HOLLYWOOD, FLA. — Flat-panel detector systems have made it possible to perform angiography with a quarter of the contrast media routinely used with conventional image intensifiers.
“Flat-panel systems represent a huge evolution in angiographic technology,” Dr. Timothy W. Clark said at ISET 2009, an international symposium on endovascular therapy. “Much less contrast is needed to generate the same image quality as conventional image intensifiers, and because image production is more efficient, there is less radiation exposure to patients” and staff, said Dr. Clark, chief of vascular and interventional radiology at New York University. The reduction cuts the risk for contrast-induced nephropathy.
Flat panels offer a “dramatically wider dynamic range across all soft tissue anatomy, a larger field of view, homogeneous and distortion-free images, and improved detector efficiency,” he said. These features improve visualization, despite less contrast and a lower radiation dose. Unlike conventional image intensifiers, they do not involve an analog conversion, there is no geometric distortion, and there is no lateral dispersion of light to reduce image sharpness. Flat panels are less bulky and allow for greater freedom of movement.
With a flat-panel detector, Dr. Clark uses iodinated contrast diluted to 25%.
The degree of dilution depends on the contrast resolution of the flat-panel system.
For renal arteriograms, he said he has produced excellent images using a total contrast volume of 7 mL. For renal stenting, he uses 15 mL. For a popliteal chronic total occlusion, he uses a total volume of 25 mL, and for an iliac chronic total occlusion, he uses 32 mL of contrast.
“We use amazingly small volumes of contrast and still get high-resolution images,” said Dr. Clark, who does not have financial relationships with the companies that make flat-panel detectors.
One caveat regarding the use of diluted contrast is that the fluid must be power injected so it can displace the blood within the imaged vessels, he said.
HOLLYWOOD, FLA. — Flat-panel detector systems have made it possible to perform angiography with a quarter of the contrast media routinely used with conventional image intensifiers.
“Flat-panel systems represent a huge evolution in angiographic technology,” Dr. Timothy W. Clark said at ISET 2009, an international symposium on endovascular therapy. “Much less contrast is needed to generate the same image quality as conventional image intensifiers, and because image production is more efficient, there is less radiation exposure to patients” and staff, said Dr. Clark, chief of vascular and interventional radiology at New York University. The reduction cuts the risk for contrast-induced nephropathy.
Flat panels offer a “dramatically wider dynamic range across all soft tissue anatomy, a larger field of view, homogeneous and distortion-free images, and improved detector efficiency,” he said. These features improve visualization, despite less contrast and a lower radiation dose. Unlike conventional image intensifiers, they do not involve an analog conversion, there is no geometric distortion, and there is no lateral dispersion of light to reduce image sharpness. Flat panels are less bulky and allow for greater freedom of movement.
With a flat-panel detector, Dr. Clark uses iodinated contrast diluted to 25%.
The degree of dilution depends on the contrast resolution of the flat-panel system.
For renal arteriograms, he said he has produced excellent images using a total contrast volume of 7 mL. For renal stenting, he uses 15 mL. For a popliteal chronic total occlusion, he uses a total volume of 25 mL, and for an iliac chronic total occlusion, he uses 32 mL of contrast.
“We use amazingly small volumes of contrast and still get high-resolution images,” said Dr. Clark, who does not have financial relationships with the companies that make flat-panel detectors.
One caveat regarding the use of diluted contrast is that the fluid must be power injected so it can displace the blood within the imaged vessels, he said.
HOLLYWOOD, FLA. — Flat-panel detector systems have made it possible to perform angiography with a quarter of the contrast media routinely used with conventional image intensifiers.
“Flat-panel systems represent a huge evolution in angiographic technology,” Dr. Timothy W. Clark said at ISET 2009, an international symposium on endovascular therapy. “Much less contrast is needed to generate the same image quality as conventional image intensifiers, and because image production is more efficient, there is less radiation exposure to patients” and staff, said Dr. Clark, chief of vascular and interventional radiology at New York University. The reduction cuts the risk for contrast-induced nephropathy.
Flat panels offer a “dramatically wider dynamic range across all soft tissue anatomy, a larger field of view, homogeneous and distortion-free images, and improved detector efficiency,” he said. These features improve visualization, despite less contrast and a lower radiation dose. Unlike conventional image intensifiers, they do not involve an analog conversion, there is no geometric distortion, and there is no lateral dispersion of light to reduce image sharpness. Flat panels are less bulky and allow for greater freedom of movement.
With a flat-panel detector, Dr. Clark uses iodinated contrast diluted to 25%.
The degree of dilution depends on the contrast resolution of the flat-panel system.
For renal arteriograms, he said he has produced excellent images using a total contrast volume of 7 mL. For renal stenting, he uses 15 mL. For a popliteal chronic total occlusion, he uses a total volume of 25 mL, and for an iliac chronic total occlusion, he uses 32 mL of contrast.
“We use amazingly small volumes of contrast and still get high-resolution images,” said Dr. Clark, who does not have financial relationships with the companies that make flat-panel detectors.
One caveat regarding the use of diluted contrast is that the fluid must be power injected so it can displace the blood within the imaged vessels, he said.
A 28-year-old woman comes in for her annual checkup. Her physician notices a palpable, painless, 1-cm, well-demarcated mass in the left breast at the 3 o’clock position 2 cm from the nipple, with no associated skin changes, nipple retraction, or discharge. The patient has no personal or family history of breast cancer.
Given the patient’s age, physical findings, and medical history, the clinician believes it unlikely that the patient has cancer. How should she proceed with the workup of this patient?
PHYSICAL FINDINGS OF A BREAST MASS ARE NOT EXCLUSIVE
Figure 1. A simple cyst in the left breast. All three mammographic views—craniocaudal (A), mediolateral oblique (B), and spot-compression (C)—show a round, well-circumscribed mass in the mid-breast. Ultrasonography (D) shows a round, well-circumscribed anechoic lesion with a sharply defined posterior wall and posterior acoustic enhancement.
Breast cancer is the most common female malignancy and the second-leading cause of cancer deaths in the United States.1 The incidence is low in young women and increases with advancing age. Benign breast disease is common in young women and less common in postmenopausal women.2,3 However, the discovery of a breast mass, whether by the woman herself or by a clinician, is a common occurrence and distressing for any woman.
Benign lesions tend to have discrete, well-defined margins and are typically mobile. Malignant lesions may be firm, may have indistinct borders, and are often immobile.2 Although most breast masses found by palpation are benign, imaging is the critical next step in the workup to help determine if the mass is benign or malignant.
Benign palpable masses include:
Figure 2. Fibroadenoma. On mammography, the craniocaudal (A) and mediolateral oblique (B) views with a bright metallic marker (arrows) show a round, well-circumscribed mass in the upper outer quadrant of the left breast. Ultrasonography (C) shows an oval, well-circumscribed, mildly heterogeneous, hypoechoic mass that is wider than tall, indicating a benign mass.
Cysts (Figure 1)
Fibroadenomas (Figure 2)
Prominent fat lobules
Lymph nodes
Oil cysts
Lipomas
Hamartomas (Figure 3)
Hematomas
Fat necrosis
Galactoceles.
Malignant palpable masses include:
Figure 3. Hamartoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the left breast show an apparently encapsulated, heterogeneous mass that contains fat mixed with fibroglandular tissue.
Invasive ductal and lobular carcinoma (Figure 4)
Ductal carcinoma in situ (which rarely presents as a palpable mass.)
HISTORY AND PHYSICAL EXAMINATION
To ensure that imaging provides the most useful information about a palpable breast lump, it is important to first do a careful history and physical examination. Important aspects of the history include family history, personal history of breast cancer, and any previous breast biopsies. The onset and duration of the palpable mass, changes in its size, the relationship of these changes to the menstrual cycle, and the presence or lack of tenderness are additional important elements of the history.
Figure 4. Infiltrating ductal carcinoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the right breast show an irregular, mildly spiculated, high-density lesion in the posterior, medial breast. Ultrasonography (C) shows an irregularly shaped hypoechoic mass which is taller than wide (a profile tending to indicate malignancy) and has mild posterior acoustic shadowing.
On examination, it is important to note the clock-face location, size, texture, tenderness, and mobility of the lump. Accompanying nipple discharge and skin erythema or retraction are also important to report. In addition to conveying the location of the mass to the radiologist, it is equally important that the patient know what features the physician feels. This way, if the clinical information from the ordering physician is not available at the time of the radiologic evaluation, the patient will be able to guide the radiologist to the region of concern.
IMAGING TECHNIQUES
Mammography and ultrasonography are the primary imaging studies for evaluating palpable breast masses. Typically, in women under age 30, ultrasonography is the first or the only test ordered to evaluate the abnormality.4 In women age 30 or older, diagnostic mammography is typically the first test ordered. If mammography indicates that the palpable mass is not benign, then ultrasonography is the next study to be done.3 Although a powerful tool, magnetic resonance imaging of the breast does not currently have a role in the workup of a palpable abnormality and should not be used as a decision-delaying tactic or in place of biopsy.
Screening or diagnostic mammography?
Mammography is used in both screening and diagnosis. Screening mammography consists of two standard views of each breast—craniocaudal and mediolateral oblique—and is appropriate for asymptomatic women.
Women age 30 or older who present with a palpable breast mass require diagnostic mammography, in which standard mammographic views are obtained, as well as additional views (eg, tangential or spot-compression views) to better define the area of clinical concern. In a tangential view, a metallic skin marker is placed on the skin overlying the site of the palpable abnormality.
On mammography, a suspicious palpable mass has an irregular shape with spiculated margins. A benign mass typically has a round shape with well-circumscribed margins. If the palpable abnormality is not mammographically benign (eg, if it does not look like a lymph node, lipoma, or degenerating fibroadenoma), then ultrasonography is performed.
Mammography is less sensitive in younger women (ie, under age 30) because their breast tissue tends to be dense and glandular, whereas the tissue becomes more “fat-replaced” with age.3
Ultrasonography plays a complementary role
Ultrasonography complements diagnostic mammography and can be used as a first imaging study to evaluate a palpable breast mass in a young woman (ie, under age 30) with dense breast tissue. Ultrasonography is helpful in distinguishing cystic lesions from solid masses. It helps the radiologist delineate the shape, borders, and acoustic properties of the mass. It is also performed when a palpable mass is mammographically occult. When a mass appears suspicious on either mammography or ultrasonography, ultrasonography can be used to guide biopsy.
A suspicious mass on ultrasonography classically appears “taller than wide” and has posterior acoustic shadowing. Microlobulations and a spiculated margin also raise concern for malignancy. A benign sonographic appearance of a palpable mass includes a “wider than tall” (ellipsoid) shape, with homogeneous echogenicity, and four or fewer gentle lobulations. A thin, echogenic capsule also suggests the mass is benign.
Core-needle biopsy with ultrasonographic guidance
Core-needle biopsy is performed with a large-diameter (14-gauge to 18-gauge) needle to obtain tissue cores for histologic analysis. It has gained popularity over fine-needle aspiration because it includes surrounding tissue architecture, thus providing a more definitive histologic diagnosis.
Pathologic information obtained from core-needle biopsy allows the radiologist and surgeon to counsel the patient and determine the best surgical management or follow-up imaging study. If a clinician performs fine-needle biopsy in the office, it should be preceded by an imaging workup of the palpable finding.
WHAT IS APPROPRIATE FOR OUR 28-YEAR-OLD PATIENT?
Because she is under age 30, ultrasonography is the initial study of choice to evaluate the mass. If a simple cyst is detected, she can be reassured that the lesion is benign, and no subsequent follow-up is required. If the lesion is a solid mass with benign features, mammography may be considered, the patient may be followed with short-interval imaging (every 6 months) depending on patient-specific factors such as family history, or the mass can be biopsied. If the lesion is a solid mass with suspicious or malignant features, mammography with spot-compression views should be performed, and the patient should undergo core-needle biopsy with ultrasonographic guidance.
In a patient age 30 or older, diagnostic mammography is the imaging study of first choice.3 If the mass is clearly benign on mammography, no additional imaging would be necessary. If mammography fails to image the mass or shows it to have benign features such as fat, then the patient can undergo ultrasonography for further evaluation and confirmation of the clinical and mammographic findings. If the mass appears suspicious or malignant on mammography, ultrasonography is the next step, as it can help characterize the lesion and be used to guide core-needle biopsy.
IF A PREGNANT WOMAN HAS A PALPABLE BREAST MASS
Most publications on breast cancer in pregnancy report a prevalence of 3 per 10,000 pregnancies, accounting for 3% of all breast cancers diagnosed.5 Therefore, imaging evaluation of a palpable mass should not be postponed.
Hormonal changes throughout pregnancy may increase the nodularity of breast tissue, raising the concern of palpable masses. Additionally, there is a higher prevalence of galactoceles and lactating adenomas in these patients. Because contrasting fatty breast tissue is lost during pregnancy and because of the need to minimize radiation exposure, ultrasonography is often the imaging test of first choice. If mammography is required, the radiation dose is very low and the patient’s abdomen and pelvis can be shielded.6 In this situation, the patient can be reassured that the imaging test is not jeopardizing her fetus.
WHAT WORKUP IS REQUIRED IN MEN?
Breast cancer in men is rare, accounting for less than 0.5% of all cases.7 Most often, a palpable breast mass in a man presents as unilateral gynecomastia. Gynecomastia occurs in a bimodal age distribution (in the 2nd and 7th decades) and has a variety of hormonal and drug-related causes. Despite the low prevalence of breast cancer in men, the combination of mammography and ultrasonography is recommended for evaluation at all ages.
References
Klein S. Evaluation of palpable breast masses. Am Fam Physician2005; 71:1731–1738.
Pruthi S. Detection and evaluation of a palpable breast mass. Mayo Clin Proc2001; 76:641–648.
Harvey JA. Sonography of palpable breast masses. Semin Ultrasound CT MR2006; 27:284–297.
Mehta TS. Current uses of ultrasound in the evaluation of the breast. Radiol Clin North Am2003; 41:841–856.
Gallenberg MM, Lopines CL. Breast cancer and pregnancy. Semin Oncol1989; 16:369–376.
Barnavon Y, Wallack MK. Management of the pregnant patient with carcinoma of the breast. Surg Gynecol Obstet1990; 171:347–352.
Cardenosa G. The Core Curriculum: Breast Imaging. Philadelphia: Lippincott Williams and Wilkins, 2003;304.
Lauren Stein, MD Imaging Institute, Cleveland Clinic
Melanie Chellman-Jeffers, MD Center for Specialized Women’s Health and Section of Breast Imaging, Department of Diagnostic Radiology, Imaging Institute, Cleveland Clinic
Address: Melanie Chellman-Jeffers, MD, Imaging Institute, Section of Breast Imaging, A10, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail [email protected]
Lauren Stein, MD Imaging Institute, Cleveland Clinic
Melanie Chellman-Jeffers, MD Center for Specialized Women’s Health and Section of Breast Imaging, Department of Diagnostic Radiology, Imaging Institute, Cleveland Clinic
Address: Melanie Chellman-Jeffers, MD, Imaging Institute, Section of Breast Imaging, A10, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail [email protected]
Author and Disclosure Information
Lauren Stein, MD Imaging Institute, Cleveland Clinic
Melanie Chellman-Jeffers, MD Center for Specialized Women’s Health and Section of Breast Imaging, Department of Diagnostic Radiology, Imaging Institute, Cleveland Clinic
Address: Melanie Chellman-Jeffers, MD, Imaging Institute, Section of Breast Imaging, A10, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail [email protected]
A 28-year-old woman comes in for her annual checkup. Her physician notices a palpable, painless, 1-cm, well-demarcated mass in the left breast at the 3 o’clock position 2 cm from the nipple, with no associated skin changes, nipple retraction, or discharge. The patient has no personal or family history of breast cancer.
Given the patient’s age, physical findings, and medical history, the clinician believes it unlikely that the patient has cancer. How should she proceed with the workup of this patient?
PHYSICAL FINDINGS OF A BREAST MASS ARE NOT EXCLUSIVE
Figure 1. A simple cyst in the left breast. All three mammographic views—craniocaudal (A), mediolateral oblique (B), and spot-compression (C)—show a round, well-circumscribed mass in the mid-breast. Ultrasonography (D) shows a round, well-circumscribed anechoic lesion with a sharply defined posterior wall and posterior acoustic enhancement.
Breast cancer is the most common female malignancy and the second-leading cause of cancer deaths in the United States.1 The incidence is low in young women and increases with advancing age. Benign breast disease is common in young women and less common in postmenopausal women.2,3 However, the discovery of a breast mass, whether by the woman herself or by a clinician, is a common occurrence and distressing for any woman.
Benign lesions tend to have discrete, well-defined margins and are typically mobile. Malignant lesions may be firm, may have indistinct borders, and are often immobile.2 Although most breast masses found by palpation are benign, imaging is the critical next step in the workup to help determine if the mass is benign or malignant.
Benign palpable masses include:
Figure 2. Fibroadenoma. On mammography, the craniocaudal (A) and mediolateral oblique (B) views with a bright metallic marker (arrows) show a round, well-circumscribed mass in the upper outer quadrant of the left breast. Ultrasonography (C) shows an oval, well-circumscribed, mildly heterogeneous, hypoechoic mass that is wider than tall, indicating a benign mass.
Cysts (Figure 1)
Fibroadenomas (Figure 2)
Prominent fat lobules
Lymph nodes
Oil cysts
Lipomas
Hamartomas (Figure 3)
Hematomas
Fat necrosis
Galactoceles.
Malignant palpable masses include:
Figure 3. Hamartoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the left breast show an apparently encapsulated, heterogeneous mass that contains fat mixed with fibroglandular tissue.
Invasive ductal and lobular carcinoma (Figure 4)
Ductal carcinoma in situ (which rarely presents as a palpable mass.)
HISTORY AND PHYSICAL EXAMINATION
To ensure that imaging provides the most useful information about a palpable breast lump, it is important to first do a careful history and physical examination. Important aspects of the history include family history, personal history of breast cancer, and any previous breast biopsies. The onset and duration of the palpable mass, changes in its size, the relationship of these changes to the menstrual cycle, and the presence or lack of tenderness are additional important elements of the history.
Figure 4. Infiltrating ductal carcinoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the right breast show an irregular, mildly spiculated, high-density lesion in the posterior, medial breast. Ultrasonography (C) shows an irregularly shaped hypoechoic mass which is taller than wide (a profile tending to indicate malignancy) and has mild posterior acoustic shadowing.
On examination, it is important to note the clock-face location, size, texture, tenderness, and mobility of the lump. Accompanying nipple discharge and skin erythema or retraction are also important to report. In addition to conveying the location of the mass to the radiologist, it is equally important that the patient know what features the physician feels. This way, if the clinical information from the ordering physician is not available at the time of the radiologic evaluation, the patient will be able to guide the radiologist to the region of concern.
IMAGING TECHNIQUES
Mammography and ultrasonography are the primary imaging studies for evaluating palpable breast masses. Typically, in women under age 30, ultrasonography is the first or the only test ordered to evaluate the abnormality.4 In women age 30 or older, diagnostic mammography is typically the first test ordered. If mammography indicates that the palpable mass is not benign, then ultrasonography is the next study to be done.3 Although a powerful tool, magnetic resonance imaging of the breast does not currently have a role in the workup of a palpable abnormality and should not be used as a decision-delaying tactic or in place of biopsy.
Screening or diagnostic mammography?
Mammography is used in both screening and diagnosis. Screening mammography consists of two standard views of each breast—craniocaudal and mediolateral oblique—and is appropriate for asymptomatic women.
Women age 30 or older who present with a palpable breast mass require diagnostic mammography, in which standard mammographic views are obtained, as well as additional views (eg, tangential or spot-compression views) to better define the area of clinical concern. In a tangential view, a metallic skin marker is placed on the skin overlying the site of the palpable abnormality.
On mammography, a suspicious palpable mass has an irregular shape with spiculated margins. A benign mass typically has a round shape with well-circumscribed margins. If the palpable abnormality is not mammographically benign (eg, if it does not look like a lymph node, lipoma, or degenerating fibroadenoma), then ultrasonography is performed.
Mammography is less sensitive in younger women (ie, under age 30) because their breast tissue tends to be dense and glandular, whereas the tissue becomes more “fat-replaced” with age.3
Ultrasonography plays a complementary role
Ultrasonography complements diagnostic mammography and can be used as a first imaging study to evaluate a palpable breast mass in a young woman (ie, under age 30) with dense breast tissue. Ultrasonography is helpful in distinguishing cystic lesions from solid masses. It helps the radiologist delineate the shape, borders, and acoustic properties of the mass. It is also performed when a palpable mass is mammographically occult. When a mass appears suspicious on either mammography or ultrasonography, ultrasonography can be used to guide biopsy.
A suspicious mass on ultrasonography classically appears “taller than wide” and has posterior acoustic shadowing. Microlobulations and a spiculated margin also raise concern for malignancy. A benign sonographic appearance of a palpable mass includes a “wider than tall” (ellipsoid) shape, with homogeneous echogenicity, and four or fewer gentle lobulations. A thin, echogenic capsule also suggests the mass is benign.
Core-needle biopsy with ultrasonographic guidance
Core-needle biopsy is performed with a large-diameter (14-gauge to 18-gauge) needle to obtain tissue cores for histologic analysis. It has gained popularity over fine-needle aspiration because it includes surrounding tissue architecture, thus providing a more definitive histologic diagnosis.
Pathologic information obtained from core-needle biopsy allows the radiologist and surgeon to counsel the patient and determine the best surgical management or follow-up imaging study. If a clinician performs fine-needle biopsy in the office, it should be preceded by an imaging workup of the palpable finding.
WHAT IS APPROPRIATE FOR OUR 28-YEAR-OLD PATIENT?
Because she is under age 30, ultrasonography is the initial study of choice to evaluate the mass. If a simple cyst is detected, she can be reassured that the lesion is benign, and no subsequent follow-up is required. If the lesion is a solid mass with benign features, mammography may be considered, the patient may be followed with short-interval imaging (every 6 months) depending on patient-specific factors such as family history, or the mass can be biopsied. If the lesion is a solid mass with suspicious or malignant features, mammography with spot-compression views should be performed, and the patient should undergo core-needle biopsy with ultrasonographic guidance.
In a patient age 30 or older, diagnostic mammography is the imaging study of first choice.3 If the mass is clearly benign on mammography, no additional imaging would be necessary. If mammography fails to image the mass or shows it to have benign features such as fat, then the patient can undergo ultrasonography for further evaluation and confirmation of the clinical and mammographic findings. If the mass appears suspicious or malignant on mammography, ultrasonography is the next step, as it can help characterize the lesion and be used to guide core-needle biopsy.
IF A PREGNANT WOMAN HAS A PALPABLE BREAST MASS
Most publications on breast cancer in pregnancy report a prevalence of 3 per 10,000 pregnancies, accounting for 3% of all breast cancers diagnosed.5 Therefore, imaging evaluation of a palpable mass should not be postponed.
Hormonal changes throughout pregnancy may increase the nodularity of breast tissue, raising the concern of palpable masses. Additionally, there is a higher prevalence of galactoceles and lactating adenomas in these patients. Because contrasting fatty breast tissue is lost during pregnancy and because of the need to minimize radiation exposure, ultrasonography is often the imaging test of first choice. If mammography is required, the radiation dose is very low and the patient’s abdomen and pelvis can be shielded.6 In this situation, the patient can be reassured that the imaging test is not jeopardizing her fetus.
WHAT WORKUP IS REQUIRED IN MEN?
Breast cancer in men is rare, accounting for less than 0.5% of all cases.7 Most often, a palpable breast mass in a man presents as unilateral gynecomastia. Gynecomastia occurs in a bimodal age distribution (in the 2nd and 7th decades) and has a variety of hormonal and drug-related causes. Despite the low prevalence of breast cancer in men, the combination of mammography and ultrasonography is recommended for evaluation at all ages.
A 28-year-old woman comes in for her annual checkup. Her physician notices a palpable, painless, 1-cm, well-demarcated mass in the left breast at the 3 o’clock position 2 cm from the nipple, with no associated skin changes, nipple retraction, or discharge. The patient has no personal or family history of breast cancer.
Given the patient’s age, physical findings, and medical history, the clinician believes it unlikely that the patient has cancer. How should she proceed with the workup of this patient?
PHYSICAL FINDINGS OF A BREAST MASS ARE NOT EXCLUSIVE
Figure 1. A simple cyst in the left breast. All three mammographic views—craniocaudal (A), mediolateral oblique (B), and spot-compression (C)—show a round, well-circumscribed mass in the mid-breast. Ultrasonography (D) shows a round, well-circumscribed anechoic lesion with a sharply defined posterior wall and posterior acoustic enhancement.
Breast cancer is the most common female malignancy and the second-leading cause of cancer deaths in the United States.1 The incidence is low in young women and increases with advancing age. Benign breast disease is common in young women and less common in postmenopausal women.2,3 However, the discovery of a breast mass, whether by the woman herself or by a clinician, is a common occurrence and distressing for any woman.
Benign lesions tend to have discrete, well-defined margins and are typically mobile. Malignant lesions may be firm, may have indistinct borders, and are often immobile.2 Although most breast masses found by palpation are benign, imaging is the critical next step in the workup to help determine if the mass is benign or malignant.
Benign palpable masses include:
Figure 2. Fibroadenoma. On mammography, the craniocaudal (A) and mediolateral oblique (B) views with a bright metallic marker (arrows) show a round, well-circumscribed mass in the upper outer quadrant of the left breast. Ultrasonography (C) shows an oval, well-circumscribed, mildly heterogeneous, hypoechoic mass that is wider than tall, indicating a benign mass.
Cysts (Figure 1)
Fibroadenomas (Figure 2)
Prominent fat lobules
Lymph nodes
Oil cysts
Lipomas
Hamartomas (Figure 3)
Hematomas
Fat necrosis
Galactoceles.
Malignant palpable masses include:
Figure 3. Hamartoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the left breast show an apparently encapsulated, heterogeneous mass that contains fat mixed with fibroglandular tissue.
Invasive ductal and lobular carcinoma (Figure 4)
Ductal carcinoma in situ (which rarely presents as a palpable mass.)
HISTORY AND PHYSICAL EXAMINATION
To ensure that imaging provides the most useful information about a palpable breast lump, it is important to first do a careful history and physical examination. Important aspects of the history include family history, personal history of breast cancer, and any previous breast biopsies. The onset and duration of the palpable mass, changes in its size, the relationship of these changes to the menstrual cycle, and the presence or lack of tenderness are additional important elements of the history.
Figure 4. Infiltrating ductal carcinoma. Craniocaudal (A) and mediolateral oblique (B) mammographic views of the right breast show an irregular, mildly spiculated, high-density lesion in the posterior, medial breast. Ultrasonography (C) shows an irregularly shaped hypoechoic mass which is taller than wide (a profile tending to indicate malignancy) and has mild posterior acoustic shadowing.
On examination, it is important to note the clock-face location, size, texture, tenderness, and mobility of the lump. Accompanying nipple discharge and skin erythema or retraction are also important to report. In addition to conveying the location of the mass to the radiologist, it is equally important that the patient know what features the physician feels. This way, if the clinical information from the ordering physician is not available at the time of the radiologic evaluation, the patient will be able to guide the radiologist to the region of concern.
IMAGING TECHNIQUES
Mammography and ultrasonography are the primary imaging studies for evaluating palpable breast masses. Typically, in women under age 30, ultrasonography is the first or the only test ordered to evaluate the abnormality.4 In women age 30 or older, diagnostic mammography is typically the first test ordered. If mammography indicates that the palpable mass is not benign, then ultrasonography is the next study to be done.3 Although a powerful tool, magnetic resonance imaging of the breast does not currently have a role in the workup of a palpable abnormality and should not be used as a decision-delaying tactic or in place of biopsy.
Screening or diagnostic mammography?
Mammography is used in both screening and diagnosis. Screening mammography consists of two standard views of each breast—craniocaudal and mediolateral oblique—and is appropriate for asymptomatic women.
Women age 30 or older who present with a palpable breast mass require diagnostic mammography, in which standard mammographic views are obtained, as well as additional views (eg, tangential or spot-compression views) to better define the area of clinical concern. In a tangential view, a metallic skin marker is placed on the skin overlying the site of the palpable abnormality.
On mammography, a suspicious palpable mass has an irregular shape with spiculated margins. A benign mass typically has a round shape with well-circumscribed margins. If the palpable abnormality is not mammographically benign (eg, if it does not look like a lymph node, lipoma, or degenerating fibroadenoma), then ultrasonography is performed.
Mammography is less sensitive in younger women (ie, under age 30) because their breast tissue tends to be dense and glandular, whereas the tissue becomes more “fat-replaced” with age.3
Ultrasonography plays a complementary role
Ultrasonography complements diagnostic mammography and can be used as a first imaging study to evaluate a palpable breast mass in a young woman (ie, under age 30) with dense breast tissue. Ultrasonography is helpful in distinguishing cystic lesions from solid masses. It helps the radiologist delineate the shape, borders, and acoustic properties of the mass. It is also performed when a palpable mass is mammographically occult. When a mass appears suspicious on either mammography or ultrasonography, ultrasonography can be used to guide biopsy.
A suspicious mass on ultrasonography classically appears “taller than wide” and has posterior acoustic shadowing. Microlobulations and a spiculated margin also raise concern for malignancy. A benign sonographic appearance of a palpable mass includes a “wider than tall” (ellipsoid) shape, with homogeneous echogenicity, and four or fewer gentle lobulations. A thin, echogenic capsule also suggests the mass is benign.
Core-needle biopsy with ultrasonographic guidance
Core-needle biopsy is performed with a large-diameter (14-gauge to 18-gauge) needle to obtain tissue cores for histologic analysis. It has gained popularity over fine-needle aspiration because it includes surrounding tissue architecture, thus providing a more definitive histologic diagnosis.
Pathologic information obtained from core-needle biopsy allows the radiologist and surgeon to counsel the patient and determine the best surgical management or follow-up imaging study. If a clinician performs fine-needle biopsy in the office, it should be preceded by an imaging workup of the palpable finding.
WHAT IS APPROPRIATE FOR OUR 28-YEAR-OLD PATIENT?
Because she is under age 30, ultrasonography is the initial study of choice to evaluate the mass. If a simple cyst is detected, she can be reassured that the lesion is benign, and no subsequent follow-up is required. If the lesion is a solid mass with benign features, mammography may be considered, the patient may be followed with short-interval imaging (every 6 months) depending on patient-specific factors such as family history, or the mass can be biopsied. If the lesion is a solid mass with suspicious or malignant features, mammography with spot-compression views should be performed, and the patient should undergo core-needle biopsy with ultrasonographic guidance.
In a patient age 30 or older, diagnostic mammography is the imaging study of first choice.3 If the mass is clearly benign on mammography, no additional imaging would be necessary. If mammography fails to image the mass or shows it to have benign features such as fat, then the patient can undergo ultrasonography for further evaluation and confirmation of the clinical and mammographic findings. If the mass appears suspicious or malignant on mammography, ultrasonography is the next step, as it can help characterize the lesion and be used to guide core-needle biopsy.
IF A PREGNANT WOMAN HAS A PALPABLE BREAST MASS
Most publications on breast cancer in pregnancy report a prevalence of 3 per 10,000 pregnancies, accounting for 3% of all breast cancers diagnosed.5 Therefore, imaging evaluation of a palpable mass should not be postponed.
Hormonal changes throughout pregnancy may increase the nodularity of breast tissue, raising the concern of palpable masses. Additionally, there is a higher prevalence of galactoceles and lactating adenomas in these patients. Because contrasting fatty breast tissue is lost during pregnancy and because of the need to minimize radiation exposure, ultrasonography is often the imaging test of first choice. If mammography is required, the radiation dose is very low and the patient’s abdomen and pelvis can be shielded.6 In this situation, the patient can be reassured that the imaging test is not jeopardizing her fetus.
WHAT WORKUP IS REQUIRED IN MEN?
Breast cancer in men is rare, accounting for less than 0.5% of all cases.7 Most often, a palpable breast mass in a man presents as unilateral gynecomastia. Gynecomastia occurs in a bimodal age distribution (in the 2nd and 7th decades) and has a variety of hormonal and drug-related causes. Despite the low prevalence of breast cancer in men, the combination of mammography and ultrasonography is recommended for evaluation at all ages.
References
Klein S. Evaluation of palpable breast masses. Am Fam Physician2005; 71:1731–1738.
Pruthi S. Detection and evaluation of a palpable breast mass. Mayo Clin Proc2001; 76:641–648.
Harvey JA. Sonography of palpable breast masses. Semin Ultrasound CT MR2006; 27:284–297.
Mehta TS. Current uses of ultrasound in the evaluation of the breast. Radiol Clin North Am2003; 41:841–856.
Gallenberg MM, Lopines CL. Breast cancer and pregnancy. Semin Oncol1989; 16:369–376.
Barnavon Y, Wallack MK. Management of the pregnant patient with carcinoma of the breast. Surg Gynecol Obstet1990; 171:347–352.
Cardenosa G. The Core Curriculum: Breast Imaging. Philadelphia: Lippincott Williams and Wilkins, 2003;304.
References
Klein S. Evaluation of palpable breast masses. Am Fam Physician2005; 71:1731–1738.
Pruthi S. Detection and evaluation of a palpable breast mass. Mayo Clin Proc2001; 76:641–648.
Harvey JA. Sonography of palpable breast masses. Semin Ultrasound CT MR2006; 27:284–297.
Mehta TS. Current uses of ultrasound in the evaluation of the breast. Radiol Clin North Am2003; 41:841–856.
Gallenberg MM, Lopines CL. Breast cancer and pregnancy. Semin Oncol1989; 16:369–376.
Barnavon Y, Wallack MK. Management of the pregnant patient with carcinoma of the breast. Surg Gynecol Obstet1990; 171:347–352.
Cardenosa G. The Core Curriculum: Breast Imaging. Philadelphia: Lippincott Williams and Wilkins, 2003;304.
Typically, in women under age 30, ultrasonography is the first or the only test ordered to evaluate the abnormality. In women age 30 or older, diagnostic mammography is typically the first test ordered.
On mammography, a suspicious palpable mass has an irregular shape with spiculated margins. A benign mass typically has a round shape with well-circumscribed margins.
When mammography is required during pregnancy, the patient can be reassured that it will not jeopardize her fetus because the radiation dose is very low and the abdomen and pelvis can be shielded.
Use of Single-Photon Emission Computed Tomography/Low-Resolution Computed Tomography Fusion Imaging in Detecting an Unusually Presenting Osteoid Osteoma of the Lumbar Vertebra
Dr. Hephzibah is Lecturer, Dr. Theodore is Registrar, and Dr. Oommen is Professor and Head, Department of Nuclear Medicine, Christian Medical College, Vellore, India.
Dr. David is Reader, Department of Orthopedics, Christian Medical College, Vellore, India.
Dr. Moses is Lecturer, Department of Radiology, Christian Medical College, Vellore, India.
Dr. Shah is Lecturer, and Dr. Panicker is Registrar, Department of Pathology, Christian Medical College, Vellore, India.
Dr. Hephzibah is Lecturer, Dr. Theodore is Registrar, and Dr. Oommen is Professor and Head, Department of Nuclear Medicine, Christian Medical College, Vellore, India.
Dr. David is Reader, Department of Orthopedics, Christian Medical College, Vellore, India.
Dr. Moses is Lecturer, Department of Radiology, Christian Medical College, Vellore, India.
Dr. Shah is Lecturer, and Dr. Panicker is Registrar, Department of Pathology, Christian Medical College, Vellore, India.
Dr. Hephzibah is Lecturer, Dr. Theodore is Registrar, and Dr. Oommen is Professor and Head, Department of Nuclear Medicine, Christian Medical College, Vellore, India.
Dr. David is Reader, Department of Orthopedics, Christian Medical College, Vellore, India.
Dr. Moses is Lecturer, Department of Radiology, Christian Medical College, Vellore, India.
Dr. Shah is Lecturer, and Dr. Panicker is Registrar, Department of Pathology, Christian Medical College, Vellore, India.
Use of Single-Photon Emission Computed Tomography/Low-Resolution Computed Tomography Fusion Imaging in Detecting an Unusually Presenting Osteoid Osteoma of the Lumbar Vertebra
Display Headline
Use of Single-Photon Emission Computed Tomography/Low-Resolution Computed Tomography Fusion Imaging in Detecting an Unusually Presenting Osteoid Osteoma of the Lumbar Vertebra
Magnetic resonance imaging and other advanced imaging modalities have a long way to go before they become accepted parts of the diagnostic work-up for ankylosing spondylitis. History, physical examination, and conventional radiography form its existing diagnostic criteria.
Dr. Helena Marzo-Ortega is a consultant rheumatologist at the University of Leeds (England). She has been studying the use of MRI in the diagnosis and treatment of AS. Here are her thoughts on what roles different imaging modalities can play in better diagnosing and managing AS.
X-Ray
With x-ray, which is the imaging tool used by the main AS classification, only abnormalities affecting the bone structure can be seen. This means that “it may take up to 8–10 years of symptoms before somebody develops changes that are picked up by conventional x-ray,” Dr. Marzo-Ortega noted.
Still, x-ray has a place in AS. “Young patients, who [make up] most of our population, may not [present as soon as] pain starts. It usually takes them a few months, and sometimes years, to come in,” she said. The first line of investigation with such patients could be an x-ray because if positive, the diagnosis of AS can be made.
MRI
MRI is mainly used in the research setting. The strength of MRIis its ability to reveal abnormalities in the synovium, the soft tissues, and the entheses, said Dr. Marzo-Ortega.
MRI picks up inflammation and bone edema, which may be identified in about 80% of patients. “This means that there are still another 20% of cases, where we are left with a negative MRI and uncertainty about the diagnosis,” she said.
AS diagnosis is based on involvement of the sacroiliac joint. “The majority of patients will have the sacroiliac joints affected before the spine.”
Most research done to date using MRI in AS has looked at the sacroiliac joints to see if there are any signs of active inflammation. However, MRI equipment, limited by its reliance on the commonly used T1.5 magnets, is not sensitive enough to reveal such changes.
“The SI joints are very small and the abnormalities happen within the bone marrow. … It's really the bone marrow that we're looking at.” A positive MRI would indicate inflammation within the bone marrow.
The use of biologics requires patients be followed with x-ray according to the treatment guidelines in both the United States and Europe, which follow the New York criteria.
“However, we all know that we're not prepared to wait 8–10 years so we can make the diagnosis and then treat the patient.” Instead, if the MRI is positive, “we follow criteria, as recently proposed by the ASAS [Assessment in Ankylosing Spondylitis] international working group. This allows for the diagnosis of axial SpA (or preradiographic AS) to be made if sacroiliitis is found by any imaging method with at least one clinical parameter, or if there is HLA-B27 positivity plus at least two clinical parameters,” Dr. Marzo-Ortega noted.
Data from a study following AS patients for 8 years show that “the MRI signal determines the development of radiographic structural damage. It is the intensity of the signal that matters. … The more severe the edema, the greater the chance to develop radiographic sacroiliitis at a year's time [Arthritis Rheum. 2008;58:3413–8].
MRI has a role to play in the evaluation of therapies for AS. In this disease, inflammation may lead to erosive disease but it may also lead to new bone formation, which may result in spinal fusion. “We don't really know what the relationship between inflammation and new bone formation is. Even if we use very potent agents, such as tumor necrosis factor [TNF]-alpha blockers that can control inflammation, we're not really sure whether that's making any big impact on new bone formation as an outcome,” said Dr. Marzo-Ortega. MRI could be used to follow patients treated with TNF-blockers to understand what effect the drugs have on erosions and new bone formation.
CT
Computed tomography has a place in the diagnosis of AS, particularly established disease, because it has the ability to detect erosions at an early time, compared with conventional radiograph, said Dr. Marzo-Ortega. The main problem with CT is radiation exposure. “So it won't be something that we would be doing on a daily basis.”
However, “there is a place for it when we have an x-ray that shows sort of borderline changes. Then we do a CT to confirm that it's definitely established abnormalities. … We're looking for erosions, we're looking for sclerosis, we're looking for ankylosis to establish changes.”
Ultrasound
“Ultrasound does not have a role in spinal diseases as yet. There are no data to suggest that it is good for visualizing any structures in the spine,” Dr. Marzo-Ortega said.
Where ultrasound does have a role is in evaluating peripheral joints. “There is definitely a place in spondyloarthritis/ankylosing spondylitis to look for enthesitis in the peripheral joints, and also—as in rheumatoid arthritis—to assess bone damage or synovitis.” So when patients present with axial and peripheral disease, ultrasound can be useful to look for subclinical or entheseal disease in the peripheral joints.
Magnetic resonance imaging and other advanced imaging modalities have a long way to go before they become accepted parts of the diagnostic work-up for ankylosing spondylitis. History, physical examination, and conventional radiography form its existing diagnostic criteria.
Dr. Helena Marzo-Ortega is a consultant rheumatologist at the University of Leeds (England). She has been studying the use of MRI in the diagnosis and treatment of AS. Here are her thoughts on what roles different imaging modalities can play in better diagnosing and managing AS.
X-Ray
With x-ray, which is the imaging tool used by the main AS classification, only abnormalities affecting the bone structure can be seen. This means that “it may take up to 8–10 years of symptoms before somebody develops changes that are picked up by conventional x-ray,” Dr. Marzo-Ortega noted.
Still, x-ray has a place in AS. “Young patients, who [make up] most of our population, may not [present as soon as] pain starts. It usually takes them a few months, and sometimes years, to come in,” she said. The first line of investigation with such patients could be an x-ray because if positive, the diagnosis of AS can be made.
MRI
MRI is mainly used in the research setting. The strength of MRIis its ability to reveal abnormalities in the synovium, the soft tissues, and the entheses, said Dr. Marzo-Ortega.
MRI picks up inflammation and bone edema, which may be identified in about 80% of patients. “This means that there are still another 20% of cases, where we are left with a negative MRI and uncertainty about the diagnosis,” she said.
AS diagnosis is based on involvement of the sacroiliac joint. “The majority of patients will have the sacroiliac joints affected before the spine.”
Most research done to date using MRI in AS has looked at the sacroiliac joints to see if there are any signs of active inflammation. However, MRI equipment, limited by its reliance on the commonly used T1.5 magnets, is not sensitive enough to reveal such changes.
“The SI joints are very small and the abnormalities happen within the bone marrow. … It's really the bone marrow that we're looking at.” A positive MRI would indicate inflammation within the bone marrow.
The use of biologics requires patients be followed with x-ray according to the treatment guidelines in both the United States and Europe, which follow the New York criteria.
“However, we all know that we're not prepared to wait 8–10 years so we can make the diagnosis and then treat the patient.” Instead, if the MRI is positive, “we follow criteria, as recently proposed by the ASAS [Assessment in Ankylosing Spondylitis] international working group. This allows for the diagnosis of axial SpA (or preradiographic AS) to be made if sacroiliitis is found by any imaging method with at least one clinical parameter, or if there is HLA-B27 positivity plus at least two clinical parameters,” Dr. Marzo-Ortega noted.
Data from a study following AS patients for 8 years show that “the MRI signal determines the development of radiographic structural damage. It is the intensity of the signal that matters. … The more severe the edema, the greater the chance to develop radiographic sacroiliitis at a year's time [Arthritis Rheum. 2008;58:3413–8].
MRI has a role to play in the evaluation of therapies for AS. In this disease, inflammation may lead to erosive disease but it may also lead to new bone formation, which may result in spinal fusion. “We don't really know what the relationship between inflammation and new bone formation is. Even if we use very potent agents, such as tumor necrosis factor [TNF]-alpha blockers that can control inflammation, we're not really sure whether that's making any big impact on new bone formation as an outcome,” said Dr. Marzo-Ortega. MRI could be used to follow patients treated with TNF-blockers to understand what effect the drugs have on erosions and new bone formation.
CT
Computed tomography has a place in the diagnosis of AS, particularly established disease, because it has the ability to detect erosions at an early time, compared with conventional radiograph, said Dr. Marzo-Ortega. The main problem with CT is radiation exposure. “So it won't be something that we would be doing on a daily basis.”
However, “there is a place for it when we have an x-ray that shows sort of borderline changes. Then we do a CT to confirm that it's definitely established abnormalities. … We're looking for erosions, we're looking for sclerosis, we're looking for ankylosis to establish changes.”
Ultrasound
“Ultrasound does not have a role in spinal diseases as yet. There are no data to suggest that it is good for visualizing any structures in the spine,” Dr. Marzo-Ortega said.
Where ultrasound does have a role is in evaluating peripheral joints. “There is definitely a place in spondyloarthritis/ankylosing spondylitis to look for enthesitis in the peripheral joints, and also—as in rheumatoid arthritis—to assess bone damage or synovitis.” So when patients present with axial and peripheral disease, ultrasound can be useful to look for subclinical or entheseal disease in the peripheral joints.
MRI shows bone marrow edema (white arrows) in the same patient. PHOTOS COURTESY DR. HELENA MARZO-ORTEGA
Magnetic resonance imaging and other advanced imaging modalities have a long way to go before they become accepted parts of the diagnostic work-up for ankylosing spondylitis. History, physical examination, and conventional radiography form its existing diagnostic criteria.
Dr. Helena Marzo-Ortega is a consultant rheumatologist at the University of Leeds (England). She has been studying the use of MRI in the diagnosis and treatment of AS. Here are her thoughts on what roles different imaging modalities can play in better diagnosing and managing AS.
X-Ray
With x-ray, which is the imaging tool used by the main AS classification, only abnormalities affecting the bone structure can be seen. This means that “it may take up to 8–10 years of symptoms before somebody develops changes that are picked up by conventional x-ray,” Dr. Marzo-Ortega noted.
Still, x-ray has a place in AS. “Young patients, who [make up] most of our population, may not [present as soon as] pain starts. It usually takes them a few months, and sometimes years, to come in,” she said. The first line of investigation with such patients could be an x-ray because if positive, the diagnosis of AS can be made.
MRI
MRI is mainly used in the research setting. The strength of MRIis its ability to reveal abnormalities in the synovium, the soft tissues, and the entheses, said Dr. Marzo-Ortega.
MRI picks up inflammation and bone edema, which may be identified in about 80% of patients. “This means that there are still another 20% of cases, where we are left with a negative MRI and uncertainty about the diagnosis,” she said.
AS diagnosis is based on involvement of the sacroiliac joint. “The majority of patients will have the sacroiliac joints affected before the spine.”
Most research done to date using MRI in AS has looked at the sacroiliac joints to see if there are any signs of active inflammation. However, MRI equipment, limited by its reliance on the commonly used T1.5 magnets, is not sensitive enough to reveal such changes.
“The SI joints are very small and the abnormalities happen within the bone marrow. … It's really the bone marrow that we're looking at.” A positive MRI would indicate inflammation within the bone marrow.
The use of biologics requires patients be followed with x-ray according to the treatment guidelines in both the United States and Europe, which follow the New York criteria.
“However, we all know that we're not prepared to wait 8–10 years so we can make the diagnosis and then treat the patient.” Instead, if the MRI is positive, “we follow criteria, as recently proposed by the ASAS [Assessment in Ankylosing Spondylitis] international working group. This allows for the diagnosis of axial SpA (or preradiographic AS) to be made if sacroiliitis is found by any imaging method with at least one clinical parameter, or if there is HLA-B27 positivity plus at least two clinical parameters,” Dr. Marzo-Ortega noted.
Data from a study following AS patients for 8 years show that “the MRI signal determines the development of radiographic structural damage. It is the intensity of the signal that matters. … The more severe the edema, the greater the chance to develop radiographic sacroiliitis at a year's time [Arthritis Rheum. 2008;58:3413–8].
MRI has a role to play in the evaluation of therapies for AS. In this disease, inflammation may lead to erosive disease but it may also lead to new bone formation, which may result in spinal fusion. “We don't really know what the relationship between inflammation and new bone formation is. Even if we use very potent agents, such as tumor necrosis factor [TNF]-alpha blockers that can control inflammation, we're not really sure whether that's making any big impact on new bone formation as an outcome,” said Dr. Marzo-Ortega. MRI could be used to follow patients treated with TNF-blockers to understand what effect the drugs have on erosions and new bone formation.
CT
Computed tomography has a place in the diagnosis of AS, particularly established disease, because it has the ability to detect erosions at an early time, compared with conventional radiograph, said Dr. Marzo-Ortega. The main problem with CT is radiation exposure. “So it won't be something that we would be doing on a daily basis.”
However, “there is a place for it when we have an x-ray that shows sort of borderline changes. Then we do a CT to confirm that it's definitely established abnormalities. … We're looking for erosions, we're looking for sclerosis, we're looking for ankylosis to establish changes.”
Ultrasound
“Ultrasound does not have a role in spinal diseases as yet. There are no data to suggest that it is good for visualizing any structures in the spine,” Dr. Marzo-Ortega said.
Where ultrasound does have a role is in evaluating peripheral joints. “There is definitely a place in spondyloarthritis/ankylosing spondylitis to look for enthesitis in the peripheral joints, and also—as in rheumatoid arthritis—to assess bone damage or synovitis.” So when patients present with axial and peripheral disease, ultrasound can be useful to look for subclinical or entheseal disease in the peripheral joints.
A 55-year-old woman presents with an intermittent sensation of food getting stuck in her mid to lower chest. The symptoms have occurred several times per year over the last 2 or 3 years and appear to be slowly worsening. She says she has no trouble swallowing liquids. She has a history of gastroesophageal reflux disease, for which she takes a proton pump inhibitor once a day. She says she has had no odynophagia, cough, regurgitation, or weight loss.
How should her symptoms best be evaluated?
DYSPHAGIA CAN BE OROPHARYNGEAL OR ESOPHAGEAL
Dysphagia is the subjective sensation of difficulty swallowing solids, liquids, or both. Symptoms can range from the inability to initiate a swallow to the sensation of esophageal obstruction. Other symptoms of esophageal disease may also be present, such as chest pain, heartburn, and regurgitation. There may also be nonesophageal symptoms related to the disease process causing the dysphagia.
Dysphagia can be separated into oropharyngeal and esophageal types.
Oropharyngeal dysphagia arises from problems in the oropharynx and cervical esophagus and is commonly caused by neurologic disorders of the central or peripheral nervous system (eg, stroke, myasthenia gravis), inflammatory myopathy, or a structural abnormality of the oropharynx, hypopharynx, or cervical esophagus such as a cricopharyngeal bar or tumor (Table 1). Patients typically complain of not being able to initiate a swallow or of food getting stuck in the cervical region immediately upon swallowing, accompanied by nasal regurgitation.1
Interestingly, many patients with symptoms of oropharyngeal dysphagia in fact have referred symptoms from primary esophageal dysphagia2; many patients with a distal mucosal ring describe a sense of something sticking in the cervical esophagus.
Esophageal dysphagia arises in the mid to distal esophagus or gastric cardia, and as a result, the symptoms are typically retrosternal.1 It can be caused by structural problems such as strictures, rings, webs, extrinsic compression, or a primary esophageal or gastroesophageal neoplasm, or by a primary motility abnormality such as achalasia (Table 1). Eosinophilic esophagitis is now a frequent cause of esophageal dysphagia, especially in white men.3
ESOPHAGOGRAPHY VS ENDOSCOPY IN EVALUATING DYSPHAGIA
Many gastroenterologists recommend endoscopy rather than barium esophagography as the initial examination in patients with dysphagia.4–8 Each test has certain advantages.
Advantages of endoscopy. Endoscopy is superior to esophagography in detecting milder grades of esophagitis. Further, interventions can be performed endoscopically (eg, dilation, biopsy, attachment of a wireless pH testing probe) that cannot be done during a radiographic procedure, and endoscopy does not expose the patient to radiation.
Advantages of esophagography. Endoscopy cannot detect evidence of gastroesophageal reflux disease unless mucosal injury is present. In dysphagia, the radiologic findings correlate well with endoscopic findings, including the detection of esophageal malignancy and moderate to severe esophagitis. Further, motility disorders can be detected with barium esophagography but not with endoscopy.9,10
Subtle abnormalities, especially rings and strictures, may be missed by narrow-diameter (9.8–10 mm) modern upper-endoscopic equipment. Further, esophagography is noninvasive, costs less, and may be more convenient (it does not require sedation and a chaperone for the patient after sedation). This examination also provides dynamic evaluation of the complex process of swallowing. Causes of dysphagia external to the esophagus can also be determined.
In view of the respective advantages and disadvantages of the two methods, we believe that in most instances barium esophagography should be the initial examination,1,9,11–15 and at our institution most patients presenting with dysphagia undergo barium esophagography before they undergo other examinations.14
OBTAIN A HISTORY BEFORE ORDERING ESOPHAGOGRAPHY
Before a barium examination of the esophagus is done, a focused medical history should be obtained, as it can guide the further workup as well as the esophageal study itself.
An attempt should be made to determine whether the dysphagia is oropharyngeal or if it is esophageal, as the former is generally best initially evaluated by a speech and language pathologist. Generally, the physician who orders the test judges whether the patient has oropharyngeal or esophageal dysphagia. Often, both an oropharyngeal examination, performed by a speech and language pathologist, and an esophageal examination, performed by a radiologist, are ordered.
Rapidly progressive symptoms, especially if accompanied by weight loss, should make one suspect cancer. Chronic symptoms usually point to gastroesophageal reflux disease or a motility disorder such as achalasia. Liquid dysphagia almost always means the patient has a motility disorder such as achalasia.
In view of the possibility of eosinophilic esophagitis, one should ask about food or seasonal allergies, especially in young patients with intermittent difficulty swallowing solids.3
BARIUM ESOPHAGOGRAPHY HAS EIGHT SEPARATE PHASES
Barium esophagography is tailored to the patient with dysphagia on the basis of his or her history. The standard examination is divided into eight separate phases (see below).14 Each phase addresses a specific question or questions concerning the structure and function of the esophagus.
At our institution, the first phase of the examination is determined by the presenting symptoms. If the patient has liquid dysphagia, we start with a timed barium swallow to assess esophageal emptying. If the patient does not have liquid dysphagia, we start with an air-contrast mucosal examination.
The patient must be cooperative and mobile to complete all phases of the examination.
Timed barium swallow to measure esophageal emptying
The timed barium swallow is an objective measure of esophageal emptying.16–18 This technique is essential in the initial evaluation of a patient with liquid dysphagia, a symptom common in patients with severe dysmotility, usually achalasia.
Figure 1. Timed barium swallow in a patient with achalasia. The patient consumed 140 mL of low-density barium. There is no emptying of barium between the 1-minute and 5-minute films.
In the upright position, the patient is asked to ingest up to 250 mL of low-density barium, as tolerated. The height and width of the barium column at 1 minute and 5 minutes are measured and recorded (Figure 1).
We use this examination in our patients with suspected or confirmed achalasia and to follow up patients who have been treated with pneumatic dilatation, botulinum toxin injection, and Heller myotomy.17,18 In addition, this timed test is an objective measure of emptying in patients who have undergone intervention but whose symptoms have not subjectively improved, and can suggest that further intervention may be required.
Air-contrast or mucosal phase
Figure 2. Esophagographic phases in a patient with solid-food dysphagia and a significant distal mucosal ring. A. The upright, mucosal phase of the examination shows no abnormalities. B. The distended or full-column phase of the examination shows the distal mucosal ring (arrow) as a sharply defined, ridge-like filling defect in the barium column above a small, sliding-type hiatal hernia (HH) (brought out by the increased intra-abdominal pressure with the patient in the semiprone position). C. The mucosal relief phase again shows the circumferential nature of the distal ring (arrows), as well as the hiatal hernia. D. Spontaneous reflux of gastric barium (arrows) with the patient in the supine position. The barium refluxed to the level of the thoracic inlet. E. Obstruction of the ingested 13-mm tablet (T) at the level of the distal mucosal ring. Barium above the tablet was given to precisely identify the location of the obstruction.
The air-contrast phase of the examination is designed to evaluate the esophageal mucosa and to determine if there is a fixed (nonreducible) hernia. In the upright position, the patient ingests CO2 gas-producing crystals with a small amount of water and then ingests high-density barium in order to coat the mucosa. Spot films are taken of the gas-distended, barium-coated esophagus (Figure 2A).
Although this phase is not as sensitive as endoscopy, it can detect masses, mucosal erosions, ulcers, and—most importantly in our experience—fixed hernias. Patients with a fixed hernia have a foreshortened esophagus, which is important to know about before repairing the hernia. Many esophageal surgeons believe that a foreshortened esophagus precludes a standard Nissen fundoplication and necessitates an esophageal lengthening procedure (ie, Collis gastroplasty with a Nissen fundoplication).14
Motility phase
The third phase examines esophageal motility. With the patient in a semiprone position, low-density barium is given in single swallows, separated by 25 to 30 seconds. The images are recorded on digital media to allow one to review them frame by frame.
The findings on this phase correlate well with those of manometry.19 This portion of the examination also uses impedance monitoring to assess bolus transfer, an aspect not evaluated by manometry.20,21 Impedance monitoring detects changes in resistance to current flow and correlates well with esophagraphic findings regarding bolus transfer.
While many patients with dysphagia also undergo esophageal manometry, the findings from this phase of the esophagographic examination may be the first indication of an esophageal motility disorder. In fact, this portion of the examination shows the distinct advantage of esophagography over endoscopy as the initial test in patients with dysphagia, as endoscopy may not identify patients with achalasia, especially early on.4
Single-contrast (full-column) phase to detect strictures, rings
The fourth phase of the esophagographic evaluation is the distended, single-contrast examination (Figure 2B). This is performed in the semiprone position with the patient rapidly drinking thin barium. It is done to detect esophageal strictures, rings, and contour abnormalities caused by extrinsic processes. Subtle abnormalities shown by this technique, including benign strictures and rings, are often not visualized with endoscopy.
Mucosal relief phase
The fifth phase is performed with a collapsed esophagus immediately after the distended, single-contrast phase, where spot films are taken of the barium-coated, collapsed esophagus (Figure 2C). This phase is used to evaluate thickened mucosal folds, a common finding in moderate to severe reflux esophagitis.
Reflux evaluation
Provocative maneuvers are used in the sixth phase to elicit gastroesophageal reflux (Figure 2D). With the patient supine, he or she is asked to roll side to side, do a Valsalva maneuver, and do a straight-leg raise. The patient then sips water in the supine position to assess for reflux (the water siphon test). If reflux is seen, the cause, the height of the reflux, and the duration of reflux retention are recorded.
Solid-bolus phase to assess strictures
In the seventh phase, the patient swallows a 13-mm barium tablet (Figure 2E). This allows one to assess the significance of a ring or stricture and to assess if dysphagia symptoms recur as a result of tablet obstruction. Subtle strictures that were not detected during the prior phases can also be detected using a tablet. If obstruction or impaired passage occurs, the site of obstruction and the presence or absence of symptoms are recorded.
Modified esophagography to assess the oropharynx
The final or eighth phase of barium esophagography is called “modified barium esophagography” or the modified barium swallow. However, it may be the first phase of the examination performed or the only portion of the examination performed, or it may not be performed at all.
Modified barium esophagography is used to define the anatomy of the oropharynx and to assess its function in swallowing.12 It may also guide rehabilitation strategies aimed at eliminating a patient’s swallowing symptoms.
Most patients referred for this test have sustained damage to the central nervous system or structures of the oropharynx, such as stroke or radiation therapy for laryngeal cancer. Many have difficulty in starting to swallow, aspirate when they try to swallow, or both.
In this test, thin liquids are given to the patient in escalating amounts. The patient is then given thicker foods, including thick liquids, purees, and food requiring chewing. If the patient has difficulty swallowing, intervention and therapeutic strategies are initiated. If the test is done by itself and the speech pathologist cannot find a cause of the patient’s symptoms, then barium esophagography should be performed by a radiologist.
The final esophagographic report should document the findings of each phase of the examination (Table 2).
WHAT HAPPENED TO OUR PATIENT?
Our patient underwent barium esophagography (Figure 2). A distal mucosal ring that transiently obstructed a 13-mm tablet was found. The patient underwent endoscopy and the ring was dilated. No biopsies were necessary.
References
Levine MS, Rubesin SE. Radiologic investigation of dysphagia. AJR Am J Roentgenol1990; 154:1157–1163.
Smith DF, Ott DJ, Gelfand DW, Chen MY. Lower esophageal mucosal ring: correlation of referred symptoms with radiographic findings using a marshmallow bolus. AJR Am J Roentgenol1998; 171:1361–1365.
Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology2007; 133:1342–1363.
Spechler SJ. American Gastroenterological Association medical position statement on treatment of patients with dysphagia caused by benign disorders of the distal esophagus. Gastroenterology1999; 117:229–233.
American Society for Gastrointestinal Endoscopy. Appropriate use of gastrointestinal endoscopy. Gastrointest Endosc2000; 52:831–837.
Esfandyari T, Potter JW, Vaezi MF. Dysphagia: a cost analysis of the diagnostic approach. Am J Gastroenterol2002; 97:2733–2737.
Varadarajulu S, Eloubeidi MA, Patel RS, et al. The yield and the predictors of esophageal pathology when upper endoscopy is used for the initial evaluation of dysphagia. Gastrointest Endosc2005; 61:804–808.
Standards of Practice Committee. Role of endoscopy in the management of GERD. Gastrointest Endosc2007; 66:219–224.
Halpert RD, Feczko PJ, Spickler EM, Ackerman LV. Radiological assessment of dysphagia with endoscopic correlation. Radiology1985; 157:599–602.
Ott DJ. Gastroesophageal reflux disease. Radiol Clin North Am1994; 32:1147–1166.
Ekberg O, Pokieser P. Radiologic evaluation of the dysphagic patient. Eur Radiol1997; 7:1285–1295.
Logemann JA. Role of the modified barium swallow in management of patients with dysphagia. Otolaryngol Head Neck Surg1997; 116:335–338.
Baker ME, Rice TW. Radiologic evaluation of the esophagus: methods and value in motility disorders and GERD. Semin Thorac Cardiovasc Surg2001; 13:201–225.
Baker ME, Einstein DM, Herts BR, et al. Gastroesophageal reflux disease: integrating the barium esophagram before and after antire-flux surgery. Radiology2007; 243:329–339.
Levine MS, Rubesin SE, Laufer I. Barium esophagography: a study for all seasons. Clin Gastroenterol Hepatol2008; 6:11–25.
deOliveira JM, Birgisson S, Doinoff C, et al. Timed barium swallow: a simple technique for evaluating esophageal emptying in patients with achalasia. AJR Am J Roentgenol1997; 169:473–479.
Kostic SV, Rice TW, Baker ME, et al. Time barium esophagram: a simple physiologic assessment for achalasia. J Thorac Cardiovasc Surg2000; 120:935–943.
Vaezi MF, Baker ME, Achkar E, Richter JE. Timed barium oesophagram: better predictor of long term success after pneumatic dilation in achalasia than symptom assessment. Gut2002; 50:765–770.
Hewson EG, Ott DJ, Dalton CB, Chen YM, Wu WC, Richter JE. Manometry and radiology. Complementary studies in the assessment of esophageal motility disorders. Gastroenterology1990; 98:626–632.
Imam H, Shay S, Ali A, Baker M. Bolus transit patterns in healthy subjects: a study using simultaneous impedance monitoring, video-esophagram, and esophageal manometry. Am J Physiol Gastrointest Liver Physiol2005;G1000–G1006.
Imam H, Baker M, Shay S. Simultaneous barium esophagram, impedance monitoring and manometry in patients with dysphagia due to a tight fundoplication [abstract]. Gastroenterology2004; 126:A-639.
Brian C. Allen, MD Imaging Institute, Cleveland Clinic
Mark E. Baker, MD Imaging Institute and Taussig Cancer Institute, Cleveland Clinic
Gary W. Falk, MD, MS Center for Swallowing and Esophageal Disorders, Digestive Disease Institute, and Taussig Cancer Institute, Cleveland Clinic; Professor of Medicine, Cleveland Clinic Lerner College of Medicine of Case, Western Reserve University
Address: Brian C. Allen, MD, Imaging Institute, Hb6, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH; e-mail [email protected]
Brian C. Allen, MD Imaging Institute, Cleveland Clinic
Mark E. Baker, MD Imaging Institute and Taussig Cancer Institute, Cleveland Clinic
Gary W. Falk, MD, MS Center for Swallowing and Esophageal Disorders, Digestive Disease Institute, and Taussig Cancer Institute, Cleveland Clinic; Professor of Medicine, Cleveland Clinic Lerner College of Medicine of Case, Western Reserve University
Address: Brian C. Allen, MD, Imaging Institute, Hb6, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH; e-mail [email protected]
Author and Disclosure Information
Brian C. Allen, MD Imaging Institute, Cleveland Clinic
Mark E. Baker, MD Imaging Institute and Taussig Cancer Institute, Cleveland Clinic
Gary W. Falk, MD, MS Center for Swallowing and Esophageal Disorders, Digestive Disease Institute, and Taussig Cancer Institute, Cleveland Clinic; Professor of Medicine, Cleveland Clinic Lerner College of Medicine of Case, Western Reserve University
Address: Brian C. Allen, MD, Imaging Institute, Hb6, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH; e-mail [email protected]
A 55-year-old woman presents with an intermittent sensation of food getting stuck in her mid to lower chest. The symptoms have occurred several times per year over the last 2 or 3 years and appear to be slowly worsening. She says she has no trouble swallowing liquids. She has a history of gastroesophageal reflux disease, for which she takes a proton pump inhibitor once a day. She says she has had no odynophagia, cough, regurgitation, or weight loss.
How should her symptoms best be evaluated?
DYSPHAGIA CAN BE OROPHARYNGEAL OR ESOPHAGEAL
Dysphagia is the subjective sensation of difficulty swallowing solids, liquids, or both. Symptoms can range from the inability to initiate a swallow to the sensation of esophageal obstruction. Other symptoms of esophageal disease may also be present, such as chest pain, heartburn, and regurgitation. There may also be nonesophageal symptoms related to the disease process causing the dysphagia.
Dysphagia can be separated into oropharyngeal and esophageal types.
Oropharyngeal dysphagia arises from problems in the oropharynx and cervical esophagus and is commonly caused by neurologic disorders of the central or peripheral nervous system (eg, stroke, myasthenia gravis), inflammatory myopathy, or a structural abnormality of the oropharynx, hypopharynx, or cervical esophagus such as a cricopharyngeal bar or tumor (Table 1). Patients typically complain of not being able to initiate a swallow or of food getting stuck in the cervical region immediately upon swallowing, accompanied by nasal regurgitation.1
Interestingly, many patients with symptoms of oropharyngeal dysphagia in fact have referred symptoms from primary esophageal dysphagia2; many patients with a distal mucosal ring describe a sense of something sticking in the cervical esophagus.
Esophageal dysphagia arises in the mid to distal esophagus or gastric cardia, and as a result, the symptoms are typically retrosternal.1 It can be caused by structural problems such as strictures, rings, webs, extrinsic compression, or a primary esophageal or gastroesophageal neoplasm, or by a primary motility abnormality such as achalasia (Table 1). Eosinophilic esophagitis is now a frequent cause of esophageal dysphagia, especially in white men.3
ESOPHAGOGRAPHY VS ENDOSCOPY IN EVALUATING DYSPHAGIA
Many gastroenterologists recommend endoscopy rather than barium esophagography as the initial examination in patients with dysphagia.4–8 Each test has certain advantages.
Advantages of endoscopy. Endoscopy is superior to esophagography in detecting milder grades of esophagitis. Further, interventions can be performed endoscopically (eg, dilation, biopsy, attachment of a wireless pH testing probe) that cannot be done during a radiographic procedure, and endoscopy does not expose the patient to radiation.
Advantages of esophagography. Endoscopy cannot detect evidence of gastroesophageal reflux disease unless mucosal injury is present. In dysphagia, the radiologic findings correlate well with endoscopic findings, including the detection of esophageal malignancy and moderate to severe esophagitis. Further, motility disorders can be detected with barium esophagography but not with endoscopy.9,10
Subtle abnormalities, especially rings and strictures, may be missed by narrow-diameter (9.8–10 mm) modern upper-endoscopic equipment. Further, esophagography is noninvasive, costs less, and may be more convenient (it does not require sedation and a chaperone for the patient after sedation). This examination also provides dynamic evaluation of the complex process of swallowing. Causes of dysphagia external to the esophagus can also be determined.
In view of the respective advantages and disadvantages of the two methods, we believe that in most instances barium esophagography should be the initial examination,1,9,11–15 and at our institution most patients presenting with dysphagia undergo barium esophagography before they undergo other examinations.14
OBTAIN A HISTORY BEFORE ORDERING ESOPHAGOGRAPHY
Before a barium examination of the esophagus is done, a focused medical history should be obtained, as it can guide the further workup as well as the esophageal study itself.
An attempt should be made to determine whether the dysphagia is oropharyngeal or if it is esophageal, as the former is generally best initially evaluated by a speech and language pathologist. Generally, the physician who orders the test judges whether the patient has oropharyngeal or esophageal dysphagia. Often, both an oropharyngeal examination, performed by a speech and language pathologist, and an esophageal examination, performed by a radiologist, are ordered.
Rapidly progressive symptoms, especially if accompanied by weight loss, should make one suspect cancer. Chronic symptoms usually point to gastroesophageal reflux disease or a motility disorder such as achalasia. Liquid dysphagia almost always means the patient has a motility disorder such as achalasia.
In view of the possibility of eosinophilic esophagitis, one should ask about food or seasonal allergies, especially in young patients with intermittent difficulty swallowing solids.3
BARIUM ESOPHAGOGRAPHY HAS EIGHT SEPARATE PHASES
Barium esophagography is tailored to the patient with dysphagia on the basis of his or her history. The standard examination is divided into eight separate phases (see below).14 Each phase addresses a specific question or questions concerning the structure and function of the esophagus.
At our institution, the first phase of the examination is determined by the presenting symptoms. If the patient has liquid dysphagia, we start with a timed barium swallow to assess esophageal emptying. If the patient does not have liquid dysphagia, we start with an air-contrast mucosal examination.
The patient must be cooperative and mobile to complete all phases of the examination.
Timed barium swallow to measure esophageal emptying
The timed barium swallow is an objective measure of esophageal emptying.16–18 This technique is essential in the initial evaluation of a patient with liquid dysphagia, a symptom common in patients with severe dysmotility, usually achalasia.
Figure 1. Timed barium swallow in a patient with achalasia. The patient consumed 140 mL of low-density barium. There is no emptying of barium between the 1-minute and 5-minute films.
In the upright position, the patient is asked to ingest up to 250 mL of low-density barium, as tolerated. The height and width of the barium column at 1 minute and 5 minutes are measured and recorded (Figure 1).
We use this examination in our patients with suspected or confirmed achalasia and to follow up patients who have been treated with pneumatic dilatation, botulinum toxin injection, and Heller myotomy.17,18 In addition, this timed test is an objective measure of emptying in patients who have undergone intervention but whose symptoms have not subjectively improved, and can suggest that further intervention may be required.
Air-contrast or mucosal phase
Figure 2. Esophagographic phases in a patient with solid-food dysphagia and a significant distal mucosal ring. A. The upright, mucosal phase of the examination shows no abnormalities. B. The distended or full-column phase of the examination shows the distal mucosal ring (arrow) as a sharply defined, ridge-like filling defect in the barium column above a small, sliding-type hiatal hernia (HH) (brought out by the increased intra-abdominal pressure with the patient in the semiprone position). C. The mucosal relief phase again shows the circumferential nature of the distal ring (arrows), as well as the hiatal hernia. D. Spontaneous reflux of gastric barium (arrows) with the patient in the supine position. The barium refluxed to the level of the thoracic inlet. E. Obstruction of the ingested 13-mm tablet (T) at the level of the distal mucosal ring. Barium above the tablet was given to precisely identify the location of the obstruction.
The air-contrast phase of the examination is designed to evaluate the esophageal mucosa and to determine if there is a fixed (nonreducible) hernia. In the upright position, the patient ingests CO2 gas-producing crystals with a small amount of water and then ingests high-density barium in order to coat the mucosa. Spot films are taken of the gas-distended, barium-coated esophagus (Figure 2A).
Although this phase is not as sensitive as endoscopy, it can detect masses, mucosal erosions, ulcers, and—most importantly in our experience—fixed hernias. Patients with a fixed hernia have a foreshortened esophagus, which is important to know about before repairing the hernia. Many esophageal surgeons believe that a foreshortened esophagus precludes a standard Nissen fundoplication and necessitates an esophageal lengthening procedure (ie, Collis gastroplasty with a Nissen fundoplication).14
Motility phase
The third phase examines esophageal motility. With the patient in a semiprone position, low-density barium is given in single swallows, separated by 25 to 30 seconds. The images are recorded on digital media to allow one to review them frame by frame.
The findings on this phase correlate well with those of manometry.19 This portion of the examination also uses impedance monitoring to assess bolus transfer, an aspect not evaluated by manometry.20,21 Impedance monitoring detects changes in resistance to current flow and correlates well with esophagraphic findings regarding bolus transfer.
While many patients with dysphagia also undergo esophageal manometry, the findings from this phase of the esophagographic examination may be the first indication of an esophageal motility disorder. In fact, this portion of the examination shows the distinct advantage of esophagography over endoscopy as the initial test in patients with dysphagia, as endoscopy may not identify patients with achalasia, especially early on.4
Single-contrast (full-column) phase to detect strictures, rings
The fourth phase of the esophagographic evaluation is the distended, single-contrast examination (Figure 2B). This is performed in the semiprone position with the patient rapidly drinking thin barium. It is done to detect esophageal strictures, rings, and contour abnormalities caused by extrinsic processes. Subtle abnormalities shown by this technique, including benign strictures and rings, are often not visualized with endoscopy.
Mucosal relief phase
The fifth phase is performed with a collapsed esophagus immediately after the distended, single-contrast phase, where spot films are taken of the barium-coated, collapsed esophagus (Figure 2C). This phase is used to evaluate thickened mucosal folds, a common finding in moderate to severe reflux esophagitis.
Reflux evaluation
Provocative maneuvers are used in the sixth phase to elicit gastroesophageal reflux (Figure 2D). With the patient supine, he or she is asked to roll side to side, do a Valsalva maneuver, and do a straight-leg raise. The patient then sips water in the supine position to assess for reflux (the water siphon test). If reflux is seen, the cause, the height of the reflux, and the duration of reflux retention are recorded.
Solid-bolus phase to assess strictures
In the seventh phase, the patient swallows a 13-mm barium tablet (Figure 2E). This allows one to assess the significance of a ring or stricture and to assess if dysphagia symptoms recur as a result of tablet obstruction. Subtle strictures that were not detected during the prior phases can also be detected using a tablet. If obstruction or impaired passage occurs, the site of obstruction and the presence or absence of symptoms are recorded.
Modified esophagography to assess the oropharynx
The final or eighth phase of barium esophagography is called “modified barium esophagography” or the modified barium swallow. However, it may be the first phase of the examination performed or the only portion of the examination performed, or it may not be performed at all.
Modified barium esophagography is used to define the anatomy of the oropharynx and to assess its function in swallowing.12 It may also guide rehabilitation strategies aimed at eliminating a patient’s swallowing symptoms.
Most patients referred for this test have sustained damage to the central nervous system or structures of the oropharynx, such as stroke or radiation therapy for laryngeal cancer. Many have difficulty in starting to swallow, aspirate when they try to swallow, or both.
In this test, thin liquids are given to the patient in escalating amounts. The patient is then given thicker foods, including thick liquids, purees, and food requiring chewing. If the patient has difficulty swallowing, intervention and therapeutic strategies are initiated. If the test is done by itself and the speech pathologist cannot find a cause of the patient’s symptoms, then barium esophagography should be performed by a radiologist.
The final esophagographic report should document the findings of each phase of the examination (Table 2).
WHAT HAPPENED TO OUR PATIENT?
Our patient underwent barium esophagography (Figure 2). A distal mucosal ring that transiently obstructed a 13-mm tablet was found. The patient underwent endoscopy and the ring was dilated. No biopsies were necessary.
A 55-year-old woman presents with an intermittent sensation of food getting stuck in her mid to lower chest. The symptoms have occurred several times per year over the last 2 or 3 years and appear to be slowly worsening. She says she has no trouble swallowing liquids. She has a history of gastroesophageal reflux disease, for which she takes a proton pump inhibitor once a day. She says she has had no odynophagia, cough, regurgitation, or weight loss.
How should her symptoms best be evaluated?
DYSPHAGIA CAN BE OROPHARYNGEAL OR ESOPHAGEAL
Dysphagia is the subjective sensation of difficulty swallowing solids, liquids, or both. Symptoms can range from the inability to initiate a swallow to the sensation of esophageal obstruction. Other symptoms of esophageal disease may also be present, such as chest pain, heartburn, and regurgitation. There may also be nonesophageal symptoms related to the disease process causing the dysphagia.
Dysphagia can be separated into oropharyngeal and esophageal types.
Oropharyngeal dysphagia arises from problems in the oropharynx and cervical esophagus and is commonly caused by neurologic disorders of the central or peripheral nervous system (eg, stroke, myasthenia gravis), inflammatory myopathy, or a structural abnormality of the oropharynx, hypopharynx, or cervical esophagus such as a cricopharyngeal bar or tumor (Table 1). Patients typically complain of not being able to initiate a swallow or of food getting stuck in the cervical region immediately upon swallowing, accompanied by nasal regurgitation.1
Interestingly, many patients with symptoms of oropharyngeal dysphagia in fact have referred symptoms from primary esophageal dysphagia2; many patients with a distal mucosal ring describe a sense of something sticking in the cervical esophagus.
Esophageal dysphagia arises in the mid to distal esophagus or gastric cardia, and as a result, the symptoms are typically retrosternal.1 It can be caused by structural problems such as strictures, rings, webs, extrinsic compression, or a primary esophageal or gastroesophageal neoplasm, or by a primary motility abnormality such as achalasia (Table 1). Eosinophilic esophagitis is now a frequent cause of esophageal dysphagia, especially in white men.3
ESOPHAGOGRAPHY VS ENDOSCOPY IN EVALUATING DYSPHAGIA
Many gastroenterologists recommend endoscopy rather than barium esophagography as the initial examination in patients with dysphagia.4–8 Each test has certain advantages.
Advantages of endoscopy. Endoscopy is superior to esophagography in detecting milder grades of esophagitis. Further, interventions can be performed endoscopically (eg, dilation, biopsy, attachment of a wireless pH testing probe) that cannot be done during a radiographic procedure, and endoscopy does not expose the patient to radiation.
Advantages of esophagography. Endoscopy cannot detect evidence of gastroesophageal reflux disease unless mucosal injury is present. In dysphagia, the radiologic findings correlate well with endoscopic findings, including the detection of esophageal malignancy and moderate to severe esophagitis. Further, motility disorders can be detected with barium esophagography but not with endoscopy.9,10
Subtle abnormalities, especially rings and strictures, may be missed by narrow-diameter (9.8–10 mm) modern upper-endoscopic equipment. Further, esophagography is noninvasive, costs less, and may be more convenient (it does not require sedation and a chaperone for the patient after sedation). This examination also provides dynamic evaluation of the complex process of swallowing. Causes of dysphagia external to the esophagus can also be determined.
In view of the respective advantages and disadvantages of the two methods, we believe that in most instances barium esophagography should be the initial examination,1,9,11–15 and at our institution most patients presenting with dysphagia undergo barium esophagography before they undergo other examinations.14
OBTAIN A HISTORY BEFORE ORDERING ESOPHAGOGRAPHY
Before a barium examination of the esophagus is done, a focused medical history should be obtained, as it can guide the further workup as well as the esophageal study itself.
An attempt should be made to determine whether the dysphagia is oropharyngeal or if it is esophageal, as the former is generally best initially evaluated by a speech and language pathologist. Generally, the physician who orders the test judges whether the patient has oropharyngeal or esophageal dysphagia. Often, both an oropharyngeal examination, performed by a speech and language pathologist, and an esophageal examination, performed by a radiologist, are ordered.
Rapidly progressive symptoms, especially if accompanied by weight loss, should make one suspect cancer. Chronic symptoms usually point to gastroesophageal reflux disease or a motility disorder such as achalasia. Liquid dysphagia almost always means the patient has a motility disorder such as achalasia.
In view of the possibility of eosinophilic esophagitis, one should ask about food or seasonal allergies, especially in young patients with intermittent difficulty swallowing solids.3
BARIUM ESOPHAGOGRAPHY HAS EIGHT SEPARATE PHASES
Barium esophagography is tailored to the patient with dysphagia on the basis of his or her history. The standard examination is divided into eight separate phases (see below).14 Each phase addresses a specific question or questions concerning the structure and function of the esophagus.
At our institution, the first phase of the examination is determined by the presenting symptoms. If the patient has liquid dysphagia, we start with a timed barium swallow to assess esophageal emptying. If the patient does not have liquid dysphagia, we start with an air-contrast mucosal examination.
The patient must be cooperative and mobile to complete all phases of the examination.
Timed barium swallow to measure esophageal emptying
The timed barium swallow is an objective measure of esophageal emptying.16–18 This technique is essential in the initial evaluation of a patient with liquid dysphagia, a symptom common in patients with severe dysmotility, usually achalasia.
Figure 1. Timed barium swallow in a patient with achalasia. The patient consumed 140 mL of low-density barium. There is no emptying of barium between the 1-minute and 5-minute films.
In the upright position, the patient is asked to ingest up to 250 mL of low-density barium, as tolerated. The height and width of the barium column at 1 minute and 5 minutes are measured and recorded (Figure 1).
We use this examination in our patients with suspected or confirmed achalasia and to follow up patients who have been treated with pneumatic dilatation, botulinum toxin injection, and Heller myotomy.17,18 In addition, this timed test is an objective measure of emptying in patients who have undergone intervention but whose symptoms have not subjectively improved, and can suggest that further intervention may be required.
Air-contrast or mucosal phase
Figure 2. Esophagographic phases in a patient with solid-food dysphagia and a significant distal mucosal ring. A. The upright, mucosal phase of the examination shows no abnormalities. B. The distended or full-column phase of the examination shows the distal mucosal ring (arrow) as a sharply defined, ridge-like filling defect in the barium column above a small, sliding-type hiatal hernia (HH) (brought out by the increased intra-abdominal pressure with the patient in the semiprone position). C. The mucosal relief phase again shows the circumferential nature of the distal ring (arrows), as well as the hiatal hernia. D. Spontaneous reflux of gastric barium (arrows) with the patient in the supine position. The barium refluxed to the level of the thoracic inlet. E. Obstruction of the ingested 13-mm tablet (T) at the level of the distal mucosal ring. Barium above the tablet was given to precisely identify the location of the obstruction.
The air-contrast phase of the examination is designed to evaluate the esophageal mucosa and to determine if there is a fixed (nonreducible) hernia. In the upright position, the patient ingests CO2 gas-producing crystals with a small amount of water and then ingests high-density barium in order to coat the mucosa. Spot films are taken of the gas-distended, barium-coated esophagus (Figure 2A).
Although this phase is not as sensitive as endoscopy, it can detect masses, mucosal erosions, ulcers, and—most importantly in our experience—fixed hernias. Patients with a fixed hernia have a foreshortened esophagus, which is important to know about before repairing the hernia. Many esophageal surgeons believe that a foreshortened esophagus precludes a standard Nissen fundoplication and necessitates an esophageal lengthening procedure (ie, Collis gastroplasty with a Nissen fundoplication).14
Motility phase
The third phase examines esophageal motility. With the patient in a semiprone position, low-density barium is given in single swallows, separated by 25 to 30 seconds. The images are recorded on digital media to allow one to review them frame by frame.
The findings on this phase correlate well with those of manometry.19 This portion of the examination also uses impedance monitoring to assess bolus transfer, an aspect not evaluated by manometry.20,21 Impedance monitoring detects changes in resistance to current flow and correlates well with esophagraphic findings regarding bolus transfer.
While many patients with dysphagia also undergo esophageal manometry, the findings from this phase of the esophagographic examination may be the first indication of an esophageal motility disorder. In fact, this portion of the examination shows the distinct advantage of esophagography over endoscopy as the initial test in patients with dysphagia, as endoscopy may not identify patients with achalasia, especially early on.4
Single-contrast (full-column) phase to detect strictures, rings
The fourth phase of the esophagographic evaluation is the distended, single-contrast examination (Figure 2B). This is performed in the semiprone position with the patient rapidly drinking thin barium. It is done to detect esophageal strictures, rings, and contour abnormalities caused by extrinsic processes. Subtle abnormalities shown by this technique, including benign strictures and rings, are often not visualized with endoscopy.
Mucosal relief phase
The fifth phase is performed with a collapsed esophagus immediately after the distended, single-contrast phase, where spot films are taken of the barium-coated, collapsed esophagus (Figure 2C). This phase is used to evaluate thickened mucosal folds, a common finding in moderate to severe reflux esophagitis.
Reflux evaluation
Provocative maneuvers are used in the sixth phase to elicit gastroesophageal reflux (Figure 2D). With the patient supine, he or she is asked to roll side to side, do a Valsalva maneuver, and do a straight-leg raise. The patient then sips water in the supine position to assess for reflux (the water siphon test). If reflux is seen, the cause, the height of the reflux, and the duration of reflux retention are recorded.
Solid-bolus phase to assess strictures
In the seventh phase, the patient swallows a 13-mm barium tablet (Figure 2E). This allows one to assess the significance of a ring or stricture and to assess if dysphagia symptoms recur as a result of tablet obstruction. Subtle strictures that were not detected during the prior phases can also be detected using a tablet. If obstruction or impaired passage occurs, the site of obstruction and the presence or absence of symptoms are recorded.
Modified esophagography to assess the oropharynx
The final or eighth phase of barium esophagography is called “modified barium esophagography” or the modified barium swallow. However, it may be the first phase of the examination performed or the only portion of the examination performed, or it may not be performed at all.
Modified barium esophagography is used to define the anatomy of the oropharynx and to assess its function in swallowing.12 It may also guide rehabilitation strategies aimed at eliminating a patient’s swallowing symptoms.
Most patients referred for this test have sustained damage to the central nervous system or structures of the oropharynx, such as stroke or radiation therapy for laryngeal cancer. Many have difficulty in starting to swallow, aspirate when they try to swallow, or both.
In this test, thin liquids are given to the patient in escalating amounts. The patient is then given thicker foods, including thick liquids, purees, and food requiring chewing. If the patient has difficulty swallowing, intervention and therapeutic strategies are initiated. If the test is done by itself and the speech pathologist cannot find a cause of the patient’s symptoms, then barium esophagography should be performed by a radiologist.
The final esophagographic report should document the findings of each phase of the examination (Table 2).
WHAT HAPPENED TO OUR PATIENT?
Our patient underwent barium esophagography (Figure 2). A distal mucosal ring that transiently obstructed a 13-mm tablet was found. The patient underwent endoscopy and the ring was dilated. No biopsies were necessary.
References
Levine MS, Rubesin SE. Radiologic investigation of dysphagia. AJR Am J Roentgenol1990; 154:1157–1163.
Smith DF, Ott DJ, Gelfand DW, Chen MY. Lower esophageal mucosal ring: correlation of referred symptoms with radiographic findings using a marshmallow bolus. AJR Am J Roentgenol1998; 171:1361–1365.
Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology2007; 133:1342–1363.
Spechler SJ. American Gastroenterological Association medical position statement on treatment of patients with dysphagia caused by benign disorders of the distal esophagus. Gastroenterology1999; 117:229–233.
American Society for Gastrointestinal Endoscopy. Appropriate use of gastrointestinal endoscopy. Gastrointest Endosc2000; 52:831–837.
Esfandyari T, Potter JW, Vaezi MF. Dysphagia: a cost analysis of the diagnostic approach. Am J Gastroenterol2002; 97:2733–2737.
Varadarajulu S, Eloubeidi MA, Patel RS, et al. The yield and the predictors of esophageal pathology when upper endoscopy is used for the initial evaluation of dysphagia. Gastrointest Endosc2005; 61:804–808.
Standards of Practice Committee. Role of endoscopy in the management of GERD. Gastrointest Endosc2007; 66:219–224.
Halpert RD, Feczko PJ, Spickler EM, Ackerman LV. Radiological assessment of dysphagia with endoscopic correlation. Radiology1985; 157:599–602.
Ott DJ. Gastroesophageal reflux disease. Radiol Clin North Am1994; 32:1147–1166.
Ekberg O, Pokieser P. Radiologic evaluation of the dysphagic patient. Eur Radiol1997; 7:1285–1295.
Logemann JA. Role of the modified barium swallow in management of patients with dysphagia. Otolaryngol Head Neck Surg1997; 116:335–338.
Baker ME, Rice TW. Radiologic evaluation of the esophagus: methods and value in motility disorders and GERD. Semin Thorac Cardiovasc Surg2001; 13:201–225.
Baker ME, Einstein DM, Herts BR, et al. Gastroesophageal reflux disease: integrating the barium esophagram before and after antire-flux surgery. Radiology2007; 243:329–339.
Levine MS, Rubesin SE, Laufer I. Barium esophagography: a study for all seasons. Clin Gastroenterol Hepatol2008; 6:11–25.
deOliveira JM, Birgisson S, Doinoff C, et al. Timed barium swallow: a simple technique for evaluating esophageal emptying in patients with achalasia. AJR Am J Roentgenol1997; 169:473–479.
Kostic SV, Rice TW, Baker ME, et al. Time barium esophagram: a simple physiologic assessment for achalasia. J Thorac Cardiovasc Surg2000; 120:935–943.
Vaezi MF, Baker ME, Achkar E, Richter JE. Timed barium oesophagram: better predictor of long term success after pneumatic dilation in achalasia than symptom assessment. Gut2002; 50:765–770.
Hewson EG, Ott DJ, Dalton CB, Chen YM, Wu WC, Richter JE. Manometry and radiology. Complementary studies in the assessment of esophageal motility disorders. Gastroenterology1990; 98:626–632.
Imam H, Shay S, Ali A, Baker M. Bolus transit patterns in healthy subjects: a study using simultaneous impedance monitoring, video-esophagram, and esophageal manometry. Am J Physiol Gastrointest Liver Physiol2005;G1000–G1006.
Imam H, Baker M, Shay S. Simultaneous barium esophagram, impedance monitoring and manometry in patients with dysphagia due to a tight fundoplication [abstract]. Gastroenterology2004; 126:A-639.
References
Levine MS, Rubesin SE. Radiologic investigation of dysphagia. AJR Am J Roentgenol1990; 154:1157–1163.
Smith DF, Ott DJ, Gelfand DW, Chen MY. Lower esophageal mucosal ring: correlation of referred symptoms with radiographic findings using a marshmallow bolus. AJR Am J Roentgenol1998; 171:1361–1365.
Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology2007; 133:1342–1363.
Spechler SJ. American Gastroenterological Association medical position statement on treatment of patients with dysphagia caused by benign disorders of the distal esophagus. Gastroenterology1999; 117:229–233.
American Society for Gastrointestinal Endoscopy. Appropriate use of gastrointestinal endoscopy. Gastrointest Endosc2000; 52:831–837.
Esfandyari T, Potter JW, Vaezi MF. Dysphagia: a cost analysis of the diagnostic approach. Am J Gastroenterol2002; 97:2733–2737.
Varadarajulu S, Eloubeidi MA, Patel RS, et al. The yield and the predictors of esophageal pathology when upper endoscopy is used for the initial evaluation of dysphagia. Gastrointest Endosc2005; 61:804–808.
Standards of Practice Committee. Role of endoscopy in the management of GERD. Gastrointest Endosc2007; 66:219–224.
Halpert RD, Feczko PJ, Spickler EM, Ackerman LV. Radiological assessment of dysphagia with endoscopic correlation. Radiology1985; 157:599–602.
Ott DJ. Gastroesophageal reflux disease. Radiol Clin North Am1994; 32:1147–1166.
Ekberg O, Pokieser P. Radiologic evaluation of the dysphagic patient. Eur Radiol1997; 7:1285–1295.
Logemann JA. Role of the modified barium swallow in management of patients with dysphagia. Otolaryngol Head Neck Surg1997; 116:335–338.
Baker ME, Rice TW. Radiologic evaluation of the esophagus: methods and value in motility disorders and GERD. Semin Thorac Cardiovasc Surg2001; 13:201–225.
Baker ME, Einstein DM, Herts BR, et al. Gastroesophageal reflux disease: integrating the barium esophagram before and after antire-flux surgery. Radiology2007; 243:329–339.
Levine MS, Rubesin SE, Laufer I. Barium esophagography: a study for all seasons. Clin Gastroenterol Hepatol2008; 6:11–25.
deOliveira JM, Birgisson S, Doinoff C, et al. Timed barium swallow: a simple technique for evaluating esophageal emptying in patients with achalasia. AJR Am J Roentgenol1997; 169:473–479.
Kostic SV, Rice TW, Baker ME, et al. Time barium esophagram: a simple physiologic assessment for achalasia. J Thorac Cardiovasc Surg2000; 120:935–943.
Vaezi MF, Baker ME, Achkar E, Richter JE. Timed barium oesophagram: better predictor of long term success after pneumatic dilation in achalasia than symptom assessment. Gut2002; 50:765–770.
Hewson EG, Ott DJ, Dalton CB, Chen YM, Wu WC, Richter JE. Manometry and radiology. Complementary studies in the assessment of esophageal motility disorders. Gastroenterology1990; 98:626–632.
Imam H, Shay S, Ali A, Baker M. Bolus transit patterns in healthy subjects: a study using simultaneous impedance monitoring, video-esophagram, and esophageal manometry. Am J Physiol Gastrointest Liver Physiol2005;G1000–G1006.
Imam H, Baker M, Shay S. Simultaneous barium esophagram, impedance monitoring and manometry in patients with dysphagia due to a tight fundoplication [abstract]. Gastroenterology2004; 126:A-639.
Dysphagia can be due to problems in the oropharynx and cervical esophagus or in the distal esophagus.
Radiologic evaluation of dysphagia has distinct advantages over endoscopy, including its ability to diagnose both structural changes and motility disorders.
A barium evaluation can include a modified barium-swallowing study to evaluate the oropharynx, barium esophagography to evaluate the esophagus, and a timed study to evaluate esophageal emptying.
Often, the true cause of dysphagia is best approached with a combination of radiographic and endoscopic studies.
Nicholas Jouriles, MD, FACEP, Knox H. Todd, MD, MPH, Keith D. Hentel, MD, Corey M. Slovis, MD, Larry B. Goldstein, MD, FAAN, FAHA, Susan Stone, MD, Carl H. Schultz, MD, FACEP, and Joseph D. Toscano, MD
Nicholas Jouriles, MD, FACEP, Knox H. Todd, MD, MPH, Keith D. Hentel, MD, Corey M. Slovis, MD, Larry B. Goldstein, MD, FAAN, FAHA, Susan Stone, MD, Carl H. Schultz, MD, FACEP, and Joseph D. Toscano, MD
Author and Disclosure Information
Nicholas Jouriles, MD, FACEP, Knox H. Todd, MD, MPH, Keith D. Hentel, MD, Corey M. Slovis, MD, Larry B. Goldstein, MD, FAAN, FAHA, Susan Stone, MD, Carl H. Schultz, MD, FACEP, and Joseph D. Toscano, MD

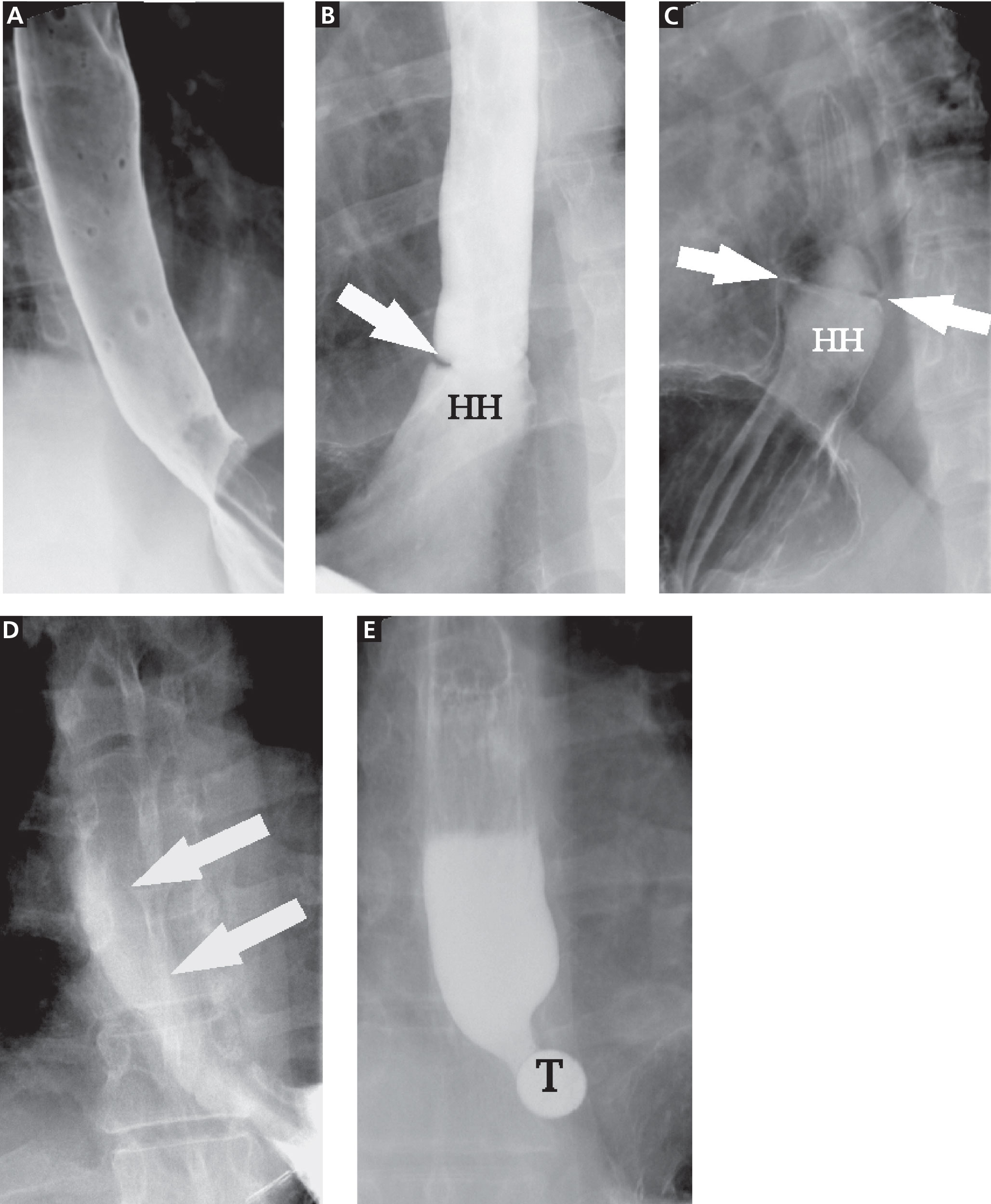
{kind=link}
{kind=link}