it.
Dr. Ricotta reported that recruitment numbers have been fairly steady at Beth Israel Deaconess over the last few years. “In addition to the critical care physicians, hospital medicine was really the front line of this pandemic and so in some ways, we gained some recognition that we may not have had otherwise,” said Dr. Ricotta. He believes this has the benefit of attracting some residents, but at the same time, it could potentially scare others away from what they perceive as a demanding, grueling job. “I think it has been mixed. It’s dependent on the person.”
At UC Denver, Dr. Gottenborg said they are seeing a rapid rise in the number of applications and interest in their programs. Still, “I think this could go both ways,” she acknowledged. With the focus on hospital medicine in the media, medical students are more aware of the specialty and what it involves. “I think the sense of mission is really exemplified and everyone is talking about it,” she said. This is evident in the arrival this summer of the first new class of interns since the pandemic. “They’re incredibly passionate about the work,” said Dr. Gottenborg.
However, there is also the notable increase in physician burnout since the pandemic started. That this has been regularly featured in the media leaves Dr. Gottenborg to wonder if prospective residents will shy away from hospital medicine because they believe it is an area that leads to burnout. “I hope that’s not the case,” she said.
“I would actually argue [recruitment] is easier,” said Dr. Rawal. Like Dr. Hall, she sees virtual interviews as a big benefit to prospective trainees because they don’t have to spend a large amount of money on travel, food, and other expenses like they did before, a welcome relief for residents with significant debt. “I think that is one very big positive from the pandemic,” she said. Her trainees were advised to make a final list and consider going to see the top two or three in person, but “at this point, there’s really no expectation to go see all 15 places that you look into.”
Dr. Rawal also pointed out that recruitment is affected by whether or not trainees are expected to see COVID patients. “I know in some places they aren’t and in some places they are, so it just depends on where you are and what you’re looking for,” she said.
Shifts in education
It remains to be seen if all the educational changes will be permanent, though it appears that many will remain. Dr. Hall hopes that virtual visits to provide care to patients who have difficulty getting to physical clinics will continue to be a focus for hospital medicine trainees. “For medical students, I think this will allow us to better assess what content can best be delivered in person, synchronously online, or asynchronously through recorded content,” he said.
Dr. Ricotta predicts that virtual conferences will become more pervasive as academic hospitals continue to acquire more community hospitals, especially for grand rounds. “The virtual teaching that occurred in the residency program because it’s required by the [Accreditation Council for Graduate Medical Education] has, I think, informed how academic centers do ongoing faculty development, professional development, and obviously education for the residents,” Dr. Ricotta said. “I think virtual teaching is here to stay.” This includes telehealth training, which had not been a widespread part of residency education before now.
Trainees have been given tools to handle high patient censuses and learned a whole new set of communication skills, thanks to the pandemic, said Dr. Rawal. There has been a focus on learning how to advocate for the vaccine, along with education on situations like how to have conversations with patients who don’t believe they have COVID, even when their tests are positive. “Learning to handle these situations and still be a physician and provide appropriate care regardless of the patient’s views is very important. This is not something I learned in my training because it never came up,” she said.
Dr. Gottenborg has been impressed by the resident workforce’s response across all specialties throughout these difficult days. “They were universally ready to dive in and work long hours and care for these very sick patients and ultimately share their experiences so that we could do it better as these patients continue to flow through our systems,” she said. “It has been very invigorating.”
The pandemic has also put a spotlight on the importance of being flexible, as well as various problems with how health care systems operate, “which, for people in our field, gets us both excited and gives us a lot of work to do,” said Dr. Gottenborg. “Our residents see that and feel that and will hopefully continue to hold that torch in hospital medicine.”
In spite of everything, Dr. Rawal believes this is an exhilarating time to be a trainee. “They’re getting an opportunity that none of us got. Usually, when policies are made, we really don’t see the immediate impact.” But with recent mandates like masks and social distancing, “the rate of change that they get to see things happen is exciting. They’re going to be a very exciting group of physicians.”
Misinterpretation is a science, not an art
It isn’t autocorrect’s fault this time, we swear
We’ve come a long way with communication technology. Back in the day, when Gondor needed to call for aid, they had to pull off the greatest signal fire montage of all time. Now we can send each other texts back and forth in an instant. (“Hey Theoden, send army, need help pls” doesn’t quite have the same gravitas though.) The question is, how do our brains keep up with such rapidly advancing technology?

Er, they don’t. Not really. Instead, our brains create shortcuts called “good-enough language processing,” which is exactly what it sounds like.
Psychologists and psycholinguists have been studying misinterpretations such as good-enough language processing since the 1970s. Recently, however, psycholinguists from the Centre for Language and Brain at Higher School of Economics in Moscow have found that, when it comes to reading comprehension over text, older adults are using their knowledge of the world over how it’s grammatically formed in the sentence.
In the study, 349 people were asked to read and interpret four sentences, the third of which (translated from Russian) was: “Misha met the firefighter’s dentist, who had put out a fire in the warehouse.” When asked who put the fire out, 79% of older adults (aged 55 years and older), utilizing good-enough language processing, said the firefighter put out the fire. You probably glossed over that sentence and assumed the same thing. But this time, the dentist was the real hero.
That said, adolescents (aged 13-17) and young adults (aged 20-30) weren’t much better, and got that particular sentence wrong 63%-68% of the time. According to the researchers, good-enough language processing forms in adolescence and intensifies throughout adulthood.
Moral of the story? We should utilize signal fires more often. Less room for misinterpretation. When the beacons of Minas Tirith were lit, Rohan answered.
Singing … your … lungs … out
There’s nothing quite like a karaoke bar to unleash your inner rock star. Hey, why not just go for it, everyone is just as bad at singing as you. That’s part of the fun.

A 25-year-old man named Wang Zhe may have taken the karaoke concept a bit too far, however. While out with friends at a birthday party, Mr. Zhe let loose on a song with a particularly large number of high notes. He tried his best, gamely attacking the song until he felt a pain in his chest. He didn’t think much of it, although he did cut his performance short, but then he awoke the next morning unable to breathe properly.
After a trip to the hospital, he explained the sequence of events to the doctors, and an x-ray found that the culprit of the pain and difficulty breathing was a life-threatening condition in which air bubbles are created between the chest and lung. All the force Mr. Zhe had used trying to sing made air sacks in his lung burst, causing the air bubbles and his lung to be compressed to 15% of what it should be. Mr. Zhe needed surgery to remove the air bubbles, but fortunately turned out just fine.
So, if you’re ever at a karaoke bar, looking for a song to sing, maybe avoid the ones with super high notes and stick with something a little lower. We’re picturing something like Paul Robeson singing Ol’ Man River. That oughta do the trick.
And the word of the year is …
Flibbertigibbet. Bamboozle. Gobbledygook. If the LOTME staff had any say, those would be the words of the year every year, but sadly, we’re not in charge of such things. Instead, we’ll just have to defer to Oxford and Merriam-Webster, both of whom have recently chosen their words of the year. No word yet on whether or not they made their announcement at a red carpet gala dinner attended by all the most fashionable and powerful words out there, but we’re hoping that’s what happened.

We’ll start with Oxford, since they did choose first. We all know Oxford is the bad boy of the dictionary world, so they’ve chosen a casual colloquialism related to the big COVID-sized elephant in the room (or should it be elephant-sized COVID in the room?): Vax. According to them, while vax has been hanging around since the 1980s, it’s only been in the past year that it’s exploded in popularity in a wide range of contexts (we can’t imagine what those would be). According to Oxford, “as a short pithy word, it appeals, perhaps especially to media commentators, when more formal alternatives are much more long-winded.”
Speaking of long-winded, that brings us to Merriam-Webster, the sheltered nerd of the dictionary world. Clearly they’re too good for vax, so they’ve gone with vaccine as their 2021 word of the year. Vaccine, according to Merriam-Webster, carries two big stories: The impressive and herculean feat of bringing a COVID-19 vaccine so quickly to so many people, and the complex political and social upheaval between vaccine supporters and deniers.
Vaccine also serves as a great bookend for Merriam-Webster’s 2020 word of the year: Pandemic. In 2020, the pandemic started, and in 2021, thanks to the vaccine, the pandemic ends. That’s how it works, right? We have a vaccine, it’s all over now. What’s that? Omicron? No! Bad COVID! You do that outside, not on the carpet!
It isn’t autocorrect’s fault this time, we swear
We’ve come a long way with communication technology. Back in the day, when Gondor needed to call for aid, they had to pull off the greatest signal fire montage of all time. Now we can send each other texts back and forth in an instant. (“Hey Theoden, send army, need help pls” doesn’t quite have the same gravitas though.) The question is, how do our brains keep up with such rapidly advancing technology?
Er, they don’t. Not really. Instead, our brains create shortcuts called “good-enough language processing,” which is exactly what it sounds like.
Psychologists and psycholinguists have been studying misinterpretations such as good-enough language processing since the 1970s. Recently, however, psycholinguists from the Centre for Language and Brain at Higher School of Economics in Moscow have found that, when it comes to reading comprehension over text, older adults are using their knowledge of the world over how it’s grammatically formed in the sentence.
In the study, 349 people were asked to read and interpret four sentences, the third of which (translated from Russian) was: “Misha met the firefighter’s dentist, who had put out a fire in the warehouse.” When asked who put the fire out, 79% of older adults (aged 55 years and older), utilizing good-enough language processing, said the firefighter put out the fire. You probably glossed over that sentence and assumed the same thing. But this time, the dentist was the real hero.
That said, adolescents (aged 13-17) and young adults (aged 20-30) weren’t much better, and got that particular sentence wrong 63%-68% of the time. According to the researchers, good-enough language processing forms in adolescence and intensifies throughout adulthood.
Moral of the story? We should utilize signal fires more often. Less room for misinterpretation. When the beacons of Minas Tirith were lit, Rohan answered.
Singing … your … lungs … out
There’s nothing quite like a karaoke bar to unleash your inner rock star. Hey, why not just go for it, everyone is just as bad at singing as you. That’s part of the fun.
A 25-year-old man named Wang Zhe may have taken the karaoke concept a bit too far, however. While out with friends at a birthday party, Mr. Zhe let loose on a song with a particularly large number of high notes. He tried his best, gamely attacking the song until he felt a pain in his chest. He didn’t think much of it, although he did cut his performance short, but then he awoke the next morning unable to breathe properly.
After a trip to the hospital, he explained the sequence of events to the doctors, and an x-ray found that the culprit of the pain and difficulty breathing was a life-threatening condition in which air bubbles are created between the chest and lung. All the force Mr. Zhe had used trying to sing made air sacks in his lung burst, causing the air bubbles and his lung to be compressed to 15% of what it should be. Mr. Zhe needed surgery to remove the air bubbles, but fortunately turned out just fine.
So, if you’re ever at a karaoke bar, looking for a song to sing, maybe avoid the ones with super high notes and stick with something a little lower. We’re picturing something like Paul Robeson singing Ol’ Man River. That oughta do the trick.
And the word of the year is …
Flibbertigibbet. Bamboozle. Gobbledygook. If the LOTME staff had any say, those would be the words of the year every year, but sadly, we’re not in charge of such things. Instead, we’ll just have to defer to Oxford and Merriam-Webster, both of whom have recently chosen their words of the year. No word yet on whether or not they made their announcement at a red carpet gala dinner attended by all the most fashionable and powerful words out there, but we’re hoping that’s what happened.
We’ll start with Oxford, since they did choose first. We all know Oxford is the bad boy of the dictionary world, so they’ve chosen a casual colloquialism related to the big COVID-sized elephant in the room (or should it be elephant-sized COVID in the room?): Vax. According to them, while vax has been hanging around since the 1980s, it’s only been in the past year that it’s exploded in popularity in a wide range of contexts (we can’t imagine what those would be). According to Oxford, “as a short pithy word, it appeals, perhaps especially to media commentators, when more formal alternatives are much more long-winded.”
Speaking of long-winded, that brings us to Merriam-Webster, the sheltered nerd of the dictionary world. Clearly they’re too good for vax, so they’ve gone with vaccine as their 2021 word of the year. Vaccine, according to Merriam-Webster, carries two big stories: The impressive and herculean feat of bringing a COVID-19 vaccine so quickly to so many people, and the complex political and social upheaval between vaccine supporters and deniers.
Vaccine also serves as a great bookend for Merriam-Webster’s 2020 word of the year: Pandemic. In 2020, the pandemic started, and in 2021, thanks to the vaccine, the pandemic ends. That’s how it works, right? We have a vaccine, it’s all over now. What’s that? Omicron? No! Bad COVID! You do that outside, not on the carpet!
It isn’t autocorrect’s fault this time, we swear
We’ve come a long way with communication technology. Back in the day, when Gondor needed to call for aid, they had to pull off the greatest signal fire montage of all time. Now we can send each other texts back and forth in an instant. (“Hey Theoden, send army, need help pls” doesn’t quite have the same gravitas though.) The question is, how do our brains keep up with such rapidly advancing technology?
Er, they don’t. Not really. Instead, our brains create shortcuts called “good-enough language processing,” which is exactly what it sounds like.
Psychologists and psycholinguists have been studying misinterpretations such as good-enough language processing since the 1970s. Recently, however, psycholinguists from the Centre for Language and Brain at Higher School of Economics in Moscow have found that, when it comes to reading comprehension over text, older adults are using their knowledge of the world over how it’s grammatically formed in the sentence.
In the study, 349 people were asked to read and interpret four sentences, the third of which (translated from Russian) was: “Misha met the firefighter’s dentist, who had put out a fire in the warehouse.” When asked who put the fire out, 79% of older adults (aged 55 years and older), utilizing good-enough language processing, said the firefighter put out the fire. You probably glossed over that sentence and assumed the same thing. But this time, the dentist was the real hero.
That said, adolescents (aged 13-17) and young adults (aged 20-30) weren’t much better, and got that particular sentence wrong 63%-68% of the time. According to the researchers, good-enough language processing forms in adolescence and intensifies throughout adulthood.
Moral of the story? We should utilize signal fires more often. Less room for misinterpretation. When the beacons of Minas Tirith were lit, Rohan answered.
Singing … your … lungs … out
There’s nothing quite like a karaoke bar to unleash your inner rock star. Hey, why not just go for it, everyone is just as bad at singing as you. That’s part of the fun.
A 25-year-old man named Wang Zhe may have taken the karaoke concept a bit too far, however. While out with friends at a birthday party, Mr. Zhe let loose on a song with a particularly large number of high notes. He tried his best, gamely attacking the song until he felt a pain in his chest. He didn’t think much of it, although he did cut his performance short, but then he awoke the next morning unable to breathe properly.
After a trip to the hospital, he explained the sequence of events to the doctors, and an x-ray found that the culprit of the pain and difficulty breathing was a life-threatening condition in which air bubbles are created between the chest and lung. All the force Mr. Zhe had used trying to sing made air sacks in his lung burst, causing the air bubbles and his lung to be compressed to 15% of what it should be. Mr. Zhe needed surgery to remove the air bubbles, but fortunately turned out just fine.
So, if you’re ever at a karaoke bar, looking for a song to sing, maybe avoid the ones with super high notes and stick with something a little lower. We’re picturing something like Paul Robeson singing Ol’ Man River. That oughta do the trick.
And the word of the year is …
Flibbertigibbet. Bamboozle. Gobbledygook. If the LOTME staff had any say, those would be the words of the year every year, but sadly, we’re not in charge of such things. Instead, we’ll just have to defer to Oxford and Merriam-Webster, both of whom have recently chosen their words of the year. No word yet on whether or not they made their announcement at a red carpet gala dinner attended by all the most fashionable and powerful words out there, but we’re hoping that’s what happened.
We’ll start with Oxford, since they did choose first. We all know Oxford is the bad boy of the dictionary world, so they’ve chosen a casual colloquialism related to the big COVID-sized elephant in the room (or should it be elephant-sized COVID in the room?): Vax. According to them, while vax has been hanging around since the 1980s, it’s only been in the past year that it’s exploded in popularity in a wide range of contexts (we can’t imagine what those would be). According to Oxford, “as a short pithy word, it appeals, perhaps especially to media commentators, when more formal alternatives are much more long-winded.”
Speaking of long-winded, that brings us to Merriam-Webster, the sheltered nerd of the dictionary world. Clearly they’re too good for vax, so they’ve gone with vaccine as their 2021 word of the year. Vaccine, according to Merriam-Webster, carries two big stories: The impressive and herculean feat of bringing a COVID-19 vaccine so quickly to so many people, and the complex political and social upheaval between vaccine supporters and deniers.
Vaccine also serves as a great bookend for Merriam-Webster’s 2020 word of the year: Pandemic. In 2020, the pandemic started, and in 2021, thanks to the vaccine, the pandemic ends. That’s how it works, right? We have a vaccine, it’s all over now. What’s that? Omicron? No! Bad COVID! You do that outside, not on the carpet!
‘Top’ surgery for trans youth: Advance or dangerous medicine?
Is the gender-affirmative treatment approach an example of “medicine continuing on its progressive march of improving human life” or “a manifestation of dangerous medicine that ... will cause more harm than benefit to vulnerable youths?” wonders an Australian psychiatrist in a newly published letter that addresses the controversial procedure of masculinizing chest surgery – a double mastectomy – in young people with gender dysphoria (GD).
Alison Clayton, MBBS, explores the evidence for masculinizing chest surgery and looks back at examples of “dangerous medicine” in the past century while looking forward, wondering how future medics will retrospectively view gender affirmative treatment, especially so-called “top” or masculinizing chest surgery, which is in actual fact a double mastectomy, in a letter published Nov. 22 in the Archives of Sexual Behavior.
“It is surprising that clinicians and researchers claim chest surgery for GD youth is an evidence-based intervention, rather than acknowledging it is an experimental treatment that requires more rigorous and human research ethics committee [HREC] approved research,” she writes.
“The medical profession needs to consider whether, in its championing of the gender-affirmative approach for GD youth, it is also acting brashly and making mistakes that will negatively impact some young people for the rest of their lives,” she continues.
Ms. Clayton, after many years of experience as a psychiatrist, has recently returned to postgraduate research into the history of 20th-century psychiatry at the School of Historical and Philosophical Studies, University of Melbourne.
Meanwhile, the authors of a viewpoint published online Dec. 1 in JAMA Surgery, agree with Ms. Clayton on the issue of a lack of long-term studies on which to base decisions, particularly when it comes to insurance coverage for gender surgeries in the United States.
Nnenaya Agochukwu-Mmonu, MD, and colleagues recommend use of the coverage with evidence development (CED) approach, which would, they say, provide a “rigorous evidence base for gender-affirming interventions and surgery while simultaneously allowing access and provisional coverage for these services.”
Threefold increase in gender-affirming surgeries in past decade
There has been a threefold rise in the rate of gender-affirming surgeries in the United States in the past decade, which can be attributed to increased recognition of gender dysphoria, decreasing social stigma toward these individuals, greater clinical experience, and expanding insurance coverage, according to Dr. Agochukwu-Mmonu, of the department of urology, NYU School of Medicine, and coauthors.
Ms. Clayton meanwhile notes that of the increasing number of adolescents being referred for treatment for gender dysphoria in the Western world, most were born female and many have “a history of psychiatric illness or neurodevelopmental disorders.”
Many of these youngsters also show a “high demand” for surgical removal of breasts, she adds, noting that this operation is being undertaken as routine treatment in patients as young as 13, with some clinicians arguing that “this surgery is an evidence-based intervention that improves mental health outcomes, and that it is discriminatory for it not to be available.”
She also notes that “chest dysphoria” is “a recently created term meaning discomfort with one’s breasts.” The term “breast” is therefore largely absent in publications talking about this surgery as it “may cause distress for transgender males,” to quote one source, Ms. Clayton says, and “this seems part of a broader pattern of removing this term from clinical language,” according to another article on the subject.
Ms. Clayton also says, “There are only a handful of published studies focusing on the potential benefits of masculinizing chest surgery,” and notes that these mostly report on surgery for individuals younger than 21 years old.
Significant methodological flaws in existing research
One study of 14 postsurgical youth (nine of whom were under 18 years) found that “all reported high aesthetic satisfaction and most self-reported low complication rates and improvement in mood.”
Another cross-sectional retrospective survey looked at 68 postsurgical transmasculine youth (72% of the eligible postsurgical population); 49% had surgery when younger than age 18, with the youngest being age 13 and the oldest age 24. At the time of the survey, only 14% of participants were more than 2 years postsurgery. The postsurgical participants were found to have reduced chest dysphoria (the outcome) compared with a convenience and nonmatched comparison sample of nonsurgical transmasculine youth.
And a 2021 qualitative study of 30 transmale youth – about half of whom had undergone chest surgery – concluded that the postsurgical cohort experienced “tremendous” benefits in chest dysphoria and a range of psychological outcomes.
On this particular study, Ms. Clayton notes that “in my opinion, they did not provide enough detail for the reader to make an informed judgment regarding this latter claim.”
She goes on to discuss genital surgery, sometimes called full gender-affirming surgery (or “bottom surgery”), and says proponents of these operations point out that the main objections to them in minors is to “surgical sterilization, and people get super worked up about that ... it is a barrier we have to overcome, and I think we are going to.”
Ms. Clayton asserts that it seems “this barrier is already being overcome, as it has been reported that in the United States, genital surgery is being undertaken on gender dysphoric minors as young as 15 years old.”
Reflecting on the available evidence, Ms. Clayton highlights the significant methodological flaws that limit the extent to which surgery can be linked to short-term improved mental health outcomes and adds that information on long-term outcomes and rates of regret is unavailable.
She also asserts that the research fails to assess “a role for psychological interventions which could be utilized, as a least-harm intervention, until maturity is reached.”
Historical examples of experimental medicine
Ms. Clayton goes on to draw parallels with experimental medicine performed on homosexuals in the 20th century, highlighting the medical and surgical interventions, which included metrazol convulsive therapy, chemical castration with estrogens, surgical castration, clitoridectomy, brain operations, and aversive electrotherapy.
She also refers to the historical practice of hormonal treatment for “tall girls” and “short boys” between the 1960s and 1980s. Hormones were given to young people who did not have any medical reason underpinning their stature but were distressed, and society considered their height to have a negative social impact.
“With the encouragement of physicians and school nurses, enthusiastic media promotion, and pharmaceutical companies’ advertising, parents sought hormonal interventions,” she writes, adding that, at the time the hormones were considered safe, but long-term adverse effects emerged, including impaired fertility and increased risk of cancers.
“This seems another part of the story of medicine acting to reinforce society’s sex stereotypes, and for some patients it came at disastrous personal cost,” writes Ms. Clayton.
The gender-affirming approach is based on endorsing the adolescent’s stated gender identity with minimal questioning and “that they should be supported to undertake social transition, medical transition, masculinizing chest surgery, and, some also argue, genital surgery,” she writes.
Objectors to this approach pinpoint the “limited and low-quality evidence base for the benefits” but also “the irreversible and long-term adverse impacts of these treatments on fertility and sexual function, as well as on bone, brain, and cardiovascular functioning.”
Current studies of gender-affirming surgeries lack standardization
In their viewpoint, Dr. Agochukwu-Mmonu and colleagues state that use of a CED would not only help provide an evidence base but would also ensure better-informed policy access and coverage decisions to help standardize approaches to gender surgery in the United States.
Currently, they note, “Studies examining the mental health benefit for patients undergoing gender-affirming surgeries include measures that lack standardization, evaluate different interventions (that is, surgeries are rarely done with concurrent hormone administration), include dissimilar patient populations, and use different study designs.”
This difference in study design leads to variation in reported outcomes. Although many studies have shown benefit, others report that patients have unrealistic expectations or experience regret, Dr. Agochukwu-Mmonu and coauthors conclude.
CED provides an option that would enable informed decisions. “It allows the deliberate use of innovative therapies, explicit integration of transgender and nonbinary patient input, and ongoing systematic evaluation aimed to identify specific patient groups who would or would not benefit from their use.”
This leads back to Ms. Clayton’s central question around whether the gender-affirmative approach is a medical advance or dangerous medicine.
“Why are these experimental interventions, with inherent risks and scarce, low-quality evidence for benefits being implemented outside HREC-regulated clinical trial settings?’” she wonders.
Ms. Clayton has declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
Is the gender-affirmative treatment approach an example of “medicine continuing on its progressive march of improving human life” or “a manifestation of dangerous medicine that ... will cause more harm than benefit to vulnerable youths?” wonders an Australian psychiatrist in a newly published letter that addresses the controversial procedure of masculinizing chest surgery – a double mastectomy – in young people with gender dysphoria (GD).
Alison Clayton, MBBS, explores the evidence for masculinizing chest surgery and looks back at examples of “dangerous medicine” in the past century while looking forward, wondering how future medics will retrospectively view gender affirmative treatment, especially so-called “top” or masculinizing chest surgery, which is in actual fact a double mastectomy, in a letter published Nov. 22 in the Archives of Sexual Behavior.
“It is surprising that clinicians and researchers claim chest surgery for GD youth is an evidence-based intervention, rather than acknowledging it is an experimental treatment that requires more rigorous and human research ethics committee [HREC] approved research,” she writes.
“The medical profession needs to consider whether, in its championing of the gender-affirmative approach for GD youth, it is also acting brashly and making mistakes that will negatively impact some young people for the rest of their lives,” she continues.
Ms. Clayton, after many years of experience as a psychiatrist, has recently returned to postgraduate research into the history of 20th-century psychiatry at the School of Historical and Philosophical Studies, University of Melbourne.
Meanwhile, the authors of a viewpoint published online Dec. 1 in JAMA Surgery, agree with Ms. Clayton on the issue of a lack of long-term studies on which to base decisions, particularly when it comes to insurance coverage for gender surgeries in the United States.
Nnenaya Agochukwu-Mmonu, MD, and colleagues recommend use of the coverage with evidence development (CED) approach, which would, they say, provide a “rigorous evidence base for gender-affirming interventions and surgery while simultaneously allowing access and provisional coverage for these services.”
Threefold increase in gender-affirming surgeries in past decade
There has been a threefold rise in the rate of gender-affirming surgeries in the United States in the past decade, which can be attributed to increased recognition of gender dysphoria, decreasing social stigma toward these individuals, greater clinical experience, and expanding insurance coverage, according to Dr. Agochukwu-Mmonu, of the department of urology, NYU School of Medicine, and coauthors.
Ms. Clayton meanwhile notes that of the increasing number of adolescents being referred for treatment for gender dysphoria in the Western world, most were born female and many have “a history of psychiatric illness or neurodevelopmental disorders.”
Many of these youngsters also show a “high demand” for surgical removal of breasts, she adds, noting that this operation is being undertaken as routine treatment in patients as young as 13, with some clinicians arguing that “this surgery is an evidence-based intervention that improves mental health outcomes, and that it is discriminatory for it not to be available.”
She also notes that “chest dysphoria” is “a recently created term meaning discomfort with one’s breasts.” The term “breast” is therefore largely absent in publications talking about this surgery as it “may cause distress for transgender males,” to quote one source, Ms. Clayton says, and “this seems part of a broader pattern of removing this term from clinical language,” according to another article on the subject.
Ms. Clayton also says, “There are only a handful of published studies focusing on the potential benefits of masculinizing chest surgery,” and notes that these mostly report on surgery for individuals younger than 21 years old.
Significant methodological flaws in existing research
One study of 14 postsurgical youth (nine of whom were under 18 years) found that “all reported high aesthetic satisfaction and most self-reported low complication rates and improvement in mood.”
Another cross-sectional retrospective survey looked at 68 postsurgical transmasculine youth (72% of the eligible postsurgical population); 49% had surgery when younger than age 18, with the youngest being age 13 and the oldest age 24. At the time of the survey, only 14% of participants were more than 2 years postsurgery. The postsurgical participants were found to have reduced chest dysphoria (the outcome) compared with a convenience and nonmatched comparison sample of nonsurgical transmasculine youth.
And a 2021 qualitative study of 30 transmale youth – about half of whom had undergone chest surgery – concluded that the postsurgical cohort experienced “tremendous” benefits in chest dysphoria and a range of psychological outcomes.
On this particular study, Ms. Clayton notes that “in my opinion, they did not provide enough detail for the reader to make an informed judgment regarding this latter claim.”
She goes on to discuss genital surgery, sometimes called full gender-affirming surgery (or “bottom surgery”), and says proponents of these operations point out that the main objections to them in minors is to “surgical sterilization, and people get super worked up about that ... it is a barrier we have to overcome, and I think we are going to.”
Ms. Clayton asserts that it seems “this barrier is already being overcome, as it has been reported that in the United States, genital surgery is being undertaken on gender dysphoric minors as young as 15 years old.”
Reflecting on the available evidence, Ms. Clayton highlights the significant methodological flaws that limit the extent to which surgery can be linked to short-term improved mental health outcomes and adds that information on long-term outcomes and rates of regret is unavailable.
She also asserts that the research fails to assess “a role for psychological interventions which could be utilized, as a least-harm intervention, until maturity is reached.”
Historical examples of experimental medicine
Ms. Clayton goes on to draw parallels with experimental medicine performed on homosexuals in the 20th century, highlighting the medical and surgical interventions, which included metrazol convulsive therapy, chemical castration with estrogens, surgical castration, clitoridectomy, brain operations, and aversive electrotherapy.
She also refers to the historical practice of hormonal treatment for “tall girls” and “short boys” between the 1960s and 1980s. Hormones were given to young people who did not have any medical reason underpinning their stature but were distressed, and society considered their height to have a negative social impact.
“With the encouragement of physicians and school nurses, enthusiastic media promotion, and pharmaceutical companies’ advertising, parents sought hormonal interventions,” she writes, adding that, at the time the hormones were considered safe, but long-term adverse effects emerged, including impaired fertility and increased risk of cancers.
“This seems another part of the story of medicine acting to reinforce society’s sex stereotypes, and for some patients it came at disastrous personal cost,” writes Ms. Clayton.
The gender-affirming approach is based on endorsing the adolescent’s stated gender identity with minimal questioning and “that they should be supported to undertake social transition, medical transition, masculinizing chest surgery, and, some also argue, genital surgery,” she writes.
Objectors to this approach pinpoint the “limited and low-quality evidence base for the benefits” but also “the irreversible and long-term adverse impacts of these treatments on fertility and sexual function, as well as on bone, brain, and cardiovascular functioning.”
Current studies of gender-affirming surgeries lack standardization
In their viewpoint, Dr. Agochukwu-Mmonu and colleagues state that use of a CED would not only help provide an evidence base but would also ensure better-informed policy access and coverage decisions to help standardize approaches to gender surgery in the United States.
Currently, they note, “Studies examining the mental health benefit for patients undergoing gender-affirming surgeries include measures that lack standardization, evaluate different interventions (that is, surgeries are rarely done with concurrent hormone administration), include dissimilar patient populations, and use different study designs.”
This difference in study design leads to variation in reported outcomes. Although many studies have shown benefit, others report that patients have unrealistic expectations or experience regret, Dr. Agochukwu-Mmonu and coauthors conclude.
CED provides an option that would enable informed decisions. “It allows the deliberate use of innovative therapies, explicit integration of transgender and nonbinary patient input, and ongoing systematic evaluation aimed to identify specific patient groups who would or would not benefit from their use.”
This leads back to Ms. Clayton’s central question around whether the gender-affirmative approach is a medical advance or dangerous medicine.
“Why are these experimental interventions, with inherent risks and scarce, low-quality evidence for benefits being implemented outside HREC-regulated clinical trial settings?’” she wonders.
Ms. Clayton has declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
Is the gender-affirmative treatment approach an example of “medicine continuing on its progressive march of improving human life” or “a manifestation of dangerous medicine that ... will cause more harm than benefit to vulnerable youths?” wonders an Australian psychiatrist in a newly published letter that addresses the controversial procedure of masculinizing chest surgery – a double mastectomy – in young people with gender dysphoria (GD).
Alison Clayton, MBBS, explores the evidence for masculinizing chest surgery and looks back at examples of “dangerous medicine” in the past century while looking forward, wondering how future medics will retrospectively view gender affirmative treatment, especially so-called “top” or masculinizing chest surgery, which is in actual fact a double mastectomy, in a letter published Nov. 22 in the Archives of Sexual Behavior.
“It is surprising that clinicians and researchers claim chest surgery for GD youth is an evidence-based intervention, rather than acknowledging it is an experimental treatment that requires more rigorous and human research ethics committee [HREC] approved research,” she writes.
“The medical profession needs to consider whether, in its championing of the gender-affirmative approach for GD youth, it is also acting brashly and making mistakes that will negatively impact some young people for the rest of their lives,” she continues.
Ms. Clayton, after many years of experience as a psychiatrist, has recently returned to postgraduate research into the history of 20th-century psychiatry at the School of Historical and Philosophical Studies, University of Melbourne.
Meanwhile, the authors of a viewpoint published online Dec. 1 in JAMA Surgery, agree with Ms. Clayton on the issue of a lack of long-term studies on which to base decisions, particularly when it comes to insurance coverage for gender surgeries in the United States.
Nnenaya Agochukwu-Mmonu, MD, and colleagues recommend use of the coverage with evidence development (CED) approach, which would, they say, provide a “rigorous evidence base for gender-affirming interventions and surgery while simultaneously allowing access and provisional coverage for these services.”
Threefold increase in gender-affirming surgeries in past decade
There has been a threefold rise in the rate of gender-affirming surgeries in the United States in the past decade, which can be attributed to increased recognition of gender dysphoria, decreasing social stigma toward these individuals, greater clinical experience, and expanding insurance coverage, according to Dr. Agochukwu-Mmonu, of the department of urology, NYU School of Medicine, and coauthors.
Ms. Clayton meanwhile notes that of the increasing number of adolescents being referred for treatment for gender dysphoria in the Western world, most were born female and many have “a history of psychiatric illness or neurodevelopmental disorders.”
Many of these youngsters also show a “high demand” for surgical removal of breasts, she adds, noting that this operation is being undertaken as routine treatment in patients as young as 13, with some clinicians arguing that “this surgery is an evidence-based intervention that improves mental health outcomes, and that it is discriminatory for it not to be available.”
She also notes that “chest dysphoria” is “a recently created term meaning discomfort with one’s breasts.” The term “breast” is therefore largely absent in publications talking about this surgery as it “may cause distress for transgender males,” to quote one source, Ms. Clayton says, and “this seems part of a broader pattern of removing this term from clinical language,” according to another article on the subject.
Ms. Clayton also says, “There are only a handful of published studies focusing on the potential benefits of masculinizing chest surgery,” and notes that these mostly report on surgery for individuals younger than 21 years old.
Significant methodological flaws in existing research
One study of 14 postsurgical youth (nine of whom were under 18 years) found that “all reported high aesthetic satisfaction and most self-reported low complication rates and improvement in mood.”
Another cross-sectional retrospective survey looked at 68 postsurgical transmasculine youth (72% of the eligible postsurgical population); 49% had surgery when younger than age 18, with the youngest being age 13 and the oldest age 24. At the time of the survey, only 14% of participants were more than 2 years postsurgery. The postsurgical participants were found to have reduced chest dysphoria (the outcome) compared with a convenience and nonmatched comparison sample of nonsurgical transmasculine youth.
And a 2021 qualitative study of 30 transmale youth – about half of whom had undergone chest surgery – concluded that the postsurgical cohort experienced “tremendous” benefits in chest dysphoria and a range of psychological outcomes.
On this particular study, Ms. Clayton notes that “in my opinion, they did not provide enough detail for the reader to make an informed judgment regarding this latter claim.”
She goes on to discuss genital surgery, sometimes called full gender-affirming surgery (or “bottom surgery”), and says proponents of these operations point out that the main objections to them in minors is to “surgical sterilization, and people get super worked up about that ... it is a barrier we have to overcome, and I think we are going to.”
Ms. Clayton asserts that it seems “this barrier is already being overcome, as it has been reported that in the United States, genital surgery is being undertaken on gender dysphoric minors as young as 15 years old.”
Reflecting on the available evidence, Ms. Clayton highlights the significant methodological flaws that limit the extent to which surgery can be linked to short-term improved mental health outcomes and adds that information on long-term outcomes and rates of regret is unavailable.
She also asserts that the research fails to assess “a role for psychological interventions which could be utilized, as a least-harm intervention, until maturity is reached.”
Historical examples of experimental medicine
Ms. Clayton goes on to draw parallels with experimental medicine performed on homosexuals in the 20th century, highlighting the medical and surgical interventions, which included metrazol convulsive therapy, chemical castration with estrogens, surgical castration, clitoridectomy, brain operations, and aversive electrotherapy.
She also refers to the historical practice of hormonal treatment for “tall girls” and “short boys” between the 1960s and 1980s. Hormones were given to young people who did not have any medical reason underpinning their stature but were distressed, and society considered their height to have a negative social impact.
“With the encouragement of physicians and school nurses, enthusiastic media promotion, and pharmaceutical companies’ advertising, parents sought hormonal interventions,” she writes, adding that, at the time the hormones were considered safe, but long-term adverse effects emerged, including impaired fertility and increased risk of cancers.
“This seems another part of the story of medicine acting to reinforce society’s sex stereotypes, and for some patients it came at disastrous personal cost,” writes Ms. Clayton.
The gender-affirming approach is based on endorsing the adolescent’s stated gender identity with minimal questioning and “that they should be supported to undertake social transition, medical transition, masculinizing chest surgery, and, some also argue, genital surgery,” she writes.
Objectors to this approach pinpoint the “limited and low-quality evidence base for the benefits” but also “the irreversible and long-term adverse impacts of these treatments on fertility and sexual function, as well as on bone, brain, and cardiovascular functioning.”
Current studies of gender-affirming surgeries lack standardization
In their viewpoint, Dr. Agochukwu-Mmonu and colleagues state that use of a CED would not only help provide an evidence base but would also ensure better-informed policy access and coverage decisions to help standardize approaches to gender surgery in the United States.
Currently, they note, “Studies examining the mental health benefit for patients undergoing gender-affirming surgeries include measures that lack standardization, evaluate different interventions (that is, surgeries are rarely done with concurrent hormone administration), include dissimilar patient populations, and use different study designs.”
This difference in study design leads to variation in reported outcomes. Although many studies have shown benefit, others report that patients have unrealistic expectations or experience regret, Dr. Agochukwu-Mmonu and coauthors conclude.
CED provides an option that would enable informed decisions. “It allows the deliberate use of innovative therapies, explicit integration of transgender and nonbinary patient input, and ongoing systematic evaluation aimed to identify specific patient groups who would or would not benefit from their use.”
This leads back to Ms. Clayton’s central question around whether the gender-affirmative approach is a medical advance or dangerous medicine.
“Why are these experimental interventions, with inherent risks and scarce, low-quality evidence for benefits being implemented outside HREC-regulated clinical trial settings?’” she wonders.
Ms. Clayton has declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM JAMA SURGERY
Supporting clinician wellbeing and organizational resilience

In a 2020 report, the National Academy of Medicine advocated for “fixing the workplace,” rather than “fixing the worker,” as a more sustainable mechanism to advance physician wellbeing and foster organizational resilience. According to the report, “A resilient organization, or one that has matched job demands with job resources for its workers and that has created a culture of connection, transparency, and improvement, is better positioned to achieve organizational objectives during ordinary times and also to weather challenges during times of crisis” (Sinsky CA et al. “Organizational Evidence-Based and Promising Practices for Improving Clinician Well-Being.” National Academy of Medicine. Nov. 2, 2020.
The report highlights six domains of evidence-based practices to support organizational resilience and improve clinician well-being: organizational commitment, workforce assessment (such as measurement of physician wellbeing and burnout); leadership (including shared accountability, distributed leadership, and the emerging role of a chief wellness officer), policy (such as eliminating and/or re-envisioning policies and practices that interfere with clinicians’ ability to provide high-quality patient care), (5) efficiency (such as minimizing administrative tasks to allow clinicians to focus on patient care), and (6) support (such as providing resources and/or policies to support work-life balance, fostering a culture of connection at work). While many organizations (including both academic and community practices) already have begun to invest in this transformation, I urge you to think creatively about whether there is more your practice can do at an organizational level to support and sustain clinician wellbeing and prevent burnout.
In this month’s issue of GIHN, we highlight AGA’s new Clinical Practice Guideline on Coagulation in Cirrhosis, as well as results from a study confirming the benefits of coffee for liver health (welcome news to the caffeine-lovers among us!). We also report on a novel text-based patient-education intervention that aims to connect patients newly diagnosed with colorectal cancer to valuable resources and support.
Thank you for your dedicated readership – we look forward to continuing to bring you engaging, clinically-relevant content in 2022!
Megan A. Adams, MD, JD, MSc
Editor in Chief
In a 2020 report, the National Academy of Medicine advocated for “fixing the workplace,” rather than “fixing the worker,” as a more sustainable mechanism to advance physician wellbeing and foster organizational resilience. According to the report, “A resilient organization, or one that has matched job demands with job resources for its workers and that has created a culture of connection, transparency, and improvement, is better positioned to achieve organizational objectives during ordinary times and also to weather challenges during times of crisis” (Sinsky CA et al. “Organizational Evidence-Based and Promising Practices for Improving Clinician Well-Being.” National Academy of Medicine. Nov. 2, 2020.
The report highlights six domains of evidence-based practices to support organizational resilience and improve clinician well-being: organizational commitment, workforce assessment (such as measurement of physician wellbeing and burnout); leadership (including shared accountability, distributed leadership, and the emerging role of a chief wellness officer), policy (such as eliminating and/or re-envisioning policies and practices that interfere with clinicians’ ability to provide high-quality patient care), (5) efficiency (such as minimizing administrative tasks to allow clinicians to focus on patient care), and (6) support (such as providing resources and/or policies to support work-life balance, fostering a culture of connection at work). While many organizations (including both academic and community practices) already have begun to invest in this transformation, I urge you to think creatively about whether there is more your practice can do at an organizational level to support and sustain clinician wellbeing and prevent burnout.
In this month’s issue of GIHN, we highlight AGA’s new Clinical Practice Guideline on Coagulation in Cirrhosis, as well as results from a study confirming the benefits of coffee for liver health (welcome news to the caffeine-lovers among us!). We also report on a novel text-based patient-education intervention that aims to connect patients newly diagnosed with colorectal cancer to valuable resources and support.
Thank you for your dedicated readership – we look forward to continuing to bring you engaging, clinically-relevant content in 2022!
Megan A. Adams, MD, JD, MSc
Editor in Chief
In a 2020 report, the National Academy of Medicine advocated for “fixing the workplace,” rather than “fixing the worker,” as a more sustainable mechanism to advance physician wellbeing and foster organizational resilience. According to the report, “A resilient organization, or one that has matched job demands with job resources for its workers and that has created a culture of connection, transparency, and improvement, is better positioned to achieve organizational objectives during ordinary times and also to weather challenges during times of crisis” (Sinsky CA et al. “Organizational Evidence-Based and Promising Practices for Improving Clinician Well-Being.” National Academy of Medicine. Nov. 2, 2020.
The report highlights six domains of evidence-based practices to support organizational resilience and improve clinician well-being: organizational commitment, workforce assessment (such as measurement of physician wellbeing and burnout); leadership (including shared accountability, distributed leadership, and the emerging role of a chief wellness officer), policy (such as eliminating and/or re-envisioning policies and practices that interfere with clinicians’ ability to provide high-quality patient care), (5) efficiency (such as minimizing administrative tasks to allow clinicians to focus on patient care), and (6) support (such as providing resources and/or policies to support work-life balance, fostering a culture of connection at work). While many organizations (including both academic and community practices) already have begun to invest in this transformation, I urge you to think creatively about whether there is more your practice can do at an organizational level to support and sustain clinician wellbeing and prevent burnout.
In this month’s issue of GIHN, we highlight AGA’s new Clinical Practice Guideline on Coagulation in Cirrhosis, as well as results from a study confirming the benefits of coffee for liver health (welcome news to the caffeine-lovers among us!). We also report on a novel text-based patient-education intervention that aims to connect patients newly diagnosed with colorectal cancer to valuable resources and support.
Thank you for your dedicated readership – we look forward to continuing to bring you engaging, clinically-relevant content in 2022!
Megan A. Adams, MD, JD, MSc
Editor in Chief
Question 2
Correct answer: A. Intravenous proton pump inhibitor drip.
Rationale
It is important to understand the initial management of patients with bleeding esophageal varices. With voluminous hematemesis, especially from a proximal source like the esophagus, airway protection is crucial so this patient should be intubated. Patients like this are at high risk to develop infected ascites so IV antibiotics should be given. Antibiotics have been shown to decrease mortality in cirrhotic patients admitted with GI bleeding. Somatostatin analogs decrease portal inflow by causing splanchnic vasoconstriction and have been proven to achieve hemostasis and decrease the risk of rebleeding. One has to be cautious with resuscitation efforts, as excessive resuscitation can lead to accelerated bleeding due to increased portal pressures. However, this patient's Hemoglobin concentration is well below the threshold that warrants transfusion, so giving him PRBCs is appropriate. In the acute setting of an upper GI bleed, proton pump inhibitors work to help optimize platelet function by increasing gastric pH. Since the source here is varices in the more pH neutral esophageal environment, intravenous PPI likely has little effect in the acute setting. However after band ligation is performed, it may help decrease the risk of forming post-banding ulcers. Since this patient's banding was performed a month ago, this episode of bleeding is more likely to be from recurrent varices than from a post-banding ulcer.
References
Garcia-Tsao G et al. Hepatology. 2007 Sep;46(3):922-38.
Tripathi D et al. Gut. 2015 Nov;64(11):1680-704.
Correct answer: A. Intravenous proton pump inhibitor drip.
Rationale
It is important to understand the initial management of patients with bleeding esophageal varices. With voluminous hematemesis, especially from a proximal source like the esophagus, airway protection is crucial so this patient should be intubated. Patients like this are at high risk to develop infected ascites so IV antibiotics should be given. Antibiotics have been shown to decrease mortality in cirrhotic patients admitted with GI bleeding. Somatostatin analogs decrease portal inflow by causing splanchnic vasoconstriction and have been proven to achieve hemostasis and decrease the risk of rebleeding. One has to be cautious with resuscitation efforts, as excessive resuscitation can lead to accelerated bleeding due to increased portal pressures. However, this patient's Hemoglobin concentration is well below the threshold that warrants transfusion, so giving him PRBCs is appropriate. In the acute setting of an upper GI bleed, proton pump inhibitors work to help optimize platelet function by increasing gastric pH. Since the source here is varices in the more pH neutral esophageal environment, intravenous PPI likely has little effect in the acute setting. However after band ligation is performed, it may help decrease the risk of forming post-banding ulcers. Since this patient's banding was performed a month ago, this episode of bleeding is more likely to be from recurrent varices than from a post-banding ulcer.
References
Garcia-Tsao G et al. Hepatology. 2007 Sep;46(3):922-38.
Tripathi D et al. Gut. 2015 Nov;64(11):1680-704.
Correct answer: A. Intravenous proton pump inhibitor drip.
Rationale
It is important to understand the initial management of patients with bleeding esophageal varices. With voluminous hematemesis, especially from a proximal source like the esophagus, airway protection is crucial so this patient should be intubated. Patients like this are at high risk to develop infected ascites so IV antibiotics should be given. Antibiotics have been shown to decrease mortality in cirrhotic patients admitted with GI bleeding. Somatostatin analogs decrease portal inflow by causing splanchnic vasoconstriction and have been proven to achieve hemostasis and decrease the risk of rebleeding. One has to be cautious with resuscitation efforts, as excessive resuscitation can lead to accelerated bleeding due to increased portal pressures. However, this patient's Hemoglobin concentration is well below the threshold that warrants transfusion, so giving him PRBCs is appropriate. In the acute setting of an upper GI bleed, proton pump inhibitors work to help optimize platelet function by increasing gastric pH. Since the source here is varices in the more pH neutral esophageal environment, intravenous PPI likely has little effect in the acute setting. However after band ligation is performed, it may help decrease the risk of forming post-banding ulcers. Since this patient's banding was performed a month ago, this episode of bleeding is more likely to be from recurrent varices than from a post-banding ulcer.
References
Garcia-Tsao G et al. Hepatology. 2007 Sep;46(3):922-38.
Tripathi D et al. Gut. 2015 Nov;64(11):1680-704.
Q2. A 52-year-old man with NASH-cirrhosis is admitted to the ICU with red hematemesis and hemodynamic instability. For the past few months, he has been maintained on diuretics but has still required frequent paracenteses for ascites management. An upper endoscopy 44 weeks ago revealed only large esophageal varices that were incompletely eradicated with banding, but the patient did not show up for his scheduled repeat upper endoscopy last week. His initial hemoglobin is 5.8 g/dL. His INR is 1.8, and his platelet count is 94K.
Question 1
Correct answer: A. Diphyllobothrium latum.
Rationale
This is likely a tapeworm infection with Diphyllobothrium latum. D. latum infection can be acquired from ingesting certain forms of freshwater fish, and those who consume raw fish, including sushi, are at increased risk. The classical manifestation of infection with D. latum is megaloblastic anemia due to vitamin B12 deficiency. D. latum has a unique affinity for vitamin B12 and therefore competes with the host for absorption. Humans become infected with Taenia by ingesting raw or undercooked infected meat containing cysticerci. Infection with Hymenolepis is common in children secondary to breaches in fecal-oral hygiene. Most infections are asymptomatic.
Reference
Webb C, Cabada MM. Curr Opin Infect Dis. 2017 Oct;30(5):504-10.
Correct answer: A. Diphyllobothrium latum.
Rationale
This is likely a tapeworm infection with Diphyllobothrium latum. D. latum infection can be acquired from ingesting certain forms of freshwater fish, and those who consume raw fish, including sushi, are at increased risk. The classical manifestation of infection with D. latum is megaloblastic anemia due to vitamin B12 deficiency. D. latum has a unique affinity for vitamin B12 and therefore competes with the host for absorption. Humans become infected with Taenia by ingesting raw or undercooked infected meat containing cysticerci. Infection with Hymenolepis is common in children secondary to breaches in fecal-oral hygiene. Most infections are asymptomatic.
Reference
Webb C, Cabada MM. Curr Opin Infect Dis. 2017 Oct;30(5):504-10.
Correct answer: A. Diphyllobothrium latum.
Rationale
This is likely a tapeworm infection with Diphyllobothrium latum. D. latum infection can be acquired from ingesting certain forms of freshwater fish, and those who consume raw fish, including sushi, are at increased risk. The classical manifestation of infection with D. latum is megaloblastic anemia due to vitamin B12 deficiency. D. latum has a unique affinity for vitamin B12 and therefore competes with the host for absorption. Humans become infected with Taenia by ingesting raw or undercooked infected meat containing cysticerci. Infection with Hymenolepis is common in children secondary to breaches in fecal-oral hygiene. Most infections are asymptomatic.
Reference
Webb C, Cabada MM. Curr Opin Infect Dis. 2017 Oct;30(5):504-10.
Q1. A 36-year-old man presents to the clinic with a history of diarrhea and significant fatigue for the last 2 months. He has no significant past medical history and works as a chef in a local sushi bar. He complains of six to seven watery stools daily with nocturnal symptoms. Diarrhea is associated with abdominal cramps, and he denies any passage of blood. His physical examination, including vital signs, is unremarkable. Laboratory investigation reveals 9.8 g/dL hemoglobin, with a mean corpuscular volume 110 fL. Peripheral eosinophilia is also noted. A stool sample is sent to the lab and is pending.
Pediatric insomnia: Assessment and diagnosis
FIRST OF 2 PARTS
A thorough evaluation can identify modifiable factors and guide treatment
Sleep problems are common among children and adolescents,1 with prevalence rates of 25% to 40%.2-4 Young children most commonly exhibit what is referred to as bedtime problems and night wakenings, whereas children in middle childhood (age 4 to 12) through adolescence (age 13 to 17) report insomnia. For many children, these problems persist.3 Insufficient sleep in children and adolescents worsens inattention, daytime fatigue, and cognitive and behavioral deficits.5 Assessment and treatment of sleep problems in children and adolescents is critical because poor sleep among youth increases the risk for depression, self-harm, and suicide,6,7 increases family stress, and decreases parental well-being.1
This 2-part article describes the assessment, diagnosis, and treatment of sleep problems among children and adolescents. In part 1, we focus on:
- sleep architecture (circadian rhythms, stages of sleep)
- sleep in healthy youth (age 6 to 17) and those with attention-deficit/hyperactivity disorder (ADHD), depressive disorders, and anxiety
- how to assess sleep, and the differential diagnosis of behavioral sleep problems in pediatric patients.
In Part 2, we will cover psychotherapeutic and psychopharmacologic interventions for youth with insomnia, and describe an effective approach to consultation with pediatric sleep medicine specialists.
How much sleep do children and adolescents need?
Throughout their development, children spend 40% to 50% of their time asleep. Sleep schedules are based on circadian rhythms, which are physical, mental, and behavioral changes that follow an approximately 24-hour cycle. Human circadian rhythm varies between 24 and 25 hours and is vital in determining our sleep patterns. Exposure to sunlight drives our circadian rhythm, sending signals to our bodies to “turn on” melatonin production at night (ie, 9
Box
Sleep architecture consists of 3 states: wake; non-rapid eye movement (NREM) sleep; and rapid eye movement (REM) sleep (“dreaming” sleep).2 These stages have distinct polysomnographic features of electroencephalographic EEG patterns, eye movements, and muscle tone.2 NREM sleep can be further divided into 3 stages: stage 1 (N1), stage 2 (N2), and stage 3 (N3). Stage 1 is the lightest stage and lasts for 30 seconds to 5 minutes; it is easy to wake up from stage 1 sleep. During stage 2 sleep, the body moves into a deeper sleep stage that is considered “true” sleep. This sleep stage is characterized by bursts of rhythmic rapid EEG activity known as spindles, as well as high-amplitude slow-wave spikes called K complexes.2 Stage 2 sleep lasts for 10 to 45 minutes. Stage 3, better known as “deep sleep,” slow-wave sleep, or delta sleep, is the most restorative sleep.2 Respiration is low and parasympathetic activity is high.2 It is difficult to be awakened during deep sleep, and if aroused, the person likely will feel confused or groggy. Deep sleep is followed by a return to lighter stage of sleep before the first REM sleep period begins.
REM sleep is the active stage of sleep. Breathing and heart rate become irregular, and the body experiences muscle atonia, or temporary paralysis, of arms and legs. When in REM sleep, individuals have the highest brain metabolic rates, and periodic bursts of eye movements.2 Most individuals move through stages of NREM and REM sleep in predicable ways, meaning they experience NREM sleep, return to a lighter stage of sleep after deep sleep, then move into REM sleep before the cycle repeats. It takes approximately 90 minutes for most adults to complete the NREM sleep cycle, and then REM sleep occurs before returning to NREM sleep.
In children, especially in infants and babies, sleep cycles are closer to 50 to 60 minutes. Newborns spend approximately 50% of their sleep in REM sleep, whereas adults spend 20% to 25% of their sleep in REM sleep. Children will spend more time in REM sleep until the third and fourth years of life, at which point REM gradually decreases to 20% to 25% by adulthood.
Sleep needs also change predictably throughout the lifespan. The National Sleep Foundation guidelines for sleep duration provide clinicians and parents with a range of recommended sleep for each stage of development. Infants require 14 to 17 hours of sleep, whereas adolescents need 8 to 10 hours by age 14 to 17.8 The key for clinicians is to determine if the child is within the recommended range, and how they are functioning on the number of hours of sleep they report. This allows for variation in how much sleep an individual child might need while acknowledging that some children within a specific age group might need more or less sleep than other children of the same age.
Sleep in healthy youth: Middle childhood
School-age children (age 6 to 12) typically need 9 to 10 hours of sleep over a 24-hour period.2 This developmental period is especially important for children to develop healthy sleep habits; however, developmentally appropriate cognitive and social/emotional factors might interfere with the quality and quantity of sleep. Middle childhood is a time when children can understand the dangers of the outside world (ie, violence, health problems) and resulting anxiety can disrupt sleep. Parents usually are less involved in bedtime as children approach adolescence, which leads to later bedtimes. At this stage, many children begin to take on more serious roles in their academics and extracurricular activities, peer relationships become more important, and use of electronics (eg, television, video games, internet, and handheld devices) increases—all of which compete with sleep.9 Frequent sleep issues during middle childhood include:
- irregular sleep-wake schedules
- later bedtimes
- decreased nighttime sleep
- increased caffeine intake
- reduced parental presence at bedtime
- daytime sleepiness.3
In school-age children, regular napping, falling asleep during short car rides, and daytime fatigue at school or home are cause for concern. When these symptoms are present, an evaluation is warranted.
Sleep in healthy youth: Adolescence
The National Sleep Foundation recommends adolescents obtain 8 to 10 hours of sleep per night; for some adolescents, as much as 11 hours of sleep per night might be appropriate.8 However, this contrasts with findings from the National Sleep Foundation’s Sleep in America Poll, which revealed that 75% of 12th graders report <8 hours of sleep nightly.10 Many adolescents experience delayed sleep phase syndrome or delayed sleep-wake phase disorder, which involves a persistent phase shift of >2 hours in the sleep-wake schedule that conflicts with the adolescent’s school, work, or lifestyle demands.11 Such circadian rhythm disorders typically result from a poor match between the sleep-wake schedule and the demands of the adolescent’s life, or a failure to synchronize their internal clock with a 24-hour circadian clock.12 Children typically become tired after sunset, but puberty is associated with reduced slow-wave sleep and changes in circadian rhythms. As a result, a 3-hour delay (delayed phase preference) is common among adolescents. At approximately age 20, people start to become tired after sunset and awaken earlier in the morning—a pattern driven by sunlight and the timing of melatonin release that will remain stable until the sixth decade of life.
Continue to: Effects of chronic sleep deprivation...
Effects of chronic sleep deprivation
Most older studies of sleep loss examined the impact of total sleep loss (sleep deprivation) rather than the effect of partial sleep loss or sleep restriction, a more commonly experienced phenomenon. More recent research shows that a cumulative sleep deficit could cause the body to override voluntary wakefulness and a sleep-deprived individual can experience brief “microsleeps” where they are unaware and lose attention/wakefulness for several seconds.2 This can be deadly if a sleep-deprived adolescent experiences microsleeps while driving.13
There is a well-studied correlation between chronic sleep deprivation and increased body mass index in children.14 This might be caused by reduction in physical activity as well as alterations in the “hunger hormones”—ghrelin and leptin—that have been observed with sleep deprivation.15-17 Other studies have noted decreased glucose tolerance, reduced insulin sensitivity, and catecholamine and cortisol secretion abnormalities, which place children at higher risk for metabolic syndrome and hypertension.13,18 Sleep deprivation also is associated with mood and anxiety disorders and is an independent risk factor for substance use and suicidal ideation among adolescents.19 Sleep deprivation increases impairments in impulse control, concentration, and attention, which could be especially problematic in school-age children.
How sleep is assessed
The sleep history is the first step in evaluating a child or adolescent for a sleep disorder. The sleep history includes exploring the chief complaint, sleep patterns and schedules, bedtime routines, and nocturnal and daytime behaviors (Table).

Chief complaint
Behavioral sleep specialists will assess the primary problem with everyone involved in the child’s bedtime.20 This might include parents (custodial and noncustodial), grandparents, or stepparents as well as the child/adolescent. This important step can reveal a sleep disorder or an inappropriately early bedtime relative to the child’s development. During this assessment, ask detailed questions about how long the sleep problem has persisted, the frequency of sleep problems, and any precipitating stressors. Parents and caregivers can review strategies they have tried, and for how long and to what extent interventions were implemented consistently to result in change.
Sleep patterns and schedules
Review the child/adolescent’s typical sleep patterns and behaviors. Ask parents and caregivers, as well as the patient, about general sleep schedules for the past few weeks or a typical 2-week time period.2 A behavioral assessment of sleep should include asking families about how the child/adolescent sleeps during the week and over the weekend, and if school-year sleep differs from summer or holiday sleep schedules. These questions can illuminate how long a sleep problem has been occurring and what sleep habits might be contributing to the problem. Bedtime
Determine if there is a set bedtime or if the child goes to bed when they wish. It is important to ascertain if the bedtime is age-appropriate, if weekday and weekend bedtimes differ, and to what extent extracurricular activities or school demands impact bedtime. Assess the consistency of the bedtime, the nature of bedtime routines (eg, is the child engaging in stimulating activities before bed), where the bedtime routine occurs (eg, sibling’s room, parents’ room, child’s room), and what role (if any) electronic devices play.2
Nocturnal behaviors
Assessment should include a series of questions and age-specific questionnaires to focus on what behaviors occur at night, including awakenings. Parents should be asked how frequent night awakenings occur, how long arousals last, and how the child signals for the parent (eg, calling out, climbing into parents’ bed).2 Additionally, ask how parents respond and what is required to help the child fall back asleep (eg, rocking, soothing, feeding). The presence of nightmares, night terrors, parasomnias, and sleep-related breathing disorders also must be assessed.20
Daytime behaviors
A sleep history should include assessment of daytime functioning, including daytime sleepiness, fatigue, morning waking, and functioning during school, extracurriculars, and homework. For children and teens, falling asleep in the car, while in school, or during passive activities (meals, conversation) suggests insufficient sleep, sleep disruption, or excessive daytime sleepiness.2
Continue to: Sleep disruption in youth with psychiatric disorders...
Sleep disruption in youth with psychiatric disorders
Disordered sleep is common across psychiatric disorders. The National Comorbidity Survey Adolescent Supplement—a nationally representative cross-sectional survey of adolescents (N = 10,123)—found that a later weeknight bedtime, shorter weeknight sleep duration, and greater weekend bedtime delay increased the risk of developing a mood, anxiety, or substance use (including nicotine) disorder, and suicidality. These risk factors also were associated with lower “perceived mental and physical health.”21 Clinicians should routinely obtain a sleep history in children and adolescents with these disorders. Consider using the sleep screening tool BEARS:
- Bedtime issues
- Excessive daytime sleepiness
- Awakenings
- Regularity and duration of sleep
- Snoring.
ADHD
Up to one-half of children and adolescents with ADHD experience sleep problems,22,23 including delayed sleep onset, bedtime resistance, daytime fatigue, and feeling groggy in the morning beyond what is typical (>20 minutes). Pharmacotherapy for ADHD contributes to sleep disturbances24,25 while sleep deprivation exacerbates inattention and hyperactivity. In youth with ADHD, restless leg syndrome, periodic limb movement disorder, and sleep-disordered breathing disorder are more common than in the general population.
Depressive disorders
Up to three-quarters of depressed children and 90% of depressed adolescents report sleep disturbances, including initial, middle, and terminal insomnia as well as hypersomnia.26 Disrupted sleep in pediatric patients with major depressive disorder could be moderated by the patient’s age, with depressive symptoms more common among adolescents (age 12 to 17) than among younger children (age 6 to 11).27 Successful treatment of depression fails to relieve dyssomnia in 10% of children. Sleep problems that persist after successfully treating a depressive episode could increase the risk of another depressive episode.28
Anxiety disorders
Sleep problems are common among children and adolescents with anxiety disorders.29 Longitudinal data from >900 children found that symptoms of sleep disturbance in early childhood were correlated with experiencing an anxiety disorder 20 years later.30 Fears related to the dark or monsters under the bed that are developmentally appropriate for younger children may interfere with sleep. However, in anxious children, fears might also be related to separation, sleeping alone, worry about the loss of a loved one, concerns about personal safety, fear of frightening dreams, or concerns about academics and social relationships. Anxious individuals ruminate about their worries, and this might be especially true for children at bedtime, when there are limited distractions from ruminative fears.31 Bedtime resistance, parental involvement in bedtime rituals, and cultural factors related to sleep also could play a role for children with anxiety symptoms and sleep problems.
Having an anxiety disorder is significantly associated with an increased risk of insomnia; however, 73% of the time anxiety symptoms precede an insomnia diagnosis.29 Sleep problems and anxiety symptoms might have a reciprocal influence on one another; tiredness that results from sleep problems could exacerbate anxiety, which further worsens sleep problems.
A bridge to treatment
A thorough assessment can help identify modifiable factors and guide treatment selections. In Part 2 of this article, we will describe healthy sleep practices, cognitive-behavioral therapy for insomnia, when pharmacotherapy might be indicated, and the evidence supporting several medications commonly used to treat pediatric insomnia. We also will discuss factors to consider when seeking consultation with a pediatric behavioral sleep specialist.
1. Meltzer LJ, Mindell JA. Systematic review and meta-analysis of behavioral interventions for pediatric insomnia. J Pediatr Psychol. 2014;39(8):932-948. doi:10.1093/jpepsy/jsu041
2. Owens JA, Mindell JA. Pediatric insomnia. Pediatr Clin North Am. 2011;58(3):555-569. doi:10.1016/j.pcl.2011.03.011
3. Meltzer LJ, Plaufcan MR, Thomas JH, et al. Sleep problems and sleep disorders in pediatric primary care: treatment recommendations, persistence, and health care utilization. J Clin Sleep Med. 2014;10(4):421-426. doi:10.5664/jcsm.3620
4. Moore M, Meltzer LJ, Mindell JA. Bedtime problems and night wakings in children. Prim Care. 2008;35(3):569-581, viii. doi:10.1016/j.pop.2008.06.002
5. Williamson AA, Mindell JA, Hiscock H, et al. Longitudinal sleep problem trajectories are associated with multiple impairments in child well-being. J Child Psychol Psychiatry. 2020;61(10):1092-1103. doi:10.1111/jcpp.13303
6. Roberts RE, Roberts CR, Chen IG. Impact of insomnia on future functioning of adolescents. J Psychosom Res. 2002; 53(1):561-569. doi:10.1016/s0022-3999(02)00446-4
7. Singareddy R, Krishnamurthy VB, Vgontzas AN, et al. Subjective and objective sleep and self-harm behaviors in young children: a general population study. Psychiatry Res. 2013;209(3):549-553. doi:10.1016/j.psychres.2013.03.036
8. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1(4):233-243. doi:10.1016/j.sleh.2015.10.004
9. Calamaro CJ, Mason TBA, Ratcliffe SJ. Adolescents living the 24/7 lifestyle: Effects of caffeine and technology on sleep duration and daytime functioning. Pediatrics. 2009;123(6):e1005-1010. doi:10.1542/peds.2008-3641
10. Mindell JA, Owens JA, Carskadon MA. Developmental features of sleep. Child Adolesc Psychiatr Clin N Am. 1999;8(4):695-725.
11. Moore M, Meltzer LJ. The sleepy adolescent: causes and consequences of sleepiness in teens. Paediatr Respir Rev. 2008;9(2):114-120. doi:10.1016/j.prrv.2008.01.001
12. Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med. 2007;8(6):602-612. doi:10.1016/j.sleep.2006.12.002
13. Millman RP; Working Group on Sleepiness in Adolescents/Young Adults; AAP Committee on Adolescence. Excessive sleepiness in adolescents and young adults: causes, consequences, and treatment strategies. Pediatrics. 2005;115(6):1774-1786. doi:10.1542/peds.2005-0772
14. Kaczor M, Skalski M. Prevalence and consequences of insomnia in pediatric population. Psychiatr Pol. 2016;50(3):555-569. doi:10.12740/PP/61226
15. Gomes TN, Dos Santos FK, Santos D, et al. Correlates of sedentary time in children: a multilevel modelling approach. BMC Public Health. 2014;14:890. doi:10.1186/1471-2458-14-890
16. Stone MR, Stevens D, Faulkner GEJ. Maintaining recommended sleep throughout the week is associated with increased physical activity in children. Prev Med. 2013;56(2):112-117. doi:10.1016/j.ypmed.2012.11.015
17. Hart CN, Fava JL, Subak LL, et al. Time in bed is associated with decreased physical activity and higher BMI in women seeking weight loss treatment. ISRN Obes. 2012;2012:320157. doi:10.5402/2012/320157
18. Tasali E, Leproult R, Ehrmann DA, et al. Slow-wave sleep and the risk of type 2 diabetes in humans. Proc Natl Acad Sci U S A. 2008;105(3):1044-1049. doi:10.1073/pnas.0706446105
19. de Zambotti M, Goldstone A, Colrain IM, et al. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. 2018;39:12-24. doi:10.1016/j.smrv.2017.06.009
20. Mindell JA, Owens JA. A clinical guide to pediatric sleep: diagnosis and management of sleep problems. 3rd ed. Lippincott Williams & Wilkins; 2015.
21. Zhang J, Paksarian D, Lamers F, et al. Sleep patterns and mental health correlates in US adolescents. J Pediatr. 2017;182:137-143. doi:10.1016/j.jpeds.2016.11.007
22. Gregory AM, Agnew-Blais JC, Matthews T, et al. ADHD and sleep quality: longitudinal analyses from childhood to early adulthood in a twin cohort. J Clin Child Adolesc Psychol. 2017;46(2):284-294. doi:10.1080/15374416.2016.1183499
23. Weiss MD, Salpekar J. Sleep problems in the child with attention-deficit hyperactivity disorder: Defining aetiology and appropriate treatments. CNS Drugs. 2010;24(10):811-828. doi:10.2165/11538990-000000000-00000
24. Galland BC, Tripp EG, Taylor BJ. The sleep of children with attention deficit hyperactivity disorder on and off methylphenidate: a matched case-control study. J Sleep Res. 2010;19(2):366-373. doi:10.1111/j.1365-2869.2009.00795.x
25. Becker SP, Froehlich TE, Epstein JN. Effects of methylphenidate on sleep functioning in children with attention-deficit/hyperactivity disorder. J Dev Behav Pediatr. 2016;37(5):395-404. doi:10.1097/DBP.0000000000000285
26. Roberts RE, Duong HT. Depression and insomnia among adolescents: a prospective perspective. J Affect Disord. 2013;148(1):66-71. doi:10.1016/j.jad.2012.11.049
27. Emslie GJ, Rush AJ, Weinberg WA, et al. Sleep EEG features of adolescents with major depression. Biol Psychiatry. 1994;36(9):573-581. doi:10.1016/0006-3223(94)90067-1
28. Alfano CA, Zakem AH, Costa NM, et al. Sleep problems and their relation to cognitive factors, anxiety, and depressive symptoms in children and adolescents. Depress Anxiety. 2009;26(6):503-512. doi:10.1002/da.20443
29. Alfano CA, Ginsburg GS, Kingery JN. Sleep-related problems among children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry. 2007;46(2):224-232. doi:10.1097/01.chi.0000242233.06011.8e
30. Gregory AM, Caspi A, Eley TC, et al. Prospective longitudinal associations between persistent sleep problems in childhood and anxiety and depression disorders in adulthood. J Abnorm Child Psychol. 2005;33(2):157-163. doi: 10.1007/s10802-005-1824-0
31. Chorney DB, Detweiler MF, Morris TL, et al. The interplay of sleep disturbance, anxiety, and depression in children. J Pediatr Psychol. 2008;33(4):339-348. doi:10.1093/jpepsy/jsm105
32. Sadeh A. Stress, trauma, and sleep in children. Child Adolesc Psychiatr Clin N Am. 1996;5(3):685-700. doi:10.1016/S1056-4993(18)30356-0

33. Glod CA, Teicher MH, Hartman CR, et al. Increased nocturnal activity and impaired sleep maintenance in abused children. J Am Acad Child Adolesc Psychiatry. 1997;36(9):1236-1243. doi:10.1097/00004583-199709000-00016
34. Strawn JR, Lu L, Peris TS, et al. Research review: pediatric anxiety disorders: what have we learnt in the last 10 years? J Child Psychol Psychiatry. 2021;62(2):114-139. doi:10.1111/jcpp.13262
35. Wehry AM, Beesdo-Baum K, Hennelly MM, et al. Assessment and treatment of anxiety disorders in children and adolescents. Curr Psychiatry Rep. 2015;17(7):52. doi:10.1007/s11920-015-0591-z
36. Hamill Skoch S, Mills JA, Ramsey L, et al. Letter to editor: sleep disturbances in selective serotonin reuptake inhibitor-treated youth with anxiety disorders and obsessive compulsive disorder— a bayesian hierarchical modeling meta-analysis. J Child Adolesc Psychopharmacol. 2021;31(5):387-388. doi:10.1089/cap.2020.0169
FIRST OF 2 PARTS
A thorough evaluation can identify modifiable factors and guide treatment
Sleep problems are common among children and adolescents,1 with prevalence rates of 25% to 40%.2-4 Young children most commonly exhibit what is referred to as bedtime problems and night wakenings, whereas children in middle childhood (age 4 to 12) through adolescence (age 13 to 17) report insomnia. For many children, these problems persist.3 Insufficient sleep in children and adolescents worsens inattention, daytime fatigue, and cognitive and behavioral deficits.5 Assessment and treatment of sleep problems in children and adolescents is critical because poor sleep among youth increases the risk for depression, self-harm, and suicide,6,7 increases family stress, and decreases parental well-being.1
This 2-part article describes the assessment, diagnosis, and treatment of sleep problems among children and adolescents. In part 1, we focus on:
- sleep architecture (circadian rhythms, stages of sleep)
- sleep in healthy youth (age 6 to 17) and those with attention-deficit/hyperactivity disorder (ADHD), depressive disorders, and anxiety
- how to assess sleep, and the differential diagnosis of behavioral sleep problems in pediatric patients.
In Part 2, we will cover psychotherapeutic and psychopharmacologic interventions for youth with insomnia, and describe an effective approach to consultation with pediatric sleep medicine specialists.
How much sleep do children and adolescents need?
Throughout their development, children spend 40% to 50% of their time asleep. Sleep schedules are based on circadian rhythms, which are physical, mental, and behavioral changes that follow an approximately 24-hour cycle. Human circadian rhythm varies between 24 and 25 hours and is vital in determining our sleep patterns. Exposure to sunlight drives our circadian rhythm, sending signals to our bodies to “turn on” melatonin production at night (ie, 9
Box
Sleep architecture consists of 3 states: wake; non-rapid eye movement (NREM) sleep; and rapid eye movement (REM) sleep (“dreaming” sleep).2 These stages have distinct polysomnographic features of electroencephalographic EEG patterns, eye movements, and muscle tone.2 NREM sleep can be further divided into 3 stages: stage 1 (N1), stage 2 (N2), and stage 3 (N3). Stage 1 is the lightest stage and lasts for 30 seconds to 5 minutes; it is easy to wake up from stage 1 sleep. During stage 2 sleep, the body moves into a deeper sleep stage that is considered “true” sleep. This sleep stage is characterized by bursts of rhythmic rapid EEG activity known as spindles, as well as high-amplitude slow-wave spikes called K complexes.2 Stage 2 sleep lasts for 10 to 45 minutes. Stage 3, better known as “deep sleep,” slow-wave sleep, or delta sleep, is the most restorative sleep.2 Respiration is low and parasympathetic activity is high.2 It is difficult to be awakened during deep sleep, and if aroused, the person likely will feel confused or groggy. Deep sleep is followed by a return to lighter stage of sleep before the first REM sleep period begins.
REM sleep is the active stage of sleep. Breathing and heart rate become irregular, and the body experiences muscle atonia, or temporary paralysis, of arms and legs. When in REM sleep, individuals have the highest brain metabolic rates, and periodic bursts of eye movements.2 Most individuals move through stages of NREM and REM sleep in predicable ways, meaning they experience NREM sleep, return to a lighter stage of sleep after deep sleep, then move into REM sleep before the cycle repeats. It takes approximately 90 minutes for most adults to complete the NREM sleep cycle, and then REM sleep occurs before returning to NREM sleep.
In children, especially in infants and babies, sleep cycles are closer to 50 to 60 minutes. Newborns spend approximately 50% of their sleep in REM sleep, whereas adults spend 20% to 25% of their sleep in REM sleep. Children will spend more time in REM sleep until the third and fourth years of life, at which point REM gradually decreases to 20% to 25% by adulthood.
Sleep needs also change predictably throughout the lifespan. The National Sleep Foundation guidelines for sleep duration provide clinicians and parents with a range of recommended sleep for each stage of development. Infants require 14 to 17 hours of sleep, whereas adolescents need 8 to 10 hours by age 14 to 17.8 The key for clinicians is to determine if the child is within the recommended range, and how they are functioning on the number of hours of sleep they report. This allows for variation in how much sleep an individual child might need while acknowledging that some children within a specific age group might need more or less sleep than other children of the same age.
Sleep in healthy youth: Middle childhood
School-age children (age 6 to 12) typically need 9 to 10 hours of sleep over a 24-hour period.2 This developmental period is especially important for children to develop healthy sleep habits; however, developmentally appropriate cognitive and social/emotional factors might interfere with the quality and quantity of sleep. Middle childhood is a time when children can understand the dangers of the outside world (ie, violence, health problems) and resulting anxiety can disrupt sleep. Parents usually are less involved in bedtime as children approach adolescence, which leads to later bedtimes. At this stage, many children begin to take on more serious roles in their academics and extracurricular activities, peer relationships become more important, and use of electronics (eg, television, video games, internet, and handheld devices) increases—all of which compete with sleep.9 Frequent sleep issues during middle childhood include:
- irregular sleep-wake schedules
- later bedtimes
- decreased nighttime sleep
- increased caffeine intake
- reduced parental presence at bedtime
- daytime sleepiness.3
In school-age children, regular napping, falling asleep during short car rides, and daytime fatigue at school or home are cause for concern. When these symptoms are present, an evaluation is warranted.
Sleep in healthy youth: Adolescence
The National Sleep Foundation recommends adolescents obtain 8 to 10 hours of sleep per night; for some adolescents, as much as 11 hours of sleep per night might be appropriate.8 However, this contrasts with findings from the National Sleep Foundation’s Sleep in America Poll, which revealed that 75% of 12th graders report <8 hours of sleep nightly.10 Many adolescents experience delayed sleep phase syndrome or delayed sleep-wake phase disorder, which involves a persistent phase shift of >2 hours in the sleep-wake schedule that conflicts with the adolescent’s school, work, or lifestyle demands.11 Such circadian rhythm disorders typically result from a poor match between the sleep-wake schedule and the demands of the adolescent’s life, or a failure to synchronize their internal clock with a 24-hour circadian clock.12 Children typically become tired after sunset, but puberty is associated with reduced slow-wave sleep and changes in circadian rhythms. As a result, a 3-hour delay (delayed phase preference) is common among adolescents. At approximately age 20, people start to become tired after sunset and awaken earlier in the morning—a pattern driven by sunlight and the timing of melatonin release that will remain stable until the sixth decade of life.
Continue to: Effects of chronic sleep deprivation...
Effects of chronic sleep deprivation
Most older studies of sleep loss examined the impact of total sleep loss (sleep deprivation) rather than the effect of partial sleep loss or sleep restriction, a more commonly experienced phenomenon. More recent research shows that a cumulative sleep deficit could cause the body to override voluntary wakefulness and a sleep-deprived individual can experience brief “microsleeps” where they are unaware and lose attention/wakefulness for several seconds.2 This can be deadly if a sleep-deprived adolescent experiences microsleeps while driving.13
There is a well-studied correlation between chronic sleep deprivation and increased body mass index in children.14 This might be caused by reduction in physical activity as well as alterations in the “hunger hormones”—ghrelin and leptin—that have been observed with sleep deprivation.15-17 Other studies have noted decreased glucose tolerance, reduced insulin sensitivity, and catecholamine and cortisol secretion abnormalities, which place children at higher risk for metabolic syndrome and hypertension.13,18 Sleep deprivation also is associated with mood and anxiety disorders and is an independent risk factor for substance use and suicidal ideation among adolescents.19 Sleep deprivation increases impairments in impulse control, concentration, and attention, which could be especially problematic in school-age children.
How sleep is assessed
The sleep history is the first step in evaluating a child or adolescent for a sleep disorder. The sleep history includes exploring the chief complaint, sleep patterns and schedules, bedtime routines, and nocturnal and daytime behaviors (Table).
Chief complaint
Behavioral sleep specialists will assess the primary problem with everyone involved in the child’s bedtime.20 This might include parents (custodial and noncustodial), grandparents, or stepparents as well as the child/adolescent. This important step can reveal a sleep disorder or an inappropriately early bedtime relative to the child’s development. During this assessment, ask detailed questions about how long the sleep problem has persisted, the frequency of sleep problems, and any precipitating stressors. Parents and caregivers can review strategies they have tried, and for how long and to what extent interventions were implemented consistently to result in change.
Sleep patterns and schedules
Review the child/adolescent’s typical sleep patterns and behaviors. Ask parents and caregivers, as well as the patient, about general sleep schedules for the past few weeks or a typical 2-week time period.2 A behavioral assessment of sleep should include asking families about how the child/adolescent sleeps during the week and over the weekend, and if school-year sleep differs from summer or holiday sleep schedules. These questions can illuminate how long a sleep problem has been occurring and what sleep habits might be contributing to the problem. Bedtime
Determine if there is a set bedtime or if the child goes to bed when they wish. It is important to ascertain if the bedtime is age-appropriate, if weekday and weekend bedtimes differ, and to what extent extracurricular activities or school demands impact bedtime. Assess the consistency of the bedtime, the nature of bedtime routines (eg, is the child engaging in stimulating activities before bed), where the bedtime routine occurs (eg, sibling’s room, parents’ room, child’s room), and what role (if any) electronic devices play.2
Nocturnal behaviors
Assessment should include a series of questions and age-specific questionnaires to focus on what behaviors occur at night, including awakenings. Parents should be asked how frequent night awakenings occur, how long arousals last, and how the child signals for the parent (eg, calling out, climbing into parents’ bed).2 Additionally, ask how parents respond and what is required to help the child fall back asleep (eg, rocking, soothing, feeding). The presence of nightmares, night terrors, parasomnias, and sleep-related breathing disorders also must be assessed.20
Daytime behaviors
A sleep history should include assessment of daytime functioning, including daytime sleepiness, fatigue, morning waking, and functioning during school, extracurriculars, and homework. For children and teens, falling asleep in the car, while in school, or during passive activities (meals, conversation) suggests insufficient sleep, sleep disruption, or excessive daytime sleepiness.2
Continue to: Sleep disruption in youth with psychiatric disorders...
Sleep disruption in youth with psychiatric disorders
Disordered sleep is common across psychiatric disorders. The National Comorbidity Survey Adolescent Supplement—a nationally representative cross-sectional survey of adolescents (N = 10,123)—found that a later weeknight bedtime, shorter weeknight sleep duration, and greater weekend bedtime delay increased the risk of developing a mood, anxiety, or substance use (including nicotine) disorder, and suicidality. These risk factors also were associated with lower “perceived mental and physical health.”21 Clinicians should routinely obtain a sleep history in children and adolescents with these disorders. Consider using the sleep screening tool BEARS:
- Bedtime issues
- Excessive daytime sleepiness
- Awakenings
- Regularity and duration of sleep
- Snoring.
ADHD
Up to one-half of children and adolescents with ADHD experience sleep problems,22,23 including delayed sleep onset, bedtime resistance, daytime fatigue, and feeling groggy in the morning beyond what is typical (>20 minutes). Pharmacotherapy for ADHD contributes to sleep disturbances24,25 while sleep deprivation exacerbates inattention and hyperactivity. In youth with ADHD, restless leg syndrome, periodic limb movement disorder, and sleep-disordered breathing disorder are more common than in the general population.
Depressive disorders
Up to three-quarters of depressed children and 90% of depressed adolescents report sleep disturbances, including initial, middle, and terminal insomnia as well as hypersomnia.26 Disrupted sleep in pediatric patients with major depressive disorder could be moderated by the patient’s age, with depressive symptoms more common among adolescents (age 12 to 17) than among younger children (age 6 to 11).27 Successful treatment of depression fails to relieve dyssomnia in 10% of children. Sleep problems that persist after successfully treating a depressive episode could increase the risk of another depressive episode.28
Anxiety disorders
Sleep problems are common among children and adolescents with anxiety disorders.29 Longitudinal data from >900 children found that symptoms of sleep disturbance in early childhood were correlated with experiencing an anxiety disorder 20 years later.30 Fears related to the dark or monsters under the bed that are developmentally appropriate for younger children may interfere with sleep. However, in anxious children, fears might also be related to separation, sleeping alone, worry about the loss of a loved one, concerns about personal safety, fear of frightening dreams, or concerns about academics and social relationships. Anxious individuals ruminate about their worries, and this might be especially true for children at bedtime, when there are limited distractions from ruminative fears.31 Bedtime resistance, parental involvement in bedtime rituals, and cultural factors related to sleep also could play a role for children with anxiety symptoms and sleep problems.
Having an anxiety disorder is significantly associated with an increased risk of insomnia; however, 73% of the time anxiety symptoms precede an insomnia diagnosis.29 Sleep problems and anxiety symptoms might have a reciprocal influence on one another; tiredness that results from sleep problems could exacerbate anxiety, which further worsens sleep problems.
A bridge to treatment
A thorough assessment can help identify modifiable factors and guide treatment selections. In Part 2 of this article, we will describe healthy sleep practices, cognitive-behavioral therapy for insomnia, when pharmacotherapy might be indicated, and the evidence supporting several medications commonly used to treat pediatric insomnia. We also will discuss factors to consider when seeking consultation with a pediatric behavioral sleep specialist.
FIRST OF 2 PARTS
A thorough evaluation can identify modifiable factors and guide treatment
Sleep problems are common among children and adolescents,1 with prevalence rates of 25% to 40%.2-4 Young children most commonly exhibit what is referred to as bedtime problems and night wakenings, whereas children in middle childhood (age 4 to 12) through adolescence (age 13 to 17) report insomnia. For many children, these problems persist.3 Insufficient sleep in children and adolescents worsens inattention, daytime fatigue, and cognitive and behavioral deficits.5 Assessment and treatment of sleep problems in children and adolescents is critical because poor sleep among youth increases the risk for depression, self-harm, and suicide,6,7 increases family stress, and decreases parental well-being.1
This 2-part article describes the assessment, diagnosis, and treatment of sleep problems among children and adolescents. In part 1, we focus on:
- sleep architecture (circadian rhythms, stages of sleep)
- sleep in healthy youth (age 6 to 17) and those with attention-deficit/hyperactivity disorder (ADHD), depressive disorders, and anxiety
- how to assess sleep, and the differential diagnosis of behavioral sleep problems in pediatric patients.
In Part 2, we will cover psychotherapeutic and psychopharmacologic interventions for youth with insomnia, and describe an effective approach to consultation with pediatric sleep medicine specialists.
How much sleep do children and adolescents need?
Throughout their development, children spend 40% to 50% of their time asleep. Sleep schedules are based on circadian rhythms, which are physical, mental, and behavioral changes that follow an approximately 24-hour cycle. Human circadian rhythm varies between 24 and 25 hours and is vital in determining our sleep patterns. Exposure to sunlight drives our circadian rhythm, sending signals to our bodies to “turn on” melatonin production at night (ie, 9
Box
Sleep architecture consists of 3 states: wake; non-rapid eye movement (NREM) sleep; and rapid eye movement (REM) sleep (“dreaming” sleep).2 These stages have distinct polysomnographic features of electroencephalographic EEG patterns, eye movements, and muscle tone.2 NREM sleep can be further divided into 3 stages: stage 1 (N1), stage 2 (N2), and stage 3 (N3). Stage 1 is the lightest stage and lasts for 30 seconds to 5 minutes; it is easy to wake up from stage 1 sleep. During stage 2 sleep, the body moves into a deeper sleep stage that is considered “true” sleep. This sleep stage is characterized by bursts of rhythmic rapid EEG activity known as spindles, as well as high-amplitude slow-wave spikes called K complexes.2 Stage 2 sleep lasts for 10 to 45 minutes. Stage 3, better known as “deep sleep,” slow-wave sleep, or delta sleep, is the most restorative sleep.2 Respiration is low and parasympathetic activity is high.2 It is difficult to be awakened during deep sleep, and if aroused, the person likely will feel confused or groggy. Deep sleep is followed by a return to lighter stage of sleep before the first REM sleep period begins.
REM sleep is the active stage of sleep. Breathing and heart rate become irregular, and the body experiences muscle atonia, or temporary paralysis, of arms and legs. When in REM sleep, individuals have the highest brain metabolic rates, and periodic bursts of eye movements.2 Most individuals move through stages of NREM and REM sleep in predicable ways, meaning they experience NREM sleep, return to a lighter stage of sleep after deep sleep, then move into REM sleep before the cycle repeats. It takes approximately 90 minutes for most adults to complete the NREM sleep cycle, and then REM sleep occurs before returning to NREM sleep.
In children, especially in infants and babies, sleep cycles are closer to 50 to 60 minutes. Newborns spend approximately 50% of their sleep in REM sleep, whereas adults spend 20% to 25% of their sleep in REM sleep. Children will spend more time in REM sleep until the third and fourth years of life, at which point REM gradually decreases to 20% to 25% by adulthood.
Sleep needs also change predictably throughout the lifespan. The National Sleep Foundation guidelines for sleep duration provide clinicians and parents with a range of recommended sleep for each stage of development. Infants require 14 to 17 hours of sleep, whereas adolescents need 8 to 10 hours by age 14 to 17.8 The key for clinicians is to determine if the child is within the recommended range, and how they are functioning on the number of hours of sleep they report. This allows for variation in how much sleep an individual child might need while acknowledging that some children within a specific age group might need more or less sleep than other children of the same age.
Sleep in healthy youth: Middle childhood
School-age children (age 6 to 12) typically need 9 to 10 hours of sleep over a 24-hour period.2 This developmental period is especially important for children to develop healthy sleep habits; however, developmentally appropriate cognitive and social/emotional factors might interfere with the quality and quantity of sleep. Middle childhood is a time when children can understand the dangers of the outside world (ie, violence, health problems) and resulting anxiety can disrupt sleep. Parents usually are less involved in bedtime as children approach adolescence, which leads to later bedtimes. At this stage, many children begin to take on more serious roles in their academics and extracurricular activities, peer relationships become more important, and use of electronics (eg, television, video games, internet, and handheld devices) increases—all of which compete with sleep.9 Frequent sleep issues during middle childhood include:
- irregular sleep-wake schedules
- later bedtimes
- decreased nighttime sleep
- increased caffeine intake
- reduced parental presence at bedtime
- daytime sleepiness.3
In school-age children, regular napping, falling asleep during short car rides, and daytime fatigue at school or home are cause for concern. When these symptoms are present, an evaluation is warranted.
Sleep in healthy youth: Adolescence
The National Sleep Foundation recommends adolescents obtain 8 to 10 hours of sleep per night; for some adolescents, as much as 11 hours of sleep per night might be appropriate.8 However, this contrasts with findings from the National Sleep Foundation’s Sleep in America Poll, which revealed that 75% of 12th graders report <8 hours of sleep nightly.10 Many adolescents experience delayed sleep phase syndrome or delayed sleep-wake phase disorder, which involves a persistent phase shift of >2 hours in the sleep-wake schedule that conflicts with the adolescent’s school, work, or lifestyle demands.11 Such circadian rhythm disorders typically result from a poor match between the sleep-wake schedule and the demands of the adolescent’s life, or a failure to synchronize their internal clock with a 24-hour circadian clock.12 Children typically become tired after sunset, but puberty is associated with reduced slow-wave sleep and changes in circadian rhythms. As a result, a 3-hour delay (delayed phase preference) is common among adolescents. At approximately age 20, people start to become tired after sunset and awaken earlier in the morning—a pattern driven by sunlight and the timing of melatonin release that will remain stable until the sixth decade of life.
Continue to: Effects of chronic sleep deprivation...
Effects of chronic sleep deprivation
Most older studies of sleep loss examined the impact of total sleep loss (sleep deprivation) rather than the effect of partial sleep loss or sleep restriction, a more commonly experienced phenomenon. More recent research shows that a cumulative sleep deficit could cause the body to override voluntary wakefulness and a sleep-deprived individual can experience brief “microsleeps” where they are unaware and lose attention/wakefulness for several seconds.2 This can be deadly if a sleep-deprived adolescent experiences microsleeps while driving.13
There is a well-studied correlation between chronic sleep deprivation and increased body mass index in children.14 This might be caused by reduction in physical activity as well as alterations in the “hunger hormones”—ghrelin and leptin—that have been observed with sleep deprivation.15-17 Other studies have noted decreased glucose tolerance, reduced insulin sensitivity, and catecholamine and cortisol secretion abnormalities, which place children at higher risk for metabolic syndrome and hypertension.13,18 Sleep deprivation also is associated with mood and anxiety disorders and is an independent risk factor for substance use and suicidal ideation among adolescents.19 Sleep deprivation increases impairments in impulse control, concentration, and attention, which could be especially problematic in school-age children.
How sleep is assessed
The sleep history is the first step in evaluating a child or adolescent for a sleep disorder. The sleep history includes exploring the chief complaint, sleep patterns and schedules, bedtime routines, and nocturnal and daytime behaviors (Table).
Chief complaint
Behavioral sleep specialists will assess the primary problem with everyone involved in the child’s bedtime.20 This might include parents (custodial and noncustodial), grandparents, or stepparents as well as the child/adolescent. This important step can reveal a sleep disorder or an inappropriately early bedtime relative to the child’s development. During this assessment, ask detailed questions about how long the sleep problem has persisted, the frequency of sleep problems, and any precipitating stressors. Parents and caregivers can review strategies they have tried, and for how long and to what extent interventions were implemented consistently to result in change.
Sleep patterns and schedules
Review the child/adolescent’s typical sleep patterns and behaviors. Ask parents and caregivers, as well as the patient, about general sleep schedules for the past few weeks or a typical 2-week time period.2 A behavioral assessment of sleep should include asking families about how the child/adolescent sleeps during the week and over the weekend, and if school-year sleep differs from summer or holiday sleep schedules. These questions can illuminate how long a sleep problem has been occurring and what sleep habits might be contributing to the problem. Bedtime
Determine if there is a set bedtime or if the child goes to bed when they wish. It is important to ascertain if the bedtime is age-appropriate, if weekday and weekend bedtimes differ, and to what extent extracurricular activities or school demands impact bedtime. Assess the consistency of the bedtime, the nature of bedtime routines (eg, is the child engaging in stimulating activities before bed), where the bedtime routine occurs (eg, sibling’s room, parents’ room, child’s room), and what role (if any) electronic devices play.2
Nocturnal behaviors
Assessment should include a series of questions and age-specific questionnaires to focus on what behaviors occur at night, including awakenings. Parents should be asked how frequent night awakenings occur, how long arousals last, and how the child signals for the parent (eg, calling out, climbing into parents’ bed).2 Additionally, ask how parents respond and what is required to help the child fall back asleep (eg, rocking, soothing, feeding). The presence of nightmares, night terrors, parasomnias, and sleep-related breathing disorders also must be assessed.20
Daytime behaviors
A sleep history should include assessment of daytime functioning, including daytime sleepiness, fatigue, morning waking, and functioning during school, extracurriculars, and homework. For children and teens, falling asleep in the car, while in school, or during passive activities (meals, conversation) suggests insufficient sleep, sleep disruption, or excessive daytime sleepiness.2
Continue to: Sleep disruption in youth with psychiatric disorders...
Sleep disruption in youth with psychiatric disorders
Disordered sleep is common across psychiatric disorders. The National Comorbidity Survey Adolescent Supplement—a nationally representative cross-sectional survey of adolescents (N = 10,123)—found that a later weeknight bedtime, shorter weeknight sleep duration, and greater weekend bedtime delay increased the risk of developing a mood, anxiety, or substance use (including nicotine) disorder, and suicidality. These risk factors also were associated with lower “perceived mental and physical health.”21 Clinicians should routinely obtain a sleep history in children and adolescents with these disorders. Consider using the sleep screening tool BEARS:
- Bedtime issues
- Excessive daytime sleepiness
- Awakenings
- Regularity and duration of sleep
- Snoring.
ADHD
Up to one-half of children and adolescents with ADHD experience sleep problems,22,23 including delayed sleep onset, bedtime resistance, daytime fatigue, and feeling groggy in the morning beyond what is typical (>20 minutes). Pharmacotherapy for ADHD contributes to sleep disturbances24,25 while sleep deprivation exacerbates inattention and hyperactivity. In youth with ADHD, restless leg syndrome, periodic limb movement disorder, and sleep-disordered breathing disorder are more common than in the general population.
Depressive disorders
Up to three-quarters of depressed children and 90% of depressed adolescents report sleep disturbances, including initial, middle, and terminal insomnia as well as hypersomnia.26 Disrupted sleep in pediatric patients with major depressive disorder could be moderated by the patient’s age, with depressive symptoms more common among adolescents (age 12 to 17) than among younger children (age 6 to 11).27 Successful treatment of depression fails to relieve dyssomnia in 10% of children. Sleep problems that persist after successfully treating a depressive episode could increase the risk of another depressive episode.28
Anxiety disorders
Sleep problems are common among children and adolescents with anxiety disorders.29 Longitudinal data from >900 children found that symptoms of sleep disturbance in early childhood were correlated with experiencing an anxiety disorder 20 years later.30 Fears related to the dark or monsters under the bed that are developmentally appropriate for younger children may interfere with sleep. However, in anxious children, fears might also be related to separation, sleeping alone, worry about the loss of a loved one, concerns about personal safety, fear of frightening dreams, or concerns about academics and social relationships. Anxious individuals ruminate about their worries, and this might be especially true for children at bedtime, when there are limited distractions from ruminative fears.31 Bedtime resistance, parental involvement in bedtime rituals, and cultural factors related to sleep also could play a role for children with anxiety symptoms and sleep problems.
Having an anxiety disorder is significantly associated with an increased risk of insomnia; however, 73% of the time anxiety symptoms precede an insomnia diagnosis.29 Sleep problems and anxiety symptoms might have a reciprocal influence on one another; tiredness that results from sleep problems could exacerbate anxiety, which further worsens sleep problems.
A bridge to treatment
A thorough assessment can help identify modifiable factors and guide treatment selections. In Part 2 of this article, we will describe healthy sleep practices, cognitive-behavioral therapy for insomnia, when pharmacotherapy might be indicated, and the evidence supporting several medications commonly used to treat pediatric insomnia. We also will discuss factors to consider when seeking consultation with a pediatric behavioral sleep specialist.
1. Meltzer LJ, Mindell JA. Systematic review and meta-analysis of behavioral interventions for pediatric insomnia. J Pediatr Psychol. 2014;39(8):932-948. doi:10.1093/jpepsy/jsu041
2. Owens JA, Mindell JA. Pediatric insomnia. Pediatr Clin North Am. 2011;58(3):555-569. doi:10.1016/j.pcl.2011.03.011
3. Meltzer LJ, Plaufcan MR, Thomas JH, et al. Sleep problems and sleep disorders in pediatric primary care: treatment recommendations, persistence, and health care utilization. J Clin Sleep Med. 2014;10(4):421-426. doi:10.5664/jcsm.3620
4. Moore M, Meltzer LJ, Mindell JA. Bedtime problems and night wakings in children. Prim Care. 2008;35(3):569-581, viii. doi:10.1016/j.pop.2008.06.002
5. Williamson AA, Mindell JA, Hiscock H, et al. Longitudinal sleep problem trajectories are associated with multiple impairments in child well-being. J Child Psychol Psychiatry. 2020;61(10):1092-1103. doi:10.1111/jcpp.13303
6. Roberts RE, Roberts CR, Chen IG. Impact of insomnia on future functioning of adolescents. J Psychosom Res. 2002; 53(1):561-569. doi:10.1016/s0022-3999(02)00446-4
7. Singareddy R, Krishnamurthy VB, Vgontzas AN, et al. Subjective and objective sleep and self-harm behaviors in young children: a general population study. Psychiatry Res. 2013;209(3):549-553. doi:10.1016/j.psychres.2013.03.036
8. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1(4):233-243. doi:10.1016/j.sleh.2015.10.004
9. Calamaro CJ, Mason TBA, Ratcliffe SJ. Adolescents living the 24/7 lifestyle: Effects of caffeine and technology on sleep duration and daytime functioning. Pediatrics. 2009;123(6):e1005-1010. doi:10.1542/peds.2008-3641
10. Mindell JA, Owens JA, Carskadon MA. Developmental features of sleep. Child Adolesc Psychiatr Clin N Am. 1999;8(4):695-725.
11. Moore M, Meltzer LJ. The sleepy adolescent: causes and consequences of sleepiness in teens. Paediatr Respir Rev. 2008;9(2):114-120. doi:10.1016/j.prrv.2008.01.001
12. Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med. 2007;8(6):602-612. doi:10.1016/j.sleep.2006.12.002
13. Millman RP; Working Group on Sleepiness in Adolescents/Young Adults; AAP Committee on Adolescence. Excessive sleepiness in adolescents and young adults: causes, consequences, and treatment strategies. Pediatrics. 2005;115(6):1774-1786. doi:10.1542/peds.2005-0772
14. Kaczor M, Skalski M. Prevalence and consequences of insomnia in pediatric population. Psychiatr Pol. 2016;50(3):555-569. doi:10.12740/PP/61226
15. Gomes TN, Dos Santos FK, Santos D, et al. Correlates of sedentary time in children: a multilevel modelling approach. BMC Public Health. 2014;14:890. doi:10.1186/1471-2458-14-890
16. Stone MR, Stevens D, Faulkner GEJ. Maintaining recommended sleep throughout the week is associated with increased physical activity in children. Prev Med. 2013;56(2):112-117. doi:10.1016/j.ypmed.2012.11.015
17. Hart CN, Fava JL, Subak LL, et al. Time in bed is associated with decreased physical activity and higher BMI in women seeking weight loss treatment. ISRN Obes. 2012;2012:320157. doi:10.5402/2012/320157
18. Tasali E, Leproult R, Ehrmann DA, et al. Slow-wave sleep and the risk of type 2 diabetes in humans. Proc Natl Acad Sci U S A. 2008;105(3):1044-1049. doi:10.1073/pnas.0706446105
19. de Zambotti M, Goldstone A, Colrain IM, et al. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. 2018;39:12-24. doi:10.1016/j.smrv.2017.06.009
20. Mindell JA, Owens JA. A clinical guide to pediatric sleep: diagnosis and management of sleep problems. 3rd ed. Lippincott Williams & Wilkins; 2015.
21. Zhang J, Paksarian D, Lamers F, et al. Sleep patterns and mental health correlates in US adolescents. J Pediatr. 2017;182:137-143. doi:10.1016/j.jpeds.2016.11.007
22. Gregory AM, Agnew-Blais JC, Matthews T, et al. ADHD and sleep quality: longitudinal analyses from childhood to early adulthood in a twin cohort. J Clin Child Adolesc Psychol. 2017;46(2):284-294. doi:10.1080/15374416.2016.1183499
23. Weiss MD, Salpekar J. Sleep problems in the child with attention-deficit hyperactivity disorder: Defining aetiology and appropriate treatments. CNS Drugs. 2010;24(10):811-828. doi:10.2165/11538990-000000000-00000
24. Galland BC, Tripp EG, Taylor BJ. The sleep of children with attention deficit hyperactivity disorder on and off methylphenidate: a matched case-control study. J Sleep Res. 2010;19(2):366-373. doi:10.1111/j.1365-2869.2009.00795.x
25. Becker SP, Froehlich TE, Epstein JN. Effects of methylphenidate on sleep functioning in children with attention-deficit/hyperactivity disorder. J Dev Behav Pediatr. 2016;37(5):395-404. doi:10.1097/DBP.0000000000000285
26. Roberts RE, Duong HT. Depression and insomnia among adolescents: a prospective perspective. J Affect Disord. 2013;148(1):66-71. doi:10.1016/j.jad.2012.11.049
27. Emslie GJ, Rush AJ, Weinberg WA, et al. Sleep EEG features of adolescents with major depression. Biol Psychiatry. 1994;36(9):573-581. doi:10.1016/0006-3223(94)90067-1
28. Alfano CA, Zakem AH, Costa NM, et al. Sleep problems and their relation to cognitive factors, anxiety, and depressive symptoms in children and adolescents. Depress Anxiety. 2009;26(6):503-512. doi:10.1002/da.20443
29. Alfano CA, Ginsburg GS, Kingery JN. Sleep-related problems among children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry. 2007;46(2):224-232. doi:10.1097/01.chi.0000242233.06011.8e
30. Gregory AM, Caspi A, Eley TC, et al. Prospective longitudinal associations between persistent sleep problems in childhood and anxiety and depression disorders in adulthood. J Abnorm Child Psychol. 2005;33(2):157-163. doi: 10.1007/s10802-005-1824-0
31. Chorney DB, Detweiler MF, Morris TL, et al. The interplay of sleep disturbance, anxiety, and depression in children. J Pediatr Psychol. 2008;33(4):339-348. doi:10.1093/jpepsy/jsm105
32. Sadeh A. Stress, trauma, and sleep in children. Child Adolesc Psychiatr Clin N Am. 1996;5(3):685-700. doi:10.1016/S1056-4993(18)30356-0
33. Glod CA, Teicher MH, Hartman CR, et al. Increased nocturnal activity and impaired sleep maintenance in abused children. J Am Acad Child Adolesc Psychiatry. 1997;36(9):1236-1243. doi:10.1097/00004583-199709000-00016
34. Strawn JR, Lu L, Peris TS, et al. Research review: pediatric anxiety disorders: what have we learnt in the last 10 years? J Child Psychol Psychiatry. 2021;62(2):114-139. doi:10.1111/jcpp.13262
35. Wehry AM, Beesdo-Baum K, Hennelly MM, et al. Assessment and treatment of anxiety disorders in children and adolescents. Curr Psychiatry Rep. 2015;17(7):52. doi:10.1007/s11920-015-0591-z
36. Hamill Skoch S, Mills JA, Ramsey L, et al. Letter to editor: sleep disturbances in selective serotonin reuptake inhibitor-treated youth with anxiety disorders and obsessive compulsive disorder— a bayesian hierarchical modeling meta-analysis. J Child Adolesc Psychopharmacol. 2021;31(5):387-388. doi:10.1089/cap.2020.0169
1. Meltzer LJ, Mindell JA. Systematic review and meta-analysis of behavioral interventions for pediatric insomnia. J Pediatr Psychol. 2014;39(8):932-948. doi:10.1093/jpepsy/jsu041
2. Owens JA, Mindell JA. Pediatric insomnia. Pediatr Clin North Am. 2011;58(3):555-569. doi:10.1016/j.pcl.2011.03.011
3. Meltzer LJ, Plaufcan MR, Thomas JH, et al. Sleep problems and sleep disorders in pediatric primary care: treatment recommendations, persistence, and health care utilization. J Clin Sleep Med. 2014;10(4):421-426. doi:10.5664/jcsm.3620
4. Moore M, Meltzer LJ, Mindell JA. Bedtime problems and night wakings in children. Prim Care. 2008;35(3):569-581, viii. doi:10.1016/j.pop.2008.06.002
5. Williamson AA, Mindell JA, Hiscock H, et al. Longitudinal sleep problem trajectories are associated with multiple impairments in child well-being. J Child Psychol Psychiatry. 2020;61(10):1092-1103. doi:10.1111/jcpp.13303
6. Roberts RE, Roberts CR, Chen IG. Impact of insomnia on future functioning of adolescents. J Psychosom Res. 2002; 53(1):561-569. doi:10.1016/s0022-3999(02)00446-4
7. Singareddy R, Krishnamurthy VB, Vgontzas AN, et al. Subjective and objective sleep and self-harm behaviors in young children: a general population study. Psychiatry Res. 2013;209(3):549-553. doi:10.1016/j.psychres.2013.03.036
8. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1(4):233-243. doi:10.1016/j.sleh.2015.10.004
9. Calamaro CJ, Mason TBA, Ratcliffe SJ. Adolescents living the 24/7 lifestyle: Effects of caffeine and technology on sleep duration and daytime functioning. Pediatrics. 2009;123(6):e1005-1010. doi:10.1542/peds.2008-3641
10. Mindell JA, Owens JA, Carskadon MA. Developmental features of sleep. Child Adolesc Psychiatr Clin N Am. 1999;8(4):695-725.
11. Moore M, Meltzer LJ. The sleepy adolescent: causes and consequences of sleepiness in teens. Paediatr Respir Rev. 2008;9(2):114-120. doi:10.1016/j.prrv.2008.01.001
12. Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med. 2007;8(6):602-612. doi:10.1016/j.sleep.2006.12.002
13. Millman RP; Working Group on Sleepiness in Adolescents/Young Adults; AAP Committee on Adolescence. Excessive sleepiness in adolescents and young adults: causes, consequences, and treatment strategies. Pediatrics. 2005;115(6):1774-1786. doi:10.1542/peds.2005-0772
14. Kaczor M, Skalski M. Prevalence and consequences of insomnia in pediatric population. Psychiatr Pol. 2016;50(3):555-569. doi:10.12740/PP/61226
15. Gomes TN, Dos Santos FK, Santos D, et al. Correlates of sedentary time in children: a multilevel modelling approach. BMC Public Health. 2014;14:890. doi:10.1186/1471-2458-14-890
16. Stone MR, Stevens D, Faulkner GEJ. Maintaining recommended sleep throughout the week is associated with increased physical activity in children. Prev Med. 2013;56(2):112-117. doi:10.1016/j.ypmed.2012.11.015
17. Hart CN, Fava JL, Subak LL, et al. Time in bed is associated with decreased physical activity and higher BMI in women seeking weight loss treatment. ISRN Obes. 2012;2012:320157. doi:10.5402/2012/320157
18. Tasali E, Leproult R, Ehrmann DA, et al. Slow-wave sleep and the risk of type 2 diabetes in humans. Proc Natl Acad Sci U S A. 2008;105(3):1044-1049. doi:10.1073/pnas.0706446105
19. de Zambotti M, Goldstone A, Colrain IM, et al. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. 2018;39:12-24. doi:10.1016/j.smrv.2017.06.009
20. Mindell JA, Owens JA. A clinical guide to pediatric sleep: diagnosis and management of sleep problems. 3rd ed. Lippincott Williams & Wilkins; 2015.
21. Zhang J, Paksarian D, Lamers F, et al. Sleep patterns and mental health correlates in US adolescents. J Pediatr. 2017;182:137-143. doi:10.1016/j.jpeds.2016.11.007
22. Gregory AM, Agnew-Blais JC, Matthews T, et al. ADHD and sleep quality: longitudinal analyses from childhood to early adulthood in a twin cohort. J Clin Child Adolesc Psychol. 2017;46(2):284-294. doi:10.1080/15374416.2016.1183499
23. Weiss MD, Salpekar J. Sleep problems in the child with attention-deficit hyperactivity disorder: Defining aetiology and appropriate treatments. CNS Drugs. 2010;24(10):811-828. doi:10.2165/11538990-000000000-00000
24. Galland BC, Tripp EG, Taylor BJ. The sleep of children with attention deficit hyperactivity disorder on and off methylphenidate: a matched case-control study. J Sleep Res. 2010;19(2):366-373. doi:10.1111/j.1365-2869.2009.00795.x
25. Becker SP, Froehlich TE, Epstein JN. Effects of methylphenidate on sleep functioning in children with attention-deficit/hyperactivity disorder. J Dev Behav Pediatr. 2016;37(5):395-404. doi:10.1097/DBP.0000000000000285
26. Roberts RE, Duong HT. Depression and insomnia among adolescents: a prospective perspective. J Affect Disord. 2013;148(1):66-71. doi:10.1016/j.jad.2012.11.049
27. Emslie GJ, Rush AJ, Weinberg WA, et al. Sleep EEG features of adolescents with major depression. Biol Psychiatry. 1994;36(9):573-581. doi:10.1016/0006-3223(94)90067-1
28. Alfano CA, Zakem AH, Costa NM, et al. Sleep problems and their relation to cognitive factors, anxiety, and depressive symptoms in children and adolescents. Depress Anxiety. 2009;26(6):503-512. doi:10.1002/da.20443
29. Alfano CA, Ginsburg GS, Kingery JN. Sleep-related problems among children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry. 2007;46(2):224-232. doi:10.1097/01.chi.0000242233.06011.8e
30. Gregory AM, Caspi A, Eley TC, et al. Prospective longitudinal associations between persistent sleep problems in childhood and anxiety and depression disorders in adulthood. J Abnorm Child Psychol. 2005;33(2):157-163. doi: 10.1007/s10802-005-1824-0
31. Chorney DB, Detweiler MF, Morris TL, et al. The interplay of sleep disturbance, anxiety, and depression in children. J Pediatr Psychol. 2008;33(4):339-348. doi:10.1093/jpepsy/jsm105
32. Sadeh A. Stress, trauma, and sleep in children. Child Adolesc Psychiatr Clin N Am. 1996;5(3):685-700. doi:10.1016/S1056-4993(18)30356-0
33. Glod CA, Teicher MH, Hartman CR, et al. Increased nocturnal activity and impaired sleep maintenance in abused children. J Am Acad Child Adolesc Psychiatry. 1997;36(9):1236-1243. doi:10.1097/00004583-199709000-00016
34. Strawn JR, Lu L, Peris TS, et al. Research review: pediatric anxiety disorders: what have we learnt in the last 10 years? J Child Psychol Psychiatry. 2021;62(2):114-139. doi:10.1111/jcpp.13262
35. Wehry AM, Beesdo-Baum K, Hennelly MM, et al. Assessment and treatment of anxiety disorders in children and adolescents. Curr Psychiatry Rep. 2015;17(7):52. doi:10.1007/s11920-015-0591-z
36. Hamill Skoch S, Mills JA, Ramsey L, et al. Letter to editor: sleep disturbances in selective serotonin reuptake inhibitor-treated youth with anxiety disorders and obsessive compulsive disorder— a bayesian hierarchical modeling meta-analysis. J Child Adolesc Psychopharmacol. 2021;31(5):387-388. doi:10.1089/cap.2020.0169
