User login
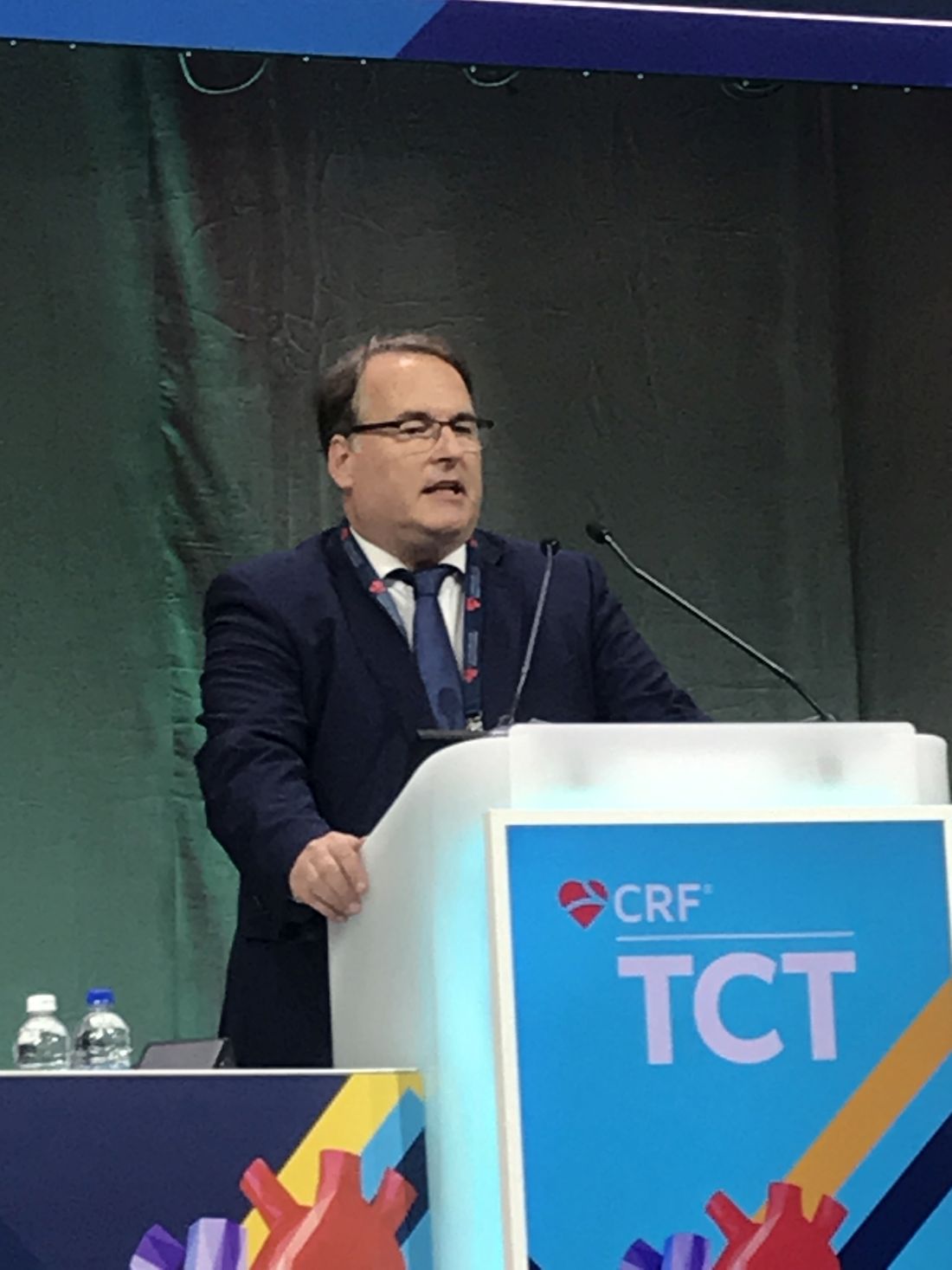
In cardiogenic shock, edge-to-edge mitral valve repair improves outcome
In patients with severe mitral regurgitation (MR) and cardiogenic shock, successful transcatheter edge-to-edge repair (TEER) is associated with a substantial reduction in all-cause mortality and lower morbidity at 1 year, according to an analysis of registry data.
The data from this analysis also confirm that “successful reduction of MR is achievable with TEER in most patients with cardiogenic shock,” reported Mohamad A. Alkhouli, MD, an interventional cardiologist and professor of medicine at the Mayo Clinic, Rochester, Minn.

In those with device success, achieved in 85.6% of patients, all-cause mortality was about 21% lower (34.6% vs. 55.5%; P < .001) at 1 year than in those who were not successfully repaired, according to Dr. Alkhouli, who presented the findings at the Transcatheter Cardiovascular Therapeutics annual meeting in Boston. This translated into a reduction in the hazard ratio for death of nearly 50% (hazard ratio, 0.52; 95% confidence interval, 0.43-0.63).
A similar relative benefit was found for the composite endpoint of mortality and heart failure admissions at 1 year. Whether unadjusted (HR, 0.54; 95% CI, 0.45-0.66) or adjusted (HR, 0.51; 95% CI, 0.42-0.62), risk reductions with successful MR reduction, defined as greater than or equal to 1 grade improvement and a final MR grade of less than or equal to 2+, indicated that major adverse outcomes are reduced by about half.
STS/ACC TCT registry data queried
Drawn from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry, 3,797 patients with cardiogenic shock underwent MR repair between November 2013 and December 2021. Outcomes at 1 year were evaluable in 2,773 of these patients. For inclusion, all had to meet at least one of the definitions of cardiogenic shock, such as inotrope use or mechanical circulatory support.
At baseline, 94.5% had a MR severity of at least 3+, and most of these had 4+. Thirty days after treatment, 88.8% had MR severity of 2+ or less, the majority of which had a severity of 1+.
These data address an important question not previously well studied, according to Dr. Alkhouli. In MR patients, cardiogenic shock is associated with a high risk of death, but there has been little evidence that valve repair does not exacerbate, let alone modify, this risk.
These data support the value of intervention, which was performed in almost all patients with MitraClipä (Abbott), the only device available for most of the period in which the registry was queried. However, Dr. Alkhouli cautioned that his data are best considered “hypothesis generating.”
“We need a randomized trial,” he said at the meeting sponsored by the Cardiovascular Research Foundation. He pointed out that this is a complex population for which multiple variables might have skewed results when data are analyzed retrospectively. Not least, those MR patients with cardiogenic shock in the database considered for TEER might well have been relatively healthy and not representative of an unselected population with both MR and cardiogenic shock.
The question might be better answered by the multicenter Canadian trial CAPITAL MINOS, which has just started. Described in an article in the American Heart Journal, it has a planned enrollment of about 150 MR patients with cardiogenic shock randomized to TEER or medical therapy. Results are expected in about 1 year, according to Dr. Alkhouli.
But regarding the present analysis, Dr. Alkhouli did note that sensitivity analyses conducted within his data across risk factors, such as degenerative versus nondegenerative MR, low (< 30%) versus higher left ventricular ejection fraction (LVEF), and presence or absence of an acute coronary syndrome (ACS), consistently supported a benefit from intervention.
Also, cardiogenic shock did not appear to be a factor in device failure, according to Dr. Alkhouli, addressing a potential criticism that cardiogenic shock was an underlying reason for device failure.
More than 90% in NYHA class III or IV heart failure
In this study, the mean age was 73 years. More than 90% were in class III or IV heart failure in the 2 weeks prior to TEER. More than half had established coronary artery disease. Other concomitant cardiovascular morbidities, including atrial fibrillation or flutter (65%), prior MI (39%), and prior stroke or transient ischemic attach (> 10%) were well represented.
When those with device success were compared with those with device failure, the risk profile was comparable. The predicted STS (Society of Thoracic Surgeons) mortality for mitral valve repair among these two groups was 14.8% versus 15% (P = 0.97), respectively.
However, those with device failure did have a lower baseline left ventricular ejection fraction (40.7% vs. 42.9%; P = .009) and a greater prevalence of moderate-to-severe or severe MR (96.1% vs. 84.9%; P < 0.001).
The growing experience with TEER means that benefit has now been shown in several complicated MR groups, such as those with severe ventricular dysfunction, renal insufficiency, and obstructive lung disease. This was a rationale for looking at the impact or repairing MR in patients with cardiogenic shock.
It is a pressing question, according to Dr. Alkhouli. He cited studies suggesting that up to 20% of patients hospitalized for cardiogenic shock have at least moderate-to-severe MR. Conversely, cardiogenic shock is not an uncommon finding in patients with MR.
While Dr. Alkhouli acknowledged that the many variables influencing outcome in patients with MR and cardiogenic shock will make a randomized trial “challenging,” many experts echoed this concern and even expressed some skepticism about the potential for an unbiased trial.
Data confirm MR repair is safe during shock
“These data do show that repair of MR is safe in patients safe in patients with cardiogenic shock,” said Anita W. Asgar, MD, an interventional cardiologist associated with the Montreal Heart Institute. She noted that there was a 5- to 6-day delay among the cardiogenic shock patients prior to undergoing MR repair in this analysis, potentially reflecting an elimination of those at very high risk. Similarly, she suggested that many interventionalists are likely to consider multiple variables before proceeding.
As a result, MR repair may not be amenable to randomization in a cardiogenic shock population, given that this decision is not typically undertaken out of the context of multiple variables.
“I am not sure that a clinical trial is ethical,” she said. She would expect that clinicians enrolling patients would only do so on a selective basis.
Alexandra J. Lansky, MD, Director of the Yale Heart and Vascular Research Program, Yale University, New Haven, Conn., also emphasized the difficulty of controlling for variables, such as the duration of cardiogenic shock, that influence decision-making.
Nevertheless, she called the data “very important” in that they at least lend some objective data for deciding whether to intervene a group of “challenging” patients not uncommonly faced in clinical practice.
Dr. Alkhouli reports financial relationships with Abbott Vascular, Boston Scientific, Johnson & Johnson, and Phillips. Dr. Asgar reports financial relationships with Abbott Vascular, Edwards Lifesciences, W.L. Gore & Associates, and Medtronic. Dr. Lasky reports no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
In patients with severe mitral regurgitation (MR) and cardiogenic shock, successful transcatheter edge-to-edge repair (TEER) is associated with a substantial reduction in all-cause mortality and lower morbidity at 1 year, according to an analysis of registry data.
The data from this analysis also confirm that “successful reduction of MR is achievable with TEER in most patients with cardiogenic shock,” reported Mohamad A. Alkhouli, MD, an interventional cardiologist and professor of medicine at the Mayo Clinic, Rochester, Minn.
In those with device success, achieved in 85.6% of patients, all-cause mortality was about 21% lower (34.6% vs. 55.5%; P < .001) at 1 year than in those who were not successfully repaired, according to Dr. Alkhouli, who presented the findings at the Transcatheter Cardiovascular Therapeutics annual meeting in Boston. This translated into a reduction in the hazard ratio for death of nearly 50% (hazard ratio, 0.52; 95% confidence interval, 0.43-0.63).
A similar relative benefit was found for the composite endpoint of mortality and heart failure admissions at 1 year. Whether unadjusted (HR, 0.54; 95% CI, 0.45-0.66) or adjusted (HR, 0.51; 95% CI, 0.42-0.62), risk reductions with successful MR reduction, defined as greater than or equal to 1 grade improvement and a final MR grade of less than or equal to 2+, indicated that major adverse outcomes are reduced by about half.
STS/ACC TCT registry data queried
Drawn from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry, 3,797 patients with cardiogenic shock underwent MR repair between November 2013 and December 2021. Outcomes at 1 year were evaluable in 2,773 of these patients. For inclusion, all had to meet at least one of the definitions of cardiogenic shock, such as inotrope use or mechanical circulatory support.
At baseline, 94.5% had a MR severity of at least 3+, and most of these had 4+. Thirty days after treatment, 88.8% had MR severity of 2+ or less, the majority of which had a severity of 1+.
These data address an important question not previously well studied, according to Dr. Alkhouli. In MR patients, cardiogenic shock is associated with a high risk of death, but there has been little evidence that valve repair does not exacerbate, let alone modify, this risk.
These data support the value of intervention, which was performed in almost all patients with MitraClipä (Abbott), the only device available for most of the period in which the registry was queried. However, Dr. Alkhouli cautioned that his data are best considered “hypothesis generating.”
“We need a randomized trial,” he said at the meeting sponsored by the Cardiovascular Research Foundation. He pointed out that this is a complex population for which multiple variables might have skewed results when data are analyzed retrospectively. Not least, those MR patients with cardiogenic shock in the database considered for TEER might well have been relatively healthy and not representative of an unselected population with both MR and cardiogenic shock.
The question might be better answered by the multicenter Canadian trial CAPITAL MINOS, which has just started. Described in an article in the American Heart Journal, it has a planned enrollment of about 150 MR patients with cardiogenic shock randomized to TEER or medical therapy. Results are expected in about 1 year, according to Dr. Alkhouli.
But regarding the present analysis, Dr. Alkhouli did note that sensitivity analyses conducted within his data across risk factors, such as degenerative versus nondegenerative MR, low (< 30%) versus higher left ventricular ejection fraction (LVEF), and presence or absence of an acute coronary syndrome (ACS), consistently supported a benefit from intervention.
Also, cardiogenic shock did not appear to be a factor in device failure, according to Dr. Alkhouli, addressing a potential criticism that cardiogenic shock was an underlying reason for device failure.
More than 90% in NYHA class III or IV heart failure
In this study, the mean age was 73 years. More than 90% were in class III or IV heart failure in the 2 weeks prior to TEER. More than half had established coronary artery disease. Other concomitant cardiovascular morbidities, including atrial fibrillation or flutter (65%), prior MI (39%), and prior stroke or transient ischemic attach (> 10%) were well represented.
When those with device success were compared with those with device failure, the risk profile was comparable. The predicted STS (Society of Thoracic Surgeons) mortality for mitral valve repair among these two groups was 14.8% versus 15% (P = 0.97), respectively.
However, those with device failure did have a lower baseline left ventricular ejection fraction (40.7% vs. 42.9%; P = .009) and a greater prevalence of moderate-to-severe or severe MR (96.1% vs. 84.9%; P < 0.001).
The growing experience with TEER means that benefit has now been shown in several complicated MR groups, such as those with severe ventricular dysfunction, renal insufficiency, and obstructive lung disease. This was a rationale for looking at the impact or repairing MR in patients with cardiogenic shock.
It is a pressing question, according to Dr. Alkhouli. He cited studies suggesting that up to 20% of patients hospitalized for cardiogenic shock have at least moderate-to-severe MR. Conversely, cardiogenic shock is not an uncommon finding in patients with MR.
While Dr. Alkhouli acknowledged that the many variables influencing outcome in patients with MR and cardiogenic shock will make a randomized trial “challenging,” many experts echoed this concern and even expressed some skepticism about the potential for an unbiased trial.
Data confirm MR repair is safe during shock
“These data do show that repair of MR is safe in patients safe in patients with cardiogenic shock,” said Anita W. Asgar, MD, an interventional cardiologist associated with the Montreal Heart Institute. She noted that there was a 5- to 6-day delay among the cardiogenic shock patients prior to undergoing MR repair in this analysis, potentially reflecting an elimination of those at very high risk. Similarly, she suggested that many interventionalists are likely to consider multiple variables before proceeding.
As a result, MR repair may not be amenable to randomization in a cardiogenic shock population, given that this decision is not typically undertaken out of the context of multiple variables.
“I am not sure that a clinical trial is ethical,” she said. She would expect that clinicians enrolling patients would only do so on a selective basis.
Alexandra J. Lansky, MD, Director of the Yale Heart and Vascular Research Program, Yale University, New Haven, Conn., also emphasized the difficulty of controlling for variables, such as the duration of cardiogenic shock, that influence decision-making.
Nevertheless, she called the data “very important” in that they at least lend some objective data for deciding whether to intervene a group of “challenging” patients not uncommonly faced in clinical practice.
Dr. Alkhouli reports financial relationships with Abbott Vascular, Boston Scientific, Johnson & Johnson, and Phillips. Dr. Asgar reports financial relationships with Abbott Vascular, Edwards Lifesciences, W.L. Gore & Associates, and Medtronic. Dr. Lasky reports no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
In patients with severe mitral regurgitation (MR) and cardiogenic shock, successful transcatheter edge-to-edge repair (TEER) is associated with a substantial reduction in all-cause mortality and lower morbidity at 1 year, according to an analysis of registry data.
The data from this analysis also confirm that “successful reduction of MR is achievable with TEER in most patients with cardiogenic shock,” reported Mohamad A. Alkhouli, MD, an interventional cardiologist and professor of medicine at the Mayo Clinic, Rochester, Minn.
In those with device success, achieved in 85.6% of patients, all-cause mortality was about 21% lower (34.6% vs. 55.5%; P < .001) at 1 year than in those who were not successfully repaired, according to Dr. Alkhouli, who presented the findings at the Transcatheter Cardiovascular Therapeutics annual meeting in Boston. This translated into a reduction in the hazard ratio for death of nearly 50% (hazard ratio, 0.52; 95% confidence interval, 0.43-0.63).
A similar relative benefit was found for the composite endpoint of mortality and heart failure admissions at 1 year. Whether unadjusted (HR, 0.54; 95% CI, 0.45-0.66) or adjusted (HR, 0.51; 95% CI, 0.42-0.62), risk reductions with successful MR reduction, defined as greater than or equal to 1 grade improvement and a final MR grade of less than or equal to 2+, indicated that major adverse outcomes are reduced by about half.
STS/ACC TCT registry data queried
Drawn from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry, 3,797 patients with cardiogenic shock underwent MR repair between November 2013 and December 2021. Outcomes at 1 year were evaluable in 2,773 of these patients. For inclusion, all had to meet at least one of the definitions of cardiogenic shock, such as inotrope use or mechanical circulatory support.
At baseline, 94.5% had a MR severity of at least 3+, and most of these had 4+. Thirty days after treatment, 88.8% had MR severity of 2+ or less, the majority of which had a severity of 1+.
These data address an important question not previously well studied, according to Dr. Alkhouli. In MR patients, cardiogenic shock is associated with a high risk of death, but there has been little evidence that valve repair does not exacerbate, let alone modify, this risk.
These data support the value of intervention, which was performed in almost all patients with MitraClipä (Abbott), the only device available for most of the period in which the registry was queried. However, Dr. Alkhouli cautioned that his data are best considered “hypothesis generating.”
“We need a randomized trial,” he said at the meeting sponsored by the Cardiovascular Research Foundation. He pointed out that this is a complex population for which multiple variables might have skewed results when data are analyzed retrospectively. Not least, those MR patients with cardiogenic shock in the database considered for TEER might well have been relatively healthy and not representative of an unselected population with both MR and cardiogenic shock.
The question might be better answered by the multicenter Canadian trial CAPITAL MINOS, which has just started. Described in an article in the American Heart Journal, it has a planned enrollment of about 150 MR patients with cardiogenic shock randomized to TEER or medical therapy. Results are expected in about 1 year, according to Dr. Alkhouli.
But regarding the present analysis, Dr. Alkhouli did note that sensitivity analyses conducted within his data across risk factors, such as degenerative versus nondegenerative MR, low (< 30%) versus higher left ventricular ejection fraction (LVEF), and presence or absence of an acute coronary syndrome (ACS), consistently supported a benefit from intervention.
Also, cardiogenic shock did not appear to be a factor in device failure, according to Dr. Alkhouli, addressing a potential criticism that cardiogenic shock was an underlying reason for device failure.
More than 90% in NYHA class III or IV heart failure
In this study, the mean age was 73 years. More than 90% were in class III or IV heart failure in the 2 weeks prior to TEER. More than half had established coronary artery disease. Other concomitant cardiovascular morbidities, including atrial fibrillation or flutter (65%), prior MI (39%), and prior stroke or transient ischemic attach (> 10%) were well represented.
When those with device success were compared with those with device failure, the risk profile was comparable. The predicted STS (Society of Thoracic Surgeons) mortality for mitral valve repair among these two groups was 14.8% versus 15% (P = 0.97), respectively.
However, those with device failure did have a lower baseline left ventricular ejection fraction (40.7% vs. 42.9%; P = .009) and a greater prevalence of moderate-to-severe or severe MR (96.1% vs. 84.9%; P < 0.001).
The growing experience with TEER means that benefit has now been shown in several complicated MR groups, such as those with severe ventricular dysfunction, renal insufficiency, and obstructive lung disease. This was a rationale for looking at the impact or repairing MR in patients with cardiogenic shock.
It is a pressing question, according to Dr. Alkhouli. He cited studies suggesting that up to 20% of patients hospitalized for cardiogenic shock have at least moderate-to-severe MR. Conversely, cardiogenic shock is not an uncommon finding in patients with MR.
While Dr. Alkhouli acknowledged that the many variables influencing outcome in patients with MR and cardiogenic shock will make a randomized trial “challenging,” many experts echoed this concern and even expressed some skepticism about the potential for an unbiased trial.
Data confirm MR repair is safe during shock
“These data do show that repair of MR is safe in patients safe in patients with cardiogenic shock,” said Anita W. Asgar, MD, an interventional cardiologist associated with the Montreal Heart Institute. She noted that there was a 5- to 6-day delay among the cardiogenic shock patients prior to undergoing MR repair in this analysis, potentially reflecting an elimination of those at very high risk. Similarly, she suggested that many interventionalists are likely to consider multiple variables before proceeding.
As a result, MR repair may not be amenable to randomization in a cardiogenic shock population, given that this decision is not typically undertaken out of the context of multiple variables.
“I am not sure that a clinical trial is ethical,” she said. She would expect that clinicians enrolling patients would only do so on a selective basis.
Alexandra J. Lansky, MD, Director of the Yale Heart and Vascular Research Program, Yale University, New Haven, Conn., also emphasized the difficulty of controlling for variables, such as the duration of cardiogenic shock, that influence decision-making.
Nevertheless, she called the data “very important” in that they at least lend some objective data for deciding whether to intervene a group of “challenging” patients not uncommonly faced in clinical practice.
Dr. Alkhouli reports financial relationships with Abbott Vascular, Boston Scientific, Johnson & Johnson, and Phillips. Dr. Asgar reports financial relationships with Abbott Vascular, Edwards Lifesciences, W.L. Gore & Associates, and Medtronic. Dr. Lasky reports no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM TCT 2022
Fourth-gen transcatheter mitral valve shows clinical, procedural improvements
The design improvements introduced in the fourth-generation device for transcatheter mitral valve repair, called the MitraClip G4 (Abbott), appears to yield better outcomes than previous iterations, according to a multinational postapproval study with more than 1,000 patients.
Not least, the 1.3% all-cause mortality at 30 days in this series, called EXPAND G4, “is the lowest that has been reported to date,” reported Ralph Stephan von Bardeleben, MD, at the Transcatheter Cardiovascular Therapeutics annual meeting, sponsored by the Cardiovascular Research Foundation.
The evidence of relative advantages was based on comparisons with historical data and a similar study of the previous-generation device. That previous study, called EXPAND, evaluated the MitraClip NTR and ETR systems.
Device times shorter with new device
“There were shorter device times with MitraClip G4,” said Dr. von Bardeleben, referring to a more than 10-minute advantage over the previous generation device (35 minutes in EXPAND G4 vs. 46 min in EXPAND). Although the reduction in overall median procedure time was more modest (77 vs. 80 minutes), Dr. von Bardeleben said these are “the shortest device and procedural times reported to date.”
He also reported what appeared to be incremental advantages across multiple other endpoints, such as procedural success (96.2% vs. 95.8%) and a reduction in the mean clip rate (1.4 vs. 1.5).
Compared with historical outcomes with other devices employed in transcatheter edge-to-edge repair (TEER) of mitral valves, Dr. von Bardeleben contended that the results support the premise that the MitraClip G4 system is a meaningful advance by incorporating such features as an expanded choice of clip sizes, a greater coaptation area, and a more advanced gripper actuation for leaflet grasping.
Over 90% achieve MR 1+
Not least, it appears to increase the proportion of patients who achieve a mitral regurgitation grade of 1+ (MR1+) or lower, which is increasingly recognized as the goal of TEER, said Dr. von Bardeleben, head of the Centre of Structure Heart Disease Interventions, Heart Valve Centre, Mainz, Germany.
He said the rates of 91% achieving MR1+ or less and 98% achieved 2+ or lower compare favorably with most other series and exceeds levels achieved with surgery.
Dr. von Bardeleben also contended that, because of its design features, the MitraClip G4 “expands the spectrum of TEER-suitable patients.” He noted that 5% of the patients in this real-world series had a high risk of stenosis owing to such issues as severe annular or leaflet calcification and another 5% had factors that would predict inadequate MR reduction, such as Barlow’s disease, bi-leaflet prolapse, and severe leaflet degeneration.
The 1,164 patients in EXPAND G4 were enrolled from sites in the United States, Europe, Canada, and Japan. For the key outcome measure of procedural success, echocardiograms were assessed by an independent core laboratory. Of the 1,164 patients enrolled, 1,044 (91%) had complete follow-up data at 30 days.
The procedural success rates were reflected in improvements in New York Heart Association (NYHA) functional classes and in the Kansas City Cardiomyopathy Questionnaire (KCCQ), a quality of life instrument. Prior to treatment, 69% were in NYHA class III or greater. Following treatment, the proportion was 17% (P < .0001). The 18-point improvement in the KCCQ was characterized by Dr. von Bardeleben as “both clinically and statistically significant [P < .0001].”
There were no strokes in this series, and the 30-day incidence of myocardial infarction was 0.2%. The proportion requiring cardiovascular surgery within 30 days was less than 1%. The rate of bleeding episodes, all of which were nonserious, was 7%.
The “EXPAND G4 study confirms the safety and effectiveness of the next generation MitraClip G4 system,” according to Dr. von Bardeleben, and it did so “in a contemporary real-world setting.”
Outcome data characterized as ‘excellent’
Several invited panelists participating in a discussion following the presentation agreed.
“These results are excellent,” said Raj Makkar, MD, associate director of interventional technologies at Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles. While he was impressed with the fact that only 2% missed the primary endpoint of MR 2+ or lower, he indicated that the 91% achieving MR 1+ or lower might be an even more apt signal that newer-generation devices are improving.
This was echoed by other panelists who appeared to form a general consensus over the premise that the target in TEER should no longer be MR 2+ for most patients.
“We should now be aiming for MR grade of 0-1,” stated panelist Stephan Windecker, MD, chairman, department of cardiology, University of Bern (Switzerland). He indicated that this goal is increasingly reasonable given the advances in device design and greater operator experience.
Dr. von Bardeleben reported financial relationships with Abbott Vascular, Edwards Lifesciences, Medtronic, and Neochord. Dr. Makkar reported financial relationships with Abbott Vascular, Cordis, Edwards Lifesciences, and Medtronic. Dr. Windecker reported financial relationships with more than 30 pharmaceutical companies, including Abbott Vascular, which manufactures MitraClip G4.
The design improvements introduced in the fourth-generation device for transcatheter mitral valve repair, called the MitraClip G4 (Abbott), appears to yield better outcomes than previous iterations, according to a multinational postapproval study with more than 1,000 patients.
Not least, the 1.3% all-cause mortality at 30 days in this series, called EXPAND G4, “is the lowest that has been reported to date,” reported Ralph Stephan von Bardeleben, MD, at the Transcatheter Cardiovascular Therapeutics annual meeting, sponsored by the Cardiovascular Research Foundation.
The evidence of relative advantages was based on comparisons with historical data and a similar study of the previous-generation device. That previous study, called EXPAND, evaluated the MitraClip NTR and ETR systems.
Device times shorter with new device
“There were shorter device times with MitraClip G4,” said Dr. von Bardeleben, referring to a more than 10-minute advantage over the previous generation device (35 minutes in EXPAND G4 vs. 46 min in EXPAND). Although the reduction in overall median procedure time was more modest (77 vs. 80 minutes), Dr. von Bardeleben said these are “the shortest device and procedural times reported to date.”
He also reported what appeared to be incremental advantages across multiple other endpoints, such as procedural success (96.2% vs. 95.8%) and a reduction in the mean clip rate (1.4 vs. 1.5).
Compared with historical outcomes with other devices employed in transcatheter edge-to-edge repair (TEER) of mitral valves, Dr. von Bardeleben contended that the results support the premise that the MitraClip G4 system is a meaningful advance by incorporating such features as an expanded choice of clip sizes, a greater coaptation area, and a more advanced gripper actuation for leaflet grasping.
Over 90% achieve MR 1+
Not least, it appears to increase the proportion of patients who achieve a mitral regurgitation grade of 1+ (MR1+) or lower, which is increasingly recognized as the goal of TEER, said Dr. von Bardeleben, head of the Centre of Structure Heart Disease Interventions, Heart Valve Centre, Mainz, Germany.
He said the rates of 91% achieving MR1+ or less and 98% achieved 2+ or lower compare favorably with most other series and exceeds levels achieved with surgery.
Dr. von Bardeleben also contended that, because of its design features, the MitraClip G4 “expands the spectrum of TEER-suitable patients.” He noted that 5% of the patients in this real-world series had a high risk of stenosis owing to such issues as severe annular or leaflet calcification and another 5% had factors that would predict inadequate MR reduction, such as Barlow’s disease, bi-leaflet prolapse, and severe leaflet degeneration.
The 1,164 patients in EXPAND G4 were enrolled from sites in the United States, Europe, Canada, and Japan. For the key outcome measure of procedural success, echocardiograms were assessed by an independent core laboratory. Of the 1,164 patients enrolled, 1,044 (91%) had complete follow-up data at 30 days.
The procedural success rates were reflected in improvements in New York Heart Association (NYHA) functional classes and in the Kansas City Cardiomyopathy Questionnaire (KCCQ), a quality of life instrument. Prior to treatment, 69% were in NYHA class III or greater. Following treatment, the proportion was 17% (P < .0001). The 18-point improvement in the KCCQ was characterized by Dr. von Bardeleben as “both clinically and statistically significant [P < .0001].”
There were no strokes in this series, and the 30-day incidence of myocardial infarction was 0.2%. The proportion requiring cardiovascular surgery within 30 days was less than 1%. The rate of bleeding episodes, all of which were nonserious, was 7%.
The “EXPAND G4 study confirms the safety and effectiveness of the next generation MitraClip G4 system,” according to Dr. von Bardeleben, and it did so “in a contemporary real-world setting.”
Outcome data characterized as ‘excellent’
Several invited panelists participating in a discussion following the presentation agreed.
“These results are excellent,” said Raj Makkar, MD, associate director of interventional technologies at Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles. While he was impressed with the fact that only 2% missed the primary endpoint of MR 2+ or lower, he indicated that the 91% achieving MR 1+ or lower might be an even more apt signal that newer-generation devices are improving.
This was echoed by other panelists who appeared to form a general consensus over the premise that the target in TEER should no longer be MR 2+ for most patients.
“We should now be aiming for MR grade of 0-1,” stated panelist Stephan Windecker, MD, chairman, department of cardiology, University of Bern (Switzerland). He indicated that this goal is increasingly reasonable given the advances in device design and greater operator experience.
Dr. von Bardeleben reported financial relationships with Abbott Vascular, Edwards Lifesciences, Medtronic, and Neochord. Dr. Makkar reported financial relationships with Abbott Vascular, Cordis, Edwards Lifesciences, and Medtronic. Dr. Windecker reported financial relationships with more than 30 pharmaceutical companies, including Abbott Vascular, which manufactures MitraClip G4.
The design improvements introduced in the fourth-generation device for transcatheter mitral valve repair, called the MitraClip G4 (Abbott), appears to yield better outcomes than previous iterations, according to a multinational postapproval study with more than 1,000 patients.
Not least, the 1.3% all-cause mortality at 30 days in this series, called EXPAND G4, “is the lowest that has been reported to date,” reported Ralph Stephan von Bardeleben, MD, at the Transcatheter Cardiovascular Therapeutics annual meeting, sponsored by the Cardiovascular Research Foundation.
The evidence of relative advantages was based on comparisons with historical data and a similar study of the previous-generation device. That previous study, called EXPAND, evaluated the MitraClip NTR and ETR systems.
Device times shorter with new device
“There were shorter device times with MitraClip G4,” said Dr. von Bardeleben, referring to a more than 10-minute advantage over the previous generation device (35 minutes in EXPAND G4 vs. 46 min in EXPAND). Although the reduction in overall median procedure time was more modest (77 vs. 80 minutes), Dr. von Bardeleben said these are “the shortest device and procedural times reported to date.”
He also reported what appeared to be incremental advantages across multiple other endpoints, such as procedural success (96.2% vs. 95.8%) and a reduction in the mean clip rate (1.4 vs. 1.5).
Compared with historical outcomes with other devices employed in transcatheter edge-to-edge repair (TEER) of mitral valves, Dr. von Bardeleben contended that the results support the premise that the MitraClip G4 system is a meaningful advance by incorporating such features as an expanded choice of clip sizes, a greater coaptation area, and a more advanced gripper actuation for leaflet grasping.
Over 90% achieve MR 1+
Not least, it appears to increase the proportion of patients who achieve a mitral regurgitation grade of 1+ (MR1+) or lower, which is increasingly recognized as the goal of TEER, said Dr. von Bardeleben, head of the Centre of Structure Heart Disease Interventions, Heart Valve Centre, Mainz, Germany.
He said the rates of 91% achieving MR1+ or less and 98% achieved 2+ or lower compare favorably with most other series and exceeds levels achieved with surgery.
Dr. von Bardeleben also contended that, because of its design features, the MitraClip G4 “expands the spectrum of TEER-suitable patients.” He noted that 5% of the patients in this real-world series had a high risk of stenosis owing to such issues as severe annular or leaflet calcification and another 5% had factors that would predict inadequate MR reduction, such as Barlow’s disease, bi-leaflet prolapse, and severe leaflet degeneration.
The 1,164 patients in EXPAND G4 were enrolled from sites in the United States, Europe, Canada, and Japan. For the key outcome measure of procedural success, echocardiograms were assessed by an independent core laboratory. Of the 1,164 patients enrolled, 1,044 (91%) had complete follow-up data at 30 days.
The procedural success rates were reflected in improvements in New York Heart Association (NYHA) functional classes and in the Kansas City Cardiomyopathy Questionnaire (KCCQ), a quality of life instrument. Prior to treatment, 69% were in NYHA class III or greater. Following treatment, the proportion was 17% (P < .0001). The 18-point improvement in the KCCQ was characterized by Dr. von Bardeleben as “both clinically and statistically significant [P < .0001].”
There were no strokes in this series, and the 30-day incidence of myocardial infarction was 0.2%. The proportion requiring cardiovascular surgery within 30 days was less than 1%. The rate of bleeding episodes, all of which were nonserious, was 7%.
The “EXPAND G4 study confirms the safety and effectiveness of the next generation MitraClip G4 system,” according to Dr. von Bardeleben, and it did so “in a contemporary real-world setting.”
Outcome data characterized as ‘excellent’
Several invited panelists participating in a discussion following the presentation agreed.
“These results are excellent,” said Raj Makkar, MD, associate director of interventional technologies at Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles. While he was impressed with the fact that only 2% missed the primary endpoint of MR 2+ or lower, he indicated that the 91% achieving MR 1+ or lower might be an even more apt signal that newer-generation devices are improving.
This was echoed by other panelists who appeared to form a general consensus over the premise that the target in TEER should no longer be MR 2+ for most patients.
“We should now be aiming for MR grade of 0-1,” stated panelist Stephan Windecker, MD, chairman, department of cardiology, University of Bern (Switzerland). He indicated that this goal is increasingly reasonable given the advances in device design and greater operator experience.
Dr. von Bardeleben reported financial relationships with Abbott Vascular, Edwards Lifesciences, Medtronic, and Neochord. Dr. Makkar reported financial relationships with Abbott Vascular, Cordis, Edwards Lifesciences, and Medtronic. Dr. Windecker reported financial relationships with more than 30 pharmaceutical companies, including Abbott Vascular, which manufactures MitraClip G4.
FROM TCT 2022
Extravascular ICD surpasses goals in pivotal trial
BARCELONA – A novel “extravascular” implantable cardioverter defibrillator (ICD) that uses substernally placed electrodes surpassed its prespecified efficacy and safety targets in the device’s pivotal trial with 299 patients who received an implant.
The results showed that the extravascular ICD “provides antitachycardia pacing and low energy defibrillation while avoiding the vascular space” for lead placement, Ian Crozier, MD, said at the annual congress of the European Society of Cardiology.

“The results are fantastic; they exceeded our expectations,” said Dr. Crozier in an interview, adding that he expects the new device to receive marketing approval from regulatory agencies based on the findings. “This will be the next generation of ICD going forward,” predicted Dr. Crozier, an electrophysiologist cardiologist at Christchurch (New Zealand) Hospital.
Moving beyond transvenous and subcutaneous ICDs
Traditional ICDs use transvenous leads, which can cause vascular injury, are prone to lead fracture over time, and can produce serious infections as well as other potential complications. The U.S. Food and Drug Administration first approved an alternative-design, subcutaneous ICD in 2012 that avoids the need for transvenous leads and the risks they pose. But subcutaneous ICDs have their own limitations: an inability to provide antitachycardia pacing or chronic pacing; a limited ability to provide bradycardia pacing; and an increased device size with shorter battery life, because of the high shock power needed for effective performance. These drawbacks have collectively hindered uptake, Dr. Crozier said.
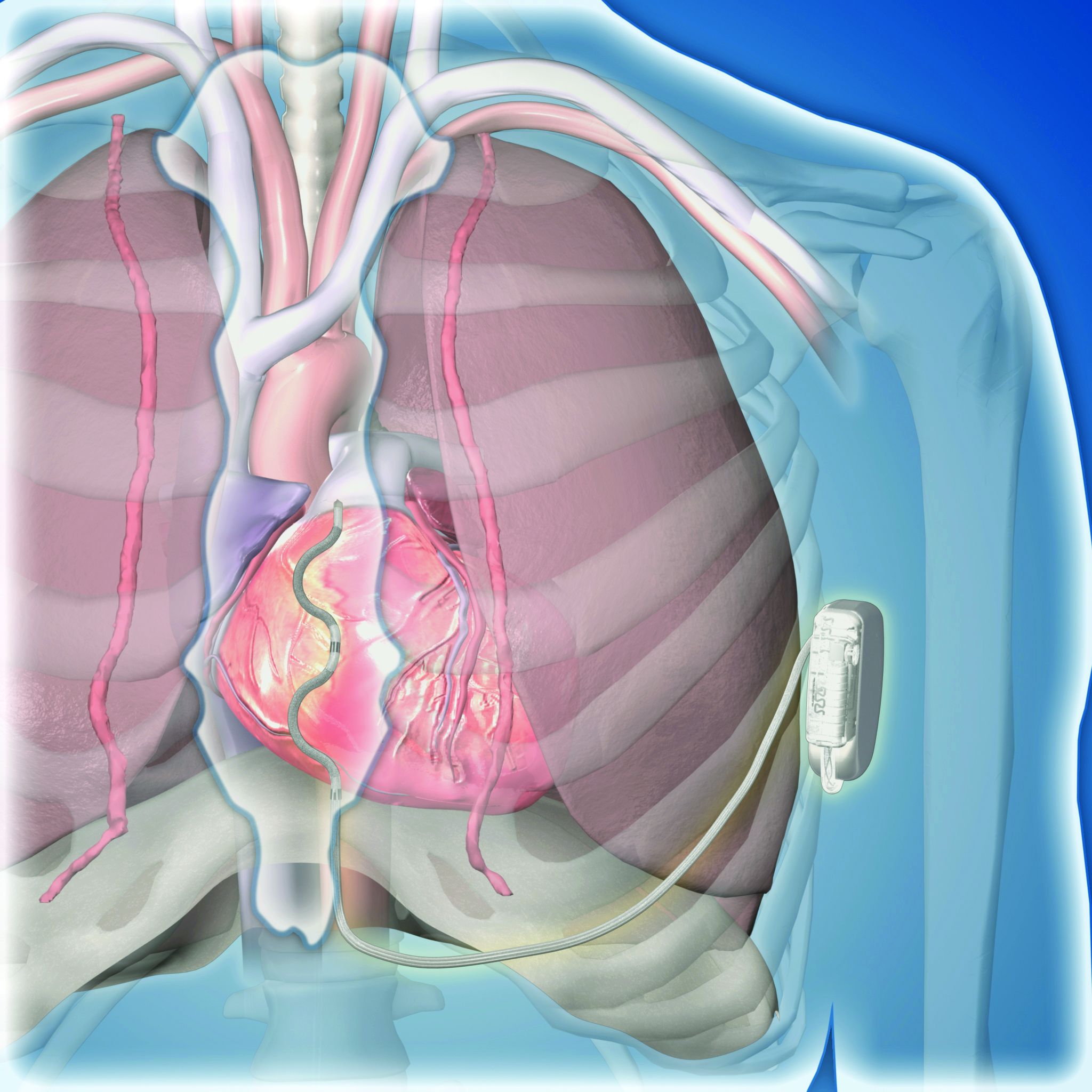
This led to development of the extravascular ICD – 10 years in the making – which uses substernally placed leads that allow antitachycardia pacing and backup pacing in a device with the size of and the anticipated battery longevity of a transvenous ICD device, noted Dr. Crozier.
A 98.7% rate of arrhythmia termination at implant
The pivotal trial’s primary efficacy endpoint was successful defibrillation based on terminating an induced, sustained, shockable ventricular arrhythmia at the time of implantation. The rate was 98.7%, compared with a prespecified target of 88%. All patients had a class I or IIa indication for an ICD.
The primary safety endpoint was freedom from major system- or procedure-related complications at 6 months, which occurred at a rate of 92.6%, compared with the study’s prespecified target rate of 79%. Both targets were derived from the historical rates of ICDs with transvenous leads.
Simultaneously with Dr. Crozier’s report at the congress, the results also appeared online in the New England Journal of Medicine.
Although the pivotal study met both prespecified endpoints, the evidence has limitations that make it likely that regulatory bodies will seek additional data, commented Fred Kusumoto, MD, director of heart rhythm services for the Mayo Clinic in Jacksonville, Fla.
Short follow-up; questions remain
“Follow-up was relatively short, less than a year,” and “questions remain” about the extravascular ICD’s performance, Dr. Kusumoto said in an interview. “Inappropriate shocks occurred in nearly 10% of patients after 11 month follow-up,” he noted, and also cited the 29 patients who needed revisions including two cases with lead fractures.
“The extravascular lead strategy has an advantage over transvenous systems because of the lower risk for extraction or explant,” and it also provides the antitachycardia pacing that’s not available with subcutaneous ICDs, he granted. But in the new study, antitachycardia termination was delivered to only 10 patients and had “reasonable” effectiveness by resolving 70% of these episodes. “Wide adoption by clinicians will depend on results from larger studies with longer follow-up,” Dr. Kusumoto maintained. He also wanted to see confirmation of the ease of lead removal after longer periods of implantation.
Implantation ‘is not difficult’
The trial ran at 46 sites in 17 countries during September 2019 to October 2021. It enrolled patients with a class I or IIa indication for an ICD, excluding patients with a prior sternotomy or need for chronic pacing, and those unable to undergo defibrillation testing.
Clinicians attempted an implantation in 316 patients and had successful placement in 299 (314 had successful placement of their substernal leads), with 292 having a functional device after 6 months, and 284 completing their planned 6-month follow-up. The median procedure time was 66 minutes, including the time for defibrillation testing.
All of the cardiologists who did the implants had received a full day of training prior to performing the procedure. “This is not a difficult procedure, but it is not a region [the substernal space] that cardiologists are familiar working in,” noted Dr. Crozier, explaining the rationale behind a policy of required implantation training.
Twenty-five adverse events occurred in 23 patients. Eighteen of these events required a system revision, including nine lead dislodgments and five infections. The seven adverse events that did not require a revision included three wound-related episodes and three hospitalizations for inappropriate shock. No patients died, nor were there any cardiac injuries as result of the implant.
During average follow-up of 10.6 months, the implanted devices delivered antitachycardia pacing to 10 patients, successfully terminating 32 of 46 episodes (70%), a rate that Dr. Crozier called “very good, and very comparable to transvenous devices.” The devices also delivered 18 appropriate shocks that successfully converted all 18 episodes.
A 10% rate of inappropriate shocks
However, 29 patients (10% of the study cohort) received inappropriate shocks in 81 episodes, with a total of 118 inappropriate shocks delivered, including 34 episodes (42%) triggered by oversensing of a P wave.
“We fully acknowledge that the inappropriate shock rate is higher than what’s seen with transvenous ICDs, but the rate is comparable to what was seen in the early trials with subcutaneous ICDs,” said Dr. Crozier. “We have a number of strategies to reduce the inappropriate shock rate to what we’d expect with conventional devices,” such as making sure that P waves are not detected by the device at the time of implantation, using new algorithms to mitigate P wave sensing, and other programming changes, he added.
Two patients had lead fractures that Dr. Crozier attributed to atypical lead locations and that are likely avoidable in the future. He expressed optimism that the extravascular ICD will avoid the high lead fracture rate over time that remains a problem for ICDs with transvenous leads.
The study also followed a subgroup of 36 patients who underwent a prespecified protocol of chronic defibrillation testing that was successful in all 36.
Dr. Crozier conceded that the extravascular ICD cannot currently deliver chronic pacing, but he expressed optimism that this capability will be available in the future.
“This innovative [extravascular] ICD system would be particularly beneficial for patients with ventricular arrhythmias that can be reliably pace terminated and avoid a transvenous endocardial lead, but more information is required,” concluded Dr. Kusumoto.
The study was sponsored by Medtronic, the company that is developing the extravascular ICD. Dr. Crozier is a consultant to and has received research funding from Medtronic. Dr. Kusumoto had no disclosures.
BARCELONA – A novel “extravascular” implantable cardioverter defibrillator (ICD) that uses substernally placed electrodes surpassed its prespecified efficacy and safety targets in the device’s pivotal trial with 299 patients who received an implant.
The results showed that the extravascular ICD “provides antitachycardia pacing and low energy defibrillation while avoiding the vascular space” for lead placement, Ian Crozier, MD, said at the annual congress of the European Society of Cardiology.
“The results are fantastic; they exceeded our expectations,” said Dr. Crozier in an interview, adding that he expects the new device to receive marketing approval from regulatory agencies based on the findings. “This will be the next generation of ICD going forward,” predicted Dr. Crozier, an electrophysiologist cardiologist at Christchurch (New Zealand) Hospital.
Moving beyond transvenous and subcutaneous ICDs
Traditional ICDs use transvenous leads, which can cause vascular injury, are prone to lead fracture over time, and can produce serious infections as well as other potential complications. The U.S. Food and Drug Administration first approved an alternative-design, subcutaneous ICD in 2012 that avoids the need for transvenous leads and the risks they pose. But subcutaneous ICDs have their own limitations: an inability to provide antitachycardia pacing or chronic pacing; a limited ability to provide bradycardia pacing; and an increased device size with shorter battery life, because of the high shock power needed for effective performance. These drawbacks have collectively hindered uptake, Dr. Crozier said.
This led to development of the extravascular ICD – 10 years in the making – which uses substernally placed leads that allow antitachycardia pacing and backup pacing in a device with the size of and the anticipated battery longevity of a transvenous ICD device, noted Dr. Crozier.
A 98.7% rate of arrhythmia termination at implant
The pivotal trial’s primary efficacy endpoint was successful defibrillation based on terminating an induced, sustained, shockable ventricular arrhythmia at the time of implantation. The rate was 98.7%, compared with a prespecified target of 88%. All patients had a class I or IIa indication for an ICD.
The primary safety endpoint was freedom from major system- or procedure-related complications at 6 months, which occurred at a rate of 92.6%, compared with the study’s prespecified target rate of 79%. Both targets were derived from the historical rates of ICDs with transvenous leads.
Simultaneously with Dr. Crozier’s report at the congress, the results also appeared online in the New England Journal of Medicine.
Although the pivotal study met both prespecified endpoints, the evidence has limitations that make it likely that regulatory bodies will seek additional data, commented Fred Kusumoto, MD, director of heart rhythm services for the Mayo Clinic in Jacksonville, Fla.
Short follow-up; questions remain
“Follow-up was relatively short, less than a year,” and “questions remain” about the extravascular ICD’s performance, Dr. Kusumoto said in an interview. “Inappropriate shocks occurred in nearly 10% of patients after 11 month follow-up,” he noted, and also cited the 29 patients who needed revisions including two cases with lead fractures.
“The extravascular lead strategy has an advantage over transvenous systems because of the lower risk for extraction or explant,” and it also provides the antitachycardia pacing that’s not available with subcutaneous ICDs, he granted. But in the new study, antitachycardia termination was delivered to only 10 patients and had “reasonable” effectiveness by resolving 70% of these episodes. “Wide adoption by clinicians will depend on results from larger studies with longer follow-up,” Dr. Kusumoto maintained. He also wanted to see confirmation of the ease of lead removal after longer periods of implantation.
Implantation ‘is not difficult’
The trial ran at 46 sites in 17 countries during September 2019 to October 2021. It enrolled patients with a class I or IIa indication for an ICD, excluding patients with a prior sternotomy or need for chronic pacing, and those unable to undergo defibrillation testing.
Clinicians attempted an implantation in 316 patients and had successful placement in 299 (314 had successful placement of their substernal leads), with 292 having a functional device after 6 months, and 284 completing their planned 6-month follow-up. The median procedure time was 66 minutes, including the time for defibrillation testing.
All of the cardiologists who did the implants had received a full day of training prior to performing the procedure. “This is not a difficult procedure, but it is not a region [the substernal space] that cardiologists are familiar working in,” noted Dr. Crozier, explaining the rationale behind a policy of required implantation training.
Twenty-five adverse events occurred in 23 patients. Eighteen of these events required a system revision, including nine lead dislodgments and five infections. The seven adverse events that did not require a revision included three wound-related episodes and three hospitalizations for inappropriate shock. No patients died, nor were there any cardiac injuries as result of the implant.
During average follow-up of 10.6 months, the implanted devices delivered antitachycardia pacing to 10 patients, successfully terminating 32 of 46 episodes (70%), a rate that Dr. Crozier called “very good, and very comparable to transvenous devices.” The devices also delivered 18 appropriate shocks that successfully converted all 18 episodes.
A 10% rate of inappropriate shocks
However, 29 patients (10% of the study cohort) received inappropriate shocks in 81 episodes, with a total of 118 inappropriate shocks delivered, including 34 episodes (42%) triggered by oversensing of a P wave.
“We fully acknowledge that the inappropriate shock rate is higher than what’s seen with transvenous ICDs, but the rate is comparable to what was seen in the early trials with subcutaneous ICDs,” said Dr. Crozier. “We have a number of strategies to reduce the inappropriate shock rate to what we’d expect with conventional devices,” such as making sure that P waves are not detected by the device at the time of implantation, using new algorithms to mitigate P wave sensing, and other programming changes, he added.
Two patients had lead fractures that Dr. Crozier attributed to atypical lead locations and that are likely avoidable in the future. He expressed optimism that the extravascular ICD will avoid the high lead fracture rate over time that remains a problem for ICDs with transvenous leads.
The study also followed a subgroup of 36 patients who underwent a prespecified protocol of chronic defibrillation testing that was successful in all 36.
Dr. Crozier conceded that the extravascular ICD cannot currently deliver chronic pacing, but he expressed optimism that this capability will be available in the future.
“This innovative [extravascular] ICD system would be particularly beneficial for patients with ventricular arrhythmias that can be reliably pace terminated and avoid a transvenous endocardial lead, but more information is required,” concluded Dr. Kusumoto.
The study was sponsored by Medtronic, the company that is developing the extravascular ICD. Dr. Crozier is a consultant to and has received research funding from Medtronic. Dr. Kusumoto had no disclosures.
BARCELONA – A novel “extravascular” implantable cardioverter defibrillator (ICD) that uses substernally placed electrodes surpassed its prespecified efficacy and safety targets in the device’s pivotal trial with 299 patients who received an implant.
The results showed that the extravascular ICD “provides antitachycardia pacing and low energy defibrillation while avoiding the vascular space” for lead placement, Ian Crozier, MD, said at the annual congress of the European Society of Cardiology.
“The results are fantastic; they exceeded our expectations,” said Dr. Crozier in an interview, adding that he expects the new device to receive marketing approval from regulatory agencies based on the findings. “This will be the next generation of ICD going forward,” predicted Dr. Crozier, an electrophysiologist cardiologist at Christchurch (New Zealand) Hospital.
Moving beyond transvenous and subcutaneous ICDs
Traditional ICDs use transvenous leads, which can cause vascular injury, are prone to lead fracture over time, and can produce serious infections as well as other potential complications. The U.S. Food and Drug Administration first approved an alternative-design, subcutaneous ICD in 2012 that avoids the need for transvenous leads and the risks they pose. But subcutaneous ICDs have their own limitations: an inability to provide antitachycardia pacing or chronic pacing; a limited ability to provide bradycardia pacing; and an increased device size with shorter battery life, because of the high shock power needed for effective performance. These drawbacks have collectively hindered uptake, Dr. Crozier said.
This led to development of the extravascular ICD – 10 years in the making – which uses substernally placed leads that allow antitachycardia pacing and backup pacing in a device with the size of and the anticipated battery longevity of a transvenous ICD device, noted Dr. Crozier.
A 98.7% rate of arrhythmia termination at implant
The pivotal trial’s primary efficacy endpoint was successful defibrillation based on terminating an induced, sustained, shockable ventricular arrhythmia at the time of implantation. The rate was 98.7%, compared with a prespecified target of 88%. All patients had a class I or IIa indication for an ICD.
The primary safety endpoint was freedom from major system- or procedure-related complications at 6 months, which occurred at a rate of 92.6%, compared with the study’s prespecified target rate of 79%. Both targets were derived from the historical rates of ICDs with transvenous leads.
Simultaneously with Dr. Crozier’s report at the congress, the results also appeared online in the New England Journal of Medicine.
Although the pivotal study met both prespecified endpoints, the evidence has limitations that make it likely that regulatory bodies will seek additional data, commented Fred Kusumoto, MD, director of heart rhythm services for the Mayo Clinic in Jacksonville, Fla.
Short follow-up; questions remain
“Follow-up was relatively short, less than a year,” and “questions remain” about the extravascular ICD’s performance, Dr. Kusumoto said in an interview. “Inappropriate shocks occurred in nearly 10% of patients after 11 month follow-up,” he noted, and also cited the 29 patients who needed revisions including two cases with lead fractures.
“The extravascular lead strategy has an advantage over transvenous systems because of the lower risk for extraction or explant,” and it also provides the antitachycardia pacing that’s not available with subcutaneous ICDs, he granted. But in the new study, antitachycardia termination was delivered to only 10 patients and had “reasonable” effectiveness by resolving 70% of these episodes. “Wide adoption by clinicians will depend on results from larger studies with longer follow-up,” Dr. Kusumoto maintained. He also wanted to see confirmation of the ease of lead removal after longer periods of implantation.
Implantation ‘is not difficult’
The trial ran at 46 sites in 17 countries during September 2019 to October 2021. It enrolled patients with a class I or IIa indication for an ICD, excluding patients with a prior sternotomy or need for chronic pacing, and those unable to undergo defibrillation testing.
Clinicians attempted an implantation in 316 patients and had successful placement in 299 (314 had successful placement of their substernal leads), with 292 having a functional device after 6 months, and 284 completing their planned 6-month follow-up. The median procedure time was 66 minutes, including the time for defibrillation testing.
All of the cardiologists who did the implants had received a full day of training prior to performing the procedure. “This is not a difficult procedure, but it is not a region [the substernal space] that cardiologists are familiar working in,” noted Dr. Crozier, explaining the rationale behind a policy of required implantation training.
Twenty-five adverse events occurred in 23 patients. Eighteen of these events required a system revision, including nine lead dislodgments and five infections. The seven adverse events that did not require a revision included three wound-related episodes and three hospitalizations for inappropriate shock. No patients died, nor were there any cardiac injuries as result of the implant.
During average follow-up of 10.6 months, the implanted devices delivered antitachycardia pacing to 10 patients, successfully terminating 32 of 46 episodes (70%), a rate that Dr. Crozier called “very good, and very comparable to transvenous devices.” The devices also delivered 18 appropriate shocks that successfully converted all 18 episodes.
A 10% rate of inappropriate shocks
However, 29 patients (10% of the study cohort) received inappropriate shocks in 81 episodes, with a total of 118 inappropriate shocks delivered, including 34 episodes (42%) triggered by oversensing of a P wave.
“We fully acknowledge that the inappropriate shock rate is higher than what’s seen with transvenous ICDs, but the rate is comparable to what was seen in the early trials with subcutaneous ICDs,” said Dr. Crozier. “We have a number of strategies to reduce the inappropriate shock rate to what we’d expect with conventional devices,” such as making sure that P waves are not detected by the device at the time of implantation, using new algorithms to mitigate P wave sensing, and other programming changes, he added.
Two patients had lead fractures that Dr. Crozier attributed to atypical lead locations and that are likely avoidable in the future. He expressed optimism that the extravascular ICD will avoid the high lead fracture rate over time that remains a problem for ICDs with transvenous leads.
The study also followed a subgroup of 36 patients who underwent a prespecified protocol of chronic defibrillation testing that was successful in all 36.
Dr. Crozier conceded that the extravascular ICD cannot currently deliver chronic pacing, but he expressed optimism that this capability will be available in the future.
“This innovative [extravascular] ICD system would be particularly beneficial for patients with ventricular arrhythmias that can be reliably pace terminated and avoid a transvenous endocardial lead, but more information is required,” concluded Dr. Kusumoto.
The study was sponsored by Medtronic, the company that is developing the extravascular ICD. Dr. Crozier is a consultant to and has received research funding from Medtronic. Dr. Kusumoto had no disclosures.
AT ESC CONGRESS 2022
Heparin pretreatment may safely open arteries before STEMI cath
, suggests a large registry study.
An open infarct-related artery (IRA) at angiography on cath-lab arrival presents STEMI patients an opportunity for earlier reperfusion and a chance, in theory at least, for smaller infarcts and maybe improved clinical outcomes.
In the new analysis, which covers more than 40,000 patients with STEMI in Sweden, the 38% who received heparin before cath-lab arrival were 11% less likely to show IRA occlusion at angiography prior to direct percutaneous coronary intervention (PCI). They also showed a 13% lower 30-day mortality compared with patients who were started on heparin in the cath lab. Importantly, their risk of major bleeding in the hospital did not increase.
The “early reperfusion” associated with IRA patency at angiography “could have long-term benefit due to smaller infarct size,” potentially explaining the observed 30-day survival gain in the pretreatment group, Oskar Love Emilsson, Lund (Sweden) University, said in an interview.
Mr. Emilsson, a third-year medical student, reported the analysis at the annual congress of the European Society of Cardiology, and is lead author on its same-day publication in the journal EuroIntervention.
He mentioned a few cautions in interpreting the study, which is based primarily on data from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR). It included several sensitivity analyses that continued to back pretreatment heparin as a significant predictor of an unoccluded IRA but didn’t consistently support the 30-day mortality benefit seen in the primary analysis.
And, although the pretreatment group overall didn’t have more major bleeds, the risk did go up significantly for those older than 75 or those who weighed less than 60 kg (132 pounds) or underwent catheterization with an access route other than the radial artery. Extra caution should be exercised in such patients who receive heparin before cath-lab arrival for PCI, Mr. Emilsson observed.
“Our results suggest that heparin pretreatment might be a good option to improve patency of infarct related arteries in STEMI,” and potentially clinical outcomes, he said. “However, a definite answer would require a randomized controlled trial.”
Meanwhile, the current study may be the largest yet to look at clinical outcomes after pretreatment with unfractionated heparin before PCI for acute STEMI, the report states. There have been some observational studies, subanalyses of STEMI trials, and even a few limited randomized trials – including the HEAP trial published in 2000 – to weigh in on the subject. Some have supported the strategy, others have not.
“With rapid door-to-balloon times in STEMI, it can be challenging to show a significant difference between a prehospital heparin approach and heparin given in the lab,” observed Sunil V. Rao, MD, NYU Langone Health System, New York, who is not connected with the current study.
Many EDs in the United States have “a STEMI protocol that calls for an IV bolus of heparin. It would be tougher in the U.S. to give it in the ambulance but again, it’s not clear how much advantage that would really provide,” he told this news organization.
Support from randomized trials would be needed before the practice could be formally recommended. “The SCAAR registries have set the standard for how registries should be conducted,” Dr. Rao said. “This is a very well done observational study, but it is observational.”
The priority for STEMI patients, he added, “really should be to get them to the lab as fast as possible. If the ED protocol includes heparin before the cath lab, that’s great, but I don’t think we should delay getting these patients to the lab to accommodate pre–cath-lab heparin.”
The current analysis covered 41,631 patients with STEMI from 2008 through to 2016, of whom 38% were pretreated with heparin in an ambulance or the ED. The remaining 62% initiated heparin in the cath lab.
About one-third of the group had an open IRA at angiography. The adjusted risk ratio (RR) for IRA occlusion at angiography for patients pretreated vs. not pretreated with heparin was 0.89 (95% confidence interval [CI], 0.87-0.90).
The corresponding RR for death within 30 days was 0.87 (95% CI, 0.77-0.99), and for major in-hospital bleeding it was 1.01 (95% CI, 0.86-1.18).
The analysis was adjusted for other medications received before cath-lab arrival, especially a long list of antiplatelets and non-heparin antithrombins. That strengthens the case for heparin pretreatment as an independent predictor of an open IRA at initial angiography, Mr. Emilsson said.
Comparisons of propensity-score–matched subgroups of the total cohort, conducted separately for the IRA-occlusion endpoint and the endpoints of 30-day mortality and major bleeding, produced similar results.
Some observational data suggest that antiplatelet pretreatment with a P2Y12 inhibitor may promote IRA patency on angiography after cath lab arrival, Dr. Rao observed. “This indicates that there probably is a role of earlier antithrombotic therapy in STEMI patients, but the randomized trials have not shown a consistent benefit,” he said, referring in particular to the ATLANTIC trial.
Mr. Emilsson and Dr. Rao disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, suggests a large registry study.
An open infarct-related artery (IRA) at angiography on cath-lab arrival presents STEMI patients an opportunity for earlier reperfusion and a chance, in theory at least, for smaller infarcts and maybe improved clinical outcomes.
In the new analysis, which covers more than 40,000 patients with STEMI in Sweden, the 38% who received heparin before cath-lab arrival were 11% less likely to show IRA occlusion at angiography prior to direct percutaneous coronary intervention (PCI). They also showed a 13% lower 30-day mortality compared with patients who were started on heparin in the cath lab. Importantly, their risk of major bleeding in the hospital did not increase.
The “early reperfusion” associated with IRA patency at angiography “could have long-term benefit due to smaller infarct size,” potentially explaining the observed 30-day survival gain in the pretreatment group, Oskar Love Emilsson, Lund (Sweden) University, said in an interview.
Mr. Emilsson, a third-year medical student, reported the analysis at the annual congress of the European Society of Cardiology, and is lead author on its same-day publication in the journal EuroIntervention.
He mentioned a few cautions in interpreting the study, which is based primarily on data from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR). It included several sensitivity analyses that continued to back pretreatment heparin as a significant predictor of an unoccluded IRA but didn’t consistently support the 30-day mortality benefit seen in the primary analysis.
And, although the pretreatment group overall didn’t have more major bleeds, the risk did go up significantly for those older than 75 or those who weighed less than 60 kg (132 pounds) or underwent catheterization with an access route other than the radial artery. Extra caution should be exercised in such patients who receive heparin before cath-lab arrival for PCI, Mr. Emilsson observed.
“Our results suggest that heparin pretreatment might be a good option to improve patency of infarct related arteries in STEMI,” and potentially clinical outcomes, he said. “However, a definite answer would require a randomized controlled trial.”
Meanwhile, the current study may be the largest yet to look at clinical outcomes after pretreatment with unfractionated heparin before PCI for acute STEMI, the report states. There have been some observational studies, subanalyses of STEMI trials, and even a few limited randomized trials – including the HEAP trial published in 2000 – to weigh in on the subject. Some have supported the strategy, others have not.
“With rapid door-to-balloon times in STEMI, it can be challenging to show a significant difference between a prehospital heparin approach and heparin given in the lab,” observed Sunil V. Rao, MD, NYU Langone Health System, New York, who is not connected with the current study.
Many EDs in the United States have “a STEMI protocol that calls for an IV bolus of heparin. It would be tougher in the U.S. to give it in the ambulance but again, it’s not clear how much advantage that would really provide,” he told this news organization.
Support from randomized trials would be needed before the practice could be formally recommended. “The SCAAR registries have set the standard for how registries should be conducted,” Dr. Rao said. “This is a very well done observational study, but it is observational.”
The priority for STEMI patients, he added, “really should be to get them to the lab as fast as possible. If the ED protocol includes heparin before the cath lab, that’s great, but I don’t think we should delay getting these patients to the lab to accommodate pre–cath-lab heparin.”
The current analysis covered 41,631 patients with STEMI from 2008 through to 2016, of whom 38% were pretreated with heparin in an ambulance or the ED. The remaining 62% initiated heparin in the cath lab.
About one-third of the group had an open IRA at angiography. The adjusted risk ratio (RR) for IRA occlusion at angiography for patients pretreated vs. not pretreated with heparin was 0.89 (95% confidence interval [CI], 0.87-0.90).
The corresponding RR for death within 30 days was 0.87 (95% CI, 0.77-0.99), and for major in-hospital bleeding it was 1.01 (95% CI, 0.86-1.18).
The analysis was adjusted for other medications received before cath-lab arrival, especially a long list of antiplatelets and non-heparin antithrombins. That strengthens the case for heparin pretreatment as an independent predictor of an open IRA at initial angiography, Mr. Emilsson said.
Comparisons of propensity-score–matched subgroups of the total cohort, conducted separately for the IRA-occlusion endpoint and the endpoints of 30-day mortality and major bleeding, produced similar results.
Some observational data suggest that antiplatelet pretreatment with a P2Y12 inhibitor may promote IRA patency on angiography after cath lab arrival, Dr. Rao observed. “This indicates that there probably is a role of earlier antithrombotic therapy in STEMI patients, but the randomized trials have not shown a consistent benefit,” he said, referring in particular to the ATLANTIC trial.
Mr. Emilsson and Dr. Rao disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, suggests a large registry study.
An open infarct-related artery (IRA) at angiography on cath-lab arrival presents STEMI patients an opportunity for earlier reperfusion and a chance, in theory at least, for smaller infarcts and maybe improved clinical outcomes.
In the new analysis, which covers more than 40,000 patients with STEMI in Sweden, the 38% who received heparin before cath-lab arrival were 11% less likely to show IRA occlusion at angiography prior to direct percutaneous coronary intervention (PCI). They also showed a 13% lower 30-day mortality compared with patients who were started on heparin in the cath lab. Importantly, their risk of major bleeding in the hospital did not increase.
The “early reperfusion” associated with IRA patency at angiography “could have long-term benefit due to smaller infarct size,” potentially explaining the observed 30-day survival gain in the pretreatment group, Oskar Love Emilsson, Lund (Sweden) University, said in an interview.
Mr. Emilsson, a third-year medical student, reported the analysis at the annual congress of the European Society of Cardiology, and is lead author on its same-day publication in the journal EuroIntervention.
He mentioned a few cautions in interpreting the study, which is based primarily on data from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR). It included several sensitivity analyses that continued to back pretreatment heparin as a significant predictor of an unoccluded IRA but didn’t consistently support the 30-day mortality benefit seen in the primary analysis.
And, although the pretreatment group overall didn’t have more major bleeds, the risk did go up significantly for those older than 75 or those who weighed less than 60 kg (132 pounds) or underwent catheterization with an access route other than the radial artery. Extra caution should be exercised in such patients who receive heparin before cath-lab arrival for PCI, Mr. Emilsson observed.
“Our results suggest that heparin pretreatment might be a good option to improve patency of infarct related arteries in STEMI,” and potentially clinical outcomes, he said. “However, a definite answer would require a randomized controlled trial.”
Meanwhile, the current study may be the largest yet to look at clinical outcomes after pretreatment with unfractionated heparin before PCI for acute STEMI, the report states. There have been some observational studies, subanalyses of STEMI trials, and even a few limited randomized trials – including the HEAP trial published in 2000 – to weigh in on the subject. Some have supported the strategy, others have not.
“With rapid door-to-balloon times in STEMI, it can be challenging to show a significant difference between a prehospital heparin approach and heparin given in the lab,” observed Sunil V. Rao, MD, NYU Langone Health System, New York, who is not connected with the current study.
Many EDs in the United States have “a STEMI protocol that calls for an IV bolus of heparin. It would be tougher in the U.S. to give it in the ambulance but again, it’s not clear how much advantage that would really provide,” he told this news organization.
Support from randomized trials would be needed before the practice could be formally recommended. “The SCAAR registries have set the standard for how registries should be conducted,” Dr. Rao said. “This is a very well done observational study, but it is observational.”
The priority for STEMI patients, he added, “really should be to get them to the lab as fast as possible. If the ED protocol includes heparin before the cath lab, that’s great, but I don’t think we should delay getting these patients to the lab to accommodate pre–cath-lab heparin.”
The current analysis covered 41,631 patients with STEMI from 2008 through to 2016, of whom 38% were pretreated with heparin in an ambulance or the ED. The remaining 62% initiated heparin in the cath lab.
About one-third of the group had an open IRA at angiography. The adjusted risk ratio (RR) for IRA occlusion at angiography for patients pretreated vs. not pretreated with heparin was 0.89 (95% confidence interval [CI], 0.87-0.90).
The corresponding RR for death within 30 days was 0.87 (95% CI, 0.77-0.99), and for major in-hospital bleeding it was 1.01 (95% CI, 0.86-1.18).
The analysis was adjusted for other medications received before cath-lab arrival, especially a long list of antiplatelets and non-heparin antithrombins. That strengthens the case for heparin pretreatment as an independent predictor of an open IRA at initial angiography, Mr. Emilsson said.
Comparisons of propensity-score–matched subgroups of the total cohort, conducted separately for the IRA-occlusion endpoint and the endpoints of 30-day mortality and major bleeding, produced similar results.
Some observational data suggest that antiplatelet pretreatment with a P2Y12 inhibitor may promote IRA patency on angiography after cath lab arrival, Dr. Rao observed. “This indicates that there probably is a role of earlier antithrombotic therapy in STEMI patients, but the randomized trials have not shown a consistent benefit,” he said, referring in particular to the ATLANTIC trial.
Mr. Emilsson and Dr. Rao disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2022
PARADISE-MI results obscured as post hoc analysis finds flaws
A post hoc analysis of the PARADISE-MI trial, although not intended to alter the conclusions generated by the published data, suggests that clinically relevant benefits were obscured, providing the basis for recommending different analyses for future studies that are more suited to capture the most clinically significant endpoints.
“What these data show us is that we need clinical trial designs moving towards more pragmatic information that better reflect clinical practice,” reported Otavio Berwanger, MD, PhD, director of the Academic Research Organization at Hospital Israelita Albert Einstein, São Paulo, Brazil.

The reevaluation of the PARADISE-MI data, presented at the annual congress of the European Society of Cardiology in Barcelona, was based on a win ratio analysis and on the inclusion of investigator-reported endpoints, not just adjudicated events. Both appear to reveal clinically meaningful benefits not reflected in the published study, according to Dr. Berwanger.
In PARADISE-MI, which was published in the New England Journal of Medicine last year, more than 5,500 patients were randomized to the angiotensin receptor neprilysin inhibitor (ARNI) sacubitril/valsartan or the ACE inhibitor ramipril after a myocardial infarction. A reduced left ventricular ejection fraction (LVEF), pulmonary congestion, or both were required for enrollment.
For the primary composite outcomes of death from cardiovascular (CV) causes or incident heart failure, the ARNI had a 10% numerical advantage, but it did not reach statistical significance (hazard ratio [HR], 0.90; P = .17).
“PARADISE-MI was a neutral trial. This post hoc analysis will not change that result,” Dr. Berwanger emphasized. However, the post hoc analysis does provide a basis for exploring why conventional trial designs might not be providing answers that are relevant and helpful for clinical practice.
New analysis provides positive trial result
When the data from PARADISE-MI are reevaluated in a hierarchical win ratio analysis with CV death serving as the most severe and important outcome, the principal conclusion changes. Whether events are reevaluated in this format by the clinical events committee (CEC) or by investigators, there is a greater number of total wins than total losses for the ARNI. Combined, sacubitril/valsartan was associated with a win ratio of 1.17 (95% confidence interval, 1.03-1.33; P = 0.015) over ramipril.
Using a sports analogy, Dr. Berwanger explained that the win ratio analysis divides the total number of wins to the total number of losses to provide a much more clinically relevant approach to keeping score. It also used a hierarchical analysis so that the most serious and important events are considered first.
In addition to CV death, this analysis included first hospitalization for heart failure and first outpatient heart failure events. CEC-defined events and events reported by investigators were evaluated separately.
The ARNI had more wins than losses in every category for all outcomes, whether CEC adjudicated or investigator reported, but most of this benefit was generated by the endpoint of CEC-adjudicated CV deaths. This accounted for 36.9% of all events (investigator-documented CV death accounted for 0.7%). This is important because PARADISE-MI, like many standard trials, was conducted on a time-to-primary event basis.
“In this type of analysis, the first event is what counts. Usually time-to-first-event analyses are dominated by nonfatal events,” Dr. Berwanger explained. He believes that placing more weight on the most serious events results in an emphasis on what outcomes are of greatest clinical interest.
In addition, Dr. Berwanger argued that it is important to consider investigator-reported events, not just CEC-adjudicated events. While adjudicated events improve the rigor of the data, Dr. Berwanger suggested it omits outcomes with which clinicians are most concerned.
Investigator, adjudicated outcomes differ
Again, using PARADISE-MI as an example, he reevaluated the primary outcome based on investigator reports. When investigator-reported events are included, the number of events increased in both the ARNI (443 vs. 338) and ramipril (516 vs. 373) arms, but the advantage of the ARNI over the ACE inhibitors now reached statistical significance (HR, 0.85; P = .01).
“The data suggest that maybe we should find definitions for adjudication that are closer to clinical judgment in the real world and clinical practice,” Dr. Berwanger said.
One possible explanation for the neutral result in PARADISE-MI is that benefit of an ARNI over an ACE inhibitor would only be expected in those at risk for progressive left ventricular dysfunction, and it is likely that a substantial proportion of patients enrolled in this trial recovered, according to Johann Bauersachs, MD, PhD, professor and head of cardiology at Hannover (Germany) Medical School.
“You cannot predict which patients with reduced LV function following an MI will go on to chronic remodeling and which will recover,” said Dr. Bauersachs, who was an ESC-invited discussant of Dr. Berwanger’s post hoc analysis.

He agreed that Dr. Berwanger has raised several important issues in standard trial design that might have prevented PARADISE-MI from showing a benefit from an ARNI, but he pointed out that there are other potential issues, such as the low use of mineralocorticoid antagonists in PARADISE-MI, that may have skewed results.
However, he agreed generally with the premise that there is a need for trial design likely to generate more clinically useful information.
“We have now seen the win-ratio approach used in several studies,” said Dr. Bauersachs, citing in particular the EMPULSE trial presented at the 2022 meeting of the American College of Cardiology. “It is a very useful tool, and I think we will be seeing it used more in the future.”
However, he indicated that the issues raised by Dr. Berwanger are not necessarily easily resolved. Dr. Bauersachs endorsed the effort to consider trial designs that generate data that are more immediately clinically applicable but suggested that different types of designs may be required for different types of clinical questions.
Dr. Berwanger reports financial relationships with Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Pfizer, Servier, and Novartis, which provided funding for the PARADISE-MI trial. Dr. Bauersachs reports financial relationships with Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Boehringer Ingelheim, Cardior, Corvia, CVRx, Novartis, Pfizer, Vifor, and Zoll.
A post hoc analysis of the PARADISE-MI trial, although not intended to alter the conclusions generated by the published data, suggests that clinically relevant benefits were obscured, providing the basis for recommending different analyses for future studies that are more suited to capture the most clinically significant endpoints.
“What these data show us is that we need clinical trial designs moving towards more pragmatic information that better reflect clinical practice,” reported Otavio Berwanger, MD, PhD, director of the Academic Research Organization at Hospital Israelita Albert Einstein, São Paulo, Brazil.
The reevaluation of the PARADISE-MI data, presented at the annual congress of the European Society of Cardiology in Barcelona, was based on a win ratio analysis and on the inclusion of investigator-reported endpoints, not just adjudicated events. Both appear to reveal clinically meaningful benefits not reflected in the published study, according to Dr. Berwanger.
In PARADISE-MI, which was published in the New England Journal of Medicine last year, more than 5,500 patients were randomized to the angiotensin receptor neprilysin inhibitor (ARNI) sacubitril/valsartan or the ACE inhibitor ramipril after a myocardial infarction. A reduced left ventricular ejection fraction (LVEF), pulmonary congestion, or both were required for enrollment.
For the primary composite outcomes of death from cardiovascular (CV) causes or incident heart failure, the ARNI had a 10% numerical advantage, but it did not reach statistical significance (hazard ratio [HR], 0.90; P = .17).
“PARADISE-MI was a neutral trial. This post hoc analysis will not change that result,” Dr. Berwanger emphasized. However, the post hoc analysis does provide a basis for exploring why conventional trial designs might not be providing answers that are relevant and helpful for clinical practice.
New analysis provides positive trial result
When the data from PARADISE-MI are reevaluated in a hierarchical win ratio analysis with CV death serving as the most severe and important outcome, the principal conclusion changes. Whether events are reevaluated in this format by the clinical events committee (CEC) or by investigators, there is a greater number of total wins than total losses for the ARNI. Combined, sacubitril/valsartan was associated with a win ratio of 1.17 (95% confidence interval, 1.03-1.33; P = 0.015) over ramipril.
Using a sports analogy, Dr. Berwanger explained that the win ratio analysis divides the total number of wins to the total number of losses to provide a much more clinically relevant approach to keeping score. It also used a hierarchical analysis so that the most serious and important events are considered first.
In addition to CV death, this analysis included first hospitalization for heart failure and first outpatient heart failure events. CEC-defined events and events reported by investigators were evaluated separately.
The ARNI had more wins than losses in every category for all outcomes, whether CEC adjudicated or investigator reported, but most of this benefit was generated by the endpoint of CEC-adjudicated CV deaths. This accounted for 36.9% of all events (investigator-documented CV death accounted for 0.7%). This is important because PARADISE-MI, like many standard trials, was conducted on a time-to-primary event basis.
“In this type of analysis, the first event is what counts. Usually time-to-first-event analyses are dominated by nonfatal events,” Dr. Berwanger explained. He believes that placing more weight on the most serious events results in an emphasis on what outcomes are of greatest clinical interest.
In addition, Dr. Berwanger argued that it is important to consider investigator-reported events, not just CEC-adjudicated events. While adjudicated events improve the rigor of the data, Dr. Berwanger suggested it omits outcomes with which clinicians are most concerned.
Investigator, adjudicated outcomes differ
Again, using PARADISE-MI as an example, he reevaluated the primary outcome based on investigator reports. When investigator-reported events are included, the number of events increased in both the ARNI (443 vs. 338) and ramipril (516 vs. 373) arms, but the advantage of the ARNI over the ACE inhibitors now reached statistical significance (HR, 0.85; P = .01).
“The data suggest that maybe we should find definitions for adjudication that are closer to clinical judgment in the real world and clinical practice,” Dr. Berwanger said.
One possible explanation for the neutral result in PARADISE-MI is that benefit of an ARNI over an ACE inhibitor would only be expected in those at risk for progressive left ventricular dysfunction, and it is likely that a substantial proportion of patients enrolled in this trial recovered, according to Johann Bauersachs, MD, PhD, professor and head of cardiology at Hannover (Germany) Medical School.
“You cannot predict which patients with reduced LV function following an MI will go on to chronic remodeling and which will recover,” said Dr. Bauersachs, who was an ESC-invited discussant of Dr. Berwanger’s post hoc analysis.
He agreed that Dr. Berwanger has raised several important issues in standard trial design that might have prevented PARADISE-MI from showing a benefit from an ARNI, but he pointed out that there are other potential issues, such as the low use of mineralocorticoid antagonists in PARADISE-MI, that may have skewed results.
However, he agreed generally with the premise that there is a need for trial design likely to generate more clinically useful information.
“We have now seen the win-ratio approach used in several studies,” said Dr. Bauersachs, citing in particular the EMPULSE trial presented at the 2022 meeting of the American College of Cardiology. “It is a very useful tool, and I think we will be seeing it used more in the future.”
However, he indicated that the issues raised by Dr. Berwanger are not necessarily easily resolved. Dr. Bauersachs endorsed the effort to consider trial designs that generate data that are more immediately clinically applicable but suggested that different types of designs may be required for different types of clinical questions.
Dr. Berwanger reports financial relationships with Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Pfizer, Servier, and Novartis, which provided funding for the PARADISE-MI trial. Dr. Bauersachs reports financial relationships with Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Boehringer Ingelheim, Cardior, Corvia, CVRx, Novartis, Pfizer, Vifor, and Zoll.
A post hoc analysis of the PARADISE-MI trial, although not intended to alter the conclusions generated by the published data, suggests that clinically relevant benefits were obscured, providing the basis for recommending different analyses for future studies that are more suited to capture the most clinically significant endpoints.
“What these data show us is that we need clinical trial designs moving towards more pragmatic information that better reflect clinical practice,” reported Otavio Berwanger, MD, PhD, director of the Academic Research Organization at Hospital Israelita Albert Einstein, São Paulo, Brazil.
The reevaluation of the PARADISE-MI data, presented at the annual congress of the European Society of Cardiology in Barcelona, was based on a win ratio analysis and on the inclusion of investigator-reported endpoints, not just adjudicated events. Both appear to reveal clinically meaningful benefits not reflected in the published study, according to Dr. Berwanger.
In PARADISE-MI, which was published in the New England Journal of Medicine last year, more than 5,500 patients were randomized to the angiotensin receptor neprilysin inhibitor (ARNI) sacubitril/valsartan or the ACE inhibitor ramipril after a myocardial infarction. A reduced left ventricular ejection fraction (LVEF), pulmonary congestion, or both were required for enrollment.
For the primary composite outcomes of death from cardiovascular (CV) causes or incident heart failure, the ARNI had a 10% numerical advantage, but it did not reach statistical significance (hazard ratio [HR], 0.90; P = .17).
“PARADISE-MI was a neutral trial. This post hoc analysis will not change that result,” Dr. Berwanger emphasized. However, the post hoc analysis does provide a basis for exploring why conventional trial designs might not be providing answers that are relevant and helpful for clinical practice.
New analysis provides positive trial result
When the data from PARADISE-MI are reevaluated in a hierarchical win ratio analysis with CV death serving as the most severe and important outcome, the principal conclusion changes. Whether events are reevaluated in this format by the clinical events committee (CEC) or by investigators, there is a greater number of total wins than total losses for the ARNI. Combined, sacubitril/valsartan was associated with a win ratio of 1.17 (95% confidence interval, 1.03-1.33; P = 0.015) over ramipril.
Using a sports analogy, Dr. Berwanger explained that the win ratio analysis divides the total number of wins to the total number of losses to provide a much more clinically relevant approach to keeping score. It also used a hierarchical analysis so that the most serious and important events are considered first.
In addition to CV death, this analysis included first hospitalization for heart failure and first outpatient heart failure events. CEC-defined events and events reported by investigators were evaluated separately.
The ARNI had more wins than losses in every category for all outcomes, whether CEC adjudicated or investigator reported, but most of this benefit was generated by the endpoint of CEC-adjudicated CV deaths. This accounted for 36.9% of all events (investigator-documented CV death accounted for 0.7%). This is important because PARADISE-MI, like many standard trials, was conducted on a time-to-primary event basis.
“In this type of analysis, the first event is what counts. Usually time-to-first-event analyses are dominated by nonfatal events,” Dr. Berwanger explained. He believes that placing more weight on the most serious events results in an emphasis on what outcomes are of greatest clinical interest.
In addition, Dr. Berwanger argued that it is important to consider investigator-reported events, not just CEC-adjudicated events. While adjudicated events improve the rigor of the data, Dr. Berwanger suggested it omits outcomes with which clinicians are most concerned.
Investigator, adjudicated outcomes differ
Again, using PARADISE-MI as an example, he reevaluated the primary outcome based on investigator reports. When investigator-reported events are included, the number of events increased in both the ARNI (443 vs. 338) and ramipril (516 vs. 373) arms, but the advantage of the ARNI over the ACE inhibitors now reached statistical significance (HR, 0.85; P = .01).
“The data suggest that maybe we should find definitions for adjudication that are closer to clinical judgment in the real world and clinical practice,” Dr. Berwanger said.
One possible explanation for the neutral result in PARADISE-MI is that benefit of an ARNI over an ACE inhibitor would only be expected in those at risk for progressive left ventricular dysfunction, and it is likely that a substantial proportion of patients enrolled in this trial recovered, according to Johann Bauersachs, MD, PhD, professor and head of cardiology at Hannover (Germany) Medical School.
“You cannot predict which patients with reduced LV function following an MI will go on to chronic remodeling and which will recover,” said Dr. Bauersachs, who was an ESC-invited discussant of Dr. Berwanger’s post hoc analysis.
He agreed that Dr. Berwanger has raised several important issues in standard trial design that might have prevented PARADISE-MI from showing a benefit from an ARNI, but he pointed out that there are other potential issues, such as the low use of mineralocorticoid antagonists in PARADISE-MI, that may have skewed results.
However, he agreed generally with the premise that there is a need for trial design likely to generate more clinically useful information.
“We have now seen the win-ratio approach used in several studies,” said Dr. Bauersachs, citing in particular the EMPULSE trial presented at the 2022 meeting of the American College of Cardiology. “It is a very useful tool, and I think we will be seeing it used more in the future.”
However, he indicated that the issues raised by Dr. Berwanger are not necessarily easily resolved. Dr. Bauersachs endorsed the effort to consider trial designs that generate data that are more immediately clinically applicable but suggested that different types of designs may be required for different types of clinical questions.
Dr. Berwanger reports financial relationships with Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Pfizer, Servier, and Novartis, which provided funding for the PARADISE-MI trial. Dr. Bauersachs reports financial relationships with Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Boehringer Ingelheim, Cardior, Corvia, CVRx, Novartis, Pfizer, Vifor, and Zoll.
FROM ESC CONGRESS 2022
No invasive strategy benefit at 5 years in ISCHEMIA-CKD extension study
A trip to the cath lab for possible revascularization after a positive stress test, compared with a wait-and-see approach backed by optimal medications, did not improve 5-year survival for patients with advanced chronic kidney disease (CKD) in the ISCHEMIA-CKD trial’s extension study, ISCHEMIA-CKD EXTEND.
The long-term results, from the same 777 patients followed for an average of 2.2 years in the main trial, are consistent with the overall findings of no survival advantage with an initially invasive strategy, compared with one that is initially conservative. The finding applies to patients like those in the trial who had moderate to severe ischemia at stress testing and whose CKD put them in an especially high-risk and little-studied coronary artery disease (CAD) category.
Indeed, in a reflection of that high-risk status, 5-year all-cause mortality reached about 40% and cardiovascular (CV) mortality approached 30%, with no significant differences between patients in the invasive- and conservative-strategy groups.

Those numbers arguably put CKD’s effect on CAD survival in about the same league as an ejection fraction (EF) of 35% or less. For context, all-cause mortality over 3-4 years was about 32% in the REVIVED-BCIS2 trial of such patients with ischemic reduced-EF cardiomyopathy, whether or not they were revascularized, observed Sripal Bangalore, MD, MHA.
Yet in ISCHEMIA-CKD EXTEND, “you’re seeing in a group of patients, with largely preserved EF but advanced CKD, a mortality rate close to 40% at 5 years,” said Dr. Bangalore of New York University.
Although the study doesn’t show benefit from the initially invasive approach in CKD patients with stable CAD, for those with acute coronary syndromes (ACS), it seems to suggest that “at least the invasive strategy is safe,” Dr. Bangalore said during a press conference preceding his presentation of the study Aug. 29 at the annual congress of the European Society of Cardiology, held in Barcelona.
REVIVED-BCIS2 was also presented at the ESC sessions on Aug. 27, as reported by this news organization.
ISCHEMIA-CKD EXTEND “is a large trial and a very well-done trial. The results are robust, and they should influence clinical practice,” Deepak L. Bhatt, MD, MPH, Brigham and Women’s Hospital Heart & Vascular Center, Boston, said as the invited discussant after Dr. Bangalore’s presentation.
“The main message here, really, is don’t just go looking for ischemia, at least with the modalities used in this trial, in your CKD patients as a routine practice, and then try to stomp out that ischemia with revascularization,” Dr. Bhatt said. “The right thing to do in these high-risk patients is to focus on lifestyle modification and intensive medical therapy.”
A caveat, he said, is that the trial’s results don’t apply to the types of patients excluded from it, including those with recent ACS and those who are highly symptomatic or have an EF of less than 35%.
“Those CKD patients likely benefit from an invasive strategy with anatomically appropriate revascularization,” whether percutaneous coronary intervention (PCI) or coronary bypass surgery, Dr. Bhatt said.
At a median follow-up of 5 years in the extension study, the rates of death from any cause were 40.6% for patients in the invasive-strategy group and 37.4% for those in the conservative-strategy group. That yielded a hazard ratio of 1.12 (95% confidence interval, 0.89-1.41; P = .32) after adjustment for age, sex, diabetes status, EF, dialysis status, and – for patients not on dialysis – baseline estimated glomerular filtration rate.
The rates of CV death were 29% for patients managed invasively and 27% for those initially managed conservatively, for a similarly adjusted HR of 1.04 (95% CI, 0.80-1.37; P = .75).
In subgroup analyses, Dr. Bangalore reported, there were no significant differences in all-cause or CV mortality by diabetes status, by severity of baseline ischemia, or by whether the patient had recently experienced new or more frequent angina at study entry, was on guideline-directed medical therapy at baseline, or was on dialysis.
Among the contributions of ISCHEMIA-CKD and its 5-year extension study, Dr. Bangalore told this news organization, is that the relative safety of revascularization they showed may help to counter “renalism,” that is, the aversion to invasive intervention in patients with advanced CKD in clinical practice.
For example, if a patient with advanced CKD presents with an acute myocardial infarction, “people are hesitant to take them to the cath lab,” Dr. Bangalore said. But “if you follow protocols, if you follow strategies to minimize the risk, you can safely go ahead and do it.”
But in patients with stable CAD, as the ISCHEMIA-CKD studies show, “routinely revascularizing them may not have significant benefits.”
ISCHEMIC-CKD and its extension study were funded by the National Heart, Lung, and Blood Institute. Dr. Bangalore discloses receiving research grants from NHLBI and serving as a consultant for Abbott Vascular, Biotronik, Boston Scientific, Amgen, Pfizer, Merck, and Reata. Dr. Bhatt has disclosed grants and/or personal fees from many companies; personal fees from WebMD and other publications or organizations; and having other relationships with Medscape Cardiology and other publications or organizations.
A version of this article first appeared on Medscape.com.
A trip to the cath lab for possible revascularization after a positive stress test, compared with a wait-and-see approach backed by optimal medications, did not improve 5-year survival for patients with advanced chronic kidney disease (CKD) in the ISCHEMIA-CKD trial’s extension study, ISCHEMIA-CKD EXTEND.
The long-term results, from the same 777 patients followed for an average of 2.2 years in the main trial, are consistent with the overall findings of no survival advantage with an initially invasive strategy, compared with one that is initially conservative. The finding applies to patients like those in the trial who had moderate to severe ischemia at stress testing and whose CKD put them in an especially high-risk and little-studied coronary artery disease (CAD) category.
Indeed, in a reflection of that high-risk status, 5-year all-cause mortality reached about 40% and cardiovascular (CV) mortality approached 30%, with no significant differences between patients in the invasive- and conservative-strategy groups.
Those numbers arguably put CKD’s effect on CAD survival in about the same league as an ejection fraction (EF) of 35% or less. For context, all-cause mortality over 3-4 years was about 32% in the REVIVED-BCIS2 trial of such patients with ischemic reduced-EF cardiomyopathy, whether or not they were revascularized, observed Sripal Bangalore, MD, MHA.
Yet in ISCHEMIA-CKD EXTEND, “you’re seeing in a group of patients, with largely preserved EF but advanced CKD, a mortality rate close to 40% at 5 years,” said Dr. Bangalore of New York University.
Although the study doesn’t show benefit from the initially invasive approach in CKD patients with stable CAD, for those with acute coronary syndromes (ACS), it seems to suggest that “at least the invasive strategy is safe,” Dr. Bangalore said during a press conference preceding his presentation of the study Aug. 29 at the annual congress of the European Society of Cardiology, held in Barcelona.
REVIVED-BCIS2 was also presented at the ESC sessions on Aug. 27, as reported by this news organization.
ISCHEMIA-CKD EXTEND “is a large trial and a very well-done trial. The results are robust, and they should influence clinical practice,” Deepak L. Bhatt, MD, MPH, Brigham and Women’s Hospital Heart & Vascular Center, Boston, said as the invited discussant after Dr. Bangalore’s presentation.
“The main message here, really, is don’t just go looking for ischemia, at least with the modalities used in this trial, in your CKD patients as a routine practice, and then try to stomp out that ischemia with revascularization,” Dr. Bhatt said. “The right thing to do in these high-risk patients is to focus on lifestyle modification and intensive medical therapy.”
A caveat, he said, is that the trial’s results don’t apply to the types of patients excluded from it, including those with recent ACS and those who are highly symptomatic or have an EF of less than 35%.
“Those CKD patients likely benefit from an invasive strategy with anatomically appropriate revascularization,” whether percutaneous coronary intervention (PCI) or coronary bypass surgery, Dr. Bhatt said.
At a median follow-up of 5 years in the extension study, the rates of death from any cause were 40.6% for patients in the invasive-strategy group and 37.4% for those in the conservative-strategy group. That yielded a hazard ratio of 1.12 (95% confidence interval, 0.89-1.41; P = .32) after adjustment for age, sex, diabetes status, EF, dialysis status, and – for patients not on dialysis – baseline estimated glomerular filtration rate.
The rates of CV death were 29% for patients managed invasively and 27% for those initially managed conservatively, for a similarly adjusted HR of 1.04 (95% CI, 0.80-1.37; P = .75).
In subgroup analyses, Dr. Bangalore reported, there were no significant differences in all-cause or CV mortality by diabetes status, by severity of baseline ischemia, or by whether the patient had recently experienced new or more frequent angina at study entry, was on guideline-directed medical therapy at baseline, or was on dialysis.
Among the contributions of ISCHEMIA-CKD and its 5-year extension study, Dr. Bangalore told this news organization, is that the relative safety of revascularization they showed may help to counter “renalism,” that is, the aversion to invasive intervention in patients with advanced CKD in clinical practice.
For example, if a patient with advanced CKD presents with an acute myocardial infarction, “people are hesitant to take them to the cath lab,” Dr. Bangalore said. But “if you follow protocols, if you follow strategies to minimize the risk, you can safely go ahead and do it.”
But in patients with stable CAD, as the ISCHEMIA-CKD studies show, “routinely revascularizing them may not have significant benefits.”
ISCHEMIC-CKD and its extension study were funded by the National Heart, Lung, and Blood Institute. Dr. Bangalore discloses receiving research grants from NHLBI and serving as a consultant for Abbott Vascular, Biotronik, Boston Scientific, Amgen, Pfizer, Merck, and Reata. Dr. Bhatt has disclosed grants and/or personal fees from many companies; personal fees from WebMD and other publications or organizations; and having other relationships with Medscape Cardiology and other publications or organizations.
A version of this article first appeared on Medscape.com.
A trip to the cath lab for possible revascularization after a positive stress test, compared with a wait-and-see approach backed by optimal medications, did not improve 5-year survival for patients with advanced chronic kidney disease (CKD) in the ISCHEMIA-CKD trial’s extension study, ISCHEMIA-CKD EXTEND.
The long-term results, from the same 777 patients followed for an average of 2.2 years in the main trial, are consistent with the overall findings of no survival advantage with an initially invasive strategy, compared with one that is initially conservative. The finding applies to patients like those in the trial who had moderate to severe ischemia at stress testing and whose CKD put them in an especially high-risk and little-studied coronary artery disease (CAD) category.
Indeed, in a reflection of that high-risk status, 5-year all-cause mortality reached about 40% and cardiovascular (CV) mortality approached 30%, with no significant differences between patients in the invasive- and conservative-strategy groups.
Those numbers arguably put CKD’s effect on CAD survival in about the same league as an ejection fraction (EF) of 35% or less. For context, all-cause mortality over 3-4 years was about 32% in the REVIVED-BCIS2 trial of such patients with ischemic reduced-EF cardiomyopathy, whether or not they were revascularized, observed Sripal Bangalore, MD, MHA.
Yet in ISCHEMIA-CKD EXTEND, “you’re seeing in a group of patients, with largely preserved EF but advanced CKD, a mortality rate close to 40% at 5 years,” said Dr. Bangalore of New York University.
Although the study doesn’t show benefit from the initially invasive approach in CKD patients with stable CAD, for those with acute coronary syndromes (ACS), it seems to suggest that “at least the invasive strategy is safe,” Dr. Bangalore said during a press conference preceding his presentation of the study Aug. 29 at the annual congress of the European Society of Cardiology, held in Barcelona.
REVIVED-BCIS2 was also presented at the ESC sessions on Aug. 27, as reported by this news organization.
ISCHEMIA-CKD EXTEND “is a large trial and a very well-done trial. The results are robust, and they should influence clinical practice,” Deepak L. Bhatt, MD, MPH, Brigham and Women’s Hospital Heart & Vascular Center, Boston, said as the invited discussant after Dr. Bangalore’s presentation.
“The main message here, really, is don’t just go looking for ischemia, at least with the modalities used in this trial, in your CKD patients as a routine practice, and then try to stomp out that ischemia with revascularization,” Dr. Bhatt said. “The right thing to do in these high-risk patients is to focus on lifestyle modification and intensive medical therapy.”
A caveat, he said, is that the trial’s results don’t apply to the types of patients excluded from it, including those with recent ACS and those who are highly symptomatic or have an EF of less than 35%.
“Those CKD patients likely benefit from an invasive strategy with anatomically appropriate revascularization,” whether percutaneous coronary intervention (PCI) or coronary bypass surgery, Dr. Bhatt said.
At a median follow-up of 5 years in the extension study, the rates of death from any cause were 40.6% for patients in the invasive-strategy group and 37.4% for those in the conservative-strategy group. That yielded a hazard ratio of 1.12 (95% confidence interval, 0.89-1.41; P = .32) after adjustment for age, sex, diabetes status, EF, dialysis status, and – for patients not on dialysis – baseline estimated glomerular filtration rate.
The rates of CV death were 29% for patients managed invasively and 27% for those initially managed conservatively, for a similarly adjusted HR of 1.04 (95% CI, 0.80-1.37; P = .75).
In subgroup analyses, Dr. Bangalore reported, there were no significant differences in all-cause or CV mortality by diabetes status, by severity of baseline ischemia, or by whether the patient had recently experienced new or more frequent angina at study entry, was on guideline-directed medical therapy at baseline, or was on dialysis.
Among the contributions of ISCHEMIA-CKD and its 5-year extension study, Dr. Bangalore told this news organization, is that the relative safety of revascularization they showed may help to counter “renalism,” that is, the aversion to invasive intervention in patients with advanced CKD in clinical practice.
For example, if a patient with advanced CKD presents with an acute myocardial infarction, “people are hesitant to take them to the cath lab,” Dr. Bangalore said. But “if you follow protocols, if you follow strategies to minimize the risk, you can safely go ahead and do it.”
But in patients with stable CAD, as the ISCHEMIA-CKD studies show, “routinely revascularizing them may not have significant benefits.”
ISCHEMIC-CKD and its extension study were funded by the National Heart, Lung, and Blood Institute. Dr. Bangalore discloses receiving research grants from NHLBI and serving as a consultant for Abbott Vascular, Biotronik, Boston Scientific, Amgen, Pfizer, Merck, and Reata. Dr. Bhatt has disclosed grants and/or personal fees from many companies; personal fees from WebMD and other publications or organizations; and having other relationships with Medscape Cardiology and other publications or organizations.
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2022
ACC/AHA issue chest pain data standards update to 2021 guideline
The American College of Cardiology/American Heart Association have issued a set of data standards for chest pain and acute myocardial infarction to accompany the 2021 guidelines for evaluation and diagnosis of chest pain.
In October 2021, the AHA/ACC issued a joint clinical practice guideline encouraging clinicians to use standardized risk assessments, clinical pathways, and tools to evaluate and communicate with patients who present with chest pain, as reported by this news organization.
The writing group underscored the need to reach a consensus for the definitions of chest pain. The new document standardizes related data elements for consistent reporting on chest pain syndromes.
“This is an appendix to the guidelines and a planned effort to try to harmonize and bring uniformity to the language applied,” writing committee chair H.V. “Skip” Anderson, MD, with UT Health Science Center, Houston, told this news organization.
“You want heart attack to mean the same thing in Miami Beach as in Western Pennsylvania, as in Oregon and Washington and every place in between,” Dr. Anderson explained. “You want everybody to be using the same language, so that’s what these data standards are meant to do.”
In the document, data elements are grouped into three broad categories: chest pain, myocardial injury, and MI.
“We deliberately followed the plans contained in the new guideline and focused on potentially serious cardiovascular causes of chest pain as might be encountered in emergency departments,” the writing group notes in the document.
The terms “typical” and “atypical” as descriptors of chest pain or anginal syndromes are not used in the new document, in line with the 2021 guidance to abandon these terms.
Instead, the new document divides chest pain syndromes into three categories: “cardiac,” “possible cardiac,” and “noncardiac” – again, in keeping with the chest pain guideline.
The document also includes data elements for risk stratification scoring according to several common risk scoring algorithms and for procedure-related myocardial injury and procedure-related MI.
Each year, chest pain sends more than 7 million adults to the emergency department in the United States. Although noncardiac causes of chest pain make up a large majority of these cases, there are several life-threatening causes of chest pain that must be identified and treated promptly.
Distinguishing between serious and nonserious causes of chest pain is an urgent imperative, the writing group says.
Overall, they say this new clinical lexicon and set of data standards should be “broadly applicable” in various settings, including clinical trials and observational studies, patient care, electronic health records (EHRs), quality and performance improvement initiatives, registries, and public reporting programs.
The 2022 ACC/AHA Key Data Elements and Definitions for Chest Pain and Acute Myocardial Infarction was simultaneously published online in the Journal of the American College of Cardiology and Circulation: Cardiovascular Quality and Outcomes.
It was developed in collaboration with the American College of Emergency Physicians and the Society for Cardiac Angiography and Interventions and endorsed by the Society for Academic Emergency Medicine.
Dr. Anderson noted that “almost all of the guidelines that come out now, certainly in the last few years, have been followed after a certain interval by a set of data standards applicable to the guidelines.”
“It would be really great if it could actually be attached as an appendix, but the nature of the development of these things is such that there will always be a bit of a time lag between the writing group that develops the guidelines and the work group that develops the data standards; you can’t really have them working in parallel at the same time,” Dr. Anderson said in an interview.
This research had no commercial funding. The authors have no relevant disclosures.
A version of this article first appeared on Medscape.com.
The American College of Cardiology/American Heart Association have issued a set of data standards for chest pain and acute myocardial infarction to accompany the 2021 guidelines for evaluation and diagnosis of chest pain.
In October 2021, the AHA/ACC issued a joint clinical practice guideline encouraging clinicians to use standardized risk assessments, clinical pathways, and tools to evaluate and communicate with patients who present with chest pain, as reported by this news organization.
The writing group underscored the need to reach a consensus for the definitions of chest pain. The new document standardizes related data elements for consistent reporting on chest pain syndromes.
“This is an appendix to the guidelines and a planned effort to try to harmonize and bring uniformity to the language applied,” writing committee chair H.V. “Skip” Anderson, MD, with UT Health Science Center, Houston, told this news organization.
“You want heart attack to mean the same thing in Miami Beach as in Western Pennsylvania, as in Oregon and Washington and every place in between,” Dr. Anderson explained. “You want everybody to be using the same language, so that’s what these data standards are meant to do.”
In the document, data elements are grouped into three broad categories: chest pain, myocardial injury, and MI.
“We deliberately followed the plans contained in the new guideline and focused on potentially serious cardiovascular causes of chest pain as might be encountered in emergency departments,” the writing group notes in the document.
The terms “typical” and “atypical” as descriptors of chest pain or anginal syndromes are not used in the new document, in line with the 2021 guidance to abandon these terms.
Instead, the new document divides chest pain syndromes into three categories: “cardiac,” “possible cardiac,” and “noncardiac” – again, in keeping with the chest pain guideline.
The document also includes data elements for risk stratification scoring according to several common risk scoring algorithms and for procedure-related myocardial injury and procedure-related MI.
Each year, chest pain sends more than 7 million adults to the emergency department in the United States. Although noncardiac causes of chest pain make up a large majority of these cases, there are several life-threatening causes of chest pain that must be identified and treated promptly.
Distinguishing between serious and nonserious causes of chest pain is an urgent imperative, the writing group says.
Overall, they say this new clinical lexicon and set of data standards should be “broadly applicable” in various settings, including clinical trials and observational studies, patient care, electronic health records (EHRs), quality and performance improvement initiatives, registries, and public reporting programs.
The 2022 ACC/AHA Key Data Elements and Definitions for Chest Pain and Acute Myocardial Infarction was simultaneously published online in the Journal of the American College of Cardiology and Circulation: Cardiovascular Quality and Outcomes.
It was developed in collaboration with the American College of Emergency Physicians and the Society for Cardiac Angiography and Interventions and endorsed by the Society for Academic Emergency Medicine.
Dr. Anderson noted that “almost all of the guidelines that come out now, certainly in the last few years, have been followed after a certain interval by a set of data standards applicable to the guidelines.”
“It would be really great if it could actually be attached as an appendix, but the nature of the development of these things is such that there will always be a bit of a time lag between the writing group that develops the guidelines and the work group that develops the data standards; you can’t really have them working in parallel at the same time,” Dr. Anderson said in an interview.
This research had no commercial funding. The authors have no relevant disclosures.
A version of this article first appeared on Medscape.com.
The American College of Cardiology/American Heart Association have issued a set of data standards for chest pain and acute myocardial infarction to accompany the 2021 guidelines for evaluation and diagnosis of chest pain.
In October 2021, the AHA/ACC issued a joint clinical practice guideline encouraging clinicians to use standardized risk assessments, clinical pathways, and tools to evaluate and communicate with patients who present with chest pain, as reported by this news organization.
The writing group underscored the need to reach a consensus for the definitions of chest pain. The new document standardizes related data elements for consistent reporting on chest pain syndromes.
“This is an appendix to the guidelines and a planned effort to try to harmonize and bring uniformity to the language applied,” writing committee chair H.V. “Skip” Anderson, MD, with UT Health Science Center, Houston, told this news organization.
“You want heart attack to mean the same thing in Miami Beach as in Western Pennsylvania, as in Oregon and Washington and every place in between,” Dr. Anderson explained. “You want everybody to be using the same language, so that’s what these data standards are meant to do.”
In the document, data elements are grouped into three broad categories: chest pain, myocardial injury, and MI.
“We deliberately followed the plans contained in the new guideline and focused on potentially serious cardiovascular causes of chest pain as might be encountered in emergency departments,” the writing group notes in the document.
The terms “typical” and “atypical” as descriptors of chest pain or anginal syndromes are not used in the new document, in line with the 2021 guidance to abandon these terms.
Instead, the new document divides chest pain syndromes into three categories: “cardiac,” “possible cardiac,” and “noncardiac” – again, in keeping with the chest pain guideline.
The document also includes data elements for risk stratification scoring according to several common risk scoring algorithms and for procedure-related myocardial injury and procedure-related MI.
Each year, chest pain sends more than 7 million adults to the emergency department in the United States. Although noncardiac causes of chest pain make up a large majority of these cases, there are several life-threatening causes of chest pain that must be identified and treated promptly.
Distinguishing between serious and nonserious causes of chest pain is an urgent imperative, the writing group says.
Overall, they say this new clinical lexicon and set of data standards should be “broadly applicable” in various settings, including clinical trials and observational studies, patient care, electronic health records (EHRs), quality and performance improvement initiatives, registries, and public reporting programs.
The 2022 ACC/AHA Key Data Elements and Definitions for Chest Pain and Acute Myocardial Infarction was simultaneously published online in the Journal of the American College of Cardiology and Circulation: Cardiovascular Quality and Outcomes.
It was developed in collaboration with the American College of Emergency Physicians and the Society for Cardiac Angiography and Interventions and endorsed by the Society for Academic Emergency Medicine.
Dr. Anderson noted that “almost all of the guidelines that come out now, certainly in the last few years, have been followed after a certain interval by a set of data standards applicable to the guidelines.”
“It would be really great if it could actually be attached as an appendix, but the nature of the development of these things is such that there will always be a bit of a time lag between the writing group that develops the guidelines and the work group that develops the data standards; you can’t really have them working in parallel at the same time,” Dr. Anderson said in an interview.
This research had no commercial funding. The authors have no relevant disclosures.
A version of this article first appeared on Medscape.com.
Patisiran benefits ATTR amyloidosis with cardiomyopathy: APOLLO-B
The RNA interference (RNAi) therapeutic, patisiran (Onpattro, Alnylam), showed a statistically significant and clinically meaningful benefit on functional capacity, as measured by the 6-minute walk test (6-MWT), compared with placebo, in the treatment of transthyretin-mediated amyloidosis with cardiomyopathy, in the APOLLO-B trial.
The study also met its first secondary endpoint, demonstrating a statistically significant and clinically meaningful benefit on health status and quality of life.
These positive results, their first formal presentation, were announced Sept. 8 at the 18th International Symposium on Amyloidosis. However, the company announced positive top-line results from the trial in early August.
Transthyretin-mediated (ATTR) amyloidosis is a rare, rapidly progressive, debilitating disease caused by misfolded transthyretin (TTR) proteins which accumulate as amyloid fibrils in multiple tissues including the nerves, heart, and gastrointestinal tract.
There are two different types of ATTR amyloidosis: hereditary ATTR (hATTR) amyloidosis, caused by a TTR gene variant, and wild-type ATTR (wtATTR) amyloidosis, which occurs without a TTR gene variant. hATTR amyloidosis affects approximately 50,000 people worldwide, whereas wtATTR amyloidosis is estimated to affect 200,000-300,000 people worldwide.
Patisiran is an intravenously administered RNAi therapeutic that is approved in the United States and Canada for the treatment of the polyneuropathy of hATTR amyloidosis in adults. It is also approved in the European Union, Switzerland, Brazil, and Japan for a similar indication. It is designed to target and silence TTR messenger RNA, thereby reducing the production of TTR protein before it is made. Reducing the pathogenic protein leads to a reduction in amyloid deposits in tissues.
“The results of the APOLLO-B phase 3 study are impressive, as I believe they underscore the potential for patisiran to provide a benefit on functional capacity and quality of life in patients living with ATTR amyloidosis with cardiomyopathy. Furthermore, these results were seen after only 12 months of treatment,” Mathew Maurer, MD, Arnold and Arlene Goldstein Professor of Cardiology at Columbia University Irving Medical Center, New York, said in an Alnylam press release.
“The cardiac manifestations associated with ATTR amyloidosis can have a devastating impact on patients’ lives and current treatment options are limited. With the rapidly progressive nature of the disease, there is a significant need for treatments like patisiran, which has the potential to be a new option for patients and physicians to treat the cardiomyopathy of ATTR amyloidosis,” Dr. Maurer added.
APOLLO-B is a phase 3, randomized, double-blind study evaluating the effects of patisiran on functional capacity and quality of life in patients with ATTR amyloidosis with cardiomyopathy. The study enrolled 360 adult patients with ATTR amyloidosis (hereditary or wild-type) with cardiomyopathy who were randomly assigned 1:1 to receive 0.3 mg/kg of patisiran or placebo intravenously administered every 3 weeks over a 12-month treatment period. After 12 months, all patients will receive patisiran in an open-label extension.
Results at 12 months, reported by Alnylam, found that the primary endpoint, the 6-MWT, showed a median change from baseline of –8.15 m for the patisiran group and –21.34 m for the placebo group, a significant difference favoring patisiran.
The first secondary endpoint was health status and quality of life, as measured by the Kansas City Cardiomyopathy Questionnaire Overall Summary score. This showed a mean change from baseline of +0.300 for the patisiran group and –3.408 for the placebo group, a significant difference favoring patisiran.
Secondary composite outcome endpoints did not achieve statistical significance.
A nonsignificant result (win ratio, 1.27; P = .0574) was found on the secondary composite endpoint of all-cause mortality, frequency of cardiovascular events, and change from baseline in 6-MWT over 12 months, compared with placebo.
The final two composite endpoints were not powered for statistical significance, given the sample size and short duration of the study – all-cause mortality and frequency of all-cause hospitalizations and urgent heart failure visits in patients not on tafamidis at baseline (hazard ratio, 0.997) and in the overall study population (HR, 0.883).
Patisiran achieved a rapid and sustained reduction in serum TTR levels, with a mean percent reduction from baseline in serum TTR reduction of 87% at month 12.
A beneficial effect on the exploratory endpoint, N-terminal of the prohormone brain natriuretic peptide, a measure of cardiac stress, was observed in the patisiran arm, with a 20% reduction in the adjusted geometric mean fold change from baseline, compared with placebo.
Patisiran also demonstrated an encouraging safety and tolerability profile, including no cardiac safety concerns relative to placebo, during the 12-month treatment period, Alnylam reported.
The majority of adverse events were mild or moderate in severity. Treatment emergent adverse events in the patisiran group included infusion-related reactions, arthralgia, and muscle spasms.
In the safety analysis, there were five deaths (2.8%) observed in patisiran-treated patients and eight deaths (4.5%) observed in the placebo group.
Pushkal Garg, MD, chief medical officer at Alnylam, said: “We believe these data validate the therapeutic hypothesis that TTR silencing by an RNAi therapeutic may be an effective approach to treating cardiomyopathy of both wild-type and hereditary ATTR amyloidosis.”
Alnylam plans to file a supplemental new drug application for patisiran as a potential treatment for ATTR amyloidosis with cardiomyopathy in the United States in late 2022.
A version of this article first appeared on Medscape.com.
The RNA interference (RNAi) therapeutic, patisiran (Onpattro, Alnylam), showed a statistically significant and clinically meaningful benefit on functional capacity, as measured by the 6-minute walk test (6-MWT), compared with placebo, in the treatment of transthyretin-mediated amyloidosis with cardiomyopathy, in the APOLLO-B trial.
The study also met its first secondary endpoint, demonstrating a statistically significant and clinically meaningful benefit on health status and quality of life.
These positive results, their first formal presentation, were announced Sept. 8 at the 18th International Symposium on Amyloidosis. However, the company announced positive top-line results from the trial in early August.
Transthyretin-mediated (ATTR) amyloidosis is a rare, rapidly progressive, debilitating disease caused by misfolded transthyretin (TTR) proteins which accumulate as amyloid fibrils in multiple tissues including the nerves, heart, and gastrointestinal tract.
There are two different types of ATTR amyloidosis: hereditary ATTR (hATTR) amyloidosis, caused by a TTR gene variant, and wild-type ATTR (wtATTR) amyloidosis, which occurs without a TTR gene variant. hATTR amyloidosis affects approximately 50,000 people worldwide, whereas wtATTR amyloidosis is estimated to affect 200,000-300,000 people worldwide.
Patisiran is an intravenously administered RNAi therapeutic that is approved in the United States and Canada for the treatment of the polyneuropathy of hATTR amyloidosis in adults. It is also approved in the European Union, Switzerland, Brazil, and Japan for a similar indication. It is designed to target and silence TTR messenger RNA, thereby reducing the production of TTR protein before it is made. Reducing the pathogenic protein leads to a reduction in amyloid deposits in tissues.
“The results of the APOLLO-B phase 3 study are impressive, as I believe they underscore the potential for patisiran to provide a benefit on functional capacity and quality of life in patients living with ATTR amyloidosis with cardiomyopathy. Furthermore, these results were seen after only 12 months of treatment,” Mathew Maurer, MD, Arnold and Arlene Goldstein Professor of Cardiology at Columbia University Irving Medical Center, New York, said in an Alnylam press release.
“The cardiac manifestations associated with ATTR amyloidosis can have a devastating impact on patients’ lives and current treatment options are limited. With the rapidly progressive nature of the disease, there is a significant need for treatments like patisiran, which has the potential to be a new option for patients and physicians to treat the cardiomyopathy of ATTR amyloidosis,” Dr. Maurer added.
APOLLO-B is a phase 3, randomized, double-blind study evaluating the effects of patisiran on functional capacity and quality of life in patients with ATTR amyloidosis with cardiomyopathy. The study enrolled 360 adult patients with ATTR amyloidosis (hereditary or wild-type) with cardiomyopathy who were randomly assigned 1:1 to receive 0.3 mg/kg of patisiran or placebo intravenously administered every 3 weeks over a 12-month treatment period. After 12 months, all patients will receive patisiran in an open-label extension.
Results at 12 months, reported by Alnylam, found that the primary endpoint, the 6-MWT, showed a median change from baseline of –8.15 m for the patisiran group and –21.34 m for the placebo group, a significant difference favoring patisiran.
The first secondary endpoint was health status and quality of life, as measured by the Kansas City Cardiomyopathy Questionnaire Overall Summary score. This showed a mean change from baseline of +0.300 for the patisiran group and –3.408 for the placebo group, a significant difference favoring patisiran.
Secondary composite outcome endpoints did not achieve statistical significance.
A nonsignificant result (win ratio, 1.27; P = .0574) was found on the secondary composite endpoint of all-cause mortality, frequency of cardiovascular events, and change from baseline in 6-MWT over 12 months, compared with placebo.
The final two composite endpoints were not powered for statistical significance, given the sample size and short duration of the study – all-cause mortality and frequency of all-cause hospitalizations and urgent heart failure visits in patients not on tafamidis at baseline (hazard ratio, 0.997) and in the overall study population (HR, 0.883).
Patisiran achieved a rapid and sustained reduction in serum TTR levels, with a mean percent reduction from baseline in serum TTR reduction of 87% at month 12.
A beneficial effect on the exploratory endpoint, N-terminal of the prohormone brain natriuretic peptide, a measure of cardiac stress, was observed in the patisiran arm, with a 20% reduction in the adjusted geometric mean fold change from baseline, compared with placebo.
Patisiran also demonstrated an encouraging safety and tolerability profile, including no cardiac safety concerns relative to placebo, during the 12-month treatment period, Alnylam reported.
The majority of adverse events were mild or moderate in severity. Treatment emergent adverse events in the patisiran group included infusion-related reactions, arthralgia, and muscle spasms.
In the safety analysis, there were five deaths (2.8%) observed in patisiran-treated patients and eight deaths (4.5%) observed in the placebo group.
Pushkal Garg, MD, chief medical officer at Alnylam, said: “We believe these data validate the therapeutic hypothesis that TTR silencing by an RNAi therapeutic may be an effective approach to treating cardiomyopathy of both wild-type and hereditary ATTR amyloidosis.”
Alnylam plans to file a supplemental new drug application for patisiran as a potential treatment for ATTR amyloidosis with cardiomyopathy in the United States in late 2022.
A version of this article first appeared on Medscape.com.
The RNA interference (RNAi) therapeutic, patisiran (Onpattro, Alnylam), showed a statistically significant and clinically meaningful benefit on functional capacity, as measured by the 6-minute walk test (6-MWT), compared with placebo, in the treatment of transthyretin-mediated amyloidosis with cardiomyopathy, in the APOLLO-B trial.
The study also met its first secondary endpoint, demonstrating a statistically significant and clinically meaningful benefit on health status and quality of life.
These positive results, their first formal presentation, were announced Sept. 8 at the 18th International Symposium on Amyloidosis. However, the company announced positive top-line results from the trial in early August.
Transthyretin-mediated (ATTR) amyloidosis is a rare, rapidly progressive, debilitating disease caused by misfolded transthyretin (TTR) proteins which accumulate as amyloid fibrils in multiple tissues including the nerves, heart, and gastrointestinal tract.
There are two different types of ATTR amyloidosis: hereditary ATTR (hATTR) amyloidosis, caused by a TTR gene variant, and wild-type ATTR (wtATTR) amyloidosis, which occurs without a TTR gene variant. hATTR amyloidosis affects approximately 50,000 people worldwide, whereas wtATTR amyloidosis is estimated to affect 200,000-300,000 people worldwide.
Patisiran is an intravenously administered RNAi therapeutic that is approved in the United States and Canada for the treatment of the polyneuropathy of hATTR amyloidosis in adults. It is also approved in the European Union, Switzerland, Brazil, and Japan for a similar indication. It is designed to target and silence TTR messenger RNA, thereby reducing the production of TTR protein before it is made. Reducing the pathogenic protein leads to a reduction in amyloid deposits in tissues.
“The results of the APOLLO-B phase 3 study are impressive, as I believe they underscore the potential for patisiran to provide a benefit on functional capacity and quality of life in patients living with ATTR amyloidosis with cardiomyopathy. Furthermore, these results were seen after only 12 months of treatment,” Mathew Maurer, MD, Arnold and Arlene Goldstein Professor of Cardiology at Columbia University Irving Medical Center, New York, said in an Alnylam press release.
“The cardiac manifestations associated with ATTR amyloidosis can have a devastating impact on patients’ lives and current treatment options are limited. With the rapidly progressive nature of the disease, there is a significant need for treatments like patisiran, which has the potential to be a new option for patients and physicians to treat the cardiomyopathy of ATTR amyloidosis,” Dr. Maurer added.
APOLLO-B is a phase 3, randomized, double-blind study evaluating the effects of patisiran on functional capacity and quality of life in patients with ATTR amyloidosis with cardiomyopathy. The study enrolled 360 adult patients with ATTR amyloidosis (hereditary or wild-type) with cardiomyopathy who were randomly assigned 1:1 to receive 0.3 mg/kg of patisiran or placebo intravenously administered every 3 weeks over a 12-month treatment period. After 12 months, all patients will receive patisiran in an open-label extension.
Results at 12 months, reported by Alnylam, found that the primary endpoint, the 6-MWT, showed a median change from baseline of –8.15 m for the patisiran group and –21.34 m for the placebo group, a significant difference favoring patisiran.
The first secondary endpoint was health status and quality of life, as measured by the Kansas City Cardiomyopathy Questionnaire Overall Summary score. This showed a mean change from baseline of +0.300 for the patisiran group and –3.408 for the placebo group, a significant difference favoring patisiran.
Secondary composite outcome endpoints did not achieve statistical significance.
A nonsignificant result (win ratio, 1.27; P = .0574) was found on the secondary composite endpoint of all-cause mortality, frequency of cardiovascular events, and change from baseline in 6-MWT over 12 months, compared with placebo.
The final two composite endpoints were not powered for statistical significance, given the sample size and short duration of the study – all-cause mortality and frequency of all-cause hospitalizations and urgent heart failure visits in patients not on tafamidis at baseline (hazard ratio, 0.997) and in the overall study population (HR, 0.883).
Patisiran achieved a rapid and sustained reduction in serum TTR levels, with a mean percent reduction from baseline in serum TTR reduction of 87% at month 12.
A beneficial effect on the exploratory endpoint, N-terminal of the prohormone brain natriuretic peptide, a measure of cardiac stress, was observed in the patisiran arm, with a 20% reduction in the adjusted geometric mean fold change from baseline, compared with placebo.
Patisiran also demonstrated an encouraging safety and tolerability profile, including no cardiac safety concerns relative to placebo, during the 12-month treatment period, Alnylam reported.
The majority of adverse events were mild or moderate in severity. Treatment emergent adverse events in the patisiran group included infusion-related reactions, arthralgia, and muscle spasms.
In the safety analysis, there were five deaths (2.8%) observed in patisiran-treated patients and eight deaths (4.5%) observed in the placebo group.
Pushkal Garg, MD, chief medical officer at Alnylam, said: “We believe these data validate the therapeutic hypothesis that TTR silencing by an RNAi therapeutic may be an effective approach to treating cardiomyopathy of both wild-type and hereditary ATTR amyloidosis.”
Alnylam plans to file a supplemental new drug application for patisiran as a potential treatment for ATTR amyloidosis with cardiomyopathy in the United States in late 2022.
A version of this article first appeared on Medscape.com.
FDA warns of clip lock malfunctions with MitraClip devices
The Food and Drug Administration is alerting health care providers about the potential for clip lock malfunctions with Abbott’s MitraClip’s delivery system.
“These events appear to occur in approximately 1.3% of MitraClip procedures and have been observed with all device models,” the FDA says in a letter posted on its website.
The MitraClip device was approved in 2013 for patients with symptomatic, degenerative mitral regurgitation (MR) deemed high risk for mitral-valve surgery.
In its own “urgent medical device correction letter” to providers, Abbott reports a recent increase in reports of the clips failing to “establish final arm angle (EFAA)” and of “clip opening while locked (COWL)” events.
During device preparation and prior to clip deployment, the operator intentionally attempts to open a locked clip to verify that the locking mechanism is engaged.
COWL describes when the clip arm angle increases postdeployment. “In these cases, users observe a slippage in the lock, resulting in an arm angle greater than 10 degrees from the angle observed at deployment,” which can be identified through fluoroscopy, Abbott says.
From February 2021 to January 2022, the EFAA failure rate was 0.51% and COWL rate 0.28%, increasing to 0.80% and 0.50%, respectively, from February 2022 to July 2022, according to the company.
Despite the increase in reports, the acute procedural success rate remains consistent with historical data, according to Abbott. “Further, EFAA failure or COWL most often results in no adverse patient outcomes. COWL may lead to less MR reduction, which is often treated with the use of one or more additional clips.”
Abbott says there is also a “low incidence” of required additional interventions. No immediate open surgical conversions have occurred as a result of EFAA/COWL events, whereas 0.53% of such events have resulted in nonurgent surgical conversions.
“In any case where significant residual MR is observed after clip deployment, a second clip should be considered and implanted in accordance with the IFU [instructions for use],” it advises.
Abbott says that a “change in the material properties of one of the clip locking components” has been identified as a contributing cause of EFAA/COWL events. It is working on producing new lots with updated manufacturing processing and raw material to mitigate the risk.
Certain use conditions can also contribute to EFAA/COWL events, and are referenced in the IFU, Appendix A, it notes.
The FDA is working with Abbott and recommends that health care providers do the following:
- Review the recall notice from Abbott for all MitraClip Clip Delivery Systems.
- Be aware of the potential for clip lock malfunctions before or after deployment with this device.
- Read and carefully follow the instructions for use and the recommendations provided in the recall notice to help minimize the chance of the clip failing to lock. These include recommendations about procedural steps for implant positioning, locking sequences, establishing clip arm angle, preparation for clip release, and avoiding excessive force and manipulation when unlocking the clip during device preparation and during the procedure.
Health care professionals can also report adverse reactions or quality problems they experience using these devices to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration is alerting health care providers about the potential for clip lock malfunctions with Abbott’s MitraClip’s delivery system.
“These events appear to occur in approximately 1.3% of MitraClip procedures and have been observed with all device models,” the FDA says in a letter posted on its website.
The MitraClip device was approved in 2013 for patients with symptomatic, degenerative mitral regurgitation (MR) deemed high risk for mitral-valve surgery.
In its own “urgent medical device correction letter” to providers, Abbott reports a recent increase in reports of the clips failing to “establish final arm angle (EFAA)” and of “clip opening while locked (COWL)” events.
During device preparation and prior to clip deployment, the operator intentionally attempts to open a locked clip to verify that the locking mechanism is engaged.
COWL describes when the clip arm angle increases postdeployment. “In these cases, users observe a slippage in the lock, resulting in an arm angle greater than 10 degrees from the angle observed at deployment,” which can be identified through fluoroscopy, Abbott says.
From February 2021 to January 2022, the EFAA failure rate was 0.51% and COWL rate 0.28%, increasing to 0.80% and 0.50%, respectively, from February 2022 to July 2022, according to the company.
Despite the increase in reports, the acute procedural success rate remains consistent with historical data, according to Abbott. “Further, EFAA failure or COWL most often results in no adverse patient outcomes. COWL may lead to less MR reduction, which is often treated with the use of one or more additional clips.”
Abbott says there is also a “low incidence” of required additional interventions. No immediate open surgical conversions have occurred as a result of EFAA/COWL events, whereas 0.53% of such events have resulted in nonurgent surgical conversions.
“In any case where significant residual MR is observed after clip deployment, a second clip should be considered and implanted in accordance with the IFU [instructions for use],” it advises.
Abbott says that a “change in the material properties of one of the clip locking components” has been identified as a contributing cause of EFAA/COWL events. It is working on producing new lots with updated manufacturing processing and raw material to mitigate the risk.
Certain use conditions can also contribute to EFAA/COWL events, and are referenced in the IFU, Appendix A, it notes.
The FDA is working with Abbott and recommends that health care providers do the following:
- Review the recall notice from Abbott for all MitraClip Clip Delivery Systems.
- Be aware of the potential for clip lock malfunctions before or after deployment with this device.
- Read and carefully follow the instructions for use and the recommendations provided in the recall notice to help minimize the chance of the clip failing to lock. These include recommendations about procedural steps for implant positioning, locking sequences, establishing clip arm angle, preparation for clip release, and avoiding excessive force and manipulation when unlocking the clip during device preparation and during the procedure.
Health care professionals can also report adverse reactions or quality problems they experience using these devices to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration is alerting health care providers about the potential for clip lock malfunctions with Abbott’s MitraClip’s delivery system.
“These events appear to occur in approximately 1.3% of MitraClip procedures and have been observed with all device models,” the FDA says in a letter posted on its website.
The MitraClip device was approved in 2013 for patients with symptomatic, degenerative mitral regurgitation (MR) deemed high risk for mitral-valve surgery.
In its own “urgent medical device correction letter” to providers, Abbott reports a recent increase in reports of the clips failing to “establish final arm angle (EFAA)” and of “clip opening while locked (COWL)” events.
During device preparation and prior to clip deployment, the operator intentionally attempts to open a locked clip to verify that the locking mechanism is engaged.
COWL describes when the clip arm angle increases postdeployment. “In these cases, users observe a slippage in the lock, resulting in an arm angle greater than 10 degrees from the angle observed at deployment,” which can be identified through fluoroscopy, Abbott says.
From February 2021 to January 2022, the EFAA failure rate was 0.51% and COWL rate 0.28%, increasing to 0.80% and 0.50%, respectively, from February 2022 to July 2022, according to the company.
Despite the increase in reports, the acute procedural success rate remains consistent with historical data, according to Abbott. “Further, EFAA failure or COWL most often results in no adverse patient outcomes. COWL may lead to less MR reduction, which is often treated with the use of one or more additional clips.”
Abbott says there is also a “low incidence” of required additional interventions. No immediate open surgical conversions have occurred as a result of EFAA/COWL events, whereas 0.53% of such events have resulted in nonurgent surgical conversions.
“In any case where significant residual MR is observed after clip deployment, a second clip should be considered and implanted in accordance with the IFU [instructions for use],” it advises.
Abbott says that a “change in the material properties of one of the clip locking components” has been identified as a contributing cause of EFAA/COWL events. It is working on producing new lots with updated manufacturing processing and raw material to mitigate the risk.
Certain use conditions can also contribute to EFAA/COWL events, and are referenced in the IFU, Appendix A, it notes.
The FDA is working with Abbott and recommends that health care providers do the following:
- Review the recall notice from Abbott for all MitraClip Clip Delivery Systems.
- Be aware of the potential for clip lock malfunctions before or after deployment with this device.
- Read and carefully follow the instructions for use and the recommendations provided in the recall notice to help minimize the chance of the clip failing to lock. These include recommendations about procedural steps for implant positioning, locking sequences, establishing clip arm angle, preparation for clip release, and avoiding excessive force and manipulation when unlocking the clip during device preparation and during the procedure.
Health care professionals can also report adverse reactions or quality problems they experience using these devices to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
Artificial sweeteners linked to higher CV event risk
Health concerns about the consumption of artificial sweeteners could be strengthened with the publication of a new study linking their intake to increased risk of heart disease and stroke events.
In this latest large-scale, prospective study of French adults, total artificial sweetener intake from all sources was associated with increased risk overall of cardiovascular and cerebrovascular disease.
The study was published online in the BMJ.
The current study differs from those done previously in that it includes artificial sweetener intake from both food and drinks, whereas previous studies have focused mainly on artificial sweetener content of beverages alone.
“Here we have quantified for the first time the global exposure to artificial sweeteners. This is not just beverages but includes the use of tabletop sweeteners, and other foods that include artificial sweeteners such as yogurts and desserts. This is the first time this information has been correlated to risk of heart disease,” senior author Mathilde Touvier, MD, Sorbonne Paris Nord University, told this news organization.
Just over half of the artificial sweetener intake in the study came from drinks, with the rest coming from tabletop sweeteners and foods.
“We included hard cardio- and cerebrovascular clinical endpoints such as a heart attack or stroke, and our results suggest that the amount of artificial sweetener in less than one can of soda could increase the risk of such events,” Dr. Touvier noted.
“This is an important and statistically significant association which shows robustness in all models after adjusting for many other possible confounding factors,” she said.
“There is now mounting evidence correlating artificial sweeteners to weight gain and heart disease,” she concluded. “My advice would be that we all need to try to limit sugar intake, but we should not consider artificial sweeteners as safe alternatives. Rather, we need to try to reduce our need for a sugary taste in our diet.”
But another leading researcher in the field urges caution in interpreting these results.
John Sievenpiper, MD, departments of nutritional sciences and medicine, University of Toronto, commented: “This paper shows the same relationship seen by many other large prospective cohorts which model the intake of artificial sweeteners as baseline or prevalent exposures.
“These observations are well recognized to be at high risk of residual confounding from behavior clustering and reverse causality in which being at risk for cardiovascular disease causes people to consume artificial sweeteners as a strategy to mitigate this risk as opposed to the other way around.”
Risk increased by 9%
The current study included 103,388 French adults from the NutriNet-Sante cohort, of whom 37.1% reported consumption of artificial sweeteners. The sweeteners assessed were mainly aspartame (58% of sweetener intake), acesulfame potassium (29%), and sucralose (10%), with the other 3% made up of various other sweeteners including cyclamates and saccharin.
Results showed that over an average 9 years of follow-up, artificial sweetener intake was associated with a 9% increased risk of cardiovascular or cerebrovascular events, including myocardial infarction, acute coronary syndrome, angioplasty, angina, stroke, or transient ischemic attack, with a hazard ratio of 1.09 (95% confidence interval, 1.01-1.18; P = .03).
The average intake of artificial sweeteners among those who reported consuming them was 42.46 mg/day, which corresponds to approximately one individual packet of tabletop sweetener or 100 mL of diet soda.
“We don’t have enough evidence to work out an amount of artificial sweetener that is harmful, but we did show a dose-effect association, with a higher risk of cardiovascular events with higher consumption,” Dr. Touvier said.
“Higher consumption in this study was a mean of 77 mg/day artificial sweetener, which is about 200 mL of soda – just a bit less than one standard can of soda,” she added.
The absolute incidence rate of cardiovascular or cerebrovascular events in higher consumers was 346 per 100,000 person-years vs. 314 per 100,000 person-years in nonconsumers.
Further analysis suggested that aspartame intake was particularly associated with increased risk of cerebrovascular events, while acesulfame potassium and sucralose were associated with increased coronary heart disease risk.
Study strengths
Dr. Touvier acknowledged that dietary studies, which generally rely on individuals self-reporting food and drink intake, are always hard to interpret. But she said this study used a more reliable method of dietary assessment, with repeated 24-hour dietary records, which were validated by interviews with a trained dietitian and against blood and urinary biomarkers.
And whereas residual confounding cannot be totally excluded, she pointed out that models were adjusted for a wide range of potential sociodemographic, anthropometric, dietary, and lifestyle confounders.
Dr. Touvier also noted that cases of cardiovascular disease in the first 2 years of follow-up were excluded to minimize the bias caused by individuals who maybe have switched to artificial sweeteners because of a cardiovascular issue.
“While this study has many strengths, it cannot on its own prove a causal relationship between artificial sweetener and increased cardiovascular risk,” she added. “We need health agencies to examine all the literature in the field. This is however another important piece of evidence.”
Dr. Touvier says that although observational studies have their issues, they will form the basis of the evidence on the effects of artificial sweeteners on health.
“Randomized studies in this area can only really look at short-term outcomes such as weight gain or biomarker changes. So, we will have to use observational studies together with experimental research to build the evidence. This is what happened with cigarette smoking and lung cancer. That link was not established by randomized trials, but by the accumulation of observational and experimental data.”
Different artificial sweeteners may be better?
Commenting on the study, Kim Williams Sr., MD, University of Louisville (Ky.), pointed out that this study included artificial sweeteners that increase insulin or decrease insulin sensitivity, and that insulin spikes increase obesity, insulin resistance, hypertension, and atherosclerosis.
“There are some safer artificial sweeteners that do not increase insulin much or at all, such as erythritol, yacon root/yacon syrup, stevia root, but they weren’t included in the analysis,” Dr. Williams added.
Dr. Sievenpiper explained that most studies on artificial sweeteners look at their consumption in isolation without considering how they compare to the intake of the sugars that they are intended to replace.
“The comparator matters as no food is consumed in a vacuum,” he said.
To address this, Dr. Sievenpiper and colleagues have recently published a systematic review and meta-analysis of the prospective cohort study evidence that shows if exposure to artificially sweetened beverages is modeled in substitution for sugar-sweetened beverages, then they are associated with less coronary heart disease, cardiovascular mortality, and all-cause mortality.
On the other hand, if exposure to artificially sweetened beverages is compared with water, then no difference in these outcomes was seen.
“These observations are more biologically plausible, robust, and reproducible and agree with the evidence for the effect of artificial sweeteners on intermediate risk factors in randomized trials,” Dr. Sievenpiper notes.
His group has also recently published a review of randomized studies showing that when compared with sugar-sweetened beverages, intake of artificially sweetened beverages was associated with small improvements in body weight and cardiometabolic risk factors without evidence of harm.
“I think the context provided by these studies is important, and taken together, the totality of the evidence suggests that artificial sweeteners are likely to be a useful tool in sugar reduction strategies,” Dr. Sievenpiper concludes.
The current study was funded by the European Research Council under the European Union’s Horizon 2020 research and innovation program, French National Cancer Institute, French Ministry of Health, IdEx Université de Paris Cité, Bettencourt-Schueller Foundation Research Prize 2021. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Health concerns about the consumption of artificial sweeteners could be strengthened with the publication of a new study linking their intake to increased risk of heart disease and stroke events.
In this latest large-scale, prospective study of French adults, total artificial sweetener intake from all sources was associated with increased risk overall of cardiovascular and cerebrovascular disease.
The study was published online in the BMJ.
The current study differs from those done previously in that it includes artificial sweetener intake from both food and drinks, whereas previous studies have focused mainly on artificial sweetener content of beverages alone.
“Here we have quantified for the first time the global exposure to artificial sweeteners. This is not just beverages but includes the use of tabletop sweeteners, and other foods that include artificial sweeteners such as yogurts and desserts. This is the first time this information has been correlated to risk of heart disease,” senior author Mathilde Touvier, MD, Sorbonne Paris Nord University, told this news organization.
Just over half of the artificial sweetener intake in the study came from drinks, with the rest coming from tabletop sweeteners and foods.
“We included hard cardio- and cerebrovascular clinical endpoints such as a heart attack or stroke, and our results suggest that the amount of artificial sweetener in less than one can of soda could increase the risk of such events,” Dr. Touvier noted.
“This is an important and statistically significant association which shows robustness in all models after adjusting for many other possible confounding factors,” she said.
“There is now mounting evidence correlating artificial sweeteners to weight gain and heart disease,” she concluded. “My advice would be that we all need to try to limit sugar intake, but we should not consider artificial sweeteners as safe alternatives. Rather, we need to try to reduce our need for a sugary taste in our diet.”
But another leading researcher in the field urges caution in interpreting these results.
John Sievenpiper, MD, departments of nutritional sciences and medicine, University of Toronto, commented: “This paper shows the same relationship seen by many other large prospective cohorts which model the intake of artificial sweeteners as baseline or prevalent exposures.
“These observations are well recognized to be at high risk of residual confounding from behavior clustering and reverse causality in which being at risk for cardiovascular disease causes people to consume artificial sweeteners as a strategy to mitigate this risk as opposed to the other way around.”
Risk increased by 9%
The current study included 103,388 French adults from the NutriNet-Sante cohort, of whom 37.1% reported consumption of artificial sweeteners. The sweeteners assessed were mainly aspartame (58% of sweetener intake), acesulfame potassium (29%), and sucralose (10%), with the other 3% made up of various other sweeteners including cyclamates and saccharin.
Results showed that over an average 9 years of follow-up, artificial sweetener intake was associated with a 9% increased risk of cardiovascular or cerebrovascular events, including myocardial infarction, acute coronary syndrome, angioplasty, angina, stroke, or transient ischemic attack, with a hazard ratio of 1.09 (95% confidence interval, 1.01-1.18; P = .03).
The average intake of artificial sweeteners among those who reported consuming them was 42.46 mg/day, which corresponds to approximately one individual packet of tabletop sweetener or 100 mL of diet soda.
“We don’t have enough evidence to work out an amount of artificial sweetener that is harmful, but we did show a dose-effect association, with a higher risk of cardiovascular events with higher consumption,” Dr. Touvier said.
“Higher consumption in this study was a mean of 77 mg/day artificial sweetener, which is about 200 mL of soda – just a bit less than one standard can of soda,” she added.
The absolute incidence rate of cardiovascular or cerebrovascular events in higher consumers was 346 per 100,000 person-years vs. 314 per 100,000 person-years in nonconsumers.
Further analysis suggested that aspartame intake was particularly associated with increased risk of cerebrovascular events, while acesulfame potassium and sucralose were associated with increased coronary heart disease risk.
Study strengths
Dr. Touvier acknowledged that dietary studies, which generally rely on individuals self-reporting food and drink intake, are always hard to interpret. But she said this study used a more reliable method of dietary assessment, with repeated 24-hour dietary records, which were validated by interviews with a trained dietitian and against blood and urinary biomarkers.
And whereas residual confounding cannot be totally excluded, she pointed out that models were adjusted for a wide range of potential sociodemographic, anthropometric, dietary, and lifestyle confounders.
Dr. Touvier also noted that cases of cardiovascular disease in the first 2 years of follow-up were excluded to minimize the bias caused by individuals who maybe have switched to artificial sweeteners because of a cardiovascular issue.
“While this study has many strengths, it cannot on its own prove a causal relationship between artificial sweetener and increased cardiovascular risk,” she added. “We need health agencies to examine all the literature in the field. This is however another important piece of evidence.”
Dr. Touvier says that although observational studies have their issues, they will form the basis of the evidence on the effects of artificial sweeteners on health.
“Randomized studies in this area can only really look at short-term outcomes such as weight gain or biomarker changes. So, we will have to use observational studies together with experimental research to build the evidence. This is what happened with cigarette smoking and lung cancer. That link was not established by randomized trials, but by the accumulation of observational and experimental data.”
Different artificial sweeteners may be better?
Commenting on the study, Kim Williams Sr., MD, University of Louisville (Ky.), pointed out that this study included artificial sweeteners that increase insulin or decrease insulin sensitivity, and that insulin spikes increase obesity, insulin resistance, hypertension, and atherosclerosis.
“There are some safer artificial sweeteners that do not increase insulin much or at all, such as erythritol, yacon root/yacon syrup, stevia root, but they weren’t included in the analysis,” Dr. Williams added.
Dr. Sievenpiper explained that most studies on artificial sweeteners look at their consumption in isolation without considering how they compare to the intake of the sugars that they are intended to replace.
“The comparator matters as no food is consumed in a vacuum,” he said.
To address this, Dr. Sievenpiper and colleagues have recently published a systematic review and meta-analysis of the prospective cohort study evidence that shows if exposure to artificially sweetened beverages is modeled in substitution for sugar-sweetened beverages, then they are associated with less coronary heart disease, cardiovascular mortality, and all-cause mortality.
On the other hand, if exposure to artificially sweetened beverages is compared with water, then no difference in these outcomes was seen.
“These observations are more biologically plausible, robust, and reproducible and agree with the evidence for the effect of artificial sweeteners on intermediate risk factors in randomized trials,” Dr. Sievenpiper notes.
His group has also recently published a review of randomized studies showing that when compared with sugar-sweetened beverages, intake of artificially sweetened beverages was associated with small improvements in body weight and cardiometabolic risk factors without evidence of harm.
“I think the context provided by these studies is important, and taken together, the totality of the evidence suggests that artificial sweeteners are likely to be a useful tool in sugar reduction strategies,” Dr. Sievenpiper concludes.
The current study was funded by the European Research Council under the European Union’s Horizon 2020 research and innovation program, French National Cancer Institute, French Ministry of Health, IdEx Université de Paris Cité, Bettencourt-Schueller Foundation Research Prize 2021. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Health concerns about the consumption of artificial sweeteners could be strengthened with the publication of a new study linking their intake to increased risk of heart disease and stroke events.
In this latest large-scale, prospective study of French adults, total artificial sweetener intake from all sources was associated with increased risk overall of cardiovascular and cerebrovascular disease.
The study was published online in the BMJ.
The current study differs from those done previously in that it includes artificial sweetener intake from both food and drinks, whereas previous studies have focused mainly on artificial sweetener content of beverages alone.
“Here we have quantified for the first time the global exposure to artificial sweeteners. This is not just beverages but includes the use of tabletop sweeteners, and other foods that include artificial sweeteners such as yogurts and desserts. This is the first time this information has been correlated to risk of heart disease,” senior author Mathilde Touvier, MD, Sorbonne Paris Nord University, told this news organization.
Just over half of the artificial sweetener intake in the study came from drinks, with the rest coming from tabletop sweeteners and foods.
“We included hard cardio- and cerebrovascular clinical endpoints such as a heart attack or stroke, and our results suggest that the amount of artificial sweetener in less than one can of soda could increase the risk of such events,” Dr. Touvier noted.
“This is an important and statistically significant association which shows robustness in all models after adjusting for many other possible confounding factors,” she said.
“There is now mounting evidence correlating artificial sweeteners to weight gain and heart disease,” she concluded. “My advice would be that we all need to try to limit sugar intake, but we should not consider artificial sweeteners as safe alternatives. Rather, we need to try to reduce our need for a sugary taste in our diet.”
But another leading researcher in the field urges caution in interpreting these results.
John Sievenpiper, MD, departments of nutritional sciences and medicine, University of Toronto, commented: “This paper shows the same relationship seen by many other large prospective cohorts which model the intake of artificial sweeteners as baseline or prevalent exposures.
“These observations are well recognized to be at high risk of residual confounding from behavior clustering and reverse causality in which being at risk for cardiovascular disease causes people to consume artificial sweeteners as a strategy to mitigate this risk as opposed to the other way around.”
Risk increased by 9%
The current study included 103,388 French adults from the NutriNet-Sante cohort, of whom 37.1% reported consumption of artificial sweeteners. The sweeteners assessed were mainly aspartame (58% of sweetener intake), acesulfame potassium (29%), and sucralose (10%), with the other 3% made up of various other sweeteners including cyclamates and saccharin.
Results showed that over an average 9 years of follow-up, artificial sweetener intake was associated with a 9% increased risk of cardiovascular or cerebrovascular events, including myocardial infarction, acute coronary syndrome, angioplasty, angina, stroke, or transient ischemic attack, with a hazard ratio of 1.09 (95% confidence interval, 1.01-1.18; P = .03).
The average intake of artificial sweeteners among those who reported consuming them was 42.46 mg/day, which corresponds to approximately one individual packet of tabletop sweetener or 100 mL of diet soda.
“We don’t have enough evidence to work out an amount of artificial sweetener that is harmful, but we did show a dose-effect association, with a higher risk of cardiovascular events with higher consumption,” Dr. Touvier said.
“Higher consumption in this study was a mean of 77 mg/day artificial sweetener, which is about 200 mL of soda – just a bit less than one standard can of soda,” she added.
The absolute incidence rate of cardiovascular or cerebrovascular events in higher consumers was 346 per 100,000 person-years vs. 314 per 100,000 person-years in nonconsumers.
Further analysis suggested that aspartame intake was particularly associated with increased risk of cerebrovascular events, while acesulfame potassium and sucralose were associated with increased coronary heart disease risk.
Study strengths
Dr. Touvier acknowledged that dietary studies, which generally rely on individuals self-reporting food and drink intake, are always hard to interpret. But she said this study used a more reliable method of dietary assessment, with repeated 24-hour dietary records, which were validated by interviews with a trained dietitian and against blood and urinary biomarkers.
And whereas residual confounding cannot be totally excluded, she pointed out that models were adjusted for a wide range of potential sociodemographic, anthropometric, dietary, and lifestyle confounders.
Dr. Touvier also noted that cases of cardiovascular disease in the first 2 years of follow-up were excluded to minimize the bias caused by individuals who maybe have switched to artificial sweeteners because of a cardiovascular issue.
“While this study has many strengths, it cannot on its own prove a causal relationship between artificial sweetener and increased cardiovascular risk,” she added. “We need health agencies to examine all the literature in the field. This is however another important piece of evidence.”
Dr. Touvier says that although observational studies have their issues, they will form the basis of the evidence on the effects of artificial sweeteners on health.
“Randomized studies in this area can only really look at short-term outcomes such as weight gain or biomarker changes. So, we will have to use observational studies together with experimental research to build the evidence. This is what happened with cigarette smoking and lung cancer. That link was not established by randomized trials, but by the accumulation of observational and experimental data.”
Different artificial sweeteners may be better?
Commenting on the study, Kim Williams Sr., MD, University of Louisville (Ky.), pointed out that this study included artificial sweeteners that increase insulin or decrease insulin sensitivity, and that insulin spikes increase obesity, insulin resistance, hypertension, and atherosclerosis.
“There are some safer artificial sweeteners that do not increase insulin much or at all, such as erythritol, yacon root/yacon syrup, stevia root, but they weren’t included in the analysis,” Dr. Williams added.
Dr. Sievenpiper explained that most studies on artificial sweeteners look at their consumption in isolation without considering how they compare to the intake of the sugars that they are intended to replace.
“The comparator matters as no food is consumed in a vacuum,” he said.
To address this, Dr. Sievenpiper and colleagues have recently published a systematic review and meta-analysis of the prospective cohort study evidence that shows if exposure to artificially sweetened beverages is modeled in substitution for sugar-sweetened beverages, then they are associated with less coronary heart disease, cardiovascular mortality, and all-cause mortality.
On the other hand, if exposure to artificially sweetened beverages is compared with water, then no difference in these outcomes was seen.
“These observations are more biologically plausible, robust, and reproducible and agree with the evidence for the effect of artificial sweeteners on intermediate risk factors in randomized trials,” Dr. Sievenpiper notes.
His group has also recently published a review of randomized studies showing that when compared with sugar-sweetened beverages, intake of artificially sweetened beverages was associated with small improvements in body weight and cardiometabolic risk factors without evidence of harm.
“I think the context provided by these studies is important, and taken together, the totality of the evidence suggests that artificial sweeteners are likely to be a useful tool in sugar reduction strategies,” Dr. Sievenpiper concludes.
The current study was funded by the European Research Council under the European Union’s Horizon 2020 research and innovation program, French National Cancer Institute, French Ministry of Health, IdEx Université de Paris Cité, Bettencourt-Schueller Foundation Research Prize 2021. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM BMJ